Embed Size (px)
Citation preview

www.elsevier.com/locate/jcf
Journal of Cystic Fibrosis xx (2014) xxx–xxx
JCF-01033; No of Pages 9
Original Article
Neutrophil elastase-mediated increase in airway temperatureduring inflammation
Annika Schmidt a,1, Azzaq Belaaouaj b,1, Rosi Bissinger a, Garrit Koller c, Laurette Malleret b,Ciro D'Orazio d, Martino Facchinelli e, Bernhard Schulte-Hubbert f, Antonio Molinaro g,
Otto Holst h, Jutta Hammermann i, Monika Schniederjans j, Keith C. Meyer k, Soeren Damkiaer l,Giorgio Piacentini e, Baroukh Assael d, Kenneth Bruce c, Susanne Häußler h, John J. LiPuma m,
Joachim Seelig n, Dieter Worlitzsch o,⁎, Gerd Döring a,1
a Institute of Medical Microbiology and Hygiene, German Center for Infection Research, University Clinic Tübingen, Germanyb INSERM U-1111, Centre International de Recherche en Infectiologie (CIRI), Lyon, France
c King's College, London, Englandd Department of Pediatrics, Verona, Italye Ospedale Civile Maggiore, Verona, Italy
f Medical Clinic und Policlinic I Pneumology, Technical University Dresden, Dresden, Germanyg Department of Chemical Sciences, Università di Napoli Federico II, Italy
h Research Center Borstel, Center for Medicine and Biosciences, Airway Research Center North (ARCN), Member of the German Center for Lung Research (DZL),Borstel, Germany
i Department of Pediatrics, Technical University Dresden, Dresden, Germanyj Helmholtz-Centre for Infection Research, Braunschweig, Germany
k University of Wisconsin School of Medicine, Madison, USAl Department of Systems Biology and Center for Biosustainability, Technical University of Denmark, Lyngby, Denmark
m Department of Paediatrics, University of Michigan, Ann Arbor, USAn Biophysical Chemistry, University of Basel, Basel Switzerland
o Institute of Hygiene, University of Halle, Germany
Received 3 January 2014; received in revised form 13 March 2014; accepted 13 March 2014Available online xxxx
Abstract
Background: How elevated temperature is generated during airway infections represents a hitherto unresolved physiological question. Wehypothesized that innate immune defence mechanisms would increase luminal airway temperature during pulmonary infection.Methods: We determined the temperature in the exhaled air of cystic fibrosis (CF) patients. To further test our hypothesis, a pouch inflammatory modelusing neutrophil elastase-deficient mice was employed. Next, the impact of temperature changes on the dominant CF pathogen Pseudomonas aeruginosagrowth was tested by plating method and RNAseq.Results: Here we show a temperature of ~38 °C in neutrophil-dominated mucus plugs of chronically infected CF patients and implicateneutrophil elastase:α1-proteinase inhibitor complex formation as a relevant mechanism for the local temperature rise. Gene expression of themain pathogen in CF, P. aeruginosa, under anaerobic conditions at 38 °C vs 30 °C revealed increased virulence traits and characteristic cell wallchanges.
⁎ Corresponding author at: Institute of Hygiene, University Hospital, Martin-Luther-University Halle, Magdeburger Str. 24, 06097 Halle/Saale, Germany. Tel.: +49345 557 1103; fax: +49 345 557 1093.
E-mail address: [email protected] (D. Worlitzsch).1 A.S. and A.B. contributed equally to this work. This study is dedicated to the memory of Gerd Döring and his commitment to CF research.
http://dx.doi.org/10.1016/j.jcf.2014.03.0041569-1993/© 2014 European Cystic Fibrosis Society. Published by Elsevier B.V. All rights reserved.
Please cite this article as: Schmidt A, et al, Neutrophil elastase-mediated increase in airway temperature during inflammation, J Cyst Fibros (2014), http://dx.doi.org/10.1016/j.jcf.2014.03.004

2 A. Schmidt et al. / Journal of Cystic Fibrosis xx (2014) xxx–xxx
Conclusion: Neutrophil elastase mediates increase in airway temperature, which may contribute to P. aeruginosa selection during the course of chronicinfection in CF.© 2014 European Cystic Fibrosis Society. Published by Elsevier B.V. All rights reserved.
Keywords: Neutrophil elastase; Temperature; Inflammation; Pseudomonas aeruginosa
1. Introduction
Mammals maintain and closely regulate elevated core bodytemperature (TB) by the hypothalamus via a complex feedbacksystem [1]. Besides their evolutionary importance [2,3], endother-my and homeothermy provide mammals with increased fitnessagainst fungal infections over a tight range of temperature from35.9 °C to 37.7 °C [4]. Whilst this “thermal exclusion zone”does not affect bacterial pathogens, which generally grow well atphysiological temperature in mammals, the elevated human coreTB provides optimal metabolic conditions for phagocytic cellactivity. For instance, maximum killing of the opportunisticpathogen, Staphylococcus aureus, by human neutrophils has beenobserved at 36–40 °C [5].
The airways are formally considered “outside” of the body,and, therefore, it is unclear how core TB [1] is regulated inhuman airways, particularly during pulmonary infection. Wehypothesized that innate immune defence mechanisms, activatedas a consequence of bacterial lung infection, would contribute tothe increase of luminal airway temperature during pulmonaryinfection. We tested this hypothesis in patients with the hereditarydisease cystic fibrosis (CF). CF patients suffer from chronicbacterial airway infections that are characterized by a largeinflux of polymorphonuclear leukocytes (neutrophils), whichform highly viscous mucus plugs around the bacterial pathogensthat persist in the airway lumen [6,7]. Our studies revealed that thebinding of neutrophil elastase (NE), to its physiologic inhibitor,α1-proteinase inhibitor (α1-PI), contributes to temperature rise ininflamed airways.
2. Methods
2.1. Patients
We determined the temperature in the exhaled air of 56 CFpatients, aged 6–17 years, attending the outpatient clinic of theCF centre in Verona, Italy. Patients with fever (3 times dailyauricular temperature measurement N38 °C) were excluded. Inaddition, we recruited 20 healthy subjects, aged 7–17 years,from the outpatient clinic of the Department of Paediatrics,Policlinico G. B. Rossi, Verona, Italy. Individuals with a previousdiagnosis of asthma or another respiratory disease were excluded.All controls were free from any respiratory infection for aminimum of 3 weeks prior to the study. For bronchial temperaturemeasurements, 5 CF patients (3 males, mean age 32.6 years,forced expiratory volume in one second % predicted, FEV1%:63% and 2 females, mean age: 26 years, FEV1%: 40.5%)
Please cite this article as: Schmidt A, et al, Neutrophil elastase-mediated increase in a10.1016/j.jcf.2014.03.004
attending the CF centre of the University of Dresden, Germany,and the CF centre of the University of Wisconsin, Schoolof Medicine, Madison, USA, were included. Additionally, wedetermined the bronchial temperature in 3 non-CF individualswith diagnosis of an unknown solitary pulmonary node, attendingthe Medical Clinic und Policlinic I Pneumology of the TechnicalUniversity Dresden. Body core temperature in the CF patientswas 36.7 ± 0.4 °C, in the healthy individuals 36.5 ± 0.4 °C.Informed consent was obtained from all patients and/or parents,and all parts of the study were approved by the local ethicalcommittees.
Data, which were normally distributed, were analysed usingpaired Student's t test. Results with inhomogeneous variancesin the Student's t test were analysed using the non-parametricMann–Whitney test. A p value of 0.05 or less was consideredsignificant.
2.2. Fiberoptic bronchoscopy and temperature measurementsin patients
Fiberoptic bronchoscopy was performed as described previ-ously [8] with minor modifications. The exhaled breath temper-ature test was performed using a CareFusion respiratory functionequipment (Vmax, SensorMedics,Yorba Linda, USA) [9]. Arespiratory filter (Mada, Milano, Italy) was attached to the massflow sensor for each participant to avoid microbiological con-tamination. Furthermore, a recently updated software applicationwas used to increase the sensitiveness of the measurementwhich resulted in an intra-subject variability of b1%, comparedto 2.35% using the previous software [10]. We applied theend-expiratory manoeuver plateau temperature (PLET) method[11]. PLET values depict the exhaled gas temperature withinthe device and therefore may differ from airway temperaturedepending on the type of device, respiratory filters and othertechnological items.
For measurements of the temperature in the bronchial lumenand in mucopurulent material within the bronchi, a computer-ized Clark type oxygen probe (length: 65 cm; outer diameter:2 mm; inner diameter: 0.4 mm; Licox pO2; GMS, Kiel, Germany)was inserted in the working channel of the bronchoscope andguided under video control into the right upper lobe, obstructedwith a mucopurulent material. Additionally, temperature mea-surements were conducted using a prototype thermistor basedprobe (Exacon Scientific, Roskilde, Denmark) with a confirmedtolerance of less than ±0.1 °C between 25° and 45 °C (length:200 cm; outer diameter: 2 mm; shieldedwith autoclavablemedicalgrade silicone). The base unit used was a DATEX CARDIOCAP
irway temperature during inflammation, J Cyst Fibros (2014), http://dx.doi.org/

3A. Schmidt et al. / Journal of Cystic Fibrosis xx (2014) xxx–xxx
II Patient Monitor (Datex Ohmeda, GE Healthcare, Salt LakeCity, USA) with a calibrated A type adapter and a presetmeasuring reference of 2252 Ohms at 25 °C. Patients weremildly sedated. Temperature measurements were made in theairway lumen and in mucopurulent material when present.
2.3. Isothermal titration calorimetry
For isothermal titration calorimetry, we incubated purifiedhuman NE and α1-PI at ratios of 1:10 or 10:1 w/w assumingextinction coefficients (E) and molecular masses (Mr) for NE ofE = 9.85 (1%, 1 cm pathway, 280 nm) andMr = 30,000 Da [12]and for α1-PI E = 0.433 (0.1%, 1 cm pathway, 280 nm) andMr = 52,000 Da [13], for 5 min and determined the enthalpy ofthe reaction mixtures. NE into α1-PI titrations and oppositetitrations was performed using an ITC-200 calorimeter (Microcal,Northampton, MA, USA). Titration experiments were performedin the range of 10 °C to 40 °C. Experiments were analysed usingthe ORIGIN software provided with the calorimeter. A bindingmodel with identical and independent binding sites was used to fitthe data.
2.4. Pouch temperature in mouse strains
NE-deficient (NE−/−) mice were generated by targetedmutagenesis as previously described [14]. Mouse strains wereback-crossed (8 generations) on a pure C57BL6/J background.C57BL/6 NE−/− mice and their wild-type (WT) littermates wereused in this study. Mice were sex and age (8–10 weeks) matchedand maintained in the animal barrier facility with a 12 h light/dark cycle and provided with water and food ad libitum. Animalhandling and procedures were approved by the InstitutionalAnimal Studies Committee (Health and Animal ProtectionOffice, Châlons-en-Champagne, Authorisation number: 51-31)in accordance with the guidelines of the Federation ofEuropean Laboratory Animal Science Associations (FELASA)and following the European Directive 2010/63/EU on theprotection of animals used in scientific procedures. Airpouches were generated as previously described [15]. Briefly,1 ml of sterile air was injected subcutaneously into the back ofmice (n = 5 per genotype), followed by instillation of 1 × 107
Pseudomonas aeruginosa colony forming units (CFU) perpouch to induce an inflammatory response. We used theP. aeruginosa strain H103, kindly provided by Dr. R. Hancock,Vancouver, BC, Canada, which was grown overnight in LuriaBertani broth at 37 °C to late exponential phase and washed twicewith PBS, pH 7.4. Control mice (n = 5) were challenged withsterile PBS alone. At designated time points (three dayspost-challenge), temperature in the pouch airspace was de-termined using a temperature probe (C8.B; GMS, Milkendorf,Germany), attached to a Licox CMP temperature monitor(Integra, Plainsboro, NJ, USA) which was introduced into thepouch via an 18 gauge needle. Next, the air pouch was lavagedwith PBS, and total and differential counts were performedimmediately [16].
Please cite this article as: Schmidt A, et al, Neutrophil elastase-mediated increase in a10.1016/j.jcf.2014.03.004
2.5. P. aeruginosa densities at different temperature
The following P. aeruginosa strains were used: PAO1 [17],PAO1 SD4 (Δ mucA), and PAO1 SD40 (Δ mucA algT), bothDTU Lyngby, Denmark [18]. Strains were grown in trypticasesoy broth (TSB) overnight. An aliquot was inoculated in freshmedium to an optical density (OD578) of 0.05, corresponding tocolony forming units (CFU) of 1 ×107 to 1 × 108. Then thebacterial suspensions were grown anaerobically in a anaerobicbox (Anaerocult®, Merck KGaA, Darmstadt, Germany) usingAnaeroGen (Oxoid Ltd., Basingstoke, England) under shakingat 30 °C, 37 °C, 38 °C and 39 °C (Infors, Bottmingen,Switzerland) for 96 h and CFU was determined by platingmethod.
2.6. P. aeruginosa transcript analysis at different temperatures
For P. aeruginosa transcript analysis at different tempera-tures and aerobic versus anaerobic growth conditions, strainPAO1 was incubated overnight at 30 °C and 38 °C in an100 ml Erlenmeyer flask, filled with 50 ml TSB medium undershaking at 180 rpm. An aliquot (OD578 0.05) is transferred to aBiostat B plus bioreactor (Sartorius, Melsungen, Germany)containing 1.5 l TSB medium, and incubated at 30 °C and38 °C aerobically with pH control for 6 h leading to a celldensity of 1 × 1010 CFU (OD578 8.0). Then the bioreactor wasflushed with nitrogen for 1 h to obtain anaerobic cultureconditions. Fifty millilitres of the suspension is harvested andmixed with an equal volume of RNA-Protect buffer (Qiagen,Hilden, Germany). After 10 min incubation at room tempera-ture, 1 ml aliquots are centrifuged at 6000 ×g for 5 min, thesupernatant removed and the pellets stored at −70 °C untiltranscript analysis.
2.7. Preparation and sequencing of cDNA libraries
The preparation and sequencing of the cDNA libraries weredone as described previously [19] with some modifications.The libraries were sequenced on an Illumina HiSeq 2000.Barcoded 59-adapters [19] enabled the pooling of multiplesamples on one lane of the Illumina flow cell. Libraries weresequenced with 50 cycles in single end mode. Computationalanalysis was done as described previously [19] with somemodifications. The reads were aligned to the PAO1 referencegenome using stampy, a short-read aligner that allows for gappedalignments [20]. The reported gene read counts were used toestimate the differential gene expression making use of thepackage DESeq in R (Project for statistical computing). Fordetails, see [19].
2.8. LPS analysis
For analysis by gel electrophoresis and silver staining, LPSwas prepared and visualized as previously described [21].Monosaccharides (as alditol acetates), total fatty acids (as methylesters) and organic phosphate contents were determined asreported [21]. GLC analyses were performed either on an Agilent
irway temperature during inflammation, J Cyst Fibros (2014), http://dx.doi.org/

35
34PL
ET
[°C
]
R2 = 0.3071
3320 40 60 80 100 120
FEV1%
35
p=0.001
p=0.004
34
PL
ET
[°C
]
33
FEV1%
20-60 60-80 80-120 90-12032
CF Control
39 p<0.05
p<0.05
37
38
tem
per
atu
re °
C
36CF Sputum CF Lumen healthy Lumen
0.0
-0.4
-0.2
0 1000 2000 3000 4000
-0.6
Time [sec]
Hea
t fl
ow
[µ
cal/s
ec]
0
-10
0 1 2
-20
Kca
l/Mo
l in
ject
ant
Molar ratio α1-PI:NE
105 CFUP. aeruginosa
32
34p<0.0005
30
WT
105 CFUP. aeruginosa
tem
per
atu
re °
C
WT NE -/-26
28
NE-/-
/WT PMN: 73.2% MNC: 26.8% NE-/- PMN: 67.2 MNC: 32.8%
50n.s.
30
40
20
0
10
To
tal f
luid
po
uch
cel
ls (
x10
5 /m
l)
WT NE-/-WT NE
A B
C
E F
G H
D
4 A. Schmidt et al. / Journal of Cystic Fibrosis xx (2014) xxx–xxx
Please cite this article as: Schmidt A, et al, Neutrophil elastase-mediated increase in airway temperature during inflammation, J Cyst Fibros (2014), http://dx.doi.org/10.1016/j.jcf.2014.03.004
5A. Schmidt et al. / Journal of Cystic Fibrosis xx (2014) xxx–xxx
7890A (sugars) or Agilent 6890 N instrument (fatty acids)(Agilent, Waldbronn, Germany), equipped with an AgilentHP-5MS capillary column (0.25 mm × 30 m). Matrix-assistedlaser desorption/ionization time-of-flight mass spectrometry(MALDI-TOF-MS) of lipid A were performed on a 4800Proteomic analyser (Applied Biosystems) supplied with a Nd:YAG laser at the wavelength of 355 nm. External calibrationwas performed and mass accuracy was better than 75 ppm[22].
3. Results
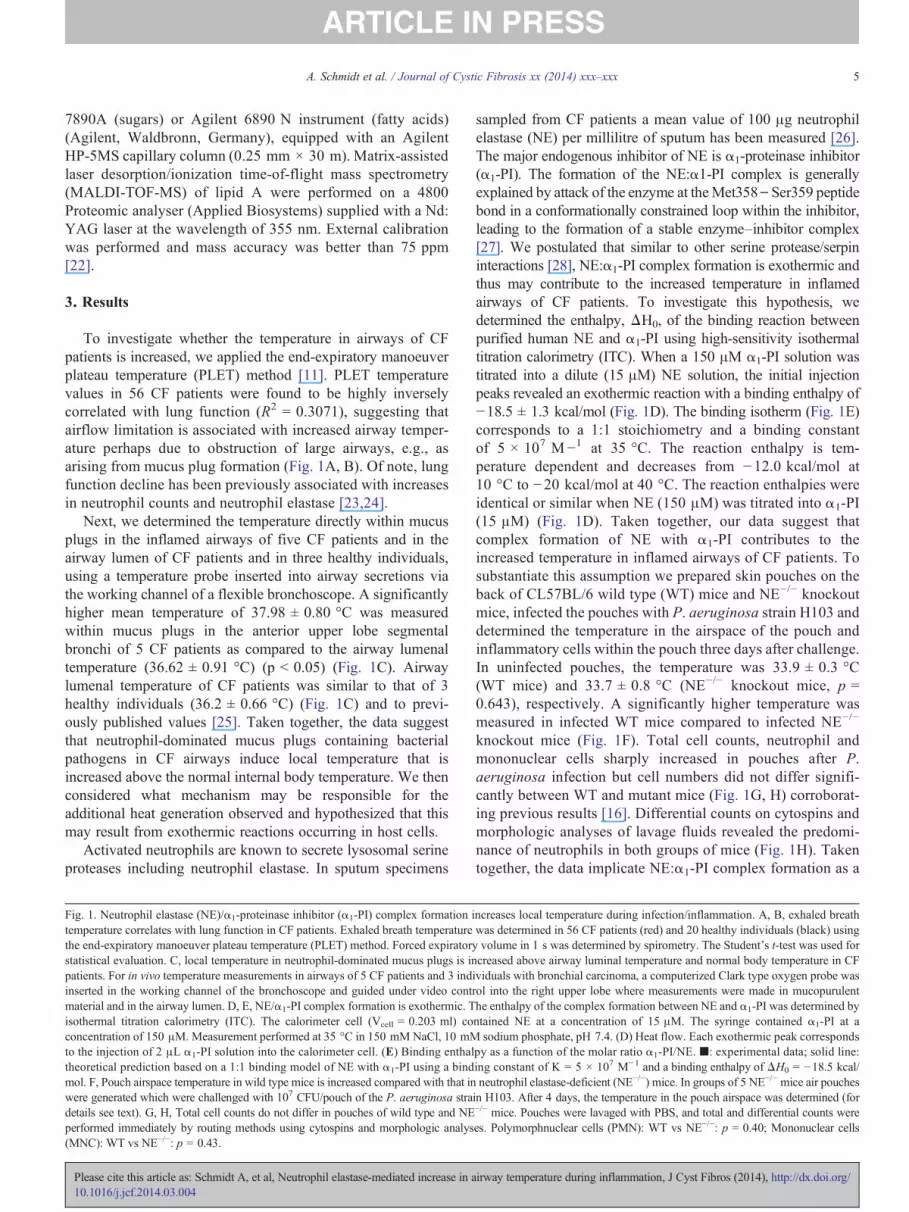
To investigate whether the temperature in airways of CFpatients is increased, we applied the end-expiratory manoeuverplateau temperature (PLET) method [11]. PLET temperaturevalues in 56 CF patients were found to be highly inverselycorrelated with lung function (R2 = 0.3071), suggesting thatairflow limitation is associated with increased airway temper-ature perhaps due to obstruction of large airways, e.g., asarising from mucus plug formation (Fig. 1A, B). Of note, lungfunction decline has been previously associated with increasesin neutrophil counts and neutrophil elastase [23,24].
Next, we determined the temperature directly within mucusplugs in the inflamed airways of five CF patients and in theairway lumen of CF patients and in three healthy individuals,using a temperature probe inserted into airway secretions viathe working channel of a flexible bronchoscope. A significantlyhigher mean temperature of 37.98 ± 0.80 °C was measuredwithin mucus plugs in the anterior upper lobe segmentalbronchi of 5 CF patients as compared to the airway lumenaltemperature (36.62 ± 0.91 °C) (p b 0.05) (Fig. 1C). Airwaylumenal temperature of CF patients was similar to that of 3healthy individuals (36.2 ± 0.66 °C) (Fig. 1C) and to previ-ously published values [25]. Taken together, the data suggestthat neutrophil-dominated mucus plugs containing bacterialpathogens in CF airways induce local temperature that isincreased above the normal internal body temperature. We thenconsidered what mechanism may be responsible for theadditional heat generation observed and hypothesized that thismay result from exothermic reactions occurring in host cells.
Activated neutrophils are known to secrete lysosomal serineproteases including neutrophil elastase. In sputum specimens
Fig. 1. Neutrophil elastase (NE)/α1-proteinase inhibitor (α1-PI) complex formation itemperature correlates with lung function in CF patients. Exhaled breath temperaturethe end-expiratory manoeuver plateau temperature (PLET) method. Forced expiratorystatistical evaluation. C, local temperature in neutrophil-dominated mucus plugs is inpatients. For in vivo temperature measurements in airways of 5 CF patients and 3 indinserted in the working channel of the bronchoscope and guided under video contmaterial and in the airway lumen. D, E, NE/α1-PI complex formation is exothermic. Tisothermal titration calorimetry (ITC). The calorimeter cell (Vcell = 0.203 ml) coconcentration of 150 μM. Measurement performed at 35 °C in 150 mM NaCl, 10 mMto the injection of 2 μL α1-PI solution into the calorimeter cell. (E) Binding enthaltheoretical prediction based on a 1:1 binding model of NE with α1-PI using a bindmol. F, Pouch airspace temperature in wild type mice is increased compared with that inwere generated which were challenged with 107 CFU/pouch of the P. aeruginosa stradetails see text). G, H, Total cell counts do not differ in pouches of wild type and NEperformed immediately by routing methods using cytospins and morphologic analys(MNC): WT vs NE−/−: p = 0.43.
Please cite this article as: Schmidt A, et al, Neutrophil elastase-mediated increase in a10.1016/j.jcf.2014.03.004
sampled from CF patients a mean value of 100 μg neutrophilelastase (NE) per millilitre of sputum has been measured [26].The major endogenous inhibitor of NE is α1-proteinase inhibitor(α1-PI). The formation of the NE:α1-PI complex is generallyexplained by attack of the enzyme at theMet358\Ser359 peptidebond in a conformationally constrained loop within the inhibitor,leading to the formation of a stable enzyme–inhibitor complex[27]. We postulated that similar to other serine protease/serpininteractions [28], NE:α1-PI complex formation is exothermic andthus may contribute to the increased temperature in inflamedairways of CF patients. To investigate this hypothesis, wedetermined the enthalpy, ΔH0, of the binding reaction betweenpurified human NE and α1-PI using high-sensitivity isothermaltitration calorimetry (ITC). When a 150 μM α1-PI solution wastitrated into a dilute (15 μM) NE solution, the initial injectionpeaks revealed an exothermic reaction with a binding enthalpy of−18.5 ± 1.3 kcal/mol (Fig. 1D). The binding isotherm (Fig. 1E)corresponds to a 1:1 stoichiometry and a binding constantof 5 × 107 M−1 at 35 °C. The reaction enthalpy is tem-perature dependent and decreases from −12.0 kcal/mol at10 °C to −20 kcal/mol at 40 °C. The reaction enthalpies wereidentical or similar when NE (150 μM) was titrated into α1-PI(15 μM) (Fig. 1D). Taken together, our data suggest thatcomplex formation of NE with α1-PI contributes to theincreased temperature in inflamed airways of CF patients. Tosubstantiate this assumption we prepared skin pouches on theback of CL57BL/6 wild type (WT) mice and NE−/− knockoutmice, infected the pouches with P. aeruginosa strain H103 anddetermined the temperature in the airspace of the pouch andinflammatory cells within the pouch three days after challenge.In uninfected pouches, the temperature was 33.9 ± 0.3 °C(WT mice) and 33.7 ± 0.8 °C (NE−/− knockout mice, p =0.643), respectively. A significantly higher temperature wasmeasured in infected WT mice compared to infected NE−/−
knockout mice (Fig. 1F). Total cell counts, neutrophil andmononuclear cells sharply increased in pouches after P.aeruginosa infection but cell numbers did not differ signifi-cantly between WT and mutant mice (Fig. 1G, H) corroborat-ing previous results [16]. Differential counts on cytospins andmorphologic analyses of lavage fluids revealed the predomi-nance of neutrophils in both groups of mice (Fig. 1H). Takentogether, the data implicate NE:α1-PI complex formation as a
ncreases local temperature during infection/inflammation. A, B, exhaled breathwas determined in 56 CF patients (red) and 20 healthy individuals (black) usingvolume in 1 s was determined by spirometry. The Student's t-test was used forcreased above airway luminal temperature and normal body temperature in CFividuals with bronchial carcinoma, a computerized Clark type oxygen probe wasrol into the right upper lobe where measurements were made in mucopurulenthe enthalpy of the complex formation between NE and α1-PI was determined byntained NE at a concentration of 15 μM. The syringe contained α1-PI at asodium phosphate, pH 7.4. (D) Heat flow. Each exothermic peak corresponds
py as a function of the molar ratio α1-PI/NE. ■: experimental data; solid line:ing constant of K = 5 × 107 M−1 and a binding enthalpy ofΔH0 = −18.5 kcal/neutrophil elastase-deficient (NE−/−) mice. In groups of 5 NE−/−mice air pouches
in H103. After 4 days, the temperature in the pouch airspace was determined (for−/− mice. Pouches were lavaged with PBS, and total and differential counts werees. Polymorphnuclear cells (PMN): WT vs NE−/−: p = 0.40; Mononuclear cells
irway temperature during inflammation, J Cyst Fibros (2014), http://dx.doi.org/

109
1010A Bp < 0.0001
CF
U/m
l
108
Start 30°C 37°C 38°C106
107
109
1010
108
106
107
p < 0.0001
p < 0.002
CF
U/m
l
PAO1 PAO1 mucA PAO1 mucA/algT
Fig. 2. P. aeruginosa grown anaerobically at an elevated temperature. A, The P. aeruginosa strain PAO1 was grown in liquid media at 30 °C, 37 °C, 38 °C and39 °C under anaerobic conditions for 96 h and bacterial CFU were determined using routine methods. B, At 39 °C the P. aeruginosa strain PAO1 and the alginateoverexpressing mutant PAO1 SD4 (Δ mucA) were significantly compromised compared to the nonmucoid strain PAO1 SD40 (Δ mucA/algT) under anaerobicconditions after 96 h incubation.
6 A. Schmidt et al. / Journal of Cystic Fibrosis xx (2014) xxx–xxx
relevant mechanism for temperature rise in lungs and otherareas outside of endothermic mammal bodies.
In contrast to mammals, bacteria are ectotherms, i.e., theirTB is dependent on the ambient temperature (TA). To successfullycope with extremely differences in TA, bacteria alter theirmembrane structures and the rates of many physiologicalprocesses. Here we assessed the survival of the dominantbacterial pathogen in CF airways, P. aeruginosa, at an arbitrarilyset low temperature of 30 °C, at human TB (37 °C), as well as at38 °C under anaerobic conditions which prevail within mucusplugs in the CF lung [6]. P. aeruginosa grew well at all elevatedtemperature compared to the inoculum for an extended timeperiod of 96 h (Fig. 2A). At 39 °C, growth of the alginateproducing WT strain PAO1 and the alginate overexpressingisogenic mutant PAO1 SD4 (Δ mucA) was significantly com-promised when compared to the isogenic non-mucoid variantPAO1 SD40 (Δ mucA algT) (Fig. 2B), suggesting an increasedfitness of algT mutants under these conditions. Of noteP. aeruginosa mucA/algT mutants are frequently observed inthe infected airways of CF patients [29]. Collectively the datashow that P. aeruginosa is capable not only to survive but togrow at elevated temperature under anaerobic conditions.
To investigate temperature-dependent gene expression, wedetermined the transcriptome of P. aeruginosa PAO1 at 30 °Cand 38 °C under anaerobic growth conditions (Table 1; TableS1). We identified a total of 575 genes that showed statisticallysignificant over-expression of transcripts at 38 °C, and 448genes whose mRNA levels were reduced at 38 °C compared to30 °C (Table S1, Fig. S1). Growth at 38 °C resulted in anextremely increased expression of proteins involved in Mg2+
transport (cluster PA4822–4826) (Table 1, Fig. S2). Increasedcytosolic Mg2+ concentrations are thought to increase thestability of cell membranes and proteins as well as protein–nucleic acid interactions, thus preventing cell damage at highertemperature [30]. In addition, various virulence genes, includ-ing regulators, secretion machinery components and effectorsof the Type III secretion system (T3SS) such as ExoS, ExoYand ExoT [31], and components of the LasR regulated quorumsensing system [32] such as rhamnolipid, LasA and phenazinepigments [33], were found to be significantly up-regulated at38 °C compared to 30 °C, suggesting that P. aeruginosa
Please cite this article as: Schmidt A, et al, Neutrophil elastase-mediated increase in a10.1016/j.jcf.2014.03.004
particularly activates its protective armoury at higher environ-mental temperature under anaerobic growth as present duringinfection in mucus plugs of CF patients [6] (Table 1, Table S1).
In contrast, many genes of four different clusters annotatedto the anti-bacterial Type VI secretion system (T6SS) [34] andthe Type II secretion system (T2SS) cluster of P. aeruginosawere significantly down-regulated at 38 °C (Table 1) as well asvarious genes involved in lipopolysaccharide (LPS) produc-tion [35] (Table 1). Phenotypic analysis demonstrated thatP. aeruginosa did not express the polysaccharide O-sidechain under anaerobic growth at 38 °C (Fig. 3), suggestingan optimal exposure of the up-regulated 60–120 nm longtoxigenic T3SS needle of P. aeruginosa [31] towardseukaryotic cell surfaces [10]. Loss of the polysaccharideO-side chain was not observed at any temperature whenP. aeruginosa was grown aerobically (Fig. 3, Fig. S3).Analysis of the aerobic PAO1 transcriptome at 30 °C and38 °C revealed a total of 1116 genes that showed statisticallysignificant over-expression of transcripts at 38 °C, and 1209genes whose mRNA levels were reduced at 38 °C compared to30 °C (Table 1, Table S1, Fig. S2). The comparison of ouraerobic differentially expressed genes with that of previousinvestigations [36] revealed only a small overlap (Fig. S4),suggesting that strain characteristic or minimal temperaturedifferences play an important role in gene expression.
4. Discussion
Our data demonstrate that the temperature within theinflamed airways of CF patients is increased to ~38 °C andthat an exothermic reaction between NE and its endogenousinhibitor, α1-PI, highly likely contributes to this increase.Similar to the NE:α1-PI interaction also proteinase 3 (PR3) andcathepsin G (CG) are able to interact with α1-PI [37]. However,PR3 and CG are almost not inhibited by α1-PI as long as activeNE is present in the solution [38]. Once NE was saturated,α1-PI bound PR3 faster than CG [38]. So we hypothesized thatthe contribution of NE:α1-PI interaction to the temperatureincrease is the main mechanism, followed by PR3 and CG.
To counteract the neutrophil released proteases the airwaysare equipped not only with α1-PI, but with two other physiologic
irway temperature during inflammation, J Cyst Fibros (2014), http://dx.doi.org/

30 38 30
O2
[°C] 30 38 30 38 38
+ + + +- - - -PAO1 Environmental strain
Fig. 3. P. aeruginosa does not produce a polysaccharide O-antigen chain whengrown at 38 °C under anaerobic conditions. The LPS fractions of P. aeruginosaPAO1 and an environmental P. aeruginosa isolate, grown at 30 °C and 38 °Caerobically or anaerobically, were extracted from whole cell lysate andsubjected to SDS gel electrophoresis. LPS analysis reveals lack of the O-sidechain at 38 °C under anaerobic growth.
Table 1Selected differentially expressed gene clusters of P. aeruginosa PAO1 at 38 °Ccompared to 30 °C under anaerobic or aerobic conditions. Grey: not significantlyregulated. Red: significantly up-regulated at 38 °C. Green: significantly down-regulated at 38 °C. Values represent means of four single values of twoindependent cultures. The replicates clustered in the principal component analysis.Significance pval N20.
Anaerobic Aerobic
Group ID Gene
name
log2fold
change
pval log2fold
change
pval
T3SS PA1697 3305 0.077 0,55
PA1705 pcrG 3350 1675 4,68
PA1706 pcrV 3101 2055 33,30
PA1707 pcrH 3155 1430 9,33
PA1708 popB 2127 0.306 1,77
PA1710 exsC 2879 0.823 6,55PA1711 exsE 2908 0.609 1,80
PA1712 exsB 1754 0.113 1,41
PA1713 exsA 1680 0.124 1,68
PA1714 exsD 1756 0.222 1,79
T3SS PA3841 exoS 2399 2351 49,47
effect. PA0044 exoT 2172 1497 16,05
PA2191 exoY 2357 0.047 1,91
QS PA1430 lasR 1816 2211 52,73PA1432 lasI 5963 4906 163,76
QS PA1871 lasA 2866 3679 113,72
effect. PA1249 aprA 2175 1002 18,01
PA2193 hcnA 2246 1695 15,28
PA2194 hcnB 2186 0.930 8,97
PA4209 phzM 1502 2401 35,23
PA4217 phzS 2737 2793 50,83PA2399 pvdD 2111 1251 18,58
PA0051 phzH 3463 2670 58,21
PA3479 rhlA 1340 2198 50,25
PA3478 rhlB 1989 2058 48,30
PA0411 pilJ 2198 2.357 53,76
PA5044 pilM 1756 0518 6,07PA0396 pilU 1797 1613 29,80
T2SS PA3097 xcpX 2200 1841 32,18
PA3099 xcpV 1906 1556 21,35
PA3100 xcpU 1522 1563 27,96
PA3101 xcpT 2574 1,213 17,20
PA3102 xcpS 1661 0.231 2,08
PA3105 xcpQ 1826 1256 18,50
T6SS PA0072 tagS1 4298 4077 62,407PA0074 ppkA 3137 3755 108,60
PA0075 pppA 3302 4066 91,93
PA0076 tagF1 1928 4754 84,64
PA0077 tssM1 2089 2776 72,22
PA0078 tssL1 2525 2958 61,86
PA0079 tssK1 1631 1954 35,81PA0083 tssB1 2883 2939 77,79
PA0084 tssC1 3183 3628 115,27
PA0085 hcp1 3174 2929 77,52
PA0263 hcpC 6655 5987 219,28
PA1512 hcpA 6374 6211 227,83
PA5267 hcpB 6473 6431 228,96PA1656 hsiA2 2573 4593 165,95
PA1657 hsiB2 4698 5248 201,59
PA1658 hsiC2 5213 5850 238,95
PA1659 hsiF2 4488 5364 204,22
PA1660 hsiG2 4079 4674 167,34
PA1661 hsiH2 4344 5025 185,36PA1662 clpV2 4458 4824 177,87
PA1663 sfa2 4581 5605 209,92
PA1664 orfX 7788 5095 139,58
PA1665 fha2 5441 5444 200,66
PA1666 lip2 5363 5251 189,55
PA1667 hsiJ2 4550 4327 145,32PA1668 dotU2 4408 4701 168,87
PA1669 icmF2 4621 4606 170,82
PA1670 stp1 3237 4916 161,51
PA1671 stk1 4234 5524 185,56
LPS PA5009 waaP 1535 0.983 15,25
PA3146 wbpK 1990 1956 34,14
PA3147 wbpJ 2181 2045 34,92PA3148 wbpI 3359 2183 25,66
PA3149 wbpH 3529 2174 10,40
PA3150 wbpG 3673 1665 14,76
PA3151 hisF2 2724 1252 9,03
PA3152 hisH2 2423 1350 11,04
PA3153 wzx 2284 1829 12,68PA3154 wzy 1813 1.148 4,98
PA3158 wbpB 1670 0.997 10,99
Mg PA4822 8799 6,826 237,40
PA4823 8727 999.00 56,98
PA4824 1025 8452 86,94
PA4825 mgtA 101 9993 117,55
PA4826 9593 9058 132,91PA1179 phoP 1666 1333 17,54
PA1180 phoQ 0.054 0.391 2,40
PA4635 8055 6681 41,94
43.67
34.27
58.08
28.32
27.99
63.5829.53
21.28
23.00
23.63
39.79
31.43
31.81
30.97190.2
67.39
40.78
25.88
26.55
24.53
54.5135.27
69.69
24.51
41.33
35.81
21.0924.88
34.45
22.05
22.92
41.22
25.51
29.82
31.9152.32
38.79
23.00
42.10
25.00
22.9651.62
67.87
70.51
166.23
165.68
160.0758.95
124.19
146.39
104.58
100.72
107.16116.82
116.20
116.43
136.81
147.36
117.43117.80
121.77
66.54
88.48
20.57
37.69
43.2672.23
81.90
84.14
53.22
46.92
41.9329.63
23.50
305.2
96.35
232.4
187
197.120.94
0.412
56.55
7A. Schmidt et al. / Journal of Cystic Fibrosis xx (2014) xxx–xxx
Please cite this article as: Schmidt A, et al, Neutrophil elastase-mediated increase in a10.1016/j.jcf.2014.03.004
inhibitors, the secretory leucoprotease inhibitor (SLPI) and elafin[28,38]. A study looking at the status of elafin in CF sputum foundthat elafin was cleaved in sputum of CF patients [39]. However,elafin was still able to interact with NE, but it has been shown thatthere is no heat release when truncated versions of inhibitors bindto proteinases [28]. Whether interaction of NE with SLPIparticipates to temperature rise remains to be determined.However, the interaction between proteases and protease inhibitorsmay be used as a target for speculative therapies: reduction of theabundant proteases or blocking of the active binding sites couldinduce a decrease of the exothermic reaction and via normalizationof the increased temperature a reduction of the P. aeruginosaselection.
For many opportunistic bacterial pathogens, a temperatureof 38 °C may be deleterious in conjunction with anaerobicgrowth conditions in mucus plugs of CF patients. However, theopportunistic pathogen P. aeruginosa is not negatively affectedin growth by a temperature up to 42 °C due to its extraordinaryability to adapt to specific environmental conditions, which islinked to a large number of differential expressed regulatorygenes [35]. Although a large number of different bacterialpathogens can be detected in sputum specimens from CFpatients [40], recent reports demonstrate a substantially reduceddiversity of this microbiota during the course of chronic lunginfections, with P. aeruginosa often becoming the dominant, ifnot the sole, pathogen in patients with advanced CF lungdisease [40]. The higher temperature in mucus plugs triggeredby NE binding to α1-PI may thus explain at least in part thedominance of P. aeruginosa in the airways of CF patients [41].Our findings also suggest that airway temperature in otherinflammatory lung diseases that are characterized by aprofound neutrophil influx, such as in patients with severebronchial asthma [42], is increased. Indeed, increased expira-tory breath temperature has also been demonstrated in patientswith bronchial asthma [9,11]. However, the influence of
irway temperature during inflammation, J Cyst Fibros (2014), http://dx.doi.org/

8 A. Schmidt et al. / Journal of Cystic Fibrosis xx (2014) xxx–xxx
respiration on airways and mucus temperature has to be takeninto consideration. Taken together, our findings suggest anovel inflammatory function for NE in neutrophil rich-diseasedsituations.
Acknowledgments
We thank Joseph Bieth and Christian Boudier, INSERMU392, Strasbourg, France, for valuable discussions, SylviaDüpow (RCB) for technical assistance, and Melvin Berger,Cleveland, OH, USA, for a gift of α1-antitrypsin. G.D., O.H.and A.M. acknowledge COST Action BM1003 “Microbial cellsurface determinants of virulence as targets for new thera-peutics in Cystic Fibrosis.”. AS acknowledge DFG-fundedGRK 1708 “Molecular principles of bacterial survivalstrategies”. AB acknowledges funds from Inserm AvenirProgram, Fondation pour la Recherche Médicale (FRM), AgenceNationale de la Recherche (ANR), and Contrats ProjetsEtat-Région (CPER). This study is dedicated to the memoryof Gerd Döring and his commitment to CF research.
Appendix A. Supplementary data
Supplementary data to this article can be found online athttp://dx.doi.org/10.1016/j.jcf.2014.03.004.
References
[1] Dinarello CA. Interleukin-1 and the pathogenesis of the acute-phaseresponse. N Engl J Med 1984;311(22):1413–8.
[2] Bennett AF, Ruben JA. Endothermy and activity in vertebrates. Science1979;206(4419):649–54.
[3] Clarke A, Portner HO. Temperature, metabolic power and the evolution ofendothermy. Biol Rev Camb Philos Soc 2010;85(4):703–27.
[4] Bergman A, Casadevall A. Mammalian endothermy optimally restrictsfungi and metabolic costs. mBio 2010;1(5).
[5] Craig CP, Suter E. Extracellular factors influencing staphylocidal capacityof human polymorphonuclear leukocytes. J Immunol 1966;97(2):287–96.
[6] Worlitzsch D, Tarran R, Ulrich M, Schwab U, Cekici A, Meyer KC, et al.Effects of reduced mucus oxygen concentration in airway Pseudomonasinfections of cystic fibrosis patients. J Clin Invest 2002;109(3):317–25.
[7] Ratjen F, Doring G. Cystic fibrosis. Lancet 2003;361(9358):681–9.[8] Meyer KC, Zimmerman J. Neutrophil mediators, Pseudomonas, and
pulmonary dysfunction in cystic fibrosis. J Lab Clin Med 1993;121(5):654–61.
[9] Piacentini GL, Peroni D, Crestani E, Zardini F, Bodini A, Costella S, et al.Exhaled air temperature in asthma: methods and relationship with markersof disease. Clin Exp Allergy 2007;37(3):415–9.
[10] Niu C, Shang N, Liao X, Feng E, Liu X, Wang D, et al. Analysis ofsoluble protein complexes in Shigella flexneri reveals the influence oftemperature on the amount of lipopolysaccharide. Mol Cell Proteomics2013;12(5):1250–8.
[11] Piacentini GL, Bodini A, Zerman L, Costella S, Zanolla L, Peroni DG,et al. Relationship between exhaled air temperature and exhaled nitricoxide in childhood asthma. Eur Respir J 2002;20(1):108–11.
[12] Baugh RJ, Travis J. Human leukocyte granule elastase: rapid isolation andcharacterization. Biochemistry 1976;15(4):836–41.
[13] Mills K, Mills PB, Clayton PT, Johnson AW,Whitehouse DB, WinchesterBG. Identification of alpha(1)-antitrypsin variants in plasma with the useof proteomic technology. Clin Chem 2001;47(11):2012–22.
Please cite this article as: Schmidt A, et al, Neutrophil elastase-mediated increase in a10.1016/j.jcf.2014.03.004
[14] Belaaouaj A, McCarthy R, Baumann M, Gao Z, Ley TJ, Abraham SN,et al. Mice lacking neutrophil elastase reveal impaired host defense againstgram negative bacterial sepsis. Nat Med 1998;4(5):615–8.
[15] Dalhoff A. The granuloma pouch. In: Sande MA, Zak O, editors.Experimental models in antimicrobial chemotherapy, Vol. 1. London:Academic Press; 1986. p. 123.
[16] Hirche TO, Benabid R, Deslee G, Gangloff S, Achilefu S, Guenounou M,et al. Neutrophil elastase mediates innate host protection againstPseudomonas aeruginosa. J Immunol 2008;181(7):4945–54.
[17] Holloway BW, Romling U, Tummler B. Genomic mapping of Pseudo-monas aeruginosa PAO. Microbiology 1994;140(Pt 11):2907–29.
[18] Damkiaer S, Yang L, Molin S, Jelsbak L. Evolutionary remodeling ofglobal regulatory networks during long-term bacterial adaptation to humanhosts. Proc Natl Acad Sci U S A 2013;110(19):7766–71.
[19] Dotsch A, Eckweiler D, Schniederjans M, Zimmermann A, Jensen V,Scharfe M, et al. The Pseudomonas aeruginosa transcriptome in planktoniccultures and static biofilms using RNA sequencing. PLoS One 2012;7(2):e31092.
[20] Lunter G, Goodson M. Stampy: a statistical algorithm for sensitive andfast mapping of Illumina sequence reads. Genome Res 2011;21(6):936–9.
[21] De Castro C, Parrilli M, Holst O, Molinaro A. Microbe-associated molecularpatterns in innate immunity: extraction and chemical analysis of gram-negative bacterial lipopolysaccharides. Methods Enzymol 2010;480:89–115.
[22] Sturiale L, Palmigiano A, Silipo A, Knirel YA, Anisimov AP, Lanzetta R,et al. Reflectron MALDI TOF and MALDI TOF/TOF mass spectrometryreveal novel structural details of native lipooligosaccharides. J MassSpectrom 2011;46(11):1135–42.
[23] Sagel SD, Wagner BD, Anthony MM, Emmett P, Zemanick ET. Sputumbiomarkers of inflammation and lung function decline in children withcystic fibrosis. Am J Respir Crit Care Med 2012;186(9):857–65.
[24] Mayer-Hamblett N, Aitken ML, Accurso FJ, Kronmal RA, Konstan MW,Burns JL, et al. Association between pulmonary function and sputumbiomarkers in cystic fibrosis. Am J Respir Crit Care Med 2007;175(8):822–8.
[25] Gilbert IA, Fouke JM, McFadden Jr ER. The effect of repetitive exerciseon airway temperatures. Am Rev Respir Dis 1990;142(4):826–31.
[26] Goldstein W, Doring G. Lysosomal enzymes from polymorphonuclearleukocytes and proteinase inhibitors in patients with cystic fibrosis. AmRev Respir Dis 1986;134(1):49–56.
[27] Carrell RW, Boswell DR, Brennan SO, Owen MC. Active site of alpha 1-antitrypsin: homologous site in antithrombin-III. Biochem Biophys ResCommun 1980;93(2):399–402.
[28] Boudier C, Bieth JG. The reaction of serpins with proteinases involvesimportant enthalpy changes. Biochemistry 2001;40(33):9962–7.
[29] Folkesson A, Jelsbak L, Yang L, Johansen HK, Ciofu O, Hoiby N, et al.Adaptation of Pseudomonas aeruginosa to the cystic fibrosis airway: anevolutionary perspective. Nat Rev Microbiol 2012;10(12):841–51.
[30] O'Connor K, Fletcher SA, Csonka LN. Increased expression of Mg(2+)transport proteins enhances the survival of Salmonella enterica at hightemperature. Proc Natl Acad Sci U S A 2009;106(41):17522–7.
[31] Hauser AR. The type III secretion system of Pseudomonas aeruginosa:infection by injection. Nat Rev Microbiol 2009;7(9):654–65.
[32] Williams P, Camara M. Quorum sensing and environmental adaptation inPseudomonas aeruginosa: a tale of regulatory networks and multifunc-tional signal molecules. Curr Opin Microbiol 2009;12(2):182–91.
[33] Dietrich LE, Price-Whelan A, Petersen A, Whiteley M, Newman DK. Thephenazine pyocyanin is a terminal signalling factor in the quorum sensingnetwork of Pseudomonas aeruginosa. Mol Microbiol 2006;61(5):1308–21.
[34] Silverman JM, Brunet YR, Cascales E, Mougous JD. Structure andregulation of the type VI secretion system. Annu Rev Microbiol 2012;66:453–72.
[35] Stover CK, Pham XQ, Erwin AL, Mizoguchi SD, Warrener P, Hickey MJ,et al. Complete genome sequence of Pseudomonas aeruginosa PAO1, anopportunistic pathogen. Nature 2000;406(6799):959–64.
irway temperature during inflammation, J Cyst Fibros (2014), http://dx.doi.org/

9A. Schmidt et al. / Journal of Cystic Fibrosis xx (2014) xxx–xxx
[36] Wurtzel O, Yoder-Himes DR, Han K, Dandekar AA, Edelheit S,Greenberg EP, et al. The single-nucleotide resolution transcriptome ofPseudomonas aeruginosa grown in body temperature. PLoS Pathog2012;8(9):e1002945.
[37] Quinn DJ, Weldon S, Taggart CC. Antiproteases as therapeutics totarget inflammation in cystic fibrosis. Open Respir Med J 2010;4:20–31.
[38] Korkmaz B, Poutrain P, Hazouard E, de Monte M, Attucci S, Gauthier FL.Competition between elastase and related proteases from human neutrophilfor binding to alpha1-protease inhibitor. Am J Respir Cell Mol Biol2005;32(6):553–9.
Please cite this article as: Schmidt A, et al, Neutrophil elastase-mediated increase in a10.1016/j.jcf.2014.03.004
[39] Guyot N, Butler MW, McNally P, Weldon S, Greene CM, Levine RL,et al. Elafin, an elastase-specific inhibitor, is cleaved by its cognateenzyme neutrophil elastase in sputum from individuals with cysticfibrosis. J Biol Chem 2008;283(47):32377–85.
[40] Zhao J, Schloss PD, Kalikin LM, Carmody LA, Foster BK, Petrosino JF,et al. Decade-long bacterial community dynamics in cystic fibrosisairways. Proc Natl Acad Sci U S A 2012;109(15):5809–14.
[41] Cystic fibrosis foundation patient registry 2009 annual data report.Bethesda, MD, USA: Cystic Fibrosis Foundation; 2010.
[42] Fahy JV. Eosinophilic and neutrophilic inflammation in asthma: insightsfrom clinical studies. Proc Am Thorac Soc 2009;6(3):256–9.
irway temperature during inflammation, J Cyst Fibros (2014), http://dx.doi.org/















![[Rapid airway access]](https://img.pdfslide.net/doc/110x75/6354cd1b765a645b3106d438/rapid-airway-access.jpg)













