Embed Size (px)
Citation preview

It is now well accepted that HIV/AIDS is a challenge for the world community as it transcendsboundaries of nation, class, ethnicity and sexual preference.
Over the years, research has shown that HIV is not random in its spread or its impact. An intersectionof several variables—poverty, urbanisation, gender inequality and stereotypical gender roles—impacts upon vulnerabilities. Significant factors—such as lack of autonomy for women and girls,discrimination against sexual minorities, abuse of power, lack of basic services, and violence againstwomen—play a key role in determining the most vulnerable constituencies in society.
Human poverty reduces the ability of people to control their circumstances and make choices.Poor people are forced by economic imperatives into living conditions and occupations in whichrisks to life and health are endemic. In countries that are experiencing widespread impacts ofHIV/AIDS, it has been found that prevention initiatives can work only if enabling environmentsare created for people to effect change in their lives that would help them practice safe behaviourconsistently.
Linking HIV/AIDS-related indicators to human development parameters representing long andhealthy life, knowledge and a decent standard of living, would support dialogue with policy-makers and stakeholders to set the course for considered action.
This report highlights South Asia’s substantial challenge, both in terms of human deprivation andvulnerability to the epidemic. It argues for a comprehensive intersectoral response based on therecognition of the linkages between human development and HIV/AIDS.
This document has been prepared by the UNDP’s Human Development Resource Centre and theRegional HIV and Development Programme in collaboration with UNAIDS.
ointhe debate!http://hdrc.undp.org.inhttp://www.youandaids.org
J

andDevelopment in South Asia 2003
������������ ����������������
HIV/AIDS

ii
© United Nations Development Programme, 2003
All rights are reserved. The document may, however, be freely reviewed, quoted,reproduced or translated, in part or in full, provided the source is acknowledged. Thedocument may not be sold or used in conjunction with commercial purposes withoutprior written approval from UNDP. The views expressed in documents by namedauthors are solely the responsibility of those authors.
The analysis and policy recommendations of this Report do not necessarily representthe views of the United Nations Development Programme, its Executive Board or itsMember States.
Designed and Printed by New Concept Information Systems Pvt. Ltd., New Delhi
ISBN No. 81-88788-03-1
Price: INR 395.00

iii
The Regional Human DevelopmentReport on “HIV/AIDS and HumanDevelopment in South Asia 2003” is thefirst report prepared under the aegis ofUNDP’s Asia Pacific Regional Initiativeon Human Development Reports(HDRC) and the Regional Programmeon HIV and Development (REACHBeyond Borders).
This Report builds upon an extensivecorpus of research on humandevelopment in South Asia, pioneeredby the late Dr Mahbub-ul-Haq andstrengthened by successive national andsub-national HDRs. The challenge of HIVin South Asia has been examined inseveral documents prepared by UNorganizations, national Governments,research institutions, NGOs, activistsworking with HIV programmes andpositive people’s networks.
It is heartening that this complex anddifficult issue is being addressed by a largenumber of people who recognise thepressing importance of fighting thisepidemic before it reaches catastrophicproportions. We do not have the luxuryof waiting for a crisis to be thrust uponus before we devise solutions for it.
The Report argues that just as HIV canreverse the gains of human developmentin the region, largely through the
vector of life expectancy, morbidityand prejudice, the lack of humandevelopment can also trump the fightagainst HIV. This Report is the first attemptto examine the dynamics of HIV andhuman development through a commonlens, and suggests possible arenas foraction that may lie outside a strictlyepidemiological approach. It is also truethat a classic public health response thatfocuses upon “disease control”,important as that is, may not be adequategiven the fact that there is thus far novaccine against HIV and the health careinfrastructure in the region is in need ofever greater reform and rejuvenation.
The analysis in the Report indicates thatthe two-way relationship between ill-health and poverty holds particularly truein South Asia. In this context, humandevelopment concerns, particularlythose of social security, livelihood andhuman dignity are required to bemainstreamed into efforts to combatthe epidemic. As a corollary, it wouldbe essential to include HIV concernsinto policies and programmes forhuman development. A comprehensiveresponse cannot be a mere catch-word orslogan, it needs to become a living reality —on this hinges the success of the struggleagainst human deprivation and theepidemic in South Asia.
Hafiz PashaUN Assistant Secretary GeneralUNDP Assistant Administrator
Director, Regional Bureau for Asia and the Pacific
��������

iv
�������
Globally, the Human DevelopmentReports (HDRs) have placed people at thecentre of development discourse andflagged the urgency of focused public actiontowards international development goals.Several regional, national, and indeed sub-national HDRs pioneered in India havecontributed to a worldwide alliance towiden people’s choices and meet thechallenges of poverty, ill-health andignorance.
The Regional HDR on HIV/AIDS andDevelopment in South Asia examines thecomplex interplay between disease anddeprivation in a scenario where majorsuccesses in human development areundermined by persistent challenges. TheReport brings together for the first timean analysis of HIV and humandevelopment under a common lens inSouth Asia. The linkages between the twoare mutually reinforcing in the sense thatHIV can undo gains of humandevelopment, and the lack of humandevelopment can trump any strategyagainst HIV.
The Report assesses the adverse impactof HIV on the Human Development Index(HDI) and also the parameters of the HDIviz. literacy, school enrollment, lifeexpectancy and per capita income. It alsopoints out that successful humandevelopment in terms of improvedliteracy, a more functional health systemand enhanced livelihoods make for a moreeffective response to the epidemic inSouth Asia.
It is vital that dialogue in the region,between statesmen, governments andcivil society, be harnessed to focus uponcooperation in arenas such as affordabledrugs and treatment through tradeagreements, sharing best practices inharm reduction and an enabling policyenvironment where the struggle againstthe epidemic is an integral part of the roadmap for human development.
The Report documents the price of inertiain the fight against HIV and showsthat the micro-level impacts at thelevel of individuals, households andcommunities are more significant thanthe macro-level impact, given the currentrates of HIV prevalence. It points out thatthe impact of HIV on firms and businessesaffects not only corporate profits but alsothe livelihoods of workers and theprospects of social security for organisedand unorganised workers.
The case is made in the Report thatsuccessful outcomes for HIV may alsorequire an enabling framework whererights of people living with HIV/AIDS(PLWHA) are guaranteed and stigma anddiscrimination are minimised. Itanalyses the legislative and judicialframework of HIV in South Asiaand argues for a closer integrationwith mainstream constitutional and rightto development mandates andinstitutions.
The Report examines the debate overprevention versus treatment and

v
overturns the argument that the former isthe responsibility of the state and thelatter is to be taken care of by privateprovisioning and market forces. It arguesthat the success of prevention efforts oftendepends on effective care and supportespecially in the light of the principles ofGreater Involvement of People with AIDS(GIPA). It also shows the feasibility ofaccess to Highly Active Anti-retroviralTherapy (HAART) in resource-poorsettings. It examines the issues pertainingto provision of drugs at affordable pricesthrough mechanisms such as compulsorylicensing and parallel country importing,an issue which could be taken up forregional cooperation in South Asia.
The Report points out that the formidablechallenge of HIV in the region can be metonly when the credo of multi-sectoralresponses is translated into reality byensuring that the concerns of positivepeople are reflected not only in dedicatedpublic health interventions but also inprogrammes and policies for livelihood
promotion, social security and access tobasic services.
While this Report does not purport toconvey the views of any of the nationalGovernments in the region, it doessignpost, however, the urgency of meetingthe challenge of HIV and humandeprivation in a region that is critical tothe world’s ability to meet the MillenniumDevelopment Goals. It is hoped that thefindings of the Report could spark publicdebate and help build an enabling policyenvironment for more effective action.
We look forward to wider discussions inSouth Asia, within and across countries,which could provide policy options onpractical modalities of a multi-sectoralresponse, access to treatment in resource-poor settings, demystifying the epidemicby building advocacy and informationnetworks for advocacy and ensuring a highpriority for HIV and human developmentin the political agenda.
Brenda Gael McSweeneyUNDP Resident Representative &
UN Resident Coordinator
�������

vi
�� ��������� ��
Combating HIV/AIDS is a criticalchallenge for human development inSouth Asia, and as such one of the keyMillennium Development Goals that theworld community has set for itself. Thereis now a consensus that public policy isrequired to address not only the medicalor public health issues, but also the socio-economic context, including issuespertaining to human dignity andelimination of stigma and discrimination.
This Report is an attempt to utiliseUNDP’s principal advocacy platform tomake a compelling case for coherent,practical action across sectors andstakeholders, keeping in mind the groundrealities of South Asia and the possibilityof the epidemic reversing the gains ofhuman development in the region. Itmarshalls relevant facts and evidence andanalyses the two-way linkage betweenhuman development outcomes and thetrajectory of the epidemic. It is hoped thatthis would help widen the currentdevelopment debate on the subject andpromote experience sharing acrosscountries and contribute to the ‘humandevelopment movement’ worldwide.
The leadership of Mark Malloch Brown,UNDP Administrator and his vision of thenew UNDP as a knowledge network hasinspired the preparation of this Report inone of UNDP’s key practice areas.
The encouragement by the RegionalBureau for Asia Pacific (RBAP), under theleadership of Hafiz Pasha was valuable.
This is the first Report funded under RBAP’sRegional Initiative on HDRs in Asia andthe Pacific. This Report has been preparedby the Human Development ResourceCentre (HDRC), and Regional HIV andDevelopment Programme (REACHBeyond Borders), New Delhi incollaboration with UNAIDS. SubinayNandy, Joanna Merlin-Scholtes, KanniWignaraja and Arusha Stanislaus at theBureau have extended useful support.Sarah Burd-Sharps and SharmilaKurukulasuriya from the National HDR(NHDR) Unit at the Human DevelopmentReport Office (HDRO) have been ourcomrades-in-arms, not only facilitating apresentation on the Report at the XIVInternational HIV/AIDS Conference atBarcelona, but also in facilitatingdiscussions on the NHDR network. We aregrateful to members of the NHDRNetwork, particularly the CambodiaNHDR team and Hakan Bjorkman fortheir detailed comments, which helpedimprove the draft. Gillman Rebello andBarbara Lemoine at the United NationsOffice for Project Services (UNOPS) weremost helpful.
The support from the country offices ofUNDP and UNAIDS in the regionincluding the HIV/AIDS focal points forfacilitating the sharing of the draft isacknowledged. David Miller, K. Pradeep,Pernilla Berlin from UNAIDS IndiaCountry Office, Vidya Ganesh fromUNAIDS, South Asia Inter-Country Team(SAICT), Sunita Dhar from UNIFEM,South Asian Regional Office (SARO),

vii
Jai Narain, Subhash Hira from WHO,South-East Asia Regional Office (SEARO)and Roma Bhattacharjea from UNDP,Sub-Regional Resource Facility (SURF),Kathmandu, deserve special thanks.
The Asia Pacific Regional HumanDevelopment Reports Initiative andREACH Beyond Borders Programme,both hosted by the Government of India,New Delhi, have in the course ofpreparation of this Report benefitedfrom the continuous advice and supportof Meenakshi Datta Ghosh and herteam from National AIDS ControlOrganisation, India.
This Report would not have been possiblewithout the contribution, support andencouragement from a large number ofpeople and institutions. Theircontribution is acknowledged without inany way making them responsible for thecontents. The guidance of the membersof the Advisory and TechnicalCommittees is gratefully acknowledged.Thanks to all the resource persons andinstitutions who contributed backgroundpapers. Special thanks are due to EileenStillwaggon and Robert Cassen for theirintellectual guidance that helped sharpenthe perspectives in the Report.
The process of preparing this Report wasas fruitful as the end product. Theparticipants at the regional NGOconsultation at Goa enriched the contentsof the Report and provided a grass-rootsperspective of activists and people livingwith HIV/AIDS. We wish to put onrecord our appreciation of Caitlin Wiesenand the CSO Division for there supportof the partnership initiatives, and ofIshwar Shrestha, Sharmini Boyle,
U. Nobokishore Singh, Rohan Edrisinha,Gunjan Sharma, Shyamala Ashok, BitraGeorge, Elizabeth Sivakumar, Priya Dias,John Pinheiro, Prakash Nadkarni, MariottCorrea, Sangita Sonak, Ashwin Tombatand Sabina Martin. We wish toacknowledge the following groups andnetworks of people living with HIV/AIDS(PLWHA) in South Asia for deepening ourknowledge and analysis: Asia PacificNetwork of PLWHA (APN+), IndianNetwork for PLWHA (INP+), PositiveWomen Network of South India (PWN+),En-Joy, Affected Infected Women’sAssociation in Churachandpur (AIWAC),Nepal Plus, Makwanur Group of Infectedand Affected women, Lanka+, Ashar AloSociety and New Light AIDS ControlAction Awareness Group.
Draft versions of the Report were sharedwith several experts whose feedback isacknowledged. We would particularly liketo mention Michael Hahn, P.L. Joshi, RajivSadanandan, Julie Hamblin, DesmondCohen, D.C.S. Reddy and Mukul Saxena.Readers including policy-makers andplanners from across the region, helpedin improving the presentation andsharpening the analysis. This process,though time consuming, helped inbuilding a constituency for theperspectives and messages of the Report.A special thanks to our fellow travellerswho have already initiated the process ofsharing the human developmentconcept and messages arising fromthis analysis.
Editorial inputs from SeethaParthasarathy and Jaya Shreedhar, andprinting by New Concept InformationSystems Pvt. Ltd against very tightdeadlines are duly acknowledged.
�� ��������� ��
viii
�������
HDRC: K. Seeta Prabhu, Suraj Kumar, Trishna Satpathy, Alka Narang, AnuradhaRajivan, Kalyani Menon-Sen
REACH Beyond Borders Programme: Sonam Yangchen Rana, G. Pramod Kumar,Uffe Gartner, Rie Debabrata, Clare Castillejo, Chandrika Bahadur, Meera Mishra
Advisory Board Technical Committee
David Bloom Meenakshi Datta GhoshRobert Cassen Reeta DeviKhadija Haq Rohan EdrisinhaS.R. Osmani Anand GroverPeter Piot D.C. JayasuriyaNihal Rodrigo David MillerWerasit Sittitrai S.V. Joga Rao
Prema RamachandranElizabeth ReidSwarup SarkarMonica SharmaGita Sen

ix
���� ������������������������ �� �
UNDP’s Human Development Resource Centre (HDRC) is a centre of excellencededicated to human development research, training and advocacy since August 2000.The Centre’s objectives are (1) translating the concept of human development intopolicy-oriented action; (2) creating awareness among national and local policy makersabout tools and techniques to mainstream Human Development Report (HDR)analyses into policies and programmes; and (3) facilitating learning and exchange ofideas by strengthening regional and local networks and capacity building. This Reporthas been prepared under the Regional Initiative on HDRs in Asia and the Pacific, aproject sponsored by the Regional Bureau of Asia and Pacific (RBAP), UNDP, New York.
����!�"��#!��#������$����� �� �
REACH Beyond Borders is UNDP’s Regional HIV and Development Programmecovering 13 countries in the South and North-East Asia region. The programmeaddresses the development and trans-border challenges of HIV/AIDS in the regionand supports integrated and rights based responses that promote gender equality,sustainable livelihoods and community participation. Focus areas of work includepolicy advocacy and outreach, mobility and HIV/AIDS, capacity development andGreater Involvement of People Living with HIV/AIDS (GIPA) and human rights.
���� %
The Joint United Nations Programme on HIV/AIDS (UNAIDS) brings together the effortsand resources of eight United Nations organisations. As the main advocate for globalaction on HIV/AIDS, UNAIDS leads, strengthens and supports an expanded responseaimed at preventing the transmission of HIV, providing care and support, reducing thevulnerability of individuals and communities to HIV/AIDS, and alleviating the impactof the epidemic.
���� ������������������

x
�� �� ��
CHAPTER 1
Introduction��� ��������� �
��� ���� !"�#������ �$�%�����&��$'������ ��'�� (
��� ���� ���������� %�� �)�������� ��������� *
��+ !",!)$�� �� %�� �)�������� �������� � -
��. �%������������������� /
CHAPTER 2
Nexus between Human Development and HIV/AIDS��� ! ����%��� �.
��� 0 ����� �*
��� ������������! ����&�������������� !"��������$��������� ��1��� ���0���� ��
��+ !������� ��������� ��'�� �.
��. �� ��%�� �*
CHAPTER 3
The HIV/AIDS Epidemics of South Asia��� $���%���������#����� +�
��� �� ������ ��)�������� �� �$�%����� .2
��� �%��� ������� ������ !",!)$� �$�%����� .(
��+ ������ ����� ��!��������� ((
CHAPTER 4
Human Rights and HIV/AIDS+�� ! ����%��� *�
+�� !",!)$3�$������ ��)���� ��� �� �� %�� ������� �$�%����� **
+�� $�����"��� ���� �� %�� �������"����� � -2
+�+ ����$�������� %�� ������ --
+�. ���������������� �3������� ��$%����� /�
+�( ! ��� ��� ��� %�� ���������������� �2+
+�* ����������������$���� �2-
+�- ������� ���� � �2-
+�/ �� ��%�� ��+
CHAPTER 5
The Way Forward.�� ������ ��4����� !"�� �� %�� �)�������� �&
����'������� ��������$�%����� ��*
.�� ����'���� ����� !",!)$ ��-
.�� #���� ������'�!��%������� !",!)$�� �� %�� �)�������� ��
$�%����� ��/
.�+ ������ ��)�%��5�� ��+

xi
�� �� ��
.�. ������� ��$�4%��� ������1���� ��.
.�( ��������6� ����7%������ ��#�������� � ��.
.�* $��� ���� ������ ������ ��*
.�- ��� ����������������� &������ �� 3������� ��)�������� � ���
.�/ ����8�������'�! �������� � !",!)$ ���
.��2 ���� ����� �� ��.
.��� �� ��%�� ��(
Annexures �4%���� �� ��%� ���8������� ��8'������'��� ��� � �./
8������ ���%��������� ������������������������� �����
����� ������ !",!)$
�4%���� ! ��� ��� ���6%��� ���� � !",!)$�� �� %�� ������ �(�
���� ����1���� 9���������'���������%���� ���� ����� ����� )� �(+
���� ����1����: ����� ��������������� !",!)$�� � %�� �)�������� � �(*
Statistical Tables��8����� %�� ���������� �� ��������� �� ���� �-(
��8����8 ��� ��� � )! �-(
��8���� )����������������� ������� �-*
��8���� ���������� �����3�������'�� �� �;%���' �--
��8���+ ! ������� �� ������% ���� � ������� �--
��8���. ���������������'���� � � �-/
Country Fact Sheets���� ��� �/�
:� ������� �/+
:�%�� �/.
! �� �/(
!���������%8������!�� �/*
9������ �/-
1���� �//
������ �22
$��0� �� �2�
Boxes��� #���%�� ���� !"����������' �
��� 5 ������ � ���%�� ���������� � -
��� 9��� %��)�������� ��6������ �� !",!)$ �2
��� :��� �������������%�� ���������� ��� �� !"� �$�%����� �*
��� #4��%�� ���� !"<������������� ������������� ������ ������8�'���� �/
��� ����6�������! ������� ������������0� ������ !",!)$�=6!�> ��
��+ ?��� �� �� !" �.
��. ��� ������ !"&������� ��������� �-
��( ������'3��� ����� �� !",!)$ �/
��* ���������8��'������������������� ������ �%�� �� �2
��- !"������ �� ���������� ���%�� ���������� �&�16���4���� ��
�����$� �� ��
��/ �������������!)$&�8%� �������%�%��@ �+
���2 )��������'���� ����� ������'@ �(
��� ���� ��� &�8�������� ��%�� 3� A��� ����%��%��������%�������
��� ����� ���� � +�

xii
�� �� ��
��� ���� �!)$��� ���������������� ++
��� ! ��������������������8�������% �����8�������� ��%�� � +.
��+ ������������������������� ��������%���� +(
��. !",!)$��%� ���8��'���� �������� ���%��%���� +*
��( ������� ��������� ���������%�����8���� �$�%����� +-
��* �������������� ��� ���� �%������ ������ !"��������
���� ����� ��� �������@ .�
��- �� ������������ !"������ �� .�
��/ ���������� ��8%� ������������������� !"� ��� �������%��� � .+
���2 ����! �� ���'����������� !" ..
���� $�4���%���� �����$��0� �� �������� .(
���� ����'������ ������ !"� �$�%����� .-
���� �������������� ��� ����'������0? � �! �� (�
���+ ����6��8����% ����������!)$3��%8���%������ ��9������=6��9> (+
���. ��������������������������������� ���������� ������ !",!)$�
$�%����� (-
+�� $�4%��� ������� ������������� �&�����$� �������������� *(
+�� #��������%�������������� !",!)$ **
+�� $������ ������� ��� � �$�%�����&�� ���%����������%�' */
+�+ ������������������������!)$������� -2
+�. :�������% ���� �1����&��%��� ������������������ ������ �� -�
+�( ! ��������������������8�������������� ��������� -*
+�* 9� �����'����� � --
+�- ! �� ���%�����4�8���� ����'����������0? /�
+�/ $�4��������� �:� �������&��%�� ������������� ��� ��������������� /�
+��2 "��� ����������� � /+
+��� ! ��� ��� ���������� �������������� /.
+��� 9��� ������������ ��������%����� � /*
+��� 0���� �����������:��B���4���� �� /-
+��+ �������������;%��8������ �� �� �%� �������� �22
+��. ��������� ��% ��������)����)�������� �2�
+��( ����5 ����1��� ��6� ���������8�'�$������$���� �=516$$>
� � !",!)$�� ������516$$�)�������� ����������� � �2*
+��* %�� ������������� ��� ���'�������������� � �2/
Tables��� ���� ��������������� !",!)$C�22� +
��� #����������� !",!)$� �$�%�����C�22� .
��� %�� ���������� ��� �� !",!)$� �$�%�������=8'���% ��'> �(
��� %�� ���������� �� �������� �$�%�����3��222�=8'���% ��'> �(
��� )�%��%���� �� !"� ����� �� �$�%����� +-
��� ����� ������� ��� ����51 ��� �$�%����� .�
��� ����'������ ������� !",!)$� �$�%�����3���22� (.
��+ �������� ������������ ���������� !",!)$<����������%�� (*
+�� 0������ ���%�� �������������������������8'� !",!)$ *-
+�� !������ ���%�� �� ��������������� ������������� ���� -/
+�� ������������� �<����������������� �� �������� ����% ����3
)����8����22�D /.
+�+ ������������ ��'���������� ������ �2+
+�. $���%������������� ������� � ��� ��� ����%�� ������� ���%�� �� �2.

xiii
88������ �AIDS Acquired Immuno-
deficiency SyndromeANC Antenatal clinicART Anti-retroviral therapyARV Anti-retroviral drugsCEDAW Convention on the
Elimination of All forms ofDiscrimination AgainstWomen
CGE Computable GeneralEquilibrium
GDI Gender Development IndexGDP Gross Domestic ProductGNP Gross National ProductGIPA Greater Involvement of
People Living WithHIV/AIDS
HAART Highly Active Anti-retroviralTherapy
HD Human DevelopmentHDI Human Development IndexHDR Human Development
ReportHIV Human Immuno-deficiency
VirusIDU Intravenous drug users/
Injecting drug usersILO International Labour
OrganizationIMF International Monetary FundMDG Millennium Development
GoalsMSM Men who have sex with menMTCT Mother to child transmissionNACO National AIDS Control
OrganisationNACP National AIDS Control
Programme/s
NGO Non-governmentalorganisation
OLS Ordinary Least SquaresPPP Purchasing Power ParityPLWHA People Living With
HIV/AIDSSAARC South Asian Association for
Regional CooperationSACS State AIDS Control SocietySHIP STD/HIV Intervention
ProjectSTD Sexually Transmitted
DiseaseSTI Sexually Transmitted
InfectionTRIPS Trade-Related Intellectual
Property RightsUN United NationsUNAIDS Joint United Nations
Programme on HIV/AIDSUNDP United Nations
Development ProgrammeUNDCP United Nations Drug
Control ProgrammeUNFPA United Nations Population
FundUNGASS United Nations General
Assembly Special Session onHIV/AIDS
UNICEF United NationsInternational Children’sEducation Fund
UNIFEM United NationsDevelopment Fund forWomen
VCT Voluntary Counselling andTesting
WHO World Health OrganizationWTO World Trade Organization

xiv
6������'�� %
Acquired Immuno-deficiency Syndromeis a physiological or medical conditionwhereby the body’s immune system isweakened by Human Immuno-deficiency Virus (HIV ) to the extentthat it is no longer able to defend itselfagainst attacks by ordinary (and other)ailments. A cure for AIDS has not beenfound, although research is underway fordeveloping an AIDS vaccine.
�� %&������# #�����
Deaths linked to AIDS-related diseasessuch as tuberculosis, pneumonia anddiarrhoea.
���������
Occurring before birth
���'&������'��� ��$�
Substances used to kill or inhibit themultiplication of retroviruses such as HIV.
������
In epidemiology, a group of individualswith some characteristics in common.
���('���'�� ������"
Two or more drugs or treatments usedtogether to achieve optimum results.
��#��'�
The standard epidemiological definitionof the term endemic is the constantpresence of a disease in a given geographicarea or within a given population.
��'#��'�
An epidemic is the occurrence of a greaternumber of cases of a disease than wouldnormally be expected to occur in apopulation, community or region.
��'#��'���$"
Study of the occurrence, distribution anddetermining factors associated with healthevents and diseases in a population.
����� �����'� ���#��� )� �*
The total output of goods and services forfinal use produced by a economy, by bothresidents and non-residents, regardless ofthe allocation to domestic and foreignclaims. It does not include deductions fordepreciation of physical capital ordepletion and degradation of naturalresources.
���#������+�������������)���*
A composite index measuring averageachievement in the three basic dimensionsof empowerment: economic participationand decision-making, political participa-tion and decision-making and power overeconomic resources.
'$��" ���'�� ���'&������'���
������" )����*
Treatment regimens that suppress viralreplication and progress of the HIV. Thesetreatment regimens have been shown toreduce the amount of virus so that itbecomes undetectable in the blood.

xv
������ �,'�'���"
Inability of certain parts of the immunesystem to function, thus making a personmore susceptible to infections.
���'#����
The number of new cases (e.g., of adisease) occurring in a given populationover a certain period of time.
HIV incidence is the number of new HIVinfections occurring in a specified periodof time in a specified population.
���'#���� ����
The incidence rate is the rate at which newevents, or new cases, occur in a specifiedtime in a defined population that is “at risk”of experiencing the condition or event.
existing cases of a disease at a specifiedtime divided by a defined population thatis “at risk” of experiencing the condition
���+��������-+'�����
This includes men who report eitherhomosexual or bisexual contact.
�������'�$ ��+�� ���'�"
A rate of exchange that accounts for pricedifferentials across countries allowinginternational comparison of real outputand incomes
����������
Total number of people cumulative witha specific disease or health conditionliving in a defined population at aparticular time.
���������� ����
The prevalence rate is the number of
%���'��� %����'������
Sentinel surveillance is a type ofsurveillance activity in which specificfacilities such as offices of certain healthcare providers, hospitals or clinics acrossa geographical region are designated tocollect data about a disease, such as HIVinfection. These data are reported to acentral database for analysis andinterpretation.
%����������'��
In HIV/AIDS research, seroconversionrefers to the development of detectableantibodies to HIV in the blood as a result ofHIV infection.
%�������������
The term seroprevalence refers to theprevalence or prevalence rate of a diseasedetermined by testing blood rather thanby testing saliva, urine, or sputum.
%����'������
Surveillance is the ongoing collection,analysis and interpretation of data abouta disease such as HIV or about a healthcondition. The objective of surveillanceis to assess the health status ofpopulations, detect changes in diseasetrends or changes in how the disease isdistributed, define priorities, assist in theprevention and control of the disease, andmonitor and evaluate related treatmentand prevention programmes.
Number of existing eventsin a specified period
Number of people exposedto risk in this period
Prevalence Rate =
6������'
Number of new events ina specified period of time
Number of people exposedto risk in this period
Incidence Rate =
������&� 51)�3� �22��E��� ��� �!)$� $����'3� �22�



������������ ����������������
����� ���� ���������� ���������������2
������������

������������ ����������������
����� ���� ���������� ���������������3
������������
������� �
������������
��� ���� �����
In a span of less than three decades,HIV/AIDS has emerged as the single mostformidable challenge to public health,human rights and development in thenew millennium. Already, over 25 millionpeople have died of AIDS worldwide, with3.1 million deaths in 2002. The number ofdeaths is certain to rise in the future. Anestimated 42 million people are presentlyliving with HIV/AIDS (with womenaccounting for 50 per cent of adults livingwith HIV/AIDS worldwide) and 5 million
�������������� �������������������������������������
������������
new infections occurred in 2002 alone(See Table 1.1).1 The Global Commissionon Macroeconomics of Health hasrecommended that the strategic responseto HIV be invested with the seriousnessof a mission whose philosophy is oneof approaching health as ‘globalpublic good’.2
The South Asian region may have onlyaround 25 per cent of the world’spopulation but it is home to 40 per centof the world’s absolute poor subsisting onless than $1 a day.3 Besides, at 4.2 million
���!����������������� �������"#����������
$������$�����$%��������&���'�����$���'�������%��
������(������������������$���‘��������)*������'�������!������������$������� ���������‘+�!������� ������, �$������! �!������)' �����%!
���������������!������-���������.����������!*
��%��/�����!'����������-��$����$���%!���$�������
�����,���������������.������-�����������������
��������$�����������������������������������$$��
$�����������*������--�������������������� �
������������$�����-������������!���-���������
������������%����������$������'�����'��������!���
��.������$������*
0������!����'��������������-���������������
������������������������������*��������������$
������� �����%���-������!'���������' ��%���������'
���/�����! &�����������! ������ ���/�����!( ���
Evolution of HIV epidemiology
�������!����������������1��$�������������%�������*
�����$�����$���������������2�$�������!$��-����
��������'���������������-����'���������������������
��.�������������'�%����$��-��������2�$��������
�����������������!�2�!��������������������-����,
�$$���������������������������!*
�����'�������������� ������������������!
�����������������������$�����������!'�������
�����������������������$��$������������*3��
������!$�������%���������������$���-�������
�����%������������'�����-�����%���������������
����������������������������'����������'������
������! ������ ���������� ��%��� $�� healthcare���������* �-����' ��� ����� �$ ���������� ��
����� �����%�-������'��������$����������
�����������������������.�����������������,�����
��$$������������������%����!������������$��������*
Box 1.1

������������ ����������������
����� ���� ���������� ���������������4
������������
cases, the region has the second largestprevalence of HIV/AIDS in the world(because of the large population base), aproblem that can get exacerbated by thehigh levels of inequality, poverty, socialstigma and discrimination that couldenhance the vulnerability of people to theinfection. There are several reasons forthis. Low and inappropriate compositionof public expenditure on basic services in
most countries limits the access of thepoor to health facilities. This reflects thepressure of competing priorities onlimited public resources. The quality ofpublic services is also a matter of concern.The high proportion of the informal sectorin economic activity and lack of adequatesocial security also add to the vulnerabilityof the poor. There is very high mobility ofpeople in the region, especially as
3�%���*�
��� ������������ ����������–����
��� ������ �� ������ �� �� !��������� � "��� ��#�$� �
������� ��������%� ���%����� & ����� � ������� �� ���� ���
&����������� ����'#($ ���)�� ��%� �%��&�����������
�� ���
��%,������� �����"4��1 �"'5��'��� #*# 6# �������.��� ��.
�$���� ����!�"#��
7�����$������� �����"#�� 66�'��� �*� 66 �������.��� ��.'
8������� ��9�������������
� ������� �� ������*+�� ,-���-��� ��, ., ����� ��/ �����/-
�������� 0������� �� ��
���������� �����"#�� �'���'��� �*� �5 �������.��� ��.'
:���$�� ��9�������������'
��.��� ������������
��������-������
��.-������
;����������� �����"4��1 �'6��'��� �*< �� �������.��� ��.'
����!�"#�� ��9�������������'
��.��� ������������
��������-������
��.-������
����%%��� �����"4��1 55�'��� �*5 6� �������.��� ��.'
����!�"#�� ��.��� ������������
��������-������
��.-������
������ �����= ����!�""�� �'���'��� �*< �4 ��9�������������
�����������
8������ ����� �����"4��1 64�'��� �*� �6 ��.��� ������������
����!�"#�� ��������-������
��.-������'��9������
�������
7����������� �����"4��1 "#�'��� �*< �� �������.��� ��.'
����!�"#�� ��9�������������'
��.��� ������������
��������-������
��.-������
������������ �����"4��1 �6'��� �*� 4 ��.��� ������������
7�->������ ����!�"#�� ��������-������
��.-������
� ��� 1�-���-��� ��� 2�
?3�������������$������ &�6��5"!�����$���( ������-�������� � ������'����������������������%���*
������� @7�� ��80' ����

������������ ����������������
����� ���� ���������� ���������������5
������������
migrant labour, and this creates a largeconstituency whose movement—in theabsence of adequate information, servicesand choices—increases their vulnerabilityto HIV.
Table 1.1 compares the magnitude of HIVprevalence in South Asia with that of otherregions of the world. It shows that HIVprevalence rates in South Asia (which,for the purposes of this report, includesIran and Afghanistan) and South East Asiaare significantly lower than in regionslike sub-Saharan Africa where theepidemic is rampant.
Table 1.2 shows that the estimates of HIVprevalence among adults aged 15–49years in the nine countries that this studycovers range from negligible levels inBhutan to 0.8 per cent in India, figuresthat are well below the 8.8 per centprevalence rate among similar agegroups in sub-Saharan Africa.4
These low prevalence rates, however,mask a more complex picture and shouldnot be a source of complacency, forseveral reasons.
� The first relates to scale. Nine South andAsian countries account for nearly25 per cent of the world’s population,so that even small rates of HIVincidence translate into large absolutenumbers. With an estimated 3.97million infections, India alone hasnearly 10 per cent of all the peopleliving with HIV/AIDS (PLWHA) in theworld, with sentinel surveillancesurveys showing an advance ofHIV/AIDS in several parts of thecountry.5 Several urban areas in thewestern state of Maharashtra and insouthern India already have HIVincidence rates among pregnantwomen coming to antenatal clinics inexcess of 2 per cent.6
� The second reason is growth rates. Thetotal number of PLWHA in Asia andthe Pacific grew by 10 per cent since2001 to 7.2 million.7 Nepal has seenrapid increases in HIV prevalencerates among sex workers and injectingdrug users in recent years.8 Althoughthe proportion of pregnant womenwho are HIV-positive – a barometer ofthe spread of HIV into the generalpopulation—in Nepal is negligible, it
������
����������� �����
� �����������
������������
����������������
�����������������
������������
3�%���*�
��������� ������������� ������3����
4 ��5 6 �7��� � 6 �7�� �������%����� 6 �7��� � 6 �7��� � 6 �7��� �
�� ������ ���� ��� ������� � & �� ������ �������#�� ���
������ #�231* �� ����#($ #�231*���� #�3�1���� ���������$
������ �$ �� �$ �� �$
�$��������� 7*�* 7*�* 7*�* 7*�* 7*�* 7*�*
A��������� ��'��� ��'��� B�*� �'��� ��� <6�
A����� B��� B��� B�*� 7*�* 7*�* 7*�*
����� �'"4�'��� �'#��'��� �*# �'6��'��� �4�'��� 7*�*
����&�*�*( ��'��� ��'��� B�*� 6'��� B��� �"�
C������� B��� B��� �*� 7*�* 7*�* 7*�*
7���� 6#'��� 6<'��� �*6 �5'��� �'6�� �'5��
:�2����� 4#'��� 4<'��� �*� �<'��� �'��� 56��
���;��2� 5'#�� 5'4�� B�*� �'5�� B��� �6�
7���D 7*�* ��������� ��� ������%��
������� @7�� �' �����

������������ ����������������
����� ���� ���������� ���������������6
������������
would be only a matter of time beforeHIV moves from vulnerable groupsinto its general population.
� Third, the epidemic is still relativelyrecent in South Asia, at least incomparison to sub-Saharan Africa. Sothe current relatively low HIVprevalence rate in the seven countriesother than India and Nepal may just bea temporary reprieve. Fortunately, thisgives the South Asian countries anopportunity to arrest the epidemic atits present stage rather than waiting forit to become generalised in nature.
The following features are associated withthe spread of HIV in all these countries.� High rates of poverty and consequent
poor living conditions.� Gender inequality.� Incomplete epidemiological
transition with high prevalence ofcommunicable diseases such astuberculosis (TB).
� Low levels of knowledge as a result ofwhich populations will be less thanfully aware about methods of reducingrisk of HIV infection.
� Migrant and displaced populations.
These relationships will be examined infurther detail subsequently.
��� ���������������� ������8����5��������5��
Both immediate and structural factorscontribute to the spread of HIV/AIDS. Mostof the responses to date, including acrossSouth Asia, have dealt with the immediatefactors. These include sexual and socialbehaviors that place people at risk,inadequate screening of donated blood andmultiple uses of invasive instrumentswithout effective cleaning between uses.Most information and behaviour changeinterventions focus on sexual and drug
taking habits and primarily targetindividuals. In effect, such interventionsrespond to the consequences of theepidemic rather than addressing the rootcauses. The persistence of the vulnerablegroup approach demonstrates that thereis still a lack of understanding about theactual dynamics of the epidemic,especially for the general population.Clearly, a systems analysis within a humandevelopment framework—rather than anarrower medical or health approach—would be useful here.
Structural factors that contribute to theepidemic are associated with prevailingsocio-economic conditions, access toquality health facilities, and the opennessof society to face the epidemic and itssexual and behavioural attributes. Socio-economic inequalities (along class,gender, and ethnic lines) have long beenknown to be constraints to development.Those inequalities shape the patterns ofHIV/AIDS as well.
Although the HIV/AIDS infection cutsacross socio-economic groups, itstransmission follows the paths createdby economic, social and politicalinequalities between women and men.Over the past three decades, as the processof economic liberalisation gathered steam,the inequalities that foster the spread ofHIV/AIDS have intensified. Some of thoseinequalities may appear unrelated—lackof easy access to diagnosis and treatmentof sexually transmitted infections (STIs);living away from a family; or working tosurvive in marginal and insecure jobs—butthey are extremely conducive to the rapidspread of HIV/AIDS.
These inequalities present majorchallenges to policy makers in all sectorsand at all levels. It is well known thatpolitical decisions about resourceallocation and response to diverse needs
���������
� !"� #�����������
�������������$
���������������
������������
����� �������
����������
���������������
�������������
���%�������
��� ���� ����
��������

������������ ����������������
����� ���� ���������� ���������������7
������������
and interests have a profound influenceon socio-economic conditions. Pastexperience across the region indicates acertain reluctance on the part of policymakers to tackle these inequalities and atendency to postpone action because theproblems appear insurmountable.However, the issues can be broken downinto more manageable and actionablecomponents.
Policy makers should be more sensitive tothe importance of creating an appropriate‘enabling environment’ for a moreeffective response to the epidemic. Thiswill include policy changes in areas suchas human rights that may not strictly liewithin the domain of ‘public health’. Forexample, the shift from public-supportedhealth systems to a mixture of public andprivate services and cost-recoverymeasures, such as user charges for once freeor low-cost services, is an essential part ofthe economic liberalisation process,stemming from the decision to reducepublic expenditures on health. However,this limits access to health facilities formany people or forces them to re-prioritisetheir spending to pay for services. It hasbeen argued that the use of health facilities,especially by the lower income groups,tends to decline sharply with increases infees at public facilities. Thus, the revenuemodel of ‘health sector reforms’ mayfurther exclude the poor from adequatehealthcare. In India, privatisation isincreasing corporate involvement in theprovision of healthcare, and there is a riskthat concerns of profitability could seelow-income groups being left out ofquality healthcare.9
��. ��� ����� ����� ����%�� ��������� ���
Human poverty10 reduces the ability ofpeople to control their circumstances andmake choices. Poor people are forced by
economic necessity into living conditionsand occupations with a high level of risk tolife and health. It has increasingly beenfound in countries that are experiencingwidespread impact of HIV/AIDS thatprevention initiatives can work only ifenabling environments are created forpeople to change their lives in a mannerthat would help them practise safe andprotective behaviour consistently. There is,therefore, a need to look at the epidemicfrom the perspective of its socio-economiccauses and consequences, and analyse itsimpact on the overall development indicesat the national and regional level.
Analysis of HIV/AIDS within a humandevelopment framework can offer newinsights not only for determining issuesfor ‘bridge populations’ (groups that linkthe vulnerable groups with the generalpopulation), but also to offer mainstreamdevelopment solutions to the challengeof the epidemic.
There are two sets of issues relating to thelinkages of HIV/AIDS with poverty:(a) the combined effect of poverty and
income inequalities on socialinteractions including sex, patterns ofvulnerability and patterns of riskbehaviour; and
(b) HIV/AIDS as a cause of furtherimpoverishment of poor people,which can have a devastating impacton communities and the potentialto reverse any gains in humandevelopment.
Studies indicate that gender issues are atthe heart of the epidemic, as women areincreasingly being infected. Women aredoubly vulnerable to HIV/AIDS. Forbiological reasons, they are four timesmore prone to STIs than men.11 Inaddition, their low social and economicstatus and their dependence on men limittheir control over their lives, including
&�����$�����
������������
�������������
�������������
�����������
�����������
'��������
�����������(������
����� ���������
������������
���������

������������ ����������������
����� ���� ���������� ���������������8
������������
)����$�����
����������������
����������������
������������������
��������������
���������������
� ������������
�����������
��������
����������������
over exposure to HIV. It has also beenobserved that the vulnerability ofpopulations to the virus increases inregions where macro policies are lesssensitive to gender issues. Furthermore,HIV/AIDS prevention efforts need toaddress culturally rooted ideas of maleidentity and behaviour. These areintrinsically linked to gender issues andneed to be addressed within theprevention strategies for the epidemic.
��1 ������������� ����%�� ����� ��� ���
Several authors and policy makers haveargued that, apart from the obvious
implications for the health of PLWHA,HIV/AIDS will have significant impactson the affected countries, along a numberof dimensions. These effects includeadverse implications for the rate of growthof real income per capita.13 Potentialeffects could also include impacts onthe distribution of economic resources,the educational achievements ofpopulations, and other freedoms thatpeople value, including basic humanrights such as life and liberty. 14
In short, HIV/AIDS influences societiesin ways that go beyond the purely healthor purely economic dimension and intothe realm of human development, a goal
�������������������%�!��������������������
�$ �������� ����������� ���� ��� ���� �� %�
�!���!����-������-�����������������������*��
������������������������2��-�����&���������(���
��������!������$�������,����������������$‘���/�����!�$ ��$�)* A���� �� ��� ��������� �� ���������)�
*����������+���������E-������-��������$�����
�-���2�%��$�������2��$�������������F��������
�����������$����-��2����-�$�������������������,
���������������%�����������������������$-���
%����*3���'��������������������'%������%����
�����%��������������'�����������������$�.�������
�������� ������������� $�� ��� ����������' ��� ����
������%�����������������������%���������������*
����������������������������'��������!'������%���
�������������������������������'%���������%����
��������������%�����-����'-������%!���������%���
��������������������)���������$����$�����)�
�������������%���������*�����'��������������%����
������1������'���������$������'��$������%���!1���
�.�������$������������%�����������-����%��������
�����������������������$����������������������
%!�����!����*
3�������������������$�������������������
������� ������ ����.'��$����������������
���������� ����. & �(* 3��� ���%���� �����
��������1��$� �.�������! �� %����' �����������
����������&�-���������������$������������!���
���%����G������!'��������!����������!-���������
�����(������������+���� �������:������&+ :(*
3���'��������� ������������������������������
����-������������!�������%�����������������$
‘�����������)����$�����%���1������'������������������* 3� ��������� �' ���� �$ ��� �����
�����������������������������������.'�������
%��-��������'�������������������������������
�$�������������������������� �*
��������������� �'@7 :����������������%��
�$�������������������������������$‘�����������)����������������������$��������$���*3�����������
���������,����������������������.&+ �(����-�
���������$�������:�����!����.&:�(&���$��
��������� ��������� ��� ������� $�� ����������
���������(*��3�������������!����.$������������
�������������������������������$������������!����'
������%�%����!�$�����������������5�'������
����������$���������$������&������$�������������
�$����������-����������������$�-�������������
����������������������$�����,6��������-�����
�����-�����(*��������������� �������:�'���
+ �$�����������/��������-����������������1������
����������/��������%��-���������-����*3��
������$�����������������$������!�������������
�������������'���������.������!%����-�!��-����
����.��������$����%����������%������������*A����
��������������!�������2��!��%��%��������������
������������$$�����������������������2�$��
���������‘�����������)*
Understanding human developmentBox 1.2

������������ ����������������
����� ���� ���������� ���������������9
������������
that societies cherish. Linking HIV/AIDS-related indicators to development andpoverty alleviation indicators wouldprovide necessary information foradvocacy with policy makers as well asstrategic direction for action.
Political commitment has been shown tobe essential for the success of preventionprogrammes for HIV. Multi-levelinterventions that seek to involve a varietyof partners in coordinated action havebeen shown to be more successful thanisolated, segmented efforts. Moreover, anenhanced and coordinated political,economic and social effort is required toreduce societal vulnerability alongsideprogrammes operating at the individualand community levels.
Mainstreaming HIV and the issues thatexacerbate the effect of the epidemic intonational poverty reduction programmesas well as gender programmes has beenrecognised as the key to reducing itsimpact. This can happen only througheffective advocacy tools that will spurground-level action by the policy-makers.
Since 1990, UNDP’s HumanDevelopment Reports (HDRs) haveemerged as the principal advocacyplatform for Sustainable HumanDevelopment for UNDP and otheragencies. Global, regional and nationalHDRs have contributed towards raisingawareness and generating debates onpolicies and activities. It has been anextremely useful tool for policy makers,agencies working in the field ofdevelopment as well as multilateral andbilateral donors to assess the efficacy ofcurrent approaches and strategies inorder to implement innovative andbetter programmes. A case in point isthe Botswana National HumanDevelopment Report on HIV/AIDS,
which spurred a public discussion on theaccessibility of anti-retroviral (ARV )drugs and the responsibility of thegovernment in providing them. Thisultimately led to a decision in 2001 bythe country’s President to provide freeaccess to ARV drugs. The President alsohad an abridged version of the reportproduced for distribution in all seniorprimary and junior secondary schools.
��2 ! �� ��� ��������� ��
This report, which is also the first RegionalHDR on HIV/AIDS, attempts to examinethe connection between the epidemicand the larger challenge of humandeprivation in South Asia. In the light ofthe United Nations General AssemblySpecial Session on HIV/AIDS (UNGASS)Declaration and the MillenniumDevelopment Goals (MDGs) (See Box1.3), it is especially imperative that theattempt to halt and reverse the spread ofHIV goes hand in hand with theeradication of human poverty in theregion. However, policy analysis on HIVand human development has, thus far,treated the two separately. This reportattempts to explore the conceptual andempirical links between HIV and humandevelopment. The objectives of thisreport, therefore, are:� to create an understanding of the
causes and consequences of HIVwithin a development framework andthereby to advocate for a shift indevelopment priorities andapproaches to HIV;
� analyse convincing data and evidenceregarding the socio-economicdimensions of HIV/AIDS, includingfactors that heighten vulnerability;
� in the light of the analysis andexperiences, identify key points forHIV/AIDS and development strategiesin the region;
)����$�����
����������������
����������������
������������������
��������������
���������������
� ������������
�����������
��������
����������������

������������ ����������������
����� ���� ���������� ���������������10
������������
� document good practices inindividual countries and create a casefor adapting those that are relevant tothe region; and
� to advocate integrated approaches topolicy makers and implementers inthe region for reducing the spread andimpact of the epidemic by main-streaming HIV response into poverty
alleviation, gender equality and otherdevelopment programmes.
The subsequent report structurehighlights the complex interrelation-ships between dimensions of humandevelopment and HIV/AIDS issues,based upon multi-variate regressionanalysis in Chapter 2. A treatment of the
3�� C��������� ���������� +���� &C +�(
����������� ��� ����������� ������� ������ ��
�����������������������$����������-�����������
����������""��*�����C����������������$���
@�����7������&@7(������������%������'-����
���������������������2�!����������������������
HC��������� ����������H'-����-���������%!�54
�����$��������+�������������"��������*
A��������� ����������'@7 :���-��2��-���
�����@7�����������'$�����������������'���
8����A��2'�������������C������!I���������
0����������� $�� ������� ����������� ���
������������������������$�����'���������
����������/�����$��%����������������������������*
3����C +������������������'�#��������������
5�����������*
3������������������$����� �-�����������%��
��������������������%��������������������.��
C +'-����������������7���� ���%���������������
�����������75����2*�-����'������!�����������
����������$����� �������������$'%����������
������������2����%��-����������� ���������
�����������C +�*���������������������������
�$������C +���������������������������������
�������������� ���������'-����������������
���������������������-������%������%��-������
���������������$��������C +�*3�������2����
$�������������������������������������%��-�����
�������������������'��-��������������������
$��%����,%���������,�����������������*
9:�����7��&������������������� �����"�;�8
�������������/������� %���5����� ���
3�������$�����������������!�����$��������$$�����
%!����� �������9���������������������-��'
$������������� ��������������-��� %���� &�� ���
�������,������������'�����������-�����$�����%!5
������������%��������������!���%������%!����
6��������(*
�������%�� %�����������5��� ���
3��/�����!�$�������������������������������$$�����
%�������$�������%���������������������������
�������*C��������������������������$����������2
����������������������%�������$�����������������
�$������*�� �,����������������������$����!%������'
��2�����������$$���������!������$���*
.��!� � ����������< ���5������� &���& ��
+�������������2��!��%�2�������$���������������
����'��-����������������������*8������2���
����������%������$���������$������������������
���������!-���-����������$������*8����������
�/���!'%��������������������'�����������$�������
�����������2'����� ��.����%�������������/��������
���%��������-����*
1����� ��������� �����5
��$�������������������!-���������������������$��
�����.�������'��������%�!������'�����������,��,
���������$������*
2������ %����������������
����� � �� �����������!�������$����������
�������*
,���� ����%� ������� ����7��5
�������'�����������%����������$��������$����������'
��� ���� ��%��� ������ ���� $�� $�������-����'
���������!$��-����*���������������������
����� ��-���������!���������$$����������!���
����������������$��������������������*
=����%�� ������ 7�������������� ����%�� ����
����� � ��������� �� ����� ���������� ��������
%���������������������������*
Millennium Development Goals and HIV/AIDSBox 1.3

������������ ����������������
����� ���� ���������� ���������������11
������������
status, trends and prospects of theepidemic in the context of humandeprivation and inadequacy of publichealth systems in South Asia isundertaken in Chapter 3. It indicates thatthe region cannot avoid potentiallycatastrophic consequences unless thereis a political will to galvanise resourcesand catalyse reform for placing highpriority on health and humandevelopment. The creation of an‘enabling environment’ that guaranteeshuman rights and eliminates socialstigma and discrimination againstPLWHA is imperative. Chapter 4examines the legal and human rightsframework for a response to HIV in SouthAsia. It argues that there is a need toensure that the strategies for ‘harmreduction’ are backed by suitablemodifications of laws so that the PLWHAare guaranteed a life with dignity andcare, free of social stigma and dailyharassment. Emerging issues such asstigma and discrimination, conflictsituations and affordability of HighlyActive Anti-retroviral Therapy (HAART)in the resource-poor setting of SouthAsia, dealt with in the previous chapters,form the backdrop of discussion on theway forward in Chapter 5. In the case oftreatment, it is argued that there is notrade-off between prevention and careand support. Indeed, effective care andsupport based on the principles of
Greater Involvement of People withAIDS (GIPA) can guarantee more effectiveprevention strategies. The chapterconcludes with a call for greater regionalcooperation on HIV issues such as drugpricing, mobility and the integration ofHIV into mainstream developmentprogrammes. It provides specificrecommendations for policy action andprogramme implementation to furtherstrengthen the public agenda on HIV andhuman development in South Asia.Building on the analysis of the foregoingchapters, the way forward on thisimportant issue involves buildingalliances of national, state and localgovernance with civil societyorganisations, media and researchinstitutions. A comprehensive responseto the challenge of human deprivationin general and the epidemic in particularmust involve a widening of the debateacross disciplines, specialisations and“single focus” initiatives.
This report does not claim to offer auniversal solution or monolithic strategyto tackle what is admittedly a very largechallenge. It does however emphasise theurgency of mainstreaming HIV responsein all human development-relatedprogrammes and, conversely, the criticalimportance of combatting the epidemicthrough an integrated human develop-ment framework.
������������������������������������������� �������������� ����������������� ������� ������� ������������������������������������������������ ������ ������!������������ ������������������ ���"������#���������������������������"������� ����
�$�%������ ��� �������������������&��� ������ �������������' ������( �������������� ����������� ��������� ������������������ ���"����)������������������������ ����������������������������������"�� ��
�� ����������������� ������������� �����������������������������
����!��"�� #��������������������������$��%��&''&



������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 14

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 15
!� ����� �
��������������� ����������� ����������
��� ����������
This chapter brings out the mutuallyreinforcing relationship between thevulnerability to HIV and the persistenceof human deprivation and the manner inwhich the HIV/AIDS epidemic shapes,and is, in turn, shaped by the patterns ofdevelopment in South Asia. “Thesituation is worst in regions and countrieswhere poverty is extensive, genderinequality is pervasive, and public servicesare weak. In fact, the spread of HIV/AIDSat the turn of the twenty-first century is asign of maldevelopment-an indicatorof the failure to create more equitableand prosperous societies over large partsof the world.”1
Conventionally, the analyses of theepidemic and human development inSouth Asia have been done in a segregatedmanner. The former has focusedprimarily on the identification ofvulnerable groups, seropositivityestimates and concomitant socio-economic profiles of ‘people at risk’. TheHDRs, for their part, have analysedliteracy, vital statistics and indicators ofincome, employment and poverty,albeit within an integrated framework.There is, however, a growingrecognition that HIV/AIDS is not just ahealth issue but a fundamental issueunderlying the sustainability of human
������������ � ������ ���������� ���������������� ����������������� ������� ��������� ������������ ���� ������������ ��������� ����������� �������� ������� ����������� ����� �������������� ��������������� �!"
������������ ����
������������������
�������� �����������
����� ����������� development. This has widened the scopeof the present discourse.
����� ����������������������� ���������������������� ��������Where do the countries in the region rankin terms of development achievements?Tables 2.1 and 2.2 shed light on some of thecomponents of HDI, and HIV prevalence.
There appears to be considerablevariation in achievement, in terms ofaggregate indicators such as the HDI andGDI and in individual components ofHDI, across even this small group of ninecountries. Sri Lanka, Maldives and Iranare at the upper end of the spectrum, withIndia in the middle and the others(Bangladesh, Bhutan, Nepal and Pakistan)at the lower end.
The same appears to hold true for SouthAsia’s economic indicators such as theproportion of population living below theinternational poverty line of $1 (1993PPP), with the exception of Sri Lanka.These already low levels of developmentindicators are likely to be furtheraffected by HIV, with recent gains indevelopment reversed.
Table T1 (see Technical Note B) highlightschanges in some of the indicators ofhuman development in the last two

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 16
decades in the countries of South Asia. Thedata show that Sri Lanka’s HDI, adultliteracy rate and life expectancy at birthhave grown at somewhat slower rates thanthat of the other countries, given its already
high rates of achievement. With theexception of Pakistan, most of thecountries have experienced robust growthin per capita income. The table alsohighlights Pakistan’s economic difficulties
" �����#$
�������������������������� ���� ��������������������
!����� ��� "��������������������# ��� $%&�������
����������������"�� ���������� �������������
����� ���� ������� ��������� �������� ���������
��������� �����''� �''� ��()*+������
���������
�%�� ��� �#�# �#�# �#�# �#�# �#�# �#�#
& �� ���� �#'() $'* �#'+) $�$ $ ,��� -�#$
&��� �#'.' $'� �#�# �#�# -$�� -�#$
��� �#*(( $�' �#*+ $�* ,.(�,��� �#)
�� �/�#�#0 �#(�$ .) �#(� ) ��,��� -�#$
1 ������ �#(' )' �#( . +) -$�� �#$
��� � �#'.� $'� �#'( $$. *),��� �#*
2 3��� �#'.. $ ) �#'+) $�� (),��� �#$
����4 3 �#('$ ). �#( ( (� ',)�� -�#$
5����� � 3��� ��������%�$( �6�������#
7�8���� 3��� ��������%�$'+�6�������
����9� �#�#� ���6 ���� ��� � �� ���
�������� �!�����$�:��9�;��2,�����<�!����� :'9�;�����,������!
" �����#�
����������������������������� ��������,��'''�����������
!����� %��� ���������������� ���� �������� $��������� $�������������-
�#�������� �����������,''' ������.��/� "�$�$$$ �������$�������������.
������������������ ����������� �(������ 0 $ $���������++1�$$$
�������� 0 $ ��+21)�'''3
�%�� ��� �#�# �#�# �#�# �#�# �#�#
& �� ���� *.#' *' '$# $,+�� �.#$
&��� +�#� (( '(#� $,'$� �#�#
��� + # +. *(#� �, *) ''#�
�� �/�#�#0 +)#. + (+# *,))' �#�#
1 ������ ++#* *. .+#( ',')* �#�#
��� � *)#+ (� '$#) $, �( (#(
2 3��� +�#� )* ' #� $,.�) $#�
����4 3 (�#$ $( .$#+ ,* � +#+
7�� � � ��%��� ��� ��������� ��6���=� �� � �� ���������� ��������������6�%���
����9� �#�#� ���6 ���� ��� � �� ���
�������� ;��2,� ����

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 17
in recent years. The low rate of growth ofadult literacy in the Maldives reflects, asin the case of Sri Lanka, its already highliteracy rate of about 92 per cent.
��� %��4�/��
����� �������������������������������The HIV/AIDS epidemic has profoundconsequences for human development inSouth Asia. This is because HIV affects notjust the health of individuals, but has botha direct and indirect effect on theircapabilities, their family and kinshipstructures, and consequently, on theeconomic, social and institutionalarrangements. These nuanced effects ofHIV make it imperative to look at it from a
development perspective, rather than apurely public health one. It is alsoimportant that the impact be examinedprimarily through the individuals andhouseholds it affects, using a humandevelopment framework. Such a broaderapproach is more conducive to theprevention and management of theepidemic, a combination of which wouldreverse the incidence.
������� ���������� ��������
���������� ��� ����� ����������
Human development is, very simply, theprocess of enlarging choices. The humandevelopment framework looks at howthese choices are enlarged by enhancingthe capabilities of individuals, and at theoutcomes of these enlarged choices. The
������������
� ������ �����%���������� =�6�������������������
����������� ��������6 ���#���� � ������%����
���% �������������6�������������$..��,����
������ ����6�������������� ���
� � ������������������6 ���,���%������6� 6=� �
��������� ������������ �� ��������������
� ���%������6 ���
� ��66���� �%� ����6� ��6� ����� 6�� �������
6� ��������%�����6��=� ������6��� �������������=
� >�����6���%� ����� ���8?��������@�A���%��
��� �� ����� ����� ���� �� � ��=� $�������� �
��� � ����
� "� �������%�6������=�6 ���� ��6��� ������� �
���� ������6������������ ������6� ��������%����� �
���������������
� B��� ���� �%� ����6 ����� ��� �� 2���� ����,
��6��� ����� =��� �� C����������6�� �������
����� �����=�������� ��6��� ����������$..��,
���� ������ �������������������
!������/��
� ��D���%��6���������� ����� ��@����6������
8�2��%�������������� �6������������������ �(�
����6����%�����8�2��%�!�� � ����A��������� �
�%�E � #�"�������6 ��� �8�2��%��� ,������������
���������������������� ��*�����6����%��������
6 ��� �8�2��%�E �
� �������������%��6���� ����� �������=�� ���%
6������ ��������,� ����� � �� �����=� �%� � ��6
% 6�������@���3��� ���,� � �� ���,� ��� �
�%� ����6����
� �������� � ���� ��������,� ���� ��� ��� � ���
����������� 6�����������������6�������������
������% ���% ���������%�������������������6�����
������> ������ �6������������� ������ ���������
� 2�����������������F� ���=@�������������%�%�� ��
������� 6=��� ���6����������6��������4 3 � �����
1 ������
� ��6�����������������6������������%�����6� �
��6�����������$..��,��������%��6 ��������6=� �
����6��� �� �C����������������
� ��6����������� ���������������%�������������
�����������������
Balance sheet of human development and HIV in South AsiaBox 2.1

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 18
HIV epidemic affects the manner andextent to which these choices are eitherenlarged or constrained for individuals,groups of individuals and societyas a whole.
Incomes, poverty and earningcapabilitiesThere are several ways in which individualsand their households are likely to beeconomically affected by AIDS. The mostvisible and immediate impact is on theearnings and incomes of households ofPLWHA, especially since HIV affectsindividuals in their most productive years.As seen in Chapter 1, more than 90 per centof the world’s PLWHA are in the age groupof 15–49 years. This group is likely to be partof the labour force, or provide in-kindsupport to the household. The impact cantake the form of lost earnings whenindividuals are sick or die prematurely dueto AIDS. In South Asia, the earnings lossesare staggering. Bloom and Mahal (1996)estimate that in Sri Lanka, lost lifetimeearnings due to an AIDS death werenearly eleven times the annual treatmentcosts.4 In Nepal, they suggest that similarlosses were more than four times the percapita income.5 Prolonged illness alsoresults in loss in savings and assetholdings, both due to an increase in costs,as well as a decrease in the propensity tosave due to lower life expectancy.
A second, key immediate impact is thechange in the disposable income becauseof increased expenditure on treatment.Several studies have documented thecosts of treatment as being more thantwice the per capita incomes in selectedAsian countries.6 In India, for instance,the ratio of treatment costs to per capitaincome was 2.2 while in Sri Lanka it was1.5. These estimates did not include thecosts of ARVs, which could be expectedto further push up the economic burdenon families and households.
Loss of incomes and earnings can alsooccur due to the loss of a job because ofthe stigma associated with HIV infection,even if the HIV-positive individual is notlaid up with any of the opportunisticinfections associated with HIV/AIDS. Inthese cases, the discounted value of lostearnings is even greater than in the caseof an AIDS death, because treatmentcosts are incurred without any incomebeing earned. It is apparent that the lossof a job for a young adult has negativeeconomic and, possibly, psychologicalconsequences both for PLWHA and theirdependants. It is not the consequencesof job loss, however, but the relationshipbetween an individual’s HIV-status andjob loss that is of concern here. AMumbai-based NGO in India took up thecase of an individual who was dismissedfrom a public sector company after beingfound to be HIV-positive during medicalfitness tests that included testing hisblood for HIV, without obtaining priorconsent.7 A similar example washighlighted in the Middle East Times8 thatnoted the dismissal of a factory workerin Iran after he was found to be HIV-positive. This discrimination is notconfined to South Asia but exists in manyother countries as well. In Australia andCanada, for example, individuals weredischarged from the armed forces onmedical grounds after being found to beHIV-positive.9
At the same time, however, there arepromising signs of change in this attitude,with examples of how judicial, legislativeor policy action can readily mitigatestigma and discrimination. There havebeen several instances where the courtshave ruled in favour of reinstating HIV-affected people in jobs in India.10 In othercountries, there are statutes orinjunctions against dismissal solely forbeing HIV-positive. In Iran, for example,the health ministry appears to have
������� ����
��� ������ � ���
� ������ ��
����� �������
���� ��� �� �
������� � ������
�� �� �� �
�������� � ���
��������� �� ����
��� �� ���� ���
����������

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 19
“banned the expulsion of people sufferingfrom AIDS”.11 However, it is extremelylikely that these cases are more theexception than the rule. Since stigma anddiscrimination are deeply rooted insocietal attitudes, legislative and judicialsanctions alone will not be sufficient.Bharat (1999) documents a number ofcases where individuals resigned fromtheir jobs where they feared the reactionof other employees if found to be HIV-positive. In one case, the resignation wasprompted by the threat of a strike fromthe labour union.
The HIV/AIDS epidemic also perpetuatespoverty across generations, by reducingthe economic, social and educationalopportunities available to children inaffected households. It also increases theburden on the elderly, many of whombecome responsible for orphanedgrandchildren and other dependentrelatives. This burden is now significantlyaltering social arrangements in sub-Saharan Africa. While this impact of theepidemic has not yet been documentedin the South Asian context, as theepidemic spreads, extended socialnetworks will certainly have to bear theburden of care. High levels of ignoranceleading to stigma and discriminationcould further strain these networks,
leading to possible breakdowns incommunity ties and social capital asinfected people and their families facerejection and isolation.
Human capabilitiesApart from affecting income, theepidemic significantly affects bothexisting capabilities of PLWHA and theopportunities available to them and theirfamily members to further enhance thesecapabilities. There is some evidence tosuggest that members of householdsaffected by HIV/AIDS, especially children,would have lower educational and healthlevels. This can happen if children haveto prematurely leave school to care forthe sick, or if the family can no longerafford to educate them after the death ofa breadwinner. Within the region,studies12 indicate the difficulties thatchildren of HIV-positive persons face atschool, owing to stigma (See Box 2.2).Further, high rates of HIV/AIDS can alsoindirectly reduce education levels, ifpeople are unwilling to invest ineducation if there is little expectation ofchildren living long enough to benefitsubstantially from it.
Spending on HIV treatment also crowdsout spending on nutritional intake andother health inputs, especially as
Box 2.2
��B���� �=���� ,����������A���������6������,
����%���� �������=� ��,����� ������������ ��� ��A
����6�������������� ��� ����%�G�� � ,����� ��������
���6 ������ ������� ������%�����������$$.��������
�����������������6�����������6�������6 �����%�%� ��
�� �����=������6��� 6�����������#������������������
���� ������=6����%��������������6������,� �����
����%�6 ������ � ��������� �������6�����,�����G�� �
��������� ��6����� ���������6�����������
��� �6������� �� ����� �� �� ��� ������#� �8?�
����������=�6� ������� ������ �����������H�
��6�������������������6�������%���������6����,� �����
�� �����=�� ��� �6�� �����������������6 �������������
6������#
"����6 ���� �������������F�������� ����������6��%����
�%���6� ��=�� 6������ �����6����������66���������
�����=����6 ���� ������������6������=,� ��������=
6 ���� ��������#�������6�� ���� ����������� ����������
%���6�� ������������������ ���������=����� ����� �
������� ���� ���� 6��������� �%�������������=��
�����%�,������ ��� ����������6���������� ����
������ ���� ������������������6��������������%
�������������������������/24I��0�6 ����������#
Exclusion of HIV-positive children from school in response to boycott

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 20
household resources become increasinglylimited. HIV also affects the averageproductivity levels of PLWHA, as well ascommunities and firms. At the workplace,individual morale and productivitylevels are affected by the economicenvironment in which they operate.
HIV/AIDS also limits the access of PLWHAto health services, other public servicesand financial and social resources. All thisaffects their capabilities to developthemselves. In an intensive study of twocities in India, Mumbai and Bangalore,Bharat (1999) documented cases wherePLWHA had difficulty in accessinghealthcare and support, even from familymembers. In some cases, familycaregivers simply abandoned them, whilein others, hospitals and medical carepersonnel actively discriminated againstthem. This included isolating HIV-positive individuals from other patients,delaying or avoiding surgery, replacingintravenous procedures by oralprocedures, and early discharge ofpatients from hospitals. The studyalso noted the inability of medicalpersonnel to preserve the confidentialityof PLWHA. As a result, some patientschose to voluntarily discharge themselvesrather than allow their HIV status to bewidely disclosed.
In a small survey conducted amongmedical personnel in Sri Lanka in 1994,Bloom et al.13 found that 75 per cent ofhospital staff agreed with the statementthat “AIDS patients are very infectious andshould, therefore, be isolated in separatewards to reduce the risk of infectingmedical personnel and other patients.”Thirty-six per cent also said that ifinformed about a patient’s HIV-positivestatus, they would inform otherindividuals without obtaining thepatient’s consent.
HIV positive status can also deny accessto life and health insurance. This willseriously limit the ability of the affectedperson (or household members) to affordcare that is needed, and will have severefinancial implications for the family giventhe high treatment costs and thepremature death of a possiblebreadwinner. In a region where publicexpenditure on health is limited, and theprivate sector is the dominant provider ofhealth services, every incidence of ill-health could lead to a debt trap for poorhouseholds. This situation is furtheraggravated in the absence of universalcoverage by an affordable health insurancescheme to provide for the health needs ofthe poorest sections of society.
Individual libertiesHIV/AIDS and its associated stigma anddiscrimination have significantlycurtailed individual liberties in theeconomic, social and political lives ofPLWHA. Social ostracism has often beenaccompanied by State-sponsoredrestriction of liberties as well. In theIndian state of Goa, Dominic D’Souza,who had donated blood and was found tobe HIV positive, was kept in solitaryconfinement under the Goa Public HealthAmendment Act (GPHAA), 1985, whichput anyone testing positive for HIV undermandatory isolation. D’Souza wasreleased from confinement after a lengthycourt battle, in which the court held that“it would no longer be mandatory todetain positive people, except in‘justifiable’ cases”. The GPHAA was lateramended and such isolation was madediscretionary. Similarly, in Pakistan, anHIV-positive housemaid was sentencedto a three-month stay in isolation at aprison hospital in 1988.14
Such official policies also restrictindividuals’ freedom of movement and
���� �!� ���
�"��� ��� ������ ��
�#$� �� �����
��������� �����
����� �������� ��
������ �� �����
����������

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 21
their ability to travel, within the region andbeyond, whether for employment, refuge,education or, simply, pleasure. Testingmigrants and those seeking residence forHIV is a common practice globally andthere is mandatory testing for certainpopulations. A study undertaken for theWHO’s Global Programme on AIDS,15
analysed the then existing immigrationlaws in 40 countries, in terms of their abilityto influence mobility across nationalborders. It concluded that countries have
used one or more of two sets ofjustifications–reducing public financialburden and reducing risks to publichealth–to restrict entry on health grounds.Such restrictions are common in theSouth Asian region. In Iran the standardvisa application form inquires whether theapplicant has previously suffered from acontagious illness. A worldwide survey ofimmigration restrictions suggests thatcurbs on PLWHA are also present inBangladesh, Maldives, Sri Lanka and
"���8�2�����6������������� �������� ������2 ��������
�����������6������$..',� ������ ���6�� �����
����2 ������������������6� � ���#����������6� � ���,
�������� ������ %����'�� 6�������� 6��������� ��
��������������� �������������%�����������������
���������/24I��0�������6�������������������
�������6� �� ���������#�"���� ��6�����������%����
��6� � ����������9
� ��������������� ���������������%�24I����������
���� ����������������������6 � 6��=� ��6����� ���
�%�����3���%�24I��� �� 6������=A� ���
��� �� �����/!&?�0,������� ��������6�� �����%
�����������������6 �,���� �� ����6� ����������
� B���=� ������� 24I��� �� ��6����� � 3��,
%����� ���� ���������� �����%������6�����6���
� 2����6�� ����������������������%� ������� ��,
� ���6�� ��=������������������������������ ������
��������,������������ �� ����6� ���� �����
� 1 3�� � �� ���� �6��� �=� ������6��� ��� ������
6��� �������������6��6������ ��F� ����������
%��� 24I��,� �8?�� �� !&?����3������
����� ���� ��� ��� ����������� ����
� ��������� ��� �� ������ ��� ����6� ����
�� �� ���6�6�����������������,���� �������
������6�
��6������������ �� �����������6���%�24I��� �
���������� 6���%��������� ��%��������������
����=� ���6���%���������������� �6��6� ����������
����������� �����������������6� ������� ������
��� 6���%���������#�"������ ���������������%�������
�������������������/8�2�0� �������6�� ����� 6�
�������6���=�%��� 6������ ���6�� �����%�24I��� �
��� ������@%���� ����6=� �� ��6����A� 3��� ��
�������� ���#
8�2��� ���%������������������ �������� ����
% 6�� �����6��������������������6#�������,� �������
�������� �%��������������6�� ����������� �� �����
����6��������� �� ���������� ��,�6���������� �
��6������� ��� �� ���3� %�������,� ���� ���%��� ���� ��
��3����������24I���� �����6������C�6���� ����
�� ����C�6��������������������������������6#��
���������� ����� � ���6�� ��=,� ������ ��%��
�����������%����A���������������� � ����%�������
�����������%�24I��,�� =��%����� ���%���
� ��� ������������� �� ��� �=��������6��������=,
������������ �����6���� ���#����������������
6�����,� �����%���,� 8�2�� ��� �6�� ����=� ����
����������� �����������������%��24I��������6���
������%�6� ���������������� �%������������� �
� ������� ��6 ��������� � �����6���� ���,��������
�����6��%������ �������� ���6�� �������F� ���=��%
������������,�6 ��,��������� ����� �������������#
������,����������������� �� 66��� 6���%�����8�2�
���6�����,������������������� 6��6����� ��� ������
6� �����#� �� ������ ��� ,� �� � ���6�� �,� 24I��
��� �� ����,�������� ������3��� �������������
�����������������������6� ���������6�� ��������� �
������� ������� � �����6���� ���,���������6 � 6��=
�����=��6 �6��������6��#
�����������������=�������%�������24I������ �� ����
�� �� ������ ��������������������������� �� ��
�6�� ����=���=�������%���6������6=A� 3��� �����
����3�������� 6��6������=A��������������#
The Greater Involvement of People Living with HIV/AIDS (GIPA)Box 2.3

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 22
Pakistan.16 Given that South Asiacontributes a large number of workers anddomicile residents, these restrictivepolicies curtail livelihood options forpeople in the region and violate humanrights of migrants and travellers. SouthAsian migrants working overseas are oftendeported because of their HIV status withno support or counselling provided.
Marginalisation and discriminationof vulnerable groupsThe fact that it is marginalised groups—sex workers, migrants, injecting drugusers and men who have sex with men—who have so far been most severelyaffected by HIV/AIDS in South Asia hasresulted in these groups being blamedfor its spread. This has led to theirfurther marginalisation, stigmatisation,harassment and discrimination. Apartfrom violations of their rights, this alsomakes them face greater social exclusion.This, in turn, only increases theirvulnerability to HIV and allows theepidemic to spread because they are thenless able to access the information,services and support needed to protectthemselves and others from infection.They also become more vulnerable toabuse and exploitation, as seen in thesexual abuse experienced by men whohave sex with men in Bangladesh.17 Suchincreased marginalisation also reducesthe livelihood security and opportunitiesof these groups, thereby heightening theirvulnerability to HIV/AIDS by promptingunsafe migration or sex work.
Impact on womenNearly 36 per cent of all PLWHA in Southand South East Asia are women.18 Thespread of the epidemic in a region withalready highly unequal gender relationsaffects men and women differently. Theimpact of the epidemic falls primarilyon women in four different, thoughrelated, ways:
� women shoulder the increased burdenof care within the household andthe community, in addition to theirdomestic work and economicresponsibilities;
� this increased care or the disease itselflessens the ability of women to workin the formal, informal or agriculturalsectors, leading to a further loss ofincome, reduction in child care andfood security;
� in cases where the male members ofthe household stop earning or die ofAIDS, the women are left to providefor the rest of the family, and this caninclude being pushed into the sextrade; and
� finally, women are often blamed fortheir family’s and their own sickness,and are ostracised by the extendedfamily and community, leading to theirbearing the social and psychologicalburden of the disease as well.19
5������/� ���� ����������������
����� ����������
There have been several attempts tomeasure the aggregated impact ofHIV/AIDS on human development. Thissection assesses the statistical relationshipbetween HIV and human developmentand some of its components—lifeexpectancy, educational achievements,and real GDP per capita,20 particularly forSouth Asia.
The estimates show that HIV/AIDS has anegative association with HDI, mainlythrough a decline in life expectancy atbirth. For the countries in South Asia,however, the estimated impact ofHIV/AIDS on overall human develop-ment is likely to have been small, owingsimply to the relatively small scale of theepidemic thus far. For instance, in Indiaas a whole, the effect of the AIDS epidemicbetween 1980 and 1998 would havebeen to reduce the HDI in 1999 by about
���� �!� ��� �
�������
���������� ����
�!�� "���
������� � �����
� ��� ���������
�� ������

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 23
0.003—or about 0.6 per cent below whatit would have been in the absence of AIDS.For other countries in the region, with thepossible exception of Nepal where itwould be 0.4 per cent, the effects will beeven smaller, given the currently smallscale of the epidemic there.21
Given the comparatively sparse coverageof data on HIV, this is likely to be anunderestimation and reflects a lower limitof the impact spectrum. Tables T3, T4a and b and T5 (see Technical Note B)examine three individual components ofHDI and their relationship to HIV toidentify the main ways by which HIV hasinfluenced HDI, thus far. The HIV/AIDSepidemic has a statistically significantassociation with life expectancyat birth.22
In India, the country most affected byHIV/AIDS in the region, the adverseeffect on life expectancy at birth is milder,given the relatively recent origin of theepidemic (about 0.4 years). For India andNepal, the reductions in life expectancydue to HIV/AIDS turn out to be small,relative to what they would have been inthe absence of HIV/AIDS—0.7 per centand 0.35 per cent, respectively of theno-AIDS case life expectancy.23
Table T4 presents Ordinary Least Squares(OLS) results of regressions of adultliteracy rates in 1998 on its lagged valuesand indicators of the HIV/AIDS epidemic.This relationship tends to go in a directionopposite to what intuition mightsuggest—that is, towards increasing themeasured levels of average achievement.24
On the other hand, disproportionatenumbers of AIDS deaths among peoplewho are educated (and rich), as some haveargued, may also cause average levels ofeducational achievement to decline. Atthe same time, average educationalcapital might also go up on account of
HIV, if the epidemic is disproportionatelyconcentrated among the poor who mayhave less than average amounts ofeducational capital in the short term. Thisis consistent with the hypothesis that HIVis disproportionately concentratedamong the poor, but further analyses totest the robustness of these findings areobviously warranted. Careful reflectionwould suggest, however, that thedirection of influence could go eitherway. In the case of children who are HIVpositive, a reduced expected length oflife, by reducing the returns that theymight receive over their lifetime,might cause parents to spend less oneducational capital.
In an exercise to study the relationshipof HIV/AIDS with the GenderDevelopment Index (GDI), it is clear thatHIV/AIDS has a statistically significantnegative association with GDI. TablesT7, T8, T9 (see Technical Note B)demonstrate that, as in the case of theHDI, the influence of the AIDS epidemicon GDI is primarily through the lifeexpectancy index, and not by measuresof educational achievement. The abovefinding is not surprising given that boththe HDI and GDI values in the SouthAsian region are comparatively low andthe vector of patriarchy is common to allthe countries of the region.
These low levels of association are notsurprising given the current stage of theepidemic in the region. However, asindicated earlier, this should not be asource for complacency. Examples fromother regions, ranging from sub-SaharanAfrica to Eastern Europe, have shownthat the epidemic spreads rapidly, andonce it reaches a certain scale in acountry, it has a devastating effect on theeconomy, the productive capacity of itspeople and the sustainability of itseconomic growth.
� ��� ���� ��
������ ��� ���
��� ��������� �
������� ��������
���� �� ���� ��
������� ���
������ ���� ����
"���� ������� ����
����� �����"��
"���� �����
������ �� ����
��� � ���������
�������

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 24
����� ����������������������������������� In this section, the focus is on theobverse of the relationship highlightedpreviously—the role that variables relatedto human development play ininfluencing the spread of HIV, as well asthe possible linkages between humandevelopment strategies and the responseto HIV.
������� ��� ��������� ���������� ��
����� ����������� ��� ���
There are several ways in which humandevelopment can influence HIVtransmission—the level of economic andeducational achievement, standards ofhealth and access to health services,income inequalities, gender relations andthe treatment of vulnerable subgroups ofthe population and basic legal rights toprivacy, life and liberty.
It has been argued that the differentdimensions of human development affectthe vector of HIV transmission. “Therate of HIV transmission is not simplya function of sexual behaviour.Epidemiological, clinical and laboratoryevidence shows that HIV infection isevidenced by the same factors thatpromote the transmission of otherinfectious diseases. There is an establishedliterature in public health and a centuryof clinical practice demonstrating thatpersons with nutritional deficiencies,with parasitic diseases whose generalhealth is poor, who have little access tohealth services, or who are otherwiseeconomically disadvantaged have greatersusceptibility to infectious diseases,whether they are transmitted sexually, byfood, water, air or other means.”25
Socio-economic conditionsWithin South Asia, there are four sets ofanalyses whose findings relating to theimpact of income levels and educational
attainment on protection measuresagainst HIV risk are especially instructive.Basu, Gupta and Krishna (1997), in theirexamination of the impact of adult deathon households in India, foundconsiderable socio-economic variation inAIDS awareness among individuals.Within the South Asian region, they foundthat although there are adverse impactsof the epidemic, the responsemechanisms tend to vary according to thecharacteristics of the household. Richerhouseholds tend to be able to cope betterthan poorer households, and householdswhere the adult was ‘self-employed’ tendto cope better than where the adult wasemployed as wage or salary-worker.
Specifically, indicators such as income,asset holdings, quality of housing,occupation and the level of educationalachievement were all strongly andpositively associated with awareness ofHIV/AIDS. The study also found that theuse of disposable needles for injections inthe sampled households increased withsocio-economic status. Studies of thegeneral population, sex workers, overseasmigrant returnee workers in Sri Lanka allshowed that HIV/AIDS awareness wasmuch lower among individuals with lowerlevels of economic and educationalachievement. Sex workers in Sri Lanka whoearn higher wages (and who were alsorelatively better educated) were muchbetter informed about HIV/AIDS thanbrothel-based sex workers andstreetwalkers who serve the lower end ofthe sex market. This was reflected incondom use—only 44 per cent of thestreetwalkers used condoms “always”,compared to 87 per cent for those whoearned more.26 Another study, using datafrom a 1993 survey of nearly 600 sex workersin Kolkata, India, found that condom useis negatively linked to the price of a sexualact and positively associated with thelevel of education. This suggests the key
�����������
��������� ���� ��
���"�� �����
������� %����� ��
�������
��������� �� ���
��� �� ���������
�������"�� ����
� ������ ��
���������
���������� ����
�������� ��
���� �!��

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 25
role that economic returns and educationplay in the implementation of HIVprevention policies.27
It is not always clear to those engaging inmulti-partner sex that sexual activity canbe safe if condoms are always used.Education and awareness levels matter,as indicated in a recent survey of theliterature on the roots of HIV.28 Schoolenrolment rates and illiteracy rates in themajority of the developing world, andparticularly in Africa, are substantiallylower than in richer countries. Analysesof household data from Cambodia,Vietnam, Nicaragua and Tanzania showsa strong correlation between both wealthand education on the one hand andknowledge that condoms prevent AIDS,of where condoms can be obtained, anduse of condoms on the other.29
Gender inequalityLiving as they do on the margins of society,poor men, women and girls have to cope
with vulnerable environments. Genderdiscrimination and inequality expressthemselves in many forms acrosssocieties. It is also established now thatvulnerability to the infection is notrandom, nor is the impact. Theseinequalities not only facilitate the spreadof HIV but they also get reinforced in thoseinfected and affected.
There is a growing recognition that thedisempowerment of women—because ofwhich they have no control over decisionsabout their bodies or sexual health—islargely responsible for the pace at whichthe infection is spreading in this group. UNSecretary General Kofi Annan summed upthe problem in his ‘Report of the Secretary-General’, 2001: “The gender dynamics ofthe epidemic are far-reaching due towomen's weaker ability to negotiate safesex and their generally lower socio-economic status.” Girls and youngwomen show a higher rate of acquisitioncompared to men of similar ages.
&��� �� ��� ���'��"���6 ����%�% ���=������������% ��
��63� �� ���������%���������� ������������������������
�%��������6� ���6����6�������#
#��� �� #���������� ���6 ����%�������63��%��=���� 3��
���H������,���� ��� ���6�������63�������%,����
� =����%��6������ � �����3���%��� ������%��� �
��6����,�����6���F��������6������% ���=��6���
��%������6����=#�4 63��%������ ��������6��,���63���
����� ������� =��� �������������6���%�6������#
(���"�� ������� �� ��� ��"��� I����������%��6���� �
���������%������������� ����%������ ����������,����
����%������������������% ���=� ��6���������� �����
=����=�6 #�"����� =��6�������������� ������%����
%�� �������%��6����6�������������������#
������ �� ����"�����������������%���������
�������� ����%����������� �� �����6�����% �������63,
������ �������� �����%����������%�6���,��� ������
��C�6���� ������������=�����% ���=� ��6������=#
��6��A�6����6,�6����� �� ����� ��6���������%���6�
������������%���6������ 3���6 � 6��=� ��� �� �
��� ����
� ���������� �� ������%��������6 ���<
� ���������� �� ������%�����������%��������� �
6�����=<
� ������,���� ����������� �����<
� ���� ������%��������� ����� ��������<
� ������,���� �� ��� �%��� ���� ��6����
���� �<
� �������������� ���������3��������%�� ���6����<
� ������� �������������6��������� �����%��
�������6������� ������������<
� ������� ���� ��� �%������ �������������� �
�����������6 � 6���%��%�����<� �
� �����������������6����6 ��=#
����6�� �6�����,����6 � ��� ������������
�����6��������%� �����������6�����%���������%�6���#
Women and HIVBox 2.4
����6�9������ ����������� 9��� ����������� 6� �����,�;��2����� ������������� 2���� ���,����$

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 26
The gendered face of HIV/AIDS isintegrally connected to the fact thatwomen bear the major brunt of thepsychological, social and economiconslaught related to loss of livelihoods,poverty and care of the sick. Gendernorms impact the way in which infectedmen and women are perceived, thusinfluencing ways in which individualscope with HIV/AIDS.30 Effectiveimplementation of gender sensitiveprogrammes in HIV/AIDS requires ananalysis of the differential politicaleconomy of risk in the region.
Women constitute the most deprivedsections of society and have very limitedaccess to resources, education, trainingand labour markets. A total of 44 per centof the world's illiterate women are inSouth Asia and the region accounts forone-third of the world's maternal deaths.31
Only some countries like Bhutan havebeen able to achieve some gender parity,particularly in issues of property andinheritance and women are, therefore,seen to have a greater role in decision-making. However the impact of this is yetto be seen in the context of HIV/AIDS inthe country.
The low economic and social position ofwomen in the South Asian region hasprofound implications on the HIVepidemic. Women typically have limitedaccess to reproductive health services andare often ignorant about HIV, the ways inwhich it can spread and preventionoptions. Social and cultural norms oftenprevent them from insisting onprevention methods such as use ofcondoms in their relations with theirhusbands. The congruence betweenindicators of women’s poor status andtheir vulnerability to HIV demonstratesthe close link between patriarchy and HIVin South Asia. The lack of decision-makingis reflected in the increasingly high rates
of infection among what are traditionallyconsidered low risk population groups.
The vulnerability of women is evident inthe high rates of unwanted pregnanciesand high prevalence of SexuallyTransmitted Diseases (STDs).32 Womenare thrown out of their homes or desertedby their husbands and are forced intosituations where they are sexuallyexploited, whether for work or foodsecurity. Employers and recruiters ofwomen working outside their homecountry often withhold passports andearnings. In Sri Lanka, girls left in the careof friends and relatives, when theirmothers have gone abroad as maids, areoften vulnerable to sexual abuse.33
The impact of HIV is also more severelyfelt by the women in the family. Positiveand affected women end up fending forthe family, repaying debts, and meetinghospital costs of the spouse. A study oftheir clients by Lawyer's Collective, anNGO in Mumbai, India, found that out ofthe 67 positive women respondents, atleast 60 per cent were economicallydependent and unemployed and 56 percent were widows.34
In several cases, it is the natal family thatprovides more support to the positiveperson than the marital family. Thisseems an extension of the dowry demandsmade on the wife's family. As such, theeconomic costs incurred by the natalfamily tend to be invisible.35
A study conducted by UNICEF indicatesthat most HIV-positive women becameaware of their status only after theirhusbands are diagnosed to be HIV-positive or even as late as the death oftheir husbands. Such female-headedhouseholds are unable to afford evenbasic medicines to treat opportunisticinfections. A woman experiences dual
�������� ��
�������� ��"�
�� �� ����� ���
��� ��"���
������� ������
�� "�����
������� ����� ��
��� �������

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 27
stigmatisation—as a widow andespecially a widow of a positive man.Discriminatory access to property rights,shelter and care facilities are some issueswith which single and widowed womenare confronted. If the child is alsodiagnosed as HIV positive (a likelihood,given the increase in mother to childtransmission), the burden on themother increases.
Studies indicate that the level ofeducation in women is linked tothe information they access aboutHIV/AIDS. A study analysing HIV/AIDSawareness and prevention amongstwomen in India from the SecondNational Family Health Survey (NFHS-II, 1998) found that only 18 per cent ofnon-literate women had heard of HIVwhile 54 per cent of women with aprimary level of education had heard ofit. Even here there are regional variations.Women in states such as Tamil Nadu andKerala with higher rates of female literacyreported higher awareness as comparedto states like Bihar.36
Unequal access to resourcesThe dualistic pattern of development inSouth Asia has meant an incompleteepidemiological transition, with thesimultaneous prevalence of diseases ofpoverty (caused due to poor livingconditions and poor nutrition) along withdiseases induced by affluent lifestyles.This is reflected in the skeweddevelopment of health infrastructure andfacilities in these countries. Thus, the richin South Asia access the relatively better-equipped private hospitals while the poorrely to a greater extent on public hospitals.Since the services rendered there areunsatisfactory, they turn to privatehospitals for curative treatment thoughthe costs are far higher. Primary healthcareis, thus, a neglected area as is thetreatment of communicable diseases.
More often than not, the lack of insurancecoverage has serious implications foraffordability of care (see Box 2.7).The study by Bloom et al. (1996), usinginterviews with the staff of insurancecompanies in Sri Lanka, demonstratedthat, as of 1995, individuals withHIV/AIDS were excluded from health andlife insurance schemes, with limitedexceptions in circumstances wherepremium requirements had been fulfilled.
Rural–urban economic differences,unequal opportunities, conflict, naturalcalamities, social factors and exploitationare the main factors behind migration. Inmany cases, the economic inequalityreflects an underlying social inequality –like the lower status of women relative tomen, which is reflected in their lowereducational status, fewer remunerativeopportunities and assets, and access tohealth. Migration, in itself, does not havean inevitable correlation with HIV, but inthe absence of information and access toservices and adequate preparedness,mobile populations become vulnerableto exploitation, trafficking and HIV.
Economic deprivationEconomic deprivation and HIV/AIDSincidence appear to be linked, and thereare a number of reasons why one canexpect low levels of economicachievement to be rooted in HIV.37 Thedynamics of the sex industry, for example,illustrates this linkage starkly. Extremepoverty often forces women and younggirls into the sex trade, which increasestheir risk of exposure to HIV. In one studyof female sex workers in Sri Lanka, nearly37 per cent of the women intervieweddescribed the need for “survival” as amajor reason for their entry into the sextrade. The numbers were even higher—48 per cent—for streetwalkers.38 One studyin Ichok village in the Sindhupalchowkdistrict of Nepal quotes an interviewee as
)��� ���� ���
��� ��� ��'
�� �������
�������� ���
�������
�"�������� ���
������������ ��
�����

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 28
saying, “No one can survive on farmingonly…There would be a famine herewithout the sex trade.”39 Examples ofeconomic need leading to entry into sexwork can be found in Bangladesh andPakistan as well.40
Of course, as the Sri Lankan study suggests,not all women enter the trade for ‘survival’.Levels of remuneration are also a
determining factor, especially if alternativeeconomic opportunities are not asattractive. For instance, a study of Bangkokmassage parlours in 1980 indicated that theaverage earnings of masseuses exceededwhat they earn in occupations elsewhereby nearly 1,700 per cent.41 This alsoindicates that quality of employment is asimportant as the quantity in the context ofexpanding employment opportunities.
I����������������������������6������ ����@�����
����,�6� ����,������,�����6��=����6������@��������
����� �����=�������� ������ �����=����6����������� ��
�%���6����� � ��6 ��=��=���������%��6���#�"������ 6�
�%�������������� ��������� �6��� �������=�����6#
E�����>���! �����%�����������%��6 ����6��������
���� 66�������������� ���6 ��� ����� ������ ����
��������� �� � 6����,��� ���=� �������6�������%�9
J��6 �� 3��������� ��������6 �����%������ � �=���� �
�� �C����#��� �� ������� %%����������6���K�=������6�
�������������������C����6����%���������%��6 �K�
��6���.����������%��6 ������������������� ��$�;�$ �� =,���6 � %%���������=�����6 ����6������%� ����
;�$�'�����������#������������������=��%��%��6 ���� ����%����=�����6 ������ �� ����������6� ����� ���
��������#��� ���������6 ������6 � %%�������� =�%��
4�%�������%L#
������3���6��� ����������%��������������=��%�� �3
1 = ,� ��� �%���� ��������� ��������������#
J1=�������H�����������������A����������������#
�������������=� ����� ��=� �������������H�� �������
���#�������=���,��=����������� ������%%����#�I�����H�
3��� ������� �,�������������������� ����
����� ��� 6����� ����=��� �����������=� %��
��� ����#�I�� �������3�����������������M �� ��������
��� N�%������ ����������������������� ���������
� 3������%%���6���������������3�����6���������#
I����� �3�������� �������������,����� ����� �
��6��������6����� ��� �������6������������� 3��
��%%���6�,������������� 3������#���H������ 3��
����6��������������������������������������� ��=#
>���=�%��� =�,�)�A.���������� ��������������
� � ���� ���������%������#����� ���%������6����,
��H�������������#�1=�������������%������������#����
���� ������� ���������������=#�I ����������%���
����,����� �����������������6���,� ����������
������������#�����=������������H��� ��������������
�� =�����������#
J�6����� ��������#��������%����=� ��������
���������� ������#�2����������� ����������%� ���6��������
���6 ����6����� ���6������ ���� �,�����%������
� 3�,���� ������� 3�����������#�?�������,����6����
%��������#����� �� =,� ������%����=� ������#����
����������������3��� �� ���������������#������������� �
���� ������ ��� ����������%�������%������������,��������,
��������#����� =�OA� =������� 3�#��������������=
� �������� �� �����3��������� �������������� �6 ��,
�������������=� ��������6�����OA� =��#
J"��=�� ����������������������������%���������#�I��� �
��� ��� %���� &�� � � �� ��� �� � ,� ��� ���������
�� ����� �����������#������ �� �������,������
������ ����������6������ � #����� ������������
%�����C�6����� �� =� �����=�6���������������� 6�#
"�����������������6�����%�����6��� �������� �
�������#�"���� ������ ������ ������������������ �@
%����������,�B � ,�=������#�"����H�����6���,�C���
�������#�1=�����������%�����#�&�%�����������%������63,
����� ������������%������������%#�����=����������
������=�����������#L
!�� ��=�������� 6���%������ �� �6� ����� �,��������
����� �� ���� ����� �� � ���������6��������6����
�������������6�����%���� ����� ������������%�����������#
���������������������������������� ��������� ��
��� 3��������=��%�������� �����%���������� ��� ���=
%�����������������,�6���������� ����6���=#
Coping with HIV: different realitiesBox 2.5
��������� & ����� ��I��������,� ����<� B���� ,� ����

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 29
Global economic processes and macro-economic policies serve as a factor inincreasing the vulnerability of certainsections of society. Increasing mobility inresponse to demands for cheap labour andthe absence of safe mobility options createsituations of vulnerability for migrantworkers. Long periods of separation fromthe family, marginalisation withinreceiving communities and absence ofsocial capital often lead to the migrantworkers seeking multi-partner sex inorder to meet their physical andemotional needs. Infection rates amongNepalese workers who had worked inIndia were found to be substantiallyhigher (10 per cent) than those who hadnot (2 per cent).42
Indeed, a study of the region found thattruck drivers routinely “stop at roadsidehotels which provide food, rest, alcohol,drugs and sex.”43 Some countries in theregion—for example, Bangladesh,Pakistan and Sri Lanka—have notexperienced high rates of HIV infectionamong truck drivers thus far. The evidenceavailable indicates, however, that truckdrivers, even in these countries, are at highrisk of HIV infection, with some 60 percent in a recent sample of Bangladeshitruck drivers reporting engaging incommercial sex twice a month.46 There isalso evidence that, based on the relativelysignificant numbers of reported cases ofHIV infection, overseas migrant workersmay be at high risk of HIV infection inBangladesh, Pakistan and Sri Lanka.47
Evidence of high-risk sexual behavioramong domestic migrant workers in Indiacan be found in one study of the Wazirpurindustrial area in Delhi.48
Institutional development andpolitical freedomsIn all of the above cases, it could be arguedthat punitive measures associated withHIV status, the role of legal and other
restrictions related to the practice of sexwork or drug use actually contribute to thespread of HIV, rather than curtailing it. Forsex workers under the control of madams,this is self-evident, as the former havelittle choice in terms of partners andprotection from HIV infection. Inaddition to the anecdotal evidence citedabove, a study of sex workers in Nepalfound that women who had been ‘coerced’into entering the sex trade were threetimes as likely to be HIV-positive thanthose who had not.49 The incarceration ofsex workers in rehabilitation homes andprisons is also likely to result in theirremaining “underground”, an approachthat could prevent them from accessinghealth messages.50
The impact of coercive laws can beexpected to increase the risk potential ofdrug user behaviour for three reasons.� The illegality of drug possession
means that drug users might prefer tostay underground, and so are unableto obtain ready access to preventionmessages associated with HIV
Poverty, gender and HIV/AIDSBox 2.6
������9� >��� 6�� %����!������ ��� �,� ����
������3��� ������������=�������=������3��=����%��������� ������
�� �� �����������3A� 3����� �����������������������6 ��#���2�����=
��� �6����������� ������ 66���� �6����������%������������
6����#�"���C��� �� ���6����=�I ������ �#�������������=��%
6�����6� ��������3������"� �� ��F����������� �������3��
��� =��9��J���������������� �������/�����������6����0#
������������#��%���� ����� ���� ����,������=������=�%���,��
����� 66������L#''�������3������� �������� �����3��=������3��
��A6� ������ �������������������������#�"��=� ����������3��=���
� ��� 66���������� �����%����������"��,�������6������ ���
�%�6���������� �3�=�6�A% 6���������6���������=�������#�"�����6�����
����������3��=������� ����%�������� 3����������=��������3���%����
���������"��� ������ 3�����6 �������=������ �6����#��"����
��������=������������� =� ����������#��� ��������������6 ���
�%����3A� 3������ ���������6����=������� ���������%�������=,
�����6�����6� ��������3����� ������������=����������������
�%�6��������������������� �����6���������������� ������6�����,
���������6���������� �������� ���������%�6�����#'*

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 30
� Drug users might prefer to move tomore efficient methods of drug use—injection as against inhalation orsmoking—so as to reduce thetransaction costs of being caught whilepossessing drugs.51
� When either drug or paraphernaliapossession is illegal, it would bebeneficial for injecting drug users toshare injecting equipment, and nothave everyone carry their ownequipment in order to reduce the riskof being suspected of carrying drugs.
Family and community health levelsHealth status too, can affect HIVtransmission. There could be behaviouralfactors as individuals with a lower life
expectancy may have low self-esteem andlow levels of health-seeking behaviour andmight take risks with their health—including exposure to HIV infection—compared to those in better health. Thishas adverse implications not only for theindividual but the household andcommunity as well. Lower investmentin human development in terms ofhealth and education would lead to lowerhuman capital. Thus, even from thenarrower human capital perspective, “thelower the optimal investment in healthhuman capital, the fewer are the periodsin which a return to the investment canbe expected”.52 This indicates that theconstraints and opportunities in theenabling environment of humandevelopment have a direct bearing on theongoing relation to HIV (See Box 2.8 as abest practice example).
����1 �������������������������������6������7�������������At a macro level, there is a systemic linkbetween human development and HIVacross countries. The analysis showsthat human development achieve-ments, including a higher real incomeper capita and lower degree of economicinequality as measured by the ginicoefficient,54 tend to contain the extentto which HIV prevalence is increasedowing to the duration of its presence ina population.
Treating the time span of the epidemic asconstant, the analysis also indicates thatthe major indicators of humandevelopment achievements are alsostrongly associated with HIV incidence,and their effect is to lower HIV incidence.The other variable that has a statisticallysignificant effect on the HIV prevalencerate (at 5 per cent or 10 per cent levels ofsignificance) is economic inequality asmeasured by the gini coefficient. The
������ �,�%��� ������ 6�������� 66���������������������
���������������� �� ����=��%���6��� �����=�6� ����* #���� =�����,
���� ������� 6��6���� �������=��6 ��=�F��������������������
��� �6�������,� �� ���� %��=������%%������=����������6���6���,
��������6� ��6���� ���� 6��6���� ��#�>��� ���� ��� ��������%
6���� ��� ���� ��������=����������%��6 ������ ������� =��%
������ 6�������� �� ���� ������� 6�� �%� �%��� �� ��6���
�����=������ ������������������� ������%�����%��� �������6���6���#
?���%�����%�� =������6�������������6 �����6��������� 6�
�%����������=�����������6���6������ ����% 6���������� �� ����%��
� �� ���� �� ����������� � ���� ��� ���� ����#� ������,� ���
�� ���% 6���=�%�6�������%����������6��� �����=������������
6������������������ ������������ =������� ������� 66�������
��F��������� ����� ��������% 6�������#�>��� �������������F�����
��� ����� ��� � �� ���,� �� ���� �������6� ���� ��,� ��� �� 6��
6������ ������� �������� ��� �=������6����6 � 6��=��%����������6
�� �����=����#�"��������������%��������������������6�������
���� � �� 6�������������������6,���������� ������������
����������������6 � 6��=��%����������6��� ������6���#�����A��� ���
�����66�� 6=�� �����������6������� ���������� ��6���������
���A� � � ��%��6 �� ���%�����*A(������6��,������������
�����6 �����%��������� ����������#���� =�����,���� ��� ����� �
��� ��������������6 � 66���������6��� �������������� ���#��
� ��� ��������66���������=���� � ����6 ������ ���������
������6����%���������A %%�6���������������� ���������������
�� ���6 ������ ���������������������%������������������6��#
Box 2.7 The availability of formal healthand life insurance
������� 8������ ����� ,� ����

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 31
results of Table T6 (see Technical Note B)indicate that, all else being the same, agreater degree of economic inequality isassociated with higher HIV incidence andprevalence in the adult population.Further, the effects of all these variablesbecome larger in size the greater the lengthof time an epidemic is prevalent in a givenpopulation. This is a desirable outcome,given that an initial infection of HIV islikely to be associated with severalsecondary infections.55
��1 8���$���������������6�8��!������������������� ����������9��������%����
In addition to impacts at the level of theindividual and the household, HIV/AIDScan also have implications at the level ofspecific sectors and national economies,
which, in turn, have direct and indirecteffects on human development. The highcosts to the government in the form oflost services, lower national productivityand output, loss in skills and experience,depletion of workforce in specificsectors, increased demands on healthand social sectors, and loss of humancapital can push the country into avicious circle of poverty. The epidemiccan lower human developmentoutcomes as resources are used up incombating the disease, leaving futuregenerations worse off, and underminingthe premise of sustainable humandevelopment. This section presents adiscussion of the impacts of HIV on foursectors—health (including healthinsurance), agriculture, private industryand transport—and the costs to thecountry as a whole.
"���6 ����%�� ���= ������1�F �� �2 ���� ���/��120
%��������$..+�����������1 � � ���� ������ ���������
�������%��� ����������������������%���������� ���
6�����6� ��������3���#��"����� ������6����6�����P
�����,������� ,����������3�������������� 6�������P
����� �������� ���� �%� ������3� �%� ��8?� 6 ����
���8��1�� ������� ���,�1 � � ���� #
���8��1H���� �� �����6�� ��� ����� � �����������
�������������������6��=���� ����������������3� �
������� ������6��������������������6� ��������
6��6���� 6��#����� ������� ���������������%��� ��������3���
6�������6���� �����%���6� ���%������������������� �
������� ����6������=#��"��� 6����������%���12� �
���8��1����������������6 ��������� ���������6�
������3����������� �����%��� ���� ����������������
��������������� ��,��������������%�6�����,��� ���� �
6��������������������� ��������%��6��6����
�����=�6������ ����������������� 66�����������6 �
6 ��#�?�������� ������6��������� �����������%���12
������ ���3��%� ����������� ����6��������� � ����� �
HIV prevention efforts and human development:NGO experience from Sangli
���������%� �6������=��������� ��=����%�6� ���� ��#
�� ��� %���� ����� ���� 6����� �����������
����� ���,���12������������������������������
�%�������6������=�����%%����� =�#�"��=� ����� ��
6������=� ��������,� ����=����� ��������6�,� ����
���� 66������������������ ����� ���������
�� �������������� �#�B����� ����,����=�%��F����=
���� ��� ��������� ������ ������3���� �� ���
����%���������������#��"����������6����������
����6������������ ����������%������� ��� ����6 �
����6�,�� ������������3������ ����������� ������
��� ��=�����6��7#��&=�����=��������� �6�����������=
����������������������3,���12��������� ��
������������ 6������������� ���������6=��� �%����#
"�������� ��������A6���� ��� �����%�������3,�������
����6 ��6 ��� �������6������� �������������������12
���� ���,� �����������6��� ��������������#�1�������,
���3�=����A��� �������6���� ��� ������� �����������
� �����%�6����A����� ���������%A���������� ���6��
�����=�6 ���������� ����+���������3������ �� ������
��12����� ���#
Box 2.8
7� 6�����6 ��������1�� � �����,� ���8��1
������9�1 � �� ��� �#,� ���$<�1��� ,�1 � �� ���� �,� ����

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 32
Health sectorThe relationship between HIV and healthis obvious. But have its impacts beenreflected at the sector-level, say, in termsof an increased burden on health services,increased share of health budgets, and onthe health insurance sector? Publicexpenditures on HIV/AIDS for countriesin the South Asian region are small, as inSri Lanka and India.56 Scenario analysesundertaken in Bloom et al. (1997) indicatethat the effect of HIV/AIDS on bedoccupancy, while small in magnitude,could still be severe given that excesscapacity (supply of inpatient days relativeto demand) appears to be extremelylimited at present. This study also pointsout that an expanded HIV/AIDSepidemic could constrain the supply ofmedical personnel, many of whomrevealed that they would need to becompensated monetarily for increasedrisk of HIV infection.57
There is more evidence from countrieswith a longer experience with theepidemic, particularly from sub-SaharanAfrica, which hold useful lessons for SouthAsia. Guinness and Alban (2000) citestudies from Burkina Faso, the DemocraticRepublic of Congo, Uganda and Tanzaniaindicating that bed occupancyattributable to HIV/AIDS exceeded 50 percent in selected hospitals in countrieswith HIV-prevalence rates of 5-10 per centaround the time the study was conducted.For countries with HIV prevalence ratesin excess of 10 per cent (Cote d’Ivoire,South Africa, Swaziland, Zambia andZimbabwe), available data suggests thatbed occupancy due to AIDS ranged from25-70 per cent in urban hospitals.58
Guinness and Alban also summarisestudies that indicate significant shares ofthe health budget being accounted for byHIV/AIDS—20 per cent of the Malawihealth budget in 1996 and 13 per cent ofthe Swaziland health budget in 1994. In
Cote d’Ivoire, about 5.7 per cent of publichealth spending in 1995 was AIDS-related, the corresponding figure forTanzania being 3.1 per cent.59
Public health spending is not the onlycasualty. A national AIDS accountingexercise recently conducted for Rwandasuggests that nearly 10 per cent of allhealth spending, public or private, wasaccounted for by HIV/AIDS. Besides,over 90 per cent of all spending ontreatment and prevention of HIV/AIDStook the form of out-of-pocket spendingby households.60
Compared to studies on the impact ofHIV/AIDS on health services and publichealth spending, there are very fewanalyses of the effect on the private healthinsurance sector. A major reason for thiscould be the exclusion of HIV-positiveindividuals from the pool of insurableindividuals, as suggested by a study for SriLanka.61 Examples from other regionsmay be instructive in this regard. OneZimbabwean insurance companyestimated that 45 per cent of its healthinsurance claims in 1995-96 were AIDS-related.62 Insurance companies’ reactionto HIV/AIDS is another way to discernpotential impacts of the epidemic.Thailand’s American InternationalAssurance (AIA) works with NGOs topromote HIV-prevention among factoryowners. The company gives financialincentives and discounts to companieswith strong workplace and communityprevention programmes.
Agricultural sectorGiven its disproportionately high impacton young adults, it is safe to assume thatHIV/AIDS will have a significant impacton agricultural activities, which are largelylabour intensive. Studies from Africa maynot be completely indicative for the region,but they illustrate possible scenarios for the
����� �!�
��������
�������� ������
�������� ���
*���� ��������
���� ����
+, ��� ��� �� �
����� �������
����� �� ��������
��� �������� ���
�� ���� �!��

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 33
future. A study for Rwanda estimated thatthe loss of a female adult member of anagricultural household could lead to anearly 50 per cent decline in its farm labourinputs, and similar results have beendocumented elsewhere in sub-SaharanAfrica.63 Some of the consequences of thishas been a shift to less labour-intensivecash crops, declines in cultivated areas,and less animal husbandry.64 In Zimbabwe,household survey results suggest thatAIDS-affected households experiencedsignificant declines in production onaverage—61 per cent in maize production,47 per cent in cotton production, and37 per cent in groundnut production.65
The effects of HIV/AIDS on national orregional agricultural production levels,however, have not been as welldocumented. A major reason couldsimply be the substitution of this lostproduction by increased agriculturalproduction among households notaffected by AIDS, a process facilitated byland transfers/sales from AIDS-affectedfamilies to such households. The onlysector-level estimates available are fromcomputable general equilibrium (CGE)model-based simulations undertaken byArndt and Lewis (2001) for South Africa,which show that value added in theagricultural sector in that country wouldbe 17 per cent lower in 2010 under aprojected AIDS scenario compared to asituation of no AIDS.
Private sectorHIV/AIDS has the potential ofinfluencing private firms’ operating innon-agricultural sectors along these samelines—costs of worker replacement,absenteeism, insurance expenses, andhealthcare expenditures. In addition,there is the possibility of legal actionrelated to discrimination against HIV-infected employees and possible loss ofcustomer base. Non-economic factors, in
the form of loss of morale in the work forceas workers lose many of their colleaguesto AIDS or if HIV-positive workersare stigmatised, could also affectproductivity.66 The evidence on theeconomic impact of HIV/AIDS on theprivate sector thus far is, however, mixed.Using data from a survey of nearly 1,000firms in sub-Saharan Africa, Biggs andShah (1997) concluded that the impact ofAIDS on staff turnover was minimal.However, they did find that replacingprofessional staff—often thought to be athigh risk, based on early studies in Africa—to be a significant problem, with firmstaking 24 weeks to replace a deceasedprofessional, compared to two to threeweeks for less skilled staff. Indeed, thereare examples of multinationals in SouthAfrica hiring three workers for each skilledposition to ensure that replacements areon hand when trained workers die.67
HIV/AIDS could adversely affect thecustomer base of companies, since thegroup hardest hit by AIDS—young adultsof working age—is also the group withmore purchasing power. Spending willbe redirected away from a host of sectorsto the health sector, which could seeincreased demand. Such effects are notreadily detected by individual firmsbecause of the dissipation of spendingimplications across local and inter-national economies. Effects on thecustomer base are more likely to betransparent if there are dominant firms, orfirms organised into business associations.
Transport sectorSeveral analyses have focused on the roleof people involved in the truckingindustry as a facilitating factor in HIVtransmission.68 There are also a fewanalyses of the impact of HIV/AIDS onthe transport sector, relating to railwaysand the trucking industry. A study69 of thesocio-economic impact of HIV on the
����� ���
*���� ����"����
���� ��� ��� �� �
��"�� ����
"�"��� �� �
����������
�������� ����
��� �� � ����
-, ��� ��� �����
� ��� ���" �����
������

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 34
transport sector in India identified anumber of economic weaknesses withinthe industry, influenced by thedetrimental effects of HIV/AIDS. It arguesthat the loss of productivity of drivers withHIV will lead to revenue losses, forcingcompanies out of business since the“cost of maintaining the current level ofdeath benefits may overwhelm manybusinesses”. The study also noted that onlya few companies are prepared to cope withHIV and may insist on mandatory testingor end medical benefits.
Giraud (1993) developed a methodology toassess and predict the impact of HIVamong long-haul truck drivers onThailand’s trucking industry in the 1991 to2000 period. The scenario undertaken inthat study led to Giraud concluding thatHIV/AIDS-related costs to the truckingindustry would increase from an estimated$40,000 to nearly $14.5 million by 2000.Another more recent study, of the Uganda
Railway Corporation, concluded thatHIV/AIDS had substantially increased thelabour turnover rate for the Corporationand that nearly 10 per cent of itsemployees had died of AIDS in the yearspreceding the study.70 Another set ofresults is available from the CGE analysisof Arndt and Lewis, who report that thetransport sector in South Africawould have 20 per cent lower value addedin 2001 under a projected scenario of theAIDS epidemic, relative to a no-AIDSscenario. Although few in number, thesestudies taken together suggest that thetransport sector could be a possiblemajor casualty of HIV/AIDS. Availabledata do indicate, however, high riskbehaviour being common among truckdrivers in the region.71
!���� ��� �������
Impacts on national economiesTwo types of impacts are worth notinghere—on aggregate outputs (or outputsper capita) and the distribution ofnational income. The two, taken together,have implications for the proportion ofnational population living below thepoverty line, as well. This sub-sectionassesses primarily the impact ofHIV/AIDS on national economic growthfor the countries of the region.
Impacts on growth of real income percapita: some new evidenceNew evidence on the links betweenHIV/AIDS and growth of real income percapita, shows that the epidemic wouldhave reduced the worldwide annual rateof growth of real GDP per capita by nearly0.06 percentage points below what itwould have been in the absence of AIDSduring the 1980-98 period. In the countriesof sub-Saharan Africa, the reduction in theannual rate of growth of income per capitais estimated to be of the order of 0.15percentage points in this same period.Given the exceedingly small rate of growth
The impact of AIDS: business as usual?
������� ��=�=� ����%����������� ����6���������������� ������
�������������� �������������������� =���������������,� �����
��3�� 6�� ��������� �� �� C��������%�������������#
8��� ��=,� ��������� 6���%�������6�����������������,��������
�� ����� ��� �6�� ����=� ������ ���� �� � ���� �%� 6�� ���
�������������� ����#����������� ����������,����������� ��
���������� ������������ ����� ���=��%� ��������3���� �
6��������� ��#�����������6�� ��������6�����%�������������,
����6��������6�����=� ���������������� ������ �#��"����������
�%%�6���%������ ��������3�� 6����� �6�6���%���� ����� �� ��
������,�%�������������%����������������������������� �����#
�� ���%����������%��������6����������,��6�� ������6�������
���� ����6����� ���������� ������������,���������� ���������6�
�%� ���������������������A��� ������������,������������6 ��
%���������,� ����� �����%��� ��#���!�� �,�6 ��� ���%���� H�
���������� ����%�" ����� ��,�������� ��� ����� ���������� �
����6����������������6 �����%�����#�8������������� �����=��%
%�����������,�������������� ����3���� ����������������� �
6���������������6�����=������,����� 3����������������
������������������6 ��� ��������������� ���������������6����
�������������6�����=,����%�� �����=� ����3���H��6����#
�������� ;�����,� $..)
Box 2.9

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 35
of course, policies in other areas aresimilarly evaluated.
������������������������������:���
It is true that 95 per cent of those infectedwith HIV live in developing countries,home to 80 per cent of the world’spopulation. At the global level, there is astatistically significant associationbetween low income and HIV prevalencerates—the poorer the country, the greaterHIV prevalence rate. Moreover, absolutepoverty rates across countries—definedas the proportion of population livingbelow the poverty line of $1 per day—arepositively associated with national HIVprevalence rates. There is a positive andstatistically significant correlationbetween HIV and economic inequality aswell.75 Nonetheless, beyond thesecorrelations, the direct impact of HIV onpoverty and inequality has not beendemonstrated empirically at the nationallevel. This is remarkable, given the globaltwo-way links between the HIV andindicators of economic well being.76
Education is not the only factor highlightedby micro-data. There is evidence thatpoverty forces people to make sub-optimalchoices and this puts them at risk of HIVinfection. As already mentioned, a seriesof small-scale studies from Sri Lanka,Brazil, sub-Saharan Africa and Haiti showhow poor women can be forced into sexwork, or be sexually exploited, and are lessable to insist on condoms use.77
��* ���������������������������
The sections of this chapter highlighted thegamut of human development dimensionsthat are affected by, and in turn, impactHIV/AIDS. These, additionally, demons-trated the effects of HIV on incomes, assetholdings, education, health, liberty andother elements of human development.
of cumulative AIDS prevalence amongcountries in the South Asian regionduring 1980-98, the AIDS epidemic has hada negligible impact on economic growththus far, even in India, the country withthe highest number of HIV cases inthe region.
The returns to policy action inHIV/AIDSThe tools of cost-benefit and cost-effectiveness analyses—that compare thebenefits of a policy to its opportunitycosts—are standard methods usedby economists to evaluate alternativepolicy options.
Cost-benefit analysis compares thebenefits of a policy action to its costs, bothof them evaluated in monetary terms. InSri Lanka, studies have shown thatpreventing HIV transmission via thescreening of blood used for transfusion,and the use of disposable, instead ofreusable, injecting equipment in hospitalsettings can yield benefits that are muchgreater relative to costs.72
Cost-effectiveness analysis typicallycompares an outcome indicator such aslives saved and disability adjusted lifeyears averted73 that is not measured inmonetary units, with costs that aremeasured in monetary units. There arestudies demonstrating the potentiallyhigh cost-effectiveness ratio ofprogrammes such as needle exchanges,STD prevention, informationprovision.74 Cost-effectiveness analysesfor health interventions (includingHIV/AIDS) are not always useful forpolicymakers when comparing withpolicies in sectors other than health,since the former have outcomeindicators in units other than money.Thus, cost-benefit analyses are typicallypreferred since both benefits and costsare reduced to monetary units, provided,
.���� ��� �������
��"�������� ���
�������� ����
����/������������
����� ��
������""�� ����
�� ����
��������� �.!
��������� ��
����"����
���������

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 36
The subsequent cross-country data areconsistent with this two-way linkage. Afirst set of analyses show that the HIVepidemic has a statistically significantassociation with human development asmeasured by the HDI, primarily throughits influence on life expectancy at birth.The effects of HIV/AIDS on literacy and
other indicators of educationalachievement and GDP per capita are notapparent, at least statistically, for theperiod of the study. A second set of cross-country econometric analyses highlightedthe relationship between humandevelopment and HIV prevalence,specifically indicating the role of literacy,
���� ������ ��� ���� ������� %���� ��������� � �����,
� ������� �� ���,�����������������������6Q�"������ �
����������� �=�����%���������% �,� ����������������������
������� ���������6� �������%�6���������������� �������
�%� ����6=� �� � ��6��6 �� ������������ ������ 3�=
6�������#�"����� ��9
� "�������6������6�����/������������6������� ���
�����0� �%� ����� �������� ������� ���� �� �%
�������������������6=������� ���=<
� ���� ��������%�����%� �������������������6=
������ ���=����������%�����������������%����
�%�6�����������6������������<� �
� ������%%���6���������������%������%�6�����/�%
=0�%�����������������������6=������������
�������� ���,��� ���%���������������� �����6�����
������#
"�������������6�������������6�� ��=,����������� ��
6����=�� ������������%�6�������������������$,
���� �������������%����%�6�������������� 6�
=� �������� ���6���%� =����������#����������� ��
����������%�6�������=� ��$,�%������=� ���,������
��=� �� ,�$+���=� ��',� ����=� ��*,� ������#����
�������,���������� ������������� ��6�����!���� 6�
=� ���� �����%��������� ���������%���������������� �
��6������6��������������%����%�6������=�� �%
� 6��=� �#��"��,��%������������������������6����
=� ��$,�������������%�����%�������6 �������$,$,$,$,$K
�%������������������������6���������%�����=� �#���%
%�����������6�����������6���=� �,�������������%������
�,�,�,�,�K���%��������=�� �����%� � ����������
6 �������,������������������%� �������������������
��%���� ����������� ���� ����6=� ��6����� ��� �%
6��� ��������/������������6����� ��� ������������
��������6���������%����%��������������������6=
������ ���=�������� �������������������0� ��!#���%
������6�����!,�������������6=������������������ 3�
������ ���=#�?�������,������������������������� ��
��������������#
"��� ������� ���������������� ������ ������%���������6=
������������� ������3��=������� �6��6� ��% 6���������
��6����������������������� �����%��������������
�����6=#��I������������ ����� ����������������3��=������
������ ������������������6=,�� ��=������������ =
������%��,� ���������������6����������� ����#��?
����������� �,��� ���������%������������ ��6��� ��,
������������� ������������%��� ���� ����� ������
�������3�%����������6�������� �� 6�����=�� =������
���=����%������%���6�������A���3���� �������%�������
���6������������3��������� ��#��� ���������� ��6��� ��
������,���6���%��� �������������� =� 6�� ��=��%���6�
��� ������ �� ���� 6��������� �� ����� ���3� �%����
�%�6���#�"� ��� =�6 ���%�����6�����������������
������6��� ������ ���#��������,���������������� ��������
����������3��=��������� 3��‘���� ��H����������� 6�����=��������������������6��� ������6���������
�������,������6�=����������������������������� ����
� =�� ���������������6���� ��=#��"�������%%�6�������
�������%�����6=��������������������� �������������
�%�����������%%�6��#
� �=����6���6����%�������4 3 �/ �������A���� ��6�
� ���6����=0����������� ������ =����6���A���%�6� ����
��������������6����������� ����� �����������6�
������ ���,����� ���%����� ����6�������F����������
��������%�6����� ���� �����������=���,� ���#�)
����6��#()��"�������=�6��� ���������������%���
������6��� ������� ����������������A�6������ �
������������ ������� ����6����� �� ������ ������A
���� ��6��������� ��%������ ������� ����%�����������
6���� ��$+�����6��,���������������� ���%�6����
�����6������%��������������=� ��#��"���,���������6=
�%� ������6��� � �6������ ����� ���� 6����� ��
����������� ��� =����� ����� ������������������6�
��������� ���������� ���=,��%�������=�6��� ��������
�����6=�������������6������=� ���� ���#
Does it pay to intervene early?Box 2.10

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 37
health and economic status, economicinequality and indicators of internationalmobility as possible factors ininfluencing HIV prevalence. Thesequalitative analyses also showed that theexposure of individuals to, and adoptionof, many of the standard preventionmethods for HIV—condom use, the useof clean needles, contacts with the formalhealth system and healthcare andprevention messages—appear to becontingent on achievements in thehuman development arena.
The two-way link noted above should notbe taken to mean support for aprogramme that focuses solely on HIVprevention, with the idea that this wouldpromote human development, in turnleading to reduction in HIV transmission,and so on. Rather, the key point to note isthat these relationships suggest that thesuccess of the prevention programmesthemselves may depend on gains in thehuman development arena. This isreflected in the discussion on thepotential influences on condom usepatterns, needle sharing habits and accessto healthcare and information. It is bestperceived as lending support to HIVprevention efforts that go beyond anarrow technical focus on preventionand attempt to integrate such effortswithin a broader programme of humandevelopment.
The popular misconception that humandevelopment approaches to the epidemicare too time-consuming need to bereviewed and revised. On the one hand,key elements on the human developmentfront can be addressed in the short run.These include, for example, thefunctioning of law enforcement agents ina manner that protects the rights of thosevulnerable to, or living with, HIV, and oftenjust require a fairer application of existinglaws or a revision of laws that are not
enabling. On the other hand, humandevelopment responses provide effectiveentry points to contain the spread of theepidemic and mitigate its impact in aregion where the epidemic is not visibleand denial and stigma and discriminationare high. They also provide sustainablesolutions having multiplier effects that gobeyond the epidemic itself.
��( !��������
While the AIDS epidemic has a definiteeconomic impact, it has not always beenpossible to measure it empirically with areasonable degree of precision. Moreover,while there is some evidence of negativeindividual, household and firm level-impacts, the empirical evidence on theimpacts at the sector and national levelsis weak. Much of the evidence available iswith respect to sub-Saharan Africa andevidence for the countries being studiedin this report is scarce. Further work maybe necessary to provide conclusiveevidence of the size and nature of theeffects in the region.
A more fundamental aspect that thisdiscussion raises is that of viewing themacro impact, which is an instrumentalapproach, located in the conceptualframework of human capital whereinvestments in people’s skills is seen asproviding a greater return in terms ofincreased productivity, improvedworkforce management etc. On the otherhand, our analysis has demonstrated that,within South Asia the micro-economicimpact of HIV—at the level of individualhousehold, communities and firms—ismore significant than the macroeconomic impact. It would, therefore,be appropriate to go beyond the cost-to-national economies discourse and focusstrongly on the psycho-social dimensionsat the grass-roots level – for the individualsand households that directly confront the
.�� '�� ���� ��
��� �� ���� �����
�����������
������� ���� ���
������� �� ���
��������
������""��
���"����� "��
����� � ���� �
��� ��"�
������"��
�����

������ ��������� ������������ ����������
����� ����� ������������������
��������� ������������� ����������� ���� 38
epidemic and live with the virus on a dailybasis. Clearly the human developmentframework, which places people at thecentre as empowered beings and not asfactory inputs is well suited to enshrinethe principle of GIPA. It may beinstructive at this point to listen to the
voices of PLWHA and build their concernssystematically into not only programmespertaining to HIV and public health butalso address their concerns regardinglivelihood, social security and a publicexistence cleansed of stigma anddiscrimination.
�#�������� ��������������������� �� � ������������ ������������������������������������� ������� �������������� �� � � ������ ����������� ������ ��� ������ ������������������������� ������������ ������� ������������������� �� � ����� ���� �����$������� ���������� �� ��������� ��������� ������������ ������������ �������������� �� ���� �������������������������� � �� ���� ������������ ������� ����%������ ��������������� ������������������� � �� ��������� � ������ ������������� ���������������� ������������������������ ��������� ���������� ��� �������������&������������� �"
!�����!����������������"���� ���'�����������
��� ������(����� ����� ��

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 39

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 40

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 41
!�� ����
������������ �������������������
��� ��������� ���� ���
����� ������ �������� ��� ����Any analysis of the HIV/AIDS epidemicsof South Asia is limited by the sparsenessof epidemiological data. HIV is believedto have entered South Asia in the early tomid 1980s. By the late 1980s, it was clearthat HIV transmission among variousSouth Asian populations was escalatingand with disturbing rapidity in some ofthem. From all obtainable data, it appearsthat the region is a collage of mini-epidemics displaying considerablevariation in scope and intensity.
Some 700,000 new HIV infections areestimated to have occurred in South andSouth East Asia in 2002.1 By the end of2002, an estimated 6 million adults andchildren are living with HIV in theseregions, less than half the adults beingwomen. The South and South East Asiaregion accounted for an estimated440,000 child and adult deaths due toHIV/AIDS in 2002.2
The earliest detection of HIV infectionin South Asia was in 1986 in India. Thenext year, Iran, Nepal, Pakistan andSri Lanka also reported the presence ofHIV in their countries, followed byBangladesh in 1989. Since then, nearlyall the countries of the region have
������������������� ������������������������������������������������ ���������������������������������������������������������������������������������������� ������������������� �����!������������"#������������������������������ ������������������ ���������������� ���$�
����� ���� ��������� �� �
���������������� ��
��������������������
����� ������ ����������
������������ ���
�� ���� ��������!����
������� �"#$�"%�� ��
������ ���&�� '�� �(��
)�*��� !�+����� ,--.
recorded increases in HIV prevalence.
In Afghanistan, the lack of reliable datain general—and epidemiological datain particular—precludes a realisticassessment of the HIV/AIDS situation. Itis clear, however, that the many factorscontributing to aggressive HIV/AIDSepidemics elsewhere are present in thiscountry as well. Afghanistan has long beena cradle of conflict and the resultantinstability has shredded the fabric ofAfghan society. The presence of local andinternational military forces, thewidespread availability of heroin and itsuse by young people, the vulnerable statusof women and the high levels of mobilityof large, displaced populations conspireto create a situation of heightenedsusceptibility to HIV.
Under-reporting may be the cause of thelow estimates of HIV infections and AIDSfrom Bangladesh, Sri Lanka, Iran andelsewhere in the region. For many years,Bhutan and the Maldives remained in theranks of countries that had not reported asingle case of HIV or AIDS. Both have,however, begun to report increases inthe number of HIV infections. Apartfrom inadequacies and difficulties insurveillance and voluntary testing andcounselling, ignorance and stigmatisa-tion obscure the true extent of HIV/AIDSin South Asia.

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 42
India, the most populous country in theregion, accounts for the vast majority ofPLWHA, not just in South Asia but thewhole of Asia and the Pacific. India’s lownational HIV prevalence rate of less than1 per cent translates into millions ofinfections in absolute numbers, given theenormous size of the population.Globally, India’s HIV positive populationof nearly 4 million ranks second only tothat of South Africa.3
Though the HIV/AIDS profile of SouthAsia is biased towards both men andwomen in the 15–49 years age group,which is the prime working period andthe age in which a person is sexuallyactive, the majority of PLWHA in theregion are men in this age group. To givejust one example, the ratio of HIV positivemen to women in Pakistan in 2000 was7:1.4 The fewer numbers of HIV positivewomen in some South Asian countriescould, however, also be due to bias insample size of the sexes. In Sri Lanka, forexample, the reported HIV infectionsamong women and men are nearly equalbecause the large numbers of womenwho form the bulk of workers travellingto the West in search of work are routinelyscreened for HIV. In any case, this trendof more HIV positive men than womenappears to be changing. By December2002, women accounted for 36 per centof all new infections reported in Southand South East Asia.5 In the “older”6
epidemics of many African countries,women account for the majority of newHIV infections.
����� �� ��������� ��� ���Apart from data problems, the lowprevalence rate may have something todo with the fact that the HIV epidemics ofSouth Asia are relatively young andHIV/AIDS related illnesses and deaths areonly just beginning to surface. Adult HIV
prevalence rates reported from SouthAsian countries are yet to touch 1 per centand, therefore, the region imparts areassuring impression of low HIVprevalence rates.
However, this ‘low prevalence rate’situation may be short-lived. AllHIV/AIDS affected countries – includingthe severely affected ones in sub-SaharanAfrica—were low prevalence ratecountries in the early years of theirepidemics. HIV prevalence rates amongpregnant women attending antenatalclinics in South Africa was less than 1 percent in 1990. By 2001, the figure had risento 24.8 per cent and the country is now inthe grip of a fast-growing HIV epidemic.
The urgency of launching preventiveprogrammes is the other (albeitunintended) factor perpetuating abehavioural explanation for high levels ofHIV/AIDS in Africa. The use of condomscan directly prevent cases of HIVtransmission. Consequently, the provisionof condoms becomes the most immediateshort-term programme for HIV/AIDSprevention. Often prevention essentiallystops there, given the expense of anyprevention programme, the complexitiesof dealing with host governments withdiffering political agendas and the seemingenormity of resolving the morefundamental causes of HIV/AIDS.HIV/AIDS, like other infectious diseases,is the result of all the complex andinterrelated factors that exist in poorcountries. Leaving prevention essentiallyto condom provision (and treatment ofSTIs) reinforces the notion that HIVtransmission is narrowly the result of levelsof sexual activity and fails to address otherdeterminants, such as general health, theeffects of poverty, and gender relations.
The ‘low prevalence rate’ label is alsodeceptive as it obscures the reality of sub-
% �����������������������������������������������������������������&���������������������������������������������������������������������������������������������������� ��������������������������������������'������������������������(�������������������������������������������������������������������������������������������)�����)������ ������������������������������������������������������������������������������������������������������������������'�������(���(������*������������������������������������������������������������������ ����������������������������������� ������������$
������� �����/����� ��
�"#� 0��� ������� ��
����� � ����1
�� *������ /���� �����
�(� *������ � *���������
0��� ������ ������
2������ ��� ����� ����
%��� +��� ,---

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 43
epidemics of greater degree amongsizeable segments of the populations.7
For example, though India’s HIVprevalence rate among adults isreported to be 0.8 per cent, the states ofMaharashtra, Andhra Pradesh and TamilNadu have reported prevalence rates ofover 1 per cent among pregnant womencoming to antenatal clinics, a statisticconsidered indicative of its spread intothe general population.8
Thus, even within this overall lowprevalence rate setting, many SouthAsian countries have both concentratedand generalised epidemics in respectivesituations of high risk such as injectingdrug use, commercial sex and sexbetween men. The prevalence rateamong female sex workers in Nepal alsoincreased from less than 2 per cent in1990 to current rate of 20 per cent.9
However, the epidemic is not restrictedto these groups, and expectant mothersand children are now increasinglyvulnerable. Indeed, MTCT rates are onthe upswing across the region.
It is virtually impossible to predictprecisely how the HIV epidemics of SouthAsia could expand and intensify.Generalised epidemics have beenreported from six Indian states and severaldistricts in these states have prevalencerates of more than 5 per cent. This showsthat the epidemic can emerge quickly andunexpectedly.
Although the epidemics in individualSouth Asian countries are varied andgrowing at different rates, it is clear thatthe factors playing a key role indetermining their course are similar.These are:� the magnitude of people in risk
situations;� the frequency and numbers of
unprotected risk behaviours such as
sex without condoms or sharing ofinjecting equipment;
� the extent of networking among the sexand injecting drug use circuits, and thesize of bridge populations that share riskbehaviours with these circuits and thegeneral population; and
� the reach and effectiveness ofprotective responses by governmentsand civil society.
In India, the virus was foundpredominantly among sex workers andinjecting drug users in the early years. Itthen started spreading into segments ofsociety not recognised as being at risksuch as wives who were monogamousbut whose spouses had contracted thevirus from sex workers or other sexpartners belonging to the bridgepopulations. It is argued that whatmakes married women vulnerable isbasically their inability to negotiate safersex, a problem that is part of thegeneralised lack of control over theirsexual and reproductive decisions, which
�����������������������������������������������"���������������#���
���� ����������������������������������������$�"�����������������%
�&�'��������� ����������������������(������������)�����*�����
+(�),���#�����������������-��$���"���������������������������������
�������������%�����������#.������������"������������#���-�����
�������"�������������������������%�)�������������������������"���
�������� �������������������������������"���������������������� �����
�������������/ ����������� ���#�� �����������"���-�����������%
0��������������������#1����������#���������������������#����2
�� �� ��� "����� ��������������#� ����� ���"�� �� ��-��#� ��������
������������%�(�)��� ������������������"������� �������������������
�� ��������� ������� ��� ������ ��������� ���������%� 0������2
������������������������$����1���������� ������������� ���� � ���
�����$�����������2���������������#���3�����2�����������%
Afghanistan: blood transfusion, injectingdrug use are suspected transmission means
Box 3.1
�������� )������ ��� �������������� ������������ 4�������2� 5%��� �������
��������
+��� ��������%�����%���,

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 44
is also reflected in other indicators ofpatriarchy, such as high fertility rates.
����� ���� ����� �������� ������ �� ����� �In South Asia, vulnerability to HIV is a‘shared reality’. Hundreds of refugees andmobile populations in search oflivelihoods who move within andbetween Afghanistan, Bangladesh, Nepal,Pakistan, Bhutan and Sri Lanka areexposed to situations that increase theirvulnerability to HIV/AIDS.
����� ��� ����������� ���
��� �����
According to a WHO estimate, more than50 per cent of blood transfusions in theregion were not screened for HIV in 1995.
Mandatory HIV screening of blood has yetto establish itself in many countries in theregion, despite the enormous volume ofblood transfusions. Bangladesh, whichtransfuses close to 200,000 units of bloodeach year, does not screen for HIV,according to the provisional report of theMonitoring of AIDS Pandemic (MAP)Network Symposium, 1997. In Pakistan,an estimated 40 per cent of about1.5 million annual blood transfusionselude HIV screening.11 Maldives has thehighest incidence in the world ofThalassaemia minor. This hereditaryblood disorder requires frequent bloodtransfusions, rendering the countryvulnerable to HIV if blood is not tested forHIV. However, there are examples ofpositive State action on this issue, such
������������������������������(�����������������
������������������������������������� ��������������
�������#� ���� 6���-�#� ��� ����"��� ���� �������� ���
�� ����������������������������� ����������%�(������
�������# ���������������/�����#������� ����������
��������������������$�������������$��������������
��������������$�����"����6�����������������������
$��-%���������$��-���������� �������������������
���������������������� ��������������$������� ��������
���������� �����������# �������%������������ �����
���� ����� ���������������"������� ���������"�����
���� ��������#� ����������� ���� �� "��������7"����
��� ����#%
�������2�������������� ������������������#�������� ����#
��-����������������������������������������������#
�������������������������������� ������%��������"���
����������������� ����������������������������7��������2
������ ���� ������������ ��� "��������� �������� ��
��� �������$�����������������%
��������������������/�������������6����������������#
����������%�58�����������$������-�"������������#
����� ��������������� �����������������������������
$�������#��������������� ���������������%��9����/�� ��2
���"��������5������:�������+��������2��%�&� �������,
����;��"���+��������2�<&%�=� �������,2��=� ����������
������ ������������������7����������/� ������%���������#2
�$��*�������+��������2��% �� �������,���������#�!����
+��������2�<�%�>� �������,��� ��������������#����������
�� �������������������$�����$�������7����������/
�������%<�
����������#�������������� ���������� ����������������
������ +��"���� ����������,� ������� �� ��������� �
"������������/ ���������������������������������������%
������������������������������#� �������������������
������������%�!����6�����#2����� �������������������
"�������������������������������7����� ��������
������� ���������%�)����� ��������������������#���� �
�����2������������/ ����������#� ���������� ��������2
������� ��/�����������������$���������������������$���
���������� ����������������������������������������#���
�������������������������������������������%���2
��-���������������������������2�������������������������
��� ��/��������������������������������/������� ���
���������%�?������� ��������������������#����������
���������+���������������������,����������������������
������������������������������$�#���������������������
��� ��/���� �������#� ���� ������ ��� �������� �����
������������2�����������������������2���������������
�����#2���������������������%
African AIDS is not a special caseBox 3.2
�������� �����$�����2� ����

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 45
as the improvement in the blood safetyprogramme and quality of blood bankingservices in India (see Box 3.3).
Injections are a popular method ofmedical treatment in South Asia and areoften given or demanded even when notnecessary. Studies show that Pakistanhas a high annual ratio of 4.5 injectionsper capita and used injectingequipment is re-used for 94 per cent ofthe injections. According to WHOestimates, unsafe injections accountfor 62 per cent of cases of Hepatitis B,84 per cent of Hepatitis C, and 3 per centof new HIV cases.12
�� ����� ���� �� ��
HIV infection is common amonginjecting drug users since the sharing ofneedles rapidly spreads the infection.Injecting drug use followed theintroduction of heroin and has expandedsignificantly in South Asia since the 1990s.It is replacing traditional modes of drugintake such as smoking. The shift fromtraditional drugs such as opium to life-endangering drugs such as heroin andbrown sugar and further to pharma-
ceutical drugs is linked with the legal,social and economic developments in thelast few decades. The fall in the availabilityand quality of drugs and rise in prices areamong the factors that have led toincreasing levels of injecting drug use. Todate, the most serious co-existence ofinjecting drug use and HIV-positivepeople is seen in the states of northeasternIndia, notably Manipur (See Box 3.4).
VulnerablePopulations
� ��/�$��-���
� �������-���$����
� @���$����������/
$�������
� ��3���������������
BridgePopulations
� !������������/
$��-���
� @�"���� � ��������
� 4� �����������
��������
Affected populations
India addresses the problem ofunsafe blood transfusions
������������!�����������������������������+ �����������,2
����2���-��� �������������� �������������"����������� ���� ����
����������"��������������A����2��� �������02��� �������!2��# �����
������������A���������#%������������������� �����������"�����"��-�
����"������� ����#��������"������������������������������ �����
��������#�������������������������"������$�����������������������%
�������2�����B������������������������� ��������8��������0����
4����#2�$�������������������������#��������"����#��������6����
�� �#�������������6�����#�"���������"�������� ����������������
�����$���7����������������7��������������������"��������������
$���7�6�� ��� �������%�8�����������!�������)�����������
+8!),���������������� �������� ����������������4���7����
����������7$������ �������������������������������������$��������
8��������0�����4����#������ ������"�������7"�����������%
Box 3.3
General population� C����
� (����
� @��

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 46
The rapid spread to the general population
���/�� ����������� ��������������������������������� ���������
����� ������#��������"������� ���������������� � ����������#�"�
���������@��� ��2������������������������������%��������� ���������
�������������3��������������������������������������������������"��
����������<&DD�����������$��������=�� ����������������#����%����
��"��6�����#�� �������������������/�����������������$��������
��/� �������������3����������������������"#�<&&&2����� ���������
����������� ��������$��������@��� ������������%�� �������%
��������58��� �����
Numerous drug users began usinginjections as heroin became moreavailable from fields in Afghanistan andtrade networks in that country andPakistan. In eastern India andBangladesh, drug trade with Myanmarcontributed to increases in injecting druguse. There are an estimated 60,000 to100,000 injecting drug users (IDUs) inPakistan, 20,000 to 25,000 in Bangladesh,98,000 to 118,000 in India and nearly300,000 in Iran.13 In the Maldives, too,rising drug use among youth is a causefor concern. The Maldives HumanDevelopment Report, 2000, says that theislands reported a 40-fold increase in druguse between 1977 and 1995.
Injecting drug use does not seem to be afactor in Bhutan and Sri Lanka, and onlya minor factor in Bangladesh. Thoughthere is limited evidence about HIVinfection among injecting drug users inBangladesh, the potential certainly existsas needle sharing among injecting drugusers is at a very high rate of up to 97 percent.14 In central Bangladesh, needlesharing was found to be a routine matteramong 93.4 per cent of over 500 injectingdrug users. These drug injectors are notinsulated from the general population—they are often married and are sometimescommercial sex workers or professionalblood sellers.15
In Pakistan, an initial study16 of injectingdrug users found no cases of HIV infection.However, it was found that 63.3 per centshared needles and half of them weresexually active. Among the latter group,49.5 per cent had sex with commercialsex workers.17
Iran also has a major drug problem thathas led some authorities to suggest thatthe number of HIV infections is greaterthan available data indicate. In fact, themajority of HIV infections have beendetected among injecting drug users. AnIslamic Republic News Agency (IRNA)report, “More than 3000 people affectedby AIDS” quotes recent estimates thatsuggest that some 300,000 people injectdrugs. Besides, prisons pose a high riskenvironment for the spread of HIVbecause of the sharing of smuggledinjecting equipment. Rates of HIVinfection rose from 1.37 per cent in 1999to 2.28 per cent in 2000.
� !"�# ��
In South Asia, the magnitude of men andwomen offering, or forced to offer, sexualservices for payment or other forms ofbenefit is unknown. Besides sex workersthemselves, there are a large number ofpeople who make an indirect living fromthe sex trade. It should be noted thatestimating numbers is difficult because ofthe covert manner in which the trade takesplace. In Nepal, for example, there are noidentifiable red light areas and sex workersoften shift their operations upondiscovery, which leads to theirpersecution by society and the police.18
Street children are also vulnerable.Enforcement of existing internationalagreements and national laws has beenlax, in part because of the perception thatmany of the children drawn into the sextrade are willing participants or belong tosocially marginal groups.19
Box 3.4

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 47
The notion that young girls are less likelyto be infected with HIV than women whoare more experienced sexually hasincreased the recruitment of minor girlsinto the sex trade. A 1998 InternationalLabour Organization (ILO) studyestimated that there were 30,000 childrenwho are sexually exploited in Sri Lanka.20
Male child sex workers—also referred toas `beach boys’ because they operate inthe coastal resort areas patronised, inparticular, by European nationals-figurein travel advertisements.
$ �"���� � !"���� �%$�$&
Sex between men is not uncommon inSouth Asian societies.21 Studies such asthose carried out by the NAZ Foundation,a New Delhi-based NGO, highlight thewidespread occurrence of such sexualpractices in India, Bangladesh, Pakistanand Sri Lanka.
HIV prevention efforts among men who
have sex with men have focused onproviding information on safer sex, in thehope that an awareness of the risk of HIVwould enable them to choose saferoptions. Bandhu, a community-basedorganisation in Bangladesh, carriedprevention information to the generalpopulation through public campaignsand to MSM populations throughpeer educators. These efforts weresupplemented with the provision of STIdiagnoses and treatment, condoms andlubricants. Studies from India andBangladesh show that while theavailability of increased informationcertainly leads to greater awarenessamong MSM, it has not necessarilyresulted in safer behaviour. The failureto effect behaviour change has beenattributed to poverty and the lack ofskills to negotiate safer sex, as well assexual abuse, stigmatisation andthe criminalisation of homosexualbehaviours.
������������������������������"����#�����������������
�����������������������������������������4�-���������$�
���E�����2����8B)2�8���;������2���������������������
����#����@�#��������������"��������$����584%����������
�����������#�$���������� ����������������-#�"��������
��������������� ��������#������������������������������
$������������������"����7"�������������%
)������<F����������������������������������������$���
���������"����2�<F� ��������$����������$�����������
���4�-�������������������������� �����������������#2���
�� ���������� ����$��7��-�� ���������� �������������%�
��3����#����������� ��������$������������������������
�����2�����$������������������������� ����������������
"������2������2������������3��-�����������$��-%���������2
�%�� ������������������ ��������������3��������������
����� ������������2����#�<F� ���������������������#�$���
��3����������������������������������������$%���$����2
���������������3��������������������������������������
���� ��������������"����������������������#����=>� ��
HIV/AIDS vulnerability amongst Afghan drug users
��������������3������������������$�������������#������%
���3����#������� ���������������������������������
������#�$��� �������� ���������� ���� ���� ��� �����%
��$����2��������������������$���������������������
���#������ �����2������������������������������������
"����������������������"���������#� ����7���������
���������� ��������������-����������������%
��/�����������#�$�����������������/�$��-���2�������
�����������������$����������/�$����������� ��������
����������������������%����#���$����������������
���2��������-����-��$�������"���������#���������
�/ �����������������-�����������2�����������������%
(������������������������������������F�� ��������������
��� �������������������������"������%�����������
����� � ����������� ��������$�������������������#�-��$
��$����������� ��������2�������3����#�����������$��
$������-������������������������������������ ���������%
��������8���;������� G����#� ������������������������"����#�"���� ����������/���� ������������ ��3���������������������� ���
��������������������������� ���E�����.2�@�#�����
Box 3.5

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 48
Trafficking of women is a seriousproblem in South Asia
� �� ����H����<&&I2��2����$�����$�����������-��������/�������
��������%����������������2����$����������"�����������-�����
4�-��������������� ����<��#����2����������������-�������������
����������������������I���$���������������%
� ����H�)����������������$����������/�$��-���������2��FA �� ��
���������������%������������������������������������������<2���
G���������������.��������������������#%
� ��� H�F2���A<�2��������������$����������������-�������������
����#�#���%
�������� !�(2� ����
Governmental policies for HIVprevention are often at odds with thepenal laws. For instance, homosexualbehaviour is a cognizable offence in SouthAsian countries such as India. At the sametime, governmental AIDS programmesare committed to protect the rights anddignity of people living with HIV,irrespective of their sexual orientation.These conflicting governmental policiesand programmes detract from theeffective utilisation of HIV preventive
services by men who have sex with menwho fear exposure and subsequent legalpersecution.
'��� � !�����(
A related problem is the denial of youthsexuality and of their reproductive healthneeds. A large number of young peoplealso form part of mobile populations, withassociated vulnerabilities. A recent surveyin Bangladesh showed that adolescentsin both rural and urban settings hadlimited knowledge of STIs/ReproductiveTract Infections (RTIs). Urban youth weresomewhat more aware, though notnecessarily better informed, than theirrural counterparts, a good understandingof STI and HIV was limited.22 Thegovernment and a small number of NGOshave begun an information, education,communication (IEC) programme toinform adolescents about STI and havebegun to improve reproductive healthservices for the youth. In India, some pilotcurricula for ‘life skills’ education, whichincludes sex education, have begun.However, across South Asia there is awidespread view among influential
Box 3.6
��"��� %<
)����� ���* +��� ���������������
,����( -��� �� �� �����)����� �� * +�� ��� �� ��� �����
% )��& )��%.&
����������� 8%% 8%%
/������ �� ��2���A�F2��� <%=
/����� 8%% 8%%
���� &D2���A<<D2��� 8%%
���% �0�& ���2������� ��2��� =F
$����� � 8%% 8%%
- ��� ��2��� �J����<&&����/�������F�J
���<&&&
1�#����� >�2���A<��2��� <<
���2��#� >�� 8���� �����������
������8%%� ���������� ���� ������"��
����������������0���������H�(�����0��-2��������������������!�������2�����K�������� ����H�����
����!������������K��������8� ��H�(�����0��-������K��������4�-�����H�(�����0��-������K����
�������?��-�H�(�����0��-�����"

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 49
groups (teachers, parents, spiritualleaders, some politicians) that sexeducation for young people onlycontributes to the early onset of sexualrelations.
India’s reproductive health policies, whileusing the latest jargon and concepts, arestill influenced by traditional attitudesand mindsets. The reason often given bygovernment authorities for not addressingadolescent sexuality and sexual healthneeds is that these issues are not relevantas young people are not sexually active.23
In Iran, social and policy changes haveaffected youth (including adolescent)sexual health, although no aspect ofnational policy explicitly speaks aboutsexual health. Both young men andwomen are marrying later than inprevious decades, in part because ofcontinuing formal education, in partbecause of economic constraints, and inpart because of national policy raising thepermitted age of marriage.24 Couples whoregister to marry are required to undergomedical tests for STIs. Premarital sexualrelations and pregnancy amongadolescents (particularly amongunmarried girls) are strictly censured andsubject to severe punishment.
Sri Lanka, like India, has adopted aPopulation and Reproductive Healthpolicy. However, the Sri Lankan policyhas specific provisions aboutadolescents. The strategies includethe following:� providing adequate information on
population, family life includingethical human behavior, sexuality, anddrug abuse in school curricula at theappropriate levels;
� strengthening youth-workereducation by including informationabout drug abuse and sex-relatedproblems at vocational training
centres, institutions of higher learning,work places, and free trade zones;
� encouraging counselling on drug andsubstance abuse, human sexuality,and psychosocial problems,especially by NGOs, CBOs, and theNational Youth Services Council;
� promoting informed constructivemedia coverage of youth-related socialproblems; and
� promoting productive employmentopportunities for youth.
The country has moved ahead withimplementing the policy and relatedstrategies. An interesting objective withinthe programme is to contribute to creatinga socio-political and value climate, clearlyan activity within which policy makers andinfluential authorities will play a role,especially with parents and conservativeelements in society.25
Many Nepalese adolescents are aware ofHIV/AIDS and the means of transmissionand prevention, indicating activecampaigns to reach youth and adults withbasic messages. Young people in Nepalare, in general, sexually active in theirteenage years, according to surveyfindings. However, without extensivehealth services targeted towardsadolescents, to complement awarenessand information, the vulnerability to HIVcould be significant.26
$������ ��� ���� ���������
Mobility and migration is often a survivalimperative in South Asia, as abject povertyand lack of employment opportunities athome compel people to migrate.Although there has been little research onthe impact of intra-and inter-countrymigration on the spread of HIV, and itwould be wrong to label migrant andmobile populations as being a source ofinfection, the fact remains that this groupis vulnerable to HIV. The link between
���� ������
������������������
������ � ���������
���������������
����������������
�����
��� ������
���������������
����������
���� �����������

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 50
HIV and mobility is shown by the rise inHIV incidence in remote areas of Nepalwhose contacts with the outside world areconfined to people who frequentlymigrate for work to cities like Mumbai andDelhi in India.27
HIV prevention efforts focusingexclusively or extensively on especiallyvulnerable people might worsen thestigmatisation of some groups. Vulnerableand bridge populations such as sexworkers, migrant workers and longdistance truckers struggle to survive withina hostile social structure that shapes theirbehaviour and that of the authorities whointeract with them. Sex workers mightrequire a large number of clients to earn alivelihood and do not have the ability tonegotiate safer sex and better payment.For mobile populations, long absencesfrom the home environment, housing insingle-sex hostels, lack of access to STItreatment, the use of alcohol or drugs inorder to ‘belong’ to the peer group andharassment or indifference from serviceproviders are all factors over which theyhave no control. The preventionapproaches of many HIV programmes inSouth Asia assume that raising awarenessabout HIV and providing condoms orclean needles will enable people to switchto safer behaviours. Given the situationalnature of risk, however, it is clear thatpeople are more likely to adopt–and sustain–safer behaviours whenthe underlying risk situation issimultaneously made safer. This isespecially true wherever individuals arepowerless to protect themselves, despitebeing aware about HIV/AIDS.
The challenge, then, is to bring aboutsocietal changes to reduce HIV risk amonghighly vulnerable populations and lessenthe social stigma surrounding them. Thisentails the inculcation of caring socialattitudes, improving the availability,
accessibility and sensitivity of HIVservices and introducing legal andregulatory measures that can protect thesegroups. Vulnerable groups may then feelencouraged to avail of healthcare servicesand support mechanisms offered bygovernments and NGOs. The usage ofnon-judgmental language in expandedmedia coverage of the epidemic, forinstance, can help transform negativeattitudes to people in risk situations.
��� ,������ ���) � ��� ������������
Human security, a concept thatcombines peace and development, isgaining relevance in the policy agendasof South Asia due to its critical rolein building human capabilities. Thelinks between human security anddevelopment are increasingly being feltin the area of health and are acquiringpre-eminence in research.28 In a scenarioof fiscal constraints and often misplacedspending priorities, the notion ofguaranteeing human security can be aneffective way of placing the concerns ofpoverty eradication, universal literacyand health for all at the forefront of SouthAsia’s public agenda.
Human security presumes freedom fromwant and from fear, as well as access to andcontrol of resources and opportunities. Thebasic elements of human security includesurvival, safety, opportunity, dignity,agency and autonomy. Thesepreconditions for human security areessential in reducing vulnerability to HIVinfection and to its impact.
The underlying causes of internalconflicts have seldom been addressed.The most contentious issues revolvearound ethnic status, religion, language,demarcation of land, distribution ofassets, and the absence of meaningful
��������������
���� �����������
��������
���� ���
��������������������
�������������
����������
�������������
�������
����������!����
� ��������
�����������
�������
����������
������� � ������
����� �������
������������������
���������"����� ��
����

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 51
employment. The unequal distribution ofwealth and imbalances in regional growthhave routinely fuelled discontent. “Whentimes are hard, the sense of injustice isoften borne along ethnic, religious, andcaste lines. Violence thrives in poorsocieties where politics is weaklyinstitutionalised, law and order is fragile,and where the parallel economy is strong.South Asia, at least for the moment, fitsthe bill perfectly.”29
In the South Asian context, the potentialof conflict to disrupt development andviolate human rights needs to be closelymonitored to enable pre-emptivecountermeasures. Conflict may also beviewed as an aggravated form of socialtension, which clouds constructivethinking and prevents people from the fullenjoyment of their human right to a long,healthy and productive life. Conflict andviolence in South Asia are often viewed aslaw and order problems and theirdevelopment implications are usuallyneglected.30 UN documents view conflictas a violent physical and social
confrontation between inter-state orintra-state entities, inhibiting peoplefrom the full enjoyment of their humanrights in terms of the UN InternationalCovenant on Economic, Social andCultural Rights (1966).
Conflict has become a crucialdevelopment concern in South Asiatoday. The region is torn by both inter-state as well as intra-state conflicts. Intra-state conflicts, which are larger innumber, are socially divisive andundermine the integrity of the nationstates leading to a vicious cycle of violenceand social disintegration. Warring factionsresort to looting, drug trafficking,arms smuggling, plundering of theenvironment and other internationalcrimes. Much of this escapes notice inliterature on development.
The South Asian countries have largepopulations living in or fleeing fromconflict situations. The situation is causingconcern to the affected countries, theirneighbours and humanitarian aid
� *������#�����H�!����������������������� �� �����
���������������"��������������������������������
����������������#���������������� � �������%
� 1��������� ������H�����������#����������
��-�����������3����������"���� �� ��.��"��������%
� )������� ��H������������������������ ���������
����� ������ ����"������#�������� ������ ���� ����
��������������"����������������$������������%
� 1������� ��������3�������H�'���������������
$����������������#������������������������������"��
���������������"��� � ��������%
� 1" �� ���������H��������� �� �����"3��������
How do perceptions and language reinforce HIV-relatedmisconceptions and stigma?
�����������/ �����������-���� ������������-������
�������������������$���������������������������
��������������%
� * +���� ���H������������������������ �� ���$���
�������������������2�������#������%
� ���� � ���� �� �����H����/���������#����������
����� �� ������L������.���������������������������
������ �������������������������$������ �������
������������������%
� �� #��� ���� �� 4������7"�������������$����
�����������#�"���� ������������������"������������
��������� ���� ������������ ����� ������� ������
����������$���� �� ����������$����������%
Box 3.7

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 52
organisations. Any form of civil conflictthat results in the displacement of peoplewill fuel the epidemic.
����� ���� ���������Conflict in South Asia is aggravated by avariety of factors such as ambitiousprojects of ‘nation-building’, the failureof representative democracies andinadequate governance. The latter halfof the twentieth century has witnessedthe parallel emergence of sectarianand fundamentalist ideologies andglobalisation, which have beenaccompanied by the wide dispersal ofarms and narcotics, the progressivemilitarisation of the establishment andof subversive groups, and increasedmilitary spending. At the same time,natural resources have been grosslydepleted and certain developmentinterventions have led to communitiesbeing displaced from their naturalhabitats. Large parts of the region, whichtoday consist of independent nation-states, were once part of one colonial
empire. Besides, the political, ecological,social and human security implicationsof conflicts in one country are carriedover into neighbouring countries, a readyexample being the movement of hugenumbers of Afghan refugees across thefrontiers into Iran and Pakistan.
The region is an ethnic and culturalmosaic characterised by the traditionallyclose interaction of indigenouscommunities, castes, races and religions.Porous borders enable the movement ofpeople across frontiers, facilitating notonly cultural and social contact but alsothe movement of drugs, arms, moneyand insurgent groups. These have abearing on internal developments in theadjoining countries.
In development terms, wide-rangingmaterial and psychological deprivationsare associated with conflict, includingentitlement failures, health crises,physical violence and forceddisplacements. Conflict also disruptsdevelopment prospects by destroying theproductive infrastructure, public services,settlement patterns, environmentalresources, social capital and theinstitutions of governance.33 Given theenormity of the task of providing foodsupplies, shelter and basic medicines toan ever-growing refugee population,there is need for the mobilisation ofresources on an unprecedented scale.
Competing demands on limited publicrevenues in South Asia result in influentialgroups accessing a larger share ofresources. Besides, non-merit subsidies,making for losses of public sectorcorporations and external defence alsoabsorb a significant portion of resources.With the notable exception of Maldives,social sector expenditures in South Asiaremain low at less then 5 per cent of GDP.Endemic deprivation that becomes the
Conflict impedes HIV prevention
�����$��������� ����������$��-���������$�#2��������"�������#
����� ����"#���������%��������������������$���������"����������
���8� ��.����������������������"�������������"#����������"��$���
@������ ��"���� ���� ����������� ������%� ���� ��������� ���
���������������������7�������������������������������"#����������
����������%� ��� �� ���"��� ���<2� ���� ��������� ���� DF>
����������2����������������������%�������9�"����#�����2��������
�����������������"����������@�������������%����8B)�������������
"����"�������$�K��������������������������������������������"���
������#��%�8B)�$��-���������������������������������$��-2����
���� ��������.���� �������������������%��������������������#7
"����� ���������$������������� ���������������2��������� �������
���������$�������������������������%����� �� �����������
��������������������������������� ���������$��������#�������"���
������% <
���� ���������� �������� ������ ��������� ��� ����� ��������$���
���������#%� ��� ���� ����#� <&&��������� ��"���� ���� �� ������#
�����������$������������������� �����4�-���������������������
����"������������������������������������% �
Box 3.8
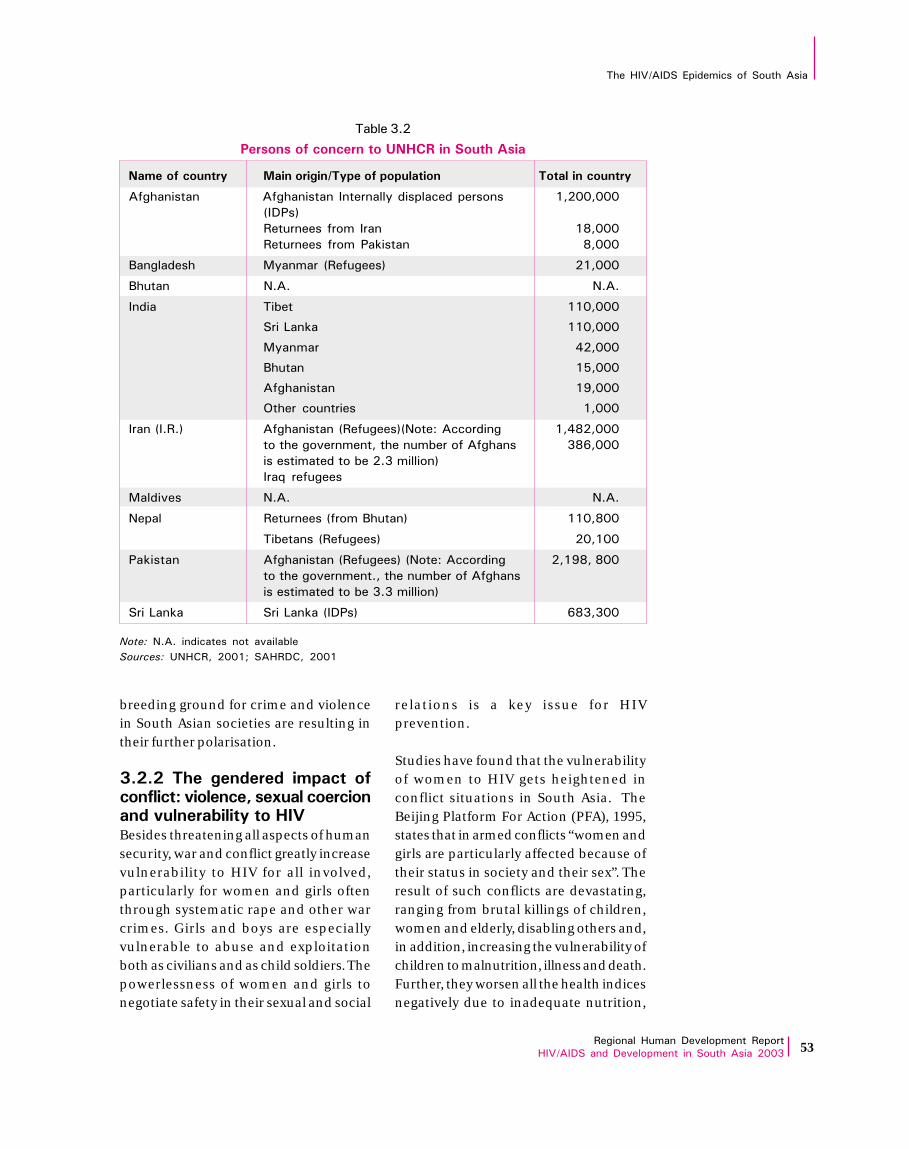
������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 53
breeding ground for crime and violencein South Asian societies are resulting intheir further polarisation.
����� �� � �� � � ������ ��������4��� �� �� !���� ����������� �������(�* +Besides threatening all aspects of humansecurity, war and conflict greatly increasevulnerability to HIV for all involved,particularly for women and girls oftenthrough systematic rape and other warcrimes. Girls and boys are especiallyvulnerable to abuse and exploitationboth as civilians and as child soldiers. Thepowerlessness of women and girls tonegotiate safety in their sexual and social
relations is a key issue for HIVprevention.
Studies have found that the vulnerabilityof women to HIV gets heightened inconflict situations in South Asia. TheBeijing Platform For Action (PFA), 1995,states that in armed conflicts “women andgirls are particularly affected because oftheir status in society and their sex”. Theresult of such conflicts are devastating,ranging from brutal killings of children,women and elderly, disabling others and,in addition, increasing the vulnerability ofchildren to malnutrition, illness and death.Further, they worsen all the health indicesnegatively due to inadequate nutrition,
��"��� %�
1 �������� ����-*,0����������
-�� ������( $��������5�(� ��������� �����������(
���������� ��������������������#���� ������ ������ <2���2���
+�4�,
������������������� <D2���
���������� �����4�-����� D2���
0��������� @#������+��������, �<2���
0����� 8%% 8%%
����� ��"�� <<�2���
����?��-� <<�2���
@#����� I�2���
0����� <F2���
���������� <&2���
)����� ��������� <2���
�����+�%�%, �����������+��������,+8���H��������� <2ID�2���
�����������������2��������"������������ D>2���
����������������"���% ��������,
���6� ��������
@������� 8%% 8%%
8� �� ����������+�����0�����, <<�2D��
��"������+��������, ��2<��
4�-����� �����������+��������,�+8���H��������� �2<&D2�D��
�����������������%2��������"������������
����������������"�� % ��������,
����?��-� ����?��-��+�4�, >D 2 ��
������8%%� ���������� ���� ������"��
���������58�!�2� ���<K� ���!2� ���<

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 54
unsafe drinking water and inadequatematernal and child healthcare.
Violence against women contributesdirectly and indirectly to women’svulnerability to HIV and their ability tocope with it. In population-basedstudies world wide, 10 per cent to morethan 50 per cent of women reportphysical assault by an intimate partner.Physical violence, the threat of violence,and the fear of abandonment act assignificant barriers for women innegotiating the use of a condom,
discussing fidelity with their partners, orleaving relationships that they perceiveto be unsafe. Those who are especiallyvulnerable to violence are women knownor suspected to be HIV positive, youngwomen and girls, sex workers, traffickedwomen, street children and orphanswhose parents have died of an AIDS-related illness.
Women play several roles in armedconflict situations: as armed activists, asrelatives of armed activists, as relatives ofstate armed forces, as shelter providers,
� � !��� ��� �� 4� ��� �������� ��� �� ���� �����
������������$������� ������ �� ��2�$��������������
���-������������� ���������������#�����������������
����������#�������������������������������$������
$����%
� /� �#�"���������������� ����� ������ ����4
��/��������������� ��"��������������������#����
��#����������������������"������ �������%��C����
�� ���"��������/����#����������������#����������
��������������������"����������������2��������������
�� ��#������ ����������%�����������������������
$���������#�����������������������/����#��"����
�������� ����������������/������������
� * ����������������� 4������� ����������������������
������������������������������������"�������#�"�
�����������$������� �� ��� ���������2� ������� ��
������������������2�������������������������������
���� ���� ������"��� ��� �������������7��7�����
������������%�����2���������������������������������#
����������������������������������� ������������ �������
������%� ����� ��� �� ������#� ����� ��� ��� ����#
���������������������2�@�������2�����������������"���
������������������������������� ��-��#� ��� �������
��������������������������������������������%��(����
����������������� ������#�������������������������
������������������������� �"�������������������"������
��������"������������������������������ ���%
� 6 �� ��� 7���(4������"����#����$�����������������
������������������/�����"���������"�����������
Factors contributing to the spread of HIV in conflict situations
��������������������������������������#�����������2
��������������������������������"�����������������
������ ��� ��/���� ���� ������7"����� ��������2
��������������������������������%
� /����� ����� �������������� �4�(����
������������������������/���������/���������2
�����������������2� ������������������#%�����2���
�����"����������������������#2�����������������
����"�����������������/�$��-%
� ������������#������������4�@����$��������������
������� ��� ���-#� "���������� "������� �� ���-� ��
���������������-��������������������������$������$
� ����������������7������������ ����������%
� )������ � ��4� ������ ������ ��������2� �����
� ���������������������� �����2�$���������������
��������� ���� ����� ���2� ������� ��� "�����
��������"��%��@�����������������������������������
����������� ���������� ����� ����� ��$�2� �������
������������"����������������#�����������������������
���� ����� ��� ������� ��������� ���� �����������%
@�������2� �� ��� ����� ���������� �������� ���
"��-�������� ���� ����$�� ��������� �������� ��
��3�������� ��"����2� ���������������#�������������
$�������/������������������������"�����������
���6������������������������� ������������ ��������
������2���������������2�"#�������� ���������������
����� �� �������%��(����������������������������$�2
"���������������������"���������������������������
�����������2���������������#�������������%
Box 3.9
������H� 58942� ����

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 55
as victims of sexual and physical abuseand as peace-builders.34 While thepowerlessness of women in conflictsituations is to be emphasised, their abilityto cope with adverse situations shouldalso be highlighted. Often, the formationof self-help groups, supportivecounselling groups and other trainingallow women avenues to negotiatesafety in their relationships. Thesevectors of change need to be consideredwhile addressing issues of violence,gender inequalities, trafficking andHIV/AIDS.35
Throughout South Asia, men, women,boys and girls are trafficked within theirown countries and across internationalborders in a clandestine trade. Conflictsituations are found to aggravate theunderlying factors leading to trafficking,including the heightening of existing socio-economic disparities, class and genderbias, lack of transparency in regulationsgoverning labour migration and poor
enforcement of human rights standards.36
In the conflict-affected areas in South Asia,many issues arise in relation to womenaffected by armed conflict. These includethe lack of protection of reproductiveand sexual health rights of refugeeand displaced women; the non-representation of women in conflictresolution activities; and the failure of stateand non-state actors to adhere tohumanitarian norms in regard to thetreatment of women and children inconflict. However, some post factomeasures for women affected by conflictare in evidence. In Pakistan, a pilotproject, Women in Crisis Home,coordinates inputs for women affected byconflict. In Bangladesh, a project for poorwomen who suffered due to the unrest inthe Chittagong Hill tracts was developed.In India, financial compensation for warwidows was offered. In Sri Lanka, womenhave been participating in conflictresolution activities.37
����#��������2����������$�����������������������$���
�������������#� ���������� ����� ������ ����������� ���
�� ������%������������#�$����������$�#�����������2
��������������������������$�������6�����#�� ���#���� ��#��%
����#��������������������"�#���������������������"���
������������������������������������������#��"����������
�����������������#2��������������$�������� ���������
�����"��������������%���������#�!����������������������
!������� ���� "����� � ����2� ��� ��� ���������
�������������"���������������������������9�����
�����������������������#��#��������"�����"��-�����"����
����������%�9��������������������������������������
8!)2�$������"������������<������������<F��������
+$� �>2���,%
������3��������$��������������������2��������������������
�����/ ���������"���$������2�������� ������2���#� �������
The Indian Army addresses HIV
��"������������������������������2����������������������
���� �������������7���-�"��������%�9����������2��������
�����-�����������+��������.���������,����� ���������
����!����������)��������+!)�,����������������-�$���
��������������#��"�������2�$���������!).��$�����������
���� ��� ����$����� ��� ���� ��������%���$����2� ����
����������������������$�#��� �����������-%�)�������
��#������������#����-��"������/�$��������������������#
�����������������#������������������������ ����%�)�����
��������.� ���2��������������������������������������� ������
��-�6��������������#%�M��.����-���������7������������%�C��
����3������������������������%N�4����#�������������������
"������� ���������� ����������������<%<��������7������
��#2��������"����������������������$���������������
��$%�������������������������+<&&&,����$�<2I������#
����������������������������������2�$�����������������
���"��� ��� ����8��#� ���� ������� 9����%� ��������
��������������"�����7 �������������������������2�"��
�����������������$��-%
Box 3.10
�������� �/������ ��������������-�(����$���2� ����

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 56
����� ��� ���� ������������������������ ������ �������(Without strengthened HIV preventionefforts, the presence of internationalpeacekeeping forces and other mobilepersonnel in post-conflict settings mayprovide a focus for a new local epidemic.The impact of peacekeeping operationson the HIV/AIDS epidemic is of suchconcern that in July 2000 the UNSecurity Council addressed the issueand adopted resolution 1308 with specialrecommendations for states onprevention measures to be taken. InBangladesh, authorities believe that theHIV/AIDS education programmesorganised by the Army prior to overseasdeployment were successful in alertingthe personnel to the vital need to avoidbehavours that put people at risk.38
Boxes 3.10 and 3.11 illustrate the SouthAsian success stories in addressing HIVamong soldiers, through a compassionateand caring approach, as distinct from oneof discipline and punishment.
��� ,��� ��0 ���� �* +5� )�����������
There is frequent debate about whether theHIV response should be focused especiallyon vulnerable groups in the hope ofcontaining the epidemic at an early stage,or whether all citizens must be involvedearly on to reduce the potential for rapidspread of the epidemic. The issue here,however, is that of scale rather than focus,considering that both approaches entailthe delivery of HIV preventive informationand services, the active inclusion of
����������������������� ��������!�������#����������
+�8�!)�,��������������������������������������?��-��
���#�������-�������� ������������7� ������������������
��/����������� ������������������������������%����
���������$������ ����������2�$����������������#2
��������������������������������%����#������ �����������
���������������%
)��7���7�7�������#� ����������$��������������$���
���� ����� �����I�� ������ ����������"������/����������
�������$����������������������������%���������������#
������������������ �$��-2������������2���������7 ��#2��
��������� �������� ��� ������� ���� ���� ����
���������������������������������%�!������������
������6����$������������������������ ������ �������
������������������������#��"������/�����������������%
���������$�����������-������������"�����/ �����������
���������������K�������$������� ������������"��-
��� ����� �������%� ���� ���������$��� ������� �����
�/ ���������$����������������#���#%
������&������������������������� ���������%����#
$������������������������ ��-����� ��/������#�����
������%���#���"���$��������������"���������$���������
Sex education for Sri Lankan soldiers
8B)�%� ����� ���� ��� ������� ��� ���� ��������2
��6�����������"����������������������������������$
��������%
������������������������ ��������2����"������� �����
�������������������������-��$�����������/�����������������%
��$����2����#�$�������#�-�����������������������������
������� ���2��������������#� �������%
����G�������������.���������A��������� ������ ����
��� ����������������������#��������A$���������������
����������� ��������%����$���������������� ������
���������������������������������#�����������������
���� ����� ���� ���� ���������� ����� ��� ����� �����
���������%��#� ��"������������������������������
�������"#��������������/�����������$�����������
"#�����$���� ������ ��������$��-�������������� �����
�������������������������������������$��������������
��-�6��������%
)����"��6����������������������#���� �2����������$���
������ ��� "�� ����#���� �������2� ������#���� �����
������������������$�������������� �����������������
�����������������%
Box 3.11
�������� �/������ �����58��2� �����

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 57
stigmatised people and an honestdiscussion of issues pertaining to sociallystigmatised behaviours. Governmentsmust intelligently apportion scarceresources and efforts between theespecially vulnerable groups and thegeneral population because the reality isthat HIV prevention must be available toeverybody regardless of their degree ofvulnerability. The extent and intensity ofsuch efforts, however, must be judiciouslytailored to each group’s scale of need.
The stigmatisation of people living withHIV may hasten the spread of the virusdue to denial of medical attention or theunavailability or unaffordability oftreatment. Social stigma can also increasevulnerability to HIV by deterring peopleat risk from accessing education,information, counseling and testing.
With support from the WHO, UNAIDS,World Bank, UN agencies and other bi/multilateral agencies, most of theSouth Asian countries have establishednational AIDS policies39 and coordinatingbodies through their Ministries of Health(Tables 3.3, 3.4). The national policieshave helped set programme priorities andprovided justification for unconventionalmeasures such as sex education in schoolsor condom promotion. However,prevailing HIV/AIDS-related policies andstrategies focus on those considered tobe most marginalised and thoseconsidered likely to ‘spread the infection’and largely pertain to injecting drugusers, sex workers and truckers.
The advantages of early prevention,where many lives can be saved andhealthcare and other costs can be averted,have yet to be fully agreed upon. Thepredominantly health-focused context ofthe epidemic and prevailing social normsand political imperatives have, in fact,resulted in the HIV/AIDS epidemic being
labelled as someone else’s concern or aforeign-driven agenda. Governmentshave yet to take the full responsibility toprotect disempowered people from thestigma related to HIV/AIDS and to preventits spread by including HIV-relatedstrategies and budgets in the NationalPlans or enforcing legislation aimed atprotecting the rights of PLWHA.
����� 0��� �� ���� �Within South Asia, there is considerablevariation in the national policy responsesto HIV/AIDS, mirroring the diverse natureof the multiple epidemics. Lessons canbe drawn from countries such as Thailand,which have achieved notable successes inmitigating the spread and impact of HIVby expanding their responses beyond theconfines of a health approach to one thatembraces a broad spectrum of humanrights and development needs. Theconceptual shift reflected the new globalrecognition that HIV took root andflourished wherever human rights wereviolated and wherever communities weredisadvantaged by poor development.During the initial years of the epidemic,the health sector took the lead role,instituting epidemiological monitoringand surveillance systems, introducingsystems for blood screening and the useof sterile equipment and providing careand treatment facilities. As the epidemicprogressed and a more comprehensiveresponse evolved, other sectors suchas education, industry and transportcame to the forefront. An inclusive,comprehensive response to HIV/AIDS isstill not readily discernible in thecountries of South Asia, for variousreasons. These include:
Over-identification of National AIDSProgrammes with SexuallyTransmitted Infections ControlProgrammesThe relationship between national STI
#����������
��������� ����� �
��������������
������������
�����������!���
���������� �
�� ���� ��������
������������
���� ����
����������
�� �����������$�%
���������������
����� � ����
���������
����� ������������
���������
�� ����� ���

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 58
programmes and national AIDSprogrammes took time to be defined andarticulated in national AIDS policies andvaries between countries. In Sri Lanka, forinstance, the STI programme became thefocus for national AIDS control andprevention activities. In India, however,while the implementation component ofthe STI programme was merged with theNational AIDS Programme, thecomponents of teaching, training,research and epidemiology have remainedindependent.40 In Nepal, the NationalSTI Programme is a special division underthe National AIDS Programme. In somecountries, STI programmes wereestablished many years before the adventof the HIV epidemic. The integration ofefforts against HIV with established STIprogrammes, thus, enabled speedy accessto an already existing, albeit not yet fullydeveloped, network of health personneland institutions.
Health ‘heavy’ programme prioritiesIt was long assumed that a ‘miracle’ drugor vaccine would be found and thatHIV/AIDS would not assume intractabledimensions. Ministries of Health thus
adopted a traditional public healthapproach. Monitoring the epidemicthrough HIV sero-surveillance assumedhigh priority. HIV testing with pre-andpost-counselling was followed by adviceto use condoms, clean needles andsyringes etc. Screening blood for HIV wasidentified as an important means ofpreventing its further transmission. Apoor grasp of the scale of the HIV/AIDScrisis made medical and otherestablishments reluctant to broaden thefocus of the AIDS programme to includethe participation of agencies outside thehealth sector.
Welfare-based, instrumentalistapproachesThe bulk of responses embody narrowbio-medical and instrumentalistapproaches centred on epidemiology,‘target’ populations and strategies tochange individual behaviours. It was soonclear that much more is needed to meetthe challenges of the epidemic in SouthAsia as most vulnerable people are unableto protect themselves in the absence ofthe power to influence their sexual, socialor healthcare circumstances. The low
���� ����#7����������� �����������������������������
��������������"#����������$���H
� ���"��������� ����������������������������������
�������%
� ������������ �"���������������������������������
�������������������������������������� ������
��������������������������������������������������
����������� ������%
� ������������� ���� ���������7��������� ��� �����
$����������6������/ ������������$����������������
������$����#�����"����������%
� "������������6��������������#�������������������$
� ������� ������� �������%
Policy response to HIV in South Asia
� ?��-� ��� �������� �� ���� ����� ����������
�� ������������������������������������� ����
������������2����������������������������������������#
$��-������� �����#2�����������������������������%
B���������������������������������������#� ��#���
�� ������������������������������� ��������������
$���������������������������������%���������������������2
�/�� �������2�������������������"�������������#� �������
����� ������2�����������#���������������������������
���������������$���"#������������������������ ����
�������������%����������� ������6�����#������� ���#
�������������������2��02����-�����������������������-���
$����2������ ���2����6������������2����������#2������
��"���2���������2����%
Box 3.12

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 59
socio-economic status of women, younggirls and boys, rampant child labour andsocially sanctioned norms that violatehuman rights and promote subservienceand stratification (whether in terms ofclass or caste) facilitate the spread of HIV.Those working to contain HIV/AIDS havemostly supported welfare-based,isolationist and vertical responses thatfocus on ferrying HIV-related services tothose perceived as needing them. Thedearth of appropriate attention to theinterfacing issues of poverty, livelihoods,empowerment, gender and human rightsguarantees that such responses have littleimpact. Successful HIV prevention andcare challenges human and societal valuesand norms, intimate human behaviourand relationships and demands changesin norms relating to class, gender,sexuality and power. It cannot but involveall of society. Besides continueddependence on rational behaviour,incentives and subsidies to arrest thespread of HIV are increasingly beingchallenged by growing poverty andinequality, mismanagement andtransaction costs and growingfundamentalism in South Asia.
Lack of operational tools forimplementing the developmentagendaReducing poverty, improving genderrelations and preventing human rightsviolations as well as initiating an overallimprovement in the quality of human life formed the thrust of the newdevelopmental approach to tackleHIV/AIDS. The agenda gained importanceas prospects of a vaccine or cure for HIVinfection receded. However, such a broadagenda does not fall within the scope ormandate of a single ministry or agency butcuts across several of them, none beingindividually equipped to take on thedaunting task of developing an overallresponse. Yet, it was the ministries of health
alone that were burdened with theresponsibility of developing planswithout help from other ministries andagencies.
The predominant responses supportedby countries in South Asia to addressHIV/AIDS fall into two broad categories–individual and community-levelinitiatives.
���������3� � � ��������� �
� Mass and small group education: Asinformation was initially thought to bethe key to behavioural change, HIVprevention programmes began witha focus on transmission andprevention. Several mass educationefforts successfully raised publicawareness of AIDS. Some educationprogrammes even helped initiatebehavioural change as evidencedby a rise in condom sales. Suchprogrammes have fetched appreciableresults in India and Nepal, amongpopulations perceived as beingvulnerable.
� Peer education: Trained peer educatorsrecruit leaders from communities toeducate their peers. This approachhas helped increase communityparticipation and engage diversegroups in the HIV/AIDS preventionefforts. Peer educators help developand discuss safer sex, distributecondoms as well as IEC materials suchas video clips and pamphlets andencourage meaningful engagement toimprove community empowerment,health and human rights. The peerprogrammes carried out by sex workersin India and Bangladesh arenoteworthy examples of the success ofsuch initiatives.
� Voluntary Counselling and Testing(VCT): VCT has gained value as aservice that can potentially helpchange negative attitudes about HIV
��������� �$�%
�������������
���� �� �����
��������������
� �������������
������������
�����������
�� ������������
�������������
����������� �������
� �����������
��&� ������
��!��

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 60
and AIDS. However, testing is oftengiven precedence over counselling inmost South Asian countries.Promoting constructive attitudesamong healthcare providers andimproving the quality of counsellingare public health imperatives. A FamilyHealth International (FHI) sponsoredevaluation of counselling initiatives inthe South Asian countries in 2001found that the quality of counselling,including counselling skills, werecause for concern.
,������(3� � � ��������� �
� Outreach initiatives: Outreachprogrammes enable individuals tocirculate HIV-related informationwithin existing social networks.Outreach workers help stimulatebehavioural change in marginalisedgroups such as drug users, sex workersand their sexual partners. Outreachwork is characterised by harmreduction strategies such as providingcondoms to sex workers and does notnecessarily consider the vulnerabilityfactors associated with sex work.Outreach workers in South Asiaface difficulties in working withmarginalised and excludedcommunities given the environmentof stigma and discrimination.
� School-based programmes: AIDSeducation has yet to find legitimacy inmany schools in the countries of theregion. Existing programmes providebasic AIDS information in theclassroom, and discussions ofsexuality and peer pressure arelimited. Some educators may sufferinhibitions during such discussionswhile others may consider sucheducation unnecessary and aspolluting young minds. Besides, thevast majority of children vulnerable toHIV/AIDS are outside the formalsystem of education.
� Condom promotion and socialmarketing: Several studies fromvarious South Asian countriesidentify lack of access and poorcommunication with sexual partnersas major barriers to condom use. As aresult, most HIV preventionprogrammes include the distributionof free condoms with the aim ofimproving their availability. The poorsustainability and reliability of freecondom distribution programmesprompted the introduction of socialmarketing as a more viablealternative. In an effort to increasetheir social acceptability, condomswere made available at non-traditional outlets such as truck stops,bars and hotels. Social marketing hasalso helped promote voluntarycounselling and testing. Bangladeshand India have reported that thesimultaneous empowerment of sexworkers has helped expand the scopeof traditional condom distribution.SHAKTI, a HIV project of CAREBangladesh working with street-based female sex workers, helpedorganise sex workers into the DurjoyNari Shanga (Undefeatable Women’sCommittee) in 1988.41 The groupassumed the responsibility ofmarketing condoms to sex workers.Though sales declined during periodsof police harassment, the group wasable to increase the overall sales withina short period. In December 1998, only39 per cent of all vaginal and anal sexualintercourse episodes had entailedcondom use, but the figure rose to 52.4per cent and 65.6 per cent over thesubsequent two years.
� Blood safety: Unsafe blood and bloodproducts have been major challengesto the containment of HIV sincethe beginning of the epidemic.Governmental efforts to prevent thespread of HIV through this route
'��������
������������
�������������
�� �����
������������
�������������
(� ������
������ ������
��� ����� ��
����������

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 61
include the provision of guidelines forthe treatment of blood disorders andthe rational use of blood, and thescreening of blood for HIV. Blooddonation is promoted to help reducedependency on professional bloodsellers. Despite monitoring, however,poor compliance to uniformstandards of blood safety is commonin South Asia.
����� -������� ���� �
�����������
Afghanistan has yet to formulate itsNational AIDS policy or national plan onHIV/AIDS.42 The government has neithermade attempts to confirm or rule out thepresence of HIV/AIDS nor has it initiatedsteps to lower vulnerability to HIV amongits peoples. The number of HIV/AIDScases in Afghanistan is not known but isprobably less than 100.43
/������ ��
Bangladesh established a National AIDSCommittee (NAC) in 1985, with aTechnical and Coordination Committeeat the central level and other committeesat various peripheral levels. The Ministryof Health and Family Welfare formulated aNational Policy Document on HIV/AIDSand STI that received cabinet approvalin 1997 and a framework for itsimplementation was developed between1997 and 2002. Bangladesh’s HIV/AIDSpolicy documents pay special attention toinjecting drug use and approve harmreduction as an appropriate strategy.However, the Ministry of Home Affairs,which is concerned with implementationof the Act, does not approve of harmreduction as it conflicts with existingdrug laws. Under the StrategicImplementation Plan (SIP) for HIV/AIDSPrevention and Control under the Ministryof Health and Family Welfare, Bangladeshinitiated HIV prevention efforts among its
prisoners. Acknowledging that militaryand police personnel also buy sex, the SIPgave near-equal importance to HIVprevention among the police, the militaryand sex workers. The SIP aims to achieveabout 80 per cent condom usage amongbrothel-based sex workers.
In Bangladesh, there is no specificlegislation to protect the rights ofPLWHA. The Constitution of Bangladeshhowever, confers fundamental rightssuch as the right to equality, non-discrimination, life, liberty and privacy44
to all its citizens. The National Policy onHIV/AIDS and STD related issuesendorses the Universal Declaration ofHuman Rights (UDHR) as a standard forpolicy making and action at all levels inthe response to HIV/AIDS and STDs inBangladesh. In the context of access tohealthcare, the policy states that “healthprofessionals must treat all personsseeking medical attention withoutdiscrimination and prejudice”.
/�����
The National STD/AIDS ControlProgramme in Bhutan, begun in 1988, hasadopted a multi-sectoral initiativeinvolving all sections of society. Theprogramme is integrated into thecountry's decentralised national healthsystem. HIV education has been taken torural communities and integrated with theeducation curriculum. The momentum ofthese efforts has been sustained by theHealth Ministry's information educationactivities.45 According to UNAIDS, morethan 25 per cent of the government’s totalbudget is allocated to healthcare andeducation, both of which are provided freein Bhutan.46
����
The Indian Government formed aNational AIDS Committee in 1986 andlaunched its National AIDS Control
)������
�����������
��!����������
���� �������
���������������
���� ������������
���������
���������

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 62
Programme in 1987. In 1992, the NationalAIDS Control Organisation (NACO) wasestablished to implement the strategicplan for prevention and control of AIDSin India for 1992-97. State AIDS Cells wereset up in each State for the expeditiousimplementation of the programme.Currently, Government of India isimplementing a comprehensive NationalAIDS Control Programme – Phase IIthrough autonomous State AIDS ControlSociety (SACS) in all States and UnionTerritories. A multi-sectoral response hasbeen launched involving variousministries. In addition an innovativestrategy through Family Health AwarenessCampaign has been initiative tomainstream HIV/AIDS into the country’shealth care system.
In the absence of an anti-discriminationlegislation, courts in India havefollowed the principles enshrined inthe Constitution, which guaranteefundamental rights including the right to
equality, the right against discriminationand the right to protection of life andliberty.47 While these provisions havebeen interpreted to protect againstdiscrimination by the State48 on the basisof HIV status,49 the juridical interpretationnow also needs to provide protection fromdiscrimination in the private sector. Afterall, fundamental rights are enforceable notonly against the State but also applicableto all citizens and non-State actors.
Although the right to health is afundamental right, PLWHAs do facediscrimination in healthcare settings. Thisis particularly true for injecting drug users,who are easily identified by needle marksand abscesses. Discrimination takesmany forms including outright denial oftreatment, physical isolation in wards,early and inappropriate discharges,delays in treatment, higher treatmentcharges and prejudicial comments andbehaviour. Confidentiality about HIVstatus is often breached.50
���<&&D2���������������3�����������@�%�O��%���� �����;2
������ �����!���������������������������������������7
���������������������#�$��� ��������������������������
������2��� ������.�� ������ �����������������#�$������
��������"����������������$������� ������������ ������
���-�������������������������������������� ��� ������
� ����%�@�%�O1������������������������������"��������
��������������#�������� ���������1�����7 ��������������
"#������ �����"�����"��-�������� ���������1�����������%
���������7�������������������������������������������
� ����2�����!���������������������������� �����#�������
���������������"�������������������������������#�"�
����������%� ���� ������ ����� ������ ����� ������ ������
������������ ��$�� ����$� ��������� ���������� ��� "�
������������������������������2��� ��������������������
��������������������������������������������������������
�������#���������������������������"��������������
G��� �����������.%�������������"����������������������
��-��#����� ��������������"�����������������������
The right to confidentiality for PLWHA in India
�����������������4�����!���2����������������������� ����
��������������� ��������������������$�������-����
������������������%
?����2�����?�$#���.�!���������.���������5�����������
��������"���������@�%�O2����-����������������������
����������������<&&D�3�������%�)��<������"�������2
������ �����!��������������������"�������������������
���������������������������3���������$��������$��������
������#�$���������������"����������!����%������� ����
!��������2���$����2���������������� �������������
������������������������� �����������-���������������
���� �����������������������3���������������������#
$��������%����������2����������2�����<&&D�3�������2
��������/���������������� �������������������4?(����
����#���������������������$��������������������������%
��$����2����������������-���$�#�������������#���
������$���-��$����������7 �������������������"����
���������������������������� ��� �������� ����� ����
�����������%
Box 3.13

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 63
���
The National Committee to CombatHIV/AIDS, chaired by the Minister ofHealth, was established in 1987. TheCommittee provides policy guidance tothe National AIDS Programme. TheNational Strategic Plan, though basedon multi-sectoral collaboration andcoordination, largely focuses onprevention.51
- ���
Nepal’s National AIDS Prevention andControl Programme was established in1995. The same year, the Ministry ofHealth adopted a National Policy onHIV/AIDS/STDs, establishing amulti-sectoral approach involving 12government ministries.
The Constitution guarantees citizenscertain fundamental rights. These includethe right to equality, which prohibits thestate from discriminating on the basis ofreligion, race, sex, caste, tribe, ideologicalconviction or any of these.52 Although thisprinciple has not been tested in courts asyet in the context of HIV/AIDS, thisprovision would oblige State-runhealthcare institutions to provide non-discriminatory treatment to PLWHA.Further, there is a provision that enablesthe State to take affirmative legislative orpolicy action to protect and advance theinterests of special groups, includingthose who are physically or mentallyincapacitated.53 Whether HIV/AIDSwould qualify for such a provision issubject to judicial interpretation. TheConstitution allows restrictions to beimposed on the right to freedom andpersonal liberty on the grounds of publichealth and morality54 and proponents ofisolationist public health strategies mayseek to apply this principle to PLWHA.The right to privacy is consideredinviolable except as provided by law55 and,as in India, assumes special significance
in the context of doctor-patientconfidentiality about HIV status.
Notwithstanding constitutionalguarantees, healthcare professionalsroutinely discriminate against PLWHA,often refusing to treat people with HIV.Moreover, Nepal's healthcare system isinadequately equipped to handleHIV/AIDS cases56. The Infectious DiseaseAct, 1963, the Prisons Act, 1963, and theHotel Management and Sales andDistribution of Liquor (Control) Act, 1966all discriminate against PLWHA,segregating them on the basis of theirsero-status. PLWHA are forced to carrytheir burden alone to avoid beingalienated by their families and in order toretain their jobs.57
1�#�����
Pakistan’s Federal Ministry of Healthinitiated a National AIDS Prevention andControl Programme (NACP) in 1987. Inearly 2001, NACP developed a NationalHIV/AIDS Strategic Framework to guidethe activities of the HIV/AIDSstakeholders in Pakistan. This frameworkencompasses nine priority areas,including coordinated, multi-sectoralresponses, reduction of risk amongvulnerable groups, reduction ofvulnerability among youth and improvedquality of care for PLWHA.58
The Constitution of Pakistan prohibits theState from discriminating on grounds ofsex, caste, race, religion, residence andplace of birth in matters pertaining toaccess to public spaces andemployment.59 In principle, this wouldapply to discrimination on the basis ofHIV status in State-run medicalinstitutions. There is, however, nolegislation to cover discriminatorypractices in private healthcare settings.Increased knowledge and compliancewith universal precautions within the

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 64
healthcare setting and improved qualityof care for PLWHA60 are among the priorityareas identified in the National HIV/AIDSStrategic Framework. In spite of this,there are reports that PLWHA in Pakistannot only suffer the physical anguish of thedisease but also experience isolation,discrimination, and abuse.61 Clearly, thelegal principles and fundamental rightsenshrined in the Constitution do notalways ensure access to healthcareservices for PLWHA and othermarginalised communities. This onlyunderscores the need for the involvementof other agencies in the HIV/AIDSprevention efforts. An ILO project onHIV/AIDS education for workers aims toimprove their understanding of the socialand labour implications of HIV/AIDS atthe workplace.
Pakistan also has a Disabled Persons'(Employment and Rehabilitation)Ordinance 1981,62 which provides forrehabilitation and employment ofpersons who are disabled due to disease.It remains to be seen, however, if PLWHAqualify to be covered under its provisions.Moreover, the ordinance does not dealwith discrimination.
��� 2��#�
The Constitution of Sri Lanka guaranteesthe fundamental right to accesshealthcare services to all its citizens.63 Italso ensures the fundamental right toequality and prohibits discrimination onthe grounds of ethnicity, religion,language, caste, gender, sex, maritalstatus etc.64 There has been at least onecase of termination of employment onthe basis of HIV status in Sri Lanka.65
There have been efforts to urgeemployers not to fire employees solelyon the basis of their HIV positive status.66
Tables 3.3 and 3.4 indicate that the SouthAsian nations, with the notable exceptionof Afghanistan, have taken steps to tackleHIV/AIDS. An evaluation needs to bedone of the coverage and effectiveness ofgovernmental and non-governmentalprogrammes in prevention and theirimpact on poor and marginalisedpopulations. Data on patterns of HIVinfection and sexual behaviour continuesto be scarce and most countries withnascent epidemics need to expand datacollection and analysis. Crafting cost-effective programmes and identifyingpolicy and programme needs isalso essential.
*+������������������,������������������������
���������������� ����������������������!���� ��-
����������������������!� ������������� ����
�������������������������������������������������������
� �����������������������������������������������
���$�%.��)���������� ��������� ������������������
���������������������������������������������������
������ �������)��� �������#� � /PB9�@
@���������$ �"�����������"���� ��������������B��"��9���2���������� ����� ������� ���������� �������� ���
9������������� %����'�����#���� 2�����B��"���9���
� �����������������������������������������������
$D>>2���2����������$��#����2����"��������������������
The Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM)
������� �������"�%� ��� ����"�������������� ����� ��
�������������"������ ���������������������������$����
�����$<��"���������#���%�(���������B��"���9����$����"���
-�#� ��#���������������������� �����2��������������
������� ���������������������������9����$�������#������
�� ��������� ��� ���� ������ ����%� 9���� ������ ���2
�� ��������������������������$=�2�<F2I�������������24�-�����2�8� ��2�0���������2�����2���������������
$����� ���������'�����#���� %����������������������
�������������������������������������������%����
�� �����������0�����2�@����������������?��-�����
��������������������������������������"������������
�������������������������������� ����������������
����B9�@%
Box 3.14

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 65
This chapter analysed policy responsesthat directly relate to HIV/AIDS and thosethat influence the socio-economic contextof the epidemic. Clearly, the latter willdetermine the course of the epidemic inSouth Asia. While countries wage acontinual struggle to upgrade the socialand economic status of their peoples andagree that vulnerability to HIV/AIDS islinked to poverty, these linkages have neverbeen clearly analysed or articulated. Povertyis viewed as a static condition rather thanas an outcome of the various pressures thatimpinge on people’s capacity to achieve
economic and social security. The term‘impoverishment’ is preferable, as it issuggestive of the dynamic processesleading to poverty. Impoverishment canresult from long-term or suddenunemployment, loss of assets (such asland), lack of access to basic social services(e.g., education, health, security, andtransportation), or lack of control overeveryday decisions. Impoverishment isoften characterised by inequalitiesbetween socio-economic groups.
In almost all the countries, ministries
��"��� %
1���(� ���� ��* +5� )�������������88�
�����������9 /������ �� /�����:; ����:< ���% �0�&:= - ��� 1�#�����;8 ���2��#�;�
8������� 8%% C�� C��2������ C�� C��2����� C�� C��2�"�� C��
������ �����$����� ���������2 �������
4�������� @������#��� ����� ���������
������ �������� ������ ���
8������� 8%% C��2 ?������ C��2 C�� C��2 8%% C��
4����# ���"����� ����# ���"����� ��������
����# ��� ������ ����# �����
�������;� ������
+;���������,
��� �������
$�����$���
���
8������� 8%% C��2 �������7 C�� C�� C�� ������<2 C��
��������� ��������� ����� ��� "�����6�����
�������� � ����������� �������������
4��� �������
������
��������� 8%% B��������� ����� C��2�$��� �����2 C�� C��2�"�� C��2
������"�� ������-���� �$������� ���������� ���#����7 ������2
+���������� (�����0��- (���� ��������� �������� (����
���������, ����K��������� 0��-������ ��� $����$�� 0��-
��������� ����B��"�� B��"�� ���������# ����
9��� 9��� "�������
4�������� 8%% )�������� C��2����� C��2�"�� 8%% 8������� C��2��� 8�������
������7 ���������� ���� �������# �������� �������#
������ �������� ������ ��������2
������ �������� ���$����
��������� �������� �$�����
���� �����������
������
Q ������ ��� ������� ��������� ��� ����������� ����� ��������������%� 9����������2� ������� ������)���"��� ���<���-�� ��#
��������� �"���� M����������N� ����#� ��"�������2� ��� ���� ����������%
����H� 8%%� ���������� ���� ������"��2� ���� ����������#� ���� �"������ ��� �� ����#� ��� ����%

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 66
other than health have seldom beeninvolved in the HIV-related policy-making process. Some countries haveinvolved the ministries of education andwomen’s affairs. The organisationalstructure of ministries and departmentsvaries from country to country and sodoes the relative influence wielded by oneministry vis-à-vis another. Sri Lanka, forinstance, had, at one time, a combinedMinistry of Health and Women’s Affairsand the issue of HIV and women wasapproached with a health bias. On theother hand, India and Pakistan, eachwith a separate ministry for women, wereable to bring to the problem a sharperfocus on developmental concerns ofwomen.
A multi-sectoral approach has also beenslow to emerge in budgetary allocationand programme development withinministries other than health, as theseministries have been reluctant to prisefunds away from tightly controlled orlimited budgets and competing demands.Yet, countries like Bangladesh wererelatively pro-active in attempting todevelop multi-pronged programmes evenat a time when the infection rates werelow. UNAIDS estimated that at the end of2001, there were 13,000 persons withHIV/AIDS, and that 1,000 deaths due toAIDS-related infections had occurred inthat year.72 The rates are higher in specificgroups such as injecting drug users(2.5 per cent) and commercial sex workers(0.6 per cent).73
HIV/AIDS came to be accorded highnational priority only in recent times inSouth Asia, whereas in Africa, theDeclaration on the AIDS Epidemic wasendorsed by the Heads of State andGovernment of the Organisation of AfricanUnity (OAU) in June/July 1992 itself. TheDeclaration adopted the target that: “Bythe end of 1992, each one of us will be
publicly recognised as the leader of thefight against AIDS in our country.”
��> ,���� �� � ��� �� ����� �
South Asian countries face variouschallenges in the implementation of theirnational plans of action to tackleHIV/AIDS. These challenges areheightened by the persistence of thefactors that constrain development ingeneral. The mechanism to deliver‘public goods’ for national HIV/AIDSprevention programmes can move nofaster than any other and NGOs thatadopt a fast track often find themselvesin conflict with the law or with theauthorities concerned.
People living with HIV/AIDS continue tofeel isolated, neglected and deprived ofthe benefits intended for them.Urbanisation and post-liberalisationpublic culture – consumerism fuelled bygreater media exposure and a tendencytowards increased commodification ofwomen – have prompted changes in thelifestyles of the younger generation. Theseonly make them more vulnerable toinfection, underscoring the need forurgent preventive measures. Even the bestplanned programmes face formidableproblems in the South Asian region. Thesheer magnitude of the geographical anddemographic challenges in some of thecountries, the staggering numbers ofpeople below the poverty line, low levelsof literacy, large migrant populations,inadequate health infrastructures andcompeting demands for scarce resourcesmay all conspire to relegate HIV/AIDS tothe backburner.
The South Asian Association for RegionalCooperation (SAARC) Secretariat has yetto accord HIV/AIDS priority status. SouthAsian countries can benefit through
+��������������
�� �����0��� ��
�����"����������
$�%.��)�
����������
������������
�������������
���������������
�#1�����������
��������������
����������� ������
���� ����!�������
!����!�������
����������
���������

������������ ��������������������
�������������������� ������� ���
���������������� ���������������������
67
��"��� %I
1���� ����������� ��� � �� �* +5� )�3� ��� ����� �
����������� /������ �� /����� ���� ���% �0�& - ��� 1�#����� ���2��#�
��������� 8�������������K 8��������� 8�� ����# @�3����������H �������� ������������� @������ (�����
�� ��������� ������������� ������#K������� ������2�"�� ����������� ����������� �����������# ����# ��������
�������4����#� ����������� �������������� ���� ����������������� �����������K �������2�"�� ����������� �� ���������
4����������=I �������#�������� ����"��� ���������� ����������������2 ����������� ����#���� �������� ������� ����#�
������K�������� ������������� ���������K �������� ���������
����������/ !������������ ��������� ���������
������������ ��������#
���������������� ������
����������
�������������� ���� ��������� 8%% 8%% ����������������� ������� 8%% 8%% 8%%
������������ ��������� ������������� �������K������
������������"# ������������������ ������������
��$������ ��������������7 �5��$��
��������� ����# ��������������5� ����3���������
���"���������
�������=F
�������-��� 8%% ?�$���/������ 4����"���� 4����"����2�"�� 4����"���� 4����#���� �������2�"�� �������
������ �������-�� ������� ��� ������
�������-��� $���������� �/������
��������� ����"��
������# �������-�������
������/������K
�������
���������
4������������� 8%% 8%% 8%% 5 �����"#�������2 ������ 8%% 8%% ���#��������
���� ������� "����������������� �������#
�� ��#��� ���������� �������=> ����"���
�������� ��# ����������
���������������� ����������
���� �������
�� ��#���==
������8%%� ���������� ���� ������"��

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 68
technical exchange with developingcountries that have much to offer.With concerns that India might emergeas the global epicentre of the secondwave of HIV infections, HIV/AIDSbecomes a matter of serious concern forthe entire region.
The South Asian countries must nowaddress the implications of the WorldTrade Organization ( WTO) regimesregarding Intellectual Property Rights
and patent systems on ARV drug pricingand the growing demand for such drugs.The impact of growing conflictsituations and the limited availability ofresources in the countries of the regionmay well be compounded by imminentglobal recession. Health ministries andNGOs that are dependent on donorsmay find funding for HIV/AIDS dryingup as wealthy nations re-adjustdevelopmental aid programmes andpriorities.
����������������������� �������������������������������
������#�������� ������� ��������������������������������
���������������/��������������� ��"�����������������
������������6��������������$������%���������2�������������2
���$������#��������B��"������?�$�!�������������<&&F
���������4��������2�4�����@����������������@����������
���������������� ������������ ��-����������%��������2
����4�����@���������������������������������������� ��"���
����������������������������%�����������2�������������
���"����������� ������������������ ���������%������.�
4�����@����������������������$��������!�����@��������
���������/��������$��������� ��������������������������
���� ���� ��� �� ������������ ��� ������ �������� ���
�������������%
�������������������������$���� �"�����#2��������������
���������������#�������������"����#����������������
�����7������������%�����4�����@�����������������$���
"���������������������� ����������������������"�������
��0��������!������������������������������� ���"��
���<%��������"���<&&D2�����4�����@������������0�����
��3 �#�������������������������������8��������4������
����4��������������!������������������������������
M��������������������������� �"����������� ��"���
������������N%�!������"�"��8����2�����!�����@����������
�������������������4������2��������������������H�M�
����������������"�����������#�����������#%����$�
������������$2�$��$��������� ��"����%���������$�#�$�
��������"���-������������N%�����������������������������
58�B�����������"�#�� ��������������������������
'�������<�$�������"#�����5������������@�����������
��������� ���� ������� ��� ���� � �������%��8�������
!���������� ���������������� �����������$��
�������������8����"��������"#�8!)���������"�������
Critical role of political leadership in the response toHIV/AIDS in South Asia
$����58�������� ���������������������� ����58
�#����%
���4�-�����2�����4�����@�������.�����������������������
���<&&D��������������������������8��������4������������
���(����������� ���"#�����@������#����(����.�
����� ����%�����4���������������������#�������2
"������������"�����������������$��������� �����#2����
�� ���������������� �����������$����2���/������������2
�������������#���$������ �������������������������%
���8� ��2����F�����"�������2��������������!��$�
4���������������-�������H�M�������������$�"�����
�� ��"������������������������������������N%=D�����
�������@�������� ����� ������2� ��� ����2� ����� ���
�� ����������������������� ������������������������
�� ��������������������������� ����������8� ��%����
E��������0�����2��������������#�(������-���������
"������ �$���������������������������������4?(�
��������� �-���������������������������� �������������
�������������������/�����������������!�������������
�����������4�������+�!4,%
���@�������2��������8��������!�����������������@��������
!�������������'��#2�<&&<2�����4���������@�������"���
B�#���������������H�MR��$�������-������� ����������
������������������������� ����"����������������� �������
��������#���*������������������������ ��������������
�� ���%�������������2����������2�"�������������#���
��#���������������������������������� ���������������
����#�������� ���� ������ � ������ ���� �����#� �������
���������N%=&����������������"������ ����������#
�������$��������@������#�����������"�����������������
������������������������������������� ���������%
Box 3.15

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 69
Countries in South Asia, being in the earlyphase of the HIV epidemic, still haveample opportunity to avert large-scalefuture infections. An environmentsupportive of broad-based governmentalinitiatives is emerging, albeit slowly. Themultiplier effect of efforts against AIDSthrough developmental responses such asliteracy programmes, income generation
schemes and reproductive healthinitiatives is gaining ground. NGOparticipation is being increasinglyrecognised as being critical to the successof such efforts. In the first decade of thisnew century, there is more hope than everbefore that countries in South Asia will bebetter placed to come to grips with theepidemic.
%+���,������������-��� ��������������������������������������������������������������������������+����������������������������������������������������������������������������������������������,������������-������������������������������� ������ ��������������������������������������������
+������� ������������������������ �������������� ������������ ��������������������������.��������������������������������������������������������+���/�����������������������������������������������������������������������������������0�����������������������������������122�222���������������'�������$
�((�����+�����������������+��3�� ������*��������������������(�����������
4����(�)������������4����(�)����������������� +����*���������������
�"#$�"%�� 54)����6�� ,---

������������ ��������������������
�������������������� ������� ���
���������������� ����� ���������������� 70


����������� �� ���������
��������������������������������
����������� ������������� �����������������72

����������� �� ���������
��������������������������������
����������� ������������� �����������������73
������� �
������������� ���������
��� ����������
This chapter looks at the necessity of usinga human rights approach in the fightagainst HIV/AIDS. It argues that theepidemic can be combated effectively onthe one hand only with an enabling legalenvironment, and on the other, societalacceptance through sustained sensitisa-tion and the elimination of stigma anddiscrimination.
Many of the key strategies against HIV—especially those dealing with behaviourchange among vulnerable groups—require a set of legal and statutory changesthat make it feasible for PLWHA to have agreater voice in decisions affecting theirown lives, without fear of beingstigmatised and discriminated against.Treating HIV prevention as a corecomponent of the policy frameworkof human development can helpaccomplish this task, since the objectiveof a ‘caring society’ is common tothe concerns of human rights andAIDS activists.
����� �������������������������������������������������������Human rights are now widely acceptedas being central to any community ornation’s effective response to HIV/AIDS.
�������������� ������������������������ ��� �� �� ��������� ����������������� ������ ���� ��� ������������ ������ ���� � ��������� ��� ���� ������ ����� ��� ��� � ��!���� ����� ����� ��� �!����"���������������� �� ���� ������� ���������������� ��� � ���������������������������� �����������������#�
���������������� ���
������� �������������� ��
������������������������
����������������
��������� �!�������
������"��#$$%
This has been acknowledged both ininternational documents and nationalresponses.1 It is important, then, to assessthe role and importance of a human rightsframework in responding to HIV/AIDS.
Human rights are inherent in andinalienable to every individual. They renderthe government and the larger societyaccountable to the citizen. Every individualhas a right to live with freedom and dignityand ‘citizens’ are the ‘duty holders’obligated to respect, protect and addressthis fundamental need. Human rights arenot given or bestowed upon people byindividual governments or society butare earned by virtue of being born ̀ human’.As Justice J.S. Verma, former chairpersonof India’s National Human RightsCommission so aptly put it, “dignity is theentitlement of all as long as life exists.”2
HDR 2000 defines human rights as “therights possessed by all persons, by virtueof their common humanity, to live a life offreedom and dignity. They give peoplemoral claims on the behaviour ofindividuals and in the design of socialarrangements–and are universal,inalienable and indivisible.” The value of ahuman rights approach lies not only inprinciples such as state accountability andpopular participation, but also in thenormative potential of rights to alleviateinjustice, inequality and poverty.3

����������� �� ���������
��������������������������������
����������� ������������� �����������������74
The conceptual framework of humandevelopment places people at the centreas empowered beings. It embodies arights-based approach to developmentthat could serve as the appropriate frameof reference for integrating the humanrights concerns in the struggle against HIV.Principles of GIPA are, therefore, intrinsicto the human development approach.“The protection of human rights isessential to safeguard human dignity inthe context of HIV/AIDS and to ensurean effective, rights-based response toHIV/AIDS. An effective response requiresthe implementation of all human rights,civil and political, economic, social andcultural, and fundamental freedoms of allpeople, in accordance with existinginternational human rights standards…”.4
Addressing the epidemic within a humanrights framework involves a strongemphasis on acceptance and non-discrimination of populations perceivedto be more vulnerable to HIV. The lastdecade has witnessed the increasingconcentration of the epidemic in thedeveloping world where the responseneeds to not only protect individual rightsand privacy, but must also deal with widerdevelopmental concerns like poverty,gender and inequality. Such an approachwill encompass the InternationalCovenant on Economic and Social Rights,the Convention on the Elimination of AllForms of Discrimination Against Women(CEDAW) and the Convention on Rightsof the Child (CRC). In sum, it will capturethe spirit of the Universal Declaration ofHuman Rights, which talks about povertybeing the greatest denial of human rights.
����� ��������������������������������������������� �!"It has been argued that protecting therights of those affected and at risk is thebest public health strategy to cope withan epidemic. A rights-based approach
recognises vulnerability to the epidemicnot just in terms of individual behaviourbut also the social, cultural and economicconditions that lead to this vulnerability.It also recognises that the vulnerability ofwomen, children, migrant workers, menwho have sex with men, injecting drugusers and sex workers can be reducedthrough the protection of their humanrights. It is only when the stigma anddiscrimination faced by PLWHA iseliminated, that they can be empoweredto take control of their lives. Protection ofhuman rights helps to create a supportiveenvironment, encouraging PLWHA toaccess the various health and HIV/AIDS-related social services and, consequently,stimulating behaviour change. Thisposition has been vindicated by theexperiences of several countries.5
The international response to HIV/AIDShas been characterised by twodiametrically opposed public healthapproaches-the isolationist approachand the integrationist approach. Theisolationist response proposes three basicstrategies for HIV/AIDS prevention:compulsory and universal HIV screening,the disclosure of the HIV status of thosetesting positive and their isolation fromlarger society through discriminatorypractices. The integrationist strategy, onthe other hand, proposes voluntarytesting following informed consent, thenon-disclosure of a person’s HIV-positivestatus and the equitable treatment ofPLWHA in healthcare, employment andall other facets of life.
Integrationist policies were based on thefundamental human rights of individualsto self-autonomy, privacy and equality.The basis of this philosophy was that,in the long term, voluntary testing,confidentiality and non-discriminationwould encourage people to come out andaccess health services. This, in turn, would
��������������
��� �����
����������������
������������ ��
��������������
���� �����
������ ������
�������������
����������
������������
����

����������� �� ���������
��������������������������������
����������� ������������� �����������������75
increase the possibility of bringing aboutbehaviour change and instilling a sense ofpersonal responsibility through counse-lling, thus helping retard the spread of thevirus. The integrationist approach,therefore, sought to battle and reducestigma whereas the isolationist approachsought to increase it, thus pushing theepidemic further underground.
Initially, the isolationist response,requiring as it did the disclosure of thepositive status of persons in order toprotect the rest of society from the spreadof the epidemic,6 was felt to be mostappropriate in South Asia. However, thisapproach was given up when it was seento be violating people’s human rights andfuelling stigmatisation.7 HIV-relateddiscrimination first attracted attention inthe region when India announced thetesting of foreign students, mainly thoseof African origin.8 This was followed by anannouncement that certain categories oflong-term residents also had to be testedfor HIV. Concerns that foreigners mighttransmit the infection to the localpopulation prompted the preparation ofa draft bill prohibiting marriage betweenforeigners and Indian nationals.Fortunately, the proposed legislation didnot see the light of day.
The realisation gradually dawned that theisolation versus integration debate couldnot be perceived as an issue of publicinterest versus individual rights. It cameto be acknowledged that the protectionof the individual was itself in the publicinterest as it increased accessibility toservices and brought the epidemic intothe open. This enabled concerted andeffective public health interventions thatwere ultimately beneficial to societyat large.
An outstanding example of a successful,integrationist rights-based approach is
that of the STD/HIV Intervention Project(SHIP) in the red-light area of Sonagachiin the Indian city of Kolkata (See Box 4.1).The empowerment of sex workers in SHIPbrought about significant improvementsin their health as evidenced by a drasticdecline in STD rates and the marginal risein HIV infection.
Certain key legal issues arose in the contextof HIV/AIDS, which the human rightsframework had to consider. The threeissues at the core of any response to HIV—consent to testing, non-disclosure of HIVstatus and anti-discrimination–requiredthat policies be informed by threefundamental human rights— those of self-autonomy, confidentiality/privacy andequality.
The issue of consent to testing addressedthe question of whether testing should bevoluntary or mandatory. Consent,therefore, dealt with the right to self-autonomy, to decide for oneself what canbe done to one’s own body.
The issue of non-disclosure was based onthe right to privacy/confidentiality. It wasalso based on the very pragmaticconsideration that disclosure (since thatmight lead to stigma and discrimination)would make people distrust healthcareand shy away from it, thereby driving theepidemic underground.
Anti-discrimination was based on thefundamental right to equality – that HIVpositive status should not preventpersons from accessing services(healthcare, education, employment,insurance, travel etc.) and lead to theirbeing treated unequally from others.
These issues also exemplified the famousparadox—that the best way to controlHIV/AIDS is to protect those mostvulnerable and those affected.9 Help,
�������������
������
������� ��������
������������
�������� � �� �
��������������
!�������
������������

����������� �� ���������
��������������������������������
����������� ������������� �����������������76
����������� ���� ����!���������������������"����������
#��������������������������������$���������������� ��
�������� ������������%�����$&��� ����!���������%
��$� ��'������������#�����(��'����������##���%���)
������������%�����$�������������� ���#���������� ���
���"����������������%������#���)!���#�� ���%������
����#�&����*++�!�����,�������������������-��.�#��/���-0
�����������,��#����#�%�����$� ��'��������������� ������
#��������� �#�� ��� �����"�����&���� ����!����%�#��
�%������������������"��� ��� ����� ���������#�����
��������%��� ��!�#������� ���$�����)&
���-���������"��� ���$� ��'���1�#���"����)����2�������
���#���������������)�����%� �������#���)!��� �"���
� ���������%��� ����� � ���������� ��&�,����$
��'�������������� �#� �������������1�����������&
, ���)3%��������#�����%��������������������������
���.�#������������� �%�����$� ��'������ ���)��� ����)
'�)����������&����������������������������%!���)� ���
������ �����#����������� �#�����!�#����#��������������
#����#������ ��������������.�#���,��#����#�&
�,�����.�#�� ���"���������� ����%���� ���� ������
���������4
� ,�������� �#������ ��������� � � ��������%���
�%������#����!��� ����%%�� �����)�#�� �!� �#����
���� ��#���� ��#�������&� �� ������� �%� �������
�#��������� ����������� !� �����������%���������
���%3������#���� �#��%� ��#������������$� ��'���!
�� �������������#��%�������#�������)����������
��������������������� ��������)� ����5%�����1
����
� ��$�)3%���������� �#������ ����%����������������
�������� 3���������!��2����� � �����%�����������
�,����������������!�����!�� �����##������ �#��
#������ � �)���%�2������������ �������#���������
������� �������#�
� -����� �#������#�� �#�� ��������)� ���"�"���/���3
������������#������0&�6��)�7*&7�����#�����%���
#�������� ���� ��%������������ �8�&8�����#���
� ���������� ���#�� ��&������������!�������#��
����%���� �"�� ���������$� ��'������ ���
#��������������������%�����$�������#��#��!���#�� ��
����������������%���$����������#������������
� �� �������� �������� %��� ����#�� ���������� ��
������� �")���������� ��������������%���������
�)����&�9)������ ��%�������*++:!��"����*;������#�
�%%�#����� ������ � �����������������������
� ���*++7!�������"���<������������)�����������
/�<��0!���������%�����$� ��'���!� ���%���� ���
�������� �� � ��%��#�� ����� ����&� ,�� �����
����������%������)���#������������������)
"��� ������<������"����������� �������������
����������&� ,��� "��� � �������� ���� ���
���'��� ���� ��� ��� �� � ���� ����� � ���� ��� �
�������)����� �#� ���%�#�� �#�!���#������������
#�� �������%%�#'� ������������������������
�� ��������%���������)�#��#������� ���$� ��'���
� �%����%�������������������� !����"�������-
��������������1������������� �����)���������
��#�������".�#����
� ,�����.�#�������� � ���������� ���%������$
��'���������)������&������$�����!����-������ �
���3�%������� �#������ ������ ���� �%���������#)
�����!���� ���������#�������������������������
%�����$� ��'����#��#���� ��"������#����)������
��&� �� #�� ��� �� � ������� �#���� ��� ����
����"���� � ��� ���� ��$� ��'���� ���� ��� ���%3
�����)������#����
� ,��(�����=�� ����������������������")���$
��'���� ��� ���"�� � ���� ��� #������#���
���� ���%�������������%�����$� ���#������!
�����!��������#���� �"������� �������������3
���������������������
� ���-������������ � ����������%�/�����)0����!
��#�� ��������!�"������� ����!�#��������� ���
����#�!����#�����#�������%������������#���%�����
#������� �� � ����� ������� � ����� �������� %��
������� ������%�����$� ��'���&�,�������������
�� ���#�� #������� ��� ����������� �������#��
����#�����
� ��##���%�������������������%�������.�#���������.���
�"����#�����"��������"�������������� �����'�
��� �)�������#���)���� ����$�����)!������#'��%
��#���� �##�����#�� �%� ��$� ��'� �� � ��� ����
��"���������������������
� ,����$� ��'������������ �����������%���������!
�� ����� ������� ������� �������������������
��$� ��'��������������)� �%%������%��������������
�%������ �������������%��������#���&�,���������
������������������#)��� � ���������
Sexual negotiation as empowerment: the Sonagachi approachBox 4.1
������� >$���#�� %����?��!� ����

����������� �� ���������
��������������������������������
����������� ������������� �����������������77
support and protection for the infectedand their carers has been identified as akey strand of the campaign againstHIV/AIDS. “Protecting the groups andindividuals at risk is a moral obligation, apriority strategy owed to brothers andsisters because, like us, they are human.They feel. They suffer. They and theirfamilies are cruelly burdened when thisinfection takes hold, and nowhere moreso than in poorer, developing countrieswhere palliative drugs are generallyunavailable, social support outsidethe family, is negligible and wherestigmatisation based on ignorance andprejudice is rife. Prevention is not theonly strategy.”10
There are certain ethical issues that areimportant considerations in the humanrights-based approach to HIV/AIDS(See Box 4.2).
With the realisation that the denial offundamental human rights had to betackled for HIV/AIDS to be effectivelycontrolled, other key legal issuesaddressing the fundamental right to liferequired consideration. It was noticedthat those most susceptible to HIV/AIDSwere persons who were legally andsocially disempowered and whose basicrights were denied to them. These groupsdid not have the basic human rights tolead a wholesome life, which could guardthem against public health crises,particularly HIV/AIDS. These popula-tions included injecting drug users,prisoners, sex workers, women, womenexperiencing gender violence, children,migrant workers and men who have sexwith men.
Therefore, it was understood thatenforcing positive rights (the entire rangeof socio-economic rights), law reform anddecriminalising behaviours would help incontrolling the spread of HIV/AIDS
�������� ������
�������������
���"��������
����������������
�����������
��������������
��� �����
���������
within these groups and, thereby, itsspread within the general population aswell. In order to achieve this, reviewingand amending laws that prejudice,criminalise and marginalise these groupsis essential, and this needs to be supportedby changes in underlying cultural andsocial attitudes.
It is important to demonstrate the linkbetween globally recognised humanrights standards and the response toHIV/AIDS. Table 4.1 attempts to highlightthe practical aspects of human rights inthe context of HIV/AIDS.
��� ���� �!"#�"��������!�������������� �����������������"���� ���
“Research shows that discrimination ismost frequently associated with diseasesthat have severe (incurable andprogressive) outcomes and modes oftransmission that are perceived tobe under an individual’s personalbehavioural control.11 UnfortunatelyHIV/AIDS fits the criteria perfectly.HIV/AIDS discrimination has led to theuse of such terms as ‘leper’ to label thosethat are infected with disease as well asto brand them as ‘others’ or ‘deviants’.12
Metaphors portraying AIDS asretribution or punishment for a sinful lifeor moral failure are a powerful indication
� �#��������� ������������#���!���#�� ����#��������%��������
����
� ���%� ��������)��� ������#)
� ���#����������������� ��'���#�
� 9��� ���%��)��� ������� �������
� �##��������� � ������)��%�����#���
� 9��3�� �#���������#�/�&&� ������������%���##������ � ���
�� �������@�����������������%���"��#����������#�����������������
�� �#������0
Ethical issues related to HIV/AIDSBox 4.2

����������� �� ���������
��������������������������������
����������� ������������� �����������������78
of the stigma attached to HIV/AIDS.Through stigma, society often blamesinfected people for being ill and assertsthe innocence and health of thestigmatisers”.13
While many serious diseases attractstigma and discrimination, HIV/AIDS isparticularly open to generate responseswhich ‘discredit’14 those who are infected.This is both because the routes of HIV
transmission include sexual behaviourand the sharing of injecting equipmentby drugs users—behaviours that areconsidered shameful or illegal in manysocieties—and because many of thegroups that have been most affected arealready marginalised and stigmatisedwithin society. This stigma has beencompounded by fear due to lack ofknowledge within South Asian societiesabout the modes of HIV transmission.
������� A?����&� ����#
,�"����&*
$�������������������������������������%&����� �!"
"������&����������������������� ���� �!"'������������� �������������������������������
,������������������������"�� >�������������3���������������� � ����#����7��%����A��������
���� �� ��%��)��#����� ������������ �� ������#���/��#������������� ��#����������%�����������
%����,��!������������%�������� � ����#���*���%�����������������
%������#�� ���!��� ���������) ����������%�>#�����#!���#���
#������������ �������0���� �� ��������������
������"��!�������� ��� ����%�� � ����#���*���%�����������������
������������#���%�#�����!�������� >������������%������������%
��%%����!��� �����3�����������& ���#������������������B����
>�����������������%������#�����) ����#��������� ��7��%���
�������%������#������� ����������& �����������������������%
������
,�����������%����������� �� �#����� -���� ����%����������� �� �#����� � ����#���*+��%����A��������
�������������$����������� ���� ��#����������������������
����������& � ����#���*8��%�����������������
�������������������� �-�����#��
����
� ����#����8��%�����������������
���������%�������
,��������������#) >����������#������������ � ����#���*���%����A��������
�������������������)!��� ���� ��#����������������������
���������������������#��%� ������@ � ����#���*8��%�����������������
�����������������%����3 �������������������� �-�����#��
��#���������������� ��������& ����
� ����#����8��%�����������������
���������%�������
,����������������� ��� ������ ��#����������%����"����)����#��#�� � ����#�������� ��7��%���
��� ����) �� ���������##������������"�� A�����������#����������%������
��%��������� ������� ��� ����
�������"����)��������������� � �C6������������+8!�����#���*��%
���%%�#'��!�����#����)�%��� ���� ���<��������%���>����)����
�� �#�� ��� ����������
� ����#�����:��� ��+��%���
�����������������������%
������

����������� �� ���������
��������������������������������
����������� ������������� �����������������79
This lack of knowledge is evident evenamong policymakers and healthcareworkers who have often appliedunnecessary and restrictive measures toPLWHA, thereby fuelling the misconcep-tions, fear and stigma relating to thedisease as well as violating individualrights.
HIV-related stigma is built upon, andserves to strengthen and legitimise,existing social inequalities. The powerimbalances and socio-economic andgender inequalities within South Asiansocieties combine with taboos aroundsexuality, fear and ignorance about HIVtransmission, and inappropriate mediareports, to create a powerful stigma
attached to HIV/AIDS. Marginalisedgroups are also stigmatised partly becausethere is little general understanding of thestructural factors that make themvulnerable to HIV. Therefore, betterunderstanding of the developmentaspects of HIV would help reduce stigmasurrounding them.
Throughout the region, PLWHA haveexperienced violent attacks, refusal ofmedical treatment, rejection fromfamilies, communities and from theworkplace, denial of last rites and manyother rights violations. In Bangladesh,there have been cases of PLWHA beingheld in police custody,15 while in India aSupreme Court judgement had
��A?�-���� )!��������������� ���%����?=6�!�#�� �#��
�������)�������������#����� �������#����� ���)!���
� ����%)��� ������������#����������������%����#�����3
������ � �����!� ��#����������� �� �������� ����� ��
� �2�����)�#����%������������������������� �������������
���9���� ��!��� ��!�?����!�-�'�������� �����C��'�&
������#� ����� ����'�������������������� �� ����"��#
��������������#��%�%����#������/�����"�!�����!���'�!
(���#�!��� �(����� �0&�,��*���������� ����� ���
�� ��%����%�������%%������� �������#��������4
�#����!� ������!� �� � ����������� �� � ��"������)
��#��#����&��,������������� �#� ������"����%��#����
���� ������� ��� "�� '�)� #�����������%� ��������
��#������������� ������������� �%%����#��������������
�� ���'�� ��� �%� ������ �� � ��#����������� ����
�%%������������������������ ������ �%%������������
�%������������%%&
,����� )������ ����#�����������������"�� ���
����������������� ����� � ��#���������)����#��#�����
��������� ��� ���������%�'�� �� �!�� ����������
���%����������$������#���%���������������������%%���
�������&�,���������� ����� ����#��#����������%���
�����#������� %��� ���2�����)��%�����#���� �������
��������������������#����&�<������ �#������%%�����"���
")�#� ����%����#���������� ����� ������������������
������������������� ��2����)&�D��!�������%�#���%���
��%�#������ ������!�������%%1��#��#����%��������� �
��%��)� #��� #��"���� ��� ������ � '�� �� �� ��
�$������#���%����������� ��������������������� �����
��#���������)� ���#��#��� ����� ��������&� ��#
�����������"������������������������%%!�����#����)
������"��������������%������� ���#!�����������
������ ����%���#���)��������&
,�������������)���� )��� ������������"��������"��
�� ���#�����)�������������� � ������������3������
�������� � ��#����������&�,������������ �#����������
��.���#�����������%��������� � ��#������������� �� �
-CB��������������������������������#���"�������
��������������� �%�����%����#����2���#����%���%�#����&
������� ������#� ��� ��� � � ��� �� ������ � ��
�����#��������%��������� � ��#���������������������
������ #����$�� �� � ����� �������������� ��� �� �#�
��#������� ��&
������ �����"������ !�� ����!����������� )� �������
����)�����#����3��3"��� !�� �������� �#�������%���
������)�����������������&������#���������������
�����#������� ���� ��'��� ��� �%%�#����#�� ���������
����������� ����� �"�������� ��� ���%��#�������%
��#���)� ���������&� ��� ���������������������������
"������������������2��������������&
Stigma and discrimination in South Asia: an illustrative studyBox 4.3
������� >$���#�� %����?��!� ����

����������� �� ���������
��������������������������������
����������� ������������� �����������������80
‘suspended’ HIV-positive people’s right tomarry in 1998, though that right has nowbeen restored.16 This is happening despitethe UN Commission on Human Rightsclearly stating: “Discrimination on thebasis of HIV or AIDS status, actual orpresumed, is prohibited by existinginternational human rights standards,and the term, ‘or other status’ in non-discrimination provisions in inter-national human rights texts should beinterpreted to cover health status,including HIV/AIDS”.17
A recent study of the attitudes andbehaviour of health service providersindicates that stigma and discriminationpervades the hospital system as well(See Box 4.3).
The stigma and discrimination attachedto HIV/AIDS also hampers preventionefforts, as people are less willing to test forHIV or to admit to their positive status.Many PLWHA, therefore, do not receive thesupport needed for behaviour change andare not involved in HIV-related responses.This also results in a lack of accurateinformation about levels of HIVprevalence, making informed preparationand responses impossible. Such denial and
secrecy takes place not just at a personal,but also at a social level, with communitiesand nations across the region refusing toadmit the scale of the problem.
��( "���������������������������������������
The active role of civil society, includingthat of local decision-policy-makers, inprotecting the rights of individualcommunity members is crucial insustaining the socio-cultural fabric ofany community. Given the existingenvironment of intolerance, stigma anddiscrimination, societal acceptance isparticularly crucial for the effectiveimplementation of HIV-related legis-lation. There is evidence within SouthAsia that human rights violations andviolence against individuals (includingthose who have been traditionallymarginalised, especially the poor anddisempowered, women, those belongingto Scheduled Castes/Scheduled Tribes,religious minorities, migrants andstigmatised groups) are often aggravatedwithin existing community structures.
Studies in South Asia reveal that morewomen die from violence-induced causesthan from maternal mortality (the regionhas one of the world’s highest rates ofmaternal mortality18). The lives ofmillions of women in this region aredefined by traditions that enforcesubmission to men and endorse unequaltreatment. In some countries, forexample, it is reported that young girlsand women are sometimes killed by theirrelatives even if they are raped, as they areblamed for bringing dishonour to thefamily.19 Women from Bangladesh whohave been in the sex trade also fear beingkilled by their families. Apart fromtraditional mindset, another reason forsuch manifestations of violations is thelack of access that women have over
,��������������������������������� ���#������)���#���)�
,����������������� ���#��%�������%�#�����/�����������#�������)
�������)��� �������#� 0&
�������������� ���#��%�����!� �#��������� �������������
��%�3������������%�#����&
�������������� ���#��%������!� ��#����������!�"������� �#����#����
�����!� �#���'���������� �%%�#��������%%�#�����)���#'������%����
� �&
#�����$��%� ���� ������������!� ����&����'��������
����%� ()*+
The three phases of the AIDS epidemicBox 4.4

����������� �� ���������
��������������������������������
����������� ������������� �����������������81
familial assets, exacerbating socio-economic insecurities. Since youngwomen and girls lack education, thereare limited livelihood opportunitiesavailable to them, especially since theexisting social support mechanismaround them is inadequate. Such skewedsocio-cultural realities and trendsseriously challenge the right todevelopment for many, besides infringingtheir basic human rights. Women livingin these insecure conditions arevulnerable to trafficking and sexualviolence and, therefore, to HIV.
Gender inequities and stereotypes inSouth Asia increase the vulnerability ofyoung women, and to a lesser extentyoung men, to HIV and create anenvironment in which it is easy for HIV tospread.20 The taboos around the opendiscussion of sex and the social value thatis placed on the ignorance of women andgirls with regards to sexuality, safer sex andrelationships creates a situation in which
women and girls engage in sexualrelationships without the basicinformation, resources, confidence andskills needed to protect themselvesfrom HIV.
The strong pressure on women and mento conform to widely held gender idealscreates a situation in which it is oftensocially unacceptable for both women andmen to seek information on sex thatwould empower them to protectthemselves from HIV. For women,ignorance of sexual matters is valued asa sign of ‘purity’ and ‘innocence’, whileknowledge about sex is seen as a sign of‘immorality’, making it difficult for themto seek information on sexual matters.Men, on the other hand, are expected toconform to a masculine ideal whichvalues sexual knowledge and experiencewith a variety of partners, often makingit hard for them to admit ignoranceon sexual matters and seek informationand support.
9� ���%��������#������%����5�����#�"��1���� ��#����
���?����&�9� �� ������������ ��������)���� ���$!���
�������#�����%�9� �������� ������������������� ����
��������������$���� �!��##�� �������$�����&����?=6!
��#����� ������������> �#������/���>0!����.����������
#�� ���� ���������� � �����"�������������$� ��'���
�� ������#������&
6������������%����)����!��������� ���#���"� �����%�5�����
����#�1� #���� � ,��� �� ��� ������� /?��"�����
���������������������0!�������)�#�����������#����
���!�������'��������#����������5�$����������������1!
�#!������������ !� ����)���)����� ������9� �
#�������)&�6������"����%����#���������� ����
,�������'���������������*!�EB��� ��%��� ����
���9� �� ����1�������!� ��"���� ������� ���
����#����!� ������������������&F����������� ��#�������
�%���$� ��'���� ��� �������)�")� ������#�������&
<��.�!���#�������)���"������� ��'��� %������>!
�����"������������%)�����������������"��'������
���������� �"����������"�#��������� �#��������
�������������#��������&�������'���%�����������#��
����#���������&���,����$�� �)!����%��� ����������
"������� ����� &�<��.�� ���%��#� ���������������
������� �������������������"����� &�?������!
�������9� �� ����!���#���������������������%�9� �
����� ����������� �����������#����������%����
��#������&�E,���� ������ ��#������!F������)�&
E,�)������ � ����"��#'�������%�#����� ����� ����
����� ��� �� ������#�� ����� ��!�5������� ���1&F
-�����������#�%������%���#����)����#����� �����������!
9� �� �����%������������ �����#������'�������������
���#������������#��"�������������������������#�
���#�� �������&
Badi communities in Nepal: surviving social ostracism and violenceBox 4.5
������� 9��� � ��� �������� ��� -�� �������� �����!� ������ �!� *++�!� G��3,������"��!� ,����� ���%%�B�����@�.� ��� �����!
G��)� 73**!� ����!�?��"��� *�*

����������� �� ���������
��������������������������������
����������� ������������� �����������������82
In addition to the existing cultural valueplaced on sexual inexperience in women,it has been seen that the HIV epidemiccan prompt older men to seek everyounger partners who they believe will beless sexually experienced and thereforeless likely to be infected by HIV.21 Thismakes young women more vulnerable tobeing infected by older men with widersexual experience.22
��(�� "�)����&���������%�������*���������������)���������Sex between men is common withinSouth Asia, as it is in other societies.However, such sex is generally not viewedas ‘homosexual’ and those men engagingin it are rarely part of any ‘gay’community.23 Moreover, such activitiesare taboo and not widely talked about, andare also officially outlawed in most SouthAsian countries, often by old Britishcolonial laws that have been left in place.Despite this, it appears that in manycountries young men have their earlysexual experiences with other young menand that many go on to continuedbisexual activity in later life. For example,50 per cent of male university studentsinterviewed in Sri Lanka reported thattheir first sexual experience had been withanother man.24 While male bisexualitycannot be understood simply as aresponse to men’s lack of access towomen, it is likely that restrictions oncontact between men and women inmany South Asian cultures do play a partin the widespread nature of sex betweenmen as an alternative means of sexualexpression.
A study conducted in the Bangladeshicapital of Dhaka25 found that the rights ofmen who have sex with men, includingmale sex workers, were being violated withincreasing frequency. The study went onto establish that such violations affected
their self-esteem, negotiating power, andultimately increased their vulnerability toHIV/AIDS. For men, selling sex is bothhighly stigmatised and illegal in most ofSouth Asia. Although male sex workers areoften more aware of their vulnerabilitiesto HIV and STIs than their peers, the factthat they are an extremely marginalisedgroup, and are forced to operate incircumstances over which they have verylittle control, makes it extremely difficultfor them to protect themselves. It isparticularly difficult for young men tonegotiate safer sex with older and morepowerful male partners, and when analsex is practised, the unavailability ofcondoms and lubricants can exacerbatethe vulnerabilities that they face.
��(�� +�%��������������Migration is a survival strategy for manyindividuals in search of work within SouthAsia. The region is currently undergoingmajor macro economic changes as partof the process of globalisation, which hasopened up many avenues for large-scalelabour mobility. Poverty, absence ofadequate or appropriate livelihoodoptions, depleting rural employmentopportunities, caste and gender-basedexploitation and oppression, violenceand conflict, the hope of finding betteropportunities elsewhere and the searchfor a better life are among the key factorsthat make people move in search oflivelihoods. Migration patterns from theregion include internal and inter-countrymobility, as well as overseas migration.The migration trends depend upon socio-economic and geographical factorsas well as tradition/past migrationexperiences in the source community,availability of local livelihood options andproximity to metropolitan cities.
According to figures from the Bureau ofManpower and Employment andTraining of Bangladesh, the average
��������������/
��"�������!���
��������!
������ ��������������
�������������
���������� ����%
����!�����������
������/�������
����������
��� �����"�����
�/�������� ��!!�����
!��������� �����
�����������

����������� �� ���������
��������������������������������
����������� ������������� �����������������83
number of documented migrant workers,both skilled and unskilled, is about 200,000per year. In India, according to theNational Sample Survey (1993), 24.68 percent of the population—approximately200 million people—were recorded ashaving migrated, either within India, toneighbouring countries or overseas.Recent studies have estimated the annualflow of workers overseas to be well over100,000, 80 per cent of them from theunskilled sector. Nepal’s Department ofLabour has registered 52,170 overseasmigrant workers, and this figure does notinclude the vast numbers crossing theopen border into India, for whichestimates are as high as one million.Figures provided by the Bureau ofEmigration and Overseas Employment ofPakistan for 1999 show 2,790,221 migrantworkers working abroad. Its major citieshouse vast migrant populations both fromwithin Pakistan and outside. Roughly20 per cent of the population of Karachiconsists of individuals who have comefrom other provinces or are migrants fromAfghanistan, Bangladesh, Myanmar,Philippines and the Central Asian states.The total number of Sri Lankans abroad isestimated to be around 788,000, of whom90 per cent are in West Asia, includingSaudi Arabia, Kuwait and the United ArabEmirates. In 1999 alone, almost 180,000people are recorded as having leftSri Lanka for employment abroad, out ofwhich 64.5 per cent were females. Besidesofficial data on number of departuresand arrivals at ports of entry, there issubstantial movement by peopleunofficially, by refugees, immigrants andtemporary residents.
A factor that significantly influences thedecisions of potential migrants is thenarrative of returning migrants, who, intheir desire to create a favourableimpression, highlight monetary gains andunderplay or gloss over experiences of
exploitation and abuse. The decisionto migrate, therefore, is often based onlittle more than an ill-defined impressionthat life will offer more elsewhere,with very little information about theground realities.
Migrants contribute to the developmentof local economies in both the source anddestination countries. Earnings fromwork abroad are a vital source of incomefor migrants’ families back home. In manycases, the remittances from foreignmigrant workers are one of the mainsources of foreign exchange for countriesin the region. In Sri Lanka, for example,such remittances form the bulk of foreignexchange earnings.26 In Pakistan,remittances in 1993 were estimated to be44 per cent of the total earnings fromexports. In Bangladesh, foreign employ-ment is the second highest source offoreign exchange earnings after garmentexports. Migrant workers are a source ofcheap labour in destination countries,since many of them work for lower wagesthan the resident workers.
It is, however, paradoxical that in spite ofthis, a majority of these migrants are poor,do not have access to health services andare exploited and neglected. They residein squatter settlements and urban slumsand are employed in the informal sector.Being ‘foreign workers’, they are often notcovered by the same legal protections astheir local counterparts, and are generallyunaware of their rights as workers. A largenumber among them have to cope withinsecurities in their jobs, unsteadyincomes, cultural alienation, lack ofaccess to social support systems andsocial capital and loneliness. It is thesevery challenges that make migrants morevulnerable to HIV infection.
However, attempts to establish intuitivelinks between mobility and HIV/AIDS
�������������
0!��������1����
��� ������
���������������������
2��%��������
������%��������
�������%���"�!
������������
�� ����������
��������� ���
�������������

����������� �� ���������
��������������������������������
����������� ������������� �����������������84
have often resulted in stigmatisation ofmigrants as well as restrictions on them,including forced testing for HIV anddeportation of those found positive andlimitations on the rights of women tomove in some countries. The inhumaneand exploitative conditions that mostmigrants face in source areas, duringtransit and within host communities indestination countries need to be changedand a comprehensive response needs tobe developed to facilitate safe migration,thereby reducing HIV/AIDS relatedvulnerabilities.
It must be stressed that migrants areneither ‘carriers’ of the virus nor are theyresponsible for the spread of theepidemic. They are often unaware ofwhether they have been exposed to HIVand of the potential harm this poses totheir spouse and unborn children. Mostof those returning home because of illnessarising from various opportunisticinfections are not aware that HIV is thecause of their poor health. Many,especially those in West Asia, are deportedwithout explanation if found to be HIVpositive. In the rare cases where they mayhave knowledge about their HIV status,the climate of stigma and discriminationmakes them reluctant to disclose theirstatus within their communities and evenfamilies. Importantly, the femalespouses/partners of male migrants arefurther disadvantaged because existingasymmetrical power and genderequations make it difficult for them toprotect themselves against HIV infection.
������%����&� �����������������
The gender dimension of migration-related vulnerability presents a complexpicture. The number of women migratingis increasing within South Asia. Globally,the percentage share of female labour inthe total agricultural labour force isreported to have increased from 44 per
cent to 48 per cent within the last 50 years,in spite of the share of agricultural labourwithin the total labour force decliningby over 20 per cent within the sametime period.27 Such gender-specific trendsalso give rise to particular migratorypatterns, leading to what may be termedthe ‘feminisation of migration’ acrossthe region.
For many women, migration—inaddition to being a livelihood strategy—is also an escape route from limitationsimposed by traditional societies,oppressive laws and abuse or violence. Astudy in Bangladesh has shown thatfamilies tend to urge women to migratewhen they are perceived as being a burdento the family.28 There are also higherexpectations from women to send backremittances, compared to young men.
The circumstances of such migrationprocesses, coupled with the limitedpreparedness, may create conditions thatlead to women—especially young girls—being lured with false promises ofemployment and marriage and beingtrafficked into the sex trade, slavery andexploitation. Gender biases limit theaccess of women migrants to informationand services that could make theirmovement safer. These women also lacksupport mechanisms within their source-communities, thus confining theirknowledge to hearsay. All these factorsexacerbate women’s vulnerability to HIV.
Women migrants are often victims ofviolence and harassment. Reports of sexualassault by employers and others arecommon both within the region andoverseas, and legal redress is rarely availableor availed of. Further, pressure from thefamily to send more money may often leadwomen migrants to supplement theirearnings through sex work. In all of thesesituations, the ability of women to
�������������������
��������������
��������3������� �!
���������������
�������� �������!�
����� ����!����
� �������

����������� �� ���������
��������������������������������
����������� ������������� �����������������85
negotiate safer sex remains low, even if theyare aware that they might be exposed toHIV. Contrary to popular belief, thevulnerability to HIV remains high for thosemigrating with families as well. When menmigrate in search of work, women leftbehind are often exploited includingsexually. As sole caretakers of the childrenand family they are especially vulnerableas the expected incomes from malemigrants are often unstable or inadequate.
Apart from women who move, even thosewhose partners move, leaving thembehind, are vulnerable to HIV/AIDS to theextent that they are vulnerable toexploitation and denial of rights. Theirlower position in society and their limitedcontrol over their lives heighten theirvulnerability to sexual exploitation,particularly when debts have beenincurred for covering migration costsand remittances fail to come. Wherewomen move alone, leaving their spouseand children behind, the men are ofteninvolved in multi-partner sexualrelationships and girl children are knownto become exposed to situations of sexualexploitation, abuse, rape and incest.
The region has several examples of effectiveresponses aimed at reducing thevulnerability of migrant populations.Formal pre-departure trainings in SriLanka, initiatives for interactionsbetween returnee migrants and out-goingmigrants in Bangladesh, multi-sectoralresponses to address the broad spectrumof needs of migrants in selected sourceareas in Nepal and India are someexamples. However, there is need forconcerted and more comprehensiveresponses. All efforts to reduce the HIVvulnerabilities associated with mobilityneed to address the broader issues ofpoverty, livelihoods, education, access toinformation and services and the need fora rights-sensitive legal environment.
Effective responses would necessarilyreflect the voices of migrants and theirneeds and would involve returneemigrants, spouses, youth, key enforce-ment personnel, recruiting agencies andPLWHA, addressing vulnerabilities atsource, during transit and in destinationcountries. Most importantly, all efforts toreduce the vulnerability of migrantpopulations must be careful not tostigmatise the migrants or their familiesand communities.
��(�( ,�����������������������For a large number of people in the region,migration has become a key survivalstrategy. However, the lack of safe, secureand legal channels for migration driveunsuspecting and uninformed womenand girls into the hands of unscrupulousagents and traffickers who promise them‘good jobs’ and ‘safe travel’ into sites ofwork. These are usually young men,themselves from poor families, who arelured into the trafficking networks in orderto support their own families.
Because trafficking is an illegal andconcealed activity, it is difficult to beprecise about the exact numbers ofwomen and children involved. Estimatesare based on the reports of lawenforcement agencies, researchers andgroups working with survivors andcommunities, and indicate that hundredsof thousands of women and children havebeen or are vulnerable to being traffickedfrom South Asia. Sources estimate that10,000-20,000 women and children aretrafficked from Bangladesh every year.29
NGOs have estimated that 5,000-7,000girls from Nepal are annually traffickedinto Indian brothels.30
The factors contributing to an increase inthe trafficking of women are as follows:� increased demand and supply of
trafficked persons;
4�������
���������������
!���"%�����
��!�����������
!�����/ �����
������������/�����

����������� �� ���������
��������������������������������
����������� ������������� �����������������86
� professionalisation of the traffickersand syndicates;
� modern transport, technology and theInternet;
� the growth of sex tourism;� the feminisation of poverty;� trading in human organs;� the changing nature of sex work; and� the erosion of social capital.
The all-pervasive neglect, discriminationand sexual abuse of women and girls in theregion are responsible for their increasedvulnerability to being trafficked, and toHIV/AIDS. Research shows that womenand girls often end up bearing the tripleburden of exploitation – they are poor, theyform a marginalised group and they arewomen.31 HIV prevalence rates has beenestimated to be as high as 60 per cent inthe brothels of Mumbai, India, wherecondom usage is very low.32 It is extremelydifficult for sex workers who are HIVpositive to get medical treatment, andonce found to be HIV positive, or too sickto receive customers, they are thrown outof the brothels. This often forces them intoinformal and unsafe sex work for survival.
Significantly, the region is witnessing adangerous trend of younger girls beingtrafficked increasingly to satisfy consumerdemand. According to the CoalitionAgainst Trafficking in Women (CATW),the average age of girls trafficked fromNepal into India has fallen over the pastdecade from 14–16 years to 10–14 years.One common myth fuelling the demandfor young girls in South Asia and West Asiais that sex with a virgin girl can cure STIsand HIV/AIDS. This means that theyoungest girls, biologically the mostvulnerable to HIV infection, are especiallysought out for unprotected sex by the menmost likely to infect them.
Women in Afghanistan have endured aparticularly difficult environment, having
been, until recently, denied even the mostbasic rights, including employment andeducation. The female literacy rate is oneof the world’s lowest—15 per cent in1995.33 Decades of political and civil unrestand conflict had heightened theirvulnerability to violence. Emerginginformation, reported, for example, byAmnesty International, indicates thatAfghan women and girls had been treatedas the spoils of war, and were beingsystematically kidnapped and rapedby fighters.
Orphans, women with disabilities, andwidows, who are often very young, havebeen noted as being particularlyvulnerable. Poor widowed women withlittle or no financial support or means ofearning a livelihood are forced to resort tobeggary to feed their children, thus gettingexposed to abuse, including sexual abuse.In an atmosphere of silence and taboosabout sex, this only heightens thevulnerability of women and girls toHIV/AIDS. Furthermore, there arereports of rising levels of drug use amongdisplaced Afghan men, unsafe sexualrelationships, and the migration of malerefugees to metropolitan centres, such asKarachi in Pakistan to find work. Many ofthese men are uninformed about safe sexpractices and are themselves vulnerableto HIV/AIDS. On their return, theyincrease the vulnerability of their wives/female partners to HIV/AIDS.
Trafficking and HIV/AIDS are presentingserious threats to the health, dignity andlives of young women and girls across theregion. The nexus of poverty, HIV and themarketing of youth within and acrossborders is creating ever-widening circlesof desperate insecurity and dispropor-tionately threatens the lives of young girls,making poor people poorer throughsickness, loss of livelihoods and rejectionby society. The epidemic is severely
�������/�������
��!!������!����/
��"���������
���� ������������
������� ��������%
�������!�����
������� ������%��
�����"����������
��������%��������
���������!����
��������

����������� �� ���������
��������������������������������
����������� ������������� �����������������87
undermining human security and humanrights, destroying the lives of individualsand families and posing a serious threatto the social capital and the overalldevelopment of the region.
Trafficked persons in South Asia are oftendiscriminated against even by their owncommunities, once they return or arerepatriated from destination countries.The process of re-integration for traffickedsurvivors is an uphill task, since theircommunities ostracise them. This is evenmore pronounced in the case of traffickedsurvivors who are HIV-positive. Studies inNepal have documented that HIV positivesurvivors of trafficking are oftenstigmatised and find it impossible tore-integrate themselves into theircommunities.34
Urgent and integrated action at thenational and regional levels is required toaddress the multiple and complex waysin which the security and rights of younggirls are threatened. The integralconnection between HIV/AIDS, genderand trafficking through the nexus ofvulnerability and sexual violence, can besummed up as follows:� the factors, which determine the
context of trafficking, are also the
factors, which are associated with theincreased vulnerability of women andgirls to HIV/AIDS. Specifically, theserelate to gender-related social andeconomic disempowerment, lack ofsocial capital formation and unequalaccess to all the indicators ofdevelopment, including health,information and education. Suchcircumstances severely underminethe basic rights to social protectionand the right to the highest attainablestandard of living;35
� trafficking is part of a pattern ofmigration within and acrosscountries, which removes personsfrom the protection of theircommunities and severs them fromtheir systems of social support. Thesevery factors are recognised as causesfuelling the continued spread of theHIV epidemic, and which, in turn,violate a person’s right to a standard ofliving adequate for the health andwellbeing of oneself and one’s family;
� those caught in the web of traffickingface an increased vulnerability toHIV/AIDS on account of their inabilityto control their working and livingconditions, including sexual relations,as well as their inability to come out ofit. Such situations grossly violate a
������#�������%� ��#��������������� ���#�������%
�����������78��A?�=������������"�)����6#��"��
����!���������������%��� ����%%���� �����#���������
�� �� ��������� ��������%� ����!���%�����������
?��������-���#)�%������>��� ��������%�B�����/���*0&
�&�&���� ����!�<��"����%�-������������ ����"����%
��� �� ���� ��������� ��� � ���� ��� ��������,��%%�#
/-���������0��#���%�*+7:�/�,-�0!������������ �")���
�� ����-������� �!�����"�������%%�#'�����������"����&
��� ����� ��� � �������� ����� �����!� ������������
�������������������#����� ���� ���������������������%
���%%�#'��&�,��?�������������������%���B����!��
��������)�"� )!����"�������%������#��#�����������������
%��#��������������� �����������&��������������������!
�� ������ � ���!� ��� ������ ������� %������� � ��
��������������,��%%�#'�����#�����������������������)
������%��#����&�,��-����#������,��%%�#'������-������!
����#����)� ������� �#�� ���!��%����A?�����������
�������,�������������6������ �����������$��#�� ���
����%��#������������%%��������� ������������"���&
India addresses the problem of trafficking of womenBox 4.6
�����������������")����1"���<�&��&����� ����!�<&-��� �<��"����%� ��� �� �������������!�,�� ����������!�78��A?
=������� �����"�)!� ?� �D��'!� *��6#��"��� ����

����������� �� ���������
��������������������������������
����������� ������������� �����������������88
person’s right to freedom from slaveryor servitude and the right to physicalintegrity (security of person); and
� common societal responses to thoseaffected by HIV/AIDS as well astrafficking are strongly influenced bystigmatisation, discrimination andfurther marginalisation. Theseresponses, in turn, undermine thebasic rights and freedoms of theseaffected individuals, includingthe right to mobility and residence,the right to essential services, rightto confidentiality, right to freeassociation, and sexual andreproductive rights.
��� ,���"������������������
It is important to briefly explain the legalframeworks within which most PLWHAin South Asia live. As mentioned inChapter 3, some of the fundamentalhuman rights are covered under several ofSouth Asia’s national constitutions,although the scope of these rights variesfrom country to country, as does theirapplication in the context of PLWHA.Nations who are signatories tointernational documents/agreements/conventions (such as the Universal
Declaration of Human Rights) are boundby the standards laid down therein,depending on the binding nature of thedocument and the manner in which eachcountry codifies it within its national laws.
Very few nations in the world—and nonein South Asia—have specific statutorylaws governing HIV/AIDS or ensuringprotections to PLWHA. Fundamentalrights guaranteed by national constitu-tions are, therefore, the prime source oflaw in South Asia. However, there are alsocustomary and personal laws, particularlyin South Asia, that determine the rights ofindividuals, especially women.
Apart from constitutional guarantees,policies and guidelines on HIV/AIDSdrawn up by national governments oftenbecome the prime basis on which therights of PLWHA are defined. However, inIndia, governmental policies/guidelinescannot be enforced by the courts, thoughmany rights of PLWHA are defined throughcourt judgments as India is governed bythe system of English common law.36
Recently, widely published cases of lawenforcement interventions involvingharassment of vulnerable group outreachworkers created an uproar within civil
����4�A� ����� ��1����������,��%%�#�/-���������0��#�!
*+7:�/�,-�0!������$���� �������%��������#���� ��� ���
��������#�����)!�������"������'�������� �����#����
�����"��#����#������&��-�������)!�����������9������� ��
"�%�������-��������������� ���������� ��,-�&�,��9���
����� ���%���������"�����������%���$� ��'���&��� ����!
��������#�������������������%������ ����)���������%���$
��'���� %����,����� ����&� ���� �����!���#�����;
�������������������������������������������#����#����
������������ ��������������������������� ����)�����
#�#'�������� �������������$���� �&�,������#������)
�����������������#)��%��� ��1��?��6!� �#���#������
��������)��� ���%���� �������&
5���������,��*++7�?��������-���#)���������������
�,�������� �����������������������3"��� �������#
�� ��� ���������A�����������#����������%�����������
�����"��#���'�%�������#)���'����� ��#������������������
����������������������������� ��,��&��� ����!���
����#)���'��������� ����)�%������������� ���"��#���#���
����#����������������!������)�����#����#���� ���
���� �%��#��������#����������%)��������#�������=������
�����������#����"��������������������� �����������
/-CB��0��� ������ ��#���� ������&����������������!
��� ����#)����������� ���� ����%�#����������� "�
����)������� �#��%� ��������)������"����������� ���
����������&
Mandatory testingBox 4.7

����������� �� ���������
��������������������������������
����������� ������������� �����������������89
,�"����&�
������������������������������������������������������
-����������������
-������$��������������� �!"�.-$/� 0
� ,�� ���� ��� ��%�H���������� ��
����#���!� �����)����!� #��%�3
��������)� �� � �����#)!� �����#����
%���� ������#�!� %���� ������ ��
����#�������
� ,�� ���� ��� �2�����)� �� � ���3
��#����������H��� ����#���!
�����)����!��������#�!����������
��������!������#��!�����������
%����)
� ,�� ���� ��� ��%��������H��
���������!���%�����$��������!����
�� �#��������� �
� ,�� ���� ��� �����#)� ��
#��%� ��������)H��� ����#���!
�����)����!�������.� �#�����)�����
� ,�� ���� ��� "� ��)� �������)� ��
�������)H#������� ��� ���������
�� �������
� ,�������������H�##���������
"���� ������"��� �� �#������ ��
�%%�� �"��� ���#��
� ,�� ���� ��� ����� �#����� #��#��
�� � �#��������'��H#�����������
����������� ������#)!� �#�����
�"���� %�������)� /��� ��� #����$�� �%
�������������� ���� ���3��������
����� ���� ��".�#�� � ��� �����
#������0
��0��������������
� ,�����������%�H#����������������
��"�����)���������� �����������")
�� � ��%��#������ �� � �����!
����������������"���������
� ,�� ���� ��� ����H��%��������!
���������!� ���3 ��#����������� ��
����#���!� �##���� ��� ���
�� �#���������������/#�������� ���!
�)�������� �������������0
������������
1�������������������������������������������"���� ���
,��������������#�%�#�����������������������������������#������
��%��������������������%�-CB��&��� ����!����)�#������������
����� ��#������� %�� �������� ����� ��#�� ��� ��� ���� ����2�����)
�� ����3 ��#����������!����������%���� ���"���)���� ������������#)!�8
�#��������������� ������#����$���%���������&�,�������� ��
��#'��%������#����� ����������!����)�������������������������� ���
-CB������� ������� � ��� %�� �������� ����� ����� �� � %��� ��!
��#�� �������������#��%� ��������)����������%����������������#)&
���?������������� ���#���� ��� ��������"����$#������������ � �")
�� &�;��-�"��#���������������������������#��������������"����� ����
��� ��#���������"�� �������������������"������%�������������� ���
����� �� ���������� %��� ������������#� ��%�#�����&� �������� ��#
���������!� ��#������������%�-CB����������#������������������
�����#�������$������#�&�9���#��%�#��%� ��������)��"��������������
��������������%�#���� ������ ������#����$���%�����#�����������&
���"����)�����##���������#��� ������%�����%��������� � ��#����������
���������%�#����#��#����%���-CB�������������� &�,���������������
�$��������������������%�����������������������.�"��"�#�������)
����� ����� ��������� ���<�� ����!� � ���������������������� ��)��
������������� �"����� ��#������������������-CB��� �������
��������)����������������)������������#����������#���� ����������3
� �� � #��������&�+� -CB��� ���� ����� �)�������#���)� ����
�������#�!�����������#���#����������������$#�� �����"����)�%������3
������ � �$������&
1�������������������������������������������"���� ���
�������� ������#������������ �#����"���������� ��������)�"���
�����!� ���'�������'� ���������#����������%���������&��������� ��
��� ����� �#����� �%� �����!� � ����!� ��.�#���� ��� ���� ��� ��
#�����&�,����������#���%���.�#���� ��������������#���� ���"�)
������� �"�� ����#��������!�%�������)� �� ���������������� � ��
�%�����������������+������#���� �����������#��� ���9���� ��&
<�����%���������������#����������������������������������������
�����������#���,��%%�#����?��#���#�������� �-�)#������#���"����#��!
*+;;��� ������������������������?��#���#�����!�*+:*&�,������
����� �� ����������������� ���?��#���#������ �� � -�)#������#
��"����#��

����������� �� ���������
��������������������������������
����������� ������������� �����������������90
���� ����*++;&�,��#����������������������� ��� ������#����������
������!����#������������%�����������)��� �#����"��@���� �#����!
���#�����!�"�)��!�������!���� ��!�'�������� ����%%�#'����%� ���&
,��������)� %��������������%� �� �������� ���� ����#������)� %���
�������� ������ �%� ������������� ��� ���� ������#�� ��� �������
#�������!���#�� �������C��'���� ��� ��&�C� ��%������������������
���"�����������%� ������������������)�"����� ���� ����������%
������������������ ��� �%��������*� %��� ����#��� ��� ���� ��
������������%� ���&�,�������������������� ��������#'��%����������
%�#�����������?����!�����������"����%� �������������"�������� �
����� ��������������� �������5#�� ����'�)1������� ��%����������
���%���� � &����.�#���� �������������"����������� �����������
������%���#���)������ ������ ��)���������� ����������������� ���
���� ����� �� ���#�� %��� ��� ��������������� �%� ���� �� �#����
���������&�?�� ����$#������������������"��������� �#�
�� �����%�� � �")����������������!���#���������%�����������%
<������������ ��!�������� �?����&��� ����!������)!���#������������
��)������������"��������%��%%��#����� ������ ����� ���%���
#�����)&����������%����#��������������������!��%%�� �����%� ��
�� ����'����������)���"���������������%�������������������&
1�������������������������������������������"���� ���
>���� ���� ��� � �������� �%���������� ����� ��$� ��'���� ��
���������)������#����������%���������!�#�� ����������������� &
C�������#�������%���$� ��'���� ��������)�#���������������������
�����������%�� �%��������%������������ �����������"�� ������$
��'���� �� � �� ���%��#�������%%�#����&�B���� ��$� ��'� ������� �
#�������� �����%� ������)��%����#��������!�"�������� �������3"���
��$� ��'����������&�������������$#������!� �����$�#������/")�%����
�2�� ����������0���������$�����������)�%�����$� ��'������ ���#
�$�#�����������#�����&��
� ��#����������������%� ���������
��%���� �%� ������ � �� �� ��� � ��
�$��������A�
� ,�� ���� ��� �2�����)� �� � ���3
��#����������H��������#�����#�� ��
����#���
"�)��������
� ,�����������%�H#����������������
��"�����)���������� �����������")
�� � ��%��#������ ���#���� ��
�����!� ���� ��� %���� ������ ��
����#�������!�������������"��
� ���� ����%�����#��� ��$��������H
��� ��"���� � �#�������� ��
��%������������������
� ,�� ���� ��� ����H��%��������!
���������!� ���3 ��#����������� ��
����#���!� �##���� ��� ���
�� �#����� ���������� /#�� ��
�����"�����!� ��%��� ��$!� � �#�����
���������0
� ��#��������������� �%� �����$���
�����#������ �� � ��%���� ��� ������
�� ����� �����$���������� �����
��$� ������
� ,�� ���� ��� �2�����)� �� � ���3
��#�������������������#�����#�� ��
����#���!� �����#����� %���
�"�#����)��� �

����������� �� ���������
��������������������������������
����������� ������������� �����������������91
society in India.45 Implementation ofinterventions gets delayed in such a non-enabling environment and lives are lost.The published cases reveal that nationalguidelines clash with legislation and lawenforcers’ instructions. For instance,criminal laws affecting vulnerablepopulations have impeded sexual healthinterventions among them. Harmreduction methods like condomdistribution and needle exchangeprogrammes could be, and have been,seen as abetting crimes (homosexual sex,sex work, drug use). As a result, theireffective implementation has beenimpossible in many countries.
Clearly, clarification, understanding andsensitisation of the particularities of theHIV/AIDS response is needed within lawenforcement agencies at first, but also inthe judicial administration and thelegislature. There has been someinteresting development in this regard inIndia. (see Box 4.8)
������2�����������Apart from the United States and Australia,the highest number of HIV/AIDS-related litigation has perhaps taken placein India. In 1997, the Lawyers’ Collectivechallenged the termination of the servicesof a worker on the ground of being
HIV-positive though the person wasotherwise functionally healthy. In alandmark judgement of the Mumbai HighCourt, the worker was reinstated and paidback wages. More importantly, theCollective was able to obtain an order ofsuppression of identity because of whichthe HIV-positive person could sue undera pseudonym.
A study of 130 cases handled by theLawyers’ Collective between 1998 and2001 found that the most important legalissue for men related to employment. Inthe case of women, the major problemrelated to maintenance, custody ofchildren and property rights (such asmatrimonial or joint property rights).48
An increase in the number of divorcecases was also noted. It has beensuggested that women remain vulnerablewithin the institution of marriage due tothe unjust gender construction ofsexuality in various Indian laws.49
Many of the South Asian countries haveundertaken several measures to reform thelegal climate surrounding HIV/AIDS.Some of them are:� organising and training a nation-wide
network of lawyers to handleindividual complaints;
� providing free legal services;
,����������������#����������� ���������������� ��
����� ����#������:��� ����#�����������$�"�������#������
����������)� ��� ��� ��� � %��� -CB��� �����������
#��%� ��������)&�������)�#����!���)���������� ��� ���
�%�5�������������%�� �����)1�������������"������#��#����
�������������'����#������������������)����� �����
%�����%�"����� ����%�� ��� ���������� &����#������%
�������������%�� �����)!������������������������%��� ���
���%����������%����-CB��&���%����������� ��)�
�� ������������� !����������� ������%������������
'�������������� �#������������$#�������#���� )��%���
��������� �%� ��� #����� ���� ��� #����� %����� ���
��"������� �")�������� ��)�&����)����������� �����
���%�����.� ������%����#������������� ��� �����
���� ��)�&
���?����"�������!����������������������� �����#��
���"������A����������������� ������������������
���'��� ����� ����������� ��� ��%����� �%� �������� #��)
������������������������3���������������&�?���#��� ���
���������� ��������������������� ���������������
����%������������!����)����"������� �� �)&�8
Indian courts exhibit sensitivity towards PLWHABox 4.8

����������� �� ���������
��������������������������������
����������� ������������� �����������������92
� organising workshops to formulatepolicies for the protection of the rightsof PLWHA and their families; and
� campaigning for the decriminalisationof homosexuality and sex work and forthe formulation of laws covering issuessuch as HIV testing, confidentiality ofHIV test results and discriminationagainst people with HIV.50
Sex workers have used legal redress andaccess to the justice system to addressrights violation, as happened inBangladesh (see Box 4.9).
����� $������������������The need for legislative reforms has beenunderlined at regional workshops on HIVlaw, ethics and human rights organised inthe early and mid-1990s by the UNDPRegional Project on StrengtheningResponses to the HIV Epidemic in Asiaand the Pacific.51 The issue still remains
to be adequately addressed by mostcountries.
In most countries of the region, doctors whowish to prescribe ARVs to survivors of rapefind themselves torn between governmentpolicy and medical ethics. These drugs areused as ‘Post Exposure Prophylaxis’ (PEP)for occupational exposure52 and to reducemother-to-child transmission of HIV. Ithas been contended that they should alsoprove effective for rape survivors.53
However, many countries limit the use ofPEP to occupational exposure and not torape. This violates the rights of personssurviving sexual violence, compromisestheir treatment and care and infringesupon doctors’ ethical duties. Moreover,even in countries that have policies forPEP provisions in occupationalexposure, there is limited knowledgeabout such provisions, reducing theiroperational efficacy.
,��"�I���������� 3���������������9���� ��������������
�� ���%�?���)����.!��7�'��������%����#�������#��)
�%���'�&�?����)��������#�����%��������"�����3"���
��$� ��'�������9���� ���������������������� ������
���� �������� ����*!:��� ��$� ��'���� �� � ����
#�� ���&� ��� ������ � ���� �����������%����"������
���������������)������#�����#�����#��������� �������
"������/����!���#&0�"���������$��� � �%���������%���
��$� ��'���&� ��� G��)� *+++!� ��#��� �%%�#����� ���#��
�����������$� ��'����%�������"����������,��"�I��&
��"������������ ��������� ���%�<����� ���������
���� ������� �7���%������#�� ������������� �������
#���� � � �&
,����$� ��'���������#�������������� ����'������
���������%���'������������!�#���)��������#�� ������
���#�� �� ��� ���E���"������������������"�#'����
����F&�,����$� ��'������� �������)�� �"����%��#�
������������������������ ������'�&��EB������ ����
������������� �%���� %������ ��� ��� ��)� ���� %���
����������!F���� �<����I�9���!�-���� �����%������$
B��'���1�?�� ��'��%�9���� ��&��������� �������
��$� ��'���� �������#�� ������������)� ���
��������������)��� ���� ���$���������"�������������)&
6����%���$� ��'������� �������)� ����%��#� ������)
�����#���������)�����������#���� ���#������&�E,�)
��� �����������)�%�������������������"�����"��� ��
�����%������$&�?� ���)�������)��������� �������
�� ���'��������������#������!F���� �����!�����$� ��'��&
������������#�������������"���������������������� ���
"��*7�����*�����������!��� �����)��������������#�
���������"����7������#���&��>$�����!�����%���!�%����
��������#���������%������ ��'���� ��� � ����������
%�����##������������"�����#������ ������������#��
�� � ��� �������'�������������"���������&
�������� ���'�.� ���������<��#�����!��%������#���
���%��� �")������*�����$� ��'������ ����������
������������!����9���� ���������������� ����
������#������%���$� ��'���� ������� %����� ���)
� �������������'�������������������� �&
Sex workers in Bangladesh: human rights violations and legal redressBox 4.9
������� 9��� ���� �������� %������ � ��� �������� ���!� 9���� ��!� G��)3������*+++��� �99��?� �!�<��#3G��)�����

����������� �� ���������
��������������������������������
����������� ������������� �����������������93
Reforms concerning gender equality andthe empowerment of women do notalways receive the much-needed supportin male-dominated legislative assemblies.Entrenched conservative attitudes inmost countries in the region renders theliberalisation of laws relating tohomosexuality difficult. Laws concerningsex work, the availability of condoms inprisons and needle exchange pro-grammes are also treated as being far toocontroversial by legislators, who prefer tosupport only what are perceived as ‘safe’and conservative measures.
One issue that has dominated the lawreform scene in India and Sri Lanka isthe proposed repeal of the provision inthe respective penal codes making it anoffence to engage in “carnal intercourseagainst the order of nature with any man,woman or animal”. This section appliesto homosexual as well as heterosexualoral and anal sex, with consent not seena valid excuse.54 In 1995, Sri Lankaamended certain sections of the PenalCode and the repeal of the provisiondealing with homosexual acts wasrecommended.55 In passing theamendment, however, the legislature notonly decided to retain the section makinghomosexuality an offence but widenedits scope to cover sexual relationsbetween females by replacing the word“males” with “persons”. Such incidenceshave led to greater harassment of sexualminorities.
��3 ���������,��������#4�������"�����
A crucial aspect of the human rights ofPLWHA is their access to treatment.Denial or lack of such access amounts toa violation of the basic human right to life.
The last decade has witnessed a numberof significant advances in the under-
standing of the HIV infection and how itcan lead to AIDS. These advances haveled to the development of a range ofpotent drugs to control HIV infection (seeBox 4.10). Both these developments havesubstantially altered the way in whichHIV/AIDS is regarded and treated. Thefatal course of HIV infection can now bealtered to a chronic manageable conditionthat allows a person living with HIV tolead a relatively normal life.
The drugs that control HIV infection,known as Anti-retroviral drugs (ARVs),are a recent phenomenon and haveradically changed the HIV care landscapewithin a short span of a few years. Acombination of three or more differentARVs in various regimens, that as a groupare known as Highly Active Anti-Retroviral Therapy (HAART), form thestaple of HIV treatment today indeveloped countries.56
HIV is one of the most rapidly mutatingviruses and its immense capacity forgenetic variation enables it to sometimesproduce forms that are unresponsive tothe drugs that interfere with viralreplication. Treating HIV infection with asingle ARV drug-monotherapy – quicklyleads to drug resistance. The chances ofdrug resistance are also present in the caseof dual therapy. The rule, therefore, is toprovide for triple therapy or HAART,where the chances of drug resistance aregreatly reduced. In the United States, thewidespread use of HAART since 1996 hasled to a 50 per cent decline in AIDSincidence, hospital admissions andrelated deaths.
��3�� � �,*�������%����&���������Developing countries are home to 95 percent of PLWHA57 and WHO estimates that6 million people in these countries arein immediate need of HAART. However,
�������������
���������
��!�����%�"�����
���6��������
�����%�����������
����������
���� �������
��������������
���� ����� �
�������������� �
!��!��������

����������� �� ���������
��������������������������������
����������� ������������� �����������������94
62 per cent or 500,000 of the 800,000people estimated to be receiving HAARTin 2001 live in developed countries. Only230,000 people from developingcountries were on HAART in 2002, withBrazil accounting for half this number.HAART reaches only 5 per cent of thosewho need it in the developing world (SeeTable 4.3). In December 2002, around43,000 people in Asia were receivingHAART, barely 4 per cent of theestimated 1,000,000 who neededtherapy. “These drugs have savedhundreds of thousands of lives in Europeand the United States. They could do thesame for millions more in developing
countries. If we can get cold Coca Colaand beer to every remote corner ofAfrica, it should not be impossible to dothe same with drugs.”58
,��� �����%����&����� �,� ��
�������'������� ��������
There are two perspectives on the issueof access to treatment–theinstrumentalist perspective of thehuman capital approach and the humanrights perspective of the humandevelopment approach. The humancapital approach, with its focus on ratesof return and affordability by individuals,is against public provisioning of HAART.
,����<�)�����!������� �"���������:��-���������#����#��
��������%�������������#�� � ����������##����&�,���
�������� ������� ���� ����� � ��� ����� ��� ��%��)� ��
���������#��)��%����#�� � ������##����&
,��?��������������������%�������/?��0!�������������������
��##���������������/����0��� ����������%��#�������
��##���������������/�����0�����������%���� ��� 1����.��
������#�����%����������##���&�?��6!��� ��!��� ���
����#����%�<� �#���������#��� �������������������
��##��������������������������� � ��'���� ���������
�� ���������##������������������"�����������%����3*&
������##����������������2���#���� ���������%������ �#�
�� �#����#��� ������������� �#���%����������������� �
%�������������)� ����������&�,��������������������
���� ���� � ��#�� �� ��� �#�� #���#����������� ��
����%�#�����!�����#������������� ���%�%������������
�� ��##�����������%%�#�������%��)!����������#��)���
�%%�#�#)� ���� �����#����#��� ����������&
�������� �����������"��#��������� !�������##���
������#�������"������2��������"���%����#��������������&
,�� �#�����%�#� #�������� ���� ������!� �� � ��
���������������������������)!��$���������� �������&
���� �����!�����������.����)��%�������� ����� �������
��##������������������#�3����� ���������#��������&�,��
#��#�����"���������#'��%�����)������'������ ��������
#��������� ��#���������������#�������������%�� ����
��##����������#�%����������������������#������� �#��
�����#�����)������"���%����� ��3��#����#��������&
��������'��)������������������3�#������������%��������
���� ��##����� ���� "�� ��#�����)� "�%���� �� ��)
�%%�#�������� �#������ ����%�� &�,����������� �����������
������ ���%����������������� ���� ��� �������������
)����&������#�����������%�������##��������������������
#��#������"���������#�����������#�������� �������#
���#�&
9�#�����������##����������)���� ���#� ���#����)
��)�"���$�������!�#������ � ���#���������##����!���
�������)������� �����#����������#�������������#��������
�������.����������%�#��#���&������ �����!������� �2����
����#������%������#������������)� ���������#��������
������� ������ �%%�#������� �����"��������##���&��9��� ��!
��##������������������ �����������"��� ���� �������#
������'�������������� ����������##���������������)&
�������� ������������� ���������� ��� ��������
#���������%�#���������#���#�� ���!�"��������������$����)
�#������ ����#������� �� ��������� ������������� �����)
��� �����##����%������&�-�����%����#��������������
� ��������������#���#��������������%����)�#��������
����#'�� �� ������)�����������������$����)��#����&
,�����"�����%����#�����)���"������� �����#�
������������ ����������������"���$����� &
������J�/��� �#� �")���$=��0����������)���������
��##��������������#� ����������#����#���������� �����
��� ��������� �#����� ����������� �%%�#�#)� ��� ����
"����&�,����##���� ���������� �)�8;&������#���
�%%�#����������������%��%��#����������� �:;�����#���
�%%�#��������������&
Vaccine developmentBox 4.10

����������� �� ���������
��������������������������������
����������� ������������� �����������������95
This school argues that the efforts to stepup access to treatment may dilute thefocus on HIV prevention while the highcosts of HAART may divert scarce resourcesaway from HIV prevention efforts andother competing require-ments within thehealth sector. In other words, HIVprevention and health priorities such asgastro-enteritis, tuberculosis, malaria,malnutrition, and population control maymerit greater consideration than themedication requirements of a smaller,albeit vocal, special ‘interest group’ ofPLWHA and their advocates.
However, if public health action on HIV—especially the care and support regime—is perceived as being an example for otherhealth challenges, then it would no longerbe viable to see HIV/AIDS as a specialinterest of a few people. Instead, theapproaches and lessons of theHIV/AIDS strategy would help augmentthe capabilities of the existing publichealth system at all levels. Indeed, itwould be essential to strengthen theprimary health centres and local hospitalseven to meet the challenge of HIV at itspresent scale in South Asia, in addition toongoing work of the NGOs, voluntarycounselling and testing centres etc.In other words, the agenda for healthsector reforms in South Asia would be
greatly strengthened by mainstreamingHIV/AIDS. Therefore, there is nounavoidable trade-off between theprovision of HAART and other healthpriorities.
The second argument of the humancapital school is that HAART involvesrather complex regimens of expensivedrugs that have serious side effects.HAART, therefore, calls for additionalinvestments in training medicalpersonnel in the long term treatment,monitoring and care of PLWHA.
�������B�6��,��!� ����
,�"����&�
4���������������'������������������������������������������#�!����%����55�6
0���������������1
������ 7�%������������ 8������� 4�������
���� �, ��� .9:
��"3��������%��#� 7�!��� �!*��!��� *
���� ��!��� *!���!��� �
?�����%��#�!�B�������� �!��� 8!��� �+
>�������>�����!������������� 8!��� ;�!��� +
C����������#�!�����""��� *+:!��� �8�!��� 7�
���������� ���!��� 7!7��!��� 7
6��*����#��"��� ����!� ��� �������������� ,����������##���
����������/�,��0��%����������7����������� ���%���� ��������#���
���#���������%��$��� ����##����������� ���&�,����������
��#�� � �?=6�!� �������� �����������!�-CB������ �����
� ��#����!��������������#���!��#� ���#��� �������#�������������
�� ���������������������������&��,�����������������������%%�#����
�������%���%����������� ���#��#��� �����"���� ��� ��'����
��##���%������������!���������������"���������%������"��� ��
���#���������)�����!��� �������������#���� ��'���&�,������
������������������������ �#��� ������ ������#������� ������ �
��#3��� � � ��#��#�����������#�� ���������������� ���������
���������&���� ����"������� �")�����������#������������B�61�
��� 2�����������=�����&
International TreatmentAccess Coalition
Box 4.11
������� �,��
/���4�� &���#��������&���#������&���0

����������� �� ���������
��������������������������������
����������� ������������� �����������������96
Moreover, HAART has to be taken on afairly regular basis, life-long, implyingregular treatment expenditures for severalyears. In addition, a person living withHIV has to spend on regular medicalevaluation to monitor disease progressionas well as on treatment for themanagement of the side effects of HAART.
In all the countries of South Asia, the costof HAART is significantly higher than theaverage per capita income. Access totreatment is, thus, a luxury that most SouthAsian governments and the large majorityof their PLWHA cannot afford. The highcost often results in frequent interruptionof treatment, especially among the poorerpatients and this could lead to drugresistance. Presently, the private sector isthe only provider of anti-HIV treatmentsthat include ARV drugs and, in certaincases, even little understood indigenouspreparations. The haphazard provision ofARVs further underscores the urgency forgovernmental initiatives to standardiseHAART, train the health sector—bothpublic and private—and provide affordabletreatment.
With South Asia bearing more than one-third of the world’s TB burden,comprehensive national programmesbased on the free distribution of anti-TBdrugs have been in operation for severalyears. In recent times, TB controlprogrammes have also absorbed theadded cost of Directly ObservedTreatment (DOT). The TB programmesin Bangladesh, Indonesia, Nepal andMyanmar have made considerable stridesin achieving high rates of cure throughDOT, thus providing the rationale forconsidering a similar approach in the caseof HAART. Though there are few studies todemonstrate the feasibility of DOT forHAART, the approach can work amongsome groups such as sex workers orinjecting drug users.
The human capital school also focuses onthe difficulties in implementing initiativesthat promote the use of HAART in aresource limited setting. The majority ofthe population, its advocates argue, is notliterate, and good health is not animmediate pre-occupation of poorhouseholds. The problem is compoundedwhen the intervention calls for complexpatterns of healthcare, in terms of thetimings and dosage of drugs, the need forancillary services such as periodic medicalreview, counselling and the managementof side-effects. The discrimination againstPLWHA even by healthcare providers andthe healthcare system in general cangreatly complicate access to HAART.
This line of thinking can be countered,first, by the public obligation argument.PLWHA may be a small fraction of thetotal population in the region but, at4.2 million, their numbers are still largeand it would be a dereliction of dutynot to address the treatment, careand support of such a large number ofpeople. This argument could also bestrengthened if the morbidity and thefatality associated with HIV/AIDS is takeninto consideration. Approximately 1,000people are estimated to die every day inthe South and South East Asian region, anumber that could be compared to twofully loaded jumbo jets crashing everyday.At 400,000 deaths in a year, the death tollfrom HIV/AIDS is nearly 400 times thecombined annual death toll from railwayaccidents. Ignoring the requirements fortreatment would involve accepting adeath toll that would be unacceptable inother contexts. Clearly, then, the ‘silentemergency’ of HIV/AIDS in South Asiarequires urgent attention in ensuringaffordable and universal access totreatment, care and support.
It would also be erroneous to look atprevention, care and support as mutually
�����2�����!
���� �����%
�������!����
������ ���
���������%���
����������%���
��������������
����������
����� ����!
�����������

����������� �� ���������
��������������������������������
����������� ������������� �����������������97
exclusive responses to HIV/AIDS. Thereis enough evidence from variousinitiatives to show that the availability ofcare and support has enhanced thesuccess of prevention. The experience ofBrazil shows that a policy of providing freeor subsidised HAART to PLWHA hashelped de-stigmatise AIDS and facilitatedthe mainstreaming of HIV-related care(see Box 4.13). As a result, PLWHA had theopportunity to access counselling on notonly treatment but also on preventionand protection for themselves and theirfamilies. This inclusive approachembodies the principle of GIPA, byaccepting them as partners with
healthcare providers in mitigating theimpact of HIV and slowing its spread.
The humane approach of providinghealthcare and prevention services ensuresgreater credibility, acceptance, sustainabi-lity and involvement on the part of bothprovider and recipient of care. In the caseof SHIP in Sonagachi in the Indian city ofKolkata, sex workers were not approachedwith isolated messages on HIV prevention,but were simply offered free treatment forSTIs. Similarly, the Community HealthEducation Society (CHES) in the Indiancity of Chennai provided STI treatment tosex workers with no mention of HIV unless
A��������*!� ������#��� �����%���� �"��� ���������%��
��������������#���� ��������"��#��������������%���%�3
�$��� ��������)����������� ������&�����,�#���
����������"�����$*�!�������$*�!������)�����������)�����&�����"� ������'��������%%�� �"�������������!�A?����
�� �����'�����##������� ��##�������������������� 3
����&�,�������������"��������������������"�� ���
%���� �����#����#��� #��������H=��$�����(����!
9���������������!�9������3<)�����2��""!�<��#'���
��%%���3C����#�K�� ����A���� �?����������#���&
,�� ����������� ������� �������������"�� ��������
#����������� � ���������#�����)��������������
�����)������������ �#���������� �#� ����#��&�6%���
%����#��������!����)�=��$�����(�����������#� ���+�
����#������ �#���������������#��&����������2��������
�� ������#������� ������������##�������������������!
������%��������������#� ����%������� �� ���
�����#����#���#�����)!������!������� �������'��&
B����� ��'�!�������#����%�"��� � �����3���� ���
�������� ����$7������$;���%����� 3�� ��� ��3��#���#��������&
�����"����)����*!��������%%��� ���������)������ ���
%������������$*��� �)!��E�����������������#�F��%���%��#�!�#���� ��������������)�������������������������
��� ����,������ ����"�#����� ��������%�#���� �")
��������������#����������������#� �"�)�� ���������#&
����������1�����������#��������� ���<� �#��������
����������!�����"���#�����"����������������%� �#����!
�#�"����"�)�����������#������%���$�7�������������)���!� �#� ��������������%������������������#��
���#�&� ���� ��� �� �������'��!� � ����!� �����1�
#��"�������������)�������#� ����&�>�����%�����
�� �#�����������#�������������"����)����*!������1��������
���#�#'������%�C����� ���!������ ������ �?���������
#�������������������� �����&��!����/$+�&:�0�������! �#�����������������%��#������#�&
������������*!�����������#� �,�������!���#�#'����
�%������ ���!�C����� ������ �?��������������������
"�3��)��� �%����������&�,��������#������������������
����$���������&�,����������%�������� ���������������)� #�������� � ")� �%%������ #��������&
=��$�����(������� ���������������C����� ���!
9�������������������?������������ �9������3<)���
�2��""��������� ���&������������������� �?�������
����������!� �� %����������� �%� ?���������� ��
L� ��� ������ �C����� ����%���#�� ���&�,�����%
�����1�������#������ ����� � ����B�61��������%
��%�� �������<��#�����&
,��%�#�������������#� �������%�#�������������
�����#��� ���##���%���)��� ���"���������)�"���� � �
���#������%�����������"3��������%��#���� �����
��������%���������������##���%����� ������%� ������#��
�����������&�<�������!��������%�#���� �%%������������
���#�����%�����,�������#����������%���������!���
��������%�#���������#���#��)��������%�#���������
��� ������"��� ���)� ��� �� %� � #��������!� �%%���� ��
����������)�%�������������� ���� �#����������&�,�����)
�����"�����"�������������������� �� ��%����������!�#���
�� ����������#�������������&
Meeting the challenge of drug pricingBox 4.12

����������� �� ���������
��������������������������������
����������� ������������� �����������������98
the women brought it up themselves.Once sex workers found that they couldreceive care in a non-judgmental andnon-discriminatory manner, theydeveloped enough trust in the providersto share their intimate concerns aboutunsafe sexual practices and HIV.Condoms, made available at this point,were more likely to be accepted with adegree of understanding of why and howthey needed to be used. Providing HAARTto those in need, along similar lines, is likelyto enhance HIV prevention besidesproviding care. HAART may alsocontribute to lowering the efficacy of HIVtransmission by greatly reducing thenumbers of viral particles in the semen andvaginal fluids.
The argument that HAART is beyond thereach of people in South Asia also has itslimitations. It is true that the cost of thetherapy, multiplied by the total numberof PLWHA in the region, appear daunting,more so because these are recurringlifetime costs. However, a carefulexamination of global experiencesindicates that affordable treatment need
not be an unrealisable dream fordeveloping countries (see Box 4.12).
The WHO has also made efforts to dealwith the issue of access. In 2002, it issuedguidelines for scaling up ART in resource-limited settings, as part of a commitmentfor expanding the coverage of ART to 3million people by 2005. The guidelineswere developed through a consensualprocess of consultations with healthcareproviders from developed and developingcountries and propose a public healthapproach to the issue. Such an approachincorporates the following elements:� the scaling up of treatment
programmes to meet the needs ofPLWHA in resource limited settings;
� the standardisation and simplifica-tion of ARV regimens to support theefficient implementation of treatmentprogrammes; and
� ensuring that ARV treatmentprogrammes are based on the bestscientific evidence in order to avoidthe use of substandard treatmentprotocols which compromise thetreatment outcome of individual
����*++�!����B��� �9��'�� ����.�#�� ���������� ���
"��*&����������������������� ����������9��I���")�����&
9��I��1������������%������������##�������'������������
���������� ��� ���������&� ,�� ��������� �%
#��������)���#�����!��� ��� �#�������%��������
��������%�#���� ���#���)��� ������ � �������%������
�����"�� ��� ��������������������� ��%����������!���
�������� ���������������� �:��!������ ���%�#�����&
������������������������� �����%����*++���������!
7;!�8������� #����� �� � �!�8*� #����� �%� �����#��
��������������%����� ������������ ��� �����+�!+:�
����� %��������3������ � ���������� ���� ���� � &
>2����)������������������:�H;������#������ �#�������
������� ��������3%�� ��� �#����������������� ��������&
,��������������������� ���������%�$*�"����������#���������*++��&
,��9��I�������$������#��������2����������)�%��� ���
�����������##����"��������%������������%������#� ���
����%�#���� ����9��I��&�A����%������#� ���� �#�����
�� ��� ���� ���#�����")�8������#������ �")�:�����
#����%���� �3 ��3��� �����3 ��3������ ���������
�����#�����)!�"�� ����*++8��� �����&�����������
��#����������"����%���������!�����������������#�����%
�����)� �#����� �;�����#����%����*+++�����������
� ������$#�� �������������"� ����%�$�����������&�������������%���������������� �#������%������#�!���
#�����%������������������������#����� ������#���
)����!���'�����������"��������������������������##���
������������)&�,��9��I�������� ����%%�������������
��������%��� ���������#��������!�"�#���������� �����
��������������3����������)��������#����"������!�����
������� 3��#����#�����)&
Lessons from the Brazil experienceBox 4.13
��������������!� ����

����������� �� ���������
��������������������������������
����������� ������������� �����������������99
clients and create the potential for theemergence of drug resistant virus.
There are also examples of successfulgovernment action to ensure affordableor free treatment from developingcountries, notably Brazil (See Box 4.13).Though Brazil’s per capita income issignificantly higher than that of the SouthAsian countries, it is still instructive to seehow governments can make treatmentavailable to even those from the lowerincome groups by according the rightpriority to treatment. The provision ofHAART and care, consistent with theframeworks of human development andhuman rights, help establish the necessityof ensuring affordable and universalaccess to treatment, care and support forPLWHA in South Asia.
A study by British medical journal, Lancet,comparing the costs of HIV preventionversus treatment reported that for everylife-year purchased with treatment drugs,28 life-years could have been purchasedwith prevention. The study59 used Cipla’sARV costing of $350 a patient a year anddid not include drug distribution costs. Theimplication is that the scarce resourcesavailable to fight AIDS should go toprevention programmes rather thantreatment. Similar arguments that thepotential savings of investments inprevention far outweigh the monies savedeven with low cost ARV treatmentintervention in developing countries, raiseserious questions regarding the principlesthat are needed to guide policy makers inadopting public health strategies. Theglobal debate on whether to accord equalfunding priority to treatment andprevention continues, even as there isemerging consensus that a judicious mixof both are needed to achieve any measureof success in dealing with HIV/AIDS.Meanwhile, a number of field-based studiesfrom developing countries are demon-
strating the feasibility and benefits ofHAART. They show that treatment andprevention can both be achieved in asimple and low cost manner.
A study of a model employer-fundedprogramme for South Africa concludedthat a programme that focused only onthe prevention and treatment ofopportunistic infections would be cost-effective for all companies and all gradesof workers. If it was to prove profitable,HAART would have to be provided at$500 to $750 per patient per year. WithCipla making ARVs available in Africafor less than $370 a year, the potentialviability of such a model is greatlyenhanced.
The widespread introduction of HAARTin low-income countries is dependent onthe provision of generic ARV drugs thatare either free or heavily subsidised.Meanwhile, HAART, accompanied by lowcost options with regard to the routinelaboratory monitoring of CD4 cell countsand viral loads, is already beingattempted in some resource-limitedsettings. In the last two years, smallgroups of people living with HIV arereceiving HAART because of the modestefforts of the few small-scale initiativesthat exist in the Caribbean, India andAfrica. They serve as beacons of hope forthe millions in need of ART in thedeveloping world.
��3�� /�&������������������������ ����������"���� ���The access to ARV treatment is severelylimited in developing countries in generaland South Asia in particular because ofseveral reasons: lack of proper guidelineson the correct selection and use of drugs,lack of adequate and competent healthservices, lack of affordable drugs on asustainable basis, high price of patenteddrugs and low purchasing power.
��������� ���
�����������!
���7�������6
�����������������
�� ������������
�������!
���������7�������
��������������!���
��������
�����������

����������� �� ���������
��������������������������������
����������� ������������� �����������������100
There have been several attempts bypublic-private collaborations to offer ARTdrugs at decreased prices, the mostimportant of these being the AcceleratingAccess Initiative. Till March 2002, 78countries had expressed interest inparticipating in the Initiative. Each ofthese countries has committed itself to,and is in the process of, developingnational care and treatment plans. So far,18 countries (12 from Africa, five fromLatin America and the Caribbean
countries and one from Europe) haveactually reached an agreement with thedrug companies. While the initiative is auseful attempt to lower the price of drugs,it clearly needs to be supplemented byother measures as well.
��3�(�,������������������Patents are a major factor in restrictingaccess to ARV drugs. Pharmaceuticalcompanies in high-income countriesdevelop these drugs after years of research
>2����"������#��K��� �%%����������������� ����#��K��%���
������#��#�����%����#������ �#������ �%%���������'���
�##�� ���������#��������1��"����)������)�����������
")��������#����������&�9)����#������� ������� �%%�����
���#���%��� �%%������#��������!�#���������#������
�����������)���#�����#����� ���!����������������!
��'�������� ����������"������������)������������
�����"��&��������������%����'����%���������������%
�2����"��� ���#��� #��� "�� ���� ����� ��� �����
������������ �� �#��� /���0� ��� �� #��� ����� � ��
������������������!����#�������������� ��� �%�#���
�����"��#������������%����������� ����� ��� �����"����)
�����)&���%%������������#������#�����"���%������ ����'�&
�� ����!�������'��#���"��������� ������#���%��
����#)��������&
;878<�,"
���������������4�,���#���"�������� ������������
�%%�� �"����)&����#���%%�� �"����)�������� � !��� ������
I���3���!�#��#���!� �%%������������#������������##���
���%��������������������� ��� ����� ����"�������"��&
�������� �� �!�����)�� �������� �������� �#� ���
���#�����'������ ���������%%�� �"���%�������
�������&
����������������4��������!��������������#�� ����'���
�����#����#���#��������������%��� 3��#����#��������!
�#������������������'���&�9)�������2����"������#��!
#���������#�����#�������������������"������������&
,��%����#��������#���%����#���������'��!�����%���!
���� �"�����������������%������������� �%�����������
���'������������� �����������������%����#������� ��
���#��&
��"="
-����������'�����������4�,��������"���������'�������
�%����'���&�-����#����#���#����������������#�
��� ������ �%� �� 3���#� � ���� "���� �������)
���������� � "�#'� ��� ������� � #�����)����'���!
����")��� ��������#����������3���#� ����'���&
������)!��%����'������������������� !����#���#���%���
���"������'������������ ��������&
�� ����!� ���� ���'� #��� "�� #������� � ")� ��������
����������������#���%���)� ����� �����#�������
����������3�����������:���%������ ������� �������
���'���&�,���$������#��%��������� �%%���������)����#�
������ ���� �#������"������#��������� �����
��� "���� ������� ��� ��#�� �%� ����3�#���� ��3����)� �%
#��������� �#���"�#'���� ������� ����'���&
"������%����&���������4����#�� �%%������������#�����
��������)������ �#��3 ����������������!����������#��#����
����� ��������#���"���������������� 3��������������&
,�������������������������������#��� ����"������� ���
�����"��!����#����� ���� ������������)������� ��#������
�%����%����&���������%�#������ ������%�"������� ���
��"�����������������$���#����#����#���#��#����������
�������#������������)������/�-�0��� � ����!��� �����
#����#���������&
������%����������#������#��� �"��������� ��%
�%%������������#������������%�����"�������������� ���#����!
������������ �����&� ,�� �������!� ���3%��� ���%��� ��
������������#����� ������� ���� ��'�����������������
�������#������"��� ������������#����%�������������
#��������!������������������� ��������#����� ��� ����
�2����"������#������.�������!��� �����������)!�������)
�����������##������� ���&:*
The role of equitable pricing in ensuring accessBox 4.14

����������� �� ���������
��������������������������������
����������� ������������� �����������������101
and development at high costs.62 Patentson these drugs preserve monopoly rightson producing them for a minimumnumber of years and the selling priceincludes a premium that helps recoup theresearch costs. Generic versions of thesedrugs are much cheaper to produce.
The cost of these drugs in a particularcountry depends on several factors. Someof these are related to patents: whetherthe pharmaceutical companies haveapplied for patents in that country(which, in turn, depends on the size andvalue of the potential market); whetherthe country permits product patents onpharmaceuticals; and whether it has thetechnical capacity, market size and thelegal framework to produce genericversions of these drugs. Pricing policieswithin these countries also determine thecost. India, for example, has beenimposing price controls on bulk drugsthrough the Drug Price Control Order(DPCO), 1995. However, the number ofdrugs under this order have been steadilydecreasing after complaints by theindustry over loss in profitability.Combined with the change in the patentregime, this has adverse implications foraccess to affordable drugs.
Till 1995, individual country patent lawswere determined by domestic policy.However, the global system of intellectualproperty rights (IPR) is today much morestructured than before. With theestablishment of the World TradeOrganisation ( WTO) Agreement onTrade-Related Intellectual Property Rights(TRIPS), most countries are required tostrengthen their intellectual propertylaws. TRIPS has profound implications forthe availability of and access to medicinesfor the South Asian countries, especiallyin the context of HIV/AIDS since most ofthese medicines are the products ofongoing research, and their supply will
be immediately affected by changes inpatent laws.
,���,��-"� ������������������
��� ���
The TRIPS Agreement, which came intoeffect in 1995, requires all member-countries to extend intellectual propertyrights to all technologies, covering bothproducts and processes.63 TRIPS requirescountries to recognise product andprocess patent rights in the pharma-ceutical sector and offer patents for aminimum of 20 years in order to protectthe rights of innovators and balance themwith the rights of consumers.
India, Pakistan, Maldives, Bangladesh andSri Lanka together account for 98.7 percent of all HIV/AIDS cases in the region.All five of them are members of the WTO.Nepal and Bhutan currently haveobserver status at the WTO. Nepal hasbegun negotiations for accession andBhutan needs to begin accessionnegotiations within the next five years.Iran’s application for accession has notbeen unanimously approved by the WTOGeneral Council, and Afghanistan has notyet applied for membership.
Despite their varying official WTO status,all countries in the region are affected bythe TRIPS Agreement, since (barringIndia) all of them lack the capacity tomanufacture drugs locally and aredependent on imports from countriesthat are signatories to TRIPS.
The single-most important implicationof TRIPS for access to treatment is theimpact of patent protection on drugprices. In the case of India, several studieshave shown that the introduction ofpatents once TRIPS is implemented canraise the prices of drugs by as much as 200per cent.64

����������� �� ���������
��������������������������������
����������� ������������� �����������������102
TRIPS also affects the production ofgeneric versions of drugs. Countries inSouth Asia have different levels ofproduction capacity. India has innovativecapabilities and the technical capacity toproduce generic versions of drugs.Pakistan, Nepal, Sri Lanka, Afghanistan,Bangladesh and Iran have reproductivecapabilities to differing degrees, since thepharmaceutical industry in thesecountries can manufacture finishedproducts from imported ingredientsonly. Bhutan and the Maldives dependentirely on imports to fulfil their drugrequirements.65
TRIPS restricts ‘reverse engineering’ ofpatented products and increases thewaiting time to market generic versionsof these products to the 20-year period ofpatent protection. The generic drugsindustry in India owes its existence to theabsence of product patents in thepharmaceutical sector and comprises,along with indigenous research-basedfirms, up to 74 per cent of the totalpharmaceutical market. With the adventof TRIPS, the industry will be unable toproduce generic versions of new drugs tillthe patent term expires or a compulsorylicense is issued.66
Apart from TRIPS, several bilateralagreements between developed anddeveloping countries on intellectualproperty rights have restrictive clausesthat sometimes negate the advantagesnegotiated under the multilateralframework. The United States and SriLanka signed a bilateral agreement in1991, under which the terms for issuing acompulsory license are significantly morestringent than under TRIPS. For examplethe government is required to negotiatecompensation to the companies in allcases of compulsory licenses except whenthose licenses are granted to remedyviolations of competition laws. Also, all
decisions regarding compulsory licensesare subject to judicial review. Such termsmake many of the flexibilities negotiatedunder TRIPS redundant.
TRIPS has serious implications for publichealth outcomes in poor countries sinceit not only affects medicines for HIV/AIDSbut also research in other diseases.Recognising this problem, the TRIPSAgreement provided for exceptions tothese rights under certain specificconditions. However, it becameincreasingly clear that this was notenough. The exceptions could bechallenged under the WTO DisputeSettlement Procedures, and developingcountries lacked the legal expertise andthe resources to fight these often lengthyand expensive battles.
As the implications of TRIPS for HIV/AIDSmedicines became clearer in the yearssince the Agreement was signed, civilsociety groups and HIV/AIDS activistsacross the world launched aninternational campaign against therestrictive provisions of the agreement.Developing country governments also feltincreasingly constrained by the TRIPSprovisions and demanded more flexibilityto address their public health concerns.In response to these concerns, the DohaDeclaration on TRIPS and Public Healthwas adopted at the Fourth WTOMinisterial Conference in 2001.
,���!����!����������
The Declaration reaffirmed thecommitment of the WTO members topublic health goals. Specifically, membersagreed “that the TRIPS Agreement does notand should not prevent Members fromtaking measures to protect publichealth…that the Agreement can andshould be interpreted and implementedin a manner supportive of WTO Members’right to protect public health and, in
�7�'�����������
�� ��������!�
�����������
���������� �
�����������������
�������!!����
����������!�
���������������
���������������
��������

����������� �� ���������
��������������������������������
����������� ������������� �����������������103
particular, to promote access to medicinesfor all.”
While the Doha Declaration was primarilya political statement, it lays down clearlegal guidelines for dealing with cases inthe dispute settlement process, and is animportant and necessary reaffirmation ofthe precedence of public health concernsover patents. Since the Declaration,however, WTO members have found itdifficult to reach an agreement on ways ofoperationalising it. Following thediscussions at the mini-ministerial inSydney, Australia, in 2002, the chairmanof the WTO TRIPS Council released a drafton 19 November 2002 for a decision bythe General Council. Most countriesagreed with the chair’s proposal of amoratorium on disputes regarding TRIPStill the Agreement is amended. However,disagreements remain over certainelements of the solution such as coverage,scope of eligible countries, etc.
The Doha Declaration was particularlyimportant for the South Asian region,because most countries are dependent onimported HIV/AIDS drugs, and, giventhe low purchasing power in thesecountries, the cost of drugs is an importantconcern in the provision of treatment.However, the Declaration and theflexibilities in TRIPS at the internationallevel will only partially help in ensuringaccess. Eventually, implementation ofthese provisions will be done throughnational legislation and appropriatedomestic policy.
Most WTO members in the South Asianregion have already altered their patentlaws to make them TRIPS-compliant.India, Pakistan and Sri Lanka have timeuntil 1 January 2005 before bringing thepharmaceutical sector under TRIPS.However, it is not clear if all theamendments carried out fully takeadvantage of the flexibilities under the
�������(�4�,��,��-����������!��� �������#����*!
���� ��%���#��������)���#�������� ����������%�#�� ������&
,��������#�����������#����������%��$�"����)�������"��
������"��3#������������ �%�������#��#������#����� ��
�#�#��������)���#������������#�����)&�A� ���,��-�!
����������������$��#�� ������������� ���������
�� ����%�����������)���#����������������"���������"�%���
�������#��������)� ��#�����!� �$#���� ��� ���#�����%
���������������#���&�,��������#������������������
�%���������� ��#�����%����������������#���������
����������!������������� ��#����������#��������
��"��#������#������������������������#�����%���#�����)&
����#��� �*/%0� �%� ��� ,��-����������� ������� ���
#��������)���#���������� �"������� ���������)�%��
�����)������� ������#����'��&�,��������#��������
��#��������������� ��������� �����������"�����%
#��������� ��������������������%�#������#���#��)!���
�������%%�#����� ������#� ���� ���������#��������)
���� ��������������&�����������������������#�������)
�� ��� ��#���������� ���B,6� ��� � ����%)����������
��������%������������%������#� ���&
�������(54�,�����#���������� ���%��������� ��$#�������
����$#�����������:8������ � ��� ����������&��������
#����������� ��$����������������� ����������������
����������������� �������#�������������������������
���"�����%����� ��������#� ����%����$�����:;����
������������������ ��� �� �������������)�����������
�$�#������������#����*&
�������>4�,��,��-������������������#���������%���
��� �#� ���������#������%��$���������%��-���������
��)� ������%���� !���".�#��������������������������
�����%������ �������������#�����&�,������#������%
�$�������� �%���������������%��������� �#���
��� �#��1����������������� �#���$�����&�,�����
��#��������� ���%%���� � ��� ���� �%� #��������� ��
���#������������#������%����������������$���������%
�-��� �!����� ���%��������������#������ ���������%
������� ���� �#����#�����#����������������������
�������&�B����������������������������������%����������
�����������%� ���!���� ����������������������"�����%
����3�#�������#�����%� ��������%%�� �"��������&
Clarifications under the Doha DeclarationBox 4.15

����������� �� ���������
��������������������������������
����������� ������������� �����������������104
TRIPS Agreement and the DohaDeclaration. Maldives and Bangladesh,along with other least developedcountries have time until 2016 toimplement the patent provisions ofTRIPS for pharmaceutical products.
The challenge of providing access to goodquality drugs to PLWHA is, indeed, adaunting one, dealing as it does withissues of medical research, pricing andintellectual property rights. However,facing the challenge is an integral part ofdealing with HIV/AIDS in a rights-basedframework.
��> �������������� ����������� <��������
The Universal Declaration of HumanRights has been recognised as the MagnaCarta of human rights all over the world.The basic tenets of this declaration are theright to liberty, security and freedom ofmovement, the right to work, the right toeducation, the right to social security andservices, the right to equality-equalprotection before the law, the right tomarriage and family and the right to health.
International human rights have beenfurther codified in a number of legallybinding international covenants anddeclarations such as the following:� International Convention on the
Elimination of All Forms of RacialDiscrimination (CERD-1965)
� International Covenant on Civil andPolitical Rights (ICCPR-1966)
� International Covenant onEconomic, Social and Cultural Rights(ICESCR-1966)
� Convention on the Elimination of Allforms of Discrimination AgainstWomen (CEDAW-1979)
� Convention Against Torture andother Cruel, Inhuman or DegradingTreatment or Punishment (CAT –1984)
� Convention on the Rights of the Child(CRC-1989)
International human rights instrumentsplay an important role in respect ofHIV/AIDS and human rights, since theirnorms may guide the establishment ofprocedural, institutional and socialmechanisms to counter the HIV/AIDSepidemic. In addition to the legally
,�"����&�
4���������������&������������������
4����& -������$��
�� �� �� ����-��������#�!���#�� ����� ���������4�-���� ���������������#�����%����������#��������
��� �#���������������E��������������F��� �#���"����%�E�� �������������#�����F&�,���#���$�����
�����#����#������ �#����������#��"�������!��� �#����%����������%����������#��������)���#�����&
�� ����!����9���������������#������!� �#����������"�������� � ������� �#����%�#������"�%���
�� ����##� ������,��-��������7&
-�'����� -�������6� ����#�!�����4�-�������� ����"�������#�����)1����������� ����������� ���,��-�!���
�� ��� ���#������������������������� �#����� ����#������ �#������� !���������������������
������� �����#���"����%��� �������������#�����!������ ��������������%���#��������)���#��������
��������� �������&
����C��'� �� ���%��������#�����-������)!��#��?�&�7���%�*+8+�,���#������� ��������#�����%�����������%����
����� ��%�*7�)����&���� ��������#����)� ���,��-���� ��� ������������ ����"�����#�� �"�%���
G�����)����7&� �����C��'�� ���!�� ����!�����"��������� �-����������� /�&&� ������A����
������0��� ��� �#�����##�� �����������#����������������%���������#��������&

����������� �� ���������
��������������������������������
����������� ������������� �����������������105
binding instruments listed above, theinternational community, through itsestablished mechanisms, like the UNGeneral Assembly and the Commissionon Human Rights, has issued morallybinding declarations and resolutions onemerging issues and interpretations of thecodified human rights standards.
State parties to most of the human rightsinstruments need to submit reports totreaty monitoring bodies to receiveguidance on more effective implementa-tion. This also serves the purpose ofenabling the international community topressurise state parties to speed up theimplementation, by publishing therespective implementation statuses andscenarios. The treaty monitoring bodies,such as the Human Rights Committee, theCommittee on the Rights of the Child, theCEDAW Committee etc. issue commentsand concluding observations on the
reports submitted by the state parties(See Annex I). These bodies also take intoconsideration information submittedby non-governmental sources in therespective countries.
Two prominent HIV/AIDS-specificinternational agreements are theDeclaration of Commitment passed atthe United Nations General AssemblySpecial Session on HIV/AIDS(UNGASS), June 2001 and the Inter-national Guidelines of HIV/AIDS, 1996(See Annex II). There are other importantdocuments as well.70
As member states of the United Nations,South Asian nations are obliged topromote respect for human rightswithout discrimination. Moreover,international human rights law andcovenants are binding on state partiesthat have signed and ratified them.
?���4—�� �#����� #�����)� ��� ���� ����%��
�������6%%�#�� �%� ���A���� �?����������������������� %�������������
/���4�� &��#�&#�� %�������&� %0
,�"����&7
"������������������������������������������������������������������>?
4����& ������������� ������������� 4������������ 4������������ 4��������� 4������������
4���������� 4���������� ����8���������� ����8���������� ������ �������������
8�������# 4������� ��� ���<������� ��� ���<������� ,�������� ����4���
"�������� -��������������� ������ !������������� ������4���#
4����� !������������� �������/���� ���������
������ !�������
,�����������
-��������
���������� J J J K J J
;�������� J J J J J J
;���� K K K J K J
���� J J J J J J
�����.����: J J J K K J
+������ K K J J K J
7���� J J J J J J
-������� K K J J K J
"���$���� J J J J J J

����������� �� ���������
��������������������������������
����������� ������������� �����������������106
Despite South Asian nations beingsignatories to all of these agreements, thesituation on the human rights front isnot satisfactory.
��>�� ����������������������������� �!"In September 1996, the SecondInternational Consultation on HIV/AIDSand Human Rights, convened byUNAIDS and the Office of the UN HighCommissioner for Human Rights, led tothe formulation of the InternationalGuidelines on HIV/AIDS and HumanRights.71 The Guidelines address multi-sectoral responsibilities and accounta-bility, including improving the roles of thegovernment and private sector. Inaddition, they stress the duty of the Statesto engage in law reform and identify legalobstacles to an effective HIV/AIDSstrategy of prevention and care. Theattendant difficulties in the actualimplementation of the Guidelines mustnow be addressed.
����� 7������� !����������� ��
4���������
The UN Declaration of Commitment isof particular interest since all countries ofthe region, barring Afghanistan, aresignatories to it. The UNGASS was the firstevent of its kind organised by the UnitedNations to address HIV/AIDS andincluded participation by civil society(See Box 4.16).
The Declaration addresses issues ofprevention, care, support and treatment;leadership at the national, regional andsub-regional level; reducing vulnerability;alleviating social and economic impact;research and development; respectingimplementation of multi-sectoralstrategies; conflict and disaster-affectedregions; resources; and follow-up at thenational, regional and global levels.
However, the need for a human rights-based approach to deal with HIV/AIDSfinds only brief mention in theDeclaration.
Thus, it is not surprising that thedocument fails to comprehensivelyaddress the needs of vulnerablepopulations such as men who have sexwith men, sex workers and injecting drugusers. This oversight is of concern to thecountries where the promotion of rightsof vulnerable populations is largelyabsent. Empowerment through humanrights initiatives has been difficult toinitiate due to social stigma and culturalpressures. It is evident that greaterinternational initiatives are required todraw attention to these deficiencies andadvocate for human rights protections aspart of HIV/AIDS strategies.
��>�� �������������������The SAARC Convention on Preventingand Combating Trafficking in Women andChildren for Prostitution, held in January2002 marked an important step towardsaddressing the concerns of gender, sexwork and human rights. The SAARCmember states—Bangladesh, Bhutan,India, Maldives, Nepal, Pakistan and SriLanka—were signatories to theConvention, which requires all stateparties to enact legislation that providespunishment for the offence of trafficking,including for keeping, maintaining,managing, knowingly financing, orknowingly renting a place used fortrafficking. A major drawback of theConvention is that it considers traffickingsolely for the purpose of ‘prostitution’thereby limiting the scope of thelegislation. Further, the Conventionadopts a predominantly welfare-basedapproach in dealing with trafficking, asopposed to one based on protectinghuman rights.
���������%����
&����������������
���������!����
����������������
�����!�����
������!������
�����������
�!!���������������
��������!
�����������
����

����������� �� ���������
��������������������������������
����������� ������������� �����������������107
The Asia Pacific Forum (APF) of NationalHuman Rights Institutions, a regionalnetwork comprising the Human RightsCommissions of Australia, Fiji, India,Indonesia, Mongolia, Nepal, NewZealand, Philippines and Sri Lanka, has acrucial role to play in ensuring respect forhuman rights in the context of HIV/AIDS.The APF members can ensure theprotection of the human rights of PLWHAand consequently the creation of anenabling environment throughcooperation; information sharing;training and development for institutionmembers and staff; developing andsharing technical expertise; andbenefiting from the ‘best practice’experiences of other institutions.72 At thesixth annual meeting of the APF held inMelbourne in September 2001, themembers “committed themselves to
combat discrimination and human rightsviolations on the basis of HIV/AIDS andcalled upon the assistance of the UnitedNations, governments and NGOs in theperformance of this task”.
��>�(��������������������������������%����������������������*�������������������Sex workers, men who have sex with men,injecting drug users, peer educators andoutreach workers make essential partnerswithin national HIV prevention efforts. Ifthey possess accurate information, themeans of protection and a supportiveenvironment amongst their peers, familyand the surrounding community(including administration of justiceand law enforcement agencies), theycan contribute effectively to the reduction
���G�������*!���� ���%��������� ������������������%
=������������%�*;+�������������������A���� �?������
=������� �����"�)� ���#���� ��������6?���������
/A?=���0&�,���������� �����������#���� ���'!���
�#����"������������#����� �������� ��� �%�#�
��������#� ���� ��� ��##���������#�����!� �#� ��
��������)��� �������� ������������#������������
�������������#���� ���#����)!��� � �#���2����
��"����#����&
����#����������%������������ ���� ���� �")���
�������!� �#����A?���#�����)3=�������(�%�������
��#��"� ����E��"���������%���%�������%%�����")����A����
?��������)������� �<��"��������������� �#����������
�%������������ �������������������#�F�/���G��)����*!
������� ���A?����� �������� �������0&�,���A?=���
��#����������%����������������� �����%���� ��'�%��
����$��� � ������������������"��������������� ���#&
���� ����� �� � ������� ���� ����� � ��� � ����� ���
�����������%������� ���#��� ��������������������� �
%���#������ ���"��#���'�%�����"����#����&
,����#��������� �%� ����������� ��#������� ���
�������������� �����������#��������� �� ������
��������������������"�����������'� ������� �������
��"��#������������#������������ ���#!���#�� �����
��� �������� ��� ����!������������#���%�����
�������������� ����������#�����"�� ��������������
�� �#���&���������#����!������#�������������������
E�������������� �������������!�������������������
!�����!!���������� ����������� ������8��� �#����
%������� ��)����%���� ��������������������������
����#�����!� ������%�����������������%�#�������#���)!
�������������#������ �-CB���
,�����������%������#����������%�����������������
�������3��#������ ������#&�B����� �����#��������!
���#�%�#� #����������� ������ �� ��� ��� ������ �%
����#� ���� �����@�����������!�#���!�����������
���������@������#�������������!������#�����)�����
�%�-CB��@��� �#����������"����)!�����#����)��%� ����@
���������#�� ���� ������"���������� ��� ��� �
�������"���")���������@������������ �����#������
�#�����#�����#���%���������@�%������������#���
����������@�� �������������������#��%��#��I����
�� � �������3�%%�#�� � ������@� �������� �� � ��
�������� �������#��@��� �����������������������
�� �����������������������%����������&
The United Nations General Assembly Special Session (UNGASS) onHIV/AIDS and the UNGASS Declaration of Commitment
Box 4.16

����������� �� ���������
��������������������������������
����������� ������������� �����������������108
of transmission of HIV to the generalpopulation.
The mobilisation and empowerment ofwomen and men working in the sexindustry, the MSM community and drugusers to access basic services andinformation has strengthened efforts forthe management of the HIV/AIDSepidemic. Such empowerment andmobilisation should be seen as anessential ingredient to an effectiveHIV/AIDS response, as it contributes tosaving lives. Those within the vulnerableand marginalised groups who are workingto this end are actively defending humanrights and principles.
The international community has, inrecent years, established that humanrights defenders deserve recognition andprotection by the state.73 This responsi-bility is outlined in the General Assemblyresolution, ‘Declaration on the Right andResponsibility of Individuals, Groups andOrgans of Society to Promote and ProtectUniversally Recognised Human Rightsand Fundamental Freedoms’.74 It is,therefore, critical that all governmentsembrace this responsibility and protectthose key partners in the response toHIV/AIDS.
��@ ,���������������"����
The legislatures and judiciaries in SouthAsia have had an uneven record inprotecting human rights of PLWHA. Thispartially reflects the lack of understandingof the epidemic within these branches ofthe government themselves. It alsohighlights the additional challenges thatface PLWHA in countries where the Stateis insensitive to their needs. Even moreworrying are the well-documentedincidents of systemic harassment ofPLWHAs and designated human rightsdefenders.75 The lack of an enabling State
structure, along with active discrimina-tion and harassment by officials acts as afurther disincentive for people to disclosetheir HIV status, making it harder tocontain the epidemic.
��A ��������������
An overview of the legal frameworks in theSouth Asian countries clearly brings outseveral lacunae in the law and humanrights guarantees that have an adverseimpact on PLWHA and those mostvulnerable to the epidemic. Certainunequivocal measures, therefore, needto be taken at the policy and legislativelevel to effectively control the spread ofthe epidemic.
,�������������������������������������������������������������It is clear that all South Asian legal regimescriminalise those most vulnerable to theepidemic. It is because of the legalsanctions and social marginalisation andstigma that these groups face that they findthemselves vulnerable to public healthcrises such as HIV/AIDS. Removing theselegal sanctions will go a long way inaddressing the problem of vulnerabilityand stigma faced by these groups and willcheck the spread of HIV/AIDS not only intheir communities but in the generalpopulation as well. The empowerment ofindividuals is the best way to reducevulnerabilities to HIV/AIDS and this canbe done not just through the provision ofinformation and education but alsothrough the guarantee of legal protection.
Protecting the human rights of those mostvulnerable to HIV/AIDS—a centralcomponent of an effective controlstrategy—will firstly require thedecriminalisation of vulnerable groupsthrough a serious and committed attemptat law reform and sensitisation of law
������"�!��
������������
���������%����
����������
���������������
�����������
!!������������
!������
�������������!�
� ������������
���������������%
�"��������������
���������
� �������

����������� �� ���������
��������������������������������
����������� ������������� �����������������109
enforcement, healthcare and otherauthorities. However, this should only bea first step. In addition, it will be necessaryto endow these communities with therange of positive rights that allow for thefull realisation of human potential. Theseinclude rights that guarantee life andliberty in all its varied forms (includingthe rights to sexual orientation, foundingof family, marriage and other civil rights),equality and non-discrimination, employ-ment, access to services (includinghealthcare, social security, education,
civic amenities, housing, transport etc.)and freedoms of speech, expression,movement and organisation.
However, any attempt at decriminalisa-tion must be sensitive to the differencesamong the various groups vulnerable toHIV/AIDS, as a universally applicableapproach is not possible. Additionally,there is debate within these communitiesand groups on the appropriate legalresponse to their situation. Any effectivelegal response, then, must be undertaken
5�������4�,��9����������#)��#�!�*+��� �%����
��5������1����E���������%��� ���'���%�������������)
��"��#����#����� �� ������"��������������������
��"��#����#�������#�#�� ����������������������'�����
��'��)�������#�����������$�����")���'���%�������F
/��#�����80&�,�����#����<����������������� �����
��'����������)���2���)��� !��%�������������������!
#��� �#��������������"����������&�,�����������
������ � ������������#���� )��%�����%%�#������#���
�%��������������#������#�����&�,���� �#����%%�#��
������#������������� ��� �����$���������������
�� ��������� �#���������� �#�����!����������
����!� ������ ����� ��� ������� ��� ���������)
�%�#����!� �� ������ ��� ��%%���� %���� ��)� ����
#������#�"��� ������&�C�����!������������������)
�%�#����� �������� �� � ����� ��%%����� %���
#������#�"��� ���������� �#�� ���������������
%������#�����&��,���#����������)������� ��� ���
����#���%������������������ ������ �������������#
��� #�����#���� ��$� ��'���!� ��� ���!� ������#
������!� �)���"������!�������#�� �����������������
�� � �������������������������������������
#�� ������&��##�� ����������� )8:�����.����)��%���
������������������������������ ������� �������%
��������#�����#������$� ��'���&
�������������!���$� ��'����%�#������$�����������)��%
�$�#������")�%������2�� ������������� ���#��$�#������
����#�����&��,��������"����#������%������)����
"���� ��������� � ��� ��� ���� �� �%� ���� ������&
�� ����!������������"����������� ������������
�������)���!����#��6#��"������*!�"���� �����$�������
�%�-CB���%���� ��'&�,���$�#���$������� ������#������
�%�����������������������"��������%�� &
����4��� ��)�������E�����������%%��#�F��� �����#����
�88��%������ ����-������� �!���� �� ����%� �#���
� ����#��� ��������%����-������� ���%�9���� ��&
A����������%%��#�����#�� ��#�����������#������#�������
������������ ����%��������")���������� �����������
��������")���������� ����������)�������� �����
������&���#������88����"������ ��������"�������
�����#��������� ���&��� ����!���������*++��!���
�����%������#��������"�������#�%�#�������#����$���%
#�� ���$�����������!�%��� �#��������������������������
���������&�,��������������������"������� ���������
�� ���#������������$����!���#�� ������� ��������$
������&����#������+���%������ ����-������� �!� �#
������������)�'�� ��%�E�"�#����"�������������"��#F!���
���������#���-���#���#������������"������� �������
���� ������ ��$� ������&��#�������� �� �?=6
��'�����%����%�#������������")�����#������������!
��������� ��������� ���%�C�#'�� ����G��)����*!� ��
�������#����� � �����%%�#����%�� ��?=6�� ��'��� ��
���<�<�#�������)&��������#�������� ����������� ��� ��
��#������88��� �#��� � ���#��������#�������#)!
�"��������� ������������������%��"�#�������������&
,�)� ���� ���� �"����")�������������1��#����������
���� �������)� ������E#����������#���)F&��,����
����������������� �"�����%�����7� �)���%�������������&
,���#�������%������#�������#���������#�����$�������
����"�� ������������������#)��� ��������#����&���
�������������������������?�����������%����#����������
������� �������������?����"�������!����?�������
���������������������������#����� � ���������
�� �����������%���#������88������ ���������� ���<�<
�� ������%%�#���������������������������&��,��������
�������#����� � �����������������%���$�����#��������
"�� ����#���������� ����&
Human rights violations and systemic harassmentBox 4.17

����������� �� ���������
��������������������������������
����������� ������������� �����������������110
after consultation with the stakeholdersfrom within these communities.
The exercise of collective power by sexworkers can be one strategy that cansuccessfully minimise HIV/AIDS vulnera-bilities and human rights violations, as canbe seen in the case of the SHIP projectand Durbar Mahila Samanvay Committee(DMSC) in Kolkata, India.
The argument that sex work should bedecriminalised stems from rights-basedand public health perspectives. Fear ofprosecution has been seen to inhibit sexworkers from accessing information andservices including healthcare andHIV/AIDS information. Further, the illegalstatus of sex work makes negotiation withclients difficult. It also makes sex workersvulnerable to abuse both within the sexwork setting (madams, pimps, brotheloperators and owners) and outside(clients, law enforcers, lawyers, themagistracy etc.). Decriminalisationimplies that sex work, including solicitingand earnings from sex work, must not beconsidered criminal in so far as theypertain to consenting adults. There havebeen growing demands for this from sexworkers’ collectives, organisationsworking with sex workers, HIV/AIDSintervention groups, public healthspecialists and rights activists. Suchdemands have come in contexts wheresex workers have been able to presenttheir perspectives and where the adversepublic health implications of criminalisa-tion of sex work have been recognised.
There are other perspectives on thequestion of decriminalisation of sexwork, including the view that sex work,but not the sex worker, should becriminalised. These ideas largely arise outof the view that sex work itself amountsto exploitation of women. It is not clearhow sex work can be criminalised
without having an adverse impact on thelives of sex workers. The primary issue inadvocacy around these issues is theinvolvement of sex workers in thedecision-making processes. This itself isbound to be a difficult task, consideringthat there are a wide range of contexts inwhich sex work is carried out in theregion and even within countries.Decriminalisation, however, seems tobe a prerequisite for the participationof sex workers in such decision-making processes.
It is important to note, however, thatdecriminalisation of these groups doesnot mean ignoring the root causeswhich put people in positions ofvulnerability (such as the mafia behindthe trafficking of humans or smugglingof narcotics). It only means that lawsmust begin to target those who are, inreality, behind the crimes.
-������������������������������������Until the time that a human rights-friendly legal regime is put into place, itwill be necessary to introduce legalprovisions that will allow harm reductionprogrammes (providing clean needles toinjecting drug users and condoms to sexworkers and men who have sex with men)to be carried out among vulnerablegroups. In the absence of legal provisions,such programmes could easily beinterpreted as abetting crimes, as theyalready have been in India, despitegovernment support of such interven-tions. Even here, law reform must go handin hand with the sensitisation of statemachinery. Such law reform will requirethat NGO and community-basedorganisations working on harm reductionthrough advocacy, education andcounselling be allowed to functionoutside the purview of criminal laws suchas those relating to obscenity and public
�������� ������
���%�������%����
���������������!
��������� �����
��������������
������������
������ ��� � �����
�������!
�������������

����������� �� ���������
��������������������������������
����������� ������������� �����������������111
nuisance. Such harm reductionprogrammes must, however, lead tothe ultimate goal of law reform todecriminalise the behaviour of variousvulnerable groups.
,���������������������'�������������������������As has been observed earlier, legal regimesin South Asia that guarantee equalityapply only to the public sector. As a result,private healthcare or employment fallsoutside the scope of the non-discrimination legislation and they are,therefore, free to refuse treatment or jobsto PLWHA. PLWHA, therefore, have nolegal recourse when they face suchdiscrimination in the private sector. Thisis a huge lacuna in the law that requires tobe filled urgently.
$�����������������-$/� Apart from specifically protecting therights of PLWHA and those mostvulnerable to HIV/AIDS, it is alsonecessary to ensure that appropriate andaccessible legal remedies are available tothem. This can be done by insertingrelevant provisions in the respectiveconstitutions and the civil and criminallaws, where such safeguards and remediesdo not already exist.
The remainder of this section will look atlegal remedies available to PLWHA in thecontext of the Indian legal system.
To ensure that the rights of PLWHA areprotected and they are able to takerecourse to legal remedies, it is necessary(a) to ensure that the rule of law exists;and (b) to build an enabling environmentso that fear, discrimination and stigma donot hinder access to the judicial system.
Constitutional remediesArticle 32 of the Indian Constitution has aremedial provision for the violation of
fundamental rights by the State and forthe enforcement of fundamental rightsagainst the State. The Supreme Court ofIndia has the power to issue directions,orders, writs or any appropriatedirections for the enforcement offundamental rights. Similar powers havealso been conferred by the Constitutionon the High Courts of each state. The rightto move the courts for the enforcementand/or protection of fundamental rightsrelates only to violation by the State orState-run organisations or agencies.Therefore, if discriminatory treatment ismeted out to PLWHA working in thepublic sector or accessing publichospitals, they can approach the courtsfor the enforcement of their fundamentalright to equality guaranteed underArticle 14.
It is important to note that certainfundamental rights under the IndianConstitution (Articles 17, 23 and 24dealing with untouchability, traffic inhumans and forced/ child labour) can alsobe enforced against private individuals ifthere are violations. However, there is nosimilar provision for HIV positive status.
Civil remediesThere are certain other rights of peoplethat may not be fundamental rights, butare legal rights or civil rights conferred bya statute, e.g. custody rights, maintenanceetc. Such rights are enforceable throughthe civil courts in the country. Therefore,if a private employer discriminates againsta PLWHA, then, subject to the existinglaws, the employer can be taken to courtfor the violation of the rights of theemployee. Persons who have beenillegally and unlawfully dispossessed fromtheir homes can file a suit for repossession.Similarly, issues relating to land, propertyrights, tenancy, maintenance, custody,divorce, dues from the employer, etc. canfind legal recourse through the civil courts.
-��������������
������������
���������9�����
������������
������������

����������� �� ���������
��������������������������������
����������� ������������� �����������������112
Criminal law remediesThe penal code and other penal statuteslay down acts or omissions thatconstitute an offence. Once a complaintis made and is recorded as cognizable ornon-cognizable depending on the gravityof the offence, investigation and trialsfollow. A person is considered innocentuntil proven guilty. Victims of violence,persons who have been thrown out oftheir house because of their HIV positivestatus, individuals from vulnerable groupswho are being extorted, exploited etc. canfile a complaint in the police station. Ifthe complaints are not registered at thepolice station, they can send writtencomplaints to the senior officials and alsomake a complaint to the magistrate.
Other foraIn India, certain statutory fora likeconsumer courts, AdministrativeTribunals, Lok Adalats (people’s courts)etc. have been set up to facilitate speedydisposal of cases on issues ranging fromconsumer disputes to grievances withgovernment departments and adminis-trative matters within the civil services.These have not yet been accessed byPLWHA and their networks. Theirusefulness for issues relating to PLWHAneeds to be explored.
7������������������������������While commitment at the internationaland regional level is extremely crucial ininitiating debate and setting guidelinesfor building a human rights framework,their implementation can be ensuredonly when backed by effective legalmechanisms at the national level.National human rights institutions areone such mechanism. These areindependent bodies established by theState for the effective promotion andprotection of human rights issues thatarise in the context of HIV/AIDS.
In his address to the international meetingof human rights institutions in Geneva inApril 2001, the Executive Director ofUNAIDS identified five practical ways inwhich national human rights institutionscan strengthen their work regardingHIV/AIDS:� by investigating violations of human
rights that occur in the context ofHIV/AIDS;
� by conducting public inquiriesfocusing on these violations;
� by receiving and, where appropriate,redressing complaints of HIV/AIDS-related human rights violations;
� by providing advice and assistance togovernments in the area of humanrights and HIV/AIDS; and
� conducting human rights educationin the context of HIV/AIDS.
These commitments require theintegration of HIV/AIDS-related humanrights into institutional strategies andprogrammes at the national level.77
In India, the National Human RightsCommission78 and the State HumanRights Commissions are empowered toinquire into complaints of violation ofhuman rights either suo moto or on apetition by a victim or someone actingon his behalf. They can also inquire intoinstances of negligence in the preventionof such violation by a public servant. TheCommissions have powers to review thesafeguards provided under the Consti-tution or any law for the protection ofhuman rights and recommend measuresfor their effective implementation. TheCommissions may undertake research inthe field of human rights and takemeasures to promote awareness ofhuman rights among all sections ofsociety.
In Nepal, the Human Rights CommissionAct (1997) established an independent
4��������������
����������������
���������������
����/�������
�������������������
����������������
�����������!�
��������������6
�������!�����"%
�����
�� ���������
�������������
�����������"��
����!!�����������
���������������
������������

����������� �� ���������
��������������������������������
����������� ������������� �����������������113
and autonomous National Human RightsCommission for the effective enforcementas well as protection and promotion ofhuman rights conferred by the Consti-tution and other prevailing laws.
Bangladesh has also initiated moves toconstitute an independent Human RightsCommission. The law, justice andparliamentary affairs ministry is in theprocess of finalising a draft legislation,which will also fix the terms of referenceof the proposed commission. Accordingto the draft, the commission wouldinvestigate the allegations of human rightsviolation and take necessary actions asper the existing provisions of law.
Since 1986, the Human RightsCommission of Pakistan (HRCP) hasplayed a leading role in providing a highlyinformed and independent voice in thestruggle for human rights and democraticdevelopment in the country. It is anindependent, voluntary, non-political,non-profit making, non-governmentalorganisation. One of the main functionsof HRPC is to work for the ratification andimplementation by Pakistan of theUniversal Declaration of Human Rightsand of other related charters, covenants,protocols, resolutions, recommendationsand internationally adopted norms.
"������������������������������The poor development of social capitalin South Asia has severely limitedthe progress with regard to dealingwith HIV/AIDS, as societies remainentrenched in gender inequities, casteand class-based violence, religiousfundamentalism, violations of the rightsof marginalised populations and anoverall environment of intolerance.Provisions for strengthening, for example,educational systems, infrastructuralfacilities and local governancemechanisms would contribute signi-
ficantly to enriching the social, cultural andeconomic environment of communities.This, in turn, would have a favourableimpact upon the indices for developmentat macro levels.
������������������������8+
Parliamentarians can play a key role atthe local, national and regional levelsin initiating dialogue and legislativeaction on HIV/AIDS and human rightsissues, as well as mobilising financialresources to support HIV/AIDSprogrammes. They can work at severallevels.� As political leaders, they can influence
public opinion, and can increasepublic knowledge of relevant issues.
� As legislators, they vote on acts ofParliament and can ensure thatlegislation protects human rights, andadvances effective prevention andcare programmes.
� As advocates, they can mobilise theinvolvement of government, privatesector and civil society to dischargetheir societal responsibilities inresponding appropriately to theepidemic.
� As resource mobilisers, they canallocate financial resources to supportand enhance effective HIV/AIDSprogrammes that are consistent withhuman rights principles.
An important regional initiative is thesetting up of the SAARC MedicalParliamentarians, which held a meetingon reproductive health, STDs andHIV/AIDS in Kathmandu, Nepal, in May1998. The meeting issued a Declarationon the Prevention and Control ofHIV/AIDS. The Declaration asked parlia-mentarians to take a stronger role inadvocacy at the regional, national,and community levels. The meetingalso recommended the establishmentof a regional forum of SAARC
���� �
����� �����!
������ ������
�����������
��������������������
�����������
��������������
�������������%��
��������� �����
�������������
����������9������%
������������6
������������%
��������
!�����������%
��������!����
�������!
����������
�����������
����������������
!�����������

����������� �� ���������
��������������������������������
����������� ������������� �����������������114
Parliamentarians and mechanisms toreview and reform national laws andpolicies.
In Dhaka, a successful workshop onHIV/AIDS and STDs for parliamentarianswas held in September-October 1997by ACTIONAID, an NGO, and thegovernment AIDS Prevention and ControlProgramme. It included a presentation bypeer educators of sex workers at theTangail brothel.80 The objectives were tocreate an environment where partici-pants felt at ease to talk, to bridge the gapbetween lawmakers and activists, to shareprevention and management interven-tions, and to identify areas where law-makers could contribute at the policylevel, in Parliament and in the local areathey represent.
Democratically elected parliamentariansare in a unique position to influencepublic opinion and lead theirconstituents towards attitudes that aresupportive of an effective national and
�$ ���� ���� ��� ���� ����������������!�� ��������� !���� �� ��������������$ ����������� ���� ����������������� �� ��������� ������� � ���� �������#
&�����������' ������� ()�������*����������� �
%������"��#$$#
regional response to the epidemic.Political commitment is an essentialingredient to a rights-based response toHIV/AIDS and to the allocation ofadequate resources to implement it.
��?�4��������
The impact of the epidemics of HIV/AIDSon individuals and communities hasthrown light on the complex intersectionsbetween human development, humanrights and health. While these domains areorganically intertwined, there has been atendency to lose sight of this inter-dependence. This has led to the evolutionof philosophies, vocabularies, researchand activism that have virtually excludedone domain from the other. The emergingglobal recognition that human rights area potent approach to defining andadvancing human development andwell being, calls for increasedcommunication and interaction betweenthe fields of human development, rightsand health.

������������
������������������������ ���
������������������������ �������������� !115

������������
������������������������ ���
������������������������ �������������� !116

������������
������������������������ ���
������������������������ �������������� !117
"������ #
������������
��� ���������� ����������������������� ��������������� �!����"���
The foregoing chapters have highlightedthe gravity of the challenge of HIV/AIDSin South Asia and the urgency ofaddressing the epidemic within a humandevelopment framework and a rights-based approach. It is, therefore,imperative that HIV be treated as amainstream issue rather than a purelyhealth issue. An effective responsetowards the epidemic must be based onthe realisation that South Asia is indeedon the threshold of an unparalleledAIDS epidemic.
The epidemic is becoming generalised inmany parts of the region, and focusedpublic action that goes beyond a purelymedical or communicable diseaseapproach is needed to tackle it. HIV/AIDShas a major impact on humandevelopment attainments, especially ofthe poor and marginalised communities/groups, including women. At the micro-level, it has a significant impact onindividuals, households and firms. Tillnow, the macro-economic impact of theepidemic in South Asia has been relativelylow compared to the situation in sub-Saharan Africa. However, since thestructural determinants of HIV prevalencesuch as high levels of poverty, migration,
illiteracy, ill-health, gender inequality andurbanisation are widely present in SouthAsia, the region can ill-afford to wait for afull-blown crisis. The mutually reinforcingrelationship between HIV and humandeprivation in South Asia needs to bebrought at the centre of all efforts tocombat the epidemic.
The most important lesson for South Asiais about fighting the epidemic right nowto prevent it from reaching catastrophicproportions. National responses shouldnot wait for HIV/AIDS cases to soar.Commitment to checking the spread ofHIV has to be imbued with a sense ofurgency. The cost of trying to reverse theupward trend of the epidemic once itreaches the 1 per cent level will haveserious implications in terms of humanlives and resources.1
Given the early stage of the epidemic inSouth Asia, it is important to address thestructural factors such as poverty andlivelihood, gender and human rights, foreffective prevention, care and support. Inorder to do this, it is essential to get theepidemic out of the “public health”box and address it as a mainstreamdevelopment issue. The elements of sucha response would include:� provision of livelihood and social
security for PLWHA and vulnerablegroups;
����������� ������������������������������������������������������������������������������������������ ����������������������
�������������� �����
�� ��� �����
�� ������ ������� � � � �
�� ���������������
����������������� �
������� � ����� ���!"#
$���� ����������������
�����%��! �� ��� ��
�� ������� ��!&��� ���
����� '������� (!���')�
*��+���,--.
���������������� ���������������������������������� �!�"������������������������������������������ ���#��������� �#���� ����!������� ��������������������$���� �������������������$��!!!�%��&���� ������������ ����������$���&��������������������������� ��������� ������������������������!
&��/����� ������� �������
0 1��������2/
�������3 � ����� ��
�!"4�!&��� ����������
���������������$�1��
�� ���� ��� 5��������� �
������� ���� ���
6�������� ���!"4�!&�
� � ���������78
9���� ����/�����
6�+����� ,--:

������������
������������������������ ���
������������������������ �������������� !118
� empowerment of women to ensuregreater control over their bodies, bettersexual negotiation and avoidance ofopportunistic infection;
� public education to reduce ‘fear andloathing’, which is at the heart ofstigma and discrimination and linkmobilisation of positive people withwider social movements; and
� improved management of theeconomy to address issues stemmingfrom globalisation like vulnerability oflocal livelihoods, healthcare accessand affordability and drug pricingregimes in the age of TRIPS.
The policy and regulatory frameworkmust be simultaneously widened, toensure that:� access to basic services for positive
people is guaranteed;� AIDS strategies go beyond public
communication and media advocacy;and
� human rights of PLWHA are respected,with changes in laws and penal codesto ensure their decriminalisation.
��# ������"���� ���$"��!
While there is general agreement that theHIV/AIDS epidemic calls for policyintervention, there is considerably lessclarity about the appropriate content ofany such policy response. Should it be apurely technical intervention? Shouldother goals be pursued as well? Whoshould participate in “delivering” theintervention?
Countries have experimented witha number of policy approaches,incorporating one or more of the abovecharacteristics, in the two decades sincethe onset of the epidemic. These haveranged from the screening of donatedblood, HIV testing of individuals
(voluntary or forced), counselling,subsidised provision of ARV drugs, needleexchange programmes, removal ofPLWHA from proximity to populations atrisk, subsidised condom distribution,prevention messages (through the massmedia and peer groups), and social andeconomic empowerment schemes.Sometimes, the primary goal has been toreduce HIV infection, but at other times,additional goals—such as economicbetterment and protection of humanrights—appear to have been incorporatedas well. The government has played acentral role in executing someinterventions, whereas others have beenconducted under the auspices of theprivate for-profit and non-profit sectors.Still others have been undertaken aspartnerships between the private sector,the government and NGOs. Groupstargeted for intervention have beeninvolved in the design and execution ofpolicy in some cases, while that has notbeen the case in others.
To the extent that HIV/AIDS has anadverse impact on economic indicatorsand other socially desirable goals, policyaction is necessary early in the epidemic,rather than later. The question ofappropriate policy is also relevant here.One objection to policy action is thatindividual (or private) actions act toneutralise government policy, so the netoutcome of the policy intervention endsup being rather small. For example, acountry may have a policy of subsidisingHIV testing of blood for transfusion.Assuming that, in the absence of anygovernment policy, individuals wouldactually have paid for testing of blood, theonly impact of the policy of subsidisingHIV tests is a transfer of public resourcesto individuals using transfused blood,with no influence on HIV. Therefore,unless there is a clear assessment that sucha transfer is beneficial to society, the policy
�������������
������� ���� ���
�����������������
����� �����������
��������������������
�������
��������������
�����������������
�����������
��������������
����������
�������

������������
������������������������ ���
������������������������ �������������� !119
is not a desirable one. Sometimes theeffects of a policy can even be the oppositeof the intended effects as, for examplepolicies that seek to identify and imprisonPLWHA.2 In this case, individuals whomight otherwise have visited formal healthfacilities avail of HIV counselling andlearn methods to reduce the risk ofinfection to others, may choose not to doso. This may, therefore, enhance HIVtransmission, instead of the intendedpolicy effect of reducing it.3
Even if concrete evidence on someaspects of the economic impact ofHIV/AIDS is not readily available, thereare enough reasons for makinginvestments in an HIV/AIDS policy. Thefirst is, simply, the human developmentcosts of the epidemic, as indicated by thenegative effects of stigma and the lossof key adult members of individualhouseholds at the micro-level, and overalldeclines in life expectancy at birth inthe worst-affected countries at themacro level. There are also measurableeconomic impacts such as large medicalexpenditures on treating PLWHA that useup resources that could have been usedelsewhere in the absence of AIDS.
However, to justify spending more onpolicies to address HIV/AIDS, it isimportant that investments in AIDSprevention and treatment be comparedto investments in other (health and non-health) sectors.
��% &�� ���������� ������ ����$"��!��������������������!����"���
The future of public policy on HIV/AIDSand efforts to combat the epidemic inSouth Asia will increasingly be influencedby a number of emerging critical issues,three of which are highlighted in thissection. The first is the role of stigma and
discrimination in affecting care andprevention strategies. The second is thespecial requirements of policy initiativesin regions of conflict, and the ways inwhich conflict affects the spread ofHIV/AIDS. The third issue is the questionof access to ARV drugs as the regionbattles the disease.
��%�� !������������� ������� ������� �����The stigma and taboos surrounding HIVin most South Asian societies haveprevented open discussion of HIV/AIDS,making the epidemic socially invisibleand leaving individuals ignorant aboutthe causes and how they can protectthemselves and others. It has also madelarge sections of society considerthemselves behaviourally immune to HIV,a disease they perceive as only attackingstigmatised ‘others’ like sex workers, menwho have sex with men, injecting drugusers etc.
In the light of these damagingconsequences, it is clear that stigma anddiscrimination need to be urgentlyaddressed both in order to ensure effectiveresponses to the epidemic, as well as toguarantee the human rights of PLWHA.Challenging stigma and discrimination isthus increasingly becoming a priority forgovernments, civil society and inter-governmental organisations.4
& ������� �������� ��������
����� ����� ��� ������ �����
There have been relatively few sustainedor effective responses aimed atchallenging stigma and discriminationwithin the region. This is partly because ithas been difficult to measure and proveresults in this area and also because thefactors that influence stigma anddiscrimination, and the interplaybetween them, are rarely explored. As aresult, responses have not addressed the
��!������������
�����������������
���������������
������ ������������
����� ������
���������������
��������� ������
�� ��������
����� ������
������"����������
���#������$
������

������������
������������������������ ���
������������������������ �������������� !120
root causes of stigmatising attitudes ordiscriminatory practices and, therefore,have limited effectiveness.
The gap in useful data on stigma anddiscrimination is now being recognisedas a serious problem. A UNAIDS researchstudy on HIV-related stigma anddiscrimination in India and Uganda notedthat “relatively little systematic researchhas taken place on the forms thatHIV/AIDS related stigmatisation anddiscrimination take, the different contextsin which they occur and their varyingdeterminants”.5 Current interventions,initiated largely by NGOs, tackle stigmaand discrimination by applying thehuman rights standards as outlined byvarious human rights mechanisms. They,however, require benchmarks for actionso that progress can be monitored moresystematically.6
Besides, by focusing on the humanrights approach, many stigma anddiscrimination-related initiatives lose thepriority of the two main public healtheffects:� stigma results in denial, leading to
inaccurate disease surveillance,severely restricting the ability toassess and plan health needsappropriately; and
� stigma and discrimination decreasethe access to treatment andcounselling services.7
In order to effectively tackle the problem,simple research methods are needed thatwill provide precise and measurable dataabout the levels of stigma anddiscrimination and the underlyingcomponents (e.g. fear, moral judgementetc.) that inform them, as well as thecorrelations and linkages between thesecomponents. Such a disaggregated anddetailed understanding of both thelevels and operation of stigma and
discrimination would allow thedevelopment of tailored, effectivesensitisation programmes.
The key elements of successfulprogrammes tackling stigma anddiscrimination are8
� analysing of the causes and effects ofstigma and discrimination;
� communication and education aimedat changing attitudes and behaviour,not just imparting knowledge;
� establishing a more equitable policycontext;
� giving top priority to tackling legalchallenges;
� safeguarding the dignity and rights ofindividuals and marginalised groups;
� addressing the issue from a humanrights framework;
� empowering communities through aparticipatory process;
� social marketing;� social mobilisation;� sensitising and involving leaders
(government, religious andcommunity) to create a more opensociety;
� involving marginalised groups andPLWHA networks in forming policy,designing and implementingprogrammes and allowing themto build ‘new identities’ withinsociety; and
� identifying both prevention and care/support.
��%�# � �������������������!����"���The South Asian region is torn by civil andmilitary conflict, both within countriesand across borders, and has large refugeepopulations. Though there have been fewstudies that establish a direct link betweenconflict situations and the spread of HIV,civil and military strife do aggravate thevarious factors that fuel the epidemic. Ata general level, conflict situations disrupt
%����������
���������������
������������
�� �����
�����������
����� �������
�������������
���������������
�� ����
������������

������������
������������������������ ���
������������������������ �������������� !121
development, divert scarce resourcesaway from social and developmentalspending to military expenditure, displacepeople, throw normal administrativestructures and processes out of gear, andviolate human rights. All these factorsaggravate the conditions that contributedirectly to the spread of HIV. Women andgirls become more vulnerable to genderviolence and sexual exploitation and theyare less able to negotiate safer sex. Multi-partner sex is common, as sexualrelationships become more transitory.Such sexual activity is often withoutcondoms, the easy availability of whichbecomes a problem. The breakdown ofhealth infrastructure results in STIs notbeing treated, testing of blood not beingdone and drugs not being available. Thepresence of international peacekeepingforces can also be the source of a newlocal epidemic. Conflict also placesinnumerable hurdles in existingHIV/AIDS prevention efforts.
& ������� �������� ��� ������ ���
��� ����� ������
The spread of HIV/AIDS in conflictsituations cannot be addressed inisolation. As in the case of other responsesto the epidemic, this too has to be locatedwithin a larger developmental framework.Thus, any response will have to firstaddress the underlying causes of conflict.It must also deal with providing care andsupport to PLWHA in conflict situations.The key elements of such a strategywould be:� undertake research to analyse the link
between conflict situations and thespread of HIV;
� Address the underlying causes ofconflict and social tension by:� dealing with issues relating to
livelihoods, ethnic, religious andlinguistic minorities;
� promoting developmentalpolicies that do not lead to
displacement, ensure balancedregional development and donot harm the environment; and
� ensuring a more meaningfuland participatory democracyby strengthening grassrootspolitical institutions.
� Undertake focused action using acompassionate and caring approachto HIV/AIDS in actual conflictsituations. Such programmes mustdeal with:� educating women about their
reproductive and sexual healthrights;
� ensuring representation forwomen in conflict resolutionactivities;
� designing awareness pro-grammes regarding HIV/AIDSand sexual health for both sexes;
� ensuring humanitarian normsin regard to treatment of womenand children in conflictsituations; and
� enhancing awareness in thearmed forces about HIV/AIDS
��%�% � ������'��� �������� �The mainstay of efforts to respond to theepidemic in the South Asian region at thepresent time consists of public education,voluntary counselling and testing,condom promotion and the treatment ofSTIs and opportunistic infections.However, in the absence of a vaccine or acure for HIV infection, the need for takingup access to treatment as an integral partof the common agenda for humandevelopment and HIV prevention isincreasingly being recognised. Access totreatment comprises several elements,including the quality and scope ofhealthcare infrastructure and equipment,the availability of trained medicalpersonnel and the availability of highquality affordable medicines.
�������&��'����
������
�������������
�����������(�����
��� �����
�����������������
�����������������
��������������
����������������
����� ���
����������

������������
������������������������ ���
������������������������ �������������� !122
Significant strides have been made overthe last decade in developing a range ofARV drugs to control HIV infection andthis has made an enormous difference tothe way HIV/AIDS is treated. However,the high cost of these drugs makes accessto them a major problem in developingcountries, including those in the SouthAsian region. Till December 2002, only4 per cent of the 1 million people whoneeded therapy had access to HAART. Thesituation is likely to get exacerbatedwith the coming into effect of theTRIPS Agreement. The Agreementwill require countries to legislate strictpatent laws, which will only furtherrestrict the availability of drugs and makethem more expensive.
There is also concern over theeffectiveness of ARV treatment withoutadequate supervision or health infra-structure. Fears of drug resistance fuelledthese concerns and led to questionsregarding whether ARV treatment wasan appropriate policy response inpoor countries.
& ������� �������� ���������
��� ����� ��� (������� ����������
The UN Declaration of Commitmentendorses HIV prevention and care asbeing at the core of the larger responseto the epidemic. This suggests that thedetection and treatment of HIV infectionand associated opportunistic diseases isimportant. The increasing availability ofARV drugs also makes it clear that itwould be unethical to withhold life-saving therapy. Most importantly, theDeclaration endorses the commitmentof countries to come to terms with theissue of providing HIV treatment.
ARV drugs are not a cure for HIV infection.Improving access to ART and care forHIV infection and AIDS needs to belogically integrated with HIV prevention
programmes. Offering a mix of voluntarycounselling and testing, ART andtreatment for opportunistic illnesses willbe a stepping stone to expandingprevention efforts, as this larger gamut ofservices will cover a larger number of thoseinfected and those at risk.
Developing countries standing on thethreshold of ART need to ensure that theirprevention programmes do not getisolated from care programmes. In somedeveloped countries, the gains of ART interms of reduced morbidity and mortalityis being neutralised by stable or evenincreasing rates of HIV transmission.
In addition, treatment for HIV needs tobe utilised as an additional impetus forupgrading sustainable health delivery intoto, rather than being seen as an extraburden on the health budget.
The WHO Commission on Macro-economics and Health calculated that anoutlay of $66 billion per year onhealthcare and services in developingcountries would save about eight millionlives a year by preventing or treatingdiseases such as HIV/AIDS, malaria andTB. The resultant economic benefits ofsustaining the health of the workingpopulation and lowering future medicalcosts were estimated to touch $360billion a year by 2020.
There is a mounting body of evidenceregarding the positive associationbetween investments in health andeconomic growth, indicating that ahealthy population is as much aprecondition for growth as a product ofit. The response to HIV/AIDS, includingHIV treatments, needs to be at the core ofpublic policy, poverty reductionstrategies, action for sustainabledevelopment and the preservation ofhuman security.
� �����������
�������#����������
���������������
�����������������
����������������
�����������
����������'���
��������������
����� ��

������������
������������������������ ���
������������������������ �������������� !123
Providing ARV treatment in resourcelimited settings is possible, once theright capacities are built up. A stronggenerics drug industry provides much-needed competition to brandedproducts and is a key element in ensuringaffordable access to medicines. There isscope for technical cooperationamong countries within and outside theregion. In 2001, one such attempt wasmade with discussions between thePakistani and Indian pharmaceuticalindustry on transfer of technology,machinery and plant equipment fromIndia to Pakistan for bulk production ofgeneric drugs.
Countries like Bhutan and the Maldives,which do not provide the economies ofscale for mass production and dependentirely on imports, must collaborate withgeneric drug producers in the region tosource their requirements. Compatiblelegislation in both producing andimporting countries is essential to allowfor such collaborations. Countries thatrequire import of ingredients also need toensure that their laws are in compliancewith international agreements and, at thesame time, allow imports from genericproducers without violating theseagreements.
Issues of quality control also need to beaddressed. The WHO, together withUNAIDS and UNICEF, took an importantstep in this direction in March 2002, whenit released the first list of safe HIV/AIDSdrugs and suppliers. The list, which isbeing regularly updated, includes bothgeneric and research-based companies,ARVs and drugs for opportunisticinfections. Two Indian generic producerswere included, reducing concerns over thequality of locally produced HIV/AIDSdrugs. The WHO list highlighted theimportance of quality control being anintegral part of the technical capacity
building exercise to set up a competitivegeneric industry.
Issues relating to drug quality andeffectiveness of ARV in resource-limitedsettings have been addressed in severalstudies by the WHO and independentmedical researchers. The WHO, whichestimates that ART can be extended to3 million people by 2005, hasdocumented treatment regimens that aredesigned specifically for resource-poorsettings and set out guidelines for suchtreatment. These guidelines outline whento start ART and describe recommendedfirst-line and second-line ARV regimensfor specific subgroups of patients. Theguidelines also recommend the setting upof a parallel HIV drug resistance sentinelsurveillance system and “innovativestrategies for enhancing adherenceto ART”.
There are lessons to be drawn fromthe success of DOT in TB controlprogrammes. While there are few studiesto show that adopting a DOT approachwill work in HIV/AIDS programmes, itcould be attempted for some subgroupsof PLWHA.
UNAIDS has documented a number ofcase studies that show that theeffectiveness of ART in reducingmorbidity and mortality in developingcountries such as Thailand, Uganda, Braziland Senegal is comparable to that in highincome countries. Managing ARVtreatments at district-level hospitals inSouth Africa, Kenya, Uganda and Senegalhas proven to be feasible, though notsimple.9 Further, research on ARVregimens in resource-poor settings iscontinuously evolving. Though thesample sizes in pilot projects have beensmall, the evidence so far has beenencouraging and needs further work. Forthe South Asian region, this is particularly
�������������
�����������
�������� ���#
������
�� �����������
���������������
��������&��
��� ������
�����������������
�������
��������

������������
������������������������ ���
������������������������ �������������� !124
important since evidence from otherregions, though useful, is not adequate todevise appropriate ART strategies.
Along with care and prevention, access totreatment is an essential part of the battleagainst HIV/AIDS. The implications ofinternational trade treaties such as TRIPSand technological capabilities underscorethe need for a multi-pronged approach totackle the disease. The elements of such anapproach are:� ensuring prevention programmes and
care programmes work in tandem andnot in an isolated manner;
� studying the feasibility of providingHAART through DOT and applying itwhere it is found to be successful;
� encouraging technical cooperationamong countries in the region to makeARV drugs available;
� encouraging public-private partner-ships to offer ARV drugs at reasonableprices;
� encouraging pharmaceuticalcompanies to take up differentialpricing for developing countries tomake the drugs more affordable;
� adopting a larger public healthapproach and strengthening thegeneral health infrastructure; and
� placing HIV/AIDS at the centre ofdevelopment strategies and publicpolicy.
��) "�� ������� ���*��
The expansion of injecting drug use inSouth Asia has been a factor in the spreadof HIV/AIDS in the region. The infectionspreads through the use of shared needlesand also through the sexual route to thewives and sexual partners of injectingdrug users.
Much of the official response to injectingdrug use has been to de-emphasise its socialimportance and stigmatise users as
marginal members of society. Womeninjecting drug users are heavily stigmatised.As with other aspects of HIV/AIDS, the drugconnection has not yet become a part ofthe official dialogue and response in manycountries. Throughout the region, drug useis illegal and this leads to harassment bythe police. This only prevents injectingdrug users from availing of counselling andtreatment services.
Most countries offer some detoxificationservices, but a wider set of harm-reductionprogrammes that focus on both drugabuse and HIV infection hardly exist, withjust one notable exception. Despite druguse being illegal in India, the northeasternstate of Manipur has undertaken harm-reduction services on an experimentalbasis in an attempt to reduce thevulnerability of injecting drug users. Theprogramme includes needle exchangeand education about sterilising drugequipment. This is the only needleexchange programme operating in thecountry.10 The results have been positive,with a one-third decline in HIV infectionsamong injecting drug users between themid and late-1990s.
& ������� �������� ������
�� �� ������
Given this background, the potentialexists both for HIV to spread beyondinjecting drug users and for a range ofactions by policy makers and influentialauthorities. The policy response mustinvolve the following:� recognising that injecting drug use is
a factor in national HIV epidemics;� ending the prevailing discrimination
and marginalisation of injecting drugusers, with legal reforms, wherenecessary; and
� taking up harm reduction strategies,including needle exchange program-mes and education about sterilisinginjecting equipment.
���� ������������
�������������� �����
�������������
%�)�����
������������
�����������
�������������
����������� ����#
���������������
������&������
������

������������
������������������������ ���
������������������������ �������������� !125
��� "�������� !������������+����
The fact that adolescents are sexuallyactive is a reality most South Asian societiestend to deny. Despite high levels of sexualactivity, adolescents were found to havelimited knowledge about STDs, RTIs andHIV. Ignorance about sexual health issuesmakes them less able to make informedchoices about safer sex and, hence,increases their vulnerability to HIV/AIDS.The problem is compounded by the factthat, across the region, policy makers andopinion leaders disapprove of efforts toincrease adolescents’ knowledge aboutsexual health and see it as polluting youngminds. Girls are especially vulnerable sincethey have little control in sexualrelationships and are not supposed to beaware of sexual matters. Some countrieslike India, Bangladesh, Sri Lanka and Nepalare making attempts to make youth awareof sexual health issues and improvereproductive health services but suchefforts are not systematic. Sri Lanka standsout as the only country whose Populationand Reproductive Health Policy hasspecific provisions about adolescents.
Moreover, a large number of young peoplealso form part of mobile populations, withassociated vulnerabilities.
& ������� �������� ��,-������
���� � (������� ��� ������ ��
Any effort to check the spread of HIVamong the youth has to first acknowledgethe fact of adolescent sexuality. The otherelements of the strategy to reduce thevulnerability of youth should be:� Undertaking IEC programmes that
will increase the awareness of youthabout matters relating to sexual health;and
� addressing gender inequalities anddisempowering norms in life skillsprogrammes.
��. �-� ���/��� 0����������&��-� ���
Over the last two decades, responses toissues related to gender and HIV have beenintensified to address the problem multi-sectorally and to take on more issues asthe epidemic continues to spread. Issuessuch as mother-to-child transmission,access to treatment, access to moreinformation and legal rights havebeen taken up at various levels bygovernments, civil society organisationsand international bodies. While gender isthe underlying issue inevitably addressedby most of these interventions, a specificanalysis of gender-centred responses isnecessary.
The inequalities in societies in South Asiaare most manifest in the field of genderrelations. Policies and practices designedby or enforced by men curtail female accessto education and information, healthcare,decent work, proper nutrition, andsecurity. Though many South Asiancountries are making progress inpromoting women’s access to socialservices and involvement in decision-making, there is still strong socialresistance to such changes both withingovernments and major social institutionssuch as religious groups and businesses.
One area in which limited progress hasbeen made is the violence againstwomen, especially by men. From publicbeatings and executions (Afghanistan), totrafficking in young women (seemingly,in all the countries of South Asia), todomestic violence (in all the countries),women are regularly sexually intimidatedand sexually abused. In Bangladesh, as inother countries, “male authority overwomen’s sexuality is socially accepted…and reflected in violent behaviour withinmarriage.”11 In Pakistan, a 1987 study bythe Ministry of Women’s Development
�������������
����&����������
�������� ������
����������������
��&��'��������
�����������������
�(�������

������������
������������������������ ���
������������������������ �������������� !126
indicated that domestic violence takesplace in approximately 80 per cent of thehouseholds.12 Violence also is expressedin less direct ways, such as denyingwomen and adolescent girls adequateand appropriate information about RTIsand STIs, about the female condom, orabout risks of HIV infection. Theassociation of commercial sex workerswith HIV transmission, without referenceto the reasons why women are involvedin sex work, contains built-in biases andcontributes to further discrimination inproviding them with various services.For women and girls from low-incomegroups, the violence of sexualexploitation is a real or potential out-come of struggling to survive in difficulteconomic circumstances. Social andeconomic disruptions increase thelikelihood of what is sometimes called“survival sex”—exchanging sexual favorsfor food, small amounts of money, ortemporary security.
The result of inequitable gender relationsis higher risk of HIV transmission, forwomen and men, and countries as awhole. Limited literacy and access to non-written forms of information preventsboth men and women from becomingaware about HIV/AIDS and how it can beprevented. These factors also increasethe likelihood of misunderstandings,setting the stage for stigma anddiscrimination and the further spread ofHIV. If the pattern seen in Africa issubsequently replicated in South Asia,women are likely to suffer increaseddomestic violence and stigma if and whenthey reveal they are HIV positive.
The prevention, care and support needsof men and women are different, not justbecause of their physiology but moreimportantly in the context of gender rolesand relations. Programmes that foster thedevelopment of women-controlled
prevention technologies is one suchexample. Providing women with femalecondoms and micobicides are gendersensitive efforts which need moreencouragement in the region.
On the other hand, there are alsoprogrammes that have recognised theunique vulnerabilities that men are facedwith. The Healthy Highways project inIndia was one such effort to reducethe vulnerability of truck drivers, crewmembers and their paid sexual partnersto STDs and HIV/AIDS. The response tothe programme was positive as menwelcomed the services and expressed aneagerness to get more information. Theproject is implemented through 30 NGOsand 18 transport companies.
It is well accepted now that a multi-sectoral response is the need of the hour.This, in turn, demands that policies andprogrammes comprehensively addressissues that foster gender inequality andvulnerability. Coercive programmesand policies not only violate individualrights but invariably do not elicit thedesired results. There is need to providegreater access for women and girls toproductive resources such as education,employment, legal assistance, dispel theculture of silence and shame thatsurrounds sexuality, and protect girls andboys from adverse effects of genderstereotyping.
Much of the analysis and description ofHIV and women is couched in thelanguage of “vulnerability”, which is notan operationally useful concept if thereality of women’s lives have to bechanged.13 Focusing on those issues thatdisempower women runs the risk ofdiverting attention away from those areasof women’s lives where they are capableof ordering the world differently. It hasbeen argued that if the conditions of
*�������������
��������
��� ��'��
'� ����������
��&������������
�����������'��
��� ����������
���'� ��+�����
'�������������
������������������
����'����
������������

������������
������������������������ ���
������������������������ �������������� !127
women’s lives are to be changed in waysthat will make a fundamental differenceto the global experience of HIV/AIDS, itwould be desirable to learn from policyareas where outcomes are clearlybeneficial and apply these to the globalresponse to HIV.14 The population policyin parts of South Asia has been cited as agood example of this. However, theselessons cannot be directly applied todifferent situations. At best, they point theway forward and are evidence of what canbe achieved through policies andprogrammes that are relevant andeffective.
There is general agreement that highfertility imposes unreasonable burdens onwomen and that reductions in family sizelead to improved standards of living forall members of the family. Moreover, thereare gains for society in general throughreductions in the level of poverty and abetter educated and more healthy youngergeneration who grow into moreproductive adults. There are also gains tothe State in the form of faster economicgrowth and lower rates of publicexpenditure (in areas such as educationand primary healthcare).
As in policies for HIV/AIDS, the problemlay, in part, in putting in place thosepolicies that would be effective insupporting women—and to some extentmen—in limiting family size. This meantchanging a world in which women havetraditionally had little or no voice overmatters relating to fertility. The argument,quite simply, is that if women were givenmore voice and more power they wouldchoose lower rates of fertility, as a result ofwhich there would be profound outcomesfor women and children and substantialsocial benefits. Similar arguments couldbe made in the case of HIV/AIDSresponses as well.
& ������� �������� ������� ���
�������� � ���� � ������
As long as gender inequality exists,women’s rights and opportunities to resistthe infection, to assert their reproductivechoices, to demand safer sex and tosupport their families will be threatenedand the epidemic will grow in scope andimpact. A range of policy-makers andservice providers need to take up strategicgender interests and power dynamics toseek effective solutions. Some of thesesteps would include:� creating gender-specific information
in simple language;� providing gender-sensitive individual
and group counselling services;� providing widespread sex education
services and programmes withadolescents;
� sensitising and training healthcareprofessionals;
� imparting more information to theaffected groups on women’s rights;
� empowering women through capacitybuilding interventions;
� involving men as partners; and� ensuring that programmes
encompassing care take into accountthe fact that women have no supportand care facilities, and providingadequate care and support services
��1 !� ��������� �� �����
The challenge of HIV/AIDS, and the needto address the epidemic at multiple levelsin order to ensure a comprehensiveresponse, requires the development ofinnovative partnerships and dynamicnetworks that will work in a collaboratedmanner. This involves bringing togetherpartners from different sections ofsociety—government, media, civil societyorganisations, private sector, UNagencies, donors and PLWHA—andmoving beyond the focus on traditional
�������������
� ���
�����������
����������'� ��
��������
������������
�� �����,���������
� ������
����������������
�������� � ������
������ ����

������������
������������������������ ���
������������������������ �������������� !128
public–private partnerships. Such anapproach will, for example, explore howthe private sector and media can supportthe work of civil society organisationsor how PLWHA can play a role ingovernment initiatives.
The field of HIV/AIDS has seen examplesof collaborative initiatives, although farmore needs to be done. These initiativeshave clearly demonstrated that innovativepartnerships can enhance outreach andeffectiveness by pooling differentstrengths and reaching multipleconstituencies through coordinatedaction. Such examples include the path-breaking work done by advocacy groups,PLWHA groups, research institutions,service providers, NGOs and the media.
Social mobilisation is at the heart of anystrategy for reducing the spread andimpact of the epidemic. Lessonsemerging from implementation havedemonstrated the need to link theseefforts at the micro-level with broaderissues of poverty, gender equality andgovernance at the macro-level. This canonly be done through creative anddynamic partnerships within andbetween sectors that allow multipleactors to work together to produce results.
"��������-����� ������ ������
The issue of access to treatment is a clearexample of civil society organisationscoming together to form strong andeffective alliances. In April 2001, 39pharmaceutical companies dropped theircase against the Government of SouthAfrica,15 allowing the government toimport ARV drugs. This withdrawal cameafter unprecedented public pressure dueto the campaign for access launched byseveral national and international civilsociety organisations. Prominent amongthese were Medicins Sans Frontiereswhich won the Nobel Peace Prize in 2000,
Treatment Action Campaign (TAC) andOxfam International. The work of civilsociety partnerships in this area alsoextended this pressure to policy makersand the sustained campaign world-wideto provide affordable drugs to poor peoplepaved the way for the Doha Declarationon TRIPS and Public Health in November2001. In December 2001, TAC won a courtcase against the Government of SouthAfrica, leading to a governmentcommitment to provide Nevrapine toprevent MTCT, another example of civilsociety collaborating across borders toinform public policy.
South Asia has seen the development ofseveral innovative partnerships betweensex workers’ organisations and NGOs/community-based organisations workingon several gender-related issues, such asanti-trafficking. These partnerships haveresulted in the formation of regionallyreplicable models of ‘self regulatorymechanisms’ at destination sites, whichcurtail the trafficking of minors andpersons coerced into sex work and reducetheir vulnerability to HIV. The success ofthe Sonagachi project in Kolkata, India,and the various sex workers’ collectives inBangladesh in strengthening HIV/AIDSresponses have demonstrated thesignificant impact such partnershipshave on sustaining integrated and rights-based responses.
�!23� ������ ���� � �� �� �����
A non-profit organisation, Family HealthInternational’s (FHI) manual titled,Workplace HIV/AIDS Programs: AnAction Guide for Managers (2002)aims to develop and sustain effectivepartnerships between the privatesector, labour unions, managers andmedical personnel. The manual isdesigned for use by companies’ humanresources managers, medical officers andunion representatives. It provides
����������
��������������
����������������
���������������
���������
����������������
�����������
�������
������������
������
�����������
�������

������������
������������������������ ���
������������������������ �������������� !129
comprehensive guidance in assessingthe real and potential impact ofHIV/AIDS on companies, in developingan HIV/AIDS policy to cover theworkplace and in designing andimplementing HIV/AIDS preventionand care programmes for the workplace.The guide also includes examples andcase studies of how other companieshave responded to the epidemic.
The ILO has also undertaken initiativesto address the issue of HIV/AIDS at theworkplace. It formally launched apioneering Code of Practice on HIV/AIDSand the World of Work at the UNGASS.“This code focuses on the world of workbecause so many people with HIV can befound there,” the director-general JuanSomavia said on the occasion. “Of the 36million people infected with HIVworldwide, we estimate at least 23 million,or three-quarters, are working people aged15 to 49 years, often our most productivepeople, people in the prime of their lives.”
The ILO Code of Practice is aimed atproviding workers, employers andgovernments with new globalguidelines—based on internationallabour standards—for addressingHIV/AIDS and its impact at theenterprise, community and nationallevels where most infections occur. It willalso help boost efforts to prevent thespread of HIV, manage its impact, providecare and support for those suffering fromits effects and reduce stigma anddiscrimination, which arise from it.
The Code of Practice is part of newILO efforts to mitigate the impact ofHIV/AIDS in the workplace. Whileseeking to promote prevention incountries where the epidemic alreadyhas a strong grip, it is also designed tohelp prevent an increase in infectionrates in relatively unaffected countries.
What is more, it also provides guidance onsuch issues as testing, screening andconfidentiality, non-discrimination inemployment, and gender issues.
Governments and NGOs in South Asiahave not made major efforts to stimulatethe private corporate sector in HIV/AIDSprevention efforts. Nepal and Sri Lankahave initiated limited programmes to reachworkers within the private sector. Overall,however, there has not been an effectiveanalysis in the region of:� how business policies and practices
(such as requiring employees to travelfor extended periods or operatingconstruction projects that attract singlemen and commercial sex workers) maycontribute to the risk of HIV/AIDS risk;
� initiatives by government, businessesand labour to stimulate collectivedialogue about HIV/AIDS prevention;or
� advocacy with businesses to stimulateeffective workplace responses.
Although several efforts have been made inIndia to stimulate greater awareness andinvolvement of the private corporate sectorin HIV/AIDS prevention, most companiesremain without workplace policies orprogrammes. The Corporate sector in Indiahas established the Indian Business Trust forHIV/AIDS (IBT) in 2001 to address criticalissues related to HIV/AIDS through multi-level partnerships. The Confederation ofIndian Industry (CII) and ILO in partnershipwith NACO, India, are implementingworkplace intervention. CII has alsoadopted workplace guidelines for membercompanies, but progress towardimplementation is limited. Trade unions,too, have been slow to respond; theirattention is instead focused on job securityissues in the context of economicliberalisation.16 Nevertheless, national andstate governments and some internationaldonors, continue to urge the private sector
-����� �������
.-/���������
������������
���� �!���������
����� ���������
�������� ���������
�����������������
������������������

������������
������������������������ ���
������������������������ �������������� !130
and unions to adopt a more aggressiveresponse to the growing HIV/AIDSepidemic.
There are limited examples within SouthAsia of company polices and practicesdesigned to reduce the risks of HIV amongemployees and to reinforce non-discriminatory practices toward HIV-infected employees. Some companies inIndia have begun formulating HIV/AIDSpolicies and, with assistance from NGOs,implementing prevention programmesfor workers. As a part of Sri Lanka’sreproductive health policy, inter-ministerial collaboration is beginning toprovide health information to femaleworkers in the Free Trade Zones. Workers’leaders, supervisors, and managers offactories all receive training in dealingwith a variety of risk reduction strategiesand potential problems on shop floors.
Indian steel major, Tata Steel, took animportant initiative in corporate sectorinvolvement in HIV/AIDS programmes inthe town of Jamshedpur, Jharkhand.17 Thecompany established a group of doctors,educationists and community workers todevelop and implement education andinformation programmes and undertakecounselling and medical guidance. Thecompany went beyond its workers and theirfamilies and developed an outreachprogramme to cater to the needs of migrantlabourers, truckers and army and policepersonnel. Condom vending machineswere installed at various places. Completemedical care is provided to all employees.Emphasis is also given to prevention ofopportunistic infections as well as nutritionfor good health. Counselling and socialsupport is also provided. The programmeis extended to the larger community and allother companies in the town.
In general, governments have not madeworker health and safety a priority. Existing
laws and regulations are not enforced andnew collaborations with businesses are notpursued. Rather, NGOs have been theprimary initiators within India in terms ofengaging both urban and rural-basedbusinesses to address HIV/AIDS. Indeed,businesses themselves find limitedguidance or dialogue with governmentauthorities. For example, a study ofcorporate attitudes and practices inMumbai, India, found that businesses“rated support from community leadershigher than campaigns by government….”.18 Thus, there is a basis for coordination andcollaboration. Businesses often feel theyare expected to initiate HIV/AIDS policiesand programmes on their own. In reality,governments and NGOs can offer a wealthof experiences in the design and implemen-tation of prevention and care programmes,assist in shaping policies, and monitoreffectiveness of implementation.
Leveraging private sector changes canexpand overall prevention and careresponses. This can take two forms:regulatory actions and financial incentives.Regulations are likely to be a result ofgovernment action to set standards andmechanisms to ensure adherence to thosestandards. Governments can requirecompanies not to test potential or existingemployees, to keep medical data onemployees confidential, or can levy a taxto help pay for HIV/AIDS programmes.Regulations relating to benefit coverageand workplace rights can also beformulated as a result of negotiations withunions or worker associations.
Financial leveraging can result when onecompany encourages (or requires) acontractor to take action on HIV/AIDS inreturn for continued business or discounts.Insurance companies can offer premiumdiscounts to company policyholders thatmaintain effective HIV/AIDS preventionprogrammes for all or some employees.
�����������
����� �������
.-/������������
'��������
�(���������������
��������
� ��� �����������
�������������������
����� ������
�����������������
���� ������
��������������
� ��� ���������

������������
������������������������ ���
������������������������ �������������� !131
������� �������� ����� ��4
Involving religious leaders in campaignsrelating to HIV/AIDS can be quiteeffective. In the region there are examplesof Christian and Muslim religious leadersbeing involved in AIDS awarenesscampaigns. Both India and Bangladeshhave attempted to enlist imams in theHIV/AIDS campaign. The choice ofimams probably stems from the fact that,by virtue of leading prayers at a mosque,they carry authority, enjoy mass reach,possess the power to convince and theyhave a captive audience every Friday.Before prayers, they deliver the khutba,or sermon, during which, in addition toreligious topics, they may choose toeducate their congregations on education,civic sense, hygiene or health.
The plan to enlist imams has beeninspired by a hugely successfulexperiment in Africa. It involvedmotivating and training imams inUganda, Senegal and Ghana who thenwent to their mosques and told people ofways to avoid HIV/AIDS. In Uganda, thiseffort was called the “Jihad AgainstHIV/AIDS”. The model, hailed by the UN,is now inspiring other countries with largeMuslim populations to devise a specificallyIslamic approach to HIV/AIDS preventionthat combines health information withKoranic teachings proscribing adulteryand pre-marital sex.
But a contentious issue is the useof condoms. Imams fear thatrecommending them could promote sexoutside marriage. It took HIV/AIDSproject leaders in Africa a year to convinceimams that the condom was only beingpromoted after the failure of the first twolines of protection—abstaining from sexand having sex only within marriage.“Don’t forget that human beings haveweaknesses,” Islamic leaders were told.However, the message was ignored.
Then campaigners tried another tactic,pointing out that knowledge of condomsdid not imply that they would be usedirresponsibly. After all, they argued,Muslims know all about alcohol but itdoesn’t mean they drink withoutrestraint. This argument seemed to work.Finally, after much deliberation, Islamicleaders consented to let imams promotecondom use.
Another vital message the imams will beexpected to put across is the need forhumane behavior towards those who areHIV-positive. The imams will be urged toteach compassion and to condemn thetendency to stigmatise.
��5 "�6��-�������� "������ �����'��� �������������
This section focuses on two aspects ofpolicy responses: policies directly relatedto HIV/AIDS and policies that form thesocio-economic context of the epidemic.The latter are particularly important,given that HIV/AIDS arises fromdevelopmental failures and canexacerbate those shortcomings, if notaddressed in a holistic manner. Mostcountries in the region have policies todeal with a variety of social, economic,and cultural development issues,including poverty. Thus, there is soundprecedent for adapting andimplementing existing policies anddesigning new policies to controlHIV/AIDS and mitigate the impact of thedisease on individuals, households,communities, and nations. “What theHIV epidemic does is to illustrate onlytoo well the costs of previous failure, andthe fact that if we are to prevent anexpanding epidemic which hasenormous potential to disrupt not onlydevelopment but also social, economicand political structures, then we have to
������������
� � ���������
�� ���� ����
��������������������
����������������
����� �0��������
����������������
��!��� ��������
����������'��
���������������
�����������
����������������
������*������

������������
������������������������ ���
������������������������ �������������� !132
ensure better overall developmentperformance.”20
There is widespread agreement that thevulnerability to HIV/AIDS is linked topoverty. Unfortunately, the linkages havenot been adequately analysed to assistpolicy makers or advocacy groups inoutlining policy and programmaticresponses that alleviate conditions ofpoverty and reduce HIV vulnerability. Partof this problem stems from poverty beingviewed as a static condition rather thanas an outcome of processes of change. Asmentioned earlier, ‘impoverishment’ is amore comprehensive concept, suggestingas it does a dynamic set of processesleading to poverty. In previous sections,we have shown how some of theseconditions (unemployment, loss ofassets, lack of access to social services etc.)relate to HIV/AIDS.
6��� � � ������ �� �������
Given the human development deficit inSouth Asia, in terms of levels ofachievement in literacy, longevity andlivelihood, as also fiscal compression ofthe 1990s, it is essential to put preventionstrategies at the forefront of the policyresponse to HIV. Providing knowledge,awareness and skills to the population atlarge is absolutely necessary to containthe spread of the epidemic.
Prevention strategies must:� address sustainable behaviour change;� address the gap between knowledge
and practice;� integrate care and support for its
successful implementation;� must be tailored to specific
populations such as:� men who have sex with men;� women and children;� injecting drug users;� armed forces /uniformed forces;� brothel and non-brothel-based
sex workers and their clients; and� mobile populations (migrants,
refugees, people displaced inconflict)
� incorporate principles of GIPA andinvolve PLWHA in such actions; and
� Integrate HIV prevention strategieswith development actions such asenhancing livelihood opportunities,providing information and support forsafe mobility etc.
It must be borne in mind that preventionstrategies have traditionally evolved in adeveloped country context, and,therefore, focused on individual behaviourchange, especially sexual behaviour.Given that household and communityvalues play a major role in South Asiansociety, it would be essential to tailorprevention strategies to addresscommunity concerns relating to HIV.This would ensure that prevention stepsfor ‘safer sex’ such as condom use are notseen as an endorsement of individualpromiscuity, but as agents for socialresponsibility.
It would, thus, be important to enlist theSouth Asian communitarian traditionsand religious sanctions as allies in thebattle against HIV.
�� �� ��� ���� �
The apprehensions regarding access totreatment and care arise from theselective calculation of the costs ofproviding treatment and care, whileignoring the need to assess the cost of notdoing this. Treatment, care and supportare part of the prevention continuum andeach element is incomplete without theother. Focusing primarily on prevention,without giving equal attention to care andtreatment, creates barriers in the way ofthe complete and active involvement ofPLWHA, thus weakening the effectivenessof responses. Moreover, community
)�������
&��'�����
�'���������
&����������
������������������
�����������
����������
�����������������
������������ ���

������������
������������������������ ���
������������������������ �������������� !133
concerns and extended family structuresin South Asia offer ample opportunitiesfor involving communities and familiesin providing home-based care, especiallysince the health infrastructure in thesecountries are unable to cope withcontinuous and long term care. Thequestion, therefore, is not whether toprovide care and access to treatment ornot, but rather how to do it. The followingissues must, therefore, be kept in mindwhen designing strategies for care,support and treatment:� understand the importance of
voluntary counselling and testing;� act to prevent mother to child
transmission;� identify appropriate financing
mechanisms;� seek support from the private sector;� manage TB as a major opportunistic
infection; and� aim towards treatment for all.
��4 ����(��� ��������������������$"��!
The following are some of requisite policy-oriented steps to address HIV/AIDS inSouth Asia:� Collection and quick dissemination
of relevant data. Given the currentlow prevalence rates of HIV in thecountries of South Asia, it is most costeffective to track prevalence throughselective surveillance systems that willmonitor changes in HIV/STI andbehaviour in the vulnerable groupswhere the disease tends tobe seen early on. Any policy intendedto gather HIV data from selectgroups must be accompanied byconfidentiality and by effectivecommunication to the public in orderto reduce stigma and to avoid thesense of complacency that theepidemic is associated only with thegroups from which data is obtained
� Demonstrate strong leadership,through commitment and action,and foster networks of leaders drawnfrom all levels of society, who willwork together to address theunderlying causes of HIV/AIDS andrevolutionise responses. Pioneeringleadership by governments is essentialfor containing the epidemic atnational, regional and global levels,as emphasised in the UNGASSdeclaration, and should becomplemented and enhanced byleadership from civil society and theprivate sector
� Reinforce commitments to the GIPAprinciples. This will also involve theprovision of substantive resources andsupport to national and regionalorganisations, groups and networks ofPLWHA, as well as to civil societyorganisations that work to supportand empower those vulnerable andmarginalised communities mostaffected by HIV/AIDS. This will playan important part in ensuring effectiveand rights-based responses bybuilding the capacity of those who aremost affected to play a central role inall responses to the epidemic.
� Encouraging political, social,economic, religious and culturalleaders to openly discuss HIV/AIDSwith their constituents. UNAIDS andothers speak of “breaking the silence”that surrounds HIV/AIDS, sexuality,and inequalities that drive theepidemic. The family planningprogrammes provide a ready examplein which leaders with diverseperspectives joined in the discussion.In the case of HIV/AIDS, these leaderswill need reliable information in orderto offer clear, non-stigmatisingmessages
� Adapt lessons and examples fromother countries in the region andAfrica. Policy makers and opinion
���0�������
����������������
'�����������������
����������������
����� �����������
�������������'���
������

������������
������������������������ ���
������������������������ �������������� !134
leaders need to be aware of theimpact of HIV/AIDS on families,communities, businesses and nationsin other countries in order tounderstand the grave proportions theproblem can assume if not tackled
� Learn from NGOs that have beenactive in prevention and care. NGOshave taken the lead in addressingHIV/AIDS, injecting drug use, genderequity, youth outreach, transportworkers health needs, and a variety ofother issues. Their experiences areinvaluable guides for informing policy-makers and for strategic planning
� Include consideration of the causes ofHIV/AIDS in the design andimplementation of all socio-economic projects. This will beespecially important for the regionwhere the epidemic is growing rapidly.This issue especially needs to be a partof any reconstruction programme inAfghanistan and in Afghan refugeecamps in Pakistan and Iran
� Accord priority to policies andprogrammes for sex education foryoung people and adolescentreproductive health services. Caremust be taken to see that such effortscover all young people in formal andnon-formal settings as well as marriedadolescents
� Implement policies and statementson multi-sectoral responses toHIV/AIDS within a humandevelopment paradigm. Such policiesalso need to complement andstrengthen inter-ministerial workinggroups. Multi-sectoral responseswill include government and civilsociety responses at all levels.Implementation of such multi-sectoralresponses will be a combination ofnational responses at various levelsand diverse forms of communitymobilisation
� Continue to advocate innovative
policies and the implementation ofexisting policies promoting greatergender equality. This will involve notonly achieving greater equity insociety for women, but re-definingappropriate and responsible malenorms and behaviours (includingcondom use within marriage) thathinder equity.21 Continued progresson revising inheritance laws, withreinforcement for changes in socialattitudes about inheritance rights, isessential for gender equality and forlong term response to women andchildren affected by HIV/AIDS.
� Draw up policies and potential lawsfor the protection of PLWHA fromdiscrimination. Other policies andlaws are likely to be needed to supportpeople affected by HIV/AIDS, e.g.,widows, orphaned children, traffickedwomen, who may lose property, beunable to attend school, or beexcluded from certain jobs because oftheir association with a person orgroup who is infected.
� Greatly expand business involvementin the arena of HIV/AIDS responsesas part of corporate socialresponsibility, including formulationof business and union policies.Governments can more aggressivelyengage businesses to develop policiesand prevention programmes, as hasbeen done in the Free Trade Zones ofSri Lanka. Standards of behaviour andresponsible sexual and socialpractices within the workplacecan have a significant influenceon behaviours outside the jobenvironment.
� Develop comprehensive responsesto reduce mobility-relatedvulnerabilities. Comprehensivestrategies and action on the ground toreduce such vulnerability at source,transit and destination areas need tobe developed on a priority basis.
.������ ��
�������
�������������������
����������������
���������������
� ��� �����������
��������#����� ��
���!����

������������
������������������������ ���
������������������������ �������������� !135
Involvement of government sectorsdealing with armed personnel, para-military forces, railways, mining,labour etc. which generate large-scalemovement is crucial to sustainableHIV/AIDS prevention and careamong mobile populations.Responses and strategies must ensurethat the migrant population is notstigmatised as a result of focusedinitiatives and that the rights ofindividuals to move are upheld as abasic human right.
� Develop polices and laws that operatein synergy to protect and enhance therights of those infected or affectedand recognise the centralimportance of a rights-basedapproach to effective responses. Inaddition, comprehensive efforts mustbe made—through sensitisation andawareness programmes and creativepartnerships with the media—to fostera normative environment in whichHIV-related stigma and discriminationare reduced and values of tolerance,acceptance and human dignity arepromoted. Only in such an environ-ment will the full implementation ofrights-based laws and policies bepossible.
���7 6������ "����
In South Asia, as in many other parts ofthe world, the underlying factors thatmake people vulnerable to HIV/AIDStranscend borders. Hence, containing theepidemic within national borders aloneis not enough to make the response to theepidemic meaningful. There are alsodaunting challenges, ranging from acutegender inequality to severe stigma anddiscrimination of PLWHA, within theregion. This collective vulnerability of theregion—particularly that which arisesfrom the mobility of people, trafficking inwomen and children and conflicts—calls
for integrated, inter-country responses.Regional cooperation, a shared agendaand sharing of knowledge and experiencewill also strengthen the national-levelinitiatives and help cost-effectiveprogramming. To gainfully use thewindow of opportunity provided by theseemingly low prevalence rates in theregion, the following regional level actionsare required:� enhance regional cooperation and
shared political commitment onHIV/AIDS issues among nations andgovernments;
� promote regional networks betweencivil society partners across South Asiafor shared learning, capacityenhancement and the developmentof a strong, regional, civil society voice;
� foster sustained, committedleadership in the region to raiseconcerns regarding HIV in South Asiaat regional and global fora, in order tomobilise international support andresources;
� undertake concerted internationaladvocacy for the recognition of thevisibility and gravity of the epidemicin the region at the global level;
� develop inter-country dialogue andcollaboration between governmentsto address issues of trans-borderconcern, such as migration, traffickingand conflict;
� undertake advocacy to ensure theratification and implementation ofrelevant conventions and commit-ments, as well as develop newcommitments through regional forasuch as SAARC, particularly to protectthe rights of PLWHA and vulnerablepopulations;
� develop regional-level strategies toaddress the common norms, valuesand taboos that fuel the epidemic andfeed the stigma and discriminationfaced by PLWHA and vulnerablegroups within the region;
%������
��������������
���������������
��������
&��'��������
�(���������'���
����������������
��������#�����
�������������������
���#���������
����� ���

������������
������������������������ ���
������������������������ �������������� !136
� share best practices from around theregion for learning and scaling upefforts;
� enhance scope for South-Southcooperation and developmechanisms for mentoring and on-going technical support for enhancingcapacity;
� provide support in enhancing accessto treatment through inter-countrymemorandums of understanding(MoUs) and trade agreements for thesupply of cheap generic drugs; and
� provide support for regional PLWHAnetworks and fora that will enable HIVpositive people across South Asiadevelop shared agendas and strategiesin order to advocate for the needs andrights of those infected and affected atregional and global levels.
���� ������
In a region as diverse and complex asSouth Asia, HIV/AIDS policy responsesand needs cannot fit into a single mouldand it is not appropriate to say what isadequate or needed for each country. Evenwithin countries, different socio-economic conditions and past policyresponses shape how HIV/AIDS is viewedand addressed. The goal is to identify bothstrengths and gaps in policy responses inorder to guide further effective initiativesin this area. Special attention must begiven to policy responses relating tostigma and discrimination of PLWHA. Infact, these factors offer insights into howgovernments, businesses, and social andreligious groups address some of the keyfeatures of the epidemic, such as payingattention to the needs and interests ofalready marginalised socio-economicgroups or enforcement of legalprotections.
The relative incipience—or evenabsence—of a coherent regional policy
framework for HIV/AIDS in South Asia isstriking, given the long history of regionaldialogue on key development issues andthe existence of entities such as SAARC.Clearly, the debate on regional cooperationin South Asia needs to be broadenedbeyond trade and development to includean explicit recognition of HIV as a majorchallenge to development, peace andstability in the region.
The countries of South Asia have begunthe process of creating policies torespond to HIV/AIDS. Within nationalAIDS programmes and ministries ofhealth, there is a sense of urgency toexpand the scope of policies andprogrammes. International donoragencies have played a facilitating role innational responses. NGOs possessgrowing experience in preventionprogrammes. Thus, a foundation exists inmost South Asian countries for shapingnew policies, particularly those that willdiscourage stigma and discrimination. Therole of existing inter-governmentalmechanisms and institutions for regionalcooperation, such as SAARC, would becritical. It would also be important todevelop regional strategies with regard tothe provision of HAART and the entiregamut of care and support services,customised to the requirements ofresource poor settings. Mechanismssuch as the South Asia Free Trade Area(SAFTA) and also bilateral tradecooperation agreements could addressthe concern of affordable drug pricing,especially in the post-Doha scenariowhere developing countries have awindow of opportunity in terms ofcompulsory licensing and parallelcountry importation.
This could be the foundation for buildingnew responses, particularly those thatwill keep the epidemic at low levels andwill provide adequate care and support
������������
����������
�� ���(��������
�������������
�������������
���������������
���������������
�����������������
�����������������
'���������0����
������������������
��������

������������
������������������������ ���
������������������������ �������������� !137
policy-makers and opinion-shapers in allsectors ignore or deny the power of theepidemic, they are clearing thesepathways. Rather than serving theirconstituents, they are putting them at risk.
Above all, there is a need to recognisethat the challenge of HIV in South Asiacan be met more effectively through ahuman development framework and notsolely through a public healthperspective. More importantly, there isneed to go beyond rhetoric and actuallychange the methodology through whichHIV/AIDS is currently being addressedin South Asia.
for people who are and will becomeinfected. The overriding unknown is notwhether the epidemic will spread, for itsurely will. Rather, the unknown is thewillingness of groups at all levels of societyto openly address the disease, its causes,and effective means to control it. Thus, apart of the response is to speed up thetimetable for generating public andpolitical will. The level of motivation todo so is very mixed. HIV/AIDS can spreadrapidly, especially given the rightconditions. Across South Asia, thoseconditions exist and form pathwaysthrough which the epidemic can explodewithin the next several years. So long as
�'�����������������������������������������#���#���������� �&�����(��� �����)�����#���������#����#����������!�
9����� � ��2/;�������� � ������ 2/ ����&�������� � ��� �������
� ��!"4�!&�

��������
������ ����� ����������� �������������� ��� ����������� � ����� ��� ���� 139
��������
��������
� ���� ��� � �!��� ����� ��" #�
���#��� � ��#$������� � �!�% ���� ��
&� ��� !��� � ����� � �!��� '�� ���
����% ����" #�!���� ��������" �' ��$
��( �������� ����� ��� �!���% ���
�����! � ���� ��'� � ����� ����� �
��� '����) ����� ��' �����" � *� ���
!��� �!����� � ��� � �!���� � ����%
��� ��� ���#�� � !���� � ������� ������
��� +������ ��� ��� ���� #" ���� ����
���$���� ,-.�������/% ����% ����0)
+��!���� ���� ���� #��� ��!�� ����
!�����!��!" � ��� ���� ,'�� ���
���#��� ���� ���� ����� � "���
��� � ��� -���� ������ ��' �������� ��
#� � �!��� '�� ��� ��� �����"0 ��� �
���)
� ��/% ����1 2���% 3���#�� 4 �����%
�555
� 6��#�#$��$��7 ����� �����������
+�����% ����)
8 ������% ��� ��������!� ����� ����
������ � ���� � ��� ��#$������� � �!��
!������� ��� �9������" ��% ��% ��
�9�����% � :���'��� '�� �;); ��� !���
��� ����� � �!� '�� �� ��� !���
,-.�������/% ����0)
* �� ��� #��� ������ ��� ���� ����
������� �� ��� ������� � ��������
���% �� #���% �������� ��� ��� �9�!�
!��!�������) <���� � ��� ��� ���� ��
#� ���� �#��� ����) <�� �9���� � ����
���� � ���� � ��� �����" (��'� ���
����� ��� ���" ������� ��� � ���#�� �
���������!� !������) <�� ���� ��������!�
��� �!���!� ���� !���� #� � �����)
�� ������� � ��� -� .������
��������!� +������� ���=�!�� � ���"
�� ���#�� � ��� ���� �����) ��'����%
� � � !����������� ����)
> .�+/ ,����0% ����
& -.�������/% ����
; ����� :��(% �����
5 ?�����% ����1 3������ ��� ������%
�55&1 @�� �� ��)% ����
�� ����� ������" � ���� ���� �!���
������") �� � ��� ����� � !��!�� ���
����������� �� ��� �� �!!����#�� � �
,-.�? ����� ����������� ������%
�55&0
�� ��/% ����
�� -.�?% ����#
�� :���� ��� 6����% �55&1 :�����% ����1
6�!A����� ��� �����% ����1 /���% �55�
�8 :������ ��� :��(�% �55�1 :�����% �5551
:���� ��� 6����% �55*1 6����% �55>1
?"��% �55;% :��(�$�����% ����
��������
� +����� ��� ���% ����
� -.�?% ����
� -.�+�A% ����
8 � ����" #" ?��"���� �� ��) �55& �
<������ ��� ���� B��� �!����! ���!�
� �� ����� ���� ����� � �C��#�� ���
�� !��� ������ ��� ��� !���
�������� �����"��) <�� ����� �#�� ��
!��� '��� ��� ������� ��� ����� ���!����
���������� ����� � ��!������� '��()
<�� �!����! ���!� � �� ����� ����
����� '�� ���� ������ ���� ��� ���!� �
����� ��� ����� !�����) <�� � �����"
#�!���� ���� � �!�� � ���! !
���������% ����" ����� ������"
����������� ��� ���� �#�� �� !��� '��
��� ������� �������"D)
* :���� ��� 6����% �55>1 �)�5
> :���� ��� 6����% �55> ��� :���� ���
3���% �55�
& ����'��% ����
; ������� ��� ����% 8 @�����" ����
5 �����$��#������% ����
�� ����'��% ����1 �����$��#������% ����
�� ������� ��� ����% 8 @�����" ����
�� :�����%�5551 ����� �� ��)% ����
�� :���� �� ��)% �55&% �)�5&
�8 �����% �55&
�* 6����% �55>
�> ��� ����E��''')������)!�

��������
������ ����� ����������� �������������� ��� ����������� � ����� ��� ����140
�& :�����% ����
�; -.�������/% ����
�5 <����% �55;
�� <�� ����"���% '��� ���" ����� �� ��
������ '��( #" :���� �� ��) ,�55>0% ���(
� �� !��� ���� ��'���% � ����� � ���
����� ���#�� � !������� �� '�!� ����
��� �����#��% ��� �!������ ����� � ���
��� ����� ���� '�!� ��� ���!�� � ���
�����! !�� #� ��������% ��� ���
�����#��" � #����� �������� � ���
��������!� ��� ���� !����)
�� -� ���������"% ��!( � ��� �������
���������!� ���� �� ��� ������ �
������!� � �#���� ���� !���
�������� �� .����)
�� <�� ������� ���! !���� ����� ,���
<�!��!�� .��� :0 ��=�!� ��� ����
�"������� � �� ������� � �!� �����
��� � � �9��!���!" �� ��������)
�� /�� ������� ��� ��!����� ���� '�
�9!���� ��� ��#$������� � �!�� !�������
��� ��� ������)
�8 ������% ��� ���� ������� ���� ���� ���
����� �����!" ���� ����#�� � �����!�� #"
�����" ������ ��!�����" ��������� �����%
�� #" ���� "���� � �!����� � ���
��������� ��� �* "���� ��� �#���)
�* ����'���% ����
�> :���� �� ��)% �55&
�& ��� �� ��)% ����
�; :����% 6����% ������ ��� ���� ?���
����!����% ����
�5 ��!��� ������!� � +��#���% ��� !�����"
'�� ��� ���� �����!�� �����! � ���%
������������ ��� ������� ������� �
��!��" ���� ��!� ���� (��'���� � ��'
���� � ���������� ��� ���������) ?�����
��� ��� !���� ��� ���� �(��" �� ����
��9 �� � "����� �� ��� ��� !������
���� ��7�����") � ����" � :��C� ���'��
���� �����$7������� � ������ ��'�"
������� '�� ��� � ��� ����" �5;��
��� � �������" �� ��!�����" ���!����%
#�� #" ��� ����" �55�� ��� ����� ���
����� �� ���$����)
�� :�����% �555
�� ����� :��(% ����
�� -.A?�% ����
�� -.�?% ����
�8 F�'"���G +����!���% ����
�* -.�A�6% ����
�> <�� :��������� ���������!� �"����
,:��0 !����!��� #" .�+/ � ���� �������
���� ��� ������� �'������� '�� ����
����� '���� � ���� ������ ��!� �� :���
,��)> ��� !���0 ��� -���� ?������ ,�5)8
��� !���0) ,:�� �����"% .�+/% ����0
�& H����� �� ��)% ���� �� �����!� ��� ���
����� � 6����!������� � ��� -����
������ ���� �!����! ��������� ��� �
����� ������ ����!���� '�� ���
�!���!� � ����)
�; :���� �� ��)% �55&
�5 +?� ����% ����% �)�)
8� @� ��"�% ����1 2�(�% ����1 �����
������ /���C����% �����
8� ?�����!��% �5;�1 6!�����% ����
8� 6�? ����% �)��
8� �����% �555% �)�1 :�"��% A���� ���
:��C��% ����
88 ��'�� �� ��)% �55>
8* A��� ��� 2�����'��% �55�
8> .������ ������<� ?�����% :��������%
����
8& :���� �� ��% �55&1 .������ ������<�
?�����% :��������% ����% ?�(����
���� ?�������� ��!��" ����1 -.�?%
����1 ����� :��(% ����
8; ���% ����
85 6�?% ����% �)�&
*� <�� ������!� � ����#���C% A�!� ���
.�=��� ,�55�% ��)8�>$&0 ����� ������
������� �� ��� !��!����� #" ���� ���
����� � ������� �!��� �� �������
��� ���������� � ����� �� !������
�"���� � ��� ����" �'������ !�����")
*� 6����% �55*1 +������ �������� F���
.��'��(% ����
*� ?������ ��� ?�����% �55*% �);�&
*� :���� �� ��)% �55&1 /���% ����
*8 3� !�$� !��� � �� ��!���� � �!���
��7����" �� ��!�� ��� ����#���� �
�!��� ��������� ��� ���������) �
�!��� � ����#���� �7����" �!���� ���
���������% ��� !�$� !��� � �7��� ��
C��� ��� � �' ��������
�����������" ���� ��� '�����% ��� !�$
� !��� � !���� �� ���)
** A�� ���� ������% ��� <�!��!�� .��� :
*> :���� �� ��)% �55&
*& :���� �� ��)% �55&
*; 3������ ��� ��#��% ����% �)��
*5 �������% �55;% �)�8&
>� :������ �� ��)% ����
>� :���� �� ��)% �55&
>� :����% 6���� ��� ���� ?��� ����!����%
����
>� 3������ ��� ��#�� ����% ��� �� ����!��
!��� ������
>8 :������ ��� :��(�% �55�1 3������ ���
��#��% ����% ��)&$;
>* 2'����#�% �55&
>> :����% 6���� ��� ���� ?��� ����!����
����
>& :����% 6���� ��� ���� ?��� ����!����
����% �)&
>; :���� ��� 6����% �55> ��� �� ����!��
!��� ������1 3����% �55�
>5 2��=��� ��� A���"���% �55&
&� :������% ������ ��� 2#��% �555
&� 6����% ����
&� :���� �� ��)% �55&
&� ����� :��(% �55�
&8 2����� ��� /G 2�� �% �55�1 /��� ���
?��% �55�

��������
������ ����� ����������� �������������� ��� ����������� � ����� ��� ���� 141
&* :���� �� ��)% ����1 /���% �55;
&> �� ��� �!��$����� ����� � ����
�����!�% �����" ��� ��#$�������
� �!�% �� ������� ��� �������� ���� ���
���� ��� ��� ���� ���!���� ��� �� ������
��( ��� ��� � �!��� ,:���� �� ��)%
����0) ��'����% /��� ,�55�0 ����
��������� �����!� � ������ ���
��������!� ���� ��� �!����!���" #�����
� � ����� ������� � ��������) :��
����� � �����!� ���� ��� ��" !����
���� ���) � ����" � ����� -����% �� ���
����� ����% ���� ���� � � !����� �
�����" ��%��� ������ ��� �*$*5 "����
����'�� ���� ����� ��� � ��� "����% ���$
����!���� �������" '�� ����� ����
��� #����� ���!����) <�� ��!��� � �(��"
�� #� �� ������� ���� ��� ����" �����
� ��� �����!% #�� � �!��� ����� ���
��' ���� 7�!(��� ���� ���� ,:����
�� ��)% �55;0) <�� ��� ��������
���!����� �� ����� ��� �� '���%
����!���" �� ���� !������� ����
��������" ��' ������ ���!���� ������)
&& :���� ��� 6����% �55>1 :���� �� ��)%
�55&1 :���� �� ��)% ����
&; :���� �� ��) �55&
���������
� -.�������/% ����
� -.�������/% ����
� -.�������/% ����
8 ����� :��(% ����
* -.�������/% ����
> � ����� �������
& �� ������ #� ����� ���� '��� ��� ��������
���������!� ���� ������ �����$#����
�������� �� ��� ��������!�% ��� ���� ��
��� ��������!� ��� ��� ������ ��� �9�!�
!��!�������) �� ��� ���� #��� ������ ���
���� ��� �������� ���� !���� ��" #� �
���� ��� �� ��� ������" � ��� �����!%
�� � ���" !���� ��� ����� � �� ���
������ ������ ��" ���� �!�����" #���
����#���� �� �� ����������! � �!���
��!� �� <:)
; .�+/% ����
5 ����� :��(% ����#
�� -.����% �55;)
�� ����� :��(% ����#
�� ����� :��(% ����#
�� ��� ��� +�����% ����1 ����� :��( �����
�8 ����� :��(% ����#
�* ����� :��(% �����
�> <�� ����" '�� !����!��� �� ��������
��� ���������� #��'��� �=�!�� ���
���% ��� ��� ������� + ���� ����
�=�!�� ��� ����� � F�����% .� H���
'�� !��������� #" -.�+? ���
-.���� � @�����" �555 �� � #������
����") ���� '�� !����!��� ��� ��� ����
��-� � F�����)
�& -.�+?�-.����% �555
�; �������� �� ��)% �55;
�5 .������� ������ ���� ��!�������
��� !(� � '���� ��� !������ � �����
���) .���� ����� ����������� ������%
�55;1 -.�+�% �5581 ����'�% �55;
�� ���������% ����
�� -.����% ����#
�� .����% <����% :��(��$�$2����% ����
�� ����!�������% �555
�8 ��������% �555
�* I�(����'��� ��� ���������% �555
�> �����" ������!� 3����% �555
�& -.�?% �����
�; ���% ����
�5 6���+% �555
�� ��#�������% �55�1 ���C�% ����
�� ������������ ���� ��� +������% ����
�� A�C����!(% �558)
�� ���C�% ����
�8 3��'�� ��� �����% �5551 6��!�����%
����1 +����"% ����1 :�����% ����
�* ����% ����
�> ��������% ����1 �������% �)�)
�& -.�A�6% ����
�; ������% ����
�5 J.������ ?��!��G ��� ������" ��7���� ��
#� �������� #" ��� �������� #���� �
!������� ��� ������� �� J��������G%
���� �� ���� ������������
8� 2�����% .��(��� ��� :�����% �55;
8� :���� �� ��)% �555
8� �� ������� ������� #" 6�) �����%
-.�?% � ������� #���� � ������#��) �$
��� ����� �� ����� ����)
8� -.�������/% ����
88 ���!��� �&% �;% �� ��� 8�% +���������
� ��� ?�����G� ����#�! � :��������
8* ''')"��������)������������
��K#�����)���L
8> ''')"��������)������������
��K#�����)���L
8& ���!��� �8% �*% ��% <�� +��������� �
����
8; J�����G �� ��� �� ���������% ���!���
#����% ����� !��������� #���� 4
!���������� 4 #���� !������ #" �������
85 6M � HI% ��� �55& :�� 8�>
*� .��+% ����
*� ��������� #" ��) �� �(#�� ��""��%
�����" 6����� �� ������ 4 6��!��
���!����% �����! ����#�! � ���� �� ���
-.3��� � ��������% @��� ����
*� ���!�� ��,�0% ?��� �% <�� +��������� �
��� 2���� � .����
*� ���!�� ��,�0% ?��� �% <�� +��������� �
��� 2���� � .����
*8 ���!�� ��,*0% ?��� �% <�� +��������� �
��� 2���� � .����
** ���!�� ��% ?��� �% <�� +��������� � ���
2���� � .����

��������
������ ����� ����������� �������������� ��� ����������� � ����� ��� ����142
*> ?������% �55;
*& 6����% ����
*; ����� :��( ����#
*5 ���!��� �*% �> ��� �&% ?��� ��%
+��������� � ��� �����! ����#�! �
?�(����
>� ����� :��( ����#
>� ����� :��( ����#
>� /�����!� ��) MF � �5;�
>� ���!�� �*,�0 ,�0 +������ ���% <��
+��������� � ��� ����#�! � �� F��(�
>8 ���!�� ��,�0 +������ ���% <�� +���������
� ��� ����#�! � �� F��(�
>* � ��!��� '�� �!7���� ��� ��� � #����
����� ���� � � ���$��������� �������
'�� ���� �� �� ������� =�#) ,������%
�55&0
>> ������% ����
>& ''')"��������)��
>; ����� :��(% ����#
>5 ��������� #" ��$�(#�� ��""�� % �����!
����#�! � ���� �� ��� ���!�� ������ �
��� -���� .����� 3������ �����#�" ��
��������% �* @��� ����
&� 3��������� � ?�(����% 6����" �
������ ��� -.����% ���� ����� :��(%
����
&� ����� :��(% ����#
&� -.����% ����
&� ����� :��(% ����� !�� �55;$55
.������ ����$���������!� ����
&8 ���� � ��� � ������� � ������� ���
��7�� ���) 3�#��=�% ����
&* ���� .�'�% @��" �8% ����
&> <���% �555
&& �������% /!��#�� ��% ����
&; ���!� A���!�$?�����% ����
&5 6������ ����� ����������� ������%
����
���������
� ���� �9������ ��� ��� -���� .�����
��!������� � +��������% @��� ����
��� ��� 3��������� � ����G� .������
���� ?�������� ��� +������ ?��!"
� �* .����#�� ����
� ��#���"�% ����
8 -)� +������� �� -. ?�������� A���%
���� ,����E��'''���!�������)���
����*K�)����0
* ��������% �� �����!�% ��' � ����
��!����� � �������� �!���!� '��� �
������!�� � ���� ���� ���� �����!���
��� ���� � ����� ���� �� ��( N ��9
'��(���% �=�!�� ��� ����� N ���
�������� ?F��� ��� �������#�� �����
#" ����'��� ���� '�� � �������%
�!!��� �� ����!��% ��!����������%
���� ����!��� ��!)
> <�� 3�� ?�#�! ������ ,���������0 �!�%
�5;* � ��� ����� ����� � 3�� ���
��"��� ����� ������ �� ��� �����
��������" �������) <�� '�� �����
������� �� ��(� ��!� �������
��!�������")
& <�� ����� ��������� ��� ��' �������
�� ���������� ����� � �� .������
��� ?�������� ��� +������ ?��!")
; ��#����% �5;;
5 2�#"% ����
�� @���!� 6!���� 2�#" � ��� �� +���� �
�������� �� ��� ������" ������ ��
B?���������� �!���� :������ �����
��������D% 8�� ������������ +������ ��
���� � ��� ��� ��� ?�! !% 6����%
?�������% �; /!��#�� �55&
�� +������� ��� 6�����"% �55*
�� :�����% �5551 3����� ��� ���������%
�558
�� +��.3� 4 �+��% ����
�8 3� ���% �5>�% �� ��� ���� �� �
J�� !����" ��!�����G ����#���)
�* -.�? 4 ������% ����
�> 6�) M �) ������� H% O�55;P ; �++ �5>
�& ��������� 85��555
�; �!!���� �� 6���+ ����% 6�������
6������" ���� ,��� ���%��� ��� #����0
�5;*$�555 '����� ������ � 85� ��
����� ��� ,�9!���� � ������� ���
����0
�5 �!!���� �� ��� ?�(����$#���� F�'"���
�� ����� ���� ��� F��� �� ,F��F�0%
����" "��� �������� � '����% � ���
��� ��� � ��� ����� � ��� !�����"% ���
�������� (���� � ��� ���� � ������)
���� ��� ��� ��� ������ � ����%
*85 '���� #�!��� ��� �!��� �
#��#��! !����� � 2��� 2�� ,�������"
#��!( ���% #��!( '����0 � ?�(���� ���
��� ��� !���� ��!���� '�� ��#�!�")
������!� #" F��F� ���'�� ���� ��� ����
���#�� � ��!� (���� � �� ������ ����
��� ���#�� �������� � ��� ������� ����
����) ������ (���� ��� �� ����� ���"
�������� ��� ������ ����� ����� #�� ����-����� ���� ��7�����"- ��� ��'�� ���
!���) <�� ����� � (��� ���"% '��
������ #�� ��!(�� �� ��!�� � ����%
� ��� � ��' � ��� '�� ��� ���!� ��
�9��!� ���!��� � ��� !������") �� ���
�����!� � ?��=�#% ��!� (���� �!!�� �
�� ��#�� ����� ��� ������ #���� ����
�� ������� ��!����) <�� (���� ���
������" !����� ��� #" ������ ��� ��� ���
��'�"� !����� ��� � ��#�!)
�� <�� ��9� � ��� ��� ��� ��#��7����
��!��� ���'� �����" ��� ����� ���
������% �555
�� ?��!���(" 4 @���% �55;
�� +����!(% �55>
�� 6!2����% �55>
�8 ���� �� ��)% �55&
�* :�����% ����

��������
������ ����� ����������� �������������� ��� ����������� � ����� ��� ���� 143
�> �F/% ����
�& A�/% �55*
�; -.�?% �����
�5 -���� :��������% ����
�� +�<�% ����
�� �</?% ����
�� ����� :��(% ����#
�� -.����) �� ���� #� ����� ���� ��� ����
7����� ���� ��� ��� �55* #�!���� ��
�������!���� ���� ��� �����#�� ��
� ������� ��!� �55*)
�8 ��(����% ����
�* /��% �555
�> F�' ���� #" =���� ������ ����
��!���� � ��� �#���!� � ��������%
'�!� ���� #�!��� ���!������ ���
#��� ��'
�& ���!��� �&% �;% �� ��� 8�% +���������
� ��� ?�����G� ����#�! � :��������
�; ���!�� ��% ?��� �% <�� +��������� � ���
2���� � .����
�5 ��$�����% �55*
8� ��� ��� +�����% ����
8� ���!�� �% F�' �� +��#��� ����%
�55�)
8� <�(� �������� ��� ����� � ����
'����� ��!����� ����� ���'�" �������
� ������ '�����'�� �"������
8� -.�+?% �555#
88 ��) :�"��� I�����% ���!���% ����
.������ ���� ?�������� +�������
,''')���)!�����'����������
�?������)����$0
8* ����� ���� ���!�% ����
8> F�'"��� +����!��� �������� -��% ��
����� .3/% ��� ���� ��� �����9�����"
;� ��!� !���� � ��� ���� ��� "���� �
������ ����� !�����)
8& �������� ������.����#�� ��% ����
8; @����% �) ��� ����% �)% ����
85 2�����% �) ��� ����% �)% ����
*� ��������� ��� +���!�% �55>
*� 3�!(% �55�1 @�"����"�% �55*)
*� ������!��� '��(��� ��� �� ��( �
�!!�������� �9������ �� ���) �9�������
�!!�� ������ ������$��!(� �� !��� ���
����� ����� ���������� ,���!��������
�9�������0 !���������� '�� �� � �!���
������G� #���� �� ������ !����!� � ���
�"�% ����% �� ����� ,��!��� ���#����0
�� �(� '�� � ������G� #����)
*� ''')���������(!��!)!���
?���K�9������K?����"��9�K���)���
*8 3�����% �55�
** 3������(���% �55;
*> ����< ���������� ���� ����!���� ��
�������" ������!��#�� ������ � #����
�����) ����< ���� ����� �� ��� ������
�����!����� � +�8 �"����!"���)
<�����" � ������" #��� '��� ��� ������
� ������� '�� !��!�� ����%
������!��� � +�8 !��� !����% �� ��� �
+�8 !��� !���� #���' ��� !��������% ��
� ������� '�� ��/ ����� �� �� ���
��� ������ '�� � ����� �"����!"�� !����
#���' �������)�) <���% ���" � !�����
��������� � � !�����"G� ��������� �
������ ��� '�� ��� '�� ��7��� ����
�� ��" ��� ���) ���� '��( �
� ����� '�"�) ���� ��#� ��� ����
����!���� ���!���) /����� ������� ���
����" � ��� ��� +�8 �"����!"���) ���
����!���� ���� '�� ��� ���� � �'�
��C"��� (��'� �� ������� �����!������
��� ��������) <�� ��� !���� � ���$
��������� ���� '��( #" ��#�� ��� ��
����� � ����� ���� ��C"��� ��� ���%
����� ���% (��'� �� ������� �����!������
��� �������� ��#����) +����� �����
���� #����� �� ��� ��!��� !�����"
�������� ��������" ����" � ��� � �!���
���!���) <���� ����% (��'� �� ����
��#����% '��( #" #��!(� ��� ���� �
��� '�� ��� +�8 < �"����!"��% ����
�������� ��� ����" � ��� ���� ��� ��� <
!���)
*& -.�������/% ����
*; �� @��� F���% ?�������% ������������
���� ��!��"% �� ��� ����!� � ���
������������ ��� <�������� �!!���
+������ � 3�����% ��!��#�� ����
*5 6������� �� ��)% ����
>� ?������� ��������� � ���� ����'�
�������� �� #���� �� ����� ����!
���� �� ��� !�����" � ���� � #������
���� � ��� ���� ����! #�� ���� �
��� !�����" #" ����� � ��� ���
�����!��) <�� �������� ��� ���������
����'� ��� !������� ��� !��!� � � '��
���� � ����! ���� �� � ��'�� ��!�
>� -.�?% ����
>� ?�����!���!�� ������!� ���
6��� �!������ � ����!� �������� �4�
!���� �� Q*��$;�� �����
>� <�� �"��� � ������!���� �������"
�����!��� ����� <��?� �!���� !��"����%
��������(�% ������!�� ��!�����%
�������� �����% �������� !�!���%
������� ��� ����� ��!����)
>8 A�(% ����1 �����% ����
>* +�����% ����
>> +��������" �!����� ��� �!����� �����
#" �� ����������� �������" ��
������������ ����� ���� ����' ���$������
������� �� �����!� � �������� �����!�)
>& B6��#��� ��" ������ ����� �9!������
�� ��� �9!����� ���� !�� ����� #" �
������ ������� ��!� �9!������ �� ���
���������#�" !�� �!� '�� � ������
�9�������� � ��� ������ ��� �� ���
���������#�" ���=��!� ��� �������
�������� � ��� ������ �'���% ��(�
�!!���� � ��� ������� �������� � ����
������D) <��?� ��������% ���!�� ��)
>; F��� ����% +����� ���� ��!)
>5 / !� � ��� -. �� +��������� ��
����� ����% ����) ,+��+�-+�������

��������
������ ����� ����������� �������������� ��� ����������� � ����� ��� ����144
�� �!����!% ��!�� ��� +������� ����%
++?�$+������� �� +�� ��� ?���!��
����% +���-+�������� �� ���
�������� � ��!�� ��!�������%
+����-+�������� �� ��� �������� �
��� ���� � ��!������� �����
�����% +�<N+�������� ����� <������
��� ����� +����% ������� �� ������
<�������� � ?��������% +�+-+�������� �� ��� ���� � ��� +���)
&� <�� +������ ���� ��!������� �� ����
����% �; 6�" ����) <�� �������� -���
?������� �� �!���E �!!�������� �!���
�� ��������% ������ ��� ��#��!����� �
��� !����9� � ������" ����!���% �8 6�"
����1 <�� �#�=� ��!������� ���
A����'��( �� �!��� �� ��� �� �����
��������% ��#��!����� ��� ����� �������
� �!���� ������� � � �!�% �& ����
����1 <�� ������ !��� �� �!��� �� ��
�������� � ��� ��� ��� ?�! !% �* ����
����1 <�� ?��$+��##��� ?���������
����� ��������% �8 A�#����" ����1 <��
��!������� � ��� <���� �#���$����!��
����� � ����� � �����% �; .����#��
����1 <�� -���� .����� 6�������
��!�������% ; ������#�� ����1 <��
����!�� ��!������� ��� ������ �!����
��� ������� �� �������� ���
!��������� ���� �� ��� ����� �����
�� ��!�� �����������% � @��" ����1 <��
����!�� ��!������� ��� ������ �!��� ���
������� �� �������� ��� :�=�
��!������� ��� ?��� ��� �� �!���% ��
@��� ����1 <�� :���! ��� ��!������� ��
�������� ?��������% 8 6�" ����1 2�"
�!���� �� ��� ������ ������������ �
��� ?������� � �!��� � ���
������������ +�� ����!� �� ?�������� ���
�����������% � @��" �5551 <��
������������ +������� �� +�� ���
?���!�� ����1 ��� ��� -���� .�����
-������� ��!������� �� ����� ����)
&� ���� � ����#��( �� F�������� '��
����#���� � �555% ��� ���������� �
��� 3������� ��� #��� !��!��� ��
#�� ����7���� ��� ���������
��������� ���� #��� ������
���������) � ��!����� �� �������
��� ������������ � ��� 3������� ���
#��� ��������)
&� �9���!� ��� >�� ������������ +������ ��
���� � ��� ��� ��� ?�! !% ����%
������ ���(���� �� B� �� ������
�������������������������������
����������� ������� ��� ��� ����� ���
�!���!"
&� +������� �� ����� ���� ���������
�����>� ��� �!����! ��� ��!�� +���!�
��!��� ��������)
&8 -. 3������ �����#�" ��������� *���88
,������*���880% ; 6��!� �555)
&* F�'"���% �!����� ��� ����������
'��(� �� �� ��� ����� ���� ������
��� '����
&> ����:% �555
&& �9���!� ��� ��� >�� ������������
+������ �� ���� � ��� ��� ��� ?�! !%
����% #���������$��%��&� ���� �� ��
�����������������������������������
����������� ������� ��� ��� ����� ���
�!���!D)
&; ������ � ��� .������ +�� ����!� ��
����� ���� ��� ��������% .�' ����%
�8$�* .����#�� ����)
<�� +�� ����!� '�� ������� #" .��+%
� ?��������� '�� .�+/% F�'"��G�
+����!���% -.�+�A ��� -.����) <��
�#=�!��� � ��� !�� ����!� '�� �� �����
��� ���!��� � �������� � ����$#����
�������� �� ��� �������� �����! '���
����% �� #� ��(�� ��'��� #" ������
����� ����� ���� +�������% ���!�
�����������% �������������� ��� ���
������$��!��� ��� ����� ���� +������
��!���� � !���� !����#������ '�� !��
��!����)
A�� ������ � ������� ������ �� �� ��E
,����E�����!)�!)� � ������ ��R���)���0
&5 -.������?-% �555
;� -.������?-% �555
��������
� ����� ��� �� ����� !�� ����!� ��
J�!!��������� ����������� ��� ��� ����
������ � �'� ��G �$8 A�#����" ����%
-.����4-.�+�A
� 6����% ����
� 6���% 6���� ��� ����% ����1 ?������
��� ?�����% �55�1 2�����% �55;
8 <�� ���� '�� ���� ��� ����� �� �����
���� ��" ����
* ������% ����
> -.����% �����
& -.����% �����
; <���� ��!����������� ��� ���'� ������
������" ��� � �'� ��� ������� �����
������!������������� ��(���� ���
��������$�)�*������� ������������%
-.����% �����
5 -.����% �����
�� ���% ����1 ����!������% ����1 ��"
��� ������% �55;
�� :���� ��� ��!�% �55;
�� 6����" � �����G� �����������% �5;&)
�� ���� ��� +����% ����
�8 ���� ��� +����% ����
�* +?<�!�% ����
�> �)�) 2��(���% ��� ���� ?��� ��� ��!(
���(��� A��������% ��������
!�����!����)
�& <��� �����% ����
�; .���% �55;
�5 ������% ����
�� ���� ��� +����% ����
�� � ��� ������" � ��� �������� �
������� ����� �7��" � 3����% ����

������������ ����������������
����� ���� ���������� ���������������157
���������

������������ ����������������
����� ���� ���������� ���������������158
���������

������������ ����������������
����� ���� ���������� ���������������159
���������
���������
������������ ��!��!������"������#�!�������������
��������$�����#�����������$������������������������
������"��������$����������������!���������������!��
�������������%��������#������!!����"��������&�����
��������������� ����'(�������&#����$��������
�����!������������$�������� ����&������������
���!�������������������"����$���������!�������"���
�������!��'��������������!����������)����������#
*������������������������������$���������
�������!���������������!�����������"���������$
��������������������� ���"�����# ����'
���������������#������ ��������##�!������������
����"������������������� ���������� ��������#
�������!�������������������#�������������&����������
!��!������������!+�#���%��������$�������!��������
#�����#�������������� ��+��� ������#��!�������&
��!������,�����&�� $���&�� ��#��!��������������&
���������#���������&���!����&��!��� ��+���&���������
��+�����!����-!���������������#��!��������������!�
�##�!���'.�����������������������������#����!���/���
���-���!����������!�����0�#�������������&������������
������������!��!�����������������!��#���!���������$
����������������#�����!��!���##�!���������&�������������
"$������������������&�������������������"�������
�##�!���������,�$�����#�������������������&������&
���������������!�����'������������������������
���������!��#����#�����!��!����!����� �$�������$
��������' ��!���������$����������� ����!�������"���
����# ����!+&!������� ����������������� ��+�����
���������&!������!�����#������������������&!������� ���
����"�������&��#����!����������!�������"�������������"��
�������������������������#!��!���'
��������������!��!��������� ���������������
�������������������������������-��������!����-"�����
���##�!+���'��������!��!�������������� �������
�������������� �������������+����������������
�������������!���������������$�������������������'
����������������� ���!��!�������������������
����������#�������##���#�����"���$���������������
��������$������"����$�������������������$�����#�����
��������������
1�����������#���#�����#
��!�����������������
.����&��2���3����'4&
5��� ��&�����'6�78696
:4�������477;<'
���������������������#
��������&������42�
���';6&:43=���477;<'
��������������
1�����������#���#�����#
��!�����������������
.����� ���$-��!���
�������&4;=�����$8
6>�"����$����'
��������������
1�����������#���#�����#
��!�����������������
*���������
*���������
�����
(�������
�1 �.
���
�1 �.
�1 �.
������������ ������������ ���������������� ������� �
� � �������� ������� ��������� � ����� ����������
������� �� ��� ������������ ������������� ��� �����

������������ ����������������
����� ���� ���������� ���������������160
���������
������� �� ��� ������������ ������������� ��� �����
.����&� ���$-#�����
�������&��29�
�3&�����'4468469:42
=�����$8�>�"����$���4<
���������������������#
��������&������42�
���'74:2=���4773<
��������������
1�����������#���#�����#
��!�����������������
.����&� ���$-#����
�������&��26��3&
�����'44;849�
:;8�2=���4777<
������������##���$�������������������#�!���$������'
������������������!��!����������������!������
�������$��!����������������������������!��� ����?�
������������������'
������������������$?��##����������!��������#���
��������$���������!�������!����������������&���
�����������!��!������������������!��#������������
:�����������������#�!���!$<�����������������������$����&
�� ����������������!!�������#� ����������%����
����������@������������������!��!��������������
���"�����#������!���������&�������!��������������
��!������������#����$�������!���&�����!+�#�!!���"$
������������������!����-���������!�������������!��&���
�������##�!���������������������������������� �@
>����������&������������������������!��!��������
����##�!���������������������"�����-#�������#!�������&
����!����$��������#�!�������'��������������!�������
����������������$�������������!�������������!������
����������"$&����������&��������������������!����-������
���!��������!���������������!���� ��������������
��������������������!��"������� �@������������
#�������������������!��������������������-���!�������$
����$"��������+������������������!����#���
�����������#������!������������"����&��!���������
������������!��#����$���������@����������������
��!�����������#�������##����&"���#����!�����������&
��!������������������#!���������������!��#��"���
$������������������#�������&"��������+��#�����
�������������!����#������!����?���������"�������#��
�������"����������#��!����'
��������������������)���������������!�������
��������������������!�!$��������������������!����
�����!������������������&������!����!�������+���&������
���#�������������� ��#��!������##�!����������������
�����!������������������#����"�����������������
�������������!������'���������������������!��!�����
���!�������� & ��!�!������������"������&��!��������
!�����#�������!$���������������!���'������������
!���������������!�������� ���"������!�����"����"�����
�����������������������$������A����������������
���"���# ������������������������'��������!��!�����
������������������������������!�������� !���������
"�������!����&���� ����"���������$ ������������?�
����������������'��������������������)�����������
��������������������������������!������������������
����������������������������!��#����#��"�������'���
�����������!��������������)�������������������
�����������#�� ������������!$�������#����$��������
�����!�����������!�����'��������##����&������������
���������������)�����������+��!!�����#�������
��!������������6������!��4�&B.�������������C'
���
�1 �.
(�������
A����

������������ ����������������
����� ���� ���������� ���������������161
���������
������� �� ��� ������������ ������������� ��� �����
�����������1!�����!&
��!��������������������&
� ���$-�����
:������������$< �������
:4�8�4���������4<
���������������������#
��������&������42����'43
:�2�����4776<'
�����������1!�����!&
��!��������������������&
1��'4��4����'�6
:49=���4773<
�����������������������������$����+���������
�!�������������������"�����#!�����������"�������&
�� ������������!������������������#��������
��������$'������������&�������������������������
����$������#��!��������!�������������������
����������&�������!����������������&‘��������� �"������ ����������!��������#���������������������
�#��������!���@��������������%������������
���������$&����������������!������&������������"���
�������-��������������������������������#��������
�"����������$����"��������������!!������������
������������������������"$�������������������
��!�����#�������������@�������������������$
!��!����������������� ��������!��������������$
��������������������������������!�����!������
������##�!+����# �������!�������&�������������'
��������������!��!�����������������������������
����������������������������������#��!����������
�����#�����������������������������&��!������
��������!�'�������������������"������ ������
����������!+�#!�����$��������������#��������"�������
"�� ������������!������#������������#�����
������������#�������������$healthcare�$����@�!����������������"���+��&�������� �#���
���������&����+� ����$+�� �����������������
����!������#������������������������!����������+�'
����������������##����&�����������������������!��&
������������!�������$�������������"���!���������
��+����!���������������������##�����������!���
��������������!��!����!������ ��!����!��������
�������!�������&�����!�����$�������!����&���������#��
�������������� ��#����#!�������'����������&����
��!���������������������"���!����������������"�
������������������#��������������'
����������������� ���!��!�������������!��#
�����������"�� �����������$�� ���!�������$�� '���
���#��������������������$�� ��43$�������"�������
��$������4�$�����#�������"��������$�����
!�������$�� &������������������!������'���
������������#������ ����������!��!��#����$
�����������������������!��������������������&�����
�����!������������������ ��+&�����!�����$�#�������
!����'����������$�� &��������%�����$�#���������!�
�������"����� ����!�������$�� ���!����������������
������� ���� ��&����+�����������&��$����������
#����$�������$'������ ���!�������$�� �������������
��������$�� ������������&���)��������������
!����$��� �������"���������������!�����������#
��������������!����������'
��1���
���
��1���
A����
5�+�����
���D��+�

������������ ����������������
����� ���� ���������� ���������������162
���������
4 )��������9 �� ��������� ���� ������ ������ �������������������������������� ��������
������& )�����& �28�9 =��$ ���� :E���FA�� �<'
��� ��������� ��� ��� � ������������������!����
Guideline 1: States should establish aneffective national framework for theirresponse to HIV/AIDS which ensures acoordinated, participatory, transparentand accountable approach, integratingHIV/AIDS policy and programmeresponsibilities across all branches ofGovernment.
Guideline 2: States should ensure,through political and financial support,that community consultation occurs inall phases of HIV/AIDS policy design,programme implementation andevaluation and that communityorganisations are enabled to carry out theiractivities, including in the field of ethics,law and human rights, effectively.
Guideline 3: States should review andreform public health laws to ensure thatthey adequately address public healthissues raised by HIV/AIDS, that theirprovisions applicable to casuallytransmitted diseases are notinappropriately applied to HIV/AIDS andthat they are consistent with internationalhuman rights obligations.
Guideline 4: States should review andreform criminal laws and correctionalsystems to ensure that they are consistentwith international human rightsobligations and are not misused in thecontext of HIV/AIDS or targeted againstvulnerable groups.
Guideline 5: States should enact orstrengthen anti-discrimination and otherprotective laws that protect vulnerablegroups, people living with HIV/AIDSand people with disabilities fromdiscrimination in both the public andprivate sectors, ensure privacy andconfidentiality and ethics in researchinvolving human subjects, emphasiseeducation and conciliation, and providefor speedy and effective administrativeand civil remedies.
Guideline 6: States should enactlegislation to provide for the regulationof HIV-related goods, services andinformation, so as to ensure widespreadavailability of qualitative preventionmeasures and services, adequate HIVprevention and care information andsafe and effective medication at anaffordable price. States should also takemeasures necessary to ensure for allpersons on a sustained and equal basis,the availability and accessibility ofquality goods, services and informationfor HIV/AIDS prevention, treatment,care and support, including anti-retroviral and other safe and effectivemedicines, diagnostics and relatedtechnologies for preventive, curativeand palliative care of HIV/AIDS andrelated opportunistic infections andconditions. States should take suchmeasures at both domestic andinternational levels, with particularattention to vulnerable individuals andpopulations.1
����������

������������ ����������������
����� ���� ���������� ���������������163
���������
Guideline 7: States should implementand support legal support services thatwill educate people affected by HIV/AIDSabout their rights, provide free legalservices to enforce those rights, developexpertise on HIV-related legal issues andutilise means of protection in addition tothe courts, such as offices of ministries ofjustice, ombudspersons, health complaintunits and human rights commissions.
Guideline 8: States, in collaboration withand through the community, shouldpromote a supportive and enablingenvironment for women, children andother vulnerable groups by addressingunderlying prejudices and inequalitiesthrough community dialogue, speciallydesigned social and health services andsupport to community groups.
Guideline 9: States should promote thewide and ongoing distribution of creativeeducation, training and mediaprogrammes explicitly designed tochange attitudes of discrimination andstigmatisation associated with HIV/AIDS
to understanding and acceptance.
Guideline 10: States should ensure thatgovernment and private sectors developcodes of conduct regarding HIV/AIDSissues that translate human rightsprinciples into codes of professionalresponsibility and practice, withaccompanying mechanisms toimplement and enforce these codes.
Guideline 11: States should ensuremonitoring and enforcement mechan-isms to guarantee the protection of HIV-related human rights, including those ofpeople living with HIV/AIDS, theirfamilies and communities.
Guideline 12: States should cooperatethrough all relevant programmes andagencies of the United Nations system,including UNAIDS, to share knowledgeand experience concerning HIV-relatedhuman rights issues and should ensureeffective mechanisms to protect humanrights in the context of HIV/AIDS atinternational level.
����������

������������ �
������������������������������
���������������������� �������������� 164
actual value – minimum value
maximum value – minimum valueDimension index =
������������ �
���������� ��� ���������������� ����������
������������������������
�����
The HDI is a summary measure of humandevelopment. It measures the averageachievements in a country in three basicdimensions of human development:� A long and healthy life, as measured
by life expectancy at birth.� Knowledge, as measured by the adult
literacy rate (with two-thirds weight)and the combined primary,secondary and tertiary grossenrolment ratio (with one-thirdweight).
� A decent standard of living, asmeasured by gross domestic product(GDP) per capita (PPP US$).
Before the HDI itself is calculated, anindex needs to be created for each of thesedimensions. To calculate thesedimensions indices—the life expectancy,education and GDP indices—minimumand maximum values (goalposts) arechosen for each underlying indicator.Performance in each dimension isexpressed as a value between 0 and 1 byapplying the general formula:
The HDI is then calculated as a simpleaverage of the dimension indices. Thegoalposts are as under:
actual value – minimum value
maximum value – minimum valueDimension index =
����������������������������
����������
While the HDI measures averageachievement, the GDI adjusts the averageachievement to reflect the inequalitiesbetween men and women in the followingdimensions:� A long and healthy life, as measured
by life expectancy at birth.� Knowledge as measured by the adult
literacy rate and the combinedprimary, secondary and tertiary grossenrolment ratio.
� A decent standard of living, asmeasured by estimated earned income(PPP US$).
The calculation of the GDI involves threesteps. First, female and male indices ineach dimension are calculated accordingto this general formula:
������������ �� �������������
���� ���� ������� �������
����� �����
!�"��#�������$ %& �&
��'����($����)
����� �������$ *�� �
����(+)
,��'��������� *�� �
���������
�����(+)
-�.��������� /�0��� *��
(...1�2)

������������ �
������������������������������
���������������������� �������������� 165
Second, the female and male indices ineach dimension are combined in a waythat penalises differences in achievementbetween men and women. The resultingindex, referred to as the equally distributedindex, is calculated according to thisgeneral formula:
Equally distributed index = {[female population
share (female index1-ε)] + [male population
share(male index 1-ε )]}1/1-ε
ε measures the aversion to inequality. Inthe GDI ε = 2. Thus the general equationbecomes
Equally distributed index ={[female population share
(female index -1 )]+[ male population share (male
index -1 )]}-1
which gives the harmonic mean of thefemale and male indices.
Third, the GDI is calculated combining thethree equally distributed indices in anunweighted average.
��������� ���!������
��������� ��
Focusing on women’s opportunities ratherthan their capabilities, the GEM capturesgender inequality in three key areas:
1 Political participation and decision-making power, as measured bywomen’s and men’s percentage sharesof parliamentary seats.
2 Economic participation anddecision—making power, asmeasured by two indicators—women’s and men’s percentage sharesof positions as legislators, seniorofficers and managers and women’sand men’s percentage shares ofprofessional and technical positions.
3 Power over economic resources, asmeasured by women’s and men’sestimated earned income (PPP US$).
For each of these three dimensions, anequally distributed equivalent percentage
������������ �� �������������
���� ��������� ������������ �������
3�������"��#�������$��'����($����) %45& �45&
6�����"��#�������$��'����($����) %�5& ��5&
������������$����(+) *�� �
,��'�����������������������(+) *�� �
7��������������������(...1�2) /�0��� *��
���8 �����#���� ���������� ������ (���������) "�� ��"� �#�������$ ��� "��� $����
������ "��9������ ��:� ����������� ����� ������ ��"��#�������$5
Why ε= 2 in calculating the GDI���������"ε�������;��"���������$"�����������<�����$5�����������������0�������������$�������$�����������"��������
���<��������5
�"ε=�0���������<�����$��������������(�������������-��
9����������������������������)5������������9������"����$0�����������9�������������������������������������5
�������������������������������-��(��9��������-76)5
������������������������������$�������� ���<�����$ ��
�����������5

������������ �
������������������������������
���������������������� �������������� 166
(EDEP) is calculated, as a population-weighted average, according to thefollowing general formula:
EDEP = {[female population share
(female index1-ε)]
+[male population share
(male index1-ε)]} 1/1-ε
ε measures the aversion to inequality. Inthe GEM (as in the GDI) ε = 2, which placesa moderate penalty on inequality. Theformula is thus:
EDEP ={[female population share (female index -1)]
+ [male population share (male index-1)]} -1
For political and economic participationand decision making, the EDEP is thenindexed by dividing it by 50. The rationalefor this indexation: in an ideal society,with equal empowerment of the sexes, theGEM variables would equal 50 per cent,that is, women’s share would equal men’sshare for each variable.
Finally, the GEM is calculated as a simpleaverage of the three indexed EDEPs.
��������1�.0 ����

������������ �
������������������������������
���������������������� ������������ !167
��������������� ������������������ ������������
Our approach to assessing the impact ofthe HIV/AIDS epidemic on humandevelopment involves (1) estimating itsimpact on the HDI or GDI in theaggregate; (2) assessing the impact onindividual components of HDI and/orGDI; and (3) using the results from (a) and(b) to assess what the value of HDI wouldbe if there were no HIV/AIDS.
One way to estimate the effect of theAIDS epidemic on the HDI (or GDI) andits component variables would be toestimate the correlation across countriesbetween these variables and/orindicators of the HIV/AIDS epidemic –adult HIV prevalence and number ofreported AIDS cases. However, thisprocedure does not adequately controlfor other factors that might legitimatelyaffect life expectancy, literacy, schoolenrolment, and income and mightpossibly also be correlated withindicators of HIV/AIDS. To avoid thispotential bias, we must also account forthese other factors. This can be done in avariety of ways, one of which is simplycontrolling for pre-AIDS epidemic valuesof each component of HDI and GDI. Inother words, we are effectively trying todetermine whether HDI improved lessrapidly from 1980 to 1999 in countriesthat had to contend with more severeHIV/AIDS epidemics, relative to othersthat did not. This was the approachadopted by Bloom et al. (1996) and is theone that we adopt here.
Specifically, our goal is to obtain anestimate in the context of the followingmodel:
(1) Yit
= ß0 + ß
1Y
i0 + ß
2Y
i02 + π*AIDS
i + ε
i
[i = 1, 2, …N]
Here, N is the number of countries in thesample and Y
it refers to the value of the
dependent variable in country “i” at time“t”. Y
i0 refers to the value of the dependent
variable in country “i” at some pre-AIDSepidemic base year, labeled “0”. AIDSrefers to an indicator of the severity of theHIV/AIDS epidemic. The dependentvariable could be the value of the humandevelopment index (or the genderdevelopment index), or its components.The error-term ε
i (i = 1, 2, …N) is an
independently and identically distributedrandom variable with zero mean andconstant variance. There is, of course, thepossibility of reverse causality if, as oneexpects, improvements in humandevelopment to influence thetransmission of HIV, and we consider thatin our analysis as well.
A few points are worth noting about thespecification (1). The first is the nature ofthe relationship between the dependentvariable and its lagged quadraticcounterpart on the right hand side ofequation (1). In the case of at least thehuman development index, the genderdevelopment index, the adult literacyrates and the like that have well definedupper and lower bounds, one wouldexpect the following, all else being thesame: countries with greater initial valuesof the Y variable (Y
0), ought to have higher
values of Yt. However, the closer the initial
������������ �

������������ �
������������������������������
���������������������� ������������ !168
value is to the upper bound, the smallerthe degree of improvement that ispossible, so that in regimes where suchhuman development indicators areimproving over time, one might expect aconcave relationship between the initialvalue Y
0 and Y
t. Indeed, given that one
might also reasonably expect lifeexpectancy at birth to have an upperbound, so the concave relationshiphypothesized previously ought to hold forlife expectancy as well. Although it is lessapparent that same concave relationshipought to hold for the real GDP per capitacomponent, the well-known Solow-Swan growth model suggests that it must.1
In sum, one would prefer(a) ß
2 < 0; and (b) ß
1 > -2ß
2. Second, the
non-negativity of the sum of thedependent variables that are bound byunity suggests the desirable property that(c) 1 ≥"ß
0 + ß
1 + ß
2 ≥ 0. Ideally, one would
like to undertake the estimation proceduretaking account of these constraints on theparameters, but this was renderedunnecessary owing to the estimatedunconstrained coefficients satisfyingthem anyway.
�������The results of estimating differentversions of our specifications arehighlighted in Tables T2 to T5 and can besummarised as follows. First, HIV appearsto have a statistically significantassociation with progress in humandevelopment as indicated by the HDI (seeTables T2a – b). This result holds true bothin the case of HIV prevalence rates andincrease in the number of AIDS cases. Thisis the case whether one uses HIVprevalence rates (among those aged15–64 years in 1998), or indicators of theeffect of the AIDS epidemic, such as theaverage annual increase in the cumulativenumber of AIDS cases over the 1980-1998
period, normalised by the populationaged 15–64 years in 1998. Although AIDSis more likely to be relevant in terms ofinfluencing life expectancy at birth asmeasured by the United Nationspopulation division, in practice, the useof either of the indicators—HIVprevalence or AIDS—does not seem toinfluence the results significantly. This isnot surprising, since the correlationcoefficient between the two is 0.87.2
Despite the much larger sample ofcountries, our OLS results are similar tothe findings of Bloom et al. (1996) that theHIV/AIDS epidemic has a statisticallysignificant negative association with theHDI. Our estimated coefficient of theAIDS variable is, however, much larger inabsolute magnitude (nearly five times theestimate of Bloom et al. (1996),presumably reflecting the fact that theeffect of a much larger AIDS epidemic,relative to the 1980–92 period (the focusof their study) is now beginning to be felton human development.
The negative influence of the AIDSepidemic on human developmentbecomes even more apparent when oneallows for the possibility of reversecausality – that is, on the impact fromHDI to the spread of HIV. Table T2breports the results of estimates based onan instrumental variable (IV) approach.According to column (5) of the IVestimates reported in Table T2b, a 1 percent increase in the average annual rateof growth of cumulative AIDS prevalenceover the 1980–98 period has the potentialof reducing HDI by 0.17. This is apreferred estimate. For the full sampleof countries for which AIDS data wereavailable, we find that on average, thespread of the HIV/AIDS epidemicduring 1980-98 reduced HDI in 1999 byabout four per cent, relative to what it

������������ �
������������������������������
���������������������� ������������ !169
would have otherwise been – 0.715, asagainst 0.686.
��� ������������������������ ���� ����
This sub-section assesses the influence ofHIV/AIDS on key gender dimensions ofhuman development. The indicatorsused are the GDI and two of its keycomponents – the ratio of female to malelife expectancy at birth, and the ratio offemale to male educational achievements(literacy rates, mean years of schooling inthe 15+ population, and female to maleratios of primary and secondaryenrolment rates).
��� ��������
The GDI is the un-weighted average ofthree “inequality” indices correspondingto each of its three components.Specifically, each component index, Xi(i = 1,2,3) is calculated to be the followingformula
(2) Xi = [θ X
if1-α + (1-θ) X
im1-α]1/1-α (i= 1,2,3)
Here, Xif is the index of female
achievements in component “i”, and Xim
is the index of male achievements incomponent “i” and θ is the female sharein total population. The parameter “α”indicates the preferred degree ofinequality aversion. In GDI calculations,it is taken to be equal to 2 (UNDP 2001).
The GDI combines the relativeachievements of females and males inearned income, education and lifeexpectancy at birth, in such a way as topenalise gender-related inequalities in‘either’ direction. The GDI is the un-weighted average of three ‘inequality’indices corresponding to each of its threecomponents.3 The main results are
summarised in Tables T7–T9, whichpresent OLS estimates.
The key dependent variable in theempirical analysis of this section isnational-level HIV prevalence estimatesin 1999 provided by UNAIDS. In terms ofexplanatory variables, we have previouslydiscussed the potential role of differentindicators of human development ininfluencing HIV transmission, such asincome, education, health, inequality,and civil liberties. Indicators ofinequality used in this paper include theratio of female to male literacy andfemale to male life expectancy at birth.In estimating some of the specificationswe also used an indicator for politicalrights and civil liberties developed byFreedom House (2002).
Analysis also emphasises the role ofmigrant populations as a key factor in HIVtransmission. However, other factors alsomatter. One of them is the time elapsedsince the start of the epidemic.
�������� �������������Table T10 provides descriptive statisticson the variables used in the analysis of thissection, and lists the countries for whichthe full set of such data were available. Thedata indicate that there is substantialvariation in the variables of interest acrossthe sample countries, with two keyexceptions – the ratio of female to malelife expectancy at birth and the ratio offemales to males in the age group 15-49years. Particularly noteworthy is that theestimated length of the epidemic variedfrom eight years in some countries to 21.5years in others.4 This suggests that a‘steady state’ HIV prevalence will not be auseful assumption for estimationpurposes, a hunch that is confirmed bythe econometric results that are discussedfurther below. The data indicate a

������������ �
������������������������������
���������������������� ������������ !170
substantial degree of gender inequality ineducational achievement as measured byratio of the female to male adult literacyrates in 1980. The gender inequality inliteracy rates was highly correlated with thehuman development achievement of acountry in 1980 – with a correlationcoefficient of 0.91. Gender inequality inliteracy was correlated to a somewhat lesserdegree with economic achievement, witha correlation coefficient of 0.79.
The difference between the rate of growthof the urban population and the totalpopulation of a country during the periodfrom 1980 to 1990 was used as a roughproxy for the rate of growth of migrantpopulations from rural to urban areas overthe decade. The rate varied significantlybetween countries, with a mean annualaverage of growth of about 1.28 per centfor the full sample of 73 countries, a low of–0.14 per cent for Sri Lanka and a high of7.08 per cent for Mozambique.
������ �������������Additional estimates of the effects ofHIV/AIDS on health spending patterns isavailable from a study by Arndt and Lewis(2000) who used a 14-sector CGE modelto assess the economic impact of HIV inSouth Africa. In their framework, andunlike previous work, the health sectorwas explicitly accounted for along withassumptions on household andgovernment spending on health due toHIV/AIDS. Their paper suggests that thehealth sector in South Africa would notsuffer as much as the other sectors onaccount of HIV/AIDS over the 2001-2010period. They estimate the GDP in 2010under projected AIDS scenarios beingnearly 6.5 per cent higher than it wouldbe if the health sector was excluded fromthe GDP computations.5 In fact,compared to the no-AIDS scenario, theoverall GDP under AIDS would be nearly17 per cent lower in 2010, whereas the
corresponding figure for value added inthe health sector would be 10 per cent asper their simulation results.6
��������� �����Early work on the impact of HIV/AIDS ongrowth of real income (or real income percapita) inferred, rather than directlydemonstrated, the aggregate economicimpact of HIV/AIDS from thecombination of large projected numbersof prime-age HIV-positive individualsand the relatively high costs of treatingaffected people.
More recent work on the aggregateeconomic impact of AIDS has essentiallytaken a more rigorous methodologicalroute and falls into mainly two groups.The first group derives its conclusionsfrom well-established economic models,customised in various ways to account forkey aspects of the AIDS epidemic. Itincludes analyses that use CGE models,as well as those using a neoclassical growthmodel. Kambou, Devarajan and Over(1992) simulated the economic impact ofthe AIDS epidemic using an 11-sectorCGE model of Cameroon. In theiranalysis, they assumed that the AIDSepidemic would claim the life of 30,000workers (or 0.8 per cent of the labour force)each year from 1987 to 1990, with deathsoccurring disproportionately among themore skilled segments of the work force.Thus, 6.0 per cent of the skilled urban workforce was assumed to die of AIDS eachyear, compared to 0.4 per cent of theunskilled rural labour force. In theirsimulations, the AIDS epidemic loweredthe rate of growth of real GDP by nearlytwo percentage points per year. Theirmodel did not suggest any significantchange in the growth of real incomeper capita.
Arndt and Lewis’ model was intended tobe more comprehensive than that of

������������ �
������������������������������
���������������������� ������������ !171
Kambou, Devarajan and Over. It includedthe health sector, allowed for impacts onsavings on account of medicalexpenditures undertaken by thegovernment and households, labour forceimpacts, household and governmentallocations to health sector spending andexogenously given assumptions on trendsin sector productivity. Moreover, in theirmodel, the impact of the AIDS epidemicwas assumed to fall disproportionately onlow-skill segments of the labour force, inline with available evidence from SouthAfrica.7 Dynamic elements wereincorporated by using outputs from theone-period CGE model as inputs into theCGE framework for subsequent years. Themain conclusion was that over the2000-2010 period, the annual rate ofgrowth of real GDP in South Africa undertheir projected AIDS-scenario would besubstantially lower in comparison to ano-AIDS scenario, with the differenceranging from 1 percentage point to2.6 percentage points, depending on theyear. The net effect would be a real GDPin 2010 that would be 17 per cent lower insize, compared to a no-AIDS case. Theyfound that per capita real GDP would alsosuffer on account of HIV/AIDS althoughnot as much as real GDP, being about8 per cent lower in 2010 compared to ano-AIDS scenario.
In contrast to the studies above that relyon simulations conducted under variousassumptions of HIV/AIDS, an alternativeapproach is to econometrically estimatethe link between HIV/AIDS and nationaleconomic performance. Bloom andMahal (1997) used standard empiricalequations of the form found in Barro(1991) and Mankiw, Romer and Weil (1992)to measure the nature and strength ofstatistical associations between theprevalence of AIDS and the rate of growthof real GDP per capita, using cross-country data for 51 countries. The main
rationale for using an empirical approachis its potential use in taking account ofstandard influences of AIDS, as reflectedin simulation models of the typediscussed above, as well as others (suchas community responses to AIDS, lifecycle savings behavior by individuals andthe like) not readily captured by the latter.Indeed, one obvious benefit is in avoidingthe pitfalls of simulation models that relyon assumptions that often lack anempirical justification. The econometricapproach adopted by Bloom and Mahaltook into account the possibility ofsimultaneity bias resulting from the effectof economic growth on HIV transmission,as well as the possible non-linear natureof the relationship between HIVprevalence and economic growth. Theirmain finding was that the AIDS epidemichad a statistically insignificant effect onthe growth of real income per capita, withno evidence of reverse causality during theperiod 1980 to 1992.
There are factors that can potentiallyconfound the results found in Bloom andMahal’s analysis. The first is the possibilitythat their study was undertaken at a timewhen HIV-prevalence rates were still toolow to have a detectable economic effectat the national level.8 To be sure, Bloomand Mahal (1997) also presented resultsfor the impact of HIV/AIDS over theperiod 1987–92, when HIV might havebeen expected to have a greater effect oneconomies, relative to earlier years, butthe prevalence rates at the time wereobviously much lower than at present.Bonnel (2000) examined the associationbetween rate of growth of real income percapita during the period 1990–97 and aquadratic term in HIV prevalence (aftercontrolling for factors that couldpotentially confound the relationship)and found it to be negative andstatistically significant. He also concludedthat the HIV/AIDS epidemic depressed

������������ �
������������������������������
���������������������� ������������ !172
the rate of growth of real income per capitain Africa during the period 1990–97 bynearly 0.7 percentage points per year, atruly remarkable decline.
McDonald and Roberts (2001) sought toaddress some of the above concerns, byusing panel data methods to estimate theimpact of HIV/AIDS, and using amodified version of the Mankiw, Romerand Weil (1992) empirical elaboration ofthe neoclassical growth model. Theirmain modeling contribution was inlinking HIV/AIDS to economic growth viaits impact on life expectancy, the latterserving as an indicator of health capital inan empirical equation of the link betweengrowth of real income per capita and itsdeterminants. They report the finding ofa statistically significant effect of theHIV/AIDS epidemic on life expectancyand, via life expectancy, on growth of realincome per capita. Their empiricalapproach of emphasising the role ofHIV/AIDS in influencing per capitaincome via life expectancy serves tohighlight the role of one major pathwaythrough which the AIDS epidemic willhave an effect on national economicperformance. Recent empirical work byBhargava et al. (2001) and Bloom,Canning and Sevilla (2001) using paneldata techniques also highlights the linkbetween life expectancy and economicgrowth, and could potentially be modifiedto serve as a means to understand the linksbetween HIV and economic growth.
This note studies the link betweenHIV/AIDS and the growth of real GDP percapita. This is a useful exercise for threereasons. First, compared to the situationa decade ago, data is available for a muchgreater set of countries, a fact highlightedin the work of Bonnel (2000) andMcDonald and Roberts (2001). At thetime of Bloom and Mahal’s work, data foronly about 51 countries were available.
Now, however, UNAIDS providesestimates of HIV prevalence in more than200 countries. Second, the quality of datahas improved compared to a decade ago.In particular, sentinel surveillance datafor women visiting antenatal clinics inmany countries offers a glimpse into HIV-prevalence rates in a group reasonablyrepresentative of trends in the generalpopulation.9
A third factor has to do with the use of AIDScase estimates, instead of HIV, in ouranalysis. Use of AIDS data is desirable,because many of the adverseconsequences of the HIV/AIDS epidemicfor aggregate economic performance havedirectly to do with effects on the labourforce via premature death or morbidity,treatment costs and the fact that many ofthe individual responses to HIV are likelyto kick in at the AIDS stage when they aremore likely to be aware of their HIV status.Most developing countries have poorrecord-keeping systems, so, in alllikelihood, recorded AIDS cases will bebiased downwards. Thus model-basedapproaches to estimating AIDS cases havebeen used for developing countries.
� � � ������������ ����� �����!
The data used in the analysis wereobtained from several sources.Information about the HDI, its gender-adjusted counterpart, the GDI, lifeexpectancy at birth, literacy rates amongpeople aged 15 years and above,enrolment rates and real per capita GDPwas obtained from the HumanDevelopment Report 200110 and the WorldBank’s World Development IndicatorsDatabase.11 In addition, we have utiliseddata on average years of schooling forpeople aged 15 years and above describedin Barro and Lee (2000), the degree ofopenness of an economy as measured by

������������ �
������������������������������
���������������������� ������������ !173
the ratio of exports and imports to GDPin World Bank (2001), population growthrates (World Bank 2001), proportion of thatpopulation that is Muslim and/or Judeo-Christian (Central Intelligence Agency(CIA) 2001), date of the first reported HIVand AIDS cases (United States Bureau ofthe Census 2001; Mann, Tarantola andNetter 1992), indicators of political freedom(Freedom House 2002) and urbanpopulation growth (World Bank 2001).
Estimates of HIV prevalence for 1999 wereobtained from the UNAIDS countryepidemiological fact sheets.12 These HIVprevalence estimates were obtained bycareful examination of sentinelsurveillance data sources among womenvisiting antenatal clinics in manycountries and other sources of HIV data,coupled with an extensive process ofdouble-checking and verifying estimatesof HIV so obtained. As a consequence,the full sample (as indicated in Table T10)had HIV prevalence data for 112countries, nearly double the number ofcountries for which HIV estimates wereavailable in 1996.13
Estimates of cumulative AIDS cases wereobtained as follows. For developingcountries, multi-year and multi-site HIV-prevalence information for womenvisiting antenatal clinics in sentinelsurveillance data was used. The numberof countries for which such data wasavailable was somewhat less than thecountries for which UNAIDS HIV-prevalence data were available, given thatthe analyses were restricted only tocountries for which several years (andseveral sites) of sentinel surveillance HIV-prevalence data were available for womenvisiting antenatal clinics. This was donein two steps, with the help of a set ofsoftware packages recently developed byUNAIDS.14 First, data points obtainedfrom HIV sentinel surveillance were used
to fit a curve for the time profile for HIVprevalence with the Epidemic ProjectionPackage (EPP) developed by UNAIDS.15
Having obtained the times series of HIVprevalence rates, the second part of themethod involved using the SPECTRUMsoftware package that combinedpopulation estimates and projectionswith HIV prevalence rates to arrive atestimates of the incidence of AIDS casesand deaths, after taking into account theprogression rate from HIV to AIDS todeath.16 The model also provides separateestimates of AIDS cases and deaths formales and females, if additional inputregarding the nature of the epidemic –primarily heterosexual, homo- or bi-sexual, or injecting drug use driven – isprovided. The computation assumed themedian time from infection to death ofabout nine years in developing countries,and involves the assumption of no ARVdrug use.17 This assumption appearsreasonably valid for the developing world,most of which is not in a position to affordARVs, but not for developed countries.For the latter set of countries, we useddirectly the estimates of AIDS casesprovided by their governments, given thatthe reporting errors for AIDS cases in thedeveloped world can be expected to besmall, and nowhere near as large as thedeveloping countries, a group thatincludes the countries of South Asia, withpoor AIDS reporting systems. For thelatter group, indirect estimation via EPPand SPECTRUM, along the linesindicated above, was obviously moredesirable. In sum we were able to obtainAIDS incidence and cumulative AIDScase data for a total of 76 developing anddeveloped countries.
Table T10 summarises, for the samplecountries, the main descriptive statisticsrelevant to our analysis of the potentialimpact of HIV on human development.

������������ �
������������������������������
���������������������� ������������ !174
The full list of countries is provided in thenotes to Table T10. The data indicate thesubstantial variation in HIV prevalenceamong adults, from negligible levels insome countries, to a high prevalence ofnearly 34 per cent in Botswana. The meanHIV prevalence in the full cross-sectionof countries, in contrast to Botswana’scase, is three per cent. As anotherexample of the variation in the spread ofthe HIV/AIDS epidemic across countries,the average annual increase in AIDS cases(taken as a proportion of per 100population aged 15–64 years in 1998)during the period from 1980 to 1998 wasabout 0.18 for the full sample, but rangedfrom 0 in some, to 1.93 in Botswana. Oursample of countries includes those withextremely low levels of humandevelopment in 1999—0.258 for SierraLeone –as also countries such as Norway,with an HDI of 0.939 in 1999. Similarvariation is apparent from data oneducation variables such as adult literacy,mean years of schooling and schoolingenrolment, life expectancy at birth andreal GDP per capita.
"�#���������������������������� ����������� ���������The starting point of our discussion is thefollowing simple equation that can beused to describe the dynamics of HIVtransmission in an adult population,whose HIV prevalence rate is denotedby H.18
(3) dH/dt = (1 – H)*Hp *ß *T - θ*H
Here dH/dt is the derivative of H withrespect to time “t” and equation (3)describes the movement of HIVprevalence over time. H
p is the infection
rate among the “sexual” partners of theabove population, ß is the proportion ofunprotected sexual interactions in anygiven interval and T is the rate oftransmission of HIV during unprotected
sex. θ denotes the proportion exiting fromthe infected pool in any time period.
The HIV prevalence rate among partners,the proportion of people in thepopulation of interest who haveunprotected sex and the rate oftransmission of HIV will depend on anumber of variables, such as the level ofknowledge people possess about risk ofinfection, income levels and hence theopportunity cost of infection, concernsabout health (including one’s owninfection status, especially if there isassortative matching), opportunity,inequalities that allow some people to payoff others to incur increased risk as well asindicative of poverty, cultural norms thatgovern the practice of unprotected sexand the like. Specifically, let us assumethat the impact of these other forces is feltin such a way that
(4) Hp *ß *T = (α + π*x)*ρ*H
Here x indicates all variables other thanan average individual’s HIV-status, H.H is taken to enter multiplicatively in thisformulation. Thus, we can write
(5) dH/dt =(1 - H) * (α + π*x) *ρ*H - θ*H
and
(6) dH/dt = (α*ρ + ρ*π*x - θ)*H -(α + π*x)*ρ*H2
This formulation, under differentassumptions, leads to three relatedeconometric specifications, as isdemonstrated below. The differentialequation in (6) has a readily obtainablesolution given by,
(7) Z(t) = exp(-k*t) * z(0) + (m/k)*(1 - exp(-k*t))

������������ �
������������������������������
���������������������� ������������ !175
Where
k = (α∗ρ + ρ∗π∗ x − θ)m = (α + π*x)*ρz(t) = 1/H(t)
As k→∞, Z(t) tends to the steady state“m/k”. We can also see that
(8) Z(t) - (m/k) =[Z(0) - (m/k)]* exp(-k*t)
Case I: In the special case whereθ = 0 (implying that m/k = 1), we havefrom (8), after taking logs on both sidesand substituting for z = (1/H)
(9) ln(H/(1-H)) =ln (H(0)/(1-H(0))) + k*t
or,
(9’) ln(H/(1-H)) =ln (H(0)/(1-H(0))) + α∗ρ∗ t + ρ∗π∗τ *x
Assuming all countries start from roughlya similar sized epidemic (roughly 1 percent of some segment of the population),we can set forth the first version of oureconometric formulation as
(10) ln(H/(1-H)) = δ + β*t + λ*t*x + ε
Here, δ, β and λ are parameters (orvectors of parameters) to be estimatedand ε is an “error” term with the usualproperties.
Notice that the assumption of θ = 0 is astringent one, because it is effectivelyruling out a faster rate of exits, relative tothe rest of the population, from theinfected population in the model.Moreover, the assumption implies thatthe population heads to a steady stateHIV-prevalence level of unity, but with theproviso that the rate at which it get there
depends on the parameters and thex variables characteristic of each group.
Case II: An alternative formulation is oneis where θ ≠ 0. If so, we can write fromabove
(8’) Z(t) = exp(-k*t) * z(0) + (m/k)*(1- exp(-k*t))
If we work with the assumption that weare still early in the epidemic, using alinear approximation around t=0 we canwrite
(11) Z(t) ≈ Z(0)(1 – k*t) + m*t
From this we have,
(12) Z(t) ≈ Z(0) + (m – Z(0)*k)*t
The resulting econometric specificationis:
(12’) 1/H(t) =Z(0) + ϕ + χ*t + µ*t*x + ν
Where ν is an error term and (Z(0)+ ϕ) isconstant. Given that (12’) is the outcomeof a linear approximation, the estimationexercise also considered anotherspecification that allowed for the naturallog transform of (1/H) as the dependentvariable of interest.
Case III: At the other extreme, one canfocus on the steady state outcomes forpurposes of estimation if one believes thatthe country HIV/AIDS epidemics are farenough advanced. In particular, goingback to
(4) dH/dt =(α∗ρ + ρ∗π*x - θ)*H - (α + π*x)*ρ*H2
Putting dH/dt = 0, we have that in thesteady state

������������ �
������������������������������
���������������������� ������������ !176
(13) H =(α∗ρ + ρ∗π∗ x - θ)/[(α + π*x)*ρ]
and
(13’) (1 - H) = θ/[(α + π*x)*ρ]
This gives rise to the followingeconometric specification
(14) H*(1 – H)-1 = δ + λ*x + ε
The statistical analysis of this paper onthe determinants of HIV prevalenceinvolves primarily the estimation of (9’),(12’) and its logarithmic counterpart, and(14). However, as discussed below thepaper also presents the results ofspecifications of the form in (15) below tocompare the results using national levelHIV prevalence data with those obtainedby Over (1998) who used this specificationto analyse urban HIV prevalence rates indeveloping countries.
(15) ln (H*(1 – H)-1) = δ + λ*x + η*t + ε
$" ��������� ��������� ���������� ��������The standard approach has been to usedata on HIV prevalence (taken to berepresentative of the whole population),combine it with a description of the rateat which HIV cases progress to AIDS andto death (normally approximated by aWeibull distribution, Bloom and Mahal,1997), along with a further assumptionabout the start date of the epidemic.Unfortunately, an infinite number of timeprofiles of HIV prevalence that canachieve the HIV prevalence at a point intime exist, even with these requirements.Thus the typical approach to derive thetime profile of HIV/AIDS cases has beento make an assumption that HIVincidence follows a gamma function ofone (or, two) parameter variety, add tothat a further statement about the peak
year of incidence, and then to choose thevalue of the gamma distributionparameter itself.19 Bloom and Mahal(1997) introduced the methodologicalinnovation in a maximum likelihoodframework whereby the gammadistribution parameter was chosensimultaneously as part of the econometricspecification linking AIDS to economicgrowth. However, owing to data fromsentinel surveillance sites being availablefor several recent years and developingcountries, it is possible to directly derivethe time profile of HIV incidence usingcurve-fitting techniques and softwareprovided by UNAIDS for these countries.The methodology is more fully discussedin UNAIDS (2002b).
For the purpose of examining the impactof AIDS on economic growth, were-estimated two empirical equations —(1) modified version of the empiricalspecification used in Bloom and Mahal(1997) with new data, for the period 1980to 1998, for 69 countries; and (2) a modifiedversion of the equation used by Bloom andWilliamson (1998). The set of countrieschosen was smaller than the countries forwhich UNAIDS provides HIV prevalencedata, in order to include only thosedeveloping countries for which a largenumber of sentinel surveillance data wereavailable for some years, for reasonablysized samples. The sample of countriesalso included developed nations fromEurope and North America, as well asAustralia, Japan and New Zealand, wherereported AIDS cases can be expected tobe a reasonably accurate indicator of thetrue AIDS cases. These were combinedwith data on range of geographicdemographic and socio-economicvariables as additional explanatoryfactors — real GDP per capita in 1980,government expenditures on educationand defence as a proportion of GDP, meanyears of schooling, the ratio of exports and

������������ �
������������������������������
���������������������� ������������ !177
imports to GDP, rate of growth ofpopulation, the rate of growth of workingage population (15–64 years), whether thecountry was landlocked, quality ofinstitutions, whether located in tropicalregions, life expectancy at birth in 1980and the rate of growth of lagged per capitaincome. The sources of this data includedthe World Development Indicatorsdatabase,20 the Penn World Tables,21 Barro-Lee database on education indicators,Human Development Reports for variousyears, and Gallup and Sachs (2000).
Our empirical approach was to estimatethe following equation, the same asequation (1) in Bloom and Mahal (1997,p.112), and equation (5) in Bloom andWilliamson (1998, p.431) after including aterm for AIDS.
(16) Yi
= α + βAIDSi + X
iπ + ε
i
(i=1,2, ..., N).
Here Yi is the rate of growth of real income
per capita, AIDSi is the average annual
increase in the cumulative adultprevalence of AIDS (the average annualincrease in the number of AIDS cases overthe estimation period, taken as aproportion of the population aged 15–64years in 1998), X
i is a vector of variables
that influence economic growth and εi are
independently and identically distributederror terms, each with zero mean; α, βand π are parameters to be estimated. Amajor goal of our analysis is to obtain aconsistent estimate of the coefficient ofthe AIDS variable, β.
The results of estimation of equation (1)by ordinary least squares, given the findingboth in Bloom and Mahal (1997) andBonnel (2000) of there being no statisticalevidence of a reverse causality going fromgrowth of real income per capita toHIV/AIDS. Estimation of equation (1) byinstrumental variable methods (resultsnot reported here) confirmed these earlierfindings. The estimation method does notrely on panel data methods and thus isopen to the methodological objectionsnoted previously. This is proposed to berectified in future work, as more HIVprevalence data becomes available. Theresults as reported here are also open tothe objection that they may becontaminated by the effects of classicalmeasurement error in the AIDS variable,which can influence the coefficient tobecoming statistically insignificant. Thisis more readily addressed by the use of IVmethods. However, as noted previously,the use of IV methods does not influencethe main results of this paper. Anotheraspect of the estimation method (for bothBloom and Williamson and Bloom andMahal specifications) is that thepopulation growth rate variable has beenadjusted to compensate for any AIDSdeaths that may have occurred. Doing soraises the “adjusted” rate of populationgrowth over that actually observed. Thisadjustment permits the coefficient of theAIDS variable to be interpreted as the sumof the direct effect of AIDS on growth ofreal income per capita, plus any indirecteffect on growth of real income per capita,working via the impact of AIDS onpopulation growth.

������������ �
������������������������������
���������������������� ������������ !178
��#����$�%
������� ��������� �����������������%&�'()*+((&�,���� � �-� ����.� ���
���������� ������������ �����������������%�'(((
/'" /!" /0" /1" /2"
&������� ' ($ ' (% ' �$ ' )% ' *$ ' !% ' ($ ' !*% ' �$ ' (%
���+ ,',-$ ',)% ,'� $ '� % ,'��$ ',,% ,'(,$ ',!% ,'!)$ ',(%
���+ .���+ ',-$ ',�% ',-$ ',*% '�)$ ' /% '!/$ ',,% '!($ ',,%
�������������,//+
$���, ���������� ' (! ' ()
����,)0*(��,//+% $ ' ,*% $ ' ,*%
�������������
����������
�������������� ',
�����,/+ /+ $ ' �%
$���, ����������
����,)0*(��,//+%
��#���1
�#���������� /! *- /! *- *-
� �2����� '/)- '/** '/-( '/+! '/+(
������3 ������4� ������������' �������5���������6 ��������� �������� ������ �������� �� �����������'
��#���,
��� �������������������������������� &�$ �������
������ ���� ��� �� ���� ��� �� ���� ��� �� ���� ��� �� ���� ��� ��
�������3� �������3� �������3� �������3� �������3�
���/4" ��5���� -��� ������ ����� � 6������������
'((*+(( � ��� �/4" �%���� �� � ��/4" ����%�/4"
'((*7(( '()*7(( '()*7(( '()*7!***
�1��������� '�' '�' '-, '�' '
���������� ,'(� �'// ,',/ ,'-* '--
������ '�' !',* '�' '�' ,'!�
����� ,'�* !'-! '-/ ,'- '
���� ,',( �'!, '+/ �',* '/�
7������� '�' '�' ,' '!( '(+
���� ,'*! �'�- ,' � !' ( �'�!
8�5����� ,'!* ,'(, '*- �'), '(!
���9��5� '*� !'+( '!/ '!- ,'-
����3 '�' ��������� ��� ������#��
������3 ������4� ������������ �����:���� ���5; � ����'

������������ �
������������������������������
���������������������� ������������ !179
��#����$#%
������� ��������� �����������������%&�'()*7((&�������� ���
���������� ������������ �����������������%�'(((
/'" /!" /0" /1" /2"
&������� ' ($ ' (% ' �$ ' )% ' *$ ' !% ' ,$ ' (% ' �$ ' )%
���+ ,',-$ ',)% ,'� $ '� % ,'�)$ ',,% ,'),$ ',!% ,'(*$ ',-%
���+ .���+ ',-$ ',�% ',-$ ',*% '�/$ ' /% ') $ ',,% '(*$ ',!%
�������������,//+
$���, ���������� ' *, ' *)
����,)0*(��,//+% $ ' ,�% $ ' ,,%
�������������
��������������������
���������,/+ /+ ',-
$���, ���������� $ ' !%
����,)0*(��,//+%
��#���1
�#���������� /! *- /! *- *-
�����������
���������&�� �2$!% ,*',* � '+, !!'-*
� �2����� '/)- '/** '/- '/-/ '/-)
����3 ��#��� �������� ������ �������� �� �����������' �����1�������� $!% $)% ��� ��������� ����� ������������
�����#��� 1�� ��� �������� �����#���'
��������3 ���+ ;���+ �2�����;<����1 ��� ������1 ���������������;�����������1���������� ���� ��
7�����;����������1���������1��������6$������1 �������1 �����������=����� ��>�8 ��,/+ %; ���
����6�����1 ��������� ����������������,)6��������#��� $,/+ %; ��� ������1 ��1� �=�������6�1 1������
�������1�����;�����������1���?���1����������������,/- + '
��#���!$�%
������� ���������%���� �� � ��$���&�'()*7()&�,-������� ���
���������� �������-����8%���� �� � ��9���&�'(()
/'" /!" /0" /1" /2"
&������� ! '(+ ,�'/( �*',- �!'+) �,'+)
$,�' *% $,)'/ % $+' % $/'!�% $/'-/%
9�1��=�������6;,/+ $6����% �'�( ,')( �'! �',) �' -
$ '(�% $ ')*% $ '�*% $ '!�% $ '!�%
9�1��=�������6;,/+ �2����� ' ,, ' ( ' ,� ' , ' ,
$ ' (% $ ' )% $ ' �% $ ' !% $ ' !%
�������������,//+$���, ')+ ')(
��������������,)0*(��,//+% $ ' +% $ ' /%
�����������������������
�������������������,/+ /+ ,,'(
���, ��������������,) *( $!'�)%
��,//+%
��#���1�#���������� ,,� -* ,,� -* -*
� �2����� '+-( '+/, '/!* '/(! '/(-
������3 ������4� ������������' �������5���������6 ��������� �������� ������ �������� �� �����������'

������������ �
������������������������������
���������������������� ������������ !180
��#���!$#%
������� ���������%���� �� � ��$���&�'()*7()&�������� ���
���������� �������-����8%���� �� � ��9���&�'(()
/'" /!" /0" /1" /2"
&������� ! '(+ ,�'/( !,'�, !�'(( �/'*)
$,�' *% $,)'/ % $+'*�% $/')!% $,�'!)%
9�1��=�������6;,/+ $6����% �'�( ,')( �')! �')( �'(/
$ '(�% $ ')*% $ '�+% $ '!,% $ '(,%
9�1��=�������6;,/+ �2����� ' ,, ' ( ' ,( ' ,( ' ,(
$ ' (% $ ' )% $ ' �% $ ' !% $ ' !%
�������������,//+$���, '-+ '-)
��������������,)0*(��,//+% $ ',)% $ ',(%
�����������������������
�������������������,/+ /+ ,+'*,
$���, ��������������,) *( $�'/+%
��,//+%
��#���1�#���������� ,,� -* , ) -! -!
����������� ��������� )',, '+ )-'�/
� �2����� '+-( '+/, '/�+ '/!) '/�!
������3 ������4� ������������' �������5���������6 ��������� �������� ������ �������� �� �����������'
�����1�������� $!% $)% ��� ��������� ����� ������������ �����#��� 1�� ��� �������� �����#���'
��������3 ���+ ;���+ �2�����;<����1 ���������1 ���������������;�����������1���������� ����
��7�����; ����������1���������1��������6$������1 �������1 �����������=����� ��>�8 ��
,/+ %; �������6�����1��������� ����������������,)6��������#��� $,/+ %; ��� ������1 ��1�
�=�������6�1 1������ �� �����1�����;������ �����1���?���1����������������,/- + '
��#���(
������� ������ ���������� � �� ��&�'()*7()&�,-������� ���
���������� �������������-���� � �� ��&�'(()
/'" /!" /0" /1" /2"
&������� , '!) , '( , '*) ,,',( , '/-
$!' -% $!'*�% $!', % $!'*!% $!'*(%
������������6����;,/+ ,'(( ,'(� ,'!/ ,'!( ,'!*
$ ',,% $ ',!% $ ',,% $ ',!% $ ',!%
������������6�����2�����; ' * ' )% ' ) ' ) ' )
,/+ $ ' ,% $ ' , $ ' ,% $ ' ,% $ ' ,%
�������������,//+$���, ' / ',�
��������������,)0*(��,//+% $ ' *% $ ' *%
�����������������������
�������������������,/+ 0/+ �'�!
$���, ��������������,)0*( $,' )%
��,//+%
��#���1�#���������� ,,� -) ,,� -) -)
� �2����� '/*) '/*) '/** '/** '/*)
������3 ������4� ������������' �������5���������6 ��������� �������� ������ �������� �� �����������'
�� �����1������� 1���� �� #� ������������6 ��������������#�� 1���@9� �����1������� ����� �������� ����'

������������ �
������������������������������
���������������������� ������������ !181
��#���)
������� �������� ��� ��� ����5&�'()*7()&�,-������� ���
���������� ��������� ����5������ ��� &�'(()
/'" /!" /0" /1" /2"
&������� ((('!- �-(' / (�/' * , )' ,!)'(�
$,) '/-% $,!!',*% $,+!'+)% $� /')�% $,+ ')!%
����>�8���������,/+ ,'*( ,'-, ,'*( ,'- ,'-
$,//)A�B% $ ',!% $ ',,% $ ',!% $ ',,% $ ',,%
����>�8���������,/+ ' , ' , ' , ' , ' ,
�2�����$,//)A�B% $ ' % $ ' % $ ' % $ ' % $ ' %
���8���������,//+
$���, �������������� !'� �*')�
,)0*(��,//+% $�,'**% $�-'/*%
���������������������
���������������������
,/+ 0/+ (- ' �
$���, �������������� $!- '/+%
,)0*(��,//+%
��#���1�#���������� , � -( , � -( -(
� �2����� '/) '/* '/) '/* '/*
������3 ������4� ������������' �������5���������6 ��������� �������� ������ �������� �� �����������
��#���*
�������������� ��������/������� ������.� ��� ��������"
� �� $�� � �� � �� �� �� ������� � %����
���� ����
�������������;,/// ,,� �'/-- )'-)) ' ! !!'+!,
$���, ������,)0*(%
���������������������������������
����$���, ������;,)0*(6����% -* ',+ '!,/ ,'/!(
>��������������������=;,/// , + '*+, ',/( '�* '/!-
���2�����6����=
9������6����������������,)C;,//+ ,, '--+ '�!� ',, ,'
���2�����6����=
9�1��=�������6��#����;,//+ ,,) '*-+ ',/+ '� ( '/�*
����3 ��1��� �� ������#���1��������� �� ���������'
������3 :���� ���5; � DA�8; �
&��������3 ���� ����� ��� ������3 �������; �����; ����?���; ���5��� E���; �������; &�������; &������
�1����� ����#���; &���; &��� �4������; &6����; �F�#����; G�6��; G�������; >�#��; ���>��#��;>����; ������
H�����; I��6�; 9�#6�;7���������;7���?�;7���;7������;7��������;7�J��#�2��; ���#��; ����;
������; �?����; ����� ���#��; �������; ������ 9����; ������1����; �?�J�����; �6���; ���J����; �������;
A�����; K����; K��#��; K��#�#?�' ����3 ����������; &��#����; &����; ����I���; �����; ���������;
����; H����; ����#��� �1 I����;7���6���;7�������;76�����; ����; 8�5�����; 8����������; ���������; ���
9��5�; ��������; �������' ����� �������� ��� ��������3 ���������; ��� �������; ���#����; �������;
���J��; &����; &����#��; &���� ����; ��������� ����#���; G������; G� ��������; >��������; >�6���; �����;
��������; H������; ��������; 8�����; 8������6; 8���; �������� ��� ��#���; A�����6; ����J����'�����
�������3 &�����;7�=���; A����� ������'������3 ���������; �? K������
������3 �������; �������;������5; E������; E�����; >�����6;>�����; ������6; �������; �������; ����6;
7����; ����������; �? K������; ��?�6; 8�������; �����; �?����; �?��J������; ���5�6; A����� I������

������������ �
������������������������������
���������������������� ������������ !182
��#���-
������� ����������������������������%&�'()*7!***&�,-�
���������� ����������������������%�!***
/'" /!" /0" /1" /2"
&������� ' + ' ) ',� ', ',,
$ ' �% $ ' �% $ ' �% $ ' �% $ ' �%
���2�����6����= '-/ '+, '-, '*/ '*-
9�1��=�������6��#����,/+ $ ' *% $ ' -% $ ' *% $ ' -% $ ' -%
���2�����6����= ',- ',/ '� '�) '�)
������������6����,/+ $ ' (% $ ' (% $ ' (% $ ' (% $ ' (%
�������������,//+ ' �+ ' �)
$���, ��������������,)0*(��,//+% $ ' /% $ ' +%
�����������������������
�������������������,/+ /+ ' *
$���, ��������������,)0*(��,//+% $ ' �%
��#���1�#���������� , - -( , - -( -(
� �2����� '/(- '/-( '/)! '/-- '/-/
������3 ������4� ������������' �������5���������6 ��������� �������� ������ �������� �� �����������'
��#���+
������� ������.� ��� �����%�����������%���� �� � ��$���&�'()*7()&�,-������� ���
���������� ��.� ��� ����%�����-����8%���� �� � ��9���&�'(()
/'" /!" /0" /1" /2"
&������� ' + ' ) ' � ' � ' �
$ ' +% $ ' /!% $ ' )% $ ' *% $ ' */%
���2�����6����= ,')� ,',( ,')- ,')� ,'(!
9�1��=�������6;,/+ $ '�+% $ '!)% $ ',-% $ '� % $ '��%
���2�����6����= '(( ' - '* ')� '((
9�1��=�������6;,/+ �2����� $ '�!% $ '�/% $ ',!% $ ',)% $ ',-%
�������������,//+ ' /- ' /�
$���, ��������������,)0*(��,//+% $ ' ,!% $ ' ,(%
���������������������������������
���������,/+ 0/+ ',/
$���, ��������������,)0*(��,//+% $ ' *%
��#���1�#���������� ,,� -* ,,� -* -*
� �2����� '++* '/ '/(+ '/)) '/)(
������3 ������4� ������������' �������5���������6 ��������� �������� ������ �������� �� �����������'

������������ �
������������������������������
���������������������� ������������ !183
��#���/
������� ���������.� ��� �����%����� ���������� � �� ��&�'()*7()&�,-������� ���
���������� ��.� ��� ����%����������-���� � �� ��&�'(()
/'" /!" /0" /1" /2"
&������� ',) ',( ',( ',( ',(
$ ' �% $ ' �% $ ' �% $ ' �% $ ' �%
���2�����6����= ,'( ,'(! ,'!/ ,'(� ,'(�
������������6����;,/+ $ ' +% $ ' /% $ ' +% $ ', % $ ', %
���2�����6����= ')* ')+ ')) ')* ')*
������������6�����2�����;,/+ $ ' *% $ ' -% $ ' -% $ ' +% $ ' +%
�������������,//+ ' ) ' )
$���, ��������������,)0*(��,//+% $ ' *% $ ' -%
���������������������������������
���������,/+ /+ ' ,
$���, ��������������,)0*(��,//+% $ ' ,%
��#���1�#���������� , / -( , / -( -(
� �2����� '/-) '/+ '/-) '/+ '/+
������3 ������4� ������������' �������5���������6 ��������� �������� ������ �������� �� �����������'
�� �����1������� 1���� �� #� ������������6 ��������������#�� 1���@9� �����1������� ����� �������� ����'
��#���,
�������������� �������
� �� $�� � �� � �� �� �� ������� � %����
���� ����
�������������;,///$���,
������,)0*(% ,,� �'/-- )'-)) ' ! !!'+!,
���������������������������������
����$���, ������;,)0*(% -* ',+ '!,/ ,'/!(
��������������������=;,/// ,,� '*+( ',/) '�)+ '/!/
�������������������;,//+$,//)A�B% ,, -;)!( ,,;,)) ,, ((;/ *
9������6����������������,)C;
,//+$�������% ,,� -+'!( ��',, ,)'! ,
7���6�����1���������,)C;
,//)$6����% /! *' ) �'+/ '*/ ,�',+
>������������6���������;
,//)$�������% /, *-'�- !*'�/ )'( ,(*
>����������6���������;,//)$�������% , /-'** ��'!/ �/' ,*�'
9�1��=�������6��#����;,//+$6����% ,,) *)'*) ,,'++ !-'( + ')(
����3 ��1��� �� ������#���1��������� �� ���������'
������3 :���� ���5; � DA�8; �
&��������3 ���� ����� ��� ������3 �������; �����; ����?���; ���5��� E���; �������; &�������; &������ �1�����
����#���; &���;&��� �4������; &6����;�F�#����; G�6��; G�������;>�#��; ���>��#��;>����; ������ H�����;
I��6�; 9�#6�;7���������;7���?�;7���;7������;7��������;7�J��#�2��; ���#��; ����; ������; �?����;
����� ���#��; �������; ������ 9����; ������1����; �?�J�����; �6���; ���J����; �������; A�����; K����; K��#��;
K��#�#?�' ����3 ����������;&��#����;&����;����I���; �����; ���������; ����; H����;����#��� �1I����;
7���6���;7�������;76�����; ����; 8�5�����; 8����������; ���������; ��� 9��5�; ��������; �������' ����
�������� ��� ��������3 ���������; ��� �������; ���#����; �������; ���J��; &����; &����#��; &���� ����;

������������ �
������������������������������
���������������������� ������������ !184
8�������
, ���5�6 �������� �� ������������� ������� ��������6 ������ $���� ��;?����������� ������� ����
>�8���������%���?������?���������������?��� ��?�� �������1>�8���������0���
�� ������ "����������� �6�������� L $1�� �=�����; ����� ,//,%'��1��� ��� � 6��� ���?�� ����
�1 ����>�8 ��� ������ �� M<$�% 0<$ %N�<$ %' ���� ���?�� �� ���������6 ����������?���<$ %;
��������� �� ��� ������������6��������; �'�'; �������� ��6; 1�� �=����� M<$�%0<$ %N�<$ %O
$.<$ %;?��� $P ' ��� ���� ���������������6 ���������� ������������?� ��1�� �� �� �������
��=�'
� ����;�� ��������������#���������������#���������������������#������������������
��� ���������� �1 ������#����6 �����������6 ����������?��� ����������� ��������'
! �����1�����6; ������������� ����=;Q� $�O,;�;!% �� ���������� ��#� ��� 1����?��� 1������
Q�OMRQ
�1, SC$, R%Q
��, SN,�, S$�O,;�;!%
����; Q�1 �� ��� ����= �1 1����� ������������ �� ��������� "�L; ���Q
�� �� ��� ����= �1����
������������ �� ��������� "�L ��� R �� ��� 1����� ����� �� ����� ����������' ��� ���������
"SL���������������1������������1 �����������������' ��>��������������; �� ����5����#�
�2������$A�8� ,%'��1����������>����� ?���#������1����������������������
������ $� ,%;��� ��1������������������������#������ ��1��=�������6�����#���;���������6
#6 ������; 1��� ���:���� ����������� ���������� ����#��� �1 ���:���� ���5 $:���� ���5
� %'�������������1��1��������?��������������������������������2�����6�������1��
��1� �=�������6 �� #���� �� ,/+ ��� ,//+; ��� ����� �������6 ����� 1�� ,/+ ��� ,//+'
�����1�������� ������� �� $,%?��� ��������� �� ������ ��� ������ �1 �������� �� ���2�����6
�������;?�������=�������'�������>����1��������1��,/+ ?����������#��;,/+ �������1
������������ ����=1�� �������� �������6 ������������������� ����=1�� ��1��=�������6��
#����?����������=��������6�����#������������1����1���������������������������������
�����#�6 ��1������>��'
( �������������1�����������?�����������#����6������1������������?������������
����������6;�������������������1����?�����������������=������� ')�������;1������
��F�����#6 ����������6����������������6����1 ����������� 1������ ������'
) ����� ��� 9�?��; � ; �',�D����� ��� 9�?��; � ,
* ����� ��� 9�?�� � ,; �',*
- ����� ��� 9�?��; � ; �'/
+ ������� ; �'!;7������� �����#����;� ,; �'*
/ ���� 2����1�������� �� ���� ����� ��� ��������6' �� �� ��� �#������6 ���� ���� ��� ����������
����� �����?���� �������� ��������� ������� ��� �������������� �1 ���������� ����� �����
���' ��� ����� ����� �������#�6 �������������� �1 ��� ���������� ����� �����?���� �� ���
��������������������T 7��6��������������������������������;�����1?������� �������
��������� ����#���; G������; G� ��������; >��������; >�6���; �����; ��������; H������;
��������; 8�����; 8������6; 8���; �������� ��� ��#���; A�����6; ����J����'������ �������3
&�����;7�=���; A����� ������'������3 ���������; �? K������
������3 �������; �������;������5; E������; E�����; >�����6;>�����; ������6; �������; �������;
����6;7����; ����������; �? K������; ��?�6; 8�������; �����; �?����; �?��J������; ���5�6;
A�����I������

������������ �
������������������������������
���������������������� ������������ !185
�� ��#�� �����; �� ���6 ��� ��5��6 �� ���� ��?�� ����������� �1 �����?����' ������; 6����
?�������������51��������1������������������������������������������1������'�����;
��� ����� �� ���� �� ��?�� 1�������6 �����; �� ���� �������� �� ��������� ������� ?����
�����������������6 ��������� �����������?��� ��?����� ����������; �������� �� ���?���� �����'
E�����6;�����1������������������������������������������#���1���������;�����������?����
#� ����� �������� ��11������� #��?���?����?���� #���� �� ������ 1�� ��� �� ��� ��������
������������ �����; ��� �����?�� ����� ������� 1���������; ��� ��� ��� �������' ����� �������
������� ���� �������� ������������ ����?���� ������������� ��� ���������� �����?���� ��
������������ ��� ������' ��� ���������6 ������� ����?���?������� �� ����������� ��?����;
�������� �����;��� ��� ���������� �����1��������=�����= ����������������� ������������
���������; �������� ��?����; �� ����� ��� 1����� ������� �� � #��� �� ��� ����� ���������?���
����� ���� ����� ������ ��� ���� �� ��������� ���������� ����� ����� ��� ������'
, A�8; � ,
,, :���� ���5; � ,
,� A�����:�@; � ,;A����; � # ��� �
,! ����� �� ��'; ,//*
,( A����; � �#
,) ������� ���������� �1 ��� G88 ���� ��� �����������; G8�7@�G9; �� ��� �#����6 ����5�����
�����11����������1����������1��������������� ����������;�����#��#����?��5?����
���� #������ ��� �1 �����#��� ��1�������� ��� ���������� $&��� ��� 9?���� ,// ; A����
� �#%' �� ����������; G88 �������� ��� ���������� �1 1��� ���������� ���� ������#� ��� ����
���1����1��������������������������0����������6����1�����������;���������������������1
������������������51����� ��1������;���������#������1������������� ��������� ���5�����
���5����������;������������?��������� ���5�������������� ��1�����?������'E��������
������� �1 ����������� 1������ ������; ����� ����� ���� ����� ����������� ��� ��1�����?���
���; #���� ����� �1 ��� �������� ��������; �������� ����� �� ��� ,) �������� ��1����� ��������;
1�������6 ��������� ��� �� ��� ��� ��� ���� �1 ��������� ������������; ��� G88 1���� ��� $1���%
��������� ��������� ��� ��� ��������� �������� ������� �1 ��� ���������� ���� "#��� 1���L ���
�#������ ��� ���������� ���� 1��� �������� �����' G���������6; ���� ������� �� �������� ���
���������� �� �� ���������� ��� ����� ��� �1 �2����� �1 ��� 1����� ����� $A���� � �#;
�'(,%'������������6������������������1G88�����������������������������#�����������������
���� ���������� �������� $������#����%���������������������� 1�� ����� �����#�� �������'
,* E�� ���������� �������; ���A���� � �#
,- ����������������������������#����������� �� 1�������6 ������?��� ����� ��1�����������
������������ ���?����'
,+ ���; 1�� ��������;�������� ���7�6,//,DI�����,//*
,/ &��� ���9?����;,//,
� :���� ���5; �
�, ������� ���������; ,//,

������������ ����
�� ������������������������������
������������������������� ������������������186
����������������
���� �
�������������� ������� ���������������
���� ����� ��� ���� ��� �������� ����� ��� ���
��� � ��� ���� � ����� �������! �"���#$% ��� "���
&''' � ���� ( �� ��#$ ���������
#�����% �)���* ���� �� ����
�&''' ��� )����
����% �������
&''' �� ��#$%
�+++
�! �������� "#�# "#�# "#�# "#�# "#�# "#�# "#�#
$�� ������ �#%&' ()#% % #� �& %�#% �#%*' �#���
$����� �#%)% *� %& �� "#�# "#�# "#�#
����� �#(&& *�#� (&#� (( ��# �#(*� "#�#
�����+�#�#, �#&� *'#) &*#� &� &#� �#&�� "#�#
-������� �#&%� **#( )*#& && (#' �#&�) �#�*
"���� �#%)� ('#* % #' *� %�#% �#%&� "#�#
.�/����� �#%)) *� %�#� %� % #� �#%*' "#�#
����0��/� �#&% &�# ) #* &� &#* �#&�& �#�&%
"���1� "#�#� ���������� ���� ��������
�������� 2"�.3� ����
����
,������������
���� �� �+-* �+.' �+.* �++' �++* &'''
�! �������� "#�# "#�# "#�# "#�# "#�# "#�#
$�� ������ �#��( �#�(� �#�'* �#% * �#%%( �#%&'
$����� "#�# "#�# "#�# "#�# "#�# �#%)%
����� �#%�& �#%�% �#%&� �#( �#(%( �#(&&
�����+�#�#, �#((* �#(*� �#*�& �#*%( �#*'' �#&�
-������� "#�# "#�# �#*�) �#*&* �#&�& �#&%�
"���� �#�') �#��' �#�&� �#% * �#%(� �#%)�
.�/����� �#�%( �#�&� �#%�% �#%%� �#%&� �#%))
����0��/� �#* * �#*(� �#*&* �#*)& �#& ) �#&%

����������������
�� ������������������������������
���������������������������
����������������
187
�����
����)���(���(�� (������� ���
���� �� ����� ����� ,� � ��� ����� �� /�� (� ��(�������� ������ ,���������� ����� �� ���� ����� ���� � ���
��� ( /�� ( 0�� �� � �������� � ����� #��� ������ ����� ��� �� � ��� �� � (�� ( (�� ( ���� �
1� � 1� � 1� � #$%�� ����2��� �''!''' #��� #��� 1� � �1� �� � ����� ��� � ����� ��� (�� (
#��� #�����''' �++*3 �++*4&''' (�� ( �����% �''!''' �''!''' #����''' ����� �� #���$ #���$ � ����� ���
�''' ����� ���% &''' � ����#$% �++'3 �����% �����% ������� (�% #��� ������% ������% #���
����4 �+++ �++*3 �+++�� &''' �+++ &''' �''!''' �++. �++. 56$%
� ���% &'''��� ������ (�% ��++.
�+++ �+.*3++
�! �������� )#% %'#) "#�# "#�# "#�# "#�# "#�# "#�# "#�# '��� "#�# "#�# "#�#
+ ))(,
$�� ������ %#' )#' �#' (% � �� %� *� (% �(� #& #) �
$����� 4)#� �)#) (#( "#�# "#�# * �'� (& && �'� �#� �#* �*
����� '#( �(#' �#� %' %� %' )� �� *) (%� "#�# %#� "#�#
�����+�#�#, *#� '#& �#� &� "#�# '( �& ' �* �& #& �#( �'
-������� 4%#� ��#� (#' "#�# "#�# %� "#�# (( () �(� �#& %#� (�
"���� �#� ��#* %#' �' � % �� & &� (%� #� %#�
.�/����� )#( ��# (#( �% �� (& (' % '( "#�# �#&� �# '
����0��/� (#& &#� �# "#�# "#�# �* �' & *� #&� #' �)�
"���1� "#�#� ���������� ���� ��������
� 5 ����� ��!���� ��� )))
�� 5������ ��!���� �����������6������ ��� (5%)3���� ������������ �� ��� ������������7����7���6�������������
�� 5������ ��!���� ��� ��������� �������7������������������ � ����������������!���
�� 5� ������� 5� 2"� ����������� ��������3�-���������� ����������� �������3� ����
������1� 2"�.3� ����

������������ ����
�� ������������������������������
������������������������� ������������������188
������
�����������������!����� ���������7��� �
��)(���� �� /��)����( /(� �� �������������#�818% ������ 9��� ��2�� �� 6������2�
8�.�+2�$ "#�# %&# �#( %(& �%#) �#* (#( * #* *#�
������,�
����
8�.�.�� "#�# 3*�� 3% � �3�(' (3''% %3%'( 3��& 3)�' �3(��
9������+...$,����
.��������� "#�# �)# "#�# %%#� "#�# "#�# �&#& � *#*
���6�������
������7
�����+:,
5�$ �����7��+ ))��...
��$,�+ )'�;������,<
8��������=<< "#�# ��#* "#�# �&#' "#�# �*#& "#�# � #� �%#%
<����� ��!��� ��� ��������� ������� 7���� ��������
<<����8���� ����=���������� ���>�����7������ ������������������������!� ���������������������#����������!��� ��������������!���
���>�����73��������������!� ������!���� ���>�����7#
"���1� "#�#� ���������� ���� ��������
�������� 2"�.3� ����
�����%
������� ����������������� ���������� ���
/��)����( /(� �� ����� �����#�818% ������ 9��� ��2�� �� 6������2�
������������������ % �� �� %) ) � �� %�
+���� ����������,�����
?�=��������� "#�# #&� �#� "#�# %#� �#% � "#�#
+���� 3����������,� )))
.�������� ��������� �# ) �#(' �#(' *#)& �# ) �#�( �#% �#)�
+���� �������#,�����
��������� ����� "#�# *#%* �#' �#�' "#�# �#*& �#&' #��
+���� �3��������#,����
9����������������������� � % ( �' "#�# � ��
+���� ����������,�����
���������� "#�# &( "#�# %�� & ) �� "#�#
+���� 3����������,� ))) &
9���� ��������� "#�# "#�# �&# "#�# "#�# �#) �# �
+���� 3����������,� )))
����7���6������� ) "#�# �� "#�# � � �)
+���� 3����������,� ))*
"���1� "#�#� ���������� ���� ��������@� ����� ;� ����������
�������� ��6� �A�(1�2"�.3� ����@���6���A�%1� �23� ����� ����1��666#���#�����25�����������������@� ��6��3*3&�A�'1� �-���93����
<������ ��!��� ��� ��������� �������7������������������ � ���������!����������@��1�7���� ))*@�1�7���� ))(@��1�7���� ))&

����������������
�� ������������������������������
���������������������������
����������������
189
�����(
������������� �����������)
��)(���� �� /��)����( /(� �� ����� �����#�818% ������ 9��� ��2�� �� 6������2�
��!������=���������
+2�$��������3� ))��������,
; )'( "#�# ��' "#�# &3��& "#�# "#�# �� �3�'' � %
; ))) (�� )3(�� (� �3'�� (&�
��!������=��������� "#�# ��#( "#�# ��#� "#�# "#�# *#� ��#� �&#�
�������:����������;
+ )'(; ))),
-������7��=��������� "#�# #� "#�# �#% �#' "#�# �#) %#( %#(
+�����:��!�8�.,�����
��!������=���������
+�����:��!��������
�����������=���������,
; )'� "#�# )#% "#�# )#' "#�# "#�# *#& ���#* #&
; ))) �#) )#( �# �� #� ��#�
.������=���5 "#�# �#�B %# �#� %#� *#% �#� �#& �#%
���������
���������
+���:��!
8"., ))(;)&
.������=���5 "#�# #& �#� "#�# #& �#& #� �#&C #&C
���������
������
+���:��!�8�., ))'
��!������=���������
+�����:��!��������������
��������=���������,
; )*� "#�# "#�# "#�# *' "#�# "#�# *& �)� &
; ))( %* (& �� ' ��
"���1� "#�#� ���������� ���� ��������
������1� ��6�� 3�3%1�-���93� ����@� ��6�� �3� (3� *1� 2"�.3� ����@� ��6�&1�-���93� ���

������������ ����
�� ������������������������������
������������������������� ������������������190
������������ ����
�������������������������������
������������������������ ������� �������� 191

������������ ����
�������������������������������
������������������������ ������� �������� 192

������������ ����
�������������������������������
������������������������ ������� �������� 193
�������� ����
� One of the poorest countries in the region.� Devastated by protracted armed conflicts since
1978.� Large number of internally displaced persons.� Women’s rights suppressed for several years.� Lack of social and health infrastructure, which
impedes access to essential services.� Placed at 173 out of a list of 191 countries by WHO
in its June 2000 ranking of healthcare.� More than 2 million Afghan refugees in Pakistan.� More than 1.5 million Afghan refugees in Iran.
��������� �� �����
� Information on HIV/AIDS is scant.� Vulnerability factors indicate the possibility of
rapid spread of the epidemic if preventive effortsare not taken immediately.
� Low socio-political and economic status ofwomen.
� Large numbers of displaced people.� Extremely poor social and public health
infrastructure.� World’s largest producer of opium, from which
heroin is derived.� Drug trafficking, use of injecting drugs and lack of
blood safety practices identified as factors thatcould fuel the epidemic.
����� !� �������� "��#���� ������������ �������� �$����� #���� %� �&&&'��������'���
��������������� ��
(���! ('�'� ��������� ���� ���)��
* ���������� +��)��,� #��� ���� ��� � �� "��#��� -�+�"./� 0������(������ 1�������� ��� ������ ����������� #��� ���
��� � �� "��#��� -0(1���"./� ���2
�����������
��������� � �� ���� �� �����
"���������-��������. ���� �2'33 �+�"/�0(�1���"*/����2
"������������&� �-24445���2. ('�' ('�' 6
�������������������&� �-7. ���� �'3 �+�"/�0(�1���"/����2
"�����������������-�����8'�,�. 2434-������. �� �+�"/�0(�1���"/����2
��$������-#����������2/��������. ('�' ('�' 6
������9��� �����-����2���. 2444 :;'4 �+�"/�0(�1���"/����2
��������� �����-����2���. 2444 24': �+�"/�0(�1���"/����2
<�����������������-����&���. ('�' ('�' 6
��#���=������������-����2���������)��� �. ('�' ('�' 6
=������=�������������-����2��/�������� 244> ;�� 0(�������������������/
)��� �. =�������������������
��)��/�����
���������������������$���, ('�' ('�' 6
�������������������-7����2>����)���. ('�' ('�' 6
"���������)���&��������������������-7. ('�' ('�' 6
-$�2����.�-244 .�-"""�0�$.0�)������������-7.* ('�' ('�' 6
?�#���$��������-����. ('�' ('�' 6
@�"����������-"""�0�$. ('�' ('�' 6
"�����������������8������������ ���� 2� 0(�������������������/
#���������-7. =�������������������
��)��/�����
"������������������������&������������-7. ���� 2 0(�������������������/
=�������������������
��)��/�����
"�)�����$������������� ��� �-��7��#�@�". ('�' ('�' 6
"������ ��� ��$����������-7��#�@�". ('�' ('�' 6
" ������������2��/������������� ('�' ('�' 6
"���������&�� �������������������������-7. ('�' ('�' 6
�������������������������-7. ('�' ('�' 6

������������ ����
�������������������������������
������������������������ ������� �������� 194
�������� ����
� Highest population density in the world.� Topography makes it highly vulnerable to
devastating cyclones and floods, which, combinedwith high population densities, results in highlevel of damages and loss of life.
� Agriculture is the mainstay of economy.� Urban population has grown from 6 million in
1974 to 24 million in 1996, about one-fifth of thecountry’s population.
� By 2020, the urban population is expected to reach80 million.
��������� �� �����
� Limited information on HIV prevalence.� Available data suggests that overall prevalence
low.� Several socio-economic factors make the country
vulnerable to the epidemic.� Evidence of a high rate of syphilis (approximately
60 per cent) and other STDs among sex workers.� Condom use among Bangladesh’s 36,000 sex
workers varies between 4 and 28 per cent.� Awareness levels among the youth very low. Over
95 per cent of 15-19 year-old Bangladeshis do notknow a single method of HIV prevention.
����� !� �������� "��#���� ������������ �������� �$����� #���� %� �&&&'��������'���
!���"�����
��������� � �� ���� �� �����
"���������-��������. ���� 2 3': @��)����������
"������������&� �-24445���2. ('�' ('�' 6
�������������������&� �-7. 243>5���� �': @��)����������
"�����������������-�����8'�,�. ���2�-������. ; : �+�"/�0(�1���"/����2
��$������-#����������2/��������. ���2 4 A�����9�,
������9��� �����-����2���. 2444 24'; �+�"/�0(�1���"/����2
��������� �����-����2���. 2444 :'; �+�"/�0(�1���"/����2
<�����������������-����&���. 244>5���� '; @��)����������
��#���=������������-����2���������)��� �. ���� >: @��)����������
=������=�������������-����2��/���������)��� �. 24;>544 >� @��)����������
���������������������$���, ���� 2:> @��)����������
�������������������-7����2>����)���. ���� :2' @��)����������
"���������)���&��������������������-7. 24; 5���� �4'2 @��)����������
-$�2����.�-244 .�-"""�0�$.0�)������������-7. ���� �>'� @��)����������
?�#���$����������)��� �-����. ���� >4': @��)����������
@�"����������-"""�0�$. ���� 2B�� @��)����������
"�����������������8�������������#���������-7. ���� > @��)����������
"������������������������&������������-7. ���� 43 @��)����������
"�)�����$������������� ��� �-��7��#�@�". 244; 2'3 @��)����������
"������ ��� ��$����������-7��#�@�". 244; 2'4 @��)����������
" ������������2��/������������� 244�544 �� @��)����������
"���������&�� �������������������������-7. 2444 >�%34 @��)����������
�������������������������-7. ���2 C�'2 0(����������
(���!� ('�'� ��������� ���� ���)��

������������ ����
�������������������������������
������������������������ ������� �������� 195
�������� ����
� Around 96,000 Bhutanese refugees present inNepal.
� Marked rural–urban migration.� One of the world’s smallest and least developed
economies, based on subsistence farming, animalhusbandry and forestry.
��������� �� �����
� Epidemic at a very early stage. ( The first HIVinfection was detected in 1993.)
� Only nine out of approximately 75,000 bloodsamples screened from all over the country havebeen identified as HIV positive.
� STIs pose a substantial problem in the country.� There is significant risk of a widespread epidemic
if interventions are not intensified.
����� !� �������� "��#���� ������������ �������� �$����� #���� %� �&&&'��������'���
!�#���
��������� � �� ���� �� �����
"���������-��������. ���� �'2 @��)����������
"������������&� �-24445���2. ('�' ('�' 6
�������������������&� �-7. 243>5���� �' @��)����������
"�����������������-�����8'�,�. 24;��-������. �> �+�"/�0(�1���"/����2
��$������-#����������2/��������. ('�' ('�' 6
������9��� �����-����2���. ���� 4'4 �+�"/�0(�1���"/����2
��������� �����-����2���. ���� 4'� �+�"/�0(�1���"/����2
<�����������������-����&���. 244>5���� >'> @��)����������
��#���=������������-����2���������)��� �. ���� 33 @��)����������
=������=�������������-����2��/���������)��� �. 24;>544 ;� @��)����������
���������������������$���, ���� 2:� @��)����������
�������������������-7����2>����)���. ���� :3'� @��)����������
"���������)���&��������������������-7. 24; 5���� ('�' @��)����������
-$�2����.�-244 .�-"""�0�$.
0�)������������-7. ���� 3'2 @��)����������
?�#���$����������)��� �-����. ���� B�'� @��)����������
@�"����������-"""�0�$. ���� 2:2� @��)����������
"�����������������8�������������#���������-7. ���� B4 @��)����������
"������������������������&������������-7. ���� B� @��)����������
"�)�����$������������� ��� �-��7��#�@�". 244; '� @��)����������
"������ ��� ��$����������-7��#�@�". 244; 'B @��)����������
" ������������2��/������������� 244�544 2B @��)����������
"���������&�� �������������������������-7. 2444 ;�54: @��)����������
�������������������������-7. ���2 C�'2 0(����������
(���!� ('�'� ��������� ���� ���)��
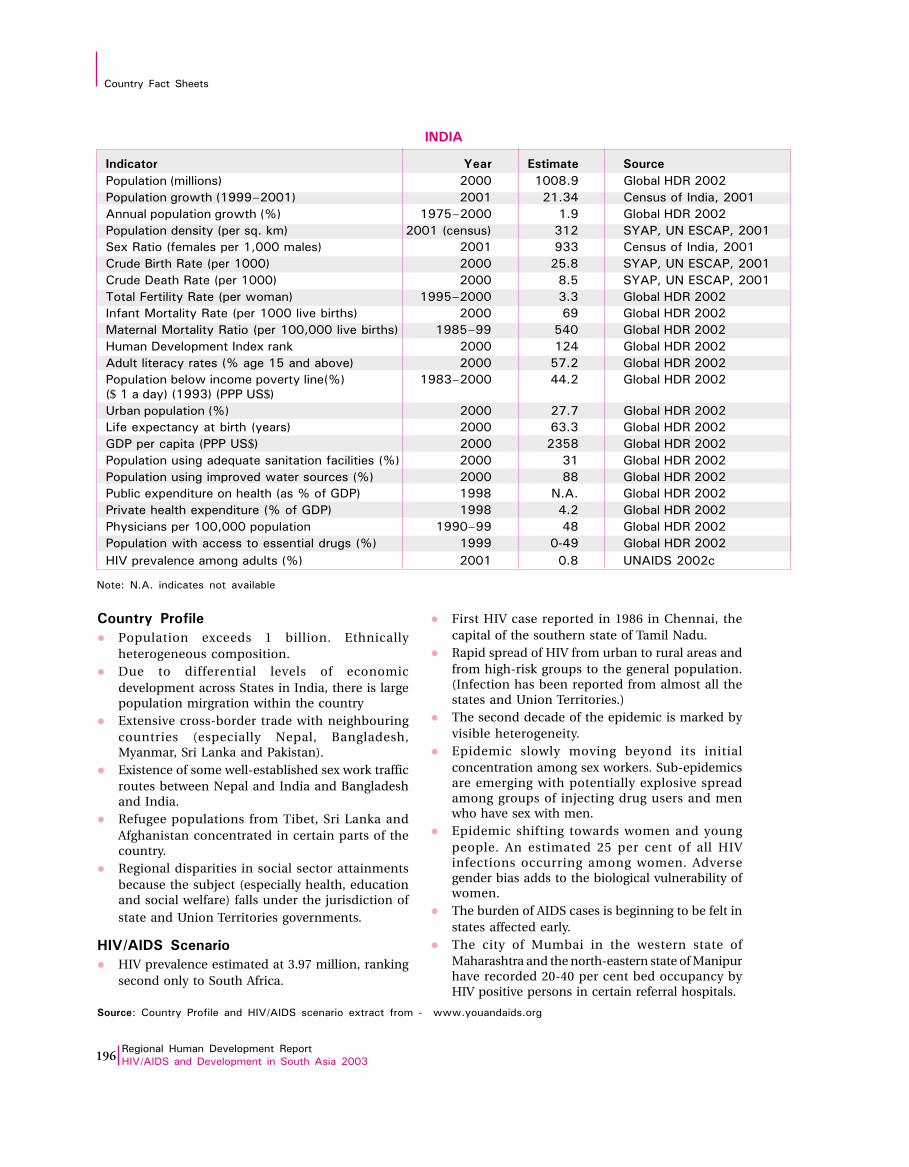
������������ ����
�������������������������������
������������������������ ������� �������� 196
� First HIV case reported in 1986 in Chennai, thecapital of the southern state of Tamil Nadu.
� Rapid spread of HIV from urban to rural areas andfrom high-risk groups to the general population.(Infection has been reported from almost all thestates and Union Territories.)
� The second decade of the epidemic is marked byvisible heterogeneity.
� Epidemic slowly moving beyond its initialconcentration among sex workers. Sub-epidemicsare emerging with potentially explosive spreadamong groups of injecting drug users and menwho have sex with men.
� Epidemic shifting towards women and youngpeople. An estimated 25 per cent of all HIVinfections occurring among women. Adversegender bias adds to the biological vulnerability ofwomen.
� The burden of AIDS cases is beginning to be felt instates affected early.
� The city of Mumbai in the western state ofMaharashtra and the north-eastern state of Manipurhave recorded 20-40 per cent bed occupancy byHIV positive persons in certain referral hospitals.
�������� ����
� Population exceeds 1 billion. Ethnicallyheterogeneous composition.
� Due to differential levels of economicdevelopment across States in India, there is largepopulation mirgration within the country
� Extensive cross-border trade with neighbouringcountries (especially Nepal, Bangladesh,Myanmar, Sri Lanka and Pakistan).
� Existence of some well-established sex work trafficroutes between Nepal and India and Bangladeshand India.
� Refugee populations from Tibet, Sri Lanka andAfghanistan concentrated in certain parts of thecountry.
� Regional disparities in social sector attainmentsbecause the subject (especially health, educationand social welfare) falls under the jurisdiction ofstate and Union Territories governments.
��������� �� �����
� HIV prevalence estimated at 3.97 million, rankingsecond only to South Africa.
����� !� �������� "��#���� ������������ �������� �$����� #���� %� �&&&'��������'���
�����
��������� � �� ���� �� �����
"���������-��������. ���� 2��;'4 @��)����������
"������������&� �-24445���2. ���2 �2' : ��������#�����/����2
�������������������&� �-7. 243>5���� 2'4 @��)����������
"�����������������-�����8'�,�. ���2�-������. 2� �+�"/�0(�1���"/����2
��$������-#����������2/��������. ���2 4 ��������#�����/����2
������9��� �����-����2���. ���� �>'; �+�"/�0(�1���"/����2
��������� �����-����2���. ���� ;'> �+�"/�0(�1���"/����2
<�����������������-����&���. 244>5���� ' @��)����������
��#���=������������-����2���������)��� �. ���� B4 @��)����������
=������=�������������-����2��/���������)��� �. 24;>544 >:� @��)����������
���������������������$���, ���� 2�: @��)����������
�������������������-7����2>����)���. ���� >3'� @��)����������
"���������)���&��������������������-7. 24; 5���� ::'� @��)����������
-$�2����.�-244 .�-"""�0�$.0�)������������-7. ���� �3'3 @��)����������
?�#���$����������)��� �-����. ���� B ' @��)����������
@�"����������-"""�0�$. ���� � >; @��)����������
"�����������������8�������������#���������-7. ���� 2 @��)����������
"������������������������&������������-7. ���� ;; @��)����������
"�)�����$������������� ��� �-��7��#�@�". 244; ('�' @��)����������
"������ ��� ��$����������-7��#�@�". 244; :'� @��)����������
" ������������2��/������������� 244�544 :; @��)����������
"���������&�� �������������������������-7. 2444 �����%:4 @��)����������
�������������������������-7. ���2 �'; 0(����������
(���!� ('�'� ��������� ���� ���)��

������������ ����
�������������������������������
������������������������ ������� �������� 197
�������� ����
� One of the world’s largest oil rich countries.� Alarming drug use problem that directly affects
nearly 2 per cent of the population.� Marked migration, heterogeneous population.� Significant level of unemployment.� Major route for drug trafficking.
��������� �� �����
� First HIV case identified in 1987.� An estimated 2271 PLWHA at the beginning of 2001.� Out of this, 2167 are male and 104 female.� Nearly 65 per cent of the infected are injecting drug
users.� Heterosexual route accounts for 12 per cent of HIV
cases.� Iranian nationals working in high-prevalence
countries classified by the government as being atrisk.
� HIV/AIDS situation apprehended to be moreserious than generally believed.
� The potential spread of infection from injectingdrug users to the general population is the mainconcern
����� !� �������� "��#���� ������������ �������� �$����� #���� %� �&&&'��������'���
(���!� ('�'� ��������� ���� ���)��
��"�$���%�#!"���&���%��
��������� � �� ���� �� �����
"���������-��������. ���� 3�' @��)����������
"������������&� �-24445���2. ('�' ('�' 6
�������������������&� �-7. 243>5���� '� @��)����������
"�����������������-�����8'�,�. 244B�-������. 3 �+�"/�0(�1���"/����2
��$������-#����������2/��������. ('�' ('�' 6
������9��� �����-����2���. ���� 2;'3 �+�"/�0(�1���"/����2
��������� �����-����2���. ���� B' �+�"/�0(�1���"/����2
<�����������������-����&���. 244>5���� '� @��)����������
��#���=������������-����2���������)��� �. ���� B @��)����������
=������=�������������-����2��/���������)��� �. 24;>544 3 @��)����������
���������������������$���, ���� 4; @��)����������
�������������������-7����2>����)���. ���� 3B' @��)����������
"���������)���&��������������������-7. 24; 5���� ('�' @��)����������
-$�2����.�-244 .�-"""�0�$.
0�)������������-7. ���� B:'� @��)����������
?�#���$����������)��� �-����. ���� B;'4 @��)����������
@�"����������-"""�0�$. ���� >;;: @��)����������
"�����������������8�������������#���������-7. ���� ;2 @��)����������
"������������������������&������������-7. ���� 4> @��)����������
"�)�����$������������� ��� �-��7��#�@�". 244; 2'3 @��)����������
"������ ��� ��$����������-7��#�@�". 244; �'> @��)����������
" ������������2��/������������� 244�544 ;> @��)����������
"���������&�� �������������������������-7. 2444 ;�54: @��)����������
�������������������������-7. ���2 C�'2 0(����������

������������ ����
�������������������������������
������������������������ ������� �������� 198
�������� ����
� Tourism is the main industry, accounting for 20per cent of the GDP and more than 60 per cent offoreign exchange receipts.
� Over 90 per cent of government tax revenue comes
from import duties and tourism-related taxes.
��������� �� �����
� First case of HIV in the country confirmed in 1991.
� The reported number of people with HIV, as of 31December 1998, was 58, of which 48 wereforeigners.
� All the ten Maldivians were in the 15–49 years agegroup, the youngest being 23 and the oldest 42years of age.
� Six persons have died of AIDS. Two appear to havecontracted the infection while working at touristresorts.
� A number of factors make the country vulnerableto the spread of HIV, and the government has takenthe threat to a small population very seriously.
����� !� �������� "��#���� ������������ �������� �$����� #���� %� �&&&'��������'���
$�"�����
��������� � �� ���� �� �����
"���������-��������. ���� �' @��)����������
"������������&� �-24445���2. ('�' ('�' 6
�������������������&� �-7. 243>5���� '� @��)����������
"�����������������-�����8'�,�. �����-������. 4�B �+�"/�0(�1���"/����2
��$������-#����������2/��������. ('�' ('�' 6
������9��� �����-����2���. ���� ��'� �+�"/�0(�1���"/����2
��������� �����-����2���. ���� :'� �+�"/�0(�1���"/����2
<�����������������-����&���. 244>5���� >'; @��)����������
��#���=������������-����2���������)��� �. ���� >4 @��)����������
=������=�������������-����2��/���������)��� �. 24;>544 >� @��)����������
���������������������$���, ���� ;: @��)����������
�������������������-7����2>����)���. ���� 4B'3 @��)����������
"���������)���&��������������������-7. 24; 5���� ('�' @��)����������
-$�2����.�-244 .�-"""�0�$.
0�)������������-7. ���� �3'B @��)����������
?�#���$����������)��� �-����. ���� BB'> @��)����������
@�"����������-"""�0�$. ���� ::;> @��)����������
"�����������������8�������������#���������-7. ���� >B @��)����������
"������������������������&������������-7. ���� 2�� @��)����������
"�)�����$������������� ��� �-��7��#�@�". 244; '3 @��)����������
"������ ��� ��$����������-7��#�@�". 244; :'� @��)����������
" ������������2��/������������� 244�544 :� @��)����������
"���������&�� �������������������������-7. 2444 >�534 @��)����������
�������������������������-7. ���2 �'2 0(����������
(���!� ('�'� ��������� ���� ���)��

������������ ����
�������������������������������
������������������������ ������� �������� 199
��������� �� �����
� HIV epidemic characterised by high prevalenceamong groups involved in high-risk behaviour.
� Prevalence among street sex workers inKathmandu rose from 1 per cent in 1992 to 16 percent in 1998.
� Prevalence among injecting drug users rose froman estimated 2 per cent in 1991 to 50 per cent in1997. There are an estimated 20,000 IDUs in Nepal.
� Prevalence among STD patients has beenfluctuating, ranging from 1 per cent to5 per cent in Kathmandu in 1998.
� In essence, the prevalence ranged from noevidence to 3 per cent.
� Sentinel surveys in pregnant women in 1991 and1992 in eight districts showed no evidence. (USCensus Bureau, HIV/AIDS Surveillance Data Base,June 2000)
� The HIV situation is rapidly deteriorating from low
prevalence to concentrated epidemic.
�������� ����
� Among the poorest and least developed countriesin the world.
� Nearly half of its population lives below thepoverty line.
� One of the two countries in the world where lifeexpectancy of men is longer than that of women.
� Ethnically and geographically diverse.� Seasonal and long-term mobility and migration
abroad is common.� Consumption of drugs is widespread.� No identifiable red light areas. The sex trade is
covert and takes place on the streets and in theparks of Kathmandu and major towns.
� Trafficking of girls to India a major problem.� Number of Nepalese sex workers in India
estimated to range from 20,000 to 100,000 or more.
����� !� �������� "��#���� ������������ �������� �$����� #���� %� �&&&'��������'���
���"
��������� � �� ���� �� �����
"���������-��������. ���� � '� @��)����������
"������������&� �-24445���2. ('�' ('�' 6
�������������������&� �-7. 243>5���� �'� @��)����������
"�����������������-�����8'�,�. 2442-������. 2�B �+�"/�0(�1���"/����2
��$������-#����������2/��������. ('�' ('�' 6
������9��� �����-����2���. ���� 'B �+�"/�0(�1���"/����2
��������� �����-����2���. ���� 2�'� �+�"/�0(�1���"/����2
<�����������������-����&���. 244>5���� :'; @��)����������
��#���=������������-����2���������)��� �. ���� 3� @��)����������
=������=�������������-����2��/���������)��� �. 24;>544 >:� @��)����������
���������������������$���, ���� 2:� @��)����������
�������������������-7����2>����)���. ���� :2'; @��)����������
"���������)���&��������������������-7. 24; 5���� 3'3 @��)����������
-$�2����.�-244 .�-"""�0�$.
0�)������������-7. ���� 22'; @��)����������
?�#���$����������)��� �-����. ���� >;'B @��)����������
@�"����������-"""�0�$. ���� 2 �3 @��)����������
"�����������������8�������������#���������-7. ���� �3 @��)����������
"������������������������&������������-7. ���� ;2 @��)����������
"�)�����$������������� ��� �-��7��#�@�". 244; 2' @��)����������
"������ ��� ��$����������-7��#�@�". 244; :'� @��)����������
" ������������2��/������������� 244�544 : @��)����������
"���������&�� �������������������������-7. 2444 �5:4 @��)����������
�������������������������-7. ���2 �'> 0(����������
(���!� ('�'� ��������� ���� ���)��

������������ ����
�������������������������������
������������������������ ������� �������� 200
��������� �� �����
� Estimated HIV prevalence remains low at about0.1 per cent of the population.
� Cases have been reported from all provinces butappear to have been confined mainly to peopleengaged in high-risk behaviour.
� Most of the infected persons belong to the 20 to 49years age group
� Infection through the heterosexual route is themost common cause.
� Infection through contaminated blood and bloodproducts and through IDU also prevalent.
� An estimated 11 per cent of 60,000-100,000 injectingdrug users living with HIV/AIDS.
�������� ����
� Among the low HDI countries, with poor indicatorsof social development and high levels of externaldebt.
� One million Afghan refugees living in the borderareas.
� Labour migration within and outside the countryis common.
� Commercial sex work is widely prevalent.
� Males too engage in sex work.
� Injecting drug use is widespread.
� Absence of universal screening of blood and bloodproducts.
� Low condom usage.
� Low education and literacy levels.
� Low status of women and high rate of femaleilliteracy.
����� !� �������� "��#���� ������������ �������� �$����� #���� %� �&&&'��������'���
�'�����
��������� � �� ���� �� �����
"���������-��������. ���� 2:2' @��)����������
"������������&� �-24445���2. ('�' ('�' 6
�������������������&� �-7. 243>5���� �'; @��)����������
"�����������������-�����8'�,�. 244;�-������. 2BB �+�"/�0(�1���"/����2
��$������-���������2���#�����. 244; 2�;'2 @�����������#
",����/� ���������
��������/�"��������
�������D���������/
����
������9��� �����-����2���. ���� �'2 �+�"/�0(�1���"/����2
��������� �����-����2���. ���� 4'> �+�"/�0(�1���"/����2
<�����������������-����&���. 244>5���� >'> @��)����������
��#���=������������-����2���������)��� �. ���� ;> @��)����������
=������=�������������-����2��/���������)��� �. 24;>544 ('�' @��)����������
���������������������$���, ���� 2 ; @��)����������
�������������������-7����2>����)���. ���� : '� @��)����������
"���������)���&��������������������-7. 24; 5���� 2'� @��)����������
-$�2����.�-244 .�-"""�0�$.
0�)������������-7. ���� '2 @��)����������
?�#���$����������)��� �-����. ���� B�'� @��)����������
@�"����������-"""�0�$. ���� 24�; @��)����������
"�����������������8�������������#���������-7. ���� B2 @��)����������
"������������������������&������������-7. ���� ;; @��)����������
"�)�����$������������� ��� �-��7��#�@�". 2444 �'3 @��)����������
"������ ��� ��$����������-7��#�@�". 244; '2 @��)����������
" ������������2��/������������� 244�544 >3 @��)����������
"���������&�� �������������������������-7. 2444 >�534 @��)����������
�������������������������-7. ���2 �'2 0(����������
(���!� ('�'� ��������� ���� ���)��

������������ ����
�������������������������������
������������������������ ������� �������� 201
�������� ����
� Good health parameters.
� High literacy rate of 90 per cent.
� About 160,000 seek employment abroad annually.
� Significant number of persons employed in WestAsia.
� Good immunisation coverage of children againstpotentially life threatening childhood diseases.
� Unrest in north and the east because of a separatist
rebellion.
��������� �� �����
� Low prevalence of HIV/AIDS.
� First case of HIV reported in 1987.
� Fifty-two new cases of infection reported betweenJanuary and December 1998. However, the numberof cases reported falls short of the projectionsmade some years ago.
� Infection still thought to be largely limited toindividuals engaging in risk-taking behaviour
� Condom promotion is a sensitive issue, withopposition from the Buddhist and Christian clergy.
� Ninety-eight per cent of blood and blood productsscreened for HIV; collection of blood fromprofessional donors virtually stopped.
� IDU is not yet a problem.
� Large-scale emigration
������!� �������� "��#���� ������������ �������� �$����� #���� %� �&&&'��������'���
�%��"��'�
��������� � �� ���� �� �����
"���������-��������. ���� 2;'4 @��)����������
"������������&� �-24445���2. ('�' ('�' 6
�������������������&� �-7. 243>5���� 2' @��)����������
"�����������������-�����8'�,�. 244:-������. ��4 �+�"/�0(�1���"/����2
��$������-#����������2/��������. ('�' ('�' 6
������9��� �����-����2���. ���� 23' �+�"/�0(�1���"/����2
��������� �����-����2���. ���� >'3 �+�"/�0(�1���"/����2
<�����������������-����&���. 244>5���� �'2 @��)����������
��#���=������������-����2���������)��� �. ���� 23 @��)����������
=������=�������������-����2��/���������)��� �. 24;>544 B� @��)����������
���������������������$���, ���� ;4 @��)����������
�������������������-7����2>����)���. ���� 42'B @��)����������
"���������)���&���������������������-7. 24; 5���� B'B @��)����������
-$�2����.�-244 .�-"""�0�$.
0�)������������-7. ���� ��'; @��)����������
?�#���$����������)��� �-����. ���� 3�'2 @��)����������
@�"����������-"""�0�$. ���� > � @��)����������
"�����������������8�������������#���������-7. ���� ; @��)����������
"������������������������&������������-7. ���� ; @��)����������
"�)�����$������������� ��� �-��7��#�@�". 244; 2'3* @��)����������
"������ ��� ��$����������-7��#�@�". 244; 2'; @��)����������
" ������������2��/������������� 244�544 B @��)����������
"���������&�� �������������������������-7. 2444 4>52�� @��)����������
�������������������������-7. ���2 C�'2 0(����������
*���� ��#���� ���2444
(���!� ('�'� ��������� ���� ���)��

������������ ����
�������������������������������
������������������������ ������� �������� 202





























