Embed Size (px)
Citation preview

SURGERY
SPINE Volume 37, Number 6, pp E381–E386©2012, Lippincott Williams & Wilkins
Spine www.spinejournal.com E381
Osteosarcoma of the Mobile Spine Joseph Schwab , MD , * Alessandro Gasbarrini , MD , † Stefano Bandiera , MD , † Luca Boriani , MD , † Luca Amendola , MD , † Piero Picci , MD , ‡ Stefano Ferrari , MD , § and Stefano Boriani , MD †
Study Design. Retrospective case series. Objective. Our goal was to assess whether en bloc resection had an impact on survival. Summary of Background Data. Osteogenic sarcoma occurs rarely in the mobile spine, but when it does, the prognosis is poor. Wide resection is recommended for osteogenic sarcoma of the extremities, but wide resection is diffi cult and often dangerous in the spine. The goal of this study was to examine whether en bloc removal of osteogenic sarcomas in the mobile spine improves survival. Methods. We performed a retrospective review of all cases of high-grade, osteogenic sarcoma of the mobile spine treated with high-dose methotrexate and adrimaycin–based chemotherapy between 1985 through 2005. There were 9 male patients and 8 female patients. Patients were followed for a median of 38 months or until death, and surviving patients were followed for a minimum of 6.4 years. Patients were grouped on the basis of whether they underwent en bloc spondylectomy. The Enneking stage and Weinstein, Boriani, and Biagini stage, as well as the pre- and postoperative Frankel grades, were collected on all patients. Local recurrence and metastasis data were collected for all patients. Overall survival was calculated using Kaplan-Meier methods with the log rank test utilized to evaluate the effect of en bloc resection on survival. Results. Twelve (71%) of 17 patients with osteogenic sarcoma of the mobile spine died. Median disease-specifi c survival for the entire cohort was 38.1 months (standard error 29.6; 95% confi dence interval 0–96). Nine patients underwent en bloc resection. Median overall survival for patients after en bloc resection was 77.3 months (standard error 62; 95% confi dence interval 96) versus 17 months (standard error 6.5; 95% confi dence interval 4–29.6) ( P = 0.09).
The spine accounts for less than 3% of all primary cases of osteogenic sarcoma (OGS). 1 – 4 The spine poses partic-ularly diffi cult challenges with regard to wide resection.
As such, the outcomes of patients prior to modern chemother-apy were particularly dismal, with all patients succumbing to their disease in 2 of the larger series (n = 10 and n = 16). 1 , 2 Ozaki et al. 5 reported on 7 patients suffering from OGS of the spine among another 15 with OGS of the sacrum who were treated with modern chemotherapy including high-dose methotrexate and adriamycin. The authors reported that 4 of the 7 patients with OGS of the spine were alive at last follow-up in spite of only 2 having a marginal or wide resection. The authors concluded that patients suffering from OGS of the spine ought to be treated with chemotherapy and at least a marginal excision. 5 Schoenfeld et al. 6 reported the results of 26 patients with OGS of the spine (18 mobile spine, 8 sacrum) treated with multimodal therapy including chemotherapy, radiation, and surgery with median survival of 29 months. En bloc resection was performed in 7 cases, with negative mar-gins in 3 cases. The study was underpowered to demonstrate a difference in outcome based on en bloc excision plus/minus negative margins. 6
A wide resection has been shown to improve survival in patients with extremity OGS. However, there have been no large series demonstrating the effects of en bloc excision on survival in OGS of the mobile spine alone. The goal of our study was to determine whether en bloc excision for OGS of the spine improved survival. Our hypothesis was that en bloc
From the * Department of Orthopedic Surgery, Massachusetts General Hospital, Boston, MA ; and † Department of Medical Oncology , ‡ Laboratory of Experimental Oncology , and § Department of Orthopedic Oncologic and Degenerative Spine Surgery, Rizzoli Institute, University of Bologna, Bologna, Italy.
Acknowledgment date: December 6, 2010. First revision date: May 11, 2011. Second revision date: July 19, 2011. Acceptance date: July 22, 2011.
The manuscript submitted does not contain information about medical device(s)/drug(s).
No funds were received in support of this work. No benefi ts in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Address correspondence and reprint requests to Joseph Schwab, MD, Department of Orthopedic Surgery, Yawkey 3, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114; E-mail: [email protected]
Eleven (65%) of 17 patients developed pulmonary metastasis, and 9 of those 11 died from their disease ( P = 0.04). Six (35%) patients developed a local recurrence, and all 6 died from their disease ( P = 0.07). Conclusion. Osteogenic sarcoma of the mobile spine presents a signifi cant challenge, and most patients die from their disease in spite of aggressive surgery and chemotherapy. Metastastic disease is associated with a worse prognosis. There is a trend toward improved survival with en bloc resection when compared with intralesional resection. Osteogenic sarcoma of the mobile spine is rare and historically has a very poor prognosis. We reviewed our cases of osteogenic sarcoma of the mobile spine to assess whether modern en bloc resection improved survival. Survival remains poor, but there is a trend toward improved survival with en bloc resection. Key words: en bloc resection , mobile spine , osteosarcoma. Spine 2012 ; 37 : E381 – E386
DOI: 10.1097/BRS.0b013e31822fb1a7
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS204675.indd E381BRS204675.indd E381 26/02/12 10:39 AM26/02/12 10:39 AM

SURGERY Osteosarcoma of the Mobile Spine • Schwab et al
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.E382 www.spinejournal.com March 2012
resection combined with chemotherapy would have a positive impact on survival.
MATERIALS AND METHODS After receiving our institutional equivalent of institutional review board approval, we performed a retrospective review of all high-grade OGSs occurring in the mobile spine that we managed between 1985 and 2005. We excluded cases of high-grade OGS that were not treated with high-dose metho-trexate and adriamycin–based chemotherapy, which began in the mid-1980s at our institution. The clinical, pathologic, and radiographic data were reviewed in all cases. All of the histologic specimens were originally graded at the Rizzoli Institute by a musculoskeletal pathologist, and the surgical margins were determined by them. All cases were classifi ed according to the classifi cation proposed by Enneking 7 and also the Wienstein, Boriani, Biagini (WBB) classifi cation. 8 Pre- and postoperative Frankel grades were recorded for all patients. Nonsurgical means of treatment including radiation therapy and chemotherapy were also collected. Follow-up including data on local and distant recurrences and survival was recorded for all patients. Seventeen patients including 9 male and 8 female patients were included. The average age was 35 years (range 18–63). The median follow-up was 38 months or until death. All living patients were followed for a minimum of 5 years.
Weinstein, Boriani, Biagini Classifi cation En bloc spondylectomy was performed in 9 cases. We have been prospectively applying the WBB system since 1990. The system aids the surgeon who is trying to decide whether a patient is a candidate for en bloc resection from a techni-cal standpoint. The WBB system is based on axial images upon which a clock face can be superimposed. The spinous process is split by the 12 o’clock and 1 o’clock positions, the pedicles occur at the 4 o’clock and 9 o’clock positions, and the center of the vertebral body is split by 6 o’clock and 7 o’clock. The anatomy of the tumor is further classifi ed based on the depth of invasion and categorized from “a” to “e”. A tumor involving zone a involved only the soft tissues adjacent to the spine. Zone b involves the bone superfi cially, whereas zone c delineates deep bony involvement. Zone d corresponds to the epidural space, and zone e is indradural. Approaching en bloc resection with this radial map can be useful because it helps guide the angle the surgeon must uti-lize with his chisel to avoid tumor contamination. When one is planning on obtaining a negative margin, it is important that 1 pedicle remain tumor free to allow appropriate dis-section along the nontumor side with excision of the healthy pedicle. In general, we approach these cases with an ante-rior and a posterior-only approach. However, there are cases in which we have performed en bloc resections through a posterior-only approach. If the tumor is in the posterior ele-ments only or if the tumor is relatively superifi cial in the ver-tebrae, then one might consider a posterior-only approach. It is important to note that en bloc resection defi nes a surgical approach to a tumor, and it is not synonymous with a wide
resection. The fi nal oncologic margin must be determined by the pathologist. Thus, one can have an intralesional margin and still have performed an en bloc removal of the tumor. The goal is to obtain a wide margin whenever possible.
Treatment A frank discussion occurs with each patient in the preopera-tive setting regarding surgery. Adjuvant treatments including chemotherapy and radiation therapy are discussed with the medical oncologist and radiation oncologist, respectively. The goal of our surgical approach is to obtain a negative margin. Chemotherapy is delivered in the neoadjuvant setting except in cases in which the patient presents with progressive spinal cord compromise. Radiation is used as an adjuvant to sur-gery, and its use is tailored to each patient. We generally use convential, fractionated photon radiation at a dose between 4000 and 4500 Gy. Higher doses are not used, to avoid spinal cord toxicity.
We reconstruct the spine using segmental, pedicle fi xa-tion posteriorly. The vertebral body defect is replaced with a stackable carbon fi ber system or a mesh cage fi lled with auto and/or allograft.
Overall survival was calculated using Kaplan-Meier meth-ods ( Figure 1 ). The log rank test was used to determine whether en bloc resection infl uenced survival or not. A P value of less than 0.05 was considered statistically signifi cant.
RESULTS Seventeen patients treated between 1985 and 2005 for OGS of the mobile spine were included in our study. The
Figure 1. This is a Kaplan-Meier curve comparing en bloc resections with intralesional resections with regard to disease-specifi c survival. En bloc resections are represented with a blue line, and the red line represents intralesional resections. There was a trend toward improved disease-specifi c survival for en bloc resections over intralesional resections ( P = 0.09).
BRS204675.indd E382BRS204675.indd E382 26/02/12 10:39 AM26/02/12 10:39 AM

SURGERY Osteosarcoma of the Mobile Spine • Schwab et al
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.Spine www.spinejournal.com E383
median disease-specifi c survival was 38.1 months (standard error [SE] 29.6; 95% confi dence interval [CI] 0–96). Twelve (71%) of 17 had died at fi nal follow-up. The 1- and 5-year survival rates for the entire cohort were 76% and 45%, respectively.
Pulmonary metastasis occurred in 11 (65%) of 17 patients. Three patients presented with pulmonary metastasis, and 8 developed metastasis later in the course of their disease. Nine (82%) of the 11 patients with pulmonary metastasis died from their disease, whereas 1 (17%) of the 6 patients without pulmonary metastasis died from their disease ( P = 0.04).
Local recurrence occurred in 6 (35%) of 17 patients. Five of the 6 cases of local recurrence occurred in patients who had positive surgical margins, and 1 occurred after a marginal margin. All patients with local recurrences died from their dis-ease, whereas 4 (36%) of the 11 patients who did not develop a local recurrence died from their disease ( P = 0.07).
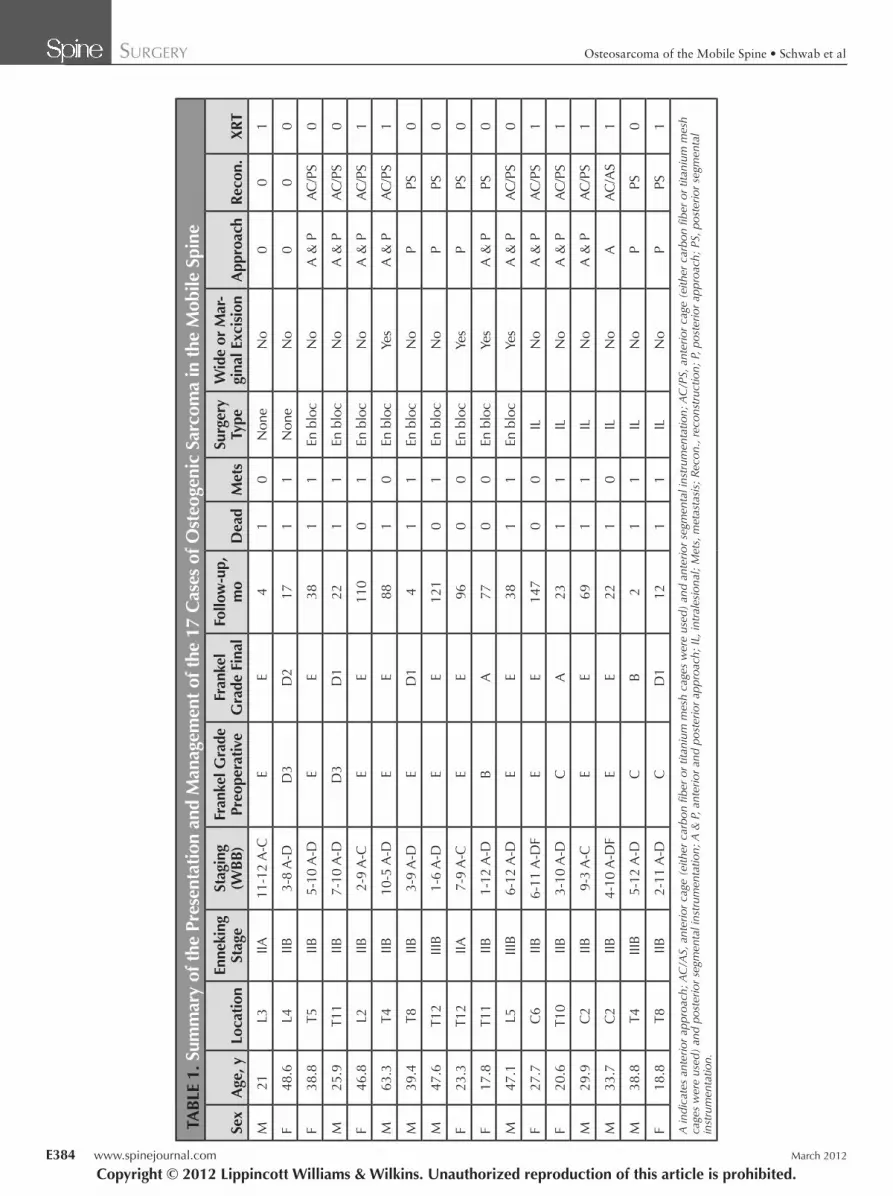
Two (12%) out of 17 patients refused surgery ( Table 1 ). They were both treated with high-dose methotrexate and adriamycin–based chemotherapy. One of them was also treated with radiation. They both developed metastatic dis-ease, and both of them died from their disease. One patient died at 4 months after presenting to our clinic, and the other died at 17 months.
Nine patients underwent en bloc spondylectomy ( Figure 2 ) including 5 male and 4 female patients with an average age of 39 years. Two patients presented with metastasis. All 9 patients had primarily vertebral body involvement, with some having posterior element involvement as well (Table 1). Seven of 9 involved zone d, and the other 2 extended to zone c (Table 1). Four of the 9 patients who underwent en bloc resection had a negative margin. The remaining 5 patients who underwent en bloc resection had contaminated margins noted in surgery. They had gross total resection of their tumors.
Six patients underwent intralesional resections. The aver-age age of this group including 3 male and 3 female patients was 28 years. One patient presented with metastasis, and the other 5 had local disease only on presentation. Three of the 6 patients had both anterior and posterior approaches to their spine. One patient had an anterior-only approach, and the other had a posterior-only approach. Five of 6 involved zone d, and the other involved zone c (Table 1). Four of the 6 patients died from their disease, and all 4 had devel-oped pulmonary metastasis. Two patients did not develop metastasis, and they were both alive at last follow-up without evidence of disease.
Nine patients underwent en bloc resection of their high-grade OGS, and 6 patients underwent intralesional, gross total resections. The median survival for patients who underwent intralesional, gross total resection was 16.8 months (SE 6.5 months; 95% CI 4.0–29.6). The median overall survival for patients who underwent en bloc resection was 77.3 months (SE 62.3; 95% CI 0–96) ( P = 0.09).
Four patients had negative surgical margins, and 11 patients had either an intralesional resection or a positive mar-gin after en bloc resection. The median survival for patients
who had positive margins or an intralesional resection was 22.7 months (SE 8.9 months; 95% CI 5.3–40.0). The median overall survival for patients who had negative surgical margins was 82.5 months (SE 38.2; 95% CI 13.2–163.0) ( P = 0.1).
Overall, 5 of 17 patients were alive at last follow up. All 5 had no evidence of disease. Four of the 5 had been treated with en bloc excision, and the other with intralesional resec-tion. Three of the 4 en bloc patients with no evidence of dis-ease at last follow-up had a wide or marginal margin. The lone survivor in the non–en bloc group had undergone an aggressive, extracapsular intralesional excision with both an anterior and posterior approach. They were also treated with 4500 Gy of postoperative radiation and high-dose methotrex-ate- and adriamycin-based chemotherapy.
DISCUSSION We are presenting the results of 17 patients treated for high-grade OGS of the mobile spine. The results indicate that survival for this subgroup of patients with OGS continues to lag behind what is reported for OGS in the extremity. There seems to be a trend toward improved survival with en bloc resection with negative margins. Although this is in keeping with what is known in the extremity, the paucity of cases makes more defi nitive statistical analysis diffi cult. The stan-dard treatment for OGS occurring in the extremities is with the combination of chemotherapy and wide surgical excision. Survival rates with this approach have improved by roughly 50% when one compares the results of amputation and no chemotherapy with the results reported during the modern era of chemotherapy. 9 , 10 The treatment of OGS of the spine has lagged behind that of the extremity. Reports from the 1980s documented a death rate from disease of more than 90% for OGS of the spine. 1 , 2 However, these reports pre-dated current chemotherapeutic treatment modalities. A more recent report on 7 cases of OGS in the spine and 15 from the sacrum treated with current chemotherapy proto-cols indicated a less dim picture with a median survival rate of 23 months. Ten of the 22 patients in that series were not treated surgically, and 5 of the 22 were treated with a wide or marginal margin. Their report indicated that a wide or marginal margin coupled with chemotherapy had a positive impact on survival in OGS of the spine including the sarcum. 5 Schoenfeld et al. 6 reported on 18 cases of the mobile spine and 8 of the sacrum treated with multimodal therapy with median survival of 29.5 months. They included 4 patients with Paget-associated sarcoma, which is known to carry a particularly poor prognosis. 11 , 12 They had 7 cases treated with en bloc resection including 3 with negative margins; however, they were underpowered to demonstrate an improvement in survival with en bloc resection.
There have been several other reports of en bloc resec-tion for the management of primary spine tumors. The concept of obtaining a wide or marginal margin in the spine has gained acceptance as the techniques needed to per-form these procedures have evolved. 13 We have published our experience with treating chordoma and chondrosar-coma with en bloc excision with positive results. 14 , 15 It is
BRS204675.indd E383BRS204675.indd E383 26/02/12 10:39 AM26/02/12 10:39 AM
SURGERY Osteosarcoma of the Mobile Spine • Schwab et al
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.E384 www.spinejournal.com March 2012
TAB
LE 1
. Sum
mar
y of
the
Pres
enta
tion
and
Man
agem
ent o
f the
17
Cas
es o
f Ost
eoge
nic
Sarc
oma
in th
e M
obile
Spi
ne
Sex
Age
, yLo
catio
nEn
neki
ng
Stag
eSt
agin
g (W
BB
)Fr
anke
l Gra
de
Preo
pera
tive
Fran
kel
Gra
de F
inal
Follo
w-u
p,
mo
Dea
dM
ets
Surg
ery
Type
Wid
e or
Mar
-gi
nal E
xcis
ion
App
roac
hR
econ
.X
RT
M21
L3IIA
11-1
2 A
-CE
E4
10
Non
eN
o0
01
F48
.6L4
IIB3-
8 A
-DD
3D
217
11
Non
eN
o0
00
F38
.8T5
IIB5-
10 A
-DE
E38
11
En b
loc
No
A &
PA
C/P
S0
M25
.9T1
1IIB
7-10
A-D
D3
D1
221
1En
blo
cN
oA
& P
AC
/PS
0
F46
.8L2
IIB2-
9 A
-CE
E11
00
1En
blo
cN
oA
& P
AC
/PS
1
M63
.3T4
IIB10
-5 A
-DE
E88
10
En b
loc
Yes
A &
PA
C/P
S1
M39
.4T8
IIB3-
9 A
-DE
D1
41
1En
blo
cN
oP
PS0
M47
.6T1
2III
B1-
6 A
-DE
E12
10
1En
blo
cN
oP
PS0
F23
.3T1
2IIA
7-9
A-C
EE
960
0En
blo
cYe
sP
PS0
F17
.8T1
1IIB
1-12
A-D
BA
770
0En
blo
cYe
sA
& P
PS0
M47
.1L5
IIIB
6-12
A-D
EE
381
1En
blo
cYe
sA
& P
AC
/PS
0
F27
.7C
6IIB
6-11
A-D
FE
E14
70
0IL
No
A &
PA
C/P
S1
F20
.6T1
0IIB
3-10
A-D
CA
231
1IL
No
A &
PA
C/P
S1
M29
.9C
2IIB
9-3
A-C
EE
691
1IL
No
A &
PA
C/P
S1
M33
.7C
2IIB
4-10
A-D
FE
E22
10
ILN
oA
AC
/AS
1
M38
.8T4
IIIB
5-12
A-D
CB
21
1IL
No
PPS
0
F18
.8T8
IIB2-
11 A
-DC
D1
121
1IL
No
PPS
1
A in
dica
tes
ante
rior
appr
oach
; AC
/AS,
ant
erio
r ca
ge (
eith
er c
arbo
n fi b
er o
r tit
aniu
m m
esh
cage
s w
ere
used
) an
d an
terio
r se
gmen
tal i
nstr
umen
tatio
n; A
C/P
S, a
nter
ior
cage
(ei
ther
car
bon fi b
er o
r tit
aniu
m m
esh
cage
s w
ere
used
) an
d po
ster
ior
segm
enta
l ins
trum
enta
tion;
A &
P, a
nter
ior
and
post
erio
r ap
proa
ch;
IL, i
ntra
lesi
onal
; M
ets,
met
asta
sis;
Rec
on.,
reco
nstr
uctio
n; P
, pos
terio
r ap
proa
ch;
PS, p
oste
rior
segm
enta
l in
stru
men
tatio
n.
BRS204675.indd E384BRS204675.indd E384 26/02/12 10:39 AM26/02/12 10:39 AM

SURGERY Osteosarcoma of the Mobile Spine • Schwab et al
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.Spine www.spinejournal.com E385
Figure 2. This case is representative of our series of en bloc resections. This is a 38-year-old male patient who presented to an outside hospital with back pain. He was thought to have a traumatic fracture, and he underwent anterior stabilization with vertebral body screws. Pathology was sent, which revealed high-grade osteogenic sarcoma. He underwent a posterior en bloc spondylectomy with marginal margins. He later developed metastatic disease and died. A, This is a lateral, plain x-ray of the thoracic spine demonstrating a fracture with a mixed lytic and blastic lesion. B, An axial CT of the same lesion revealing the lytic and blastic nature of the lesion as well as retropulsion into the spinal canal. C, These sagittal, T2-weighted images of the lesion demonstrate the fracture as well as the canal involvement. D, This is an anterior posterior (a/p), plain x-ray after the lesion was treated at an outside facility. E, This is an intraoperative photograph of our posterior thoracic approach with fi ber wires in place in preparation for a posterior en bloc spondylectomy. F, This is a gross photograph of the resected specimen. G, This is an a/p, plain x-ray of the resected specimen demonstrating the lesion as well as the vertebral body screws placed in the normal vertebrae above and below the tumor. H, This is an axial, plain x-ray of the resected specimen. I, This is a lateral, plain x-ray of the reconstructed spine including carbon fi ber cages used to reconstruct the anterior column.
important to understand that en bloc excision describes a surgical technique and not synonymous with a wide margin. In fact, margins are often close and may be contaminated with en bloc excisions. The necessity to obtain a wide patho-logic margin or to approach a tumor in an en bloc fashion is based in part on the tumor itself. One should be much more aggressive with malignant tumors than with benign
tumors. For instance, it is our experience that an intrale-sional excision can provide adequate control for Enneking stage II giant cell tumors, whereas a wide margin is neces-sary to control a chordoma.
The literature strongly supports an aggressive surgical approach to OGSs of the extremity and pelvis. 16 , 17 In the spine, this implies that OGSs should be approached with an
BRS204675.indd E385BRS204675.indd E385 26/02/12 10:39 AM26/02/12 10:39 AM

SURGERY Osteosarcoma of the Mobile Spine • Schwab et al
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.E386 www.spinejournal.com March 2012
en bloc strategy. We have developed the WBB spine tumor staging system as a means to help surgeons in preparation of their surgical strategy. We have been using the WBB system since 1990 and have found it quite useful as a means to develop a surgical plan. In addition, the WBB system pro-vides a means of communication between surgeons. This is particularly important in our fi eld because the incidence of primary spine tumors is very low. If meaningful compari-sons are going to be made, then a common language needs to be adopted.
Our study suffers from low numbers along with all of the published reports on OGS of the spine. The low num-bers weaken our statistical analysis. However, the concept of removing these tumors en bloc with a wide margin is in keeping with what has been defi nitively shown to be effective in the extremities. Our report includes patients who had a contaminated margin with their en bloc exci-sion. Several of these patients have not developed local or distant recurrences. It is unclear whether this is due to a positive response to chemotherapy or whether the postop-erative radiation used in some of the patients helped with the local control. Another plausible means to explain the good results even with a contaminated margin is that the tumor is transgressed in a controlled manner as opposed to inadvertently. The contaminated margins were predictable preoperatively based on using the WBB system. Again, this is speculation because the data are not supportive of any 1 explanation. In fact, a contaminated margin is known to portend a poor prognosis in the extremity.
The contaminated margin is often at the dura. The most oncologically sound surgical procedure to perform in these cases is a dural resection or a transaction of the neuraxis above and below the tumor. The patient must be an active participant in this decision because neurologic defi cits are common after dural resection and predictable after spinal cord transaction. Still, it should be considered, and a frank conversation must take place. It is not fair to the patient to take this option off the table without speaking with him or her about it because it may be the patient’s best chance for survival. In fact, one of our long-term survivors has undergone planned cord transaction of the thoracic spine to achieve a wide margin. This patient lives independently and uses a wheelchair for mobilization.
In summary, en bloc resection of OGS in the mobile spine is associated with a trend toward improved survival. A large, multicenter study will be necessary if one hopes to obtain enough power to demonstrate clear superiority of wide resection over intralesional resection in the spine. It remains our practice to achieve a wide surgical margin in these cases when possible.
➢ Key Points
Osteogenic sarcoma of the mobile spine has histori-cally been associated with a poor prognosis.
En bloc resection has been shown to improve survival in the extremities, but there are scarce data demon-strating its utility in the mobile spine.
Survival with osteogenic sarcoma of the mobile spine lags behind what has been reported in the literature.
There was a trend toward improved survival with en bloc resection versus intralesional resection.
References 1. Barwick KW , Huvos AG , Smith J . Primary osteogenic sarcoma of
the vertebral column: a clinicopathologic correlation of ten patients . Cancer 1980 ; 46 : 595 – 604 .
2. Shives TC , Dahlin DC , Sim FH , et al . Osteosarcoma of the spine . J Bone Joint Surg Am 1986 ; 68 : 660 – 8 .
3. Campanacci M , Cervellati G . Osteosarcoma: a review of 345 cases . Ital J Orthop Traumatol 1975 ; 1 : 5 – 22 .
4. Tigani D , Pignatti G , Picci P , et al . Vertebral osteosarcoma . Ital J Orthop Traumatol 1988 ; 14 : 5 – 13 .
5. Ozaki T , Flege S , Liljenqvist U , et al. Osteosarcoma of the spine: experience of the Cooperative Osteosarcoma Study Group . Cancer 2002 ; 94 : 1069 – 77 .
6. Schoenfeld AJ , Hornicek FJ , Pedlow FX , et al. Osteosarcoma of the spine: experience in 26 patients treated at the Massachusetts General Hospital . Spine J 2010 ; 10 : 708 – 14 .
7. Enneking WF . A system of staging musculoskeletal neoplasms . Clin Orthop Relat Res 1986 : 9 – 24 .
8. Boriani S , Weinstein JN , Biagini R . Primary bone tumors of the spine. Terminology and surgical staging . Spine (Phila Pa 1976) 1997 ; 22 : 1036 – 44 .
9. Marcove RC , Mike V , Hajek JV , et al . Osteogenic sarcoma under the age of twenty-one. A review of one hundred and forty-fi ve oper-ative cases . J Bone Joint Surg Am 1970 ; 52 : 411 – 23 .
10. Meyers PA , Heller G , Healey J , et al. Chemotherapy for nonmeta-static osteogenic sarcoma: the Memorial Sloan-Kettering experi-ence . J Clin Oncol 1992 ; 10 : 5 – 15 .
11. Dray MS , Miller MV . Paget’s osteosarcoma and post-radiation osteosarcoma: secondary osteosarcoma at Middlemore Hospital, New Zealand . Pathology 2008 ; 40 : 604 – 10 .
12. Shaylor PJ , Peake D , Grimer RJ , et al . Paget’s osteosarcoma—no cure in sight . Sarcoma 1999 ; 3 : 191 – 2 .
13. Fisher CG , Saravanja DD , Dvorak MF , et al. Surgical management of primary bone tumors of the spine: validation of an approach to enhance cure and reduce local recurrence . Spine (Phila Pa 1976) 36 : 830 – 6 .
14. Boriani S , Bandiera S , Biagini R , et al. Chordoma of the mobile spine: fi fty years of experience . Spine (Phila Pa 1976) 2006 ; 31 : 493 – 503 .
15. Boriani S , De Iure F , Bandiera S , et al. Chondrosarcoma of the mobile spine: report on 22 cases . Spine (Phila Pa 1976) 2000 ; 25 : 804 – 12 .
16. Jaffe N , Carrasco H , Raymond K , et al . Can cure in patients with osteosarcoma be achieved exclusively with chemotherapy and abrogation of surgery? Cancer 2002 ; 95 : 2202 – 10 .
17. Kawai A , Huvos AG , Meyers PA , et al . Osteosarcoma of the pel-vis. Oncologic results of 40 patients . Clin Orthop Relat Res 1998 : 196 – 207 .
BRS204675.indd E386BRS204675.indd E386 26/02/12 10:39 AM26/02/12 10:39 AM





























