Embed Size (px)
Citation preview

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Persistent dysfunction of viable myocardium afterrevascularization in chronic ischaemic heartdisease: implications for dobutamine stressechocardiography with longitudinal systolicstrain and strain rate measurementsAssami Rosner1,2*, Derk Avenarius1, Siri Malm1, Amjid Iqbal1, Aigul Baltabaeva3,George R. Sutherland4, Bart Bijnens5,6, and Truls Myrmel1,2
1University Hospital North Norway, Tromsø and Harstad, Norway; 2Department of Clinical Medicine, University of Tromsø, 9037 Tromsø, Norway; 3Department of Cardiology,St George’s Hospital, London, UK; 4Heart Institute, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia; 5ICREA-Universitat Pompeu Fabra, Barcelona, Spain;and 6K.U.Leuven, Leuven, Belgium
Received 5 September 2011; accepted after revision 30 January 2012; online publish-ahead-of-print 28 February 2012
Aims Studies of functional recovery after revascularization in chronic coronary artery disease are contradictory and mark alack of knowledge of persistent dysfunction in the non-scarred myocardium. Based on tissue Doppler-derived regionallongitudinal systolic strain and strain rate (SR), both at rest and during dobutamine stress (DS), we assessed to whatextent ischaemia-related reduced myocardial function would recover after revascularization in hearts with predomin-antly viable myocardium.
Methodsand results
Reference peak systolic strain and SR values were determined from tissue Doppler imaging in 15 healthy volunteers.Fifty-seven patients scheduled for coronary artery bypass grafting (CABG), with an average ejection fraction of 49%,underwent pre-operative magnetic resonance imaging (MRI) with late enhancement, resting echocardiography, andDS echocardiography (DSE), with assessment of systolic strain and SR and post-systolic strain (PSS). Eight to 10months after CABG, myocardial function was reassessed. Forty per cent of all segments had reduced longitudinalsystolic strain pre-operatively despite only 1.4% of segments with transmural infarctions on MRI. After revasculariza-tion, 38% of prior dysfunctional segments improved their resting strain, whereas 72% were improved by DS. Positiveresting systolic strain indicated the absence of significant scar tissue. Resting systolic strain and DS strain responseswere good prognosticators for functional improvement with areas under the receiver operating characteristic curveof 0.753 (0.646–0.860) and 0.790 (0.685–0.895), respectively.
Conclusion Persistently reduced longitudinal function was observed in more than half of pre-operatively viable but dysfunctionalsegments after CABG. We propose that such a functional impairment marks a regional remodelling process notamendable to re-established blood flow.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Strain rate imaging † Viability † Coronary artery disease † Dobutamine stress † Echocardiography
IntroductionThe effects of chronic coronary artery disease (CAD) on myocar-dial function in humans are complex and difficult to predict. The
consequences for muscle function depends on a number offactors including the severity of coronary flow reduction, timeaspects of flow deprivation, medical treatment of ventriculardysfunction, and coronary dysregulation.1 –8 Importantly,
* Corresponding author. Tel: +47 95990071; fax: +47 77628298, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2012. For permissions please email: [email protected]
European Heart Journal Cardiovascular Imaging (2012) 13, 745–755doi:10.1093/ehjci/jes036
at University of T
romsoe on D
ecember 17, 2012
http://ehjcimaging.oxfordjournals.org/
Dow
nloaded from

determination of myocardial viability and functional contractilereserve has been assumed to be necessary to predict recoveryof function after various revascularization procedures and there-fore the merit of clinical revascularization.1 Recently, however,the randomized STICH trial found no clinical benefit of revascular-ization of dysfunctional but viable myocardium compared withmodern medical heart failure treatment alone.9 This study thusadds to the accumulating number of observations pointing to alack of understanding of the functional and mechanistic aspectsof flow deprivation and treatment effects in human chronic CAD.
Dobutamine stress echocardiography (DSE) has emerged as aversatile and simple tool to assess myocardial function and hasbeen used extensively to determine myocardial viability andpredict reversibility of ischaemia-induced reduction in functionalparameters.1– 3 Recently, regional myocardial function has beenmeasured by the deformation parameters strain and strain rate(SR). Using tissue Doppler imaging (TDI) to assess these deform-ation parameters,10 –15 we determined segmental systolic longitu-dinal function of the left ventricle (LV) in patients with chronicCAD and predominately viable myocardium. Also, pre- andpost-operative segmental responses to inotropic stimulation andrevascularization were determined using longitudinal deformationparameters. We observed a limited normalization of longitudinalsegmental function in the viable myocardium, indicating persistentdysfunction after revascularization in chronic coronary heartdisease.
MethodsAll patients were studied at the University Hospital of North Norway.Each underwent resting echocardiography, DSE, and late gadoliniumenhancement-magnetic resonance imaging (LGE-MRI), 1–7 daysbefore and 8–10 months after coronary artery bypass grafting(CABG), with assessment of global and regional LV functionalparameters.
PatientsBetween November 2005 and December 2007, 67 patients with CADscheduled for CABG were included in the study. All patients gavewritten informed consent. The study was approved by the InstitutionalReview Board for Clinical Research. Exclusion criteria were valvularheart disease, chronic obstructive lung disease or asthma, atrial fibril-lation, unstable angina, myocardial infarction within 3 months priorto CABG, left bundle branch block or any contraindications to MRIsuch as claustrophobia, pacemaker implants, or significantly reducedrenal function as assessed by glomerular filtration rate. However,due to limited MR capacity, a maximum of two patients per weekcould be recruited. We aimed to include patients with both normaland moderately reduced ejection fraction (EF) and 20 patients hadprevious myocardial infarctions. Additionally, 15 healthy volunteers(age 44+ 10 years, 67% male) underwent echocardiography at restto define our normal TDI values for normokinetic myocardialsegments.
Magnetic resonance imagingAll LGE-MRI images were acquired using a 1.5 T scanner (Philips Interarelease 2.1, Best, The Netherlands). Fifteen minutes after infusion of0.1 mmol/kg gadoversetamide (Optimark, Mallinckrodt, St Louis, MO,USA), LGE images were obtained, using an inversion recovery
turbo-field-echo (TFE) gradient echo sequence. A five-element heartcoil was used. LGE images were obtained in four-chamber, leftventricle outflow tract, and short-axis views. Imaging parameters ofthis 15-slice breath-hold TFE (GE) sequence were: repetition time/echo time 4.2/1.33, field of view 330 × 105 mm, 1.3 × 1.3 × 7 mmrecon voxel size, TFE factor 40, number of signals averaged 1, flipangle 158, and no parallel imaging were used. Images were analysedaccording to the standard 16-myocardial-segment model used forechocardiography.16 Care was taken to ensure correct alignment ofthe apex, mitral annulus, aortic valve, and septum. Quantification ofthe extent of myocardial scar tissue was performed by visual assess-ment of LGE images. The extent of myocardial scar tissue wasgrouped into three categories: ‘no scar’ (LGE ¼ 0), ‘subendocardialscar’ (LGE ¼ 1–49%), and ‘transmural scar’ (LGE ¼ 50–100%). Seg-ments were defined as viable when LGE was lower than 50%.
EchocardiographyEcho data acquisitionAll echocardiographic studies were performed using an iE33 scanner(S5-1 probe, iE33, Philips Medical Systems, Andover, MA, USA) witha 1–5 MHz transducer in the left lateral decubital position. Both atbaseline and during DS, conventional two-dimensional (2D) grey-scaleimages and TDI data were obtained in the apical two-, three-, and four-chamber views.
Acquisitions of TDI loops of five consecutive cardiac cycles wereperformed wall by wall in the three standard apical views, using asector angle of 25–308 and a frame rate of 120–170 s21. Wallswere carefully aligned with the ultrasound beam. The cineloopswere obtained in the DICOM format and digitally stored for off-lineanalysis.
Dobutamine stress protocolb-Blockers were withdrawn 36–48 h before DSE. The test was per-formed using infusion rates of 2.5, 5, 10, and 20 mg/kg/min, withcontinuous 12-lead ECG monitoring and blood pressure measure-ments at the end of every 3 min stage. Conventional 2D and TDIdata were acquired at baseline and at the end of each dobutamineincrement. Criteria for terminating the test were completion of theprotocol when 85% of the maximal heart rate (HR) was reached,severe ischaemia evidenced by extensive new wall motion abnormal-ities, horizontal or down-sloping ST-segment depression .2 mm,ST-segment elevation .1 mm in patients without prior myocardialinfarction, severe angina, systolic blood pressure .240 or,100 mmHg, or serious ventricular arrhythmias. During DSE, themaximal Doppler velocities were increased manually from 15 to25 cm/s in order to avoid aliasing, whereas frame rates were notchanged.
Echo image analysisThe investigators of both echocardiographic and MRI data wereblinded for mutual test results. All 2D and TDI measurements wereanalysed by a single experienced observer using commercially availablesoftware (QLAB, Philips Medical Systems). Global LV function wasassessed by calculating end-systolic volume, end-diastolic volume(EDV), and EF, using the biplane Simpson’ method. Stroke volume(SV) and cardiac output were derived from the calculatedvolumes and HR. Left atrial areas (LAA) were measured at end-systolein the four-chamber view.
Regional LV function was evaluated using the 16-segment model asdefined by the American Society of Echocardiography.16 As in earlierSR imaging (SRI) studies, in the conventional 2D grey-scale loops,myocardial segments were scored as normal (score ¼ 1), moderately
A. Rosner et al.746
at University of T
romsoe on D
ecember 17, 2012
http://ehjcimaging.oxfordjournals.org/
Dow
nloaded from

hypokinetic (2), severely hypokinetic (2.5), akinetic (3), ordyskinetic (4).11 Data from segments with poor image quality were dis-carded. All septal segments, non-revascularized segments (accordingto the surgical report), and segments with increased post-proceduralLGE were excluded from statistical analyses.
For TDI strain analysis, each segment was tracked manually by posi-tioning a region of interest (ROI) with a length between 1.0 and1.8 cm, and a width of 0.25 cm in the centre of the myocardial wallthroughout five cardiac cycles. The system calculates cosines’ a cor-rected SR. Axial averaging of SR at a length of 1 cm and weightedtemporal smoothing were applied. Measurements were discarded insegments with aliasing, missing Doppler data for more than 50% ofthe cardiac cycle, large reverberations, and angle deviation over 258,when velocity and SR curves lacked E-waves and when curve shapeand peak values changed more than 20% from beat to beat. Addition-ally, the uniformity of strain curves derived from five to eight divisionsalong the ROI served to assess visually data quality.
The aortic valve opening and closure, and thereby the ejection time(ET) period, were determined by Doppler detection of the aortic valve
clicks. SR was expressed as the mean of all SR values during ET, and ETstrain was defined as the highest positive or negative peak strain valueduring ET. Post-systolic strain (PSS) was then defined as the differencebetween peak ET strain and peak strain. The ratio PSS/ET strain wasexpressed as the post-systolic strain index (PSI). In a cineloop of fivecardiac cycles, the first cycle was analysed, except in the case of extra-systoles or insufficient quality of the first beat. Then, the second or fol-lowing cycles were analysed.
For wall motion scores (WMS), ET strain, SR, and PSI, the highestvalues from all dobutamine doses and the peak increment betweenthe resting value and maximal values were extracted. In the healthyvolunteers, 97.5% of ET strain values were less than or equal to210.3%. This 97.5% percentile for segments in normal individualswas chosen as a cut-off to define dysfunctional myocardium. The his-tograms of both groups are shown in Figure 1. Definitions of differentischaemic substrates and cut-off values are listed in Table 1. The cut-offfor akinesia was arbitrarily set at ET strain greater than 24.0%. Conse-quently, hypokinesia was defined as ET strain between 210.3 and24.0%. Four groups of DSE strain increments were defined as
Figure 1 Histograms of resting ejection time strain in the normal population and coronary artery disease patients. A cut-off a 97.5 percentileat ejection time strain of 210.3% reveals 39% of dyskinetic segments in coronary artery disease patients.
Persistent dysfunction of viable myocardium 747
at University of T
romsoe on D
ecember 17, 2012
http://ehjcimaging.oxfordjournals.org/
Dow
nloaded from

described in Table 1, whereas the cut-off of 27.5% between moderateDS increment (DSE+) and low DS increment (DSE2) was extractedfrom the receiver operating characteristic (ROC) curve for functionalimprovement of all dysfunctional segments. Cut-offs for ‘no DS strainincrement’ (DSE2 2) (21%) and ‘high DS strain increment’(DSE++) (215%) were selected arbitrarily.
Regional functional improvement was defined as the pre- and post-operative difference in ET strain of at least 4.4% [¼1 standard devi-ation (SD) of the Bland–Altman plot for intraobserver variability].Segments not improving beyond strain values of 24% were also con-sidered ‘unimproved’.
ReproducibilityTo determine interobserver variability for TDI strain and SR, 15patients with moderately reduced EF (44+9%) were randomlyselected, and another independent, experienced observer (S.M.),who was blinded to all other data, analysed the pre-operative data atrest and peak dobutamine dose. For assessing intraobserver variability,data from the same 15 patients were reanalysed by the main observer(A.R.) in a new random order after at least 6 months.
Statistical analysesIf not stated otherwise, all data are expressed as mean+ SD. PairedStudent’s t-tests were used to test changes before and after CABG.Differences between functional parameters of normokinetic, hypoki-netic, and akinetic segments or parameters of healthy individuals andCAD patients with normal and reduced EF were tested by one-wayANOVA with the Bonferroni post hoc analysis. The differencebetween improved and unimproved groups was analysed by a Stu-dent’s t-test. General estimated equations with binary logistic regres-sion were used to test segmental differences between these groupsfor global parameters, correcting for the same data distributed indifferent groups. Univariate linear regression analyses were performedto test the ability of segmental parameters in predicting strain improve-ment. x2 tests were used to compare the number of improved and notimproved segments of different ischaemic subgroups. Cut-off valuesfrom one-half of the data set were extracted using ROC curves. Sensi-tivity and specificity were calculated from the other half of the data.Sequential Cox’s proportional hazard models were used to correctROC curves for clustered data. Results are expressed as area underthe curve (AUC), P-value, and 95% confidence interval (CI) forAUC. Probability values ,0.05 were considered statistically significant.
Inter- and intraobserver variabilities for strain and SR wereexpressed as the absolute difference between two measurements inper cent of their mean.17 To avoid the problem of increasing variationwith a denominator close to 0, a constant of 225 was added to allmeasured strain and 22.5 to all measured SR2 values. In assessingvariability, percentages of less than 20% were regarded as fair andless than 15% as good results. All statistics were performed by SPSSversion 16.0 (SPSS Inc., Chicago, IL, USA).
Results
Patient and myocardial segmentexclusionsOf the 67 enrolled patients, five were excluded from the studyprior to CABG due to atrial fibrillation (n ¼ 1), claustrophobia(n ¼ 2), or logistic problems (n ¼ 2). Additionally, five patientsdid not complete the post-operative protocol; one due to lossof data, one refused a second MRI, and three had declininghealth after the surgical procedure. Thus, 57 patients wereincluded in the final analysis. Table 2 displays the patientcharacteristics.
We excluded the following segments from data analyses: allseptal segments, due to their known deterioration after cardio-thoracic surgery18 (285/912 segments), segments with increasedLGE post-CABG indicating peri- or post-operative infarctions,defined as increments exceeding 25% LGE (28/627 segments),and diseased segments not revascularized according to the surgicalreport (60/627 segments). Due to low quality, in LGE-MRI, 4 seg-ments were discarded before and 24 segments after CABG, while87/912 (9.54%) segments were discarded after DSE and beforeCABG and, finally, 128/912 (14.0%) post-operatively. All together,428 segments were left for statistical analyses.
Longitudinal ejection time strain inpatients with high-grade coronaryartery diseaseCompared with the 97.5% percentile obtained from the healthyreference group, longitudinal resting ET strain was reduced in
Table 1 Overview over definitions of segmental ischaemic substrates
Viable segment LE-MRI ,50%
Transmural scar LE-MRI 50–100%
Subendocardial scar LE-MRI 1–49%
Hypokinesia Resting ET strain: 210.3 to 24%
Akinesia Resting ET strain: greater than 24%
Dysfunctional segment Resting ET strain: greater than 210.3%
DSE2 2 (no DS response) DSE strain increment: 21.0–0.0%
DSE2 (low DS response) DSE strain increment: 27.5 to 21.01%
DSE+ (moderate DS response) DSE strain increment: 215.0 to 27.51%
DSE++ (high DS response) DSE strain increment: less than 215.0%
ET strain improvement after CABG (ET strain post-CABG) – (ET strain pre-CABG) ≤ 24.4 and ET strain post-CABG ≤ 24.4
No ET strain improvement after CABG (ET strain post-CABG) – (ET strain pre-CABG) . 24.4 or ET strain post-CABG . 24
DSE improvement after CABG (DSE strain increment post-CABG) 2 (DSE strain increment pre-CABG) ≤ 24
The first 10 definitions are based on pre-operative data only, while the last 3 rows express the difference between pre- and post-operative ET strain.
A. Rosner et al.748
at University of T
romsoe on D
ecember 17, 2012
http://ehjcimaging.oxfordjournals.org/
Dow
nloaded from
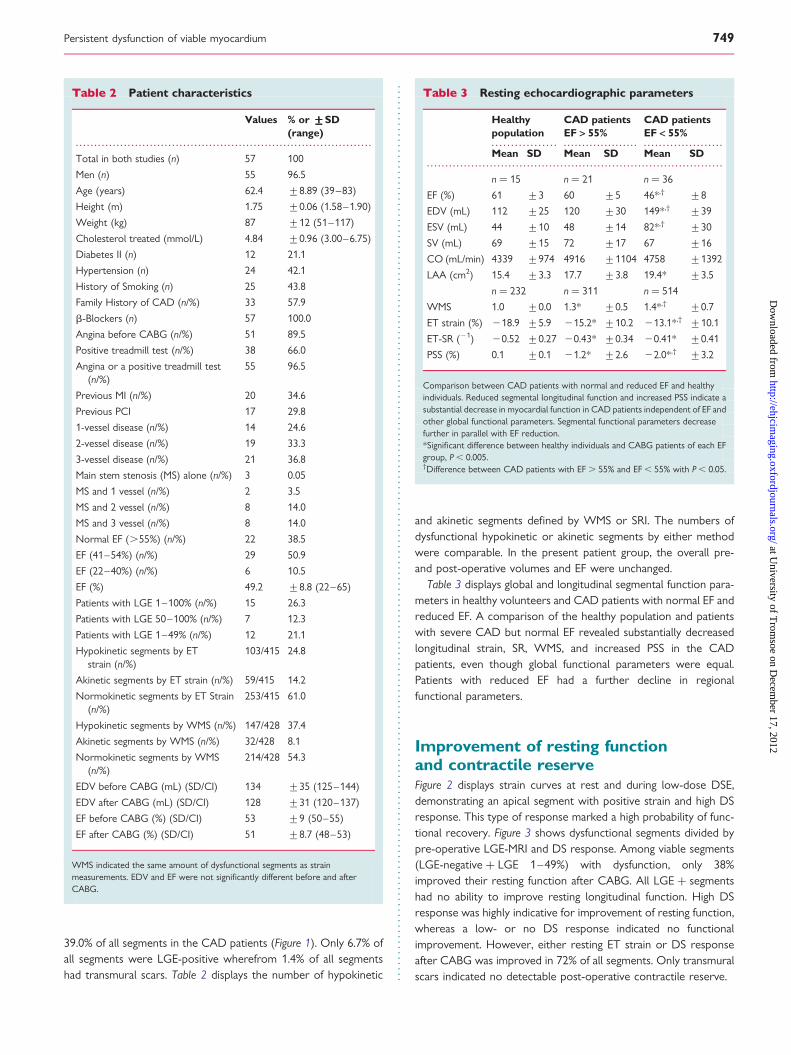
39.0% of all segments in the CAD patients (Figure 1). Only 6.7% ofall segments were LGE-positive wherefrom 1.4% of all segmentshad transmural scars. Table 2 displays the number of hypokinetic
and akinetic segments defined by WMS or SRI. The numbers ofdysfunctional hypokinetic or akinetic segments by either methodwere comparable. In the present patient group, the overall pre-and post-operative volumes and EF were unchanged.
Table 3 displays global and longitudinal segmental function para-meters in healthy volunteers and CAD patients with normal EF andreduced EF. A comparison of the healthy population and patientswith severe CAD but normal EF revealed substantially decreasedlongitudinal strain, SR, WMS, and increased PSS in the CADpatients, even though global functional parameters were equal.Patients with reduced EF had a further decline in regionalfunctional parameters.
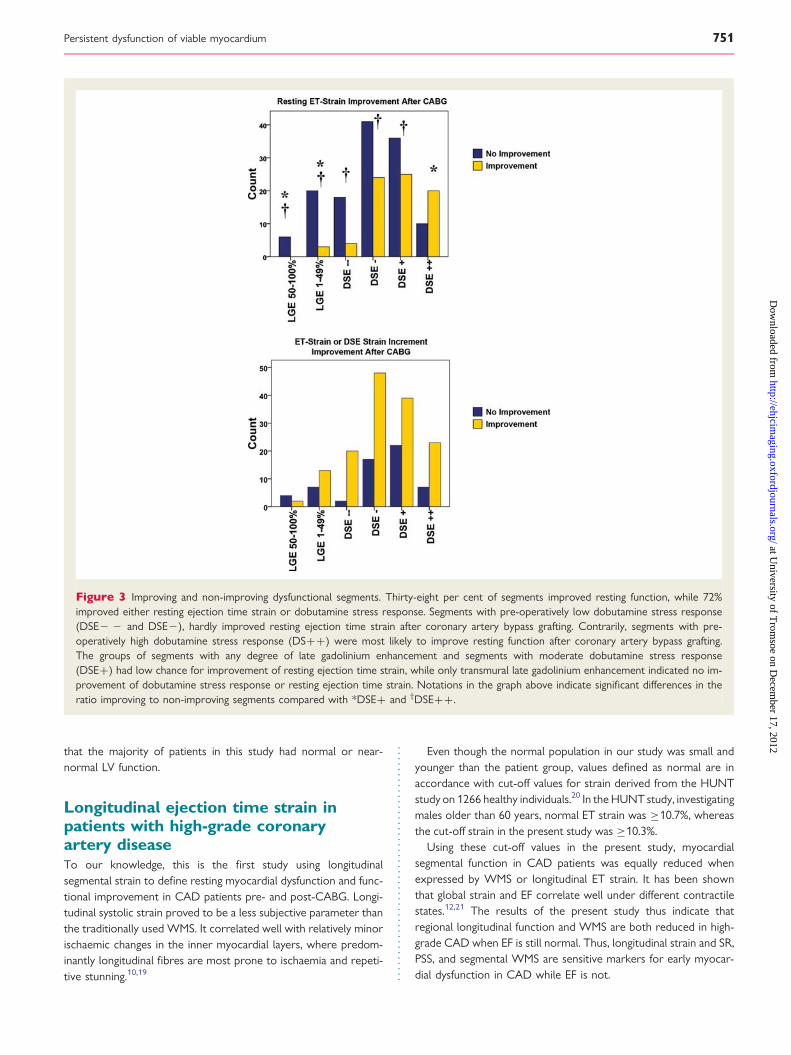
Improvement of resting functionand contractile reserveFigure 2 displays strain curves at rest and during low-dose DSE,demonstrating an apical segment with positive strain and high DSresponse. This type of response marked a high probability of func-tional recovery. Figure 3 shows dysfunctional segments divided bypre-operative LGE-MRI and DS response. Among viable segments(LGE-negative + LGE 1–49%) with dysfunction, only 38%improved their resting function after CABG. All LGE + segmentshad no ability to improve resting longitudinal function. High DSresponse was highly indicative for improvement of resting function,whereas a low- or no DS response indicated no functionalimprovement. However, either resting ET strain or DS responseafter CABG was improved in 72% of all segments. Only transmuralscars indicated no detectable post-operative contractile reserve.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 3 Resting echocardiographic parameters
Healthypopulation
CAD patientsEF > 55%
CAD patientsEF < 55%
Mean SD Mean SD Mean SD
n ¼ 15 n ¼ 21 n ¼ 36
EF (%) 61 +3 60 +5 46*,† +8
EDV (mL) 112 +25 120 +30 149*,† +39
ESV (mL) 44 +10 48 +14 82*,† +30
SV (mL) 69 +15 72 +17 67 +16
CO (mL/min) 4339 +974 4916 +1104 4758 +1392
LAA (cm2) 15.4 +3.3 17.7 +3.8 19.4* +3.5
n ¼ 232 n ¼ 311 n ¼ 514
WMS 1.0 +0.0 1.3* +0.5 1.4*,† +0.7
ET strain (%) 218.9 +5.9 215.2* +10.2 213.1*,† +10.1
ET-SR (21) 20.52 +0.27 20.43* +0.34 20.41* +0.41
PSS (%) 0.1 +0.1 21.2* +2.6 22.0*,† +3.2
Comparison between CAD patients with normal and reduced EF and healthyindividuals. Reduced segmental longitudinal function and increased PSS indicate asubstantial decrease in myocardial function in CAD patients independent of EF andother global functional parameters. Segmental functional parameters decreasefurther in parallel with EF reduction.*Significant difference between healthy individuals and CABG patients of each EFgroup, P , 0.005.†Difference between CAD patients with EF . 55% and EF , 55% with P , 0.05.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Patient characteristics
Values % or +++++SD(range)
Total in both studies (n) 57 100
Men (n) 55 96.5
Age (years) 62.4 +8.89 (39–83)
Height (m) 1.75 +0.06 (1.58–1.90)
Weight (kg) 87 +12 (51–117)
Cholesterol treated (mmol/L) 4.84 +0.96 (3.00–6.75)
Diabetes II (n) 12 21.1
Hypertension (n) 24 42.1
History of Smoking (n) 25 43.8
Family History of CAD (n/%) 33 57.9
b-Blockers (n) 57 100.0
Angina before CABG (n/%) 51 89.5
Positive treadmill test (n/%) 38 66.0
Angina or a positive treadmill test(n/%)
55 96.5
Previous MI (n/%) 20 34.6
Previous PCI 17 29.8
1-vessel disease (n/%) 14 24.6
2-vessel disease (n/%) 19 33.3
3-vessel disease (n/%) 21 36.8
Main stem stenosis (MS) alone (n/%) 3 0.05
MS and 1 vessel (n/%) 2 3.5
MS and 2 vessel (n/%) 8 14.0
MS and 3 vessel (n/%) 8 14.0
Normal EF (.55%) (n/%) 22 38.5
EF (41–54%) (n/%) 29 50.9
EF (22–40%) (n/%) 6 10.5
EF (%) 49.2 +8.8 (22–65)
Patients with LGE 1–100% (n/%) 15 26.3
Patients with LGE 50–100% (n/%) 7 12.3
Patients with LGE 1–49% (n/%) 12 21.1
Hypokinetic segments by ETstrain (n/%)
103/415 24.8
Akinetic segments by ET strain (n/%) 59/415 14.2
Normokinetic segments by ET Strain(n/%)
253/415 61.0
Hypokinetic segments by WMS (n/%) 147/428 37.4
Akinetic segments by WMS (n/%) 32/428 8.1
Normokinetic segments by WMS(n/%)
214/428 54.3
EDV before CABG (mL) (SD/CI) 134 +35 (125–144)
EDV after CABG (mL) (SD/CI) 128 +31 (120–137)
EF before CABG (%) (SD/CI) 53 +9 (50–55)
EF after CABG (%) (SD/CI) 51 +8.7 (48–53)
WMS indicated the same amount of dysfunctional segments as strainmeasurements. EDV and EF were not significantly different before and afterCABG.
Persistent dysfunction of viable myocardium 749
at University of T
romsoe on D
ecember 17, 2012
http://ehjcimaging.oxfordjournals.org/
Dow
nloaded from

Prediction of functional improvementTable 4 displays the values of global and segmental parameters inpatients with varying degrees of myocardial dysfunction and con-tains an analysis of factors predicting functional improvementafter revascularization. ‘DSE highest strain’ and ‘DSE strain incre-ment’ were the only segmental parameters predicting improve-ment after CABG in pre-operatively hypokinetic segments. Inpre-operatively akinetic segments, however, PSS, DSE peakvalues of strain and SR, DSE strain and SR increments, lowerLAA, and higher EF all indicated higher probabilities for functionalimprovement. Interestingly, positive peak ET strain indicated highprobabilities for functional improvement.
Table 5 presents the results of a univariate linear regressionanalysis of segmental function parameters. Preoperative ET strainand DSE strain increments correlated best with the improvementof post-operative ET strain. Only these two parameters were inde-pendent predictors of functional improvement in a multiple regres-sion analysis. However, creating a combined parameter: ‘Sum: ETstrain and DSE strain increment’ ¼ (0.59 × ET strain) 2 (0.65 ×DSE strain increment), did not significantly improve the correlationcoefficient. Figure 4 shows ROC curves for ET strain improvementafter CABG. The prognostic values of the three tested parameters(ET strain, DSE strain increment, and ‘Sum: ET strain and DSEstrain increment’) were fair in akinetic segments and poor inhypokinesia.
Positive strain as an indicator for viabilityFigure 5 demonstrates that positive strain is a significant predictorfor functional improvement. Segments with LGE and segmentswith no or low DS response were not represented in this
functional group, indicating preserved tissue elasticity in segmentswith positive strain, viability, and a high ability to improve restingfunction. All segments with positive strain improved eitherresting function or DS response.
ReproducibilityFor intra- and interobserver variability, 386 segments were ana-lysed; half were segments at rest and half analysed during DS atthe highest dobutamine dose used. The coefficient of variationfor intraobserver variability for ET strain and mean SR was 9.6and 6.5%, respectively. The repetition coefficient (2 × SD) forET strain values in the Bland–Altman plot was +8.8% (see Supple-mentary data online, Figure S1). The coefficient of variation for theinterobserver variability was 10.3% for ET strain and 7.6% formean SR.
DiscussionThis study demonstrates that longitudinal function was reduced ina high amount of segments in hearts with diffuse CAD. In thisrepresentative surgical CAD patient population, only 38% of seg-ments subsequently improved their resting longitudinal functionafter grafting. However, contractile reserve improved in themajority (72%) of viable segments as demonstrated by a positiveresponse to inotropic drugs. Functional improvement was pre-dicted by DS in non-scarred segments. Additionally, restingsegmental positive strain proved to be a good indicator of thepre-operative absence of scar tissue and a predictor of functionalimprovement after successful grafting. It is important to notice
Figure 2 Strain curves with positive longitudinal ejection time strain in the apex and strain increment during dobutamine stress echocardi-ography, indicating preserved tissue elasticity and the ability to improve function after revascularization.
A. Rosner et al.750
at University of T
romsoe on D
ecember 17, 2012
http://ehjcimaging.oxfordjournals.org/
Dow
nloaded from
that the majority of patients in this study had normal or near-normal LV function.
Longitudinal ejection time strain inpatients with high-grade coronaryartery diseaseTo our knowledge, this is the first study using longitudinalsegmental strain to define resting myocardial dysfunction and func-tional improvement in CAD patients pre- and post-CABG. Longi-tudinal systolic strain proved to be a less subjective parameter thanthe traditionally used WMS. It correlated well with relatively minorischaemic changes in the inner myocardial layers, where predom-inantly longitudinal fibres are most prone to ischaemia and repeti-tive stunning.10,19
Even though the normal population in our study was small andyounger than the patient group, values defined as normal are inaccordance with cut-off values for strain derived from the HUNTstudy on 1266 healthy individuals.20 In the HUNT study, investigatingmales older than 60 years, normal ET strain was ≥10.7%, whereasthe cut-off strain in the present study was ≥10.3%.
Using these cut-off values in the present study, myocardialsegmental function in CAD patients was equally reduced whenexpressed by WMS or longitudinal ET strain. It has been shownthat global strain and EF correlate well under different contractilestates.12,21 The results of the present study thus indicate thatregional longitudinal function and WMS are both reduced in high-grade CAD when EF is still normal. Thus, longitudinal strain and SR,PSS, and segmental WMS are sensitive markers for early myocar-dial dysfunction in CAD while EF is not.
Figure 3 Improving and non-improving dysfunctional segments. Thirty-eight per cent of segments improved resting function, while 72%improved either resting ejection time strain or dobutamine stress response. Segments with pre-operatively low dobutamine stress response(DSE2 2 and DSE2), hardly improved resting ejection time strain after coronary artery bypass grafting. Contrarily, segments with pre-operatively high dobutamine stress response (DS++) were most likely to improve resting function after coronary artery bypass grafting.The groups of segments with any degree of late gadolinium enhancement and segments with moderate dobutamine stress response(DSE+) had low chance for improvement of resting ejection time strain, while only transmural late gadolinium enhancement indicated no im-provement of dobutamine stress response or resting ejection time strain. Notations in the graph above indicate significant differences in theratio improving to non-improving segments compared with *DSE+ and †DSE++.
Persistent dysfunction of viable myocardium 751
at University of T
romsoe on D
ecember 17, 2012
http://ehjcimaging.oxfordjournals.org/
Dow
nloaded from

Improvement of resting function andcontractile reserveTraditionally, improvement of resting function after revasculariza-tion has been thought to reflect the absence of transmural scarsand thus indicating viability. Earlier studies on the effect ofCABG in heart failure patients with high percentages of scartissue have reported an improvement in 78–83% of viable seg-ments already 6–9 months after surgery.14,22,23 In contrast, inthe present study, the percentage of recovering dysfunctional seg-ments was much lower (38%). This discrepancy could possibly beexplained by the associated major changes in loading in dilatedfailing hearts.24 LVs with low EF have increased wall stress thatoften is reduced post-operatively through re-remodelling and theeffect of drug therapy.3 In the present study, however, most ofthe patients had normal or nearly normal EF with low potentialfor improvement of global function measured by SV or EF. Post-operative re-remodelling was therefore not prominent. In accord-ance with this hypothesis, an unchanged post-operative EDV andblood pressure indicate unchanged ventricular geometry and wallstress. Thus, in our patients, strain improvements had a higherprobability of expressing ‘true functional improvement’ meaningrecovery of contractile force in contrast to ‘pseudo-functionalimprovement’ due to reduced wall stress at unchanged contractileforce at rest.
The present study showed that any improvement in DSresponse (72% of dysfunctional segments) in addition to improve-ment at rest (38% of dysfunctional segments) better reflected a
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 4 Preoperative resting and dobutamine stress echocardiographic parameters in left ventricular segments
Normokinesia Hypokinesia Akinesia
Improved Not improved Improved Not improvedn 5 253 n 5 39 n 5 64 n 5 29 n 5 30
Stroke volume (mL) 71+16 67+17 66+17† 68+16 67+17
Cardiac output (mL/min) 4934+1274 4551+1147 4700+1243 4761+1005 4601+1200
EF Simpson (%) 54+8 54+++++9 51+++++11* ,† 52+10 47+11
End-diastolic volume (mL) 134+34 127+42 134+42 136+36 146+39
End-systolic volume (mL) 62+24 61+31 69+33 68+29 79+33
Left atrial area (mL) 18.5+3.8 17.9+++++3.5 19.2+++++3.5* 17.7+++++4.1 20.1+++++3.0*
Wall motion score (WMS) 1.3+0.5 1.4+0.4 1.6+0.7† 1.8+0.8† 1.8+0.9†
ET strain (%) 220.1+6.1 28.4+2.4† 28.4+2.3† 3.9+++++5.4† 21.1+++++2.8* ,†
ET-SR (21) 20.61+0.41 20.24+0.13† 20.21+0.14† 0.04+++++0.23† 20.05+++++0.10* ,†
Post-systolic index 0.1+0.1 0.2+0.4 0.2+0.3 3.0+34.4 3.7+13.0
Post-systolic strain (%) 21.2+2.2 21.8+2.9 21.6+2.6 24.4+++++4.9† 22.4+++++2.4* ,†
DSE: highest WMS 1.1+0.3 1.2+0.4 1.3+0.6† 2.5+0.8† 2.4+0.7†
DSE: highest strain (%) 226.7+8.2 217.7+++++7.1† 215.0+++++5.9* ,† 211.8+++++10.9† 26.2+++++4.7* ,†
DSE: highest SR (21) 21.19+0.57 20.75+0.44† 20.66+0.36† 20.54+++++0.49† 20.29+++++0.21* ,†
DSE: WMS increment 0.2+0.4 0.3+0.4 0.3+0.4 0.3+0.5† 0.3+0.4
DSE: strain increment (%) 26.6+6.6 29.3+++++6.6 26.7+++++5.7* 215.8+++++13.2† 25.0+++++4.0*
DSE: SR increment (21) 20.58+0.48 20.51+0.41 20.45+0.36 20.59+++++0.57 20.24+++++0.21*
DSE: PSI increment 20.5+1.5 20.8+2.1 21.1+1.7 6.0+13.0 12.0+43.3†
Mean values and SD of improved and not improved segments in hypokinesia vs. akinesia for echocardiographic global and segmental functional parameters. Highest DSE valuesindicate the peak value of the whole DSE test; DSE increments: difference between highest values and the resting value. Notations: significant differences in groups with improvedand not improved segmental resting strain after CABG (bold and *); significant differences comparing akinetic or hypokinetic segments with normokinetic segments (†).
. . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 5 Univariate regression analysis for ejectiontime strain improvement after coronary artery bypassgrafting
R R2 P-value CI
Lowerbound
Upperbound
ET strain (%) 0.570 0.325 ,0.001 20.7 20.6
ET-SR (21) 0.455 0.207 ,0.001 214.46 29.90
Post-systolic strain (%) 0.144 0.021 0.003 0.2 0.9
Wall motion score (WMS) 0.143 0.021 0.004 0.9 4.5
DSE: highest WMS 0.110 0.012 0.026 0.3 4.7
DSE: highest strain (%) 0.224 0.050 ,0.001 20.3 20.1
DSE: highest SR (21) 0.151 0.023 0.002 24.67 21.08
DSE: WMS increment 0.084 0.005 n.s. 25.1 0.4
DSE: strain increment (%) 0.415 0.172 ,0.001 0.5 0.7
DSE: SR increment (21) 0.221 0.049 ,0.001 3.13 7.69
DSE: PSI increment 0.064 0.004 n.s. 20.0 0.2
Sum: ET strain + DSEstrain
0.613 0.375 ,0.001 0.98 1.25
Resting and DSE parameters and the correlation between the amount of DSEstrain improvement after CABG. ET strain and DSE strain increment had thehighest correlation coefficients showing significant results in regression analysis.The sum of ET strain and DSE strain increment showed improved correlationcoefficients.
A. Rosner et al.752
at University of T
romsoe on D
ecember 17, 2012
http://ehjcimaging.oxfordjournals.org/
Dow
nloaded from

recovery potential than resting function alone in segments withouttransmural infarction. This finding also indicates that the absence oftransmural scar tissues does not necessarily implicate improvingfunction at rest. For example, viable segments with no or lowDS response have probably no flow reserve and suffer high-gradeischaemia before revascularization.25 These viable segments withlow DS response had no ability to improve resting function.However, nearly all segments with low DS response beforeCABG regained contractile reserve after revascularization.
Prediction of functional improvementIn the present study, DS response and resting strain were the bestpredictors for functional improvement in longitudinal strain. Inaccordance with previous studies,10,11,13,14,26,27 no DS responsewas a highly accurate predictor for no functional improvement
and a high DS response indicated a high probability of functionalimprovement. However, intermediate results led to low test accur-acies in hypokinetic segments. The relatively low number of seg-ments with subendocardial and transmural scars andconsecutively high EF in our patient population might have a highimpact on predictivity in terms of lower test accuracies. Addition-ally, the medication with b-blockers might also influence theprediction of functional improvement. Even though all patientswere medicated with b-blockers, the DS test was performed36–48 h after withdrawal. However, high b-blocker dosagemight have caused blunted test results. Anyhow, a previous studyon patients without b-blocker withdrawal has shown that perform-ing low dose DS at maximal doses of 20 mg/kg/min significantlyimproved test accuracies.28 Interestingly, we could demonstratethat both the presence of subendocardial scars and no DS
Figure 4 Receiver operating characteristic curves, sensitivities, and specificities for the identification of functional improvement after coron-ary artery bypass grafting in all segments and segments with hypokinesia or akinesia. Unexpectedly, dobutamine stress and resting strain weregood predictors of functional improvement in hearts with low amount of scar tissue. This effect is probably due to inclusion of positive strain inakinetic/dyskinetic segments.
Persistent dysfunction of viable myocardium 753
at University of T
romsoe on D
ecember 17, 2012
http://ehjcimaging.oxfordjournals.org/
Dow
nloaded from

response (in viable tissue indicating no flow reserve) were goodpredictors for functional non-recovery in viable segments asdefined by the MR technique.
Positive strain as an indicator for viabilityExpressing ET strain by the highest negative or positive valueduring ET is a novel approach applied under the assumption thatpositive strain might express preserved tissue elasticity. Tradition-ally, strain has been expressed as the maximal negative value duringET.10,11,13,14,26,27 By distinguishing predominantly positive ‘dyski-netic’ or akinetic strain, we found positive strain to be a markerfor the absence of LGE. Segments with LGE have probablyreduced tissue elasticity and thus behave hypokinetic or akineticinstead of ‘dyskinetic’ giving positive strain. Of note, when positivelongitudinal strain was present, segments had not only high prob-ability of functional improvement; the majority of segments evennormalized their function.
Limitations of the studySegmental tissue-flow measurements with sufficiently high spatialresolution are difficult to apply in the clinical setting and werenot attempted in our study. The measurement of tissue flowwould have been advantageous to differentiate reduced segmentalflow reserve and segmental dysfunction with normal flow. Further-more, segmental biopsies could have been able to demonstratestructural myocardial damage in the absence of myocardial scarsdetectable by MRI. Contrarily to other viability strainstudies,10,11,13,14,26,27 we have studied CABG patients only.CABG itself might have deteriorating influence on post-
interventional strain, especially in the septum.18 However, weexcluded the septal segments, in which long-term decreased longi-tudinal function is a known phenomenon.
In spite of these methodological limitations, the reducedrecovery of deformation indexes was demonstrated in thelimited number of 57 patients with small amounts of scar tissue.Thus, the study indicates that more in-depth studies can be donewith selected methodology in relatively small number of patients.A 2-year follow-up might have revealed a higher percentage ofrecovering segments as demonstrated by Bondarenko et al.(95%).22 However, such a prolonged observation period couldhave seen a disease progression with functional deterioration.Resting ET strain has probably only prognostic relevance whendifferentiating positive strain from negative to zero strain. Thecut-offs for group definitions were more or less set arbitrarily.Therefore, the favoured test parameters were chosen accordingto the regression analysis.
Implications and conclusionResults from the ‘STICH’ trial9 indicate that the traditional viabilitytesting before medical or surgical treatment has no significantimpact on the patient prognosis. Additionally, our study indicatesthat resting regional functional parameters are particularly unre-sponsive to revascularization in hearts with near-normal globalLV function. The pathophysiological substrate for these observa-tions remains to be clarified, but the observations point to acomplex relation between the degree and time course of chronic-ally reduced blood flow and recovery of myocardial function, alsoin hearts with well-preserved global function.
Figure 5 Percentage of all segments with lesion characteristics in different ejection time strain groups. Yellow to red: indicating improvementof function; violet to blue: indicating no functional improvement. The probability of functional improvement was highest in segments with posi-tive ‘dyskinetic’ ejection time strain. Segments with late gadolinium enhancement and segments with low or no dobutamine stress responsewere not ‘dyskinetic’, indicating preserved tissue elasticity in this group with positive ejection time strain.
A. Rosner et al.754
at University of T
romsoe on D
ecember 17, 2012
http://ehjcimaging.oxfordjournals.org/
Dow
nloaded from
Supplementary dataSupplementary data are available at European Heart Journal –Cardiovascular Imaging online.
References1. Bax JJ, Visser FC, Poldermans D, Elhendy A, Cornel JH, Boersma E et al. Time
course of functional recovery of stunned and hibernating segments after surgicalrevascularization. Circulation 2001;104(12 Suppl. 1):I314–8.
2. Bax JJ, Poldermans D, Elhendy A, Boersma E, Rahimtoola SH. Sensitivity, specifi-city, and predictive accuracies of various noninvasive techniques for detecting hi-bernating myocardium. Curr Probl Cardiol 2001;26:147–86.
3. Bax JJ, Poldermans D, Elhendy A, Cornel JH, Boersma E, Rambaldi R et al. Im-provement of left ventricular ejection fraction, heart failure symptoms and prog-nosis after revascularization in patients with chronic coronary artery disease andviable myocardium detected by dobutamine stress echocardiography. J Am CollCardiol 1999;34:163–9.
4. Bito V, Heinzel FR, Weidemann F, Dommke C, van der Velden J, Verbeken E et al.Cellular mechanisms of contractile dysfunction in hibernating myocardium. CircRes 2004;94:794–801.
5. Gallagher KP, Matsuzaki M, Koziol JA, Kemper WS, Ross J Jr. Regional myocardialperfusion and wall thickening during ischemia in conscious dogs. Am J Physiol 1984;247(5 Pt 2):H727–38.
6. Heyndrickx GR, Millard RW, McRitchie RJ, Maroko PR, Vatner SF. Regional myo-cardial functional and electrophysiological alterations after brief coronary arteryocclusion in conscious dogs. J Clin Invest 1975;56:978–85.
7. Takayama M, Norris RM, Brown MA, Armiger LC, Rivers JT, White HD. Postsys-tolic shortening of acutely ischemic canine myocardium predicts early and late re-covery of function after coronary artery reperfusion. Circulation 1988;78:994–1007.
8. Theroux P, Ross J Jr, Franklin D, Kemper WS, Sasyama S. Regional myocardialfunction in the conscious dog during acute coronary occlusion and responsesto morphine, propranolol, nitroglycerin, and lidocaine. Circulation 1976;53:302–14.
9. Bonow RO, Maurer G, Lee KL, Holly TA, Binkley PF, Desvigne-Nickens P et al.Myocardial viability and survival in ischemic left ventricular dysfunction. N Engl JMed 2011;364:1617–25.
10. Chan J, Hanekom L, Wong C, Leano R, Cho GY, Marwick TH. Differentiation ofsubendocardial and transmural infarction using two-dimensional strain rateimaging to assess short-axis and long-axis myocardial function. J Am Coll Cardiol2006;48:2026–33.
11. Hanekom L, Jenkins C, Jeffries L, Case C, Mundy J, Hawley C et al. Incrementalvalue of strain rate analysis as an adjunct to wall-motion scoring for assessmentof myocardial viability by dobutamine echocardiography: a follow-up study afterrevascularization. Circulation 2005;112:3892–900.
12. Stoylen A, Heimdal A, Bjornstad K, Wiseth R, Vik-Mo H, Torp H et al. Strain rateimaging by ultrasonography in the diagnosis of coronary artery disease. J Am SocEchocardiogr 2000;13:1053–64.
13. Vitarelli A, Montesano T, Gaudio C, Conde Y, Cimino E, D’angeli I et al. Strain ratedobutamine echocardiography for prediction of recovery after revascularizationin patients with ischemic left ventricular dysfunction. J Card Fail 2006;12:268–75.
14. Becker M, Lenzen A, Ocklenburg C, Stempel K, Kuhl H, Neizel M et al. Myocardialdeformation imaging based on ultrasonic pixel tracking to identify reversible myo-cardial dysfunction. J Am Coll Cardiol 2008;51:1473–81.
15. Hoffmann R, Altiok E, Nowak B, Heussen N, Kuhl H, Kaiser HJ et al. Strain ratemeasurement by Doppler echocardiography allows improved assessment of myo-cardial viability inpatients with depressed left ventricular function. J Am Coll Cardiol2002;39:443–9.
16. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA et al.Recommendations for chamber quantification: a report from the AmericanSociety of Echocardiography’s Guidelines and Standards Committee and theChamber Quantification Writing Group, developed in conjunction with the Euro-pean Association of Echocardiography, a branch of the European Society of Car-diology. J Am Soc Echocardiogr 2005;18:1440–63.
17. Bland JM, Altman DG. Statistical methods for assessing agreement between twomethods of clinical measurement. Lancet 1986;1:307–10.
18. Toyoda T, Akasaka T, Watanabe N, Akiyama M, Neishi Y, Kume T et al. Evaluationof abnormal motion of interventricular septum after coronary artery bypass graft-ing operation: assessment by ultrasonic strain rate imaging. J Am Soc Echocardiogr2004;17:711–6.
19. Sjoli B, Orn S, Grenne B, Ihlen H, Edvardsen T, Brunvand H. Diagnostic capabilityand reproducibility of strain by Doppler and by speckle tracking in patients withacute myocardial infarction. JACC Cardiovasc Imaging 2009;2:24–33.
20. Dalen H, Thorstensen A, Aase SA, Ingul CB, Torp H, Vatten LJ et al. Segmentaland global longitudinal strain and strain rate based on echocardiography of1266 healthy individuals: the HUNT study in Norway. Eur J Echocardiogr 2010;11:176–83.
21. Weidemann F, Jamal F, Sutherland GR, Claus P, Kowalski M, Hatle L et al. Myo-cardial function defined by strain rate and strain during alterations in inotropicstates and heart rate. Am J Physiol Heart Circ Physiol 2002;283:H792–9.
22. Bondarenko O, Beek AM, Twisk JW, Visser CA, van Rossum AC. Time course offunctional recovery after revascularization of hibernating myocardium: acontrast-enhanced cardiovascular magnetic resonance study. Eur Heart J 2008;29:2000–5.
23. Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O et al. The use ofcontrast-enhanced magnetic resonance imaging to identify reversible myocardialdysfunction. N Engl J Med 2000;343:1445–53.
24. Rosner A, Bijnens B, Hansen M, How OJ, Aarsaether E, Muller S et al. Left ven-tricular size determines tissue Doppler-derived longitudinal strain and strain rate.Eur J Echocardiogr 2009;10:271–7.
25. Bijnens B, Claus P, Weidemann F, Strotmann J, Sutherland GR. Investigatingcardiac function using motion and deformation analysis in the setting of coronaryartery disease. Circulation 2007;116:2453–64.
26. Hoffmann R, Stempel K, Kuhl H, Balzer J, Kramer N, Krombach G et al. Integratedanalysis of cardiac tissue structure and function for improved identification of re-versible myocardial dysfunction. Coron Artery Dis 2009;20:21–6.
27. Zhang Y, Chan AK, Yu CM, Yip GW, Fung JW, Lam WW et al. Strain rate imagingdifferentiates transmural from non-transmural myocardial infarction: a validationstudy using delayed-enhancement magnetic resonance imaging. J Am Coll Cardiol2005;46:864–71.
28. Zaglavara T, Haaverstad R, Cumberledge B, Irvine T, Karvounis H, Parharidis Get al. Dobutamine stress echocardiography for the detection of myocardial viabil-ity in patients with left ventricular dysfunction taking beta blockers: accuracy andoptimal dose. Heart 2002;87:329–35.
Persistent dysfunction of viable myocardium 755
at University of T
romsoe on D
ecember 17, 2012
http://ehjcimaging.oxfordjournals.org/
Dow
nloaded from





























