Embed Size (px)
Citation preview

PHARMACOKINETICS OF ORALLY ADMINISTERED
TERBINAFINE IN AFRICAN PENGUINS (SPHENISCUS
DEMERSUS) FOR POTENTIAL TREATMENT OF ASPERGILLOSIS
Ursula Bechert, D.V.M., Ph.D., J. Mark Christensen, Ph.D., Robert Poppenga, D.V.M., Ph.D.,
Hang Le, Ph.D., Jeff Wyatt, D.V.M., M.P.H., and Todd Schmitt, D.V.M.
Abstract: The objective of this study was to determine the pharmacokinetic parameters of orally administered
terbinafine hydrochloride based on 3, 7, and 15 mg/kg single- as well as multiple-dosage trials in order to calculate
dosing requirements for potential treatment of aspergillosis in African penguins (Spheniscus demersus). Ten adult
African penguins were used in each of these trials, with a 2-wk washout period between trials. Mean plasma
concentrations of terbinafine peaked in approximately 4 hrs at 0.11 6 0.017 mg/ml (mean 6 SD) following
administration of 3 mg/kg terbinafine, while 7 mg/kg and 15 mg/kg dosages resulted in peak plasma concentrations
of 0.37 6 0.105 and 0.33 6 0.054 mg/ml, respectively. The volume of distribution increased with increasing dosages,
being 37 6 28.5, 40 6 28.1, and 52 6 18.6 mg/L for 3, 7, and 15 mg/kg doses, respectively. The mean half-life was
biphasic with initial terminal half-life (tK) values of 9.9 6 4.5, 17.2 6 4.9 and 16.9 6 5.4 hrs, for 3, 7, and 15 mg/kg
doses, respectively. A rapid first elimination phase was followed by a slower second phase, and final elimination
was estimated to be 136 6 9.7 and 131 6 9.9 hrs, for 7 and 15 mg/kg doses, respectively. Linearity was
demonstrated for area under the curve but not for peak plasma concentrations for the three dosages used.
Calculations based on pharmacokinetic parameter values indicate that a 15 mg/kg terbinafine q24h dosage regimen
would result in steady-state trough plasma concentrations above the minimum inhibitory concentration (0.8–1.6 mg/
ml), and this dosage is recommended as a potential treatment option for aspergillosis in penguins. However,
additional research is required to determine both treatment efficacy and safety.
Key words: Terbinafine, pharmacokinetics, African penguins, aspergillosis.
INTRODUCTION
Aspergillosis is a common respiratory disease
of birds in both wild and captive environments
caused by a saprophytic mold found worldwide.
In wild penguin populations, aspergillosis has
been reported in association with stress or
challenging environmental conditions.10,35 In
New Zealand and Antarctica, 60% of 184
penguins were seropositive for aspergillosis by
indirect ELISA testing.31 African penguin (Sphe-
niscus demersus) populations in the wild are
endangered, and this species represents the
greatest percentage of captive penguins in North
America.18 In zoologic collections, aspergillosis is
a main health concern for waterfowl, raptors,
psittacines, and passerines and is considered to be
the most-important airborne disease of captive
indoor penguins.62 The most common aspergillo-
sis pathogen is Aspergillus fumigatus, followed by
infections with Aspergillus flavus and Aspergillus
niger.9,79,84 These fungi are prevalent in humid
environments and accumulate in the air-handling
systems and soil substrates of many institutional
exhibits.
Individual birds become susceptible to Asper-
gillus spp. when exposed to high concentrations
of fungal spores or when inherent immune
defenses are compromised due to stress, malnu-
trition, or pre-existing disease.18,41 The majority of
aspergillosis outbreaks in the northern hemi-
sphere occur during the summer (July–Septem-
ber).21 There is also evidence that the occurrence
of aspergillosis has been age-dependent in captive
penguin populations, occurring most commonly
in 2–3-mo-old chicks and only sporadically in
adults.21
The three stages of infection are an acute,
overwhelming dissemination of fungal spores to
critical organs that may be characterized by
anorexia, dyspnea, or occasionally, sudden death
without signs; subacute infection with respiratory
From the Oregon State University, College of
Science, 2082 Cordley Hall, Corvallis, Oregon 97331,
USA (Bechert); Oregon State University, College of
Pharmacy, 229 Pharmacy Building, Corvallis, Oregon
97331, USA (Christensen, Le); University of Pennsyl-
vania, New Bolton Center, 382 West Street Road,
Kennett Square, Pennsylvania 19348, USA (Poppenga);
Seneca Park Zoo, 2222 Saint Paul Street, Rochester,
New York 14621, USA (Wyatt); and SeaWorld, 500
Sea World Drive, San Diego, California 92109, USA
(Schmitt). Present address (Poppenga): University of
California–Davis, CAHFS Toxicology Laboratory,
Davis, California 95616, USA. Correspondence
should be directed to: Dr. Bechert (ursula.bechert@
oregonstate.edu).
Journal of Zoo and Wildlife Medicine 41(2): 263–274, 2010
Copyright 2010 by American Association of Zoo Veterinarians
263

tract granulomas over several weeks duration;
and chronic, granulomatous infection continuing
for several months.61,62,87 Mycotic granulomas are
frequently found near the tracheal bifurcation,
but can also develop in other areas of the
respiratory tract, liver, kidneys, eyes, and brain.54
Chronic aspergillosis is the more-common form,
and affected birds exhibit voice change, anorexia,
biliverdinuria, lethargy or depression, dyspnea,
emaciation, and, occasionally, ataxia or paralysis
if the central nervous system is involved.88
Because of the ubiquitous nature of Aspergillus
spp., establishing a definitive diagnosis of asper-
gillosis is difficult. Identification of cases is
usually based on initial observations, but clinical
signs are not diagnostic and, if chronic, resemble
other debilitating diseases. Antemortem diagno-
ses are typically made using a combination of
radiographs, complete blood counts (CBC),
serum biochemistry panels, serum electrophoresis
to detect b and c globulin elevations, and
determination of Aspergillus antigen and anti-
body levels.47,87 Blood, cerebrospinal fluid, and
bone marrow specimens rarely yield Aspergillus
spp., and radiographic findings alone are not
diagnostic because other conditions can produce
similar images. Quantification of antibody titers
against Aspergillus to diagnose aspergillosis has
produced conflicting results, and serial assays are
recommended over isolated tests.81 Definitive
diagnosis requires both histologic evidence of
Aspergillus hyphae and cultures from specimens
obtained by biopsy or aspiration from involved
organs.79 Bronchoalveolar lavage, with assay of
the fluid by smear, culture, or antigen (or both),
detection has excellent specificity for invasive
aspergillosis.42,44
Currently, there are four classes of antifungal
agents with activity against Aspergillus; the
polyenes, such as amphotericin B; the triazoles,
including itraconazole, fluconazole, and vorico-
nazole; the echinocandins, such as caspofungin
and micofungin; and the allylamines, including
terbinafine. Although amphotericin B is the
human standard for treatment of aspergillosis,79
it must be administered by injection and there are
concerns about its nephrotoxic side effects.23 The
triazoles are currently a more-popular choice for
treatment of birds due to their broad spectrum of
activity, relative ease of administration, and low
toxicity.19,22,25,63 However, treatment failures re-
main a concern,76 and differences in absorption
between generic, bulk-compounded itraconazole
powder and Sporanox ready-made doses (Torpac
Inc., Fairfield, New Jersey 07004, USA) have
been demonstrated.8 Some drug therapies can
cause adverse side effects (e.g., flucytosine has the
potential to cause bone marrow toxicity13), and
most drugs are fungistatic in nature. In most
instances, dosing schedules for these drugs,
derived from pharmacokinetic data to maintain
blood levels above the minimum inhibitory
concentration (MIC), have not been established
for birds. Therefore, it is not known whether lack
of treatment success is due to the inherent
inability of fungistatic drugs to effectively inhibit
Aspergillus spp. in vivo, to inadequate dosing, or
to both.
Terbinafine hydrochloride (LamisilH, Novartis,
East Hanover, New Jersey 07936, USA) was
released in 1996 for treatment of human mycotic
nail infections (onychomyscosis).33,46 The allyl-
amines are a relatively new class of antifungal
agents which have a different mechanism of
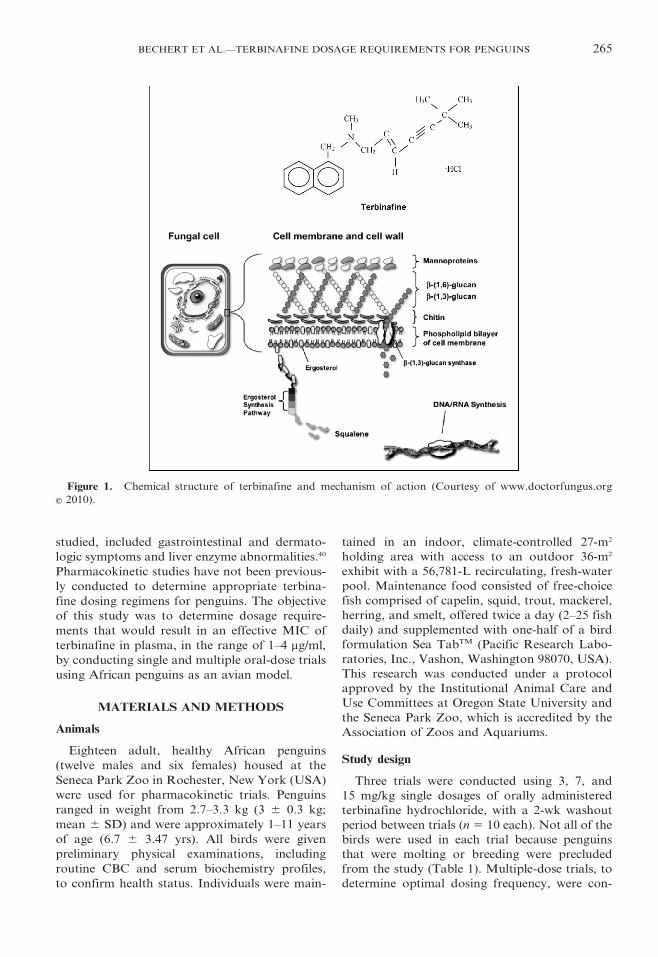
action as compared to the azoles.2,60 Terbinafine
(Fig. 1) is thought to have fungicidal activity59 by
inhibiting squalene epoxidases, thereby causing
cytotoxic accumulation of intracellular squa-
lene.68 Secondarily, enzyme inhibition results in
a depletion of ergosterol, which is the fungal
counterpart of cholesterol in mammalian cells.
This interferes with membrane function and cell
growth, resulting in a fungistatic action.67 The
different mechanisms of action provide terbina-
fine with a comparative advantage over other
drugs that are either fungistatic or fungicidal in
nature, and because the metabolism of terbina-
fine utilizes less than 5% of the cytochrome P450
capacity of the liver,82 there is less interference
with other drugs that could potentially result in
negative side effects.1,20 In humans, it is estimated
that approximately 10% of terbinafine metabo-
lites initially eliminated in bile undergo entero-
hepatic recycling.4
Terbinafine can be given orally or topically,
has excellent absorption rates between 70% and
80%,16 a bioavailability of approximately 40% in
humans, and approximately 70% of the metab-
olites are eliminated in the urine.2,40 Potential use
of terbinafine as a treatment for aspergillosis in
penguins is of interest because high concentra-
tions of terbinafine accumulate in connective
tissues, and air sacs have a relatively poor blood
supply, making delivery of most therapeutic
agents to this region difficult.
The published MIC range of terbinafine
against A. fumigatus in humans is broad, ranging
from 0.02–5 mg/ml for dosages ranging from
62.5–250 mg/day.12,28,29,36,74,75 Potential adverse
reactions, reported in up to 5.6% of 465 humans
264 JOURNAL OF ZOO AND WILDLIFE MEDICINE
studied, included gastrointestinal and dermato-
logic symptoms and liver enzyme abnormalities.40
Pharmacokinetic studies have not been previous-
ly conducted to determine appropriate terbina-
fine dosing regimens for penguins. The objective
of this study was to determine dosage require-
ments that would result in an effective MIC of
terbinafine in plasma, in the range of 1–4 mg/ml,
by conducting single and multiple oral-dose trials
using African penguins as an avian model.
MATERIALS AND METHODS
Animals
Eighteen adult, healthy African penguins
(twelve males and six females) housed at the
Seneca Park Zoo in Rochester, New York (USA)
were used for pharmacokinetic trials. Penguins
ranged in weight from 2.7–3.3 kg (3 6 0.3 kg;
mean 6 SD) and were approximately 1–11 years
of age (6.7 6 3.47 yrs). All birds were given
preliminary physical examinations, including
routine CBC and serum biochemistry profiles,
to confirm health status. Individuals were main-
tained in an indoor, climate-controlled 27-m2
holding area with access to an outdoor 36-m2
exhibit with a 56,781-L recirculating, fresh-water
pool. Maintenance food consisted of free-choice
fish comprised of capelin, squid, trout, mackerel,
herring, and smelt, offered twice a day (2–25 fish
daily) and supplemented with one-half of a bird
formulation Sea TabTM (Pacific Research Labo-
ratories, Inc., Vashon, Washington 98070, USA).
This research was conducted under a protocol
approved by the Institutional Animal Care and
Use Committees at Oregon State University and
the Seneca Park Zoo, which is accredited by the
Association of Zoos and Aquariums.
Study design
Three trials were conducted using 3, 7, and
15 mg/kg single dosages of orally administered
terbinafine hydrochloride, with a 2-wk washout
period between trials (n 5 10 each). Not all of the
birds were used in each trial because penguins
that were molting or breeding were precluded
from the study (Table 1). Multiple-dose trials, to
determine optimal dosing frequency, were con-
Figure 1. Chemical structure of terbinafine and mechanism of action (Courtesy of www.doctorfungus.org
E 2010).
BECHERT ET AL.—TERBINAFINE DOSAGE REQUIREMENTS FOR PENGUINS 265
ducted with ten penguins using 15 mg/kg dosages
administered once daily for 4 days. Terbinafine
tablets were compounded into slurry, at a
concentration of 45 mg/ml, by Animal Pharmacy
(Canandaigua, New York 14424, USA). Drug
dosages were based on body weights determined
prior to the initiation of each trial. Each penguin
was manually restrained, as terbinafine was
administered orally using a syringe placed in the
throat past the epiglottis.
Penguins were manually restrained while blood
samples were taken from the right or left jugular
vein, using 22-gauge needles and collected in 5-ml
heparinized VacutainerTM tubes (BD Diagnostics,
Franklin Lakes, New Jersey 07417, USA). One-
milliliter blood samples for initial, single-dose
trials were collected at 25, 15, 30, 45 min, 1, 2, 4,
10, 12, and 24 hr postadministration (10 ml total
over 24 hr). Blood samples for multiple-dose
trials were collected in heparin hourly for 4 hr
after each administration, and then every 6 hr,
plus 1 hr prior to the next administration, in
order to detect peak and trough concentrations.
Samples were placed into glass tubes and
centrifuged for 10 min at 1,300 g (International
Equipment Company, Needham, Maryland
02494, USA). Plasma was decanted into plastic,
screw-cap vials (VWR International, West Ches-
ter, Pennsylvania 19380, USA), frozen, and sent
to the New Bolton Center, University of Penn-
sylvania in Kennett Square, where they were
maintained at 24uC until time of analysis.
Terbinafine analysis
Plasma drug concentrations were quantified
within 30 days of receipt by high-performance
liquid chromatography (HPLC) after sample
preparation.17,86 Ten microliters internal standard
(50 ng/ml; Sandoz #85-190, Batch #79901) was
added to 0.5 ml plasma in a glass tube. To this
plasma mixture, 1 ml 0.2 M borate buffer (pH 9)
and 8 ml n-hexane were added. Each tube was
horizontally shaken for 25 min at 200 oscillations/
min, followed by centrifugation for 10 min at 750 g
at room temperature. Seven milliliters superna-
tant (n-hexane) was transferred to a 16 3 125 mm
glass tube, and 1 ml 1.0 N sulfuric acid 2-propanol
solution (85:15 v/v) was added. Each tube was
shaken horizontally for 15 min at 200 oscillations/
min and then centrifuged for 5 min at 750 g. The
upper organic phase was discarded, and 800 ml of
the aqueous phase was transferred to an amber
glass mini-injection vial. The sample was injected
into a Spectra System HPLC with a P4000
gradient pump and a UV3000 UV-VIS detector
set at a wavelength of 225 (Thermo Separation
Products, Piscataway, New Jersey 08854, USA)
and a Keystone Betasil C18 column (250 3
4.6 mm, particle diameter 5 mm; Thermo Fischer
Scientific, Waltham, Maryland 02451, USA). The
flow rate was 0.9 ml/min, the injection volume was
20 ml, and the column temperature was 30uC. The
mobile phase was an aqueous solution of 0.012 M
triethylamine/0.020 M orthophosphoric acid with
acetonitrile (57:43 v/v).
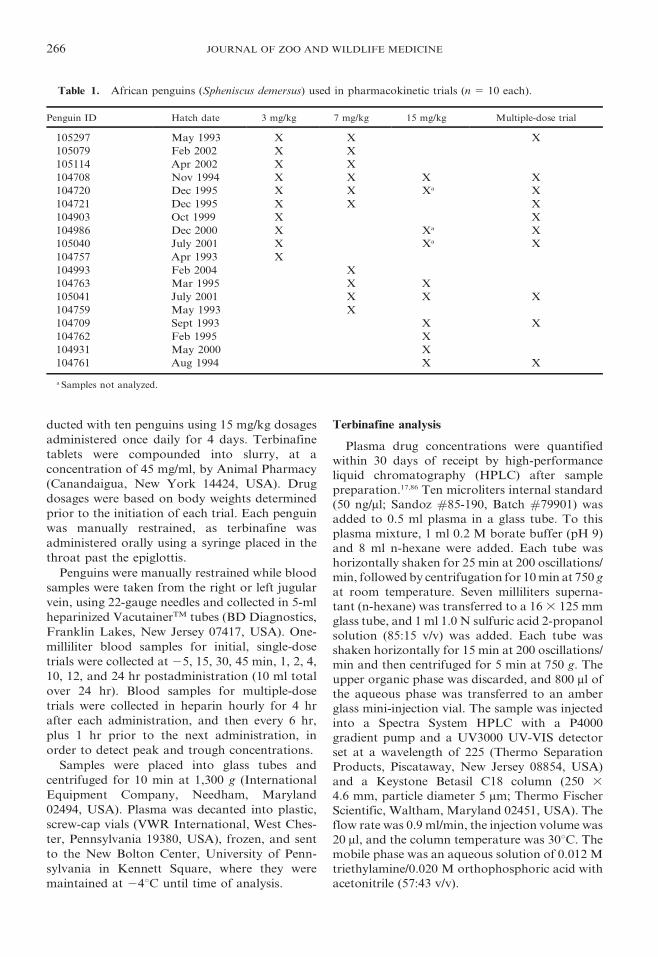
Table 1. African penguins (Spheniscus demersus) used in pharmacokinetic trials (n 5 10 each).
Penguin ID Hatch date 3 mg/kg 7 mg/kg 15 mg/kg Multiple-dose trial
105297 May 1993 X X X
105079 Feb 2002 X X
105114 Apr 2002 X X
104708 Nov 1994 X X X X
104720 Dec 1995 X X Xa X
104721 Dec 1995 X X X
104903 Oct 1999 X X
104986 Dec 2000 X Xa X
105040 July 2001 X Xa X
104757 Apr 1993 X
104993 Feb 2004 X
104763 Mar 1995 X X
105041 July 2001 X X X
104759 May 1993 X
104709 Sept 1993 X X
104762 Feb 1995 X
104931 May 2000 X
104761 Aug 1994 X X
a Samples not analyzed.
266 JOURNAL OF ZOO AND WILDLIFE MEDICINE

A standard curve for terbinafine was generated
using 0.01, 0.1, 0.5, 1.0, and 5 ppm standards in
plasma, and plasma concentrations of terbinafine
were quantified using this standard curve. A
linear fit, forced through zero, was achieved by
evaluating the signal area of the samples com-
pared to the matrix-matched, identically handled,
spiked plasma samples. A correlation coefficient
for calibration curves was calculated (r2 5 0.975;
range 0.926–0.999). The limit of detection (LOD)
and limit of quantitation (LOQ)s were deter-
mined to be 0.01 ppm and 0.1 ppm based upon
the matrix-matched spikes. Spike recoveries were
80% or greater. The interassay coefficient of
variation was 10.7%. The internal standard, at
1 ppm, was added to all blanks, standards, spikes,
and samples. Separate 0.5- and 1.0-ppm spikes
were run to check run precision (80% recovery or
greater required), and a duplicate plasma sample
was run every ten samples (80% or greater
precision required).
Pharmacokinetic and statistical analyses
Pharmacokinetic data were modeled and fitted
for individual birds using compartmental and
noncompartmental approaches with Win Nonlin
(2002 Version 3.2, Pharsight Corporation, Moun-
tain View, California 94040, USA). Parameters
determined for each penguin (mean 6 SD)
included the maximal concentration (Cmax), time
of maximal concentration (Tmax), volume of
distribution (Vd/F), area under the curve
(AUC), mean residence time (MRT), clearance
rate (Cl/F), terminal half-life (tK), and the
elimination rate constant (Kel). The AUC was
calculated using the linear trapezoidal rule
method, or from integration of the fitted
equation to the concentration time curve. The
elimination half-life for terbinafine (tKel) was
determined by dividing the natural logarithm of
2 (0.693) by Kel. For the 7 and 15 mg/kg single-
dose trials, the 3-wk washout period was
insufficient to completely eliminate terbinafine
from the system of all penguins. Plasma terbin-
afine concentrations were corrected for any
residual carryover remaining in effected penguins
from the washout period of the previous dose in
the manner detailed by Girolamo et al.27
Terbinafine was administered as a single, daily
dose basis for the 3, 7, and 15 mg/kg doses, allowing
terbinafine accumulation after multiple dosing to
be calculated according to the following equation:77
Accumulation factor~1
1{e{lT,
where l is the terminal elimination rate constant,
and T is the dosing interval.
Estimates predicting appropriate doses, and
dosing intervals, for terbinafine were based on
the published range for MIC against A. fumiga-
tus. Because the MIC range of terbinafine against
A. fumigatus in humans is 0.02–5 mg/ml, initial
target peak therapeutic serum concentrations
were 1–4 mg/ml.
Dose proportionality of terbinafine was deter-
mined using AUC0–t, AUC0R‘, and Cmax, with
respect to the AUC0–t value, AUC0R‘ value, and
Cmax value of the lowest dose (3 mg/kg), according
to the following equations:
R~AUC0?t, 3, 7, or 15 mg=kg
AUC0?t, 3 mg=kg
and
R~C max3, 7, or 15 mg=kg
C max3 mg=kg
,
where R is the dose-proportionality ratio. Line-
arity was tested using a lack-of-fit F-test. In
addition, a power function relationship was used
to describe the relationship between AUC0–t,
AUC0R‘, Cmax, and Dose:
AUC~a(Dose)band C max~a(Dose)b,
where a represents the coefficient, and b repre-
sents the exponent of the power function
determined by regression (Excel, Microsoft, Red-
mond, Washington 98052, USA). If the AUC0–t
and AUC0R‘ dose relationship is linear, then the
exponent b should be in unity. Linearity was
indicated if the 95% confidence interval for the
exponent b included the value of 1.0.77
Following the oral administration of terbinafine
at three different doses, statistical comparisons of
mean plasma concentrations, at each sampling
time, and estimates of the pharmacokinetic pa-
rameters among the three doses, were made using
an analysis of variance. Statistical software was
used for analysis (SAS, Version 8.0, InnaPhase
Corporation, Cary, North Carolina 27513, USA).
RESULTS
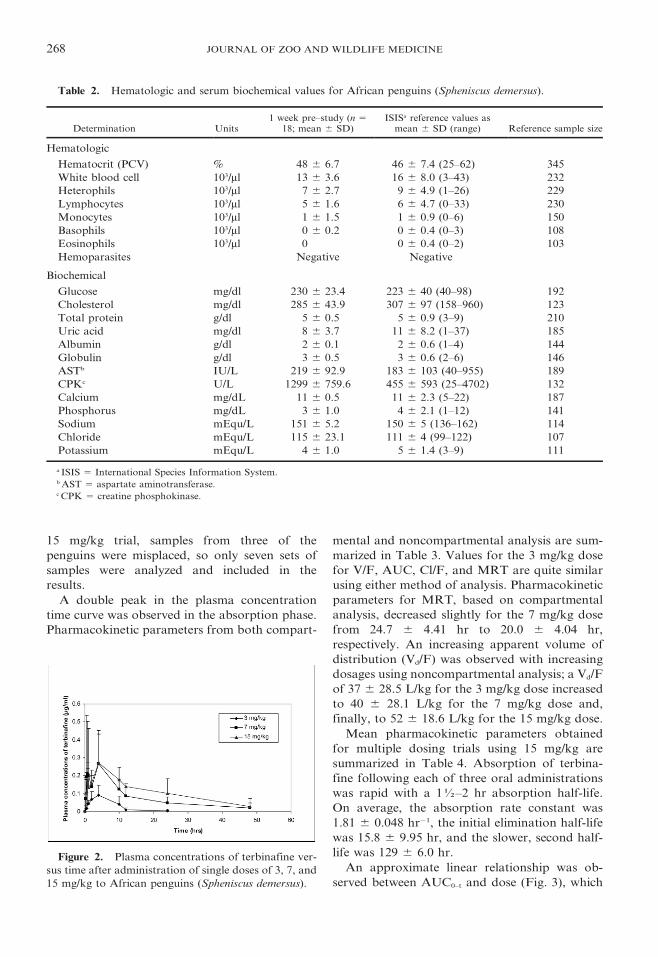
Results for initial penguin CBC and biochem-
istry analyses were within the normal range
described for this species (Table 2), with the
exception of slightly elevated creatine phospho-
kinase levels, and all birds were healthy through-
out the duration of the study.
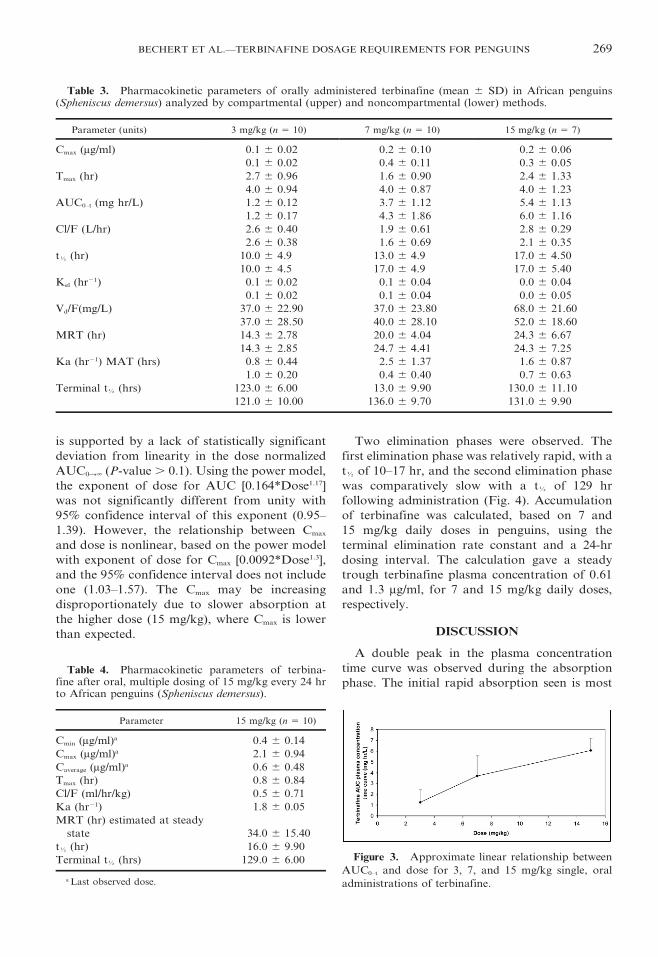
Plasma concentrations of terbinafine versus
time, after administration of single doses of 3, 7,
and 15 mg/kg, are presented in Figure 2. For the
BECHERT ET AL.—TERBINAFINE DOSAGE REQUIREMENTS FOR PENGUINS 267
15 mg/kg trial, samples from three of the
penguins were misplaced, so only seven sets of
samples were analyzed and included in the
results.
A double peak in the plasma concentration
time curve was observed in the absorption phase.
Pharmacokinetic parameters from both compart-
mental and noncompartmental analysis are sum-
marized in Table 3. Values for the 3 mg/kg dose
for V/F, AUC, Cl/F, and MRT are quite similar
using either method of analysis. Pharmacokinetic
parameters for MRT, based on compartmental
analysis, decreased slightly for the 7 mg/kg dose
from 24.7 6 4.41 hr to 20.0 6 4.04 hr,
respectively. An increasing apparent volume of
distribution (Vd/F) was observed with increasing
dosages using noncompartmental analysis; a Vd/F
of 37 6 28.5 L/kg for the 3 mg/kg dose increased
to 40 6 28.1 L/kg for the 7 mg/kg dose and,
finally, to 52 6 18.6 L/kg for the 15 mg/kg dose.
Mean pharmacokinetic parameters obtained
for multiple dosing trials using 15 mg/kg are
summarized in Table 4. Absorption of terbina-
fine following each of three oral administrations
was rapid with a 1K–2 hr absorption half-life.
On average, the absorption rate constant was
1.81 6 0.048 hr21, the initial elimination half-life
was 15.8 6 9.95 hr, and the slower, second half-
life was 129 6 6.0 hr.
An approximate linear relationship was ob-
served between AUC0–t and dose (Fig. 3), which
Table 2. Hematologic and serum biochemical values for African penguins (Spheniscus demersus).
Determination Units1 week pre–study (n 5
18; mean 6 SD)ISISa reference values as
mean 6 SD (range) Reference sample size
Hematologic
Hematocrit (PCV) % 48 6 6.7 46 6 7.4 (25–62) 345
White blood cell 103/ml 13 6 3.6 16 6 8.0 (3–43) 232
Heterophils 103/ml 7 6 2.7 9 6 4.9 (1–26) 229
Lymphocytes 103/ml 5 6 1.6 6 6 4.7 (0–33) 230
Monocytes 103/ml 1 6 1.5 1 6 0.9 (0–6) 150
Basophils 103/ml 0 6 0.2 0 6 0.4 (0–3) 108
Eosinophils 103/ml 0 0 6 0.4 (0–2) 103
Hemoparasites Negative Negative
Biochemical
Glucose mg/dl 230 6 23.4 223 6 40 (40–98) 192
Cholesterol mg/dl 285 6 43.9 307 6 97 (158–960) 123
Total protein g/dl 5 6 0.5 5 6 0.9 (3–9) 210
Uric acid mg/dl 8 6 3.7 11 6 8.2 (1–37) 185
Albumin g/dl 2 6 0.1 2 6 0.6 (1–4) 144
Globulin g/dl 3 6 0.5 3 6 0.6 (2–6) 146
ASTb IU/L 219 6 92.9 183 6 103 (40–955) 189
CPKc U/L 1299 6 759.6 455 6 593 (25–4702) 132
Calcium mg/dL 11 6 0.5 11 6 2.3 (5–22) 187
Phosphorus mg/dL 3 6 1.0 4 6 2.1 (1–12) 141
Sodium mEqu/L 151 6 5.2 150 6 5 (136–162) 114
Chloride mEqu/L 115 6 23.1 111 6 4 (99–122) 107
Potassium mEqu/L 4 6 1.0 5 6 1.4 (3–9) 111
a ISIS 5 International Species Information System.b AST 5 aspartate aminotransferase.c CPK 5 creatine phosphokinase.
Figure 2. Plasma concentrations of terbinafine ver-
sus time after administration of single doses of 3, 7, and
15 mg/kg to African penguins (Spheniscus demersus).
268 JOURNAL OF ZOO AND WILDLIFE MEDICINE
is supported by a lack of statistically significant
deviation from linearity in the dose normalized
AUC0R‘ (P-value . 0.1). Using the power model,
the exponent of dose for AUC [0.164*Dose1.17]
was not significantly different from unity with
95% confidence interval of this exponent (0.95–
1.39). However, the relationship between Cmax
and dose is nonlinear, based on the power model
with exponent of dose for Cmax [0.0092*Dose1.3],
and the 95% confidence interval does not include
one (1.03–1.57). The Cmax may be increasing
disproportionately due to slower absorption at
the higher dose (15 mg/kg), where Cmax is lower
than expected.
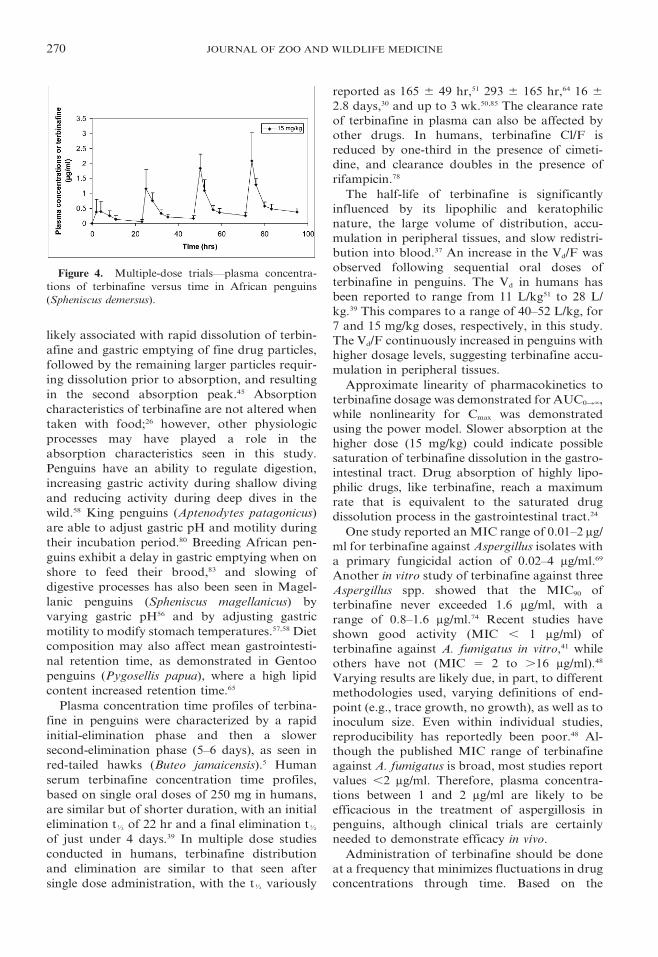
Two elimination phases were observed. The
first elimination phase was relatively rapid, with a
tK of 10–17 hr, and the second elimination phase
was comparatively slow with a tK of 129 hr
following administration (Fig. 4). Accumulation
of terbinafine was calculated, based on 7 and
15 mg/kg daily doses in penguins, using the
terminal elimination rate constant and a 24-hr
dosing interval. The calculation gave a steady
trough terbinafine plasma concentration of 0.61
and 1.3 mg/ml, for 7 and 15 mg/kg daily doses,
respectively.
DISCUSSION
A double peak in the plasma concentration
time curve was observed during the absorption
phase. The initial rapid absorption seen is most
Table 3. Pharmacokinetic parameters of orally administered terbinafine (mean 6 SD) in African penguins(Spheniscus demersus) analyzed by compartmental (upper) and noncompartmental (lower) methods.
Parameter (units) 3 mg/kg (n 5 10) 7 mg/kg (n 5 10) 15 mg/kg (n 5 7)
Cmax (mg/ml) 0.1 6 0.02 0.2 6 0.10 0.2 6 0.06
0.1 6 0.02 0.4 6 0.11 0.3 6 0.05
Tmax (hr) 2.7 6 0.96 1.6 6 0.90 2.4 6 1.33
4.0 6 0.94 4.0 6 0.87 4.0 6 1.23
AUC0–t (mg hr/L) 1.2 6 0.12 3.7 6 1.12 5.4 6 1.13
1.2 6 0.17 4.3 6 1.86 6.0 6 1.16
Cl/F (L/hr) 2.6 6 0.40 1.9 6 0.61 2.8 6 0.29
2.6 6 0.38 1.6 6 0.69 2.1 6 0.35
tK (hr) 10.0 6 4.9 13.0 6 4.9 17.0 6 4.50
10.0 6 4.5 17.0 6 4.9 17.0 6 5.40
Kel (hr21) 0.1 6 0.02 0.1 6 0.04 0.0 6 0.04
0.1 6 0.02 0.1 6 0.04 0.0 6 0.05
Vd/F(mg/L) 37.0 6 22.90 37.0 6 23.80 68.0 6 21.60
37.0 6 28.50 40.0 6 28.10 52.0 6 18.60
MRT (hr) 14.3 6 2.78 20.0 6 4.04 24.3 6 6.67
14.3 6 2.85 24.7 6 4.41 24.3 6 7.25
Ka (hr21) MAT (hrs) 0.8 6 0.44 2.5 6 1.37 1.6 6 0.87
1.0 6 0.20 0.4 6 0.40 0.7 6 0.63
Terminal tK (hrs) 123.0 6 6.00 13.0 6 9.90 130.0 6 11.10
121.0 6 10.00 136.0 6 9.70 131.0 6 9.90
Table 4. Pharmacokinetic parameters of terbina-fine after oral, multiple dosing of 15 mg/kg every 24 hrto African penguins (Spheniscus demersus).
Parameter 15 mg/kg (n 5 10)
Cmin (mg/ml)a 0.4 6 0.14
Cmax (mg/ml)a 2.1 6 0.94
Caverage (mg/ml)a 0.6 6 0.48
Tmax (hr) 0.8 6 0.84
Cl/F (ml/hr/kg) 0.5 6 0.71
Ka (hr21) 1.8 6 0.05
MRT (hr) estimated at steady
state 34.0 6 15.40
tK (hr) 16.0 6 9.90
Terminal tK (hrs) 129.0 6 6.00
a Last observed dose.
Figure 3. Approximate linear relationship between
AUC0–t and dose for 3, 7, and 15 mg/kg single, oral
administrations of terbinafine.
BECHERT ET AL.—TERBINAFINE DOSAGE REQUIREMENTS FOR PENGUINS 269
likely associated with rapid dissolution of terbin-
afine and gastric emptying of fine drug particles,
followed by the remaining larger particles requir-
ing dissolution prior to absorption, and resulting
in the second absorption peak.45 Absorption
characteristics of terbinafine are not altered when
taken with food;26 however, other physiologic
processes may have played a role in the
absorption characteristics seen in this study.
Penguins have an ability to regulate digestion,
increasing gastric activity during shallow diving
and reducing activity during deep dives in the
wild.58 King penguins (Aptenodytes patagonicus)
are able to adjust gastric pH and motility during
their incubation period.80 Breeding African pen-
guins exhibit a delay in gastric emptying when on
shore to feed their brood,83 and slowing of
digestive processes has also been seen in Magel-
lanic penguins (Spheniscus magellanicus) by
varying gastric pH56 and by adjusting gastric
motility to modify stomach temperatures.57,58 Diet
composition may also affect mean gastrointesti-
nal retention time, as demonstrated in Gentoo
penguins (Pygosellis papua), where a high lipid
content increased retention time.65
Plasma concentration time profiles of terbina-
fine in penguins were characterized by a rapid
initial-elimination phase and then a slower
second-elimination phase (5–6 days), as seen in
red-tailed hawks (Buteo jamaicensis).5 Human
serum terbinafine concentration time profiles,
based on single oral doses of 250 mg in humans,
are similar but of shorter duration, with an initial
elimination tK of 22 hr and a final elimination tK
of just under 4 days.39 In multiple dose studies
conducted in humans, terbinafine distribution
and elimination are similar to that seen after
single dose administration, with the tK variously
reported as 165 6 49 hr,51 293 6 165 hr,64 16 6
2.8 days,30 and up to 3 wk.50,85 The clearance rate
of terbinafine in plasma can also be affected by
other drugs. In humans, terbinafine Cl/F is
reduced by one-third in the presence of cimeti-
dine, and clearance doubles in the presence of
rifampicin.78
The half-life of terbinafine is significantly
influenced by its lipophilic and keratophilic
nature, the large volume of distribution, accu-
mulation in peripheral tissues, and slow redistri-
bution into blood.37 An increase in the Vd/F was
observed following sequential oral doses of
terbinafine in penguins. The Vd in humans has
been reported to range from 11 L/kg51 to 28 L/
kg.39 This compares to a range of 40–52 L/kg, for
7 and 15 mg/kg doses, respectively, in this study.
The Vd/F continuously increased in penguins with
higher dosage levels, suggesting terbinafine accu-
mulation in peripheral tissues.
Approximate linearity of pharmacokinetics to
terbinafine dosage was demonstrated for AUC0R‘,
while nonlinearity for Cmax was demonstrated
using the power model. Slower absorption at the
higher dose (15 mg/kg) could indicate possible
saturation of terbinafine dissolution in the gastro-
intestinal tract. Drug absorption of highly lipo-
philic drugs, like terbinafine, reach a maximum
rate that is equivalent to the saturated drug
dissolution process in the gastrointestinal tract.24
One study reported an MIC range of 0.01–2 mg/
ml for terbinafine against Aspergillus isolates with
a primary fungicidal action of 0.02–4 mg/ml.69
Another in vitro study of terbinafine against three
Aspergillus spp. showed that the MIC90 of
terbinafine never exceeded 1.6 mg/ml, with a
range of 0.8–1.6 mg/ml.74 Recent studies have
shown good activity (MIC , 1 mg/ml) of
terbinafine against A. fumigatus in vitro,41 while
others have not (MIC 5 2 to .16 mg/ml).48
Varying results are likely due, in part, to different
methodologies used, varying definitions of end-
point (e.g., trace growth, no growth), as well as to
inoculum size. Even within individual studies,
reproducibility has reportedly been poor.48 Al-
though the published MIC range of terbinafine
against A. fumigatus is broad, most studies report
values ,2 mg/ml. Therefore, plasma concentra-
tions between 1 and 2 mg/ml are likely to be
efficacious in the treatment of aspergillosis in
penguins, although clinical trials are certainly
needed to demonstrate efficacy in vivo.
Administration of terbinafine should be done
at a frequency that minimizes fluctuations in drug
concentrations through time. Based on the
Figure 4. Multiple-dose trials—plasma concentra-
tions of terbinafine versus time in African penguins
(Spheniscus demersus).
270 JOURNAL OF ZOO AND WILDLIFE MEDICINE

pharmacokinetic parameters of terbinafine calcu-
lated in this study, steady-state trough levels in
African penguins are predicted to occur in 2 wk
at 1.2 mg/ml, using 15 mg/kg dosages s.i.d., which
falls within the reported in vitro MIC90 range of
0.8–1.6 mg/ml for terbinafine against A. fumiga-
tus.74 This is less than the recommended dose of
30 mg terbinafine/kg given orally every 24 hr for
cats (Felis catus) and dogs (Canis lupus famil-
iaris),26 but is the same dosage recommended for
red-tailed hawks,5 and approximates the oral
dosage of 10–15 mg/kg given every 12–24 hr
generically recommended for avian species.15
Steady-state plasma levels of terbinafine in
humans are also reached within 10–14 days of
treatment.34
In vitro tests have demonstrated an additive or
synergistic effect when terbinafine was used in
combination with itraconazole or fluconazole49,69
and amphotericin B.69 However, negative results
of terbinafine and amphotericin B in vitro have
also been reported,14,49 and one study demon-
strated a difference of effect based on time of
administration.3 Data are sparse on the efficacy
of combination therapy, and several combina-
tions that demonstrated synergy in vitro failed to
do so in animal models.3 Clearly, again, in vivo
trials are needed to determine actual efficacy of
potential additive or synergistic effects, or both,
of drug combinations.73
Human clinical trials have yielded some
promising results for treatment of lower respira-
tory tract Aspergillus infections using terbinafine.
In one study, fourteen patients given between 5
and 15 mg terbinafine/kg/day for 84–264 days
were all considered microbiologically cured, and
eight were clinically cured.71 Other clinical case
reports have also demonstrated the efficacy of
terbinafine for treatment of refractory pulmonary
aspergillosis,55,70,72 as well as for treatment and
prevention of Aspergillus infection in lung-trans-
plant patients.34 However, controlled trials and
prospective observational studies are still needed
to establish the correlation of in vitro susceptibil-
ity with the clinical outcome.11 Similarly, recom-
mended dosages of terbinafine for treatment of
aspergillosis in penguins need to be used, in
controlled trials, to demonstrate actual clinical
efficacy.
Future alternative therapeutic treatments for
A. fumigatus infections may include vaccinations
that boost cell-mediated immunity.6,7,38,43 Mater-
nal or parental antibody passage in birds can be
achieved through egg yolk or crop milk.66
Prenatal transfer of Aspergillus spp. antibodies
has been demonstrated in African black-footed
penguins, and evidence supported a potential
protective role of maternal antibodies against
aspergillosis for S. demersus chicks during the
first 4 wk posthatch.32 Additionally, because of
the significant correlation of Aspergillus antibody
levels between female penguins and their eggs, it
was suggested that penguin eggs could be used to
predict the prevalence of Aspergillus in wild
penguin populations.32 Alternative drug therapies
are also likely to emerge in the future. Recent
sequencing of the A. fumigatus genome,52 coupled
with the genetic tools now available for research
on antifungal drug resistance mechanisms, may
eventually lead to a shift from random screens for
antifungal agents to screens against specific
molecular targets.53
CONCLUSIONS
Based on these results, it is recommended that
a 15 mg/kg per day oral dose of terbinafine be
used for the treatment of aspergillosis in penguins
to provide steady-state trough plasma concentra-
tions above the MIC of 1 mg/ml. Patients with
either liver or renal impairment should receive
lower dosages. Terbinafine has few side effects
and has no reported interactions with other
agents, although cimetidine and rifampin may
alter the clearance rate of terbinafine. However,
because the drug is eliminated so slowly over time
and accumulates in tissues, long-term multiple
dosing, as well as clinical efficacy trials for
treatment of aspergillosis, should be conducted
with penguins before safe and therapeutic dosing
regimens can be confirmed.
Acknowledgments: The authors thank the staff
at the Seneca Park Zoo, especially Garrett
Caulkins, B.S., L.V.T., Seneca Park Zoo Animal
Health Center Supervisor, for conducting the
dosing trials in African penguins. They also
acknowledge the work of Carol Buckley, who
analyzed plasma samples at the University of
Pennsylvania, New Bolton Center. This study
was funded by the Morris Animal Foundation.
LITERATURE CITED
1. Back, D., and J. Tija. 1990. Azoles and allyl-
amines: the clinical implications of interaction with
cytochrome P-450 enzymes. J. Dermatol. Treat. 1: 11–
13.
2. Balfour, J. A., and D. Faulds. 1992. Terbinafine.
A review of its pharmacodynamic and pharmacokinetic
properties, and therapeutic potential in superficial
mycoses. Drugs 43: 259–284.
BECHERT ET AL.—TERBINAFINE DOSAGE REQUIREMENTS FOR PENGUINS 271
3. Barchiese, F., L. F. Di Francisco, P. Compag-
nucci, D. Arzeni, A. Giacometti, and G. Scalise. 1998.
In vitro interaction of terbinafine with amphotericin B,
fluconazole and itraconazole against clinical isolates of
Candida albicans. J. Antimicrob. Chemother. 41: 59–65.
4. Battig, F., M. Nefzger, and G. Schulz. 1987.
Major biotransformation routes of some allylamine
antimycotics. In: Fromtling, R. A. (ed.). Recent Trends
in the Discovery, Development and Evaluation of
Antifungal Agents. JR Prous Science Publishers,
Barcelona, Spain. Pp. 479–495.
5. Bechert, U. S., J. M. Christensen, R. Poppenga, S.
A. Fahmy, P. Redig. (In Press for June 2010)
Pharmacokinetics of terbinafine after single dose
administration in red-tailed hawks (Buteo jamaicensis).
J. Avian Med. Surg.
6. Bellocchio, S., S. Bozza, C. Montagnoli, K.
Perruccio, R. Gaziano, L. Pitzurra, and L. Romani.
2005. Immunity to Aspergillus fumigatus: the basis
for immunotherapy and vaccination. Med. Mycol.
43(Suppl. 1): 181–188.
7. Brown, S., C. Andreasen, A. Monroe, and P.
Noah. 1996. Results of Aspergillus vaccine trial in tufted
puffins. Proc. Int. Assoc. Aqua. Anim. Med. Pp. 10–12.
8. Bunting, E. M., N. A. Madi, S. Cox, T. Martin-
Jimenez, H. Fox, and G. V. Kollias. 2009. Evaluation
of oral itraconazole administration in captive Hum-
boldt penguins (Spheniscus humboldti). J. Zoo Wildl.
Med. 40: 508–518.
9. Campbell, T. W. 1986. Mycotic diseases. In:
Harrison, G. J., and L. R. Harrison (eds.), Clinical
Avian Medicine and Surgery. W. B. Saunders Co.,
Philadelphia, Pennsylvania. Pp. 464–466.
10. Carrasco, L., J. S. Lima, Jr., D. C. Halfen, F. J.
Salguero, P. Sanchez-Cordon, and G. Becker. 2001.
Systemic aspergillosis in an oiled Magallanic penguin
(Spheniscus magellanicus). J. Vet. Med. B 48: 551–554.
11. Chamilos, G., and D. P. Kontoyiannis. 2005.
Update on antifungal drug resistance mechanism of
Aspergillus fumigatus. Drug Resist. Updates 8: 344–358.
12. Clayton, Y. M. 1987. The in vitro activity of
terbinafine against uncommon fungal pathogens. In:
Fromtling, R. A. (ed.). Recent Trends in the Discovery,
Development and Evaluation of Antifungal Agents. JR
Prous Science Publishers, Barcelona, Spain. Pp. 433–439.
13. Clubb, S. L. 1986. Therapeutics: individual and
flock treatment regimens. In: Harrison, G. J., and L. R.
Harrison (eds.). Clinical Avian Medicine and Surgery.
W. B. Saunders Co., Philadelphia, Pennsylvania. Pp.
338–339.
14. Cuenca-Estrella, M. 2004. Combinations of
antifungal agents in therapy—what value are they? J.
Antimicrob. Chemother. 54: 854–869.
15. Dahlhausen, B., J. G. Lindstrom, and S.
Radabaugh. 2002. The use of terbinafine hydrochloride
in the treatment of avian fungal disease. Proc. Assoc.
Avian Vet. Pp. 35–39.
16. Debruyne, D., and A. Coquerel. 2001. Pharma-
cokinetics of antifungal agents in onychomycoses. Clin.
Pharmacokinet. 40: 441–472.
17. Denouel, J., H. P. Keller, P. Schaub, C.
Delaborde, and H. Humbert. 1995. Determination of
terbinafine and its desmethyl metabolite in human
plasma by high performance liquid chromatography. J.
Chromato. Biomed. Applic. 663: 353–359.
18. Diebold, E. N., S. Branch, and L. Henry. 1999.
Management of penguin populations in North Amer-
ican zoos and aquariums. Marine Ornithol. 27: 171–
176.
19. Di Somma, A., T. Bailey, C. Silvanose, and C.
Garcia-Martinez. 2007. The use of voriconazole for the
treatment of aspergillosis in falcons (Falco species). J.
Avian Med. Surg. 21: 307–316.
20. Elewski, B., and A. Tavakkol. 2005. Safety and
tolerability of oral antifungal agents in the treatment of
fungal nail disease: a proven reality. Ther. Clin. Risk
Manage. 1: 299–306.
21. Flach, E. J., M. F. Stevenson, and G. M.
Henderson. 1990. Aspergillosis in gentoo penguins
(Pygoscelis papua) at Endinburgh Zoo, 1964 to 1988.
Vet. Rec. 126: 81–85.
22. Flammer, J. 1994. Antimicrobial therapy. In:
Ritchie, B. W., G. J. Harrison, and L. R. Harrison
(eds.). Avian Medicine: Principles and Application.
Wingers Publishing, Lake Worth, Florida. Pp. 434–456.
23. Furebring, M., G. Oberg, and J. Sjolin. 2000.
Side-effects of amphotericin B lipid complex (Abelcet)
in the Scandinavian population. Bone Marrow Trans.
25: 341–343.
24. Gao, J. Z., M. A. Husain, R. Motheram, D. A.
Gray, W. D. Benedek, W. D. Fiske, W. J. Doll, E.
Sandefer, R. C. Page, and G. A. Digenis. 2007.
Investigation of human pharmacoscintigraphic behav-
ior of two tablets and a capsule of a high dose, poorly
soluble/highly permeable drug (Efavirenz). J. Pharm.
Sci. 96: 2970–2977.
25. Ghannoum, M. A., and L. B. Rice. 1999.
Antifungal agents: mode of action, mechanisms or
resistance, and correlation of these mechanisms with
bacterial resistance. Clin. Microbiol. Rev. 12: 501–
517.
26. Giguere, S., and P. M. Dowling. 2007. Antimi-
crobial Therapy in Veterinary Medicine, 4th ed. Black-
well Publishing, Hoboken, New Jersey. Pp. 301–320.
27. Girolamo, G. D., G. A. Keller, A. R. de Los
Santos, D. Schere, and C. D. Gonzales. 2008. Bio-
equivalence of two tablet formulations without and
with mathematical adjustment for basal thyroxine levels
in healthy Argentinean volunteers: a single-dose,
randomized, open-label, crossover study. Clin. Thera.
30: 2015–2023.
28. Goudard, M., Y. Buffard, H. Ferrari, and P.
Regli. 1986. Spectre d’action in vitro d’un nouvel
anrifongique derive de la naftifine: la terbinafine (SF
86-327). Pathol. Biol. (Paris) 34: 680–683.
29. Goudard, M., P. Regli, Y. Buffard, and B.
Gabriel. 1988. Sensibilite in vitro des Aspergillus a la
terbinafine: etude comparative avec l’amphotericine B,
la 5-fluorcytosine et le ketoconazole. Pathol. Biol.
(Paris) 36: 139–143.
272 JOURNAL OF ZOO AND WILDLIFE MEDICINE
30. Gough, K., M. Hutchison, O. Keene, B. Byrom,
S. Ellis, L. Lacey, and J. Mckellar. 1995. Assessment of
dose proportionality: report from the statisticians in the
pharmaceutical industry/pharmacokinetics UK joint
working party. Drug Info. J. 29: 1039–1048.
31. Graczyk, T. K., and J. F. Cockrem. 1995.
Aspergillus spp. seropositivity in New Zealand pen-
guins. Mycopathologia 131: 179–184.
32. Graczyk, T. K., and M. R. Cranfield. 1995.
Maternal transfer of anti-Aspergillus spp. immunoglob-
ulins in African black-footed penguins (Spheniscus
demersus). J. Wildl. Dis. 31: 545–549.
33. Gupta, A. K., R. K. Scher, and P. DeDoncker.
1997. Current management of onychomycosis. Derma-
tol. Clin. 15: 121–135.
34. Harari, S., E. DeJuli, G. Ziglio, G. Cimino, and
G. F. Schiraldi. 1996. Is terbinafine an alternative
treatment for non-invasive Aspergillus bronchitis in
lung transplant recipients? Eur. Respir. J. 9: 367.
35. Hawkey, C. M., S. L. Pugsley, and J. A. Knight.
1984. Abnormal heterophils in a king shag with
aspergillosis. Vet. Rec. 114: 322–324.
36. Hiratani, T., Y. Asagi, and H. Yamaguchi. 1991.
Evaluation of in vitro anti-mycotic activity of terbina-
fine, a new allylamine agent. Jpn. J. Med. Mycol. 32:
323–332.
37. Hosseini-Yeganeh, M., and A. J. McLachlan.
2002. Physiologically based pharmacokinetic model for
terbinafine in rats and humans. Antimicrob. Agents
Chemother. 46: 2219–2228.
38. Ito, J. I., and J. M. Lyons. 2002. Vaccination of
corticosteroid immunosuppressed mice against invasive
pulmonary aspergillosis. J. Infect. Dis. 186: 869–871.
39. Jensen, J. 1989. Clinical pharmacokinetics of
terbinafine. Clin. Exper. Dermatol. 14: 110–113.
40. Jensen, J. C. 1990. Pharmacokinetics of Lamisil
in humans. J. Dermatol. Treat. 2: 15–18.
41. Jessup, C. J., M. A. Ghannoum, and N. S.
Ryder. 2000. An evaluation of the in vitro activity of
terbinafine. Med. Mycol. 38: 155–159.
42. Khan, Z. U., M. Pal, D. K. Paliwal, and V. N.
Damodaran. 1977. Aspergillosis in imported penguins.
Sabouraudia 15: 43–45.
43. Kisch, A. I., R. M. Echols, and R. P. Maydew.
1979. Protective efficacy of antifungal immunization in
opportunistic murine pulmonary aspergillosis. Clin.
Res. 27: 83–88.
44. Levy, H., D. A. Horak, B. R. Tegtmeier, S. B.
Yokota, and S. J. Forman. 1992. The value of
bronchoalveolar lavage and bronchial washings in the
diagnosis of invasive pulmonary aspergillosis. Respir.
Med. 86: 243–248.
45. Li, J., H. Huynh, and E. Chan. 2002. Evidence
for dissolution rate-limited absorption of COL-3, a
matrix metalloproteinase inhibitor, leading to the
irregular absorption profile in rats after oral adminis-
tration. Pharm. Res. 19: 1655–1662.
46. McClellan, K. J., L. R. Wiseman, and A.
Markham. 1999. Terbinafine: an update of its use in
superficial mycoses. Drugs 58: 179–202.
47. Monroe, A., P. Noah, and S. Brown. 1994.
Comparison of medical treatment regimes for aspergil-
losis in captive tufted puffins (Lunda cirrhata). Penguin
Conserv. 7: 1–5.
48. Moore, C., C. Walls, and D. Denning. 2001. In
vitro activities of terbinafine against Aspergillus species
in comparison with those of itraconazole and ampho-
tericin B. Antimicrob. Agents Chemother. 45: 1882–
1885.
49. Mosquera, J., A. Sharp, C. B. Moore, P. A.
Warn, and D. W. Denning. 2002. In vitro interaction of
terbinafine with itraconazole, fluconazole, amphotericin
B and 5-flucytosine against Aspergillus spp. J. Anti-
microb. Chemother. 50: 189–194.
50. Nedelman, J., E. Gibiansky, B. Robbins, J.
Cramer, J. Riefler, T. Lin, and J. Meligeni. Pharmaco-
kinetics and pharmacodynamics of multiple-dose ter-
binafine. J. Clin. Pharmacol. 36: 452–461.
51. Nejjam, F., M. Zagula, M. Cabiac, N. Guessous,
H. Humbert, and H. Lakhdar. 1995. Pilot study of
terbinafine in children suffering from tinea capitis:
evaluation of efficacy, safety and pharmacokinetics.
Brit. J. Dermatol. 132: 98–105.
52. Nierman, W. C., A. Pain, M. J. Anderson, J. R.
Wortman, H. S. Kim, and J. Arroyo. 2006. Genome
sequence of the pathogenic and allergenic filamentous
fungus Aspergillus fumigatus. Nature 438: 1151–1156.
53. Odds, F. C., A. J. Brown, and N. A. Gow. 2003.
Antifungal agents: mechanisms of action. Trends
Microbiol. 11: 279–299.
54. Orosz, S., and D. L. Frazier. 1995. Antifungal
agents: a review of their pharmacology and therapeutic
indications. J. Avian Med. Surg. 9: 8–18.
55. Perez, A. 1999. Terbinafine: broad new spec-
trum of indications in several subcutaneous and
systemic and parasitic diseases. Mycoses. 42(Suppl. 2):
111–114.
56. Peters, G. 1997. A new device for monitoring
gastric pH in free-ranging animals. Am. J. Physiol. 273:
G748–G753.
57. Peters, G. 1997. A reference electrode with free-
diffusion liquid junction for electrochemical measure-
ments under changing pressure conditions. Anal. Chem.
69: 2362–2366.
58. Peters, G. 2004. Measurement of digestive
variables in free-living animals: gastric motility in
penguins during foraging. Mem. Natl. Inst. Polar Res.
Spec. 58: 203–209.
59. Petranyi, G., J. Meingassner, and H. Mieth.
1987. Antifungal activity of allylamine derivative
terbinafine in vitro. Antimicrob. Agents Chemother.
31: 1365–1368.
60. Petranyi, G., N. Ryder, and A. Stutz. 1984.
Allylamine derivatives: new class of synthetic antifungal
agents inhibiting fungal squalene epoxidase. Science
224: 1239–1241.
61. Redig, P. 1983. Aspergillosis. In: Kirk, R. W.
(ed.). Current Veterinary Therapy VIII. Small Animal
Practice, W. B. Saunders Co., Philadelphia, Pennsylva-
nia. Pp. 611–613.
BECHERT ET AL.—TERBINAFINE DOSAGE REQUIREMENTS FOR PENGUINS 273
62. Redig, P. 2000. Fungal diseases. In: Samour, J.
(ed.), Avian Medicine. Mosby, London, United King-
dom. P. 275–291.
63. Ritchie, B. W., and G. J. Harrison. 1994.
Formulary. In: Ritchie, B. W., G. J. Harrison, and L.
R. Harrison (eds.). Avian Medicine: Principles and
Application. Wingers Publishing, Lake Worth, Florida.
Pp. 457–478.
64. Robbins, B., C. Chang, J. Cramer, S. Garreffa,
B. Hafkin, T. Hunt, and J. Meligeni. 1996. Safe co-
administration of terbinafine and terfenadine: a place-
bo-controlled crossover study of pharmacokinetic and
pharmacodynamic interactions in healthy volunteers.
Clin. Pharmacol. Therap. 59: 275–283.
65. Roby, D. D., K. L. Brink, and A. R. Place. 1989.
Relative passage rates of lipid and aqueous digesta in
the formation of stomach oils. Auk 106: 303–313.
66. Rose, M. E., and E. Orleans. 1981. Immuno-
globulins in the egg, embryo and young chick. Dev.
Comp. Immunol. 5: 15–20.
67. Ryder, N. S. 1992. Terbinafine: mode of action
and properties of the squalene epoxidase inhibition.
Brit. J. Dermatol. 126: 2–7.
68. Ryder, N. S., and B. Favre. 1997. Antifungal
activity and mechanism of action of terbinafine. Rev.
Contemp. Pharmacother. 8: 275–287.
69. Ryder, N. S., and I. Leitner. 2001. Synergistic
interaction of terbinafine with triazoles or amphotericin
B against Aspergillus species. Med. Mycol. 39: 91–95.
70. Schiraldi, G. F., S. L. Cicero, M. D. Colombo,
D. Rossato, M. Ferrarese, and E. Soresi. 1996.
Refractory pulmonary aspergillosis: compassionate trial
with terbinafine. Brit. J. Dermatol. 134(Suppl. 46): 25–
29.
71. Schiraldi, G., and M. Colombo. 1997. Potential
use of terbinafine in the treatment of aspergillosis. Rev.
Contemp. Pharmacother. 8: 349–356.
72. Schiraldi, G. F., M. D. Colombo, S. Harari, S.
Lo Cicero, G. Ziglio, M. Ferrarese, D. Rossato, and E.
Soresi. 1996. Terbinafine in the treatment of non-
immunocompromised compassionate cases of broncho-
pulmonary aspergillosis. Mycoses 39: 5–12.
73. Schiraldi, G. F., G. Gramegna, C. DeRosa, S. L.
Cicero, P. Capone, M. Ferrarese, and E. Sbicego. 2003.
Chronic pulmonary aspergillosis: current classification
and therapy. Curr. Opin. Investig. Drugs 4: 186–191.
74. Schmitt, H., E. Bernard, J. Andrade, F. Ed-
wards, B. Schmitt, and D. Armstrong. 1988. MIC and
antifungal activity of terbinafine against clinical isolates
of Aspergillus spp. Antimicrob. Agents Chemother. 32:
780–781.
75. Shadomy, S., A. Espinell-Ingroff, and R. J.
Gebhart. 1985. In vitro studies with SF 86-327, a new
orally active allylamine derivative. Sabouraudia 23:
125–132.
76. Shannon, D. 1992. Treatment with itraconazole
of penguins suffering from aspergillosis. Vet. Rec. 130:
479.
77. Shargel, L., S. Wu-Pong, and A. B. Yu. 2005.
Applied Biopharmaceutics and Pharmacokinetics, 5th
ed. McGraw Hill, New York, New York. Pp. 185–196.
78. Shear, N., L. Drake, A. K. Gupta, J. Lambert,
and R. Yaniv. 2000. The implications and management
of drug interactions with itraconazole, fluconazole and
terbinafine. Dermatology 201: 196–203.
79. Stevens, D. A., V. L. Kan, M. A. Judson, V. A.
Morrison, S. Dummer, D. W. Denning, J. E. Bennett,
T. J. Walsh, T. F. Patterson, and G. A. Pankey. 2000.
Practice guidelines for diseases caused by Aspergillus.
Clin. Inf. Dis. 30: 696–709.
80. Thouzeau, C., G. Peters, C. Le Bohec, and Y. Le
Maho. 2004. Adjustments of gastric pH, motility and
temperature during long-term preservation of stomach
contents in free-ranging incubating king penguins. J.
Exper. Biol. 207: 2715–2724.
81. Tomee, J. F., G. P. Mannes, W. van der Bij, T.
S. van der Werf, W. J. de Boer, G. H. Koeter, and H. K.
Kauffman. 1996. Serodiagnosis and monitoring of
Aspergillus infections after lung transplantation. Ann.
Intern. Med. 125: 197–201.
82. Vickers, A. E., J. R. Sinclair, M. Zollinger, F.
Heitz, U. Glanzel, L. Johanson, and V. Fischer. 1999.
Multiple cytochrome P-450sb involved in the metabolis
of terbinafine suggest a limited potential for drug-drug
interactions. Drug Metab. Dispos. 27: 1029–1038.
83. Wilson, R. P., P. G. Ryan, and M. P. Wilson.
1989. Sharing food in the stomachs of seabirds between
adults and chicks: a case for delayed gastric emptying.
Comp. Biochem. Physiol. 94A: 461–466.
84. Xavier, M. O., M. P. Soares, A. R. Meinerz, M.
O. Nobre, L. G. Osorio, R. P. da Silva Filho, and M. C.
Meireles. 2007. Aspergillosis: a limiting factor during
recovery of captive Magellanic penguins. Braz. J.
Microbiol. 38: 480–484.
85. Zehender, H., M. Cabiac, J. Denouel, J.
Faergemann, P. Donatsch, K. Kutz, and H. Humbert.
1994. Elimination kinetics of terbinafine from human
plasma and tissues following multiple-dose administra-
tion, and comparison with 3 main metabolites. Drug
Invest. 8: 203–210.
86. Zehender, H., J. Denouel, M. Roy, L. Saux, and
P. Schaub. 1995. Simultaneous determination of
terbinafine (Lamisil) and five metabolites in human
plasma and urine by high-performance liquid chroma-
tography using on-line solid-phase extraction. J. Chro-
mato. Biomed. Applic. 664: 347–355.
87. Zielozienski-Roberts, K., and C. Cray. 1998. An
update on the application of aspergillosis antigen
diagnostic testing. Proc. Ann. Conf. Assoc. Avian
Vet. Pp. 95–97.
88. Zucca, P. 2000. Infectious diseases. In: Samour,
J. (ed.). Avian Medicine. Mosby, London, United
Kingdom. Pp. 275–287.
Received for publication 16 October 2009
274 JOURNAL OF ZOO AND WILDLIFE MEDICINE




























