Embed Size (px)
Citation preview

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
Journal of Clinical Psychology in Medical Settings, Vol. 8, No. 4, December 2001 ( c© 2001)
Posttraumatic Stress in Survivors of Childhood Cancer and Mothers:Development and Validation of the Impact of Traumatic StressorsInterview Schedule (ITSIS)
Anne E. Kazak,1,3,6 Lamia P. Barakat,2 Melissa Alderfer,3 Mary T. Rourke,3 Kathleen Meeske,4 Paul R. Gallagher,3
Avital Cnaan,1,3 and Margaret L. Stuber5
This study presents initial data validating the use of a new instrument, the Impact of TraumaticStressors Interview Schedule (ITSIS), to assess the occurrence of cancer-related posttraumaticstress in childhood cancer survivors and their mothers. Sixty-six child/adolescent cancer sur-vivors and 64 of their mothers, as well as 130 young adult survivors, completed the ITSISand other measures of posttraumatic stress and general distress. Five ITSIS factors wereidentified for the mothers and for the young adult survivors, and three ITSIS factors wereidentified for the child/adolescent survivors. Factors in all three samples reflected symptomsof posttraumatic distress, concern over medical late effects, communication, and changes inself due to cancer. Only young adult survivors had a factor reflecting a positive engagementwith the cancer history. Factors correlated with validation measures in predicted ways. Thefindings further the conceptualization of posttraumatic stress in pediatric cancer by describ-ing the traumatic experience for survivors and mothers. Comparing factors across samplesallows an examination of different influences of cancer within families and over the course ofdevelopment.
KEY WORDS: childhood cancer; posttraumatic stress disorder (PTSD); families; survival.
Symptoms consistent with posttraumatic stressdisorder (PTSD) have been noted clinically in childand adolescent cancer patients (Nir, 1987), and em-pirical studies have documented its occurrence inchildhood cancer survivors and their parents. For
1The University of Pennsylvania, Department of Pediatrics,Philadelphia, Pennsylvania.
2Department of Psychology, Drexel University, Philadelphia,Pennsylvania.
3The Children’s Hospital of Philadelphia, Philadelphia,Pennsylvania.
4Children’s Hospital of Los Angeles, Los Angeles, California.5The University of California at Los Angeles, Los Angeles,California.
6Correspondence should be addressed to Anne E. Kazak, Divi-sion of Oncology, The Children’s Hospital of Philadelphia, WoodBuilding, 4th Floor, 324 S. 34th Street, Philadelphia, Pennsylvania19104-4399; e-mail: [email protected].
example, Pelcovitz and colleagues found, in a smallsample, that 17% of adolescent cancer survivors and25% of their mothers fulfilled diagnostic criteria forPTSD (Pelcovitz et al., 1996; 1998). Other estimateshave been more modest (e.g., Manne, Du Hamel,Gallelli, Sorgen, & Redd, 1998), but most reports re-veal clinically significant levels of posttraumatic stresssymptoms in survivors of childhood cancer and theirparents (PTSS; Barakat et al., 1997; Hobbie et al.,2000; Kazak et al., 1997, 1998). These findings sup-port the applicability of a trauma model to childhoodcancer (Stuber, Kazak, Meeske, & Barakat, 1998), butthey do not provide the level of detail necessary to un-derstand specifics of the traumatic reaction to child-hood cancer, or to guide interventions aimed at theprevention or reduction of posttraumatic symptoms.
To provide a viable and practical approach to theassessment of ongoing, distressing aspects of cancer
307
1068-9583/01/1200-0307$19.50/0 C© 2001 Plenum Publishing Corporation

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
308 Kazak, Barakat, Alderfer, Rourke, Meeske, Gallagher, Cnaan, and Stuber
for survivors and their parents, we created the Impactof Traumatic Stressors Interview Schedule (ITSIS;Kazak, Stuber, Barakat, & Meeske, 1996). The ITSIScan be used as a supplement to pencil-and-papermeasures assessing generic posttraumatic stress sym-ptoms and to structured psychiatric interviews. It pro-vides a way to assess (a) which aspects of cancerdiagnosis and treatment contribute to the experi-ence of posttraumatic stress, (b) perceptions of on-going and future medical problems related to cancer,(c) perceptions of changes in self due to cancer andtreatment, (d) communication among family mem-bers and others regarding cancer and its treatment,and (e) attributions of causality related to the can-cer. Each of these areas was selected to provide use-ful information for the elaboration of a conceptualunderstanding of childhood cancer as a traumaticstressor, and to guide the development and evalua-tion of intervention approaches to prevent or reduceposttraumatic stress in families of childhood cancersurvivors.
A previous report (Kazak et al., 1996) providedinformation on the development of the ITSIS, as wellas on its utility in describing the specific forms ofposttraumatic stress in a group of survivors and theirmothers. That report gave promising evidence for as-sociations between ITSIS responses and paper-and-pencil measures of posttraumatic stress symptoms,and demonstrated that the ITSIS can procure de-tailed information from individuals and within fami-lies about content areas pertinent to adjustment afterchildhood cancer and treatment.
This report represents a next step in ITSIS devel-opment and validation. A primary goal was to demon-strate validity of the ITSIS by reporting the resultsof a factor analysis with three different samples. Weaimed to demonstrate convergent validity by examin-ing correlations between obtained factor scores andother measures of distress. In addition, the use of mul-tiple samples allowed us to examine two questions ofinterest. First, the meaning of cancer and survivor-ship appears to differ for different family members.Comparing factor structures in samples of mothersand survivors allows an exploration of similarities anddifferences in ways in which cancer affects individualswith different roles in the family, and can further de-velop a family-based understanding of the effects ofchildhood cancer. Second, because we believe that themeaning of having had cancer is likely to change overthe course of development, we planned to use the IT-SIS to explore developmental variables. ComparingITSIS factor structure in a sample of young adults
with that in a sample of children and adolescents al-lows a first, albeit preliminary, look at this issue.
METHOD
The data reported in this paper were obtainedfrom two separate studies of survivors of childhoodcancer. The first sample, a group of 130 young adultsurvivors, was part of a larger study of long-term psy-chological effects of cancer diagnosis and treatmentbeing conducted at a large East Coast major teachinghospital. Patients were included if they were between18 and 36 years old, were at least 2 years from the endof their treatment, and had been disease-free for atleast 5 years. Young adult survivors who met the in-clusion criteria listed here were sent a letter describ-ing the study. Follow-up telephone calls were made todescribe the study in more detail and to schedule aninterview.7
The second sample was drawn from the second,(interview) phase of a larger two-site study at ma-jor teaching hospitals on the east and west coasts ofthe United States. Childhood cancer survivors andtheir parents (n = 309) and comparison families (n =219) participated in the first (questionnaire) phase(Barakat et al., 1997; Kazak et al., 1997, 1998; Stuberet al., 1997). Patients were included in that study ifthey were English-speaking, between the ages of 8 and20 (or the mother of such a child), and off cancer treat-ment for a minimum of 1 year. All mother and survivorparticipants from the first phase of the study who livedwithin a 2-hour drive of the hospitals were sent a letterdescribing the second phase. They had been informedthat the study had two phases at the time of their orig-inal consent. Follow-up telephone calls were made todescribe the second phase in more detail and to sched-ule an interview. A subset of participants (66 child sur-vivors and 64 of their mothers) from the first phaseparticipated in this second phase of that study (seeKazak et al., 1997, for a summary of recruitment statis-tics). Data from the first phase indicated comparabil-ity between the sites with regard to patient recruit-ment, participation rates, and lack of significant sitedifferences on demographic and outcome variables.
7Four hundred seventy seven eligible young adults were identifiedfrom hospital records. Of those, 257 were lost to follow up. Ninetyof the eligible participants contacted refused to participate, and130 participated. The participation rate was 59%. Reasons givenfor not participating included scheduling difficulties (young adultswere too busy, work schedules were inflexible, too far to travel),lack of interest, and not wanting to revisit the past.

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
Impact of Traumatic Stressors 309
Participants
Participants were 130 young adult survivors ofchildhood cancer, 66 children and adolescent sur-vivors of cancer who previously completed the first(questionnaire) phase of the larger study, and 64 ofthe child/adolescent survivors’ mothers.
Young Adult Survivors
Sixty-four males (49.2%) and 66 females (50.2%)participated. Participants ranged in age from 18to 36 (M = 25, SD = 4.04). Their mean age atthe time of cancer diagnosis was 10 (SD = 4.96,range = 0–19). Survivors had been off treatmentranging from 3 to 29 years (M = 13, SD = 5.40).Participant diagnoses generally reflect the distri-bution of diseases treated at our pediatric can-cer center: 25.2% acute lymphoblastic leukemia,14.6% non-Hodgkin’s lymphoma, 13.0% Hodgkin’slymphoma, 13.0% sarcomas, 8.9% brain tumor, 8.1%Wilms tumor, and the remaining 17.2% bone tu-mors, neuroblastoma, and other cancers. Most pa-tients were Caucasian (87.8%), with 4.6% Black,2.3% Hispanic, 1.5% Asian, and 3.1% describingthemselves as “other.” An overwhelming majority(98.5%) had at least graduated from high school,with 58% having attended at least some of a 4-yearcollege. Approximately half (48.9%) were employedfull-time, with 18.3% reporting part-time employ-ment, 21.4% reporting full-time student status, 4.6%reporting to be homemakers, and 6.9% reporting un-employment. The young adults’ median income was$10,000–19,000.
Mothers and Child Survivors
Half (47%) of the child/adolescent survivor par-ticipants were females. At the time of this study,the survivor participants ranged in age from 6 to 19(M = 12.74, SD = 3.73). Their mean age at the timeof cancer diagnosis was 5.55 years (SD= 3.84). Theirmean off-treatment period was 4.86 years, (SD= 3.31years). Participant diagnoses generally reflect the dis-eases treated at our pediatric cancer centers and are asfollows: 45.5% acute lymphoblastic leukemia, 12.1%non-Hodgkin’s lymphoma, 9.1% Wilms tumor, 9.1%acute non-lymphoblastic leukemia, 6.1% sarcomas,with the remaining 18.1% bone tumors, Hodgkin’slymphoma, and other cancers. Mothers’ age averagedin the early 40s; 84.5% were married. The majority
of participants were Caucasian (90.9%) with 4.5%Hispanic and 4.5% Asian. Most mothers had grad-uated from high school or had some college educa-tion (58.5%) whereas 41.6% had completed collegeor graduate school. The median household incomewas $50,000–75,000/year.
Procedure
Young adults met alone with the interviewer todiscuss the procedure and to obtain informed con-sent. Mothers and survivors met together for this step.All participants were then interviewed separately, andaudiotaped to establish procedural reliability. Youngadult survivors, mothers, and child survivors all com-pleted a measure of life stress, a structured diagnos-tic interview for PTSD, the ITSIS, and a measureof general functioning in the stated order. Mothersalso completed a diagnostic interview for PTSD fortheir children and a scale measuring the child’s gen-eral functioning. Interviews took approximately 2 hrfor young adult survivors and mothers and 1 1
2 -hrs forchild/adolescent survivors. Families who completedthe interviews as the second phase of a larger studyreceived $20 for their participation, whereas youngadults received $50 for their participation. The pro-cedures were approved by the Human Subjects Com-mittees of both sites.
Measures
Structured Interviews
The ITSIS (Kazak et al., 1996) was constructedspecifically for this project. It is a semistructuredinterview involving a total of 45 questions thatinclude open-ended questions, structured responseformats, dichotomous card sorts, and Likert-typescales. Parallel versions of the ITSIS, young adultsurvivor, child survivor, and survivor mother, wereadministered. Each version covers the following con-tent areas related to cancer diagnosis and treat-ment: memory for cancer and treatment (for sur-vivors), reexperiencing, reminders, avoidance, lifethreat, intense fear/horror/helplessness, attributionsfor causality, medical effects, perceptions of changesin self, and communication. ITSIS takes approxi-mately 45–60 min. In this first phase of analysisof this new instrument, only items appropriate forquantitative analysis were included in the factoranalysis (n = 25 for child and adolescent survivors,

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
310 Kazak, Barakat, Alderfer, Rourke, Meeske, Gallagher, Cnaan, and Stuber
26 for mothers, 27 for young adult survivors). Re-maining items (e.g., “What do you remember fromthat time [when you had cancer]?”) include open-ended narratives that are primarily intended forclinical use.
The ITSIS was developed by a multidisciplinaryresearch team. Items were derived from our previ-ous research and clinical experience, and focused to-ward clarifying the relationship between PTSD andchildhood cancer. Generally, items are presented inthe following structured order: a yes/no question isasked to introduce a symptom cluster (in this exam-ple, about intrusive memories): “Many people willremember things that they don’t really want to re-member. Sometimes they will find themselves think-ing about things when they don’t want to think aboutthem. Sometimes it may seem as if they are happeningagain. That is, they may see pictures, hear sounds, orsmell or feel things that happened to them. Are thereany memories about your/your child’s cancer and itstreatment that come into your mind when you don’twant them to?” Following the participant’s yes or noresponse, a probe is asked to elicit open-ended nar-rative information (e.g., “What specific memories doyou have?”). The final step is a card sort. The par-ticipant is given a stack of 31 cards. Each card hasan example of a symptom (in this example, a poten-tially intrusive memory) written on it (e.g., “Findingout I/my child had cancer,” “Pain,” “Being worriedabout (my child) getting sick again,” “I/My child los-ing hair”). The participant sorts the cards into “Yes”and “No” piles with regard to whether each repre-sents something that she or he experiences. In addi-tion, for some items, participants rate on a Likert-likescale how applicable different symptoms or experi-ences are to them (e.g., “On a scale of 1 to 5, howbothered are you by these memories?”). Basic scor-ing procedures for the ITSIS include dichotomousscoring of yes/no items, mean number of items en-dorsed on card sorts, and means from Likert-typeitems.
The Structured Clinical Interview for DSM-IV(SCID, First, Spitzer, Gibbon, & Williams, 1995) isa well-established semistructured interview for usewith adults to establish Axis I and II diagnoses consis-tent with the Diagnostic and Statistical Manual for theAmerican Psychiatric Association (1994). The PTSDsection was administered to young adult survivors andmothers. Previous versions of the SCID have ade-quate reliability and validity for clinical and researchpurposes.
The Diagnostic Interview Schedule for Children(DISC 2.3, Fisher et al., 1993) is a highly struc-tured interview with parallel parent and child ver-sions. The PTSD section was administered to boththe child/adolescent survivors and their mothers. Thechild/adolescent DISC data are presented in this pa-per. The DISC has adequate reliability and validity.
Training and Reliability for the Structured Interview Measures
Training in the administration of the ITSIS,SCID, and DISC was conducted before the first stageof interviewing (mothers and child survivors) at theWest Coast site in a 6-hr session with all interview-ers from both sites present. A subsequent series offour 2-hr training sessions was held at each site sepa-rately. At the start of the second stage of interviewing(young adult survivors), a series of five 2-hr trainingmeetings was held at the interview site. Throughoutall phases of data collection, monthly meetings wereheld with the teams at each site to discuss questions,clarify issues, and provide feedback from the reliabil-ity procedures. Notes from the training sessions andthe monthly team meetings were shared between thetwo sites by the Project Directors. Interviewers weremaster’s and doctoral level psychologists and master’slevel nurses.
For a subset of the data (mothers and child sur-vivors), every fifth SCID, DISC, and ITSIS was re-coded by a trained interviewer who listened to au-diotapes of the interviews. For the ITSIS, proceduralreliability was checked to assess deviations from thesemistructured protocol. The structure of the ITSISdoes not lend itself to other reliability checks becausethe responses provided are straightforward and donot require interpretation for scoring (structured re-sponses, card sorting methodologies, and Likert-typescales). The reliability coder completed a checklist foreach session reviewed. Using these written feedbacksheets, the Project Directors at each site reviewedcompliance with the procedure with each interviewer.This feedback process was continuous and allowedfor easy refinements in the procedure. No major de-viations from the ITSIS protocol were noted, and theITSIS and overall procedures were felt to be highlyreliable.
For the SCID and the DISC, Cohen’s Kappa wascomputed for each question based on the agreementof scores assigned by the interviewer and those as-signed by the reliability coder. For the SCID, kappasranged from .34 to 1.00 with an overall kappa of .86.

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
Impact of Traumatic Stressors 311
Fig. 1. A comparison of ITSIS factors for young adult survivors, mothers of child/adolescent survivors, and child/adolescent survivors.

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
312 Kazak, Barakat, Alderfer, Rourke, Meeske, Gallagher, Cnaan, and Stuber
For the DISC, kappas ranged from .63 to 1.00, with anoverall kappa of .97. These kappas provide evidencefor the reliability of SCID and DISC administrationacross sites and over time.
Self-Report Scales
Impact of Event Scale (IES). The IES (Horowitz,Wilber, & Alvarez, 1979) consists of 15 items ratedon a 4-point scale for frequency of occurrence dur-ing the previous week. It assesses two clusters ofexperiences that occur in response to a traumatic in-cident: intrusion and avoidance. The IES has high in-ternal consistency, has test-retest reliability, discrimi-nates different populations and symptom levels, andhas been supported in factor analyses (Schwarzwald,Solomon, Weisenberg, & Mikulincer, 1987) and inmedical samples (Epping-Jordan, Compas, & Howell,1994). Mothers and child survivors completed the IESin the Phase 1 study; young adults completed theIES during the interview in which they completed theITSIS.
Posttraumatic Stress Disorder Reaction Index.The Reaction Index is a 20-item self report question-naire that assesses symptoms of posttraumatic stress(Pynoos, Frederick, Nader, & Arroyo, 1987). Itemsinclude intrusion, avoidance, and arousal. The scalehas been used with children (La Greca et al., 1996)and adults (Goenjian et al., 1994) exposed to a va-riety of natural disasters and other traumatic events.The frequency of each item is endorsed on a 4-pointscale; the total score was used. Data indicate a strongassociation of empirically derived categories with clin-ical diagnoses of PTSD based on diagnostic measures(Pynoos et al., 1993). The categories are mild (12–24), moderate (25–39), and severe (≥40). Two items,which were stated in the reverse, were dropped fromcomputation of children’s scores because of difficultyunderstanding these items. Mothers and child sur-vivors completed the Reaction Index in the first phase;young adults completed the Reaction Index duringthe interview in which they completed the ITSIS.
Appraisal of Life Threat and Treatment Inten-sity Questionnaire (ALTTIQ). The ALTTIQ was con-structed for the larger study (Phase I) and is composedof seven questions rated on a 5-point Likert-type scale(Kazak et al., 1998; Stuber, Christakis, Houskamp,Pynoos, & Kozak, 1996). Mothers and child survivorscompleted it during the first phase of the project;young adults completed it during the interview inwhich they completed the ITSIS. Questions addressthe extent to which the cancer and its treatment are
believed to be intense and life threatening. Exami-nation of responses to the seven ALTTIQ questionsshowed little variance in three items, and they weretherefore removed from further consideration. Itemsretained assess perceived past life threat, current lifethreat, and treatment intensity.
Youth Self-Report (YSR). The YSR (Achenbach,1991) is a well-established paper-and-pencil measureof general functioning, behavior problems, and socialcompetence in children and adolescents completedby child survivors at the time of the ITSIS interview.The internalizing problems, externalizing problems,and total competence scales were used. For the inter-nalizing and externalizing behavior problem scales, Tscores above 63 are in the clinical range. For the totalcompetence scale, a T score below 37 is in the clinicalrange.
The Brief Symptom Inventory (BSI). The BSI(Derogatis, 1993) is a 53-item self-report measureassessing the presence and intensity of symptomsrelated to psychopathology in adults. The BSI hasbeen shown to have adequate reliability and valid-ity (Derogatis & Slavitz, 1999; Tennen, Affleck, &Herzberger, 1984). The Global Severity Index (GSI)as well as the following subscales related to depres-sion and general anxiety were used, with norms from anonpatient sample in parentheses: somatization (.29),interpersonal sensitivity (.32), depression (.28), andanxiety (.35). The norm for the GSI is .30 (Derogatis,1993). Mothers completed the BSI in the secondphase, and young adults completed it during their one-time interview.
Ratings of Intensity of Treatment and Severityof Medical Late Effects
For mother and child participants, intensity oftreatment and medical late effects were based on chartreview and rated by a pediatric oncologist and a pe-diatric oncology nurse practitioner blind to patientidentity. Treatment intensity ratings were made ona 3-point scale, with 1 – surgery only or six monthschemotherapy only or both; 2 – treatment for low oraverage risk cancer according to Children’s CancerGroup (CCG) treatment protocol, 3 – bone marrowtransplantation, high risk CCG protocol. The kappafor interrater reliability was .94. For medical late ef-fects ratings, a score of 1 – no limitation in activity andno special medical attention required; 2 – mild restric-tion of activity, mild cosmetic changes, and some med-ical attention (e.g., mild hearing loss, abnormally shortstature); 3 – significant restriction in daily activity and
P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
Impact of Traumatic Stressors 313
Table I. Descriptive Statistics for Validation Measures
Young adult Mother Child/adolescent
Measure Median Range Median Range Median Range
Impact of Event ScaleIntrusion 2.0 0.0–33.0 7.0 0.0–35.0 3.0 0.0–29.0Avoidance 1.0 0.0–27.0 5.0 0.0–36.0 3.0 0.0–32.0Total score 4.0 0.0–59.0 17.0 0.0–71.0 9.0 0.0–61.0PTSD Reaction Index 11.0 1.0–55.0 20.0 0.0–64.0 14.5 0.0–45.0
SCID/DISCCriterion B (Reexperiencing) 1.0 0.0–5.0 3.0 0.0–5.0 0.5 0.0–6.0Criterion C (Avoidance) 1.0 0.0–5.0 1.5 0.0–6.0 1.0 0.0–4.0Criterion D (Arousal) 0.0 0.0–5.0 2.0 0.0–5.0 1.0 0.0–5.0
Brief Symptom inventorySomatization 0.14 0.0–2.29 0.0 0.0–2.43 na naInterpersonal sensitivity 0.25 0.0–3.75 0.25 0.0–3.00 na naDepression 0.17 0.0–3.17 0.17 0.0–2.67 na naAnxiety 0.17 0.0–3.83 0.33 0.0–2.00 na naGlobal Severity Index 0.25 0.0–3.06 0.25 0.0–1.87 na na
Youth Self ReportInternalizing na na na na 47.5 16.0–67.0Externalizing na na na na 46.5 25.0–72.0Total competence na na na na 51.0 30.0–71.0
ALTTIQLife threat, current 1.0 1.0–5.0 2.5 1.0–5.0 1.0 1.0–4.0Life threat, past 2.0 1.0–5.0 5.0 1.0–5.0 5.0 1.0–5.0Perceived treatment intensity 8.0 2.0–10.0 10.0 5.0–10.0 9.0 3.0–10.0Severity of medical life effects rating na na 1.0 1.0–3.0 1.0 1.0–3.0Treatment intensity rating na na 2.0 1.0–3.0 2.0 1.0–3.0
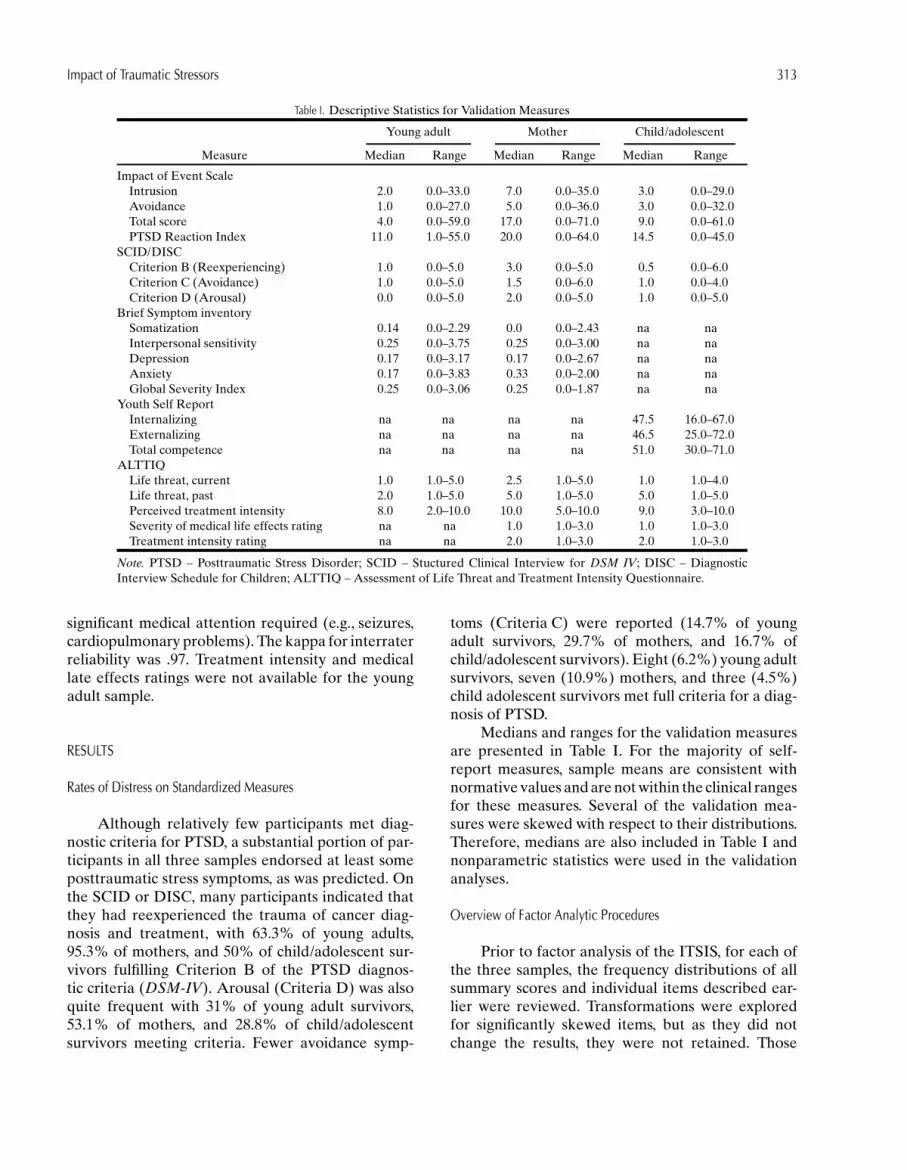
Note. PTSD – Posttraumatic Stress Disorder; SCID – Stuctured Clinical Interview for DSM IV; DISC – DiagnosticInterview Schedule for Children; ALTTIQ – Assessment of Life Threat and Treatment Intensity Questionnaire.
significant medical attention required (e.g., seizures,cardiopulmonary problems). The kappa for interraterreliability was .97. Treatment intensity and medicallate effects ratings were not available for the youngadult sample.
RESULTS
Rates of Distress on Standardized Measures
Although relatively few participants met diag-nostic criteria for PTSD, a substantial portion of par-ticipants in all three samples endorsed at least someposttraumatic stress symptoms, as was predicted. Onthe SCID or DISC, many participants indicated thatthey had reexperienced the trauma of cancer diag-nosis and treatment, with 63.3% of young adults,95.3% of mothers, and 50% of child/adolescent sur-vivors fulfilling Criterion B of the PTSD diagnos-tic criteria (DSM-IV). Arousal (Criteria D) was alsoquite frequent with 31% of young adult survivors,53.1% of mothers, and 28.8% of child/adolescentsurvivors meeting criteria. Fewer avoidance symp-
toms (Criteria C) were reported (14.7% of youngadult survivors, 29.7% of mothers, and 16.7% ofchild/adolescent survivors). Eight (6.2%) young adultsurvivors, seven (10.9%) mothers, and three (4.5%)child adolescent survivors met full criteria for a diag-nosis of PTSD.
Medians and ranges for the validation measuresare presented in Table I. For the majority of self-report measures, sample means are consistent withnormative values and are not within the clinical rangesfor these measures. Several of the validation mea-sures were skewed with respect to their distributions.Therefore, medians are also included in Table I andnonparametric statistics were used in the validationanalyses.
Overview of Factor Analytic Procedures
Prior to factor analysis of the ITSIS, for each ofthe three samples, the frequency distributions of allsummary scores and individual items described ear-lier were reviewed. Transformations were exploredfor significantly skewed items, but as they did notchange the results, they were not retained. Those

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
314 Kazak, Barakat, Alderfer, Rourke, Meeske, Gallagher, Cnaan, and Stuber
Table II. Factor Structure for Young Adults’ ITSIS
Factor
1 (Distress 1) 2 (Distress 2) 3 (Communication) 4 (Changes) 5 (Engagement)
Number of events causing helplessness .820Number of events causing intense fear .812Number of events causing horror .766Extent of helplessness .492Extent of fear .563Extent of horror .558Number of events reexperienced .660Number of reminders .537Number of events avoided .475 −.582Number of memories .416 .455Negative feelings from talking .500 .462 −.433Extent life is harder due to medical problems .852Extent of distress felt regarding medical problems .693Presence of medical late effects .488Number of medical problems .777Obviousness of medical problems .599Worry about future medical problems .629Extent life is harder due to memories .694Extent of distress felt regarding memories .440Average frequency of discussing cancer with others .910Number of people with whom cancer is discussed .888Frequency of cancer being topic of discussion .733Number of cancer events discussed within family .523Number of changes due to cancer .783Extent of changes due to cancer .764Positive valence of changes .709Extent of danger felt during cancer experience .460
Eigenvalues 4.63 4.29 2.78 2.21 1.67Percent variance explained 17.16 15.87 10.31 8.20 6.19
scores with little or no variability were excluded fromfurther analysis. All variables remaining were sub-jected to exploratory principal components factoranalysis with varimax rotation. Factors with fewerthan two items and eigenvalues less than 1.0 wereeliminated. Further refinement of the number andcontent of factors was determined based upon inspec-tion of scree plots, number of items per factor load-ing .400 or higher, amount of variance explained, andinterpretability (Tabachnick & Fidell, 1996). For theyoung adult survivors and mothers’ samples, five-factor solutions best captured the data, accounting for57.7 and 54.7% of the variance in the measure, respec-tively. A three-factor solution best captured the datafor the child/adolescent survivor sample, accountingfor 48.8% of the measure’s variance. Factor scoreswere calculated for each participant in each sample bysumming scores on the items retained on each factor.These scores were utilized in the validation analyses.Figure 1 provides a global summary and comparisonof the factor solutions identified for each of the threesamples examined.
Young Adult Survivors of Childhood Cancer
Table II provides the item composition, rotatedfactor loadings for the items in each factor, eigenval-ues, and percentage of variance accounted for by eachfactor. Table III provides correlations of factor scoreswith the validation measures.
Factor 1. Distress 1: PTSD A2 Criteria, Reexperiencing,and Avoiding
Factor 1 appears to be a strong measure of dis-tress specific to cancer in its association with bothposttraumatic stress symptoms and a broad spectrumof psychological distress. Items on this factor tappedA2 criteria for PTSD (feeling intense fear, horror,and helplessness), number of cancer-related mem-ories, events reexperienced, reminders and stimuliavoided, and arousal of negative feelings when talk-ing about the cancer experience. Cronbach’s alphafor summed scores on this scale was .84. Scores on

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
Impact of Traumatic Stressors 315
Table III. Spearman’s Rho Correlates of Young Adult Survivors ITSIS Factor Scores With Validation Measures
Factor
1 (Distress 1) 2 (Distress 2) 3 (Communication) 4 (Changes) 5 (Engagement)
Posttraumatic stress measuresIES Intrusion .43∗∗∗ .43∗∗∗ .19∗ .24∗∗ −.21∗IES Avoidance .36∗∗∗ .38∗∗∗ .03 .11 −.37∗∗∗IES Total .44∗∗∗ .44∗∗∗ .14 .22∗ −.26∗∗∗Reaction Index .54∗∗∗ .64∗∗∗ .13∗ .32∗∗∗ −.28∗∗∗SCID B: Reexperiencing .42∗∗∗ .33∗∗∗ .06 .23∗∗∗ −.17SCID C: Avoidance .33∗∗∗ .33∗∗∗ −.14 .10 −.34∗∗∗SCID D: Arousal .21∗∗∗ .48∗∗∗ .13 .28∗∗∗ −.17SCID PTSD Dx .25∗∗∗ .32∗∗∗ −.09 .19∗ −.14
General functioningBSI Anxiety .40∗∗∗ .49∗∗∗ .00 .21∗ −.32∗∗∗BSI Depression .34∗∗∗ .55∗∗∗ −.07 .18∗ −.35∗∗∗BSI Interpersonal Sensitivity .33∗∗∗ .47∗∗∗ −.04 .18∗ −.39∗∗∗BSI Somatization .34∗∗∗ .53∗∗∗ .07 .21∗ −.23∗∗BSI GSI .36∗∗∗ .53∗∗∗ −.05 .21∗ −.40∗∗∗
Treatment-related variablesALTTIQ present life threat .28∗∗∗ .36∗∗∗ .10 .13 .04ALTTIQ past life threat .52∗∗∗ .17 .03 .17 .27∗∗∗ALTTIQ treatment intensity .63∗∗∗ .29∗∗∗ .00 .33∗∗∗ −.02
Note. IES – Impact of Events Scale; SCID – Structure Clinical Interview for DSM IV; BSI – Brief Symptom Inventory; ALTTIQ –Assessment of Life Threat and Treatment Intensity Questionnaire.∗p < .05. ∗∗p < .01. ∗∗∗p < .005.
this factor were significantly correlated with the self-report and interview measures of posttraumatic stressat both the global and specific symptom cluster levels(i.e., reexperiencing, avoidance, and arousal). Higherscores on this factor were significantly associated withdepression, anxiety, interpersonal sensitivity, somati-zation, and global severity of emotional symptoms.They were also highly correlated with the belief thatone could have died from cancer and that cancer treat-ment was intense, and moderately correlated with thebelief that one could still die from cancer.
Factor 2. Distress 2: Medical Late Effects, Hardship, and Distress
The second factor also captured elements ofdistress, but with emphasis on perceived negativechanges and hardship because of these changes. Theitems on this factor mainly tapped issues related tocurrent and potential future medical problems, butalso tapped hardship and distress associated withmemories of the cancer experience. Cronbach’s alphafor this scale was .84. Scores on this factor were associ-ated with both global and specific symptom clusters ofposttraumatic stress. They were moderately to highlycorrelated with general distress, depression, anxiety,interpersonal sensitivity, and somatization. There wasalso a significant association between scores on thisfactor and current perceived life threat and treat-
ment intensity. The pattern of correlations is simi-lar to Factor 1 scores; however, correlations betweenFactor 2 scores and the general distress items seem ofgreater magnitude, suggesting that this factor focusesmore on general distress than on cancer-specific dis-tress. Factor 1 and Factor 2 scores were significantlycorrelated (r = .43, p < .001).
Factor 3. Communication
This 4-item factor was composed of variables as-sessing how often the respondent talks about can-cer, the number of people with whom they talk, andthe number of cancer-related events their family dis-cusses. Cronbach’s alpha for this Communication fac-tor scale was .79. Scores on this factor had only onesignificant correlation with a validation measure, andthis correlation was quite small. This pattern of resultswas expected as our validation measures did not di-rectly assess communication patterns. Factor 3 scoreswere not significantly correlated with Factor 1 and 2scores.
Factor 4. Positive Changes in Self
The three items on this factor assessed the num-ber of ways and extent to which the respondenthas changed because of the cancer experience and

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
316 Kazak, Barakat, Alderfer, Rourke, Meeske, Gallagher, Cnaan, and Stuber
the valence of these changes. The positive corre-lation indicated positive change. Cronbach’s alphafor this scale was .77. Higher scores on this factorwere associated with higher scores on global indicesof PTSD symptoms and the posttraumatic symptomclusters of reexperiencing and arousal, but not avoid-ance. Factor 4 scores were also associated mildly withdepression, anxiety, interpersonal sensitivity, soma-tization, and the global index of emotional func-tioning. Factor 4 scores were significantly correlatedwith scores on Factors 1 (r = .31, p < .001), 2 (r =.25, p < .005), and 3 (r = .21, p < .05).
Factor 5: Engagement
This scale appears to capture an approach ori-entation or engagement with the experience of can-cer (α = .38). Specifically, the four items that loadedon this factor assessed the amount of life danger per-ceived at the time of cancer diagnosis, the absenceof avoidance of cancer-related stimuli, the number ofmemories of the cancer experience, and the absence ofarousal of negative feelings when talking about can-cer. Factor 5 scores were correlated negatively with
Table IV. Factor Structure for Mothers’ ITSIS
Factor
1 (Distress 1) 2 (Distress 2) 3 (Changes) 4 (Communication) 5 (Vigilance)
Number of events causing helplessness .862Number of events causing intense fear .809Number of events causing horror .697Extent of helplessness .601Extent of fear .421Extent of horror .614Number of events reexperienced .711Number of reminders .467Negative feelings from talking .436Extent life is harder due to medical problems .701Extent of distress felt regarding medical problems .754Presence of medical late effects .443Number of medical problems .595 .407Obviousness of medical problems .607Worry about future medical problems .586Extent life is harder due to memories .722Extent of distress felt regarding memories .418 .563Average frequency of discussing cancer .440Number of people with whom cancer is discussed .888Frequency of cancer being topic of discussion .871Positive feelings result from discussions .418Number of changes due to cancer .774Extent of changes due to cancer .743Positive valence of changes .680Extent of danger felt during cancer experience .670
Eigenvalues 3.74 3.42 2.44 2.34 1.74Percent variance explained 14.96 13.67 9.76 9.35 6.96
self-report indices of global posttraumatic stress, re-experiencing and avoidance, as well as with depres-sion, anxiety, interpersonal sensitivity, somatization,and the global emotional functioning index. Factor 5scores correlated negatively with scores on Factor2 (r = −.22, p < .05), but positively with scores onFactor 3 (r = .27, p < .005), suggesting that thosescoring high on Factor 5 experience less generaldistress and communicate more about their cancerexperience.
Mothers of Child and Adolescent Survivors of Cancer
Table IV provides the item composition, rotatedfactor loadings for items on each factor, eigenvalues,and percentage of variance accounted for by each ofthe five factors. Table V provides correlations betweenthe factor scores and validation measures.
Factor 1. Distress 1: PTSD A2 Criteria, Reminders,and Reexperiencing
Similar to Factor 1 for the Young Adult sample,Factor 1 for mothers of adolescents appeared to be a

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
Impact of Traumatic Stressors 317
Table V. Spearman’s Rho Correlates of Mothers’ ITSIS Factor Scores With Validation Measures
Factor
1 (Distress 1) 2 (Distress 2) 3 (Changes) 4 (Communication) 5 (Vigilance)
Posttraumatic stress measuresIES Intrusion .29∗ .23 .25∗ .11 −.03IES Avoidance .42∗∗∗ .35∗∗∗ .25∗ .09 .06IES Total .38∗∗∗ .32∗∗ .25∗ .09 .03Reaction Index .43∗∗∗ .55∗∗∗ .15 −.12 .12SCID B: Reexperiencing .44∗∗∗ .15 .19 .24 .23SCID C: Avoidance .33∗∗ .45∗∗∗ .36∗∗∗ −.22 .24SCID D: Arousal .31∗∗∗ .39∗∗∗ .35∗∗∗ −.01 .36∗∗∗SCID PTSD Dx .09 .35∗∗∗ .17 .36∗∗∗ .09
General functioningBSI Anxiety .38∗∗∗ .35∗∗∗ .26∗ −.15 .15BSI Depression .46∗∗∗ .44∗∗∗ .35∗∗ −.13 .29BSI Interpersonal sensitivity .28∗ .33∗∗ .22 −.08 .29∗BSI Somatization .19 .28∗ .31∗ .07 .23BSI GSI .44∗∗∗ .41∗∗∗ .31∗ −.10 .23
Treatment-related variablesALTTIQ present life threat .31∗ .21 .17 −.05 .18ALTTIQ past life threat .02 .12 .10 −.09 .23ALTTIQ treatment intensity .33∗ .34∗ .29∗ .09 .02
Note. IES – Impact of Events Scale; SCID – Structure Clinical Interview for DSM IV; BSI – Brief Symptom Inventory; ALTTIQ –Assessment of Life Threat and Treatment Intensity Questionnaire.∗p < .05. ∗∗p < .01. ∗∗∗p < .005.
strong measure of distress specific to cancer in its asso-ciation with both posttraumatic stress symptoms and abroader spectrum of psychological distress. The sevenitems loading on this factor assessed A2 criteria forPTSD (feeling intense fear, horror, and helplessness),the number of cancer-related events reexperiencedand reminders, and distress associated with cancer-related memories. Cronbach’s alpha for this scale was.78. Scores on this factor were significantly correlatedwith the global self-report measures of posttraumaticstress symptoms and with the specific self-report andinterview-derived symptom clusters of reexperienc-ing, avoidance, and arousal. They were also signifi-cantly associated with items of the BSI indicative ofdepression, anxiety, interpersonal sensitivity, and gen-eral emotional distress. Finally, Factor 1 scores weresignificantly correlated with the belief that one’s childcould still die from cancer and perceived treatmentintensity.
Factor 2. Distress 2: Medical Late Effects, Hardship, and Distress
As in the Young Adult sample, the second factorfor the mothers captured aspects of distress with em-phasis upon hardship and worry in regard to medicallate effects and memories of the cancer experience.The remaining items tapped negative feelings whentalking of cancer and amount of fear felt at diagno-
sis. Cronbach’s alpha for this scale was .79. Scoreson this factor were associated with global measuresof posttraumatic stress and with the specific symp-tom clusters of avoidance and arousal. They weresignificantly and moderately correlated with BSI de-pression, anxiety, interpersonal sensitivity, somatiza-tion, and the global emotional distress index. Therewas also a significant association between scores onthis factor and perceived treatment intensity. Factor 1and Factor 2 scores were moderated correlated (r =.50, p < .001) indicating their shared association withdistress.
Factor 3. Changes in Self
This 4-item factor closely paralleled Factor 4 ofthe Young Adult sample. The items assessed the num-ber of ways and extent to which the respondent haschanged because of the cancer experience (includingnumber of medical late effects) and the valence ofthese changes. Cronbach’s alpha for this scale was .64.Scores on this factor had significant associations withsome of the indices tapping the global and specificsymptom clusters of posttraumatic stress. Significantcorrelations were found between scores on this factorand most of the symptomatology scales of the BSI.This pattern of intercorrelations was similar to thatfound for the Changes in Self factor in the young adult

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
318 Kazak, Barakat, Alderfer, Rourke, Meeske, Gallagher, Cnaan, and Stuber
survivor sample. Factor 3 scores were moderatelycorrelated with Factor 2 scores (r = .40, p < .005).
Factor 4. Communication
The 4-item fourth factor for the mothers corre-sponded closely to Factor 3 for the young adults. Itincluded items tapping how often and with how manypeople the respondent talks about the cancer expe-rience and number of positive feelings arising fromtalking. Cronbach’s alpha for this scale was .63. Thisfactor had no statistically significant associations withour measures of posttraumatic stress or emotionalsymptomatology, much like the young adult survivor’scommunication factor. Factor 4 was not significantlycorrelated with other factors (rs < .17, ps > .17).
Factor 5. Vigilance to Threat
The final factor arising from the mothers’ datacaptured feelings of danger and horror during the can-cer experience and obviousness of medical problems
Table VI. Factor Structure for Child/Teen Survivors’ ITSIS
Factor
1 (Distress) 2 (Communication and changes) 3 (Vigilance)
Number of events causing helplessness .710Number of events causing intense fear .668Number of events causing horror .828Extent of helplessness .410Extent of horror .437 .498Number of events reexperienced .538Number of reminders .547Number of events avoided .687Number of memories .475Negative feelings from talking .564Extent life is harder due to medical problems .570Extent of distress felt regarding medical problems .451Presence of medical late effects .463Number of medical problems .524Obviousness of medical problems −.617Worry about future medical problems .623Extent life is harder due to memories .491 .479Extent of distress felt regarding memories .694Average frequency of discussing cancer with others .749Number of people with whom cancer is discussed .736Frequency of cancer being topic of discussion .557Number of cancer events discussed within family .750Number of changes due to cancer .538 .689Extent of changes due to cancer .636Positive valence of changes .596Extent of danger felt during cancer experience .533
Eigenvalues 5.27 5.08 2.33Percent variance explained 20.27 19.55 8.95
related to the cancer diagnosis. Cronbach’s alpha forthis factor was .37. Scores on this factor were posi-tively associated with fulfilling criteria for arousal perthe SCID and for interpersonal sensitivity per the BSI.Factor 5 scores were not significantly correlated withthe other factor scores arising from the mother’s data(rs < .22, ps > .08).
Child and Adolescent Survivors of Cancer
Item composition, rotated factor loadings, eigen-values, and variance accounted for by each of the threefactors are presented in Table VI. Table VII displayscorrelations between the factor scores and validationmeasures.
Factor 1. Distress: PTSD A2 Criteria, Reexperiencing,Avoiding, and Hardship
As can be seen in Fig. 1, this 13-item factorcorresponded to Factor 1 in the young adult sur-vivor and mother analyses. Items captured PTSD A2

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
Impact of Traumatic Stressors 319
Table VII. Spearman’s Rho Correlates of Child ITSIS Factor With Validation Measures
Factor
1 (Distress) 2 (Communication and changes) 3 (Vigilance)
Posttraumatic stress measuresIES Intrusion .43∗∗∗ .50∗∗∗ .23IES Avoidance .44∗∗∗ .33∗∗∗ .25∗IES Total .47∗∗∗ .44∗∗ .26∗Reaction Index .32∗ .27∗ .17DISC B: Reexperiencing .45∗∗∗ .25∗ .23DISC C: Avoidance .27∗ .12 .29∗DISC D: Arousal .41∗∗∗ .31∗ .19DISC PTSD Dx .20 .19 .28∗
General functioningYSR Internal .50∗∗∗ .36∗ .23YSR External .16 .17 .10YSR Competence .00 .10 .07
Treatment-related variablesALTTIQ Current Life Threat .07 .13 −.04ALTTIQ Past Life Threat .28∗ .49∗∗∗ .32∗ALTTIQ Treatment Intensity .35∗∗ .26∗ .29∗
Note. IES – Impact of Events Scale; DISC – Diagnostic Interview Schedule for Children; YSR Internal –Youth Self-Report Internalizing Problem Scale; YSR External – Youth Self-Report Externalizing ProblemScale; YSR Competence – Youth Self-Report Total Competence; ALTTIQ – Assessment of Life Threat andTreatment Intensity Questionnaire.∗p < .05. ∗∗p < .01. ∗∗∗p < .005.
criteria (fear, horror, and helpless), number of cancer-related events reexperienced and reminders avoided,and hardship and perceived danger. Cronbach’s al-pha for this scale was .85. Scores on this factor weresignificantly correlated with self-reported measuresof posttraumatic stress and with all symptom clusterindicators. Significant associations were also foundbetween scores on this factor and the CBCL inter-nalizing behavior problems score (e.g., anxiety, de-pression). Participants scoring higher on this factoralso indicated greater perceived past life threat andgreater perceived intensity of treatment.
Factor 2. Communication and Changes in Self
The second factor was composed of 10 items tap-ping how often and with how many people the re-spondent talks about their cancer experience, positivechanges in the self resulting from the cancer experi-ence, and number of memories, reminders, and medi-cal late effects. This factor corresponded to Factors 3and 4 in the young adult and mother data. Cronbach’salpha for this scale was .89. Scores on this factor wereassociated with self-reported measures of posttrau-matic stress symptoms and with most of the symptomcluster measures. Scores on this factor were also asso-ciated with internalizing problems, perceived treat-
ment intensity, and perceived previous life threat.Factor 2 scores were highly correlated with Factor 1scores (r = .72, p < .001).
Factor 3. Vigilance to Distress and Perceived Threat
The final factor consisted of six items tapping ex-tent of horror and helplessness felt during cancer di-agnosis and treatment, distress and hardship resultingfrom memories of cancer, and issues related to med-ical late effects. As seen in Fig. 1, some aspects ofthis factor parallel Factor 2 in the young adult andmother samples. Cronbach’s alpha for this factor was.67. Factor scores were correlated with fulfilling crite-ria for PTSD per the DISC, scoring high on the IESglobal index and experiencing avoidance symptoms.They were also significantly associated with perceivedlife threat in the past and perceived intensity of treat-ment. Factor 3 scores were significantly correlatedwith both Factor 1 (r = .64, p < .001) and Factor 2scores (r = .56, p < .001).
DISCUSSION
The goal of this study was to provide prelimi-nary evidence for the utility of a measure, the ITSIS,

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
320 Kazak, Barakat, Alderfer, Rourke, Meeske, Gallagher, Cnaan, and Stuber
that moves beyond a simple screening for distress orcounting of PTSD symptoms. As hoped, our data in-dicate that the ITSIS can provide a more elaboratedunderstanding of traumatic reactions to childhoodcancer, which can ultimately guide the developmentof interventions for childhood cancer survivors andtheir families.
A goal of the ITSIS is to assess five categoriesof information: forms of posttraumatic stress particu-lar to the cancer/treatment experience, perceptions ofongoing medical late effects, perceived changes in selfdue to cancer, communication about the cancer expe-rience, and perceived causality. Results of the factoranalyses with all three of our samples suggest that theITSIS does gather information in all of these cate-gories except for the last (perceived causality). Thematch is most clear for the five-factor solutions ob-tained for young adult survivors and for mothers ofchild/adolescent survivors. In both groups, separatefactors were obtained that correspond to posttrau-matic symptoms related to the cancer experience, con-cerns over medical late effects, perceived changes inself, and communication about the cancer experience.The child data, although less clear and still some-what tentative, demonstrate a three-factor solutionthat includes posttraumatic stress symptoms relatedto cancer (Factor 1), as well as positive changes in selfand communication (Factor 2), and distress related tomedical late effects (Factor 3). The concordance be-tween the categories of information we intended theITSIS to tap and the obtained ITSIS factor structuresoffers some support for the validity of the instrument.
Consistent with our earlier research (Kazak et al.,1996), the factors we obtained offer further supportfor the use of the ITSIS to gain a uniquely targeted un-derstanding of the forms of posttraumatic stress expe-rienced by childhood cancer survivors and their fam-ilies. Like other instruments, the ITSIS demonstratesthat mothers, their adolescent cancer survivors, andyoung adult survivors all express general posttrau-matic stress symptoms, such as reexperiencing diffi-cult moments and upsetting reminders, perceiving lifedanger, and having feelings of intense fear, horror,and helplessness related to their trauma (i.e., the can-cer). The ITSIS, however, tells us that returning tooncology clinic for follow-up appointments and see-ing children with no hair are specific examples of fre-quently distressing reminders for survivors. Horrorfor mothers was associated with witnessing one’s childgetting tests (such as bone marrow aspirations) andtreatments. Concerns over medical late effects in-clude distress over the existence of current problems,
feelings that life is much harder because of late ef-fects, and worry that future late effects will emerge.The findings have important clinical implications andsupport the importance of furthering our understand-ing of subdiagnostic or partial PTSD, in the contextof illness and of targeting intervention strategies tothese symptom clusters.
Further support for validity of the ITSIS is foundin the patterns of correlation between the derivedITSIS factors and other measures, including diagnos-tic interview measures and self- and parent-reportscales of posttraumatic stress symptoms, measures ofgeneral adjustment, and subjective perceptions of lifethreat and treatment intensity. As was expected, fac-tors tapping cancer-related posttraumatic stress andmedical late effects correlated with most standard-ized measures of posttraumatic stress, other psycho-logical distress, and perceived treatment intensity andlife threat for all three samples. Those young adultswho were positively engaged with their memories ofcancer (i.e., did not avoiding reminders of treatment,did not become overwhelmed by negative emotionwhen talking about cancer) reported higher levels ofperceived life threat, but also, as expected, reportedlower levels of posttraumatic stress and other distress.
Communication factors for the mothers andyoung adult survivors, on the other hand, correlatedwith relatively few of our measures. This lack of rela-tionship is not surprising, given that this study did notinclude any formal measures of communication. Iden-tifying relationships between this factor and morespecific measures of communication or, given theassociation between talking and improved levels ofsymptoms (Foa, 1997), adaptive functioning, is a fu-ture aim.
For all groups, factors reflecting positive changesin self due to cancer—including gains in compe-tence, improved social relationships, and having amore positive outlook on life—were significantly neg-atively associated with symptoms of distress and withavoidance on the structured interviews and self-reportmeasures. This may reflect that positive and negativeoutcomes of the experience may be accepted and bal-anced. That is, part of adaptive coping is finding asilver lining to stressful experiences while acceptingand addressing the distressing aspects.
The current data also suggest the utility of theITSIS in understanding how the meaning of cancerand survivorship appears to differ for different fam-ily members. A primary difference found betweenthe five-factor solution of the young adult versus themother samples, for example, is that the young adults

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
Impact of Traumatic Stressors 321
have a positive engagement factor, whereas mothershave an additional distress factor. This difference infactor structures between young adult survivors andmothers of survivors indicates that just as the traumaof childhood cancer differs for the patient versus theparents of a patient, so will the experience of can-cer survivorship. The ITSIS can help to inform thesedifferences.
A final goal in this study was to begin an ex-ploration of developmental issues in cancer survivor-ship by comparing the young adult survivors with theyounger sample of adolescent survivors. The youngadult survivors had a more differentiated and specificfactor structure. Although the child/adolescent sur-vivors’ factor structure contained most of the specificelements of the young adults’ structure, the organi-zation was different: for younger survivors, posttrau-matic stress and concern over late effects grouped to-gether in a single factor, as did communication andchanges in the self. Our sample size for the chil-dren was considerably smaller than that of the youngadults, which may explain the differences. Develop-mental issues may also contribute to this difference,however. Younger survivors are closer to their cancerexperience and lack the cognitive sophistication andlife experience that may lead older survivors to a moreexistential consideration of what it means to have sur-vived their cancer. This developmental issue may alsoexplain why young adults have developed an “engage-ment” factor that represents a positive understandingof the ways in which their illness and treatment havecontributed to “who they are.” Younger survivors maynot have had the life experience, or simply the timesince diagnosis, to come to this kind of understanding.Future longitudinal examinations of survivors, usingthe ITSIS, can lend a more thorough understandingof the ways in which the meaning of the cancer expe-rience changes across development.
Although the current results are promising, sev-eral issues necessitate future research to confirm thepatterns seen here. First, the generalizability of theITSIS is limited by the lack of father data. It is notclear whether fathers’ responses would be similar toor at variance with that of their spouses. Although fa-thers have shown similar levels of posttraumatic stresssymptoms as mothers (Barakat et al., 1997; Kazaket al., 1997), the focus of these symptoms may dif-fer from their spouses reflecting the differing rolesthey play in their families and in their children’s treat-ment. Indeed, mother participants often reported thatthey would be interested in knowing their spouses’responses on the ITSIS, believing that their spouses’
responses would differ from their own. Comparingthe ITSIS responses of all family members—mothers,fathers, survivors, and siblings—is critical to develop-ing a more definitive conceptualization of the familycontext of posttraumatic stress in cancer survivorship.Further, although we have demonstrated convergentvalidity for several factors, demonstrating divergentrelationships between factors and other theoreticallyunrelated constructs is an important next step.
An additional issue to consider in the interpreta-tion of these findings is that the significantly higherrated intensity of treatment for mother and ado-lescent participants compared with nonparticipantsmay mean that this study overestimates posttraumaticstress symptoms in these survivors and their families.However, our previous finding of a lack of associa-tion between objective measures of intensity and post-traumatic stress makes this consideration less tenable(Barakat et al., 1997). A practical limitation of theITSIS is the time and personnel necessary for admin-istration. Although a shorter form of the ITSIS maybe feasible (given the exclusion of items in the cur-rent analyses), participants appeared to benefit fromthe opportunity to discuss their experiences and thevariety in format of responses engaged children andadolescents, as expected.
Although the sample sizes we report are mod-est, the adequacy of sample size in factor analy-sis, contrary to other analytical approaches, can of-ten be determined only after the fact (MacCallum,Widaman, Zhang, & Hong, 1999). The ability of thesample to represent the population is based on thecommunalities of the factors and the ratio of numberof items to number of factors. Although our ratio ofitems to factors is sufficiently high (22 items and nomore than five factors), the variability in the commu-nalities we obtained would suggest that a sample of100–150 participants is necessary to clarify the stabil-ity of the factors. Our young adult sample (n = 130)meets this criterion, whereas our mother and childsamples fall somewhat short of this ideal. The simi-larity between the mother and young adult findings,however, support the validity of the analyses in bothgroups. The findings in the child group are somewhatless clear, and rely on replication with a larger numberof participants.
Despite these limitations, the validity data pre-sented here indicate that the ITSIS provides valid in-formation about the constellation of cancer-specificposttraumatic stress symptoms in mothers and sur-vivors. The data also indicate that the ITSIS canbe used to understand differences in posttraumatic

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
322 Kazak, Barakat, Alderfer, Rourke, Meeske, Gallagher, Cnaan, and Stuber
reactions in different family members, as well as dif-ferences in the experience of cancer survivorship overdevelopment. For example, our research team hasincluded the ITSIS as part of a randomized clinicaltrial of a cognitive–behavioral-family therapy inter-vention for adolescent cancer survivors and their fam-ilies. Information extrapolated from the ITSIS hasbeen used successfully to tailor these interventions tothe specific needs of different family members (Kazaket al., 1999). The current data are therefore offered aspreliminary evidence of the value of the ITSIS notonly in understanding individual and family develop-ment after childhood cancer, but also in informinginterventions aimed at reducing or preventing long-term symptoms of posttraumatic stress in individualsand families. Future research with additional samples,including many members of the same family, will con-tinue to delineate the uses of the instrument.
ACKNOWLEDGMENTS
This research was supported, in part, by grantsfrom the National Cancer Institute (R01-63930,5-U10-CA15488-23) and the National Institute ofMental Health (K07-01604). The authors thank thefollowing for assistance with data collection: DianneDarbasie, Violet Hovsepian Mesrkhani, BiancamariaPenati, Deborah Seacord, Steven Simms, Scott Ward.We also thank Anna Meadows and Wendy Hobbie forproviding ratings of treatment intensity and medicallate effects.
REFERENCES
Achenbach, T. (1991). Manual for the Child Behavior Check-list. Burlington, VT: Department of Psychiatry, University ofVermont.
American Psychiatric Association. (1994). Diagnostic and statisticalmanual of mental disorders (4th ed.). Washington, DC: Author.
Barakat, L., Kazak, A., Meadows, A., Casey, R., Meeske, K., &Stuber, M. (1997). Families surviving childhood cancer: Acomparison of posttraumatic stress symptoms with families ofhealthy children. Journal of Pediatric Psychology, 22, 843–859.
Derogatis, L. (1993). Administration, scoring, and procedures man-ual for the BSI-I. Minneapolis, MN: National ComputerSystems.
Derogatis, L., & Savitz, K. L. (1999). The SCL-90-R, Brief Symp-tom Inventory, and Matching Clinical Rating Scales. In M. E.Maruish (Ed.), The use of psychological testing for treatmentplanning and outcome assessment (2nd ed.). Mahwah, NJ:Erlbaum.
Epping-Jordan, J., Compas, B., & Howell, D. (1994). Predictors ofcancer progression in young adult men and women: Avoid-ance, intrusive thoughts, and psychological symptoms. HealthPsychology, 13, 539–547.
First, M., Spitzer, R., Gibbon, M., & Williams, J. (1995). Struc-tured Clinical Interview for DSM-IV (Nonpatient Edition).
New York: Biometrics Research Department, New York StatePsychiatric Institute.
Fisher, P., Shaffer, D., Piacentini, J., Lapkin, J., Kafantaris,V., Leonard, H., & Herzog, D. (1993). Sensitivity of the Diag-nostic Interview Schedule for Children (DISC2.1) for specificdiagnoses of children and adolescents. Journal of the Amer-ican Academy of Child and Adolescent Psychiatry, 32, 666–673.
Foa, E. B. (1997). Psychological processes related to recovery froma trauma and an effective treatment for PTSD. In R. Yehuda &A. McFarlane (Eds.), Psychobiology of posttraumatic stressdisorder (pp. 410–424). New York: New York Academy ofScience.
Goenjian, A., Najarian, L., Pynoos, R., Steinberg, A., Manoukian,G., Tavosian, A., & Fairbanks, L. (1994). Posttraumatic stressdisorder in elderly and younger adults after the 1988 earth-quake in Armenia. American Journal of Psychiatry, 151, 895–901.
Hobbie, W. L., Stuber, M., Meeske, K., Wissler, K., Rourke, M. T.,Ruccione, K., Hinkle, A., & Kazak, A. E. (2000). Symptomsof posttraumatic stress in young adult survivors of childhoodcancer. Journal of Clinical Oncology, 18(24), 4060–4066.
Horowitz, M., Wilner, N., & Alvarez, W. (1979). Impact of EventScale: A measure of subjective stress. Psychosomatic Medicine,41, 209–218.
Kazak, A., Barakat, L., Meeske, K., Christakis, D., Meadows,A., Casey, R., Penati, B., & Stuber, M. (1997). Posttraumaticstress, family functioning, and social support in survivors ofchildhood leukemia and their mothers and fathers. Journal ofConsulting and Clinical Psychology, 65, 120–129.
Kazak, A. E., Simms, S., Barakat, L., Hobbie, W., Foley, B.,Golomb, V., & Best, M. (1999). Surviving Cancer CompetentlyIntervention Program (SCCIP): A cognitive–behavioral andfamily therapy intervention for adolescent survivors of child-hood cancer and their families. Family Process, 38(2), 175–191.
Kazak, A., Stuber, M., Barakat, L., & Meeske, K. (1996). Assess-ing posttraumatic stress related to medical illness and treat-ment: The Impact of Traumatic Stressors Interview Schedule(ITSIS). Families, Systems, and Health, 14, 365–380.
Kazak, A., Stuber, M., Barakat, L., Meeske, K., Guthrie, D., &Meadows, A. (1998). Predicting posttraumatic stress symp-toms in mothers and fathers of survivors of childhood cancer.Journal of the American Academy of Child and AdolescentPsychiatry, 37, 823–831.
La Greca, A., Silverman, W., Vernberg, E., & Prinstein, M. (1996).Symptoms of posttraumatic stress in children after HurricaneAndrew: A prospective study. Journal of Consulting and Clin-ical Psychology, 64, 712–723.
MacCallum, R. C., Widaman, K. F., Zhang, S., & Hong, S. (1999).Sample size in factor analysis. Psychological Methods, 4(1),84–99.
Manne, S., Du Hamel, K., Gallelli, K., Sorgen, K., & Redd, W.(1998). Posttraumatic stress disorder among mothers of pedi-atric cancer survivors: Diagnosis, comorbidity, and utility ofthe PTSD Checklist as a screening instrument. Journal of Pe-diatric Psychology, 23, 357–366.
Nir, Y. (1997). Post-traumatic stress disorder in children with can-cer. In J. E. Schowalter, P. Buschmann, et al. (Eds.), Childrenand death: Perspectives from birth through adolescence (pp. 63–72). New York, NY: Praeger Publishers.
Pelcovitz, D., Goldenberg, B., Kaplan, S., Weinblatt, H., Madel,F., Meyers, B., & Vinciguerra, V. (1996). Posttraumatic stressdisorder in mothers of pediatric cancer survivors. Psychoso-matics, 37, 116–126.
Pelcovitz, D., Libov, B. G., Mandel, F., Kaplan, S., Weinblatt, M., &Septimus, A. (1998). Posttraumatic stress disorder and familyfunctioning in adolescent cancer. Journal of Traumatic Stress,11, 205–221.

P1: LMD/GYQ/LOV/GQT P2: GFU/GCP/LMD
Journal of Clinical Psychology in Medical Settings PP245-344443 August 29, 2001 14:12 Style file version Oct. 19, 2000
Impact of Traumatic Stressors 323
Pynoos, R., Frederick, C., Nader, K., & Arroyo, W. (1987). Lifethreat and posttraumatic stress in school age children. Archivesof General Psychiatry, 44, 1057–1063.
Pynoos, R., Goenjian, A., Tashjian, M., Karakashian, M.,Manjikian, R., Manoukian, G., Steinberg, A., & Fairbanks, L.(1993). Posttraumatic stress reactions in children after the 1988Armenian earthquake. British Journal of Psychiatry, 163, 239–247.
Schwarzwald, J., Solomon, Z., Weisenberg, M., & Mikulincer, M.,(1987). Validation of the Impact of Event Scale for psycholog-ical sequellae of combat. Journal of Consulting and ClinicalPsychology, 55, 251–256.
Stuber, M., Christakis, D., Houskamp, B., Pynoos, R., & Kazak, A.(1996). Posttrauma symptoms in childhood leukemia survivorsand their parents. Psychosomatics, 37, 254–261.
Stuber, M., Kazak, A., Meeske, K., Barakat, L., Guthrie,D., Garnier, H., Pynoos, R., & Meadows, A. (1997). Predic-tors of posttraumatic stress in childhood cancer survivors.Pediatrics, 100, 958–964.
Stuber, M., Kazak, A., Meeske, K., & Barakat, L. (1998). Is post-traumatic stress a viable model for understanding responsesto childhood cancer? Child and Adolescent Psychiatric Clinicsof North America, 7(1), 169–182.
Tabachnick, B. G., & Fidell, L. S. (1996). Using multivari-ate statistics (3rd ed.). New York: Harper Collins CollegePublishers.
Tennen, H., Affleck, G., & Herzberger, S. (1984). SCL-90R. InD. J. Keyser & R. C. Sweetland (Eds.), Test critiques (Vol. 3,pp. 583–594). Kansas City, MO: Test Corporation ofAmerica.





























