Embed Size (px)
Citation preview
JUNE 2003, VOL 77, NO 6 9 Oetker-Black Jones * Estok
Ryan 8 Gale Parker
Preoperative Teaching and Hysterectomy Outcomes
ysterectomy is the second most common major surgery performed in the United States.’ Hysterectomy, therefore, represents a serious concern for women’s health.2 The long-term personal, psychological, and
social costs of uncomplicated and complicated expe- riences with hysterectomy require study.
Adequate health assessment and intervention before the surgery may improve hysterectomy out- c o m e ~ . ~ Preoperative preparation for hysterectomy using a teaching protocol based on self-efficacy, post- operative measures to improve short- and long-term outcomes, and specific postoperative behaviors designed to decrease postoperative complications has not been studied. This is especially relevant because preoperative instruction has been researched for years, yet individuals who receive preoperative
A B S T R A C T
instruction do not always remember it.4 Although preoperative instruction, in general,
has been found to yield better immediate postopera- tive outcomes than no preoperative instruction, the magnitude and consistency of benefits have been smalL5 In addition, there remains a lack of knowledge regarding the effects of preoperative instruction on long-term outcomes. Theoretical links between pre- operative preparation and outcome measures rarely have been presented!
PURFOSE The purpose of this study was to use a theoreti-
cal model to determine whether an eficacy-enhanc- ing teaching protocol was effective in improving immediate postoperative behaviors and selected short- and long-term health outcomes in women who
underwent abdominal hysterec- tomies. The model used was the self-efficacy theory of Albert Bandura, PhD.7
This study used a theoretical model to determine whether an efficacy-enhancing teaching protocol was effective in improving immediate postoperative behaviors and selected short- and long- term health outcomes in women who underwent abdominal hys- terectomies. The model used was the self-efficacy theory of Albert Bandura, PhD. One hundred eight patients in a 486-bed teaching hospital in the Midwest who underwent hysterectomies participated. The participation rate was 85%, and the attrition rate was 17% dur- ing the slx-month study. The major finding was that participants in the efficacy-enhancing teaching group ambulated significantly longer than participants in the usual care group. This is an important finding because the most prevalent postoperative complications after hys- terectomy are atelectasis, pneumonia, paralytic ileus, and deep vein thrombosis, and postoperative ambulatlon has been shown to decrease or prevent all of these complications. This finding could affect the overall health status of women undergoing hysterectomies. AORNJ77 (June 2003) 1215-1231.
The hypotheses guiding this study were as follows. 1. Patients who received the efi-
cacy-enhancing teaching pro- tocol will have higher scores on the preoperative self-efEca- cy scale (PSES), while control- ling for postintervention self- efficacy, than patients who did not receive the protocol.
2. Patients who received the eR- cacy-enhancing teaching pro- tocol will have lower preopera- tive and postoperative scores on the State Anxiety Inventory (SAI) than patients who did not receive the protocol, while
O E T K E R - B L A C K , J O N E S , E S T O K , R Y A N , G A L E , P A R K E R
1215 AORN JOURNAL
JUNE 2003, VOL 77, NO 6 Oetker-Black Jones Estok
9 Ryan Gale Parker
controlling for postintervention anxiety, preopera- tively, at discharge, at six weeks after surgery, and at six months after surgery.*
3. Patients who received the efficacy-enhancing teaching protocol will have lower pain scores on the visual analog scale (VAS) immediately after surgery than patients who did not receive the protocol.
4. Patients who received the efficacy-enhancing teaching protocol will have a higher level of per- formance of ambulation immediately after surgery than patients who did not receive the protocol, when controlling for postoperative pain.
5. Patients who received the efficacy-enhancing teaching protocol will have a higher vital capacity immediately after surgery, while controlling for postintervention vital capacity and postoperative pain, than patients who did not receive the protocol.
6. Patients who received the efficacy-enhancing teaching protocol will have fewer preventable complications (ie, atelectasis, pneumonia, paralyt- ic ileus, deep vein thrombosis) while hospitalized than patients who did not receive the protocol.
7. Patients who received the efficacy-enhancing teaching protocol will have shorter hospital stays than patients who did not receive the protocol.
8. Patients who received the efficacy-enhancing teaching protocol will have higher scores on the health status questionnaire (HSQ) at discharge, six weeks after surgery, and six months after surgery than patients who did not receive the protocol?
9. Preoperative efficacy expectations, preoperative instruction method, and anxiety are significant pre- dictors of immediate postoperative behaviors (eg, ambulation, vital capacity), preventable complica- tions, and selected health outcomes in women who undergo total abdominal hysterectomies.
REVIEW OF THE LITERATURE Approximately 600,000 women have hysterec-
tomies annually in the United States. Hysterectomy reaches its peak occurrence rate in women who are between 45 and 54 years of age.” Although the imme- diate physical complications associated with hysterec- tomy are similar to those of any major abdominal sur- gery, even the prospect of hysterectomy is said to engender more stress than other comparable surger- ies.” The physiological response to stress puts women at risk for more negative surgical outcomes. In response to the stressor of an impending surgery, anx- iety often occurs and has been shown to be related to
the effect size of preoperative instruction.l* Preoperative instruction A surgical procedure
constitutes an aversive situation in which a patient faces pain, serious body damage, and possibly death.” Preoperative instruction has been shown to help patients deal more effectively with surgery.14 Preoperative instruction tends to decrease complica- tions, increase patient satisfaction, shorten the length of hospitalization, and promote psychological well- being.15 Two researchers found that psychoeducation- al interventions with an average duration of only 42 minutes enhanced recovery.16 Other researchers con- cluded that the overall mean effect size of preopera- tive teaching on positive postoperative outcomes ranged fiom 0.39’’ to 0.44.’*
One group of researchers found that preoperative instruction improved posthysterectomy outcomes.19 Structured preoperative teaching by a nurse clinician resulted in women performing more self-care activi- ties in the immediate postoperative period and at one month after discharge. Instruction was not related to the incidence of preventable complications. No analysis was presented regarding the relationship between performance of self-care activities and the incidence of preventable complications.
Other studies have indicated that appropriate preoperative preparation and counseling can alleviate the anxiety and concerns that women have about their response to hysterectomy.” Two researchers studied educational needs and found that women undergoing hysterectomies wanted more explanation related to all areas of surgery?’ The area most often rated as very important (ie, by 92% of participants) was phys- ical effects of surgery. Ninety-four percent stated that they wanted to receive preoperative information about hysterectomy before hospitalization. These researchers concluded that
women had a need for structured preoperative information, more information on physical effects should be included, and information should be provided before hospitalization.
Same day surgeries and shorter hospital stays demand that health care professionals find ways to provide patient education that effectively addresses the physical and psychological concerns of women undergoing hysterectomies. In general, surgical patients, and in particular, women undergoing hys- terectomies, need more support and information than they receive?*
1216 AORN JOURNAL
JUNE 2003, VOL 77, NO 6 Oetker-Black 9 Jones Estok
Ryan Gale Parker 9
Although any preoperative teaching tends to be more effective than no teaching, research is needed to determine how preoperative instruction exerts its effects. One researcher concluded that patient knowledge alone is not sufficient to ensure perform- ance of behaviors necessary to prevent postoperative complication^.^^
One study suggests that additional theory-based research is required to understand the processes of coping with surgery?‘ Two researchers noted that comprehensive psychoeducational interventions for preoperative patients need to be improved and, by doing so, the physical, personal, and social costs to patients and their family members could be reduced enormou~ly?~
SelJeflcaacy theov. Self-efficacy theory offers a link between self-perceptions and behavior and has been found to be effective in explaining health pro- motive behaviors in Self-efficacy is concerned with individuals’ beliefs in their capabili- ties to mobilize motivation, cognitive resources, and courses of action required to exercise control over the environment and bring about a desired o~tcome.~’ There are two components of self-efficacy-out- come expectations and efficacy expectations. An outcome expectation is a person’s estimate that a given behavior will lead to certain outcomes. An efficacy expectation is a person’s conviction that he or she successfilly can execute behavior that is required to produce desired outcomes. Efficacy expectations vary on three dimensions-magnitude, generality, and strength. Magnitude refers to the level of difficulty, generality refers to the number of behavioral domains in which individuals judge themselves to be efficacious, and strength refers to the confidence individuals have in their ability to complete a specific task.**
According to Bandura, self-efficacy is based on four sources of information-performance accom- plishments, vicarious experiences, oral persuasion, and physiological states.29 Performance accomplish- ments are based on mastery experiences or those behaviors that individuals actually have performed themselves. Vicarious experiences involve seeing others perform activities. Oral persuasion happens when people are given information orally about their capability to perform a specific behavior. Physio- logical states (eg, emotional arousal) describe the experience of personally painfil situations. The amount of anxiety experienced is a cue to an individ- ual’s ability to master a situation and how much effort
will be required to master an experience.’O Self-efficacy has been found to determine moti-
vational levels,” and individuals who believe they can exert control over potential threats are not as stressed by them as those who feel they cannot man- age threat^.'^ Researchers found that restoring self- efficacy to perform normal everyday activities was essential for recovery of patients who had undergone cardiac surgery and that lack of confidence in their abilities to resume normal activities slowed recovery, even when physical healing was present.” High lev- els of stress, autonomic activation, and plasma cate- cholamine secretion are related to inefficacy in con- trolling psychological stressors.M
Eflcacy expectations and health promotion. In 1990, two researchers found that inpatient educa- tion and telephone monitoring during convalescence between four and eight weeks and between eight and 24 weeks after surgery increased efficacy expectations of 149 patients who had undergone cardiac surgery.35 The efficacy expectations for all physical activities were summed at eight weeks and found to be predictive for activities. Another group of researchers revealed that efficacy expectations were the best predictors of physical status and sociaVleisure hctioning six months after coronary bypass surgery in a study of 125 men.36 Efficacy expectations explained more variance in functional status outcomes than did measures of disease sever- ity, hctional capacity, comorbidity, or preoperative function. In addition, even when physical healing was present, recovery was slow for patients who lacked confidence in their abilities to resume normal activities. In 1991, two researchers found that effi- cacy expectations were a significant predictor of exercise levels in sedentary adult females.” In a review of determinants of health promotive behav- ior, another researcher noted that efficacy expecta- tions have a positive influence on physical activity and exer~ise.)~
Self-efficacy scores were found to be signifi- cantly related to distress during endoscopy in a study of 48 men.3g As hypothesized, pre-endoscopy efica- cy expectations predicted coping outcomes, regard- less of whether participants had prior experience with endoscopy, which supports the idea that self-efficacy is a mediator of performance and arousal in a stress- laden medical context.
Efficacy expectations were related to improved function and lower self-report of pain at a six-month follow-up in 45 people participating in a three-week
1218 AORN JOURNAL
JUNE 2003, VOL 77, NO 6 Oeiker-Black Jones 8 Esiok 8
Ryan Gale Parker
rehabilitation program for low back paina Self-effi- cacy also has been shown to be related to the per- formance of health promotive behaviors in patients with chronic diseases. A 1993 study found that improved self-management of disability and adher- ence to health recommendations in 86 patients with rheumatoid arthritis was related to efficacy expecta- tions:' The study concluded that patient education should be aimed at strengthening efficacy expecta- tions. Another group of researchers found that effi- cacy expectations were a significant predictor of patients' adherence to diabetes treatment during an eight-week and one-year time period>*
In regard to health promotion, efficacy expecta- tions have been related to more effective outcomes in smoking cessation, weight reduction, and exercise compliance. Furthermore, efficacy expectations can be increased through patient education and are relat- ed to positive postoperative outcomes."
Summary. Although it has been demonstrated that self-efficacy is a reliable predictor of physical and social functioning six months after cardiac sur- gery, no research was found that examined the rela- tionship between efficacy expectations and health promotion, complication prevention, or recovery in women undergoing hysterectomies.M Additional research is needed to fill the knowledge gap that exists about the relationships between short- and long-term posthysterectomy outcomes, preoperative preparation, and self-efficacy theory. Hysterectomy affects the lives of many women. Findings regarding the short- and long-term personal, psychological, and social effects of hysterectomy are not well-estab- Iished, and those that do exist often are inconsistent.
Although preoperative preparation has the potential to increase efficacy expectations, decrease anxiety, and improve postoperative outcomes, the mechanism by which preoperative instruction exerts its effect is unknown. The paucity of theoretically based research regarding preoperative instruction may explain the discrepancies in findings. The use of a self-efficacy based educational program may be effective in improving physical, psychosocial, and financial outcomes related to hysterectomy.
This study is important for the 600,000 women who undergo hysterectomies annually, their family members, and those who provide their health care. Given same day admissions and shortened hospital stays, nurses who are responsible for providing pre- operative instruction should study new ways to improve the outcomes related to such surgery.
M M O D This experimental study was designed to deter-
mine whether an efficacy-enhancing teaching proto- col was effective in improving preoperative efficacy expectations, performance of postoperative behaviors, and selected short- and long-term health outcomes for women who underwent hysterectomies. A sample of 108 women admitted to a 486-bed teaching hospital in the Midwest for same day total abdominal hysterec- tomies (ie, removal of uterus, ovaries, and fallopian tubes) was obtained by convenience sampling.
For hypotheses one through seven using a sig- nificance level of 0.05, a power of 0.8, and an effect size of 0.3 for a standard deviation difference in means, it was determined that 90 participants were needed.45 Assumption of 0.3 effect size is the same for each variable and consistent with previous psycho- educational studies.q Criteria for participant selection were that they be
I 8 to 54 years of age; able to read and write English; premenopausal; oriented to person, place, and time; able to do deep breathing exercises three times per hour; able to walk for five minutes without assistance; and undergoing total abdominal hysterectomy for non- malignant reasons under general anesthesia.
Data collectors used the OR schedule to identify potential participants. n o s e willing to participate were assigned via a table of random numbers to one of the study groups and received either the usual care protocol or the efficacy-enhancing teaching protocol. Preoperative instruction was given during partici- pants' preassessment testing period, which occurred before surgery.
Ethical considerations. Permission to conduct the study was obtained from the Human Subjects Review Board of Kent State University, Ohio, and the institution where data were collected. Written permission was obtained from all participants. Patients were approached to participate on the day of preassessment testing, and a thorough explanation of the study was provided. Patients then were given time to read the consent form and ask questions before consenting to participate.
Implementation of eficacy-enhancing teach- ingprotocoL The teaching protocol was based on the theory of self-efficacy, and it prepared patients for surgery and postoperative recovery. The protocol
1221 AORN JOURNAL
JUNE 2003, VOL 77, NO 6 Oetker-Black ‘Jones Estok 9
Ryan Gale Parker
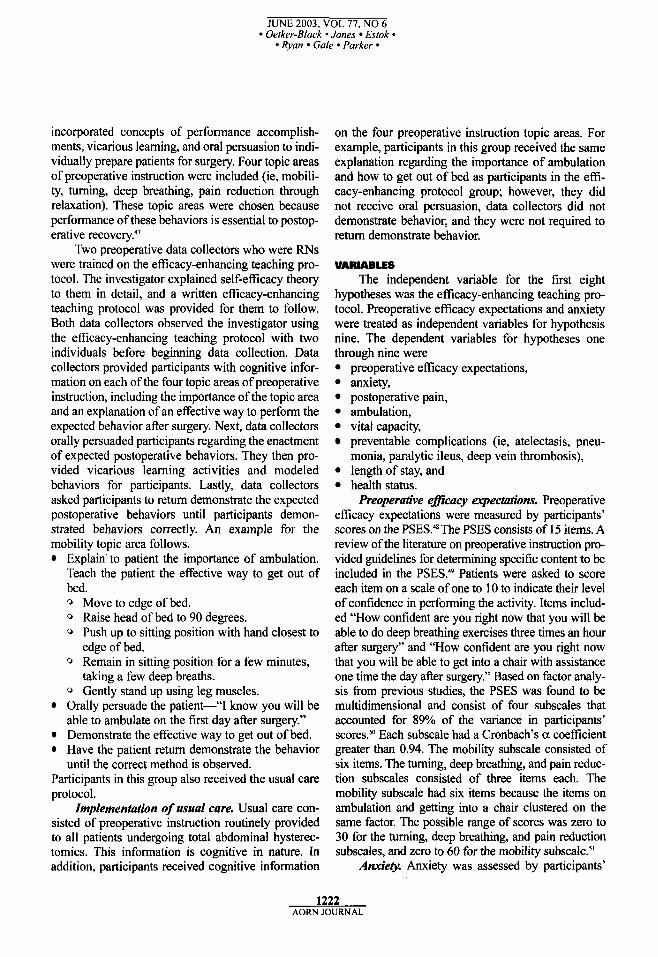
incorporated concepts of performance accomplish- ments, vicarious learning, and oral persuasion to indi- vidually prepare patients for surgery. Four topic areas of preoperative instruction were included (ie, mobili- ty, turning, deep breathing, pain reduction through relaxation). These topic areas were chosen because performance of these behaviors is essential to postop- erative recovery.4’
Two preoperative data collectors who were RNs were trained on the efficacy-enhancing teaching pro- tocol. The investigator explained self-efficacy theory to them in detail, and a written efficacy-enhancing teaching protocol was provided for them to follow. Both data collectors observed the investigator using the efficacy-enhancing teaching protocol with two individuals before beginning data collection. Data collectors provided participants with cognitive infor- mation on each of the four topic areas of preoperative instruction, including the importance of the topic area and an explanation of an effective way to perform the expected behavior after surgery. Next, data collectors orally persuaded participants regarding the enactment of expected postoperative behaviors. They then pro- vided vicarious learning activities and modeled behaviors for participants. Lastly, data collectors asked participants to return demonstrate the expected postoperative behaviors until participants demon- strated behaviors correctly. An example for the mobility topic area follows.
Explain. to patient the importance of ambulation. Teach the patient the effective way to get out of bed. Q Move to edge of bed. Q Raise head of bed to 90 degrees. Q Push up to sitting position with hand closest to
edge of bed. 0 Remain in sitting position for a few minutes,
taking a few deep breaths. Q Gently stand up using leg muscles. Orally persuade the patient-“I know you will be able to ambulate on the first day after surgery.” Demonstrate the effective way to get out of bed. Have the patient return demonstrate the behavior until the correct method is observed.
Participants in this group also received the usual care protocol.
Implementation of usual care. Usual care con- sisted of preoperative instruction routinely provided to all patients undergoing total abdominal hysterec- tomies. This information is cognitive in nature. In addition, participants received cognitive information
on the four preoperative instruction topic areas. For example, participants in this group received the same explanation regarding the importance of ambulation and how to get out of bed as participants in the effi- cacy-enhancing protocol group; however, they did not receive oral persuasion, data collectors did not demonstrate behavior, and they were not required to return demonstrate behavior.
VARIABLES The independent variable for the first eight
hypotheses was the efficacy-enhancing teaching pro- tocol. Preoperative efficacy expectations and anxiety were treated as independent variables for hypothesis nine. The dependent variables for hypotheses one through nine were
preoperative efficacy expectations, anxiety, postoperative pain, ambulation, vital capacity, preventable complications (ie, atelectasis, pneu- monia, paralytic ileus, deep vein thrombosis), length of stay, and health status.
Preoperative e#Zcacy expectations. Preoperative efficacy expectations were measured by participants’ scores on the PSES.4’ The PSES consists of 15 items. A review of the literature on preoperative instruction pro- vided guidelines for determining specific content to be included in the PSES.49 Patients were asked to score each item on a scale of one to 10 to indicate their level of confidence in performing the activity. Items includ- ed “HOW confident are you right now that you will be able to do deep breathing exercises three times an hour after surgery” and “How confident are you right now that you will be able to get into a chair with assistance one time the day after surgery.” Based on factor analy- sis from previous studies, the PSES was found to be multidimensional and consist of four subscales that accounted for 89% of the variance in participants’ scores.5O Each subscale had a Cronbach’s a coefficient greater than 0.94. The mobility subscale consisted of six items. The turning, deep breathing, and pain reduc- tion subscales consisted of three items each. The mobility subscale had six items because the items on ambulation and getting into a chair clustered on the same factor. The possible range of scores was zero to 30 for the turning, deep breathing, and pain reduction subscales, and zero to 60 for the mobility subscale.”
Anxiety. Anxiety was assessed by participants’
1222 AORN JOURNAL
JUNE 2003, VOL 77, NO 6
Ryan Gale Parker Oetker-Black Jones Estok
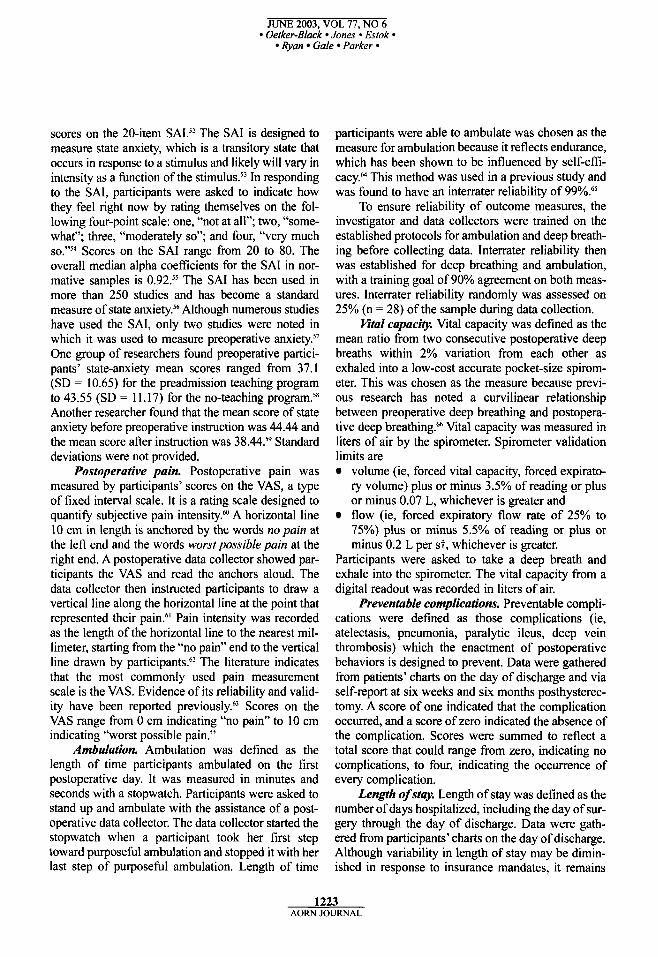
scores on the 20-item SAL5’ The SAI is designed to measure state anxiety, which is a transitory state that occurs in response to a stimulus and likely will vary in intensity as a function of the In responding to the SAI, participants were asked to indicate how they feel right now by rating themselves on the fol- lowing four-point scale: one, “not at all”; two, “some- what”; three, “moderately so”; and four, “very much
Scores on the SAI range from 20 to 80. The overall median alpha coefficients for the SAI in nor- mative samples is 0.92.55 The SAI has been used in more than 250 studies and has become a standard measure of state Although numerous studies have used the SAI, only two studies were noted in which it was used to measure preoperative an~iety.~’ One group of researchers found preoperative partici- pants’ state-anxiety mean scores ranged from 37.1 (SD = 10.65) for the preadmission teaching program to 43.55 (SD = 1 1.17) for the no-teaching pr~gram.’~ Another researcher found that the mean score of state anxiety before preoperative instruction was 44.44 and the mean score after instruction was 3 8 M s 9 Standard deviations were not provided.
Postoperative pain. Postoperative pain was measured by participants’ scores on the VAS, a type of fixed interval scale. It is a rating scale designed to quantify subjective pain intensity.” A horizontal line 10 cm in length is anchored by the words no pain at the left end and the words worst possible pain at the right end. A postoperative data collector showed par- ticipants the VAS and read the anchors aloud. The data collector then instructed participants to draw a vertical line along the horizontal line at the point that represented their pain.6’ Pain intensity was recorded as the length of the horizontal line to the nearest mil- limeter, starting from the “no pain” end to the vertical line drawn by participants?’ The literature indicates that the most commonly used pain measurement scale is the VAS. Evidence of its reliability and valid- ity have been reported previou~ly.~~ Scores on the VAS range from 0 cm indicating “no pain” to 10 cm indicating “worst possible pain.”
Ambulation. Ambulation was defined as the length of time participants ambulated on the first postoperative day. It was measured in minutes and seconds with a stopwatch. Participants were asked to stand up and ambulate with the assistance of a post- operative data collector. The data collector started the stopwatch when a participant took her first step toward purposeful ambulation and stopped it with her last step of purposefbl ambulation. Length of time
participants were able to ambulate was chosen as the measure for ambulation because it reflects endurance, which has been shown to be influenced by self-efi- cacy.M This method was used in a previous study and was found to have an interrater reliability of 99%?5
To ensure reliability of outcome measures, the investigator and data collectors were trained on the established protocols for ambulation and deep breath- ing before collecting data. Interrater reliability then was established for deep breathing and ambulation, with a training goal of 90% agreement on both meas- ures. Interrater reliability randomly was assessed on 25% (n = 28) of the sample during data collection.
Htal capacity. Vital capacity was defined as the mean ratio from two consecutive postoperative deep breaths within 2% variation from each other as exhaled into a low-cost accurate pocket-size spirom- eter. This was chosen as the measure because previ- ous research has noted a curvilinear relationship between preoperative deep breathing and postopera- tive deep breathing.% Vital capacity was measured in liters of air by the spirometer. Spirometer validation limits are
volume (ie, forced vital capacity, forced expirato- ry volume) plus or minus 3.5% of reading or plus or minus 0.07 L, whichever is greater and flow (ie. forced expiratory flow rate of 25% to 75%) plus or minus 5.5% of reading or plus or minus 0.2 L per st, whichever is greater.
Participants were asked to take a deep breath and exhale into the spirometer. The vital capacity from a digital readout was recorded in liters of air.
Preventable complications. Preventable compli- cations were defined as those complications (ie, atelectasis, pneumonia, paralytic ileus, deep vein thrombosis) which the enactment of postoperative behaviors is designed to prevent. Data were gathered from patients’ charts on the day of discharge and via self-report at six weeks and six months posthysterec- tomy. A score of one indicated that the complication occurred, and a score of zero indicated the absence of the complication. Scores were summed to reflect a total score that could range from zero, indicating no complications, to four, indicating the occurrence of every complication.
Length of stay. Length of stay was defined as the number of days hospitalized, including the day of sur- gery through the day of discharge. Data were gath- ered from participants’ charts on the day of discharge. Although variability in length of stay may be dimin- ished in response to insurance mandates, it remains
1223 AORN JOURNAL
JUNE 2003, VOL 77, NO 6 Oetker-Black 9 Jones Estok 8
9 Ryan Gale Parker
an important variable to be assessed because of its relationship to postoperative complications and costs.
Health sfafus. Health status was obtained from participants' scores on the HSQ.6' There are eight sub- scales of the HSQ (ie, health perception, physical functioning, social functioning, role limitations attrib- uted to physical health, role limitations attributed to emotional problems, bodily pain, mental health, ener- gy/fatigue) grouped into three health dimensions (ie, overall evaluation of health, functional status, well- being). This is a 39-item questionnaire that measures health across populations, both with and without dis- ease. Each item has response options ranging from one to six. Responses were scored in two steps. The first step involved the recoding of questionnaire items. In the second step, an average of these recoded items was taken, giving a summated score for each of the eight health concepts. Subscales were scored so that the higher numbers represent more positive health attributes. Reliability estimates via alpha were greater than 0.7 for all subscales. The instrument has estab- lished content and construct validity."
DATA COLLECTION During data collection, the primary investigator
observed the data collectors initially, after half the participants were entered in the study, and every two months while data collectors instructed participants. Using a checklist, the investigator determined whether key points were being included and ensured consistency of the teaching protocols. Inclusion of less than 90% of the content items of the teaching protocols indicated a need for further training to reestablish consistency.
To ensure that data collectors were not biased, each implemented both the eacacy-enhancing and usual care teaching protocols. After half of the partic- ipants were entered in the study, data collectors were retrained and then switched teaching protocols. All participants followed the same postoperative protocol. Two different data collectors, blind to the experimen- tal condition of participants, collected data on the postoperative measures of anxiety, pain, ambulation, vital capacity, preventable complication rates, length of stay, and health status. Postoperative data were col- lected at six weeks and six months because six weeks after surgery is when physiological healing is near completion and six months provides time to assess long-term outcomes found to be less positive."
Eflcacy-enhancing group. Participants in this group completed the SAI and PSES, and data collec-
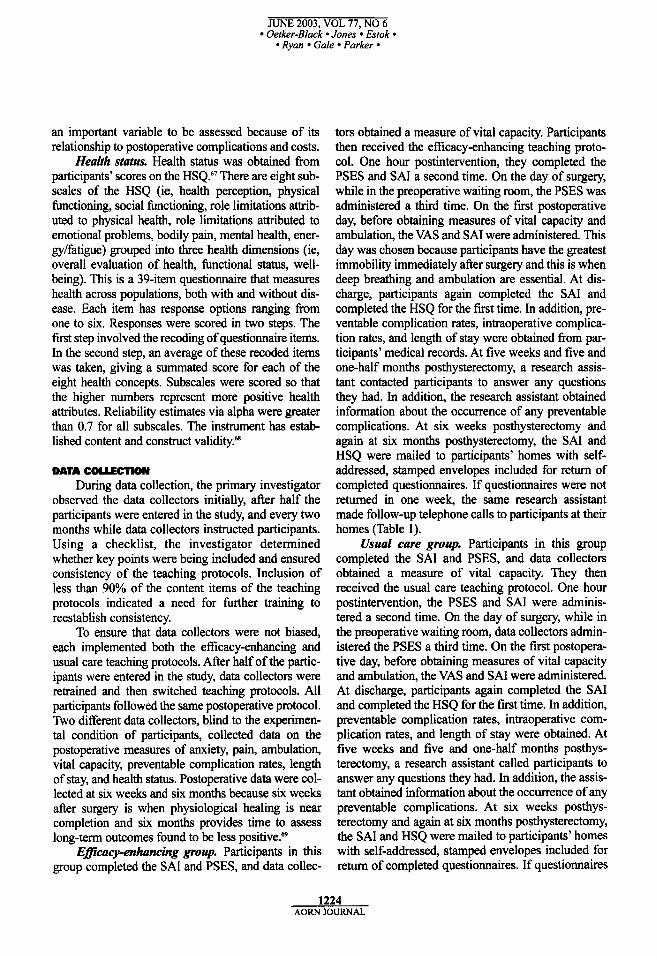
tors obtained a measure of vital capacity. Participants then received the efticacy-enhancing teaching proto- col. One hour postintervention, they completed the PSES and SAI a second time. On the day of surgery, while in the preoperative waiting room, the PSES was administered a third time. On the first postoperative day, before obtaining measures of vital capacity and ambulation, the VAS and SAI were administered. This day was chosen because participants have the greatest immobility immediately after surgery and this is when deep breathing and ambulation are essential. At dis- charge, participants again completed the SAI and completed the HSQ for the first time. In addition, pre- ventable complication rates, intraoperative complica- tion rates, and length of stay were obtained from par- ticipants' medical records. At five weeks and five and one-half months posthysterectomy, a research assis- tant contacted participants to answer any questions they had. In addition, the research assistant obtained information about the occurrence of any preventable complications. At six weeks posthysterectomy and again at six months posthysterectomy, the SAI and HSQ were mailed to participants' homes with self- addressed, stamped envelopes included for return of completed questionnaires. If questionnaires were not returned in one week, the same research assistant made follow-up telephone calls to participants at their homes (Table 1).
Usual care group. Participants in this group completed the SAI and PSES, and data collectors obtained a measure of vital capacity. They then received the usual care teaching protocol. One hour postintervention, the PSES and SAI were adminis- tered a second time. On the day of surgery, while in the preoperative waiting room, data collectors admin- istered the PSES a third time. On the first postopera- tive day, before obtaining measures of vital capacity and ambulation, the VAS and SAI were administered. At discharge, participants again completed the SAI and completed the HSQ for the first time. In addition, preventable complication rates, intraoperative com- plication rates, and length of stay were obtained. At five weeks and five and one-half months posthys- terectomy, a research assistant called participants to answer any questions they had. In addition, the assis- tant obtained information about the occurrence of any preventable complications. At six weeks posthys- terectomy and again at six months posthysterectomy, the SAI and HSQ were mailed to participants' homes with self-addressed, stamped envelopes included for return of completed questionnaires. If questionnaires
1224 AORN JOURNAL
JUNE 2003, VOL 77, NO 6 9 Oetker-Black Jones Estok
Ryan Gale Parker
Table 1 MODEL OF RESEARCH DESIGN FOR EFFICACY-ENHANCING AND USUAL CARE PROTOCOU
Preoperative Hrst postintenrention postoperattve Discharge 6-week 6-month
outcome Preintenrention outcome Dayof dayoutcome outcome outcome measures measures surgery measures measures measures measures State Anxiety PSES PSES Visual analog SAI Preventable Preventable Inventory (SAI) scale Health status complication complication Preoperative SAI questionnaire rates self-efficacy scale (PSES)
Vital capacity complication rates lntraoperative complication rates Length of
rates SAI SAI vital capacity (HSQ)
hbulation Preventable HSQ HSQ
Stay
were not returned in one week, the same research assistant made follow-up telephone calls to partici- pants at their homes.
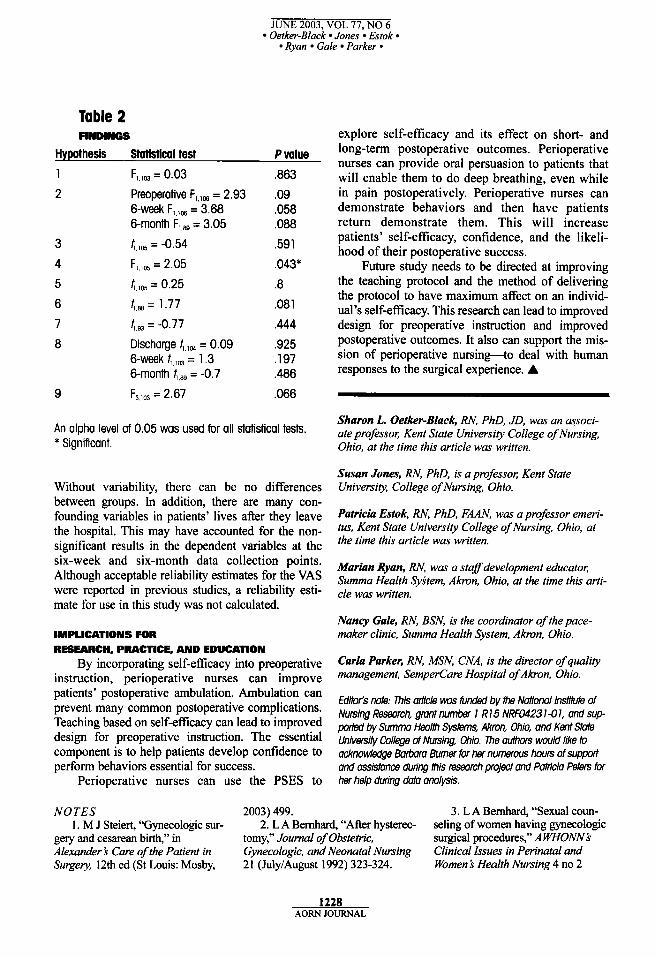
RESULTS The age of participants ranged from 25 to 52
years (mean [MI = 41; standard deviation [SD] = 5.87). Educational level ranged from 10 to 20 years (M = 13.64, SD = 2.3). Approximate family income ranged from $5,000 to $170,000 per year (M = $5 1,3 12; SD = $3 1,778). Hypotheses one, two, three, five, six, seven, eight, and nine were rejected because no significant difference was found between groups (Table 2). The fourth hypothesis was analyzed using analysis of covariance to test for mean ambulation score differences between patients who received the efficacy-enhancing protocol and those who did not, while controlling for postoperative pain. Ambulation was the only variable that showed significant differ- ences. Patients in the efficacy-enhancing teaching group ambulated significantly longer than patients in the usual care group (F,.,,, = 2.05, P = .043). They ambulated for a mean of 330 seconds (SD = 615), whereas patients in the usual care group ambulated for a mean of 156 seconds (SD = 97).
DISCUSSION The significant finding of this study cannot be
underestimated. The most common postoperative complications of hysterectomy (ie, atelectasis, pneu-
monia, paralytic ileus, deep vein thrombosis) are sim- ilar to those of any major abdominal surgery. Postoperative ambulation has been shown to decrease or prevent all of these complications. This could have a major affect on the overall health status of women undergoing hysterectomies.
Participants in the efficacy-enhancing group did not vary significantly from those in the usual care group in regard to eight of the hypotheses. This may have been due to the teaching protocol. It may need to be revised or started at an earlier period in the surgical experience to affect preoperative patients’ self-efficacy in areas other than ambula- tion. The majority of participants had a positive attitude regarding the study and believed it benefit- ed them, as evidenced by only a 17% attrition rate during the six-month study.
The major finding of the study is an important one. Ambulation is the key to postoperative recovery in many abdominal surgeries. Increasing self-efficacy preoperatively increases postoperative ambulation with the current teaching method. The next step is to discover what teaching method will affect the other dependent variables.
STUDY LIMITATIONS The current health care system, diagnosis-related
groups, and other factors may have affected the results. Every patient is treated using a clinical path- way. These pathways do not allow for variability.
1226 AORN JOURNAL
JUNE 2003, VOL 77, NO 6 Oerker-Black Jones Estok
Ryan Gale Parker 9
Table 2 FINDINGS
Hypothesis Statistical test P value 1 F,,,, = 0.03 ,863 2 Preoperative F,,,, = 2.93 .09
6-wek F,,,, = 3.68 ,058 6-month Fl,w = 3.05 .088
3 t,lm = -0.54 .591 4 F,,,,, = 2.05 .043* 5 t,,% = 0.25 .8 6 (,, = 1.77 .08 1
7 f1,93 = -0.77 ,444
8 Discharge fi,104 = 0.09 ,925 6 - w ~ k 4,,, = 1.3 ,197 6-month 4,= = -0.7 ,486
9 F,,,, = 2.67 ,066
An alpha level of 0.05 was used for all statistical tests. * Significant.
Without variability, there can be no differences between groups. In addition, there are many con- founding variables in patients’ lives after they leave the hospital. This may have accounted for the non- significant results in the dependent variables at the six-week and six-month data collection points. Although acceptable reliability estimates for the VAS were reported in previous studies, a reliability esti- mate for use in this study was not calculated.
IMPLICATIONS FOR RESEARCH, PRACTICE, AND EDUCATION
By incorporating self-eficacy into preoperative instruction, perioperative nurses can improve patients’ postoperative ambulation. Ambulation can prevent many common postoperative complications. Teaching based on self-eficacy can lead to improved design for preoperative instruction. The essential component is to help patients develop confidence to perform behaviors essential for success.
Perioperative nurses can use the PSES to
NOTES 2003) 499.
explore self-efficacy and its effect on short- and long-term postoperative outcomes. Perioperative nurses can provide oral persuasion to patients that will enable them to do deep breathing, even while in pain postoperatively. Perioperative nurses can demonstrate behaviors and then have patients return demonstrate them. This will increase patients’ self-efficacy, confidence, and the likeli- hood of their postoperative success.
Future study needs to be directed at improving the teaching protocol and the method of delivering the protocol to have maximum affect on an individ- ual’s self-efficacy. This research can lead to improved design for preoperative instruction and improved postoperative outcomes. It also can support the mis- sion of perioperative nursing-to deal with human responses to the surgical experience. A
Sharon L. Oetker-Black, RN, PhD, JD, was an associ- ate professor; Kent State University College of Nursing, Ohio, at the time this article was written.
Susan Jones, RN, PhD, is a professor; Kent State University, College of Nursing, Ohio.
Patricia Estok, RN, PhD, FAAN. was a professor emeri- tus, Kent State University College of Nursing, Ohio, at the time this article was written.
Marian Ryan, RN, was a staff development educator; Summa Health System, Akron, Ohio, at the time this arti- cle was written.
Nancy Gale, RN, BSN, is the coordinator of the pace- maker clinic, Summa Health System, Akron, Ohio.
Carla Parker, RN, MSN, CNA, is the director of quality management, SemperCare Hospital of A h n , Ohio.
EdMs note: mis an’icle w s Rlnded by the National InstiiMe of Nursing Research, grant number 1 R 15 NRW423 1-0 I , and sup- ported by Summa Hmlth Systems, Akron, Ohio, and Kent state Univmw Call@e of Nursing, Ohio. The aulhors would like to acknowledge Barbara Burner far her numerous hours of support and assistance during this research project and W c l a Peters for her help during data analysis.
3. L A Bemhard, “Sexual coun- 1. M J Steiert, “Gynecologic sur- 2: L A Bemhard, “After hysterec- seling of women having gynecologic
surgical procedures,” A WHONNb Clinical Issues in Perinatal and Women b Health Nursing 4 no 2
gery and cesarean birth,” in Alexander b Care of the Patient in Surgey, 12th ed (St Louis: Mosby,
tomy,” Journal of Obstetric, Gynecologic, and Neonatal Nursing 21 (July/August 1992) 323-324.
1228 AORN JOURNAL
JUNE 2003, VOL 77, NO 6 Oetker-Black Jones Estok
Ryan Gale Parker
(1993) 250-257. 4. E C Devine, T D Cook, “A
meta-analytic analysis of effects of psychoeducational interventions on length of postsurgical hospital stay,” Nursing Research 32 (September/ October 1983) 267-274; E C Devine, T D Cook, “Clinical and cost-saving effects of psychoeducational inter- ventions with surgical patients: A meta-analysis,” Research in Nursing and Health 9 (June 1986) 89- 105; D Hathaway, “Effect of preoperative instruction on postoperative out- comes: A meta-analysis,” Nursing Research 35 (September/October 1986) 269-275; K M Healy, “Does preoperative instruction make a dif- ference?“ American Journal of Nursing 68 (January 1968) 62-67; J E Johnson, N J Christman, C Stitt, “Personal control interventions: Short- and long-term effects on sur- gical patients,” Research in Nursing andHealth 8 (June 1985) 131-145; I King, B Tarsitano, “The effect of structured and unstructured pre-oper- ative teaching: A replication,” Nursing Research 3 1 (November/ December 1982) 324-329; F E Schmitt, P J Wooldridge, “Psycho- logical preparation of surgical patients,” Nursing Research 22 (March/April 1973) 108-116.
5. Hathaway, “Effect of preopera- tive instruction on postoperative out- comes: A meta-analysis,” 269-275; J E Johnson, “Coping with elective surgery,” Annual Review of Nursing Research 2 (1984) 107-132.
6. Johnson, Christman, Stitt, “Personal control interventions: Short- and long-term effects on sur- gical patients,” 131-145.
7. A Bandura, “Self-efficacy: Toward a unifLing theory of behav- ioral change,” Psychological Review
8. C D Spielberger, R L Gorsuch, 84 (March 1977) 191-215.
Manual for the State-Trait Anxiety Inventory, revised ed (Palo Alto, Calif: Consulting Psychologists Press, Inc, 1983); C D Spielberger, R L Gorsuch, R E Lushene, STM Manual for the State-Trait Anxiety Inventory (Palo Alto, Calif:
Consulting Psychologist Press, 1970).
2.0 (Bloomington, Minn; Health Outcomes Institute, 1993).
10. N C Sharts, “Hysterectomy for nonmalignant conditions,” American Journal of Nursing 101 (September 2001) 32-40.
Englesmann, J Marino, “Depression after hysterectomy: A comparative study,” Psychosomatics 29 (Summer
12. Hathaway, “Effect of preoper-
9. Health Status Questionnaire
1 1. M Lalinec-Michaud, F
1988) 307-314.
ative instruction on postoperative outcomes: A meta-analysis,” 269- 275.
13. I L Janis, Psychological Stress; Psychoanalytic and Behavioral Studies of Surgical Patients (New York Wiley, 1958).
14. Ibid; Healy, “Does preopera- tive instruction make a difference?” 62-67; King, Tarsitano, ‘The effect of structured and unstructured pre- operative teaching: A replication,” 324-329; D Klos et al, “A compari- son of two methods of delivering presurgical instructions,” Patient Counselling and Health Education 2 (First quarter 1980) 6-13; L Levesque et al, “Evaluation of a presurgical group program given at two different times,” Research in Nursing and Health 7 (September 1984) 227-236; C Shimko, “The effect of preoperative instruction on state anxiety,” Journal of Neum- surgical Nursing 13 (December 1981) 3 18-322; Schmitt, Wooldridge, “Psychological preparation of surgi- cal patients.” 108- 1 16.
15. Devine, Cook, “A meta-analyt- ic analysis of effects of psychoeduca- tional interventions on length of postsurgical hospital stay,” 267-274; Devine, Cook, “Clinical and cost- saving effects of psychoeducational interventions with surgical patients: A meta-analysis,” 89-105; Hathaway, “Effect of preoperative instruction on postoperative outcomes: A meta- analysis,” 269-275; Healy, “Does preoperative instruction make a dif- ference?” 62-67; Johnson, Christ-
man, Stitt, “Personal control inter- ventions: Short- and long-term effects on surgical patients,’’ 1 3 1 - 145; King, Tarsitano, “The effect of structured and unstructured pre-oper- ative teaching: A replication,” 324- 329; Schmitt, Wooldridge, “Psycho- logical preparation of surgical patients,” 1 08- 1 16.
16. Devine, Cook, “Clinical and cost-saving effects of psychoeduca- tional interventions with surgical patients: A meta-analysis,” 89-105.
17. Ibid. 18. Hathaway, “Effect of preoper-
ative instruction on postoperative outcomes: A meta-analysis,” 269- 275.
19. P D Williams et al, “Effects of preparation for mastectomyhysterec- tomy on women’s post-operative self-care behaviors,” International Journal of Nursing Studies 25 no 3 (1988) 191-206.
20. Bemhard, “Sexual counseling of women having gynecologic surgi-
“Hidden problems after a hysterecto- my,” Nursing f i m a 82 (June 4- 10, 1986) 4346.
2 1. M S N e e h , M E Taylor, “Educational needs of hysterectomy patients,’’ Patient Counselling and Health Education 3 (Fourth quarter
cal P ~ O C ~ U R S , ” 250-257; D Gould,
1981) 150-155. 22. P E Dulaney, V C Crawford, G
Turner, “A comprehensive education and support program for women experiencing hysterectomies,” Journal of Obstetric, Gynecologic, and Neonatal Nursing 19 (JUly/Au~St 1990) 3 19-325.
23. N L Risser, “Preoperative and postoperative care to prevent pul- monary complications,” Heart and Lung 9 (JanwyFebruary 1980) 57- 67.
24. Johnson “Coping with elective
25. Devine, Cook, “A meta-analyt- ic analysis of effects of psychoeduca- tional interventions on length of postsurgical hospital stay,” 267-274.
26. S M Gattuso, M D Litt, T E Fitzgerald, “Coping with gastroin- testinal endoscopy: Self-efficacy
surgery,” 107-132.
1229 AORN JOURNAL
JUNE 2003, VOL 77, NO 6 Oetker-Black Jones - Estok .
Ryan Gale - Parker
enhancement and coping style,” Journal of Consulting and Clinical Psychology 60 (February 1992) 133- 139; D J Kavanaugh, S Gooley, P H Wilson, “Prediction of adherence and control in diabetes,” Journal of Behavioral Medicine I6 (October 1993) 509-522; E McAuley, L Jacobson, “Self-efficacy and exercise participation in sedentary adult females,” American Journal of Health Promotion 5 (January/ February 1991) 185-191.
regulatory mechanisms governing the impact of social comparison on complex decision making,” Journal of Personality and Social Psychology 60 (June 1991) 941-951.
Toward a unifying theory of behav- ioral change,” 191-215.
27. A Bandura, F J Jourden, “Self-
28. Bandura, “Self-efficacy:
29. [bid 30. A Bandura, “Human agency in
social cognitive theory,” American Psychologist 44 (September 1989) I 175-1 184.
3 I . Ibid. 32. S A Wiedenfeld et al, “Impact
of perceived self-efficacy in coping with stressors on components of the immune system,” Journal of Personality and Social Psychology 59 (November 1990) 1082-1094.
33. J K Allen, D M Becker, R T Swank, “Factors related to functional status after coronary artery bypass surgery,” Heart and Lung 19 (July
34. A Bandura, L Reese, N E 1990) 337-343.
Adams, “Microanalysis of action and fear arousal as a function of differen- tial levels of perceived self-efficacy” Journal of Personali& and Social
Bandura et al, “Catecholamine secre- tion as a function of perceived cop- ing self-efficacy,” Journal of Consulting and Clinical Psychology 53 (June 1985) 406-414; E M Ozer, A Bandura, “Mechanisms governing empowering effects: A self-efficacy analysis,” Journal of Personality and Social P.sychology 58 (March 1990)
35. S R Gortner, L S Jenkins,
Psychology 43 (July 1982) 5-21; A
472-486.
“Self-efficacy and activity level fol- lowing cardiac surgery,” Journal of Advanced Nursing 15 (October
36. Allen, Becker, Swank, “Factors related to hnctional status after coronary artery bypass SUT- gery,” 337-343.
cacy and exercise participation in sedentary adult females,” 185- 19 1.
38. C L Palank, “Determinants of health-promotive behavior. A review of current research,” Nursing Clinics of North America 26 (December
39. Gattuso, Litt, Fitzgerald, “Coping with gastrointestinal endoscopy: Self-efficacy enhance- ment and coping style,” 133-1 39.
self-efficacy in rehabilitation out- come among chronic low back patients,” Journal of Counseling
1990) 1132-1138.
37. McAuley, Jacobson, “Self-effi-
1991) 815-832.
40. E M Altmaier et al, “Role of
Psychology 40 (July 1993) 335-339. 4 1 . E Taal et al, “Health status,
adherence with health recommenda- tions, self-efficacy and social support in patients with rheumatoid arthritis,” Patient Education and Counseling 20 (May 1993) 63-76.
42. Kavanaugh, Gooley, Wilson, “Prediction of adherence and control in diabetes,” 509-522.
43. Allen, Becker, Swank, “Factors related to hnctional status after coronary artery bypass sur- gery,” 337-343; Gortner, Jenkins, “Self-efficacy and activity level fol- lowing cardiac surgery,” 132-1 138. 44. Allen, Becker, Swank,
“Factors related to functional status after coronary artery bypass sur- gery,” 337-343.
45. J Cohen, Statistical Power Analysis for the Behavioral Sciences, second ed (Hillsdale, NJ: L Erlbaum Associates, 1988).
46. Devine, Cook, “A meta-analyt- ic analysis of effects of psychoeduca- tional interventions on length of postsurgical hospital stay,” 267-274; Hathaway, “Effect of preoperative instruction on postoperative out- comes: A meta-analysis,” 269-275.
47. Devine, Cook, “A meta-analyt-
ic analysis of effects of psychoeduca- tional interventions on length of postsurgical hospital stay,” 267-274; Devine, Cook, “Clinical and cost- saving effects of psychoeducational interventions with surgical patients: A meta-analysis,” 89-1 05; King, Tarsitano, “The effect of structured and unstructured pre-operative teach- ing: A replication,” 324-329; S L Oetker-Black, “Generalizability of the preoperative self-efficacy scale,” Applied Nursing Research 9 (February 1996) 40-44; S L Oetker- Black, C Kauth, “Evaluating a revised self-efficacy scale for preop- erative patients,” AORN Journal 62 (August 1995) 244-250; S L Oetker- Black, R L Taunton, “Evaluation of a self-efficacy scale for preoperative patients,” AORN Journal 60 (July 1994) 43-50; S L Oetker-Black et al, “Preoperative self-efficacy and post- operative behaviors,” Applied Nursing Research 5 (August 1992)
48. Oetker-Black, “Generaliz- 134-139.
ability of the preoperative self-efica- cy scale,” 40-44; Oetker-Black, Kauth, “Evaluating a revised self- efficacy scale for preoperative patients,” 244-250; Oetker-Black, Taunton, “Evaluation of self-efficacy scale for preoperative patients,” 43- 50; Oetker-Black et al, “Preoperative self-efficacy and postoperative behaviors,” 134-1 39.
49. Healy, “Does preoperative instruction make a difference?” 62- 679; King, Tarsitano, “The effect of structured and unstructured pre- operative teaching: A replication,” 324-329; Klos et al, “A comparison of two methods of delivering presur- gical instructions,” 6- 13; Levesque et al, “Evaluation of a presurgical group program given at two differ- ent times,” 227-236; C A Lindeman, “Nursing intervention with the presurgical patient: Effectiveness and efficiency of group and individ- ual preoperative teaching,” Nursing Research 2 1 (May/June 1972) 196- 209; J Morgan, N Wells, E Robertson, “Effects of preoperative teaching on postoperative pain: A
1230 AORN JOURNAL
JUNE 2003, VOL 77, NO 6 8 Oetker-Black Jones Estok
Ryan Gale Parker
replication and expansion,” International Journal of Nursing Studies 22 no 3 (1 985) 267-280; J Wong, S Wong, “A randomized con- trolled trial of a new approach to preoperative teaching and patient compliance,” International Journal of Nursing Studies 22 no 2 ( I 985) 105- 1 I 5; M M Ziemer, “Effects of information on postsurgical coping,” Nursing Research 32 (September/ October 1983) 282-287.
50. Oetker-Black, “Generaliz- ability of the preoperative self-efica- cy scale,” 40-44; Oetker-Black, Kauth, “Evaluating a revised self- eficacy scale for preoperative patients,” 244-250; Oetker-Black, Taunton, “Evaluation of a self-efica- cy scale for preoperative patients,” 43-50; Oetker-Black et al, “Preoperative self-eficacy and post- operative behaviors,” 134- 139.
5 I . Oetker-Black, “Generaliz- ability of the preoperative self-efica- cy scale,” 40-44; Oetker-Black, Kauth, “Evaluating a revised self- efficacy scale for preoperative patients,” 244-250; Oetker-Black, Taunton, “Evaluation of a self-efica- cy scale for preoperative patients,” 43-50.
52. Spielberger, Gorsuch, Lushene, STAI Manual for the State-
Trait Anxiety Inven tory.
“Effects of music on patient anxi- ety,” AORN Journal 77 (February 2003) 396-410.
Lushene, STAI Manual for the State- Trait Anxiety Inventory.
55. Spielberger, Gorsuch, Manual for the State-Trait Anxiety Inventory, revised ed.
56. Ibid. 57. J R Graham, R S Lilly,
Psychological Testing (Englewood Cliffs, NJ: Prentice Hall, 1984); Spielberger, Gorsuch, Manual for the State-Trait Anxiety Inventory, revised ed.
58. Levesque et al, “Evaluation of a presurgical group program given at two different times,” 227-236.
59. Shimko, “The effect of preop- erative instruction on state anxiety,”
60. J S Carpenter, D Brockopp, “Comparison of patients’ ratings and examination of nurses’ responses to pain intensity rating scales,” Cancer Nursing 18 (August 1995) 292-298.
53. Ibid: E Mok, K Wong,
54. Spielberger, Gorsuch,
3 18-322.
6 1. Ibid 62. Ibid. 63. A G Gift, “Visual analog
scales: Measurement of subjective phenomena,” Nursing Research 38
(September/October 1989) 286-288.
cacy and exercise participation in sedentary adult females,” 185-1 91 ; Oetker-Black et al, “Preoperative self-eficacy and postoperative behaviors,” 134- 139.
“Preoperative self-efficacy and post- operative behaviors,” 134- 139.
64. McAuley, Jacobson, “Self-efi-
65. Oetker-Black et al,
66. Ibid. 67. Health Status Questionnaire
2.0. 68. C A McHomey, J E Ware, Jr,
A E Raczek, “The MOS 36-item Short-form Health Survey (SF-36): 11. Psychometric and clinical tests of validity in measuring physical and mental health constructs,” Medical Care 3 1 (March 1993) 247-263; Health Status Questionnaire 2.0; J E Ware, Jr, C D Sherbourne, “The MOS 36-item short-form health sur- vey (SF-36). I. Conceptual fkame- work and item selection,” Medical Care 30 (June 1992) 473-483.
69. Bemhard, “Sexual counseling of women having gynecologic surgi- cal procedures,” 250-257; D Gould, J Wilson-Bamett, “A comparison of recovery following hysterectomy and major cardiac surgery,” Journal of Advanced Nursing 10 (July 1985) 3 15-323.
Health Care Working Conditions Mect Patient Safety A report detailing the effects of health care working conditions on patient safety recommends increasing nurse staffing and improving communication sys- tems in health care facilities, according to a May 2, 2003, news release from the Agency for Healthcare Research and Quality (AHRQ). Researchers from the Oregon Health & Science University Evidence- based Practice Center, Portland, reviewed 1 15 stud- ies conducted in health care and nonhealth care set- tings, and they concluded that the literature supports specific recommendations to improve patient safety.
Among the researchers’ findings are that pre- ventable complications are less likely to occur when complex procedures are performed by physicians who perform them regularly. In addition, errors are
less likely to occur when staff members are subject to fewer interruptions and distractions. Improved communications systems for exchanging information when patient care is transferred from a hospital to a nonhospital setting can decrease medication errors.
Researchers did not find sufficient evidence to make recommendations regarding workplace stress, lighting, and several organizational factors. A sum- mary of the report is available from AHRQ at http://www.ahrq.gov/clinic/epcsums/worksum. htm.
AHRQ Report Describes Enhancements to Health Care Working Conditions that Could Improve Patient Safety (news release, Rmkville, Md: Agency for Healthcare Research and Qualily, May 2, 2003).
1231 AORN JOURNAL

![[Uterus preserving surgery versus vaginal hysterectomy in treatment of uterine descent: a systematic review]](https://img.pdfslide.net/doc/110x75/635a7925ef8fb73aab01c2e2/uterus-preserving-surgery-versus-vaginal-hysterectomy-in-treatment-of-uterine-descent.jpg)



























