Embed Size (px)
Citation preview
ORIGINAL PAPER
Preparing MSW Students for Integrative Mind–Body-SpiritPractice
Salome Raheim • Jack J. Lu
Published online: 16 March 2014
� Springer Science+Business Media New York 2014
Abstract Knowledge of new developments in social
work education supports clinical practitioners’ professional
development and their supervision of students and early
career social workers. Integrative mind–body-spirit (IMBS)
practice is a holistic paradigm that is emerging in social
work education and the profession. IMBS modalities have
a growing evidence base and are congruent with the heal-
ing practices of many cultures, thereby supporting cultur-
ally competent practice. This article explores the
development, implementation, and outcomes of an elective
MSW course designed to critically examine the IMBS and
biomedical paradigms and introduce students to IMBS
practice. Two sections of this course were piloted (n = 35)
and pre- and post-assessments administered. Findings
suggest that experienced clinicians can support the pro-
fessional development of novice practitioners by encour-
aging ongoing exploration and critical assessment of the
IMBS and biomedical paradigms and incorporation of
evidence-based mind–body-spirit practices in their clinical
work and self-care.
Keywords Integrative practice � Mind–body-spirit
paradigm � Social work education � Complementary and
alternative medicine
Introduction
Western scientific discoveries during the past 20 years
align with conceptualizations of healing, health, and well-
being held by Eastern traditions, indigenous peoples of the
Americas and many U.S. racial-ethnic groups. Findings
from neuroscience (Froeliger et al. 2012; Siegel 2007,
2012; Siegel et al. 2010), psychoneuroimmunology (Irwin
2008; Irwin and Miller 2007), psychosocial genomics
(Garland and Howard 2009; Rossi 2002a, b), and epige-
netics (Curley et al. 2011) affirm the mind–body-spirit
(MBS) connection and the dynamic interplay between
individual well-being and the physical and social envi-
ronment—principles that are common among many ancient
cultural traditions (Cassidy 2011). Studies have also shown
the efficacy of healing modalities that arise from these
traditions, such as acupuncture, mindfulness meditation
(Froeliger et al. 2012; Garland et al. 2012; Gaylord et al.
2011; Garland and Roberts-Lewis 2013), qi gong, and yoga
(Coffey and Hartman 2008; Coffey et al. 2010; Greeson
2009). This growing evidence base and the profession’s
commitment to effective practice across of a wide range of
human differences (i.e., culturally competent practice)
require that social workers increase their knowledge of
MBS approaches and their ability to work with clients who
use or may benefit from these practices.
From the standpoint of conventional practice, these
modalities and the healing systems from which they
emerge are decentered and viewed as ‘‘complementary and
alternative medicine,’’ defined by the National Center for
Complementary and Alternative Medicine (NCCAM) as ‘‘a
group of diverse medical and health care systems, prac-
tices, and products that are not generally considered part of
conventional medicine’’ (U.S. Department of Health and
Human Services 2011, para. 1). This perspective privileges
S. Raheim (&) � J. J. Lu
School of Social Work, University of Connecticut, 1798 Asylum
Avenue, West Hartford, CT 06117, USA
e-mail: [email protected]
J. J. Lu
e-mail: [email protected]
123
Clin Soc Work J (2014) 42:288–301
DOI 10.1007/s10615-014-0484-3

the allopathic tradition, more commonly referred to as
biomedicine. When not subjugated by the dominant bio-
medical paradigm, these practices can be understood within
a MBS framework and may be used independently or in
tandem with, but not subordinate to, conventional approa-
ches. In this paper, the term MBS practice will be used
instead of complementary and alternative medicine (CAM)
to refer to these healing systems and modalities, unless
citing literature or the context requires use of the term
CAM. The authors use the term MBS in this paper to center
this paradigm and related practices rather than subordinate
them to biomedicine.
The integrative mind–body-spirit (IMBS) paradigm
supports the use of all appropriate approaches within a
holistic framework to promote health and healing. Few
social workers have had the opportunity to study this par-
adigm and related modalities during their graduate training.
Despite the documented efficacy of MBS practices, such as
acupuncture, mindfulness meditation, qi gong, and yoga,
these modalities are not widely incorporated into social
work education or clinical practice. Clinical social workers
are positioned to practice more effectively when they have
a critical understanding of the philosophical and theoretical
foundations of the biomedical and IMBS paradigms and
related modalities, as well as the power and privilege
dynamics that promote or constrain their use. These critical
and analytic tools allow clinicians to recognize personal,
institutional, and societal biases for or against specific
practice methods. With these prejudices uncovered, clini-
cians are enabled to use a range of evidence to select or
advocate for efficacious approaches and attend to ethical
considerations, contraindications, and risks related to all
modalities and interventions in which they may engage or
use for referral.
This article discusses an elective MSW course the
authors designed to address the need for greater inclusion
of IMBS practice in social work education and support
development of critical and analytic tools to recognize and
assess practice paradigms. Descriptions of the content,
pedagogical approach, and outcomes of the course are
intended to increase clinicians’ awareness of this emerging
trend in social work education. With knowledge of the
training that some students and earlier career practitioners
are receiving, experienced clinicians are poised to provide
clinical supervision that supports and encourages their
ongoing learning and professional development.
Contrasting Paradigms
Prior to the mid-1800s, diverse approaches to health and
healing were commonly used in North America, and
diverse types of practitioners engaged in treating health and
behavioral health problems. Indigenous spiritual and herbal
healing practices, homeopathy, naturopathy, and allopathic
medicine co-existed and were practiced without regulation.
Of these, allopathy or biomedicine was distinct in its bio-
logically based approach to healing. With the 1848 for-
mation of the American Medical Association (AMA) by
allopathic physicians and their subsequent success in
advocacy for legislation and standards that privileged their
approach to treating disease, allopathic medicine’s rise to
dominance began. The Flexner (1910) Report of North
American medical education played a decisive role in
advancing the biomedical approach and discrediting any
approach not based on the scientific paradigm. The result
was the closure of medical schools that did not use allo-
pathic methods (Stahnisch and Verhoef 2012; Wheatley
1989). Biomedicine was positioned as mainstream health
care, and other approaches to healing were dismissed as
ineffective.
Biomedicine is rooted in the Western materialist
worldview, which holds that ‘‘everything that exists is
material’’ and all phenomena, including consciousness, are
the results of material interactions (Mosher and Trout 2002,
p. 1). The biomedical model is conceptually grounded in
Newtonian physics and Cartesian dualism that inform
understanding the body as a mechanism that is separate
from mind. Together, the materialist world view, Newto-
nian mechanics, and Cartesian dualism reduce conscious-
ness to electro-magnetic impulses of the brain and ‘‘spirit’’
is relegated to the domain of philosophy and religion.
Arising from the Western scientific paradigm, biomed-
ical approaches to health care are guided by the paradigm’s
four core principles:
(1) objectivism—the observer is separate from the
observed; (2) reductionism—complex phenomena are
explainable in terms of simpler, component phe-
nomena; (3) positivism—all information can be
derived from physically measureable data; and (4)
determinism—phenomena can be predicted from a
knowledge of scientific law and initial conditions
(Micozzi 2011, p. 8).
The application of these principles has led to the rise of
pharmaceutical health solutions and significant advances in
health care during the last century. Concurrently, biomed-
icine’s advocates have constrained the development and
use of competing approaches to health and healing through
aggressive lobbying efforts to restrict or prohibit these
practices. While the scientific paradigm is only one con-
struction of how human knowledge is generated, it has
risen to such dominance that other ways of knowing are
ignored, discredited, or even worse, vilified.
Despite historical opposition of biomedicine’s propo-
nents, non-allopathic approaches to healing have persisted
Clin Soc Work J (2014) 42:288–301 289
123

and interest in these approaches has grown significantly
over the past 30 years (Centers for Disease Control and
Prevention 2011; Eisenberg et al. 1993). In 1991, United
States (U.S.) legislation established an office within the
National Institutes of Health (NIH), the forerunner of
NCCAM, to ‘‘investigate and evaluate promising uncon-
ventional medical practices’’ (National Center for Com-
plementary and Alternative Medicine 2013). The
establishment of this NIH center created a space for non-
allopathic practices to gain legitimacy, while at the same
time, decentering these practices as ‘‘complementary and
alternative’’ to biomedicine.
The IMBS paradigm is guided by the principles of
holism, multi-systemic connectedness, and balance.
These principles are at odds with the principles of
objectivism, reductionism, positivism, and determinism
that guide the biomedical model. Holism is ‘‘an eco-
logical concept that the totality of biological phenom-
ena in a living organism or system cannot be reduced,
observed or measured at a level below that of the whole
organism or system’’ (Smuts 1926 as cited in Micozzi
2011, p. 10). Gant et al. (2009) define this connected-
ness as:
The dynamic interdependence of micro and macro
units of analysis at multiple interacting levels (e.g.,
person, cultural, organ system, cellular structure,
work organization); connectedness of mind, body,
and spirit, social, kin, or business relationships;
physical elements; neural circuitry; and health care
practices.
The IMBS paradigm is not simply using modalities
that are not embraced by biomedicine. Instead, practice
guided by this paradigm seeks to restore connectedness
and facilitate a ‘‘state of harmony and balance between
MBS and between individual and other individuals,
community, and cosmos’’ (Lee et al. 2009, p. 53). The
practitioner’s role is to support clients to regain harmony
and balance in all dimensions of their lives—physical,
mental, emotional and spiritual. The principle of con-
nectedness in the IMBS paradigm also acknowledges the
influence of the practitioner’s state of well-being in the
healing process. Consequently, self-care that helps restore
the practitioner’s sense of harmony, balance, and con-
nectedness is essential for the practitioner to be able to
engage in effective practice.
The IMBS paradigm aligns with health practices of
U.S. racial-ethnic groups that biomedical dominance has
undermined (Goodkind et al. 2010). The IMBS wellness
orientation, reliance on self-healing, focus on the bio-
energetic aspects of healing, and emphasis on spiritual
growth (Lee et al. 2009) are more consistent with the
cultural orientation of many groups than biomedicine’s
focus on disease diagnosis and use of pharmaceutical
interventions to treat illness. Resisting a ‘‘one-size fits
all’’ approach to health care, IMBS practice advances
cultural competence by recognizing the importance of
unique personal and cultural histories and acknowledg-
ing the healing practices of communities of color that
have been historically marginalized (Brown 2008).
Integrative MBS Practice, Social Work, and Social
Work Education
Lee et al. (2009) argue for a fundamental paradigm shift in
social work to IMBS practice that maintains a client-cen-
tered, strengths-based perspective, and:
[F]ocuses on the mind–body-spirit relationship, rec-
ognizes spirituality as a fundamental domain of
human existence, acknowledges and utilizes the
mind’s power as well as the body’s, and reaches
beyond self-actualization or symptom reduction to
broaden a perception of self that connects individuals
to a larger sense of themselves and their communities
(p. 39).
Integrative mind–body-spirit practice addresses the
spiritual dimension of human experience, over which social
work has historically stumbled.
Beyond the ground-breaking work of Lee et al. (2009),
the IMBS practice paradigm has not been addressed in the
social work literature. Social work scholars have explored
‘‘CAM,’’ in general, or specific modalities in a variety of
practice contexts—health and mental health settings (Block
2006; Cook et al. 2000; Dziegielewski and Sherman 2004;
Finger and Arnold 2002; Henderson 2000), social work
(Hicks 2009), and substance abuse treatment agencies
(Larkin et al. 2012); with specific populations—children
(Van Pelt 2011), families (Becvar 2010), older adults
(Behrman and Tebb 2009; Wang 2010), oncology patients
(Runfola et al. 2006), trauma survivors (Lee et al. 2011)
and youth sex offenders (Derezotes 2000); and for specific
health and behavioral health conditions—addiction (Carl-
son and Larkin 2009; Kissman and Maurer 2002; Plasse
2002; Temme et al. 2012), depression (Hicks 2009), and
schizophrenic disorders (Leahy 2005). Other scholars have
addressed the use of specific modalities in social work
education (Birnbaum 2008; Brenner 2009; Lynn 2010;
Mensinga 2011; Napoli and Bonifas 2011; Shier and
Graham 2011), with mindfulness and other meditation
approaches being the most frequent type of modality
explored.
Gant et al. (2009) assert the need for social work
education to prepare social workers for practice in the
290 Clin Soc Work J (2014) 42:288–301
123
growing context of ‘‘integrative health services.’’ The
authors identify several roles that social workers may
play in relation to integrative health services, including
CAM-related health educator, client advocate for CAM
services, and CAM practitioner. Data on national trends
affirm the need that Gant and colleagues identify. The
2010 Complementary and Alternative Medicine Survey
of Hospitals found that 42 % of hospitals surveyed
offered one or more CAM therapies (Ananth 2011).
Additionally, the number of integrative health programs
in academic medical centers has grown substantially
over the past decade (Consortium of Academic Health
Centers for Integrative Medicine 2013). Whether in
medical centers, non-academic integrative health care
programs, or other practice contexts, the need for edu-
cation and training to support social workers in these
settings is compelling.
Gant et al. (2009) define integrative health services as an
evidenced-based approach that uses:
(1) a biopsychosocial/spiritual, non-pharmacologi-
cally limited framework of health that affirms the
importance of considering conventional, comple-
mentary, and alternative medical modalities in
developing plans for health and wellness; (2) client
education, advocacy skills, and services that help
people (a) make better informed health decisions,
(b) communicate with health care practitioners, and
(c) explore health-related decisions and choices in
the context of personal history, meaning, beliefs,
and lifestyles; and (3) a simple set of vetted mind–
body skills for teaching basic coping and stress
reduction approaches to clients (p. 410).
Gant and colleagues describe a foundation course
designed to build knowledge about ‘‘CAM systems and
modalities’’ used by U.S. ‘‘ethnic subcultures’’ and increase
awareness that ‘‘forms of healing [are] central to an indi-
vidual’s cultural values’’ (p. 413). The course used a
knowledge-building strategy to increase cultural sensitivity
and willingness to collaborate with ‘‘alternative healing
practitioners.’’ The description the authors provide does not
indicate that the course analyzed issues of power and
dominance that may influence individual and societal
perceptions of healing systems and modalities that are not
biomedically based. It is also not apparent that the course
critically examined how these healing systems and
modalities may be constrained if used subordinately to the
biomedical model. Although the course developed by the
authors of the current paper is similar in aim to the one
Gant and colleagues described, we incorporated critical
analysis to achieve learning objectives, coupled with
knowledge-building to advance social work and social
justice.
The Course
The authors designed a special topics MSW course entitled
Integrative Social Work Practice—Mind–Body-Spirit-
Approaches, which was offered as a one-semester, three-
credit elective. The course introduced students to IMBS
practice and encouraged critical reflection on the underly-
ing assumptions related to integrative and allopathic
approaches to health and well-being. In the course design
process, the authors were guided by the literature and their
experience as MBS practitioners. One author has many
years of clinical practice experience in several community
hospital settings and uses a range of MBS modalities in
private clinical practice, including family constellation
therapy (see Cohen 2006 for description of family con-
stellation therapy). The other author is trained in yoga, as
well as Reiki and other energy healing modalities, has over
20 years of experience with energy therapies, and provides
these services at a local healing center. Both authors are
trained in mindfulness-based stress reduction (MBSR) and
maintain a personal meditation practice for self-care.
The intended learning outcomes of the course were for
students to: be able to critically examine the biomedical
and IMBS paradigms; gain knowledge of MBS approaches,
patterns of usage, current research on their efficacy, con-
traindications, and risks; be able to critically examine the
expansion of MBS approaches in the U.S, their historical
and cultural origins, and responses of allopathic health care
systems and practitioners; demonstrate understanding of
the integration of MBS approaches in social work practice
and related ethical considerations; and demonstrate com-
mitment to culturally competent practice with client sys-
tems who use MBS approaches. Learning was facilitated
through lectures, discussion, presentations by guest MBS
practitioners, demonstrations of MBS modalities, videos,
experiential exercises, reading assignments, and written
assignments that required critical analysis and self-
reflection.
Several written and electronic resources supported this
course. Integrative body–mind-spirit social work: An
empirically based approach to assessment and treatment
(Lee et al. 2009) was used as the primary textbook. The
text was supplemented by conceptual and empirical arti-
cles. Two web resources were of particular value for def-
initions of practices and empirical research: NCCAM
(2013) and the Stanford Health Library—Stanford Uni-
versity Hospital (2013). The technology, entertainment,
design (TED) website was a valuable resource for short
lectures by international experts, such as Daniel J. Siegel,
MD, Executive Director of Mindsight Institute (2009).
These resources present IMBS concepts and empirical
studies that examine the efficacy, contraindications, bene-
fits, and risks of a wide range of MBS modalities.
Clin Soc Work J (2014) 42:288–301 291
123

The course examined the theoretical and philosophical
foundations of the IMBS paradigm and the biomedical
paradigm, in which social work’s bio-psycho-social
approach is rooted. In addition, the course critically
examined the socio-political-economic forces that enable
the dominance of the biomedical paradigm, as well as those
that have promoted and constrained MBS approaches.
Students were introduced to Ayurveda, Traditional Chinese
Medicine, and the National Indian Child Welfare Associ-
ation’s Relational Worldview Model (Cross 2013) as
exemplars of MBS health and healing systems that are
rooted in non-Western conceptualizations. The course
provided an overview of types of MBS modalities,
including meditation, body movement and manipulation,
and energy therapies, and explored specific modalities,
such as acupuncture, mindfulness meditation, Reiki, and
yoga. Research on the applications, efficacy, contraindi-
cations, and risks of each modality were presented. The
instructors stressed that the introductory content provided
was not sufficient preparation to practice specific modali-
ties with clients and emphasized the ethical responsibility
for training and licensure, where appropriate, to practice
the modalities discussed.
Held during the late afternoon, each class session began
with a brief mindfulness exercise led by one of the
instructors to assist students to be fully present and enhance
their ability to release the stresses and concerns of the day,
as well as provide experiential learning of mindfulness.
These exercises generally began by inviting students to
become still, notice their body, focus on their breathing and
notice thoughts that emerged without attachment or judg-
ment. Variations were introduced, such as mindfully eating
a raisin, which is used in MBSR training. After each
exercise, students were invited to reflect on their experi-
ence in a brief discussion.
As students became more familiar with mindfulness
practices, they discussed applications to their self-care, as
well as their work in field placements. Students reported
using grounding exercises before stressful meetings and
teaching clients simple grounding exercises. For example,
one student introduced breathing exercises at the begin-
ning of an open-ended adolescent skills group to manage
hyperactivity and difficulty with focus in a school envi-
ronment. The student recounted experiencing some ner-
vousness about ‘‘starting something new and different’’
with clients, but found that with practice in class and on
her own, she was able to bring a playful curiosity to the
group. Furthermore, she reported that her focus and
patience with her adolescent group improved and
observed greater attentiveness and ability to focus among
group members.
The in-class exercises and discussions were important
aspects of the experiential learning process and provided
insights about applications to social work practice. Stu-
dents were able to gain perspective on the benefits and
challenges of mindfulness and potential uses for self-care
and clinical practice.
The instructors and guest speakers used lectures, dem-
onstrations, and exercises, when appropriate, to introduce
MBS principles and modalities. For example, the guest
practitioner who discussed energy therapies presented
information on the connection between thoughts, difficult
emotions, and physical discomfort in specific locations of
the body and guided a meditation to assist students to
increase awareness of this link. The conceptual information
combined with experiential learning promoted an embod-
ied understanding of an otherwise abstract idea of mind and
body connection.
Guest speakers also discussed their education, training,
and licensure, when relevant, that prepared them for
IMBS practice. They addressed legal and ethical issues
relevant to specific practice modalities. One master’s level
social work guest speaker discussed her difficulties as a
biofeedback practitioner because of legal challenges from
the American Medical Association regarding the use of
biofeedback for medical conditions. This guest speaker
discussed the advocacy efforts of an organization she co-
founded to demystify MBS practices and facilitate
awareness and understanding between federal elected
officials, MBS practitioners, and communities that utilize
these practices. Other guest speakers, who were also
licensed clinical social workers, discussed their MBS
approach to social work practice. Each of them empha-
sized the importance of maintaining their own balance
and well-being in their work with clients and stressed the
critical role of self-care in the effectiveness of their
practice.
The authors were explicit with students about the values
that guided their teaching and the themes that served as
common threads throughout the course. These values and
themes directed course design, interaction with students
and interaction with each other:
• Centrality of self-care for effective practice
• Holism in practice
• Importance of mindful practice that includes on-going
self-reflection
• Value of maintaining awareness of the operations of
power and privilege that normalize dominant groups
and practices, while marginalizing practices not rooted
in or embraced by the dominant group
• Importance of practicing ‘‘beginners mind’’ when
292 Clin Soc Work J (2014) 42:288–301
123

learning about new, unfamiliar practices, as well as
familiar, conventional practices
• Value of openness and critical analysis of healing
systems and modalities, whether indigenous/traditional,
MBS, or biomedical, and the importance of recognizing
their benefits and limitations
• Importance of recognizing the implications of the
paradigm in which healing systems and modalities are
situated
Consistent with these values and themes, self-care, self-
reflection, mindfulness, and ethical practice were encour-
aged throughout the course in lectures, classroom discus-
sions, and written assignments. To facilitate self-reflection,
as well as analysis and synthesis of course material, several
writing assignments required students to identify insights
that emerged from exploration of course topics, applica-
tions to students’ personal development and self-care, and
implications for social work practice. The final paper
required students to complete a critical analysis of one
MBS modality, including its historical, cultural, and
philosophical foundations, and examine the evidence-base
regarding its use. Students were also required to analyze
the level of acceptance of the modality within the allo-
pathic health care system and among insurance providers,
as well as critique the power and privilege dynamics
related to the modality’s availability and accessibility.
Finally, students were asked to reflect on ways that the
practice was consistent or in conflict with their personal
conceptual framework and beliefs about how to maintain
and/or achieve health and wellness.
Methodology
Sample
Thirty-seven students enrolled in the MSW course ‘‘Inte-
grative Social Work Practice: A MBS Approach’’ during
the spring terms of 2012 and 2013. The course was a
special topics, 14-session elective offered at a graduate
school of social work program in the U.S. All enrolled
students were invited to complete a pre- and post-course
survey, which the instructors designed to assess students’
prior knowledge and course outcomes. Participation was
voluntary. All 37 enrolled students completed the pre-
course survey. Of these, 35 completed the course and 32
completed the post-course survey.
Demographic data were not collected to protect stu-
dents’ privacy, since they could easily be identified in these
small classes. However, instructors’ observations estab-
lished that both classes were predominately white and
female, but with some racial-ethnic and gender diversity.
Students’ voluntary verbal self-reports during the semester
indicated a diverse mix of micro and macro concentrations
were represented in the class.
Data Collection
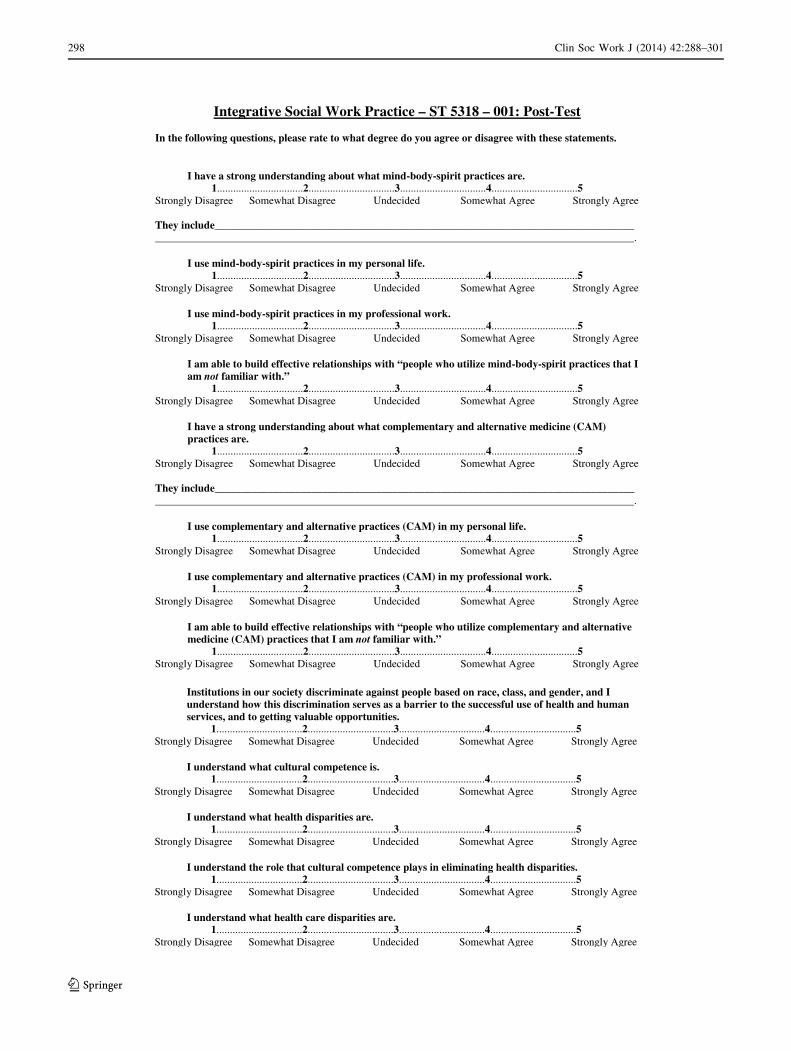
The pre- and post-course survey instrument contained
fourteen quantitative and four qualitative items (see
‘‘Appendix’’). Data collected consisted of 37 pre-test and
32 post-test surveys. Pre-test surveys were conducted at
the end of the first class session each semester, while
post-test data were collected at the end of the final
session. Surveys had no personal identifiers when col-
lected. Quantitative survey items explored knowledge,
skills, and behaviors related to MBS and CAM practices,
and cultural competence. Each item was measured on a
five-point Likert scale, ranging from: strongly disagree,
somewhat disagree, undecided, somewhat agree, and
strongly agree. Qualitative items focused on students’
prior experience with MBS and CAM practices, reasons
for electing the course, expectations of and actual
learning, and understanding of how MBS and CAM
practices relate to social work.
Results
Survey responses revealed that most students had some
prior experience with MBS and/or CAM practices. These
included acupuncture, energy therapies, including Reiki,
herbal medicines, homeopathy, massage, meditation,
reflexology, and yoga. Means and standard deviations
scores were calculated for each survey item to measure
central tendency. The non-parametric Mann–Whitney U
test was used to determine if differences existed between
pre-test and post-test scores. Statistically significant levels
are reported for p values less than or equal to .05. Highly
significant levels are p values B.001.
The Mann–Whitney U test revealed significant dif-
ferences in scores for items that measured knowledge
and use of MBS practices, knowledge and use of CAM
practices, and knowledge of cultural competence.
Scores indicated an increase in students’ perceptions of
their knowledge of MBS practices, CAM practices,
applications of MBS and CAM in professional practice,
and cultural competence. Scores did not change sig-
nificantly for items that measured personal practice of
Clin Soc Work J (2014) 42:288–301 293
123
MBS modalities, CAM practices, and the ability to
effectively work with people who utilize unfamiliar
MBS modalities and CAM practices.
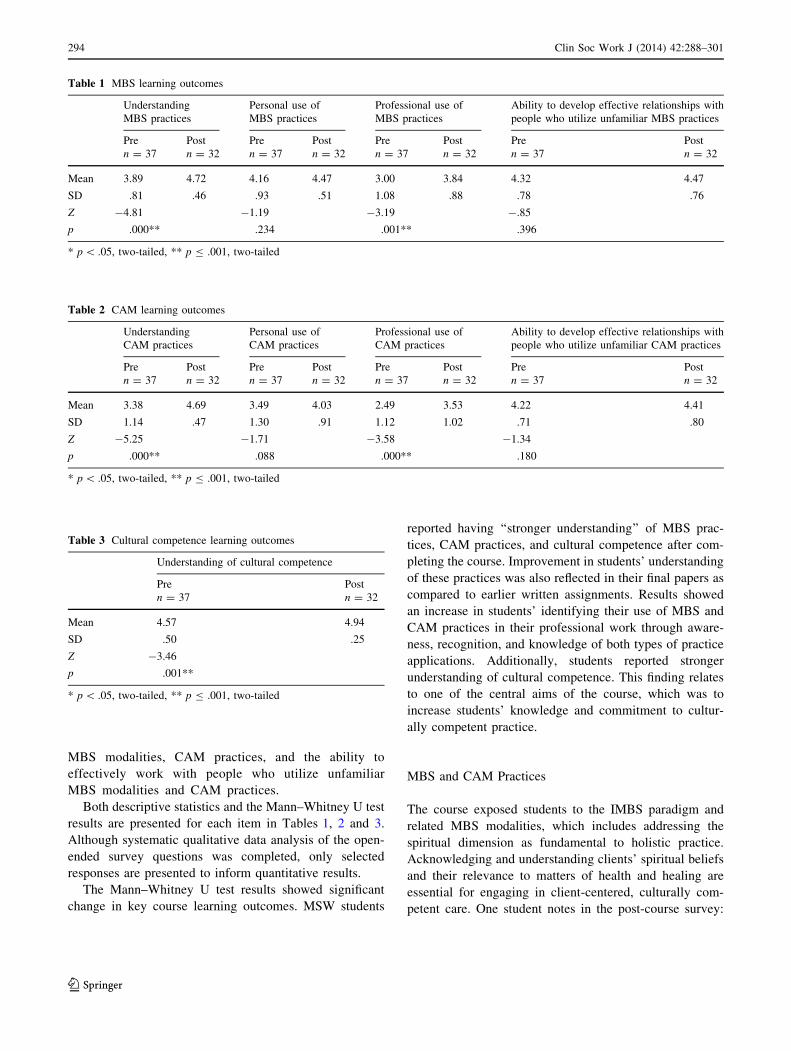
Both descriptive statistics and the Mann–Whitney U test
results are presented for each item in Tables 1, 2 and 3.
Although systematic qualitative data analysis of the open-
ended survey questions was completed, only selected
responses are presented to inform quantitative results.
The Mann–Whitney U test results showed significant
change in key course learning outcomes. MSW students
reported having ‘‘stronger understanding’’ of MBS prac-
tices, CAM practices, and cultural competence after com-
pleting the course. Improvement in students’ understanding
of these practices was also reflected in their final papers as
compared to earlier written assignments. Results showed
an increase in students’ identifying their use of MBS and
CAM practices in their professional work through aware-
ness, recognition, and knowledge of both types of practice
applications. Additionally, students reported stronger
understanding of cultural competence. This finding relates
to one of the central aims of the course, which was to
increase students’ knowledge and commitment to cultur-
ally competent practice.
MBS and CAM Practices
The course exposed students to the IMBS paradigm and
related MBS modalities, which includes addressing the
spiritual dimension as fundamental to holistic practice.
Acknowledging and understanding clients’ spiritual beliefs
and their relevance to matters of health and healing are
essential for engaging in client-centered, culturally com-
petent care. One student notes in the post-course survey:
Table 1 MBS learning outcomes
Understanding
MBS practices
Personal use of
MBS practices
Professional use of
MBS practices
Ability to develop effective relationships with
people who utilize unfamiliar MBS practices
Pre Post Pre Post Pre Post Pre Post
n = 37 n = 32 n = 37 n = 32 n = 37 n = 32 n = 37 n = 32
Mean 3.89 4.72 4.16 4.47 3.00 3.84 4.32 4.47
SD .81 .46 .93 .51 1.08 .88 .78 .76
Z -4.81 -1.19 -3.19 -.85
p .000** .234 .001** .396
* p \ .05, two-tailed, ** p B .001, two-tailed
Table 2 CAM learning outcomes
Understanding
CAM practices
Personal use of
CAM practices
Professional use of
CAM practices
Ability to develop effective relationships with
people who utilize unfamiliar CAM practices
Pre Post Pre Post Pre Post Pre Post
n = 37 n = 32 n = 37 n = 32 n = 37 n = 32 n = 37 n = 32
Mean 3.38 4.69 3.49 4.03 2.49 3.53 4.22 4.41
SD 1.14 .47 1.30 .91 1.12 1.02 .71 .80
Z -5.25 -1.71 -3.58 -1.34
p .000** .088 .000** .180
* p \ .05, two-tailed, ** p B .001, two-tailed
Table 3 Cultural competence learning outcomes
Understanding of cultural competence
Pre Post
n = 37 n = 32
Mean 4.57 4.94
SD .50 .25
Z -3.46
p .001**
* p \ .05, two-tailed, ** p B .001, two-tailed
294 Clin Soc Work J (2014) 42:288–301
123

‘‘Adding the spiritual aspect to mind and body practices
completes an individual and therefore society as a whole. I
also learned to be more sensitive to client’s voices because
everyone is different.’’ Survey results showed that students
perceived that their understanding of MBS practices
increased (pre-test mean = 3.89, post-test mean = 4.72,
p = .000). These results suggest that students learned to
recognize the holistic framework of MBS practices.
Complementary and alternative medicine modalities
were discussed as holistic in their origin and that their
application may or may not be holistic, depending upon
the broader paradigm that guides their use. Health and
behavioral health professionals who practice within a
biomedical paradigm may use CAM modalities in ways
that are not holistic. For example, yoga may be
understood in ways that are disconnected from the
traditional practice, for example, as simply a series of
stretching exercises. Used in this way, the practice is a
reflection of the biomedical mechanistic view of the
body, which is likely to be beneficial for clients who
are sedentary. However, if yoga is conceptualized and
used in this way, clients may not benefit fully from the
MBS connection and balance that this modality is
designed to facilitate when properly practiced. Since the
field of biomedicine frames CAM practices through a
biological lens, CAM practices used in this context may
not be used holistically nor accomplish the intended
outcomes of a MBS approach. Although survey results
showed that students perceived that their understanding
of MBS (pre-test mean = 3.89, post-test mean = 4.72,
p = .000) and CAM practices (pre-test mean = 3.38,
post-test mean = 4.69, p = .000) had increased, open-
ended post-test responses indicated some students were
not clear about the distinction between the two. One
student wrote: ‘‘Honestly I don’t know how to differ-
entiate between MBS and CAM except that CAM is
more based in health and medicine.’’ Since most liter-
ature makes no distinction between MBS and CAM
practices, students likely received inconsistent messages
about the potential differences between these practices,
despite course lectures and discussion.
Cultural Competence, IMBS Practice, and Engaging
Diverse Populations
Effective practice in the context of cultural and ethnic
diversity is a core commitment of social work. The
National Association of Social Workers Code of Ethics
(2008) takes a strong stand on cultural competence and
outlines social work’s commitment to vulnerable,
oppressed, and marginalized populations. These popula-
tions may have cultural healing practices that conflict with
the dominant biomedical approach to healing. For example,
Goodkind et al. (2010) assert that for American Indian/
Native American youth, the divergence of western and
traditional indigenous approaches to health and behavioral
health is a major impediment to improving services, and
that the impact of prohibiting, disregarding, and discredit-
ing traditional and indigenous health practices has been
detrimental. The profession’s value of cultural competence
and commitment to social justice compel social workers to
address barriers in the U.S. health care system to effective
work with diverse populations (National Association of
Social Workers 2008). The value of using a holistic
framework with diverse cultures is interwoven within the
fabric of IMBS practice.
IMBS’s holistic approach is in greater alignment with
indigenous and traditional healing approaches than con-
ventional biomedicine because of similarities in their
underlying conceptualizations of the healing process.
Implicit to IMBS practice is recognition of the centrality of
the client’s role in the healing process. Centering the client
in this way makes cultural competence an essential aspect
of IMBS practice. Student post-test surveys indicated a
self-reported increase in their understanding of cultural
competence. While the change was significant (p = .001),
mean scores were high at the outset of the course (pre-test
mean = 4.57; post-test mean = 4.94). However, students’
open-ended responses indicated that some understood the
link between IMBS and cultural competence:
‘‘In our [social work] practice it [mind–body-spirit
practices] matches as more culturally competent
when dealing with diverse populations.’’
‘‘I learned about many practices which I was not
familiar with before taking this class as well as the
barriers for treatment based on how our system is set
up.’’
Since students were simultaneously enrolled in other
graduate courses that likely focused on cultural compe-
tence, it is impossible to know with certainty what con-
tribution this course made to the increase in their general
understanding of cultural competence.
Although students reported that their knowledge and
application of MBS modalities (p = .000 and p = .001
respectively) and CAM (p = .000 and p = .000 respec-
tively) to professional practice significantly increased, sur-
vey responses did not reflect an increase in students’
perceived ability to build effective relationships with people
who use MBS and/or CAM modalities unfamiliar to the
Clin Soc Work J (2014) 42:288–301 295
123

student. Pre-test scores on this item were high (MSB
mean = 4.32, CAM mean = 4.22). Since most students
reported prior experience with MBS and/or CAM practices,
knowledge gained in the course was unlikely to increase their
skills in this area. Perhaps a more skills-based practice
course would be needed to increase student competencies
in working with people who use unfamiliar healing
modalities.
Personal Practice
Finally, indicators to measure students’ changes in personal
use of MBS and CAM modalities did not yield significant
results: MBS modalities (pre-test mean = 4.16, post-test
mean = 4.47, p = .234) and CAM modalities (pre-test
mean = 3.49, post-test mean = 4.03, p = .088). The main
purpose of this class was not to enhance students’ personal
practice. However, the authors believed it was important to
measure if a change occurred as a result of exposure to
course content, especially the experiential learning.
Although the class did not require students to actively
engage in MBS modalities or CAM practices outside of
class, the literature supports the value of social work stu-
dents and practitioners using MBS modalities for self-care
and to strengthen their professional practice by enhancing
mindfulness with themselves, colleagues, and clients
(Birnbaum 2008; McGarrigle and Walsh 2011; Napoli and
Bonifas 2011; Shier and Graham 2011).
Reflections
Using the IMBS paradigm to guide course development
and implementation, we engaged in an on-going process of
mindful reflection, peer-debriefing, and shared learning. As
co-instructors, we met weekly prior to and after each class
session. Post-session meetings were used to share obser-
vations, insights, and reflections about the content and
dynamics of the session, with particular attention to how
effectively the shared values and common themes (stated in
‘‘The Course’’ section) were reflected in the session. Our
self-reflections and feedback included focus on self-care,
our degree of ‘‘presence’’ in the classroom, and strategies
for improvement, when needed. These discussions
informed areas of growth and were helpful to fine-tune
plans for future class sessions. When guest speakers lec-
tured, they were invited to join these reflective discussions.
Analogous to clinical peer supervision, this shared, safe
space to process the classroom experience enhanced our
learning. From a holistic perspective, creating this safe
space for interactions outside the classroom supported our
mindful interactions inside the classroom to enhance stu-
dent learning. We shared selected self-reflections from our
peer-debriefing sessions with students, which encouraged
them to share insights and experiences, both positive and
negative, about their personal and professional growth. The
safe space allowed for an open and honest dialogue to
respect diversity in professional and personal realms.
As co-instructors, we developed keen awareness that
experiential learning and reflection are as important as
conventional teaching tools (e.g., reading assignments and
lectures accompanied by PowerPoint presentations) in
building knowledge about IMBS practice. Demonstrations
and simulations led by guest speakers who are expert
practitioners in their fields were vital for accomplishing the
aims of the course. Consistent with the Kolb Experiential
Learning Model (Kolb 1984), the combination of reading
assignments, lectures, guest speakers, experiential exer-
cises, and self-reflective discussions moved learning
beyond abstract concepts to active experimentation, con-
crete experience, and reflective observation.
We noted in classroom discussions early in the
semester that students tended to harshly criticize bio-
medicine and favored familiar MBS modalities. Their
acceptance of familiar MBS modalities was often without
critical analysis of their benefits and contraindications.
Since students who enrolled in this elective course were
likely to be positively pre-disposed to MBS modalities,
we encouraged critical assessment of all practice
approaches and encouraged an unbiased view of their
benefits and risks. By the end of the course, students
expressed a deeper appreciation for the critical role of
biomedical interventions and their use within an integra-
tive approach to health and healing. This stance is con-
sistent with the IMBS paradigm, which supports the use
of all effective and appropriate approaches to maintain
and restore health and well-being.
Maintaining focus on self-care throughout the course
was an important pedagogical strategy for fostering
understanding of the personal and professional relevance
of course content. Given the high rates of burnout or
‘‘compassion fatigue’’ that social workers and other
helping professionals experience (Gillespie 2013), this
self-care focus had practical, as well as pedagogical
benefits. We found that students recognized the signifi-
cance of a holistic paradigm when they understood how
self-care affected them and those around them in their
personal and professional lives. We placed a higher pri-
ority on self-care than is common in the traditional
classroom setting by beginning each class session with a
mindfulness exercise (as described earlier), as well as on-
296 Clin Soc Work J (2014) 42:288–301
123

going discussion during the semester of students’ expe-
riences with self-care.
Recognizing that self-care may be different and unique
for each person, a range of self-care practices were
encouraged, including attention to mind (e.g., guided
imagery and positive reflection), body (e.g., breathing
exercises, gentle stretching, nutrition, and hydration), and
spirit (e.g., seeking meaning, purpose, and connection;
engaging in one’s own spiritual practices). In class dis-
cussions, students commented that their experiences with
self-care exercises introduced in class validated the critical
need for attending to their own well-being, unlike classes
that focused primarily on their intellectual development.
Students also reported that their self-care practices
informed their work with clients. For example, students
indicated that the benefits (e.g., feeling more relaxed) and
barriers (e.g., time, resources, and space) they experienced
in their efforts to engage in self-care increased their
appreciation of clients’ efforts and challenges. Students
said that these new insights helped them to support clients
more effectively in their self-care efforts. For example, one
student reflected upon how his response to a client’s
established self-care practice changed after developing his
own self-care experience. The client had been using
breathing exercises and positive, spiritual affirmations to
calm her anxieties during stressful times. However, the
student had given the client no acknowledgment of these
efforts she was making, because they did not seem sig-
nificant. Once the student had a greater awareness of the
usefulness of these self-care strategies, he was able to
acknowledge their value and affirm the strengths the client
was demonstrating by using these practices. The student
expressed greater understanding of the connection between
his self-awareness and the effectiveness of his practice with
clients.
As co-instructors, our intentions were to create a
learning environment that was shaped by the IMBS para-
digm and use all appropriate pedagogical tools to promote
a critical and experiential perspective on MBS approaches
in social work practice.
Conclusion
Master’s level social work education is designed to
enhance students’ knowledge and abilities to use effective,
culturally competent practices. While the course discussed
in this paper contributed to students’ practice knowledge,
skills, and values, training for IMBS practice requires far
more than this course was intended to accomplish. The
results reported here suggest that an introductory IMBS
course is best used as a platform to engage in an explora-
tion of a holistic paradigm that appropriately and ethically
employees MBS and conventional modalities. Despite the
breadth of knowledge provided in the course, students
noted that there is much more to learn:
‘‘[T]here is a vast amount of alternative methods that
I was unaware of. I learned about the importance of
knowledge in these areas to be able to provide our
clients with the most effective service.’’
‘‘I learned a lot about how many different types of
MBS and CAM practices there are. I know there are
far more than were covered in this class.’’
Lessons learned from implementing the course suggest
that experienced clinicians can support the professional
development of novice practitioners by encouraging (1)
ongoing exploration and critical assessment of the IMBS
and biomedical paradigms; and (2) incorporation of evi-
dence-based MBS practices in their clinical work and self-
care. Details presented in this paper on the content, peda-
gogical approach, and outcomes of the course may also
support clinicians to reexamine the paradigm that guides
their practice, consider a wider range of evidence-based
practices in their clinical work, and recommit to their own
self-care.
Appendix: Integrative Social Work Practice—ST
5318-001: Post-test
Clin Soc Work J (2014) 42:288–301 297
123
Integrative Social Work Practice – ST 5318 – 001: Post-Test
In the following questions, please rate to what degree do you agree or disagree with these statements.
• I have a strong understanding about what mind-body-spirit practices are.1................................2................................3................................4................................5
Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
They include_______________________________________________________________________________________________________________________________________________________________________.
• I use mind-body-spirit practices in my personal life.1................................2................................3................................4................................5
Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
• I use mind-body-spirit practices in my professional work.1................................2................................3................................4................................5
Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
• I am able to build effective relationships with “people who utilize mind-body-spirit practices that I am not familiar with.”
1................................2................................3................................4................................5Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
• I have a strong understanding about what complementary and alternative medicine (CAM) practices are.
1................................2................................3................................4................................5Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
They include_______________________________________________________________________________________________________________________________________________________________________.
• I use complementary and alternative practices (CAM) in my personal life.1................................2................................3................................4................................5
Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
• I use complementary and alternative practices (CAM) in my professional work.1................................2................................3................................4................................5
Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
• I am able to build effective relationships with “people who utilize complementary and alternative medicine (CAM) practices that I am not familiar with.”
1................................2................................3................................4................................5Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
• Institutions in our society discriminate against people based on race, class, and gender, and I understand how this discrimination serves as a barrier to the successful use of health and human services, and to getting valuable opportunities.
1................................2................................3................................4................................5Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
• I understand what cultural competence is.1................................2................................3................................4................................5
Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
• I understand what health disparities are.1................................2................................3................................4................................5
Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
• I understand the role that cultural competence plays in eliminating health disparities.1................................2................................3................................4................................5
Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
• I understand what health care disparities are.1................................2................................3................................4................................5
Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
298 Clin Soc Work J (2014) 42:288–301
123

References
Ananth, S. (2011). 2010 complementary and alternative medicine
survey of hospitals: The Samueli Institute and Health Forum. An
American Hospital Association Company.
Becvar, D. S. (2010). What marriage and family therapists need to
know about complementary and alternative medicine. Family
Therapy, 9(2), 23–25.
Behrman, G., & Tebb, S. (2009). The use of complementary and
alternative interventions as a holistic approach with older adults.
Journal of Religion & Spirituality in Social Work: Social
Thought, 28(1–2), 127–140.
Birnbaum, L. (2008). The use of mindfulness training to create an
‘accompanying place’ for social work students. Social Work
Education, 27(8), 837–852. doi:10.1080/2615470701538330.
Block, P. (2006). Alternative, complementary, and integrative
medicine in a conventional setting. In S. Gehlert & T.
A. Browne (Eds.), Handbook of health social work (pp.
673–707). Hoboken, NJ: Wiley.
Brenner, M. J. (2009). Zen practice: A training method to enhance the
skills of clinical social workers. Social Work in Health Care,
48(4), 462–470. doi:10.1080/00981380802589860.
Brown, L. S. (2008). Cultural competence in trauma therapy: Beyond the
flashback. Washington, DC: American Psychological Association.
Carlson, B. E., & Larkin, H. (2009). Meditation as a coping
intervention for treatment of addiction. Journal of Religion &
Spirituality in Social Work: Social Thought, 28(4), 379–392.
doi:10.1080/15426430903263260.
Cassidy, C. M. (2011). Social and cultural factors in medicine. In M.
S. Micozzi (Ed.), Fundamentals of complementary and alternative
medicine (4th ed., pp. 42–60). St. Louis, MO: Saunders Elsevier.
Centers for Disease Control and Prevention. (2011). National health
interview survey. 2007 Data Release. Retrieved from http://
www.cdc.gov/NCHS/nhis/nhis_2007_data_release.htm.
Coffey, K. A., & Hartman, M. (2008). Mechanisms of action in the
inverse relationship between mindfulness and psychological
distress. Complementary Health Practice Review, 13(2), 79–91.
doi:10.1177/1533210108316307.
Coffey, K. A., Hartman, M., & Fredrickson, B. L. (2010). Decon-
structing mindfulness and constructing mental health: Under-
standing mindfulness and its mechanisms of action. Mindfulness,
1(4), 235–253. doi:10.1007/s12671-010-0033-2.
Cohen, D. B. (2006). ‘‘Family constellations’’: An innovative
systemic phenomenological group process from Germany. The
Family Journal, 14, 226–233. doi:10.1177/1066480706287279.
Consortium of Academic Health Centers for Integrative Medicine.
(2013). Retrieved from http://ww.imconsortium.org.
Cook, C. A. L., Becvar, D. S., & Pontious, S. L. (2000). Comple-
mentary alternative medicine in health and mental health:
Implications for social work practice. Social Work in Health
Care, 31(3), 39–57.
Cross, T. L. (2013). Relational world view model. National Indian
child welfare association. Retrieved from www.nicwa.org/
relational_worldview/.
Curley, J. P., Jensen, C. L., Mashoodh, R., & Champagne, F. A.
(2011). Social influences on neurobiology and behavior: Epige-
netic effects during development. Psychoneuroendocrinology,
36(3), 352–371. doi:10.1016/j.psyneuen.2010.06.005.
Derezotes, D. (2000). Evaluation of yoga and meditation trainings
with adolescent sex offenders. Child and Adolescent Social Work
Journal, 17(2), 97–113.
Dziegielewski, S., & Sherman, P. (2004). Complementary therapies: Tips
and techniques. In S. Dziegielewski (Ed.), The changing face of
health care social work: Professional practice in managed
behavioral healthcare (2nd ed., pp. 422–438). New York: Springer.
Eisenberg, D. M., Kessler, R. C., Foster, C., Norlock, F. E., Calkins,
D. R., & Delbanco, T. L. (1993). Unconventional medicine in the
United States: Prevalence, costs and patterns of use. New
England Journal of Medicine, 328, 246–252.
Finger, W., & Arnold, E. M. (2002). Mind–body interventions:
Applications for social work practice. Social Work in Health
Care, 35(4), 57–78. doi:10.1300/J010v35n04_04.
Flexner, A. (1910). Medical education in the United States and
Canada: A report to the Carnegie Foundation for the advance-
ment of teaching. New York City: The Carnegie Foundation for
the Advancement of Teaching.
Froeliger, B., Garland, E. L., & McClernon, F. J. (2012). Yoga meditation
practitioners exhibit greater gray matter volume and fewer reported
cognitive failures: Results of a preliminary voxel-based morpho-
metric analysis. Evidence-Based Complementary and Alternative
Medicine, Article ID 821307, 8. doi: 10.1155/2012/821307.
Froeliger, B. E., Garland, E. L., Modlin, L. A., & McClernon, F. J.
(2012b). Neurocognitive correlates of the effects of yoga
meditation practice on emotion and cognition: A pilot study.
• I understand the role that cultural competence plays in eliminating health care disparities.1................................2................................3................................4................................5
Strongly Disagree Somewhat Disagree Undecided Somewhat Agree Strongly Agree
Please respond to the open-ended questions with your own words.
1. What are the reasons you signed up for this course?
2. What do you hope to learn by the end of this course?
3. How do you think mind-body-spirit practices relate to social work practice?
4. How do you think complementary and alternative medicine practices relate to social work practice?
Clin Soc Work J (2014) 42:288–301 299
123
Frontiers in Integrative Neuroscience, 6, 48. doi:10.3389/fnint.
2012.00048.
Gant, L., Benn, R., Gioia, D., & Seabury, B. (2009). Incorporating
integrative health services in social work education. Journal of
Social Work Education, 45(3), 407–425.
Garland, E. L., & Howard, M. O. (2009). Neuroplasticity, psycho-
social genomics, and the biopsychosocial paradigm in the 21st
century. Health Social Work, 34(3), 191–199.
Garland, E. L., & Roberts-Lewis, A. (2013). Differential roles of
thought suppression and dispositional mindfulness in posttrau-
matic stress symptoms and craving. Addictive Behaviors, 38(2),
1555–1562. doi:10.1016/j.addbeh.2012.02.004.
Garland, E. L., Schwarz, N. M., Kelly, A., Whitt, A., & Howard, M. O.
(2012). Mindfulness-oriented recovery enhancement for alcohol
dependence: Therapeutic mechanisms and intervention accept-
ability. Social Work Practice in the Addictions, 12(3), 242–263.
Gaylord, S. A., Palsson, O. S., Garland, E. L., Faurot, K. R., Coble, R.
S., Mann, J. D., et al. (2011). Mindfulness training reduces the
severity of irritable bowel syndrome in women: Results of a
randomized controlled trial. American Journal of Gastroenter-
ology, 106(9), 1678–1688. doi:10.1038/ajg.2011.184.
Gillespie, D. F. (2013). Burnout among social workers. New York:
Routledge.
Goodkind, J. R., Ross-Toledo, K., John, S., Hall, J. L., Ross, L.,
Freeland, L., et al. (2010). Promoting healing and restoring trust:
Policy recommendations for improving behavioral health care
for American Indian/Alaska Native adolescents. American
Journal of Community Psychology, 46(3–4), 386–394. doi:10.
1007/s10464-010-9347-4.
Greeson, J. M. (2009). Mindfulness research update: 2008. Comple-
mentary Health Practice Review, 14(1), 10–18. doi:10.1177/
1533210108329862.
Henderson, L. (2000). The knowledge and use of alternative
therapeutic techniques by social work practitioners. Social Work
in Health Care, 30(3), 55–71. doi:10.1300/J010v30n03_04.
Hick, S. F. (2009). Mindfulness and social work. Chicago, IL:
Lyceum Books.
Irwin, M. R. (2008). Human psychoneuroimmunology: 20 years of
discovery. Brain, Behavior, and Immunity, 22(2), 129–139.
Irwin, M. R., & Miller, A. H. (2007). Depressive disorders and
immunity: 20 years of progress and discovery. Brain, Behavior,
and Immunity, 21(4), 374–383.
Kissman, K., & Maurer, L. (2002). East meets west: Therapeutic
aspects of spirituality in health, mental health and addiction
recovery. International Social Work, 45(1), 35–43.
Kolb, D. A. (1984). Experiential learning: Experience as the source
of learning and development (Vol. 1). Englewood Cliffs, NJ:
Prentice Hall.
Larkin, H., Hardiman, E. R., Weldon, T., & Kim, H. C. (2012).
Program characteristics as factors influencing the implementa-
tion of mindfulness meditation in substance abuse treatment
agencies. Journal of Religion & Spirituality in Social Work,
31(4), 311–327.
Leahy, D. (2005). How and why movement works: A movement
workshop for adults with schizophrenic disorders. Social Work
with Groups, 27(2–3), 113–127. doi:10.1300/J009v27n02_08.
Lee, M. Y., Siu-man, N., Leung, P. P. Y., & Chan, C. L. W. (2009).
Integrative body–mind-spirit social work: An empirically based
approach to assessment and treatment. New York: Oxford
University Press.
Lee, M. Y., Zaharlick, A., & Akers, D. (2011). Meditation and
treatment of female trauma survivors of interpersonal abuses:
Utilizing clients’ strengths. Families in Society: The Journal of
Contemporary Social Services, 92(1), 41–49. doi:10.1606/1044-
3894.4053.
Lynn, R. (2010). Mindfulness in social work education. Social Work
Education, 29(3), 289–304. doi:10.1080/02615470902930351.
McGarrigle, T., & Walsh, C. A. (2011). Mindfulness, self-care, and
wellness in social work: Effects of contemplative training.
Journal of Religion & Spirituality in Social Work: Social
Thought, 30(3), 212–233. doi:10.1080/15426432.2011.687384.
Mensinga, J. (2011). The feeling of being a social worker: Including
yoga as an embodied practice in social work education. Social
Work Education, 30(6), 650–662.
Micozzi, M. (2011). Fundamentals of complementary and alternative
medicine (4th ed.). St. Louis, MO: Saunders Elsevier.
Mosher, P. K., & Trout, J. D. (Eds.). (2002). Contemporary
materialism: A reader. New York: Routledge.
Napoli, M., & Bonifas, R. (2011). From theory toward empathic self-
care: Creating a mindful classroom for social work students.
Social Work Education, 30(6), 635–649. doi:10.1080/02615479.
2011.586560.
National Association of Social Workers. (2008). Code of ethics.
Retrieved from http://www.socialworkers.org/pubs/code/code.
asp?print=1&.
National Center for Complementary and Alternative Medicine.
(2013). Retrieved from http://nccam.nih.gov/.
Plasse, B. R. (2002). A stress reduction and self-care group for
homeless and addicted women: Meditation, relaxation and
cognitive methods. Social Work with Groups, 24(3–4),
117–133. doi:10.1300/J009v24n03_09.
Rossi, E. L. (2002a). Psychosocial genomics: Gene expression,
neurogenesis, and human experience in mind–body medicine.
Advances in Mind Body Medicine, 18(2), 22–30.
Rossi, E. L. (2002b). The psychobiology of gene expression. New
York: W.W. Norton & Company.
Runfola, J. F., Levine, E., & Sherman, P. (2006). Helping patients
make decisions about complementary and alternative treatments.
Journal of Psychosocial Oncology, 24(1), 81–106.
Shier, M. L., & Graham, J. R. (2011). Mindfulness, subjective well-
being, and social work: Insight into their interconnection from
social work practitioners. Social Work Education, 30(1), 29–44.
doi:10.1080/02615471003763188.
Siegel, D. J. (2007). The mindful brain: Reflection and attunement in
the cultivation of well-being. New York: W. W. Norton &
Company.
Siegel, D. J. (2009). The power of mindsight. TEDxBlue. Retrieved
from http://www.youtube.com/watch?v=Nu7wEr8AnHw&fea
ture=youtube_gdata_player.
Siegel, D. J. (2012). The developing mind: How relationships and the
brain interact to shape who we are (2nd ed.). New York:
Guildford Press.
Siegel, D. J., Fosha, D., & Solomon, M. F. (Eds.). (2010). The healing
power of emotion: Affective neuroscience, development and
clinical practice. New York: W. W. Norton & Company.
Stahnisch, F. W., & Verhoef, M. (2012). The flexner report of 1910
and its impact on complementary and alternative medicine and
psychiatry in North America in the 20th century. Evidence-
Based Complementary and Alternative Medicine. doi:10.1155/
2012/647896.
Stanford Health Library—Stanford University Hospital and Clinics.
(2013). Treatment: CAM therapies and modalities. Retrieved
from http://healthlibrary.stanford.edu/resources/treatment/treat
ment_cam2.html.
Temme, L. J., Fenster, J., & Ream, G. L. (2012). Evaluation of
meditation in the treatment of chemical dependency. Journal of
Social Work Practice in the Addictions, 12(3), 264–281. doi:10.
1080/1533256X.2012.702632.
U.S. Department of Health and Human Services, National Institutes
of Health, National Center for Complementary and Alternative
300 Clin Soc Work J (2014) 42:288–301
123

Medicine. (2011). What is complementary and alternative
medicine? Retrieved from http://nccam.nih.gov/.
Van Pelt, J. (2011). Yoga and children’s mental health. Social Work
Today, 11(6), 8.
Wang, D. S. (2010). Feasibility of a yoga intervention for enhancing
the mental well-being and physical functioning of older adults
living in the community. Activities, Adaptation & Aging, 34,
85–97. doi:10.1080/01924781003772559.
Wheatley, S. C. (1989). The politics of philanthropy: Abraham
Flexner and medical education. Wisconsin: University of
Wisconsin Press.
Salome Raheim Ph.D., ACSW, Dean, UConn School of Social Work
is a Reiki and yoga practitioner. She is trained in mindfulness-based
stress reduction and maintains a personal meditation practice.
Jack J. Lu MSW, LCSW is a family constellation therapist,
maintains a private clinical practice, and is a doctoral candidate. He
is trained in mindfulness-based stress reduction and maintains a
personal meditation practice.
Clin Soc Work J (2014) 42:288–301 301
123




























