Embed Size (px)
Citation preview
1
Vol 21 No 1 February 2004
continued on page 3
Peter Sainsbury, PHAA President
Extremely belatedly I’d like to express mythanks and congratulations to theQueensland Branch for organising a reallyenjoyable and interesting annualconference last September. Brisbane in the
spring - the river, the non-stop activities on the South Bank,the weather - was just spectacular and conference delegateswere treated to a parade of stimulating speakers. SenatorPatterson opened the conference for us and within an hourof the opening ceremony we, and the rest of Australia,heard that she would shortly no longer be the Minister forHealth - that set tongues wagging furiously. Especially whenit became clear that Tony Abbott was to be the new HealthMinister. The conference settled into a more predictablepattern after that, I’m pleased to say.Almost immediately after the conference I left for six weeksin the USA - a combination of conferences in New York,Atlanta, Washington and San Francisco and some holidaytime. I won’t bore you with my verbal holiday snapshots butI do want to make two observations. Firstly, Americansseem to love cinnamon, spitting, the stars and stripes andGod - evidence of each of them is everywhere. Secondly, Iwas struck by how often I read or heard reference touniversal health insurance. I was last in the USA about fiveyears ago and I don’t think that then I once heard mentionof universal health insurance - certainly not in the contextof the USA’s own health care system. On my recent visit,
however, the need for universal health insurance in the USA
was mentioned by at least one speaker at every conference Iwent to and was frequently discussed in the press by
journalists, commentators and politicians (see for instance
http://www.iom.edu/report.asp?id=17632). Now I wouldn’tbe silly enough to imply that universal health insurance isjust around the corner for Americans or that it will be amajor feature of this year’s presidential election but therecertainly was a suggestion that many critical thinkers haverealised that the current health system in the USA is
unsustainable, financially, socially and morally, in thelonger term and that it is just a matter of time beforesomething changes.In Australia Medicare continues to be a politicalbattleground, although ‘battleground’ is not quite thecorrect metaphor. A genuine political and public ‘battle’,i.e. a well informed and open debate with a clear outcome,about what Australians want from their health system and
President’s message
The Public Health Association of Australia is the major organisation for public health practitioners in Australia with more than 40health related disciplines represented in its membership. The Association makes a major contribution to health policy in Australia and has branches in every state and territory. Any person who supports the objectives of the Association is invited to join.
In this IssuePresident’s message ................................................................... 1Hotham Mission launches research proving community basedasylum processing .................................................................... 2Office Bearers .......................................................................... 2Eye Care .................................................................................. 3Death Blow for Kyoto? ............................................................ 4The lives of millions are at stake .............................................. 6Public Health Promotion - a Conference Challenge ................. 7Tai-Chi boosts immunity: study ............................................... 8War in Iraq will have health consequences for many years ........ 9Record Number of Donors support UN PopulationAgency this year ....................................................................... 9First “Green-Friendly” Refrigerator .......................................... 10Immigration ‘ignored brothel raids’ .......................................... 11Global warming kills 150,000 a year ....................................... 12Agency certifies new generic HIV drug .................................... 13Global trade keeps a billion children in poverty, says Unicef .... 14TNC GLAXO chief says drugs do not work on patients .......... 15The Ecology of Energy Transformations .................................. 16Western Australia Reports on Injuries ................................. 17-18Ozone layer ‘sacrificed’ to lift Bush’s re-election prospects ........ 19Farmers say food must be dropped from Governmentsdeal-making ............................................................................. 20Letter to the Editor .................................................................. 21Australia Day Honours List ...................................................... 22Bush impedes Aid for Global AIDS Pandemic ......................... 23Developing a primary health care perspective on cancer ........... 24PHAA Advocacy update ........................................................... 25Items of Interest ....................................................................... 26What’s On ............................................................................... 28New Members ......................................................................... 28l
2
Office Bearers
The BoardPresidentPeter Sainsbury: Ph (02) 9515 3270 [email protected] President - (Policy),Jane Freemantle: Ph (08) 9489 7754, [email protected] President - (Development)Leonie Short: Ph (07) 3371 4360 [email protected] President (Finance)Peter Trebilco: Ph (02) 9319 1993, [email protected] Convenors’ representativeFran McFadzen: Ph (07) 4920 6980,[email protected] Welch: (07) 3284 5155, [email protected] Presidents’ representativeJim Hyde: Ph (02) 9256 9602, [email protected] Heard:Ph (08) 8226 6384, [email protected], ANZJPHJudith Lumley: Ph (03) 8341 8500 [email protected] ANDJeanne Daly: Ph (03) 9285 5273 [email protected]
Branch PresidentsACT Cathy Banwell: Ph (02) 6125 0016, [email protected] Jim Hyde: Ph (02) 9256 9602, [email protected] Vicki Taylor: Ph (08) 8951 4713, [email protected] Peter Anderson: Ph(07) 3864 3526, [email protected] Adrian Heard: Ph (08) 8226 6384, [email protected] Michael Wilson: Ph (03) 6228 2921, [email protected] Margaret Stebbing, Ph (03) 9903 0960,[email protected] Ilse O’Ferrall: Ph (08) 9224 1620 [email protected]
SIG ConvenorsAboriginal & Torres Strait Islander HealthTBAChild HealthTBAEnvironmental HealthElizabeth Hanna: (03) 5761 1248, [email protected] & NutritionMark Lawrence: (03) 9244 3789, [email protected] PromotionFran McFadzen: Ph (07) 4920 6980, [email protected] PreventionAngela Wallace: Ph (07) 3864 4675, [email protected] HealthAnna Whelan: Ph (02)9385 3593, [email protected] HealthValerie Gerrand: ph 9326 7776 [email protected] HealthChristine Morris: Ph (08) 8295 2311, [email protected] Economy of HealthDoug Welch: (07) 3284 5155, [email protected] Health CareLaurann Yen: (02) 6207 1212, [email protected] Health Research EthicsTBARural HealthTBAWomen’s Health Co-ConvenorsKelsey Hegarty: Ph (03) 8344 4992 [email protected] Taft: Ph (03) 8341 8571, [email protected] DirectorPieta Laut: ph (02) 6285 2373, [email protected]
Australian Human Rights News
The Uniting Church agency, Hotham Mission, launched onSaturday a new report which proves that a community-based system for all asylum seekers can work in Australia . Ithas called on the Federal Government to consider thiscommunity-based system.
The Asylum Seeker Project based at Hotham Mission hasoperated a project for seven years, assisting more than 300asylum seekers who live in the community on bridgingvisas. “We have found in the seven years of workingwith hundreds of asylum seekers, that not one person hasabsconded or failed to report or comply with theDepartment of Immigration requirements,” UnitingChurch Victorian moderator Reverend Sue Gorman said.“We are saying that this project is saying that we believethat a community-based way of helping people that wewould normally put in detention centres is a far moredignified and honorable way to look after these people.”
The project researched the 200 asylum seekers they haveworked with for the past 2 years. The findings included:• No asylum seeker absconded;• All asylum seekers complied with their reporting
requirements; and• Appropriate welfare and social support assisted asylum
seekers significantly in the steps towards settlement orreturn, depending on their final decision.
The research also highlighted the welfare impact on asylumseekers left in the community with no Medicare, workrights or welfare payment support.
The report was launched on Saturday, 13th December, andhas received coverage from ABC, SBS and 3AW.
See some of the news coverage below: http://www.abc.net.au/news/newsitems/s1009343.htmFor a copy of the report: http://www.hothammission.org.au/index.cgi?tid=3
Hotham Mission launches research proving communitybased asylum processing

3
Presidents message - continued from page 1
how it can be delivered most equitably and most cost-effectively, would be a real advance. What has masqueradedas political debate on this topic in Australia in recent yearsthough might be more accurately described as a series ofmessy, noisy, skirmishes in the dark that have resolvednothing of any long term significance. We currently have aSenate Inquiry into the Commonwealth Government’slatest proposals for Medicare and while this allows thecombatants, including the PHAA, another welcomeopportunity to shoulder arms it is unlikely to change theGovernment’s basic position and approach. Whether aLabor government would take a more strategic approach isdifficult to say in view of their policy timidity.For the public it must be all extremely confusing. On theone hand we have very good health in Australia comparedwith the past and the rest of the world; we spend a lot onhealth care; we have very well trained and committedhealth professionals; for the most part, we have excellenthealth care facilities; every week sees a new researchbreakthrough reported in the media; and, in general, mostpeople get pretty good health care most of the time. On theother hand bad news about health and health care is hardlyever off the front pages of the newspapers; disgruntleddoctors are resigning; nurses complain they are underpaid;hospitals face funding ‘crises’; people are reported as dyingbecause of second rate care; out of pocket expenses areincreasing; queues for surgery, emergency departments and
Nean McKenzieResearch Officer, Optometrists Association Victoria
Vision is a very precious sense. It is invaluable early on inlife when we are learning about the world. It is necessaryfor our work and for good socialisation. Getting aroundand being active requires good vision. Without sight wewould experience a very different life.
To maximise our chances of having and keeping goodvision, it is important to have regular eye checks. Childrenshould be tested around the age of three and a half, then inGrades 1 and 3, and again at the start of secondary school.Over the age of forty, many degenerative eye conditionsbecome more common, and regular eye tests become veryimportant.
Increasing community awareness of eye problems will savemany people from unnecessary loss of vision. Currently theOptometrists Association is conducting a children’s visioncampaign. The key message is that recent Australianresearch shows that one in four children has some kind of
visual problem before they finishschool, and a large number of theseproblems are going undetected. Thismessage is being conveyed throughseveral methods: optometrists goingout into the community to talk toteachers, advertising in the printmedia and information booklets for teachers and parents.
Many ageing conditions of the eyes can be treated or preventedif picked up early. The Optometrists Association Victoria hasalso instituted a series of talks to elderly groups to increasetheir knowledge of eye problems. Glaucoma, cataracts, aged-related macular degeneration and refractive error are all easilypicked up in an optometric examination. Victorianoptometrists have also become more involved in increasingcommunity awareness of the important role of vision in fallsprevention, driving and exercise. Medicare covers eyeexaminations by optometrists, and no referral is required.
For more information about eye care, please contact theOptometrists Association Victoria on 03 9486 1700 or at theirweb site www.vicoptom.asn.au
Eye Care
GPs are increasing; and those public health people,whatever they do, are forever whinging that they don’t get abig enough slice of the cake. What is a voter to think? I amnot one to suggest that ‘health should be taken out ofpolitics’ - on the contrary, health and health care areintensely political and anyone who says otherwise is eitheruninformed or mischievous - but Australia must developsome mechanisms by which all of these issues can beconsidered by politicians and bureaucrats from all thejurisdictions, by health professionals in all parts of thesystem, and by the public. Otherwise we condemnourselves to another decade of indecisive yet energy sappingand damaging skirmishes. I am convinced that eventuallychange, good change, will occur but how much unnecessarydamage will we do to Australians’ health in the meantime?On that note, I’ll wish you a happy, productive and healthy2004 and remind you that early bird registrations for theconference in Melbourne in April close very soon. Thispromises to be a very exciting meeting with something foreveryone who works in public health, health promotionand population health. I look forward to seeing manyPHAA members there.
4
By Francesca Colombo
“ The European Union, which has been the driving forcedbehind the Kyoto Protocol, was forced to admit that itwould not meet its ambitious target of reducing emissionsto eight percent below 1990 levels by 2010.”
Delegates to the ninth conference on climate change inItaly are discussing alternatives in case the Kyoto Protocol isdone in by a “no” from Russia, which would doom 11 yearsof efforts.
The future of the Kyoto Protocol has been thrown intodoubt by Russia’s recent wavering on whether it will ratifythe treaty. The question has divided the delegates at theninth conference on climate change and given rise todiscussions of alternative mechanisms, like a new globalconvention.
Recent statements by Russian officials raised questions as towhat that country would eventually decide with respect tothe Protocol aimed at cutting emissions of greenhouse gasesthat cause global warming, which is being discussed at theninth Conference of the Parties (COP-9) to the U.N.framework Convention on Climate Change, meeting untilDec. 12 in the northern Italian city of Milan.
If Moscow joins the United States, Canada and Australia inrejecting the Protocol, “it will condemn the world to asituation worse than the one we have today,” Burkina Faso’sdirector-general of the environment, Honore Toe, toldTierramérica.
Tens of millions of people around the world are directly orindirectly affected by climate change, which most of thescientific community agrees is caused when greenhousegases, especially carbon dioxide generated by the burning offossil fuels – oil, gas and coal — are trapped in theatmosphere by the “greenhouse effect”.
The global temperature increased between 0.2 and 0.6degrees in the 20th century, the sea level rose between 10and 20 cms, the glaciers are melting (up to 40 percent inthe Arctic Ocean), and water resources are drying up.
The Protocol, originally signed in 1997 in Kyoto, Japan toset targets for cutting the greenhouse gas emissions ofindustrialized countries, cannot go into effect unless it isratified by countries representing 55 percent of 1990emissions.
That means Russia’s ratification is essential, given the factthat the United States pulled out of the treaty in 2001.On Dec. 2, Russian President Vladimir Putin’s adviser oneconomic issues, Andrei Illarionov, said Moscow would notratify the Protocol “in its current format” because it couldhamper future opportunities for Russia’s economic growth.
But the next day, Deputy Minister of the EconomyMukhamed Tsikhanov said that no final decision had beenreached yet, and that the Russian parliament may ratify thetreaty in 2004.
The wavering by Russia, which accounts for six percent ofthe world’s greenhouse gas emissions, “sends a negativesignal to the international markets,” the director of Japan’sInstitute for Global Environmental Strategies (IGES),Srinivasan Ancha, told Tierramérica.
Kyoto is “only one step towards cutting emissions. A newtreaty would mean the loss of 11 years of efforts made sincethis initiative emerged in Rio de Janeiro,” said Ancha,referring to the 1992 Earth Summit.
“The world’s indigenous and peasant communities are themost vulnerable to climate change,” said the representativeof Costa Rica’s Bri-Bri indigenous community, FlorMorales.
“We have lost harvests, our soil is flooded or eroded. Wehave a certain order for agriculture, a time for harvesting,which is being broken because of humanity’s practicesagainst the environment,” she added.
The Kyoto Protocol is aimed at forcing the industrializedworld to cut carbon dioxide emissions to five percent below1990 levels by 2012.
But the outlook is not promising. The European Union,which has been the driving forced behind the Protocol, wasforced to admit that it would not meet its ambitious targetof reducing emissions to eight percent below 1990 levels by2010. According to projections by the EuropeanEnvironment Agency, emissions will only have been cut by0.5 percent by 2010.
At the current pace, only Britain and Sweden will meet thetarget, while Spain will reach 2010 with 30 percent higheremissions and the rest of the EU countries with emissions atleast 20 percent higher than the goal.
The EU is divided on the issue. Some members of the blocare calling for voluntary projects like research into the useof hydrogen in transportation, renewable energy sources,and improving the energy efficiency of fossil fuels.
Among the EU nations that support the United States in itswithdrawal from the pact is Italy, whose emissions increased7.3 percent between 1990 and 2003, and which is pushing
continued next page
Death Blow for Kyoto?

5
2004 General Practice & Primary Health CareResearch Conference
What’s [not] working? How do we know?
Sheraton Brisbane Hotel2-4 June 2004
CALL FOR ABSTRACTSThe GP & PHC Research Conference is an importantannual forum where investigators can present researchfunded through a variety of primary health care fundingsources. It also provides a unique opportunity for delegatesto meet, share ideas and explore general practice & primaryhealth care issues.
The conference will enable investigators at various stagesof their research to interact with and learn from each otherthrough presentation and networking opportunities. Theconference program will include pre-conference workshops,keynote and plenary sessions, a hypothetical and paper andposter presentations and displays.
Abstracts for paper of poster presentations or display postersare invited from individuals or groups working in the fieldof general practice/primary health care research. Closingdate for receipt of abstracts is Monday 1 March 2004.
On-line abstract submission & registrationAre available at
www.phcris.org.au
Enquiries should be directed to:Conference Logistics
PO Box 201Deakin West ACT 2600
Tel: (02) 6281 6624Fax: (02) 6285 1336
Email: [email protected]
- continued from page 4
for emission reduction programmes without binding rules.
Some areas like the northern Italian region of Lombardy,one of the richest and most industrialized parts of Europe,are focusing on domestic policies: low energy-consumptionhome appliances, new systems for controlling greenhousegases, and the planting of trees to create carbon sinks.
But Germany, Sweden and Finland are calling for strictenforcement of the Protocol even without the “renegade”countries (the United States, Canada and Australia).
“We will need to negotiate other options to implement theaccords that have already been approved in the frameworkof Kyoto. We have a committee that can apply pressure andcan seek new routes forward. Perhaps we can make newrules, but we have to debate them,” Aulikki Kauppila,adviser on international affairs to Finland’s Ministry ofAgriculture and Forests, told Tierramérica.
Other nations like the Netherlands are in favor of comingup with a new global agreement. “We all hope Russia willratify the Protocol. If it doesn’t, we have to think of othermechanisms. A small group of states is discussing thepossibility of a new treaty, but we can’t talk about that yet,”Dutch Foreign Ministry official Sara Affermans remarkedto Tierramérica.
But for the representatives of Asia and Africa, where themajority of poor nations exempt from the Kyoto Protocol’semissions reduction targets are located, the Protocol isirreplaceable.
“If Russia fails to ratify it, we cannot move ahead. We don’tneed another protocol. Kyoto is a global effort, and it tookthe international community a long time to come up withthe Protocol. Creating a new one would not be an easytask,” Li Liyan, with China’s National Office on ClimateChange, said to Tierramérica.
Since it withdrew from the treaty in 2001, Washington hastried to convince developing nations that bilateralagreements are a better option.
Prior to the start of the two-week meeting taking place inMilan, environmental groups warned of the U.S. intentionto promote a 1.7 billion dollar investment in studyingclimate change, and a one billion dollars investment inobtaining hydrogen from coal and creating newtechnologies to eliminate greenhouse gases.
From: http://www.tierramerica.org/english/2003/1208/iarticulo.shtml
Death Blow for Kyoto? Report on the Evaluation of the NationalMinimum Data Set for Admitted Patient Care.
Catalogue No. HSE 29, $30.00, Available fromCanPrintThis report presents the Institute’s mostcomprehensive evaluation to date of the quality andconsistency of data collected under the NationalMinimum Data Set for Admitted Patient Care. Thereport is a useful resource for health informationmanagers, researchers, state and territory dataproviders and all users of data based on this NationalMinimum Data Set.
http://www.aihw.gov.au/publications/index.cfm?type=new

6
Reprinted By: William Maclean, Reuters
”The World Health Organization and UNAIDS promisedcheaper drugs, simpler treatment regimens and more money aspart of a campaign launched in Nairobi to provide threemillion HIV-infected people with the latest drugs available bythe end of 2005 in a $5.5-billion US effort.”
Tens of thousands of activists and health workers ralliedworldwide today to mark World AIDS Day and officials hailednew initiatives, new funding and a new pill to fight the diseasethat has infected 40 million people and kills more than 8,000every day. The World Health Organization and UNAIDSpromised cheaper drugs, simpler treatment regimens and moremoney as part of a campaign launched in Nairobi to providethree million HIV-infected people with the latest drugsavailable by the end of 2005 in a $5.5-billion US effort.
WHO also certified an innovative, generic drug for treatingHIV that combines three essential anti-retroviral drugs intoone pill to be taken twice a day. WHO and UNAIDSpromised to promote international agreements to streamlinetreatment programs. “In two short decades, HIV/AIDS hasbecome the premier disease of mass destruction,” said Dr. JackChow, the assistant director general of WHO. “The deathodometer is spinning at 8,000 lives a day and accelerating.”
Medecins Sans Frontieres, an aid agency that has led efforts tosimplify HIV treatment, welcomed the announcement but saidfunding will be critical.“The treatment has to be free; if the treatment is not free, theywill not meet their goals,” said Dr. Morten Rostrup, presidentof the group’s international council.
Thousands of activists marched and rallied in Nairobi to showsupport for people infected with HIV and to demand access toessential drugs. “It is depleting our stock of knowledge andreallocating family and national budgets,” President MwaiKibaki said. “Indeed, this disease could lead to the collapse ofsome economies in the next few generations. We, therefore,owe it to humanity to fight this disease relentlessly.”
Tommy Thompson, U.S. health and human services secretary,appealed in Zambia for redoubling efforts against HIV. Africa,the hardest-hit continent, cannot fight the pandemic alone, hesaid. “This war has caused more casualties than any other war,”Thompson said. “We need America, the European Union andeverybody. Nobody is going to be spared unless we all cometogether in the fight against this disease.”Former South African president Nelson Mandela urged theworld to fight the stigma associated with HIV, saying it wasstopping people from being tested and treated. “That is a tragicmistake, because when you do that, you make the people thatare suffering feel like they are not human beings,” Mandelasaid in Cape Town. “Many will die because of feeling less thanhuman.”
UNAIDS estimates three million people have died this yearfrom AIDS. WHO says more than five million HIV patientsneed anti-retroviral drugs, but fewer than 400,000 have access
to them. Anti-retroviral drugs allow HIV patients to live arelatively normal life by preventing the development of AIDS.The drugs improve their health, but they remain infected andcan transmit the disease.
India announced plans to spend $44 million to provide freeanti-retroviral drugs to 100,000 AIDS patients, a “significantscale-up” in the fight against the disease in a country that hasthe world’s second-highest number of HIV-infected people.Until now, India has focused on prevention, but starting April1, 2004, it will offer free drugs at government hospitals.
Health workers hit Beijing’s streets to teach prevention in acountry whose leaders have promised to fight the diseaseaggressively. The China Daily newspaper, citing a survey bythe Health Ministry, WHO and UNAIDS, said 840,000Chinese are HIV-positive and 80,000 have developed AIDS.But Siri Tellier, head of the UN Theme Group on HIV/AIDSin China, said it was not known whether that figure wasaccurate. She said there has been no widespread blood testingin the country, and she urged Beijing to improve itsmonitoring.
The British government said it will double its funding toUNAIDS next year to $10.2 million. “HIV/AIDS destroysfamilies and threatens to break down the fabric of wholesocieties, but I believe the challenges ahead can be met,” saidInternational Development Secretary Hilary Benn.
Botswana President Festus Mogae said people must takeresponsibility for utilizing the free anti-retroviral therapy, HIVtesting and the prevention of mother-to-child transmissionservices that are available. “Unless we take it upon ourselves touse condoms and prevent HIV infection, we have onlyourselves to blame for our plight,” Mogae said.
Malawi’s government pledged to provide free AIDS medicineto 50,000 people by 2005, paid for by the Geneva-basedGlobal Fund to Fight AIDS, Tuberculosis and Malaria, Vice-President Justin Malewezi said.
In Liberia, which is struggling to emerge from 14 years ofconflict, U.S. Ambassador John Blaney called peace the mainprerequisite, since AIDS is spread in warring West Africancountries by troops and the rape of women and girls.
Swedish activists organized a conference called Hope, Insightand Vision that included conferences on children and HIV, themedical outlook for a vaccine and treatments.
Even countries with a smattering of AIDS cases held eventsMonday aimed at boosting awareness. In Albania, with only116 registered cases since 1993, scores of high school studentsmarched in Tirana with candles and a banner that read, ProtectYourself and Others.
From: http://www.thestar.com/NASApp/cs/ContentServer?pagename=thestar/Layout/Article_Type1&c=Article&cid=1070233810424&call_pageid=968332188854&col=968350060724
The lives of millions are at stake

7
As many In Touch readers are aware, in 2004 the annualPHAA conference will be incorporated into the 18th WorldConference on Health Promotion and Health Education,Health2004, Melbourne April 26-30. The conference isauspiced by the International Union of Health Promotionand Education (IUHPE), based in Paris.
PHAA decided to join Health2004 for a number of reasons.The conference title ‘Valuing diversity, reshaping power:exploring pathways for health and wellbeing’ encapsulateschallenges for public health critical to the future health ofthe populations of the world and to the health of ourplanet. Increasing concern over widening inequalities inhealth led to the identification of globalisation, indigenoushealth, and the distribution of power over social decision-making as major themes for the conference. Many of theseissues are multifaceted and multi-layered, requiringcomplex responses on the part of communities, sectors andgovernments. Key public health topics covered over the fourdays include physical activity, indigenous health, mentalhealth, evidence/effectiveness, tobacco, cancer, healthyageing, youth, HIV/AIDS and blood-borne diseases.
Another reason for joining this international conference isthe significant learning and liaison opportunities it willprovide for members. The line-up of speakers and events atthe conference is first class. Featured amongst the 12plenary speakers are Professor Mason Durie (Assistant ViceChancellor and Professor of Maori Research Development,Massey University, New Zealand); Dr Jeff Koplan (EmoryUniversity, Georgia USA and former Director of the Centerfor Disease Control and Prevention); Datin Paduka MarinaMahathir (President Malaysian AIDS Foundation andExecutive Producer ‘3R’ television); Dr David Satcher(National Center for Primary Care; Morehouse School ofMedicine, Georgia, USA and former United States SurgeonGeneral); Anna Tibaijuka (Executive Director: UN –Habitat), Dr Nafis Sadik (UN Special Envoy on AIDS inAsia, Pakistan and former head of UNFPA HealthPromotion and Urban Governance); and Prof. FionaStanley, (Department of Paediatric Medicine, University ofWA).
The participation of delegates from a variety of countriesprovides members with an opportunity to understandinternational perspectives, to form and strengthenrelationships with international colleagues, and to showcasethe public health achievements of Australians to aninternational audience. Further learning and liaisonopportunities are offered by a series of associated meetingsand conferences, including the international Conference onthe Reduction of Drug Related Harm (April 21-24) andthe WHO Mega-Country Meeting (April 22-25). Alsounique to the conference will be three one-day conferenceson HIV/AIDS, cervical screening, and health promoting
schools, co-organised by the AIDS Society of Asia and thePacific, the Cancer Council of Victoria and the AustralianHealth Promoting Schools Association respectively.A strategic advantage in PHAA joining the conference is itspotential to strengthen relationships between PHAA, theAustralian Health Promotion Association (AHPA) andIUHPE. The history of the public health and healthpromotion professions has been characterised by a contestabout the nature of health itself, the causes of ill-health,appropriate interventions to reduce disease and promotehealth and motivations for intervention (a rights basedverses utilitarian view of health).1 Although both fieldsshare the aim of population health gain, they havetolerated, and to some extent defined themselves, byconceptual, definitional, methodological and operationaldifferences.2 Increasingly complex understandings of thedeterminants of health, for example the contribution ofsocial inequalities and political boundaries to the emergenceand spread of communicable disease3, are challenging bothfields to revisit and question the importance of thesedifferences in view of significant commonalities. Sharing inValuing Diversity, Reshaping Power is an opportunity for usto examine how further collaboration between the fieldsmay be useful in promoting public health.
PHAA has contributed to developing the generalconference program, developed some specific sessions andpreserved some of the networking benefits of the nationalconference, including a separate PHAA dinner, pre-conference SIG workshops, and informal meeting spacesfor PHAA members. The conference committee is makingevery effort to ensure that the conference is inclusive,challenging, and a positive experience for all.
Further details on registrations are available on the WorldConference website: http://www.health2004.com.au Takeadvantage of the discounted PHAA membershipregistration fee.
EARLY REGISTRATION CLOSES15TH FEBRUARY 2004.
Ali Barr (Victorian Branch) and Peter Ryan (Health2004Media Committee)
(Footnotes)1 Webster C, and French J. The cycle of conflict: the history of thepublic health and health promotion movements. In Sidell M, Jones L,Katz J, Peberdy A and Douglas J. Debates and Dilemmas inPromoting Health. Hampshire: Palgrave MacMillan, 2003: 9 – 18.2 Ibid.3 Farmer, P. Social inequalities and emerging infectious diseases.Emerging Infectious Diseases 1996; 2: 259-269.
Public Health Promotion - a Conference Challenge

8
Bob BealeReprinted from: ABC Science Online
The Chinese exercise practice of Tai-Chi can significantlyboost the body’s immune system response to virus infectionand may, in particular, help ward off painful shinglesoutbreaks in older people, a new study has found.
The research, by Dr Michael Irwin of the University ofCalifornia Los Angeles and colleagues is reported in thecurrent issue of the journal Psychosomatic Medicine.
The controlled study in the U.S. on 36 men and womenwith an average age of 70, showed that those who used Tai-Chi’s combined elements of movement and meditation overseveral months enjoyed a 50% increase in immune cellsthat target the shingles virus. The research is thought to bethe first to show that a behavioural intervention canpositively influence a virus-specific immune response: “Ourfindings offer a unique and exciting example of mind overmatter,” Irwin said.
The herpes virus - known as varicella - that causeschickenpox in younger people remains alive in nerve cells inthe body and is the cause of shingles later in life. Shinglesoutbreaks can occur when an infected individual’s immunesystem is weakened by stress, illness or advancing age,allowing the virus to re-emerge and cause skin rashes thatcan remain painful for months or years.
”There is no standard medical treatment to preventshingles, or medical means to boost the immune system anddecrease the risk of shingles,” Irwin told ABC ScienceOnline. “Novel interventions or treatments are needed todecrease the risk of shingles in older adults at risk for thisviral disease.”
None of the study subjects had suffered from shingles butall had chickenpox earlier in life. Half were randomlyselected to take a Tai-Chi course for 45 minutes, three daysa week, for 15 weeks, while the remaining half acted as acontrol group and did not do Tai-Chi.
A week after the end of the study period, physical check-ups and immune-system tests showed that on average theTai-Chi group did not simply feel healthier but had sharplyincreased levels of memory T-cells that specifically recogniseand attack the varicella virus, although individual responsesvaried.
Tai-Chi involves making slow and precise movements co-ordinated with controlled breathing. Subjects in the Tai-Chigroup also showed improvements in physical functioning,especially those who before the study had problems withcommon tasks, such as walking and climbing stairs. Forthem, Tai-Chi’s benefits were “comparable or exceeded thatreported for hip-replacement surgery or for heart-valvereplacement in older adults,” said the researchers.
Tai-Chi boosts immunity: studyTai-Chi Chih - as it is formally known - is a westernisedversion of Tai-Chi Chuan, an exercise form that has existedas a martial art in the Chinese culture for 2,000 years andas an exercise for elderly people for around 300 years, Irwintold ABC Science Online.
Irwin cautions that the study group was small and that aplacebo effect might account for the results: “What isimportant about this study is [the effect] that this ‘power ofthe mind’ - if that is the effect of Tai-Chi Chih - had onobjective measures of immune function.”
More research is needed to discover whether Tai-Chi’seffects on specific immunity are long-lasting and whether itmight be useful in boosting the immune response to otherinfectious diseases.
The study was supported by the U.S. National Institutes ofHealth
The Australian Forum for Textile Arts, South Australia
Yarn needed for Baxter Detention Centre. Of the womenbeing held in the Baxter Centre, Port Augusta, there are atleast twelve keen knitters. There is very little for them to doand they enjoy knitting garments for themselves, theirchildren and their visitors. Unfortunately, they have verylimited supplies of wool. This is a problem as a garmentcan be knitted in only 10 days. The knitters then have tounpick their finished work so they can use the wool againto be able to keep knitting.
There is a need for yarn so that the women can makegarments which can be used, rather than continuallyunpicked. As there are four babies due soon, baby woolwould be very useful. Dark royal blue and maroon wouldbe appreciated as they are the Port Augusta High Schoolcolours and can be used for garments for students attendingfrom Baxter. However, yarns of any colour will be welcome.
Yarn and knitting patterns are needed by the knitters(plastic knitting needles could also be useful but it may beeasier if they were sent separately). If you or people youknow are interested in donating these items, the bestapproach is to contact the Rural Australians for Refugeesgroup at Port Augusta by either sending an email [email protected] or phoning Jenny Bourne on 088642 4414 (after hours). They will be able to providenames and addresses of knitters in Baxter so parcels can besent directly to them. It is suggested that contact details areincluded so the recipient has the opportunity to send a
thank you letter.
http://www.ggcreations.com.au/tafta/news.html
continued on page 13

9
New York, Dec 19 2003 10:00AMThe United Nations Population Fund (UNFPA) receivedcontributions from a record 142 countries in 2003 - thelargest number in its history, the agency said today.
The top six donors were the Netherlands, Japan, Norway,the United Kingdom, Denmark and Sweden. The UnitedStates was not among the countries backing the Fund thisyear.
UNFPA Executive Director Thoraya Ahmed Obaid saidlevel of support had surpassed the agency’s expectations.“This is strong evidence that countries, from every region ofthe world, have confidence in the Fund.” Regular resourcesfor UNFPA in 2003 were approximately $294 million.
The number of donors more than doubled since 1999when the agency received funding from just 69 States. Newdonors in 2003 included Armenia, Azerbaijan, Estonia,Hungary, the Former Yugoslav Republic of Macedonia,Moldova, Somalia, Swaziland, Tajikistan, Timor-Leste andUzbekistan.
“UNFPA works hard to make pregnancy and childbirthsafer for women in developing countries, to prevent HIVinfections and to help couples plan their families and avoidunintended pregnancies,” said Ms. Obaid. “We can nowmeet more of the demands for reproductive health care inthe 150 countries where we work.”
The health consequences of the war in Iraq will be felt foryears and perhaps even generations, according to a recentreport.
Released in November by the health charity Medact, the reportestimates that more than 20,000 Iraqis have died since thewar began. Although the official end of the war was declaredmonths ago, children and adults continue to be maimed andkilled by mines, those needing medical care are now even lesslikely to receive it, and the country’s residents will face physicaland mental illnesses for years as a result of ongoing violence,poor sanitation and a weakened health service, according tothe report.
“Limited access to clean water and sanitation, poverty,malnutrition and disruption of public services, includinghealth services, continue to have a negative impact on thehealth of the Iraqi people,” said the report’s lead author SabyaFarooq, PhD.
Medact members spoke out against the military conflict beforeit began last year, warning of long-term health consequences.Medact is calling on the United Nations and occupying forcesto further investigate the long-term health impact of the war.
War in Iraq will have health consequences for many years
According to the agency, about 350 million couples stilllack access to a range of safe, effective and affordablecontraceptive methods, while only half of all births indeveloping countries take place with a trained attendant.
For more details go to UN News Centre at http://www.un.org/news
They also urge fully funding the reconstruction of publichealth services and continued efforts to provide law and orderin the country.
Main health concerns outlined in the report include clusterweapons, which contain ammunition called “bomblets”designed to separate and explode when released.They often are colourful and attract children who are especiallyvulnerable to injury. Hidden and deadly landmines have beenfound in stockpiles around the country, in locations thatinclude civilian buildings and mosques. In addition, depleteduranium used in anti-tank ammunition could leave cancer-causing residue countrywide.
Malnutrition is a major concern, with many Iraqis selling theirfood rations to buy clothing and medicine. While Iraq’s pre-war electricity supply was “erratic and weak,” as described inthe report, some regions still lack power and others have nearnormal power supplies for the first time in years.
“Continuing Collateral Damage: The Health andEnvironmental Costs of War on Iraq 2003” was published inconjunction with International Physicians for the Preventionof Nuclear War and is available fromwww.medact.org or www.ippnw.org
Record Number of Donors support UN Population Agency this Year
Alcohol and Other Drug Treatment Services:findings from the National Minimum Data Set(NMDS) 2001-02
Drug Treatment Data Briefings (for each State andTerritory except Queensland)Free, Available from AIHW
These data briefings summarise the main findings fromthe 2001-02 alcohol and other drug treatment servicesNMDS data for each State and Territory (exceptQueensland). More detailed information about the 2001-02 collection and its findings can be found in thepublication titled Alcohol and Other Drug TreatmentServices in Australia 2001-02: report on the NationalMinimum Data Set which can be accessed on line at http://www.aihw.gov.au/drugs
Click on the link to view http://www.aihw.gov.au/publications/index.cfm?type=new.
10
“ By year-end, a small company in Argentina will put a newkind of refrigerator on the market, which will go down inhistory as the first in South America to operate withoutdamaging the ozone layer or contributing to globalwarming.”
The ozone-safe model has been used in Europe for nearly adecade. But the transnational corporations thatmanufacture the refrigerators there have been reluctant tomake the investment necessary to adopt the new technologyin the Americas.
Firms in Argentina and other Latin American countrieshave attempted to develop products using the technology,but without success until this year when the goal wasachieved by Autosal, an Argentine company with180 employees that produces merchandise carrying theColumbia and Koh-i-noor brand-names.
The price, traditional style and white color of therefrigerators will remain the same. The revolutionary aspectof the units is that they use a new refrigerant, isobutane, toreplace the ozone-depleting chlorofluorocarbons (CFCs)that destroy the ozone layer that protects life on earth fromharmful ultraviolet radiation from the sun.
Nor do the new refrigerators use hydrochlorofluorocarbons(HCFCs), which do not deplete the ozone layer but aregreenhouse gases that contribute to global warming.
Isobutane is a gas from the family of the hydrocarbons thathas the approval of the Montreal Protocol, the internationalagreement aimed at eliminating ozone-depleting gases.
HCFCs were seen as a step forward from CFCs, until theywere found to aggravate global warming. Isobutane, on theother hand, passes muster with the Kyoto Protocol , theinternational treaty aimed at reducing emissions of gasesthat contribute to climate change, which has not yet goneinto effect.
The new model also replaces hydrofluorocarbon (HFC),used as a foaming agent in insulation, with cyclopentane,another hydrocarbon gas.
Thus, the new units meet the requirements of both theMontreal and Kyoto protocols, as do most refrigerators soldtoday in Europe.
The world’s first climate- and ozone-safe refrigeratortechnology replacing CFCs and HCFCs with hydrocarbongases was developed in the early 1990s by the internationalenvironmental organisation Greenpeace, which named thenew technology “greenfreeze”. To ensure maximum
diffusion, it did not patent the invention.
The idea was initially rejected by Germany’s leadingrefrigerator manufacturers, which had just invested inreplacing CFCs with HCFCs. The companies also allegedsafety reasons, since the hydrocarbon gases are flammable.
But a company on the verge of bankruptcy, located in theformer East Germany, embraced the idea, the head ofGreenpeace International’s Renewable Solutions Campaignin Argentina, Mariana Walter, told Tierramérica.
The German company, Foron, saw its sales increaseconsiderably almost overnight, and within a few months,Germany’s major manufacturers began to convert theirplants to incorporate the new technology, under pressurefrom consumer demand.
Transnational corporations like Whirlpool, Bosch andElectrolux began to produce refrigerators employing thenew green technology in Europe, but not in the Americas.
Not even the most-developed countries in the hemisphere,the United States and Canada, have adopted the newtechnology, which would require extra investment.
Only Cuba, unable to import chemical refrigerants due tothe four-decade U.S. embargo, is manufacturingrefrigerators using hydrocarbon gases.
Several other Argentine manufacturers tried to adapt theirfactories to the new green technology, but their attemptsended in failure.
”Of the four firms that set out on the new endeavor, threewent under,” said Walter. Only Autosal, in the northeasternArgentine province of San Luis, which supplies 12 percentof the national market, was left.
Up to now, the company has been selling 12,000 units ayear. But it hopes to sell 5,000 of the new units a month,Autosal’s marketing director, Guillermo Moro, toldTierramérica.
The firm invested 1.5 million dollars in the reconversionprocess, including 800,000 dollars that came from theMontreal Protocol Multilateral Fund created to helpdeveloping countries meet the target of eliminating CFCsby 2010.
According to Moro, the safety measures that must beadopted in the manufacturing of appliances using isobutane
First “Green-Friendly” Refrigerator
continued on page 11
11
and cyclopentane are no greater than those required forproducing traditional refrigerators. “We install detectorscapable of detecting any gas leak,” said the executive.
Although the new units are slightly more expensive toproduce, the company decided to absorb the difference incost to order to hold prices steady.
The new clean technology will not be publicised by thecompany. “We are putting it out on the market practicallyat the end of the refrigerator-buying season (from Octoberto January), which is not a good time to launch anadvertising campaign. Maybe next year,” said Moro.
Greenpeace, however, will take on the task of publicisingthe new product. “This is a key development for openingup the game in the region to other companies that want tojoin in and use this technology,” said Walter.
Environmentalists hope to see a repeat of what happened inGermany: that consumers in Argentina - and other
countries in Latin America - will begin to demandrefrigerators using the new green technology.
(* Marcela Valente is a Tierramérica contributor. Originallypublished Dec. 6 by Latin American newspapers that arepart of the Tierramérica network. Tierramérica is aspecialised news service produced by IPS with the backingof the United Nations Development Programme and theUnited Nations Environment Programme.)
By:Marcela ValenteReprinted From: http://www.ipsnews.net/
interna.asp?idnews=21538
First “Green-Friendly” Refrigerator - continued from page 10
THE Immigration Department has come under fire at theopening of a parliamentary inquiry into sexual slavery.
A council officer for inner-Melbourne’s Yarra City Council,Ken Wolfe, told the committee he had closed 23 illegalbrothels in the past year, most of which contained suspectedillegal Asian workers, but he could not get any officers fromthe department to attend the raids.
“I have never been able to get people to come with me,” MrWolfe told the committee. “I haven’t called Immigration for18 months because they always say the raids are ‘too basic’and they haven’t got anyone available.” Mr Wolfe said mostof the women at the illegal brothels produced temporaryvisas for identification.
The Victorian police also told the committee yesterday thedepartment had been “unable” to supply them with anyfigures about the numbers of women who had beendeported after they were discovered working in sexualservitude.
Mr Wolfe said most of the women arrived in Australia ontourist visas and then claimed protection visas, whichallowed them to work in Australia while their claim wasconsidered by the Refugee Review Tribunal. Committeemember and federal Labor MP Duncan Kerr questionedhow the women involved in the illegal industry hadobtained tourist visas in the first place.
Immigration ‘ignored brothel raids’Mr Kerr said experience with his electorate had shown himthat tourist visas from places such as Thailand, where manyof the women came from, were almost impossible to obtain.“Something stinks because these women seem to be comingin relatively easily when normally people from thesecountries, even if they have entirely legitimate reasons forvisiting Australia, can’t get visas because they are considereda high risk of not returning home,” he said outside thehearing.
“Unless there is some explanation that emerges, it’s an issuewe are going to have to seriously address.” TheParliamentary Joint Committee on the Australian CrimeCommission inquiry into trafficking in women for sexualservitude is conducting public hearings around the country.
Kathleen Maltzhan of Project Respect, an anti-traffickingorganisation, told the committee an estimated 1000 womenworked in Australia in sexual servitude at any one time.
In October, the federal Government announced a$20million plan to fight the trade in sex slaves to Australia.A new 23-member police strike force based in Canberrawith an officer in Bangkok is part of the plan to target theflourishing illegal trade.
By Barclay CrawfordThe Australianhttp://www.news.com.au/common/story_page/0,4057,7912963%255E26462,00.html

12
“But beside the deaths, there was a large increase in otherillnesses. Many children were admitted to hospital in Englandwith kidney problems due to dehydration. Parents and childrenhad failed to realise that they needed to drink more to survivethe heat.”
At least 150,000 people die needlessly each year as a directresult of global warming, three major UN organisationswarned yesterday. The belief that the effects of climatechange would become apparent in 10, 20 or 50 years timewas misplaced, they said in a report. The changes hadalready brought about a noticeable increase in malnutrition,as well as outbreaks of diarrhoea and malaria, the three “bigkillers” in the poorest countries of the world.
The report was published at the climate talks in Milan,where ministers are trying to put the finishing touches tothe Kyoto protocol, designed to put legal limits ondeveloped countries’ greenhouse gas emissions. Russia’sratification of the protocol is needed for it to come intoforce.
Diarmid Campbell-Lendrum, a World Health Organisationscientist, said the estimates of deaths were extremelyconservative and the reality was probably far higher. Theywere expected to double in the next 30 years. “People maysay that this is a small total compared with the totals whodie anyway, but these are needless deaths. We must do ourbest to take preventative measures,” he said.
Although the rises in death and diseases were most markedin poorest states, they were worldwide. Global warming ledto drought and a shorter growing season, and malnutritionweakened people, particularly children, making themsusceptible to killer diseases.
The most recent example of people being caught unawareswas the summer heat wave in Europe, where the initialestimates of excess deaths are still being revised upwards,with 25,482 people now known to have died in theunusually high temperatures, 2,045 of them in Englandand Wales. In some badly affected countries, such asGermany, the results have still not been made public.
But beside the deaths, there was a large increase in otherillnesses. Many children were admitted to hospital inEngland with kidney problems due to dehydration. Parentsand children had failed to realise that they needed to drinkmore to survive the heat.
Bettina Menne, a medical officer with the WHO, said theFrench were caught by surprise. Many of the 14,802 whodied, 60% more than expected, were in institutions.Research is under way to establish whether air conditioningshould be a necessity for parts of hospitals, or whether a‘cold room’ should be established for vulnerable patientsduring heat waves in residential homes.
Global warming kills 150,000 a year The report, produced by the WHO, the UN EnvironmentProgramme and the World Meteorological Programme,details how the increased warmth has intensified the spreadof diseases. Diarrhoeal diseases spread by bacteria, mostlyvia unclean water and food, spread and develop morequickly in warmer temperatures and humidity. Dirty wateris the largest killer of children under five.
In Lima, Peru, a six-year study at a clinic set up to treatdiarrhoeal complaints showed a 12% increase in cases forevery 1C rise in temperature in cooler months and a 4%increase in the hotter months. Similar results were found ina survey of 18 Pacific islands. The problem is made worseby high rainfall or drought, where water supplies becomecontaminated.
Diseases spread by rats and insects are also more commonin warmer weather. Malaria, dengue fever and Lyme diseaseare all on the increase. Many threats can be curtailed bydispensing preventive medicine and providing clean waterand sanitation. Climate change makes these issues moreurgent, the report said.
The combined effects of increased warmth and the greatervolume of standing water brought by storms create malariaepidemics by providing breeding sites and a speeded-up lifecycle. In Africa, where the death toll from malaria ishighest, mosquitoes carrying the disease are spreading intomountain areas previously too cool for them to thrive.
Hot and bothered...
Malaria Acutely sensitive to climate change. Thought to be1m extra cases because of climate change in 2000.Epidemics also triggered by high soil moisture content,allowing insects to survive long after floods have receded.Report predicts malaria spreading north and south intocurrently temperate regions, particularly those with highrainfall
Heat stroke Kills old and vulnerable; 25,842 extra peopledied in August in Europe
Salmonella In UK, a 12% increase in salmonella foodpoisoning is reported to health authorities for every 1C risein temperature, starting as low as 5C. Rises steeply in hotmonths
Malnutrition Climate change is already increasingmalnutrition because of crop losses
By Paul Brown
ReprintedFrom: http://www.guardian.co.uk/international/story/0,3604,1105118,00.html

13
” Pharmaceutical companies holding patents for AIDSdrugs have fiercely fought to block generic manufacturersfrom impinging on their patent rights, often lobbyinggovernments to reject the vastly cheaper alternatives inreturn for discounted prices.”
Promising cheaper drugs, simpler regimens and moremoney, two U.N. agencies launched a campaign Monday toprovide 3 million HIV-infected people with the latest drugsavailable by the end of 2005, potentially revolutionizingtreatment of the disease.
In marking World AIDS Day, the World HealthOrganization also certified a new, innovative generic drugfor use in treating HIV. The tablet combines three essentialanti-retroviral drugs into one pill that is taken twice a day.The pills are manufactured by two India-based generic drugmakers and cost patients only $270 a year, but violatespatents held by two major drug manufacturers. In order tolegally import the drugs, countries must suspend the rightsof the patent holder.
The WHO’s approval of simplified treatment regimens andgeneric anti-retroviral drugs is only one part of the agency’sstrategy, dubbed 3x5. WHO also joined UNAIDS inencouraging greater financial aid to poor countries.The detailed plan released Monday also focuses onestablishing the United Nations as a global leader infighting HIV, ensuring a reliable source for essential drugsand creating a system for disseminating the latestinformation on HIV, the virus that causes AIDS.
”In two short decades, HIV/AIDS has become the premieredisease of mass destruction,” Dr. Jack Chow, the assistantdirector-general of WHO, said. The death odometer isspinning at 8,000 lives a day and accelerating.” Treating 3
Agency certifies new generic HIV drugmillion patients with anti-retroviral drugs by 2005 will costabout $5.5 billion over the next two years, Chow said.
More than 40 million people are infected with HIV andmore than 3 million have died in 2003, UNAIDS reportedlast week. WHO estimates more than 5 million HIVpatients need anti-retroviral drugs, but fewer than 400,000currently have access to them.
Anti-retroviral drug combinations, often called triple-therapy cocktails, allow HIV patients to live a relativelynormal life by preventing them from developing full-blownAIDS. While the drugs improve the health of patients, theyremain infected with the virus and can transmit the disease.High prices have kept the drugs out of reach of mostpatients, but recent initiatives have made the drugs moreaffordable. The WHO and UNAIDS initiative will improvedrug distribution channels and train health professionals inpoor countries. Noticeably absent from the program’slaunch in Nairobi were representatives from the world’sdrug manufacturers. Pharmaceutical companies holding patents for AIDS drugshave fiercely fought to block generic manufacturers fromimpinging on their patent rights, often lobbyinggovernments to reject the vastly cheaper alternatives inreturn for discounted prices. Chow said they have heldmeetings with patent holders and generic companies butsaid no major agreements have been reached. Expandingproduction of the drugs will be critical to meeting the 3x5goals, he said.
By: Chris Tomlinson, APReprinted From: http://www.thestate.com/mld/thestate/news/world/7386534.htm
continued from page 8
So often it is the little things that matter in detention. This was sent to me by a wonderful friend. Apart from being a skilled ITManager, she has a wide range of interests including native Australian birds. She has surprised me of late with her intenseintellectual interest in knitting machines. She came across this important item during her research and forwarded it to me - I willnever laugh at her interest in knitting machines again.
For me this sums up the indomitable courage of women in detention. How brave those Baxter knitters are, how determined, howfull of hope. We all, in our priviledged lives outside the wire, can learn so much about what matters in life from the knitters ofBaxter. They won’t give up and nor can we however determined the government is to unravel the hopes of these valiant knitters. The media needs to be told about this and should run with it - it says so much:-
The Australian Forum for Textile Arts, Ltd, http://www.ggcreations.com.au/tafta/news.html
AustHumanRightsNews
Knitting in Detention
14
CLIMATE CHANGE AND HEALTH
Symposium and Short-course: Research Methods and Policy Issues
29th September - 2nd October 2003, Australian National University, Canberra
The one-day Symposium (Sept 29) on international and Australian perspectives onclimate change and health will bring together key international experts (with assistancefrom the International Society for Environmental Epidemiology) actively researchingthese issues. Speakers from the US, UK, New Zealand and Australia will present whatis currently known about the impact of climate change on health, globally and inAustralia.
The four-day short course (incorporating the symposium) will focus on researchmethods and policy issues in climate change and health. The presenters, includingsymposium speakers, will further elaborate on the latest methods and explore therelationships between science and policy applications.
Further details about symposium, short-course, speakersand registration is available at http://nceph.anu.edu.au/Envir_Collab/Climate_Change_course.htm.
Global trade keeps a billion children in poverty, saysUnicefBy Maxine Frith; The Independent
International targets to reduce child poverty are going to bemissed because globalized trade and cuts to aid budgets arecreating an ever- greater chasm between the richest andpoorest countries.
More than one billion young people in the developingworld are now living in conditions of severe deprivation,according to a report for the United Nations Children’sFund (Unicef ). Tens of millions of children in developingcountries still do not have access to basic human needs suchas food, water and sanitation, the study found.
The report is the first attempt to scientifically measureworld poverty, and paints a grim picture of how little thelives of the world’s poorest people have improved in the lastfew years.
A UN declaration in 2000 pledged that by 2015, it wouldhalve the proportion of people whose income was less thanone dollar a day and achieve a similar reduction in thenumber of people suffering from hunger. The declarationalso pledged to cut the death rate among the under-fives bytwo thirds and ensure that all children could complete
primary school.
Shailen Nandy, a co-author of the report, said: “At this rate,the goals are unlikely to be met, given declininginternational commitment to development aid. The resultsof cutting public spending on basic social services have beenan increase in poverty and inequality, a fact whichorganizations like the World Bank need toacknowledge.”
Campaigners warned that globalization and pressure ondeveloping countries to liberalize trade were adding topoverty.
Judith Melby, spokeswoman for the charity Christian Aid,said: “In many countries, poverty is increasing rather thandecreasing, particularly in relation to things likemalnutrition among the under- fives.
”We have to look at how globalisation has affected thesecountries. There is a real link between that and povertylevels. They are put under enormous pressure to liberalisetheir markets, then they lose their indigenous trade tosubsidised markets in the EU and the US; and the poorest
continued on page 21
15
“Dr Roses said doctors treating patients routinely appliedthe trial-and-error approach which says that if one drugdoes not work there is always another one.”
A senior executive with Britain’s biggest drugs company hasadmitted that most prescription medicines do not work onmost people who take them.
Allen Roses, worldwide vice-president of genetics atGlaxoSmithKline (GSK), said fewer than half of thepatients prescribed some of the most expensive drugsactually derived any benefit from them.
It is an open secret within the drugs industry that most ofits products are ineffective in most patients but this is thefirst time that such a senior drugs boss has gone public. Hiscomments come days after it emerged that the NHS drugsbill has soared by nearly 50 per cent in three years, rising by£2.3bn a year to an annual cost to the taxpayer of £7.2bn.GSK announced last week that it had 20 or more newdrugs under development that could each earn thecompany up to $1bn (£600m) a year.
Dr Roses, an academic geneticist from Duke University inNorth Carolina, spoke at a recent scientific meeting inLondon where he cited figures on how well different classesof drugs work in real patients.
Drugs for Alzheimer’s disease work in fewer than one inthree patients, whereas those for cancer are only effective ina quarter of patients. Drugs for migraines, for osteoporosis,and arthritis work in about half the patients, Dr Roses said.Most drugs work in fewer than one in two patients mainlybecause the recipients carry genes that interfere in some waywith the medicine, he said.
“The vast majority of drugs - more than 90 per cent - onlywork in 30 or 50 per cent of the people,” Dr Roses said. “Iwouldn’t say that most drugs don’t work. I would say thatmost drugs work in 30 to 50 per cent of people. Drugs outthere on the market work, but they don’t work ineverybody.”
Some industry analysts said Dr Roses’s comments werereminiscent of the 1991 gaffe by Gerald Ratner, the jewelryboss, who famously said that his high street shops aresuccessful because they sold ‘total crap’. But others believeDr Roses deserves credit for being honest about a little-publicized fact known to the drugs industry for many years.
“Roses is a smart guy and what he is saying will surprise thepublic but not his colleagues,” said one industry scientist.“He is a pioneer of a new culture within the drugs businessbased on using genes to test for who can benefit from aparticular drug.”
Dr Roses has a formidable reputation in the field of‘pharmacogenomics’ - the application of human genetics todrug development - and his comments can be seen as an
attempt to make theindustry realize that itsfuture rests on beingable to target drugs to asmaller number ofpatients with specificgenes. The idea is toidentify ‘responders’ -people who benefitfrom the drug - with asimple and cheapgenetic test that can be used to eliminate those non-responders who might benefit from another drug.
This goes against a marketing culture within the industrythat has relied on selling as many drugs as possible to thewidest number of patients - a culture that has made GSKone of the most profitable pharmaceuticals companies, butwhich has also meant that most of its drugs are at bestuseless, and even possibly dangerous, for many patients.
Dr Roses said doctors treating patients routinely applied thetrial-and-error approach which says that if one drug doesnot work there is always another one. “I think everybodyhas it in their experience that multiple drugs have been usedfor their headache or multiple drugs have been used fortheir backache or whatever.It’s in their experience, but they don’t quite understand why.The reason why is because they have differentsusceptibilities to the effect of that drug and that’s genetic,”he said.
“Neither those who pay for medical care nor patients wantdrugs to be prescribed that do not benefit the recipient.Pharmacogenetics has the promise of removing much of theuncertainty.”
Response ratesTherapeutic area: drug efficacy rate in per centAlzheimer’s: 30Analgesics (Cox-2): 80Asthma: 60Cardiac Arrhythmias: 60Depression (SSRI): 62Diabetes: 57Hepatitis C (HCV): 47Incontinence: 40Migraine (acute): 52Migraine (prophylaxis)50Oncology: 25Rheumatoid arthritis: 50Schizophrenia: 60
From: http://www.commondreams.org/headlines03/1208-02.htmBy: Steve Connor; Independent Newspaper, UK
TNC GLAXO chief says drugs do not work on patients

16
The Ecology of Energy TransformationsDr Frank FisherProfessor of Environmental StudiesMonash UniversityReprinted from ETHICAL INVESTOR ISSUE 27
Pacific ocean levels are rising due to global warming. FrankFisher says the problem for all societies is our misplacedemphasis on renewable energy rather than energyconservation.
At the rate industrialised peoples have grown used to usingenergy, no energy form can be used, and no energytransformation to electricity can occur, withoutenvironmental problems. While most of us are aware ofissues such as greenhouse gases, global warming and risingsea levels threatening low-lying islands in the Pacific region,on the whole, all societies are profoundly ignorant of energyas engineers understand it and even less aware of energy asecologists understand it.
The very idea of renewables fosters the illusion that ourpresent ignorant ways with energy can continue. The moreviable renewables become and the more they are able tocompete with fossil fuels - most of whose costs are simplyignored - the more they suppress energy conservation.Energy conservation is our cheapest and most socially andenvironmentally benign energy source.Conservation can be mined just like coal! If we could seethis, it would become exciting as an opportunity for venturecapitalists and be reflected in our economic and regulatorystructures.Renewables, not conservation, are sold as a panacea.Renewables are marketed on the basis that they will permitus to continue to live in the ways we have grownaccustomed to, but with ‘zero emissions’. This is amischievous and dangerous illusion. On average, eachAustralian demands some 2kW (three horsepower) ofelectricity-generating capacity and much more than thatfrom our other energy systems, such as heating andtransport. Most of these systems are based on fossil fuels,which are of course not renewable and place a tremendousburden on the environment in transformation to electricity.
Large-scale renewable systems involve mining sunshine viaplants and the heat and movement the sun gives to theatmosphere and the oceans; hence hydro and wind power.Attempting to fill the current demand with renewablescreates a raft of environmental, social and even moralconcerns. Take, for example, ‘energy cropping’ for electricityand automotive fuels. Energy cropping means ‘growing’fuels and burning them directly to generate electricity,distilling alcohol from sugar cane or squeezing oils fromother plant materials and then burning these liquids ininternal combustion engines to drive vehicles or, again, in
boilers to generate electricity. In the case of electricity, itmeans wasting 60-80 per cent of the crop because theprocess is at best only 40 per cent efficient. As auto fuel,however, it means wasting more than 99 per cent becausemost of it then goes to drive the auto-system, rather thanthe motorist.
Solar energies may seem benign; but when they are minedthrough hydroelectric plants (solar energy lifts the water),wind generators and natural draft towers, they generate abroad range of ecological implications. If all humans wereto demand the same 2kW from the wind say, as we inAustralia currently expect from fossil fuels, the energetics ofthe atmosphere would change as surely as through burningfossil fuels. It also needs to be said that solar cell electricityor photovoltaics is not the answer, because the quantitiesavailable per square metre per day are small, especially afterdeducting the energy costs of production and installation.
All energy infrastructure costs energy to create, transport,install, and maintain; to dismantle when its life is done;and to defend. If these costs are greater than the returns (inthe form of energy), one can be excused for askingquestions. That is almost certainly the case with nuclearpower and therefore the sanity of its use has to bequestioned even before we concern ourselves with issues ofradiation and the potential of nuclear terrorism.
Wind generators and natural draft towers willunequivocally deliver more electricity than their energycosts. However, they are patently not zero emissiongenerators. Even in service, they suck energy frommeteorological and ecological processes with various, as yetlargely unknown, effects. In construction, monitoring,maintaining and dismantling, they have the usualmultifarious energy and ecological implications.
There simply are no such things as energy andenvironmental cost-free energy forms. Even conservationinvolves cost. Driver-only automotive commuting is acategory of energy use so wasteful that it deserves specialmention. This is a task that a bicycle coupled with trainscould do faster, more healthily and more ecologicallysustainably for a tiny fraction of the energy cost. Issues suchas these however, simply do not figure on the public’s radarbecause energy and efficiency indicators are not given highpriority. Few of us actually read our electricity bills, letalone graph the efficiency of our cars. The price of energy istoo low, joules and kWh are still too obscure as measures,and most of the really large scale pollutants associated withenergy transformations such as water, carbon dioxide and
Energy conservation is our cheapest and most socially andenvironmentally benign energy source.
continued on page 18

17
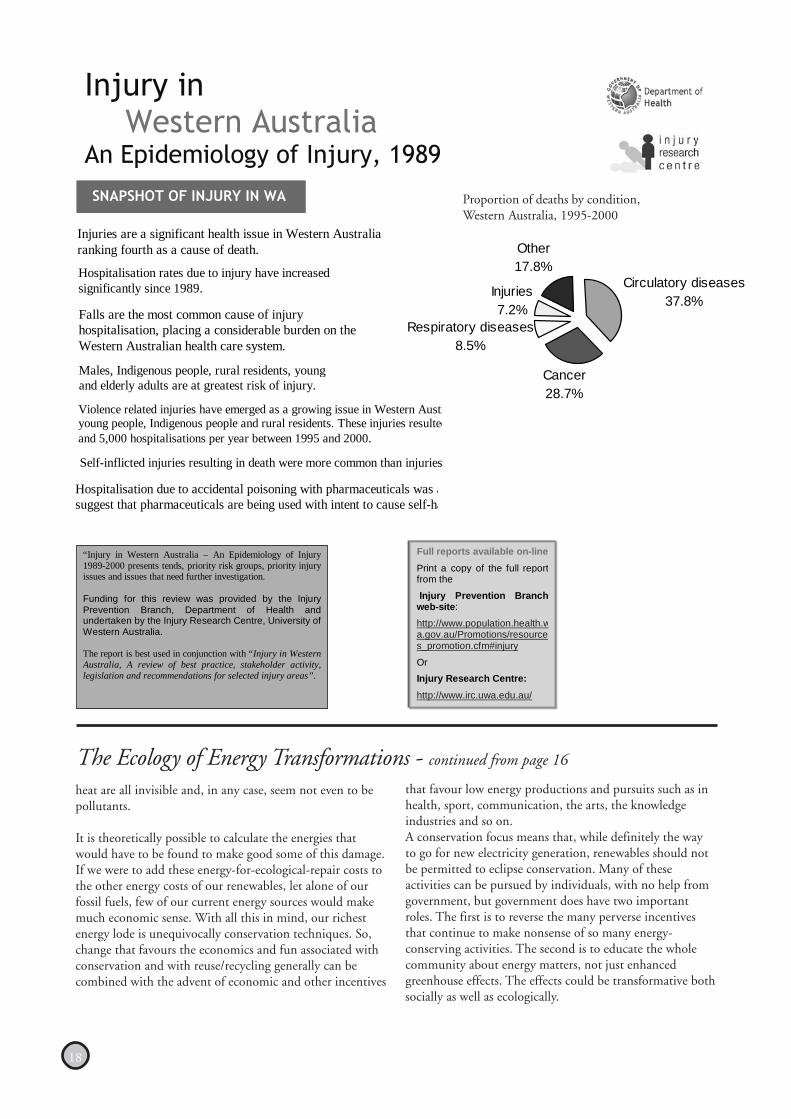
New statistics released by the Department of Health revealthe projected costs of accidental falls in West Australian’s aged65 and over will more than double in less than 20 years.
By the year 2021 it is forecast falls will cost the WA healthsystem $174 million. In the year 2001/2002 falls cost thehealth system $83 million.
The research was released for the first time at the seminar‘Falls – Costly? How much do we know?’ and highlights thecurrent and future impact on health system resources ofaccidental falls by seniors.
Conducted by the UWA Injury Research Centre incollaboration with the Department of Health InjuryPrevention Branch, the research also shows the pressure offalls on emergency departments and hospital admissions. Thekey findings include:
• The number of people presenting at emergencydepartments as a result of falls will be 39 000, more thandouble the current number of 18 706; and
• The number of hospital admissions following a fall willbe 12 300, compared to the current admissions of 5 923.
Seniors falls prevention is a state health priority andcollaborative falls prevention programs play an important roleto reduce the incidence and severity of fall-related injuries.
To download a copy of “Injury in Western Australia, The HealthSystem Cost of Falls in Older Adults in Western Australia” visit:
http://www.population.health.wa.gov.au/Promotion/resources_promotion.cfm#injury
Reports are listed under “Injury in Western Australia”
The Health System Cost of Falls in Older Adults in Western Australia
The Injury Prevention Branch, Department of Health andthe Injury Research Centre – The University of WesternAustralia, have released a new report, Injury in WesternAustralia: Family Violence – A review of best practice,stakeholder activity, legislation and recommendations.
The report investigates the epidemiology, stakeholderactivity, legislation and ‘best practice’ interventions forinjurious behaviour in Western Australia and:
Focuses on primary/ early prevention strategies toreduce family violence related injuries, as opposed toa risk management or treatment perspective.
Provides policy makers, researchers, healthprofessionals, advocates and volunteers involved inviolence prevention with a snapshot of the level ofinjury associated with family violenceProvides an overview of the prevention andmanagement strategies currently undertaken in WesternAustralia.
Provides practitioners new to the field of familyviolence a useful starting point for identifying priorities,stakeholders and recommendations for futureaction.
It is best used in conjunction with the recently releasedInjury in Western Australia: An Epidemiology of Injury, 1989– 2000 , which identifies intentional injury (ie. Violence-related injuries) as a growing issue in Western Australia.
Together these reports can be used as a platform forprofiling intentional injury and to promote support forresearch and early intervention strategies to reduce domesticviolence in Western Australia. To download a copy of‘Injury in Western Australia, Family Violence - A review ofbest practice, stakeholder activity, legislation andrecommendations’ visit:
http://www.population.health.wa.gov.au/Promotion/resources_promotion.cfm#injury
Reports are listed under “Injury in Western Australia”.
Injury in Western Australia: Family Violence
18
heat are all invisible and, in any case, seem not even to bepollutants.
It is theoretically possible to calculate the energies thatwould have to be found to make good some of this damage.If we were to add these energy-for-ecological-repair costs tothe other energy costs of our renewables, let alone of ourfossil fuels, few of our current energy sources would makemuch economic sense. With all this in mind, our richestenergy lode is unequivocally conservation techniques. So,change that favours the economics and fun associated withconservation and with reuse/recycling generally can becombined with the advent of economic and other incentives
that favour low energy productions and pursuits such as inhealth, sport, communication, the arts, the knowledgeindustries and so on.A conservation focus means that, while definitely the wayto go for new electricity generation, renewables should notbe permitted to eclipse conservation. Many of theseactivities can be pursued by individuals, with no help fromgovernment, but government does have two importantroles. The first is to reverse the many perverse incentivesthat continue to make nonsense of so many energy-conserving activities. The second is to educate the wholecommunity about energy matters, not just enhancedgreenhouse effects. The effects could be transformative bothsocially as well as ecologically.
Circulatory diseases37.8%
Cancer28.7%
Respiratory diseases8.5%
Injuries7.2%
Other17.8%
Injury in Western Australia
An Epidemiology of Injury, 1989
SNAPSHOT OF INJURY IN WA
Injuries are a significant health issue in Western Australia ranking fourth as a cause of death.
Hospitalisation rates due to injury have increased significantly since 1989.
Falls are the most common cause of injury hospitalisation, placing a considerable burden on the Western Australian health care system.
Males, Indigenous people, rural residents, young and elderly adults are at greatest risk of injury.
“Injury in Western Australia – An Epidemiology of Injury 1989-2000 presents tends, priority risk groups, priority injury issues and issues that need further investigation. Funding for this review was provided by the Injury Prevention Branch, Department of Health and undertaken by the Injury Research Centre, University of Western Australia. The report is best used in conjunction with “Injury in Western Australia, A review of best practice, stakeholder activity, legislation and recommendations for selected injury areas”.
Full reports available on-line
Print a copy of the full report from the
Injury Prevention Branch web-site:
http://www.population.health.wa.gov.au/Promotions/resources_promotion.cfm#injury
Or
Injury Research Centre:
http://www.irc.uwa.edu.au/
Proportion of deaths by condition,Western Australia, 1995-2000
The Ecology of Energy Transformations - continued from page 16
Violence related injuries have emerged as a growing issue in Western Austryoung people, Indigenous people and rural residents. These injuries resultedand 5,000 hospitalisations per year between 1995 and 2000.
Self-inflicted injuries resulting in death were more common than injuries
Hospitalisation due to accidental poisoning with pharmaceuticals was asuggest that pharmaceuticals are being used with intent to cause self-ha

19
By: Geoffrey Lean
“ The provisions of the treaty, forecast to prevent twomillion cancers in the West alone, have been progressivelytightened as the use of ozone-destroying chemicals has beenphased out in industrialized countries. Developingcountries follow after a period of grace.”
President George Bush has broughtthe international treaty aimed atrepairing the Earth’s vital ozonelayer close to breakdown, riskingmillions of cancers, to benefitstrawberry and tomato growers inthe electorally critical state ofFlorida, The Independent onSunday can reveal.
His administration is insisting on a sharp increase inspraying of the most dangerous ozone-destroying chemicalstill in use, the pesticide methyl bromide, even though it isdue to be phased out under the Montreal Protocol in littlemore than a year. And it has threatened that the UnitedStates could withdraw from the treaty’s provisionsaltogether if its demand is not met.
Talks on the unprecedented demand broke down withoutagreement at the conference in Nairobi this month as USdelegates refused to consider any compromise. They evenrejected a European Union proposal that would haveallowed farmers to use the same amount of the pesticide asat present, even though this, itself, would violate the spiritof the protocol.
The crisis has come to a head at a particularly embarrassingmoment for Tony Blair, who this week played host toGeorge Bush on the first state visit by a US President. Forthree years, the Prime Minister has been quietly attemptingto persuade him to stop trying to kill the Kyoto Protocol,designed to combat global warming. But now Mr Bush istrying to emasculate what the UN regards as the mostsuccessful international environmental agreement evermade.
It also comes at a critical time for the ozone layer. Scientistshad hoped that it would be beginning to heal by now, butthis autumn the ozone hole over Antarctica was at near-record levels.
Ironically the MontrealProtocol, agreed in 1987,was only brought aboutthrough the drive andcommitment of theReagan administration -in which George Bush Sr.served as Vice-President.It was rapidly agreed after
the shock of the discovery of the ozone hole - the size of theUS - and findings that the layer had thinned worldwide.
The layer is made up of a type of oxygen so thinly scatteredthough the upper atmosphere that, if gathered together, itwould girdle the globe with a ring no thicker than the soleof a shoe. But it screens out harmful ultraviolet rays fromthe sun that otherwise would wipe out life. As the layerweakens, increasing amounts of rays get through, causingskin cancer and blindness from cataracts.
The provisions of the treaty, forecast to prevent two millioncancers in the West alone, have been progressively tightenedas the use of ozone-destroying chemicals has been phasedout in industrialized countries. Developing countries followafter a period of grace. Methyl bromide, which has alsobeen linked with prostate cancer, is one of the last to becontrolled; developed countries agreed in 1997 to stopusing it by the end of next year. So far they have succeededin reducing it to 30 per cent of its former level byintroducing substitutes.
Several countries, however, foresee difficulties in completingthe phase-out in time, and have asked for year-long “criticalexemptions” for some limited uses, as permitted under thetreaty. But uniquely, the US, which already accounts for aquarter of the world’s use of the pesticide, is demandingthat it should indefinitely increase its use.
It is responding to pressure from farmers, particularly inFlorida and California. While the election of ArnoldSchwarzenegger as Governor has bolstered the Republicans’hopes in California, Florida is expected to be critical in nextyear’s presidential poll - as it was in 2000.
When EU and Third World governments refused to agreeto the demand at the meeting, the US said legislation hadbeen introduced into Congress to exempt it from thetreaty’s provisions on the pesticide altogether. ClaudiaMcMurray, the head of its delegation, said that this would“either put us out of compliance or would lead us to violatethe protocol”.
When all attempts at compromise failed, the meetingagreed to defer negotiations to a special “extraordinary”conference in Montreal in March. But unless Mr Bush hasa change of heart, the world will then be faced withchoosing between two alternative means of underminingthe treaty: allowing the US to reverse the process of phase-out, with the risk other nations will follow; or seeing itignore the agreement altogether.
From: http://news.independent.co.uk/low_res/story.jsp?story=466406&host=3&dir=507
Ozone layer ‘sacrificed’ to lift Bush’s re-election prospects
20
“ Farmers and peasant groups around the world are pressingthe concept of ‘food sovereignty’ as a challenge to the WorldTrade Organisation’s agriculture policies, which they say pushmillions of small farmers off their land and lead to foodinsecurity.”
Described by the international farmers network ViaCampesina as “the right of peoples to define their own foodand agriculture; (and) to protect and regulate domesticagricultural production and trade”, food sovereignty, itsproponents say, is the only way to alleviate poverty and achievesustainable development in the developing world.
The People’s Food Sovereignty network, a coalition of non-governmental organisations and movements from the Northand South, released a Food and Agriculture statement on itswebsite demanding that “governments remove agriculture andfood from the World Trade Organisation (WTO) and establishan alternative international framework for the sustainableproduction and trade of food and agriculture”.
”Millions of peasants in the third world have been activelyworking to develop food sovereignty as a movement for thepast five to 10 years,” said Dr. Raj Patel, a policy analyst at theOakland-based Institute for Food and Development Policy(Food First) in a telephone interview.
A new report released by Food First claims that food security— the goal championed by multilateral agencies to ensure thatpeople have enough to eat each day — does nothing to secureproductive land for rural farmers or stable prices for theircrops.
”Food security says that every child, woman, and man musthave the certainty of having enough to eat each day, but it saysnothing about where that food comes from or how it isproduced,” said Dr. Peter Rosset, author of the Food Firstreport, in a statement.
”Thus in trade negotiations underway in the WTO, NAFTAand the proposed Free Trade Area of the Americas (FTAA),Washington is able to argue that importing cheap food fromthe U.S. is a better way for poor countries to achieve foodsecurity than producing it themselves.”
NAFTA, or the North American Free Trade Agreement, wascreated in 1992 and includes the United States, Canada andMexico. The FTAA, a much larger version of NAFTA, is set tobe launched in 2005, but has come under intense criticism byfarmers, trade unions and activists from North and SouthAmerica who fear the deal will entrench neo-liberal tradepolicies harmful to developing countries.
The World Bank, which is highly influential in shaping foodand agriculture policy and projects in developing countries,identifies on its website three dimensions of food security asfood availability, affordability, and stability of access. The Banksays that free trade is essential to food security because it makesthe most efficient use of world resources.
Patel disagrees with this interpretation, and says that free tradeas espoused by the World Bank does not exist because ofsubsidies, disguised taxes, and hidden environmental and socialcosts.
”There is no such thing as free trade,” he said, “The WorldBank can have all the theories they want, but the evidenceshows that poor people are not helped by liberalising trade.”
Via Campesina says that by prioritising international tradeover local food production, the WTO’s free trade agendaincreases the dependence of developing countries on cheapimports of subsidised grains from the North, causing hundredsof millions of farmers to abandon traditional agriculturalpractices.
Patel, an expert in rural development, explained that U.S. cornis sold below the cost of production due to massivegovernment subsidies, and that exporting it to Mexicodevastates peasant farmers who cannot compete with theartificially low prices. He said that subsidising and dumpingcorn in Mexico is “almost like targeting the impoverishedfarmers”.
”It’s bitter and cruel to say free trade is enhancing foodsecurity,” he added.
According to Patel, there are three areas of Chiapas, Mexicowhere peasants are demanding food sovereignty as ademocratic process to allow them to define and control thelocal food system, and to protect their land and livelihoodsfrom foreign agribusinesses and the vagaries of the globalmarketplace.
Via Campesina is pressuring the United Nations HumanRights Commission to recognise the right of peasants toproduce food as a fundamental human right, and is using thepower of the Internet to challenge entrenched positions intrade negotiations.
Patel said that agriculture should be removed from WTOnegotiations because the millions of farmers who are mostaffected are not represented. He claims that even thoughorganisations like Via Campesina appear at WTOnegotiations, they are not given a true voice in the proceedings,which are exclusively the domain of governments andcorporate lobbyists.
”Until there is genuine democracy and transparency in trade,agriculture should be left out of negotiations,” he said.
Farmers Say Food Must Be Dropped From GovernmentsDeal-Making
21
people, such as subsistence farmers, are left with absolutelynothing.”
The report was prepared for Unicef by the TownsendCentre for International Poverty Research at the Universityof Bristol.
It is the first time child poverty in the developing worldhas been scientifically measured. The lives of more than1.2 million children from 46 of the world’s poorestcountries were analysed for the study.
The report defines children who lack one basic humanneed, such as food, safe drinking water, sanitation facilities,health, shelter and education are defined as living in severedeprivation, while those without two basic needs are saidto be in absolute poverty.
The report found that more than half of all children livingin the developing world are living in severe deprivation,while 674 million are in absolute poverty. A third of allchildren in the survey lived in a dwelling with more thanfive people to a room, or with only a mud floor.
A similar proportion had no kind of toilet facility and onein five had no access to safe drinking water. More than onein ten children aged seven to eighteen had never been toschool, and one in seven was severely malnourished.
Ms Melby said: “We need to make sure that money iscarefully targeted and gets to the people who need it most,such as women and children. Health and education are the
most important factors, and are closely linked toglobalisation.
”If these countries lose income from their own markets, theycut social services and people are forced to pay for healthand education. This has a huge impact on the future healthand prospects for children.”
Countries in sub-Saharan Africa have the highest rates ofdeprivation, according to the report. In some countries, 90per cent of children in rural areas were assessed as living inabsolute poverty.
Professor Dave Gordon from the University of Bristol andanother of the report’s authors, said: “Many of the childrensurveyed who were living in absolute poverty will have diedor had their health profoundly damaged by the time thisreport is published, as a direct consequence of theirappalling living conditions.
”Many others will have had their development so severelyimpaired that they will be unable to escape from a lifetimeof grinding poverty. The UN targets were quite modestanyway and yet we are still not going to hit them.
”The Romans managed to provide sanitation for peoplethousands of years ago, and yet millions of people today stilldo not have access to a toilet.”http://www.zmag.org/content/print_article.cfm?itemID=4389§ionID=13
Global trade keeps a billion children in poverty, says Unicef- continued from page 14
Letter to the Editor
Dear Editor,
The November/December 2003 edition had an article entitled A Children’s Vision Campaign recommending frequentchecks of children’s vision. This is contrary to the NH&MRC recommendations in their document Child Health Screeningand Surveillance: A Critical Review of the Evidence. March 2002. The document is available at the following website:http://www.health.gov.au/nhmrc/publications/synopses/ch42syn.htm
Garth Alperstein, Area Community Paediatrician
Dear Garth
Thank you for drawing our attention to this matter. We appreciate that screening with disregard to evidence-basedrecommendations has little benefit.
Editor
22
It is always a pleasure to see individuals commended fortheir dedication to the Australian Community. Thatpleasure is even greater when the individuals are members ofthe PHAA. This year five members have been recognized.
Professor Lesley Margaret Barclay from Rozelle NSW.Professor Barclay was recognized for her service to nursing,particularly in the fields of midwifery and child health inAustralia and internationally through participation indevelopment assistance activities.
Emeritus Professor Charles Baldwin Kerr, from FarMeadow, NSW. Emeritus Professor Baldwin wasrecognized for service to medicine in the fields of publichealth and human genetics, and to education.
Professor Charles Roger Watson, from Freemantle WA.Professor Watson was recognized for service to public healthand education as an administrator and educator, toneuroscience, particularly as a contributor to work on brainmapping, and to the community.
Associate Professor Francis Leo Archer, from Guys Hill,VIC. Associate Professor Archer was recognized for serviceto medicine, particularly in the development and delivery ofeducational programs for ambulance officers andparamedics.
Major Peter McDonald Trebilco, Waterloo, NSW. MajorTrebilco was recognized for his service to communitythrough a range of health, welfare and social justiceorganizations.
Our congratulations go to all five recipients of AustraliaDay honours.
Australia Day Honours List
USA: Vitamin E may be key to listeria-freeturkey meat - research
Adding vitamin E to the diets of turkeys may furtherreduce the likelihood of consumers contracting aserious food borne illness from eating turkey meat,according to the US Agricultural Research Service.
Scientists from the Agricultural Research Service, whichis the chief scientific research agency of the USDepartment of Agriculture (USDA), were studyingways to control Listeria monocytogenes, a major humanbacterial food borne pathogen found in poultry.
Microbiologist Irene Wesley of the ARS NationalAnimal Disease Center (NADC) in Ames, Iowa, foundthat supplementing turkeys’ diets with vitamin Estimulates their immune responses, helping them clearthe gut of the microorganism that causes the disease.This can in turn lead to reduced contamination ofcarcasses at slaughter and during processing, the ARSsaid.
The ARS plans to test the effectiveness of vitamin E against
Salmonella and Campylobacter, two other food borne
pathogens.
Source: just-food.com
China: China cracks down on soy saucemade from human hair
China has ordered a crackdown on domestic ingredientmakers after it was discovered one plant had beenillegally producing a base for soy sauce made out ofhuman hair.
A recent China Central Television report uncovered afactory in Hubei province that had been processing overten tons of human hair daily into edible amino acidssuitable for turning into soy sauce.
Rich in proteins and amino acids human hair was until
recently widely used to make food ingredient L-cysteineworldwide. Such products pose no human health risks so
it is unclear why China has banned their use in food.
Source: Michael Fitzpatrick
Andrology Australia has released the above report. Thereport highlights findings from the literature regardinginformation needs, men’s information-seeking and healthaccess behaviours, and community education strategiesin regards to male reproductive health issues. There arealso five accompanying disease-specific supplements.Copies can be obtained on (03) 9594 7134 or by emailon [email protected]
Needs Analysis of Community Education inAustralia on Male Reproductive Health

23
From the radio newsmagazine, Between The Lines
Global AIDS Pandemic Spreading at Alarming Rate WhileBush Administration Impedes Access to Life-Saving Treatment
Dec. 1 marked World AIDS Day, and the big news this yearwas that the government of China has finally publiclyacknowledged its AIDS crisis and promised to take steps tocombat it. Less than a week before World AIDS Day this year,the U.N. released its annual report on the state of the HIV/AIDS crisis, which revealed that the pandemic is continuing tospread at an alarming rate worldwide. New figures show thatmore people were infected with HIV, and more people died ofAIDS, this year than ever before. Currently, more than 40million people are living with HIV/AIDS across the globe,with two-thirds of them on the African continent.
Africa Action, a non-governmental organization based inWashington, D.C., organized World AIDS Day events on 20U.S. university campuses as part of the group’s Africa’s Rightto Health campaign, which seeks to end the social injusticesthat have given rise to the HIV/AIDS crisis. Africa Action’s“Most Wanted” campaign has condemned the Bushadministration’s policies for failing to improve access to life-saving AIDS treatment.
Between The Lines’ Melinda Tuhus spoke with Salih Booker,executive director of Africa Action, about how his organizationobserved World AIDS Day and their goal of tearing down theobstacles which stand in the way of more progress incombating the AIDS pandemic.
Salih Booker: The main thrust was to add sort of a politicalthrust to World AIDS Day. Traditionally the day has been aday of remembrance of those fallen to the HIV/AIDSpandemic, and we felt very much that one of the mostimportant ways to mourn the fallen was to fight for the living.We wanted to use the day to point to those who are mostresponsible as obstacles to the much-accelerated fight againstthe AIDS pandemic. We targeted George Bush and a numberof his key advisers, because he’s made very significant promisesabout increasing the U.S. role in the fight against AIDS, buthe’s been reneging on those promises ever since he’s made themin his State of the Union address in January of this year.
Between The Lines: In what way has he reneged on it? Myunderstanding is that much of the funding has been passed inCongress. Is your understanding that the money has beenappropriated but is not going through maybe the channels thatyou think are the right channels?
Salih Booker: The president made his promise in January2003. He referred to it as an emergency plan for AIDS relief.And it is indeed an emergency. And yet he asked for no newfunding for the entire year of 2003. So here we are at the endof the year, looking at a death toll due to AIDS of almost threemillion people worldwide, many of whom could have beensaved if they’d had access to anti-retroviral treatment. So thefirst problem is that he didn’t give this initiative the urgencythat is required. He promised $15 billion over five years, whichworks out to $3 billion a year for U.S. funding to fight AIDS.
Bush Impedes Aid for Global AIDS PandemicIn his budget request that he sent out after his speech, he onlyasked for $2 billion.
Now the Congress did better than the president. Theyauthorized an annual expenditure of $3 billion a year to fightAIDS, but that’s just the authorization, the Congress actuallyhas to appropriate the money. And in recent weeks, theCongress has provided more than the administrationrequested. They have prepared to appropriate $2.4 billion fornext year, for 2003, which is more than the $2 billion the Bushadministration requested. That money, of course, is tied upwith all these appropriations bills that the Congress is going toconsider as an omnibus package. So it’s not enough funding. Itcertainly is more than the U.S. provided in previous years. Butwhen one considers how much the U.S. is spending in Iraq —$4 billion a month for the war and the occupation of Iraq —$4 billion a month, and yet the White House is unwilling tospend $3 billion a year that it promised for fighting globalAIDS.
AIDS is the greatest global threat to human security right now— it’s a greater threat than terrorism or even weapons of massdestruction. It’s killing some three million people a year,undermining even more families and destabilizing countries’economies, particularly in Africa. And the U.S. is creating anentirely new bureaucracy to manage the AIDS money, and thisis most unfortunate because the Global Fund to Fight AIDS,TB and Malaria was established in 2001 with U.S. support,and yet the U.S. has been reluctant to provide it with adequatefunding such that the global fund is almost bankrupt torespond to the proposals it is receiving, and yet the U.S. hasonly been willing to provide it with a mere $200 million ayear.
When President Bush announced his new initiative of $15billion over a five-year period, he decided to create a new,duplicative bureaucracy — I would say wasteful bureaucracy— and he then appointed the former head of a pharmaceuticalgiant, Eli Lilly, to direct this global AIDS initiative out of theState Department. So you have this new bureaucracy at theState Department to handle AIDS money, you have a NewMillennium Challenge Account initiative which is separate,and both of these are examples of American unilateralism, anunwillingness to pool our resources with other resources fromdonor countries in order to ensure that the poor countries canfocus on the fight at hand, that they don’t spend all their timedealing with dozens of different donors, but that they canaccess resources in the most straightforward, simple andtransparent way.
Interview with Salih Booker, executive director of Africa Action,conducted by Melinda Tuhus, Listen in RealAudio: http://www.btlonline.org/booker121903.ram
For more information, call Africa Action at (202) 546-7961 or visittheir website at http://www.africaaction.org
Related links: The Global Health Access Gap athttp://www.healthgap.org World AIDS Day athttp://www.worldaidsday.org

24
The National Cancer Control Initiative (NCCI) hasrecently commenced work on a project to develop a primaryhealth care perspective on cancer. The project aims toenable general practitioners, nurses and other primaryhealth care professionals to (i) optimise their contributionto the full spectrum of cancer control from prevention topalliation, and (ii) to contribute further to improving thequality of cancer care for patients and carers. It is intendedthat the primary health care perspective on cancer will alsoinform, complement and strengthen the National ServiceImprovement Framework (NSIF) for cancer beingdeveloped by the Australian Government.
A preliminary meeting on the topic was held at the NCCI inMarch 2003. A report on this meeting is available from theNCCI website (see www.ncci.org.au).
Why develop a primary health care perspective on cancer?
Cancer is a major health burden in Australia. It is theleading cause of death among Australians, currentlyaccounting for 28% of all deaths.1 A major cancer willaffect one in three Australian men and one in fourAustralian women before they reach the age of 75 years, andthe number of new diagnoses is increasing.1 In addition,some 360,000 people have a non-melanoma skin cancertreated each year.
Primary health care professionals, especially generalpractitioners and community nurses, have a critical role toplay in cancer control in Australia. Their work spans thefull spectrum of cancer care - prevention, detection,treatment and palliation, including psychological support ofpatients and carers. Primary health care practitionerspractise clinical medicine in a very different setting andcontext from hospital specialists. Problems are oftenundifferentiated and illness is more common than disease.From a primary health care perspective, patients with a newdiagnosis of cancer can be infrequent, but providingongoing care for patients with an established diagnosis ofcancer and their carers poses substantial challenges.
Possibly the largest component of a general practitioner’sworkload related to cancer involves dealing with patientswho have suspicious symptoms, concerns about possiblecancer or who are at increased risk due to family history orlifestyle factors such as smoking, sun exposure oroccupation. Although hospitalisation and specialisttreatment are critical components in combating cancer,most of the cancer patient’s ‘journey’ takes place in thecommunity, where primary health care professionals are thecornerstone of continuing care.
Developing a primary health care perspective on cancer istherefore of strategic and practical importance. It is particularlytimely in the context of the recently published OptimisingCancer Care in Australia (OCCA) report2, the AustralianGovernment’s plans for the development of a NSIF for cancerand the development of new approaches to cancer control byvarious states.
Developing a primary health care perspective on cancer:an NCCI initiative
Scoping exercise-your chance to contribute
The project to develop a primary health care perspective oncancer is taking an incremental approach. As an initial activity,the NCCI is conducting a scoping exercise to identify thepriorities, existing resources, and needs and gaps in support forprimary health care professionals on cancer issues. In particular,the NCCI is interested in obtaining information and opinions onprimary health care support and services, and training andeducation in relation to cancer.
As a first step for the scoping exercise, the NCCI is seekingexpressions of interest from individuals or groups who wish tocontribute information. Further details about the project,including how to contribute to the scoping exercise, are availableon the NCCI website at www.ncci.org.au. Expressions of interestshould be returned to the NCCI by Monday 16 February 2004.Alternatively, further information about the project and scopingexercise is available from Dr Karen Pedersen at the NCCI(Karen.Pedersen @ neci.org.au).
Reference1. Australian Institute of Health and Welfare and Australasian
Association of Cancer Registries. Cancer in Australia 2000.Canberra, Australian Institute of Health and Welfare, 2003.
2. Clinical Oncological Society of Australia, The CancerCouncil Australia, National Cancer Control Initiative.Optimising Cancer Care in Australia. Melbourne, NationalCancer Control Initiative, 2003.
Agent Orange, used in Vietnam 30 years ago, is responsiblefor high blood dioxin levels among residents who haveeaten the substance in their food, according to a study inthe August Journal of Occupational and EnvironmentalMedicine.
Researchers collected samples of food animals from BienHoa City, located north of Ho Chi Minh City, which wasbelieved to be a hot spot for dioxin contamination.Very high levels of TCDD, the highly toxic dioxincontaminant of Agent Orange, were found in most typesof animals studied. The highest levels were found in duckswho showed up to 343 parts per trillion, compared with ausual level of less than .1 per trillion. Other contaminantfood sources included fish, free-range chickens and even atoad. Samples of pork and beef did not show elevatedlevels of TCDD.
A previous study showed high dioxin levels in the blood ofBien Hoa City residents. A spill from underground storagetanks at an airbase near the city in 1971 released thousandsof gallons of Agent Orange into the environment
Vietnamese food has agent orange residue
25
PPHA Advocacy Update - December/January
Free Trade Agreement
The national office has continued to maintain its advocacyrole on the free trade agreement (FTA) between the US andAustralia, both alone and in partnership with other groups.In late November - December it was revealed that cost ofpharmaceuticals issues currently regulated under the PBS werebeing handled by the negotiating team via a ‘backdoor’. Thenegotiators were reported as leaving the PBS alone, but werechanging intellectual property rights and how they are treatedunder the PBS as a means of increasing pharmaceutical profitsfor US and global companies.
In both December and January, media releases were providedon this subject asking the Federal Government to come cleanon the changes. In addition, emails were sent to all FederalMembers of Parliament asking them to insist that the contentof the FTA be debated in Parliament and only ratified withthe agreement of Parliament rather than simply being ratifiedby the Cabinet.
To date we have received a reply from the Greens who havethis stance as their policy. The e-mails and the media releasesare on the PHAA web-site. Replies will be placed there asthey are received.
Refugees
The major focus of the PHAA’s work on refugees continuesthrough the participation of the International Health SIG inthe ARC Linkage Grant, “An examination of Refugee Womenat risk in Australia’s Refugee Policy”. Our contact on thiswork is Dr Anna Whelan.
In December, a letter of support and congratulations was sentto Mark Latham in reaction to his calling for the release ofwomen and children from refugee centres, as one of his firstactions in his new position as leader of the Federal Opposition.A copy of the letter can be found on the PHAA website.
In January, a letter was sent to Dr Carman Lawrence in relationto a Western Australian survey that indicated a lower thananticipated community support for allowing refugees to livein the community. The letter sought for Dr Lawrence tomaintain her stance on this issue, and provided a list of the44 local government areas that have declared themselves asrefugee welcome zones. Dr Lawrence has replied, thankingus for the information supplied.
International Health – Bali
The International SIG has continued to provide support forthe yAKKUM Bali project, that supports poor young peopleand children who have a permanent disability and who arenot receiving help from any other organization. $3,000 hasbeen raised for the project to date.
More information on this project can be found under SIGs,International Health, on the PHAA web-site.
Tax deductible donations can be made to PHERT – Bali.Receipts will be issued for all donations.
Oral Health
In January, a media release wasprovided on the continuing problemof oral health care in Australia. Themedia release focused on the inabilityof the poor, elderly and unemployedto access dental care in a timely andappropriate manner, while the FederalGovernment subsidises it through theprivate health insurance rebate to thetune of approximately $300 million
a year. This mainly benefits middle and high incomeAustralians who can already afford good dental care. A copyof this media release is on the PHAA website under Advocacy.
Food and Nutrition
The PHAA has been invited tomeet with the Food Policy area ofthe Department of Health andAgeing late in January, prior to aconsultative meeting to be held inFebruary. Points for discussion are
being collected from members of the Food and Nutrition SIG.A report on the discussions will be placed on the Food andNutrition page on the web-site early in February.
Dioxins
Pieta Laut has continued to be the PHAA representative(observer) on the National Dioxins Stakeholders Group. Sheis currently preparing input to the national risk managementguidelines.
Western Australia
Population Health Discussion Paper - The Western AustralianBranch and the national office provided comments on theWestern Australian Government’s discussion paper onPopulation Health. Comments largely focused on the need,during a period of limited resources, to develop government,NGO, and business relationships that have the capacity toextend the effect of limited resources. Copies of the commentscan be found on the PHAA website on the Western AustralianBranch page.

26
Items of InterestBreastScreen Australia Monitoring Report 2000-2001
This report is the fifth annual report based on key programactivity, performance and outcome indicators to monitorthe achievements of the BreastScreen Australia Program.The report presents the most recent information onparticipation in breast screening, cancer detection, programsensitivity and recall to assessment and rescreening rates. Inaddition, the report presents national breast cancerincidence and mortality data to provide a context for theseindicators of screening activity. Where possible, the data arepresented by state and territory as well as nationally.Catalogue No. CAN 20, Available from CanPrint (toll free1300 889 873); $24.00
Cervical Screening in Australia 2000-2001 and 1999-2000 This is the third annual report based on key programactivity, performance and outcome indicators to monitorthe achievements of the National Cervical ScreeningProgram. The report provides a comprehensive nationalpicture of cervical screening in Australia for 2000-2001 and1999-2000. The report presents most recent informationon participation in cervical screening, rate of earlyrescreening, low-grade and high-grade abnormalitiesdetected, incidence of cervical cancer and mortality.Analysis of incidence and mortality data by location (rural,remote and metropolitan) as well as mortality byIndigenous status are also presented. Where possible, dataare presented by state and territory stratification.Catalogue No. CAN 19, Available from CanPrint (toll free1300 889 873); $24.00
Spinal Cord Injury, Australia 2001-2002
Australia was the first country to implement a nationalpopulation-based register to enable surveillance of spinalcord injury cases to help prevent and control this problem.This report provides information on case registrations forthe year 2001-02.Catalogue No. INJCAT 58, Available from CanPrint (tollfree 1300 889 873); $25.00
Homeless People in SAAP - SAAP NDC Annual Report2002-03 Australia
Catalogue No. HOU 91, Available from CanPrint (toll free1300 889 873); $25.00
This is the eighth annual report on the SupportedAccommodation Assistance Program (SAAP) National DataCollection. The reports provide information on people whoare homeless and people who are at risk of being homeless,and an overview of assistance given to clients by the SAAP.
This report is accompanied by supplementary tables foreach individual state and territory. These are available onthe AIHW website.http://www.aihw.gov.au/publications/index.cfm?type=new
Commonwealth-State Housing Agreement National DataReports 2002-03:
State and Territory Owned and Managed IndigenousHousing - Catalogue No. HOU 102This report provides the data items and performanceindicators collected for annual reporting for State andTerritory owned and managed Indigenous housing underthe 1999 Commonwealth-State Housing Agreement(CSHA). The Indigenous housing report providesinformation on one of six programs under the 1999Agreement. For more information:http://www.aihw.gov.au/publications/index.cfm?type=new
CSHA Community Housing
- Catalogue No. HOU 101This report provides the data items and performanceindicators collected for annual reporting for communityhousing under the 1999 Commonwealth-State HousingAgreement (CSHA). The community housing reportprovides information on one of six programs under the1999 Agreement. For more information:http://www.aihw.gov.au/publications/index.cfm?type=new
Public Rental Housing
- Catalogue No. HOU 100This report provides the data items and performanceindicators collected for annual reporting for public rentalhousing under the 1999 Commonwealth-State HousingAgreement (CSHA). The public rental housing reportprovides information on one of six programs under the1999 Agreement.These publications are currently available on the internet.http://www.aihw.gov.au/publications/index.cfm?type=new
Cancer Incidence Study 2003: Australian Veterans of theKorean War.
This study was commissioned by the Department ofVeterans’ Affairs. It investigated the incidence rates ofcancer among Australian male veterans of the Korean Warbetween 1982 and 1999 and compared these with theincidence rates over the same period for male members ofthe general Australian population of the same age.Catalogue No. PHE 48, free, Available from: Mr Denis

27
Items of InterestMurphy, Department of Veteran’s Affairs, Ph: 6289 4806http://www.aihw.gov.au/publications/index.cfm?type=new
The Future Supply of Informal Care 203 to 2013
Catalogue No. AGE 32,
This publication is currently available on the internet andwill be available in hard copy through CanPrint in the nearfuture.
This report looks at factors that may affect the futuresupply of informal care. These include Australia’s ageingpopulation, an increase in female labour force participation,and changed living arrangements. The report was jointlyfunded by the Australian Government Department ofHealth and Ageing and the AIHW. Hard copies of thisreport will be available for sale shortly.http://www.aihw.gov.au/publications/index.cfm?type=new
Australia’s Young People: their health and wellbeing
This is the second national report on the health andwellbeing of young people in Australia. It providescomprehensive information on the health status of youngpeople including causes of hospitalisations and deaths,chronic diseases, infectious diseases, injury, disability,reproductive and sexual health. The behavioural risk andprotective factors influencing young people’s health andwellbeing that are covered in this report include substanceuse, diet and nutrition, physical activity and overweight andobesity. Social conditions are also important determinantsof health. The report therefore includes information on thefamily environment, relationships and social participation,education, employment and income. An overview of thehealth and welfare of Aboriginal and Torres Strait Islanderyoung people is also presentedCatalogue No. PHE 50 Available from CanPrint (toll free1300 889 873); $40.00http://www.aihw.gov.au/publications/index.cfm?type=new
Australia’s Welfare 2003
Catalogue No. AUS 41, Available from CanPrint for$45.00 (Ph: 1300 889 873)
Australia’s Welfare is the most comprehensive andauthoritative source of national information on welfareservices in Australia. Topics include welfare servicesexpenditure, the welfare services labour force, children’s andfamily services, child protection, housing assistance, servicesfor homeless people, ageing and aged care services anddisability services. Australia’s Welfare 2003 also featuresspecial chapters on informal care and indicators of thewelfare of Australia’s population.
http://www.aihw.gov.au/publications/index.cfm?type=new
General Practice Activity in Australia 2002-03
This publication reports the results of the fifth year of theBEACH program, April 2002 to March 2003. Datareported by 1,008 general practitioners on 100,800 GP-patient encounters are used to describe aspects of generalpractice in Australia: the general practitioners and theirpatients; the problems managed and the treatmentprovided. Information is also reported on body weight toheight ratio, smoking status and alcohol use of a subsampleof patients. For the period April 1998-March 2003, anoverview of more than 5,000 encounters with Indigenouspeople provides an indication of the role of GPs in theprovision of care to these people. Changes in relative ratesof selected problems and management techniques are alsoinvestigated over this period. Data for each of the five yearsof BEACH are summarised in the appendix to this report.Catalogue No. GEP 14, Available from CanPrint for$25.00 (Ph: 1300 889 873)http://www.aihw.gov.au/publications/index.cfm?type=new
Adoptions Australia 2002-03
Adoptions Australia 2002-03 presents adoptions statisticsprovided by the state and territory community servicesdepartments for the period 1 July 2002 to 30 June 2003.These cover all finalised adoptions reported to state andterritory community services departments during that year.The report provides information on adopted children,adoptive families and birth mothers. It also provides dataon the number of requests for information and the numberof contact and information vetoes lodged by parties to theadoption.Catalogue No. CWS-21, Available from CanPrint(Ph:1300 889 873); $24.00http://www.aihw.gov.au/publications/index.cfm?type=new
Nursing Labour Force 2002
This report presents statistics on trends in the employmentof nurses in Australia. It is based on the main findings ofthe 2001 national survey of registered and enrolled nurses,and includes registration and enrolment data for 2002.Information presented in this report includes the numberand characteristics of registered and enrolled nurses in eachgeographic region and in each state and territory, their ageand sex profiles, type of nurse, area of clinical nursing, worksetting and hours worked.Catalogue No. HWL-29, Available from CanPrint(Ph:1300 889 873); $21.00http://www.aihw.gov.au/media/2003/mr031217.html
28
Editor: Executive Director Design: Design Direction
Articles appearing in intouch do not necessarily reflect the views of thePHAA but are intended to inform and stimulate thought, discussion andcomment. Contributions are welcome and should be sent to:
The Editor, intouch, PHAAPO Box 319, Curtin ACT 2605or email [email protected]
How to join PHAA
Membership enquiries to:
Membership Coordinator, PHAAPO Box 319, Curtin ACT 2605Tel 02 6285 2373 Fax 02 6282 5438email [email protected] http://www.phaa.net.au
Advertising Rates
1/4 page ............................... $100
1/2 page ............................... $150
Full page ............................... $200
PDF format preferred but PHAA
staff can prepare your
advertisement (rate of $20 p/h)
Conference listing (5cmcolumn)
up to 5 lines ............................ $35
up to 10 lines .......................... $58
*after booking, send to PHAA,
attention:
Vicki Thompson20 Napier CloseDeakin ACT 2605
. If further information is required
please contact PHAA via email:
or phone 02 6285 2373
25-27 March 2004“The Path Forward”, NationalConvention Centre, Canberra ACTPre-Summit Workshops 24 March 2004Registration brochures can bedownloaded from the websitewww.injurymanagement.consec.com.au
21-22 May 2004Viral Hepatitis Workshop 2004,Whakatane, NZ. The workshop willcover the prevention and managementof hepatitis B and C, includingtreatment of chronic carriers. Contact:Alan Henderson: phone64 7 307 1259; [email protected];or www.hepfoundation.org.nz.
What’s on New Members
EDITORS: Elizabeth Proude and Susan Stratigos
New MembersNEW SOUTH WALES
Craig SmithRobert Margloire Zoa MangaLeah Maree FinneyRebecca GeeYe RongTanya JochelsonCassandra WilkinsonJan CarterJames David HarrisonJan FizzellAndrew GeorgiouJo RyanJane LloydAnne Catriona EdwardsTherese Jones
VICTORIA
Paul JacksonMohammad Siahpush
Todd HarperDominique Ann-Michele CadilhacSandra FalconerSue DaveyWendy ThomasCarmel Brady
SOUTH AUSTRALIA
Helene DimitriEmily SteeleAndrea Church
QUEENSLAND
Maxine ChaselingJoanne RiskCarolyn ChappleKaeleen Deanne DingleBarbara FordMichelle SmithKirsten McKenzieJacqueline CaskeyCraig HansenSally AustinKaren Harmon
WESTERN AUSTRALIA
Ana ToqueroRani ParamBarry EvensKynan Feeney
AUSTRALIAN CAPITAL TERRITORY
Ruth ParslowJulia Patricia SmithSamantha M Salvaneschi
TASMANIA
Lynne Andrewartha
This new free resource available athttp://www.participateinhealth.org.au/train can help primary care andconsumer organisations run trainingin consumer participation forconsumers and service staff. TheResource includes a guide and fourmodules. For more information call1800 625 619.
Consumer Participation inPrimary Care Training Resource





























