Embed Size (px)
Citation preview

Preventing occupational stress in healthcare workers (Review)
Marine A, Ruotsalainen J, Serra C, Verbeek J
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2006, Issue 4
http://www.thecochranelibrary.com
1Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

T A B L E O F C O N T E N T S
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW . . . . . . . . . . . . . . . . . .
3SEARCH METHODS FOR IDENTIFICATION OF STUDIES . . . . . . . . . . . . . . . . . . .
4METHODS OF THE REVIEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5DESCRIPTION OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7METHODOLOGICAL QUALITY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10NOTES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10POTENTIAL CONFLICT OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . .
10ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14Characteristics of included studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19Characteristics of excluded studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19Table 01. Search strategy (MEDLINE) . . . . . . . . . . . . . . . . . . . . . . . . . . .
21Table 02. Study quality and intervention type . . . . . . . . . . . . . . . . . . . . . . . . .
22Table 03. Levels of evidence: legend . . . . . . . . . . . . . . . . . . . . . . . . . . . .
22Table 04. Levels of evidence: Person-directed interventions: Stress . . . . . . . . . . . . . . . . . .
22Table 05. Levels of evidence: Person-directed interventions: Maslach Burnout Inventory . . . . . . . . . .
23Table 06. Levels of evidence: Person-directed interventions: State Trait Anxiety Inventory . . . . . . . . . .
23Table 07. Levels of evidence: Person-directed interventions: general symptoms . . . . . . . . . . . . . .
23Table 08. Levels of evidence: Work-directed interventions: Stress . . . . . . . . . . . . . . . . . .
23Table 09. Levels of evidence: Work-directed interventions: Maslach Burnout Inventory . . . . . . . . . . .
23Table 10. Levels of evidence: Work-directed interventions: general symptoms . . . . . . . . . . . . . .
24ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
24Comparison 01. Person-directed intervention vs no intervention (Short Term) . . . . . . . . . . . . . .
24Comparison 02. Person-directed intervention vs no intervention (Medium and Long Term) . . . . . . . . .
24Comparison 03. Work-directed intervention vs no intervention (Short Term) . . . . . . . . . . . . . .
24Comparison 04. Work-directed intervention vs no intervention (Medium Term) . . . . . . . . . . . . .
24COVER SHEET . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
26GRAPHS AND OTHER TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
26Analysis 01.01. Comparison 01 Person-directed intervention vs no intervention (Short Term), Outcome 01 Beck &
Srivastava Stress Scale and Perceived Stress Scale . . . . . . . . . . . . . . . . . . . . . .
26Analysis 01.02. Comparison 01 Person-directed intervention vs no intervention (Short Term), Outcome 02 Maslach
Burnout Inventory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
27Analysis 01.03. Comparison 01 Person-directed intervention vs no intervention (Short Term), Outcome 03 State Trait
Anxiety Inventory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
28Analysis 01.04. Comparison 01 Person-directed intervention vs no intervention (Short Term), Outcome 04 General
Health Questionnaire . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
28Analysis 02.01. Comparison 02 Person-directed intervention vs no intervention (Medium and Long Term), Outcome
01 Maslach Burnout Inventory (at 2 years) . . . . . . . . . . . . . . . . . . . . . . . .
29Analysis 02.02. Comparison 02 Person-directed intervention vs no intervention (Medium and Long Term), Outcome
02 Stait Trait Anxiety Inventory (Jones at 3 months and Yung at 1 month) . . . . . . . . . . . . .
iPreventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

29Analysis 02.03. Comparison 02 Person-directed intervention vs no intervention (Medium and Long Term), Outcome
03 Perceived Stress Scale (at 1 month) . . . . . . . . . . . . . . . . . . . . . . . . .
30Analysis 02.04. Comparison 02 Person-directed intervention vs no intervention (Medium and Long Term), Outcome
04 General Health Questionnaire (at 1 month) . . . . . . . . . . . . . . . . . . . . . .
30Analysis 03.01. Comparison 03 Work-directed intervention vs no intervention (Short Term), Outcome 01 Maslach
Burnout Inventory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31Analysis 03.02. Comparison 03 Work-directed intervention vs no intervention (Short Term), Outcome 02 Nursing
Stress Scale . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31Analysis 03.03. Comparison 03 Work-directed intervention vs no intervention (Short Term), Outcome 03 General
symptoms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31Analysis 04.01. Comparison 04 Work-directed intervention vs no intervention (Medium Term), Outcome 01 Nursing
Stress Scale (at 6 months) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iiPreventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Preventing occupational stress in healthcare workers (Review)
Marine A, Ruotsalainen J, Serra C, Verbeek J
Status: New
This record should be cited as:
Marine A, Ruotsalainen J, Serra C, Verbeek J. Preventing occupational stress in healthcare workers. Cochrane Database of SystematicReviews 2006, Issue 4. Art. No.: CD002892. DOI: 10.1002/14651858.CD002892.pub2.
This version first published online: 18 October 2006 in Issue 4, 2006.
Date of most recent substantive amendment: 21 August 2006
A B S T R A C T
Background
Healthcare workers can suffer from occupational stress which may lead to serious mental and physical health problems.
Objectives
To evaluate the effectiveness of work and person-directed interventions in preventing stress at work in healthcare workers.
Search strategy
We searched the Cochrane Depression Anxiety and Neurosis Group trials Specialised Register, MEDLINE, PsychInfo and Cochrane
Occupational Health Field database.
Selection criteria
Randomised controlled clinical trials (RCT) of interventions aimed at preventing psychological stress in healthcare workers. For work-
directed interventions interrupted time series and prospective cohort were also eligible.
Data collection and analysis
Two authors independently extracted data and assessed trial quality. Meta-analysis and qualitative synthesis were performed where
appropriate.
Main results
We identified 14 RCTs, three cluster-randomised trials and two crossover trials, including a total of 1,564 participants in intervention
groups and 1,248 controls. Two trials were of high quality.
Interventions were grouped into 1) person-directed: cognitive-behavioural, relaxation, music-making, therapeutic massage and mul-
ticomponent; and 2) work-directed: attitude change and communication, support from colleagues and participatory problem solving
and decision-making, and changes in work organisation.
There is limited evidence that person-directed interventions can reduce stress (standardised mean difference or SMD -0.85; 95%CI
-1.21, -0.49); burnout: Emotional Exhaustion (weighted mean difference or WMD -5.82; 95%CI -11.02, -0.63) and lack of Personal
Accomplishment (WMD -3.61; 95%CI -4.65, -2.58); and anxiety: state anxiety (WMD -9.42; 95%CI -16.92, -1.93) and trait anxiety
(WMD -6.91; 95%CI -12.80, -1.01). One trial showed that stress remained low a month after intervention (WMD -6.10; 95%CI
-8.44, -3.76). Another trial showed a reduction in Emotional Exhaustion (Mean Difference or MD -2.69; 95%CI -4.20, -1.17) and
in lack of Personal Accomplishment (MD -2.41; 95%CI -3.83, -0.99) maintained up to two years when the intervention was boosted
with refresher sessions. Two studies showed a reduction that was maintained up to a month in state anxiety (WMD -8.31; 95%CI
-11.49, -5.13) and trait anxiety (WMD -4.09; 95%CI -7.60, -0.58).
There is limited evidence that work-directed interventions can reduce stress symptoms (Mean Difference or MD -0.34; 95% CI -0.62,
-0.06); Depersonalization (MD -1.14; 95% CI -2.18, -0.10), and general symptoms (MD -2.90; 95% CI -5.16, -0.64). One study
showed that the difference in stress symptom level was nonsignificant at six months (MD -0.19; 95%CI -0.49, 0.11).
1Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Authors’ conclusions
Limited evidence is available for the effectiveness of interventions to reduce stress levels in healthcare workers. Larger and better quality
trials are needed.
P L A I N L A N G U A G E S U M M A R Y
Preventing occupational stress in healthcare workers
Healthcare workers suffer from work-related or occupational stress often resulting from high expectations coupled with insufficient
time, skills and/or social support at work. This can lead to severe distress, burnout or physical illness, and finally to a decrease in quality
of life and service provision. The costs of stress and burnout are high due to increased absenteeism and turnover.
We conducted a systematic search of the literature on preventing stress or burnout in healthcare workers. We then appraised the quality
of the studies found and combined their results.
Person-directed interventions that include a cognitive-behavioural approach (e.g. coping skills training), combined with relaxation
techniques or not, can be effective in reducing burnout, anxiety, stress and general symptoms in healthcare workers when compared to
no intervention. Work-directed interventions that include communication or nursing delivery change can also be effective in reducing
burnout, stress and general symptoms in healthcare workers when compared to no intervention. At best, the results of stress or burnout
reducing interventions may still be apparent from six months to two years after the end of the interventions.
Most of the studies are small and of poor quality, and it is not clear how large a change in a stress or burnout score is meaningful.
B A C K G R O U N D
Healthcare workers can suffer from work-related or occupational
stress as a result of organisational factors and an imbalance of de-
mands, skills and/or social support at work. Under some condi-
tions this can lead to severe distress, burnout or psychosomatic
diseases, and the resulting deterioration in quality of life and ser-
vice provision (Weinberg 2000). Burnout has been defined as “a
persistent, negative, work-related state of mind in ’normal’ indi-
viduals that is primarily characterized by exhaustion, which is ac-
companied by distress, a sense of reduced effectiveness, decreased
motivation, and the development of dysfunctional attitudes and
behaviours at work. This psychological condition develops grad-
ually but may remain unnoticed for a long time for the individual
involved. It results from a misfit between intentions and reality at
the job. Often burnout is self-perpetuating because of inadequate
coping strategies that are associated with the syndrome” (Schaufeli
2003). Burnout and occupational stress are both considered to
result from exposure to stressors at work, the effects of which are
mediated by personal coping or the ability to deal with environ-
mental stressors at a personal level (Cooper 2001; Schaufeli 2003).
Burnout is considered here as a specific form of psychological stress
and not as a clinical diagnosis (Firth-Cozens 1999). The economic
impact of such conditions is high, as can be inferred from data on
absenteeism and turnover (Jacobson 1996; Raiger 2005). More
than 10% of total claims for occupational diseases are attributed to
stress at work (Williamson 1994). There are a variety of stress fac-
tors in the workplace of healthcare workers that have been shown
to increase the risk of distress and burnout such as increasing
workload, emotional response to contact with suffering and dying
patients, and organisational problems and conflicts (Payne 1987;
McNeely 2005). In addition, many studies have shown that levels
of dissatisfaction, distress and burnout at work are quite high in
healthcare workers (Deckard 1994; Karasek 1992; Maslach 1982;
Ramirez 1996; Raiger 2005).
In order to lessen the impact of different psychosocial risk fac-
tors, programs and intervention activities have been designed with
many focussing on healthcare workers. These interventions are
either directed at risk factors in the working environment, or at
individual persons - such as increasing the individual’s ability to
cope with stress - or at both the working environment and the
individual person.
An extensive number of reviews have been published on the effec-
tiveness of interventions to prevent or treat stress (DeFrank 1987;
Murphy 1995; van der Hek 1997; van der Klink 2001). However,
apart from Mimura 2003, there are no other reviews that focus
specifically on interventions directed at stress prevention in health-
care workers. According to Michie 2003, the levels of psycholog-
ical ill health may be higher in healthcare than in non-healthcare
workers. Therefore, because the characteristics of interventions
designed for healthcare workers may be different from those of
other occupations, the aim of this review is to determine the effec-
tiveness of interventions to reduce stress specifically in healthcare
workers.
2Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

O B J E C T I V E S
1. To evaluate the effectiveness of work- and person-directed in-
terventions in preventing stress in healthcare workers.
2. To compare the effectiveness of different kinds of interventions
in preventing stress in healthcare workers.
C R I T E R I A F O R C O N S I D E R I N G
S T U D I E S F O R T H I S R E V I E W
Types of studies
For person-directed interventions we considered only randomised
controlled trials.
For work-directed interventions (see types of interventions) it is
usually unfeasible to randomise study participants because the in-
terventions are usually brought about at the environmental or
group level. This can be overcome by using the cluster-randomised
design where work places or departments are randomised to the
intervention or control groups. However, as this is a difficult and
fairly new design, we also considered additional study designs
for inclusion that allow for environmental interventions at the
group level: controlled before and after studies (otherwise known
as prospective cohort studies or quasi-experimental studies) and
interrupted time-series. The interrupted time-series design is de-
fined by the Cochrane Effective Practice and Organisation of Care
review group as a series of at least three outcome measurements
before and at least three after the implementation of an interven-
tion (EPOC 1998).
Types of participants
We included studies in which the interventions were directed at
workers who had not actively sought help for conditions such
as burnout, depression or anxiety disorder. This included inter-
ventions directed at healthcare workers officially employed in any
healthcare setting or at student nurses or physicians otherwise in
training to become a professional who were also doing clinical
work. This excluded studies in which the participants were just
caregivers and were not employed by a healthcare organisation.
Types of intervention
We included studies with any kind of intervention aimed at pre-
venting or reducing stress arising from work. Prevention was de-
fined as an intervention directed at healthy individuals not diag-
nosed with a specific disease.
Interventions were categorised into two groups:
1. Interventions directed at factors at work, or work-directed inter-
ventions containing measures to change the working environment,
work tasks or working methods. For example, interventions aimed
at decreasing workload or changing the organisation of work.
2. Interventions focusing on people, or person-directed interven-
tions, aimed at teaching personal skills, techniques or remedies
to decrease the effects of stressors at the individual level. For ex-
ample, interventions aimed at mitigating the effects of stress by
relaxation techniques or cognitive-behavioural techniques that in-
creased coping skills, without changing the work environment or
work tasks.
For both work- and person-directed interventions we included
studies with both non-intervention controls and with one or more
alternative intervention as a control group.
Types of outcome measures
Primary outcome measures
As primary outcomes we considered all validated self-report ques-
tionnaires measuring stress or burnout. These included mea-
sures such as: Karasek’s job content questionnaire (Karasek 1998),
Maslach Burnout Inventory (MBI) (Maslach 1982) and the Nurs-
ing Stress Scale (Gray-Toft 1981).
Secondary outcome measures
As secondary outcomes we considered all outcome measures of the
detrimental effects of stress or burnout. These included measures
such as:
(a) psychological symptoms: anxiety and depression, such as
the State Trait Anxiety Inventory (Spielberger 1970), General
Health Questionnaire (Goldberg 1991), Beck Depression Inven-
tory (Beck 1961)
(b) physical symptoms and physiological parameters, such as hor-
mone levels such as prolactin, corticosteroids or others.
We considered the effects measured with all the above instruments
on the following time-scales:
(i) Short Term: up to one month
(ii) Medium Term: from one month to a year
(iii) Long Term: over a year
All other outcomes that did not measure stress or its effects on
individuals were deemed beyond the scope of this review and were
thus excluded from analyses. Examples of excluded outcomes are:
coping skills, knowledge or attitude change, work-performance,
patient satisfaction and claims from clients, employee absenteeism
and turnover.
S E A R C H M E T H O D S F O R
I D E N T I F I C A T I O N O F S T U D I E S
See: Cochrane Depression, Anxiety and Neurosis Group methods
used in reviews.
See Collaborative Review Group search strategy for the search
strategy in the CCDAN database.
1. Electronic databases
(a) MEDLINE (1966- May 2005): see strategy in Table 01.
3Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(b) PsycINFO: we used the following strategy up to May 2005:
(((“Nursery-School-Students” in MJ,MN) or (“Nursery-Schools”
in MJ,MN) or (“Nurses-” in MJ,MN) or (“Nursing-” in
MJ,MN) or (“Nursing-Education” in MJ,MN) or (“Nursing-
Homes” in MJ,MN) or (“Nursing-Students” in MJ,MN) or
(“Psychiatric-Nurses” in MJ,MN) or (“Public-Health-Service-
Nurses” in MJ,MN) or (“School-Nurses” in MJ,MN)) or
(“Health-Personnel” in MJ,MN)) and ((“Stress-Management” in
MJ,MN) or (“Occupational-Stress” in MJ,MN)))
and (intervention or effectiveness or evaluation)
(c) Cochrane Collaboration Specialised Registry of Clinical Trials
of the Depression, Anxiety and Neurosis Group (CCDANCTR):
latest search, February 2002, using the following strategy:
Keyword = burnout or “psychological stress”
and
Free-text = healthcare or staff or employ* or job or work* or nurs*
(d) Cochrane Occupational Health Field database
2. Reference lists
Reference lists from articles and reviews were also carefully
reviewed.
3. Handsearch
All issues between January 1987 and March 2000 of Work &
Stress were handsearched.
M E T H O D S O F T H E R E V I E W
Selection of studies
Two reviewers independently selected the studies to include
in the review according to the inclusion criteria. If there was
any disagreement concerning the inclusion of a study, this was
discussed jointly, and where necessary a third reviewer resolved the
disagreement.
Data extraction and management
The extraction of data was carried out using a made-to-measure
data extraction form filled in independently by two reviewers for
each study.
(a) If studies used a cross-over design we used the results from just
after the implementation of the intervention in the intervention
group, compared to the results in the concurrent waiting-list
control group.
(b) If studies used continuous measures and reported only means
and p-values, we calculated standard deviations from p-values in
the article to be used in the meta-analysis, according to the method
stated in the Cochrane Handbook for Reviewers.
(c) If studies compared more than one active intervention we chose
which of the active interventions to enter into the meta-analysis.
Assessment of methodological quality of included studies
Evaluation of the quality of clinical trials included in the review
was done by means of the checklist developed by Downs 1998.
We had clear reasons for using the Downs 1998 checklist. Since
we needed to include non-randomised studies of work-directed
interventions, we wanted to have an instrument that could assess
the quality of both randomised and non-randomised studies.
According to the review by Deeks 2003, the Downs 1998 checklist
was the best choice for this specific purpose. The checklist contains
separate subscales for reporting, external validity, internal validity
and power with a maximum number of points respectively 10,
2, 13 and 5, and a total maximum score of 30. The individual
items of the check list were rated either as yes (=1) or no/
unable to determine (=0). Two evaluators independently evaluated
the quality of the studies. Where necessary, study authors were
contacted for clarification. The scales of internal validity were used
to rate the quality of studies. Studies were considered to have high
internal validity if they scored higher than 75% of the maximum
score of the two scales combined. The other scales of the checklist
were reported separately.
Measures of treatment effect
The results of each trial were plotted as means and standard
deviations (SD) for continuous outcomes. For continuous
measures, in cases where the same instrument was used, preference
was given to analysing the results with weighted mean differences
(WMD) because these results are easier to interpret for clinicians
and other readers. If this was not possible because different
instruments were used, then standardised mean differences (SMD)
or effect sizes were used.
Unit of analysis issues
For studies that employed a cluster-randomised design and that
reported sufficient data to be included in the meta-analysis and
that did not make an allowance for the design effect we calculated
the design effect based on a fairly large assumed intra-cluster
correlation of 0.10. Even though we did not find information
for the intra-cluster correlation for these types of studies we
assumed that 0.10 would be a realistic estimate. We based
this assumption by analogy on studies about implementation
research (Campbell 2001). We followed the methods stated in the
Cochrane Handbook for the calculations.
Dealing with missing data
Where necessary, missing statistics data (means and standard
deviations) were sought from authors. Since all studies used
questionnaires to measure outcomes using continuous data, we
were unable to conduct an intention-to-treat analysis. We refrained
from standard approaches such as last observation carried forward
or imputing baseline outcomes since we did not have access to
raw patient data. Therefore all results were based on available case
analysis.
Assessment of heterogeneity
We tested for statistical heterogeneity by means of the I2 in
the meta-analysis graphs. If this is greater than 50% there is
4Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

substantial heterogeneity between studies. When studies were
statistically heterogeneous, a random-effects model was used;
otherwise a fixed-effect model was used. All estimates included a
95% confidence interval (95% CI).
Data synthesis
The choice between qualitative and quantitative pooling was based
first on clinical homogeneity. Clinically homogeneous studies
were defined as those with similar populations, interventions,
and outcomes measured at the same follow-up point. All studies
concerned healthcare workers. Interventions were divided into
person- and work-directed interventions. Outcomes were judged
similar if they used the same instrument such as the Maslach
Burnout Inventory (Maslach 1982). Statistical pooling was then
done for each subscale of the instrument with RevMan 4.2
software. If different instruments were used but the instruments
measured the same concept such as exposure to stressors, the results
were pooled as well.
Analysis of the data
The results were summarised within the two main categories of
interventions: work-directed interventions and person-directed
interventions. We used weighted mean differences (WMD) to
combine the results of studies that used similar questionnaires
to measure the outcome. For similar outcomes that were
measured with different questionnaires we used standardised mean
differences (SMD) to combine the results.
In addition, because only a proportion of the studies reported data
in sufficient detail for meta-analysis, we used a qualitative synthesis
to grade the evidence according to the methods suggested by the
Cochrane Back Review Group (van Tulder 2003). Although levels
of evidence are essentially subjective and arbitrary they are explicit
and reproducible by giving exact meaning to labels like strong
and limited evidence (de Vet 2003). In other words, this method
allows one to make a judgement (level) of the entirety of results
(evidence) presented in the included studies. We adapted the van
Tulder 2003 grading as follows (see also Table 03):
(i) Strong evidence: if there are two or more high quality studies
with similar positive or negative effects that are confirmed by the
quantitative analysis
(ii) Limited evidence: if there is only one high quality study and/or
multiple low quality studies with similar positive or negative effects
or the results of the high quality studies are not confirmed by the
quantitative analysis
(iii) No evidence: if there are no studies available
(iv) Conflicting evidence: if the results of studies point in opposite
directions.
Outcomes are defined as positive if there is a significant positive
effect at the p = 0.05 level, and negative if there is a significant
negative effect at the p = 0.05 level. If there is no significant effect
this will not be considered as a conflicting outcome.
We followed Van Tulder’s advice to explicitly describe conflicting
outcomes and criteria for high quality studies. We simplified
the levels of evidence as originally described by Van Tulder by
combining the levels of moderate and limited evidence into one
level of limited evidence. Moreover, we added the requirement of
confirmation by meta-analysis as an extra criterion to be met to
reach the level of strong evidence.
Publication bias
We planned to assess publication bias by means of funnel plots.
Methods for future updates
We will expand this review to also cover the cost-effectiveness of
interventions. The search strategy will also be updated to better
reflect the variety in healthcare job titles outside nursing. The
present sample is nonetheless the largest and most specific of
systematic reviews so far conducted. Therefore we feel that even
though our search strategy was initially developed with a different
set of inclusion criteria (all hospital staff including e.g. cleaners),
it still provided an effective and comprehensive search of all the
relevant literature.
D E S C R I P T I O N O F S T U D I E S
From the initial references, a set of 51 potentially eligible studies
were identified. These were then scrutinized further, and another
32 studies were excluded leaving a total of 20 studies. However, we
noticed that two studies (Lökk 1997; Lökk 2000) actually reported
separate sets of results of a single study so we included them as one
study. Thus, our final sample consisted of 19 studies (see table of
included studies).
Additional information regarding study details and/or statistical
data was sought from 10 authors and was received from six. Three
of the authors provided statistical data that had not been published
in their articles which enabled two of these three studies to be
entered into meta-analyses.
Study designs
Of the 19 included studies, 14 were randomised controlled trials,
three were cluster-randomised trials and two were cross-over stud-
ies. All three included cluster-randomized trials had a unit of anal-
ysis error. We calculated the design effect as 2.2 for the Lökk 1997
and Lökk 2000 study (r=2, m=13); 2.73 for the Schrijnemaekers
2003 study (r=16, m=18.3) and 1.72 for the Proctor 1998 study
(r=12, m=8.2). We used the design effect to diminish the actual
number of participants in both intervention and control groups
if quantitative outcomes were used. We were aiming to also in-
clude studies with interrupted time-series and controlled before-
after designs but the final sample contained none of these.
Country and time period
Eleven of the included studies had been conducted before the year
2000 and eight at or after the year 2000. Eight studies had been
5Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

carried out in Europe, another eight in North America and three
in Asia.
Type of settings and participants
Altogether 12 of the studies had been run in hospitals and the
remaining seven in varying settings ranging from a secure forensic
mental health unit to residential care homes for the elderly or the
disabled.
Sample sizes
The total number of participants in various intervention groups
was 1564, and in control groups 1248. The number of partici-
pants in the smallest study groups was less than 20 in seven stud-
ies, between 21 and 50 in six studies, between 51 and 100 in four
studies and more than 101 in two studies (Heaney 1995; Schri-
jnemaekers 2003). These two studies were the only ones deemed
a priori to have sufficient power to detect relevant differences.
Interventions
1. Person-directed interventions
Some interventions were quite straightforward but many used dif-
ferent methods.
(a) Cognitive-behavioural training: Lee 1994, Rowe 1999; von
Baeyer 1983; West 1984.
(b) Relaxation training: Tsai 1993; Yung 2004
(c) Music-making: Bittman 2003. The intervention consisted of
recreational music-making where participants engaged in playing
various drum and percussion instruments in response to questions
that had been designed to inspire deep thought and mutual respect.
(d) AMMA touch therapy (a form of therapeutic massage): McEl-
ligott 2003.
(e) Multicomponent interventions: Cohen-Katz 2005 employed
a pre-existing Mindfulness-Based Stress Reduction program con-
taining group sessions of formal didactic instruction and exercises
to enhance communication skills, stress reactivity and self-com-
passion. Ewers 2002 used a regime of training about practical skills
in reducing distress and improving functioning with schizophrenic
patients. In the Lökk study (Lökk 1997 and Lökk 2000) the inter-
vention consisted of cognitive-behavioural training coupled with
group therapy. Jones 2000 and Norvell 1987 both employed in-
terventions combining cognitive-behavioural and relaxation skills
training.
2. Work-directed interventions
Delvaux 2004 and Razavi 1993 used psychological training pro-
grams with theory, role-playing and experiential exchanges in-
tended to improve attitudes, communication skills and occupa-
tional stress. Heaney 1995 ran a training program about mobi-
lizing support from colleagues and about learning participatory
problem solving and decision-making skills. Melchior 1996, Proc-
tor 1998 and Schrijnemaekers 2003 employed interventions that
introduced innovations in nursing delivery via changes in work
organisation, knowledge and skills training and support and ad-
vice from supervisors.
Multiple interventions
Three studies compared more than one active intervention against
no intervention (Rowe 1999; West 1984; Yung 2004). The re-
sults of two studies could be entered into meta-analyses. Rowe
1999 compared an adaptive coping training condition with the
same training coupled with refresher sessions. Yung 2004 com-
pared stretch-release relaxation with cognitive relaxation. With
these two studies a choice had to be made regarding which active
interventions to enter into the meta-analyses. In the case of Rowe
1999, we chose the training with booster sessions condition as it
was the more intensive option of the two interventions, and with
Yung 2004 we chose the cognitive relaxation condition because
we felt that a cognitive intervention for a cognitive problem was
conceptually on firmer ground.
Type of control group (no intervention vs. other active or “pas-
sive” interventions)
Almost all (n=15) of the included studies used a no intervention
or waiting list control group (Bittman 2003; Cohen-Katz 2005;
Delvaux 2004; Ewers 2002; Heaney 1995; Jones 2000; Melchior
1996; Norvell 1987; Proctor 1998; Razavi 1993; Rowe 1999;
Schrijnemaekers 2003; von Baeyer 1983; West 1984; Yung 2004).
Four studies used another, “passive” intervention aiming to control
for the Hawthorne effect etc. (Lee 1994; Lökk 1997 & Lökk 2000;
McElligott 2003; Tsai 1993). Finally, three studies also compared
one or more active interventions (Rowe 1999; West 1984; Yung
2004).
Follow-up
(i)Short Term:
There were six studies in which the last outcome measurement
was either at the end of the intervention (Ewers 2002; McElligott
2003; Norvell 1987; Proctor 1998; von Baeyer 1983) or at less
than a month after intervention (Tsai 1993).
(ii) Medium Term:
In nine studies the last follow-up measurement was between one
and six months after intervention (Heaney 1995; Lee 1994; Razavi
1993; Yung 2004; Bittman 2003; Cohen-Katz 2005; Delvaux
2004; Lökk 1997 & Lökk 2000; West 1984).
(iii) Long Term:
There were also four studies in which the last follow-up measure-
ment was at twelve months after intervention or later (Jones 2000;
Melchior 1996; Rowe 1999; Schrijnemaekers 2003).
Excluded studies
Reasons for excluding the 32 studies were the following (see table
of excluded studies):
(a) No intervention (Bradley 2002; Fernandez 1995; Teasdale
2001).
(b) No intention to prevent or treat stress or burnout (Schinke
1977).
(c) No stress or burnout or health effects outcome (Calomeni
1999; McPhail 1990; Nissen 1997; Taylor 2001; Weir 1997).
6Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(d) Non-randomised study design (Beddoe 2004; Berg 1994;
Bruneau 2004; Bunce 1996; Freedy 1994; Jones 1998; Keyes
1988; Kushnir 1998; McCue 1991; Murphy 1983; Pålsson 1996;
van Dierendonck 1998; Young 2001; Zimber 2001).
(e) Participants were not healthcare workers or nursing students
with clinical duties (Drain 1991; Lloyd 2002; Toivanen 1993).
(f ) Participants were nursing students but did not have clinical
duties (Godbey 1994; Heaman 1995; Hughes 2003; Johansson
1991; Mancini 1983; Sharif 2004).
M E T H O D O L O G I C A L Q U A L I T Y
Allocation concealment and randomisation
Only one study (Jones 2000) reported concealing intervention
versus control group allocation until it was completed and irrevo-
cable. This was also the only study that described an acceptable
method of randomisation, using random number tables. One fur-
ther study (Tsai 1993) reported having used coin tossing as the
method of randomisation whereas the rest did not describe their
choice of randomisation method.
Blinding
There was mention in only one of the studies (Delvaux 2004)
of blinding those rating the outcome measurements i.e. Nursing
Stress Scale questionnaires. In all but one of the included studies
(McElligott 2003), the blinding of participants to the interven-
tions they were receiving would have been impossible due to the
nature and aims of interventions being self-evident.
Attrition
The loss of participants was low throughout, with only two of the
studies (Norvell 1987; Tsai 1993) suffering a loss exceeding 20%
of the initial sample.
Quality assessment with the Downs 1998quality checklist
Two reviewers (JR and JV) independently rated all included studies
with the Downs 1998 quality checklist. The overall Cohen’s Kappa
of agreement for the entire checklist was 0.54 and for items 13-
25 (internal validity) it was 0.62. The two reviewers then rated all
studies a second time but now working together. All disagreements
were solved by discussion and better definition of the criteria used
for assessment.
The results of the second rating are presented broken down into
the five subscales of the checklist:
A: reporting,
B: external validity,
C: internal validity - bias,
D: internal validity - confounding/ selection bias
E: power (see Table 02: Study quality and intervention type).
The overall mean score (± standard deviation) of the 19 included
studies for the checklist was 17.4 ± 3.8 out of a maximum attain-
able score of 30, which means that on average 58% of the max-
imum attainable score was achieved. The minimum score was 9
and the maximum score 23.
A: The mean score of the quality of reporting scale was 6.6 ± 0.4
out of a maximum of 10.
B: For the external validity subscale the mean score was 0.5 ± 0.1
out of a maximum of two.
C+D: For the combined internal validity subscales the mean score
was 7.9 ± 0.3 out of a maximum of 13. There were only two
studies that got more than 75% on the internal validity subscales
and were therefore rated as high quality studies (Delvaux 2004;
Schrijnemaekers 2003).
E: For statistical power the mean score was 2.4 ± 0.4 out of a
maximum of five.
Studies on work-directed interventions scored on average higher
than studies on person-directed interventions on the checklist as
a whole and on all the subscales. This difference was, however,
only significant for the subscale of statistical power. Most person-
directed studies were fairly small in contrast to the work-directed
interventions that had much bigger numbers of participants. The
two studies that were rated as being high quality were both studies
on work-directed interventions.
R E S U L T S
1. Person-directed interventions
1.1 Primary outcome Stress and Burnout symptoms
(a) Stress symptoms
There were two studies (Jones 2000; Lee 1994) that measured
stress directly and were thus included in a meta-analysis. Since
both used different scales (Jones 2000: Beck and Srivastava Stress
Inventory (Beck 1991); Lee 1994; Perceived Stress Scale (Cohen
1983)) we used standardised mean differences (SMD) in the analy-
sis instead of weighted mean differences (WMD). Person-directed
interventions reduced stress significantly when compared to no in-
tervention and when measured by the abovementioned two stress
scales (SMD -0.85; 95% CI -1.21 to -0.49).
In the medium term, stress remained lower in the intervention
group than it did in the control group in one study (Lee 1994),
(mean difference -6.10; 95% CI -8.44 to -3.76).
The levels of evidence table showed a positive effect in four stud-
ies of person-directed interventions on stress and one inconclu-
sive outcome (Rowe 1999) (Table 04). The scales used to measure
stress that produced results which could not be entered into meta-
analysis were: Stress Assessment Inventory (Rowe 1999), Nursing
Stress Checklist (Benoliel 1990) and the Job-Related Tension In-
dex (Kahn 1964).
(b) Burnout symptoms
Altogether three studies (Cohen-Katz 2005; Ewers 2002; Rowe
1999) were included in a meta-analysis of person-directed inter-
7Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

ventions intended to reduce burnout symptoms measured at the
short term with the Maslach Burnout Inventory (MBI) (Maslach
1996). The summary effect of two subscales of the Maslach
Burnout Inventory was in favour of the intervention: Emotional
Exhaustion (WMD -5.82; 95% CI: -11.02 to -0.63), and lack
of Personal Accomplishment (WMD -4.89; 95% CI: -8.71 to
-1.07). The Depersonalization subscale confidence interval just
overlapped with zero: (WMD -2.44; 95% CI: -5.06 to 0.17).
There was considerable heterogeneity between the three studies in
the meta-analysis (I2 ranged from 67.6% to 86.7%; p=0.05 and
p=0.0005 respectively), with Rowe 1999 having a smaller decrease
in the MBI scores (respectively -2, -2, -0.6) than the other two
studies.
For the long term, the results of Rowe 1999 showed that when
compared to six weeks of cognitive-behavioural training, having
refresher sessions at 5, 11 and 17 months led to significantly lower
Emotional Exhaustion (mean difference -6.00; 95% CI -8.16 to
-3.84) and lack of Personal Accomplishment (mean difference
-5.82; 95% CI -7.89 to -3.75) at two years.
The levels of evidence table showed a positive effect in two studies
(Ewers 2002; Rowe 1999) with person-directed interventions on
all burnout subscales as measured with the Maslach Burnout In-
ventory (Maslach 1996) and in three other studies (Cohen-Katz
2005; Norvell 1987; West 1984) on one or two subscales (Table
05). For one study (Bittman 2003), the results were inconclusive
for all subscales.
1.2 Secondary outcomes: Anxiety and General Health com-
plaints
(a) Anxiety
Three studies (Jones 2000; von Baeyer 1983; Yung 2004) were
included in a meta-analysis of person-directed interventions with
the State-Trait Anxiety Inventory (Spielberger 1970) as the out-
come. The data of two studies could not be entered into the analy-
sis because Rowe 1999 did not report the results of the State-Trait
Anxiety Inventory measurements and in the case of West 1984
the results were not in a useable format. Based on Jones 2000, von
Baeyer 1983, Yung 2004, person-directed interventions signifi-
cantly reduced both state anxiety (WMD -9.42; 95% CI -16.92
to -1.93) as well as trait anxiety (WMD -6.91; 95% CI -12.80
to -1.01) when compared to no intervention and when measured
by the State-Trait Anxiety Inventory. There was considerable het-
erogeneity (I2 = 83.1%; p=0.003) with the study of Yung 2004
having a smaller decrease on both scales (respectively -5 and -2)
than the other two studies in the meta-analysis.
In the medium term, based on the studies of Jones 2000 and Yung
2004 state-anxiety and trait-anxiety scores (WMD -8.31; 95% CI
-11.49 to -5.13) and trait anxiety scores (WMD -4.09; 95% CI
-7.60 to -0.58) remain lower in the intervention group than in the
control group.
The levels of evidence table showed a positive effect in three in-
cluded studies (Jones 2000; von Baeyer 1983; West 1984) of per-
son-directed interventions on both state and trait anxiety and one
study (Yung 2004) was positive in the state anxiety domain and
inconclusive in the trait anxiety domain (Table 06).
(b) General symptoms
There were two studies (Jones 2000; Yung 2004) that employed
the General Health Questionnaire (Goldberg 1991) and could
therefore be included in a meta-analysis. In the meta-analysis of
these studies person-directed interventions did not reduce general
symptoms significantly more than no intervention (WMD -11.87;
95% CI -27.24 to 3.49).
Three other studies used general health symptoms as an outcome
but their results could not be used for meta-analysis. They also did
not contribute to the levels of evidence because of inconclusive re-
sults (Cohen-Katz 2005; Norvell 1987; Tsai 1993). In the levels of
evidence tables the same studies as in the meta-analysis contribute
positive results based on the authors conclusions (Table 07).
In the medium term, based on the results of Yung 2004 cogni-
tive relaxation training maintains the reduction in General Health
Questionnaire scores for at least one month whereas stretch-re-
lease relaxation training does not (mean difference -7.10; 95% CI
-10.58 to -3.62).
2. Work-directed interventions
Three of the five studies on work-directed interventions reported
results that could be quantified. The other two studies only re-
ported the results of multivariate analysis.
2.1 Primary outcome: Stress and Burnout symptoms
(a) Stress symptoms
The results of Delvaux 2004 show that psychological training on
attitudes, communication skills and occupational stress alleviate
stress (mean difference -0.34; 95% CI -0.62 to -0.06) when com-
pared to no intervention and when measured with the Nursing
Stress Scale (Gray-Toft 1981). This difference became non-signifi-
cant at six-months (mean difference -0.19; 95% CI -0.49 to 0.11)
The addition of the study by Proctor 1998 in the levels of evidence
tables did not change this result because it was inconclusive (Table
08).
(b) Burnout symptoms
According to the results of Melchior 1996, support and advice
given by nurse managers or quality care coordinators alleviate
symptoms on one of the subscales of the Maslach Burnout Inven-
tory: Depersonalization (mean difference -1.14; 95% CI -2.18 to
-0.10) when compared to no intervention. The other two sub-
scales of the Maslach Burnout Inventory, Emotional Exhaustion
and lack of Personal Accomplishment, were non-significant.
The addition of the study by Schrijnemaekers 2003 in the levels
of evidence table showed positive study results for the Maslach
8Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Burnout Inventory subscale lack of Personal Accomplishment,
whereas the Melchior 1996 study was inconclusive (Table 09).
2.2 Secondary outcome: Anxiety and General Health com-
plaints
Anxiety was not used as an outcome measure in any of the studies
on work-directed interventions.
Proctor 1998 used a combination of training of knowledge and
skills and individual programme planning to decrease general
symptoms (mean difference -2.90; 95% CI -5.16 to -0.64) when
compared to no intervention and when measured with the Gen-
eral Health Questionnaire (Goldberg 1991).
Adding the study by Heaney 1995, which measured general health
complaints with the Symptom Checklist-90-Revised (Derogatis
1976), into the levels of evidence tables did not change the results
(Table 10).
Publication bias
We planned to assed publication bias using funnel plots, but no
more than three studies could have been included, making it diffi-
cult draw conclusions. However, as most studies had only a small
sample size and all reported positive outcomes, it is conceivable
that there may have been publication bias. If there are more studies
included in future updates, we will assess the extent of publication
bias by means of funnel plots.
D I S C U S S I O N
The meta-analyses and the qualitative analyses in this review show
that there is limited evidence that person-directed interventions
in healthcare workers effectively reduce the levels of burnout, anx-
iety, stress and general symptoms. With regard to work-directed
interventions, we also found limited evidence that work-directed
interventions in healthcare workers effectively reduce the levels of
stress, general symptoms and burnout on the Depersonalization
and lack of Personal Accomplishment subscales of the Maslach
Burnout Inventory (Maslach 1996).
The programmes for managing stress at work vary greatly with
respect to objectives, types of interventions, duration and the pro-
fessional group at which they are aimed. It therefore makes sense
to try to classify the different types of interventions in order to
compare them in terms of efficacy. Person-directed interventions
are the most common interventions to have been evaluated.
We did not find it feasible to further subdivide the person-directed
interventions because almost all studies used several different in-
gredients. Most claim that it is possible to change the participants’
cognitions about stressful elements at work. We refrained from a
further sensitivity analysis based on differences in quality because
most studies scored about average on the quality scale. Nor did we
perform a sensitivity analysis based on differences in the content
of the interventions such as relaxation techniques versus cogni-
tive behavioural techniques because most interventions comprised
both elements.
We also examined interventions aimed at changing the organi-
sation of work. Although broad organisational interventions are
generally regarded as being more useful and appropriate in terms
of primary prevention, studies evaluating them are very scarce or
lack a robust evaluative design.This has not been confirmed in
this review since on average studies on work-directed interventions
scored higher on the quality checklist, and the two studies with
the highest quality scores were evaluations of work-directed inter-
ventions. Since there were no direct comparisons between work-
directed and person-directed interventions, we did not attempt
to compare the outcomes of the work-directed with the person-
directed interventions. It is clear however, that the problem of at-
trition is greater in the evaluation of work-directed intervention
studies in which the personal interest of participants is apparently
different.
In the meta-analysis of person-directed interventions there was
considerable heterogeneity with Rowe 1999 showing a smaller
decrease in MBI scores in the short term. The same holds for
the Yung 2004 study that showed less decrease in anxiety scores.
However, in the medium and long term follow-up these differences
disappeared. We could not find a plausible explanation for the
heterogeneity in the short term.
The quality of the evidence that we found was not very high.
Some studies applied rigorous methods but contended with attri-
tion problems. Most RCTs were small and in all but one of the
included RCT studies (Jones 2000) the method of randomisation
was not reported or not valid. It was also difficult to get a good
impression of the concealment of allocation to researchers. We as-
sumed that outcomes that were measured by questionnaire were
reported blind to the researchers but we could not be certain about
this assumption. The reporting of most studies was of low quality
as well which is reflected in the low number of studies that could
be used for the meta-analysis. All in all, according to our classifi-
cation of the studies, only two of 19 studies were high quality in
terms of internal validity.
Even though we found significant results it is not possible to say
how this is related to the clinical relevance of the changes achieved
in the studies. With the Maslach Burnout Inventory (Maslach
1996) for example, there is no generally accepted change that
would be regarded as clinically relevant. The authors of the ques-
tionnaire were contacted but could not help clarify this issue for
us.
Since most studies had only a small sample size and all reported
positive outcomes, it is conceivable that there may have been pub-
lication bias. However, it was not possible to assess the extent to
which publication bias may have been present due to the small
9Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

number of studies that reported outcomes that could be used for
statistical analysis.
Comparison with other reviews
When compared to the Mimura 2003 review, the present review
used more rigorous inclusion criteria ,only accepting randomised
controlled trials and randomised crossover trials. We found twice as
many (14) RCTs than Mimura 2003 (7). Where Mimura 2003 re-
frained from drawing clear conclusions based on the studies found,
we could make better inferences. The quality of the evidence that
we found was also better than Michie 2003 found, as their sample
consisted almost entirely of cross-sectional studies. Another review
by van der Klink 2001 involved a meta-analysis of interventions
to prevent or treat stress in all occupations. They synthesized all
study outcomes regardless of how they were measured and used all
possible figures available in primary studies to be included in their
meta-analysis. This made it difficult to decipher the meaning of
their findings. Compared to van der Klink’s review, we managed to
relate our results to concrete outcomes such as the Nursing Stress
Scale (Gray-Toft 1981), the Maslach Burnout Inventory (Maslach
1996) or the State-Trait Anxiety Inventory (Spielberger 1970). In
contrast with our review, van der Klink 2001 concluded that there
was no evidence for work-directed interventions. Due to the differ-
ent methods used it is difficult to explain this contrasting finding.
A recent review by Gilbody 2006 about interventions to improve
morale of staff was restricted to mental healthcare workers only.
It reached more or less the same conclusion as the present review,
even though the number of studies included was fewer and they
used a wider range of outcome measures and study designs. We
were more precise in our outcome measures and were therefore
better able to quantify our results.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
Limited evidence is available for the effectiveness of person- and
work-directed interventions to reduce stress levels in healthcare
settings. At best, the results of these interventions are still apparent
six months to two years after the end of interventions. There is
evidence from one trial that interventions which contain cognitive
elements yield better results than those with behavioural elements.
Implications for research
For person-directed interventions, larger studies with adequate
randomisation and blinding of allocation for the researchers are
needed to confirm the results of this systematic review. More stud-
ies are needed that contrast various stress or burnout reducing tech-
niques with one another. For work-directed interventions cluster-
randomised studies are feasible, but care should be taken to avoid
attrition. Studies that contrast work-directed interventions with
person-directed interventions will show if one type of intervention
is more effective in reducing stress levels than the other. Studies
are also needed comparing different person- and work-directed
interventions with one another.
N O T E S
The title of this review has changed from ’Effectiveness of occu-
pational stress management programmes’ to ’Preventing occupa-
tional stress in healthcare workers’.
P O T E N T I A L C O N F L I C T O F
I N T E R E S T
None known.
A C K N O W L E D G E M E N T S
Ingalill Rahm Hallberg, Dirk von Dierendonck, Martyn Jones,
Deborah McElligott, Michelle Rowe and Joanne Cohen-Katz for
providing further information about their studies; to Albert West-
ergren for kindly facilitating contact with one of the authors. To
Wilmar Schaufeli for his expertise on burnout. To Joan Martí and
to Hugh McGuire for their support in identifying studies for this
review. To Elinor Thompson for technical editing. We thank the
Cochrane Occupational Health Field for help and enthusiastic in-
volvement in finalizing the review.
S O U R C E S O F S U P P O R T
External sources of support
• Ministry of Social Affairs and Health FINLAND
Internal sources of support
• Cochrane Occupational Health Field FINLAND
• Finnish Institute of Occupational Health FINLAND
• Corporació Parc Taulí (Sabadell) SPAIN
• Network of Centers for Research on Epidemiology and Public
Health SPAIN
10Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

R E F E R E N C E S
References to studies included in this review
Bittman 2003 {published data only}
Bittman B, Bruhn KT, Stevens C, Westengard J, Umbach PO. Recre-
ational music-making: a cost-effective group interdisciplinary strat-
egy for reducing burnout and improving mood states in long-term
care workers. Advances in Mind-Body Medicine 2003;19(3-4):4–15.
Cohen-Katz 2005 {unpublished data only}
Cohen-Katz J, Wiley SD, Capuano T, Baker DM, Kimmel S, Shapiro
S. The effects of mindfulness-based stress reduction on nurse stress
and burnout, Part II: A quantitative and qualitative study. Holistic
Nursing Practice 2005;19(1):26–35.
Delvaux 2004 {published data only}
Delvaux N, Razavi D, Marchal S, Bredart A, Farvacques C, Slach-
muylder JL. Effects of a 105 hours psychological training program on
attitudes, communication skills and occupational stress in oncology:
a randomised study. British Journal of Cancer 2004;90(1):106–14.
Ewers 2002 {published data only}
Ewers P, Bradshaw T, McGovern J, Ewers B. Does training in psy-
chosocial interventions reduce burnout rates in forensic nurses?. Jour-
nal of Advanced Nursing 2002;37(5):470–6.
Heaney 1995 {published data only}
Heaney CA, Price RH, Rafferty J. Increasing coping resources at
work: a field experiment to increase social support, improve work
team functioning, and enhance employee mental health. Journal of
Organizational Behavior 1995;16:335–52.
Jones 2000 {unpublished data only}
Jones MC, Johnston DW. Evaluating the impact of a worksite stress
management programme for distressed students: a randomised con-
trolled trial. Psychology and Health 2000;15:689–706.
Lee 1994 {published data only}
Lee S, Crockett MS. Effect of assertiveness training on levels of stress
and assertiveness experienced by nurses in Taiwan, Republic of China.
Issues in Mental Health Nursing 1994;15(4):419–32.
Lökk 1997 {published data only}
Lökk J, Arnetz B. Psychophysiological concomitants of organiza-
tional change in health care personnel: effects of a controlled inter-
vention study. Psychotherapy and Psychosomatics 1997;66(2):74–7.
Lökk 2000 {published data only}
Lökk J, Arnetz B. Impact of management Change and an Interven-
tion Program on Health Care Personnel. Psychotherapy and Psychoso-
matics 2000;69:79–85.
McElligott 2003 {unpublished data only}
McElligott D, Holz MB, Carollo L, Somerville S, Baggett M,
Kuzniewski S, et al. A pilot feasibility study of the effects of touch
therapy on nurses. Journal of the New York State Nurses Association
2003;34(1):16–24.
Melchior 1996 {published data only}
Melchior ME, Philipsen H, bu-Saad HH, Halfens RJ, van de Berg
AA, Gassman P. The effectiveness of primary nursing on burnout
among psychiatric nurses in long-stay settings. Journal of Advanced
Nursing 1996;24(4):694–702.
Norvell 1987 {published data only}
Norvell N, Belles D, Brody S, Freund A. Worksite Stress Management
for Medical Care Personnel: Results from a Pilot Program. Journal
for Specialists in Group Work 1987;57:118–26.
Proctor 1998 {published data only}
Proctor R, Stratton-Powell H, Tarrier N, Burns A. The impact of
training and support on stress among care staffin nursing and res-
idential homes for the elderly. Journal of Mental Health 1998;7(1):
59–71.
Razavi 1993
Razavi D, Delvaux N, Marchal S, Bredart A, Farvacques C, Paes-
mans M. The effects of a 24-h psychological training program on at-
titudes, communication skills and occupational stress in oncology: a
randomised study. European Journal of Cancer 1993;29A(13):1858–
63.
Rowe 1999 {published data only}
Rowe MM. Teaching health-care providers coping: results of a two-
year study. Journal of Behavioral Medicine 1999;22(5):511–27.
Schrijnemaekers 2003 {published data only}
Schrijnemaekers VJ, Van Rossum E, Candel MJ, Frederiks CM, De-
rix MM, Sielhorst H, et al. Effects of emotion-oriented care on work-
related outcomes of professional caregivers in homes for elderly per-
sons. Journals of Gerontology Series B-Psychological Sciences & Social
Sciences 2003;58(1):50–7.
Tsai 1993 {published data only}
Tsai SL, Crockett MS. Effects of relaxation training, combining im-
agery, and meditation on the stress level of Chinese nurses working
in modern hospitals in Taiwan. Issues in Mental Health Nursing 1993;
14(1):51–66.
von Baeyer 1983 {published data only}
von Baeyer C, Krause L. Effectiveness of stress management training
for nurses working in a burn treatment unit. International Journal of
Psychiatry in Medicine 1983;13(2):113–26.
West 1984 {published data only}
West DJ Jr, Horan JJ, Games PA. Component Analysis of Occupa-
tional Stress Inoculation Apllied to Registered Nurses in an Acute
Care Hospital Setting. Journal of Counseling Psychology 1984;31(2):
209–18.
Yung 2004 {published data only}
Yung PM, Fung MY, Chan TM, Lau BW. Relaxation training meth-
ods for nurse managers in Hong Kong: a controlled study. Interna-
tional Journal of Mental Health Nursing 2004;13(4):255–61.
References to studies excluded from this reviewBeddoe 2004
Beddoe AE, Murphy SO. Does mindfulness decrease stress and foster
empathy among nursing students?. The Journal of Nursing Education
2004;43(7):305–12.
Berg 1994
Berg A, Hansson UW, Hallberg IR. Nurses creativity, tedium and
burnout during 1 year of clinical supervision and implementation
of individually planned nursing care: comparisons between a ward
for severely demented patients and a similar control ward. Journal of
Advanced Nursing 1994;20(4):742–9.
11Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Bradley 2002
Bradley JR, Cartwright S. Social support, job stress, health, and job
satisfaction among nurses in the United Kingdom. International Jour-
nal of Stress Management 2002;9(3):163–81.
Bruneau 2004
Bruneau BM, Ellison GT. Palliative care stress in a UK community
hospital: evaluation of a stress-reduction programme. International
Journal of Palliative Nursing 2004;10(6):296–304.
Bunce 1996
Bunce D, West MA. Stress management and innovation interven-
tions at work. Human Relations 1996;49(2):209–32.
Calomeni 1999
Calomeni CA, Solberg LI, Conn SA. Nurses on quality improvement
teams: how do they benefit?. Journal of Nursing Care Quality 1999;
13(5):75–90.
Drain 1991
Drain CB, Dirks KR, Jenkins OC, Campbell JK, Finstuen K, John-
son GR. Comparison of two instructional methods on the levels of
physiologic and psychologic stress as measured by blood cortisol and
the State-Trait Anxiety Inventory. Nurse Anesthesia 1991;2(4):172–
83.
Fernandez 1995
Fernandez San Martin MI, Villagrasa F Jr, Fe GM, Vazquez GJ, Cruz
CE, guirre Trigo MV, et al. The study of occupational satisfaction
and its determining factors among health professionals working in
one of the areas in Madrid. Revista Espanola de Salud Publica 1995;
69(6):487–97.
Freedy 1994
Freedy JR, Hobfoll SE. Stress inoculation for reduction of burnout: a
conservation of resources approach. Anxiety, Stress, and Coping 1994;
6:311–25.
Godbey 1994
Godbey KL, Courage MM. Stress-management program: interven-
tion in nursing student performance anxiety. Archives of Psychiatric
Nursing 1994;8(3):190–9.
Heaman 1995
Heaman D. The quieting response (QR): a modality for reduction
of psychophysiologic stress in nursing students. Journal of Nursing
Education 1995;34(1):5–10.
Hughes 2003
Hughes LC, Romick P, Sandor MK, Phillips CA, Glaister J, Levy K, et
al. Evaluation of an informal peer group experience on baccalaureate
nursing students’ emotional well-being and professional socialization.
Journal of Professional Nursing 2003;19(1):38–48.
Johansson 1991
Johansson N. Effectiveness of a stress management program in reduc-
ing anxiety and depression in nursing students. Journal of American
College Health 1991;40(3):125–9.
Jones 1998
Jones JW, Barge BN, Steffy BD, Fay LM, Kunz LK, Wuebker LJ.
Stress and medical malpractice: organizational risc assessment and
intervention. Journal of Applied Psychology 1998;7:727–35.
Keyes 1988
Keyes JB, Dean SF. Stress inoculation training for direct contact
staff working with mentally retarded persons. Behavioral Residential
Treatment 1988;3:315–23.
Kushnir 1998
Kushnir T, Malkinson R, Ribak J. Rational thinking and stress man-
agement in health workers: a psychoeducational program. Interna-
tional Journal of Stress Management 1998;5(3):169–78.
Lloyd 2002
Lloyd C, King R, Chenoweth L. Social work, stress and burnout: A
review. Journal of Mental Health 2002;11(3):255–65.
Mancini 1983
Mancini J, Lavecchia C, Clegg R. Graduate nursing students and
stress. Journal of Nursing Education 1983;22(8):329–34.
McCue 1991
McCue JD, Sachs CL. A stress management workshop improves res-
ident’s coping skills. Archives of Internal Medicine 1991;151:2273–7.
McPhail 1990
McPhail A, Pikula H, Roberts J, Browne G, Harper D. Primary
nursing. A randomized crossover trial. Western Journal of Nursing
Research 1990;12(2):188–97.
Murphy 1983
Murphy LR. A comparision of relaxation methods for reducing stress
in nursing personnel. Human Factors 1983;25:413–40.
Nissen 1997
Nissen JM, Boumans NP, Landeweerd JA. Primary nursing and qual-
ity of care: a Dutch study. International Journal of Nursing Studies
1997;34(2):93–102.
Pålsson 1996
Palsson MB, Hallberg IR, Norberg A, Björvell H. Burnout, empathy
and sense of coherence among Swedish district nurses before and
after systematic clinical supervision. Scandinavian Journal of Caring
Sciences 1996;10(1):19–26.
Schinke 1977
Schinke SP, Wong SE. Evaluation of staff training in group homes
for retarded persons. American Journal of Mental Deficiency 1977;82
(2):130–6.
Sharif 2004
Sharif F, Armitage P. The effect of psychological and educational
counselling in reducing anxiety in nursing students. Journal of Psy-
chiatric and Mental Health Nursing 2004;11(4):386–92.
Taylor 2001
Taylor B, Lo R. The effects of Healing Touch on the coping ability,
self esteem and general health of undergraduate nursing students.
Complementary Therapies in Nursing & Midwifery 2001;7(1):34–42.
Teasdale 2001
Teasdale K, Brocklehurst N, Thom N. Clinical supervision and sup-
port for nurses: an evaluation study. Nursing and Health Care Man-
agement 2001;33(2):216–24.
Toivanen 1993
Toivanen H, Helin P, Hänninen O. Impact of regular relaxation
training and psychosocial working factors on neck-shoulder tension
and absenteeism in hospital cleaners. Journal of Occupational Medicine
1993;35(11):1123–30.
12Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

van Dierendonck 1998
van Dierendonck D, Schaufeli W, Buunk BP. The evaluation of an
individual burnout intervention program: the role of inequity and
social support. Journal of Applied Psychology 1998;83(3):392–407.
Weir 1997
Weir R, Stewart L, Browne G, Roberts J, Gafni A, Easton S, Seymour
L. The efficacy and effectiveness of process consultation in improving
staff morale and absenteeism. Medical Care 1997;35(4):334–53.
Young 2001
Young LE, Bruce A, Turner L, Linden W. Evaluation of mindfulness-
based stress reduction intervention. The Canadian Nurse 2001;97(6):
23–6.
Zimber 2001
Zimber A, Rudolf A, Teufel S. A training program to reduce distress
among geriatric caregivers [Arbeitsbelastungen in der Altenpflege re-
duzieren: Ein Trainingsprogramm für Mitarbeiter und Leitugskräfte].
Zeitschrift fur Gerontologie und Geriatrie 2001;34(5):401–7.
References to studies awaiting assessment
Carson 1999
Carson J, Cavagin J, Bunclark J. Effective communication in men-
tal health nurses: did social support save the psychiatric nurse?. NT
Research 1999;4:31–42.
Additional references
Beck 1961
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory
for measuring depression. Archives of General Psychiatry 1961;4:561–
71.
Beck 1991
Beck DL, Srivastava R. Perceived level and sources of stress in bac-
calaureate nursing students. Journal of Nursing Education 1991;30
(3):127–33.
Benoliel 1990
Benoliel JQ, McCorkle R, Georgiadou F, Denton T, Spitzer A. Mea-
surement of stress in clinical nursing. Cancer Nursing 1990;13(4):
221–28.
Campbell 2001
Campbell MK, Mollison J, Grimshaw JM. Cluster trials in imple-
mentation research: estimation of intra-cluster correlation and sam-
ple size. Statistics in Medicine 2001;20:391–9.
Cohen 1982
Cohen S, Hoberman HM. Positive events and social supports as
buffers of life change stress. Journal of Applied Social Psychology 1982;
13:99–125.
Cohen 1983
Cohen S, Kamarck T, Mermelstein R. A global measure of perceived
stress. Journal of Health and Social Behavior 1983;24(4):385–96.
Cooper 1988
Cooper CL, Sloane SJ, Williams S. The Occupational Stress Indicator.
Windsor, Berkshire: NFER-Nelson, 1988.
Cooper 2001
Cooper CL, Dewe P, O’Driscoll MP. Organizational stress. London:
SAGE, 2001.
de Vet 2003
de Vet HCW, van Tulder MW, Bouter LM. Levels of evidence: Intel-
lectual aid or absolute judgement?. Journal of Clinical Epidemiology
2003;56:917–8.
Deckard 1994
Deckard G, Meterko M, Field D. Physician burnout: an examination
of personal, professional, and organizational relationships. Medical
Care 1994;32(7):745–54.
Deeks 2003
Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F,
et al. Evaluating non-randomised intervention studies. Health Tech-
nology Assessment 2003;7(27):1–173.
DeFrank 1987
DeFrank RS, Cooper CL. Worksite stress management interventions:
their effectiveness and conceptualisation. Journal of Managerial Psy-
chology 1987;2:4–10.
Derogatis 1976
Derogatis L, Rikels K, Rock A. The SCL-90 and MMPI: A step in
the validation of a new self-report scale. British Journal of Psychiatry
1976;128:280–9.
Derogatis 1983
Derogatis LR, Melisaratos N. The Brief Symptom Inventory: an in-
troductory report. Psycholical Medicine 1983;13(3):595–605.
Downs 1998
Downs SH, Black N. The feasibility of creating a checklist for the
assessment of the methodological quality both of randomised and
non-randomised studies of health care interventions. Journal of Epi-
demiology and Community Health 1998;52(6):377–84.
Dunnette 1990
Dunnette MD, Hough LM. Handbook of industrial and organiza-
tional psychology. 2nd Edition. Palo Alto, CA: Consulting Psycholo-
gists Press, 1990.
EPOC 1998
Cochrane Effective Practice and Organisation of Care Group. In-
cluding Interrupted Time Series (ITS) Designs in a EPOC Review.
http://www.epoc.uottawa.ca/methods.htm 1998:1–5.
Firth 1989
Firth H, Britton P. Burnout, absence and turnover amongst British
nursing staff. Journal of Occupational Psychology 1989;62(1):55–9.
Firth-Cozens 1999
Firth-Cozens J, Payne R. Stress in health professionals. Chichester:
Wiley, 1999.
Gilbody 2006
Gilbody S, Cahill J, Barkham M, Richards D, Bee P, Glanville J.
Can we improve the morale of staff working in psychiatric units? A
systematic review. Journal of Mental Health 2006;15(1):7–17.
Goldberg 1991
Goldberg D, Williams P. A User’s Guide to the General Health Ques-
tionnaire. London: NFER–Nelson, 1991.
Gray-Toft 1981
Gray-Toft P, Anderson JG. The Nursing Stress Scale: Development
of an instrument. Journal of Psychopathology and Behavioral Assessment
1981;3(1):11–23.
13Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Jacobson 1996
Jacobson BH, Aldana SG, Goetzel RZ, Vardell KD, Adams TB,
Piedras RJ. The relationship between perceived stress and self-re-
ported illness-related absenteeism. American Journal of Health Pro-
motion 1996;11(1):54–61.
Kahn 1964
Kahn R, Wolfe D, Quinn R, Snoek JD, Rosenthal R. Organizational
Stress: Studies in role conflict and role ambiguity. New York, NY: Wiley,
1964.
Karasek 1992
Karasek R. Stress prevention through work reorganization: a sum-
mary of 19 international case studies. Conditions of Work Digest 1992;
11:23–42.
Karasek 1998
Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick
B. The Job Content Questionnaire (JCQ): an instrument for inter-
nationally comparative assessments of psychosocial job characteris-
tics. Journal of Occupational Health Psychology 1998;3(4):322–55.
Maslach 1982
Maslach C. Burnout: the cost of caring. New York, NY: Prentice-Hall,
1982.
Maslach 1996
Maslach C, Jackson SE, Leiter SP. Maslach Burnout Inventory manual.
3rd Edition. Palo Alto, CA: Consulting Psychologists Press, 1996.
McNeely 2005
McNeely E. The consequences of job stress for nurses’ health: Time
for a check-up. NursING Outlook 2005;53:291–9.
Michie 2003
Michie S, Williams S. Reducing work related psychological ill health
and sickness absence: a systematic literature review. Occupational and
Environmental Medicine 2003;60(1):3–9.
Mimura 2003
Mimura C, Griffiths P. The effectiveness of current approaches to
workplace stress management in the nursing profession: an evidence
based literature review. Occupational and Environmental Medicine
2003;60(1):10–5.
Murphy 1995
Murphy S. Stress management in work settings: a critical review of
the health effects. American Journal of Health Promotion 1995;11(2):
112–35.
Payne 1987
Payne RL, Firth-Cozens J. Stress in health professionals. Chichester:
Wiley, 1987.
Raiger 2005
Raiger J. Applying a Cultural Lens to the Concept of Burnout. Journal
of Transcultural Nursing 2005;16(1):71–6.
Ramirez 1996
Ramirez AJ, Graham J, Richards MA, Cull A, Gregory WM. Mental
health of hospital consultants: the effects of stress and satisfaction at
work. Lancet 1996;347(9003):724–8.
Schaufeli 2003
Schaufeli WB, Buunk BP. Burnout: An Overview of 25 Years of Re-
search and Theorizing. In: SchabracqMJ, WinnubstJAM, CooperCL
editor(s). The handbook of Work and Health Psychology. 2nd Edition.
Chichester: Wiley, 2003:383–424.
Spielberger 1970
Spielberger CD, Gorsuch RL, Lushene RE. Manual for the State-
Trait Anxiety Inventory (Self-Evaluation Questionnaire). Palo Alto, CA:
Mind Garden, 1970.
van der Hek 1997
van der Hek H, Plomp HN. Occupational stress management pro-
grammes: a practical overview of published effect studies. Occupa-
tional Medicine [London] 1997;47(3):133–41.
van der Klink 2001
van der Klink JJ, Blonk RW, Schene AH, van Dijk FJ. The benefits
of interventions for work-related stress. American Journal of Public
Health 2001;91(2):270–6.
van Tulder 2003
van Tulder M, Furlan A, Bombardier C, Bouter L. Updated method
guidelines for systematic reviews in the cochrane collaboration back
review group. Spine 2003;28(12):1290–9.
Weinberg 2000
Weinberg A, Creed F. Stress and psychiatric disorder in healthcare
professionals and hospital staff. Lancet 2000;355(9203):533–7.
Williamson 1994
Williamson AM. Managing Stress in the Workplace .2. the Scien-
tific Basis (Knowledge-Base) for the Guide. International Journal of
Industrial Ergonomics 1994;14(1-2):171–96.
T A B L E S
Characteristics of included studies
Study Bittman 2003
Methods Cross-over study
Participants 112 randomly selected staff of a retirement community in the USA
Interventions 1) Recreational music making
2) No intervention -control
14Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Outcomes Maslach Burnout Inventory, Profile of Mood States
Notes Person-directed
Allocation concealment D – Not used
Study Cohen-Katz 2005
Methods RCT
Participants 25 nurses, pastoral care, respiratory therapy and social work personnel in the USA
Interventions 1) Mindfulness-based stress reduction programme
2) No intervention -control
Outcomes Maslach Burnout Inventory, Brief Symptom Inventory
Notes Person-directed
Allocation concealment D – Not used
Study Delvaux 2004
Methods RCT
Participants 115 oncology nurses in Belgium
Interventions 1) Psychological Training Program
2) No intervention -control
Outcomes Nursing Stress Scale
Notes Organisational
Allocation concealment D – Not used
Study Ewers 2002
Methods RCT
Participants 20 forensic mental health nurses in the UK
Interventions 1) Psychosocial Intervention Training
2) No intervention -control
Outcomes Maslach Burnout Inventory
Notes Person-directed
Allocation concealment D – Not used
Study Heaney 1995
Methods RCT
Participants 1375 direct care staff and home managers in the USA
Interventions 1) Caregiver support program
2) No intervention -control
Outcomes Social support, Organisational climate, SCL-90-R, Confidence in coping ability
Notes Organisational
Allocation concealment D – Not used
Study Jones 2000
Methods RCT
Participants 79 student nurses reporting significant levels of affective distress at screen in the UK
Interventions 1) multi-modal stress management
15Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
2) No intervention -control
Outcomes Derogatis Stress profile, B&S Stress Inventory, GHQ, STAI, BDI, ways of coping, absenteeism
Notes Person-directed
Allocation concealment A – Adequate
Study Lee 1994
Methods RCT
Participants 60 hospital nurses suffering from either: insomnia, headache or gastrointestinal discomfort in Taiwan
Interventions 1) assertiveness training
2) traditional inservice program about computer applications in nursing
Outcomes Perceived Stress Scale, Rathus Assertiveness Schedule
Notes Person-directed
Allocation concealment D – Not used
Study Lökk 1997
Methods Cluster-randomised trial
Participants 26 health care personnel in a geriatric hospital in Sweden
Interventions 1) support and advice from a psychologist
2) passive attendance by psychologist
Outcomes Blood pressure and pulse rate, prolactin, cortisol, DHEA, estradiol
Notes Person-directed
Allocation concealment D – Not used
Study Lökk 2000
Methods Cluster-randomised trial
Participants 26 health care personnel in a geriatric hospital in Sweden
Interventions 1) support and advice from a psychologist
2) passive attendance by psychologist
Outcomes A structured made-to-measure stress questionnaire
Notes Person-directed
Allocation concealment D – Not used
Study McElligott 2003
Methods RCT
Participants 20 nurses working at a tertiary care center in the USA
Interventions 1) AMMA therapy
2) a standardised touch therapy protocol
Outcomes VAS of anxiety, blood pressure, heart rate, pulse oximetry, skin temperature
Notes Person-directed
Allocation concealment D – Not used
Study Melchior 1996
Methods RCT
16Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Participants 161 psychiatric nurses in long-stay settings in the Netherlands
Interventions 1) support and advice given by nurse managers or quality care coordinators
2) No intervention -control
Outcomes Maslach Burnout Inventory
Notes Organisational
Allocation concealment D – Not used
Study Norvell 1987
Methods RCT
Participants 12 respiratory therapists in the USA
Interventions 1) stress management program
2) No intervention -control
Outcomes MBI, C-H Inventory of Phys Symptoms, The Hassles Scale, The Uplifts Scale
Notes Person-directed
Allocation concealment D – Not used
Study Proctor 1998
Methods Cluster-randomised trial
Participants 98 care staff in residential nursing homes in the UK
Interventions 1) developing knowledge and skills and individual programme planning
2) No intervention -control
Outcomes The Occupational Stress Indicator, GHQ
Notes Organisational
Allocation concealment D – Not used
Study Razavi 1993
Methods RCT
Participants 72 oncology nurses in Belgium and France
Interventions 1) a 24-h Psychological Training Program
2) No intervention -control
Outcomes The Nursing Stress Scale
Notes Organisational
Allocation concealment D – Not used
Study Rowe 1999
Methods RCT
Participants 126 health-care professionals from the USA
Interventions 1) Stress management/ adaptive coping training, with refresher sessions
2) No intervention -control
Outcomes Maslach Burnout Inventory
Notes Person-directed
Allocation concealment D – Not used
17Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Schrijnemaekers 2003
Methods Cluster-randomised trial
Participants 300 professional caregivers in homes for elderly persons in the Netherlands
Interventions 1) Emotion-oriented care training, clinical lessons and supervision meetings
2) No intervention -control
Outcomes Maslach Burnout Inventory, Job satisfaction
Notes Organisational
Allocation concealment D – Not used
Study Tsai 1993
Methods RCT
Participants 137 nurses in Taiwan
Interventions 1) Training about stress at work, relaxation, breathing, imagery and meditation
2) traditional in-service education about theory analysis
Outcomes Nurse Stress Checklist, Chinese General Health Questionnaire
Notes Person-directed
Allocation concealment D – Not used
Study West 1984
Methods RCT
Participants 60 acute care hospital nurses in the USA
Interventions 1) Stress Inoculation (SI) training
2) No intervention -control
Outcomes MBI, Job-related tension, Life satisfaction STAI, RAS, Systolic and diastolic blood pressure
Notes Person-directed
Allocation concealment D – Not used
Study Yung 2004
Methods RCT
Participants 65 nurse managers in China
Interventions 1) Cognitive relaxation
2) Stretch-release relaxation
3) No intervention -control
Outcomes C-STAI, C-GHQ
Notes Person-directed
Allocation concealment D – Not used
Study von Baeyer 1983
Methods Cross-over study
Participants 14 nurses in a burn treatment unit in Canada
Interventions 1) Cognitive-behavioural stress management training
2) No intervention -control
Outcomes STAI
Notes Person-directed
18Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Allocation concealment D – Not used
Characteristics of excluded studies
Study Reason for exclusion
Beddoe 2004 The study does not employ a control group.
Berg 1994 The study is non-randomised by design.
Bradley 2002 The study does not employ an intervention. It is an aetiological study.
Bruneau 2004 The study is non-randomised by design.
Bunce 1996 The study is non-randomised by design.
Calomeni 1999 The study does not have a stress outcome.
Drain 1991 The participants of the study are not health care personnel or nursing students with clinical duties.
Fernandez 1995 The study does not employ an intervention.
Freedy 1994 The study is non-randomised by design.
Godbey 1994 The participants are nursing students but do not have clinical duties.
Heaman 1995 The participants are nursing students but do not have clinical duties.
Hughes 2003 The participants are nursing students but do not have clinical duties.
Johansson 1991 The participants are nursing students but do not have clinical duties.
Jones 1998 The study is non-randomised by design.
Keyes 1988 The study is non-randomised by design.
Kushnir 1998 The study is non-randomised by design.
Lloyd 2002 The participants of the study are not health care personnel or nursing students with clinical duties.
Mancini 1983 The participants are nursing students but do not have clinical duties.
McCue 1991 The study is non-randomised by design.
McPhail 1990 The study does not have a stress outcome.
Murphy 1983 The study is non-randomised by design.
Nissen 1997 The study does not have a stress outcome.
Pålsson 1996 The study is non-randomised by design.
Schinke 1977 The study does not intend to prevent or treat stress or burnout.
Sharif 2004 The participants are nursing students but do not have clinical duties.
Taylor 2001 The study does not have a stress outcome.
Teasdale 2001 The study does not employ an intervention.
Toivanen 1993 The participants of the study are not health care personnel or nursing students with clinical duties.
Weir 1997 The study does not have a stress outcome.
Young 2001 The study is non-randomised by design.
Zimber 2001 The study is non-randomised by design.
van Dierendonck 1998 The study is non-randomised by design.
A D D I T I O N A L T A B L E S
Table 01. Search strategy (MEDLINE)
Search strategy
19Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

1 exp Burnout, professional
2 burnout.tw.
3 exp job satisfaction
4 job satisfaction.tw.
5 (mental adj25 health adj25 professional$) .ab,ti.
6 (stress adj25 professional$) .ab,ti.
7 (stress adj25 occupational) .ab,ti.
8 randomised controlled trial.pt.
9 controlled clinical trial.pt.
10 randomised controlled trials
11 random allocation
12 double blind method
13 single blind method
14 or/8-13
15 clinical trial.pt.
16 exp Clinical trial
17 (clin$ adj25 trial$) .ti,ab.
18 ((singl$ or doubl$ or trebl$ or tripl$) adj25 (blind $ or 12010 mask$)) .ti,ab.
19 19 placebos
20 placebos.ti,ab.
21 random.ti,ab.
22 research design
23 or/15-22
24 comparative study
25 exp “Evaluation and Follow Up”
26 follow up studies
27 prospective studies
28 (control$ or prospectiv$ or volunteer$) .ti,ab.
29 or/24-28
30 14 or 23 or 29
31 animal
32 human
33 31 and 32
34 31 not 33
35 or/1-7
36 exp anxiety/ or exp anxiety disorders
37 anxiety.ti.
38 exp Depression
39 depression.ti.
40 or/35-39
41 exp Health personnel
42 health.mp. and personnel.ti,ab. [mp=title, abstract, registry]
43 Nursing
44 nurse.mp. or nursing.ti,ab. [mp=title, abstract, registry]
20Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 01. Search strategy (MEDLINE) (Continued )
Search strategy
45 limit 44 to human
46 or/41-45
47 40 and 46
48 34
49 limit 48 to human
50 30
51 limit 50 to human
52 47 and 51
53 52 and 8
54 41 or 42
55 54 and 51 and 40
56 health.mp. and personnel.tw. [mp=title, abstract, registry]
57 54 and 56
58 54 or 56
59 58 and 51 and 40
60 (health and related and occupation$) .ab,tw,ti.
61 cleaners.mp. [mp=title, abstract, registry]
62 exp Occupational diseases
63 58 and 62
64 58 or 62
65 from 64 keep 8
Table 02. Study quality and intervention type
Study ID Intervention type Intervention content Reporting External validity Internal validity Power
Bittman Person-directed 8 2 8 4
Cohen-Katz Person-directed 3 0 8 1
Delvaux Organisational communication skills 8 1 10 4
Ewers Person-directed 8 1 9 0
Heaney Organisational participatory problem solving 5 0 6 5
Jones Person-directed 7 0 8 3
Lee Person-directed 8 0 8 3
Lökk Person-directed 7 1 8 1
McElligott Person-directed 5 0 6 0
Melchior Organisational primary nursing 7 1 7 4
Norvell Person-directed 3 0 6 0
Proctor Organisational coping with difficult residents 6 0 7 3
Razavi Organisational communication skills 7 0 8 3
Rowe Person-directed 8 0 9 3
21Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 02. Study quality and intervention type (Continued )
Study ID Intervention type Intervention content Reporting External validity Internal validity Power
Schrijnemaekers Organisational emotion-oriented care 7 1 10 5
Tsai Person-directed 5 1 6 4
von-Baeyer Person-directed 8 1 9 0
West Person-directed 6 0 8 1
Yung Person-directed 10 0 9 2
Table 03. Levels of evidence: legend
HQ+ LQ+ HQ- LQ- HQinc LQinc
High quality
positive effect
(strong evidence)
Low quality,
positive effect
(limited evidence)
High quality,
negative effect
(strong evidence)
Low quality,
negative effect
(limited evidence)
High quality,
inconsistent effect
Low quality,
inconsistent effect
Table 04. Levels of evidence: Person-directed interventions: Stress
Stress scale HQ+ LQ+ HQ- LQ- HQinc LQinc
Beck and Srivastava Stress Inventory Jones
Perceived Stress Scale Lee
Stress Assessment Inventory Rowe 1999
Nursing Stress Checklist Tsai
Job-Related Tension Index West
Table 05. Levels of evidence: Person-directed interventions: Maslach Burnout Inventory
MBI subscales HQ+ LQ+ HQ- LQ- HQinc LQinc
Emotional Exhaustion Cohen-Katz
Ewers
Norvell
Rowe
West
Bittman
Depersonalisation Ewers
Rowe
Bittman
Cohen-Katz
Norvell
West
Personal Accomplishment Cohen-Katz
Ewers
Rowe
West
Bittman
Norvell
22Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 06. Levels of evidence: Person-directed interventions: State Trait Anxiety Inventory
STAI facets HQ+ LQ+ HQ- LQ- HQinc LQinc
State Jones
von Baeyer
West
Yung
Trait Jones
von Baeyer
West
Yung
Table 07. Levels of evidence: Person-directed interventions: general symptoms
Scale HQ+ LQ+ HQ- LQ- HQinc LQinc
Brief Symptom Inventory Cohen-Katz
GHQ General Health Questionnaire Jones
C-H Inventory of Physical Symptoms Norvell
Chinese GHQ Tsai
Chinese GHQ Yung
Table 08. Levels of evidence: Work-directed interventions: Stress
Stress scale HQ+ LQ+ HQ- LQ- HQinc LQinc
Nursing Stress Scale Delvaux
Occupational Stress Indicator Proctor
Table 09. Levels of evidence: Work-directed interventions: Maslach Burnout Inventory
MBI subscales HQ+ LQ+ HQ- LQ- HQinc LQinc
Emotional Exhaustion Schrijnemaekers Melchior
Depersonalisation Schrijnemaekers Melchior
Personal Accomplishment Schrijnemaekers Melchior
Table 10. Levels of evidence: Work-directed interventions: general symptoms
Scale HQ+ LQ+ HQ- LQ- HQinc LQinc
Symptom Checklist-90-Revised Heaney
GHQ General Health Questionnaire (somatic symptoms) Proctor
23Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

A N A L Y S E S
Comparison 01. Person-directed intervention vs no intervention (Short Term)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Beck & Srivastava Stress Scale
and Perceived Stress Scale
2 130 Standardised Mean Difference (Fixed) 95% CI -0.85 [-1.21, -0.49]
02 Maslach Burnout Inventory Weighted Mean Difference (Random) 95% CI Subtotals only
03 State Trait Anxiety Inventory Weighted Mean Difference (Random) 95% CI Subtotals only
04 General Health Questionnaire 2 127 Weighted Mean Difference (Random) 95% CI -11.87 [-27.24,
3.49]
Comparison 02. Person-directed intervention vs no intervention (Medium and Long Term)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Maslach Burnout Inventory (at
2 years)
Weighted Mean Difference (Random) 95% CI Subtotals only
02 Stait Trait Anxiety Inventory
(Jones at 3 months and Yung at
1 month)
Weighted Mean Difference (Random) 95% CI Subtotals only
03 Perceived Stress Scale (at 1
month)
1 57 Weighted Mean Difference (Fixed) 95% CI -6.10 [-8.44, -3.76]
04 General Health Questionnaire
(at 1 month)
1 48 Weighted Mean Difference (Fixed) 95% CI -7.10 [-10.58, -3.62]
Comparison 03. Work-directed intervention vs no intervention (Short Term)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Maslach Burnout Inventory Weighted Mean Difference (Random) 95% CI Subtotals only
02 Nursing Stress Scale 1 115 Weighted Mean Difference (Fixed) 95% CI -0.34 [-0.62, -0.06]
03 General symptoms 1 57 Weighted Mean Difference (Fixed) 95% CI -2.90 [-5.16, -0.64]
Comparison 04. Work-directed intervention vs no intervention (Medium Term)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Nursing Stress Scale (at 6
months)
1 111 Weighted Mean Difference (Fixed) 95% CI -0.19 [-0.49, 0.11]
C O V E R S H E E T
Title Preventing occupational stress in healthcare workers
Authors Marine A, Ruotsalainen J, Serra C, Verbeek J
Contribution of author(s) Albert Marine and Consol Serra conceived the review, gathered the data and wrote the first
draft.
Jani Ruotsalainen and Jos Verbeek updated the searches two years later. Jani Ruotsalainen
and Consol Serra re-analysed the new material. Jani Ruotsalainen rewrote the second draft.
Jos Verbeek was responsible for the statistical calculations.
All authors commented on the final draft.
24Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
Issue protocol first published 2000/2
Review first published 2006/4
Date of most recent amendment 23 August 2006
Date of most recent
SUBSTANTIVE amendment
21 August 2006
What’s New Information not supplied by author
Date new studies sought but
none found
Information not supplied by author
Date new studies found but not
yet included/excluded
14 August 2006
Date new studies found and
included/excluded
01 May 2005
Date authors’ conclusions
section amended
Information not supplied by author
Contact address Dr Albert Marine
Head of Counselling Programme for Health Professionals
Prevention Service
Corporacio Sanitaria Parc Tauli de Sabadell
Parc Tauli s/n
Sabadell
Catalonia
08208
SPAIN
E-mail: [email protected]
Tel: 34-93-7231010
Fax: 34-93-7233804
DOI 10.1002/14651858.CD002892.pub2
Cochrane Library number CD002892
Editorial group Cochrane Depression, Anxiety and Neurosis Group
Editorial group code HM-DEPRESSN
25Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

G R A P H S A N D O T H E R T A B L E S
Analysis 01.01. Comparison 01 Person-directed intervention vs no intervention (Short Term), Outcome 01
Beck & Srivastava Stress Scale and Perceived Stress Scale
Review: Preventing occupational stress in healthcare workers
Comparison: 01 Person-directed intervention vs no intervention (Short Term)
Outcome: 01 Beck % Srivastava Stress Scale and Perceived Stress Scale
Study Intervention Control Standardised Mean Difference (Fixed) Weight Standardised Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Jones 2000 39 56.33 (12.74) 34 69.43 (16.40) 55.7 -0.89 [ -1.37, -0.41 ]
Lee 1994 29 22.80 (4.90) 28 26.80 (4.90) 44.3 -0.81 [ -1.35, -0.26 ]
Total (95% CI) 68 62 100.0 -0.85 [ -1.21, -0.49 ]
Test for heterogeneity chi-square=0.05 df=1 p=0.82 I² =0.0%
Test for overall effect z=4.64 p<0.00001
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control
Analysis 01.02. Comparison 01 Person-directed intervention vs no intervention (Short Term), Outcome 02
Maslach Burnout Inventory
Review: Preventing occupational stress in healthcare workers
Comparison: 01 Person-directed intervention vs no intervention (Short Term)
Outcome: 02 Maslach Burnout Inventory
Study Intervention Control Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Emotional Exhaustion
Cohen-Katz 2005 12 15.00 (10.21) 13 23.31 (9.88) 21.5 -8.31 [ -16.20, -0.42 ]
Ewers 2002 10 10.51 (3.14) 10 18.91 (3.14) 38.1 -8.40 [ -11.15, -5.65 ]
Rowe 1999 42 23.53 (4.09) 42 25.60 (4.60) 40.4 -2.07 [ -3.93, -0.21 ]
Subtotal (95% CI) 64 65 100.0 -5.82 [ -11.02, -0.63 ]
Test for heterogeneity chi-square=15.02 df=2 p=0.0005 I² =86.7%
Test for overall effect z=2.20 p=0.03
02 Depersonalization
Cohen-Katz 2005 12 1.58 (1.78) 13 5.54 (6.78) 24.2 -3.96 [ -7.78, -0.14 ]
Ewers 2002 10 2.04 (3.26) 10 5.96 (3.26) 31.4 -3.92 [ -6.78, -1.06 ]
Rowe 1999 42 6.73 (2.84) 42 7.30 (3.41) 44.4 -0.57 [ -1.91, 0.77 ]
Subtotal (95% CI) 64 65 100.0 -2.44 [ -5.06, 0.17 ]
Test for heterogeneity chi-square=6.18 df=2 p=0.05 I² =67.6%
Test for overall effect z=1.83 p=0.07
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control (Continued . . . )
26Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(. . . Continued)
Study Intervention Control Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
03 Personal Accomplishment (lack of)
Cohen-Katz 2005 12 -42.33 (3.96) 13 -36.92 (5.92) 28.0 -5.41 [ -9.33, -1.49 ]
Ewers 2002 10 -39.64 (2.45) 10 -32.21 (2.45) 35.3 -7.43 [ -9.58, -5.28 ]
Rowe 1999 42 35.33 (3.86) 42 37.38 (4.28) 36.7 -2.05 [ -3.79, -0.31 ]
Subtotal (95% CI) 64 65 100.0 -4.89 [ -8.71, -1.07 ]
Test for heterogeneity chi-square=14.87 df=2 p=0.0006 I² =86.5%
Test for overall effect z=2.51 p=0.01
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control
Analysis 01.03. Comparison 01 Person-directed intervention vs no intervention (Short Term), Outcome 03
State Trait Anxiety Inventory
Review: Preventing occupational stress in healthcare workers
Comparison: 01 Person-directed intervention vs no intervention (Short Term)
Outcome: 03 State Trait Anxiety Inventory
Study Intervention Control Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 State anxiety
Jones 2000 39 30.77 (7.46) 34 46.35 (12.69) 35.0 -15.58 [ -20.45, -10.71 ]
Yung 2004 18 36.89 (5.75) 30 41.48 (8.16) 36.9 -4.59 [ -8.54, -0.64 ]
von Baeyer 1983 7 27.00 (6.50) 7 35.10 (8.50) 28.1 -8.10 [ -16.03, -0.17 ]
Subtotal (95% CI) 64 71 100.0 -9.42 [ -16.92, -1.93 ]
Test for heterogeneity chi-square=11.86 df=2 p=0.003 I² =83.1%
Test for overall effect z=2.46 p=0.01
02 Trait anxiety
Jones 2000 39 37.29 (7.90) 34 45.68 (9.81) 38.3 -8.39 [ -12.52, -4.26 ]
Yung 2004 18 42.06 (6.26) 30 43.90 (7.93) 38.6 -1.84 [ -5.89, 2.21 ]
von Baeyer 1983 7 24.10 (4.80) 7 37.00 (10.80) 23.1 -12.90 [ -21.66, -4.14 ]
Subtotal (95% CI) 64 71 100.0 -6.91 [ -12.80, -1.01 ]
Test for heterogeneity chi-square=7.71 df=2 p=0.02 I² =74.1%
Test for overall effect z=2.30 p=0.02
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control
27Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 01.04. Comparison 01 Person-directed intervention vs no intervention (Short Term), Outcome 04
General Health Questionnaire
Review: Preventing occupational stress in healthcare workers
Comparison: 01 Person-directed intervention vs no intervention (Short Term)
Outcome: 04 General Health Questionnaire
Study Intervention Control Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Jones 2000 40 15.00 (8.54) 39 34.73 (14.00) 49.9 -19.73 [ -24.86, -14.60 ]
Yung 2004 18 24.78 (7.03) 30 28.83 (10.35) 50.1 -4.05 [ -8.98, 0.88 ]
Total (95% CI) 58 69 100.0 -11.87 [ -27.24, 3.49 ]
Test for heterogeneity chi-square=18.68 df=1 p=<0.0001 I² =94.6%
Test for overall effect z=1.51 p=0.1
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control
Analysis 02.01. Comparison 02 Person-directed intervention vs no intervention (Medium and Long Term),
Outcome 01 Maslach Burnout Inventory (at 2 years)
Review: Preventing occupational stress in healthcare workers
Comparison: 02 Person-directed intervention vs no intervention (Medium and Long Term)
Outcome: 01 Maslach Burnout Inventory (at 2 years)
Study Intervention Control Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Emotional Exhaustion
Rowe 1999 42 19.38 (4.67) 42 25.38 (5.41) 100.0 -6.00 [ -8.16, -3.84 ]
Subtotal (95% CI) 42 42 100.0 -6.00 [ -8.16, -3.84 ]
Test for heterogeneity: not applicable
Test for overall effect z=5.44 p<0.00001
02 Depersonalisation
Rowe 1999 42 6.87 (2.47) 42 7.49 (3.39) 100.0 -0.62 [ -1.89, 0.65 ]
Subtotal (95% CI) 42 42 100.0 -0.62 [ -1.89, 0.65 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.96 p=0.3
03 Personal Accomplishment (lack of)
Rowe 1999 42 31.21 (4.61) 42 37.03 (5.04) 100.0 -5.82 [ -7.89, -3.75 ]
Subtotal (95% CI) 42 42 100.0 -5.82 [ -7.89, -3.75 ]
Test for heterogeneity: not applicable
Test for overall effect z=5.52 p<0.00001
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control
28Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
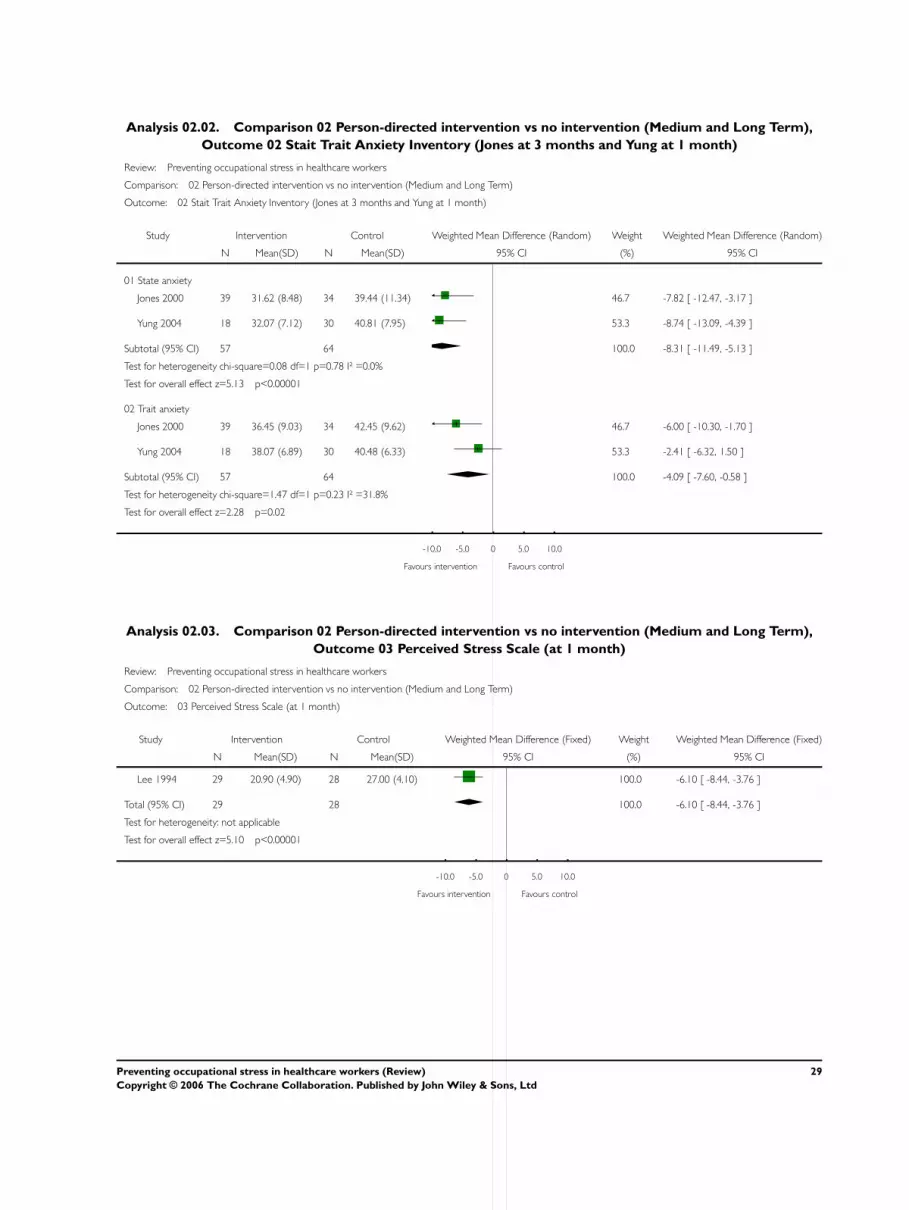
Analysis 02.02. Comparison 02 Person-directed intervention vs no intervention (Medium and Long Term),
Outcome 02 Stait Trait Anxiety Inventory (Jones at 3 months and Yung at 1 month)
Review: Preventing occupational stress in healthcare workers
Comparison: 02 Person-directed intervention vs no intervention (Medium and Long Term)
Outcome: 02 Stait Trait Anxiety Inventory (Jones at 3 months and Yung at 1 month)
Study Intervention Control Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 State anxiety
Jones 2000 39 31.62 (8.48) 34 39.44 (11.34) 46.7 -7.82 [ -12.47, -3.17 ]
Yung 2004 18 32.07 (7.12) 30 40.81 (7.95) 53.3 -8.74 [ -13.09, -4.39 ]
Subtotal (95% CI) 57 64 100.0 -8.31 [ -11.49, -5.13 ]
Test for heterogeneity chi-square=0.08 df=1 p=0.78 I² =0.0%
Test for overall effect z=5.13 p<0.00001
02 Trait anxiety
Jones 2000 39 36.45 (9.03) 34 42.45 (9.62) 46.7 -6.00 [ -10.30, -1.70 ]
Yung 2004 18 38.07 (6.89) 30 40.48 (6.33) 53.3 -2.41 [ -6.32, 1.50 ]
Subtotal (95% CI) 57 64 100.0 -4.09 [ -7.60, -0.58 ]
Test for heterogeneity chi-square=1.47 df=1 p=0.23 I² =31.8%
Test for overall effect z=2.28 p=0.02
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control
Analysis 02.03. Comparison 02 Person-directed intervention vs no intervention (Medium and Long Term),
Outcome 03 Perceived Stress Scale (at 1 month)
Review: Preventing occupational stress in healthcare workers
Comparison: 02 Person-directed intervention vs no intervention (Medium and Long Term)
Outcome: 03 Perceived Stress Scale (at 1 month)
Study Intervention Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Lee 1994 29 20.90 (4.90) 28 27.00 (4.10) 100.0 -6.10 [ -8.44, -3.76 ]
Total (95% CI) 29 28 100.0 -6.10 [ -8.44, -3.76 ]
Test for heterogeneity: not applicable
Test for overall effect z=5.10 p<0.00001
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control
29Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 02.04. Comparison 02 Person-directed intervention vs no intervention (Medium and Long Term),
Outcome 04 General Health Questionnaire (at 1 month)
Review: Preventing occupational stress in healthcare workers
Comparison: 02 Person-directed intervention vs no intervention (Medium and Long Term)
Outcome: 04 General Health Questionnaire (at 1 month)
Study Intervention Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Yung 2004 18 20.47 (5.23) 30 27.57 (7.00) 100.0 -7.10 [ -10.58, -3.62 ]
Total (95% CI) 18 30 100.0 -7.10 [ -10.58, -3.62 ]
Test for heterogeneity: not applicable
Test for overall effect z=4.00 p=0.00006
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control
Analysis 03.01. Comparison 03 Work-directed intervention vs no intervention (Short Term), Outcome 01
Maslach Burnout Inventory
Review: Preventing occupational stress in healthcare workers
Comparison: 03 Work-directed intervention vs no intervention (Short Term)
Outcome: 01 Maslach Burnout Inventory
Study Intervention Control Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Emotional Exhaustion
Melchior 1996 60 14.45 (6.47) 101 15.97 (6.66) 100.0 -1.52 [ -3.61, 0.57 ]
Subtotal (95% CI) 60 101 100.0 -1.52 [ -3.61, 0.57 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.43 p=0.2
02 Depersonalisation
Melchior 1996 60 5.61 (2.96) 101 6.75 (3.68) 100.0 -1.14 [ -2.18, -0.10 ]
Subtotal (95% CI) 60 101 100.0 -1.14 [ -2.18, -0.10 ]
Test for heterogeneity: not applicable
Test for overall effect z=2.15 p=0.03
03 Personal Accomplishment (lack of)
Melchior 1996 60 32.28 (3.55) 101 32.21 (3.98) 100.0 0.07 [ -1.12, 1.26 ]
Subtotal (95% CI) 60 101 100.0 0.07 [ -1.12, 1.26 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.12 p=0.9
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control
30Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 03.02. Comparison 03 Work-directed intervention vs no intervention (Short Term), Outcome 02
Nursing Stress Scale
Review: Preventing occupational stress in healthcare workers
Comparison: 03 Work-directed intervention vs no intervention (Short Term)
Outcome: 02 Nursing Stress Scale
Study Intervention Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Delvaux 2004 57 1.70 (0.76) 58 2.04 (0.78) 100.0 -0.34 [ -0.62, -0.06 ]
Total (95% CI) 57 58 100.0 -0.34 [ -0.62, -0.06 ]
Test for heterogeneity: not applicable
Test for overall effect z=2.37 p=0.02
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control
Analysis 03.03. Comparison 03 Work-directed intervention vs no intervention (Short Term), Outcome 03
General symptoms
Review: Preventing occupational stress in healthcare workers
Comparison: 03 Work-directed intervention vs no intervention (Short Term)
Outcome: 03 General symptoms
Study Intervention Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Proctor 1998 30 5.55 (3.77) 27 8.45 (4.80) 100.0 -2.90 [ -5.16, -0.64 ]
Total (95% CI) 30 27 100.0 -2.90 [ -5.16, -0.64 ]
Test for heterogeneity: not applicable
Test for overall effect z=2.52 p=0.01
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control
Analysis 04.01. Comparison 04 Work-directed intervention vs no intervention (Medium Term), Outcome 01
Nursing Stress Scale (at 6 months)
Review: Preventing occupational stress in healthcare workers
Comparison: 04 Work-directed intervention vs no intervention (Medium Term)
Outcome: 01 Nursing Stress Scale (at 6 months)
Study Intervention Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Delvaux 2004 53 1.62 (0.73) 58 1.81 (0.87) 100.0 -0.19 [ -0.49, 0.11 ]
Total (95% CI) 53 58 100.0 -0.19 [ -0.49, 0.11 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.25 p=0.2
-10.0 -5.0 0 5.0 10.0
Favours intervention Favours control
31Preventing occupational stress in healthcare workers (Review)
Copyright © 2006 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd





























