Embed Size (px)
Citation preview
M A J O R A R T I C L E
Prevention of Antibiotic-NonsusceptibleStreptococcus pneumoniae With ConjugateVaccines
Lee M. Hampton,1,2 Monica M. Farley,3 William Schaffner,4 Ann Thomas,5 Arthur Reingold,6 Lee H. Harrison,7
Ruth Lynfield,8 Nancy M. Bennett,9 Susan Petit,10 Kenneth Gershman,11 Joan Baumbach,12 Bernard Beall,2
James Jorgensen,13 Anita Glennen,8 Elizabeth R. Zell,2 and Matthew Moore2
1Epidemic Intelligence Service, and 2Respiratory Disease Branch, Centers for Disease Control and Prevention; and 3Emory University School of Medicineand Veterans Affairs Medical Center, Atlanta, Georgia; 4Department of Preventive Medicine, Vanderbilt University School of Medicine, Nashville,Tennessee; 5Health Division, Oregon Public Health Division, Portland; 6The School of Public Health, University of California, Berkeley; 7Johns HopkinsBloomberg School of Public Health, Baltimore, Maryland; 8Minnesota Department of Health, St. Paul; 9University of Rochester, New York;10Connecticut Department of Public Health, Hartford; 11Colorado Department of Public Health and Environment, Denver; 12New Mexico Department ofHealth, Santa Fe; and 13University of Texas, San Antonio
Background. Streptococcus pneumoniae (pneumococcus) caused approximately 44 000 US invasive pneumo-
coccal disease (IPD) cases in 2008. Antibiotic nonsusceptibility complicates IPD treatment. Using penicillin
susceptibility breakpoints adopted in 2008, we evaluated antibiotic-nonsusceptible IPD trends in light of the
introductions of a 7-valent pneumococcal conjugate vaccine (PCV7) in 2000 and a 13-valent pneumococcal
conjugate vaccine (PCV13) in 2010.
Methods. IPD cases were defined by isolation of pneumococcus from a normally sterile site in individuals
residing in Active Bacterial Core surveillance (ABCs) areas during 1998–2008. Pneumococci were serotyped and
tested for antibiotic susceptibility using broth microdilution.
Results. During 1998–2008, ABCs identified 43198 IPD cases. Penicillin-nonsusceptible strains caused 6%–14%
of IPD cases, depending on age. Between 1998–1999 and 2008, penicillin-nonsusceptible IPD rates declined 64% for
children aged,5 years (12.1–4.4 cases per 100 000), and 45% for adults aged$65 (4.8–2.6 cases per 100 000). Rates of
IPD nonsusceptible to multiple antibiotics mirrored these trends. During 2007–2008, serotypes in PCV13 but not
PCV7 caused 78%–97% of penicillin-nonsusceptible IPD, depending on age.
Conclusions. Antibiotic-nonsusceptible IPD rates remain below pre-PCV7 rates for children ,5 and adults
$65 years old. PCV13 vaccines hold promise for further nonsusceptibility reductions.
Streptococcus pneumoniae (pneumococcus) caused ap-
proximately 63 000 invasive pneumococcal disease
(IPD) cases annually in the late 1990s in the United States,
leading to about 6100 deaths [1]. During the first
7 years after the introduction in the United States of a
7-valent pneumococcal conjugate vaccine (PCV7) for
children, an estimated 211 000 fewer cases of IPD oc-
curred among all ages than would have occurred without
the vaccine [2]; however, approximately 44 000 IPD
cases continue to occur annually [3]. Antibiotic resistance
and intermediate susceptibility, together termed non-
susceptibility, complicate management of pneumococcal
disease [4–6]. Despite increasing during the 1990s [7],
the incidence of antibiotic-nonsusceptible IPD in the
United States fell following the introduction of PCV7
[8, 9]. The 7 serotypes covered by PCV7 accounted for
78% of nonsusceptible serotypes in 1998 [7], and the
incidence rate of these serotypes decreased 78% among
children aged ,2 years by 2001 [9]. However, by 2003,
the incidence of antibiotic-nonsusceptible IPD in chil-
dren aged ,5 years was increasing again [8], coinciding
with the emergence of serotypes not included in PCV7,
Received 11 March 2011; accepted 16 September 2011.Presented in part: 7th International Conference on Emerging Infectious
Diseases, Atlanta, Georgia, 11–14 July 2010.Correspondence: Lee Hampton, MD, Epidemic Intelligence Service and
Respiratory Disease Branch, Centers for Disease Control and Prevention, 1600Clifton Rd, MS A-24, Atlanta, GA 30329 ([email protected]).
The Journal of Infectious DiseasesPublished by Oxford University Press on behalf of the Infectious Diseases Society ofAmerica 2011.DOI: 10.1093/infdis/jir755
Prevention of S. pneumoniae With Conjugate Vaccines d JID d 1
Journal of Infectious Diseases Advance Access published December 7, 2011 at C
DC
Public Health L
ibrary & Inform
ation Center on D
ecember 7, 2011
http://jid.oxfordjournals.org/D
ownloaded from

particularly serotype 19A [10]. A new 13-valent pneumococcal
conjugate vaccine (PCV13) [11] could help reverse the rise in
antibiotic-nonsusceptible IPD, depending in part on the pro-
portion of antibiotic-nonsusceptible IPD caused by PCV13
serotypes.
Rates and proportions of antibiotic-nonsusceptible IPD de-
pend on the definition of antibiotic nonsusceptibility used. In
2008, the Clinical and Laboratory Standards Institute (CLSI)
established new, higher minimum inhibitory concentration
(MIC) breakpoints for defining pneumococcal susceptibility to
parenterally administered penicillin when treating pneumococ-
cal disease other than meningitis [12–14]. The breakpoints for
orally administered penicillin and for parenterally administered
penicillin for the treatment of meningitis did not change
[12, 13]. Since penicillin is the drug of choice for treatment of
penicillin-susceptible pneumococcal disease [4], this break-
point change could impact both individual clinical treatment
and public health surveillance for pneumococcal disease. We
used a population-based surveillance system to determine how
trends in antibiotic-nonsusceptible IPD in the United States
had changed since 1998, howmuch IPDwas caused by individual
serotypes, and how large was the impact of the revised penicillin
susceptibility breakpoints on nonsusceptible IPD trends.
METHODS
The Active Bacterial Core surveillance (ABCs) system performs
active, population-based surveillance for IPD, defined as oc-
curring when pneumococcus is isolated from a normally sterile
site, such as blood, cerebrospinal fluid (CSF), or pleural fluid,
from a person who is a resident of an ABCs area on the date of
culture [1, 7, 8, 15]. We analyzed IPD cases detected using the
ABCs system from 1 January 1998 through 31 December 2008.
In 1998, ABCs pneumococcal surveillance covered the entire
state of Connecticut and 49 counties in California, Georgia,
Maryland, Minnesota, New York, Oregon, and Tennessee [15].
By 2008, the ABCs pneumococcal surveillance system had
added 2 California counties, 5 Colorado counties, the rest of
Minnesota, all of New Mexico, 8 New York counties, and
6 Tennessee counties. The total population under surveillance
was 16 515 110 in 1998 and 28 856 774 in 2008. Before begin-
ning our analysis and to better characterize trends in IPD from
less common serotypes, we chose to use data from all counties
in the ABCs system, not just those with continuous surveillance
since 1998. We calculated annual IPD incidence rates (cases per
100 000 population) using the total number of cases identified by
ABCs in a given year and the population of the areas under
surveillance as reported by the US Census Bureau.
We abstracted case medical records for demographic and
clinical information, including diagnoses. S. pneumoniae isolates
were serotyped by the Quellung method at the Centers for
Disease Control and Prevention (CDC) or the Minnesota
Department of Health and classified in 1 of 6 ways: (1) serotypes
in PCV7 (4, 6B, 9V, 14, 18C, 19F, 23F); (2) additional PCV13
serotypes (1, 3, 5, 6A, 7F, 19A); (3) serotypes in PCV13 (PCV7
serotypes plus serotypes 1, 3, 5, 6A, 7F, 19A); (4) serotype 6A;
(5) serotype 19A, which, like serotype 6A, was analyzed separately
because of its unique epidemiology [2, 16]; and (6) serotypes not
found in PCV13, including the newly identified 6C [17, 18].
Serotype 6C was distinguished from serotype 6A using multiplex
polymerase chain reaction (PCR) containing primer pairs spe-
cific for cpsA, serogroup 6, and a wciN6C gene fragment [19].
Pneumococcal isolates were tested for antibiotic susceptibility
using reference broth microdilution at the CDC, the Minnesota
Department of Health, or the University of Texas Health Science
Center at San Antonio. We determined penicillin susceptibility
for all isolates using the new CLSI standard that recommends
different sets of breakpoints depending on whether penicillin is
administered orally, parenterally for meningitis, or parenterally
for nonmeninigitis disease [13], and using the single set of old
breakpoints that applied to all administration routes and clinical
syndromes [14]. The old breakpoints classified isolates as peni-
cillin susceptible (S; MIC#0.06 lg/mL), penicillin intermediate
(I; MIC 0.12–1.0 lg/mL), or penicillin resistant (R; MIC
$2 lg/mL), regardless of the clinical syndrome. The new CLSI
standards still specify these breakpoints for pneumococcal
disease treated orally. The new parenteral breakpoints classify
isolates from nonmeningitis cases as penicillin susceptible,
intermediate, or resistant at MICs of #2, 4, and $8 lg/mL,
respectively; isolates from meningitis cases are considered
penicillin susceptible (MIC #0.06 lg/mL) or resistant (MIC
$0.12 lg/mL). We considered intermediate and resistant iso-
lates to be nonsusceptible, so isolates were nonsusceptible under
the old/oral/meningitis breakpoints with an MIC$0.12 lg/mL
and nonsusceptible under the new parenteral-nonmeningitis
breakpoints with an MIC $4 lg/mL. The new meningitis
breakpoints were applied to all isolates from CSF and to iso-
lates from blood if the case had a clinical diagnosis of men-
ingitis. The new nonmeningitis breakpoints were applied to
all other isolates. To estimate the total number of penicillin-
nonsusceptible IPD cases under the new parenteral break-
points, we added the number of penicillin-nonmeningitis IPD
cases that were nonsusceptible under the new parenteral-
nonmeningitis breakpoints (MIC $4 lg/mL) to the number
of meningitis cases with a penicillin MIC $0.12 lg/mL.
Susceptibilities to all other antibiotics were determined using
only the 2008 CLSI susceptibility standards [13].
We considered an isolate to be nonsusceptible to multiple
drugs if it was not susceptible to 3 or more of the following
drugs: penicillin, clindamycin, cotrimoxazole, erythromycin,
tetracycline, levofloxacin, vancomycin, and chloramphenicol.
Cases with missing isolates (12%) were assumed to have the
same distribution among the different age groups as cases with
known antibiotic susceptibility and serotypes. We estimated
2 d JID d Hampton et al
at CD
C Public H
ealth Library &
Information C
enter on Decem
ber 7, 2011http://jid.oxfordjournals.org/
Dow
nloaded from

changes in rates of penicillin-nonsusceptible IPD since the in-
troduction of PCV7 by comparing the average rate during the
1998–1999 prevaccine baseline period with the rate in 2008, the
most recent year for which data are available (v2 test). We
examined the effect of replacement disease by comparing the
lowest rates of penicillin-nonsusceptible IPD (2002 for children
aged ,5 years as previously reported [8], 2004 for all other
age groups) with the rates in 2008. We considered 2-sided
P values #.05 to be statistically significant and did not adjust
for multiple comparisons. The proportions of penicillin-non-
susceptible IPD caused by different serotypes were determined
for the 1998–1999 prevaccine period and 2007–2008; the years
were combined to compensate for annual random variation
due to the small numbers of cases involved for many serotypes.
We analyzed all data using SAS 9.2 (SAS Institute, Cary, NC).
ABCs case reporting and isolate collection were considered to
be public health surveillance activities exempt from CDC in-
stitutional review. Each participating surveillance site evaluated
the surveillance protocol and either decided the protocol was
exempt from review or obtained appropriate local institutional
review board approval. Neither the CDC nor individual site
institutional review boards required informed consent.
RESULTS
Overall Incidence RatesDuring 1998–2008, ABCs identified 43 198 IPD cases, of which
7273 (17%) were among children aged ,5 years. Meningitis
accounted for 2485 cases, 483 (19%) of which were in children
aged ,5 years. Strains not susceptible to penicillin caused
6%–14% of IPD cases under the new parenteral breakpoints
and 19%–35% of IPD cases under the old/oral/meningitis
breakpoints, varying with age. Depending on which set of
breakpoints was used, the 2008 rates of penicillin-nonsusceptible
IPD among children aged ,5 years and adults aged $65 years
were 64%–78% and 30%–45% below the 1998–1999 baseline
period rates, respectively (Table 1). However, the 2008 rates of
penicillin-nonsusceptible IPD were 33%–137% higher than the
2002 rates among children aged,5 years and 23%–84% higher
than the 2004 rates among adults aged $65 years, depending
on the breakpoints used (Figure 1). Both the baseline levels
of and the magnitudes of the subsequent changes in the
penicillin-nonsusceptible IPD rates among individuals aged
5–17, 18–49, and 50–64 years were less than those among young
children and older adults under both the old/oral/meningitis
and new parenteral breakpoints (Figure 1). Rates of penicillin-
nonsusceptible IPD were higher under the old/oral/meningitis
breakpoints than under the new parenteral breakpoints, but
the trends were similar. Rates of IPD by penicillin MIC showed
declines between 1998–1999 and 2008, similar to the declines
seen in rates of penicillin-nonsusceptible IPD (Figure 2),
especially in children aged ,5 years.
Incidence Rates by SerotypeTo assess the impact of PCV7 and the possible future impact of
PCV13, we stratified penicillin-nonsusceptible IPD rates by se-
rotype. The rate of penicillin-nonsusceptible disease caused by
serotypes in PCV7 dropped substantially among all age groups
between 1998–1999 and 2008 (Table 1), especially among young
children and older adults. In contrast, the rate of penicillin-
nonsusceptible IPD from serotypes not in PCV7 increased for
all age groups. In each age group, these absolute rate increases
were larger under the new parenteral breakpoints for the ad-
ditional serotypes in PCV13 than for the serotypes not included
in PCV13 despite substantial decreases in the rate of penicillin-
nonsusceptible IPD caused by serotype 6A, one of the additional
serotypes in PCV13. Almost all of the increase in penicillin-
nonsusceptible IPD caused by the additional PCV13 serotypes
during 1998–2008 was due to serotype 19A (Table 1).
The increase in penicillin-nonsusceptible IPD from serotype
19A resulted from both an increase in the incidence of IPD from
serotype 19A [2] and an increase in the proportion of serotype
19A that was penicillin-nonsusceptible. Depending on age, the
proportion of serotype 19A IPD that was not susceptible to
penicillin increased from 0%–7% in 1998–1999 to 20%–53%
in 2008 under the new parenteral breakpoints, and went
from 52%–71% to 50%–77% under the old/oral/meningitis
breakpoints. We observed generally similar trends among
other serotypes, such as serotypes 6C, 15A, 23A, and 35B
(data not shown), which had smaller increases in their rates
of penicillin-nonsusceptible IPD than serotype 19A.
Association Between Penicillin Nonsusceptibility and SerotypeBy 2007–2008, the proportion of penicillin-nonsusceptible IPD
cases caused by serotypes in PCV7 had fallen dramatically in all
age groups (Table 2). In contrast, in 2007–2008, the additional
PCV13 serotypes caused $77.8% of penicillin-nonsusceptible
IPD cases among all groups under the new parenteral breakpoints
and 42.5%–78.5% under the old/oral/meningitis breakpoints,
depending on age (Table 2). Serotype 19A alone accounted for
82.0% of all penicillin-nonsusceptible IPD for all ages com-
bined under the new parenteral breakpoints, and 52.1% of all
cases under the old/oral/meningitis breakpoints in 2007–2008.
Unlike the additional PCV13 serotypes, in 2007–2008, the se-
rotypes not included in PCV13 caused a lower proportion of
cases (3.1%–15.6%) in the different age groups under the new
parenteral breakpoints than the 16.0%–49.0% of cases they
caused under the old/oral/meningitis breakpoints.
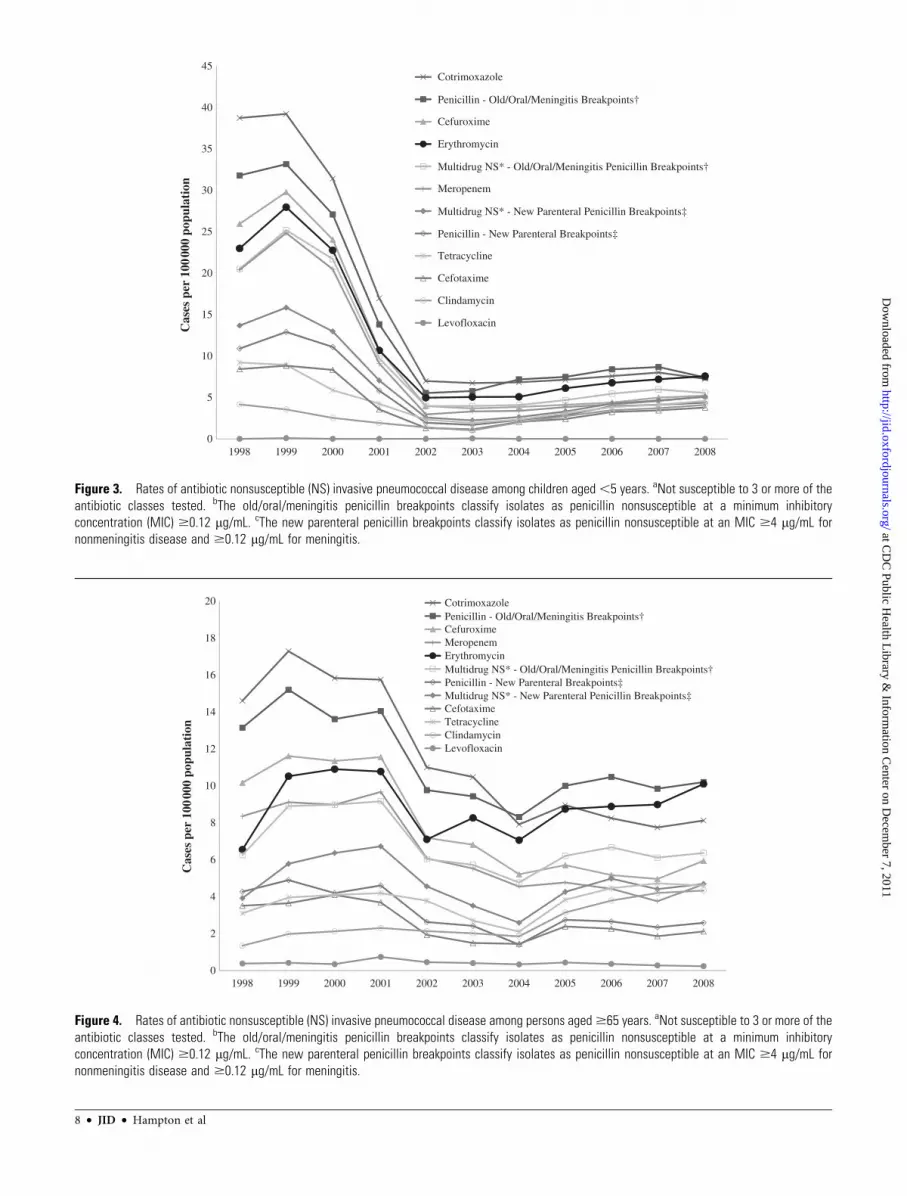
Nonsusceptibility to Other AntibioticsRates of IPD caused by strains not susceptible to antibiotics
other than penicillin dropped after 1999 in children aged
,5 years (Figure 3) and after 2001 in adults aged $65 years
(Figure 4). Despite increases in rates of nonsusceptible IPD that
were evident by 2003–2004 in children aged ,5 years and in
Prevention of S. pneumoniae With Conjugate Vaccines d JID d 3
at CD
C Public H
ealth Library &
Information C
enter on Decem
ber 7, 2011http://jid.oxfordjournals.org/
Dow
nloaded from
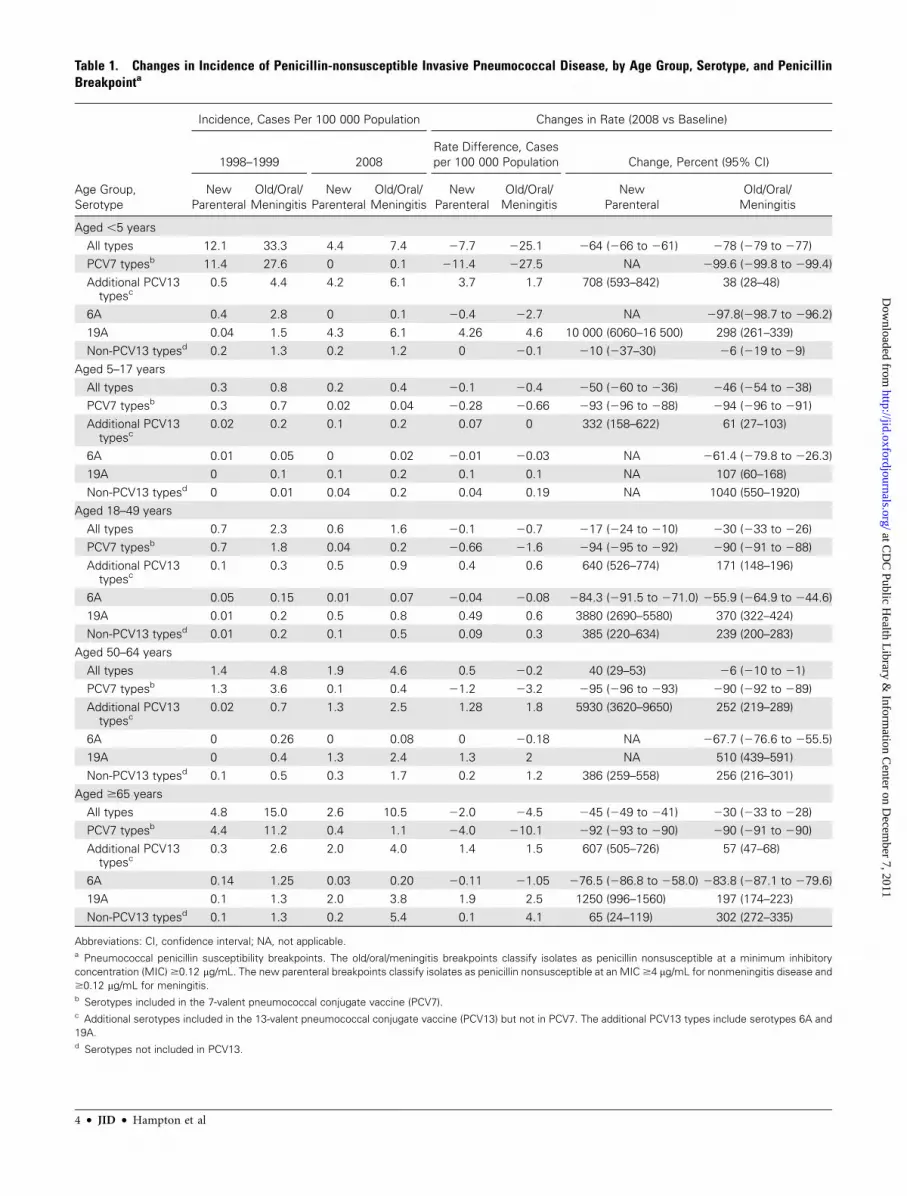
Table 1. Changes in Incidence of Penicillin-nonsusceptible Invasive Pneumococcal Disease, by Age Group, Serotype, and PenicillinBreakpointa
Age Group,
Serotype
Incidence, Cases Per 100 000 Population Changes in Rate (2008 vs Baseline)
1998–1999 2008
Rate Difference, Cases
per 100 000 Population Change, Percent (95% CI)
New
Parenteral
Old/Oral/
Meningitis
New
Parenteral
Old/Oral/
Meningitis
New
Parenteral
Old/Oral/
Meningitis
New
Parenteral
Old/Oral/
Meningitis
Aged ,5 years
All types 12.1 33.3 4.4 7.4 27.7 225.1 264 (266 to 261) 278 (279 to 277)
PCV7 typesb 11.4 27.6 0 0.1 211.4 227.5 NA 299.6 (299.8 to 299.4)
Additional PCV13typesc
0.5 4.4 4.2 6.1 3.7 1.7 708 (593–842) 38 (28–48)
6A 0.4 2.8 0 0.1 20.4 22.7 NA 297.8(298.7 to 296.2)
19A 0.04 1.5 4.3 6.1 4.26 4.6 10 000 (6060–16 500) 298 (261–339)
Non-PCV13 typesd 0.2 1.3 0.2 1.2 0 20.1 210 (237–30) 26 (219 to 29)
Aged 5–17 years
All types 0.3 0.8 0.2 0.4 20.1 20.4 250 (260 to 236) 246 (254 to 238)
PCV7 typesb 0.3 0.7 0.02 0.04 20.28 20.66 293 (296 to 288) 294 (296 to 291)
Additional PCV13typesc
0.02 0.2 0.1 0.2 0.07 0 332 (158–622) 61 (27–103)
6A 0.01 0.05 0 0.02 20.01 20.03 NA 261.4 (279.8 to 226.3)
19A 0 0.1 0.1 0.2 0.1 0.1 NA 107 (60–168)
Non-PCV13 typesd 0 0.01 0.04 0.2 0.04 0.19 NA 1040 (550–1920)
Aged 18–49 years
All types 0.7 2.3 0.6 1.6 20.1 20.7 217 (224 to 210) 230 (233 to 226)
PCV7 typesb 0.7 1.8 0.04 0.2 20.66 21.6 294 (295 to 292) 290 (291 to 288)
Additional PCV13typesc
0.1 0.3 0.5 0.9 0.4 0.6 640 (526–774) 171 (148–196)
6A 0.05 0.15 0.01 0.07 20.04 20.08 284.3 (291.5 to 271.0) 255.9 (264.9 to 244.6)
19A 0.01 0.2 0.5 0.8 0.49 0.6 3880 (2690–5580) 370 (322–424)
Non-PCV13 typesd 0.01 0.2 0.1 0.5 0.09 0.3 385 (220–634) 239 (200–283)
Aged 50–64 years
All types 1.4 4.8 1.9 4.6 0.5 20.2 40 (29–53) 26 (210 to 21)
PCV7 typesb 1.3 3.6 0.1 0.4 21.2 23.2 295 (296 to 293) 290 (292 to 289)
Additional PCV13typesc
0.02 0.7 1.3 2.5 1.28 1.8 5930 (3620–9650) 252 (219–289)
6A 0 0.26 0 0.08 0 20.18 NA 267.7 (276.6 to 255.5)
19A 0 0.4 1.3 2.4 1.3 2 NA 510 (439–591)
Non-PCV13 typesd 0.1 0.5 0.3 1.7 0.2 1.2 386 (259–558) 256 (216–301)
Aged $65 years
All types 4.8 15.0 2.6 10.5 22.0 24.5 245 (249 to 241) 230 (233 to 228)
PCV7 typesb 4.4 11.2 0.4 1.1 24.0 210.1 292 (293 to 290) 290 (291 to 290)
Additional PCV13typesc
0.3 2.6 2.0 4.0 1.4 1.5 607 (505–726) 57 (47–68)
6A 0.14 1.25 0.03 0.20 20.11 21.05 276.5 (286.8 to 258.0) 283.8 (287.1 to 279.6)
19A 0.1 1.3 2.0 3.8 1.9 2.5 1250 (996–1560) 197 (174–223)
Non-PCV13 typesd 0.1 1.3 0.2 5.4 0.1 4.1 65 (24–119) 302 (272–335)
Abbreviations: CI, confidence interval; NA, not applicable.a Pneumococcal penicillin susceptibility breakpoints. The old/oral/meningitis breakpoints classify isolates as penicillin nonsusceptible at a minimum inhibitory
concentration (MIC) $0.12 lg/mL. The new parenteral breakpoints classify isolates as penicillin nonsusceptible at an MIC $4 lg/mL for nonmeningitis disease and
$0.12 lg/mL for meningitis.b Serotypes included in the 7-valent pneumococcal conjugate vaccine (PCV7).c Additional serotypes included in the 13-valent pneumococcal conjugate vaccine (PCV13) but not in PCV7. The additional PCV13 types include serotypes 6A and
19A.d Serotypes not included in PCV13.
4 d JID d Hampton et al
at CD
C Public H
ealth Library &
Information C
enter on Decem
ber 7, 2011http://jid.oxfordjournals.org/
Dow
nloaded from

2005 in adults aged$65 years, the 2008 rates of nonsusceptible
IPD were below the 1999–2001 rates for almost all antibiotics
tested in both age groups (Figures 3 and 4) as well as in youth
aged 5–17 years (data not shown). The 2008 rates of non-
susceptible IPD were less than the 1999–2001 rates for most
antibiotics tested in adults aged 18–49 years but were higher
than the 1999–2001 rates for all antibiotics tested in adults
aged 50–64 years (data not shown). Rates of multidrug-
nonsusceptible IPD, which were lower under the new parenteral
breakpoints than under the old ones, were less in 2008 than in
1999–2001 under all breakpoints among all age groups except
adults aged 50–64 years. In contrast to these general trends,
all isolates were fully susceptible to vancomycin, rates of
levofloxacin-nonsusceptible IPD remained very low for all age
groups between 1998 and 2008, and the 2008 rates of
clindamycin-nonsusceptible IPD among all age groups aged
$5 years were higher than the 2001 rates.
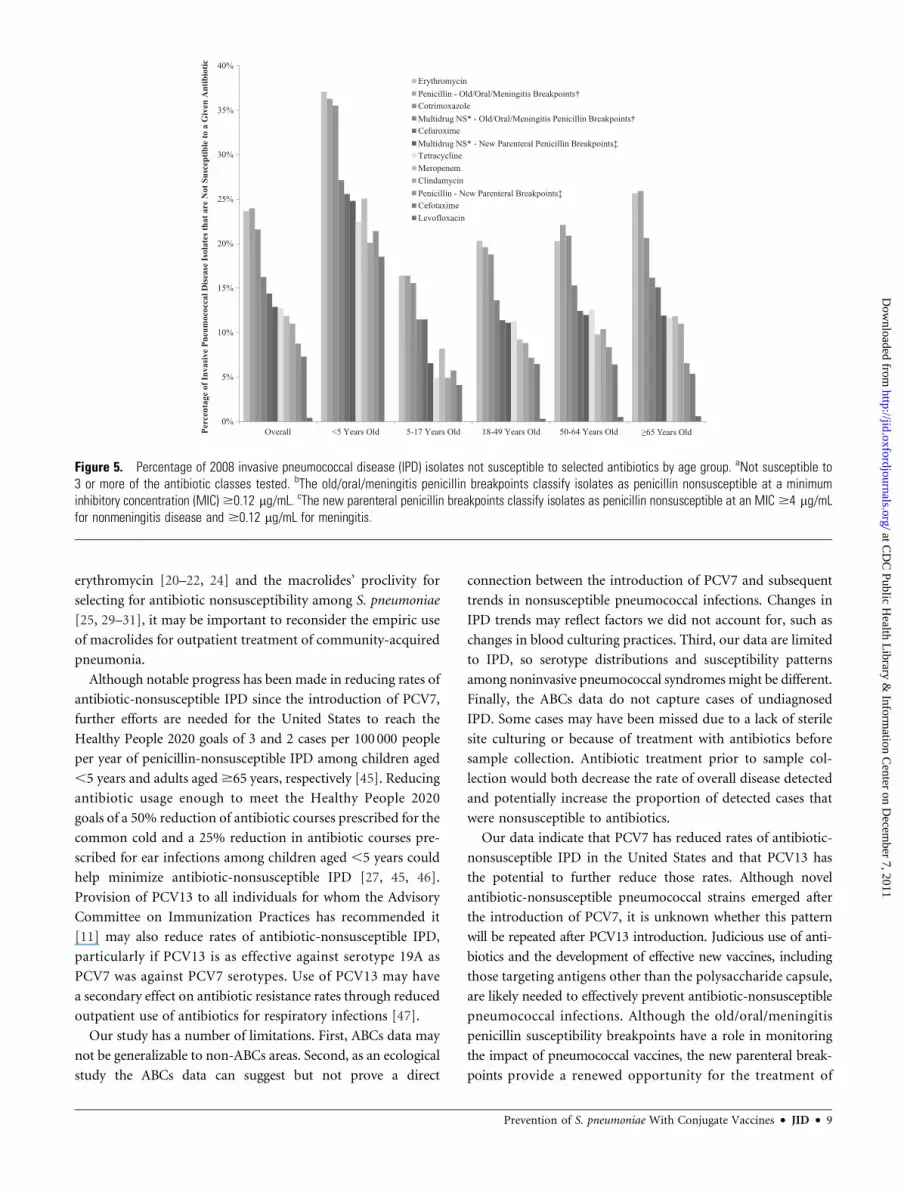
Regardless of the choice of penicillin breakpoints, 2008 IPD
isolates were most likely to be susceptible to vancomycin,
levofloxacin, and cefotaxime (Figure 5). Under the old/oral/
meningitis breakpoints, isolates were most likely to be non-
susceptible to erythromycin and penicillin, but under the new
parenteral breakpoints, isolates were more likely to be non-
susceptible to erythromycin, cotrimoxazole, cefuroxime, and
meropenem than to penicillin. Isolates were most likely to be
nonsusceptible to erythromycin under the new parenteral
breakpoints for all age groups except adults aged 50–64 years.
DISCUSSION
Regardless of whether the old/oral/meningitis or new paren-
teral penicillin susceptibility breakpoints are used, penicillin-
nonsusceptible IPD caused by PCV7 serotypes has decreased
significantly for all age groups and has almost disappeared except
A All Ages
0
1
2
3
4
5
6
7
1998 2000 2002 2004 2006 2008
Cas
es p
er 1
00 0
00 p
opul
atio
n NS IPD Old/Oral/MeningitisBreakpoints
NS IPD New ParenteralBreakpoints
B Children <5 Years Old
0
5
10
15
20
25
30
35
1998 2000 2002 2004 2006 2008
Cas
es p
er 1
00 0
00 p
opul
atio
n
NS IPD Old/Oral/MeningitisBreakpoints
NS IPD New ParenteralBreakpoints
C Children 5–17 Years Old
0
1
2
3
4
5
6
7
1998 2000 2002 2004 2006 2008
Cas
es p
er 1
00 0
00 p
opul
atio
n
NS IPD Old/Oral/Meningitis Breakpoints
NS IPD New Parenteral Breakpoints
D Individuals 18–49 Years Old
0
1
2
3
4
5
6
7
1998 2000 2002 2004 2006 2008
Cas
es p
er 1
00 0
00 p
opul
atio
n
NS IPD Old/Oral/Meningitis Breakpoints
NS IPD New Parenteral Breakpoints
E Adults 50–64 Years Old
0
1
2
3
4
5
6
7
1998 2000 2002 2004 2006 2008
Cas
es p
er 1
00 0
00 p
opul
atio
n NS IPD Old/Oral/Meningitis Breakpoints
NS IPD New Parenteral Breakpoints
F Adults 65 Years Old
0
2
4
6
8
10
12
14
16
1998 2000 2002 2004 2006 2008
Cas
es p
er 1
00 0
00 p
opul
atio
n NS IPD Old/Oral/MeningitisBreakpoints
NS IPD New ParenteralBreakpoints
Figure 1. Penicillin-nonsusceptible (NS) invasive pneumococcal disease (IPD) rates using old/oral/meningitis and new parenteral breakpoints for allages (A), children aged,5 years (B ), children aged 5–17 years (C ), adults aged 18–49 years (D ), adults aged 50–64 years (E ), and adults aged$65 years(E ). The old/oral/meningitis penicillin breakpoints classify isolates as penicillin nonsusceptible at a minimum inhibitory concentration (MIC) $0.12 lg/mL.The new parenteral penicillin breakpoints classify isolates as penicillin nonsusceptible at an MIC$4 lg/mL for nonmeningitis disease and$0.12 lg/mL formeningitis.
Prevention of S. pneumoniae With Conjugate Vaccines d JID d 5
at CD
C Public H
ealth Library &
Information C
enter on Decem
ber 7, 2011http://jid.oxfordjournals.org/
Dow
nloaded from

among adults aged$65 years. Rates of penicillin-nonsusceptible
IPD remain markedly below the rates that existed before PCV7
introduction for all age groups except adults aged 50–64 year
under the new parenteral breakpoints. These findings highlight
the dramatic herd effects of PCV7 resulting from decreased
nasopharyngeal colonization of children and, subsequently,
decreased transmission from children to older persons of sero-
types in PCV7 [2]. The incidence of IPD caused by strains not
susceptible to antibiotics besides penicillin also generally re-
mains below pre-PCV7 levels for all age groups except adults
aged 50–64 years. The serotypes included in PCV13 accounted
for the majority of penicillin-nonsusceptible disease in 2008
($78% depending on age under the new parenteral break-
points). Our results are consistent with trends in nonsusceptible
IPD seen elsewhere in the United States [20–24].
Despite continued use of PCV7, rates of penicillin-
nonsusceptible IPD have been gradually increasing since
2002–2004, largely because of higher rates of IPD caused by
serotype 19A and increases in the proportion of serotype 19A
IPD that is penicillin nonsusceptible. The rise of penicillin-
nonsusceptible 19A may be due, in part, to continued selective
pressure from antibiotic use among children and transmission
to adults [25–28]. Azalides such as azithromycin may be
particularly effective in selecting for nonsusceptible strains
[25, 29–31]. Even countries that have not introduced PCV7
have observed increases in the proportion of pneumococcal
carriers colonized by serotype 19A coinciding with extensive
antibiotic use [30]. However, it is also possible that the major
emergent clonal complex 320, which causes the majority of
penicillin-nonsusceptible 19A IPD in the United States [16],
has additional advantageous traits that have contributed to
the increased proportion of pneumococcal carriage and IPD
attributable to serotype 19A. Other serotype 19A clonal com-
plexes in the Netherlands have replaced the serotypes pre-
viously associated with nasopharyngeal colonization among
young children, despite being generally susceptible to anti-
biotics [32]. The ability of serotype 19A to cause both in-
vasive disease [33–37] and nasopharyngeal carriage [33, 37]
may also have played a role in the rise of 19A.
The new parenteral CLSI penicillin pneumococcal susceptibility
breakpoints offer an opportunity to increase use of penicillin,
which may reduce antimicrobial costs, decrease risk of
healthcare-associated infections, and possibly forestall re-
sistance to broader-spectrum antibiotics [5]. The CLSI changed
the breakpoints for nonmeningitis pneumococcal disease in
2008 because recent data indicated that parenteral penicillin
could be effective even if isolates had MICs above the old/oral/
meningitis breakpoints [14]. In our study, under the new par-
enteral CLSI breakpoints the probability that a pneumococcus
from an individual with IPD in an ABCs area was susceptible
to parenteral penicillin was comparable to the probability that
it was susceptible to carbapenems, cephalosporins, and other
b-lactams and higher than the probability that it was susceptible
to macrolides or cotrimoxazole. Whether the use of parenteral
penicillin increases as a result of this change in breakpoints
remains to be seen.
Clinicians and surveillance staff need to be aware of the effects
on apparent penicillin susceptibility of applying the old/oral/
meningitis breakpoints versus the new parenteral breakpoints
because the incidence of penicillin nonsusceptible IPD is much
lower with the new parenteral CLSI breakpoints [12]. Although
the new breakpoints are more appropriate for guiding parenteral
treatment of nonmeningitis pneumococcal disease, the old/oral/
meningitis breakpoints are still useful in monitoring emerging
pneumococcal antibiotic resistance. The old/oral/meningitis
breakpoints are more suitable for identifying strains with MICs
between 0.12 and 1 lg/mL that perhaps have more potential to
accumulate additional penicillin-binding protein gene mutations
that could lead to full penicillin resistance [38, 39]. For example,
the proportion of penicillin-nonsusceptible IPD caused by se-
rotypes not included in PCV13 is more prominent under the
old breakpoints because many isolates from these serotypes
were classified as intermediate under the old breakpoints but
susceptible under the new breakpoints. In addition, the break-
points recommended for choosing oral treatment are unchanged
from the ones used prior to the 2008 revision of the CLSI
standards for antibiotic susceptibility [29]. The relatively high
proportions of IPD isolates not susceptible to cotrimoxazole
and cefuroxime support the recommendations for choosing
other agents as first-line empiric therapy for diseases that can be
caused by pneumococcus [40–43], recommendations that have
contributed to declines in outpatient use of sulfonamides and
cephalosporins for acute respiratory tract infections [44]. Given
the even higher proportions of IPD isolates not susceptible to
0
2
4
6
8
10
12
14
16
18
0.03 0.06 0.12 0.25 0.5 1 2 4 8 16
Cas
es p
er 1
00,0
00 p
opul
atio
n
Minimum Inhibitory Concentration (MIC) Value
1998-1999 2008
Susceptible Intermediate Resistant
Susceptible Resistant
Intermediate
Susceptible Resistant
Old/Oral Penicillin
Parenteral Penicillin, Non-meningitis
Parenteral Penicillin, Meningitis
Figure 2. Rates of 1998–1999 and 2008 invasive pneumococcal diseasecases among all ages by minimum inhibitory concentration (MIC) andpenicillin breakpoints.
6 d JID d Hampton et al
at CD
C Public H
ealth Library &
Information C
enter on Decem
ber 7, 2011http://jid.oxfordjournals.org/
Dow
nloaded from

Table 2. Proportion of Penicillin-Nonsusceptible Strains by Age Group, Year, Penicillin Susceptibility Breakpoints,a and Serotype
Vaccine
Serotype
and
Formulation
Aged ,5 Years Aged 5–64 Years Aged .65 Years Old
1998–1999 2007–2008 1998–1999 2007–2008 1998–1999 2007–2008
New
Parenteral
(n 5 259)
Old/Oral/
Meningitis
(n 5 703)
New
Parenteral
(n 5 161)
Old/Oral/
Meningitis
(n 5 307)
New
Parenteral
(n 5 183)
Old/Oral/
Meningitis
(n 5 597)
New
Parenteral
(n 5 275)
Old/Oral/
Meningitis
(n 5 822)
New
Parenteral
(n 5 167)
Old/Oral/
Meningitis
(n 5 516)
New
Parenteral
(n 5 144)
Old/Oral/
Meningitis
(n 5 588)
14 49.4% 38.1% 0.0% 0.3% 32.2% 21.6% 1.8% 1.3% 39.5% 23.1% 4.2% 1.4%
19F 12.7% 12.1% 0.0% 0.3% 7.7% 5.5% 1.8% 0.9% 6.0% 4.3% 4.2% 1.4%
06B 8.9% 11.9% 0.0% 0.3% 4.9% 9.0% 0.0% 2.1% 4.2% 11.2% 2.1% 2.7%
18C 0.0% 0.6% 0.0% 0.0% 0.0% 0.3% 0.0% 0.0% 0.6% 0.4% 0.0% 0.0%
23F 17.4% 10.7% 0.0% 0.0% 21.3% 13.9% 1.1% 1.0% 23.4% 12.8% 0.7% 0.7%
4 0.4% 0.1% 0.0% 0.0% 0.5% 1.3% 0.0% 0.0% 0.0% 0.8% 0.0% 0.0%
09V 4.6% 9.1% 0.0% 0.0% 23.5% 26.1% 1.8% 4.1% 17.4% 22.1% 0.0% 2.4%
PCV7b 93.4% 82.6% 0.0% 1.0% 90.2% 77.9% 6.5% 9.4% 91.0% 74.6% 11.1% 8.5%
1 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
07F 0.0% 0.0% 0.0% 0.3% 0.0% 0.0% 0.0% 0.2% 0.0% 0.2% 0.0% 0.0%
5 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
3 0.4% 0.3% 0.0% 0.0% 1.1% 0.5% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
06A 3.9% 8.5% 0.0% 0.7% 4.4% 5.9% 0.4% 3.5% 3.0% 8.3% 2.1% 4.1%
19A 0.4% 4.6% 96.9% 82.1% 1.1% 8.0% 77.5% 51.0% 3.0% 8.5% 76.4% 38.4%
AdditionalPCV13c
4.6% 13.4% 96.9% 83.1% 6.6% 14.4% 77.8% 54.7% 6.0% 17.1% 78.5% 42.5%
06C 0.0% 0.0% 0.6% 1.3% 0.0% 0.2% 1.5% 5.6% 0.0% 0.4% 1.4% 8.0%
09A 1.5% 2.1% 0.0% 0.0% 1.6% 3.2% 0.0% 0.1% 0.0% 2.5% 0.0% 0.2%
15A 0.0% 0.0% 0.0% 4.2% 0.0% 0.0% 2.5% 10.7% 0.0% 0.4% 2.8% 12.8%
22F 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
23A 0.4% 0.4% 0.6% 2.0% 0.5% 0.3% 4.0% 7.8% 0.6% 0.4% 4.2% 12.9%
23B 0.0% 0.0% 0.0% 1.6% 0.0% 0.0% 2.2% 1.7% 0.0% 0.0% 0.0% 0.5%
35B 0.0% 0.6% 1.2% 4.9% 0.0% 1.2% 3.3% 6.9% 1.8% 2.5% 1.4% 12.6%
NT 0.0% 0.1% 0.0% 0.3% 0.0% 0.3% 0.4% 0.4% 0.0% 0.4% 0.0% 0.3%
Other 0.0% 0.8% 0.7% 1.7% 1.2% 2.5% 1.7% 2.6% 0.6% 1.8% 0.6% 1.7%
Non-PCV13d 1.9% 4.0% 3.1% 16.0% 3.3% 7.7% 15.6% 35.8% 3.0% 8.4% 10.4% 49.0%
a Pneumococcal penicillin susceptibility breakpoints. The old/oral/meningitis breakpoints classify isolates as penicillin nonsusceptible at a minimum inhibitory concentration (MIC) $0.12 lg/mL. The new parenteral
breakpoints classify isolates as penicillin nonsusceptible at an MIC $4 lg/mL for nonmeningitis disease and $0.12 lg/mL for meningitis.b Serotypes included in the 7-valent pneumococcal conjugate vaccine (PCV7).c Additional serotypes included in the 13-valent pneumococcal conjugate vaccine (PCV13) but not in PCV7. The additional PCV13 types include serotype 19A.d Serotypes not included in PCV13.
Preven
tionofS.
pneumoniae
With
Conjugate
Vaccin
esdJID
d7
at CDC Public Health Library & Information Center on December 7, 2011 http://jid.oxfordjournals.org/ Downloaded from
0
2
4
6
8
10
12
14
16
18
20
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Cas
es p
er 1
0000
0 po
pula
tion
CotrimoxazolePenicillin - Old/Oral/Meningitis Breakpoints†CefuroximeMeropenemErythromycinMultidrug NS* - Old/Oral/Meningitis Penicillin Breakpoints†Penicillin - New Parenteral Breakpoints‡Multidrug NS* - New Parenteral Penicillin Breakpoints‡CefotaximeTetracyclineClindamycinLevofloxacin
Figure 4. Rates of antibiotic nonsusceptible (NS) invasive pneumococcal disease among persons aged$65 years. aNot susceptible to 3 or more of theantibiotic classes tested. bThe old/oral/meningitis penicillin breakpoints classify isolates as penicillin nonsusceptible at a minimum inhibitoryconcentration (MIC) $0.12 lg/mL. cThe new parenteral penicillin breakpoints classify isolates as penicillin nonsusceptible at an MIC $4 lg/mL fornonmeningitis disease and $0.12 lg/mL for meningitis.
0
5
10
15
20
25
30
35
40
45
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Cas
es p
er 1
0000
0 po
pula
tion
Cotrimoxazole
Penicillin - Old/Oral/Meningitis Breakpoints†
Cefuroxime
Erythromycin
Multidrug NS* - Old/Oral/Meningitis Penicillin Breakpoints†
Meropenem
Multidrug NS* - New Parenteral Penicillin Breakpoints‡
Penicillin - New Parenteral Breakpoints‡
Tetracycline
Cefotaxime
Clindamycin
Levofloxacin
Figure 3. Rates of antibiotic nonsusceptible (NS) invasive pneumococcal disease among children aged,5 years. aNot susceptible to 3 or more of theantibiotic classes tested. bThe old/oral/meningitis penicillin breakpoints classify isolates as penicillin nonsusceptible at a minimum inhibitoryconcentration (MIC) $0.12 lg/mL. cThe new parenteral penicillin breakpoints classify isolates as penicillin nonsusceptible at an MIC $4 lg/mL fornonmeningitis disease and $0.12 lg/mL for meningitis.
8 d JID d Hampton et al
at CD
C Public H
ealth Library &
Information C
enter on Decem
ber 7, 2011http://jid.oxfordjournals.org/
Dow
nloaded from
erythromycin [20–22, 24] and the macrolides’ proclivity for
selecting for antibiotic nonsusceptibility among S. pneumoniae
[25, 29–31], it may be important to reconsider the empiric use
of macrolides for outpatient treatment of community-acquired
pneumonia.
Although notable progress has been made in reducing rates of
antibiotic-nonsusceptible IPD since the introduction of PCV7,
further efforts are needed for the United States to reach the
Healthy People 2020 goals of 3 and 2 cases per 100000 people
per year of penicillin-nonsusceptible IPD among children aged
,5 years and adults aged$65 years, respectively [45]. Reducing
antibiotic usage enough to meet the Healthy People 2020
goals of a 50% reduction of antibiotic courses prescribed for the
common cold and a 25% reduction in antibiotic courses pre-
scribed for ear infections among children aged ,5 years could
help minimize antibiotic-nonsusceptible IPD [27, 45, 46].
Provision of PCV13 to all individuals for whom the Advisory
Committee on Immunization Practices has recommended it
[11] may also reduce rates of antibiotic-nonsusceptible IPD,
particularly if PCV13 is as effective against serotype 19A as
PCV7 was against PCV7 serotypes. Use of PCV13 may have
a secondary effect on antibiotic resistance rates through reduced
outpatient use of antibiotics for respiratory infections [47].
Our study has a number of limitations. First, ABCs data may
not be generalizable to non-ABCs areas. Second, as an ecological
study the ABCs data can suggest but not prove a direct
connection between the introduction of PCV7 and subsequent
trends in nonsusceptible pneumococcal infections. Changes in
IPD trends may reflect factors we did not account for, such as
changes in blood culturing practices. Third, our data are limited
to IPD, so serotype distributions and susceptibility patterns
among noninvasive pneumococcal syndromes might be different.
Finally, the ABCs data do not capture cases of undiagnosed
IPD. Some cases may have been missed due to a lack of sterile
site culturing or because of treatment with antibiotics before
sample collection. Antibiotic treatment prior to sample col-
lection would both decrease the rate of overall disease detected
and potentially increase the proportion of detected cases that
were nonsusceptible to antibiotics.
Our data indicate that PCV7 has reduced rates of antibiotic-
nonsusceptible IPD in the United States and that PCV13 has
the potential to further reduce those rates. Although novel
antibiotic-nonsusceptible pneumococcal strains emerged after
the introduction of PCV7, it is unknown whether this pattern
will be repeated after PCV13 introduction. Judicious use of anti-
biotics and the development of effective new vaccines, including
those targeting antigens other than the polysaccharide capsule,
are likely needed to effectively prevent antibiotic-nonsusceptible
pneumococcal infections. Although the old/oral/meningitis
penicillin susceptibility breakpoints have a role in monitoring
the impact of pneumococcal vaccines, the new parenteral break-
points provide a renewed opportunity for the treatment of
Figure 5. Percentage of 2008 invasive pneumococcal disease (IPD) isolates not susceptible to selected antibiotics by age group. aNot susceptible to3 or more of the antibiotic classes tested. bThe old/oral/meningitis penicillin breakpoints classify isolates as penicillin nonsusceptible at a minimuminhibitory concentration (MIC) $0.12 lg/mL. cThe new parenteral penicillin breakpoints classify isolates as penicillin nonsusceptible at an MIC $4 lg/mLfor nonmeningitis disease and $0.12 lg/mL for meningitis.
Prevention of S. pneumoniae With Conjugate Vaccines d JID d 9
at CD
C Public H
ealth Library &
Information C
enter on Decem
ber 7, 2011http://jid.oxfordjournals.org/
Dow
nloaded from

nonmeningitis pneumococcal infections with a safe, effective,
and narrow-spectrum antibiotic.
Notes
Acknowledgments. We thank the following members of the Active
Bacterial Core surveillance/Emerging Infections Program Network for
their assistance with this project:
California Emerging Infections Program: Mirasol Apostol, Susan
Brooks, Pam Daily Kirley, Joelle Nadle, and Lauren Pasutti.
Colorado Emerging Infections Program: Deborah Aragon.
Connecticut Emerging Infections Program: Zack Fraser and James L.
Hadler.
Georgia Emerging Infections Program: Wendy Baughman, Amy Holst,
and Stephanie Thomas.
Maryland Emerging Infections Program: Kim D. Holmes, Rosemary
Hollick, and Kathleen Shutt.
Minnesota Emerging Infections Program: Brenda Jewell, Billie Ann
Juni, Catherine Lexau, Lindsey Lesher, and Lori Triden.
New Mexico Emerging Infections Program: Kathy Angeles, Joseph
Bareta, Lisa Butler, Sarah Khanlian, Robert Mansmann, andMegin Nichols.
New York Emerging Infections Program: Geetha Nattanmai, Glenda
Smith, Suzanne Solghan, and Nancy Spina.
Oregon Emerging Infections Program: Karen Stefonek.
Tennessee Emerging Infections Program: Brenda G. Barnes and Terry
McMinn.
University of Texas Health Sciences Center, San Antonio: Letitia C.
Fulcher, M. Leticia McElmeel, and Christa Trippy.
CDC: Felicita David, Melissa Lewis, Tamara Pilishvili, Karrie-Ann
Toews, Chris Van Beneden, Carolyn Wright, and the entire staff of the CDC
Streptococcus laboratory.
Financial support. This work was supported by the Emerging In-
fections Programs and the Office of Antimicrobial Resistance of the Centers
for Disease Control and Prevention. The Centers for Disease Control and
Prevention’s Emerging Infections Programs provided funding but made no
other contributions to the design and conduct of this study; the collection,
management, analysis, and interpretation of the data; or the preparation,
review, or approval of this manuscript.
Potential conflicts of interest. W. S. has served as a consultant to Pfizer,
Novartis, GSK, Sanofi-Pasteur, and Dynavex, and is a member of Data
Safety Monitoring Boards for Merck. L. H. H. has served as a consultant to
and received lecture fees from Merck and Pfizer. J. H. J. has been a member
of advisory boards for BD Microbiology Systems and for Rib-X Pharma-
ceuticals and has received research funding from BD, bioMerieux, Merck,
Pfizer, and Siemens Healthcare. E. Z. owns stock in Pfizer, Merck, and
Johnson and Johnson. All other authors report no potential conflicts.
All authors have submitted the ICMJE Form for Disclosure of Potential
Conflicts of Interest. Conflicts that the editors consider relevant to the
content of the manuscript have been disclosed.
References
1. Robinson KA, BaughmanW, Rothrock G, et al. Epidemiology of invasive
Streptococcus pneumoniae infections in the United States, 1995–1998:
opportunities for prevention in the conjugate vaccine era. JAMA 2001;
285:1729–35.
2. Pilishvili T, Lexau C, Farley MM, et al. Sustained reductions in invasive
pneumococcal disease in the era of conjugate vaccine. J Infect Dis 2010;
201:32–41.
3. CDC. Active Bacterial Core surveillance report, Emerging Infections
Program Network, Streptococcus pneumoniae, 2008. 2009. http://www.
cdc.gov/abcs/reports-findings/survreports/spneu08.html. Accessed 29
November 2011.
4. van der Poll T, Opal SM. Pathogenesis, treatment, and prevention of
pneumococcal pneumonia. Lancet 2009; 374:1543–56.
5. Dellit TH, Owens RC, McGowan JE, et al. Infectious Diseases Society
of America and the Society for Healthcare Epidemiology of America
guidelines for developing an institutional program to enhance anti-
microbial stewardship. Clin Infect Dis 2007; 44:159–77.
6. Smolinski MS, Hamburg MA, Lederberg J, eds. Microbial threats to
health: emergence, detection, and response. Washington, DC: National
Academies Press, 2003.
7. Whitney CG, Farley MM, Hadler J, et al. Increasing prevalence
of multidrug-resistant Streptococcus pneumoniae in the United States.
N Engl J Med 2000; 343:1917–24.
8. Kyaw MH, Lynfield R, Schaffner W, et al. Effect of introduction of the
pneumococcal conjugate vaccine on drug-resistant Streptococcus
pneumoniae. N Engl J Med 2006; 354:1455–63.
9. Whitney CG, Farley MM, Hadler J, et al. Decline in invasive pneu-
mococcal disease after the introduction of protein-polysaccharide
conjugate vaccine. N Engl J Med 2003; 348:1737–46.
10. Hicks LA, Harrison LH, Flannery B, et al. Incidence of pneumococcal
disease due to non-pneumococcal conjugate vaccine (PCV7) serotypes
in the United States during the era of widespread PCV7 vaccination,
1998–2004. J Infect Dis 2007; 196:1346–54.
11. CDC. Licensure of a 13-valent pneumococcal conjugate vaccine (PCV13)
and recommendations for use among childrendAdvisory Committee
on Immunization Practices (ACIP), 2010. MMWR Morb Mortal Wkly
Rep 2010; 59:258–61.
12. CDC. Effects of new penicillin susceptibility breakpoints for Streptococcus
pneumoniaedUnited States, 2006–2007. MMWR Morb Mortal Wkly
Rep 2008; 57:1353–5.
13. Clinical and Laboratory Standards Institute. Performance standards for
antimicrobial susceptibility testing; eighteenth informational supple-
ment. CLSI document M100–S18. Wayne, PA: Clinical and Laboratory
Standards Institute, 2008.
14. Weinstein MP, Klugman KP, Jones RN. Rationale for revised penicillin
susceptibility breakpoints versus Streptococcus pneumoniae: coping
with antimicrobial susceptibility in an era of resistance. Clin Infect Dis
2009; 48:1596–600.
15. Schuchat A, Hilger T, Zell ER, et al. Active bacterial core surveillance
of the emerging infections program network. Emerg Infect Dis 2001; 7:
92–9.
16. Moore MR, Gertz RE, Woodbury RL, et al. Population snapshot of
emergent Streptococcus pneumoniae serotype 19A in the United States,
2005. J Infect Dis 2008; 197:1016–27.
17. Park IH, Pritchard DG, Cartee R, Brandao A, Brandileone MC,
NahmMH. Discovery of a new capsular serotype (6C) within serogroup 6
of Streptococcus pneumoniae. J Clin Microbiol 2007; 45:1225–33.
18. Park IH, Moore MR, Treanor JJ, et al. Differential effects of pneu-
mococcal vaccines against serotypes 6A and 6C. J Infect Dis 2008;
198:1818–22.
19. Carvalho Mda G, Pimenta FC, Gertz RE, et al. PCR-based quantitation
and clonal diversity of the current prevalent invasive serogroup
6 pneumococcal serotype, 6C, in the United States in 1999 and 2006 to
2007. J Clin Microbiol 2009; 47:554–9.
20. Kaplan SL, Barson WJ, Lin PL, et al. Serotype 19A is the most com-
mon serotype causing invasive pneumococcal infections in children.
Pediatrics 2010; 125:429–36.
21. Farrell DJ, Klugman KP, PichicheroM. Increased antimicrobial resistance
among nonvaccine serotypes of Streptococcus pneumoniae in the pediatric
population after the introduction of 7-valent pneumococcal vaccine in
the United States. Pediatr Infect Dis J 2007; 26:123–8.
22. Mera R, Miller LA, Fritsche TR, Jones RN. Serotype replacement and
multiple resistance in Streptococcus pneumoniae after the introduction
of the conjugate pneumococcal vaccine. Microb Drug Resist 2008;
14:101–7.
23. Hsu KK, Shea KM, Stevenson AE, et al. Changing serotypes causing
childhood invasive pneumococcal disease: Massachusetts, 2001–2007.
Pediatr Infect Dis J 2010; 29:289–93.
24. Jenkins SG, Farrell DJ. Increase in pneumococcus macrolide resistance,
United States. Emerg Infect Dis 2009; 15:1260–4.
25. Moore MR. Rethinking replacement and resistance. J Infect Dis 2009;
199:771–3.
10 d JID d Hampton et al
at CD
C Public H
ealth Library &
Information C
enter on Decem
ber 7, 2011http://jid.oxfordjournals.org/
Dow
nloaded from

26. Hanage WP, Huang SS, Lipsitch M, et al. Diversity and antibiotic
resistance among nonvaccine serotypes of Streptococcus pneumoniae
carriage isolates in the post-heptavalent conjugate vaccine era. J Infect
Dis 2007; 195:347–52.
27. Dagan R, Barkai G, Givon-Lavi N, et al. Seasonality of antibiotic-
resistant Streptococcus pneumoniae that causes acute otitis media: a clue
for an antibiotic-restriction policy? J Infect Dis 2008; 197:1094–102.
28. Van Effelterre T, Moore MR, Fierens F, et al. A dynamic model of
pneumococcal infection in the United States: implications for prevention
through vaccination. Vaccine 2010; 28:3650–60.
29. Dagan R, Klugman KP. Impact of conjugate pneumococcal vaccines on
antibiotic resistance. Lancet Infect Dis 2008; 8:785–95.
30. Dagan R, Givon-Lavi N, Leibovitz E, Greenberg D, Porat N. In-
troduction and proliferation of multidrug-resistant Streptococcus
pneumoniae serotype 19A clones that cause acute otitis media in an
unvaccinated population. J Infect Dis 2009; 199:776–85.
31. Barkai G, Greenberg D, Givon-Lavi N, Dreifuss E, Vardy D, Dagan R.
Community prescribing and resistant Streptococcus pneumoniae. Emerg
Infect Dis 2005; 11:829–37.
32. van Gils EJ, Veenhoven RH, Hak E, et al. Pneumococcal conjugate
vaccination and nasopharyngeal acquisition of pneumococcal serotype
19A strains. JAMA 2010; 304:1099–106.
33. Sleeman KL, Griffiths D, Shackley F, et al. Capsular serotype-specific
attack rates and duration of carriage of Streptococcus pneumoniae in
a population of children. J Infect Dis 2006; 194:682–8.
34. Lagos R, Munoz A, San Martin O, et al. Age- and serotype-specific
pediatric invasive pneumococcal disease: insights from systematic sur-
veillance in Santiago, Chile, 1994–2007. J Infect Dis 2008; 198:1809–17.
35. Hsieh YC, Lin PY, Chiu CH, et al. National survey of invasive pneu-
mococcal diseases in Taiwan under partial PCV7 vaccination in 2007:
emergence of serotype 19A with high invasive potential. Vaccine 2009;
27:5513–18.
36. Hanage WP, Kaijalainen TH, Syrjanen RK, et al. Invasiveness of sero-
types and clones of Streptococcus pneumoniae among children in Finland.
Infect Immun 2005; 73:431–5.
37. Sa-Leao R, Pinto F, Aguiar S, et al. Analysis of invasiveness of pneu-
mococcal serotypes and clones circulating in Portugal before widespread
use of conjugate vaccines reveals heterogeneous behavior of clones ex-
pressing the same serotype. J Clin Microbiol 2011; 49:1369–75.
38. Tomasz A. Antibiotic resistance in Streptococcus pneumoniae. Clin
Infect Dis 1997; 24:S85–8.
39. Hakenbeck R, Kaminski K, Konig A, et al. Penicillin-binding proteins
in beta-lactam-resistant Streptococcus pneumoniae. Microb Drug Resist
1999; 5:91–9.
40. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases
Society of America/American Thoracic Society consensus guidelines on
the management of community-acquired pneumonia in adults. Clin
Infect Dis 2007; 44:S27–72.
41. American Academy of Pediatrics Subcommittee on Management of
Acute Otitis Media. Diagnosis and management of acute otitis media.
Pediatrics 2004; 113:1451–65.
42. American Academy of Pediatrics. Pneumococcal infections. In:
Pickering LK, Baker CJ, Kimberlin DW, Long SS, eds. Red Book: 2009
Report of the Committee on Infectious Diseases. 28th ed. Elk Grove
Village, IL: American Academy of Pediatrics, 2009:524–35.
43. American Thoracic Society, Infectious Diseases Society of America.
Guidelines for the management of adults with hospital-acquired,
ventilator-associated, and healthcare-associated pneumonia. Am J Respir
Crit Care Med 2005; 171:388–416.
44. Grijalva CG, Nuorti JP, Griffin MR. Antibiotic prescription rates
for acute respiratory tract infections in U.S. ambulatory settings. JAMA
2009; 302:758–66.
45. Healthy People 2020. Healthy People 2020 summary of objectivesdimmunization and infectious diseases. http://www.healthypeople.
gov/2020/topicsobjectives2020/pdfs/Immunization.pdf. Accessed 29
November 2011.
46. Guillemot D, Varon E, Bernede C, et al. Reduction of antibiotic use
in the community reduces the rate of colonization with penicillin G
nonsusceptible Streptococcus pneumoniae. Clin Infect Dis 2005; 41:
930–8.
47. Dagan R, Sikuler-Cohen M, Zamir O, Janco J, Givon-Lavi N, Fraser D.
Effect of a conjugate pneumococcal vaccine on the occurrence of re-
spiratory infections and antibiotic use in day-care center attendees.
Pediatr Infect Dis J 2001; 20:951–8.
Prevention of S. pneumoniae With Conjugate Vaccines d JID d 11
at CD
C Public H
ealth Library &
Information C
enter on Decem
ber 7, 2011http://jid.oxfordjournals.org/
Dow
nloaded from





























