Embed Size (px)
Citation preview

mykosen 19 (8) 259-264 0 Grosse Verlag 1976
Eingegangen am 13. Juni 1975
From the Hospital Universitario de Los Andes, MCrida, Venezuela, S.A.
Primary cutaneous histoplasmosis * R. ALVARADO, R. AVENDARO and K. SALFELDER
Summary Biopsy of a swollen, painful, right inguinal lymph node of a 15-year-old boy revealed
histoplasmic lymphadenitis. Histoplasmic granulomas were also observed a t biopsy of right plantar skin ulcer, thought traumatic in origin. The patient was asymptomatic and had a normal chest x-ray.
The subject of primary inoculation of mucocutaneous histoplasmosis is being reviewed. Four previous cases with bona fide extra pulmonary primary mucocutaneous histoplas- mosis with a benign course have been reported.
Zusarnrnenfassung Die Biopsie eines geschwollenen und schmerzhaften rechtsseitigen Leistenlymphknotens
eines 15 Jahre alten Jungen ergab eine histoplasmotische Lymphadenitis. Als daraufhin die Probeexcision von einem vermutlich traumatischen Hautulkus an der rechten Fuflsohle untersucht wurde, fanden sich auch histoplasmotische Granulome. Der Patient war asym- ptomatisch und hatte ein normales Rontgenbild der Lungen.
Nur vier ,bona fide"-Falle von primarer mucokutaner Histoplasmose sind bisher mit- geteilt worden.
Introduction Mucocutaneous lesions in histoplasmosis are not as prominent as in other deep mycoses
and primary inoculation is rare (6). Only four acceptable reports on primary cutaneous histoplasmosis are available (7, 8, 10, 11). A traumatic inoculation of skin with regional lymphadenitis due to infection with Histoplasma capsulatum is herein reported.
Report of the case
For a period of six weeks, a 15-year-old boy from a village near the town MCrida had a painful swelling of the right inguinal lymph nodes. Tumorous nodules had grown slowly. On October 2, 1974 a biopsy was performed to rule out a suspected lymphoproliferative disorder.
Three specimens were submitted; the largest was a lymph node of 2.5 cm. in diameter surrounded by fat tissue. The two smaller specimens were also lymph nodes. I n all three lymph nodes, necrotic foci of different sizes were seen grossly. Microscopically, the lymph
* This work was supported in part by the CONICIT (Concejo Nacional de Investigaciones Cienti- ficas y Tecnolbgicas), Caracas, and the Concejo de Desarrollo Cientifico y Humanistic0 de la ULA, MCrida I Venezuela, S. A.
Key words: Histo lasmosis, cutaneous histoplasmosis, histoplasmic lymphadenitis, histoplasmic granufomas, Histoplasma capsulatum.
260 R. ALVARADO, R. AVENDARO and K. SALFELDER
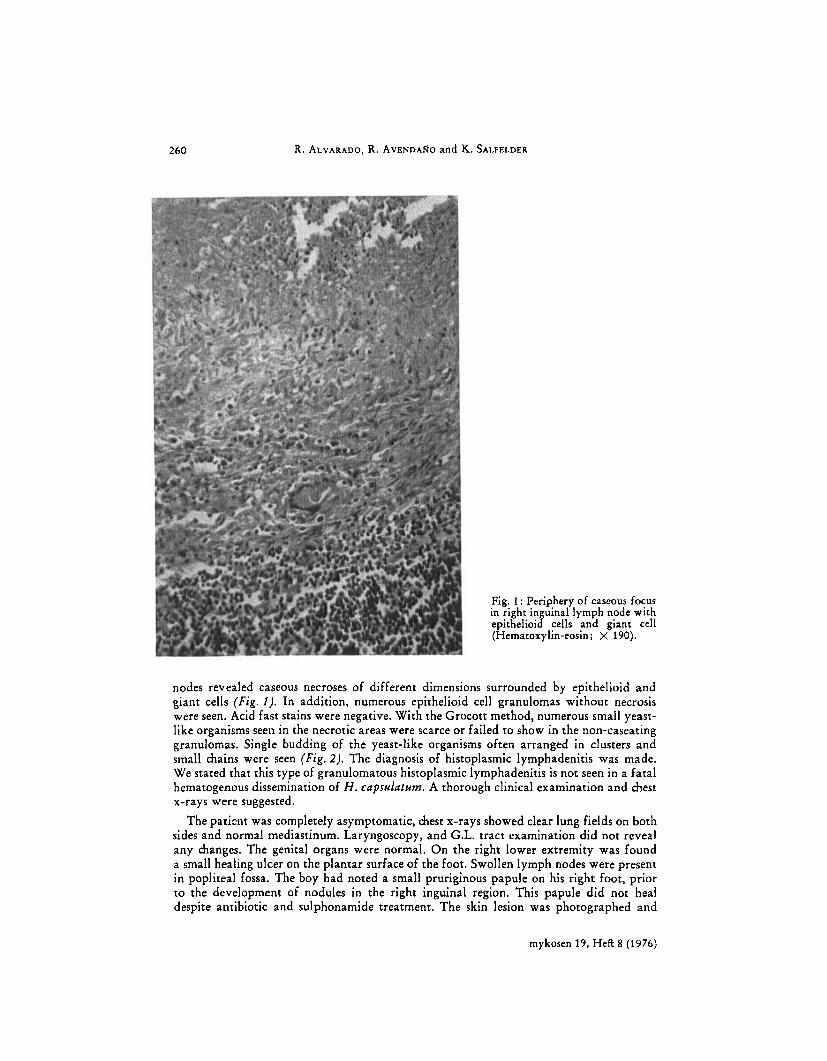
Fig. 1 : Periphery of caseous focus in right inguinal lymph node with epithelioid cells and giant cell (Hematoxylin-eosin; X 190).
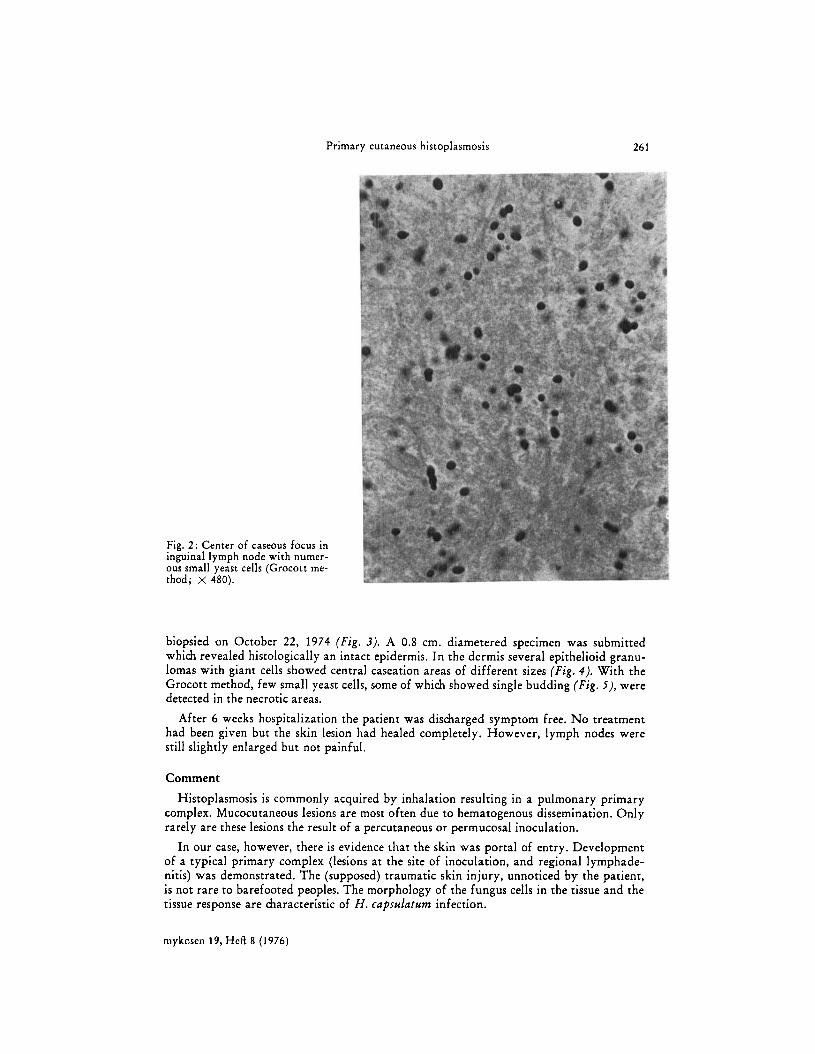
nodes revealed caseous necroses of different dimensions surrounded by epithelioid and giant cells ( F i g . I). In addition, numerous epithelioid cell granulomas without necrosis were seen. Acid fast stains were negative. With the Grocott method, numerous small yeast- like organisms seen in the necrotic areas were scarce or failed to show in the non-caseating granulomas. Single budding of the yeast-like organisms often arranged in clusters and small chains were seen (Fig. 2). The diagnosis of histoplasmic lymphadenitis was made. We stated that this type of granulomatous histoplasmic lymphadenitis is not seen in a fatal hematogenous dissemination of H . capsulatum. A thorough clinical examination and chest x-rays were suggested.
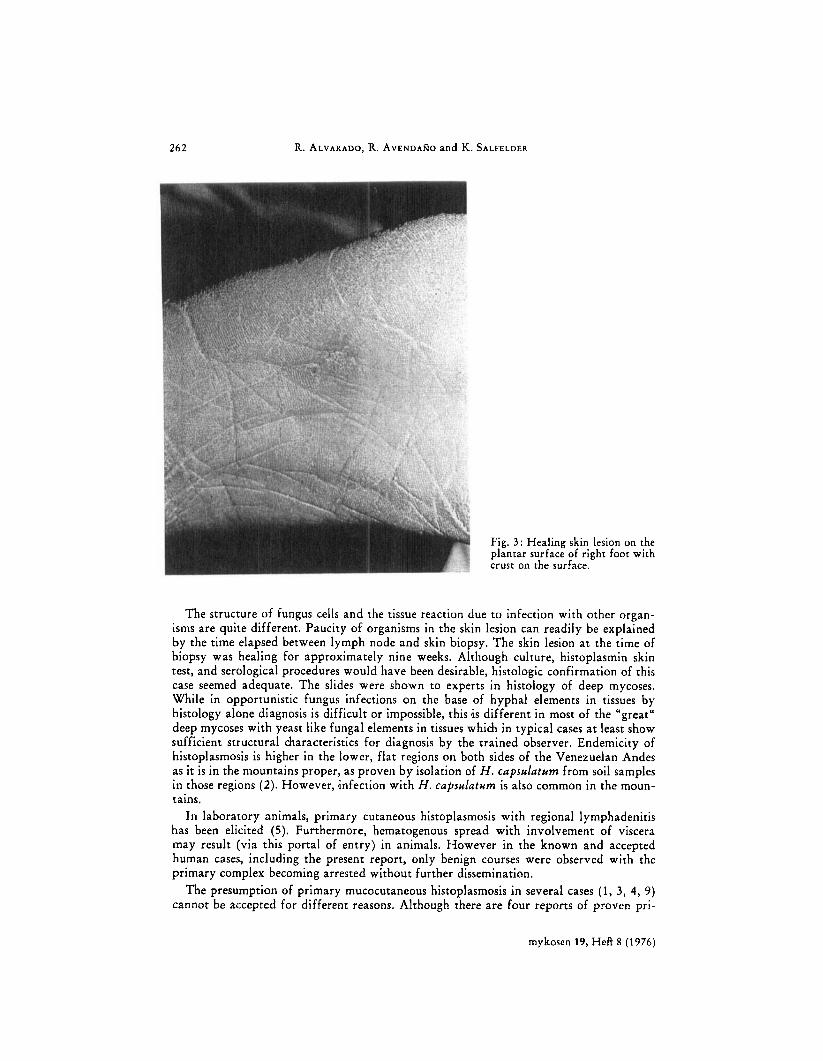
The patimt was completely asymptomatic, chest x-rays showed clear lung fields on both sides and normal mediastinum. Laryngoscopy, and G.L. tract examination did not reveal any cfianges. The genital organs were normal. On the right lower extremity was found a small healing ulcer on the plantar surface of the foot. Swollen lymph nodes were present in popliteal fossa. The boy had noted a small pruriginous papule on his right foot, prior to the development of nodules in the right inguinal region. This papule did not heal despite antibiotic and sulphonamide treatment. The skin lesion was photographed and
mykosen 19, Hefl 8 (1976)
Primary cutaneous histoplasmosis 261
Fig. 2: Center of caseous focus in inguinal lymph node with numer- ous small yeast cells (Grocott me- thod; x 480).
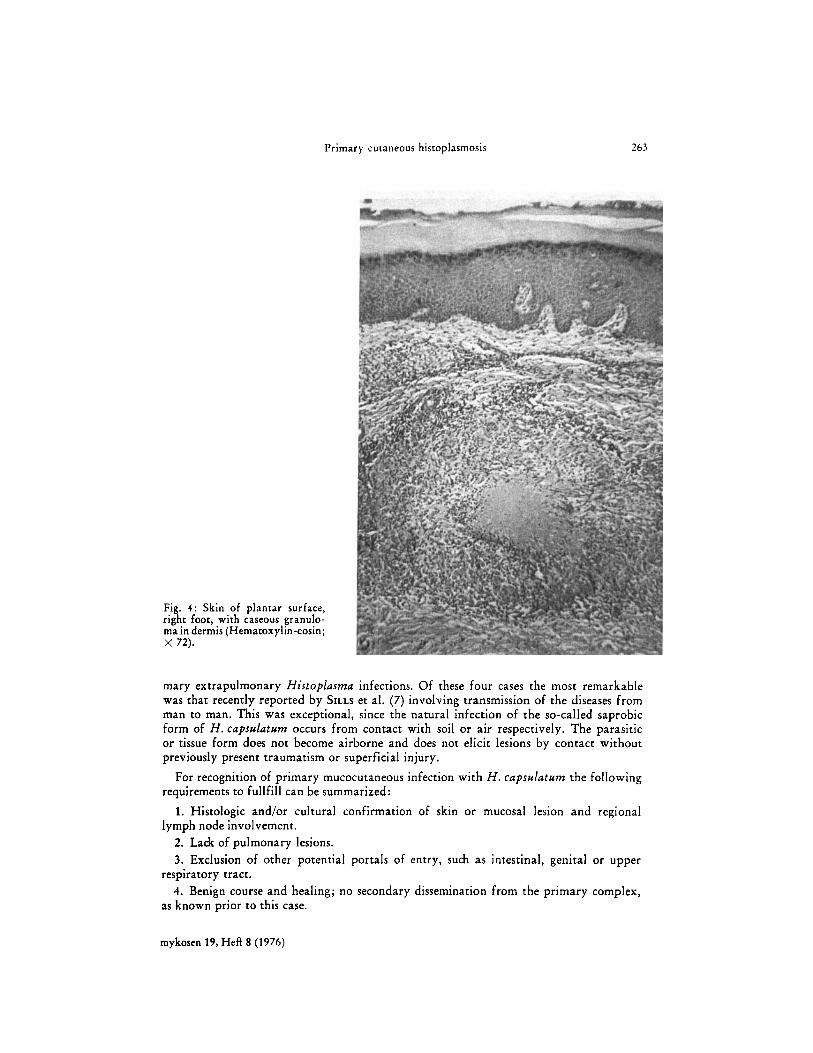
biopsied on October 22, 1974 ( F i g . 3). A 0.8 cm. diametered specimen was submitted which revealed histologically an intact epidermis. In the dermis several epithelioid granu- lomas with giant cells showed central caseation areas of different sizes ( F i g . 4) . With the Grocott method, few small yeast cells, some of which showed single budding (Fig . j), were detected in the necrotic areas.
After 6 weeks hospitalization the patient was discharged symptom free. No treatment had been given but the skin lesion had healed completely. However, lymph nodes were still slightly enlarged but not painful.
Comment
Histoplasmosis is commonly acquired by inhalation resulting in a pulmonary primary complex. Mucocutaneous lesions are most often due to hematogenous dissemination. Only rarely are these lesions the result of a percutaneous or permucosal inoculation.
In our case, however, there is evidence that the skin was portal of entry. Development of a typical primary complex (lesions at the site of inoculation, and regional lymphade- nitis) was demonstrated. The (supposed) traumatic skin injury, unnoticed by the patient, is not rare to barefooted peoples. The morphology of the fungus cells in the tissue and the tissue response are characteristic of H . capsulat~m infection.
niykcsen 19, Heft 8 (1976)
262 R. ALVARADO, R. AVENDARO and K. SALFELDER
Fig. 3 : Healing skin lesion on the plantar surface of right foot with crust on the surface.
The structure of fungus cells and the tissue reaction due to infection with other organ- isms are quite different. Paucity of organisms in the skin lesion can readily be explained by the time elapsed between lymph node and skin biopsy. The skin lesion a t the time of biopsy was healing for approximately nine weeks. Although culture, histoplasmin skin test, and serological procedures would have been desirable, histologic confirmation of this case seemed adequate. The slides were shown to experts in histology of deep mycoses. While in opportunistic fungus infections on the base of hyphal elements in tissues by histology alone diagnosis is difficult or impossible, this I s different in most of the "great" deep mycoses with yeast like fungal elements in tissues which in typical cases at least show sufficient structural characteristics for diagnosis by the trained observer. Endemicity of histoplasmosis is higher in the lower, flat regions on both sides of the Venezuelan Andes as it is in the mountains proper, as proven by isolation of H . capsulatum from soil samples in those regions (2). However, ,infection with H . capsulatum is also common in the moun- tains.
In laboratory animals, primary cutaneous histoplasmosis with regional lymphadenitis has been elicited (5). Furthermore, hematogenous spread with involvement of viscera may result (via this portal of entry) in animals. However in the known and accepted human cases, including the present report, only benign courses were observed with the primary complex becoming arrested without further dissemination.
The presumption of primary mucocutaneous histoplasmosis in several cases (1, 3, 4, 9) cannot be accepted for different reasons. Although there are four reports of proven pri-
mykosen 19, Heft 8 (1976)
Primary cutaneous histoplasmosis 263
Fig. 4 : Skin of plantar surface, right foor, with caseous granulo- ma in dermis (Hematoxylin-eosin; X 72).
mary extrapulmonary Histoplusma infections. Of these four cases the most remarkable was that recently reported by SILLS et al. (7) involving transmission of the diseases f rom man to man. This was exceptional, since the natural infection of the so-called saprobic form of H . capsuluturn occurs from contact with soil or air respectively. The parasitic or tissue form does not become airborne and does not elicit lesions by contact without previously present traumatism or superficial injury.
For recognition of primary mucocutaneous infection with H . capsulnturn the following requirements to fullfill can be summarized:
1. Histologic and/or cultural confirmation of skin o r mucosal lesion and regional lymph node involvement.
2. Lack of pulmonary lesions. 3. Exclusion of other potential portals of entry, such as intestinal, genital o r upper
4. Benign course and healing; no secondary dissemination from the primary complex, respiratory tract.
as known prior to this case.
mykosen 19, Heft 8 (1976)
264 R. ALVARADO, R. AVENDARO and K. S A L P E L D ~ R
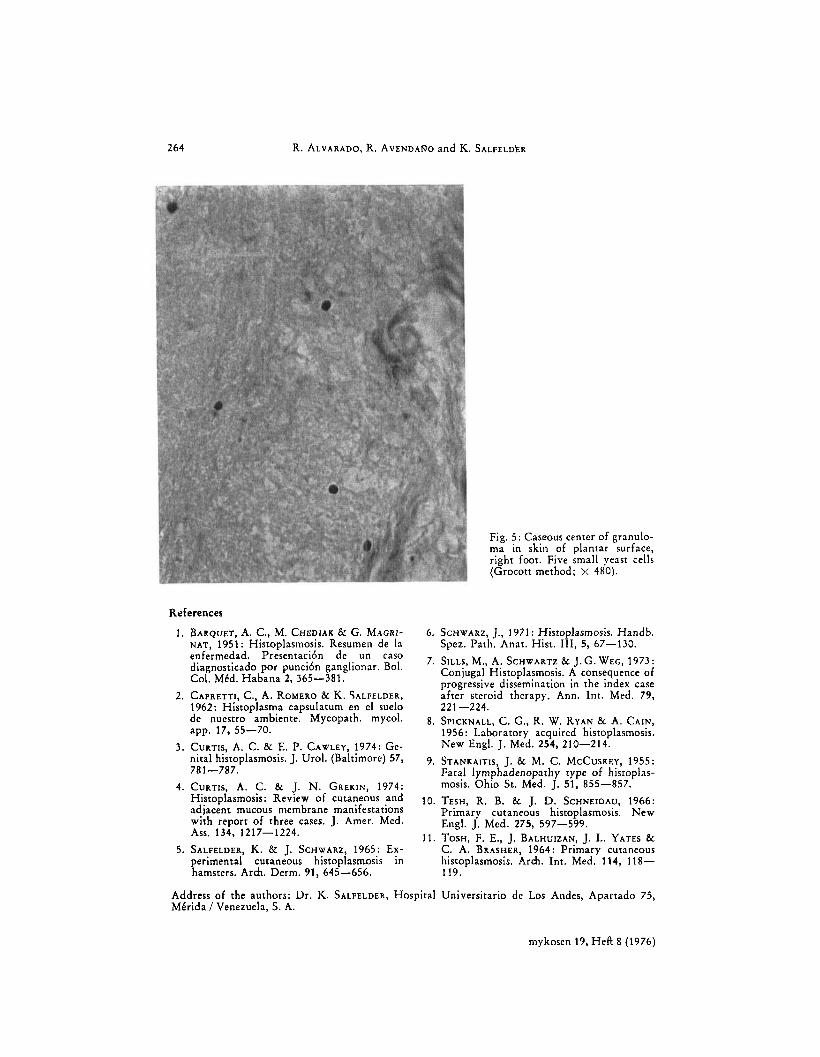
Fig. 5: Caseous center of granulo- ma in skin of plantar surface, right foot. Five small yeast cells (Grocott method; >: 480).
References
1.
2.
3.
4.
5.
BARQUET, A. C., M. CHEDIAK & G. MAGRI- NAT, 1951 : Histoplasmosis. Resumen de In enfermedad. Presentaci6n de un caso diagnosticado por punci6n ganglionar. Bol. Col. MCd. Habana 2, 365-381.
1962: Histoplasma capsulatum en el suelo de nuestro ambiente. Mycopath. mycol. app. 17, 55-70.
CURTIS, A. C. & E. P. CAWLEY, 1974: Ge- nital histoplasmosis. J. Urol. (Baltimore) 57,
CURTIS, A. C. & J. N. GREKIN, 1974: Histoplasmosis: Review of cutaneous and adjacent mucous membrane manifestations with report of three cases. J. Amer. Med.
SALFELDER, K. & J. SCHWARZ, 1965: Ex- perimental cutaneous histoplasmosis in hamsters. Arch. Derm. 91, 645-656.
CAPRETTI, c . , A. ROMERO & K. SALFELDER,
781-787.
ASS. 134, 1217-1224.
6. SCHWARZ, J., 1971 : Histoplasmosis. Handb. Spez. Path. Anat. Hist. 111, 5, 67-130.
Conjugal Histoplasmosis. A consequence of progressive dissemination in the index case after steroid therapy. Ann. Int. Med. 79,
7. SILLS, M., A. SCHWARTZ & J.G.WEG, 1973:
221 -224. 8. SPICKNALL, C. G., R. W. RYAN & A. CAIN,
1956: Laboratory acquired histoplasmosis. New Engl. J. Med. 254, 210-214.
9. STANKAITIS, J. & M. C. MCCUSKEY, 1955: Fatal lymphadenopathy type of histoplas- mosis. Ohio Sr. Med. J. 51, 855-857.
10. TESH, R. B. & J. D. SCHNEIDAU, 1966: Primary cutaneous histoplasmosis. New Engl. J. Med. 275, 597-599.
11. TOSH, F. E., J. BALHUIZAN, J. L. YATES & C. A. BRASHER, 1964: Primary cutaneous histoplasmosis. Arch. Int. Med. 114, 118- 119.
Address of the authors: Dr. K. SALFELDEn, Hospital Universitario dc Los Andes, Apartado 75, MCrida I Venezuela, S. A.
niykoscn 19, Heft 8 (1976)





























