Embed Size (px)
Citation preview

Simultaneous and Differential Fronto-orbital and MidfaceDistraction Osteogenesis for Syndromic Craniosynostosis
Using Rigid External Distractor II
Ahmed Mohamed Medra, MD,* Ahmed Gaber Marei, MD,Þ Ehab Ali Shehata, MD,*Mark McGurk, MD,þ and Ahmed Habib, MD*
Abstract: In syndromic craniosynostosis, the relation between thesupraorbital area and the frontal bone is not good, and it is not possibleto reform this area with 1-block advancement. To avoid this problem,the frontal bone is separated from the fronto-orbital bandeau, each isreshaped and remodeled separately, and then both are reattached.
The retrusion of the midface, especially in syndromic craniosy-nostosis, is usually greater than that of cranial bones, so the tech-nique usually separating the midface from the cranium is Le Fort IIIosteotomy, which allows differential distraction of each part.
In this procedure, the cranial and midfacial bones are advancedsimultaneously and differentially, both to the planned extent, in asingle-stage operation, using rigid external distractor II, correctingexorbitism, respiratory embarrassment, and cranial structures andavoiding eye complications in the future. This procedure was used,with a follow-up, in 10 patients with syndromic craniosynostosisfrom 2 to 5 years.
Key Words: Simultaneous, fronto-orbital, midface, distractionosteogenesis, syndromic cranial stenosis
(J Craniofac Surg 2012;23: 1306Y1313)
P irouzmand and Muhajarine1 stated that the skull configurationis the end result of intricate interaction of genetics and environ-
mental factors. Their study revealed certain common factors ex-plaining the topographic organization of the skull with reasonableaccuracy. These factors suggest an important role for the coronal
suture region in the formation of the final skull shape. It seems thatthe timing and speed by which this area contributes to the osteo-genesis and subsequently halting of the growth using suture fusionare important determinants of the skull configuration. The finalshape is determined mainly by the overall brain size (acting as theexpansile force) and the coronal suture region final inhibitory force.1
The surgical treatment of craniosynostosis aims at restorationof both form and function. To achieve this, patients with syndromiccraniosynostosis have traditionally undergone the traditional firstfronto-orbital advancement at 6 to 9 months, whereas most treatmentprotocols address the midfacial hypoplasia between 4 and 7 years.1
During the last decade, different methods for gradual midfaceadvancement have been presented,2Y22 whereby the surgeon can ob-tain unlimited skeletal advancement, thereby lending hope to promiseof fewer reoperations.1
The technique of fronto-orbital advancement and cranial vaultremodeling has beenwidely used all over theworld tomanage childrenwith cranial stenosis both syndromic and nonsyndromic. In mostchildren who undergo this technique, the results are excellent.23Y26
However, some patients with syndromic craniosynostosis mayrequire secondary surgical intervention for increased intracranialpressure and/or unsatisfactory craniofacial form or structure.27,28 Inaddition, the extent of advancement is limited by skin flap restric-tion and the risk of production of persistent extradural dead spacewith its possible sequelae.
Sugawara et al29,30 introduced fronto-orbital advancement withgradual distraction. The advantages of this technique include no re-quirement of bone grafting, ease of suturing overlying skin and softtissues, unlimited advancement length, less possibility of develop-ment of extradural dead space, and lower risk of retrofrontal abscess.
In syndromic craniosynostosis, the relation between the su-praorbital area and the frontal bone is not optimum, and it is notpossible to reform this area with 1-block advancement. To avoid thisproblem, the frontal bone is separated from the fronto-orbital ban-deau, each is reshaped and remodeled separately, and then both arereattached for advancement in more optimal relation.1Y9
The retrusion of the midface, especially in syndromic cra-niosynostosis, is usually different in severity compared with thatof cranial bones, so our technique usually separating the midfacefrom the cranium is Le Fort III osteotomy, which allows differentialdistraction of each part. Overcorrection (3Y4 mm) at the level ofocclusion was performed in all patients as a guard for any possiblerelapse in the future.
In this procedure, the cranial and midfacial bones are ad-vanced simultaneously, both to the planned extent, in a single stage.We aimed to correct exorbitism, respiratory embarrassment, andcranial and midface bone shape and position, and to avoid future eyecomplications.
We hereby present our experience with this bone-lengtheningtechnique using rigid external distraction device after simultaneous
ORIGINAL ARTICLE
1306 The Journal of Craniofacial Surgery & Volume 23, Number 5, September 2012
What Is This Box?AQRCode is amatrix barcode readable byQR scanners, mobile phones with cam-eras, and smartphones. The QR Codelinks to the online version of the article.
From the *Department of Maxillofacial and Plastic Surgery, Faculty ofDentistry, †Department of Neurosurgery, Faculty of Medicine, Alexan-dria University, Alexandria, Egypt; and ‡Department of Oral and Max-illofacial Surgery, Guy’s Hospital, University of London, UK.
Received September 23, 2011.Accepted for publication March 19, 2012.Address correspondence and reprint requests to Prof. Ahmed Mohamed
Medra, Department of Maxillofacial and Plastic Surgery, Faculty ofDentistry, Alexandria University, Shamplioon Street, Azarita, Alexandria,21599 Egypt; E-mail: [email protected]
The authors report no conflicts of interest.Copyright * 2012 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3182565599
Copyright © 2012 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

fronto-orbital and Le Fort III osteotomies, with a follow-up, in 10patients with syndromic craniosynostosis from 2 to 5 years.
MATERIALS AND METHODSFrom January 2005 to December 2009, 10 patients with
syndromic craniosynostosis were treated in the Department ofCranio-Maxillofacial and Plastic Surgery, Faculty of Dentistry,Alexandria University, Egypt. The clinical profile is presented inTable 1.
All patients had preoperative dental casts and dental cepha-lometric tracing (when possible), radiographic evaluation, three-dimensional computed tomographic (CT) scan, and orthodonticassessment. Cephalometric tracing and dental casts were obtainedimmediately and 6 months and 1 year postoperatively. Preoperativeophthalmologic assessment was carried out in all patients.
Surgical TechniqueThree patients underwent nasotracheal intubation, and the
other seven (with severe narrowing of the nasal airway) underwenta submental intubation. All patients were kept intubated for thefirst postoperative 24 hours in the intensive care unit.
Surgeries were carried out by a team consisting of neuro-surgeons, cranio-maxillofacial surgeons, and pediatric anesthetistafter conjoint evaluation by the operating team.
Fronto-orbital OsteotomyExposure of the cranium and upper facewas carried out through
a coronal approach. Any preexisting coronal scar from previous sur-gery was observed for the incision, and subcillary incisions were usedin 6 patients.
Simple standard fronto-orbital osteotomy was performed, butwithout the tongue-in groove extension, this leaves intact skull bonefor proper fixation of the distractor.
Through a coronal incision, dissection was conducted in asupraperiostal plane. Two inches above the superior orbital margin,subperiosteal dissection was made down to the inferior border of theorbits. If the supraorbital nerve was enclosed in bony canal, then itwas freed so as to expose the lateral and medial canthus. A crani-otomy was made to remove frontal bone, including all the deformedpart. The inferior border of the bifrontal bone flap was about 1 cm
above the orbital rim, and its superior limitation was beyond thecoronal suture. The dura was carefully elevated from the anteriorskull base to show the orbital roof and the sphenoid edge at the lateralsides, while avoiding any exposure of the cribriform plate. Fronto-orbital osteotomy with remodeling of the frontal osteoblastic flapwas performed with an osteotomy across the floor of the anteriorcranial fossa and was extended laterally through the thick sphenoidbone, downward along the lateral orbital walls, and laterally throughthe frontozygomatic sutures. The supraorbital bar was removed inone piece. The supraorbital bar was remolded to correct the defor-mity where it existed. In severely deformed cases, the frontal bonewas cut into smaller pieces, completely or in greenstick fashion byperforming multiple osteotomies in the inner surface of the bone tohave a more symmetrical and protruded configuration of the frontalbone. These osteotomized bony segments were held together by theoverlying periostium.
After remolding, the frontal bone was fixed loosely with finewires (0.3 mm) to the remolded supraorbital bandeau. Properrepositioning of the supraorbital bar was attempted to create a near-normal frontonasal angle.
Two miniplates were applied, one on each side, to the fronto-orbital bandeau, and a wire loop of 0.5 mm was passed aroundeach plate to exit via the skin, in the upper eyebrow region. Thesewire loops were attached to the upper horizontal bar of the distractorafter its assembly. The temporalis muscles were brought back andresuspended in the temporal ridge, and lateral canthopexy was car-ried out. By advancing the supraorbital bone, the frontal bone waspulled forward.
Le Fort III OsteotomyA modified Le Fort III osteotomy was performed using the
same approach, and a small vestibular incision was added to help inseparation of the pterygomaxillary suture and fixation of the mini-plate or microplate on each side. In some patients, additional sub-cillary incisions were also used.
The osteotomy line runs across the zygomatic arch, from thesphenozygomatic suture along the posterior floor of orbit, behindthe nasolacrimal duct, along the lacrimomaxillary suture to the nasalbone. Three to 5 mm of the root of the nose were left untouchedto serve as a barrier against ascending infections, especially in olderchildren. If the frontal sinus was present, then it was obliterated andcovered with a periosteal flap. The pterygoid plates were separatedwith a chisel placed in the pterygomaxillary region via the vestibularincision. The same procedure was carried out on the other side, andthe midface was mobilized.
Down-rotation of the midface may be helped using Rowedisimpaction forceps. One miniplate was placed on the anterior wallof maxillary sinus lateral to the pyriform aperture. Two 0.5-mmstainless steel wire loops were twisted and passed around the mini-plates, through the skin, and in the paranasal area, and attached tothe rigid external distractor II device.
The distraction device was tested to ensure that Le Fort III wasadequately mobilized and that the distraction vectors were optimal.The distractor was assembled. The wounds were closed in layerswith suction drainage.
All patients received prophylactic antibiotics perioperativelyand postoperatively. To minimize the postoperative swelling, 2 sub-cutaneous vacuum drains were used during the first postoperative24 hours, as well as corticosteroids perioperatively and postop-eratively. In addition, bags with ice water were used to keep thefronto-orbital area cool. Using these maneuvers, swelling has beendramatically reduced compared with our earlier results before adopt-ing this protocol. Topical wound care was applied to the pin sitestwice daily.
TABLE 1. Clinical Profile of the Patients
Demographics n
Age, y Range, 1.5Y13 Mean, 6.2
Sex
Male 4
Female 6
Clinical indications
Moderate to severe exorbitism 10
Impending corneal ulceration 7
Recurrent globe subluxation 5
Respiratory embarrassment 9
Severe sleep apnea 5
Surgery
Primary 5
Secondary 5
Syndrome
Apert 5
Crouzon 5
The Journal of Craniofacial Surgery & Volume 23, Number 5, September 2012 Simultaneous Craniofacial Distraction
* 2012 Mutaz B. Habal, MD 1307
Copyright © 2012 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Distraction PhaseDistraction was started 5 days after the operation, at the rate
of 1 mm/d. A change of the direction of the distraction (distractionvector) was possible by changing the direction of the pulling forces,for example, downward or using differential speeds of distraction oneach side, or at each level (cranial or occlusal).
The profile, the clinical aspect, and the dental occlusion wereused to evaluate the extent of distraction. Slight overcorrection by3 to 4 mm turned out to be advisable at the dental occlusion levelbecause a certain degree of relapse may occur.
Consolidation PhaseAfter 8 weeks of end of distraction, the device, the plates,
and the screws were taken out under general anesthesia throughinitial incisions.
RESULTSThe age of the patients ranged from 1.5 to 13 years with
the mean age of 6.2 years. Two patients were younger than 4 years,another 2 patients were older than 8 years, and the remaining 6patients were from 4 to 8 years. Four patients (40%) were male, and6 patients (60%) were female (Table 1).
Ten patients complained of snoring and interrupted sleep;9 patients, bulging eyes; 10 patients, abnormal shape of the head;7 patients, facial disfigurement; 7 patients, improper dental rela-tion; 3 patients, impaired vision; and 1 patient, headache (Table 1).
Five patients had history of skull vault remodeling and fronto-orbital advancement, 1 patient had ventriculoperitoneal (VP) shunt.In these patients, we consider our procedure as secondary surgery.The other 5 patients had no history, so our procedure was primarysurgery (Table 1).
Skull and face examination revealed an abnormal shape ofthe skull in all patients in the form of brachycephaly. In addition, allthe patients had flat and retruded forehead relative to orbital bones,concave face, midface retrusion, and incompetent lips. Five patientshad small peaked nose. Five patients had scalp scars from previoussurgeries; one of them had palpable button of VP shunt. Two patientshad craniofacial asymmetry.
Upon intraoral evaluation, all patients were found to havehigh arched palate and two of them had submucous cleft palate. Allpatients had Class III malocclusion secondary to midface retrusionwith bilateral posterior crossbite in 8 patients and total open bite in1 patient.
Upon evaluation of the extremities, it was revealed that 5patients had syndactyly, whereas the other five had normal extremities.
Ophthalmological examination revealed that one had com-plete eye closure without force, five had complete eye closure withforce, and four had incomplete eye closure with force. Eye closureduring sleep was complete only in 1 patient, whereas the remaining9 patients had lagophthalmos.
All had proptosis, which was moderate in 1 patient, and 9patients had severe proptosis. In addition, CT scan showed proptosisand shallow orbits in all patients.
Visual acuity was more than 6/60 in 7 patients. Conjunctivalchemosis was found in all patients, 9 patients had exposure kera-topathy, and 1 patient had abnormal eye movement in the form ofnystagmus.
Fundus examination revealed that 7 patients had papilledema,whereas primary optic atrophy was detected in the other 3 patients.
All the 10 patients had upper airway obstruction that wasmanifested in all of by snoring, mouth breathing, nasal obstruction,and obstructive sleep apnea.
Neurological evaluation revealed raised intracranial pressuredue to restriction of cranial vault growth and midface retrusion thatwas manifested by headache in 1 patient, presence of VP shuntin another patient, papilledema in 7 patients, and optic atrophy in3 patients. Plain skull x-ray examination showed finger printing in9 patients, whereas brain CT scan showed increased intracranialpressure in all patients.
Genetic counseling reported that 5 patients (50%) had Apertsyndrome and the other 5 patients (50%) had Crouzon syndrome(Table 1).
Three-dimensional CT scan showed that all patients had cra-niosynostosis, raised intracranial pressure, shallow orbits, proptosis,
TABLE 2. Evaluation of the Outcome
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6 Patient 7 Patient 8 Patient 9 Patient 10 Total Mean SD
Type of surgery 2ry 1ry 2ry 1ry 2ry 2ry 1ry 1ry 1ry 2ry 5:5 V V
Operative time, min 345 300 330 270 315 300 260 240 250 300 2910 291 34.9
Estimated blood loss, mL 530 600 550 480 450 570 400 370 380 520 4850 485 67.2
Perioperative blood transfusion, U 2 2 2 2 1 2 1 1 1 2 14 1.4 0.56
Hospital stay, d 13 15 11 15 8 18 12 20 14 16 142 14.2 3.4
1ry indicates primary; 2ry, secondary.
TABLE 3. Distraction Patterns
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6 Patient 7 Patient 8 Patient 9 Patient 10 Total Mean SD
Fronto-orbitaldistraction
8 12 10 14 12 12 14 (right, 15; left, 13) 13 11 12 118 11.8 1.8
Midfacedistraction
15 18.5 (right, 21; left, 16) 16 20 18 19 21.5 (right, 23; left, 20) 20 15 17 180 18 2.2
TABLE 4. Ophthalmologic Evaluation
Findings n
Complete eye closure without force 10
Complete eye closure during sleep 10
Absence of conjunctival chemosis 10
Disappearance of nystagmus 1
Resolution of papilledema 7
Persistence of optic atrophy 3
Medra et al The Journal of Craniofacial Surgery & Volume 23, Number 5, September 2012
1308 * 2012 Mutaz B. Habal, MD
Copyright © 2012 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
and midface hypoplasia. In addition, it reported the presence of theabnormal skull shape in all patients who had brachycephaly.
Evaluation of the OutcomeType of surgery, operative time, blood loss, perioperative
blood transfusion, and duration of hospital stay are shown in Table 2.Distraction period (in days), distance (in mm), and pattern are shownin Table 3.
Disappearance of snoring was gained within a week afterstart of distraction, continued during distraction, and remained aftercompletion of distraction and during follow-up period (up to 5 years).
Improvement of both eye closure without force and eye clo-sure during sleep was achieved postoperatively with absence ofconjunctival ecchymosis. The 7 patients with preoperative papille-dema had resolution of papilledema postoperatively (Table 4).
The patient with preoperative nystagmus did not improvepostoperatively.
The 3 patients with preoperative optic nerve atrophy did notobviously improve postoperatively.
After removal of the distractor, all patients showed im-provement in dental relationship. They gained Class I molar rela-tionship. The incisal relationship was over jet in 1 patient, edge toedge in another, and anterior open bite in 8 patients.
At the end of follow-up period, occlusion was maintainedas class I molar relationship in 9 patients. The incisal relationshipremained over jet in 1 patient, whereas it changed to Class I withreversed over jet in another patient. Long-term follow-up of the
TABLE 5. Aesthetic Outcome
Aesthetic OutcomeNo. Good (Very
Satisfied)No. Fair(Satisfied)
No. Bad(Dissatisfied)
Skull shape 5 5 0
Scalp and face scars 3 7 0
Facial symmetry 10 0 0
Profile view (convexity) 10 0 0
Appearance and projectionof forehead
10 0 0
Improvement of proptosis 10 0 0
Midface advancement 10 0 0
Lip competence 9 1 0
Dental relation 9 1 0
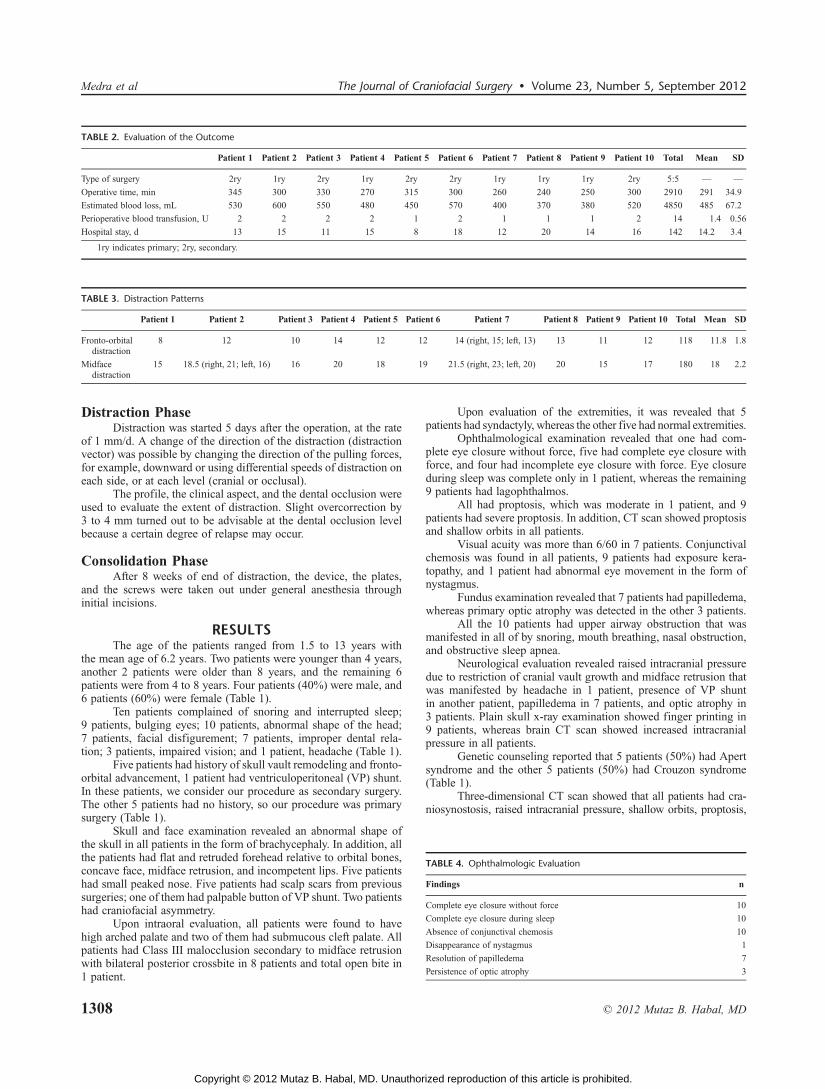
FIGURE 1. Patient 4: preoperative (A, B, and C), 2 months postoperative(D, E, and F), and 2 years postoperative (G, H, and J).
FIGURE 2. Patient 4: occlusion before distraction (A, B, and C), at the endof distraction with overcorrection (D), and 1 year after distraction (E).
FIGURE 3. Patient 4: preoperative lateral cephalometry (A) and cephalometrictracing (B), and 1 year postdistraction lateral cephalometry (C) andcephalometric tracing (D).
FIGURE 4. Patient 2: preoperative (A, B, and C), 2 weeks after end of distraction(D, E, and F), and 2 years postoperative (G, H, and J).
FIGURE 5. Patient 2: preoperative (A, B, and C), 2 weeks after end of distraction(D, E, and F), and 2 years postdistraction (G, H, and J).
The Journal of Craniofacial Surgery & Volume 23, Number 5, September 2012 Simultaneous Craniofacial Distraction
* 2012 Mutaz B. Habal, MD 1309
Copyright © 2012 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
occlusion in the 10th patient could not be achieved as she died2 months postoperatively.
The patients and/or their families participated in the aestheticoutcome assessment. Subjective aesthetic outcome was judged bythe parents of patients as good, fair, or bad (Table 5).
Questionnaire results demonstrated that all the patients foundthat the aesthetic outcome was good as regarding facial symmetry,profile view, appearance, and projection of the forehead; improve-ment of proptosis; and midface advancement. The lip competencewas good in 9 patients, whereas it was fair in 1 patient. In addition,dental relation was good in 9 patients and fair in 1 patient. Regard-ing scalp and face scars, 3 patients found that the aesthetic outcomewas good, whereas in the other 7 patients, it was fair. The skull shape
was good in 5 patients, whereas it was fair in the other 5 patients. Theclinical results are shown in Figures 1 to 6.
Preoperative and postoperative lateral cephalometry was car-ried out for all patients except for two (patients 5 and 8) in whom itwas not feasible to perform the lateral cephalometry because both ofthem were young and uncooperative.
Cephalograms were traced, with the anterior cranial base usedfor overall superimposition. Measurements were taken preopera-tively (T1) and postdistraction at follow-up (Table 6 and Figure 7).
The resultant fronto-orbital advancement achieved by dis-traction ranged from 5 to 9 mmwith a mean (SD) of 7.75 (1.38) mm.The resultant midface advancement achieved by distraction rangedfrom 9 to 14 mm with a mean (SD) of 10.12 (1.7) mm. The resultant
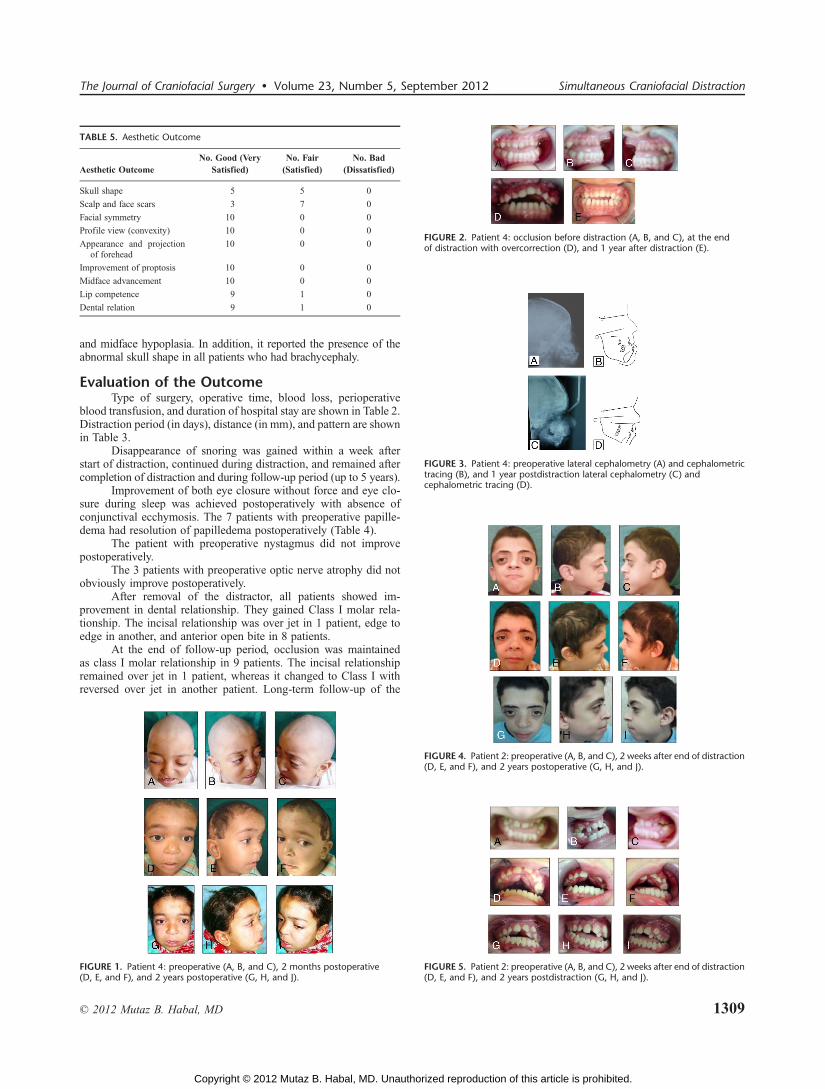
FIGURE 6. Patient 2: preoperative lateral cephalometry (A) and cephalometrictracing (B), and 2 years postdistraction lateral cephalometry (C) andcephalometric tracing (D).
TABLE 6. Clinical and Cephalometric Advancement and Ratio Between Them
Fronto-orbital Distraction (Forehead $W), mm Mid-face Distraction (Midface $W), mm Maxilla Distraction (Maxilla $W), mm
Patient Clinical Cephalometric Ceph/clinical Clinical Cephalometric Ceph/clinical Clinical Cephalometric Ceph/clinical
1 8 5 0.625 15 9 0.6 15 11 0.733
2 12 9 0.75 18.5 (right, 21; left, 16) 10 0.54 18.5 (right, 21; left, 16) 14 0.756
3 10 7 0.7 16 9 0.56 16 11 0.688
4 14 8 0.571 20 9 0.45 20 11 0.55
5 12 V V 18 V V 18 V V
6 12 9 0.75 19 11 0.58 19 12 0.632
7 14 (right, 15; left, 13) 8 0.571 21.5 (right, 23; left, 20) 14 0.65 21.5 (right, 23; left, 20) 11 0.511
8 13 V V 20 V V 20 V V
9 11 7 0.63 15 9 0.6 15 10 0.66
10 12 9 0.75 17 10 0.59 17 11 0.65
Sum 118 62 5.347 180 81 4.396 180 91 3.87
Mean 11.8 7.75 0.66 18 10.12 0.55 18 11.38 0.647
SD 1.8 1.38 V 2.2 1.7 V 2.2 1.3 V
FIGURE 7. Cephalometric tracing of advancement.
FIGURE 8. Changes in the SNA angle.
FIGURE 9. Change in the SNOr angle.
Medra et al The Journal of Craniofacial Surgery & Volume 23, Number 5, September 2012
1310 * 2012 Mutaz B. Habal, MD
Copyright © 2012 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

maxillary advancement achieved by distraction ranged from 11 to14 mm with a mean of 11.38 (1.3) mm.
Cephalometric analysis revealed that the resultant advance-ment is less than the clinical distraction distance. The mean ratiobetween the resultant advancement and the distraction distance was66% in the fronto-orbital region, 55% in the midface, and 64.7% inthe maxilla.
Preoperative lateral cephalometric analysis showed the con-stant findings of mid face retrusion. The mean preoperativeSNA and SNOr were 70.4 and 46.6 degrees, respectively (Table 7and Figures 8 and 9).
In the postoperative lateral cephalometric analysis, the find-ings showed successful midface advancement that was shown bythe increase in both SNA and SNOr. The mean postoperative SNAand SNOr were 79.1 and 54.2 degrees, respectively.
Complications encountered in the stages of surgery areshown in Table 8. Using a visual analog scale for measuring theoverall satisfaction of the outcome, 9 patients were very satisfied,whereas only 1 patient was very dissatisfied (Table 9). The clinicalresults are shown in Figures 1 to 6.
DISCUSSIONFronto-orbital advancement and cranial vault remodeling
have been widely performed to treat brachycephaly associated withsyndromic and nonsyndromic craniosynostosis since the early1960s.23Y27 Performing this procedure at an early age in childrenhas been carried out in the hope that it would result not only inimproving craniofacial function and structure but also in satisfactorygrowth and development of the craniofacial region.
The fronto-orbital advancement and cranial vault remodelinggave excellent results in most patients, in expert hands. However,some of these children who undergo fronto-orbital advancement, atan early age, require secondary surgical interventions for increasedintracranial pressure or unsatisfactory craniofacial structure, espe-
cially in patients with syndromic craniosynostosis. In addition, whenconventional fronto-orbital advancement is carried out, extraduraldead space forms behind the frontal bone, which is considered amajor disadvantage of this procedure, although rapid expansion ofthe brain could obliterate this retrofrontal extradural dead spacewithin a few days.31,32 However, Spinelli et al32 reported that thedead space remained in 90% of patients on the seventh day aftersurgery and was still present in 50% of patients on the 14th dayafter surgery.
Although the dead space exists, revascularization to the frontalbone occurs only from the skin flap side. The longer the dead spacelasts, the less likely the bone is to be vascularized from the dura. Thechance of infection increases.33,34 Tessier35 originally recommendedadvancing the frontal bone no more than 10 to 12 mm to avoid leavinga large dead space behind it.
In frontofacial monobloc advancement, the dead space is amuch more serious problem. Retrofrontal dead space has commu-nication with the nasal cavity. It is much more likely to be in-fected.36Y38 High infection rates led many experienced craniofacialsurgeons to discontinue use of this procedure. Marchac et al39
published the excellent idea of floating forehead. They let the frontalbone float on the brain (dura), leaving no dead space between them.They let the brain decide the shape of the cranial vault, and thetechnique works very well. However, the advancement length of thesupraorbital bone is limited because of the limited amount of bonegraft and covering skin. When the advancement length is relativelyshort for the patient’s intracranial pressure, the cranium will becometurricephalic.
Since McCarthy et al40 applied distraction osteogenesis inlengthening the mandible, craniofacial distraction has virtuallyboomed. Successful experimental expansions of the cranium havebeen reported. There have been several successful reports of ex-perimental and clinical use of gradual advancement in expandingthe cranial vault.22Y26 The Sugawara/Hirabayashi group applied
TABLE 7. Changes in SNA and SNOr Angles
SNA, degree SNOr, degree
Patient T1 T2 $T2jT1 T1 T2 $T2jT1
1 73 86 13 53 66 13
2 64 72 8 49 55 6
3 79 83 4 45 49 4
4 72 80 8 45 54 9
5 V V V V V V
6 76 82 6 60 64 4
7 61 77 16 37 46 9
8 V V V V V V
9 67 75 8 41 47 6
10 71 78 7 43 53 10
Sum 563 633 70 373 434 61
Mean 70.4 79.1 8.75 46.6 54.2 7.6
SD 6 4.5 V 7.2 7.4 V
Or indicates orbital.
TABLE 8. Complications Encountered in the Stages of Surgery
Timing Complications n
Intraoperative Dural tear 6
Brain contusion 1
Separation of supraorbital bandeau 1
Palatal split 2
Early postoperative (first wk) Edema of forehead, eyelids, and face 10
Feeding difficulties 10
Cerebrospinal fluid leak (stopped spontaneously) 2
Intermediate postoperative(first mo)
Wires and pin site infection 10
Cerebrospinal fluid rhinorrhea 2
Scalp abscess 1
Device loosening 1
Premature removal of rigid external distractor II 1
Late postoperative (91 y) Scalp scar and localized alopecia 10
Step deformity of skull 7
Anterior open bite 7
Reversed over jet 1
Death 1
TABLE 9. Overall Patient Satisfaction
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6 Patient 7 Patient 8 Patient 9 Patient 10 Total Mean
Very satisfied * * * * * V * * * * 9 V
Very dissatisfied V V V V V * V V V V 1 V
Measurement of visual analog scale 9 9 9 9 9 5 8 9 8 9 82 8.2
The Journal of Craniofacial Surgery & Volume 23, Number 5, September 2012 Simultaneous Craniofacial Distraction
* 2012 Mutaz B. Habal, MD 1311
Copyright © 2012 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

gradual distraction for fronto-orbital advancement. They cut thefrontal and supraorbital bone as 1 block without elevating from thedura. A certain amount of vascularity from the dura to the cut boneblock was maintained. They applied the distraction device betweenthe block and temporal or parietal bone. The fronto-orbital boneblock was advanced gradually. Retrofrontal dead space will notappear in this procedure.29,30
Bone graft is not required. Cho et al41 reported a similar pro-cedure and successful cases. They stress that the best way to preventpostoperative complication is to prevent the formation of extraduraldead space. Surgeons who are supporting 1-block distraction stressthat the connection between the bone and the dura is important toprevent resorption of the advanced fronto-orbital bone.
It is definitely truewhen the conventional 1-stage advancement isconcerned. McCarthy et al42 reported that only 1 of 8 patients whounderwent bilateral fronto-orbital advancement experienced a frontalsinus, although in their experience with the floating forehead, minimumresorption of the once-removed frontal bone is observed unless infectionoccurs. Formation of frontal sinuses is observed in most patients whounderwent the floating forehead technique, which correlates with thereport by Locher et al.43
In early experimental reports, craniums were taken off once andplaced back to the original area, and successful distractions were carriedout.22,23 It was reported that gradual distraction of a frontoparietal boneprevents extradural dead space formation, regardless ofwhether the durais kept attached to or is separated from the distracted bone segment.They also reported that no evidence of bony resorption was observed ineither of the groups. Thus, we believe that it is not so important topreserve vascularity of the bone if the patient is operated on in thefloating forehead fashion in his early childhood, when the cranium isthin and easy to be revascularized. Wewere able to advance frontofacialmonobloc successfully with gradual distraction, allowing the frontalbone to float on the dura.26
In some patients, especially in those with syndromic cra-niosynostosis, the relation between the supraorbital area and thefrontal bone is not good. Frontal bossing will not be improved by1-block advancement. So by separating the fronto-orbital ban-deau from the midface via Le Fort III osteotomy, we can advanceeach part, separately, to the exact required extent without jeop-ardizing the facial esthetics. A depressed sphenoidal greater wingarea also will not be improved. We think it is technically difficultto cut the anterior cranial base without taking off the frontalbone, especially in patients with frontal bossing. Cutting thesupralateral portion of orbit is very difficult when temporalbossing is obvious. Torn dura may not be realized during theoperation because it may be hidden beneath the bone. To re-model the supraorbital area into a better shape, the bone should becut out. It is easier to cut frontal bone into smaller pieces when itis removed.
In comparison with the original 1-block gradual distraction ofthe Sugawara/Hirabayashi group, our technique produces a smoothcontour with appropriate cranial volume regulated by intracranialpressure. Because we once removed and remolded bones, the inva-sion level is not much different from that of conventional fronto-orbital advancement, except for avoiding bone grafts.
Although our follow-up period is relatively short, most ofthe craniums of surgically treated patients continued to grow after anormal growth curve. But in 1 patient, digital impression on the skullbecame obvious again. That patient required secondary cranium ex-pansion. This implies that this technique alone is not the perfectsolution for syndromic craniosynostosis.
How much the bones should be advanced remains unknown.A large amount of advancement may give good room for the brain,but the facial appearance may be disfigured with too much pro-truding forehead, especially for the patient with a small skull.
Some complications were experienced. Infantile cranium isthin and too fragile to hold screws, especially in patients withlacunar skulls.
Cranium remodeling with gradual distraction certainly hasdrawbacks. The treatment period is longer than 1-stage remodeling.A second operation to remove distractors is required. Treatmentcosts rise. Complications with the devices may occur. However,the possibility of avoiding major complication should b stressed,especially for patients with syndromic craniosynostosis who re-quire relatively greater advancements.
Improvement of the distraction devices is needed. Most ofthe internal devices on the market cannot change distraction direc-tion after the operation. External devices can do this, but infantile skullsare too fragile for device fixation, so external devices are used for olderchildren older than 4 years. Devices madewith absorbable material maybe an improvement. Because cranium remodeling with gradual dis-traction is a new technique, long-term follow-up is necessary to de-termine its advantages.
Preoperative lateral cephalometric analysis showed the con-stant finding of midface retrusion. The mean preoperative SNA andSNOr were 70.8 and 48.1 degrees, respectively. In the postopera-tive lateral cephalometric analysis, the findings showed successfulmidface advancement that was shown by the increase in both SNAand SNOr. The mean postoperative SNA and SNOr were 80 and55.6 degrees, respectively.
This technique showed significant advancement of the fore-head,midface, andmaxilla by performing lateral cephalometric tracingin 8 patients (2 patients were too young to have lateral cephalogram).This tracing was carried out preoperatively, after removal of distractor,and after surgery.
Fronto-orbital advancement ranged from 6 to 12 mm with amean of 9.8 mm. Although midface advancement ranged from 11 to14 mm with a mean of 12.33 mm. Maxillary advancement rangedfrom 11 to 16 mm with a mean of 14 mm (Tables 6 and 7). However,cephalometric analysis revealed that the resultant advancement isless than the clinical distraction distance. The mean ratio betweenthe resultant advancement and distraction distance was 80% in thefronto-orbital region, 68% in the midface, and 77% in the maxilla.
CONCLUSIONSSimultaneous, differential cranial and midface advancement
by distraction osteogenesis, using rigid external distractor, is a ver-satile technique in selected patients with syndromic craniofacial ste-nosis. However, being a recent technique, long-term results andfollow-up of this technique has to be evaluated.
REFERENCES1. Pirouzmand F, Muhajarine N. Definition of topographic organization
of skull profile in normal population and its implications on therole of sutures in skull morphology. J Craniofacial Surg2008;19:27Y36
2. Bruner E. Geometric morphometrics and paleoneurology: brain shapeevolution in the genus Homo. J Hum Evol 2004;47:279Y303
3. Axelsson S, Kjaer I, Bjornland T, et al. Longitudinal cephalometricstandards for the neurocranium in Norwegians from 6 to 21 years of age.Eur J Orthod 2003;25:185Y198
4. Ogle RC, Tholpady SS, McGlynn KA, et al. Regulation of cranialsuture morphogenesis. Cells Tissues Organs 2004;176:54Y66
5. Jiang X, Iseki S, Maxson RE, et al. Tissue origins and interactionsin the mammalian skull vault. Dev Biol 2002;241:106Y116
6. Alden TD, Lin KY, Jane JA. Mechanisms of premature closure ofcranial sutures. Childs Nerv Syst 1999;15:670Y675
7. Opperman LA, Passarelli RW, Morgan EP, et al. Cranial suturesrequire tissue interactions with dura mater to resist osseous obliterationin vitro. J Bone Miner Res 1995;10:1978Y1987
Medra et al The Journal of Craniofacial Surgery & Volume 23, Number 5, September 2012
1312 * 2012 Mutaz B. Habal, MD
Copyright © 2012 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
8. Kabbani H, Raghuveer TS. Craniosynostosis. Am Fam Phys2004;69:2863Y2870
9. Mao JJ, Nah HD. Growth and development: hereditary and mechanicalmodulations. Am J Orthod Dentofacial Orthop 2004;125:676Y689
10. Meling TR, Orstavik KH, Heiberg A. Complex craniofacial synostoses.Tidsskr Nor Laegeforen 2004;124:1230Y1234
11. Ridgway EB, Weiner HL. Skull deformities. Pediatr Clin North Am2004;51:359Y387
12. Mooney MP, Moursi AM, Opperman LA, et al. Cytokine therapy forcraniosynostosis. Expert Opin Biol Ther 2004;4:279Y299
13. Matsumoto K, Nakanishi H, Kubo Y, et al. Advances in distractiontechniques for craniofacial surgery. J Med Invest 2003;50:117Y125
14. Abuelo D. Genetic evaluation and counseling for craniofacial anomalies.Med Health R I 2002;85:373Y378
15. Flores-Sarnat L. New insights into craniosynostosis. Semin Pediatr Neurol2002;9:274Y291
16. Wilkie AO, Patey SJ, Kan SH, et al. FGFs, their receptors,and human limb malformations: clinical and molecular correlations.Am J Med Genet 2002;112:266Y278
17. Warren SM, Greenwald JA, Spector JA, et al. New developments incranial suture research. Plast Reconstr Surg 2001;107:523Y540
18. Opperman LA. Cranial sutures as intramembranous bone growth sites.Dev Dyn 2000;219:472Y485
19. McIntyre GT, Mossey PA. Size and shape measurement in contemporarycephalometrics. Eur J Orthod 2003;25:231Y242
20. Chen SY, Lestrel PE, Kerr WJ, et al. Describing shape changes in thehuman mandible using elliptical Fourier functions. Eur J Orthod2000;22:205Y216
21. Moyers RE, Bookstein FL. The inappropriateness of conventionalcephalometrics. Am J Orthod 1979;75:599Y617
22. Morriss-Kay GM. Derivation of the mammalian skull vault. J Anat2001;199:143Y151
23. Tessier P. Relationship of craniostenoses to craniofacialdysostoses,and to faciostenoses: a study with therapeutic implications.Plast Reconstr Surg 1971;48:224Y237
24. McCarthy JG, Glasberg SB, Cutting CB, et al. Twenty-year experiencewith early surgery for craniosynostosis: I. Isolated craniofacialsynostosisVresults and unsolved problems. Plast Reconstr Surg1995;96:272Y283
25. McCarthy JG, Glasberg SB, Cutting CB, et al. Twenty-year experiencewith early surgery for craniosynostosis: II. The craniofacial synostosissyndromes and pansynostosisVresults and unsolved problems.Plast Reconstr Surg 1995;96:284Y295
26. Muhlbauer W, Anderl H, Heeckt P, et al. Early operation in craniofacialdysostosis. World J Surg 1989;13:366Y372
27. Whitaker LA, Bartlett SP, Schut L, et al. Craniosynostosis: an analysis ofthe timing, treatment, and complications in164 consecutive patients.Plast Reconstr Surg 1987;80:195Y212
28. Wall SA, Goldin JH, Hockley AD, et al. Fronto-orbital re-operation incraniosynostosis. Br J Plast Surg 1994;47:180Y184
29. Sugawara Y, Hirabayashi S, Sakurai A, et al. Gradual cranial vaultexpansion for the treatment of craniofacial synostosis: a preliminaryreport. Ann Plast Surg 1998;40:554Y565
30. Hirabayashi S, Sugawara Y, Sakurai A, et al. Fronto-orbitaladvancement by gradual distraction. Technical note. J Neurosurg1998;89:1058Y1061
31. Munro IR. Current surgery of craniofacial anomalies. Otolaryngol ClinNorth Am 1981;14:157Y166
32. Spinelli HM, Irizarry D, McCarthy JG, et al. An analysis of extraduraldead space after fronto-orbital surgery. Plast Reconstr Surg1994;93:1372Y1377
33. David DJ, Cooter RD. Craniofacial infection in 10 years of transcranialsurgery. Plast Reconstr Surg 1987;80:213Y225
34. Fisher J, Jackson IT. Microvascular surgery as an adjunct tocraniomaxillofacial reconstruction. Br J Plast Surg 1989;42:146Y154
35. Tessier P. Recent Improvements in Treatment of Facial and CranialDeformities of Crouzon’s and Apert’s syndrome. St Louis, Mo: Mosby;271Y293
36. Whitaker LA, Bartlett SP, Schut L, et al. Craniosynostosis: an analysis ofthe timing, treatment, and complications in 164 consecutive patients.Plast Reconstr Surg 1987;80:195Y212
37. Fearon JA, Whitaker LA. Complications with facial advancement:a comparison between the Le Fort III and monobloc advancements.Plast Reconstr Surg 1993;91:990Y995
38. Gosain AK, Santoro TD, Havlik RJ, et al. Midface Distraction followingLe Fort III and monobloc osteotomies: problems and solutions. PlastReconstr Surg 2002;109:1797Y1808
39. Marchac D, Renier D, Jones BM. Experience with the floating forehead.Br J Plast Surg 1988;41:1Y15
40. McCarthy JG, Schreiber J, Karp N, et al. Lengthening the humanmandible by gradual distraction. Plast Reconstr Surg 1992;89:1Y8
41. Cho BC, Hwang SK, Uhm KI. Distraction osteogenesis of the cranialvault for the treatment of craniofacial synostosis. J Craniofac Surg2004;15:135Y144
42. McCarthy JG, Karp NS, LaTrenta GS, et al. The effect of earlyfronto-orbital advancement on frontal sinus development and foreheadaesthetics. Plast Reconstr Surg 1990;86:1078Y1084
43. Locher MC, Sailer HF, Haers PE, et al. Development of the frontalsinus following bilateral fronto-orbital osteotomies.J Craniomaxillofac Surg 1998;26:129Y135
The Journal of Craniofacial Surgery & Volume 23, Number 5, September 2012 Simultaneous Craniofacial Distraction
* 2012 Mutaz B. Habal, MD 1313
Copyright © 2012 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.





























