Embed Size (px)
Citation preview

characteristic alterations remains unclear. Immunological injuryto the endothelium has to be considered (2—4).
Histologic studies and recently intravascular ultrasonographyhave revealed intimal thickening and vascular sclerosis despiteseemingly normal angiographic findings as early as 1 yr aftertransplantation in nearly all patients (1,5—7).A major problemis the lack of a valid “goldstandard―in the early detection ofthis widespread diffuse disease: coronary angiography is quiteinsensitive in this setting. Intravascular ultrasonography is anew, sensitive imaging modality that has the potential to depictthe vessel wall morphology, but it is limited to the largeepicardial vessels.
The role of201Tl myocardial scintigraphy in the follow-up ofheart transplant recipients was repeatedly evaluated (8—12).With regard to critical stenosis (comparable to coronary arterydisease ofthe native heart) 201T1SPECT after treadmill exerciseyielded satisfying results: sensitivity ranged between 77% and100% (8,10). In our experience, contrast to the reported smallnumber of false-positive findings, 201Tl SPECT of the transplanted heart often shows inhomogeneous patterns, areas withredistribution or reverse redistribution and persistent defectswithout any correlation to coronary territories.
To evaluate our observations systematically we developed ascore that indicates the degree of inhomogeneity or the severityof regional perfusion defects, respectively. We compared results obtained in 43 consecutive transplant recipients withoutcritical or diffuse stenotic segments to 12 patients with singlevessel disease of their native heart and to 13 controls. In asubgroup of 27 heart transplant recipients, we prospectivelycompared the SPECT findings to results of intracoronaryultrasonography.
Our study should answer the following questions: Does thedegree of 201Tl SPECT abnormalities in transplant recipientsreach statistical significance in comparison to a control group?Is there any influence of former rejection episodes oninhomogeneity? Do 201T1myocardial SPECT findings reflectprogressive disease? Can SPECT findings be explained bysonographically detected wall alterations of epicardial coronaryarteries?
MATERIALSAND METhODS
PatentsForty-three consecutive orthotopic heart recipients (34 men, age
range 26—70yr, mean age 53.7 ±10.7 yr; body surface area (BSA)1.90 ±0.19 (1.51—2.45)m2; donor age 10—55yr, mean age 28.9 ±12.7 yr) have been included in the study if coronary angiographywas normal (no stenosis > 50%, no loss of middle sized vessels,absence of pruning effects) and 201Tl SPECT after treadmillexercise was available at the same time. Eighty-one scans havebeen evaluated. Thirty-three investigations were performed in
Progressivegraft atherosclerosisis a serious complication in longterm survivors after heart transplantation.Coronary angiographyisinsensitivewith regardto the earlyand characteristicafteratlonS.Weevaluatedthe progressionof these abnormalitiesand the influenceof former rejection episodes. Methods Early after transplantation,43 patients(34 men,meanage53.7 ±10.7yr)underwentstressandredistribution 201@flmyocardiai SPECT after treadmill exercise.Twenty patientswere followed-up to the second postoperativeyear,and 13 patients to the third postoperativeyear.Thallium-201distribution and kinetic abnormalities were documented in a schemeenclosing20 myocardialsegments.Mdi@onally,a score was developed that measuredthe degree of inhomogeneityof 201@fldistributionandthe severityof perfusiondefects,respectively.Results:Regardingscintigraphy,pathologic resultscould be found in 40% ofsegments (redistribution,25%; reverse redistribution,30%; persistent defects, 49%). Score values in heart transplant recipientsdiffered significantly from normal controls (p < 0.001) and werecomparable to patients with single vessel disease of their nativehearts. Thallium-201 inhomogeneity in recipients after treatablerejectionepisodesdid not differfrom resuttsin recipientswithout anybiopsy-provenrejection.Thefollow-up of cardiactransplantpatientsrevealeda significant increaseof score values up to the third yearaftertransplantation(p < 0.02),despite reproduciblenormalangiography. There was no direct correlation between score values andIVUS results, although there was a parallel trend in 10 of 12follow-ups. Conclusion: Despite normal coronary angiography,2O1@fl myocardial SPECT frequently revealed pathOlogIC results in
heart transplant recipients. Scintigraphic resutts dkl not correlatewith intimal thickening of epicardialcoronary arteries accessibletointravascularuttrasonographyin the early phase after transplantstion.Thepresentedscoreof inhomogeneitymightrevealprogressive disease possibly caused by small vessel alterations.Key Words thallium-201; SPECT;heart transplantation;graft atheroscierosis;intravascularultrasound
J NuciMed1997;38760-765
A fterthefirstpostoperativeyear,progressivegraftatheroscierosis accounts for 36% of deaths and 60% of retransplantationprocedures after primarily successful cardiac transplantation(1). The pattern in graft vasculopathy is quite different fromcoronary artery disease of the native heart; diffuse concentricintimal proliferation leads to luminal narrowing throughout thecoronary tree with distal obliteration and extensive coronaryartery stenosis. Although the influence of cytomegalovirusinfection is proven, and the role of severe hypercholesterinemiaand rejection is under discussion, the defmitive cause of these
Received Mar. 12. 1996; revision accepted Sep. 11, 1996.For correspondence or reprints cont@t Corneha Puskás,Department of Medicine
and Nuclear Medicine, Hospital OfWeStfaliScheWilheIms-University of MUnster,AlbertSchweitzer Sb'. 33, 48129 MUnster, Germany.
760 THEJOURNALOFNUCLEARMEDICINE•Vol. 38 •No. 5 •May 1997
Progressive Heterogeneity of Myocardial Perfusionin Heart Transplant Recipients Detected byThallium-201 Myocardial SPECTCornelia Puskás,Markus Kosch, Sebastian Kerber, Margot Jonas, Michael Weyand, GünterBreithardt, Hans H. Scheld andOtmar SchoberDepartments ofNuclear Medicine, Cardiology and Angiology, and Cardiovascular Surgery, Wes@dlische Wilhelms University,Miinster, Germany
by on November 28, 2015. For personal use only. jnm.snmjournals.org Downloaded from

the first, 27 in the second and 21 in the third postoperative years(3.9 ±2.7, 17.1 ±3.3 and 30.1 ±3.7 mo after transplantation,respectively), including 20 who underwent follow-up from the firstto the second year and 13 who underwent follow-up from thesecond to the third year.
Twelve patients with angiographically proven single-vesseldisease of the left anterior descending artery (LAD) (10 men, agerange 44—71yr, mean age 61.5 ±7.6 yr) were evaluated forcomparison and validation of the inhomogeneity score. Patients withprevious infarctionor cardiovascularsurgeryhad been excluded.
Thirteenpatientswith atypicalchest pain and low risk for coronaryartery disease (4 men, age range 46—68yr, mean age 57.5 ±8.7 yr.BSA 1.80 ± 0.15 (1.59—2.12)m2) served as control subjects.Angiography and clinical follow-up excluded underlying cardiacdisease.
In a subgroup of 27 heart recipients (21 men, age range 24—69yr, mean age 520 ±11.0 yr), intravascular ultrasonography wasperformed in the first postoperative year; 12 patients underwentfollow-up in the second year.
In transplant recipients, immunosuppression consisted of prednisolone, azathioprine and cyclosponne. In the first year, endomyocardial biopsy was routinely performed once per week duringthe first month, monthly in the following 5 mo and then at intervalsof 6—8wk up to 1 yr. Patients underwent angiography 3.9 ±2.7mo after transplantation and thereafter in yearly intervals. Scintigraphy was performed on the occasion of these routine surveysincluding endomyocardial biopsy and angiography within 1 wk.Acute rejection episodes at the time of investigation were excludedby endomyocardial biopsy.
ScintigraphyVasoactive drugs were withdrawn 24 hr before the study. All
patients underwent a maximal symptom-limited bicycle ergometerexercise test in the sitting position in a fasting state. The initialworkload of 50 W for 2 mm was subsequently increased by 25 Wevery 2 mm. One hundred megabecquerels of 201T1-chloridewasinjected intravenously during maximal treadmill exercise andexercise was continued for 1 mm. Imaging was started 5—10mmand 3 hr after exercise. Thirty-two views (30 sec) on a 180°rotation(starting in the 45°right anterior oblique position) were acquired ina 64 X 64 matrix. Long and short projections of the heart wereobtained using standard SPECT software with filtered backprojection (Butterworth filter of fifth order and 0.5 Nyquist cutofffrequency).
Deta M@A target scheme was overlaid on the short axis slices represent
ing best the apical, medial and basal myocardium. Thus, the leftventricular myocardium was divided into 20 segments (Fig. 1). Theshort-axis slices of the stress and redistribution study of eachindividual were realigned using the apex of the left ventricle andthe anteroseptal insertion of the right ventricle visible on theimages without background subtraction. The segment with themaximal uptake was defmed for each scan. Segments having lessthan 40% of the maximal uptake were categorized as Grade 0 (=threshold). Segments with uptake between 40% and 55% werecategorized as Grade 1; segments with uptake between 55% and70% were categorized as Grade 2; segments with uptake of morethan 70% were categorized as Grade 3. Thus, intensity of 201T1accumulation in each segment of the stress and redistribution scanwas scored as 0 (no uptake), 1 (severely reduced uptake), 2(moderately reduced uptake) or 3 (normal uptake) with regard tograduation on the color scale. To avoid the influence of wellknown absorption artifacts in 201Tlscintigraphy, the five inferiorwall segments were excluded, and the remaining 15 segments were
FIGURE1.DMsionof leftventricularmyocardiumin20segments.Segments1-4 = apicalmyocardium;segments5-12 = midventricularmyocardium;segments13—20= basalmyocardium.
evaluated. Scoring was done by two independent observers. If adiscrepancy in scoring was present, score values were averaged.
The score of inhomogeneity was calculated as follows:
15
Score = 45 —
15
+ @lS@—R11 i = 1,-••,l5Eq. 1i=l i=l
ScoreScore (%) = x 100%
90Eq. 2
@l,- .@ ‘ @l5= grade of201Tl accumulation in the 15 segments of
the stress image. R1, . . . , R15 = grade of201Tl accumulation in the15 segments of the redistribution image. Si —R1 = differencebetween grades given in corresponding segments in stress andredistribution image (in positive values).
The first term of Equation 1 results from the stress image: 15 X3 score points are possible, yielding an ideal value of 45 —45 =0. The second term represents the sum ofthe segmental differences(positive values) comparing stress and redistribution images. Withregard to the highest possible score of 90, the score is ultimatelyexpressed in percent (Eq. 2).
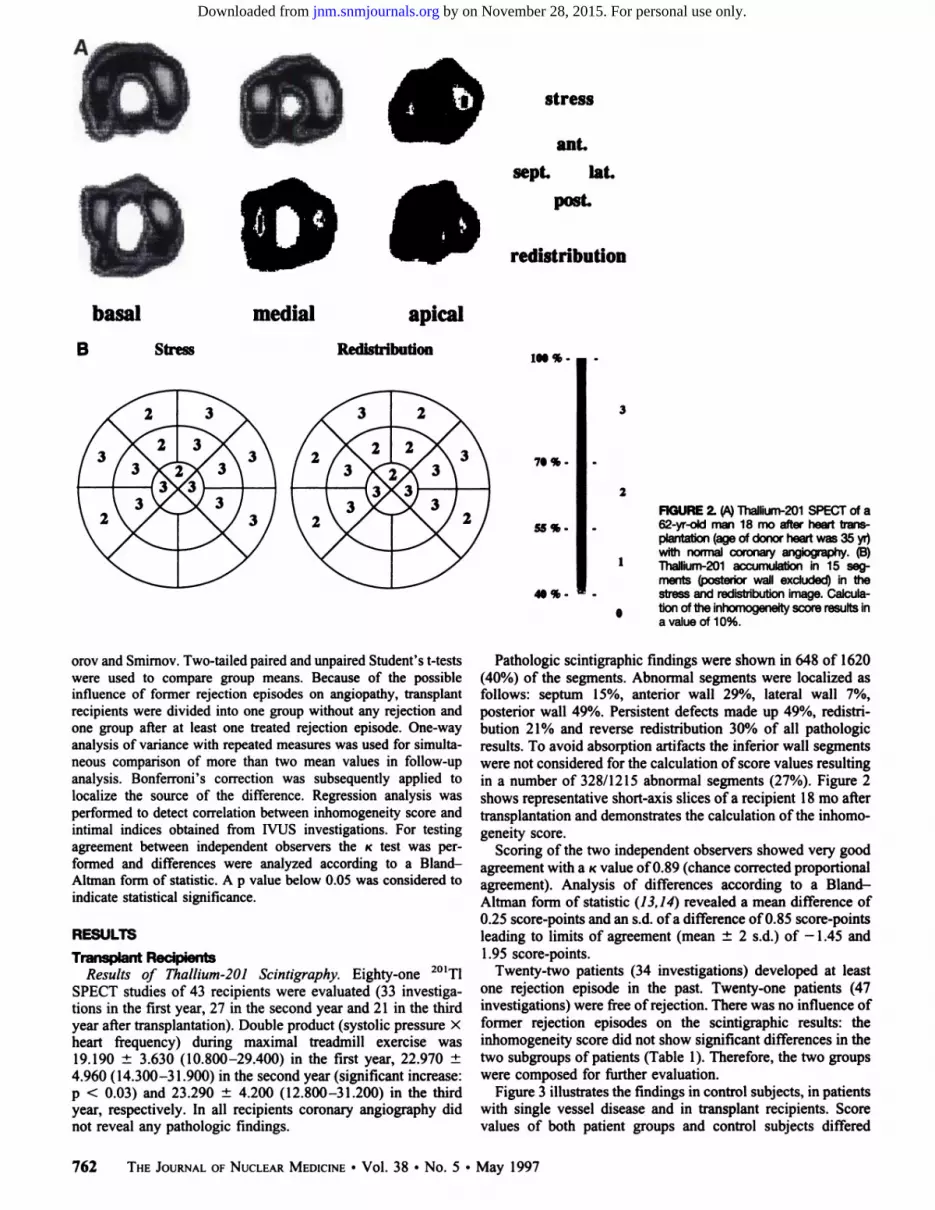
Figure 2 gives an example and demonstrates grading of 201Tlaccumulation.
Intravascular ultrasonography was confmed to one coronaryartery (see below). For comparison of scintigraphic results withintravascular ultrasound (WUS) findings related to the corresponding coronary territory a regional score value was calculated, e.g.,including the five anterior segments [1, 5, 6, 13 and 14 (Fig. 1)] incorrelation to LAD WUS findings.
NUSDuring routine coronary angiography using the Judkin's tech
nique by means of the right femoral artery, a guide wire (0.0 14inch) was advanced into the mmdportionof the LAD. Using thisguide wire, a 3.5 French somcath-catheter was advanced usingcontinuous biplane fluoroscopic control. The 30 MHz transducer ofthe ultrasound catheter (monorail system) was connected to theimaging system Sonos 1000. During withdrawal of the transducerfrom the midportion of the LAD to the stem, cross-sectional areasof coronary segments were depicted and the vessel morphologyincluding intima-media-boundary was visualized. All intravascularimages were stored on VHS videotapes for later analysis.
Data Analysis. Measurement of cross-sectional lumen andplaque was performed off-line. The outer boundaries of plaqueareas were determined after the internal elastic lamina. Intimalindex (intimal index = plaque area/lumen area) as a parameter ofgraft atherosclerosis was calculated for each cross-sectional area.
Ststistical An@All values are expressed as means ±s.d. Normal distribution of
score values in each subgroup was proven by the test of Kolmog
[email protected] SPECT IN CARDIACALLOGRAFTS•Puskás et al. 761
by on November 28, 2015. For personal use only. jnm.snmjournals.org Downloaded from
basal medial apical
B Stress Redistribution iN % -
70%-
55%-
41%-
2RGURE2. (i@4Thallium-201SPECTof a62-yr-oldmen 18 me afterhearttransp@ntatlon(ageof donorheartwas35yr)wfth normalcoronaryangkgraphy.(B)
1 Thallium-201accumulationin 15 sagmerits (posteriorwall excluded)in thestressandredistributionimage.Calcula
0 tlon of the inhomogeneltyscore resultsina valueof10%.
orov and Smimov. Two-tailed paired and unpaired Student's t-testswere used to compare group means. Because of the possibleinfluence of former rejection episodes on angiopathy, transplantrecipients were divided into one group without any rejection andone group after at least one treated rejection episode. One-wayanalysis of variance with repeated measures was used for simultaneous comparison of more than two mean values in follow-upanalysis. Bonferroni's correction was subsequently applied tolocalize the source of the difference. Regression analysis wasperformed to detect correlation between inhomogeneity score andintimal indices obtained from IVUS investigations. For testingagreement between independent observers the K test was performed and differences were analyzed according to a BlandAltman form of statistic. A p value below 0.05 was considered toindicate statistical significance.
RESULTS
Transplant RecipientsResults of Thallium-201 Scintigraphy. Eighty-one 201T1
SPECT studies of 43 recipients were evaluated (33 investigations in the first year, 27 in the second year and 21 in the thirdyear after transplantation). Double product (systolic pressure Xheart frequency) during maximal treadmill exercise was19.190±3.630(10.800—29.400)inthefirstyear,22.970±4.960 (14.300—31.900) in the second year (significant increase:p < 0.03) and 23.290 ±4.200 (12.800—31.200) in the thirdyear, respectively. In all recipients coronary angiography didnot reveal any pathologic findings.
Pathologic scintigraphic findings were shown in 648 of 1620(40%) of the segments. Abnormal segments were localized asfollows: septum 15%, anterior wall 29%, lateral wall 7%,posterior wall 49%. Persistent defects made up 49%, redistribution 21% and reverse redistribution 30% of all pathologicresults. To avoid absorption artifacts the inferior wall segmentswere not considered for the calculation ofscore values resultingin a number of 328/1215 abnormal segments (27%). Figure 2shows representative short-axis slices of a recipient 18 mo aftertransplantation and demonstrates the calculation ofthe inhomogeneity score.
Scoring of the two independent observers showed very goodagreement with a Kvalue ofO.89 (chance corrected proportionalagreement). Analysis of differences according to a BlandAltman form of statistic (13, 14) revealed a mean difference of0.25 score-points and an s.d. ofa difference ofO.85 score-pointsleading to limits of agreement (mean ±2 s.d.) of —1.45 and1.95score-points.
Twenty-two patients (34 investigations) developed at leastone rejection episode in the past. Twenty-one patients (47investigations) were free ofrejection. There was no influence offormer rejection episodes on the scintigraphic results: theinhomogeneity score did not show significant differences in thetwo subgroups of patients (Table 1). Therefore, the two groupswere composed for further evaluation.
Figure 3 illustrates the findings in control subjects, in patientswith single vessel disease and in transplant recipients. Scorevalues of both patient groups and control subjects differed
762 THEJOURNALOFNUCLEARMEDICINE•Vol. 38 •No. 5 •May 1997
stress
ant.
sept. lat.
post.
redistribution
3
by on November 28, 2015. For personal use only. jnm.snmjournals.org Downloaded from

Score of inhomogeneity(%)Yearafter
transplantation Mean±s.d. RangeNo.
of investigationsandsignificanceofdifferencesrvs.t)5.3±2.8
First5.8±2.31.1—9.93.0—11.0fl*19
ns@ 14 (p=0.4)6.5
±3.9Second7.1±3.72.2—15.41.1—14.3n@
11 ns@ 16 (p=0.5)5.8
±3.6Third6.9±4.23.3—1
1.01.1—15.6n*
4@ 17 (p =0.5)Without
rejection.tAftartreatablerejection.ns
= not significant.
TABLE IThallium-201 lnhomogenelty in Heart RecipientsWith and Without
RejectionEpisodes
year and of 7.8% ±4.3% in the second year was calculated. Inthe 12 patients who underwent follow-up, paired t-test revealeda significant increase of score values (j < 0.03).
Results of IVUS. In 39 IVUS investigations (including 12patients who underwent follow-up), a three-layer appearance ofthe vessel wall indicating significant intimal thickening wasdemonstrated in 112/283 (39%) of all cross-sectional areas. Atfirst investigation (n = 27), mean intimal index of all crosssectional areas was 0.08 ±0.1 (range: 0.0—0.314). At secondinvestigation (n = 12), mean intimal index was 0.09 ±0.1(range: 0.0—0.346). The increase was not significant.
Comparison Between Thallium-201 SPECT Results andIVUS Findings. There was no correlation either between theinhomogeneity score values, including 15 myocardial segmentsand the intimal indices (r = 0.06, p = 0.72), or betweenregional inhomogeneity score and corresponding intimal mdices (r = 0.143, p = 0.49).
In 10 of 12 follow-ups, there was a parallel change in bothintimal index and inhomogeneity score. In six patients, bothparameters increased, in four patients both parameters decreased, in two patients there were discordant developments.
Patients with CAD (Single-VesselDisease of the LAD)In each patient, scintigraphy showed persistent perfusion
defects or redistribution in accordance with angiographic results(more than 70% luminal narrowing of the LAD). Score valuesranged from 3.3%—9.9%(mean 65% ±2.2%).
Control SubjectsIn 13 normal control subjects, score values ranged from
0%—3.3%(mean 1.1% ±1.4%). The difference between scorevalues of control subjects and heart recipients proved to behighly significant (j' < 0.001).
significantly (p < 0.001). The degree of abnormality in patientswith single vessel disease and transplant recipients was on thesame level, given the fact that score values do not depend ondistribution of pathologic segments. The score values of patientscovered a wide range (mean values and s.d. in year 1, 2 and 3:5.5% ±2.6%,6.6% ±3.7%and6.8% ±4.6%,respectively).
Follow-up studies in 20 patients from the first to the secondyear and in 13 patients from the second to the third year couldbe obtained. Results are listed in Table 2. Analysis of variancewith repeated measures showed significantly increasing scorevalues in course oftime (p < 0.05). Bonferroni corrected pairedt-test revealed a significant increase from the first to the secondyear and from the first to the third year (p < 0.04).
In the subgroup of the 27 patients with 39 P/US investigations a mean inhomogeneity score of 5.8% ±2.6% in the first
20
@l 15 0
EC 00
.E0
hi
00 0 J 000 0c@@ 00
00
010@ c@@ 00
5-@ I @° c@a@
00@@ 00 0 0
00@ I@ i 0
aD 0@ 00
0 J 0 00 aD
aD 0
0- trrvrri I 00 00 0
Controls CAD â€1̃2mo 13 - 24 mo > 24 mo
(n= 13) (n= 12) (n= 33) (n= 27) (n= 21)
Transplant recipients
FIGURE3@Distributionof score values in controls, in patients with singlevessel d@ease(CAD)and heart transplant recipients.Posteriorsegments wereexcluded.
Th@&LLIuI@i-20lSPECT n@CARDIACALLOGRAFTS. Puskáset al. 763
by on November 28, 2015. For personal use only. jnm.snmjournals.org Downloaded from

YearafterScore
of inhomogeneity(%)Significanceofdifferencelstto2ndyeantransplantationMean
±s.d.Range2nd to 3rdyear1st to 3rdyearFirst6.0
±3.01.1—11.0n= 20; p <0.05Second7.0
±3.32.4—15.4n = 10;p <0.04n=13;p=0.066Third7.4
±3.71.1—13.2
TABLE2Thallium-201 Inhomogeneityin Follow-up Patients
DISCUSSIONProgressive graft atherosclerosis has a strong impact on the
long-term survival of heart transplant recipients. Coronaryangiography reveals atherosclerotic lesions in 2O%—4O%ofpatients 3 yr after transplantation (8). After 5 yr, about 50% oftransplant recipients are concerned, whereas 20% have criticalstenosis of more than 75% (15). However, transplant vasculopathy is different from coronary atherosclerosis of the nativeheart because its diffuse nature of concentric narrowing affecting the small endocardial vessels as well as the large epicardialarteries. Therefore, sensitivity of coronary angiography is lowwith regard to the early characteristic alterations ofgraft vessels.Histologic studies and intravascular ultrasonography have revealeda high percentage of patients with at least diffuse intimal thickening as early as 1 yr after transplantation(1,6, 7).
The evaluation of 201Tl myocardial scintigraphy in the follow-up of heart transplant recipients has focused on the detection of circumscribed coronary artery stenoses comparable toCAD of the native heart. The reported sensitivity of exercise201T1scintigraphy ranged from 77% (10) to 100% (8), wherebythe particular investigations were based on small numbers ofpatients. Oral application of dipyridamole is a questionablemethod of pharmacological stressing and resulted in a lowsensitivity of2l% (11). The degree ofresorption of dipyridamole is probably a poor controlled factor in this protocol andkinetics of 201Tlare different from exercise studies (16).
Thallium-201 distribution does not only depend on patencyof coronary arteries and their branches. It rather reflectsperfusion throughout the coronary tree up to the capillary bed.McKillop et al. (1 7) reported on four patients without coronaryartery stenoses of their transplants and fixed defects in planar201T1scintigraphy. The authors discussed small vessel diseaseas a possible cause. Apart from that, the reported small numberof false-positive results in the working groups of Ciliberto,Rodney and Ambrosi is surprising (8, 10, 12). In contrast to thesefindings, we frequently observed pathologic 201Tl SPECTresults in patients with normal angiography after heart transplantation. The distribution of abnormalities was arbitrary anddid not correlate to coronary territories as in CAD of the nativeheart. One possible explanation for this contradiction could bethe criteria for a pathologic scan used by other investigators:most authors focused on the typical scintigraphic equivalent ofischemic myocardium, i.e., redistribution or persistent defects.However, the diffuse nature of graft vasculopathy may notresult in scintigraphic abnormalities depicting coronary territories (18).
To objectify our visual impression, we analyzed 81 scans of43 transplant recipients semiquantitatively in a 20-segmentscheme. The evaluation by two independent observers demonstrated high reproducibility. We observed abnormalities in 40%of all segments of the angiographically normal hearts.
To measure the degree of 20'Tl inhomogeneity and severity
of regional perfusion defects, a score was developed based on201T1accumulation in 15 left ventricular myocardial segments.The loss of information about the localization of defects wasaccepted because of the diffuse nature of graft atherosclerosis.Even if the posterior wall was excluded, score values oftransplant recipients without significant angiographic findingsdiffered significantly from normal control subjects. The degreeof abnormality in terms of inhomogeneity score was comparable to patients with angiographically proven-single vesseldisease (Fig. 3). It is difficult to exclude soft-tissue artifactspossibly caused by breast absorption. It has to be consideredthat 9 women in the group of 13 control subjects may at mostraise the mean score value and increase variability in inhomogeneity scores, respectively. Nevertheless, the difference between controls and recipients reached a high grade of significancy. On the other hand, the longitudinal study evaluatingintraindividual changes is not influenced by breast absorption.Therefore, we did not exclude women from our investigation.
The degree of exercise in transplant recipients was comparable to those reported by other authors (19). The group aroundSchelbert demonstrated that the absolute myocardial flow understress in heart transplant recipients is not significantly differentfrom normal control subjects, although the level ofexercise waslower in patients (20,21). The exercise protocol used in thatquantitative PET study was identical to that used in our study.Therefore, 201T1SPECT abnormalities in our patients cannot beexplained by suboptimal exercise levels.
An influence of acute rejection episodes on 201Tl uptake hasbeen repeatedly demonstrated in experimental and clinicalstudies (22—24).Apart from impaired myocardial perfusion, thealteration of membrane integrity by immunological processesseems to be of importance. Therefore, acute rejection wasexcluded by biopsy in our study.
Effects of former rejection episodes on graft artherosclerosisare under controversial discussion. We compared one subgroupof patients without any rejection episode in the history with asubgroup with at least one treatable rejection crisis. Scorevalues did not differ significantly in both groups. This result isin accordance with the studies of Nitenberg and Richter whofound a rapid normalization of coronary flow reserve and 201Tlscintigraphy after recovery from acute rejections (25,26). Gaoet al. (27) did not find any correlation between frequency andseverity of rejection episodes and accelerated graft atheroscierosis. However, chronic rejection that is not proven by biopsycould not be excluded in our study.
In the course of time, transplant recipients showed significantly increasing inhomogeneity scores (p < 0.04), despitereproducible normal angiographic findings. The observed abnormalities in the 201Tl SPECT studies do obviously indicate aprogressive course.
For interpretation of these results, morphology and distribulion of the disease may be important: histologic studies dem
764 THEJOURNALOFNUCLEARMEDICINE•Vol. 38 •No. 5 •May 1997
by on November 28, 2015. For personal use only. jnm.snmjournals.org Downloaded from

onstrated graft vasculopathy as an accelerated, diffuse processof intimal hyperplasia of the whole coronary tree (18). Johnsonet a!. (6) found intimal alterations in all explanted hearts asearly as 1 yr after transplantation. Billingham et al. (28) showedearly occlusion of small distal vessels without sufficient collateralization leading to microinfarction of the myocardium. Mason et al. (29) reported the case of a patient who died shortlyafter a normal coronary angiography because of multiplemicroinfarctions. Autopsy showed normal epicardial vessels,but intimal proliferation and occlusion of the small distalvessels. Therefore, the progressive abnormalities demonstratedin our study may well be early signs of accelerated graftvasculopathy of the small vessels. This would be in line withfindings of a PET study of coronary flow in transplant recipients with angiographically proven graft atherosclerosis (30).Coronary resistance was homogeneously increased not only inthe coronary territory of the narrowed vessel. Wolpers et al.(30) explain this discrepancy between morphological and functional findings by microvascular obliterations.
Another factor contributing to inhomogeneity of 201Tluptakemay be endothelial dysfunction leading to altered microvascularcirculation. Angiography demonstrated a high percentage ofpatients with abnormal endothelial reaction on intracoronaryacetylcholine in the first year after transplantation (7).
Contrary to expectation, there was no direct correlationbetween intimal indices calculated from IVUS images and theinhomogeneity scores from 201Tl SPECT. There are someexplanations for this discrepancy: the mean extent of intimalhyperplasia measured by IVUS in the LAD was discrete. Inaddition to this, the findings in the proximal and mid-portion ofthe LAD do not necessarily represent the extent of vasculopathythroughout the coronary tree. Klauss et al. (31 ) demonstratedthe differences in degree and extent of the disease betweendifferent coronary segments and arteries by intravascular ultrasonography. However, there was a parallel change (predominantly deterioration) of 10 of 12 follow-up patients. Long-termfollow-up studies should focus on this trend.
CONCLUSIONOne problem in the evaluation of follow-up procedures in
heart transplant recipients is the lack ofa valid gold standard forthe early state of graft vasculopathy. Sensitivity of coronaryangiography is low with regard to early, diffuse changes invessel morphology. IVUS is certainly an accurate imagingtechnique of vessel morphology, but it is limited to the largeepicardial arteries. Biopsy does normally not depict relevantvessels. Possibly the observed progressive scintigraphic abnormalities may be early signs of beginning graft vasculopathy,i.e., angiographically silent small vessel disease that is notnecessarily correlated to IVUS findings in epicardial coronaryarteries. However, possible influences of chronic rejection orendothelial dysfunction could not be excluded. The prognosticrelevance of °1TlSPECT findings, the possibility of identifying “highrisk patients,―has to be evaluated in a furtherlong-term follow-up study.
REFERENCES1. St Goar FG, Fausto JP, Alderman EL, et al. Intracoronary ultrasound in cardiac
transplant recipients: in vivo evidence of―angiographically silent―intimal thickening.Circulation 1992;85:979—987.
2. Olivari MT, Kubo SH, Braunlin EA, Bolman RM, Ring WS. Five-year experience withtriple-drug immunosuppressive therapy in cardiac transplantation. Circulation 1990;82(suppl):1V276—1V280.
3. McDonaldK, RectorIS, BraunlinEA, Kubo SH,Olivari MT. Associationof coronaryartery disease in cardiac transplant recipients with cytomegalovirus infection. Am JCardiol1989;64:359—362.
4. Eich D, Thompson J, Ko D, et al. Hypercholesterinemia in long term survivors of hearttransplantation: an early marker of accelerated coronary artery disease. J Heart LungTransplant 1991 ;l0:45—49.
5. Pinto FJ, Chenzbraun A, Botas J, Ct al. Feasibility of serial intracoronaiy ultrasoundimaging for assessment of progression of intimal proliferation in cardiac transplantrecipients. Circulation 1994;90:2348—2355.
6. JohnsonDE, AldermanEL, SchroederJS,et al. Transplantcoronaryartery disease:histopathologic correlations with angiographic morphology. J Am Coil Cardioll991;17:449—457.
7. Kerber 5, Rahmel A, Karbenn U, et al. Early allograft vasculopathy in orthotopic hearttransplantrecipients:angiographic,intravascularultrasoundand functional in vivofindings. Z Kardioi 1994;83:215—224.
8. Ciliberto GR, Mangiavacchi M, Banfi F, et al. Coronary artery disease after hearttransplantation: noninvasive evaluation with exercise thallium scintigraphy. EurHeart J 1993;l4:226—229.
9. Rodney RA, Johnson LL. Myocardial perfusion scintigraphy to assess heart transplantvasculopathy. J Heart Lung Transplant 1992;l l:S74—S78.
10. Rodney RA, Johnson LL, Blood DK, Barr ML. Myocardial perfusion scintigraphy inheart transplant recipients with and without allograft atherosclerosis: a comparison ofthallium-201 and technetium-99m-sestamibi. J Heart Lung Transplant 1994;l3:173—180.
11. Smart FW, Ballantyne CM, Cocanougher B, et al. Insensitivity of noninvasive tests todetect coronary artery vasculopathy after heart transplant. Am J Cardiol 1991;67:243—247.
12. Ambrosi P, Habib G, Kreitman B, et al. Thallium perfusion and myocardialhypertrophy in transplanted heart recipients with normal or near normal coronaryarteriograms. EurHeartf 1994;l5:lll9—1123.
13. Altman DO. Inter-rater agreement. In: Altman DO, ed. Practical statisticsfor medicalresearch. London: Chapman and Hall; 1991:403—409.
14. Bland JM, Altman DO. Statisticalmethodsfor assessingagreementbetweentwomethods of clinical measurement. Lancet 1986;i:307—310:.
15. von Scheidt W, ErdmannE. Dilated angiography:a specific subtype of allograftcoronary disease. J Heart Lung Transplant 1991;I0:698-703.
16. Lee J, Shung C, Chae C, Lee K, Hen J, Iskandrian AS. Biokinetics ofthallium-20I innormal subjects: comparison between adenosine, dipyridamole, dobutamine andexercise. JNuci Med 1994;35:535—54l.
17. MeKillop JH, Goris ML. Thallium-201 myocardial imaging in patients with previouscardiac transplantation. Clin Radiology 1981;32:447—449.
18. Hosenpud JD, Shipley GD, wagn@ CR. Cardiac allograft vasculopathy: currentconcepts, recent developments and future directions. J Heart Lung Transplant1992;l 1:9—23.
19. Mandá JS, Aaronson KD, Mancini DA. Serial assessment of exercise capacity afterheart transplantation. J Heart Lung Transplant l995;l4:468—478.
20. Krivokapich J, Stevenson LW, Kobashigawa J, Sung-Cheng H, Schelbert HR.Quantification of absolute myocardial perfusion at rest and during exercise withpositron emission tomography after human cardiac transplantation. J Am Coil Cardiol199l;18:512—5l7.
21. McGinn AL, wilson RF, Olivari MT, Homans DC, V@'hiteC%V.Coronary. vasodilatorreserve after human orthotopic cardiac transplantation. Circulation 1988;78:l200—1209.
22. PinedoJI, Golitsin A, CienfuegosJA, et al. Roleof thallium-20l in the managementof cardiactransplantation.EurJ Nuci Med l985;l0:203—207.
23. Bergsland J, CarrEA, Caroll M, et al. Uptake ofmyocardial imaging agents by rejectedhearts. J Heart Transplant 1985;4:536—540.
24. RichterJA, HerrerosJ, SerenaA. Thallium-201myocardialimagingin cardiacrejectionepisode.EurJNuclMed I986;I 1:368—370.
25. Nitenberg A, Tavolaro 0, Benvenuti C, et al. Recovery ofa normal coronary vascularreserve after rejection therapy in acute human cardiac allograft rejection. Circulation1990;8l:l312—1318.
26. RichterJA,HerrerosJ,SerenaA. DomperM, RamirezJC,AreasR.Thalliumscintigraphyin human transplants: a way to detect myocardial damage. J Heart Lung Thanspiant199l;l0:33—37.
27. Gao SZ, Schroeder iS, Hunt SA, Valantine HA, Hill IR, Stinson EB. Influence of graftrejection on incidence of accelerated graft coronary artery disease: a new approach toanalysis. J Heart Lung Transplant 1993;12:1029—l035.
28. Billingham ME. The pathologic changes in long.term heart and lung transplantsurvivors. J Heart Lung Transplant 1992;l 1:252—257.
29. Mason JW, Strefling A. Small vessel disease of the heart resulting in myocardialnecrosis and death despite angiographicallynormalcoronaryarteries.Am J Cardiol1979;44:171—176.
30. wolp@raHG, KösterC, Burchertw, et al. Dipyridamole coronary reserve afterorthotopic heart transplantation: measurement by ‘3Nammonia and positron emissiontomography. ZKardiol 1995;84:1I2—120.
31. Klauss V, Rieber J, UberfuhrP. Theisen K, MudraH. Variabilityof cardiac graftvasculopathy: a study with intravascular ultrasonography. Z Kardiol 1995;84: 121—129.
[email protected] SPECT m@CARDIACALLOGRAFTS@ Puskáset al. 765
by on November 28, 2015. For personal use only. jnm.snmjournals.org Downloaded from

1997;38:760-765.J Nucl Med. and Otmar SchoberCornelia Puskás, Markus Kosch, Sebastian Kerber, Margot Jonas, Michael Weyand, Günter Breithardt, Hans H. Scheld Detected by Thallium-201 Myocardial SPECTProgressive Heterogeneity of Myocardial Perfusion in Heart Transplant Recipients
http://jnm.snmjournals.org/content/38/5/760This article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1997 SNMMI; all rights reserved.
by on November 28, 2015. For personal use only. jnm.snmjournals.org Downloaded from





























