Embed Size (px)
Citation preview

Prospective Randomized Controlled Trial of OperativeRib Fixation in Traumatic Flail Chest
Silvana F Marasco MSurg FRACS Andrew R Davies FRACP FCICM Jamie Cooper FRACP FCICM MDDinesh Varma FRANZCR Victoria Bennett BNSc CCRN Rachael Nevill BNurs Geraldine Lee MPhilMichael Bailey PhD MSc (statistics) Mark Fitzgerald FACEM
BACKGROUND Traumatic flail chest injury is a potentially life threatening condition traditionally treatedwith invasive mechanical ventilation to splint the chest wall Longer-term sequelae of paindeformity and physical restriction are well described This study investigated the impact ofoperative fixation in these patients
STUDY DESIGN A prospective randomized study compared operative fixation of fractured ribs in the flailsegment with current best practice mechanical ventilator management In-hospital data3-month follow-up review spirometry and CT and 6-month quality of life (Short Form-36)questionnaire were collected
RESULTS Patients in the operative fixation group had significantly shorter ICU stay (hours) postran-domization (285 hours [range 191 to 319 hours] for the surgical group vs 359 hours [range270 to 581 hours] for the conservative group p frac14 003) and lesser requirement for nonin-vasive ventilation after extubation (3 hours [range 0 to 25 hours] in the surgical group vs 50hours [range 17 to 102 hours] in the conservative group p frac14 001) No differences inspirometry at 3 months or quality of life at 6 months were noted
CONCLUSIONS Operative fixation of fractured ribs reduces ventilation requirement and intensive carestay in a cohort of multitrauma patients with severe flail chest injury (J Am Coll Surg2013-1e9 2013 by the American College of Surgeons)
Flail chest is a severe thoracic injury associated with signif-icant morbidity and mortality Mortality rates of up to33 have been reported reflecting the severity of theinjury as well as the likelihood of associated life threateninginjuries such as splenic liver myocardial and lung lacera-tions1 Risk of death is significantly higher in both youngpatients (18 to 45 years) with rib fractures of AbbreviatedInjury Score (AIS) of 3 or greater (odds ratio 14 95
CME questions for this article available athttpjacscmefacsorg
Disclosure InformationAuthors havenothing todiscloseTimothy JEberleinEditor-in-Chief has nothing to disclose
Support This study was funded by a grant from the Transport AccidentCommission Victoria Australia
Received October 25 2012 Revised December 3 2012 AcceptedDecember 11 2012From the CJOB Cardiothoracic Surgery Department (Marasco Lee) theIntensive Care Unit (Davies Cooper Bennet Nevill) the Department ofRadiology (Varma Bailey) and the Trauma Service (Fitzgerald) The AlfredHospital the Department of Surgery (Marasco Varma) Monash Univer-sity The Alfred Hospital and the Department of Epidemiology amp Preven-tive Medicine Monash University Melbourne AustraliaCorrespondence address AProf Silvana F Marasco CJOB CardiothoracicDepartment The Alfred Hospital Commercial Rd Prahran 3181 Australiaemail smarascoalfredorgau
FLA 510 DTD ACS6738_proof 8
1ordf 2013 by the American College of Surgeons
Published by Elsevier Inc
CI 13 to 16) and older patients (over 64 years) (odds ratio25 95CI 23 to 28)2 Patients with flail chest often havesevere acute respiratory failure requiring mechanical venti-lation and prolonged ICU stay Long-term morbidityincluding chronic pain deformity disability and respira-tory compromise have been well documented34
Despite some promising prospective trials operative ribfixation of flail chest is not considered standard manage-ment and is not practiced widely Currently rib fixationtends to be used in specialty trauma centers and is practicedby a minority of cardiothoracic trauma or orthopaedicsurgeons Reasons for this include lack of familiarity withexisting evidence and until recently a lack of specific ribfixation prostheses5
We conducted a prospective randomized controlled trialinvolving traumatic flail chest patients receivingmechanicalventilation comparing operative rib fixation to nonopera-tive management This single institution study was per-formed at The Alfred Hospital 1 of 2 adult major traumacenters in Victoria Australia6 More than 1200 majortrauma patients with an overall mortality of 8 are treatedeach year including approximately 580 adult thoracictrauma (Maximum Abbreviated Injury Score [1998version] gt2) patients with an overall mortality of 5
February 2013 354 pm
ISSN 1072-751512$3600
httpdxdoiorg101016jjamcollsurg201212024
2 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
The primary aim of the study was to investigate theeffect of operative rib fixation of flail chest on mechanicalventilation time and ICU stay
METHODSEnrolment for the study took place between January 2007and December 2011 Informed consent was obtainedfrom the next of kin initially and consent sought fromthe patient for follow-up once sufficiently recoveredInstitutional ethics committee approval was obtainedThe trial was registered under Clinical Trials Gov withregistration number NCT00298259Patients were screened for enrollment into the trial on
hospital admission Forty-six patients with traumatic flailchest injury receiving invasive mechanical ventilationwere enrolled in the study Patients were enrolled only ifthey were ventilator dependent with no prospect of success-ful weaning within the next 48 hours Inclusion criteriawere the presence of a flail segment defined as 3 or moreconsecutive ribs fractured in more than 1 place producinga free floating segment of chest wall Diagnosis was madeclinically with confirmation on 3-dimensional CTimaging Exclusion criteria were age greater than 80 years(it was considered that osteoporotic bones precluded fixa-tion with the available prostheses) spinal injuries (whichprecluded placement of the patient in a lateral decubitusposition) open rib fractures with soiling or infectionsepsis severe traumatic brain injury (Glasgow Coma Scalelt10 at the scene of accident or at presentation to thehospital as its management may have received priorityover the study protocol) and uncorrected coagulopathyRandomization was via a computer generated code using
block randomizationwith block size of 4 After consent andenrollment an opaque envelope with the treatment assign-ment was opened and the time of enrollment documentedPatients were randomized to either operative rib fixa-
tion or nonoperative management Surgery was plannedafter viewing 3-dimensional CT chest reconstructionsand was performed within 48 hours of enrollmentOnly rib fractures between the levels of ribs 3 and 10were fixed Usually 1 or 2 incisions were used to achieveaccess to multiple ribs Wherever possible chest wallmuscles were preserved splitting them along the lengthof their fibers The periosteum was also preserved Ribsfractured more than once were usually addressed by fixing1 fracture per rib converting a flail segment to simplefractured ribs Ribs with a single fracture were not fixedunless there was gross deformity mandating interventionAnterior and lateral rib fractures were preferentially fixedover posterior rib fractures due to more reliable fixationand easier access compared with posterior rib fractures78
FLA 510 DTD ACS6738_proof 8
Inion resorbable (Inion OTPS) 6- or 8-hole plates andbicortical screws were used for every rib fixation Theseplates and screws are made of a polylactide copolymerthat resorbs over 18 to 24 months The plates were appliedto the external cortical surface of the rib after reducing thefracture The screws traversed both the outer and innercortex of the ribs and were inserted after tapping the drillhole and using a depth gauge to determine the length ofscrew to be usedPatients assigned to nonoperative management were
treated with current best practice mechanical ventilatormanagement Weaning from ventilation was via a protocolused for all patients irrespective of assigned group and irre-spective of mode of ventilation Commencing from the dayafter surgery or 24 hours after enrollment in the conserva-tive management group patients had sedation (notanalgesia) cessation considered every morning and a spon-taneous breathing trial conducted if patients met appro-priate criteria If the patient was comfortable witha respiratory rate lt25 breathsminute after 4 hours ofthe spontaneous breathing trial mechanical ventilationwas weaned If the patientrsquos respiratory rate was gt25breathsminute appropriate sedation and mechanicalventilation were recommenced for another 24 hoursTracheostomy insertion was also protocol driven andoccurred at day 7 if it appeared to the treating physicianthat weaning of mechanical ventilation was not likelywithin the next 2 to 3 daysThe primary endpoints of the study were duration of
mechanical ventilation and ICU stay The secondaryendpoints were number of respiratory complications(pneumonia pneumothorax intercostal catheter usage)rate of failed extubation rate of tracheostomy readmis-sion to intensive care duration of hospital stay andcost assessment of the operation Pneumonia was definedas a new infiltrate on chest x-ray with positive sputumculture Intensive care unit discharge time was recordedas the time the patient was deemed ready for dischargeso that ward bed access did not affect the resultsPatients were reviewed at 3 months postoperatively for
clinical assessment spirometry and CT scan of chestimaging with 3-dimensional reconstructions of thethoracic cage All patients were sent a Short Form 36-item Health Status Questionnaire (SF-36) at 6 monthsto assess physical functioning role limitations owing tophysical problems role limitations owing to emotionalproblems social functioning mental health generalhealth perceptions vitality and bodily painSample size estimation was based on duration of
mechanical ventilation Calculations were performed usingduration of mechanical ventilation values from patientswith traumatic flail chest treated at The Alfred Hospital
February 2013 354 pm
printampweb4C=FPO
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 3
over the 4 years before commencement of this studyAssuming an alpha of 005 power of 08 and a standarddeviation of 140 hours to detect a difference in durationof mechanical ventilation of 120 hours (5 days) 23patients per group were required to be enrolled
Statistical analysis
Statistical analysis was performed using SAS version 92(SAS Institute Inc) All variables were initially assessedfor normality Group comparisons of proportions weremade using chi-square tests or Fishers exact tests wherenumbers were small and were reported as numbers ()Continuously normally distributed variables were com-pared using Student t-tests and reported as mean (stan-dard deviation) non-normally distributed data werecompared using Wilcoxon rank sum tests and reportedas medians (interquartile range) To ensure that allobserved results were not due to baseline imbalancesmultivariate modelling was used adjusting for the covar-iate of ldquoother surgical interventionsrdquo In order to facilitatethis duration variables were log-transformed andanalyzed using generalized linear modelling with resultsreported as geometric means (95 CI) The need for
Assessed for e
Analysed (n=23 for in hospital data and 59 for postoperative data)
Lost to follow-up (n=4)
Allocated to intervention (n= 23) diams Received allocated intervention (n=22)
Randomi
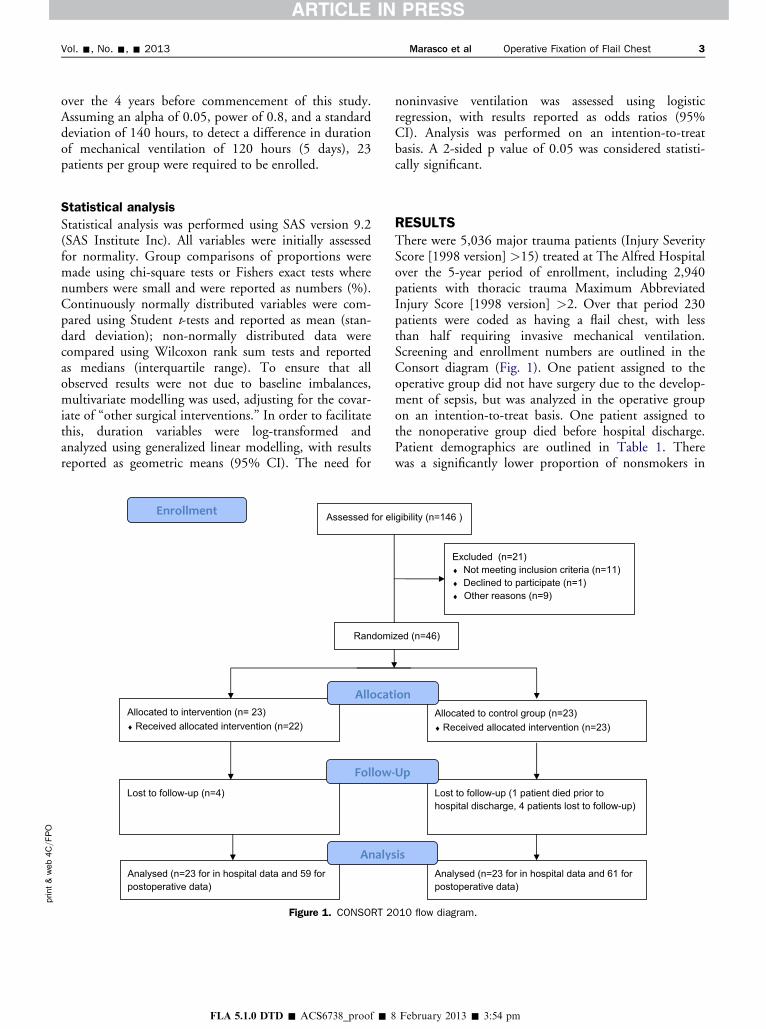
Figure 1 CONSORT 2
FLA 510 DTD ACS6738_proof 8
noninvasive ventilation was assessed using logisticregression with results reported as odds ratios (95CI) Analysis was performed on an intention-to-treatbasis A 2-sided p value of 005 was considered statisti-cally significant
RESULTSThere were 5036 major trauma patients (Injury SeverityScore [1998 version] gt15) treated at The Alfred Hospitalover the 5-year period of enrollment including 2940patients with thoracic trauma Maximum AbbreviatedInjury Score [1998 version] gt2 Over that period 230patients were coded as having a flail chest with lessthan half requiring invasive mechanical ventilationScreening and enrollment numbers are outlined in theConsort diagram (Fig 1) One patient assigned to theoperative group did not have surgery due to the develop-ment of sepsis but was analyzed in the operative groupon an intention-to-treat basis One patient assigned tothe nonoperative group died before hospital dischargePatient demographics are outlined in Table 1 Therewas a significantly lower proportion of nonsmokers in
ligibility (n=146 )
Excluded (n=21) diams Not meeting inclusion criteria (n=11) diams Declined to participate (n=1) diams Other reasons (n=9)
Lost to follow-up (1 patient died prior to hospital discharge 4 patients lost to follow-up)
Allocated to control group (n=23) diams Received allocated intervention (n=23)
Analysed (n=23 for in hospital data and 61 for postoperative data)
zed (n=46)
010 flow diagram
February 2013 354 pm
Table 1 Patient Demographics
Variable Operative group (n frac14 23) Nonoperative group (n frac14 23) p Value
Age y mean SD 578 171 593 104 072
Sex malefemale n 203 203 100
Body mass index kgm2 mean SD 279 46 290 68 055
Smoking history n ()
Ex smoker 5 (22) 2 (9) 022
Current smoker 8 (35) 3 (13) 008
Nonsmoker 10 (43) 18 (78) 002
Underlying lung disease n ()
Asthma 3 (13) 1 (4)
COPD 2 (9) 1 (4)
Mechanism of injury n () 086
Motor vehicle accident 17 (74) 14 (61)
Pedestrian vs car 2 (9) 3 (13)
Crush injury 1 (4) 2 (9)
Fall from height 3 (13) 4 (17)
NISS mean SD 364 103 429 133 007
ISS mean SD 350 114 300 63 013
TRISS mean SD 08 02 08 02 077
GCS at scene mean SD 134 28 136 26 074
Best GCS within first 48 h mean SD 110 45 99 47 043
Head injury AIS code 2 or above n () 0 (0) 2 (9) 049
Bony spinal injury n () 15 (65) 14 (61) 076
AIS Abbreviated Injury Score GCS Glasgow Coma Scale ISS Injury Severity Score NISS New Injury Severity Score TRISS Trauma and Injury SeverityScore
4 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
the operative group (43 vs 78 p frac14 002) but other-wise both groups were adequately matchedThere were no differences between groups in the
number of ribs fractured or the degree of underlyinglung contusion (measured at time of enrollment)(Table 2) There was a difference between groups in termsof other nonthoracic surgical interventions performed Thenonoperative group had a higher number of orthopaedicand general surgical operative procedures (74 vs 48p frac14 007) (Table 2)Twenty-two patients underwent operative rib fixation
Most (13 of 22 59) patients had 4 ribs fixed (range 2 to7 ribs) Two (9) patients had bilateral rib fixationAnterior and lateral fractures were most commonly fixedOnly 1 patient had posterior rib fractures fixedThe early postoperative outcomes are outlined in
Table 3 There was no difference between groups in theduration of invasive mechanical ventilation but noninva-sive ventilation was used in a greater number of patientsand for a longer duration in the nonoperative manage-ment group The nonoperative group had a longer dura-tion of ICU stay More patients in the nonoperativegroup required tracheostomy There was a trend towardmore patients in the nonoperative group developingpneumonia (p frac14 007 Table 3) There were no
FLA 510 DTD ACS6738_proof 8
significant differences between groups in packed celltransfusion requirements or total blood products trans-fused during their inpatient stay (Table 3) Althoughthe median packed cell volume transfused in the nonop-erative group appears to be twice that of the operativegroup this was largely driven by a single patient whorequired 58 units of packed cells during his inpatientstay He was also the only mortality in the entire cohortwhich occurred due to sepsis at day 92 postinjuryMultivariate modelling was used to adjust for the co-
variate of ldquoother surgical interventionsrdquo which althoughnot significantly different on univariate analysis showeda higher incidence in the nonoperative group (Table 2)For all of the significantly different outcomes reportedearlier statistical significance remained after adjustmentduration of ICU stay postrandomization (mean hours[95 CI] 255 [201 to 323] vs 372 [294 to 470]p frac14 003) total ICU stay (mean hours [95 CI] 317[257 to 390] vs 456 [371 to 562] p frac14 002) durationof noninvasive ventilation postextubation (mean hours[95 CI] 22 [11 to 45] vs 67 [37 to 121] p frac14 003)received noninvasive ventilation postextubation (oddsratio [95 CI] 44 [104 to 186] p frac14 004)The difference between groups in the ICU of 124 hours
equates to a saving of 517 days in the operative group
February 2013 354 pm
Table 2 Injury Description
Variable Operative group (n frac14 23) Nonoperative group (n frac14 23) p Value
Total no fractured ribs mean SD 110 31 113 47 079
No of ribs in flail segment mean SD 51 17 55 20 043
No of patients with bilateral vs unilateral rib fractures 1211 1310
Underlying lung contusion n ()
None 3 (13) 2 (9) 100
Mild 16 (70) 16 (70) 100
Moderate 4 (17) 4 (17) 100
Severe 0 (0) 1 (4) 100
Pneumothorax n () 20 (90) 21 (91) 064
Other surgical interventions required n ()y 11 (48) 17 (74) 007
Thoracotomy n 0 2
Laparotomy n 1 2
ORIF clavicle n 3 5
Pelvic external fixation n 0 2
Spinal fusion n 2 0
ORIF limb fracture n 5 6
Plastics n 2z 4
Determined on chest x-ray on day of enrollment into trialySome patients underwent more than 1 surgical interventionzIncludes ORIF facial fractures in 1 patientORIF open reduction internal fixation
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 5
The cost of running an ICU bed in our hospital is esti-mated to be $4109 per day This potential cost savingof $21243 per operatively managed patient is offset bythe average cost of the operation which in this cohortwas $6800 per patient The breakdown of these costsare $4200 for the prostheses ($1050 per fracture fixed)and $2600 for approximately 25 hours of operating
Table 3 Outcomes
Outcomes Op
Duration of ICU stay prerandomization h mean SD
Duration of ICU stay between randomization and surgery hmean SD
Duration of IMV postrandomization h mean SD
Duration of ICU stay postrandomization h median (IQR)
Total ICU stay h median (IQR)
Failed extubation n ()
Received NIV postextubation n ()
Duration of NIV postextubation h median (IQR)
Tracheostomy n ()
Patients requiring blood product transfusion n
Packed cell transfusion during inpatient stay mL median (IQR)
Total blood products transfused mL median (IQR)
Readmission to ICU n ()
ICCs required n median (IQR)
Pneumonia n ()
Duration of hospital stay d median (IQR)
In hospital mortality n
ICC intercostal catheter IMV invasive mechanical ventilation IQR interquar
FLA 510 DTD ACS6738_proof 8
room time This equates to a cost saving of $14443 perpatient who underwent rib fixationFollow-up at 3 months showed no significant differ-
ences between groups in spirometry results (Table 4)Clinical review at 3 months revealed 2 patients witha visible flail segment Both had an anterior flail segmentand were in the nonoperative group The flail segment
erative group (n frac14 23) Nonoperative group (n frac14 23) p Value
616 361 813 842 031
494 359 NA
1518 831 1810 1302 037
285 (191e319) 359 (270e581) 003
324 (238e380) 448 (323e647) 003
3 (13) 1 (4) 061
13 (57) 19 (83) 005
3 (0e25) 50 (17e102) 001
9 (39) 1623 (70) 004
18 19 078
620 (0e3100) 1240 (620e3100) 039
930 (620e1860) 900 (500e1395) 057
223 (9) 223 (9) 099
2 (1e4) 2 (1e4) 099
1123 (48) 1723 (74) 007
20 (18e28) 25 (18e38) 024
0 1 087
tile range NIV noninvasive ventilation
February 2013 354 pm
Table 4 Spirometry Results at 3-Month Follow-Up
Percentpredicted value
Operative group(n frac14 17)
Nonoperative group(n frac14 17) p Value
FEV1 743 150 802 183 031
FVC 779 157 848 140 019
MMEF 762 369 821 350 064
PEF 628 285 681 365 063
TLC 840 244 882 234 061
FEV1FVC 956 98 950 173 092
Data are reported as mean SDFEV1 forced expiratory volume in one second FVC forced vital capacityMMEF maximal mid expiratory flow PEF peak expiratory flow TLCtotal lung capacity
Table 5 Three-Dimensional CT Results at 3 Months
3D CT appearance
Operativegroup
n (n frac14 21)
Nonoperativegroup
n (n frac14 17)p
Value
Complete healing 11 8 050
Partial healing 7 8 051
Nonhealing 3 1 038
Preoperative overlapping ribends 14 10 086
Residual overlapping rib ends 8 10 035
Improvement in overlappingbone ends 6 0 072
Preoperative displacement(gt1 rib gtrib width) 9 13 005
Residual displacement(gt1 rib gtrib width) 4 7 016
Improvement in ribdisplacement 5 6 012
Preoperative angulation(gt5 degrees gt1 rib) 9 12 009
Residual angulation(gt5 degrees gt1 rib) 3 9 001
Improvement in angulation 6 3 015
Table 6 Short Form-36 Quality of Life QuestionnaireResults at 6 Months Postinjury
SF-36 domainsOperative group
(n frac14 19)Nonoperative group
(n frac14 18) p Value
Physical functioning 334 130 384 120 024
Physical role 321 79 351 114 036
Bodily pain 422 94 379 110 022
General health 452 118 440 122 077
Vitalityenergy 441 108 463 82 049
Social functioning 360 150 372 125 079
Emotional role 376 145 378 135 097
Mental health 459 132 465 91 087
PCS 336 98 352 107 065
MCS 451 138 452 92 098
Scores are reported as mean SDMCS mental component summary score PCS physical componentsummary score
6 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
was not causing either patient any pain or restriction ofactivity Most (60) patients complained of ongoinglimitation in their daily work and home lives (15 of 21[71] in the nonoperative group vs 10 of 21[48] inthe operative group) However the majority of theserestrictions were due to injuries other than the flail chestinjury Only 2 patients (1 in each group) reportedconcerns about the cosmetic appearance of their chestat follow-up Chest CTs with 3-dimensional reconstruc-tions performed at 3 months were analyzed for degreeof healing and residual deformity in the fixed ribs(Table 5) Short Form-36 quality of life questionnaireat 6 months showed no differences between groups inany of the domains or the component summary scores(Table 6)
DISCUSSIONIn this prospective randomized trial comparing operativerib fixation and nonoperative management for traumaticflail chest we demonstrated reduced duration of ICU stayand reduced use of noninvasive ventilation and tracheos-tomy in the operative group The duration of invasivemechanical ventilation (IMV) from randomization wasnot significantly different between groups although itdid trend to a lesser duration in the conservative manage-ment group If the duration of IMV in the surgical groupis analyzed from the time of operation the differencesbetween groups becomes quite marked with significantlyless requirement for IMV in the surgical group Althoughthe treating intensivists were not blinded to the treatmentgroup ventilatory weaning and requirement for tracheos-tomy were protocol driven A spontaneous breathing trialwas considered in every patient on a daily basis After day7 postintubation tracheostomy was considered if itappeared the patient would not reach extubation withinthe next 2 to 3 days Although IMV time between groupswas not significantly different it was 30 hours shorter inthe surgical group which helps to explain why those
FLA 510 DTD ACS6738_proof 8
patients were less likely to receive a tracheostomyFurther the increased requirement for noninvasive venti-lation in the nonoperative group indicates that the trache-ostomy protocol was appropriately followed because thosepatients did require ongoing ventilatory support albeitnoninvasiveThe duration of hospital stay was 5 days shorter in the
surgical group which reflects the 5-day shorter ICU stayHowever the difference in overall hospital stay (20 daysvs 25 days) was not significantly different between groupsIt is also possible that this length of stay was affected by
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 7
a delay in transfer to rehabilitation hospitals due to bedblock which often tends to occur in our area Howeverthis would occur equally between groups so does notexplain the difference in length of stay seen in this studycohort The reduction in ICU stay in the operative groupreduced the ICU costs by more than $14000 per patient(a considerable cost savings to the health system) andsaved 5 ICU bed days per patientShort-term follow-up of our patients demonstrated no
significant differences in spirometry at 3 months betweengroups This result contrasts with previous studies thathave demonstrated improvements in percent predictedforced vital capacity total lung capacity and forced expi-ratory flow at 75 of vital capacity from 2-monthfollow-up49
We were unable to demonstrate any difference betweengroups in terms of Short Form-36 quality of life question-naire outcomes at 6 months postinjury The physicalsummary score was lower in both groups than the mentalsummary score This finding suggests that the patientsmade appropriate psychological adjustments to theirinjuries as has been previously reported10 Normativedata from the Australian population show a mental healthsummary score of 508 which is similar to the scores inour study population The reported physical summaryscore in the general Australian population is 498 whichis quite a bit higher than the scores in the groups in thisstudy11
We did not specifically assess pain in this study becauseall of the enrolled patients were sedated and ventilated atthe time of enrollment So the main indication forsurgery was mechanical stabilization not pain Furtherbecause these patients were a true multitrauma cohortwith multiple system injuries it was thought that anyassessment of analgesic requirement would beconfounded by the many other injuries also requiringanalgesia Indeed that is what we found at 3-monthfollow-up As outlined in the results patients who com-plained of ongoing physical limitation reported thatthey were limited by pain and stiffness from otherinjuries particularly shoulder girdle injuries rather thanrib injuries themselvesOnly 2 other prospective randomized trials have been
reported investigating the impact of operative fixationof flail chest injury49 Both studies slightly smaller thanthis one demonstrated significantly reduced mechanicalventilation time ICU stay incidence of pneumoniaand improved spirometry at follow-up in the operativegroup Tanaka and colleagues4 also demonstrated earlierreturn to work in the surgical cohort at 6-monthfollow-up The average age of the patients in our study(58 years) was older than that reported in both previous
FLA 510 DTD ACS6738_proof 8
randomized controlled trials of 45 years4 and 38 years9
This is likely to explain the seemingly slower recoveryin our patients and the lower rates of return to work(many of our patients were retired) Our failure to iden-tify differences in spirometry results at 3 months may alsobe related to the older age cohort in our studyThe study by Grantezny and associates9 also had
a cohort of patients with much lower Injury SeverityScores (ISS) (average 174) compared with those in ourstudy group (average 333) Again this reflects a seeminglydifferent study populationdyounger patients with singlesystem injuriesdcompared with our population of olderpatients with multiple system injuries (as evidenced bythe number of nonthoracic operations required) Wehave also reported the New Injury Severity Score(NISS) and the Trauma and Injury Severity Scores(TRISS) to give a more comprehensive picture of theinjury severity of this group of patients The higher ISSscores and multisystem nature of the injuries in ourcohort of patients may explain our failure to identifyany differences in quality of life between groupsOther previous research on operative fixation of frac-
tured ribs has consisted of retrospective reviews and casereports The retrospective review by Voggenreiter andcoworkers12 was the only one to subdivide the treatmentgroups into those with and without significant contusionAlthough they found benefits in the operative treatmentgroup they also found that these benefits were negatedby the presence of significant pulmonary contusion Inour study the majority of patients had only mild contu-sion on chest x-ray at the time of enrollmentAlmost all of the published studies have used metal
implants for operative fixation of the ribs Granetznyand colleagues9 used Kirschner and stainless steel wiresTanaka and associates4 used Judet struts In contrast weused a polylactide copolymer prosthesis applied as a 6-or 8-hole plate and screws These prostheses degrade byhydrolysis and are metabolized by the body into carbondioxide and water They maintain at least 40 of theirstrength at 3 months by which time the fractures wouldbe expected to have completely healed and arecompletely absorbed without toxicity over 1 to 3 yearsAnimal models using these absorbable plates have shownfaster and stronger healing compared with traditionalmetal plates which may actually slow bone healing13
This occurs because the metal plate protects the bonefrom any load but in doing so it removes the stimulusfor new bone growth (known as stress-shielding) Incontrast the absorbable plates allow gradual transfer ofstress loads to the bone stimulating faster bone growth13
Because the plates and screws are absorbable there is noneed to remove plates which confers a potential cost
February 2013 354 pm
8 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
savings to this procedure Also it minimizes the sequelae ofpossible prosthesis-related complications such as migrationpalpability (especially in thin patients) or thermal sensi-tivity Metal prostheses usually require removal if thesecomplications occur while a more conservative approachcan be adopted with absorbable prostheses Furthermorethere is no contraindication to future MRI in patientswho have had absorbable plates implantedDespite the existing evidence of patient and hospital
benefits with operative fixation of flail chest injury clinicalequipoise within the Western surgical community has per-sisted (operative rib fixation seems to have been taken upmore readily in East Asia14) This study is now the thirdstudy (in 3 different countries) to show similar benefitsin this patient population and we hope that it will influ-ence management change in these critically ill traumapatients Another reason why surgeons have been slow toembrace this type of surgery is probably related to thelack of specific prostheses designed for rib fixation Inthis study we used a prosthesis designed for the fibulaHowever over the last few years a number of productshave come onto the market specifically designed for ribfixation15 This demonstrates the increasing awarenessand interest in this type of surgery and also acknowledgesthat in the past surgical results when using nonspecificprostheses have been very variable16-18
Ribs present a number of surgical difficulties notencountered with other bony injuries Ribs are subjectto continual movement with breathing as well as suddenmore forceful movements during coughing and sneezingRibs have a thin inner and outer cortex making pros-thesis fixation difficult and at times unreliable Typicalrib fractures often involve splintering of the ribsmandating that bone fixation be undertaken at a sitefurther away from the fracture Each rib differs slightlyin its shape and in particular in the radius of its curva-ture which means that a ldquoone size fits allrdquo approachparticularly with less malleable prostheses is unlikely tobe successful19
A wide variety of prostheses have been tried in rib fixa-tion Many have flaws Kirschner wires provide little rota-tional stability and are prone to migration Metal platesborrowed from other applications are able to be curved inone direction only Because rib curvature is quitecomplex these metal plates are prone to ldquolifting offrdquothe rib Although the ribs do not carry a heavy loadthey are affected by torque in multiple directions due tothe layers of intercostal muscles inserting onto the ribsas well as multiple chest wall muscles Few authors havecommented on the impact of the chest wall musculatureon the dislocation and distraction of fractured ribs Bor-relly and Aazami20 in their retrospective review of flail
FLA 510 DTD ACS6738_proof 8
chest patients noted that the actions of serratus anteriortend to distract anterolateral fractures while impactingthe ribs in posterolateral fractures Analysis of the effectof intercostal muscle forces on rib fractures and fixationmethod has recently been analyzed and could assist indevelopment of specific rib prostheses78
CONCLUSIONSThis study shows clinical benefit and cost savings to thehealth system for flail chest patients who undergo rib fixa-tion Hopefully this study will help to change operativemanagement protocols for these critically ill patientsFurther trials into nonventilator-dependent patients alsoneed to be performed to assess in more detail potentialpatient benefits of pain reduction and functionalimprovements
Author Contributions
Study conception and design Marasco Davies CooperFitzgerald
Acquisition of data Marasco Bennet Nevill LeeAnalysis and interpretation of data Marasco DaviesCooper Varma Lee Bailey Fitzgerald
Drafting of manuscript Marasco Davies CooperVarma Bennet Nevill Lee Bailey Fitzgerald
Critical revision Marasco Davies Cooper VarmaBennet Nevill Lee Bailey Fitzgerald
REFERENCES
1 Ciraulo DL Elliott DMitchell KA et al Flail chest as a markerfor significant injuries J Am Coll Surg 1994178466e470
2 Kent R Woods W Bostrom O Fatality risk and the presenceof rib fractures Annu Proc Assoc Adv Automot Med 20085273e82
3 Kerr-Valentic MA Arthur M Mullins RJ et al Rib fracturepain and disability can we do better J Trauma 2003541058e1063
4 Tanaka H Yukioka T Yamaguti Y et al Surgical stabilizationof internal pneumatic stabilization A prospective randomizedstudy of management of severe flail chest patients J Trauma200252727e732
5 Mayberry JC Ham LB Schipper PH et al Surveyed opinionof American trauma orthopaedic and thoracic surgeons on riband sternal fracture repair J Trauma 200966875e879
6 Atkin C Freedman I Rosenfeld JV et al The evolution of anintegrated state trauma system in Victoria Australia Injury2005361277e1287
7 Marasco SF Sutalo ID Bui AV Mode of failure of rib fixationwith absorbable plates a clinical and numerical modellingstudy J Trauma 2010681225e1233
8 Marasco SF Liovic P Sutalo ID Structural integrity of intra-medullary rib fixation using a single bioresorbable screw AcuteCare Surg 201273668e673
9 Granetzny A El-Aal MA Emam E et al Surgical versus conser-vative treatment of flail chest Evaluation of the pulmonarystatus Interact Cardiovasc Thorac Surg 20054583e587
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 9
10 Singer MA Hopman WM MacKenzie TA Physical func-tioning and mental health in patients with chronic medicalconditions Qual Life Res 19998687e691
11 Australian Bureau of Statistics National health survey SF-36population norms Australia Canberra ACT Australian Bureauof Statistics 1995
12 Voggenreiter G Neudeck F Aufmkolk M et al Operative chestwall stabilisation in flail chest e outcomes of patients with orwithout pulmonary contusion J Am Coll Surg 1998187130e138
13 Viljanen J Pihlajamaki H Kinnunen J et al Comparison ofabsorbable poly-L-lactide and metallic intramedullary rods inthe fixation of femoral shaft osteotomies an experimentalstudy in rabbits J Orthop Sci 20016160e166
14 Yang Y Dong LW Wang J Memory alloy embracing fixatorin treatment of multiple fractured ribs and flail chest World JEmerg Med 20101212e215
FLA 510 DTD ACS6738_proof 8
15 Marasco SF Open surgical fixation of fractured ribs RecentPatents Biomed Eng 201031e6
16 Balci AE Eren S Cakir O Eren MN Open fixation in flailchest review of 64 patients Asian Cardiovasc Thorac Ann20041211e15
17 Mayberry JC Terhes JT Ellis TJ et al Absorbable plates forrib fracture repair preliminary experience J Trauma 200355835e839
18 Marasco S Cooper J Pick A Kossmann T Pilot study ofoperative fixation of fractured ribs in patients with flail chestANZ J Surg 200979804e808
19 Mohr M Abrams E Engel C et al Geometry of human ribspertinent to orthopaedic chest-wall reconstruction J Biomech2007401310e1317
20 Borrelly J Aazami MH New insights into the pathophysiologyof flail segment the implications of anterior serratus muscle inparietal failure Eur J Cardiothorac Surg 200528742e749
February 2013 354 pm

2 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
The primary aim of the study was to investigate theeffect of operative rib fixation of flail chest on mechanicalventilation time and ICU stay
METHODSEnrolment for the study took place between January 2007and December 2011 Informed consent was obtainedfrom the next of kin initially and consent sought fromthe patient for follow-up once sufficiently recoveredInstitutional ethics committee approval was obtainedThe trial was registered under Clinical Trials Gov withregistration number NCT00298259Patients were screened for enrollment into the trial on
hospital admission Forty-six patients with traumatic flailchest injury receiving invasive mechanical ventilationwere enrolled in the study Patients were enrolled only ifthey were ventilator dependent with no prospect of success-ful weaning within the next 48 hours Inclusion criteriawere the presence of a flail segment defined as 3 or moreconsecutive ribs fractured in more than 1 place producinga free floating segment of chest wall Diagnosis was madeclinically with confirmation on 3-dimensional CTimaging Exclusion criteria were age greater than 80 years(it was considered that osteoporotic bones precluded fixa-tion with the available prostheses) spinal injuries (whichprecluded placement of the patient in a lateral decubitusposition) open rib fractures with soiling or infectionsepsis severe traumatic brain injury (Glasgow Coma Scalelt10 at the scene of accident or at presentation to thehospital as its management may have received priorityover the study protocol) and uncorrected coagulopathyRandomization was via a computer generated code using
block randomizationwith block size of 4 After consent andenrollment an opaque envelope with the treatment assign-ment was opened and the time of enrollment documentedPatients were randomized to either operative rib fixa-
tion or nonoperative management Surgery was plannedafter viewing 3-dimensional CT chest reconstructionsand was performed within 48 hours of enrollmentOnly rib fractures between the levels of ribs 3 and 10were fixed Usually 1 or 2 incisions were used to achieveaccess to multiple ribs Wherever possible chest wallmuscles were preserved splitting them along the lengthof their fibers The periosteum was also preserved Ribsfractured more than once were usually addressed by fixing1 fracture per rib converting a flail segment to simplefractured ribs Ribs with a single fracture were not fixedunless there was gross deformity mandating interventionAnterior and lateral rib fractures were preferentially fixedover posterior rib fractures due to more reliable fixationand easier access compared with posterior rib fractures78
FLA 510 DTD ACS6738_proof 8
Inion resorbable (Inion OTPS) 6- or 8-hole plates andbicortical screws were used for every rib fixation Theseplates and screws are made of a polylactide copolymerthat resorbs over 18 to 24 months The plates were appliedto the external cortical surface of the rib after reducing thefracture The screws traversed both the outer and innercortex of the ribs and were inserted after tapping the drillhole and using a depth gauge to determine the length ofscrew to be usedPatients assigned to nonoperative management were
treated with current best practice mechanical ventilatormanagement Weaning from ventilation was via a protocolused for all patients irrespective of assigned group and irre-spective of mode of ventilation Commencing from the dayafter surgery or 24 hours after enrollment in the conserva-tive management group patients had sedation (notanalgesia) cessation considered every morning and a spon-taneous breathing trial conducted if patients met appro-priate criteria If the patient was comfortable witha respiratory rate lt25 breathsminute after 4 hours ofthe spontaneous breathing trial mechanical ventilationwas weaned If the patientrsquos respiratory rate was gt25breathsminute appropriate sedation and mechanicalventilation were recommenced for another 24 hoursTracheostomy insertion was also protocol driven andoccurred at day 7 if it appeared to the treating physicianthat weaning of mechanical ventilation was not likelywithin the next 2 to 3 daysThe primary endpoints of the study were duration of
mechanical ventilation and ICU stay The secondaryendpoints were number of respiratory complications(pneumonia pneumothorax intercostal catheter usage)rate of failed extubation rate of tracheostomy readmis-sion to intensive care duration of hospital stay andcost assessment of the operation Pneumonia was definedas a new infiltrate on chest x-ray with positive sputumculture Intensive care unit discharge time was recordedas the time the patient was deemed ready for dischargeso that ward bed access did not affect the resultsPatients were reviewed at 3 months postoperatively for
clinical assessment spirometry and CT scan of chestimaging with 3-dimensional reconstructions of thethoracic cage All patients were sent a Short Form 36-item Health Status Questionnaire (SF-36) at 6 monthsto assess physical functioning role limitations owing tophysical problems role limitations owing to emotionalproblems social functioning mental health generalhealth perceptions vitality and bodily painSample size estimation was based on duration of
mechanical ventilation Calculations were performed usingduration of mechanical ventilation values from patientswith traumatic flail chest treated at The Alfred Hospital
February 2013 354 pm
printampweb4C=FPO
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 3
over the 4 years before commencement of this studyAssuming an alpha of 005 power of 08 and a standarddeviation of 140 hours to detect a difference in durationof mechanical ventilation of 120 hours (5 days) 23patients per group were required to be enrolled
Statistical analysis
Statistical analysis was performed using SAS version 92(SAS Institute Inc) All variables were initially assessedfor normality Group comparisons of proportions weremade using chi-square tests or Fishers exact tests wherenumbers were small and were reported as numbers ()Continuously normally distributed variables were com-pared using Student t-tests and reported as mean (stan-dard deviation) non-normally distributed data werecompared using Wilcoxon rank sum tests and reportedas medians (interquartile range) To ensure that allobserved results were not due to baseline imbalancesmultivariate modelling was used adjusting for the covar-iate of ldquoother surgical interventionsrdquo In order to facilitatethis duration variables were log-transformed andanalyzed using generalized linear modelling with resultsreported as geometric means (95 CI) The need for
Assessed for e
Analysed (n=23 for in hospital data and 59 for postoperative data)
Lost to follow-up (n=4)
Allocated to intervention (n= 23) diams Received allocated intervention (n=22)
Randomi
Figure 1 CONSORT 2
FLA 510 DTD ACS6738_proof 8
noninvasive ventilation was assessed using logisticregression with results reported as odds ratios (95CI) Analysis was performed on an intention-to-treatbasis A 2-sided p value of 005 was considered statisti-cally significant
RESULTSThere were 5036 major trauma patients (Injury SeverityScore [1998 version] gt15) treated at The Alfred Hospitalover the 5-year period of enrollment including 2940patients with thoracic trauma Maximum AbbreviatedInjury Score [1998 version] gt2 Over that period 230patients were coded as having a flail chest with lessthan half requiring invasive mechanical ventilationScreening and enrollment numbers are outlined in theConsort diagram (Fig 1) One patient assigned to theoperative group did not have surgery due to the develop-ment of sepsis but was analyzed in the operative groupon an intention-to-treat basis One patient assigned tothe nonoperative group died before hospital dischargePatient demographics are outlined in Table 1 Therewas a significantly lower proportion of nonsmokers in
ligibility (n=146 )
Excluded (n=21) diams Not meeting inclusion criteria (n=11) diams Declined to participate (n=1) diams Other reasons (n=9)
Lost to follow-up (1 patient died prior to hospital discharge 4 patients lost to follow-up)
Allocated to control group (n=23) diams Received allocated intervention (n=23)
Analysed (n=23 for in hospital data and 61 for postoperative data)
zed (n=46)
010 flow diagram
February 2013 354 pm
Table 1 Patient Demographics
Variable Operative group (n frac14 23) Nonoperative group (n frac14 23) p Value
Age y mean SD 578 171 593 104 072
Sex malefemale n 203 203 100
Body mass index kgm2 mean SD 279 46 290 68 055
Smoking history n ()
Ex smoker 5 (22) 2 (9) 022
Current smoker 8 (35) 3 (13) 008
Nonsmoker 10 (43) 18 (78) 002
Underlying lung disease n ()
Asthma 3 (13) 1 (4)
COPD 2 (9) 1 (4)
Mechanism of injury n () 086
Motor vehicle accident 17 (74) 14 (61)
Pedestrian vs car 2 (9) 3 (13)
Crush injury 1 (4) 2 (9)
Fall from height 3 (13) 4 (17)
NISS mean SD 364 103 429 133 007
ISS mean SD 350 114 300 63 013
TRISS mean SD 08 02 08 02 077
GCS at scene mean SD 134 28 136 26 074
Best GCS within first 48 h mean SD 110 45 99 47 043
Head injury AIS code 2 or above n () 0 (0) 2 (9) 049
Bony spinal injury n () 15 (65) 14 (61) 076
AIS Abbreviated Injury Score GCS Glasgow Coma Scale ISS Injury Severity Score NISS New Injury Severity Score TRISS Trauma and Injury SeverityScore
4 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
the operative group (43 vs 78 p frac14 002) but other-wise both groups were adequately matchedThere were no differences between groups in the
number of ribs fractured or the degree of underlyinglung contusion (measured at time of enrollment)(Table 2) There was a difference between groups in termsof other nonthoracic surgical interventions performed Thenonoperative group had a higher number of orthopaedicand general surgical operative procedures (74 vs 48p frac14 007) (Table 2)Twenty-two patients underwent operative rib fixation
Most (13 of 22 59) patients had 4 ribs fixed (range 2 to7 ribs) Two (9) patients had bilateral rib fixationAnterior and lateral fractures were most commonly fixedOnly 1 patient had posterior rib fractures fixedThe early postoperative outcomes are outlined in
Table 3 There was no difference between groups in theduration of invasive mechanical ventilation but noninva-sive ventilation was used in a greater number of patientsand for a longer duration in the nonoperative manage-ment group The nonoperative group had a longer dura-tion of ICU stay More patients in the nonoperativegroup required tracheostomy There was a trend towardmore patients in the nonoperative group developingpneumonia (p frac14 007 Table 3) There were no
FLA 510 DTD ACS6738_proof 8
significant differences between groups in packed celltransfusion requirements or total blood products trans-fused during their inpatient stay (Table 3) Althoughthe median packed cell volume transfused in the nonop-erative group appears to be twice that of the operativegroup this was largely driven by a single patient whorequired 58 units of packed cells during his inpatientstay He was also the only mortality in the entire cohortwhich occurred due to sepsis at day 92 postinjuryMultivariate modelling was used to adjust for the co-
variate of ldquoother surgical interventionsrdquo which althoughnot significantly different on univariate analysis showeda higher incidence in the nonoperative group (Table 2)For all of the significantly different outcomes reportedearlier statistical significance remained after adjustmentduration of ICU stay postrandomization (mean hours[95 CI] 255 [201 to 323] vs 372 [294 to 470]p frac14 003) total ICU stay (mean hours [95 CI] 317[257 to 390] vs 456 [371 to 562] p frac14 002) durationof noninvasive ventilation postextubation (mean hours[95 CI] 22 [11 to 45] vs 67 [37 to 121] p frac14 003)received noninvasive ventilation postextubation (oddsratio [95 CI] 44 [104 to 186] p frac14 004)The difference between groups in the ICU of 124 hours
equates to a saving of 517 days in the operative group
February 2013 354 pm
Table 2 Injury Description
Variable Operative group (n frac14 23) Nonoperative group (n frac14 23) p Value
Total no fractured ribs mean SD 110 31 113 47 079
No of ribs in flail segment mean SD 51 17 55 20 043
No of patients with bilateral vs unilateral rib fractures 1211 1310
Underlying lung contusion n ()
None 3 (13) 2 (9) 100
Mild 16 (70) 16 (70) 100
Moderate 4 (17) 4 (17) 100
Severe 0 (0) 1 (4) 100
Pneumothorax n () 20 (90) 21 (91) 064
Other surgical interventions required n ()y 11 (48) 17 (74) 007
Thoracotomy n 0 2
Laparotomy n 1 2
ORIF clavicle n 3 5
Pelvic external fixation n 0 2
Spinal fusion n 2 0
ORIF limb fracture n 5 6
Plastics n 2z 4
Determined on chest x-ray on day of enrollment into trialySome patients underwent more than 1 surgical interventionzIncludes ORIF facial fractures in 1 patientORIF open reduction internal fixation
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 5
The cost of running an ICU bed in our hospital is esti-mated to be $4109 per day This potential cost savingof $21243 per operatively managed patient is offset bythe average cost of the operation which in this cohortwas $6800 per patient The breakdown of these costsare $4200 for the prostheses ($1050 per fracture fixed)and $2600 for approximately 25 hours of operating
Table 3 Outcomes
Outcomes Op
Duration of ICU stay prerandomization h mean SD
Duration of ICU stay between randomization and surgery hmean SD
Duration of IMV postrandomization h mean SD
Duration of ICU stay postrandomization h median (IQR)
Total ICU stay h median (IQR)
Failed extubation n ()
Received NIV postextubation n ()
Duration of NIV postextubation h median (IQR)
Tracheostomy n ()
Patients requiring blood product transfusion n
Packed cell transfusion during inpatient stay mL median (IQR)
Total blood products transfused mL median (IQR)
Readmission to ICU n ()
ICCs required n median (IQR)
Pneumonia n ()
Duration of hospital stay d median (IQR)
In hospital mortality n
ICC intercostal catheter IMV invasive mechanical ventilation IQR interquar
FLA 510 DTD ACS6738_proof 8
room time This equates to a cost saving of $14443 perpatient who underwent rib fixationFollow-up at 3 months showed no significant differ-
ences between groups in spirometry results (Table 4)Clinical review at 3 months revealed 2 patients witha visible flail segment Both had an anterior flail segmentand were in the nonoperative group The flail segment
erative group (n frac14 23) Nonoperative group (n frac14 23) p Value
616 361 813 842 031
494 359 NA
1518 831 1810 1302 037
285 (191e319) 359 (270e581) 003
324 (238e380) 448 (323e647) 003
3 (13) 1 (4) 061
13 (57) 19 (83) 005
3 (0e25) 50 (17e102) 001
9 (39) 1623 (70) 004
18 19 078
620 (0e3100) 1240 (620e3100) 039
930 (620e1860) 900 (500e1395) 057
223 (9) 223 (9) 099
2 (1e4) 2 (1e4) 099
1123 (48) 1723 (74) 007
20 (18e28) 25 (18e38) 024
0 1 087
tile range NIV noninvasive ventilation
February 2013 354 pm
Table 4 Spirometry Results at 3-Month Follow-Up
Percentpredicted value
Operative group(n frac14 17)
Nonoperative group(n frac14 17) p Value
FEV1 743 150 802 183 031
FVC 779 157 848 140 019
MMEF 762 369 821 350 064
PEF 628 285 681 365 063
TLC 840 244 882 234 061
FEV1FVC 956 98 950 173 092
Data are reported as mean SDFEV1 forced expiratory volume in one second FVC forced vital capacityMMEF maximal mid expiratory flow PEF peak expiratory flow TLCtotal lung capacity
Table 5 Three-Dimensional CT Results at 3 Months
3D CT appearance
Operativegroup
n (n frac14 21)
Nonoperativegroup
n (n frac14 17)p
Value
Complete healing 11 8 050
Partial healing 7 8 051
Nonhealing 3 1 038
Preoperative overlapping ribends 14 10 086
Residual overlapping rib ends 8 10 035
Improvement in overlappingbone ends 6 0 072
Preoperative displacement(gt1 rib gtrib width) 9 13 005
Residual displacement(gt1 rib gtrib width) 4 7 016
Improvement in ribdisplacement 5 6 012
Preoperative angulation(gt5 degrees gt1 rib) 9 12 009
Residual angulation(gt5 degrees gt1 rib) 3 9 001
Improvement in angulation 6 3 015
Table 6 Short Form-36 Quality of Life QuestionnaireResults at 6 Months Postinjury
SF-36 domainsOperative group
(n frac14 19)Nonoperative group
(n frac14 18) p Value
Physical functioning 334 130 384 120 024
Physical role 321 79 351 114 036
Bodily pain 422 94 379 110 022
General health 452 118 440 122 077
Vitalityenergy 441 108 463 82 049
Social functioning 360 150 372 125 079
Emotional role 376 145 378 135 097
Mental health 459 132 465 91 087
PCS 336 98 352 107 065
MCS 451 138 452 92 098
Scores are reported as mean SDMCS mental component summary score PCS physical componentsummary score
6 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
was not causing either patient any pain or restriction ofactivity Most (60) patients complained of ongoinglimitation in their daily work and home lives (15 of 21[71] in the nonoperative group vs 10 of 21[48] inthe operative group) However the majority of theserestrictions were due to injuries other than the flail chestinjury Only 2 patients (1 in each group) reportedconcerns about the cosmetic appearance of their chestat follow-up Chest CTs with 3-dimensional reconstruc-tions performed at 3 months were analyzed for degreeof healing and residual deformity in the fixed ribs(Table 5) Short Form-36 quality of life questionnaireat 6 months showed no differences between groups inany of the domains or the component summary scores(Table 6)
DISCUSSIONIn this prospective randomized trial comparing operativerib fixation and nonoperative management for traumaticflail chest we demonstrated reduced duration of ICU stayand reduced use of noninvasive ventilation and tracheos-tomy in the operative group The duration of invasivemechanical ventilation (IMV) from randomization wasnot significantly different between groups although itdid trend to a lesser duration in the conservative manage-ment group If the duration of IMV in the surgical groupis analyzed from the time of operation the differencesbetween groups becomes quite marked with significantlyless requirement for IMV in the surgical group Althoughthe treating intensivists were not blinded to the treatmentgroup ventilatory weaning and requirement for tracheos-tomy were protocol driven A spontaneous breathing trialwas considered in every patient on a daily basis After day7 postintubation tracheostomy was considered if itappeared the patient would not reach extubation withinthe next 2 to 3 days Although IMV time between groupswas not significantly different it was 30 hours shorter inthe surgical group which helps to explain why those
FLA 510 DTD ACS6738_proof 8
patients were less likely to receive a tracheostomyFurther the increased requirement for noninvasive venti-lation in the nonoperative group indicates that the trache-ostomy protocol was appropriately followed because thosepatients did require ongoing ventilatory support albeitnoninvasiveThe duration of hospital stay was 5 days shorter in the
surgical group which reflects the 5-day shorter ICU stayHowever the difference in overall hospital stay (20 daysvs 25 days) was not significantly different between groupsIt is also possible that this length of stay was affected by
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 7
a delay in transfer to rehabilitation hospitals due to bedblock which often tends to occur in our area Howeverthis would occur equally between groups so does notexplain the difference in length of stay seen in this studycohort The reduction in ICU stay in the operative groupreduced the ICU costs by more than $14000 per patient(a considerable cost savings to the health system) andsaved 5 ICU bed days per patientShort-term follow-up of our patients demonstrated no
significant differences in spirometry at 3 months betweengroups This result contrasts with previous studies thathave demonstrated improvements in percent predictedforced vital capacity total lung capacity and forced expi-ratory flow at 75 of vital capacity from 2-monthfollow-up49
We were unable to demonstrate any difference betweengroups in terms of Short Form-36 quality of life question-naire outcomes at 6 months postinjury The physicalsummary score was lower in both groups than the mentalsummary score This finding suggests that the patientsmade appropriate psychological adjustments to theirinjuries as has been previously reported10 Normativedata from the Australian population show a mental healthsummary score of 508 which is similar to the scores inour study population The reported physical summaryscore in the general Australian population is 498 whichis quite a bit higher than the scores in the groups in thisstudy11
We did not specifically assess pain in this study becauseall of the enrolled patients were sedated and ventilated atthe time of enrollment So the main indication forsurgery was mechanical stabilization not pain Furtherbecause these patients were a true multitrauma cohortwith multiple system injuries it was thought that anyassessment of analgesic requirement would beconfounded by the many other injuries also requiringanalgesia Indeed that is what we found at 3-monthfollow-up As outlined in the results patients who com-plained of ongoing physical limitation reported thatthey were limited by pain and stiffness from otherinjuries particularly shoulder girdle injuries rather thanrib injuries themselvesOnly 2 other prospective randomized trials have been
reported investigating the impact of operative fixationof flail chest injury49 Both studies slightly smaller thanthis one demonstrated significantly reduced mechanicalventilation time ICU stay incidence of pneumoniaand improved spirometry at follow-up in the operativegroup Tanaka and colleagues4 also demonstrated earlierreturn to work in the surgical cohort at 6-monthfollow-up The average age of the patients in our study(58 years) was older than that reported in both previous
FLA 510 DTD ACS6738_proof 8
randomized controlled trials of 45 years4 and 38 years9
This is likely to explain the seemingly slower recoveryin our patients and the lower rates of return to work(many of our patients were retired) Our failure to iden-tify differences in spirometry results at 3 months may alsobe related to the older age cohort in our studyThe study by Grantezny and associates9 also had
a cohort of patients with much lower Injury SeverityScores (ISS) (average 174) compared with those in ourstudy group (average 333) Again this reflects a seeminglydifferent study populationdyounger patients with singlesystem injuriesdcompared with our population of olderpatients with multiple system injuries (as evidenced bythe number of nonthoracic operations required) Wehave also reported the New Injury Severity Score(NISS) and the Trauma and Injury Severity Scores(TRISS) to give a more comprehensive picture of theinjury severity of this group of patients The higher ISSscores and multisystem nature of the injuries in ourcohort of patients may explain our failure to identifyany differences in quality of life between groupsOther previous research on operative fixation of frac-
tured ribs has consisted of retrospective reviews and casereports The retrospective review by Voggenreiter andcoworkers12 was the only one to subdivide the treatmentgroups into those with and without significant contusionAlthough they found benefits in the operative treatmentgroup they also found that these benefits were negatedby the presence of significant pulmonary contusion Inour study the majority of patients had only mild contu-sion on chest x-ray at the time of enrollmentAlmost all of the published studies have used metal
implants for operative fixation of the ribs Granetznyand colleagues9 used Kirschner and stainless steel wiresTanaka and associates4 used Judet struts In contrast weused a polylactide copolymer prosthesis applied as a 6-or 8-hole plate and screws These prostheses degrade byhydrolysis and are metabolized by the body into carbondioxide and water They maintain at least 40 of theirstrength at 3 months by which time the fractures wouldbe expected to have completely healed and arecompletely absorbed without toxicity over 1 to 3 yearsAnimal models using these absorbable plates have shownfaster and stronger healing compared with traditionalmetal plates which may actually slow bone healing13
This occurs because the metal plate protects the bonefrom any load but in doing so it removes the stimulusfor new bone growth (known as stress-shielding) Incontrast the absorbable plates allow gradual transfer ofstress loads to the bone stimulating faster bone growth13
Because the plates and screws are absorbable there is noneed to remove plates which confers a potential cost
February 2013 354 pm
8 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
savings to this procedure Also it minimizes the sequelae ofpossible prosthesis-related complications such as migrationpalpability (especially in thin patients) or thermal sensi-tivity Metal prostheses usually require removal if thesecomplications occur while a more conservative approachcan be adopted with absorbable prostheses Furthermorethere is no contraindication to future MRI in patientswho have had absorbable plates implantedDespite the existing evidence of patient and hospital
benefits with operative fixation of flail chest injury clinicalequipoise within the Western surgical community has per-sisted (operative rib fixation seems to have been taken upmore readily in East Asia14) This study is now the thirdstudy (in 3 different countries) to show similar benefitsin this patient population and we hope that it will influ-ence management change in these critically ill traumapatients Another reason why surgeons have been slow toembrace this type of surgery is probably related to thelack of specific prostheses designed for rib fixation Inthis study we used a prosthesis designed for the fibulaHowever over the last few years a number of productshave come onto the market specifically designed for ribfixation15 This demonstrates the increasing awarenessand interest in this type of surgery and also acknowledgesthat in the past surgical results when using nonspecificprostheses have been very variable16-18
Ribs present a number of surgical difficulties notencountered with other bony injuries Ribs are subjectto continual movement with breathing as well as suddenmore forceful movements during coughing and sneezingRibs have a thin inner and outer cortex making pros-thesis fixation difficult and at times unreliable Typicalrib fractures often involve splintering of the ribsmandating that bone fixation be undertaken at a sitefurther away from the fracture Each rib differs slightlyin its shape and in particular in the radius of its curva-ture which means that a ldquoone size fits allrdquo approachparticularly with less malleable prostheses is unlikely tobe successful19
A wide variety of prostheses have been tried in rib fixa-tion Many have flaws Kirschner wires provide little rota-tional stability and are prone to migration Metal platesborrowed from other applications are able to be curved inone direction only Because rib curvature is quitecomplex these metal plates are prone to ldquolifting offrdquothe rib Although the ribs do not carry a heavy loadthey are affected by torque in multiple directions due tothe layers of intercostal muscles inserting onto the ribsas well as multiple chest wall muscles Few authors havecommented on the impact of the chest wall musculatureon the dislocation and distraction of fractured ribs Bor-relly and Aazami20 in their retrospective review of flail
FLA 510 DTD ACS6738_proof 8
chest patients noted that the actions of serratus anteriortend to distract anterolateral fractures while impactingthe ribs in posterolateral fractures Analysis of the effectof intercostal muscle forces on rib fractures and fixationmethod has recently been analyzed and could assist indevelopment of specific rib prostheses78
CONCLUSIONSThis study shows clinical benefit and cost savings to thehealth system for flail chest patients who undergo rib fixa-tion Hopefully this study will help to change operativemanagement protocols for these critically ill patientsFurther trials into nonventilator-dependent patients alsoneed to be performed to assess in more detail potentialpatient benefits of pain reduction and functionalimprovements
Author Contributions
Study conception and design Marasco Davies CooperFitzgerald
Acquisition of data Marasco Bennet Nevill LeeAnalysis and interpretation of data Marasco DaviesCooper Varma Lee Bailey Fitzgerald
Drafting of manuscript Marasco Davies CooperVarma Bennet Nevill Lee Bailey Fitzgerald
Critical revision Marasco Davies Cooper VarmaBennet Nevill Lee Bailey Fitzgerald
REFERENCES
1 Ciraulo DL Elliott DMitchell KA et al Flail chest as a markerfor significant injuries J Am Coll Surg 1994178466e470
2 Kent R Woods W Bostrom O Fatality risk and the presenceof rib fractures Annu Proc Assoc Adv Automot Med 20085273e82
3 Kerr-Valentic MA Arthur M Mullins RJ et al Rib fracturepain and disability can we do better J Trauma 2003541058e1063
4 Tanaka H Yukioka T Yamaguti Y et al Surgical stabilizationof internal pneumatic stabilization A prospective randomizedstudy of management of severe flail chest patients J Trauma200252727e732
5 Mayberry JC Ham LB Schipper PH et al Surveyed opinionof American trauma orthopaedic and thoracic surgeons on riband sternal fracture repair J Trauma 200966875e879
6 Atkin C Freedman I Rosenfeld JV et al The evolution of anintegrated state trauma system in Victoria Australia Injury2005361277e1287
7 Marasco SF Sutalo ID Bui AV Mode of failure of rib fixationwith absorbable plates a clinical and numerical modellingstudy J Trauma 2010681225e1233
8 Marasco SF Liovic P Sutalo ID Structural integrity of intra-medullary rib fixation using a single bioresorbable screw AcuteCare Surg 201273668e673
9 Granetzny A El-Aal MA Emam E et al Surgical versus conser-vative treatment of flail chest Evaluation of the pulmonarystatus Interact Cardiovasc Thorac Surg 20054583e587
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 9
10 Singer MA Hopman WM MacKenzie TA Physical func-tioning and mental health in patients with chronic medicalconditions Qual Life Res 19998687e691
11 Australian Bureau of Statistics National health survey SF-36population norms Australia Canberra ACT Australian Bureauof Statistics 1995
12 Voggenreiter G Neudeck F Aufmkolk M et al Operative chestwall stabilisation in flail chest e outcomes of patients with orwithout pulmonary contusion J Am Coll Surg 1998187130e138
13 Viljanen J Pihlajamaki H Kinnunen J et al Comparison ofabsorbable poly-L-lactide and metallic intramedullary rods inthe fixation of femoral shaft osteotomies an experimentalstudy in rabbits J Orthop Sci 20016160e166
14 Yang Y Dong LW Wang J Memory alloy embracing fixatorin treatment of multiple fractured ribs and flail chest World JEmerg Med 20101212e215
FLA 510 DTD ACS6738_proof 8
15 Marasco SF Open surgical fixation of fractured ribs RecentPatents Biomed Eng 201031e6
16 Balci AE Eren S Cakir O Eren MN Open fixation in flailchest review of 64 patients Asian Cardiovasc Thorac Ann20041211e15
17 Mayberry JC Terhes JT Ellis TJ et al Absorbable plates forrib fracture repair preliminary experience J Trauma 200355835e839
18 Marasco S Cooper J Pick A Kossmann T Pilot study ofoperative fixation of fractured ribs in patients with flail chestANZ J Surg 200979804e808
19 Mohr M Abrams E Engel C et al Geometry of human ribspertinent to orthopaedic chest-wall reconstruction J Biomech2007401310e1317
20 Borrelly J Aazami MH New insights into the pathophysiologyof flail segment the implications of anterior serratus muscle inparietal failure Eur J Cardiothorac Surg 200528742e749
February 2013 354 pm
printampweb4C=FPO
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 3
over the 4 years before commencement of this studyAssuming an alpha of 005 power of 08 and a standarddeviation of 140 hours to detect a difference in durationof mechanical ventilation of 120 hours (5 days) 23patients per group were required to be enrolled
Statistical analysis
Statistical analysis was performed using SAS version 92(SAS Institute Inc) All variables were initially assessedfor normality Group comparisons of proportions weremade using chi-square tests or Fishers exact tests wherenumbers were small and were reported as numbers ()Continuously normally distributed variables were com-pared using Student t-tests and reported as mean (stan-dard deviation) non-normally distributed data werecompared using Wilcoxon rank sum tests and reportedas medians (interquartile range) To ensure that allobserved results were not due to baseline imbalancesmultivariate modelling was used adjusting for the covar-iate of ldquoother surgical interventionsrdquo In order to facilitatethis duration variables were log-transformed andanalyzed using generalized linear modelling with resultsreported as geometric means (95 CI) The need for
Assessed for e
Analysed (n=23 for in hospital data and 59 for postoperative data)
Lost to follow-up (n=4)
Allocated to intervention (n= 23) diams Received allocated intervention (n=22)
Randomi
Figure 1 CONSORT 2
FLA 510 DTD ACS6738_proof 8
noninvasive ventilation was assessed using logisticregression with results reported as odds ratios (95CI) Analysis was performed on an intention-to-treatbasis A 2-sided p value of 005 was considered statisti-cally significant
RESULTSThere were 5036 major trauma patients (Injury SeverityScore [1998 version] gt15) treated at The Alfred Hospitalover the 5-year period of enrollment including 2940patients with thoracic trauma Maximum AbbreviatedInjury Score [1998 version] gt2 Over that period 230patients were coded as having a flail chest with lessthan half requiring invasive mechanical ventilationScreening and enrollment numbers are outlined in theConsort diagram (Fig 1) One patient assigned to theoperative group did not have surgery due to the develop-ment of sepsis but was analyzed in the operative groupon an intention-to-treat basis One patient assigned tothe nonoperative group died before hospital dischargePatient demographics are outlined in Table 1 Therewas a significantly lower proportion of nonsmokers in
ligibility (n=146 )
Excluded (n=21) diams Not meeting inclusion criteria (n=11) diams Declined to participate (n=1) diams Other reasons (n=9)
Lost to follow-up (1 patient died prior to hospital discharge 4 patients lost to follow-up)
Allocated to control group (n=23) diams Received allocated intervention (n=23)
Analysed (n=23 for in hospital data and 61 for postoperative data)
zed (n=46)
010 flow diagram
February 2013 354 pm
Table 1 Patient Demographics
Variable Operative group (n frac14 23) Nonoperative group (n frac14 23) p Value
Age y mean SD 578 171 593 104 072
Sex malefemale n 203 203 100
Body mass index kgm2 mean SD 279 46 290 68 055
Smoking history n ()
Ex smoker 5 (22) 2 (9) 022
Current smoker 8 (35) 3 (13) 008
Nonsmoker 10 (43) 18 (78) 002
Underlying lung disease n ()
Asthma 3 (13) 1 (4)
COPD 2 (9) 1 (4)
Mechanism of injury n () 086
Motor vehicle accident 17 (74) 14 (61)
Pedestrian vs car 2 (9) 3 (13)
Crush injury 1 (4) 2 (9)
Fall from height 3 (13) 4 (17)
NISS mean SD 364 103 429 133 007
ISS mean SD 350 114 300 63 013
TRISS mean SD 08 02 08 02 077
GCS at scene mean SD 134 28 136 26 074
Best GCS within first 48 h mean SD 110 45 99 47 043
Head injury AIS code 2 or above n () 0 (0) 2 (9) 049
Bony spinal injury n () 15 (65) 14 (61) 076
AIS Abbreviated Injury Score GCS Glasgow Coma Scale ISS Injury Severity Score NISS New Injury Severity Score TRISS Trauma and Injury SeverityScore
4 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
the operative group (43 vs 78 p frac14 002) but other-wise both groups were adequately matchedThere were no differences between groups in the
number of ribs fractured or the degree of underlyinglung contusion (measured at time of enrollment)(Table 2) There was a difference between groups in termsof other nonthoracic surgical interventions performed Thenonoperative group had a higher number of orthopaedicand general surgical operative procedures (74 vs 48p frac14 007) (Table 2)Twenty-two patients underwent operative rib fixation
Most (13 of 22 59) patients had 4 ribs fixed (range 2 to7 ribs) Two (9) patients had bilateral rib fixationAnterior and lateral fractures were most commonly fixedOnly 1 patient had posterior rib fractures fixedThe early postoperative outcomes are outlined in
Table 3 There was no difference between groups in theduration of invasive mechanical ventilation but noninva-sive ventilation was used in a greater number of patientsand for a longer duration in the nonoperative manage-ment group The nonoperative group had a longer dura-tion of ICU stay More patients in the nonoperativegroup required tracheostomy There was a trend towardmore patients in the nonoperative group developingpneumonia (p frac14 007 Table 3) There were no
FLA 510 DTD ACS6738_proof 8
significant differences between groups in packed celltransfusion requirements or total blood products trans-fused during their inpatient stay (Table 3) Althoughthe median packed cell volume transfused in the nonop-erative group appears to be twice that of the operativegroup this was largely driven by a single patient whorequired 58 units of packed cells during his inpatientstay He was also the only mortality in the entire cohortwhich occurred due to sepsis at day 92 postinjuryMultivariate modelling was used to adjust for the co-
variate of ldquoother surgical interventionsrdquo which althoughnot significantly different on univariate analysis showeda higher incidence in the nonoperative group (Table 2)For all of the significantly different outcomes reportedearlier statistical significance remained after adjustmentduration of ICU stay postrandomization (mean hours[95 CI] 255 [201 to 323] vs 372 [294 to 470]p frac14 003) total ICU stay (mean hours [95 CI] 317[257 to 390] vs 456 [371 to 562] p frac14 002) durationof noninvasive ventilation postextubation (mean hours[95 CI] 22 [11 to 45] vs 67 [37 to 121] p frac14 003)received noninvasive ventilation postextubation (oddsratio [95 CI] 44 [104 to 186] p frac14 004)The difference between groups in the ICU of 124 hours
equates to a saving of 517 days in the operative group
February 2013 354 pm
Table 2 Injury Description
Variable Operative group (n frac14 23) Nonoperative group (n frac14 23) p Value
Total no fractured ribs mean SD 110 31 113 47 079
No of ribs in flail segment mean SD 51 17 55 20 043
No of patients with bilateral vs unilateral rib fractures 1211 1310
Underlying lung contusion n ()
None 3 (13) 2 (9) 100
Mild 16 (70) 16 (70) 100
Moderate 4 (17) 4 (17) 100
Severe 0 (0) 1 (4) 100
Pneumothorax n () 20 (90) 21 (91) 064
Other surgical interventions required n ()y 11 (48) 17 (74) 007
Thoracotomy n 0 2
Laparotomy n 1 2
ORIF clavicle n 3 5
Pelvic external fixation n 0 2
Spinal fusion n 2 0
ORIF limb fracture n 5 6
Plastics n 2z 4
Determined on chest x-ray on day of enrollment into trialySome patients underwent more than 1 surgical interventionzIncludes ORIF facial fractures in 1 patientORIF open reduction internal fixation
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 5
The cost of running an ICU bed in our hospital is esti-mated to be $4109 per day This potential cost savingof $21243 per operatively managed patient is offset bythe average cost of the operation which in this cohortwas $6800 per patient The breakdown of these costsare $4200 for the prostheses ($1050 per fracture fixed)and $2600 for approximately 25 hours of operating
Table 3 Outcomes
Outcomes Op
Duration of ICU stay prerandomization h mean SD
Duration of ICU stay between randomization and surgery hmean SD
Duration of IMV postrandomization h mean SD
Duration of ICU stay postrandomization h median (IQR)
Total ICU stay h median (IQR)
Failed extubation n ()
Received NIV postextubation n ()
Duration of NIV postextubation h median (IQR)
Tracheostomy n ()
Patients requiring blood product transfusion n
Packed cell transfusion during inpatient stay mL median (IQR)
Total blood products transfused mL median (IQR)
Readmission to ICU n ()
ICCs required n median (IQR)
Pneumonia n ()
Duration of hospital stay d median (IQR)
In hospital mortality n
ICC intercostal catheter IMV invasive mechanical ventilation IQR interquar
FLA 510 DTD ACS6738_proof 8
room time This equates to a cost saving of $14443 perpatient who underwent rib fixationFollow-up at 3 months showed no significant differ-
ences between groups in spirometry results (Table 4)Clinical review at 3 months revealed 2 patients witha visible flail segment Both had an anterior flail segmentand were in the nonoperative group The flail segment
erative group (n frac14 23) Nonoperative group (n frac14 23) p Value
616 361 813 842 031
494 359 NA
1518 831 1810 1302 037
285 (191e319) 359 (270e581) 003
324 (238e380) 448 (323e647) 003
3 (13) 1 (4) 061
13 (57) 19 (83) 005
3 (0e25) 50 (17e102) 001
9 (39) 1623 (70) 004
18 19 078
620 (0e3100) 1240 (620e3100) 039
930 (620e1860) 900 (500e1395) 057
223 (9) 223 (9) 099
2 (1e4) 2 (1e4) 099
1123 (48) 1723 (74) 007
20 (18e28) 25 (18e38) 024
0 1 087
tile range NIV noninvasive ventilation
February 2013 354 pm
Table 4 Spirometry Results at 3-Month Follow-Up
Percentpredicted value
Operative group(n frac14 17)
Nonoperative group(n frac14 17) p Value
FEV1 743 150 802 183 031
FVC 779 157 848 140 019
MMEF 762 369 821 350 064
PEF 628 285 681 365 063
TLC 840 244 882 234 061
FEV1FVC 956 98 950 173 092
Data are reported as mean SDFEV1 forced expiratory volume in one second FVC forced vital capacityMMEF maximal mid expiratory flow PEF peak expiratory flow TLCtotal lung capacity
Table 5 Three-Dimensional CT Results at 3 Months
3D CT appearance
Operativegroup
n (n frac14 21)
Nonoperativegroup
n (n frac14 17)p
Value
Complete healing 11 8 050
Partial healing 7 8 051
Nonhealing 3 1 038
Preoperative overlapping ribends 14 10 086
Residual overlapping rib ends 8 10 035
Improvement in overlappingbone ends 6 0 072
Preoperative displacement(gt1 rib gtrib width) 9 13 005
Residual displacement(gt1 rib gtrib width) 4 7 016
Improvement in ribdisplacement 5 6 012
Preoperative angulation(gt5 degrees gt1 rib) 9 12 009
Residual angulation(gt5 degrees gt1 rib) 3 9 001
Improvement in angulation 6 3 015
Table 6 Short Form-36 Quality of Life QuestionnaireResults at 6 Months Postinjury
SF-36 domainsOperative group
(n frac14 19)Nonoperative group
(n frac14 18) p Value
Physical functioning 334 130 384 120 024
Physical role 321 79 351 114 036
Bodily pain 422 94 379 110 022
General health 452 118 440 122 077
Vitalityenergy 441 108 463 82 049
Social functioning 360 150 372 125 079
Emotional role 376 145 378 135 097
Mental health 459 132 465 91 087
PCS 336 98 352 107 065
MCS 451 138 452 92 098
Scores are reported as mean SDMCS mental component summary score PCS physical componentsummary score
6 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
was not causing either patient any pain or restriction ofactivity Most (60) patients complained of ongoinglimitation in their daily work and home lives (15 of 21[71] in the nonoperative group vs 10 of 21[48] inthe operative group) However the majority of theserestrictions were due to injuries other than the flail chestinjury Only 2 patients (1 in each group) reportedconcerns about the cosmetic appearance of their chestat follow-up Chest CTs with 3-dimensional reconstruc-tions performed at 3 months were analyzed for degreeof healing and residual deformity in the fixed ribs(Table 5) Short Form-36 quality of life questionnaireat 6 months showed no differences between groups inany of the domains or the component summary scores(Table 6)
DISCUSSIONIn this prospective randomized trial comparing operativerib fixation and nonoperative management for traumaticflail chest we demonstrated reduced duration of ICU stayand reduced use of noninvasive ventilation and tracheos-tomy in the operative group The duration of invasivemechanical ventilation (IMV) from randomization wasnot significantly different between groups although itdid trend to a lesser duration in the conservative manage-ment group If the duration of IMV in the surgical groupis analyzed from the time of operation the differencesbetween groups becomes quite marked with significantlyless requirement for IMV in the surgical group Althoughthe treating intensivists were not blinded to the treatmentgroup ventilatory weaning and requirement for tracheos-tomy were protocol driven A spontaneous breathing trialwas considered in every patient on a daily basis After day7 postintubation tracheostomy was considered if itappeared the patient would not reach extubation withinthe next 2 to 3 days Although IMV time between groupswas not significantly different it was 30 hours shorter inthe surgical group which helps to explain why those
FLA 510 DTD ACS6738_proof 8
patients were less likely to receive a tracheostomyFurther the increased requirement for noninvasive venti-lation in the nonoperative group indicates that the trache-ostomy protocol was appropriately followed because thosepatients did require ongoing ventilatory support albeitnoninvasiveThe duration of hospital stay was 5 days shorter in the
surgical group which reflects the 5-day shorter ICU stayHowever the difference in overall hospital stay (20 daysvs 25 days) was not significantly different between groupsIt is also possible that this length of stay was affected by
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 7
a delay in transfer to rehabilitation hospitals due to bedblock which often tends to occur in our area Howeverthis would occur equally between groups so does notexplain the difference in length of stay seen in this studycohort The reduction in ICU stay in the operative groupreduced the ICU costs by more than $14000 per patient(a considerable cost savings to the health system) andsaved 5 ICU bed days per patientShort-term follow-up of our patients demonstrated no
significant differences in spirometry at 3 months betweengroups This result contrasts with previous studies thathave demonstrated improvements in percent predictedforced vital capacity total lung capacity and forced expi-ratory flow at 75 of vital capacity from 2-monthfollow-up49
We were unable to demonstrate any difference betweengroups in terms of Short Form-36 quality of life question-naire outcomes at 6 months postinjury The physicalsummary score was lower in both groups than the mentalsummary score This finding suggests that the patientsmade appropriate psychological adjustments to theirinjuries as has been previously reported10 Normativedata from the Australian population show a mental healthsummary score of 508 which is similar to the scores inour study population The reported physical summaryscore in the general Australian population is 498 whichis quite a bit higher than the scores in the groups in thisstudy11
We did not specifically assess pain in this study becauseall of the enrolled patients were sedated and ventilated atthe time of enrollment So the main indication forsurgery was mechanical stabilization not pain Furtherbecause these patients were a true multitrauma cohortwith multiple system injuries it was thought that anyassessment of analgesic requirement would beconfounded by the many other injuries also requiringanalgesia Indeed that is what we found at 3-monthfollow-up As outlined in the results patients who com-plained of ongoing physical limitation reported thatthey were limited by pain and stiffness from otherinjuries particularly shoulder girdle injuries rather thanrib injuries themselvesOnly 2 other prospective randomized trials have been
reported investigating the impact of operative fixationof flail chest injury49 Both studies slightly smaller thanthis one demonstrated significantly reduced mechanicalventilation time ICU stay incidence of pneumoniaand improved spirometry at follow-up in the operativegroup Tanaka and colleagues4 also demonstrated earlierreturn to work in the surgical cohort at 6-monthfollow-up The average age of the patients in our study(58 years) was older than that reported in both previous
FLA 510 DTD ACS6738_proof 8
randomized controlled trials of 45 years4 and 38 years9
This is likely to explain the seemingly slower recoveryin our patients and the lower rates of return to work(many of our patients were retired) Our failure to iden-tify differences in spirometry results at 3 months may alsobe related to the older age cohort in our studyThe study by Grantezny and associates9 also had
a cohort of patients with much lower Injury SeverityScores (ISS) (average 174) compared with those in ourstudy group (average 333) Again this reflects a seeminglydifferent study populationdyounger patients with singlesystem injuriesdcompared with our population of olderpatients with multiple system injuries (as evidenced bythe number of nonthoracic operations required) Wehave also reported the New Injury Severity Score(NISS) and the Trauma and Injury Severity Scores(TRISS) to give a more comprehensive picture of theinjury severity of this group of patients The higher ISSscores and multisystem nature of the injuries in ourcohort of patients may explain our failure to identifyany differences in quality of life between groupsOther previous research on operative fixation of frac-
tured ribs has consisted of retrospective reviews and casereports The retrospective review by Voggenreiter andcoworkers12 was the only one to subdivide the treatmentgroups into those with and without significant contusionAlthough they found benefits in the operative treatmentgroup they also found that these benefits were negatedby the presence of significant pulmonary contusion Inour study the majority of patients had only mild contu-sion on chest x-ray at the time of enrollmentAlmost all of the published studies have used metal
implants for operative fixation of the ribs Granetznyand colleagues9 used Kirschner and stainless steel wiresTanaka and associates4 used Judet struts In contrast weused a polylactide copolymer prosthesis applied as a 6-or 8-hole plate and screws These prostheses degrade byhydrolysis and are metabolized by the body into carbondioxide and water They maintain at least 40 of theirstrength at 3 months by which time the fractures wouldbe expected to have completely healed and arecompletely absorbed without toxicity over 1 to 3 yearsAnimal models using these absorbable plates have shownfaster and stronger healing compared with traditionalmetal plates which may actually slow bone healing13
This occurs because the metal plate protects the bonefrom any load but in doing so it removes the stimulusfor new bone growth (known as stress-shielding) Incontrast the absorbable plates allow gradual transfer ofstress loads to the bone stimulating faster bone growth13
Because the plates and screws are absorbable there is noneed to remove plates which confers a potential cost
February 2013 354 pm
8 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
savings to this procedure Also it minimizes the sequelae ofpossible prosthesis-related complications such as migrationpalpability (especially in thin patients) or thermal sensi-tivity Metal prostheses usually require removal if thesecomplications occur while a more conservative approachcan be adopted with absorbable prostheses Furthermorethere is no contraindication to future MRI in patientswho have had absorbable plates implantedDespite the existing evidence of patient and hospital
benefits with operative fixation of flail chest injury clinicalequipoise within the Western surgical community has per-sisted (operative rib fixation seems to have been taken upmore readily in East Asia14) This study is now the thirdstudy (in 3 different countries) to show similar benefitsin this patient population and we hope that it will influ-ence management change in these critically ill traumapatients Another reason why surgeons have been slow toembrace this type of surgery is probably related to thelack of specific prostheses designed for rib fixation Inthis study we used a prosthesis designed for the fibulaHowever over the last few years a number of productshave come onto the market specifically designed for ribfixation15 This demonstrates the increasing awarenessand interest in this type of surgery and also acknowledgesthat in the past surgical results when using nonspecificprostheses have been very variable16-18
Ribs present a number of surgical difficulties notencountered with other bony injuries Ribs are subjectto continual movement with breathing as well as suddenmore forceful movements during coughing and sneezingRibs have a thin inner and outer cortex making pros-thesis fixation difficult and at times unreliable Typicalrib fractures often involve splintering of the ribsmandating that bone fixation be undertaken at a sitefurther away from the fracture Each rib differs slightlyin its shape and in particular in the radius of its curva-ture which means that a ldquoone size fits allrdquo approachparticularly with less malleable prostheses is unlikely tobe successful19
A wide variety of prostheses have been tried in rib fixa-tion Many have flaws Kirschner wires provide little rota-tional stability and are prone to migration Metal platesborrowed from other applications are able to be curved inone direction only Because rib curvature is quitecomplex these metal plates are prone to ldquolifting offrdquothe rib Although the ribs do not carry a heavy loadthey are affected by torque in multiple directions due tothe layers of intercostal muscles inserting onto the ribsas well as multiple chest wall muscles Few authors havecommented on the impact of the chest wall musculatureon the dislocation and distraction of fractured ribs Bor-relly and Aazami20 in their retrospective review of flail
FLA 510 DTD ACS6738_proof 8
chest patients noted that the actions of serratus anteriortend to distract anterolateral fractures while impactingthe ribs in posterolateral fractures Analysis of the effectof intercostal muscle forces on rib fractures and fixationmethod has recently been analyzed and could assist indevelopment of specific rib prostheses78
CONCLUSIONSThis study shows clinical benefit and cost savings to thehealth system for flail chest patients who undergo rib fixa-tion Hopefully this study will help to change operativemanagement protocols for these critically ill patientsFurther trials into nonventilator-dependent patients alsoneed to be performed to assess in more detail potentialpatient benefits of pain reduction and functionalimprovements
Author Contributions
Study conception and design Marasco Davies CooperFitzgerald
Acquisition of data Marasco Bennet Nevill LeeAnalysis and interpretation of data Marasco DaviesCooper Varma Lee Bailey Fitzgerald
Drafting of manuscript Marasco Davies CooperVarma Bennet Nevill Lee Bailey Fitzgerald
Critical revision Marasco Davies Cooper VarmaBennet Nevill Lee Bailey Fitzgerald
REFERENCES
1 Ciraulo DL Elliott DMitchell KA et al Flail chest as a markerfor significant injuries J Am Coll Surg 1994178466e470
2 Kent R Woods W Bostrom O Fatality risk and the presenceof rib fractures Annu Proc Assoc Adv Automot Med 20085273e82
3 Kerr-Valentic MA Arthur M Mullins RJ et al Rib fracturepain and disability can we do better J Trauma 2003541058e1063
4 Tanaka H Yukioka T Yamaguti Y et al Surgical stabilizationof internal pneumatic stabilization A prospective randomizedstudy of management of severe flail chest patients J Trauma200252727e732
5 Mayberry JC Ham LB Schipper PH et al Surveyed opinionof American trauma orthopaedic and thoracic surgeons on riband sternal fracture repair J Trauma 200966875e879
6 Atkin C Freedman I Rosenfeld JV et al The evolution of anintegrated state trauma system in Victoria Australia Injury2005361277e1287
7 Marasco SF Sutalo ID Bui AV Mode of failure of rib fixationwith absorbable plates a clinical and numerical modellingstudy J Trauma 2010681225e1233
8 Marasco SF Liovic P Sutalo ID Structural integrity of intra-medullary rib fixation using a single bioresorbable screw AcuteCare Surg 201273668e673
9 Granetzny A El-Aal MA Emam E et al Surgical versus conser-vative treatment of flail chest Evaluation of the pulmonarystatus Interact Cardiovasc Thorac Surg 20054583e587
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 9
10 Singer MA Hopman WM MacKenzie TA Physical func-tioning and mental health in patients with chronic medicalconditions Qual Life Res 19998687e691
11 Australian Bureau of Statistics National health survey SF-36population norms Australia Canberra ACT Australian Bureauof Statistics 1995
12 Voggenreiter G Neudeck F Aufmkolk M et al Operative chestwall stabilisation in flail chest e outcomes of patients with orwithout pulmonary contusion J Am Coll Surg 1998187130e138
13 Viljanen J Pihlajamaki H Kinnunen J et al Comparison ofabsorbable poly-L-lactide and metallic intramedullary rods inthe fixation of femoral shaft osteotomies an experimentalstudy in rabbits J Orthop Sci 20016160e166
14 Yang Y Dong LW Wang J Memory alloy embracing fixatorin treatment of multiple fractured ribs and flail chest World JEmerg Med 20101212e215
FLA 510 DTD ACS6738_proof 8
15 Marasco SF Open surgical fixation of fractured ribs RecentPatents Biomed Eng 201031e6
16 Balci AE Eren S Cakir O Eren MN Open fixation in flailchest review of 64 patients Asian Cardiovasc Thorac Ann20041211e15
17 Mayberry JC Terhes JT Ellis TJ et al Absorbable plates forrib fracture repair preliminary experience J Trauma 200355835e839
18 Marasco S Cooper J Pick A Kossmann T Pilot study ofoperative fixation of fractured ribs in patients with flail chestANZ J Surg 200979804e808
19 Mohr M Abrams E Engel C et al Geometry of human ribspertinent to orthopaedic chest-wall reconstruction J Biomech2007401310e1317
20 Borrelly J Aazami MH New insights into the pathophysiologyof flail segment the implications of anterior serratus muscle inparietal failure Eur J Cardiothorac Surg 200528742e749
February 2013 354 pm
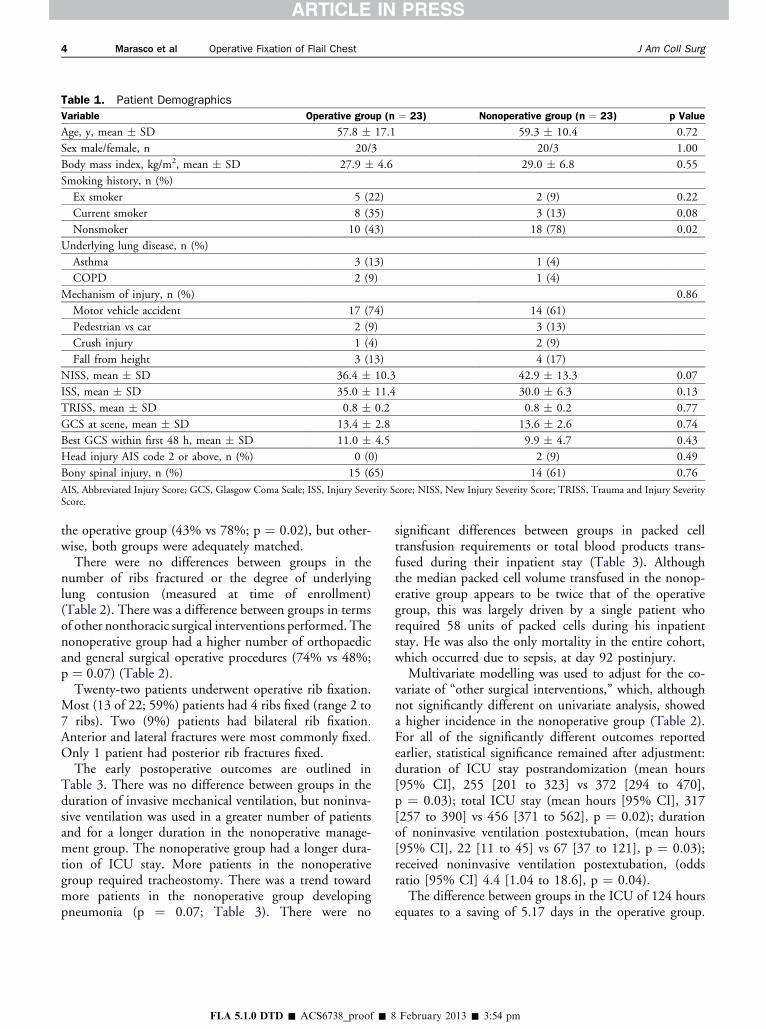
Table 1 Patient Demographics
Variable Operative group (n frac14 23) Nonoperative group (n frac14 23) p Value
Age y mean SD 578 171 593 104 072
Sex malefemale n 203 203 100
Body mass index kgm2 mean SD 279 46 290 68 055
Smoking history n ()
Ex smoker 5 (22) 2 (9) 022
Current smoker 8 (35) 3 (13) 008
Nonsmoker 10 (43) 18 (78) 002
Underlying lung disease n ()
Asthma 3 (13) 1 (4)
COPD 2 (9) 1 (4)
Mechanism of injury n () 086
Motor vehicle accident 17 (74) 14 (61)
Pedestrian vs car 2 (9) 3 (13)
Crush injury 1 (4) 2 (9)
Fall from height 3 (13) 4 (17)
NISS mean SD 364 103 429 133 007
ISS mean SD 350 114 300 63 013
TRISS mean SD 08 02 08 02 077
GCS at scene mean SD 134 28 136 26 074
Best GCS within first 48 h mean SD 110 45 99 47 043
Head injury AIS code 2 or above n () 0 (0) 2 (9) 049
Bony spinal injury n () 15 (65) 14 (61) 076
AIS Abbreviated Injury Score GCS Glasgow Coma Scale ISS Injury Severity Score NISS New Injury Severity Score TRISS Trauma and Injury SeverityScore
4 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
the operative group (43 vs 78 p frac14 002) but other-wise both groups were adequately matchedThere were no differences between groups in the
number of ribs fractured or the degree of underlyinglung contusion (measured at time of enrollment)(Table 2) There was a difference between groups in termsof other nonthoracic surgical interventions performed Thenonoperative group had a higher number of orthopaedicand general surgical operative procedures (74 vs 48p frac14 007) (Table 2)Twenty-two patients underwent operative rib fixation
Most (13 of 22 59) patients had 4 ribs fixed (range 2 to7 ribs) Two (9) patients had bilateral rib fixationAnterior and lateral fractures were most commonly fixedOnly 1 patient had posterior rib fractures fixedThe early postoperative outcomes are outlined in
Table 3 There was no difference between groups in theduration of invasive mechanical ventilation but noninva-sive ventilation was used in a greater number of patientsand for a longer duration in the nonoperative manage-ment group The nonoperative group had a longer dura-tion of ICU stay More patients in the nonoperativegroup required tracheostomy There was a trend towardmore patients in the nonoperative group developingpneumonia (p frac14 007 Table 3) There were no
FLA 510 DTD ACS6738_proof 8
significant differences between groups in packed celltransfusion requirements or total blood products trans-fused during their inpatient stay (Table 3) Althoughthe median packed cell volume transfused in the nonop-erative group appears to be twice that of the operativegroup this was largely driven by a single patient whorequired 58 units of packed cells during his inpatientstay He was also the only mortality in the entire cohortwhich occurred due to sepsis at day 92 postinjuryMultivariate modelling was used to adjust for the co-
variate of ldquoother surgical interventionsrdquo which althoughnot significantly different on univariate analysis showeda higher incidence in the nonoperative group (Table 2)For all of the significantly different outcomes reportedearlier statistical significance remained after adjustmentduration of ICU stay postrandomization (mean hours[95 CI] 255 [201 to 323] vs 372 [294 to 470]p frac14 003) total ICU stay (mean hours [95 CI] 317[257 to 390] vs 456 [371 to 562] p frac14 002) durationof noninvasive ventilation postextubation (mean hours[95 CI] 22 [11 to 45] vs 67 [37 to 121] p frac14 003)received noninvasive ventilation postextubation (oddsratio [95 CI] 44 [104 to 186] p frac14 004)The difference between groups in the ICU of 124 hours
equates to a saving of 517 days in the operative group
February 2013 354 pm
Table 2 Injury Description
Variable Operative group (n frac14 23) Nonoperative group (n frac14 23) p Value
Total no fractured ribs mean SD 110 31 113 47 079
No of ribs in flail segment mean SD 51 17 55 20 043
No of patients with bilateral vs unilateral rib fractures 1211 1310
Underlying lung contusion n ()
None 3 (13) 2 (9) 100
Mild 16 (70) 16 (70) 100
Moderate 4 (17) 4 (17) 100
Severe 0 (0) 1 (4) 100
Pneumothorax n () 20 (90) 21 (91) 064
Other surgical interventions required n ()y 11 (48) 17 (74) 007
Thoracotomy n 0 2
Laparotomy n 1 2
ORIF clavicle n 3 5
Pelvic external fixation n 0 2
Spinal fusion n 2 0
ORIF limb fracture n 5 6
Plastics n 2z 4
Determined on chest x-ray on day of enrollment into trialySome patients underwent more than 1 surgical interventionzIncludes ORIF facial fractures in 1 patientORIF open reduction internal fixation
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 5
The cost of running an ICU bed in our hospital is esti-mated to be $4109 per day This potential cost savingof $21243 per operatively managed patient is offset bythe average cost of the operation which in this cohortwas $6800 per patient The breakdown of these costsare $4200 for the prostheses ($1050 per fracture fixed)and $2600 for approximately 25 hours of operating
Table 3 Outcomes
Outcomes Op
Duration of ICU stay prerandomization h mean SD
Duration of ICU stay between randomization and surgery hmean SD
Duration of IMV postrandomization h mean SD
Duration of ICU stay postrandomization h median (IQR)
Total ICU stay h median (IQR)
Failed extubation n ()
Received NIV postextubation n ()
Duration of NIV postextubation h median (IQR)
Tracheostomy n ()
Patients requiring blood product transfusion n
Packed cell transfusion during inpatient stay mL median (IQR)
Total blood products transfused mL median (IQR)
Readmission to ICU n ()
ICCs required n median (IQR)
Pneumonia n ()
Duration of hospital stay d median (IQR)
In hospital mortality n
ICC intercostal catheter IMV invasive mechanical ventilation IQR interquar
FLA 510 DTD ACS6738_proof 8
room time This equates to a cost saving of $14443 perpatient who underwent rib fixationFollow-up at 3 months showed no significant differ-
ences between groups in spirometry results (Table 4)Clinical review at 3 months revealed 2 patients witha visible flail segment Both had an anterior flail segmentand were in the nonoperative group The flail segment
erative group (n frac14 23) Nonoperative group (n frac14 23) p Value
616 361 813 842 031
494 359 NA
1518 831 1810 1302 037
285 (191e319) 359 (270e581) 003
324 (238e380) 448 (323e647) 003
3 (13) 1 (4) 061
13 (57) 19 (83) 005
3 (0e25) 50 (17e102) 001
9 (39) 1623 (70) 004
18 19 078
620 (0e3100) 1240 (620e3100) 039
930 (620e1860) 900 (500e1395) 057
223 (9) 223 (9) 099
2 (1e4) 2 (1e4) 099
1123 (48) 1723 (74) 007
20 (18e28) 25 (18e38) 024
0 1 087
tile range NIV noninvasive ventilation
February 2013 354 pm
Table 4 Spirometry Results at 3-Month Follow-Up
Percentpredicted value
Operative group(n frac14 17)
Nonoperative group(n frac14 17) p Value
FEV1 743 150 802 183 031
FVC 779 157 848 140 019
MMEF 762 369 821 350 064
PEF 628 285 681 365 063
TLC 840 244 882 234 061
FEV1FVC 956 98 950 173 092
Data are reported as mean SDFEV1 forced expiratory volume in one second FVC forced vital capacityMMEF maximal mid expiratory flow PEF peak expiratory flow TLCtotal lung capacity
Table 5 Three-Dimensional CT Results at 3 Months
3D CT appearance
Operativegroup
n (n frac14 21)
Nonoperativegroup
n (n frac14 17)p
Value
Complete healing 11 8 050
Partial healing 7 8 051
Nonhealing 3 1 038
Preoperative overlapping ribends 14 10 086
Residual overlapping rib ends 8 10 035
Improvement in overlappingbone ends 6 0 072
Preoperative displacement(gt1 rib gtrib width) 9 13 005
Residual displacement(gt1 rib gtrib width) 4 7 016
Improvement in ribdisplacement 5 6 012
Preoperative angulation(gt5 degrees gt1 rib) 9 12 009
Residual angulation(gt5 degrees gt1 rib) 3 9 001
Improvement in angulation 6 3 015
Table 6 Short Form-36 Quality of Life QuestionnaireResults at 6 Months Postinjury
SF-36 domainsOperative group
(n frac14 19)Nonoperative group
(n frac14 18) p Value
Physical functioning 334 130 384 120 024
Physical role 321 79 351 114 036
Bodily pain 422 94 379 110 022
General health 452 118 440 122 077
Vitalityenergy 441 108 463 82 049
Social functioning 360 150 372 125 079
Emotional role 376 145 378 135 097
Mental health 459 132 465 91 087
PCS 336 98 352 107 065
MCS 451 138 452 92 098
Scores are reported as mean SDMCS mental component summary score PCS physical componentsummary score
6 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
was not causing either patient any pain or restriction ofactivity Most (60) patients complained of ongoinglimitation in their daily work and home lives (15 of 21[71] in the nonoperative group vs 10 of 21[48] inthe operative group) However the majority of theserestrictions were due to injuries other than the flail chestinjury Only 2 patients (1 in each group) reportedconcerns about the cosmetic appearance of their chestat follow-up Chest CTs with 3-dimensional reconstruc-tions performed at 3 months were analyzed for degreeof healing and residual deformity in the fixed ribs(Table 5) Short Form-36 quality of life questionnaireat 6 months showed no differences between groups inany of the domains or the component summary scores(Table 6)
DISCUSSIONIn this prospective randomized trial comparing operativerib fixation and nonoperative management for traumaticflail chest we demonstrated reduced duration of ICU stayand reduced use of noninvasive ventilation and tracheos-tomy in the operative group The duration of invasivemechanical ventilation (IMV) from randomization wasnot significantly different between groups although itdid trend to a lesser duration in the conservative manage-ment group If the duration of IMV in the surgical groupis analyzed from the time of operation the differencesbetween groups becomes quite marked with significantlyless requirement for IMV in the surgical group Althoughthe treating intensivists were not blinded to the treatmentgroup ventilatory weaning and requirement for tracheos-tomy were protocol driven A spontaneous breathing trialwas considered in every patient on a daily basis After day7 postintubation tracheostomy was considered if itappeared the patient would not reach extubation withinthe next 2 to 3 days Although IMV time between groupswas not significantly different it was 30 hours shorter inthe surgical group which helps to explain why those
FLA 510 DTD ACS6738_proof 8
patients were less likely to receive a tracheostomyFurther the increased requirement for noninvasive venti-lation in the nonoperative group indicates that the trache-ostomy protocol was appropriately followed because thosepatients did require ongoing ventilatory support albeitnoninvasiveThe duration of hospital stay was 5 days shorter in the
surgical group which reflects the 5-day shorter ICU stayHowever the difference in overall hospital stay (20 daysvs 25 days) was not significantly different between groupsIt is also possible that this length of stay was affected by
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 7
a delay in transfer to rehabilitation hospitals due to bedblock which often tends to occur in our area Howeverthis would occur equally between groups so does notexplain the difference in length of stay seen in this studycohort The reduction in ICU stay in the operative groupreduced the ICU costs by more than $14000 per patient(a considerable cost savings to the health system) andsaved 5 ICU bed days per patientShort-term follow-up of our patients demonstrated no
significant differences in spirometry at 3 months betweengroups This result contrasts with previous studies thathave demonstrated improvements in percent predictedforced vital capacity total lung capacity and forced expi-ratory flow at 75 of vital capacity from 2-monthfollow-up49
We were unable to demonstrate any difference betweengroups in terms of Short Form-36 quality of life question-naire outcomes at 6 months postinjury The physicalsummary score was lower in both groups than the mentalsummary score This finding suggests that the patientsmade appropriate psychological adjustments to theirinjuries as has been previously reported10 Normativedata from the Australian population show a mental healthsummary score of 508 which is similar to the scores inour study population The reported physical summaryscore in the general Australian population is 498 whichis quite a bit higher than the scores in the groups in thisstudy11
We did not specifically assess pain in this study becauseall of the enrolled patients were sedated and ventilated atthe time of enrollment So the main indication forsurgery was mechanical stabilization not pain Furtherbecause these patients were a true multitrauma cohortwith multiple system injuries it was thought that anyassessment of analgesic requirement would beconfounded by the many other injuries also requiringanalgesia Indeed that is what we found at 3-monthfollow-up As outlined in the results patients who com-plained of ongoing physical limitation reported thatthey were limited by pain and stiffness from otherinjuries particularly shoulder girdle injuries rather thanrib injuries themselvesOnly 2 other prospective randomized trials have been
reported investigating the impact of operative fixationof flail chest injury49 Both studies slightly smaller thanthis one demonstrated significantly reduced mechanicalventilation time ICU stay incidence of pneumoniaand improved spirometry at follow-up in the operativegroup Tanaka and colleagues4 also demonstrated earlierreturn to work in the surgical cohort at 6-monthfollow-up The average age of the patients in our study(58 years) was older than that reported in both previous
FLA 510 DTD ACS6738_proof 8
randomized controlled trials of 45 years4 and 38 years9
This is likely to explain the seemingly slower recoveryin our patients and the lower rates of return to work(many of our patients were retired) Our failure to iden-tify differences in spirometry results at 3 months may alsobe related to the older age cohort in our studyThe study by Grantezny and associates9 also had
a cohort of patients with much lower Injury SeverityScores (ISS) (average 174) compared with those in ourstudy group (average 333) Again this reflects a seeminglydifferent study populationdyounger patients with singlesystem injuriesdcompared with our population of olderpatients with multiple system injuries (as evidenced bythe number of nonthoracic operations required) Wehave also reported the New Injury Severity Score(NISS) and the Trauma and Injury Severity Scores(TRISS) to give a more comprehensive picture of theinjury severity of this group of patients The higher ISSscores and multisystem nature of the injuries in ourcohort of patients may explain our failure to identifyany differences in quality of life between groupsOther previous research on operative fixation of frac-
tured ribs has consisted of retrospective reviews and casereports The retrospective review by Voggenreiter andcoworkers12 was the only one to subdivide the treatmentgroups into those with and without significant contusionAlthough they found benefits in the operative treatmentgroup they also found that these benefits were negatedby the presence of significant pulmonary contusion Inour study the majority of patients had only mild contu-sion on chest x-ray at the time of enrollmentAlmost all of the published studies have used metal
implants for operative fixation of the ribs Granetznyand colleagues9 used Kirschner and stainless steel wiresTanaka and associates4 used Judet struts In contrast weused a polylactide copolymer prosthesis applied as a 6-or 8-hole plate and screws These prostheses degrade byhydrolysis and are metabolized by the body into carbondioxide and water They maintain at least 40 of theirstrength at 3 months by which time the fractures wouldbe expected to have completely healed and arecompletely absorbed without toxicity over 1 to 3 yearsAnimal models using these absorbable plates have shownfaster and stronger healing compared with traditionalmetal plates which may actually slow bone healing13
This occurs because the metal plate protects the bonefrom any load but in doing so it removes the stimulusfor new bone growth (known as stress-shielding) Incontrast the absorbable plates allow gradual transfer ofstress loads to the bone stimulating faster bone growth13
Because the plates and screws are absorbable there is noneed to remove plates which confers a potential cost
February 2013 354 pm
8 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
savings to this procedure Also it minimizes the sequelae ofpossible prosthesis-related complications such as migrationpalpability (especially in thin patients) or thermal sensi-tivity Metal prostheses usually require removal if thesecomplications occur while a more conservative approachcan be adopted with absorbable prostheses Furthermorethere is no contraindication to future MRI in patientswho have had absorbable plates implantedDespite the existing evidence of patient and hospital
benefits with operative fixation of flail chest injury clinicalequipoise within the Western surgical community has per-sisted (operative rib fixation seems to have been taken upmore readily in East Asia14) This study is now the thirdstudy (in 3 different countries) to show similar benefitsin this patient population and we hope that it will influ-ence management change in these critically ill traumapatients Another reason why surgeons have been slow toembrace this type of surgery is probably related to thelack of specific prostheses designed for rib fixation Inthis study we used a prosthesis designed for the fibulaHowever over the last few years a number of productshave come onto the market specifically designed for ribfixation15 This demonstrates the increasing awarenessand interest in this type of surgery and also acknowledgesthat in the past surgical results when using nonspecificprostheses have been very variable16-18
Ribs present a number of surgical difficulties notencountered with other bony injuries Ribs are subjectto continual movement with breathing as well as suddenmore forceful movements during coughing and sneezingRibs have a thin inner and outer cortex making pros-thesis fixation difficult and at times unreliable Typicalrib fractures often involve splintering of the ribsmandating that bone fixation be undertaken at a sitefurther away from the fracture Each rib differs slightlyin its shape and in particular in the radius of its curva-ture which means that a ldquoone size fits allrdquo approachparticularly with less malleable prostheses is unlikely tobe successful19
A wide variety of prostheses have been tried in rib fixa-tion Many have flaws Kirschner wires provide little rota-tional stability and are prone to migration Metal platesborrowed from other applications are able to be curved inone direction only Because rib curvature is quitecomplex these metal plates are prone to ldquolifting offrdquothe rib Although the ribs do not carry a heavy loadthey are affected by torque in multiple directions due tothe layers of intercostal muscles inserting onto the ribsas well as multiple chest wall muscles Few authors havecommented on the impact of the chest wall musculatureon the dislocation and distraction of fractured ribs Bor-relly and Aazami20 in their retrospective review of flail
FLA 510 DTD ACS6738_proof 8
chest patients noted that the actions of serratus anteriortend to distract anterolateral fractures while impactingthe ribs in posterolateral fractures Analysis of the effectof intercostal muscle forces on rib fractures and fixationmethod has recently been analyzed and could assist indevelopment of specific rib prostheses78
CONCLUSIONSThis study shows clinical benefit and cost savings to thehealth system for flail chest patients who undergo rib fixa-tion Hopefully this study will help to change operativemanagement protocols for these critically ill patientsFurther trials into nonventilator-dependent patients alsoneed to be performed to assess in more detail potentialpatient benefits of pain reduction and functionalimprovements
Author Contributions
Study conception and design Marasco Davies CooperFitzgerald
Acquisition of data Marasco Bennet Nevill LeeAnalysis and interpretation of data Marasco DaviesCooper Varma Lee Bailey Fitzgerald
Drafting of manuscript Marasco Davies CooperVarma Bennet Nevill Lee Bailey Fitzgerald
Critical revision Marasco Davies Cooper VarmaBennet Nevill Lee Bailey Fitzgerald
REFERENCES
1 Ciraulo DL Elliott DMitchell KA et al Flail chest as a markerfor significant injuries J Am Coll Surg 1994178466e470
2 Kent R Woods W Bostrom O Fatality risk and the presenceof rib fractures Annu Proc Assoc Adv Automot Med 20085273e82
3 Kerr-Valentic MA Arthur M Mullins RJ et al Rib fracturepain and disability can we do better J Trauma 2003541058e1063
4 Tanaka H Yukioka T Yamaguti Y et al Surgical stabilizationof internal pneumatic stabilization A prospective randomizedstudy of management of severe flail chest patients J Trauma200252727e732
5 Mayberry JC Ham LB Schipper PH et al Surveyed opinionof American trauma orthopaedic and thoracic surgeons on riband sternal fracture repair J Trauma 200966875e879
6 Atkin C Freedman I Rosenfeld JV et al The evolution of anintegrated state trauma system in Victoria Australia Injury2005361277e1287
7 Marasco SF Sutalo ID Bui AV Mode of failure of rib fixationwith absorbable plates a clinical and numerical modellingstudy J Trauma 2010681225e1233
8 Marasco SF Liovic P Sutalo ID Structural integrity of intra-medullary rib fixation using a single bioresorbable screw AcuteCare Surg 201273668e673
9 Granetzny A El-Aal MA Emam E et al Surgical versus conser-vative treatment of flail chest Evaluation of the pulmonarystatus Interact Cardiovasc Thorac Surg 20054583e587
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 9
10 Singer MA Hopman WM MacKenzie TA Physical func-tioning and mental health in patients with chronic medicalconditions Qual Life Res 19998687e691
11 Australian Bureau of Statistics National health survey SF-36population norms Australia Canberra ACT Australian Bureauof Statistics 1995
12 Voggenreiter G Neudeck F Aufmkolk M et al Operative chestwall stabilisation in flail chest e outcomes of patients with orwithout pulmonary contusion J Am Coll Surg 1998187130e138
13 Viljanen J Pihlajamaki H Kinnunen J et al Comparison ofabsorbable poly-L-lactide and metallic intramedullary rods inthe fixation of femoral shaft osteotomies an experimentalstudy in rabbits J Orthop Sci 20016160e166
14 Yang Y Dong LW Wang J Memory alloy embracing fixatorin treatment of multiple fractured ribs and flail chest World JEmerg Med 20101212e215
FLA 510 DTD ACS6738_proof 8
15 Marasco SF Open surgical fixation of fractured ribs RecentPatents Biomed Eng 201031e6
16 Balci AE Eren S Cakir O Eren MN Open fixation in flailchest review of 64 patients Asian Cardiovasc Thorac Ann20041211e15
17 Mayberry JC Terhes JT Ellis TJ et al Absorbable plates forrib fracture repair preliminary experience J Trauma 200355835e839
18 Marasco S Cooper J Pick A Kossmann T Pilot study ofoperative fixation of fractured ribs in patients with flail chestANZ J Surg 200979804e808
19 Mohr M Abrams E Engel C et al Geometry of human ribspertinent to orthopaedic chest-wall reconstruction J Biomech2007401310e1317
20 Borrelly J Aazami MH New insights into the pathophysiologyof flail segment the implications of anterior serratus muscle inparietal failure Eur J Cardiothorac Surg 200528742e749
February 2013 354 pm
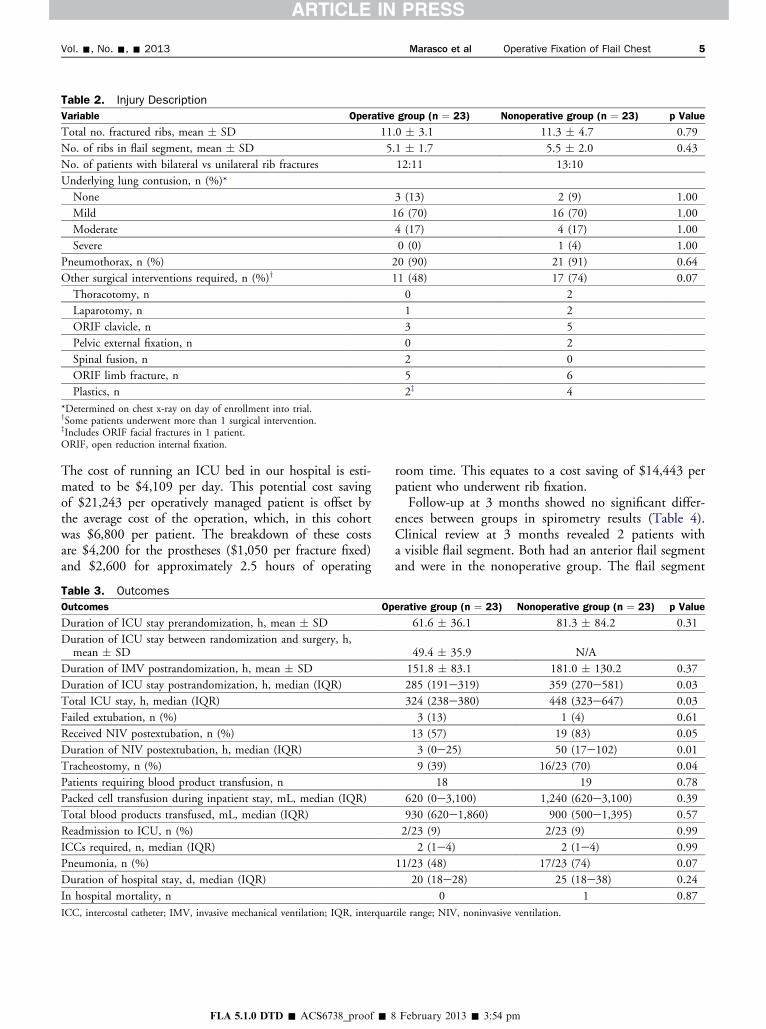
Table 2 Injury Description
Variable Operative group (n frac14 23) Nonoperative group (n frac14 23) p Value
Total no fractured ribs mean SD 110 31 113 47 079
No of ribs in flail segment mean SD 51 17 55 20 043
No of patients with bilateral vs unilateral rib fractures 1211 1310
Underlying lung contusion n ()
None 3 (13) 2 (9) 100
Mild 16 (70) 16 (70) 100
Moderate 4 (17) 4 (17) 100
Severe 0 (0) 1 (4) 100
Pneumothorax n () 20 (90) 21 (91) 064
Other surgical interventions required n ()y 11 (48) 17 (74) 007
Thoracotomy n 0 2
Laparotomy n 1 2
ORIF clavicle n 3 5
Pelvic external fixation n 0 2
Spinal fusion n 2 0
ORIF limb fracture n 5 6
Plastics n 2z 4
Determined on chest x-ray on day of enrollment into trialySome patients underwent more than 1 surgical interventionzIncludes ORIF facial fractures in 1 patientORIF open reduction internal fixation
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 5
The cost of running an ICU bed in our hospital is esti-mated to be $4109 per day This potential cost savingof $21243 per operatively managed patient is offset bythe average cost of the operation which in this cohortwas $6800 per patient The breakdown of these costsare $4200 for the prostheses ($1050 per fracture fixed)and $2600 for approximately 25 hours of operating
Table 3 Outcomes
Outcomes Op
Duration of ICU stay prerandomization h mean SD
Duration of ICU stay between randomization and surgery hmean SD
Duration of IMV postrandomization h mean SD
Duration of ICU stay postrandomization h median (IQR)
Total ICU stay h median (IQR)
Failed extubation n ()
Received NIV postextubation n ()
Duration of NIV postextubation h median (IQR)
Tracheostomy n ()
Patients requiring blood product transfusion n
Packed cell transfusion during inpatient stay mL median (IQR)
Total blood products transfused mL median (IQR)
Readmission to ICU n ()
ICCs required n median (IQR)
Pneumonia n ()
Duration of hospital stay d median (IQR)
In hospital mortality n
ICC intercostal catheter IMV invasive mechanical ventilation IQR interquar
FLA 510 DTD ACS6738_proof 8
room time This equates to a cost saving of $14443 perpatient who underwent rib fixationFollow-up at 3 months showed no significant differ-
ences between groups in spirometry results (Table 4)Clinical review at 3 months revealed 2 patients witha visible flail segment Both had an anterior flail segmentand were in the nonoperative group The flail segment
erative group (n frac14 23) Nonoperative group (n frac14 23) p Value
616 361 813 842 031
494 359 NA
1518 831 1810 1302 037
285 (191e319) 359 (270e581) 003
324 (238e380) 448 (323e647) 003
3 (13) 1 (4) 061
13 (57) 19 (83) 005
3 (0e25) 50 (17e102) 001
9 (39) 1623 (70) 004
18 19 078
620 (0e3100) 1240 (620e3100) 039
930 (620e1860) 900 (500e1395) 057
223 (9) 223 (9) 099
2 (1e4) 2 (1e4) 099
1123 (48) 1723 (74) 007
20 (18e28) 25 (18e38) 024
0 1 087
tile range NIV noninvasive ventilation
February 2013 354 pm
Table 4 Spirometry Results at 3-Month Follow-Up
Percentpredicted value
Operative group(n frac14 17)
Nonoperative group(n frac14 17) p Value
FEV1 743 150 802 183 031
FVC 779 157 848 140 019
MMEF 762 369 821 350 064
PEF 628 285 681 365 063
TLC 840 244 882 234 061
FEV1FVC 956 98 950 173 092
Data are reported as mean SDFEV1 forced expiratory volume in one second FVC forced vital capacityMMEF maximal mid expiratory flow PEF peak expiratory flow TLCtotal lung capacity
Table 5 Three-Dimensional CT Results at 3 Months
3D CT appearance
Operativegroup
n (n frac14 21)
Nonoperativegroup
n (n frac14 17)p
Value
Complete healing 11 8 050
Partial healing 7 8 051
Nonhealing 3 1 038
Preoperative overlapping ribends 14 10 086
Residual overlapping rib ends 8 10 035
Improvement in overlappingbone ends 6 0 072
Preoperative displacement(gt1 rib gtrib width) 9 13 005
Residual displacement(gt1 rib gtrib width) 4 7 016
Improvement in ribdisplacement 5 6 012
Preoperative angulation(gt5 degrees gt1 rib) 9 12 009
Residual angulation(gt5 degrees gt1 rib) 3 9 001
Improvement in angulation 6 3 015
Table 6 Short Form-36 Quality of Life QuestionnaireResults at 6 Months Postinjury
SF-36 domainsOperative group
(n frac14 19)Nonoperative group
(n frac14 18) p Value
Physical functioning 334 130 384 120 024
Physical role 321 79 351 114 036
Bodily pain 422 94 379 110 022
General health 452 118 440 122 077
Vitalityenergy 441 108 463 82 049
Social functioning 360 150 372 125 079
Emotional role 376 145 378 135 097
Mental health 459 132 465 91 087
PCS 336 98 352 107 065
MCS 451 138 452 92 098
Scores are reported as mean SDMCS mental component summary score PCS physical componentsummary score
6 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
was not causing either patient any pain or restriction ofactivity Most (60) patients complained of ongoinglimitation in their daily work and home lives (15 of 21[71] in the nonoperative group vs 10 of 21[48] inthe operative group) However the majority of theserestrictions were due to injuries other than the flail chestinjury Only 2 patients (1 in each group) reportedconcerns about the cosmetic appearance of their chestat follow-up Chest CTs with 3-dimensional reconstruc-tions performed at 3 months were analyzed for degreeof healing and residual deformity in the fixed ribs(Table 5) Short Form-36 quality of life questionnaireat 6 months showed no differences between groups inany of the domains or the component summary scores(Table 6)
DISCUSSIONIn this prospective randomized trial comparing operativerib fixation and nonoperative management for traumaticflail chest we demonstrated reduced duration of ICU stayand reduced use of noninvasive ventilation and tracheos-tomy in the operative group The duration of invasivemechanical ventilation (IMV) from randomization wasnot significantly different between groups although itdid trend to a lesser duration in the conservative manage-ment group If the duration of IMV in the surgical groupis analyzed from the time of operation the differencesbetween groups becomes quite marked with significantlyless requirement for IMV in the surgical group Althoughthe treating intensivists were not blinded to the treatmentgroup ventilatory weaning and requirement for tracheos-tomy were protocol driven A spontaneous breathing trialwas considered in every patient on a daily basis After day7 postintubation tracheostomy was considered if itappeared the patient would not reach extubation withinthe next 2 to 3 days Although IMV time between groupswas not significantly different it was 30 hours shorter inthe surgical group which helps to explain why those
FLA 510 DTD ACS6738_proof 8
patients were less likely to receive a tracheostomyFurther the increased requirement for noninvasive venti-lation in the nonoperative group indicates that the trache-ostomy protocol was appropriately followed because thosepatients did require ongoing ventilatory support albeitnoninvasiveThe duration of hospital stay was 5 days shorter in the
surgical group which reflects the 5-day shorter ICU stayHowever the difference in overall hospital stay (20 daysvs 25 days) was not significantly different between groupsIt is also possible that this length of stay was affected by
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 7
a delay in transfer to rehabilitation hospitals due to bedblock which often tends to occur in our area Howeverthis would occur equally between groups so does notexplain the difference in length of stay seen in this studycohort The reduction in ICU stay in the operative groupreduced the ICU costs by more than $14000 per patient(a considerable cost savings to the health system) andsaved 5 ICU bed days per patientShort-term follow-up of our patients demonstrated no
significant differences in spirometry at 3 months betweengroups This result contrasts with previous studies thathave demonstrated improvements in percent predictedforced vital capacity total lung capacity and forced expi-ratory flow at 75 of vital capacity from 2-monthfollow-up49
We were unable to demonstrate any difference betweengroups in terms of Short Form-36 quality of life question-naire outcomes at 6 months postinjury The physicalsummary score was lower in both groups than the mentalsummary score This finding suggests that the patientsmade appropriate psychological adjustments to theirinjuries as has been previously reported10 Normativedata from the Australian population show a mental healthsummary score of 508 which is similar to the scores inour study population The reported physical summaryscore in the general Australian population is 498 whichis quite a bit higher than the scores in the groups in thisstudy11
We did not specifically assess pain in this study becauseall of the enrolled patients were sedated and ventilated atthe time of enrollment So the main indication forsurgery was mechanical stabilization not pain Furtherbecause these patients were a true multitrauma cohortwith multiple system injuries it was thought that anyassessment of analgesic requirement would beconfounded by the many other injuries also requiringanalgesia Indeed that is what we found at 3-monthfollow-up As outlined in the results patients who com-plained of ongoing physical limitation reported thatthey were limited by pain and stiffness from otherinjuries particularly shoulder girdle injuries rather thanrib injuries themselvesOnly 2 other prospective randomized trials have been
reported investigating the impact of operative fixationof flail chest injury49 Both studies slightly smaller thanthis one demonstrated significantly reduced mechanicalventilation time ICU stay incidence of pneumoniaand improved spirometry at follow-up in the operativegroup Tanaka and colleagues4 also demonstrated earlierreturn to work in the surgical cohort at 6-monthfollow-up The average age of the patients in our study(58 years) was older than that reported in both previous
FLA 510 DTD ACS6738_proof 8
randomized controlled trials of 45 years4 and 38 years9
This is likely to explain the seemingly slower recoveryin our patients and the lower rates of return to work(many of our patients were retired) Our failure to iden-tify differences in spirometry results at 3 months may alsobe related to the older age cohort in our studyThe study by Grantezny and associates9 also had
a cohort of patients with much lower Injury SeverityScores (ISS) (average 174) compared with those in ourstudy group (average 333) Again this reflects a seeminglydifferent study populationdyounger patients with singlesystem injuriesdcompared with our population of olderpatients with multiple system injuries (as evidenced bythe number of nonthoracic operations required) Wehave also reported the New Injury Severity Score(NISS) and the Trauma and Injury Severity Scores(TRISS) to give a more comprehensive picture of theinjury severity of this group of patients The higher ISSscores and multisystem nature of the injuries in ourcohort of patients may explain our failure to identifyany differences in quality of life between groupsOther previous research on operative fixation of frac-
tured ribs has consisted of retrospective reviews and casereports The retrospective review by Voggenreiter andcoworkers12 was the only one to subdivide the treatmentgroups into those with and without significant contusionAlthough they found benefits in the operative treatmentgroup they also found that these benefits were negatedby the presence of significant pulmonary contusion Inour study the majority of patients had only mild contu-sion on chest x-ray at the time of enrollmentAlmost all of the published studies have used metal
implants for operative fixation of the ribs Granetznyand colleagues9 used Kirschner and stainless steel wiresTanaka and associates4 used Judet struts In contrast weused a polylactide copolymer prosthesis applied as a 6-or 8-hole plate and screws These prostheses degrade byhydrolysis and are metabolized by the body into carbondioxide and water They maintain at least 40 of theirstrength at 3 months by which time the fractures wouldbe expected to have completely healed and arecompletely absorbed without toxicity over 1 to 3 yearsAnimal models using these absorbable plates have shownfaster and stronger healing compared with traditionalmetal plates which may actually slow bone healing13
This occurs because the metal plate protects the bonefrom any load but in doing so it removes the stimulusfor new bone growth (known as stress-shielding) Incontrast the absorbable plates allow gradual transfer ofstress loads to the bone stimulating faster bone growth13
Because the plates and screws are absorbable there is noneed to remove plates which confers a potential cost
February 2013 354 pm
8 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
savings to this procedure Also it minimizes the sequelae ofpossible prosthesis-related complications such as migrationpalpability (especially in thin patients) or thermal sensi-tivity Metal prostheses usually require removal if thesecomplications occur while a more conservative approachcan be adopted with absorbable prostheses Furthermorethere is no contraindication to future MRI in patientswho have had absorbable plates implantedDespite the existing evidence of patient and hospital
benefits with operative fixation of flail chest injury clinicalequipoise within the Western surgical community has per-sisted (operative rib fixation seems to have been taken upmore readily in East Asia14) This study is now the thirdstudy (in 3 different countries) to show similar benefitsin this patient population and we hope that it will influ-ence management change in these critically ill traumapatients Another reason why surgeons have been slow toembrace this type of surgery is probably related to thelack of specific prostheses designed for rib fixation Inthis study we used a prosthesis designed for the fibulaHowever over the last few years a number of productshave come onto the market specifically designed for ribfixation15 This demonstrates the increasing awarenessand interest in this type of surgery and also acknowledgesthat in the past surgical results when using nonspecificprostheses have been very variable16-18
Ribs present a number of surgical difficulties notencountered with other bony injuries Ribs are subjectto continual movement with breathing as well as suddenmore forceful movements during coughing and sneezingRibs have a thin inner and outer cortex making pros-thesis fixation difficult and at times unreliable Typicalrib fractures often involve splintering of the ribsmandating that bone fixation be undertaken at a sitefurther away from the fracture Each rib differs slightlyin its shape and in particular in the radius of its curva-ture which means that a ldquoone size fits allrdquo approachparticularly with less malleable prostheses is unlikely tobe successful19
A wide variety of prostheses have been tried in rib fixa-tion Many have flaws Kirschner wires provide little rota-tional stability and are prone to migration Metal platesborrowed from other applications are able to be curved inone direction only Because rib curvature is quitecomplex these metal plates are prone to ldquolifting offrdquothe rib Although the ribs do not carry a heavy loadthey are affected by torque in multiple directions due tothe layers of intercostal muscles inserting onto the ribsas well as multiple chest wall muscles Few authors havecommented on the impact of the chest wall musculatureon the dislocation and distraction of fractured ribs Bor-relly and Aazami20 in their retrospective review of flail
FLA 510 DTD ACS6738_proof 8
chest patients noted that the actions of serratus anteriortend to distract anterolateral fractures while impactingthe ribs in posterolateral fractures Analysis of the effectof intercostal muscle forces on rib fractures and fixationmethod has recently been analyzed and could assist indevelopment of specific rib prostheses78
CONCLUSIONSThis study shows clinical benefit and cost savings to thehealth system for flail chest patients who undergo rib fixa-tion Hopefully this study will help to change operativemanagement protocols for these critically ill patientsFurther trials into nonventilator-dependent patients alsoneed to be performed to assess in more detail potentialpatient benefits of pain reduction and functionalimprovements
Author Contributions
Study conception and design Marasco Davies CooperFitzgerald
Acquisition of data Marasco Bennet Nevill LeeAnalysis and interpretation of data Marasco DaviesCooper Varma Lee Bailey Fitzgerald
Drafting of manuscript Marasco Davies CooperVarma Bennet Nevill Lee Bailey Fitzgerald
Critical revision Marasco Davies Cooper VarmaBennet Nevill Lee Bailey Fitzgerald
REFERENCES
1 Ciraulo DL Elliott DMitchell KA et al Flail chest as a markerfor significant injuries J Am Coll Surg 1994178466e470
2 Kent R Woods W Bostrom O Fatality risk and the presenceof rib fractures Annu Proc Assoc Adv Automot Med 20085273e82
3 Kerr-Valentic MA Arthur M Mullins RJ et al Rib fracturepain and disability can we do better J Trauma 2003541058e1063
4 Tanaka H Yukioka T Yamaguti Y et al Surgical stabilizationof internal pneumatic stabilization A prospective randomizedstudy of management of severe flail chest patients J Trauma200252727e732
5 Mayberry JC Ham LB Schipper PH et al Surveyed opinionof American trauma orthopaedic and thoracic surgeons on riband sternal fracture repair J Trauma 200966875e879
6 Atkin C Freedman I Rosenfeld JV et al The evolution of anintegrated state trauma system in Victoria Australia Injury2005361277e1287
7 Marasco SF Sutalo ID Bui AV Mode of failure of rib fixationwith absorbable plates a clinical and numerical modellingstudy J Trauma 2010681225e1233
8 Marasco SF Liovic P Sutalo ID Structural integrity of intra-medullary rib fixation using a single bioresorbable screw AcuteCare Surg 201273668e673
9 Granetzny A El-Aal MA Emam E et al Surgical versus conser-vative treatment of flail chest Evaluation of the pulmonarystatus Interact Cardiovasc Thorac Surg 20054583e587
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 9
10 Singer MA Hopman WM MacKenzie TA Physical func-tioning and mental health in patients with chronic medicalconditions Qual Life Res 19998687e691
11 Australian Bureau of Statistics National health survey SF-36population norms Australia Canberra ACT Australian Bureauof Statistics 1995
12 Voggenreiter G Neudeck F Aufmkolk M et al Operative chestwall stabilisation in flail chest e outcomes of patients with orwithout pulmonary contusion J Am Coll Surg 1998187130e138
13 Viljanen J Pihlajamaki H Kinnunen J et al Comparison ofabsorbable poly-L-lactide and metallic intramedullary rods inthe fixation of femoral shaft osteotomies an experimentalstudy in rabbits J Orthop Sci 20016160e166
14 Yang Y Dong LW Wang J Memory alloy embracing fixatorin treatment of multiple fractured ribs and flail chest World JEmerg Med 20101212e215
FLA 510 DTD ACS6738_proof 8
15 Marasco SF Open surgical fixation of fractured ribs RecentPatents Biomed Eng 201031e6
16 Balci AE Eren S Cakir O Eren MN Open fixation in flailchest review of 64 patients Asian Cardiovasc Thorac Ann20041211e15
17 Mayberry JC Terhes JT Ellis TJ et al Absorbable plates forrib fracture repair preliminary experience J Trauma 200355835e839
18 Marasco S Cooper J Pick A Kossmann T Pilot study ofoperative fixation of fractured ribs in patients with flail chestANZ J Surg 200979804e808
19 Mohr M Abrams E Engel C et al Geometry of human ribspertinent to orthopaedic chest-wall reconstruction J Biomech2007401310e1317
20 Borrelly J Aazami MH New insights into the pathophysiologyof flail segment the implications of anterior serratus muscle inparietal failure Eur J Cardiothorac Surg 200528742e749
February 2013 354 pm
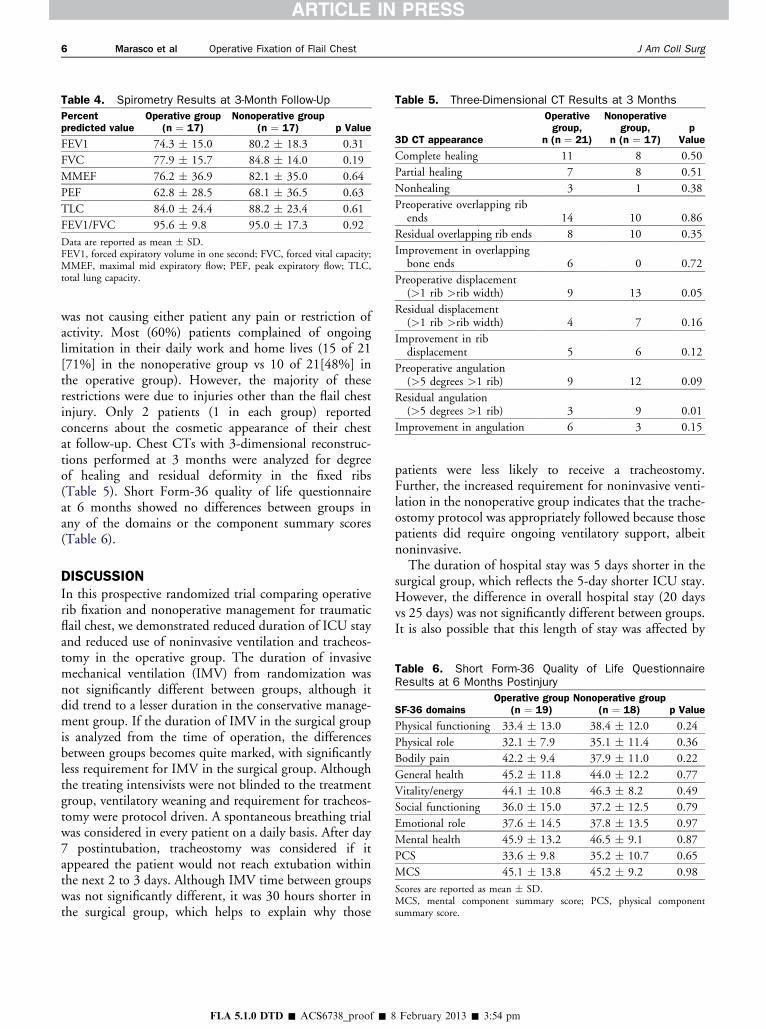
Table 4 Spirometry Results at 3-Month Follow-Up
Percentpredicted value
Operative group(n frac14 17)
Nonoperative group(n frac14 17) p Value
FEV1 743 150 802 183 031
FVC 779 157 848 140 019
MMEF 762 369 821 350 064
PEF 628 285 681 365 063
TLC 840 244 882 234 061
FEV1FVC 956 98 950 173 092
Data are reported as mean SDFEV1 forced expiratory volume in one second FVC forced vital capacityMMEF maximal mid expiratory flow PEF peak expiratory flow TLCtotal lung capacity
Table 5 Three-Dimensional CT Results at 3 Months
3D CT appearance
Operativegroup
n (n frac14 21)
Nonoperativegroup
n (n frac14 17)p
Value
Complete healing 11 8 050
Partial healing 7 8 051
Nonhealing 3 1 038
Preoperative overlapping ribends 14 10 086
Residual overlapping rib ends 8 10 035
Improvement in overlappingbone ends 6 0 072
Preoperative displacement(gt1 rib gtrib width) 9 13 005
Residual displacement(gt1 rib gtrib width) 4 7 016
Improvement in ribdisplacement 5 6 012
Preoperative angulation(gt5 degrees gt1 rib) 9 12 009
Residual angulation(gt5 degrees gt1 rib) 3 9 001
Improvement in angulation 6 3 015
Table 6 Short Form-36 Quality of Life QuestionnaireResults at 6 Months Postinjury
SF-36 domainsOperative group
(n frac14 19)Nonoperative group
(n frac14 18) p Value
Physical functioning 334 130 384 120 024
Physical role 321 79 351 114 036
Bodily pain 422 94 379 110 022
General health 452 118 440 122 077
Vitalityenergy 441 108 463 82 049
Social functioning 360 150 372 125 079
Emotional role 376 145 378 135 097
Mental health 459 132 465 91 087
PCS 336 98 352 107 065
MCS 451 138 452 92 098
Scores are reported as mean SDMCS mental component summary score PCS physical componentsummary score
6 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
was not causing either patient any pain or restriction ofactivity Most (60) patients complained of ongoinglimitation in their daily work and home lives (15 of 21[71] in the nonoperative group vs 10 of 21[48] inthe operative group) However the majority of theserestrictions were due to injuries other than the flail chestinjury Only 2 patients (1 in each group) reportedconcerns about the cosmetic appearance of their chestat follow-up Chest CTs with 3-dimensional reconstruc-tions performed at 3 months were analyzed for degreeof healing and residual deformity in the fixed ribs(Table 5) Short Form-36 quality of life questionnaireat 6 months showed no differences between groups inany of the domains or the component summary scores(Table 6)
DISCUSSIONIn this prospective randomized trial comparing operativerib fixation and nonoperative management for traumaticflail chest we demonstrated reduced duration of ICU stayand reduced use of noninvasive ventilation and tracheos-tomy in the operative group The duration of invasivemechanical ventilation (IMV) from randomization wasnot significantly different between groups although itdid trend to a lesser duration in the conservative manage-ment group If the duration of IMV in the surgical groupis analyzed from the time of operation the differencesbetween groups becomes quite marked with significantlyless requirement for IMV in the surgical group Althoughthe treating intensivists were not blinded to the treatmentgroup ventilatory weaning and requirement for tracheos-tomy were protocol driven A spontaneous breathing trialwas considered in every patient on a daily basis After day7 postintubation tracheostomy was considered if itappeared the patient would not reach extubation withinthe next 2 to 3 days Although IMV time between groupswas not significantly different it was 30 hours shorter inthe surgical group which helps to explain why those
FLA 510 DTD ACS6738_proof 8
patients were less likely to receive a tracheostomyFurther the increased requirement for noninvasive venti-lation in the nonoperative group indicates that the trache-ostomy protocol was appropriately followed because thosepatients did require ongoing ventilatory support albeitnoninvasiveThe duration of hospital stay was 5 days shorter in the
surgical group which reflects the 5-day shorter ICU stayHowever the difference in overall hospital stay (20 daysvs 25 days) was not significantly different between groupsIt is also possible that this length of stay was affected by
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 7
a delay in transfer to rehabilitation hospitals due to bedblock which often tends to occur in our area Howeverthis would occur equally between groups so does notexplain the difference in length of stay seen in this studycohort The reduction in ICU stay in the operative groupreduced the ICU costs by more than $14000 per patient(a considerable cost savings to the health system) andsaved 5 ICU bed days per patientShort-term follow-up of our patients demonstrated no
significant differences in spirometry at 3 months betweengroups This result contrasts with previous studies thathave demonstrated improvements in percent predictedforced vital capacity total lung capacity and forced expi-ratory flow at 75 of vital capacity from 2-monthfollow-up49
We were unable to demonstrate any difference betweengroups in terms of Short Form-36 quality of life question-naire outcomes at 6 months postinjury The physicalsummary score was lower in both groups than the mentalsummary score This finding suggests that the patientsmade appropriate psychological adjustments to theirinjuries as has been previously reported10 Normativedata from the Australian population show a mental healthsummary score of 508 which is similar to the scores inour study population The reported physical summaryscore in the general Australian population is 498 whichis quite a bit higher than the scores in the groups in thisstudy11
We did not specifically assess pain in this study becauseall of the enrolled patients were sedated and ventilated atthe time of enrollment So the main indication forsurgery was mechanical stabilization not pain Furtherbecause these patients were a true multitrauma cohortwith multiple system injuries it was thought that anyassessment of analgesic requirement would beconfounded by the many other injuries also requiringanalgesia Indeed that is what we found at 3-monthfollow-up As outlined in the results patients who com-plained of ongoing physical limitation reported thatthey were limited by pain and stiffness from otherinjuries particularly shoulder girdle injuries rather thanrib injuries themselvesOnly 2 other prospective randomized trials have been
reported investigating the impact of operative fixationof flail chest injury49 Both studies slightly smaller thanthis one demonstrated significantly reduced mechanicalventilation time ICU stay incidence of pneumoniaand improved spirometry at follow-up in the operativegroup Tanaka and colleagues4 also demonstrated earlierreturn to work in the surgical cohort at 6-monthfollow-up The average age of the patients in our study(58 years) was older than that reported in both previous
FLA 510 DTD ACS6738_proof 8
randomized controlled trials of 45 years4 and 38 years9
This is likely to explain the seemingly slower recoveryin our patients and the lower rates of return to work(many of our patients were retired) Our failure to iden-tify differences in spirometry results at 3 months may alsobe related to the older age cohort in our studyThe study by Grantezny and associates9 also had
a cohort of patients with much lower Injury SeverityScores (ISS) (average 174) compared with those in ourstudy group (average 333) Again this reflects a seeminglydifferent study populationdyounger patients with singlesystem injuriesdcompared with our population of olderpatients with multiple system injuries (as evidenced bythe number of nonthoracic operations required) Wehave also reported the New Injury Severity Score(NISS) and the Trauma and Injury Severity Scores(TRISS) to give a more comprehensive picture of theinjury severity of this group of patients The higher ISSscores and multisystem nature of the injuries in ourcohort of patients may explain our failure to identifyany differences in quality of life between groupsOther previous research on operative fixation of frac-
tured ribs has consisted of retrospective reviews and casereports The retrospective review by Voggenreiter andcoworkers12 was the only one to subdivide the treatmentgroups into those with and without significant contusionAlthough they found benefits in the operative treatmentgroup they also found that these benefits were negatedby the presence of significant pulmonary contusion Inour study the majority of patients had only mild contu-sion on chest x-ray at the time of enrollmentAlmost all of the published studies have used metal
implants for operative fixation of the ribs Granetznyand colleagues9 used Kirschner and stainless steel wiresTanaka and associates4 used Judet struts In contrast weused a polylactide copolymer prosthesis applied as a 6-or 8-hole plate and screws These prostheses degrade byhydrolysis and are metabolized by the body into carbondioxide and water They maintain at least 40 of theirstrength at 3 months by which time the fractures wouldbe expected to have completely healed and arecompletely absorbed without toxicity over 1 to 3 yearsAnimal models using these absorbable plates have shownfaster and stronger healing compared with traditionalmetal plates which may actually slow bone healing13
This occurs because the metal plate protects the bonefrom any load but in doing so it removes the stimulusfor new bone growth (known as stress-shielding) Incontrast the absorbable plates allow gradual transfer ofstress loads to the bone stimulating faster bone growth13
Because the plates and screws are absorbable there is noneed to remove plates which confers a potential cost
February 2013 354 pm
8 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
savings to this procedure Also it minimizes the sequelae ofpossible prosthesis-related complications such as migrationpalpability (especially in thin patients) or thermal sensi-tivity Metal prostheses usually require removal if thesecomplications occur while a more conservative approachcan be adopted with absorbable prostheses Furthermorethere is no contraindication to future MRI in patientswho have had absorbable plates implantedDespite the existing evidence of patient and hospital
benefits with operative fixation of flail chest injury clinicalequipoise within the Western surgical community has per-sisted (operative rib fixation seems to have been taken upmore readily in East Asia14) This study is now the thirdstudy (in 3 different countries) to show similar benefitsin this patient population and we hope that it will influ-ence management change in these critically ill traumapatients Another reason why surgeons have been slow toembrace this type of surgery is probably related to thelack of specific prostheses designed for rib fixation Inthis study we used a prosthesis designed for the fibulaHowever over the last few years a number of productshave come onto the market specifically designed for ribfixation15 This demonstrates the increasing awarenessand interest in this type of surgery and also acknowledgesthat in the past surgical results when using nonspecificprostheses have been very variable16-18
Ribs present a number of surgical difficulties notencountered with other bony injuries Ribs are subjectto continual movement with breathing as well as suddenmore forceful movements during coughing and sneezingRibs have a thin inner and outer cortex making pros-thesis fixation difficult and at times unreliable Typicalrib fractures often involve splintering of the ribsmandating that bone fixation be undertaken at a sitefurther away from the fracture Each rib differs slightlyin its shape and in particular in the radius of its curva-ture which means that a ldquoone size fits allrdquo approachparticularly with less malleable prostheses is unlikely tobe successful19
A wide variety of prostheses have been tried in rib fixa-tion Many have flaws Kirschner wires provide little rota-tional stability and are prone to migration Metal platesborrowed from other applications are able to be curved inone direction only Because rib curvature is quitecomplex these metal plates are prone to ldquolifting offrdquothe rib Although the ribs do not carry a heavy loadthey are affected by torque in multiple directions due tothe layers of intercostal muscles inserting onto the ribsas well as multiple chest wall muscles Few authors havecommented on the impact of the chest wall musculatureon the dislocation and distraction of fractured ribs Bor-relly and Aazami20 in their retrospective review of flail
FLA 510 DTD ACS6738_proof 8
chest patients noted that the actions of serratus anteriortend to distract anterolateral fractures while impactingthe ribs in posterolateral fractures Analysis of the effectof intercostal muscle forces on rib fractures and fixationmethod has recently been analyzed and could assist indevelopment of specific rib prostheses78
CONCLUSIONSThis study shows clinical benefit and cost savings to thehealth system for flail chest patients who undergo rib fixa-tion Hopefully this study will help to change operativemanagement protocols for these critically ill patientsFurther trials into nonventilator-dependent patients alsoneed to be performed to assess in more detail potentialpatient benefits of pain reduction and functionalimprovements
Author Contributions
Study conception and design Marasco Davies CooperFitzgerald
Acquisition of data Marasco Bennet Nevill LeeAnalysis and interpretation of data Marasco DaviesCooper Varma Lee Bailey Fitzgerald
Drafting of manuscript Marasco Davies CooperVarma Bennet Nevill Lee Bailey Fitzgerald
Critical revision Marasco Davies Cooper VarmaBennet Nevill Lee Bailey Fitzgerald
REFERENCES
1 Ciraulo DL Elliott DMitchell KA et al Flail chest as a markerfor significant injuries J Am Coll Surg 1994178466e470
2 Kent R Woods W Bostrom O Fatality risk and the presenceof rib fractures Annu Proc Assoc Adv Automot Med 20085273e82
3 Kerr-Valentic MA Arthur M Mullins RJ et al Rib fracturepain and disability can we do better J Trauma 2003541058e1063
4 Tanaka H Yukioka T Yamaguti Y et al Surgical stabilizationof internal pneumatic stabilization A prospective randomizedstudy of management of severe flail chest patients J Trauma200252727e732
5 Mayberry JC Ham LB Schipper PH et al Surveyed opinionof American trauma orthopaedic and thoracic surgeons on riband sternal fracture repair J Trauma 200966875e879
6 Atkin C Freedman I Rosenfeld JV et al The evolution of anintegrated state trauma system in Victoria Australia Injury2005361277e1287
7 Marasco SF Sutalo ID Bui AV Mode of failure of rib fixationwith absorbable plates a clinical and numerical modellingstudy J Trauma 2010681225e1233
8 Marasco SF Liovic P Sutalo ID Structural integrity of intra-medullary rib fixation using a single bioresorbable screw AcuteCare Surg 201273668e673
9 Granetzny A El-Aal MA Emam E et al Surgical versus conser-vative treatment of flail chest Evaluation of the pulmonarystatus Interact Cardiovasc Thorac Surg 20054583e587
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 9
10 Singer MA Hopman WM MacKenzie TA Physical func-tioning and mental health in patients with chronic medicalconditions Qual Life Res 19998687e691
11 Australian Bureau of Statistics National health survey SF-36population norms Australia Canberra ACT Australian Bureauof Statistics 1995
12 Voggenreiter G Neudeck F Aufmkolk M et al Operative chestwall stabilisation in flail chest e outcomes of patients with orwithout pulmonary contusion J Am Coll Surg 1998187130e138
13 Viljanen J Pihlajamaki H Kinnunen J et al Comparison ofabsorbable poly-L-lactide and metallic intramedullary rods inthe fixation of femoral shaft osteotomies an experimentalstudy in rabbits J Orthop Sci 20016160e166
14 Yang Y Dong LW Wang J Memory alloy embracing fixatorin treatment of multiple fractured ribs and flail chest World JEmerg Med 20101212e215
FLA 510 DTD ACS6738_proof 8
15 Marasco SF Open surgical fixation of fractured ribs RecentPatents Biomed Eng 201031e6
16 Balci AE Eren S Cakir O Eren MN Open fixation in flailchest review of 64 patients Asian Cardiovasc Thorac Ann20041211e15
17 Mayberry JC Terhes JT Ellis TJ et al Absorbable plates forrib fracture repair preliminary experience J Trauma 200355835e839
18 Marasco S Cooper J Pick A Kossmann T Pilot study ofoperative fixation of fractured ribs in patients with flail chestANZ J Surg 200979804e808
19 Mohr M Abrams E Engel C et al Geometry of human ribspertinent to orthopaedic chest-wall reconstruction J Biomech2007401310e1317
20 Borrelly J Aazami MH New insights into the pathophysiologyof flail segment the implications of anterior serratus muscle inparietal failure Eur J Cardiothorac Surg 200528742e749
February 2013 354 pm

Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 7
a delay in transfer to rehabilitation hospitals due to bedblock which often tends to occur in our area Howeverthis would occur equally between groups so does notexplain the difference in length of stay seen in this studycohort The reduction in ICU stay in the operative groupreduced the ICU costs by more than $14000 per patient(a considerable cost savings to the health system) andsaved 5 ICU bed days per patientShort-term follow-up of our patients demonstrated no
significant differences in spirometry at 3 months betweengroups This result contrasts with previous studies thathave demonstrated improvements in percent predictedforced vital capacity total lung capacity and forced expi-ratory flow at 75 of vital capacity from 2-monthfollow-up49
We were unable to demonstrate any difference betweengroups in terms of Short Form-36 quality of life question-naire outcomes at 6 months postinjury The physicalsummary score was lower in both groups than the mentalsummary score This finding suggests that the patientsmade appropriate psychological adjustments to theirinjuries as has been previously reported10 Normativedata from the Australian population show a mental healthsummary score of 508 which is similar to the scores inour study population The reported physical summaryscore in the general Australian population is 498 whichis quite a bit higher than the scores in the groups in thisstudy11
We did not specifically assess pain in this study becauseall of the enrolled patients were sedated and ventilated atthe time of enrollment So the main indication forsurgery was mechanical stabilization not pain Furtherbecause these patients were a true multitrauma cohortwith multiple system injuries it was thought that anyassessment of analgesic requirement would beconfounded by the many other injuries also requiringanalgesia Indeed that is what we found at 3-monthfollow-up As outlined in the results patients who com-plained of ongoing physical limitation reported thatthey were limited by pain and stiffness from otherinjuries particularly shoulder girdle injuries rather thanrib injuries themselvesOnly 2 other prospective randomized trials have been
reported investigating the impact of operative fixationof flail chest injury49 Both studies slightly smaller thanthis one demonstrated significantly reduced mechanicalventilation time ICU stay incidence of pneumoniaand improved spirometry at follow-up in the operativegroup Tanaka and colleagues4 also demonstrated earlierreturn to work in the surgical cohort at 6-monthfollow-up The average age of the patients in our study(58 years) was older than that reported in both previous
FLA 510 DTD ACS6738_proof 8
randomized controlled trials of 45 years4 and 38 years9
This is likely to explain the seemingly slower recoveryin our patients and the lower rates of return to work(many of our patients were retired) Our failure to iden-tify differences in spirometry results at 3 months may alsobe related to the older age cohort in our studyThe study by Grantezny and associates9 also had
a cohort of patients with much lower Injury SeverityScores (ISS) (average 174) compared with those in ourstudy group (average 333) Again this reflects a seeminglydifferent study populationdyounger patients with singlesystem injuriesdcompared with our population of olderpatients with multiple system injuries (as evidenced bythe number of nonthoracic operations required) Wehave also reported the New Injury Severity Score(NISS) and the Trauma and Injury Severity Scores(TRISS) to give a more comprehensive picture of theinjury severity of this group of patients The higher ISSscores and multisystem nature of the injuries in ourcohort of patients may explain our failure to identifyany differences in quality of life between groupsOther previous research on operative fixation of frac-
tured ribs has consisted of retrospective reviews and casereports The retrospective review by Voggenreiter andcoworkers12 was the only one to subdivide the treatmentgroups into those with and without significant contusionAlthough they found benefits in the operative treatmentgroup they also found that these benefits were negatedby the presence of significant pulmonary contusion Inour study the majority of patients had only mild contu-sion on chest x-ray at the time of enrollmentAlmost all of the published studies have used metal
implants for operative fixation of the ribs Granetznyand colleagues9 used Kirschner and stainless steel wiresTanaka and associates4 used Judet struts In contrast weused a polylactide copolymer prosthesis applied as a 6-or 8-hole plate and screws These prostheses degrade byhydrolysis and are metabolized by the body into carbondioxide and water They maintain at least 40 of theirstrength at 3 months by which time the fractures wouldbe expected to have completely healed and arecompletely absorbed without toxicity over 1 to 3 yearsAnimal models using these absorbable plates have shownfaster and stronger healing compared with traditionalmetal plates which may actually slow bone healing13
This occurs because the metal plate protects the bonefrom any load but in doing so it removes the stimulusfor new bone growth (known as stress-shielding) Incontrast the absorbable plates allow gradual transfer ofstress loads to the bone stimulating faster bone growth13
Because the plates and screws are absorbable there is noneed to remove plates which confers a potential cost
February 2013 354 pm
8 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
savings to this procedure Also it minimizes the sequelae ofpossible prosthesis-related complications such as migrationpalpability (especially in thin patients) or thermal sensi-tivity Metal prostheses usually require removal if thesecomplications occur while a more conservative approachcan be adopted with absorbable prostheses Furthermorethere is no contraindication to future MRI in patientswho have had absorbable plates implantedDespite the existing evidence of patient and hospital
benefits with operative fixation of flail chest injury clinicalequipoise within the Western surgical community has per-sisted (operative rib fixation seems to have been taken upmore readily in East Asia14) This study is now the thirdstudy (in 3 different countries) to show similar benefitsin this patient population and we hope that it will influ-ence management change in these critically ill traumapatients Another reason why surgeons have been slow toembrace this type of surgery is probably related to thelack of specific prostheses designed for rib fixation Inthis study we used a prosthesis designed for the fibulaHowever over the last few years a number of productshave come onto the market specifically designed for ribfixation15 This demonstrates the increasing awarenessand interest in this type of surgery and also acknowledgesthat in the past surgical results when using nonspecificprostheses have been very variable16-18
Ribs present a number of surgical difficulties notencountered with other bony injuries Ribs are subjectto continual movement with breathing as well as suddenmore forceful movements during coughing and sneezingRibs have a thin inner and outer cortex making pros-thesis fixation difficult and at times unreliable Typicalrib fractures often involve splintering of the ribsmandating that bone fixation be undertaken at a sitefurther away from the fracture Each rib differs slightlyin its shape and in particular in the radius of its curva-ture which means that a ldquoone size fits allrdquo approachparticularly with less malleable prostheses is unlikely tobe successful19
A wide variety of prostheses have been tried in rib fixa-tion Many have flaws Kirschner wires provide little rota-tional stability and are prone to migration Metal platesborrowed from other applications are able to be curved inone direction only Because rib curvature is quitecomplex these metal plates are prone to ldquolifting offrdquothe rib Although the ribs do not carry a heavy loadthey are affected by torque in multiple directions due tothe layers of intercostal muscles inserting onto the ribsas well as multiple chest wall muscles Few authors havecommented on the impact of the chest wall musculatureon the dislocation and distraction of fractured ribs Bor-relly and Aazami20 in their retrospective review of flail
FLA 510 DTD ACS6738_proof 8
chest patients noted that the actions of serratus anteriortend to distract anterolateral fractures while impactingthe ribs in posterolateral fractures Analysis of the effectof intercostal muscle forces on rib fractures and fixationmethod has recently been analyzed and could assist indevelopment of specific rib prostheses78
CONCLUSIONSThis study shows clinical benefit and cost savings to thehealth system for flail chest patients who undergo rib fixa-tion Hopefully this study will help to change operativemanagement protocols for these critically ill patientsFurther trials into nonventilator-dependent patients alsoneed to be performed to assess in more detail potentialpatient benefits of pain reduction and functionalimprovements
Author Contributions
Study conception and design Marasco Davies CooperFitzgerald
Acquisition of data Marasco Bennet Nevill LeeAnalysis and interpretation of data Marasco DaviesCooper Varma Lee Bailey Fitzgerald
Drafting of manuscript Marasco Davies CooperVarma Bennet Nevill Lee Bailey Fitzgerald
Critical revision Marasco Davies Cooper VarmaBennet Nevill Lee Bailey Fitzgerald
REFERENCES
1 Ciraulo DL Elliott DMitchell KA et al Flail chest as a markerfor significant injuries J Am Coll Surg 1994178466e470
2 Kent R Woods W Bostrom O Fatality risk and the presenceof rib fractures Annu Proc Assoc Adv Automot Med 20085273e82
3 Kerr-Valentic MA Arthur M Mullins RJ et al Rib fracturepain and disability can we do better J Trauma 2003541058e1063
4 Tanaka H Yukioka T Yamaguti Y et al Surgical stabilizationof internal pneumatic stabilization A prospective randomizedstudy of management of severe flail chest patients J Trauma200252727e732
5 Mayberry JC Ham LB Schipper PH et al Surveyed opinionof American trauma orthopaedic and thoracic surgeons on riband sternal fracture repair J Trauma 200966875e879
6 Atkin C Freedman I Rosenfeld JV et al The evolution of anintegrated state trauma system in Victoria Australia Injury2005361277e1287
7 Marasco SF Sutalo ID Bui AV Mode of failure of rib fixationwith absorbable plates a clinical and numerical modellingstudy J Trauma 2010681225e1233
8 Marasco SF Liovic P Sutalo ID Structural integrity of intra-medullary rib fixation using a single bioresorbable screw AcuteCare Surg 201273668e673
9 Granetzny A El-Aal MA Emam E et al Surgical versus conser-vative treatment of flail chest Evaluation of the pulmonarystatus Interact Cardiovasc Thorac Surg 20054583e587
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 9
10 Singer MA Hopman WM MacKenzie TA Physical func-tioning and mental health in patients with chronic medicalconditions Qual Life Res 19998687e691
11 Australian Bureau of Statistics National health survey SF-36population norms Australia Canberra ACT Australian Bureauof Statistics 1995
12 Voggenreiter G Neudeck F Aufmkolk M et al Operative chestwall stabilisation in flail chest e outcomes of patients with orwithout pulmonary contusion J Am Coll Surg 1998187130e138
13 Viljanen J Pihlajamaki H Kinnunen J et al Comparison ofabsorbable poly-L-lactide and metallic intramedullary rods inthe fixation of femoral shaft osteotomies an experimentalstudy in rabbits J Orthop Sci 20016160e166
14 Yang Y Dong LW Wang J Memory alloy embracing fixatorin treatment of multiple fractured ribs and flail chest World JEmerg Med 20101212e215
FLA 510 DTD ACS6738_proof 8
15 Marasco SF Open surgical fixation of fractured ribs RecentPatents Biomed Eng 201031e6
16 Balci AE Eren S Cakir O Eren MN Open fixation in flailchest review of 64 patients Asian Cardiovasc Thorac Ann20041211e15
17 Mayberry JC Terhes JT Ellis TJ et al Absorbable plates forrib fracture repair preliminary experience J Trauma 200355835e839
18 Marasco S Cooper J Pick A Kossmann T Pilot study ofoperative fixation of fractured ribs in patients with flail chestANZ J Surg 200979804e808
19 Mohr M Abrams E Engel C et al Geometry of human ribspertinent to orthopaedic chest-wall reconstruction J Biomech2007401310e1317
20 Borrelly J Aazami MH New insights into the pathophysiologyof flail segment the implications of anterior serratus muscle inparietal failure Eur J Cardiothorac Surg 200528742e749
February 2013 354 pm

8 Marasco et al Operative Fixation of Flail Chest J Am Coll Surg
savings to this procedure Also it minimizes the sequelae ofpossible prosthesis-related complications such as migrationpalpability (especially in thin patients) or thermal sensi-tivity Metal prostheses usually require removal if thesecomplications occur while a more conservative approachcan be adopted with absorbable prostheses Furthermorethere is no contraindication to future MRI in patientswho have had absorbable plates implantedDespite the existing evidence of patient and hospital
benefits with operative fixation of flail chest injury clinicalequipoise within the Western surgical community has per-sisted (operative rib fixation seems to have been taken upmore readily in East Asia14) This study is now the thirdstudy (in 3 different countries) to show similar benefitsin this patient population and we hope that it will influ-ence management change in these critically ill traumapatients Another reason why surgeons have been slow toembrace this type of surgery is probably related to thelack of specific prostheses designed for rib fixation Inthis study we used a prosthesis designed for the fibulaHowever over the last few years a number of productshave come onto the market specifically designed for ribfixation15 This demonstrates the increasing awarenessand interest in this type of surgery and also acknowledgesthat in the past surgical results when using nonspecificprostheses have been very variable16-18
Ribs present a number of surgical difficulties notencountered with other bony injuries Ribs are subjectto continual movement with breathing as well as suddenmore forceful movements during coughing and sneezingRibs have a thin inner and outer cortex making pros-thesis fixation difficult and at times unreliable Typicalrib fractures often involve splintering of the ribsmandating that bone fixation be undertaken at a sitefurther away from the fracture Each rib differs slightlyin its shape and in particular in the radius of its curva-ture which means that a ldquoone size fits allrdquo approachparticularly with less malleable prostheses is unlikely tobe successful19
A wide variety of prostheses have been tried in rib fixa-tion Many have flaws Kirschner wires provide little rota-tional stability and are prone to migration Metal platesborrowed from other applications are able to be curved inone direction only Because rib curvature is quitecomplex these metal plates are prone to ldquolifting offrdquothe rib Although the ribs do not carry a heavy loadthey are affected by torque in multiple directions due tothe layers of intercostal muscles inserting onto the ribsas well as multiple chest wall muscles Few authors havecommented on the impact of the chest wall musculatureon the dislocation and distraction of fractured ribs Bor-relly and Aazami20 in their retrospective review of flail
FLA 510 DTD ACS6738_proof 8
chest patients noted that the actions of serratus anteriortend to distract anterolateral fractures while impactingthe ribs in posterolateral fractures Analysis of the effectof intercostal muscle forces on rib fractures and fixationmethod has recently been analyzed and could assist indevelopment of specific rib prostheses78
CONCLUSIONSThis study shows clinical benefit and cost savings to thehealth system for flail chest patients who undergo rib fixa-tion Hopefully this study will help to change operativemanagement protocols for these critically ill patientsFurther trials into nonventilator-dependent patients alsoneed to be performed to assess in more detail potentialpatient benefits of pain reduction and functionalimprovements
Author Contributions
Study conception and design Marasco Davies CooperFitzgerald
Acquisition of data Marasco Bennet Nevill LeeAnalysis and interpretation of data Marasco DaviesCooper Varma Lee Bailey Fitzgerald
Drafting of manuscript Marasco Davies CooperVarma Bennet Nevill Lee Bailey Fitzgerald
Critical revision Marasco Davies Cooper VarmaBennet Nevill Lee Bailey Fitzgerald
REFERENCES
1 Ciraulo DL Elliott DMitchell KA et al Flail chest as a markerfor significant injuries J Am Coll Surg 1994178466e470
2 Kent R Woods W Bostrom O Fatality risk and the presenceof rib fractures Annu Proc Assoc Adv Automot Med 20085273e82
3 Kerr-Valentic MA Arthur M Mullins RJ et al Rib fracturepain and disability can we do better J Trauma 2003541058e1063
4 Tanaka H Yukioka T Yamaguti Y et al Surgical stabilizationof internal pneumatic stabilization A prospective randomizedstudy of management of severe flail chest patients J Trauma200252727e732
5 Mayberry JC Ham LB Schipper PH et al Surveyed opinionof American trauma orthopaedic and thoracic surgeons on riband sternal fracture repair J Trauma 200966875e879
6 Atkin C Freedman I Rosenfeld JV et al The evolution of anintegrated state trauma system in Victoria Australia Injury2005361277e1287
7 Marasco SF Sutalo ID Bui AV Mode of failure of rib fixationwith absorbable plates a clinical and numerical modellingstudy J Trauma 2010681225e1233
8 Marasco SF Liovic P Sutalo ID Structural integrity of intra-medullary rib fixation using a single bioresorbable screw AcuteCare Surg 201273668e673
9 Granetzny A El-Aal MA Emam E et al Surgical versus conser-vative treatment of flail chest Evaluation of the pulmonarystatus Interact Cardiovasc Thorac Surg 20054583e587
February 2013 354 pm
Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 9
10 Singer MA Hopman WM MacKenzie TA Physical func-tioning and mental health in patients with chronic medicalconditions Qual Life Res 19998687e691
11 Australian Bureau of Statistics National health survey SF-36population norms Australia Canberra ACT Australian Bureauof Statistics 1995
12 Voggenreiter G Neudeck F Aufmkolk M et al Operative chestwall stabilisation in flail chest e outcomes of patients with orwithout pulmonary contusion J Am Coll Surg 1998187130e138
13 Viljanen J Pihlajamaki H Kinnunen J et al Comparison ofabsorbable poly-L-lactide and metallic intramedullary rods inthe fixation of femoral shaft osteotomies an experimentalstudy in rabbits J Orthop Sci 20016160e166
14 Yang Y Dong LW Wang J Memory alloy embracing fixatorin treatment of multiple fractured ribs and flail chest World JEmerg Med 20101212e215
FLA 510 DTD ACS6738_proof 8
15 Marasco SF Open surgical fixation of fractured ribs RecentPatents Biomed Eng 201031e6
16 Balci AE Eren S Cakir O Eren MN Open fixation in flailchest review of 64 patients Asian Cardiovasc Thorac Ann20041211e15
17 Mayberry JC Terhes JT Ellis TJ et al Absorbable plates forrib fracture repair preliminary experience J Trauma 200355835e839
18 Marasco S Cooper J Pick A Kossmann T Pilot study ofoperative fixation of fractured ribs in patients with flail chestANZ J Surg 200979804e808
19 Mohr M Abrams E Engel C et al Geometry of human ribspertinent to orthopaedic chest-wall reconstruction J Biomech2007401310e1317
20 Borrelly J Aazami MH New insights into the pathophysiologyof flail segment the implications of anterior serratus muscle inparietal failure Eur J Cardiothorac Surg 200528742e749
February 2013 354 pm

Vol - No - - 2013 Marasco et al Operative Fixation of Flail Chest 9
10 Singer MA Hopman WM MacKenzie TA Physical func-tioning and mental health in patients with chronic medicalconditions Qual Life Res 19998687e691
11 Australian Bureau of Statistics National health survey SF-36population norms Australia Canberra ACT Australian Bureauof Statistics 1995
12 Voggenreiter G Neudeck F Aufmkolk M et al Operative chestwall stabilisation in flail chest e outcomes of patients with orwithout pulmonary contusion J Am Coll Surg 1998187130e138
13 Viljanen J Pihlajamaki H Kinnunen J et al Comparison ofabsorbable poly-L-lactide and metallic intramedullary rods inthe fixation of femoral shaft osteotomies an experimentalstudy in rabbits J Orthop Sci 20016160e166
14 Yang Y Dong LW Wang J Memory alloy embracing fixatorin treatment of multiple fractured ribs and flail chest World JEmerg Med 20101212e215
FLA 510 DTD ACS6738_proof 8
15 Marasco SF Open surgical fixation of fractured ribs RecentPatents Biomed Eng 201031e6
16 Balci AE Eren S Cakir O Eren MN Open fixation in flailchest review of 64 patients Asian Cardiovasc Thorac Ann20041211e15
17 Mayberry JC Terhes JT Ellis TJ et al Absorbable plates forrib fracture repair preliminary experience J Trauma 200355835e839
18 Marasco S Cooper J Pick A Kossmann T Pilot study ofoperative fixation of fractured ribs in patients with flail chestANZ J Surg 200979804e808
19 Mohr M Abrams E Engel C et al Geometry of human ribspertinent to orthopaedic chest-wall reconstruction J Biomech2007401310e1317
20 Borrelly J Aazami MH New insights into the pathophysiologyof flail segment the implications of anterior serratus muscle inparietal failure Eur J Cardiothorac Surg 200528742e749
February 2013 354 pm





























