Embed Size (px)
Citation preview
vier.com/locate/ijpsycho
International Journal of Psychop
Psychophysiological responses of adults who do not stutter while
listening to stuttering
Vijaya K. Guntupalli a, Joseph Kalinowski a,*, Chayadevie Nanjundeswaran a,
Tim Saltuklaroglu b, D. Erik Everhart c
a Department of Communication Sciences and Disorders, East Carolina University, Oglesby Drive, Greenville, NC, USAb Department of Audiology and Speech Pathology, University of Tennessee, Knoxville, TN, USA
c Department of Psychology, East Carolina University, Greenville, NC, USA
Received 20 April 2005; received in revised form 30 August 2005; accepted 2 November 2005
Available online 18 January 2006
Abstract
The present study examined the psychophysiological responses of fluent listeners to stuttered speech. Specifically, skin conductance and heart
rate changes were measured from adults who do not stutter while watching one-minute video speech samples of persons stutter read aloud. Fifteen
adult participants observed three stuttered and three fluent speech samples, presented in random order with a two-minute interstimulus intervals.
Results revealed that observing stuttered speech evoked a significant increase in skin conductance and a significant deceleration in heart rate
relative to watching fluent speech samples. These findings suggest that listeners are physiologically aroused by stuttering and appear to maintain
feelings of unpleasantness to stuttered speech. Further, deceleration in heart rate during stuttered samples also suggest that listeners may be paying
more attention to the stuttered speech samples as compared to the fluent speech samples. We speculate that aberrant and anomalous stuttering
behaviors probably simulate the mirror neuronal mechanism eliciting the emotional arousal associated within them. Such physiological arousal
may provide the emotional genesis to the listener’s negative stereotypical perceptions towards people who stutter.
D 2005 Elsevier B.V. All rights reserved.
Keywords: Skin conductance; Heart rate; Stuttering; Arousal; Deceleration; Emotion; Mirror neurons; Speech therapy
1. Introduction
Stuttering is an involuntary, intermittent and debilitating
speech disorder that afflicts approximately 1% of the popula-
tion. Its primary manifestations include aberrant sound
prolongations and syllabic repetitions that are interspersed
with otherwise perceptually normal speech patterns (Blood-
stein, 1995). In other words, a person who stutters may begin
oral communication normally without disruption and then
suddenly and uncontrollably, begins to produce unexpected
rapid oscillatory syllabic repetitions (Kalinowski et al., 2004).
Oftentimes, syllable repetitions are intermixed with audible
(i.e., sound prolongations) and inaudible oscillatory fixations
(i.e., no sound), producing intermittent and aberrant interrup-
tions in the communicative process. However, these overt
speech disruptions often end just as abruptly as they started,
0167-8760/$ - see front matter D 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.ijpsycho.2005.11.001
* Corresponding author.
E-mail address: [email protected] (J. Kalinowski).
with the return of normal-sounding speech. The sudden onset
and offset of stuttering continues throughout oral communica-
tion and differentiates the speech of those who stutter from
those who do not. Along with these perceptual/acoustic
manifestations, people who stutter oftentimes exhibit oscilla-
tory, ancillary behaviors that transcend the speech mechanism.
These aberrant behaviors may include involuntary head jerks,
arm jerks, finger tapping, foot tapping, postural fixations, facial
grimaces, lip bites, clavicular breathing, and other struggle
behaviors (Bloodstein, 1995; Woolf, 1967). The ancillary
stuttering behaviors occur at the same time as speech related
behaviors suggesting that the block has spread and that
stuttering has necessarily become more severe. Oftentimes
the rapid onset and offset of these aberrant symptoms of loss of
control can be disconcerting to the listener, and the listener’s
unfavorable emotional reactions such as nervousness, impa-
tience, embarrassment, pity, shock, etc. to stuttered speech can
directly influence the speech of a person who stutters (Blood-
stein, 1995).
hysiology 62 (2006) 1 – 8
www.else
V.K. Guntupalli et al. / International Journal of Psychophysiology 62 (2006) 1–82
Numerous researchers have reported that people who stutter
have been thought to be nervous, tense, shy, quiet, reticent,
guarded, avoiding, introverted, afraid, passive, self-derogatory
and more sensitive relative to people who do not stutter. These
stereotypic attitudes towards stuttering were found to exist
among various groups including students (Dorsey and
Guenther, 2000; St. Louis and Lass, 1981; White and Collins,
1984), teachers and professors (Crowe and Walton, 1981;
Dorsey and Guenther, 2000; Lass et al., 1992; Yeakle and
Cooper, 1986), parents (Crowe and Cooper, 1977; Fowlie and
Cooper, 1978; Woods and Williams, 1976), speech-language
clinicians (Cooper and Cooper, 1985; Cooper and Rustin,
1985; Kalinowski et al., 1993; Lass et al., 1989, Rami et al.,
2003; Turnbaugh et al., 1979; Woods and Williams, 1971; Yairi
and Williams, 1970), people who stutter (Lass et al., 1995;
Kalinowski et al., 1987), vocational rehabilitation counselors
(Hurst and Cooper, 1983), special educators (Ruscello and
Lass, 1994), people who have never had any direct contact with
a person who stutters (Craig et al., 2003), and even residents of
small rural communities who had close contact with people
who stutter such as relatives and family members (Doody et al.,
1993). These findings suggest that stuttering stereotypes are
persistent and omnipresent in many populations. However,
after reviewing hundreds of studies that investigated the
personality differences between people who stutter and who
do not stutter, Bloodstein (1995: 236) states that Fthere is littleconclusive evidence of any specific kind of character structure
or broad-set of basic personality traits that is typical of
stutterers as a group._ Simply put, although people who stutter
have been perceived as nervous, tense, anxious, afraid, etc.
relative to people who do not stutter, there is little evidence to
support this notion.
Studying listener’s opinions about the personality or
character traits of hypothetical persons who stutter relative to
the hypothetical persons who do not stutter is important with
regards to the acquired insights into stuttering stereotypes.
However, they only provide this subjective information via
Fpaper–pencil_ tasks. They fail to reveal the actual physiolog-
ical state of listeners during the observation of stuttered speech.
In other words, though we know much about the negative
stereotypes, we know little about the physiological state of
those who listen to stuttering. Simply put, there is a paucity of
physiological data with regards to how persons who do not
stutter react when witnessing aberrant and disruptive stuttering
behaviors. Hence, the aim of the present study is to uncover
physiological effects associated with the observing and hearing
stuttering.
Researchers have frequently used measures such as electro-
dermal response (EDR), heart rate (HR), blood pressure, blood
volume and flow as a general indicator of physiological anxiety
both in people who stutter and those who do not stutter. Among
these physiological measures, EDR has been used extensively
as a sensitive and reliable measure of physiological arousal to
various emotional or affective stimuli, such as fear, anxiety,
excitement etc. (Ashcroft et al., 1991; Dietrich and Roaman,
2001; Lang et al., 1993). EDR measurement is simple,
repeatable, and fast. It can be a useful method for acquiring
data that describes autonomic nerve activity, specifically the
responses of sympathetic nervous system to various kinds of
arousal evoking emotional stimuli (Tarvainen et al., 2001).
EDR has been found to increase monotonically with intensi-
fying stimulation and the apparent trend in the data is that skin
conductance increases proportionately with autonomic arousal
(Bradley et al., 2001; Lang et al., 1993).
Heart rate is another physiological measure that is com-
monly used as a tool for measuring physiological anxiety
(Caruso et al., 1994; Peters and Hulstijn, 1984; Weber and
Smith, 1990). Unlike skin conductance, which is under the
control of the sympathetic nervous system, heart rate is under
the influence of both sympathetic and parasympathetic
systems. In contrast to EDR responses to stressors, differential
effects on HR have depended on the strength of the related
stimuli. In cases that have examined the impact of fearful
stimuli or strong stressors, an increase in HR has been
observed, due to the systemwide activation of sympathetic
nervous system. However, in cases of mild to moderate
stressors, greater variety in HR patterns have been observed
(e.g., either an acceleration or deceleration, depending on the
situation) (Stern et al., 2001). In other words, no unidimen-
sional pattern has been found to exist among Farousal-related_responses, such as increased EDR responses that are accom-
panied by an increase in HR or breathing rate. Lacey (1967)
noted that on some occasions deceleration in heart rate was
accompanied by increases in skin conductance. A recent model
of autonomic function suggests that sympathetic and parasym-
pathetic branches of the autonomic nervous system can act
independently, reciprocally, or even coactively (i.e., increase or
decrease together) to an external stimulus (Bernston et al.,
1991, 1993). In people who stutter, a deceleration in heart rate
prior to stuttering has been attributed to the coactivation pattern
of both sympathetic and parasympathetic activations (Alm,
2004). Therefore, due to the variability in physiological
responses, generalizing the physiological data from a single
channel (e.g., EDR) to the entire autonomic system in a
unidimensional continuum of Farousal_ may lack accuracy and
may be misleading (Weber and Smith, 1990; Stern et al., 2001;
Alm, 2004). Hence, in the present study, to provide more
consistency in data interpretation, we recorded the changes in
both EDR and HR through independent channels to indicate
the autonomic activity to fluent and stuttered speech.
The purpose of the present study was to measure electro-
dermal response and heart rate of listeners to stuttered and
fluent speech. The importance of comparing the physiological
responses of normal listeners to stuttered and fluent speech has
several purposes. Firstly, to the best of our knowledge, no real-
time objective physiological data to this effect has ever been
collected. Such measures provide objective and quantifiable
data about listener’s arousal states in response to distinctly
different patterns of speech (i.e., normal versus aberrantly
disrupted). It is suspected that the rapid onset and offset of
stuttering symptoms, which is indicative of a Floss of control_while speaking, may create an increased state of physiological
arousal in listeners who are not used to experiencing such
symptoms. Secondly, these data can help clinicians accurately

V.K. Guntupalli et al. / International Journal of Psychophysiology 62 (2006) 1–8 3
understand the listener’s psychophysiological or emotional
responses while witnessing the stuttered speech. With the
empirical evidence, clinicians can counsel their clients about
any visceral response to stuttered speech and assist in
developing appropriate coping strategies with potential nega-
tive emotional reactions of listeners. Oftentimes, people who
stutter and clinicians have anecdotally reported that nonverbal
responses are sometimes filled with signs of discomfort and
duress on the part of the listener when stuttering behaviors
occurs during interactions. It was also observed that listeners
lost their mobility and eye contact and reduced their speech
behavior when they were confronted with a person who stutters
suggesting that listeners could be having altered emotional and
physiological reactions while talking with a person who stutters
(Bloodstein, 1995; Van Riper, 1971).
Finally, differences in physiological responses of listeners to
stuttered and fluent speechmay help to understand sources of the
strong negative stereotypes that exist towards people who stutter.
In other words, is it possible for uncontrollable physiological
responses to sow the seeds for stereotypical attitudes towards
people who stutter? Though stereotypes are thought to manifest
through cognitive processes, listeners’ emotional reactions are
thought to play a strong role in the early conception of social
groups, prior to the addition of a cognitive component. Simply
put, if a particular group of people or a stimulus (e.g., people who
stutter or aberrant stuttering behaviors associated with struggle
behaviors) possesses the capability of evoking emotional or
visceral responses in those perceiving them, these feelings can
be transferred to beliefs about the group (Mackie et al., 1996).
Recently, Gallese et al. (2004) posited a neural mechanism
known as Fmirror neurons_ that allows us to understand the
actions and emotions of others by internally Fsimulating_ thoseactions or emotions. In other words, observed events are directly
simulated or mimicked in the listeners brain creating a direct link
between sender and receiver and be able to understand the
actions and experience the emotions associated with those
events (Carr et al., 2003; Leslie et al., 2004). Therefore, when
listeners observe the stuttered speech suddenly, those events can
be simulated in their mind and may experience a physiological
arousal and other emotional responses due to the aberrant nature
of stuttering. Listeners may then be transferring these emotional
responses towards the person who stutters. Simply put, listeners
make such inferences because they experience the similar Flossof control_ and emotions when they execute the similar actions.
Hence, understanding the physiological responses of listeners to
stuttered speech provides physiological evidence to the gener-
alized stereotypic attitudes towards people who stutter.
2. Method
2.1. Participants
Participants in this study consisted of 15 normally fluent
adults (7 males and 8 females) with no diagnosed history of
hearing difficulty or any other speech or language disorder. The
age range for the participants varied from 18 to 33 years with
mean age of 27.3 years (SD=3.40). All the participants
presented with normal or corrected vision. Participants were
recruited from the population of college students, staff and
faculty enrolled at East Carolina University and from the
surrounding area. For inclusion in the experiment, (1)
participants should have no training in the area of speech,
language and hearing disorders, (2) no self-report of a family
member or acquaintance with a communication disorder(s),
including fluency disorders, (3) no self-report of any speech,
language, cognitive, and/or hearing impairment(s). Prior to the
experiment, informed consent (approved by University Med-
ical Center Institutional Review Board, East Carolina Univer-
sity) was obtained from all the participants.
2.2. Stimulus materials
The stimuli consisted of three fluent and three stuttered
speech samples. The stuttered speech samples were recorded
from two males and one female who stutter while they read
different junior-high level passages with similar themes and
complexity. All the three individuals who stutter were rated as
Fsevere_ (SSI-3, Riley, 1994), exhibiting high levels of struggle
filled with overt stuttering behaviors such as repetitions,
prolongations and silent postural fixations on speech sounds,
in addition to tension-filled secondary behaviors such as head
jerks, lip protrusion and facial grimaces. Three fluent speech
samples were recorded from gender matched fluent speakers
while they read different sets of three junior-high level passages
with similar themes and complexity. Stuttered and fluent
samples were recorded in a sound treated room using a digital
video camera (JVC miniDV GR-D70U). The recorded stuttered
and fluent speech samples were digitized and approximately
50–60 s of stimulus of three fluent and three stuttered tokens
were copied onto a DVD for playback to the listeners.
2.3. Apparatus
The speech stimulus was played through a Panasonic DVD
video recorder (model DMR-E30). The participants wore the
glasstron home theatre system (SONY personal LCD monitor
PLM-A35), consisting of a personal monitor with special
viewing lenses for video presentation (Saltuklaroglu et al.,
2004). Video output from the DVD player was also sent to the
color television for the experimenter to view and monitor the
stimulus. The audio output was routed through a Mackie 1202
mixer and presented to the listeners via E-A-R 3A insert
earphones at a comfortable listening level. PSYLAB computer
instrumentation (Contact Precision Instruments) was used to
record the autonomic responses (i.e., SCR and HR).
2.4. Physiological recording and measurement
Skin conductance response to speech stimuli was recorded
with a pair of 8 mm2 pre-wired Ag/AgCl electrodes (TD-22
EL1, Med associates Inc.) attached to the palmer surface of the
distal phalanges of the second and third fingers of the left hand.
Electrodes were filled with 0.05-M NaCl electrolyte material.
The PSYLAB SC5 coupler provides a 0.5-V constant voltage

0
0.2
0.4
0.6
0.8
Cha
nge
in S
C (
mic
roS
iem
ens)
FLU1 FLU2 FLU3 STU1 STU2 STU3
Stimulus Condition
Fig. 1. Changes in skin conductance as a function of stimulus condition. _FLU_refers to fluent speech conditions, and FSTU_ refers to stuttered speech
conditions. Error bars represent Tone standard error.
V.K. Guntupalli et al. / International Journal of Psychophysiology 62 (2006) 1–84
across the two electrodes and measures the skin conductance
directly. SC5 skin conductance coupler provides a 24-bit
accuracy A–D converter built into the Amplifier (SCR-B
06). SC signals were recorded at a sampling rate of 100 Hz and
the accuracy of skin conductance measurement was checked
with the two calibrator buttons (20 and 0.1 AS) provided in the
pre-amplifier.
Electrocardiogram (ECG) measures were used to detect
changes in heart rate. ECG was recorded using two disposable
Ag/AgCl monitoring electrodes with solid gel (3M Red dot,
2239) placed one at the base of neck on the right side and other
on the left ankle. ECG was recorded using a Bioamplifier (Bio-
C 03) with high pass filter set at 10 Hz and low pass filter set at
40 Hz. Gain was adjusted to 1 mV with Hum filter on. ECG
signals were recorded with a sampling rate of 100 Hz and
quantized at 12 bits accuracy.
2.5. Procedure
Participants were given a brief description of the stimuli, the
recording techniques and then were asked to sign an informed
consent form approved by the UMCIRB. At the beginning of
the experiment, participants were asked to wash their hands
with soap and water and dry them thoroughly. This is to
maintain an equal degree of skin hydration across all
participants for the measurement of skin conductance. Partici-
pants were then seated in a comfortable chair and the required
transducers for collecting autonomic response data were
applied to the appropriate areas by the investigator. The
glasstron home theatre system was placed over the participants’
eyes and disposable foam ear tips were used to insert the E-A-R
3A insert earphones.
All the participants were given a five-minute adaptation
period before viewing the first experimental video stimulus.
They were asked to remain comfortable and rest quietly.
Following the adaptation period, the investigator collected
baseline autonomic responses for 30 s before presenting the first
speech token. After the presentation of stimulus, a two-minute
recovery period was given before measuring the baseline for the
next stimulus. During the two-minute recovery period, partici-
pants were instructed to rest quietly. The two-minute time
period was given to allow physiological measures to return to
baseline levels. Skin conductance and ECG responses during
the baseline and experimental tasks were continuously recorded
throughout the procedure. However, the investigator placed
event markers in order to indicate onset of stimulus presenta-
tion. The presentation of fluent and stuttered speech samples
were randomized (using http://www.randomizer.org/) for each
participant.
2.6. Data quantification and analysis
Measurement was completed during a sixty-second window
for each stuttered and fluent speech sample. That is, a 30 s
period before the presentation of the stimulus (baseline) and a
30 s period during the presentation of the stimulus (response).
The average amplitude of skin conductance (in microsiemens)
was measured during baselines and during the presentation of
all the stimulus tokens. Heart rate was calculated from ECG by
manually counting the number of R waves for 30 s baseline and
stimulus periods. In addition, a complete beat was considered
only when the partial beats appeared both in the beginning and
end of the assessment period. The differences between baseline
and stimulus response was calculated for skin conductance and
heart rate for all speech samples. Descriptive and inferential
statistical analysis was performed using the statistical software
package SPSS PC (version 11.0). SC and HR data were entered
in the order that participants viewed the fluent and stuttered
speech samples, not to the specific stimulus token. That is,
responses were entered in the order of first viewed stuttered
sample to the last viewed stuttered sample (STU1, STU2,
STU3) and similarly first viewed fluent speech sample to last
viewed fluent speech sample (FLU1, FLU2, FLU3). A 2�3
repeated measures ANOVA was performed to investigate the
difference in skin conductance and heart rate responses as a
function of speech condition (fluent versus stuttered) and order
of stimulus (i.e., first, second and third). Results were
considered significant at the level of p <0.05. Greenhouse–
Geisser adjustment of the degrees of freedom was used for the
violations of sphericity assumptions.
3. Results
The mean and standard errors for change in skin conduc-
tance (in microsiemens) as a function of six stimulus conditions
(three fluent and three stuttered speech samples) are shown in
Fig. 1.
The mean change (response�baseline) in skin conductance
values to the first, second and third stuttered speech samples
was 0.527 (SE=0.109), 0.184 (SE=0.066), 0.120 (SE=0.060),
respectively. In contrast, the mean change in skin conductance
values to the first, second and third fluent speech samples
was only 0.107 (SE=0.066), 0.104 (SE=0.054), 0.050
V.K. Guntupalli et al. / International Journal of Psychophysiology 62 (2006) 1–8 5
(SE=0.053), respectively. A 2�3 repeated measures ANOVA
revealed a significant main effect for both speech conditions
[F(1, 14)=9.83, Greenhouse–Geisser p =0.007, g2=0.41,
/ =0.83 at a =0.05], and order of stimulus [F(2,28)=4.56,
Greenhouse–Geisser p =0.031, g2=0.25, / =0.63 at a =0.05].Further, the interaction of speech condition and order of
stimulus was also significant [F(2,28)=5.81, Greenhouse–
Geisser p =0.013, g2=0.29, / =0.77 at a=0.05]. To under-
stand the interaction effects, five planned single-df contrasts
were performed: a significant difference was found between
the conditions of (1) first stuttered and first fluent speech
samples [F(1, 14)=10.54, p =0.006, g2=0.43, / =0.86 at
a =0.05] and (2) first and third order of stimulus presenta-
tions [F(1,14)=7.75, p =0.015, g2=0.36, / =0.74 at a =0.05].The mean and standard errors for change in heart rate
(number of beats per 30 s) as a function of three fluent (FLU1,
FLU2, FLU3) and three stuttered (STU1, STU2, STU3) speech
samples are shown in Fig. 2.
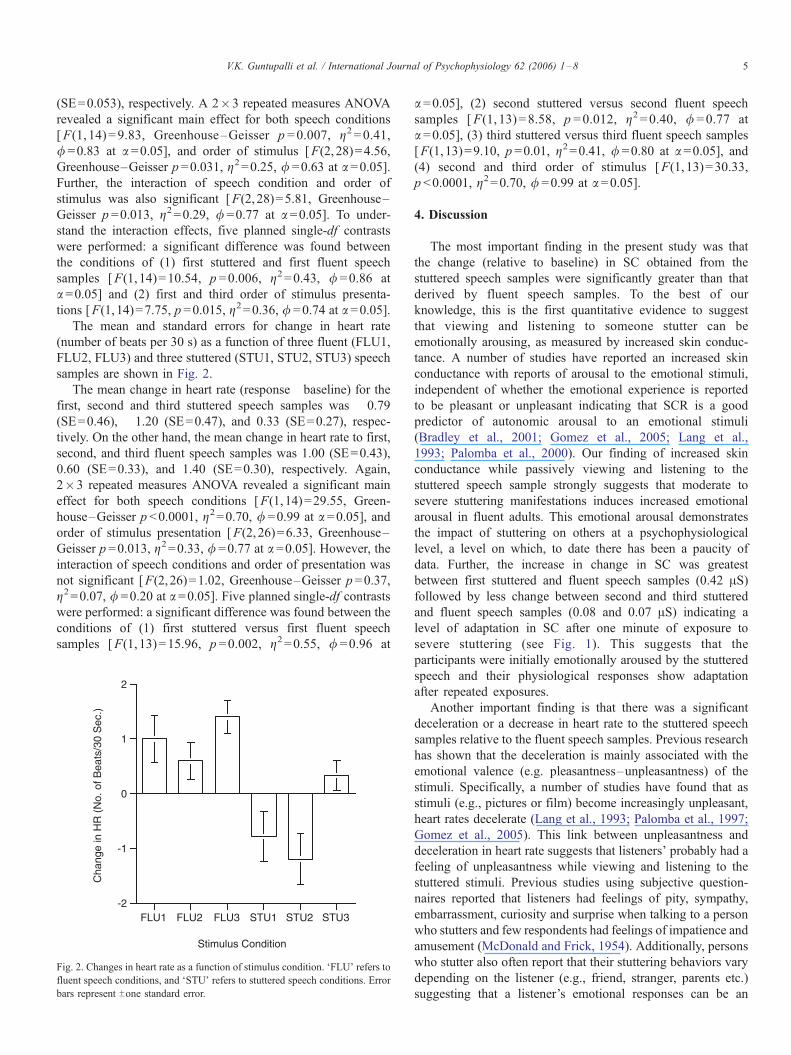
The mean change in heart rate (response�baseline) for the
first, second and third stuttered speech samples was �0.79(SE=0.46), �1.20 (SE=0.47), and 0.33 (SE=0.27), respec-
tively. On the other hand, the mean change in heart rate to first,
second, and third fluent speech samples was 1.00 (SE=0.43),
0.60 (SE=0.33), and 1.40 (SE=0.30), respectively. Again,
2�3 repeated measures ANOVA revealed a significant main
effect for both speech conditions [F(1,14)=29.55, Green-
house–Geisser p <0.0001, g2=0.70, / =0.99 at a =0.05], andorder of stimulus presentation [F(2,26)=6.33, Greenhouse–
Geisser p =0.013, g2=0.33, / =0.77 at a =0.05]. However, theinteraction of speech conditions and order of presentation was
not significant [F(2,26)=1.02, Greenhouse–Geisser p =0.37,
g2=0.07, / =0.20 at a =0.05]. Five planned single-df contrasts
were performed: a significant difference was found between the
conditions of (1) first stuttered versus first fluent speech
samples [F(1, 13)=15.96, p =0.002, g2=0.55, / =0.96 at
-2
-1
0
1
2
Cha
nge
in H
R (
No.
of B
eats
/30
Sec
.)
FLU1 FLU2 FLU3 STU1 STU2 STU3
Stimulus Condition
Fig. 2. Changes in heart rate as a function of stimulus condition. FFLU_ refers to
fluent speech conditions, and FSTU_ refers to stuttered speech conditions. Error
bars represent Tone standard error.
a =0.05], (2) second stuttered versus second fluent speech
samples [F(1, 13)=8.58, p =0.012, g2=0.40, / =0.77 at
a =0.05], (3) third stuttered versus third fluent speech samples
[F(1,13)=9.10, p =0.01, g2=0.41, / =0.80 at a =0.05], and(4) second and third order of stimulus [F(1, 13)=30.33,
p <0.0001, g2=0.70, / =0.99 at a=0.05].
4. Discussion
The most important finding in the present study was that
the change (relative to baseline) in SC obtained from the
stuttered speech samples were significantly greater than that
derived by fluent speech samples. To the best of our
knowledge, this is the first quantitative evidence to suggest
that viewing and listening to someone stutter can be
emotionally arousing, as measured by increased skin conduc-
tance. A number of studies have reported an increased skin
conductance with reports of arousal to the emotional stimuli,
independent of whether the emotional experience is reported
to be pleasant or unpleasant indicating that SCR is a good
predictor of autonomic arousal to an emotional stimuli
(Bradley et al., 2001; Gomez et al., 2005; Lang et al.,
1993; Palomba et al., 2000). Our finding of increased skin
conductance while passively viewing and listening to the
stuttered speech sample strongly suggests that moderate to
severe stuttering manifestations induces increased emotional
arousal in fluent adults. This emotional arousal demonstrates
the impact of stuttering on others at a psychophysiological
level, a level on which, to date there has been a paucity of
data. Further, the increase in change in SC was greatest
between first stuttered and fluent speech samples (0.42 AS)followed by less change between second and third stuttered
and fluent speech samples (0.08 and 0.07 AS) indicating a
level of adaptation in SC after one minute of exposure to
severe stuttering (see Fig. 1). This suggests that the
participants were initially emotionally aroused by the stuttered
speech and their physiological responses show adaptation
after repeated exposures.
Another important finding is that there was a significant
deceleration or a decrease in heart rate to the stuttered speech
samples relative to the fluent speech samples. Previous research
has shown that the deceleration is mainly associated with the
emotional valence (e.g. pleasantness–unpleasantness) of the
stimuli. Specifically, a number of studies have found that as
stimuli (e.g., pictures or film) become increasingly unpleasant,
heart rates decelerate (Lang et al., 1993; Palomba et al., 1997;
Gomez et al., 2005). This link between unpleasantness and
deceleration in heart rate suggests that listeners’ probably had a
feeling of unpleasantness while viewing and listening to the
stuttered stimuli. Previous studies using subjective question-
naires reported that listeners had feelings of pity, sympathy,
embarrassment, curiosity and surprise when talking to a person
who stutters and few respondents had feelings of impatience and
amusement (McDonald and Frick, 1954). Additionally, persons
who stutter also often report that their stuttering behaviors vary
depending on the listener (e.g., friend, stranger, parents etc.)
suggesting that a listener’s emotional responses can be an

V.K. Guntupalli et al. / International Journal of Psychophysiology 62 (2006) 1–86
important factor contributing to the variability in stuttering
behaviors (Bloodstein, 1995). Finally, when the participants in
this study were asked about their feelings, more than half of them
stated that they felt anxious or uneasy. Some even described
themselves as feeling Fshocked_ while viewing the stuttered
samples, which is consistent with the HR deceleration. Further,
the change in heart rate was significantly lower for all the three
stuttered samples compared to the fluent speech samples (see
Fig. 2).
Thus, upon witnessing the first episode of stuttering, an
increase in skin conductance and decrease in heart rate was
found relative to witnessing the first episode of fluent speech,
suggesting that stuttered speech stimuli evoked the differential
pattern of autonomic activation. This kind of differential
fractionation has been generally observed when blood-related
stimuli such as surgical operations, bloody wounds, etc. were
used as visual elicitors (Palomba et al., 2000). These authors
also reported an increase in skin conductance and cardiac
deceleration while watching a surgery film. In contrast, they
observed an increase in SC and cardiac acceleration during the
threat film, suggesting that autonomic response patterns were
related to the specific content of the unpleasant films (i.e.,
threat versus surgery). In other words, unpleasant stimulus, that
is commonly associated with the sympathetic activation, may
evoke both sympathetic and parasympathetic autonomic
system (co-activation), thus causing the differential autonomic
response patterns (i.e., increased SC and decreased HR).
Additionally, this kind of directional-fractionation was also
observed when participants focused their attention on the
stimulus and received increased sensory intake (Lacey, 1967;
Stern et al., 2001). Therefore, based on the available subjective
data from both listeners and people who stutter, our findings of
increased skin conductance and decreased heart rate to the
stuttered speech samples suggest that participants were more
attentive, while having feelings of unpleasantness due to
witnessing the stuttered speech samples. These findings
demonstrate the natural physiological response of people who
do not stutter to the aberrant nature of stuttering moment that is
often associated with physical tension and struggle behaviors
that include head jerks, facial grimaces, clavicular breathing,
and involuntary arm, torso, and leg movements.
The results of the present study could be helpful to both
clinicians and people who stutter. Clinicians should be acutely
aware of this reality and understand listener’s emotional and
visceral responses to stuttered speech. Clinicians can further
counsel their clients with regards to listeners’ negative
emotional reactions and help them to develop coping strategies
to deal with the host of potential social penalties associated
with stuttering (Kalinowski et al., 1996). It is also important to
eliminate or inhibit the aberrant stuttering behaviors early on in
the treatment protocol, as listener’s negative emotional reac-
tions could be detrimental to the overall communication.
Further, present psychophysiological data may provide basis
to the emotional genesis of negative stuttering stereotypes.
Recent neuroimaging studies have shed light on how the
actions or emotions of others are internally mimicked and can
be mapped directly onto our own nervous system allowing the
perception of a particular emotion in others to be Ffelt_ by the
passive observer (Leslie et al., 2004). Simply put, in this study
the participants were not just passively Fseeing and hearing_stuttering; they could also feel the speech breakdown and
experienced the negative emotions associated involuntary
blocking of the speech mechanism, such as feelings of
discomfort, unpleasantness associated with those involuntary
blocks (Gallese et al., 2004). Therefore, we hypothesize that
listeners may have attributed their emotional responses to the
aberrant stuttered speech to the person who is producing them.
Additionally, as previously stated, if a particular group of
people or a stimulus (i.e., stutterers or stuttering) possesses the
capability of evoking emotional arousal in those perceiving
them, these feelings can be transferred to beliefs about the
group (Mackie et al., 1996). In this case, the sources of
emotional arousal were the overtly disrupted speech patterns of
those who stutter. When stuttering occurs, an unexplainable
hitch is introduced to the flow of verbal and non-verbal
information between speaker and listener. Though, it may only
increase the physiological arousal initially, the unpleasantness
is pervasive throughout the exchange as the person perceiving
this aberrant speech witnesses a simple motor process gone
awry with aberrant productions resulting from a loss of
voluntary control. Thus, the listener leaves the communicative
exchange with a negative feeling about the interaction. With
repeated exposures to stuttering and its continued impact on the
communicative process, the negative stereotypes about people
who stutter seemingly begin to arise. In other words, these
stereotypes do not manifest because of what stuttering does to
the stutterer. Instead, they appear to arise because of what
stuttering does to the listener, beginning with simple involun-
tary autonomic arousal.
It should be noted that in this experiment, participants only
viewed and listened to videotapes of people stuttering and the
reactions of the participants were detected using psychophys-
iological measures. It is likely that these changes in autonomic
measures were also accompanied by subtle behaviors such as
wanting to turn away from the stimulus or flinching. Thus, in a
live interaction, a continuous cycle of negative emotions may
be present that is felt both by the stutterer and the listener,
further contributing to the stutterer’s negative reactions to
stuttering and to the listener’s stereotypical views of people
who stutter. The presence of mirror systems for providing
perception–production links supports our proposal regarding
negativity towards people who stutter. These neural mechan-
isms are thought to play a role in understanding and
experiencing the emotional states of others by internally
simulating the others emotions (empathy). In a recent fMRI
study, researchers have found that anterior insula was
selectively activated both when participants were exposed to
disgusting odorants and also mere observation of facial
expression of disgust of others, suggesting that the anterior
insula may play a key role in the mirror system for empathy
(Wicker et al., 2003).
In summary, the present study demonstrates that stuttering
manifestations can induce increased emotional arousal as well
as a pervasive feeling of unpleasantness while witnessing

V.K. Guntupalli et al. / International Journal of Psychophysiology 62 (2006) 1–8 7
stuttering in fluently speaking adults. This is the first empirical
study to demonstrate this phenomenon at a psychophysiolog-
ical level. People who do not stutter simply react differently to
overt stuttering behaviors than they do to fluent speech. A
psychophysiological response to stuttering suggests that our
therapeutic response must incorporate this reality and under-
stand that the listener can become emotionally aroused when
presented with stuttering. Listeners are not to be blamed for
their response as they are only reacting at a very basic
physiological level to a speakers’ atypical speech behavior.
Further, clinicians should be aware that increased emotional
arousal and feelings of unpleasantness in listeners may severely
impair the communicative capabilities of those who stutter as
they sense the emotional arousal and feelings of unpleasantness
in their listeners when they begin to stutter. We also advise
people who stutter to join support groups (e.g., National
Stuttering Association, Stuttering Foundation of America,
British Stammering Association, etc.) who share the similar
emotional experiences and that can be a source of counseling
for those who stutter.
Acknowledgement
We would like to thank Dr. Al Porterfield, Associate
Professor, Oberlin College for his invaluable time spent in
expanding our knowledge on the recording and measurement
procedures of psychophysiological responses.
References
Alm, P.A., 2004. Stuttering, emotions, and heart rate during anticipatory
anxiety: a critical review. J. Fluen. Disord. 29, 123–133.
Ashcroft, K.R., Guimaraes, F.S., Wang, M., Deakin, J.F., 1991. Evaluation of a
psychophysiological model of classical fear conditioning in anxious
patients. Psychopharmacology 104, 215–219.
Bernston, G.G., Cacioppo, J.T., Quigley, K.S., 1991. Autonomic determinism:
The modes of autonomic control, the doctrine of autonomic space, and the
laws of autonomic control, the doctrine of autonomic space, and the laws of
autonomic constraint. Psychol. Rev. 98, 459–487.
Bernston, G.G., Cacioppo, J.T., Quigley, K.S., 1993. Respiratory sinus
arrhythmia: autonomic origins, physiological mechanisms, and psycho-
physiological implications. Psychophysiology 30, 183–196.
Bloodstein, O., 1995. A Handbook on Stuttering, 5th ednR Singular Publishing
Group, San Diego. 107 pp.
Bradley, M.M., Codispoti, M., Cuthbert, B.N., Lang, P.J., 2001. Emotion and
motivation I: defensive and appetitive reactions in picture processing.
Emotion 1, 276–298.
Carr, L., Iacoboni, M., Dubeau, M.C., Mazziotta, J.C., Lenzi, G.L., 2003.
Neural mechanisms of empathy in humans: a relay from neural systems for
imitation to limbic areas. Proc. Natl. Acad. Sci. 100, 5497–5502.
Caruso, A.J., Chodzko-Zajko, W.J., Bidinger, D.A., Sommers, R.K., 1994.
Adults who stutter: responses to cognitive stress. J. Speech Hear. Res. 37,
746–754.
Cooper, E.B., Cooper, C.S., 1985. Clinician attitudes toward stuttering: a
decade of change (1973–1983). J. Fluen. Disord. 10, 19–33.
Cooper, E.B., Rustin, L., 1985. Clinician attitudes toward stuttering in the United
States and Great Britain: a cross-cultural study. J. Fluen. Disord. 10, 1–17.
Craig, A., Tran, Y., Craig, M., 2003. Stereotypes towards stuttering for those
who have never had direct contact with people who stutter: a randomized
and stratified study. Percept. Mot. Skills 97, 235–245.
Crowe, T.A., Cooper, E.B., 1977. Parental attitudes toward and knowledge of
stuttering. J. Fluen. Disord. 10, 343–357.
Crowe, T.A., Walton, J.H., 1981. Teacher attitudes toward stuttering. J. Fluen.
Disord. 6, 163–174.
Dietrich, S., Roaman, M.H., 2001. Physiologic arousal and predictions of
anxiety by people who stutter. J. Fluen. Disord. 26, 207–225.
Doody, I., Kalinowski, J., Armson, J., Stuart, A., 1993. Stereotypes of stutterers
and nonstutterers in three rural communities in Newfoundland. J. Fluen.
Disord. 18, 363–373.
Dorsey, M., Guenther, R.K., 2000. Attitudes of professors and students toward
college students who stutter. J. Fluen. Disord. 25, 77–83.
Fowlie, G.M., Cooper, E.B., 1978. Traits attributed to stuttering and
nonstuttering children by their mothers. J. Fluen. Disord. 3, 233–246.
Gallese, V., Keysers, C., Rizzolatti, G., 2004. A unifying view of the basis of
social cognition. Trends Cogn. Sci. 8, 396–403.
Gomez, P., Zimmermann, P., Guttormsen-Schar, S., Danuser, B., 2005.
Respiratory responses associated with affective processing of film stimuli.
Biol. Psychol. 68, 223–235.
Hurst, M.A., Cooper, E.B., 1983. Vocational rehabilitation counselors’ attitudes
toward stuttering. J. Fluen. Disord. 8, 13–27.
Kalinowski, J.S., Lerman, J.W., Watt, J., 1987. A preliminary examination of
the perceptions of self and others in stutterers and nonstutterers. J. Fluen.
Disord. 12, 317–331.
Kalinowski, J., Armson, J., Stuart, A., Lerman, J., 1993. Speech clinicians’ and
the general public’s perception of self and stutterers. J. Speech-Lang.
Pathol. Audiol. 17, 79–85.
Kalinowski, J., Stuart, A., Armson, J., 1996. Perceptions of stutterers and
nonstutterers during speaking and nonspeaking situations. J. Speech-Lang.
Pathol. Audiol. 5, 61–67.
Kalinowski, J., Saltuklaroglu, T., Guntupalli, V.K., Stuart, A., 2004. Gestural
recovery and the role of forward and reversed syllabic repetitions as
stuttering inhibitors in adults. Neurosci. Lett. 363, 144–149.
Lacey, J.T., 1967. Somatic response patterning and stress: some revision of
activation theory. In: Appley, M.H., Trumbell, T. (Eds.), Psychological
Stress. Appleton Century Crofts, New York, pp. 14–37.
Lang, P.J., Greenwald, M.K., Bradley, M.M., Hamm, A.O., 1993. Looking at
pictures: affective, facial, visceral, and behavioral reactions. Psychophys-
iology 30, 261–273.
Lass, N.J., Ruscello, D.M., Pannbacker, M., Schmitt, J.F., Everly-Myers, D.S.,
1989. Speech-language pathologists’ perceptions of child and adult female
and male stutterers. J. Fluen. Disord. 14, 127–134.
Lass, N.J., Ruscello, D.M., Schmitt, J.F., Pannbacker, M., Orlando, M.B.,
Dean, K.A., Ruziska, J.C., Bradshaw, K.H., 1992. Teachers’ perceptions of
stutterers. Lang. Speech Hear. Serv. Sch. 23, 78–81.
Lass, N.J., Ruscello, D.M., Pannbacker, M., Schmitt, J.F., Middleton, G.F.,
Schweppenheiser, K., 1995. The perceptions of stutterers by people who
stutter. Folia Phoniatr. Logop. 47, 247–251.
Leslie, K.R., Johnson-Frey, S.H., Grafton, S.T., 2004. Functional imaging of
face and hand imitation: towards a motor theory of empathy. Neuroimage
21, 601–607.
Mackie, D.M., Hamilton, D.L., Suskind, J., Rosselli, F., 1996. Social
psychological foundations of stereotype formation. In: Macrae, C.N.,
Stangor, C., Hewstone, M. (Eds.), Stereotypes and Stereotyping. The
Guilford Press, New York.
McDonald, E.T., Frick, J.V., 1954. Store clerks’ reaction to stuttering. J. Speech
Hear. Disord. 19, 306–311.
Palomba, D., Angrilli, A., Mini, A., 1997. Visual evoked potentials, heart rate
responses and memory to emotional pictorial stimuli. Int. J. Psychophysiol.
27, 55–67.
Palomba, D., Sarlo, M., Angrilli, A., Mini, A., Stegagno, L., 2000. Cardiac
responses associated with affective processing of unpleasant film stimuli.
Int. J. Psychophysiol. 36, 45–57.
Peters, H.F.M., Hulstijn, W., 1984. Stuttering and anxiety: the difference
between stutterers and nonstutterers in verbal apprehension and physiologic
arousal during the anticipation of speech and non-speech tasks. J. Fluen.
Disord. 9, 67–84.
Rami, M.K., Kalinowski, J., Stuart, A., Rastatter, M.P., 2003. Self-
perceptions of speech language pathologists-in-training before and
after pseudostuttering experiences on the telephone. Disabil. Rehabil. 6,
491–496.

V.K. Guntupalli et al. / International Journal of Psychophysiology 62 (2006) 1–88
Riley, G.D., 1994. Stuttering Severity Instrument for children and adults, 3rd
ednR Pro-Ed, Austin.
Ruscello, D.M., Lass, N.J., 1994. Special educators’ perceptions of stutterers. J.
Fluen. Disord. 19, 306–311.
Saltuklaroglu, T., Kalinowski, J., Dayalu, V.N., Stuart, A., Rastatter, M.P.,
2004. Voluntary stuttering suppresses true stuttering: a window on the
speech perception–production link. Percept. Psychophys. 66, 249–254.
Stern, R.M., Ray, W.J., Quigley, K.S., 2001. Psychophysiological Recording,
2nd ednR Oxford University Press, New York.
St. Louis, K.O., Lass, N.J., 1981. A survey of communicative disorders
students’ attitudes toward stuttering. J. Fluen. Disord. 6, 49–79.
Tarvainen, M.P., Koistinen, A.S., Valkonen-Korhonen, M., Partanen, J.,
Karjalainen, P.A., 2001. Analysis of galvanic skin responses with principal
components and clustering techniques. IEEE Trans. Biomed. Eng. 48,
1071–1079.
Turnbaugh, K.R., Guitar, B.E., Hoffman, P.R., 1979. Speech clinicians’
attribution of personality traits as a function of stuttering severity. J. Speech
Hear. Res. 22, 37–45.
Van Riper, C., 1971. The Nature of Stuttering. Prentice-Hall, Englewood
Cliffs, NJ.
Weber, C.M., Smith, A., 1990. Autonomic correlates of stuttering and
speech assessed in a range of experimental tasks. J. Speech Hear. Res.
33, 690–706.
White, P.A., Collins, S.R.C., 1984. Stereotype formation by inference: a
possible explanation for the ‘‘stutterer’’ stereotype. J. Speech Hear. Res. 27,
567–570.
Wicker, B., Keysers, C., Plailly, J., Royet, J.P., Gallese, V., Rizzolatti, G., 2003.
Both of us disgusted in My insula: the common neural basis of seeing and
feeling disgust. Neuron 40, 655–664.
Woods, C.L., Williams, D.E., 1971. Speech clinicians’ conceptions of boys and
men who stutter. J. Speech Hear. Disord. 36, 225–234.
Woods, C.L., Williams, D.E., 1976. Traits attributed to stuttering and normally
fluent males. J. Speech Hear. Res. 19, 267–278.
Woolf, G., 1967. The assessment of stuttering as struggle, avoidance, and
expectancy. Br. J. Disord. Commun. 2, 158–171.
Yairi, E., Williams, D.E., 1970. Speech clinician’s stereotypes of elementary-
school boys who stutter. J. Commun. Disord. 3, 161–170.
Yeakle, M.K., Cooper, E.B., 1986. Teacher perceptions of stuttering. J. Fluen.
Disord. 11, 345–359.





























