Embed Size (px)
Citation preview
283
Raynaud’s phenomenon
Report of a Meeting of Physicians and Scientists, University College London Medical School, London
Division of Dermatology, Department of Medicine(Pauline M Dowd FRCP, Portia C Goldsmith MRCP,Helen A Bull PhD), Department of Anatomy andDevelopmental Biology (Prof Geoffrey Burnstock FRS), andDepartment of Pharmacology (Prof John C Foreman, DSc,Ian Marshall PhD), University College London Medical School
Correspondence to: Dr Pauline Dowd, Department of Medicine,Rayne Institute, 5 University Street, London WC1E 6JJ
IntroductionPauline Dowd
In 1862 Maurice Raynaud described the phenomenon ofcold-induced digital pallor followed by cyanosis and
erythema which has since borne his name.’ In 1888 hehypothesised that it resulted from a contraction of theterminal vascular ramifications. Raynaud regarded thestate as one of "local syncope" due to an exaggeration ofthe normal reflex response to cooling. He believed theabnormality to be in the central nervous system, wherethere was "increased irritability of the central parts of thecord presiding over vascular innervation".By the turn of the century, Jonathan Hutchinson2 had
realised that Raynaud’s phenomenon might have morethan one cause, and now it is well known that Raynaud’sphenomenon can be primary and innocent or the
harbinger of serious associated diseases, most commonlysystemic sclerosis. Raynaud’s phenomenon can also bedrug-provoked or occupationally induced. Sir ThomasLewis was amongst the first physician/scientists to
investigate the pathophysiology of the phenomenon.3 Hisexperiments in 1930 showed that, even when reflexvasodilation had been produced by warming the body,vasospasm could be induced by putting the hands in coldwater; conversely, vasospasm could not be produced bybody cooling if the hands were kept warm. Lewisconcluded that the fault lay in abnormal susceptibility ofthe digital cutaneous vasculature to stimulation by localcooling-a "local fault".Cutaneous vascular tone, which was considered to be
solely under al-adrenergic vasoconstrictor control, withvasodilation as a reflex event, is now known to be
controlled by neural and biochemical mechanisms inwhich endothelium is an active participant. Anatomicalstudies have identified an array of new neurotransmittersand have highlighted the importance of peptidergic nervesin the control of vascular tone.4 Investigations into tissue-specific gene splicing led to the discovery of calcitonin-gene-related peptide (CGRP)/ the most potentvasodilator yet identified.6 Subsequent immuno-histochemical studies have shown that CGRP is the mostabundant neuropeptide in sensory primary afferent nervesthat are closely associated with the dermalmicrovasculature in human skin.7,8 Pharmacologicalstudies have identified novel endothelium-derivedmediators of vascular tone, including the vasodilator nitric
oxide9 and the vasoconstrictor endothelin-1.10 In this
grand round we examine, in the light of these advances,the contributions of neurological and vascular
pharmacological abnormalities to the pathophysiology ofRaynaud’s phenomenon.
Case-presentationsPortia Goldsmith
Patient 1
A 32-year-old nurse was first referred at age 22 in 1984.She gave a history of cold hands and feet since childhood.Her fingers would turn white and numb, then blue, andeventually red and painful. She was otherwise well. Therewas no family history of Raynaud’s phenomenon.Examination, including nail-fold capillary microscopy,was normal. Full blood count, urea and electrolytes,liver-function tests, and radiographs (to exclude thoracicoutlet obstruction) were normal. Blood cryoglobulinsand autoantibodies, including antinuclear factor,anticentromere, and anti-Scl-70 antibodies, were
negative. Primary Raynaud’s phenomenon was diagnosed,and the patient was treated with calcium-channel
blockers. She experienced adverse effects at doses
insufficient to control the attacks of Raynaud’sphenomenon, but conservative measures and topicalvasodilators adequately controlled the symptoms.
Patient 2
The second patient, a 68-year-old housewife, initiallypresented 20 years ago to the rheumatologists. At thattime she gave a year’s history of blanching attacks in herfingers triggered by the cold, a general tightness of theskin of her fingers and face, painful hard lumps under theskin of her fingers, and difficulty with swallowing andheartburn. A year later she developed painful ulcerationof her finger tips. Over the next 2 years she underwent leftand then right cervical sympathectomies with only short-lived benefit and was treated with a-blockers andantacids. Between 1978 and 1988 she was admitted to
hospital seven times for episodes of digital ulceration
necessitating, among other treatments, repeatedprostacyclin infusions. She had frequent attacks of
Raynaud’s phenomenon between these episodes despitelarge doses of oral nifedipine (80 mg daily) and longcourses of antibiotics. On examination, she hadscleroderma of the fingers, hands, and face, calcinosis onher fingers and elbows, ulceration of the tips of most ofthe fingers, profuse matt telangiectases on the hands andface, and abnormal nail-fold capillary microscopy. Chestradiography was normal, with no evidence of cervical rib.The full blood count, liver-function tests, urea and
electrolytes, and serum creatinine concentrations were
normal; erythrocyte sedimentation rate (ESR) was
24 mm/h. Antinuclear antibody was present at a titre of1:260; anti-Scl-70 antibody, anticentromere antibodies,and antimitochondrial antibody (titre 1:640) were all
284
positive. Pulmonary-function tests indicated the existenceof a restrictive deficit and decreased transfer factor. The
diagnosis was systemic sclerosis with severe secondaryRaynaud’s phenomenon and peripheral vascularischaemia leading to tissue necrosis.
Patient 3
A 32-year-old man, who worked as a road breaker for awater company, presented with a 2-year history of "whiteattacks" in the index and middle fingers of both handstriggered by the cold or wet. During attacks his handswere numb and clumsy, and attacks could last an hour ormore until he was able to warm up his hands. The fingerabnormalities interfered with his work and his hobby offly fishing. For a year he had also had aching andparaesthesiae in both arms. These occurred independentlyof the "white attacks" and were especially troublesome atnight. He had worked with a water company for 17 years,using hand-held vibrating machinery such as pneumaticdrills and power hammers regularly. He was a non-
smoker. Physical examination was normal. There was noevidence of carpal-tunnel syndrome, and investigations,including full blood count, ESR, urea and electrolytes,and liver-function tests, were normal. The chest
radiograph was normal and cervical rib was not present.Autoantibodies, including antinuclear antibody, anti-Scl-70 antibody, and anticentromere antibodies, were
negative. Nerve-conduction studies (kindly done by DrClare Fowler) were also normal. Hence, these
investigations excluded as far as possible any underlyingcause of Raynaud’s phenomenon. The diagnosis wasvibration white finger (hand-arm vibration syndrome).
Recent advances in vascular controlmechanisms
Geoffrey BurnstockKnowledge of local regulation of blood flow hasaccumulated rapidly in recent years and we now recognisethat regulation of blood-vessel tone involves both
perivascular nerves and the endothelium4 (figure 1).
Perivascular nerves
The vascular neuroeffector junction consists of varicosenerve fibres within a plexus at the adventitial-medialborder. Transmitter is released "en passage" fromvaricosities to reach vascular smooth-muscle cells that arein electrical continuity with each other via gap junctions.The varicosities do not have a fixed relation with
particular smooth-muscle cells and the junctional cleftvaries between about 60 nm and as much as 2 µm in
some large arteries. Neuromodulation as well as
neurotransmission occurs at these junctions. A
prejunctional neuromodulator acts by decreasing or
increasing the amount of transmitter released by the nervevaricosities, whereas a postjunctional neuromodulator actsby altering the time-course or extent of action of theneurotransmitter. Neuromodulators may be circulatingneurohormones, local agents such as prostanoids,bradykinin, or histamine, or neurotransmitter substancesreleased from other nerves nearby, or even from the samenerve varicosities.
For over 50 years, the only transmitters considered inperivascular nerves were noradrenaline and acetylcholine(ACh). Since the discovery of non-adrenergic, non-
cholinergic nerves in the early 1960s, more than twelve
new chemical messengers have been identified, includingmonoamines, purines, aminoacids, polypeptides, and
nitric oxide. The concept of co-transmission-namely,that nerves synthesise, store, and release more than onetransmitter-was first proposed in 1976, and this
hypothesis is now generally accepted. Although at first
sight the multiplicity of transmitters released in variouscomputations from different perivascular nerves seems
formidable and unnecessary, a pattern is now emergingwhich clarifies the situation. The pattern suggests thatautonomic nerves have a "chemical coding"-ie,individual neurons contain a particular combination oftransmitter substances, have processes that project to
identifiable target sites, and have defined centralconnections.
Sympathetic perivascular nervesThere is now substantial evidence that noradrenaline and
adenosine-5’-triphosphate (ATP) act as co-transmitters insympathetic perivascular nerves." The proportions of theco-transmitters noradrenaline and ATP vary considerablybetween different vessels. Neuropeptide Y is also storedin, and released from, sympathetic nerves. In many vesselsit has little direct post-junctional action; however, it doeshave neuromodulatory actions. In a study of blood vesselsin guineapig skin, a different chemical coding has beendemonstrated: the sympathetic nerves in the distributingarteries contain neuropeptide Y and noradrenaline; insmaller arteries, they contain dynorphin, as well as
neuropeptide Y and noradrenaline; and in the pre-
capillary arteries, only dynorphin and noradrenaline arepresent.’2
Parasympathetic perivascular nervesVasoactive intestinal peptide (VIP) seems to be stored
together with ACh in some parasympathetic nerves,
probably in separate vesicles; ATP and ACh are co-
transmitters in others.
Sensory-motor perivascular nervesThe potent vasodilator peptides CGRP and substance Phave been shown to co-exist in sensory nerve varicositiesin perivascular nerves. By analogy with other systems, it
seems likely that ATP co-exists in different proportionswith these peptides, perhaps cooperating in "axon reflex"vasodilation. Since these nerves have a motor rather than
sensory function during axon reflex dilation in manyorgans, they have been termed "sensory-motor nerves" todistinguish them from afferent fibres that are entirelysensory and whose terminals contain few vesicles and a
predominance of mitochondria.
Endothelium
Furchgott and Zawadzki" reported that the vasodilatorresponse to ACh requires the presence of an intactendothelium. Occupation of endothelial receptors byseveral vasoactive substances stimulates the productionof endothelium-derived relaxing factor (EDRF) or
constricting factors or both. EDRF has been identified asnitric oxide9, and prostaglandins also contribute to
relaxation, whereas the peptide endothelin is consideredone of the constricting factors. There is considerable
heterogeneity in the endothelium-dependent responses ofmammalian blood vessels, with variations betweenarteries and veins and between different vascular beds.
285
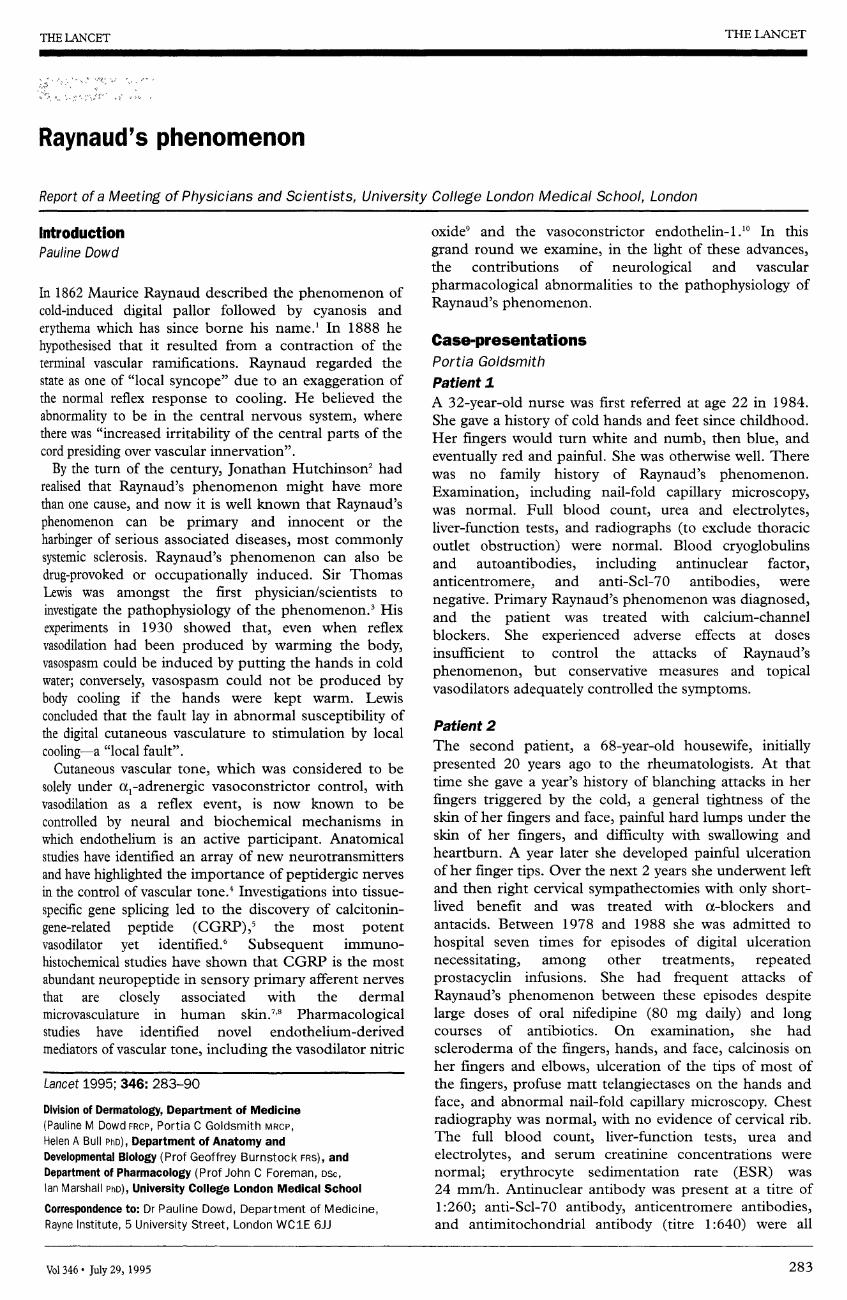
Figure 1: Regulation of vascular tone by perivascular nerves and endothelial cellsNPY, noradrenaline, ATP, CGRP, substance P, and VIP from nerve varicosities in the adventitia act on receptors in the media, causing vasoconstriction(+) or vasodilation (-). ATP, ACh, 5-HT, and substance P, released from endothelial cells by shear stress or hypoxia, act on their receptors onendothelial cells to release EDRF/nitric oxide or prostaglandins which, in turn, induce smooth muscle relaxation. Angiotensin II, vasopressin, andhistamine are also contained in, and may be released from, subpopulations of endothelial cells. In areas denuded of endothelial cells, opposite effectsmay be produced by substances released from endothelial cells acting on receptors on the smooth muscle cells; for example, ACh and ATP will causevasoconstriction.
NPY=neuropeptide Y; NA=noradrenaline; CGRP=calcitonin-gene-related peptide; SP=substance P; VIP=vasoactive intestinal peptide;5HT=5-hydroxytryptamine; EDRF=endothelium-derived relaxing factor; ATII=angiotensin II; VP=vasopressin; H=histamine; a=adrenoceptor;P2X=P2X purinoceptor; P2Y=P2Y purinoceptor; M=muscarinic receptor.
Endothelium-mediated vasodilation
In addition to ACh, endothelium-dependent vasodilationhas been shown to occur in response to ATP, adenosine 5’-diphosphate (ADP), arachidonic acid, substance P,neurokinin A, 5-hydroxytryptamine (5-HT), bradykinin,histamine, neurotensin, vasopressin, angiotensin II, andthrombin. Different subtypes of the receptors to suchvasoactive substances occur on the endothelium andon the vascular smooth muscle. For example,P2X-purinoceptors are present on the vascular smoothmuscle and are acted on by ATP released from
perivascular nerves to produce vasoconstriction, whereasATP released from endothelial cells can cause vasodilationvia P 2y-purinoceptors on the endothelial cells.Although some of these substances would reach
endothelial cells in the microcirculation after release from
nerves, transmitter released from nerves would probablybe degraded before it could reach endothelial cells in theintima of large vessels. It is now known that endothelialcells themselves are a source of these substances; cholineacetyltransferase (ChAT), the enzyme responsible for thesynthesis of ACh, has been shown to be localised inendothelial cells lining capillaries and small vessels in ratcortex. Subsequently, by use of the same technique ofimmunocytochemical staining combined with electron-microscopy, ChAT, substance P, 5-HT, vasopressin,histamine, and angiotensin II were all found inendothelial cells from a variety of blood vessels.4,14,15
Endothelium-mediated vasoconstrictionIt has been proposed that the endothelium mediatesvasoconstriction by producing a constricting factor in
response to various chemical and physical stimuli such asnoradrenaline, thrombin, high extracellular K’, hypoxia,
and stretch. In response to stretch, it has been suggestedthat endothelial Ca2+ channels operate as mechano-transducers. Thus, the role of endothelial cells is two-fold-sensory and effector-such that vasoconstriction mayoccur independently of the action of extraneous
vasoactive substances. Some endothelial vasoconstrictorsubstances have been recognised, includingendothelin-1.’"
Spontaneous release of nitric oxide may be responsiblefor a resting endothelium-mediated vasodilator tone in
opposition to a resting vasoconstrictor tone. Underdifferent physiological and pathophysiological circum-
stances, the balance may be altered so that one or theother dominates. Endothelial release of vasoactivesubstances is probably of greatest importance in
mediating the response of blood vessels to local changesin their internal environment, such as hypoxia andincreased blood flow. In contrast, perivascular nerves maybe more concerned with the integrative control of bloodflow in the organism’s response to its externalenvironment.
Molecular mechanisms of CGRP-mediatedvasodilation
Ian Marshall
Calcitonin-gene-related peptide is a 37 aminoacid peptidefirst identified as a tissue-specific post-transcriptionalsplicing product of the calcitonin gene in the rat brain.’CGRP-like immunoreactivity is found widely in thecentral and peripheral nervous systems. It is present inbeaded fibres around blood vessels, including those of thecerebral, mesenteric, and skin vasculature.7,8 The peptideis known to circulate in human plasma and acts on
receptors on the blood vessels to evoke vasodilation.6
286
CGRP can induce vasodilation via both endothelium-
dependent and endothelium-independent mechanisms.Endothelium-independent vasorelaxation is associatedwith an increase in cyclic-AMP,16 whereas endothelium-dependent vasodilation is associated with an increase inboth cyclic-AMP and cyclic-GMP.CGRP evokes a concentration-dependent fall in the
tone of isolated rings of rat thoracic aorta and pulmonaryand renal artery. It seems that CGRP activates nitricoxide synthase in endothelium, since its relaxant responseis inhibited by NG-monomethyl-L-arginine or by NG-nitro-L-arginine (L-NOArg), both inhibitors of nitricoxide formation. Furthermore this inhibition is
stereospecifically reversed by L-arginine but not by theinactive isomer D-arginine."The endothelium-dependent mechanism of vaso-
relaxation by CGRP is associated with a rise in cyclic-AMP and cyclic-GMP and provides the first example ofvasorelaxation involving both cyclic nucleotides.
L-NOArg pretreatment prevents the CGRP-inducedincrease in cyclic-GMP but not in cyclic-AMP.18These findings are consistent with the explanation that
CGRP acts on the receptors on the endothelium to
activate adenylate cyclase and raise cyclic-AMP. Thisleads to activation of nitric oxide synthase, with
production of nitric oxide, which diffuses to the smoothmuscle of the blood vessel and stimulates guanylatecyclase, thereby increasing cyclic-GMP levels and
stimulating vasorelaxation.
Human dermal microvascular endothelial cellsand vasoactive mediators
Helen Bull
In view of the technical difficulties in investigatingneurological and pharmacological interactions withendothelium in human digital cutaneous vasculature andbecause we were loath to extrapolate the results of large-vessel experiments to small-vessel pathophysiology, weestablished human dermal microvascular endothelial cells
(HDMEC) in culturel9 to facilitate investigation of humancutaneous endothelial cell biology and pathophysiology.
Prostaglandin production and endothelin-1Initially we showed that prostaglandin E 2 (PGE,), notprostacyclin, was the major arachidonic acid metaboliteproduced by HDMEC in response to several agonists,including histamine, interleukin-1, and the calcium
ionophore A23187.19 However, neither CGRP nor
substance P stimulated release of PGE2 from HDMEC.2ONormal serum reduced the ionophore-stimulated
release of prostaglandins in a concentration-dependentmanner, and serum from patients with Raynaud’sphenomenon, whether primary or secondary to systemicsclerosis, exerted a greater inhibitory effect.21 These
findings raised the possibility that a circulating inhibitorof prostaglandin release might contribute to the
vasoconstriction.We have since reported that endothelin-1 attenuates the
basal release of PGEz from HDMEC, and that this effectis associated with an increase in cyclic-AMP concentrations.2= The endothelin-1 receptor is
closely associated with the dihydropyridine Ca2+ channels,and our data have shown that inhibitors of Ca2’
mobilisation, including 8-(diethylamino)-octyl-3,4,5-trimethoxybenzoate (TMB-8), nifedipine, and ethylene
glycol-bis-(ßamino ethyl)-N,N,N’,N’-tetra acetic acid,block the increase in cyclic-AMP accumulation.
Furthermore, we have identified immunoreactiveendothelin-1 in the skin microvasculature and endothelin-
1 mRNA in HDMEC by in-situ hybridisation andnorthern blot analysis. These data indicate that HDMECare both a source of and a target for endothelin-1 and thatendothelin-1 may have autocrine and paracrine effectsand provide a neuron-independent vasoconstrictormechanism in human skin.
Subsequently, increased circulating levels ofendothelin-1 have been reported in primary Raynaud’sphenomenon following cold challenge23 and in Raynaud’sphenomenon secondary to systemic sclerosis,24 and it isconceivable that the circulating serum factor that weidentified in these two forms of Raynaud’s phenomenon isendothelin-1.
Nitric oxide productionIn addition to vasodilator prostaglandins, HDMEC alsorelease nitric oxide. Indomethacin-treated unstimulatedHDMEC inhibited aggregation of washed human
platelets, and the inhibitory effect of the HDMEC wasblocked by haemoglobin, which binds and inactivatesnitric oxide.25 Substance P potentiated HDMECinhibition of platelet aggregation, an effect that was
blocked by haemoglobin. CGRP inhibited plateletaggregation per se, and the inhibitory effect was so
pronounced that further potentiation in the presence ofHDMEC could not be detected. In more recent studies,nitrite production by HDMEC has been measured, andboth CGRP and substance P increased nitrite formation
(unpublished data), indicating that their vasodilatoraction in the microvasculature is mediated by nitric oxide.The constitutively expressed endothelial nitric oxide
synthase has been identified in the microvasculature innormal human skin and in HDMEC by use of antibodiesto endothelial nitric oxide synthase.26 The presence ofimmunoreactive endothelial nitric oxide synthase hasbeen confirmed on western blots of protein extracts
prepared from HDMEC in which the antibodies to
endothelial nitric oxide synthase detected a band with amolecular weight of approximately 135 kDa.Hence HDMEC produce the vasodilators PGEz and
nitric oxide, and CGRP and substance P both inducerelease of nitric oxide from HDMEC. These data indicatethat the cutaneous microvascular endothelium is able to
respond to vasoactive neuropeptides that have beenidentified in human skin and that the endothelium itself isa source of vasoactive mediators. Furthermore, theyindicate that neuropeptide-induced vasodilation is
mediated, at least in part, by release of nitric oxide, thusidentifying the importance of this molecule as a
vasodilator in the microvasculature of human skin.
Immunohistochemistry and in-vivopharmacology of human digital skinJohn Foreman
To test the hypothesis that there might be an abnormalityof the peripheral "sensory-motor" vasodilationmechanisms in Raynaud’s phenomenon, and to elucidatewhether there was a deficient response to or release ofhistamine in Raynaud’s phenomenon, as has been
proposed by Lafferty,27 we conducted a study to determinethe sensitivity of patients with Raynaud’s phenomenon to
287
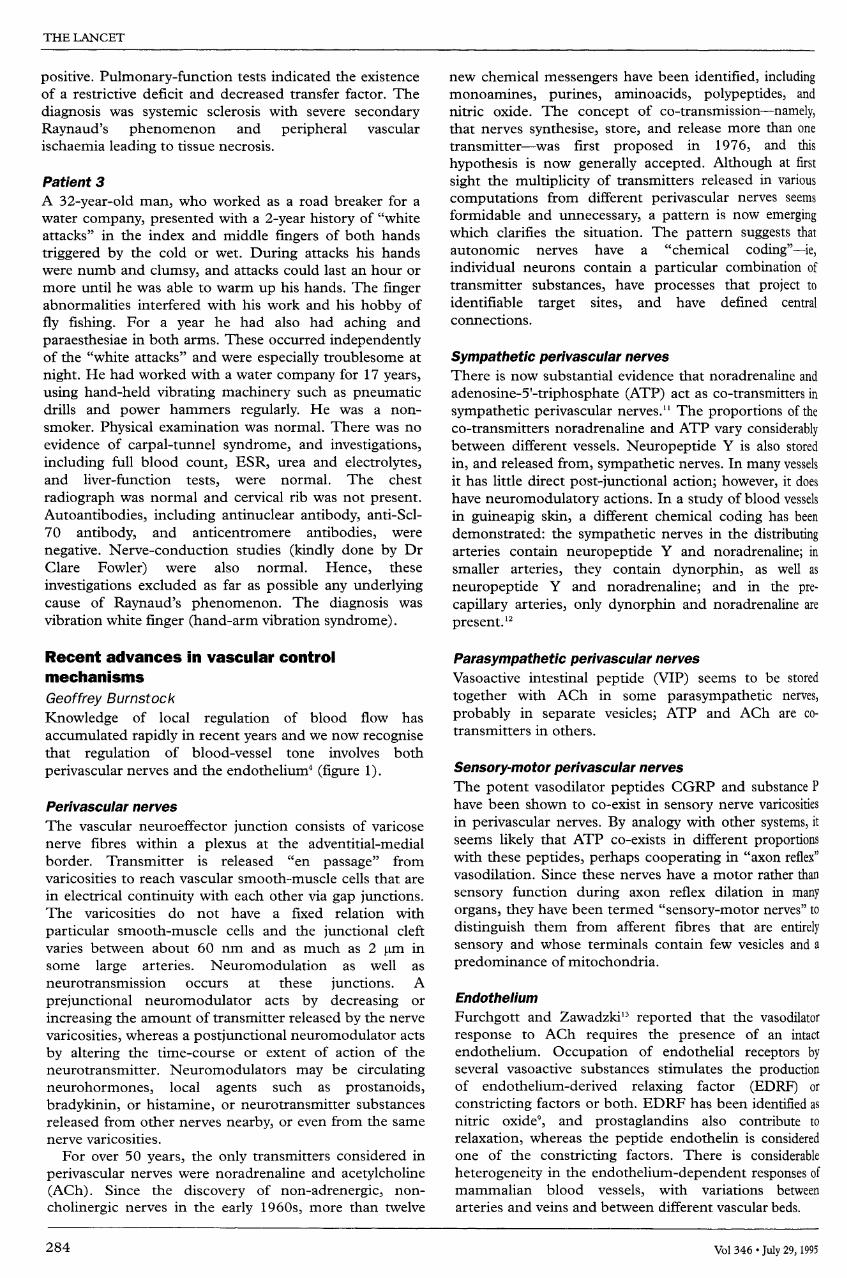
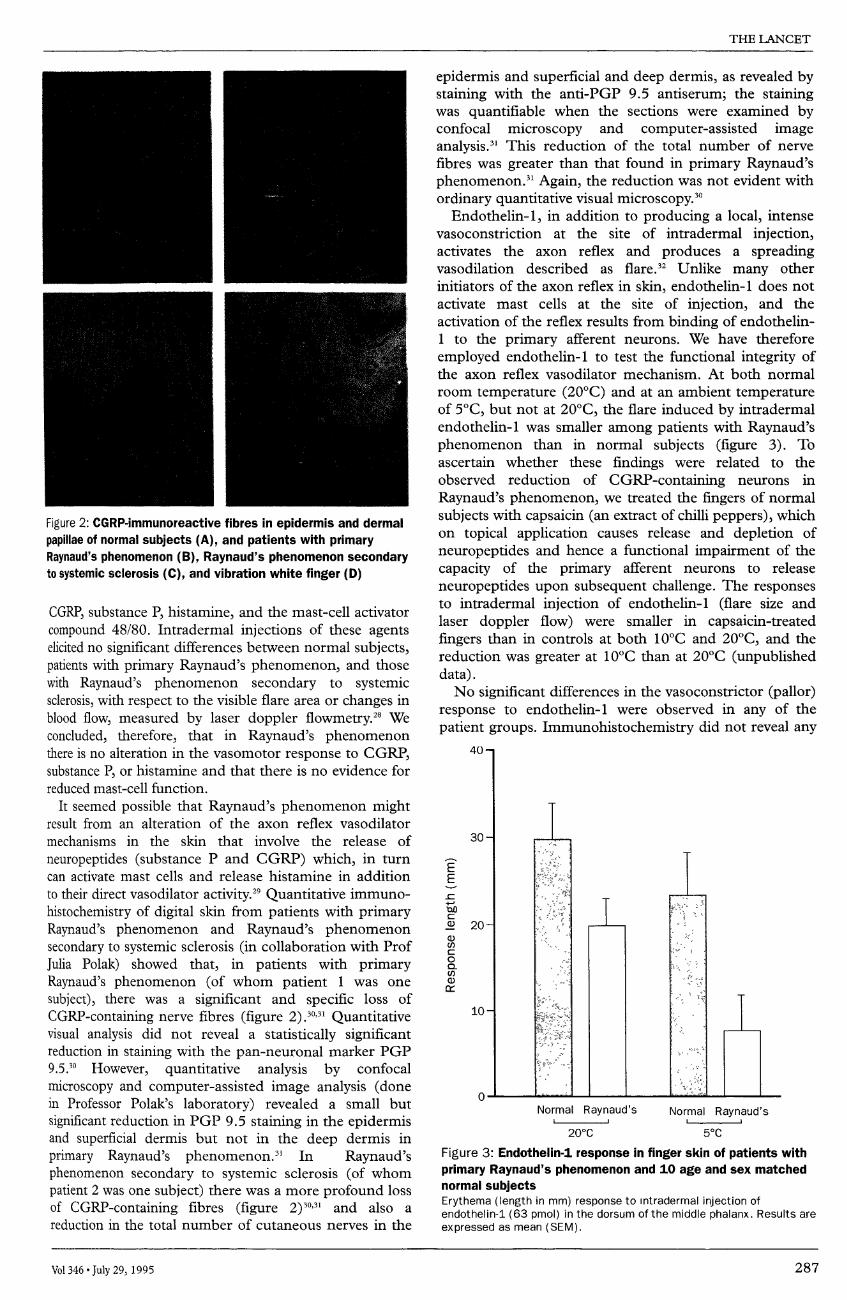
Figure 2: CGRP-immunoreactive fibres in epidermis and dermalpapillae of normal subjects (A), and patients with primaryRaynaud’s phenomenon (B), Raynaud’s phenomenon secondaryto systemic sclerosis (C), and vibration white finger (D)
CGRP, substance P, histamine, and the mast-cell activatorcompound 48/80. Intradermal injections of these agentselicited no significant differences between normal subjects,patients with primary Raynaud’s phenomenon, and thosewith Raynaud’s phenomenon secondary to systemicsclerosis, with respect to the visible flare area or changes inblood flow, measured by laser doppler flowmetry.28 Weconcluded, therefore, that in Raynaud’s phenomenonthere is no alteration in the vasomotor response to CGRP,substance P, or histamine and that there is no evidence forreduced mast-cell function.
It seemed possible that Raynaud’s phenomenon mightresult from an alteration of the axon reflex vasodilatormechanisms in the skin that involve the release of
neuropeptides (substance P and CGRP) which, in turncan activate mast cells and release histamine in additionto their direct vasodilator activity.29 Quantitative immuno-histochemistry of digital skin from patients with primaryRaynaud’s phenomenon and Raynaud’s phenomenonsecondary to systemic sclerosis (in collaboration with ProfJulia Polak) showed that, in patients with primaryRaynaud’s phenomenon (of whom patient 1 was one
subject), there was a significant and specific loss of
CGRP-containing nerve fibres (figure 2).30,31 Quantitativevisual analysis did not reveal a statistically significantreduction in staining with the pan-neuronal marker PGP9.5.30 However, quantitative analysis by confocal
microscopy and computer-assisted image analysis (donein Professor Polak’s laboratory) revealed a small but
significant reduction in PGP 9.5 staining in the epidermisand superficial dermis but not in the deep dermis in
primary Raynaud’s phenomenon.3’ In Raynaud’sphenomenon secondary to systemic sclerosis (of whompatient 2 was one subject) there was a more profound lossof CGRP-containing fibres (figure 2)30,31 and also a
reduction in the total number of cutaneous nerves in the
epidermis and superficial and deep dermis, as revealed bystaining with the anti-PGP 9.5 antiserum; the stainingwas quantifiable when the sections were examined byconfocal microscopy and computer-assisted imageanalysis.3’ This reduction of the total number of nervefibres was greater than that found in primary Raynaud’sphenomenon.3’ Again, the reduction was not evident withordinary quantitative visual microscopy."
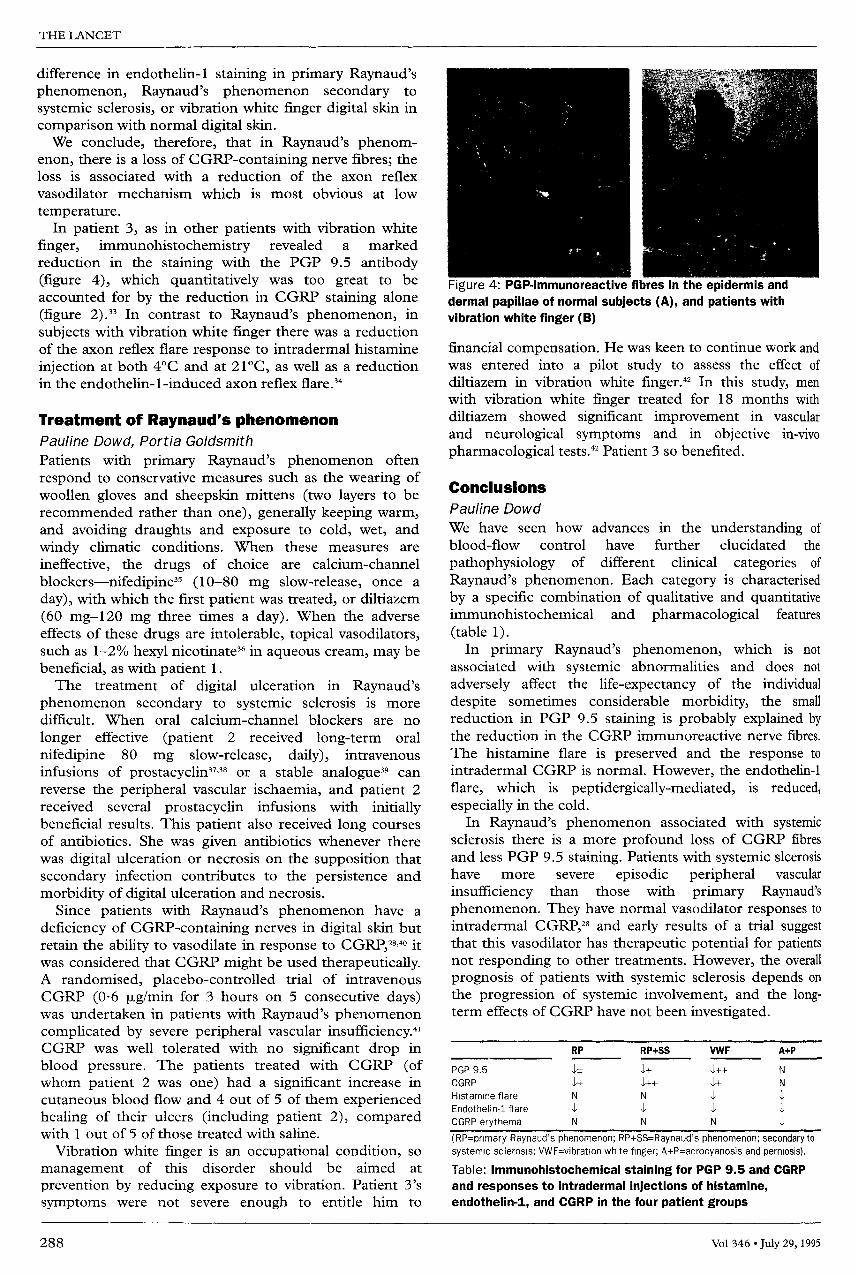
Endothelin-1, in addition to producing a local, intensevasoconstriction at the site of intradermal injection,activates the axon reflex and produces a spreadingvasodilation described as flare.32 Unlike many otherinitiators of the axon reflex in skin, endothelin-1 does notactivate mast cells at the site of injection, and theactivation of the reflex results from binding of endothelin-1 to the primary afferent neurons. We have therefore
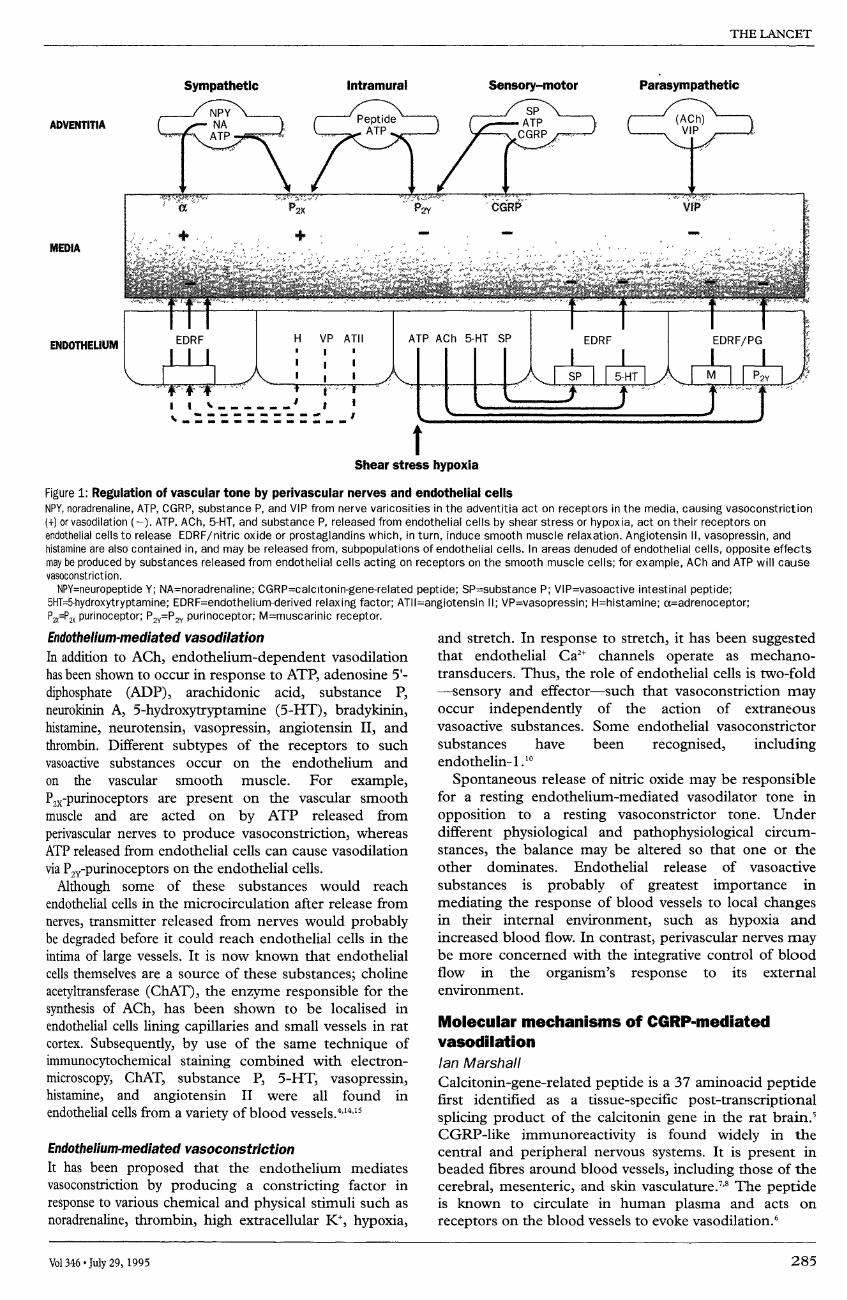
employed endothelin-1 to test the functional integrity ofthe axon reflex vasodilator mechanism. At both normalroom temperature (20°C) and at an ambient temperatureof 5°C, but not at 20°C, the flare induced by intradermalendothelin-1 was smaller among patients with Raynaud’sphenomenon than in normal subjects (figure 3). Toascertain whether these findings were related to theobserved reduction of CGRP-containing neurons in
Raynaud’s phenomenon, we treated the fingers of normalsubjects with capsaicin (an extract of chilli peppers), whichon topical application causes release and depletion of
neuropeptides and hence a functional impairment of thecapacity of the primary afferent neurons to release
neuropeptides upon subsequent challenge. The responsesto intradermal injection of endothelin-1 (flare size andlaser doppler flow) were smaller in capsaicin-treatedfingers than in controls at both 10°C and 20°C, and thereduction was greater at 10°C than at 20°C (unpublisheddata).No significant differences in the vasoconstrictor (pallor)
response to endothelin-1 were observed in any of the
patient groups. Immunohistochemistry did not reveal any
20°C 5°C
Figure 3: Endothelin-1 response in finger skin of patients withprimary Raynaud’s phenomenon and 10 age and sex matchednormal subjectsErythema (length in mm) response to Intradermal injection ofendothelin-1 (63 pmol) in the dorsum of the middle phalanx. Results areexpressed as mean (SEM).
288
difference in endothelin-1 staining in primary Raynaud’sphenomenon, Raynaud’s phenomenon secondary to
systemic sclerosis, or vibration white finger digital skin incomparison with normal digital skin.We conclude, therefore, that in Raynaud’s phenom-
enon, there is a loss of CGRP-containing nerve fibres; theloss is associated with a reduction of the axon reflexvasodilator mechanism which is most obvious at low
temperature.In patient 3, as in other patients with vibration white
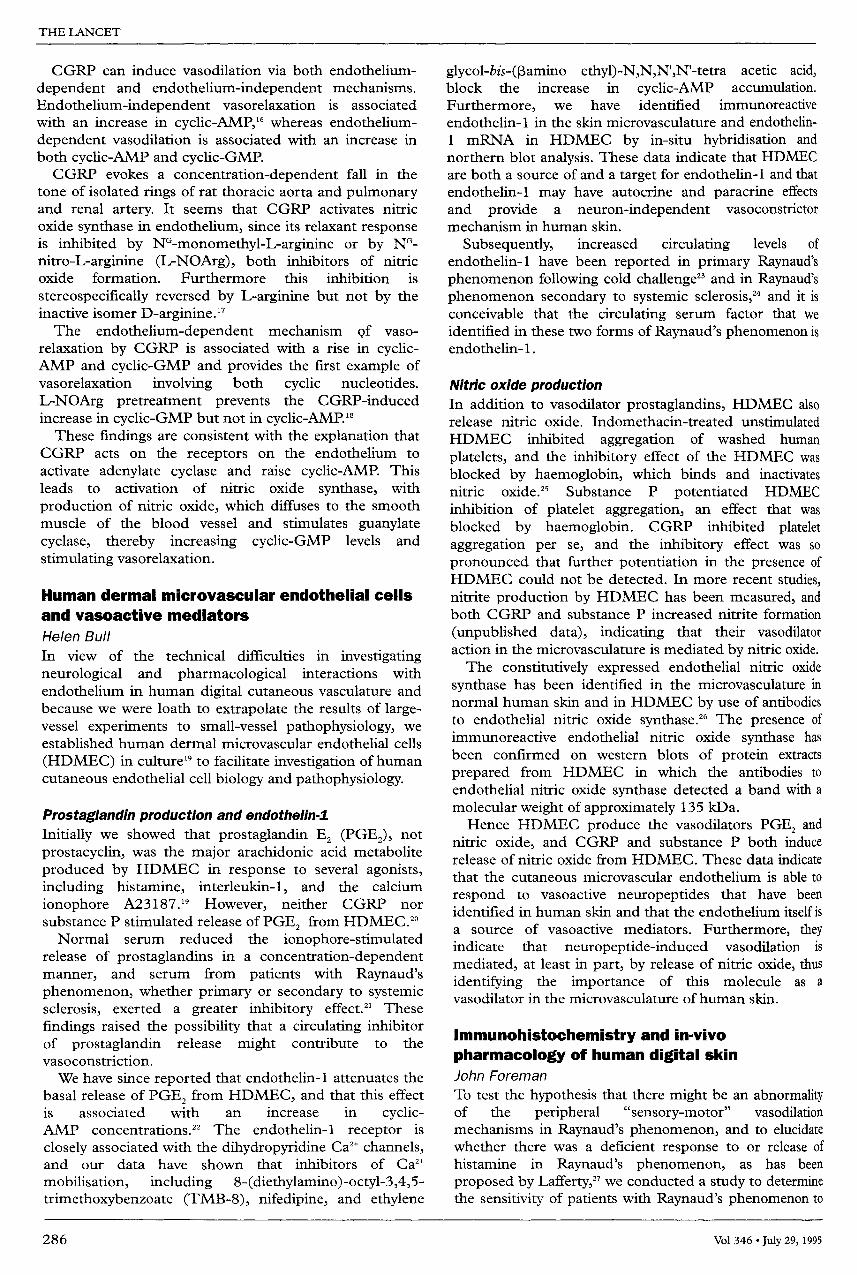
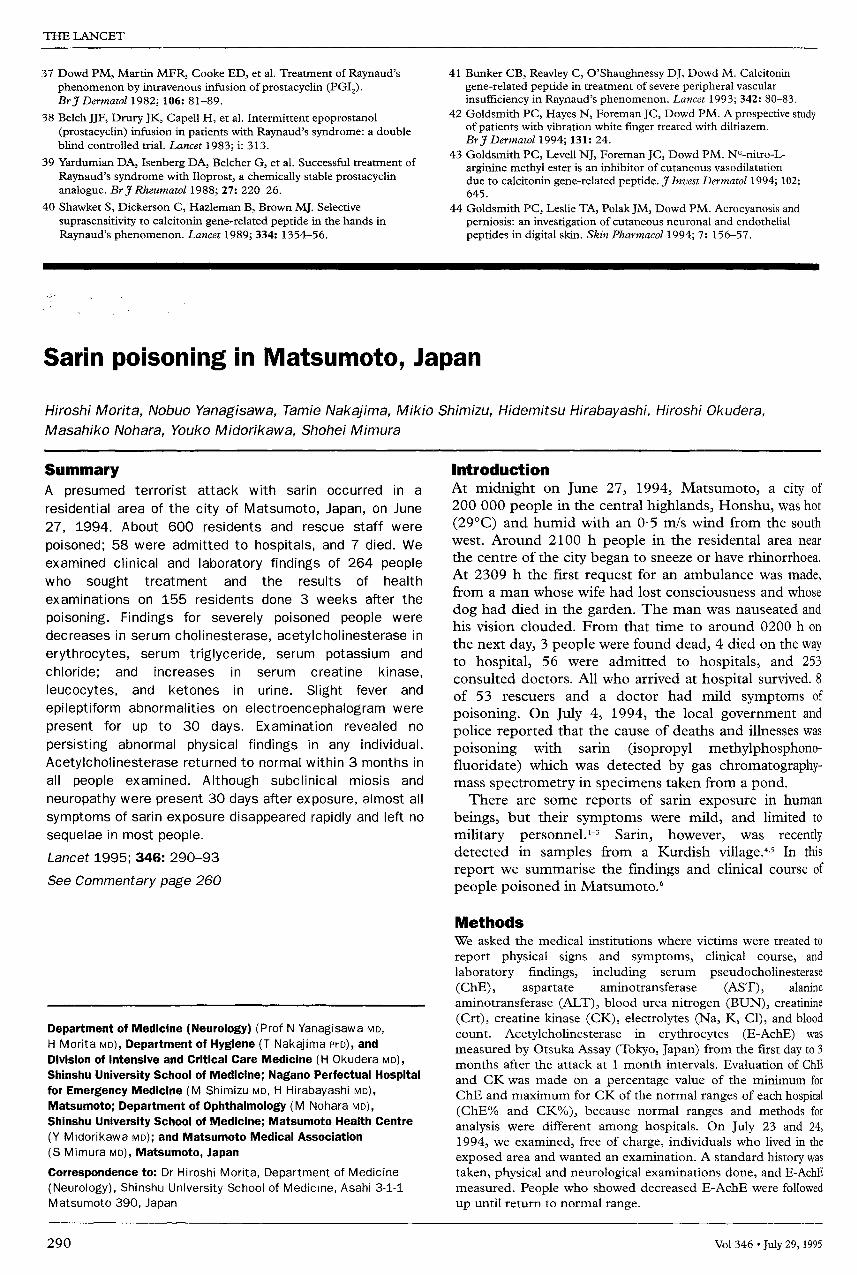
finger, immunohistochemistry revealed a markedreduction in the staining with the PGP 9.5 antibody(figure 4), which quantitatively was too great to beaccounted for by the reduction in CGRP staining alone(figure 2).33 In contrast to Raynaud’s phenomenon, in
subjects with vibration white finger there was a reductionof the axon reflex flare response to intradermal histamine
injection at both 4°C and at 21°C, as well as a reductionin the endothelin-1-induced axon reflex flare.34
Treatment of Raynaud’s phenomenonPauline Dowd, Portia GoldsmithPatients with primary Raynaud’s phenomenon often
respond to conservative measures such as the wearing ofwoollen gloves and sheepskin mittens (two layers to berecommended rather than one), generally keeping warm,and avoiding draughts and exposure to cold, wet, andwindy climatic conditions. When these measures are
ineffective, the drugs of choice are calcium-channel
blockers-nifedipine35 (10-80 mg slow-release, once a
day), with which the first patient was treated, or diltiazem(60 mg-120 mg three times a day). When the adverseeffects of these drugs are intolerable, topical vasodilators,such as 1-2% hexyl nicotinate 36 in aqueous cream, may bebeneficial, as with patient 1.The treatment of digital ulceration in Raynaud’s
phenomenon secondary to systemic sclerosis is moredifficult. When oral calcium-channel blockers are no
longer effective (patient 2 received long-term oral
nifedipine 80 mg slow-release, daily), intravenousinfusions of prostacyclin37,38 or a stable analogue 39 canreverse the peripheral vascular ischaemia, and patient 2received several prostacyclin infusions with initiallybeneficial results. This patient also received long coursesof antibiotics. She was given antibiotics whenever therewas digital ulceration or necrosis on the supposition thatsecondary infection contributes to the persistence andmorbidity of digital ulceration and necrosis.
Since patients with Raynaud’s phenomenon have a
deficiency of CGRP-containing nerves in digital skin butretain the ability to vasodilate in response to CGRP,28,40 itwas considered that CGRP might be used therapeutically.A randomised, placebo-controlled trial of intravenousCGRP (0-6 (JLg/min for 3 hours on 5 consecutive days)was undertaken in patients with Raynaud’s phenomenoncomplicated by severe peripheral vascular insufficiency. 41CGRP was well tolerated with no significant drop in
blood pressure. The patients treated with CGRP (ofwhom patient 2 was one) had a significant increase incutaneous blood flow and 4 out of 5 of them experiencedhealing of their ulcers (including patient 2), comparedwith 1 out of 5 of those treated with saline.
Vibration white finger is an occupational condition, somanagement of this disorder should be aimed at
prevention by reducing exposure to vibration. Patient 3’ssymptoms were not severe enough to entitle him to
Figure 4: PGP-immunoreactive fibres in the epidermis anddermal papillae of normal subjects (A), and patients withvibration white finger (B)
financial compensation. He was keen to continue work andwas entered into a pilot study to assess the effect ofdiltiazem in vibration white finger.42 In this study, menwith vibration white finger treated for 18 months withdiltiazem showed significant improvement in vascularand neurological symptoms and in objective in-vivo
pharmacological tests.42 Patient 3 so benefited.
Conclusions
Pauline Dowd
We have seen how advances in the understanding of
blood-flow control have further elucidated the
pathophysiology of different clinical categories of
Raynaud’s phenomenon. Each category is characterised
by a specific combination of qualitative and quantitativeimmunohistochemical and pharmacological features
(table 1).In primary Raynaud’s phenomenon, which is not
associated with systemic abnormalities and does not
adversely affect the life-expectancy of the individual
despite sometimes considerable morbidity, the smallreduction in PGP 9.5 staining is probably explained bythe reduction in the CGRP immunoreactive nerve fibres.The histamine flare is preserved and the response to
intradermal CGRP is normal. However, the endothelin-1flare, which is peptidergically-mediated, is reduced,especially in the cold.
In Raynaud’s phenomenon associated with systemicsclerosis there is a more profound loss of CGRP fibresand less PGP 9.5 staining. Patients with systemic slcerosishave more severe episodic peripheral vascular
insufficiency than those with primary Raynaud’sphenomenon. They have normal vasodilator responses tointradermal CGRP,28 and early results of a trial suggestthat this vasodilator has therapeutic potential for patientsnot responding to other treatments. However, the overallprognosis of patients with systemic sclerosis depends onthe progression of systemic involvement, and the long-term effects of CGRP have not been investigated.
(RP=pnmary Raynaud’s phenomenon; RP+SS=Raynaud’s phenomenon; secondary tosystemic sclerosis; VWF=v!brat!on white finger; A+P=acrocyanosis and perniosis).
Table: Immunohistochemical staining for PGP 9.5 and CGRPand responses to intradermal injections of histamine,endothelin-1, and CGRP in the four patient groups

289
In vibration white finger, the reduction in PGP 9.5
staining is quantitatively too great to be explained solelyby the decrease in the CGRP fibres, which is of the sameorder as that in primary Raynaud’s phenomenon.33 Thisfinding is indicative of a more general neuronal loss,which might account for the reduced histamine and
endothelin-1 flares at normal temperatures since the
histamine flare is not totally mediated by peptidergicfibres. As in the other two categories of primaryRaynaud’s phenomenon, the responses of the vessels toCGRP are preserved in vibration white finger. The
prognosis in vibration white finger is variable, and theprospect of recovery after avoidance of exposure to
vibration is being investigated. Whether recovery is
promoted by oral vasodilators such as calcium-channelblockers requires further investigation.
In Raynaud’s phenomenon there is therefore a specificdeficit of CGRP in the neurons in digital skin. In additionto the in-vitro experiments with HDMEC, which
demonstrate that CGRP induces release of nitric oxide
from the cutaneous microvascular endothelium, we havenow been able to demonstrate that the erythema producedby intradermal injection of CGRP is attenuated by thenitric oxide synthase inhibitor, NG-nitro-L-arginine methylester (L-NAME), which in our experiments is the most
potent such inhibitor in human skin. Its inactive
stereoisomer, D-NAME, does not attenuate the erythema.The effect of L-NAME on the erythema is at least partlyreversible by L-arginine,43 indicating that in human skinCGRP-induced vasodilation is partly mediated by nitricoxide. The deficit of CGRP in the various types of
Raynaud’s phenomenon thus seems to result in a
functional deficit of nitric oxide synthase-vasodilation inthe skin of the digits during a cold-induced vasoconstrictorresponse, mediated by endothelin-1. Whether this deficitalone is sufficient to account for the vasospasm of
Raynaud’s phenomenon requires further elucidation.In other cutaneous disorders characterised by abnormal
sensitivity to cold, such as perniosis and acrocyanosis, theimmunohistochemistry is qualitatively and quantitativelynormal.’4 However, in these disorders, the histamine andET-1 flares are both reduced, as is the response to
intradermal CGRP and to compound 48/80 and
phenylephrine. These responses indicate that there is a
general vascular hyporeactivity in these conditions that
probably reflects a primary vascular disorder and offerfurther evidence that the deficit of CGRP-containing nervefibres in digital skin is specific to Raynaud’s phenomenon.
References
1 Raynaud M. On local asphyxia and symmetrical gangrene of theextremities, 1862, and New research on the nature and treatment oflocal asphyxia of the extremities, 1872. Barlow T, trans. In:Selected monographs, vol 121. London, New Sydenham Society,1988.
2 Hutchinson J. Raynaud’s phenomenon. Medical Press Circular 1901; 72:403-05.
3 Lewis T. Observations upon the reaction of the vessels of the humanskin to cold. Heart 1929; 15: 177-208.
4 Burnstock G. Integration of factors controlling vascular tone.Overview. Anesthesiology 1993; 79: 1368-80.
5 Rosenfeld MG, Mermod TJ, Amara SG, et al. Production of a novelneuropeptide encoded by the calcitonin gene via tissue-specific RNAprocessing. Nature 1983; 304: 129-35.
6 Gennari C, Fischer JA. Cardiovascular action of calcitonin gene-relatedpeptide in humans. Calcif Tissue Int 1985; 37: 581-84.
7 Wallengren J, Ekman R, Sundler F. Occurrence and distribution ofneuropeptides in the human skin: an immunocytochemical andimmunohistochemical study on normal skin and blister fluid frominflamed skin. Acta Derm Venereol 1987; 67: 185-92.
8 Dalsgaard CJ, Jernbeck J, Stains W, et al. Calcitonin gene-relatedpeptide-like immunoreactivity in nerve fibres in the human skin:relation to fibres containing substance P-, somatostatin- and vasoactiveintestinal peptide-like immunoreactivity. Histochemistry 1989; 91:35-46.
9 Palmer RMJ, Ferrige AG, Moncada S. Nitric oxide release accounts forthe biological activity of endothelium-dependent responses inmammalian blood vessels. Nature 1986; 327: 524-26.
10 Yanigasawa M, Kurihara H, Kimura S, et al. A novel potentvasoconstrictor peptide produced by endothelial cells. Nature 1988;332: 411-15.
11 Burnstock G. The Fifth Heymans Lectures, Ghent. Co-transmission.Arch Int Pharmacodyn Ther 1990; 304: 7-33.
12 Gibbins IL, Morris JL. Sympathetic noradrenergic neurons containingdynorphin but not neuropeptide Y innervate small cutaneous bloodvessels of guinea-pigs. J Auton Nerv Syst 1990; 29: 137-50.
13 Furchgott RF, Zawadski JV. The obligatory role of endothelial cells inthe relaxation of arterial smooth by acetylcholine. Nature 1980; 288:373-76.
14 Parnavelas JG, Kelly W, Burnstock G. Ultrastructural localization ofcholine acetyltransferase in vascular endothelial cells in rat brain.Nature 1985; 316: 724-25.
15 Lincoln J, Loesch A, Burnstock G. Localization of vasopressin,serotonin, and angiotensin II in endothelial cells of the renal andmesenteric arteries. Anat Embryol 1988; 178: 137-42.
16 Gray DW, Marshall I. Nitric oxide synthesis inhibitors attenuatecalcitonin gene-related peptide endothelium-dependent vasorelaxationin rat aorta. Europ J Pharmacol 1992; 212: 37-42.
17 Gray DW, Marshall I. Human &agr;-calcitonin gene-related peptidestimulates adenylate cyclase and guanylate cyclase and relaxes ratthoracic aorta by releasing nitric oxide. Br J Pharmacol 1992; 107:691-96.
18 Marshall I. Mechanism of vascular relaxation by the calcitoningene-related peptide. Ann NY Acad Sci 1992; 657: 204-15.
19 Bull HA, Rustin MHA, Spaul J, et al. Pro-inflammatorymediators induce sustained release of prostaglandin E2 from humandermal microvascular endothelial cells. Br J Dermatol 1990; 122: 153-64.
20 Bull HA, Bunker CB, Dowd PM. Action of vasoactive neuropeptides inmicrovascular endothelium. Int J Microcirc: Clin Exp 1991; 25: 224.
21 Rustin MHA, Bull HA, Machin SJ, et al. Serum from patients withRaynaud’s phenomenon inhibits prostaglandin release. J Invest Dermatol1987; 89: 555-59.
22 Bull HA, Dowd PM. Endothelin-1 in the skin. Dermatology 1992; 187:1-5.
23 Zamora MR, O’Brien RF, Rutherford RB, Weil JV. Serum endothelin-1concentrations and cold provocation in primary Raynaud’sphenomenon. Lancet 1990; 336: 1144-47.
24 Yamane K, Miyanchi T, Suzuki N, et al. Significance of plasmaendothelin-1 levels in patients with systemic sclerosis. J Rheumatol1992; 19: 1566-71.
25 Bull HA, Dowd PM. Mechanisms of vasodilatation in the cutaneousmicrovasculature. Br J Dermatol 1991; 125: 482.
26 Bull HA, Springall DR, Polak JM, Dowd PM. Nitric oxide synthaseisoforms in the human dermal microvasculature. J Invest Dermatol1994; 103: 435.
27 Lafferty K, Roberts VC, de Trafford JC, et al. On the nature ofRaynaud’s phenomenon: the role of histamine. Lancet 1983; 322:313-15.
28 Bunker CB, Foreman JC, Dowd PM. Digital cutaneous responses tohistamine and neuropeptides in Raynaud’s phenomenon.J Invest Dermatol 1991; 96: 314-17.
29 Foreman JC. Peptides and neurogenic inflammation. Br Med Bull1987; 43: 386-400.
30 Bunker CB, Terenghi G, Springall DR, et al. Deficiency of calcitoningene-related peptide in Raynaud’s phenomenon. Lancet 1990; 336:1530-33.
31 Terenghi G, Bunker CB, Liu Y-F, et al. Image analysis quantification ofpeptide-immunoreactive nerves in the skin of patients with Raynaud’sphenomenon. J Pathol 1991; 164: 245-52.
32 Bunker CB, Coulson ML, Hayes NA, et al. Further studies on theaction of endothelin-1 on blood flow in human skin. Br J Dermatol1992; 127: 85-90.
33 Goldsmith PC, Abadia Molina F, Bunker CB, et al. Cutaneous nervedepletion and vibration white finger. J Roy Soc Med 1994; 87: 377-81.
34 Goldsmith PC, Leslie TA, Hayes N, et al. Impaired responses tointeradermal injections of histamine and endothelin-1 indicating smallnerve fibre dysfunction in vibration white finger. Br J Dermatol 1993;129: 488.
35 Smith CD, McKendry RJR. Controlled trial of nifedipine in thetreatment of Raynaud’s phenomenon. Lancet 1982; ii: 1299-301.
36 Bunker CB, Lanigan S, Rustin MHA, Dowd PM. The effects oftopically applied hexyl nicotinate lotion on the cutaneous blood flow inpatients with Raynaud’s phenomenon. Br J Dermatol 1988; 199: 771-76.
290
37 Dowd PM, Martin MFR, Cooke ED, et al. Treatment of Raynaud’sphenomenon by intravenous infusion of prostacyclin (PGI2).Br J Dermatol 1982; 106: 81-89.
38 Belch JJF, Drury JK, Capell H, et al. Intermittent epoprostanol(prostacyclin) infusion in patients with Raynaud’s syndrome: a doubleblind controlled trial. Lancet 1983; i: 313.
39 Yardumian DA, Isenberg DA, Belcher G, et al. Successful treatment ofRaynaud’s syndrome with Iloprost, a chemically stable prostacyclinanalogue. Br J Rheumatol 1988; 27: 220-26.
40 Shawket S, Dickerson C, Hazleman B, Brown MJ. Selectivesuprasensitivity to calcitonin gene-related peptide in the hands inRaynaud’s phenomenon. Lancet 1989; 334: 1354-56.
41 Bunker CB, Reavley C, O’Shaughnessy DJ, Dowd M. Calcitoningene-related peptide in treatment of severe peripheral vascularinsufficiency in Raynaud’s phenomenon. Lancet 1993; 342: 80-83.
42 Goldsmith PC, Hayes N, Foreman JC, Dowd PM. A prospective studyof patients with vibration white finger treated with diltiazem.Br J Dermatol 1994; 131: 24.
43 Goldsmith PC, Levell NJ, Foreman JC, Dowd PM. NG-nitro-L-arginine methyl ester is an inhibitor of cutaneous vasodilatationdue to calcitonin gene-related peptide. J Invest Dermatol 1994; 102:645.
44 Goldsmith PC, Leslie TA, Polak JM, Dowd PM. Acrocyanosis andperniosis: an investigation of cutaneous neuronal and endothelialpeptides in digital skin. Skin Pharmacol 1994; 7: 156-57.
Sarin poisoning in Matsumoto, Japan
Department of Medicine (Neurology) (Prof N Yanagisawa MD,H Morita MD), Department of Hygiene (T Nakajima PhD), andDivision of Intensive and Critical Care Medicine (H Okudera MD),Shinshu University School of Medicine; Nagano Perfectual Hospitalfor Emergency Medicine (M Shimizu MD, H Hirabayashi MD),Matsumoto; Department of Ophthalmology (M Nohara MD),Shinshu University School of Medicine; Matsumoto Health Centre(Y Midorikawa MD); and Matsumoto Medical Association(S Mimura MD), Matsumoto, Japan
Correspondence to: Dr Hiroshi Morita, Department of Medicine(Neurology), Shinshu University School of Medicine, Asahi 3-1-1Matsumoto 390, Japan
SummaryA presumed terrorist attack with sarin occurred in a
residential area of the city of Matsumoto, Japan, on June27, 1994. About 600 residents and rescue staff were
poisoned; 58 were admitted to hospitals, and 7 died. Weexamined clinical and laboratory findings of 264 peoplewho sought treatment and the results of health
examinations on 155 residents done 3 weeks after the
poisoning. Findings for severely poisoned people weredecreases in serum cholinesterase, acetylcholinesterase inerythrocytes, serum triglyceride, serum potassium and
chloride; and increases in serum creatine kinase,leucocytes, and ketones in urine. Slight fever and
epileptiform abnormalities on electroencephalogram werepresent for up to 30 days. Examination revealed no
persisting abnormal physical findings in any individual.
Acetylcholinesterase returned to normal within 3 months inall people examined. Although subclinical miosis and
neuropathy were present 30 days after exposure, almost allsymptoms of sarin exposure disappeared rapidly and left nosequelae in most people.
IntroductionAt midnight on June 27, 1994, Matsumoto, a city of200 000 people in the central highlands, Honshu, was hot(29 °C) and humid with an 0-5 m/s wind from the southwest. Around 2100 h people in the residental area nearthe centre of the city began to sneeze or have rhinorrhoea.At 2309 h the first request for an ambulance was made,from a man whose wife had lost consciousness and whose
dog had died in the garden. The man was nauseated andhis vision clouded. From that time to around 0200 h onthe next day, 3 people were found dead, 4 died on the wayto hospital, 56 were admitted to hospitals, and 253
consulted doctors. All who arrived at hospital survived. 8of 53 rescuers and a doctor had mild symptoms of
poisoning. On July 4, 1994, the local government andpolice reported that the cause of deaths and illnesses waspoisoning with sarin (isopropyl methylphosphono-fluoridate) which was detected by gas chromatography-mass spectrometry in specimens taken from a pond.There are some reports of sarin exposure in human
beings, but their symptoms were mild, and limited tomilitary personnel.’-3 Sarin, however, was recentlydetected in samples from a Kurdish village.45 In this
report we summarise the findings and clinical course ofpeople poisoned in Matsumoto. 6
MethodsWe asked the medical institutions where victims were treated to
report physical signs and symptoms, clinical course, and
laboratory findings, including serum pseudocholinesterase(ChE), aspartate aminotransferase (AST), alanineaminotransferase (ALT), blood urea nitrogen (BUN), creatinine(Crt), creatine kinase (CK), electrolytes (Na, K, CI), and bloodcount. Acetylcholinesterase in erythrocytes (E-AchE) was
measured by Otsuka Assay (Tokyo, Japan) from the first day to 3months after the attack at 1 month intervals. Evaluation of ChEand CK was made on a percentage value of the minimum forChE and maximum for CK of the normal ranges of each hospital(ChE% and CK%), because normal ranges and methods for
analysis were different among hospitals. On July 23 and 24,1994, we examined, free of charge, individuals who lived in theexposed area and wanted an examination. A standard history wastaken, physical and neurological examinations done, and E-AchEmeasured. People who showed decreased E-AchE were followedup until return to normal range.





























