Embed Size (px)
Citation preview

In-Depth Review
Regional Citrate Anticoagulation for RRTs in CriticallyIll Patients with AKI
Santo Morabito,* Valentina Pistolesi,* Luigi Tritapepe,† and Enrico Fiaccadori‡
AbstractHemorrhagic complications have been reported in up to 30% of critically ill patients with AKI undergoing RRTwith systemic anticoagulation. Because bleeding is associated with significantly increased mortality risk,strategies aimed at reducing hemorrhagic complications while maintaining extracorporeal circulation should beimplemented. Among the alternatives to systemic anticoagulation, regional citrate anticoagulation has beenshown to prolong circuit life while reducing the incidence of hemorrhagic complications and lowering transfusionneeds. For these reasons, the recently published Kidney Disease Improving Global Outcomes Clinical PracticeGuidelines for Acute Kidney Injury have recommended regional citrate anticoagulation as the preferredanticoagulation modality for continuous RRT in critically ill patients in whom it is not contraindicated. However,the use of regional citrate anticoagulation is still limited because of concerns related to the risk of metaboliccomplications, the complexity of the proposed protocols, and the need for customized solutions. The introductionof simplified anticoagulation protocols based on citrate and the development of dialysis monitors with integratedinfusion systems and dedicated software could lead to the wider use of regional citrate anticoagulation inupcoming years.
Clin J Am Soc Nephrol 9: 2173–2188, 2014. doi: 10.2215/CJN.01280214
IntroductionAlthough AKI is a well recognized high–bleeding riskcondition (1), the patency of the extracorporeal circuitfor RRT is usually maintained by the use of systemicanticoagulation with unfractionated heparin (2,3).However, a high incidence of hemorrhagic complica-tions has been documented in patients undergoingRRT in the intensive care unit (ICU), with wide var-iability (5%–30%) related to differences in patientpopulations and anticoagulation protocols (4–7).Thus, the choice of the anticoagulant strategy, possi-bly limited to the extracorporeal circuit (i.e., regionalanticoagulation), represents a key issue for safe andeffective RRT in AKI. Although RRT can be per-formed without anticoagulation (8–11), this approachincreases the risk of delivering low RRT doses in upto 30% of patients (12) because of shorter circuit life,increased downtime, and reduced filter performance(12–14).
A number of recent clinical studies has shownadvantages of regional citrate anticoagulation (RCA)compared with heparin in terms of prolonged circuitlife, reduced incidence of hemorrhagic complications,and lower transfusion needs (14–19). On the basis ofthese data, the 2012 Kidney Disease ImprovingGlobal Outcomes (KDIGO) Clinical Practice Guide-lines for Acute Kidney Injury recommend use ofRCA as the preferred anticoagulation modality forcontinuous RRT (CRRT) in patients without contra-indications for citrate, even in the absence of an in-creased bleeding risk or deranged coagulation (20). Inaddition, the same guidelines also recommend using
RCA rather than no anticoagulation in patients with ahigh risk of bleeding (20). These KDIGO guidelineswere also endorsed by the Canadian Society of Ne-phrology (21). However, issues remain regardingthe use of citrate for RRT in AKI, including a cleardefinition of potential contraindications to its use,heterogeneity of RCA protocols, optimal bedsidemonitoring, and cost.This review provides a critical overview of the use
of RCA in patients undergoing RRT for AKI. Themetabolism and kinetics of citrate will be discussedalong with the advantages and potential drawbacksof RCA in the clinical setting of AKI in the ICU.Moreover, the practical application of RCA for variousRRT modalities will be discussed in depth, includingfuture perspectives for simplification of RCA proto-cols.
RCA: Basic Principles and Citrate MetabolismCitrate, the anionic salt of citric acid, is available at
various concentrations of the trisodium salt. Citrateanticoagulates the extracorporeal circuit by chelatingionized calcium (10,11,22), the key cofactor of manysteps of the clotting cascade (23). Additional antihe-mostatic and anti-inflammatory activities of citratemay indirectly derive from its effects on blood cellcomponents, including reduced activation of whiteblood cells and platelets (24–29), and protective ef-fects against endothelial-cell inflammation and dys-function (30). Furthermore, citrate may be directlyinvolved as a signal molecule in several cellular
*Department ofNephrology andUrology,Hemodialysis Unitand †Department ofAnesthesiology andIntensive Care,Sapienza University,Rome, Italy; and‡Department ofClinical andExperimentalMedicine, Acute andChronic Renal FailureUnit, ParmaUniversity, Parma,Italy
Correspondence:Dr. Santo Morabito,Department ofNephrology andUrology, Umberto I,Policlinico di Roma,Sapienza University,Viale del Policlinico,155 00161 Rome,Italy. Email: [email protected]
www.cjasn.org Vol 9 December, 2014 Copyright © 2014 by the American Society of Nephrology 2173

processes related to inflammation and balance of oxidativespecies (31). On this basis, citrate may behave as a trueanti-inflammatory agent (10,18).Citrate is infused in the most proximal portion of the RRT
circuit at rates proportional to blood flow. The infusionrates also vary with the concentration of the citrate solutionused and the target blood citrate concentration (Figure 1)(11,22). The citrate infusion rate is titrated to maintain lowionized calcium levels in the extracorporeal circuit that aresufficient to achieve full blood anticoagulation (i.e., 0.3–0.4mmol/L) (11,22); this target is generally attained with acitrate level in the extracorporeal circuit of approximately3 mmol/L (Figure 1) (32). Because both citrate anion andtrisodium citrate complexes have low molecular weight(198 and 258, respectively), high sieving coefficients(0.85–1), and high diffusive/convective clearances, a sig-nificant quantity of the citrate anions and calcium-citratecomplexes is lost in the effluent fluid (33,34). As a result,calcium infusion is usually needed to replace calciumlosses and maintain systemic ionized calcium levelswithin the normal range (Figure 1). Although some re-ports suggest possible differences in the rapidity of cal-cium release from calcium chloride (CaCl2) comparedwith calcium gluconate (35), chemically equivalent dosesof these formulations produce equally rapid increases insystemic ionized calcium during the anhepatic stage ofliver transplantation (36). Thus, simple dissociation ratherthan hepatic metabolism is probably the main mecha-nism for the release of ionized calcium from both prep-arations (36). In practice, 10% CaCl2 and 10% calciumgluconate solutions provide 0.68 and 0.226 mmol/mlelemental calcium, respectively.
Specific clinical situations, such as severe rhabdomyol-ysis, can potentially complicate the management of serumionized calcium concentrations during RCA (22,37). Al-though hypocalcemia is a common complication in theearly phase of rhabdomyolysis, full correction of calciumlevels is not recommended because of potentially harmfuleffects of excessive calcium supplementation (e.g., tissuecalcium deposition and episodes of late hypercalcemia)(38). Thus, a lower than usual systemic ionized calciumlevel (0.9–1 mmol/L) should be considered a reasonabletarget while performing RCA CRRT in this clinical sce-nario (22,37).Because ionized magnesium is also chelated by citrate,
this cation is also removed by RRT. However, magnesiumis partially replaced with dialysate and/or replacementfluid; therefore, the need for supplementation is related toexchanged volumes and the magnesium concentration inCRRT solutions (22,39).The metabolic load of citrate is the difference between the
citrate infused into the extracorporeal circuit and theamount of citrate lost in the effluent. This citrate load israpidly metabolized through the aerobic pathways of theKrebs cycle (tricarboxylic acid cycle) in the liver and to alesser extent, the skeletal muscle and the kidney (11,22).Thus, the final whole-body citrate balance, which is themain determinant of systemic citrate levels, results fromthe difference between the citrate load and metabolic dis-posal. Although the metabolic clearance of citrate is re-duced and the half-life is prolonged in patients withliver disease (40), no major differences in citrate kineticshave been documented in patients with AKI comparedwith subjects with normal renal function (41).
Figure 1. | RCA in continuous RRT: basic principles. *Sampling for systemic ionized calcium is from the circuit arterial line or the patient’sarterial line (to avoid the effects of vascular access recirculation). Systemic total calcium can be measured from a central venous line. CVVH,continuous venovenous hemofiltration; CVVHD, continuous venovenous hemodialysis; CVVHDF, continuous venovenous hemodiafiltration;Qb, blood flow rate; RCA, regional citrate anticoagulation.
2174 Clinical Journal of the American Society of Nephrology

The ensuing bicarbonate production from citrate metab-olism along with bicarbonate in replacement/dialysisfluids provides the buffer supply to the patient. Indeed,for each 1 mmol citrate metabolized in the Krebs cycle,3 mmol hydrogen ions are consumed, and 3 mmol bicar-bonate is generated (11,22). In citrate solutions containingcitric acid, 3 mmol hydrogen ions are generated from each1 mmol citric acid, counterbalancing the ensuing 3 mmolbicarbonate. Therefore, although the citric acid contained insome citrate solutions contributes to attaining the targetblood citrate concentration and extracorporeal circuit anti-coagulation, it should not be considered as a buffer source.Finally, citrate also represents a source of carbohydrate-
like energy, providing 0.59 kcal/mmol (10,42). Thus, withthe more commonly reported citrate protocols, whichprovide a citrate load of 11–20 mmol/h, the energy de-rived from citrate is approximately 150–280 kcal/24 h.Moreover, when anticoagulant citrate dextrose solutionA (ACD-A) is used, which contains 2.5% dextrose, an ad-ditional caloric load is derived from dextrose metabolism(0.73 kcal/mmol), therefore providing 350–600 kcal/24 h.Lastly, in RCA protocols using lactate-buffered CRRT solu-tions, an additional supply of energy (500–600 kcal/24 h)may be derived from lactate (0.33 kcal/mmol). Therefore,the energy delivered from RRT fluid components (bothanticoagulation and replacement fluid) should be takeninto account when calculating the nutritional needs of crit-ically ill patients undergoing RRT (10,42,43).
Citrate Accumulation Risk and RCA MonitoringCitrate accumulation represents the most common com-
plication of RCA, with a reported incidence of 0%–12% ofpatients depending on the RCA protocol used and the pa-tient case mix (14,16,18,19,44–51). Because hepatic clear-ance represents the main metabolic fate of endogenousand exogenous citrate, citrate metabolism may be signifi-cantly slowed in clinical conditions where liver function isimpaired, with a higher risk of citrate accumulation andconsequent acid-base and electrolyte complications. Inclinical conditions such as severe liver failure or septic/cardiogenic shock, impaired citrate metabolism may pre-vent bicarbonate generation from citrate, leading to nega-tive buffer balance and metabolic acidosis during RCARRT. Moreover, inadequate citrate metabolism may be as-sociated with a fall in ionized serum calcium levels as theresult of impaired calcium release from the calcium-citratecomplexes. As a consequence, progressively higher cal-cium infusion rates may be required to maintain the ion-ized calcium concentration within physiologic limits, andthere may be a disproportionate rise in both the total sys-temic calcium concentration and the total-to-ionized cal-cium ratio (the calcium ratio) (11,22,44,52). In clinicalpractice, because the calcium ratio is related to the bloodcitrate concentration, it is commonly accepted as an indi-rect index of citrate accumulation during RCA (45,48,53–55). A calcium ratio.2.5 is considered the critical thresholdfor increased risk of metabolic complications caused byimpaired citrate metabolism (54). However, it has beenreported that a lower cutoff of 2.1 seems to accurately pre-dict citrate overdose (systemic citrate concentration.1mmol/L) with high sensitivity and specificity (89% and
100%, respectively) (55). It should be recognized that thesuggested cutoff values for the calcium ratio were obtainedwithout any adjustment of total systemic calcium for serumalbumin.The suitability of the calcium ratio as a surrogate for
blood citrate accumulation has only been partially con-firmed (34,40). However, the measurement of blood orplasma citrate concentration is not widely available andgenerally cannot be obtained in a timely manner for rapidbedside clinical decision making. Thus, assessment of thecalcium ratio along with accurate monitoring of acid-basestatus, systemic ionized calcium levels, and changes in cal-cium substitution requirements is the most reasonable ap-proach for early detection of citrate accumulation. Closeattention to the early signs of citrate accumulation is man-datory in high-risk patients (21); in particular, because themain risk of citrate accumulation is a rapid fall in the sys-temic ionized calcium level, potentially resulting in seriouscomplications, such as hypotension and arrhythmias(10,52), the usual calcium monitoring intervals (4–6 hours)as well as the timing of the calcium ratio assessmentshould be shortened in patients who may have impairedcitrate metabolism (e.g., those with severe liver failure andtissue hypoperfusion). Despite these concerns, there is in-creasing evidence of the safety of RCA in patients withsevere liver failure/liver transplant with or without mo-lecular adsorbent recirculating system support (53,56–58)or severe septic shock with liver hypoperfusion (47). Inthese clinical settings, strategies for the prevention of cit-rate accumulation should be targeted to reduce the citrateload by decreasing citrate administration (lower bloodflow rates and higher ionized calcium targets) and/or in-creasing citrate clearance (higher convective and/or dif-fusive dialysis dose) (59). Moreover, because liberaladministration of citrate-containing blood products (i.e.,blood transfusions and fresh frozen plasma) may signifi-cantly increase the citrate metabolic load, this potentialsource of additional exogenous citrate should be takeninto account in any strategy aimed at preventing citrateaccumulation (59).Finally, because the value of conventional liver function
tests is poor at predicting metabolic clearance in critically illpatients with decompensated liver cirrhosis or acute liverfailure, it may be difficult to identify subjects at increasedrisk for citrate accumulation (53). Instead, a prothrombintime#26%, roughly corresponding to $33 seconds, andelevation of the serum lactate to $3.4 mmol/L seem tobe the best predictors of RCA-related metabolic complica-tions (53), serving as surrogates of the liver’s capacity forcitrate metabolism.
Solutions and Protocols for RCARCA was first described for intermittent hemodialysis
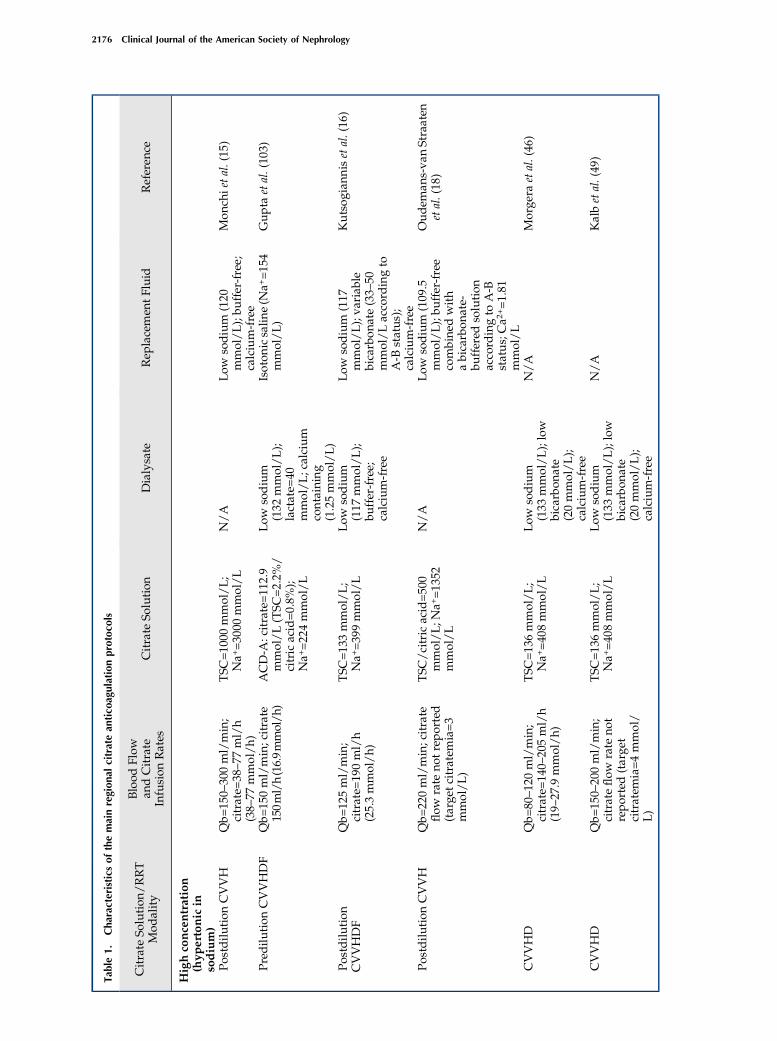
in the 1960s (60), and it was later applied to CRRT (61). Us-ing commercially available or pharmacy-made citrate so-lutions, which generally were not specifically intendedfor RRT use (i.e., ACD solutions), multiple RCA proto-cols were developed for different RRT modalities (14–19,46,47,49,50,61–67) (Table 1). The wide array of citratesolutions and dialysate/replacement fluids as well as thewidely changing operational parameters are associated
Clin J Am Soc Nephrol 9: 2173–2188, December, 2014 Regional Citrate Anticoagulation in Patients with AKI, Morabito et al. 2175
Tab
le1.
Characteristicsofthemainregional
citratean
tico
agulationprotoco
ls
Citrate
Solution
/RRT
Mod
ality
Blood
Flow
andCitrate
Infusion
Rates
Citrate
Solution
Dialysate
Rep
lacemen
tFluid
Referen
ce
Highco
ncentration
(hyp
ertonic
insodium)
Postdilu
tion
CVVH
Qb=
150–
300ml/min;
citrate=
38–77
ml/h
(38–
77mmol/h)
TSC
=10
00mmol/L;
Na+=30
00mmol/L
N/A
Low
sodium
(120
mmol/L);bu
ffer-free;
calcium-free
Mon
chietal.(15
)
Pred
ilution
CVVHDF
Qb=
150ml/min;citrate
150ml/h(16.9mmol/h
)ACD-A
:citrate=11
2.9
mmol/L(TSC
=2.2%
/citric
acid=0.8%
);Na+=22
4mmol/L
Low
sodium
(132
mmol/L);
lactate=
40mmol/L;calcium
containing
(1.25mmol/L)
Isoton
icsalin
e(N
a+=15
4mmol/L)
Gup
taetal.(10
3)
Postdilu
tion
CVVHDF
Qb=
125ml/min;
citrate=
190ml/h
(25.3mmol/h)
TSC
=13
3mmol/L;
Na+=39
9mmol/L
Low
sodium
(117
mmol/L);
buffer-free;
calcium-free
Low
sodium
(117
mmol/L);va
riab
lebicarbon
ate(33–
50mmol/Laccord
ingto
A-B
status
);calcium-free
Kutsog
iann
isetal.(16
)
Postdilu
tion
CVVH
Qb=
220ml/min;citrate
flow
rate
notreported
(targe
tcitratemia=3
mmol/L)
TSC
/citricacid=50
0mmol/L;N
a+=13
52mmol/L
N/A
Low
sodium
(109
.5mmol/L);bu
ffer-free
combine
dwith
abicarbon
ate-
buffered
solution
acco
rdingto
A-B
status;Ca2
+=1.81
mmol/L
Oudem
ans-va
nStraaten
etal.(18
)
CVVHD
Qb=
80–12
0ml/min;
citrate=
140–
205ml/h
(19–
27.9
mmol/h)
TSC
=13
6mmol/L;
Na+=40
8mmol/L
Low
sodium
(133
mmol/L);low
bicarbon
ate
(20mmol/L);
calcium-free
N/A
Morge
raetal.(46
)
CVVHD
Qb=
150–
200ml/min;
citrateflow
rate
not
reported(targe
tcitratem
ia=4mmol/
L)
TSC
=13
6mmol/L;
Na+=40
8mmol/L
Low
sodium
(133
mmol/L);low
bicarbon
ate
(20mmol/L);
calcium-free
N/A
Kalbetal.(49
)
2176 Clinical Journal of the American Society of Nephrology

Tab
le1.(Continued
)
Citrate
Solution
/RRT
Mod
ality
Blood
Flow
andCitrate
Infusion
Rates
Citrate
Solution
Dialysate
Rep
lacemen
tFluid
Referen
ce
Pred
ilution
CVVHDF
Qb=
120ml/min;
citrate=
700ml/h
(19.75
mmol/h)
ACD-A
–ba
seddilu
ted
citratesolution
=28
.22
mmol/L;N
a+=16
3.3
mmol/L;
bicarbon
ate=
30mmol/L
Low
sodium
(133
mmol/L);low
bicarbon
ate
(20mmol/L);
calcium-free
N/A
Mariano
etal.(47
)
CVVHD
Qb=
75–10
0ml/min;
citrate=
35–45
ml/h
(39.3–
50.6
mmol/h)
TSC
/citricacid=74
3/38
1mmol/L;
Na+=22
29mmol/L
Low
tostan
dardsodium
(129
–14
0mmol/L);
variab
lebicarbon
ate
(13.2–
34.3
mmol/L
accord
ingto
A-B
status
);calcium
containing
(1.75mmol/L)
N/A
Sane
retal.(57
)
SLED
Qb20
0ml/min;citrate
180ml/h(24.5
mmol/h)
TSC
=13
6mmol/L;
Na+=40
8mmol/L
Stan
darddialysate
(Gen
iussystem
;18
0–20
0ml/min);
calcium
containing
(1.0
mmol/L)
N/A
Morge
raetal.(10
5)
SLED
Qb=
250ml/min;
citrate=
231–
261ml/h
(31.4–
35.5
mmol/h)
TSC
=13
6mmol/L;
Na+=40
8mmol/L
Stan
dardsodium
and
bicarbon
atedialysate
(300
ml/min);
calcium-free
N/A
Clark
etal.(86
)
SLED-H
DF
Qb=
130ml/min;
citrate=
1350
ml/h
(38.1mmol/h)
ACD-A
–ba
seddilu
ted
citratesolution
=28
.22
mmol/L;N
a+=16
3.3
mmol/L;
bicarbon
ate=
30mmol/L
Low
sodium
(133
mmol/L);low
bicarbon
ate
(20mmol/L);
calcium-free
N/A
Mariano
etal.(47
)
SLED
Qb=
200ml/min;
citrate=
200–
400ml/h
(22.6–
45.2
mmol/h)
ACD-A
:citrate=11
2.9
mmol/L(TSC
=2.2%
/citric
acid=0.8%
);Na+=22
4mmol/L
Cocurrent
flow
stan
dard
dialysate
(300
ml/
min);calcium
containing
(1.25mmol/L)
N/A
Fiaccadorietal.(51
)
Low
concentration
(iso
tonic
insodium)
Pred
ilution
CVVHDF
Qb=
100–
150ml/min;
citrate=
1000
–20
00ml/h(18–
46mmol/h)
TSC
=18
or23
mmol/L
obtained
bydilu
ting
aTSC
4%citrate
solution
;Na+=14
0mmol/L
Stan
dardsodium
(140
mmol/L);low
bicarbon
ate
(25mmol/L);
calcium-free
N/A
Tolwan
ietal.(62
)
Clin J Am Soc Nephrol 9: 2173–2188, December, 2014 Regional Citrate Anticoagulation in Patients with AKI, Morabito et al. 2177

Tab
le1.(Continued
)
Citrate
Solution
/RRT
Mod
ality
Blood
Flow
andCitrate
Infusion
Rates
Citrate
Solution
Dialysate
Rep
lacemen
tFluid
Referen
ce
Pred
ilution
CVVH
Qb=
100–
200ml/min;
citrate=
2000
–40
00ml/h(26–
52mmol/h)
TSC
=13
mmol/L;
Na+=14
0mmol/L
N/A
N/A
Hetzeletal.(19
)
Pre-
andpo
stdilu
tion
CVVH
Qb=
130–
150ml/min;
citrate=
1560
–18
00ml/h(18.7–
21.6
mmol/h)
TSC
/citricacid=10
/2
mmol/L;N
a+=13
6mmol/L
N/A
Stan
dardsodium
(140
mmol/L);stan
dard
bicarbon
ate
(32mmol/L);calcium
containing
(1.75mmol/L)
Morab
itoetal.(14
)
Pred
ilution
CVVH
Qb=
150ml/min;
citrate=
2500
ml/h
(30mmol/h)
TSC
/citricacid=10
/2
mmol/L;N
a+=13
6mmol/L
N/A
N/A
Shum
etal.(64
)
Pred
ilution
CVVH
Qb=
180ml/min;
citrate=
2400
ml/h
(31.9mmol/h)
TSC
=13
.3mmol/L;
Na+=14
0mmol/L
N/A
N/A
Nurmoh
amed
etal.(50
)
Pre-
andpo
stdilu
tion
CVVHDF
Qb=
140ml/min;
citrate=
1000
ml/h
(18mmol/h)
TSC
=18
mmol/L;
Na+=14
0mmol/L
Stan
dardsodium
(140
mmol/L);stan
dard
bicarbon
ate
(30mmol/L);calcium
containing
(1.25mmol/L);
phosph
atecontaining
(HPO42
+=1.2
mmol/L)
Stan
dardsodium
(140
mmol/L);stan
dard
bicarbon
ate
(30mmol/L);calcium
containing
(1.25mmol/L);
phospha
tecontaining
(HPO
422=1.2
mmol/L)
Morab
itoetal.(66
)
The
defi
nition
sSL
ED
andSL
ED-H
DFha
vebe
enmaintaine
das
intheoriginal
articles;b
othtreatm
entm
odalitiesmay
beinclud
edun
der
theterm
prolon
gedinterm
ittent
RRT(PIR
RT).CVVH,
continuo
usve
nove
nous
hemofi
ltration
;CVVHDF,
continuo
usve
nove
nous
hemod
iafiltration
;CVVHD,con
tinu
ousve
nove
nous
hemod
ialysis;SL
ED,sus
tained
low-efficien
cydialysis;SL
ED-
HDF,
sustaine
dlow-efficien
cyhe
mod
iafiltration
;Qb,
bloo
dflow
rate;T
SC,trisodium
citrate;ACD-A
,anticoa
gulant
citratedextrosesolution
A;N
/A,n
otap
plicab
le.
2178 Clinical Journal of the American Society of Nephrology

with exposure of patients to different electrolyte andbuffer combinations, significantly affecting acid-base sta-tus and electrolyte balance during RCA (46,62,65,66).For the sake of simplicity, RCA solutions may be clas-
sified on the basis of citrate concentration as high- and low-concentration solutions, with high citrate concentrationscorresponding to hypertonicity with regard to sodium.
High-Concentration Citrate Solutions (Hypertonic inSodium)High-concentration citrate solutions are also known as
hypertonic citrate solutions because of their high sodiumcontent as trisodium citrate. Although the use of standardsodium concentration CRRT solutions has also been re-ported in RCA protocols adopting hypertonic citrate for-mulations (68,69), these solutions are usually combinedwith customized low-sodium dialysis/replacement fluidsto prevent hypernatremia. As long as a well designed pro-tocol is implemented, hypertonic citrate solutions can beused to perform RCA with all modalities of CRRT (Figure2, Table 1) (15,16,18,46,47,49). RCA protocols based on hy-pertonic citrate solutions use citrate as the primary buffer,regardless of CRRT modality. In the case of continuous
venovenous hemodialysis (CVVHD), a custom-made orcommercially available low-bicarbonate concentration di-alysate is commonly used to obtain a negative bicarbonatemass balance to compensate for the indirect bicarbonateload derived from citrate (46). Therefore, in these proto-cols, the optimization of acid-base status and prevention/treatment of metabolic alkalosis can be achieved by en-hancing the diffusive removal of citrate and bicarbonatethrough increased flow rates of a low-bicarbonate dialy-sate. Conversely, as in the case of metabolic acidosis, anincrease in the buffer supply to the patient can be achievedby increasing the citrate load throughout a parallel rise ofblood and citrate flow rates (46). This approach permitsflexibility in the management of acid-base status, but itmay result in the development of metabolic acidosis if ahigh dialysis dose is required (high diffusive removal ofbuffers related to the increase of low-bicarbonate dialysateflow rate) (46,49). A different approach, using pharmacy-made solutions, was adopted to perform RCA in continu-ous venovenous hemofiltration (CVVH). This approachused a very high-concentration citrate solution (500mmol/L) along with a variable bicarbonate concentrationin the replacement fluid (18). Specifically, a buffer-free
Figure 2. | Schematic representation of RCA for the different continuous RRT modalities. In protocols adopting high-concentration citratesolutions, the use of a low-sodiumdialysate and/or replacement fluid is generally required to prevent hypernatremia. In protocols adopting low-concentration citrate solutions, citrate acts as both an anticoagulant and a predilution replacement fluid, thus contributing to the total con-tinuous RRT dose. Sections A and C display RCA circuits in predilution-only CVVH and CVVHDmodalities, respectively. The dotted boxes inB andD indicate the possibility of using a calcium-free predilution replacement fluid alongwith a separate hypertonic citrate solution to obtainpredilution and postdilution CVVH or CVVHDF.
Clin J Am Soc Nephrol 9: 2173–2188, December, 2014 Regional Citrate Anticoagulation in Patients with AKI, Morabito et al. 2179

replacement solution was mixed in various proportionswith bicarbonate-buffered fluids to modulate the postdilu-tion buffer supply on the basis of clinical needs (18). A sim-ilar approach was described for continuous venovenoushemodiafiltration (CVVHDF), combining a hypertonic cit-rate solution with buffer-free dialysate and postdilution re-placement fluid with variable bicarbonate concentrations(33.3–50 mmol/L) (16).In an alternative approach, hypertonic ACD-A has been
used to prepare a custom-made replacement solution:ACD-A was diluted with a commercially available CRRTsolution, making a hypertonic citrate-containing predilu-tion replacement fluid (28.22 mmol/L citrate, 163.3 mmol/L Na, 77.2 mmol/L chloride, and 30 mmol/L NaHCO3
2),which was combined with a low-bicarbonate dialysate(20 mmol/L) to perform RCA in CVVHDF (47).
Low-Concentration Citrate Solutions (Isotonic in Sodium)In protocols using low-concentration citrate solutions, a
higher citrate flow rate is required to achieve the targetcitrate levels in the extracorporeal circuit. As a conse-quence, citrate acts as both an anticoagulant and a pre-dilution replacement fluid (citrate-buffered replacementsolutions), thus contributing significantly to the total di-alysis dose (Figure 2). The physiologic sodium content ofisotonic solutions allows RCA CVVH or RCA CVVHDFwithout the need of a low-sodium replacement fluid and/or dialysate (Table 1). In protocols using citrate-bufferedreplacement solutions, the buffer supply derives from cit-rate (predilution CVVH) or citrate and bicarbonate in var-ious proportions (predilution and postdilution CVVH andCVVHDF) in relation to the composition and the combi-nation of the solutions that are used (14,19,50,62,64–67). Asimplification on the basis of the use of solutions with anappropriately low citrate concentration allows RCA CRRTas CVVH in the predilution-only modality (19,50). Thisapproach has the advantage of allowing RCA despite theuse of CRRT equipment without a dedicated citrate infu-sion pump, but the downside is that the CRRT dose isintimately linked to the citrate dose (50). The buffer supplyto the patient is exclusively derived from citrate, makinghandling of acid-base status more difficult and potentiallyincreasing the risk of citrate accumulation when a highdialysis dose is used or in other specific clinical settings(50). The use of standard sodium and bicarbonate replace-ment fluids in addition to the citrate-buffered solutionprovides a simplified method for RCA CVVH when predi-lution and postdilution replacement fluids are used withoutrequiring customized CRRT solutions (14,67); a standard(66) or lower than usual bicarbonate (62) dialysate can beused to design an RCA CVVHDF protocol with the advan-tage of operating at lower filtration fractions (Table 1).
Safety and Efficacy of RCASeveral studies comparing citrate-based protocols with
heparin-based protocols have reported better filter survivaland/or fewer bleeding events during RCA (14–19). Twoseparate meta-analyses, including six randomized trialscomparing RCA with systemic anticoagulation with hep-arin, confirmed a significant decrease of bleeding events inthe citrate arm (70,71); however, they provided slightly
different results about filter survival. In particular, Zhangand Hongying (70) showed a significantly prolonged filterlife (mean difference.20 hours) and a highly significantreduction of bleeding risk with RCA (0.28 risk ratio com-pared with heparin). The meta-analysis of Wu et al. (71),which excluded one of six randomized controlled trialsfrom the analysis of filter life, confirmed the lower riskof bleeding with RCA without showing significant advan-tages in terms of circuit survival. Transfusion needs werealso reduced with the use of RCA (14,15,17). Comparedwith unfractioned heparin, RCA was associated with amarked reduction in transfusion requirements in 20 pa-tients treated with CVVH (0.2 versus 1.0 blood units/d,P,0.001) (15). More recently, in patients with high-bleedingrisk cardiac surgery switched to citrate from heparin or noanticoagulation at all, no bleeding complications were ob-served with RCA, and the transfusion rate was significantlylower compared with the other anticoagulation modalities(P,0.02) (14). In addition, RCA was associated with anincrease in platelet count and antithrombin-III activity,thus avoiding platelet concentrate administration andantithrombin-III supplementation (14). At the same time,RCA safely prolonged filter life in the absence of CRRT in-terruption for filter clotting, minimizing CRRT downtime(mean delivered dose around 95%) (14).No robust demonstration is currently available concern-
ing the possible positive effects of RCA on patient survival.In a large single-center randomized trial including 200critically ill patients on CRRT using nadroparin or citrateanticoagulation, RCA was associated with an unexpected15% absolute increase in 3-month survival, which was notcompletely explained by the lower incidence of bleeding(18). Post hoc analysis showed that RCA might be particu-larly beneficial in specific clinical conditions (e.g., surgery,sepsis, severe multiple organ dysfunction syndrome, andyounger age). To explain the survival benefit of RCA, thepreviously discussed interference of citrate with the acti-vation of the inflammatory cascade was suggested (18).However, although RCA was associated with prolongedcircuit patency and a marked reduction in bleeding com-plications, no survival benefit of citrate was shown in asubsequent multicenter randomized trial comparing un-fractioned heparin with RCA in 170 patients undergoingCVVH (19).
RCA in Prolonged Intermittent RRTSustained low-efficiency dialysis, also known as ex-
tended daily dialysis, is a prolonged intermittent RRT(PIRRT) usually lasting 8–12 hours that is increasinglyused in patients with AKI in the ICU (12,72–76). PIRRTis considered a hybrid RRT modality; it combines the mainadvantages of conventional intermittent forms of RRT (e.g.,standard hemodialysis equipment, online-produced dialy-sate, flexible scheduling, and lower costs) with those ofCRRT (e.g., better hemodynamic tolerance, excellent meta-bolic control, and gentle osmotic fluctuation and fluid re-moval capacity) (74,77–81).Despite shorter treatment duration, even with PIRRT,
anticoagulation of the extracorporeal circuit is often re-quired. The optimal strategy for anticoagulation duringPIRRT is still a matter of debate (13,82). Saline flushes
2180 Clinical Journal of the American Society of Nephrology

without a antihemostatic agent (81,83,84), unfractionedheparin (79,81,83,85), or prostacyclin (80) are among thedifferent options proposed thus far for the maintenance ofthe extracorporeal PIRRT circuit. Treatment interruptionbecause of circuit clotting is found in 26%–46% of caseswith saline flushes and 17%–26% of cases with standardheparin (500–1000 IU/h) (81,83,84). A 10% incidence ofcircuit interruption (one half for circuit coagulation) hasbeen reported when relatively low doses of epoprostenol,a synthetic analog of the antiaggregant and vasodilatoryprostacyclin PGI2, are used (80). In parallel to the expand-ing use of citrate as a regional anticoagulation method inCRRT, increasing interest has been devoted to the appli-cation of this anticoagulant strategy to PIRRT. Protocolsfor RCA have been proposed for PIRRT on the basis of theuse of different citrate solutions and the use of eitherCRRT or standard dialysis machines (86,87) (Table 1). Inone of these studies, in 30 patients undergoing 117 PIRRTsessions with citrate, treatment interruption caused by cir-cuit clotting never occurred, with an average treatmentduration of 6.7–7.3 h (86). However, the protocol requiredcalcium-free dialysis fluid and CaCl2 supplementation,with a stepwise titration protocol for both citrate and cal-cium administration (86). Recently, a simple RCA protocolfor PIRRT was proposed and validated in a single-institutionobservational study of 116 patients in the ICU with AKI whounderwent 807 PIRRT sessions (51). The protocol usedACD-A solution and standard dialysis equipment withmaintenance of blood calcium levels provided by calciumback-transport from calcium-containing dialysis fluid(1.25 mmol/L) (Figure 3). Interruptions of PIRRT caused
by impending/irreversible clotting were recorded in 19sessions (2.4%); blood restitution was complete in 98%of the cases. Major bleeding was observed in six patients(5.2% or 0.4 episodes per 100 person-days on PIRRT),with a hemorrhagic complication rate similar or even lowerto that reported in previous studies (4,5,70,71,88–91). Nocitrate accumulation was observed, even in patients withsevere liver dysfunction (51). Intravenous calcium for sys-temic hypocalcemia (ionized calcium levels,0.90 mmol/L)was needed during 28 treatment sessions (3.4%); however,in eight of 28 sessions, low ionized calcium was alreadypresent before starting PIRRT. Systemic coagulation of pa-tients remained unchanged, and metabolic/fluid controlwas easily achieved. These results suggest that simplifiedprotocols with commercially available citrate solutions al-low safe and effective RCA for PIRRT with limited labora-tory monitoring and without the need for systemic calciuminfusion in most patients.
RCA: Electrolyte Balance, Acid-Base Status, andEffects on Bone MetabolismDespite its recognized advantages, concerns about the
risk of electrolyte and acid-base disorders are probablyamong the main factors still precluding the more wide-spread use of RCA in critically ill patients undergoing RRT.Although reported issueswith citrate include hypernatremiaor hyponatremia, hypercalcemia or hypocalcemia, hyper-magnesemia or hypomagnesemia, and metabolic acidosis oralkalosis (Table 2), these complications are quite uncommonwhen strict adherence to the RCA protocol and accurate
Figure 3. | Schematic representation of a simplified regional citrate anticoagulation protocol for SLED using a calcium-containing dialysate.Detailed protocol is shown as supplemental material in ref. 51. *Sampling for systemic ionized calcium is from the circuit arterial line or thepatient’s arterial line (to avoid the effects of vascular access recirculation). Systemic total calcium can be measured from a central venous line.ACD-A, anticoagulant citrate dextrose solution A; SLED, sustained low-efficiency dialysis; Uf, ultrafiltration.
Clin J Am Soc Nephrol 9: 2173–2188, December, 2014 Regional Citrate Anticoagulation in Patients with AKI, Morabito et al. 2181
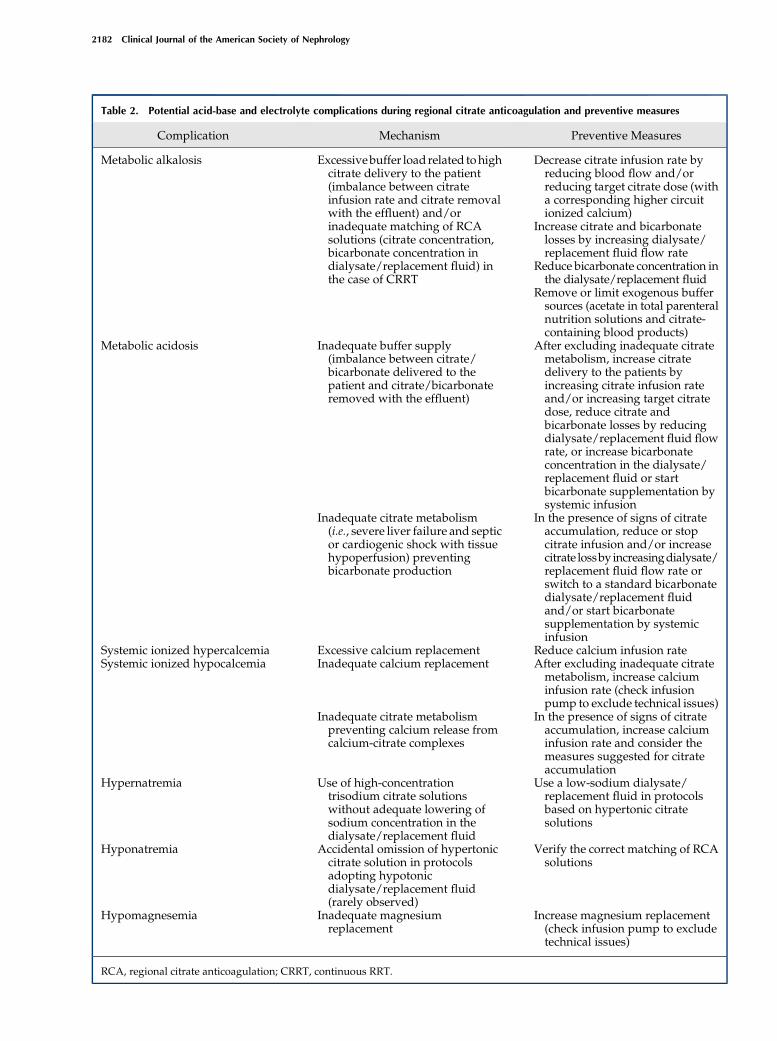
Table 2. Potential acid-base and electrolyte complications during regional citrate anticoagulation and preventive measures
Complication Mechanism Preventive Measures
Metabolic alkalosis Excessivebuffer load related tohighcitrate delivery to the patient(imbalance between citrateinfusion rate and citrate removalwith the effluent) and/orinadequate matching of RCAsolutions (citrate concentration,bicarbonate concentration indialysate/replacement fluid) inthe case of CRRT
Decrease citrate infusion rate byreducing blood flow and/orreducing target citrate dose (witha corresponding higher circuitionized calcium)
Increase citrate and bicarbonatelosses by increasing dialysate/replacement fluid flow rate
Reduce bicarbonate concentration inthe dialysate/replacement fluid
Remove or limit exogenous buffersources (acetate in total parenteralnutrition solutions and citrate-containing blood products)
Metabolic acidosis Inadequate buffer supply(imbalance between citrate/bicarbonate delivered to thepatient and citrate/bicarbonateremoved with the effluent)
After excluding inadequate citratemetabolism, increase citratedelivery to the patients byincreasing citrate infusion rateand/or increasing target citratedose, reduce citrate andbicarbonate losses by reducingdialysate/replacement fluid flowrate, or increase bicarbonateconcentration in the dialysate/replacement fluid or startbicarbonate supplementation bysystemic infusion
Inadequate citrate metabolism(i.e., severe liver failure and septicor cardiogenic shock with tissuehypoperfusion) preventingbicarbonate production
In the presence of signs of citrateaccumulation, reduce or stopcitrate infusion and/or increasecitrate lossby increasingdialysate/replacement fluid flow rate orswitch to a standard bicarbonatedialysate/replacement fluidand/or start bicarbonatesupplementation by systemicinfusion
Systemic ionized hypercalcemia Excessive calcium replacement Reduce calcium infusion rateSystemic ionized hypocalcemia Inadequate calcium replacement After excluding inadequate citrate
metabolism, increase calciuminfusion rate (check infusionpump to exclude technical issues)
Inadequate citrate metabolismpreventing calcium release fromcalcium-citrate complexes
In the presence of signs of citrateaccumulation, increase calciuminfusion rate and consider themeasures suggested for citrateaccumulation
Hypernatremia Use of high-concentrationtrisodium citrate solutionswithout adequate lowering ofsodium concentration in thedialysate/replacement fluid
Use a low-sodium dialysate/replacement fluid in protocolsbased on hypertonic citratesolutions
Hyponatremia Accidental omission of hypertoniccitrate solution in protocolsadopting hypotonicdialysate/replacement fluid(rarely observed)
Verify the correct matching of RCAsolutions
Hypomagnesemia Inadequate magnesiumreplacement
Increase magnesium replacement(check infusion pump to excludetechnical issues)
RCA, regional citrate anticoagulation; CRRT, continuous RRT.
2182 Clinical Journal of the American Society of Nephrology

monitoring of the procedure by an adequately trained staffare ensured (Table 3) (22,92).Hypernatremia represents a potential but rarely ob-
served complication related to the use of hypertonic solu-tions without low-sodium concentration dialysate and/orreplacement fluids (22,92). Calcium and magnesium imbal-ances are usually caused by effluent losses of both electro-lytes, mainly in the form of citrate complexes, not adequatelycounterbalanced by systemic supplementation (22,92).As previously discussed, alterations of ionized calciumlevels may also occur as a consequence of accumulation ofcalcium-citrate complexes in patients with impaired cit-rate metabolism. In this situation, increasing levels of totalserum calcium coexist with low systemic ionized calciumlevels, leading to high–calcium ratio values (10,54). Met-abolic acidosis may develop when impaired citrate metab-olism prevents bicarbonate generation or, alternatively,from an insufficient buffer supply. The latter may be re-lated to the suboptimal setting of RCA CRRT parametersand/or an inadequate combination of CRRT fluids result-ing in an imbalance between the amount of buffers (citrate/bicarbonate) delivered to the patients and the amount re-moved with the effluent fluid (Table 2). Conversely, meta-bolic alkalosis may develop when buffer overload is caused
by inappropriate setting of RCA parameters and/or inade-quate matching of RCA CRRT solutions (Table 2) (10,22). Inpatients receiving significant amounts of citrate-containingblood products, the exogenous citrate load may increase therisk of buffer overload and metabolic alkalosis and must betaken into account in the RCA protocol (10).The development of well designed RCA protocols, char-
acterized by a balanced combination of citrate and CRRTsolutions, facilitates the modulation of the buffer supplyaccording to clinical needs, minimizing the risk of acid-baseimbalances. For example, the combination of a highly con-centrated trisodium citrate solution (136 mmol/L) with acustomized low-bicarbonate dialysate (20 mmol/L) hasbeen successfully used for CVVHD (46). Acid-base andelectrolyte control was excellent in the majority of patients,and any occurrence of metabolic imbalances was rapidlycorrected by modifying either the dialysate or the bloodflow rate (46). An appropriate matching of citrate and CRRTsolutions is also required with the use of isotonic solutions.In a comparison between two different low-concentrationcitrate solutions in RCA CVVHDF, the use of a citrate con-centration of 23 mmol/L was frequently associated withmetabolic alkalosis, whereas a lower citrate concentration(18 mmol/L) provided more appropriate acid-base balance
Table 3. Monitoring of regional citrate anticoagulation for continuous RRT
Parameter Monitoring Intervals Aim
Circuit ionized calcium(postfilter)
Within 1 h from the start of thetreatment and then at leastevery 6–8 h
To evaluate the maintenance ofcircuit ionized calcium withinthe intended target and modifycitrate dose accordingly
Systemic ionized calcium Baseline (before starting RRT) To check baseline levels and setinitial calcium infusion rate
Within 1 h from the start of thetreatment and then at leastevery 4–6 h
To evaluate the maintenance ofsystemic ionized calciumwithin the physiologic rangeand modulate calcium infusionrate accordingly
Systemic total calcium At least every 12–24 h(simultaneous to systemicionized calcium)
To calculate calcium ratio (total-to-ionized systemic calcium) asan indirect index of citrateaccumulation ($2.5)
Acid-base parameters (pH andbicarbonate)a
Baseline (before starting RRT) To exclude acid-base imbalances(metabolic acidosis or alkalosis)and modify RCA and RRTparameters setting if needed
Within 1 h from the start of thetreatment and then at leastevery 4–6 h
Magnesium At least every 24 h To modulate the amount ofmagnesium supplementation ifneeded
Serum sodium Once daily To exclude hypernatremia orhyponatremia (rarely observedwith a correct matching of RCAsolutions)
Citratemia (if available) Not routinely used for clinicalpurposes
To confirm hypercitratemia in thepresence of indirect signs ofcitrate accumulation
Serum lactate Baseline (before starting RRT) To identify patients at higher riskfor citrate accumulation andmonitor lactate levels duringRCA
At least every 6–12 h or accordingto clinical needs
aSample drawn from an arterial line.
Clin J Am Soc Nephrol 9: 2173–2188, December, 2014 Regional Citrate Anticoagulation in Patients with AKI, Morabito et al. 2183

(62). In both cases, the target CRRT dose was 35 ml/kg perhour, and a lower than usual dialysate bicarbonate concen-tration (25 mmol/L) was adopted to optimize the buffersupply to the patient (62). Aside from fluid composition,citrate and dialysis dose may significantly affect acid-basestatus. Indeed, by adopting a lower target blood citrateconcentration (2.5–3 mmol/L) along with a CRRT doseof 30 ml/kg per hour, the above-mentioned 18-mmol/Lcitrate solution was successfully combined with a phosphate-containing dialysate/replacement fluid with a standard bi-carbonate concentration (30 mmol/L). This combinationafforded adequate acid-base control without the occurrenceof metabolic alkalosis. At the same time, it minimizedCRRT-related phosphate depletion (66,67). The use of alower-concentration isotonic citrate solution (12 or 13mmol/L) alone (predilution CVVH) (19,64) or combinedwith postdilution conventional replacement fluid (predilu-tion and postdilution CVVH) (14) may be associated with asuboptimal buffer supply, which is not easily balancedthrough the optimization of RCA settings and frequentlyrequires additional bicarbonate supplementation directly tothe patient.Abnormalities of parathyroid hormone (PTH) release
during RCA have been reported (93,94) and seem to bemainly related to calcium balance during RRT. In particu-lar, negative calcium balance during RCA CRRT seems tostimulate PTH release (93,95). Although the significance ofPTH secretion in this setting is still unclear, concerns aboutthe potential harmful effects on bone metabolism havebeen expressed (10). Indeed, recruitment of body calciumstores as compensation for negative calcium balance couldlead to severe bone reabsorption during prolonged RCACRRT, which was reported after discontinuation of calciumsupplementation in patients with immobilization-relatedhypercalcemia, possibly masked by calcium chelation duringRCA (96). Although additional investigations are required toestablish the most appropriate calcium substitution strate-gies, adequate calcium replacement aimed at avoiding epi-sodes of hypocalcemia should help prevent bone loss duringprolonged RCA (10,93). Strict maintenance of systemic ion-ized calcium within physiologic values has been shown toprevent a short-term increase in PTH levels in acutely illpatients on maintenance hemodialysis undergoing RCA(93). In addition to the potential effects of RCA on PTHlevels, other factors (i.e., immobilization, vitamin D defi-ciency, and cytokine effects) may negatively affect boneturnover rates in critically ill patients (10,93).
RCA Protocols Simplification: Future PerspectivesDespite positive reports about the safety and efficacy of
RCA, use of this alternative method of anticoagulation isstill relatively limited. The Beginning and Ending Support-ive Therapy for the Kidney study, an international surveyof RRT in critically ill patients involving 54 ICUs, reportedthe use of RCA in only about 10% of CRRT treatments (97).More recently, in the multicenter randomized VeteransAffairs/National Institutes of Health Acute Renal FailureTrial Network study, RCA was used in only 20% ofCVVHDF treatments (12). It is likely that many reasonslimit the widespread use of RCA: complexity of publishedprotocols, concerns about the risk of metabolic complications,
and lack of commercially available CRRT-specific citratesolutions and/or custom-designed dialysis equipment(98). However, the growing availability of dedicated com-mercial solutions (Figure 4), along with the introduction oftechnologically advanced CRRT equipment with inte-grated infusion systems and RCA-dedicated software,could help to simplify RCA delivery, improving the safetyof RCA and facilitating a more expanded use of citrate(46,99). In this regard, the use of mathematical modelsand the application of target-oriented algorithms specifi-cally developed for different RRT modalities (87,95,100–102) could provide an estimation of calcium balance duringRCA, allowing modulation of calcium infusion rates onthe basis of variations in treatment- and patient-relatedparameters (i.e., blood flow rate, citrate dose, hematocrit,albumin, and serum calcium). The latest generation ofCRRT equipment partially fulfills the characteristics re-quired for near-automated RCA by keeping the citratedose stable even when blood flow changes and adjustingcalcium replacement according to the estimated RCACRRT calcium balance (46,99). In particular, the initial cal-cium infusion rate as well as subsequent adjustmentscould be calculated according to RCA CRRT operationalparameters, taking into account the estimated calciumlosses with the effluent and the calcium supply possiblyderiving from the optional use of calcium-containingCRRT solutions.Finally, additional refinements of the composition of
RCA CRRT solutions could help minimize the need forsupplementation of calcium, magnesium, potassium, andphosphate, with the aim of simplifying RRT management.For example, the adoption of RCA protocols in whichpredilution citrate is combined with a calcium-containingdialysate and/or replacement fluid may reduce the calciuminfusion requirements and minimize the risks of errorsrelated to the handling of calcium-free solutions(14,51,66,67,103). These protocols seem to be able to pro-vide prolonged filter survival without any increase in ve-nous drip chamber clotting rates or the need to increasethe initial citrate dose (14,66,67). However, in any protocol,variations in operational parameters and calcium concen-tration in the CRRT solutions could significantly affect theneed for citrate dose adjustments.
Costs of RCAConcerns related to cost issues could represent another
potential drawback for a wider use of RCA. Currently,comparative data on the cost-effectiveness ratio of differ-ent anticoagulation methods for RRT in AKI are lacking(21). RCA could be more costly than heparin-based anti-coagulation because of the higher cost of citrate solutions(especially commercial solutions developed specificallyfor CRRT) and the need for more intensive monitoringof metabolic parameters (85). However, it is likely thatsavings related to both the lower incidence of bleedingcomplications and the lower frequency of circuit replace-ment could shift the balance toward RCA (104). Finally, inthe cost-benefit evaluation of RCA, indirect costs shouldbe taken into account, such as platelet and red cell trans-fusions, as well as the need for antithrombin-III supple-mentation (14).
2184 Clinical Journal of the American Society of Nephrology

ConclusionsIn conclusion, several studies on RCA use have docu-
mented prolonged filter survival associated with lowerbleeding risk and transfusion needs in critically ill patientswith AKI on RRT. On the basis of these results, the 2012KDIGO Clinical Practice Guidelines for Acute KidneyInjury recommended RCA as the preferred anticoagulation
modality in patients without contraindications for citrate(20). Recently, the Canadian Society of Nephrology com-mentary on these KDIGO guidelines endorsed this state-ment, suggesting the possibility of cautiously extendingRCA use in patients with relative contraindications for cit-rate (21). In this regard, the adoption of well designedRCA protocols, characterized by reduced citrate load and
Figure 4. | Composition of commercially available citrate and CRRT solutions for RCA. To design the appropriate RCA protocol (CVVHD,CVVH, CVVHDF), each citrate solution should be combined with the correctly matched dialysate and/or replacement fluid. Availability andtrade name of each solution may vary according to different countries. The list of commercially available citrate and CRRT solutions derivesfrom the more recently reported RCA protocols and could be partial. N/A, not applicable or not available.
Clin J Am Soc Nephrol 9: 2173–2188, December, 2014 Regional Citrate Anticoagulation in Patients with AKI, Morabito et al. 2185

careful monitoring, could permit safe delivery of RCA inpatients with severely impaired liver function and/orshock with tissue hypoperfusion (47,53,56–58). Moreover,although the incidence of metabolic and/or electrolyte dis-orders with RCA is low, operational parameters and com-binations of different CRRT solutions with either isotonicor hypertonic citrate formulations may significantly affectelectrolyte and buffer balance during RCA.Finally, the introduction of simplified protocols and the
development of RRT equipment with RCA-dedicated soft-ware couldminimize the risk of errors in RCA handling, thusimproving the safety of citrate use and facilitating a moreexpanded use of this highly effective anticoagulation mo-dality for RRT.
DisclosuresNone.
References1. Fiaccadori E, Maggiore U, Clima B,Melfa L, Rotelli C, Borghetti
A: Incidence, risk factors, and prognosis of gastrointestinalhemorrhage complicating acute renal failure. Kidney Int 59:1510–1519, 2001
2. Mehta RL: Anticoagulation during continuous renal re-placement therapy. ASAIO J 40: 931–935, 1994
3. van deWetering J,Westendorp RG, van der Hoeven JG, Stolk B,Feuth JD, Chang PC: Heparin use in continuous renal re-placement procedures: The struggle between filter coagulationand patient hemorrhage. J Am Soc Nephrol 7: 145–150, 1996
4. Ward DM, Mehta RL: Extracorporeal management of acute re-nal failure patients at high risk of bleeding. Kidney Int Suppl 41:S237–S244, 1993
5. Brophy PD, Somers MJ, Baum MA, Symons JM, McAfee N,Fortenberry JD, Rogers K, Barnett J, Blowey D, Baker C,Bunchman TE, Goldstein SL: Multi-centre evaluation of anti-coagulation in patients receiving continuous renal re-placement therapy (CRRT).Nephrol Dial Transplant 20: 1416–1421, 2005
6. Oudemans-van StraatenHM,Wester JP, de Pont AC, SchetzMR:Anticoagulation strategies in continuous renal replacementtherapy: Can the choice be evidence based? Intensive CareMed32: 188–202, 2006
7. Tolwani AJ, Wille KM: Anticoagulation for continuous renalreplacement therapy. Semin Dial 22: 141–145, 2009
8. Tan HK, Baldwin I, Bellomo R: Continuous veno-venous he-mofiltration without anticoagulation in high-risk patients. In-tensive Care Med 26: 1652–1657, 2000
9. Morabito S, Guzzo I, Solazzo A, Muzi L, Luciani R, Pierucci A:Continuous renal replacement therapies: Anticoagulation in thecritically ill at high risk of bleeding. J Nephrol 16: 566–571,2003
10. Oudemans-van Straaten HM, Ostermann M: Bench-to-bedsidereview: Citrate for continuous renal replacement therapy, fromscience to practice. Crit Care 16: 249, 2012
11. Tolwani A, Wille KM: Advances in continuous renal re-placement therapy: Citrate anticoagulation update. Blood Purif34: 88–93, 2012
12. Palevsky PM, Zhang JH, O’Connor TZ, Chertow GM, CrowleyST, Choudhury D, Finkel K, Kellum JA, Paganini E, Schein RM,Smith MW, Swanson KM, Thompson BT, Vijayan A, Watnick S,Star RA, Peduzzi P; VA/NIH Acute Renal Failure Trial Network:Intensity of renal support in critically ill patients with acutekidney injury. N Engl J Med 359: 7–20, 2008
13. Joannidis M, Oudemans-van Straaten HM: Clinical review:Patency of the circuit in continuous renal replacement therapy.Crit Care 11: 218, 2007
14. Morabito S, Pistolesi V, Tritapepe L, Zeppilli L, Polistena F,Strampelli E, Pierucci A: Regional citrate anticoagulation incardiac surgery patients at high risk of bleeding: A continuousveno-venous hemofiltration protocol with a low concentrationcitrate solution. Crit Care 16: R111, 2012
15. Monchi M, Berghmans D, Ledoux D, Canivet JL, Dubois B,Damas P: Citrate vs. heparin for anticoagulation in continuousvenovenous hemofiltration: A prospective randomized study.Intensive Care Med 30: 260–265, 2004
16. Kutsogiannis DJ, Gibney RT, Stollery D, Gao J: Regional citrateversus systemic heparin anticoagulation for continuous renalreplacement in critically ill patients. Kidney Int 67: 2361–2367,2005
17. Betjes MG, van OosteromD, van AgterenM, van deWetering J:Regional citrate versus heparin anticoagulation duringvenovenous hemofiltration in patients at low risk for bleeding:Similar hemofilter survival but significantly less bleeding.J Nephrol 20: 602–608, 2007
18. Oudemans-van Straaten HM, Bosman RJ, KoopmansM, van derVoort PH, Wester JP, van der Spoel JI, Dijksman LM, ZandstraDF: Citrate anticoagulation for continuous venovenous hemo-filtration. Crit Care Med 37: 545–552, 2009
19. HetzelGR, SchmitzM,WissingH, RiesW, SchottG,Heering PJ,Isgro F, Kribben A, Himmele R, Grabensee B, Rump LC: Re-gional citrate versus systemic heparin for anticoagulation incritically ill patients on continuous venovenous haemofiltra-tion: A prospective randomized multicentre trial. Nephrol DialTransplant 26: 232–239, 2011
20. Kidney Disease: Improving Global Outcomes (KDIGO) AcuteKidney InjuryWork Group: KDIGOClinical Practice Guidelinefor Acute Kidney Injury. Kidney Int [Suppl 2]: 1–138, 2012
21. James M, Bouchard J, Ho J, Klarenbach S, LaFrance JP, RigattoC, Wald R, Zappitelli M, Pannu N: Canadian Society of Ne-phrology commentary on the 2012 KDIGO clinical practiceguideline for acute kidney injury. Am J Kidney Dis 61: 673–685, 2013
22. Davenport A, Tolwani A: Citrate anticoagulation for continuousrenal replacement therapy (CRRT) in patients with acute kidneyinjury admitted to the intensive care unit.NDTPlus 2: 439–447,2009
23. Abramson S, Niles JL: Anticoagulation in continuous renal re-placement therapy. Curr Opin Nephrol Hypertens 8: 701–707,1999
24. Bohler J, Schollmeyer P, Dressel B, Dobos G, Horl WH: Re-duction of granulocyte activation during hemodialysis with re-gional citrate anticoagulation: Dissociation of complementactivation and neutropenia from neutrophil degranulation. J AmSoc Nephrol 7: 234–241, 1996
25. Bos JC, Grooteman MP, van Houte AJ, Schoorl M, van LimbeekJ, Nube MJ: Low polymorphonuclear cell degranulation duringcitrate anticoagulation: A comparison between citrate andheparin dialysis.NephrolDial Transplant 12: 1387–1393, 1997
26. Dhondt A, Vanholder R, Tielemans C, Glorieux G, WaterloosMA, De Smet R, Lameire N: Effect of regional citrate anti-coagulation on leukopenia, complement activation, and ex-pression of leukocyte surface molecules during hemodialysiswith unmodified cellulose membranes.Nephron 85: 334–342,2000
27. Gabutti L, Ferrari N, Mombelli G, Keller F, Marone C: The fa-vorable effect of regional citrate anticoagulation on interleukin-1beta release is dissociated frombothcoagulationandcomplementactivation. J Nephrol 17: 819–825, 2004
28. Gritters M, Grooteman MP, Schoorl M, Schoorl M, Bartels PC,Scheffer PG, Teerlink T, Schalkwijk CG, Spreeuwenberg M,Nube MJ: Citrate anticoagulation abolishes degranulation ofpolymorphonuclear cells and platelets and reduces oxidativestress during haemodialysis. Nephrol Dial Transplant 21: 153–159, 2006
29. Schilder L, Nurmohamed SA, ter Wee PM, Paauw NJ, GirbesAR, Beishuizen A, Beelen RH, Groeneveld AB: Citrate confersless filter-induced complement activation and neutrophil de-granulation than heparin when used for anticoagulation duringcontinuous venovenous haemofiltration in critically ill patients.BMC Nephrol 15: 19, 2014
30. Bryland A, Wieslander A, Carlsson O, Hellmark T, Godaly G:Citrate treatment reduces endothelial death and inflammationunder hyperglycaemic conditions.Diab Vasc Dis Res 9: 42–51,2012
31. Iacobazzi V, Infantino V: Citrate - new functions for an oldmetabolite. Biol Chem 395: 387–399, 2014
2186 Clinical Journal of the American Society of Nephrology

32. Oudemans-van Straaten HM, Kellum JA, Bellomo R: Clinicalreview: Anticoagulation for continuous renal replacementtherapy—heparin or citrate? Crit Care 15: 202, 2011
33. Swartz R, Pasko D, O’Toole J, Starmann B: Improving the de-livery of continuous renal replacement therapy using regionalcitrate anticoagulation. Clin Nephrol 61: 134–143, 2004
34. Mariano F, Morselli M, Bergamo D, Hollo Z, Scella S, Maio M,Tetta C, Dellavalle A, Stella M, Triolo G: Blood and ultrafiltratedosage of citrate as a useful and routine tool during continuousvenovenous haemodiafiltration in septic shock patients.Nephrol Dial Transplant 26: 3882–3888, 2011
35. White RD, Goldsmith RS, Rodriguez R, Moffitt EA, Pluth JR:Plasma ionic calcium levels following injection of chloride,gluconate, and gluceptate salts of calcium. J Thorac CardiovascSurg 71: 609–613, 1976
36. Martin TJ, Kang Y, Robertson KM, Virji MA, Marquez JM: Ioni-zation and hemodynamic effects of calcium chloride and cal-cium gluconate in the absence of hepatic function.Anesthesiology 73: 62–65, 1990
37. MorganDJ, Ho KM: Profound hypocalcaemia in a patient beinganticoagulated with citrate for continuous renal replacementtherapy. Anaesthesia 64: 1363–1366, 2009
38. Vanholder R, Sever MS, Erek E, Lameire N: Rhabdomyolysis.J Am Soc Nephrol 11: 1553–1561, 2000
39. BrainM, Anderson M, Parkes S, Fowler P: Magnesium flux duringcontinuous venovenous haemodiafiltration with heparin and cit-rate anticoagulation. Crit Care Resusc 14: 274–282, 2012
40. Kramer L, Bauer E, Joukhadar C, Strobl W, Gendo A, Madl C,Gangl A: Citrate pharmacokinetics and metabolism in cirrhoticand noncirrhotic critically ill patients. Crit Care Med 31: 2450–2455, 2003
41. Zheng Y, Xu Z, Zhu Q, Liu J, Qian J, You H, Gu Y, Hao C, Jiao Z,Ding F: Citrate pharmacokinetics in critically ill patients withacute kidney injury. PLoS ONE 8: e65992, 2013
42. Balik M, Zakharchenko M, Leden P, Otahal M, Hruby J, Polak F,RusinovaK, StachZ, TokarikM,Vavrova J, Jabor A,Oudemans-vanStraaten HM: Bioenergetic gain of citrate anticoagulated continu-ous hemodiafiltration—a comparison between 2 citratemodalitiesand unfractionated heparin. J Crit Care 28: 87–95, 2013
43. Fiaccadori E, Regolisti G, Maggiore U: Specialized nutritionalsupport interventions in critically ill patients on renal re-placement therapy. Curr Opin Clin Nutr Metab Care 16: 217–224, 2013
44. Meier-Kriesche HU, Gitomer J, Finkel K, DuBose T: Increasedtotal to ionized calcium ratio during continuous venovenoushemodialysis with regional citrate anticoagulation. Crit CareMed 29: 748–752, 2001
45. Khadzhynov D, Schelter C, Lieker I, Mika A, Staeck O,Neumayer HH, Peters H, Slowinski T: Incidence and out-come of metabolic disarrangements consistent with citrateaccumulation in critically ill patients undergoing continuousvenovenous hemodialysiswith regional citrate anticoagulation.J Crit Care 29: 265–271, 2014
46. Morgera S, Schneider M, Slowinski T, Vargas-Hein O,Zuckermann-Becker H, Peters H, Kindgen-Milles D, NeumayerHH: A safe citrate anticoagulation protocol with variabletreatment efficacy and excellent control of the acid-base status.Crit Care Med 37: 2018–2024, 2009
47. Mariano F, Tedeschi L, Morselli M, Stella M, Triolo G: Normalcitratemia and metabolic tolerance of citrate anticoagulationfor hemodiafiltration in severe septic shock burn patients. In-tensive Care Med 36: 1735–1743, 2010
48. Link A, Klingele M, Speer T, Rbah R, Poss J, Lerner-Graber A,Fliser D, Bohm M: Total-to-ionized calcium ratio predictsmortality in continuous renal replacement therapy with citrateanticoagulation in critically ill patients.Crit Care 16: R97, 2012
49. Kalb R, Kram R, Morgera S, Slowinski T, Kindgen-Milles D:Regional citrate anticoagulation for high volume continuousvenovenous hemodialysis in surgical patients with high bleed-ing risk. Ther Apher Dial 17: 202–212, 2013
50. Nurmohamed SA, Jallah BP, Vervloet MG, Yldirim G, ter WeePM, Groeneveld AB: Continuous venovenous haemofiltrationwith citrate-buffered replacement solution is safe and effica-cious in patients with a bleeding tendency: A prospective ob-servational study. BMC Nephrol 14: 89, 2013
51. Fiaccadori E, Regolisti G, Cademartiri C, Cabassi A, Picetti E,Barbagallo M, Gherli T, Castellano G, Morabito S, Maggiore U:Efficacy and safety of a citrate-based protocol for sustained low-efficiency dialysis in AKI using standard dialysis equipment.Clin J Am Soc Nephrol 8: 1670–1678, 2013
52. Meier-Kriesche HU, Finkel KW, Gitomer JJ, DuBose TD Jr.:Unexpected severe hypocalcemiaduring continuous venovenoushemodialysis with regional citrate anticoagulation. Am J KidneyDis 33: e8, 1999
53. Schultheiß C, Saugel B, Phillip V, Thies P, Noe S, Mayr U, HallerB, Einwachter H, Schmid RM, Huber W: Continuous venove-nous hemodialysis with regional citrate anticoagulation in pa-tients with liver failure: A prospective observational study. CritCare 16: R162, 2012
54. Hetzel GR, Taskaya G, Sucker C, Hennersdorf M, Grabensee B,Schmitz M: Citrate plasma levels in patients under regionalanticoagulation in continuous venovenous hemofiltration.Am JKidney Dis 48: 806–811, 2006
55. Bakker AJ, Boerma EC, Keidel H, Kingma P, van der Voort PH:Detection of citrate overdose in critically ill patients on citrate-anticoagulated venovenous haemofiltration: Use of ionisedand total/ionised calcium. Clin Chem Lab Med 44: 962–966,2006
56. Faybik P, Hetz H, Mitterer G, Krenn CG, Schiefer J, Funk GC,Bacher A: Regional citrate anticoagulation in patients with liverfailure supported by a molecular adsorbent recirculating sys-tem. Crit Care Med 39: 273–279, 2011
57. Saner FH, Treckmann JW,Geis A, LoschC,WitzkeO,CanbayA,Herget-Rosenthal S, KribbenA, Paul A, FeldkampT: Efficacyandsafety of regional citrate anticoagulation in liver transplant pa-tients requiring post-operative renal replacement therapy.Nephrol Dial Transplant 27: 1651–1657, 2012
58. Meijers B, Laleman W, Vermeersch P, Nevens F, Wilmer A,Evenepoel P: A prospective randomized open-label crossovertrial of regional citrate anticoagulation vs. anticoagulation freeliver dialysis by the Molecular Adsorbents Recirculating Sys-tem. Crit Care 16: R20, 2012
59. Bouchard J, Madore F: Role of citrate and other methods ofanticoagulation in patients with severe liver failure requiringcontinuous renal replacement therapy. NDT Plus 2: 11–19,2009
60. Morita Y, Johnson RW, Dorn RE, Hall DS: Regional anti-coagulation during hemodialysis using citrate. Am J Med Sci242: 32–43, 1961
61. Mehta RL, McDonald BR, Aguilar MM, Ward DM: Regionalcitrate anticoagulation for continuous arteriovenous hemodi-alysis in critically ill patients. Kidney Int 38: 976–981, 1990
62. Tolwani AJ, Prendergast MB, Speer RR, Stofan BS, Wille KM: Apractical citrate anticoagulation continuous venovenous he-modiafiltration protocol for metabolic control and high soluteclearance. Clin J Am Soc Nephrol 1: 79–87, 2006
63. Cubattoli L, Teruzzi M, Cormio M, Lampati L, Pesenti A: Citrateanticoagulation during CVVH in high risk bleeding patients. IntJ Artif Organs 30: 244–252, 2007
64. Shum HP, Chan KC, Yan WW: Regional citrate anticoagulationin predilution continuous venovenous hemofiltration usingprismocitrate 10/2 solution. Ther Apher Dial 16: 81–86, 2012
65. Morabito S, Pistolesi V, Tritapepe L, Zeppilli L, Polistena F,Fiaccadori E, Pierucci A: Regional citrate anticoagulation inCVVH: A new protocol combining citrate solution with aphosphate-containing replacement fluid. Hemodial Int 17:313–320, 2013
66. Morabito S, Pistolesi V, Tritapepe L, Vitaliano E, Zeppilli L,Polistena F, Fiaccadori E, Pierucci A: Continuous venovenoushemodiafiltration with a low citrate dose regional anti-coagulation protocol and a phosphate-containing solution: Ef-fects on acid-base status and phosphate supplementationneeds. BMC Nephrol 14: 232, 2013
67. Morabito S, Pistolesi V, Tritapepe L, Vitaliano E, Zeppilli L,Polistena F, Fiaccadori E, Pierucci A: Continuous veno-venoushemofiltration using a phosphate-containing replacement fluidin the setting of regional citrate anticoagulation. Int J Artif Or-gans 36: 845–852, 2013
68. Tobe SW, Aujla P, Walele AA, Oliver MJ, Naimark DM, PerkinsNJ, Beardsall M: A novel regional citrate anticoagulation
Clin J Am Soc Nephrol 9: 2173–2188, December, 2014 Regional Citrate Anticoagulation in Patients with AKI, Morabito et al. 2187

protocol for CRRTusing only commercially available solutions.J Crit Care 18: 121–129, 2003
69. Munjal S, Ejaz AA: Regional citrate anticoagulation in contin-uous venovenous haemofiltration using commercial prepara-tions. Nephrology (Carlton) 11: 405–409, 2006
70. Zhang Z, Hongying N: Efficacy and safety of regional citrateanticoagulation in critically ill patients undergoing continuousrenal replacement therapy. Intensive CareMed 38: 20–28, 2012
71. Wu MY, Hsu YH, Bai CH, Lin YF, Wu CH, Tam KW: Regionalcitrate versus heparin anticoagulation for continuous renal re-placement therapy: A meta-analysis of randomized controlledtrials. Am J Kidney Dis 59: 810–818, 2012
72. Fliser D, Kielstein JT: Technology insight: Treatment of renalfailure in the intensive care unit with extended dialysis.Nat ClinPract Nephrol 2: 32–39, 2006
73. Mariano F, Pozzato M, Canepari G, Vitale C, Bermond F, SaccoC, Amore A, Manes M, Navino C; Piedmont and Aosta ValleySection of Italian Society of Nephrology: Renal replacementtherapy in intensive care units: A survey of nephrologicalpractice in northwest Italy. J Nephrol 24: 165–176, 2011
74. Marshall MR, Golper TA: Low-efficiency acute renal re-placement therapy: Role in acute kidney injury. Semin Dial 24:142–148, 2011
75. Marshall MR, Creamer JM, Foster M, Ma TM, Mann SL,Fiaccadori E, Maggiore U, Richards B,Wilson VL,Williams AB,Rankin AP: Mortality rate comparison after switching fromcontinuous to prolonged intermittent renal replacement foracute kidney injury in three intensive care units from differentcountries. Nephrol Dial Transplant 26: 2169–2175, 2011
76. Schwenger V, Weigand MA, Hoffmann O, Dikow R, Kihm LP,Seckinger J, Miftari N, Schaier M, Hofer S, Haar C, Nawroth PP,Zeier M, Martin E, Morath C: Sustained low efficiency dialysisusing a single-pass batch system in acute kidney injury - a ran-domized interventional trial: The REnal Replacement TherapyStudy in Intensive Care Unit PatiEnts. Crit Care 16: R140, 2012
77. FieghenHE, Friedrich JO, Burns KE,NisenbaumR, AdhikariNK,Hladunewich MA, Lapinsky SE, Richardson RM, Wald R; Uni-versity of Toronto Acute Kidney Injury Research Group: Thehemodynamic tolerability and feasibility of sustained low effi-ciency dialysis in the management of critically ill patients withacute kidney injury. BMC Nephrol 11: 32, 2010
78. Kron J, Kron S, Wenkel R, Schuhmacher HU, Thieme U,Leimbach T, Kern H, Neumayer HH, Slowinski T: Extendeddaily on-line high-volume haemodiafiltration in septic multipleorgan failure: Awell-tolerated and feasible procedure.NephrolDial Transplant 27: 146–152, 2012
79. Kielstein JT, Kretschmer U, Ernst T, Hafer C, Bahr MJ, Haller H,Fliser D: Efficacy and cardiovascular tolerability of extendeddialysis in critically ill patients: A randomized controlled study.Am J Kidney Dis 43: 342–349, 2004
80. Fiaccadori E, MaggioreU, Parenti E, Giacosa R, Picetti E, RotelliC, Tagliavini D, Cabassi A: Sustained low-efficiency dialysis(SLED)with prostacyclin in critically ill patientswith acute renalfailure. Nephrol Dial Transplant 22: 529–537, 2007
81. Marshall MR, Golper TA, Shaver MJ, Alam MG, Chatoth DK:Sustained low-efficiency dialysis for critically ill patients re-quiring renal replacement therapy. Kidney Int 60: 777–785,2001
82. Oudemans-Van Straaten HM: Review and guidelines for re-gional anticoagulation with citrate in continuous hemofiltra-tion. Neth J Crit Care 8: 146–156, 2004
83. Kumar VA, Craig M, Depner TA, Yeun JY: Extended daily di-alysis: A new approach to renal replacement for acute renalfailure in the intensive care unit. Am J Kidney Dis 36: 294–300,2000
84. Marshall MR, Ma T, Galler D, Rankin AP, Williams AB: Sus-tained low-efficiency daily diafiltration (SLEDD-f) for criticallyill patients requiring renal replacement therapy: Towards anadequate therapy. Nephrol Dial Transplant 19: 877–884, 2004
85. Berbece AN, Richardson RM: Sustained low-efficiency dialysisin the ICU: Cost, anticoagulation, and solute removal. KidneyInt 70: 963–968, 2006
86. Clark JA, Schulman G, Golper TA: Safety and efficacy of re-gional citrate anticoagulation during 8-hour sustained low-efficiency dialysis. Clin J Am Soc Nephrol 3: 736–742, 2008
87. Szamosfalvi B, Frinak S, Yee J: Automated regional citrate an-ticoagulation: Technological barriers and possible solutions.Blood Purif 29: 204–209, 2010
88. Fiaccadori E, Lombardi M, Leonardi S, Rotelli CF, Tortorella G,Borghetti A: Prevalence and clinical outcome associated withpreexisting malnutrition in acute renal failure: A prospectivecohort study. J Am Soc Nephrol 10: 581–593, 1999
89. Ronco C, Bellomo R, Homel P, Brendolan A, DanM, Piccinni P,La Greca G: Effects of different doses in continuous veno-venous haemofiltration on outcomes of acute renal failure:A prospective randomised trial. Lancet 356: 26–30, 2000
90. Schiffl H, Lang SM, Fischer R: Daily hemodialysis and the out-come of acute renal failure. N Engl J Med 346: 305–310, 2002
91. Bouman CS, Oudemans-Van Straaten HM, Tijssen JG, ZandstraDF, Kesecioglu J: Effects of early high-volume continuousvenovenous hemofiltration on survival and recovery of renalfunction in intensive care patients with acute renal failure: A pro-spective, randomized trial. Crit Care Med 30: 2205–2211, 2002
92. Fall P, Szerlip HM: Continuous renal replacement therapy:Cause and treatment of electrolyte complications. Semin Dial23: 581–585, 2010
93. Apsner R, Gruber D, Horl WH, Sunder-Plassmann G: Para-thyroid hormone secretion during citrate anticoagulated he-modialysis in acutely ill maintenance hemodialysis patients.Anesth Analg 99: 1199–1204, 2004
94. van der Voort PH, Postma SR, KingmaWP, Boerma EC, de HeideLJ, Bakker AJ: An observational study on the effects of nadroparin-based andcitrate-based continuous venovenous hemofiltrationoncalcium metabolism. Blood Purif 25: 267–273, 2007
95. Brain M, Parkes S, Fowler P, Robertson I, Brown A: Calcium fluxin continuous venovenous haemodiafiltration with heparin andcitrate anticoagulation. Crit Care Resusc 13: 72–81, 2011
96. Wang PL, Meyer MM, Orloff SL, Anderson S: Bone resorptionand “relative” immobilization hypercalcemia with prolongedcontinuous renal replacement therapy and citrate anti-coagulation. Am J Kidney Dis 44: 1110–1114, 2004
97. Uchino S, Bellomo R,Morimatsu H,Morgera S, SchetzM, Tan I,Bouman C, Macedo E, Gibney N, Tolwani A, Oudemans-vanStraaten H, Ronco C, Kellum JA: Continuous renal replacementtherapy: A worldwide practice survey. The beginning and end-ing supportive therapy for the kidney (B.E.S.T. kidney) inves-tigators. Intensive Care Med 33: 1563–1570, 2007
98. Morabito S, Pistolesi V, Pierucci A: Regional citrate anti-coagulation: Towards a first-choice treatment. G Ital Nefrol 29:14–19, 2012
99. Liet JM, Allain-Launay E, Gaillard-Leroux B, Barriere F,Chenouard A, Dejode JM, Joram N: Regional citrate anti-coagulation for pediatric CRRTusing integrated citrate softwareand physiological sodium concentration solutions [publishedonline ahead of print February 15, 2014]. Pediatr Nephrol10.1007/s00467-014-2770-2
100. Thijssen S, Kruse A, Raimann J, Bhalani V, LevinNW, Kotanko P:A mathematical model of regional citrate anticoagulation inhemodialysis. Blood Purif 29: 197–203, 2010
101. Brandl M, Strobl K, Hartmann J, Kellner K, Posnicek T,Falkenhagen D: A target-orientated algorithm for regionalcitrate-calcium anticoagulation in extracorporeal therapies.Blood Purif 33: 7–20, 2012
102. Strobl K, Hartmann J, Wallner M, Brandl M, Falkenhagen D: Atarget-oriented algorithm for citrate-calcium anticoagulation inclinical practice. Blood Purif 36: 136–145, 2013
103. Gupta M, Wadhwa NK, Bukovsky R: Regional citrate anti-coagulation for continuous venovenous hemodiafiltration usingcalcium-containing dialysate.Am J KidneyDis 43: 67–73, 2004
104. Park JS, Kim GH, Kang CM, Lee CH: Regional anticoagulationwith citrate is superior to systemic anticoagulation with heparinin critically ill patients undergoing continuous venovenoushemodiafiltration. Korean J Intern Med 26: 68–75, 2011
105. Morgera S, Scholle C, Melzer C, Slowinski T, Liefeld L, BaumannG, Peters H, Neumayer HH: A simple, safe and effective citrateanticoagulation protocol for the genius dialysis system in acuterenal failure. Nephron Clin Pract 98: c35–c40, 2004
Published online ahead of print. Publication date available at www.cjasn.org.
2188 Clinical Journal of the American Society of Nephrology


!["Ételnek idején, aki mely asztalhoz rendeltetett, oda menjen". [In] 2000 19 (2007) 8. sz. 12-20](https://img.pdfslide.net/doc/110x75/6344284aeb730715bb0e191a/etelnek-idejen-aki-mely-asztalhoz-rendeltetett-oda-menjen-in-2000-19-2007.jpg)


























