Embed Size (px)
Citation preview
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
1
Rehabilitation following UCL Rehabilitation following UCL Reconstruction/Repair in
AthletesKevin E. Wilk, PT, DPT,FAPTA
Kevin E Wilk, PT, DPT,FAPTA2017 Injuries in Football
Faculty Disclosure:• Theralase Laser – Medical Advisory Board
• LiteCure Laser – Consultant
• AlterG – Medical Advisory Board
• Intelliskin USA – Medical Advisory Board
• Zetroz Medical – Medical Advisory Brd
• Throw Like A Pro – Co-Owner
• Dr PRP – Rehab Advisor
• Educational Grants:
» Empi Medical
» Joint Active System
» ERMI
» Bauerfeind Brace
• Book Royalties:
» CV Mosby, Lippincott, Human Kinetics
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
2
American Sports Medicine InstituteBirmingham, Alabama
asmi.org
Elbow Injuries in SportsIntroduction
• Number of elbow injuries
appear to be increasing
• Repetitive high forces –
overhead athlete
�22% of all baseball injuries
• Macrotraumatic forces –dislocation / fractures / tears
• Thrower’s “not all or none”
Rehabilitation Program Must Be Specific For Each Type of Athlete
Elbow Dislocation
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
3
J Sports Health ‘12 J Sports Health ‘12
UCL Rehabilitation Rehab Plan
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
4
Beckett et al: AJSM ‘14
• Assessment of scapular & hip joint
in preadolescent (7-12 yrs) &
adolescent (13-18 yrs) in baseball
players
�High rate of scapular dyskinesis in
adolescent players compared to
pre-adolescent
�Also poor single leg squat test
�Higher coracoid process distance
– correlated to dyskinesis
UCL RECONSTRUCTION REHABLower Extremity Strengthening
UCL RECONSTRUCTION REHABLower Extremity Strengthening Linking UE & LE
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
5
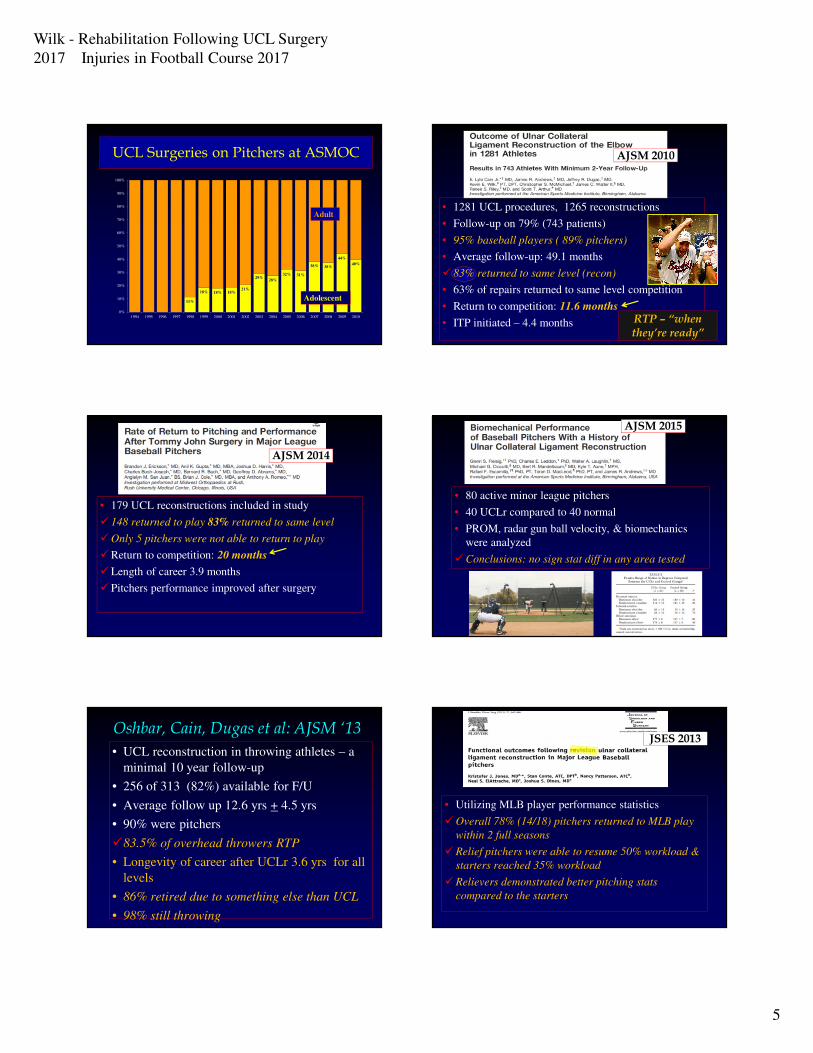
11%
18% 18% 18%21%
29%28%
32% 31%
38% 38%
44%
40%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
UCL Surgeries on Pitchers at ASMOC
Adolescent
Adult• 1281 UCL procedures, 1265 reconstructions
• Follow-up on 79% (743 patients)
• 95% baseball players ( 89% pitchers)
• Average follow-up: 49.1 months
� 83% returned to same level (recon)
• 63% of repairs returned to same level competition
• Return to competition: 11.6 months
• ITP initiated – 4.4 months
AJSM 2010
RTP – “when they’re ready”
• 179 UCL reconstructions included in study
� 148 returned to play 83% returned to same level
�Only 5 pitchers were not able to return to play
�Return to competition: 20 months
�Length of career 3.9 months
� Pitchers performance improved after surgery
AJSM 2014
• 80 active minor league pitchers
• 40 UCLr compared to 40 normal
• PROM, radar gun ball velocity, & biomechanics
were analyzed
�Conclusions: no sign stat diff in any area tested
AJSM 2015
Oshbar, Cain, Dugas et al: AJSM ‘13
• UCL reconstruction in throwing athletes – a
minimal 10 year follow-up
• 256 of 313 (82%) available for F/U
• Average follow up 12.6 yrs + 4.5 yrs
• 90% were pitchers
�83.5% of overhead throwers RTP
• Longevity of career after UCLr 3.6 yrs for all
levels
• 86% retired due to something else than UCL
• 98% still throwing
• Utilizing MLB player performance statistics
�Overall 78% (14/18) pitchers returned to MLB play
within 2 full seasons
�Relief pitchers were able to resume 50% workload &
starters reached 35% workload
�Relievers demonstrated better pitching stats
compared to the starters
JSES 2013

Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
6
Fleisig, Bolt, Fortenbaugh, Wilk: JOSPT ‘11
• 17 healthy college pitchers
• Biomechanical analysis of long & short throwing
• Threw 18.4m , 37m, 55m & maximal distance on a
line
• Shoulder line was horizontal for mound distance but
gradually went uphill as distance increased
�Maximal throwing distance resulted in more ER,
more Elb Flexion, more shoulder IR torque & more
varus elbow torque
• Trunk tilt gradually increased with distance
Biomechanics change with increase distance
Interval Throwing Programs
�Go slow
�Don’t be in a big hurry
�Stay at reasonable distances
�Crow Hop – use your legs
�Watch mechanics
�Watch mechanics
�Slow to go off mound
�Don’t throw high velocity or distance –until ready
UCL ReconstructionReturn to Play & PerformanceVitale & Ahmad: AJSM ‘08
• Systematic review of UCLr in overhead athletes
� 83% excellent result
• 10% complication rate
• Muscle splitting,decr handling UN, & docking improved outcomes
• 41 MLB pitchers underwent UCL reconstruction – pair
matched group
• 8 did not return to MLB play
• No sign change in velocity following UCL
• No sign diff in innings pitched, ERA, walks, SO etc
• No sign diff in UCL group
Jiang & Leland: AJSM ‘14
Elbow Injuries in BaseballUCL Surgeries – Conte, Wilk: AJSM ‘15
�Surveyed all Minor League Baseball Players
�4,052 respondents (2,145 pitchers)
�29/30 teams responded
�100% responses in 29 teams
�331 players had UCLr (8%)
�Pitchers: 300/2145 (14%)
�Position players: 31/1907 (2%)
�Avg age at time of surgery 21
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
7
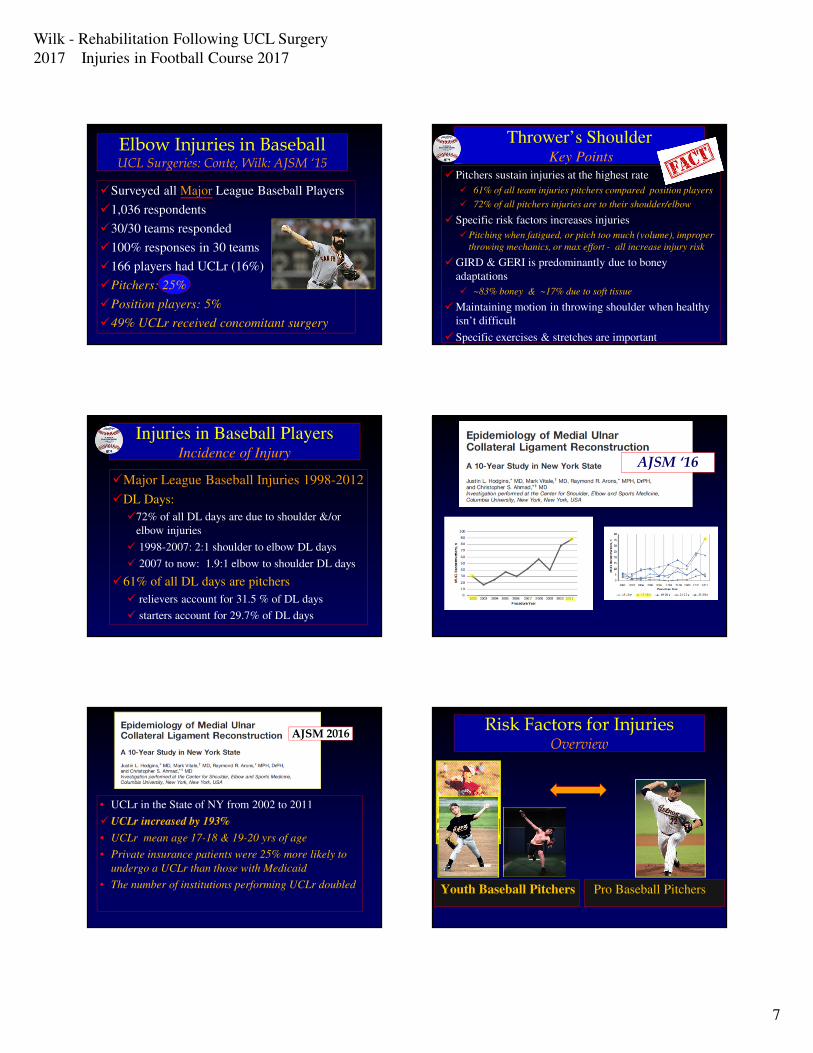
Elbow Injuries in BaseballUCL Surgeries: Conte, Wilk: AJSM ‘15
�Surveyed all Major League Baseball Players
�1,036 respondents
�30/30 teams responded
�100% responses in 30 teams
�166 players had UCLr (16%)
�Pitchers: 25%
�Position players: 5%
�49% UCLr received concomitant surgery
Thrower’s ShoulderKey Points
� Pitchers sustain injuries at the highest rate
� 61% of all team injuries pitchers compared position players
� 72% of all pitchers injuries are to their shoulder/elbow
� Specific risk factors increases injuries
�Pitching when fatigued, or pitch too much (volume), improper
throwing mechanics, or max effort - all increase injury risk
�GIRD & GERI is predominantly due to boney
adaptations
� ~83% boney & ~17% due to soft tissue
�Maintaining motion in throwing shoulder when healthy
isn’t difficult
� Specific exercises & stretches are important
Injuries in Baseball PlayersIncidence of Injury
�Major League Baseball Injuries 1998-2012
�DL Days:
�72% of all DL days are due to shoulder &/or
elbow injuries
� 1998-2007: 2:1 shoulder to elbow DL days
� 2007 to now: 1.9:1 elbow to shoulder DL days
�61% of all DL days are pitchers
� relievers account for 31.5 % of DL days
� starters account for 29.7% of DL days
AJSM ‘16
• UCLr in the State of NY from 2002 to 2011
�UCLr increased by 193%
• UCLr mean age 17-18 & 19-20 yrs of age
• Private insurance patients were 25% more likely to
undergo a UCLr than those with Medicaid
• The number of institutions performing UCLr doubled
AJSM 2016Risk Factors for Injuries
Overview
Youth Baseball Pitchers Pro Baseball Pitchers
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
8
�Pitching when fatigued
�Pitching too many innings/year
�Not enough rest from throwing at end season
�Too many pitches in game, week, year
�Pitching consecutive days
�Poor pitching or throwing mechanics
�Playing on multiple teams, leagues
Youth Baseball PlayerRisk Factors
Don’t Throw When Fatigued !�Excessive throwing when not pitching
�Throwing curveballs or sliders
�Too much Pitching
� Improper conditioning
� Not following proper conditioning guidelines
� Not following safe practice guidelines at
showcases
� Too much throwing with not enough rest !
Youth Baseball PlayerRisk Factors
Don’t Rush Through the Interval Throwing Program
� Pitching at maximum effort
“ too many pitches at 100% effort”
�Excessive retrotorsion
“excessive ER – increases velocity”
� Pitching too many innings
“over utilization”
� Pitching when fatigued
“alteration in normal throwing mechanics”
� Pitching beyond the player’s capabilities
“types of pitches, velocity, innings, reliever vs”
Elite Baseball PitcherRisk Factors for Injury
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
9
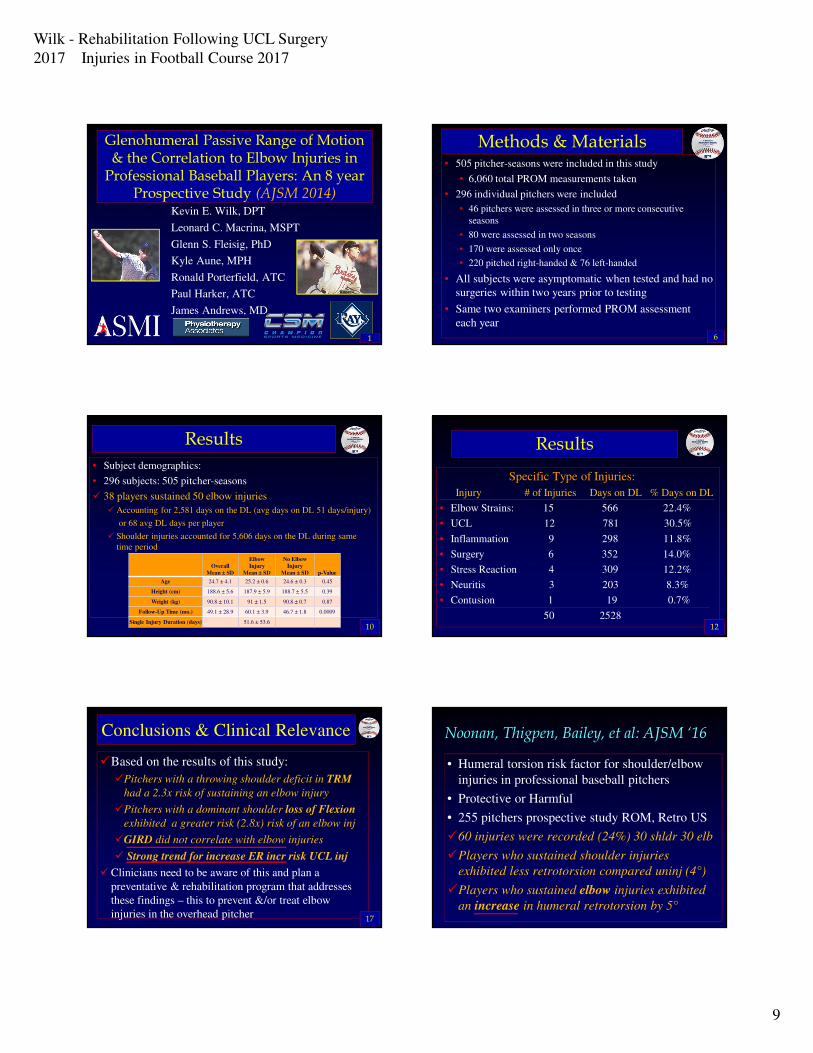
Glenohumeral Passive Range of Motion & the Correlation to Elbow Injuries in
Professional Baseball Players: An 8 year Prospective Study (AJSM 2014)
Kevin E. Wilk, DPT
Leonard C. Macrina, MSPT
Glenn S. Fleisig, PhD
Kyle Aune, MPH
Ronald Porterfield, ATC
Paul Harker, ATC
James Andrews, MD
1
Methods & Materials• 505 pitcher-seasons were included in this study
• 6,060 total PROM measurements taken
• 296 individual pitchers were included
• 46 pitchers were assessed in three or more consecutive
seasons
• 80 were assessed in two seasons
• 170 were assessed only once
• 220 pitched right-handed & 76 left-handed
• All subjects were asymptomatic when tested and had no
surgeries within two years prior to testing
• Same two examiners performed PROM assessment
each year
6
Results
• Subject demographics:
• 296 subjects: 505 pitcher-seasons
� 38 players sustained 50 elbow injuries
� Accounting for 2,581 days on the DL (avg days on DL 51 days/injury)
or 68 avg DL days per player
� Shoulder injuries accounted for 5,606 days on the DL during same
time period
10
Overall
Mean ± SD
Elbow
Injury
Mean ± SD
No Elbow
Injury
Mean ± SD p-Value
Age 24.7 ± 4.1 25.2 ± 0.6 24.6 ± 0.3 0.45
Height (cm) 188.6 ± 5.6 187.9 ± 5.9 188.7 ± 5.5 0.39
Weight (kg) 90.8 ± 10.1 91 ± 1.5 90.8 ± 0.7 0.87
Follow-Up Time (mo.) 49.1 ± 28.9 60.1 ± 3.9 46.7 ± 1.8 0.0009
Single Injury Duration (days) 51.6 ± 53.6
Results
Specific Type of Injuries:
Injury # of Injuries Days on DL % Days on DL
• Elbow Strains: 15 566 22.4%
• UCL 12 781 30.5%
• Inflammation 9 298 11.8%
• Surgery 6 352 14.0%
• Stress Reaction 4 309 12.2%
• Neuritis 3 203 8.3%
• Contusion 1 19 0.7%
50 252812
Conclusions & Clinical Relevance
�Based on the results of this study:
�Pitchers with a throwing shoulder deficit in TRM
had a 2.3x risk of sustaining an elbow injury
�Pitchers with a dominant shoulder loss of Flexion
exhibited a greater risk (2.8x) risk of an elbow inj
�GIRD did not correlate with elbow injuries
� Strong trend for increase ER incr risk UCL inj
�Clinicians need to be aware of this and plan a
preventative & rehabilitation program that addresses
these findings – this to prevent &/or treat elbow
injuries in the overhead pitcher 17
Noonan, Thigpen, Bailey, et al: AJSM ‘16
• Humeral torsion risk factor for shoulder/elbow
injuries in professional baseball pitchers
• Protective or Harmful
• 255 pitchers prospective study ROM, Retro US
�60 injuries were recorded (24%) 30 shldr 30 elb
�Players who sustained shoulder injuries
exhibited less retrotorsion compared uninj (4°)
�Players who sustained elbow injuries exhibited
an increase in humeral retrotorsion by 5°
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
10
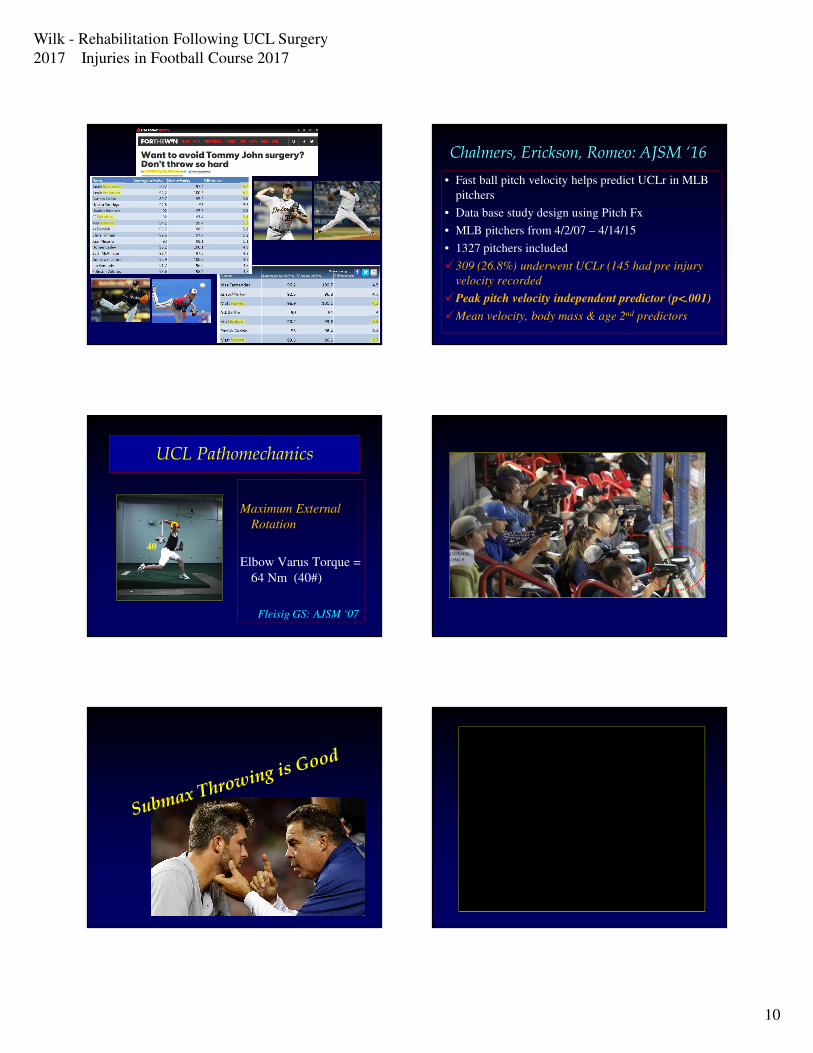
Chalmers, Erickson, Romeo: AJSM ‘16
• Fast ball pitch velocity helps predict UCLr in MLB
pitchers
• Data base study design using Pitch Fx
• MLB pitchers from 4/2/07 – 4/14/15
• 1327 pitchers included
�309 (26.8%) underwent UCLr (145 had pre injury
velocity recorded
�Peak pitch velocity independent predictor (p<.001)
�Mean velocity, body mass & age 2nd predictors
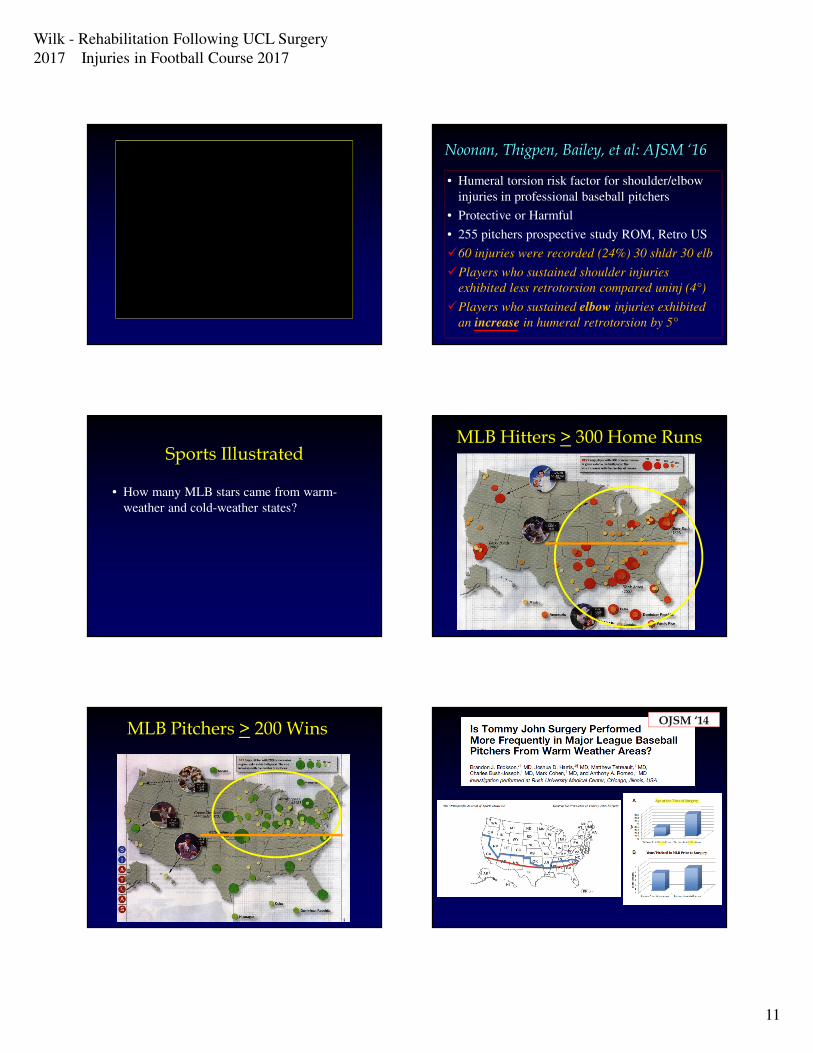
UCL Pathomechanics
40
Maximum External
Rotation
Elbow Varus Torque =
64 Nm (40#)
Fleisig GS: AJSM ‘07
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
11
Noonan, Thigpen, Bailey, et al: AJSM ‘16
• Humeral torsion risk factor for shoulder/elbow
injuries in professional baseball pitchers
• Protective or Harmful
• 255 pitchers prospective study ROM, Retro US
�60 injuries were recorded (24%) 30 shldr 30 elb
�Players who sustained shoulder injuries
exhibited less retrotorsion compared uninj (4°)
�Players who sustained elbow injuries exhibited
an increase in humeral retrotorsion by 5°
Sports Illustrated
• How many MLB stars came from warm-
weather and cold-weather states?
MLB Hitters > 300 Home Runs
MLB Pitchers > 200 WinsOJSM ‘14
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
12
Elbow Injuries in SportsUCL Injuries
Traumatic UCL Injuries Repetitive Overhead
Stresses
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
13
Elbow Dislocation
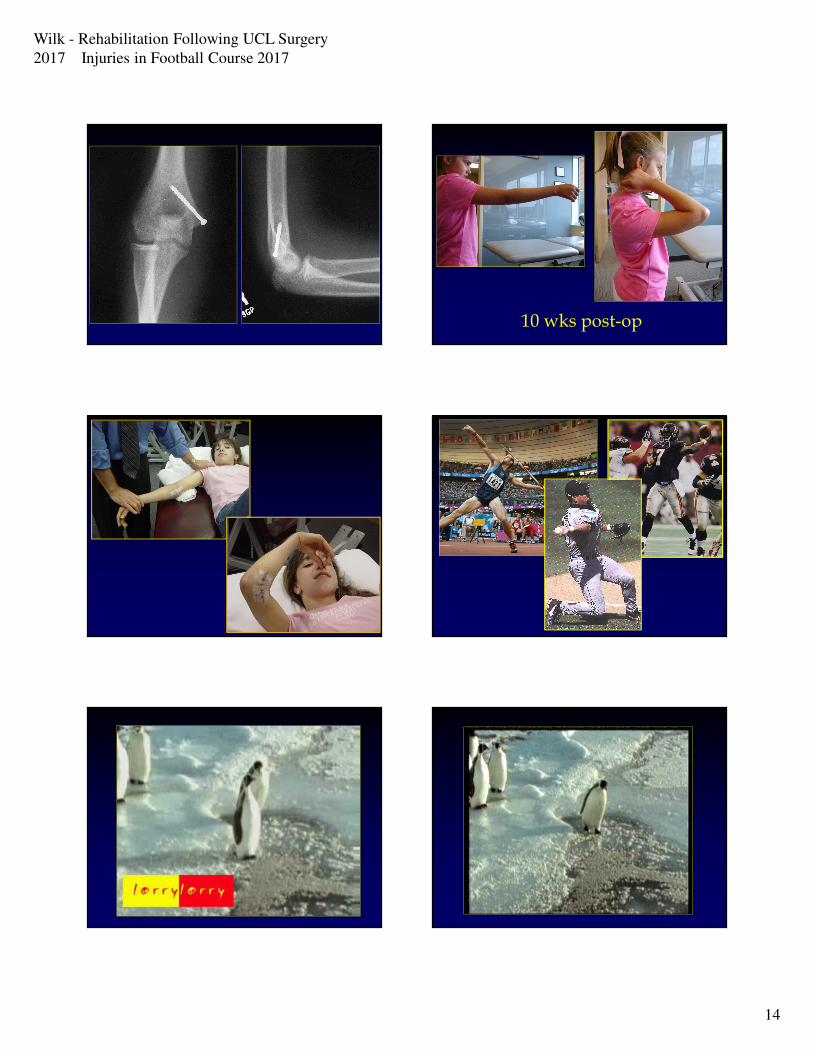
Flexor/Pronator AvulsionUCL Avulsion (10 yr old)
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
14
10 wks post-op
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
15
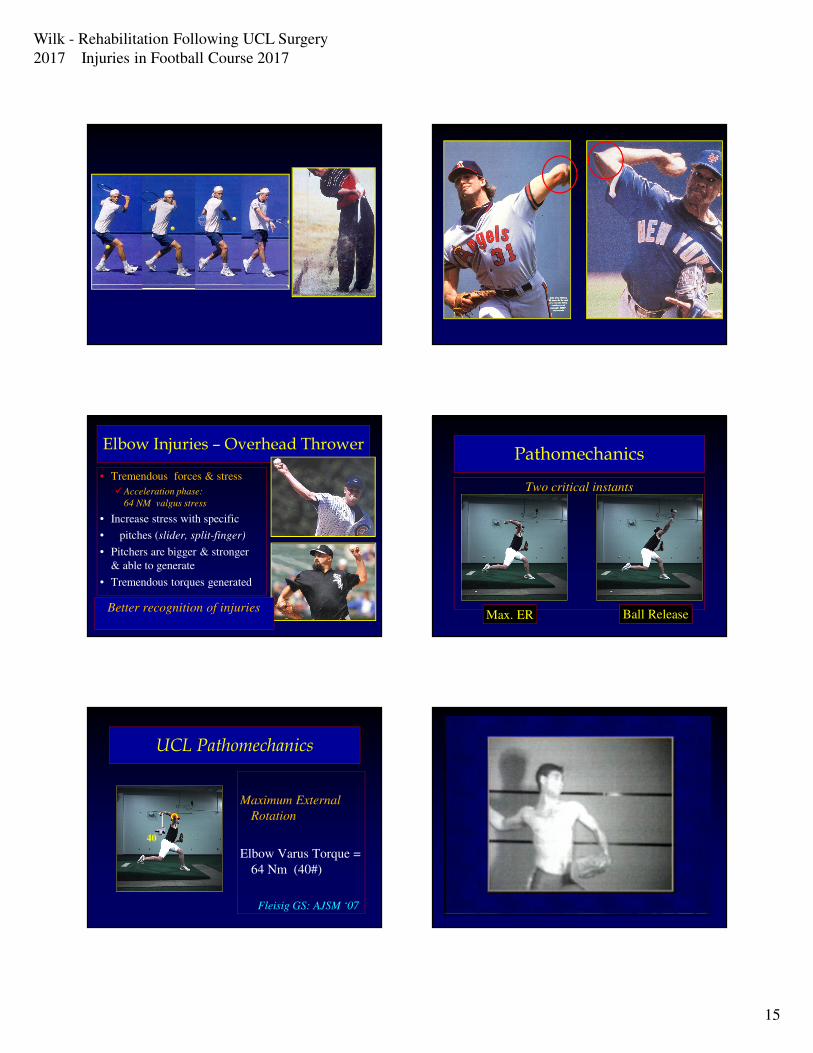
Elbow Injuries – Overhead Thrower
• Tremendous forces & stress
�Acceleration phase:
64 NM valgus stress
• Increase stress with specific
• pitches (slider, split-finger)
• Pitchers are bigger & stronger
& able to generate
• Tremendous torques generated
Better recognition of injuries
Pathomechanics
Two critical instants
Max. ER Ball Release
UCL Pathomechanics
40
Maximum External
Rotation
Elbow Varus Torque =
64 Nm (40#)
Fleisig GS: AJSM ‘07

Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
16
Fleisig, Bolt, Fortenbaugh, Wilk: JOSPT ‘11
• 17 healthy college pitchers
• Biomechanical analysis of long & short throwing
• Threw 18.4m , 37m, 55m & maximal distance on a
line
• Shoulder line was horizontal for mound distance but
gradually went uphill as distance increased
�Maximal throwing distance resulted in more ER,
more Elb Flexion, more shoulder IR torque & more
varus elbow torque
• Trunk tilt gradually increased with distance
UCL Reconstructions in Youth Baseball Players (JRA)
Fleisig et al: Curr Spts Med Reports ‘09
Youth & High School Total % Youth & HS
• 1994 0 6 0%
• 1995 2 21 10%
• 1998 5 43 12%
• 2000 17 93 18%
• 2004 35 174 20%
• 2006 36 140 26%
• 2007 38 125 30%
• 2008 33 103 32%
• 2009 34 121 28%
Total 333 1476 23%
Prevention Programs for the Throwing Athlete
Prevention Programs for the Throwing Athlete
www.asmi.org
www.aossm.org

Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
17
“Throw Like A Pro” App The Overhead ThrowerIntroduction
• Why the increase in injuries at all levels of baseball???
• Factors that influence injury rates:�Arm fatigue
�Technique & Skill level
�Size of players
�Number of pitches per game
�Number of games per year
�Number of years throwing
�Type of pitches
Lyman, Fleisig, et al: AJSM ’02
Lyman, Fleisig, et al: Med Sci Spts Ex ’01
Olsen, Fleisig, et al: AJSM ‘06
» Pitches allowed per game
• 17-18 yrs 105 pitches
• 13-16 yrs 95 pitches
• 11-12 yrs 85 pitches
• 9-10 75 pitches
• 7-8 50 pitches
Injury Prevention
� Little League Pitch Count Rule (since 2007)
• Days rest after pitching (14 and under)
•66 or more pitches 4 days
•51-65 pitches 3 days
•36-50 pitches 2 days
•21-35 pitches 1 day
Olsen, Fleisig, Dun, Loftice, Andrews: Am J Sports Med ‘06
• Risk factors for developing shoulder & elbow injuries in adolescent baseball pitchers
• Compared 95 pitchers who had surgery to 45 pitchers who never had a significant injury
• Risk factors:» Pitched more months per year
» Games per year
» Innings per game
» Pitches per game
» More starting pitchers
» Participated in showcases
» Pitched at higher velocity
» Pitched more often & when fatigued
» Used NSAIDs & ice
» Injured group was taller & heavier
Biomechanics of the Elbow
Throwing
Biomechanics of the Elbow Joint Complex During
Throwing
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
18
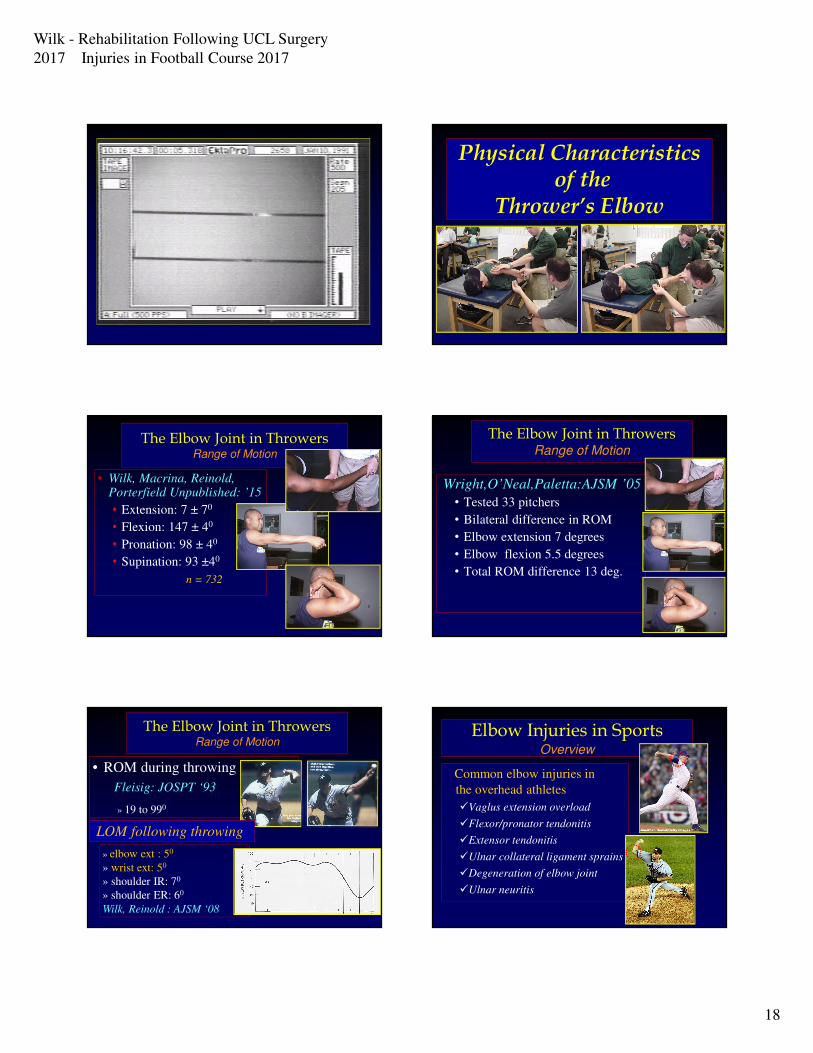
Physical Characteristicsof the
Thrower’s Elbow
The Elbow Joint in ThrowersRange of Motion
• Wilk, Macrina, Reinold, Porterfield Unpublished: ’15
• Extension: 7 ± 70
• Flexion: 147 ± 40
• Pronation: 98 ± 40
• Supination: 93 ±40
n = 732
The Elbow Joint in ThrowersRange of Motion
Wright,O’Neal,Paletta:AJSM ’05
• Tested 33 pitchers
• Bilateral difference in ROM
• Elbow extension 7 degrees
• Elbow flexion 5.5 degrees
• Total ROM difference 13 deg.
The Elbow Joint in ThrowersRange of Motion
• ROM during throwing
Fleisig: JOSPT ‘93
» 19 to 990
» elbow ext : 50
» wrist ext: 50
» shoulder IR: 70
» shoulder ER: 60
Wilk, Reinold : AJSM ‘08
LOM following throwing
Elbow Injuries in SportsOverview
Common elbow injuries in
the overhead athletes
�Vaglus extension overload
�Flexor/pronator tendonitis
�Extensor tendonitis
�Ulnar collateral ligament sprains
�Degeneration of elbow joint
�Ulnar neuritis
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
19
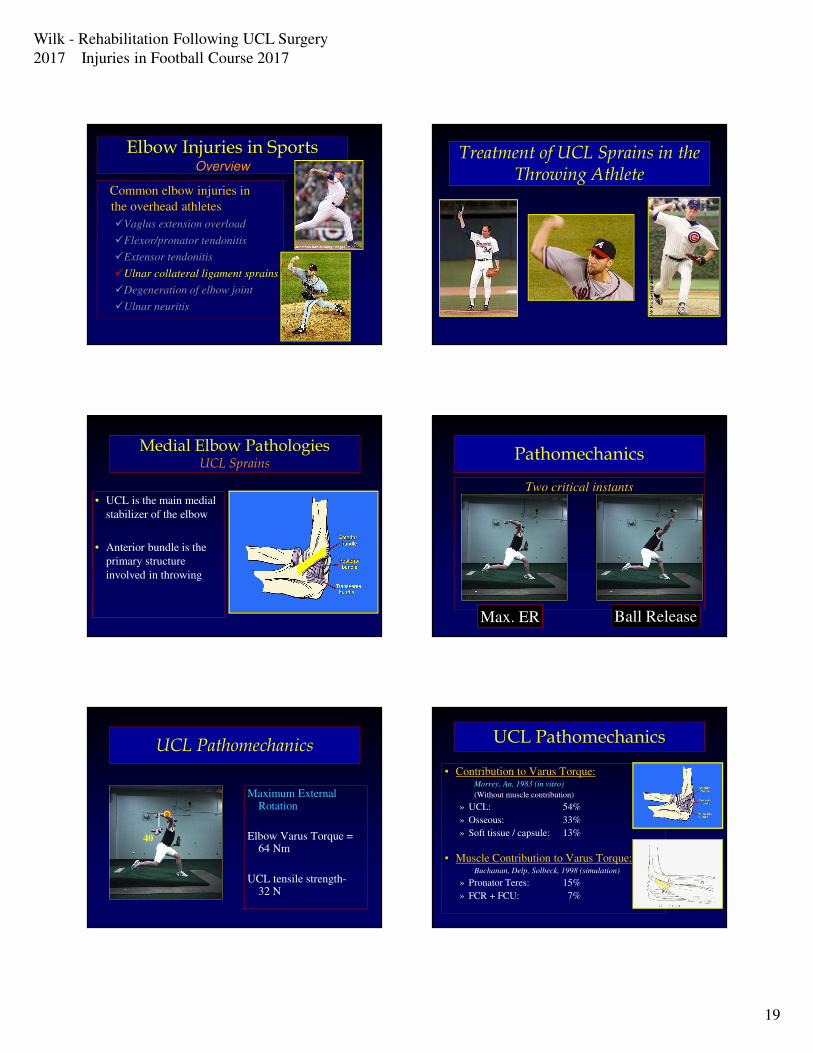
Elbow Injuries in SportsOverview
Common elbow injuries in
the overhead athletes
�Vaglus extension overload
�Flexor/pronator tendonitis
�Extensor tendonitis
�Ulnar collateral ligament sprains
�Degeneration of elbow joint
�Ulnar neuritis
Treatment of UCL Sprains in the Throwing Athlete
Medial Elbow PathologiesUCL Sprains
• UCL is the main medial
stabilizer of the elbow
• Anterior bundle is the
primary structure
involved in throwing
Pathomechanics
Two critical instants
Max. ER Ball Release
UCL Pathomechanics
40
Maximum External Rotation
Elbow Varus Torque = 64 Nm
UCL tensile strength-32 N
UCL Pathomechanics
• Contribution to Varus Torque:Morrey, An, 1983 (in vitro)
(Without muscle contribution)
» UCL: 54%
» Osseous: 33%
» Soft tissue / capsule: 13%
• Muscle Contribution to Varus Torque:Buchanan, Delp, Solbeck, 1998 (simulation)
» Pronator Teres: 15%
» FCR + FCU: 7%
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
20
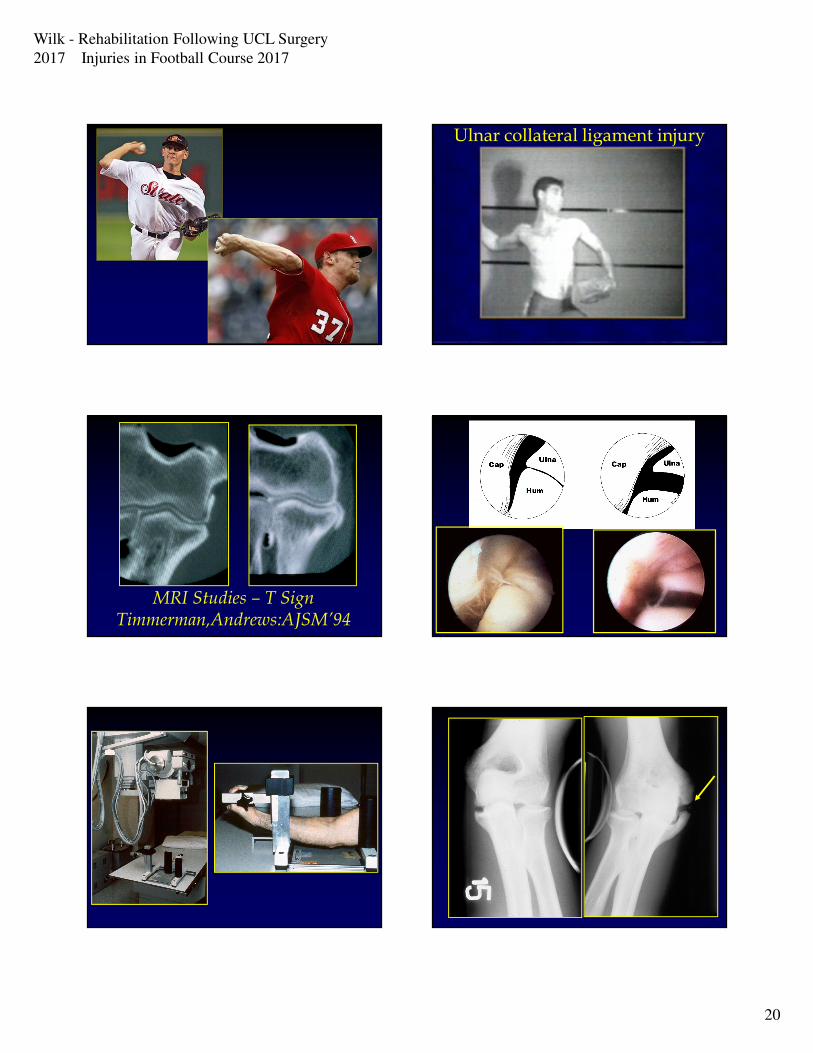
Ulnar collateral ligament injury
MRI Studies – T SignTimmerman,Andrews:AJSM’94
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
21
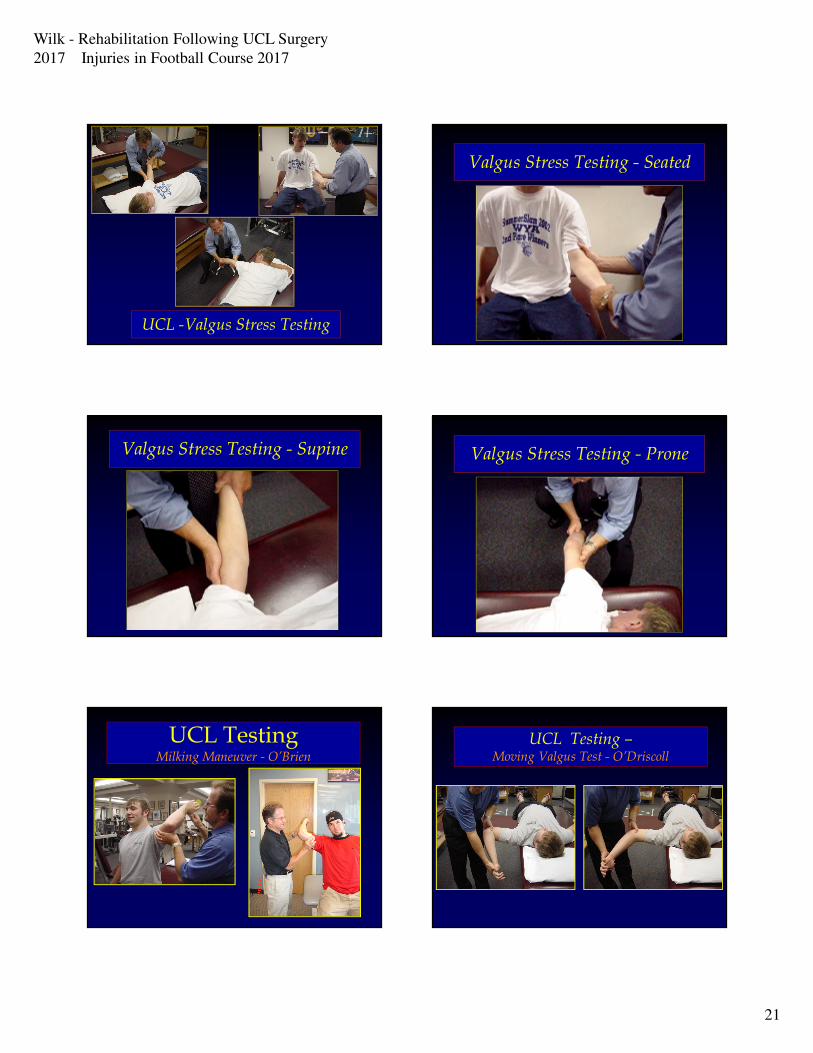
UCL -Valgus Stress Testing
Valgus Stress Testing - Seated
Valgus Stress Testing - Supine Valgus Stress Testing - Prone
UCL TestingMilking Maneuver - O’Brien
UCL Testing –Moving Valgus Test - O’Driscoll

Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
22
Bruce, Joyner, Andrews: JSES’15
• Stress radiograghs performed on
273 baseball players pre-operative
prior to surgery
• How much joint opening present in
UCL insufficient throwing elbows
• Elbow tested at 20 to 30 with 15
daN force
�UCL injured elbow: 0.4mm
�UCL complete tears: 0.7 mm
Elbow Laxity in Professional Baseball Players/Pitchers
Ellenbecker, Mattalino:
AJSM ’98
• 40 uninjured professional
pitchers
• Stress radiograghs 15daN
• D: 1.20mm ND: 0.88
�Bilateral Diff: 0.32 mm
Ciccotti et al: AJSM ’14
• 368 asymptomatic
professional baseball
pitchers (10 yrs)
• Stress US assessment
�UCL thicker on D elbow
� Joint opening:
D 4.5mm
ND: 3.72mm
Diff: 0.8mm
Treatment of UCL Injuries in The Overhead Throwing Athlete
Non-Operative Rx Operative Rx
Stop Pitching
Treatment of UCL Injuries in The Overhead Throwing Athlete
Non-Operative Rx Operative Rx
Stop Pitching Rehab
Successful Outcome
Treatment of UCL Injuries in The Overhead Throwing Athlete
Non-Operative Rx Operative Rx
Stop Pitching Rehab Reconstruction Repair
Successful Outcome
Non-Operative Rehab Partial Thickness UCL Tears in Throwers
Rehab ProgramJobe: Clin Spts Med ’86
Yocum: Clin Spts Med ’89
Jobe: Instr Course Lect ’91
Wilk & Andrews: Spts Med Arth Rev ’95
Azar & Wilk Op Tech Spts Med ’96
Wilk & Andrews: JOSPT ‘93
Rettig: AJSM ’01*
Podesta et al: AJSM ‘13
Effective Treatment Plan – What % of Patients
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
23
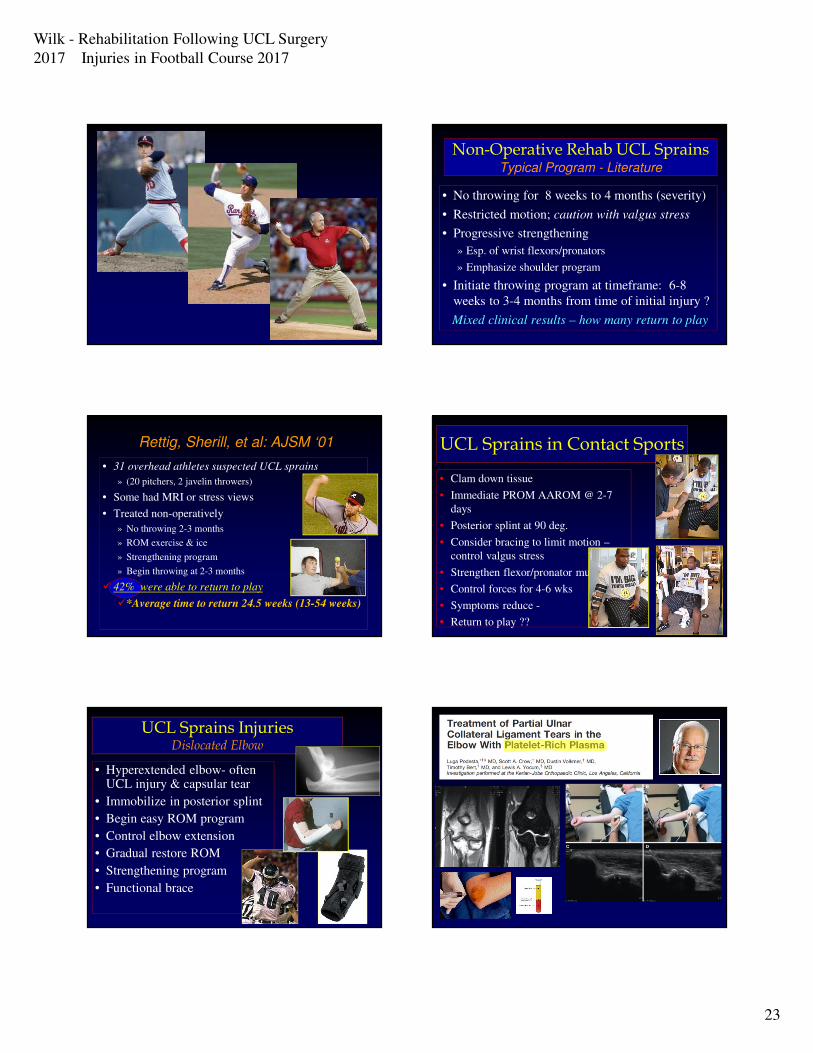
Non-Operative Rehab UCL SprainsTypical Program - Literature
• No throwing for 8 weeks to 4 months (severity)
• Restricted motion; caution with valgus stress
• Progressive strengthening
» Esp. of wrist flexors/pronators
» Emphasize shoulder program
• Initiate throwing program at timeframe: 6-8
weeks to 3-4 months from time of initial injury ?
Mixed clinical results – how many return to play
Rettig, Sherill, et al: AJSM ‘01
• 31 overhead athletes suspected UCL sprains
» (20 pitchers, 2 javelin throwers)
• Some had MRI or stress views
• Treated non-operatively
» No throwing 2-3 months
» ROM exercise & ice
» Strengthening program
» Begin throwing at 2-3 months
� 42% were able to return to play
�*Average time to return 24.5 weeks (13-54 weeks)
UCL Sprains in Contact Sports
• Clam down tissue
• Immediate PROM AAROM @ 2-7
days
• Posterior splint at 90 deg.
• Consider bracing to limit motion –
control valgus stress
• Strengthen flexor/pronator muscles
• Control forces for 4-6 wks
• Symptoms reduce -
• Return to play ??
UCL Sprains InjuriesDislocated Elbow
• Hyperextended elbow- often UCL injury & capsular tear
• Immobilize in posterior splint
• Begin easy ROM program
• Control elbow extension
• Gradual restore ROM
• Strengthening program
• Functional brace
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
24
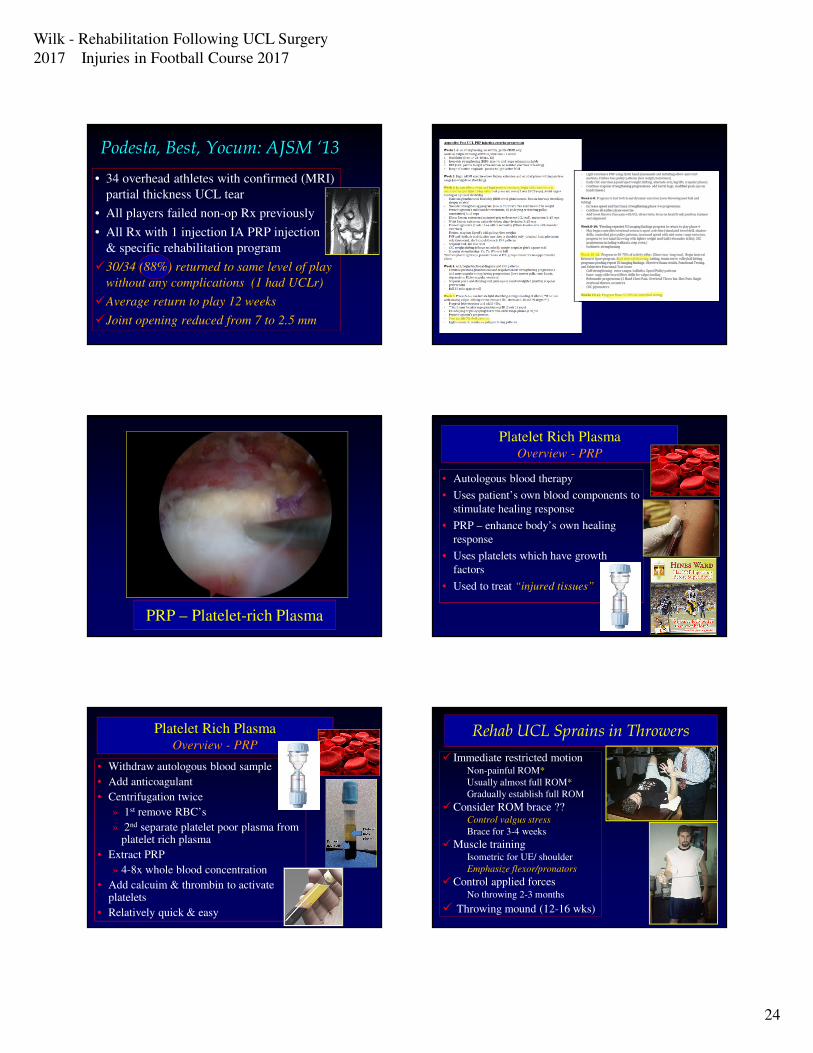
Podesta, Best, Yocum: AJSM ‘13
• 34 overhead athletes with confirmed (MRI)
partial thickness UCL tear
• All players failed non-op Rx previously
• All Rx with 1 injection IA PRP injection
& specific rehabilitation program
�30/34 (88%) returned to same level of play
without any complications (1 had UCLr)
�Average return to play 12 weeks
�Joint opening reduced from 7 to 2.5 mm
PRP – Platelet-rich Plasma
Platelet Rich PlasmaOverview - PRP
• Autologous blood therapy
• Uses patient’s own blood components to
stimulate healing response
• PRP – enhance body’s own healing
response
• Uses platelets which have growth
factors
• Used to treat “injured tissues”
Platelet Rich PlasmaOverview - PRP
• Withdraw autologous blood sample
• Add anticoagulant
• Centrifugation twice
» 1st remove RBC’s
» 2nd separate platelet poor plasma from platelet rich plasma
• Extract PRP
» 4-8x whole blood concentration
• Add calcuim & thrombin to activate platelets
• Relatively quick & easy
Rehab UCL Sprains in Throwers
� Immediate restricted motionNon-painful ROM*
Usually almost full ROM*
Gradually establish full ROM
�Consider ROM brace ??Control valgus stress
Brace for 3-4 weeks
�Muscle trainingIsometric for UE/ shoulder
Emphasize flexor/pronators
�Control applied forcesNo throwing 2-3 months
� Throwing mound (12-16 wks)

Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
25
UCL SPRAINS REHABMuscular Strength Training
• Wrist & hand isometrics day 1
• Isometrics UE week 1-2
• Isotonics program week 3-4
• Thrower’s Ten program week 4
• Advanced Thrower’s Ten wk 6-8
• Weight lifting week 8
• Sports (golf) week 8-12
• Plyometrics
» Two hand drills week 6-8
» One hand drills week 8-12
Manual Resistance Techniques
Elbow Rehabilitation in Athletes
Dynamic Stabilization
Davidson et al: AJSM ‘95
Rehab UCL Sprains in Throwers
Advanced phase:
�Gradually increase applied
stresses & forces
» Thrower’s ten program
» Plyometrics
�Initiate Throwing Program
(criteria-based)
�Mild sprain 6-8 wks
�Moderate sprain 3-4 mos
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
26
Rehab UCL Sprains in Throwers
Advanced phase:
�Gradually increase applied
stresses & forces
» Thrower’s ten program
» Plyometrics
�Initiate Throwing Program
(criteria-based)
�Mild sprain 6-8 wks
�Moderate sprain 3-4 mos
UCL Sprains in Contact Sports
• Immediate following injury
• Posterior splint at 90 deg.
• Consider bracing to limit motion
– control valgus stress
• Strengthen flexor/pronator
muscles
• Control forces for 4-6 wks
• Symptoms reduce -
• Return to play ??
UCL Sprains InjuriesDislocated Elbow
• Hyperextended elbow- often UCL injury & capsular tear
• Immobilize in posterior splint for 1-2 weeks
• Begin easy ROM program
• Control elbow extension
• Gradual restore ROM
• Strengthening program
• Functional brace
Rehabilitation FollowingUCL Reconstruction
Our Current Program (2017)
UCL RECONSTRUCTION REHABRecent Adaptations in Our Program
�Earlier restoration of motion
• Previous: 7-8 wks FROM
• Present: 4-6 wks FROM
• More present: Full ext ASAP *
Acute Injury Chronic Injury
• Emphasis on wrist flexors, shoulder strength
• Preparation phase of throwing –plyometrics longer
� Throwing programs – long toss (more time)…
delay hard throwing for longer –return to games delayed
• Phase I: Acute Post-Op Phase:
• Phase II: Subacute Phase:
• Phase III: Advanced Phase:
• Phase IV: Return to Activity Phase:
Rehabilitation Following UCLrin Throwers
Rehabilitation – 4 Phases Program
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
27
• Phase I: Post-Op Phase (weeks 0-8):
�Protect the healing tissue (UCL)
�Gradually restore motion
�Decrease inflammation & pain
�Prevent muscular atrophy
� Scapular, GH joint, leg, core program
• Phase II: Subacute Phase (weeks 9-12
�Continue ROM & stretching
� Isotonic strengthening program (Throw 10�Scapular & Glenohumeral joint
�Fine tune muscular ratios
�Core & Leg program
Rehabilitation UCLr ThrowersRehabilitation – 4 Phases Program
• Phase III: Advanced Phase(weeks 13-16
�Advanced isotonic program�Strength, power, & endurance
�Advanced thrower’s ten program
�Plyometrics
�Continue stretching & ROM program
• Phase IV: Return to Activity Phase: 4 mos
�Thrower’s ten program
�Plyometrics
� Interval throwing program (ITP)
�Light stretching program
Rehabilitation UCLr ThrowersRehabilitation – 4 Phases Program
Reconstruction of the UCL Surgical Overview
�Modification of Jobe procedure
Jobe: JBJS ’86
Andrews: Op Tech Spts Med ’96
Andrews et al: Am J Sports Med ‘10
• Subcutaneous ulnar nerve transposition
• fascial sling
• Graft source
• Palmaris longus
• Gracilis
Reconstruction of the UCL Surgical Technique Update
Graft location:
• UCL reconstruction - 2386
�Palmaris longus 62%
ipsilateral:(78%) contralateral: (22%)
�Gracilis 38%
Reconstruction of the UCL Surgical Technique
• Graft location: (from 1989 – present)
» Palmaris longus 81%
ipsilateral (84%) contralateral (16%)
» Plantaris 10%
» Gracilis 6%
» Toe extensors 3%
» Patellar tendon n=1
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
28
Reconstruction of the UCL Surgical Technique Update*
• Graft location:
• UCL reconstruction -
» Palmaris longus 65%
ipsilateral:(78%) contralateral: (22%)
» Gracilis 33%
» Anterior tibialis n=1
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
29
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
30
Reconstruction of the UCL Surgical Technique
• Docking Procedure
Altchek DW: HSS
• Muscle split
• Single huneral tunnel
• Smaller tunnels (?)
• No ulnar nerve transposition
Rohrbough & Altchek: AJSM ’02
Dodson: AJSM ‘06
UCL RECONSTRUCTION REHAB
Range of Motion Progression
�Week one: splint at 90 degrees
�Week two: brace 30-100 degrees
�Week three: brace 15-115
degrees
�Progress program 5 degrees
of extension and 10 degrees
of flexion per week
�Full ROM at week 5-6
More Aggressive with ROM
UCL RECONSTRUCTION REHAB
UCL Strain with PROM
Bernas: AJSM ‘09
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
31
Wrist & hand ROM / gripping
Rehab of Graft Site
• Palmaris tendon graft:» Ice & compression first 5-7 days
» Immediate wrist motion, no aggressive stretching 2 weeks
» Immediate hand gripping exercises
» Soft tissue (scar) mobilization at 2 wks
» If scars: US, stretch, tissue tissue
» Begin strengthening program for wrist flexors
• Isometrics immediate
• Isotonics at 3 weeks
» Progress to stretch with open hand & digits extended
• Gracilis tendon graft
» Ice & compression first 5-7 days
» No stretching of hamstrings for 2-3 weeks
» Soft tissue (scar) mobilization on day 15
» No isolated hamstrings for 3-4 wks
» May bicycle at 2-4 weeks
» Begin strengthening program for hamstrings & calf
• Isometrics at 4 weeks
• Isotonics at 6 weeks
Rehab of Graft SiteUCL RECONSTRUCTION
REHABMuscular Strength Training
• Wrist & hand isometrics day 1
• Isometrics UE week 1-2
• Active ROM week 2-3
• Isotonics program week 3-4
• Thrower’s Ten program week 4/5
• Weight lifting week 10-12
• Sports (golf) week 11
• Plyometrics
» Two hand drills week 12
» One hand drills week 14
Thrower’s Ten Program
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
32
Bilateral Extremity Exercises
UCL RECONSTRUCTION REHABUCL RECONSTRUCTION REHAB
Rotator Cuff Strengthening
UCL RECONSTRUCTION REHABRotator Cuff Strengthening UCL RECONSTRUCTION REHAB
Advanced Strengthening Phase: Week 12-16
�Progress strengthening program
�Initiate isotonic strengthening program
• Bench press (seated)
• Pull-downs
• Seated Rows
• Biceps/Triceps
�Advanced Throwers’ 10
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
33
Manual Resistance Techniques
UCL RECONSTRUCTION REHABStrengthening Drills – Elbow/Wrist Flex/Pron
UCL RECONSTRUCTION REHABStrengthening Drills- MR Elbow/Wrist Flex C/E
UCL RECONSTRUCTION REHABStrengthening Drills-MR Elbow/Wrist Flex
Elbow Rehabilitation in Athletes
Dynamic Stabilization
Davidson et al: AJSM ‘95
UCL RECONSTRUCTION REHABStrengthening Drills
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
34
UCL RECONSTRUCTION REHABStrengthening Drills- RS Shoulder/Elbow
UCL RECONSTRUCTION REHABStrengthening Drills
UCL RECONSTRUCTION REHABStrengthening Drills
UCL RECONSTRUCTION REHABStrengthening Drills
UCL RECONSTRUCTION REHABStrengthening Drills
Advanced Thrower’s Ten Program
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
35
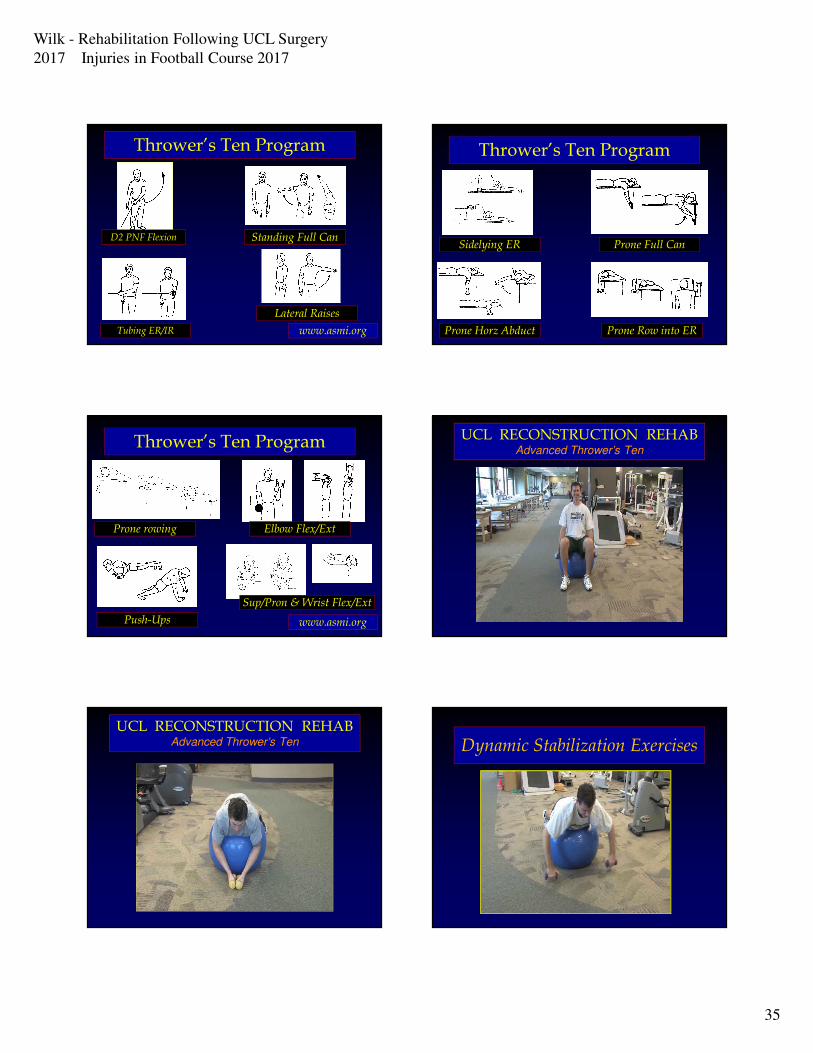
Thrower’s Ten Program
www.asmi.orgTubing ER/IR
Standing Full Can
Lateral Raises
D2 PNF Flexion
Thrower’s Ten Program
Sidelying ER
Prone Horz Abduct
Prone Full Can
Prone Row into ER
Thrower’s Ten Program
Prone rowing
Push-Ups
Elbow Flex/Ext
Sup/Pron & Wrist Flex/Ext
www.asmi.org
UCL RECONSTRUCTION REHABAdvanced Thrower’s Ten
UCL RECONSTRUCTION REHABAdvanced Thrower’s Ten Dynamic Stabilization Exercises
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
36
Dynamic Stabilization Exercises

Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
37
Scapular NM Control DrillsDynamic Stabilization Exercises
Dynamic Stabilization ExercisesUCL RECONSTRUCTION REHAB
Strengthening Drills
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
38
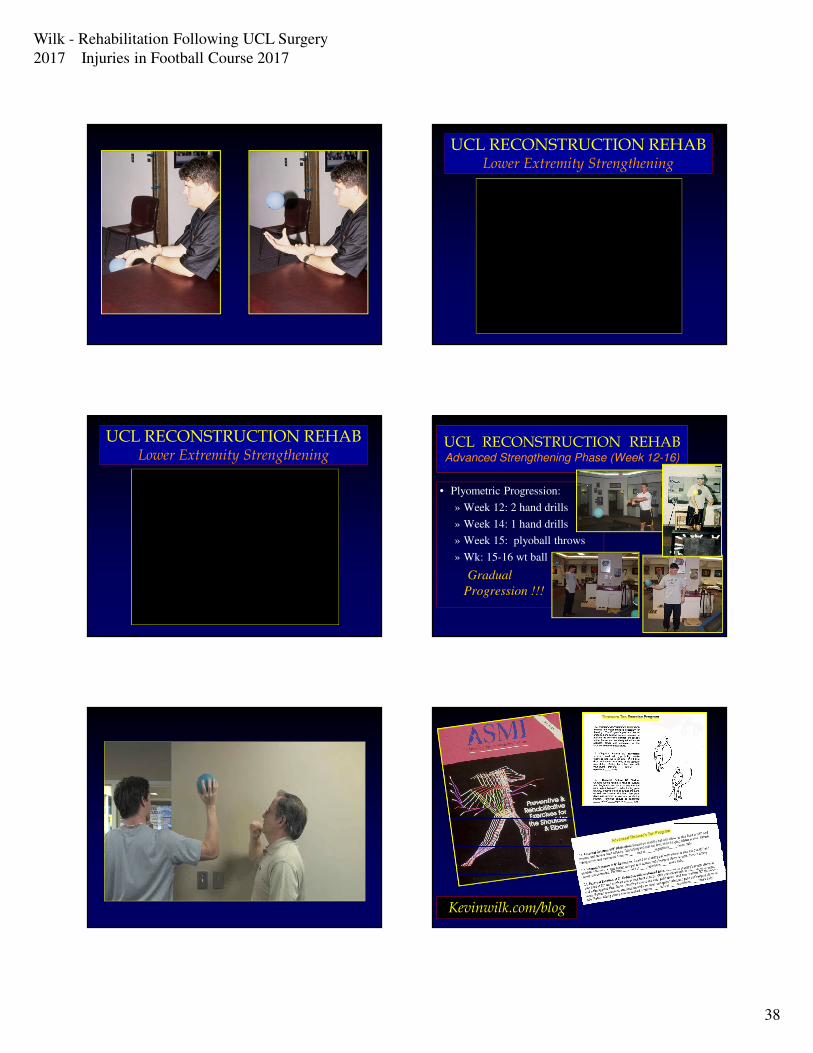
UCL RECONSTRUCTION REHABLower Extremity Strengthening
UCL RECONSTRUCTION REHABLower Extremity Strengthening
UCL RECONSTRUCTION REHABAdvanced Strengthening Phase (Week 12-16)
• Plyometric Progression:
» Week 12: 2 hand drills
» Week 14: 1 hand drills
» Week 15: plyoball throws
» Wk: 15-16 wt ball
Gradual
Progression !!!
Kevinwilk.com/blog
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
39
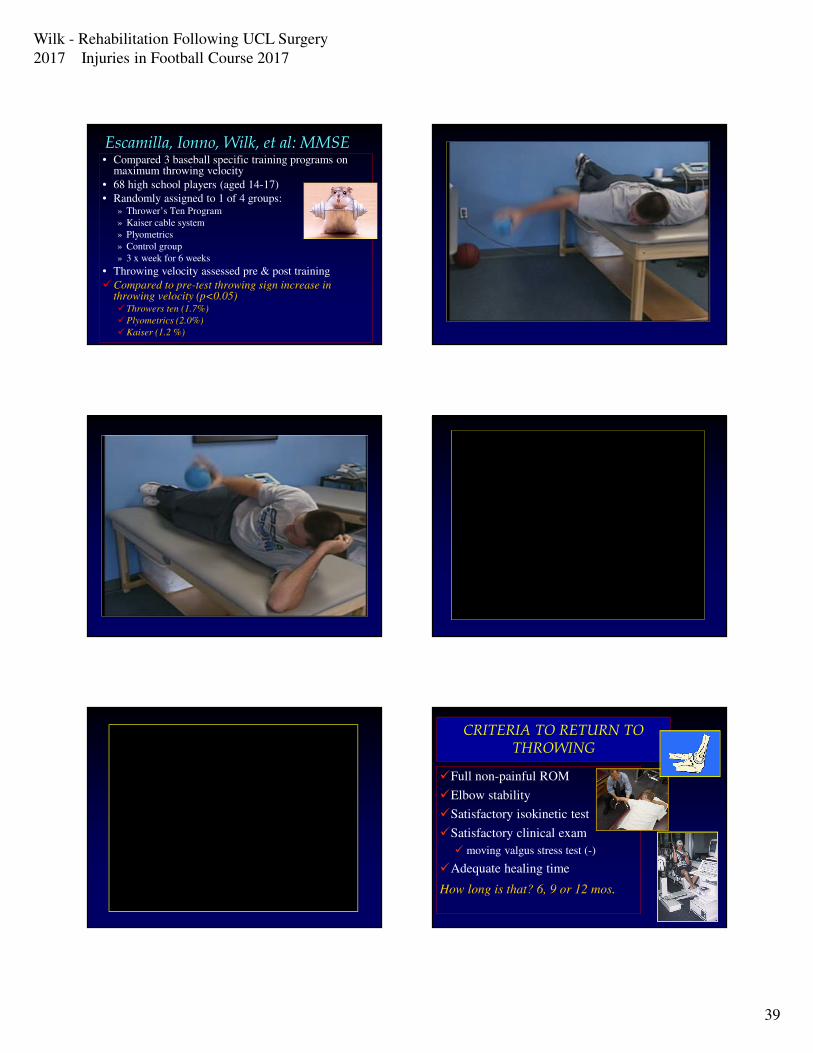
Escamilla, Ionno, Wilk, et al: MMSE• Compared 3 baseball specific training programs on
maximum throwing velocity
• 68 high school players (aged 14-17)
• Randomly assigned to 1 of 4 groups:» Thrower’s Ten Program
» Kaiser cable system
» Plyometrics
» Control group
» 3 x week for 6 weeks
• Throwing velocity assessed pre & post training
�Compared to pre-test throwing sign increase in throwing velocity (p<0.05)�Throwers ten (1.7%)
�Plyometrics (2.0%)
�Kaiser (1.2 %)
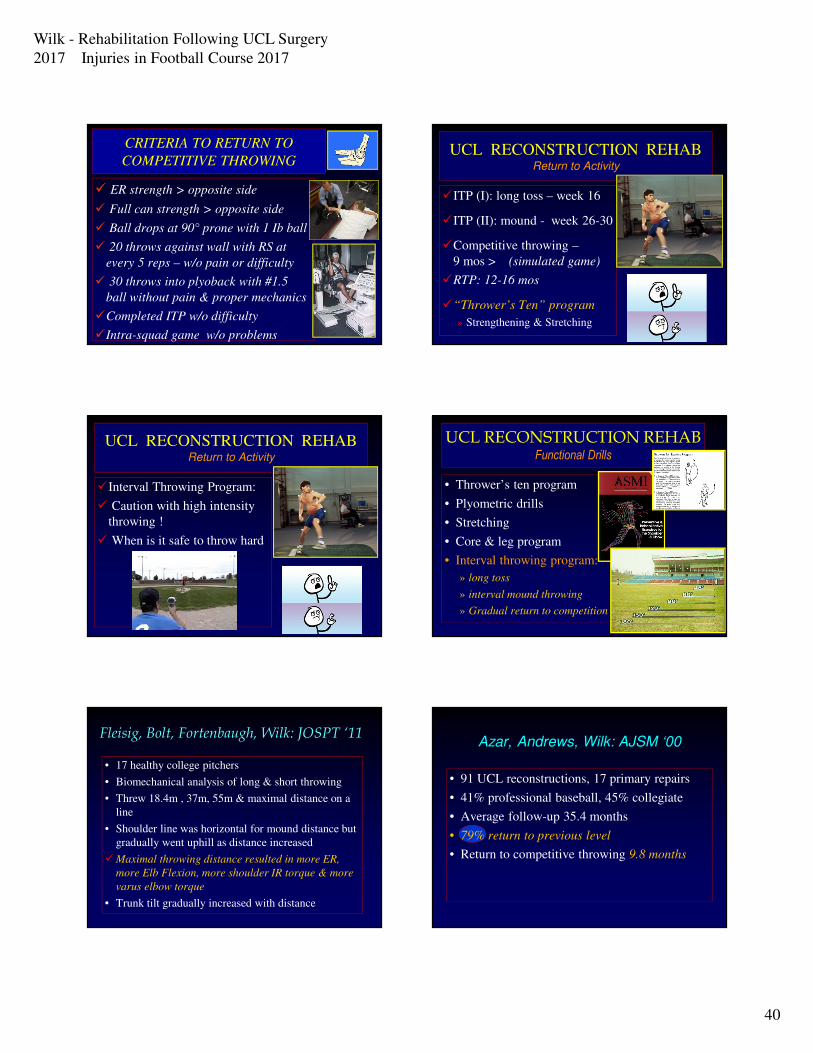
CRITERIA TO RETURN TO THROWING
�Full non-painful ROM
�Elbow stability
�Satisfactory isokinetic test
�Satisfactory clinical exam
� moving valgus stress test (-)
�Adequate healing time
How long is that? 6, 9 or 12 mos.
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
40
CRITERIA TO RETURN TO
COMPETITIVE THROWING
� ER strength > opposite side
� Full can strength > opposite side
� Ball drops at 90° prone with 1 Ib ball
� 20 throws against wall with RS at
every 5 reps – w/o pain or difficulty
� 30 throws into plyoback with #1.5
ball without pain & proper mechanics
�Completed ITP w/o difficulty
�Intra-squad game w/o problems
UCL RECONSTRUCTION REHABReturn to Activity
�ITP (I): long toss – week 16
�ITP (II): mound - week 26-30
�Competitive throwing –
9 mos > (simulated game)
�RTP: 12-16 mos
�“Thrower’s Ten” program
» Strengthening & Stretching
UCL RECONSTRUCTION REHABReturn to Activity
�Interval Throwing Program:
� Caution with high intensity
throwing !
� When is it safe to throw hard
UCL RECONSTRUCTION REHABFunctional Drills
• Thrower’s ten program
• Plyometric drills
• Stretching
• Core & leg program
• Interval throwing program:
» long toss
» interval mound throwing
» Gradual return to competition
Fleisig, Bolt, Fortenbaugh, Wilk: JOSPT ‘11
• 17 healthy college pitchers
• Biomechanical analysis of long & short throwing
• Threw 18.4m , 37m, 55m & maximal distance on a
line
• Shoulder line was horizontal for mound distance but
gradually went uphill as distance increased
�Maximal throwing distance resulted in more ER,
more Elb Flexion, more shoulder IR torque & more
varus elbow torque
• Trunk tilt gradually increased with distance
Azar, Andrews, Wilk: AJSM ‘00
• 91 UCL reconstructions, 17 primary repairs
• 41% professional baseball, 45% collegiate
• Average follow-up 35.4 months
• 79% return to previous level
• Return to competitive throwing 9.8 months
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
41
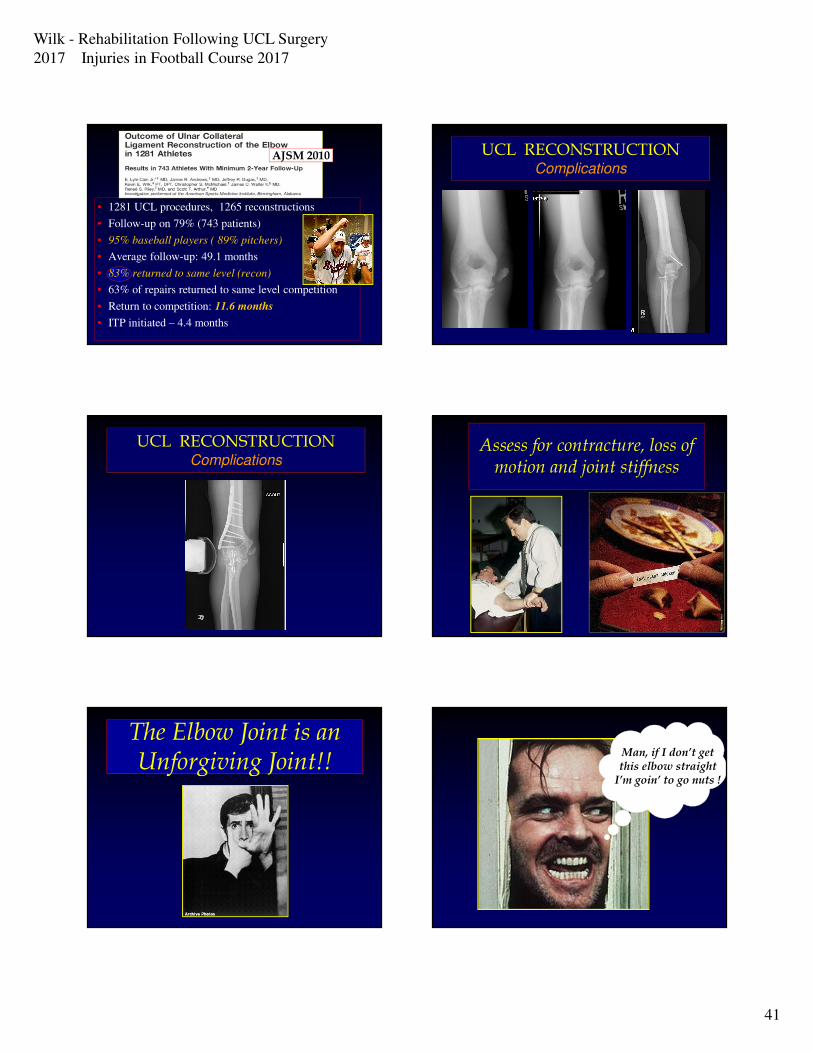
• 1281 UCL procedures, 1265 reconstructions
• Follow-up on 79% (743 patients)
• 95% baseball players ( 89% pitchers)
• Average follow-up: 49.1 months
• 83% returned to same level (recon)
• 63% of repairs returned to same level competition
• Return to competition: 11.6 months
• ITP initiated – 4.4 months
AJSM 2010 UCL RECONSTRUCTION Complications
UCL RECONSTRUCTION Complications
Assess for contracture, loss of motion and joint stiffness
The Elbow Joint is an Unforgiving Joint!!The Elbow Joint is an Unforgiving Joint!!
Man, if I don’t get this elbow straight
I’m goin’ to go nuts !
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
42
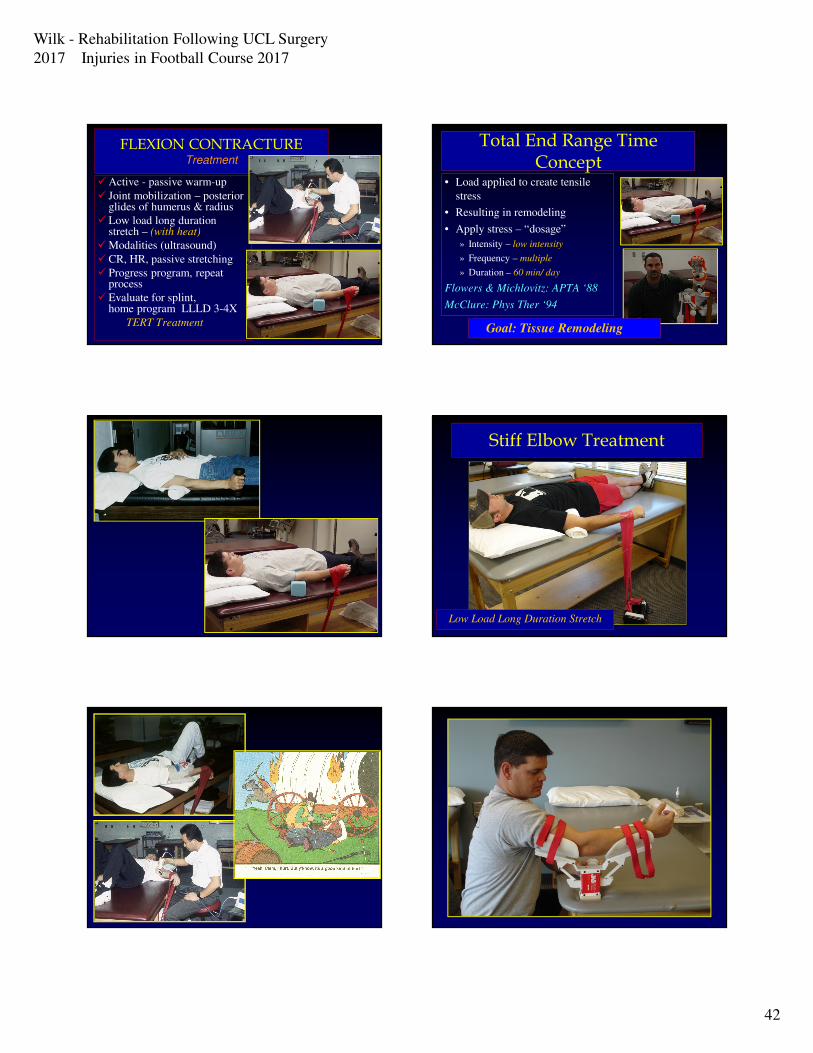
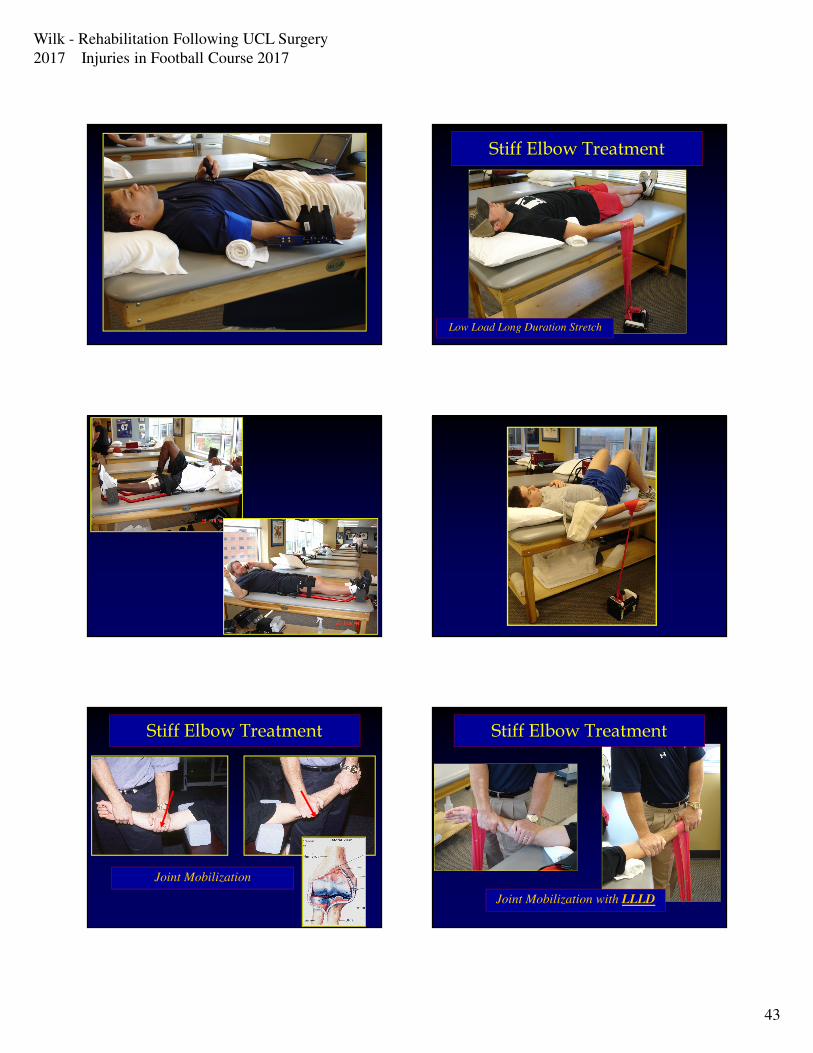
FLEXION CONTRACTURETreatment
�Active - passive warm-up
� Joint mobilization – posterior glides of humerus & radius
�Low load long duration stretch – (with heat)
�Modalities (ultrasound)
�CR, HR, passive stretching
� Progress program, repeat process
�Evaluate for splint, home program LLLD 3-4X
TERT Treatment
Total End Range Time Concept
• Load applied to create tensile
stress
• Resulting in remodeling
• Apply stress – “dosage”
» Intensity – low intensity
» Frequency – multiple
» Duration – 60 min/ day
Flowers & Michlovitz: APTA ‘88
McClure: Phys Ther ‘94
Goal: Tissue Remodeling
Stiff Elbow Treatment
Low Load Long Duration Stretch
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
43
Stiff Elbow Treatment
Low Load Long Duration Stretch
Stiff Elbow Treatment
Joint Mobilization
Stiff Elbow Treatment
Joint Mobilization with LLLD
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
44
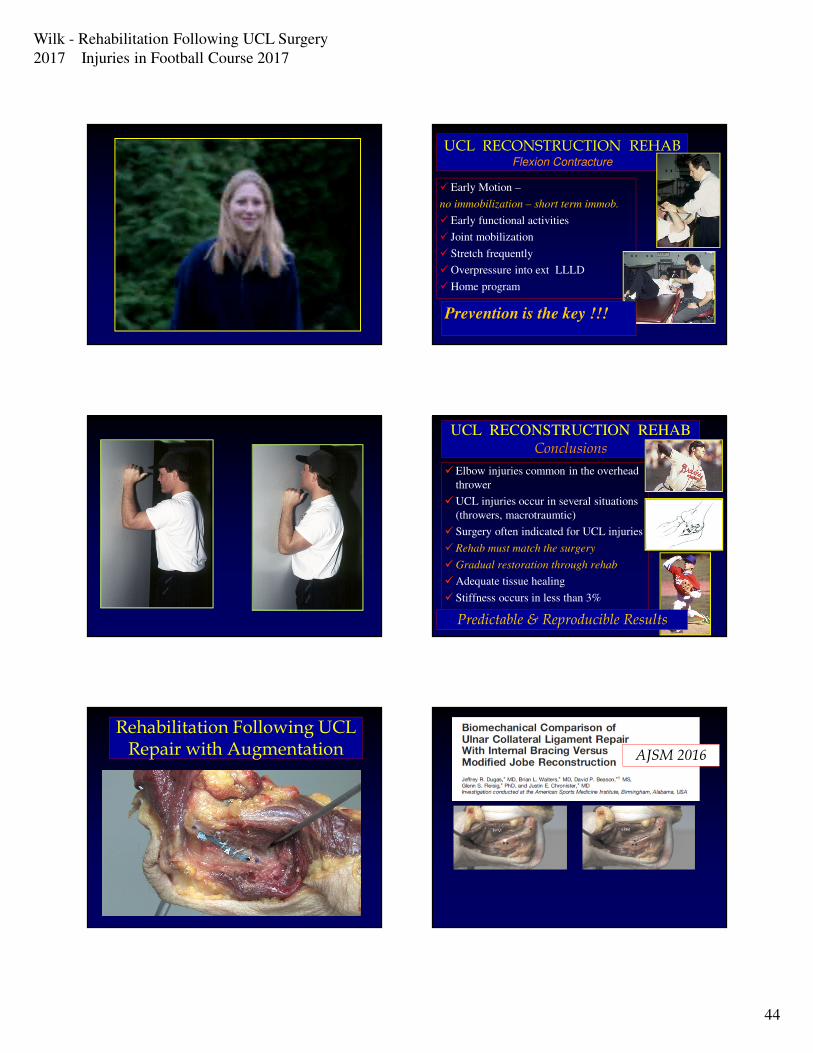
�Early Motion –
no immobilization – short term immob.
�Early functional activities
� Joint mobilization
� Stretch frequently
�Overpressure into ext LLLD
�Home program
UCL RECONSTRUCTION REHABFlexion Contracture
Prevention is the key !!!
UCL RECONSTRUCTION REHAB
Conclusions
�Elbow injuries common in the overhead
thrower
�UCL injuries occur in several situations
(throwers, macrotraumtic)
� Surgery often indicated for UCL injuries
�Rehab must match the surgery
�Gradual restoration through rehab
�Adequate tissue healing
� Stiffness occurs in less than 3%
Predictable & Reproducible Results
Rehabilitation Following UCL Repair with Augmentation AJSM 2016
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
45
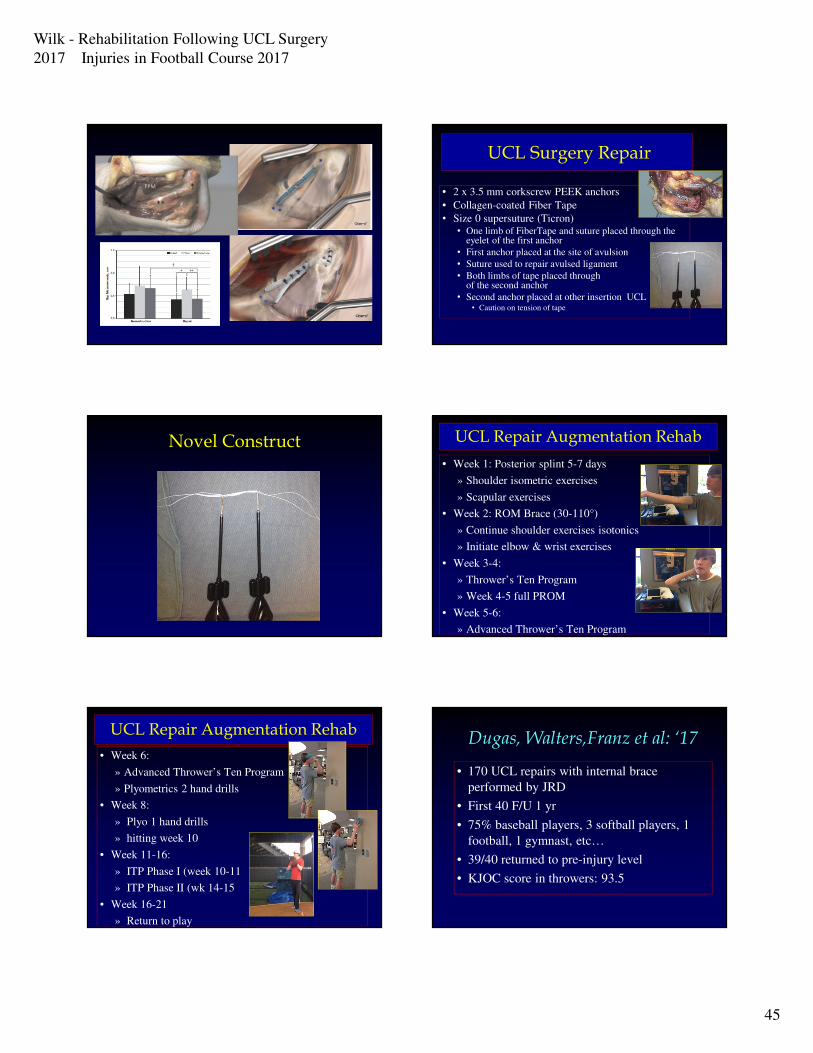
UCL Surgery Repair
• 2 x 3.5 mm corkscrew PEEK anchors
• Collagen-coated Fiber Tape
• Size 0 supersuture (Ticron)• One limb of FiberTape and suture placed through the
eyelet of the first anchor
• First anchor placed at the site of avulsion
• Suture used to repair avulsed ligament
• Both limbs of tape placed through eyelet of the second anchor
• Second anchor placed at other insertion UCL• Caution on tension of tape
Novel Construct UCL Repair Augmentation Rehab
• Week 1: Posterior splint 5-7 days
» Shoulder isometric exercises
» Scapular exercises
• Week 2: ROM Brace (30-110°)
» Continue shoulder exercises isotonics
» Initiate elbow & wrist exercises
• Week 3-4:
» Thrower’s Ten Program
» Week 4-5 full PROM
• Week 5-6:
» Advanced Thrower’s Ten Program
UCL Repair Augmentation Rehab
• Week 6:
» Advanced Thrower’s Ten Program
» Plyometrics 2 hand drills
• Week 8:
» Plyo 1 hand drills
» hitting week 10
• Week 11-16:
» ITP Phase I (week 10-11
» ITP Phase II (wk 14-15
• Week 16-21
» Return to play
Dugas, Walters,Franz et al: ‘17
• 170 UCL repairs with internal brace
performed by JRD
• First 40 F/U 1 yr
• 75% baseball players, 3 softball players, 1
football, 1 gymnast, etc…
• 39/40 returned to pre-injury level
• KJOC score in throwers: 93.5
Wilk - Rehabilitation Following UCL Surgery
2017 Injuries in Football Course 2017
46
UCL RECONSTRUCTION REHAB
Conclusions
�Elbow injuries common in the overhead
thrower
�UCL injuries occur in several situations
(throwers, macrotraumtic)
� Surgery often indicated for UCL injuries
�Rehab must match the surgery
�Gradual restoration through rehab
�Excellent outcomes: 85% > return sport
� Stiffness occurs in less than 2%
Predictable & Reproducible Results





























