Embed Size (px)
Citation preview

Journal of Leukocyte Biology Volume 52, September 1992 357
Release of active oxygen radicals by leukocytes of Fanconi
anemia patientsLudmila G. Korkina, Elena V. Samochatova, Aleksei A. Maschan, Tatjana B. Suslova,Zinaida P Cheremisina, and lgor B. Afanas’evRussian Institute of Hematology for Children, Moscow, and Vitamin Research Institute, Moscow
Abstract: The release of oxygen radicals by blood and
bone marrow leukocytes of patients with Fanconi anemia
(FA) has been studied. It was found that the nonstimulatedFA leukocytes and those stimulated by concanavalin A,
Si02, latex, and opsonized zymosan produced enhanced
levels of luminol- and lucigenin-dependent chemilumi-
nescence (CL) in comparison with normal leukocytes. At
the same time, the ratio of the intensity of lucigenin-dependent CL to that of luminol-dependent CL was sig-
nificantly smaller for FA leukocytes than for normal leu-kocytes. From these findings and from the effects of anti-
oxidative enzymes and free radical scavengers on CL, itwas concluded that FA leukocytes release enhanced
amounts of oxygen radicals and that these free radicals
contain enhanced amounts of hydroxyl or hydroxyl-like
radicals more active than superoxide ion. It was proposedthat elevated reactivity of the oxygen radicals released by
FA leukocytes may be a major factor in the development
of Fanconi anemia; this proposal is supported by the first
positive results of treatment of FA patients with rutin (a
nontoxic natural free radical scavenger and chelator).
J. Leukoc. Biol. 52: 357-362; 1992.
Key Words: oxygen radicals . superoxide . leulcocytes . chemi-
luminescence Fanconi anemia
Introduction
Oxygen radical production by leukocytcs has been widely
studied [i]. It was shown that the primary oxygen species
produced by NADPH oxidase of leukocytes and other
phagocytes is superoxide ion. Superoxide ion may be re-
leased by the cells or be converted to much more active oxy-
gen species such as hydroxyl or hydroxyl-like free radicals viathe supcroxidc-driven Fenton reaction (reactions I and 2):
02’ + Fe3� -� 0� + Fe2�
Fe2� + H2O2 : Fe3� + HO #{247}H0
Indeed, release of hydroxyl radicals by stimulated neutro-phils, monocytes, and macrophages has been shown [1].
The yields of superoxide ion and other oxygen species can
be measured by means of luminol- and lucigenin-dependent
chemiluminescence (CL); the latter is considered a specifictest for superoxide production [2]. Both methods have been
applied for measuring oxygen radical production by phago-
cytes. Thus, it has been shown [3] that human granulocytes
stimulated with phytohemagglutin did not release super-
oxide ion because they produced only luminol-dependent
CL, whereas those stimulated with concanavalin A (Con A)released superoxide ion and hydroxyl radicals simultanc-
ously because they produced both luminol- and lucigenin-
dependent CL.
One might expect the development of free radical patholo-
gies to affect the structures and amounts of oxygen radicals
released by phagocytes. A well-known example is the inabil-
ity of leukocytes of patients with chronic granulomatous dis-
ease to produce oxygen radicals due to some defects in the
structure and the activation mechanism of NADPH oxidase
[4]. Another example of free radical pathologies is Fanconi
anemia (FA). FA is an autosomal recessive disorder charac-
terized by progressive pancytopenia, chromosomal instabil-ity, growth retardation, and congenital malfunctions [5].
The erythrocytes of FA patients exhibited decreased super-
oxide dismutase (SOD) activity [6-9] and enhanced super-
oxide production [10]. Therefore, it may be proposed that
the development of FA is a consequence of overproduction of
oxygen radicals.We have studied the production of oxygen radicals by leu-
kocytcs of FA patients, using the luminol- and lucigenin-
dependent CL technique. In contrast to normal leukocytes,
which released mainly superoxide ion, leukocytes of FA pa-
tients released enhanced amounts of active hydroxyl or
hydroxyl-like free radicals. Based on the results of in vitro ex-
periments, the use of the free radical scavenger and chelator
rutin was recommended for treatment of FA patients. Long-
term rutin treatment resulted in some decrease in chro-
mosomal aberrations and improvement of hematological
characteristics and health of FA patients.
MATERIALS AND METHODS
Patients with Fanconi anemia
The diagnosis of FA was confirmed clinically and cytogeneti-
cally for nine patients (one male and eight females). Thepatients’ ages ranged from 6.5 to 14 years. All major manifesta-
(1) tions of the disease were due to pancytopenia (leukocyto-penia, 1.5-3.0 x i0� cells/L blood; erythrocytopenia, 33-
(2) 70 g Hb/L, and platelctpenia, 1-3 x i0�� cells/L). Bone
marrow was hypocellular and contained no more than
2-3 x 1010 cells/L. In all cases, lymphocytosis (more than30%), granulocytopenia, and megakariocytopenia were ob-
served. Diagnosis was confirmed cytogenetically: the total
Abbreviations: CL, chemiluminescence; Con A, concanavalin A; FA,
Fanconi anemia; HBSS, Hanks’ balanced salt solution; NDGA, nordi-
hydroguaretic acid; PMN, polymorphonuclear leukocyte; SOD, superoxide
dismutase.
Reprint requests: I. B. Afanas’ev, Vitamin Research Institute, Nauchny
pr. 14A, 117820, GSP-7, Moscow, Russia.
Received March 9, 1992; accepted April 14; 1992.

358 Journal of Leukocyte Biology Volume 52, September 1992
amount of chromosomal aberrations in blood lymphocyteswas within the range 6-56% and strongly correlated with FA
phenotype. All patients manifested physical and psychic mal-
functions.
Chemicals
Luminol, lucigenin, acctylsalicylic acid (aspirin), colchicine,
nordihydroguaretic acid (NDGA), indomethacin, and latex
were from Sigma; Si02 (DQ 12, world standard) was from
Germany; concanavalin A (Con A) was from Serva; dextranwas from Farmacia, Sweden; phytohemagglutinin P was
from Difco, USA; and rutin and taurin were of USSR
production.
Enzymes
Superoxide dismutase and catalase from bovine erythrocytes
were from Sigma, and horseradish peroxidase (HRP) was
from Rcanal, Hungary.
Preparation of leukocytes
Leukocytes were isolated from peripheral blood of healthy
donors (n = 4) and from peripheral blood and bone marrow
of FA patients (n = 9). The blood samples (5 ml) were col-
lected by venipuncture and anticoagulated with 1 ml of
heparin (20 U) in Hanks’ balanced salt solution (HBSS).
The bone marrow samples (i ml) were obtained by puncture
of sternum. The samples were then scdimcnted with 1 ml of
6% dextran solution at 37#{176}Cfor 30 mm. The white cell-rich
supernatant was centrifuged at lSOg for 10 mm. Cell pellets
were washed twice in the Ca2�, Mg�-frec HBSS. The final
suspension of 2-3 x 106 leukocyte/ml was prepared in
medium 199. The cells were counted with a Coulter counter,
and their viability was assessed by exclusion of 0.2% trypanblue dye. Cell differential count was confirmed by Giemsa
staining. It was found that the blood cell suspension isolated
from normal donors contained 70-80% polymorphonuclear
leukocytes (PMNs), 1-2% monocytes, and 20-30% lympho-
cytes; the bone marrow cell suspension had the same compo-
TABLE 1. Luminol-Dependent CL of Whole Blood, Isolated
Mononuclear Leukocytes, and Total Leukocyte Fraction of FA Patients
CL intensi ty (mV) per 106 cells’
Without Opsonisedstimulus Con A SiO, zymosan Latex
Whole blood 33 190 660 1100 1800Mononuclear leukocytes 43 86 170 250 N.A.bTotal leukocyte fraction 1280 670 2040 3120 2800
‘Average values for three FA patients.bNot analyzed.
sition. Because of neuropenia and lymphocytosis, differentialisolation of PMNs from the cell suspensions of FA patients
was not performed. All measurements of the blood samples
from FA patients and donors were carried out simultaneously.
Chemiluminescence measurements
Lucigenin- and luminol-dependent CL was measured on an
LKB luminometer (model 1251, Sweden). Leukocyte suspen-
sion (50 �jl, 2 x 106 cells/mI), luminol or lucigenin (50 �jM,
final concentration), and 0.85 ml of HBSS were mixed in the
1-ml polystyrene cell at 37#{176}C.After 5 mm, the 0.5% suspen-
sion of latex (50 gil), the suspension of Si02 (50 gil,
10 mg/mi), or Con A (50 gil, I mg/ml) in 0.9% NaC1 solution
was added and the light emission was recorded continuously.
The intensity of spontaneous CL and the difference between
the maximal values of the cellular CL response to an am-
plifier (luminol or lucigenin) and of spontaneous CL were
measured. When the effects of free radical scavengers andenzyme inhibitors were studied, 50 �tl of the solutions of cor-
responding substances (20-100 cM) was added before the be-
ginning of experiments.
Cytogenetic analysis
The whole blood of FA patients was cultured according to
the standard method [11]. The cultured mixture contained
10% blood, 15% fetal calf serum, and 75% medium 199.
Lymphocyte mitosis was stimulated by the addition of phor-
TABLE 2. Luminol-Dependent CL of a Total Fraction of Blood Leukocytes of FA Patients and Normal Donors
‘(PMN) (mV ) per 106 cells
Without
Patients/donors stimulus Con A SiO, Latex
FA patientsD-vaSh-ov
17,300 (2,900)’
1,100 (300)
4,300 (740)
NA.”
15,600 (2,600)
5,000 (1,400)
19,000 (3,300)
6,400 (1,800)
M-ko NA. 1,200 (710) 4,300 (2,500) NA.
O-ch 500 (220) 1,200 (560) 6,000 (2,700) NA.
Mi-ov 1,400 (420) NA. 11,100 (3,300) 12,200 (3,700)
Dz-ov 230 (90) NA. 2,800 (1,100) 3,400 (1,300)
G-ov 590 (200) NA. 7,200 (2,500) 14,000 (4,900)
M-ovaA. 1,300 (240) NA. 3,600 (690) 7,300 (1,400)
M-ova E. 1,200 (290) NA. 6,300 (1,500) 15,000 (3,700)
Average 3,000 -2000 6,900 ± 4,070 11,000 ± 5,500
Donorsb
1 270 (190) 360 (250) 1,140 (800) 1,010 (710)
2 300 (210) 310 (220) 760 (530) 990 (690)
.3 14 (10) 400 (280) 210 (150) NA.
4 60 (40) 600 (420) 1,160 (810) NA.
Average -200 410 ± 160 810 ± 440 1,000 ± 15
‘(Icuk) values are given in parentheses. !(PMN) values of FA patients are calculated from equation 3.
bNot analyzed.
‘For donors I(PMN) values are equal to

TABLE 3. Luminol-Dependent CL of Bone Marrow Leukocytes of FA Patients and Normal Donors
Korkina et al. Oxygen radicals in Fanconi anemia 359
Patients/donors % PMNs
‘(PMN) (mV) per 106 cells
Without
stimulus Con A SiO,Opsonized
zymosan
FA patients
D-vaM-ko
Donors
1
2
18
42
70
70
560 (100)’
240 (100)
290 (200)
110 (80)
310 (60)
360 (150)
140 (100)
210 (150)
1000 (180)
620 (260)
540 (380)
170 (120)
1600 (290)
620 (260)
510 (360)
830 (580)
‘(kuk) values are given in parentheses.
bol myristate acetate at the beginning of cultivation. The
total period of cultivation at 37#{176}Cwas 56 h. At 2.5 h beforefixation of the cells, 0.1 ml of a colchicine solution of final
concentration 0.25 mg/mI was added. Fixation was per-
formed by a standard cytological procedure. The cells were
exposed to 0.075 M KC1 solution for 10-12 mm and fixed in
ethanol-acetic acid solution (3:1 v/v).
RESULTS
Luminol- and lucigenin-dependent CL of blood andbone marrow leukocytes
The results of measurements of luminol- and lucigenin-
dependent CL of nonstimulated and stimulated blood and
bone marrow leukocytes of healthy donors and FA patients
are given in Tables 1-4. It is known [12] that PMNs make
a major contribution to the total CL response of whole blood
or isolated cell suspensions. Therefore, the intensity of non-
stimulated and stimulated CL depends linearly on the
amount of PMNs in cell suspensions. Because of this, the CL
intensity induced by PMNs can be calculated from the CL
intensity of the total leukocyte fraction, using equation 3:
100 V-1(PMNs) = ‘(leuk)
vCn
where v is the cell suspension volume, V the volume of the
cuvette, C the leukocyte concentration, and n the PMN con-
tent (%).The data in Table 1 confirm the above proposal. In all
cases the CL intensity of mononuclear leukocytes did not ex-
ceed 10% of the intensity of the total leukocyte fraction, in-
dicating a predominant contribution of PMNs in the CL re-sponse. As could be expected, the CL intensity of the whole
blood was much lower than that of the total leukocyte frac-
tion because of inhibition by erythrocytes and other blood
components. Opsonised zymosan (acting through the recep-tor of the C3 component of complement), Con A (acting
through lectin-like receptors), latex, and SiO2 (stimulatingthe phagocytes without receptor activation) significantly en-
hanced the luminol-dependent CL induced by blood leuko-
cytes of FA patients and normal donors (Tables I and 2). The
same was true for bone marrow leukocytes (Table 3),although in this case the levels of stimulated and nonstimu-
lated CL were much lower. The luminol-dependcnt CL of
leukocytes of FA patients always exceeded that of normal
donors.Similar findings were obtained for the lucigcnin-dependcnt
CL of leukocytes; however, here the difference between the
CL levels for leukocytes of FA patients and donors was sig-
nificantly smaller (Table 4).
Effects of antioxidative enzymes, free radicalscavengers, and enzyme inhibitors onchemiluminescence of leukocytes
The antioxidative enzyme SOD inhibited the luminol-
dependent CL of blood leukocytes of FA patients by 5-15%
and that of blood leukocytes of normal donors by 60-70%
(Table 5). Similarly, SOD strongly inhibited the lucigenin-
dependent CL of leukocytes (data not shown). Catalase,
another major antioxidative enzyme, had little effect on theluminol-dependent CL of leukocytes of Fanconi patients; in
three cases it even slightly enhanced the CL intensity. The
inhibitory effect of catalase on the luminol-dependent CL of
lcukocytcs of normal donors was 40-65%.
The bioflavonoid rutin, which is a free radical scavenger
and an iron chclator simultaneously [13], strongly inhibited
the luminol-dcpcndent CL of FA leukocytes in a concen-
tration-dependent manner (Fig. 1) and was a less effective
inhibitor in the case of normal donors (Table 5).
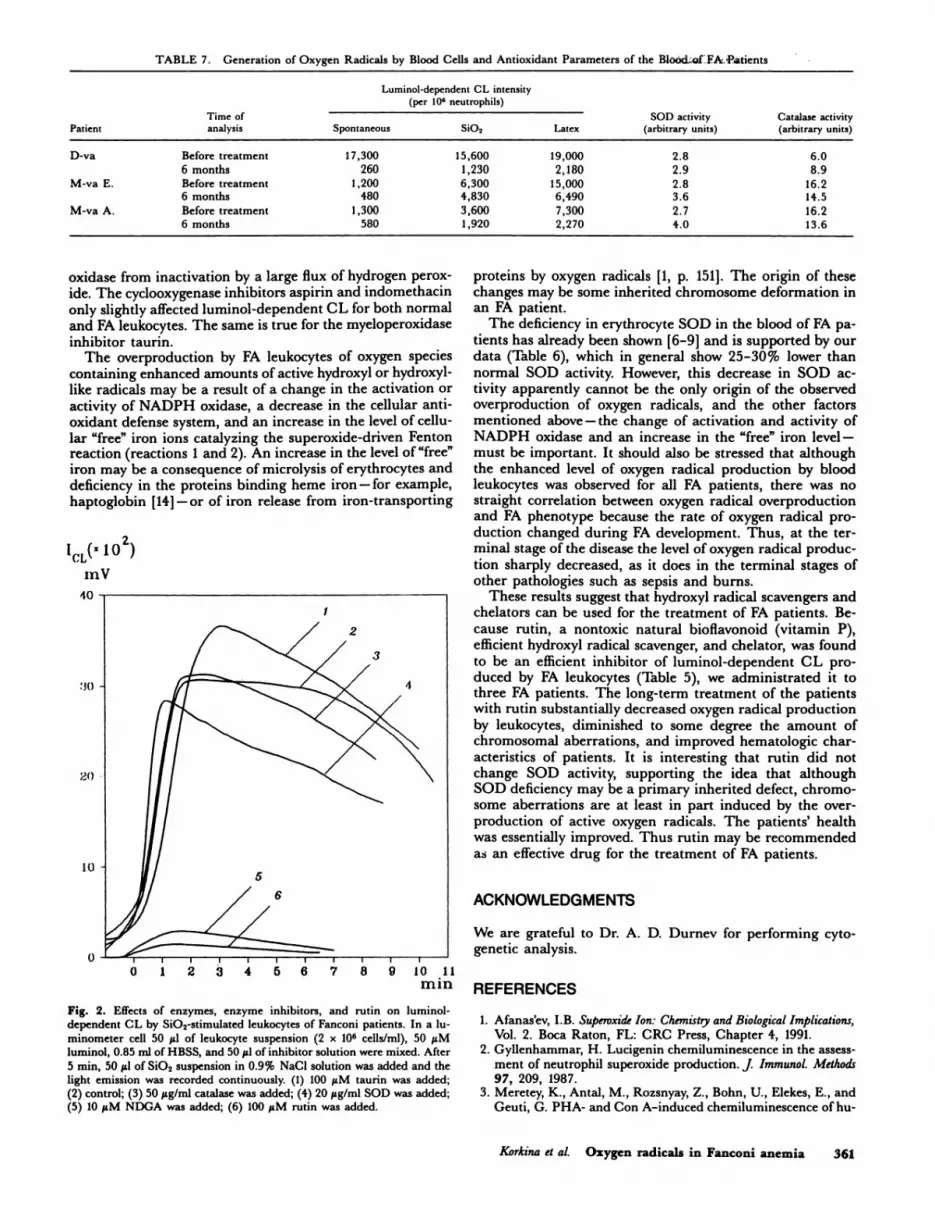
Aspirin and indomethacin, inhibitors of cyclooxygenase,
and taurin, an inhibitor of myeloperoxidase, inhibited the
luminol-dcpendcnt CL of both FA patients and donors by
only 10-30%, but NDGA, an inhibitor of lipoxygenase and
(3) a free radical scavenger, was a very strong inhibitor of
luminol-dependent CL of leukocytes of both FA patients
(Fig. 2) and normal donors (Table 5).
Therapeutic treatment
Patients were given 10 mg rutin/kg body weight three times
per day. Long-term treatment with rutin was possible only
TABLE 4. CompLatex-Stimulate
arison of Luminol- and Lucigenin-Dependent CL ofd Leukocytes of FA Patients and Normal Donors’
Patients/donors
‘(PMN) (mV) per 106 cells ‘�l,,rig,nm)
‘(Iu,mnoi)‘(i,�minoI) ��k�ig�nin)
FA patients
D-va 20,600 1,350 0.07
M-ko 29,000 750 0.03Dz-ov 3,350 130 0.04
G-ov 15,700 4,350 0.28
Donors
1 1,470 360 0.24
2 1,700 170 0.10
3 1,200 120 0.10
‘The luminol- and lucigenin-dependent CL data were obtained for sam-
ples other than those cited in Table 2. This explains the difference in the
luminol-dependent CL data presented in Tables 2 and 4.

‘Refractory to splenectomy and treatment with prednisolone and methan-
drostenolone.�‘Twins.
0 1 2 3 4 5 6 7
360 Journal of Leukocyte Biology Volume 52, September 1992
TABLE 5. Effects of Antioxidative Enzymes, Free Radical Scav
and Enzyme Inhibitors on the Luminol-Dependent CL ofBlood Leukocytes
engers,
Inhibition (%)
ConcentrationInhibitor (tiM) FA patients Donors
SOD 20 (�ig/ml) 5-15
Catalase 50 (�ig/ml) 0-7’Rutin 100 75-95
60-70
40-65
30-70NDGA 10 85-90 85-95Aspirin 50 7-15 na.
Indomethacin 50 10-20 7-30Taurin 100 0 (or activation)
Mannitol 10,000 48-5010-15
0
‘In three cases there was activation by 5-15%.
for three patients (for 3 years in the case of one female child
and for 1 year in the case of two female children). No side
effects were observed in patients during the long-term rutin
treatment. Hematological parameters and CL data for FApatients subjected to rutin treatment are given in Tables 6
and 7. Chromosome aberrations in lymphocytes of periph-
eral blood were measured for three FA patients to whom
rutin was administrated for 6 months. It was found that
chromosomal aberrations diminished from 15.5 to 7.7% for
one patient (D-va) and did not change essentially for twoothers (M-va A. and M-va E.).
There were improvements in physical conditions of FA pa-
tients. For example, D-va’s height increased by 8 cm and
I(.L( 102)
IHV
Fig. 1. Effect of rutin on luminol-dependent CL by the latex-stimulated leu-
kocytes of Fanconi patients. In a luminometer cell 50 �sl of leukocyte suspen-
sion (2 x 106 cells/mI), 50 1sM luminol, and 0.85 ml of HBSS were mixed.
After 5 mm, 50 �tl of 0.5% latex suspension in 0.9% NaCI solution was
added and the light emission was recorded continuously. (1) Without rutin;
(2-4) 10, 20, and 100 sM rutin were added, respectively; (5) without latex.
TABLE 6. Hematological Parameters of FA Patients Before and After
Long-Term Rutin Treatment
Patient
Time of
analysis Hb
Leukocytes
(% neutrophils) Platelets
D-va’
M-va E.’5
M-va A.”
Before treatment
6 months
11 months
18 months
Before treatment
6 monthsBefore treatment
6 months
56
96
93
125
34
125
25
113
3.4 (17)
6.2 (65)
3.8 (42)
5.2 (59)
3.0 (30)
4.1 (56)
1.3 (26)
2.3 (50)
28
190
48
5850
120
Single
50
body weight by 7.5 kg in 1.5 years. The secondary sexual in-
dications appeared.
DISCUSSION
The results of the study of luminol-dependent CL suggest
that blood leukocytes of FA patients produce an enhanced
level of active oxygen species in comparison with those of
normal donors (Table 2). A similar but weaker tendency is
observed for bone marrow leukocytes (Table 3). The stimula-
tion of luminol-dependent CL by zymosan, latex, SiO2, and
Con A indicates that an increase in oxygen radical produc-
tion by FA leukocytes may be a consequence of binding C3
or lectin-like receptors or of nonreceptor stimulation.
The level of lucigenin-dependent CL was also higher for
blood leukocytes of FA patients than for normal donors, but
the most significant difference was observed for a ratio of the
intensities of lucigenin- and luminol-dependent CL (Table
4). It is thought [2] that lucigenin-dependent CL is a specific
test for superoxide production, whereas luminol-dependent
CL is apparently relevant to the production of all active oxy-gen species. Therefore, one may conclude not only that the
leukocytes of FA patients produce an enhanced amount of
oxygen species but also that these species contain much more
active oxygen radicals that are different from superoxide ion.
This proposal was confirmed in the study of inhibitory
effects of SOD and hydroxyl radical scavengers on the pro-duction of oxygen radicals by Icukocytes of normal donors
and FA patients (Table 5). SOD inhibited the luminol-
dependent CL of normal leukocytes by 60-70% and that of
FA leukocytes by 5-15%. These data support the conclusion
that superoxide production is predominant in normal leuko-
cytes and relatively unimportant in FA leukocytes. On the
other hand, mannitol, a classical hydroxyl radical scavenger,
inhibited the luminol-dependent CL of FA leukocytes by50% and did not affect that of normal leukocytes. This indi-
cates that FA leukocytes produce a significant amount ofhydroxyl radicals and normal leukocytes do not.
Two other hydroxyl radical scavengers, rutin and NDGA,
were also very efficient inhibitors of oxygen radical produc-
tion by FA leukocytes (Table 5). However, they also inhibited
8 mi�� oxygen radical production by normal leukocytes, being
simultaneously a chelator and superoxide scavenger (rutin)
and a lipoxygenase inhibitor (NDGA). Catalase inhibited
luminol-dependent CL of normal leukocytes (by 40-65%)
and did not affect it or even enhanced it in the case of FA leu-
kocytes (Table 5). The last is probably explained by the fact
that exogenous catalase can protect the leukocyte NADPH
[1
10 �11mi n
TABLE 7. Generation of Oxygen Radicals by Blood Cells and Antioxidant Parameters of the Blood..of FAPatients
Korkina et a!. Oxygen radicals in Fanconi anemia 361
Time of
Luminol-
(pe
dependent CL intensity
r 106 neutrophils)
SOD activity Catalase activity
Patient analysis Spontaneous SiO, Latex (arbitrary units) (arbitrary units)
D-va Before treatment
6 months
17,300
260
15,600
1,230
19,000
2,180
2.8
2.9
6.0
8.9
M-va E. Before treatment
6 months
1,200
480
6,300
4,830
15,000
6,490
2.8
3.6
16.2
14.5
M-va A. Before treatment
6 months
1,300
580
3,600
1,920
7,300
2,270
2.7
4.0
16.2
13.6
oxidase from inactivation by a large flux of hydrogen perox-
ide. The cyclooxygenase inhibitors aspirin and indomethacin
only slightly affected luminol-dependent CL for both normal
and FA leukocytes. The same is true for the myeloperoxidase
inhibitor taurin.The overproduction by FA leukocytes of oxygen species
containing enhanced amounts of active hydroxyl or hydroxyl-
like radicals may be a result of a change in the activation or
activity of NADPH oxidase, a decrease in the cellular anti-
oxidant defense system, and an increase in the level of cellu-
lar “free” iron ions catalyzing the superoxide-driven Fentonreaction (reactions 1 and 2). An increase in the level of “free”
iron may be a consequence of microlysis of erythrocytcs and
deficiency in the proteins binding heme iron - for example,
haptoglobin [14] -or of iron release from iron-transporting
1CL( 102)
‘fly
Fig. 2. Effects of enzymes, enzyme inhibitors, and rutin on luminol-
dependent CL by SiO2-stimulated leukocytes of Fanconi patients. In a lu-
minometer cell 50 �il of leukocyte suspension (2 x 106 cells/mI), 50 �sM
luminol, 0.85 ml of HBSS, and 50 �sl of inhibitor solution were mixed. After
5 mm, 50 �sl of SiO2 suspension in 0.9% NaCI solution was added and thelight emission was recorded continuously. (1) 100 �M taurin was added;
(2) control; (3) 50 �sg/ml catalase was added; (4) 20 �ag/ml SOD was added;(5) 10 �tM NDGA was added; (6) 100 �tM rutin was added.
proteins by oxygen radicals [1, p. 151]. The origin of these
changes may be some inherited chromosome deformation in
an FA patient.
The deficiency in erythrocyte SOD in the blood of FA pa-
tients has already been shown [6-9] and is supported by our
data (Table 6), which in general show 25-30% lower than
normal SOD activity. However, this decrease in SOD ac-
tivity apparently cannot be the only origin of the observed
overproduction of oxygen radicals, and the other factorsmentioned above - the change of activation and activity of
NADPH oxidase and an increase in the “free” iron level -must be important. It should also be stressed that although
the enhanced level of oxygen radical production by blood
leukocytes was observed for all FA patients, there was nostraight correlation between oxygen radical overproduction
and FA phenotype because the rate of oxygen radical pro-
duction changed during FA development. Thus, at the ter-
minal stage of the disease the level of oxygen radical produc-
tion sharply decreased, as it does in the terminal stages of
other pathologies such as sepsis and burns.These results suggest that hydroxyl radical scavengers and
chelators can be used for the treatment of FA patients. Be-
cause rutin, a nontoxic natural bioflavonoid (vitamin P),
efficient hydroxyl radical scavenger, and chelator, was found
to be an efficient inhibitor of luminol-dependent CL pro-
duced by FA leukocytes (Table 5), we administrated it to
three FA patients. The long-term treatment of the patients
with rutin substantially decreased oxygen radical production
by leukocytcs, diminished to some degree the amount of
chromosomal aberrations, and improved hematologic char-
acteristics of patients. It is interesting that rutin did not
change SOD activity, supporting the idea that althoughSOD deficiency may be a primary inherited defect, chromo-
some aberrations are at least in part induced by the over-
production of active oxygen radicals. The patients’ health
was essentially improved. Thus rutin may be recommended
as an effective drug for the treatment of FA patients.
ACKNOWLEDGMENTS
We are grateful to Dr. A. D. Durnev for performing cyto-
genetic analysis.
REFERENCES
1. Afanas’ev, LB. Superoxide Ion: Chemistry and Biological Implications,Vol. 2. Boca Raton, FL: CRC Press, Chapter 4, 1991.
2. Gyllenhammar, H. Lucigenin chemiluminescence in the assess-ment of neutrophil superoxide production. j Immunol. Methods
97, 209, 1987.3. Meretcy, K., Antal, M., Rozsnyay, Z., Bohn, U., Elekes, E., and
Geuti, G. PHA- and Con A-induced chemiluminescence of hu-

362 Journal of Leukocyte Biology. Volume 52, September 1992
man blood mononuclear cells and granulocytes in luminol orlucigenin. Inflammation 11, 417, 1987.
4. Bellavite, P. The superoxide-forming enzymatic system of
phagocytes. Free Radicals Biol. Med. 4, 225, 1988.5. Schroeder-Kurth, TM., Auerbach, AD., and Obe, G. (Eds.)
Fanconi Anemia, Clinical, Cytogenetic and Experimental Aspects.
Berlin: Springer-Verlag, 1990.
6.Joenje, H., Eriksson, A.W., Frants, R.R., Arwert, F., and
Houwen, B. Erythrocyte superoxide dismutase deficiency in
Fanconi’s anaemia. Lancet 1, 204, 1978.
7. Mavelli, I., Ciriolo, MR., and Rotilio, G. Superoxide dismu-
tase, glutathionc peroxidase and catalase in oxidative hemoly-
sis. A study of Fanconi’s anemia erythrocytes. Biochem. Biophys.
Res. Common. 106, 286-290, 1982.
8. Okahata, S., Kobayashi, Y., and Usui, T. Erythrocyte super-
oxide dismutase in Fanconi’s anaemia. C/in. Sci. 58, 173, 1980.
9. Yoshimitsu, K., Kobayashi, Y., and Usui, T. Decreased super-oxide dismutase activity of erythrocytes and leukocytes in Fan-
coni’s anemia. Acta HaemotoL 27, 208, 1984.
10. Scarpa, M., Rmgo, A., Momo, E, Isacchi, G., Novelli, G., andDallapiccola, B. Increased rate of superoxide ion generation in
Fanconi anemia erythrocytes. Biochem. Biophys. Res. Commun.
130, 127, 1985.
11. Korkina, L.G., Durnev, AD., Suslova, TB., Cheremisina, Z.P.,
Daugel-Dauge, NO., and Afanas’ev, lB. Oxygen radical medi-ated mutagenic effect of asbestos on human lymphocytes: sup-
pression by oxygen radical scavengers. Mutat. I�es. 265, 245,1992.
12. Lindena, J., and Purkhardt, H. Separation and chemilumines-cence of human, canine and rat polymorphonuclcar cells,
j ImmunoL Methods 115, 141, 1988.13. Afanas’e� lB., Dorozhko, Al., Brodskim, A.V., Kostyuk, V.A.,
and Potapovitch, A.!. Chelating and free radical scavengingmechanisms of inhibitory action of rutin and quercetin in lipid
peroxidation. Biochein. Pharmacol. 38, 1763, 1989.
14. Gutteridge, J.M.C., Westermarck, T., and Halliwell, B. Oxygen
radical damage in biological systems. In Free Radicals, Aging andDegenerative Diseases. New York: Alan R. Liss, p. 99, 1985.





























