Embed Size (px)
Citation preview
REVIEW: Aromatase Inhibitors for Ovulation Induction
Robert F. Casper and Mohamed F. M. Mitwally
Division of Reproductive Sciences (R.F.C.), Fran and Lawrence Bloomberg Department of Obstetrics and Gynecology,Samuel Lunenfeld Research Institute, Mount Sinai Hospital and The University of Toronto, Toronto, Ontario, Canada M5S2X9; and Division of Reproductive Endocrinology and Infertility (M.F.M.M.), Department of Obstetrics and Gynecology,Wayne State University, Detroit, Michigan 48202
Context: For the last 40 yr, the first line of treatment for anovulationin infertile women has been clomiphene citrate (CC). CC is a safe,effective oral agent but is known to have relatively common anties-trogenic endometrial and cervical mucous side effects that could pre-vent pregnancy in the face of successful ovulation. In addition, thereis a significant risk of multiple pregnancy with CC, compared withnatural cycles. Because of these problems, we proposed the concept ofaromatase inhibition as a new method of ovulation induction thatcould avoid many of the adverse effects of CC. The objective of thisreview was to describe the different physiological mechanisms ofaction for CC and aromatase inhibitors (AIs) and compare studies ofefficacy for both agents for ovulation induction.
Evidence Acquisition: We conducted a systematic review of all thepublished studies, both controlled and noncontrolled, comparing CCand AI treatment, either alone or in combination with gonadotropins,for ovulation induction or augmentation, identified through the En-trez-PubMed search engine.
Evidence Synthesis: Because of the recent acceptance of the conceptof using AIs for ovulation induction, few controlled studies were iden-tified, and the rest of the studies were pilot or preliminary compar-isons. Based on these studies, it appears that AIs are as effective asCC in inducing ovulation, are devoid of any antiestrogenic side effects,result in lower serum estrogen concentrations, and are associatedwith good pregnancy rates with a lower incidence of multiple preg-nancy than CC. When combined with gonadotropins for assisted re-productive technologies, AIs reduce the dose of FSH required foroptimal follicle recruitment and improve the response to FSH in poorresponders.
Conclusions: Preliminary evidence suggests that AIs may replaceCC in the future because of similar efficacy with a reduced side effectprofile. Although worldwide experience with AIs for ovulation induc-tion is increasing, at present, definitive studies in the form of ran-domized controlled trials comparing CC with AIs are lacking. (J ClinEndocrinol Metab 91: 760–771, 2006)
FOR THE LAST 40 yr, the first line of treatment for anovu-lation in infertile women has been clomiphene citrate
(CC). The choice of CC was appropriate because the drugwas highly effective in inducing ovulation in selected pa-tients with the advantages of being orally administered, rel-atively safe, and inexpensive. In contrast, alternative treat-ments usually involved parenteral gonadotropins that weresignificantly more complicated and uncomfortable to ad-minister, expensive, and associated with more frequent andserious complications. However, CC was also found to haveadverse effects, especially in the form of common antiestro-genic endometrial and cervical mucous changes that couldprevent pregnancy in the face of successfully induced ovu-lation. We believed it was time to develop a more effectiveovulation induction agent, and we have demonstrated thataromatase inhibitors (AIs) seem to be a promising alternativeto CC for ovulation induction. The purpose of this reviewwas to outline the data collected by us and others, over thepast 5 yr, regarding the use of AIs for ovulation induction.We will start with a brief description of the physiology of thenormal ovulatory cycle, information required for the reader
to understand the mechanism of action and problems withCC as well as the mechanism of action and advantages of AIs.
Physiological Basis of Ovulation
The ovarian cortex at puberty contains hundreds of thou-sands of primordial follicles (1). In response to unknownsignals, independent of gonadotropins, a cohort (hundreds)of primordial follicles is recruited to grow (2). During thisearly follicle development, the oocyte enlarges and the gran-ulosa cells proliferate to form a preantral follicle. Over 3–6months, the follicle develops FSH receptors in the granulosacells and LH receptors in the theca cells, and the follicle formsa fluid-filled space called an antrum (1). At this stage, antralfollicles become acutely dependent on FSH for further de-velopment (1). In natural cycles just before menses, fallingestrogen levels result in withdrawal of negative feedbackcentrally leading to increased gonadotropins levels (3). FSHstimulates granulosa cell proliferation and differentiation,with the development of more FSH receptors and the pro-duction of aromatase (4). LH stimulates androstenedioneproduction by theca cells that diffuses into the granulosa cellproviding substrate for estrogen secretion. This step is cat-alyzed by the aromatase enzyme, which is induced by FSH.The so-called two-cell, two-gonadotropin theory (5, 6) pos-tulated that FSH concentrations must exceed a certain level(FSH threshold) before follicular development will proceed.The duration of this period in which the threshold is ex-ceeded (the FSH window) is limited in the normal cycle bya gradual decrease in FSH, occurring in the early-midfol-
First Published Online December 29, 2005Abbreviations: AI, Aromatase inhibitor; CC, clomiphene citrate;
COH, controlled ovarian stimulation; E2, estradiol; ER, estrogen recep-tor; hCG, human chorionic gonadotropin; IUI, intrauterine insemina-tion; IVF, in vitro fertilization; OHSS, ovarian hyperstimulation syn-drome; PCOS, polycystic ovary syndrome.JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the en-docrine community.
0021-972X/06/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 91(3):760–771Printed in U.S.A. Copyright © 2006 by The Endocrine Society
doi: 10.1210/jc.2005-1923
760
at Pakistan:Endo Jnls Sponsored on November 7, 2008 jcem.endojournals.orgDownloaded from

licular phase as a response to negative feedback from risingestrogen levels produced by the larger follicles (7). Smallerfollicles, with fewer FSH receptors, are no longer stimulatedto grow by FSH levels below the FSH threshold and undergoatresia (8). Therefore, generally only one follicle reaches thestage of ovulation each cycle, despite the fact that hundredsof primordial follicles, the number of which varies depend-ing on a woman’s age, may have begun development in thesame cohort 3–6 months earlier.
Administering exogenous FSH prolongs the time FSH lev-els are above the FSH threshold and extends the FSH win-dow. This allows multiple ovulation by rescuing smallerfollicles that would otherwise have undergone atresia. Inaddition, FSH also induces LH receptors in larger antralfollicles above 1.0 cm in diameter (9). At this point, LH cansubstitute for FSH in stimulating follicle growth and aro-matase activity (10). This observation led Sullivan et al. (11)and Filicori et al. (12) to postulate that exogenous LH/humanchorionic gonadotropin (hCG) could be used as a substitutefor FSH to continue follicular maturation before ovulation.
Rapidly increasing levels of estradiol produced by themature preovulatory follicle precede the midcycle LH andFSH surge that will initiate ovulation. The duration andcirculating level of estradiol seem to be the determinant of thetiming of the LH surge. Although the actual trigger of thesurge is unclear, there is the suggestion that it may be aresponse to a rise in both estrogen and progesterone (13),with a role for diurnal and estradiol-dependent changes inGnRH neuron firing activity (14). Angiogenesis and lutein-ization of granulosa and theca cells occur to form the corpusluteum in which an alteration of the steroidogenic pathwayresults in progesterone as the primary steroid hormone pro-duced after luteinization. The corpus luteum retains the abil-ity to produce estrogen. In addition, the demonstration ofmultiple waves of follicular growth in the majority of cycles(15) also suggests that some estrogen in the luteal phase maybe contributed by growing follicles that will subsequentlyundergo atresia. With implantation and pregnancy, hCGproduction by the trophoblast results in maintenance of cor-pus luteum function. Luteal progesterone is required untilabout 8 wk gestation when the placenta takes over proges-terone production (16). In the absence of pregnancy, LHlevels likely become too low to sustain the corpus luteum, asa result of very infrequent LH pulses (17). The corpus luteumundergoes regression with a fall in progesterone and estro-gen and the onset of menses. FSH levels rise with withdrawalof estrogen negative feedback and the next cohort of folliclesbegins to develop. The laboratory of Yen and colleagues (18)demonstrated, using naloxone (narcotic antagonist) infu-sions, that increased central endogenous opioid peptide ac-tivity is the cause of the decreased pulse frequency in theluteal phase. Such endogenous opioid activity is induced byelevated levels of progesterone.
In summary, normal follicular development culminates inovulation of a mature oocyte, followed by the developmentof a corpus luteum producing adequate amount of proges-terone. This sequence of events is orchestrated by the inter-action of local ovarian factors and endocrine factors from thepituitary and hypothalamus. The presence of subtle abnor-malities despite the occurrence of ovulation may be respon-
sible, at least in part, for unexplained infertility in somewomen, and perhaps for endometriosis-related infertility.On the other hand, overt anovulation or oligoovulation hasbeen traditionally classified into three groups: World HealthOrganization (WHO) types I, II, and III anovulation.
WHO Classification of Anovulation
Women in WHO group I suffer from a defect at the levelof the hypothalamus/pituitary. They are estrogen deficientwith normal or low FSH or prolactin levels. They typicallyhave amenorrhea and do not bleed in response to progestinchallenge. They generally require pulsatile GnRH infusionsor injectable gonadotropins to ovulate.
Women in WHO group II are not estrogen deficient. TheirFSH and prolactin levels are normal. They typically experi-ence oligomenorrhea, but they may have anovulatory cyclesor amenorrhea with bleeding in response to a progestin chal-lenge. This is the most common type of anovulation andincludes women with polycystic ovary syndrome (PCOS).For this group, oral agents such as insulin sensitizers, CC, ormore recently AIs are useful for ovulation induction.
Women in WHO group III include those with elevatedgonadotropins secondary to primary ovarian failure mainlydue to diminished ovarian reserve and loss of ovarian fol-licles. They are resistant to various methods of ovarian stim-ulation, and the best approach for their infertility is oocytedonation.
The present review will focus on the use of the oral agents,CC and AIs, to induce ovulation in women with WHO groupII anovulation.
Clomiphene Citrate
For more than 40 yr, CC has been the most commonly usedoral agent for induction of ovulation. In 1961 Greenblatt et al.(19) published the first results of ovulation inductionachieved by CC (at that time known as MRL/41). Since theearly 1960s, pregnancy rates with CC treatment have notchanged appreciably, despite advances in cycle monitoring.It is interesting to note that CC is considered pregnancy riskcategory X. This is particularly important when consideringits relatively long clearance half-life of about 5 d to 3 wk(depending on the isomer) and that CC may be stored inbody fat (20, 21).
Chemical structure and pharmacokinetics
Chemically, CC is a nonsteroidal triphenylethylene deriv-ative that exhibits both estrogen agonist and antagonist prop-erties, i.e. selective estrogen receptor modulating activity. CCis a racemic mixture of two distinct stereoisomers, enclomi-phene and zuclomiphene, having different properties. Avail-able evidence indicates that enclomiphene is the more potentantiestrogenic isomer primarily responsible for the ovula-tion-inducing actions of CC (20, 21). Currently available clo-miphene compounds are skewed toward enclomiphene pre-dominance. Levels of enclomiphene rise rapidly afteradministration and fall to undetectable concentrations aftera few days. Zuclomiphene is cleared far more slowly; levelsof this less active isomer remain detectable in the circulation
Casper and Mitwally • Aromatase Inhibitors for Ovulation Induction J Clin Endocrinol Metab, March 2006, 91(3):760–771 761
at Pakistan:Endo Jnls Sponsored on November 7, 2008 jcem.endojournals.orgDownloaded from

for more than 1 month after treatment and may actuallyaccumulate over consecutive cycles of treatment (21).
Mechanism of action of CC
CC binds to estrogen receptors (ERs) throughout thebody due to its structural similarity to estrogen. CC bind-ing to ERs occurs for an extended period of time, i.e. weeksrather than hours as with natural estrogen. Such extendedbinding ultimately depletes ER concentrations by inter-fering with the normal process of ER replenishment (19,22). The antiestrogenic effect on the hypothalamus, and thepituitary, is believed to be the main mechanism of actionfor ovarian stimulation. Depletion of hypothalamic ERsprevents correct interpretation of circulating estrogen lev-els; estrogen concentrations are falsely perceived as lowleading to reduced estrogen-negative feedback on GnRHproduction and subsequent increased gonadotropin (FSHand LH) secretion (Fig. 1). The rise of FSH promotesgrowth of ovarian follicles and ovulation in anovulatorywomen. It is believed that the hypothalamus is the mainsite of action because in normally ovulatory women, CCtreatment was found to increase GnRH pulse frequency(23). However, actions at the pituitary level may also beinvolved because CC treatment increased pulse amplitudebut not frequency in anovulatory women with PCOS, inwhom the GnRH pulse frequency is already abnormallyhigh (24).
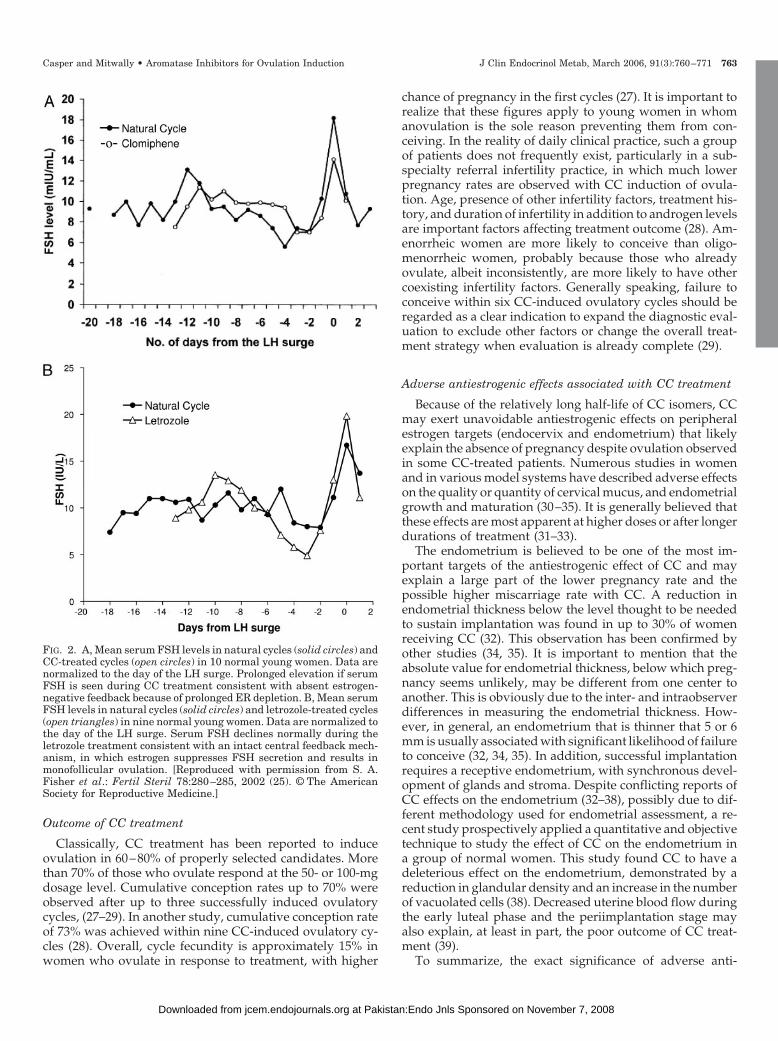
During CC treatment, levels of both LH and FSH undergoa prolonged rise, compared with a natural cycle (Fig. 2A) (25)because of the prolonged ER depletion in the brain. Supra-physiological levels of estrogen can occur without centralsuppression of FSH because the normal ER-mediated feed-back mechanisms are blocked as a result of prolonged ERdepletion (Fig. 1). This pertubation of normal negative feed-back is reflected in the FSH window being extended, leadingto multiple follicle growth and a higher multiple pregnancyrate with CC than occurs in natural cycles.
Indications
The two main indications for CC treatment are inductionof ovulation in anovulatory infertility and stimulating mul-tifollicular ovulation or enhancing ovulation in ovulatoryinfertile women, e.g. unexplained infertility. For anovulatoryinfertility, CC treatment will likely be effective only in con-ditions in which adequate levels of circulating estrogen existto exert estrogen-negative feedback on gonadotropin pro-duction, which in turn could be antagonized by the anties-trogenic effect of CC as explained above. Adequate estrogenlevels for a response to CC are hard to determine in absolutevalues. However, a withdrawal bleed after progesterone ad-ministration is usually a reasonable clinical evidence for ad-equate levels of circulating estrogen. CC is the initial treat-ment of choice for most anovulatory or oligoovulatoryinfertile women who are euthyroid and euprolactinemic buthaving adequate circulating levels of estrogen (WHO type IIanovulation, e.g. PCOS. On the other hand, women with verylow circulating estrogen levels such as (WHO types I and III)or women with a defective hypothalamic/pituitary axis such
as Sheehan’s syndrome and Kallmann’s syndrome will notrespond to CC treatment.
For ovulatory infertility, CC is believed to enhance chancesof achieving pregnancy by stimulating multifollicular devel-opment as well as alleviating possible subtle ovulation dys-function (26).
Regimens of CC administration
CC is administered orally, usually starting on the secondto fifth day of spontaneous or progestin-induced menses.Treatment typically begins with a 50-mg tablet daily for5 consecutive days, increasing by 50-mg increments insubsequent cycles until ovulation is induced. After ovulationis achieved, the same dose is repeated until pregnancy isachieved or a maximum number of around six cycles isreached. Once the effective dose of CC is established, thereis no indication for further increases in dose unless the ovu-latory response is lost.
FIG. 1. CC (d 5). Administration of CC from d 3 to 7 results in ERdepletion at the level of the pituitary and mediobasal hypothalamus.As a result, estrogen-negative feedback centrally is interrupted andFSH secretion increases from the anterior pituitary leading to mul-tiple follicular growth. D 10, By the late follicular phase, because ofthe long tissue retention of CC, there continues to be ER depletioncentrally, and increased E2 secretion from the ovary is not capable ofnormal negative feedback on FSH. The result is multiple dominantfollicle growth and multiple ovulation. AI (d 5), Administration of anAI from d 3 to 7 results in suppression of ovarian E2 secretion andreduction in estrogen-negative feedback at the pituitary and medio-basal hypothalamus. Increased FSH secretion from the anterior pi-tuitary results in stimulation of multiple ovarian follicle growth. D 10,Later in the follicular phase, the effect of the AI is reduced and E2levels increase as a result of follicular growth. Because AIs do notaffect ERs centrally, the increased E2 levels result in normal negativefeedback on FSH secretion, and follicles less than dominant folliclesize undergo atresia, with resultant monofollicular ovulation in mostcases. [Reproduced with permission from R. F. Casper: Fertil Steril80:1335–1337, 2003 (106). © The American Society for ReproductiveMedicine.]
762 J Clin Endocrinol Metab, March 2006, 91(3):760–771 Casper and Mitwally • Aromatase Inhibitors for Ovulation Induction
at Pakistan:Endo Jnls Sponsored on November 7, 2008 jcem.endojournals.orgDownloaded from
Outcome of CC treatment
Classically, CC treatment has been reported to induceovulation in 60–80% of properly selected candidates. Morethan 70% of those who ovulate respond at the 50- or 100-mgdosage level. Cumulative conception rates up to 70% wereobserved after up to three successfully induced ovulatorycycles, (27–29). In another study, cumulative conception rateof 73% was achieved within nine CC-induced ovulatory cy-cles (28). Overall, cycle fecundity is approximately 15% inwomen who ovulate in response to treatment, with higher
chance of pregnancy in the first cycles (27). It is important torealize that these figures apply to young women in whomanovulation is the sole reason preventing them from con-ceiving. In the reality of daily clinical practice, such a groupof patients does not frequently exist, particularly in a sub-specialty referral infertility practice, in which much lowerpregnancy rates are observed with CC induction of ovula-tion. Age, presence of other infertility factors, treatment his-tory, and duration of infertility in addition to androgen levelsare important factors affecting treatment outcome (28). Am-enorrheic women are more likely to conceive than oligo-menorrheic women, probably because those who alreadyovulate, albeit inconsistently, are more likely to have othercoexisting infertility factors. Generally speaking, failure toconceive within six CC-induced ovulatory cycles should beregarded as a clear indication to expand the diagnostic eval-uation to exclude other factors or change the overall treat-ment strategy when evaluation is already complete (29).
Adverse antiestrogenic effects associated with CC treatment
Because of the relatively long half-life of CC isomers, CCmay exert unavoidable antiestrogenic effects on peripheralestrogen targets (endocervix and endometrium) that likelyexplain the absence of pregnancy despite ovulation observedin some CC-treated patients. Numerous studies in womenand in various model systems have described adverse effectson the quality or quantity of cervical mucus, and endometrialgrowth and maturation (30–35). It is generally believed thatthese effects are most apparent at higher doses or after longerdurations of treatment (31–33).
The endometrium is believed to be one of the most im-portant targets of the antiestrogenic effect of CC and mayexplain a large part of the lower pregnancy rate and thepossible higher miscarriage rate with CC. A reduction inendometrial thickness below the level thought to be neededto sustain implantation was found in up to 30% of womenreceiving CC (32). This observation has been confirmed byother studies (34, 35). It is important to mention that theabsolute value for endometrial thickness, below which preg-nancy seems unlikely, may be different from one center toanother. This is obviously due to the inter- and intraobserverdifferences in measuring the endometrial thickness. How-ever, in general, an endometrium that is thinner that 5 or 6mm is usually associated with significant likelihood of failureto conceive (32, 34, 35). In addition, successful implantationrequires a receptive endometrium, with synchronous devel-opment of glands and stroma. Despite conflicting reports ofCC effects on the endometrium (32–38), possibly due to dif-ferent methodology used for endometrial assessment, a re-cent study prospectively applied a quantitative and objectivetechnique to study the effect of CC on the endometrium ina group of normal women. This study found CC to have adeleterious effect on the endometrium, demonstrated by areduction in glandular density and an increase in the numberof vacuolated cells (38). Decreased uterine blood flow duringthe early luteal phase and the periimplantation stage mayalso explain, at least in part, the poor outcome of CC treat-ment (39).
To summarize, the exact significance of adverse anti-
FIG. 2. A, Mean serum FSH levels in natural cycles (solid circles) andCC-treated cycles (open circles) in 10 normal young women. Data arenormalized to the day of the LH surge. Prolonged elevation if serumFSH is seen during CC treatment consistent with absent estrogen-negative feedback because of prolonged ER depletion. B, Mean serumFSH levels in natural cycles (solid circles) and letrozole-treated cycles(open triangles) in nine normal young women. Data are normalized tothe day of the LH surge. Serum FSH declines normally during theletrozole treatment consistent with an intact central feedback mech-anism, in which estrogen suppresses FSH secretion and results inmonofollicular ovulation. [Reproduced with permission from S. A.Fisher et al.: Fertil Steril 78:280–285, 2002 (25). © The AmericanSociety for Reproductive Medicine.]
Casper and Mitwally • Aromatase Inhibitors for Ovulation Induction J Clin Endocrinol Metab, March 2006, 91(3):760–771 763
at Pakistan:Endo Jnls Sponsored on November 7, 2008 jcem.endojournals.orgDownloaded from

estrogenic effects on pregnancy outcome in CC-treatedwomen is difficult to quantify. Individual variability exists,likely because of the complexity of ER replenishment andactivation and individual differences in the pharmacokinet-ics of CC. The discrepancy in the success rates in achievingpregnancy between women with unexplained infertility andwomen with PCOS in response to CC treatment (higher ratesin PCOS women) suggests that PCOS women may be lessvulnerable to the antiestrogenic effects of CC on peripheraltissues.
A New Method of Ovulation Induction
In our tertiary referral center for infertility, we frequentlyidentified women, especially with unexplained infertility,who had failed to conceive with up to a year of CC treatmentcycles before referral. Almost universally, we discovered anendometrial thickness less than 6 mm on transvaginal ultra-sound. As a result of the antiestrogenic effects of CC on theendometrium in these and other women, we attempted de-velopment of a novel oral ovulation method that would befree of these adverse side effects. Aromatase was identifiedas a potential target for suppressing estrogen-negative feed-back centrally and the availability of new specific AIs led toinitial studies with these drugs.
Aromatase InhibitorsChemical structure and pharmacokinetics
Aromatase is a microsomal cytochrome P450 hemopro-tein-containing enzyme (the product of the CYP19 gene) andcatalyzes the rate-limiting step in the production of estro-gens, i.e. the conversion of androstenedione and testosteroneto estrone and estradiol, respectively (40). Aromatase activityis present in many tissues, e.g. ovaries, brain, adipose tissue,muscle, liver, breast tissue, and malignant breast tumors. Themain sources of circulating estrogens are the ovaries in pre-menopausal women and adipose tissue in postmenopausalwomen (41).
Aromatase is a good target for selective inhibition becauseestrogen production is a terminal step in the biosyntheticsequence. A large number of AIs have been developed overthe last 30 yr with the most recent, third-generation AIslicensed mainly for breast cancer treatment in postmeno-pausal women. The third-generation AIs have been devel-oped over the last 10 yr after the clinical failure of the second-(Fadrozole and Formestane, developed around 15 yr ago)and first-generation (aminoglutethimide, developed morethan 30 yr ago) AIs. The clinical failure of the first twogenerations was mainly due to significant side effects asso-ciated with their use and the lack of satisfactory potency orspecificity in inhibiting the aromatase enzyme (42–44).
The third-generation AIs commercially available includetwo nonsteroidal preparations, anastrozole [ZN 1033 (Arimi-dex)] and letrozole [CGS 20267 (Femara)], and a steroidalagent, exemestane (Aromasin), and are available for clinicaluse in North America, Europe, and other parts of the worldfor treatment of postmenopausal breast cancer. Letrozoleand anastrozole are reversible, competitive AIs with consid-erably greater potency than aminoglutethimide (�1000times) and, at doses of 1–5 mg/d, reduce estrogen levels by
97% to more than 99% down to concentrations below detec-tion by most sensitive immunoassays. AIs are completelyabsorbed after oral administration with mean terminal half-life of approximately 45 h (range 30–60 h) with clearancemainly by the liver. Mild gastrointestinal disturbances ac-count for most of the adverse events, although these haveseldom limited therapy (45–47). Exemestane is a steroidal,suicide inhibitor of aromatase (aromatase inactivators) witha circulating half-life of approximately 9 h but potentially alonger effect to inhibit aromatase because it is irreversible(48).
Induction of ovulation with AIs
Mechanism of action of AIs. We postulated that it would bepossible to block estrogen-negative feedback, without de-pletion of ERs as occurs with CC, by administration of an AIin the early part of the menstrual cycle. Both circulatingestrogen (produced mainly by the ovarian follicles and pe-ripheral conversion of androgens in fat and other tissues) andlocally produced estrogen in the brain exert negative feed-back on gonadotropin release (49–52). Inhibition of aroma-tization will block estrogen production from all sources andrelease the hypothalamic/pituitary axis from estrogenic neg-ative feedback (Fig. 1). The resultant increase in gonadotro-pin secretion will stimulate growth of ovarian follicles. With-drawal of estrogen centrally also increases activins, whichare produced by a wide variety of tissues including thepituitary gland (53) and will stimulate synthesis of FSH bya direct action on the gonadotropes (54).
The selective nonsteroidal AIs have a relatively short half-life (�45 h), compared with CC, and would be ideal for thispurpose because they are eliminated from the body rapidly(55, 56). Because AIs do not deplete ERs, as does CC, normalcentral feedback mechanisms remain intact. As the dominantfollicle grows and estrogen levels rise, normal negative feed-back occurs centrally, resulting in suppression of FSH (Fig.2B) and atresia of the smaller growing follicles. A singledominant follicle, and monoovulation, should occur in mostcases (Fig. 1).
In women with PCOS, relative oversuppression of FSHmay be the result of excessive androgen produced from theovary being converted to estrogen by aromatization in thebrain. The AIs suppress estrogen production in both theovaries and brain. In the case of PCOS, therefore, AIs shouldresult in a robust increase in FSH release and subsequentfollicle stimulation and ovulation. The actual FSH release islikely to be blunted by the high levels of circulating inhibinfound in PCOS patients (57–60) that would not be altered byaromatase inhibition. In addition, as pointed out above, aro-matase inhibition does not antagonize ERs in the brain, andthe initiation of follicle growth accompanied by increasingconcentrations of both estradiol and inhibin results in a nor-mal negative feedback loop that limits FSH response, therebyavoiding the risk of high multiple ovulation and ovarianhyperstimulation syndrome (OHSS).
Peripheral mechanism of action. A second hypothesis that mayadd to the mechanism of action of the AIs in ovarian stim-ulation involves an increased follicular sensitivity to FSH.
764 J Clin Endocrinol Metab, March 2006, 91(3):760–771 Casper and Mitwally • Aromatase Inhibitors for Ovulation Induction
at Pakistan:Endo Jnls Sponsored on November 7, 2008 jcem.endojournals.orgDownloaded from

This could result from temporary accumulation of intrao-varian androgens because conversion of androgen substrateto estrogen is blocked by aromatase inhibition. Recent datasupport a stimulatory role for androgens in early folliculargrowth in primates (61). Testosterone was found to augmentfollicular FSH receptor expression in primates, suggestingthat androgens promote follicular growth and estrogen bio-synthesis indirectly by amplifying FSH effects (62, 63). Also,androgen accumulation in the follicle stimulates IGF-I, whichmay synergize with FSH to promote folliculogenesis (64–67).It is likely that women with PCOS already have a relativearomatase deficiency in the ovary, leading to increased in-traovarian androgens (68, 69) that leads to the developmentof multiple small follicles responsible for the polycystic mor-phology of the ovaries. The androgens, as described above,may also increase FSH receptors making these PCOS ovariesexquisitely sensitive to an increase in FSH through eitherexogenous administration of gonadotropins (hence the highrisk of OHSS) or endogenous increases in FSH as a result ofdecreased central estrogen feedback induced by aromataseinhibition. In the latter case, a relatively small rise in FSH,because of a normal estrogen feedback loop as describedabove, generally leads to monofollicular ovulation, thusavoiding the occurrence of OHSS.
Another part of the peripheral hypothesis involves ERs inthe endometrium. It is possible that aromatase inhibition,with suppression of estrogen concentrations in the circula-tion and peripheral target tissues, results in up-regulation ofERs in the endometrium, leading to rapid endometrialgrowth once estrogen secretion is restored. Estrogen has beenshown to decrease the level of its own receptor by stimulatingubiquitination of ERs, resulting in rapid degradation of thereceptors. In the absence of estrogen, ubiquitination is de-creased allowing up-regulation of the ER and increasingsensitivity to subsequent estrogen administration (70). Thiscould increase endometrial sensitivity to estrogen resultingin more rapid proliferation of endometrial epithelium andstroma and improved blood flow to the uterus and endo-metrium (71). As a result, normal endometrial developmentand thickness should occur by the time of follicular matu-ration, even in the face of the observed lower-than-normalestradiol concentrations in AI-treated cycles.
Indications for AIs in induction of ovulation. As a result of themechanisms of action of the AIs described above, we pro-posed that AIs could be used alone for induction of ovulationor as an adjuvant in conjunction with exogenous FSH or othermedications to improve the outcome of ovulation induction.A major advantage of an AI used alone is the ability toachieve restoration of monofollicular ovulation in anovula-tory infertility, e.g. PCOS as a result of the intact estrogen-negative feedback loop as described above. An AI could alsobe used in conjunction with FSH injections to increase thenumber of preovulatory follicles that develop and improvethe outcome of treatment. An increase in intraovarian an-drogen concentrations during aromatase inhibition couldimprove ovarian response to exogenous gonadotropins byincreasing ovarian sensitivity to FSH (peripheral mechanismof action described above).
To summarize, the AI when used alone should result in a
predictable response with the development of one or twomature follicles and a significantly reduced risk for OHSSand multiple gestation. To achieve multiple ovulation, theaddition of FSH to the AI is likely necessary.
Clinical studies of AIs for ovulation induction
Induction of ovulation after CC failure. The first study we per-formed was a proof-of-concept trial in a group of 22 womenwho had failed to respond to CC and were about to move onto injectable gonadotropin treatment with its associated costsand risks (72, 73). We defined inadequate response to CC asfailed ovulation induction or ovulation with a very thin mid-cycle endometrium (�0.5 cm). Patients who failed to respondadequately to CC were offered the option of trying the AI,letrozole, as an alternative treatment for induction ofovulation.
In the first study group, 12 women with PCOS receivedletrozole 2.5 mg daily from d 3 to 7 after a progestin-with-drawal bleed. During letrozole treatment, ovulation oc-curred in nine patients (75%), including three of the fourpatients who were anovulatory with CC. The mean endo-metrial thickness in the women receiving letrozole for ovu-lation induction was 0.81 � 0.14 cm. Pregnancy was achievedin three cycles (25%), two of which were singleton clinicalpregnancies and one was a chemical pregnancy.
Patients in the second group were ovulatory women withunexplained or mild male factor infertility and endometrialthickness 0.5 cm or less on CC. Each patient subsequentlyreceived one letrozole treatment cycle of 2.5 mg from cycled 3 to 7. During letrozole treatment, all women ovulated withendometrial thickness greater than 7 mm. A singleton clinicalpregnancy (10%) resulted from timed intrauterine insemi-nation (IUI) in one unexplained infertility couple who de-veloped two follicles greater than 1.5 cm.
A prospective, randomized, controlled trial of CC vs. an AIfor augmentation of ovulation in women with unexplainedinfertility was carried out at about the same time by Biljanand colleagues (74) in Montreal. Twenty-four patients wererandomized to receive CC 100 mg daily from cycle d 3 to 7,and 26 patients received letrozole 2.5 mg daily from d 3 to7. Using standard hormonal and ultrasound monitoring, theinvestigators showed that the CC group had a mean of twopreovulatory follicles, whereas the letrozole group produceda mean of one. Estradiol levels on the day of hCG weresignificantly elevated in the CC group (2300 pmol/liter),compared with the letrozole group (600 pmol/liter). Endo-metrial thickness and blood flow were significantly less withCC (6.9 mm and pulsatility index of 3.6), compared withletrozole (8.6 mm and pulsatility index of 3.1) on the day ofhCG. The pregnancy rate was 5.6% in the CC group vs. 16.7%in the letrozole group (nonsignificant).
We concluded from these preliminary studies that AIswere an effective alternative to CC, particularly in cases withrecurrent CC failure. However, it is important to point outthat in cases of CC resistance (failure to ovulate) due to severeinsulin resistance or the use of CC for inappropriate indica-tions (e.g. hypothalamic amenorrhea or ovarian failure), theuse of an AI is also unlikely to be successful. The correctionof insulin resistance with an insulin sensitizer is the logical
Casper and Mitwally • Aromatase Inhibitors for Ovulation Induction J Clin Endocrinol Metab, March 2006, 91(3):760–771 765
at Pakistan:Endo Jnls Sponsored on November 7, 2008 jcem.endojournals.orgDownloaded from

approach in patients with insulin resistance. Alternativetreatments should be considered for other problems such asexogenous gonadotropin injection in patients with hypogo-nadotropic hypogonadism and oocyte donation for caseswith ovarian failure.
Since this first study, evidence supporting the success ofAIs in ovulation induction for infertility treatment has beenaccumulating (74–78). Most of the studies used the AI, letro-zole. However, anastrozole, another third-generation AI sim-ilar to letrozole, was used in other studies (78, 79). It iscurrently not known whether there are any clinically signif-icant pharmacological differences between letrozole andanastrozole (80), especially regarding efficacy of ovulationinduction (81).
AIs plus gonadotropins
Reducing FSH dose required for optimum controlled ovarian hy-perstimulation. We investigated the idea of combining an AIwith FSH injection to reduce the dose of FSH required toachieve optimum controlled ovarian stimulation (COH),without adverse antiestrogenic effects. We (82–84) and oth-ers (85, 86) found a significant reduction in the FSH doserequired (from 45 to 55%).
We also compared the use of an AI in conjunction FSHwith the use of CC in conjunction with FSH or FSH alone (83).The study included women with unexplained infertility andmild male factor infertility. Thirty-six women received an AIwith FSH in 42 treatment cycles, 18 women received CC withFSH in 19 cycles, and 56 women received FSH only in 91cycles. In this study, we found that cotreatment with an AIsignificantly reduced the FSH dose required during COH tothe same extent as did CC. The AI was not associated withantiestrogenic effects as demonstrated by the significantlylower endometrial thickness noted with CC treatment de-spite the significantly higher estradiol (E2) level. In addition,the pregnancy rate with an AI and FSH was equivalent toFSH alone and almost twice the level seen with CC and FSHtreatment (83).
It is known that the cost of FSH injections constitutes asignificant part of the expense of infertility treatment, espe-cially during assisted reproduction. We believe that the AIswill markedly reduce the cost of infertility treatment bydecreasing the FSH dose required for optimum ovarian stim-ulation. This could make assisted reproductive technologyavailable to a larger group of infertile couples.
Improving ovarian response to FSH stimulation in poor respond-ers. The reduction in the dose of FSH required observed inconjunction with an AI encouraged us to explore the use ofan AI to improve response to ovarian stimulation with FSHin poor responders. In an observational cohort study (82), 12patients with unexplained infertility and a poor response toovarian stimulation with FSH in at least two cycles (total of25 cycles of FSH-only stimulation) were studied. Thesewomen underwent COH for IUI and poor response definedas less than three follicles greater than 1.8 cm in diameter onthe day of the LH surge or hCG administration. In the ex-perimental cycles, letrozole was given at a dose of 2.5 mgfrom d 3 to 7 after onset of menses, and FSH injection was
started on d 7 of the menstrual cycle at a dose of 50–225 IU/d,depending on the number of developing follicles seen onultrasound. The aim was to achieve three preovulatory fol-licles on the day of hCG injection.
During FSH plus letrozole stimulation cycles, the meannumber of mature follicles was 3.3, which was significantlyhigher than in FSH-only cycles (1.9 follicles). The amount ofFSH required was significantly lower in the letrozole plusFSH cycles than the FSH-only cycles (616 � 454 vs. 1590 �708 IU, respectively). There was no significant differencebetween FSH only or letrozole plus FSH on the day of hCGadministration or endometrial thickness on the day of hCGadministration. Although there was no difference in the levelof E2 on the day of hCG administration, the amount ofestrogen per mature follicle was significantly lower withletrozole treatment, consistent with previous studies of usingan AI for ovulation induction. Three of the women conceiveda clinical pregnancy with the combined letrozole and FSHtreatment.
In this clinical trial, we demonstrated a benefit of aro-matase inhibition in improving ovarian response to FSHstimulation in poor responders. The improved response wasclearly shown by the significantly higher number of maturefollicles and significantly lower amount of FSH needed toachieve an adequate number of preovulatory follicles. Inaddition, the endometrium sustained implantation as dem-onstrated by three clinical pregnancies in the letrozole andFSH cycles.
Optimal dose of AIs for repeated administration
The optimal dose of each AI is not yet clear. In most of thestudies to date, the dose of letrozole (2.5 mg) or anastrozole(1.0 mg) typically used for breast cancer treatment in post-menopausal women has been chosen. Biljan et al. (85) in arandomized study comparing 2.5 and 5.0 mg of letrozole inwomen with unexplained infertility suggested that thehigher dose might be associated with more follicles devel-oping. However, the study was not large enough to dem-onstrate a significant advantage. A more recent study byHealey et al. (86) used a dose of 5.0 mg of letrozole togetherwith FSH in an overlapping regimen for superovulation inwomen undergoing IUI. Compared with FSH treatmentalone, the combination of letrozole and FSH resulted in areduction of gonadotropin dose, similar pregnancy rates, buta slight negative effect on endometrial thickness, likely be-cause the overlapping regimen advanced follicle growth andovulation and did not allow time for clearance of the largerdose of letrozole by the time of hCG administration. Simi-larly, a study using 7.5 mg letrozole from cycle d 3 to 7showed, for the first time, a thinning of the endometriumsimilar to CC (76). Based on current data, it is likely that theoptimal dose of letrozole for a 5-d course of treatment isbetween 2.5 and 5.0 mg, with higher doses resulting in per-sistence of aromatase inhibition and estrogen levels too lowfor normal endometrial development by the time of ovula-tion. For anastrozole, there are not yet enough data to de-termine the preferred dose, although it appears that the stan-dard 1-mg dose is too low for optimal follicle recruitment andovulation (78).
766 J Clin Endocrinol Metab, March 2006, 91(3):760–771 Casper and Mitwally • Aromatase Inhibitors for Ovulation Induction
at Pakistan:Endo Jnls Sponsored on November 7, 2008 jcem.endojournals.orgDownloaded from
Adverse effects and concerns about using AIs for inductionof ovulation
Side effects of AIs. In clinical use, nonsteroidal AIs are gen-erally well tolerated. The main side effects are hot flushes,headaches, and leg cramps (87, 88). These adverse effectswere observed in older women with advanced breast cancerwho were given the AIs on a daily basis over several months.Fewer adverse effects would be expected in healthy youngwomen administered a short course of AI for induction ofovulation. In addition, our clinical experience with ovulationinduction has been fewer side effects such as hot flushes andpremenstrual syndrome-type symptoms with AIs, comparedwith CC.
Aromatase inhibition is associated with significantly lowerserum estrogen levels at midcycle and per mature folliclethan found with CC (73, 83). The question whether low orvery low intrafollicular estrogen is compatible with folliculardevelopment, ovulation, and corpus luteum formation hasbeen reviewed before (89). Markedly reduced to absent in-trafollicular concentrations of estrogen are known to be com-patible with follicular expansion, retrieval of fertilizable oo-cytes, and apparently normal embryo development (90–93).The rapid clearance of the AIs, the reversible nature of en-zyme inhibition, and elevated levels of FSH, which inducesnew expression of aromatase enzyme, are factors that limitaccumulation of androgens and likely result in increasingestrogen production that should be relatively normal at thetime of ovulation. This conclusion has now been confirmedby the use of AIs in in vitro fertilization (IVF) reviewed below.
Pregnancy outcome with AIs
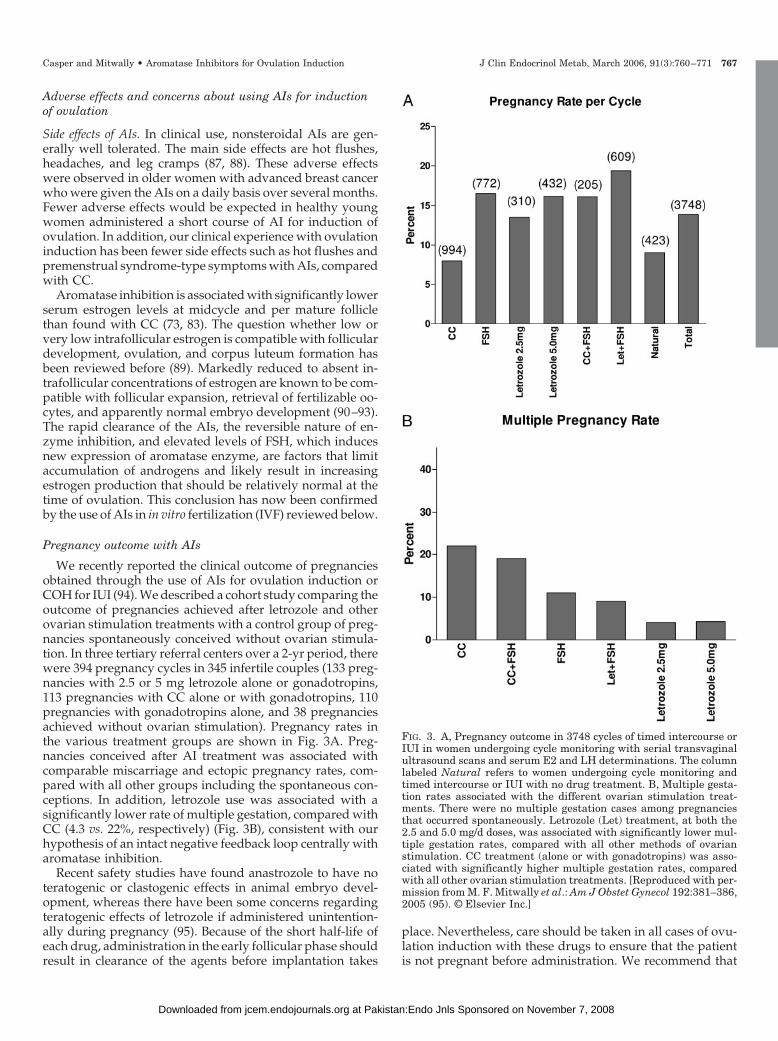
We recently reported the clinical outcome of pregnanciesobtained through the use of AIs for ovulation induction orCOH for IUI (94). We described a cohort study comparing theoutcome of pregnancies achieved after letrozole and otherovarian stimulation treatments with a control group of preg-nancies spontaneously conceived without ovarian stimula-tion. In three tertiary referral centers over a 2-yr period, therewere 394 pregnancy cycles in 345 infertile couples (133 preg-nancies with 2.5 or 5 mg letrozole alone or gonadotropins,113 pregnancies with CC alone or with gonadotropins, 110pregnancies with gonadotropins alone, and 38 pregnanciesachieved without ovarian stimulation). Pregnancy rates inthe various treatment groups are shown in Fig. 3A. Preg-nancies conceived after AI treatment was associated withcomparable miscarriage and ectopic pregnancy rates, com-pared with all other groups including the spontaneous con-ceptions. In addition, letrozole use was associated with asignificantly lower rate of multiple gestation, compared withCC (4.3 vs. 22%, respectively) (Fig. 3B), consistent with ourhypothesis of an intact negative feedback loop centrally witharomatase inhibition.
Recent safety studies have found anastrozole to have noteratogenic or clastogenic effects in animal embryo devel-opment, whereas there have been some concerns regardingteratogenic effects of letrozole if administered unintention-ally during pregnancy (95). Because of the short half-life ofeach drug, administration in the early follicular phase shouldresult in clearance of the agents before implantation takes
place. Nevertheless, care should be taken in all cases of ovu-lation induction with these drugs to ensure that the patientis not pregnant before administration. We recommend that
FIG. 3. A, Pregnancy outcome in 3748 cycles of timed intercourse orIUI in women undergoing cycle monitoring with serial transvaginalultrasound scans and serum E2 and LH determinations. The columnlabeled Natural refers to women undergoing cycle monitoring andtimed intercourse or IUI with no drug treatment. B, Multiple gesta-tion rates associated with the different ovarian stimulation treat-ments. There were no multiple gestation cases among pregnanciesthat occurred spontaneously. Letrozole (Let) treatment, at both the2.5 and 5.0 mg/d doses, was associated with significantly lower mul-tiple gestation rates, compared with all other methods of ovarianstimulation. CC treatment (alone or with gonadotropins) was asso-ciated with significantly higher multiple gestation rates, comparedwith all other ovarian stimulation treatments. [Reproduced with per-mission from M. F. Mitwally et al.: Am J Obstet Gynecol 192:381–386,2005 (95). © Elsevier Inc.]
Casper and Mitwally • Aromatase Inhibitors for Ovulation Induction J Clin Endocrinol Metab, March 2006, 91(3):760–771 767
at Pakistan:Endo Jnls Sponsored on November 7, 2008 jcem.endojournals.orgDownloaded from

a blood �hCG level be ascertained before using AIs in pre-menopausal women.
Recently, Health Canada and Novartis Pharmaceuticalsissued a warning that letrozole should not be used for ovu-lation induction because of the potential for fetal toxicity andmalformations. This warning was based on an abstract byBiljan et al. (96) in which six congenital abnormalities and onecase of hepatocellular carcinoma were reported among 150births resulting from the use of letrozole for ovulation in-duction. These 150 babies were compared with a database ofover 36,000 spontaneously conceived babies born in a low-risk community hospital in Montreal. Although the overallanomaly rate was not increased, the authors reported a sig-nificant increase in locomotor and cardiac abnormalities inthe letrozole-treated pregnancies compared to the controls.We believe a larger group of letrozole babies needs to beassembled and compared to a more suitable control group ofinfertile women before any conclusion of an increase in con-genital anomalies with letrozole can be confirmed. We arenow in the process of collecting such data.
AIs for IVF
Despite recent developments in ovarian stimulation andassisted reproductive technologies, there has not been a cor-responding increase in implantation rates. Supraphysiologi-cal levels of estrogen may explain some of the adverse effectsof ovarian stimulation on infertility treatment, including del-eterious effects on the endometrium (97, 98) and embryo (99,100). Basir et al. (101) have shown that high response to COHfor IVF results in endometrial glandular and stromal dys-synchrony as assessed by morphometric analysis. A step-down protocol has been proposed for IVF to lower E2 con-centrations and improve successful implantation (102). Analternative approach is using an AI to significantly suppressE2 levels around d 3–7 of the menstrual cycle. After stoppingthe AI, E2 levels increase steadily to reach levels high enoughto trigger an LH surge around d 12–14 of the cycle. However,preovulatory levels of estrogen remained about half to onethird the levels seen in CC- or FSH-stimulated cycles (83).This strategy may work similarly to a step-down protocolwithout jeopardizing the potential number of oocytesretrieved.
Clinical studies of AIs for ovarian stimulation in IVF
In a randomized, controlled study, Goswami et al. (103)compared an AI plus FSH protocol with a standard GnRHagonist and FSH protocol in poor responders undergoingIVF. Although this was a small pilot study including only 38patients, the results suggested that the addition of an AI toa small dose of FSH (150 IU; two injections of 75 IU on cycled 3 and 8) resulted in a similar number of oocytes retrieved,embryos transferred, and pregnancy rate as observed in thewomen on the standard protocol receiving a mean (� sem)of 2865 � 228 IU FSH. The authors concluded that AIs couldbe a low-cost alternative to natural-cycle IVF in patients whoare poor responders to FSH and that larger randomizedstudies are required to confirm their data.
A recent, larger study by Garcia-Velasco et al. (104) eval-uated the use of an AI as an adjuvant to FSH treatment in IVF
cycles of poor-responder patients. In this study, 147 lowresponders, with at least one previous canceled IVF cycle,were enrolled. The study was prospective but not random-ized. The women were divided into a control group of 76patients treated with high-dose gonadotropins in a GnRH-antagonist regimen. The experimental group of 71 patientsreceived letrozole 2.5 mg plus gonadotropins for the first 5 dof stimulation followed by the same gonadotropin/antago-nist regimen.
The study demonstrated that patients receiving an AI hadhigher numbers of oocytes retrieved and had a higher im-plantation rate despite receiving the same doses of FSH/human menopausal gonadotropin as the control group. Bothtestosterone and androstenedione were significantly in-creased in concentration in the follicular fluid in the exper-imental group, compared with the controls. Interestingly,follicular fluid E2 levels were similar to controls. These find-ings are consistent with the hypothesis that aromatase inhi-bition, by blocking androgen to estrogen conversion, in-creases intraovarian androgens and follicular FSH receptorexpression and sensitivity to FSH administration and is rap-idly reversible.
Another reason to avoid elevated estrogen levels duringovarian stimulation is fertility treatment in women withbreast cancer. Treatment for this cancer often involves che-motherapy with alkylating agents that can damage ovarianfollicle reserve leading to premature ovarian failure. With therecent success of oocyte cryopreservation, some women areopting to freeze oocytes or embryos for later use by them-selves or a gestational carrier. Oktay et al. (105) studied 60women (age range 24–43 yr) with breast cancer. Twenty-ninewomen requested IVF before chemotherapy, and 31 womendid not undergo IVF and served as the control group. The 29patients underwent 33 ovarian stimulation cycles with eithertamoxifen 60 mg/d alone or in combination with low-doseFSH (TamFSH-IVF) or letrozole 5 mg in combination withFSH (letrozole-IVF). After IVF, all resultant embryos werecryopreserved. The study was not randomized for severalreasons. Compared with women receiving tamoxifen alone(1.5 mature oocytes and 1.3 embryos), there was a significantincrease in the mean number of mature oocytes retrieved inthe group receiving letrozole-IVF (8.5) and TamFSH-IVF(5.1). The mean number of embryos cryopreserved was alsosignificantly increased (5.3 and 3.8, respectively). Peak E2levels were significantly lower with letrozole-IVF, comparedwith TamFSH-IVF (380 � 57 and 1182 � 271 pg/ml, respec-tively). After almost 2 yr of follow-up, the cancer recurrencerate was similar between IVF and control patients. The au-thors concluded that both tamoxifen and letrozole added toFSH could increase the number of oocytes retrieved for IVFin breast cancer patients, but the letrozole protocol may bepreferred because it resulted in lower peak E2 levels.
Conclusion
Preliminary studies have demonstrated that AIs are effec-tive for ovulation induction in infertile women. Based on theevidence reviewed above, these oral agents seem to be effi-cient for ovulation induction. We believe that a major ad-vantage of AIs for ovulation induction is monofollicular ovu-
768 J Clin Endocrinol Metab, March 2006, 91(3):760–771 Casper and Mitwally • Aromatase Inhibitors for Ovulation Induction
at Pakistan:Endo Jnls Sponsored on November 7, 2008 jcem.endojournals.orgDownloaded from

lation. Especially in PCOS patients, who are oftenhyperresponsive to gonadotropins, a drug that consistentlyresults in a single ovulation is very desirable. In addition,because negative effects peripherally on the endometriumare absent, a second advantage of AIs for ovulation inductionis minimal if any ultrasound monitoring is needed for en-dometrial thickness. Both of these advantages allow primarycare providers or community-based gynecologists, withoutready access to ultrasound monitoring, to participate in themanagement of PCOS and other anovulatory women.
In IUI cycles, AIs alone are probably not the optimal choicebecause, generally speaking, it is preferable to see two orthree mature follicles developing, depending on the patient’sage. To ensure multiple ovulation in IUI cycles, the additionof a low dose of FSH to the AI is required, although FSH canbe delayed (sequential protocol) until E2 levels begin to riseand when the exogenous FSH administration would over-ride negative feedback occurring centrally. This type of pro-tocol does not accelerate follicle development, and ovulationoccurs normally around cycle d 14. There is adequate time forendometrial growth to occur normally and a small dose ofgonadotropin is required, generally in the range of 50–75 IUdaily.
These advantages, if confirmed, suggest that AIs may bea viable option to replace CC in the future as the new primarytreatment for ovulation induction and in combination withFSH for assisted reproduction procedures. However, largerrandomized, controlled studies are required to determine thebest treatment regimen. If such large studies confirm effec-tiveness and safety, the use of AIs for ovulation inductionwould be the first improvement in oral ovulation inductionin decades.
Acknowledgments
Received August 29, 2005. Accepted November 29, 2005.Address all correspondence and requests for reprints to: Robert F.
Casper, M.D., F.R.C.S.(C), 150 Bloor Street West, Suite 210, Toronto,Ontario, Canada M5S 2X9. E-mail: [email protected].
This work was supported by the Canadian Institutes of Health Re-search, Ottawa, Ontario, Canada.
The authors have no conflict of interest.
References
1. Gougeon A 1998 Ovarian follicular growth in humans: ovarian ageing andpopulation of growing follicles. Maturitas 30:137–142
2. Gougeon A 1986 Dynamics of follicular growth in the human: a model frompreliminary results. Hum Reprod 1:81–87
3. Le Nestour E, Marraoui J, Lahlou N, Roger M, de Ziegler D, Bouchard P 1993Role of estradiol in the rise in follicle-stimulating hormone levels during theluteal-follicular transition. J Clin Endocrinol Metab 77:439–442
4. Marsters P, Kendall NR, Campbell BK 2003 Temporal relationships betweenFSH receptor, type 1 insulin-like growth factor receptor, and aromatase ex-pression during FSH-induced differentiation of bovine granulosa cells main-tained in serum-free culture. Mol Cell Endocrinol 203:117–127
5. Armstrong DT, Dorrington JH 1977 Estrogen biosynthesis in the ovaries andtestes. Adv Sex Horm Res 3:217–258
6. Brown JB 1978 Pituitary control of ovarian function—concepts derived fromgonadotrophin therapy. Aust N Z J Obstet Gynaecol 18:46–54
7. Fauser BCJM, van Heusden AM 1997 Manipulation of human ovarian func-tion: physiological concepts and clinical consequences. Endocr Rev 18:71–106
8. Macklon NS, Fauser BC 2000 Impact of ovarian hyperstimulation on theluteal phase. J Reprod Fertil Suppl 55:101–108
9. Shima K, Kitayama S, Nakano R 1987 Gonadotropin binding sites in humanovarian follicles and corpora lutea during the menstrual cycle. Obstet Gynecol69:800–806
10. Zeleznik AJ, Hillier SG 1984 The role of gonadotropins in the selection of thepreovulatory follicle. Clin Obstet Gynecol 27:927–940
11. Sullivan MW, StewarAkers A, Krasnow JS, Berga SL, Zeleznik AJ 1999Ovarian responses in women to recombinant follicle-stimulating hormoneand luteinizing hormone (LH): a role for LH in the final stages of follicularmaturation. J Clin Endocrinol Metab 84:228–232
12. Filicori M, Cognigni GE, Gamberini E, Parmegiani L, Troilo E, Roset B 2005Efficacy of low-dose human chorionic gonadotropin alone to complete con-trolled ovarian stimulation. Fertil Steril 84:394–401
13. Liu JH, Yen SS 1983 Induction of midcycle gonadotropin surge by ovariansteroids in women: a critical evaluation. J Clin Endocrinol Metab 57:797–802
14. Christian CA, Mobley JL, Moenter SM 2005 Diurnal and estradiol-depen-dent changes in gonadotropin-releasing hormone neuron firing activity. ProcNatl Acad Sci USA 102:15682–15687
15. Baerwald AR, Pierson RA 2004 Endometrial development in association withovarian follicular waves during the menstrual cycle. Ultrasound Obstet Gy-necol 24:453–460
16. Niswender GD, Juengel JL, Silva PJ, Rollyson MK, McIntush EW 2000Mechanisms controlling the function and life span of the corpus luteum.Physiol Rev 80:1–29
17. Finkelstein JS, Badger TM, O’Dea LS, Spratt DI, Crowley WF 1988 Effectsof decreasing the frequency of gonadotropin-releasing hormone stimulationon gonadotropin secretion in gonadotropin-releasing hormone-deficient menand perifused rat pituitary cells. J Clin Invest 81:1725–1733
18. Ropert JF, Quigley ME, Yen SS 1981 Endogenous opiates modulate pulsatileluteinizing hormone release in humans. J Clin Endocrinol Metab 52:583–585
19. Greenblatt RB, Barfield WE, Jungck EC, Ray AW 1961 Induction of ovu-lation with MRL/41. JAMA 178:101–105
20. Mikkelson TJ, Kroboth PD, Cameron WJ 1986 Single dose pharmacokineticsof clomiphene citrate in normal volunteers. Fertil Steril 46:392
21. Young SL, Opsahl MS, Fritz MA 1999 Serum concentrations of enclomipheneand zuclomiphene across consecutive cycles of clomiphene citrate therapy inanovulatory infertile women. Fertil Steril 7:639–644
22. Kurl RN, Morris ID 1978 Differential depletion of cytoplasmic high affinityoestrogen receptors after the in vivo administration of the antioestrogens,clomiphene, MER-25 and tamoxifen. Br J Pharmacol 62:487–493
23. Kerin JF, Liu JH, Phillipou G, Yen SSS 1985 Evidence for a hypothalamicsite of action of clomiphene citrate in women. J Clin Endocrinol Metab 61:265–268
24. Kettel LM, Roseff SJ, Berga SL, Mortola JF, Yen SS 1993 Hypothalamic-pituitary-ovarian response to clomiphene citrate in women with polycysticovary syndrome. Fertil Steril 59:532–538
25. Fisher SA, Reid RL, Van Vugt DA, Casper RF 2002 A randomized double-blind comparison of the effects of clomiphene citrate and the AI letrozole onovulatory function in normal women. Fertil Steril 78:280–285
26. Fisch B, Margara RA, Winston RM, Hillier SG 1989 Cellular basis of lutealsteroidogenesis in the human ovary. J Endocrinol 122:303–311
27. Garcia J, Seegar Jones G, Wentz AC 1977 The use of clomiphene citrate. FertilSteril 28:707–717
28. Imani B, Eijkemans MJ, te Velde ER, Habbema JD, Fauser BC 1999 Pre-dictors of chances to conceive in ovulatory patients during clomiphene citrateinduction of ovulation in normogonadotropic oligomenorrheic infertility.J Clin Endocrinol Metab 84:1617–1622
29. Capelo FO, Kumar A, Steinkampf MP, Azziz R 2003 Laparoscopic evalu-ation following failure to achieve pregnancy after ovulation induction withclomiphene citrate. Fertil Steril 80:1450–1453
30. Hakim RB, Gray RH, Zacur H 1995 Infertility and early pregnancy loss. Am JObstet Gynecol 1725:1510–1517
31. Check JH, Dietterich C, Lurie D 1995 The effect of consecutive cycles ofclomiphene citrate therapy on endometrial thickness and echo pattern. ObstetGynecol 86:341–345
32. Gonen Y, Casper RF 1990 Sonographic determination of an adverse effect ofclomiphene citrate on endometrial growth. Hum Reprod 5:670–674
33. Ben-Ami M, Geslevich Y, Matilsky M, Battino S, Weiner E, Shalev E 1994Exogenous estrogen therapy concurrent with clomiphene citrate: lack of effecton serum sex hormones and endometrial thickness. Gynecol Obstet Invest37:180–182
34. Nelson LM, Hershlag A, Kurl RS, Hall JL, Stillman RJ 1990 Clomiphenecitrate directly impairs endometrial receptivity in the mouse. Fertil Steril53:727–731
35. Li TC, Warren MA, Murphy C, Sargeant S, Cooke ID 1992 A prospective,randomised, cross-over study comparing the effects of clomiphene citrate andcyclofenil on endometrial morphology in the luteal phase of normal fertilewomen. Br J Obstet Gynaecol 99:1008–1013
36. Fritz MA, Holmes RT, Keenan EJ 1991 Effect of clomiphene citrate treatmenton endometrial estrogen and progesterone receptor induction in women.Am J Obstet Gynecol 165:177–185
37. Yeko TR, Nicosia SM, Maroulis GB, Bardawil WA, Dawood MY 1992Histology of midluteal corpus luteum and endometrium from clomiphenecitrate-induced cycles. Fertil Steril 57:28–32
38. Sereepapong W, Triratanachat S, Sampatanukul P, Pruksananonda K,
Casper and Mitwally • Aromatase Inhibitors for Ovulation Induction J Clin Endocrinol Metab, March 2006, 91(3):760–771 769
at Pakistan:Endo Jnls Sponsored on November 7, 2008 jcem.endojournals.orgDownloaded from

Boonkasemsanti K, Reinprayoon D 2000 Effects of clomiphene citrate on theendometrium of regularly cycling women. Fertil Steril 73:287–291
39. Hsu CC, Kuo HC, Wang ST, Huang KE 1995 Interference with uterine bloodflow by clomiphene citrate in women with unexplained infertility. ObstetGynecol 866:917–921
40. Cole PA, Robinson CH 1990 Mechanism and inhibition of cytochrome P-450aromatase. J Med Chem 33:2933–2944
41. Santen RJ, Manni A, Harvey H, Redmond C 1990 Endocrine treatment ofbreast cancer in women. Endocr Rev 11:1–45
42. Buzdar A, Howell A 2001 Advances in aromatase inhibition: clinical efficacyand tolerability in the treatment of breast cancer. Clin Cancer Res 7:2620–2635
43. Santen RJ, Lipton A, Kendall J 1974 Successful medical adrenalectomy withaminoglutethimide: role of altered drug metabolism. JAMA 230:1661–1665
44. Newsome Jr HH, Brown PW, Terz JJ, Lawrence Jr W 1977 Medical andsurgical adrenalectomy in patients with advanced breast carcinoma. Cancer39:542–546
45. Winer EP, Hudis C, Burstein HJ, Chlebowski RT, Ingle JN, Edge SB,Mamounas EP, Gralow J, Goldstein LJ, Pritchard KI, Braun S, CobleighMA, Langer AS, Perotti J, Powles TJ, Whelan TJ, Browman GP 2002 Amer-ican Society of Clinical Oncology technology assessment on the use of AIs asadjuvant therapy for women with hormone receptor-positive breast cancer:status report 2002. J Clin Oncol 2015:3317–3327
46. Buzdar A, Jonat W, Howell A, Jones SE, Blomqvist C, Vogel CL, EiermannW, Wolter JM, Azab M, Webster A, Plourde PV 1996 Anastrozole, a potentand selective AI, versus megestrol acetate in postmenopausal women withadvanced breast cancer: results of overview analysis of two phase III trials.J Clin Oncol 14:2000–2011
47. Dowsett M 1996 Biological background to aromatase inhibition. Breast 5:196–201
48. Mauras N, Lima J, Patel D, Rini A, di Salle E, Kwok A, Lippe B 2003Pharmacokinetics and dose finding of a potent AI, aromasin (exemestane), inyoung males. J Clin Endocrinol Metab 88:5951–5956
49. Kamat A, Hinshelwood MM, Murry BA, Mendelson CR 2002 Mechanismsin tissue-specific regulation of estrogen biosynthesis in humans. Trends En-docrinol Metab 133:122–128
50. Naftolin F, MacLusky NJ 1984 Aromatization hypothesis revisited. In: SerioM, ed. Differentiation: basic and clinical aspects. New York: Raven Press;79–91
51. Naftolin F, MacLusky NJ, Leranth CZ, Sakamoto HS, Garcia-Segura LM1988 The cellular effects of estrogens on neuroendocrine tissues. J SteroidBiochem 30:195–207
52. Naftolin F 1994 Brain aromatization of androgens. J Reprod Med 39:257–26153. Roberts V, Meunier H, Vaughan J, Rivier J, Rivier C, Vale W, Sawchenko
P 1989 Production and regulation of inhibin subunits in pituitary gonado-tropes. Endocrinology 124:552–554
54. Mason AJ, Berkemeier LM, Schmelzer CH, Schwall RH 1989 Activin B:precursor sequences, genomic structure and in vitro activities. Mol Endocrinol3:1352–1358
55. Sioufi A, Gauducheau N, Pineau V, Marfil F, Jaouen A, Cardot JM, God-billon J, Czendlik C, Howald H, Pfister C, Vreeland F 1997 Absolute bio-availability of letrozole in healthy post-menopausal women. Biopharm DrugDispos 18:779–789
56. Sioufi A, Sandrenan N, Godbillon J, Trunet P, Czendlik C, Howald H,Pfister C, Ezzet F 1997 Comparative bioavailability of letrozole under fed andfasting conditions in 12 healthy subjects after a 25 mg single oral adminis-tration. Biopharm Drug Dispos 186:489–497
57. Roberts VJ, Barth S, El-Roeiy A, Yen SSC 1994 Expression of inhibin/activinsystem messenger ribonucleic acids and proteins in ovarian follicles fromwomen with polycystic ovarian syndrome. J Clin Endocrinol Metab 79:1434–1439
58. Yamoto M, Minami S, Nakano R 1993 Immunohistochemical localization ofinhibin subunits in polycystic ovary. J Clin Endocrinol Metab 77:859–862
59. Anderson RA, Groome NP, Baird DT 1998 Inhibin A and inhibin B in womenwith polycystic ovarian syndrome during treatment with FSH to inducemono-ovulation. Clin Endocrinol (Oxf) 48:577–584
60. Lockwood GM, Muttukrishna S, Groome NP, Matthews DR, Ledger WL1998 Mid-follicular phase pulses of inhibin B are absent in polycystic ovariansyndrome and are initiated by successful laparoscopic ovarian diathermy: apossible mechanism regulating emergence of the dominant follicle. J ClinEndocrinol Metab 83:1730–1735
61. Weil SJ, Vendola K, Zhou J, Adesanya OO, Wang J, Okafor J, Bondy CA1998 Androgen receptor gene expression in the primate ovary: cellular lo-calization, regulation, and functional correlations. J Clin Endocrinol Metab837:2479–2485
62. Weil S, Vendola K, Zhou J, Bondy CA 1999 Androgen and follicle-stimu-lating hormone interactions in primate ovarian follicle development. J ClinEndocrinol Metab 848:2951–2956
63. Vendola KA, Zhou J, Adesanya OO, Weil SJ, Bondy CA 1998 Androgensstimulate early stages of follicular growth in the primate ovary. J Clin Invest10112:2622–2629
64. Vendola K, Zhou J, Wang J, Famuyiwa OA, Bievre M, Bondy CA 1999
Androgens promote oocyte insulin-like growth factor I expression and ini-tiation of follicle development in the primate ovary. Biol Reprod 612:353–357
65. Adashi E 1993 Intraovarian regulation the proposed role of insulin-likegrowth factors. Ann NY Acad Sci 687:10–12
66. Giudice LC 1992 Insulin-like growth factors and ovarian follicular develop-ment. Endocr Rev 13:641–669
67. Yen SSC, Laughlin GA, Morales AJ 1993 Interface between extra-and intra-ovarian factors in polycystic ovary syndrome PCOS. Ann NY Acad Science687:98–111
68. Agarwal SK, Judd HL, Magoffin DA 1996 A mechanism for the suppressionof estrogen production in polycystic ovary syndrome. J Clin EndocrinolMetab 81:3686–3691
69. Jakimiuk AJ, Weitsman SR, Brzechffa PR, Magoffin DA 1998 AromatasemRNA expression in individual follicles from polycystic ovaries. Mol HumReprod 41:1–8
70. Nirmala PB, Thampan RV 1995 Ubiquitination of the rat uterine estrogenreceptor: dependence on estradiol. Biochem Biophys Res Commun 213:24–31
71. Rosenfeld CR, Roy T, Cox BE 2002 Mechanisms modulating estrogen-in-duced uterine vasodilation. Vascul Pharmacol 382:115–125
72. Mitwally MFM, Casper RF 2000 Aromatase inhibition: a novel method ofovulation induction in women with polycystic ovarian syndrome. ReprodTechnol 10:244–247
73. Mitwally MFM, Casper RF 2000 Use of an AI for induction of ovulation inpatients with an inadequate response to clomiphene citrate. Fertil Steril 75:305–309
74. Sammour A, Biljan MM, Tan SL, Tulandi T 2001 Prospective randomizedtrial comparing the effects of letrozole (LE) and clomiphene citrate (CC) onfollicular development, endometrial thickness and pregnancy rate in patientsundergoing super-ovulation prior to intrauterine insemination (IUI). FertilSteril 76:S110
75. Cortinez A, De Carvalho I, Vantman D, Gabler F, Iniguez G, Vega M 2005Hormonal profile and endometrial morphology in letrozole-controlled ovar-ian hyperstimulation in ovulatory infertile patients. Fertil Steril 83:110–115
76. Al-Fozan H, Al-Khadouri M, Tan SL, Tulandi T 2004 A randomized trial ofletrozole versus clomiphene citrate in women undergoing superovulation.Fertil Steril 82:1561–1563
77. Fatemi HM, Kolibianakis E, Tournaye H, Camus M, Van Steirteghem AC,Devroey P 2003 Clomiphene citrate versus letrozole for ovarian stimulation:a pilot study. Reprod Biomed Online 75:543–546
78. Al-Omari WR, Sulaiman WR, Al-Hadithi N 2004 Comparison of two AIs inwomen with clomiphene-resistant polycystic ovary syndrome. Int J GynaecolObstet 853:289–291
79. Tredway DR, Buraglio M, Hemsey G, Denton G 2004 A phase I study of thepharmacokinetics, pharmacodynamics, and safety of single- and multiple-dose anastrozole in healthy, premenopausal female volunteers. Fertil Steril82:1587–1593
80. Ligibel JA, Winer EP 2003 Clinical differences among the AIs. Clin CancerRes 91:473S–479S
81. de Ziegler D, Mattenberger C, Luyet C, Romoscanu I, Irion NF, Bianchi-Demicheli F 2005 Clinical use of AIs (AI) in premenopausal women. J SteroidBiochem Mol Biol 95:121–127
82. Mitwally MFM, Casper RF 2002 Aromatase inhibition improves ovarianresponse to follicle-stimulating hormone in poor responders. Fertil Steril774:776–780
83. Mitwally MF, Casper RF 2003 Aromatase inhibition reduces gonadotrophindose required for controlled ovarian stimulation in women with unexplainedinfertility. Hum Reprod 188:1588–1597
84. Mitwally MF, Casper RF 2004 Aromatase inhibition reduces the dose ofgonadotropin required for controlled ovarian hyperstimulation. J Soc Gy-necol Investig 11:406–415
85. Biljan MM, Tan SL, Tulandi T 2002 Prospective randomized trial comparingthe effects of 2.5 and 5.0 mg of letrozole (LE) on follicular development,endometrial thickness and pregnancy rate in patients undergoing super-ovulation. Fertil Steril 78:S55
86. Healey S, Tan SL, Tulandi T, Biljan MM 2003 Effects of letrozole on su-perovulation with gonadotropins in women undergoing intrauterine insem-ination. Fertil Steril 806:1325–1329
87. Hamilton A, Piccart M 1999 The third-generation nonsteroidal AIs: a reviewof their clinical benefits in the second-line hormonal treatment of advancedbreast cancer. Ann Oncol 10:377–384
88. Goss PE 1999 Risks versus benefits in the clinical application of AIs. EndocrRelat Cancer 6:325–332
89. Palter SF, Tavares AB, Hourvitz A, Veldhuis JD, Adashi EY 2001 Areestrogens of import to primate/human ovarian folliculogenesis? Endocr Rev223:389–424
90. Yanase T, Simpson ER, Waterman M 1991 17-hydroxylase/17,20-lyase de-ficiency: from clinical investigation to molecular definition. Endocr Rev 12:91–108
91. Rabinovici J, Blankstein J, Goldman B, Rudak E, Dor Y, Pariente C, GeierA, Lunenfeld B, Mashiach S 1989 In vitro fertilization and primary embryoniccleavage are possible in 17�-hydroxylase deficiency despite extremely lowintrafollicular 17�-estradiol. J Clin Endocrinol Metab 68:693–697
770 J Clin Endocrinol Metab, March 2006, 91(3):760–771 Casper and Mitwally • Aromatase Inhibitors for Ovulation Induction
at Pakistan:Endo Jnls Sponsored on November 7, 2008 jcem.endojournals.orgDownloaded from

92. Schoot DC, Coelingh Bennink HJ, Mannaerts BM, Lamberts SW, BouchardP, Fauser BC 1992 Human recombinant FSH induced growth of preovulatoryfollicles without concomitant increase in androgen and estrogen biosynthesisin a woman with isolated GT deficiency. J Clin Endocrinol Metab 74:1471–1473
93. Shoham Z, Mannaerts B, Insler V, Coelingh HB 1993 Induction of folliculargrowth using recombinant human follicle-stimulating hormone in two vol-unteer women with hypogonadotropic hypogonadism. Fertil Steril 59:738–742
94. Mitwally MF, Biljan MM, Casper RF 2005 Pregnancy outcome after the useof an AI for induction of ovulation. Am J Obstet Gynecol 192:381–386
95. Tiboni GM 2004 AIs and teratogenesis. Fertil Steril 81:1158–115996. Biljan MM, Hemmings R, Brassard N 2005 The outcome of 150 babies
following the treatment with letrozole or letrozole and gonadotropins. FertilSteril 84 (Suppl 1):S95
97. Simon C, Cano F, Valbuena D,Remohı J, Pellicer A 1995 Clinical evidencefor a detrimental effect on uterine receptivity of high serum E2 concentrationsin high and normal responder patients. Hum Reprod 10:2432–2437
98. Paulson RJ, Sauer MV, Lobo RA 1990 Embryo implantation after human invitro fertilization: importance of endometrial receptivity. Fertil Steril 53:870–874
99. Forman R, Fries N, Testart J, Belaisch-Allart J, Hazout A, Frydman R 1988Evidence for an adverse effect of elevated serum estradiol concentration onembryo implantation. Fertil Steril 49:118–122
100. Valbuena D, Martin J, de Pablo JL, Remohi J, Pellicer A, Simon C 2001Increasing levels of estradiol are deleterious to embryonic implantation be-cause they directly affect the embryo. Fertil Steril 765:962–968
101. Basir GS, O WS, Ng EH, Ho PC 2001 Morphometric analysis of peri-im-plantation endometrium in patients having excessively high oestradiol con-centrations after ovarian stimulation. Hum Reprod 16:435–440
102. Simon C, Garcia Velasco JJ, Valbuena D, Peinado JA, Moreno C, RemohiJ, Pellicer A 1998 Increasing uterine receptivity by decreasing estradiol levelsduring the preimplantation period in high responders with the use of afollicle-stimulating hormone step-down regimen. Fertil Steril 70:234–239
103. Goswami SK, Das T, Chattopadhyay R, Sawhney V, Kumar J, ChaudhuryK, Chakravarty BN, Kabir SN 2004 A randomized single-blind controlledtrial of letrozole as a low-cost IVF protocol in women with poor ovarianresponse: a preliminary report. Hum Reprod 19:2031–2035
104. Garcia-Velasco JA, Moreno L, Pacheco A, Guillen A, Duque L, Requena A,Pellicer A 2005 The AI letrozole increases the concentration of intraovarianandrogens and improves in vitro fertilization outcome in low responderpatients: a pilot study. Fertil Steril 84:82–87
105. Oktay K, Buyuk E, Libertella N, Akar M, Rosenwaks Z 2005 Fertility pres-ervation in breast cancer patients: a prospective controlled comparison ofovarian stimulation with tamoxifen and letrozole for embryo cryopreserva-tion. J Clin Oncol 23:4347–4353
106. Casper RF 2003 Letrozole: ovulation or superovulation? Fertil Steril80:1335–1337
JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving theendocrine community.
Casper and Mitwally • Aromatase Inhibitors for Ovulation Induction J Clin Endocrinol Metab, March 2006, 91(3):760–771 771
at Pakistan:Endo Jnls Sponsored on November 7, 2008 jcem.endojournals.orgDownloaded from





























