Embed Size (px)
Citation preview

1
2
Prime University
3
PUJMQ
Prime University Journal of Multidisciplinary Quest
Editor
Profulla C. Sarker
Prime University,
Dhaka, Bangladesh
Associate Editor
M. Abul Hossain Sikder
Atish Dipankar University
Dhaka, Bangladesh
Book Review Editor
P. Dash Sharma
Ranchi University
Ranchi, India
Managing Editor
Mohammad Arshad Ali
Prime University
Dhaka, Bangladesh
Published by
Centre for Research, Human Resource Development and Publications
Prime University
2A/1 North East of Darus Salam Road
Section-1, Mirpur, Dhaka, Bangladesh
Cover Design
Amal Das
Printed by
Color Line, 01715812345
Price : Tk. 250.00 / US $ 5.00
4
Editorial Board
Bong Joo Lee
Seoul National University
South Korea
Sarah Safdar
Peshwar University
Pakistan
Ajit Kumar Singh
Ranchi University
India
Antonio Fiori
University of Bolonga
Italy
Manohar Pawar
Charles Sturt University
New South Wales, Australia
Santi Kinduka, Washington University
United States of America
Cecillia Chan
Hongkong University
China
M.A. Sobhan
Independent University
Bangladesh
M. Shahidullah
Rajshahi University
Bangladesh
Nazir M. Hossain
York University
Canada
Gareth Davey
University of Chester
United Kingdom
Durga Das Bhattacharjee
Dhaka University
Bangladesh
A. Renaweera
Colombo University
Sri Lanka
Tiong Tan
Singapore National University
Singapore
Margarita Frederico
Latrobe University
Australia
Desa Shankwan
Thamasat University
Thailand
Paul Olson
Toronto University
Canada
Sarker Ali Akkas
Jagannath University
Bangladesh
Ramesh Chandra Devnath
Rajshahi University
Bangladesh
Heinz Theisen
Catholic University of Köln
Germany

5

6
Editorial Note
Prime University Journal of Multidisciplinary Quest (PUJMQ) is an
international journal published twice a year (January and July). It is a
refereed journal designed to promote multidisciplinary inquiry on
research, education and development. PUJMQ encompasses all scientific
academic fields dealing with life, society, culture, business, law, science
and technology. The main mission and vision of PUJMQ is to make
multidisciplinary linkages that promote to inter-lock the different
disciplines in a single platform.
Prime University Journal of Multidisciplinary Quest (PUJMQ) has an
international editorial board involving the scholars of different disciplines
across the East and the West and as a result it helps to mitigate cross-
cultural issues across the globe. It is a multidisciplinary and international
forum which acts as a catalyst to promote and exchange ideas, views, and
knowledge of different disciplines that encourage scholars to enhance their
creative and innovative ideas and knowledge in global perspective. It
helps to contribute to the knowledge of the academics, researchers, policy
makers, planners, practitioners and development workers to take
appropriate policy in order to chalk out effective planning for formulating
pragmatic policies.
Eight research papers have been selected in the current volume on
different issues viz. aging and mental health in Chinese society due to
declination of filial relationship, legislative reform for the protection of the
rights of the Hindu Community in Bangladesh, health policy of India
through five year plans emphasizing the maternal and child health issues,
viscosity affects velocity and as a result it helps to determine the
parameters of temperature profiles, sensitivity study of the cumulus
parameterization scheme with planetary boundary layer options for
estimating the rainfall in Bangladesh, the health scenario of rural Bhutan
which examined the infant morbidity and mortality through SWOT

7
analysis, trend and development of advertisement through television in order
to enhance the scope of market for industrial production in Bangladesh,
and seasonal food insecurity and coping mechanisms applied by the poor
to overcome the crisis in the north western part of Bangladesh.
Profulla C. Sarker
Editor

8
Contents Changing Attitudes toward Filial Piety and Its Impact on Mental Health of Elderly People in Chinese Society 9
Kam Ping Kathy Leung Yui Huen Alex Kwan
Kai Wai Kennis Leung
The Hindu Community in need of Legislative Protection 27
Sadia Afroz Binte Siraj Tanvhir Ahmad
The five year plans in India: Overview of Public Health Policies 41
Sethuramalingam V. Selwyn Stanley Sathia S.
MHD Natural Convection Flow of Fluid with Variable Viscosity from a Porous Vertical Plate 55
Amena Ferdousi
Mohammad Salek Parvez
M. A. Alim
Sensitivity Study of the Cumulus Parameterization Schemes with Planetary Boundary Layer Options in Estimating Rainfall in Bangladesh using MM5 74
Md. A. E. Akhter Md. M. Alam
M. A. Hossain
Rural Health Scenario in Bhutan: The Social and Institutional Experiences 85
Komol Singha Lingchen
Trends and Development of Television Advertisement in Bangladesh 103
Md. Towhidul Islam
‘Monga’- A Seasonal Food Insecurity and Its Impact on Poverty in Bangladesh: A Local Issue in National Perspective 124
Profulla C. Sarker M. Abul Hossain Sikder
9

10
CHANGING ATTITUDES TOWARD FILIAL PIETY
AND ITS IMPACT ON MENTAL HEALTH OF
ELDERLY PEOPLE IN CHINESE SOCIETY
Kam Ping Kathy Leung1, Yui Huen Alex Kwan
2 &
Kai Wai Kennis Leung 3
Keywords: Attitude. Filial. Mental Health. Elderly.
Abstract: This paper is an attempt to discuss the changing attitude of the
young people of China towards elderly people and its impact on their
mental health. Filial Piety is rooted from the instinct of the Confucianism
that implies loyalty, respect and obligation among the family members to
make harmonious relationship. With the advancement of science and
technology in the age of globalization and modernization, the attitude
towards filial piety is indicative of wider cultural change in Chinese society
and thus affects the family support to the elderly and as a result the elderly
people become the victims of mental health. This paper suggests to chalk out
awareness program to make the young people to take care of the elderly.
Introduction
Filial piety is a distinctive concept in Confucianism that implies deep
loyalty, respect, and devotion of children toward their parents (Ng, Philips
& Lee, 2002, Tao, 2010). As a social norm, filial piety values family
honor and harmony more than individual interests (Yang, 1995). However,
among the Chinese in countries in the Southeast and East Asia, including
Hong Kong, mainland China, South Korea, and Singapore, attitudes
toward filial piety, particularly with respect to elderly parents, have
changed in recent decades (Ikels, 2010). Rapid sociodemographic
1 Instructor, Department of Applied Social Studies, College of Humanities and Social
Sciences, City University of Hong Kong 2 Professor, Department of Applied Social Studies, College of Humanities and Social
Sciences, City University of Hong Kong 3 Professor, Department of Applied Social Studies, College of Humanities and Social
Sciences, City University of Hong Kong

11
changes, a rapidly aging elderly population, and changes in economic
status and intergenerational expectations have all influenced filial
commitments (Caregivershome, 2007, Sung, 2008, Quah, 2010, Yi, 2010).
However, many elderly parents now understand their adult children in
terms of their individuality, rather than their obligations (Ng, Philips &
Lee, 2002, Ng, 2010), and in Hong Kong filial orientation is viewed only
as a frame of reference (Wong & Chau, 2006, Ting, 2010). In urban
China, both young and old people rank respect as the most important
aspect of filial piety and obedience as the least important (Yue & Ng,
2002, Yang, 2010). Some Koreans have modified the practice of filial
piety with respect to the constraints associated with the family context,
work situations, and social environment (Sung, 2008, Koreatimes, 2008).
In Singapore, families, welfare organizations, and governments share the
responsibility for establishing effective practices of elderly care within
families (Verbrugge & Chan, 2008).
The contemporary version of filial piety is characterized by gratitude,
respect, and reciprocal support, rather than obligation, obedience, and one-
way responsibility (Ting, 2009). Filial piety is significant to Chinese
people, but its significance is in transition, not necessarily in decline. As
stated by Ng, Philips, and Lee (2002), adult children in Hong Kong, for
example, have created acceptable substitutes for co-residency, such as
living near or maintaining close contact with elderly relatives out of
respect for filial piety. Yue and Ng (2002) showed that both younger and
older generations in Beijing and Guangzhou continue to endorse strong
filial commitment (Kwan, Cheung & Ng, 2010). Mehta and Ko (2004)
revealed that the majority (88%) of elderly people over 65 years old in
Singapore live with adult children, showing that filial obligation is still
treasured by family members. In modern Chinese families, filial piety may
serve as a buffer from the stress of being a caregiver (Lai, 2010), and may
also provide benefits by encouraging intimate relationships of equal
exchange (Kim & Kim, 2003).
To better understand these sociodemographic changes and the significance
of filial commitment in the Chinese population, this study examines the
perspective of adult children to illustrate the strain encountered by
caregivers and adult children with respect to filial piety in Southeast Asia.
Some adult children face the dilemma of fulfilling traditional values (i.e.,

12
filial piety) and actualizing their individuality (i.e., high demands at work
and at home). As such, they are not quick to accept the role of caregiver,
especially for elderly relatives who suffer from dementia or other chronic
illnesses (Knight et al., 2002, Lam, 2006). The opinions of these adults
reveal that the strain of familial obligations arises from the anticipative,
immediate, residual, and chronic stages of long-term caregiving
commitment (Kwan, Chan & Leung, 2004). Stress reactions by adult
children may include physical and psychological fatigue, self-blame, or
the disturbance of normal life patterns, and some family tragedies, such as
abuse, murder, or suicide, have occurred in recent decades (Hong Kong
Council of Social Services, 2010). In light of this trend, this study presents
a new conceptualization of filial piety that emphasizes the balancing of
societal and individual challenges to mitigate the strain on adult children.
This conceptualization should be useful in crafting government policy.
This article is organized into four parts. The first part reviews previous
studies on the meaning of filial piety in East and Southeast Asian
countries. Two perspectives on the decline of and changes in filial piety
are offered to suggest how policy-makers might assist adult children and
caregivers with respect to filial piety. The third part explains the
qualitative case study method used to conduct the study, in which two
Chinese adult children shared their experiences of interacting with their
parents. The final part presents three implications of the new reality of
elderly care outside of traditional family networks for the concept of filial
piety.
Literature review
Roots and Meanings of Filial Piety
Filial piety is a central and distinctive concept of Confucianism that
emphasizes authoritarian, family-centered care practices and the
maintenance of family harmony and cohesiveness (Hwang, 1999).
According to the doctrine of filial piety, children are expected to be loyal
to their families, mutually assist family members, sacrifice themselves for
the group, and maintain harmony with the family (Yang, 1995). The
cultural meanings of filial piety include the deep loyalty, respect, and
devotion of children toward their parents (Ng, Philips & Lee, 2002). Chow

13
(2001) classified filial piety into three levels, namely, caring for the
material needs of parents, paying attention to the wishes and preferences
of parents, and honoring parents by one‘s behavior.
From a social psychological perspective, the two essential components of
value and behavior constitute filial piety. Sung (2008) indicated that
young adult children focus on ―repayment, responsibility and sacrifice‖ as
behavioral practices and ―love/affection, harmony and respect‖ as
emotional needs. Hwang (1999) stated there are two different kinds of
filial piety: passive (e.g., obedience to authority) and active (e.g., concern
for elderly parents). Some scholars have advised that people avoid mixing
the concept of filial behavior with filial attitude because the two factors
only show a moderate correlation (Ho, 1996 & Yu, 1983). Thus,
classification schemes for filial piety often include behavior-emotional,
passive-active, and authoritarian-reciprocal binaries. Modern filial piety is
both an ideology and a practice of societal behavior that takes the form of
an individual lifestyle, an affective relationship, and reciprocal support
(Thomas, 1990).
Implications of Changes in Filial Piety for Policy-Makers
Policy-makers throughout East and Southeast Asian countries are aware of
the changing significance of filial piety, and that it must evolve to address
care that ensures the well-being of elderly parents. Implied in this
approach is a balance among private and public responsibility for elder
care and the commitment from the government (Chow, 2007, Sung, 2008),
in addition to the provision of moral education that will benefit
individuals, families, and the community (Thomas, 1990).
In this regard, there are two dimensions in which policy-makers should
focus their efforts. First, community support networks for elderly care are
in great demand but are underdeveloped in East and Southeast Asian
societies (Ng, Philips & Lee, 2002, Lam, 2006). Suggestions for
remedying this situation include a voucher system as a long-term policy
for elderly care (Chou, Chow, & Chi, 2005, Lam, 2006), the provision of
elderly care services at the community level, and public education, such as
a ―Respect for Elders Day‖ (Sung, 2008). Second, policy-makers must be

14
aware that the pressures on adult children who adopt a caregiving role
cause physical exhaustion, psychological difficulties, and conflicts within
families. Addressing the mental health of adult children and the social
support assistance available to them would be the first step to resolving the
dilemma of individuality versus cultural pressure to display filial piety
(Chan & Leong, 1994). Our societies are measured not only by the level of
affluence, but also by core values such as civic-mindedness, mental
fitness, and human rights (Policy Address, 2009).
Two Perspectives: The Decline of Filial Piety and Changes in Filial Piety
The Decline of Filial Piety
The decline of filial piety is usually evaluated by comparing current
practices with the cultural norms of filial piety and examining the
immigrant experience, particularly with respect to the dilemma between
traditional and modern values (Ting, 2009). Modernization has caused
many sociodemographic changes in East and Southeast Asia, such as an
increase in nuclear families, a decrease in extended families, better
employment opportunities for women, and better education for the
younger generations (Mehta & Ko, 2004; Census & Statistics Department,
2006; Sung, 2008). These changes are suggested to have resulted in a
decline in filial piety, as demonstrated by fewer elderly people living with
their adult children or receiving informal support from them (Lee &
Kwok, 2005, Cheung & Kwan, 2009). In Hong Kong, there has been an
increase in the number of cases of abuse of the elderly (Kwan, 1995).
The level of filial piety has decreased in the educated population in China
(Cheung & Kwan, 2009), the social position of elderly people has been
undermined in Korea (Choi, 1996), and the increasingly large aging
population is putting strain on adult children who have adopted a
caregiving role in Singapore (Mehta & Ko, 2004), all of which may have
contributed to a decline in filial piety. Filial piety is also challenged by the
cultural values and practices of Western countries (Chan & Leong, 1994).
Western scholars studying Chinese, such as those in the United States,
find that the belief and practices surrounding filial piety are not consistent,
and that belief in filial piety does not increase as children reached

15
adulthood. It has also been noted that at present there is a higher
percentage of adult daughters taking care of their elderly parents than
adult sons (Yu, 1983, Yan, 2001).
Changes in Filial Piety
Due to modernization and Westernization, people in East and Southeast
Asia express filial piety in a distinct way in response to their societal
environment and the challenges to caregiving. Hence, it can be argued that
traditional filial piety coexists with modern practice (Thomas, 1990, Ng,
Philips & Lee, 2002, Yue & Ng, 2002, Sung, 2008). As such, filial piety is
becoming about ―gratitude rather than obligation, respect rather than
obedience and reciprocal support rather than one-way responsibility in
contemporary practice‖ (Ting, 2009, pp. 8).
In Hong Kong, elderly parents and adult children express affection and
responsibility for filial piety by living near or maintaining close contact
with their parents (Ng, Philips & Lee, 2002). Some Chinese immigrants in
the United States prefer to provide material objects to parents to enhance
their happiness and regulate their development (Lin, 1985). Filial piety
may also act as a buffer against the stress encountered by caregivers (Lai,
2010). In China, both young and old people rank respect as the most
important aspect of filial piety, and obedience as the least important aspect
(Yue & Ng, 2002, Cheung & Kwan, 2009a). In South Korea, the social
meaning of filial piety is in transition (Sung, 2007 & 2008), with elderly
parents experiencing reciprocal exchange in families that have achieved a
higher quality of life (Kim & Kim, 2003). In Singapore, elderly people
who depend on adult children often provide household and childcare assistance
in exchange (Verbrugge & Chan, 2008). These examples of mutual support
describe the changing expression of filial piety today (Thomas, 1990).
A review of the relevant literature uncovers three main themes. First, the
cultural ecology of filial piety is still valued by ethnic Chinese people.
However, certain pressures, including a lack of decision-making power in
patriarchal cultures, for example, where subordinates are expected to defer
to superiors or males, make it difficult for adult children or caregivers to
fulfill the demands of the family. Second, filial piety has evolved to mean

16
gratitude, respect, and reciprocal support. These new characteristics
emphasize mutual understanding and acceptance between adult children
and elderly parents, thus allowing for reciprocity in the context of filial
piety. Third, rapid sociodemographic changes require the state or
government to provide sufficient and adequate social support for elderly
care in families under stress. Inevitably, a paid-care system must be
developed in East and Southeast Asia as a form of need-based and person-
focused support to encourage and support adult children to adopt the role
of caregiver. Here two case studies are presented to illustrate these themes.
Case Study Method and Cases
A qualitative case study method was chosen for this exploratory study.
Case studies are best suited to studying complex phenomena within real-
life contexts (Yin, 2009). Case studies are also particularly valuable for
studies on topics that are sensitive, complicated, immeasurable, and
concerned with interaction and processes in everyday life (Walker, 1995).
Further, intensive case studies can be a means of acquiring practical
knowledge (Millstein, 1993). As a social worker in Hong Kong, the author
conducted a qualitative case study to investigate the influence of filial
piety on mental stress and to understand the experiences of adult children
who are caregivers for their parents. Using a confidentiality agreement, the
author obtained consent from two respondents who voluntarily
participated in the study. Their names and details have been changed to
protect their identities. For counseling practice, the two respondents, who
were also clinical subjects, reviewed the interview transcripts and
provided valuable feedback on the final write-up. These case studies thus
provide a glimpse into the complicated process of honoring traditional values
while following one‘s individuality in a drastically changing society.
Case Study One
Wendy, a 32-year-old, unmarried, Catholic, primary school teacher,
sought assistance from a social worker in November 2008 because she felt
emotionally unstable after suddenly bursting into tears at work. She was
aware that she was losing emotional control, and thus took the initiative to
seek assistance. In April 2000, Wendy was preparing for final

17
examinations, and was frustrated because her boyfriend seemed to be on
very close terms with another girl. These factors almost pushed her to
breaking point. Frustrated by these occurrences, Wendy had a serious
quarrel with her father for the first time in her life, which brought her
long-suppressed discontentment to the surface. In addition, Wendy‘s
father had just purchased a new flat that was a long way from Wendy‘s
workplace but close to where her father‘s friends with whom he played
mah-jong lived. Wendy was extremely unhappy about her lack of
decision-making power in her father‘s choice of home. Adopting the
cultural stance that opposes unmarried daughters living alone, Wendy‘s
parents did not allow her to rent a flat near her work. Faced with these
multiple blows, Wendy began to consider suicide. Afraid that Wendy
might kill herself, her parents finally allowed her to move out, but her
mother never told her relatives and worked hard to keep it a secret.
Looking back, Wendy felt that these experiences encapsulated the phrase
―nice to see each other, but hard to live together.‖
Nevertheless, the family negotiated a new way to fulfill the demands of
filial piety. After moving out, Wendy spent less time with her parents but
continued to visit them every Sunday. Wendy began to play the role of
helper, rather than dependent child needing her parents‘ care. Her parents
in turn showed their care for her in simple ways such as ―preparing more
dishes‖ and ―worrying if I [she] had enough money to spend.‖ Here,
physical distance produced positive results by easing Wendy‘s tense
relationship with her parents. When Wendy was separated from her
parents temporarily, it allowed both parties time to calm their violent
emotions and their anger to dissipate. Eventually, Wendy was able to
treasure the intimate relationship she enjoyed with her family, and planned
to move back home after graduation.
The conflict that Wendy experienced between meeting the demands of
filial piety (e.g., maintaining a harmonious relationship) and pursuing her
individual ambitions (e.g., advancing her career) was resolved. In this
case, Wendy found that the limited space she had in the family home
interfered with her attempts to gain independence from her parents, but
she felt guilty for not fulfilling her filial responsibility. To balance the
filial daughter‘s role with the attainment of her own goals, Wendy chose

18
to live apart from her parents. Physical distance eased Wendy‘s
psychological stress and also resulted in positive changes in her parents.
Wendy enjoyed greater freedom in living alone, but still missed her
family. Wendy‘s parents learned to cherish their relationship with her, and
showed their concern for her in small ways after Wendy moved out. When
they saw one another again, they were affectionate toward each other.
Clearly, in practicing filial piety, adult children and their parents can
negotiate the meanings of that value and construct mutually acceptable
behavior, which creates a positive and supportive attitude between adult
children and their parents.
Case Study Two
Ah Ming, a 49-year-old, unmarried hairdresser, suffered from a mild
depressive disorder that included symptoms of insomnia and the loss of
25% of her body weight within three months. Once, Ming screamed
loudly at work for no particular reason. Ming‘s colleagues encouraged her
to seek psychological counseling to stabilize her mood, and she thus
sought counseling in September 2007. As a single child, Ming had taken
sole responsibility for the care of her mother following the death of her
father in 2005, and lacked support from relatives. Ming‘s mother had
suffered from diabetes and hypertension, and was hospitalized three times
due to accidents, including falling and breaking her ribs. Ming‘s mother
insisted on living at home and refused to be sent to a nursing home. Ming
went through three domestic helpers in 13 months, because her mother
found it difficult to get along with them. Ming responded to these
problems with feelings of stress, helplessness, and guilt.
After the fourth hospitalization, Ming decided to seek community support
for her elderly mother. She arranged for her mother to live in a nursing
home as she felt that she was no longer able to take care of her and be
effective at work at the same time. However, Ming still had to balance
meeting the demands of filial piety and the pursuit of personal freedom.
She lied to her mother, telling her that she was going to have surgery and
would thus be admitted to hospital for a while. Ming‘s mother moved into
a nursing home after accepting this explanation. The rent and service
charges for the nursing home accounted for 70% of Ming‘s monthly

19
income, and Ming was obliged to seek financial assistance from a medical
social worker. However, she was rejected as being ineligible for
government subsidy. Ming then took on another part-time job to ease the
financial burden, which caused her further physical strain and
psychological stress. This also resulted in her having less time to visit her
mother, and she was often obliged to ignore her mother‘s requests for
visits.
Summary: The Expected Caregiving Role
These two case studies show that the caregiver role can result in strain and
struggle for adult children and caregivers. According to traditional
Chinese family values, children are expected to be loyal to their families,
mutually assist family members, sacrifice themselves for the group, and
maintain harmony within the family (Yang, 1996). These values impose
certain rights and obligations. For example, when a family member is in
trouble, other family members are expected to assist. Some academics
have claimed that the traditional Chinese family suppresses individuality
(Pau, 2000, pp. 196).
Both Ming and Wendy contributed to their family in terms of money,
time, and energy. They gave a portion of their monthly salary to their
family although they had never been explicitly asked to do so. Ming also
took on a caregiver role due to her mother‘s chronic illness. The
dedication of Wendy and Ming reveals the culturally embedded value of
filial piety. The majority of Chinese adult children never question that they
should give care, even if they complain that the caregiver role induces
stress that affects their mental health. For instance, some feel overloaded
after weighing the costs and rewards of the role of caregiver, while others
become stressed due to the tension between fulfilling their responsibilities
to parents and achieving self-development. The caregivers in both case
studies felt suffocated and internalized their reaction to the assigned role.
The long-term commitment of the expected caregiver role undermines
adult children‘s individual development because it makes demands on
their time, emotional energy, and money. However, when parents and
children negotiate the practice of filial piety and parents come to
understand and accept the constraints faced by their adult children, the

20
situation can be improved. Caregivers with inadequate social support
could also have some of the strain alleviated by financial assistance from
the government. Providing more high-quality nursing homes and a more
flexible financial means test for subsidies, for example, would help relieve
the financial burden of caregivers, and would balance the provision of
elderly care in East and Southeast Asia between the individual and
community levels.
Discussion and Implications
1. Filial Piety in Transition: A Socially Constructed Discourse
Filial piety remains significant to Chinese families today. At the same
time, however, it is recognized that filial piety is changing into a socially
constructed discourse due to the increasing influence of the West and the
aging population in Southeast Asia (Ng, Philips & Lee, 2002, Yue & Ng,
2002). Adult children and caregivers face many challenges from urban
living and their quest to assert their individuality, which tends to
undermine the fulfillment of traditional filial commitments. This tension
results in physical and psychological strain on adult children and caregivers that
is forcing change in the meaning and practice of cultural filial piety.
Changes in the practice of filial piety emerge through the social
construction of reality, which is ―the process in which people creatively
shape reality through social interaction‖ (Macionis, 2004, pp. 89). For
instance, in Hong Kong, filial piety motivates adult children and elders to
practice gratitude, reciprocal support, and respect (Ting, 2009). Zhan and
Montgomery (2003) re-examined the caregiving behavior of adult children
within the context of economic reform and the one-child policy in urban
China. Sung (2008) noted that filial piety has become a public issue in
South Korea, which has benefited both the individual and the family
(Thomas, 1990). In this analysis, the transition of filial piety is placed
within a broad social context. Social institutions, such as the government
and communities, play an important role in socializing individuals to
adopt acceptable patterns of behavior. For instance, elderly parents may
seek social independence in old age based on mutual support from their
family, and caregivers may balance conflicting demands by making a

21
socially acceptable arrangement based on a style of filial piety that is
specific to their own family (Gigliotti & Huff, 1995).
2. Recognizing Stress in Adult Children: Changing Expectations
The culture of filial piety in East and Southeast Asia pressures adult
children to adopt a caregiver role. In 2006, around 74% of elderly people
in Hong Kong lived with their families, and over 70% of them suffered
from one or more chronic illnesses (Hong Kong Council of Social
Services, 2010). However, adult children encounter difficulties in meeting
filial demands, which often conflict with their personal goals (Wong,
2007, Kwok, Ho & Li, 2009). In the case studies presented here, Ming
found it difficult to cope with caring for a mother with chronic illness and
encountered financial difficulties as a result. Wendy was frustrated by the
demands implied by both filial piety and the pursuit of individuality. Due
to the one-child policy, in China there are now too few adult children to
care for a rapidly aging population with chronic diseases (China Concern
Over Population Aging & Health, 2006). Thus, adult children who care for
their elderly parents experience many constraints associated with family,
work, and their social environment (Sung, 2008, Liu & Kendig, 2000).
The culture of filial commitment is still valued by the Chinese (Lai, 2010),
but the culture must evolve, especially with respect to parents‘
understanding and acceptance of the constraints on their adult children.
Such acceptance will facilitate positive and supportive change for both
adult children and their elderly parents. In Hong Kong, for example,
elderly parents now accept their adult children living near them or
maintaining close contact with them as a substitute for co-residence (Ng,
Phillips & Lee, 2002). In the case study, Wendy‘s relationship with her
family improved with physical distance. As stated, both young and elderly
people rank respect as the most important aspect of filial piety and
obedience as the least important (Yue and Ng, 2002). Clearly, the
adjustment and regulation of expectations of filial piety is becoming a new
cultural focus in urban China. In Singapore, some elderly people like to
provide childcare and household assistance to alleviate the strain on adult
children arising from the norms of filial piety (Verbrugge & Chan, 2008).
Changing expectations of filial piety can thus facilitate reciprocal

22
exchange within the family to encourage a better quality of life and more
intimate relationships between adult children and their elderly parents
(Kim & Kim, 2003).
3. Accessibility and Availability of Social Support: The Role of Policy-
Makers
Having explained the strain experienced by adult children and caregivers
due to the norms of filial piety, the author suggests that policy-makers try
to strike a balanced approach between private and public responsibility for
elderly care in East and Southeast Asia (Chow, 2007; Sung, 2008).
Governments need to provide adequate support for families under stress,
while still valuing the filial orientation of the individual, family, and
society (Thomas, 1990).
A paid-care system, such as the provision of cash grants or vouchers for
elderly care, is just such a means of fulfilling filial commitments. Chou,
Chow, and Chi (2005) and Meagher (2006) suggest that a voucher system
encourages family care, integrated services, mixed-mode financing, and a
large-market approach by the government. A paid-care system also
empowers the elderly to utilize community resources to enhance their self-
esteem and self-reliance, while providing essential financial assistance. In
the case studies, Ming shouldered a large financial burden due to being
ineligible for government subsidies, which shows that caregivers are often
given inadequate social support. Financial assistance from the government
must thus include a more flexible means test to alleviate the stress on
caregivers. However, a paid-care system must also be regularly reviewed
to monitor resource allocation and the effectiveness of the system for the
elderly and their adult children.
At the community level, changes in the meaning of filial piety mean that
co-residency is not the only option for adult children. Even when children
and parents live apart, as in Wendy‘s situation, or are assisted by
community services, such as in Ming‘s case, adult children can still fulfill
their filial commitments by maintaining mutual affection within the family
(Lan, 2002, Sung, 2008). It is suggested that improved accessibility and
availability of high-quality elderly daycare centers or residential care

23
services would further help in this regard. Public education on the changes
in filial piety practice should also be provided to raise awareness of the
mental health risks for adult children and caregivers. This will help to
ensure family prosperity and engender better civic-mindedness in East and
Southeast Asia countries.
Conclusion
This study reviews previous research into current practices of filial piety
and presents two case studies of adult children trying to balance the
traditional values of filial piety with the pursuit of individuality. The key
objective of the study is to explore the changing attitudes toward filial
piety and to present the perspective of adult children of their experiences
as caregivers of elderly parents in East and Southeast Asia. This study
situates filial piety as a socially constructed discourse, and reveals that
Chinese people have evolved new meanings and practices of filial piety
that are defined by gratitude, reciprocal support, and respect. It also
highlights the strain faced by adult children in adopting a caregiving role,
as manifested by physical and emotional fatigue, self-blaming,
helplessness, guilt, and disturbance to the normal patterns of life. These
difficulties prompt new attitudes and practices based on negotiation
between adult children and their parents. For instance, parents can be more
understanding of the constraints faced by their adult children, and adult
children can be more understanding of the expectations of their parents.
Such compromises can help maintain a harmonious relationship within the
family. Government policy must also take serious account of the problem
of elderly care in East and Southeast Asia. Policy initiatives should
particularly aim to provide sufficient and adequate community support to
disadvantaged families, such as by instituting a paid-care system,
providing allowances to alleviate financial burdens, or helping individuals
to identify appropriate community services.
Given the changes in filial piety in East and Southeast Asia, the author (as
a social worker) appreciates the unique way in which Chinese
communities are finding ways of caring for the well-being of their elderly
parents while at the same time pursuing their individuality so that the

24
Chinese social orientation toward the continuation of the family and
family harmony is still valued (Yang, 1995, Cheung, Kwan & Ng, 2006). It
may not be necessary to put much effort into developing the desired attitude
toward filial piety. Instead, it will be more effective to raise awareness
about or sensitivity to parents‘ need for care (Kwan & Cheung, 2010).
Inevitably, the states and governments of East and Southeast Asia must
seriously consider providing adequate community resources for elderly
care and public education on filial commitments. The changing attitudes
toward filial piety are indicative of wider cultural changes in Chinese
societies from the humanistic and sociological perspectives. These new
attitudes emphasize the uniqueness of individuals, the interactions and
relationships among the various dimensions within each individual, and
the socio-cultural aspects of filial piety. Timely changes in family support
aimed at enhancing the quality of life of adult children and caregivers and
their elderly parents should be developed as part of the modernization of
Asian societies.
References
Caregivershome (2007) China‘s One-child Policy Could Backfire on Its Elderly:
http://www.caregivershome.com/news/article.cfm (Internet resource).
Census and Statistics Department (2006) Census reports. Hong Kong: Hong Kong
Government Printer.
Chan, S. & Leong, C.W. (1994) Chinese families in transition: Cultural conflicts and adjustment
problems. Journal of Social Distress and the Homeless, Vol. 3 (3), pp.263 – 281.
Cheung, C.K. & Kwan, Y.H. (2009) The erosion of filial piety by modernisation in
Chinese cities. Ageing and Society 29(1), pp. 179-198.
Cheung, C.K. & Kwan, Y.H. (2009a) City-level influences on Chinese filial piety
practice. Journal of Comparative Asian Development 8(1), pp.105-123.
Cheung, C.K., Kwan, Y.H. & Ng, S.H. (2006) Impacts of filial piety on preference for
kinship versus public care. Journal of Community Psychology 34(5), pp. 617-634.
Choi, S. J. (1996) The family and aging in Korea: A new concern and challenge. Aging
and Society 16(1), pp. 1-25.
Chou, K.L., Chow, N.W.S. & Chi, I. (2005) A proposal for a voucher system for long-
term care in Hong Kong. Journal of Aging and Social Policy 17(2), pp. 85-106.
Chow, N. (1991) Does filial piety exist under Chinese communism? Journal of Aging and
Social Policy, Vol.3 (1 & 2), pp. 209- 225.
Chow, N. (2001) The practice of filial piety among the Chinese in Hong Kong. In Elderly
Chinese in Pacific Rim Countries: Social Support and Integration, edited by I. Chi, N.L.

25
Chappell, & J. Lubben, pp. 125-136. Hong Kong: Hong Kong University Press.
Chow, N. (2007) Ageing and the family in Hong Kong. International Journal of
Sociology of the Family 33(1), pp. 145-155.
Gigliotti, R.J. & Huff, H.K. (1995) Role related conflicts, strains, and stresses of older-
adult college student. Sociological Factus, Vol. 28(3), pp. 329-342.
Government of the Hong Kong SAR (2009) 2009-2010 Policy Address: Breaking New
Ground Together. http://www.policyaddress.gov.hk/09-10/eng/index.html (Internet
resource).
Ho, D.Y. F. (1996) Filial piety and its psychological consequences. In The Handbook of
Chinese Psychology, edited by M.H. Bond, pp.155-165. Hong Kong: Oxford
University Press.
Hong Kong Council of Social Services (2010) Elderly population in Hong Kong.
http://www.hkcss.org.hk/download/folder/el/el eng.htm (Internet resource).
Hwang, K.K. (1999) Filial piety and loyalty: Two types of social identification in
Confucianism. Asian Journal of Social Psychology 2(1), pp.163-183.
Ikels, C. (2010) Filial piety in contemporary East Asia. Paper presented at the
Conference on Strengthening Hong Kong‘s Families: Obligations and Care across
the Generations, 9 June, 2010, HKU, Hong Kong.
Kaneda, T.(2006) China‘s Concern Over Population Aging and Health.
http://prb.org/Articles/2006/ChinasConcernOverPopulationAgingandHealth.aspx?p=
1 (Internet resource).
Kim, I.K. & Kim, C.S. (2003) Pattern of family support and the quality of life of the
elderly. Social Indicators Research, Vol. 62-63, pp.437-454.
Knight, B.G., Robinson, G.S., Longmire, C.V.F., Chun, M., Nakao, K. & Kim, J.H.
(2002) Cross cultural issues in caregiving for persons with dementia: Do familism
values reduce burden and distress? Ageing International, 27(3), pp.70-94.
Koreatimes (2008) Health Care for Elderly in Korea http://www.koreatimes.co.kr/
www/news/opinon/2008/07/202_26848.html (Internet resource).
Kwan, Y. H. (1995) Elderly abuse in Hong Kong: A new family problem for the old
East? Journal of Elderly Abuse and Neglect 6 (3-4), pp. 65-80.
Kwan, Y.H., Chan, C.M. & Leung, M.F. (2004) A reader on integrated services on
caregivers. Hong Kong: Cosmos Books Ltd.
Kwan, Y.H. & Cheung, C.K. (2010) Normative and experiential influences on filial piety
practice – A case of Hong Kong Chinese. Paper presented at the International
Federation on Ageing 10th
Global Conference, 3-6 May, 2010, Melbourne, Australia.
Kwan, Y.H., Cheung, C.K. & Ng, S.H. (2010) The impact of filial piety on the family
institution: A comparison of the younger, middle-aged and older generation in
Guangzhou. In Guangdong: Challenges in Development and Crisis Management (pp.
429-459), edited by Joseph Y.S. Cheng. Hong Kong: City University of Hong Kong
Press.
26
Kwok, T., Ho, F. & Li, J. (2009) The Effectiveness Of Day Care For Dementia People
And Their Family Caregivers – The JCCPA Experience. Hong Kong: Chinese
University of Hong Kong
Lai, D.W.L. (2010) Filial piety, caregiving appraisal and caregiving burden. Research on
Ageing, 32(2), pp. 200-223.
Lam, R.C. (2006) Contradictions between traditional Chinese values and the actual
performance: A study of the caregiving roles of the modern sandwich generation in
Hong Kong. Journal of Comparative Family Studies 37(2), pp. 299-313.
Lan, P.C. (2002) Subcontracting filial piety: Elder care in ethnic Chinese immigrant
families in California. Journal of Family Issues 23(7), pp. 812-835.
Lee, W.K.M. & Kwok, H.K. (2005) Older women and family care in Hong Kong:
Differences in filial expectation and practices. Journal of Women and Aging 17(1-2),
pp. 129-150.
Lin, C. (1985) The intergenerational relationships among Chinese immigrant families: A
study of filial piety. Unpublished doctoral dissertation, University of Illinois at Chicago.
Liu, W. T. & Kendig, H (2000) Who should care for the elderly? An East-West value.
Singapore: Singapore University Press/World Scientific.
Macionis, J.J. (2004) Society: The Basics. Upper Saddle River, New Jersey: Prentice Hall.
Meagher, G. (2006) What can we expect from paid carers? Politics and Society 34 (1),
pp. 33-54.
Mehta, K.K. & Ko, H. (2004) Filial piety revisited in the context of modernizing Asian
societies. Geriatrics and Gerontology International. Vol. 4(s1), pp. 77 -78.
Millstein, K.H. (1993) Building knowledge from the study of cases: a reflective model for
practitioner self-evaluation. Journal of Teaching in Social Work, 8(1), pp. 255-279.
Ng, A.C.Y., Phillips, D.R. & Lee, W.K.M. (2002) Persistence and challenges to filial
piety and informal support of older persons in a modern Chinese society: A case
study in Tuen Mun, Hong Kong. Journal of Ageing Studies (16), pp. 135-153.
Ng, S.H. (2010) Who will support elders best? Paper presented at the Conference on
Strengthening Hong Kong‘s Families: Obligations and Care across the Generations,
9 June, 2010, HKU, Hong Kong.
Pau, Y. K. (2000) Reconstruction family rules-from the Satir Model to the I Tao—A
trainer‘s interpretive of a personal growth group in Hong Kong. Unpublished
Doctoral dissertation, Hong Kong University.
Quah, S. (2010) Social setting and life trajectories: Challenges to obligations and care across
generation. Paper presented at the Conference on Strengthening Hong Kong‘s Families:
Obligations and Care across the Generations, 9 June, 2010, HKU, Hong Kong.
Sung, K.T. (2007) Respect and Care for the Elderly: The East Asian Way. Lanham, MD:
University Press of America.
Sung, K.T. (2008) Filial piety in modern times: Timely adaptation and practice patterns.
Australasian Journal on Ageing, Vol. 17(s1), pp.88-92.

27
Tao, J. (2010) ‗Qinging‘ in Chinese family – A Confucian perspective. Paper presented at
the Conference on Strengthening Hong Kong‘s Families: Obligations and Care
across the Generations, 9 June, 2010, HKU, Hong Kong.
Thomas, E. (1990) Filial piety, social change and Singapore youth. Journal of Moral
Education, Vol.19 (3), pp.192-205.
Ting, K.F. (2009) A Review Of The Research Literature On Filial Piety. Hong Kong:
Chinese University of Hong Kong.
Ting, K.F. (2010) Perceptions of filial piety and elderly care. Paper presented at the
Conference on Strengthening Hong Kong‘s Families: Obligations and Care across
the Generations, 9 June, 2010, HKU, Hong Kong.
Verbrugge, L.M. & Chan, A. (2008) Giving help in return: Family reciprocity by
older Singaporeans. Ageing and Society 28(1), pp.5-34.
Walker, R. (1995) Applied Qualitative Research. Aldershot: Gower Publishing Company
Limited.
Wong, D.F.K. (2007) Uncovering socio-cultural factors influencing the pathway to care
of Chinese caregivers with relatives suffering from early psychosis in Hong Kong.
Journal of Culture, Medicine and Psychiatry (31), pp.51-71.
Wong, O.M.H. & Chau, B.H.P. (2006) The evolving role of filial piety in eldercare in
Hong Kong. Asian Journal of Social Science 34(4), pp. 600-617.
Yan, F.L. (2001) A study of the experiences of single women. Unpublished Doctoral
Dissertation, University of Bristol.
Yang, K.S. (1995) Chinese social orientation: an integrative analysis. In Chinese
Societies and Mental Health (pp. 19-39), edited by T.Y. Lin, W.S. Tseng, E.K. Yeh.
Hong Kong: Oxford University Press.
Yang, K. S. (1996) The psychological transformation of the Chinese people as a result of
societal modernization. In The Handbook of Chinese Psychology (pp. 479-498),
edited by M.H. Bond. Hong Kong: Oxford University Press.
Yang, S.H. (2010) Ethical obligations and home care. Paper presented at the Conference
on Strengthening Hong Kong‘s Families: Obligations and Care across the
Generations, 9 June, 2010, HKU, Hong Kong.
Yi, C.C. (2010) The intergenerational relations and elderly care in Taiwan. Paper
presented at the Conference on Strengthening Hong Kong‘s Families: Obligations
and Care across the Generations, 9 June, 2010, HKU, Hong Kong.
Yin, R. K. (2009) Case Study Research: Design and Methods (4th edn). Los Angeles: Sage.
Yue, X. & Ng, S.H. (2002) Filial obligations and expectations in China: Current views
from young and old people in Beijing. Asian Journal of Social Psychology. Vol. 2
(2), pp.215-226.
Yu, L.C. (1983) Patterns of filial belief and behavior within the contemporary Chinese American
family. International Journal of Sociology of the Family, Vol. 13, pp. 17-36.
Zhan, H.J. & Montgomery, R.J.V. (2003) Gender and elder care in China: The influence
of filial piety and structural constraints. Gender and Society, Vol. 17(2), pp. 209-229.

28
THE HINDU COMMUNITY IN NEED OF
LEGISLATIVE PROTECTION
Sadia Afroz Binte Siraj1 & Tanvhir Ahmad
2
Keywords: Community. Reform. Inheritance. Custom. Maintenance. Adoption.
Abstract: Hindu community is the second largest community of Bangladesh.
They are guided by the age old traditional law in their personal matters.
Theses laws are very old and have not contemplated the socio-economic
changes of the society. That is why it is very difficult to implement the
laws, and because of this very fact the Hindu communities are reluctant to
have recourse to law. This large portion is deprived of their basic right of
―protection of law‖. This article has tried to suggest several reforms
mentioning the existing practice to show the huge gap. So that it gives an
idea how old and almost impossible to implement this traditional law is.
Objectives
The objective of the study is (a) to find out problems in the personal laws
for the Hindu community and (b) to examine loopholes in the implementation
of personal laws for Hindu community. Thus the community will get a law
to establish their personal rights.
Methodology: The method of the study is content analysis method .The
article is prepared by studying many previous works of different authors
published in many books and journals through the method of text analysis.
The literature on this subject matter emphasized the shortcomings of
Hindu Law because of its lacking regarding the legislative intervention,
without which a law can not ensure its complete enforcement.
Limitations: Hindu law is a vast area so this article has failed to cover
each and every area of the subject matter. It is not an exhaustive work
which left many areas untouched.
1 Lecturer, Department of Law and Justice, Southeast University
2 Lecturer, Department of Law, Prime University

29
Introduction
According to Article 27 of the Constitution of People‘s Republic of
Bangladesh all citizens are equal before law and are entitled to equal
protection of law. According to 1991 census 15 per cent of the population
of our country belong to the Hindu Community (World Directory of
Minority and Indigenous Peoples Bangladesh: Hindus). The Hindu
community is the second largest community of the State, yet they do not
have a statutory law to protect their interest in the personal matters. They
are governed by the age old traditional law in the significant subject
matters like marriage and inheritance. The protection to a greater extent
is dependant upon the accessibility to law and to get access, existence of
law is must.
Law is everywhere culture specific and that in tandem of globalization and
uniformisation of laws there are everywhere local and national
manifestation of law which are specific to particular jurisdictions
(Menski). Here lies the lacking. The Hindu community of Bangladesh are
completely guided rather by their culture than the law, taking recourse
from the aged old sruti and smriti which can work as a guiding principle
of law but not as the law itself. The society has changed, the lifestyle of
the believer of the religion has changed and the law must change also.
Now-a-days it is utterly impossible to believe that a male Hindu needs to
pay his debt full fledged and that will only happen when his son will do
the Shraddha Pravana. It is not demanded that they will not perform their
own religious performances, but it is unfortunate when the right of
inheritance (which is a legal right) is decided solely by that. Positive
changes must be brought keeping the religious belief. This is the high time
for a codified Hindu law.
Law is manifest everywhere, it is in operation all over the world, but is
certainly not the only, it is not some dead thing or a mater of past. Law is
everywhere a living reality (The funeral ceremony according to the Hindu
religion). In Bangladesh for the Hindu community Hindu Law have
become such a dead thing and failed to become a living reality which is
extremely a bare necessity.
30
Custom is considered as a very valuable source of law from the birth of
the concept of law. The reason for taking custom as a source may be that
when a rule comes from such ancestry that must have brought some
positive effect in the life of a particular community that has been attached
in the lifestyle and is not supposed to be severed. But sometimes modified
severance is required, that is why it is often said that law must be changed
keeping pace with the time. The Hindu community in Bangladesh is facing
this truth from quite a long time as no legislative action has been taken so
far. Most of the laws by which the Hindu community is guided by are the
laws of the British era. They are the largest minority community of
Bangladesh but yet there are very few reported cases regarding Hindu
personal Law. Is it because they do not face any legal problem, or they do
not have the opportunity to take assistance from the existing Hindu
personal Law of Bangladesh?
The second proposition is more appropriate. Even the Hindu community
does not find it quite logical that just because a son is offering a bigger
Pinda he is entitled to more right over the property of his father. It is
almost impossible to believe that the woman of Hindu community does
not have even the right of custody of her own son or daughter, she does
not have any right over the property of her husband or her father.
Different Stages of Development of Hindu law
1 The Basic Concept of Hindu Law
Hindu Law is considered as of divine origin. In earlier stage Hindu
Jurisprudence did not make any distinction between legal, moral and
religious rules. Moral rules have been so blended with legal rules that it
becomes very difficult to separate them. Since the Hindu law is based on
this religious belief, law is working as a branch of dharma not as a law
(Gandhi, 2003).
2 Ancient Age of Hindu Law
The Hindu law based on the religion started its application at the time of
the Veda. Hindu dharma teaches that guidance to mankind came from God
in the form of divine revelation. Divine revelation came to the people

31
through rishis, sages and saints during vedic period (3000 B.C.-1000B.C.)
(Menski, 1979). These revelations are the foundation of Hindu law. As
days passed by, these revelation were used in the form of usage and
custom and in the later part written texts were formed depending upon
these custom and usages (Jhavalah). Jhavalah has rightly pointed out that
―Hindu law was not static or staid but was empiric and progressive‖ (ibid).
Hindu law in vedic period was reasonably progressive as there was no
proved indication of caste system in this period. On the contrary, many
jurists opined that the caste system practices in last two thousand years
were non-existent in the vedic period (Alam).
3 Hindu Law at the Time of Sruti and Smriti
The Hindu law practiced in Bangladesh is primarily dependant on Sruti
and Smriti as there is no specific statutory law. Sruti and Smriti along with
custom are considered as the most authoritative source. Sruti means what
were heared. Sruti is the most authentic source of modern Hindu law
because it is believed that sruti is the reflection of divine commands.
Smriti is the second source of Hindu law, though this source contains
more legal rules than sruti. They are also divine instructions which are
remembered from ancient time. They are a combination of morals, ethics
and body of rules. Later on commentaries on these Smriti form major part
of Hindu law. Smriti was summed up for over 1500 years (ibid) Manu,
Yajnavalka and Narada are the main smritikar who developed this source,
which is still considered as a major guideline.
Commentaries on smriti are the third source though many jurists do not
agree it as an individual source as it has interpreted smriti, following the
rule of equity, justice and good conscience. Though commentaries are
explanation of smriti it has performed a great role in the reforming of
Hindu law (Firoze and Rahman). Because commentaries are the
interpretation which modified and supplemented the rules of Smriti by
reasoning and keeping pace with the changing circumstances.
Custom is the next important source, though Hindu law is not a customary
law like common law, but it is a traditional law. So custom got due
importance as they are the proof of a particular rule. Custom is defined by

32
the judicial committee in the case of Hurpurshad Vs Sheo Dayal as
―Custom is a rule, which in a particular family or in a particular district
has from long usage obtained the force of law. It must be ancient, certain
and reasonable, and being in derogation of the general rules of law, must
be construed strictly‖ (Routh). So some commentaries viewed that if a
Smriti is contradictory with custom, the Smriti should prevail, but some
commentator holds exactly opposite view. But this problem was sorted out
by the Privy Council in the case of The Collector of Madura Vs Mootoo
(12 M.I.A 397 436) (ibid). It was held that ―Under the Hindu system of
law clear proof of usage will out-weigh the written text of law.‖
4 The Legislative Development of Hindu Law
There are very few legislative intervention over the customary Hindu law
as it is emanated from the verses of Sruti and Smriti (Two basic sources of
Hindu law) and later on practices by the customs. Whatever changes have
been brought those are by the British rulers. There were a set of rules
which were enacted to eradicate some social crisis, they are the ―Racial
Inability Remission Act,1850‖, the ―Hindu Widow‘s Remarriage
Act,1856", the ―Sati Regulation,1829‖, the ―Child Marriage Restraint
Act,1929‖, the ―Earned Property Affairs Act,1930‖, the ―Inheritance
Act,1925‖, (Aktar and Syead, 2007). The question of codification of
Hindu law was first debated by the Central Law Implementation
Committee of British Government in 1937. In the same year a non-
government member proposed a bill to allot daughters right to her father‘s
property. In 1937 The Hindu Women‘s Right to Property Act was passed
(An Action Study on Proposed Reform of Hindu Law op.cit.). After that a
committee was formed in 1941 to examine various aspects of Hindu law.
The Committee recommended wide range of reforms and prepared a
single uniform code. Accordingly a draft Bill was first placed before the
Federal Legislative Assembly on April 11, 1947 and again placed in the
Indian Parliament but not as a single Code (Parashar, 1992). Unfortunately
very little effort was given after the partition. Even there is no trace of
significant initiative after the independence of Bangladesh. The Hindu
Law Hindu communities are applying is absolutely based on the shashtrik
Hindu law.

33
The Existing Practice of Hindu Law in Personal Matters
and Proposed Reforms
Many jurists find it peculiar that in the Indian Subcontinent there are
division in legal system as personal matters are guided by the respective
personal law. If a citizen is Muslim his personal matters like marriage,
dissolution of marriage, custody of child, maintenance etc are governed by
the Muslim personal law, this is the reality for the significant subject
matters like inheritance. Same is the case in Hindu Law. These personal
laws govern the institution of marriage, adoption, inheritance,
guardianship, maintenance, joint family, will, gift, partition, religious
usages and institutions, etc. subject to alteration as done by British
Legislation. (Statutes) (Mridulkanti, 2005). In this portion we will focus
on the traditional Hindu law and will propose some reforms to make it
compatible and more problem specific which can be easily enforced.
1. Marriage
Hindu Marriage law is a Samskara or religious rights or sacrament.
According to Vedas a marriage is ‗The union of flesh with flesh and bone
with bone-to be continued even in the next world.‖ It is union which is
indissoluble. One of the characteristics of a Hindu Marriage has been that
it is more connected with the performance of religious duties and
begetting of a son who enables a man to get deliverance from the
sufferings of Hell. That‘s why concept of Divorce was not recognized by
the ancient Hindu Law (Gandhi).
The ancient Hindu law specified the following requirements of a valid
marriage
Firstly, it has provided that if both parties do not belong to the same caste
then the marriage is invalid. But after the Hindu Marriage Validity Act
validity of marriage does not solely dependant on this issue. If all the other
requirements are fulfilled the marriage will not be invalid only because of
the fact that the parties belong to different religious castes and sects
(Routh).
34
Secondly, parties should be beyond the prohibited degrees. A man could
not marry a girl of the same Gotra 1 and the parties should not be
shapindas 2 of each other.
Thirdly, as Hindu marriage is defined as religious sacrament, certain
ceremonies are essential to perform for a valid marriage. Since this is a
prerequisite for marriage validity was dependant upon the performance of
these ceremonies but as there was no specific ceremony it was tough to
prove.
This particular problem was solved by judicial interpretation in the case of
AMULYA CHANDRA VS THE STATE (1983) 35 DLR, P 160. It was held
that two ceremonies are essential for a valid marriage under Hindu Law,
they are
(1) Vivah Homa Invocation before a sacred fire and
(2) The taking of seven steps before the sacred fire by the bride and
bridegroom, i.e. Saptapadi. The marriage becomes complete when the
seventh step is taken. Until then the marriage is incomplete and not
binding (Huda,1998).
Fourthly, to have legal validity marriage should be performed by any of
the approved manners.
Fifthly, consent of the guardian is a must. There is no explicit prohibition
regarding child marriage. Under Dayabhaga School a male who has
attained the age of fifteen is considered as attained his age of marriage.
The female‘s consent is not that important; guardian takes decision on her
behalf.
Certain persons are considered as the guardian of Hindu female. They are
the father, the paternal grandfather, the brother, a sakulya or a member of
the same family, the maternal grandfather, the maternal uncle, the mother.
It was held in KC Chakraborty vs Emperor (1937) that if the marriage is
otherwise valid it will not be considered as invalid only because it was
brought about by misrepresentation to the guardians or without the consent
of the guardians or in contravention of the express order of the court
(Routh).
35
Sixthly, as the guardians play the main role in Hindu marriage, child
marriage is permitted. Gurudas Banerji has described that children are not
only eligible for marriage but are the fittest to be taken in marriage.
Though the Child Marriage Restrained Act 1929 (amended in 1961 and
1984) however tried to stop child marriage this Act applies to all citizens
of Bangladesh. So it applies to the Hindus also (ibid). In the case of a
Hindu woman the consent of the bride is unnecessary.
1.1. Proposed Reforms in the Sector of Marriage
Dissolution of Marriage
The need for reform in marriage has become inevitable. Since other
personal laws have made dissolution proper same should be incorporated
in the Hindu marriage. No right of dissolution is itself a human rights
violation where equal rights of men and women are guaranteed. Not
giving the right of dissolution is making the position of the women more
vulnerable.
We can cite the example of changes brought in India by Marriages Act of
1955 applicable to Hindus permits divorce. Marriage Laws Act of 1976
brought a remarkable change. Section 13-B provides for divorce by
mutual consent of the parties. This has been added because of growing
influence of break down theory, which explains that when a marital bond
is completely broken down parties should not be compelled to live
together.
1.2. Registration of Marriage
The second area where the law can be changed in a very simple way but
has a grave effect is to make the registration of marriage mandatory. If
registration is made mandatory it will work as the proof, which can ensure
the rights of the husband and wife.
1.3. Other Reforms
Polygamy should be restricted. Hindu male should not be
permitted to keep more than one wife which is allowed by the
traditional Hindu law.
36
The mother should also be considered as the legal guardian of the
son and should be given equal rights in the matter of consent in
marriage and adoption.
Provision of consent must be incorporated as a necessary condition
both for male and female.
2 Maintenance
According to the ancient Hindu law it is the duty of a Hindu to male to
maintain his wife, minor children and aged parents. The wife can not
demand for maintenance if she leaves her husband‘s residence without a
lawful reason or if the husband is suffering from contagious diseases or if
he is guilty of cruelty according to the Hindu Women‘s Right to Separate
Residence and Maintenance Act 1946. Under this Act a Hindu wife can
institute a suit in the Family Court for maintenance against the husband; it
was decided in the case of Nirmal Kanti Das vs Sreemati Beeva Rani (47
DLR HCD pp.514) (Aktar and Syead, 2007) As there is no provision for
dissolution of marriage the question of post divorce maintenance is absent
here.
2.1 Proposed Reforms
Firstly, since divorce is suggested the women should get maintenance
until she remarries.
Secondly, the children both male and female should get maintenance upto
18 years of age.
3 Inheritance
In the matter of Hindu law the major lacuna lies in the share of women in
her father‘s or husband‘s property, since the Hindu females do not have
any absolute right. According to the Shashtric Hindu law, five female
heirs have the right of inheritance : they are wife, daughter, mother,
father‘s mother and father‘s father‘s mother. The right is restricted strictly
to enjoy the property and the female heirs are not entitled to alienate the
property. The female get only a right to enjoy the property during their
lifetime.
37
3.1 Right of Widow
The right of widow in their husband‘s property is limited. After the
marriage the wife is considered as the family member of their husband‘s
family. So after the death of the husband the father-in-law is responsible to
give maintenance from the property of her husband. The widow does not
have any specific absolute right. So she can not alienate or transfer any
portion of the property unless there is a legal necessity. Legal necessity
involves debt of the husband and religious purpose. So the widow can not
alienate the property in her extreme sickness.
3.2. Right of Daughter
Like widow, daughter gets a limited interest in her father‘s property.
Maiden daughter has a right to enjoy the property until her marriage. A
married daughter generally does not have any right but if she has a son and
does not have a brother (son of a deceased) can only enjoy the right. A
married daughter without a son or a barren widowed daughter does not get
any right.
3.3. Proposed Reforms
Firstly, it is strongly recommended that the female heir must be given an
absolute share in the property of their father and husband, which should
not be limited to enjoyment only. There should be specific share which
will be considered to be their own property and which will pass to their
heir after their death. There should not be any difference regarding
married daughter and unmarried daughter.
Secondly, both male and female must have equal share in the property of
their father. It is proposed to give equal share of mother with the son and
son should not exclude mother in the property of her husband, as it is
practiced in traditional Hindu law.
Thirdly, the doctrine of spiritual benefit should not be considered as the
only mode of deciding the right of inheritance.
4 Adoption
Adoption plays a significant role in Hindu law as by adoption a Hindu
male can secure the spiritual benefit of his own and his ancestor in

38
absence of a natural son. It was decided in Anath Bandhu vs Shudhangsu
Shekhar Dey (31 DLR 1979, pp.312) that an adopted son is considered as
a natural born son for all practical purposes. The existing practice of
adoption suggests that only the father can give a son into an adoption and
same principle is followed in case of taking a son into adoption. Another
requisite is that an adoption is only permitted in the absence of a son
grandson and great grand son. The adopted son must belong to the same
caste of his adoptive father and his mother must not be within the
prohibited degrees to his adoptive father. Generally a wife can not take an
adoption but she is permitted only if there is an expressed consent. A
widow similarly is allowed to take an adoption with the expressed or
implied permission given before the husband is dead.
4.1 Proposed Reforms
Firstly, mother should be given the status of a legal guardian and she
should have the right to give her opinion regarding the adoption. She must
be given the power to take or give a son into an adoption.
Secondly, both girls and boys should be permitted to taken in adoption.
Thirdly, the shashtric rules regarding caste disability should be abolished.
An Obligation for Bangladesh under CEDAW Convention
Bangladesh has been one of the state party to the Convention of the
Elimination of all Forms of Discrimination Against Women (CEDAW)
and has also ratified the Optional Protocol to the Convention. Under the
Convention and Protocol Bangladesh has undertaken the responsibility to
ensure the implementation of necessary mechanism to eradicate
discrimination. Thus to ensure equality between men and women, but
existing law itself is discriminating. Article 2 of CEDAW provides that
―State Parties condemn discrimination against women in all its forms,
agree to pursue by all appropriate means and without delay a policy of
eliminating discrimination against women and to this end undertake:
(a) To embody the principle of equality of men and women in their
national constitution and other appropriate legislation.
39
(b) To adopt progressive legislative and other measure including sanctions
where appropriate, prohibiting discrimination against women.
(c) To establish legal protection of the rights of women on an equal basis
with men and to ensure through competent national tribunals and
other public institutions……..
(d) To take all appropriate measures including legislation, to modify or
abolish existing laws, regulations, customs and practices which
constitute discrimination against women.
Here the Convention has mentioned thrice to protect the rights of the
women through legislative enactment and implementation of them.
Because in absence of any legal protection vulnerable groups are always
deprived of their rights.
Article 3 has even broadened the scope to social, political, economic and
cultural fields to take appropriate measures including legislation to ensure
full development.
So if we consider all these provisions it leads to only one path – that is to
reform the traditional age old Hindu law.
Conclusion
The article is a very little initiative with some major and specific
suggestions. The Hindu community is in bare need of a codified law, in
absence of which they are not getting the enforcement of their rights
accorded by different existing Hindu law. That is a gross violation of our
constitutional as well as human rights.
The study on Hindu personal law conducted by BNWLA shows that 84%
of female and76% of male respondents are not satisfied with the existing
law. On the other hand, 15.33% of female respondents are satisfied
because either they are ignorant of the legal norms or their will is
dominated by the patriarchic view. Clear dissatisfaction had reflected in
this study (Hindu Family Law: An Action Study on Proposed Reform of
Hindu Law op.cit.).

40
This is the high time to modify the traditional Hindu law reflecting the
human right thus equal rights of men and women in every aspect. It is not
suggested to follow the modification brought by India where different
Acts has dealt with different subject matters. We are suggesting a
complete codified Act which will have sufficient provision to deal with
every personal matter. If all the provisions exist in a single document it
will be easy to implement.
The community is suffering with this woe for a long time. There are not
many reported cases decided in this particular area of law. Does that
suggest that the Hindu community is reluctant to get legal assistance? On
the contrary, the legislation has failed to safeguard their interest. So the
age old traditional Hindu Law should be replaced by a self sufficient
single codified Act.
References
Agarwala R.K. (1996) Hindu Law. R.K. Sinha, (Ed) Central Law Agency, Allahabad.
Aktar, S. and Syead, M. A. A. (2007) in a Comparative study on Hindu Law between
Bangladesh and India, Asian Affairs, 29( 4): 61-95, October-December
Alam, S. M (2004); Review of Hindu Personal Law in Bangladesh Search for Reforms
Bangladesh Journal of Law (2004) , Bangladesh Institute of Law and International
Affairs: 6 (1 & 2).
Chandra, D. D. (2009) Hindu Ain: Srimati Benu Debnath, Rajshshi
Constitution of the Peoples‘ Republic of Bangladesh
Dhar, N. (1996) Hindu Ain Resisi Publishers , Basur Bazar Lane, Dhaka – 1100
Diwan, Parash, (1996) Modern Hindu Law, Allahabad Law Agency, Allahabad
Firoze, F. K. and Rahman, Z. (eds.) An Action Study on Proposed Reform of Hindu Law,
conducted by Bangladesh National Women Lawyers Association.
Gandhi, B.M (2003). Hindu Law, second edition, Lucknow, Eastern Book Company. pp.3
Gandhi B.M. op cit. pp. 207
Huda, S. (1998) Double Trouble – Hindu Women in Bangladesh A Comparative Study,
Huda, S. Dhaka University Studies F, 9 (1): 111-138.
Jhavalah, N.H. (1979) Principles of Hindu Law, C Jamnadas & Co. op. cit. p-2
Menski ,W. (2003) Public Interest Litigation Deliverance from all Evils Bangladesh
Journal of Law, Bangladesh Institute of Law and International Affairs 6 (1 & 2):03
Menski, Warner. F. (2003) Hindu Law – Beyond Tradition and Modernity, Oxford

41
University Press, op.cit., p 88-89 Jahabvlla N.H(1979). Principle of Hindu Law C.
Jamnadas & Co., pp 1-3 in Alam, S. M; Review of Hindu Personal Law in
Bangladesh Search for Reforms Bangladesh Journal of Law , Bangladesh Institute of
Law and International Affairs: 6 (1 & 2):16
Mridulkanti, R. (2005) The principle of Hindu Law ,5th
Ed.: Chittagong, Kamrul Book
House, pp.27
Mulla. (1986) The principles of Hindu Law, 15th
Edition with supplements.
Parashar, A. (1992) Women and Family Law Reform in India New Delhi: Sages
Publication pp.80
Routh S. K. (1974) Elements of Hindu Law Ideal Library, Dhaka pp-3 I.A.253-285
Routh S.K. op.cit.. pp.23-24
Routh S.K. op. cit. pp.24

42
THE FIVE YEAR PLANS IN INDIA: OVERVIEW OF
PUBLIC HEALTH POLICIES
Sethuramalingam V1, Selwyn Stanley
2 & Sathia S
3
Keywords: Plans. Public Health. Policies.
Abstract: Health policy of India is associated with the provision of safe
water and sanitation, malaria control, rural health care services through
health units and mobile units, maternal and child health care services, skill
development training for health educators, drug and equipment sufficiency
along with family planning to control the population. The main objective of
this paper is to examine how the health policy was implemented
emphasising the different issues of health through the five year plans period
of India.
Introduction
Social sector development has been the raison-d’etre of planning in India.
The Directive Principles of the State Policy, enshrined in the Constitution
form the social premises of planning in India (Gupta, 2002) The basic
objective of planning in India is ‗to initiate a process of development
which will raise living standards and open out to the people to provide
new opportunities to lead a good life‘. Keeping this objective, the public
health policies in India were formulated through various five year plans.
The public health policies in India have come a long way since 1950s. In
1946, the Health Survey and Development Committee, headed by Sir
Joseph Bhore recommended the establishment of a well-structured and
comprehensive health service with a sound primary health care
infrastructure. This report not only provided a historical landmark in the
development of the public health system but also laid down the blueprint
1 Assistant Professor, Department of Social Work, Bharathidasan University
2 Lecturer in Social Work, Faculty of Health & Social Work, School of Psychosocial
Studies, University of Plymouth 3 PhD Scholar, Department of Social Work, Bharathidasan University

43
of subsequent health planning and development in independent India
(Government of India, 1960).
First Plan (1951-1961)
The core of the public health policy enunciated in the first five year plan
was (i) provision of water-supply and sanitation; (ii) control of malaria;
(iii) preventive health care of the rural population through health units and
mobile units; (iv) health services for mothers and children; (v) education
and training, and health education; (vi) self-sufficiency in drugs and
equipment; and (vii) family planning and population control. The
emphasis was also given to construction of hospitals and dispensaries,
besides provision for medical education and training, prevention and
treatment of venereal diseases, filariasis, tuberculosis, leprosy, cancer and
up-gradation of mental hospitals (Government of India, 1952). At the
beginning of the first Five Year Plan, the B.C.G. vaccination programme
was launched in the country. A nation-wide family planning programme
was started in the year 1953. The National Malaria Control Programme
was also launched in the same year. National Water Supply and Sanitation
Programme was started in 1954 and the National Filaria Control
Programme was commenced in 1955 (Goodhealthnyou.com, 2000). The
total investment on public health during this plan period was Rs.65.30
crores which is 3.32 per cent of the total budget expenditure. Priority was
given to water supply, sanitation and health care institutions. A sum of
Rs.65.20 crore (3.33%) was invested on public health, bedsides Rs.
0.1crore (0.01%) was invested towards family planning. For the first time
in the world, family planning was adopted as a government programme in
India.
Second Plan (1956-1961)
The second plan laid more emphasis on expanding existing health
services, to bring them increasingly within the reach of all the people and
to promote a progressive improvement in the level of national health. The
specific objectives of the health policies during this plan were (i)
establishment of institutional facilities to serve as a base from which

44
services can be rendered to the people both locally and in surrounding
territories; (ii) development of technical manpower through appropriate
training programmes and employment of persons trained; (iii)
improvement of public health and institutional measures to control
communicable diseases; (iv) an active campaign for environmental
hygiene; and (v) family planning and other supporting programmes for
raising the standard of health of the people. International agencies like the
W.H.O. and the U.N.I.C.E.F. also took part in the development of medical
and public health schemes in various parts of the country (Government of
India, 1956). The Central Health Education Bureau and the Indian
Medical Council were established in the year 1956. The Demographic
Research Centres were established in 1957. The Tuberculosis Institute was
established in 1959 (Goodhealthnyou.com, 2000). A sum of Rs.146 crore
was invested during this plan period which was 3.1 per cent of the total
budget expenditure towards the health sector and was less than 0.19% of
the previous plan period. During this plan, high priority was given to
water supply, sanitation and control of communicable diseases (Rs.141
crores / 3.01%). A sum of Rs.5 crore (0.11%) was also invested on family
planning
Third Plan (1961-1966)
The Third Plan aimed at controlling and eradication of communicable
diseases, providing curative and preventive health services in rural areas
and to augment the training programmes of medical and paramedical
personnel. Emphasis was also given to family planning. Nation-wide
control campaigns were initiated against small pox and tuberculosis
(Government of India, 1960). The Central Bureau of Health Intelligence
was established in 1961. The Central Family Planning Institute was
established in the year 1962. The National Smallpox eradication and the
School Health and the District Tuberculosis Programmes were also
launched in the same year. The Applied Nutrition Programme was
launched in 1963 and the National Institute of Communicable Diseases
was also inaugurated in the same year (Goodhealthnyou.com, 2000). The
expenditure towards health sector during the third plan was Rs. 251 crores
which is 2.9 per cent of the total budget. As in the second plan, priority

45
was given to water supply, sanitation, and control of communicable
diseases (226 crores / 2.63%). A sum of Rs. 25 crore (0.29%) was invested
towards family planning.
Annual Plan (1966-1969)
The public health schemes, which had been introduced in the third plan
and earlier, were continued during the annual plan period also. In 1966-67,
the family planning programme was made target-oriented and time bound.
In 1966 a new Family Planning department was created in the Ministry of
Health. A sum of Rs 211 crore (3.2%) was invested in the health sector of
which Rs. 140 crore (2.12%) was spent for health and 71 crore (1.06%) for
family planning.
Fourth Plan (1969-1974)
During this plan period, efforts were made to provide an effective base for
health services in rural areas by strengthening the primary health centres.
These centres rendered preventive and curative health services, took over
the maintenance phase of communicable diseases control programmes.
Sub divisional and district hospitals were strengthened to serve as referral
centres for Primary Health Centres. Medical and nursing education and
training of paramedical personnel were expanded to meet the minimum
technical man power requirements. The programme of nutrition of
growing children was extended and integrated in the Fourth Plan. Family
Planning found its place in this Plan as a programme of the highest
priority (Government of India, 1970). The Nutrition Research Laboratories
were converted into the National Institute of Nutrition in 1969 and the
Central Births and Deaths Registration Act was promulgated in the same
year. The Central Council of Indian Medicine (Ayurveda, Unani and
Siddha) was formed in 1971. The Medical Termination of Pregnancy Bill
was also passed by the Parliament in the same year. The Central Council
of Homeopathy was set up in 1973. A sum of Rs. 613.5 crore was
invested in the health sector during this plan period which was 3.89
percentage of the total budget expenditure of which Rs 335.50 crore
(2.13%) was allotted for health and Rs. 278 crore (1.76%) for family
planning.
46
Fifth Plan (1974-1979)
In this plan period, the focus had been placed on research into new
methods of family planning, integrated system for delivery of health care
services to infants, and control & prevention of communicable diseases
including malaria, tuberculosis and cholera, besides provision of safe
drinking water supply. The concept of family planning was changed into
family welfare during this plan period. The country was declared free from
smallpox in April, 1977 (Government of India, 1975). The Water
(Prevention and Control of Pollution) Act and The Cigarettes Regulation
(Production, Supply and Distribution) Act were enacted in 1974 and 1975
respectively. The Integrated Child Development scheme was launched in
1975. The Central Council for Yoga and Naturopathy was established in
1976. The National Institute of Health and Family Planning was formed
and the Rural Health Scheme was launched in 1977. The Parliament
approved the Child Marriage Restraint (Amendment) Bill fixing the
minimum age of marriage of 21 years for boys and 18 years for girls in
1978. (Goodhealthnyou.com, 2000). The total budget expenditure on the
health sector during this plan was Rs. 1252.6 crores which was 3.18 per
cent of the total budget. As in the previous plan, a sum of Rs. 760.80 crore
(1.93%) was invested on public health and Rs.491.80 crore (1.25%) on
family welfare planning.
Annual Plan (1979-1980)
The Janatha Government, which came to power in 1977, terminated the
fifth plan at the end of the fourth year and formulated a draft five-year
plan for 1978-83. The country adopted the policy of ―Health for All by
2000 AD‖ enunciated in the Alma Ata Declaration of 1977. The health
care system in the country was restructured and reoriented towards these
policy objectives. Next to rural health, control of communicable diseases
was given priority. During this annual plan the total expenditure towards
the Health sector was Rs.342 crores (2.91%). A sum of Rs. 223.10 crore
(1.83%) was invested on public health and Rs. 118.50 crore (0.97%) on
family welfare.

47
Sixth Plan (1980-1985)
Sixth Five Year Plan is also referred to as the Janata Government Plan and
it was revolutionary since it marked a change from the Nehruvian model
of Five Year Plans. The government of India adopted the National Health
Policy in 1983 which reiterated India's commitment to attain "Health for
All by 2000 A.D", through the provision of comprehensive primary
healthcare services. It stressed the creation of an infrastructure for primary
healthcare; close co-ordination with health-related services and activities (like
nutrition, drinking water supply and sanitation); active involvement and
participation of voluntary organisations; provision of essential drugs and
vaccines; qualitative improvement in health and family planning services;
provision of adequate training; and medical research aimed at the common
health problems of the people (W.H.O. 2006) Health Care Programmes
were restructured and reoriented towards this policy. Priority was given to
extension and expansion of the rural health infrastructure through a
network of community health centres, primary health centres and sub-
centres, on a liberalized population norm. Efforts were made to develop
promotive and preventive services, along with curative facilities. High
priority was given to the development of primary health care located as
close to the people as possible. Improvements in living conditions of the
rural poor through the provision of protected and assured water supply
was also given priority. The family welfare programme was integrated
with the Health programme, especially Maternal and Child Health
(Government of India, 1981). The total investment in the health sector
during the sixth plan was Rs. 3412.2 crores (which was 3.12% of the total
budget expenditure) of which a sum of Rs. 2025 crores (1.9%) for health
and Rs. 1387 crores (1.3%) for family planning was invested during the
sixth plan period.
Seventh Plan (1985-1990)
The Seventh Plan which covered a time span of another five years started
in 1985 and went on till 1989. This Five Year Plan was the come back
vehicle of the Indian National Congress Party into power. The core
objective of health policy in the seventh plan was laid on preventive and

48
promotive aspects and on organising effective and efficient health services
which were comprehensive in nature, easily and widely available, freely
accessible, and generally affordable by the people. The following thrust
areas were identified: (i) Promotion of primary health measures and
improvement in quality health services; (ii) Effective coordination and
coupling of health and health- related services and activities for achieving
the goal of : ―Health for All by 2000 AD‖; (iii) Priority in community
participation and massive health education movement; (iv) Qualitative
improvements as required in Health and Family Planning services; (v)
Efforts to ensure comprehensive coverage in urban and school health
services and mental and dental health services; (vi) Control and
eradication of communicable diseases; (vii) Control and containment of
cancer, coronary heart diseases, hypertension, diabetes, and traffic and
other accidents in the area of non-communicable diseases; (viii) Training
and education of medical and paramedical personnel (ix) Medical research
of special relevance and (x) Integration and wider application of the Indian
systems of medicine particularly in the national health programme
(Government of India, 1985). A worldwide "safe motherhood" campaign,
National Diabetes Control, and the National AIDS Control Programmes
were initiated in 1987 and the Mental Health Act was also passed in the
same year. The total expenditure on Health Sector was Rs. 6809 (3.11%)
crores. A sum of Rs.3689 crores (1.69%) on public health and Rs. 3120 crores
(1.43 %) on family welfare was invested during the seventh plan period.
Annual Plan (1990-1992)
This period was of political instability and hence no five year plan was
implemented during the period; only annual plans were made for the
period between 1990 and 1992 (Indiaonline,2010) The health schemes
which had been introduced earlier were continued during this period also.
In 1990, Control of Acute Respiratory Infection Programme was initiated
as a pilot project. In 1991, the Pre-natal Diagnostic Techniques (regulation
and prevention of misuse) Act was also enacted. During this annual plan,
the total expenditure in the health sector was Rs.3644.5 crores (2.86%). A
sum of Rs. 2003.10 crores (1.57%) and Rs. 1641.5 crores (1.29%) were
invested on public health and family welfare respectively.

49
Eighth Plan (1992-1997)
Health and population control were listed as two of the six priority
objectives during the eighth plan period. Emphases were laid on provision
of safe drinking water and primary health care facilities, including
immunisation, accessibility to all the villages and the entire population,
and complete elimination of scavenging (Government of India, 1992).The
Transplantation of Human Organs Bill was passed in the year 1994 and
The Persons with Disabilities (Equal Opportunities, Protection of Rights
and Full Participation) Act passed was in 1995. The total outlay for the
health sector during this plan period was Rs. 14082.2 crores (3.24%). A
sum of Rs. 7582.20 crore (1.75%) was allotted towards public health and
Rs. 6500.00 crores (1.5%) towards family welfare.
Ninth Plan (1997-2002)
The Ninth Five Year Plan was launched in the 50th year of India‘s
Independence. During this plan, greater emphasis was provided on
primary health care, and provision of safe drinking water. Emphasis was
also given to provide integrated preventive, promotive, curative and
rehabilitative services for communicable, non-communicable and nutrition
related health problems, through appropriate strengthening of the existing
health care institutions and ensuring that they are optimally utilised.
Efforts were made to achieve substantial reduction in morbidity and
mortality rates (Government of India, 1997). In 2002, Government of India
introduced the National Health Policy (NHP). The main objective of the
NHP-2002 was to achieve an acceptable standard of good health among
the general population of the country and set goals to be achieved by the
year 2015. The major policy prescriptions were as follows: (i) Increase of
health sector expenditure to 6 percent of GDP by 2010. (ii) Increase of
allocation of public health investment in the order of 55 percent for the
primary health sector; 35 percent and 10 percent to secondary and tertiary
sectors respectively; (iii) Gradual convergence of all health programmes
under a single field administration, except the ones (such as TB, Malaria,
HIV/AIDS and universal immunisation programmes), which need to be

50
continued till moderate levels of prevalence are reached; (iv) Need to levy
user charges for certain secondary and tertiary public health services, for
those who can afford to pay; (v) Mandatory two year rural posting before
awarding the graduate medical degree; (vi) Decentralising the
implementation of health programmes to local self governing bodies by
2005; (vii) Setting up of Medical Grants Commission for funding new
Government Medical and Dental colleges; (viii) Promoting public health
discipline; (ix) Establishing two-tier urban healthcare system - Primary
Health Centre for a population of one lakh and Government General Hospital;
(x) Increase in Government funded health research to a level of 2 percent
of the total health spending by 2010; (xi) Appreciation of the role of
private sector in health, and enactment of legislation by 2003 for
regulating private clinical establishments; (xii) Formulation of procedures
for accreditation of public and private health facilities; (xiii) Co-option of
NGOs in national disease control programmes; (xiv) Promotion
of tele medicine in tertiary healthcare sector; (xv) Full operationalisation of
National Disease Surveillance Network by 2005; (xvi) Notification of
contemporary code of medical ethics by Medical Council of India; (xvii)
Encouraging setting up of private insurance instruments to bring
secondary and tertiary sectors into its purview; (xviiii) Promotion of
medical services for overseas users and (xix) Encouragement and
promotion of Indian System of Medicine (W.H.O.,2006 & Government of
India 2002). During this plan a total sum of Rs. 5314 crore (1%) was
allotted towards public health and Rs. 15088 crore (2.8%) to family
welfare. Thus, a sum of Rs. 20402 crore was allotted for the health sector
which was 3.72 per cent of the total budget of ninth plan.
Tenth Plan (2002-2007)
The major focus in the tenth plan was to improve the efficiency of the
existing health care system, quality of care, logistics of supplies of drugs
and diagnostics and promotion of the rational use of drugs. The focus was
also on evolving, implementing and evaluating systems of health care
financing so that essential health care based on need is available to all at

51
affordable cost. The reductions in fertility, mortality and population
growth rate were also the major objectives during this period (Government
of India, 2002a). The tenth plan also proposed three major initiatives in
the health sector. They are: (i) redesigning the Universal Health Insurance
scheme introduced in 2003 to make it exclusive for below poverty level
people with a reduced premium, (ii) introduction of Group Health
Insurance scheme for members of Self Help Groups and Credit Link
Groups at a premium of Rs 120 per person for an insurance cover of
Rs 10000, and (iii) exemption of income tax for hospitals working in rural
areas (W.H.O., 2006). The total outlay of Rs. 10753 crores (1.2%) for
public health and Rs. 27125 crores (3.0%) to family welfare and thus a
total sum of Rs. 37878 crore (2.4%) was allotted towards the Health
Sector during this plan period.
Eleventh Plan (2007-2012)
The Eleventh Five Year Plan provides an opportunity to restructure
policies to achieve a New Vision based on faster, broad-based, and
inclusive growth. The objectives for health sector aims (i) to achieve good
health for people, especially the poor and the underprivileged by focusing
on individual health care, public health, sanitation, clean drinking water,
access to food, and knowledge of hygiene, and feeding practices; (ii) to
facilitate convergence and development of public health systems and
services that are responsive to health needs and aspirations of people and
(iii) to give special attention to the health of marginalized groups like
adolescent girls, women of all ages, children below the age of three, older
persons, disabled, and primitive tribal groups. This Plan also facilitates
convergence and development of public health systems and services that
are responsive to health needs and aspirations of people. During this plan
major focus was given to reduce disparities in health across regions and
communities by ensuring access to affordable health care. A Sum of Rs.
Rs 136147.00 crore (3.74%) was earmarked for the health sector of which
Rs. 45589 crores for public health and Rs. 90558 crores for family welfare
were allotted during this plan (Government of India, 2007).
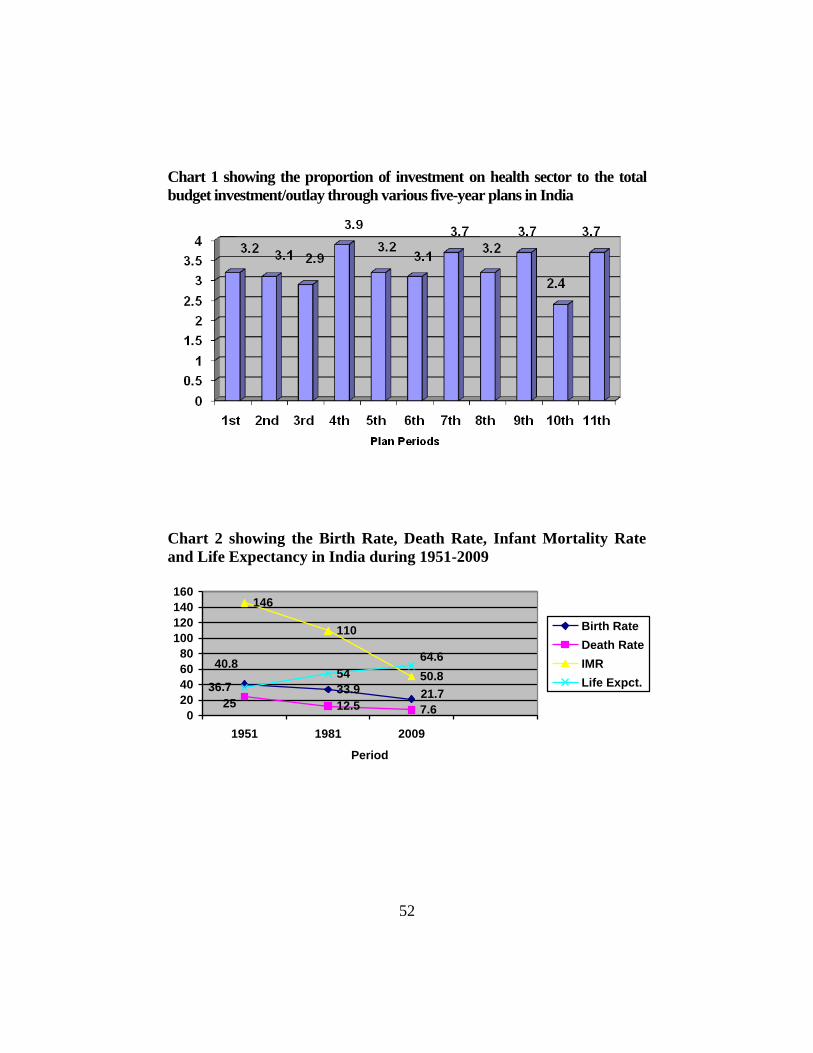
52
Chart 1 showing the proportion of investment on health sector to the total
budget investment/outlay through various five-year plans in India
Chart 2 showing the Birth Rate, Death Rate, Infant Mortality Rate
and Life Expectancy in India during 1951-2009
33.9
12.5 7.6
146
110
50.85440.8
21.725
64.6
36.7
0
20
40
60
80
100
120
140
160
1951 1981 2009
Period
Birth Rate
Death Rate
IMR
Life Expct.
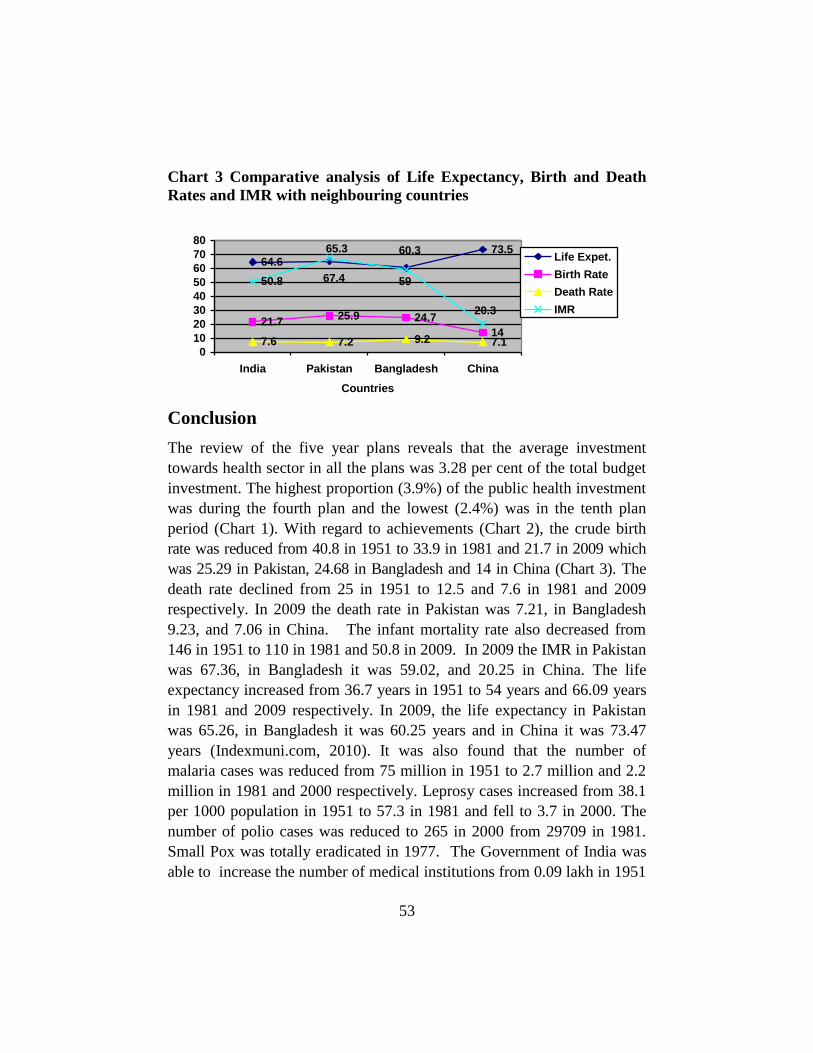
53
Chart 3 Comparative analysis of Life Expectancy, Birth and Death
Rates and IMR with neighbouring countries
64.673.5
21.725.9 24.7
147.6 7.2 9.2 7.1
50.8
60.365.3
20.3
5967.4
0
10
20
30
40
50
60
70
80
India Pakistan Bangladesh China
Countries
Life Expet.
Birth Rate
Death Rate
IMR
Conclusion
The review of the five year plans reveals that the average investment
towards health sector in all the plans was 3.28 per cent of the total budget
investment. The highest proportion (3.9%) of the public health investment
was during the fourth plan and the lowest (2.4%) was in the tenth plan
period (Chart 1). With regard to achievements (Chart 2), the crude birth
rate was reduced from 40.8 in 1951 to 33.9 in 1981 and 21.7 in 2009 which
was 25.29 in Pakistan, 24.68 in Bangladesh and 14 in China (Chart 3). The
death rate declined from 25 in 1951 to 12.5 and 7.6 in 1981 and 2009
respectively. In 2009 the death rate in Pakistan was 7.21, in Bangladesh
9.23, and 7.06 in China. The infant mortality rate also decreased from
146 in 1951 to 110 in 1981 and 50.8 in 2009. In 2009 the IMR in Pakistan
was 67.36, in Bangladesh it was 59.02, and 20.25 in China. The life
expectancy increased from 36.7 years in 1951 to 54 years and 66.09 years
in 1981 and 2009 respectively. In 2009, the life expectancy in Pakistan
was 65.26, in Bangladesh it was 60.25 years and in China it was 73.47
years (Indexmuni.com, 2010). It was also found that the number of
malaria cases was reduced from 75 million in 1951 to 2.7 million and 2.2
million in 1981 and 2000 respectively. Leprosy cases increased from 38.1
per 1000 population in 1951 to 57.3 in 1981 and fell to 3.7 in 2000. The
number of polio cases was reduced to 265 in 2000 from 29709 in 1981.
Small Pox was totally eradicated in 1977. The Government of India was
able to increase the number of medical institutions from 0.09 lakh in 1951
54
to 0.62 lakh in 1981 and 2.06 lakhs in 2000 (Government of India, 2002b).
Though there has been a marked improvement in the health status of the
people in the country, India has to go a long way towards achieving its
goal of ‗‗Health for All‖.
References
Goodhealthnyou.com., (2000) Public health milestones in independent India in in
http://good healthnyou.com/library/reading/vhai/mar_apr/mileston.asp.
Government of India (1952) The First Five Year Plan, Planning Commission, New
Delhi.
Government of India (1956) The Second Five Year Plan, Planning Commission, New
Delhi.
Government of India (1960) Third Five-Year Plan: A draft outline, Planning
Commission, New Delhi in http://planningcommission.nic.in/plans/planrel/
fiveyr/welcome.html
Government of India (1970) The Fourth Five-Year Plan, Planning commission, New
Delhi.
Government of India (1975) Draft Fifth Five Year Plan, Planning Commission, New
Delhi.
Government of India (1981) The Sixth Five Year Plan, Planning Commission, New
Delhi.
Government of India, (1985) The Seventh Five Year Plan (Vol-2), Planning
Commission, New Delhi, in http://www.planningcommission.nic.in/plans/planrel/
fiveyr/welcome.html
Government of India, (1992) The Eighth Five Year Plan (Vol-2) in http://www.planning
commission.nic.in/plans/planrel/fiveyr/welcome.html
Government of India, (1997) Ninth Five Year Plan 1997-2002, Vol.1&2, Planning
Commission, New Delhi in http://planningcommission.nic.in/plans/planrel/fiveyr/
welcome.html
Government of India, (2002) National Health Policy – 2002, Ministry of Health and
family Welfare, New Delhi in http://mohfw.nic.in/np2002. htm
Government of India, (2002a) Tenth Five Years Plan 2002-2007 (Vol.2), Planning
Commission New Delhi, 89 & 95
Government of India (2002b) Annual Report 2001-2002, Ministry of health and family
welfare, New Delhi in http://mohfw.nic.in/reports/Annual%20Report%202001-
02%20.pdf/Part%20I-2.pdf
Government of India, (2007) Eleventh Five Year Plan, - 2007-2012 (Vol.2), Planning
Commission, New Delhi, 58,107, 163 & 170
55
Gupta, V.S., (2002) Social Sector Development and the Tenth five year plan,
Employment News, Vol. XXVII, No. 1, Publication Division, Government of India,
New Delhi, 12 April.
IndexMundi, (2010) India Demography in http://www.indexmundi.com/india/
infant_mortality_ rate.html
Indiaonline, (2010) Five years plan in India in http://indiaonline.in/Profile/ Economy/
Planning Commission/five year Plans-Plans.aspx
W.H.O., (2006) Country Health System Profiles World Health Organisation in http://
www.searo.who.int/en/Section313/Section1519_10855.htm

56
MHD NATURAL CONVECTION FLOW OF FLUID
WITH VARIABLE VISCOSITY FROM A POROUS
VERTICAL PLATE
Amena Ferdousi1, Mohammad Salek Parvez
2 & M. A. Alim
3
Keywords: Porous Plate. Magnetohydrodynamic. Natural Convection.
Variable Viscosity.
Abstract: This paper presents an extension for MHD natural convection
flow with variable viscosity from a porous vertical plate. The governing
boundary layer equations are solved numerically using finite difference
method together with Keller-Box scheme. The numerical results show that
as the variable viscosity increases the surface shear stress increases and the
rate of heat transfer decreases, which are here in terms of skin friction
coefficient and local Nusselt number. It has been observed that the
inclusion of variable viscosity affects velocity as well as temperature
profiles. A comparison shows that the present result agrees well with the
published results.
Introduction The study of the flow of electrically conducting fluid in presence of
magnetic field is important from the technical point of view and such
types of problems have received much attention by many researchers. The
specific problem selected for research is the flow and heat transfer in an
electrically conducting fluid adjacent to the surface over which the fluid
flows. The interaction of the magnetic field and the moving electric charge
carried by the flowing fluid induces a force, which tends to oppose the
fluid motion. And near the leading edge of the surface the velocity is very
small so that the magnetic force, which is proportional to the magnitude of
1 Assistant Professor, Faculty of Engineering and Technology, Eastern University
2 Assistant Professor, Department of Computer Science and Engineering, Daffodil
International University 3 Associate Professor, Department of Mathematics, Bangladesh University of
Engineering and Technology

57
the longitudinal velocity of fluid acts in the opposite direction is also very
small. Consequently the influence of the magnetic field on the boundary
layer is exerted only through induced forces within the boundary layer
itself. MHD was originally applied to astrophysical and geophysical
problems but more recently to the problem of fusion power, where the
application is the creation and containment of hot plasmas by
electromagnetic forces, since material wall be destroyed. Astrophysical
problems include solar structure, especially in the outer layers, the solar
wind bathing the earth and other planets and interstellar magnetic fields.
MHD free convection flow with variable viscosity from porous vertical
plate has been drawn forth not only for its fundamental aspects but also for
its significance in the contexts of space technology and processes
involving high temperature. In the presence of variable viscosity on MHD
free convection boundary layer flow from a porous vertical plate of a
steady two dimensional viscous incompressible fluid has been considered.
The physical property, variable viscosity may change significantly with
temperature.
Merkin (1972) concluded free convection with blowing and suction. Lin
and Yu (1988) studied free convection on a horizontal plate with blowing
and suction. Hossain et al. (2001) studied the effect of radiation on free
convection flow with variable viscosity from a porous vertical plate.
Hossain et al (2000) performed flow of viscous incompressible fluid with
temperature dependent viscosity and thermal conductivity past a
permeable wedge with variable heat flux. Hossain and Takhar (2001)
studied radiation effect on mixed convection along a vertical plate with
uniform surface temperature. Molla et al. (2004)studied natural convection
flow along a vertical wavy surface with uniform surface temperature in
presence of heat generation/absorption. Akhter (2007) studied the effect of
radiations on free convection flow on sphere with isothermal surface and
uniform heat flux. Ali (2007) studied the effect of radiation on free
convection flow on sphere with heat generation. Hossain et al.
(1999)studied the effect of radiation on free convection flow from a
porous vertical plate. They (1999) analyzed a full numerical solution and
found an increase in Radiation parameter Rd causes to thin the boundary
layer and an increase in surface temperature parameter causes to thicken

58
the boundary layer. The presence of suction ensures that its ultimate fate if
vertically increased is a layer of constant thickness. Molla et al. (August
2006) studied the Magnetohydrodynamic natural convection flow on a
sphere with uniform heat flux in presence of heat generation. Gary et al.
(1982) and Mehta and Sood (1992) have concluded that when this effect is
included, the flow characteristics substantially change compared to the
constant viscosity case. Recently, Kafoussius and Williams (1995) and
Kafoussias and Rees (1998) have investigated the effect of the
temperature-dependent viscosity on the mixed convection flow past a
vertical flat plate in the region near the leading edge using the local non-
similarity method. In these studies, they concluded that when the viscosity
of a fluid is sensitive to temperature variations, the effect of temperature-
dependent viscosity has to be taken into consideration, otherwise
considerable errors may occur in the characteristics of the heat transfer
process. Hossain et al. (2002) have investigated the natural convection of
fluid with variable viscosity from a heated vertical wavy surface. Hossain
and Munir (2000) investigated the mixed convection flow from a vertical
flat plate for a temperature dependent viscosity. In above studies (Hossain
et al., 2002, Hossain & Munir, 2000) the viscosity of the fluid has been
considered to be inversely proportional to a linear function of temperature.
None of the aforementioned studies, considered variable viscosity and
MHD effects on laminar boundary layer flow of the fluids along porous
plate. In the present study, we have investigated the variable viscosity on
MHD natural convection flow from a porous vertical plate numerically.
The results will be obtained for different values of relevant physical
parameters and will be shown in graphs as well as in tables.
The governing partial differential equations are reduced to locally non-
similar partial differential forms by adopting some appropriate
transformations. The transformed boundary layer equations are solved
numerically using implicit finite difference scheme together with the
Keller Box technique (Carey & Mollendorf, 1978). Here, we have
focused our attention on the evolution of the surface shear stress in terms
of local skin friction and the rate of heat transfer in terms of local Nusselt
number, velocity profiles as well as temperature profiles for selected
values of parameters consisting of MHD M, variable viscosity , Prandtl
number Pr.
59
Nomenclatures
Cfx Local skin friction coefficient in
the direction of x-axis
Cp Specific heat at constant pressure
f Dimensionless stream function
g Acceleration due to gravity
k Thermal conductivity
Nux Local Nusselt number in
the direction of x-axis
Pr Prandtl number
M Magnetohydrodynamic parameter
qw Heat flux at the surface
cq Conduction heat flux
T Temperature of the fluid in the
boundary layer
T Temperature of the ambient fluid
Tw Temperature at the surface
( , )u v Dimensionless velocity
components along the
yx , axes
V Wall suction velocity
(x, y) Axis in the direction along and
normal to the surface
respectively
Coefficient of thermal expansion
Similarity variable
Dimensionless temperature
function
w Surface temperature parameter
Viscosity of the fluid
Kinematic viscosity
Similarity variable
Density of the fluid
Stefan-Boltzmann constant
s Scattering co-efficient
0 Electric conduction
f absolute Viscosity at the film
temperature
Coefficient of skin friction
w Shearing stress
Non-dimensional stream function
0 Strength of magnetic field
γ Viscosity parameter
Subscripts
w wall conditions
∞ Ambient temperature
Problem Description and Mathematical Model
We have investigated MHD free convection flow from a porous plate with
variable viscosity. The fluid is assumed to be a grey, emitting and
absorbing but non scattering medium. Over the work it is assumed that the
surface temperature of the porous vertical plate, Tw, is constant,
where
TTw
. The physical configuration considered is as shown in
Figure 1(a):
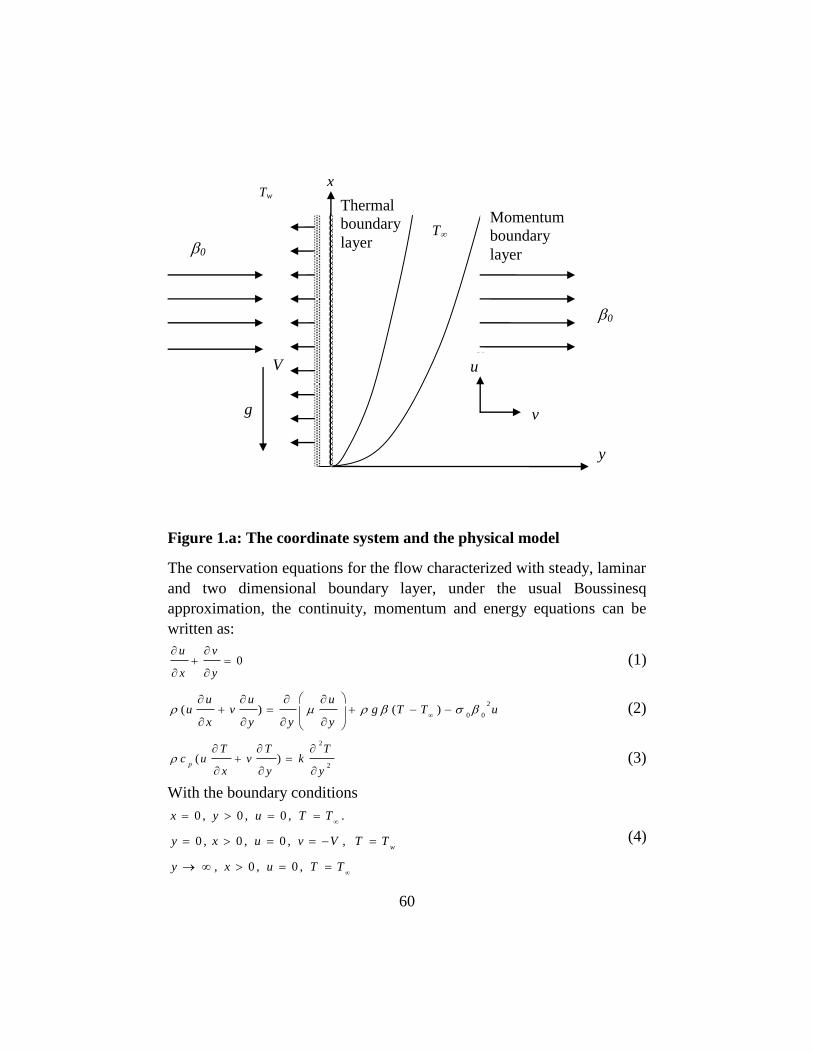
60
Figure 1.a: The coordinate system and the physical model
The conservation equations for the flow characterized with steady, laminar
and two dimensional boundary layer, under the usual Boussinesq
approximation, the continuity, momentum and energy equations can be
written as:
0u v
x y
(1)
2
0 0( ) ( )
u u uu v g T T u
x y y y
(2)
2
2( )
p
T T Tc u v k
x y y
(3)
With the boundary conditions
0 , 0 , 0 , .
0 , 0 , 0 , ,
, 0 , 0 ,
w
x y u T T
y x u v V T T
y x u T T
(4)
V
x
u u
Thermal
boundary
layer
Momentum
boundary
layer
T
v
0
0
Tw
g
y

61
where is the density, 0 is the strength of magnetic field, 0 is the
electrical conduction, k is the thermal conductivity, is the coefficient of
thermal expansion, is the reference kinematic viscosity = / , is
the viscosity of the fluid, Cp is the specific heat at constant pressure. The
absolute viscosity μ is assumed to be vary with temperature according to a
general functional form μ = μf s(T), where μf is the absolute viscosity at the
film temperature Tf and s(Tf) = 1. This form is chosen to allow definition
of the stream function based on the absolute viscosity at the film
temperature. For liquids, all transport properties vary with temperature.
However, for many liquids, petroleum oils, glycerin, glycol, silicon fluids
and some molten salt, the percent variation of absolute viscosity with
temperature is much more than that of the other properties. Under the
above conditions an analysis incorporating the above assumptions and
describing the momentum and thermal transport within the flow field are
more accurate than the usual assumption of constant properties evaluated
at some reference temperature. It should be mentioned here that there are
some fluids for which properties other than μ vary strongly with
temperature. In particular, water and methyl alcohol exhibit strong
variation of both μ and β. The analysis presented here is not applicable to
these liquids since we are considering only the variation of the absolute
viscosity as a function of temperature. However, for the case of an
isothermal surface (in an unstratified ambient fluid), the variation of the
absolute viscosity with temperature takes the form μ = μfS(θ), where θ is
the dimensionless temperature in the boundary layer defined in equation
(4), such that S(1/2) = 1. A wide variety of functional forms of S(θ)
satisfying this requirement was investigated in the literature such as
algebraic expressions, power series, exponential forms, etc. Carey and
Mollendorf (1978), the simplest form of the absolute viscosity is used in
this investigation as follows:
μ = μf[1+1/μf (dμ/dT)f (T − T∞)] (5a)
This simple form amounts to a linear variation of the absolute viscosity
with temperature, with the slope dμ/dT , evaluated at film temperature.
The assumed linear variation of viscosity with temperature gives rise to a
new parameter γ defined by
γ = 1/μf (dμ/dT) f (Tw − T∞) (5b)

62
Now introduce the following non-dimensional variables:
V y
,
1
4
2
4 xV
g T
,3 2 3
4V g T f
(6)
w
T T
T T
,
w
w
T
T
Where, is the non-dimensional temperature function, w is the surface
temperature parameter.
Substituting (6) into Equations (1), (2) and (3) leads to the following non-
dimensional equations 2
2 2 20 01
1 2 32
f ff f ff f f f v f
(7)
1
3 f
f fP r
(8)
Where Pr = μCp/k is the Prandtl number and M=020/ is the
hydromagnetic parameter .The boundary conditions (4) become
0 , 1 a t 0
0 , 0 as
f
f
0 , f (9)
The solution of equations (6), (8) enable us to calculate the
nondimensional velocity components u,v from the following
expressions 2
2
1
( , )( )
(3 )
w
u u fV g T T
fv f f
V
(10)
In practical applications, the physical quantities of principle interest are
the shearing stress w and the rate of heat transfer in terms of the skin-
friction coefficients Cfx and Nusselt number Nux respectively, which can
be written as
0 0( ) ,
x c fx
VN u q C
V T g T
(11)
00
and where
y
Tkq
y
u
cw (12)

63
qc is the conduction heat flux.
Using the Equations (6) and the boundary condition (9) into (11) and (12),
we get
1
1 , 02
, 0
f x
x
C f x
N u x
(13)
The values of the velocity and temperature distribution are calculated
respectively from the following relations:
2
( , ), ,u f x y (14)
Numerical Procedure
Solution of the local non similar partial differential equation (7) to (8)
subjected to the boundary condition (9) are obtained by using implicit
finite difference method with Keller-Box Scheme, which has been
described in details by Cebeci and Bradshaw (1984) .
The solution methodology of equations (7) and (8) with the boundary
condition given in eqn. (9) for the entire ξ values based on Keller – box
scheme is proposed here . The scheme specifically incorporated a nodal
distribution favoring the vicinity of the plate, enabling accuracy to be
maintained in this region of steep gradient. In detail equations (7) and (8)
are solved as a set of five simultaneous equations.
2 211 3 2 ( )
2
f ff f f f f M f f f
(15)
and
13
P r
ff f
(16)
To apply the aforementioned method, we first convert Equations (15)-(16)
into the following system of first order equations with dependent
variables ),( u , ),( v , ),( p and ),( g as
f = u, u
= v, g =, and
= p (17)
2 2
5 1 2 4
11
2
u fp g v p fv p u g v p u u v
(18)

64
1
1
P r
g fp p p fp u p
(19)
where
p1 =3, p2 = 2, p4 = M and p5 = γ (20)
The corresponding boundary conditions are ( , 0 ) 0 , ( , 0 ) 0 a n d ( , 0 ) 0
( , ) 0 , ( , ) 0
f u g
u g
(21)
We now consider the net rectangle on the (,) plane and denote the net
point by
0 10 1, 2 ,, ,
j j jh j J
0 10 1, 2 ,, ,
n n
nk n N
Figure 1. b: Net rectangle for difference approximations for the Box scheme
Here ‘n’ and ‘j’ are just sequence of numbers on the ),( plane, kn and hj
are the variable mesh widths.
We approximate the quantities (f, u, v, p) at the points ),(j
n of the net
by ),,,(n
j
n
j
n
j
n
jpvuf which we call net function.
1 / 2 1
1
2( )
j j j
(22)
1 / 2 11
2( )
n n n
hj
kn
ηj-1/2
ηj
ηj-1
ξn-1
ξn-1/2 ξ
n
B A
D C

65
1 / 2 11
2( )
n n n
j j jg g g
1 / 2 1
1
2( )
nn n
j j jg g g
Now we write the difference equations that are to approximate Equations
(17) - (19) by considering one mesh rectangle for the mid point
),(2
1j
nn to obtain
1
1 / 2
n n
j j n
j
j
f fu
h
(23)
n
j
j
n
j
n
j
vh
uu
2/1
1
(24)
n
j
j
n
j
n
j
ph
gg
2/1
1
(25)
Similarly Equations (18) – (19) are approximate by centering about the
midpoint ),(2
1
21
j
n
n . Centering the Equations (22) about the point
),( 21
nn
without specifying η to obtain the algebraic equations. The
difference approximation to Equations (18)-(19) become
1
1 1
5 5 5 51 1
1
2 2 2
1 1 1 2 1 1 1 4 12 2 2 2 2
2
1 1 1
1 1 1 1 1 12 2 2 2 2 2
1 0 .5 1 0 .5 1 0 .5 1 0 .52
{ ( ) } ( ) { ( ) } ( ) ( )
( ) { }
n n n nj
j j j j
nn n n n n
n nj j j j jj
n n n n n n
nj j j j j j
hp g v p g v p g v p g v
p f v p u g p u
v f v v f R
11 1 1 11 1 2 11 1 1 11 5 5 1 2 1
12 2 2 22 2
1 1 1 1 2 11
1 4 112
11 1 2 11
1 1 1
22 2 2
1 0 .5 1 0 .5
( )
( )
nn n n n nn n
j j j jj j jj j
n n n n
j j j jj
nn n n
n jj j j
w h e r e
L h p g p g p fv p u g
p h v v p u
A n d
R L u fv

66
1 1 3 3
1 3 3 1 1 12 2
1 1 1
1 1 1 1 1 12 2 2 2 2
1 1 1
1 1 1 1 1 1 1 12 2 2 2 2 2 2 2
1[ ( ) { { (1 ) } { (1 ) } } ]
P r
( ) ( ) [ ( ) ( ) ]
[ ( ) ( ) }
n n n n n n
j j j j j j j j
n n n n n
j j j j j
n n n n n n n n
n j j j j j j j j
h p p h p p g p p g p
p f p M n u g f p
u g f p u g u g p f
1
1 12 2
]n n
j jp f
1 2
1 1 1 4 1 1 1 1 12 2 2 2 2 2
1 1 1 1 1
1 1 1 1 1 1 1 1 1 12 2 2 2 2 2 2 2 2 2
1
12
1[ ( ) ] ( ) { ( ) } ( )
P r
[{ ( ) ( ) } } ]
n n n n n n n n
j j j nj j j j j j
n n n n n n n n n n
n j j j j j j j j j j
n
j
h p p p p g p f p
u g u g u g u g p f p f
T
1 1 1 1 1 1 1 1
1 1 1 1 1 1 12 2 2 2 2
1 1 1 1
1 1 1 12 2 2 2
1[ ( ) ] [ ( ) ( ) ]
P r
[ ( ) ( ) ]
n n n n n n n
j j jj j j j j
n n n n
nj j j j
w h e r e
M h p p p p f p
T M f p u g
The corresponding boundary conditions (21) become
0 0 00 0 1, ,
n n nf u g
0 0,n n
J Ju g
which just express the requirement for the boundary conditions to remain
during the iteration process. Now we will convert the momentum and
energy equations into system of linear Equations and together with the
boundary conditions can be written in matrix or vector form, where the
coefficient matrix has a block tri-diagonal structure. The whole procedure,
namely reduction to first order followed by central difference
approximations, Newton‘s quasi-linearization method and the block
Thomas algorithm, is well known as the Keller- box method.
Results and Discussion
In this exertion MHD natural convection flow from a porous vertical plate
with variable viscosity is investigated. Numerical values of local rate of
heat transfer are calculated in terms of Nusselt number Nux for the surface
of the porous vertical plate from lower stagnation point to upper
stagnation point, for different values of the aforementioned parameters and
these are shown in tabular form in Table 1 and Graphically in Figure 5-7.
The effect for different values viscosity on local skin friction coefficient
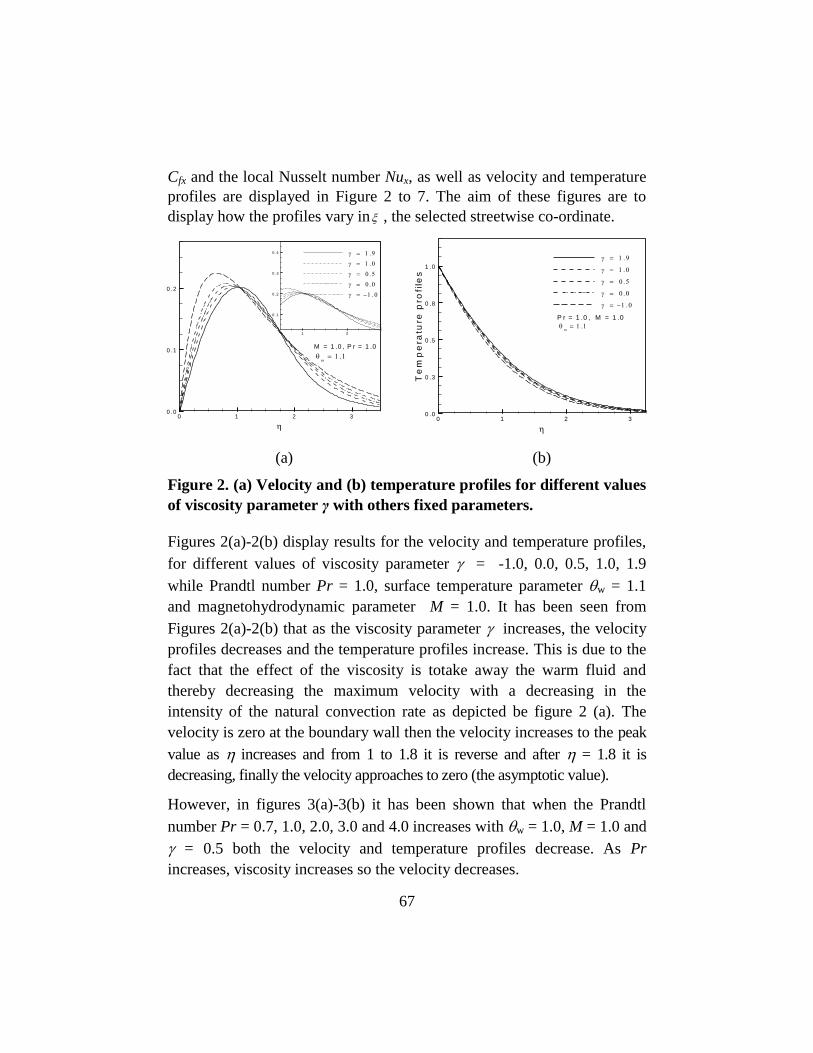
67
Cfx and the local Nusselt number Nux, as well as velocity and temperature
profiles are displayed in Figure 2 to 7. The aim of these figures are to
display how the profiles vary in , the selected streetwise co-ordinate.
(a) (b)
Figure 2. (a) Velocity and (b) temperature profiles for different values
of viscosity parameter γ with others fixed parameters.
Figures 2(a)-2(b) display results for the velocity and temperature profiles,
for different values of viscosity parameter = -1.0, 0.0, 0.5, 1.0, 1.9
while Prandtl number Pr = 1.0, surface temperature parameter w = 1.1
and magnetohydrodynamic parameter M = 1.0. It has been seen from
Figures 2(a)-2(b) that as the viscosity parameter increases, the velocity
profiles decreases and the temperature profiles increase. This is due to the
fact that the effect of the viscosity is totake away the warm fluid and
thereby decreasing the maximum velocity with a decreasing in the
intensity of the natural convection rate as depicted be figure 2 (a). The
velocity is zero at the boundary wall then the velocity increases to the peak
value as increases and from 1 to 1.8 it is reverse and after = 1.8 it is
decreasing, finally the velocity approaches to zero (the asymptotic value).
However, in figures 3(a)-3(b) it has been shown that when the Prandtl
number Pr = 0.7, 1.0, 2.0, 3.0 and 4.0 increases with w = 1.0, M = 1.0 and
= 0.5 both the velocity and temperature profiles decrease. As Pr
increases, viscosity increases so the velocity decreases.
0 1 2 3
0 .0
0 .3
0 .5
0 .8
1 .0
Te
mp
era
ture
pro
file
s
P r = 1 .0 , M = 1 .0
0 1 2 3
0 .0
0 .1
0 .2
M = 1 .0 , P r = 1 .0
1 2
0 .1
0 .2
0 .3
0 .4
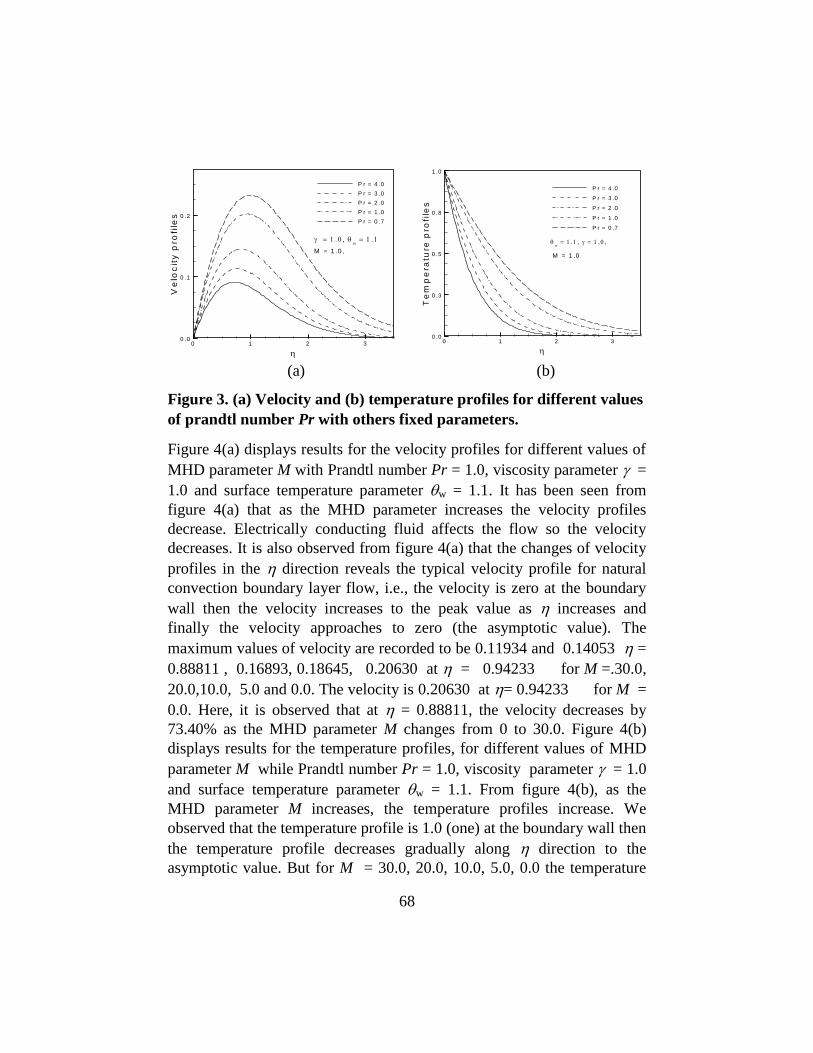
68
(a) (b)
Figure 3. (a) Velocity and (b) temperature profiles for different values
of prandtl number Pr with others fixed parameters.
Figure 4(a) displays results for the velocity profiles for different values of
MHD parameter M with Prandtl number Pr = 1.0, viscosity parameter =
1.0 and surface temperature parameter w = 1.1. It has been seen from
figure 4(a) that as the MHD parameter increases the velocity profiles
decrease. Electrically conducting fluid affects the flow so the velocity
decreases. It is also observed from figure 4(a) that the changes of velocity
profiles in the direction reveals the typical velocity profile for natural
convection boundary layer flow, i.e., the velocity is zero at the boundary
wall then the velocity increases to the peak value as increases and
finally the velocity approaches to zero (the asymptotic value). The
maximum values of velocity are recorded to be 0.11934 and 0.14053 =
0.88811 , 0.16893, 0.18645, 0.20630 at = 0.94233 for M =.30.0,
20.0,10.0, 5.0 and 0.0. The velocity is 0.20630 at = 0.94233 for M =
0.0. Here, it is observed that at = 0.88811, the velocity decreases by
73.40% as the MHD parameter M changes from 0 to 30.0. Figure 4(b)
displays results for the temperature profiles, for different values of MHD
parameter M while Prandtl number Pr = 1.0, viscosity parameter = 1.0
and surface temperature parameter w = 1.1. From figure 4(b), as the
MHD parameter M increases, the temperature profiles increase. We
observed that the temperature profile is 1.0 (one) at the boundary wall then
the temperature profile decreases gradually along direction to the
asymptotic value. But for M = 30.0, 20.0, 10.0, 5.0, 0.0 the temperature
0 1 2 3
0 .0
0 .3
0 .5
0 .8
1 .0
Te
mp
era
ture
pro
file
s
P r = 4 .0
P r = 3 .0
P r = 2 .0
P r = 1 .0
P r = 0 .7
M = 1 .0
0 1 2 3
0 .0
0 .1
0 .2
Ve
loc
ity
pro
file
sP r = 4 .0
P r = 3 .0
P r = 2 .0
P r = 1 .0
P r = 0 .7
M = 1 .0 ,
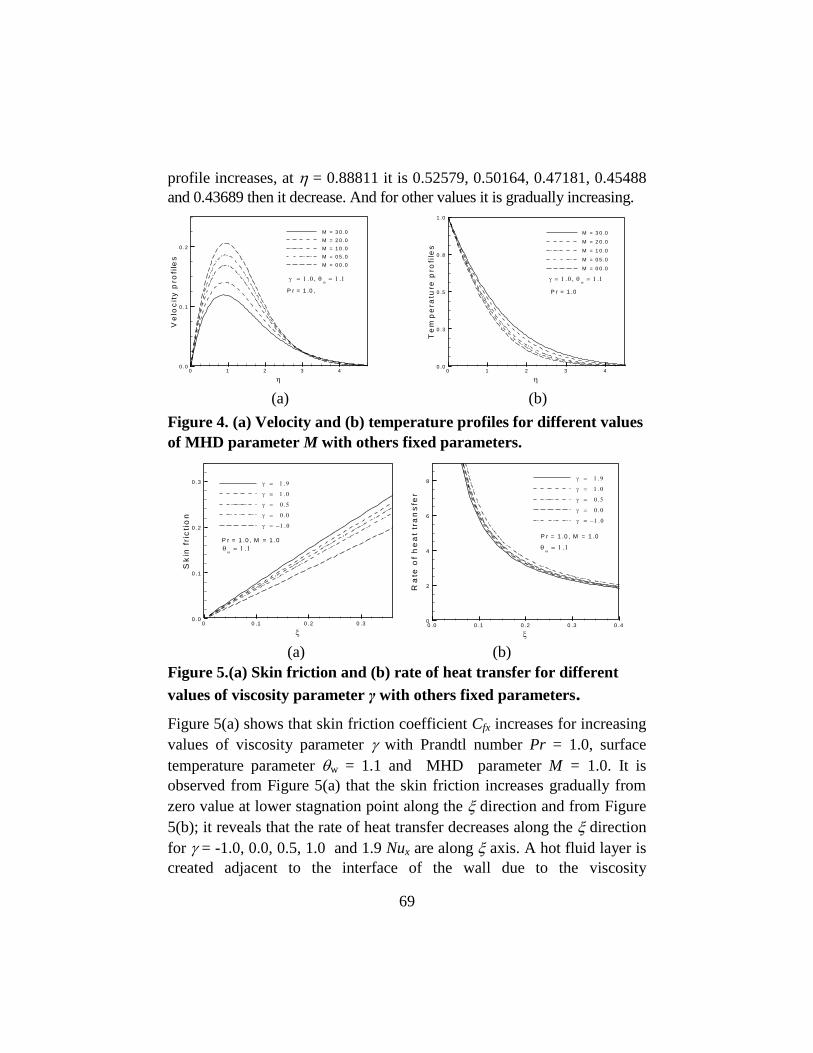
69
profile increases, at = 0.88811 it is 0.52579, 0.50164, 0.47181, 0.45488
and 0.43689 then it decrease. And for other values it is gradually increasing.
(a) (b)
Figure 4. (a) Velocity and (b) temperature profiles for different values
of MHD parameter M with others fixed parameters.
(a) (b)
Figure 5.(a) Skin friction and (b) rate of heat transfer for different
values of viscosity parameter γ with others fixed parameters.
Figure 5(a) shows that skin friction coefficient Cfx increases for increasing
values of viscosity parameter with Prandtl number Pr = 1.0, surface
temperature parameter w = 1.1 and MHD parameter M = 1.0. It is
observed from Figure 5(a) that the skin friction increases gradually from
zero value at lower stagnation point along the direction and from Figure
5(b); it reveals that the rate of heat transfer decreases along the direction
for = -1.0, 0.0, 0.5, 1.0 and 1.9 Nux are along axis. A hot fluid layer is
created adjacent to the interface of the wall due to the viscosity
0 1 2 3 4
0 .0
0 .1
0 .2
Ve
loc
ity
pro
file
s
M = 3 0 .0
M = 2 0 .0
M = 1 0 .0
M = 0 5 .0
M = 0 0 .0
P r = 1 .0 ,
0 1 2 3 4
0 .0
0 .3
0 .5
0 .8
1 .0
Te
mp
era
ture
pro
file
s
M = 3 0 .0
M = 2 0 .0
M = 1 0 .0
M = 0 5 .0
M = 0 0 .0
P r = 1 .0
0 .0 0 .1 0 .2 0 .3 0 .4
0
2
4
6
8
Ra
teo
fh
ea
ttr
an
sfe
r
P r = 1 .0 , M = 1 .0
0 0 .1 0 .2 0 .3
0 .0
0 .1
0 .2
0 .3
Sk
infr
icti
on
P r = 1 .0 , M = 1 .0
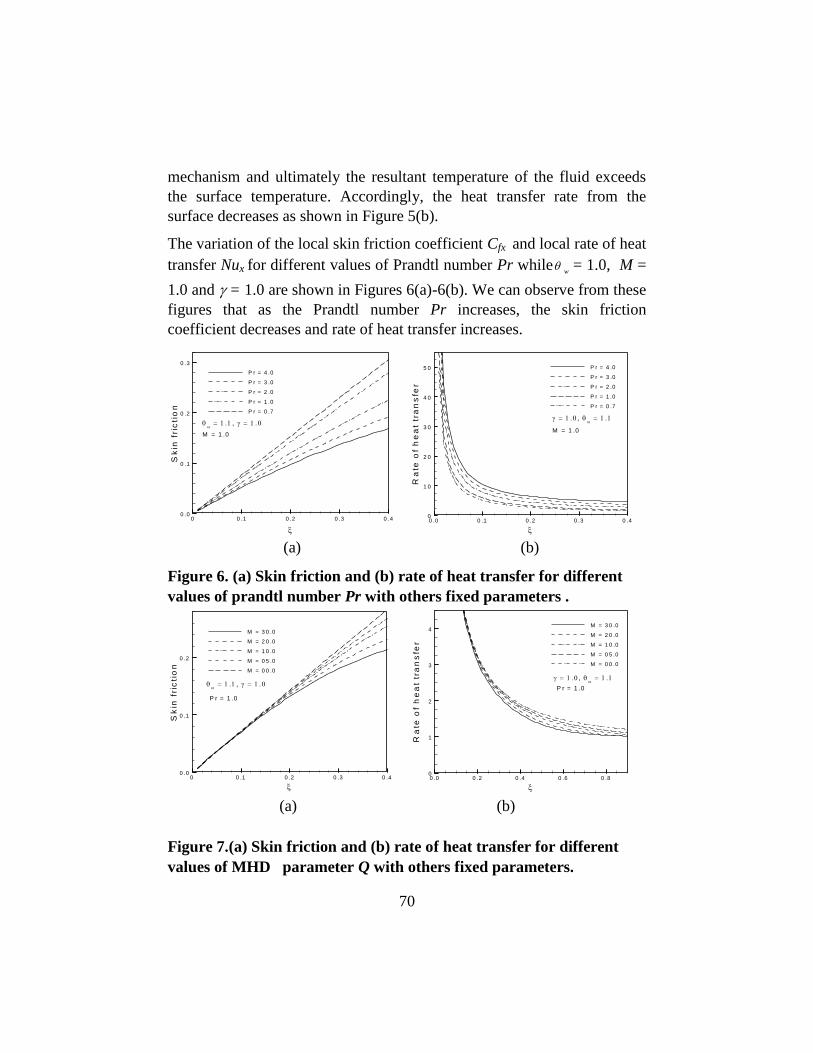
70
mechanism and ultimately the resultant temperature of the fluid exceeds
the surface temperature. Accordingly, the heat transfer rate from the
surface decreases as shown in Figure 5(b).
The variation of the local skin friction coefficient Cfx and local rate of heat
transfer Nux for different values of Prandtl number Pr whilew
= 1.0, M =
1.0 and = 1.0 are shown in Figures 6(a)-6(b). We can observe from these
figures that as the Prandtl number Pr increases, the skin friction
coefficient decreases and rate of heat transfer increases.
(a) (b)
Figure 6. (a) Skin friction and (b) rate of heat transfer for different
values of prandtl number Pr with others fixed parameters .
(a) (b)
Figure 7.(a) Skin friction and (b) rate of heat transfer for different
values of MHD parameter Q with others fixed parameters.
0 .0 0 .1 0 .2 0 .3 0 .4
0
1 0
2 0
3 0
4 0
5 0
Ra
teo
fh
ea
ttr
an
sfe
r
P r = 4 .0
P r = 3 .0
P r = 2 .0
P r = 1 .0
P r = 0 .7
M = 1 .0
0 0 .1 0 .2 0 .3 0 .4
0 .0
0 .1
0 .2
0 .3
Sk
infr
icti
on
P r = 4 .0
P r = 3 .0
P r = 2 .0
P r = 1 .0
P r = 0 .7
M = 1 .0
0 .0 0 .2 0 .4 0 .6 0 .8
0
1
2
3
4
Ra
teo
fh
ea
ttr
an
sfe
r
M = 3 0 .0
M = 2 0 .0
M = 1 0 .0
M = 0 5 .0
M = 0 0 .0
P r = 1 .0
0 0 .1 0 .2 0 .3 0 .4
0 .0
0 .1
0 .2
Sk
infr
icti
on
M = 3 0 .0
M = 2 0 .0
M = 1 0 .0
M = 0 5 .0
M = 0 0 .0
P r = 1 .0

71
Figures 7(a)-7(b) show that skin friction coefficient Cfx and heat transfer
coefficient Nux decrease for increasing values of MHD parameter M while
viscosity parameter = 1.0,.Prandtl number Pr = 1.0, and surface
temperature parameter w = 1.1. The values of skin friction coefficient Cfx
and Nusselt number Nux are recorded to be 0.25646, 0.30238, 0.39508,
0.50394. 0.87147and 1.00382, 1.00463, 1.00414, 1.00463 and 1.04285
for M = 30.0, 20.0, 10.0.5.0, 0.0 and respectively which occur at the same
point = 1.5. Here, it observed that at = 1.5, the skin friction decreases
by 70.57% and Nusselt number Nux decreases by 3.74% as the MHD
parameter M changes from 0.0 to 30.0. It is observed from figure 7(a) that
the skin friction increases gradually from zero value at lower stagnation
point along the direction and from Figure 7(b); it reveals that the rate of
heat transfer decreases along the direction.
Numerical values of rate of heat transfer Nux and skin friction coefficient
Cfx are calculated from Equations (13) from the surface of the vertical
porous plate. Numerical values of Cfx and Nux are shown in Table 1.
Table-1: Skin friction coefficient and rate of heat transfer against for
different values of MHD parameter M with other controlling parameters
Pr = 1.0, w =1.1.and = 1.0.
M = 30.0 M = 20.0 M = 10.0 M = 0.0
Cfx Nux Cfx Nux Cfx Nux Cfx Nux
0.01
0.05
0.10
0.50
1.00
1.50
0.00720
0.03579
0.07033
0.23492
0.25731
0.25646
55.24526
11.37380
5.86455
1.34271
1.01311
1.00382
0.00720
0.03586
0.07081
0.26201
0.30335
0.30238
55.25031
11.38889
5.89219
1.41711
1.01638
1.00463
0.00720
0.03593
0.07130
0.29917
0.39248
0.39508
55.25537
11.40399
5.92000
1.51681
1.03533
1.00414
0.00720
0.03600
0.07180
0.35101
0.65607
0.87147
55.26042
11.41913
5.94800
1.64306
1.16318
1.04285
In the above table the values of skin friction coefficient Cfx and Nusselt
number Nux are recorded to be 0.25646, 0.30238, 0.39508, 0.87147and
1.00382, 1.00463, 1.00414, and 1.04285 for M = 30.0, 20.0, 10.0, 5.0,
0.0 and respectively which occur at the same point = 1.5. Here, it is
observed that at = 1.5, the skin friction decreases by 70.57% and Nusselt
number Nux decreases by 3.74% as the MHD parameter M changes from
0.0 to 30.
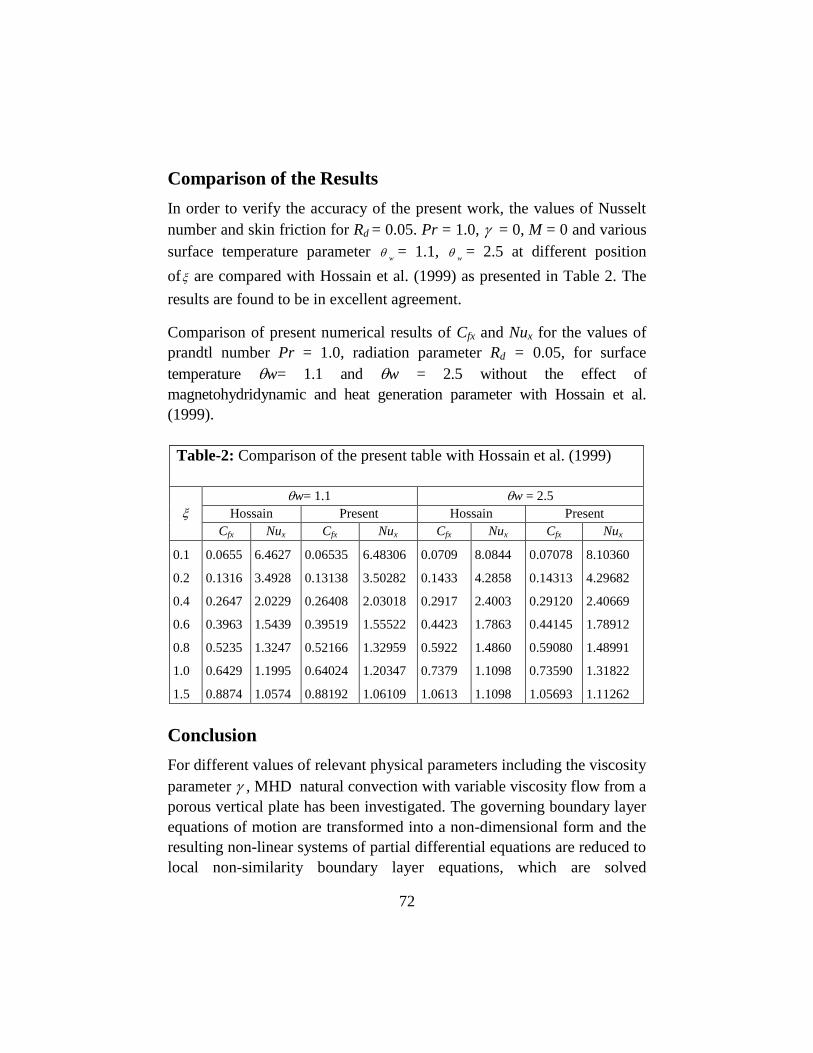
72
Comparison of the Results
In order to verify the accuracy of the present work, the values of Nusselt
number and skin friction for Rd = 0.05. Pr = 1.0, = 0, M = 0 and various
surface temperature parameter w
= 1.1, w
= 2.5 at different position
of are compared with Hossain et al. (1999) as presented in Table 2. The
results are found to be in excellent agreement.
Comparison of present numerical results of Cfx and Nux for the values of
prandtl number Pr = 1.0, radiation parameter Rd = 0.05, for surface
temperature w= 1.1 and w = 2.5 without the effect of
magnetohydridynamic and heat generation parameter with Hossain et al.
(1999).
Table-2: Comparison of the present table with Hossain et al. (1999)
w= 1.1 w = 2.5
Hossain Present Hossain Present
Cfx Nux Cfx Nux Cfx Nux Cfx Nux
0.1
0.2
0.4
0.6
0.8
1.0
1.5
0.0655
0.1316
0.2647
0.3963
0.5235
0.6429
0.8874
6.4627
3.4928
2.0229
1.5439
1.3247
1.1995
1.0574
0.06535
0.13138
0.26408
0.39519
0.52166
0.64024
0.88192
6.48306
3.50282
2.03018
1.55522
1.32959
1.20347
1.06109
0.0709
0.1433
0.2917
0.4423
0.5922
0.7379
1.0613
8.0844
4.2858
2.4003
1.7863
1.4860
1.1098
1.1098
0.07078
0.14313
0.29120
0.44145
0.59080
0.73590
1.05693
8.10360
4.29682
2.40669
1.78912
1.48991
1.31822
1.11262
Conclusion
For different values of relevant physical parameters including the viscosity
parameter , MHD natural convection with variable viscosity flow from a
porous vertical plate has been investigated. The governing boundary layer
equations of motion are transformed into a non-dimensional form and the
resulting non-linear systems of partial differential equations are reduced to
local non-similarity boundary layer equations, which are solved
73
numerically by using implicit finite difference method together with the
Keller-box scheme. From the present investigation the following
conclusions may be drawn:
Significant effects of MHD parameter M and viscosity parameter on
velocity and temperature profiles as well as on skin friction
coefficient Cfx and the rate of heat transfer Nux have been found in this
investigation but the effect of MHD parameter M and viscosity
parameter on rate of heat transfer is more significant. An increase in
the values of viscosity parameter leads to the velocity decrease and
the temperature profiles increase, the local skin friction coefficient Cfx
increase and the local rate of heat transfer Nux decreases at different
position of for Pr =1.0.
For increasing values of Prandtl number Pr leads to decrease the
velocity profile, the temperature profile and the local skin friction
coefficient Cfx but the local rate of heat transfer Nux increases.
An increase in the values of M leads to increase the temperature
profiles and the velocity profiles, the local skin friction coefficient Cfx
and the local rate of heat transfer Nux decreases.
References
Akhter, T. (2007) Effect of Radiation on Natural Convection Flow on a Sphere with
Isothermal surface and uniform Heat Flux, M.Phil Thesis, Department of
Mathematics, Bangladesh University of Engineering and Technology (BUET),
Dhaka, Bangladesh.
Ali, M. M. (2007) Numerical Study of Radiation on Natural Convection Flow on a
Sphere with Heat Generation, M.Phil Thesis, Department of Mathematics,
Bangladesh University of Engineering and Technology (BUET), Dhaka, Bangladesh.
Carey, V.P., Mollendorf, J.C. (1978) Natural convection in liquid with temperature dependent
viscosity, in: Proc. 6th Int. Heat Transfer Conference, Toronto, 2: 211–217.
Cebeci, T., Bradshaw (1984) Physical and Computational Aspects of Convective Heat
Transfer, Springer, New York.
Gary, J., Kassory, D.R., Tadjeran, H., Zebib, A., (1982) The effect of significant viscosity
variation on convective heat transport in water-saturated porous media, J. Fluid
Mech.117: 233–249.
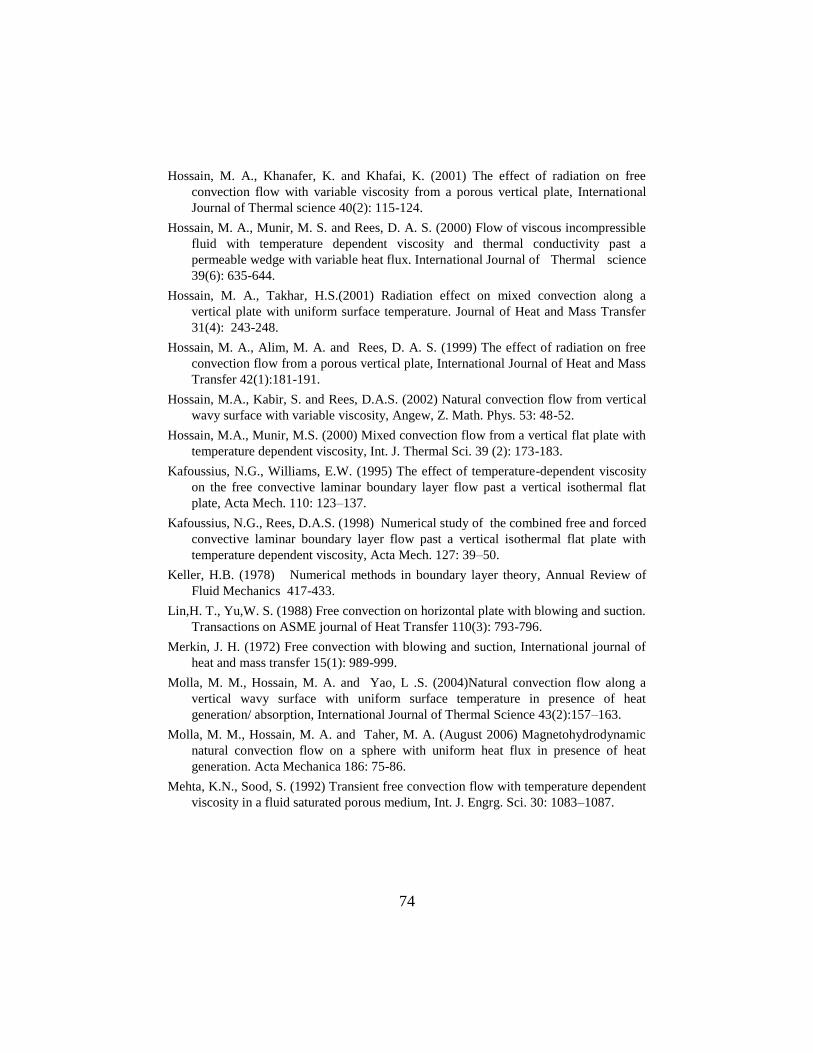
74
Hossain, M. A., Khanafer, K. and Khafai, K. (2001) The effect of radiation on free
convection flow with variable viscosity from a porous vertical plate, International
Journal of Thermal science 40(2): 115-124.
Hossain, M. A., Munir, M. S. and Rees, D. A. S. (2000) Flow of viscous incompressible
fluid with temperature dependent viscosity and thermal conductivity past a
permeable wedge with variable heat flux. International Journal of Thermal science
39(6): 635-644.
Hossain, M. A., Takhar, H.S.(2001) Radiation effect on mixed convection along a
vertical plate with uniform surface temperature. Journal of Heat and Mass Transfer
31(4): 243-248.
Hossain, M. A., Alim, M. A. and Rees, D. A. S. (1999) The effect of radiation on free
convection flow from a porous vertical plate, International Journal of Heat and Mass
Transfer 42(1):181-191.
Hossain, M.A., Kabir, S. and Rees, D.A.S. (2002) Natural convection flow from vertical
wavy surface with variable viscosity, Angew, Z. Math. Phys. 53: 48-52.
Hossain, M.A., Munir, M.S. (2000) Mixed convection flow from a vertical flat plate with
temperature dependent viscosity, Int. J. Thermal Sci. 39 (2): 173-183.
Kafoussius, N.G., Williams, E.W. (1995) The effect of temperature-dependent viscosity
on the free convective laminar boundary layer flow past a vertical isothermal flat
plate, Acta Mech. 110: 123–137.
Kafoussius, N.G., Rees, D.A.S. (1998) Numerical study of the combined free and forced
convective laminar boundary layer flow past a vertical isothermal flat plate with
temperature dependent viscosity, Acta Mech. 127: 39–50.
Keller, H.B. (1978) Numerical methods in boundary layer theory, Annual Review of
Fluid Mechanics 417-433.
Lin,H. T., Yu,W. S. (1988) Free convection on horizontal plate with blowing and suction.
Transactions on ASME journal of Heat Transfer 110(3): 793-796.
Merkin, J. H. (1972) Free convection with blowing and suction, International journal of
heat and mass transfer 15(1): 989-999.
Molla, M. M., Hossain, M. A. and Yao, L .S. (2004)Natural convection flow along a
vertical wavy surface with uniform surface temperature in presence of heat
generation/ absorption, International Journal of Thermal Science 43(2):157–163.
Molla, M. M., Hossain, M. A. and Taher, M. A. (August 2006) Magnetohydrodynamic
natural convection flow on a sphere with uniform heat flux in presence of heat
generation. Acta Mechanica 186: 75-86.
Mehta, K.N., Sood, S. (1992) Transient free convection flow with temperature dependent
viscosity in a fluid saturated porous medium, Int. J. Engrg. Sci. 30: 1083–1087.

75
SENSITIVITY STUDY OF THE CUMULUS
PARAMETERIZATION SCHEMES WITH PLANETARY
BOUNDARY LAYER OPTIONS IN ESTIMATING
RAINFALL IN BANGLADESH USING MM5
Md. A. E. Akhter1, Md. M. Alam
2 & M. A. Hossain
3
Keywords: Sensitivity. Planetary. Cumulus. Rainfall.
Abstract: The sensitivity of the cumulus parameterization schemes with
PBL options in estimating rainfall in Bangladesh has been studied using
MM5v3. Two step domains, mother domain (49 x 49) taken between
11.890-29.59
0N, 80.49
0- 99.51
0E and nested one (79 x 79) between 18.01
0-
27.570N, 85.21-95.60
0E, along with 23 sigma levels for vertical layers are
taken. The grid distances for coarse and nested domain became 45 km and
15 km respectively. We have run the model from 00 UTC of May 01 to 00
UTC of May 04, 2009 using 5 cumulus parameterization scheme Grell,
Anthe-Kuo, Kain-Fritisch, Betts-Miller and Kain-Fritisch-2 with MRF and
Blackadar PBL for both the domains and observed their effect on the
predicted rain. The predicted accumulated rainfalls are compared with the
observed rain gauge data of BMD at five different meteorological stations
over Bangladesh. It is observed that some schemes have overestimated the
rainfall and someone has underestimated that.
Introduction
Rain has always been valued by mankind, because good corps and
abundant water supplies are possible only by timely and plentiful rainfall.
Rainfall amounts generally vary from place to place and from time to
time. Predictability of weather phenomena like rainfalls, cyclones etc.
through numerical weather prediction (NWP) are very much dependent on
their physical processes. A good number of NWP models are in operation
world wide, like The European Centre for Medium-Range Weather
1 Associate Professor, Department of Physics, Khulna University of Engineering & Technology
2 Professor, Department of Physics, Khulna University of Engineering & Technology
3 Professor, Department of Mathematics, Khulna University of Engineering & Technology

76
Forecast (ECMWF), Bureau of Meteorology (BOM), Goddard Institute for
Space Studies (GISS), Geophysical Fluid Dynamics Laboratory (GFDL),
Florida State University (FSU), United Kingdom Meteorological Office
(UKMO), National Center for Atmospheric Research (NCAR), National
Meteorological Centre (NMC), Mesoscale Model (MM5), Weather
Research and Forecasting (WRF) etc. Of them the 5th generation meso-
scale model (MM5) developed by Pennsylvania State University and
National Centre for Atmospheric Research is an open source model and
we have used its version three release seven (MM5V3R7) in this study.
A number of cumulus parameterization (CP) schemes have been
developed over the years but all of them have certain limitations (Frank,
1983, Malinari et al., 1992, Emanuel & Raymond 1993, Zhang et al.,
1994, Kuo et al., 1997). Convection has long been recognized as a process
of central importance in the development of many weather events. The
scale of convective clouds is too small to be resolved by numerical models
and hence needs to be parameterized in terms of variables defined at the
grid points. With increasing computer resources, in the last half decade,
many of these NWP centers started using higher resolution models for
prediction of cyclone and cold front to reduce errors associated with finite
differencing (Dudhia, 1993) and for better representation of topographical
features and sub-grid scale physical processes.
Convective activities in the tropic play an important role. The Asian
monsoon, in particular, is composed of diurnal cycle (Nita & Sekine,
1994) and intraseasonal variation (Madden & Julian, 1972, Yasunar,
1979). During summer, the Bay of Bengal is characterized as cloudiest
oceanic area (Kodama, 2005). The monsoon wind carries water vapor
from the Bay of Bengal to the inland and produces convective systems in
and around Bangladesh and about 6000 mm rainfall occurred during
summer monsoon (Matsumoto, 1996). There are variation of rainfall with
respect to place and time (Islam, 2005). So it will be useful if we can
estimate the amount of rainfall at different places of Bangladesh. Kataoka
(2005) has used MM5 to study the diurnal variation of precipitation.
Akhter et al. (2007) has tried to select a suitable combination of PBL and
CP scheme to simulate rainfalls over Bangladesh.

77
MM5 uses many physical processes like radiation, surface layer processes,
PBL processes and precipitation (this includes CP and resolvable–scale
microphysics). In this study, Blackadar (BKD) and Medium Range
Forecast (MRF) PBL processes are combined with Anthes-Kuo (AK),
Grell, Kain-Fritsch (KF), Kain-Fritsch-2 (KF-2) and Betts-Miller (BM) CP
schemes to make ten different combinations of PBL and CP schemes and
those are used to test the sensitivity in estimating rainfall over Bangladesh
using MM5 for the rainfall during May 01 to May 04, 2009.The purpose
of this study is to select the best combination of CP scheme and PBL
process to estimate rainfall of different regions of Bangladesh. AK CP
scheme with MRF PBL is found to perform better than other
combinations.
Methodology and Description of MM5 Model
To test how well CP schemes with PBL could predict precipitation during
a rainfall event, the MM5 model was selected for several reasons.
MM5V3R7 is the most recent version of a model first developed in the
1970s by Anthes and Warner (1978). MM5 is probably one of the most
studied mesoscale atmospheric models in recent years. It features multi-
nest capability, non-hydrostatic dynamics, four-dimensional data
assimilation (FDDA), several physics options, and the ability to be run on
most UNIX platforms. A detailed description of MM5 can be found in
Grell et al. (1995) and Dudhia et al. (2004). MM5 includes several CP
schemes, five of which were used in this study: AK, Grell, KF, KF-2, and
BM and those are documented in Anthes (1977), Grell (1993), Kain and
Fritsch (1990), Kain (2002) and Betts and Miller (1986). Among the PBL
options, two PBL schemes, MRF and BKD, are taken with five CP
schemes, AK, Grell, KF, KF-2 and BM, for ten independent runs. The
common physics options which are used, other than CP and PBL,
includes: i) Dudhia Simple Ice microphysical Scheme for moisture
anticipation, ii) Cloud Radiation Schemes for radiation calculation and iii)
5- Layer Soil model to predict soil temperature.
MM5 includes the option of using nested sub-grids that can use different
parameterizations to take advantage of resolution differences. The sub-
grids can be either one way (from the coarser parent grid to the finer

78
nested grid) or two ways (feedback from the nested grid to the parent
grid). The parent and nested grids must have a 3: 1 resolution ratio. This
ensures that every point in the parent grid has a corresponding point in the
nested grid. In the model i) the governing equations are in the terrain
following sigma co-ordinate and are written in flux form and solved in
Arakawa B grid ii) Leapfrog time integration scheme with time splitting
technique is used in model integration. In time splitting technique, the
slowly varying terms are integrated with longer time step and the terms
giving rise to fast moving waves are integrated with shorter time step.
For our present study, we have used two step domains. All the options
stated earlier have been applied for both the domains. The mother domain
is taken between 11.89 – 29.590 N, 80.49-99.51
0 E and the nested one
between 18.01 -27.570 N, 85.21-95.60
0 E. The dimension of the coarse
domain, which is the mother domain, is taken as 49 x 49 and that for the
nested one as 79 x 79, thus the grid distances for coarse and nested domain
became as 45 km and 15 km respectively. 23 vertical sigma levels with
model top at 100 hPa have been used.
6 hourly and 1x1 degree resolutions data from the national Centre for
Environmental Prediction (NCEP) are used as atmospheric initial and
lateral boundary conditions data. The model is run for 72 hours from 00
UTC of 01 May to 00 UTC of 04 May 2009. Model predicted rain is taken
as output to observe the effect of physical parameterization schemes on it.
Outputs of all ten options have been produced at three hours interval and
processed through Grid Analysis and Display system (GrADS) and
Microsoft Excel. The accumulated rainfalls at five selected meteorological
stations viz Dinajpur, Sylhet, Satkhira, Teknaf and Dhaka are taken for the
plotting purpose. Using GrADS and Microsoft Excel, the model predicted
rainfall is compared with the observed rainfall as reported by Bangladesh
Meteorological Department (BMD).
Results
The rainfalls predicted by different combinations of schemes at different
stations are different. Also it is seen that maximum accumulated rainfalls
predicted at different stations are not made by the same scheme. Some
combination has overestimated and some has underestimated the rain in
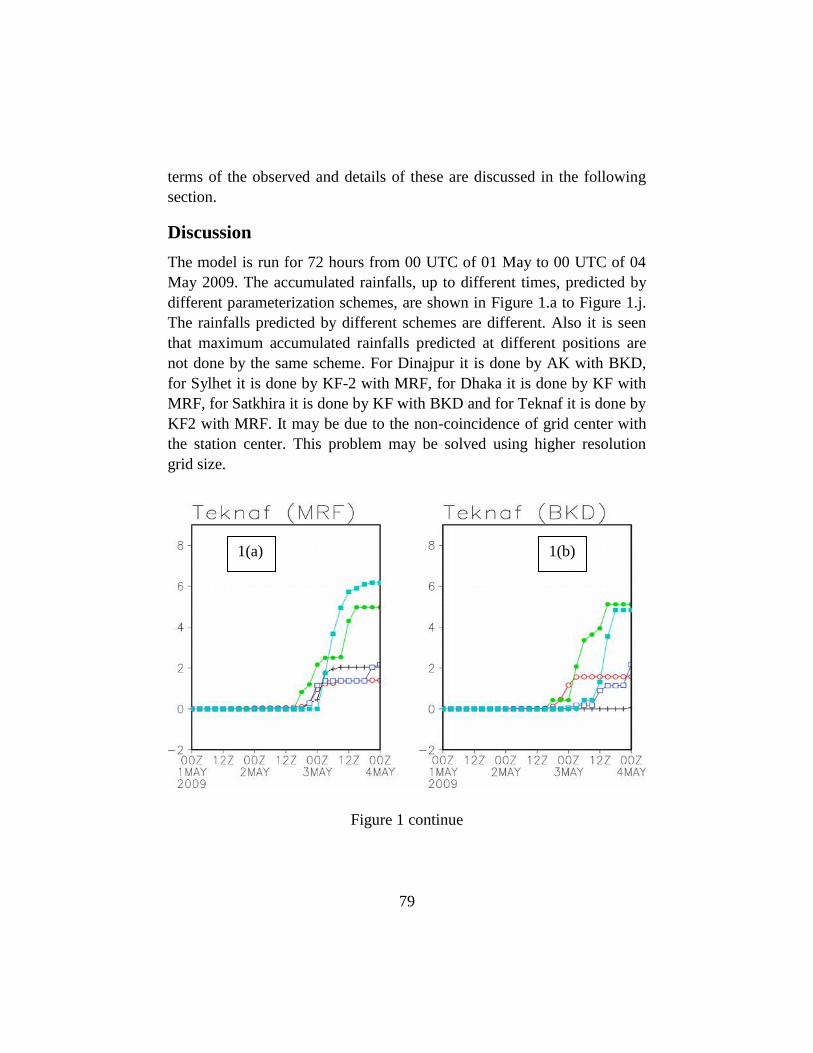
79
terms of the observed and details of these are discussed in the following
section.
Discussion
The model is run for 72 hours from 00 UTC of 01 May to 00 UTC of 04
May 2009. The accumulated rainfalls, up to different times, predicted by
different parameterization schemes, are shown in Figure 1.a to Figure 1.j.
The rainfalls predicted by different schemes are different. Also it is seen
that maximum accumulated rainfalls predicted at different positions are
not done by the same scheme. For Dinajpur it is done by AK with BKD,
for Sylhet it is done by KF-2 with MRF, for Dhaka it is done by KF with
MRF, for Satkhira it is done by KF with BKD and for Teknaf it is done by
KF2 with MRF. It may be due to the non-coincidence of grid center with
the station center. This problem may be solved using higher resolution
grid size.
Figure 1 continue
1(a) 1(b)
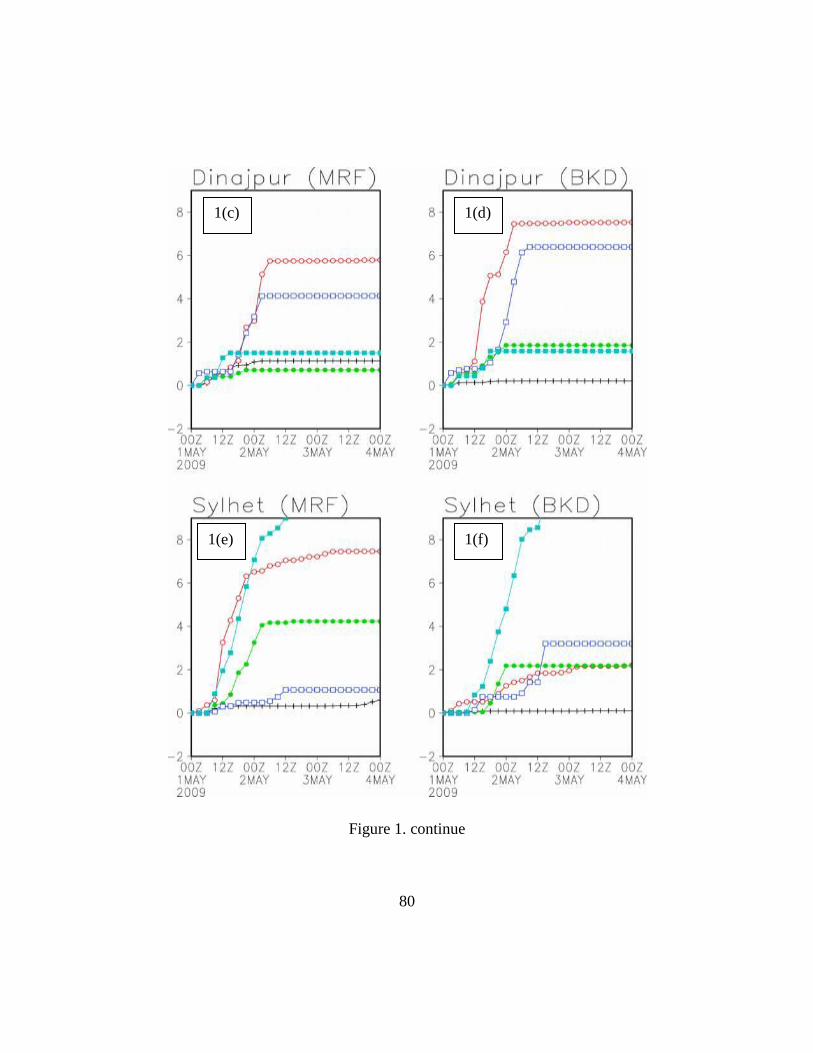
80
Figure 1. continue
1(c) 1(d)
1(f) 1(e)
81
Figure 1.a: Accumulated rainfalls at different stations with different
parameterization schemes (cross, open circle, closed circle, open
square and closed square are for Grell, AK, KF, BM and KF-2
convection scheme respectively).
1(h) 1(g)
1(j) 1(i)
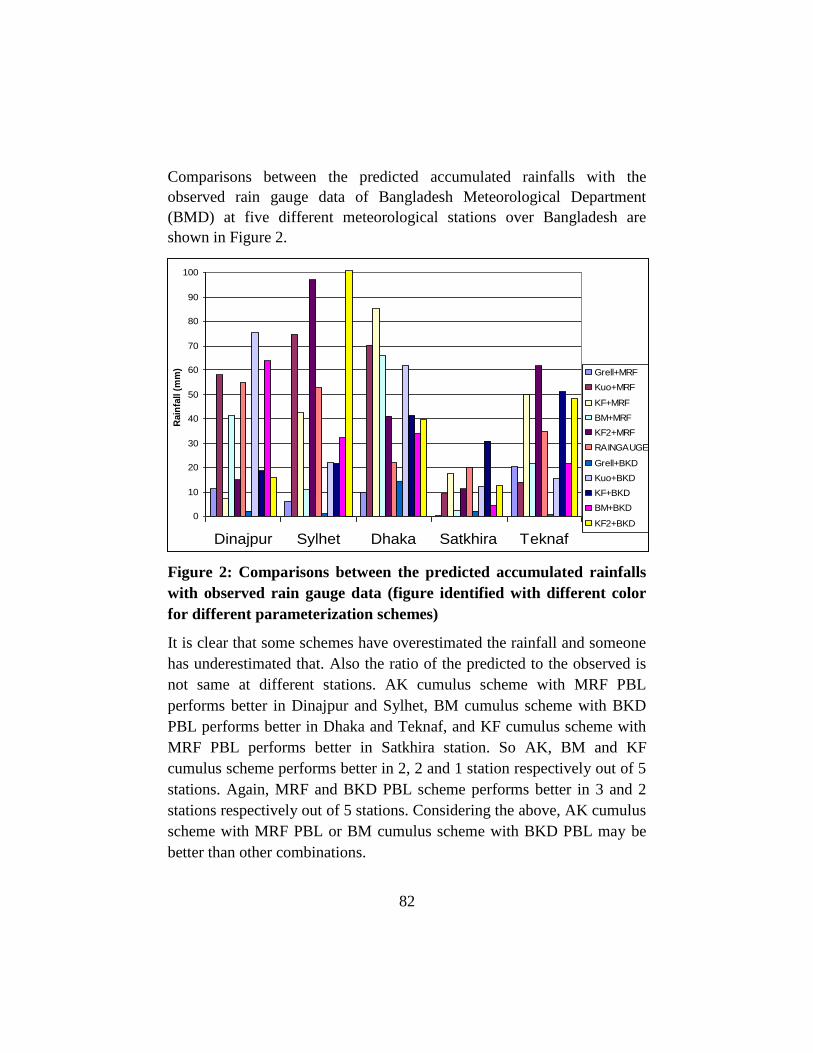
82
Comparisons between the predicted accumulated rainfalls with the
observed rain gauge data of Bangladesh Meteorological Department
(BMD) at five different meteorological stations over Bangladesh are
shown in Figure 2.
0
10
20
30
40
50
60
70
80
90
100
Dinajpur Sylhet Dhaka Satkhira Teknaf
Rain
fall (
mm
) Grell+MRF
Kuo+MRF
KF+MRF
BM+MRF
KF2+MRF
RAINGAUGE
Grell+BKD
Kuo+BKD
KF+BKD
BM+BKD
KF2+BKD
Figure 2: Comparisons between the predicted accumulated rainfalls
with observed rain gauge data (figure identified with different color
for different parameterization schemes)
It is clear that some schemes have overestimated the rainfall and someone
has underestimated that. Also the ratio of the predicted to the observed is
not same at different stations. AK cumulus scheme with MRF PBL
performs better in Dinajpur and Sylhet, BM cumulus scheme with BKD
PBL performs better in Dhaka and Teknaf, and KF cumulus scheme with
MRF PBL performs better in Satkhira station. So AK, BM and KF
cumulus scheme performs better in 2, 2 and 1 station respectively out of 5
stations. Again, MRF and BKD PBL scheme performs better in 3 and 2
stations respectively out of 5 stations. Considering the above, AK cumulus
scheme with MRF PBL or BM cumulus scheme with BKD PBL may be
better than other combinations.
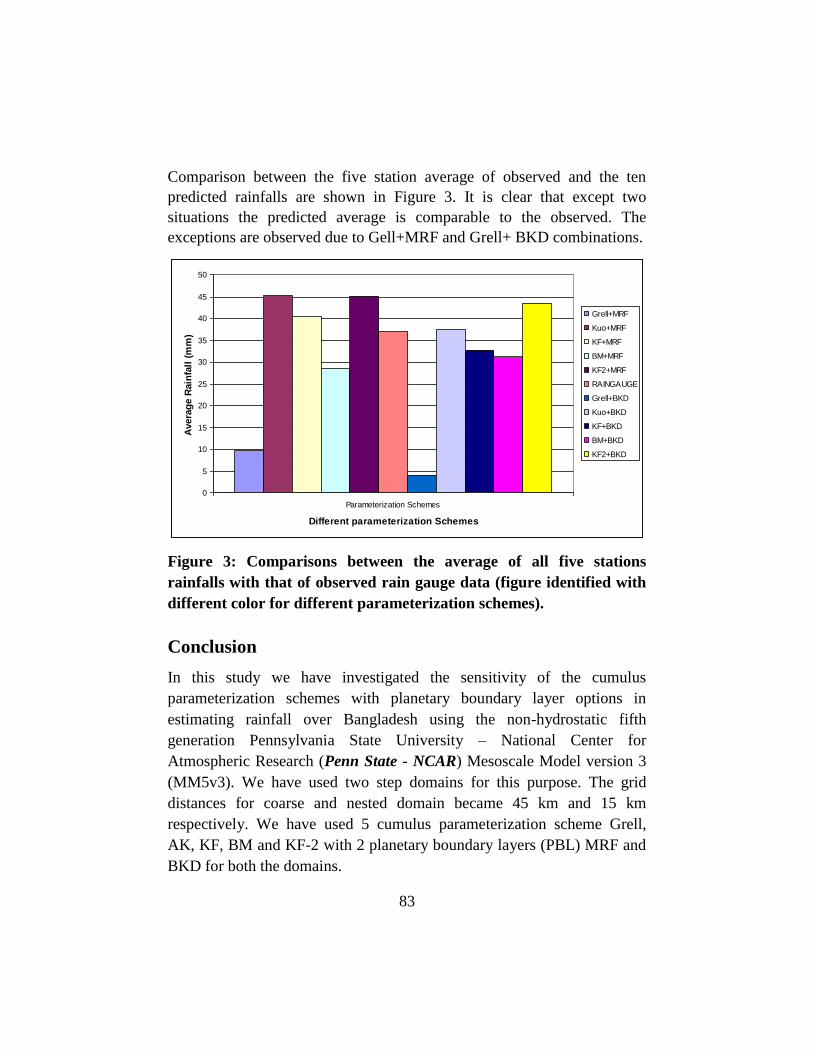
83
Comparison between the five station average of observed and the ten
predicted rainfalls are shown in Figure 3. It is clear that except two
situations the predicted average is comparable to the observed. The
exceptions are observed due to Gell+MRF and Grell+ BKD combinations.
0
5
10
15
20
25
30
35
40
45
50
Parameterization Schemes
Different parameterization Schemes
Avera
ge R
ain
fall
(m
m)
Grell+MRF
Kuo+MRF
KF+MRF
BM+MRF
KF2+MRF
RAINGAUGE
Grell+BKD
Kuo+BKD
KF+BKD
BM+BKD
KF2+BKD
Figure 3: Comparisons between the average of all five stations
rainfalls with that of observed rain gauge data (figure identified with
different color for different parameterization schemes).
Conclusion
In this study we have investigated the sensitivity of the cumulus
parameterization schemes with planetary boundary layer options in
estimating rainfall over Bangladesh using the non-hydrostatic fifth
generation Pennsylvania State University – National Center for
Atmospheric Research (Penn State - NCAR) Mesoscale Model version 3
(MM5v3). We have used two step domains for this purpose. The grid
distances for coarse and nested domain became 45 km and 15 km
respectively. We have used 5 cumulus parameterization scheme Grell,
AK, KF, BM and KF-2 with 2 planetary boundary layers (PBL) MRF and
BKD for both the domains.
84
It is observed that some schemes have overestimated the rainfall and
someone has underestimated that. The ratios of the estimated to the
observed rain are not equal for a particular physical parameterization
schemes at all stations. Simulated pattern of rainfall for individual option
agrees with observable evidences. Point to be noted that the options for
simulation rainfall with MM5 has been found dependable on resolution
and location of the area. According to our study, no single option may be
considered as the most suitable among the 10 options for the assessment of
rainfall over Bangladesh but AK CP with MRF PBL may be considered as
a better one. However, further study is required to draw the final
conclusion in choosing the best option of MM5.
References
Akhter, N., Islam, N. M., Teru, T. and Hayashi, T. (2007) Selection of Parameterization
in MM5 for the Estimation of Rainfall in Bangladesh. Bangladesh Journal of Physics
3: 75-83.
Anthes RA. (1977) A cumulus parameterization scheme utilizing a one-dimensional
cloud model. Monthly Weather Review 105: 270–286.
Anthes R.A., Warner T.T. (1978) Development of hydrodynamic models suitable for air
pollution and other mesometeorological studies. Monthly Weather Review 106:
1045-1078.
Betts A.K., Miller M.J. (1986) A new convective adjustment scheme: part II: single
column tests using GATE wave, BOMEX, ATEX and Arctic air-mass data sets.
Quarterly Journal of the Royal Meteorological Society 112: 693–709.
Dudhia, J. (1993) A nonhydrostatic version of the Penn State- NCAR mesoscale model,
Validation tests and simulation of an Atlantic cyclone and cold front. Mon, Wea.
Rev. 121: 1493-1513.
Dudhia, J., Gill D, Manning K,Wang W, Bruyere C. (2004) PSU/NCAR mesoscale
modelling system tutorial class notes and users‘ guide (MM5modelling system
version 3). National Center for Atmospheric Research, Boulder, CO.
http://www.mmm.ucar.edu/mm5/documents/ ( September 27, 2004).
Emanuel, K. A. and Raymond, D. J. (1993) The representation of cumulus convection in
numerical models. Meteorol. Monogr. Ser., Am. Meteorol. Soc., Boston, MA 46:
246.
Frank, W. M. (1983) The cumulus parameterization problem. Mon, Wea. Rev. 111:
1859-1871.
Grell, G.A. (1993) Prognostic evaluation of assumptions used by cumulus
parameterizations. Monthly Weather Review 121:765–787.

85
Grell, G.A, Dudhia J., Stauffer, D. R. (1995) A description of the fifth-generation Penn
State/NCAR mesoscale model (MM5). NCAR Technical Note 398. National Center
for Atmospheric Research, Boulder, CO.
Islam, M. N., Terao, T., Uyeda, H., Hayashi, T. and Kikuchi, K. (2005) Spatial and
temporal variation of the precipitation in and around Bangladesh. Journal of
Meteorological Society of Japan 83: 21-39.
Kain, J.S., Fritsch, J.M. (1990) A one dimensional entraining/detraining plume model and
its application in cumulus parameterization. Journal of the Atmospheric Sciences
47: 2784–2802.
Kain, J.S. (2002) The kain-Fritsch convective parameterization: An update.
http://www.mmm.ucar.edu/mm5/mm5-papers.html, to be submitted to J. Appl.
Meteor.
Kataoka, A. and Satomura, T. (2005) Numerical Simulation on the Diurnal Variation of
Precipitation over Northeastern Bangladesh, A case study of an Active Period 14-21
June 1995. Sola 1: 205-208
Kodama, Y. M., Ohta, A., Katsumata, M., Satoh, S. and Udeda, H. (2005) Seasonal
transition of predominant precipitation type and lightning activity over tropical
monsoon area derived from TRMM observations. Geophysical Research Letter, Vol,
32, L14710. DOI: 10.1029/2005GL022986.
Kuo, Y. H., Bresch,J. F., Cheng, M. -D., Kain, J., Parsons, D. B., tao, W. K. and Zhang,
D.-L.(1997) Summary of miniworkshop on cumulus parameterization for mesoscale
models. Bull. Am. Meteorol. Soc. 78: 475-491.
Madden, R.A. and Julian, P. R. (1972) Description of global –scale circulation cells in the
tropics with a 40-50 day period. Journal of Atmospheric Society 29: 1109-1123.
Matsumoto, J., Rahman, M. R., Hayashi, T., and Monji, N. (1996) Rainfall distribution
over the India Subcontinent during the 1987 and 1988 severe floods in Bangladesh.
Bulletin of Department of Geography University of Tokyo 28: 25-44.
Molinari, J., Vollaro, D., Dudek, M. and Skubis, M. (1992) Parameterization of the
convective precipitation in mesoscale numerical models, A critical review. Mon,
Wea. Rev.120: 326-344.
Nitta, T. and Sekine, S. (1994) Diurnal variation of convection activity over the tropical
western Pacific. Journal of Meteorological Society of Japan 72: 672-641.
Yasunar, T. (1979) Cloudness fluctuations associated with the Northern Hemisphere
summer monsoon. Journal of Meteorolgy Society of Japan 57: 227-242.
Zhang, D. L., Kain, J.S., Fritisch, J. M. and Gao, K. (1994) Comments on
parameterization of convective precipitation in mesoscale numerical models, A
critical review. Mon, Wea. Rev. 122: 2222-2231.

86
RURAL HEALTH SCENARIO IN BHUTAN: THE
SOCIAL AND INSTITUTIONAL EXPERIENCE
Komol Singha1 & Lingchen
2
Keywords: Health. Scenario. Institutional. Bhutan.
Abstract: This paper is an attempt to discuss the health scenario of rural
Bhutan in relation to reproductive health emphasizing the infant morbidity
and mortality along with the access to safe drinking water and sanitation
coverage. SWOT analysis method has been applied in order to find out the
strengths, weakness, opportunities and threats of health scenario of rural
Bhutan. The findings of this research reveal the honesty and sincerity in the
health care services, poor infrastructure, and social dogma among the
people of Bhutan. Despite the problems of physical infrastructure and
limited resources, the health sector has made progress in Bhutan.
Introduction
Despite Bhutan being one of the least developed nations (HDR 2006) in
the world with difficult terrains and scattered population, health sector has
made remarkable development and spread to every nook and corner of the
country, covering approximately 90% of the total population since its
establishment in 1962 (MoH 2008, NSB 2008). Development of health
sector is accorded the government‘s top priority in Bhutan and the growth
of this sector is one of the indicators of economic development. The
quality of health sector is basically population of a country; the main
indicators being morbidity and mortality (NSB 2008). However, more
factors and determinants of the country‘s health status are being discussed
in section.
The World Health Organisation (2009) places a strong emphasis on health
sector in its Millennium Development Goals (MDGs), the achievement of
1 Sr. Lecturer, Department of Economics, Royal University of Bhutan, Gaeddu College
of Business Studies, Gedu 2 Chief Librarian, Royal University of Bhutan, Gaeddu College of Business Studies, Gedu

87
which will not be possible without progress on food security, gender
equality, the empowerment of women, wider access to education and
better stewardship of the environment. With this view, the present paper is
the modest attempt to portray the health status of Bhutan, particularly in
the rural areas. It tries to identify the social and institutional role in fostering
the developing of health sector in the country. And finally, the researchers
provide some possible recommendations to strengthen the sector.
The researchers collected primary data from two adjacent villages called
Pakshikha and Alikha under Chukha Dzongkhag (district), which are
approximately 160-170 km away from the capital city Thimphu and
approximately 12 km from the Gedu town which is on the National
Highway (Thimphu-Phuentsholing highway) of Bhutan. The researchers
used SWOT analysis to determine the health status and scenario of the
country. To substantiate the study and to assess the patient‘s satisfaction
and the quality of service delivery of the country‘s health sector, 100
patients (bed-ridden) from the Jigme Dorji Wangchuk National Referral
Hospital (JDWNRH) in Thimphu were interviewed and the information
collected were analysed accordingly.
Determinants of Health Status
According to the findings of Lantz et al (1998), income or wealth is the
strongest and most robust predictor of health sector. Tshering and Sithey
(2009) claimed that ―adverse climate change is the major threat to health
sector in Bhutan‖. As South Asian Conference on Sanitation (2008)
recommended that the safe, adequate and accessible supplies of water with
proper sanitation are the foundation and essential component of primary
healthcare. Insufficient provision the communicable diseases, poor health
and environmental pollution.
Others (like, Mahapatra 1997, Nagda 2004, Dhargupta et al. 2009) opined
that education is the main factor which influences health condition of a
country. Some other scholars like Carloyn and Harphan (1992) observed
that health status of a nation is influenced by environmental conditions,
socio-economic conditions, and characteristics of the people. Similarly,
Kumar et al. (2009) also found that the health problems of any community

88
were influenced by the interplay of various factors including social,
economic and political which include people‘s beliefs, customs and
practices. Findings by Selvaraj and Lalitha (2007) reveal that better health
status is determined by many factors like: a) Literacy or education‘ b)
Economic Status; c) Environement; d) Lifestyle; e) Food habits and diet
system; and f) Size of the family etc. By and large, the development of
health sector basically depends on its infrastructure, policy and effective
delivery system in the country.
SWOT Analysis
Development of any sector needs a thorough understanding of the sector.
Therefore, to initiate development policy of health sector in rural Bhutan,
it is imperative that a clear picture and scenario of the Bhutanese health
sector is assessed first. Bhutan‘s health sector, as often portrayed in the
print and visual media, is far from the truth of the actual health scenario
prevalent in the country. A clear picture of health sector in Bhutan can be
seen with the help of SWOT analysis given below, supported by the
primary and secondary data.
SWOT Analysis of Health Sector in Bhutan
Strengths
Strength Law of the Country;
Sincerity and Honesty of the People
and the functionaries; Health as Top
Priority Policy including high budget
on Health
Weaknesses
Weak Physical Health
Infrastructure;
Less Health Expertise;
Social system and Food habits
Opportunities
Sound Environment and Eco-
systems;
Less Population;
External Aid for Health
Threats
Social Dogma;
Emergence of Dreaded
Diseases;
Rural-urban Migration

89
a. Strengths Bhutan is known for its stringent law and obedient citizens. Even if there
is limited manpower, the functionaries of health sector are obedient and
honest to the rule and policy of the country. For instance, 96 patients were
attended timely or medicated on time by the doctors out of 100 patients
interviewed in JDWNRH in the month of March 2010 and the overall
satisfaction level of the patients were also very significant. The effective
health delivery and the patients‘ satisfaction are the result of dutiful
functionaries. On the other hand, people of the country are also found to
be obedient and have great reverence to the rule of the country. Citizens of
the country especially the villagers hardly ignore the policy instructions
given by the government. It is observed from the primary survey by the
researchers. For instance, the RGoB ordered the villagers to keep their
villages/surrounding clean through proper drainage, separate livestock
place (in the traditional rural Bhutan, livestock are kept under the dwelling
house, refer to Figure 1), maintaining sanitary latrine etc. The dictate is
obeyed by the people positively. As per the survey result of the two
villages, due to the government‘s notification recently, 73% of the
households have maintained sanitary latrine (irrespective of income level);
36% maintained drainage and 89% have done away with the keeping of
livestock under the house. This obedient attitude of the villagers helps the
state functionaries to deliver effective health services to the rural areas
(even if the nation faces limited health resources).
Figure 1: A typical Bhutanese rural dwelling house with livestock
place under the house
(Livestock are kept in the gap between the terrace and surface of the earth)

90
As a result of this, despite difficult hilly terrain, around 90% of the
population have access to proper health facilities in the country with
52.3% of women are attended by trained personnel during child birth.
Maternal mortality ratio and infant mortality rate have decreased from 560
and 90 in 1990 to 2.55 (in 2005) and 53.9 in 2009 respectively. Life
expectancy at birth has increased from 45.8 for males and 49.1 for females
in 1985 to 65.9 and 66.1 respectively in 2003 (Bhutan 2007-13). The
access to safe drinking water for the rural population has increased from
about 70% to 84% and the latrine coverage has increased to 91%.
Diarrhoea and dysentery used to be the most common cause of morbidity;
it now ranks third. Improvements in the quality of drinking water in rural
areas have led to a significant decrease in the caseload of water borne
diseases in the rural community. Morbidity associated with childbirth has
significantly diminished, as a testament to the success of the reproductive
health initiatives (Nirola et al. 2006).The following tables provide clear
picture about the health indicator along with health facilities, knowledge
and use of contraceptives and infrastructure facilities related physical
health in rural Bhutan.
Table-1: Health Indicators in Bhutan
Indicators 1994 2000 2008
Infant Mortality Rate per 1000 live births 70.7 60.5 53.9
Under five Mortality Rate per 1000 live births 96.9 84.0 81
Maternal Mortality Rate per 100 live births 3.8 2.55 2.55 *
Crude Birth Rate per 1000 population 39.9 34.09 20.56
Crude Death Rate per 1000 population 9.0 8.64 7.12
Contraceptive Prevalence Rate % 18.8 30.7 35.4
Access to Safe Drinking Water % NA 77.8 83
Sanitation Coverage % NA 88.0 91
Average Life Expectancy at Birth 66 NA 65.53
Population Growth Rate % 3.1 2.5 1.3
Source: IMF (2004); UNICEF (2009); World Bank (2009)
* Population and Housing Census of Bhutan 2005
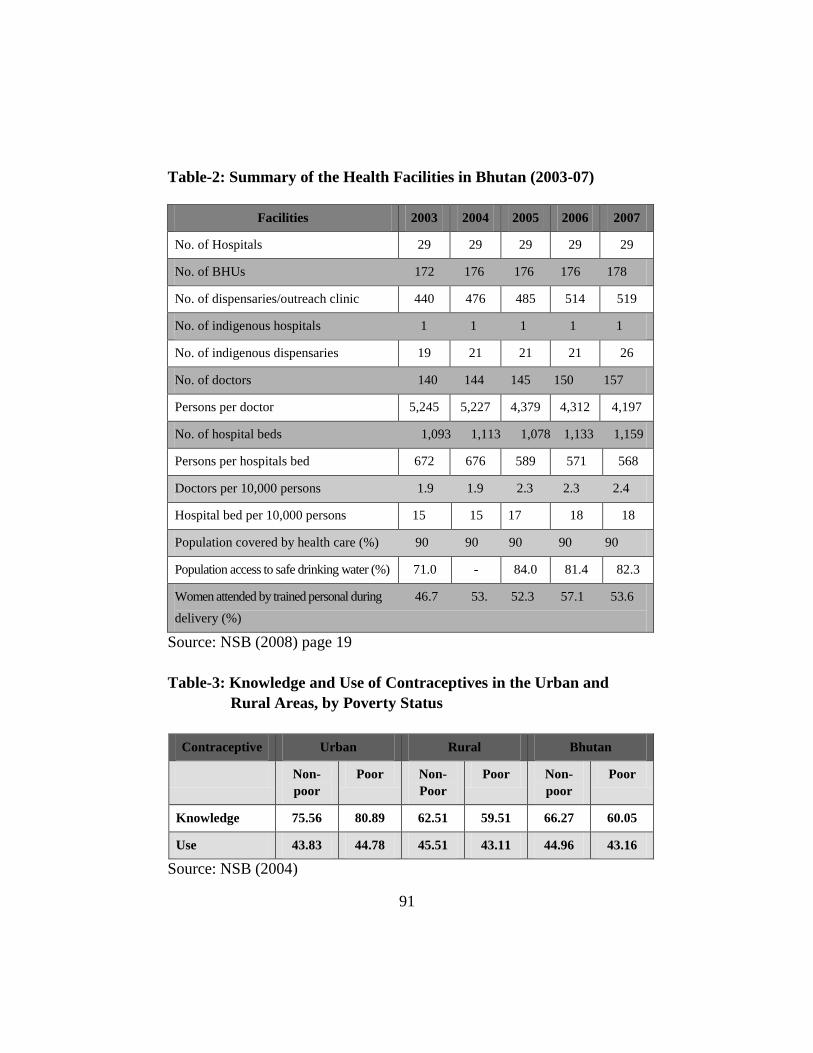
91
Table-2: Summary of the Health Facilities in Bhutan (2003-07)
Facilities 2003 2004 2005 2006 2007
No. of Hospitals 29 29 29 29 29
No. of BHUs 172 176 176 176 178
No. of dispensaries/outreach clinic 440 476 485 514 519
No. of indigenous hospitals 1 1 1 1 1
No. of indigenous dispensaries 19 21 21 21 26
No. of doctors 140 144 145 150 157
Persons per doctor 5,245 5,227 4,379 4,312 4,197
No. of hospital beds 1,093 1,113 1,078 1,133 1,159
Persons per hospitals bed 672 676 589 571 568
Doctors per 10,000 persons 1.9 1.9 2.3 2.3 2.4
Hospital bed per 10,000 persons 15 15 17 18 18
Population covered by health care (%) 90 90 90 90 90
Population access to safe drinking water (%) 71.0 - 84.0 81.4 82.3
Women attended by trained personal during 46.7 53. 52.3 57.1 53.6
delivery (%)
Source: NSB (2008) page 19
Table-3: Knowledge and Use of Contraceptives in the Urban and
Rural Areas, by Poverty Status
Contraceptive Urban Rural Bhutan
Non-
poor
Poor Non-
Poor
Poor Non-
poor
Poor
Knowledge 75.56 80.89 62.51 59.51 66.27 60.05
Use 43.83 44.78 45.51 43.11 44.96 43.16
Source: NSB (2004)
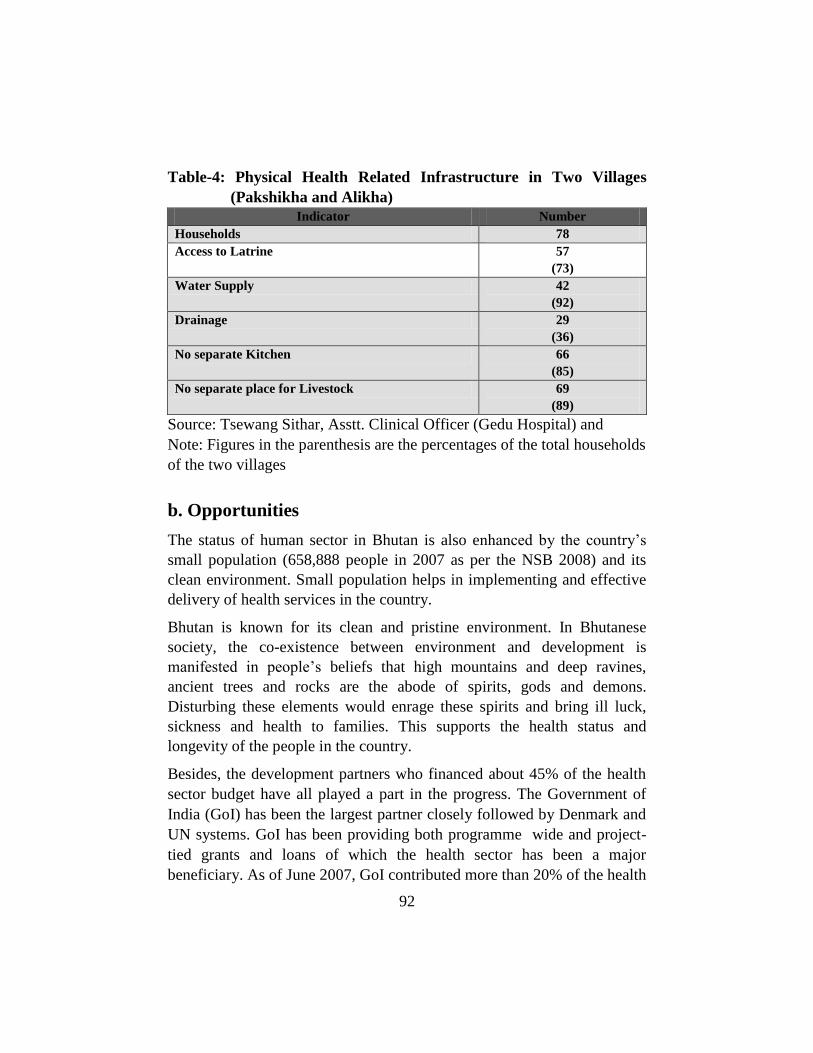
92
Table-4: Physical Health Related Infrastructure in Two Villages
(Pakshikha and Alikha)
Indicator Number
Households 78
Access to Latrine 57
(73)
Water Supply 42
(92)
Drainage 29
(36)
No separate Kitchen 66
(85)
No separate place for Livestock 69
(89)
Source: Tsewang Sithar, Asstt. Clinical Officer (Gedu Hospital) and
Note: Figures in the parenthesis are the percentages of the total households
of the two villages
b. Opportunities
The status of human sector in Bhutan is also enhanced by the country‘s
small population (658,888 people in 2007 as per the NSB 2008) and its
clean environment. Small population helps in implementing and effective
delivery of health services in the country.
Bhutan is known for its clean and pristine environment. In Bhutanese
society, the co-existence between environment and development is
manifested in people‘s beliefs that high mountains and deep ravines,
ancient trees and rocks are the abode of spirits, gods and demons.
Disturbing these elements would enrage these spirits and bring ill luck,
sickness and health to families. This supports the health status and
longevity of the people in the country.
Besides, the development partners who financed about 45% of the health
sector budget have all played a part in the progress. The Government of
India (GoI) has been the largest partner closely followed by Denmark and
UN systems. GoI has been providing both programme wide and project-
tied grants and loans of which the health sector has been a major
beneficiary. As of June 2007, GoI contributed more than 20% of the health

93
sector expenditures, mainly focusing on construction of the 350 beds JDW
National Referral Hospital, the 150 bed Eastern Regional Referral
Hospital, malaria control programme and the construction of a public
health laboratory. Denmark as of June 2007 contributed about 14% of the
health sector budget and has since 2008 switched over to providing sector
budget grant support to social sector with DKK 107 million up to 2013 in
support of the 10th
FYP policies and objectives. The UN systems, mainly
comprising UNICEF, UNFPA and WHO, have provided earmarked
support of 14% to various activities with focus on their respective UN
mandates. Together it has agreed to provide Bhutan US$9.6 million during
2008–2012 with the aim to improve the accessibility, quality and
sustainability of the health care delivery system. Since 2005m GFATM
has been providing substantial support ($3.5) to addressing malaria,
tuberculoss and HIV/AIDS. The World Bank is supporting to halt and
reverse the spread of HIV/AIDS with a total of US$ 5.77 from 2004 to
2009. Also, the bank is providing US$ 2.5 for avian flue. Furthermore, it
has provided US$ 27 million (DPG 1 for US$ 15 and DPG 2 for US$ 12)
as Development Policy Grant in support of government wide policy and
institutional reform.
c. Weaknesses
As far as the weaknesses of health sector in Bhutan are concerned,
manpower in this sector is very limited (only 157 doctors as of 2007
including hired doctors form India) (refer to Table 1 and 2). Most of the
health expertise are hired from India. Presently, most cancer cases are
referred outside the country which currently drains a large proportion of
the health budget (WHO 2003). Topographical condition (mountainous
region) and sparsely settlement of the country, made the health sector
function with a big hurdle. While the battle will continue against
HIV/AIDS, TB, malaria, etc., the problem of emerging non-communicable
diseases will require the strengthening of surveillance systems, developing
and following strategies for prevention and control of non-communicable
diseases and expanding the capacity of tertiary care facilities. Bhutan
imports 100% of its health supplies such as medical equipment, essential
drugs and vaccines. Although the quality of drugs and vaccines can be
94
assured by purchasing them from WHO authenticated suppliers in the
region, hospital equipments and other supplies are other problems (WHO
2003).
Besides, there is no training facility for medical doctors (medical college)
in Bhutan, and basically the poor health status of this country is due to the
factors given below (Jha et al 2008):
1. Food habit of the people, especially eating more chilli
2. More consumption of alcohol by male and female
3. Drugs and other substances are used by the youths
4. A kind of pan/tobacco item, fermented beetle-nut (doma) is used
by majority of the people.
5. Some weaknesses in the culture of the society like living together
without legal marriage.
Social system and food habit are also important factors for weakening the
status of this sector. Bhutanese are very much fond of chilli (emma dashi),
alcohol and tobacco products. More consumption of alcohol and tobacco
both by male and female (as it is permitted by the society) leads to a
number of dreaded diseases. More importantly, the physical infrastructure
of health sector in this country is very weak (refer to Table-2).
d. Threats
Besides the limited expertise and weak physical infrastructures of the
health sector, the Royal Government of Bhutan is struggling to prevent a
number of dreaded and communicable diseases like HIV/AIDS, bird flue
and hepatitis which are basically brought about by globalisation. Sex
related disease is also one of the serious diseases in the country now. As
the country embraces modernization and globalization, people‘s needs and
wants are becoming increasingly diversified. As a fall out of this, peoples
economic activities and behaviour have also diversified and deviated from
the traditional culturist values to a modern materialistic one, bringing drug
and sexual transmitted diseases in the country.

95
Nonetheless, it has to be acknowledged that the Bhutanese society is in the
transitional stage and hence it can neither totally ignore the traditional
system nor marry to western culture completely. Social dogma has led to
further exacerbation of dreaded diseases like HIV/AIDS and other sexual
transmitted diseases. The number of HIV cases is expected to be much
higher than the current ascertained figure in the country. Despite the
government‘s concerted effort, people are found to be less cooperative in
this context. Number of drug abuse among the young generation is
increasing rapidly (even if government cannot ascertain exact number). It
is also clear that using Marijuana1 plant as a drug is very common among
the Bhutanese youths.
Even though the country has small population, rural-urban migration is
another factor that poses a great threat to the health sector in Bhutan.
UNDP‘s HDR (2009) report states that the rural-urban migration in
Bhutan is the highest in South Asia. This is because many people move
from rural to urban areas in search of better lives. This again leads to
various unwanted diseases. Major challenges are faced mostly by young
male and female migrants who encounter difficulties of findings
employment, housing and educational opportunities as well meeting the
higher cost of living in urban areas. Those who fail to overcome these
urban challenges often resort to drugs and alcohol, and become
unproductive members of the society. The most vulnerable are the young
women who are at higher risk of exploitation and domestic violence
because of the lack of social safety (in urban areas) which otherwise is
present in their villages in the form of extended family. Of late, the
country has seen an alarming rise in the number of commercial sex
workers in towns and cities. This is one of the major factors of HIV/AIDS
problem in Bhutan.
Organism of Health Services and Delivery System
The Bhutan Medical and Health Council (BMHC) Act has been passed by
the National Assembly in 2002. The BMHC secretariat was established in
2003 with council members appointed. Health care is a public good and
completely free in Bhutan (Selvaraj and Lalitha 2007, SACOSAN 2008,
GNHC 2009). There is no private hospital or private medical practitioner

96
in the country (Nirola et al. 2006). While in neighbouring nations like
India and Pakistan, the healthcare costs, especially that of the private
healthcare services, are believed to be one of the main causes of
impoverishment (Berman et al 2010) , health care service in Bhutan,
delivered by two composite integrated systems-Modern and Traditional
medicines is free and comparatively cheaper.
The history of health services delivery in Bhutan is the introduction of
modern Allopathic system in early part of the twentieth century with the
arrival of the first batch of Indian-trained physicians and paramedics, but
its traditional Medicare was introduced in the system from Tibet in the
seventeenth century (Nirola et al. 2006). Traditional practitioners received
formal training in Tibet and apprenticed in Bhutan, despite the
introduction of western allopathic provision of health services in Bhutan.
As the traditional medicine practiced in Bhutan, Sowa Rigpa2, is a
systematic field of knowledge, traditional medical care is provided side by
side with modern allopathic health care (Nirola et al. 2006.) It was
recognised as the official medical tradition and included in the national
health system in 1967. The indigenous medical facility established in the
country is run under the Institute of Traditional Medical Services, and it
has basically three functions-medical services for out-patients; collection
and manufacturing of indigenous medicines; and research and training of
the Physicians (Drungtso) and Compounders (Menpas) (NSB 2008). Till
date, the country has one indigenous hospital (National Institute of
Traditional Medicine) and 21 indigenous dispensaries (Bhutan 2007-13).
Modern health services in Bhutan are delivered through a four-tiered
network consisting of the national Referral Hospital, the Regional Referral
Hospitals, District Hospitals and Basic Health Units to outreach clinics at
the community level. Health care is delivered in an integrated system, with
community-level basic health units (BHU) representing the initial point of
encounter for most patients. BHUs serve basically remote areas of the
country, and extended health centres- Out Reach Clinics (ORCs) and
Mobile Health Units (MHUs) support BHUs. Increasingly complicated
cases are referred to the Dzongkhag (District), Regional and National
hospitals, sequentially (Nirola et al. 2006‘ NSB 2008). The patients at the
BHU level are referred to their respective district hospitals for secondary

97
or tertiary health care. The district hospitals likewise refer to their
respective Referral Hospitals (RRHs). As it is not yet possible to have
very requiring such health care in the country, a good number of cases
requiring such health care are referred outside the country, especially in
India. As of 2007, there were 29 hospitals, 178 BHUs and over 519 ORCs
spread over 205 Gewogs (blocks) providing primary health care services
in Bhutan (NSB 2008).
In order to bridge the gap between the organised health service and the
community, the Government trains village health workers who are chosen
by the communities themselves. The Village Health Workers (VHW)
Programme was thus initiated in 1978. The VHWs are considered to be
the important link between the community and the Government in
improving basic hygiene and sanitation, prevention of vaccine preventable
diseases, family planning, nutrition, control of diarrhoeal diseases and
prevention of sexually transmitted diseases, including HIV/AIDS,
especially for communities that do not have easy access to health facilities.
As of 2009, there are 1500 village health workers, who advocate health to
the people and help in bringing the health problem of the people in the
communities to the government health workers. They are also taught and
allowed to dispense a few basic allopathic medicines. There are also the
traditional faith healers, astrologers and religious leaders in the
community.
The Ministry also takes the support of these respected people in imparting
specific health messages-ranging from the need to take iodized salt to
family planning to the people in the communities along with their routine
work. The communities also look after the development schemes like
those for drinking water supplies in their own areas. The programme
assists the communities by providing them necessary training.
Health Policy of Bhutan
In keeping with the principles of primary health care, it was seen
necessary to extend universal coverage of health services to the rural
population and encourage community participation in health activities and
awareness. To meet the need of ever increasing health care services, the

98
Royal Governments of Bhutan has announced a five year tax holiday for
the newly established pharmaceutical shops in the rural areas form 1st
January 2010 to 31st December 2015. Newly established high-end private
health services shall be eligible for 10 years tax holiday (EDP 2010).
Public health problems in rural areas have traditionally been associated
with poor hygienic conditions and a shortage of accessible health services.
Both of these root causes are currently being effectively addressed in
Bhutan with the establishment of well distributed health facilities in rural
areas, along with increasing numbers of health workers. Most of the
leading causes of death in Bhutan in the past were infectious diseases such
as diarrhoea, respiratory infections, tuberculosis and malaria (HDR 2005).
Realising the grave dangers and damaging effects of tobacco use on
health, longevity and quality of life, Bhutan has actively promoted anti-
tobacco campaigns at both national and international levels. The country
has won numerous commendations and awards for its efforts and was
among the first to sign the global Framework Convention on Tobacco
Control. On 17 December 2004, Bhutan became the world‘s first nation to
introduce a complete ban on tobacco also is now restricted to private areas
in many other countries of the world (HDR 2005).
The Royal Decree issued by His Majesty the 4th
King of Bhutan in 1992
declares water and sanitation as a basic right of all people of the country.
The Decree points out that every household in the rural areas should
construct sanitary latrine or at least a basic pit latrine, which does not have
major cost implication for the rural households (SACOSAN 2008).
In total government expenditure, health sector was carrying 12.2% in
2000. The Bhutan‘s health system as described by the WHO is ―one of the
best programs in South-East Asia,‖ and the country has won WHO 50th
anniversary awards for primary health care in 1998. Bhutan has limited
financial resources as per capita gross national product is about $ 875. The
main financial supporters to Bhutan are Denmark, India, UNICEF, the
UNPF, the World Bank and WHO. In 2004, the country spent 4.6% of its
GDP on health care with the government providing for 64.2% of that
amount according to the WHO. By comparison, India spent 5.0% of its
GDP on health while the government provided a far smaller share of that

99
amount (17.3%). The recent UNDP‘s Human Development Report (2006)
shows a life expectancy of 63.4 years, in India at 63.6 years, and
fractionally above compared to Bangladesh and Nepal. The percentage of
underweight children under 5 years of age is 19%; India‘s is 47%, with
Bangladesh and Nepal at 48%. According to UNICEF, the mortality under
5 years in Bhutan has been reduced by 55% from 166 deaths per 1000 in
1990 to 75 deaths per 1000 in 2005, and the numbers continue to drop.
Maternal mortality also dropped down to 400 per 1,00,000 live births in
1994 from 77 per 1,00,000 in 1984. India‘s maternal mortality ratio is still
floating around 400. According to UNCIF‘s State of the World‘s Children
2007, 95% of the households use iodized salt, compared with 57% in
India. Bhutan has the rate of immunization/vaccination of 93% for
tuberculosis, DPT, polio, hepatitis, and this rate is slightly better than
Bangladesh and well above the rate of India. In South Asia, only Sri
Lanka tops Bhutanese figures with near 100% immunization. According to
WHO figures, malnutrition in Bhutan is proportionately much lower than
in India and approaching the levels of Thailand. The household incomes of
Bhutan still remain the world lowest, but life expectancy rose to 63.6 years
from 46 years in 1984 to 20063.
Globally in 2006, expenditure on health was about 8.7% of gross domestic
product, with the highest level in the Americas at 12.8% and the lowest in
the South-East Asia Region at 3.4% (WHO 2009). In the finding of
Wagstaff (2005), Japan spends highest share of its GDP on health in East
Asia from 1998 to 2001, and Korea emerges as having a higher incidence
of catastrophic out-of-payments in the region.
While Bhutan allocated 8% of its 2008-09 budget for health services
(SACOSAN 2008). The Tenth Five Year Plan (2008-13) of country‘s
indicative total capital outlay for the health sector is Nu. 4394.336 million,
excluding Dzongkhag outlay for health programmes (GNHC 2009).
The main thrust of the health programs over the Ninth Plan period (2002-
07) was on the provision of primary health care services. Due attention
was also given to the relevant integration of traditional medicine services
with modern health services. Within the context of the Tenth Plan‘s (2008-
13) strategic framework, in addition to contributing to GNH and the well-
being of Bhutanese society, health is also viewed as an important
100
dimension of human capital. Health expenditures therefore are deemed to
be long term investments that are expected to provide both tangible and
intangible socio-economic returns. Additionally, continued reinvestments
into the health sector will also help protect other long term human capital
investments from erosion and enhance their impact considerably.
Reflecting this high priority, extending free basic health care has been
enshrined as a constitutional obligation. The Constitution mandates that
the Royal Government ―provide free access to basic public health services
in both modern and traditional medicines‖ and ―endeavour to provide
security in the event of sickness...‖ This constitutional commitment to
provide free basic health care for all Bhutanese has considerable positive
ramifications for the prospects of reducing both income and human
poverty in Bhutan. There is growing evidence in many countries that
health factors are closely linked to labour productivity and that
productivity gains are most prominent for those population groups with
the weakest health and nutritional status, which invariably constitute the
poorer sections of society. As such, health investments have the greatest
productivity benefits for and impact on the poor and low income groups.
Under the Tenth Plan, the Royal Government will continue to attach high
priority to maintain universal access to basic health services and ensure
that basic health services are distributed more widely throughout the
country, including the more vulnerable and isolated communities. In the
TFYP, efforts will be made to accelerate institutional as well as human
resource capacity to improve quality of service delivery, manage some of
the illness for which services are availed outside the country so far and
work in close collaboration with the Royal University of Bhutan and other
relevant agencies to increase the pool of trained health workers.4
The Policy Objectives of TFYP (2008-13)
The Constitution Mandates :
Ensure all Bhutanese have access to free basic health services for both
allopathic and traditional medicine;
Ensure efficient and effective management of the national health system
based on the tenets of quality , professionalism and equity;
Develop adequate and competent human resources to manage health
programs in line with global and national health targets and strategies;

101
Provide each Dzongkhag with at least three doctors;
Promote evidence based health planning and cost-effective interventions;
Prevent and control prevailing health problems through promotive,
preventive and rehabilitative public health services while ensuring access,
equity and quality;
Promote and enhance institutional delivery to reduce maternal mortality;
Provide each Dzongkhag with at least three doctors;
Advocate healthy lifestyle among the population;
Ensure quality delivery of primary, secondary and tertiary health care
services.
Conclusion
Despite the nation‘s weak physical infrastructure and limited manpower,
the health sector has made remarkable progress in all areas of health
developments over the last few decades since the modern health service
was introduced in the country. The Infant Mortality Rate has reduced from
102.8 in 1984 to 53.9 in 2008, and Maternal Mortality Rate has reduced
from 7.7 in 1984 to 2.55 in 2005. Population Growth Rate also has seen a
marked decrease from 3.1 in 1994 to 1.3 in 2008. The life expectancy at
birth has increased remarkably from 47.5 in 1985 to 65.53 in 2008. These
vital indicators speak well of the rapid development of health sector in the
country.
How is delivery of health care organised in rural Bhutan? With the limited
resources, a total of 90% of the population covered by effective health
services in the country is not an easy task. The secret of this achievement
in the health sector despite its limited resources in Bhutan is basically due
to the government‘s policy and the honest state functionaries on the one
hand and the people‘s support and reverence to the country‘s law on the
other. These two factors help in effective delivery of health services in the
country, while the achievement of this sector is comparatively lower in the
neighbouring nations like India.
Keeping health sector in the government‘s top priority agenda, the total
expenditures on health per capita was around 30 USD in 2004-05 rising to
around 50 USD in 2007-08 and as high as 70 USD per capita in the
2008/09 budget. This number, however, is inflated by the capital budget
102
that most likely will not be fully utilized. The corresponding numbers for
the recurrent expenditures are from roughly 20 USD to 35 USD.
Comparing the above figures to other developing countries of similar
income level, the level of health expenditure in Bhutan is definitely above
average, clearly showing the RGoB‘s willingness to invest in health.
Looking into the allocations to health in the 10th
FYP this trend continues
(RGoB 2009).
Nevertheless, the nation has to go a long way ahead in this sector. As on
the priority basis, Bhutan has to strengthen physical infrastructure and
manpower of this sector at the earliest possible time. Setting up of a
training institute, medical college is also an urgent need of this country.
References
Bhutan (2007-13) Bhutan Country Strategy Paper. http://ec. europa.eu/
external_relations/bhutan/csp/07_13_en.pdf (March 24, 2010)
Berman, P. et al. (2010) The Impoverishing Effect of Healthcare Payments in India- New
Methodology and Findings. Economic and Political Weekly, XLV (16): 65-71
Carolyn, S. and Harphan, T. (1992) The Measurement of Health in Household
Environmental Studies in Urban Areas of Developing Countries: Factors to be
Considered in the Design of Surveys. Urban Health Proramme. London: London
School of Hygiene and Tropical Medicine.
Dhargupta, A. et. al. (2009) Study on the Effect of Socio-economic Parameters on Health
Status of the Toto, Santal, Sabar and Lodha Tribes of West Bengal, India. Studies of
Tribes and Tribals 7 (1): 31-38
Economic Developing Policy (2010) Economic Development Policy of the Kingdm of
Bhutan. Royal Government of Bhutan. http://www.mti.gov.bt/Tender/edp-2010.pdf
(April 12, 2010)
HDR (2005) Bhutan National Human Development report, Royal Government of Bhutan.
IMF (2004) Bhutan- Poverty Reduction Strategy Paper. IMF Country Report No. 04/246/
(August)
Jha, N. K. et al (2008) Analysis o fIndo-Bhutan Socio-Political, Health and Economic
Situations. Sherub Doenme 8 (1 & 2): 78-91
Kumar, T. S. et al (2009) Oral Health Status and Practices of Dentate Bhil Adult Tribes
of Southern Rajasthan-India. International Dental Journal 59(30): 133-140.
Lantz, P. M. (1988) Socio-economic factors, Health Behaviours, and Mortality. Journal
of the American Medical Association (279): 1703-1708.
Mahapatra, L. K. (1997) Social change in Tribal Society in Eastern India- Supplement of
Professor Tarak Chandra Das‘ Analysis 1961. Journal o fIndian Anthropological
Society 32 (4): 201.
103
Ministry of Health (2008) Bhutan Health Information System- Review and Assessment.
Health Information and Research Unit- Policy and Planning Division, Royal
Government of Bhutan.
NSB (2004) Poverty and Inequality in Bhutan. Department of Planning (Ministry of
Finance), Royal Government of Bhutan.
NSB (2008) Statistical handbook of Bhutan. National Statistical Bureau, Royal
Government of Bhutan.
Nagda, B.L. (2004) Tribal Population and Health in Rajasthan. Studies of Tribes and
Tribals 2(1): 1-8.
Nirola, D. K. et al. (2006) The Impact of Community-oriented Primary Care in Trongsa
Dzongkhag, Kingdom of Bhutan. Indian Journal of Community Medicine (31): 18-
23. and Available from: http://www.ijcm.org.in/text.asp?2006/31/1/18/54925 (April
7,2010)
Royal Government of Bhutan (2009) Bhutan Joint Health Sector Review 2009. Ministry
of Health (Thimphu). http://www.health.gov.bt/reports/BhtJointSerctrReview
2009Rept. pdf. (April 08, 2010)
Selvaraj, M. and Lalitha, R. (2007) Environment, Demand for Health and Economic
Situation of Bhutan. Environment Informatics Archives, Vol 5, No. P002, page 700-
708 http://www.iseis.org/eia/pdfstart.asp?no=07074 (April 08, 2010)
SACOSAN (2008) Country Paper for South Asian Conference on Sanitation (Bhutan III),
18-21 November. New Delhi.
Tshering, D. and Sithey, G. (2009) Climate and Health in Bhutan. Tiempo, Issue 71
(April): 24-26.
Wagstaff, A. (2005) Health Systems in East Asia-What Can Developing Countries Learn
form Japan and the Asian Tigers?, World Bank Policy Research working Paper 3790
(December). The World Bank, Washington DC.
World Health Organisation (2003) WHO Country Cooperation Strategy-Bhutan
(January), WHO Country Office, Thimphu
World Health Organisation (2009) World Health Statistics. WHO, http://www.who.int/
whosis/whostat/2009/en/index.html (April 10, 2010)
Notes 1. The nature and usage of Marijuana plant can be studies more form the story of pop
star Bob Marley
2. The system of medicine referred to as Sowa Rigpa is practiced in many countries
today, but owing origins and development to ancient Tibet. Sowa Rigpa is known
nowadays as Tibetan medicine.
3. This section is excerpted from ―GNH, Health and Economic Status of Bhutan‖
[accessed on 08/04/10 and available at http: //www.gnhmovement.org/
papers/selvaraj.pdf]
4. See GNGC (2009) Tenth Five Year Plan (2008-13) Tenth Plan Document-Volume
1, GNHC, RGoB.
104
TRENDS AND DEVELOPMENT OF TELEVISION
ADVERTISEMENT IN BANGLADESH
Md Towhidul Islam1
Keywords: Advertisement. Abstraction. Subliminality. Pseudo-News. Attractiveness.
Abstract: The advertising industry has already passed four decades of
institutionalization in Bangladesh. At the advent of information and
telecommunications technology, the industry has experienced drastic
heave in all its vicinities such as the number of advertising agencies,
client firms, research organizations, models, production houses and
boutiques. By the way, the industry has influenced its surrounding
situations as well as adjusted to cope with the changed situation. Now it
is time to reconcile the progress and find out what it has achieved and
what yet to achieve. So far researches have concentrated on the
quantitative aspects of the industry but the qualitative appreciation yet
needs to be made. The academic and more esoteric developments have
remained less cared. This paper concentrates on the qualitative aspects of
the industry and marks the trends underway the advertising industry
while focusing on the future possibilities. Finally, it provides some
guidelines leading to an environment auguring well for the advertising
industry of Bangladesh.
Introduction
With continuous development of the size of the national economy of
Bangladesh, revolutionary ease of information and communication
systems, immense growth in the number and types of media and the
passage of time, the advertising industry here is also flourishing and
gathering multi thronged experiences. More and more ad firms of different
scopes and capabilities are joining the industry adding to the level of
competition. Genii from diverse areas of creativity are approaching the
industry with fresh talents befitting this informative and clever age.
1 Lecturer, School of Business Studies, Southeast University

105
Deeper penetration into the field along with greater mastery in the
technical fringes of the subject is adding to the proficiency of the industry.
In this small country, advertising has gone too far to create an example of
a folk singer-cum-model becoming a woman member of the parliament
(Bangladesh National Parliament Secretariat, 2009). All these facts
congeal to accentuate novel trends posing immense influence on the
culture of the nation. Some trends obviously pledge positive outcomes
while some others indicate a seizure of decadence. The growth and
potential of the industry places it in the interest list of scholars from
business studies and other fields. Business or monetary consideration of
the industry is already widespread while sparing a scope to view it from
the perspective of the art of advertising. Advertising is a kind of collage
art that makes scope for everything possible. So, it must not be considered
from monetary or structural perspectives only; rather it should be
evaluated from the perspectives of its internal aesthetics and apropism, its
adorable and abhorable effects on various segments of the population, its
ingenuity and ingeniousness, its distinctive nuances and detested
nuisances, its amity and enmity with societal forces. Above all, a holistic
evaluation should be made which is the motto of this paper. The paper
starts with a glimpse on the present state of the industry and concentrates
on the television advertisements as they create vicarious appeals to the
most of the sensory receptors of the audience and is putatively the most
effective advertising media since its inception (UTalkMarketing, 2010). It
takes into consideration advertisements from other media as well to
buttress the claims on trends underway.
Literature Review
Structure of the Industry
In Bangladesh, the size of the advertising industry is assumed to be
Tk.1200 crore (Rahman, 2010). Print media leads the industry with 43%
market share while TV stands second at 36% of the advertising market of
the country. The industry is growing at a rate of 10% per annum mainly
due to the heightened competition among the major mobile operators
(Rahman, 2010).
Before the independence, there were only a few advertisement firms in
Bangladesh, the erstwhile East Pakistan, due to inadequate industrialization
106
and limited demand for ads. The pioneers were the firm like Bitopi,
Asiatic, and Interspan who served the multinational firms like the Lever
Brothers (Anwar, 2009).
The advertisement sector is so vast in terms of nature of the firms, scope
of operation, registration status and other dimensions that it is so tough to
formally bring them into a database. Bangladesh Television shows a total
of 150 agencies in the country registered with them but the number
exceeds 500 when both the formal and informal sectors are considered
(Anwar, 2009). On the other hand, Bangladesh Yellow Pages registers a
total of 293 advertising and counseling agencies and firms today
(Bangladesh Yellow Pages, 2010).
Top nine advertising firms in descending order of market share- Adcomm,
Asiatic, Bitopi, Unitrend, Grey, Interspeed, Popular, Madona, and Matra
hold more than 70% of the formal market share while another 13% share
is held by other firms and the rest remains the domain of in-house
advertisements of business firms (Anwar, 2009).
Farhat Anwar classifies the advertisement media into two categories
namely- Above the Line and Below the Line. He includes in Above the
Line category the newspapers, magazines, radio, television, and satellite
and cable television while the Below the Line category includes event
management, in-house advertisement (company performing own advertisement)
at point of purchase, outdoor advertisement (billboards, hoarding, neon
signs, and bell signs), innovative activities (jatra, street drama) and
advertisement on vehicle bodies or fliers. The market size of the formal
advertising agencies accounted for about Tk.2 billion in 1999, while, in-
house and outdoor advertisements by manufacturing or service providing
companies and the informal agencies (non-registered agencies and
individuals) accounted for about another Tk1 billion.
The advertising agencies primarily serve the private national companies
(PNC), multinational companies (MNC) and non-government organizations
(NGO). The MNCs constitute more than 60% of the media share followed
by the PNCs constitute 25%. The major client of the print media is the
government (Anwar, 2009).

107
Monetary Performance
Bangladesh Brand Forum (BBF) studies and publishes quantitative data on
advertising spending by the companies or industries. It shows how the
industry is enlarging, how the spending shifts from one media to another,
one company to the other etc. In 2007, BBF showed the percentage of
advertisement placed in different types of media (The Daily Star, 02
March, 2008). It showed that the highest portion (43%) of advertising
went to the print media; TV covered only 36%, radio 4% and the rest by
outdoor, cinema and the Internet. They calculated a 7% increase of ad-
spending by major brands in 2007. They found out highest spending
companies in ten categories namely- telecom, bank, real-estate, education,
soft-drink, mobile-handset, personal-wash, electronics, shampoo and
snacks. It estimated that the top ten categories of industries comprised
almost 80% of total media spending that year.
Frequency of Exposure
In Bangladesh, institutions like ‗Dhaka News‘ and ‗Ryan‘s Archive‘ and
many others are doing some important work on capturing and analyzing
the advertisements and news on both news-papers and TV channels.
Dhaka News disseminates news on advertising expenditures of different
mobile phone companies of Bangladesh in 2010. It claims TV commercials
to be the most expensive form of advertising in the country (Rahman,
2010). It finds out that ‗Robi‘ surpasses Grameen Phone in July, 2010. It
also analyses the plausible reason behind the substantial increase in the
company‘s ad expense.
Ryan‘s Archive provides information on rate, time, and composition of
advertisements in different print and digital media in Bangladesh. This
archive makes available information on program rating, audience rating,
data on TV commercial monitoring and other services.
Rationale for the Research
Prior to this paper, others have ventured to analyze the background and
structure of the industry and to spot the monetary matters like expenditure,
income, market share, growth rate and the like. Yet others have been

108
trying to interpret the frequency of exposure, program rating, number of
audience etc. All these efforts serve to reveal the overt factors of
advertisements. But some of the softer, non-monetary and more esoteric
affairs of advertisements have gone unrevealed. Certainly, there is a
research gap in that the academic areas such as the factors related to
source attractiveness and credibility, abstraction of message, subliminality,
advertising influence on culture etc still remain unrevealed and unevaluated.
However, the evaluation cannot reach fulfillment until a total appraisal is
made. This paper attempts to bridge the gap.
Objectives of the Study
This paper aims to mark the recent trends in the advertisement in
Bangladesh. More specifically, it wants to spot the academic distinctions
made in the advertising arena of Bangladesh. Depending on the recent
trends and distinctions, the paper intends to project future possibilities with
caution. It intends to discern out a career path taken by the advertising
personalities. Finally, the paper undertakes to suggest some guidelines to
further upgrade the level of advertising of the country and to promote the
entire marketing environment by ensuring that all the stakeholders of the
industry can be benefited.
Methodology
At first, the ad clips from various TV channels are recorded with the help
of an internal TV card installed onto a personal computer. Then only those
clips with some considerable distinctions are spotted for analyzing. The
distinctions, either drastic or not, are enumerated under the headings such
as nuances, subliminality, shortcomings etc. Alongside, the whole range of
advertisements on the billboards and newspapers throughout the year 2008
and 2009 are observed and analyzed for distinctions. Important trends are
spotted and afterwards more ad-clips are recorded and analyzed to
highlight and accentuate the trends. No hard and fast calculations are
carried out. All is considered from a holistic, all encompassing view.

109
Findings and Discussions
Attractiveness Prevails over Credibility of Sources
Majority of the advertisements cast beautiful and attractive models rather
than the knowledgeable and experts. In fact, there are shortages of
celebrity experts in the fields of sports, culinary or engineering. Famous
culinary experts like Siddika Kabir, Keka Ferdousi, royal cook Tomy
Miah, hair expert Jawed Habib, cricketer Sakib Al Hasan, Masrafee, are
but a few. There is dearth of celebrity experts in most other fields. The
areas of health, sports other than cricket, news anchors, professionals in
teaching, dentistry or cardiology, organizational heads and others have
remained uncared and unexplored. Consequently, the ad-agencies are to
resort to the attractive models. These models in turn enjoy some sort of
transcendence and secularity with respect to the variety of product they
endorse for.
Abstraction of the Content from the Intended Message
Among the nuances in the Bangladeshi advertisements is the abstraction of
the content from the intended message. There come some advertisements
where logical claims or claims on products‘ superiority that the ads intend
to communicate never get voiced. Rather, there is an effort to create an
impression only. These ad-clips are relatively longer and relates to the
deep-set human feelings like patriotism, fraternal longing and affection,
freedom etc. For example, an ad-clip shows some children stealing flowers
from a garden early in the morning. The owner of the garden chases them
out of the garden. Later, to his utter astonishment the garden owner
discovers that they are making a replica of the Shahid Minar, the
monument resembling the martyrs of the great language movement, on
which they yearned to put the garlands of flowers as a mark of tribute to
the martyrs. Then he felt sympathetic and he himself brought garlands to
them. The scene with its serene morning panorama creates patriotic
feelings in the audience. At this very last moment the name of Grameen
Phone is just pronounced once; nothing is said about the product nor is
anything claimed. Many other clips fall in the category as in a piece where
a middle aged woman laments over the faded memory of her younger
110
brother, with his photograph in her hand, whom she left beyond a river
bank, in a dark night, in the rush days of the Independence War in 1971. A
message of condolence goes for all such aggrieved souls losing their dear
ones in the liberation war. At the very end of the scene, the company name
is quietly but clearly pronounced. Again, nothing is said about the product
nor anything claimed.
There is a notable effort from the ad-maker to apply classical learning by
casting before the audience a series of such abstract advertisements so that
they can learn to relate the advertisements to the sponsor company. All
companies cannot afford to air this type of long advertisements. Grameen
Phone, Bangla Link and other large revenue companies only step into such
ventures.
Subliminality Introduced to Advertisements
The concept of subliminal effect was first introduced in marketing by
market researcher James Vicary back in 1957. It is a proof of advancement
in advertising in Bangladesh that advertisers successfully use the concept
to create deeper imprints on audience psychology. Take for example the
advertisement claiming ―Alo ashbey‖, that is, ―light will come‖. The
advertisement re-iterates the only claim-―light will come‖ with an elusive
and deep tone redolent of something vital, more than ordinary. In
coherence to the profound tone, blurred and sublime arabesques of female
figures go on eloquently dancing and whirling with the indicative mode of
liberty of women power. Other subliminal effects like subdued voice,
songs for arousal, hypnotic poses are also in practice today.
Over-practice of Colloquialism
The advertising industry is not beyond the ambit of linguistic decadence
observed in Bangladesh. Almost all the media are using aberrant forms of
Bangla language. Vernaculars from the districts of Barisal, Noakhali,
Magura, Pabna and those from the older part of Dhaka city are endemic in
advertisements for different products. Almost invariably, these colloquies
assume some sense of humor that amuses people but the practice veritably

111
mars the linguistic knowledge base of some sects of people. Specially, the
youngsters are the most vulnerable to this malpractice. Even the students
are speaking the nonstandard forms of Bangla.
Use of Direct vs. Indirect Source/Spokesperson
Many of the advertisements exhibit the use of models who do not convey
any verbal message; rather they just appear to embellish the ad ie as
indirect sources. Female models are more frequent as indirect sources.
Appearances of pairs are also common as indirect source. The castings of
indirect sources in couple to adventurous or romantic settings are often
irrelevant to the products of interest.
Career Path of Modeling Interwoven With other Industries
The artistes have been seen to beat an apparent path consisting of some
sequential footsteps in their career. A close observation of the creative
thinkers, copy-writers, illustrators, models, producers, media planners and
others of the like may reveal a clear course of expected positions
motivating and leading these professionals at different stages of their
career. However, the path is woven into other industries in Bangladesh.
The career track has become conspicuous starting with a model and
continuing up to a film producer and beyond, to some self-actualizing
position in the state mechanism. Lately, it has become a frequently
observed phenomenon that novices start career as models in an
advertisement clips. Then they are promoted to play a role of minor
characters in some TV plays and upon rendition of several successful
episodes, get established as professional/affiliated models in
advertisements as well as characters in TV plays. Then they wait for the
auspicious moment to do something legendary in advertisements or in
short films. Afterwards, they aspire to produce ad-clips on their own and
yet later, to become a film producer or director.
Obviously, the younger performers are meticulously pursuing the course,
though not all. They seriously strive to take modeling as sole profession
but small and irregular pay makes it necessary to take it as part-time

112
(Shehreen and Karim, 2010). The following table summarizes the present
status of the media personalities in their career.
Table: Career Paths of Ad Personalities
Afjal Hossen: Character in TV play → Ad Producer → Character in move
Afsana Mimi: Model in ad clips → Character in TV play
Api Karim: Model in ad clips → Character in TV play
Apurbo: Model in ad clips → Character in TV play
Asaduzzaman Noor: Cultural worker → Character in TV play → Producer → an MP
Bipasha Hayat: Model in ad clips → Character in TV play → Co-producer of TV play
Dighi: Child model in ad clip → Character in cinema
Ferdous: Ramp model → Hero in movies → Intends to produce films in future
Mahfuj: Character in TV play → Intending to produce films
Masud Hassan: BBC reporter → Actor in short film and TV play → Ad modeling
Mim: Child model in ad clip → Character in TV play
Momotaj: Folk singer → Model in ad clips → Member of Parliament
Mou: Model in ad clips → Character in TV play
Romana: Model in ad clips → Character in TV play
Tania Ahmed: Model in ad clips → Character in TV play → Producer
Tinni: Model in ad clips → Character in TV play → Affiliated model
Source: Websites, TV channels and newspapers of Bangladesh in 2008, 2009
Directing or producing films earns them much renown and almost all the
times it becomes their life passion. At the same time, they make ad-clips
on commercial basis now and again. Models in advertisements promoting
their career to TV play to short films to cinema; then directing a piece of
ad then play then film industry and so on.
A simple diagram as follows may depict the trend-
Child
model in
radio or
TV ads
etc
→
Model in ad-
clips, or
actress in
short film or
TV plays
→
Model
affiliated
with a
commercial
→
Ad-clip or
short film
producer
→
Film
producer
or
director
→
Positions
in the State
mechanism
Figure: Career trend of ad models

113
A Sense of National and Individual Freedom
Very recently, it has become vividly conspicuous that the advertisements
are rich with a sense of independence. The most noticeable is that,
‗Jagoroner Gann‘ (reviving songs) is a buzz in the entire environment of
advertising. The telecommunications companies of Bangladesh are doing
a good thing to promote an environment auguring well for the sense of
independence. Individual freedom and self-establishment is also expressed
through recent advertisements. As already said, personal achievement,
self-consciousness and other individualistic attributes in advertisements
express a sense of personal freedom.
Exchange Relationship of Advertising with the TV, Cinema and
Choreography
There have been noticeable exchange relationships of the advertisement
industry with TV, short film and cinema in Bangladesh. As the artistes in
TV, cinema and short films are to play vital roles in creative works,
expressiveness, production, and presentation along with linguistic and
literary levels a bit similar to those necessary for advertising, they
naturally acquire the essential qualities required in the advertising
industry. The exchange relationship among these industries is easily
observed in the practices like use of common models in advertisements,
TV plays, short films and cinemas; the evolution of models to ad-
producers to film developers, and so on.
Most of the famous people in the arena are common assets to all these
industries. Mostofa Sarwar Farooki is not only a successful ad-producer
but also a producer of TV plays and the trendsetter in the present day
Bangla telefilm. Tinni is not only a super model of Bangladeshi
advertisement but also a star of TV plays. Mou was not merely an
affiliated model with Keya beauty soap; she is a master dancer indeed.
Affiliation with the Journalism Industry
The advertising industry in Bangladesh gets sincere cooperation from
journalism as an industry. All the daily newspapers along with many other
periodicals have daily or weekly pages dedicated to anchor the news and
114
pictures of advertising industry. They employ reporters and
photojournalists to that end, who are experts in reporting on such an
industry. They feel the pulse of the audience and tailor the stories to the
audiences‘ psyche. Many of the budding models get introduced to the
audience and readers through these pages.
Innovativeness
The audience has already noticed that advertisers have gone far to search
for space for ads not only physical but also digital. However, some
innovative efforts attract amazement like the TV or radio news headings
named after a commercial; the advertisers even buy TV news intervals for
promotion. It was quite novel in Bangladesh that a newspaper can use a
cover page for advertisement. The daily Prothom Alo introduced special
cover page advertisement for the City Bank when it fetched American
Express back to Bangladesh again.
Advertising in the coming days may easily enter in line with and fitted
within the daily soap or mega serials. The artistes of the daily soap or
serials will suddenly start acting ads without any type of notice to the
audience. The customers will cope themselves to the new situation and
take it for granted as they did with the intervention of the ads previously.
Not only Communicative but also Recreational
Now the advertisements not only communicate a piece of product
information but also provide the audience with much amusement and fun.
Mahfuz Ahmed, a famed actor turned director of TV play and producer of
TV ads evaluates the works of his predecessors in this way- ―Amitav Reza
and Mostofa Sarwar Farooki have heralded a distinctive dimension to the
ad-clips; now the audience even enjoys the ads. They do not seem to be
merely 30-40 second ad-clips, rather resemble complete cinemas‖
(Prothom Alo, 2009).
The claim appears correct when we see the ―Nana-nati advertisements‖
(the grand father and his grand son). They are really humorous and witty.
A Keya Ball soap advertisement cast in a setting of an election campaign
depicts a candidate to the chairmanship of Union Council feels
115
embarrassed at the brighter presence of an aide clad in a shirt whiter than
his one. Incidentally, the shirt was washed with Keya Ball soap. The facial
expression and comical threat by the candidate to his aide in the ad-piece
create much fun and enjoyment among the audience.
Motive of Making ads
The interest in making ads emanates from diverse drives. Some make ad
out of passion while others want to have a tap on creativity and production
before trying something greater. Mahfuz Ahmed says on his launching of
first TV advertisement, ―My ultimate goal is film-making. Preparing for
that, I am regularly making plays and this time I have made some
advertisements to that end.‖ (Daily Prothom Alo, Friday 6 March 2009).
On the other hand, Mostofa Sarwar Farooki is a reputed TV play and
short-film maker who produces ads often on passion.
Influence on Culture
Cultural elements put forward by advertisements today are confidence,
competition, individualism, freedom of women, self expression, self
establishment, hedonism (the eat-drink-and-enjoy stance of life), beauty-
consciousness, loquaciousness, romance etc. In the heart of today‘s
advertising industry infests greed, selfishness, ostentatiousness and
voracity. Actually, the desired qualities like fellow feeling, caring and sharing,
donating etc are nearly absent in today‘s advertisements; and though
visible ever, swallowed up and overwhelmed by the aforesaid maladies.
In addition, there are some advertisements promoting bohemian and
vagabond lifestyles. Grameen Phone promotes the urge- ‗Harie Jao‘ by the
juvenile models with abnormal lifestyles and bizarre dress-ups, which
seems to be a sinister call for the juveniles to a disastrous loss in an
ominous future. The dream of a future generation full of innocence,
responsibility, respect, study, knowledge and patience is totally
disappearing.

116
A Shift in Sponsorship
Advertising has remodeled the form of patronization today. At present,
commercial undertakings have replaced the royal patronizing authorities.
There was a time when ancient kings in Bangladesh patronized the
contemporary cultural and literary works with expense from the public
exchequer. They enthusiastically commissioned considerable amounts to
keep ‗shwabha kobis‘ (poets of the royal court) and bhars (the comedians)
in the royal palaces. Biddapoti embellished the position of ‗the poet of
Royal court of Mithila‘ under the reign of King Shibsing who awarded
Biddapoti the soubriquet ―Kobikonthahar.‖ Zamidar Roghunath
patronized the poet Mukundaram who wrote ―Chandimongol‖. Raja
Krishna Chandra Majumder patronized the poet Bharotchandra who wrote
―Biddasundor‖ and the poet was entitled ‗Raygunakor‘. Magan Thakur,
the prime minister of Arakan, placed poet Alaol at a highly respected seat
in the palace of Arakan and thus he could cotribute to the rich translated
literatute of Bangla in the middle ages. The ruler Rokonuddin Borboksha,
Ashraf Khan and many others also patronized our ancient poets and
kabials (bards). The ancient rulers Paragal Khan and Chuti Khan
patronized the great literary work Mahabharat by Kobindra Poromeshwar
and Srikor Nondi respectively in the middle ages.
Now, in the changed circumstances, national and multinational companies
are sponsoring various cultural programs. Everyday numerous concerts,
musical soirees, exhibitions, model hunting competitions, sport events etc
are taking place, backed by the sponsorships of companies. ‗Jui‘, a brand
of coconut oil, presents the recently released romantic cinema ‗Monpura‘.
Among the talent hunting programs, the Lux-Channel-i Superstar, ATN
Bangla Trokader Taroka, and Close-up-One on the ntv are some examples.
Managers of all the cricket, football, tennis and hockey matches take
special efforts to collect sponsorships.
Advertisements Turned Pseudo News
It is a very common experience to see pieces of news on the TV and come
up to features in the newspapers that bear no news value on their own
merit. They are technically placed in the flow of other news items on the
117
TV, radio or newspapers with the same natural tone of news so that the
audience takes it as news. Consider a news item on the TV that informs
that a private commercial bank opened a new branch somewhere in the
country and Mr X or Y of the management was present in the occasion.
The piece takes considerable time, far more than usual, to show the video
footage of the occasion and broadcast the recorded part of the speech by
the top management personnel. The fact is that, in Bangladesh branch
opening of different banks is a commonplace event that does not deserve
so long airtime. The same news comes in the newspapers on the following
day with sizeable space for photographic and text description.
Nevertheless, the audience cannot imagine that the entire story is paid for.
The situation resembles what the theorist and historian Daniel J. Boorstin
calls ―pseudo event‖ in one of his famous books (Boorstin,1992).
Therefore, the same news turned advertisement can easily be labeled
―pseudo-news‖.
Month and Time Based Surfeit
The industry exhibits a glut of fresh advertisements on some occasions
round the year. December, the month of victory in the fight for national
freedom, brings a row of advertisements marking victory and frenzy;
March, the month of independence, provokes an array of ads colored with
freedom and national appreciation. February, the month of language,
prompts free music and advertisements redolent of the Language
Movement. Two Eids, Puja ceremonies, sultry summers, bleak winters,
festive parliamentary elections etc turn to be good reasons to induce
streams of theme-based advertisements.
Nuisance of Advertising
Advertising also creates nuisance today. It encroaches all the openness of
the city, pollutes sound by new video display units placed at the shopping-
hubs. Some below-the-line advertisements are rampant, creating public
nuisance. They are not in the least fact-checked. Handouts and slips likely
to promote the sex pills, herbals etc are often thrown into buses through
the windows to the annoyance of the passengers.

118
Distinctive Nuances
Many of the advertisements exhibit constructive nuances contributing to
the body of Bangladeshi advertisements. ‗Fair & Lovely‘ empowers their
customers with the ability to become ‗fairness experts‘ themselves.
Advertisement of ‗Doctor Milk Candy‘ embraces characters from ‗Ek Dui
Tin Sisimpur‘, a popular TV-serial for children. ‗Wheel‘ introduces a
‗whiteness scale‘ to enable the customers to compare whiteness with.
‗Asian City‘, a construction firm, metes out fresh humor amid the
customers by incorporating a Bengali proverb ‗Nake tel die ghumao‘
tapping linguistic resources of Bangla literature. Many of the recently
released advertisements by the phone companies like Grameen Phone and
Banglalink do exhibit excellence in emancipating people from prejudice,
ignorance and lack of information. They empower their customers through
information.
Flaws and Faults
The advertisements recorded and analyzed revealed some flaws and faults.
Even the lay audience can sense them with common sense. In addition,
some are subjects to esoteric interest and deep understanding of the
subject. ‗Aktel‘ associates a picture of a huge elephant to convey the
message that ―patronizing ‗Aktel‘ is not as costly as tending an elephant‖.
However, it clearly violates the general norm of positive/direct
communication for good news. The billboard advertisement prompts to the
customer at first sight that ―the product is as costly as tending an
elephant‖; which is contrary to the intended message. Here, nonverbal
message (the picture) contradicts the written message. ‗Brittle Biscuits‘
intends to introduce a buzz ‗khaite khaite jai bela‘, that is, ‗time passed on
munching (biscuits)‘. However, in Bangladeshi culture, it hears odd if one
speaks of passing time on biscuits. It exemplifies an inappropriate
association. The expression seems appropriate to items like chewing gum,
chanachur, baked dals and peas etc. ‗Surf Excel‘ influences children to
deliberately get sullied or to draw, scratch or stain onto the interiors of
their home in order to do ‗darun kichu‘, indicating some thing excellent in
future. In reality, children can and do many excellent things in cleaner
ways. There is little need to filthify or tarnish the clean ways of learning
and living.

119
Impact on Children
Television advertisements teach children many bad habits that are contrary
to the sense of sound life. Our school texts teach children to have all types
of food items with due zeal whereas television advertisements influences
them to be choosy and problematic for the parents. ‗Eldomilk‘ shows a
boy child thrust out his mouthful of rice awkwardly and claim ‗khabo na‘,
meaning ‗I will not eat‘. It categorically violates the norms promoted in
the school texts. Another ad shows a mother who claims in a ‗Pran Orange
Juice‘ advertisement that oranges are sour and her child does not eat
natural oranges. Rather she is happy that her child drinks ‗Pran Orange
Juice‘. The reality is that the juice is packed with much preservative
dangerously harmful for the kidneys of the children. At the same time
Bangladeshi market environment is infested with unbridled adulteration
(Khan M. A. 2010). Children are sometimes depicted as greedy and
selfish. An ad for a potato-cracker encourages them to lock the door to
enjoy it alone. On the other hand a girl child model increases her friends
by distributing her chips and crackers. Clearly, one promotes selfishness
and the other openheartedness.
Prospects of Advertising in Bangladesh
Learning From More Mature Cultures
The industry is going on learning many things from more mature markets
and nations with long heritage of rich culture as Mostofa Sarwar Farooki
gets inspiration from the famous Iranian film producer Abbas Kiarostami.
The trend to follow Indian advertisements in Bangladesh will continue as
is true in the case of TV serials.
Digitization of Advertising Media
The industry will gradually shift its base to more digital communications.
Mobile, broadcast TV and Internet advertising will mar the growth of
mass media based advertising on TV, radio, newspaper, and magazine as
evident in western countries.

120
Increase in Niche Advertising
Niche advertising swells at the presence of well-defined and well-
distinguished social groups. Social media and social networking sites as
these networks usually connect smaller groups of people but clearly
defined and similar in nature as customers. Networks like ‗facebook‘ are
very popular and pools friend groups who interchange almost all thoughts
and share practical problems of daily life. Therefore, marketers will try to
knock such cost-effective, self-motivated niches. Members of the group
generally greet information from these sites more cordially and without
any business mentality.
Emergence of Freelancers
Companies will arrange competitions for the business students and
creative people of different fields to conceive innovative ideas and buy
them with instant cash and thus reduce their agency cost. Already, a group
of business students from different private universities have mastered
some technological skills to use sophisticated instruments to make
advertisements. Some of them have learnt how to conceive the innovative
ideas that get noticed. So it can be avowed with some assurance that
freelancers will boom.
A Bulging Industry
At present, the Tk.1200-crore-industry is booming at the rate of 10% per
year; the credit goes to the intense battle among the major phone
companies over winning customers (Rahman, 2010). The trend says there
will be more academic excellence in advertisements, more application of
psychological methods and conditioning. Advertisements will be still
more of fun and enjoyment. Number and types of advertising will bulge in
the coming days. Customers will gain pleasure from them but will
remember only those with greater psychological impact.

121
Demand for Full Service Agencies
In the face of heightened competition, companies will spend more on
promotion. They will make binding relations with the full service
agencies, not only for advertisements but also for other forms of
promotions, especially online promotions. As the trend of publicity is
already on, some portion of the advertising budget will be allocated to the
favorable depiction of the marketer or the products through indirect
methods like coverage in reports, magazines, films, TV plays, sponsorship
of events etc.
A Complete but Interwoven Career Path
The careers of majority advertisement personalities will follow the path
portrayed earlier in this article whereas experts from other fields will fetch
breakthroughs to the industry. Therefore, advertising will always be a
career interwoven with other highly expressive areas. The industry will
next search for experts in all walks of life. The transcendence of the
attractive models will be affected once experts in other fields realize their
potentials in advertisement just as the case of Bangladeshi cricketers
today. Competition will ease out much of today‘s inequities and
irregularities of payments and honorariums to the artists and models.
Advertising in education
Media and advertisement courses will open a door to private universities
just in the same way as journalism has given an opportunity to them in
Bangladesh. As already stated, business students of this digital age are
very alert and creative. They are very much eager to take the challenge of
creativity. The universities also will come forward to satiate the demand of
the day.
Conclusions and Policy Implications
Pursue Academic Depth
Advertisers should explore deeper in academic areas like sources from
different new fields, novel dimensions of credibility, trustworthiness and
attractiveness, message formats, new aspect rational and emotional appeal,
122
various execution styles, subliminaity, refutation, sidedness, contrast,
comparative advertisement etc. in this way they can easily avoid the
humdrums of traditional ads and attract audience more efficiently.
Reduce the Use of Indirect Sources
Advertisements in the country have long been under the spell of beauty
girls and fashion forward males. It seems that the people involved here
considered only the ‗likability‘ feature of the models. Actually, the use of
indirect models in ads is somewhat akin to the use of passive sentences in
a piece of business writing; both being boring to the audience. However,
recent advertisements have shown that persons severely lacking beauty or
likability may well prove apt/attractive to the audience by dint of
‗familiarity‘ to and more specifically ‗similarity‘ with the audience. The
use of an unfamiliar and undersized young male model in the role of
varsity-admission seeking student in a Grameen Phone ad made the clip
the most attractive. Similar other pieces prove that the industry, today, can
replace the use of indirect models for attractiveness with other models apt
for the situation.
Digitally Tap the Untapped Talents
Advertisers should utilize information technology to tap the creative
power of unfamiliar but genuine talents who are less cared and
unevaluated. These people may remain unexplored in all walks of life.
Students often do not find any scope to vent their creative ideas generated
in their course works. This digital age provides them much opportunity to
be creative but their ideas do not see the auguring face of fruition in
practical field due to the absence of opportunity.
Regularize Remuneration
The models and creative personnel work under pressure, as they do not
have regularly salaried jobs. If they have permanent jobs, modeling is
secondary. Therefore, they cannot give full concentration to their creative
work. Advertisers must ensure their regular remuneration to ensure quality
work.
123
Fetch Inter-disciplinary Cooperation
Inter-disciplinary cooperation must be encouraged to enhance advertising.
In fact advertising is like a form of collage art that makes room for almost
everything real, unreal or surreal. It offers an ample opportunity to
intermingle literary lucidity, historical evidence, fictional fantasy,
scientific precision or universal truth. Creative people from all academic
areas should be fetched to enhance the industry.
References Akter, S. (2008) Telecom operators‘ battle fuels increase in advertising spend. The Daily
Star, 02 March, Business Page
Boorstin, D. J. (1992). The Image: A Guide to Pseudo-events in America. Vintage.
ISBN:0679741801
Bangladesh National Parliament Secretariat. (2009). List of MPs in 9th
National
Parliament of Bangladesh.
http://www.parliament.gov.bd/9th_Parliament_MP%20List.pdf (January 23, 2010)
http://www.bdyellowbook.com/catalog/Business___Services/Advertising_Agencies___C
ounselors/ (February19, 2010) Bangladesh Yellow Pages.
http://www.dhakanews.info/share-of-television-advertisement-robi-crosses-grameen-
phone%E2%80%99s-cost-on-tvc/ (August 20, 2010) Rahman, M. (2010). Share of
television advertisement: Robi crosses Grameen Phone‘s cost on TVC. Dhaka News
(July 26, 2010).
http://www.utalkmarketing.com/Pages/Article.aspx?ArticleID=14500&Title=TV_is_mos
t_effective_advertising_medium_ (January 20, 2010) UTalkMarketing. (2010). ―TV
is most effective advertising medium‖. Industry Research.
http://banglapedia.search.com.bd/HT/A_0049.htm (March 09, 2010). Anwar S. F. (2006).
Advertising. Banglapedia.
Prothom Alo (2009) Bigyaponchitro Nirmata, 06 March: pp 22.
Shehreen, I. K., Karim, E. (2009) ―Facing the Spotlight‖. Stories Behind the News. The
Daily Star, 25 December
Khan, M. A. (2007) Inverse Relationship Between Price and Adulteration. The New
Nation, 20 November
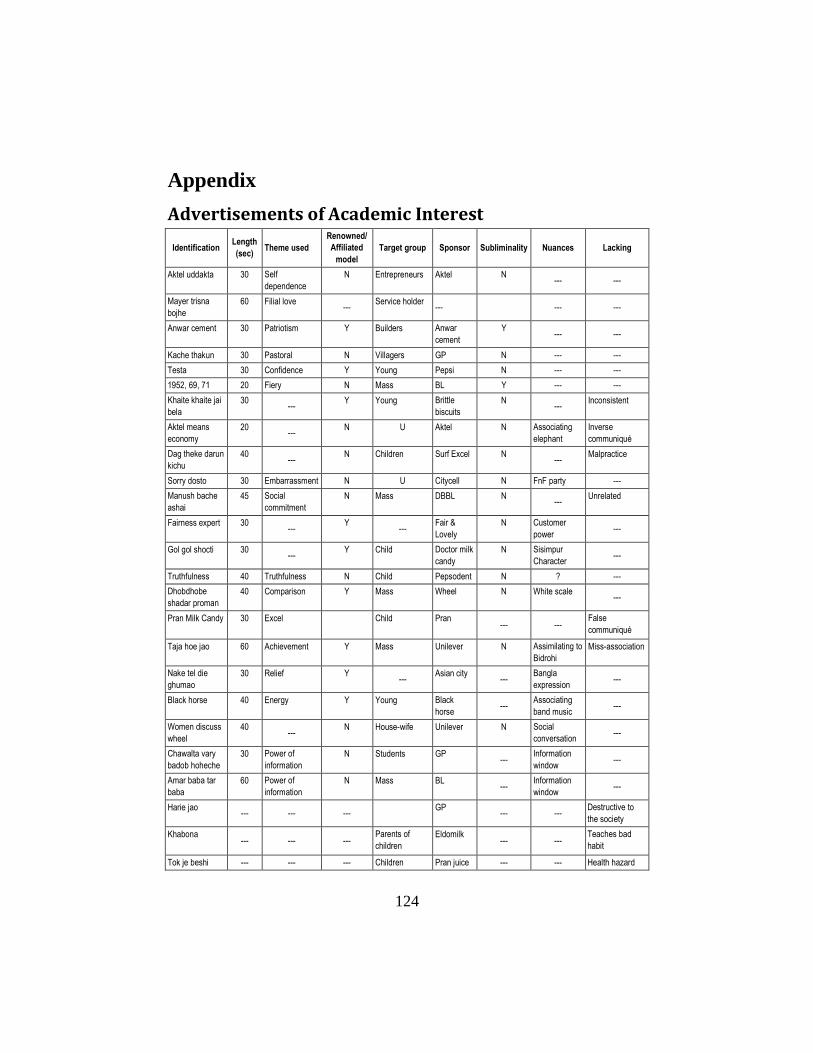
124
Appendix
Advertisements of Academic Interest
Identification Length
(sec) Theme used
Renowned/
Affiliated
model
Target group Sponsor Subliminality Nuances Lacking
Aktel uddakta 30 Self
dependence
N Entrepreneurs Aktel N --- ---
Mayer trisna
bojhe
60 Filial love ---
Service holder ---
--- ---
Anwar cement 30 Patriotism Y Builders Anwar
cement
Y --- ---
Kache thakun 30 Pastoral N Villagers GP N --- ---
Testa 30 Confidence Y Young Pepsi N --- ---
1952, 69, 71 20 Fiery N Mass BL Y --- ---
Khaite khaite jai
bela
30 ---
Y Young Brittle
biscuits
N ---
Inconsistent
Aktel means
economy
20 ---
N U Aktel N Associating
elephant
Inverse
communiqué
Dag theke darun
kichu
40 ---
N Children Surf Excel N ---
Malpractice
Sorry dosto 30 Embarrassment N U Citycell N FnF party ---
Manush bache
ashai
45 Social
commitment
N Mass DBBL N ---
Unrelated
Fairness expert 30 ---
Y ---
Fair &
Lovely
N Customer
power ---
Gol gol shocti 30 ---
Y Child Doctor milk
candy
N Sisimpur
Character ---
Truthfulness 40 Truthfulness N Child Pepsodent N ? ---
Dhobdhobe
shadar proman
40 Comparison Y Mass Wheel N White scale ---
Pran Milk Candy 30 Excel Child Pran --- ---
False
communiqué
Taja hoe jao 60 Achievement Y Mass Unilever N Assimilating to
Bidrohi
Miss-association
Nake tel die
ghumao
30 Relief Y ---
Asian city ---
Bangla
expression ---
Black horse 40 Energy Y Young Black
horse ---
Associating
band music ---
Women discuss
wheel
40 ---
N House-wife Unilever N Social
conversation ---
Chawalta vary
badob hoheche
30 Power of
information
N Students GP ---
Information
window ---
Amar baba tar
baba
60 Power of
information
N Mass BL ---
Information
window ---
Harie jao --- --- ---
GP --- ---
Destructive to
the society
Khabona
--- --- ---
Parents of
children
Eldomilk --- ---
Teaches bad
habit
Tok je beshi --- --- --- Children Pran juice --- --- Health hazard

125
‗MONGA’- A SEASONAL FOOD INSECURITY AND ITS
IMPACT ON POVERTY IN BANGLADESH: A LOCAL
ISSUE IN NATIONAL PERSPECTIVE
Profulla C. Sarker1 & M. Abul Hossain Sikder
2
Key Words: Monga. Food Insecurity. Mechanism. Poverty.
Abstract: This paper discusses the concept of ‗monga‘ and identification of
location of ‘monga’ in geo-social settings. This paper also discusses the
incidence of ‘monga’ in an analytical framework along with the main victims
of ‘monga’ and how it affects the life and society of the people in relation to
poverty. The main objectives of this paper is to examine the mechanisms that
have already been applied by the poor to exist in this crisis situation and the
services available by the GOs and NGOs to prevent as well as to reduce
poverty as a local issue in national perspective.
Introduction
The economy of Bangladesh is largely dependent on agriculture. About
21 per cent of the gross domestic product (GDP) and 23 per cent exports
of the country come from agriculture. It provides employment for about 60
per cent of the total labor force and it seems to have managed to feed 160
million people of the country. Access to land and livelihood is a crucial
factor for survival of the rural poor (BBS 2009). Hartman and James
(1979) emphasize the importance of land ownership in Bangladesh and
rightly point out that land determines who eats and who does not. Land is
a crucial asset for food production and a means for food, shelter and many
other economic activities including guarantor of employment opportunity.
Land ownership is, thus, an important contributor to food insecurity and
restricted livelihood opportunities leading to an ultimate cause of poverty
(Barkat et al. 2007). Historically, the ‘monga’ affected region was never a
food-deficit. Now this region is considered food deficit, because it is
1 Professor & Vice Chancellor, Prime University
2 Professor and Vice Chancellor (Acting), Atish Dipankar University of Science and
Technology

126
within the vulnerable grip of the mighty rivers viz. Padma, Jamuna,
Teesta, Jamunashwari, Dud Kumar, Darla etc. and as a result agricultural
production largely depends upon the adverse effect of climate change and
natural disasters.
The term ‗monga‘ is used during the food crisis in northern Bangladesh
which covers five districts viz. Rangpur, Lalmonirhat, Nilphamarri,
Kurigram, and Gaibandha of Rangpur Division in Bangladesh. The
concept of ‘monga’ is used in the other parts of Bangladesh in different
terms such as ‗akal’ or ‗ovab‘
which express scarcity. The real
connotation of those terms is
poverty. ‘Monga’ is caused by
natural disasters like floods, river
bank erosion, draughts, tropical
storms, cyclones, sediment of sand
on cultivable land and tornadoes.
Natural disasters are causing
extensive damage to crops, lives,
and properties. Consequently,
people in that area face seasonal
food insecurity due to
unemployment. Work determines
who eats and who does not during ‗monga’. A map is stated here to get
clear perception on the locations of ‗monga‘. Poverty in this region with
other poverty stricken areas show significant co-relation where people
could not afford to eat more than 1,805 kcal per day (Zug,2006:10). Due
to the character of the river Jamuna, Teesta and Padma, people of those
areas are being affected by natural disasters which are putting them in
poverty. Natural disasters limit the agricultural activities and other
employment opportunities.
The geographical, ecological, socio-economic phenomenon fueled the
prevalence of ‘monga’. This paper discusses the concept of ‗monga‘ and
identification of location of ‘monga’ in geo-social settings. This paper also
discusses the incidence of ‘monga’, in an analytical framework along with
the main victims of ‘monga’ and how it affects the life and society of the

127
people in relation to poverty. The main objectives of this paper is to
examine the mechanisms that have already been applied by the poor to
exist in this crisis situation and the services available by the GOs and
NGOs to prevent as well as to reduce poverty as a local issue in national
perspective.
Conceptual Issues
The word, ‘monga’ has been derived from Hindi language ‗mehenga’
meaning ‗expensive‘ which indicates high food price, poverty and hunger.
‗Monga’ is a word which means scarcity of food due to natural calamities
in lean season. It has been observed twice in a year in northern region of
Bangladesh when agricultural activities become off just before the
seasonal harvesting. During this period the landless agricultural laborers
become unemployed and their food stocks exhausted and job opportunities
declined and the poorer section of people fall in serious food crisis. This
situation is called ‘monga’ in local term. It indicates acute deprivation due
to erosion of purchasing capacity of the poor because of their
unemployment. As viewed by Zug (2006) ‘monga’ is a cyclical food
insecurity which occurs during the lean season that directly affects the
people who are involved in agricultural activities.
The concept of ‗monga’ is restricted in lean season (mid September to mid
November) which reduces the people‘s access to income to support the
hungry mouths. It is a seasonal deprivation of poor and they are involved
in poverty. Poverty means lack of resources, underemployment, low
income, food insecurity and hunger, lack of shelter, poor health and lack
of social security and dignity. In conventional economic sense, poverty
might be defined as lack of employment and income resulting in
incapability of providing a minimum standard of living with reference to
food, housing, cloth, health, water and sanitation, education and social safety.
Research Methodology
This paper is based on secondary data, primarily through literature review
and targeted interviews with the key informants from cross-section of
people and experts. Focus Group Discussion (FGD) method has been

128
applied to collect information on ‗manga‘ situation. In addition, case study
method is used to collect in depth information on this issue . The key
informants were the local leaders, professionals, and the people of civil
society. The data are fairly consistent and reliable, although there are some
discrepancies between government and non-government sources. The
emphasis has been given on qualitative analysis but some quantitative data
has been used to supplement the qualitative analysis.
The Victims of ‘Monga’
The main victims of ‘monga’ are the people whose incomes mainly
depend on agricultural labor and marginal farming e.g. landless and land
poor people. ‗Monga’ is a seasonal employment shortage associated with
lower intake of food. It has been observed that the people have to reduce
the number of meals during ‗monga‘. Similar findings are also found by
Ahmed (2005) in his research works of other regions of Bangladesh. The
different data shows that the ‗monga‘ affected districts are generally poor
compared to other districts. The people are largely the agricultural labor
and their wage rate is lower compared to outside of ‘monga’ area. For an
example, Kurigram is the only district across Bangladesh, where 50
percent of the total population is day laborer. It is found that the primary
group of ‗monga‘ affected people consists of those, who have to rely on
agricultural labor as their major source of income. It has been observed
that they have only income according to agricultural seasonality which is
determined by paddy cultivation. Many of them live from hand to mouth,
if they are not able to earn especially in lean season, they have to face food
insecurity.
The marginal farmers possess some amount of land and they are identified
as ‗land poor‘ people. This land is not able to provide food as required by
the owners, because of natural calamities like draughts, floods, river bank
erosion and sediment of sand. The small business men like hawkers who
sell crockery, clothes, food grains, etc. do not get customers during
‗monga’ because of less purchasing capacity and as a result their income
goes down. The female headed families are the worst sufferers of ‗monga‘
because they do not have source of income and as a result they have to live
on charity and relief. Many males migrate in search of employment as day
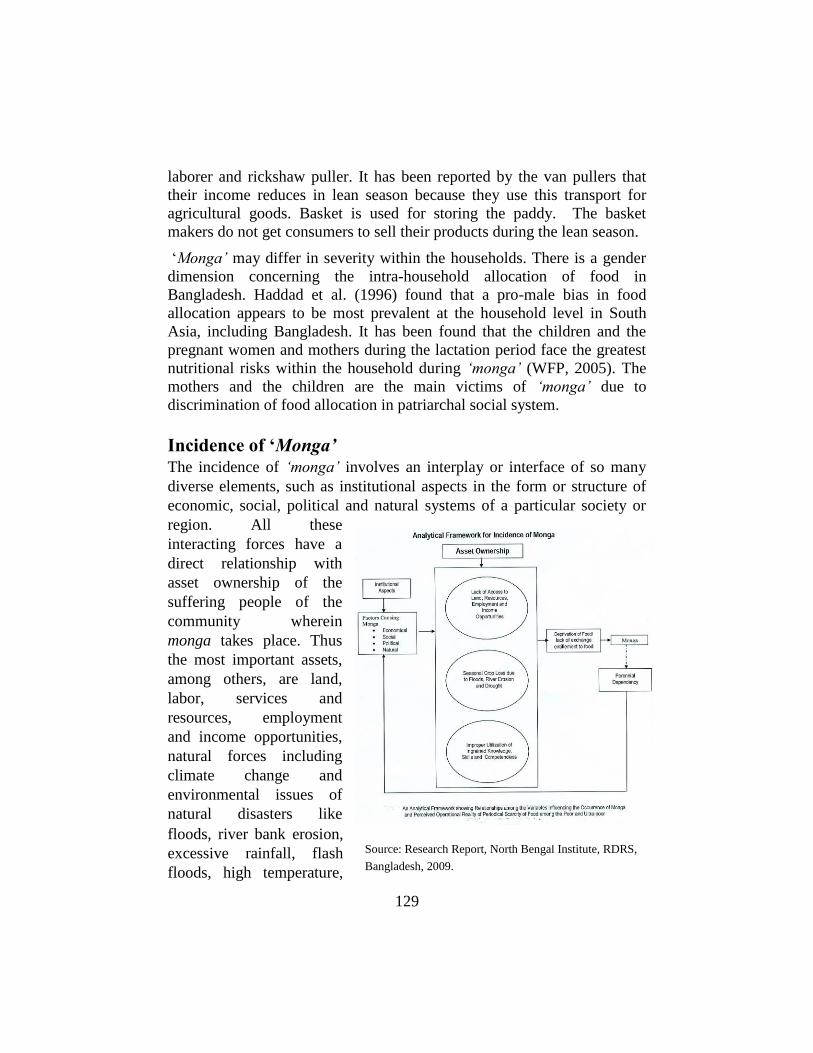
129
laborer and rickshaw puller. It has been reported by the van pullers that
their income reduces in lean season because they use this transport for
agricultural goods. Basket is used for storing the paddy. The basket
makers do not get consumers to sell their products during the lean season.
‗Monga’ may differ in severity within the households. There is a gender
dimension concerning the intra-household allocation of food in
Bangladesh. Haddad et al. (1996) found that a pro-male bias in food
allocation appears to be most prevalent at the household level in South
Asia, including Bangladesh. It has been found that the children and the
pregnant women and mothers during the lactation period face the greatest
nutritional risks within the household during ‘monga’ (WFP, 2005). The
mothers and the children are the main victims of ‘monga’ due to
discrimination of food allocation in patriarchal social system.
Incidence of ‘Monga’ The incidence of ‘monga’ involves an interplay or interface of so many
diverse elements, such as institutional aspects in the form or structure of
economic, social, political and natural systems of a particular society or
region. All these
interacting forces have a
direct relationship with
asset ownership of the
suffering people of the
community wherein
monga takes place. Thus
the most important assets,
among others, are land,
labor, services and
resources, employment
and income opportunities,
natural forces including
climate change and
environmental issues of
natural disasters like
floods, river bank erosion,
excessive rainfall, flash
floods, high temperature,
Source: Research Report, North Bengal Institute, RDRS,
Bangladesh, 2009.

130
droughts, cyclones, typhoons, water surges, severe cold, hailstorms that
directly inflict upon the community in connection with crop loss, and asset
loss which putting the community in pauperization in terms of landless,
homeless, rootless and ultimately forcing them to migrate from one place
to another. Thus the combined effects of all these factors cause deprivation
of food which leads to what is called ‘monga’ – a seasonal insecurity of
food in a lean season of a particular period of the year (see the analytical
framework of incidence of ‗monga‘). The crucial issues of ‗monga’ are the
seasonal deprivation of food due to absence of agricultural activities for
the farm labors and thus leaving no scope of income earning for them. To
a question, ‗why ‘monga’ occurs in five districts in Rangpur division only
and not in other areas, about 23 percent respondents from focus group
opined that no work opportunity is there in the lean season of ‘Ashwin-
Kartick’ (mid- September to mid- November) prior to harvesting of amon
paddy since the region is absolutely dependent on agriculture, followed by
21 percent as river erosion and floods, another 12 percent as perennial
floods destroy crops and make the victims paupers, more than 14 percent
reported as no industrial enterprises or mills and factories as an alternate
source of income and still a significant number of FGD informants viewed
it as most of the poor people are illiterate as they are unemployed, idle,
inarticulate and no scope for overseas employment. Some also expressed
resentment against the local political leaders and well-off neighbors who
do not support them in times of crisis nor do they take care of the poor
community by extending their helping hands (Bhuiyan, 2009). No
opportunities are available for skills development training making them
eligible for gainful employment either at home or abroad. Two things now
come to the fore: one is lack of work opportunity in agriculture sector, and
the other is illiteracy making them unemployed compounded with no
industrial establishment. The affluent neighbors are also not supportive to
them in times of needs and crisis thus terming them of lacking social
responsibility towards their poor neighbor (ibid).
Impact on Poverty
‘Monga’ creates disruption in the normal economic and social life and
puts the people in chaos, destroys economy and social structure and
contributes to replace social order. The breeding ground of poverty in

131
‗monga’ affected areas is lost of seasonal crops due to floods, river bank
erosion and draught. The victims are subject to absolute poverty as well as
culture of poverty. The land less agricultural laborers and the land poor
cultivators could not meet minimum requirement to survive due to
seasonal crop failure and they are considered as absolute poor. On the
other hand, women are subject to gender discrimination due to traditional
customs, beliefs and value system. They need to be satisfied with little
whatever it is food, health care, clothing and education. The culture of
feminization of poverty has great impacts on different phases of life cycle
of women and as a result the women are inborn poor. For an example, culture
of allocation of food at household level in gender perspective indicates that
the women need to be satisfied with the rest of food after taking by male
members.
During ‘monga’, the poor households suffer greater losses in terms of
physical and social assets, resulting in aggravating their poverty further.
Such losses of assets trap households in chronic poverty and affect
economic progress and social development. ‗Monga‘ affects the food and
nutrition insecurity from pediatrics to geriatrics and as a result the women
and children are the main victims. ‘Monga’ is defined as the situation
created by nature that makes people vulnerable and poor to buy adequate
quantity and quality of food. Under the circumstances, people consume
cheap and sometimes unhygienic food along with wild plants. ‗Monga‘ is
a popular expression for a severe food crisis in the lean season when most
of the people do not get employment opportunity to access adequate food
in terms of quantity, quality, safety and socio-cultural acceptablity. It
should be noted that Bangladesh has achieved much progress in
production of food grain including ‗monga‘ affected areas, but still a
significant number of people remain half-fed or ill-fed every day, because
of their extreme poverty situation, social inequality, and deprivation. A
study was conducted by RDRS Bangladesh (2004) in ‗monga’ affected
areas and found that most of the poor take inadequate amount of food
having low calorie which was less than1600 kcal per day per person
compared to minimum requirement of food for an active life is 2122 kcal.
It has been found that about 2.5 percent households went on hungry
without a single meal throughout the day, followed by 48.5 percent with

132
only one meal a day, 46 percent two meals a day, while 3 percent had
three meals a day. This indicates that more than one-half of the households
were either without meal or one meal a day affecting them to lead a life of
occasional starvation either everyday or alternate day (Bhuiyan, 2009).
About fifty percent people live under poverty line in ‗monga’ affected
areas. The number of hungry mouth is increasing at alarming rate, because
daily average income is less than one dollar. More than 56 percent people
suffer from food insecurity. About 78 percent people are illiterate and 88
percent people have no scope to get training to stand by their own. The
progress of universal primary education for all is not satisfactory and as a
result 50 percent children under 10 years of age are out of school (Action
Aid, 2010). Gender dichotomization in relation to education and health
care facilities is another important issue of poverty in ‗monga‘ affected
areas. The rate of growth of fertility is high, because 50.9% are children
(RDRS, 2004). About 74 percent poor families have single earning
member and the rest of 26 percent of them have two members. About 45
percent people are engaged in wage labor followed by 15 percent in
begging, 12 domestic work, 4 percent van pulling, 3 percent fishing, 2
percent small trading and 19 percent are engaged in share cropping,
handicraft making, boatmanship, and so on (ibid). About 97 percent
people have no land for agriculture and 68 percent have homestead. Only
5 percent people have sanitary latrine and the rest of them have hang
latrine, use dug-well and open air for defecation. The prevalence of
diseases is high at times of flood. Especially when the flood water recedes,
many water borne diseases such as diarrhoea, dysentery and other skin
diseases are common. Among others, women and children have a high
prevalence of water borne diseases.
Coping Mechanisms of the Poor
Coping refers to the thoughts and actions people use to deal with the crisis
situation. More specifically it is a process of managing to overcome the
crisis through adaptation with the resources that are available. The coping
mechanism means methods and techniques applied by the poor with
limited available resources to get rid of this crisis situation in the ‘monga’

133
affected areas. It has already been mentioned that ‗monga‘ is a cyclical
food insecurity which occurs during the lean season and directly affects
those who are involved in agricultural activities as laborers or marginal
farmers. This disadvantaged people search money in different ways for
their daily consumption during the crisis period. There are some
comparatively rich people and most of the time they take advantage from
the poor during the crisis situation. The ‗quasi-economic‘ interest is
observed behind the scenario of ‗monga’ in between the poor and the rich.
The poor people sell their assets like livestock, poultry, land, and other
movable assets cheaper than far below the market price in order to
overcome this crisis. On the other hand, the rich people take the
advantage to buy those things at cheaper prices. The main parameter of
quasi-economic interest is that the poor people want to exist by selling
their properties and the rich people are benefited by buying this property at
cheaper rate.
The poor people always try to minimize the ‗monga‘ on their livelihood
using the different coping strategies. These are preventive, resource-
opening, expenditure reduction and safety-net coping strategies. Many
people take loans from money-lender with high interest during the crisis
situation. The poor people sell their yield and labor in advance at low rate
to the better-off. The better-off people use the worse situation of the rural
poor for their personal profit. Bhattacharya (2005) pointed out that some
poor, people sold one mound of paddy for 175-200 taka in advance during
‗monga‘ 2004, which was worth about 350 taka during the following
harvest period. All mechanisms of lending money and selling labor and
crops in advance bring certain mitigation for the people during crisis
period as a temporary coping mechanism.
The selling of assets like livestock, trees, bamboo, jewellery, and furniture
is not the permanent mechanism to mitigate crisis. It has been reported
that the assets that have been built up by the poor with the intention to sell
them in times of need can be sold during ‗monga’ and these are considered
as a security source to mitigate the crisis. It has been found that many
people rely on cheaper or less preferred food. Even they depend on wild
food to eat. To quote a mother:

134
I am 42 years old widow. I have 3 young children; one is a son and others are daughters. I don’t have any land. I have a small hut beside the road and the land owned by the government which is called khas land. I am a day laborer and my two daughters were working as maid servant with little money ($ 2.00 per month along with food and accommodation) at the residence of better off people in the same village. My son is 8 years old and he is living with me. He is a student of grade two of a NGO school. He is also working in a tea stall as a part time worker without money. Just he gets two times meal. Now both the owner of the tea stall and one of the employers of my daughter refused to provide their employment, because of financial crisis. Under the circumstances, I could not find out any alternative what I should to do.
Many poor people reported that they borrow food or take help from their
relatives or friend to mitigate the crisis. Even some of the household
members eat meals at the residence of relatives or friends by rotation.
Many of them purchase food on credit. Many adult members of the family
reduce consumption to provide food for the children. It has been reported
by the law enforcement organizations that crime increases significantly
during the crisis situation. To quote a thief:
I am 38 years old and my name is Harun. I am a land less day laborer and live from hand to mouth. My family consists of five members. They are my father, wife, and one son and one daughter. My father could not work, because he is elderly and my wife is involved in house hold activities and my children are studying at secondary level. I am the only earning member of my family. Last two moths I did not get work and as a result I could not earn any money. My wife has managed because she borrowed money from my brother-in-law but this money has exhausted, so I don’t have any scope to buy food grain. My elderly father and the children are starving. I have tried to borrow money from my friends but I could not. Even I wanted to sell my labor in advance but no one has come forward to help me. Under the circumstances, I decided to be involved in stealing, otherwise I could not find out any alternative. I am not a professional thief but I have been compelled to involve myself in stealing due to extreme poverty and to provide food to the hungry mouths of children and elderly father.
It is found that some of the extreme poor people skip entire day without
eating and many of their young children are working in bidi (tobacco
stick) factories as bonded labor. It is very difficult for the poor to cross the
boundary of poverty, because most of them are in poverty trap in different
dimensions.

135
Services for the ‘Monga’ Affected Poor
The Local Government always plays an important role as the first
responder during disaster situations as well as mitigating the local people‘s
sufferings through Vulnerable Groups Development (VGD) program. This
program combines food assistance with training and credit package
keeping in view to enabling the victim women to improve their economic
and social conditions. This project is divided into four sub-projects: (1)
The Union Parishad VGD Centers; (2) The Women Training Centers; (3)
The Institutional Feeding and Development Centers; and (4) The Group
Leader/Extension Pilot Scheme.
1. The UPVGD sub-project aims to increase earning capacity of poor
and distressed women, through skill development training and
access to credit; to develop a savings habit and to increase
functional knowledge of women through training and participation
in the group activities; and to increase food intake of women and
their families. This project is implemented by the Ministry of
Relief and Rehabilitation and the local government structure at
Upazila (sub-district) and Union Parishad (lowest administrative
unit) in close cooperation of the World Food Program (WFP). The
thrust of this project is to implement the Income Generation for
Vulnerable Groups Development Program (IGVGD). It is a
collaborative effort between the Directorate of Relief and
Rehabilitation (DRR), Directorate of Livestock Services (DLS)
and Bangladesh Rural Advancement Committee (BRAC). The
program covers poorest of the poor and most disadvantaged group
in ‘monga’ areas as well as Bangladesh.
2. The IGVGD program aims to develop poultry training as well as
income earning activity for the VGD women, enabling them to
earn cash income. For a two year period, they are provided with
31.25 kg. of wheat per month as an income transfer. In addition,
they participate in a saving scheme. The VGD women who
participate in the IGVGD program also receive loans through the
DRR/BRAC Credit Scheme. The BRAC is providing motivation,
training, group organization and the delivery of inputs and services
to the VGD women.

136
Conclusion
The term “Monga‖ is, nowadays, a widely used concept in Bangladesh. It
is, in fact, a seasonal insecurity of food or in other words, it can be said as
a seasonal deprivation of food due to lack of employment in farm sector
and income earning opportunities in the monga-prone districts of greater
Rangpur region. The inner thought, insights and explanation of Monga are
embodied mainly in the agricultural arena where rural poor people cannot
find any employment opportunities and income earning, whatsoever,
between transplantation and harvesting of Amon paddy in the Bangla
months of ‗Ashwin and Kartick’ (mid September-mid November). As a
result, they used to face cash shortage to buy food items although these are
abundantly available in the market. Here lies the difference between the
concept of ‘monga’ and ‗famine‘ when money is available but not food
due to its scarcity. Monga is therefore obviously a seasonal problem of
access to food but not an analogy to famine or near-famine situation. An
attempt is thus made to address the issue with more details empirically.
References
Ali, Ahmed (2005) ― Livelihood and Food Insecurity in Rural Bangladesh-The Role of
Social Capital‖. An Unpublished Ph. D Dissertation, Washington University.
Bhuiyan, Abdul Hannan,AKM (2009) Agricultural Perspectives in terms of Access to
Land and Livelihood Patterns of Monga affected Food and Ultra Poor People.
Research Report, North Bengal Institute, RDRS, Bangladesh.
Hadded, L., J., Hoddinott and Alderson, H. (1994) Choice of Indicators for Food Security
and Nutrition Monitoring. Food Policy. 19(3): 329-343.
Hartman, Betsy and James, Boyce K. (1979) Needless Hunger, Voice from a Bangladesh
Village. Institute of Food and Development Policy, San Francisco.
Mahmuda, K. (2006) Monga in North Bengal: Causes and Remedies. An Unpublished
Research Paper.
RDRS Bangladesh (2004) Survey on Food Security and Hunger. Brot fur die Welt.
WFP (2006) Socio-Economic Profiles of WFP Operational Areas &Beneficiaries in Rural
Banglasdesh. Tango International.
Zug, Sebastian (2006) ‗Monga‘-Seasonal Food Insecurity in Bangladesh: Understanding
the Problem and Strategies to Combat it. Research Report, NETZ Partnership for
Development and Justice, Dhaka.
137
Invitation to Contributors
Office Organ Centre for Research, Human Resource Development and Publications, Prime University, 2A/1,
North East of Darussalam Road, Mirpur-1, Dhaka, Bangladesh, E-mail:
[email protected], Website: www.primeuniversity.edu.bd
Instruction for submission of papers:
Prime University Journal of Multidisciplinary Quest is an interdisciplinary
journal used to publish in January and July of each calendar year and is
registered with National Serials Data Program, Library of Congress
(ISSN. 1995-5332).The journal contains research-based articles on Social
Science, Law, Education, Business, Arts, Science and Technology.
Contributors are requested to submit articles for publication in the Journal.
The following may kindly be treated as broad guidelines for submission of
the articles.
Conditions of Submission
Manuscripts are reviewed with the understanding that they
are original;
are not under consideration by any other publisher;
have not been previously published in whole or in part;
have not been previously accepted for publication;
should not be written by more than three authors;
will not be submitted elsewhere until a decision is reached
regarding the publication
Manuscript format and style guide
When the Editor send manuscripts for external review, they are double-
blind reviewed. Thus, please ensure that no authors‘ names are given on
the first page of the manuscript and that author names have been taken out
of the "File-Properties" screen in word.
138
All manuscripts should be double-spaced. Margins should be one inch (2.5cm)
at the top, bottom and sides of the page. Font size should be 12 point or larger.
We ask that submissions be limited to 8000 words of text, unless an exception
has been granted based on discussion with the Editors in advance of
submission. This recommended word count refers to the entire content of the
article, including abstract and references. Articles with heavy use of figures
and/or tables should be correspondingly shorter to compensate for these. Please
contact the Editor at [email protected]. We give preference to shorter
pieces.
Title
The title of the article should list the title of the article and suggestions for
a short running title of no more than 40 characters (including spaces). Title
should not be in statement form. Also include the author‘s names,
affiliations and contact details (including email address) for the
corresponding author.
Abstract
Authors are requested to submit an unstructured abstract of no more than
250 words. Abstracts should be informative for non-specialists.
Please make that the abstract page does not contain any information
identifying the author(s). Also, please take care to select a title and an
abstract that are direct and ‗readers friendly‘.
Keywords
Include not more than five keywords that describe your paper for indexing
and for web searches of your manuscript.
References in the text
The citations should follow the Harvard system, marked by a superscript
number, closed up to the preceding text, but outside any punctuation that
is part of the surrounding sentence. Pairs of citations should be separated
with an unspaced comma, thus, 1, 2.
Personal communications should be listed as such where they are cited in
the text, and not listed in the references.

139
Example
Results have been reported (Don Graham, 1989, personal ommunication).
Articles not yet published should show ‗forthcoming‘ in place of the year
(in both the reference and the citation). ‗In press‘ should be used in place
of the volume, issue and page range details.
Example
1. Sharp Parker, A.M. (forthcoming) Cyberterrorism: An examination of
the preparedness of the North Carolina local law enforcement. Security
Journal, in press.
References
References are placed in a consecutive numerical list at the end of the
paper. The sequence follows the order of first-citation in the text.
References cited only in tables or captions are placed in the sequence
according to the first reference in the text to that table or figure. When a
work is cited more than once, the number of the original reference should
be repeated (not new numbers generating extra items in the reference list
cross-referring back to the original).
Examples of correct forms of references for numerical style
Book
1. Slovic, P. (2000) The Perception of Risk. London: Earthscan
Publications.
Edited volume
2. Nye Jr, J.S., Zelikow, P.D. and King D.C. (eds.) (1997) Why
People Don‘t Trust Government. Cambridge, MA: Harvard
University Press.
Chapter in book
3. Flora, P. and Alber, J. (1981) Modernization, democratization, and the
development of the welfare state. In: P. Flora and A.J. Heidenheimer
140
(eds.) The Development of Welfare States in Europe and America.
New Brunswick and London: Transaction Books, pp. 17–34.
Article in journal
4. Thompson, K., Griffith, E. and Leaf, P. (1990) A historical review
of the Madison model of community care. Hospital and
Community Psychiatry 41(6): 21–35.
Article in newspaper
5. Webster, B. (2008) Record bonus for Network Rail chief, despite
Christmas chaos. The Times, 6 June: p1.
Newspaper or magazine article (without a named author)
6. Economist (2005) The mountain man and the surgeon. 24
December, pp. 24–26.
Article Online
7. http.www.........com (April 29:15:30) Gardener, T. and Moffatt, J.
(2007) Changing behaviours in defence acquisition: a game theory
approach. Journal of the Operational Research Society, advance
online publication 28 November, doi: 10.1057/palgrave.
jors.2602476.
Conference proceedings
8. Sapin, A. (ed.) (1985) Health and the Environment. Proceeding of
the Conference on Biological Monitoring Methods for Industrial
Chemiscals; 30-31 March 1984, Chicago, IL. Chicago: American
Toxological Association.
Conference paper
9. Harley, N.H. (1981) Radon risk models. In: A.R. Knight and B.
Harrad, (eds) Indoor Air and Human Helath. Proceedings of the
Seventh Life Sciences Symposium; 29-31 October, Knoxville, TN.
Amsterdam: Elsevier, pp.69-78.
141
Papers/talks presented at a conference but not published
10. Martin, S. (2003) An exploration of factors which have an impact
on the vocal performance and vocal effectiveness of newly
qualified teachers and lectures. Paper presented at the Pan
European Voice Conference; 31 August, Graz, Austria.
Dissertation/thesis
11. Young, W.R. (1981) Effects of different tree During Democratic
Transition: The Malawi Social Action Fund 1996-2001. Brighton,
UK: Institute of Development Studies. IDS Research Report no. 5.
Figures and tables
Ensure that every table or figure is referred to in the text. The table or
figure will be placed after the first mention in the text. Legends should
be short, descriptive and define any acronyms, abbreviations or
symbols used.
Tables and figures should be submitted in their original Word format.
Number each table consecutively with Arabic numerals in order of
appearance. Avoid using vertical rules. Horizontal rules should be used only
above and below column headings and at the bottom of the table.
Distribution of Journal and reprints
One copy of journal of the article will be distributed to the concerned
contributor. The correspondence address of the contact person:
F. Nahid Huq
Secretary
Centre for Research, Human Resource Development and
Publications Prime University
2A/1, North East of Darussalam Road
Mirpur-1, Dhaka-1216
Phone: 8031810-120, Cell: 01911407266
E-mail: [email protected]





























