Embed Size (px)
Citation preview
ru\v-iumsli&711m4
voqn342556 - 61,12 11114 2557
n3-4,14t.iLvIn:.-vinlLmtf7jmumiNvilaurniitgIwIvii
LASERS IN DENTISTRY RESEARCH GROUP, KHON KAEN UNIVERSITY (LDRG-KKU)
na,v,t,1711aimvlupInZvi 3-,i1A'1711tinA-triirm.ALriu
5-1211'1Ufrfftlb'11111'1U
qfl'IF13J 2556 - 61,tfYIU14 2557
nq:3.1NtiLtYliz,1111Lfl66nn`litinYINTI-1,01LnAilltmllolvi
LASERS IN DENTISTRY RESEARCH GROUP, KHON KAEN UNIVERSITY (LDRG-KKU)
Ang,'VildfflumtiWIAVif 3.iiri7WItriA-t_IlvaULLriu
o o
TlENTIVIlTql111111,01Nr19:3TNElltYglr-IMI,VafTVItY11/1911;NWILLIAIV1E161`14Pli (fr-olm34 2556 -
6142Y1f.114 2557) l'W111141.dAtLDIMUT11.19.J215411.1119J1_1?:',1,11t1d 2557 litln0,3114IIMAI'lL'1111
3.11/111111ElATDULLrild 9'a11LIM-1aLIA9E1 Alr 1 IYVIATLIAMAT1411J1141S ATI,S1 2 ttlilidi,d1M;n1s
1J11/11T1114 tAL' 4,p_le.mrnsA11111.1111VICiltd11111ilillALLgS911CMYM)11,111,111n1M111011a.191-11.147161V11,011,5
unkilt-Alfrnwanmarvillflalt114IILLnfinfiltrITML1/1ATUbil
fltIlTWIJ 2555 sodivarninfiimwmpn-mitiilbinwil KPI lUTYlArAlon
ryinqulnumr,AuvililFings4"mngs az-SIRY114;16r1frlS r101114t1:111d411.119niLISZAEITIliiqViiii
01119AnylultnriurmullAns4-mnnTn011'uLtrilzvinl Lwaln'Alli,ornALTingilt1 tvarvinnolunnJ'
IIIIMUDwfin-ITA11,111.4111,1fritt116KUL6=r1lniltrnfifrllYMIUM.1 3.11/111112.11kraUlLrild ellnia.MuLVIN1r,
IrrIlLfilIDFNUT1 IITIl'auqtan TDinfiiikithinlviwilwalimiunlsohilulluAwihnTmumtfri
( SP1. 1/11AIr1J. (975'. Pf l C91fJG12J ) nfl'ci \IVTUVILLIAMEIVIl4frif
?ri
1101111f111141J01.911.1 191 .1A 11 2556 - iitial1t1101 2557
1 it ajAcarnumninilwigni:414iimrazwilmost iliulT114911101669171Viang 1
nrYl2ar_1141.11 4
Ab 141 fi 4
rYNCILIVA16/6th1ninti 5
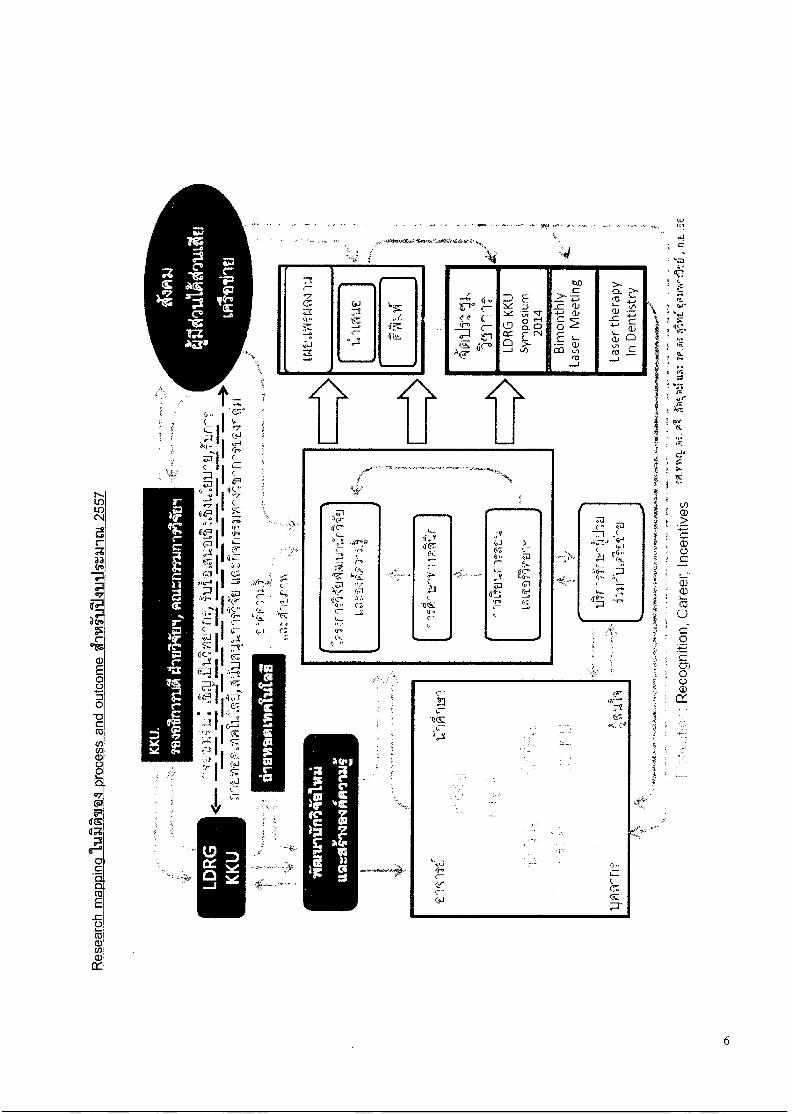
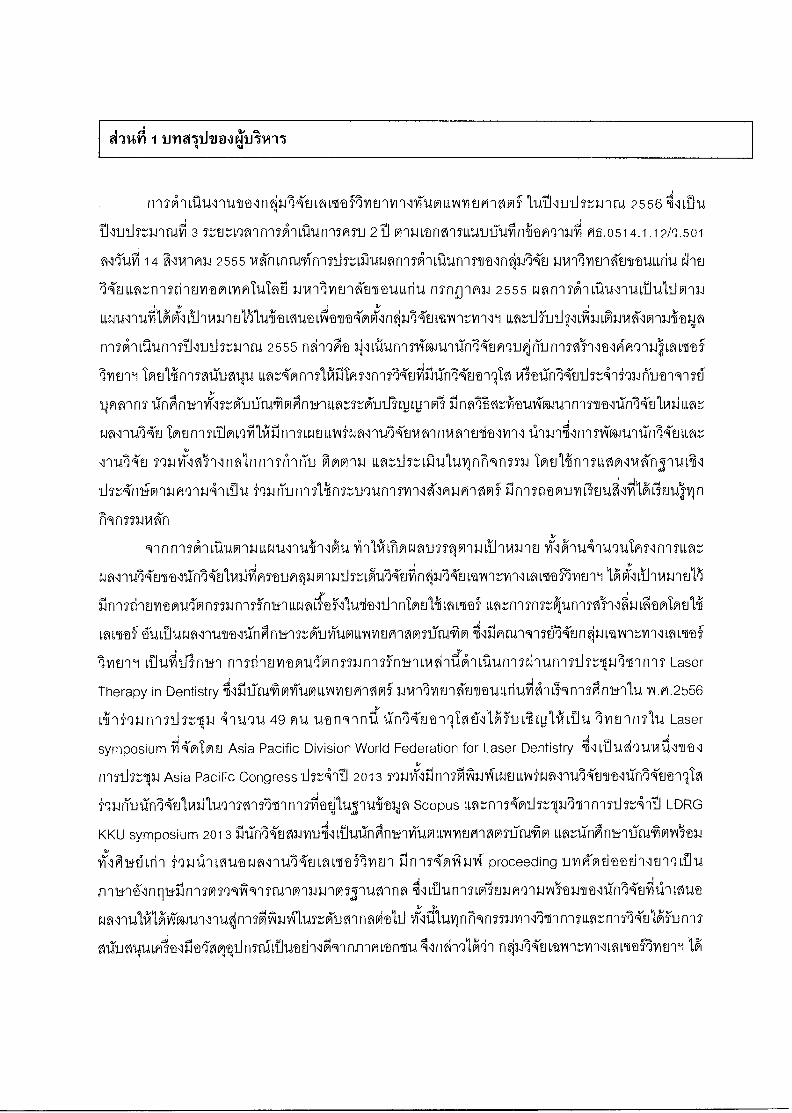
Research mapping 6
01611141MIV12.111.W14 7
rfAtP1attr1511.1111T1Int1M1rniffilfInwi
9
nuiltilnNtinvu 12
2 %Ili gl 1115. Li'414.97146balilil Intl 2557 ( 1 Oral A 34 2556 11 30 titan ma 2557 ) 14
raniggitalam. Intrakcitm (KPI) 01111111411114M1114116riall'Aial (a11.2554)
oloi-nilunil-n:414-imilg.11.111,11Z:Val 6 alit Id Ian
( 4 1411211E11 2554 114 30 trl TM 2554 )
1. pilurrnorfralumInNutoralPipranillmnstflvmminlviuntrINV1WilMlf
2. AnunnTA-pn_15-13.11ann-n Lk6LNEILLIAli Ci12.11/1tfrIt1PTAQ14LIMZINIATI-dtfifi
11(61r11.1%1,t111tVI'll IMMR112.11°1
3. AlUlAIJ3TY1511r1111T1,1111DrilErVIDPILYIATIZaL1116171E11111117114VILLYMEI-
G1101V11-4,211E1M:;1,Mr-Zei'llinl-mhti
4. lAiglIrlaL11.1111Jar,L1,141/111111S1J11/115491r1M141.17KEILtIVIZY111 LiAirdflq13.1
641ULLWAIIIJA14,14r11TH1141,11)11111traEJN-MIDA 3.11A-ilvtunkrivauuriu
- vinrmnt.1 wflrymlinlanitmuliikif.1619;1'm (KPI) V111,11M.114114mnms 15
LOUVil'a4"041 (31.H.2554) 6L8:1Th_ILIVIS'ild11.114.1914111AA'11:11,11TIV10.1
"54i_11.11LiJUS.1:11:;1>W1 6 Aldtail (4 1,119_11tAt 2554 30 t1ig.112.114, 2554)
- PVIT11111_1NrinTAliilunnsfrinikriirmt,LAmPi4nAcilrAnAlvinwen 38
Inarrin151.12:56:1144q1115ilitildirISTrd111014'fi 3.11/111VIErAT8ULLfild
MilalflIJ 2555
- P.M 1011,1i TAN von Fa4 2556 - tilant.114 2557 52
- ffrIT111,14.1141._TI.711'114 thl'A`11.191J1_151.111f1.1 2558 53

q`lt111141111141.1011114 9W1F134 2556 - riutritiu 2557
a41: 11 4114 97f11,14166W11.1V4g18
ninenran
g1 au
fliTA`lrradllintlf13.(rKEILq1,9:MfIVIE19Y1'1114-1011,1Srlit.W14Plf 1145111J11=1.11W 2557 41P1'16i1Uri1S
M'Ll 391 V11-1Ltf1A151,1,1,t1JITIAniitATIIJC4 Pi.0514.1.12/9.501 14 ii1WIAIJ 2555 VIA-mncobls
LlszillurannTAnolunnmaln3.114-ti niAllmnA-Enituitriu ehtiliTtiLiwznn.Mluvramaipabfi
1.11.11111EllAITt1.116/114 r1511g1011.1 2555 rAfrnsirlti,1141'1UL11141,1_1M11.11,1,W141101M:1111`11)11.19E11,511441ffint
6111011T1MfriflONELVIVIr,Y1111 L1,811J1-1J9411:1704;1,11A60123.1iitIOn1Tfrillgt1411111111_11J5T,W1t1,1 2555
06til9.dillTIANAId19ir114-?.01Q1JPir19J1195Ti'illtlA-ATIO6MitThlEIT1 dnunMninnviliimiu 11,W,AMn9511.11
IMT1r115114311Inityan*Va'a9ln14-tilis:541101,161.1t191TEi9p1Mrls
11,==frillInClArlfr1TY111,111U1MMINMfrlAtlfill\Y1141.1=4'111t1AWZIefl 3InflifHlr,19ial.411-fraarlt11511`61
lirl14-U1,142,ALLZ5WM-11,114-E1 tfrlf11115,TIMNfilAilf112LWEILLIIirallIA4-t.11MtnitlYralfilt1111)111U11114
riniii”;13.17rum-mv-tmFivitnvin\rviutavitifino-Ci nfriutITL-am (LDRG KKU symposium) VA"Mratill
frit Crit11,911411ii 3 ctlufriltwi4"mfriln3.11,4nvovinfillL8viltilmn-i 66~Cd~d6~S~J~1A1dn7~~1~G19b16~1d~e
1,141nutinvAT-Inlm-,friumnfiTtmsvivTuiLm,allvityvillviumumviumwspf World
Federation for Laser Dentistry IMA'161'13,11811MTVIallrlhunlvviiiallIn714'uat-iilINCtionlstLAu7IA'El
1144 13^11.111U nq 8J2`iE1M`W1vY11M66Nf_Yf1G PG1s113.1 66n1.17:-'111U11,111ni191M1.1
InElliin1SLIAPITenr1,161111T:Arlifr1131A911*10114 i‘naiungsliinstugungnnmrlAwinAg `firinTritm
ur ilmiiilf4lArInuhnryinTnran
9111f112A11,1114V11.11,13.11,111U411411417111?4'CrolVaLIS5V111.11,91_111/13,11t1 Vi\IATtAlurlutmlnqumr,
(6141175nt9J A2n 1) n-I-Nuol\tAN14TommiviA A
ugitlriunlffriblITATtnAtLitdtwitlihn nn7
Ilt1.1111DLIFAQI:ifitAIITULLGAStiCritlihn n121,611MLTafn=61unlsei-A34LMis11/1ful,Leantialu
111.11.01111,t1Mtl'iTlii'LlA-v11,fil!nfill141JINIACIAn'151,411,fl1,961frIMS1111,13191,111,113*TEITT(PlVIMMI,gtfrilu
ltd en6tJen~enld~S`~d9J1n 2) illTrira/14-Ein1S1191:1frAnrooil(INIPIginfiAtiilmmitritImItAtlihn
lkCr-Mnll,WrllVT14fr1n2nJTMJVi91L11,Illgi171Q LIM 1,1,a15fin-MittAVIATallrin`12PinY114tJ1:11'61712flltIVir'01
11,AD11.1111511,111f114i11151111MIAIWM1,1131n61,1111(61/11WMiddiumnAglyalnhni-in 3) rinTARY1MIti"
IvitnyillviuvlouruM14frifflaitNiitlriuit';atgiiatrimunrYweilomf nqsAnyMuCISOVIiM1,611tflifi.1
&rITIAIVIQT-InflUriflUnnTIVt14:',f4U61,nn111,iiiqVnfol'aiiis'imInnyritirufNviirilnrtulnumnlviumnsui
1.12tAltii,i6CiimiTtAvitrrom-nringitilitm
Ovinnalviwivaln3.11A-tn,fivivallvAntfrimtlAnnthli11119Pinna.im5inwnrrilmn'n
NM114°11t1111101n1I'In'kJYTUVILLINIMIainWISITCU6171V14131RE1,1WMJIA'tInq;3,11,VAInr,YinliAVYafIVILIT11311tili
lArl'17d'ItIVITatilfrlYi1401111,11/2.1fi'lAPIi3.114`1701EYIA-EMULLfialii'lLirIn'ITAnh''1114 Y1.1/.2556
f,V114nnni5s.°59f3.411innIT Laser Therapy in Dentistry Liili93.110TIJS113.1/4-114914 49 Piu LLatlArinuvram
LIWZ6VIN lri'191'1l1dL91G1 4 einunnni Tr,134111 WIT LDRG-Saraburi Hospital laser
2, 9.,
symposium 2014 441401 LLINV1E11,1,n'(161irlfrifila LLIA11161,41'15'(13.11JJ'Z,13.1 i'll4T14511-1111:1A1,1 72 MI,d ~dn 1S 9, 2/
1.1n11416111n0Mn't LilUrinKMiTtIPAIMManYltinYINYTIaLOAMEIVMMf '7A4'0q93,1fTl1Viliqt.M14jlani114
riTtMl?intnMgriradhAM,Wilillitlnnni'MU122151-1U1-11nlninEnTrigrb ItVan rYiniffMN'EM4?itTligli
tif tl;J L1J 117tnn5114 Laser symposium ViA-MtfrIti Asia Pacific Division World Federation for Laser
Dentistry 81107.11A9uvrtIllitliriLITnR, Asia Pacific Congress 1i5L'40111 2013 1,1,n' World Federation
for Laser Dentistry, Paris Congress 2014
A'lldt-19MIMI,VaWM11.A92.1r1`141fill.11,431n141113.114.1,NOLL'HfalTLMEITrallIt173A'UtTITMQ3.161J
111114-2J1Vi1111,ATI7Mirl'illn'ITitlq,11,1,1SnUilf650 Scopus ISI 4114714 3 LIM hOn3.11,Lflr,r1n14911.1T:',11.1
751I0tt051ii.°5401 LDRG KKU symposium 3111n14-EifolviutniMnArn±nviumLLINVIUMOVISIR146141 9,
i'D-111'11MI,Varalnli54-th,M311'aFriVIErl proceeding 1.11/A"Mtird
Mi'ME1`191,111,1111111(6'1nc11111n-MITTifmn51141013.13.1fifrlSyllMnfl 411,il1411ThffilE18aT11.1Mfl1.1611t111117KEJ
fill'11,MAWMTLIIINIAIA411,01`1140`41741141,LIStklOrlflffitil14111t1,1n1WMTLI4VITVM11rInS20111.1ii
1,111.11SJULLINAn 3 NfllntlWansnnfil,Tmelnn01,4timAntawirafIvitinvinlviioinvitimnwif
119,IL1114rvaluT2t1i0fifl'17 2005 The magazine of laser dentistry 411,11117117v0111r1n05'nt111JvrilA
World Federation for Laser Dentistry 171 0 X114 vim, LL w vieictivN
116u11-nronlalln elliin9K(91insmifit10119)Ivintill,AvnlCiullikfltl,C.IEILLMFanaiinnwY6'1nriwAtfln
ritilunn7temILMlnuiaviv6flyitriLiADYCAMmw11001(uLtlArltY1'111LattailVIEIT11Afliargi.ALAWD
(4'1U914 3 a t 1 lotutiluthn.nri4 2557
ilVi'v109n2i3.1vrierinnnsiinn-1514V1Ahinqszaimaignit151,a,T?ominst-ilLiThwati-49nn
n vanama Iblq1.111,1f1ITTAN414-1t1AA013.1P114Mell'anYIErl
110111114VILLINV1EIVI'l?lfrif latI/T4114011614VIcin1 VIMMTLIfiqtr1/111A-V111S51.111t11-11.MULtliln:11-111
kliDirknaltifildVILLIA111611nA-NIM-411Y1f1'15114TnitiMnqUitEiNAMIITVLIQUnn?114SDIJIII\TUIJIT,3.11 tld
2

2557 11 16-149:56111,111'1drgtlifid\ILA1J119;11.11/111/IFJ16211YOUL6f114 rIATII,ILI1U1APIA'1141,W,ItnY12.11Y111111.40 2/ •=1
LLIA11/121PrMfrlfY1-11,1=k1fIlflflinntluvITAlramtlX1m3.11,uvinT:Avialli
3
Q., iTial 2 1101JuathitTALLAZI1111.1iVil7,9111119:&15i96WINVATMMOPMFYIVIWY14011,61^1V194:416014
n
n0,3.111mtriTall\ILMaF1712.1111111/114P1LLME16114g
Lasers in Dentistry Research Group (LDRG) : Khon Kean University
A711167.19.4111
110142.16filAllnill6ffieHFIVILI1VINITUPLLIAIYIUM14fflf ih‘MqnnovynAolAri,a1/11111innniTtl
noln9nstim.-Apwinslumng.-,1 66qtvi1t,192.5'11.dl1.dLnivalilti maltITIalL1IVIEIGI14ffil4W111/1t1`lkIl'1UL6f11d
lArjr11Trilf.JW691(61601T11.11 91nOilir11,19111ThW1A1141ffielitrrilf.JA04141911.,111nTzki ins
r114r1W1 ffiffidtlkIlAIVITUVILLYVY16101EAlli r11AMnlsAnwilinAtnicoz-,oiutitunlorinwl
J13.11/11.11 1Avall12.111D1ralA-11SLMMF3YIEITYINITUVILLINYWWHIVIntl
nk_14111fl World Federation for Laser Dentistry 119/iP913.1tFalhiiinwillimitrifinertnnn
luttn-mihvi-Minnhlituariul,AiluintritnilAnnnilumn/rtnXtMEI 1113.10011Entl 4J1Ln
101,0141WMFNEITIVIlirlaLLINV1t1M14V1f AnMfa 411,ALmatlitA-miln014"tiLVIAIT.51/1q1WLennY101
1/1111114016611131UWIAfrif 1.11/1111/101A-nt1d66r11d tfr1U3111,114'1.4111TIATM1.11RW192T2TIMfllfIT iiwnInAnwi
3.11A'1111t1`AIVTLI66fi14 61,fl:A011:11,11,AlsMilEl
nrniriunqn\lart,nNPing-dirvinngsAnitnll'uLflvtailliwnvIll
vilanvitivinmf IALTOFIVIE113111VTLIVILLINYIUMW1f1INCrifrIlinT2.111111.1111ACIA911
Vi'111.M41160.11114 LiTurnT?ille4/ArY13.11,111a1W111/1M6EJM4'f.11,9114119'1.1:114
(Research based university) (614.L111011TM'lln`1111,11.4n111t11.11A1MVIEV4t111101d6Lrild 114111?6111,t
3.1W15111tin6.111twielL1
nmr,va-ipi-wrruni5-
n3.,714"tiLtrin..5vr-ilLfloitflyErwrilviumnyitim-mfr-ri1AlutiiarvinmAljrunknituariul,M-m
ollytannisnnnwplruwIntlairiutirai 554/2554 MrYtrill 4 61,1112114 2554 tn.% 74.11%-ti67m
kollarynt-Alfrnan4timw66 fr1SlinagAirlik11111dinVil'a\91111.17KE 3.11/111VErlftraUllii14 dlt034I1
66nfl'Ini'1LIY1f0INIAILIW.1141/111V1?J'All21411ri14 nstvini 2555 fitiluitnomumn_Tufniitfirnai
0514.1.12/Q501 M`Yldil 14 liAnna., 2555 6111:1
4
- 4 1111_41El1d 2554 ill 30 riut.nou 2554 1,11145T-Unfri+EAll'11.41,6qtthilAT19-A.111.1911%6fir19:117-Kt1
- 1 frr1P11-.1 2554 ill 30 rittElltfl4 2555 diurmkailunqicilii 1
- 1 fro`Yn9J 2554 '4.1 30 fiUtrItrld 2556 1,9711,!frnklailtil9Tilcii 2
- 1 frr 'WM 2556 30 filAllt11.1 2557 1,11WITA1LCUTIStlii 3
1 GI 3 nakrig-rmuivimin
n34,11'nvarrir,m9lim,91afTiminvrilvitwinvitomivif
MQ141TiMer1J1,flt,101111U11114171UVILLIAnnumnoimcluLlTnsmiviti umt-tiluvilminumvivanvitigvillviufri-
LLINYMPrWifrill'dlt1K1171,1,trZfriliMn
1. A11t-1ffullEl7ii1JIMIMFI11UTVINVila661taltIMA1 vilAnunlifftic19;.asnu nnnhtquilifirrwinn
atvitayunnKfrInn5174tnonnifluvrilyilann34
2. 1,12,hilrinnind2/innn5‘ LemaMmgAitiugriut,fiviraThinTvinlvi10161:141Y1W11461,LfilIflOinbl rzlifin19
141,19tNqUil'IMIILI,n6Dnqiu 7Q1.11/1141.1qP13.19T1119"11/11St011niq LIM:51,1'11,1'1111F1
3. TrAulrrninb-1(lihtamulilimvirafwilviufrinTni
5
roce
ss a
nd ou
tcom
e iiV
iiiiii4
111.1
51:34
int 2
557
Res
earc
h m
07
F
• •
CJ
C-
"Nt
•••■•••••■••••
(re-
Cie C —
MP ai • X X X e- c* 1 c ir %lc ICI V C SI p V
a at tx a
dr'
N•111■1111■1,
,
Lase
r th
era
py
In
De
nti
stry
-- Cl DR
G
( np
os
2012
Ill
0 ni
r M
E
A 67
48••••••■•
4 , '
6
TO191.11t/1114/01111,A111t1 i1ii9.11.14111J111.411t11 2556 01-13,111Ntal.WarlrlI1Vira611S4'(1g4 641.1;1.2554)
6lAttliiitIVIAtillallIViilgirlitaglall.01/113.114113,111g1145ZEIZOW1 6 altUilIn 61192nfi1.d
2554 F14 30 iiiatritna 2554) lilki4ithmu4-naurieJitiliThumailtriframivipitutqiii,41
1. vTa,14111111q111441121V1f0IMRYIEll i'AlfiLIMSIAN,11,11NA-Aq11.111,MIDFIM111/111VildVILLYIY1W111f
2. ITPIFYITI1n113.11119111TLAb1UI66M thErW01(01A(Y13.1111,n1SIATUTallItlflq:3A4-EJLVIA11:11111W1Taf
111£111
3. 112,i113M1A111nn5ArafintrirraMLYIRTUTat,fl1TaFIVIUTVInlillal,1111121PM1frlf?,illE1Tfla' 61,nAl\I
LAVIllt1
4. 1INTIZIVILLIJULLMLLUTVIllf1151.111)114Mill7r11.114'ULVIA11:11111 ISN'aPV313.1641.4,1,1Mt01119.Milil.414I2.1inti
3.11AllY1Ell'AI491-t1 TalmnIvitn6t.rwauuriu
7
0116fIldf1151111''Tt134117_11.4511tht.:VJA1 6 altuman (4 634141V11.4 2554 54 30 19(1421-1t. 2554)
1. A1Un'1514-g11,011n1A-2.10n161914ffilltnYttnYnlilUfr11,LVIMV1101f
1.1. fitmNrni7AtilAVIAIalLITWIVIt1MI lAtAll'a\101-01T1141,M'afe1112.11111,11(i1M1,1,1111EIPIWINfill(1
Lilutomn171.15stivau 11n14tyc12I4 LmnAtiln14tnistil J'93.1rimInPinwitLflr,111
lemn541.419ivatAr, 50 volImnwilikrtagilstmunq:1.114-tivannfrilLmvflrune-i
1.2. 311;f9iitnnAlbciditaimvemiNnlAnb-inviutinefifr-Any) VilvdITIVILLYIYHEPIWIMI.rleilfil
11,1ArY13.1QLLMY6111q;1114UMITIrl/1111,Mtillflf.JT1 1 altl
2. kurn74mthsr,643. 71ann1T ifAitteARLM chumwalvinqu'iLLwavintutantln3iKu MINI:n/111,MM'
11/1111 -11
2.1. 4mIlvonpAanryinwatwmalf Lm,tri'lEIVItfrit161T13.1144'1f1TWZ,'IlflZ. 1 Mil
3. AnulcrlifimnAtninTSIadnuovvoimmtuTflfitmLIDFiMilY1111;114P1ILVIVIWilAVIfOlfilMr
3.1. thErVILvimtubii tmun-nliNulnlsnblej„ilqu5',13.1riunnThlKuSilirgn-rivit;CDONnTninns
MH-120,119ETmulihm9stfvnlawInn3.1 1 14DA
3.2. Mil'IA-LsmILMealnu7ionrin5,Lw.',14'2_1 lwrniisivanwmnernnlfiitnAllfrillatkroultl f̀ri
2 Ci
3.3. AlfilnimitiLLMemni.,114ulwrivInn:..-friinnRivaninnfrNITM`1511`11'(61111,14S141111'11 2 Cital
3.4. n'Ind'ILOMWM1146114n171iTIMAT1n1nthrlintnTql 2 ilval
3.5. n-m:iniwawmnulunlnistvillinn-mthill'A 2 riN
4. 1/TaltrIp.ILLIJULL2251,11,a1111f1111.11W15'A-frIll'IM3.1NtllillAIT.;Y111 11101T13.164.114LMAITIMI141,1f1111,i11,1
3.114'11V12.1`4 2.111D1 3.11/1111/1E.Y4Inituariu
4.1. fiZLILLIJULOtfl1111141MA101141-11.4fl3.114Mt111:511111°1 171S91.1193.111`11,41,V0 1 51.11,1,1J11
4.2. 19fri5'unnwaunii.49-innntriann1411iivaiAritwil Lill,14-11.d21.d1S1.d 200,000 1.111/1
8

nre,rigniniumtnqvainirwirinui
TD1V110015-19126 G1S. pf4 viq1i9nna41A'tiLtrinvnlimvivaRviE1'1onlir9.afri-
LawitIVI1 24ffif
Ph.D. (OMFS), London University, London, United Kingdom
Tt1P11?0151915IT u
Cert. in Periodontics, MS. University of Texas at Houston USA
5Nvilofs7519-d1 ms. Owl qnrvintrge: 1.11%tatlIl'llf11411111±1
Alf151-01,11WMPTO,141TrU6k 3.114171VITI6t13.111Mq
ms.ilTfrn 41.dvifvvil:
Doctor of Science (Biomaterials) Boston University School of Dental Medicine,
Boston, MA, USA
0921P1'121V1519'n'ti PIX,111t1: 11rMtianifFrinn'IT
B.Sc Public Health Administraton, Sokhothai Thammathirat Open University,
Bangkok, Thailand
9
W191T6 1111W211,1,n111116111fl'IT
Certificate in Oral and Maxillofacial Radiology, Faculty of Dentistry,
Chulalongkorn University, Thailand
rfeihtffilAMT`191TET tIlds.11 icOld1,93T1gTT34: 9dn2'~~16t~~9dfl 11 In is
InCIAllt1/1 ?11111111-1.4frinnasmAfu ivhalrinawi7rnEn6n
6?i'19flnh,ai M11.1fIritlfl: IlrlAltaran7rtnnn7
IvitinpinAfrinnrainvilo
1.114111/1t1162HITIM`11,1011VII"
Ttlf11401T'19'1T6 MT. iTtri-flg 1117 EJI,Lfl:',11f171111112T
Doctor of Philosophy Faculty of Dentistry, Tokyo Medical and Dental
University
tTilT61715711K Wir11.4111TatI,VIN,16),11 9 d9
lltrIMNIMT3.11A9ITEAP AllITVTLIMIITT1.11,TMEM'IT 1141MrITC113.11/1111%16!.1
10
fa`19'17(1 `31E1-1 CrihElL811`114flq2
Higher Grad. Dip. (OMFS), Khon Kaen University, Thailand
unlfiAlTti 1917a AnVi,inclquannTIM8Yafttinitiftniib
Bachelor's degree in Community Development (Hons1) at Rajabhat Loei
University
1Z127g1p1 1N2312..nqu: reirlEINEI
21'11YMYIU'11115Tralfi9Lmf 1,rirrIvitr-Arnuuriu
( alalbtiown4 n.u. 56 )
v 4
qum :
wrinnnbigincp.t wonlvityAn4vrAnTnu
( 1:4111Jb1.1F14114 MCI. 56 - B.A. 56 )
1.1-11ATAriM 01:41(61 :
011I'MVIFYIWIM1fLPVI 1.1111'1171MAIIIMULIfi1,1
( 143.11.1h1JFIA'11,1 N.A. 57 )
11
t-mtairnI,Tuaarviu ejpilLiluInm-1/641 11`81r19:1414'tIlt111:111\11,MtnYIEITI
1. 1@lq1511141F111319116 3 Al
- CJ Pi. X15. iltva'm cirrisslwas
- t.vay.i■invlof qthtAiti
- CJ. II Y16Ll. lVl ltd ma41191,&I
-1/1A1.11,flAilb1-11 At-rd'D'.ff.J1-0
2. 9iim669N9/1ii66EJ9dn9iunn5-5-24 Ig4vanuiqzqn.fi 1 nu
-1111r11.t2t1,116 fr1-1Plculfrving
3. #0191541411221FF119.11grlilt
-144111.111G1117 -111i5st1.111
4. iinRmiigtiliniguilFArren 2 Pl`1.1
- 1111 41.
kuniumilro
5. Irriall12111/T1,101LINIVIii 14 All
-1.111141. LmuiVi
- uvrw.
- 1dYlYd. 67111J.114 110111Ort1
- 141(111. fl,Truto tsi,ovo
- uvrw. fAvivin 7d3.1111.1
- 1avIYV. 3V-hi Multi-11h
- uvnALl'avo' nilfr-ra?Irm u ir
- ilITIATPX11.114541/111..1
- WA. 17111E111 LIEJATYalll
- U11111. 111W1 frnItS111-114
- 1dY1W. 61NU111244
- 'owl/MI/0 `t'ULITtIAU
- 1dY11M. fr191q111-2.1 TIAr711/411X1
- U1/111. 1,111t.lUAN619
12
4114,11 44111111111,111iGii
iaLisiu
t494AFIV1119111111114i1MTVIZY1111,AMPSVItl11/111TUALLINVItIPI-111F6'
11911.1-unIMERtvuir:vrilLflrAtf-IvitywnlviuminuviumgAmf iini-iinnviuvidu 100
- t19`126Clum owe" 10 mu
- Yi1401,61NYIET 38 AU
- 9irnArnInviuoLLIA1116 31 HU
- brranviel 1 mu
- toiqtrviiaLLINVIET 5 AU
- 1‘VliAil-liiLVIMIIP1111gYINA1111,M,TafvillnmirrAtTio:,-vilarnnd 1 mu
- vilmL1,111169111fri`111J?r,INIFI 4 M1.4
6a7e 11911 umr,41'aagnit-Ful6t dl
LAIVIht1
AllInqnun3.11i-tivav - ot--yrilmvnflvitinvrilviuoulArviumnAof .9;
1114 5 V1PYITI,a3.11A15T,LrinTA 6 TrOIJ Mr1Z-Vildfr11,1,1NYMPI'Mlf 1.11,1`175YHJ'16-tnituuriu : 40002
651_11,6di: http://home.kku.ac.th/ldrg/ '710.16: Idrgakku.ac.th
TVIJANii. 043-202405 ViD 11265 rvarlt 080-3538196
- http://www.facebook.com/Idrg.kku
13
g'121111,111151.1biln411,1 Fm1F111 2556 - 2557
ivrtail 1 41cakilcir115-11411NZWIT1.111111111011`Ttili1111:',V1141MMIS'all2111114iiin111:1AITIVIT-Ifini
PI T131[111.41.1-1
1?1f.J14111 Y11.6r19
Tfrirp_J5-:Al
Research mapping
KIIVArrYMV11.11.1441.4
2gtihRtig-,11 nIngmflz-,n5111nn2vnlisnwi
rItliftla-1114-EMLIVIU
1111#1 2 ZIliMilgalli11441111141149J1.11:1111t1d 2557 ( 1 (os'1'1FIN 2556 .51 30 flinilf.11.1. 2557 )
ralliTk11,11144-11.110121614kiATO1 (KPI) 0113.111r414114LtflgillIAlniellt41g4 (i•l.2554)
imali‘n_114A4Sunii'49-mittlifil'ivrrunilnalle4111.111:i1941ZfralAq 6 131t1.116511
( 4 611141f.11.1 2554 b15 30 2554 )
1. AlUtYITIANJUTI111754t161,firINA-RT146MtFIYIUM/MAITUVILLINIMPNig
2. k11,111`154MLIT:1517)111fM2111fiLNULVIO fht..11/1(01d1419'1461=1,VIPAUTal
3. ATI,Al2,i1J111'1A9rIfYlnitatilt17110111/1PITutamiwailyiErwriAviumLLYVVIEJ-
PrIANfOltnniz,
4. ITAJIZIZLILLLJULINL'LLIXTVIqlf1151:+tir1KPIrrlfflq:dffE.16t1Arl:',VI'll VrAitH011,1
elli.1141,1,fi.°A111.14141,1r1-121,1114.11A`1DIVII'16?.17A1°11E1 ITIAliVIMA-2.111tuuriu 9, czi.zrcv
frin2q17,1-1 Wanq2AliChttlqUI012.11,611MUINA (KPI) VIM.111f-11,111,M114 9,
(31.A.2554)=',1A1115:4ChallIVIA-1911101,AA'11:11UITIThq:1-.1
14.?..13-J11,9114T1,1.1r,V)fl'l 6 atuon (4 63.111`12.19.4 2554 N 30 11146'1E114 2554) , 2' -
VIT'llMliNWAMr410`12V14.1fr1TIMLL23011MU-11)114r17t14t0111.114r1
Lnfuli rvinimiluwwnskivraunnriraln3.11AIJ 111ollYity4t1'fltu66riu
.I'lfirWt.11,1>nr11511`lf..W1(011,V1g1,1Tal rimDlni 2555
- PllrMili tif-lffrl7k11111.411-1TV1`13-JA7kfrl L1,011PiTlillTarikAlfrY11.11,1611
rn2Ll5T-6iluwfln-2in61.li,4n-myaln3i14"ti

iitlyurrnaktum-ru oplAll 2556 — IT11211V14, 2557 1,4111
.J'12.1734-EILI,W,--nnniquvramormIutthi fl5TT'lf11.1 2555
9 iumn'i5irialu\nu 1119.1quu t119,mm3. 2554
(111,(91fkr1E1111,t117ILLrielquI4noninninumnivinTutA61,69)
Vtilt441711111,1AteJq111.115cTO IT21lTIM11614 VratCJM-naL6.1.4-natrug qtuvrilthin A umrAi'm bgle0 Lag:
ni mann
6116511 INIAlli11041.1iiill
fl'ITA11,119.4111411t1t19;1A4E1681,VanYIE111/11\91711a61,1^111t011Afrlf 11411111.11.1211TICII 2556 611611U
1.111.111MTIRSI 3 nEltl,gfililllirla4rl'ISATIJ 2 111 P113.11,trIOVIT6LUIJITUIlirlitATIWili Fi8.0514.1.12/9.501
14 &WWII.] 2555 14n LnaminlnisniluwflnnTAlSaurnrvaln014-ti wurilvitnA'uttiaLriu
14EIL6Wc15r115stiltrYlt LYIPITUTal 3-J VI 11 11 trl k 61PD1.,1 n ni 2555IVISA 111.414111.d61J14stiin18J
111,11,1111.417WILIFIVIWOhlUiitlAUDLATIIV4d111014Millrlr,Y1111 lLni.11111_17,11,fi3JA.11/1A-1011,141tklp
rnsAlLti,114r11TTJ11_11JSZ-,3.1')CLA 2555 r1M9ka 11113:11,V1111/TP111411.11114UMIMriLlillS519i-ITNKPIT-11.1,i1,flIlti
11/1t1T1Tfr12.11.1411SMIUM41,161Mt4P1rmlatm\InlA4013111n7j4tyalqt
n ritv111 4rhurinannnviralilril4tilvmiLLW,'
WM11-114E1 ImunniCilmoilliArinimu61,10MTLINUIRflltTlAgiltilit1V1'111.111.11811r1171^14114-111r114£161,n
1,t141 513.131f1 1n Vinfriu
Ihtinivilwvan3ATIP14 '‘,aa.iriunnsliinnurn4n1svilloYlnw1n?svif ilnls61amuviasuAlil1̀AC4nuvzvIn
ri9nsn.n.AA'n
rinnimAlLiliallALLentmilnlAuill1,12ACAMNfilMqff111.111111)1311tIltIAMA'11,19UTM1f1151,Lat,
WM'11,1142111(611.1f114011)11.11/1PIT`61013.1N13.11_1MAU1401111.111-MV11:,111111,fl1,611'anYIEJT1111ilitIlvanti16'
iliMfiltIVIDMOVIIIMItYlS`fill±'ILLfaStfill.M11.1111Tmulii1M1,9Y6f
ovivof famluemnuvalciThArnilsrAuviufrunArnmlfrinTruilp 41iimar191Ttill'unLinvuntvilq6fl661i'af
rinninrwanutimr1Mlirlif)1±11,14111Aq1,11UtYlnilUtl'InI5T,11,11111111? Laser
Therapy in Dentistry 41311RA ValaLLAYIEJM121frlf 3.114H1111!Ilk°11tUtlfialii'lLIVIAMT11,14 IA111.2556
(4111(114 49 MU 1.4(On'llnif Ilf1)42JD'ITAFT11,Ahltiirt_ili2/iLiJulmyinflu Laser
symposium 114frlImu Asia Pacific Division World Federation for Laser Dentistry ClitiUdrri,VviillIval
nnT112.13.1 Asia Pacific Congress thr,4111 2013 511,11fflEirraiii1.114-MULLYdrall1MUTalfirlIKMTP
‘93.111'1_111-117142.11,1411,1915T0516111f11ADE41114,211441'81/41fi Scopus il,WL',nns4frnhr,oplis-in-min-4111 LDRG
KKU symposium 2013 illif11411411VIIA\91,9J1-111fliirl11/171141766701t1P112IPTLitIS91 InnIflAtIlY11.:41.1971VIVaD1J
31n1KgAiwv1 proceeding 119/01-MdflDfill?1`191,r11,1
f111.11(6-111t)1111f115TITTVIA19-1SCWIVIIIWINTS1UM11“MTJUn1SLMITI1M913.1.Mt9.111t1111114b1711:111111At
Wfll'11.41,19A,ATNIU111141111411411^11,1-InAMIlf1Mifli,li lil'AVIrrirIM11.11119111Y1111TiatflnA4tNalrrIS
fil:1110114141,M4fl1VID 41r1MQ1M1 nq;liKuLtrilL-vnlmotafIrtrri

An LCIUMITIATNAUT616AT13,19ik191LflLell'af1MY11(1-1114-1.1VILVIMJFL1Mlf 61,&n,C1g11.411:(111';'0,V13,1 PIWO1914
tiltIVIDAUTM1ITT3,1/1(611113411-2litIA,11:11'119 4,0,11D1.1"Al'llaValril,WILLIA171661M:41RIAT'lir171145T,KINI'lflelA
ati'llnTlinTr-YIUMS11-MUT119J115T-14`ltli 2556 lir6'149n,9.11411Tni'Vl'tliVillA13.111Y13414'11YIEVIA'EPIltI4L6f114
VIATIALT1WAVIA`11,ULItnliUlYINYTUVILLIAIIMPrniffIFIM:3111'101t'lgit1Ufri(611J
&mai 2 ?IOti, firi,kg-nut Lam:n-1m l'inu 11 LIMY' 09116a
nON'ivarilz-,YMMLIONUMInswiuminwitiVilAfrif
Lasers in Dentistry Research Group (LDRG) : Khon Kean University
F12'19.16911,1341
r101)1MtilltY1116M011/1tY1Y1Witil.0166YVVItOilfiNf 6N19111AQ13.111.11.1tY11\911nrIls2lt1
Plat191niatiplflln?1,1,,InWrl LI,n111119f11`11:11,11,fll'alilt1 nng5viuminimgrift-if 3.11A`1711/1E11h1VaLturiu
1AlinnTintivvafrvalK024 snn(Mnil9nnTAnwiAnumvaramnlegultIluvInv,-,friu 1113,1141 nn'
OrmOlmt-o-kanitalvairviciaLavvitilmtiviqiii rn.5-4"mn9TAn9±l2arAtniuTt-,Kutil-whilnbl nos .A
119;11A nnsThttneplatiunmnsArnt-ili-E1 'q3,11/111.11,A5st'irltriltl'NoirITIAlltfIVItIMIn1111-14P1,1,1A11/1t1P1`121V1f1,14
=fri'114-1nfl World Federation for Laser Dentistry VAATIIAID1JfIJI6fitf9d1ifi1f011111VIIVIT
61,tatillAi13.11ATIV12.14tillt141,6rildlnuInuitliiinlansilliamlvitr4u% n9;341„tiimirtjac..;
r'',01.d1,41114q1,91tflYIEJ11/11Vil,WILLAYIFJP114frlf 0)-1111Q ilalliutlya4moiln9:1iWuLt111L-1111.1061(a`flYIEll
1111VilatIVIMEPI10filf1,11Anlvm4tpnut,triu Imul'odiunnvvTmulnEu191511Limnns LL:.11r4iny-1
arvrilmtnAuni.aLiriu umr,-AnliTuvrimilu Curherwolfzilni7i 91
12.16ME111111540S1\91.11fitUlldLIT:,'LYIPAY12.1 MUdrilifrITIANJUTNA-MlilirililfrIAM.1114211,MellM11111
1110166INV1W1Wifr1f Otr1lg1Y1flM6YlnIcuId.16flL9YafIVI 1lYr1lV19.WILLINVIEIMANf INIIVILIV,5TE111111:191,111,10911
111,1,1=A1113.11114 T.19' LINflichlirMilLA3.101912,11,D1,13.11A11111t116tJk114-U XJ14119'11114
(Research based university) /A-141,111,4111SA11M13.11:1WNTV13.1VVIIVIE.r1A-UTDULLriu 1,Cdn1s69Ju
a19AilvinnkiWuka191
lamtmigivirtanig
n3414tivoln:--yriloveaflmilconlviumurnorwsmflAisiAlia9nmvillmilkvauuriuliN4'm
111611.11/11YIE142111t1,166ii WaLTIJ 554/2554 Mr5-1,0711 4 11191E114 2554 1Ltlf14 7413115'n.P,'69M
An maxi rnsilstalwannsAnalunnriyalnaAA-ti mranunAlnine 9.1ariu
unnnnintrwonvintuIdi 3.11,111ri2nA-n1, auttriu f1st-in-1mA 2555 ii111142112I-M1,1,11Jgalfrhn911.1ii P15.
0514.1.12/9.501 fl1911 14 &1;11MI 2555 01-4il
- 4 1111±12.11 2554 ill 30 ri1.allE114 2554 61114SninfrIII.12,1111466nAllf1921,11,11iD61,111112111,6fif113Mtl
- 1 qwwilA 2554 ill 30 fild2J1E114 2555 olunlikivilunnsiN 1
- 1 PO1P11.12554 30 61.1trIE114 2556 1111V1170111,radfl'ITTIVI 2
- 11P11.12556 30 tl14F11t114 2557 617.114119J1191,11141115111f/11 3
3 nat.lanililiwilnu
110111"MirillrY1111,MTaillIEFIY1117i1AVILLINVIEJMAfrlf LthAlthrIM1r11511111.1114-M6M,'IWULLIAli.
019101,d2.1911-111M1,91611/1E1M/1111/1-1,1ff11,11^11/1t1b1101FLULITZLY16311,11U1,6=111,11,A11hUffiMfIllE.11119lVil.01-
61,1111E1WMPliitItlk151,U5T,olovin8
a. LIB?19
1. nw1l4I6fit2riv6monfl1712nvillv1uo661rounwi vivlAnunn514VVIruilu
ual-,,ILILLIJ11111111TilEIWY1SAU14111111114ffIrITII4
2. 111i1J1r11/Y1111t1r11? LWEILLIA119`11.1:11,11UTTLIIMLItnYltrill-1\117110L11^11/1tIFIlARflgillar11±1 (1V1210,9
2 1/11,19211111f11M-SLIM:52111111791.1V11A3.11M3.111171111/i.9559i1J111ALLfinntr1111A
3. 1,19/'113Trn1111I1 alTm L'H FYI-11MM nsni
•
• •
4
4e-
C-C-
-C-
er.
Ce" (7", +.7
erta
q'cr C-
Las
er
t her
apy
In
Den
tist
ry
C.. t: )s
14
mm
I t
1€
cro c.—
, qco m cr
,11=1111•11111101•111•.,
CJ
A
T0191.112a114/69311)111-1t1 ACIVIM41.11.111:341t11 2556 F11116011141.146tfAingleaTVZOlf§f4 (r1.131.2554)
LIAZIH1114:4694111,FINVIi19-mi4140iMilidniTn .3.114'filliahntfitiq'ai 6 CiiMdbign (4 61112}V.114
2554 30 ifUtlifild 2554) laiTi441A9.15-114-11.illtiiiirl4iMMIglitIVItAVARTUIFILLit3
1. vTmlnilnIA-tiltwrmfrifonstflvim ''11.11I-1.111`151Aig11-0NOTAT14M 6tnVitranlifiaLLYVVIUVI'HiVri
2. 4MnqniTZ-,131riiinnTSil t6WEHATI1 ditrVitOlt,IPCM13,12i'LLnlYIRTI,ttfintlnIAA'ULVAnZ5V1111,fl191tf
trVitYri
3. 1,14ilinAlinnnSiiiitrinnYltMLYIATUTan,flL6NFIVIEMWNYTUVILLINM.IMAMflAntn7nd:,
Atainn
4. 1141147,1iLLuuLLa:,-augvnln-nulvris4"frinqsnaiKtivarri:;11'11 611111MT11,164.11.466nM111f11414141f.111qt1
111/111V1trlAVKU lituvnlvitniTintuttriu
k11,111411151134154i11.111,ThatlItTarl 6 1;1'101466511 (4 6341211t11,1 2554 30 i114t112114 2554)
1. AlLtr1171/Tglinali-E11=t1610141,q1116911t111/111711MLLINIMMOSVIf
1.1. MAS11115'NULIM:511,41UlulvinT514 11,fltAllNA-A913.111M1,161V1E.117111VTUNI,L11712.1W14frlfinjO
AltillANT111151.1TtiltUkEi 11'1114tATITA 1,1,:51/11tIlf114'f.11.1?:',41 i93,11i1.11111gfrillinr,viit
'''OE.1&.`; 50 IltlInTlf11TfifrIlL4,Ur1lAMEE-10.114b6V/11V/11\ILMItnVIEITI
1.2. alvT9.9iyanniWarrhaiguvariralnnAnwnsniinTar`vivignul vilaltilaLLYMEIF114VITiTtlehl il(8%1
11.,10VIAMLI,MINr19:3.11 -ULV/11:11111A,VaillItill 1 ritl
2. AlUngKfruisripii-innn2 LAt13.12.161,M riT.111tfrINKVY12,1161,nLYWAUTATtl1.11AIIIMA11:111111,Mtf
11'1E111
2.1. I'Mlindli171111111Wiltiwun attintivroyalA'n9144,mnsw:; 1ln 1 nis-v1
3. AM.A1911i3111A6111n`MilttintrifItMLYWTLITaLM611tnYitnIfinlYTUVILLYninFilAfrifIfiqtnTaR'.. LI,n'?125'N
3.1. tinuranalmTubfi
frILI1(irihEITKAALItfilllYilalilTS1. 1 ritl
3.2. MA13.11ATMIULLINI141-11:11ilf11TLM614?.1 llaralmiTivanmTvinervinlscit'AllAlusniulnuTirli
2 LTD1
3.3. MTAIMATLWULLIA&IM11i54't.AUTIMMAPInii/VainMY114611111n541611MA6hatfriirinii 2 ilval
3.4. nnraM,Mrar421'n.fli,dnlniV.MATMMAili.dnUTYSI 2 a'al
3.5. n'151.111,41.4(NA111,111,t11171.11°13.11111111M9i1J111frl 2 Chl
4. iimulpiLLIJLI tin'LLUT/111n9nilvinTi'mn1Tn9:1SffuLtrilL'vrw LkanynAirAcklatwano4urynAu
1.11/111112.11A-EAN 311/111111f.116f.191DULIAU
4.1. it iinumil'11,014e9i 1 51.11,0211
4.2. 1A5<unlwatatiu9nnn-inwann011i6olwiril 1,111.4411421alu 200,000 UnVI

giviltAnamminin,qtrimmililtrinv-)
T\IM10MT-19-1T6 MT. MI 1A-914111071iflitillr/1116MItillItY111111171-101-
LLYIYM FOAM:
Ph.D. (OMFS), London University, London, United Kingdom
n10110M19126 11119AbLimtfin7riinnqAtiLfInbl
Cert. in Periodontics, MS. University of Texas at Houston USA
TtivInOviriqnlif MT. finli-tnnran71-nnnfiltriniln
ons-nrimprwsvmgiTorilfri avri7vity4En.nlmq
TD1WHIP12191T6 '411111f1,111:
Doctor of Science (Biomaterials) Boston University School of Dental Medicine,
Boston, MA, USA
CJ OirAIM1AVITTI`ITei (6-1Marl AA-11/1 N:
B.Sc Public Health Administraton, Sokhothai Thammathirat Open University,
Bangkok, Thailand
cah15t1 21114611115YAi 11117A-066flt9.dn2611hnh5
Certificate in Oral and Maxillofacial Radiology, Faculty of Dentistry,
Chulalongkom University, Thailand
06/M.IM'IAMT'19'1515 N141,9111;1E511.1: 11f111bLIM:51:111711Y1MT
A`1111171"larlMlii'llitTslan
1,:i0otymonTinni nn4rU6118: 11-rM2i1,1=1,1r1111flrl'IT
IVIEI`IPMINTMV111-Wil41 W1111KM.JM`HiP1Hfalli11166fl:1:66271flilflIMA6iltifl
3.11/1'1114Enk?41°11M14131.41/1f 9ITZ:1341m
C
Tulfi'1MT-19q5t1 MT. in-pinFi M'121tIrTal: 9dn7'91~J66~° 9dn2~f In 15
Doctor of Philosophy Faculty of Dentistry, Tokyo Medical and Dental
University
t'19qT2:111?1,11P1
21TIVIVIlansn19Tm61nn5 ivinmnTramlyityiki
M91?6912.1q OliQULMITtinnT
Higher Grad. Dip. (OMFS), Khon Kaen University, Thailand
1,nqfH13Ei 191Tra: kiviiimliQanlA6TILMfahEilltlfltMain
Bachelor's degree in Community Development (Hons1) at Rajabhat Loei
University
aii-m14-u1111,-4-1/13.1
1,!'12.11FIFI I/WM.1'19,14 : rrthEMEI
Wril'171rlEnn'ITHflAQ1116 3,11ATIYItrAIMULL1114
( Lta1a,°umii, mt. 56 )
1,1114TYVTIIVII141(15' :
?i1111111W1Arltilt 1.11rMY12J1A-M.11711AnSh13.1
( alnirrum-ru n.ti. 56 - B.A. 56 )
LIS1:5k61 : A11/19:11.illiTL-41141'114,
4`111`173.1/1TIfilMfLAil 3.11)1119/1tIlAefIlltUlgil4
( C4111.1bilMi9d 34.n. 57 )

litiltirn134-tivvin9J valnai7Ku6tvunz11lltAntF)VIEIT1
1. VVI'1116.11/11.101WITYlil 3 A14
- WM. MT. 3ltv4"fr-15‘
- D.vicw.fhva
9 d9
- t.vnAg1).5:6ivu? maii°° 91Am
- vivu.7')Ukn.tra m-p4.-Ttirm
2. 'AIM Wilielili LIA141117(1401TIMI ti.4vutrn.r-montfi 1 AU
- 41, .raral,116 nnfivini
3. t1yillilifiNfilIFI4
11161111g
- 1d2M.111P1M ff°111.15'.°11
4.WI= Plantn 2 Fru
-111/14.1.FMN,J,1 W1t1.15-10.,1
- 1/1/Eu.qmq ku.varr141
5. Fi 14 Fru
- uvrw. Lu99i"fr1111,1,?il.AA
- 1.bV1VV. Anfnl
- 9,lVIVV. (11113,114 60117A
-1.-11/11. E1141rldl 8564941
- (11.11711.1
- yfffrra.
- 9dVIVV. fiid1VIS frrffP191?ItiMrEl
- ilsvinica urifivnu
- uvrw.
- urn. triari tST3.1f711(1114
- UV11^1. 1,111tmiTt-Li faMmuro
- VVITI.1/141M `LohzInu
- uvivu. mwriviti 166114141u-1
-1411111.
N 411,IniviLittr1111101419i
101:55lial
1191111.,IrliafffiltW1:::V1111,MnYltIMI'llaWILLIAMEIVIWINf riarinnmuiliu 100
- Dq915IMUVILLIA1116 10 nu
- viumniti 38 AU
-11-nAmInviuoLoArvitl 31 AU
- 6191,1:011/16 1 AU
- (111QUITUfr11,1,1^11/6 5 AU
- 1,"`11/119:rliALI/lAilA1.1114-71'11k1141M61,1'11f11J161^11161=viianna.1 1 nu
- VTUVILLY17169-1FIVI'llth':-Tirliai 4 nu
Lkqr,41'aignitilowit
nilAmoio
Anilnlnun3.,7'AntvrinfilltavnnvitiminlviufriLivIvIumwivri 9 „
IN 5 tflAlTad,11^In'IMEITA 6 Tall fUZITUNI,61^Mt1G311?105 : 40002
VIL11,11fri: http://home.kku.ac.th/ldrg/ C316: Idrgakku.ac.th
TV1TKIA41/ . 043-202405 friD 11265 re at 080-3538196
http://www.facebook.com/Idrg.kku
iTaii 4 AV waniwinfrad-nalablutInannt, 2557 (1 01,aiRaJ 2556 rhl 30 1114,91014 2557)
t•1111/0110:11,14114 TOltliAlPiPrifTh (KR) Fraillf414 lumnz-mmateraiTol A (81.A.2554) LLAZ
tlidutlIALfivihn449-mitoigivilunii.n34141213.1-ughainre.vapi 6 altIVITn (4 14.1141f.114 2554
il°4 30 Filallt114 2554)
fIlTlinli.114C4ffM*11.111,111telltlna.MuLflvraflyitn-i IiiIrrinlv,-,Lilun=ugunnsun-esiNAli
InilinFAvIntmln-nss:,-PaldnufignJstu-mt-ranIA'ErViLlimitn unvirmi,inn9;3.114'mmerallvisll rift is
dlrullumnaryAmvaltnNn12 az-SifrwrimmANI-MA'AluunInvIn 6 lk14 C.1flillTAlill,1111T11,d
9il1ATZ.1,11E1 2557 OTAM1_111,101'15-11kAlid
14
P @ .7 , V q a-.
M •zi.
ii.° Lo to
c- (NI tz C m
(a (- __ A
P .7
C-
.4° a
F -oC g Ir
ca c- r
X E O ...-. CM
M a. 116 Y (0 Ltd IC
p° in
CG ,E c- • N
-- C .7 4 ge. ro
O g (- Ti ad
F tq M aa
P
) aaE 1r dtc: tr. c- =
• .7
•
M IP
ap G c- c- 4,- ,
0C-
.G Op d S M
tr. ad p
Oa 'CG
CG E
Z M -CV"
"P g
cr- 1r C
XG X c-
O 5
......
•
a=
.7 C- (- a
s
M 1= C
co C- ca O 3 .7 ,.., c-■
N CG
.7 QS (°-
aa
• "
IX c- Xa
.7 Ir.- -A P
dcpM do, cir° —A • aa
-CV" CZ C -,
c-
dg ta
air, a -..'
C-33 3 3 Ira
.--
M -
o to.. 0 c-tr.
.7 o
KK
U
(F =
facu
lty a
nd
U =
uni
vers
ity)
0 Et 0 J
472'. (- 0 _. a
0 -'' l.' 0 C-
ir; Z. -7 co tr
a
N
co
g ag
a a (P
-11 -4g
as
Va.-
g ac. a, a (- g c- 'r
,, tr. C"
0
C°
G % .g
S
d g °P r g
g
4P cm
cc
r r
CD as (C m 3 cp
IC° 3 r g
aN V. (-
6
'flf-
oLl' 'clg
r -cr. c--. r- C- ca
cF cic° 3 M g
tr-c. tr.
.7 v. g t•-.
(1 (-
1 cr. tr.
3 3 Ca
3 t7 a C. tr. r
Ir.
r°
o aa cc m
-10 tro
((
co
z _
s
3 3
g w g
t=1 --(-°
g °
co M°-
‘—. TIC° g --.°
CD (
-0 =g (a -11M
allg
m g CC°
t.i 10 )g cl CP
-7
r Z
g —
a 1-(-0
Cra (- C-
Ilig 4-0 c- , - -
It. g
4-. „ g
, dm
F0
tr,
‘"m c- (-
tq P
X co
r -11 °& r a
A (0 t,-,,?
'cig _.(0 (- M 4 M ''
0 ,c7; a 'gs
g ''.- (P°-
'-`' ) CP 1.y.„
7, 3 tr.
.., ao
,-. tr, M
(r. 3 Ca ac° ̀r? °
ag —
°g 3
.0g ag R a a
,f- (i( ts
g 3
,..- C (7
g - I ar a- P
(II . 3 m c-
,,„
c- -e ,, -
p .-- g
.7 .- Z c-
CP lg ca"
(IC° ‘, M
le, ° -° ,m
(--- - (IF a c
" r r Ir.
. 3 4,.___C°
4-0 tr" g ‘.."
g a a
.-- Ir
c-"
c-or b=v" a a "
M
r-
c- a a ca _. g r aw, C. a
C-
aF a - tr° 'CI a a Z 1,,,-,, z d a _. ca z z co -. r IV°
--oi tr. co cm c_ "
g - (.? ...„- ar, -. ar, d=1 tr. -e .- (- 3g as
'ta Z
c? r° F a X 3 a d C-- 5 o
(-6 0
r, as D m m cir, a a
3CP ‘.1C° V° (- M (r. VI -P. 'ra d M r' _. r- tr. tr'
C5 -.- G-' Vc7 aka ,,-, g ,' gg aro 1,9
" - 11 ,_C° a_t.•
7 .7 r Iw g
cc-- c-m
,;,[r„ w
°7 (--- P
,Q-' °(•P 4c. 0,
7.,,'' C-
g &"
E'
M c-R
0 d tr. dg F—° -II
r
V*a a
<7
ca (.0 g
g lr.
0 0
-. .7 0
■.tr. 0 V r6 .--; 0
-TIV. 0
-` (5 a
c) o ° 0- 0 Cd 05
-,c- 0-.
© 0 V 0 -o (0c7
714-.
0 o co - 8 .1- - (- °,
('-
KK
U
( F =
facu
lty a
nd
U = u
nive
rsity
)
0 CC 0 _J
O 0
4 ,-.
tr
c° ,m -. c _ ,,
`- , g aa It. ,
„...., LO LO LO (N
(—
0 0 d l-
tr- a r R a)
It tr. .--
(- -P cr? .......
(0 Is) co (N
0
&- Ir. t-
ci r
°F CPa d
-11 o?
-42S 0d d
0
-- Ir.." co a
ac. d„
dC'
C- 0
Q
(I
° c-
v° r m Z
- E
r:Y
AG
lase
r co
nd
itionin
g o
f sili
ca b
ase
d, l
euc
ite b
ase
d, l
ith
ium
ba
sed,
alu
min
a b
ase
d a
nd
zirco
nia
base
d c
era
mic
for
res
in c
era
mic
ad
he
siv
e
stre
ngth
; S
Pf.G
15.1
k 2G
15 X1
611 5
6112
io
zfin
bt
im-.1
1-111-1
ilym
iali
JeuI
imA
ili-A
rn41
7: -.6'
inii
v hiq
nwra
o -un
Arri
g-ri n
r-uvi
n711
n.J7:4
14
ig
5vfli
T al6
p upc
4pllu
ni7e
lnyi
ludj
a.liu
luci
th-tla
nz4b
uiw
riri
1 1
gf.1
- 11-
17*1
14-17
,',EJZ
VA
-in-n
-wiu
ta.1 1
.1,NW
41
1tI
rlEJ
Vilt
M-1
1111
17Fl
q14
8T
ori
m. J-I
n
up:1
1u; a
.ri,a
-u.-fi
En
upt•c
r imu
miti
Ifiw
n -m
iado
19-11
-17-1
1 -114
1]-3E
JI IIM
EA-n
auaN
p.riu
lca ilihn
sliir
m-17
9
11",i'lP
7116
1 1
G15
5
IS NairI
gJIN6
IWY
11-ff
171 1
@.1 Worl
d F
aduati
on fo
r L
ase
r denti
stry
C r R
c-
c- -0
(-aa a _. 0 (-0
.((tp
,2
0 c-
g g`r (U
d ta
d va a ,-, -ate
C
as le,
.--
o?
(a c atr. g
0 c c tq (D '. -.
0
n Y
(F =
facu
lty a
nd
U = u
niv
ers
ity)
y
(-
0 0
L6
CC
_I
0
00
0
,._. c' c, ,i.
(c)
as z
(-
—e
C- _
0 co0
Lo
(- C- a2
dd
o 0 c- -,-
Lo
C \ I
0 -0 v. c- Z g
ag 7,- ''
a a P
-11
a g a a CL
v--- z 0 d
a g It.1 3 C° 0
g r. cr
ag (-- '0 tr- (-
a Co
ii(D q P d 4P Z
r° - tr." - g
ag (Tr: m '- V 5.- v.
co ,. , 0
0 4t,.1 _o -0
(-- a a - CL --. " -. C- g 2
aV _,- Ir. laz
117"*". 1:11 j
z z - C° (P -.'' QV (r.
,....? ,-, , OJ
X Jr, r C -9 ap tirro°
a-p az ,(--
a a -IrD (r. Z C ,_C-- v-
--. 'M V. r al
(r. ,__. 11(r.
a
X • is Ir,
. ,r, C°
' qn
g ''7
1,:l - tr°°-
tr. a .7
g C- °g (- g u
tr. I `" d
aa as
lip _
g C°
3F V.
d 1. (-
''
C dt,
0 TIP
t-4 ts
- 1,4
Ca . ,,
(,-- V. -
,-. ,„t
G— z ac)
r "
c° 11
*7
fr" w'"
tr. (- C
d VO a
0 IF
d (---
4g d a u-o
z 1 tg a 0
(,--.
" c
g
aCi -- .7 0 .7 (-
3 a
m Le ' - c
Ira g ,..-0
0 ts-
r `',
t=r" a a I°
-Ti
(tea 0
,- ,
cog Cody.,Z
4 g -rr: (- ---a
ar.,
`="" Z a a
V. ''. r
(1
C- 4 g
6-' 0 ar ix ,.. a a
Ir. C- C°
.---,,
cr? a -v.
_,,,
°g a'-' .' ad=
t- (- -"
cp d a
4C' °
cr. -.
r ag c
ca v
0 a-,
g _,r-
z a--
--. Ir.
C C °g
-1:1
at( ("0 gP ° t.,1 Ir. Ir.
(- (- v.
.7 a?
d 0 ) -r C 71
a ''.- C Ir. a a (-,
C .
e L.. , '7 0
0 - -11 Ica 1.o
-, - F
y< d M°-
F 111F1 4it (0 4 C.
its a.7 t,-,; .7
z g tr. Cr° 4---° _ c- C
,r? c 0
r, „..,0 , cr? --a a a m g
a 10 tr. C-
C° a .4 S ° , .7
(- • C°
"Cr. 0 Z -- , ... Ir. (-2 (0 M
v c
iM -_. (- tr. g -0 r 0 (a
4---.
0 3 _,.. 1
,..,0X
1(5 a cP
avo
-. .0
'"
1,,c- v.- .7 ts a a Ir.
'''
d _,, "-I dlr. r. _,...
-
—.
-
c'
d
0
M - 6 (a
(a ,. , Ir. (-
g
r_(,-* ‘="-
d '-
il
3'''
° 'Cl
q g 4 ,c6 *7
(7 ag c-
tr. g (.--.
g
40
tcl , .F
" r Z
(- t l̀
t l°
-11
g .7
0
C
M a v(4, V°
z .7
11V ,fr.0 (-0 V (5
at-.1 m
(,--.
a a tr°
(-
ii--
tr. (-
;-.?
(- -z a ,0 gg cll
vo (-
,.(-- d'-' ..
-3(0 %.,--
"..."
luP 0 ca
M (- - 'g
A `7
(-0 ir,
ag (-- n
r d a Ca _o
>, C
..,= C a)
17 c CO CL cz (1) _C H 43 ,,, co _1
Jr' 0
M C-
72 _a) as Ca
g d co a9
g
m c-
g
in
in do, g
S-.
c--
as VT
cD 0
ay m
Z., VT
- -7
(I
toro 0 V 0
<a -vr- 0
(-0 -(
0 0
0 2 -TIV° 0 cyi
KK
U
1
51
(F =
fa
culty
an
d
U =
uni
vers
ity)
c-
0 0 o
Iri
CC 0
C-
a-. 0 0 N- C6 C\J
g
.--,_. (-- s
g g KA 5;
-..- '7 11
CD Ir.
a d
-151 CP ,r?
ic. -
0
dr. auz, C°
a
R (-
F (-
ag
1/"' C-
c6 a
''3
0
174 c- co
ca,__..
0
V
li W g
Ito a).,
11,
fr-. (-
.7 CD
Z M
11
ntrs --
Fa*
_.,
tr.
m ac.,
,---. aka
t'T ci
0 ii(P -TIM
w;
a a Ir.
Ca w -0
cr7 S
1.1
g ̀r? Tag
o (a iro
-0 a
0 g
710 c-° ,,,g
- (-
CD p
''4 3
cr, 41W Ir.
0 (r. 1:I (-
14,.,; E 0
ars -
I, ,....,
as a 'r,
(1 '77° (-6
r̀? M Z
g,Ir. ,
m co °
•- T
i
g t,
3g
0 1i
m F
(- i
(1 1 -• (r? ca
07 c- , .cp
ars (—
eiw Ir. (-
V°o ,,_-
lox R
'M 0
a
_t a ry g
-o a.?
Ca
aa 0
M (-- (- (-
d a a ir° =,`" d a v°
-.0
M P
(-
ca a
(I (- lq C-g -p(- o-- 1r° ir. (--
-
371-11
4,Tq l
q1A
(il-
rii1,14
-)1,v
iill,,r
iia. 3r
-rnf
rnw
ilr.
An
ratch
r ern
Y1
1,11-'0
11titq
l
661N
4
aVl i
irtl
t919
1c1
d 11,6
q111
4Jql
66q1
. 101
/19:3
Aii
l Lw
ontr
i-u
a m
a fil
l En
91
Er: Y
AG
lase
r co
nditi
onin
g o
f s
ilica
ba
sed
, le
uci
te b
ase
d,
lithiu
m b
ase
d,
alu
min
a b
ase
d a
nd z
irco
nia
base
d c
era
mic
for
resi
n c
era
mic
ad
he
siv
e
stre
ngt
h ; I
91.q
1..11
51
7
LLar.
fint
::
- n
ilil
ritqf
la hr.
R-ni
kTITI
AIT
Ng -
171:d
11,R.I'6 1
1111
1./
Liq r
. 11,
MIT
Y119
1L1 C
AU
111n
-n-gf
-IAL
Lac
ri lpl a
an
gim
uffN
a5 L A
anil
li'1L
4a1v
a5ll
AII7I
aJ6 6
ug
71`i
g11
4,1ul
afl
aallu
rn7
13-I1
1(l ii-a
u ; I
91.1
11ta
it-u6
11
711
1̂114 4
, 19
1.M
./ P1i
, 1-91
. irn
Li 8.
9 ,
111̂ 1
t11.q
7q11
qin
evin
n
R c-
-c- a a C6 g
, C° ^14:4 a co
A
,m Ir. ,4- =9
et
co lu g
.ff --. -11
M 3p
aro tr. C- (D 0
- 11
C\! T-
g
°F
a 1..t ro
F m
am
3g
(0 10,
0 Ilt (IF
3a
3
d a IC°
1. (a vl - Ca (- aa (-- ,X 2,r,
r. aR 'Z' C c7 CO F ra _. a g
ltlr.
c- - C.
g 3-T-
g
a--. MC-
-MP
-11 aco
Leaf
tv, v
ia
o.1 4
1-11n
- qm
on
co
tr.
g (1
°F as ("P -TI
-4Z as fa _.,
tr..- ta (0 ap
F a c, r 3F (— F g c-‘rp g
ci -r°
°F Ir. c—
Z
- n
l Anw
ni_l
itJuL
fitn
nzuz
nain
-n-g
f1,1 5
aAga
qiIn
new
. 19%
, A
307:
.:W21
lf11
7
14U
l Taq
l,a1,61
2 f fI
TIU
L ITA
ll 80
8 1
k1 T
UL3
,191
7
nauT
11La
d1.1 5
1fJ ;
F
grr1
a.9
, 74
1.q1
7.44
14
,9/11A1
.Nrn
s im
,
- m7L
IJ IEJ
ULIIE
JUNN
/ INF1
1717
11.gla
1,1,E1f1
LaN
s@fril
lmT
ay. a
ms@
fi@
n-n
-
iildm
uLt la
rril iitl e
rnE
rna
lvt ie
Lila
dnu ia
li Jim
iazn
imr.@
q1
Im.iv
rifi ti
ttiaw
lua
ri-r a
iLia
.nav
r@f : f
rr5O
nwi lu
i(ut le
tiiirril
, wr
1AL5
7
1- ilv
v.11
11Aio
n t lN
5hsT
11L
- N
ani7
n Anu
LLLI
N9-
mn-
n-1,41
mIa
ovi saii,
mz 1
gia
LLE Ifii
a
rnol
ir ff1
7
flunw
hif irit
yrim
oin9
i- 1Jf1
1vri-m
ln-a-q
t) luv
tiaL6
@do
wim
Jin
: fl
l5Pf
f11~
11I
1J
, WiT
IA1.1
.11f4
1 b7
711E
71V
11 ,
wrm
.fri s
tin
, wrrw
.i iio
Nnr- k
aitr
vaa
- NaT
NIL
ali1
4-1i
-aurl
igi1
71.T
411.1
@fa@
n 191
411.1
1-117
3 j1
1, 41
,1,11
fIf i
CiEJI
N0i
1A
7
II1L
1 g "4
.9i- 13
all@
j 1,1.6
1,14,1
1,1q14
°11-3
1-111
11
0.11
1N11
. 1.6:1
f1f1 1
1 ,
1 111
,11̂1.1
4 , W
ill̂1.1
9111
1-19
1 , 1
-bllV A
LL9J
nzu 1
1711-
11
,
IVI II
N.q
uw
mat 4
1 a
ti
- M
icro
lea
kage
of se
lf-et
ch a
dhes i
ve s
ys t
em
in C
lass
V c
avi
ties
etc
he d
by
Er:Y
AG
lase
r w
ith d
iffere
n t p
uls
e m
odes.
: 1
1-17 4
T114
111-
1111(
0.11
. 1f1J1
irM
@.1
11"1
41.r
11̂1
7 1 A
1141
11.I'L
'ig ,
WiT
I 1.1,1
M1
1 aw
ri3J
,1'4
1A-11
3T
BLITA
L.,119L43;m164.F
.,o
19
X 6 c-
g
3
dlr. dg
a c-- . Ir.
co lir,
t=i 0 ''
(a 0
(-. v.
,,? 0
5
c, o CZ, ...„ C̀rij
c,. z
tE a a ,,, ::
o p,, . — ..?
_ 0 Itr.
''r° c- (-6 z o
0 g g .__
a a .4 fr. 0 0 0
IrZ 1.6 CV
c-
0 0 0 C5 0
KK
U
U :u
nive
r sity
)
CD cL o .__J
, •zr .--
cz; Nr
CD "g (Ir. --
(1 c- °g
a a (P -11
-atu ca
- ." 1r.
tu 6 , p g dr, an=,
3O
''' (i
°g ir. r C ca Z
a a
r
T.
a- 6 I r.
Ir. ca rl (G -0 ,,,
as
a g B 6
(Cra.
_co.
.7 0 P
TIM ("6 c,__.
C
as
e4".a
r r
, m 5 0 g 6
- r
.... 6 M O
liX Cr" r r
1'4 Cr tc aar
..Cr" s p V. r
AG Csi
.
a3 73
CN1
I° w c-
-ZP 3tr.a
C- r° 1., g
0 o o m
(— - a a
--° i-w
_. 6
-"' C i X /r
(-- r ar
-- g 3P
a a
Cr"
0
0) 7:. E) cn c co F- r 2 2 ,... cl.) /I • • -v, ... c
CD
c .- ,-,- Et2 OD -C
'5
,,,, c
t.) aro
ar r: c•-•
,-- Cc-
.7
1,:v '7
6,. 11 if-
C Ir'"
X
v .
(9
C. C (11F1
‘,. az 0 a a g tro
I.Lci lip
4x Ir° • m tr.
X ar* ,
Ii X ir.;
lovp; p
40 as
--
,,w
ir. IX
6
0
F
" Ir.
as aici
tp
• g
C-
C.-
ra
( p
F
F v. Z °- ,
X
30 r
(1 c-
4 — •(( IR Ir. g
' Z 1. 3 (:--
X tr. IX
X g
6
ca
Z '' g 31r, ltr- g
CO
3 ir.
IIP
g
4
(IC§ C- g op
aX
g
11C°
,
a
(--° -
1 ',, 3 " (Wag
g ,
dtz,
.1- 0 CV 2 D CT) 0 CL 2
CO J < H
U.) 0 I E D CO
CO oo D
Y th 121
fr- (- c r
ac. .,.- a a
g ‘7 .
g (NJ
C\I 1....
t.1.- aa Cr"
'--
0, (- F -. azp
m 6 iro
(D ds
X = LI>
M Ic„
r
d a ca _r, C 0 =. 03 C 0 E Cr) a -0 -Cs C aS
c:7) C C 0 .-S C CD c
0 z.,-. a) (r3 -I 'r7 co
ilr° 0 (- 0 r
.
,,,z .7 X
tr.
a VO ,11" (;j (
Ir.
0 c-.
t 47-; c CD
"cs . ._ >+ 2 (1)
+-C-. 4) 43 ci) Lo
a) -La _
ir-a4
-3-q1
66at'f
i1LT
hmno
as
-v. a4.,,, X -- 6 N- a as C cm
-Ti 110-1 --° a a tl- (-- 'CP " a a v„ ip -0 Ir.Z (.- aura 0 '"7 r
C- g c° (.° 1,,
t 0 67
va g (-0
p 0 ,-. (- CV -
tenT
a mie
N4. 1
1111
1E1M
11
ca V. r
,3
°g as (P
-ate 7P
-atu as
tr.- ca ao 0 3c,
'Ilt=1 .)r
r
r
cl Fr
°0 tr. r ca ca Z
- fi
lI1J7
7E. 11
U1, 7@
.1
Per
spec
tive
on
laser in
pro
stho d
ontic
s: S
c ien
ce o
f
inte
llig e
nce
Tqu l'f
f.q1
7.11
'1-01
7
- 1
1'11
-1M
L I-1
064a.9
Bas
ic las
er in
den
tistr
y Tq
12. 1
7Ff.q
1 7.f
1i
- F1
1711
71•E
YIL I6
4a
1 V
arie
ty t
echn
iqu e
s fo
r tr
eatm
ent
of o
ral
lesi
ons
IflE
.I
L111̂
111JA
M1,
R-IT
IN
- r1
171.1
1111
1E. 11:4
5. 1
P
IPS
for
roo
t can
al
trea
tment IflE
J @
:Y11 A
i.Tw
i n7
vie lm
-14a
A@
- F
1 179
J711
11E. 1
65@
.1
Man
agem
ent TM
D w
ith LLLT
Iqq.1
1,11 1
N
- n
-II1
. 177E
.11L I6
5@
Lase
r-so
ft t is
sue
surg
ery
Tq
u cri
cm-bi
. a7m
444 G 1
51N
1If1
1 fl se
LL
@. 1'
1 vt
-L.L-a i
Eri
- ri
- 119
1171
. 112.1
1ial A
ltern
ativ
e las
er t
hera
py in
oral
liche
n p
lanus
Tq1E
1
ilN
ii11 1
M114
11'0
1
- I T
IIIJ
IM1U
6 5a
Pa
in re
lieved in
min
or a
pht
hous
sto
matit
is b
y la
sers
Tqu
@A
lm-1 1
.1;1'
1,n- I
NIQ
1J "
JI:if
f
- 1-
1171
_ 111
01LI
C4N
Bas
ic of La
ser in
Den
tistr
y Tq
L1 U
. ff1̂1
.1̂1.1
91f1
f°
111_ 1
711.0
1 iL
az.
r
oiamin
tili ,
r,j a
r
as Ca g (.-L,
duzi a C.
21
g'
0 R(-
M 3 g Z
dlr. dg ----''
-li
(—
Ir.
Q
C c tr, c
C
c- b., r.
C 0 ',' -° 07 0
KK
U
( F = f
acu
lty a
nd
U =
un
ive r
sity
)
CD Ct 0 __I
r
(s) co cs) 05
cm - g Ir. c-
(i a' ' °g (Pdd
s§
CE ad Ca
11,..Z
-
CD aF
, drg aitp
C'' dg R g(-
(- "") g ct '
°g tr. (- ca a
t̂alliit
g160f4
M11,1
)
- a
. 1'1
1,U-1J
. 64
@.9 M
icro
leak
age
of
self-
etch
adh
esiv
e s
yst
em
in C
lass
V c
avi
ties
etc
hed
by
Er:
YA
G la
s er
with
diff
eren
t pul
se m
ode
s.
- a. 1
19A1
q).
Lilo-1
Alte
rnat
ive
the
rapy
fo
r oral
lich
en
pla
nus
with
low
inte
nsity
lase
r th
erap
y a
nd r
ed
lig
ht la
ser:
A c
ase
re
port
- 14Y
11N.
191
'1111
S1
LLatflf
lg; t5
a5 Effe
ct o
f blu
e li
ght a
nd
hyd
rog
en
pero
xide
on
Po
rphy
rom
onas
gin
giva
lis in
bio
film
.
-
a. 1
4,.
`1̂1. 1̂
1.1gE
7 IA
N T
he s
tudy
of
de
ntal s
tude
nt e
xperi
ence
to
lase
r in D
en
tistr
y
-
111̂1
41. 9
:1-q1-1
ql-t
1145
141
1Kl
a 64
e1
Effi
cacy
of E
ryth
rosi
ne
an
d A
n thocy
an
in -
med
iate
d P
ho
tody
nam
ic T
hera
py o
n P
orph
yrom
onas
Gin
giva
lis
bio f
ilms
- 1/1
"1. b
l-JTYl
f g
lii- 9
11,61irp
°1111
6La
n-Int
r, 6
'01
Inte
rstit
ial l
ase
r th
erap
y usin
g
Nd:
YA
G a
n d d
iode
lase
r
- i.
tim
. Lrit-
un n
7a J
bl-11
1-114
LLan
-n-wz
64a
1 A
phy
sica
l alte
ratio
n in
tis
sue
bloc
ks irr
adia
ted
by
dio
de l
aser
an
d N
d: Y
AG
lase
r irr
adia
ting to
diff
ere
nt
-ulih
nsay l
vin
lvilo
@in
JT-Io
LLar
alLa
uoir o
lrmLa
vro f 6
f1f1
,nu
tlIr4
3J -Iti
n17
BLM
13 Li
-nhvisa
Alw
ait
35 flUrr
it
- lu
vr- rtib
La
ser (P
IPS
) in E
ndo
Sta
r Wa
r gu
lf! @
.v1v
1.q5
.Ta
lnI 6ih
1i4
m
c— R c-
c- -g ca ca --g ar a,
a r
c Ca P tn -. IS (- .,
ad -Ix _ -.9 —. (-
It°
C-- C tro ci (1 ca os -11co t72: (- c-c- ar t.1 ',Ins r 0
V bq' 2ad Ir. tr.
_,,
C" ., .cp (-
..., ar m -
C- .oc
1
=
U) r R
dg U)
do> ao
-a te a , 33
1/3 3,
c ca 0
o-.
(." bq
0
bq u-. c
U) '.c 0
KK
U
1 (F
= facu
lty a
nd
U = u
niv
ers
ity)
C9 fY 0 _1
o Lc) co
C6
o LO
CO
co a)
(-6
c c) 0')
c6
in in co d- LD
df
ca -g Ir.
ag
c-
-a -ate
- a aa
(m
Va.- M
dF
& 3,,
r. a&
g
r 0? g
ra z
elit=1
a g c-.
CO co
c- .cP
, as
v-- , d(- t
'1. -a
g
2 _J
C- tP
(I r°
V° a Ir°
g c- <7
e3
r -V. I.
ca
-. (6
3'' .--- (r.
Cp
-
0? 0 1.1
(.0 -0 .
-11
-il g )
Ir. r A
Ir°
('D
aF c,
3
,_. 1
X
as U) -0
'-°g a
'c. 112
__,*? -
lir
t=1
a .
t,-.
4P (- u-. t,
4-<, 0,, tc,
TIC"
•
_... .--,
,--'' -
lag tru
as
-1:1
1„,„ g z (— M
x -,
3
Z
3-, 0-,
CR
°
a F
P c7
1 X
LO
'm
g a (-„
0
.4-
(-. .(7
=1`' a a (ro
-- d
L° -11X
e3
g
_I
ir. c- (— as
a r R tq' d a if, g r 07
-0 a)
ca "15 a)
.
c
•E CU 0 o
co _c,
c CO
C.) C .(
_c -L-
„.,' v., 4-
w a)
.5 =
LLI
(0 0 c.
3 g
.—. '
-+C' .0)
- Jo
u.)
,__— o :a
71 .
ED .0 — 0.) GO MI
' - 2 >,
_C
0 0_
0
0_
cll -C
.0 E co = >, -0 o --. 0 = 0-
-
ca
g.- (—
,t-i -
3 ,, ,-,
g tr. tg-
•
X
(,__.
, 0
•1:5 (13 c 0 0 c2
(--
'.
g 3 co
0
co
; c-
°L.P la- as
tr.
3
' 'IX ,,, q g
_.,
cr. r
(— t'.1
tIC°
'IP' a a " g
ap
c
-..=
9--
.4-
co n C
a ag c, c
0 g -C 0 0
co -F3
8 (...,- g (1) C-
*CP -'-' ,__,`9 >, ko-, t=p, ca_ ItrD „ 2 00? Ir. a) -V'''. ----
3( .0 ., (-- _ E , RI a g-ate
,-
=
-0 a a °Ir° 0 V-. g
"alP
-C •
4-. _.1 a CO c cis tg tr. 0 (r. c- 0 ,= (
„...`1-7; tq r. QC°
a
Cs'• IP'
2% a d
' >a) Ir°
:.--. g
CD 0.
>, 3 W e,
0 c as C
-0 c
•E E >, o -c
0 C 7) 2
-C -, a)
9-6 >, 0 a)
•5
LLI
a(m F
dr
a(m
r° a
g ._.
X m g
4__.
• 2 5
•c
(/) C ca
° 70-
as -0 f3 C g `-' CS) =
--2 C 0
-C .0)
=
70
7._ al
0 0
• - X • - "0
E =
a3
as
3 Q
aR
as
IR
,,,z a r
R
g arc,
...-.
0 o .4-
g (-
°CP .,..
Ir.
(- 0
co ,-•
11
a4, g
2 _J 0:1
tr. (-
-- bel
4 r' IP ,
d d ir°
<7
U) .7
U) 0
(.-.. 1,
g
C U)
"P "(1
°9 —0 CZ
-1zi 4 (--. tr.
0 -TM
CZ g
a a U)
ca --. Air.
P g tv
X
r (IR
= C°'
r ag
ca t-,
r ----°
- 3' V° Ir.
P .9
'9". C"
0
V X
(6
-., g ap G—‘. r t•—.
= a a
am - fr.
p
r, 0-' a am
g
,-. 0
0 '
X
g
Lr)
-11 .tr
t'q
'''Ir° U) tg
m
x
g
a
lits 3
CP
U) r R
r a--
F-''' -0 as
0 a
4-atq
(-.
a r
C
it D
(F =
fac
ulty
an
d
sto
matitis
pat i
ent
s. L
aser
Th
era
py 2
013;
22( 4
): 2
83
-28
9.
- S
att
ayut S
, N
akk
yo P
, P
hu
sr inuan P
, S
angia
msa
k T,
Phio
lueang R
. CO
2
- S
att
ayut S
, T
rivi
bulw
anic
h, J. b
, P
ipith
iru
nka
rn,
N.b
, Danv
irut
ai, N
.b. A
clin
ical eff
i cacy
of
usin
g C
O2
lase
r irra
dia
t ing to
tra
nsp
are
nt g
el on a
phth
ous
c-
Ko
C
CC Ca
CO a6
(
tr4 c
Ca
CD
0
Ca trir.
07 aw as
as
-CCP
'CU c-
07
<<tr° ca
am
Ca
m
"P co
la aw
aw
3.1
a-ii
Ern
oirf
i iv,Ia
il TIo
n-n- l
ivin
-IIiM
4, -)
tr.
tr. Ca
Col tV°
Fa°
aka
G-0
A r 0
0 0 '- air. tr. CO
r Cc.
07 ca
(r.
• tr. • l
`'"?
a X • 1.1r,
a
cp q=1 c-
0
• a
z,
-tr. aw r
aaP
,„, C- t , R 0
g tm <
-1- ci :,,-., 3 -, z
a g c-
Ca
at,°
a5
ac;
as a- co
11 va cG
F X ca
co ca
«,7 c fr.
ca
a
c- C-
Cn ca
a (p r as
r C- -ate 07 ca
-tr.a
X r t=1
1.;.°
g
3 CP a gc-
t7-: r 0 l'
a r c- ra a
-tr. X -.0 C
a 1
C \I cri
a
a0 a a
5-g -''
am .7
a2 --cl r v. 0t'l
a r ..?
t rr.
cm "-''... V. r Z v. r r
CM -trfr"
C‘I M r z., C g _r ..,
g`"
C c—R
d M
do,
-ate
(— R as le,
ff7
Z —
C 0
acrf m Z fp
c c 0 '00 07 CO
KK
U
(F =
fa
cul
ty a
nd
U = u
n ive
rsity
)
0 Et a --1
CD Ir° l-
(1
(- °g as ca
"a
-(It as
'-. Ir.-- t6 ca
g )co d zitz,
Co g R c- g
c—
°g cr. c— ca ca Z
- Sa t
tayu
t S, L
ow In
tens
ity L
aser
for R
educ
ing
Pa
in fr o
m A
nes t
hetic
Pa
lata
l
Inj e
ctio
n. P
ho
tom
e dic
ine
and
Lase
r Sur
gery
201
4 D
OI:
10.1
089 /
pho
.201
4.37
70
- Piji
tta C
him
tim
, Thi
tira t
Hee
bth
ama
i, Ju
tip
ond
Pha
nom
bu
ale
rt.
Mic
role
aka
ge o
f se
lf-e t
ch
a dh
es
ive
syst
em in
Cla
ss V
ca
vit i
es
etc
hed
by
Er:
YA
G la
ser
with
diff
ere
nt p
uls
e m
odes.
In T
he 4
r d inte
rnat
iona
l
LDR
G- K
KU
&S
AR
AB
UR
I HO
SP
ITA
L S
y mp
osiu
m 2
014
on L
ase
rs in
Den
tistr
y; R
esea
rch
and
Nov
el
Tec
hniq
ue; 3
1-1
r it
giflE1
1, 125
56;
IT16
65111
,1E
1', 111
1,11,U
ra i5W
aill
oinl
vigl i
; 201
4, p
. 21- 2
6.
- W
ilaira
t S
arid
eec
haig
ul,
Sa
jee
Sa
ttayu
t. A
ltern
ativ
e th
era
py
for
ora
l
lich
en
pla
nus
with
low
int
ens
ity las
er t
he
rap
y a
nd
red li
gh
t las
er: A
case
rep
ort.
In T
he 4
rd in
tern
atio
nal L
DR
G- K
KU
&S
AR
AB
UR
I
HO
SP
ITA
L S
y mp o
sium
201
4 o
n L
ase
rs in
De
n tis
try
; Res
earc
h a
nd
Nove
l Tec
hniq
ue; 3
1-1
f iLI
El'IL
IU 2
556;
TS1
1,651. 1
1,Van1
1141
,1 A146
-1 (1
1,1Rn
o i; 2
014, p
. 27
- 30.
m c—
c=a as Z g (-o
d/itg dW
'A 3
J1 EJ
LIOW1
•'"
3 Z
a afr„
,., -a
dd as t.
---
c 0
1 v. oY Q (-
k.1 4•-
o c
U) bra o
KK
U
(F =
facu
lty a
nd
U = u
niv
ers
ity)
0
0 J
e tbtuuntti ur,mktj1:,m11[LIg
err.
i6,..e.y.,to rc Llatunttti t4tt_.u
m
-C' -0 D V)
-cj5.
c a) -0
0 >, -0 ° -rn =CD I-
D E cz Q
_C (.) D 0
E
(5 -4-, co CD) c 0 0_ '
-c-fs c 0
'4=-• _CZ
cl) -.- .0
12 .._
CI) FE __C
C-- . -. u) ---- c a) 0 . (D'-• u) co _1 0_, a) 0 0
-c 0 a X a)
c ._ V) s._ a) u) CO -1 ,c .._, 71- .-- 0
E D (7) 0 a E >,
Cf) < 1- CL. u) 0 I — Et D 12°
< CI) 06 D
Y Ur' E-. 0 J
ifi LO LO (-.,
C-- 0
r- 1 c7) 6 D .0- E ..0 00 i_ TD >. 0 Z Ti c ca _C 0 s- (ip, U) a) fY . _ a-' t,) _,_, C CI) 0
o'j CO ci._ ,i: ,L' CD CN • - a
* (- o
,,,,, 0
1c, -11Cr'' 0
Cr. -az a a co E
cr,, __0 7..,
G__.
4,,7 7 >, co • ' ,,,('-1- - -• (I)
u) 6 c 0 CI as _Y (3, 4') 0 H c 0 o -," "...
_ TD o CD) 2 cO C C(5 C cc5
F-
-0 Ti 2
u) '
c -E co >, 8 _C c < -o C CZ 0
w 2
...c .,_ ?, iii ,_ 0 >, 0 3 - W
0) C co 2 ci) c 2 CO ,..,C C E co 0 Y CO „)
2 a) a) H
-
(/) E _ 0 ifi • u) To > "(7)) C 0
c 0 E 2 >,
_C 0_ " 0
0... C o 0_>'
2 a) ..c F-- .0 - ct5 c
Ti>-• 6 - c) E -0 a) _(.,,5
,-, D (1.) E
06 D Y ( r' L't"/
_ as E 0 .- C s- a) "E' - - -0 ,- d- a)
. H-C c
• 2
:'-' C
-L-' c5) -_ c cl.) 0 " 0) cs) c •c7)
'CO'
_C 2 co a) (0 CD ec ..: "C' .-. 0 f a) 0
co 0 (/) as ._, c 0
'71- ON
E . g - E >., u) -1 < I- LT u) 0 i
cc D co
<
'aT5
vro 0
1 ,, - /Cr, 0 .
e.r.. 11- Z
as
0-„ _. ',7 G... .
CO LC) I-C) CN
c-
,-,-- N- co 6 n CS . _ c -c 00
1- TD > z Ti C co
o
(6 -71- _,, 0;-)'
Cl ,t '
c) c\I a
,., (-
.,-
-; D ("3
.,._.. a5 Cf) 0 ._, CZ
Cr)
03 ..c t Cll ES 0 Z .tii C)_ CO ,_ a) 0 a. . E5 _c 0 -3 , (,)(13 E a) El) - 0 a E2 ci) a) F-
,
0
.- a) _c C -
CD CO a) -0 0 t--3 Ti = CO
0 < >_ ••• -o Z C -- u) D ›, coc)- a) -.S " ccs -
TO .-.=.. -
CO " CO E
- o
0 (N E 0 - - (r)
> CO -I -5 - a. u)
0 1
E D ca
< CI) ...„ `-'V D
(-9 Et a (-0 c 0
,=, co E " 0 c
0
(1:5' Lc) cv , C-* o
N- -,--
00 . -
CS ' E = 0 Q) i_
TD > 0 z Ti c co
_C 0 03 a)
a) Et
a) a
. ,- 0 CO
0
C
in r-'-- •sj-
0-
T--- 0 C \I --.
E bCro 0
1('-' -(1 Cr° 0
- 0 a a
(LT, 7;
3 ,-
(- e---
F1' as
d (-0 allIP a`'
g°-
m C-
s
g g' Z
ts dtr,
° -11
c aa as 1/,
Ku-0
g lq
CO '.. —`'
M
ro
‘7 ca
KK
U
U = u
niv
ers i
ty)
0 1: 0 J
0
tr° c-
g gg F2
°g as
--(1
-ate as CL
V..' t6 (-0 aF g d r, anzi C. ag c-g g (- g
(i C- °g Ir. c- ca ca a
- P
awee
na T
amm
ata
rata
rn, P
icha
ya V
ieng
tee
raw
at,
Pie
ngkh
wan
Atip
atya
kul,
Saj
ee S
atta
yut.
A p
hysi
cal a
ltera
tion
in t
issu
e b
lock
s
irrad
iate
d b
y di
ode
lase
r and
Nd:
YA
G la
s er
irrad
iatin
g to
diff
eren
t
chr
omop
hore
dye
s on
ora
l so f
t tis
sue.
In
The
4rd
in
tern
atio
nal
LDR
G- K
KU
&S
AR
AB
UR
I HO
SP
ITAL
Sym
p osi
um 2
014
on
Lase
rs in
Den
tistr
y; R
esea
rch
and
Nov
el
Tec
hniq
ue; 3
1-1
&M
IMI 2
556;
IT
1665
. 1
1,fr=
1 111,1
1,146101
611
V 1121
,1it1i
; 201
4, p
. 54
-58.
- S
atta
yut
S.
Bas
ic c
on
cep
ts o
f las
ers
in d
ent
istr
y; I
n A
PD
WF
LD
Lase
r sy
mp o
sium
an
d A
PD
C 20
13; 2
013
Ma
y 8
-9; K
ua
la L
um
pu
r.
- S
attayu
t S. L
ow
er i
nte
nsity
lase
r the
rapy
in t
he o
ral a
nd
'maxi
llofa
cia
l re
gio
n. In A
PD
WF
LD L
ase
r sym
pos
ium
an
d A
PD
C
2013
; 20
13
May
8-9
; Ku
ala
Lu
mp
ur.
- S
attayu
t S. N
ove
l tec
hnolo
gie
s fo
r soft
tis
sue s
urg
ery
: we
ldin
g fo
r
ora
l sof
t tis
sue
lesi
onan
d in
ters
titia
l las
er thera
py.
In
WF
LD
cong
ress
2014
; 2014 J
uly
2- 4
; Pari
s.
m c
c
-e* -0 as
g d angr a:
dg as Iro Ir. C-
(— tq
ar° bq' a a In,
V. c g
C—c'7 CM Z °, 0 (0 g -: t' —0 Cs1 C (1g l■-. r- c 1.1
C .-• "1- (—
c6
&°-
C- c— R
`
a ts
ay,, a
-ate a R as W
07 .?
z
qtr.co 0
0
V Ir. 0
co '.
KK
U
(F =
facu
lty a
nd
U =
un i
vers
ity)
CD CC 0 _1
0 tr.
cl
°& as
.7 'Cs as
cs .-- tro-is ca p
& ) co
anz,
r
(—
g
'r a
° Ir. ca ca z
-
Ju
nta
vee N
. In
flue
nce
of surf
ace
tre
atm
en
ts a
nd
pri
me
rs o
n s
hear
bo
nd
str
ength
of
res
in a
dhesiv
e to Y
-TZ
P c
era
mic
. T
he
Am
er ica
n
So
cie
ty of P
rost
hodo
ntic
s 2
014;
201
4 20
-21
Febru
ary
; Un
ited
Sta
tes
of A
meri
ca.
-
Ta
nta
nanug
ool
S.
Eff
ica
cy of E
ryth
rosin
e a
nd Ant h
ocya
nin
med
iate
d P
ho
tody
na
mic
Th
era
py
on
Po
rph
yro
mo
na
s G
ing
iva
lis
Bio
film
s u
sin
g g
ree
n lig
ht. In W
FLD
cong
ress
20
14
; 2
014 Ju
ly 2
-4;
Pa
ris.
-
Su
rada
Tan
tananug
ool,
Aro
on T
eera
kapo
ng
, Saj
ee S
atta
yut,
Te
era
sak
-
Wila
irat S
ar id
ee
cha
igul,
Saj
ee S
atta
yut.
Clin
ica
l out
com
e a
nd c
om
plic
atio
n
of t
reating p
ort
win
e st
ain
s w
it h dio
de la
ser:
A c
ase
re
port.
In P
roce
edin
g o
f
the 3
rd In
tern
atio
nal L
DR
G- K
KU
Sym
p osi
um 2
01
3 o
n Lase
rs in
De
n tis
try
;
Fou
ndatio
n to F
utur
e; 2
013
Sep
5-6
; Fa
culty
of D
entis
try,
Khon K
ae
n
Uni
vers
ity. K
hon
Kae
n: K
lung
nana
tha
m; 2
013, p
. 45
-48.
m
C--
d Ca _ID
dug
Co a&
cr. (—
VI ac-.3 Fr as
Cr. (--
C '7 CG 07 P
"a(r° (N
(— . cIE Cro C- <— P
a in E c6 g
C (-
a g tu
acr. aF s--" -11 a , as V".
..?
C CD (°
TW'
r tr. 0 N
D y
(F =
fac
ulty
an
d
U = u
niv
ersi
ty)
0 CC 0 _I
ca
Ir.
(1 F
c' aa p
-7
- (UG ad C(0
Ir.-- tn co
d 0
a,
r a
c-
C.
a
( ° tr. (- C (-a
g
••_:,
>, co .„
ics
0.)
.c73' Ci)
c CU -C
CD (1) 2
0 z
rtS a co
a)
a -
• - as _c 0
co 0 c0 s_ a) a) I- H- _,__, QS CL oo
0 0
05 (,)
co
a)
7:3 0
-o coic ,.- -
0,0 - c‘) - (..D < >-
73
,-, 0 c o
co ,-- 0 a (TS >
— 0 _c a - , co
C 0 = co y
0 0
CL
Cll t
Z
o
_c
o
0)
-E -0
a) 0
2 a. c - 5-, C3 D 0 ., 0
4uL
0 - -- > C .- c
a as '-' 0
_c --•
,L-- - W CO
(-zs -4.=, = 0 i•-•
'' c --
0
.., -. (7)
-_.=_ c 0
0
12
CD u) al. - - 1 c 0 (-0 ,_ cp CNI
D
.0--- 0 a_
E >, u)
0 12L r-_-.) -J
CO E 0 -- •ti') C , - - CD
- -
Co
C
C Q)
co
c o =
U) =
C a) 0 4- 0 >, - D
CU
Li- - - co 6
a 0
a° \--- cp N -as %--- D -.--,
U-
°
c 0 •- 7 .-, 03 p c
o LI_
ro E ca .= _C) CI) 0 i
18 ---
E I-
- E
-_p E --. 0 as :-C,
0:—
-E a) c,z5
-0 E 0 C a) _C a_
-.0 c
o_
"7" D -,
,
_
>, _0
D co r .S2 CD 0) °
?-=' (,3-
>
u) u) a5
(7)
c
E a)
- (7.; >, u) '3-) c7) 0
-0' 0
0 z1) I
4- -di u) y_. 0 (I) 0) ct
co 0
TD
0 - 2
D c-r) CD -c
LO
0) C -,-,-- y) _
0 L-- a_
.E
(cii 1 -0 o E
a) u)
1
02 0
- D _, ..I-4 - § 5._ 0 u) co _
(9 <
>-
iii
‘E
. _
-,, u) = c 0 0
c
,_. Q) w
-1 , 0
co .- P
E .,r
o a
>,
D
0 t:
CI -I To c 0 = co c
'07) -.-
N i
c a) co Y
c 0 -c
''' t7)
--,--- C 0
.-- o >,
0 ca
LL e5 L6
a 0
w co
Q CN1
4i-
5
LL 0 -.-, c 0 - 'Ed -0 c D o
u_
• r--- Lc)
CO I-C)
Q-- co E)
CV _ E as -c t''8 c co c
0) C
2
0 CO
E 0 -C
1, ._ u) o
-,..=> - D
,
c
>a
c
0) C a)
:,-
E
a) o) a,c
co >, co c
LT- E. L_ as
178 ,... ca -E5 E E (-0 I-
_a) - (I)
'z) co ci- ,
c as
Cr) U) co
co -0 0
--5
0
C) (D
° C m ao
> -9
t,',
2 -.- c ._
< —1 D >, CIS
ca Cr) 0 CD
.-cF co -
-5 ._. CO •._ s as a - <(
0 45
w w ..= = o u)
To b-
g a) U) >' -0
0- r a o E 0
o
--' ,02 0
0 co E -= al - .7=5 co 1- - ,c5
u) a) - 0 < >- . • 0 Z
-o
T o o_ E >, u)
a ,..- '-',-7, 1--1 _I
ca C 0 't E LD
-P_ co
5 0) c - -0 a) a) 0 o s- 0_ c -
>:, p D ii
-(5
5..
ifi >,
v a5 u_ ..__ co Lo' a
ciD Co .,- C) CN
- El2
*5 LL 0 c o
'c'Ti -0 c
.., 4-, u) 47-'- c cl) 0 .c
Lw
w (U
_1
C ° co ,_ c) c\I
(T.)
CO 00 Lo
0..
05 0 cN • - E _ c C ca C
C '
-2
,C‘ct) Y c
2
a) > - c D
C a) CO Y C
-c Y
rn Irz c a) 0
C (-
r
c= -g
as CL
a altz,,
r a
m c— A
g g°. tM
tm 3 tro g
-a te
A as tr.
ca air g
o g tq V° C '. —. .7 ca
KK
U
( F =
fa
culty
an
d
U = u
nive
rsity
)
0 CC 0 _i
Cal '-g ir, c-
ag (—
°g as
-ice -ate
as ._.. V..- t'5 co aF g dc,
411/=1 3 r°
A g g ..? g
4 g C—*g tr. C ("5 Z
- Pe n
siri
Sae
ntha
vees
uk,
Naw
ara
t S
anj a
ndee
, Tee
rapa
t Tre
era
tsa
kulc
hai,
Pee
rapa
t No
rate
etha
n, S
ajee
Sat
tayu
t. A
n in
-vitr
o st
udy
on
the
phy
s ica
l and
hist
olo
gica
l effe
cts
of w
eldi
ng te
chn
ique
with
808
nm
dio
de la
ser
In
Pro
ceed
ing
of t
he 3
rd In
tern
atio
nal
LDR
G-K
KU
Sy m
posi
um 2
013
on L
aser
s
in D
entis
try;
Fou
ndat
ion
to F
utu
re; 2
01
3 S
ep 5
-6; F
acu
lty of D
entis
try,
Kho
n
Kae
n U
niv
ersi
ty. K
hon
Kae
n: K
lung
nana
tham
; 20
13, p
. 35-
42.
hiac
usi1
i2viE
nnT
( 25 *
Ara
)
TP1.
111̂1
41.0
1T.P
il
bIt0
121- (
11'Td,1
1111
1.17'r
.4'flit1
11
:',11 n
11,fl
LeN
FiV
IEIT
V1
1 4-1,0
1
LLIAIY
MPI-M
ffl f)
-
Intr
oduc t
ion
to L
ase
r D
enti
stry
Las
er p
hys
ics
and
tissu
e int
era
ctio
n.
In L
aser
The
rapy
in D
enti
s try
: Tra
nsfe
rrin
g R
esea
rch
to P
ract
ice
;
11- 1
2 '111
.r1 11.
1 255
7; n
tizvi
umow
ito i
ngw
riwon
lviti
n kri
vauu
riu.
-
High inte
nsity
las
er t
he
rap
y in
so
ft t
issu
e In
Lase
r Th
era
py
in
Den
tistr
y: T
rans
ferr
ing R
esea
rch
to P
rac t
ice
; 1
1-1
2 Vr
t,n01
3.1 2
55
7;
Ang,41
.016
1,14111
12.1 P
1101
P1 W
1,117
j1Iltr4
21621
(aUL
Liild
.
M c— A
C -g as ca _.
ar,g
r,
C Q. Cr A
IE A
"Cl Cr: (— C
(1 F2 0E
cr. C-
ac'
Fp.,
a IP
aa-co c6
-a C" A
(—
g°-
c—
ZU
ta a y. ag
-11 g c— d a le".
-.-
77
ca 0-. #
— co
KK
U
(F =
facu
lty a
nd
U =
uni
vers
ity)
0 11 a —.1
le". C'
(2 °g as (P
-11
-CU as C-6 =r,
-.- tr., Z CD ap g 4c.
aq=,
3 (--
g # (—
ci
-'' °g ir, C-
a a
-
Low
int
ens
ity las
er t
hera
py
and a
pp
licat
ion
in
de
nta
l clin
ics.
In
Lase
r The
rapy
in D
en t
istr
y: T
rans
ferr
ing R
esea
rch
to P
ract
ice
; 11-1
2
ritn
R3. 1
2557
; A
rldt il-1
011,1
1/171
2.1W
W1 f
3.11
/11'1111
E1'1A
1611
t141,Lf
ild.
-
Bas
ic las
ers
in d
ent
istr
y. L
ase r
s in
Den
tistr
y: h
isto
ry to
up
da
te.
In
rd
The
4 in
tern
a tio
nal L
DR
G- K
KU
&S
AR
AB
UR
I HO
SP
ITA
L S
y mpo
sium
2014
on
Lase
rs in
De
ntis
try
; Re
sea
rch
and
No v
el
Tec
hniq
ue
; 31
-1
riuti h
tn.4
2556
; TT1
1,1,21. 1
wva
niuueilvith v
ravi
g i.
vm.m
.qtu
112
111,\11 an
Nut
y P)
-
Hig
h in
tens
ity la
ser
t he
rap
y in
hard
tis
sue
an d
Sel
ec t
ive
inte
nsity
lase
r thera
py.
In
Lase
r T
hera
py in
Den
tist
ry: T
ran
sfe
rrin
g R
esea
rch
to
Pra
ctic
e; 1
1-12 VI
U'IA
142
55
7; P
ILIZ
17110
161, 1
MIP
1'104
1f
rlm
nA
m
intu
ariu
.
m C-
c-
(-2 as
g ar. lit.1
36°
Z
3 g
tG
3 Ira a g
s-"' -71
as Ir.
07
(a 0 ii tr.
m bq bq
0(f--
0 b0 .° .7
co
KK
U
1 (F
= f
acu
lty a
nd
U =
un
ivers
ity)
0
Ce
0 _J
-g ir.
(1 °
d a ce .,,
ate .7 a d c6
--- tr.'
a 0 a
3 g
(— g c- .7
4
c- og o, Ca
-E .--.(1)
0 0 as —..
--7.•
CU
a) E 0) -- o_ 0
0
CO
0) c -E _C
0.) C N
>
2 0
cn _I
D CO
< CD 06 D y Y
f:
a
c 0 -.-7. co c ' a)
2
7r
—
•
CD
as -0 a D 0
(1) E
To
C
cz _C
((Pa cn cla fX •
C
(1.)
0
o)
a) 0 CO
J
d- ,•-•
0
N
a) o 0_
E >, CO
_1 <
co 0 1
,
C-
C°
Ica _.
70-
—0
Cr°
0-. c,--0
(I:5 Lo in
CN
(—
i
,— cY)
.G
.0- E 8
Oa > o Z
. - G .a
_c
-.--'
-t7)
'., -c'f-5 --, c a) a
Ef2
cts _1
"Z-.- c
C --
a 2
-,--'
U)
ir) E _,- 11•5_
CD -L- — ,
>,
_J
a-
i
D co
Cl) o5
y Y a f:
a
c
o co E C
. —
-2
.ct- cp
_c C
• tf3
-o o_ D
t,G-c.
z -C) ,.,.,c ,v _c 2
CO o a)
0
.,. -v) :i2,
c
c • —
v-2 G.) 2 _1 c
0
-1- .-- o (NI D
(/) 0_ E >, Cl)
0
E
,-
t,c,-. Co
-Pm --(ra- Co
71G-0
c as 0 z a —o
;7„
(15 10
in CN
0 e-
3
N- i
co ,■••'
0- _c
0 0 I—
< -a
--- c-
T.
(IC°
'g 1C°
6r,' 4 cr. E c,,
ag (14
•
(,-.
co a
0 .--, ?' 'CI') E
0 --, c cll a c
' — w 0 ccS
_1
--„'
c: -(7) --.7--, c
CD -0 .E
.) 0 v) 03 cp
'Fn. (75
m ,
o
E . 0
o_ >,
Cl)
—I < Cl) 0 I
n,
D ,,_, co
< U) 06 Y
a
c[ a _J
To
c o -- rz C I._
0 .0
z, - d"
a.) _c 1—
‘— CO
D 0- c _c 8
;. 0
Z
-0 c co
_, . ,...,L- a) cp ce ..._--
C
0
a
C — u) ,- (I) W
3 C 0
'71 ,- c) C \ I
-.'
-a
<6—''
(—.
66.,
-a Gm -/ (o o
L_C''
'.-- as co
L"
o-7 G-. 0— ( .6 in
L.0 C \I
(—
(—
(— ar- i--2- as Ca
a (— alita aco
0 c —
''' Z
t5
ay. av.
-ate
33 33 t°
--.
av,ca
tq tq
0 ‘.. -
0
Q
V°
.7
KK
U
U =
un
iver
sity
)
0 Ct 0 _J
e.u..ui-tw
iLtp;m14,E1
,T,wrifitg
erj.
t6e.e.e.),prEt_Lo9tuvrttl1Llp.U-lA
M
Tfai.
VIIA
LMT.11
t-l-r
ii A-
1J11'1
risfll
- M
anag
ement T
MD
with
LLLT
. L
ase r
s in
Den
tist
ry: h
isto
ry to
up
dat
e. I
n T
he
rd
4 in
tern
ati
onal L
DR
G- K
KU
&S
AR
AB
UR
I HO
SP
ITA
L S
ym
pos
ium
20
14
on
Las
ers
in D
enti
stry
; R
esea
rch a
nd
Novel T
echn
ique;
31
- 1
r11,1
2_1'1U
1d
2556; IN
66n
6m
&.5t-il
1d61 allw
afy
i -
Ca
n p
ho
tod
ynam
ic t
he
rapy t
rea
t o
ral lich
en
pla
nus
eff
ecti
ve
ly 1
, 14
nni i
Tz-,
6113.11
6-rin
n2
Bim
onth
ly L
ase
r M
eet i
ng P
21
11
16 ;
7 v
irpl
-p-in
255
7; R
altY
1 '101
61:V\
IVI t
ffil
Afri
f
11. g1
111.1A
11P I
ET
'111 J
it3.,1
11 (1
,1-fl 2
t17a
41/1 9
J)
-
Las
er s
afe
ty a
nd m
ac
hin
e. I
n L
ase
r T
her
apy i
n D
enti
stry
:
Tra
ns f
erri
ng R
ese
arc
h to
Pra
cti
ce;
11
-12
1 1141
011,I
25
57
; Arign
fila
66VIV
IE11 1
1Mlf
1. 11
K1V
IEJ1
7ti6 H
1466
1-11,1
. -
Las
er p
hys
ics
and t i
ssue
inte
rac
tio n
. In
Las
er T
her
apy i
n D
enti
s try
:
Tra
ns f
erri
ng R
esea
rch to
Pra
ctic
e; 1
1-1
2 3 1
1,11
A1. 1
2557; P
it1,1
:17 1
101
LLVI
IIEI M
AV
I f 3
.11,1
111(1
2. 11A
6N
14
1,11i1
,1.
0 C-
c ---
C-
33
C C-
tS P
d
ta
do, aF
-nom a (-
as tro
---
.7
(a
lam g C
g c"
tg r.
`‘' ..7 0
KKU
1 (F
= fac
ulty
an d
U =
univ
ersi
ty)
0 CC 0 _J
Ir. C-
a --(= °F
a a CP
,, -(Ig
wo- tU co p
F 3,- an=,
c° a
r g
c-
cf 52
°F
C -
CZ
73 C
0
-(7)
r_E •
_,-= a) N
Cs C . -
E2 0
ci) Ci3 -
0 --.-E=, a) -0 C
sU2 c/) co
0
co CO
D ' - 0 CL
E C f) < I- 0_
u) 0 1
Ca
< (I)
oe3 Y
12L 0 a _J Ta C o CO C 0 -' C
i,
a) _, I-
.- 1 CO .c6
- 0
_c m° - 1-
0.) > 0
Z
c co _C t- s U
(1) u) c:L • -
4 ./5 1,7-1 c ci.) CI .0 c./) '-- Cl.) cci _J , 0
N- c) C \ I
D
• -a
(-
s. Cr.
C° 71 (r°
7 Cr. c° g
a a co S
ST, .7 a-. C,--° -
C6 Lo C \J g o
) z
CP o r
ate r''
d =,
(- F a a
-f-J u) C 0
C
u) CO
ui , 0
0)-
2 o
0
'E'
E
(1) t--- L- 49. u.) CD C 0- E _C (1) >, — a) . s7-
> 1
-
i2 D CO
D
y
a
t:
a
Ts C 0 __, CC5 C ai .--, .c
.71-
CD -C
c - • (1) 4-' co -0 D 0 L'' o
,u) ."-
7.1 L• U) c
U)
(= ,_- -
.,-
u)
C .- s– o CI) CZ
—I c o
,- (7) CN
• D 0 D_
E > _J < I— T_
0 i
-acr°
H
-4-, C
a)
c-
6 cr. C°
-- 3/G-,,
g
10-° Z
C.
*7 C ' (:c7 LO in (N g
.- cr)
*G3-
CT _C 8
H a)
0 Z
•
,..,
_.,.
-2
U) i
.c
d g
F
c7
'" g
1(
(--
a) rE c _
(13 -0
a
2 a-,
0 ..__, . 1E
._ C 0 0 . C
e a) cn as
,--; a) E td a) ,....
76 c CO 0
2 b
12_
='. _a-
1- v-cD CN E C _ 0
0_
E (I) _J < H
0-
U)
0
- lj D CO
< CI)
D
a ct a -J To c
t , _E a)
-2 'cl-
g k-
?
CO
c7)_ - - C -C 0 0
H
-CD
0
Z D C CO _c C.) ,._
on 0
4 --(1)- C (1) a
us, a) Cr)
C
0
...
a a
%.a-. 0
--qa- g
la-. ' 0
E
,,7-.. G-.
G.--.,
Lf) C \J
C c-
C- a 3 Ca
d (-s, dq,
a c.
C- (-
ni-i',o
Rzto Rppiri 1_, re ',,m
Ft RL`
ca 5
[1,-0 ..-, c
1.1 ro c C
co '. 0
KK
U
(F =
facu
lty a
nd
U = u
niv
ers
ity)
Lt0
a _1
0 - F vo (--
F! °O ad (P
-11 77 a tu ad ra
--- 1,--- ta 0 ,, a,
ang a r ,
(1 F2
., if-c- m
T ac- c
M
b(rzi
q Cr° c.
Lo p
CO
o -' CO E
E ._ 1:2 .7j-
N _C 1- C
CD 2) = 0 CD C w
-=, 0 ({) 0 0 CO _I
CO 1
C
,—
0
CN E D - u) cD_ E (/) _ j < I- o_ u) 0 i eL D CO
< oo D
CD CL a .__,
LC) CV
,- = CO
C15. C
C _c 0 a) F_ v- > 0 z -0 c cc3 _c o CO a) a) i: -
-_- C a) 0
_ • a .--• c-
L E co
-P-.' -11(''
N --0
7 cro as 0 5
cr.' -0 04.7.
0-0
L
C
—
.c d t, ,=' ac° z
bp
4 .7 )E
,7
0 F'
as
z--
— U) c 0 -_,= ccs c t- a) C --
-2 •1- _C 1- c
C 0 o D cn
4_
°) 'cr.)
-1 I
CD
0
c
,u2 a) ct co -I C 0
T—
CD
CV E D cn 0 o_ E >,
Cl) _I I— ET_ u) 0 1
D Ca
oo D
0 _1
ci5 co co CV
N- N-CO .6 ,.--,- .- E -co Q) I
T) > 0 z -0 CO _c (2 (1:5
cll rz
-E- -(1) 0
.
LE 0 7 -V'
N -0 7 c■-,
LO
- 7,-. c
a, ac° a
(P LF
E c E cr0 t- a
kr
''-
c E
- -0- o a)
co a p E a >, C C )
_J 0 <
0 a-
tii u) 1E 0
I ,.._, LL cn D 4-=
C co -CD (__ C < -- Cl) EI2 °6
0 Y co _, . a
r2L
-E cll as D C _E -- ...) c (1) 43 cr) -4--, CO .0 o , 0 71- CO
CO ° , I-
0
,- I .,- c 0 6 C 7 E _c 0 a) I-
- a. 0 > 0 ■-" Z (- '0 C co L00 _c o s_ ii G-0 co --qcr. 0 0 W
cL . 71 Cr.
--L=. 0)
C 4
5 • - co 0 1.0 co co _1 (NJ C
-71- c- N-- 0 CV c
m C-
(-
(- a a ("6
g d r, anzi
C°
0 c-
g' ta
4g tE
4 0,
-11
(— a a ir,
op
c c 0
o-. m <— c / ro
c ro
— -7 o
KK
U
( F =
fac
ulty
an
d
U =
un
iver
sity
)
0 fY 0 J
0 -g Ir. l- g
a -( d d
-1 -am d d 0
-- fr„, F
a co 'Tctri d C°
(-- g
'r
,
Z
D.
CD 0 c — >, a 2 (1) _C I— s_ 0 u) CO _1 C — C o C.) ca
C . - a) cf) u) -7;
-0 c ,•,5 0 0 -0— >.
&.-
Q.) cn cz -1 ,
LD
E
a 1:.. ir) In CN & c-
TI CN .,_ , .--- .- a) 0
Ca s- 0-- 0 -,--, _c ,(-2 co a) u) 0 cL C s__'7 a)
c 2 1-
'°'' o 0 (— °
l'cr°
c— .&
_,,
q (-
— o dq- c- c
z- 0 4.1
111 p
's E c■-.,
.,-. q c. a
CO
(I)
iii Et C co a) g 0 C .— U) cs2 oo 0 D co co _I 6 (.5 D i2L c a3 a _.1
rp_ CO c , a) _c 0 .4-7, o (.0
7.___. C
To L.. 0.) 0 -' C . _ - - -2 >-, -,i- a CO CD &__ _c (1) F- _c _ L._ =. a) , ai ca co
-0 CI) 0_ > D .-"s= CO 0 C ,_
0 < -'<i'-) I E
-C) c as _c 0 s_ CO 0 69 _
r2
+-, co , c a) 0 C "-- ,o2 a) 0 CV
—. c 0 'q 7- o CN
E D ._ 0 0 a E
CO _i < 1--. (/) 0 2
C-
—'s 10 0-..
,,.., " 7 0-.
--a ("' CO .--/Z
7 —
0 E _.
Cr° 7; cr. c— © LO LC)
CN
C-
z
7 ,_ co 0-
.C7 E _C 0 0 F._ 0 > o Z
-a G-0
„--.., )ce (1 C°
1K a
C-.
cro
CiE CF:'
E'
Cj
172 'cr a) = H c _
,ui 0 (f)
-Lt5 >, _o
0 "4----, .-ct E o -rn
co D 0 _C :L-■ a 0 S._
o ..g_ E c ._ -o Q) >
- 0 a) 5-
c - - as a. 1
C 0
'ci-N-0 CN E
- CT) 0 a E >s U)
-1 < H
® (f)
0 i - CL D co
< c./) 06 D
a eL a — co co C 0
ITal
CZ
L_ a) -E' . _
c- 0
a z 7 x--- 0-) - - 0 4
--C- _c 0 0
I-
TO > z -o c 03 _C 2 al a) „,u) 'Li cL • - -.-,
-- -,- CD a c
.—
, co .___i
0
0
La
a)
-a.
c- --
bCro
1 T.
--(1 °
LT,
lc- z a a
—. Cr. _. sr7,
(5) LC) I-C) CN
C c-
(—
c- -g Cad d
rdg diac, C° a 0
0' m r
CaCa dg
tM ay. ag -(I
R ad (r.
P .7
11091,111-1
1tU
ps
0
11,ZU
O1
KK
U
( F = f
acu
lty a
nd
U =
un
ivers
ity)
CD CC 0 _1
co
r g ag
a) (P
-11 .? -az a a ra
,,- 0
a co q r. a
r F g r .7 g .:1 °
tro r cm a
tro
R
Wt.
'1111
.171M1
1q151-11-
-
Lase
r p
hys
ics
an
d t
issu
e int
era
ctio
n.
In L
ase
r T
he
rap
y in
De
ntis
try:
Tra
nsf
err
ing
Rese
arc
h t
o P
ract
ice
; 11
-12
9 J9r
1A3.
125
57;
Ar
LLIAI
YILI
PI1 Z
Ef1
.11,1
11111
2.11k
°H146L f
ild.
-
nnsi
zit,fl
1,6/It
iTd1
11.1M
01,6E
11.1,M
;r11T
QLLM
flY1
1,Al
valL
flviie
af I
n T
he
4rd
inte
rnatio
na
l LD
RG
- KK
U&
SA
RA
BUR
I HO
SP
ITA
L S
y mp
osiu
m 2
014 o
n
La
sers
in D
ent
istr
y; R
ese
arc
h a
nd N
ove
l Te
chniq
ue;
31
-1
414 E
1 1E1
14
255
6;
IT11
122.1
Wa:̀
, 7111
,11,144
1W
41 /
1 1,61111
,9Rnj.
.7 M F
ag M Ir c-
11P ;
1U P a IC ad m _„
.7 -a m
r 0 7-
.7 r g a t- cg
ap (r
tr, r*
apS tr. X atr° P tr. r C .7 r
r. :o° a a - ra _1,-. -' g cD P F --. M Ira m r
(— M a
r° ax ac- X
c
r
r
g°
(rstepiturcRtvriv
,Au
ttuliircu6)
9l6
.01,16131A,M,111V
IV,N
,IAL
5t,te4
egouir
escOutte
go
iR,ILS
LUV
UN
4g
g 5
cm -11g )4'4
ca
co —
g (-6
m 7.7° 0 -Ivo 0
(- _,,
‘r? m
r. z
aa Z ir.
(—
t=1 )P a" 0 ad
aA 5
cr. --*
g
cF p
§-
a a 0
Ir. co CN
.7 dop
g ,t_,, go- & IP , g
az-- 2s
Ir. c-
(- m (c°
ao
do, (- P
3 P
o
t-
0 o o 0 er co
° r R " M
, _ T- -g ra R
li-
G
Or' c- A °M r a a ca _.
ecp dr g
c_ .7
•
m c-- R r F* - a a Ca _,,
aro a=, (-, a
m )(p (Ir -cm-
—
g -- c-
,,7 Ir'P
g N---
ag a
('-' 0
tr.
(- tu --.
----* (-.
cm tr.
a a co 0 .-1
_,, .7 (— —.
IrR . a
(-a I
.4 c-
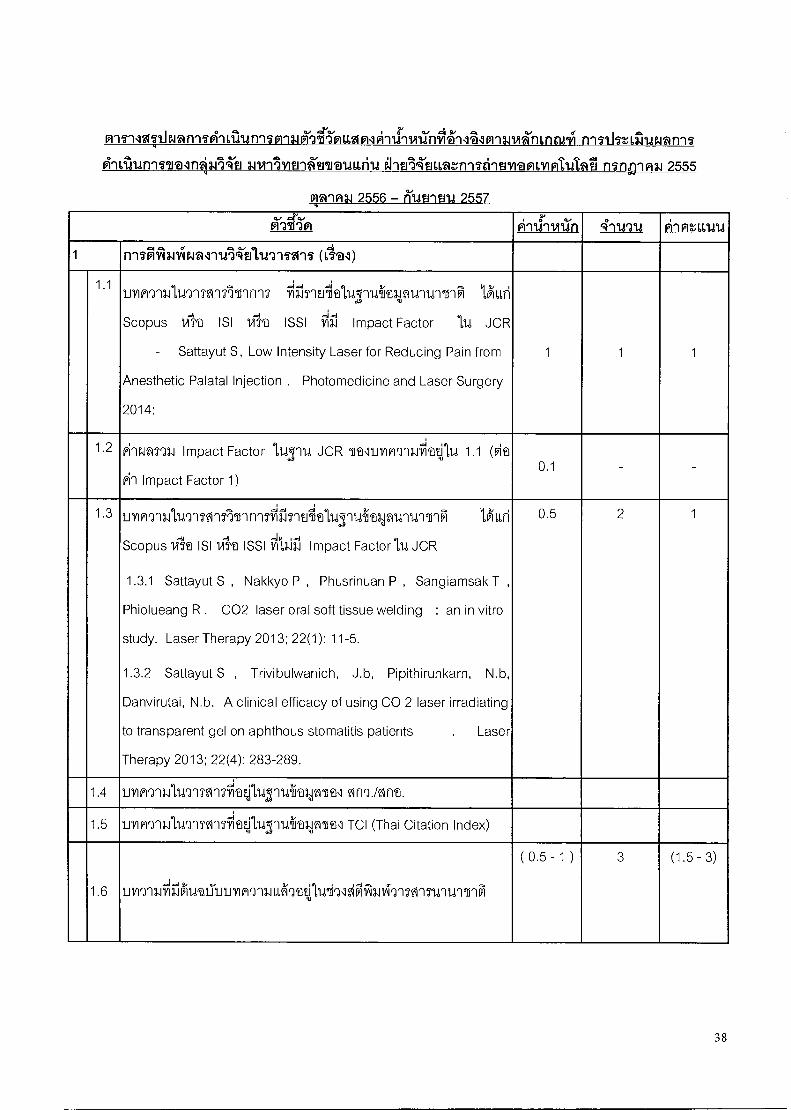
rrntlnirromn-n
a.11411511tYluvau66ri1i ehulfZuumr.rrnentruranivinti.atai n7nDipm 2555
qq9P19.1 2556 — Kum ma 2557
A'-ati'm Filtig'-wilri 4-n.2u pi-inr.iLtru 1 n-niiiiwpical-iidli'tald'IlTill (11"'@1)
1.1 UY1WY11.111,1T1SMATIMT 1711117` Eli 1,ALLri
Scopus 1,11'a ISI 1/11a ISSI frirl Impact Factor 114 JCR
- Sattayut S, Low Intensity Laser for Reducing Pain from
Anesthetic Palatal Injection . Photomedicine and Laser Surgery
2014:
1 1 1
1.2 Pinifl?93,1 Impact Factor 1,14,5q14 JCR Ttl9filA7'13AtIl1.d 1.1 (fire
vin Impact Factor 1) 0.1 _ -
1.3 uYin7ui17nni9i71innnfil8rElfal,1fs 1Araklq1'iunlinVI 1,ALLri
Scopus Vilva ISI 1if ISS11743.131 Impact Factor ILI JCR
1.3.1 Sattayut S , Nakkyo P , Phusrinuan P , Sangiamsak T ,
Phiolueang R . CO2 laser oral soft tissue welding : an in vitro
study. Laser Therapy 2013; 22(1): 11-5.
1.3.2 Sattayut S , Trivibulwanich, J.b, Pipithirunkarn, N.b,
Danvirutai, N.b. A clinical efficacy of using CO 2 laser irradiating
to transparent gel on aphthous stomatitis patients . Laser
Therapy 2013; 22(4): 283-289.
0.5 2 1
1.4 UYIAQ'llb-19'lnI'lfillq.,1111'114111(a2-0 611t1 0119Arlt.
1.5 U1IPIrnillUTITMTV;`q:11,12-11,rh1011t1 TCI (Thai Citation Index)
1.6 umna.icirAgaiTimYinqUaratitiniqlaftrirrInInnnullinM
( 0.5 - 1 ) 3 (1.5 - 3)
38
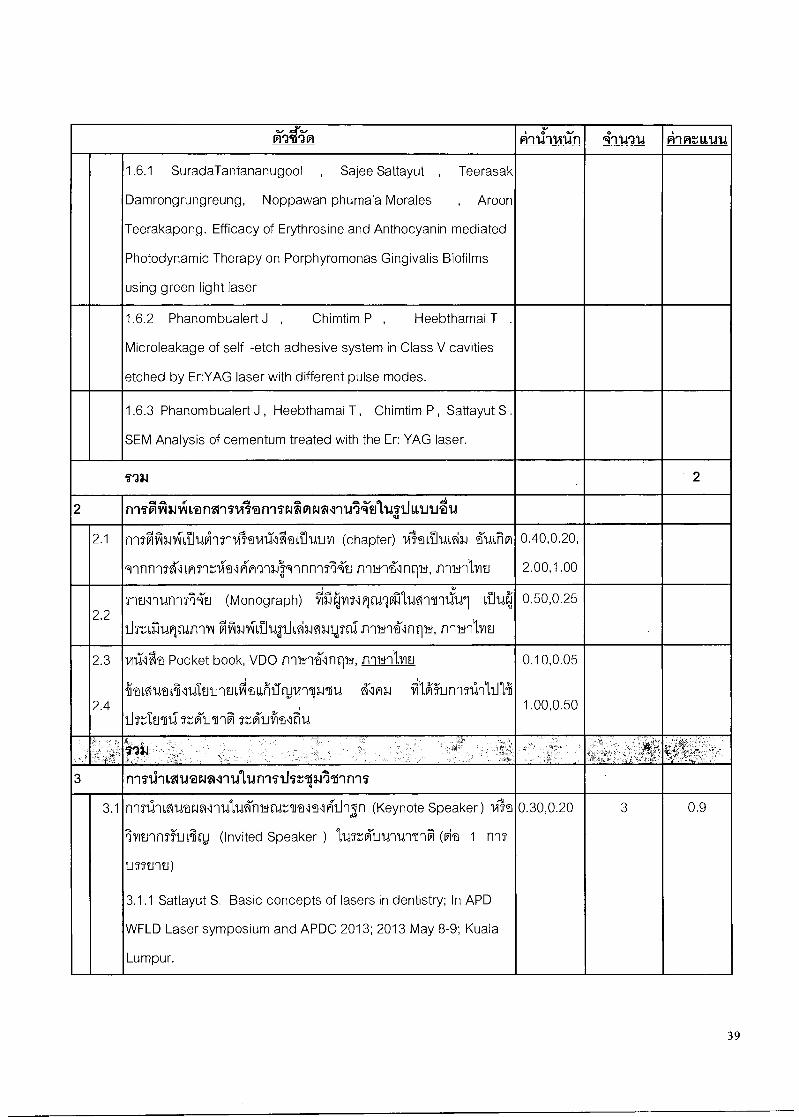
oi-atin ATLI-Ivan 4-rtrau irintavula
1.6.1 SuradaTantananugool , Sajee Sattayut , Teerasak
Damrongrungreung, Noppawan phumala Morales , Aroon
Teerakapong. Efficacy of Erythrosine and Anthocyanin mediated
Photodynamic Therapy on Porphyromonas Gingivalis Biofilms
using green light laser
1.6.2 Phanombualert J , Chimtim P , Heebthamai T .
Microleakage of self -etch adhesive system in Class V cavities
etched by Er:YAG laser with different pulse modes.
1.6.3 Phanombualert J , Heebthamai T , Chimtim P , Sattayut S .
SEM Analysis of cementum treated with the Er: YAG laser.
I'M 2
2 irngfiNiffiVanAqq`dfan'ileavlealqu'irTultiv.111,1.1141.1
2.1 nnalfmiii-SiukIrvilVA`Chltoluim (chapter) 141vOrriUlA3.1 -̀1,dein
9nnnqUrliArni-ralKM134:91rinniNTJ nqw41nri', nnb-ilYin
0.40,0.20,
2.00,1.00
2.2 rtil'llitl'177A2J (Monograph) cifillegivolqw*Terv11441 Li14,
list 0%qt-wry Mfatvl-LiluatlAwlm,,ini nnwrnntib ', frIblitiltl
0.50,0.25
2.3
2.4
Vallt Pocket book, VDO nhit'linntiiI, frThni,vm 0.10,0.05
1.00,0.50 .Tral,AUt LiillAtlinfiVALLIiIICLIV1111.11U A-1m. J frilgunnslInlillii
tkIn6l1iTtoiliqInA Ttfriirifiralriu
say , ' ..
3 rngliniZiratAlilatiniitiv,114111'mni
3.1 n'171.110Waral`11,t1,1,armarAlfalealAll'In (Keynote Speaker) IAD
111?J'111519J1.714) (Invited Speaker ) 11411'AJIVUTIVIM (cite 1 n'IS
LITSWEI)
3.1.1 Sattayut S. Basic concepts of lasers in dentistry; In APD
WFLD Laser symposium and APDC 2013; 2013 May 8-9; Kuala
Lumpur.
0.30,0.20 3 0.9
39
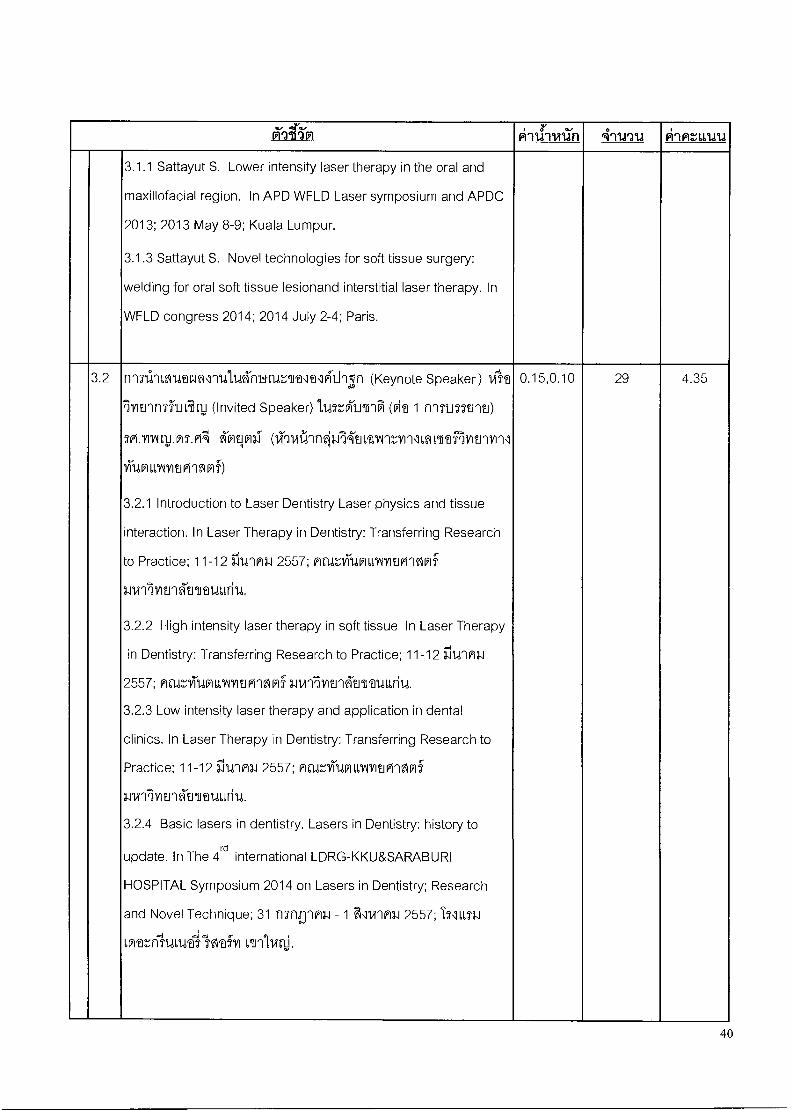
oiratim kiriviiin inv-ru Ai nutru
3.1.1 Sattayut S. Lower intensity laser therapy in the oral and
maxillofacial region. In APD WFLD Laser symposium and APDC
2013; 2013 May 8-9; Kuala Lumpur.
3.1.3 Sattayut S. Novel technologies for soft tissue surgery:
welding for oral soft tissue lesionand interstitial laser therapy. In
WFLD congress 2014; 2014 July 2-4; Paris.
3.2 filTal62114trA,InadniIrtgAt1t1A-I1'lr (Keynote Speaker) `At
Ivitinnthniinj (Invited Speaker)114=k1llnA (fit 1 r1171J51111U)
SPLITIAILIJATA 61216131- (11-9141110114'211,t1^11r,V1111,MMRIMM/111
140111,1111121P11?Ig)
3.2.1 Introduction to Laser Dentistry Laser physics and tissue
interaction. In Laser Therapy in Dentistry: Transferring Research
to Practice; 11-12 11141P13,1 2557; nar.',140111,1"11/EIGI'lgOlf
minlvitrativauLiriu.
3.2.2 High intensity laser therapy in soft tissue In Laser Therapy
in Dentistry: Transferring Research to Practice; 11-12 311,nR3.1
2557; nEIR,11TIVILLINVIUM2SPI- 3.1VilNUAblraULLril.4.
3.2.3 Low intensity laser therapy and application in dental
clinics. In Laser Therapy in Dentistry: Transferring Research to
Practice; 11-12 flu1R3.12557; AtUnrittfrniMitivin?lfrif
3.1V9'l7if121'1A-MIDULLii14.
3.2.4 Basic lasers in dentistry. Lasers in Dentistry: history to
update. In The 4rd
international LDRG-KKU&SARABURI
HOSPITAL Symposium 2014 on Lasers in Dentistry; Research
and Novel Technique; 31 nsnflnni -1 FI1WW11.12557; T216673.1
Lwan-iliaLwallwaiii vinivali.
0.15,0.10 29 4.35
40
Dig ti'm ATLI-wan 4-Ltrr1d pi-LA:alma
sm.ynALDIna ViTtrillf:f (lln1,4-E.114)
3.2.5 High intensity laser therapy in hard tissue and Selective
intensity laser therapy. In Laser Therapy in Dentistry:
Transferring Research to Practice; 11-12 illd'In1.12557; Mcig,171-101
1,11111t1G1'121P1f1.11,1'111/12.14t16M,111,111,1.
3.2.6 Laser Crown lengthening and Depigmentation . Lasers in
Dentistry: history to update. In The 4rd international
LDRG-KKU&SARABURI HOSPITAL Symposium 2014 on Lasers
in Dentistry; Research and Novel Technique; 31 mng-iml, - 1
11)1'1P1112557; I711,01.11,VaL'rii-kawallwah Vil'Avitti.
3.2.7 Interstitial lasers therapy in dentistry. Lasers in Dentistry:
history to update. In The 4rd international
LDRG-KKU&SARABURI HOSPITAL Symposium 2014 on Lasers
in Dentistry; Research and Novel Technique; 31 nst-Tnn2.1 - 1
I/1'1011.12557; IT1u,n.it,mtnisurwailwafv1 vinlinli.
TVINITI.MT.171-E2 4"1,1V61,1171 (1111NtitTjA)
3.2.8 Basic lasers in dentistry . Lasers in Dentistry : history to
update. In The 4rd
international LDRG -KKU&SARABURI
HOSPITAL Symposium 2014 on Lasers in Dentistry ; Research
and Novel Technique ; 31 1151fl'IP131 - 1 ii11A'1H1.1 2557; TN= LM'atni'uLufailwafil onlvq.
2cl.v11ALm2.lisniniAilslila,d1 (lin754-tithvin)
3.2.9 Management TMD with LLLT. Lasers in Dentistry: history to
update . In The 4rd
international LDRG -KKU&SARABURI
HOSPITAL Symposium 2014 on Lasers in Dentistry ; Research
and Novel Technique ; 31 n7nnnn34 - 1 F1114`1M31 2557; I2E,L73.1
ovatnisuarailIltfri onlvicli.
41
A2 ''f91 A11dil11M 4'11rr1d FliAtiona 3.2.10 Can photodynamic therapy treat oral lichen planus
effectively ltdinnin11,17r1Inn'17 Bimonthly Laser Meeting PIA
16 ; 7 rityN'n'inl 2557; ffigt-1/TUP11171112101`Mli"
1,11417iiii2rKUTtUiLliu.
U.M1.1AllFit7 ''''Iltin,3.0 (1,TnNtifi34111.)
3.2.11 Laser safety and machine. In Laser Therapy in Dentistry:
Transferring Research to Practice; 11-12 11141A1.12557; ALlZ
VTIWILLYMPI'Afr15 3.11.911VElnkilfauurita.
3.2.12 Laser physics and tissue interaction . In Laser Therapy in
Dentistry: Transferring Research to Practice ; 11-12 i.11.41M3.1 2557;
Patrii-UVILLMIMPInWi wirilvitrAtnuariu.
3.2.13 Basic lasers in dentistry . Lasers in Dentistry : history to
update. In The 4rd
international LDRG -KKU&SARABURI
HOSPITAL Symposium 2014 on Lasers in Dentistry ; Research
and Novel Technique ; 31 n7nEnn1 - 1 Fillrinl 2557; 17101.1
Lwal--nluilvailftfil viriliArli.
VIINC11.1:1W91171^1 i'mfiin (fin14-Em8JYlu)
3.2.14Variety techniques for treatment of oral lesions. Lasers in
rd Dentistry: history to update. In The 4 international
LDRG-KKU&SARABURI HOSPITAL Symposium 2014 on Lasers
in Dentistry; Research and Novel Technique; 31 inng-Ini - 1
filVinn3.12557; INLaalLova::n1-1,1iwallwah onlyttli.
t.villimn? CrilmnIt119 (161,4utwviu)
3.2.15 PIPS for root canal treatment. Lasers in Dentistry: history
to update. In The 4rd
international LDRG-KKU&SARABURI
HOSPITAL Symposium 2014 on Lasers in Dentistry; Research
and Novel Technique; 31 n7ngw13.1- 1 il1vi1n1.12557; INiLai
Lvantamilvafv) vinivinj.
42
oioti'm pi-rdivan 4-rin11 pilAtLitru
3.2.16 Laser (PIPS) in Endo Star War 1agin7thr11 J 1innn7 9; ...,1
Bimonthly Laser Meeting M.
V113; 2 frp1H2.12556; At1,11,11-1,!fr1
lLvIVlE1W121frlf 1.11411112Y4M141,1,614.
6. val cll. rd-S. tin 14-1,!i1iral/li (11n14t1)
3 .2.17 Laser-soft tissue surgery . In The 4rd
international
LDRG-KKU&SARABURI HOSPITAL Symposium 2014 on Lasers
in Dentistry ; Research and Novel Technique ; 31 nTnD-wm - 1
211W1P13.12557; IN anutz-,nluvallwafyi onlvgli.
valcu.t2tulK Klfiviniro (ilnIA'tnimu)
3.2.18 Laser-soft tissue surgery . In The 4rd
international
LDRG-KKU&SARABURI HOSPITAL Symposium 2014 on Lasers
in Dentistry; Research and Novel Technique; 31-1 f1lg.J12J14 2556;
IsqL1,73.11,MD:,'1111,11,1,1`641TItfil 111`111REV:.
vriNt-u.lmn krvisuni4,rp ctInNto
3.2.19 Basic lasers in dentistry . Lasers in Dentistry : history to
rd update. In The 4 international LDRG -KKU&SARABURI
HOSPITAL Symposium 2014 on Lasers in Dentistry ; Research
and Novel Technique ; 31 nmulni - 1 &VI'InIJ 2557; I516651-1
imz-,n1sumvals 14tfon onlinli.
3.2.20 Efficiencies of erythrosine and anthocyanin - mediated
photodynamic therapy of Porphyromonas gingivalis biofilms by
light fractionation 11.4nnnir.13.17riinfriT Bimonthly Laser Meeting
:J ,' . PM1115; 5 rp.innYNi 2557; PingliittPULTIMPInfigs
3.11,rilY1E1'lh'ilt1dL6r114.
3.2.21 Laser physics and tissue interaction . In Laser Therapy in
Dentistry: Transferring Research to Practice ; 11-12 311,0PM 2557;
mtigliTI,WILLIAlYitglnOlf 1.11,1`111/1E1'42111(ata6ti1d.
43
ihti'm A-lir-wan 4-rwala pi-Int111.11.1
3.2.22 Efficacy of Erythrosine and Anthocyanin mediated
Photodynamic Therapy on Porphyromonas Gingivalis Biofilms
using green light In WFLD congress 2014; 2014 July 2-4; Paris.
D.mAgull,thnl mibtoirtiro (ZlrIN'ti)
3.2.23 Alternative laser therapy in oral lichen planus . Lasers in
rd Dentistry: history to update . In The 4 international
LDRG-KKU&SARABURI HOSPITAL Symposium 2014 on Lasers
in Dentistry ; Research and Novel Technique ; 31 MnBnni - 1
&MM.] 2557; INIMILM`,11114114Vilgithl 611114
0.1111/i11.0111 Tildililliafi eirn5ito
3.2.24 Pain relieved in minor aphthous stomatitis by lasers. In
The 4rd
international LDRG-KKU&SARABURI HOSPITAL
Symposium 2014 on Lasers in Dentistry; Research and Novel
Technique; 31 nsnflnmasi -1 FIlw-Ini 2557; IN LISP 1,2`a:,1111,111A
lwafyi Linivit-d.
H9S.Y11^1.ifflitl IUStli
3.2.25 Laser physics and tissue interaction . In Laser Therapy in
Dentistry: Transferring Research to Practice ; 11-12 ilunn3.1 2557;
nrIZAWILLYIVIUMMlf 1.11/1151/1fratJTVIA66rild.
3.2.26 111T1ALMtfadNLIMfrlirtil,M1',11`1”11,LA1W1LgralIMLT61- In
The 4rd
international LDRG-KKU&SARABURI HOSPITAL
Symposium 2014 on Lasers in Dentistry; Research and Novel
Technique; 31 nTnnnHP - 1 FilVinAN 2557; bliaa.nwaz-,niuwall
-'lwofyl nrilvirl.).
44
Kgtim pilil-rvan 4-nni4 Fiimmal
3.2.27 Efficiency of erythrosine , anthocyanin and nano titanium
dioxide and blue light on killing Candida albicans in vitro %TIT
,- ..i th:,111.1)111nn7 Bimonthly Laser Meeting h7,9Y1 17; 16 n7nTni
2557; tin rogg. 3rali sur,ajlalb; nnzyiumilmvInpvmlf
wirflyiunklituarii4.
3.2.28 nnTAntinntifri-MilLtrusdrard'atrikallinnqnnnnsiziiimmtf
iralfiLIMA lunnT11S:-,13All'inn7 Bimonthly Laser Meeting OSA
14; 4 if149'1P13.1 2556; IM2.1 11111^1. lilat'l f771.1frf`lT WITIAl. cirrulp
CitAsl'anl ar,141qm. viltillrl'qj allsvitiro ilnArnlivium „
ILIWItIVilMlf 'TON 5; MOZ-Ifil4P110\11/1t1G11210- 311ATIVIfinAlrivauuriu.
3.2.29 nn71411M1,61It funTVITali1'l5LIII11141,681V.11 Vikall.hrl 1unn' ,' A
lifl,11)1(161J'In15' Bimonthly Laser Meeting ANY] 18; IME11,4111^1.YIGI1NM
76141_15zIm4, 14111,N.M1q14.1 TICARAYTfrAlrl LIV,',1,11111/.71 Vi/1211dAtl
19 111PriblVii,101,11AWIEW14fflf 111;1411til 5; ACIZY1-101111AIIMPInMlf
3,11r1IYIT.I'A1`HUIff114.
3.3 n9517,111,M,vaimmAignniTripATingra11,171111 anil abstract,
full manuscript % Proceedings
3 .3.1 S Sattayut , P Patcharanuchat , S Udompanich . An
instructional design for laser-education in dentistry for graduated
rd dentists. In Proceeding of the 2 Meeting of the International
Association of Dental Research Asia Pacific Region ; 2013 Aug
21-23; Plaza Athenee. Bangkok; p.181.
0.10,0.20 5 0.5
45
vi'ati'm Aithvan 4-itm Ain:1114U
3.3.2 P Saenthaveesuk , N Sanjandee , T Teeratsakulchai , P
Norateethan, S Sattayut . The effect of oral soft tissue welding
using diode laser . In Proceeding of the 2rd Meeting of the
International Association of Dental Research Asia Pacific Region ;
2013 Aug 21-23; Plaza Athenee. Bangkok; p.147.A78
3.3.3 Juntavee N . Influence of surface treatments and primers
on shear bond strength of resin adhesive to Y -TZP ceramic. The
American Society of Prosthodontics 2014; 2014 20-21 February;
United States of America.
3.3.4 Tantananugool S. Efficacy of Erythrosine and Anthocyanin
mediated Photodynamic Therapy on Porphyromonas Gingivalis
Biofilms using green light . In WFLD congress 2014; 2014 July 2-
4; Paris.American Society of Prosthodontics 2014; 2014 20 -21
3.3.5 V Prasongvaranon, L Thanudape, A Klungtong, S Sattayut.
An efficacy of photocoagulation using diode laser in tooth -
xtraction. In Proceeding of the 2rd Meeting of the International
Association of Dental Research Asia Pacific Region ; 2013 Aug
21-23; Plaza Athenee. Bangkok; p.148.
3.4 nnrawiLtrawmnuiunnTii5D-VnInnnTn'Ailinri unil abstract,
full manuscript1U Proceedings
3.4.1 Pijitta Chimtim, Thitirat Heebthamai, Jutipond
Phanombualert. Microleakage of self-etch adhesive system in
Class V cavities etched by Er:YAG laser with different pulse
modes. In The 4rd international LDRG-KKU&SARABURI
HOSPITAL Symposium 2014 on Lasers in Dentistry; Research
and Novel Technique; 31 nmpqmi - 1 &WM 2557; TN L1S3.1
Loazmisurwailgi'Dfm vrawli; 2014, p. 21-26.
0.05,0.10 7 0.7
46
(l`atim A-ill-wan 4-nnu Al MUM!
3.4.2 Wilairat Sarideechaigul, Sajee Sattayut. Alternative therapy
for oral lichen planus with low intensity laser therapy and red
light laser : A case report . In The 4rd international
LDRG-KKU&SARABURI HOSPITAL Symposium 2014 on Lasers
in Dentistry ; Research and Novel Technique ; 31 nTn-im3., - 1
F111/11 MI 2557; IS1LLS1.11Mr-fl-fULWal ITS'aiiil L'll'AVIElj; 2014, p.
27-30.
3.4.3 Benyawan Uea -aranchot, Chutamas Rakkhansaeng ,
Ubonwan Tapsuri , Angkhana Sangpanya , Aroon Teerakapong .
Effect of blue light and hydrogen peroxide on Porphyromonas
gingivalis in biofilm . In The 4rd international
LDRG-KKU&SARABURI HOSPITAL Symposium 2014 on Lasers
in Dentistry; Research and Novel Technique; 31-1 I-TUMULI 2556;
TS\ILMILM7111.411461TIDT-VIL611'11ViClj; 2014, p. 31-32.
3.4.4 Pongsathorn Touchpramuk. The study of dentist student
experience to Laser in Dentistry . In The 4rd international
LDRG-KKU&SARABURI HOSPITAL Symposium 2014 on Lasers
in Dentistry; Research and Novel Technique ; 31 nsnffim - 1
&Vi'lP11.1 2557; T711,01.11,Mtnl'ULIA1116-11111111)4; 2014, p. 33.
3.4.5 Surada Tantananugool , Aroon Teerakapong , Sajee
Sattayut, Teerasak Damrongrungruang . Efficacy of Erythrosine
and Anthocyanin mediated Photodynamic Therapy on
Porphyromonas Gingivalis Biofilms using green light in vitro . In
The 4rd international LDRG -KKU&SARABURI HOSPITAL
Symposium 2014 on Lasers in Dentistry ; Research and Novel
Technique; 31 nSIip'1n, - 1 FilVinn 2557; tm,Lniorm-,61-Ltiwol
Isavafil vinivitli; 2014, p. 34-46.
47
XrafTvi A 11,19'i vi iIn +lint! pi 1 pi taLtru
3.4.6 Teerapat Treeratsakulchai , Peerapat Norateethan , Sajee
Sattayut. Interstitial laser therapy using Nd :YAG and diode
laser. In The 4rd international LDRG -KKU&SARABURI
HOSPITAL Symposium 2014 on Lasers in Dentistry ; Research
and Novel Technique ; 31 risng-ini - 1 &vi"W11.1 2557; T5\161,51,1
6frratf1114614414tii1 ill'Illgt.j; 2014, p. 47-53.
3.4.7 Paweena Tammataratarn , Pichaya Viengteerawat ,
Piengkhwan Atipatyakul, Sajee Sattayut. A physical alteration in
tissue blocks irradiated by diode laser and Nd :YAG laser
irradiating to different chromophore dyes on oral soft tissue . In
The 4rd international LDRG -KKU&SARABURI HOSPITAL
Symposium 2014 on Lasers in Dentistry ; Research and Novel
Technique; 31 nTnTin2.1 - 1 illvinmasi 2557; IT11,123.10Yatr11146144
'Wahl illn11.941:; 2014, p. 54-58.
1134 6.45
4 91S9lal,11/111111.1b141
4.1 rrahrIltSfr111:1',I,VJUlifillSITVI S/ fl'Ifilialt6i1111,19/4,101/ tigilill'ITVIS 0.5
4.2 11`17111411t9frriltSitnaviltimmqTvanauurZfriritilevi 0.5
4.3 1,A5i.iryngwvitiiitnAviLlfrivnnlicainiitiuvNillai 1
4.4 Ig1.111'1S9frIVInfitne61011111TVIS 0.5
4.5 ijiliJ11979M1/1:51,i1U1AVVIi 0.2
4.6 712i1A9-iiinn2 commercialization (G1 e1 1 L6fi141J11/1) 0.1
5 eiiirruninlunquwanitatiniuilItiMIN (Witnnin)
5.1 iTtnuOuNt.vvinitVilliNcint utnnirilinnk vtiqtilm,1
fri'llth:.',01971, warmlnaLairairivil 1.0,0.50
(vita 1 kriAinvi)
3-0Phti_InnaitiigviitnVixan3A-0,1949infAnti-FirTti 3,400,000 1.52
48
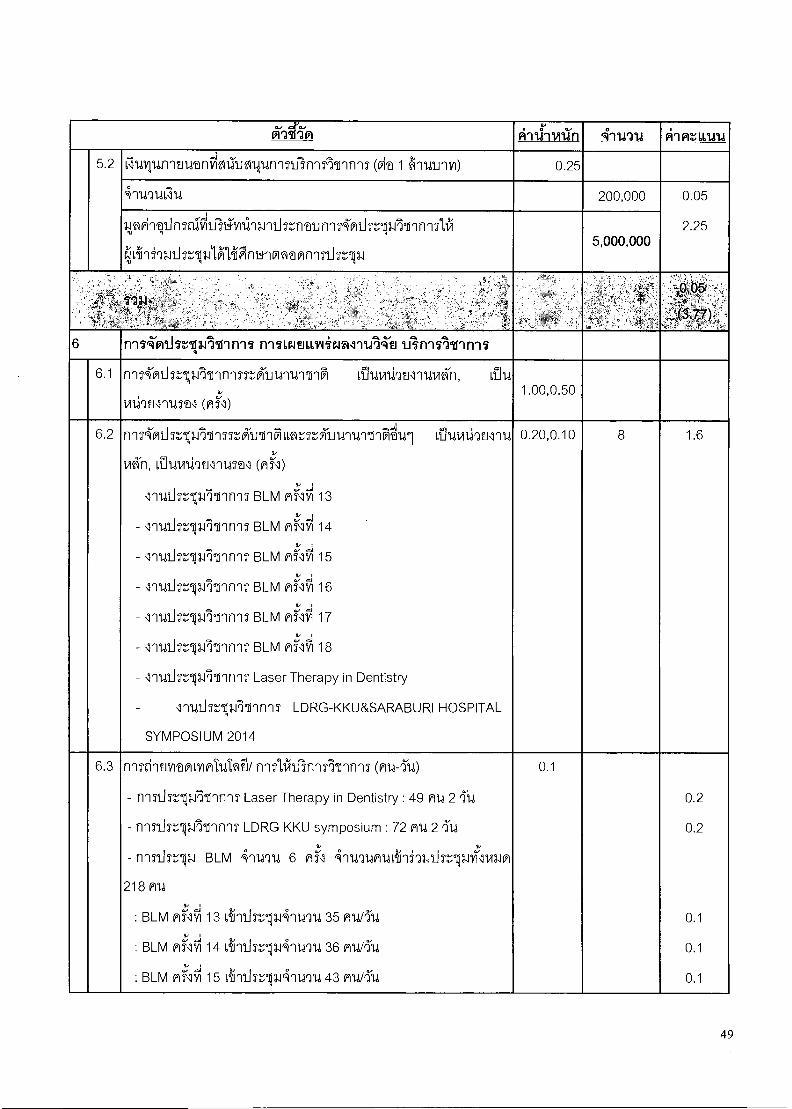
6:(45'm ATLI-Ivan 4-1n1d Alm:LIMA
5.2 Ci1411UffltlUtilfilfil:11J2NUTY1SthirlATIMS (Fit 1 6'n'tdliMil) 0.25
47U9U6JU 200,000 0.05
2.25 3zI,M9qi.inTraffitri'graq3.1nlir.,5ntlinnr4-Miin-13.171/InnnitIN
( 1Ani93.11iMplitYRignblfrifitMnq21iSrip4 5,000,000
, .
.. „.
„
7 ,
6 TYIVTP11.11:13,1111-11117 MII,r4t111141if,A1-11.11`ZEJ tat111111-1f111
6.1 nnKmthr-43.illinnnss....AloirrirSi Lawn.,19twn.,tviki, rilu v
vi1i7€ll1U•D1 (A) 1.00,0.50
6.2 nqTA'mii7:13.1111nM'fritrilq10:',5T,KliUnUTIIAW1 Li1U141.,1/22.MU ,.';
'en, 1,911441:17.11114M1 (MI)
- 111,11i7rOlinnnT BLM Mild 13
- lnUthrtilFririnq7 BLM Mi41 14
- lquii7.13AInnfiT BLM mild 15 ; -I
- lnUihsr13.17PinnnT BLM MN'tri 16
- lquii?:.',VAlinnnT BLM mili'll 17
- llutIvilFrbnnn5' BLM miA 18
- li1d1in-VAInnn7 Laser Therapy in Dentistry
lnutlriljrninn1T LDRG-KKU&SARABURI HOSPITAL
SYMPOSIUM 2014
0.20,0.10 8 1.6
6.3 nnnintnritmilfimtuIdli rinAiVisnnAlrinls (nu-2u)
- ryin17.11AinnnT Laser Therapy in Dentistry : 49 mu 2 rIU
- onniTripiliinnns LDRG KKU symposium : 72 MU 2 'YU
- nnn..151-13-4 BLM 4n14914 6 Mil 4nU9UMUL'Ili93.1klaTtniM
218 nu
.2; -I v , : BLM ANVI 13 vinuTripAnurm 35 MI,,t/rYu
; A L' IM : BLM V1711/114 L'MUIT,111.1 4-1Wri4 36 MU/`2u
:: d 9, . 1 : BLM AS\1111 15 LIY1 Li 5..',64 1.1 4 '11.4 LI 43 A 1,141,t
0.1
0.2
0.2
0.1
0.1
0 . 1
49
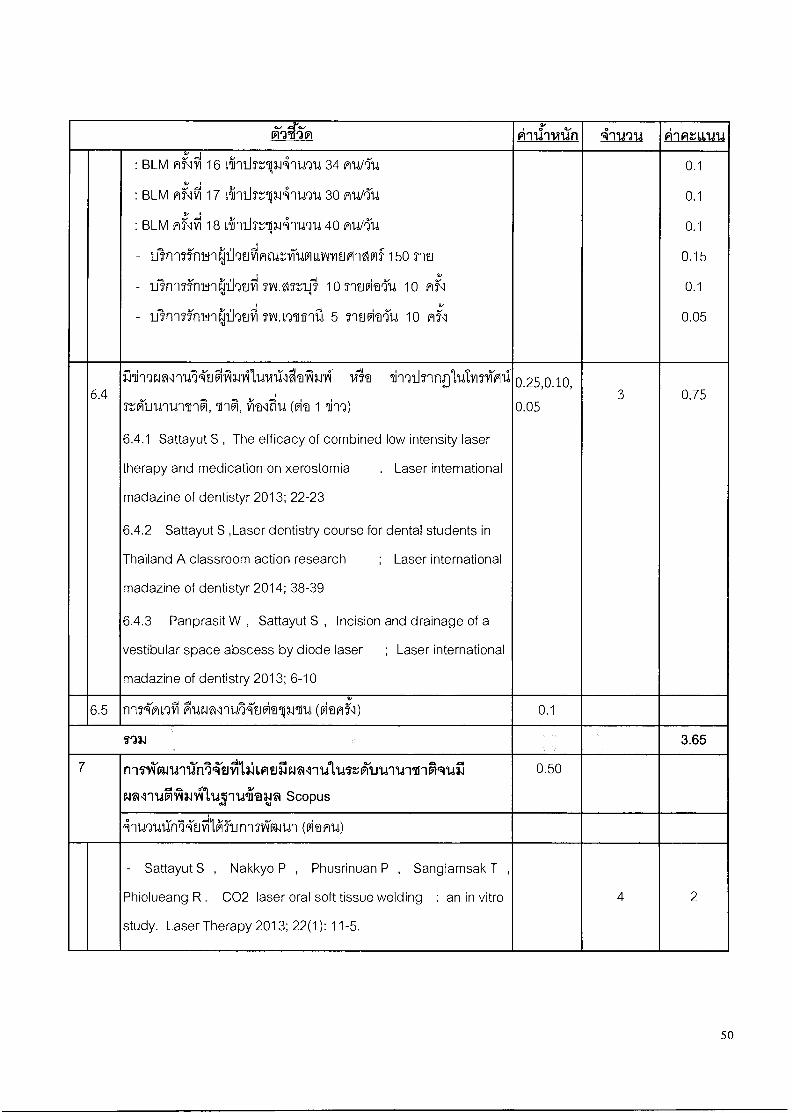
X'atim phifivan 4-m7u Pii At 111414 2, .
: BLM ni'lil 16 L41nthripJ'41ntrY14 34 AU/1'u
Mili71 : BLM 17 641` 30 Ald/1-1,1
: BLM nisiffi 18 1iin9.17:---01149U 40 RUPTU
- IliT1251rnilr,:lihniiffignril.,WILLIAIYIEJFI'AVIf 150 SIT'
- ifinn5irnInCii197.iri TIA07:51.):4 10 riuvlea714 10 n12.1
- uirrITM1/1(11h2.1Tri TIALL9611Elil 5 IsntlfricarYtd 10 n".9
0.1
0.1
0.1
0.15
0.1
0.05
6.4 illinqFA1M'll,M211c41111144111/(A.114 vis'a 11-vnJrinpluIvinficali
7:5friinnUTInr1, 611-1r1,1/1(alitil,l(ka 1 61m)
6.4.1 Sattayut S , The efficacy of combined low intensity laser
therapy and medication on xerostomia . Laser international
madazine of dentistyr 2013; 22-23
6.4.2 Sattayut S ,Laser dentistry course for dental students in
Thailand A classroom action research ; Laser international
madazine of dentistyr 2014; 38-39
6.4.3 Panprasit W , Sattayut S , Incision and drainage of a
vestibular space abscess by diode laser ; Laser international
madazine of dentistry 2013; 6-10
0.25,0.10,
0.05 3 0.75
6.5 inKnvirri PurAlnU14'tivirolp.rilU (viuS1) 0.1
I'M 3.65
7 niviartnifri'l,TthilaimuileaAntlIna,',Airtritrit-iFiquil
Wl'il.i.i1713.19,11,131144103p Scopus
0.50
411,191,11ThlibillAllinnT611141 (kanu)
- Sattayut S , Nakkyo P , Phusrinuan P , Sangiamsak T ,
Phiolueang R . CO2 laser oral soft tissue welding : an in vitro
study. Laser Therapy 2013; 22(1): 11-5.
4 2
50
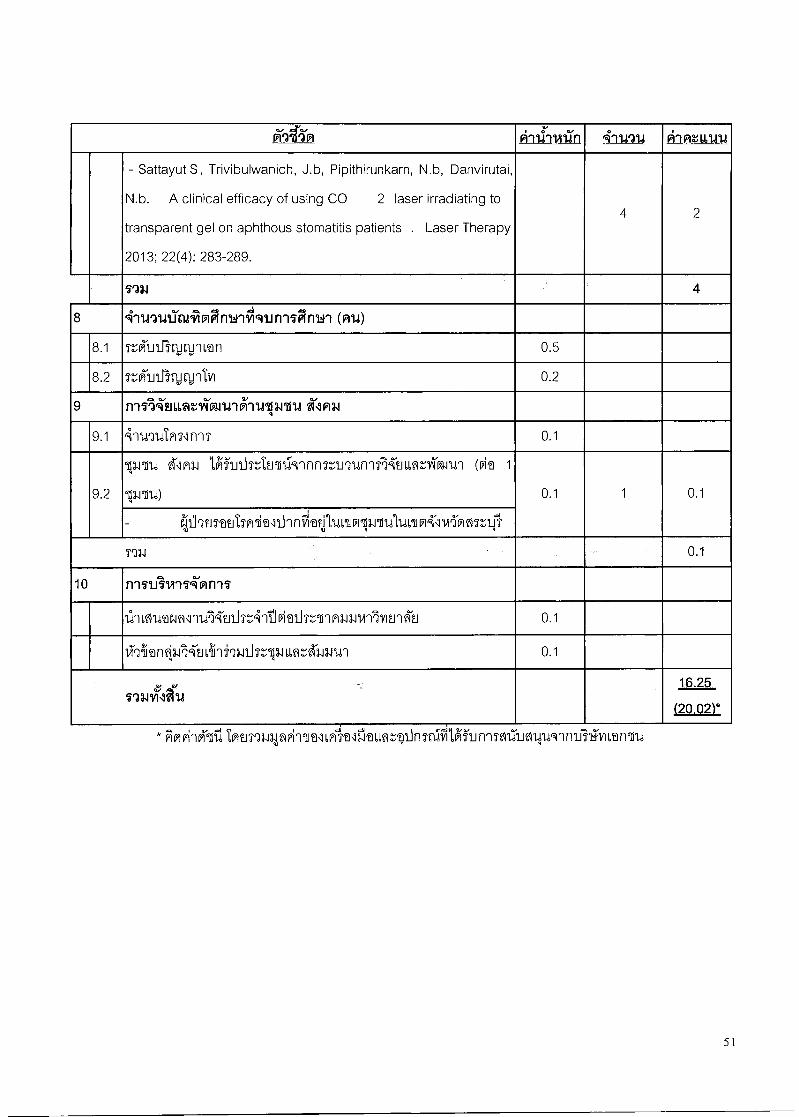
6i-a ti'm piithisiiin 4-rw2la AlAtuina
- Sattayut S, Trivibulwanich, J.b, Pipithirunkarn, N.b, Danvirutai,
N.b. A clinical efficacy of using CO 2 laser irradiating to
transparent gel on aphthous stomatitis patients . Laser Therapy
2013; 22(4): 283-289.
4 2
113.1 4
8 4-ruquirtunlimAnwrilquniiiinun (pru)
8.1 r,',KuLliwt-untian 0.5
8.2 V;,'Kuiriyuctintco 0.2
9 n -151 i-ti I, IA t Yin11,1941-11,1134711.1 irl AN
9.1 inUrnani11117 0.1
9.2
111.1111b 21:1P13.1 Ig1.11.15-ZIWIII.19`11111MaLlillTNt161,n1AigIU'l (Clef 1
60.11114) 0.1 1 0.1
- 1-ii9tiT'atiTsvrikeli_lnnii‘guilt4nfrripnallaw-I4-11,11"frnirn0
7934 0.1
10 11171A9,1114‘nr111
1111,ZIWara1lIA4'2.111nA'Itik11hT,TIP13.11,11417M.I 1 ll 0.1
irrian014-tiviindlanisr pLiqt.h3-Juq 0.1
l'IllYltl f i 16.25
(20.02)*,
*Ampi'lklidIME1511.11pM1INLvil,alliviLnqiinTn1 IgurinnaumfurInnulgitivanTu
51
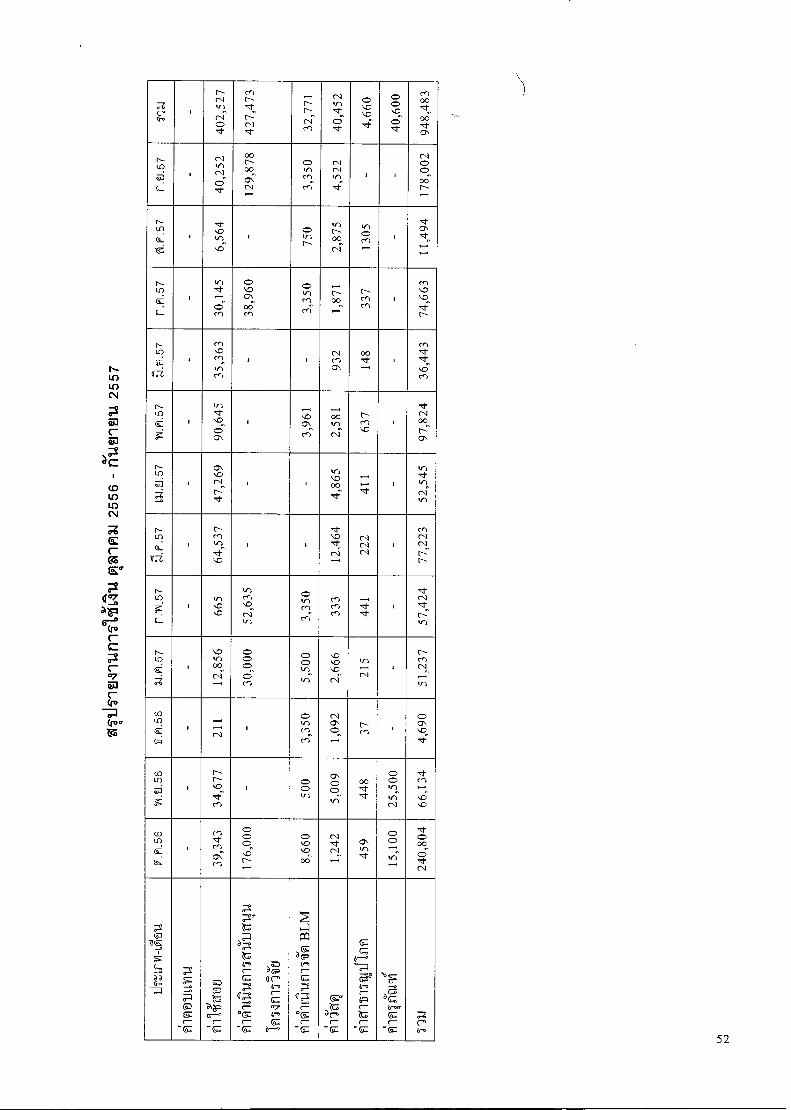
c, cr. 40,452
4,
660
948, 4
83
cr) N-
s cl 71-
. — N N c‘i rn
0 0 "c).., o 71-
3,3
50
4,5
22
I
178,0
02
I ■
2, 8
75
I 1305 cr, U) I o in N
, cr. 71:,
3, 3
50
1,8
71
1 337
O U) C) OC; cn
i
L-,-) U) U) 71-- N-
N- in
doh
I 932 1
48
36
,443
I I ,
N- Lo
, kr) 71- ‘.0
cr. 97,
824 . ,..., cr, (-,
00,... Le.1 (4
cr) c̀) ■
N-. co
. c, q:, c-4 l---- 52,
545 , , Ls-) ,..0 cxD
— ,--' 1
N- in
lg 12,464
I 222
77
,223
1 I i
N- in
3,
350 333 I 441 in ■C, ,•C) 57,
424 it) in '•CD si-irl
I
N- LO
i.0 in 00 CV- 51,
237
g
000`oE
(.0
0 0 in in-
U) 0 i0 CV
in ,,..„-4
- i
LO
6 3,350
I I N CD•■ S -
s cx)
0 c:7,
71--
co in
5,
009 . 448
I.- N- VD
Cn
I
•z1"-
oos`sz
't in ,_
U)
(.0 in
1,242
I 459
24
0, 8
04
0 i.0
00
i.0
0 0
if-;'
0 31
S )) (
--0 M 7
- M
0 cz zu a=i
0-. (— -M
Za
a Za 7
(17 tr.
(r ,--
r r7 '' ir° 7 - M 1/—'
)- XI
7 M
',1 7
'' 7
-M
- (L. 7 7
- M
M
a Ir, c-- P 7 ZU r-
- M
l'F a tr.' M 7
- M 7 Irtk
52
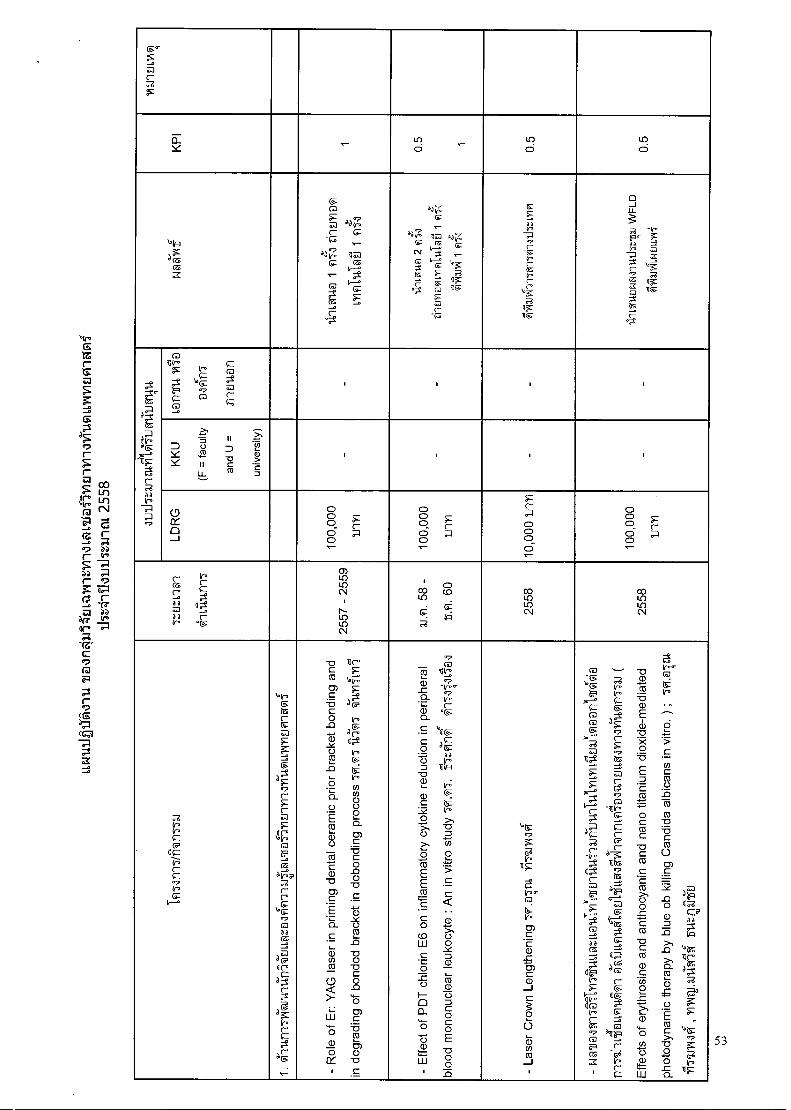
M <-
E <-- <-- Lo R ci
in d
© d
loiR
d (6 0 a
0 cr"?
0 22 C—
'' N— 3 irro? 210
tr--. — g 0 (.-5
Z -. iz''' og
aq, 0
,
', 17Q a °7 ca
dlr.
CNI <--
Cj =
(-- (r r, 0 lg
(- c
ad
.7 r-
-g ir° C- 0 v. c- C. xox
R (I ii
a _I U-
-" 1.1 °- X ad _o Iro
-- Z g '.-° .7 R c6 ei Z 31F 0 g 0 (=''
''
,,- tn
au-.P
-4_,„F
(- a a ir.
-7
Ca 114-.
g
f ("r°
1.1*-- 'T? (°
CD g m t_ C
1 1 1 1
D Y — >, 7 0 42 II
u_
II
2 ra
P ,.! a) 2 .
, . . .
0 _
u- a
o o 0 p o -
o o r 6
o
(- P
0 o cT
o 0 0 r
o ,-
rcfma
a
a. c
2 .
CD
N
ILno
0 in N
A
O
0
0
- : O o
O
V
Ir.tr.
CF (1
C-m? IP'
le--.
)0y-.
2.5 W(-
_..,
g dg .7 (-
(-
ar° 1.1r.
W o
FM°
C-C.
10 '7 0 0a a _o
d 0 CP ,e d
g(-
a 3,. a-tr. c--
g r-
- R
ole
of E
r: Y
AG
lase
r in
prim
ing
den
tal c
era
mic
prior bra
cke
t bon
din
g a
nd
in d
eg
radin
g o
f b
on
ded b
rack
et in
de
bo
ndin
g p
roce
ss 1
91.q
1
- E
ffect
of
PD
T c
hlo
rin E
6 o
n in
flam
ma
tory
cyt
oki
ne re
duct
ion in
peri
ph
era
l
blo
od
mo
no
nu
cle
ar le
uko
cyte
: A
n in v
itro s
tudy
i'7zi
;r4 k
14
96iN
- L
ase
r C
row
n L
en
gth
eni
ng
19i
.@iti
l
- Fril
-edj'A
mm
uk
i d
'ailL
I,MA
IEJ1
1111,Ra
ckil
nLf
lilan
nEJL
I,ff1
11-1
"-iai
n771
.1(
Eff
ect
s o
f e
ryth
rosi
ne
an
d a
nth
ocy
anin
an
d n
an
o t
itaniu
m d
iox
ide
-med
iate
d
phot
od
ynam
ic t
he
rap
y by b
lue
ob k
illin
g C
and
ida a
lbic
an
s in
vitr
o. )
;
111.6
111N
14, y
mitu
AnZ
ali
Eu
zajiii
'L
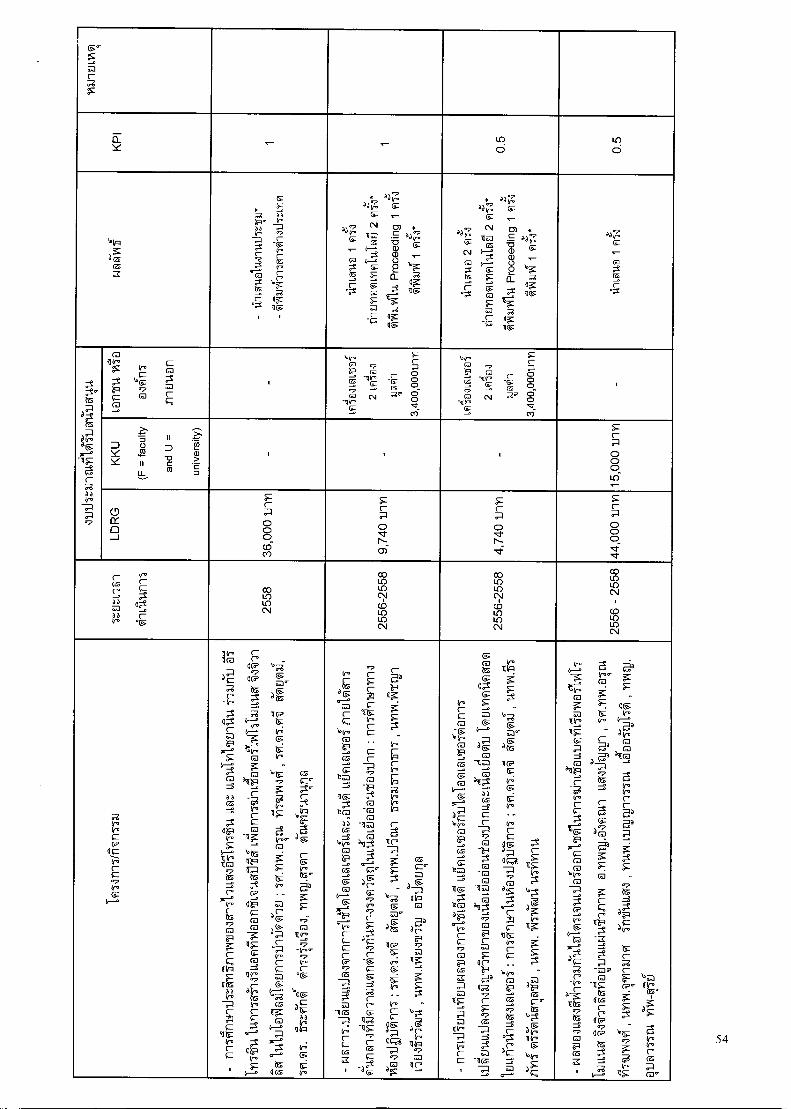
(PC m
E. Y ,_ — cc) 0
cc) d
louzi
dm ca
tr''
Ir. crr"-
7 V^ a
- c-
Ir.
°P tg
0 (—
(— CI 1g
8 . rhE
mm
ymiv
,Ig
2 F
15*
'6713
, 114.11
1, P
roce
e din
g 1
fI f.
,1
Z\ .>
filtr
iloqV
i lftila
Pg 2 f
i?1*
;11;1
1A11
,1 P
roce
edin
g 1
Fii"
l
a( g
z
t'G 31,-. g
-11
R v--aa
-7
(.0 1 IP
, ca _.,
''' (a g m (- c
.
lotro
-° C6
0 -„ g
ca
ca ,
-illr' ,-- -.- 0
csi
c-
o 0 0 _ 8 ,i- vi.
11,
ca c-
P 0 - o --D -itIt. t0
C-6 - 0
g c,-. 2, csi
-, ,t.. g co
.
D Y
= -i^
0 a 11 LL
- II D -a c ea
...-. 2 a) > -- c D
. ■
(-
. 0 0 o 1.6
° II 0 _1
(-
o o o co co
(-
o 01- N- ai
(--
o .7r N-
o o o
0::r
ra
d a M aa It-0
(-
0-1.
(- 0&
co co 0 N
cc) co c.1 Co LU uo CN
LO 1.1" c-.1 C.C) co LO CNJ
co co C NJ
co co LO C•1
Cr' v. (P (1 c-
Cr' fr--.
it (-T C'D'
(RP '(' a ac( g,
t. c-
-v° - z a
T1 g R cP ag (7,_°,, g M -- V
to V° t-o_. x -
.--c \‘ 9, '9511zi 07
(- d a Ca - g -' IF ((
g av 0 va -1 v„,
0 ,•-. ,,,t. - .7 "Cf - Z t'a =.° Ir. C° (a . .. if-. WI M
, c-0 z cm °' 7 0 CO d 0
.a 0( Cr'
as Ca (- -0
4 IC?' 4 (---
a a ay. IG-° Ir. z R
-- Cr' cm
M (r. ''_,,. c- qv .-,.
iro "
_„
c- (-- (IT
0
C- 1,.P t-, g
, Ir° tu.' as -,..
--;- 0
il tr. _,
fr."; Cr' c-
''' ,./
3
lac, W •
Jr
tr.
tr, , g ,--- m (-
'. 6-.
V a' -
'um
Ti g
Irca
il _3
loCrt . Fa°
o 1.--.
5 7/2'0
c-
C- ca cr? Ca
--E --. g M
C- cm
.
&•0
.7 c-
a
t ax
W Cr' c- g
-
. "
(- P
'-- c- a.,
t., F,
Cr'
0 (r°
-cD L
-12 (-
-' 4
);(( IC° 7 s'"
g a co
vb
7 MP d g
3
-7 1RP r-
"g tr.; (P
& n,
__,, Cr'1 _
(- '
r° tr°
-1( 7̀
(- 4
0 --
-d a
a_,
4 (014
F M 11X -°.
- ,., u
3 (-0 1 4.1t' 'p
_.
t:
' (-0
(CG
''-'
aka a
.7
- in7
Lili
EnJo
InH
atu
n-n
TiRga LIS
ALavi
sofr
ibU
llaq
l,alta
f6a
1-11I
Li Anu
irdal
ynato
rlyur
nutu
ari@
daw
ia,n
ilnu
wad
ativ IlE
.ILY1f1
1 71Mf
f@q1
: ; 7
91.1
1.ST
'4 14
,111"11
1
oricrif
,
14111
1111
4
V., 4--.
T- tr. (a
Iwo 11
...„
lit.1 (-
" t-
'-''
\ r. co
CP -. (r° &
t.-. rJ , " ; _ ,....C. . - k-
TIZ
z _„-0 7̀ 0 0 M
'
ca
`'?
a a 2- x • _
5 (IF „V°
tr. ,' a
( 4
- <a a' cm
a as ,Ii_ca
Z --0 V0
_.(- (- as
4 ca'? Ea
. --':
x g 6 _
c- =1"
C. P ilbq d in, -a
C R
-oP C-- 0 F
-ti (p.- tm • am (--
(RP 0.., - (1(7 '.0J
' x
g , -0
(,-. ((
V'M (114-0 tu' ,.,
e"
" 4-=, t."'
0°
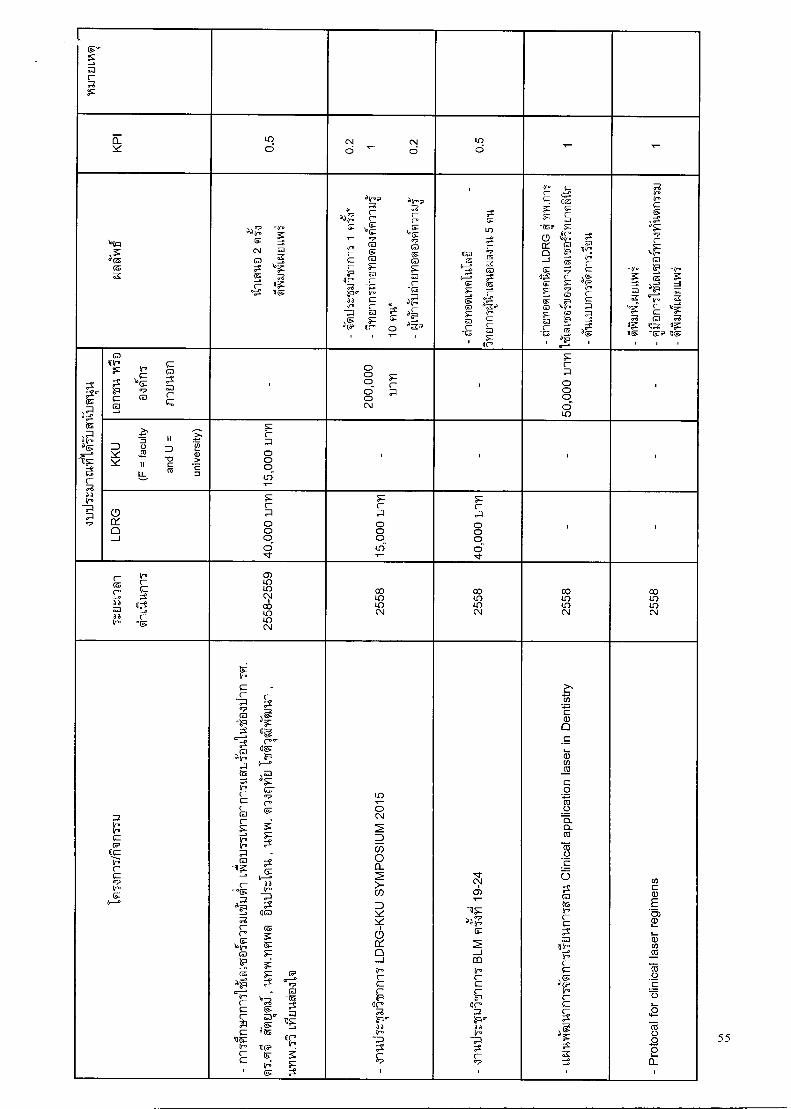
I
m r R
0_ Y
LO d
CV d '-'
CN d
ir) d
la tpi
(-6
'7 . as " W z g 10 C\I M 0 a
1g
.? ad1,-. g
tr. (-
)) Ir.
4-a c- C.' g log
g 0
tr' (-- *
tr.a
C. g lo g
ca g (a
" )1,,,
,(--
Lt)
c- am 67 (6 a
g g (0 'z
- M , ,
c-
if- c-
X
-tea
0 CC 0 --I
g g co
- I
ci do g 0 g
'CI V: 0 P (-6
Z p \--
ig9 .__„
4,„tf- i-
r z
'g ■
tr* tn,
a c7 c-
lotto a
0 Lt'
a • 1,„, a
1,,'' 2 vx
lig -gP Zg
i I
g°
tS
g
g
-.a
c- aa a a 0-*
-.?
ir.
tq
(.--O
V g
CM
M
(—
C
I
0
0
0
0 C \J
0
(—
0 0
ci IC)
.
av ., D
Y
>,
0
II Lt_
in II D -a as
12 > E m
:.-. , (-
0
LS
....... a
g
o o 0 o "1
g
o o 0 1.6
g
o o 0 0 •cr
. .
(-- Ca S.: a a 0 a a Ir.
V.
g ci — (—
‘,
0) to In c.■1 co up IC) C•1
co Lo IL) (N
co Lr) Lo C \I
co Lo IC) ( \I
co Lo IL) C \I
"
([ i-
G
tr.
• i V.
-
-- c- (—
- 1-i , 4a
o (Ig
dlr. tq
Z 0
-.. d
tr° -. g
(7,
(— g 0
(— •
--° g Ir.
0
t•—°
cg ---
-II 40
(— ca C°
lo vog g 0
V x
ca CP
a l° Tr?
* 0
g
g 11
d Z _.
VF ac-
tr. tCP ". C-
tr; g
' g - 1-1
-69hrrri7
LD
RG
-KK
U SY
MP
OS
IUM
2015
•■1- C..4 CD l-
71 as c,r_P„ g
2 ___I CO tr°
C- dr.
IP' as tr.
(— .7
I-
LLNU
IN-R
19X1
111
71
1-117
65E1
1411
17
g@
lt C
linic
al a
pp
licat
ion l
ase
r in
Den
tistr
y
- P
roto
c al
for
clin
ical
lase
r re
gim
ens
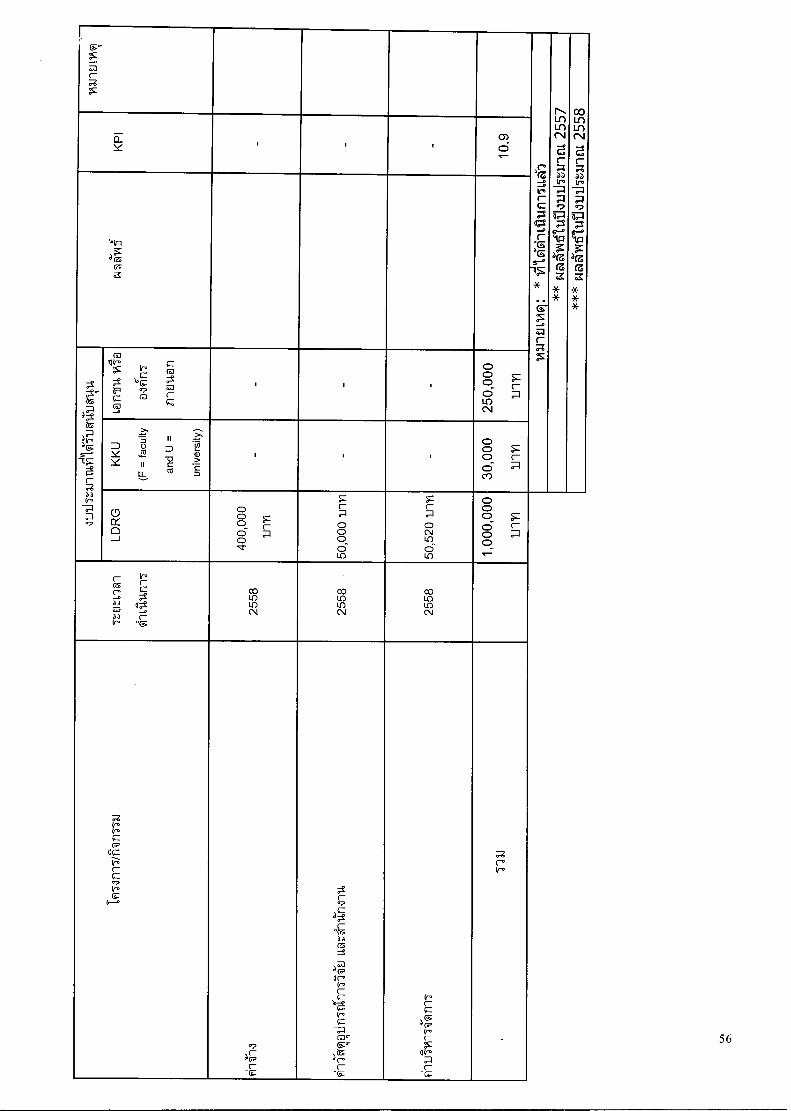
I F`r
m
cT_ . . 1
ts a 4..., aGo
lig
V.d d '--. ,,?
0
ca
Iv- tr" 0
D Y Y
> -.. = rro, 4= II IL
1 1 0 7:1 C
CO
4— >. 72. w .— C =
. .
Ct 0 J
0 0 0- 0
(—
0 0 0 0 0- in
0 C \I LO d in 1,
000,
000
1111
1
i- c6 e. - a a a a p
v-
a C2
oF
oD in in CV
co in in CN
co in in (N
Ir. tr. (P
cI Tr'. (— C tr.
t.---.
c— C-
07 c-
aC c-
°Z as
a CP ca W. tr. C-
).,, Ir.
.- C (0°- '
ZU C° C-
tr. C- F a CP tr. (—
(11r. (—
Co Ir.
.
5
n-ncriwon7mn6tnyauLiriu11244 n-)54mkn13.194ti6t111:511911 IhtlflOratIJIAnOMM VILT1M9111
TANA`116/1D1n11115111f112 1,LL'ifl.,tfrilAil'aLTVIAQ13ATIT/Iralii`1111411.1kattuz--alFIns a-IA.141.1nm
nnTOnn5I61n.i "TAT1111?" 14T:,'7111`5111f11T" 4\11,i411114A1KC11,11'6WISTill7ITTA:111,41411
CNI6191111.11.11/1111/12.142.1 fralArldr,nmirmn13.7141-1 glOulgingra.aiit1911t1J,L1,qta1191161,10112011-
Otr1=1.1(114,111A4E11,14111111111,712.1Thl IM13.1614139;f1T0t11571*.IN'ElltYtltY1111971111VMAT13.1HAralk
11.drYlVW1157111161,AillTVIT992it11 i1'11TIAMV1341371n9131LMITZ13.1 ISMAIJ`t(1915`111014fll?Vi1gilNfl
ilTrillgi'afllTiillq111111f1151,1AtTILINU 161 f11111M13.10A4961:Ifi`aLIT:',I2.11191-11'811MANA913.1i9atfit
1/11,192_111ULAtlhEMOTtaltYllilMtlf1Tr-11511ME'Mgill T93d1
finmvoturaq111511AltrIlilMr111110:-'1J14114frli1141,11UlAtlIMLItf
n1.1714uLtIAI'lVV1111,fll,91`frlYIEllY11\11ril,WILLYVVILIMAVIfilirlffEljVITQLIMPAWMAlLi1141114 1,04:531
iitl,M.,11,arAt'OCNirmiffrasiunnns14-tyati-NtlAu6nqin.ivi-MmunAmituuriu4innTLilumillmulki
n-19`A 3.11An2v1tinA'u 019TV1111141,1,nEltl.InJA911,11AMMAMWH1V11?ifrlf" Vi1114111`11,1*(113.1
VI'InVqlt.1611t1Z1i6LIJUfMNU(MethOdOlOgy)
141-01),nnfliiiimilun-nAlufrinvi-Nriu win LivivAlw-AvInma Agra AQ13.11/494'01.111.,V11TIATall.,VIVIIWal 61A15A911.1
1110111,13119M112.111(01fl1A-MlaiirlIAX1A3.11.11 LiAltriWILVW114toiflitlill'1,0.111/1911,61/14
Ltra:,-31-111 AtVAA1\914E11,1/13:1 A9:-/1111:iLlimnlyfrsimumtInl`91ulla
wonlviErAilkatiqlviaira.1 vi.ivin'ilmtrAikalfIn1TA-mnnTifiw-31",autil nqTEal.1)"1J1,1M1511.iqWilfTliillii
11141:1414frinIVINTIltlf1TZINUMTM-11111114bilf1511119113.1111°1114 rrmTim Inc/in-man imutaluvIn
VA11J 1,11Mit11111fIlTI,WEILLMWq1114142.1 LIM:',MaIJM14.1131MT114M2111t1IYITLWEILLIAth4MTIA/4b11)ipppin
61.111n14'tvalT4unlirllAi,14eilltInI4u Marl:117)91'N 3.11/91111U-IklidULlii14
wilmiltrvin.11111n1shium lAlunnn.m.ii'Lvili1X\IMIT114 L1,f19111,1,n61614
57
ni Nur) n I. thimaNalitniaz16'cria.Arvipiodo
officthindkaiuthrObtfinilw,ihrocuiti6
LDRG-KKU&SARABURI HOSPITAL
Symposium 2014 e,
IV. YIEJlitiqcdramniIi9ithr.,6p)6dini7 BLM nIlvi 13-18
V. lemicaTtinilitha,i6pillsinil Laser Therapy in Dentistry
VI. cuciinqu'dfarvi
I. 11/[email protected]@

PHO-2014-3770-ver9-Sattayut_1 P.3d 10/08/14 4:14pm Page 1
PHO-2014-3770-ver9-Sattayut_1P
Photomedicine and Laser Surgery Volume X, Number X, 2014 © Mary Ann Liebert, Inc. Pp. 1-5 DOI: 10.1089/pho.2014.3770
1.1
Low Intensity Laser for Reducing Pain from Anesthetic Palatal Injection
Sajee Sattayut
Abstract
Objective: The aim of this study was to evaluate the effectiveness of pain reduction techniques for palatal injection, namely, low intensity laser therapy (LILT), topical anesthesia, pressure, and light touch. Background data: Previous evidence indicates that LILT may prevent pain from palatal injection. However, no clinical trials evaluating this clinical question have been performed. Methods: A double-blind clinical trial was conducted using 80 healthy volunteers, 18-25 years of age. The subjects were randomly allocated into four groups with 10 females and 10 males each group. Pain reduction techniques were administered at an injection point that was 10 mm from the margin of the palatal gingiva of the upper left first molar according to the following groups: 1) a 790 nm 30 mW continuous wave with a 0.13 cm- focal spot at an applied energy of 3.6 J and fluence of 27.69 J/cm-, 2) 20% benzocaine, 3) pressure, and 4) light touch as the control. Then, 2% lidocaine with 1:100,000 epinephrine was injected using a 27 gauge needle with a pressure and volume control intraligamentary syringe. All subjects recorded pain on a 10 cm visual analog scale (VAS). Results: The pain score in the LILT group was < 50 mm. The median of pain scores of the LILT, 20% benzocaine, pressure, and light touch groups were 11 mm, 23 mm, 27 mm, and 31 mm, respectively. There was no statistically significant difference in. VAS among the groups, using Kruskal—Wallis test (p = 0.385). Conclusions: No statistically significant differences in pain scores were noted among low intensity laser, 20% benzocaine, pressure, and light touch.
Introduction
IN ADDITION TO EVIDENCE SUGGESTING the efficacy of low intensity laser for pain relief in the orofacial region, par-
ticularly for chronic myofascial pain,'-7 low intensity laser, either visible red light laser or infrared gallium aluminum arsenide laser, also exhibits clinical efficacy for pain allevi-ation and healing promotion in acute conditions, such as aphthous stomatitis and herpes simplex.9 The technique has also been applied to prevent discomfort from the surgical removal of impacted teeth,1("2 endodontic surgery,13 and mucositis after chemotherapy. I4 The explanation of these studies was related to reduction of postoperative inflamma-tion. Regarding the prevention of pain and inflammation using low intensity laser, various clinical and in vitro studies demonstrated the technique's effectiveness at reducing the severity of oral mucositis in bone marrow transplantation patients15 and head and neck cancer patients administered chemoradiotherapy.16 This activity was partially attributed to the inhibition of prostaglandin E2 production in myoblast culture, stimulated by interleukin 117 and the reduction of the mitochondrial membrane potential, resulting in decreased axonal flow in the dorsal root ganglions of the rats.18 The
fluence of the laser parameters in the previous studies as mentioned was in the range of 2.5-20 .1/cm` .
Therefore, the possibility of using low intensity laser for acute pain prevention was worth exploring. In order to prove this clinical efficacy in oral surgery, the model of pain produced by palatal local anesthetic injection, including the test for topical anesthesia application, was conducted.' )-29
The aim of this study was to compare pain scores using a visual analogue scale among the groups administered vari-ous pain reduction techniques for palatal injection as fol-lows: low intensity laser therapy (LILT), topical anesthesia using 20% benzocaine, pressure, and light touch (control).
Methods
Subjects
The sample size estimation was calculated using data from a previous study.-1 Briefly, 20 subjects were in each group, to provide 80% power for the test. The double-blind randomized parallel clinical trial was conducted using 80 healthy volun-teers 18-25 years of age. The research proposal was reviewed and approved by the Ethics Committee of Khon Kaen Uni-versity in accordance with the Helsinki Declaration. The
Oral Surgery Department, Faculty of Dentistry and Lasers in Dentistry Research Group, Khon Kaen University, Khon Kaen, Thailand.
1
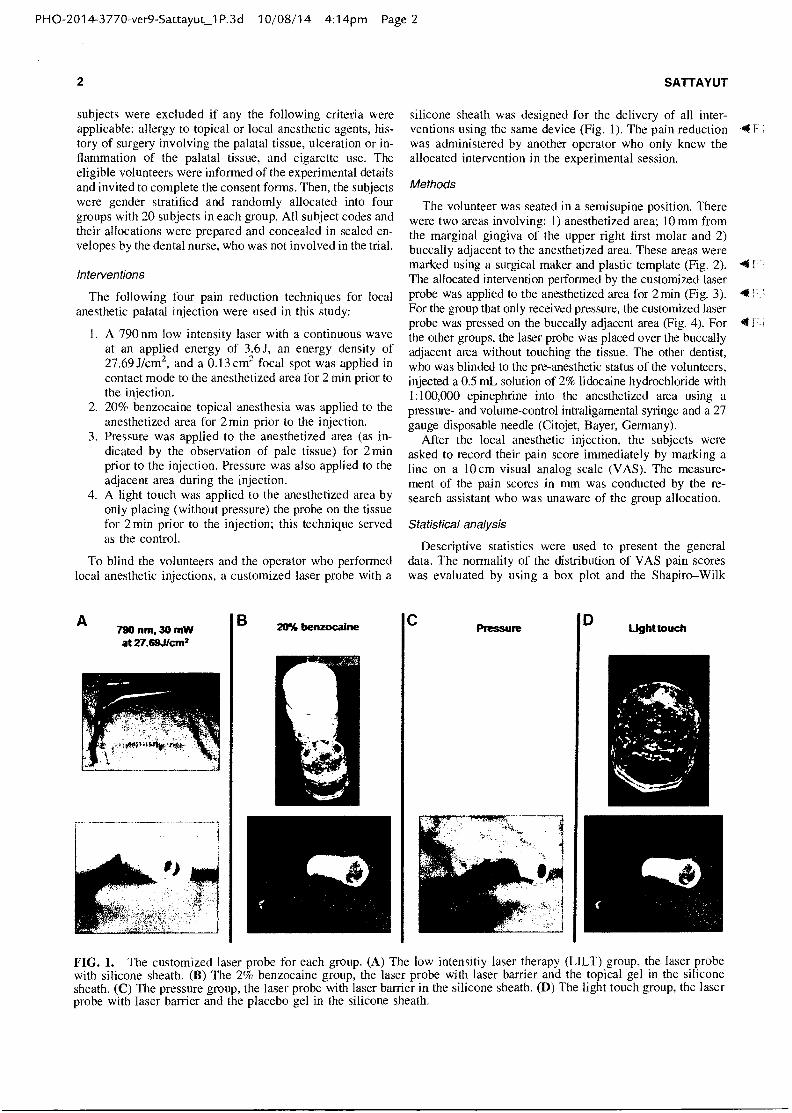
B A 790 nm, 30 mW at 27.69J/cm2
20% benzocaine Light touch D C
PHO-2014-3770-ver9-SattayuCP.3d 10/08/14 4:14pm Page 2
2
subjects were excluded if any the following criteria were applicable: allergy to topical or local anesthetic agents, his-tory of surgery involving the palatal tissue, ulceration or in-flammation of the palatal tissue, and cigarette use. The eligible volunteers were informed of the experimental details and invited to complete the consent forms. Then, the subjects were gender stratified and randomly allocated into four groups with 20 subjects in each group. All subject codes and their allocations were prepared and concealed in sealed en-velopes by the dental nurse, who was not involved in the trial.
Interventions
The following four pain reduction techniques for local anesthetic palatal injection were used in this study:
I. A 790 nm low intensity laser with a continuous wave at an applied energy of 3.6J, an energy density of 27.69 J/cm`, and a 0.13 cm2 focal spot was applied in contact mode to the anesthetized area for 2 min prior to the injection.
2. 20% benzocaine topical anesthesia was applied to the anesthetized area for 2 min prior to the injection.
3. Pressure was applied to the anesthetized area (as in-dicated by the observation of pale tissue) for 2 min prior to the injection. Pressure was also applied to the adjacent area during the injection.
4. A light touch was applied to the anesthetized area by only placing (without pressure) the probe on the tissue for 2 min prior to the injection; this technique served as the control.
To blind the volunteers and the operator who performed local anesthetic injections, a customized laser probe with a
SATTAY UT
Statistical analysis
Descriptive statistics were used to present the general data. The normality of the distribution of VAS pain scores was evaluated by using a box plot and the Shapiro—Wilk
silicone sheath was designed for the delivery of all inter-ventions using the same device (Fig. 1). The pain reduction -4 it was administered by another operator who only knew the allocated intervention in the experimental session.
Methods
The volunteer was seated in a semisupine position. There were two areas involving: 1) anesthetized area; 10 mm from the marginal gingiva of the upper right first molar and 2) buccally adjacent to the anesthetized area. These areas were marked using a surgical maker and plastic template (Fig. 2). The allocated intervention performed by the customized laser probe was applied to the anesthetized area for 2 min (Fig. 3). For the group that only received pressure, the customized laser probe was pressed on the buccally adjacent area (Fig. 4). For 4 f the other groups, the laser probe was placed over the buccally adjacent area without touching the tissue. The other dentist, who was blinded to the pre-anesthetic status of the volunteers, injected a 0.5 mL solution of 2% lidocaine hydrochloride with 1:100,000 epinephrine into the anesthetized area using a pressure- and volume-control intraligamental syringe and a 27 gauge disposable needle (Citojet, Bayer, Germany).
After the local anesthetic injection, the subjects were asked to record their pain score immediately by marking a line on a 10 cm visual analog scale (VAS). The measure-ment of the pain scores in mm was conducted by the re-search assistant who was unaware of the group allocation.
FIG. 1. The customized laser probe for each group. (A) The low intensitiy laser therapy (LILT) group, the laser probe with silicone sheath. (B) The 2% benzocaine group, the laser probe with laser barrier and the topical gel in the silicone sheath. (C) The pressure group, the laser probe with laser barrier in the silicone sheath. (D) The light touch group, the laser probe with laser barrier and the placebo gel in the silicone sheath.
PHO-2014-3770-ver9-Sattayut_1 P.3 d 10/08/14 4:15pm Page 3
LOW INTENSITY LASER FOR REDUCING PAIN
3
FIG. 2. The anesthetized area (A) and adjacent area (B) were marked.
test. The pain scores among the groups were compared by using analysis of variance (ANOVA) and multiple com-parison. In the case of a non-normal data distribution, nonparametric statistics were applied. The median and 95% confidence interval for the median were used for descriptive statistics.22'23 The Kruskal—Wallis test and the Mann—Whitney U test with Bonferroni correction were applied to compare the pain scores among the groups.
Results
General data
The trial included 80 volunteers; 10 females and 10 males were present in each group. The average age of the volun-teers was 21 years.
Main outcome: Pain scores from local anesthetic palatal injection
Based on the Shapiro—Wilk test, the pain scores from the local anesthetic palatal injection assumed a non-normal
FIG. 3. Applying the intervention via the customized laser probe to the anesthetized area, an example of applying pressure as the pale area appeared.
FIG. 4. During local anesthetic injection in the pressure group, the customized laser probe was pressed on the ad-jacent area. The pale area was also observed.
distribution. The box plot is also presented in Figure 5. The 41-' pain scored in the LILT group ranged from 0 to 50 mm, whereas the upper ranges of the pain scores were >50 mm in the other groups. The light touch group was the only group wherein the lower range of pain scores was >0. The medians and 95% confident intervals of the medians are presented in Table 1. The LILT group had lowest median pain score; 11 mm. The medians of the groups that received 20% benzocaine and pressure were 23 and 27 mm, respec-tively. The highest pain score median was observed in the control group, which received light touch. Comparing the groups using the Kruskal—Wallis test, no statistically sig-nificant differences in VAS pain scores were noted (p val-ue =0.385).
Discussion
The VAS pain scored for the various pain reduction tech-niques for palatal injection used in this study exhibited no
111 - -
LILT 20% benzocaine pressure
light touch
Group
FIG. 5. Box plots of pain scores by group.
too,
BO,
so. E E 40.
U)
20,
o.
2o,
PH 0-2014-3770 -ver9-Sattayut_ 1 P. 3 d 10/ 08/ 14 4:15pm Page 4
4
TABLE I. MEDIANS AND THEIR 95% CONFIDENT INTERVALS (CI) FOR MEDIANS OF PAIN SCORES
95% CI for Group Median (mm) median (mm)
LILT
11
10 to 30 20% benzocaine
23
18 to 39 Pressure
27
12 to 35 Light touch
31
13 to 38
LILT, low intensity laser therapy.
statistically significant differences. Compared with a similar study using the palatal injection model,21 this study had a lower median. pain score for the control group (30 mm in this trial and 56 mm in the other study). This difference is explained by the procedure used for the control. In this study, light touching was used as a placebo control, whereas the control group in the other study did not receive any in-tervention. According to the gate theory of pain,24 light touch may relieve the acute pain experienced by palatal injections by initiating larger fibers, including the A delta fiber, and closing the gate for C fiber stimulation. A previous clinical trial demonstrated that touch reduced pain produced from pulsed laser stimuli.25 Therefore, we did not observe statistically significant differences in pain scores among the groups.
In terms of clinical significance, the median pain score of the LILT group was clearly reduced compared with those of the other groups, including the use of standard topical an-esthesia, such as 20% benzocaine.26 Additionally, no vol-unteer reported a pain score > 50 mm in the LILT group. According to the cutoff point of the VAS pain score, mod-erate pain is indicated by scores > 50 mm.27 This result tended to support the advantage of LILT in preventing acute pain from palatal injection over the other methods, that is, 20% benzocaine, pressure, and light touch. The mechanism may be related to a reduced action potential of the free nerve ending of the mucosal tissue. This hypothesis is based on an in vivo study by Chow et al. that demonstrated the influence of a 830 nm low intensity laser on the reduction of mito-chondrial membrane potential and inhibition of fast axonal flow.18 This was also the reason that the infrared laser was selected in this study. Regarding the fluence of the laser parameter, this study used a higher setting than the oth-ers.w.12'18 This was supported by our in vitro experiment comparing laser fluences. It was found that the higher en-ergy density tended to provide an inhibitory effect. '
The strengths of this study included a sufficient sample size based on data from a similar previous study21 and the use of the customized laser probe for operator and subject blinding. However, the use of light touch as the control provided some pain relief. In terms of the clinical implica-tion, LILT, topical anesthesia, and pressure can also be applied to reduce the pain experienced from palatal injec-tions. In addition, light touch also provides some pain re-duction.
Conclusions
A 790 nm low intensity laser at 27.69 J/cm2 exhibited clinical efficacy regarding relief from the pain of anesthetic palatal injections. The VAS pain score ranged from 0 to
SATTAYUT
50 mm. No statistically significant differences in pain scores were noted among low intensity laser, 20% benzocaine, pressure, and light touch.
Acknowledgments
I thank the Faculty of Dentistry and Lasers in Dentistry Research Group, Khon Kaen University for a research grant. I also thank Pisake Lumbiganon for his kind advice on manuscript writing, as well as the research assistants, Kit-tiwut Hortong and Pisamai Wichan, for kindly assisting in fulfilling the double-blind methodology in this trial.
Author Disclosure Statement
No competing financial interests exist.
References
1. Fulop, A.M., Dhimmer, S., Deluca, J.R., Johanson, D.D., Lenz, R.V., Patel, K.B., Douris, P.C., and Enwemeka, C.S. (2010). A meta-analysis of the efficacy of laser photo-therapy on pain relief. Clin. J. Pain. 26, 729-736.
2. Venezian, G.C., da Silva, M.A., Mazzetto, R.G., and Mazzetto, M.O. (2010). Low level laser effects on pain to palpation and electromyographic activity in TMD patients: a double-blind, randomized, placebo-controlled study. Cranio 28, 84-91.
3. Conti, P.C. (1997). Low level laser therapy in the treatment of temporomandibular disorders (TMD): a double-blind pilot study. Cranio 15, 144-149.
4. Cetiner, S., Kahraman, S.A., and Yucetas, S. (2006). Evalua-tion of low-level laser therapy in the treatment of temporo-mandibular disorders. Photomed. Laser Surg. 24, 637-641.
5. Carvalho, C.M., de Lacerda, J.A., dos Santos, Neto, F.P., Cangussu, M.C., Marques, A.M., and Pinheiro, A.L. (2009). Wavelength effect in temporomandibular joint pain: a clin-ical experience. Lasers Med. Sci. 25, 229-232.
6. Carrasco, T.G., Mazzetto, M.O., Mazzetto, R.G., and Mestriner, W., Jr. (2008). Low intensity laser therapy in temporomandibular disorder: a phase II double-blind study. Cranio 26, 274-281.
7. Sattayut, S., and Bradley, P. (2012). A study of the influ-ence of low intensity laser therapy on painful temporo-mandibular disorder patients. Laser Ther. 21, 183-192.
8. De Souza, T.O., Martins, M.A., Bussadori, S.K., Fernandes, K.P., Tanji, E.Y., Mesquita-Ferrari, R.A., and Martins, M.D. (2010). Clinical evaluation of low-level laser treat-ment for recurring aphthous stomatitis. Photomed. Laser Surg. 28 Suppl. 2, S85-88.
9. Schindl, A., and Neumann, R. (1999). Low-intensity laser therapy is an effective treatment for recurrent herpes simplex infection. Results from a randomized double-blind placebo-controlled study. J. Invest. Dermatol. 113, 221-223.
10. Aras, M.H., and Gungormus, M. (2010). Placebo-controlled randomized clinical trial of the effect two different low-level laser therapies (LLLT) intraoral and extraoral on trismus and facial swelling following surgical extraction of the lower third molar. Lasers Med. Sci. 25, 641-645.
11. Markovic, A., and Todorovic, L. (2007). Effectiveness of dexamethasone and low-power laser in minimizing oedema after third molar surgery: a clinical trial. Int. J. Oral Max-illofac. Surg. 36, 226-229.
12. Markovic, A.B., and Todorovic, L. (2006). Postoperative analgesia after lower third molar surgery: contribution of
P H 0-2014-3770 -ver9 -Sattayut_1 P.3 d 10/ 08/ 14 4:15pm Page 5
LOW INTENSITY LASER FOR REDUCING PAIN
the use of long-acting local anesthetics, low-power laser, and diclofenac. Oral Surg. Oral Med. Oral Pathol. Oral Radio!. Endod. 102, 4-8.
13. Kreisler, M.B., Al Haj, H., Noroozi, N., Willershausen, B., and D'Hoedt, B. (2004). Efficacy of low level laser therapy in reducing postoperative pain after endodontic surgery: a randomized double blind clinical study. Int. J. Oral Max-ilifac. Surg. 33, 38-41.
14. Cauwels, R.G., and Martens, L.C. (2011). Low level laser therapy in oral mucositis: a pilot study. Eur. Arch. Paediatr. Dent. 12, 118-123.
15. Antunes, H.S., de Azevedo, A..M, da Silva Bouzas, L.F., et al. (2007). Low-power laser in the prevention of induced oral mucositis in bone marrow transplantation patients: a randomized trial. Blood 109, 2250-2255.
16. Gouvea de Lima, A., Villar, R.C., de Castro, Jr. G., Ante-quera, R., Gil, E., Rosalmeida, M.C., Federico, M.H.H., and Snitcovsky, I.M.L. (2012). Oral mucositis prevention by Low level laser therapy in head and neck cancer patients undergoing concurrent chemoradiotherapy: A phase III randomized study. Int. J. Radiat. Oncol. Biol. Phys. 82, 270-275.
17. Sattayut, S., Hughes, F., and Bradley, P. (1999). 820 nm Gallium Aluminium Arsenide Laser modulation of prosta-glandin E2 production in interleukin I stimulated myoblast. Laser Ther. 11, 88-95.
18. Chow, R.T., David, M.A., and Armati, P.J. (2007). 830 nm laser irradiation induces varicosity formation, reduces mi-tochondrial membrane potential and blocks fast axonal flow in small and medium diameter rat dorsal root ganglion neurons: implications for the analgesic effects of 830 nm laser. J. Peripher. Nerv. Syst. 12, 28-39.
19. Al-Meth, M.A., and Andersson, L. (2007). Comparison of topical anesthetics (EMLA/Oraqix vs. benzocaine) on pain
5
experienced during palatal needle injection. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 103, 16-20.
20. Harbert, H. (1989). Topical ice: A precursor to palatal in-jections. J. Endod. 15, 27-28.
21. Sattayut, S., Homdee, D., and Pol-la, A. (2002). A com-parative of painless palatal-local anesthetic injection tech-niques. Khon Kaen Dent. J. 5, 68-72.
22. Altman, D.G. (2005). Why we need confidence intervals. World J. Surg. 29, 554-556.
23. Campbell, M.J., and Gardner, M.J. (1988). Calculating confidence intervals for some non-parametric analyses. Br. Med. J. (Clin. Res. Ed.) 296, 1454-1456.
24. Mendell, L.M. (2014). Constructing and deconstructing the gate theory of pain. Pain 155, 210-216.
25. Mancini, F., Nash, T., Iannetti, G.D., and Haggard, P. (2014). Pain relief by touch: a quantitative approach. Pain 155. 635-642.
26. Meechan, J.G. (2000). Intra-oral topical anaesthetics: a review. J. Dent. 28, 3-14.
27. Collins, S.L., Moore, R.A., and McQuay, H.J. (1997). The visual analogue pain intensity scale: what is moderate pain in millimetres? Pain 72, 95-97.
Address correspondence to: Sajee Sattayut
Oral and Maxillofacial Surgery Department Faculty of Dentistry
Khon Kaen University Khon Kaen 40002
Thailand
E-mail: [email protected]
t 2

PHO-2014-3770-ver9-Sattayut_1P.3d 10/08/14 4:15pm Page 6
AUTHOR QUERY FOR PHO-2014-3770-VER9-SATTAYUT_1P
AUl: Please provide author's degree(s). AU2: Please check reference. Not in PubMed.
Official Journal of Asian-Pacific Association for Laser Medicine and Surgery (APALMS),
International Academy Laser Medicine and Surgery (IALMS), International Phototherapy Association (IPTA),
International Society for Laser Surgery and Medicine (ISLSM), Japan Association for Laser Medicine and Sports Science (JALMSS),
Japan Society for Laser Reproduction (JaSLaR), Japan Society for Laser Surgery and Medicine (JSLSM),
World Federation of Societies for Laser Medicine and Surgery (WFSLMS)
AN INTERNATIONAL JOURNAL FOR LASER SURGERY, PHOTOTHERAPY AND
PHOTOBIOACTIVATION
CONTENTS VOLUME 22 NUMBER 1
Mar 2013
Editorial It's official! LASER THERAPY has been awarded PubMed Central listing!! Toshio Ohshiro 5
Kaplan's Corner History and The CO2 surgical laser Isaac Kaplan 8
Original Article CO2 laser oral soft tissue welding: an in vitro study Sajee Sattayut, Pitinuch Nakkyo, Puntiwa Phusrinuan, Thanyaporn Sangiamsak, Ratchanee Phiolueang 11
Low level laser therapy for sports injuries Yusuke Morimoto, Akiyoshi Saito, Yasuakl Tokuhashi 17
Effect of low-level laser Therapy on blood flow and oxygen- hemoglobin saturation of the foot skin in healthy subjects: a pilot study Franziska Heu, Clemens Forster, Barbara Namer, Adrian Dragu, Werner Lang 21
Er:YAG and adhesion in conservative dentistry: clinical overview Carlo Fornaini 31
Surface enhanced Raman spectroscopy in breast cancer cells JL Gonzalez-Solis, GH Luevano-Colmenero, J Vargas-Mancilla 37
830 nm light-emitting diode low level light therapy (LED-LLL'f) enhances wound healing: a preliminary study Pak Kee Min, Boncheol Leo Goo 43
Recalcitrant molluscum contagiosum successfully treated with the pulsed dye laser Tokuya Omi, Seiji Kawana 51
The Winners of the Best/Good Paper Awards 2012 55 Profile of authors and co-authors 56 Report on Laser Florence 2012 and invitation to Laser Florence 2013 59 Announcement of IPTA 5 63 Bylaws of APALMS 64 Meeting calendar 68 Publish agreement 69 Notes for contributors 71 .Tr-dr, TCT Ql't 41 "7Q
OFFICIAL JOURNAL OF ISLSM, IPTA, APALMS, JaSLaR, JALMSS and WFSLMS

CO2 laser oral soft tissue welding: an in vitro study
Sajee Sattayut 1, Pitinuch Nakkyo 2, Puntiwa Phusrinuan 3,
'l'hanyaporn Sangiamsak 4, Ratchanee Phiolueang 5
1: Lasers in Dentistry)? Research Group, Kbon Kaen University, Thailand 2: Prasat Hospital, Prasat, Surin, Thailand
3: Payathai Sriracha Hospital, Chonburi, Thailand 4: Kantamtvichai Hospital, Mahasarakhaln, Thailand
.5: Thatoo?n Hospital, Surly, Thailand
Background and aim: Although there are some studies reporting the benefits of using laser to improve wound closure, there were a few studies in a model of oral mucosa. The aim of this in vitro study was to compare immediate tensile strength of the wound closure between suture alone and suture combined with CO2 laser welding. Materials and methods: The study was conducted in 40 samples of the tissue blocks from ventral sides of pig tongues. A 20 mm-length and 5 mm-depth incision was made in each sample. The samples were randomly allocated into 2 groups namely: the control group and the experimental group. The samples of the control group were sutured with 3- stitch of 4-0 black silk. The samples of the experimental group were irradiated with CO2 laser (ultrapulse mode, 800 Watt peak power, 10 Hz, 0.2 ms pulse duration and 2,262.62 J/cm2 energy density) before sutured. The immediate tensile strength of the wound was measured by using customized tensiometer under stereomicro-scope. Results: The median of tensile strength of the control group and the experimental group were 30.40 g/cm2 and 40.50 g/cm2, respectively. There was no statistically significant difference between the groups (P value = 0.58). The proportions of the samples without wound dehiscence at the maximum limit of the tensiometer (120 g/cm2) were 0.15 (3/20) in the control group and 0.35 (7/20) in the experimental group. Conclusion: The CO2 laser welding used in this study failed to show a greater immediate tensile strength but had a higher proportion of the wound without dehiscence at the 120 g/cm2 tensile strength by comparison with the suture alone.
Key words: Oral mucosa • Oral surgery • Tensile strength • Tensiometer • Suture • Wound closure
Introduction
There are a number of in vitro and in vivo studies in a variety of tissues such as nerve, vessel, skin, gastroin-testinal and urinary mucosa reporting the use of laser for wound approximation and closure 1-6). The results showed benefits of improving immediate tensile strength and fluid tight seal. The laser-assisted wound approximation can be divided into 2 techniques name-ly: laser tissue welding which is direct application of
Addressee for Correspondence.' Associate Professor Sajee Sattayut Lasers in Dentistry Research Group and Oral Surgery Department, Faculty of Dentistry, Khon Kaen University, Khon Kaen. 40002. Thailand
©2013 JMI,L, Tokyo, Japan
precise laser energy to the site to be welded and laser tissue soldering which is using a substrate such as pro-tein-based fluid and dye to absorb the laser energy 7).
Regarding the study in oral mucosa, there was an in vivo study by Greene et al 8) comparing immediate tensile strength between laser welding and suture of incisions on the pig tongues. Although this study showed that CO2 laser welding could produce equiva-lent or stronger tensile strength than the suture, the immediate tensile strength which was an expected result for promotion of healing in the laser welding group was less than the suture group. Owing to this potential area, it was worth exploring the benefit of combined laser tissue welding and suture to improve
Laser Therapy 22.1: 11-15 11
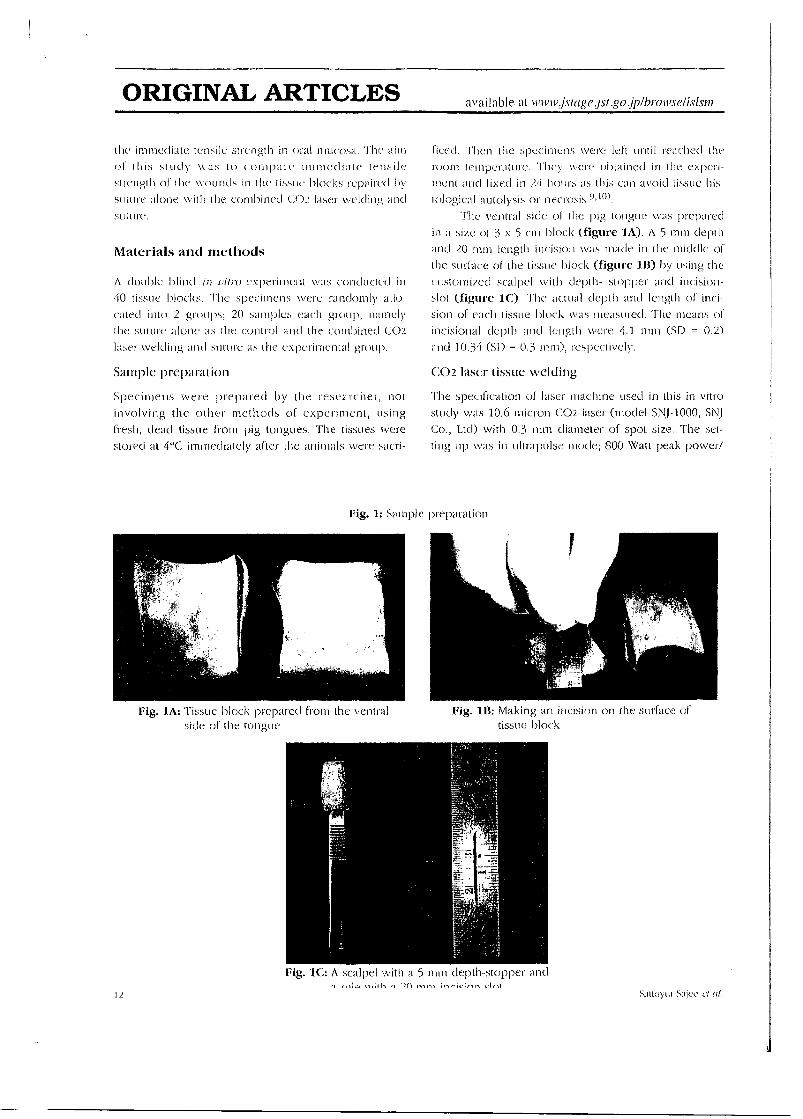
ORIGINAL ARTICLES available at wwwislagejst.gojp1bmwselisisin
the immediate tensile strength in oral mucosa. The aim
of this study was to compare immediate tensile
strength of the wounds in the tissue blocks repaired by
suture alone with the combined CO2 laser welding and
suture.
Materials and methods
A double blind ni rum experiment was conducted in
40 tissue Hocks. The specimens were randomly allo
cated into 2 groups; 20 samples each group, namely
the suture alone as the control and the combined CO2
laser welding and suture as the experimental group.
Sample preparation
Specimens were prepared by the researcher, not
involving the other methods of experiment, using
fresh, dead tissue f1011.1 pig tongues. The tissues were
stored at 4°C immediately after the animals were sacri-
ficed. 'Men the specimens were left until reached the
room temperature. They were obtained in the experi-
ment and fixed in 24 hours as this can avoid tissue his-
tological autolysis or necrosis 9, ".
The ventral side or the pig tongue was prepared in a size of 3 x 5 cm block (figure 1A). A 5 mm depth
and 20 mm length incision was made in the middle of
the surface of the tissue block (figure 1B) by using the
customized scalpel with depth- stopper and incisiori-
slot (figure 1C). The actual depth and length of inci-
sion of each tissue block was 111CISUIC(..1. 'rite means of
incisional depth and length were 4.1 nun (SD = 0.2)
and 10.34 (SD = 0.3 mm), respectively.
CO2 laser tissue welding
The specification of laser machine used in this in vitro
study was 10.6 micron CO2 laser (model SNJ-1000, SNJ
Co., Ltd) with 0.3 mm diameter of spot size. The set-
ting up was in ultrapulse mode; 800 Watt peak power/
Fig. 1: Salnple preparation
Fig. 1A: Tissue block prepared from the ventral
side of the tongue
Fig. 1B: Making an incision on the surface of tissue block.
Fig. 1C: A scalpel with a 5 mm depth-stopper and it; '1 ■,,rie;ls,-, L.1,1
12 Sallayul Sajec el al.
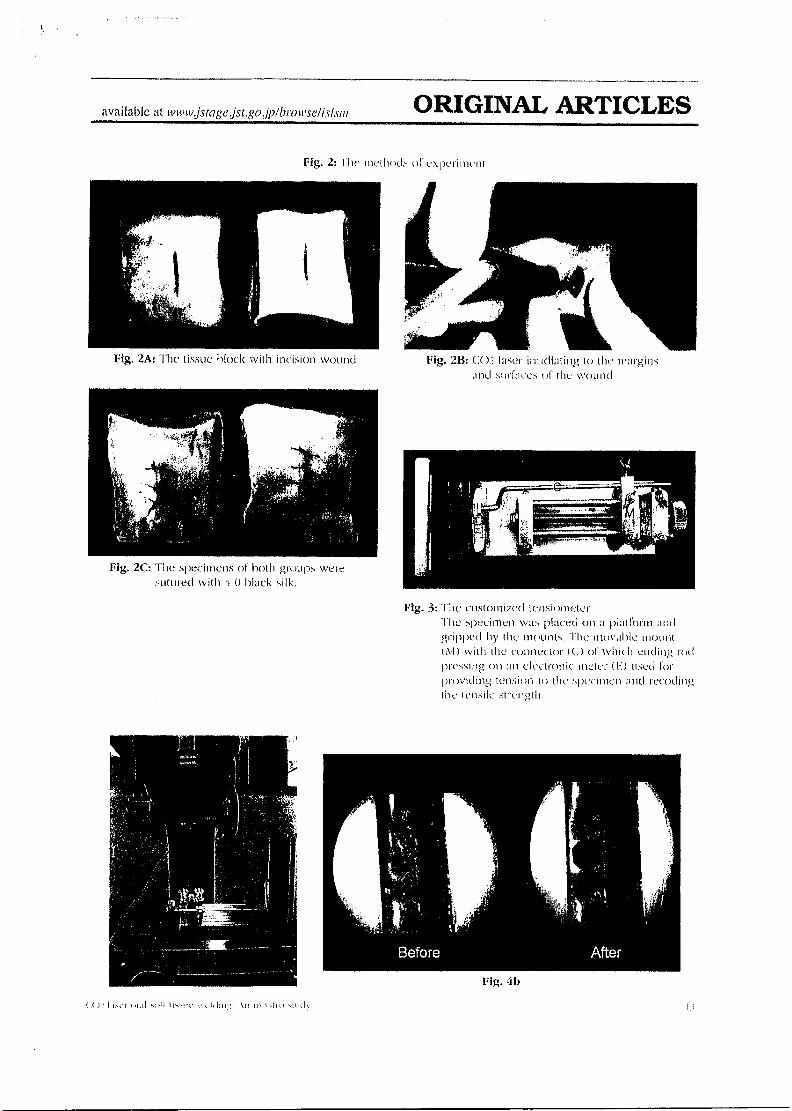
Fig. 2C: The specimens of both groups were sutured with A-0 Hack silk.
available at wwwjstage jst .go 1p/bmwse/isIsm ORIGINAL ARTICLES
Fig. 2: The methods of experiment-
Fig. 2A: The tissue block with incision wound
Fig. 213: CI)2, laser irradiating to the margins and surfaces of the wound
Fig. 3: "-Mc customized tensiometer The specimen was placed on a plattOrm gripped by the mounts. The movable inount (M) with the connector (C) of which ending rod pressing on an electronic meter (k) used for providing tension to the specimen and recoding Ilse tensile strength.
4b
Lim:r t,rAl mat Ilma.tc•
'It Iii \II 111 II

0.2 msec pulse duration/10Hz. The energy density measured by the powermeter from the dealer company (Medical Laser Thailand Co., Ltd) was 2,262.62J/cm2
per pulse. This regime was tested in a pilot study resulting no shrinkage and ablative effect of the mar-gins of the specimens.
Methods
The prepared tissue blocks were randomly allocated into 2 groups (figure 2A). The experimental group was irradiated by CO2 laser to the raw surfaces and the margins at the rate of 1 cm per second (figure 2B). Then 3 stitches of 4-0 black silk sutures were equiva-lently placed by the researcher who was blinded the groups of study (figure 2C). The control group was undertaken the same procedures apart from using the inactive CO2 laser which was the mutual setting of CO2 laser with a laser-beam blocker in the laser probe.
Measurement
The measurement of the breaking strength of wound by using tensiometer 2,11) was conducted. All speci-mens then placed in the customized tensiometer. This was mainly composed of a platform for tissue block, a movable mounting for stretching the margins of the sample and an electronic meter (figure 3). There was a connecting rod from the movable mount to the elec-tronic meter. The cnd of the rod pressing on an elec-tronic meter was designed to be a size of 1 cm2. Therefore, the tension was able to be measured in a unit of g/cm2. The maximum tension of this apparatus was 120 g/cm2. In this study, an increasing of tension was controlled by the length of movement of the mov-able mounting at the rate of 0.5 mm/min. During increasing the tension to the sample, the separation of the wound margins was inspected under a stereomi-croscope (figure 4A). The tension was recorded immediately when the dehiscence of the margins was detected (figure 4B). The measurement was undertak-en by the other researcher not involving in the irradia-tion method.
Statistical analysis
The tensile strengths between the groups were corn-pared using t-test at the significant level of 0.05 P valve. In case the data was not normal distribution, the non- parametric statistics; Mann-Whitney U test, was
used.
Results
Some samples in both groups had no separation of the wound margins at the maximum limit of che tensiome-
ter (120 g/cm2). The proportions of non-dehiscence
samples at 120 g/cm2 tension were 3/20 (0.15) in the
suture alone group and 7/20 (0.35) in the combined CO2 laser welding and suture.
The main results, the immediate tensile strengths of both groups, were not normal distribution. The cal-culation using Shapiro-Wilk test showed P value at 0.53. Therefore, the non-parametric statistics were applied. The median of the suture alone group from 17 samples was 30.40 g/cm2 while the median of the combined CO2 laser welding and suture from 13 sam-ples was 40.50 g/cm2 (table 1). There was no statisti-cally significant difference between the groups by ana-lyzing with Mann-Whitney U test (P value = 0.58).
Discussion
Even though, there was no statistically significant differ-ence of the immediate tensile strength between the suture alone and the combined CO2 laser welding, the proportion of the samples without wound dehiscence at 120 g/cm2 tension of the experimental group; com-bined CO2 laser and suture, was twice times higher than the control group; suture alone, Therefore, it tend-ed to show that combined CO2 laser welding and suture may able to increase an immediate tensile strength in the samples of simulating incision-wound in oral mucosa. It was different from the study of Greene
et al 8) in that the average of tensile strength in 1 hour
Table 1: The Medians of immediate tensile strength and the 25th and 75th percentiles by the groups
Groups Tensile strength (g/cm2)
Median 25th percentile
30.40 16.80
40.50 21.40
75th percentile 74.60 83.0
Suture alone CO2 laser welding +
14 Sattayut Sajec et al.

of the CO2 laser welding (3.30 lb) was less than the suture group (3.40 lb). This can be explained by the different settings of CO2 laser. This study used the ultra-pulse mode with the calibrated parameter showing no shrinkage of the wound margins while the other used repeated pulse mode producing some photoablation. In the previous studies 8, 12), they found that CO2 laser in repeated pulse mode provided some lateral heat dam-age of the tissue. Additionally, there was a study showed that the controlled temperature around 55°C; below the level of coagulation at 60°C, was significant for the success of welding of urinary bladder 3).
Regarding the clinical application, this tissue welding technique using CO2 can be applied for enhancing an immediate tensile strength of intraoral
suture to promote wound healing. The CO2 laser weld-ing is not able to be used solely without suture. As far as sutureless closure of oral soft tissue concerned, the tissue soldering with protein media 13,14) is suggested to be a further study.
Conclusion
The combined CO2 laser welding at ultrapulse mode and suture had no statistically significant difference in immediate tensile strength of the wound closure in oral soft tissue blocks by comparison with the suture alone but had the higher proportion of the wounds without dehiscence at the 120 g/cm2 tensile strength.
References
1: Gulsoy M, Dereli Z, Tabakoglu HO, Bozkulak 0 (2006): Closure of skin incisions by 980-nm diode laser welding. Lasers in Medical Science, 21:5-10.
2: Fried NM, Walsh yr, Jr (2000) I,aser skin welding: in vivo tensile strength and wound healing results. Lasers in Surgery and Medicine, 27:55-65.
3: Lobel B, Eyal 0, Kariv N, Katzir A (2000): Temperature controlled CO2 laser welding of soft tissues: urinary bladder welding in different animal models (rats, rabbits, and cats). Lasers in Surgery and Medicine, 26:4-12.
4: Menovsky T (2000): CO2 and Nd:YAG laser-assist-ed nerve repair: a study of bonding strength and thermal damage. Acta Chirurgiae Plasticae, 42:16-22.
5: Poppas DP, Rucker GB, Scherr DS (2000): Laser Tissue Welding - Poised for the New Millenium. Surgery Technology International, 9:33-41.
6: Bass LS, Treat MR (1995): Laser tissue welding: a comprehensive review of current and future clini-cal applications. Lasers in Surgery and Medicine,
17:315-349. • 7: Chivers RA (2000): In vitro tissue welding using
albumin solder: bond strengths and bonding tem-peratures. International Journal of Adhesion and
Adhesive, 20:179187. 8: Greene CH, Debias DA, Henderson MJ, Fair-Covely
R, Dorf B, Radin AL (1994): Healing of incisions in the tongue: a comparison of results with milliwatt
carbon dioxide laser tissue welding versus suture repair. Annals of Otology, Rhinology and Laryngology, 103:964-974.
9: Sattayut 5, Bradley P (2003): A comparative study of the central vaporization with peripheral coagula-tion of Nd YAG laser. International Congress
Series, 1248:371-376. 10: Berman B, Chen VL, France DS, Dotz WI, Petroni
G (1983): Anatomical mapping of epidermal Langerhans cell densities in adults. British Journal of Dermatology, 109:553-558.
11: Sanders DL, Reinisch L (2000): Wound healing and collagen thermal damage in 7.5-microsec pulsed CO2 laser skin incisions. Lasers in Surgery and Medicine, 26:22-32.
12: Paes-Junior TJA (2001): Clinical comparison between conventional suture and vaporization with carbon dioxide laser in rat's skin. Journal of Clinical Laser Medicine Surgery, 19:319-324.
13: Wolf-de Jonge IC, Heger M, van Marie J, Balm R, Beek JF (2008): Suture-free laser-assisted vessel repair using CO2 laser and liquid albumin solder. Journal of Biomedicine Optics, 13:044032.
14: Maitz PK, Trickett RI, Dekker P, Tos P, Dawes JM, Piper JA (1999): Sutureless microvascular anasto-moses by a biodegradable laser-activated solid pro-tein solder. Plastic and Reconstructive Surgery, 104:1726-1731.
CO2 laser oral soft tissue welding: An in vitro study 15
TRIBUTE ISSUE: Dedicated to the life and times of the late Professor Isaac Kaplan and Masha Kaplan
LASER THERAPY
1=1
Official Journal of Asian-Pacific Association for Laser Medicine and Surgery (APALMS)
European Master degree in Oral Laser applications (EMDOLA Academy) International Academy Laser Medicine and Surgery (IALMS)
International Phototherapy Association (IPTA) International Society for Laser Surgery and Medicine (ISLSM)
Japan Association for Laser Medicine and Sports Science (JALMSS) Japan Society for Laser Reproduction (JaSLaR)
Japan Society for Laser Surgery and Medicine (JSLSM) World Federation of Societies for Laser Medicine and Surgery (WFSLMS)
available at www.jstage.jst.go.jp/browse/islsm CONTENTS
AN INTERNATIONAL JOURNAL FOR LASER SURGERY, PHOTOTHERAPY AND
PHOTOBIOACTIVATION
CONTENTS VOLUME 22 NUMBER 4
December 2013
Editorial THE LAST AND FOND FAREWELL
Toshio Ohshiro 241
Announcement IMPORTANT ANNOUNCEMENT from Professor Ming-Chien Kao MD MDSc 245
Best Paper Awards 2014 246
Original Article Comparing the Effectiveness of 1064 vs. 810 nm Wavelength Endovascular Laser for Chronic Venous Insufficiency (Varicose Veins)
De-Yi Yu, Hung-Chang Chen, Shu-Ying Chang, Yen-Chang Hsiao, Cheng-Jen Chang 247
Laser Scar Management Technique
Takafumi Ohshiro, Toshio Ohshiro, Katsumi Sasaki 255
Laser doppler myography (LDMi): A novel non-contact measurement method for the muscle activity
L Scalise, S Casaccia, P Marchionni, I Ercoli, EP Tomasini 261
An update in varicose vein pathology after ten years of endovenous laser therapy (EVLT) with a 980 nm diode laser: clinical experience of a single center
Pietro Scarpelli, Annamaria Maggipinto, Marco Leopardi, Evelina Di Marco, Angelo Disabato, Michelangelo Boschetti, Giorgio Sbenaglia, Carlo Spartera, Marco Ventura 269
Laser welding and syncristallization techniques comparison: "Ex vivo" study
Fornaini Carlo, Meleti Marco, Vescovi Paolo, Merigo Elisabetta, Rocca Jean-Paul 275
A clinical efficacy of using CO2 laser irradiating to transparent gel on aphthous stomatitis patients
Sajee Sattayut, Juthamanee Trivibulwanich, Naruernon Pipithirunkarn, Nawaporn Danvirutai 283
Meeting Report World Laserology Congress 290
Joint Meeting of IPTA, ISLSM, WFSLMS, WFLD 293
Report on Laser Florence 2013 295
Profile of Authors and Co-Authors 297
Meeting Calendar 302
Indices 303
Publish Agreement 309
Notes for Contributors 311
Join ISLSM! 313
Join IPTA! 315
Official Journal of APALMS, EMDOLA Academy, !ALMS, IPTA, ISLSM, JALMSS, JaSLaR, JSLSM and WFSLMS
available at www.jstagejst.gajp/browsdislsm ORIGINAL ARTICLES
A clinical efficacy of using CO2 laser irradiating to transparent gel on aphthous stomatitis patients
Sajee Sattayut 1, Juthamanee Trivibulwanich 2,
Naruemon Pipithirunkarn 2 , Nawaporn Danvirutai 2
1: Oral Surgety Department, Faculty of Dentistly and Lasers in Dentistry Research Group, Khon Kaen University, Thailand:
2: Dental student. Faculty ty'Dentistly; Khon Kaen University
Background and aims: Regarding the laser energy delivery with non-tissue alteration when irradiating CO2 laser to the transparent gel, it was worth exploring the clinical efficacy of pain relief on oral ulceration using aphthous stomatitis as a model for painful oral ulcer. The aims of this study were to compare pain scores, daily activity-disturbance scores and sizes of the ulcers between the laser group and the placebo group. Subjects and methods: The double blind- randomized- placebo- controlled trial was conducted in 11 patients with aphthous ulcers. The subjects were allocated into 2 groups; namely, the laser group and the placebo group. The two baselines were measured on the clay before and the treatment day. Then the lesions were covered with the transparent gel and irradiated by either 2 \V defocused CO2 laser for 5 seconds or the sham laser. The outcomes were collected immediately, on clay 1, 3, 5 and 7 after treatment. Results: The means of pain and daily activity-disturbance scores of the laser group were lesser than the placebo group in every episode. A statistically significant difference between the groups was found only the pain score on day 3 after treatment (P-value<0.001, 95% CI of the difference = 8.8 to 19.20 mm). There were no statistically significant differences in the daily activity-disturbance scores and the sizes of the ulcers between the groups (P value > 0.05). Conclusion: The CO2 laser therapy used in this clinical study was able to relieve pain from aphthous stomatitis compared with the placebo on the day 3 after treatment.
Introduction
Aphthous stomatitis is a common painful and recurrent
oral ulceration disturbing patients' daily activities such
as eating, swallowing and speaking 1). Currently, there
has been no curative therapy to prevent the recurrence
of the ulcer but only to reduce the severity of
symptoms in particular pain 1,2) . The recommended
treatment modalities include topical agents such
as topical steroids and anti-inflammatory agents 1-3)
and systemic therapy such as predisone and
immunopotentiating agents 1, 2). Recently, there were a
Addressee for Correspondence: Associate Professor Sajee Sattayut Oral and Maxillofacial Surgery Department. Faculty of Dentistry. Khon Kaen University. Khon Kaen, Thailand, •i0002 Telephone: +66-8-1544-2460 e-mail: [email protected]
case report and clinical trials showing benefit of
immediate pain relief on aphthous ulcers by using CO2
laser at 0.7 to 1.5 NX: irradiating to the transparent gel.
On the basis of no clinical alteration, this was called
the non-thermal CO2 irradiation 4-7). By comparison
with laser ablation for replacing aphthous ulcer with
the lasered wound I.8), this technique appeared to be
non-invasive. However, Prasad and Pai suggested the
further study on the mechanism involving this
analgesia 4).
There was an in vitro experiment illustrated that
defocused CO2 at 1, 2 and 3 W irradiating for seconds
to a 3 mm-thickness of the high-water-contain
transparent gel providing no tissue alteration from
histological observation. This experimental study also
showed that there was no energy from CO2 laser could
Received Date: October 10th, 2013 Accepted Date: November 18th. 2013
(02013 lAJLL, Tokyo, japan Laser Therapy 22.4: 283-289
283
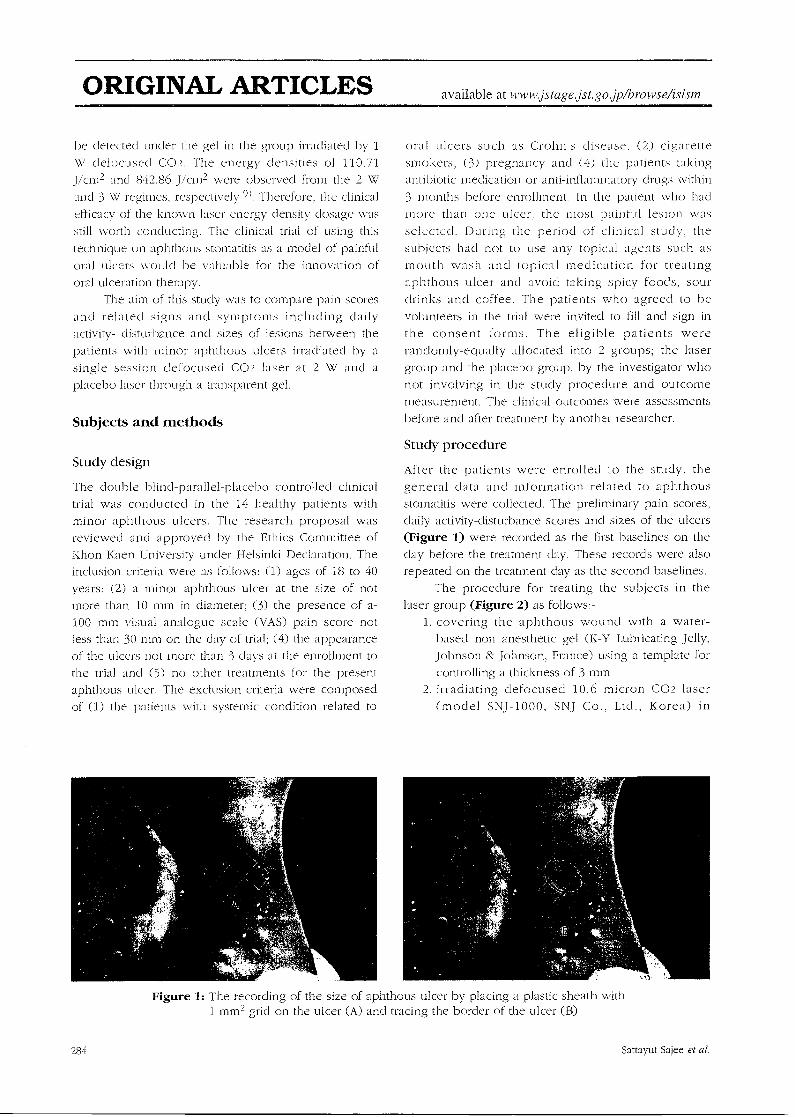
ORIGINAL ARTICLES available at www.jstagejst.go.jpArowsefislsm
he detected under the gel in the group irradiated by 1
W defocused CO2. The energy densities of 110.71
J/cm2 and 842.86 J/cm2 were observed from the 2 W
and 3 W regimes, respectively 9). Therefore, the clinical
efficacy of the known laser energy density dosage was
still worth conducting. The clinical trial of using this
technique on aphthous stomatitis as a model of painful
oral ulcers would be valuable for the innovation of
oral ulceration therapy.
The aim of this study was to compare pain scores
and related signs and symptoms including daily
activity- disturbance and sizes of lesions between the
patients with minor aphthous ulcers irradiated by a
single session defocused CO2 laser at 2 W and a
placebo laser through a transparent gel.
Subjects and methods
Study design
The double blind-parallel-placebo controlled clinical
trial was conducted in the 14 healthy patients with
minor aphthous ulcers. The research proposal was reviewed and approved by the Ethics Committee of
Khon Kaen University under Helsinki Declaration. The
inclusion criteria were as follows: (1) ages of 18 to 40
years; (2) a minor aphthous ulcer at the size of not
more than 10 mm in diameter; (3) the presence of a-100 mm visual analogue scale (VAS) pain score not
less than 30 mm on the day of trial; (4) the appearance
of the ulcers not more than 3 days at the enrollment to
the trial and (5) no other treatments for the present
aphthous ulcer. The exclusion criteria were composed
of (1) the patients with systemic condition related to
oral ulcers such as Crohn s disease, (2) cigarette
smokers, (3) pregnancy and (4) the patients taking
antibiotic medication or anti-inflammatory drugs within
3 months before enrollment. In the patient who had
more than one ulcer, the most painful lesion was
selected. During the period of clinical study. the
subjects had not to use any topical agents such as
mouth wash and topical medication for treating
aphthous ulcer and avoid taking spicy foods, sour
drinks and coffee. The patients who agreed to be
volunteers in the trial were invited to fill and sign in
the consent forms. The eligible patients were
randomly-equally allocated into 2 groups; the laser
group and the placebo group, by the investigator who
not involving in the study procedure and outcome
measurement. The clinical outcomes were assessments
before and after treatment by another researcher.
Study procedure
After the patients were enrolled to the study, the
general data and information related to aphthous
stomatitis were collected. The preliminary pain scores, daily activity-disturbance scores and sizes of the ulcers
(Figure 1) were recorded as the first baselines on the
clay before the treatment day. These records were also repeated on the treatment day as the second baselines.
The procedure for treating the subjects in the
laser group (Figure 2) as follows:-
1. covering the aphthous wound with a water-
based non anesthetic gel (K-Y Lubricating Jelly, Johnson & Johnson, France) using a template for
controlling a thickness of 3 mm
2. irradiating defocused 10.6 micron CO2 laser
(model SNJ-1000, SNJ Co., Ltd., Korea) in
Figure 1: The recording of the size of aphthous ulcer by placing a plastic sheath with 1 mm2 grid on the ulcer (A) and tracing the border of the ulcer (B)
284
Sattayut Sajee et al.
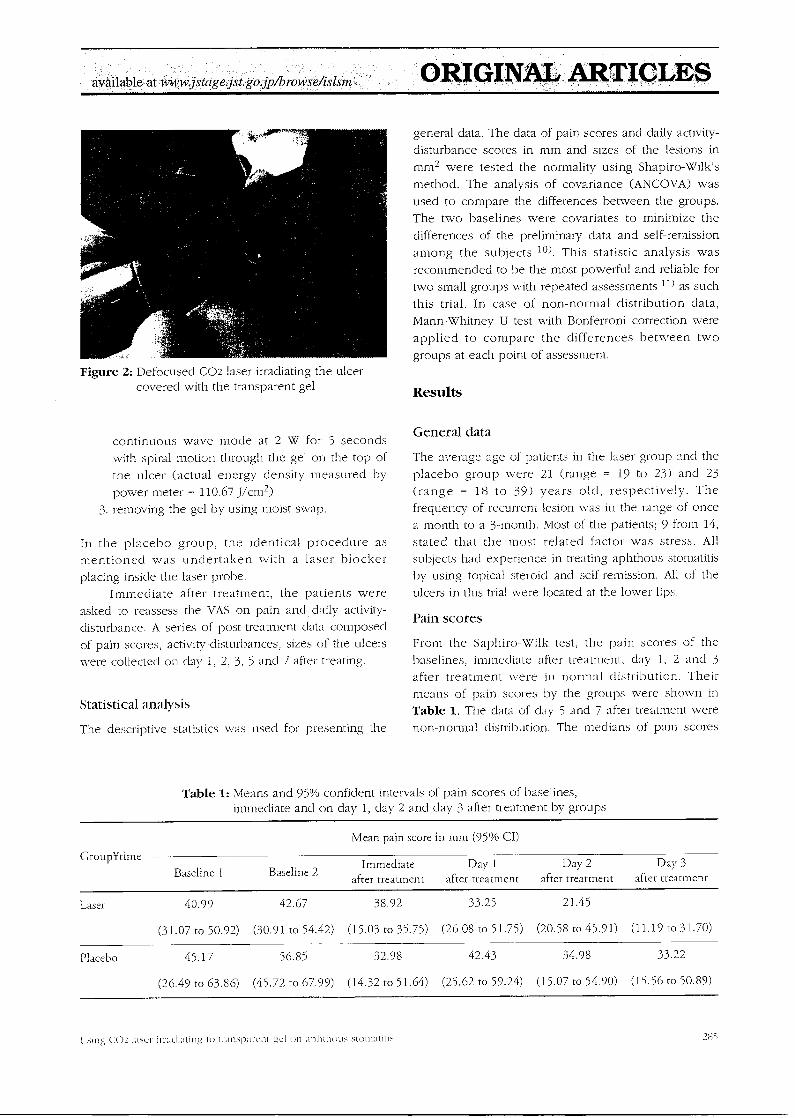
availabl&at,www,jstcige.jst.go.jp/browsdisIsm ORIGINAL ARTICLES
Figure 2: Defocused CO2 laser irradiating the ulcer covered with the transparent gel
continuous wave mode at 2 W for 5 seconds
with spiral motion through the gel on the top of
the ulcer (actual energy density measured by
power meter = 110.67 _J/cm2)
3. removing the gel by using moist swap.
In the placebo group, the identical procedure as mentioned was undertaken with a laser blocker
placing inside the laser probe. Immediate after treatment, the patients were
asked to reassess the VAS on pain and daily activity-
disturbance. A series of post-treatment data composed
of pain scores, activity-disturbances, sizes of the ulcers
were collected on clay 1, 2, 3, 5 and 7 after treating.
Statistical analysis
The descriptive statistics was used for presenting the
general data. The data of pain scores and daily activity-
disturbance scores in mm and sizes of the lesions in
mm2 were tested the normality using Shapiro-Wilk's
method. The analysis of covariance (ANCOVA) was
used to compare the differences between the groups.
The two baselines were covariates to minimize the
differences of the preliminary data and self-remission
among the subjects 10). This statistic analysis was
recommended to be the most powerful and reliable for
two small groups with repeated assessments 11) as such
this trial. In case of non-normal distribution data,
Mann-Whitney U test with Bonferroni correction were
applied to compare the differences between two
groups at each point of assessment.
Results
General data
The average age of patients in the laser group and the
placebo group were 21 (range = 19 to 23) and 23
(range = 18 to 39) years old, respectively. The
frequency of recurrent lesion was in the range of once
a month to a 3-month. Most of the patients; 9 from 14,
stated that the most related factor was stress. All
subjects had experience in treating aphthous stomatitis
by using topical steroid and self-remission. All of the
ulcers in this trial were located at the lower lips.
Pain scores
From the Saphiro-W lk test, the pain scores of the
baselines, immediate after treatment, day 1, 2 and 3
after treatment were in normal distribution. Their
means of pain scores by the groups were shown in
Table 1. The data of day 5 and 7 after treatment were
non-normal distribution. The medians of pain scores
Table 1: Means and 95% confident intervals of pain scores of baselines, immediate and on day 1, day 2 and day 3 after treatment by groups
GroupYtime
Mean pain score in mm (95% CI)
Baseline I Baseline 2 Immediate
after treatment Day 1
after treatment Day 2
after treatment Day 3
after treatment
Laser 40.99 42.67 38.92 33.25 21.45
(31.07 to 50.92) (30.91 to 54.42) (15.03 to 35.75) (26.08 to 51.75) (20.58 to 45.91) (11.19 to 31.70)
Placebo 45.17 56.85 32.98 42.43 34.98 33.22
(26.49 to 63.86) (45.72 to 67.99) (14.32 to 51.64) (25.62 to 59.24) (15.07 to 54.90) (15.56 to 50.89)
sing CO2 laser imIcIninng to Minsparcnt p.:1 on ❑ plithous stornatills 28;
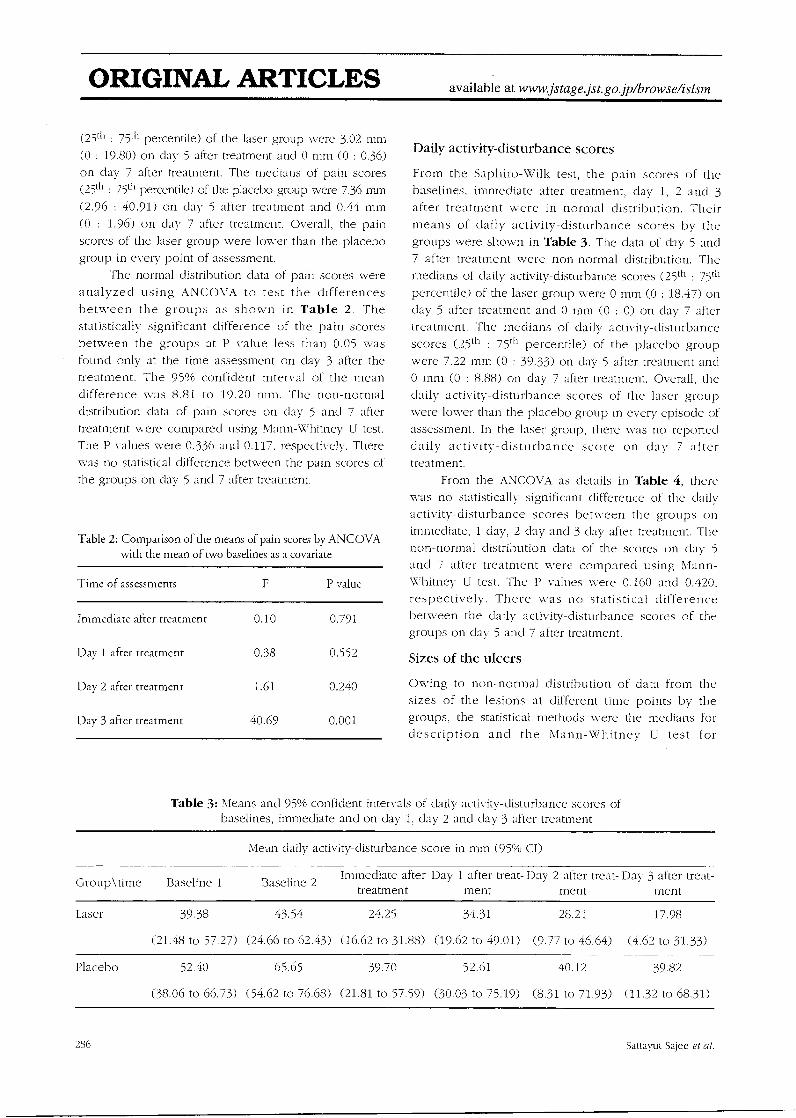
ORIGINAL ARTICLES available at www.jstage.jst.go.jp/browsefisism
(25th :75th percentile) of the laser group were 3.02 mm
(0 : 19.80) on clay 5 after treatment and 0 mm (0 : 0.36)
on day 7 after treatment. The medians of pain scores
(25th : 75th percentile) of the placebo group were 7.36 mm
(2.96: 40.91) on day 5 after treatment and 0,44 mm
(0 : 1.96) on clay 7 after treatment. Overall, the pain
scores of the laser group were lower than the placebo
group in every point of assessment.
The normal distribution data of pain scores were
analyzed using ANCOVA to test the differences
between the groups as shown in Table 2. The
statistically significant difference of the pain scores
between the groups at P value less than 0.05 was
found only at the time assessment on day 3 after the
treatment. The 95% confident interval of the mean
difference was 8.81 to 19.20 mm. The non-normal
distribution data of pain scores on clay 5 and 7 after
treatment were compared using Mann-Whitney U test.
The P values were 0.336 and 0.117, respectively. There
was no statistical difference between the pain scores of
the groups on clay 5 and 7 after treatment.
Table 2: Comparison of the means of pain scores by ANCOVA with the mean of two baselines as a covariate
Time of assessments F P value
Immediate after treatment 0.10 0.791
Day 1 after treatment 0.38 0.552
Day 2 after treatment 1.61 0.240
Day 3 after treatment 40.69 0.001
Daily activity-disturbance scores
From the Saphiro-Wilk test, the pain scores of the
baselines, immediate after treatment, day 1, 2 and 3
after treatment were in normal distribution. Their
means of daily activity-disturbance scores by the groups were shown in Table 3. The data of day 5 and 7 after treatment were non-normal distribution. The
medians of daily activity-disturbance scores (25th : 75th
percentile) of the laser group were 0 mm (0 : 18.47) on
day 5 after treatment and 0 mm (0 : 0) on clay 7 after
treatment. The medians of daily activity-disturbance
scores (25th : 75th percentile) of the placebo group
were 7.22 mm (0 : 39.33) on day 5 after treatment and 0 mm (0 : 8.88) on day 7 after treatment. Overall, the
daily activity-disturbance scores of the laser group
were lower than the placebo group in every episode of
assessment. In the laser group, there was no reported
daily activity-disturbance score on day 7 after treatment.
From the ANCOVA as details in Table 4, there was no statistically significant difference of the daily
activity-disturbance scores between the groups on
immediate, 1 day, 2 clay and 3 day after treatment. The
non-normal distribution data of the scores on day 5
and 7 after treatment were compared using Mann-
Whitney U test. The P values were 0.160 and 0.420.
respectively. There was no statistical difference between the daily activity-disturbance scores of the groups on day 5 and 7 after treatment.
Sizes of the ulcers
Owing to non-normal distribution of data from the
sizes of the lesions at different time points by the
groups, the statistical methods were the medians for
description and the Mann-Whitney U test for
Table 3: Means and 95% confident intervals of daily activity-disturbance scores of baselines, immediate and on day 1, day 2 and day 3 after treatment
Mean daily activity-disturbance score in mm (95% CI)
Group\time Baseline 1 Baseline 2 Immediate after Day 1 after treat- Day 2 after treat- Day 3 after treat-
treatment ment ment ment
Laser 39.38 43.54 24.25 34.31 28.21 17.98
(21.48 to 57.27) (24.66 to 62.43) (16.62 to 31.88) (19.62 to 49.01) (9.77 to 46.64) (4.62 to 31.33)
Placebo 52.40 65.65 39.70 52.61 40.12 39.82
(38.06 to 66.73) (54.62 to 76.68) (21.81 to 57.59) (30.03 to 75.19) (8.31 to 71.93) (11.32 to 68.31)
286 Sattayut Sajee et al.
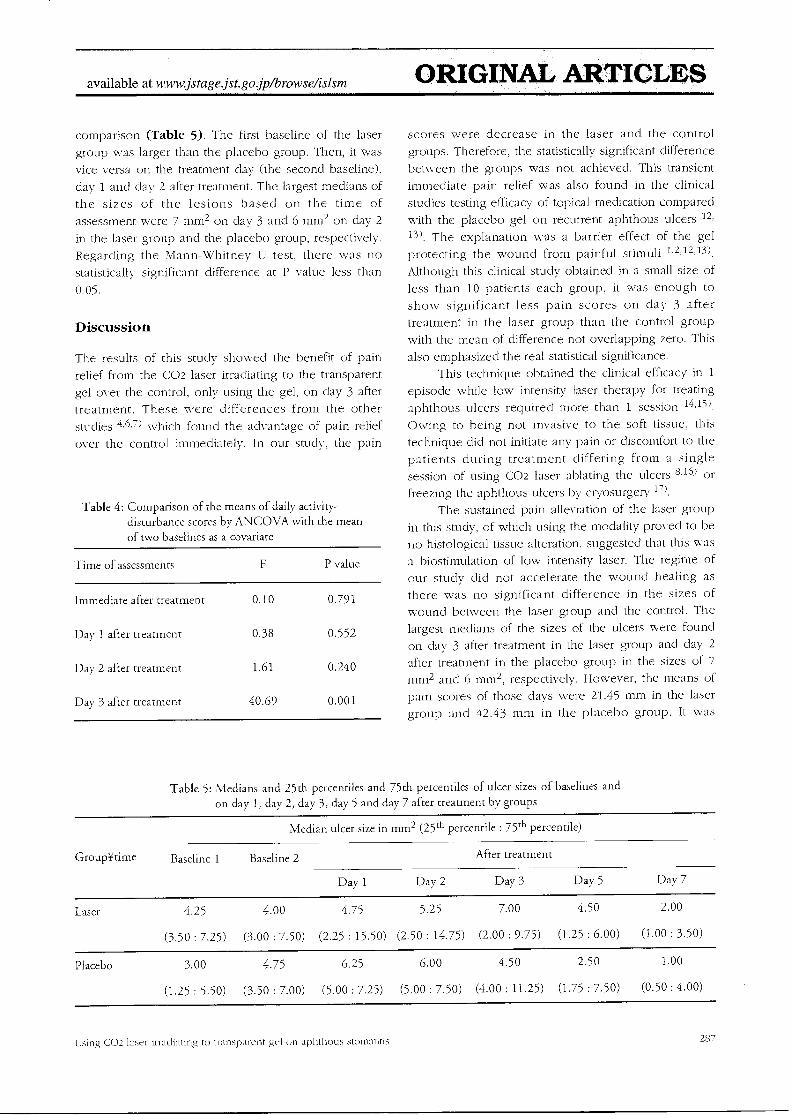
available at www.jstage jst.gajp/browsefislsm ORIGINAL ARTICLES
comparison (Table 5). The first baseline of the laser
group was larger than the placebo group. Then, it was
vice versa on the treatment day (the second baseline),
day 1 and day 2 after treatment. The largest medians of
the sizes of the lesions based on the time of
assessment were 7 mm2 on day 3 and 6 mm2 on day 2
in the laser group and the placebo group, respectively.
Regarding the Mann-Whitney U test, there was no
statistically significant difference at P value less than
0.05.
Discussion
The results of this study showed the benefit of pain
relief from the CO2 laser irradiating to the transparent
gel over the control, only using the gel, on day 3 after
treatment. These were differences from the other
studies 4,6,7) which found the advantage of pain relief
over the control immediately. In our study, the pain
Table 4: Comparison of the means of daily activity-disturbance scores by ANCOVA with the mean of two baselines as a covariate
Time of assessments P value
Immediate after treatment 0.10 0.791
Day 1 after treatment 0.38 0.552
Day 2 after treatment 1.61 0.240
Day 3 after treatment 40.69 0.001
scores were decrease in the laser and the control
groups. Therefore, the statistically significant difference
between the groups was not achieved. This transient
immediate pain relief was also found in the clinical
studies testing efficacy of topical medication compared
with the placebo gel on recurrent aphthous ulcers 12,
13). The explanation was a barrier effect of the gel
protecting the wound from painful stimuli 1,2,12,13).
Although this clinical study obtained in a small size of
less than 10 patients each group, it was enough to
show significant less pain scores on day 3 after
treatment in the laser group than the control group
with the mean of difference not overlapping zero. This
also emphasized the real statistical significance. This technique obtained the clinical efficacy in 1
episode while low intensity laser therapy for treating
aphthous ulcers required more than 1 session 14,15).
Owing to being not invasive to the soft tissue, this
technique did not initiate any pain or discomfort to the
patients during treatment differing from a single
session of using CO2 laser ablating the ulcers 8,16) or
freezing the aphthous ulcers by cryosurgery 1').
The sustained pain alleviation of the laser group
in this study, of which using the modality proved to be
no histological tissue alteration, suggested that this was a biostimulation of low intensity laser. The regime of
our study did not accelerate the wound healing as
there was no significant difference in the sizes of wound between the laser group and the control. The
largest medians of the sizes of the ulcers were found
on day 3 after treatment in the laser group and day 2
after treatment in the placebo group in the sizes of 7
mm2 and 6 mm2, respectively. However, the means of
pain scores of those days were 21.45 mm in the laser
group and 42.43 mm in the placebo group. It was
Table 5: Medians and 25th percentiles and 75th percentiles of ulcer sizes of baselines and on day 1, day 2, day 3, day 5 and day 7 after treatment by groups
Median ulcer size in mm2 (25th percentile 75th entile . 75 percentile)
GroupYtime Baseline 1 Baseline 2 After treatment
Day 1 Day 2 Day 3 Day 5 Day 7
Laser 4.25 4.00 4.75 5.25 7.00 4.50 2.00
(3.50 : 7.25) (3.00 : 7.50) (2.25 : 15.50) (2.50 : 14.75) (2.00 : 9.75) (1.25 : 6.00) (1.00 : 3.50)
Placebo 3.00 4.75 6.25 6.00 4.50 2.50 1.00
(1.25 : 5.50) (3.50 : 7.00) (5.00 : 7.25) (5.00 : 7.50) (4.00 : 11.25) (1.75 : 7.50) (0.50 : 4.00)
Using CO2 laser irradiating to transparent gel on aphthous stornatitis 287

ORIGINAL ARTICLES available at www.jstage.jstgo.jp/browse/islsm
noticed that the pain scores of the laser group was less
than the control group even though the size of the
ulcers was larger. This relation between the pain
scores and sizes of the ulcers pointed out the analgesic
effect of the laser dose and technique used in this
study. This can be explained by a biphasic effect of
dose response to low intensity laser therapy 18). There
was an in vitro study in skin fibroblast cultures show
that the close of 5 J/cm2 helium neon low intensity-
laser was able to increase cellular activity promoting
the healing. The higher closes of 10 and 16 J/cm2
decreased the substances for cellular proliferation 19).
In terms of pain inhibition, an in vitro study in
myoblast cultures showed that 820 nm low intensity
laser at energy density of 19 J/cm2 partially inhibited
prostaglandin E2 production. The lower energy density
of 4 J/cm2 had a tendency to stimulate this substance
20 '. The laser close used in this clinical trial was large amount of energy density (110.67 1/cm2). Therefore, it tended to show inhibitory effect of pain relief rather
than stimulation of wound healing. Regarding of the
advantages of pain reduction in a single session in the
model of recurrent aphthous ulcers, the application
and future study will be valuable for other painful oral
ulcerations such as traumatic ulcer, chronic
inflammation and erosive lichen plant's.
Conclusion
The defocused CO2 laser at 2 W continuous mode
irradiating to the transparent water-based gel for 5
second was able to relieve pain from the aphthous
stomatitis compared with the placebo as the results on
the day 3 after treatment.
References
1: Scully C. Porter S (2008): Oral mucosal disease:
Recurrent aphthous stomatitis. British Journal of
Oral and Maxillofacial Sitrgery, 46:198 - 206.
2: Natah SS, Konttinen YT, Enattah NS, Ashammakhi
N, Sharkey KA, Hayrinen-Immonen R (2004):
Recurrent aphthous ulcers today: a review of the
growing knowledge. International Journal of Oral
and Maxillofacial Surgery, 33:221 - 234.
3: Quijano D, Rodriguez 10 (2008): Topical
corticosteroids in recurrent aphthous stomatitis.
Systematic Review. Acta Otorrinolaringologica,
59:298 - 307.
4: Prasad R 5, Pai A (2013): Assessment of immediate
pain relief with laser treatment in recurrent
aphthous stomatitis. Oral Surgery, Oral Medicine,
Oral Pathology and Oral Radiology, 116:189 - 193.
5: Sharon-Buller A, Sela M (2004): CO2 laser
treatment of ulcerative lesions. Oral Surgery, Oral
Medicine, Oral Pathology, Oral Radiology, and
Endodontology, 97:332 - 334.
6: Zand N, Fateh M, Ataie-Fashtami L, Djavid GE,
Fatemi SM, Shirkavand A (2012): Promoting wound
healing in minor recurrent aphthous stomatitis by
non-thermal, non-ablative CO2 laser therapy: a
pilot study. Photonzedcine and Laser Surgery',
30:719 - 723.
7: Zand N, Ataie-Fashtami L, Djavid GE, Fateh 10.
Alinaghizadeh MR, Fatemi SM, Arbabi-Kalati, F
(2009): Relieving pain in minor aphthous stomatitis by a single session of non-thermal carbon dioxide
laser irradiation. Lasers in Medical Science, 24:515 -520.
8: Kotlow L (2008): Lasers and soft tissue treatments
for the pediatric dental patient. Alpha Onzegan,
101:140 - 151.
9: Sattayut S. Hortong K, Kitichaiwan C (2012): The
ablation properties of CO2 laser irradiating to
absorption media: an in vitro study. International
Journal of Dentistry, doi:10.1155/2012/230967.
10: Frison L, Pocock SJ (1992): Repeated measures in
clinical trials: analysis using mean summary
statistics and its implications for design. Statistics in
Medicine, 11:1685 - 1704. 11: Janusonis S (2009): Comparing two small samples
with an unstable, treatment-independent baseline.
Journal of Neuroscience Methods, 179:173 - 178. 12: Porter S (2007): Transient benefits for topical
hyaluronic acid in recurrent aphthous ulceration.
Evidence Based Dentistry, 8:52.
13: Nolan A, Baillie C. Badminton J, Rudralingham M,
Seymour RA (2006): The efficacy of topical
hyaluronic acid in the management of recurrent
aphthous ulceration. Journal of Oral Pathology and
Medicine, 35:461 - 465.
14: Rowell RM, Cohen DM, Powell GL, Green JG
(1988): The use of low energy laser therapy to
treat aphthous ulcers. Annual Dentistry, 47:16 - 18.
15: De Souza TO, Martins MA, Bussadori SK,
Fernandes KP, Tanji EY, Mesquita-Ferrari RA,
Martins, M. D (2010): Clinical evaluation of low-
288
Sattayut Sajee et al.

available at www.jstage.jst.go.jp/browse/islsni ORIGINAL ARTICLES
level laser treatment for recurring aphthous
stomatitis. Pbotornedicine and Laser Surgery, 28
Supplement 2:S85 - 88.
16: Loh HS, Keng SB (1989): The effectiveness of CO2
laser in dental surgery: a local experience. Annual
Academy Medicine of Singapore, 18:548 - 552.
17: Arikan OK, Birol A, Tuncez F, Erkek E, Koc C
(2006): A prospective randomized controlled trial
to determine if cryotherapy can reduce the pain of
patients with minor form of recurrent aphthous
stomatitis. Oral Surgery, Oral Medicine, Oral
Pathology, Oral Radiology, and Endodontology,
101:el - e5.
18: Huang YY, Sharma SK, Carroll J, Hamblin MR
(2011): Biphasic dose response in low level light therapy - an update. Dose-Response, 9:602 - 618.
19: Hawkins DH, Abrahamse H (2006): The role of
laser fluence in cell viability, proliferation, and
membrane integrity of wounded human skin
fibroblasts following helium-neon laser irradiation.
Lasers in Surgery and Medicine, 38:74 - 83.
20: Sattayut S, Hughes F, Bradley P (1999): 820 nm
gallium aluminium arsenide laser modulation of
prostaglandin E2 production in interleukin I
stimulated myoblasts. Laser Therapy, 11:88 - 95.
[Acknowledgements] This clinical study was granted by Faculty of Dentistry, Khon Kaen University and the Lasers in Dentistry Research Group,
Khon Kaen University. It is a deep gratitude to Professor Pisake Lumbiganon for his kind advice on manuscript writing.
Using CO2 laser irradiating to transparent gel on aphthous stomatitis
289
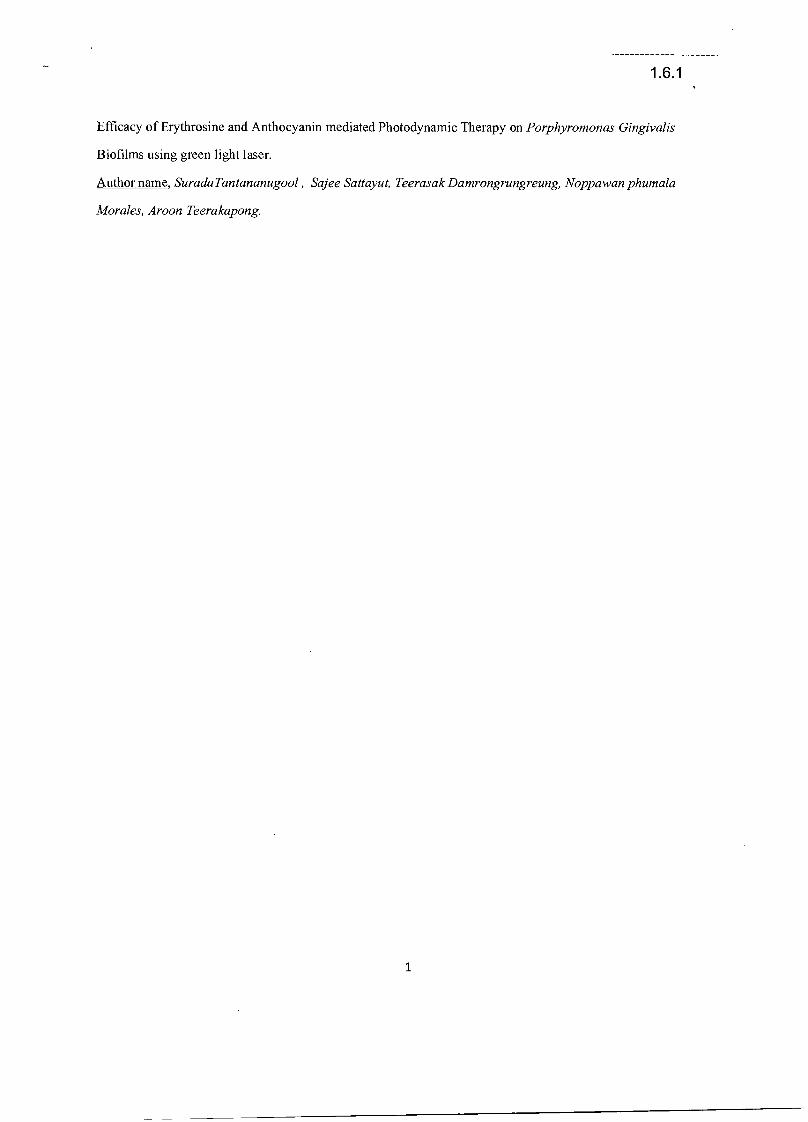
1.6.1
Efficacy of Erythrosine and Anthocyanin mediated Photodynamic Therapy on Porphyromonas Gingivalis
Biofilms using green light laser.
Author name, SuradaTantananugool , Sajee Sattayut, Teerasak Damrongrungreung, Noppawan phumala
Morales, Aroon Teerakapong.
1
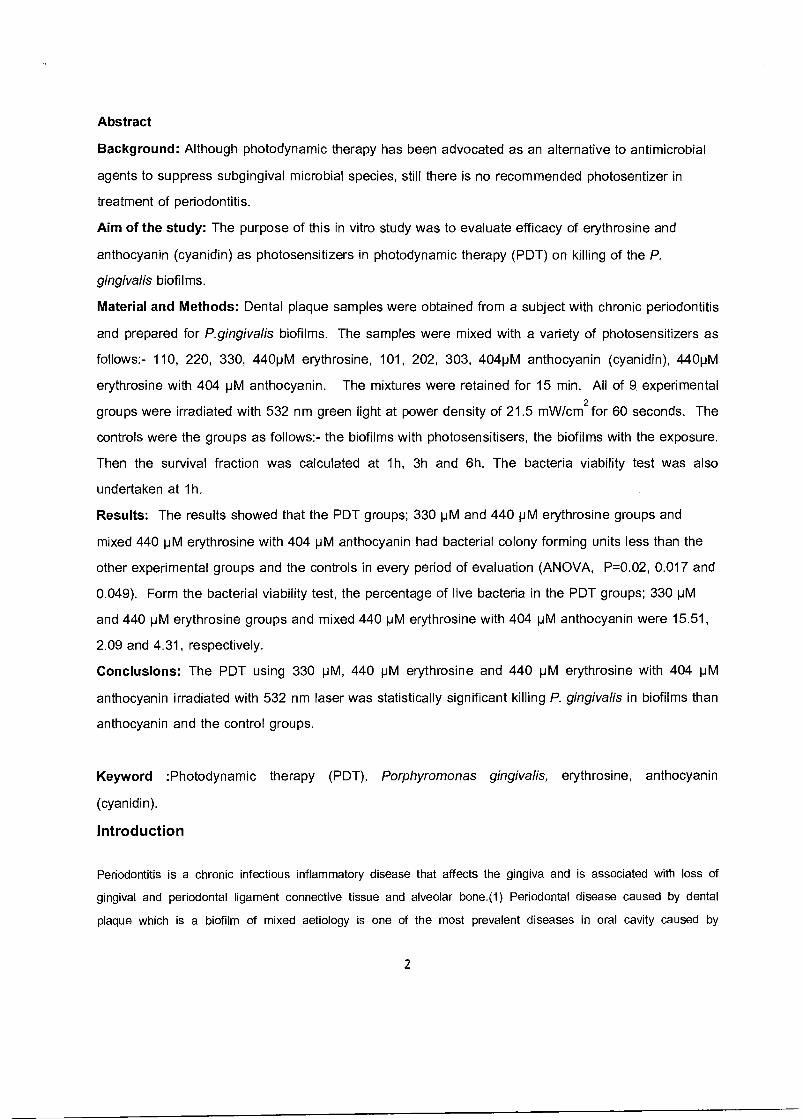
Abstract
Background: Although photodynamic therapy has been advocated as an alternative to antimicrobial
agents to suppress subgingival microbial species, still there is no recommended photosentizer in
treatment of periodontitis.
Aim of the study: The purpose of this in vitro study was to evaluate efficacy of erythrosine and
anthocyanin (cyanidin) as photosensitizers in photodynamic therapy (PDT) on killing of the P.
gingivalis biofilms.
Material and Methods: Dental plaque samples were obtained from a subject with chronic periodontitis
and prepared for P.gingivalis biofilms. The samples were mixed with a variety of photosensitizers as
follows:- 110, 220, 330, 440pM erythrosine, 101, 202, 303, 404pM anthocyanin (cyanidin), 440pM
erythrosine with 404 pM anthocyanin. The mixtures were retained for 15 min. All of 9. experimental
groups were irradiated with 532 nm green light at power density of 21.5 mW/cm2
for 60 seconds. The
controls were the groups as follows:- the biofilms with photosensitisers, the biofilms with the exposure.
Then the survival fraction was calculated at 1h, 3h and 6h. The bacteria viability test was also
undertaken at 1h.
Results: The results showed that the PDT groups; 330 pM and 440 pM erythrosine groups and
mixed 440 pM erythrosine with 404 pM anthocyanin had bacterial colony forming units less than the
other experimental groups and the controls in every period of evaluation (ANOVA, P=0.02, 0.017 and
0.049). Form the bacterial viability test, the percentage of live bacteria in the PDT groups; 330 pM
and 440 pM erythrosine groups and mixed 440 pM erythrosine with 404 pM anthocyanin were 15.51,
2.09 and 4.31, respectively.
Conclusions: The PDT using 330 pM, 440 pM erythrosine and 440 pM erythrosine with 404 pM
anthocyanin irradiated with 532 nm laser was statistically significant killing P. gingivalis in biofilms than
anthocyanin and the control groups.
Keyword :Photodynamic therapy (PDT), Porphyromonas gingivalis, erythrosine, anthocyanin
(cyanidin).
Introduction
Periodontitis is a chronic infectious inflammatory disease that affects the gingiva and is associated with loss of
gingival and periodontal ligament connective tissue and alveolar bone.(1) Periodontal disease caused by dental
plaque which is a biofilm of mixed aetiology is one of the most prevalent diseases in oral cavity caused by
2

periodontopathic bacteria. The possibility of development of resistance to antibiotics by the organisms has led to the
development of a new antimicrobial concept with fewer complications.
Photodynamic therapy (PDT) involves the use of appropriate wavelength of light, oxygen, and a suitable
photosensitizer to kill microorganisms. PDT could be a useful adjunct to mechanical as well as antibiotics in
eliminating periodontopathic bacteria.(3,4) Photodynamic therapy has been advocated as an alternative to
antimicrobial agents to suppress subgingival species and to treat periodontitis. Bacteria located within dense
biofilms, such as those encountered in dental plaque, have been found to be relatively resistant to antimicrobial
therapy.(4-6) Recently, there are some possible chemical agents can be used as photosensitizers such as
erythrosine and anthocyanins.
Erythrosine is currently used in dental practices for staining and visualizing dental plaque in the form of
disclosing solution or tablets. Erythrosine belongs to a class of cyclic compounds called xanthenes, which It's
maximum absorbance is at 500-550 nm has some reported of antimicrobial activity against Gram-positive and Gram-
negative oral bacteria. Clearly, erythrosine has an advantage over other photosensitizers in development, as it
already targets dental plaque and has full approval for use in the mouth. (7, 14, 15)
Anthocyanins are flavonoid and contribute greatly to the antioxidant properties of certain colorful. The five major
anthocyanins aglycons (delphinidin-, petunidin-, cyanidin-, peonidin- and malvidin) bound to monosaccharides
(glucose, galactose and arabinose). Cyanidin is the most common anthocyanidin, and the 3-glucoside is the most
active antioxidant anthocyanin. The cyanidin 3-glucoside has notable antioxidant and anti-inflammatory properties for
potential use in nutraceuticals. A-type cranberry proanthocyanidins (AC-PACs) possess interesting therapeutic
properties for the treatment of periodontal disease. AC-PACs reduce the virulence properties of P. gingivalis by
inhibiting biofilm formation, adhesion, proteinase activity, and invasiveness. On the other, AC-PACs exert anti-
inflammatory activity by inhibiting the P. gingivalis-induced inflammatory response in human oral epithelial cells. The
apparent specific absorption coefficients of anthocyanins at 550 nm showed no substantial dependence on the
species. Anthocyanin contribution to total light absorption at 550 nm. (8-11)
The aim of the present study is to compare the ability of erythrosine as a photosensitizers and anthocyanin
(cyanidin) as bacterial reduction upon the photodynamic therapy with light source of 532 nm green light in the in vitro
study in biofilms.
Material and methods
An in vitro study was conducted in the samples of biofilms. The structure of study design
was shown in figure 1.
3
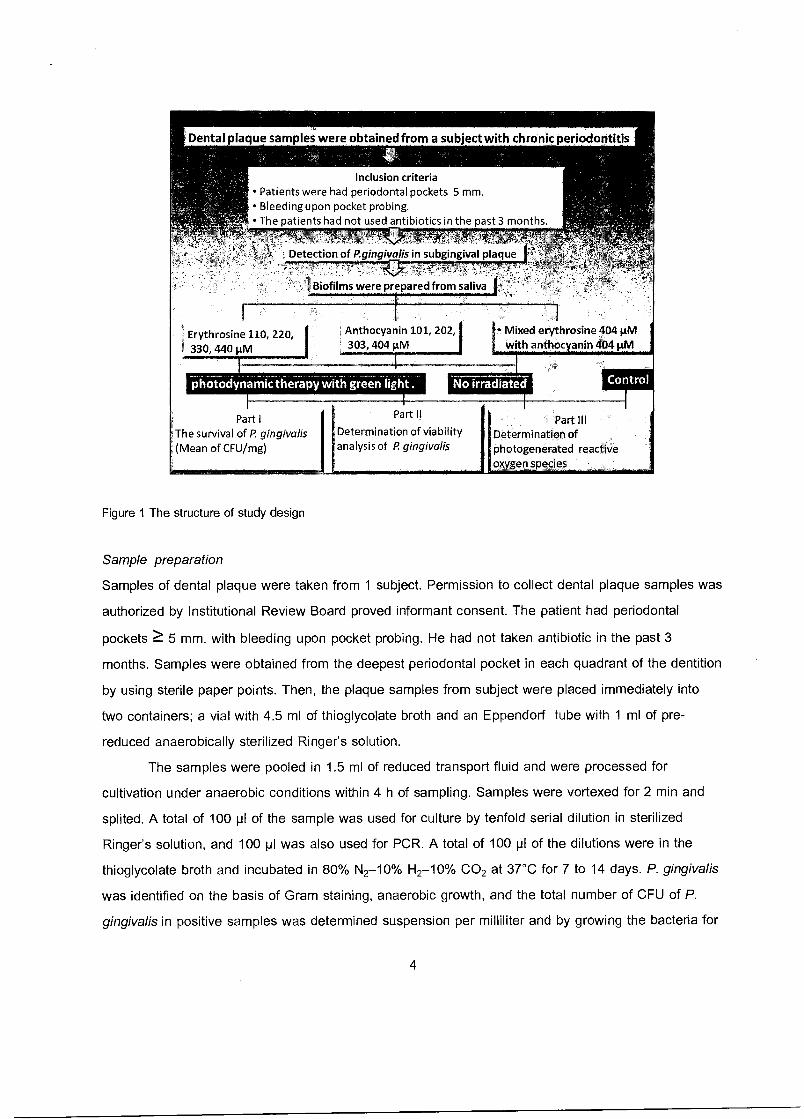
Dental plaque samples were obtained from a subject with chronic periodontitis
Inclusion criteria • Patients were had periodontal pockets 5 mm. • Bleeding upon pocket probing. • The patients had not used antibiotics in the past 3 months.
Detection of P.gingivalis in subgingival plaque
Biofilms were prepared from saliva
Erythrosine 110, 220, 330, 440 pM
Part I The survival of P. gingivalis
`(Mean of CFU/mg)
Part II
Determination of viability analysis of P gingivalis
Part Ill Determination of photogenerated reactive ox en species
Anthocyanin 101, 202, • Mixed erythrosine 404 p.M 303, 404 gM with anthoc anin 404µM
odynaMic therapy with green light . No irradiated
Figure 1 The structure of study design
Sample preparation
Samples of dental plaque were taken from 1 subject. Permission to collect dental plaque samples was
authorized by Institutional Review Board proved informant consent. The patient had periodontal
pockets ?. 5 mm. with bleeding upon pocket probing. He had not taken antibiotic in the past 3
months. Samples were obtained from the deepest periodontal pocket in each quadrant of the dentition
by using sterile paper points. Then, the plaque samples from subject were placed immediately into
two containers; a vial with 4.5 ml of thioglycolate broth and an Eppendorf tube with 1 ml of pre-
reduced anaerobically sterilized Ringer's solution.
The samples were pooled in 1.5 ml of reduced transport fluid and were processed for
cultivation under anaerobic conditions within 4 h of sampling. Samples were vortexed for 2 min and
splited. A total of 100 pl of the sample was used for culture by tenfold serial dilution in sterilized
Ringer's solution, and 100 pl was also used for PCR. A total of 100 pl of the dilutions were in the
thioglycolate broth and incubated in 80% N2-10% H2-10% CO2 at 37°C for 7 to 14 days. P. gingivalis
was identified on the basis of Gram staining, anaerobic growth, and the total number of CFU of P.
gingivalis in positive samples was determined suspension per milliliter and by growing the bacteria for
4
4 days in trypticase soy agar supplemented with blood (5% by volume), hemin (5 mg/liter), vit.K (500
pl / liter), kanamycin (400 pl / liter), and serial dilutions were inoculated on blood agar plates as
described above.
Biofilms were prepared from saliva (subject sample) and were filled in centrifuge tubes and
spin 2,000 rpm, for 5 mins, then filtered by syringe filter 0.2 pm, keep in 4°C. The cover glasses were
suspended in saliva in 6 well plates for 2 days and then discard by pipette. The cover glasses were
then suspended in 4 ml of trypticase soy broth . P.gingivalis suspension 50 pl was added with 4 pl
hemin in 6 well plates and cultured until 4 days. Plates containing the suspended slabs were
incubated in anaerobic chamber at 37°C and fresh medium with P.gingivalis culture was refilled 2
days. Biofilm formed on the upper surface of the cover glass after 4 days was treated and analyzed.
Photosensitizers
There were two photosensitizers used in this experiment. The preparations were as follows:-1)
Erythrosine (Sigma Ltd, Poole, UK) was prepared as 110,220,330,440 pM stock solutions in deionized
water, foil-covered at 25°C after filter purification (0.2 pm) and 2) Cyanidin 3-glucoside (Sigma Ltd,
Poole, UK) was prepared as 101, 202,303, 404 pM stock solutions in deionized water and 50%
ethanol, foil-covered at 25°C after filter purification (0.2 pm).
Light source and irradiation
A 532 nm green light laser at 50mW was used as a light source. The laser beam diversion was
constructed using a pair of lens with a 25 mm focus and 20 mm in diameter. This produced a
uniform circular spot of 1 cm in diameter. From a 15 cm length of irradiation to the samples, the
actual power density was 21.5 mW/cm2. The samples were irradiated for 60 second. Therefore, the
energy density was 1.2 J/ cm2.
Experimental methods
The samples were allocated into 21 groups based on the concentrations of photosensitizer and
irradiation as shown in table 1.
Then
Survival fractions in each experimental and control groups were calculated by counting the colonies
on the plates and result of bacterial viability test.
Experiment and control groups were illustrated in Table 1.
5
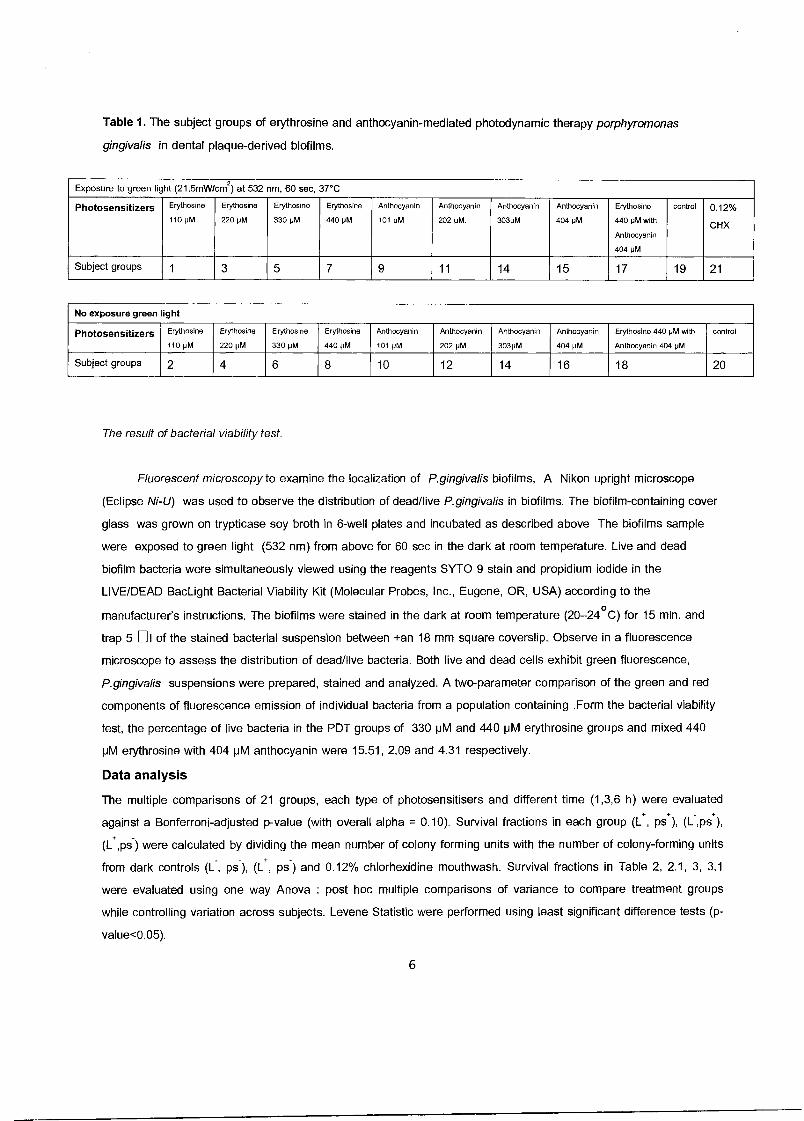
Table 1. The subject groups of erythrosine and anthocyanin-mediated photodynamic therapy porphyromonas
gingivalis in dental plaque-derived biofilms.
Exposure to green light (21.5mW/cm2) at 532 nm, 60 sec, 37°C
Photosensitizers Erythosine
110 pM
Erythosine
220 pM
Erythosino
330 pM
Erythosine
440 pM
Anthocyanin
101 pM
Anthocyanin
202 pM.
Anthocyanin
303pM
Anthocyanin
404 pM
Erythosine
440 pM with
Anthocyanin
404 pM
control 0.12%
CHX
Subject groups 1 3 5 7 9 11 14 15 17 19 21
No exposure green ight
Photosensitizers Erythosine
110 pM
Erythosine
220 pM
Erythosine
330 pM
Erythosine
440 pM
Anthocyanin
101 pM
Anthocyanin
202 pM.
Anthocyanin
303pM
Anthocyanin
404 pM
Erythosine 440 pM with
Anthocyanin 404 pM
control
Subject groups 2 4 6 8 10 12 14 16 18 20
The result of bacterial viability test.
Fluorescent microscopy to examine the localization of P.gingivalis biofilms, A Nikon upright microscope
(Eclipse Ni-U) was used to observe the distribution of dead/live P.gingivalis in biofilms. The biofilm-containing cover
glass was grown on trypticase soy broth in 6-well plates and incubated as described above The biofilms sample
were exposed to green light (532 nm) from above for 60 sec in the dark at room temperature. Live and dead
biofilm bacteria were simultaneously viewed using the reagents SYTO 9 stain and propidium iodide in the
LIVE/DEAD BacLight Bacterial Viability Kit (Molecular Probes, Inc., Eugene, OR, USA) according to the
manufacturer's instructions. The biofilms were stained in the dark at room temperature (20-24°C) for 15 min. and
trap 5 ❑1 of the stained bacterial suspension between +an 18 mm square coverslip. Observe in a fluorescence
microscope to assess the distribution of dead/live bacteria. Both live and dead cells exhibit green fluorescence,
P.gingivalis suspensions were prepared, stained and analyzed. A two-parameter comparison of the green and red
components of fluorescence emission of individual bacteria from a population containing .Form the bacterial viability
test, the percentage of live bacteria in the PDT groups of 330 pM and 440 pM erythrosine groups and mixed 440
pM erythrosine with 404 pM anthocyanin were 15.51, 2.09 and 4.31 respectively.
Data analysis
The multiple comparisons of 21 groups, each type of photosensitisers and different time (1,3,6 h) were evaluated
against a Bonferroni-adjusted p-value (with overall alpha = 0.10). Survival fractions in each group (C, ps), (r,ps.),
(L ,ps ) were calculated by dividing the mean number of colony forming units with the number of colony-forming units
from dark controls (r, ps ), (C, ps-) and 0.12% chlorhexidine mouthwash. Survival fractions in Table 2, 2.1, 3, 3.1
were evaluated using one way Anova : post hoc multiple comparisons of variance to compare treatment groups
while controlling variation across subjects. Levene Statistic were performed using least significant difference tests (p-
value<0.05).
6
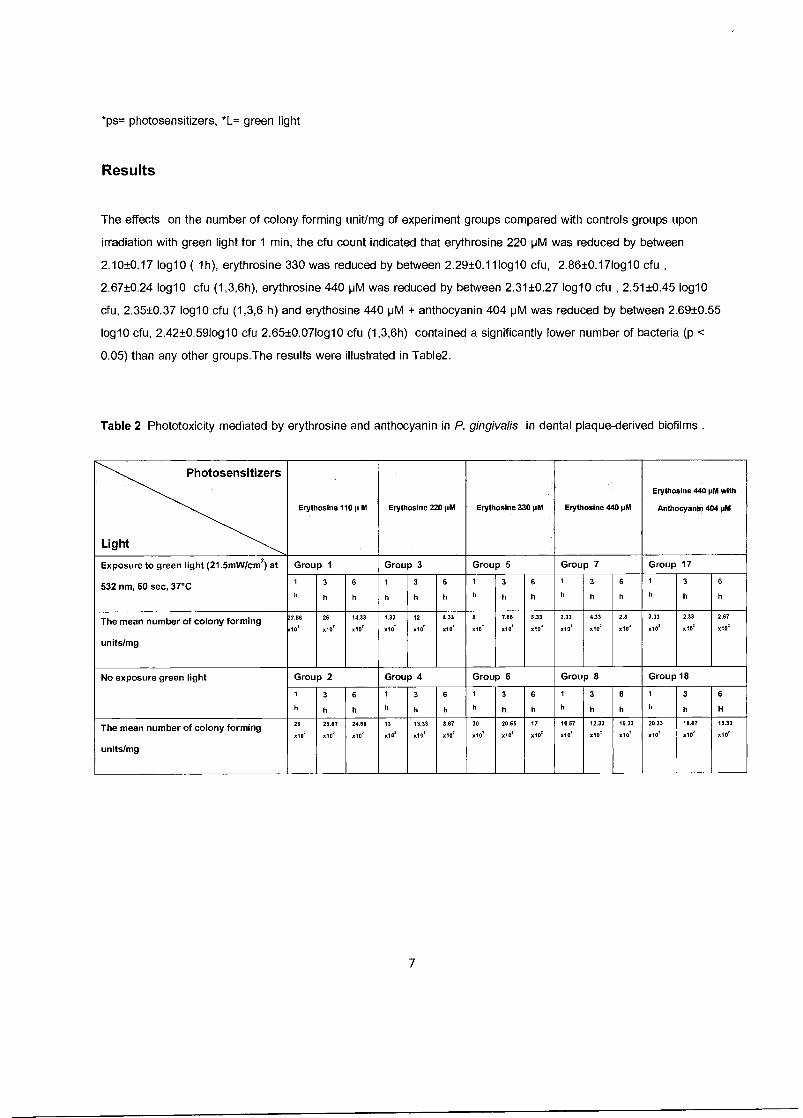
*ps= photosensitizers, *L= green light
Results
The effects on the number of colony forming unit/mg of experiment groups compared with controls groups upon
irradiation with green light for 1 min, the cfu count indicated that erythrosine 220 pM was reduced by between
2.10±0.17 log10 ( 1h), erythrosine 330 was reduced by between 2.29±0.111og10 cfu, 2.86±0.17log10 cfu ,
2.67±0.24 log10 cfu (1,3,6h), erythrosine 440 pM was reduced by between 2.31±0.27 log10 cfu , 2.51±0.45 log10
cfu, 2.35±0.37 log10 cfu (1,3,6 h) and erythosine 440 pM + anthocyanin 404 pM was reduced by between 2.69±0.55
log10 cfu, 2.42±0.591og10 cfu 2.65±0.071og10 cfu (1,3,6h) contained a significantly lower number of bacteria (p <
0.05) than any other groups.The results were illustrated in Table2.
Table 2 Phototoxicity mediated by erythrosine and anthocyanin in P. gingivalis in dental plaque-derived biofilms .
Photosensitizers
Light
Erythosine 110 p M Erythosine 220 pM Erythosine 330 pM Erythosine 440 pM
Erythosine 440 pM with
Anthocyanin 404 pM
Exposure to green light (21.5mW/cm2) at Group 1 Group 3 Group 5 Group 7 Group 17
532 nm, 60 sec, 37°C 1 3 6 1 3 6 1 3 6 1 3 6 1 3 6
h h h h h It h h h h h h h h h
The mean number of colony forming 22.66 26 14.33 1.33 12 8.33 8 7.66 5.33 2.33 4.33 2.8 3.33 2,33 2.67
units/mg
x10' x10' x10' x10' x10' x10' x10' x10' x10' x10' MO' x10' x10' x10' x10'
No exposure green light Group 2 Group 4 Group 6 Group 8 Group 18
1 3 6 1 3 6 1 3 6 1 3 6 1 3 6
h h h h h h h h h h h h h h H
The mean number of colony forming 26 26.67 24.86 13 13.33 8.67 30 28.66 17 16.67 12.33 15.33 20.33 18.67 15.33
units/mg
x102 x10' x10' x10' x10' x10' x10' x10' x10' x10' x10' x10' x10' x10' x10'
7
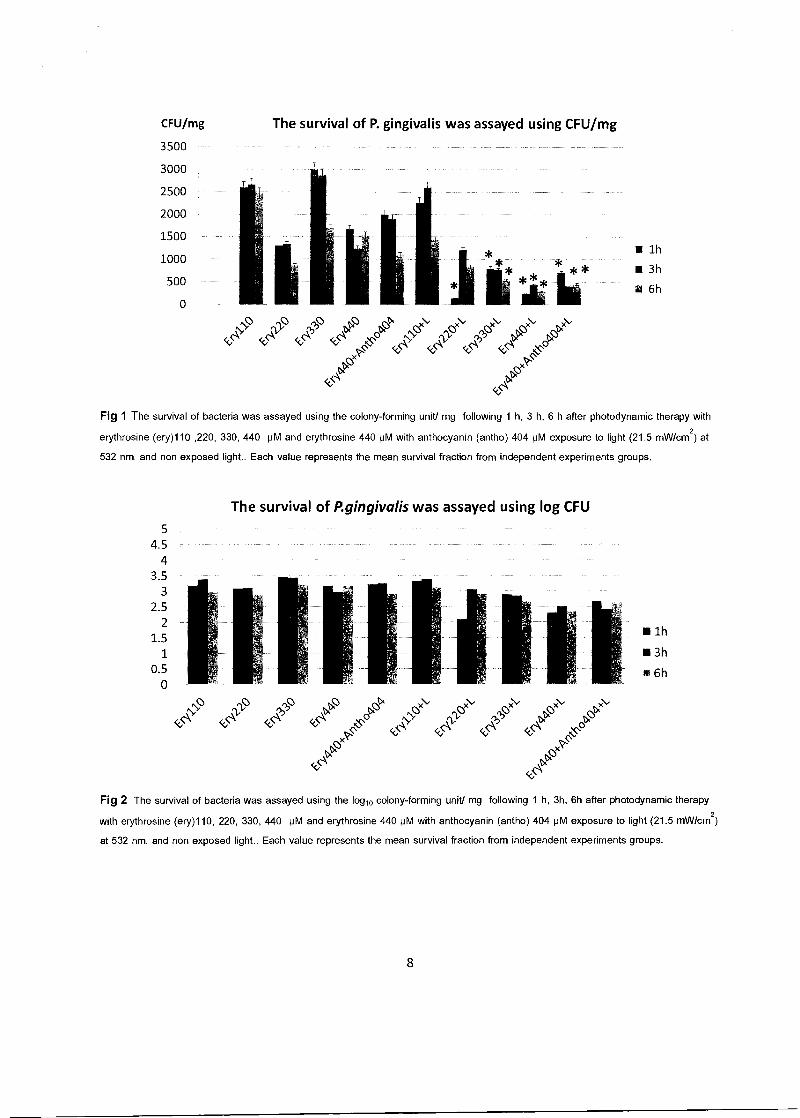
CFU/mg
3500
3000
2500
2000
1500
1000
500
0
The survival of P. gingivalis was assayed using CFU/mg
■ 1h
■ 3h
12 6h
Ntc e x\' x\, <<""\ (cKA CO '1) C4
OxP
<<C\
Fig 1 The survival of bacteria was assayed using the colony-forming unit/ mg following 1 h, 3 h, 6 h after photodynamic therapy with
erythrosine (ery)110 ,220, 330, 440 pM and erythrosine 440 pM with anthocyanin (antho) 404 pM exposure to light (21.5 mW/cm2) at
532 nm. and non exposed light.. Each value represents the mean survival fraction from independent experiments groups.
The survival of P.gingivalis was assayed using log CFU
5 4.5
4 3.5
3 2.5
2 1.5 1
0.5 0
■ 1h
■ 3h
6h
'\
.;,(
zxsy e", '1e\, Ne
•
vs,
(< - > )
S0\ 0- 0
tPox
t>,
Fig 2 The survival of bacteria was assayed using the logio colony-forming unit/ mg following 1 h, 3h, 6h after photodynamic therapy
with erythrosine (ery)110, 220, 330, 440 pM and erythrosine 440 pM with anthocyanin (antho) 404 pM exposure to light (21.5 mW/cm2)
at 532 nm. and non exposed light.. Each value represents the mean survival fraction from independent experiments groups.
<<,<'\ <Sa < •:s
ox
<<.6
eta "A
8
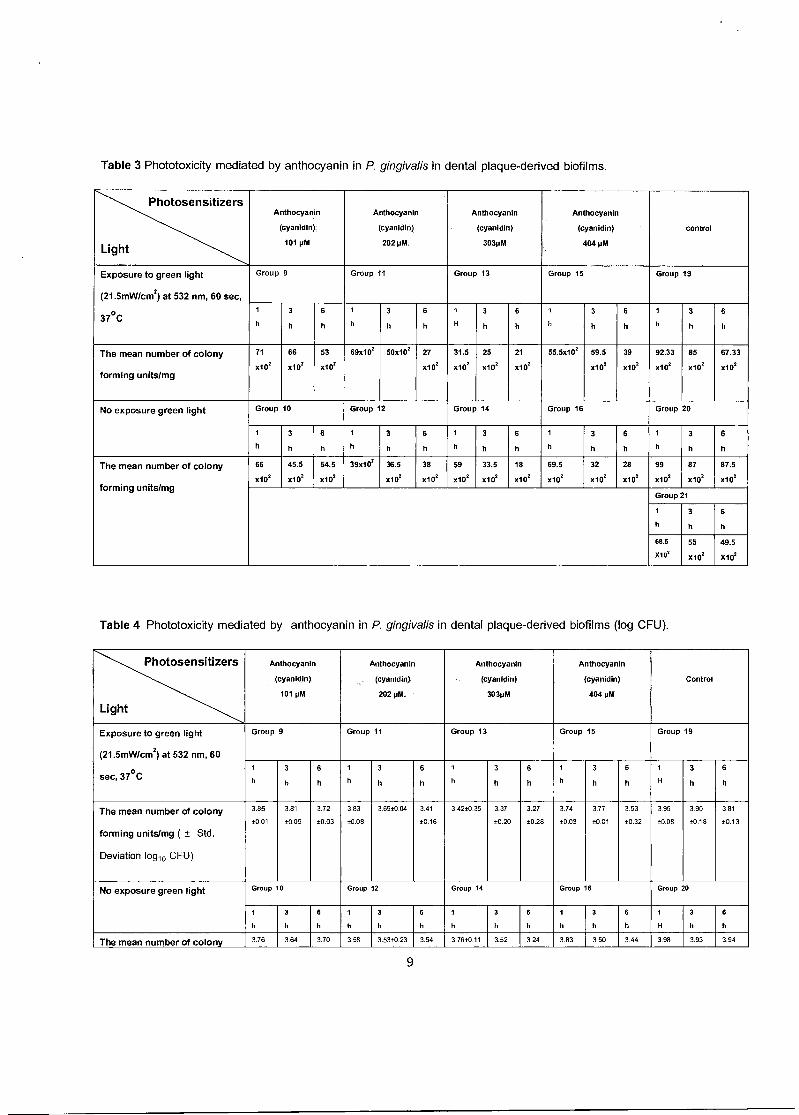
Table 3 Phototoxicity mediated by anthocyanin in P. gingivalis in dental plaque-derived biofilms.
Photosensitizers
Light
Anthocyanin
(cyanidin)
101 pM
Anthocyanin
(cyanidln)
202 pM.
Anthocyanin
(cyanidin)
303pM
Anthocyanin
(cyanidin)
404 pM
control
Exposure to green light Group 9 Group 11 Group 13 Group 15 Group 19
(21.5mW/cm2) at 532 nm, 60 sec, 1 3 6 1 3 6 1 3 6 1 3 6 1 3 6 37oc h h h h h h H h h h h h h h h
The mean number of colony 71 66 53 69x102 50x102 27 31.5 25 21 55.59102 59.5 39 92.33 85 67.33
forming units/mg x102 x1e .10' .10, xie xie xle xle .10' .10' .10' .102
No exposure green light Group 10 Group 12 Group 14 Group 16 Group 20
1 3 6 1 3 6 1 3 6 1 3 6 1 3 6
h h h h h h h h h h h h h h h
The mean number of colony 66 45.5 54.5 39x1e 36.5 38 59 33.5 18 69.5 32 28 99 87 87.5
forming units/mg x102 x102 x102 x102 x102 x102 x102 x102 x102 x102 x102 .1e .1e .102
Group 21
1 3 6
h h h
68.5 55 49.5
X102 X102 X102
Table 4 Phototoxicity mediated by anthocyanin in P. gingivalis in dental plaque-derived biofilms (log CFU).
Photosensitizers
Light
Anthocyanin
(cyanidin)
101 pM
Anthocyanin
(cyanidin)
202 pM.
Anthocyanin
(cyanidin)
303pM
Anthocyanin
(cyaniclIn)
404 pM
Control
Exposure to green light
(21.5mW/cm2) at 532 nm, 60
sec, 37°C
Group 9 Group 11 Group 13 Group 15 Group 19
1
h
3
h
6
h
1
h
3
h
6
h
1
h
3
h
6
h
1
h
3
h
6
h
1
H
3
h
6
h
The mean number of colony
forming units/mg ( ± Std.
Deviation log10 CFU)
3.85
±0.01
3.81
10.09
3.72
±0.03
3.83
10.08
3.69±0.04 3.41
±0.16
3.4210.35 3.37
10.20
3.27
±0.28
3.74
±0.03
3.77
±0.01
3.53
±0.32
3.95
10.08
3.90
±0.18
3.81
±0.13
No exposure green light Group 10 Group 12 Group 14 Group 16 Group 20
1
h
3
h
6
h
1
h
3
h
6
h
1
h
3
h
6
h
1
h
3
h
6
h
1
H
3
h
6
h
The mean number of colony 3.76 3.64 3.70 3.58 3.5340.23 3.54 3.7640.11 3.52 3.24 3.83 3.50 3.44 3.98 3.93 3.94
9
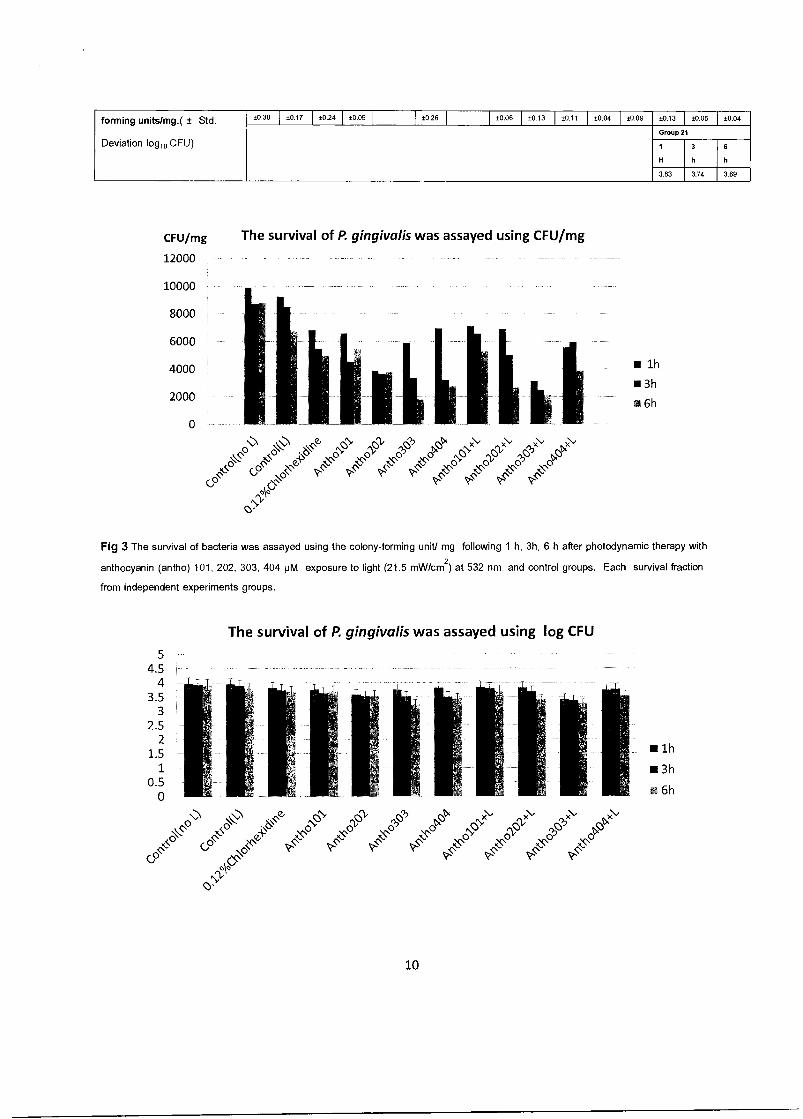
10000
8000
6000
4000
2000
0
forming units/mg.( ± Std. ±0.30 ±0.17 ±0.24 ±0.09 ±0.26 I ±0.06 ±0.13 ±0.11 ±0.04 ±0.09 ±0.13 ±0.05 ±0.04
Group 21
Deviation log10 CFU) 1 3 6
H h h
3.83 3.74 3.69
CFU/mg The survival of P. gingivalis was assayed using CFU/mg
12000
i ■ lh
is 3h
s 6h
co C\0 c40
\. 0
4, 0.N C
v
e
c-
s8
\,. s ;‘P Ic
;‹. ;,6 ,e)
04>
,
19 ,
„()
,z,o0
o.
Fig 3 The survival of bacteria was assayed using the colony-forming unit/ mg following 1 h, 3h, 6 h after photodynamic therapy with
anthocyanin (antho) 101, 202, 303, 404 pM exposure to light (21.5 mW/cm2) at 532 nm. and control groups. Each survival fraction
from independent experiments groups.
The survival of P. gingivalis was assayed using log CFU
5 4.5
4 3.5
3 2.5
2 1.5 1
0.5 0
■ lh
■ 3h
a 6h
\ .0\ ,0 _ 6>•c\q' ,c) .6\ ' _161' .2)61' _o0.‘ e fzjti .' e.'); ." ,C•s (2,-k ,ZS\ Z.01 ,_$-' e N. 81, 61,- ., .;k$o cp on
Pte- 0, ‘i..,(, ,?s, n ,n n n
. o o o o cP 0" a a- 'a a-
00 tiv
10
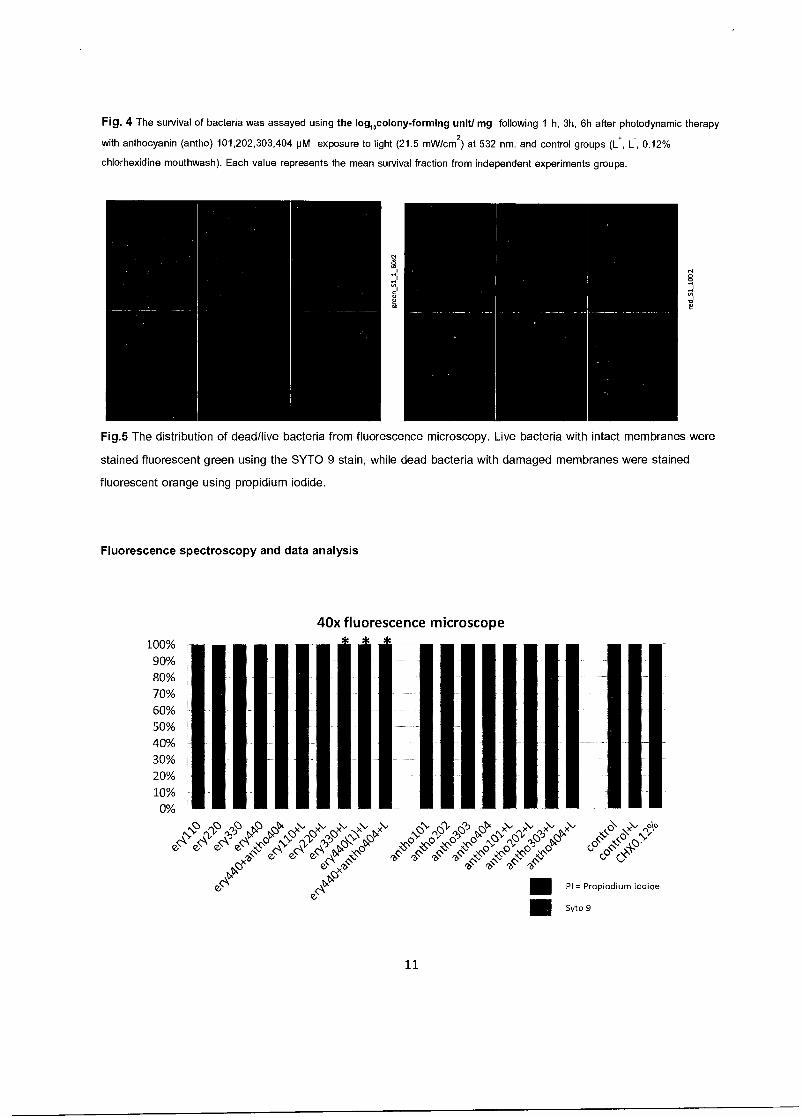
Fig. 4 The survival of bacteria was assayed using the logiocolony-forming unit/ mg following 1 h, 3h, 6h after photodynamic therapy
with anthocyanin (antho) 101,202,303,404 pM exposure to light (21.5 mW/cm2) at 532 nm. and control groups (I:, L, 0.12%
chlorhexidine mouthwash). Each value represents the mean survival fraction from independent experiments groups.
Fig.5 The distribution of dead/live bacteria from fluorescence microscopy. Live bacteria with intact membranes were
stained fluorescent green using the SYTO 9 stain, while dead bacteria with damaged membranes were stained
fluorescent orange using propidium iodide.
Fluorescence spectroscopy and data analysis
40x fluorescence microscope
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
oC) ()S>' x•• c> 5)
c> 6 6 sc.0 e, e, 0 6 e, e, e,
etas "6. ,c)x
ci`• 61 6" Ot
tC4 li)5,06 4 9 )CC'Ot t '7; C DCs e „„. ■ PI = Propiodium iodide
■ Syto 9
11
Fig 6 Analysis of relative viability of P.gingivalis suspensions in a fluorescence spectroscopy. Samples of
P.gingivalis were prepared and stained.The integrated intensities of the green (530 ± 12.5 nm) and red (620 ± 20
nm) emission of suspensions excited at 485 ± 10 nm were acquired, and the green/red fluorescence were calculated
for % population containing live/dead Each point represents the mean of 21 groups measurements.
Survival fractions in each experimental groups and control groups were carried out using SPSS version
11.5 (SPSS Inc. Chicago, IL). Data were analysed by one way ANOVA. Correlation between two parameters was
assessed by Spearman's correlation and p-value < 0.05 is considered significant. Data are presented as mean ± SD,
unless indicated otherwise.
Discussion
In the our study, we investigated the photodynamic effects of erythrosine and anthocyanin on the P.gingivalis in
human dental plaque-derived biofilms. We found erythrosine groups 330 pM, 440 pM and erythrosine 440 pM mixed
with anthocyanin 404 pM irradiated with green light laser were significantly more effective (P < 0.05) than
anthocyanin and control groups . The results of this study were confirmed the in vitro bactericidal efficacy of PDT
against the oral pathogens P. gingivalis . Several studies have reported that oral microorganisms in plaque
scrapings and biofilms are susceptible to photodynamic therapy. Recently, it was reported that photodynamic
therapy induced bacterial cell killing to a level of > 1 log10 in oral monospecies biofilms using erythrosine (7).
However some studies have demonstrated incomplete destruction of oral pathogens in plaque scrapings, mono-
species biofilms, and multi-species biofilms derived from human saliva. The reduction of P. gingivalis biofilms in
the PDT treatment with erythosine 220 pM was found at first hour ,however less reduction was found at 3 and 6
hours respectively. The P. gingivalis biofilms tended to increase in terms of colony forming units. This can be
explained that the concentration of erythosine 220 pM may be lost their ability to produce ROS in the PDT reaction.
SangWoo Kim reported P. gingivalis in agar cultures were irradiated with LED wavelengths of 625, 525, and 425 nm
at 6 mW/cm2/h. P. gingivalis viability was decreased by irradiation at 425 nm (40"60% reduction) and 525 nm
(10*20°/0 reduction) both in agar and found that green light irradiation did not have bactericidal effect.(16)
reported the biofilms of C. albicans and C. dubliniensis exposed to PDT mediated by 400 mM erythrosine and a
green LED was used as the light source with a wavelength of 532, an output power of 90 mW, a time of 3
min,exhibited statistically significant reductions in CFU/ml .Ke et al.reported the erythrosine 50 pM with 50 J/ cm2
green light emitting diode light could not killed. (15)
Gram (-) bacteria in planktonic form even after the concentration was raised up to 20,000 pM in combination of 100
J/ cm2
.The used of erythrosine 440 pM in killing micro-organisms has been shown in several studies. Costa,et al.
reported the biofilms of C.albicans and C.dubliniensis exposed to PDT mediated by erythrosine 400 pM and a green
LED exhibited statistically significant reductions in CFU/ml. Costa,et al. reported the PDT treatment with erythrosine
400 pM and green LED 14.34 J/cm2 irradiation could significantly reduce 0.73 log10 of C. albicans in vivo and
reduced the capacity of C. albicans to adhere to buccal epithelial cells in vitro. (15)
12

The role of PDT in the clinical treatment of periodontal disease, either in combination with traditional methods of
periodontal care or by itself, warrants further investigation to delivery and targeting approaches may need to be
developed to overcome the reduced susceptibility of complex dental biofilms to antimicrobial therapy.
Conclusion: PDT using erythrosine and anthocyanin as photosensitizers shows excellent potential as killing of the
P. gingivalis biofilms in the in vitro study.
13
References
1. Page RC, Schroeder HE. Pathogenesis of inflammatory periodontal disease. A summary of current
work. Lab Invest. 1976;34;235-49.
2. Newman G, Takei, H., Klokkevold, R., Carranza, A. Carranza's Clinical Periodontology Saunders; 2006.
1328 Pages p.
3. Sreenivasan P, Gaffar A. Antiplaque biocides and bacterial resistance: a review. Journal of clinical
periodontology. 2002;29(11):965-74.
4. Konopka K, Goslinski T. Photodynamic therapy in dentistry. Journal of dental research.
2007;86(8):694-707.
5. Meisel P, Kocher T. Photodynamic therapy for periodontal diseases: state of the art. Journal of
photochemistry and photobiology B, Biology. 2005;79(2):159-70.
6. Komerik N, MacRobert AJ. Photodynamic therapy as an alternative antimicrobial modality for oral
infections. Journal of environmental pathology, toxicology and oncology : official organ of the International
Society for Environmental Toxicology and Cancer. 2006;25(1-2):487-504.
7. Wood S, Metcalf D, Devine D, Robinson C. Erythrosine is a potential photosensitizer for the
photodynamic therapy of oral plaque biofilms. The Journal of antimicrobial chemotherapy. 2006;57(4):680-4.
8. Fukumoto LR, Mazza G. Assessing antioxidant and prooxidant activities of phenolic compounds.
Journal of agricultural and food chemistry. 2000;48(8):3597-604.
9. Wang J, Mazza G. Inhibitory effects of anthocyanins and other phenolic compounds on nitric oxide
production in LPS/IFN-gamma-activated RAW 264.7 macrophages. Journal of agricultural and food chemistry.
2002;50(4):850-7.
10. Matsumoto H, Nakamura Y, Tachibanaki S, Kawamura S, Hirayama M. Stimulatory effect of cyanidin 3-
glycosides on the regeneration of rhodopsin. Journal of agricultural and food chemistry. 2003;51(12):3560-3.
11. La VD, Howell AB, Grenier D. Anti-Porphyromonas gingivalis and anti-inflammatory activities of A-type
cranberry proanthocyanidins. Antimicrobial agents and chemotherapy. 2010;54(5):1778-84.
12. Street CN, Pedigo LA, Loebel NG. Energy dose parameters affect antimicrobial photodynamic therapy-
mediated eradication of periopathogenic biofilm and planktonic cultures. Photomedicine and laser surgery.
2010;28 Suppl 1:S61-6.
13. Soukos NS, Goodson JM. Photodynamic therapy in the control of oral biofilms. Periodontology 2000.
2011;55(1):143-66.
14. Fontana CR, Abernethy AD, Som S, Ruggiero K, Doucette S, Marcantonio RC, et al. The antibacterial
effect of photodynamic therapy in dental plaque-derived biofilms. Journal of periodontal research.
2009;44(6):751-9.
14
15. Ke En-Sheng, Nazzal S, Tseng Yu-Hang, Chen Chueh-Pin and Tsai Tsuimin. Erythrosine-Mediated
Photodynamic Inactivation of Bacteria and Yeast Using Green Light-Emitting Diode Light. Journal of Food &
Drug Analysis. 2012;20(4):951.
16. Kim S, Kim J, Lim W, Jeon S, Kim 0, Koh JT, et al. In vitro bactericidal effects of 625, 525, and 425 nm
wavelength (red, green, and blue) light-emitting diode irradiation. Photomedicine and laser surgery.
2013;31(11):554-62.
15

1.6.2
Microleakage of self-etch adhesive system in Class V cavities etched by Er:YAG
laser with different pulse modes.
Jutipond Phanombualert* Pijitta Chimtim** Thitirat Heebthamai**
*Lecturer, Department of Periodontitis, Faculty of Dentistry, Khon Kaen University
** Sixth year dental student, Faculty of Dentistry, Khon Kaen University
Abstract
The purpose of this study was to evaluate the effects of Er:YAG laser irradiation and diamond
bur on root cementum in Class V restored with self-etch adhesive. Sixty extracted human
premolars were prepared from extracted human periodontally-diseased teeth. All teeth were
randomly distributed into four groups (N=15). Standard Class V cavities margins were below the
cementoenamel junction on the buccal surface by diamond bur. Group 1; diamond bur, Group
2; Er:YAG laser etching with 50 mJ/ pulse/sec at 15 Hz, Group 3; 75 mJ/ pulse/sec at 15 Hz and
Group 4; 100 mJ/ pulse/sec at 15 Hz under water irrigation. Then, all cavities were restored with
AdperTM PromptTM L-PopTM self-etch adhesive (3M/ESPE) and restoration with composite resin
FiltekTM Z350 XT (3M/ESPE). After thermocycled and immersed in 0.2% methylene blue dye.
Microleakage was evaluated by polarizing microscope and analysis with NIS-Elements program
Data were analyzed by one-way ANOVA, Bonferini tests. Statistically differences were found
between groups (p<0.05) and cavities treated with the Er:YAG laser. The laser irradiation
produced uniform arrangement of spherical microstructures of the laser surface. Furthermore,
the characteristic microstructures of the root cementum surface present less microleakage at the
dentin margin and cementum margin.
Key words: Er:YAG / cementum / microleakage/ self-etch bonding
Introduction
Lasers Er: YAG (Erbium: Yttrium Aluminum Garnet) 2.94 pm wavelength emission
coincides with the main absorption peaks of water and hydroxyapatite. This device is FDA
approved and experienced significant testing involving all five Classes of cavity preparation on
both children and adults.' Laboratory research Laboratory research and clinical trials have
demonstrated the ability of Er: YAG laser to ablate enamel, dentin and cementum dental tissue
effectively, with the minimum of injury to pulp and surrounding structures.2 The energy of Er:
YAG laser-treated cementum, previous studies have demonstrated completely transformed into
an ablation effect with the minimal possible thermal effect to surrounding tissue. 3 The trend for
alternatives to the conventional method of preparation led to focus on Er: YAG laser device
within the modern "less is more" treatment strategies. 4 Thus, the aim of this study was to
investigate the microleakage and scanning electron microscopy (SEM) evaluation of class V
cavities prepared by Er:YAG laser or high-speed handpiece, using all-in-one self-etch adhesives
and respective manufacturer's nanocomposites resin.
Materials and Methods
Eighty extracted human premolars because of advanced periodontal disease. Total teeth
were washed in normal saline. The teeth were scaled by using an ultrasonic scaler to remove
residual tissues. All teeth were examined macroscopically for defects in cementum.4 Preparation
for Class V cavities were prepared on mid-buccal surface with the occlusal margins located 1
mm apical to the cemento-enamel junction (CEJ) in the cementum and the gingival margins
located 3 mm apical to the CEJ.5 The dimensional of cavity were standardized with a template 3
mm wide and 2 mm high. The cavity depth was 2 mm calibrated with periodontal probe (Hu-
Friedy CP-11.5B Dental Screening Probe).6 The teeth were randomized and divided into four
groups.
Group 1: Mechanical rotary preparation with diamond burs/ air turbine handpiece (control
group).
Group 2: Laser preparation by Er:YAG laser (Fotona®) at 50 mJ/pulse and 15 Hz.
Group 3: Laser preparation by Er:YAG laser (Fotona®) at 75 mJ/pulse and 15 Hz.
Group 4: Laser preparation by Er:YAG laser (Fotona®) at 100 mJ/pulse and 15 Hz
For group 2, 3, 4, the cavity was laser etching cavosurface at 50, 75, 100 mJ/pulse and
15 Hz. A novel laser technique, Er:YAG laser device (Fotona AT Fidelis, Fotona d.d., Slovenia)
2.94 pm wavelength, This laser system utilizes a fiber optic delivery with a non-contact
handpiece at a distance of approximately 5 mm from the cavity, very short pulse (VSP=100 ps),
tip diameter of 1.3 mm with water cooling and air for 20 seconds at a rate of 6 ml/min during
irradiation.'
After laser irradiation, all cavosurface were placed in cementum. All specimens were
immersed in ethanol concentration 70% for 10 minutes. The teeth were critical point dried in a
desiccator. The dried specimens were mounted on a metal stand and gold-coated (0.2 pm) by
cathode atomization under vacuum then examined with SEM. Photographs were taken at 100x,
500x, 3000x magnification.8 9
All cavities were restored with AdperTM PromptTM L-Pop TM self-etch adhesive (3M/ESPE)
and composite resin FiltekTM Z350 XT (3M/ESPE). The restorations were finished with fine-grit
finishing diamond burs (Diatech Dental AG), then polished with aseries of sandpaper disks (Sof-
Lex, 3 M ESPE). The same operator was performed preparation, restoration and finishing—
polishing procedures. All samples were stored in distilled water at 37°C for 24 h. After
undergoing thermocycling 10,000 times at temperatures between 5°C and 55°C and with a dwell
time of 30 s, the teeth were sealed sticky wax at the root apices, and two coats of nail varnish
were applied to the tooth within 1 mm of the restoration margins. The teeth were then immersed
in 0.2% methylene blue dye for 24 h.1° After removal from the dye, the teeth were cleaned under
running water and dried at room temperature. The specimens were sectioned longitudinally
direction on buccal to lingual, with a water-cooled, slow-speed, diamond saw (Isomed, Buehler
Ltd, Lake Bluff, IL, USA). The sectioned teeth were observed under a polarizing microscope
(x40 magnification) (Nikon, Japan). Two examiners scored the restorations independently and
calculated by NIS-Elements program (Nikon, Japan).

Results
Differences among the surfaces treated by Er:YAG laser compared with diamond bur.
At ultra-high magnification, SEM presented larger particles after Er:YAG laser irradiation. This
finding introduced a momentary temperature increase after this laser irradiation. While, this
increase in temperature was not as rearrangement of the remaining structures resulted in a very
porous superficial layer after Er:YAG irradiation.
The results of the gingival wall of cementum and occlusal wall of cementum, the
microleakage study were assessed with program calculated with using the dye penetration
method (Figs. 2). Significant differences between the cavities prepared by the Er:YAG laser and
those prepared by the diamond bur were evident, with the dental bur showing marginally
superior microleakage scores than Er:YAG laser groups (p<0.05).
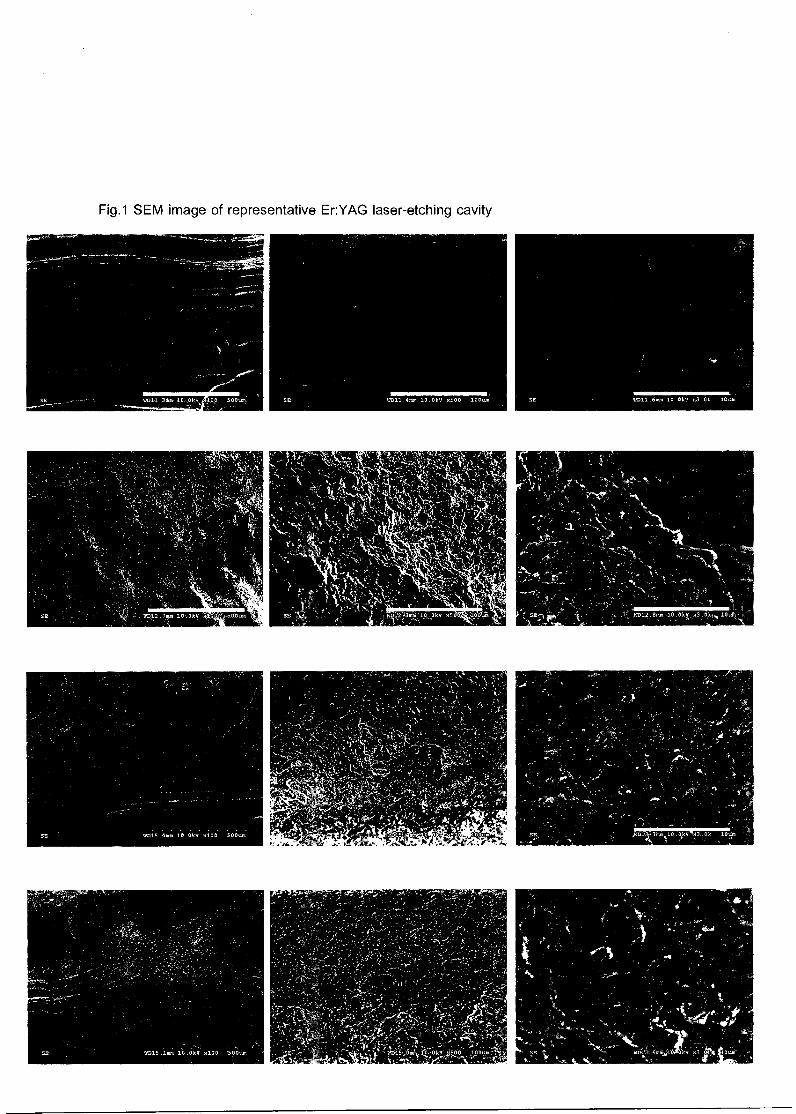
SE 1:11011.4mm 10.0kV x500 100t.m:
..15,911&A, . Opp i~00um
Fig.1 SEM image of representative Er:YAG laser-etching cavity
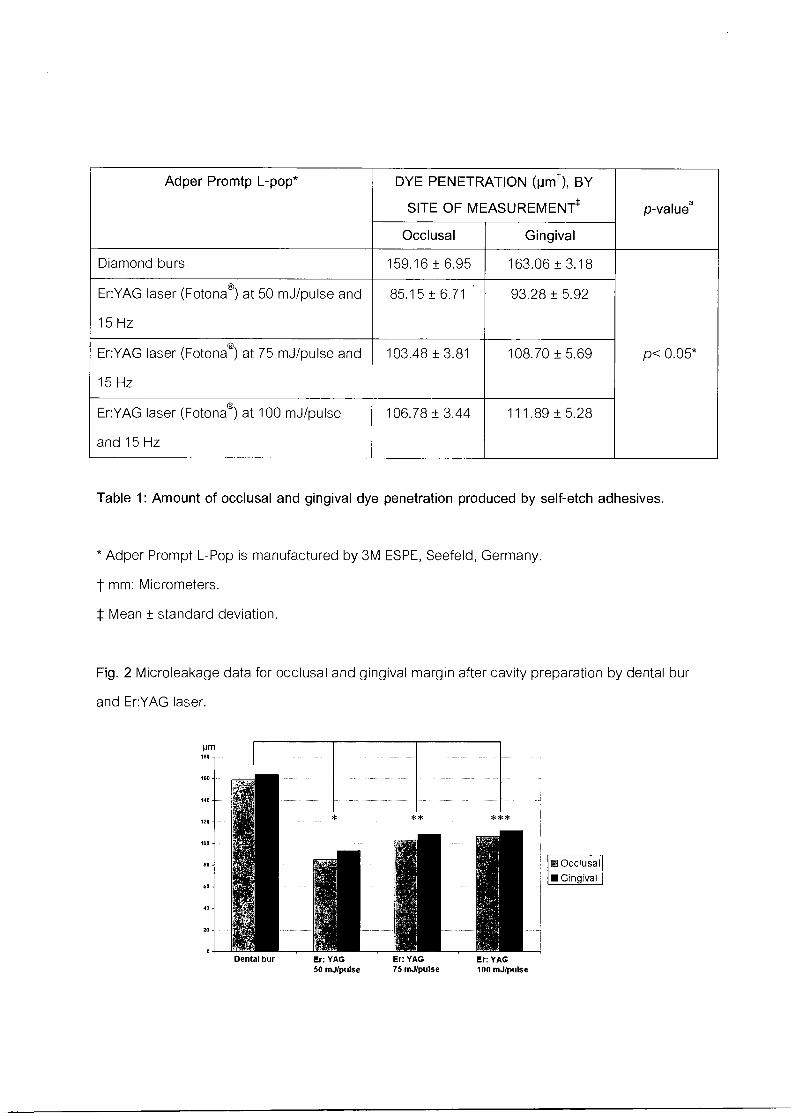
Adper Promtp L-pop* DYE PENETRATION (pmt), BY
SITE OF MEASUREMENTS p-valuea
Occlusal Gingival
Diamond burs 159.16 ± 6.95 163.06 ± 3.18
p< 0.05*
Er:YAG laser (Fotonac) at 50 mJ/pulse and
15 Hz
85.15 ± 6.71 93.28 ± 5.92
Er:YAG laser (Fotona®) at 75 mJ/pulse and
15 Hz
103.48 ± 3.81 108.70 ± 5.69
Er:YAG laser (Fotona®) at 100 mJ/pulse
and 15 Hz
106.78 ± 3.44 111.89 ± 5.28
Table 1: Amount of occlusal and gingival dye penetration produced by self-etch adhesives.
* Adper Prompt L-Pop is manufactured by 3M ESPE, Seefeld, Germany.
t mm: Micrometers.
Mean ± standard deviation.
Fig. 2 Microleakage data for occlusal and gingival margin after cavity preparation by dental bur
and Er:YAG laser.
Occlusal ■ Gingival
Dental bur
Er: YAG
Er: YAG
Er: YAG 50 mJ/pulse
75 mJ/pulse
100 mJ/pulse
Discussion
The preparation with the laser could be altering the morphological and chemical
composition of dental hard tissues, and subsequently the application of the acid material to
laser-treated teeth could affect the bonding mechanism of adhesives and microleakage
phenomenon. Therefore, penetration of the total etch adhesive to the tissue surface could
decrease microleakage.11
Laser-irradiated margins compared to conventional prepared
margins have irregular surfaces, and this fact could create microspaces and eventually more
leakage.12
Denaturation of collagen fibers has also been observed as the action of erbium
laser system relies directly upon water molecules.13 Moreover, selective removal of collagen rich
intertubular dentin in addition to photothermal effects of Er:YAG laser will cause organic loss of
dentin, collapse, and melting of collagen fibers which all can occlude dentinal tubules and
restrict resin extension into dentinal tubules.14 Current all-in-one adhesives contain co-polymers
that prevent face separation and act as wetting agents and promoters of the diffusion of resin
into exposed collagen.15 As opposed to cavity preparation by bur, which results in a layer of
debris at the surfaces, cavity preparation by Er:YAG laser results in surfaces free of smear layers
and smear plugs.16 The degree of microleakage in class V cavities was affected by the type
of adhesive restorative materials, type of self-etching adhesive, cavity margin location, and tooth
preparation method either by Er:YAG laser or dental bur. Pashley and Tay 17 reported that self-
etch dental adhesives differed in their aggressiveness. Therefore, they are classified into three
categories, according to acidity: mild, moderate and aggressive. Self-etch adhesive whose pH
is lower than 1.5 are called aggressive self-etch adhesives. On the other hand, self-etch
adhesives which have a pH higher than 1.5 are categorized as mild or moderate. The self-etch
adhesives were used in this study, the pHs of AdperTM PromptTM L-Pop TM were pH=0.5.
The reason for this finding could be single step application of this bonding system which will
reduce its technique sensitivity. The primer of this bonding agent has a lower pH than 1.5 and is
considered aggressive acidic primer. This primer could create surface demineralization to a
depth of 1 pm which creates a surface for micromechanical retention:5 In addition, more acidic
pH of AdperTM PromptTM L-PopTM may cause more micromechanical retention and a thicker
hybrid layer in dentin and thus, compensating the adverse morphologic effect of laser
irradiation. However, the least amount of gingival and occlusal microleakage for the
laser-prepared teeth was found with composite restoration.
Conclusion
To summarize, this study demonstrated that cementum and root dentin presented micro-
irregularities after Er:YAG laser irradiation. However, the performance of the Er:YAG laser for
Class V cavity preparation was showed less microleakage when compared with the diamond
bur.
Acknowledgement
Assoc. Prof. Dr. Sajee Satayut, all staffs in LDRG-KKU and Faculty of Dentistry, Khon Kaen
University.
Reference
1. Juntavee N. Laser in dentistry: Academic and practical points of view. 2011 Annual
Meeting Proceeding. The 1st International LDRG-KKU Symposium on "Laser in Dentistry:
Research and Novel Techniques" 2011; 1: 49-61.
2. Corona A, Borsatto C, Pecora D, Rocha De SA, RA RS, Palma-Dibb G. (2003) Assessing
microleakage of different class V restorations after Er:YAG laser and bur preparation. J
Oral Rehabil 30:1008-1014.
3. Teerakapong A, Chuercharuenwasuchi N, Senarasana P, Chaowaratana S, Weera-
archakul W. The comparison of morphologic of periodontitis involved root surfaces after
radiated in vitro with Er: YAG and ER,Cr : YSGG lasers. Khon Kaen Dental Journal
2007;10(2):80-90.
4. 7.IfTlalt1466t114. 6(2): p. 89-95.
5. Almehdi A, Aoki A, Ichinose S, Taniguchi Y, Sasaki KM et al. Histological and SEM
analysis of root cementum following irradiation with Er:YAG and CO(2) lasers. Lasers
Med Sci 2012;22(4): 342-50.
6. Matsumoto K, Wang X, Zhang C, Kinoshita J. Effect of a novel Er:YAG laser in caries
removal and cavity preparation: a clinical observation. Photo med Laser Surg
2007;25(1):8-13.
7. Sasaki KM, Aoki A, Ichinose S, Ishikawa I. Morphological analysis of cementum and root
dentin after Er:YAG laser irradiation. Lasers Surg Med 2002;31(2):79-85.
8. DeIme KI, Deman PJ, De Bruyne MA, De Moor RJ. Microleakage of four different
restorative glass ionomer formulations in class V cavities: Er:YAG laser versus
conventional preparation. Photomed Laser Surg 2008;26(6):541-9.
9. DeIme KI, Deman PJ, De Bruyne MA, Nammour S, De Moor RJ. Microleakage of glass
ionomer formulations after erbium:yttrium-aluminium-garnet laser preparation. Lasers
Med Sci 2010;25(2):171-80.
10. Onay EO, Orucoglu H, Kiremitci A, Korkmaz Y, Berk G. Effect of Er,Cr:YSGG laser
irradiation on the apical sealing ability of AH Plus/gutta-percha and Hybrid Root
Seal/Resilon Combinations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
2010;110(5):657-64.
11. Attar N, Korkmaz Y, Ozel E, Bicer OC, Firatli E. Microleakage of class V cavities with
different adhesive systems prepared by a diamond instrument and different parameters
of Er:YAG laser irradiation. Photomed Laser Surg 2008;26:585-91.
12. Wright GZ, McConnell RJ, Keller U. Microleakage of Class V composite restorations
prepared conventionally with those prepared with an Er:YAG laser a pilot study. Pediatr
Dent 1993;15:425-6.
13. Cozean C, Arcoria CJ, Pelagalli J, Powel GL. Dentistry for the 21st century? Erbium:YAG
laser for teeth. J Am Dent Assoc 1997;128:1080-7.
14. Hossain M, Nakamura Y, Kimura Y, Yamada Y, Ito M, Matsumuto K. Caries preventive
effect of Er:YAG laser irradiation with or without water mist. J Clin Laser Med Surg
2000;18:61-5.
15. Van Landuyt KL, De Munck J, Snauwaert J et al. Monomer-solvent phase separation in
one step self-etch adhesives. J Dent Res 2005;84:183-8.
16. Lizarelli RF, Silva PC, Neto ST, Bagnato VS. Study of microleakage at class V cavities
prepared by Er:YAG laser using rewetting surface treatment. J Clin Laser Med Surg
2004;22:51-5.
17. Pashley DH, Tay FR. Aggressiveness of contemporary self-etching adhesives. Part II:
etching effects on unground enamel. Dent Mater 2001;17:430-44.
18. Van Meerbeek B, De Munck J, Yoshida Y, et al. Buonocore memorial lecture. Adhesion
to enamel and dentin: current status and future challenges. Oper Dent 2003;28:215-35.
Correspondence author:
Jutipond Phanombualert
Department of Hospital dentistry,
Faculty of Dentistry,
Khon Kaen University,
Khon Kaen Thailand, 40002
Tel.: +66-4334-8152

1.6.3
SEM Analysis of cementum treated with the Er: YAG laser.
Authors
Jutipond Phanombualert', Thitirat Heebthamai2, Pijitta Chimtim2, Sajee Sattayut 3
Affiliations
'Hospital Dentistry Department, Faculty of Dentistry and Lasers in Dentistry Research Group,
Khon Kaen University, Thailand: 2Dental student, Faculty of Dentistry, Khon Kaen University:
3Oral Surgery Department, Faculty of Dentistry and Lasers in Dentistry Research Group, Khon
Kaen University.
Corresponding author:
Jutipond Phanombualert
'Hospital Dentistry Department, Faculty of Dentistry, Khon Kaen University, Khon Kaen,
Thailand, 40002
Telephone: +66-8-5999-6041
e-mail: [email protected]
1
Abstract
The purpose of this study was to evaluate the effects of Er:YAG laser irradiation on root
cementum by scanning electron microscopy (SEM). Twenty extracted human premolars were
prepared from extracted human periodontally-diseased teeth. Pulsed Er:YAG laser non-contact
mode was applied at various powers ranging from 50, 75 and 100 mJ/ pulse/sec at 15 Hz under
water irrigation. Following laser exposure, specimens were fixed, dehydrated, and dried. After
mounting on SEM plates and sputter-coating with gold, the cementum surface was examined by
SEM. At ultra-high magnification, SEM presented that increasing the energy parameters in Er:
YAG laser irradiation showed a difference in the surface morphology of cementum and dentine
from lack of smear layer, roughening and pattern micro-irregularities increasing depend on
energy. This study demonstrated that cementum and root dentin presented micro-retentive
features after Er: YAG laser irradiation as compared to diamond bur. The relationship between
different energies brings to increasing more irregularities cementum surface. This study
demonstrated that cementum and root dentin presented micro-irregularities after Er:YAG laser
irradiation.
2
Introduction
Er: YAG (Erbium: Yttrium Aluminum Garnet) lasers (wavelength 2940 nm) are highly
absorbed by water. This device is FDA approved and experienced significant testing involving
all five Classes of cavity preparation on both children and adults. 1
The trend for alternatives to the conventional method of preparation led to focus on Er: YAG
laser device within the modern " less is more" treatment strategies. 2
The expansion of water generates high pressures, causing the removal of hard tissue (micro-
explosions). The energy of Er: YAG laser-treated cementum, previous studies have
demonstrated completely transformed into an ablation effect with the minimal possible thermal
effect to surrounding tissue. 3
There are major variables such as energy output, pulse mode and frequency. The energy output
is varied according to an essential of high or low energy levels lead to change in the
ultrastructure of the cementum and dentin.
Therefore, the aim of this study was to precisely analyze the microstructural alterations of
human cementum resulting irradiation cavity preparation with Er: YAG laser, and to investigate
the optimal parameters energy outputs for ablating cementum and dentine with a very short
pulse (VSP=100 [is).
3
Subjects and methods
Study design
Twenty extracted human premolars because of advanced periodontal disease. Total teeth were
washed in normal saline. The teeth were scaled by using an ultrasonic scaler to remove residual
tissues. All teeth were examined macroscopically for defects in cementum.4 Preparation for
Class V cavities were prepared on mid-buccal surface with the occlusal margins located 1 mm
apical to the cemento-enamel junction (CEJ) in the cementum and the gingival margins located
3 mm apical to the CEJ.5 The dimensional of cavity were standardized with a template 3 mm
wide and 2 mm high. The cavity depth was 2 mm calibrated with periodontal probe (Hu-Friedy
CP-11.5B Dental Screening Probe).6 The teeth were randomized and divided into four groups
of 5 teeth (n=5).
Group 1: Mechanical rotary preparation with diamond burs/ air turbine handpiece (control
group).
Group 2: Laser preparation by Er: YAG laser (Fotona ) at 50 mJ/ pulse/sec at 15 Hz.
Group 3: Laser preparation by Er: YAG laser (Fotona ) at 75 mJ/ pulse/sec at 15 Hz.
Group 4: Laser preparation by Er: YAG laser (Fotona®) at 100 mJ/ pulse/sec at 15 Hz.
For group 2, 3, 4, the cavity was prepared beveling cavosurface by Er: YAG laser at 50, 75, 100
mJ/ pulse/sec at 15 Hz. A novel laser technique, Er: YAG laser device (Fotona AT Fidelis,
Fotona dd., Slovenia) 2.94 'um wavelength, This laser system utilizes a fiber optic delivery with
a non-contact handpiece at a distance of approximately 5 mm from the cavity, very short pulse
(VSP=100 ps), tip diameter of 1.3 mm with water cooling and air for 20 seconds at a rate of 6
ml/min during irradiation.'
After laser irradiation, all cavosurface were placed in cementum. All specimens were fixed for 2
hours with 2.5% glutaraldehyde fixative solution and later rinsed with 0.1 M phosphate buffer
solution overnight. After that, the plates were dehydrated in a series of graded ethanol solutions.
The teeth were critical point dried in a desiccator. The dried specimens were mounted on an
4
aluminum mount stand and gold-coated (0.2 nm) by cathode atomization under vacuum. The
prepared specimens were then observed under SEM (S-3000; Hitachi Ltd, Hitachinaka, Japan)
at a magnification of 100, 500 and 3,000 times.[8,9]
Results
The effects of laser irradiation on the cementum and dentine were found with the SEM as
follows.
In the control group treated cementum with diamond bur showed uniform pattern from diamond
ablation at a high power magnification. (Fig.la-c)
50 mJ (Fig. 2a-c).
The surface displayed a smooth appearance was showed at (100x) and the surface
treated by Er:YAG laser irradiation at higher power magnification (500x and 3000X) showed
superficial roughness without the presence of smear layer.
75 mJ (Fig. 3a-c).
The cementum surface lasered treated at 75 mJ and 15 Hz presented cutting path followed by
the Er: YAG laser beam (100x) and at higher power magnification (500x and 3000X) showed
micro-irregular (grass-like appearance), long-thin projections of equal distribution.
100 mJ (Fig. 4a-c).
The cementum surface lasered treated at 100 mJ and 15 Hz presented (100x) and at
higher power magnification (500x and 3000X) showed homogeneously distributed long-thin
projections of peritubular dentine (saucer-like cavitation).
When compare result micromorphological effects between the laser irradiation and
diamond bur conventional. The results of this study showed all of the laser-treated groups were
smear-free layer. Therefore, the morphology of the lasered cementum presented a depth of
irradiation variation as the energy output was increased.
5
Discussion
The effect of laser power related to ablation efficiency of Er: YAG resulting from
variables such as surface irradiation, laser wavelength, rate of power, duration of exposure,
wave form and utilization of a surface coolant. (10) The results of this study showed degree of
rough surface depended on increasing energy output. In the comparison of the laser treated
group with the mechanically instrumented group, not only the mechanical effect without the
production of a smear layer, effected a proper surface for bonding. Irradiation with Er: YAG
laser made rougher surface, but the use of mechanical diamond also made track and roughness.
(11)
It should be pointed out that the purpose of the present study was to investigate the
effect of morphological changes and the chemical/compositional alterations of the Er:YAG laser
treated root cementum in the laser treated root surface of those studies, the cementum layer
might have been preserved after treatment, whereas in the mechanically debrided surface the
cementum layer might have been lost completely. If such a difference had existed between both
treatments, better results might be expected with the laser treatment, which is capable of
preserving cementum on the root surface, because the cementum contains molecules that
promote chemotactic migration, adhesion and proliferation of some periodontal cells.
6
Conclusion
To summarize, this study demonstrated that cementum and root dentin presented micro-
irregularities after Er:YAG laser irradiation. However, under ultra-high magnifications,
intertubular dentine was ablated more than peri-tubular dentin that presented the dentinal
tubules appears to be better exposed. Further studies are required to investigate the
microleakage interaction between the irradiated surface and the restoration.
7

Acknowledgement
Assoc. Prof. Dr. Sajee Satayut, all staffs in LDRG-KKU and Faculty of Dentistry, Khon Kaen
University.
8
References
1: Juntavee N (2011): Laser in dentistry: Academic and practical points of view. 2011 Annual
Meeting Proceeding. The F' International LDRG-KKu Symposium on "Laser in Dentistry:
Research and Novel Techniques "Khon Kaen University, 1: 49 — 61.
2: Sattayut S (2003): Principle of lasers in dentistry. Khon Kaen Dental Journal, 6:89 — 95.
3: Teerakapong A, Chuercharuenwasuchi N, Senarasana P, Chaowaratana S, et al (2007): The
comparison of morphologic of periodontitis involved root surfaces after radiated in vitro with Er:
YAG and ER,Cr : YSGG lasers. Khon Kaen Dental Journal, 10:80 — 90.
4: Almehdi A, Aoki A, Ichinose S, Taniguchi Y, Sasaki KM, et al (2012): Histological and
SEM analysis of root cementum following irradiation with Er:YAG and CO(2) lasers. Lasers
Med Sci, 22:342 — 350.
5: Matsumoto K, Wang X, Zhang C, Kinoshita J (2007): Effect of a novel Er:YAG laser in
caries removal and cavity preparation: a clinical observation. Photomed Laser Surg, 25:8 — 13.
6: Sasaki KM, Aoki A (2002): Morphological analysis of cementum and root dentin after
Er:YAG laser irradiation. Lasers Surg Med, 31:79 — 85.
7: Delme KI, Deman PJ, De Bruyne MA, De Moor RJ (2008): Microleakage of four different
restorative glass ionomer formulations in class V cavities: Er:YAG laser versus conventional
preparation. Photomed Laser Surg, 26:541 — 549.
8: Delme KI, Deman PJ, De Bruyne MA, Nammour S, et al (2010): Microleakage of glass
ionomer formulations after erbium:yttrium-aluminium-garnet laser preparation. Lasers Med Sci,
25:171 — 180.
9: Onay EO, Orucoglu H, Kiremitci A, Korkmaz Y, et al (2010): Effect of Er, Cr:YSGG laser
irradiation on the apical sealing ability of AH Plus/gutta-percha and Hybrid Root Seal/Resilon
Combinations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 110:657 — 664.
10: Leticia HT, Patricia H, Luciano B, Valdir GG, et al (2003): Effect of Er: YAG and diode
laser irradiation on the root surface: morphological and thermal analysis. J Periodontol,
74:838843.
9
11: Katia MS, Akira A, Shizuko I, Isao I (2002): Morphological analysis of cementum and root
dentin after Er: YAG laser irradiation. Laser in Surgery and Medicine, 31:79— 85.
10
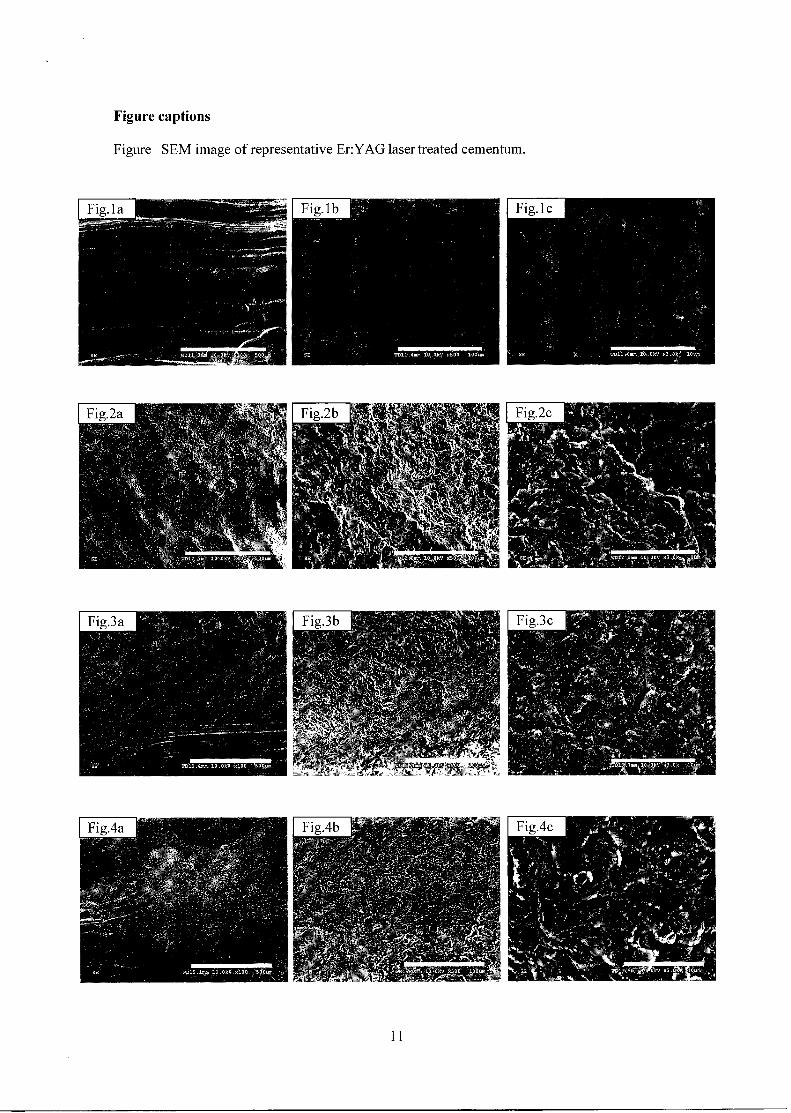
Figure captions
Figure SEM image of representative Er:YAG laser treated cementum.
11
II. Olgthiglfl11.A1'11.itiTtIVAII'lf1155rAtilirrifiF1
3.1.1 , 3.1.2
di k. World Dootal Federation fc ,
1Nt MALAYSIA' Rd
4P401° mitmcwitarm
35TH ASIA PACIFIC DENTAL CONGRESS, 7-12 MAY 2013, KUALA LUMPUR 2013 - DIAMOND JUBILEE OF MALAYSIAN DENTAL ASSOCIATION (75 YEARS)
5th February 2013
Dear Prof Sajee Sattayut Via Email : [email protected]
35th ASIA PACIFIC DENTAL CONGRESS (APDC) DATE : 7TH TO 12TH MAY 2013 VENUE : KUALA LUMPUR CONVENTION CENTRE
Greetings from the Malaysian Dental Association.
Thank you very much for accepting our invitation to lecture during the 35th APDC to be held in Kuala Lumpur this year.
We would like to confirm your schedule as follows:
Date Scientific Programme Time Venue 8-9 May 2013 (WED & THU)
Workshop : WFLD APDC Laser Symposium (Limited to 60 pax)
8.30am-5.30pm MAHSA College, Pusat Bandar Damansara, Kuala Lumpur
As it has been some time since our last communication, please do update us with:
• Your latest photograph
• Your abbreviated list of qualifications/designations (as you would like included next to your photographs on the 35th APDC flyers and website)
• ISO word curriculum vitae
• 150 word lecture title and synopsis *Email details to : mdaassoca unifi.my and [email protected]
During your lecture, you will be provided with:
• LCD projector
• Clip-on, standing microphone and laser pointer
• If you require a laptop, please let us know in advance.
• If you are using a Macbook, please kindly bring your own adaptor for the projector.
Should you require additional equipment, please write to us as soon as possible.
542, 2.d-FloorrMeelan-Setia-25-Plaza DaraansamTKuldt-Damansarar504,90 Kuala-Lumpur, Malaysia. Tel : 603-20951532 or 20951495 or 20111769 Fax : 603-20944670
We would like to cordially invite you and accompanying person/spouse to the 35th APDC social events to thank you for taking time from your busy schedule to be part of our Scientific Programme:
Social Event Date Venue Speakers' Night Thursday, 9th May 2013 TBC Citi Tour Friday, I Oth May 2013 Kuala Lumpur Opening Ceremony & Reception Dinner
Friday, I Oth May 2013 Kuala Lumpur Convention Center
We hope you would be able to RSVP as to which of these events you/your partner will be attending by 1st March 2013.
For overseas speakers, please advise our speaker welfare chairperson, Dr Eileen Koh (meiyenkohagmail.com) regarding your detailed travel itinerary to facilitate airport transfer and accommodation. She will contact you in due course.
Thank you very much.
With kind regards.
Yours sincerely,
Prof Dato Dr A Ratnanesan
Dr Shalini Kanagasingam Chairman, 35th APDC
Chairperson, Scientific Programme President-Elect of the Asia Pacific Dental Federation
35th APDC Local Organizing Committee
Past President FDI World Dental Federation email: [email protected]
Cc. - Members of the Scientific Programme Committee of 35th APDC
Terms & Conditions of Sponsorship
MDA will provide :
• Accommodation ( 3 nights at the Peninsula Residence All Suite Hotel Kuala Lumpur) • Airport transfer
• Local tours/hospitality
54-2,2a-FloarrMeitaivSetia*Plaza-DamansararRoliit-Doman-sera, 50490-Kuala-humpur, Malaysia. Tel : 603-20951532 or 20951495 or 20111769 Fax : 603-20944670
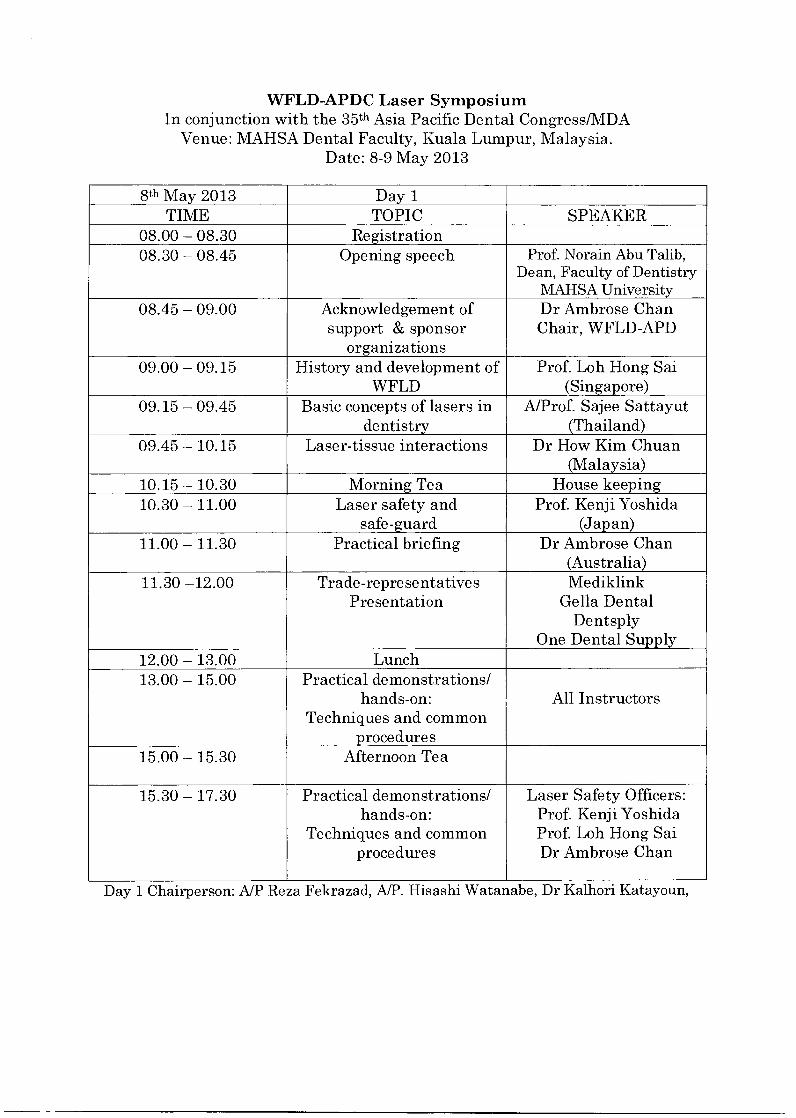
WFLD-APDC Laser Symposium In conjunction with the 35th Asia Pacific Dental Congress/MDA
Venue: MAHSA Dental Faculty, Kuala Lumpur, Malaysia. Date: 8-9 May 2013
8th May 2013 Day 1 TIME TOPIC SPEAKER
08.00 — 08.30 Registration 08.30 — 08.45 Opening speech Prof. Norain Abu Talib,
Dean, Faculty of Dentistry MAHSA University
08.45 — 09.00 Acknowledgement of support & sponsor
organizations
Dr Ambrose Chan Chair, WFLD-APD
09.00 — 09.15 History and development of WFLD
Prof. Loh Hong Sai (Singapore)
09.15 — 09.45 Basic concepts of lasers in dentistry
A/Prof. Sajee Sattayut (Thailand)
09.45 — 10.15 Laser-tissue interactions Dr How Kim Chuan (Malaysia)
10.15 — 10.30 Morning Tea House keeping 10.30 — 11.00 Laser safety and
safe-guard Prof. Kenji Yoshida
(Japan) 11.00 — 11.30 Practical briefing Dr Ambrose Chan
(Australia) 11.30 —12.00 Trade-representatives
Presentation Mediklink
Gella Dental Dentsply
One Dental Supply 12.00 — 13.00 Lunch 13.00 — 15.00 Practical demonstrations/
hands-on: Techniques and common
procedures
All Instructors
15.00 — 15.30 Afternoon Tea
15.30 — 17.30 Practical demonstrations/ hands-on:
Techniques and common procedures
Laser Safety Officers: Prof. Kenji Yoshida Prof. Loh Hong Sai Dr Ambrose Chan
Day 1 Chairperson: A/P Reza Fekrazad, A/P. Hisashi Watanabe, Dr Kalhori Katayoun,
9th May 2013 Day 2 - TIME TOPIC SPEAKER
08.00- 08.30 Registration - 08.30- 09.00 Lower intensity laser therapy in
the oral and maxillofacial region A/Prof. Sajee Sattayut
(Thailand) 09.00- 10.00 Current clinical applications of
Er:YAG laser in periodontal and peri-implant therapy
A/Prof. Akira Aoki (Japan)
10.00- 10.30 Laser osteotomy in dentistry Prof. Kenji Yoshida (Japan)
10.30 - 10.45 Question time 10.45 - 11.00 Morning Tea House keeping 11.00 - 11.30 Laser uses in periodontal surgery A/P. Hisashi Watanabe
(Japan) 11.30 - 12.00 Laser uses in implantology Dr Shigeyuki Nagai
(Japan) 12.00 - 12.30 Laser uses in endodontology Dr Kalhori Katayoun
(Iran) 12.30 - 13.00 Laser uses in oral surgery Prof. Loh Hong Sai
(Singapore) 13.00 - 14.00 Lunch Exhibition 14.00 - 14.30 Laser uses in orthodontics Dr How Kim Chuan
(Malaysia) 14.30 - 15.00 Integrate lasers in daily practice Dr Philip Tsui
(Hong Kong) 15.00 - 15.15 Afternoon Tea 15.15 - 15.45 Laser uses in Cariology :
Diagnosis and therapy Dr Ambrose Chan
(Australia) 15.45 - 16.15 Photochemistry in Dentistry A/P Reza Fekrazad
(Iran) 16.15 - 16.45 Open discussion Panel speakers 16.45 - 17.00 Closing speech Prof. Kenji Yoshida
Secretary WFLD Day 2 Morning- Chairperson: Dr How Kim Chuan, Dr Philip Tsui, Dr Ambrose Chan
Afternoon-Chairperson: A/P Sajee Sattayut, A/P Akira Aoki, Dr Shigeyuki Nagai
Practical Demon/Hands-on sessions: Technique/common procedures (4.0 hours). Rotate each station every 25 mins.
Laser Safety Officers: Prof. Kenji Yoshida, Prof. Loh hong Sai, Dr Ambrose Chan.
Station Company Instructor Si- iplus, ErCr YSGG S2- epic10 diode laser, S3- i-lase
S1-3. Mediklink Tung Soon Yong
Dr How Kim Chuan A/Prof. Akira Aoki
Dr Philip Tsui
S4- Diode laser (Zolar ) S4. Galla Dental, Adrian Wong.
A/Prof. Sajee Sattayut
S5- AMD- Diode laser 1 S6- AMD-Diode laser 2
S5-6 Dentsply- Andy William
Dr Shigeyuki Nagai A/Prof Hisashi
Watanabe
S7- Elexxion —nano
S8- Elexxion —pico Diode laser
S7-8 One Dental Supply —Ezekiel Tiew/Jonas Tan
A/P Reza Fekrazad Dr Kalhori Katayoun
Practical session Laser Safety Requirements and Instructions
• All windows should be covered with opaque materials.
• Any doors should be closed.
• Partitions (above eye level) should be placed between stations.
• Laser safety signs are to be displaced at the door entrances.
• Wavelength specific eye-wears and laser mask must be worn at
the station and at all time.
• Laser eye-wears are also placed at the door entrance.
• Implement plume and fire hazards control measures.
• Infection control and documentation.
• Keep noise level down and keep workplace tidy.
• The number of your first station is marked on your name tag.
Every 25mins, move up to the next consecutive station number.
Laser safety is everybody responsibilities
Thankyou.
3.1.3
4—)
O CU 4—)
O 5
v) CU
4-) o • t4-4 u O "c4:44
CD • • I-4 "I")
ri CD 5
• rt:$
CZ CU V) 4..) L14 Ci••=1
mod
• 0 0
o 0
••4
(1,) ;1•14
-I-4 0
;m4
(1) V) Ct
tn, fiNI!
O CD "MI 4■4 " c„,)
tx0
o • c.,) c
)■...1
g■14
1-4 (1) 4J
Prof
Fred
eric
k G
aulti
er
Loca
l Con
gres
s Cha
irman
Aw
arded t
o
Fed
era
tio
n f
or
Lase
r
Saje
e SA
TT
AY
UT
Aw
arde
d to
Saje
e SA
TTA
YU
T
rn 0 Z • p-4 a) ..4•••) C::1 Ct;-, a) • r--4 al U
1-4 ;•4 CU O ;16.4 t•I■1 r.• '44
0 r-4 all ., C) 4-4 NI RI :1`4 $■4 Rztj CD "0 Nal CD -14 >1 t•I•4 "0 Z
0 0
CZS Cli) (1) CI 14•J = •-) Ct 4.4 O U VI) 1(41 rimi CD $•-■ • rim4 bi3 Z .1.1.4 O ;'4 L.)
fJ CD r—i CM)
4-J cn 4-)
O a) 4-) 0 • t...4 Ct) v) •0 a)
47-: CU • ct
▪ c• 4-4 -43 t-4
U (I) tt.0 II—) • P-4 • r..4
al CU • "0 4-40
4—) ;■4 4—) "0 CI,) t•■••6 LA 0 0 OM V
CD
• 4-1 L1'.4 CL) cu 4.4
"C$ aPail
bA 4
▪
-)
PLO (..9 C9 cf)
"44 CZ r—i
4-1
•
Pro
f Fre
der
ick
Gau
ltie
r L
ocal
Con
gres
s C
ha
irm
an
3.2
III. liuleri,MTU th nithrti LDRG-KKU&SARABURI HOSPITAL
Symposium 2014

LDRG-KKU&SARABURI HOSPITAL Symposium 2014
Lasers in Dentistry; Integrated Fundamental and Research
ijet.,S1 31 mnTAL - 1 alviln 2557
talva4ti9J191a1lnia,
LDRG-KKU&SARABURI HOSPITAL SYMPOSIUM 2014
iian-ntinniigem
nth131triiinin550551NFJ19J1ndwiri laininTimnsoi'ln191i'fiwIrlhotliconnwithaantu
3'11 lelittfif1111911Mfa5ltAafl15if11115 Deli5f1114i01111f1 1115141,D1,910n14f11561111D10f1A1 I 197114
11151)9(1340fl 151Tionnamnfi rnriumroniaritlwanifeJiwualnuiftmiltmonvitn
11111,11d b`W1'lflff1c1t915 41f11511IMPIIM11111TIA03111011-1M113J119111-11115i'f111141hEJAMfl 3 TI '176,111,13J1
leiivfnmaurno4-114 -19sini5 alfli1-lia191f1flthl2t1tPlAllnr1111ANSD5' Y10111111/111011.11^111E1FilM15'
1114151/18-autavutivIlliflen1apo
nolf0P31/1011/1111/11401ttlAII/ElfilfrAi rlitiff1MliT1114fliffl111VIAlqbM2,'IAIR11411.11IVR16-41.1 IL
111115 a b11 fl bb fl a;Vilfid il'11.111flfl114f1151i5a;13J5951 fill' Lasers in Dentistry; Research and Novel
Technique, LDRG-KKU Symposium 2011 al014F(1111t11J 2554 OM Lasers in Dentistry; Integrated
Fundamental and Research, LDRG-KKU Symposium 2 0 1 2 16 11A 111 1 fl kl 2 5 5 5, LDRG-KKU
Symposium 2013 tgallfillE116142556 11 01 TV tflUflp
e outpcona;111AMIASON/EJTV11,11TIM,L111/1601VfOli"
1111-15)ran'Keyuovitriv4114Tufral3JVI4191f141,6tIli`)1111U,'911.191flfilflipM,10t195111L1141I5,1,11411E1
it=1152,11Iff114flIADt.it111.1iii111 f115115a,11159S1f11741ndi-) vi'llAilwrnIntinAtrutioug fnmi-nnla
52,14-i1111f6iEJLIA,'Irf1911f115611D10 14f1511452;kutaticluttiliiin mlaii'vqtrornoffirmilinhaqyffelmo
VtI11I1.ITT1191fl55111tMiluiiotwomm11imsa5'icrier1n111i11t91it11110141VOli' 1114-1111t11At19101411,f11-1
lItTWIM111i11
'
131aFrunilluni5lilifif151rilli9f1f15 LtM;f15W811111406i1EN11
r
11
f5 A A
i llf141'Nt1tPlAla11-1Mkolfe/611 01119qq19numa-nicdnfflflvfmivi i,
'lltillaJuf115V3Jf1")5i1TA11,1741,11115V11111T141FMTlflY) IqUf115611JU,11.1
1111f1151,40t11E1110W1/1414IAMail/f11 q-lfINM11,19101flafffi5111f115f19111iE19 tbflnilqi0f11V113(
tfli0911t111181140,WAWIJIV,11144111MIADP0111-IiiEMMAIS1f155111,d1.950n11011/111/11-410,1111Off1VOli'
4At2,'fiacd5,1109f117101115vionnfryniffniuttiljtrafillbMIDflY10111111T14910,111/EM1Mli'• 1'1111,152; 1J
imintnnflloctim OW0fl9141/41114111ffIllslfli5WEJA111TUflthlliEJLPIAlla,'IrillbMiDnIllE111
ilurraio
91flIATIAZr199101flIllitltUrrin/ -11LMSO5T-1019 41614AutAaimyd5?Alfilvirnrami-lio
itaT,111Vinivvill-19nni5lvoidollifittiergal ttaa,1511,1011JMff5nrilfilii711A101111fliirliT15111tM104
1/11ATT14011,61"111ElinVfli'111199S)Tf11110:`1fielitM,411,Ifilitii-nicualfluiftlY11,11M10'fiTle111/111111140111^11(16?
Sitr1152A'AfiGuaAiiV1551111Pi11,1111;11L414-19S1111111,1f19:11D14f151Y11151/1E1160 t19:11iitl U1a',
tfilogilunialuttaa;oi-mfinym inviicualfinsinfifichiluit-n54-rurpufm1604tiri 115a115'31
f11515t1iq6141,16111111f115G1115a;91114111LMOVE14111441111'11-191fl553J 1,1,=f115
14'111.1191ymailn
fl'lcavi5ournrinvm,q,13 rid.J.litlY111ML9f0f11/1611/111/1'1,1010.1^1111E1 VlthriJuni5vw-rnii
nilk11141115011111^Nfrialf1T)IMf11561115nOTITIfl15
11t1T1f1511.1f151,1/5-31d1515t1ITU tilEnfilEMOnvien umffilmt-yrnIdlilktilltmmrru
4 luvr14
1. MOMElltiAlifYillIftn111141GhttlEnfillfilliV11141i,MOnYIEJ1Y1WITIattlAIVIUMMli?' 41115-lib=
Sif-1553ril4 V113J15f113111J1JUlf1414 4int111uGbb1l J liMUMAIIJa.t61191 4 UM,'
icw010,111161V1111
2. bilDInfltilACJViinft=11nV1141114fnilli'MODT11151f11115MVISOiYIEJTVIlliTIMINIYIEJFIVIAi'
119:115i'Erl tianriiatrvivitifirffil9
3. bitiOL1719.11rIlltSDflillfl15if1111 1fl'M
M191 111E1
1. vilIMLINYI6PahLtanilleitfilfiniii-nill5Z;pilflf115 311T111,ffniuniiiwiiEnfilfriA'fltMASOi'
umaiSM551JMVISONIEJT11111YilattlIVElffiVOi'
2. Vfi'lltflIMilEJW3111i'DJfkR1ITTUfl154fIliliitlt=ffihAlliAtl55kIrdtclfOnY18111111T110
1,11111001M452,11i11115:11511V(1115flITU unnin5Y1E11A'El
3. WiAf15511t=111-11i'ElTalt193JiiEJLW11121111MiTanT10111111/i1.401,1,1111/Uff1M4 14iiin15 mottiii4iii4VILLIAITI6AM,'O'HJIT1-191111A11/16114f15a,1(15')W1115t11491
4. AJT111LEDnittni5T1111161-301,heilALVDJ-mvu ttaaifitunivi
frilviviluAna
1. 16i0111-115ifl115Z,1169f1f115
1.1 115.,'Vf11-1A11451161fl5
1.2 littrafliibillffillriltiamtllOilltVIVONfllilliif.JUM 14Sif1553J
1.3 1_17,T9SlihaNi"f115611Jnlf,9J59S11115
1.4 AUDfl15411JUI/J99f1f115
1.5 611/-11WITA0511J519JIIMMd0OtilltlIM11111AlillanflM401191enlli9J6110A1111illf115
2. 611i5a1f3J51f1f115 31 f1511q1f111-1R1911f1112557 q1111911141,1011151i5t11159f1f115
3. VIIIILMCLI5V31),INfl
ffill1491&11111111
I511t511/1f0i'MA 0.1n11M&1 9191 J~lcflSa9J1
eTi'velovoulf114f115
fl9:11111.41/41Afl5711 UM:fl9:3J -lititpcormcnilratvai'icntratilvitm
UTIVICHT1V171i' IlilliT1016nauttficw
qthr,C1111,91IdifilAf115
1111.0501,114 ) n3.11-nrvilmin551, I51Tutnu-mma,4,1
D -11511°CliT1401111Allifilifil TI'vEct.15a:avli flIllitltPlAll2;11 -111.M1fD5diYIE111/11cvii,NUIAIT1EM1M11
mil-Ivitatruatatriv
filM15115t11.1181,1,1111/1695?..48 Ifl-Kr-nitu
5alaininiirllerlienwamdioviamnividti uwilyitanauttriu
iinhtly 'Tull 31 fl5q1f111- 2557
4-nraue4rini-nidur., o
TildOlttValti Till a.1,1.1q 4 100 fill
11111CLI1 4 f111 -311 50 fill
11,111nntu
1. 1115ffITLIV10.191f1f191661,9.111,n111MNSDi?.°11/81V11AITUA
Lalliltiff1EM5 150,000 11111 (141 111V(1194 1113ATh
1111/tiT14)
2. filMIMVIIE.114 (2000x150) = 300,0001JTV1 011111V111.11116)-311)
3. C9111111.1i5lritnilMVSZ'Ari
fili9N101111115iflihnly
1 fi cl if) 1 r114 M, 750 11111 IA 'YU 150 flU = 112,500 111T1
2 filD11115illIAMAtli 04111.1 411111,1 4 3101 "d,̀f, 80 1111/1 150 f11-1 = 48,000 11191
3 fiT0111150-111 9Jeftcfla 350 111T1 ilVITW 150 MI = 52,500 IJTV1 9)
4 fil019115fid1111-1 2 VD Gl M.,' 250 1.1111 150 f11.1 = 75,000 11-111
5 filiVf9ifTaflAild = 15,0001111'1
6 till1t111111(11404(11711.4 = 30,000 MI/ o
7 filff3J141t1f1,151181fl5 = 44,300 1J11'1
8 fi1011115-illtlAnfltD141J-11(101f1ILLM'flinIfill114 iTLITIA 24'11114 &61 M.' 80 'UTh = 7,680 1J111
9 filD1111511F1115Y101flittflnlflaTi11114 4114-311 24 Tin! 1 110 61 m‘,,' 350 1JTV1 = 8,400 111V1
10 filD1111111"01AIld 51/101f1116M.11012.411111.4 4111)94 24 TiTll 2 /ID I 11 250 1JTV1 12,000 ifal
11 ti1filAiflfhlf_11115t=f1t112141111,14111-111 12 lIDA 15001111/1/h1 i11T314 2;11.1 blaild= 36,000 1JTV1
12 fi1111111A41141/11151/101f151,!=flila"VT11114 (5f199: 2 Ku 3111 41,1M; 3500 1111/1) V111,11.114= 21,000 1111'1
511A1461-1 = 462,380 MY' (atifY1411f111414V011A114V111.1fOUttlkillIJIV16)114111Tlehtl)
(1 111F16419 111111°A.114111191110ff11115061AE110)
1. 441TIJI-11501151131WII3Ji'innanikatiEllfilifl151911M9fai" 61.1111441111(41Af15511
2.VA„iiii1T1Jf111D1.151J41.19101,1f11”15-AiihielInnilttN1,1f115if1111RillivO'ihtli7111-1.319J411114D114
3. 44-611I-115D1151.1,140111; 44111 UM'Nfli9111h161101f115fflIllifltUtalfOi' s) 0,
4. FFU1T1Jf115D1J51JVf13J15flvN1151ifJtcih'ark!111114TLVMISOTTV1EJ1Y11lTi1491f1553J
A 11E1101
MI101f11 1 14116 1 5ff.fl5.111141,. fY vlowni
2 Iff.fll.1111. 11S15 51,1`V141,1/11
3 0.1111.91fflf15 ri40r11irolG1
4 50.`V111.Ditld 715%11114
5.Y111t11. D5014 14 6'11/1'1,1'41p
6 D.11111t11. 150 1 citilliflhaillrli
7 5F05.1(111:i52.,'4flil 415 1511101
8 ommtv.1" 6s1All 11111111-A1
9 0.1111qpniv 14 51-a'lu ili el
10 14.W11.1^11M5 ilf115,'1J11
11 vi1m1Ttl,P111511 italin
711J11/181f15 2 14111i 1.0.1/11141.V1501 oTt11451-111Fp
2.14.V11.11 li155 i11115,11J11
3.F191:V111.13Vfli'EJ -115ill'
4.N1S.1/11/1.fllifil lit1111fa
5.N1S.T111.1J5')5 lad if.111-1T011 d
6.F•191.1/111.btka D 11 'In al
• 99unfn9111umtinnilsa&6ania4InurniAciiinitrprnuffirm4
• 411-itallai'lmiltu viimurrneie.:61ND1-rwifu um,'NN1114114f115Tf1111
D.1111f1j.1g115 111-11111'Aff
D.111/141,.Vpol viilliibunpla
14.V11.1/4119155 itf1151,11,G1
Mr111 31 511 G1111 1-4111 11114
141/111:i7511l5? Af01,1VIMITE1
141111.i0
M11 ''' LI fill
1111111.P1T911,1 11111(i1131)
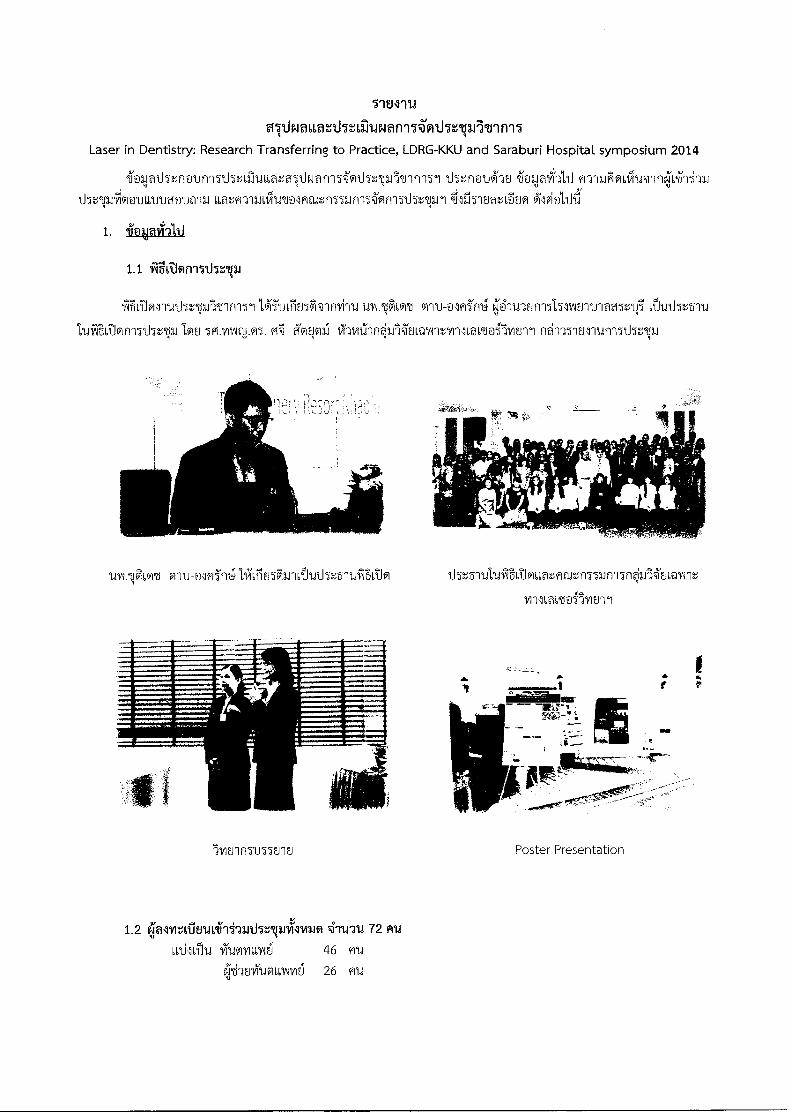
T18111.1
9Uwauattharruwani14'wdlem9 Avinil Laser in Dentistry: Research Transferring to Practice, LDRG-KKU and Saraburi Hospital symposium 2014
iimpthr,nounlIthalLilutiat?Owar -M'othrlaJltlni51 IltriuLa1-30 ifoljaih111 wrOodiulneivihi-)24
tl5e,Naniivoiatuagun-ai timm-raikraoFitut,-nmYrM'onilthallri 445-imtt:duo
1. ioapii-3111
1.1 iiitTionilthrp
fAiti,NTrutlIvuLltin-1511g.uLriza'TInvini unViLo% cru-olH'In4 P-rt.nufnmEnuiamcqi vituth.zslu
511.1/11f1J.M. A'otp12,1 vT-avrillnIfilEJLQI.AntyroLavdoilviEril nd-m-mlumnlIrp
W11.13FILMI liLilu56iLivriuti52::511.S61110 1_152',51911Sitl,t&LM'.ffIJL.TI51Jf115/0.11&,Q7CM
yl'156i964J e~5`ayl t1'1 °1
11/ITIfITU55ErlEJ
Poster Presentation
1.2 4almr.ifiErtati-ii.nrthru33viAmaim i-rtyru 72 fild
661i56N iumiLvinig 46 Flti
ezilhoitimalAimei 26 11u
1.3 Ilirnif1161,MliTIMUllErIEJ
- n15U5SEJ1EJ6591 Laser Crown lengthening and Depigmentation Interstitial lasers therapy in
dentistry
- /115U581F.1i5@5 Perspective on Laser in Prosthodontics: Science of Intelligence iou 5f31.07.i.1105
111/1i61/11 `'
11'151J1n11E.161@1 Basic laser in dentistry tou
- f1151155H1E165@1 Variety techniques for treatment of oral lesions Iii o.vimq.11f1,1%1511
n15m5Ent.d5N PIPS for root canal treatment IOEJ @.yoora1n5
- niTtnwiluilol Management TMD with LLLTiori 5FI.vil:htfTnA
fI5U550-101,1@1 Laser-soft tissue surgery iou wiltii,.@591414 11171siff-1141-p 1;1'146117t21V15
- /115115581E161@1 Alternative laser therapy in oral lichen planus mrt.441uf-la
- frITU570901,1@1 Pain relieved in minor aphthous stomatitis by lasers 191F1 @.111Alflj.NPIAI5 lAIUMTTAFI
- n15m5sluoal Basic of Laser in Dentistry In @.U.MAI.111F155 61J117t1111 yrify,.15m1 kuistrrticia
- n15u55o1u65@5 Laser safety and Hand-on Iou qt-ufleialb
w VIEJIJOkprimioNalTu
1. Poster Presentation
- @.wwqi.N;i'vu5 worIT'n,k 65o5 Microleakage of self-etch adhesive system in Class V cavities
etched by Er:YAG laser with different pulse modes.
- o.mm.11,A1i otAiftit-p IAN Alternative therapy for oral lichen planus with tow intensity
laser therapy and red light laser: A case report
- `umAI.NT12,..n 660e,flair. 61@1 Effect of blue light and hydrogen peroxide on
Porphyromonas gingivalis in biofilm
- 9.14.01A1.111f155 5"U115tar1 LIN The study of dental student experience to Laser in Dentistry
- loNt-v,m5on Aviinntifja Lij@l Efficacy of Erythrosine and Anthocyanin - mediated Photodynamic
Therapy on Porphyromonas Gingivalis Biofilms using green light in vitro.
- vamilatrilo Liatmna IAN Interstitial laser therapy using Nd:YAG and diode laser
- uvrtAuifinn 555115511/111,16Latna Ll'al A physical alteration in tissue blocks irradiated by diode
laser and Nd:YAG laser irradiating to different chromophore dyes on oral soft tissue.
1.4 Inhul-runimanitihiganJulai 31 Ml il
-1111Amiulaviumm
- 151mEntnamnimarro
- ~55tNE1 111 1c~2~~1 J5
- 17nemnaFpgrmLimi6 ufilinon
-171muitroarwrivm
- blms-rulaumumn
-15111811r1Mtn1
- Iwnitnunaa551,044115z;a14 quams-ril
-15171Erruiaejvolg alfmtlyini5
- blmtnumannLvign
-111Aionulaufilflou
- 151munrwficuvi
- blriEriunaoutar
mAr0
- bnEnula-nitrillyu quams-ril
- 15nErilnavil:1
- bvuErruwllali
-17ntriculdlluumn @qan
-I5noiviaLilu1518.1152,-mplynA.
- bnErrunamttlnLnA'n1
dTagniCAL
-
-IwivritnwumyruSail
- min'yoslA"Eilhifla
- voilms-A555annavii
- e'shErtITINIf1551.1 `ihm-rula
- Falni'fnau
-
- KNInt,@frou U9557013.1'1
- 1,W15T1'6FIL`l
- 601,1171M1N15flPtIn a5t0
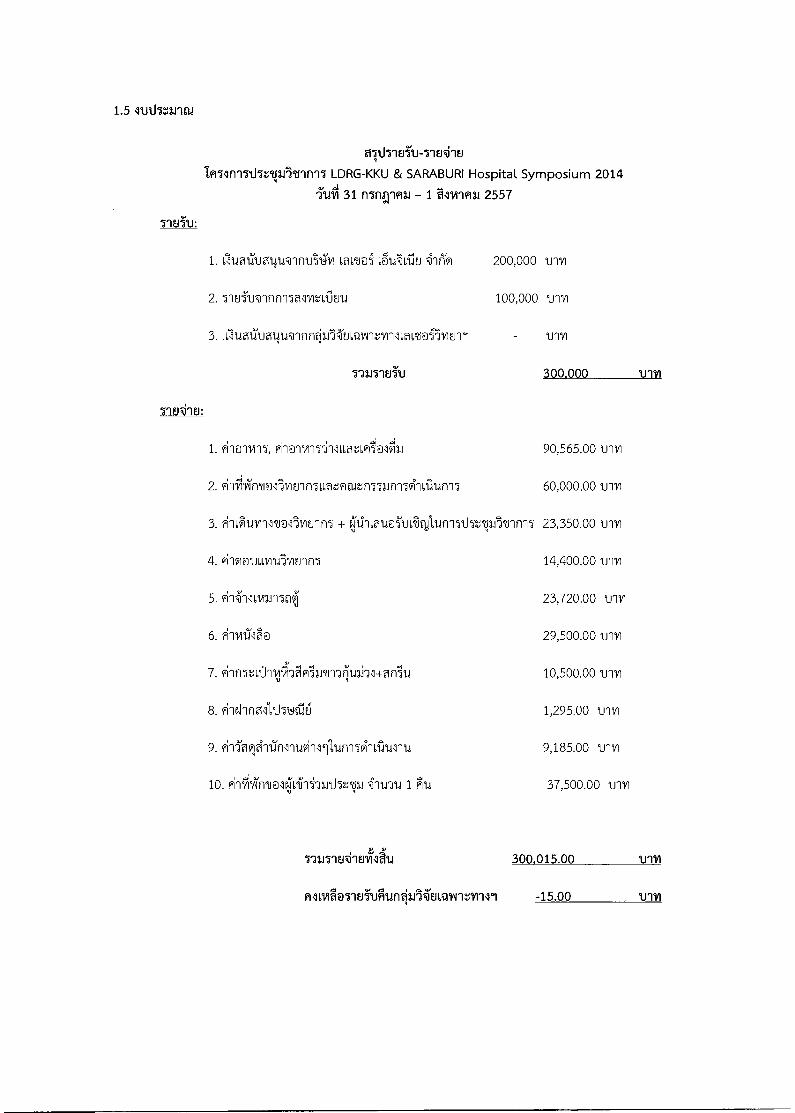
1.5 ltriiTarini
althiu5u-7-1E4-18
LDRG-KKU & SARABURI Hospital Symposium 2014
51.611 31 nInTfai - 1 alviina, 2557
1. 6lua1llmicip.,mntri4viLaLt@5 200,000 ulvl
2. 518Tulnnnwlvitvrin 100,000 trim
3. Alum:um4uvInnqL'AiLmAntvnlotmoillonci um
731171E15U 300.000 11111
1. ilo-rvi-15, 90,565.00
2. lici'vZfrii@llviuinT,Latme,n5uf-mg-IL'ilun15 60,000.00 umi
3.i'llS11.11/11111@1)1/181f15 + q1.111,01.10TULTIfaldf1151iTICrown5 23,350.00 'um
4. '1'-1Gl@cuLnit2llE1'in 14,400.00 11111
5. 23,720.00 trrn
6. 1-114111‘00 29,500.00 vqv
7. 1-InTe011111'Afli'lr'iMil:Ulj11+011i1..1 10,500.00 trivi
8. l'Iehrld1.1.151Jfilal 1,295.00 lnvi
9. 1-12?1q?1-11'.1i11-11N11111Unn5g-I6I..11.11-111 9,185.00 vim
10.iiiiikrdale;LiAii-Art.15:111 4114714 1 Au 37,500.00 'trim
111J11E41E41gl.i 300.015.00
-15.00
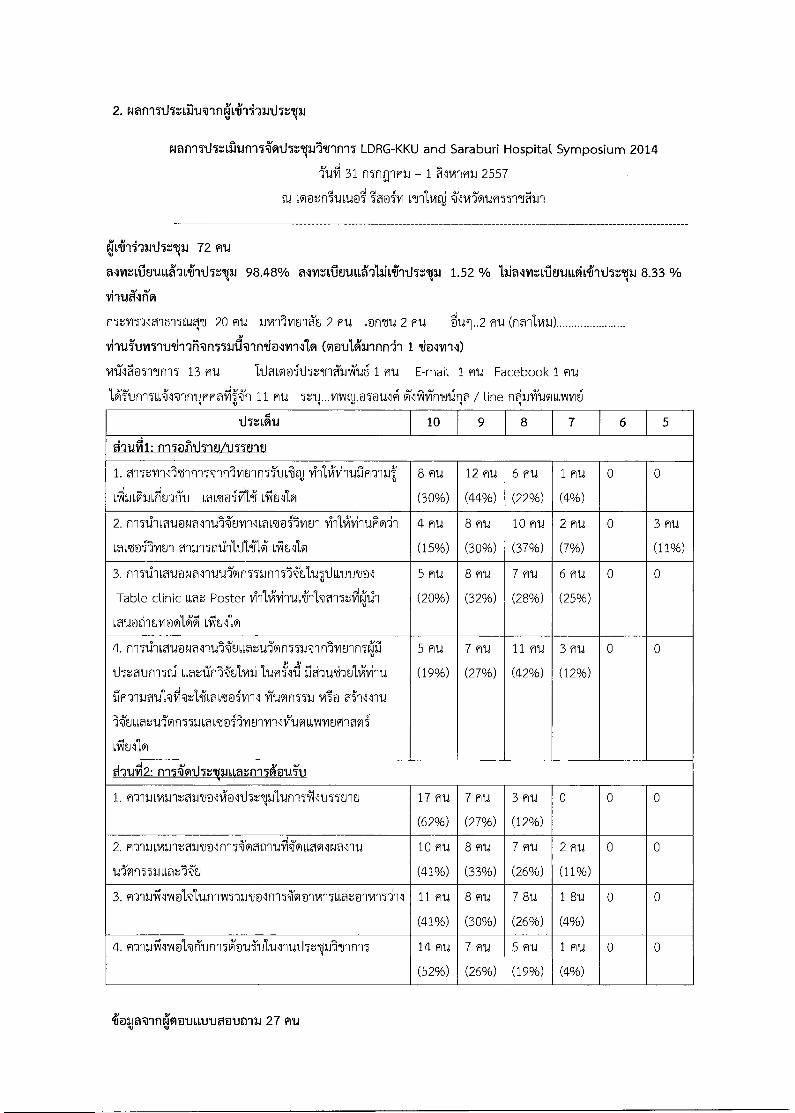
2. Nan-miniihainkitiiii-aarthrm.,
N8f1951151;1119.1f11511.11119.11661f115 LDRG-KKU and Saraburi Hospital Symposium 2014
31 mnomu - 1 2i5vinh13J 2557
oi@tniuLu@i" Ltivit '''11/1"iftA57-1/JFIL1
e.,:it,i-iiuthrtp.i 72 AU
@TVIZIA1E11.11,66%411_17,13J 98.48% NYIL611F.1U666212.164.111hZ6VJ 1.52 % lliNintrilfri.dii9iiiiii.15t6p1 8.33 %
'divaln"",1
fl5t115-JIM5'Ing14l 20 Au 3JwilliFJlk 2 HU 2ntu 2 HU '611.11..2 fw (na'1(141.1)
Vil1AUV1Ilt4il'A@f1551111@lf1410111141V1 (01a1lklinf111 1 4i@l1/191)
Vill1h5-166n-II 13 ffu 11.1001@iti5vinilivTui 1 FIU E-mail 1 flu Facebook 1 mu
Vi'un-luilvinywdpn 11 HU 5t1J...111^[email protected] 71111/Trrw.1f1 / nq;uifunam.1
tiltigru 10 9 8 7 6 5
d1Uiti1: n15@infrlotulEnEi
1. mum-111.unfn5TinTounrniuSq, Vnliviquilm-a4 8 flu 12 Hu 6 Hu 1 Hu 0 0
LitiliailiLritrViu Lmt@iitti Sitillo (30%) (44%) (22%) (4%)
2. iii51.1qau@NT-regtwrilLMEdoilliEn IfinlilfinuFwrin 4 HU 8 Hu 10 HU 2 HU 0 3 P11.1
LaLtofIvitn MI..115t111111MIALIAU11,91 (15%) (30%) (37%) (7%) (11%)
3. friTtilviu@Nalnuu-Toin5unnVgauzIluutmol 5 Fltd 8 HU 7 AU 6"114 0 0
Table clinic Loa: Poster ViiiviluLifrawri5t4.7n (20%) (32%) (28%) (25%)
Lau@tiquvioolgi vi1t111H
4. n151,1`miu@NNqu'-gULtatUiVin57/AlnlYitnn5gi 5 Hu 7 Hu 11 Hu 3 flu 0 0
115t01f115111 ILM,17/11_111/11.111.1P1112157M'Ard'AiVilld
fiEl'[email protected]/1553J M@ ?ii'lllnu
l'uitati.45'vm5m,m.dailvimvroiluviLirmumlovli
(19%) (27%) (42%) (12%)
Liu' ul'il
dqUi12: fl-l'HI.15:1%6p1148:11f1114etii.0
1. a- '1116141.11t01111@[email protected]/115.N11.155E.11E1 17 Hu 7 EU 3 Hu 0 0 0
(62%) (27%) (12%)
2. EITILLViLltn1101/1151E1`11,111,1,?1E1NallU 10 HU 8 Hu 7 E11.1 2 HU 0 0
u-TvinuLiwz-WEJ (41%) (33%) (26%) (11%)
3. fl' luiilm@IVI,unTwymialn-I5ooTvin5tor,onviwill 11 Hu 8 Hu 7 8U 1 8u 0 0
(41%) (30%) (26%) (4%)
4. FlNflJ1velv-Turn5ouTulullul.h.twIt-inq 14 Hu 7 HU 5 au 1 mu 0 0
(52%) (26%) (19%) (4%)
fokin@inqmountmougrai 27 Aid

miaJholitAui
1. 1R-aiociwraAtin-15115tvif15l@1,11 Vidlcilviquhln151inCgmonnfrilLaLtoilviugl in61unna,11
- Veneer, Crown lengthening, Implant
2. iiELOU@Laga,'LfiLL'h,
LiAnaa&I imtoi @valarilisUultivinknfanutiuv,ino-rin Umen0; Liat
nhAl ut annit
- tau rin5
MpiTy LoNnOfguiiti-miSivIoVi T,gil@U1P1VIRTIJ
Kaen of,,Social.'Devotion
th \\ The 4 Internation LDRG-KKU & Saraburi Hospital Symposium 2014 On
"Lasers in Dentistry: Research Transferring to Practice"
31 July - 1 August 2014
The Greenery Resort Khao Yai, Thailand
The 4. International LDRG - IIXU & Sarabini
Hospital Symposium 2014
P1 : Microleakage of self-etch adhesive system in Class V cavities
etched by Er:YAG laser with different pulse modes.
Pijitta Chimtim°1, Thitirat HeebthamaP, Jutipond Phanombualert2
Abstract
The purpose of this study was to evaluate the effects of Er:YAG laser irradiation and diamond
bur on root cementum in Class V restored with self-etch adhesive. Sixty extracted human premolars
were prepared from extracted human periodontally-diseased teeth. All teeth were randomly distributed
into four groups (N = 15). Standard Class V cavities margins were below the cementoenamel junction
on the buccal surface by diamond bur. Group 1; diamond bur, Group 2; Er:YAG laser etching with
50 mJ/pulse/sec at 15 Hz, Group 3; 75 mJ/pulse/sec at 15 Hz and Group 4; 100 mJ/pulse/sec at 15
Hz under water irrigation. Then, all cavities were restored with AdperTM Prompt." L-Pop" self-etch
adhesive (3M/ESPE) and restoration with composite resin Eiltek Tm Z350 XT (3M/ESPE). After thermo-
cycled and immersed in 0.2% methylene blue dye. Microleakage was evaluated by stereomicroscope
and analysis with NIS-Elements program
Data were analyzed by one-way ANOVA, Krukall-Wallis tests. Statistically differences were
found between groups (p < 0.05) and cavities treated with the Er:YAG laser presented less microleakage
than dental diamond bur.
Keywords: Er:YAG; Cementum; Microleakage; Self-etch bonding
Introduction
Lasers Er:YAG (Erbium:Yttrium Aluminum Garnet) 2.94 p.m wavelength emission coincides with the main
absorption peaks of water and hydroxyapatite. This device is FDA approved and experienced significant testing involving
all five Classes of cavity preparation on both children and adults. Laboratory research Laboratory research and clinical
trials have demonstrated the ability of Er:YAG laser to ablate enamel, dentin and cementum dental tissue effectively,
with the minimum of injury to pulp and surrounding structures (Corona A, et al., 2003). The energy of Er:YAG
laser-treated cementum, previous studies have demonstrated completely transformed into an ablation effect with the
minimal possible thermal effect to surrounding tissue (Teerakapong A, et al., 2007). The trend for alternatives to the
conventional method of preparation led to focus on Er:YAG laser device within the modern "less is more" treatment
strategies. Thus, the aim of this study was to investigate the microleakage and scanning electron microscopy (SEM)
evaluation of class V cavities prepared by Er:YAG laser or high-speed handpiece, using all-in-one self-etch adhesives
and respective manufacturer's nanocomposites resin.
Sixth year dental student, Faculty of Dentistry, Khon Kaen University, Khon Kaen Thailand
2 Lecturer, Department of Periodontology, Faculty of Dentistry, Khon Kaen University, Khon Kaen, Thailand
Correspondence author
Jutipond Phanombualert D.D.S., MSc.
Department of Hospital dentistry, Faculty of Dentistry, Khon Kaen University, Khon Kaen, 40002, Thailand
Tel: 043-348152
21
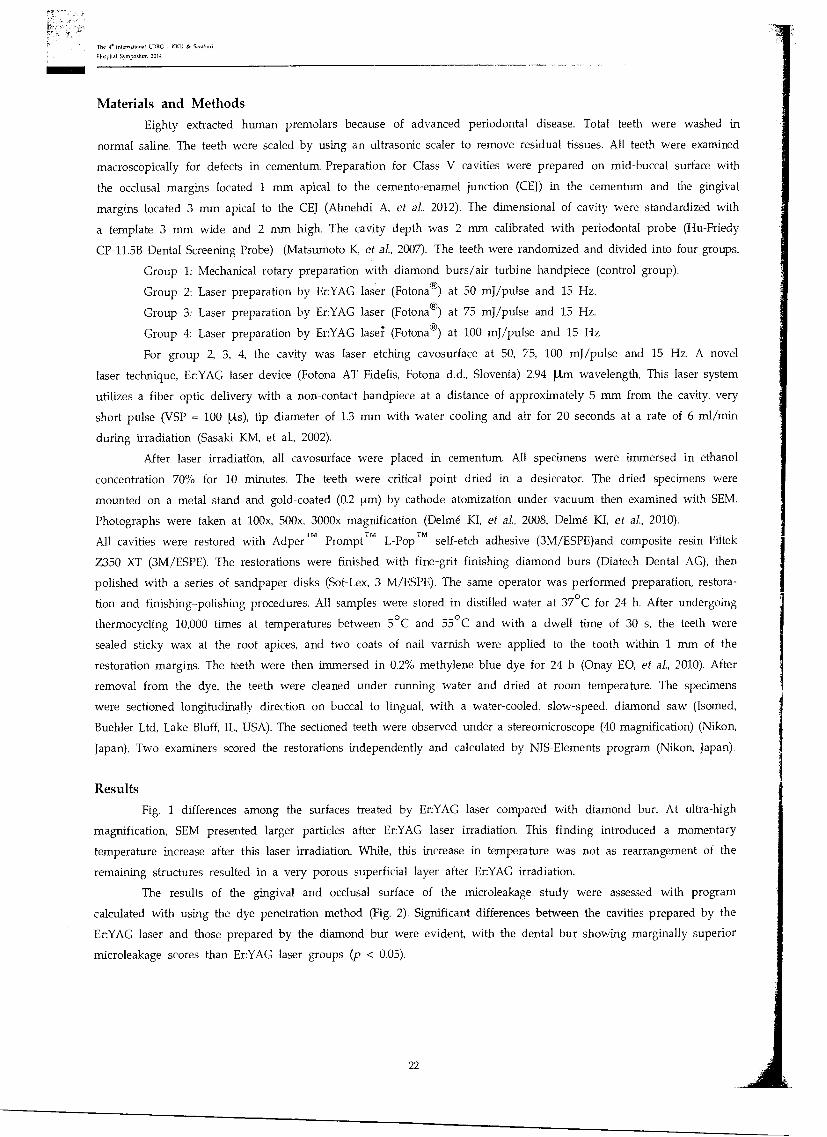
The 4. International LIDRG - Sarabori
Hospital Symposium 2014
Materials and Methods
Eighty extracted human premolars because of advanced periodontal disease. Total teeth were washed in
normal saline. The teeth were scaled by using an ultrasonic scaler to remove residual tissues. All teeth were examined
macroscopically for defects in cementum. Preparation for Class V cavities were prepared on mid-buccal surface with
the occlusal margins located 1 mm apical to the cemento-enamel junction (CEJ) in the cementum and the gingival
margins located 3 mm apical to the CEJ (Almehdi A, et al., 2012). The dimensional of cavity were standardized with
a template 3 mm wide and 2 mm high. The cavity depth was 2 mm calibrated with periodontal probe (Hu-Friedy
CP-11.5B Dental Screening Probe) (Matsumoto K, et al., 2007). The teeth were randomized and divided into four groups.
Group 1: Mechanical rotary preparation with diamond burs/air turbine handpiece (control group).
Group 2: Laser preparation by Er:YAG laser (Fotona®) at 50 mJ/pulse and 15 Hz.
Group 3: Laser preparation by Er:YAG laser (Fotona®) at 75 mJ/pulse and 15 Hz.
Group 4: Laser preparation by Er:YAG lase; (Fotona®) at 100 mJ/pulse and 15 Hz
For group 2, 3, 4, the cavity was laser etching cavosurface at 50, 75, 100 mJ/pulse and 15 Hz. A novel
laser technique, Er:YAG laser device (Fotona AT Fidelis, Fotona d.d., Slovenia) 2.94 [Lim wavelength, This laser system
utilizes a fiber optic delivery with a non-contact handpiece at a distance of approximately 5 mm from the cavity, very
short pulse (VSP = 100 ..ts), tip diameter of 1.3 mm with water cooling and air for 20 seconds at a rate of 6 ml/min
during irradiation (Sasaki KM, et al., 2002).
After laser irradiation, all cavosurface were placed in cementum. All specimens were immersed in ethanol
concentration 70% for 10 minutes. The teeth were critical point dried in a desiccator. The dried specimens were
mounted on a metal stand and gold-coated (0.2 um) by cathode atomization under vacuum then examined with SEM.
Photographs were taken at 100x, 500x, 3000x magnification (Delme KI, et al., 2008, Delme KI, et a]., 2010).
All cavities were restored with Adper TM Prompt TM L-Pop TM self-etch adhesive (3M/ESPE)and composite resin Filtek
Z350 XT (3M/ESPE). The restorations were finished with fine-grit finishing diamond burs (Diatech Dental AG), then
polished with a series of sandpaper disks (Sof-Lex, 3 M/ESPE). The same operator was performed preparation, restora-
tion and finishing-polishing procedures. All samples were stored in distilled water at 37°C for 24 h. After undergoing
thermocycling 10,000 times at temperatures between 5°C and 55°C and with a dwell time of 30 s, the teeth were
sealed sticky wax at the root apices, and two coats of nail varnish were applied to the tooth within 1 mm of the
restoration margins. The teeth were then immersed in 0.2% methylene blue dye for 24 h (Onay EO, et al., 2010). After
removal from the dye, the teeth were cleaned under running water and dried at room temperature. The specimens
were sectioned longitudinally direction on buccal to lingual, with a water-cooled, slow-speed, diamond saw (Isomed,
Buehler Ltd, Lake Bluff, IL, USA). The sectioned teeth were observed under a stereomicroscope (40 magnification) (Nikon,
Japan). Two examiners scored the restorations independently and calculated by NIS-Elements program (Nikon, Japan).
Results
Fig. 1 differences among the surfaces treated by Er:YAG laser compared with diamond bur. At ultra-high
magnification, SEM presented larger particles after Er:YAG laser irradiation. This finding introduced a momentary
temperature increase after this laser irradiation. While, this increase in temperature was not as rearrangement of the
remaining structures resulted in a very porous superficial layer after Er:YAG irradiation.
The results of the gingival and occlusal surface of the microleakage study were assessed with program
calculated with using the dye penetration method (Fig. 2). Significant differences between the cavities prepared by the
Er:YAG laser and those prepared by the diamond bur were evident, with the dental bur showing marginally superior
microleakage scores than Er:YAG laser groups (p < 0.05).
22
The e Intemattonal LDRG - KKU & Sambuci
Hosp.] Symposium 2014
Figure 1 SEM image of representative Er:YAG laser-etching cavity
23
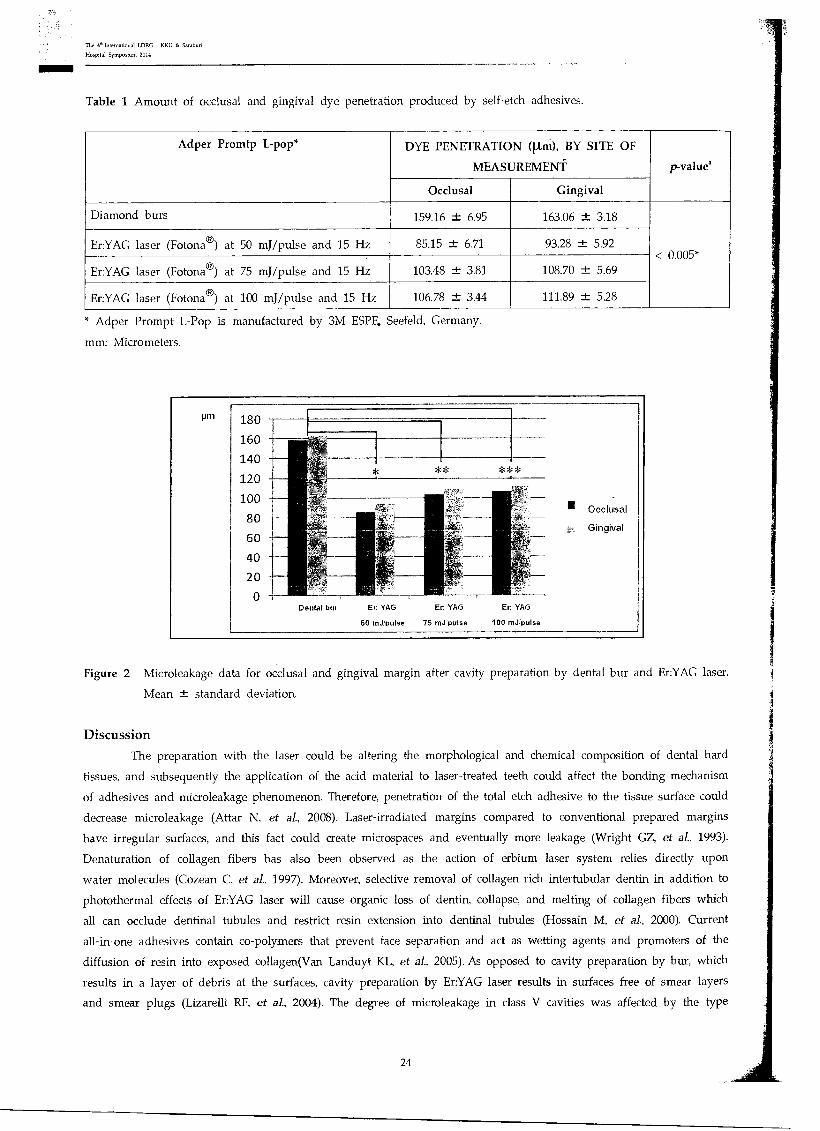
The 4" International LDRG KU & Saraburi
Hospital Symposium 2014
Table 1 Amount of occlusal and gingival dye penetration produced by self-etch adhesives.
Adper Promtp L-pop* DYE PENETRATION Wart), BY SITE OF
MEASUREMENT p-value
Occlusal Gingival
Diamond burs 159.16 -1- 6.95 163.06 ±.- 3.18
< 0.005* Er:YAG laser (Fotona®) at 50 mJ/pulse and 15 Hz 85.15 ± 6.71 93.28 1 5.92
Er:YAG laser (Fotona®) at 75 mJ/pulse and 15 Hz 103.48 -1- 3.81 108.70 -1- 5.69
Er:YAG laser (Fotona®) at 100 mJ/pulse and 15 Hz 106.78 ± 3.44 111.89 ± 5.28
Adper Prompt L-Pop is manufactured by 3M ESPE. Seefeld, Germany.
mm: Micrometers.
pm 180
160
140
120
100
80
60
40
20
*=k
* ***
III Occlusal ., .. Gingival
.----
Dental burbur Er: YAG Er. YAG Er YAG
50 mJ•pulse 75 mJ pulse 100 mJ pulse
Figure 2 Microleakage data for occlusal and gingival margin after cavity preparation by dental bur and Er:YAG laser.
Mean standard deviation.
Discussion
The preparation with the laser could be altering the morphological and chemical composition of dental hard
tissues, and subsequently the application of the acid material to laser-treated teeth could affect the bonding mechanism
of adhesives and microleakage phenomenon. Therefore, penetration of the total etch adhesive to the tissue surface could
decrease microleakage (Attar N, et al., 2008). Laser-irradiated margins compared to conventional prepared margins
have irregular surfaces, and this fact could create microspaces and eventually more leakage (Wright GZ, et al., 1993).
Denaturation of collagen fibers has also been observed as the action of erbium laser system relies directly upon
water molecules (Cozean C, et al., 1997). Moreover, selective removal of collagen rich intertubular dentin in addition to
photothermal effects of Er:YAG laser will cause organic loss of dentin, collapse, and melting of collagen fibers which
all can occlude dentinal tubules and restrict resin extension into dentinal tubules (Hossain M, et al., 2000). Current
all-in-one adhesives contain co-polymers that prevent face separation and act as wetting agents and promoters of the
diffusion of resin into exposed collagen(Van Landuyt KL, et a]., 2005). As opposed to cavity preparation by bur, which
results in a layer of debris at the surfaces, cavity preparation by Er:YAG laser results in surfaces free of smear layers
and smear plugs (Lizarelli RF, et al., 2004). The degree of microleakage in class V cavities was affected by the type
24
The 4- International IDRG - KKU & Saraburi
Hospital Symposium 2014
of adhesive restorative materials, type of self-etching adhesive, cavity margin location, and tooth preparation method
either by Er:YAG laser or dental bur. Pashley and Tay (Pashley DH and Tay FR, 2001) reported that self-etch dental
adhesives differed in their aggressiveness. Therefore, they are classified into three categories, according to acidity: mild,
moderate and aggressive. Self-etch adhesive whose pH is lower than 1.5 are called aggressive self-etch adhesives. On
the other hand, self-etch adhesives which have a pH higher than 1.5 are categorized as mild or moderate. The self-etch
adhesives were used in this study, the pHs of AdperTM
Prompt TM L-Pop TM were pH = 0.5.
The reason for this finding could be single step application of this bonding system which will reduce its
technique sensitivity. The primer of this bonding agent has a lower pH than 1.5 and is considered aggressive acidic
primer. This primer could create surface demineralization to a depth of 1 NM which creates a surface for micromechanical
retention (Van Meerbeek B, et al., 2003). In addition, more acidic pH of Adper TM Prompt TM L-Pop TM may cause more
micromechanical retention and a thicker hybrid layer in dentin and thus, compensating the adverse morphologic effect
of laser irradiation. However, the least amount of gingival and occlusal microleakage for the laser-prepared teeth was
found with composite restoration.
Conclusion
To summarize, this study demonstrated that cementum and root dentin presented micro-irregularities after
Er:YAG laser irradiation. However, the performance of the Er:YAG laser for Class V cavity preparation was showed
less microleakage when compared with the diamond bur.
Acknowledgement
Assoc. Prof. Dr. Sajee Satayut, all staffs in LDRG-KKU and Faculty of Dentistry, Khon Kaen University.
Reference
Almehdi A, Aoki A, Ichinose S, Taniguchi Y, Sasaki KM et al. Histological and SEM analysis of root cementum
following irradiation with Er:YAG and CO2 lasers. Lasers Med Sci 2012;22(4):342-50
Attar N, Korkmaz Y, Ozel E, Bicer OC, Firatli E. Microleakage of class V cavities with different adhesive systems
prepared by a diamond instrument and different parameters of Er:YAG laser irradiation. Photomed Laser Surg
2008;26:585-91.
Corona A, Borsatto C, Pecora D, Rocha De SA, RA RS, Palma-Dibb G. Assessing microleakage of different class V
Juntavee N. Laser in dentistry: Academic and practical points of view. 2011 Annual Meeting Proceeding. The 1st
Delme KI, Deman PJ, De Bruyne MA, Nammour S, De Moor RJ. Microleakage of glass ionomer formulations after
Hossain M, Nakamura Y, Kimura Y, Yamada Y, Ito M, Matsumuto K. Caries preventive effect of Er:YAG laser
Lizarelli RF, Silva PC, Neto ST, Bagnato VS. Study of microleakage at class V cavities prepared by Er:YAG laser using
Matsumoto K, Wang X, Zhang C, Kinoshita J. Effect of a novel Er:YAG laser in caries removal and cavity preparation:
Cowan C, Arcoria CJ, Pelagalli J, Powel GL. Dentistry for the 21st century? Erbium:YAG laser for teeth. J Am Dent
Delme KI, Deman PJ, De Bruyne MA, De Moor RJ. Microleakage of four different restorative glass ionomer formula-
tions 1997:128:1080-7.
tions in class V cavities: Er:YAG laser versus conventional preparation. Photomed Laser Surg 2008;26(6):541-9.
erbium:yttrium-aluminium-garnet laser preparation. Lasers Med Sci 2010;25(2):171-80.
irradiation with or without water mist. J Clin Laser Med Surg 2000;18:61-5.
restorations after Er:YAG laser and bur preparation. J Oral Rehabil 2003;30:1008-14.
International LDRG-KKU Symposium on "Laser in Dentistry: Research and Novel Techniques" 2011;1:49-61.
rewetting surface treatment. J Clin Laser Med Surg 2004;22:51-5.
a clinical observation. Photo Med Laser Surg 2007;25(1):8-13.
25
The 4- International LDRG • KIN & Saraburi
Hospital Symposium 2014
Onay EO, Orucoglu H, Kiremitci A, Korkmaz Y, Berk G. Effect of Er,CrYSGG laser irradiation on the apical sealing
ability of AH Plus/gutta-percha and Hybrid Root Seal/Resilon Combinations. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod 2010;110(5):657-64.
Pashley DH, Tay FR. Aggressiveness of contemporary self-etching adhesives. Part II: etching effects on unground enamel.
Dent Mater 2001;17:430-44.
Sattayut S. Principle of laser in Dentistry. Khon Kaen Dental Journal 2003;6(2):89-95
Sasaki KM, Aoki A, Ichinose S, Ishikawa I. Morphological analysis of cementum and root dentin after Er:YAG laser
irradiation. Lasers Surg Med 2002;31(2):79-85.
Teerakapong A, Chuercharuenwasuchi N, Senarasana P, Chaowaratana S, Weera-archakul W. The comparison of
morphologic of periodontitis involved root surfaces after radiated in vitro with Er:YAG and ER,Cr:YSGG lasers.
Khon Kaen Dental Journal 2007;10(2):80-90.
Van Landuyt KL, De Munck J, Snauwaert J et al Monomer-solvent phase separation in one step self-etch adhesives.
J Dent Res 2005;84:183-8.
Van Meerbeek B, De Munck J, Yoshida Y, et al. Buonocore memorial lecture. Adhesion to enamel and dentin: current
status and future challenges. Oper Dent 2003;28:215-35
Wright GZ, McConnell RJ, Keller U. Microleakage of Class V composite restorations prepared conventionally with those
prepared with an Er:YAG laser a pilot study. Pediatr Dent 1993;15:425-6.
26
on t ae *ears of Social
I-2.4vaulviogr-st-.43
th The 4 InternatiOn 1 LDRG-KKU & Saraburi Hospital Symposium 2014 On
"Lasers in Dentistry: Research Transferring to Practice"
31 July - 1 August 2014
The Greenery Resort Khao Yai, Thailand
The e International LDRG - KKU & Saraburi
Hmipital Symposium 2014
P2 : Alternative therapy for oral lichen planus with low intensity laser
therapy and red light laser : A case report
Wilairat Sarideechaigul'and Sajee Sattayut2
Abstract
Oral lichen planus is a chronic inflammatory oral mucosal disease, which affects oral mucosa,
skin, or other mucous membrane. Erosive, atrophic, ulcerative lesions require long-term treatment,
because of inflammation and severe pain. This is a case report of a 52-year-old female who presented
to a dentist with chief complaints of chronic ulceration and burning sensation of the lip for 5 years.
The patient had generalized erosion with white streaks and hemorrhagic crusting on the lower lip.
The laboratory investigation includes a biopsy from vermillion of the lower lip which was examined
by an oral pathologist. This case was diagnosed with lichen planus of the lip. The patient was treated
by a topical steroid, which was 0.1% fluocinolone acetonide in orabase, applying locally 4 times/day.
The OLP's patient has not been healed. The low intensity laser therapy and red light laser have been
introduced as an alternative treatment. After 6 months with 10 sessions of the treatment with lasers,
the patient's oral lesion has been improved and decreased burning sensation. As the results, the OLP
in this patient has been improved, but the lesion has not cured.
Keywords: Low intensity laser therapy; Red light laser; Oral lichen planus
Introductions
Oral lichen planus (OLP) is a chronic inflammatory oral mucosal disease, which affects oral mucosa, skin, or
other mucous membrane. The pathogenesis of OLP involving T-cells mediated disorder which the trigger factors and the
pathologic mechanism of the immune responses remain unknown (Lodi G, et al., 2005). Atrophic and erosive lesions are
severe and painful form of OLP, which are typically experience significant discomfort. The management of OLP varies
considerably between patients, and for individual patients, due to fluctuations in the disease activity (Setterfield JF, et
al., 2000, Thongprasom K, et al., 2003). Various modalities for treatment have been presented to relieve the symptoms.
These include both topical and systemic steroids, tacrolimus, systemic and topical retinoids, calcineurin inhibitors and
phototherapy (Thongprasom K, et al., 2011). However, OLP patients relapse when treatment is discontinued or resistant
to these treatments. Recently, alternative low intensity laser therapy (LILT) has been used as a treatment of OLP(Passeron
T, et al., 2004, Trehan M and Taylor CR, 2004, Miner K, et al., 2003, Mandavi 0, et al, 2013). Laser biostimulation
can obtain different intracellular biological reactions to stimulate regenerative abilities, without undesired adverse effects,
reducing also the pharmacological support and its possible invasiveness (Cafaro A, et al., 2014). The purpose of this
case report was to evaluate the effect of laser therapy in the treatment of OLP.
'Lecturer, Department of Oral Diagnosis. Faculty of Dentistry, Khon Kaen University, Thailand
2Associated Professor Dr, Lasers in Dentistry Research Group and Department of Oral Surgery, Faculty of Dentistry, Khon Kaen University,
Thailand
Correspondence author
Wilairat Sarideechaigul, D.D.S., MSc.
Department of Oral Diagnosis, Faculty of Dentistry, Khon Kaen University, Khon Kaen, 40002, Thailand.
E-mail: arindent17@hotmailcom
Tel: 043-202405
27
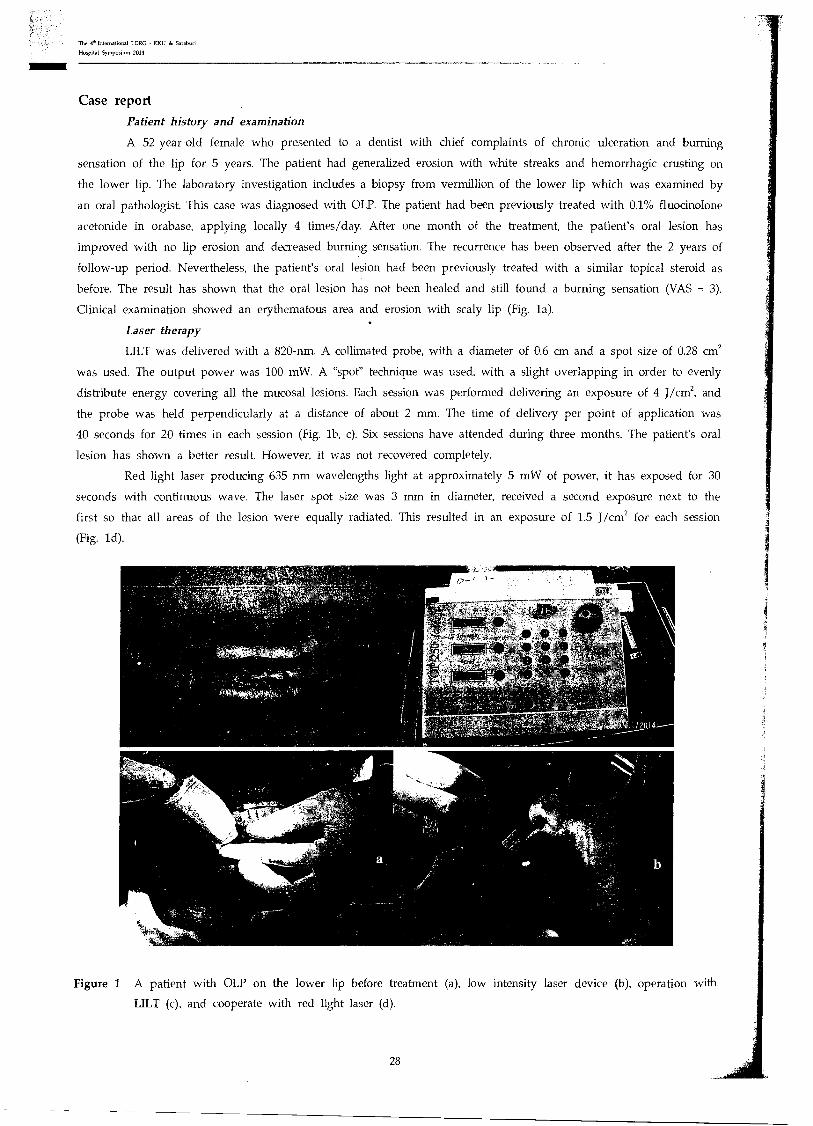
The 4^ International LORG - & Saraburi
Hospital Symposium 2019
Case report
Patient history and examination
A 52-year-old female who presented to a dentist with chief complaints of chronic ulceration and burning
sensation of the lip for 5 years. The patient had generalized erosion with white streaks and hemorrhagic crusting on
the lower lip. The laboratory investigation includes a biopsy from vermillion of the lower lip which was examined by
an oral pathologist. This case was diagnosed with OLP. The patient had been previously treated with 0.1% fluocinolone
acetonide in orabase, applying locally 4 times/day. After one month of the treatment, the patient's oral lesion has
improved with no lip erosion and decreased burning sensation. The recurrence has been observed after the 2 years of
follow-up period. Nevertheless, the patient's oral lesion had been previously treated with a similar topical steroid as
before. The result has shown that the oral lesion has not been healed and still found a burning sensation (VAS = 3).
Clinical examination showed an erythematous area and erosion with scaly lip (Fig. la).
Laser therapy
LILT was delivered with a 820-nm. A collimated probe, with a diameter of 0.6 cm and a spot size of 0.28 cm2
was used. The output power was 100 mW. A "spot" technique was used, with a slight overlapping in order to evenly
distribute energy covering all the mucosal lesions. Each session was performed delivering an exposure of 4 J/cm2, and
the probe was held perpendicularly at a distance of about 2 mm. The time of delivery per point of application was
40 seconds for 20 times in each session (Fig. lb, c). Six sessions have attended during three months. The patient's oral
lesion has shown a better result. However, it was not recovered completely.
Red light laser producing 635 nm wavelengths light at approximately 5 mW of power, it has exposed for 30
seconds with continuous wave. The laser spot size was 3 mm in diameter, received a second exposure next to the
first so that all areas of the lesion were equally radiated. This resulted in an exposure of 1.5 J/cm2 for each session
(Fig. 1d).
Figure 1 A patient with OLP on the lower lip before treatment (a), low intensity laser device (b), operation with
LILT (c), and cooperate with red light laser (d).
28
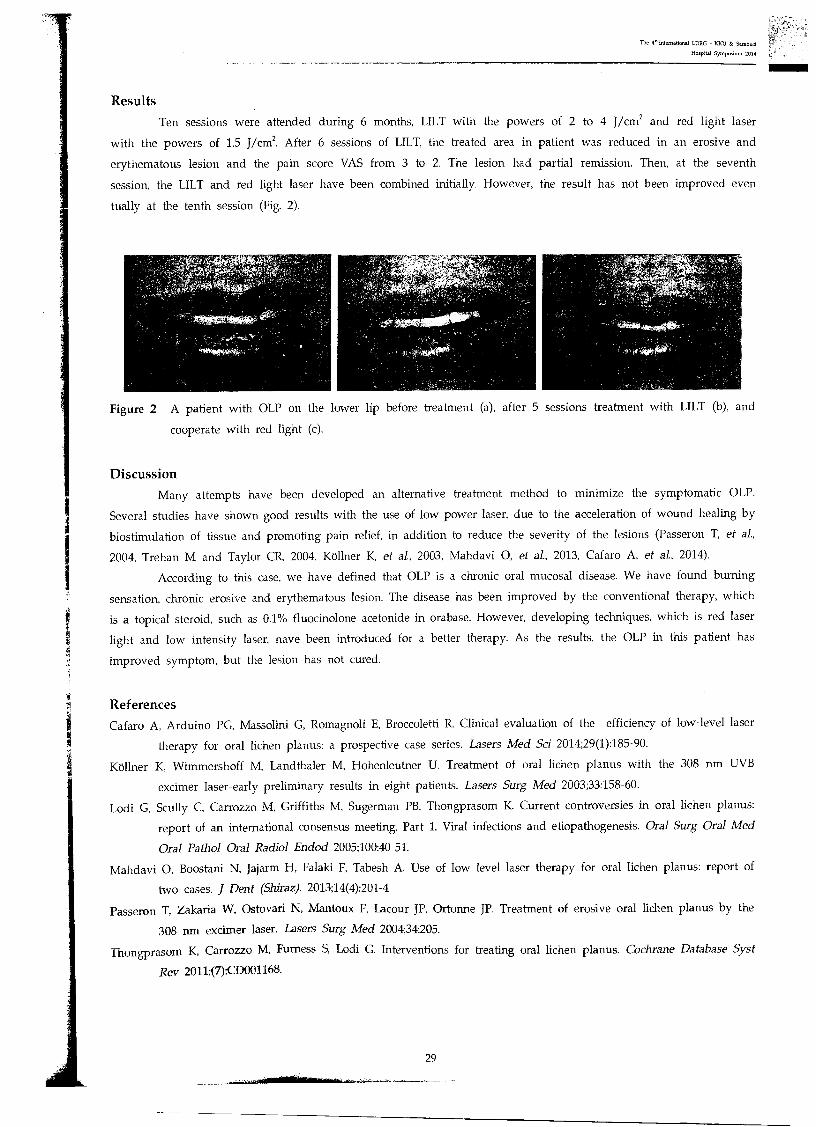
The 4" International LDRG - KKU & Saraburi
Hospital Symposium 2014
Results
Ten sessions were attended during 6 months, LILT with the powers of 2 to 4 J/cm2 and red light laser
with the powers of 1.5 J/cm2. After 6 sessions of LILT, the treated area in patient was reduced in an erosive and
erythematous lesion and the pain score VAS from 3 to 2. The lesion had partial remission. Then, at the seventh
session, the LILT and red light laser have been combined initially. However, the result has not been improved even
tually at the tenth session (Fig. 2).
Figure 2 A patient with OLP on the lower lip before treatment (a), after 5 sessions treatment with LILT (b), and
cooperate with red light (c).
Discussion Many attempts have been developed an alternative treatment method to minimize the symptomatic OLP.
Several studies have shown good results with the use of low power laser, due to the acceleration of wound healing by
biostimulation of tissue and promoting pain relief, in addition to reduce the severity of the lesions (Passeron T, et al.,
2004, Trehan M and Taylor CR, 2004, Kollner K, et al., 2003, Mandavi 0, et al, 2013, Cafaro A, et al., 2014).
According to this case, we have defined that OLP is a chronic oral mucosal disease. We have found burning
sensation, chronic erosive and erythematous lesion. The disease has been improved by the conventional therapy, which
is a topical steroid, such as 0.1% fluocinolone acetonide in orabase. However, developing techniques, which is red laser
light and low intensity laser, have been introduced for a better therapy. As the results, the OLP in this patient has
improved symptom, but the lesion has not cured.
References Cafaro A, Arduino PG, Massolini G, Romagnoli E, Broccoletti R. Clinical evaluation of the efficiency of low-level laser
therapy for oral lichen planus: a prospective case series. Lasers Med Sci 2014;29(1):185-90.
Koliner K, Wimmershoff M, Landthaler M, Hohenleutner U. Treatment of oral lichen planus with the 308 nm UVB
excimer laser-early preliminary results in eight patients. Lasers Surg Med 2003;33:158-60.
Lodi G, Scully C, Carrozzo M, Griffiths M, Sugerman PB, Thongprasom K. Current controversies in oral lichen planus:
report of an international consensus meeting. Part 1. Viral infections and etiopathogenesis. Oral Surg Oral Med
Oral Pathol Oral Radio] Endod 2005;100:40-51.
Mandavi 0, Boostani N, Jajarm H, Falaki F, Tabesh A. Use of low level laser therapy for oral lichen planus: report of
two cases. J Dent (Shiraz). 2013;14(4):201-4
Passeron T, Zakaria W, Ostovari N, Mantoux F, Lacour JP, Ortonne JP. Treatment of erosive oral lichen planus by the
308 nm excimer laser. Lasers Surg Med 2004;34:205.
Thongprasom K, Carrozzo M, Furness S, Lodi G. Interventions for treating oral lichen planus. Cochrane Database Syst
Rev 2011;(7):CD001168.
29
The 4° International LDRG KKU 0e Saraburi
Hospital Symposium 2014
Thongprasom K, Luengvisut P, Wongwatanakij A, Boonjatturus C. Clinical evaluation in treatment of oral lichen planus
with topical fluocinolone acetonide: a 2-year follow-up. J Oral Pathol Med 2003;32:315-22.
Trehan M, Taylor CR. Low-dose excimer 308-nm laser for the treatment of oral lichen planus. Arch Dermatol 2004;140:415-
20.
Setterfield JF, Black MM, Challacombe SJ. The management of oral lichen planus. Clin Exp Dermatol 2000;25:176-82.
30
Years of Social Devotio
in The 4 Interna ton ► LDRG-KKU & Saraburi Hospital Symposium 2014 On
"Lasers in Dentistry: Research Transferring to Practice"
31 July - 1 August 2014 The Greenery Resort Khao Yai Thailand

The 4-International LDRG KKU & Samburi
Hospital Symposium 2014
P3 : Effect of blue light and hydrogen peroxide on
Porphyromonas gingivalis in biofilm
Benyawan Uea-aranchotl, Chutamas Rakkhansaene, Ubonwan Tapsun
Angkhana Sangpanya2, Aroon Teerakapong3
Abstract
The phototoxic effect of blue light was found to involve the induction of reactive oxygen
species (ROS) production by the gram negative periodontal pathogens. This may result in significant
damage to cell structure of bacteria without the application of exogenous photosensitizer molecules.
Therefore, the purpose of this study was to compare between the antibacterial effect of blue light and
a combination of blue light and hydrogen peroxide on Porphyromonas gingivalis in biofilm culture.
This study was classified into 4 groups, the first group of biofilms were exposed to blue light at
wavelength of 405 nm. The distance between the light source tip and the exposed each sample was set
at 80 cm. in order to obtain a constant power dentistry of 50 mW/cm2 . The second group of biofilms
were exposed to 1% H202 without light exposure and the third group of biofilms were exposed to blue
light in the present of 1% H202. Control groups consisted of sample undergoing the same procedure
without blue light and 1% H2O. After light exposure the bacteria killing rates were calculated from
colony forming unit (CFU) count at 1, 3, 6 hours suspectively. The bacterial growth was decreasing
continuously. It tend to decrease from 1 hour after light exposure to 6 hours and dropped below the
control group. The results showed that the bacteriostatic process need to take time for reaction. The
hydrogen peroxide group and the combination of blue light and hydrogen peroxide on killing bacteria
should be discussed. We found that blue light at wavelength of 405 nm could be used for bacterial
eradication without the addition of exogenous photosensitizer.
Keywords: Blue light; Hyrogen peroxide; Porphyromonas gingivalis; Reaction oxygen species
Acknowledgement:
Laser in Dentistry Research Group (LDRG): Khon Kaen University
'Fifth year dental student, Faculty of Dentistry, Khon Kaen University, Khon Kaen, Thailand
'Lecturer, Department of Periodontology, Faculty of Dentistry, Khon Kaen University, Khon Kaen, Thailand
'Associate Professor, Department of Periodontology, Faculty of Dentistry, Khon Kaen University, Khon Kaen, Thailand
Correspondence author
Angkhana Sangpanya, D.D.S.
Department of Periodontology, Faculty of Dentistry, IThon Kaen University, Khon Kaen, 40002, Thailand.
Tel: 043-202405
31
The 4' International LDRG • KKU & Sarabun
Hospital Symposium 2014
References :
Fukui M, Yoshioka M, Satomura K, Nakanishi H, Nagayama M. Specific-wavelength visible light irradiation inhibits
bacterial growth of Porphyromonas gingivalis. I Perio Res 2008;43(2):174-8.
Sterer N, Feuerstein 0. Effect of visible light on malodour production by mixed oral microflora. I Med Microbiol 2005;
54(Pt 12):1225-9
Steinberg D, Moreinos D, Featherstone J, Shemesh M, Feuerstein 0. Genetic and physiological effects of noncoherent
visible light combined with hydrogen peroxide on Streptococcus mutans in biofilm. Antimicrob Agents Che
mother 2008;52(7):2626-31
32
Kaen Social Oevotion
th \\ The 4 Internatfon LDRG-KKU & Saraburi Hospital Symposium 2014 On
"Lasers in Dentistry: Research Transferring to Practice"
31 July - 1 August 2014
The Greenery Resort Khao Yai, Thailand

Abstract
Laser technology is an essential tool for innovative dental practitioners wishing to treat their
patients in a modern and effective manner. The specific properties of lasers enable new treatments
and operating methods to be employed, as well as complementing and supporting existing therapeutic
methods. Objective of this study: to be explored attitude of dental student for Lasers in Dentistry
course. This study is retrospective study of Basic Laser Therapy in Dentistry: Transferring Research
to Practice Continuing Education Course 2013 - 2014 B.C. 77 Dental students replied about Laser in
Dentistry course from the questionnaire. The results showed that 35 dental students (45.45%) have got
practice during laser in dentistry laser course, 42 dental students (54.54%) haven't got practice about
laser in dentistry. All of dental student were practiced and learned Laser in Dentistry course, from 45
subject (58.44%) replied about attitude of Laser in Dentistry that they were understand to principles
of laser in dentistry and they can use the application of laser systems, For confidence to use laser
application in dentistry from 15 subjects (19.48%). The proposed to apply Laser in Dentistry course
from 17 subjects (22.07%) More dentists will likely begin using Laser in Dentistry as time goes on. It
is likely that they will begin using the lasers with common, simple procedures first before using the
lasers on more complicated types of treatments. Lasers in Dentistry, has been developed in order to
enable dentists to specialize in the full range of dental laser therapies. Building upon a first higher
education degree in dentistry. The laser course enables practicing dentist student to specialize in dental
laser applications by providing both theoretical and practical training. Because of the simplicity, swift-
ness, and effectiveness of laser dentistry, it truly is the dentistry of the future.
Keywords: Laser in Dentistry; Experience
Pongsathorn Touchpramuk
The e International LDRG - 1CKU & Sanburi
Hospital Symposium 2014
P4 : The study of dental student experience to Laser in Dentistry
Faculty of Veterinary Sciences, Mahasarakham University, Mahasarakham, 44000, Thailand
Correspondence author
Pongsathorn Touchpramuk, D.VM, Dip. Small animal practice, MSc.
Department of Veterinary Clinic, Faculty of Veterinary Sciences, Mahasarakham University
Talat Subdistrict Amphur Mueang Mahasarakham, 44000, Thailand.
Email- golf vet@outlookcom
Tel: 043-742823 ext. 6182
Mobile 089-4494480
33
I-54vms-ru-rancr-svall
th The 4 Interns onLDRG-KKU & Saraburi Hospital Symposium 2014 On
"Lasers in Dentistry: Research Transferring to Practice"
31 July - 1 August 2014 The Greenery Resort Khao Yail Thailand
The 46 International LDRC - KKU & Saraburi
Hospital Symposium 2014
115 : Efficacy of erythrosine and anthocyanin mediated photodynamic
therapy on Porphyromonas gingivalis biofilms using green light in vitro.
Surada Tantananugoor Aroon Teerakapong2, Sajee Sattayut3, Teerasak Damrongrungruang4
Abstract
Photodynamic therapy has been advocated as an alternative to antimicrobial agents to suppress
subgingival species and to treat periodontitis. The purpose of this in vitro study was to evaluate
efficacy of erythrosine and anthocyanin (cyanidin) as photosensitizers in photodynamic therapy (PDT)
on killing of the P. gingivalis biofilms. To evaluate the photogenerated reactive oxygen species using
electron spin resonance (ESR) technique. Dental plaque samples were obtained from a subject with
chronic periodontitis and prepared for P. gingivalis biofilms. P. gingivalis biofilms were mixed with a
variety of photosensitizers as follows:- erythrosine 110, 220, 330, 440 flM and anthocyanin (cyanidin)
101, 202, 303, 404 1.1M and erythrosine 440 I.A,M with anthocyanin 404 LM . The mixtures were
retained for 15 min. All 9 experiment groups were exposed to 532 nm green light at power density
of 21.5 mW/cm2 for 60 seconds. The controls were the groups of the biofilms with photosensitisers
without light exposure, the biofilms with green light exposure, the biofilms with chlorhexidine and the
biofilms alone. Then the survival fraction was calculated at 1 h, 3 h and 6 h after PDT process. The
bacteria viability test was undertaken at 1 h. To evaluate photogenerated reactive oxygen species by
EPR spectroscopy that showed PDT with photosensitizers as erythrosine 330, 440 U,M and erythrosine
440 with anthocyanin 404 tA,M were mixed with Spin trap (TEMPO, DMPO). ESR spectrum were
evaluated. The results showed that the PDT groups; 330 ILIM and 440 IAM erythrosine groups and
mixed 440 tA,M erythrosine with 404 A,LM anthocyanin had bacterial colony forming units less than the
other experimental groups and the controls in every period of evaluation (ANOVA, p < 0.05). From
the bacterial viability test, the percentage of live bacteria were in the order 15.51, 2.09 and 4.31. To
evaluate photogenerated reactive oxygen species by ESR spectroscopy. The ESR spectrum of erythrosine
440 IlA,M with anthocyanin 404 t./M, erythrosine 440 fIM and erythrosine 330 IAM were decreased
when increase irradiation times.
The PDT using 330 440 tIM erythrosine and 440 [UM erythrosine with 404 !LLM
anthocyanin irradiated with green light were statistically significant killing P. gingivalis on biofilms
than anthocyanin and the control groups.
Keywords: Photodynamic therapy (PDT); Porphyromonas gingivalis; Erythrosine; Anthocyanin (cyanidin).
'Master of Science in Periodontology, Graduated School, Khon Kaen University, IGron Kaen, Thailand
2Associate Professor, Department of Periodontology, Faculty of Dentistry, Khon Kaen University, Khon Kaen, Thailand
'Associate Professor, Department of Oral Surgery, Faculty of Dentistry, Khon Kaen University, Khon Kaen, Thailand
'Associate Professor, Department of Oral Diagnosis, Faculty of Dentistry, Khon Kaen University, K/ion Kaen, Thailand
Correspondence author
Sajee Sattayut, D.D.S., Ph.D.
Department of Oral Surgery,Faculty of Dentistry, Khon Kaen University, Khon Kaen, 40002, Thailand,
E-mail: [email protected]
34
The 4. International LDRG - KM/ & Saraburi
Hospital Symposium 2014
Introduction Periodontitis is a chronic infectious inflammatory disease that affects the gingiva and is associated with loss
of gingival and periodontal ligament connective tissue and alveolar bone (Page RC and Schroeder HE, 1976). Peri-
odontal disease caused by dental plaque which is a biofilm of mixed aetiology is one of the most prevalent diseases
in oral cavity caused by periodontopathic bacteria such as Porphyromonas gingivalis. The possibility of development
of resistance to antibiotics by the organisms has led to the development of a new antimicrobial concept with fewer
complications. Photodynamic therapy (PDT) involves the use of appropriate wavelength of light, oxygen, and a
suitable photosensitizer to kill microorganisms. "PDT" could be a useful adjunct to mechanical as well as antibiotics in
eliminating periodontopathic bacteria.
Mechanical removal of the periodontal biofilms is currently the most frequently used method of periodontal
disease treatment. Antimicrobial agents are also used, but biofilm species exhibit several antibiotic-resistance mechanisms.
In addition, disruption of the oral microflora and the difficulty of maintaining therapeutic concentrations of antimicro
bials in the oral cavity are also problems associated with the use of these agents
Photodynamic therapy has been advocated as an alternative to antimicrobial agents to suppress subgingival
species and to treat periodontitis. Bacteria located within dense biofilms, such as those encountered in dental plaque,
have been found to be relatively resistant to antimicrobial therapy. The aim of the present study is to compare the
ability of erythrosine as a photosensitizers and anthocyanin (cyanidin) as bactericidal activity upon the photodynamic
therapy with green light. To determine
1. The survival of bacteria was assayed using the colony-forming unit/mg after photodynamic therapy.
2. The distribution of dead/live bacteria and relative viability analysis of P. gingivalis suspensions from
fluorescence spectroscopy.
Photosensitizers
Erythrosine
Dental practitioners currently use erythrosine to stain and visualize dental plaque in the form of disclosing
solution or tablets. Erythrosine belongs to a class of cyclic compounds called xanthenes, which It's maximum absorbance
is at 500-550 nm has some reported of antimicrobial activity against Gram-positive and Gram-negative oral bacteria.
Clearly, erythrosine has an advantage over other photosensitizers in development, as it already targets dental plaque
and has full approval for use in the mouth.
Anthocyanins
Anthocyanins are flavonoid and contribute greatly to the antioxidant properties of certain colorful. The five
major anthocyanins aglycons (delphinidin-, petunidin-, cyanidin-, peonidin- and malvidin) bound to monosaccharides
(glucose, galactose and arabinose). Cyanidin is the most common anthocyanidin, and the 3-glucoside is the most active
antioxidant anthocyanin. The cyanidin 3-glucoside has notable antioxidant and anti-inflammatory properties for potential
use in nutraceuticals. A-type cranberry proanthocyanidins (AC-PACs) possess interesting therapeutic properties for the
treatment of periodontal disease. AC-PACs reduce the virulence properties of P. gingivalis by inhibiting biofilm formation,
adhesion, proteinase activity, and invasiveness. On the other, AC-PACs exert anti-inflammatory activity by inhibiting
the P. gingivalis-induced inflammatory response in human oral epithelial cells.
The apparent specific absorption coefficients of anthocyanins at 550 nrn showed no substantial dependence on
the species. Anthocyanin contribution to total light absorption at 550 nm.
35
The 4.1nternational LORG - KKU & Samburi
Hospital Symposium 2014
Material and methods
Samples of dental plaque were taken from 1 subject. Permission to collect dental plaque samples was authorized
by Institutional Review Board proved informant consent. Patient had periodontal pockets z 5 mm. with bleeding upon
pocket probing. The patient had not used antibiotic in the past 3 months. Samples were obtained from the deepest
periodontal pocket in each quadrant of the dentition by using sterile paper points. Then, plaque sample from
subject was placed immediately into one vial containing 4.5 ml of thioglycolate broth another plaque sample was placed
immediately into an Eppendorf tube with 1 ml of pre-reduced anaerobically sterilized Ringer's solution.
The samples were pooled in 1.5 ml of reduced transport fluid and were processed for cultivation under anaerobic
conditions within 4 h of sampling. Samples were vortexed for 2 min and split. A total of 100 !ill of the sample was
used for culture by tenfold serial dilution in sterilized Ringer's solution, and 100 [11 was also used for PCR. A total
of 100 l_,L1 of the dilutions were in the thioglycollate broth and incubated in 80% N2-10% H2-10% CO2 at 37°C for 7
to 14 days. P. gingivalis was identified on the basis of Gram staining, anaerobic growth, and the total number of CFU
of P. gingivalis in positive samples was determined suspension per milliliter and by growing the bacteria for 4 days
in trypticase soy agar supplemented with blood (5% by volume), hemin (5 mg/liter), vit.K (500 1.11/liter), kanamycin
(400 IA1/liter), and serial dilutions were inoculated on blood agar plates as described above.
Biofilms were prepared from saliva (subject sample) and were filled in centrifuge tubes and spin 2,000 rpm,
for 5 mins, then filtered by syringe filter 0.2 [Am, keep in 4°C. The cover glasses were suspended in saliva in 6 well
plates for 2 days and then discard by pipette. The cover glasses were then suspended in 4 ml of trypticase soy
broth . P.gingivalis suspension 50 [4,1 was added with 4 [1,1 hemin in 6 well plates and cultured until 4 days. Plates
containing the suspended slabs were incubated in anaerobic chamber at 37°C and fresh medium with P. gingivalis
culture was refilled 2 days. Biofilm formed on the upper surface of the cover glass after 4 days was treated and analyzed.
Erythrosine (Sigma Ltd, Poole, UK) was prepared as 110, 220, 330, 440 11,M stock solutions in deionized water,
foil-covered at 25°C after filter purification (0.2 VI,m).
Cyanidin 3-glucoside (Sigma Ltd, Poole, UK) was prepared as 101, 202,303, 404 !UM stock solutions in
deionized water and 50% ethanol, foil-covered at 25°C after filter purification (0.2 1.1m).
Green light laser pointer wavelengths 532 nm 50 mW. was used as a light source. The system was coupled
to lens with a focus 25 mm, diameter 20 mm which formed a uniform circular spot 1 cm in diameter. The power
density of incident radiation was measured using a power meter. The distance between the lens and the illuminated
plates was 15 cm. with a fixed power density of 21.5 mW/cm2 (1.2 J/crn2).
The slides containing biofilms were then placed in foil-covered vials containing 4 ml of erythrosine 110, 220,
330, 440 [A,M and anthocyanin 101, 202, 303, 404 ..tM and erythrosine 440 ILIM with 404 111\A anthocyanin all served as
experiment groups were lased with green light power density 21.5 mW/cm2 for 60 sec. After 1, 3, 6 h, the wells
were added with Ringers solution in 6-well plates to be serial dilutions 1:100 and were plated on blood agar plates
and incubated under anaerobic conditions for 37°C for 4 days. Survival fractions in each well were calculated by
counting the colonies on the plates.
Subjects and plaque samples
Samples of dental plaque were taken from 1 subject. Permission to collect dental plaque samples was autho
rized by Institutional Review Board proved informant consent. Patients were had periodontal pockets 5 mm. that
showed bleeding upon pocket probing. The patients had not used antibiotics in the past 3 months. Samples were
obtained from the deepest periodontal pocket in each quadrant of the dentition by using sterile paper points. After
removal, plaque samples from subject were placed immediately into one vial containing 4.5 ml of thioglycolate broth
another plaque sample was placed immediately after its removal into an Eppendorf tube with 1 ml of pre-reduced
anaerobically sterilized Ringer's solution.
36
The 4. International LDRG - KKU & Saraburi
Hm-pital Symposium 2014
Detection of P.gingivalis in subgingival plaque
The samples were pooled in 1.5 ml of reduced transport fluid and were processed for cultivation under
anaerobic conditions within 4 h of sampling. Samples were vortexed for 2 min and split. A total of 100 [11 of the
sample was used for culture by tenfold serial dilution in sterilized Ringer's solution, and 100 111 was also used for
PCR. A total of 100 [A,1 of the dilutions were in the thioglycollate broth and incubated in 80% N2-10% H2-10% CO2
at 37°C for 7 to 14 days. P. gingivalis was identified on the basis of Gram staining, anaerobic growth, and the total
number of CFU of P. gingivalis in positive samples was determined suspension per milliliter was made by growing
the bacteria for 4 days in trypticase soy agar supplemented with blood (5% by volume), hemin (5 mg/liter), Vit.K (500
[Willer), Kanamycin (400 [11/liter), and serial dilutions were inoculated on blood agar plates as described above.
Photosensitizers
1. Erythrosine (Sigma Ltd, Poole, UK) were stored as 110, 220, 330, 440 1.1M stock solutions in deionized
water, foil-covered at 25°C after filter purification 10.2 [Am).
2. Cyanidin 3-glucoside (Sigma Ltd, Poole, UK). The chemical structures of cyanidin chlorides work are
soluble in both water and ethanol.) It were stored as 101, 202, 303, 404 [A,M stock solutions in deionized water and
50% ethanol, foil-covered at 25 °C after filter purification (0.2 tlin).
The light source
The light source used green light laser pointer, power was less than 50 mW, wavelengths 532 nm. (visible
green light) in the wavelength range 500-550 rim (region of maximal absorption by erythrosine). The system was
coupled to lens with a focus 25 mm, diameter 20 mm that delivered light into a lens, which formed a uniform
circular spot 1 cm in diameter on the base of the 6-well plate. This spot of light was able to irradiate, each time,
either onewell in a 6-well plate. The power density of incident radiation was measured using a power meter The
distance between the lensand the illuminated plates was 15 cm. to create a spot of light, 1 cm in diameter, with a
fixed power density of 21.5 mW/cm2.
Biofilms
Biofilms were prepared from saliva (subject sample) that was filled in centrifuge tube and spin 2,000 rpm,
for 5 mins, then filtered by syringe filter 0.2 [tm, keep in 4°C. The cover glass 20x20 mm were sterilized. The cover
glass were suspended in saliva in 6 well plates 2 days and then discard by pipette saliva. The cover glass were
then suspended in 4 ml of trypticase soy broth, added P.gingivalis suspension 50 [A,1 and 4 11,1 hemin in 6 well
plates with cultures of Porphyromonas gingivalis until 4 days. Plates containing the suspended slabs were incubated
in anaerobic chamber at 37°C and fresh medium with cultures of P. gingivalis was refilled 2 days. Biofilm formed on
the upper surface of the cover glass after 4 days was treated and analyzed.
Procedure
Irradiation dose parameters a non coherent green light with a wavelength of 532 nm was used and the output
power was set at 21.5 mW/cm2. Light dose was calculated by multiplying the output power by the irradiation time
as given in the following equation:
Light dose (J/cm2) = output power (mW/cm2) x irradiation time (sec)
1000
Output power = 21.5 mW/cm2 , irradiation time = 60 sec and light dose (J/cm2) = 1.29 J/cm2. The biofilm-containing
cover glass slide were then placed in foil-covered vials containing 4 ml of erythrosine 110,220,330,440 111M and anthocyanin
101, 202, 303, 404 [A,M and erythrosine 440 1.1M with anthocyanin 404 11,M. All experimental groups to photodynamic
therapy with green light untill 1, 3, 6 hrs of the appropriate wells and the control groups are stimulated with green
light, no light and 0.12% chlorhexidine mouthwash then add ringer solution in 6-well plates to serial dilutions 1:100 then
it were gently scraped on blood agar in each well using a sterile bacteriological loop and incubated under anaerobic
conditions for 37°C for 4 days. Survival fractions in each well were calculated by counting the colonies on the plates.
37
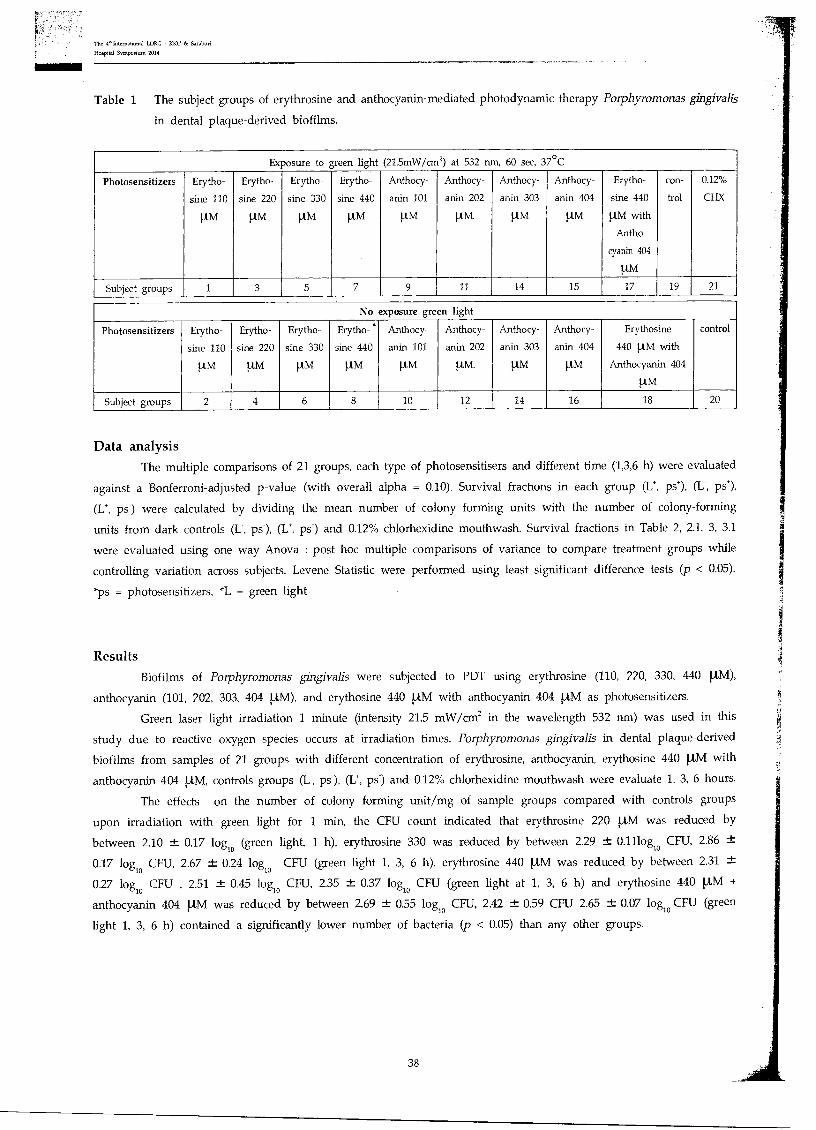
Table 1 The subject groups of erythrosine and anthocyanin-mediated photodynamic therapy Porphyromonas gingivalis
in dental plaque-derived biofilms.
Exposure to green light (21.5mW/cm2) at 532 nm, 60 sec, 37°C
Photosensitizers Erytho-
sine 110
1-AM
Erytho-
sine 220
1..tM
Erytho-
sine 330
[A,M
Erytho-
sine 440
[,LM
Anthocy-
anin 101
1.1.M
Anthocy-
anin 202
1A,M.
Anthocy-
anin 303
ttly1
Anthocy-
anin 404
ILLM
Erytho-
sine 440
!AM with
Antho
cyanin 404
p.M
con-
trol
0.12%
CI-IX
Subject groups 1 3 5 7 9 11 14 15 17 19 21
No exposure green light
Photosensitizers Erytho-
sine 110
11,M
Erytho-
sine 220
1AM
Erytho-
sine 330
1.4,M
Erytho- •
sine 440
1.0/1
Anthocy-
anin 101
1AM
Anthocy-
anin 202
[tm.
Anthocy-
anin 303
ton
Anthocy-
anin 404
[tm
Erythosine
440 1-1,M with
Anthocyanin 404
[AM
control
Subject groups 2 4 6 8 10 12 14 16 18 20
Data analysis The multiple comparisons of 21 groups, each type of photosensitisers and different time (1,3,6 h) were evaluated
against a Bonferroni-adjusted p-value (with overall alpha = 0.10). Survival fractions in each group (L*, ps'), (L-, ps'),
(L*, ps-) were calculated by dividing the mean number of colony forming units with the number of colony-forming
units from dark controls (I:, ps), (L*, ps-) and 0.12% chlorhexidine mouthwash. Survival fractions in Table 2, 2.1, 3, 3.1
were evaluated using one way Anova : post hoc multiple comparisons of variance to compare treatment groups while
controlling variation across subjects. Levene Statistic were performed using least significant difference tests (p < 0.05).
*ps = photosensitizers, *L = green light
Results
Biofilms of Porphyromonas gingivalis were subjected to PDT using erythrosine (110, 220, 330, 440 !,A,M),
anthocyanin (101, 202, 303, 404 !AM), and erythosine 440 1AM with anthocyanin 404 [A,M as photosensitizers.
Green laser light irradiation 1 minute (intensity 21.5 mW/cm2 in the wavelength 532 nm) was used in this
study due to reactive oxygen species occurs at irradiation times. Porphyromonas gingivalis in dental plaque-derived
biofilms from samples of 21 groups with different concentration of erythrosine, anthocyanin, erythosine 440 ILLM with
anthocyanin 404 tA,M, controls groups (I:, ps-), (1_7, ps-) and 0.12% chlorhexidine mouthwash were evaluate 1, 3, 6 hours.
The effects on the number of colony forming unit/mg of sample groups compared with controls groups
upon irradiation with green light for 1 min, the CFU count indicated that erythrosine 220 llA,M was reduced by
between 2.10 ± 0.17 logic (green light, 1 h), erythrosine 330 was reduced by between 2.29 ± 0.11log10 CFU, 2.86 ±
0.17 logic CFU, 2.67 ± 0.24 logic CFU (green light 1, 3, 6 h), erythrosine 440 I.A,M was reduced by between 2.31 ±
0.27 logic CFU , 2.51 ± 0.45 logic CFU, 2.35 0.37 logic CFU (green light at 1, 3, 6 h) and erythosine 440 1AM +
anthocyanin 404 1.1M was reduced by between 2.69 ± 0.55 logic CFU, 2.42 ± 0.59 CFU 2.65 0.07 logic CFU (green
light 1, 3, 6 h) contained a significantly lower number of bacteria (p < 0.05) than any other groups.
38
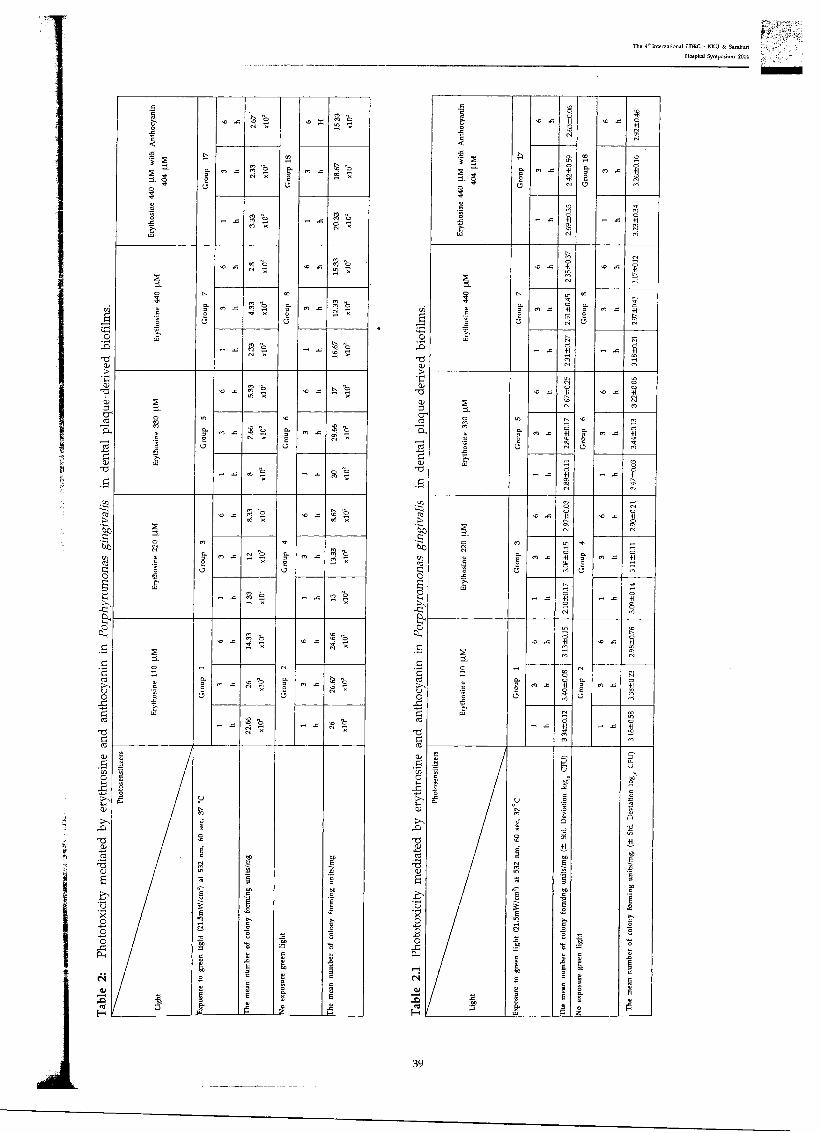
er; • .4
O
-O
O
0
O
-0 ca
0
()I 0
O
i. a)
O O 0 0
The 4' Intemational LDRG - KKU & Saraburi
Hospital Symposium 2014
Ery
thos
ine
440 1
1M w
ith
An
thoc
yan
in
404 1
1..M
.--.
o
0
.4 50 . Z M Cr' •;-i •,
M . - 6 • • ,..., N
Gro
up
1
8
m s P. ...
,76
,y.
x . . gi • , O
N .
.
Ery
tho
s ine
44
0 1
11,4
Gro
up
7
.4 ri F4
Gro
up
8
. .. M 9 „ x
tn .4 "b .-:(
cn .4 M t,
ti ,e,
T. .
r. X ..;,'4 ",'F›.9, . .4 s.1.3 , g ;:..I X
Ery
thosi
ne 3
30
1.1
M
Gro
up
5
. 2 cn. 11)
Gro
up
6
. .4 C. 0 „, 71,
01 2 fn X 45 7:,
r-I .4 a0 , 2 F '' , ,-:
Ery
thos
ine
220 1
1M
VI
4
C9
. .4 O X
Gro
up 4
. 4 '6, CO
co .4 c• ' 01 X
ob e.
''.? 2 `4 .
, .. 2 7?,,
3
'-"•.'
L_
.1
Gro
up
1
. . . i.,,,,
4 O
Gro
up
2
co .4 t..1'
"6 -• .. A °
Pho
tose
nsit
izer
s
Lig
ht
Exp
osur
e to
gr e
en
ligh
t (2
1.5m
W/c
m')
at
532 n
ni,
60
sec
. 37
°C
The
mea
n n
umber
of
colo
ny fo
rmin
g u
nit
s/m
g
No
exp
osur
e g
reen
li
ght
The
mea
n n
umber
of
colo
ny fo
rmin
g u
nit
s/m
g
Ery
thos
ine
44
0 1
1M w
ith A
nt h
ocya
nin
404 [1
M
ICI G
rou
p
17
I 2.
6 5±
0.0
6
4
+I ce cr• oi
co .4
co to eft +I or '41 oc G
rou
p 1
8
en .4 ci +1 . c't ret
2.69±
0.55
3.2
3±
0.3
4
Ery
t hosi
ne
44
0 1
.1.M
Gro
up
7
.0 x
t O +I tr. rO ,
r ')
. .4 44° R
re;
cn ..c L4l'l o 41 LI, ni G
rou
p 8
m en "el o .4 +I
cr, c...
to -4 tO +I
rel
m. 6
.4 +I ,.. rei
Ery
t hos
ine
33
0 1
.I.M
Gro
up
5
. .4
tr. t'l
+I r...
CV
Gro
up
6
.
. q o
4 +1 ev
C6 CV
co .4
,ti. d +1 ,.. c..■
0,
co
ci ..z 41
4 ,-;
mt .4
,--, 1-1 cn co ni
mt
"8 b
.4
co
Ery
t hos
ine
22
0 1
1M
5
. .4
co q o +1 ,-..
N
mom
.
Gro
up
4
.
t•71 O
.4 +I
',:?, CV
co X d -El VD
CO
co d
.4 +I
C6
m. •4
It:,■ d +I
'' oi
.. ;I': d
s +I
F3 cei
Ery
thos
ine
110 )
. LM
. .4
in ,_,
+1
M cti
d .
t''.
.4 +I
T., e..i
Gro
up
1
co X
co
+1
,l'! co G
rou
p
2
en .4
,-. X Ci +2
co eti
,-. X
C"
i"
.4 C.
Z 52P
..a
Exp
osur
e to
gre
en l
ight (2
1.5m
W/c
m)
at
532
nm
. 6
0 s
ec, 3
7°
C
F1 'he
mea
n n
umbe
r o
f co
lony
fo
rmin
g u
nit
s /m
g (-
± St
d. D
evia
tion
lo
g.
CF
U)
No
exp
osur
e g
reen
li
g ht
The
mea
n n
um
ber
of
colo
ny f
orm
ing
un
its/
mg.
(±
Std
. D
evia
tion
log.
CF
U)
39
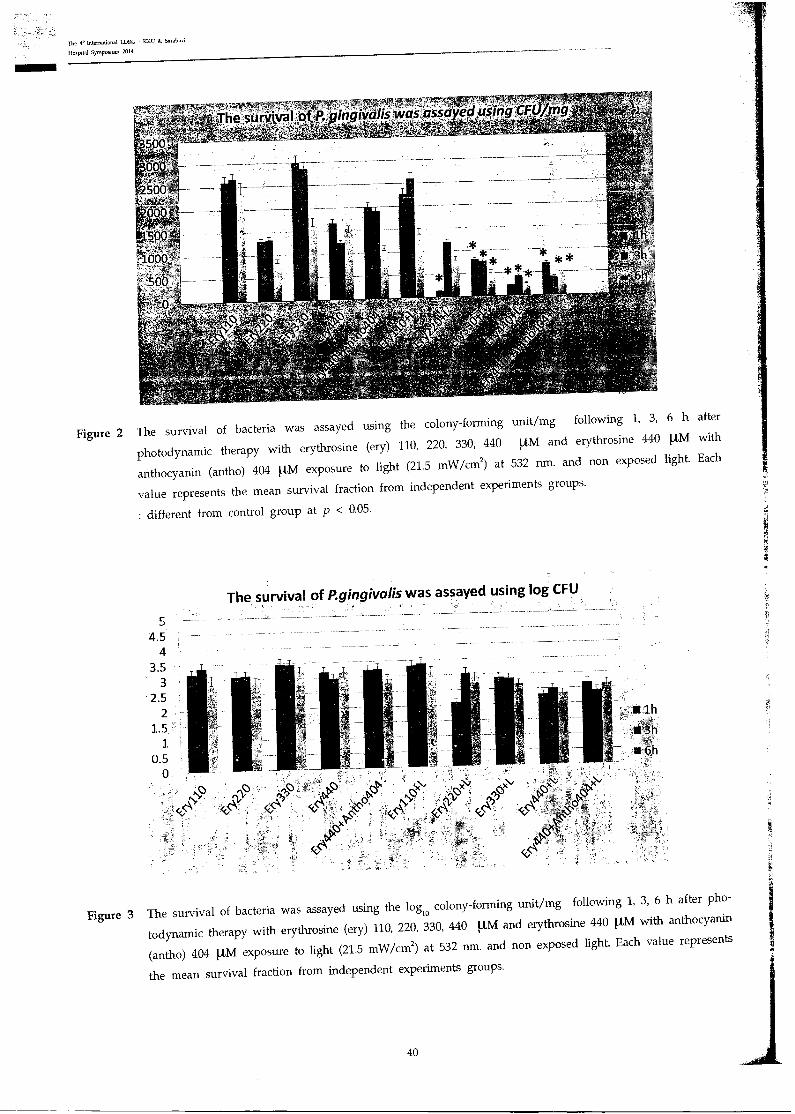
e survival of P gingivalis was assayed using CFUirn
5 4.5
4 3.5
3 2.5
2 1.5
1 0.5
lh
:If3h
.141. 6h
0
The 4" International LORC U & Saraburi
Hospital Symposium 2014
Figure 2 The survival of bacteria was assayed using the colony-forming unit/mg following 1, 3, 6 h after
photodynamic therapy with erythrosine (ery) 110, 220, 330, 440 tAM and erythrosine 440 .LM with
anthocyanin (antho) 404 I,LM exposure to light (21.5 mW/cm2) at 532 nm. and non exposed light. Each
value represents the mean survival fraction from independent experiments groups.
: different from control group at p < 0.05.
The survival of P.gingivalis was assayed using log CFU
Figure 3 The survival of bacteria was assayed using the logio colony-forming unit/mg following 1, 3, 6 h after pho-
todynamic therapy with erythrosine (ery) 110, 220, 330, 440 !AM and erythrosine 440 l,l,M with anthocyanin
(antho) 404 !AM exposure to light (21.5 mW/cm2) at 532 nm. and non exposed light. Each value represents
the mean survival fraction from independent experiments groups.
40
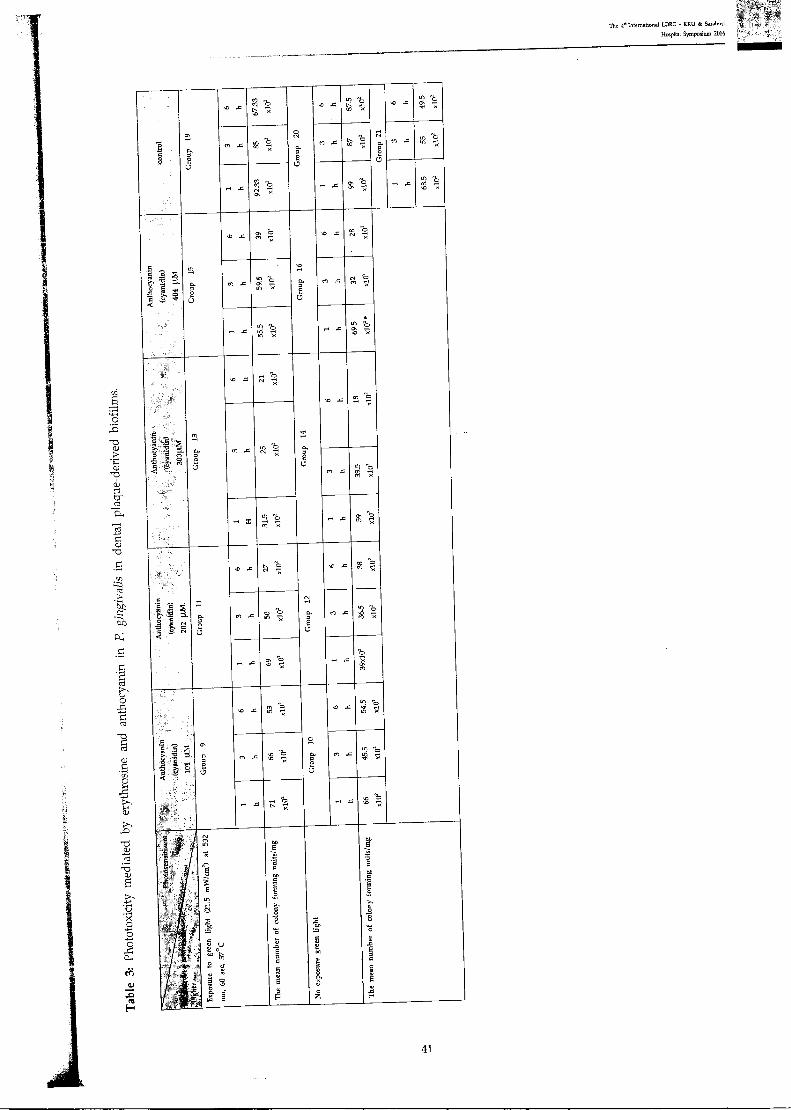
The 46 International L1DRG - KK1J & Saraburi
Hospital Symposium 2014
41
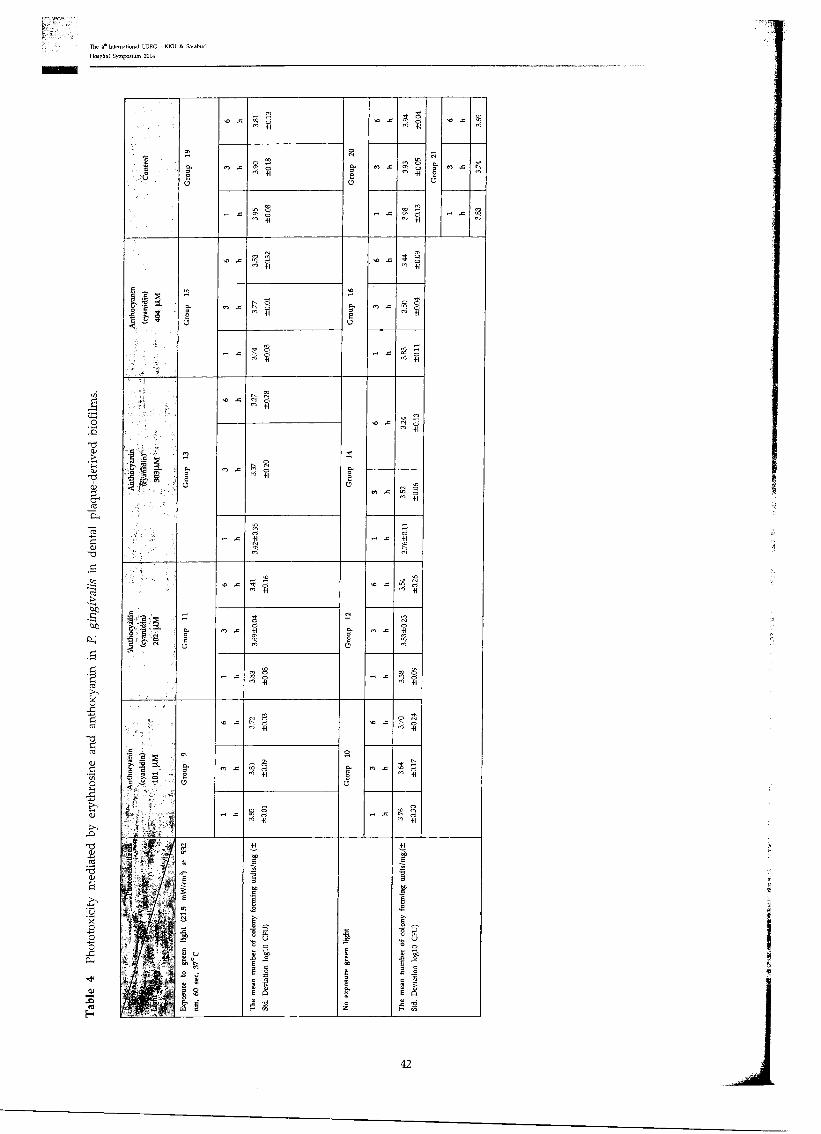
The 4. International LORG - KKU & Saraburi Hospital Symposium 2014
1)
O
TS co
s•-■
O.
O
co
.61
.0 iTo
O
O s. 0
ca
ca
co
a)
2.)
a) 5
0 0
0
dl
0
es
Gro
up
19
, 0 ..o . rn .-. , . 6
tat 0 stO .0 so
co 4 cc
o , cc, 6 M +1
Gro
up
20
cc ,4 . P
no .T1
r4 ta. g
6' 01 S
en
..-. ..= co Ln q c, 9)
co --, 6 ro .6 en cc
5 .5 ts :0 2
..
2
Gro
up
15
‘.0 .o 'ii" en 0 r, +1 • so .o .4.• g
,i 4-1
NJ .c ,.... , E.-. 2; 16 +1
Gro
up
16
,,,
cr, .4 ..,, o o
Lq 6 r' -I+
r. .. -sa q 4-- p '6 +1
.--i X oo 6 '.6 +1
1 :F. ,
t" r
Gro
up
13
... x , cc, ,s, N 6
'' +1
Gro
up
14
. .4
3.24
±0.1
3
<I, 4
o n. IN 'Il 6
+1
M +I
p
..I X
rn'.
+I
M CO
•" .
724' IP, + I
Ant
hocy
anin
(cy a
nid
in) ■---1-'
E.' c'3'
.7 s 6
Gro
up
12
‘0 .c ++. c., cc 6 '6 +l
to .o vr q o +1
I` ,i M ...
so 4'1 o 41 rri ,6
c.o. rr, . '''' 44
. c,. r6 +I
•
Gro
up
9
uSt ... 40 4.4 o
,4"-r; .161 ora = -4P o oa
4, '' +I
p
M .. q cq 0 `'.1 +1
91
g 6'
+P ,t11 6̀ +1
.4 L n 8 . 6
+I t-4 4
'.6 +1
rtF
Exp
os u
re
to g
reen
li
ght (
21
.5 m
W/c
m) a
t 5
32
run
60 s
ec.
37°
C
The
me a
n n
um
ber
of
colo
ny
fo
rmin
g u
nit
s/m
g (±
Std.
Dev
iati
on l
og10 CF
U)
No
exp
osur
e g
reen
lig
ht
The
me
an n
um
ber
of
colo
ny
form
ing u
nit
s /m
g.(-±
Std. D
e via
tion
lo
g10
CF
U)
42
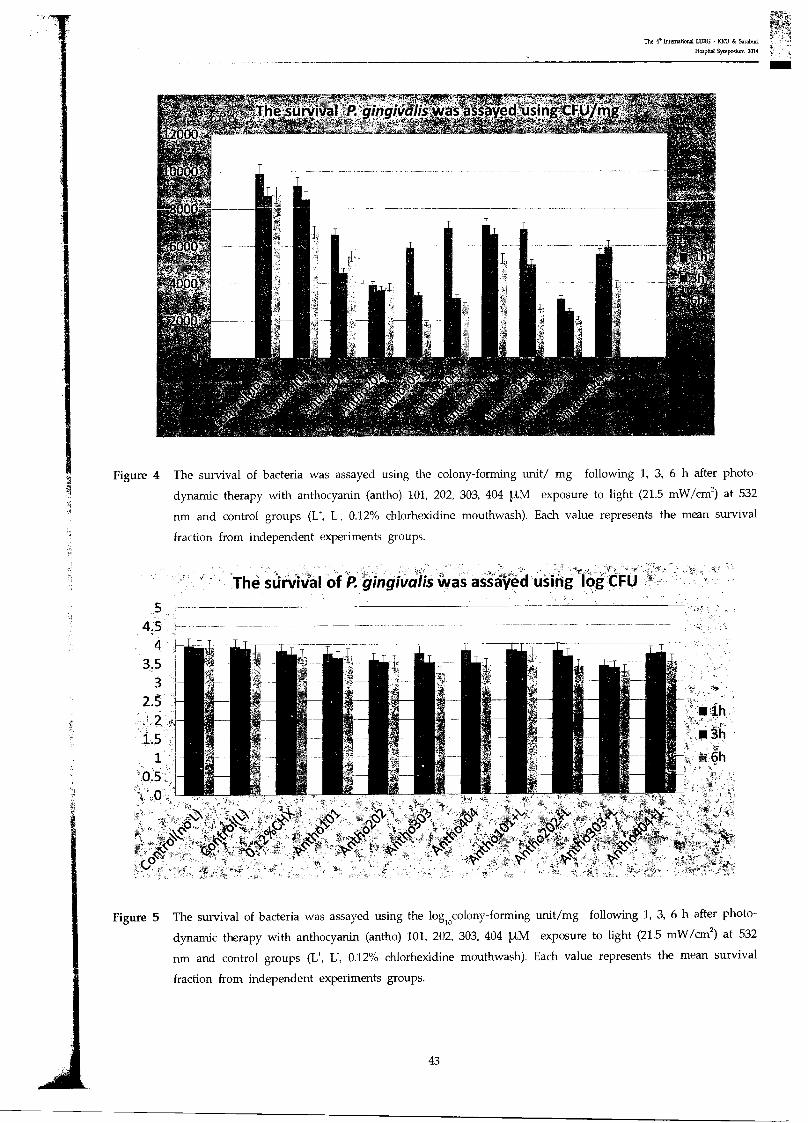
,he survival ft gingiva/iv:was ass-ayed using CFU/nig
The survival 'of P. 4ingivalis was assayed using log CFU
The 4. Inttmational I.DRG - KM) & Saraburi
Hospital Symposium 2019
Figure 4 The survival of bacteria was assayed using the colony-forming unit/ mg following 1, 3, 6 h after photo-
dynamic therapy with anthocyanin (antho) 101, 202, 303, 404 !,LM exposure to light (21.5 mW/cm2) at 532
nm and control groups (1!, I:, 0.12% chlorhexidine mouthwash). Each value represents the mean survival
fraction from independent experiments groups.
Figure 5 The survival of bacteria was assayed using the logiocolony-forming unit/mg following 1, 3, 6 h after photo-
dynamic therapy with anthocyanin (antho) 101, 202, 303, 404 !AM exposure to light (21.5 mW/cm2) at 532
nrn and control groups (L., 0.12% chlorhexidine mouthwash). Each value represents the mean survival
fraction from independent experiments groups.
43
The 4. International LDRG - ICKU & Saraburi
Hospital Symposium 2019
Discussion
In the present study, we investigated the photodynamic effects of erythrosine and anthocyanin on the
P.gingivalis in human dental plaque-derived biofilms. The results of this study were achieved by normalizing the data
from each experiment against the untreated controls and expressing the survival of bacteria was assayed using the
colony-forming unit/mg following 1 h, 3 h, 6 h respectively after photodynamic therapy. We found erythrosine groups
330 .1M, 440 fAM and erythrosine 440 IAM + anthocyanin 404 with green light were significantly more effective
(P < 0.01) than anthocyanin and control groups. The results of this study were confirmed the in vitro bactericidal
efficacy of PDT against the oral pathogens P. gingivalis. Several studies have reported that oral microorganisms in
plaque scrapings (Mark N) and biofilms (Zanin IC, et al., 2006, Zanin IC, et al., 2005) are susceptible to photodynamic
therapy. Recently, it was reported that photodynamic therapy induced bacterial cell killing to a level of > 1 logio in
oral monospecies biofilms using erythrosine (Metcalf D, et a]., 2006, Wood S, et al., 2006). However some studies have
demonstrated incomplete destruction of oral pathogen's in plaque scrapings, mono-species biofilms, and multi-species
biofilms derived from human saliva. The reduction of P. gingivalis biofilms in the PDT treatment with erythosine
220 [tM was found at first hour, however less reduction was found at 3 and 6 hours respectively. The P.gingivalis
biofilms tended to increase in terms of colony forming units.This can be explained that the concentration of erythosine
220 IAM may be lost their ability to produce ROS in the PDT reaction. SangWoo Kim reported P. gingivalis in agar
cultures were irradiated with LED wavelengths of 625, 525, and 425 nm at 6mW/cm2/h. P. gingivalis viability was
decreased by irradiation at 425 nm (40*60% reduction) and 525 run (10*20% reduction) both in agar and found that
green light irradiation did not have bactericidal effect. The reason may be a high concentration of light-induced ROS,
which are lethal to the cell, although low levels stimulate cell growth .
The reduction of P. gingivalis biofilms in the PDT treatment with erythrosine 330,440 [tM and erythosine 440
111M + anthocyanin 404 with green light at 1, 3, 6 h contained a significantly lower number of bacteria (p < 0.05)
erythosine 330, 440 IA,M. These agents are suitable for the ROS production and locally generated around the plaques
disclosed to bactericidal activity (Ishiyama K, 2012). This range of erythrosine concentration was probably suitable for
killing P. gingivalis. These concentration was confirmed by detecting ROS in the EPR spin trapping measurement
.Costa ACBP, et al. reported the biofilms of C. albicans and C dubliniensis exposed to PDT mediated by 400 mM
erythrosine and a green LED was used as the light source with a wavelength of 532, an output power of 90 mW, a
time of 3 mM, exhibited statistically significant reductions in CFU/ml. Ke et al. reported the erythrosine 50 1.1,M with
50 J/cm2 green light emitting diode light could not killed
Gram(-)bacteria in planktonic form even after the concentration was raised up to 20000 LLCM in combination
of 100 j/cm2 The used of erythrosine 440 IAM in killing micro-organisms has been shown in several studies. Costa,et
al. reported the biofilms of C albicans and C dubliniensis exposed to PDT mediated by erythrosine 400 11M and a
green LED exhibited statistically significant reductions in CFU/ml. Costa, et al. reported the PDT treatment with eryth-
rosine 400 !AM and green LED 14.34 J/cm2 irradiation could significantly reduce 0.73 logio of C albicans in vivo and
reduced the capacity of C albicans to adhere to buccal epithelial cells in vitro.
The role of PDT in the clinical treatment of periodontal disease, either in combination with traditional methods
of periodontal care or by itself, warrants further investigation to delivery and targeting approaches may need to be
developed to overcome the reduced susceptibility of complex dental biofilms to antimicrobial therapy.
Further work is now required to evaluate more clinically acceptable, perhaps to increase the light intensity or
concentration of erythrosine or the use of more efficient light delivery systems such as adaptation of light guide that
can be penetrated in the periodontal pocket depth. The future will be investigated the possibility of using erythrosine-
mediated PDT can be affected to fibroblast cell from periodontium.
44
The 4. International LDRG - KKU & 5arabuti
Hospital Symposium 2014
Conclusion: The antibacterial effect of photodynamic therapy is reduced in biofilms bacteria. PDT using erythrosine as
photosensitizer shows excellent potential as killing of the Porphyromonas gingivalis biofilms.
Reference
American Academy of Periodontology. Academy Report 2004. Position Paper Systemic Antibiotics in Periodontics.
Andersen 0 M Jordheim M. The anthocyanins. In: Anderson 0 M, Markham K R: "Flavonoids, Chemistry, biochemistry
and applications", CRC Press, Boca Raton, FL 2006;471-530.
Anderson GG, O_Toole GA. Innate and induced resistance mechanisms of bacterial biofilms. Curr Top Microbiol
Immunol 2008;322:85-105.
Athar M, Mukhtar H, Elmets CA, Zaim MT, Lloyd JR, Bickers DR. In situ evidence for the involvement of superoxide
anions in cutaneous porphyrin photosensitization. Biochem Biophys Res Commun 1988;15:1054-59.
Baab DA, Broadwell AH, Williams BL. A comparison of antimicrobial activity of four disclosant dyes. J Dent Res
1983;62:837-41.
Begue WJ, Bard RC, Koehne GW. Microbial inhibition by erythrosine. J Dent Res 1966;45:1464-7.
Bertoloni G, Lauro FM, Cortella G, Merchat M. Photosensitizing activity of hematoporphyrin on Staphylococcus aureus
cells. Biochim Biophys Acta 2000;1475:169-174.
Carranza's Clinical Periodontology. Tenth edition. Newman, Takei, Klokkevold, Carranza. Saunders Elsevier 2006.
Conlon KA, Berrios M. Light-induced proteolysis of myosin heavy chain by Rose Bengal-conjugated antibody complexes.
J Photochem Photobiol B 2001;65:22-8.
Del Pozo JL, Patel R. The challenge of treating biofilm-associated bacterial infections. ClinPharmacolTher 2007; 82:204-209.
Dougherty TJ, Gomer CJ, Henderson BW, Joni G, KesselD,nKorbelik M, Moan J, Peng Q. Photodynamic therapy. J Na tl
Cancer Inst 1998;90:889-905.
Fux CA, Costerton 1W, Stewart PS, Stoodley P. Survival strategies of infectious biofilms. Trends Microbiol 2005;13:34-40.
Huber H. Weitereveruschemitphotodynamischen, sensibilisierendenfarbstoffen (eosin, erythrosin). Pufund der wirkung
destageslichtes auf lebensfahigkeit und virulenz von bakterian, auf toxine und antitoxin und auf das labfer-
ment. Archie Hygeine 1905;54:53-88.
Ishiyama K, Nakamura K, Ikai H, Kanno T, Kohno M, et al. Bactericidal action of photogenerated singlet oxygen from
photosensitizers used in Plaque disclosing agents. PloS One 7(5):e37871. doi:10.1371/journal.pone.0037871.
Jodlbauer A, von Tappeiner H. Uber die wirkungphotodynamischer (fluoreszierender) stoffe auf bakterien. Munch
Med Wochenschr 1904;51:1096-7.
Konan YN, Gurny R, Allemann E. State of the art in the delivery of photosensitizers for photodynamic therapy. J
Photochem Photobiol B 2002;66:89-106.
Krasnoff SB, Faloon D, Williams JE et al. Toxicity of xanthenes dyes to entomopathogenic fungi. BiocontSci Tech
1999;9:215-25.
L. Santamaria, G. Prino, List of the photodynamic substances, Res Progr Org Biol Med Chem 3 (Pt 1) (1972) XI-XXXV.
Loesche WJ, Gossman NS. Periodontal Disease as a specific, albeit Chronic, Infection: Diagnosis and Treatment. Clinical
Microb Rev 2001;14:727-52.
M. Peter, Review Photodynamic therapy for periodontal diseases: State of the art. J Photochem Photobiol 2005; 79: 159-70.
Mark N. Merzlyak ,Light absorption by anthocyanins in juvenile, stressed, and senescing leaves: Journal of Exp Bota
59:3903-11. Marsh PD, Bevis RA, Newman HN et al. Antibacterial activity ofsome plaque-disclosing agents and dyes. Caries Res
1989;23:348-50.
45
The e International LDRG - KKU & Saraburi
Hospital Symposium 2014
Metcalf D, Robinson C, Devine D, Wood S. Enhancement of erythrosine-mediated photodynamic therapy of Streptococ-
cus mutans biofilms by light fractionation. J Antimicrob Chemother 2006;58:190-92.
Moan J, Berg K. The photodegradation of porphyrins in cells can be used to estimate the lifetime of singlet oxygen.
PhotochemPhotobiol 1991;53:549-53.
Moan J. Properties for optimal PDT sensitizers. J Photochem Photobiol B 1990;5:521-24.
Nikolaos S, Photodynamic therapy in the control of oral biofilms. Periodontology 2000, 2011;55:143-166.
Ochsner M. Photophysical and photobiological processes in the photodynamic therapy of tumours. J Photochem
Photobiol B 1997;39:1-18.
Page RC, Schroeder HE. Pathogenesis of inflammatory periodontal disease. A summary of current work. Lab Invest
1976;34:235-49.
Redmond RW, Gamlin JN. A compilation of singlet oxygen yields from biologically relevant molecules. Photochem
Photobiol 1999;70:391-475.
Romanova NA, Brovko LY, Moore L, Pometun E, Savitsky AP, Ugarova NN, Griffiths MW. Assessment of photody-
namicdestruction of Escherichia coli 0157:H7 and Listeria monocytogenes by using ATP bioluminescence. Appl
Environ Microbiol 2003; 69:6393-98.
Sarkar S, Wilson M. Lethal photosensitization of bacteria in subgingival plaque samples from patients with chronic
periodontitis. I Periodont Res 1993;28:204-10.
Schafer M, Schmitz C, Horneck G. High sensitivity of Deinococcusradiodurans to photodynamically-produced singlet
oxygen. Int J Radiat Biol 1998;74:249-53.
Soukos N, Ximenez-Fyvie L, Hamblin M, SocranskyS,HassanT. Tareetd Antimicrobial Photochemotherapy. Anticrobial
Agents and Chemother 1998;42:2595-601.
Steinberg D, Moreinos D. Genetic and Physiological Effects of Noncoherent Visible Light Combined with Hydrogen
Peroxide on Streptococcus mutans in Biofilm. J Antimicrob Chemother 2008:2626-31.
Tran J, Olmsted III J. Intramolecular triplet-triplet energy transfer from xanthene dyes to an anthyrl substituent. J Pho-
tochemPhotobiol A Chem 1993;71:45-9.
Von Tappeiner H. Zurkenntnis der lichtwirkenden (fluoreszierenden) Stoffe. Dtsch Med Wochen 1904;1:579-580.
Vu Dang La, Anti-Porphyromonasgingivalisand Anti-Inflammatory Activities of A-Type Cranberry Proanthocyanidins_
:Antimicrob. Agents Chemother 2010;54:1778.
Wilson M. lethal photosensitisation of oral bacteria andits potential application in the photodynamic therapy of oral
infections. Photochem Photobiol Sci 2004;3:412-18.
Wood S, Metcalf D, Devine D, Robinson C. Erythrosine is a potential photosensitizer for the photodynamic therapy of
oral plaque biofilms. I Antimicrob Chemother 2006;57:680-84.
Zanin IC, Goncalves RB, Junior AB, Hope CK, Pratten J. Susceptibility of Streptococcus mutans biofilms to photodynamic
therapy: an in vitro study. J Antimicrob Chemother 2005;56:324-30.
Zanin IC, Lobo MM, Rodrigues LK, Pimenta LA, Hofling JF, Goncalves RB. Photosensitization of in vitro biofilms by
toluidine blue 0 combined with a lightemitting diode. Eur J Oral Sci 2006;114:64-69.
46
31 July - 1 August 2014 The Greenery Resort Khao Yai, Thailand
Ilhort Kaen. Years,of Social Devotion.
misiC
th The 4 interns on =1 LDRG-KKU & Saraburi Hospital Symposium 2014 On
"Lasers in Dentistry: Research Transferring to Practice"

The 40 International IDRG KKU & Saraburi
Hospiial Symposium 7014
P6 : Interstitial laser therapy using Nd:YAG and diode laser
Teerapat TreeratsakukhaP, Peerapat Norateethan"2, Sajee Sattayut3
Abstract
This study aims to compare histOlogical change of the oral soft tissue and vascular lesion-liked
tissue specimens irradiated with Nd:YAG laser and diode laser by interstitial laser therapy technique
with a variety of the parameters. The laser settings were defined at energy density of 12,428.54 j/
cm2 with varied of powers and durations•of irradiation. The 30 tissue samples prepared from fresh
pig tongue and pig hepatic tissue were randomly allocated into 12 groups. They were irradiated by
the Nd:YAG laser at 5 watts for 2 seconds and 2 watts for 5 seconds (power density = 6,214.28 and
2,485.70 W/cm2, respectively) and the diode laser that are 5 watts for 2 seconds and 2 watts for 5
seconds (power density. 6,214.28 and 2,485.70 W/cm2, respectively). The control groups were lasered
with the Nd:YAG laser at power 0 watt for 5 seconds and diode lasers at power 0 watt for 5 seconds.
Then all samples were stained with Masson's trichrome and observed under optical microscope at a
magnification 10x. The results are not different between the group that show vaporized with coagula-
tion and the group shows only coagulation zone except two group that quite different are group two,
Nd:YAG 2 watt, 5 second and Diode 5 watt, 2 second in hepatic tissue that found amount of group
coagulation-only-zone more than group also found vaporized zone and coagulation together. This
technique need to insert fiber optic to a depth that is sufficient over the widest area of 2.4 square
millimeter to reduce laser scar on the mucosa. This research suggests using the Nd:YAG laser and
Diode laser in high power density first, but when the fiber optic perforate into the lesion should be
reduced to use Nd:YAG 2 watts 5 second, which is less power density to make coagulation zone is
optimal.
Keywords: Interstitial laser therapy; ILT; Photo ablation; Photo evaporation
General practitioner, Dental department, Paknam Lang Suan Hospital and affiliate researcher, Lasers in Dentistry Research Group, Khon
Kaen University, Thailand
2 General practitioner, Dental department, Chaturapakpiman Hospital and affiliate researcher, Lasers in Dentistry Research Group, Khon Kaen
University, Thailand
3Associate Professor in Oral and Maxillofacial Surgery, Khon Kaen University and Lasers in Dentistry Research Group, Khon Kaen University,
Thailand
Correspondence author
Sajee Sattayut, D.D.S, Ph.D.
Department of Oral Surgery, Faculty of Dentistry, Khon Kaen University, Khon Kaen, 40002, Thailand
E- mail: [email protected]
47
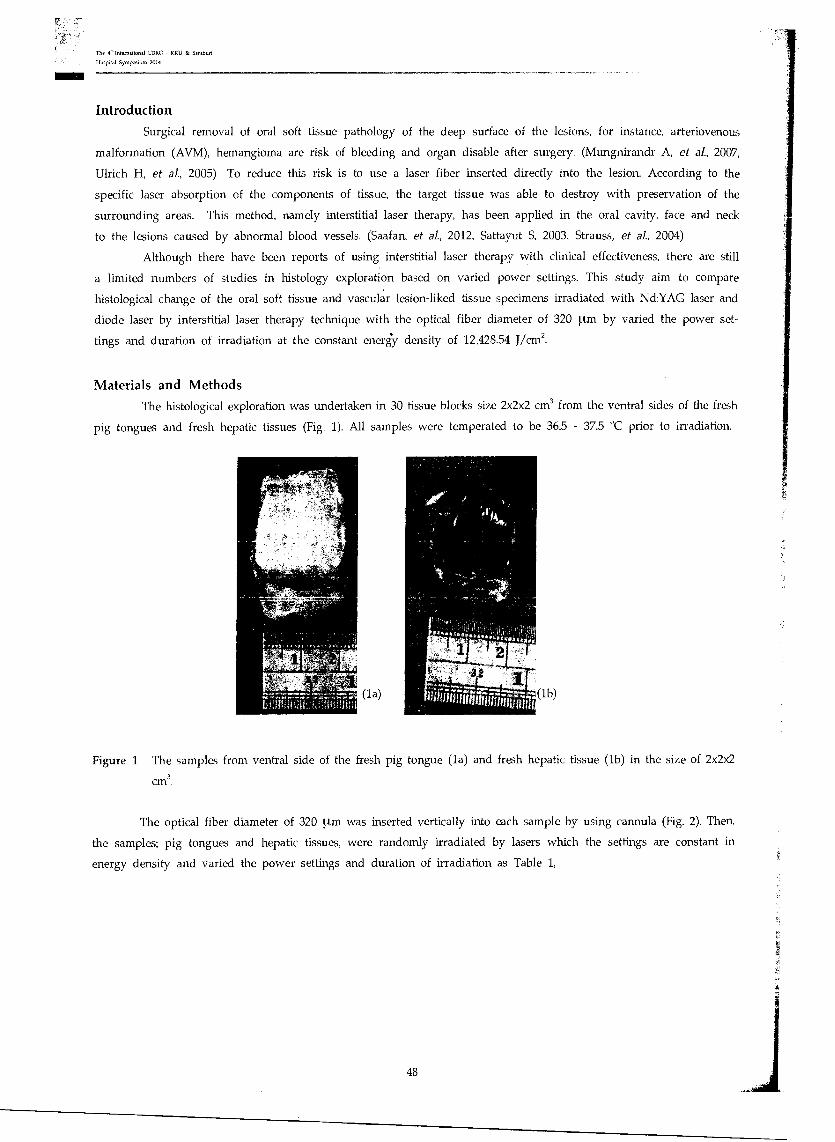
The 4' International LIJRC - KKU & Saraburi
Hospital Symposium 2014
Introduction
Surgical removal of oral soft tissue pathology of the deep surface of the lesions, for instance, arteriovenous
malformation (AVM), hemangioma are risk of bleeding and organ disable after surgery. (Mungnirandr A, et al., 2007,
Ulrich H, et al., 2005) To reduce this risk is to use a laser fiber inserted directly into the lesion. According to the
specific laser absorption of the components of tissue, the target tissue was able to destroy with preservation of the
surrounding areas. This method, namely interstitial laser therapy, has been applied in the oral cavity, face and neck
to the lesions caused by abnormal blood vessels. (Saafan, et al, 2012, Sattayut S, 2003, Strauss, et al., 2004)
Although there have been reports of using interstitial laser therapy with clinical effectiveness, there are still
a limited numbers of studies in histology exploration based on varied power settings. This study aim to compare
histological change of the oral soft tissue and vascular lesion-liked tissue specimens irradiated with Nd:YAG laser and
diode laser by interstitial laser therapy technique with the optical fiber diameter of 320 [tm by varied the power set-
tings and duration of irradiation at the constant energy density of 12,428.54 Von'.
Materials and Methods
The histological exploration was undertaken in 30 tissue blocks size 2x2x2 cm3 from the ventral sides of the fresh
pig tongues and fresh hepatic tissues (Fig. 1). All samples were temperated to be 36.5 - 37.5 °C prior to irradiation.
(1 )
-- .
(lb)
Figure 1 The samples from ventral side of the fresh pig tongue (1a) and fresh hepatic tissue (lb) in the size of 2x2x2 3
CM .
The optical fiber diameter of 320 pm was inserted vertically into each sample by using cannula (Fig. 2). Then,
the samples; pig tongues and hepatic tissues, were randomly irradiated by lasers which the settings are constant in
energy density and varied the power settings and duration of irradiation as Table 1,
48
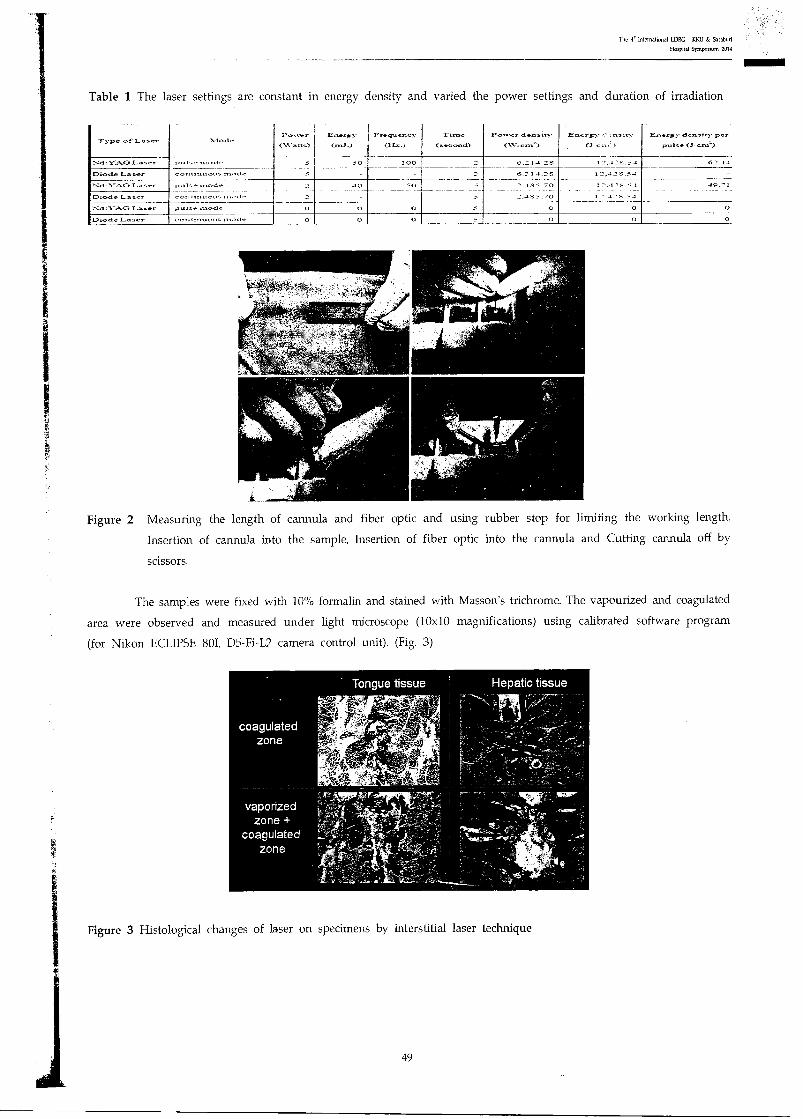
The e inteMahonal LDRG • KKU & RaLabUri • Hospital Symposium 2014
Table 1 The laser settings are constant in energy density and varied the power settings and duration of irradiation
Type of Laser :Viode Power
,-,,-241-1s)
Ener,y
(.4J.) Frequency
(11...,..)
Time
(second)
Power densit.
(W, ern')
Energy ,..9-asity
1(3.-,,,.. )
Ener,y density- per
pulse (5. cm')
.Z,(1 r-Y--4Cir La se, pLa1-.crvtod., 5 50 100 -' 6.214.2S 1 i '5.54 62.1.4
Diode Laser continno‘is ananode - - 6.2 1 4.25 12.425_54
1-,d,1-A.G.T.-..7aser p...,1,e auode 4p 50 2.455.'70 12.425.54 49.01 .. _ ..... 2.1 S -f• .70 1 ' A.' S 41 Diode Laser conlnittoLa... n,...,..,
:::3:1---1G 1.-.5,1- pulse rnode 0 0 0 0 0 0
Diode Laser convinuou, n“..,de 0 0 0 = 0 0 0
Figure 2 Measuring the length of cannula and fiber optic and using rubber stop for limiting the working length.
Insertion of cannula into the sample, Insertion of fiber optic into the cannula and Cutting cannula off by
scissors.
The samples were fixed with 10% formalin and stained with Masson's trichrome. The vapourized and coagulated
area were observed and measured under light microscope (10x10 magnifications) using calibrated software program
(for Nikon ECLIPSE 801, D5-Fi-L2 camera control unit). (Fig. 3)
Figure 3 Histological changes of laser on specimens by interstitial laser technique
49
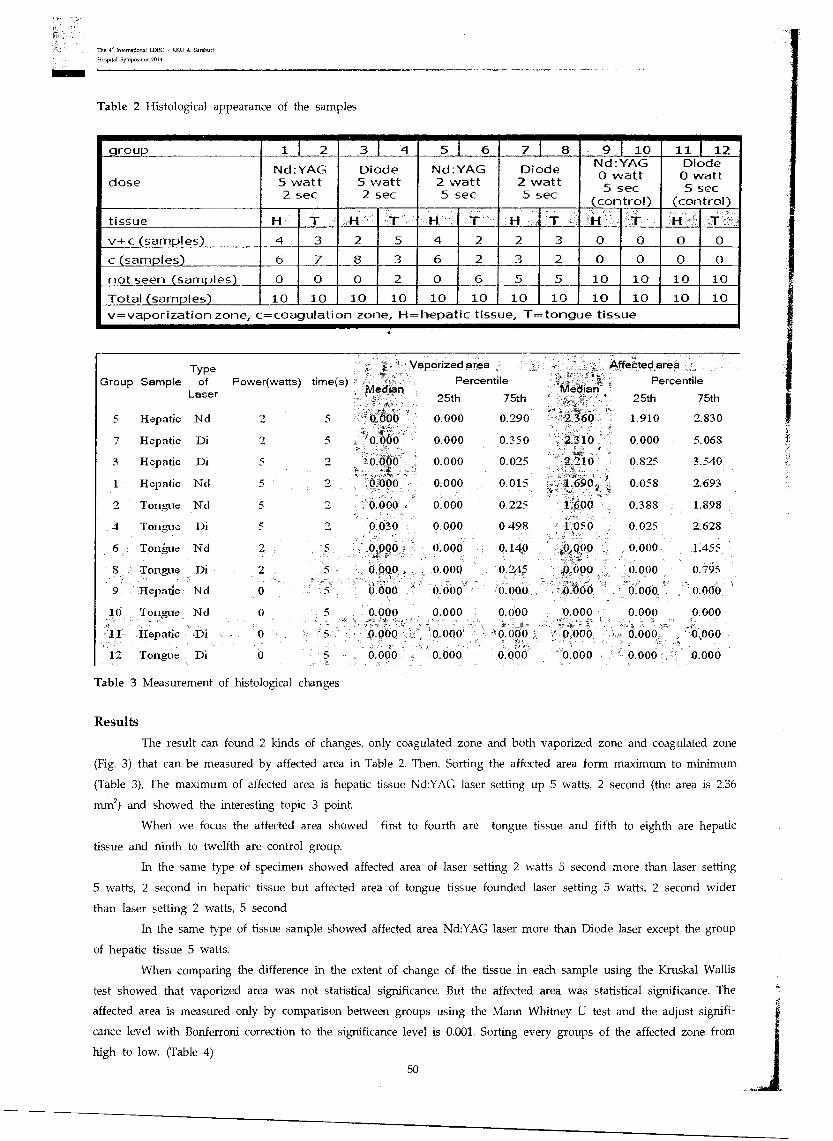
25th 75th
5 Hepatic Nd 2 5 0.000 0.290
7 Hepatic Di 2 5 o•oltio 0.000 0.350 .
3 Hepatic Di 5 2 : 0.000 0.000 0.025 .
Type Group Sample of
Laser
Vaporized area
Power(watts) time(s) - Percentile Median Median
0.000 2.360
2.310
2.210
1.690 ' ,- 1.600
, 1.050
0.000 •
. .0.090
Coo()
0.000
The 4' International LDRG KKU dr Saraburi
Hospital Symposium 2014
Table 2 Histological appearance of the samples
group 1 I 2 3 4 5 1 6 7 1 8 9 I 10 11 1 12
dose Nd:YAG 5 watt 2 sec
Diode 5 watt 2 sec
Nd:YAG 2 watt 5 sec
Diode 2 watt 5 sec
Nd:YAG 0 watt 5 sec
(control)
Diode 0 watt 5 sec
(control)
tissue HT H T T HT H T HT v-i-c (samples) 4 3 2 5 4 2 2 3 0 0 0 0
c (samples) 6 7 8 3 6 2 3 2 0 0 0 0
not seen (samples) 0 0 0 2 0 6 5 5 10 10 10 10
Total (samples) 10 10 10 10 10 _ 10 10 _ 10 10 10 10 10 v=vaporization zone, c=coagulation zone, H=hepatic tissue, T=tongue tissue
•
0.000
1 Hepatic Nd 5 2
2 Tongue Nd 5 2
4 Tongue Di 5 2 -,
6 Tongue Nd 2 5
8 - Tongue Di
Hepatic Nd 0 5
10 Tongue Nd 0 5 .. .
11 Hepatic ..Di 0
12 Tongue Di 0 5
Table 3 Measurement of histological changes
0.000 0.000 0.015
0.000 . 0.000 0.225
0.030 0.000 0.498
"..0.000 , o.000 0.140
, 0.000. > 0.000 0.245
0.000 ,. o.obo •o.000
0.000 0.000 0.000 " ...
. 0 obq '0.000 ' ' 0.000..
0.000 0.000 0.000
AffeC' ted area
Percentile
25th 75th
1.910 2.830
0.000 5.068
0.825 3.540
0.058 2.693
0.388 1.898
0.025 2.628
0.000 L455
0.000 0.795
0.000, 0.000
0.000 0.000
0.000 0.000
0.000 o.000
Results
The result can found 2 kinds of changes, only coagulated zone and both vaporized zone and coagulated zone
(Fig. 3) that can be measured by affected area in Table 2. Then, Sorting the affected area form maximum to minimum
(Table 3), The maximum of affected area is hepatic tissue Nd:YAG laser setting up 5 watts, 2 second (the area is 2.36
mm2) and showed the interesting topic 3 point.
When we focus the affected area showed first to fourth are tongue tissue and fifth to eighth are hepatic
tissue and ninth to twelfth are control group.
In the same type of specimen showed affected area of laser setting 2 watts 5 second more than laser setting
5 watts, 2 second in hepatic tissue but affected area of tongue tissue founded laser setting 5 watts, 2 second wider
than laser setting 2 watts, 5 second
In the same type of tissue sample showed affected area Nd:YAG laser more than Diode laser except the group
of hepatic tissue 5 watts.
When comparing the difference in the extent of change of the tissue in each sample using the Kruskal Wallis
test showed that vaporized area was not statistical significance. But the affected area was statistical significance. The
affected area is measured only by comparison between groups using the Mann Whitney U test and the adjust signifi-
cance level with Bonferroni correction to the significance level is 0.001. Sorting every groups of the affected zone from
high to low. (Table 4)
50
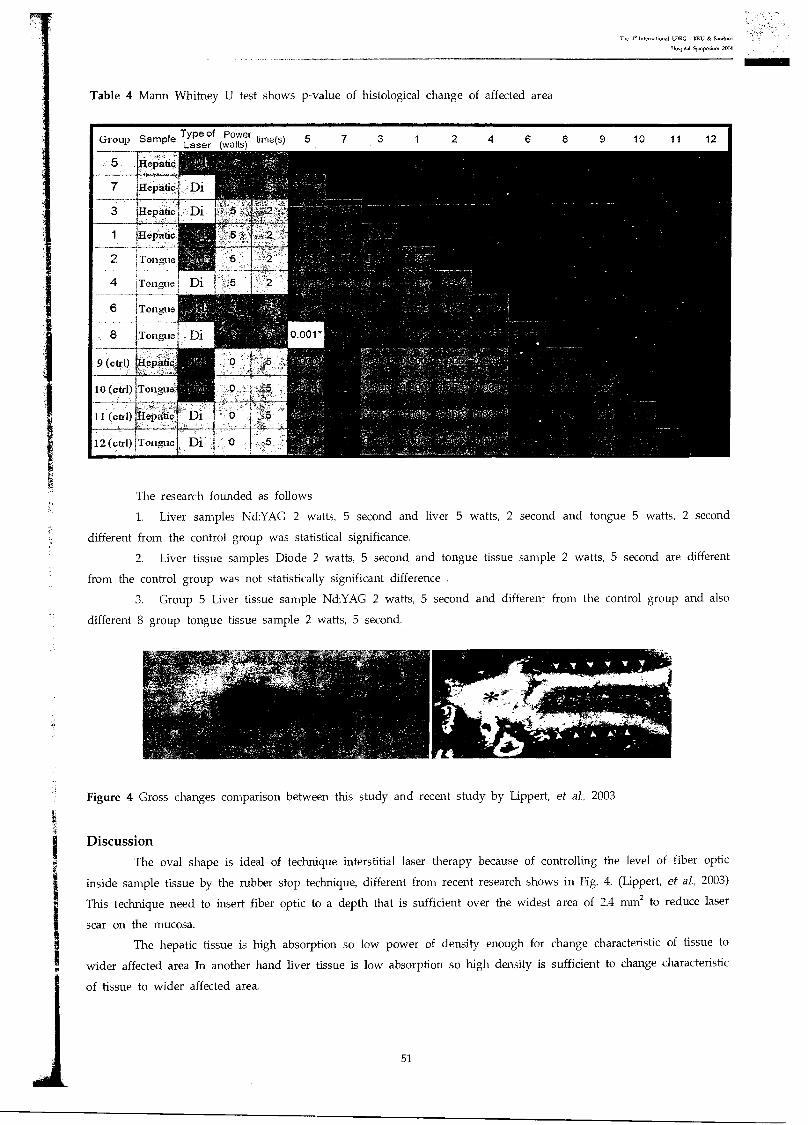
The 4.1ntemational LDRG - K1411 & Suraburi
Hospital Symposium 2014
Table 4 Mann Whitney U test shows p-value of histological change of affected area
. Hepatic.
7 Hepatic
3 epatic
1 Hepatic
2 Tongue
4 Tongue
6 Tongue
8 Tongue
9 (ail) Hepatic;
10 (ad) Tongue
The research founded as follows
1. Liver samples Nd:YAG 2 watts, 5 second and liver 5 watts, 2 second and tongue 5 watts, 2 second
different from the control group was statistical significance.
2. Liver tissue samples Diode 2 watts, 5 second and tongue tissue sample 2 watts, 5 second are different
from the control group was not statistically significant difference .
3. Group 5 Liver tissue sample Nd:YAG 2 watts, 5 second and different from the control group and also
different 8 group tongue tissue sample 2 watts, 5 second.
Figure 4 Gross changes comparison between this study and recent study by Lippert, et al., 2003
Discussion
The oval shape is ideal of technique interstitial laser therapy because of controlling the level of fiber optic
inside sample tissue by the rubber stop technique, different from recent research shows in Fig. 4. (Lippert, et al, 2003)
This technique need to insert fiber optic to a depth that is sufficient over the widest area of 2.4 mm2 to reduce laser
scar on the mucosa.
The hepatic tissue is high absorption so low power of density enough for change characteristic of tissue to
wider affected area In another hand liver tissue is low absorption so high density is sufficient to change characteristic
of tissue to wider affected area.
51
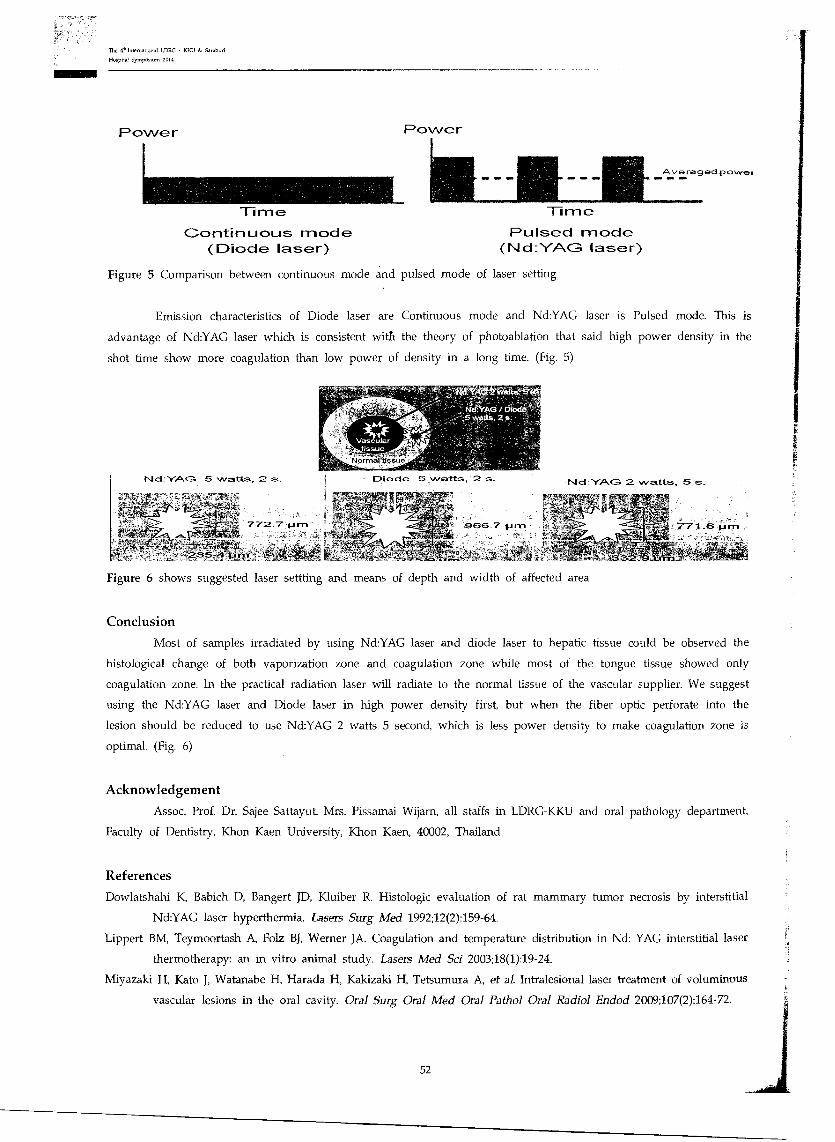
The 4- International LDRG • KKU Saraburi
Hospital Symposium 2019
Power Power
Time Time
Averaged powet 411.•
Continuous mode (Diode laser)
Pulsed mode (Nd:YAG laser)
Figure 5 Comparison between continuous mode and pulsed mode of laser setting
Emission characteristics of Diode laser are Continuous mode and Nd:YAG laser is Pulsed mode. This is
advantage of Nd:YAG laser which is consistent with the theory of photoablation that said high power density in the
shot time show more coagulation than low power of density in a long time. (Fig. 5)
Figure 6 shows suggested laser settting and means of depth and width of affected area
Conclusion
Most of samples irradiated by using Nd:YAG laser and diode laser to hepatic tissue could be observed the
histological change of both vaporization zone and coagulation zone while most of the tongue tissue showed only
coagulation zone. In the practical radiation laser will radiate to the normal tissue of the vascular supplier. We suggest
using the Nd:YAG laser and Diode laser in high power density first, but when the fiber optic perforate into the
lesion should be reduced to use Nd:YAG 2 watts 5 second, which is less power density to make coagulation zone is
optimal. (Fig. 6)
Acknowledgement
Assoc. Prof. Dr. Sajee Sattayut, Mrs. Pissamai Wijarn, all staffs in LDRG-KKU and oral pathology department,
Faculty of Dentistry, Khon Kaen University, Khon Kaen, 40002, Thailand
References
Dowlatshahi K, Babich D, Bangert JD, Kluiber R. Histologic evaluation of rat mammary tumor necrosis by interstitial
Nd:YAG laser hyperthermia. Lasers Surg Med 1992;12(2):159-64.
Lippert BM, Teymoortash A, Folz BJ, Werner JA. Coagulation and temperature distribution in Nd: YAG interstitial laser
thermotherapy: an in vitro animal study. Lasers Med Sci 2003;18(1):19-24.
Miyazaki H, Kato J, Watanabe H, Harada H, Kakizaki H, Tetsumura A, et al. Intralesional laser treatment of voluminous
vascular lesions in the oral cavity. Oral Surg Oral Med Oral Pathol Oral Radio] Endod 2009;107(2):164-72.
52
The 4. International LDRG - qRl & Saraburi
Hospital Symposium 201s
Mungnirandr A, Vajaradul Y. Treatment of Hemangioma and Vascular Malformation by Nd-YAG Laser. Siriraj Med J
2007;59:353-5.
Nikfarjam M, Malcontenti-Wilson C, Christophi C. Comparison of 980- and 1064-nm wavelengths for interstitial laser
thermotherapy of the liver. Photomed Laser Surg 2005;23(3):284-8.
Parker S. Lasers and soft tissue: 'loose' soft tissue surgery. Br Dent I 2007;202(4):185-91.
Saafan AM, Ibrahim TM. Treatment of Low-Flow Tongue Lesions by Diode Laser-Intralesional Photocoagulation (ILP).
J Am Sci 2012:8(6):247-51.
Sattayut S. Principle of laser in Dentistry. Khon Kaen Dental Journal 2003;6(2):89-95.
Sattayut S. A comparative study of the coagulative and cutting effect of Nd-YAG laser and electrosurgery. 2004,
Khon Kaen University.
Sattayut S, Hortong K, Kittichaiwan C. The histological effect of CO, laser and absorption media on oral soft tissue :
an in vitro study. Khon Kaen Dental Journal 2007;10(2):91-101.
Strauss RA, and Guttenberg SA. Lasers in oral and maxillofacial surgery. Oral maxillofac Surg Clin North Am
2004;16(2):xi-xii.
Ulrich H, Balmier W, Hohenleutner U, Landthaler M. Neodymium-YAG Laser for hemangiomas and vascular malfor-
mations - long term results. J Dtsch Dermatol Ges 2005;3(6):436-40.
53
LDRG : KKU
The 4th Intebrna r• n LDRG-KKU & Saraburi Hospital Symposium 2014 On
"Lasers in Dentistry: Research Transferring to Practice"
Khon Kaen University 50 Years of Social Devotion
31 July - 1 August 2014 The Greenery Resort Khao Yai, Thailand
ISBN 978-616-223-381-4
The 4. international I-DRG KKU h Sarabmi
Hospital Symposium 2014
P7 : A physical alteration in tissue blocks irradiated by diode laser and
Nd:YAG laser irradiating to different chromophore dyes on oral soft tissue.
Paweena Tanunataratarn'l, Pichaya Viengteerawar, Piengkhwan Atipatyakur, Sajee Sattayut2
Abstract
There was a possibility of altered ablation properties of laser by using chromophore dyes.
The aim of this was to explore physical alteration of gross specimens irradiated by 820 nm Diode
laser at 5 watt continuous wave and Nd:YAG laser at 5 watt 10 kHz for 5 seconds with a variety of
chromophore dyes. The chromophore dyes used in the experiment were lubricant gel, basic fushcin,
methylene blue and indian ink. The randomized control experimental study was conducted in fresh
tissue blocks of porcine tongues, 10 samples each group. The results showed a variety alteration in
gross specimens after irradiating each particular laser on each stained chromophore dyes. From the
group, Nd:YAG laser irradiated to Indian ink, the mostly found ablative shapes are u-shape with
eight specimens and two specimens of flat-shape were also found in this group. 820 nm diode laser
and Nd:YAG laser irradiating to tissue with the chromophore dyes provided a variety of ablative and
coagulative patterns with mostly u-shaped found.
Keywords: Nd:YAG; Chromophore; Oral soft tissue
Introduction
The technique using diode laser and Nd:YAG laser with chromophore dyes has been explored (Cox BT, Arridge
SR, Beard PC, 2009, Goldman L, 1991, Mourant JR, et al., 1997). However. there were no studies focus on different
chromophore dyes (Melato OMM, 2000, Fantini S, et al., 1994, Vinduska V, 1993), such as basic fushin, methylene
blue, Indian ink and lubricant gel in relation to laser properties. This study aimed to compare physical alteration
affected by diode laser at 5 watt continuous wave and Nd:YAG laser at 5 watt 10 kHz irradiating to oral soft tissue
blocks of porcine tongue with and without chromophore dyes for 5 seconds.
Materials and methods
A randomized control experimental study was conducted in the tissue blocks, which using fresh porcine tongues
to represent oral mucosa. The tissue blocks at a size of 2x2x2 cm3 were prepared from the fresh porcine tongue. The
total samples were 100 blocks. There were 10 samples each groups. The experimental and control groups as follows:-
820 nm diodel laser/5W/CW/5 seconds without chromophore media
820 nm diodel laser/5W/CW/5 seconds with lubricant gel
820 nm diodel laser/5W/CW/5 seconds with basic fushcin
820 nm diodel laser/5W/CW/5 seconds with methylene blue
'Fifth year dental student, faculty of dentistry Khon Kaen University and affiliate researcher, Lasers in Dentistry Research Group, Khon Kaen
University, Khon Kaen, Thailand
2Associate Professor in Oral and Maxillofacial Surgery, KhonKaen University and Lasers in Dentistry Research Group, KhonKaen University,
Khon Kaen, Thailand
Correspondence author
Sajee Sattayut, D.D.S., Ph.D.
Department of Oral Surgery, Faculty of Dentistry, Khon Kaen University, Khon Kaen, 40002, Thailand
E-mail: [email protected]
54
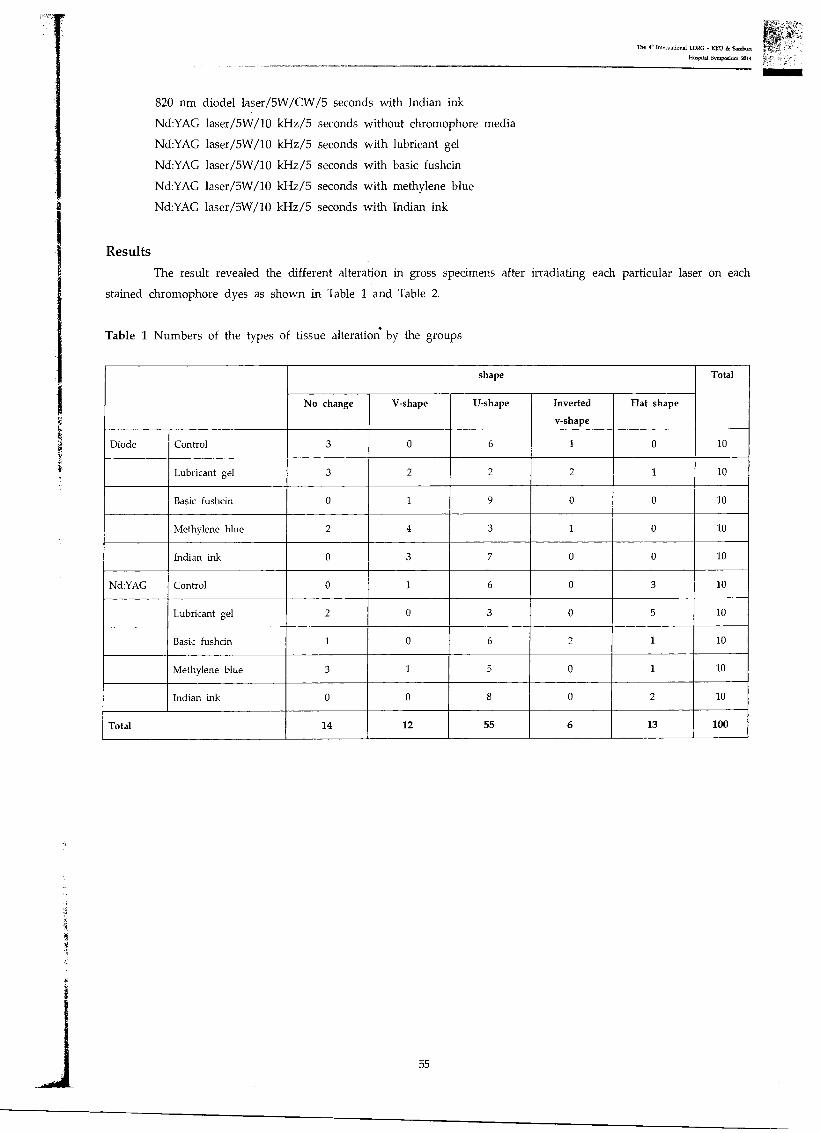
The 46 International LDRC - KICU & Saraburi
Hospital Symposium 2014
820 nm diodel laser/5W/CW/5 seconds with Indian ink
Nd:YAG laser/5W/10 kHz/5 seconds without chromophore media
Nd:YAG laser/5W/10 kHz/5 seconds with lubricant gel
Nd:YAG laser/5W/10 kHz/5 seconds with basic fushcin
Nd:YAG laser/5W/10 kHz/5 seconds with methylene blue
Nd:YAG laser/5W/10 kHz/5 seconds with Indian ink
Results The result revealed the different alteration in gross specimens after irradiating each particular laser on each
stained chromophore dyes as shown in Table 1 and Table 2.
Table 1 Numbers of the types of tissue alteration by the groups
shape Total
No change V-shape U-shape Inverted
v-shape
Flat shape
Diode Control 3 0 6 1 0 10
Lubricant gel 3 2 2 2 1 10
Basic fushcin 0 1 9 0 0 10
Methylene blue 2 4 3 1 0 10
Indian ink 0 3 7 0 0 10
Nd:YAG Control 0 1 6 0 3 10
Lubricant gel 2 0 3 0 5 10
Basic fushcin 1 0 6 2 1 10
Methylene blue 3 1 5 0 1 10
Indian ink 0 0 8 0 2 10
Total 14 12 55 6 13 100
55
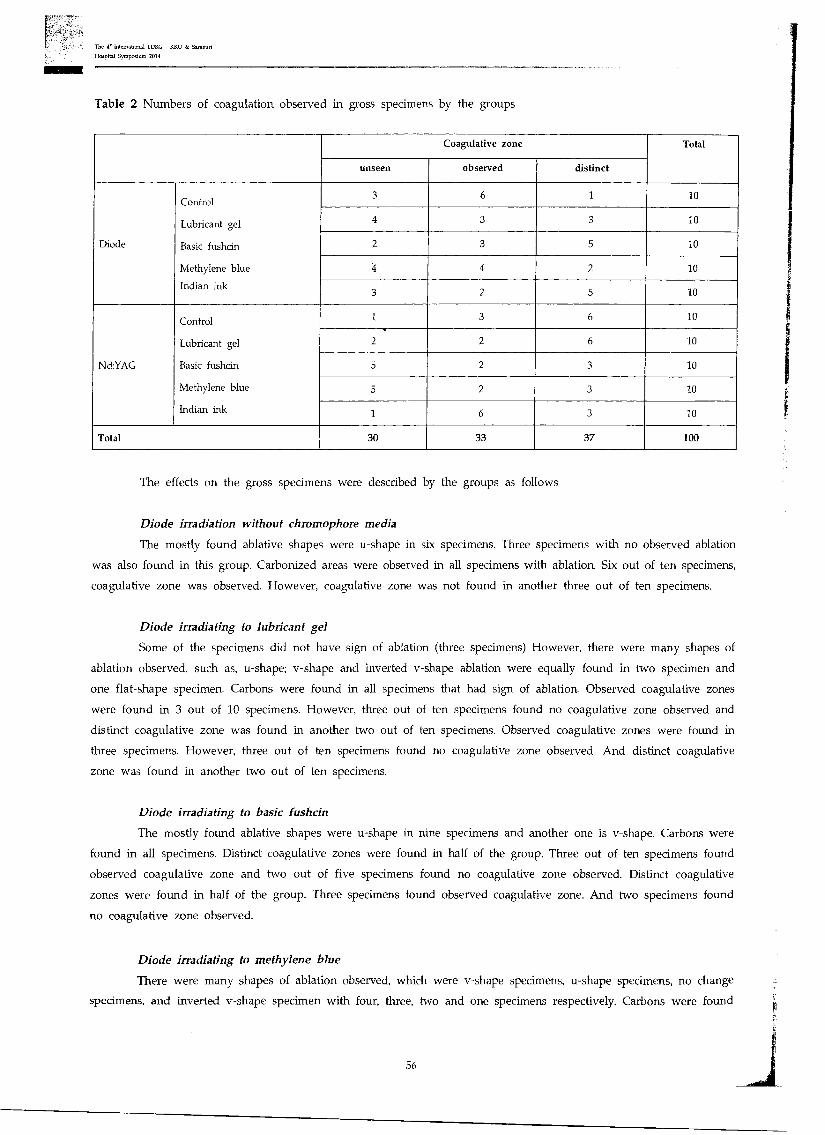
The 4. Intematonal LDRG KKU k Saraburi
Hospital Symposium 2014
Table 2 Numbers of coagulation observed in gross specimens by the groups
Coagulative zone Total
unseen observed distinct
Diode
Control
Lubricant gel
Basic fushcin
Methylene blue
Indian ink
3 6 1 10
4 3 10 3
2 3 5 10
4 4 2 10
3 2 5 10
Nd:YAG
Control
Lubricant gel
Basic fushcin
Methylene blue
Indian ink
1 3 6 10
2 2 6 10
5 2 3 10
5 2 3 10
1 6 3 10
Total 30 33 37 100
The effects on the gross specimens were described by the groups as follows
Diode irradiation without chromophore media
The mostly found ablative shapes were u-shape in six specimens. Three specimens with no observed ablation
was also found in this group. Carbonized areas were observed in all specimens with ablation. Six out of ten specimens,
coagulative zone was observed. However, coagulative zone was not found in another three out of ten specimens.
Diode irradiating to lubricant gel
Some of the specimens did not have sign of ablation (three specimens) However, there were many shapes of
ablation observed, such as, u-shape; v-shape and inverted v-shape ablation were equally found in two specimen and
one flat-shape specimen. Carbons were found in all specimens that had sign of ablation. Observed coagulative zones
were found in 3 out of 10 specimens. However, three out of ten specimens found no coagulative zone observed and
distinct coagulative zone was found in another two out of ten specimens. Observed coagulative zones were found in
three specimens. However, three out of ten specimens found no coagulative zone observed. And distinct coagulative
zone was found in another two out of ten specimens.
Diode irradiating to basic fushcin
The mostly found ablative shapes were u-shape in nine specimens and another one is v-shape. Carbons were
found in all specimens. Distinct coagulative zones were found in half of the group. Three out of ten specimens found
observed coagulative zone and two out of five specimens found no coagulative zone observed. Distinct coagulative
zones were found in half of the group. Three specimens found observed coagulative zone. And two specimens found
no coagulative zone observed.
Diode irradiating to methylene blue
There were many shapes of ablation observed, which were v-shape specimens, u-shape specimens, no change
specimens, and inverted v-shape specimen with four, three, two and one specimens respectively. Carbons were found
56
The 4.. International LDRC - KKU & Saraburi
Hospital Symposium 2014
in all specimens that had sign of ablation. Each four out of ten specimens, one coagulative zone was observed and
one coagulative zone was distinct. However, coagulative zone was not found in another two out of ten specimens.
Diode irradiating to Indian ink
The mostly found ablative shapes were u-shape with seven specimens. Secondly were v-shaped with three
specimens. Carbons were found in all specimens. Distinct coagulative zones were found in half of the group. Three
specimens found no coagulative zone observed. Two out of ten are specimens that coagulative zone was observed but
not distinct.
From the results of diode-group found every specimen with basic fushcin and specimens with Indian ink have
effected from laser which showed the abrasion in tissues.
Nd:YAG irradiation without chromophore. media
The mostly found ablative shapes were u-shape in six specimens. Flat-shape was also found in this group in
three specimens, and lastly one v-shape was found in this group. Carbons were found in all specimens. Distinct co-
agulative zones were mostly found in six specimens. Three specimens were observed coagulative zones and coagulative
zone in one specimen was unseen.
Nd:YAG irradiating to lubricant gel
Flat-shape ablations were mostly found in this group in five specimens and also have u-shape specimens in
three specimens secondly. Some specimens did not have sign of ablation (two specimens). Carbons were found in all
specimens that had sign of ablation. Distinct coagulative zones were mostly found in six specimens. The specimens
were observed coagulative zones and unseen coagulative zone were equal in two specimens.
Nd:YAG irradiating to basic fushcin
There were many shapes of ablation observed. U-shape were the mostly found in six specimens, and inverted
v-shape in two specimens. Flat-shape and no sign of ablation were equally found in one specimen. Carbons were found
in all specimens that had sign of ablation. Half of the group was not found the coagulative zones. Three specimens
found distinct coagulative zone observed. Two out of ten were specimens that coagulative zone was observed but not
distinct.
Nd:YAG irradiating to methylene blue
There were many shapes of ablation observed. U-shape was the mostly found. Secondly were no sign of ablation,
v-shape and flat-shape with five, three one and one specimens respectively. Carbons were found in all specimens that
had sign of ablation. No coagulative zone observed was found in half of the group. Three specimens were observed
distinct coagulative zones and coagulative zone in one specimen was observed but not distinct.
Nd:YAG irradiating to Indian ink
The mostly found ablative shapes were u-shape in eight specimens. Two specimens of flat-shape was also
found in this group.Carbons were found in all specimens that had sign of ablation. Six out of ten specimens, coagulative
zone was observed. Three specimens found distinct coagulative zone observed. Another one can't see the coagulative
zone.
Controlled specimens of Nd:YAG laser results in cutting shape changes. However, in lubricant, basic fushcin
and methylene blue chromophore dyes results in no change of cutting shape in some specimens. This may caused from
faultiness of laser-shooting process or some particular substances in chromophore dyes.
57

The 4- International LDRC U & Saraburi
Hospital Symposium 2014
Discussion
The chromophore dyes used in this study did not influence on the patterns of physical alteration of soft
tissue photoablation except using Indian ink as a chromophore dye with Nd:YAG laser. In this group, a majority of
the samples showed u-shaped ablative area. In diode laser groups, the results varied among the groups. There was
no particular chromophore dyes results in any distinct changes compared with the control. These may imply that the
chromophore dyes in this experiment was not able to compensate a variety of tissues among the samples.
Results were varying among specimens. Using chromophore dyes were effective in the aspect of controlling patterns
to result in the same direction, or in the aspect of supporting the results in some groups, such as, the diode laser
irradiating to basic fushcin group, the diode laser irradiating to Indian ink group or the Nd:YAG laser irradiating to
Indian ink group. In colored filters, chromophore dyes, and other such materials are designed specifically with respect
to which visible wavelengths they absorb, called absorption coefficient, which is different in each chromophore dyes.
Indian ink represents black color, which was well Imam in the best color in absorbing radiation, was showing obvious
results in both Diode and Nd:YAG laser. However, the interesting group was Diode laser irradiating to basic fushcin
group, which was found the most similar result in ablative shapes; U-shape with nine out of ten specimens. As seen
in the results, absorption coefficient could changes in some chromophore dyes when using it on specimens.
Conclusion
In conclusion, this study demonstrated differences on comparing gross specimen after irradiating each particular
laser on each stained chromophore dyes. With the dyes, irradiation both lasers provided a variety of ablative and
coagulative patterns. In both diode and Nd:YAG laser, the majority of ablative pattern was U-shaped. The inverted-
V shaped was found vice versa. The flat-shaped was mostly found in the group of Nd:YAG laser irradiation. The V-
shaped was mostly found in the group of diode laser irradiation. Coagulation was not observed, found observe and
distinct equally among all specimens.
Acknowledgement
This study was supported by Lasers in Dentistry Research Group, Khon Kaen University, and Oral and
Maxillofacial Surgery clinic. Faculty of Dentistry, Khon Kaen University.
References
Cox BT, Arridge SR, Beard PC. Estimating chromophore distributions from multiwavelength photoacoustic images. J Opt
Soc Am A Opt Image Sci Vis 2009;26(2):443-55.
Goldman L. Exogenous Chromophores for Laser Non-Surgical Photomedicine. Laser Systems for Photobiology and
Photomedicine. NATO ASI Series 1991;252:7-12.
Fantini S, Franceschini MA, Fishkin JB, Barbieri B, Gratton E. Franceschini, and Beniamino Barbieri. Quantitative
determination of the absorption spectra of chromophores in strongly scattering media: a light-emitting-diode
based technique. Appl Opt 1994;33(22):5204-213.
Melato OM.M. Tissue coloring with exogenous chromophores to extend surgical use of 808-nm diode lasers. A Window
on the Laser Medicine World 2000. 66.
Mourant JR, Bigio 1J, Jack DA, Johnson TM, Miller HD. Measuring absorption coefficients in small volumes of highly
scattering media:source-detector separations for which path lengths do not depend on scattering properties.
Appl Opt 1997;36(22):5655-61.
Vinduska V. Exogenous chromophores in Nd:YAG laser selective ablation of the model tissue. Diagnostic and Therapeutic
Cardiovascular Interventions III 1993. 214.
58
, ..i IV. 51E.1111i0Tal@flithth111116Ifif115 BLM AITVI 13-18

qt1Nain5611-11,1tht6 larinn5 Bimonthly Laser Meeting 13
iitls ci71 2 qalnl 2556
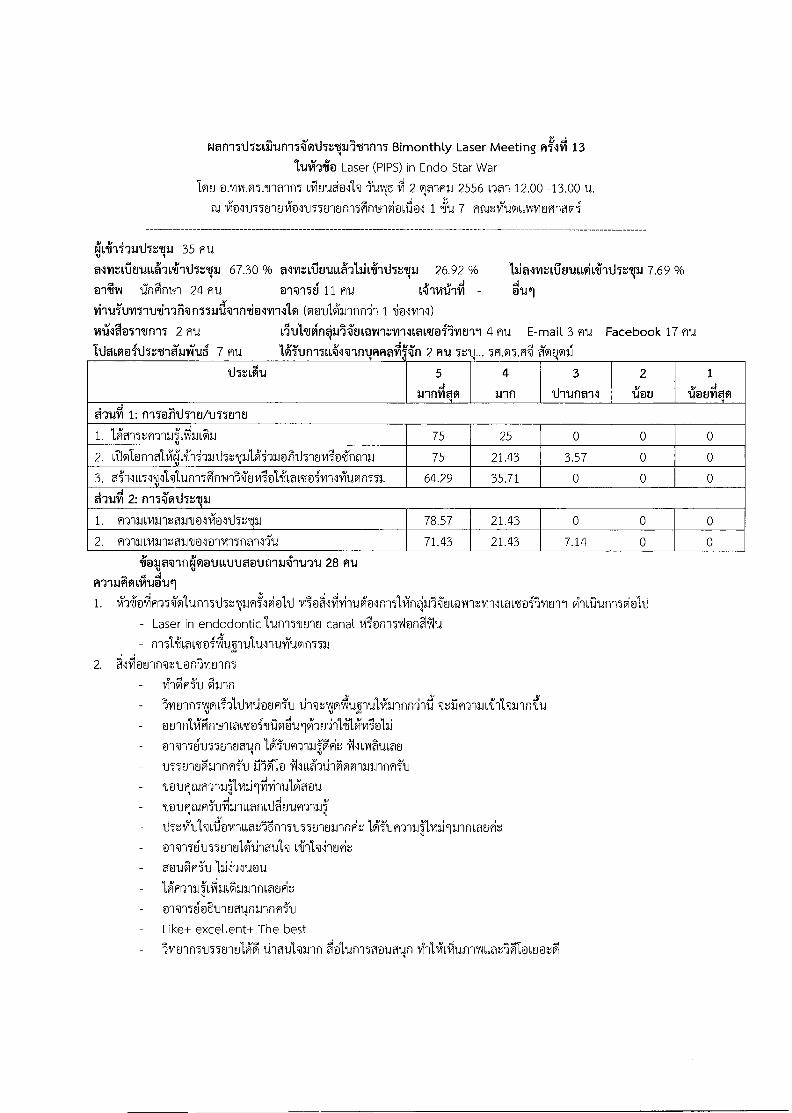
wan-milstirrianilmthnpr`tinil Bimonthly Laser Meeting fi4iti 13
Laser (PIPS) in Endo Star War Tot] LihuiiaN 71JWJ vi 2 9:1W1- 1.1 2556 6w1 12.00 -13.00 u.
tlJ [email protected]@l 1 7 miaviumtvoivwriaffli
kiLii-iiwthrqm 35 MI
mrdlouiii'ati- thrual 67.30 % almtviimiLLAULli-rthr.vi 26.92 % bialmailmniwiolithala, 7.69 % 019J141 l'InAntql 24 fitl @1@156 11 HM - @Ili
vii1d51Jmwt.rdigFinI58rd@in/imillm (moulAnnn'l 1 v19ha@51/m1l 2 FM vitillign*iiitiiMvir.VriltaitailviEn1 4 MJ E-mail 3 ffU Facebook 17 fitA
fiflail 2 fiu 5f1.05.4 ?T91
thr,t.ilu 5
annm qvi 4
Inn 3
thunail 2
iiou 1
ii@ulloi thuil 1: nileirth-mAnwilU
1. 1,kmr,m-m,t'LfimilL 75 25 0 0 0 2. vi.14@friolgiviin -31.11.17ruLlii-Jamisitlyitrviiontrai 75 21.43 3.57 0 0 3. OiNinvi,Vtufin501m4-i'sgtiviloliiaLt@imilviumn,u 64.29 35.71 0 0 0 MIA 2: nilvthrla,
1. PrialLvarmomnlioltha,11.1 78.57 21.43 0 0 0 2. ATh16viwitaLrtioloTri5nm52tl 71.43 21.43 7.14 0 0
[email protected] 28 au
1. vT-r1m41-)Tolunn51hwu8in5lviol1i - Laser in endodonticIUM511010 canal viionnTsi@nSilu - n151i066d@ill,illtal.111111711.101nu
2.ilciarinvuon/vitnnl
- .01Lin
1.11vnenivirdliannn-i-rtl @tiiRyaiLifel'hanniiu
alT1561155Enuatin laorraJPiz,' 9J55ElnahJ1nm511 3J2t a N11,1A'7111F100113,11J1flfli'11 TawIt-unTaifivai-C4i-rulA'antt Tocuqtuni'vfilinLoniliduufi-anlq
- ihtilulwilawiLLarltnnTnwrioanfwit IffunTallinilannooFir, - o'N-11(nn5EnulActinoilh
1,1N-Aunu ldifl-nal'Lciaaannniatifit @-ilwloBunuatinax-inni'v Like+ excellent+ The best
)vitrinTmunulg thaulwin aolunl5aoumv 14-NolufririatIglowoa
It1momithr.riamiuS 7 mi..1

3. ii@Lau@ivuttfiLik
- annli J. 11 -1f17 1.1-Cdf-wit (3 YITU) MTUSLIY12{iAlaigfrild

aiLINairMimncirihnpirtnim Bimonthly Laser Meeting 14
2556 IticiA),5 ci7i 4 6cLATIRL
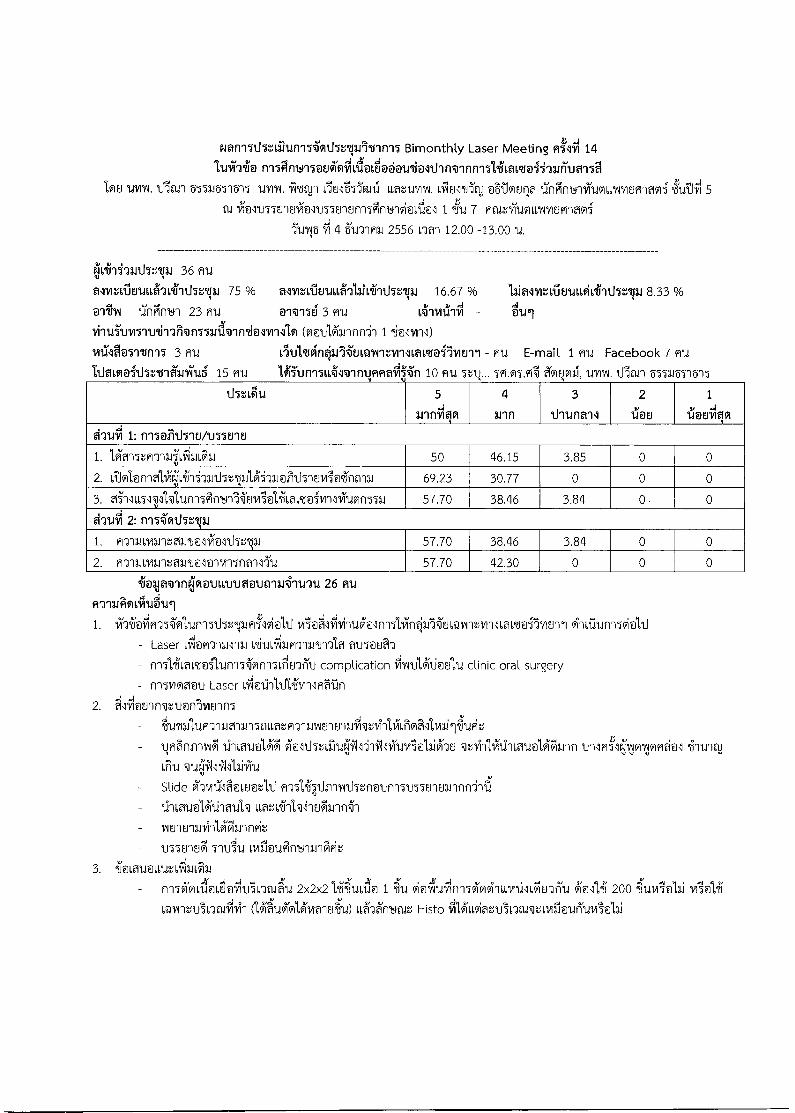
r4aniTti5taritini50115r,Vii°U'ini5 Bimonthly Laser Meeting Atrii 14
Tou td m. Ulan 55511571515 UMW fl/IN11,18a551191 Lfutmrk, oBlviuf; iTnilnyivicoiwornuenaoi.tiuTlfli 5 fid i@l1J75810@n5501Elf1150111111Vi@ISIN 1 /711 7 Fit-urriumworomaffli
luvu5 4 511-y1n8, 2556 Om 12.00 -13.00
OA-Huth:11i 36 mi..1
alitaltiluutta'aviiit15:11.1 75 % almr,vilmaiAlaiLiiiihrp, 16.67 % 11.inoiniima6o16°ilitlulli 8.33 % ,4
01'1111 1:141141 23 EU @1@156 3 Ell Ig1V1111i711 - DUI
ifill5111151U/111FlqflII111.1WM/iNT1111,91 ([email protected],41111f11 1 /1@l1111)
vraao5itn95 3 mu - fiu E-mail 1 Facebook 7 1.daimaithruiaviti6 15 Fru 10 cm ... 5P1.05.? ?TM V111,11111A1.1.lia11 55511571515
thr,Lena 5 .4
3.11f11191 4
Mil
3
odiounail
2
%Mu
1
iiatiiqo
&nal 1: nil@lithiuAnuiti
1. 1,4015*an1141,in'11113111 50 46.15 3.85 0 0
2. ttolanialiCivii-&ankelaiuolithluviaiint-m 69.23 30.77 0 0 0
3. o5-11Lm,111,41;unlFin'ill'goviialihmtoi-vnlvivain552., 57.70 38.46 3.84 0 0
&Ttiill 2: ni5i'orthr,Vi
1. E'r1.161,11.112,101.111@lVN@1`07111 57.70 38.46 3.84 0 0
2. Pranmvantnno5o1vn5nm5I1d 57.70 42.30 0 0 0
iaaja@inlmovummougnuinny 26 Ft F1 Jn8JWt16vttde7td1
1. 171-riViR-n-alunlTd5wip/lviel,11 - Laser Lil@Fraum oiuLibgrilmtml?i amooS-)
t-mliLaLt@illinnonn5itleTiu complication illArtAki@Eati clinic oral surgery
- fr157wian Laser viliotiihrlivnlmnn
2. ii'lfiotilnv,',u@nlmErin ilutillwriagramouotFramEntraSinIrctitriaillvail&it
1.11LalionlA' h1115:iii11/01-h'WliritroiolaiAcm 111194\101eE@1 .ihtriaj Criu
Slide oimirt:i1F1@wor,1111-)71,417,1inTrithEnvun151.moitannni-rti
IniunEranfragilnnie,
117701a 5111i1.11,111flUalf114111A'Et
3. i@[email protected]' Saab]
- 2x2x2 Vgidi@ 1 CI A'N141 200 4tI11i5ol8.1
aora,ViL-Jwiivin (lau9iol,(9lvimuiT11)116'"A199.fld,t Histo

aletiNannol'icutleilpitnn'l Bimonthly Laser Meeting 15
2557 ict.ar vi 5 illiiiiiilli
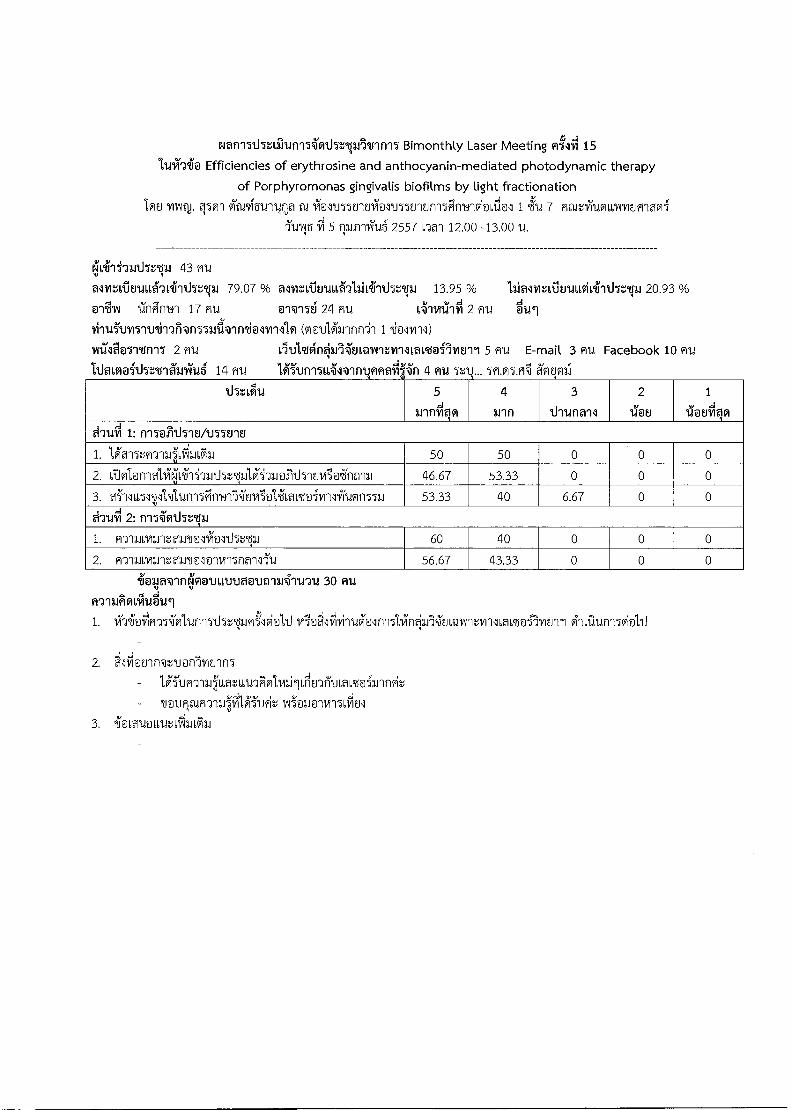
Nan15U5tirrunllifi1J5r,VA4J1m15 Bimonthly Laser Meeting ntriti 15
11.Jilli@ Efficiencies of erythrosine and anthocyanin-mediated photodynamic therapy
of Porphyromonas gingivalis biofilms by light fractionation 108 my,. viaphunioua 1,1011MEllEliallnEJlElfrl50111111V1@1:11@ 1 ifid 7 flait'ilVIIMEJFIlMli
111115 91 5 flagyruTug 2557 OM 12.00 -13.00 11.
r:.„Iviiii-Jarthalp 43 wu
asivrAouttAtifithalp 79.07 % antvriuud-alaiviiiihvgai 13.95 % laiallirAvuttviLiithrlaJ 20.93 % e11 UvV 1:1fliii1141 17 Fru @i@i16 24 mu 1,4ivrtlifli 2 nu -
vi-nifumitrti-raktiluenirmiolv-mlo willa151°Ufli5 2 Fiu itaullivinOrliumuitvn1Laivof5mErri 5 Flu E-mail 3 91.1 Facebook 10 fltd hivsloithruiarkuS 14 mu
lffunildl@inwmailiiin 4 fild 5?1.25.Fi 261D12.1
`thflaill.1 5 4
Intivilvi
4
anfl 3
thtlfl@il 2
1.9.1M 1
IbElfilfi *ran' 1: f1150711h1E1A155E11E1
1. lh-nT,HT134viru'LiFlaJ 50 50 0 0 0
2. illoInnieiliefighi'mthg.,10Mu@Fitiyi8viloint-rm 46.67 53.33 0 0 0
3. 4111,151,,[email protected] 53.33 40 6.67 0 0
Mirli 2: ni591117:13., 1. [email protected] 60 40 0 0 0
2. fiymoniummlolvil5nan151.1 56.67 43.33 0 0 0
4.1aajav-mrammotrtmouniu4-nnu 30 nu
1. 171-riiociFrM'oltininNalujoioltim10'Avinuklin5linOfguimAnniilLaiqs@fivEril
2. Slfi@onnveuonlvoin
la1Jh1n10,'66at661dahlmilLtitn6I16amiulnit,
-
3. .ki,euoLaztitiLk
oIcLINarrMjm1cul17t606nni Bimonthly Laser Meeting 16
itils CI 7 lAifict4fl'Inl 2557
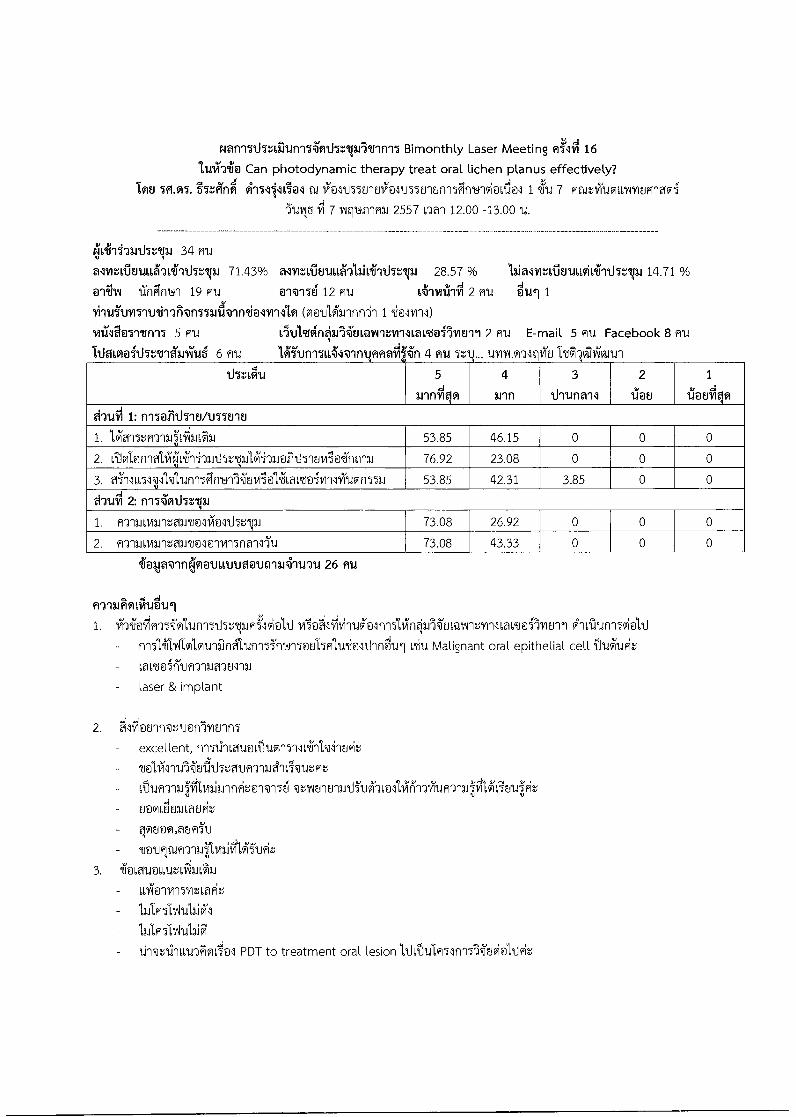
rani51.151ailignIiwthrpAlriniI Bimonthly Laser Meeting W55NI 16
lisiTti@ Can photodynamic therapy treat oral lichen planus effectively?
btu 5A.M. i5r.fifii 415,111301 cu iolv55Enuimmunsn-i5Fint4-ivioLii@l 1 7 fifuelholum.Piriwimi
JuiNS 7 vutplirwiL 2557 na-i 12.00 -13.00 IA.
4kiiiilarthrla., 34 mu
alwailuuttAcaifithrp 71.43% almAnukalaitif-rdwp, 28.57 % LialinifitnaitsiiiiiJulai 14.71 %
0-AN iingni_qh 19 flu @'@i56 12 fiu 2 mu oui 1
(voulknnfrl 1 .duifinl)
vilmoyitnil 5 R1.1 L'It.litgif105iEJLQW1VW111a16604511011 2 Ali E-mail 5 M.1 Facebook 8 nu
111M01041hritgaliihth 6 MI fifiafi in 4 uvrounItiiiu
115Z6t1ld 5 d
1.1111VITI
4
ann
3
1.1-11.1flflil
2
lk 8
1
1ThElistilffl
dlliill 1: ni5@lithitomuit,
1. 1,kri7e,mil4ikal.i 53.85 46.15 0 0 0
2. iS.101@n1AVV,hiliT.1115211.11,MT.J@T11151M,119ifilf112-.1 76.92 23.08 0 0 0
3. a5n11151v‘klunlinYil'avil@lilLait@iiillifuvinmi 53.85 42.31 3.85 0 0
MIA 2: niivit15:..1 3
1. A7'III6VIDltallTO5'il@5t15:119 3.1 73.08 26.92 0 0 0
2. fimmia.maln@laqvii5na-miu 73.08 43.33 0 0 0
foklavitiqqautttn.movniui-iuqu 26 MI
filiuknirub'tai
1. IrraiioVim-aolunl7thrwflvialliviidlihiluklni5lin*fgEiLorivollimtailmoll A'nalui-nwiplAJ
- f-v- IiilvIlm'kunfineitunl5i'm_415@s1541,u/[email protected] oiu Malignant oral epithelial cell 11`tAtig.-;
Laor nifitmlumum
- laser & implant
2. Filihointu@nlvEnn5
excellent, friTtInLauactluvr15111,41-1141Eoit,
qzlitrity-aAfTuOi'am11,1M-nifufi-na4,'Cilkin,Pit
El@liFJULWERit
- go8@oLasm5y
- Touqm-y-13.11vaiiiViiude,
3. 21@I,M.I@6L1dt6171111:6ill k19/1151fItlit
1111mtviulaiA
- 1 ;.1Wi91-1111,1g1011@1 PDT to treatment oral lesion 1,tatulfi53in570ovi@l`titi
aTIJNan-niolititht6 p16nnl Bimonthly Laser Meeting 17
it,115 CI 16 mricimad 2557
NaniTi15zirrisniintlIr.vhstin-11 Bimonthly Laser Meeting 17 1.1.1iTh Efficiency of erythrosine, anthocyanin and nano titanium dioxide and blue light on killing Candida albicans in vitro.
108 ariWad staigra, al IXNUS5EllEli@l1155Ellunl5Finwnviafi@l 1 icu 7 mare,iummuMlyimi 5Ull5 16 mnTim3.12557 nan 12.00 -13.00 u.
ejkiiii-nithrt.p.i 29 mu
almailutaqiiiiihrla, 66.67% alviziginul'alliiiiiihz.vu 33.33 % laiamifimaidili-rd5r,v, 26.92 % iinclinwl 18 mu owilti 8 mu 2 mu dui 1
[email protected]@1ntoormlo (voulk-Innl 1 tolvill)
wiliao-rtinil. 1 HU 111114111f113.1506Q`ViltY1111H611@i19/1811 1 HU E-mail 5 Hti Facebook 5 fill
TUa6@1o5llu411a8aTu6 6 mu
1 pita
ihtLiiu 5
1.11f111101
4
Intl
3
Ulla-Mil
2
`11@ 8
1
ilotriiqo
d-rthi 1: ni7@lithiutimEnv
1. 1$1015ZR'd1UVILIIL 38.46 61.54 0 0 0
2. Liiml@niali( jiLihquthelulAi'Aiorrd5loviioint-nu 38.46 61.54 0 0 0
3. eillmlvW,unn5Pirron'WEiviiolifiattoivinlvitivinu 38.46 61.54 0 0 0
d'n.iiii 2: niIivthr.V.1
1. N11f8J6HAlvtOIi`Ue1.9vie]5t15v1 53.85 46.15 0 0 0
2. m-)-aiiviantoardolo-onwalllu 46.15 53.85 0 0 0
liato@lfikiq@vittraotiniaiiiu'u 13 fru
1. ihiloi,ifi-n'alunnTt.l5t-pfii'oldill gii0un-159i0,11 I(1E1 6AIltillt11(5IAIt.) RT101,11,111P,WY151,41
wit@invi'un-M'nwn toucholivon4011111.1151vanulavroti 41.114A'' mit @i)
- nn5lif6a6t@ilto-mmoilu, remove caries 2. 'ilflounnvbuonlmunn5
iia.213im-auRia.AL PDT fitiLiira Candida albican
- vertcmimii monotone lthinio8 - til@wrdietIN
3. 41001,1@talt,iii1.1
- naTilaUlAJCIM 1,F1WA'OvtluogfilinoliNintn-H1 vm(1.11.vi5 ciou'N 6i1rI52PA80gil 11151Z6a6u0i
annliZ71vuo-runavituil2i-ruq-n.annl
(llkon'M'ol'icuthri2p16tnfm Bimonthly Laser Meeting 18
ilei.4 vi 5 cili 3 elildEllEn4 2557
emninllananiIi1vrthrprIvini7 Bimonthly Laser Meeting 18
1.1111"1.11P10 atiliStIM.1,1,11/11Al.o-gtiviu oluudol'k IThOinwnriumuctfuviumani 0Yucl!lil 5 al IXNm5EilEriiii@lm5818n-iiin1410i@a101 1 239d 7 flf1,1VVitIVI66IAIIIEFIlMli
11.115 11 3 fitiEnuu 2557 nal 12.00 - 13.00 U.
40 mu
alitudisuiawriithrtp.i 87.50 % amitiouiifillaitfrithruu 15.00 % Lialmatimausiti-nktvi 12.50 % @AIN 27 R`U 01@116 11 ff1.1 L41141214 2 mu '61`Lii
(notilk-Inn1 1 2i@ll/I11)
Vilila0111.ffilI 2 MU MulmoinOli'EnonvoilLavuoilvani 1 nu E-mail 4 fft..1 Facebook 13 Au
WVigioithrtnarauS 6 RU 1451Jn156il@in nnail 10 Rid uvrw.n-altrviu, uvirl.mmo,
thzigu 5
winC4191
4
Inn
3
itrunail
2
ilou
1
ilwriilvi
'atriti 1: nilorrthiutuIluiu
1. 1,kiltRY111:11,f1111:61J 40.74 48.15 11.11 0 0
2. LT.lmi@nwaciiiqi,ili-M.15:12,11A'i'L@TrUTIFiVii@65ntru 57.69 42.31 0 0 0
3. ai'ilM111'hi,unlFincdn'N'ErilialilLaLtoivrililumn
551.1
37.04 59.26 3.70 0 0
Mufti 2: ni7orthrzrai
1. hl'J'18J6Vf8J'1v218J21eo51Ae@5t15v2f8J 59.26 40.74 0 0 0
2. m'iaiLviLltami@lmviinall-Tu 59.26 33.33 7.41 0 0
lioaja@ineloovionaatinialuqu 27 nu
n-alliii91111141.161
1. 1Mal-41'n'&11.4111TliTglIJRI'lklli vil@FilfiviTIA@lnlitinO)ALunr,vrilLaLtEfIvioll Gl 161dun 151 J11)
- LLA'-]Loioluaain'a 61@5orl5fithaulwit
- 6a66Uoif111 Orthodontic
- initiLomoilun-M'f-n4115414/im.frintul
2. Fililalnalt@flvoln5
ilnynAankvanhtLgrucif14'Itriail -ILLue,11-1
- Tountufill''n-nallvaint
- Review anfllf'111
LdlannLaunt
1411,gine, annliLfmn-nlAuLklun-mIlLauo
3. iioviumLuttilanFai
n-an-M11..1
- anagoliouTib' 1,Am-y18JP66atl,kolugh21dikau 6-arliiii.l'hn-i-ri7NaLilEaRit (1 5 IiiLauelkviliitivilLLA'wit), ToolvimaruVilLiilu-nmvitLaikiodilt(LLii File,Pillildi)
V. 51E1111.1qclifIl5Othall3A6dini5 Laser Therapy in Dentistry

I'LJNanl .l'o111.,Alktiwl/ilnl
Laser Therapy in Dentistry : Research Transferring to Practice
lucr/1 12-15 'U'IRIJ 2556
In55n-An'auni Basic Laser Therapy in Dentistry: Transferring Research to Practice
Continuing Education Course
viinniniqr.m9wq
IMVIVOR112.111/1111fildVILLIAIYIEIMARf ISILIMARRRIA3-11M11.1AU1ALIMVIATN.11193.11ItAlkl
1.111:611fallanInnfl A'11.15'nnelunnnIT:,;60.116iinn1T Lasers in Dentistry; LDRG-KKU Symposium 2012
66M ; 2013 Ai 9wiutnnO-Ktivolltvin1,flLelitRYEJ11/1111fila,LIIIMPIWIFIf 1.1/11VItrA°11(6116,1iU Lda
Chliii11/11A1.11A111. 2555 662Vv YV.PI. 2556 611VaJRQUAU1,991n01,61niql.lthrip491nnlAkILLfl:',Lran'n
Yill,utIsnyivilviv.lii.wAJT,LvimlunOvatAnwiliTAIn War191119.til'IlIvALTIM
r11511A111,1JhUa2.114A911.14Qall nIA1111r17A't11,1,flnIr111111112°11tD1K11261,1.12:41JLEL:111EILLIRITAIn
Pffignfildfr11,61NYILIP1100151111J5151,Y1 4111f1 AVIITUYTIOIMIT tall-,n014'uLt111:11111,M6litilYIUTV1111%
L6 YIYILIWAPliMA1IV12.114-tiTt1d16111la1 61V.ranAnb-1yiuml61lvi2i ArldZ,'YTTOILLIAIYIUWHIPli
lavilmunkvauuriulA199,/i0VI1W11,1196%TallYMTVI'llYildV11,61A1116- 1ill,AAM,VITART1111274'2J TOltif.1
iln14"tivaln13.114'fil,t1^11:111111,%TanYlfMolaciiirinb-1 .111,friAmAwYmnsnit,flviitilvityrvinlaan
inlrlInlEltd1,1,1J1J Yr11114114"fP1 lAlg11,111,1AQ11.1211A'ru lunnsamIn14'utullnium:-,nnTtintwam
INIATUTa111116%9VanliltrITMEIII1114'fit1.11141.1 fr1fltfr191.4.1(TgridlIAI' 61112.11,401T11.14qatY1111911r112
1,11(aLiJULIVAU11111,1,1116/11`111111,1111M1a3'rnInKaulaiLls:Avil'n-romflt'ilplcunnvA14%.,nniiliu
VAGIATANrins4-mtumlont-rmtuynumitnvitinvinlvilownitoinwif uri.aniirrillviumummal 6
iiil16S9n1511nwl ii1U4-RilutmlnnslutuLLTn Lilt 12-15 '11,11A1-.1 2556 Ttiesiq'tAn 419nrin1T
INIAn YitatviAirticivii14q3A85\inni 21'1
AT1311AQ11.16.1119911klinkalknriLinnAlimAtutalaVIVaivinlvlianT23.iuw:,-,ilmqn01414%..51.91Rflosti
lunn5lt-nlArdwavivagmuLflostfaimInth,AlinnnintwaoImtnIn7j,4'utulini laannallnAnwn
viufrnarviai 6 iis:',/4191nnAnbl 2556 9n1-11,19n1TAnwidwiln014tri 411A4'mtuni51-Irms
41.11111116fl vivanTitnyraiimulAwityrigoi tj 2 AQEllieralU fiqr,1121'AT11.19i Win11.1V1a1 ovani3sn
rmsrstiu9S ArnIdnns ,4-u AELtuthtttrisuluvinainiiim um:',i(frart,InuTfflsninns5°'nwivi,a11.1
5-m9 -,a115414
1. 1,11t6Nt161,'MAT13118q13.1Li111,9011 2.1q61.11,Mra3-1112_1111111711JILLYIY1M110011' icptunnnTwria.11 1,;t-in5s
esinuns:,-tnUrIlT1.1512J12.1 011b11,1r1LIDITA1,1,11,1,1ILI4Wal
2. L116111,011stlilti ChUViflfrILYIAIUMILM611(6FIVIErlY1111711011,61AVV12.1WARf 1P61.11,11t1KAT-134P6TiM
1.1=Inivialluirupin 571J
1
1,11-rvilnu
1. 11'n n aN-Iiii.ou,tral
6 Tili(Valqa9nqTPinil- '0,1.411 2556 qnr1149/1911/1UnA'tiarnAlriULL.W:,',
inWnd 60 MUI,AhiAqq4 1,1,q:5W11.11Stri%1'111011'ITYI'llYTURt1511J1tiql,LITOlfflA
W66/rail,A1
2. einli.gt1192JAT-1113.1621'1VihrrisAnb--114'tilan,11"mnsnaLIEFIIIMIT111711011,61A111UPINIV1f
671.14011St@IIIA5Alliq
1101734iIIMIAMYr111,q1,6/ItnYIUTIV111711011,61AIIMMANf nzyliaLauyitimmif wirMylunkonuuriu
ni5-691,11141-ru
1. LfriltwriKm_12:3.1-rinns
1.1 tinosnlaqurnskutiunnTLiltlitRquiql.iltrilwm,-yiumouvitoym GlS
MITIYIEMA1611t111,1,11U LLVSIMVit7j112r1nAilultwan9-istiluntizviumagyitivinAfrilronlmtnAntuuriu
1.2 tls:',6iihhiltTuinhKfrILITrAllArtihnhs
1.3 Lfrisul.inhT4'm_15,1176iihnns
2. A'frr1i2:11.1llinnnT ‘5-14c4 11-12 Fjunni 2557 (NnIlii`11414frIMS)
3. ArilarihT,1,111N
irgi'aniqii51-13416gi nig
Laser physics and tissue interaction
z. Laser safety and machine
3. High intensity laser therapy in soft tissue
4. High intensity laser therapy in hard tissue
5. Selective and low intensity laser therapy
6. Hand on and Research presentation
41111113.1 ArIZITUVILLIAIVIEW14frlf 5.114`11Y1flqkVal,A61,111,1
51.121rV al 11-12 31UnRasi yV. M. 2557
491.174641-li`JWIJI:111 100 AU ISJ1,11:411Y11.11 6 iTtgyw, 60 AU Ang-,11511.111'124'1141,1 30 AU
1.:014191,11MQ5.14TLIQU 10 AU
2
4111.15-tanc1a nq;aJ14t.11,t112L1/1111,%61141112111/111VildffILLTIV1WIlAfflf
Filli'4'12111.1111VT011.1/t111
1.1 kIt'l11171ILM151,Ai15114 411,,m 2 alvtl wc1-, 30 Ir171100 w1u = 6,000 um/
1.2 incanvin5'nflql(TU(6119ntl) 1 1.1vi 70 In11 100 Au = 7,000 vnvl <N9'
1.3 kl(011/115'11Mllia(ionInAlm) 1 1.1'61 n_ 170 unll 100 Au = 17,000 unTi
1.4 kranwis(Afarim) 1 n 300 unVi 80 AU = 24,000
1.5 Pill'Aqiin'alnU = 5,000 tinVI
1.6 kvqiin511.137111,1,Mi = 3,000 inYi
Tql.figiUllU 62,000 iinfi (ViniAuArallATUirrititaU)
lvitnn7
2ymim-u5-5-v_noq-mn2 iri'vm.firailiqui91`1lirup1669Nvitwr-1140-4
ArIZVTLIVILLIAIVIUMARfITIA111/1ErAll'auuriu
ACIrATIOILLINVIUMAfrlf 15117511trAJ611tULLfil4
Atia-(91T,LINymprmfrif 1.11)11`1/1trAll'au6Lriu
RaZirldffILLYIVILIF114Pli axtriravinnknrauuriu
mm-SiumulAnummimil.nrilmunknouu,riu
ImuinillnilbueTinil ni5-146mq6villiiunnqq34 Plal.:1(IiaLLIA11/1f011Wlf 3.1111111trlkIlt`21,1,d1,1
P1[1,1LITIWILLINT1t1W121fr113.nu7jmunkvau66riu
Ang-Sicownimpingwlf wurvIvitilkVaULLfild
AnzvliaLoArimpinowil avn7vit1`4tnrau6Lriu
AtiLtbITAINV120114frlf 3.11KMVIEllk°11t1,161,fild
AfIg.',11TIA66IAIMMAfrlf IVIATIVILI4E111t1ILLF11,1
Ivitnnitimmugemlult-mig 1. 1,11111.c454N.I.CAr ld111/111
PCIraila61:1"111EIPMIFIf 1.11AllYlf.J4?J°11(61,11.1,111,1
2. uvrw.l's,rivif (1Sifr1117 flit]
ACIZYTUFILLIAIMEIMANf 1.11A111112_14tAt1,11,1,1114
3. UY111.17174PV1 (13.1113.1
Af1,1:410161,111/12MMINf
4. 141111.3M111111_11(1113.1
MaltY110166111122.1W101f 3.111'1111t14U9101,16LriU
3
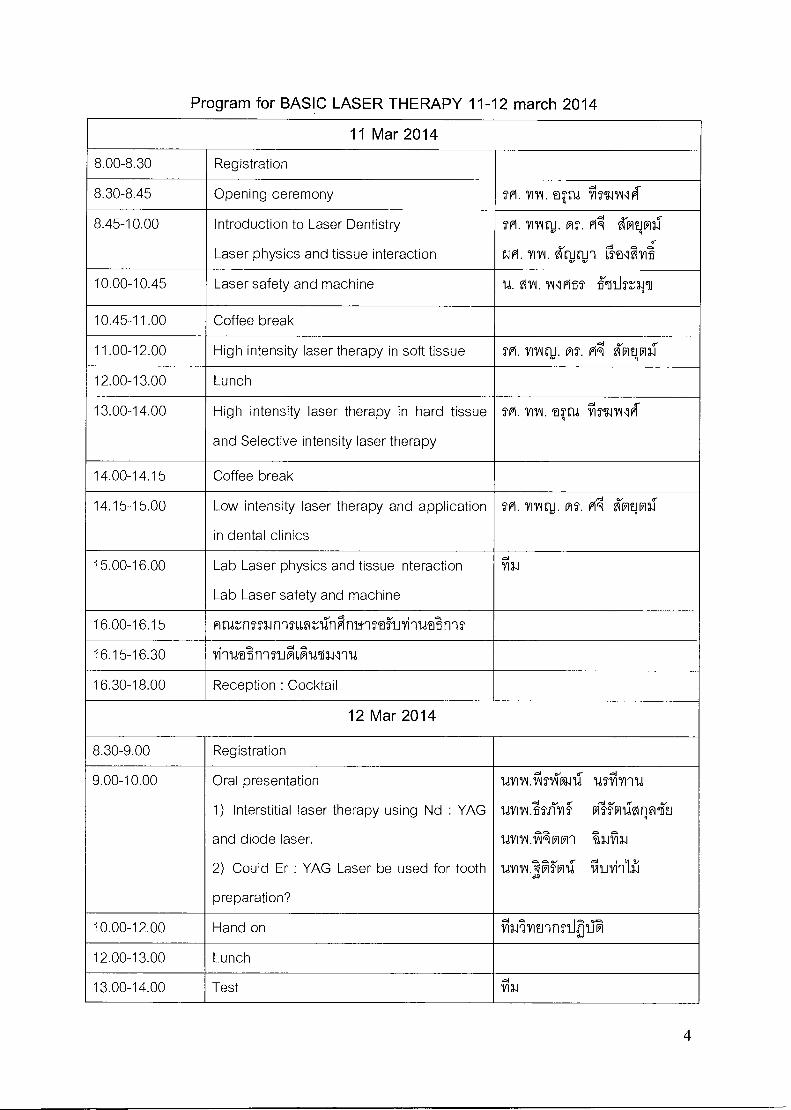
Program for BASIC LASER THERAPY 11-12 march 2014
11 Mar 2014
8.00-8.30 Registration
8.30-8.45 Opening ceremony 241.1111/1. tr4 CIMIAllfai
8.45-10.00 Introduction to Laser Dentistry
Laser physics and tissue interaction
Tm. vagru. Ms. PA 617111
N. VM.fttli1 r5El.. yit
10.00-10.45 Laser safety and machine U. N. vulmss ''.111.1v„-ar-ii
10.45-11.00 Coffee break
11.00-12.00 High intensity laser therapy in soft tissue Tpi. vrwq,J. ms. A 6-Nni
12.00-13.00 Lunch
13.00-14.00 High intensity laser therapy in hard tissue
and Selective intensity laser therapy
TM. VIAL tSrld 911 51.11114
14.00-14.15 Coffee break
14.15-15.00 Low intensity laser therapy and application
in dental clinics
TP1. Yring1),. MS. P174 hy-12.1-
15.00-16.00 Lab Laser physics and tissue interaction
Lab Laser safety and machine
'111.1
16.00-16.15 Anznmnnn,nilnPinwisfaNyinvdsnnT
16.15-16.30 YihwAnhTIA6Frina41114
16.30-18.00 Reception : Cocktail
12 Mar 2014
8.30-9.00 Registration
9.00-10.00 Oral presentation
1) Interstitial laser therapy using Nd : YAG
and diode laser.
2) Could Er : YAG Laser be used for tooth
preparation?
lalYCIATIANZ lalY1114
1471IN:bil'Ilf Plii*LIgirM6ii1J
umALTAARR1 'i2.11%
umv.:Iiii-Ril *Irvinlh
10.00-12.00 Hand on ifil.illitihnJA_Tai
12.00-13.00 Lunch
13.00-14.00 Test ch
4

14.00-15.00 Discussion VI. VIIAIrli. MT. A hq ni
15.00-16.00 Certification Tril 31
5
wanilthalirrulnwilgiartimmainlula Basic Laser Therapy in Dentistry: Transferring Research
to Practice Continuing Education Course
itril 11-12 ilinfiu 2557 tu nturhoivkaufrimii arvrainui6EJ1101161fill
4111.41,i111ht111,17T
1.1 1 11/11.10 49 MU 4`11n1,[email protected] 32 Rld
at1'1tiun-1501mm@TIMPinwn mtuz,PonaroEmlavli
6'frtltuzenen-m-runl5v7-11-nnoZnclinwl viimumnig, awn'imEnA
14'7o.stlocuu,ricu 0l 0J '114-Toqua7-16uslf.1
111150?fnaum. lctirTM'@EJL6o 11,110`05T-166S1J1 `'1111-701J11,11.15111
LIAJFITIEJ 7 ffU 11,1 25 Rt! anN 1,618 24 '11
.rs t wuthtnn-iwIliali:[email protected],1
- VIEJ621152MJ52,16 1 T'Ae.i'lll7.11 LLazaRmilualdnui,avd@flu lecture
- 6REJL411+AIMMI:31@ 1 TIfile,i11,411
LHe Observe case CIMEntiomilutTl5i11141 61,9-11j1,90011@t15212,111i@ll
- 6fit.A'Efolu5ruLamailrifivaLatvio observe case e:ohhuvitioctEaunni'irill
1
-
,1iLHEJ LmEniniflurnaavuoilui@lCimaLatladanviciquoruhalltolutavni-ml LDRG 1r166Ai-J
- me Hand on laser symposium 02,1,6Frilllmuluoi,66o4 Bimonthly meeting 2 flitl
- VIEJ6/2111111157EJ181,F1181fM101,66@ilatIMEAU assistant n1514-1 incision and drain
- Laoill1n5ensNammoliingni4-01 8-AoLtai 2
6HEJ661151/21111U Symposium Si@ 2
- LMECiEJUVI@IA 5 lat6f1E16411iUillt1550-1EJ151@1 Laser safety
- Lmellmmn-15allu9"AilnKauFrimiiii@lthn lun-ninw- v111uffiii soft tissue cession looli Diode
laser
- 6fIEJ1,411i'AllY15th111.1 Symposium 0L1d11 2555 Vilw,L5LRito-ril Loaqihiu.N1 Bimonthly meeting
- 1/7`1gulu1;h6h Interstitial laser therapy
cHwti'[email protected]'15`chtvirtnnl Laser symposium 2012-2013
Solf tissue welding
Lmmihiun-mhtiskiLLatriwn.ni Hand on 1-114 Laser symposium 2012-2013
Itichallertamn lAtilo-N-156aut.im.5EnELLvi6AlitmmihIrkS1
- Lnutlandiu-JiitiAxmluwmoivilolku Lwillimutrh.511,41@T,LRmil
- Lmuftu assistant 6thelnumwmAtinlVicac6ti@i luni55irtlne,Nu
niTtJuNnkaosoiyillviiamni,L9011-ruWEICrienel'uoLemi
- LmEnim,1411-ruLilEnficuLavuoi LoiEillaia-amt)4911unikil@e,9'1@l1,4h@LATil-11
vi@lk&I'lAME111151,6a,111114=1-11,11711ificULaLt@i 2S1611,2im-11An$hu
1
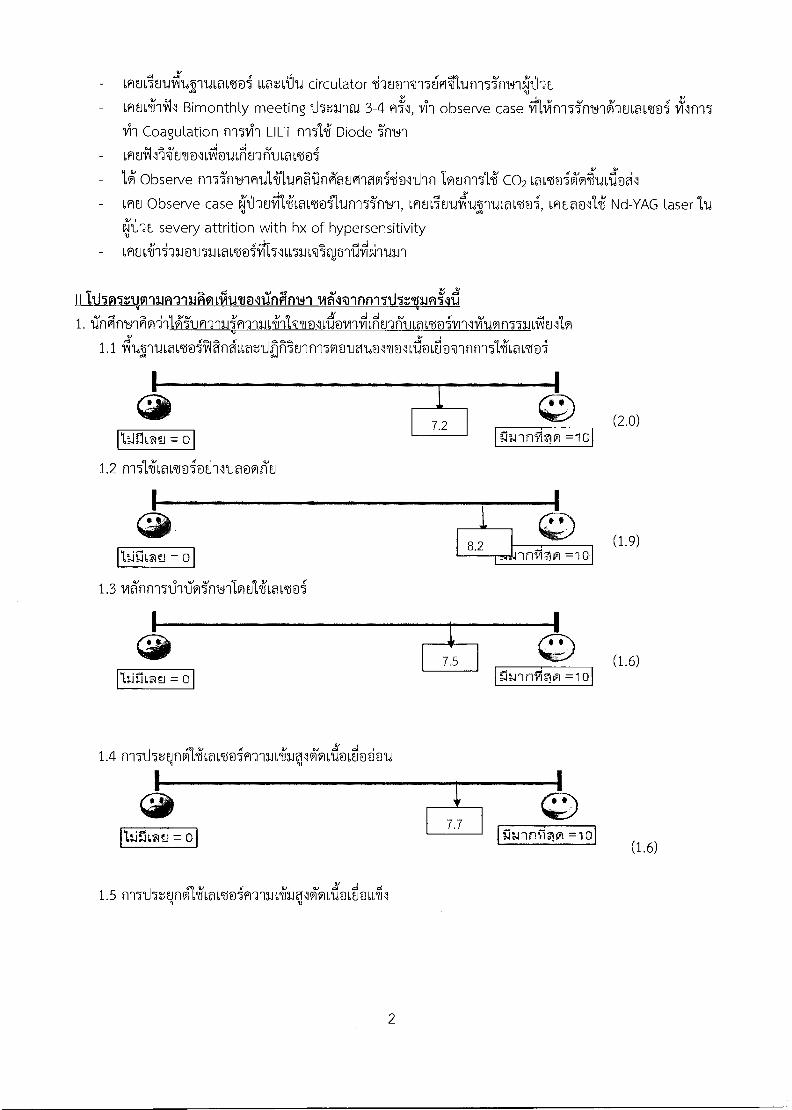
(2.0)
(1.9)
(1.6)
- VlEJCiEJ1.411-11.11,M66@i LLaalu circulator 6thEi01 -156FiTh.in-15i'f1Yy1e,),'.d2Ei
tmaniAl Bimonthly meeting 115n1'1tu 3-4 h155, VI5 observe case iilinl55ml-IPm6a62do5
Coagulation n15141 LILT fmiii Diode
- immleAlnolAutdiEnt-ivLam@i
Wi Observe rm5rrt9nmulAltimailnKauFilaffli/i@511'1n co2 La os@i6i9r7lcuLd1
Lmo Observe case eilihmtiw1,[email protected]'1, 6h1u5u1d`iL5'11d6m6mi, maNli Nd-YAG laser 1.1.1
4:thu severy attrition with hx of hypersensitivity
2'. Itholl.vragraiaionitien111-Cfint4-11461@innwilltlunIni 1. tThiinyik'ill,ffuR-314m-n3J6411'NT@ILVITVILFIEJ-3171JWLE6@imiliumn5uLfiullo
1.1 currui,amiiTangtonihiliEnnlw@aiummilajovInn-1514cLamoi
1.2 fi15l2fLavd@i@d-111Ja@i1E1
1.3 1411n-ml-rM'notlioulift,ami
1.4 n5t5qn61/216a6nim-a-m641311k9LFi@duu
(1.6)
A' 1.5 nwd5alnvitiLa1,66@i9-m1413q1V101,1J@I,0066/11
2
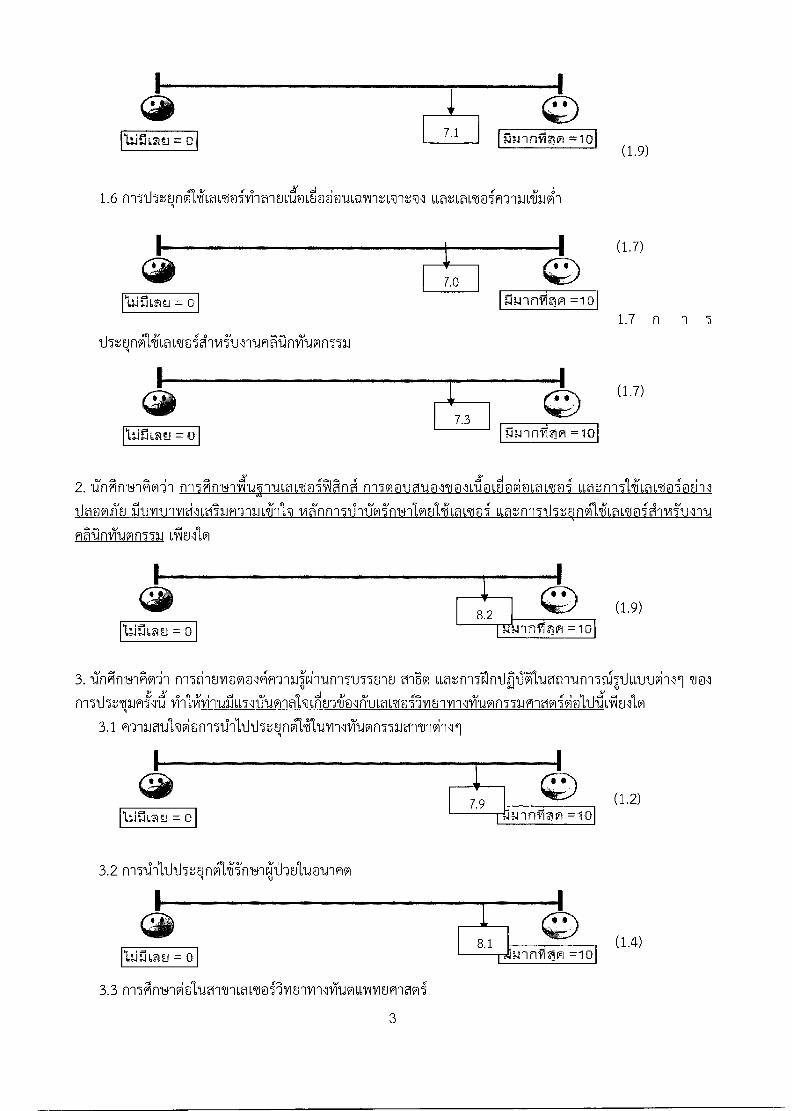
(1.9) 7.1 = 0
cd5tNnAilLavdoignmi'ul-rtmnnviumn551]
(1.9)
(1.2)
1.6 11151.i5r,qngliLavniviialuda" @d@cuLmAntLwil tLammt@im-imivraiki
2. Ilfigf1141P1O'il frITAf11.41171YWUW1,66@iiAlFing n15motaumolitailovi@Lavdoi 66atn151i6amoiail5 iluvrunvidwilmfi-r-ILLihh viA'nni513-11VimlnlAulifLavdoi LLatnn51J5LlniilifLavnienvi'vyru
flSilniumn551.1
3. iTnilinblAwin nn5d1Ern@[email protected] Lott-1511nIVIViluanntini5t-4,1Jutroilll
3.1 9-yamulwionnTailhJ5tNngHltvillviumn551grrnvilli
3.2 n1511-111JTJ5L1nvitili'ml*tillati-wwi
I •
8.1 (1.4) = 0 . ...L.nrrinlol =10
3.3 friFirrt_41viAi.,iernini,aL6tioiliiErwilliiionvormociwioli
3
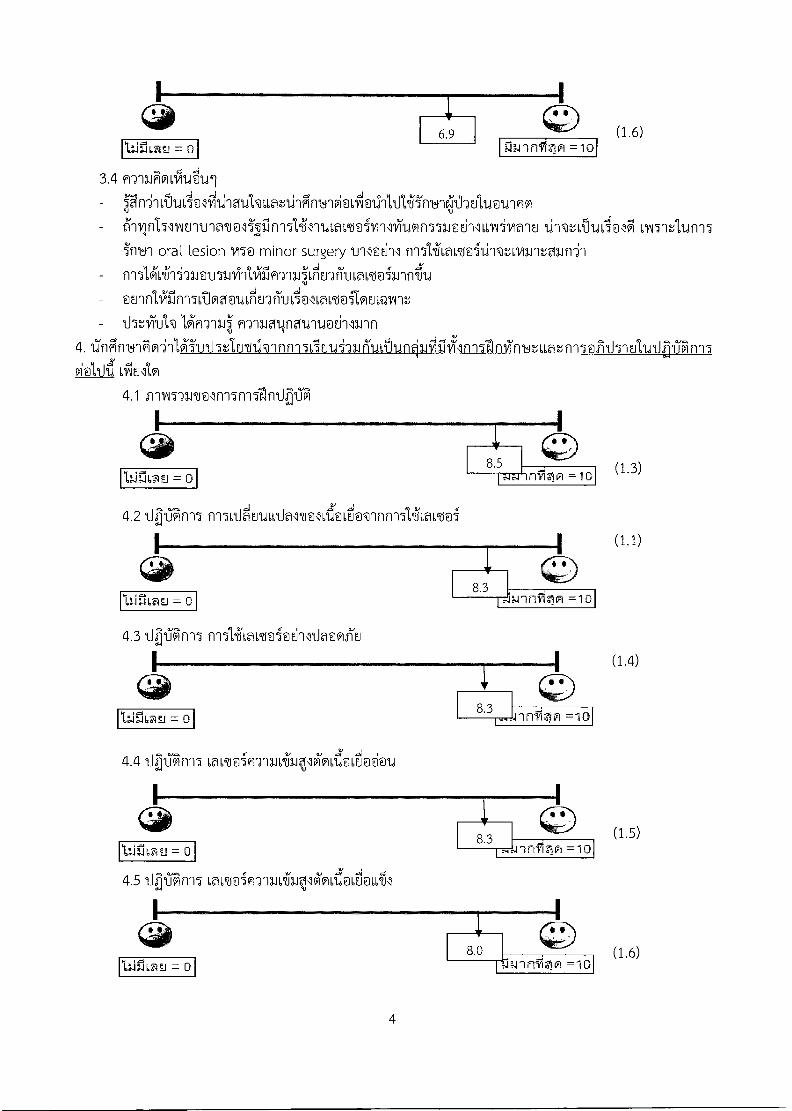
(1.6)
(1.4)
3.4 9ThiionliAuei -
[email protected]@dllogivimu 1:mtA9,ai@lg 6IA15-mAtini5 i'11141 oral lesion M@ minor surgery till@d11 ni51,41Lam51l-Nnvantaun2`1 in5livrnquvuuviiififlTIOVIEnritLamiinn.fru amfilifin-atIoanCrlEnfitill@lLa1,66@i1OEJLQ1Arlt 115V,VTUI@ fl'ilagninavrtadlurin
4. 17fIgni4Ao'inlAitrt15e,[email protected]'aguitunOitliilnll'anviirtItuatn-15@infriolvtVilin5
Lcquao
4.1 irnin-nrmln15n1511nql°16i
(1.3) tflr-I6M.1=
4.2 qan-n. m51AEruL6I1amlnlaSiavInnili6a6n5
4.3 11 1_Tkin7 n151411o1,66@iailltlooliu
( 4.4 11h1Tk-15 Lavis@iRTILLiwulM1,1a6AA @ M
I
8.3
(1.5)
= 0
=1(3
4.511 1JGlnl5 LaLtoi9-lii*I1M6A1@ L A_ ELLT1
I
8.0 w..4 n =10
(1.6)
=
4
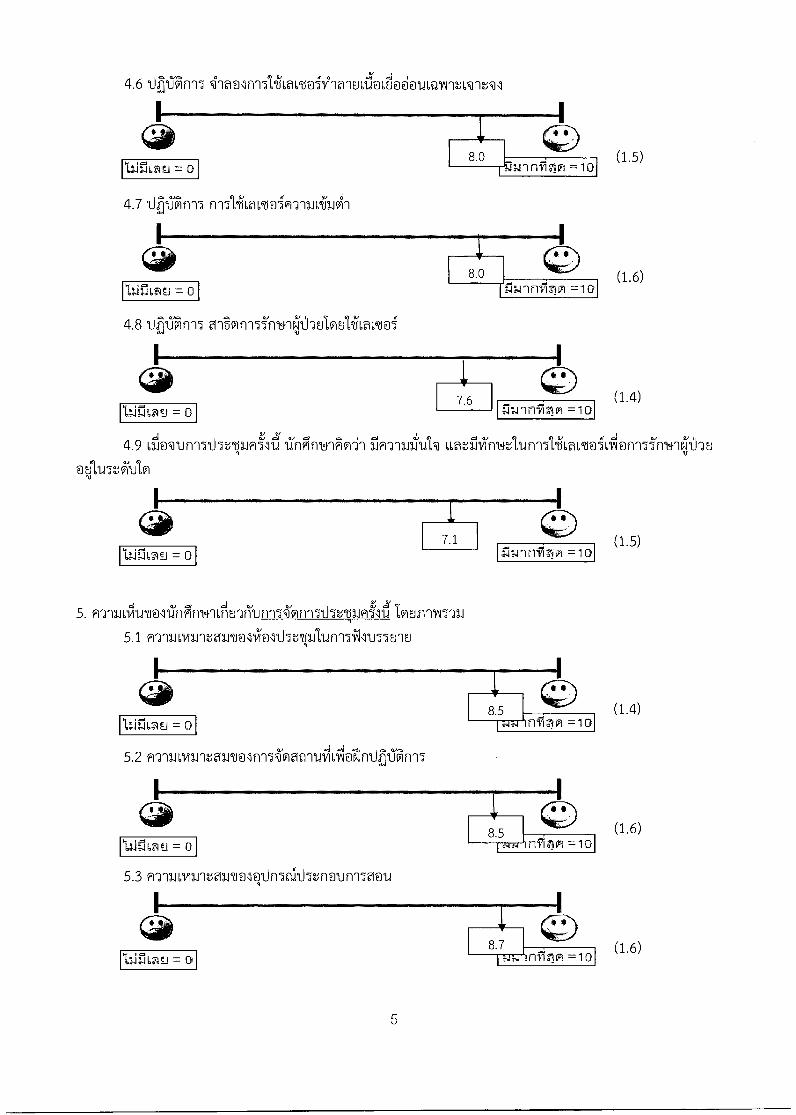
(1.6)
(1.5)
(1.4) =
8.'15 nfinn =10 "NTJ
(1.6)
(1.6)
A 4.6 1) 1J 4na@lfilitihmenivT'ialovuovi00guLmAiuLTnil
(1.5)
4.7 Ifht76ifY15 n'151,411,a1,6MicflT1111.64.1V11
4.8 eriBm-155m4-ies,WhEJIacilLaimoi
I.
7.6
(1.4)
nw-Infirin =10 =
4.9 Lilovunl5tht6pRi''Zi7nFinvlAwil rim-rwiTcul@ uatilvinblAuf-n51,41LamoiLiAl@t-mi'm9*-Jo
@ylothlo
5. A2'ILLOteti0117fignwuilE1'Jti`u8nonn5thziumiAlounTwYni
5.1 m`nli6timmaln0113i01thvil'unlA5'u5Eno
5.2 n'a-minntawnln-latrni9ASIVelnliE05in-15
5.3 9-nlionntamolq1M5althtn@unlvocu
5
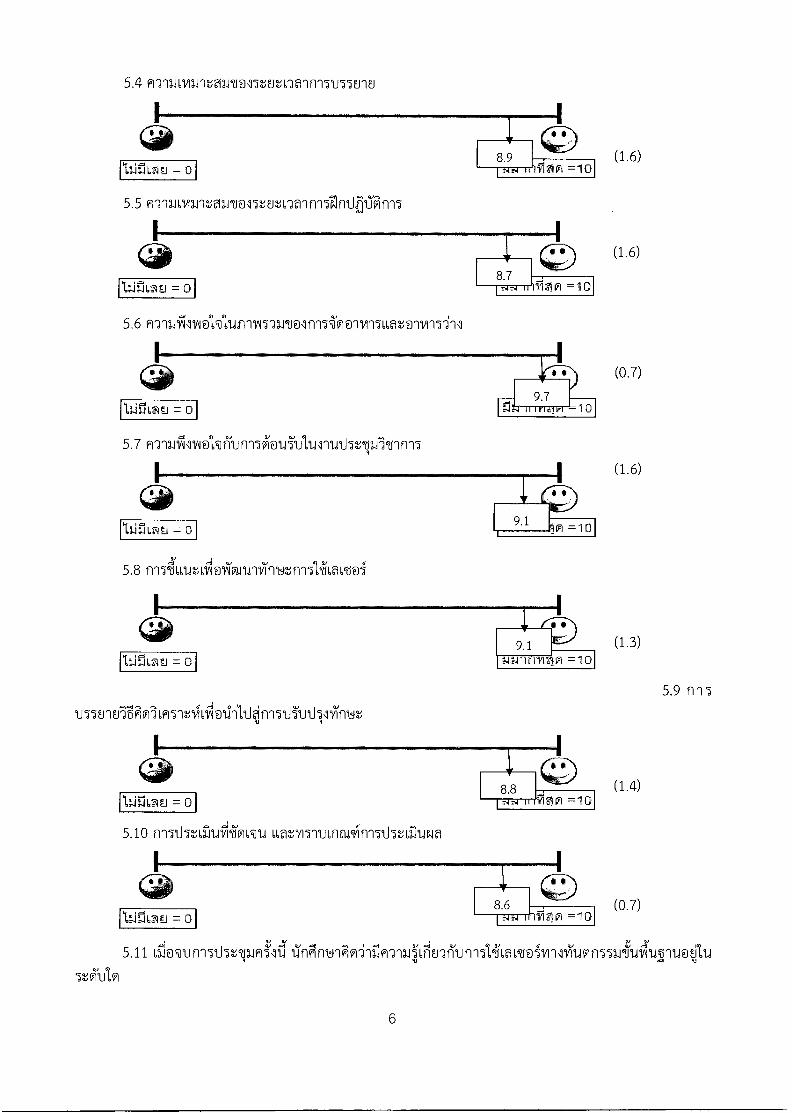
= 0
• 9.7 -10
5.5 nyoavarraimool5nv:Ialnl5elnirfran17
5.6 mnailcindkluincvl5uToln-ni(lolvn5u,atolvii5-ill
(1.6)
(1.4)
(0.7)
5.4 H'nu6vane,2{2Jrt1o55tEitna1ni155E8o
5.7 n'ywitulve'kficut-nwiguTticulluthrtil56nn15
(1.6)
(1.6)
(0.7)
5.8 n154u,cuto/okn.nifficutn-nliftoL66@i
9.1
(1.3)
~ = 0
14:,.rin 3191 =10
5.9 1115
u57EnoigNIL95-infinlvilitl)?,,in'15.tii'vdvvifrut
5.10 n15thvirticiiravu LLaro5nuLnapvIn15th2-Aih.INa
5.11 Lii@1in15thtpJ5TI 1Ingny1Ao- 1J1-ya561E2f1un-151,4LaL6boivin5i1nn556ti1ni1rwit1
5tAJ1,0
6
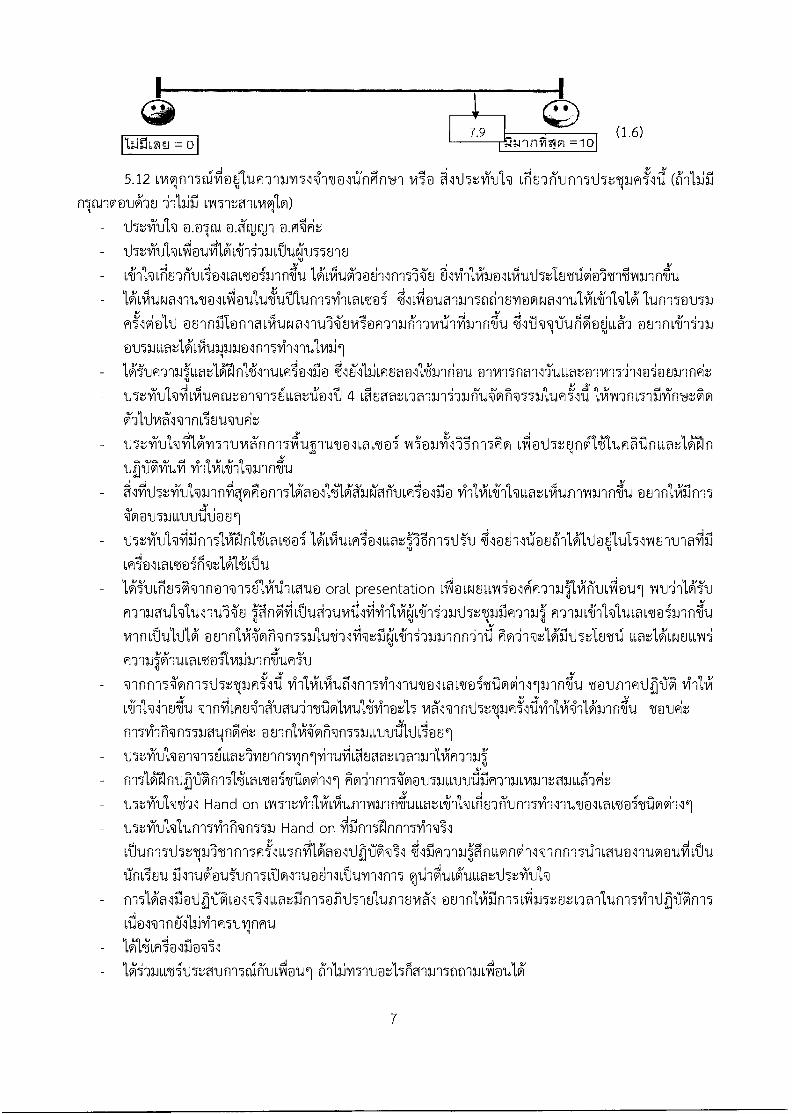
(1.6)
5.12 Li91115a1 @%illiRT1LY15141/19117f1Fif1141 CriEnfilin15115tvimi'Z(611,1iil nItool@wi-as al51:gno9lo)
115tviu'N - thotictiNolocuiilkihi-AIIN11.17501E1 - Liiv:r1Enfill1,1.1 01101,[email protected] 131'61,11.19iMEilln151E, EllviiilioldruthtlErnivierrAvanntu
1,ALOtiNalitemlviluuliAtATturnwilLamoi ;641617\11 @l10111150tilErli@nl@l1111iLillVt$i lun-15o1J51J aolnin@filartlroal-ruluvlio9-radiTrw6nfilnn'ilu ounnLihiu
ovuotlivilruNaamlnn5v1-11-nitinil 6a16113iLmuaollihnriou
115.tviculvtlivilcumng@-N156LLart7a6 4 LVIEgiatnallniufilAL'ormulumilillPiranmilim.424io
mi'mrkignn5Ao Li65z,lngliluK6iinuatlain
liithtviul%i-inorkiog@n-1513iaaRIA'A1.1101TULniNfl@ Iiiit,65-1'Num,'LVII,11111A1111f141,i ''0@l15111,1,1.11J171CJOE11
IhniTudkiiiinnThresinlifovnilkohmiolumpin-ITUTu .7il@d1Zo86-ilrbioyltil5oNantnaffiii LRINLavzsoirmaAirAu lguLtiu5A-In@-N-1561,i.tilLevia oral presentation Lilawoulli@l4rialiAiiiitiviAlaui
wingiulVtIonteA'ai m7'm641-i'hl1d6amo51nntu minvtluldUi LLatUomusui m-nLIA'[email protected]
171-11i1,111Alnwtillynnolwmirtloviillann.T7u Tuunnmihai -infiLmuil?Tcuarinvilolvraticti-i@z1,5 6JVIR1Z'
nwv4iNn55Lotin1t th.tvill'h N @-1561,LmlviEnn5vInlviliSiLhaatna-anlimm,:
Ao-111-151E1M11,1,1JVCSIJR-J11.1LvanbTfuLLA'wia; 115:,P1Jlwfil Hand on owiniiinIcuniminih4LLatLiivIluwiuni514-111146n1wdoi6trilovilli
- 115n)1Jhlun75v4li@n5531 Hand on iiMmeinn-minVil Lfkun-n-thnslt-'nnnn5mi'lu,5f-nt A'aolcdyrkil ;?il'il9-yaqinumnvillwInni511-umal-rtmotolivitu 17n65o1u viAtavitaianiuvillh
- n-nUalflatipiLolVilaatiinn5@ini5nuluillUVal @onnliiiinafilmmwilum514-rdhOinl
6-illimluatbtia-an5t-graiLfiguldi
7
- 6mulTuilul cocktail InnLaEwir,
- 131m-na4Lianhkitamt@i, fr15thalmLt1Jf11Jt,@1, lquiZiol cocktail @@En.rin
„ 5.13 6kLactawut viiom-)'13.1C101,141,11,MILVIN
- 11,1ni5vunimloi@l1J @u-inilonvoiluNayni-Nbll@H-nai-nvrt911CianniTot,4 'illNyt_Tufl'Alo%ia'-) @Erin
Liniugu5matidinIngpi@ln151411-rulvail
u,nUiLesmumli
m-naJlkuLaLtaillhnniltwit
rynlihrRn551Jat,in'kL' @EnnIARINn55pumouitiCi.oul
PwrilrM' MJ51.11,1,`U'Ufi f figrilLI,InntalILLA'wit
- ounfiliilfrmiantER,Jnaiuni5v7-11.1h05ini5LilmlnEillajlii-mTuv,in9cu
- annlifiln156iNn550-iwutnSi@Vt_lit
8
VI. umwaiaiiicria.n4
Vol.6 • Issue 2/2014
international magazine of
22014
Diclofenac, dexameth laser phototherapy?
Er,Cr:YSGG in laser- aesthetic rehabilitation. se report
Innovative pathways for extensive and efficient tissue removal with Er:YAG laser
ental students
A classroom action researc
Authors_ associate Profjl Associate Prof.
I education
_Introduction
Owing to the fact that dental students at the Khon
Kaen University (KKU) were interested in laser ther-
apy, an intensive course for laser therapy in dentistry
was introduced to the final year students. The in-
structional design was based on transferring tech-
nology and translation research to practice. A class-
room action research was conducted to evaluate this
course. The resultsshowed favourable knowledge and
attitude of the learners. This article reveals a pattern
of instructing laser dentistry to dental students.
Laser dentistry was commenced in the faculty of
dentistry, Khon Kaen University (KKU) in 1993. Conse-
quently, the lasers in dentistry research group, Khon
Kaen University, (LDRG KKU) was established in 2011.
The development of this discipline has continuously
been accomplished in basic research, clinical trial and
technical transferring. Besides this, the dental stu-
dents, KKU were also interested in conducting re-
search in laser dentistry and using laser for their gen-
eral dental practices. Therefore, we introduced an in-
tensive laser dentistry curriculum called "Laser Ther-
apy in Dentistry" for the final-year dental students. A
classroom action research was undertaken to evalu-
ate an instructional design for dental students learn-
ing laser dentistry.
_Methods
The principle of instructional design was modified
from the methods of technology transferring for pro-
fessionals." This was based on transferring laser
technology by learning both context and skills in laser
dentistry in order to utilise laser dentistry for quality
of life (Fig. 1). The instructional design (Fig. 2) com-
prised a twelve-hour interactive lecture on the basic
and application of laser dentistry, a ten-hour related
laboratory with co-operative learning after lecturing
together with clinical demonstration from the dental
students who had experiences in using lasers and a
four-hour authentic evaluation and discussion using
experiential-based learning. The laser techniques
transferred to the students were as follows: soft tis-
sue surgery', tooth preparation, laser welding for
381 ,ser
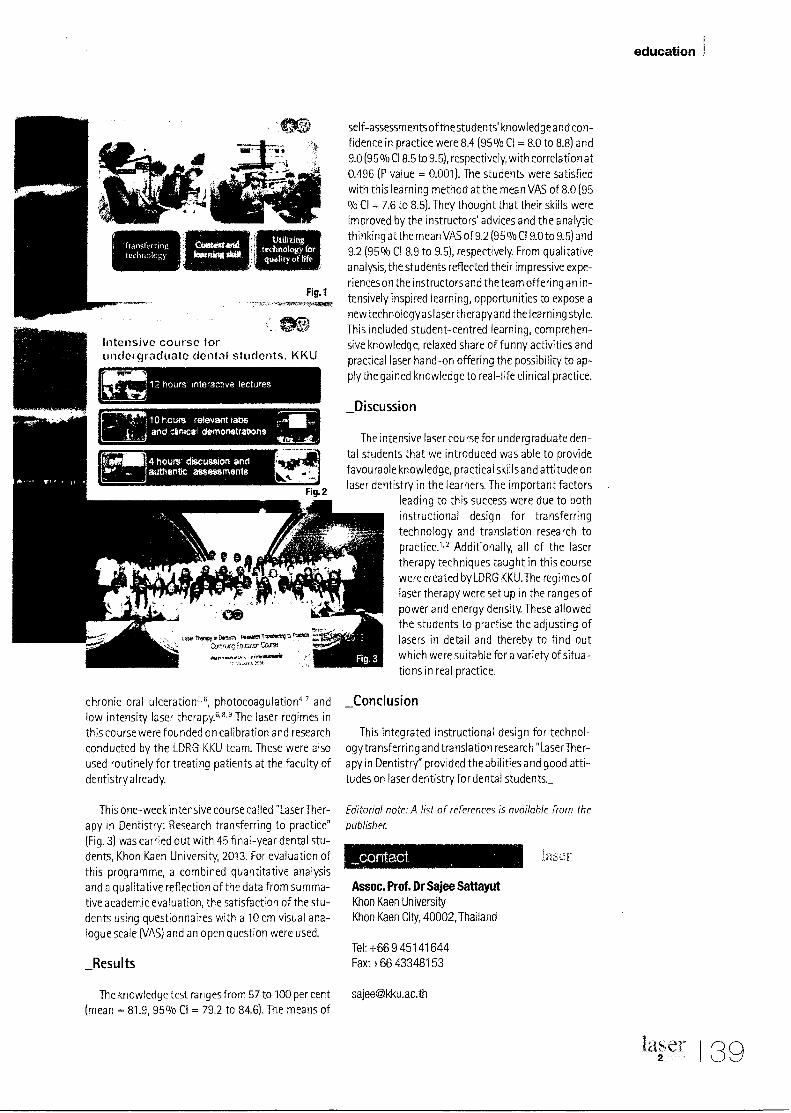
Transferring technology
utilizing technology for quality of life
education
• Intensive course for undergraduate dental students, KKU
12 hours interactive lectures
j 10 hours relevant tabs
rsfrillffi 4iff 4 hours" discussion and
authentic assessments '
Fig. 2
self-assessments of thestudents' knowledge and con-fidence in practice were 8.4 (95% CI = 8.0 to 8.8) and 9.0 (95 % C18.5 to 9.5), respectively, with correlation at 0.496 (P value = 0.001). The students were satisfied with this learning method at the mean VAS of 8.0 (95 % CI = 7.6 to 8.5). They thought that their skills were improved by the instructors' advices and the analytic thinking at the mean VAS of 9.2 (95 % CI 9.0 to 9.5) and 9.2 (95% CI 8.9 to 9.5), respectively. From qualitative
analysis, the students reflected their impressive expe-riences on the instructors and the team offering an in-
tensively inspired learning, opportunities to expose a new technologyas laser therapyand the learning style. This included student-centred learning, comprehen-sive knowledge, relaxed share of funny activities and practical laser hand-on offering the possibility to ap-ply the gained knowledge to real-life clinical practice.
_Discussion
The intensive laser course for undergraduate den-tal students that we introduced was able to provide favourable knowledge, practical skills and attitude on laser dentistry in the learners. The important factors
leading to this success were due to both instructional design for transferring technology and translation research to practice." Additionally, all of the laser therapy techniques taught in this course were created by LDRG KKU.The regimes of laser therapy were set up in the ranges of power and energy density. These allowed the students to practise the adjusting of lasers in detail and thereby to find out which were suitable for a variety of situa-tions in real practice.
_Conclusion
This integrated instructional design for technol-ogytra nsferring and translation research "LaserTher-apy in Dentistry" provided the abilities and good atti-tudes on laser dentistry for dental students_
Editorial note: A list of references is available from the
publisher.
_contact
Assoc. Prof. Dr Sajee Sattayut Khon Kaen University Khon Kaen City, 40002, Thailand
Tel: +66 9 451 41 644 Fax: +66 43348153
chronic oral ulceration5. 6, photocoagulation4' 7 and low intensity laser therapy.6, " The laser regimes in this course were founded on calibration and research conducted by the LDRG KKU team. These were also used routinely for treating patients at the faculty of dentistry already.
This one-week intensive course called "LaserTher-apy in Dentistry: Research transferring to practice" (Fig. 3) was carried out with 45 final-year dental stu-dents, Khon Kaen University, 2013. For evaluation of this programme, a combined quantitative analysis and a qualitative reflection of the data from summa-tive academic evaluation, the satisfaction of the stu-dents using questionnaires with a 10 cm visual ana-logue scale (VAS) and an open question were used.
_Results
rt DIEftrf NAM TIValerf4
Arc Ermeltr■Cruse
,INAVOOFMS1 2S%
The knowledge test ranges from 57 to 100 per cent [email protected]
(mean = 81.9, 95% CI = 79.2 to 84.6). The means of
laser 2_ 139

3.3.2 Organized by:
IADR-APR 21-23 AUGUST =013 Bangkok, Thailand %.■
2nd Meeting of the International Association for Dental Research
Asia Pacific Region Plaza Athenee, Bangkok, Thailand
PROGRAM AND ABSTRACT BO
fr,t,rnallonal As,Gcialian for O 301111,1,1A,,,,
FUTURE! The Co-Annual Scientific IADR Meetings
• 61 Meeting of Japanese Division • 53 Meeting of Australian New Zealand Division • 30 Meeting of Korean Division • 13' fvleeting of Chinese Division • 27' Meeting of Southeast.sian Division
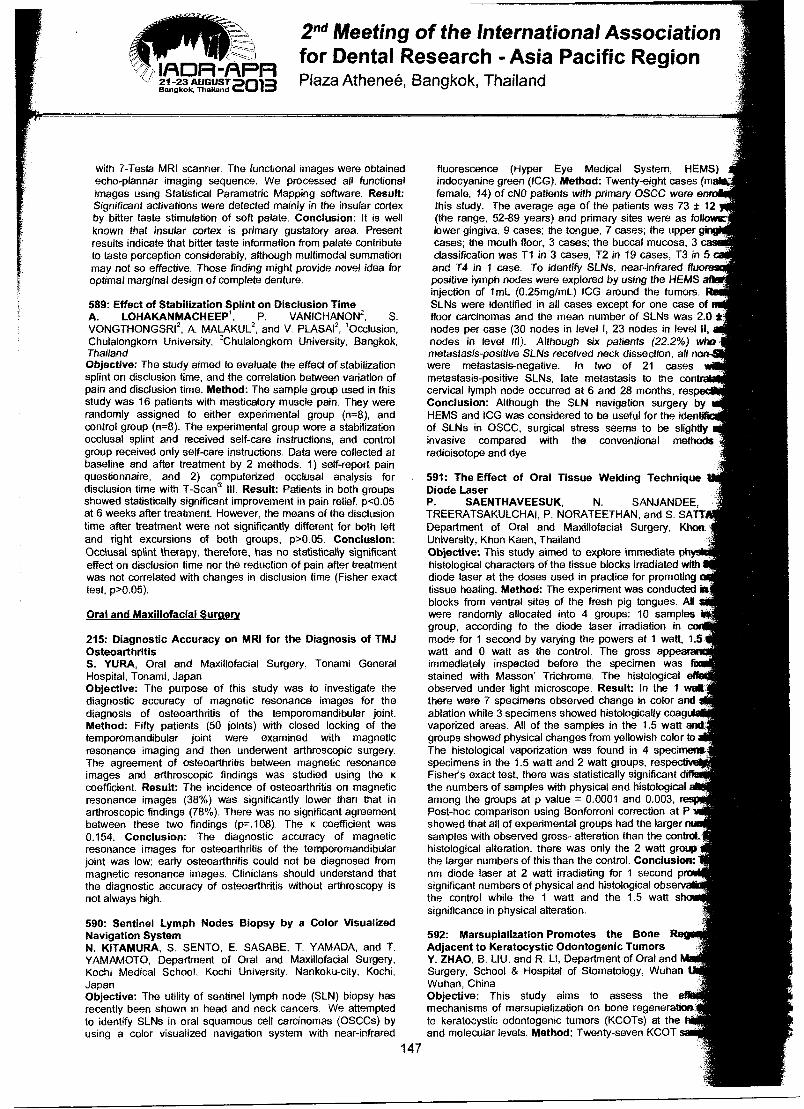
2nd Meeting of the International Association rz- for Dental Research - Asia Pacific Region
I/RDR-APR Lin-glAv2212013 Plaza Athenee, Bangkok, Thailand
with 7-Tesla MRI scanner. The functional images were obtained echo-plannar imaging sequence. We processed all functional images using Statistical Parametric Mapping software. Result: Significant activations were detected mainly in the insular cortex by bitter taste stimulation of soft palate. Conclusion: It is well known that insular cortex is primary gustatory area. Present results indicate that bitter taste information from palate contribute to taste perception considerably, although multimodal summation may not so effective. Those finding might provide novel idea for optimal marginal design of complete denture.
589: Effect of Stabilization Splint on Disciusion Time A. LOHAKANMACHEEP1, P. VANICHANON2, S. VONGTHONGSRI2, A. MALAKUL2, and V. PLASAI2, 'Occlusion, Chulalongkorn University, 2Chulalongkorn University, Bangkok, Thailand Objective: The study aimed to evaluate the effect of stabilization splint on disclusion time, and the correlation between variation of pain and disclusion time. Method: The sample group used in this study was 16 patients with masticatory muscle pain. They were randomly assigned to either experimental group (n=8), and control group (n=8). The experimental group wore a stabilization occlusal splint and received self-care instructions, and control group received only self-care instructions. Data were collected at baseline and after treatment by 2 methods. 1) self-report pain questionnaire, and 2) computerized occlusal analysis for disclusion time with T-Scan® III. Result: Patients in both groups showed statistically significant improvement in pain relief, p<0.05 at 6 weeks after treatment. However, the means of the disclusion time after treatment were not significantly different for both left and right excursions of both groups, p>0.05. Conclusion: Occlusal splint therapy, therefore, has no statistically significant effect on disclusion time nor the reduction of pain after treatment was not correlated with changes in disclusion time (Fisher exact test, p>0.05).
Oral and Maxillofacial Surgery
215: Diagnostic Accuracy on MRI for the Diagnosis of TMJ Osteoarthritis S. YURA, Oral and Maxillofacial Surgery, Tonami General Hospital, Tonami, Japan Objective: The purpose of this study was to investigate the diagnostic accuracy of magnetic resonance images for the diagnosis of osteoarthritis of the temporomandibular joint. Method: Fifty patients (50 joints) with closed locking of the temporomandibular joint were examined with magnetic resonance imaging and then underwent arthroscopic surgery. The agreement of osteoarthritis between magnetic resonance images and arthroscopic findings was studied using the K
coefficient. Result: The incidence of osteoarthritis on magnetic resonance images (38%) was significantly lower than that in arthroscopic findings (78%). There was no significant agreement between these two findings (p=.108). The K coefficient was 0.154. Conclusion: The diagnostic accuracy of magnetic resonance images for osteoarthritis of the temporomandibular joint was low; early osteoarthritis could not be diagnosed from magnetic resonance images. Clinicians should understand that the diagnostic accuracy of osteoarthritis without arthroscopy is not always high.
590: Sentinel Lymph Nodes Biopsy by a Color Visualized Navigation System N. KITAMURA, S. SENTO, E. SASABE, T. YAMADA, and T. YAMAMOTO, Department of Oral and Maxillofacial Surgery, Kochi Medical School, Kochi University, Nankoku-city, Kochi, Japan Objective: The utility of sentinel lymph node (SLN) biopsy has recently been shown in head and neck cancers. We attempted to identify SLNs in oral squamous cell carcinomas (OSCCs) by using a color visualized navigation system with near-infrared
fluorescence (Hyper Eye Medical System, HEMS) indocyanine green (ICG). Method: Twenty-eight cases (m female, 14) of cNO patients with primary OSCC were en this study. The average age of the patients was 73 ± 12 (the range, 52-89 years) and primary sites were as followir lower gingiva, 9 cases; the tongue, 7 cases; the upper g cases; the mouth floor, 3 cases; the buccal mucosa, 3 classification was T1 in 3 cases, T2 in 19 cases, T3 in 5 and T4 in 1 case. To identify SLNs, near-infrared flu positive lymph nodes were explored by using the HEMS injection of 1mL (0.25mg/mL) ICG around the tumors. SLNs were identified in all cases except for one case of floor carcinomas and the mean number of SLNs was 2.0 nodes per case (30 nodes in level I, 23 nodes in level II, nodes in level III). Although six patients (22.2%) who metastasis-positive SLNs received neck dissection, all no were metastasis-negative. In two of 21 cases metastasis-positive SLNs, late metastasis to the con cervical lymph node occurred at 6 and 28 months, res Conclusion: Although the SLN navigation surgery by HEMS and ICG was considered to be useful for the iden of SLNs in OSCC, surgical stress seems to be slightly invasive compared with the conventional methods radioisotope and dye.
591: The Effect of Oral Tissue Welding Technique Diode Laser P. SAENTHAVEESUK, N. SANJANDEE, TREERATSAKULCHAI, P. NORATEETHAN, and S. SATT Department of Oral and Maxillofacial Surgery, Khon University, Khon Kaen, Thailand Objective: This study aimed to explore immediate histological characters of the tissue blocks irradiated with diode laser at the doses used in practice for promoting tissue healing. Method: The experiment was conducted in blocks from ventral sites of the fresh pig tongues. All were randomly allocated into 4 groups; 10 samples group, according to the diode laser irradiation in mode for 1 second by varying the powers at 1 watt, 1.5 watt and 0 watt as the control. The gross appea immediately inspected before the specimen was stained with Masson' Trichrome. The histological e observed under light microscope. Result: In the 1 welt there were 7 specimens observed change in color and ablation while 3 specimens showed histologically coag vaporized areas. All of the samples in the 1.5 watt and groups showed physical changes from yellowish color to The histological vaporization was found in 4 specimen* specimens in the 1.5 watt and 2 watt groups, res Fisher's exact test, there was statistically significant d the numbers of samples with physical and histological among the groups at p value = 0.0001 and 0.003, r Post-hoc comparison using Bonforroni correction at P showed that all of experimental groups had the larger samples with observed gross- alteration than the control. histological alteration, there was only the 2 watt group the larger numbers of this than the control. Conclusion: nm diode laser at 2 watt irradiating for 1 second p significant numbers of physical and histological obsery the control while the 1 watt and the 1.5 watt s significance in physical alteration.
592: Marsupialization Promotes the Bone R Adjacent to Keratocystic Odontogenic Tumors Y. ZHAO, B. LIU, and R. LI, Department of Oral and Surgery, School & Hospital of Stomatology, Wuhan Wuhan, China Objective: This study aims to assess the mechanisms of marsupialization on bone regeneration to keratocystic odontogenic tumors (KCOTs) at the and molecular levels. Method: Twenty-seven KCOT
147
3.3.3
THQD0Ari SOCIE
EBRUARY 20.21.2014
Important Notice for Poster authors of
86th Annual Meeting of the American Prosthodontic Society
Please read carefully the instructions below
regarding the creation and submission of your e-poster.
From: (s [email protected]) on behalf of 86th Annual Meeting of the
America Prosthodontic Society ([email protected])
Sent: Mo 1/27/14 7:34 AM
To: Junta ee ([email protected])
Dear Dr. Juntavee,
The Ameri an Prosthodontic Society Sub-Committee for Abstract Selection would like to thank ydu for submitting an
abstract fo presentation at this year's Annual Meeting. There was an exceptional response to the call for abstracts
for this ye r's conference.
After a th • rough review process, its a pleasure for us to inform you that your abstract tiaiiiiteitacoetited
for a post r presentation. The Posters Program will be held in conjunction with the meeting on Thursday,
February 0, 2014 and a separate confirmation of your scheduled time to present will be sent under a separate
cover.
Wishing t use modern, environmentally friendly technologies, in this year's Meeting all posters will be
presente•electronically, as e-posters. Therefore, there will be NO NEED FOR PRINTING, carrying and pinning
posters in he conference area. Specifically, the submission, management and presentation of e-posters in the
conferenc•area and on the Internet, will be carried out using the ePostersLive system.
There is a brief overview of how to make your submission, below.
We hope ou will find the submission process simple and intuitive, and enjoy the ePoster experience.
Also, if yo are a first time presenter, your registration fee has been waived and you have already been registered for
the meeti g; there is no need to complete a registration form. If you have already presented a poster at the APS
meeting, ou must register at www.prostho.org for the meeting. If any of your co-presenters will be present at the
meeting, ey are also responsible for registering and paying the appropriate registration fee for their registration
category. our co-presenters will not be communicated with separately. Registration is available on our website.
Again, th nk you for your participation. We look forward to seeing you in Chicago at this exciting meeting!
Sincerely,
Danny R bert
Table Cli is Chair
You -eceiving this e-vtaiii ..ecause your Ostract has been accepted as a poster presentation, at the 86TH Annual
Meeting f the American Prosthodortic Societ,, which is held on February 20-21, 2014, in Swissatel Chicago, Chicago, IL.
Copyright (C) 2011 The ePostersLive team At rights reserved
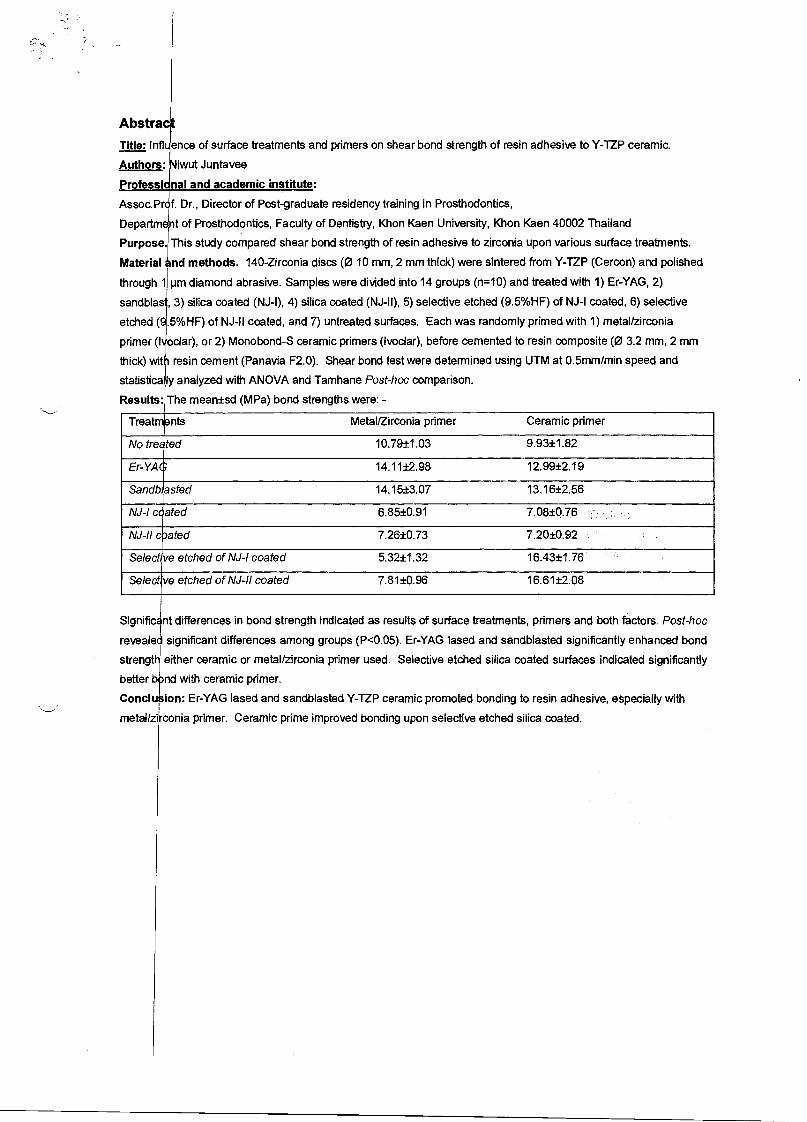
Abstra
Title: Infl ence of surface treatments and primers on shear bond strength of resin adhesive to Y-TZP ceramic.
Authors: iwut Juntavee
Professi • nal and academic institute:
Assoc.Pr f. Dr., Director of Post-graduate residency training in Prosthodontics,
Department of Prosthodontics, Faculty of Dentistry, Khon Kaen University, Khon Kaen 40002 Thailand
Purpose. This This study compared shear bond strength of resin adhesive to zirconia upon various surface treatments.
Material nd methods. 140-Zirconia discs (0 10 mm, 2 mm thick) were sintered from Y-TZP (Cercon) and polished
through 1 pm diamond abrasive. Samples were divided into 14 groups (n=10) and treated with 1) Er-YAG, 2)
sandblas , 3) silica coated (NJ-I), 4) silica coated (NJ-II), 5) selective etched (9.5%HF) of NJ-I coated, 6) selective
etched ( .5%HF) of NJ-II coated, and 7) untreated surfaces. Each was randomly primed with 1) metal/zirconia
primer (I oclar), or 2) Monobond-S ceramic primers (Ivoclar), before cemented to resin composite (0 3.2 mm, 2 mm
thick) wit resin cement (Panavia F2.0). Shear bond test were determined using UTM at 0.5mm/min speed and
statistica ly analyzed with ANOVA and Tamhane Post-hoc comparison.
Results: The meantsd (MPa) bond strengths were: -
Treatments Metal/Zirconia primer Ceramic primer
No treated 10.79±1.03 9.93±1.82
Er-YAG 14.11±2.98 12.99±2.19
Sandb,asted 14.15±3.07 13.16±2.56
NJ-I coated 6.85±0.91 7.08±0.76
NJ-II coated 7.26±0.73 7.20±0.92
Selective etched of NJ-I coated 5.32±1.32 16.43±1.76
Selective etched of NJ-II coated 7.81±0.96 16.61±2.08
Signific nt differences in bond strength indicated as results of surface treatments, primers and both factors. Post-hoc
revealed significant differences among groups (P<0.05). Er-YAG lased and sandblasted significantly enhanced bond
strengt either ceramic or metal/zirconia primer used. Selective etched silica coated surfaces indicated significantly
better bind with ceramic primer.
Conclu. ion: Er-YAG lased and sandblasted Y-TZP ceramic promoted bonding to resin adhesive, especially with
metal/zi conia primer. Ceramic prime improved bonding upon selective etched silica coated.
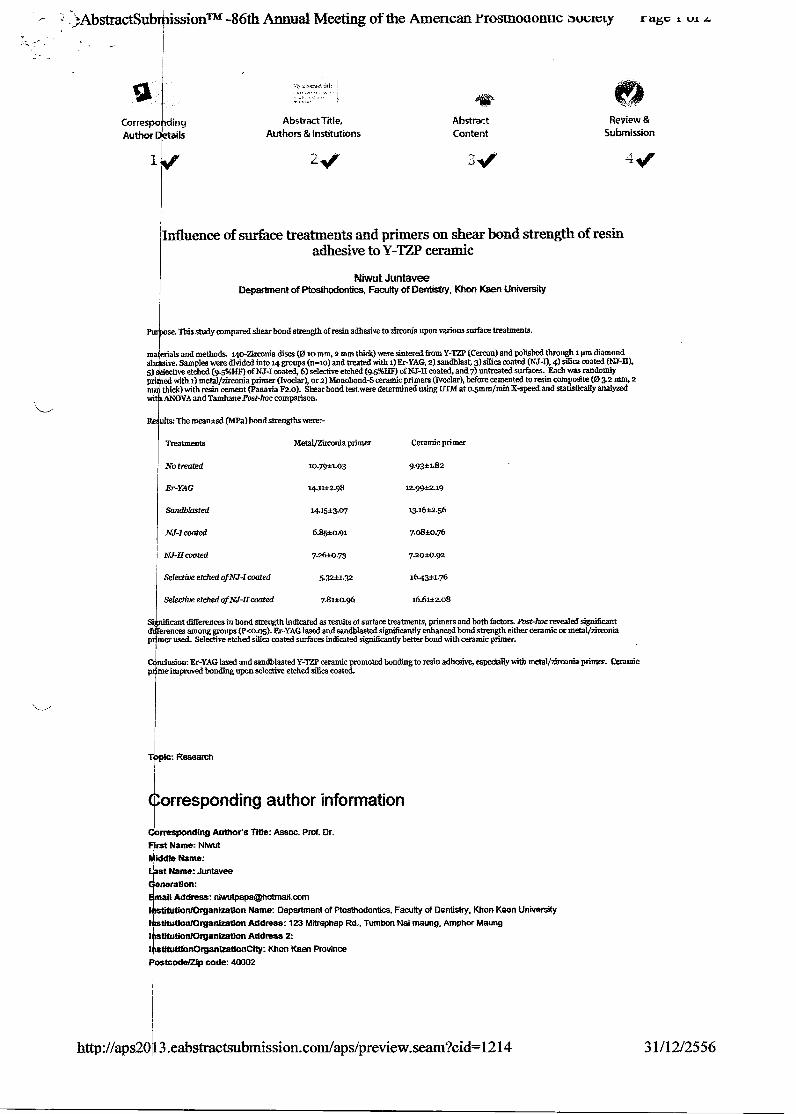
-.tAbstrdctSubr4lissionTM -86th Annual Meeting of the Amencan Yrostn000nuc 6ocavty ragc t kit
Abstract Title, Authors & Institutions
CorreSpo ding
Author ails
(10
Abstract
Review &
Content
Submission
if
Influence of surface treatments and primers on shear bond strength of resin adhesive to Y-TZP ceramic
Niwut Juntavee Department of Ptosthodantics, Faculty of Dentistry, Khon Keen University
se. This study compared shear bond strength of resin adhesive to zirconia upon various surface treatments.
ma erials and methods. 14o-Mrconia discs (0 io mm, 2 mm thick) were sintered from Y-172 (Cercon) and polished through 1 pm diamond ab 'vs. Samples were divided into 14 groups (nr--ro) and treated with 1) Er-YAG, 2) sandblast, 3) silica coated (NJ--I), 4) silica coated (NJ-II), 5) ective etched (9.5%HF) of NJ-I coated, 6) selective etched (9.5%H11) of NJ-H coated, and 7) entreated surfaces. Each was randomly pri with 1) metal/zirconia primer (Ivoclar), or 2) Monobond-S ceramic primers (Ivoclar), before cemented to resin composite (03.2 mm, 2 m thick) with resin cement (Eanavia F2.0). Shear bond test were determined using UTM at o.5mm/min X-speed and statistically analyzed mei ANOVA and Tamhane Post-hoc comparison.
ultm The mean*sd (MI's) bond strengths were:-
Treatments MetalfEnconia primer Ceramic primer
No treated 9.93±1.82
Er-YAG 14.1.1.+298
Sandblasted 1415±3.07 13.1612.56
NJ-I coated 6.85±0.91
NJ-If coated 7.26-10.73 7.20i0.92
Selective etched of NJ-I coated 5.32±1.32 16.43±1.76
Selective etched of NJ-II coated 7.81±0.96 16.61±2.08
Si cant differences in bond strength indicated as results of surface treatments, primers and both factors. Post-hoc revealed significant d erences among groups (Eco.o5). Er-YAG lased and sandblasted significantly enhanced bond strength either ceramic or metalizireonia
er used_ Selective etched silica coated surfaces indicated significantly better bond with ceramic primer.
ndusion: Er-YAG lased and sandblasted Y-172? ceramic promoted bonding to resin adhesive, especially with metal/zirconia primer. Ceramic p me improved bonding upon selective etched silica coated.
Research
orresponding author information
Corresponding Author's Title: Assoc. Prof. Dr. rst Name: Niwut fiddle Name: st Name: Juntavee
eneration: ail Address: nivoutpapa©hotrnail.corn
on/OrganIzatIon Name: Department of Ptosthodontics, Faculty of Dentistry, Khon Keen University I Mutton/Organization Address: 123 Mitraphap Rd., Tumbon Nai maung, Amphor Maung I Mutton/Organization Address 2: I tituttionOrgantzattonelty: Khon Kaen Province
ostcodef2lp code: 40002
http://aps2013.eabstractsubmission.com/aps/preview.seam?cid=1214 31/12/2556
ffline ;k ;Oka.' 0 trlfr.,-,34,:
,2Abs ractSub r issionTM -86th Annual Meeting of the American Prosthodonnc society rage z or z
: Thailand
Telephone (including country code): 66-43-2-2405
to Telephone (including country code): 66-89-7112980
Fax (including country code):
F Time APS Table Clinician: Yes
R !ration Category: Non-Member
A thors
Prof. Dr. Niwut Juntavee DDS(Hons.), GAGS, MSD, DScD
B ography of Main Presenter
A . Prof. Dr. Niwut Juntavee is program director of residency training program in Prosthodontics at the faculty of Dentistry, )01 n Keen University.
Conditions of a lication: Submission of this application obliges the applicant to present the accepted proposal, in person, and In keeping with the established regu Please read the attached regulations. Compliance with these regulations is a condition of acceptance of this application.
LI I agree
« Back to Abstract Content Confirm and Submit »
Question- or Difficulties? Chat with us li a or email us at
support@sci tech. corn
eAbstractSubmission TM by the PosterGenius® team.
Copyright 2011 SciGene Technologies. All rights reserved. Patent Pending. PosterGenius and SciGen are registered trademarks of SciGen Technologies
eAbstractSubmission T. v1.5.0
http://aps20 3.eabstractsubmission.com/aps/preview.seam?cid=1214 31/12/2556
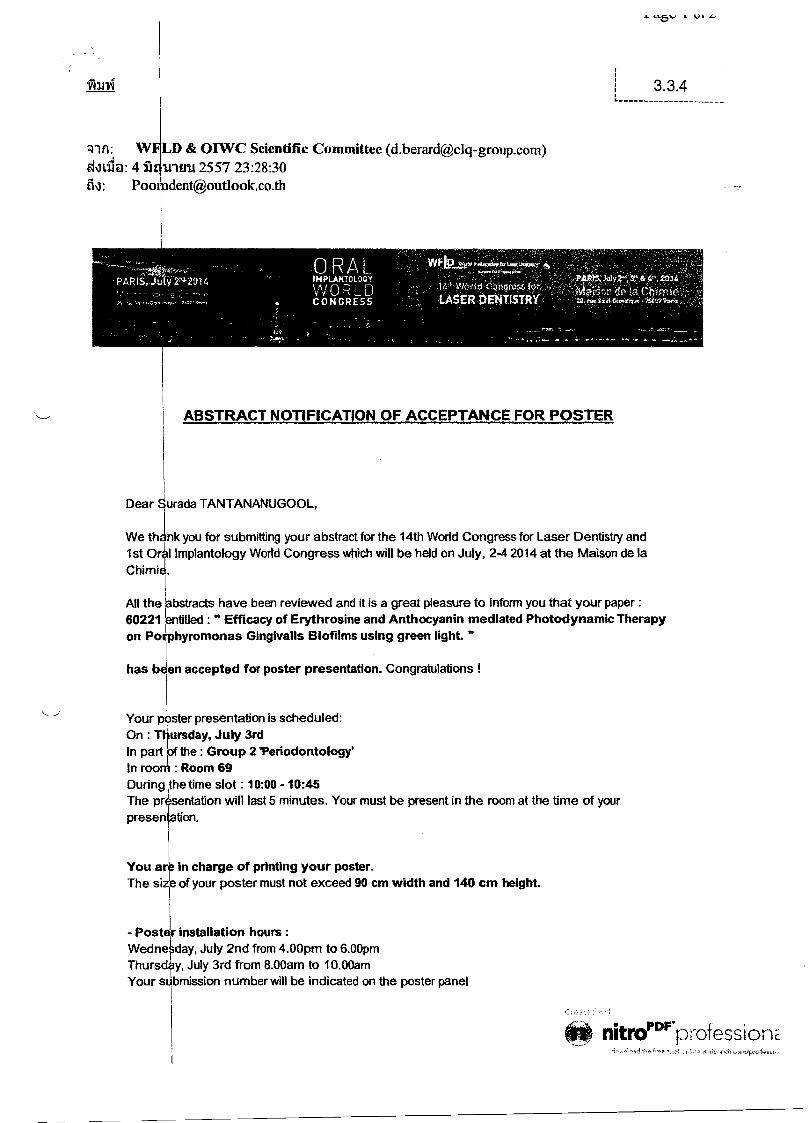
Mai
3.3.4
D & OIWC Scientific Committee ([email protected]) d4Lil@: 471 inn 2557 23:28:30
ORAL
PARIS,.JaY2,4-2014
, . 4,', 2.014
a2.3Cn de is Chimie' IMPLANTOLOGY
\A/ 0 R D CONGRESS
1 e cz)rwess tar LASER DENTISTRY
ABSTRACT NOTIFICATION OF ACCEPTANCE FOR POSTER
1st Or I Implantology World Congress which will be held on July, 2-4 2014 at the Maison de la Chimi
All the labstracts have been reviewed and it is a great pleasure to inform you that your paper : 60221 entitled : " Efficacy of Erythrosine and Anthocyanin mediated Photodynamic Therapy
on PoiLphyromonas Gingivalis Biofilms using green light "
has been accepted for poster presentation. Congratulations !
Your p ster presentation is scheduled: On : T ursday, July 3rd In part of the : Group 2 'Periodontology In roorP : Room 69 During the time slot : 10:00 - 10:45 The pr sentation will last 5 minutes. Your must be present in the room at the time of your presentation.
You ar in charge of printing your poster. The size of your poster must not exceed 90 cm width and 140 cm height.
- Poster installation hours : Wedne day, July 2nd from 4.00pm to 6.00pm Thursd y, July 3rd from 8.00am to 10.00am Your s bmission number will be indicated on the poster panel
Dear urada TANTANANtJGOOL,
We th1 nk you for submitting your abstract for the 14th World Congress for Laser Dentistry and
nitroPprprofession
L Vl L.
Frida , July 4th from 4.00pm to 5.00pm All p sters left after 5.00pm will be thrown away
We would like to remind you that registration to the congress is compulsory for all speakers. So fat, you are not registered for the congress yet. We remind you to register before June 15th. By this date, if you are not registered, your abstract will be deleted from the program.
To r gister online, please click here.
. - Shoulfd you have any modification about your title and/or the author of your abstract, please conta t us before June, 10th.
We remain at your disposal for any further information and look forward to welcoming you in Paris, Best regards,
The FLD & OIWC 2014 Scientific Committee wfld rOU .COM
To unsubscr'.e from this mailing list lease click here
PDF' tim nitro professionE
ORAL INPLANTOLOGY WnRL CONGRESS
141' World Corkgreik44:- LASER DENTISTRY
,sas.cr, d.ataClalthie - 7 42 4 Poi,
PAR Ju ■12"6,2014
Dr Surada Tantananugool LDRG KKU , Faculty of dentistry, Khon Kaen University. 40000 Khon Kaen Thailand
CERTIFICATE OF ATTENDANCE
Hereby we certify that
Dr Surada TANTANANUGOOL
has attended the 14th World Congress of Laser Dentistry, from July, 3rd to 4th 2014, which took place in the Maison de la Chimie in Paris, France.
•
Paris, France, July 4th 2014
For the Organizing Committee
Ofilheadenr COLLOQUIUM 13-1s me de Nancy -- 75010 Pad:: N, 330,11 4464 11 'S ■< 1.'at f:'41 44 641.!? 16 Ernall : infopacist9c14-zwup.eurn
47) na 317
3.3.5 Organized by:
Internahuoa, $1,11,..isr 27/ IADR-TAPR
21-23 AUGUST 2013 Bangkok, Thailand %■1
2nd Meeting of the International Association for Dental Research
Asia Pacific Region Plaza Athenee, Bangkok, Thailand
PROGRAM AND ABSTRACT BO FUTURE!
The Co-Annual Scientific IADR Meetings
• 61 Meeting of Je4,anese Drdision • 53 Meet3ng of Aist,ra; a^ Ne.', Zea and Dyson • 30 Meeting of Korean. a ✓isLon • 13 Meeting of Chinese Duuision • 27 Meeting of Southeast Asian Division
2nd Meeting of the International Association for Dental Research - Asia Pacific Region
1/ADR-APF1 21-23 AUGUST =ma Plaza Athenee, Bangkok, Thailand Bangkok, ThaHand
arsupialized and 7 marsupialized) were collected to 'gate the effects of marsupialization on bone regeneration nt to KCOTs by detecting the expression of markers of
formation. Additionally, the involvement of /RANK/RANKL signaling pathway was determined by nohistochemicai analysis and quantitative real-time PCR. It: The bone formation was significantly enhanced in pialized KCOTs, as demonstrated by the ALP activity and BMP immunostaining, respectively. Moreover, the
nohistochemical studies revealed that the number of OPG-e cells was higher in marsupialized samples, while in non-pialized samples the number of RANKL-positive cells was
r. Importantly, the real-time PCR results also demonstrated decreased expression of RANKL and increased expression of
in marsupialized samples, suggesting a modification of the RANK/RANKL signaling pathway by marsupialization. lusion: It is speculated that marsupialization might promote
bone regeneration adjacent to KCOT through its function of ating the OPG/RANK/RANKL signaling pathway.
: The Impacts of Mandibular Advancement on Mandibular and Displacement
LI, North Sichuan Medical College, Nanchong, China tive: In order to explore the best Forsus load angle and
power further, and provide the theoretical basis, this study lated changes of stress and displacement of mandible after
Forsus to protrude mandible instantaneously under nt vertical component. Method: Based on the prepared
•ible model protruded by Forsus, this study analyzed •es of stress, modification and rotation trend of mandible r three different working conditions ( horizontal component
, vertical component 2N, 4N, 1N) by using Abaqus6.5 are. Result: The torsion of condyle occurred under three ing conditions, and the stress was large. Under working •ition 1 and 3, counterclockwise rotation of mandible and the 'mum displacement of the chin occurred respectively (1.150 and 2.141 mm) .Under working Condition 2, mandible
'on was not obvious, the performance was simple •ation, the maximum displacement was only 0.18mm. clusion: With the gradual decreasing of vertical component, protrusion trend of chin increased; Forsus could promote the
ible counterclockwise rotation and modification when dible was protruded.
: An Efficacy of Photocoagulation Using Diode Laser in h-extraction Patients
PRASONGVARANON, L. THANUDAPE, A. KLUNGTONG, S. SATTAYUT' Department of Oral and Maxillofacial Surgery,
•n Kaen University, Khon Kaen, Thailand tive: This clinical study aimed to compare clinical bleeding
and pain score between using photocoagulation with diode r and local pressure technique after lower premolar action. Methods: The clinical trial was conducted on 12
" !thy patients with lower premolar extraction for orthodontic tment. The sample size was based on estimation at 80% er of the test. The patients were blocked-randomly allocated two groups, namely, the laser photocoagulation group and I pressure group as the control. The extraction sockets were iated with 808 nm diode laser at 0.5 watts continuous mode a 5-second interval until achieved hemostasis in the laser
•tocoagulation group. In the control group, the sockets were sed with cotton roll. The clinical bleeding time was recorded. visual analogue pain score was obtained every 1 hour for 4
rs. Results: The means of clinical bleeding time of the laser tocoagulation group and the control group were 95 seconds %Cl = 34.4 to 155.6 s) and 296.7 seconds (95%Cl = 179.1 to
4.2 s) respectively. The analysis of Independent sample t-test •wed that the clinical bleeding time had significant lower in the
r photocoagulation group than the control group at P value 005 (95%Cl of the difference = 87.1 to 316.3). From COVA, there was no statistically significant difference of pain
among the groups (P value = 1). Conclusion: The diode laser photocoagulation showed benefit for hemostasis of tooth-extraction socket by comparison with the local pressure technique.
595: Effect on Bone Regeneration of Lidocaine-Fibrinogen-Aprotinin(LFA)-Collagen Complex as rhBMP-2 Carriers E.J. CHOI, J. LEE, and K. KWON, Dept. of Oral and Maxillofacial surgery. School of Dentisty, Wonkwang Dental Research Institute, Wonkwang University, lksan-si, Jeollabuk-do, South Korea Objective: The aim of this study was to compare the bone-forming ability of the BMP-2 delivered by LFA to that delivered by clinically utilized BMP-2 delivery vehicle collagen membrane. Method: Twelve NewZealand White Male Rabbit were used. Four cranial defects were formed respectively, and each defect was filled with other materials. Group 1 defect was negative control, and group 2 defect was filled with collagen membrane with lidocaine, group 3 with lidocaine-rhBMP-2 with collagen, group 4 with lidocaine-fibrinogen-aprotinin-rhBMP-2 with collagen with rh-BMP. After 2, 4, 8 week, 4 animals were sacrified, and analysed radiologically and histologically. Result: LFA released 80% of the loaded BMP-2 within 20 days, whereas collagen sponge released the same amount within the first 6 days. Moreover, the BMP-2 released from the LFA showed significantly higher alkaline phosphatase activity than the BMP-2 released from collagen sponge at 2 weeks in vitro. Bone regenerated by the LEA-collagen sponge-BMP-2 had higher bone density than bone regenerated by the collagen sponge-BMP-2. Conclusion: LFA-collagen sponge as a BMP-2 delivery vehicle exerts better osteogenic ability of BMP-2 than collagen sponge alone, a clinically utilized delivery vehicle.
596: Outcome of Tongue Squamous Cell Carcinoma in Young Age Group J.H. JEON', J.Y. PARK', S.W. CHOI', J.Y. YUN2, J.H. LEE2, J.H. SHIN', and H. MYOUNG2, 'Oral Oncology Clinic, National Cancer Center of Korea, Goyang, South Korea, 2Oral and Maxillofacial Surgery, Seoul National University, Seoul, South Korea Objective: The incidence of oral squamous cell carcinoma (OSCC) in young patients has recently increased although OSCCs are rare and believed to be etiologically distinct from OSCCs in older patients owing to less exposure to risk factors such as tobacco and alcohol. There are numerous reports claiming more invasive and aggressive approaches are inevitable for OSCC patients younger than 40-years-old as localized recurrence or distant metastasis is more likely. However, the prognosis of OSCCs in young patients is still controversial. The purpose of this study was to analyze the clinical characteristics of young patients (under 40-years) with tongue OSCC and to compare them with those of an older group of patients, and to investigate if the onset age of the patient is an adverse factor for patient. Method: We retrospectively reviewed the records of 271 patients (2000-2012) who were diagnosed with squamous cell carcinoma of the oral tongue. They were divided into two age groups: over 40 years of age and under 40 years. The factors including age, sex, survival, treatment, TNM stage, loco-regional metastasis, distant metastasis were compared between the groups. Result: The results show that there are significant differences in overall, disease-free, disease-specific and distant metastasis-free survival rate between the two groups. Conclusion: In this study, young age (<40 years) patients with squamous cell carcinoma of the oral tongue had higher rate of distant metastasis and worse prognosis. An extensive therapeutic regimen should be used in all young patients
597: Aberrant Expression of Secreted Protein in Oral Squamous Cell Carcinoma T. ONDA, K. HAYASHI, H. KATO, D. HASEGAWA, S. OGANE, T. YAKUSHIJI, T. NOMURA, N. TAKANO, and T. SHIBAHARA,
148





























