Embed Size (px)
Citation preview

META-ANALYSIS
Safety of Short, In-Hospital Delays Before Surgery for AcuteAppendicitis
Multicentre Cohort Study, Systematic Review, and Meta-Analysis
The United Kingdom National Surgical Research Collaborative
Objective: To determine safety of short in-hospital delays before appendicec-tomy.Background: Short organizational delays before appendicectomy may safelyimprove provision of acute surgical services.Methods: The primary endpoint was the rate of complex appendicitis (perfo-ration, gangrene, and/or abscess). The main explanatory variable was timingof surgery, using less than 12 hours from admission as the reference. Thefirst part of this study analyzed primary data from a multicentre study onappendicectomy from 95 centers. The second part combined this data with asystematic review and meta-analysis of published data.Results: The cohort study included 2510 patients with acute appendicitis, ofwhom 812 (32.4%) had complex findings. Adjusted multivariable binary re-gression modelling showed that timing of operation was not related to risk ofcomplex appendicitis [12–24 hours odds ratio (OR) 0.98 (P = 0.869); 24–48hours OR 0.88 (P = 0.329); 48+ hours OR 0.82 (P = 0.317)]. However, after48 hours, the risk of surgical site infection and 30-day adverse events bothincreased [adjusted ORs 2.24 (P = 0.039) and 1.71 (P = 0.024), respectively].Meta-analysis of 11 nonrandomized studies (8858 patients) revealed that de-lay of 12 to 24 hours after admission did not increase the risk of complexappendicitis (OR 0.97, P = 0.750).Conclusions: Short delays of less than 24 hours before appendicectomy werenot associated with increased rates of complex pathology in selected patients.These organizational delays may aid service provision, but planned delaybeyond this should be avoided. However, where optimal surgical systemsallow for expeditious surgery, prompt appendicectomy will still aid fastestresolution of pain for the individual patient.
Keywords: appendicectomy, appendicitis, surgical outcomes, timing ofsurgery
(Ann Surg 2014;00:1–10)
A ppendicectomy for acute appendicitis is the most commonly per-formed emergency general surgical procedure. Approximately
50,000 procedures are performed annually in the United Kingdom1
and 250,000 in the United States of America.2 Traditional fears ofdelay before appendicectomy leading to perforation have led to anacceptance of the need for prompt surgery. There is little doubt that
From the West Midlands Research Collaborative, Academic Department of Surgery,Queen Elizabeth Hospital, Birmingham, UK.
The National Surgical Research Collaborative members are shown at the Acknowl-edgment section.
Disclosure: No funding was received for this study, and the authors declare noconflicts of interest.
Supplemental digital content is available for this article. Direct URL citationsappear in the printed text and are provided in the HTML and PDF versions ofthis article on the journal’s Web site (www.annalsofsurgery.com).
Reprints: Aneel Bhangu, MBChB, MRCS, West Midlands Research Collaborative,Academic Department of Surgery, Queen Elizabeth Hospital, Birmingham B152TH, UK. E-mail: [email protected].
Copyright C⃝ 2014 by Lippincott Williams & WilkinsISSN: 0003-4932/14/00000-0001DOI: 10.1097/SLA.0000000000000492
patients with peritonitis or sepsis secondary to suspected/confirmedacute appendicitis require urgent surgery. However, trials of success-ful nonoperative management of mild/moderate appendicitis havesuggested that short delays before planned surgery may be feasible.3
There is current debate surrounding the risks and benefitsof out-of-hours emergency operating. Although 24-hour operatingroom schedules have been suggested, there remain considerable per-ceived benefits to daytime surgery. Daytime operating by supervisedtrainees may improve both training and outcome compared with sleep-deprived, unsupervised nighttime trainees.4,5 It may further increaseavailability of laparoscopy and computed tomography (CT), whichreduce negative appendicectomy rates.6,7 A delay of 12 to 24 hoursafter a decision to operate may be safe, especially in the presenceof intravenous antibiotic and fluid resuscitation.8,9 This delay wouldallow cases admitted at night to be operated on the next morning, andthose admitted during the morning to be operated on before the endof the day. The converse argument is that prompt 24-hour operatingmay reduce the risk of progression to perforation while increasinghospital productivity.9
Further information is needed to support the most appropri-ate evidence-based strategy. The aim of this study was to determinewhether delaying appendicectomy by more than 12 hours increasedthe rate of complex appendicitis. This was done in 2 parts. The firstpart analyzed primary data from a multicentre study performed pre-dominantly in the British National Health Service. The second partcombined this data with a formal systematic review and meta-analysisof published studies, to provide a more globally relevant overview.
METHODSCohort StudyPatients and Data Collection
The Multicentre Appendicectomy Audit collected data onprospective patients undergoing appendicectomy from 89 centerswithin the United Kingdom and 6 centers overseas. Complete method-ology has been previously described.10 Briefly, design and data col-lection was trainee-led, protocol driven, prospective, and multicen-tered. The study period included May and June 2012, with 30-dayfollow-up for the last patient to the end of July. Results for the use oflaparoscopy, normal appendicectomy rates and adverse events rateshave been previously published, without data related to delay beforeappendicectomy.10 This study represents a subgroup analysis of pa-tients with proven appendicitis only. Permission to perform the auditwas granted from each individual site’s Clinical Audit Department.
EndpointsThe primary endpoint was the rate of complex appendicitis,
defined for this study as clinical or histopathological presence of per-foration, gangrene, and/or abscess. Secondary endpoints included (i)the rate of surgical site infection (SSI), as defined by the Centersfor Disease Control and Prevention11; (ii) the rate of 30-day ad-verse events, assessed using a composite outcome including wound
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Annals of Surgery ! Volume 00, Number 00, 2014 www.annalsofsurgery.com | 1

Bhangu and Singh Annals of Surgery ! Volume 00, Number 00, 2014
infection, intra-abdominal abscess, readmission, unscheduled postop-erative ultrasonographic scan or CT, further surgical or radiologicalintervention within 30 days and/or other unexpected postoperativeadverse events.
Statistical AnalysisMissing data were replaced using multiple imputation.12 Miss-
ing value pattern analysis revealed a non-monotone data set. Fiveimputed data sets were generated using multiple regression (Markovchain Monte Carlo method) and 10 iterations. Results from logisticregression analysis on each data set were pooled, using the SPSSmultiple imputation module.
Binary logistic regression was used to estimate odds ratios(ORs) for the main outcome measures. The main explanatory vari-able was the duration of in-hospital delay, defined as the time fromadmission in the emergency department (or as close to this time aspossible), until the time of incision. The reference group used was</≤12 hours, as stated by each study. Initially, a univariable assess-ment of the impact of time to surgery was made. To account forconfounding factors, patient and clinical care variables were then en-tered into a model to adjust these odds ratios at multivariable level.Factors entered into this model were those that were statically sig-nificant at univariable level, and also those judged to be clinicallysignificant irrespective of statistical significance. Data were analyzedusing SPSS 19 (SPSS Inc, Chicago, IL).
Systematic ReviewData Sources and Search Strategy
A systematic search of OVID SP version of Medline, Pubmedversion of Medline, the Cochrane Library, and ClinicalTrials.gov wasperformed for published studies comparing rates of complex appen-dicitis when comparing 2 time delays until operation. The search wasperformed independently by 2 researchers. No date or language lim-its were applied. The search strategies used are presented in Supple-mental Table 1, available at http://links.lww.com/SLA/A531, whereMeSH terms were used to search Medline. The last search was per-formed in January 2013. A manual search of reference lists in relevantsystematic reviews was undertaken to further identify randomized tri-als of potential interest. Abstracts and conference proceedings wereexcluded because of the high probability of incomplete data. Cita-tions were collated with EndNote Reference Manager (Version X4,Thomson Reuters) and duplicates removed. Data were extracted in-dependently by 2 authors. Discrepancies in outcome extraction wereresolved by reexamination of the relevant study until consensus wasachieved.
Inclusion/Exclusion CriteriaStudies were included on satisfaction of the following criteria:
(i) design was randomized controlled trial (RCT), prospective ob-servational or retrospective cohort study; (ii) studies compare ratesof complex appendicitis between those undergoing appendicectomybefore and after a 12-hour delay cutoff; (iii) studies presenting datafor in-hospital delays separately from other (eg, prehospital) delays;(iv) where there was overlap in patient cohorts between 2 studies,the study that contained the more recent and larger cohort was in-cluded. Studies were excluded according to the following criteria: (i)case reports, letters, reviews or comments; (ii) studies that did notprovide extractable data relating to a 12 hour cut-off; (iii) studiesthat did not provide evidence of rates of complex appendicitis; (iv)studies that provided data on pre-hospital/patient related delays wherein-hospitals delays could not separately be extracted.
Study OutcomesThe primary meta-analysis endpoint of interest was the rate
of complex appendicitis, at </≤12 hours versus >/≥12 to 24 hours.Secondary endpoints included the rate of infectious complications(wound infection and/or pelvic abscess) and overall 30-day morbidity.
Meta-analysisMeta-analysis was conducted according to guidelines from the
Meta-analysis Of Observational Studies in Epidemiology (MOOSE)group13 and Preferred Reporting Items for Systematic reviews andMeta-Analysis group (PRISMA).14 Meta-analysis was performedwhen outcome data were provided by a minimum of 3 studies. ORswere calculated from the original data and meta-analyzed using theMantel-Haenszel method. The OR represents the odds of an adverseevent (eg, complex appendicitis) occurring in the experimental group(ie, delayed appendicectomy) versus the control group (ie, early ap-pendicectomy). The point estimate of the OR was considered to bestatistically significant at the P < 0.05 level if the 95% confidenceinterval (CI) did not include the value one.
Risk of bias was assessed using the Newcastle Ottawa Scale.15
Two reviewers independently allocated study quality and disagree-ment was resolved by reexamining the relevant paper until consensuswas achieved. A score of 7 or above indicated low risk of bias.Between-study heterogeneity was assessed using the I2 and χ 2 statis-tic, and graphical exploration of funnel plots. Higher values of I2
and the χ 2 statistic signified increasing levels of inconsistency andheterogeneity between studies and P < 0.1 was considered evidencefor significant heterogeneity.16 Because of the high potential for clin-ical heterogeneity (even in the absence of statistical heterogeneity), arandom-effects model was adopted to account for differences betweenstudies. Preplanned sensitivity analysis was performed for low riskof bias studies (studies including time groups >1990, studies with>1000 patients). Meta-analysis was performed using Review Man-ager 5.1 (Copenhagen: The Nordic Cochrane Centre, The CochraneCollaboration, 2008).
RESULTSCohort StudyDemographics
The cohort study included 2510 patients from 95 centers, ofwhom 32.4% (n = 812) had complex findings. Differences betweenpatients with simple and complex appendicitis are shown in Table 1,alongside a description of missing data. Patients with complex appen-dicitis were more likely to be older, body mass index (BMI) less thanor equal to 25, American Society of Anesthesiologists (ASA) scoreIII/IV; receive an out of hours operation, open incision, and longeroperation; and have increased consultant presence in theater. How-ever, there was no significant association between delay to operationand rate of complex appendicitis (P = 0.498).
Differences in demographics between patients who receivedoperations at <12, 12–23, 24–47, and 48+ hours are shown inTable 2. Those with longer delays to operation were more likely tobe older, female, BMI ≥ 25, ASA III/IV, receive a daytime operation,receive an initially laparoscopic approach, have a consultant presentin theater, and have a longer duration of surgery.
Regression ModelsBoth univariable and adjusted multivariable analyses
(Table 3) showed that timing of operation was not related torisk of complex appendicitis [12–24 hours adjusted OR = 0.98(P = 0.869); 24–48 hours adjusted OR 0.88 (P = 0.329); 48+ hoursadjusted OR 0.82 (P = 0.317)]. After 48 hours, the risk of 30-day
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
2 | www.annalsofsurgery.com C⃝ 2014 Lippincott Williams & Wilkins

Annals of Surgery ! Volume 00, Number 00, 2014 Delay to Appendicectomy
TABLE 1. Demographics of Cohort by Simple and Complex Appendicitis
Simple Appendicitis Complex Appendicitis
Number % Number % P
Age yrs<16 345 20.3 194 23.916–50 1152 67.8 413 50.9>50 200 11.8 204 25.1 <0.001Missing 1 0.1 1 0.1
GenderMale 968 57.0 460 56.7Female 726 42.8 352 43.3 0.816Missing 4 0.2 0 0.0
BMIBMI <25 1076 63.4 438 53.9BMI ≥25 445 26.2 272 33.5 <0.001Missing 177 10.4 102 12.6
ASAI/II 1608 94.7 745 91.7III/IV 30 1.8 34 4.2 <0.001Missing 60 3.5 33 4.1
Use of preoperative imagingNone/abdominal X-ray 1240 73.0 524 64.5Ultrasonography 267 15.7 113 13.9CT 191 11.2 175 21.6 <0.001
Time of operation0800–1800 1011 59.5 411 50.61800–0000 336 19.8 194 23.90000–0800 307 18.1 180 22.2 <0.001Missing 44 2.6 27 3.3
Initial operative methodOpen 632 37.2 269 33.1Laparoscopic 1066 62.8 543 66.9 0.046
Delay to operation, h0–11 522 30.7 272 33.512–23 606 35.7 272 33.524–47 350 20.6 166 20.448+ 119 7.0 52 6.4 0.498Missing 101 5.9 50 6.2
Consultant presenceYes 357 21.0 254 31.3No 1324 78.0 552 68.0 <0.001Missing 17 1.0 6 0.7
Duration of surgery<60 min 875 51.5 298 36.760+ min 752 44.3 481 59.2 <0.001Missing 71 4.2 33 4.1
adverse events increased in both univariable and adjusted models (OR1.83, P = 0.006 and adjusted OR 1.71, P = 0.024, respectively). Inpatients operated on between 12 to 23 hours, there was no increasein the rate of adverse events based upon time of day of operation(0800–1800: reference; 1800–0000: OR 1.47, 95% CI 0.86–2.53, P= 0.160; 0000–0800: OR 0.98, 95% CI 0.54–1.77, P = 0.936). Whenpatients operated on after 12 hours were pooled, time of day was againnot associated with a change in adverse event rates (1800–0000: OR1.07, 95% CI 0.73–1.58, P = 0.730; 0000–0800: OR 1.02, 95% CI0.67–1.55, P = 0.915).
For SSI at 48 hours, univariable analysis was not significantlydifferent from reference (OR 1.79, P = 0.112) but became significantat multivariable analysis (adjusted OR 2.24, P = 0.039). Completeresults of the adjusted multivariable analyses are shown in Supple-mental Tables 2 to 4, available at http://links.lww.com/SLA/A531.There was furthermore no association between delay and pelvic ab-scess (12–23 hours: OR 0.73, 95% CI 0.40–1.31, P = 0.290; 24–47
hours: OR 0.79, 95% CI 0.42–1.51, P = 0.480; 48+ hours: OR 1.50,95% CI 0.68–3.32, P = 0.317) or increased rate of 30-day unsched-uled imaging (12–23 hours: OR 1.00, 95% CI 0.69–1.43, P = 0.986;24–47 hours: OR 1.00, 95% CI 0.68–1.49, P = 0.991; 48+ hours:OR 1.25, 95% CI 0.74–2.13, P = 0.409). All regression models wererepeated using the original (nonimputed) data set, which did not affectthe significance of results and showed similar magnitudes of effect.
Systematic ReviewDemographics of Included Studies
From 1250 screened abstracts, 14 studies were included in thefinal analysis, including the cohort study (Fig. 1). The basic demo-graphics of these studies are shown in Table 4. Two studies stateda prospective data collection strategy with an a priori aim of as-sessing delay to appendicectomy and perforation rates. One studycontained data from the American College of Surgeons’ National
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C⃝ 2014 Lippincott Williams & Wilkins www.annalsofsurgery.com | 3

Bhangu and Singh Annals of Surgery ! Volume 00, Number 00, 2014
TABLE 2. Demographics of Cohort by Timing of In-Hospital Delay
Delay to Operation, h
<12 12–23 24–47 48+ P
Age, yrs<16 237 29.8% 164 18.7% 103 20.0% 21 12.3%16–50 464 58.4% 591 67.3% 300 58.3% 103 60.2%>50 93 11.7% 123 14.0% 112 21.7% 47 27.5% <0.001
GenderMale 486 61.2% 528 60.2% 267 51.9% 65 38.0%Female 308 38.8% 349 39.8% 247 48.1% 106 62.0% <0.001
BMI<25 517 71.6% 548 70.4% 284 61.2% 95 62.5%≥25 205 28.4% 230 29.6% 180 38.8% 57 37.5% <0.001
ASAI/II 760 98.1% 833 98.0% 478 96.0% 152 93.8%III/IV 15 1.9% 17 2.0% 20 4.0% 10 6.2% 0.003
Use of preoperative imagingNone/abdominal X-ray 659 83.0% 685 78.0% 227 53.7% 30 17.5%Ultrasonography 66 8.3% 109 12.4% 125 24.2% 69 40.4%CT 69 8.7% 84 9.6% 114 22.1% 72 42.1% <0.001
Time of operation0800–1800 320 40.8% 626 72.5% 306 60.2% 112 67.1%1800–0000 240 30.6% 113 13.1% 122 24.0% 29 17.4%0000–0800 225 28.7% 124 14.4% 80 15.7% 26 15.6% <0.001
Initial operative methodsOpen 315 39.7% 318 36.2% 170 32.9% 48 28.1%Laparoscopic 479 60.3% 560 63.8% 346 67.1% 123 71.9% 0.010
Consultant presenceYes 198 25.0% 204 23.4% 140 27.2% 51 29.8%No 593 75.0% 668 76.6% 374 72.8% 120 70.2% 0.205
Duration of surgery<60 min 405 52.1% 436 51.1% 224 44.2% 65 38.5%60+ min 372 47.9% 417 48.9% 283 55.8% 104 61.5% 0.001
HistologySimple 522 65.7% 606 69.0% 350 67.8% 119 69.6%Complex 272 34.3% 272 31.0% 166 32.2% 52 30.4% 0.498
TABLE 3. Adjusted Regression Models of the Cohort Study for the Main Outcomes
Univariable Multivariable
Delay to Operation, h OR∗ P OR∗ P
Complex appendicitis†<12 Reference Reference12–23 0.87 (0.71, 1.07) 0.188 0.98 (0.78, 1.23) 0.86924–47 0.92 (0.73, 1.16) 0.476 0.88 (0.69, 1.13) 0.32948+ 0.86 (0.60, 1.23) 0.408 0.82 (0.56, 1.21) 0.317
30-d adverse events‡<12 Reference Reference12–23 1.21 (0.90, 1.63) 0.202 1.25 (0.90, 1.73) 0.18124–47 1.05 (0.74, 1.50) 0.775 0.98 (0.67, 1.41) 0.89648+ 1.83 (1.19, 2.83) 0.006 1.71 (1.07, 2.72) 0.024
SSI‡<12 Reference Reference12–23 1.04 (0.62, 1.72) 0.891 1.28 (0.75, 2.20) 0.36524–47 1.06 (0.59, 1.89) 0.846 1.15 (0.63, 2.10) 0.65848+ 1.79 (0.87, 3.65) 0.112 2.24 (1.04, 4.82) 0.039
∗With 95% CI in brackets.†Adjusted for age, gender, BMI, ASA, time of operation, time to operation.‡Adjusted for age, gender, BMI, ASA, time of operation, time to operation, histology, duration of surgery, initial operative method, and consultant
presence in theater. Complete multivariable regression models are shown in supplemental Tables 2 to 4, available at http://links.lww.com/SLA/A531.
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
4 | www.annalsofsurgery.com C⃝ 2014 Lippincott Williams & Wilkins

Annals of Surgery ! Volume 00, Number 00, 2014 Delay to Appendicectomy
TABLE 4. Characteristics of Studies Included in the Meta-analysis
Definitions
Male Minimum Time ComplexSetting Year Design Patients∗ Gender Age Delay Cutoff, h Appendicitis
Abou-Nukta etal17
Connecticut,USA
Jan2002–Dec2004
R 380 165 (43%) 18 Presentation inED to surgery
<12 Gangrenous orperforated
Bhangu 89 UK and 6overseascenters
May–June2012
R 2359 1010 (43%) 5 ED to surgery <12 Gangrenous,perforated orabscess on
histopathology orclinically
Busch et al18 11 hospitals,Switzerland
Jan2003–
Jan2006
P 1675 NS 16 Admission tooperation
≤12 Intra-operative orhistopathological
perforation
Ditillo et al19 Connecticut,USA
Feb1998–Dec2004
R 1287 615 (48%) 16 ED to operatingsuite
<12 Operative andpathologicalfindings of
gangrenous,perforated or
abscessEko et al20 Pittsfield,
USAJan
2005–Dec2007
R 354 NS 3 ED registration toskin incision
≤12 Perforation,peritonitis,
abscess,purulence
Eldar et al21 Hafia, Israel Jan1980–Dec1992
R 483 NS 5 ED to surgery ≤12 Perforated and/organgrenous by
operative and/orpathological
recordsFahim et al22 Lahore,
PakistanFeb
2002–April2002
R 102 NS 10 ED to surgery ≤12 Gangrenous/perforated by
operative findings
Giraudo et al23 Cuneo, Italy Dec2003–Dec2009
R 746 377 (51%) 3 ED to surgery <12 Clinicallygangrenous
Gupta et al24 Pokhara,Nepal
May2008–June2009
R 107 NS Unclear Presentation inemergency room
to surgery
<12 Gangrenous/perforated by
operative findings
Ingraham et al9 NSQUIP,USA
Jan2005–Dec2008
R 32782 17672 (54%) 16 Surgicaladmission toinduction ofanaesthesia
≤12 Perforation,peritonitis,abscess orrupture.
Kearney et al25 Cork,Ireland
July2005–July2006
R 115 NS 16 First hospitalpresentation to
operation
<12 Histopathologi-cally
perforated
Maroju et al26 Pondicherry,India
April1999–March2000
P 111 NS 13 Presentation tohospital casualty
to operation
≤12 Gangrenous orperforated
Teixeria et al27 Los AngelesCounty +
University ofSouthernCaliforniaMedical
Center, USA
July2003–June2011
R 4529 2745 (61%) 13 Admission tooperation
≤12 Perforation onpathology report
Yardeni et al28 Michigan,USA
1998–2001
R 126 75 (60%) <16 ED to OR ≤12 Perforated
∗No. patients with pathologically confirmed acute appendicitis.ED indicates emergency department, OR, operating room; P, prospective; R, retrospective.
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C⃝ 2014 Lippincott Williams & Wilkins www.annalsofsurgery.com | 5

Bhangu and Singh Annals of Surgery ! Volume 00, Number 00, 2014
Figure 1. PRISMA flowchart of study inclusion into the meta-analysis.
Surgical Quality Improvement Program (NSQIP9), which overlappedwith another smaller study (Teixeria et al17). However, these stud-ies provided data on different endpoints and so both were includedwhile ensuring no direct overlap. With the NSQIP study, 40,633 pa-tients were included in the analysis and with the Teixeria et al’s study,12,380 patients were included.
Studies specified delay as first hospital presentation [eitheremergency room/casualty (n = 11), surgical admission (n = 1), orunstated (n = 2)] until the time of operation (Table 4). All studiescontained a definition of complex appendicitis that contained at leastone of perforation or gangrenous finding. Five studies concerned onlyadults, 7 a mix of adults and children, 1 children only, and 1 an unclearminimum age. There was a mix of male- and female-predominantstudies, where stated (range of male patients per study: 43%–61%,Table 4). Quality assessment of included studies is shown in Supple-mental Table 5, available at http://links.lww.com/SLA/A531, with 11studies scoring 7 points or more on the Newcastle Ottawa Scale.
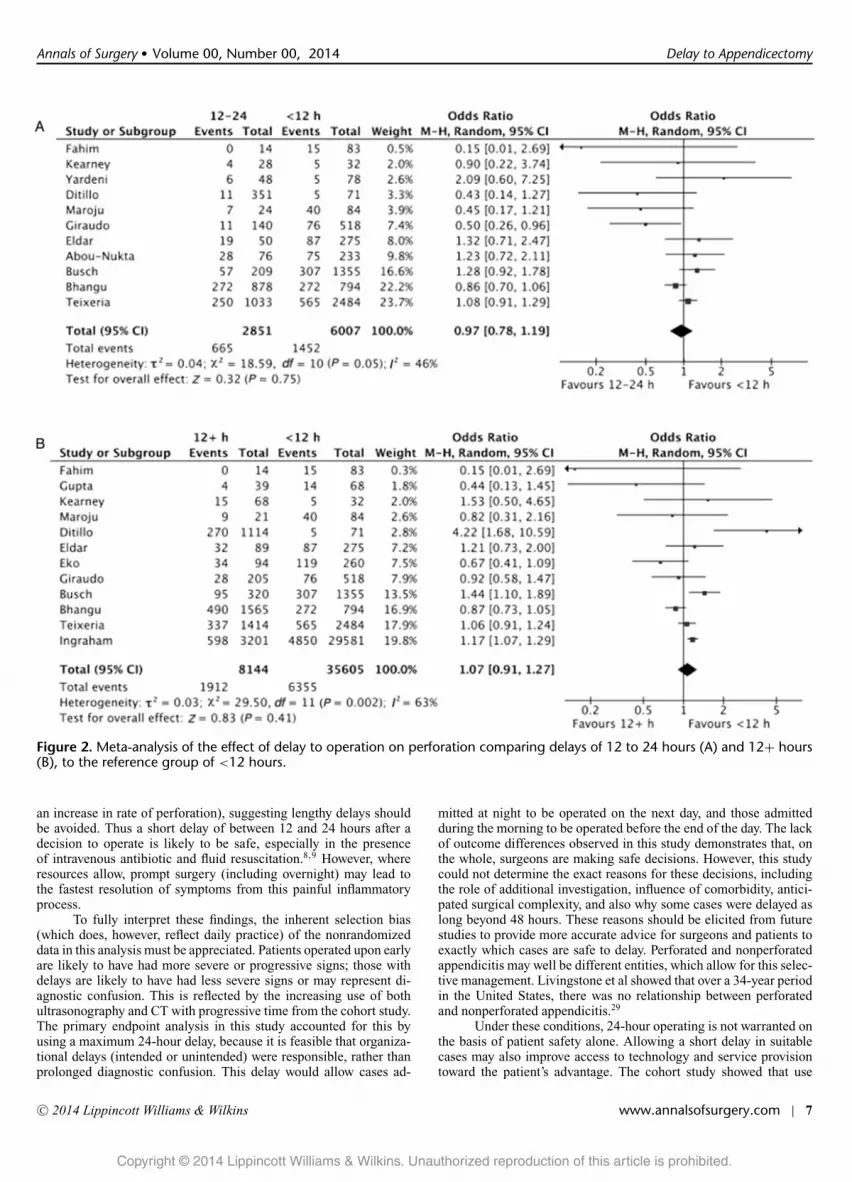
Meta-analysisFor the primary outcome, meta-analysis of 11 studies (8858
patients) revealed that delay of 12 to 24 hours after admission did
not increase the risk of complex appendicitis (OR 0.97, P = 0.750,Fig. 2A). There was no increased risk when all time periods of12 hours and beyond were combined (12 studies, 43 749 patients, OR1.07, P = 0.410, Fig. 2B).
There was no significant difference in the rate of wound infec-tion and/or intra-abdominal abscess with delay of 12 to 24 hours (3studies, 5497 patients, OR 1.03, 95% CI 0.71–1.50, P = 0.870, I2 =32%). Four studies considered postoperative morbidity. Because ofmarked heterogeneity in the definitions of morbidity, meta-analysiswas not performed.
When considering subgroup analyses (low risk of bias studies,studies including time groups >1990, studies with >1000 patients),there were no changes in significance levels for these effects.
DISCUSSIONThe main finding of both the cohort and meta-analysis phase of
this study was that a short delay of 12 to 24 hours was not associatedwith an increased rate of complex appendicitis. Meta-analysis showedthat these short delays were not associated with rates of infectiouscomplications. The cohort study showed that delays beyond 48 hourswere associated with an increased rate of wound infection (without
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
6 | www.annalsofsurgery.com C⃝ 2014 Lippincott Williams & Wilkins
Annals of Surgery ! Volume 00, Number 00, 2014 Delay to Appendicectomy
Figure 2. Meta-analysis of the effect of delay to operation on perforation comparing delays of 12 to 24 hours (A) and 12+ hours(B), to the reference group of <12 hours.
an increase in rate of perforation), suggesting lengthy delays shouldbe avoided. Thus a short delay of between 12 and 24 hours after adecision to operate is likely to be safe, especially in the presenceof intravenous antibiotic and fluid resuscitation.8,9 However, whereresources allow, prompt surgery (including overnight) may lead tothe fastest resolution of symptoms from this painful inflammatoryprocess.
To fully interpret these findings, the inherent selection bias(which does, however, reflect daily practice) of the nonrandomizeddata in this analysis must be appreciated. Patients operated upon earlyare likely to have had more severe or progressive signs; those withdelays are likely to have had less severe signs or may represent di-agnostic confusion. This is reflected by the increasing use of bothultrasonography and CT with progressive time from the cohort study.The primary endpoint analysis in this study accounted for this byusing a maximum 24-hour delay, because it is feasible that organiza-tional delays (intended or unintended) were responsible, rather thanprolonged diagnostic confusion. This delay would allow cases ad-
mitted at night to be operated on the next day, and those admittedduring the morning to be operated before the end of the day. The lackof outcome differences observed in this study demonstrates that, onthe whole, surgeons are making safe decisions. However, this studycould not determine the exact reasons for these decisions, includingthe role of additional investigation, influence of comorbidity, antici-pated surgical complexity, and also why some cases were delayed aslong beyond 48 hours. These reasons should be elicited from futurestudies to provide more accurate advice for surgeons and patients toexactly which cases are safe to delay. Perforated and nonperforatedappendicitis may well be different entities, which allow for this selec-tive management. Livingstone et al showed that over a 34-year periodin the United States, there was no relationship between perforatedand nonperforated appendicitis.29
Under these conditions, 24-hour operating is not warranted onthe basis of patient safety alone. Allowing a short delay in suitablecases may also improve access to technology and service provisiontoward the patient’s advantage. The cohort study showed that use
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C⃝ 2014 Lippincott Williams & Wilkins www.annalsofsurgery.com | 7

Bhangu and Singh Annals of Surgery ! Volume 00, Number 00, 2014
of imaging, rate of laparoscopy, and the presence of consultants intheater were all greater after 12 hours. While this may represent amore challenging case-mix, the rate of complex appendicitis did notsignificantly change over the same time periods, and so it is feasi-ble to correlate these changes to short delays. In recent years, therehave been significant changes in the management of suspected acuteappendicitis, primarily with a view to reducing negative appendicec-tomy rates.7, 30 These include the introduction of laparoscopic appen-dicectomy and increasing availability of CT for right lower quadrantpain.6, 31 The potentially variable availability of this senior supportduring the day may also impact upon the operative approach (ie,laparoscopic versus open) adopted by the operating surgeon.32 How-ever, under optimal system conditions (including qualified, restedand appropriately supervised surgical personnel, adequate systemscapacity for preoperative CT, and laparoscopy), the performance ofappendectomy should still proceed in as expeditious manner as pos-sible. Abdominal pain and suffering can be alleviated with earliersurgery and may represent the optimal treatment for the patient underthese optimal conditions.
Before recommending planned organizational delays, the rateof infectious complications and other adverse event must also beconsidered. In the cohort study, the rate of SSI increased only after48 hours. The meta-analysis showed that delays up to 24 hours werenot associated with an increased rate of infectious complications.Although the patient number was large (n = 5497), this was onlybased on 3 studies. The largest of these studies, however, showedthat although a delay of 6 or less hours did not alter the rate ofperforation, it was associated with an increased rate of wound infec-tion (adjusted OR 1.54, 95% CI 1.01–2.34, P = 0.04).27 This effectwas most marked in the nonperforated group (1.9%–3.3% with a≥6-hour delay) compared with the perforated group (3.3%–3.9%).Ingraham et al,9 in their large NSQIP analysis, found no signifi-cant difference in the adjusted rate of morbidity after 6 or 12 hours.Meta-analysis of overall morbidity was not performed because of het-erogeneity in definition of morbidity that was likely to have skewedthe result. It is reasonable to call for more evidence to fully assess theimpact of planned short delays to appendicectomy on infectious com-plications. These future studies should ensure that all infectious com-plication/morbidities have been defined and detected through soundmethodology; underdetection is a problem in reporting SSI in generalsurgery.33
There has been an increasing interest in the nonsurgical man-agement of appendicitis. In a meta-analysis of 900 patients from 4randomized trials, Varadhan et al3 showed that nonoperative man-agement was associated with a relative risk reduction of 31% forantibiotic treatment compared with appendicectomy. However, 37%of patients still required appendicectomy at 1 year, illustrating thehigh failure rate of this strategy. In this cohort study and in the meta-analysis, it is reasonable that some of the patients selected for thedelayed appendicectomy groups would be candidates for nonopera-tive management; further assessment of nonoperative strategies wasbeyond the scope of this study.
The effects of shifting away from out-of-hours operating forthe trainee should also be considered. The advantages of daytimeoperating to surgical trainees include increased supervision and de-creased sleep-disturbance patterns, both of which may improve out-comes for the patient. As surgeons increase in subspecialization, theresponsibility of emergency general surgery may fall to the acute caresurgeon, who may find being able to delay certain cases beneficialto staff and physical resources while allowing emergency cases to beprioritized.34 This study’s findings may have the greatest implicationfor the rural settings in which a single surgeon may have prolongedon-calls. In such situations, the ability to defer an operation untilmorning may make the career of such a surgeon longer and more
acceptable. Although some argue that sleep deprivation and lack ofsupervision lead to worse outcomes for the patients and training forthe surgeon,4 others argue that the introduction of full shift rotationsmean that nighttime productivity should be maintained. In England,the 2004 National Confidential Enquiry into Perioperative Deaths re-ports identified trainee-led out-of-hours surgery as a risk factor forpoor outcomes.4 However, the latest report (in 2011) suggested thatelderly age is a more important risk factor, and that 24-hour supportto emergent cases should be provided.35
The mixed methodology used a cohort analysis followed bysystematic review and meta-analysis, which has been successfullyused before to investigate other disease areas and allows for completeanalysis of the research question in a single paper.36 The limitationsof this article also need to be considered. For the cohort study, the useof a composite endpoint for adverse events may have masked under-lying significant relationships and places equal emphasis on events ofdifferent severities. However, analysis was also performed separatelyfor SSI and pelvic abscess, which are perhaps the most severe ofthese. As previously discussed, there was a lack of randomized datawith an inherent selection bias, although this preselection of patientsallows us to assess the outcome of this daily and common practice.The duration of the patient-related prehospital delay was not takeninto account, although this cannot be controlled by the physicians,unlike the relevant in-hospital delay. There were differences withinthe included studies, including definitions of delay and definitionsof complex appendicitis; this was also reflected through statisticalheterogeneity. Different time cutoffs have been used in the literatureby different studies, including Ingraham et al,9 who proved a signifi-cantly higher risk of SSI in patients with nonperforated appendicitisundergoing surgery after a delay of more than 6 hours. This studyused a 12- to 24-hour cutoff as the primary endpoint, as it representsthe most clinically relevant interval to the research questions.
CONCLUSIONSBoth the cohort and meta-analysis parts of this study found
that short delays to appendicectomy were not associated with in-creased rates of complex appendicitis. On this basis, short delays up to24 hours in selected patients are safe and are likely to aid service pro-vision, access to imaging, and/or laparoscopy. Meta-analysis showedthat these short delays were not associated with an increased rate of in-fectious complications, although further evidence should be producedto confirm this and to test the effect on overall morbidity. However,where optimal surgical systems allow for expeditious surgery, promptappendicectomy will still lead to the fastest resolution of pain for theindividual patient.
ACKNOWLEDGMENTThe authors thank Professor Dion Morton for academic
guidance.
Following is the list of members of the National Surgical ResearchCollaborative. This study was devised, performed, and written byAneel Bhangu, who acts as its guarantor. A.B. and Prashant Singhperformed the systematic review and meta-analysis. The local in-vestigators conducted the audit, including identification of patientsand data collection at 95 local centers. Local investigators (alpha-betically by centre) of the National Surgical Research Collabora-tive were as follows: I. G. Panagiotopoulou, N. Chatzizacharias, M.Rana, K. Rollins, F. Ejtehadi, B. Jha (Addenbrooke’s Hospital, Cam-bridge); Y. W. Tan, N. Fanous (Addenbrooke’s Hospital, Cambridge-–Paediatric Surgery); G. Markides, A. Tan, C. Marshal, S. Akhtar(Airedale NHS Foundation Trust, Keighley); D. Mullassery (AlderHey Children’s Hospital Foundation Trust, Liverpool); A. Ismail(Alexandra Hospital, Redditch); C. Hitchins (Ashford and St Peter’s
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
8 | www.annalsofsurgery.com C⃝ 2014 Lippincott Williams & Wilkins

Annals of Surgery ! Volume 00, Number 00, 2014 Delay to Appendicectomy
Hospitals); S. Sharif, L. Osborne (Barts Health NHS Trust, Lon-don); N. Sengupta, C. Challand, D. Pournaras, K. Bevan (BedfordHospital NHS Trust, Bedford); J. King (Birmingham Children’s Hos-pital); J. Massey, I. Sandhu (Bradford Teaching Hospitals NHS Foun-dation Trust); J. M. Wells, D. A. Teichmann (Bristol Royal Hos-pital for Children); A. Peckham-Cooper, M. Sellers (Burton Hos-pitals NHS Foundation Trust); S. E. Folaranmi, B. Davies (Cen-tral Manchester University Hospitals NHS Foundation Trust); S.Potter, D. Egbeare, C. Kallaway, S. Parsons, E. Upchurch (Chel-tenham General Hospital); A. Lazaridis, D. Cocker, D. King, N.Behar (Chelsea and Westminster Teaching Hospital, London); S. P.Loukogeorgakis (Chelsea and Westminster Hospital NHS Founda-tion Trust, London-–Paediatric Surgery); R. Kalaiselvan (Countessof Chester NHS Foundation Trust); S. Marzouk, E. J. H. Turner, S.Kaptanis, V. Kaur (Croydon University Hospital); G. Shingler, A.Bennett (Royal Glamorgan Hospital, Llantrisant); S. Shaikh (Dews-bury District Hospital); M. Aly, J. Coad, T. Khong, Z. Nouman, J.Crawford (Diana, Princess of Wales Hospital, Grimsby); P. Szatmary(East Cheshire NHS Trust, Macclesfield); H. West (Eastbourne Dis-trict General Hospital); A. MacDonald (Evelina Children’s Hospital,Guy’s and St Thomas’ NHS Foundation Trust, London); J. Lambert,K. Gash (Frenchay Hospital, North Bristol NHS Trust); K. A. Hanks,E. Griggs, L. Humphreys (Gloucester Royal Hospital); A. Torrance,J. Hardman, L. Taylor (Good Hope Hospital, Sutton Coldfield); D.Rex (Great Ormond Street Hospital NHS Foundation Trust; J. Ben-nett, N. Crowther (Great Western Hospital, Swindon); B. McAree, S.Flexer (Harrogate and District NHS Foundation Trust); P. Mistry, P.Jain, M. Hwang, J. Richardson (Heartlands Hospital, Birmingham);N. Oswald, A. Wells, H. Newsome (Hinchingbrooke Health CareNHS Trust, Cambridgeshire); P. Martinez (Hospital de San Bern-abe, Berga, Spain); C. A. B. Alvarez, J. Leon (Hospital Santos Reyes,Aranda de Duero, Spain); D. Carradice, R. Gohil, M. Mount (Hulland East Yorkshire Hospitals NHS Trust); A. Campbell (Hull andEast Yorkshire Hospitals NHS Trust—Paediatric Surgery); S. Iype, E.Dyson, T. Groot-Wassink (Ipswich Hospital NHS Trust); A. R. Ross,C. Jones (King George Hospital, Ilford); P. Charlesworth (King’sCollege Hospital, London); N. Baylem, J. Voll, T. Sian, L. Creedon(King’s Mill Hospital, Mansfield); G. Hicks (Leeds Teaching Hospi-tals NHS Trust); J. Goring, V. Ng (Leeds Teaching Hospitals NHSTrust-–Paediatric Surgery); S. Tiboni (Leicester Royal Infirmary); T.Palser, B. Rees, P. Ravindra, C. Neophytou (Lincoln County Hospi-tal); H. Dent, T. Lo (Maidstone and Tunbridge Wells NHS Trust);L. Broom, M. O’Connell (Manor Hospital, Walsall); R. Foulkes, D.Griffith (Morriston, Wales); K. Butcher, O. Mclaren, A. Tai (MusgrovePark Hospital, Taunton); H. Yano (National Centre for Global Healthand Medicine, Tokyo, Japan); H. D. T. Torrance (Newham UniversityHospital); O. Moussa, D. Mittapalli, D. Watt (Ninewells Hospital andMedical School, Dundee); S. Basson (Norfolk and Norwich Univer-sity Hospital—Paediatric Surgery); J. Gilliland, S. Pilgrim (Norfolkand Norwich University Hospitals NHS Trust); A. Wilkins, J. Yee(North Devon District Hospital, Barnstaple); H. Cain, M. Wilson, J.Pearson, E. Turnbull (North Tyneside General Hospital); A. Brigic, N.A. Yassin, J. Clarke, S. Mallappa (North West London Hospitals NHSTrust, Northwick Park); P. Jackson (Nottingham University HospitalsTrust—Paediatric Surgery); C. Jones, B. Lakshminarayanan (OxfordUniversity Hospitals NHS Trust—Paediatric Surgery); A. Sharma(Palmerston North Hospital, MidCentral District Health Board); R.Velineni (Perth Royal Infirmary); K. Fareed, G. Yip (PeterboroughCity Hospital); A. Brown, N. Patel, M. Ghisel (Plymouth HospitalsNHS Trust); N. Tanner (Prince Charles Hospital, Merthyr Tydfil);H. Jones, J. Witherspoon, M. Phillips (Princess of Wales Hospital,Bridgend); M. F. Ho, S. Ng, T. Mak (Prince of Wales Hospital, HongKong); N. Campain, D. Mukhey (Nottingham University hospitalsNHS Trust); W. K. Mitchell, F. Amawi, E. Dickson, S. Aggarwal
(Royal Derby Hospital); L. K. Satherley, F. Asprou (Royal GwentHospital, Newport); C. Keys (Royal Hospital for Sick Children, Ed-inburgh); M. Steven (Royal Hospital for Sick Children, Glasgow);M. Johnstone (Royal Liverpool and Broadgreen University HospitalTrust); J. Muhlschlegel (Royal United Hospital Bath NHS Trust); E.Hamilton, J. Yin (Royal Wolverhampton NHS Trust); M. Dilworth,A. Wright (Russells Hall Hospital, Dudley); P. Spreadborough, P.Marriott, M. Singh (Sandwell and West Birmingham Hospitals NHSTrust Hospital); K. Mockford, J. Morgan (Scunthorpe General Hos-pital); W. Ball, J. Royle, J. Lacy-Colson (Royal Shrewsbury Hospi-tal); W. Lai, S. Griffiths, S. Mitchell (South Devon Healthcare NHSFoundation Trust); C. Parsons (Southampton University HospitalsNHS Trust—Paediatric Surgery); A. S. Joel, P. F. Mason, G. J. Har-rison (Southport and Ormskirk NHS Trust); J. Steinke, H. Rafique(St George’s Hospital NHS Trust, London); C. Battersby (St Helensand Knowsley Hospitals Trust, Merseyside); W. Hawkins, D. Gur-ram (The St George Hospital, South Eastern Sydney Illawarra AreaHealth Service, Australia); C. A. Hateley, A. Penkethman, C. Lamb-den (St Mary’s Hospital, Imperial Healthcare NHS Trust, London);A. Conway, P. Dent, D. Yacob (Surrey and Sussex Healthcare NHSTrust); O. A. Oshin, A. Hargreaves, G. Gossedge (University Hospi-tal Aintree, Liverpool); J. Long, M. Walls, K. Futaba, T. Pinkney, S.Puig, D. Nepogodiev, P. Marriott (University Hospital BirminghamQueen Elizabeth NHS Trust); A. Boddy, A. Jones (University Hos-pitals Bristol, NHS Foundation Trust); C. Tennuci, N. Battersby, R.Wilkin, C. Lloyd, E. Sein (University Hospital of North Staffordshire,Stoke-on-Trent); K. McEvoy, L. Whisker, S. Austin (Warwick Hospital,South Warwickshire NHS Foundation Trust); A. Colori, P. Sinclair, M.Loughran, A. Lawrence (Watford General Hospital); J. Horsnell, J.Bagenal (Weston Area Health NHS Trust); A. Pisesky, S. Mastoridis,K. Solanki, I. Siddiq (Whipps Cross University Hospital); L. Merker,P. Sarmah, C. Richardson (Worcestershire Royal Hospital); D. Han-ratty, L. Evans, M. Mortimer (University Hospital of Wales, Cardiffand Vale University Health Board). Collaborative chairs were as fol-lows: A. Bhalla, D. Bartlett, D. Beral, N. S. Blencowe, J. Cornish, J. B.Haddow, N. J. Hall, M. Johnstone, S. Pilgrim, S Strong, R. Velineni.
REFERENCES1. Hospital Episode Statistics. Admitted Patient Care—England 2011–
2012. Total procedures and interventions. Available at: http://www.hscic.gov.uk/catalogue/PUB08288/hosp-epis-stat-admi-tot-ops-11-12-tab.xls. Ac-cessed October 2013.
2. Buckius MT, McGrath B, Monk J, et al. Changing Epidemiology of AcuteAppendicitis in the United States: study period 1993–2008. J Surg Res.2012;175:185–190.
3. Varadhan KK, Neal KR, Lobo DN. Safety and efficacy of antibiotics comparedwith appendicectomy for treatment of uncomplicated acute appendicitis: meta-analysis of randomised controlled trials. Brit Med J. 2012;344:e2156.
4. The National Confidential Enquiry into Peri-Operative Deaths (NCEPOD).Who operates when? 2003. Available at: http://www.ncepod.org.uk/pdf/2003/03full.pdf . Accessed October 2013.
5. Leff DR, Aggarwal R, Rana M, et al. Laparoscopic skills suffer on the firstshift of sequential night shifts: program directors beware and residents prepare.Ann Surg. 2008;247:530–539.
6. Sauerland S, Jaschinski T, Neugebauer EA. Laparoscopic versus open surgeryfor suspected appendicitis. Cochrane Database Syst Rev. 2004;18:CD001546.
7. Guller U, Rosella L, McCall J, et al. Negative appendicectomy and perforationrates in patients undergoing laparoscopic surgery for suspected appendicitis.Br J Surg. 2011;98:589–595.
8. Abou-Nukta F, Bakhos C, Arroyo K, et al. Effects of delaying appendectomy foracute appendicitis for 12 to 24 hours. Arch Surg. 2006;141:504–506; discussion506–507.
9. Ingraham AM, Cohen ME, Bilimoria KY, et al. Effect of delay to operation onoutcomes in adults with acute appendicitis. Arch Surg. 2010;145:886–892.
10. National Surgical Research Collaborative. Multicenter observational study ofperformance variation in provision and outcome of emergency appendicec-tomy. Brit J Surg. 2013;100:1240–1252.
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C⃝ 2014 Lippincott Williams & Wilkins www.annalsofsurgery.com | 9

Bhangu and Singh Annals of Surgery ! Volume 00, Number 00, 2014
11. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition ofhealth care–associated infection and criteria for specific types of infections inthe acute care setting. Am J Infect Contr. 2008;36:309–332.
12. Sterne JA, White IR, Carlin JB, et al. Multiple imputation for missing datain epidemiological and clinical research: potential and pitfalls. Brit Med J.2009;338:b2393.
13. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studiesin epidemiology: a proposal for reporting. Meta-analysis Of ObservationalStudies in Epidemiology (MOOSE) group. JAMA. 2000;283:2008–2012.
14. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for report-ing systematic reviews and meta-analyses of studies that evaluate health careinterventions: explanation and elaboration. J Clin Epidemiol. 2009;62:e1–e34.
15. Wells GA SB, O’Connell D, Peterson J, et al. The Newcastle-Ottawa Scale(NOS) for assessing the quality of nonrandomized studies in meta-analysis.Available at: http://www.ohri.ca/programs/clinical epidemiology/oxford web.ppt. Accessed October 2013.
16. Lau J, Ioannidis JP, Schmid CH. Quantitative synthesis in systematic reviews.Ann Intern Med. 1997;127:820–826.
17. Abou-Nukta F, Bakhos C, Arroyo K, et al. Effects of delaying appendectomyfor acute appendicitis for 12 to 24 hours. Arch Surg. 2006;141:504–506.
18. Busch M, Gutzwiller FS, Aellig S, et al. In-hospital delay increases the risk ofperforation in adults with appendicitis. World J Surg. 2011;35:1626–1633.
19. Ditillo MF, Dziura JD, Rabinovici R. Is it safe to delay appendectomy in adultswith acute appendicitis? Ann Surg. 2006;244:656–660.
20. Eko FN, Ryb GE, Drager L, et al. Ideal timing of surgery for acute uncompli-cated appendicitis. N Am J Med Sci. 2013;5:22–27.
21. Eldar S, Nash E, Sabo E, et al. Delay of surgery in acute appendicitis. Am JSurg. 1997;173:194–198.
22. Fahim F, Shirjeel S. A comparison between presentation time and delay insurgery in simple and advanced appendicitis. J Ayub Med Col Abbottabad.2005;17:37–39.
23. Giraudo G, Baracchi F, Pellegrino L, et al. Prompt or delayed appendectomy?Influence of timing of surgery for acute appendicitis. Surg Today 2013;43:392–396.
24. Gupta A, Regmi S, Hazra NK, et al. Clinically monitored delay-A valid op-tion in cases with doubtful diagnosis of acute appendicitis. Indian J Surg.2010;72:215–219.
25. Kearney D, Cahill RA, O’Brien E, et al. Influence of delays on perforation riskin adults with acute appendicitis. Dis Colon Rectum. 2008;51:1823–1827.
26. Maroju NK, Robinson Smile S, Sistla SC, et al. Delay in surgery for acuteappendicitis. ANZ J Surg. 2004;74:773–7736.
27. Teixeira PG, Sivrikoz E, Inaba K, et al. Appendectomy timing: waiting un-til the next morning increases the risk of surgical site infections. Ann Surg.2012;256:538–543.
28. Yardeni D, Hirschl RB, Drongowski RA, et al. Delayed versus immediatesurgery in acute appendicitis: do we need to operate during the night? J PediatrSurg. 2004;39:464–469.
29. Livingston EH, Woodward WA, Sarosi GA, et al. Disconnect between incidenceof nonperforated and perforated appendicitis: implications for pathophysiologyand management. Ann Surg. 2007;245:886–892.
30. Flum DR, Morris A, Koepsell T, et al. Has misdiagnosis of appendicitis de-creased over time? A population-based analysis. JAMA. 2001;286:1748–1753.
31. Terasawa T, Blackmore CC, Bent S, et al. Systematic review: computed to-mography and ultrasonography to detect acute appendicitis in adults and ado-lescents. Ann Intern Med. 2004;141:537–546.
32. Scarborough JE, Bennett KM, Pappas TN. Defining the impact of residentparticipation on outcomes after appendectomy. Ann Surg. 2012;255:577–582.
33. Anthony T, Murray BW, Sum-Ping JT, et al. Evaluating an evidence-basedbundle for preventing surgical site infection: a randomized trial. Arch Surg.2011;146:263–269.
34. Earley AS, Pryor JP, Kim PK, et al. An acute care surgery model improvesoutcomes in patients with appendicitis. Ann Surg. 2006;244:498–504.
35. The National Confidential Enquiry into Peri-Operative Deaths (NCEPOD).Knowing the risk: a review of the peri-operative care of surgical patients 2011.Available at: www.ncepod.org.uk/2011poc.htm. Accessed October 2013.
36. Czachorowski MJ, Amaral AF, Montes-Moreno S, et al. Cyclooxygenase-2expression in bladder cancer and patient prognosis: results from a large clinicalcohort and meta-analysis. PLoS ONE. 2012;7:e45025.
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
10 | www.annalsofsurgery.com C⃝ 2014 Lippincott Williams & Wilkins










![Jojo Moyes [In Before Me, #01] Me Before You](https://img.pdfslide.net/doc/110x75/635c225ca0f1eac29f0b8df7/jojo-moyes-in-before-me-01-me-before-you.jpg)


















