Embed Size (px)
Citation preview

doi:10.1182/blood-2003-04-1124Prepublished online October 23, 2003;
Christian GisselbrechtTilly, Bertrand Coiffier, Andre Bosly, Pierre Morel, Corinne Haioun, Philippe Gaulard, Felix Reyes and Marc P Andre, Nicolas Mounier, Xavier Leleu, Anne Sonet, Pauline Brice, Michel Henry-Amar, Herve on 2837 patientsnon-Hodgkin lymphoma with the ACVBP regimen. A GELA cohort study Second cancers and late toxicities after treatment of aggressive
(4217 articles)Neoplasia � (3722 articles)Clinical Trials and Observations �
Articles on similar topics can be found in the following Blood collections
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://bloodjournal.hematologylibrary.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://bloodjournal.hematologylibrary.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
articles must include the digital object identifier (DOIs) and date of initial publication. priority; they are indexed by PubMed from initial publication. Citations to Advance online prior to final publication). Advance online articles are citable and establish publicationyet appeared in the paper journal (edited, typeset versions may be posted when available Advance online articles have been peer reviewed and accepted for publication but have not
Copyright 2011 by The American Society of Hematology; all rights reserved.Washington DC 20036.by the American Society of Hematology, 2021 L St, NW, Suite 900, Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

1
Second cancers and late toxicities after treatment of aggressive non-Hodgkin lymphoma
with the ACVBP regimen. A GELA cohort study on 2837 patients.
M. André1, N. Mounier2, X. Leleu3, A. Sonet4, P. Brice2, M. Henry-Amar5, H. Tilly6, B.
Coiffier7, A. Bosly4, P. Morel8, C. Haioun9 P. Gaulard9, F. Reyes9 and C. Gisselbrecht2. For
the Groupe des Lymphomes de l’Adulte, Department of Hematology, CHNDRF, Charleroi,
Belgium.
1.Hematology department, Centre Hospitalier Notre Dame et reine Fabiola, 3 Grand Rue, 6000 Charleroi, Belgium.
2. Hematology department, Hôpital Saint-Louis, 1 avenue C. Vellefaux, 75010 Paris, France.
3. Hematology department, Centre Hospitalier Universitaire de Lille, Place de Verdun , 59037 Lille Cedex, France.
4.Hematology department, Cliniques Universitaires Mont Godinne, 1 avenue G. Thérasse, 5530 Yvoir, Belgium.
5. Clinical Research Unit and INSERM CJF 96-03/GRECAN, Centre Régional François Baclesse, route de Lion-sur-Mer, 14076 Caen Cedex 5, France.
6. Hematology department, CENTRE HENRI BECQUEREL, Rue d'Amiens, 76038 ROUEN, France.
7. Hematology Department, Centre Hospitalier Lyon-Sud, 69495 Pierre-Bénite, France.
8. Hematology Department, Centre Hospitalier de Lens, 99, route de la Bassée, 62307 Lens, France.
9 Hematology and pathology department, Hôpital Henri Mondor, Avenue du Maréchal de Lattre de Tassigny, 94010 Créteil, France.
Address for correspondence : Marc ANDRE, MD, CHNDRF, Grand-Rue 3, 6000 Charleroi,
Belgium, Tel & Fax: 00-32-71-281671 E-mail: [email protected].
Word count : Total : 4040 Abstract: 199.
Copyright (c) 2003 American Society of Hematology
Blood First Edition Paper, prepublished online October 23, 2003; DOI 10.1182/blood-2003-04-1124 For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

2
Abstract
The survival of aggressive NHL is increasing but the incidence of secondary cancer and late
toxicities is poorly defined for these patient treated with CHOP-like chemotherapy.
From 02/1984 to 01/1998, 2837 patients with aggressive NHL received the control arm
chemotherapy ACVBP in three consecutive GELA studies.
With a median follow-up of 74 months, the 5 years overall and event-free survival were 60%
and 52%. 202 non-neoplasic late toxicities were reported and this resulted in a 5.35%
cumulative probability of incidence at 7 years. 81 second tumors were observed and the 7-
years cumulative incidence rate was 2.75%. There were 64 solid tumors and 17 hematologic
malignancies. In multivariate analysis, age was the only risk factor for the development of
second cancer. An epidemiological analysis allowed a comparison of this NHL group with the
general population. Considering all tumors, no excess of second cancer was observed. But in
the male population, there was an excess of lung cancer (SIR:2.45, p<0.001) and MDS/AML
(SIR:5.65,p=0.006) and in the female population there was an excess of MDS/AML
(SIR:19.9,p<0.001).
With a long follow-up, ACVB regimen is highly effective for the treatment of aggressive
NHL. An increase of secondary MDS/AML and male lung cancer was observed.
Introduction
The late sequelae, including secondary cancers and major organ dysfunction, have been
extensively studied in Hodgkin’s disease patients as a result of the successful treatment of this
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

3
disease for many years. Second cancer, including acute non-lymphoblastic leukaemia, caused
either by chemotherapy, radiotherapy or both have been reported by different group [1,2,3].
Much less have been published about non-Hodgkin’s lymphoma (NHL) because the disease
generally occurred at a more advanced age and therapies have been less successful.
Nevertheless, recent advances in the definition of risk groups and in therapies have improved
the prognosis of the disease and an increasing number of patients can now expect relatively
long-term survival. According to the International Prognostic Index, the 5-year survival of
NHL is between 26 to 73% [4] and recent therapeutic improvements including the use of
monoclonal antibodies will probably ameliorate these results [5]. Even in case of relapse,
high-dose chemotherapy with stem cell support will allow patient to be cured and therefore
expose them to the risk of late toxicities [6].
The ACVBP regimen has been used as the control arm by the GELA Group since 1984 in
multi-centric trials to treat aggressive non-Hodgkin lymphoma and have recently shown better
results than conventional CHOP chemotherapy [7,8]. This prompted us to perform a
retrospective cohort study of an homogenous population of 2837 NHL patients included in
three different GELA protocols to evaluate the occurrence of second cancers and late
toxicities. A special attention was drawn on secondary myelodysplasia and acute leukaemia.
Patients and methods
This retrospective analysis was performed on 2837 patients included in three consecutive
GELA trials, namely LNH84, LNH87 and LNH93, between February 1984 and January 1998.
The ACVBP regimen consisted in four cycles of Adriamycine 75 mg/m2 D1,
Cyclophosphamide 1200 mg/m2 D1, Vindesine 2 mg/m2 D1 and 5, Bleomycine 10 mg D1 and
5 followed by 2 cycles of Methotrexate 3000 mg/m2, 4 cycles of Ifosfamide 1500 mg/m2 and
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

4
VP-16 300 mg/m2 and 2 cycles of Cytarabin 100 mg/m2 D1-4. Prophylactic intrathecal
administration of 15 mg of Methotrexate was performed during the first four cycles.
The first trial, LNH84, was a multicentric non-randomized trial. All the patients of this
protocol were included in the present study [9].
The second trial, LNH87, was a multicentric randomized trial based on prognostic factors
different from those of the International Index because this trial was initiated before the
publication of the International Index. Risk factors were age, ECOG >1, large tumor mass
(>10 cm), extra-nodal localization >2, bone marrow and neurological involvement. Group 1
included patient less than 70 years-old with no risk factors. The reference chemotherapy was
ACVBP and those patients were included in this study [10]. Group 2 included patients less
than 55 years-old with at least one adverse prognostic factor [11]. Only patients who received
the adriamycin-containing chemotherapy and conventional consolidation were included in the
present study. Group 3 included patients >55 and <70 years-old with at least one adverse
prognostic factor. The reference chemotherapy was ACVBP and those patients were included
in the present study [12].
The third trial, LNH93 was a multicentric randomized trial based on the International
Prognostic Index. Groups 1, 2 and 3 included patients <60 years-old. In group 1 patients
without any adverse prognostic factor were randomized between CHOP and radiotherapy vs
ACVBP [9]. The latest were included in this study. In group 2, patients with one adverse
prognostic factor were randomized between ACVBP and an epirubicin-containing regimen.
Patients from the ACVBP arm were included in the present study. In group 3, patients with 2
or more adverse prognostic factors were randomized between ACVBP and an intensive high-
dose chemotherapy with stem cell support. The patients from the ACVBP arm were included
in the present study [13]. Group 5 included patients from 61 to 69 years-old with at least one
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom
5
adverse prognostic factor. They were randomized between CHOP and ACVBP. The patients
from the ACVBP arm were included in the present study [8].
Initial staging procedure included bone marrow biopsy, CSF examination and computed
tomographic scan of chest and abdomen. Patients were classified according to the Ann Arbor
system. Serum lactate dehydrogenase (LDH) was expressed as a percentage of the highest
normal value. Central histological review was performed and B or T phenotype was
determined on deparaffinized tissue section for patient of LNH87 and LNH93. These
protocols were approved by the institutional ethics committee and all patients gave informed
consent.
Using the database of the GELA, patients assigned to the ACVBP regimen in the three
different protocols were identified. HIV positive lymphoma and non-lymphoma patients at
histological review were excluded from the study. Files were reviewed and data about
radiotherapy, occurrence of second cancer, any type of late toxicity (NCI grade II-IV) were
collected by means of a standardized form. Data were reviewed for each individual patient at
the GELA data center, if necessary additional information was requested from the responsible
investigator. Systematical review of all original files was not performed. For women less than
40 years-old occurrence of pregnancy was also recorded.
Second cancer included any tumor occurring after inclusion date. Previous cancer was an
exclusion criteria for the protocol excepted for basal skin carcinoma or non-invasive cervix
cancer. Late toxicities included any new toxicity occurring after chemotherapy completion, as
well as toxicities developing on therapy and continuing after the end of therapy [14].
Statistical methods
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

6
Follow-up started at the date of the end of the first NHL treatment and ended at the date of
death, date of second cancer or last examination whichever came first. Cancers observed were
classified by site and histological type in accordance with the oncology section of the
International Classification of Diseases [15]. Diagnoses used were those provided by centers
where the patient was followed.
The primary end point of the study was the occurrence of a solid tumour or haematological
cancer. It was calculated both as a cumulative probability or a cumulative incidence of second
cancer. The cumulative probability was calculated with a Kaplan–Meier estimate in which
data of patients who died were censored [16], curves were compared by the log-rank test [17].
Effects of potential risk factors on second cancer rates were examined in a Cox proportional-
hazards model [18]. The cumulative incidence curve, however, explicitly accounted for other
causes of death and was computed by the method of Gooley et al [19]. Demographic and
base-line laboratory data were compared for consistency among subpopulations with 2 tests
for nominal variables and t-tests for ordinal variables. All statistical tests were two-sided.
Analyses were performed with SAS software (version 8.0 , SAS Institute, Cary, N.C.) and S-
Plus (version 2000, Insightful, Seattle).
The incidence of second cancer in the NHL population was compared to the incidence of
cancer in the general population using the 1995 French registry of cancer after matching for
age and gender. In this part of the analysis, synchronous cancer, defined as cancer occurring
during the first year after diagnosis of lymphoma, were excluded and therefore, the time at
risk started 12 months after randomization and ended at the date of occurrence of second
cancer, the date of death, or the date of last known vital status. Basal skin carcinoma is not
reported to the French registry of cancer since 1990 and therefore this cancer was excluded
from this part of the analysis. Standardized incidence ratio (SIR) were calculated as the ratio
of observed to expected numbers based on cancer incidence data in France in 1995. The 95%
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

7
confidence limits were calculated assuming a binomial distribution of the observed numbers.
Finally, the excess number of cases was reported as the excess number of malignancies per
104 person-years at risk.
RESULTS
Patients characteristics and survival
Eight patients who were HIV positive lymphoma and 42 patients who were not non-
Hodgkin’s lymphoma at histological review were excluded from the analysis. LNH84,
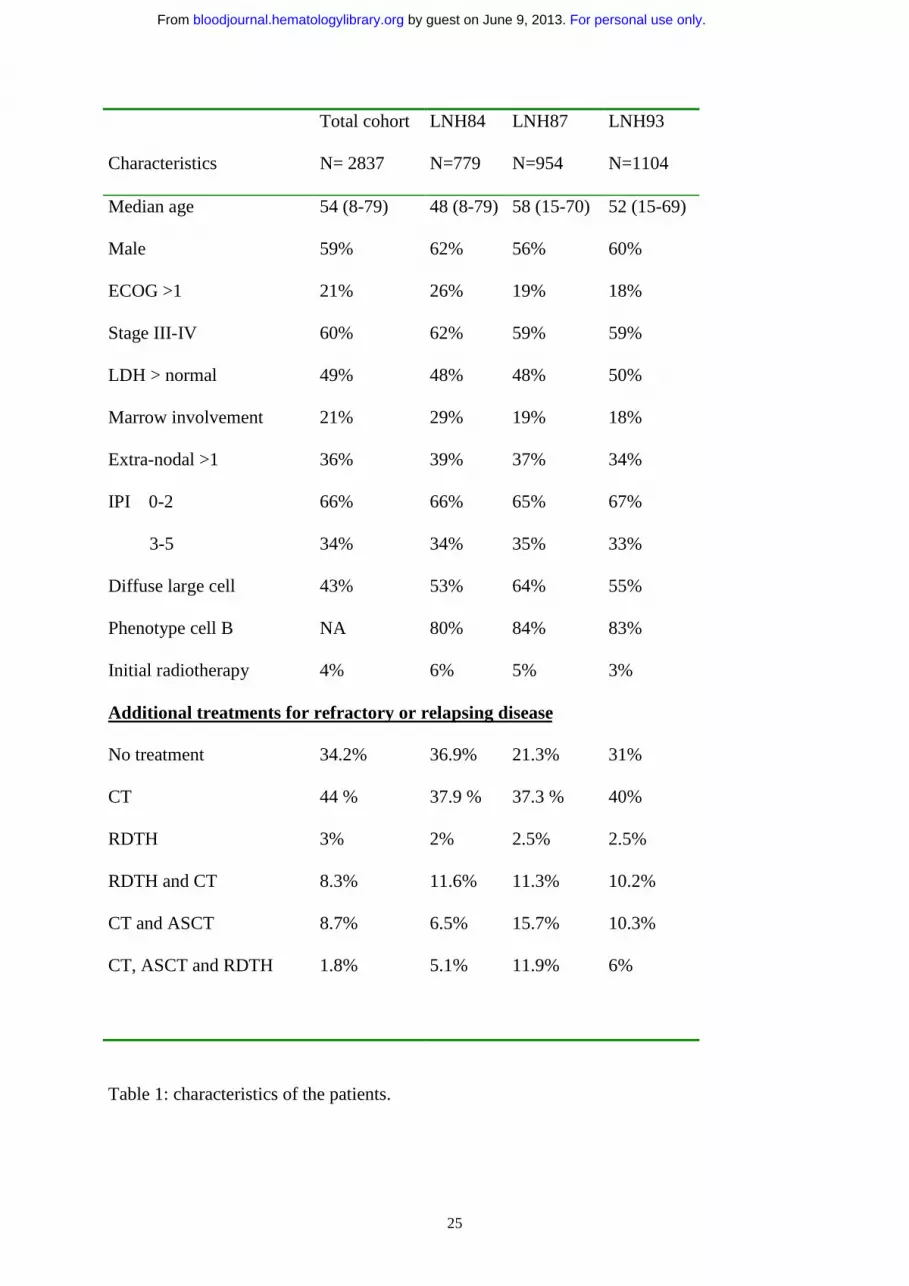
LNH87 and LNH93 contributed respectively for 26%, 34% and 40% of the total cohort. The
main patients characteristics were (Table 1): median age: 54 years (range 8-79), male: 59%,
Stage III-IV: 60%, PS >1: 21%, elevated LDH: 49%, > 1 extra-nodal involvement: 36% and
bone marrow involvement: 22%. The 5 factors of the International Prognostic Index were
distributed as 0 (19%), 1 (24%), 2 (23%), 3 17%), 4 (13%) and 5 (4%). The histology was
diffuse large cell in 55%. Phenotype was not available for the LNH84 group. In the LNH87
and LNH93 groups, 83% were B-cell lymphoma and 17% T-cell lymphoma. Additional
radiotherapy (RT) was allowed by protocols and was administered as part of the initial
treatment to 4.3% of the patient. Refractory or relapsing patients received supportive care (31
%) or additional treatments: chemotherapy alone: 40 %, radiotherapy alone: 2.5 %,
chemotherapy and radiotherapy: 10.2 %, chemotherapy and high-dose chemotherapy with
stem cell support: 10.3 %, chemotherapy, radiotherapy and high-dose chemotherapy with
stem cell support: 6 %. Among the 207 transplanted patients, 195 received an autologous
transplant and 12 an allogenic transplant.
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

8
With a median follow-up of 74 months (range: 1-203), the 5 years overall survival was 60%
(±2%) and the 5 years event-free survival was 52% (±2%) (Figure 1).
Second cancers
81 second tumors were observed and the 7-years cumulative incidence rate was 2.75%
(Figure 2). Eight (5 solid tumors and 3 MDS/AML) of these 81 second cancers occurred after
an additional treatment for relapse or progression. There were 64 solid tumors (lung 22, skin
8, head and neck 5, uterus 5, colo-rectal 4, breast 4, kidney 2, bladder 1, prostate 1, gastric 1,
biliary tract 1 esophagus 1, ovary 1 and unknown origin 5). Among the 22 lung cancers, 9
were squamous cell carcinoma, 3 were adenocarcinoma, 1 was large-cell carcinoma, 7 were
small cell lung cancer and for 3 cases the histology was not available. Among the 8 skin
tumors there were 2 melanoma end 6 non-melanoma skin cancers. Only 1 tumor, a bladder
cancer, occurred in the field of radiotherapy. Two patients developed a third solid tumor.
These two third solid tumor were not included in the present analysis.
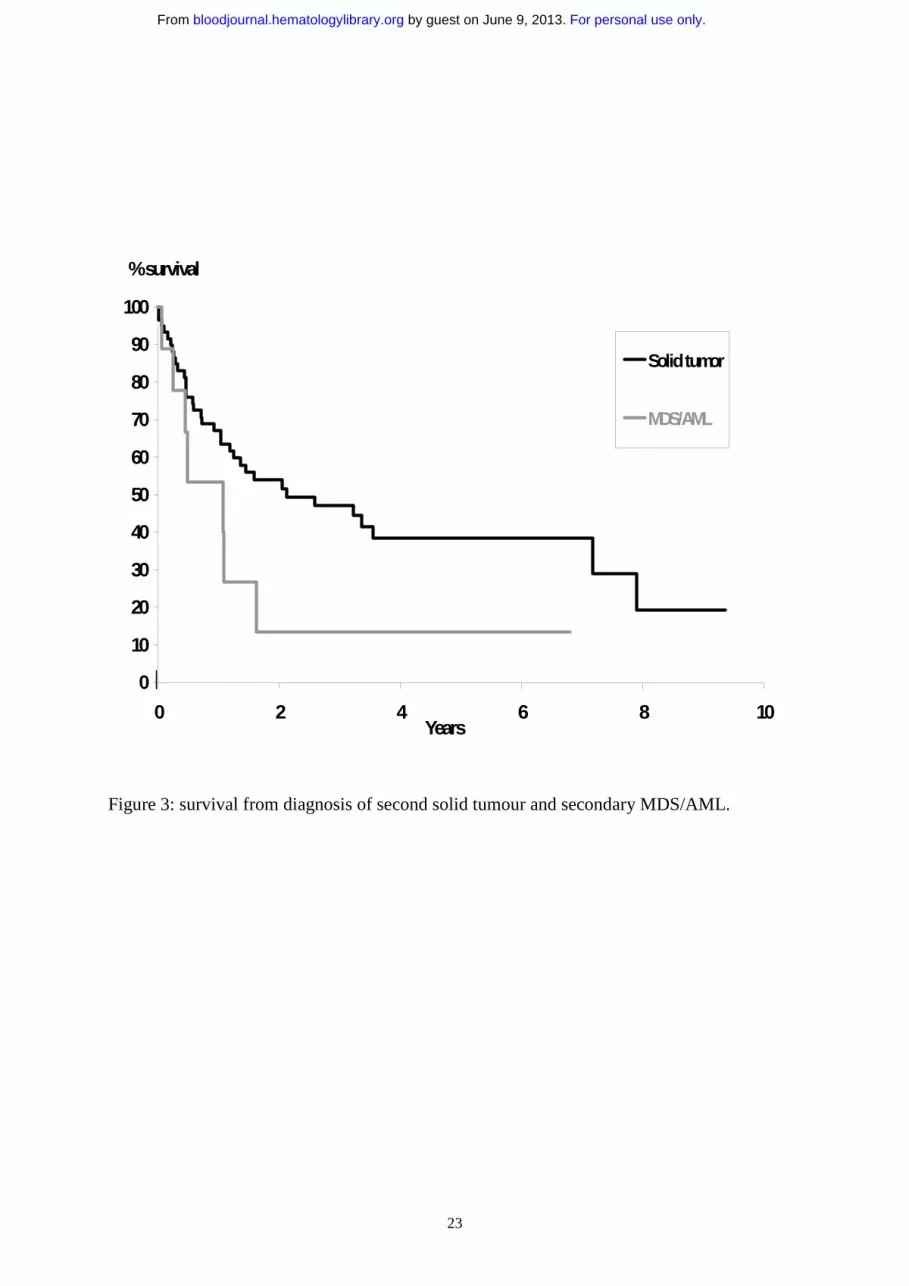
Median time from diagnosis of NHL to solid tumor was 47 months (range 2-183). Thirty-one
patients died from second solid tumor and the median time from diagnosis of solid tumor was
2.1 years (95%CI: 1.18-7.2) (figure 3).
Seventeen hematologic malignancies (AML 7, MDS 4, CML 2, CMML 1, polycythemia vera
1, essential thrombocytemia 1, myeloma 1) were observed. For the 12 cases of AML and
MDS, karyotype was available only in 2 cases of AML, showing either a monosomy 7 or a
t(8;21), and in one MDS showing a monosomy 7 associated to other abnormalities. All
patients presented with pancytopenia at diagnosis. Among them, type 2 and 4 in the FAB
classification were predominant. Of the 12 patients, 5 patients (4 AML, 1 MDS) were in first
complete remission of their NHL, 3 patients were in second complete remission. Eight out of
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

9
12 patients died from leukemia, one patient died from relapse of NHL while he was in CR
from his secondary AML, and one patient died from MDS without acutisation.
Median time from diagnosis of NHL to leukemia was 40 months (range 18-100), median
survival from diagnosis of MDS/AML was 1 years (95% CI: 0.45-1.62), and only one patient
had a prolonged survival after the diagnosis of his leukemia (figure 3).
During the course of the disease, patients experienced several competing events such as
death, second cancer or late toxicities. Risk factors associated with these different events were
evaluated. For death, prognostic factors were those of the International Prognostic Index (age,
stage, LDH, ECOG and >1 extra-nodal localization, p<0.001). In multivariate analysis, age
was the only significant risk factor for second cancer (p<0.0001). Gender, LDH, stage,
ECOG, extra-nodal involvement, relapse, stem cell transplantation at relapse, radiotherapy at
relapse and chemotherapy at relapse were not shown to have a significant influence.
Comparison to normal population
Among the 81 cases reported, 9 synchronous tumors occurring less than 12 months after the
diagnosis of NHL were excluded as well as 6 cases of basal skin cancer. Forty-nine solid
tumors (21 lung, 3 head and neck, 6 digestive, 4 breast, 7 genito-urinary, 2 melanoma and 6
miscellaneous) and all cases of hematological cancer were analyzed. This allowed us to
analyze 2,267 patients accounting for 9,847 person-year at risk. The observed second
neoplasm, SIR, and excess number are reported for male and female patients in tables 2 and 3
with various grouping of cancers . For all second cancer no excess of risk was detected for the
whole population (male, SIR 0.92; 95% CI, 0.67-1.24 and female, SIR 0.94; 95% CI, 0.59-
1.42, p value non significant for both). A significant excess of risk for secondary MDS/AML
was detected in the male population (SIR 5.65; 95% CI, 1.54-14.46, p=0.006) and was even
stronger in the female population (SIR 19.89; 95% CI, 7.98-40.97, p <0.001). For all solid
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

10
tumors, no excess of risk was identified (male, SIR 0.77; 95% CI, 0.54-1.07 and female, SIR
0.63; 95% CI, 0.35-1.06, p value non significant for both). But, in the male population only,
we observed a highly significant excess of risk of lung cancer (SIR 2.45; 95% CI, 1.48-3.83, p
<0.001). This resulted in an excess of 19.9 cases of lung cancer per 104 person-years at risk
(table 3).
Late non-neoplastic toxicities
There were 222 reported late non-neoplastic toxicities and this resulted in a 5.35 + 0.76
cumulative probability of incidence at 7 years (figure 4). 8.2 % of this late toxicities occurred
after additional treatment for refractory or relapsing lymphoma. In multivariate analysis, age
(p<0.0001) and relapse (p=0.02) were significant risk factors for late non-neoplastic
toxicities. Gender, LDH, stage, ECOG, extra-nodal involvement, stem cell transplantation at
relapse, radiotherapy at relapse and chemotherapy at relapse were not significant risk factors
in this multivariate analysys. The different causes of toxicities and death are reported in table
4. Late non-neoplastic toxicities resulted in 61 death and were the second cause of death after
NHL recurrence or progression. Late second cancers (31 deaths) were the third cause of
death. 17% of these late non-neoplastic toxic death occurred in patients who received
additional treatments after ACVBP for resistance or relapse after this first-line treatment. The
two major causes of late toxicities and death from late toxicities were infections and
cardiovascular events, resulting in 29 and 14 death respectively.
Hepatitis was the most frequent infectious complication. Because the different studies
recruited patients through the period of discovery of hepatitis C virus and HIV, several cases
of viral transmission through transfusions probably occurred. There were 12 cases of hepatitis
C transmission with one death, 2 cases of hepatitis B transmission and only one case of HIV
transmission. Two other hepatitis of unknown etiology also occurred. Seven late deaths were
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

11
attributed to aspergillosis and 4 to P. Carinii. Angina pectoris was the most frequently
reported cardiovascular complication (20 cases) but only 3 patients died from myocardial
infarction. Three other patients died from cardiac failure and 3 from arrhythmia. Ten cases of
ischemic stroke were reported resulting in 4 deaths. Eighteen patients reported disabling
peripheral neuropathy attributed to vindesine and two patient deceased from encephalopathy,
one of them after receiving brain radiotherapy. Nineteen patients experienced severe
psychological problems after treatment and this resulted in 3 deaths from suicide while in
complete remission. Three patients developed severe pulmonary fibrosis and two of them
died.
The other most frequently reported late complications were thyroid dysfunction (6 cases),
renal failure (5 cases), alcohol abuse (5 cases), benign tumor (3 cases), cataract (3 cases).
Five patients deceased from toxicity of autologous stem cell transplantation and 6 from
allogenic transplantation.
Pregnancies
Among the 2837 patients, 609 women were less than 40 years-old at the time of diagnosis of
NHL and 344 were in complete remission at the time of analysis. Thirty-one pregnancies were
reported in 26 patients. There were two therapeutic abortion and one death in utero. No
malformation was reported among the 28 children. The mean age at the time of pregnancy
was 26 years old and no pregnancy occurred after the age of 33.
DISCUSSION
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

12
In this study, the risk of second malignancies and other late toxicities was analyzed in 2837
patients treated with the same ACVBP regimen for NHL. These trials covering almost 20
years were retrospectively analyzed. With 9,847 person-year at risk, this represents one of the
largest studies ever reported on this subject. However, results must be interpreted cautiously
because of the retrospective design of this study. A total of 81 second tumors were observed
and the 7-years cumulative incidence rate was 3.5%. Overall, there was no increased risk of
developing a second cancer compared to the general population but there was a 5.6-fold risk
of developing MDS/AML in male and a 19.9-fold risk in female as compared with the general
population. In the male population, there was a strong 2.45-fold excess of risk of developing
lung cancer. However, with a median follow-up of 74 months, non-neoplastic toxicities are
accountable for much more deaths than second malignancies.
Therapy-related MDS/AML have been extensively described after treatment of Hodgkin’s
[20] disease or after use of high-dose therapy with stem cell support [21,22,23]. However, the
impact of high-dose chemotherapy by itself is unlikely to increase the risk generated by
conventional therapy [3,19]. Several investigations focused on secondary MDS/AML after
conventional chemotherapy for NHL [24, 25, 26, 27, 28, 29, 30]. In the series of Travis,
despite the excess of MDS/AML associated with therapy, secondary leukemia remained rare
events after NHL. Of 10,000 NHL patients treated for 6 months with various chemotherapy
agents and followed for 10 years, an excess of four leukemia could be expected [25]. Various
alkylating agents are used in the treatment of NHL. The increased incidence of MDS/AML
after prednimustine, chlorambucil, mechlorethamine and procarbazine for the treatment of
NHL is well known. Their risk increases with either cumulative dose and duration of therapy.
Cyclophosphamide-based regimens at a median cumulative dose of 12.5 g, were associated
with a non-significant 1.8-fold risk of AML, compared with treatments that did not include
alkylating agents. Increasing cumulative dose or duration of treatment with
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

13
cyclophosphamide was not associated with increasing risk of AML (P=0.57 and 0.33,
respectively) [25]. This weak association between small cumulative doses of
cyclophosphamide and AML is consistent with the results of other studies [31], and is
reassuring, given the frequent use of this alkylating agent in current therapy of NHL.
Epipodophyllotoxins have clearly demonstrated a leukemogenic potential after treatment of
acute lymphoblastic leukemia. In NHL and also in our studies, they were not administered
without alkylating agents and therefore the individual leukemogenic risk of
cyclophosphamide, ifosfamide and VP-16 could not be evaluated in this study. However, as
suggested by one of our patient showing a t (8;21), a possible contribution of
epipodophyllotoxins to the occurrence of secondary MDS/AML can not be ruled out.
The increased risk of lung cancer associated with radiotherapy is well known[32,33]. A recent
large study on lung cancer after Hodgkin’s disease clearly linked this cancer to alkylating
agent and distinguished this toxicity from that of radiotherapy and tabacco use [34]. Travis et
al. reported that treatment with alkylating agents without radiotherapy was associated with
increased lung cancer risk (RR=4.2). Statistically significant elevated risk was apparent
within 1-4 years after treatment with chemotherapy. In another case-control study, Kaldor et
al showed that Hodgkin’s disease patients treated with chemotherapy alone had about twice
the risk of developing lung cancer than those treated by radiotherapy and both modalities [35].
The finding that the risk of lung cancer following chemotherapy was higher than after
radiotherapy was unexplained and unexpected as it is in our study. Following alkylating agent
therapy, the risk of squamous cell lung cancer and small-cell lung cancer was statistically
significantly elevated [31]. In our series, these two histological type of tumor also represented
most of cases. A major limitation of our study, as well as of previous studies of lung cancer
in Hodgkin’s disease is the uncertainty of risk associated with treatment, in view of the great
risk conferred by tobacco use. While information on radiotherapy and chemotherapy was
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

14
consistently available in medical records, informations on smoking habits were not
systematically reported in formats used for epidemiological purposes. During the time of this
study (1984-2000), the incidence of smoking ranged between 25% and 36% (male: 30-47%,
female: 19-27%) in our countries [36]. The excess of lung cancers among male patients may
partially be explained by the consistent, 10%-higher incidence of cigarette smoking among
male. However, the difference of lung cancer among male and female population was major
in this study. Therefore, the possibility of a difference between male and female for this
tumor, despite different smoking habits, may not be ruled out. A recent review of the
literature on the association between smoking and NHL found no evidence that tobacco could
increase the risk of NHL [37]. The probability that our large NHL population would have
different smoking habits than the general population is this low and may reflect a true increase
of lung cancer secondary to chemotherapy in the male population.
Only one bladder cancer was reported in this series, although cyclophosphamide is known to
induce this late complication. This low incidence is related to the low cumulative dose (4.8
mg/m2) and short duration of treatment. In the largest study reported on bladder cancer after
cyclophosphamide, the risk was strongly associated with cumulative dose and patients
receiving less than 20 g had only a 2.4-fold increased risk [38].
Among agents used in the treatment of non-Hodgkin’s lymphoma, anthracyclines are the most
important in causing direct injury to the heart. However since the heart has considerable
compensatory reserves, a long time elapse before heart failure becomes manifest. In the study
of Miller [39], left ventricular dysfunction was found in 7 of 201 patients treated with 8 cycles
of CHOP (cumulative dose of doxorubicin 400 mg/m2), while in the group treated with 3
cycles combined with radiotherapy none of 200 patients developed left ventricular
dysfunction. Seven patients treated with the 8 cycles of CHOP but only two treated with 3
CHOP and radiotherapy subsequently died of heart disease. In our study, left ventricular
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

15
function was not systematically assessed but only 3 patients died from cardiac failure. They
received a cumulative dose of doxorucine of 300 mg/m2.
Injury to ovary by radiation or chemotherapy can cause sterilization and suppressed sexual
hormone production. In woman, the assessment of gonadal function after treatment of
lymphoma is difficult because the ova and ovary are not easily accessible for study.
Therefore, the surrogate markers of woman’s fertility are regular menses, oestrogen levels
greater than 20 pmol/L, and the ability to become pregnant. Bokemeyer [40] reported 10
women with NHL treated with CHOP and radiotherapy. One of them showed elevated level
of serum gonadotrophins and decreased oestradiol as an indicator of gonadal toxicity, with
abnormalities of the menstrual cycle. In the series of Müller, 1 of 7 woman was found to have
gonadal dysfunction after MACOP-B or VACOP-B [41]. In our series, we showed that
fertility may be preserved after 4.8 g/m2 cyclophosphamide, but no pregnancy was observed
for woman aged more than 33 years-old at time of NHL diagnosis. Several reports have
shown preservation of fertility even after high-dose chemotherapy with stem cell support [42].
NHL patients experienced after treatment elevated risks for late toxicities, therapy-related
leukemia and several solid tumors. Although, especially for second cancer occurrence, this is
substantially less frequent than for patients with Hodgkin’s disease. Genetic predisposition to
drug induced second cancers may be in the future a valuable tool to tailor therapy to
individual patients [43], but, in the meantime, a careful continuous follow-up of our
lymphoma patients is recommended to correctly evaluate late toxicities and second cancers
and to allow the design of new less toxic regimens.
Acknowledgments
Supported by grants from the Programme Hospitalier de Recherche Clinique (AOM95061)
from the Ministère de la Santé and from Amgen, Roche, Schering-Plough and Asta Medica..
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

16
References
1. Kaldor JM, Day NE, Band P et al. Second malignancies following testicular cancer,
ovarian cancer and Hodgkin's disease: an international collaborative study among
cancer registries. Int J Cancer. 1987;39:571-85.
2. Henry-Amar M. Second cancer after the treatment for Hodgkin's disease: a report
from the International Database on Hodgkin's Disease. Ann Oncol. 1992; Suppl 4:117-
28.
3. André M, Henry-Amar M, Blaise D et al. Treatment-related deaths and second cancer
risk after autologous stem-cell transplantation for Hodgkin's disease. Blood.
1998;92:1933-40.
4. Shipp M, Arrington D, Anderson J et al. A predictive model for aggressive non-
Hodgkin’s lymphoma. N Engl J Med 1993;329:987-994.
5. Coiffier B, Lepage E, Briere J et al. CHOP chemotherapy plus rituximab compared
with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J
Med. 2002;346:235-42.
6. Philip T, Guglielmi C, Hagenbeek A et al. Autologous bone marrow transplantation as
compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-
Hodgkin's lymphoma. N Engl J Med. 1995;333:1540-5.
7. Tilly H, Coiffier B, Casanovas O et al. Survival advantage of ACVBP regimen over
standart CHOP in the treatment of advanced aggressive non-Hodgkin’s lymphoma.
The LNH 93-5 study. Ann. Oncol. 2002; suppl. 2:28.
8. Reyes F, Lepage E, Munck JN et al. Superiority of the ACVBP regimen over a
combined treatment with three cycles of CHOP followed by involved field
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

17
radiotherapy in low risk localized aggressive non-Hodgkin’s lymphoma. Ann. Oncol.
2002; suppl. 2:27.
9. Coiffier B, Gisselbrecht C, Herbrecht R, Tilly H, Bosly A, Brousse N. LNH-84
regimen: a multicenter study of intensive chemotherapy in 737 patients with
aggressive malignant lymphoma. J Clin Oncol. 1989;7:1018-26.
10. Tilly H, Mounier N, Lederlin et al. Randomized comparison of ACVBP and m-
BACOD in the treatment of patients with low-risk aggressive lymphoma: the LNH87-
1 study. Groupe d'Etudes des Lymphomes de l'Adulte. J Clin Oncol. 2000;18:1309-15.
11. Haioun C, Lepage E, Gisselbrecht et al. Survival benefit of high-dose therapy in poor-
risk aggressive non-Hodgkin's lymphoma: final analysis of the prospective LNH87-2
protocol--a groupe d'Etude des lymphomes de l'Adulte study. J Clin Oncol.
2000;18:3025-30.
12. Bosly A, Lepage E, Coiffier B et al. Outcome is not improved by the use of alternating
chemotherapy in elderly patients with aggressive lymphoma. Hematol J.
2001;2(4):279-85.
13. Gisselbrecht C, Lepage E, Molina T et al. Shortened first-line high-dose chemotherapy
for patients with poor-prognosis aggressive lymphoma. J Clin Oncol. 2002;20:2472-9.
14. Haddy TB, Adde MA, McCalla J et al. Late effects in long-term survivors of high-
grade non-Hodgkin's lymphomas. J Clin Oncol. 1998;16:2070-9.
15. World Health Organisation. Manual of the International statistical classification of
disease, injuries and causes of death : based on the recommendations of the Ninth
Revision Conference, 1975, and adopted by the Twenty-ninth World Health
Assembly, Vol. I. Geneva : World Health Organisation, 1977.
16. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am
Stat Assoc 1958;53:457-481.
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

18
17. Peto R, Peto J. Asymptotically efficient rank invariant test procedures. J R Stat Soc
[A] 1972;135:185-206.
18. Cox DR. Regression models and life-tables. J R Stat Soc [B] 1972;34:187-220.
19. Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in
the presence of competing risks: new representations of old estimators. Stat Med
1999;18:695-706.
20. Van Leeuwen FE, Chorus AMJ, Van den Belt-Dusebout AW et al. Leukemia risk
following Hodgkin's disease relative to cumulative dose of alkylating agent, treatment
with Teniposide combination, number of episode of chemotherapy and bone marrow
damage. J Clin Oncol 1994;12:1063-1073.
21. Stone RM, Neuberg D, Soiffier R et al. Myelodysplastic syndrome as late
complication following autologous bone marrow transplantation for non-Hodgkin
Lymphoma. J Clin Oncol 1994;12:2535-2542.
22. Darrington DL, Vose JM, Anderson JR et al. Incidence and characterisation of
secondary myelodysplastic syndrome and acute myelogenous leukemia following
high-dose chemotherapy and autologous stem cell transplantation for lymphoid
malignancies. J Clin Oncol 1994;12:2527-2534.
23. Harrison CN, Gregory W, Hudson GV et al. High-dose BEAM chemotherapy with
autologous haemopoietic stem cell transplantation for Hodgkin's disease is unlikely to
be associated with a major increased risk of secondary MDS/AML. Br J Cancer.
1999;81:476-83.
24. Travis LB, Curtis RE, Glimelius B et al. Second cancers among long-term survivors of
non-Hodgkin's lymphoma. J Natl Cancer Inst. 1993;85:1932-7.
25. Travis LB, Curtis RE, Stovall M et al. Risk of leukemia following treatment for non-
Hodgkin's lymphoma. J Natl Cancer Inst. 1994 Oct 5;86(19):1450-7.
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom
19
26. Gomez GA, Aggarwal KK, Han T. Post-therapeutic acute malignant
myeloproliferative syndrome and acute nonlymphocytic leukemia in non-Hodgkin's
lymphoma. Cancer 1982: 50:2285-2288.
27. Greene MH, Young RC, Merrill JM, DeVita VT. Evidence of a treatment dose
response in acute nonlymphocytic leukemias which occur after therapy of non-
Hodgkin's lymphoma. Cancer Res 1983: 43:1891-1898.
28. Pedersen-Bjergaard J, Ersboll J, Sorensen HM, et al. Risk of acute nonlymphocytic
leukemia and preleukemia in patients treated with cyclophosphamide for non-
Hodgkin's lymphomas. Comparison with results obtained in patients treated for
Hodgkin's disease and ovarian carcinoma with other alkylating agents. Ann Intern
Med 1985: 103:195-200.
29. Lavey RS, Eby NL, Prosnitz LR. Impact on second malignancy risk of the combined
use of radiation and chemotherapy for lymphomas. Cancer 1990: 66:80-88.
30. Lishner M, Slingerland J, Barr J, Panzarella T, Degendorfer P, Sutcliffe S. Second
malignant neoplasms in patients with non Hodgkin's lymphoma. Hematol Oncol
1991: 9:169-179.
31. Curtis RE, Boice JD Jr, Stovall M, et al. Risk of leukemia after chemotherapy and
radiation treatment for breast cancer . N Engl J Med 1992: 326:1745-1751.
32. Abrahamsen JF, Andersen A, Hannisdal E, Nome O, Abrahamsen AF, Kvaloy S, Host
H. Second malignancies after treatment of Hodgkin's disease: the influence of
treatment, follow-up time, and age. J Clin Oncol. 1993;11:255-61.
33. van Leeuwen FE, Klokman WJ, Stovall M et al. Roles of radiotherapy and smoking in
lung cancer following Hodgkin's disease. J Natl Cancer Inst. 1995;87:1530-7.
34. Travis LB, Gospodarowicz M, Curtis RE et al. Lung cancer following chemotherapy
and radiotherapy for Hodgkin's disease. J Natl Cancer Inst. 2002;94:182-92.
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

20
35. Kaldor JM, Day NE, Bell J et al. Lung cancer following Hodgkin’s disease: a case-
control study. Int J Cancer 1992;52:677-681.
36. Joossens L. La vente de cigarette baisse, mais la consommation reste au même niveau.
Du côté des consommateurs 2002 ;107.
37. Peach HG, Barnett NE. Critical review of epidemiological studies of the association
between smoking and non-Hodgkin's lymphoma. Hematol Oncol. 2001;19:67-80.
38. Travis LB, Curtis RE, Holowaty EJ, et al. Bladder and kidney cancer following
cyclophosphamide therapy for non-Hodgkin's lymphoma. J Natl Cancer Inst 1995:
87:524-530.
39. Miller TP, Dahlberg S, Cassady JR et al. Chemotherapy alone compared with
chemotherapy plus radiotherapy for localized intermediate- and high-grade non-
Hodgkin's lymphoma. N Engl J Med. 1998;339:21-6.
40. Bokemeyer C, Schmoll HJ, van Rhee J, Kuczyk M, Schuppert F, Poliwoda H. Long-
term gonadal toxicity after therapy for Hodgkin's and non-Hodgkin's lymphoma. Ann
Hematol. 1994;68:105-110.
41. Muller U, Stahel RA. Gonadal function after MACOP-B or VACOP-B with or
without dose intensification and ABMT in young patients with aggressive non-
Hodgkin's lymphoma. Ann Oncol. 1993;4:399-402.
42. Brice P, Haioun C, Andre M, Gisselbrecht C. Pregnancies after high-dose
chemotherapy and autologous stem cell transplantation in aggressive lymphomas.
Blood. 2002;100:736.
43. Staratschek-Jox A, Shugart YY, Strom SS, Nagler A, Taylor GM. Genetic
susceptibility to Hodgkin's lymphoma and to secondary cancer: workshop report. Ann
Oncol 2002;13 (Suppl 1):30-3.
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

21
Figure 1: overall survival and event-free survival of the 2837 NHL patients treated with the
ACVBP regimen with a median follow-up of 74 months.
0
10
20
30
40
50
60
70
80
90
100
0 2 4 6 8 10 12 14 16Years
% survival
OS
EFS
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

22
0 2 5 5 0 7 5 1 0 0 1 2 50 .0 0
0 .0 2
0 .0 4
0 .0 6
0 .0 8
0 .1 0
T im e ( m o n th s )
Cum
ulat
ive
inci
denc
e
Figure 2: cumulative probability of incidence of second cancer after the ACVBP regimen in
2837 NHL patients.
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom
23
Figure 3: survival from diagnosis of second solid tumour and secondary MDS/AML.
0
10
20
30
40
50
60
70
80
90
100
0 2 4 6 8 10Years
% survival
Solid tumor
MDS/AML
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

24
0 2 5 5 0 7 5 1 0 0 1 2 50 .0 0
0 .0 2
0 .0 4
0 .0 6
0 .0 8
0 .1 0
T im e ( m o n th s )
Cum
ulat
ive
inci
denc
e
Figure 4: cumulative probability of incidence of late non-neoplastic toxicity after ACVBP
regimen in 2837 patients.
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom
25
Characteristics
Total cohort
N= 2837
LNH84
N=779
LNH87
N=954
LNH93
N=1104
Median age 54 (8-79) 48 (8-79) 58 (15-70) 52 (15-69)
Male 59% 62% 56% 60%
ECOG >1 21% 26% 19% 18%
Stage III-IV 60% 62% 59% 59%
LDH > normal 49% 48% 48% 50%
Marrow involvement 21% 29% 19% 18%
Extra-nodal >1 36% 39% 37% 34%
IPI 0-2 66% 66% 65% 67%
3-5 34% 34% 35% 33%
Diffuse large cell 43% 53% 64% 55%
Phenotype cell B NA 80% 84% 83%
Initial radiotherapy 4% 6% 5% 3%
Additional treatments for refractory or relapsing disease
No treatment 34.2% 36.9% 21.3% 31%
CT 44 % 37.9 % 37.3 % 40%
RDTH 3% 2% 2.5% 2.5%
RDTH and CT 8.3% 11.6% 11.3% 10.2%
CT and ASCT 8.7% 6.5% 15.7% 10.3%
CT, ASCT and RDTH 1.8% 5.1% 11.9% 6%
Table 1: characteristics of the patients.
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

26
Second cancer Observed SIR 95% CI P value Excess numbers
All types 22 0.94 0.59-1.42 0.64 -
Solid tumors 14 0.63 0.35-1.06 0.97 -
Breast 4 0.47 0.13-1.20 0.97 -
AML/MDS 7 19.89 7.98-40.97 <0.001 15.9
Table 2: SIR and excess number of second cancer in the female population (947 patients)
Second cancer Observed SIR 95% CI P value Excess numbers
All types 44 0.92 0.67-1.24 0.73 -
Solid tumors 35 0.77 0.54-1.07 0.95 -
- lung 19 2.45 1.48-3.83 <0.001 19.9
-head and neck 2 0.38 0.005-1.37 0.97 -
-digestive 5 0.52 0.17-1.12 0.96 -
AML/MDS 4 5.65 1.54-14.46 0.006 5.8
.
Table 3: SIR and excess number of second cancer in the male population (1320 patients)
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom

27
CAUSES N= Death
Infectious 61 29
Cardio-vascular 54 14
Neurological 20 2
Psychological 19 3
Pulmonary 12 6
Miscellaneous 36 7
TOTAL 222 61
Table 4 : late non-neoplastic toxicities and related death.
For personal use only. by guest on June 9, 2013. bloodjournal.hematologylibrary.orgFrom









![Pretransplantation [18-F]fluorodeoxyglucose positron emission tomography scan predicts outcome in patients with recurrent Hodgkin lymphoma or aggressive non-Hodgkin lymphoma undergoing](https://img.pdfslide.net/doc/110x75/63553e8721a0f893210b6bd2/pretransplantation-18-ffluorodeoxyglucose-positron-emission-tomography-scan-predicts.jpg)






![[National guidelines of diagnosis and treatment of the non-Hodgkin lymphoma]](https://img.pdfslide.net/doc/110x75/635f52f5a13521f3810d6721/national-guidelines-of-diagnosis-and-treatment-of-the-non-hodgkin-lymphoma.jpg)












