Embed Size (px)
Citation preview

Sense of coherence and socio-demographic characteristics predicting
posttraumatic stress symptoms and recovery in the aftermath
of the Second Lebanon War
Shaul Kimhia*, Yohanan Eshela,b, Leehu Zysberga,
Shira Hantmanc and Guy Enoshd
aDepartment of Psychology, Tel Hai Academic College, Tel Hai 12210, Israel; bDepartment ofPsychology, Haifa University, Haifa, Israel; cDepartment of Social Work, Tel Hai AcademicCollege, Tel Hai 12210, Israel; dDepartment of Social Work, Haifa University, Haifa, Israel
(Received 24 June 2008; final version received 15 April 2009)
This study investigated the role of sense of coherence (SOC) as a mediator betweendemographic attributes of individuals (gender, age, economic situation, andexposure to traumatic events during the war) and two war outcomes (postwarstress symptoms and perceived posttraumatic recovery). The participants were 870adults (ages ranged between 20 and 85), who were affected by the Second LebanonWar and were evacuated from their home town. They were administered theresearch questionnaire approximately one year after this war. Path analysisindicated the following: gender, age, economic situation, and exposure weresignificantly associated with level of symptoms as well as perceived recovery.However, three of these connections (age, economic, and exposure) were partiallymediated by SOC which was linked with lower levels of stress symptoms andhigher levels of perceived posttraumatic recovery. Unlike our hypothesis, exposureby age interaction was not significantly associated with SOC and the two waroutcomes. Results supported the hypotheses that SOC mediates between demo-graphic characteristics and negative (symptoms) as well as positive (perceivedrecovery) war outcomes.
Keywords: sense of coherence; stress symptoms; perceived posttraumatic recovery;mediation model; Second Lebanon War
The sense of coherence (SOC) concept comprises three interrelated components:
sense of meaningfulness, comprehensibility, and manageability. Hence, SOC affects
how individuals perceive the world and the events that happen to them as well as the
extent to which they perceive these events as controllable. According to Antonovsky,
SOC is a stable global construct, which is universally meaningful and cuts across
lines of gender, social class, and culture (Antonovsky, 1979, 1987; Sagy &
Antonovsky, 2000). Furthermore, according to Antonovsky SOC is a health-
engendering orientation that functions as a psychologically based stress-resistance
resource. Accordingly, it is a major factor determining one’s ability to cope with
harsh events such as war, as well as the rate of recovery from traumatic events and
return to normal life after experiencing distress. Other researchers have defined such
orientation as a dispositional trait: ‘‘Broad individual differences in behavior,
*Corresponding author. Email: [email protected]
ISSN 1061-5806 print/1477-2205 online
# 2010 Taylor & Francis
DOI: 10.1080/10615800902971513
http://www.informaworld.com
Anxiety, Stress, & Coping
Vol. 23, No. 2, March 2010, 139�152
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010
thought, and feeling that account for general consistencies across situations and over
time’’ (McAdams & Pals, 2006, p. 212). According to Feldt, Metsapelto, Kinnunen,
and Pulkkinen (2007), SOC and ‘‘big five factors’’ are highly interrelated. Their
study indicated significant relationships between SOC scores and both neuroticism
and conscientiousness in male adolescents (and in addition between SOC and
agreeableness in adolescent girls).
The core hypothesis of the concept is that the stronger the person’s SOC is themore
adequate will his/her capacity to be cope with distress. A recent review of the literature
(Almedom, 2005) posits further that SOC is a preferable concept for analyzing coping
with stress since it is inclusive of the related concepts of resilience and hardiness.
Sense of coherence and severe stress
Negative psychological effects of traumatic events such as wars and acts of terrorism
have been discussed widely in recent research (e.g., Ehntholt & Yule, 2006). These
effects may linger on as posttraumatic distress symptoms (PTSD; Hadi, Llabre, &
Spitzer, 2006), as well as emotional and behavioral problems.
Studies of severe stress events have also indicated the important role of SOC. For
example, Dudek and Koniarek (2000) have found that a higher level of PTSD was
associated with a lower level of SOC among firefighters. High SOC and spirituality
were positively correlated with lower stress and higher quality of life in chronic
patients (Delgado, 2007). Similarly, it was found that people with a low SOC
reported significantly slower adaptation to the adverse effects of their life experiences
than those with a higher SOC (Surtees, Wainwright, & Khaw, 2006). This study
demonstrated further that SOC was also predictive of mortality. An additional study
of displaced adult Kosovars revealed significant negative correlation between their
SOC and symptoms of depression (Roth & Ekblad, 2006), and Almedom,
Tesfamichael, Mohammed, Mascie-Taylor, and Alemu (2007) demonstrated that
SOC differentiated between displaced and non-displaced Eritreans.
Sense of coherence and positive stress-related outcomes
It has been argued further that traumatic events may also result in positive stress-
related outcomes beyond the pre-traumatic condition (Hobfoll et al., 2007). A more
modest and perhaps more realistic aim of posttraumatic growth is the ability of
people to find ‘‘some good emerging from their struggle’’ (Tedeschi & Calhoun,
1995, p. 445). Posttraumatic growth may be achieved by being able to find something
to hold onto in times of acute stress, even if people who have suffered from hardship
fail to restore previous psychological adjustment levels. Thus, it was found that
people can reestablish a positive image of postwar reality as well as a positive view of
themselves while accepting the fact that their situation has not been improved in
relation to the pre-traumatic condition (Janoff-Bulman, 1992). However, the concept
of posttraumatic growth is still equivocal and many relevant issues require further
research. These include its relation to well-being, whether growth is best conceptua-
lized as a process or an outcome, whether report of growth reflects actual behavioral
change or represents illusion or cognitive distortion supporting coping with distress
(Park & Helgeson, 2006).
140 S. Kimhi et al.
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010

We submit therefore, that recuperation from war traumas should be assessed by
allowing respondents to rate their present condition as compared with their pre-war
condition (see, Weinrib, Rothrock, Johnsen, & Lutgendorf, 2006), and will term this
recuperation ‘‘perceived posttraumatic recovery’’ (PTR). We hypothesize that level
of PTR measured this way, will be associated with improved indicators of adjustment
even when it does not exceed pre-trauma level.
The extensive research linking SOC with reactions to stress has neglected to
investigate its association with a positive outcome such as PTR (e.g., Delgado, 2007),
although Almedom and Glandon (2007) have argued forcefully that poststress
resilience is a psychological attribute in itself and not just the absence of PTSD. The
present study will address this issue.
Additionally, several studies have examined the role of SOC as a mediator
between background variables and distress. For example, demographic character-
istics and explanation of health (Eriksson & Lindstrom, 2007) and; exposure to
violence and psychological, psychosomatic, and cognitive stress reactions (Hogh &
Mikkelsen, 2005). We are not aware of a study which examined SOC as a mediator
between demographic characteristics and outcomes of war. However, based on the
literature, we hypothesized that SOC would serve as a mediator between demo-
graphic characteristics and positive as well as negative war outcomes.
Demographic characteristics predicting distress
Four demographic variables were found to be correlated in coping with traumatic
stress: level of exposure to traumatic events, age, gender, and economic situation.
Exposure to traumatic events
It has been observed that postwar psychosocial damage is substantially affected by
exposure to distressing war experiences: the greater this exposure the higher the level
of stress symptoms (Kimhi & Shamai, 2004). Furthermore, it was also found that
exposure to traumatic events was negatively associated with SOC. Hogh and
Mikkelsen (2005) have studied the relationships between exposure to violence at
work and SOC. They indicated that employees subjected to violence have a weaker
SOC than comparable peers who were not subjected to violence.
Age
Several studies have indicated that adverse postwar responses were more prevalent
and more enduring among older people (e.g., Tang, 2007). Somewhat similar results
were obtained in a longitudinal study of posttraumatic growth that studied survivors
of three disasters and retested these survivors three years later (McMillen, Smith, &
Fisher, 1997). Other studies reported that SOC tends to be relatively stable and does
not change much over the years (Hendrikx, Nilsson, &Westman, 2008). For example,
Feldt et al. (2007) reported high test-retest stability (five year follow-up) for SOC
among adults, indicating that SOC tends to be stable after the age of 30. Hakanen,
Feldt, and Leskinen’s (2007) longitudinal study has supported Antonovsky’s
hypothesis according to which SOC was more stable among high-SOC individuals
than among low-SOC individuals. Due to the wide range of respondent ages in the
Anxiety, Stress, & Coping 141
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010

present study we assumed that age would be associated with SOC as well as stress
symptoms and PTR.
Additionally, a few studies has indicated that exposure to stress affects various
ages differently (e.g., Kimhi & Shamai, 2006). Based on these studies we also
hypothesized that the exposure by age interaction would affect the two war
outcomes: PTR and stress symptoms.
Gender
Most of the studies investigating gender differences in reaction to stress (see
literature review: Tamres, Janicki, & Helgeson, 2002) have claimed that women tend
to report higher levels of war-related stress (fear, anxiety, and somatic complaints),
as well as more behavioral problems than men do (e.g., Kimhi & Shamai, 2006).
Research has failed to find gender differences in SOC scores. A recent 15-year
longitudinal study of Finnish men and women (Volanen, Souminen, Lahelma,
Koskenvuo, & Silventoinen, 2007) has found no SOC differences between men and
women. In line with these data we assumed that gender would be associated with
both stress symptoms and PTR but not with SOC.
Economic situation
Previous data indicated that poor economic conditions were associated with a larger
number of reported symptoms and a lower level of posttraumatic growth (Hobfoll
et al., 2007). Positive associations were also found between economic condition and
SOC. Thus it was found that unskilled occupations were associated with declines in
SOC (Smith, Breslin, & Beaton, 2003). Tsuno and Yamazaki (2007) reported similarly
that SOC was positively correlated with economic status among Japanese urban
residents, but not among rural residents. Economic condition is expected, therefore,
to be positively associated with PTR and negatively linked to the level of symptoms.
These and similar data on predictors of postwar symptoms assume direct links
between these four predictors and the two war outcomes (symptoms and PTR). We
submit that these associations are mediated by SOC. The fact that people who
experienced similar horrors of war respond to them differently, and most of them do
not develop chronic PTSD (Sutker, Davis, Oddo, & Ditta, 1995) which suggests that
the important predicting factors are not demographic characteristics by themselves,
but rather the connotations attached to them by the individual. Based on the
salutogenic model we hypothesized a mediation model associating four demographic
attributes with SOC, and with war outcomes. According to this model, SOC will
serve as a mediator between gender, age, exposure to adverse war experience as well
as perceived economic condition, and both positive (PTR) and negative (symptoms)
war outcomes. The indirect links of these predictors will be stronger than their direct
effects on these two war outcomes. Thus individuals with higher SOC will recover
more rapidly from traumatic stress, and will exhibit greater immunization to acute
stress symptoms. Accordingly, the main research question to be examined in the
current study is as follows: are the effects of socio-demographic variables (gender,
age, economic level, and exposure level) on postwar outcomes, mediated partially or
fully by SOC?
142 S. Kimhi et al.
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010

This expected mediation model was investigated in the present study using a large
Israeli sample of individuals living in the border town of Kiryat Shemona,
approximately one year after they had been targeted by hundreds of rockets shot
from Lebanon during the Second Lebanon War in 2006, causing a massive
destruction of the town (Israeli Ministry of Foreign Affairs, 2006). There is a reason
to believe that all the present respondents were substantially affected by stressful war
events. They were restricted for an entire month to crowded and unequipped shelters
lacking basic provisions such as food or toilets; they were constantly worrying about
the safety of relatives and friends; they risked their lives by emerging from these
shelters to breathe fresh air, to provide for daily needs, and to inspect their homes
despite the continuous shelling; and they did all this under the constant fear evoked
by the roaring of incoming and outgoing artillery. Furthermore, they had to evacuate
their homes and to become displaced persons, not knowing when they would come
back. Displacement was not employed as an additional variable predicting war
outcomes despite its importance for mental health (Almedom et al., 2007), since
practically all the town’s population was displaced during this war.
The theoretical model is presented in Figure 1.
Based on the above discussions, we formulated the following hypotheses:
1. Lower level of exposure to traumatic events during the war, young age, being a
male and a better economic situation will associate with lower level of stress
symptoms and higher level of PTR.
2. SOC will serve as a partial mediator between gender, age, economic situation,
and level of exposure to traumatic events and both stress symptoms and PTR:
higher exposure to traumatic events and lower economic situation will be
positively associated with symptoms and negatively linked to PTR. However,
higher SOC will have a negative effect on level of symptoms and a positive
effect on PTR.
Figure 1. Theoretical model � SOC as a mediator between demographic characteristics and
two war outcomes.aSOC � sense of coherence.bPTR � posttraumatic recovery.
Anxiety, Stress, & Coping 143
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010

3. Exposure by age interaction will affect SOC, stress symptoms, and PTR.
Accordingly, SOC will serve as a partial mediator between exposure by age
interaction and stress symptoms and PTR.
Method
Participants
The sample constituted 870 adults (40% men, 60% women), residents of the border
town of Kiryat Shemona. Ages ranged from 20 to 85 (M�44.12, SD�16.19). In
addition, 44% had more than 12 years of education, 50% had 9�12 years of
schooling, and 6% had studied eight years or less.
Sampling and procedure
Three sub-samples were included: (a) 36 streets (covering most of the city streets)
were sampled randomly from the map of Kiryat Shemona, about 10 months after the
2006 fighting. One research assistant covered each street, going from door to door.
In the event of absenteeism or refusal to participate, students were instructed to
move on to the next door. Less than 6% of those who were at their home during the
research assistants’ visits refused to take part in the study.
This process continued until each research assistant had completed 20
questionnaires. The sample included 747 respondents (about 15 questionnaires
were rejected as a result of incomplete responses). (b) In order to guarantee inclusion
of a wide enough range of ages in the sample, 50 elderly people (aged 65 and above)
of the daycare center for older adults in Kiryat Shemona were added. Research
assistants helped them respond individually to the research questionnaire. (c) To
ensure representation of individuals with a higher level of education, 73 teachers,
which constituted 90% of the local high-school teachers, were administered the
research questionnaire individually. The three samples were administered with the
research questionnaire concurrently. Administering the questionnaires ranged from
45 to 90 minutes each. The individual administration of the survey seems to account
for the fact that only 12 questionnaires were discarded due to missing data (more
than 20 items missing served as a cut-off point). Overall, missing data rate were less
than 3%, handled by using pair-wise exclusion method. The front page of the
questionnaire included a short explanation about the study, a consent form to
participate, and assurance of anonymity of respondents. The questionnaire was
administered after the respondent has signed the consent form.
The vast majority of the sample responded in Hebrew. A small number of older
people were administered a Russian version of the questionnaire. No differences were
found between the responses of these two versions.
Instruments
Sense of coherence
The short form of SOC scale was employed (Antonovsky, 1987). This scale,
consisting of 13 items, measures three components of SOC: meaningfulness,
manageability, and comprehensibility. Responses were indicated using a seven-point
144 S. Kimhi et al.
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010

bi-polar scale. Five of the items were reverse-scored such that higher numerical
ratings indicated higher levels of SOC for all items. A general SOC mean score was
employed. The internal reliability (Cronbach alpha coefficient) of this score in the
present study was .79. Validity and reliability data for the 13-item SOC scale are
presented in Antonovsky (1992), Gana and Garnier (2001), and Hittner (2007). In
addition, the SOC scale has been translated and adopted for use in many languages
and the scale has been found as grounded in robust primary research of cross-
cultural relevance (e.g., Almedom et al., 2007). No such translation was required in
this study since the scale was originally written in Hebrew.
Stress symptoms
The short version of the Brief Symptom Inventory (BSI; Derogatis & Savitz, 2000;
Derogatis & Spencer, 1982) was utilized. The original inventory consists of 53 items
(measuring nine symptom areas). The present study uses only three sub-scales
(anxiety, depression, and somatization) and is comprised 19 items, scored on a Likert
scale ranging from one (very low) to five (very high). Validity and reliability of this
scale have been examined in several studies, including the Hebrew version of the scale
(Derogatis & Savitz, 2000; Gilbar & Ben-Zur, 2002). These studies have indicated
that the scale is sensitive to stress situations like war. Since the overall Alpha
Cronbach reliability of the 19 items in the present study was very high (.94), a general
mean score of symptoms was employed.
Perceived posttraumatic recovery
PTRwas assessed by an eight-item ‘‘effects of war’’ inventory pertaining to perceived
war effects (Kimhi & Shamai, 2004). This scale, employed in assessing the aftermath
of the Israeli Defense Forces (IDF’s) withdrawal from Lebanon on people residing
along the Lebanese border, had reported an Alpha Cronbach of .83. In a previous
study (Kimhi, Eshel, Zysberg, & Hantman, in press), the PTR scale identified a long-
term impact of war on adolescents and adults and emerged as a solid indicator for
level of return to normal life one year after the war. Similar to Weinrib et al. (2006),
we have tapped both positive and negative possible war effects. Accordingly,
respondents were requested to compare their present situation with their pre-war
situation in eight domains of possible war effects: ‘‘In comparison with my situation
before the war, at present’’: physical-health situation, morale, social activity,
situation in my principal area of activity (studies, work), level of interest and
activity in my hobbies and/or in sports, emotional state, and level of optimism. Scale
ranged therefore from one ‘‘much worse than before the war’’ to five ‘‘much better
than before the war,’’ with three standing for ‘‘the same as before the war.’’ Inter item
correlations were all significant at level pB.001. Correlations ranged from .14 to .65,
median correlation was .39. A factor analysis (Principle component, Varimax
rotation) revealed a two factor model including a general recovery factor and an
additional rather weak specific factor pertaining to two items (optimism and hope).
Due to the relatively high reliability of the general PTR scale, a�.85 in the present
study, we decided to use an overall mean of all the items. A higher score thus
indicated a higher level of PTR or at least some degree of relapse.
Anxiety, Stress, & Coping 145
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010

Exposure to traumatic war events
This instrument, based on Palmieri, Canetti-Nisim, Galea, Johnson, and Hobfoll
(2008) scale, measures level of exposure to traumatic events. It contains four items
(witnessing death, witnessing casualties, being injured, and fear of death). A four-
point response scale determined whether each of these outcomes of war happened to
the individual personally (four), to a close family member (three), to a member of the
extended family (two), and to friends (one). An additional three items constructed
specifically for this study (Scale 1�4), pertained to the following issues: difficult/
traumatic events experienced during the last war; damage caused to one’s house
during the war; and rockets falling in the vicinity of home during the war. The sum of
all these items indicates level of exposure to traumatic war events. No internal
consistency coefficient was computed for this scale since its items refer to independent
war distresses whose accumulation indicates higher exposure to stress.
Economic condition
The economic situation was measured by three items: economic situation before the
war, economic situation today, and family income compared to average family
income in Israel (7900 NIS). The items ranged from one (‘‘very bad’’) to five (‘‘very
good’’). Alpha Cronbach reliability of the scale was .73. General economic
condition’s mean score was employed.
Gender
Women were coded as zero and men coded as one.
Results
A preliminary correlation matrix across the investigated variables (see Table 1)
indicated that in line with previous research, SOC was positively correlated with PTR
Table 1. Pearson correlations between investigated variables.
Demographic characteristics SOCa Dependent
Variables 1 2 3 4 5 6 7
1. Gender � �.058 .143*** �.054 .026 �.168*** .165***
2. Age � �.231*** .081* .029 .029*** �.121***
3. Economic � �.208*** .261*** �.396*** .263***
4. Exposure � �.142*** .244*** �.175***
5. SOCa� �.569*** .369***
6. Symptoms � �.429***
7. PTRb�
M .37 44.12 2.90 10.78 4.60 2.07 2.47
(SD) (.49) (16.15) (.90) (5.56) (1.02) (.92) (.63)
aSOC � sense of coherence.bPTR � posttraumatic recovery.*pB.05; ***pB.001.
146 S. Kimhi et al.
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010

and economic condition, and negatively correlated with stress symptoms and
exposure to war traumas. PTR was also positively linked with economic condition
and gender, and negatively correlated with the rest of the investigated variables,
whereas symptoms were negatively related to economic condition and gender
(women reported more symptoms) and positively connected with exposure to
traumatic events and age.
To examine our hypotheses, a path analysis (AMOS 16, Arbuckle, 2007) was
used. We used the maximum-likelihood estimation procedures and missing data were
used with multiple imputations (full information, maximum-likelihood method). As
the hypotheses have assumed a mediating role of SOC between the demographic
variables and the outcome variables, and further, assumed an interaction between
age and exposure, the default model to be examined allowed for all these effects (see
Figure 1). This default model was first compared with a model fixing all the
interaction effects to zero � a no interaction model. The model comparison yielded no
significant differences between the two models (^x2�4.016, ^df�3, p�.260),
indicating the preference for more parsimonious no interaction model. Thus, the third
hypothesis was rejected, and the analysis was continued assuming no age by exposure
interaction effect.
In order to examine the mediation effect of SOC, we compared the no interaction
model with a third model fixing all the paths between the demographic variables and
SOC to zero, to be called model without mediations. The difference between the two
models proved to be significant (^x2�75.746, ^df�4, pB.001), thus indicating
the rejection of the model without mediations in favor of the more inclusive
no interaction model. Further, as one of the mediation paths (the effects of gender
on SOC) was not significant, we constrained this insignificant path to zero, and
examined the final model. The model was not significantly different from the
no interaction model (^x2�.107, ^df�1, p�.744). The fit indices for the final
model have proved to be excellent (x2�4.12, df�4, p�.39; x2/df�1.031; Normal fit
index (NFI)�.999, Relative fit index (RFI)�.988, Incremental fit index (IFI)�
1.00, Comparative fit index (CFI)�1.00; Root mean square error of approximation
(RMSEA)�.006). The model is presented in Figure 2.
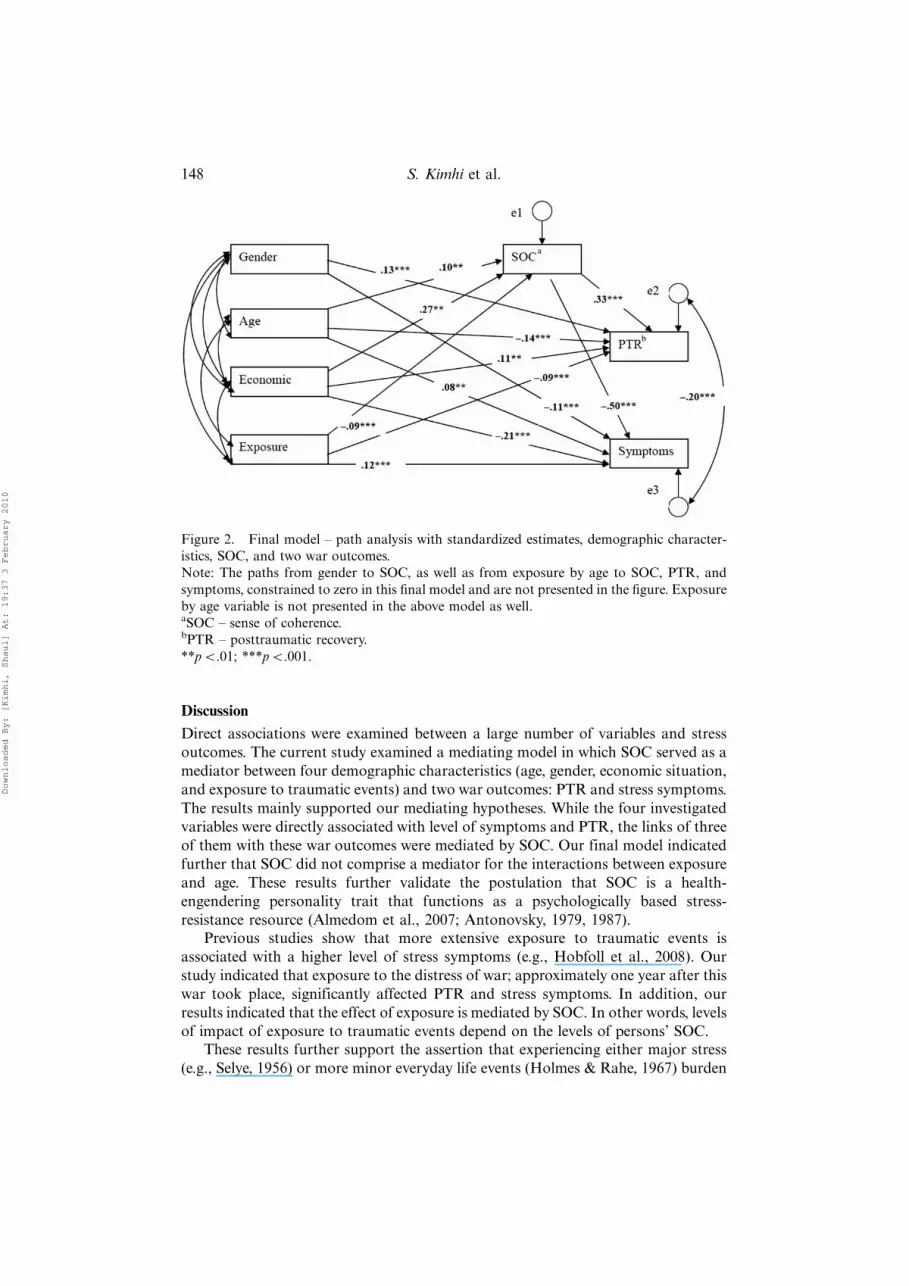
Looking further at our final model (Figure 2) indicates the following: (a) gender,
age, economic situation, and exposure to traumatic events significantly predicted
PTR as well as symptoms. Women, older persons, as well as those with a lower
economic situation and higher exposure to traumatic events reported lower level of
PTR and a higher level of stress symptoms one year after the end of the war. These
results generally support Hypothesis 1. (b) SOC served as a partial mediator between
age, economic situation, exposure to traumatic events and the two war outcomes.
However, unlike our hypothesis, SOC did not serve as a mediator for gender.
Moreover, SOC was the best predictor of PTR as well as stress symptoms.
Accordingly, those with higher SOC were less affected by age, exposure, and
economic situation, and they reported higher PTR and a lower level of symptoms.
These results mainly support our second hypothesis. (c) As indicated above, the
exposure by age interaction did not significantly predict SOC, PTR, or symptoms.
These results did not support Hypothesis 3.
Anxiety, Stress, & Coping 147
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010
Discussion
Direct associations were examined between a large number of variables and stress
outcomes. The current study examined a mediating model in which SOC served as a
mediator between four demographic characteristics (age, gender, economic situation,
and exposure to traumatic events) and two war outcomes: PTR and stress symptoms.
The results mainly supported our mediating hypotheses. While the four investigated
variables were directly associated with level of symptoms and PTR, the links of three
of them with these war outcomes were mediated by SOC. Our final model indicated
further that SOC did not comprise a mediator for the interactions between exposure
and age. These results further validate the postulation that SOC is a health-
engendering personality trait that functions as a psychologically based stress-
resistance resource (Almedom et al., 2007; Antonovsky, 1979, 1987).
Previous studies show that more extensive exposure to traumatic events is
associated with a higher level of stress symptoms (e.g., Hobfoll et al., 2008). Our
study indicated that exposure to the distress of war; approximately one year after this
war took place, significantly affected PTR and stress symptoms. In addition, our
results indicated that the effect of exposure is mediated by SOC. In other words, levels
of impact of exposure to traumatic events depend on the levels of persons’ SOC.
These results further support the assertion that experiencing either major stress
(e.g., Selye, 1956) or more minor everyday life events (Holmes & Rahe, 1967) burden
Figure 2. Final model � path analysis with standardized estimates, demographic character-
istics, SOC, and two war outcomes.
Note: The paths from gender to SOC, as well as from exposure by age to SOC, PTR, and
symptoms, constrained to zero in this final model and are not presented in the figure. Exposure
by age variable is not presented in the above model as well.aSOC � sense of coherence.bPTR � posttraumatic recovery.
**pB.01; ***pB.001.
148 S. Kimhi et al.
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010

individuals continuously, and their accumulation reduces the ability to cope with
further stressful events. Our study shows further that traumatic events have differential
effects on different individuals. Greater vulnerability seems to be associated with
a higher effect: older age and lower economic situation had a detrimental effect
on people’s ability to cope with stressful events such as war, even a year after its
termination.
The present results are in line with previous studies reporting negative
associations between stress and SOC (Darling, McWey, Howar, & Olmstead, 2007;
Delgado, 2007), and positive correlations between SOC and measures of well-being
(Ekwall & Halberg, 2007), and quality of life (Eriksson & Lindstom, 2007). Results
also support the assertion that a year after experiencing a traumatic event,
symptoms, and PTR constitute two concurrent and different way of responding to
this trauma (Antonovsky, 1987; Jacoby & Keinan, 2003).
In the current study, SOC positively affected PTR and negatively affected
symptoms. It may be concluded, therefore, that people with higher SOC have a better
chance of suffering a lower level of stress symptoms, as well as enjoying higher levels
of PTR after experiencing the hardship of war. Somewhat similar results were
reported by Hart, Wilson, and Hittner (2006) who have found that SOC was
positively correlated with measures tapping psychosocial resilience/protection, and
inversely correlated with measures tapping psychosocial risk/vulnerability.
In addition, the present study seems to suggest that SOC may constitute a
potential predictor for people’s ability to cope with traumatic events, for screening
those who are at the risk of being overwhelmed by stressful conditions, or for
selecting people for special jobs which require high resilience to severe stress (see also
Almedom et al., 2007).
Two conclusions may be drawn from the present data. Firstly, SOC may be
instrumental in decreasing the impact of age, economic situation, and exposure to
traumatic events on the development of stress symptoms. Secondly, by the same
token SOC determines, to some extent, the impact of these variables on PTR. A
possible practical conclusion may suggest that helping people to cope with stress
should aim at adopting general cognitive appraisals such as meaningfulness of life,
accepting life disappointments, or appreciating what life offers, which are determi-
nants of SOC. It appears that developing such cognitive appraisals may constitute
efficient determinants of training people to cope with stress.
Limitations of the study and directions for future research
Three limitations of this study should be mentioned. Firstly, the data presented
above are based solely on self reports. Future research may benefit from adding
behavioral measures of reasserted autonomy, sense of competence, or relations with
others. Secondly, both postwar symptoms and PTR seem to change with time. The
correlational design of the present study does not allow for drawing conclusions
concerning causal relations among the investigated variables. A longitudinal design
is required to point out cause and effect relations between these variables. Thirdly,
this study investigated a single community which had to cope with the aftermath of
war. Additional studies of war afflicted communities as well as those which were not
affected to a greater extent by war should also be conducted to substantiate the
present findings.
Anxiety, Stress, & Coping 149
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010

Acknowledgements
This study was supported by grant from the UJA Federation of New York.
References
Almedom, A.M. (2005). Resilience, hardiness, sense of coherence, and posttraumatic growth:All paths leading to light at the end of the tunnel. Journal of Loss & Trauma, 10, 253�265.
Almedom, A.M., & Glandon, D. (2007). Resilience is not the absence of PTSD any more thanhealth is the absence of disease. Journal of Loss and Trauma, 12, 127�143.
Almedom, A.M., Tesfamichael, B., Mohammed, Z.S., Mascie-Taylor, C.G.N., & Alemu, Z.(2007). Use of ‘sense of coherence (SOC)’ scale to measure resilience in Eritrea:Interrogating both the data and the scale. Journal of Biosocial Science, 39, 91�107.
Antonovsky, A. (1979). Health, stress and coping. San Francisco, CA: Jossey-Bass.Antonovsky, A. (1987). Unraveling the mystery of health. San Francisco, CA: Jossey-Bass.Antonovsky, A. (1992). Can attitude contribute to health? Advances. Journal of Mind-Body
Health, 8, 33�49.Arbuckle, J.L. (2007). Amos 16.0 user’s guide. Chicago, IL: SPSS.Darling, C.A., McWey, L.M., Howar, S.N., & Olmstead, S.B. (2007). College student stress:
The influence of interpersonal relationships on sense of coherence. Stress and Health:Journal of the International Society for the Investigation of Stress, 23, 215�229.
Delgado, C. (2007). Sense of coherence, spirituality, stress and quality of life in chronic illness.Journal of Nursing Scholarship, 39, 229�234.
Derogatis, L.R., & Savitz, K.L. (2000). The SCL-90-R and Brief Symptom Inventory (BSI) inprimary care. In M.E. Maruish (Ed.), Handbook of psychological assessment in primary caresettings (pp. 297�334). Mahwah, NJ: Lawrence Erlbaum.
Derogatis, L.R., & Spencer, P.M. (1982). The brief symptom inventory: Administration, scoringand procedures manual � I. Baltimore, MD: Clinical Psychometric Research.
Dudek, B., & Koniarek, J. (2000). Relationship between sense of coherence and post-traumaticstress disorder symptoms among firefighters. International Journal of Occupational Medicineand Environmental Health, 13, 299�305.
Ehntholt, K.A., & Yule, W. (2006). Practitioner review: Assessment and treatment of refugeechildren and adolescents who have experienced war-related trauma. Journal of ChildPsychology and Psychiatry, 47, 1197�1210.
Ekwall, A.K., & Halberg, I.R. (2007). Older caregivers’ coping strategies and sense ofcoherence in relation to quality of life. Journal of Advanced Nursing, 57, 584�596.
Eriksson, M., & Lindstrom, B. (2007). Antonovsky’s sense of coherence scale and its relationwith quality of life: A systematic review. Journal of Epidemiology and Community Health, 61,938�944.
Feldt, T., Lintula, H., Suominen, S., Doskenvuo, M., Vahtera, J., & Kivimaki, M. (2007).Structural validity and temporal stability of the 13-item sense of coherence scale:Prospective evidence from the population-based HeSSup study. Qulity of Life Research,16, 483�493.
Feldt, T., Metsapelto, R.L., Kinnunen, U., & Pulkkinen, L. (2007). Sense of coherence andfive-factor approach to personality. European Psychologist, 12, 165�172.
Gana, K., & Garnier, S. (2001). Latent structure of the sense of coherence scale in a Frenchsample. Personality and Individual Differences, 31, 1079�1090.
Gilbar, O., & Ben-Zur, H. (2002). Cancer and the family caregiver: Distress and coping.Springfield, IL: Charles C. Thomas.
Hadi, F., Llabre, M.M., & Spitzer, S. (2006). Gulf War-related trauma and psychologicaldistress of Kuwaiti children and their mothers. Journal of Traumatic Stress, 19, 653�662.
Hakanen, J.J., Feldt, T., & Leskinen, E. (2007). Change and stability of sense of coherence inadulthood: Longitudinal evidence from the healthy child study. Journal of Research inPersonality, 41, 602�617.
Hart, K.E., Wilson, T.L., & Hittner, J.B. (2006). A psychosocial resilience model to accountfor medical well-being in relation to sense of coherence. Journal of Health Psychology, 111,857�862.
150 S. Kimhi et al.
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010

Hendrikx, T., Nilsson, M., & Westman, T. (2008). Sense of coherence in three cross-sectionalstudies in Northern Sweden 1994, 1999 and 2004-patterns among men and women.Scandinavian Journal of Public Health, 36, 340�345.
Hittner, J.B. (2007). Factorial invariance of the 13-item sense of coherence scale across gender.Journal of Health Psychology, 12, 273�280.
Hobfoll, S.E., Canetti-Nisim, D., Johnson, R.J., Varley, J., Palmieri, P.A., & Galea, S. (2008).The association of exposure, risk and resiliency factors with PTSD among Jews and Arabsexposed to repeated acts of terrorism in Israel. Journal of Traumatic Stress, 21, 9�21.
Hobfoll, S.E., Hall, B.J., Canetti-Nisim, D., Galea, S., Johnson, R.J., & Palmieri, P.A. (2007).Refining our understanding of traumatic growth in the face of terrorism: Moving frommeaning cognitions to doing what is meaningful. Applied Psychology: An InternationalReview, 56, 345�366.
Hogh, A., & Mikkelsen, E.G. (2005). Is sense of coherence a mediator or moderator ofrelationships between violence at work and stress reactions? Scandinavian Journal ofPsychology, 46, 429�437.
Holmes, T.H., & Rahe, R.H. (1967). Assessment and psychological management of recurrentheadache disorders. Journal of Psychosomatic Research, 11, 213�218.
Israeli Ministry of Foreign Affairs. (last updated 14 August 2006). Hizbullah attacks NorthernIsrael and Israel’s response. Retrieved October 21, 2006, from http:mfa.gov.il/ FA/Terrorism-�Obstacle�to�Peace/Terrorism�from�Lebanon-�Hizbullah/ Hizbullah�attack�in�northern�Israel�and�Israels�response�12-Jul-2006.htm
Jacoby, R., & Keinan, G. (2003). Between stress and hope: From a disease-centered to a health-centered perspective. Westport, CT: Prager.
Janoff-Bulman, R. (1992). Shattered assumptions: Toward a new psychology of trauma.New York: Free Press.
Kimhi, S., Eshel, Y., Zysberg, L., & Hantman, S. (in press). Postwar winners and losers in thelong run: Determinants of war related stress symptoms and posttraumatic recovery.Community Mental Health Journal.
Kimhi, S., & Shamai, M. (2004). Community resilience and the impact of stress: Adultresponse to Israel’s withdrawal from Lebanon. Journal of Community Psychology, 32,439�451.
Kimhi, S., & Shamai, M. (2006). Are women at higher risk than man? Gender differencesamong teenagers and adults in their response to threat of war and terror. Women & Health,43, 1�19.
McAdams, D.P., & Pals, J.L. (2006). A new big fine: Fundamental principles for an integrativescience of personality. American Psychologist, 61, 204�217.
McMillen, J.C., Smith, E.M., & Fisher, R.H. (1997). Perceived benefit and mental health afterthree types of disaster. Journal of Consulting and Clinical Psychology, 65, 733�739.
Palmieri, P.A., Canetti-Nisim, D., Galea, S., Johnson, R.J., & Hobfoll, S.E. (2008). Thepsychological impact of the Israel-Hezbollah War on Jews and Arabs in Israel: The impactof risk and resilience factors. Social Science & Medicine, 67, 1208�1216.
Park, C.L., & Helgeson, V.S. (2006). Introduction to the special section: Growth followinghighly stressful life events � current status and future directions. Journal of Consulting andClinical Psychology, 74, 791�796.
Roth, G., & Ekblad, S. (2006). A longitudinal perspective on depression and sense ofcoherence in a sample of mass-evacuated adults from Kosovo. Journal of Nervous andMental Disease, 194, 378�381.
Sagy, S., & Antonovsky, H. (2000). The development of the sense of coherence: A retrospectivestudy of early life experiences in the family. Journal of Aging and Human Development, 51,155�166.
Selye, H. (1956). The stress of life. New York: McGraw-Hill.Smith, P.M., Breslin, F.C., & Beaton, D.E. (2003). Questioning the stability of sense of
coherence: The impact of socio-economic status and working conditions in the Canadianpopulation. Social Psychiatry and Psychiatric Epidemiology, 38, 475�484.
Surtees, P.G., Wainwright, N.W.J., & Khaw, K.T. (2006). Resilience, misfortune, and mortality:Evidence that sense of coherence is a marker of social stress adaptive capacity. Journal ofPsychosomatic Research, 61, 221�227.
Anxiety, Stress, & Coping 151
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010

Sutker, P.B., Davis, J.M., Oddo, M., & Ditta, S.R. (1995). War zone stress, personal resources,and PTSD in Persian Gulf War returnees. Journal of Abnormal Psychology, 104, 444�452.
Tamres, L.K., Janicki, D., & Helgeson, V.S. (2002). Sex differences in coping behavior: Ameta-analytic review. Personality and Social Psychology Review, 6, 2�30.
Tang, C.S. (2007). Trajectory of traumatic stress symptoms in the aftermath of extreme naturaldisaster: A study of adult Thai survivors of the 2004 Southeast Asian earthquake andtsunami. The Journal of Nervous and Mental disease, 195, 54�59.
Tedeschi, R.G., & Calhoun, L.G. (1995). Trauma and transformation: Growing in the aftermathof suffering. Thousand Oaks, CA: Sage.
Tsuno, Y.S., & Yamazaki, Y. (2007). A comparative study of sense of coherence (SOC) andrelated psychosocial factors among urban versus rural residents in Japan. Personality andIndividual Differences, 43, 449�461.
Volanen, S.M., Souminen, S., Lahelma, E., Koskenvuo, M., & Silventoinen, K. (2007).Negative life events and stability of sense of coherence: A five-year follow-up study ofFinnish women and men. Scandinavian Journal of Psychology, 48, 433�441.
Weinrib, A., Rothrock, N.E., Johnsen, E.L., & Lutgendorf, S.K. (2006). The assessment andvalidity of stress-related growth in a community based sample. Journal of Consulting andClinical Psychology, 74, 851�858.
152 S. Kimhi et al.
Downloaded By: [Kimhi, Shaul] At: 19:37 3 February 2010





























