Embed Size (px)
Citation preview
J. Cranio-Max.-Fac. Surg. 18 (1990) 237
j. Cranio-Max.-Fac. Surg. 18 (1990) 237-242 © Georg Thieme Verlag Stuttgart - New York
Sensibility and Cutaneous Reinnervation of Pectoralis Major Myocutaneous Island Flaps A Preliminary Clinical Report
Theo J. M. Hoppenreijs 1, Hans Peter M. Freihofer 1, John J.A. Brouns I, Ingolv Bruasefl, Johannes J. Manni 2
1 Dept. of Oral and Maxillofacial Surgery (Head: Prof. H. P. M. Freihofer, M.D., D.M.D.) Dept. of Oto-Rhino-Laryngology, Head and Neck Surgery (Head: Prof. P. van den Broek, M.D.), Academic Hospital University Nijmegen, The Netherlands
Submitted 15.2. 90; accepted 20.3.90
Introduction
Myocutaneous island flaps have become the mainstay of reconstructive techniques of large soft tissue defects in the head and neck area after ablative cancer surgery (Withers et al., 1979; Ariyan, 1979a; Magee et al., 1980; Manni and Bruaset, 1986). Favourable results and a low incidence of complications are reported by many (Ariyan, 1979b; Beah et al., 1982; Nicolai et al., 1983). However, the extent of the return of the sensibility of the skin island of these myo- cutaneous flaps has not been reported in the literature. In an effort to increase knowledge, a retrospective study has been undertaken to investigate the extent and quality of sensibility of the cutaneous portion of the pectoralis major myocutaneous island flaps used particularly for intraoral reconstruction. The factors which may influence the pat- tern of sensory reinnervation will be discussed.
Anatomy
By definition, the pectoralis major myocutaneous island flap includes an isolated skin paddle along with the under-
, lying muscle and its intact vascular supply. The pectoralis major muscle has a rich vascular supply from the pectoral branch of the thoraco-acromial artery and the lateral thor- acic artery (Freeman et al., 1981; Moloy and Gonzales, 1986). The muscle receives its motor innervation from the lateral and medial pectoral nerve. These nerves arise from the lateral and medial cords of the brachial plexus, and con- tain nerve fibres from C5-C7 and C8-T1 respectively. The overlying skin vascular supply is by multiple skin perfora- tors, and it has a rich sensory innervation. Cutaneous nerves contain myelinated A alpha, beta, gamma and delta fibres and unmyelinated C fibres (Lance and McLeod, 1981). The sensibility of the surface of the body can be divided in- to deep and superficial modalities. Deep sensibility, which is mediated by the muscular branches, elicits sensation of deep pressure and movements from the deeper tissues. The
Summary
The cutaneous sensibility of 13 pectoralis major myo- cutaneous island flaps has been investigated retrospec- tively. Although in raising the pectoralis major myocu- taneous island flap sensory denervation of the skin is produced, after a mean follow-up period of 29 months (range 5 to 71 months), 68 % of the cutaneous portion of the flap revealed sensibility to touch, suggesting a reinnervation from the surrounding intact oral mucosa or skin. The rate of reinnervation was found to be relat- ed to the sensibility present in the surrounding tissue.
Key words
Oral cavity - Surgical flaps - Pectoralis major myocu- taneous island flap - Sensibility - Reinnervation - Reconstruction
superficial sensibility of the skin of the anterior thoracic wall, which is mediated by medial mammary branches of the anterior cutaneous nerves and anterior and dorsal branches of the lateral cutaneous nerves, is receptive to touch, light pressure, heat or cold and painful nociceptive stimuli (Monnier, 1975). The afferent sensory nerve fibres from a thoracic segment including the given skin area covering the pectoralis muscle, converge upon an intercos- tal nerve (Truex and Carpenter, 1969). The intercostal nerve runs below the corresponding vessels in the costal groove and enters the vertebral column as a spinal nerve. The sensation of touch in particular is mediated by A delta fibres and is conducted by the ventral spinothalamic tract centrally.
Material and Methods
Patients with a pectoralis major myocutaneous island flap used in a one-stage reconstructive procedure after ablative cancer surgery, were examined at random during the rou- tine check-up by members of the head and neck oncology group. The scar tissue of a per secundam healing could in- fluence the results, therefore, only flaps which healed-in without complications are included. The patient group consisted of ten men and three women, with a mean age of 56 years (range 39 to 76 years). The de- tails are summarized in table 1. All tumours were histologi- cally proven squamous cell carcinomas except case 12 which was an Ewing sarcoma. The primary tumour was re- moved en bloc with the supraomohyoid or radical neck dis- section specimen in all patients except case 12. The site and size of the flap on the chest wall were deter- mined by the location and extent of the defect to be recon- structed after mmour ablation. Donor sites had a mean area of 29 cm ~ (range 12 to 54 cm 2) and were situated in the skin area of the fourth, fifth and sixth dermatomes (Fig. 1). The costosternal and clavicular portion of the pec- toralis major muscle were freed medially and lateral to the thoraco-acromial artery and transposed over the clavicle. The neurovascular pedicle was not skeletonized to prevent injury or spasm of the vessels, to improve the contour deft-

23 8 J. Cranio-Max.-Fac. Surg. 18 (1990) Th. J. M. Hoppenreijs et aL
Fig, 1 Design of the cutaneous part of the flap on the anterior thor- acic wall, in relation to the location of the thoraco-acromial artery. The distal part of the artery lies on the acromion-xiphoid line.
Posterior
L
V
Anterior Fig. 2 Division of the flap into 5 sectors and its surrounding area into 4 sectors.
cit of the neck and to protect the carotid artery. Postopera- tive irradiation to a total dose of 50 to 64 Gy was applied in seven patients on the basis of either the nodal status or su- spected marginal resection of the primary tumour. The mean follow-up period after surgery was 29 months (range 5 to 71 months). All patients were asked to define the general sensation of the flap. Their experiences were classified as anaesthesia, dysaesthesia or normaesthesia. For the clinical examination the flap is divided into five sectors, one central and four pe- ripheral. The surrounding tissue was divided into four sec- tors analogous to the periphery of the flap (Fig. 2). The su- perficial sensibility of each sector of the flap and its corre- sponding sector of the periphery were evaluated by testing the sensation to touch with a blunt needle (Fig. 3). Any fur-
ther analysis of the quality of tactile sensation was not made.
Results
During preparation of the cutaneous portion of the pecto- ralis major myocutaneous island flap, the cutaneous affer- ent nerve fibres were transsected, thereby leaving no sensi- tivity in the skin. The lateral pectoral nerve is a part of neu- rovascular bundle in the pedicle, and frequently the major motor nerve supply of the pectoralis major muscle was pre- served. In the patient interview, 2 patients reported anaesthesia, 8 patients dysaesthesia and 3 patients normal sensation in the cutaneous surface of the flap. Neither in the anaesthesia
Table1 Detaits of Individual Patients
Case Age Sex Follow-up Site of the PMMI flap Neck Post-op. No. (months) Dissection Irradiation
1 42 F 35 Floor of the mouth Radical No 2 58 F 34 Floor of the mouth Radical Yes 3 45 M 22 Floor of the mouth Conservative Yes 4 76 M 30 Floor of the mouth Conservative No 5 39 M 49 Floor of the mouth Radical Yes 6 75 M 7 Floor of the mouth Radical No 7 47 M 5 Pterygo-mand. region Radical Yes 8 60 M 28 Pterygo-mand. region Radical No 9 43 M 45 Pterygo-mand. region Radical Yes
10 54 M 20 Pterygo-mand. region Radical Yes 11 62 F 17 Pterygo-mand. region Radicai Yes 12 73 M 20 Cheek - No 13 60 M 71 Submental region Radical right No
Conserv. left
PMMl=Pectoralis Major Myocutaneous Island
Reinnervation of Pectoralis Major Myocutaneous Island Flaps J. Cranio-Max.-Fac. Surg. 18 (1990) 239
Fig.3 Sensat ion of touch elicited by a blunt
needle,
Posterior Posterior
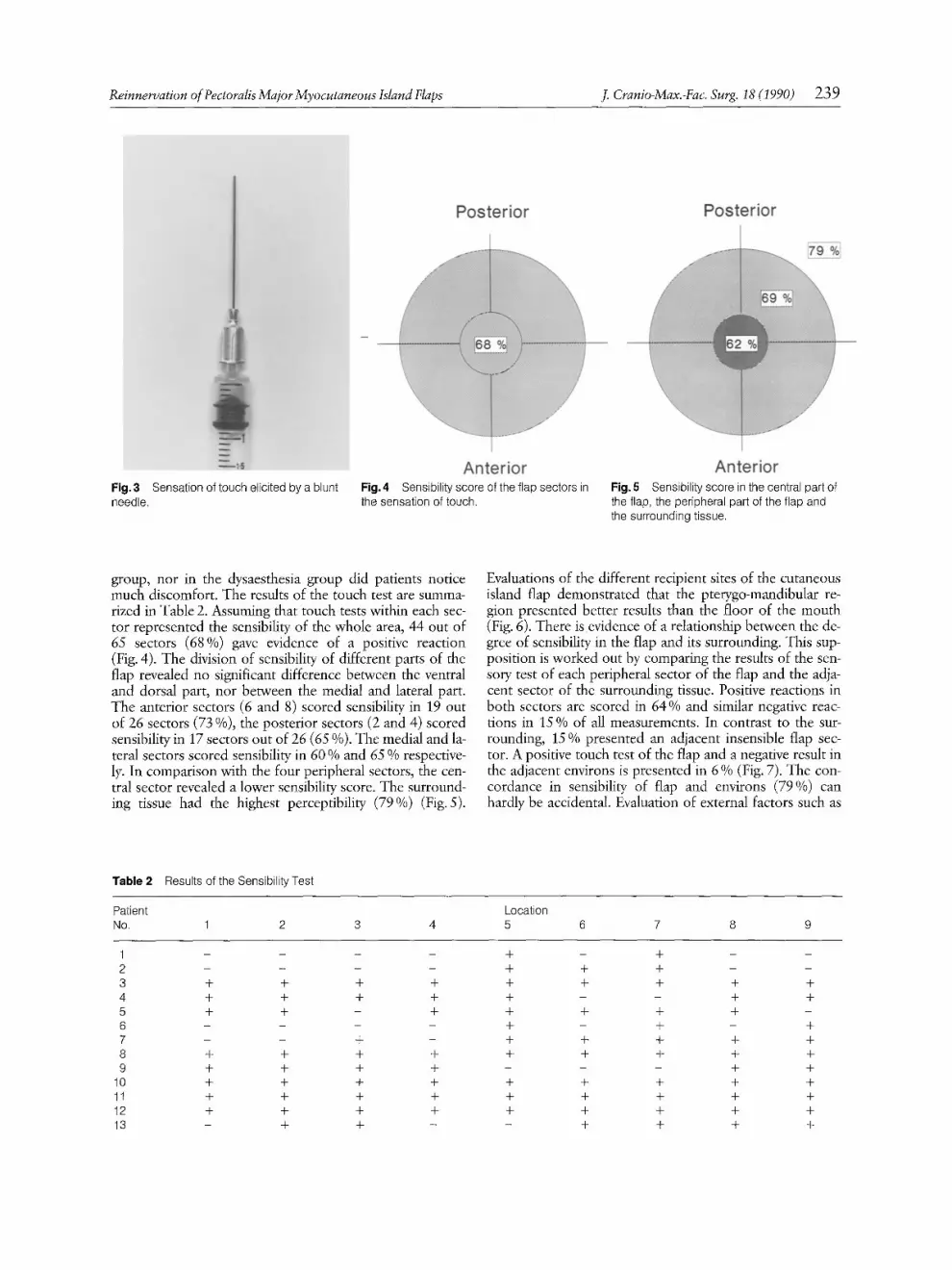
Anterior F ig .4 Sensibi l i ty score of the f lap sectors in
the sensat ion of touch.
Anterior F ig .5 Sensibi l i ty score in the central part of
the flap, the peripheral part of the f lap and
the surrounding tissue.
group, nor in the dysaesthesia group did patients notice much discomfort. The results of the touch test are summa- rized in Table 2. Assuming that touch tests within each sec- tor represented the sensibility of the whole area, 44 out of 65 sectors (68%) gave evidence of a positive reaction (Fig. 4). The division of sensibility of different parts of the flap revealed no significant difference between the ventral and dorsal part, nor between the medial and lateral part. The anterior sectors (6 and 8) scored sensibility in 19 out of 26 sectors (73 %), the posterior sectors (2 and 4) scored sensibility in 17 sectors out of 26 (65 %). The medial and la- teral sectors scored sensibility in 60 % and 65 % respective- ly. In comparison with the four peripheral sectors, the cen- tral sector revealed a lower sensibility score. The surround- ing tissue had the highest perceptibility (79%) (Fig. 5).
Evaluations of the different recipient sites of the cutaneous island flap demonstrated that the pterygo-mandibular re- gion presented better results than the floor of the mouth (Fig. 6). There is evidence of a relationship between the de- gree of sensibility in the flap and its surrounding. This sup- position is worked out by comparing the results of the sen- sory test of each peripheral sector of the flap and the adja- cent sector of the surrounding tissue. Positive reactions in both sectors are scored in 64 % and similar negative reac- tions in 15 % of all measurements. In contrast to the sur- rounding, 15 % presented an adjacent insensible flap sec- tor. A positive touch test of the flap and a negative result in the adjacent environs is presented in 6 % (Fig. 7). The con- cordance in sensibility of flap and environs (79 %) can hardly be accidental. Evaluation of external factors such as
T a b l e 2 Results of the Sensibi l i ty Test
Patient Locat ion
No. 1 2 3 4 5 6 7 8 9
1 . . . . + - + - -
2 . . . . + + + - - 3 + + 4- + + + 4- + 4-
4 + + + + + - - + + 5 + + - + + + -F + -
6 . . . . + - + - + 7 - - "4- - + + + -4- +
8 + + + ÷ + + + + +
9 + + + + - - - + + 10 + + + + + + + + + 11 + + + + + + + + +
12 + + + + + + + + + 13 - + + - - + + + +

240 J. Cranio-Max.-Fac. Surg. 18 (1990) Th. J. M. Hoppenreijs et al.
Posterior
, ^ ^
Posterior
Anterior Fig.6 a Sensibility score of flap and its surrounding in the pterygo- mandibular region (n=5).
Anterior Fig. 6 b Sensibility score of flap and its surrounding in the floor of the mouth (n=6)
70
60
50
40
30
20
10
O - -
Fig. 7
[ ~ 1 Sens surf ~ Sans. flap [ ~ Anaesth i
Results of the sensory test of each peripheral sector (right part of each column) and its adjacent surrounding sector (left part of each column).
postoperative irradiation demonstrated that the group of 7 patients who had received radiotherapy revealed a high score of sensibility (Fig. 8). This result, however, was not significant.
Discussion
The protopathic sensations such as heat, cold or pain de- pend to a varying degree upon the subject experiencing them. The analytical properties of the sense organs are best demonstrated in the epicritic sensation of touch. Percep- tion of touch is, therefore, used to obtain an impression of possible sensibility in the pectoralis major myocutaneous is- land flap. Mechanoreceptors give maximal responses to in- nocuous mechanical stimulation. The sensation of touch is caused by minimal displacement of the tissue. This superfi- cial type of sensation should not be influenced by transmit- ted sensation due to deformity of adjacent or underlying structures.
To the best of our knowledge, publications on the subject of sensibility and its recovery with regard to the pectoralis major myocutaneous island flap are not available. Reports are restricted to the vascular anatomy of the flap, the tech- nique and the results of reconstructive surgery. In the surgi- cal treatment of head and neck turnouts, radical resection of the tumour and functional reconstruction of the defect are of the utmost importance. David (1977) has promoted the use of an innervated deho- pectoral flap for intraoral reconstruction, because the quali- ty of speech, swallowing, and oral hygiene depend to some degree on the quality of sensation inside the mouth. Most articles on the subject of reinnervation concern re- construction with free flaps in the extremities. After finger or foot reconstruction, the sensation present in the flaps appears to be of protective value, therefore, restoration of sensibility in the reconstructed surface is desirable to achieve an optimal functional result and rehabilitation. Hermanson et al. (1987) investigated sensibility and senso- ry reinnervation in 12 free latissimus dorsi and 2 free graci- lis flaps predominantly located on the lower extremities. Al- though all patients showed deep pressure sensibility in the flaps, none had superficial sensibility to such stimuli as pin- prick, heat, or cold. Most patients had normal sensibility of the adjacent skin. Chang et al. (1986) described six sensory reinnervation techniques in 10 patients who underwent re- construction of the heel by microsurgical free-tissue trans- fer to correct the shortcomings of the superficial type of sensation. Surgical intervention produced a considerably more extensive sensate area than spontaneous neurotiza- tion of a non-innervated skin flap, and reinnervation took much less time. Dabb and Conldin (1981) reported sensa- tion to pinprick and pressure in the central portion of a sensory innervated latissimus dorsi musculocutaneous free flap after 6 months. The cutaneous branches of the dorsal rami and the intercostal nerve were anastomosed to the an- terior tibial nerve and the medial plantar branch of the pos- terior tibial nerve respectively. In our study, two patients showed no superficial touch sen- sibility of any sector of the flap, and in another two patients it was less than three out of five sectors. Even after a few

Reinnervation of Pectoralis Major Myocutaneous Island Flaps J. Cranio-Max.-Fac. Surg. 18 (1990) 241
Posterior
I ~ ^ ^ , i
Posterior
I n ^ ^ , I
Fig.8a (n=6).
Anterior Sensibility score of flap and its surrounding, after surgery
Anterior Fig. 8 b Sensibility score of flap and its surrounding, after surgery and additional radiotherapy (n=7).
months, some recovery may occur, but in the course of time a reasonable improvement is noticed. There are some differing opinions concerning the cutaneous reinnervation. Chang et al. (1986) reported spontaneous neurotization of a non-innervated skin flap in two patients and stated that it was presumably due to nerve ingrowth from the surround- ing normal skin. Hermanson et al. (1987) ascribed heat pain sensations to possible subcutaneous reinnervation of the flap nociceptors. Waris et al. (1983) investigated rein- nervation of human skin grafts histochemically. Their re- suits showed that nerves regenerated into the graft from the margins and at the subdermal level under the graft. It is sug- gested that the randomly regenerated sensory nerves at the periphery are under the control of the epidermis and its ap- pendages via chemotactic factors. Only free sensory nerve endings or nerves in association with hair follicles were ob- served in the grafts. In the present study, the remarkable declining sensibility from the periphery to the centre, points to a reinnervation from the margins. A similar sensibility recovery pattern is found after resection or division of mental and mandibular nerves (Wanner, 1979). A better sensibility of the peripher- al regions is assumed to be the result of nerve anastomoses from the undisturbed environs. Recovery of sensibility is expected to be dependent on the size of the flap. Because of the small number of flaps exam- ined, differing in magnitude, we are diffident about pro- nouncing upon the relationship between the area of the flap and recovery of sensibility. As a well-innervated graft bed seems to be important for optimal reinnervation of skin grafts (Waris et al., 1983), the innervation of the surrounding tissue seems to play an im- portant role in the nerve regeneration into the graft. Poor recovery is noticed in cases in which the surroundings give evidence of anaesthesia. The floor of the mouth and the an- terior part of the tongue are innervated by the lingual nerve. Not infrequently this nerve is in contact with the turnout and resected. The considerable sensory disturbance of the surrounding tissue is an unfavourable base for recovery of sensibility in the flap situated in the floor of the mouth. Fibrosis and scars surrounding the flap seem to hamper
nerve regeneration (Waris et al., 1983), however irradiation seems to be of only minor influence. The pectoralis major myocutaneous island flap possesses a well-vascularized full-thickness skin with different types of sensory receptor cells and nerve endings, which is a favou- rable point of departure in the cutaneous reinnervation (Chang and Buncke, 1986). Without biopsy samples it is difficult to define whether the neurilemmal structures of the cutaneous part of the flap are reinnervated or the nerves grow into the skin independent of these structures.
Conclusions
The use of pectoralis major myocutaneous island flaps of- fers many advantages. The predictable vascular supply, en- hances tissue survival and succesful healing. Although pre- paration of these flaps results in a sensibility denervation, the sense of touch gradually returns again. This is presum- ably due to nerve ingrowth from the surrounding tissue. The rate of recovery is dependent on the sensibility present in the surrounding tissue. Detrimental influence of radio- therapy on the cutaneous reinnervation is not observed.
References
Ariyan, S.: The pectoralis major myocutaneous flap. A versatile flap for reconstruction in head and neck. Hast. Reconstr. Surg. 63 (1979a) 73
Ariyan, S.: Further experience with the pectoralis major myocutane- ous flap for the immediate repair of defects from excision of head and neck cancers. Plast. Reconstr. Surg. 64 (1979b) 605
Baek,, S.-M., W. Lawson, H.F. Biller: An analysis of 133 pectoralis major myocutaneous flaps. Hast. Reconstr. Surg. 69 (1982) 460
Chang, K. N., H. J. Buncke: Sensory reinnervation in reconstruction of the foot. Foot Ankle 7 (1986) 124
Chang, K.N., S.J. DeArmond, H.J. Buncke: Sensory reinnervation in microsurgical reconstruction of the heel. Hast. Reconstr. Surg. 78 (1986) 652
Dabb, R.W., W.T. Conk_lin: A sensory innervated latissimus dorsi musculocutaneous free flap. J. Microsurg. 2 (1981) 289
David, D.J.: Use of an innervated deltopectoral flap for intraoral reconstruction. Hast. Reconstr. Surg. 60 (1977) 377

242 J. Cranio-Max.-Fac. Surg. 18 (1990) Th. J. M. Hoppenreijs et al.: Reinnervation of Pectoralis Major Island Flaps
Freeman, J. L., E. P. Walker, J. S. P. Wilson, H. J. Shaw: The vascular anatomy of the pectoralis major myocutaneous flap. Br. J. Plast. Surg. 34 (1981) 3
Hermanson, A., C.-J. Dalsgaard, C. Arnander, U. Lindblom: Sensib- ility and cutaneous reinnervation in free flaps. Plast. Reconstr. Surg. 79 (1987) 422
Lance, J. W., J. G. McLeod: Pain and other sensations. In: Lance, J.W., J.G. McLeod (eds): A physiological approach to clinical neurology. 3rd ed., Butterworths, London 1981, 1
Magee, W, P., D.A. Gilbert, W.D. McInnis: Extended muscle and musculocutaneous flaps. Clin. Plast. Surg. 7 (1980) 57
Manni, J.J., I. Bruaset: Reconstruction of the anterior oral cavity using the platysma myocutaneous island flap. Laryngoscope 96 (1986) 564
Moloy, P.J., F.E. Gonzales: Vascular anatomy of the pectoralis ma- jor myocutaneous flap. Otolaryngol. Head Neck Surg. 112 (1986) 66
Monnier, M., M. Fallert, M. Meulers, R. Tissot: Principles of general sensory physiology. In: Monnier, M. (ed.): Functions of the ner- vous system, vol 3: Sensory functions and perception. Elsevier, Amsterdam (1975) 3
Nicolai, J.-P., I. Bruaset, J.J. Manni: Experience with myocutaneous
island flaps of the pectoralis major muscle for reconstruction of defects in the bucco-pharyngeal cavity. Neth.J. Surg. 35 (1983) 1
Truex, R.C., M.B. Carpenter: Segmental and peripheral innerva- tion. In: Truex, R. C., M.B. Carpenter (eds.): Human Neuroana- tomy. 6th ed., Williams and Will(ins, Baltimore 1969, 194
Wanner, P.-A.: Die Sensibilit~it der Unterlippe nach Durchtrennung des Nervus mentalis oder Nervus mandibularis. Thesis, University of Z~rich (1979)
Waris, T., L. Rechardt, K. Ky6sola: Reinnervation of human skin grafts: a histochemical study. Plast. Reconstr. Surg. 72 (1983) 439
Withers, H.W., J.D. Franklin, J.J. Madden, J.B. Lynch: Pectoralis major myocutaneous flap: a new flap in head and neck reconstruc- tion. Am.J. Surg. 138 (1979) 537
Th. J. M. Hoppenreijs, D.M.D. Afdeling Mond-en Kaakchirurgie Academic Hospital Postbus 9101 NL-6500 FIB Nijmegen The Netherlands





























