Embed Size (px)
Citation preview

Chapter 32
Severe Epistaxis: Micro-endoscopic Surgical Techniques ALDO CASSOL STAMM, GLAURA FERREIRA, JOAO A. CALDAS NAVARRO, and LUIZ A.S. FREIRE
Introduction
Epistaxis is a frequent emergency in medical practice. Approximately 10% of the normal population has suffered at least one significant episode of nasal bleeding [5]. In most cases, the bleeding is anterior (90%), from the anterior portion of the nasal septum (Little's area, or Kiesselbach's plexus), and the diagnosis is made by anterior rhinoscopy. It is stopped by local chemical cautery, electrocautery or anterior packing with gauze or other agents.
Different methods of treatment are usually necessary for severe epistaxis. The classical treatment is anteroposterior nasal packing using different materials, such as gauze, a Foley catheter, inflatable nasal packs, a sponge, Avitene or Merocel, depending on the physician's experience. Alternative treatments include pterygopalatine-fossa injection, septoplasty, posterior endoscopic cautery, vessel ligation and angiography with selective embolization.
In our department, surgery is used to manage posterior epistaxis unresponsive to conservative treatment, including properly placed packs. To be effective, surgical management of epistaxis requires precise identification of the bleeding sites and adequate knowledge of the vascular anatomy of the nose.
Anatomic Features of the Nasal Blood Supply
The sources of the nasal blood supply are the branches of the internal and external carotid arteries (ECAs). The anterior and posterior ethmoidal arteries, both of which are branches of the ophthalmic artery of the internal carotid system, provide blood to the nasal bones, septal cartilage, roof of the nose, nasal areas related to the pituitary region and the lateral and medial superior nasal mucosa. The nasal blood supply from the external carotid-artery system is provided by two terminal branches of the
maxillary artery: the posterior lateral nasal artery and the septal artery [21, 23].
The anterior ethmoidal artery leaves the orbit by passing through the anterior ethmoidal canal to reach the area adjacent to the cribriform plate [17] near the crista galli, where it turns inferiorly to supply the middle and anterior ethmoid cells, the infundibulum of the frontal sinus, the anterior nasal cavity (septum and lateral walls) and the skin over the cartilaginous part of the nose. The posterior ethmoidal artery passes through the posterior ethmoidal canal to the region of the cribriform plate and has branches that descend to the posterior upper part of the nasal cavity. There is anastomosis between the ethmoidal arteries and the septal and lateral posterior nasal arteries and between both ethmoidal arteries. The posterior ethmoidal artery is 4-7 mm anterior to the optic nerve (Fig. 32.1) [18].
The maxillary artery is one of the two terminal branches of the ECA. It arises behind the neck of the mandible and is divided into three parts: the mandibular portion (between the mandibular neck and the sphenomandibular ligament), the pterygoid portion (which passes in an upward and forward direction lateral and medial to the lateral pterygoid muscle) and the pterygopalatine portion (which passes into the homonymous fossa) [23]. Branches from the first division supply the tympanic membrane, the auricle, the temporomandibular joint, the mandible, the teeth and the dura. Branches from the second division supply the masticatory muscles and, close to the tuberosity of the maxilla, the artery gives rise to the superior and inferior alveolar branches, the infraorbital branches and the descending palatine branches. After a short medial course, the maxillary artery enters the pterygopalatine fossa, where its third division is located (Fig. 32.2). The third division gives rise to orbital branches, branches to the foramen rotundum, and the pterygopalatine canal (Boeck's canal). Passing medially through the fossa, the third division splits into the posterior lateral nasal artery and the posterior septal artery, both entering the nasal cavity through the sphenopalatine
32
A. C. Stamm et al. (eds.), Micro-endoscopic Surgery of the Paranasal Sinuses and the Skull Base© Springer-Verlag Berlin Heidelberg 2000

394 ALDo CASSOL STAMM et al.
it
Fig. 32.1 a,b. Intracranial view of the anterior and posterior ethmoidal arteries running through the ethmoidal roof and cribriform plate. a Schematic drawing. b Anatomic dissection. AEA, anterior ethmoidal artery; ETC, ethmoid cells; FN, frontal nerve; lCA, internal carotid artery; OA, ophthalmic artery; ON, optic nerve; PEA, posterior ethmoidal artery
foramen, just above the caudal, bony end of the middIe turbinate. In 6.6% of the cases, Navarro et al. [21] describe an accessory foramen (located a little superior the sphenopalatine foramen) through which a branch of the posterior lateral nasal artery enters the
Fig. 32.2. The maxillary artery at the tuberosity of the maxilla. 1, Maxillary artery; 2, infraorbital/posterosuperior alveolar branch; 3, infraorbital artery; 4, posterosuperior alveolar artery; 5, descending palatine artery; 6, maxillary nerve; 7, posterosuperior alveolar nerve
nasal cavity. The septal artery passes through the sphenopalatine foramen and courses along the roof of the nasal cavity toward the sphenoid rostrum and divides into a number of vessels that extend to the septum and the superior nasal walls. The posterior lateral nasal artery splits in the lateral wall of the nasal cavity, thus providing arterial supply to the turbinates and meatal spaces (primarily the middle and the inferior meati; Fig. 32.3).
The descending palatine artery, as a terminal buccal branch of the maxillary artery, courses between the middle, posterior and anterior walls of the fossa, divides into major and minor branches (which enter their respective canals) and reaches the buccal cavity through the homonymous foramen. The greater palatine artery courses through the palate to the incisive foramen, where it joins the nasopalatine artery, which comes from the septum. Anastomosis between the contralateral branches of these arteries can occur.
The anterior and inferior septa are supplied by the superior labial branch of the facial artery. An area of multiple arterial anastomosis of the three sources of vascular supply to the nose is found superficially in

Fig. 32.3. Lateral nasal wall, demonstrating the terminal branches of the maxillary artery. The posterior lateral nasal artery and the septal artery are identified close to the sphenopalatine foramen. IT, inferior turbinate; MT, middle turbinate; S, nasal septum
the anterior nasal septum (Kiesselbach's plexus or Little's area). This area is responsible for most anterior nosebleeds.
Classification of Epistaxis
Epistaxis can be classified according to its location or its etiology. According to Montgomery [IS], epistaxis is best classified according to its location: anterior, superior or posterior. Anterior bleeding occurs in Kisselbach's plexus (or Little's area) from a branch of the anterior ethmoidal artery, the septal branch of the superior labial artery, the septal branch of the maxillary artery and/or the nasal branch of the greater palatine artery. Superior bleeding occurs from either the anterior and/or posterior ethmoidal arteries or the septal artery, a branch of the maxillary artery. Posterior bleeding occurs from either the posterior lateral nasal artery or the septal arteries, both branches of the maxillary artery.
There are many different causes of epistaxis, and they can be divided into four groups, according to Younkers et al. [39]: (1) local causes, (2) causes associated with neoplastic disorders, (3) causes associated with hematological disorders and (4) other causes. Local causes include nasal allergy, trauma, infection, ulcers, nasal surgery, intranasal medications, nose-picking habits and foreign-body reactions. Epistaxis-associated with neoplasms include mainly angiofibroma and malignant tumors. Epistaxis associated with primary hematological disorders include leukemia, anemia, purpura, polycytemia, hemophilia, lymphoma and Hodgkin's disease. Other causes include hypertension, smoking, familial telangiecta-
Severe Epistaxis: Micro-endoscopic Surgical Techniques 395
sia, liver disorders, chronic nephritis, sudden atmospheric-pressure changes, psychopathies and medications, such as aspirin or chemotherapeutic agents.
Treatment of Severe Epistaxis
Several modalities of treatment have been proposed to control epistaxis. Their use is based mainly on the location and etiology of the bleeding and on the physician's experience (Table 32.1).
During the initial evaluation, a brief history must be collected while initial measures to control the bleeding are taken. The examination of the nasal cavity requires a good source of illumination (headlight or telescopes), an appropriate nasal speculum and strong suction. It is best done using topical anesthesia containing a vasoconstrictor. This examination is of prime importance in order to locate the bleeding site and to choose the most appropriate treatment. In case of anterior nasal bleeding, anterior nasal packing and/or chemical cautery or direct electrocautery of the bleeding site are the usual procedures. Severe nasal bleeding of posterior, posterosuperior or superior origin requires posterior nasal packing (gauze, inflatable nasal packs, sponge or other packing; Fig. 32.4). The use of antibiotics is advisable, because the impaired sinus drainage caused by the pack can lead to sinus infection. The packing remains in place for 4S-72 h. Many patients with an anterior-posterior packing require hospitalization, consultation with an internist and hematological evaluation. Because of the risk of sedation with posterior packing, only cautious use of sedatives and analgesics is advisable.
Nasal packing can produce local, regional and general complications. The most common general complication is the modification of arterial p02 and peoz' leading to serious hypoxemia and hemodynamic changes in patients with decreased cardiopulmonary reserves [4, S, 22, 35]. Sleep apnea can occur as a complication of nasal packing [36].
One of the principallocallregional complications is sinusitis, occurring because of the impairment of drainage of the paranasal sinuses [16]. Swallowing problems, aspiration, septal perforation, tubal obstruction, alar necrosis, sepsis and secretory otitis media have all been described [S, 16,35,37].
Inflatable nasal packs are easy to place, both for the patient and the physician, compared with conventional posterior packs. The inflatable pack consists of two balloons of different sizes. The smaller of them, which has a volume of 10 ml, is placed at the level of the choana. The second is bigger and oblong shaped and has a volume of 30 ml; it is placed inside the nasal cavity. Once positioned
396 ALDo CASSOL STAMM et al.
Table 32.1. Severe epistaxis: topographic diagnosis and surgical treatment
--
Origin Arterial system Surgical treatment
Anterior Branches of anterior ethmoidal artery, septal branch of the superior labial artery, septal branch of the maxillary artery and nasal branch of the greater palatine artery
Cauterization (chemical or electrical) SeptopJasty Dermoplasty
Superior
Posterior
Anterior and posterior ethmoidal arteries
Posterior lateral nasal and septal arteries (branches of the maxillary artery)
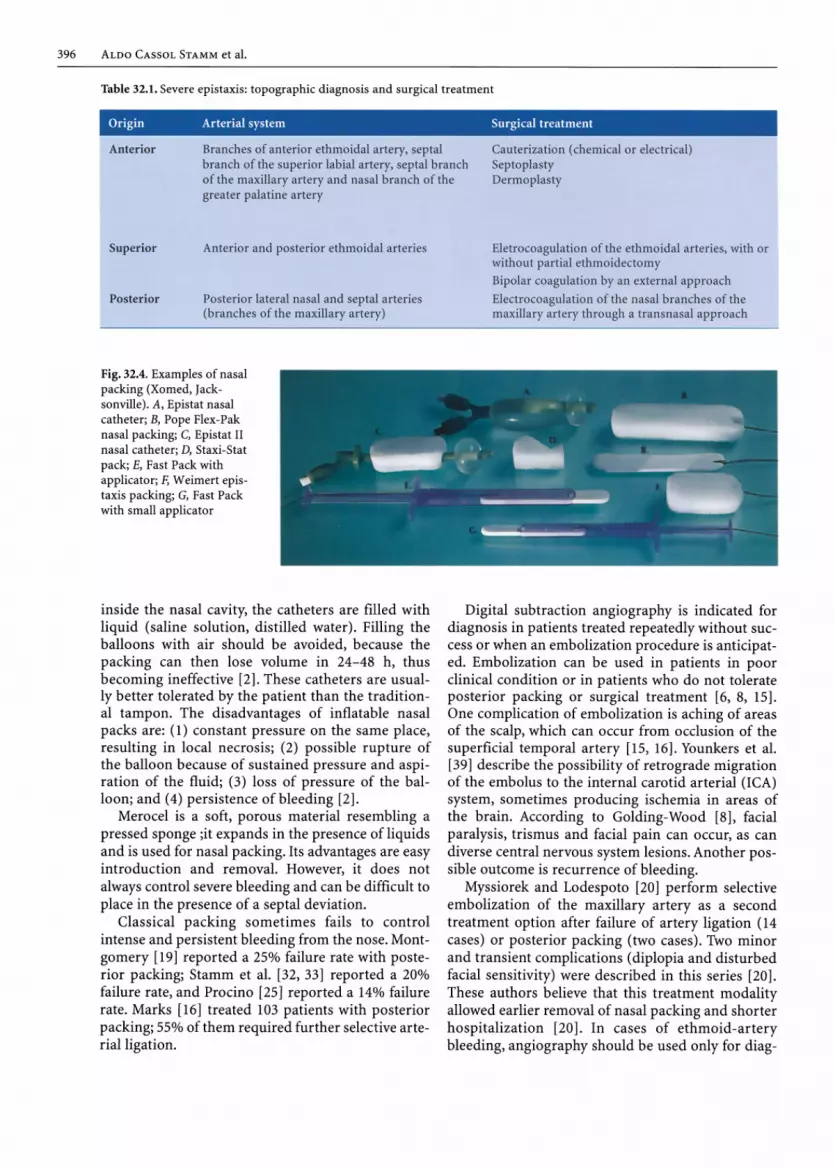
Fig. 32.4. Examples of nasal packing (Xomed, Jacksonville). A, Epistat nasal catheter; B, Pope Flex-Pak nasal packing; C, Epistat II nasal catheter; D, Staxi-Stat pack; E, Fast Pack with applicator; F, Weimert epistaxis packing; G, Fast Pack with small applicator
inside the nasal cavity, the catheters are filled with liquid (saline solution, distilled water). Filling the balloons with air should be avoided, because the packing can then lose volume in 24-48 h, thus becoming ineffective [2]. These catheters are usually better tolerated by the patient than the traditional tampon. The disadvantages of inflatable nasal packs are: (1) constant pressure on the same place, resulting in local necrosis; (2) possible rupture of the balloon because of sustained pressure and aspiration of the fluid; (3) loss of pressure of the balloon; and (4) persistence of bleeding [2].
Merocel is a soft, porous material resembling a pressed sponge ;it expands in the presence of liquids and is used for nasal packing. Its advantages are easy introduction and removal. However, it does not always control severe bleeding and can be difficult to place in the presence of a septal deviation.
Classical packing sometimes fails to control intense and persistent bleeding from the nose. Montgomery [19] reported a 25% failure rate with posterior packing; Stamm et al. [32, 33] reported a 20% failure rate, and Procino [25] reported a 14% failure rate. Marks [16] treated 103 patients with posterior packing; 55% of them required further selective arterial ligation.
Eletrocoagulalion of the ethmoidal arteries, with or without partial ethmoidectomy Bipolar coagulation by an external approach
Electrocoagulation of the nasal branches of the maxillary artery through a transnasal approach
Digital subtraction angiography is indicated for diagnosis in patients treated repeatedly without success or when an embolization procedure is anticipated. Embolization can be used in patients in poor clinical condition or in patients who do not tolerate posterior packing or surgical treatment [6, 8, 15] . One complication of embolization is aching of areas of the scalp, which can occur from occlusion of the superficial temporal artery [15, 16]. Younkers et al. [39] describe the possibility of retrograde migration of the embolus to the internal carotid arterial (lCA) system, sometimes producing ischemia in areas of the brain. According to Golding-Wood [8], facial paralysis, trismus and facial pain can occur, as can diverse central nervous system lesions. Another possible outcome is recurrence of bleeding.
Myssiorek and Lodespoto [20] perform selective embolization of the maxillary artery as a second treatment option after failure of artery ligation (14 cases) or posterior packing (two cases). Two minor and transient complications (diplopia and disturbed facial sensitivity) were described in this series [20]. These authors believe that this treatment modality allowed earlier removal of nasal packing and shorter hospitalization [20]. In cases of ethmoid-artery bleeding, angiography should be used only for diag-

nostic purposes because of the high risk of ophthalmic complications from embolization [1,20].
Pterygopalatine-fossa injection of vasoconstrictor substances through the greater palatine foramen has also been advocated as a method for the treatment of epistaxis [15]. This injection can result in infraorbital anesthesia, visual losses of variable extent and recurrence of bleeding after dissipation of the vasoconstrictor. The use of cryosurgery [15] at the site of bleeding is a secondary option because, although it can be effective when performed by experienced surgeons, it can also lead to crust formation and atrophic rhinitis. Septoplasty can be used to control recurrent bleeding from the nasal septum. Septal dermoplasty is considered for the treatment of familial telangiectasia [15,27].
Arterial ligation is indicated when non-surgical methods of treatment fail [32-34, 37], especially when nasal bleeding persists or recurs after properly placed nasal packing. Montgomery [18] advocates early surgical intervention for epistaxis [26]. Maris and Werth [15] propose some general principles for the surgical treatment of epistaxis. 1. Patients in poor clinical condition who have pul
monary or cardiovascular problems or disorders of the central nervous system should not be treated with nasal tamponade. Early vessel ligation is indicated in these cases.
2. Young patients should be treated with conservative measures, with vessel ligation indicated only in cases of failure.
3. Packing is preferred in children because of the size of the nasal cavities and maxillary sinus.
According to Small and Maran [29], surgical treatment should not be delayed for a long time. The morbidity of vessel ligation is not much greater than that of posterior nasal packing and causes less discomfort.
External carotid-artery ligation was used by Hide [12] for the treatment of epistaxis, but now the use of the microscope, endoscope and other technological improvements has displaced it, especially because of the frequency of anastomosis between the ECA and ICA systems and the distance between the site of bleeding and the location of the ligature, which severely reduces its effectiveness [15,17].
Transmaxillary ligation of the maxillary artery in the zygomatic fossa is frequently effective in controlling bleeding arising from nasal branches [19,31]. Using the surgical microscope, the artery is dissected in the zygomatic fossa close to the tuberosity of the maxilla. Difficulty identifying the artery and all its branches is usually due to poor technique [21, 37], but there is also considerable variation in the number and size of the branches arising from the maxil-
Severe Epistaxis: Micro-endoscopic Surgical Techniques 397
lary artery [25,37]. This can result in an ineffective ligation and persistence of bleeding [8,29]. Complications have included oro antral fistula and hemifacial anesthesia [19], and the method itself sometimes fails to control bleeding. This technique was initially proposed by Seiffert in 1928 [26] and was improved by Chandler and Serrins in 1965 [3]; Montgomery [18,19] deserves credit for its popularization in 1980. Macery, in 1984 [14], proposed the transoralligation of the maxillary artery in the zygomatic region without opening the maxillary sinus. Postoperative trismus, dental or facial dysesthesia and the distance between the ligature and the bleeding point are disadvantages of this method.
As implied by the etymological meaning of the word epistaxis (bleeding that comes from above) bleeding can originate in the ethmoid arterial system and, although less frequent, can be remarkably severe and impressive [8,10, 11]. According to Golding-Wood [8], ethmoidal bleeding occurs most often in young people following trauma to the face. The external ligation of the anterior ethmoidal artery and septal artery, as recommended by Silverblatt [28] in 1955, appeared to be effective in controlling epistaxis but did not gain popular favor because of technical difficulties. External ligation can result in permanent or transient loss of vision because of the close relationship of the posterior ethmoidal canal and the optic canal (3-8 mm) [7]; it can also lead to diplopia [4, 16]. These complications are uncommon, and an external approach using a surgical microscope is an excellent approach to the ethmoidal artery, with a high rate of success [34]. Snyderman and Carrau [30] performed simultaneous ligation of the anterior ethmoid and sphenopalatine arteries in 67% of their patients due to difficulty localizing the site of bleeding.
Heermann (1986) [10,11] reported treating all his patients with severe epistaxis by monopolar electrocoagulation of the anterior and posterior ethmoidal arteries in their osseous canals in the roof of the ethmoid sinus, using a microscopic intranasal approach. The most significant problem of the intranasal arterial electrocoagulation is the possibility of a CSF fistula when cautery is applied to the interior of the ethmoidal canals because the surgeon does not properly identify the vessels [10, 11, 34].
Intranasal electrocoagulation of the nasal branches of the maxillary artery, combined with bipolar electrocoagulation of the anterior and posterior ethmoidal arteries (with or without partial ethmoidectomy using an operating microscope or endoscopes) appears to be an effective method for the treatment of severe epistaxis [9-11, 13, 22, 30, 32-34, 38]. Advantages of this method are the proximity of the arterial ligation and the bleeding site, and direct

398 ALDO CAS SOL STAMM et al.
visualization of the involved vessels [5, 10, 11, 13, 32-34, 38]. Associated disorders, such as polyps, sinusitis, septal deformity and tumors can be treated with the same approach.
Nasal endoscopy can also be used in the treatment of posterior epistaxis. Authors using nasal endoscopy as an adjunct report a success rate between 82% and 90%, depending on the surgeon's experience [5,24,30,38]. Sedation and the use of topical anesthesia are advised. The patient should be in a semi-recumbent position with the head elevated, allowing visualization of the bleeding point without the use of a vasoconstrictor. After identifying the bleeding site, local vasoconstriction and local and regional anesthesia must be used. Wurman [38] rec;ommends this procedure, using 4-mm-diameter endoscopes of 0° and 30°. Prechamandra, using the endoscope [24], places small nasal packs at the bleeding area, in addition to using local electrocautery or chemical cautery. Snyderman and Carrau [30], using a transnasal endoscopic technique, approached the sphenopalatine foramen. Resecting the anterior inferior portion of the middle turbinate can also be performed to maximize surgical access to the middle meatus. A large middle-meatus antrostomy is created, and the sphenopalatine foramen (with its artery) are identified. The terminal branches of the maxillary artery are dissected and may be coagulated or ligated.
Transnasal Micro-Endoscopic Electrocoagulation of the Nasal Branches of the Maxillary Artery
The surgery can be performed with either the operating microscope or endoscopes using general anesthesia. The patient is placed in a supine position, with the dorsum elevated approximately 30°.
The nasal cavity is prepared with cottonoids soaked with a vasoconstrictor solution to reduce the bleeding and the size of the turbinates. The middle turbinate is fractured toward the nasal septum very carefully in order to avoid damaging its arterial supply. When the operating microscope is used, a number-two self-retaining speculum is placed to maintain good exposure of the surgical field. Usually the surgery is done with a 4-mm, 0° endoscope attached to a video camera system. The caudal end of the middle turbinate is an important anatomic landmark because of its close relationship with the sphenopalatine foramen, through which the nasal branches of the maxillary artery arise. Another landmark is the posterior wall of the maxillary sinus. Using micro cautery or a microknife, a vertical inci-
sion is made approximately 1 cm anterior to the caudal end of the middle turbinate through the mucosa and periostium (Fig. 32.5). A mucoperiosteal flap is elevated until the edges of the sphenopalatine foramen are exposed, identifying the posterior lateral nasal artery and the septal artery, which arise from the maxillary artery and enter the nasal cavity from the pterygopalatine fossa (Fig. 32.6). Once identified, both arterial branches are isolated by blunt dissection and are coagulated with a monopolar or bipolar
Fig. 32.5. Location of the incision at the middle meatus (mucosa and periosteum), approximately 1 cm anterior to the caudal end of the middle turbinate. A Self-retaining speculum number two in place, exposing the middle meatus and prechoanal area. B Endoscopic view
Fig. 32.6. The sphenopalatine foramen and its arteries after elevation of the mucoperiosteal flap. A Lateral view of the surgical procedure, as provided by a self-retaining speculum and operating microscope. B Endoscopic view of the surgical field

system (Fig. 32.7) as far from the edges of the foramen as possible (to avoid any possible retraction of the proximal segment into the pterygopalatine fossa; Fig. 32.8). At the end of the procedure, the mucoperiostial flap is replaced and packed in place with pieces of Gelfoam or Surgicel. The packing also minimizes oozing from the surgical area. The middle and inferior turbinates are replaced, and loose gauze packing inside a glove finger or a Merocel pack is placed into the nose for 24 h to prevent any minor bleeding caused by surgical manipulation. When it is necessary to ligate the terminal branches of the maxillary artery by the trans nasal, transmaxillary
Fig. 32.7. Electrically shielded monopolar cauteries. A, Plain. E, Alligator forceps handle
Fig. 32.8. Terminal branches of the maxillary artery arising from the sphenopalatine foramen and being coagulated separately with monopolar forceps under endoscopic control. IT, inferior turbinate; MT, middle turbinate; PLNA, posterior lateral nasal artery; SA, septal artery
Severe Epistaxis: Micro-endoscopic Surgical Techniques 399
approach, it is desirable to make a wide middle-meatus antrostomy to help identify the sphenopalatine foramen (Fig. 32.9A). A Kerrison punch is then inserted into the sphenopalatine foramen to remove the bone of the posterior wall of the maxillary sinus (Fig. 32.9B). Finally, the maxillary artery and its branches are identified, individually isolated and bipolarly electro coagulated or clipped (Fig. 32.9C).
Transnasal Microendoscopic Electrocoagulation of the Anterior and Posterior Ethmoidal Arteries
The nasal cavity is prepared with a vasoconstrictor solution, as described above. The patient is placed in a supine position, and the head is hyperextended in order to have the ethmoidal complex in a plane parallel to the light from the microscope. Using a selfretaining, properly placed speculum, the surgical microscope and continuous aspiration, the bleeding point is identified at the confluence of the roof of the nose and the superior portion of the septum. This technique can also be performed using endoscopes (mostly 0°, 4-mm-diameter endoscopes).
Anterosuperior bleeding comes from the lateral and medial branches of the anterior ethmoidal artery or from a branch of the posterior ethmoidal

400 ALDo CASSOL STAMM et al.
Fig. 32.9 a-c. Endoscopic, trans nasal, trans maxillary eletrocoagulation of the maxillary artery after a wide middle-meatus antrostomy. a Identification of the sphenopalatine foramen and its arteries. b Enlargement of the sphenopalatine foramen toward the posterior maxillary-sinus wall. c Coagulation of the maxillary artery
artery. Posterosuperior bleeding comes from branches of the posterior ethmoidal artery or the septal artery. Posterosuperior bleeding from both arterial systems (internal and external carotid) is controlled by direct coagulation of the bleeding point and the surrounding nasal mucosa (Fig. 32.10).
If there is any persistence of bleeding after this procedure, coagulation of the ethmoidal arteries should be performed at the level of their osseous canals in the roof of the ethmoid sinus, by approaching them through a transnasal partial ethmoidectomy. To perform the trans ethmoidal approach, the uncinate process and the ethmoidal bulla are identified and removed to gain complete exposure of the ethmoidal complex. The ethmoidectomy is performed until the level of the floor of the anterior cranial fossa and the ethmoidal canals is reached. The next step is coagulation of the arteries when they emerge from their canals (Fig. 32.11). Bipolar coagu-
Fig. 32.10. a Eletrocoagulation, with endoscopic assistance, of the branches of the anterior ethmoidal artery (AEA) located at the junction of the upper septum and the roof of the nose. PEA, posterior ethmoidal artery; 55, sphenoid sinus. b Arterial supply of the nasal septum

AEA
Severe Epistaxis: Micro-endoscopic Surgical Techniques 401
lation is used, if possible. Pieces of Gelfoam or Surgicel are placed close to the area. At the time of coagulation of the ethmoidal arteries, the introduction of electrocautery deep in the canals must be avoided to prevent the development of a CSF fistula [10, 11, 33].
Microsurgical External Electrocoagulation of the Anterior and Posterior Ethmoidal Arteries
When bleeding from the ethmoidal arteries system cannot be controlled trans nasally, the use of the external approach under a surgical microscope is necessary. An incision is made close to the inner canthus, similar to that for an external ethmoidectomy. A subperiostial dissection of the orbital contents from the internal osseous wall is performed until reaching the level of the fronto-ethmoidal junction, where the anterior ethmoidal artery can be found and coagulated with a bipolar system after adequate dissection and isolation of the vessel (Fig. 32.12). To keep the orbital contents away from the soft tissues of the inner canthus and the nose, a Stamm selfretaining retractor, which has a blade on one side and a hook on the other side, is used (Fig. 32.13).
To coagulate the posterior ethmoidal artery, the elevation of the soft tissues of the orbit is continued posteriorly for approximately 1 cm. The close relationship of the posterior ethmoidal artery to the optic nerve (4-7 mm) should be recalled during the bipolar electrocoagulation of this vessel. As a practical landmark, the "two-one-one half rule" is useful; the anterior ethmoidal artery is found approximately 2 cm posterior to the skin incision, the posterior ethmoidal artery is found 1 cm behind the anterior, and the optic nerve is 0.5 cm from the posterior ethmoidal artery.
Results and Complications
Between 1985-1999,173 patients were treated surgically to control severe epistaxis. The techniques consisted of selective microscopic or endoscopic electrocoagulation of the nasal branches of the maxillary
Fig. 32.11 a,b. Electrocoagulation of the anterior ethmoidal artery (ABA) after an ethmoidectomy. a Performed with an operating microscope, self-retaining speculum and plain monopolar cautery. b Performed with an endoscope and monopolar-forceps-type cautery. MT, middle turbinate

402 ALDO CASSOL STAMM et al.
Fig. 32.12. External approach for bipolar coagulation of the anterior ethmoidal artery (AEA)
Fig. 32.13. Stamm's self-retaining retractor with two arms, a blade in one side and a hook in the other side
artery transnasally or monopolar or bipolar electrocoagulation of the ethmoidal arteries through an intranasal or external approach (Table 32.2)"
Because of an error in the topodiagnosis of the bleeding sites, failure to control the bleeding occurred in six patients (3.4%) during the immediate postoperative period. Failure also occurred during the late postoperative period in four patients (2.3%) because of inadequate surgery (one of the terminal branches of the maxillary artery was not coagulated).
Complications have been infrequent and were usually related to either failure in the localization of the site of bleeding or inadequate surgical technique
[33,34]. According to Legent et al. [13], satisfactory results were obtained with intranasal ligation of branches of the maxillary artery alone in 30 patients, and only eight patients required ligation treatment of the ethmoidal arteries. Snyderman and Carrau [30] had recurrences of epistaxis after transnasal endoscopic ligation of the terminal branches of the maxillary artery in 13% of their cases.
Adhesion between the middle turbinate and the lateral nasal wall or nasal septum, transient or permanent unilateral hyposmia or anosmia, crust formation and local infection are complications related to surgical trauma or extensive coagulation of the nasal mucosa. Orbital ecchymosis and edema were the most common complications of the external approach to anterior and posterior ethmoidal-artery ligation.
Conclusions
The results of surgical treatment for severe epistaxis by intranasal micro-endoscopic ligation of the nasal branches of the maxillary artery and/or intranasal or external ligation of the ethmoid arteries lead to the following considerations: 1. Micro-endoscopic surgical technique results in
minimal surgical trauma, decreased surgical time and morbidity and improved visualization.
2. Electrocoagulation of the main nasal branches of the maxillary arteries must be selective, thus avoiding the development of collateral circulation.
3. Electrocoagulation of the ethmoidal arteries must be performed at the sites of bleeding into the nasal cavity.
4. Bipolar coagulation of the ethmoidal arteries through an external approach using a surgical microscope is effective in controlling severe epistaxis.
5. The surgical treatment of severe epistaxis can result in shorter hospitalization time, is well tolerated by patients and can also be performed in children.
References
1. Breda SD, Choi IS, Persky MS, Weiss M (1989) Embolization in the treatment of epistaxis after failure of internal maxillary artery ligation. Laryngoscope 99:809-813
2. Cannon RC (1993) Effective treatment protocol for posterior epistaxis. A lO-year experience. Otolaryngol Head Neck Surg 109:722-725
3. Chandler JR, Serrins AI (1965) Transantralligation of the internal maxillary artery. Laryngoscope 75:151-159

Severe Epistaxis: Micro-endoscopic Surgical Techniques 403
Table 32.2. Distribution of patients with severe epistaxis by the involved arteries and surgical approach (n= 173)
Arterial supply Surgical approach Number Percentage
Maxillary-artery branches/ethmoid arteries Intranasal/external 92 53 Maxillary-artery branches/ethmoid arteries r ntranasalfin tranasal 38 22
Maxillary-artery branches only Intranasal 27 16
Ethmoid arteries External 10 6
Ethmoid arteries Intranasal 6 3
4. Cooke ETM (1985) An evaluation and clinical study of severe epistaxis treated by artery ligation. J Laryngol Otol 99:745-749
5. EI-Silimy 0 (1993) Endonasal endoscopy and posterior epistaxis. Rhinology 31:119-120
6. Felker CE III (1981) Angiography and embolization of epistaxis. Ear Nose Throat J 60:57
7. Friedman WH, Rosenblum BN (1987) Epistaxis. In: Goldman JL (ed) The principles and practice of rhinology. Wiley, New York, pp 375-383
8. Golding-Wood PH (1983) The role of arterial ligation in intractable epistaxis. J Laryngol Otol SuppI8:120-122
9. Heermann H (1958) Endonasal surgery with the use of the binocular Zeiss operating microscope. Arch Klin Exp Ohren Nasen Kehlkopfheilkd 171:295-297
10. Heermann, J (1986) Intranasales mikrochirurgikes vorgehen bei epistaxis der riechspalte und weitere eingreffe mit hypotension. HNO 34:208-215
11. Heermann I, Neues D (1986) Intranasal microsurgery of all paranasal sinuses, the septum, and the lacrimal sac with hypotensive anesthesia. Ann Otol Rhinol Laryngol 35:631-638
12. Hide FT (1925) Ligation of the external carotid artery for control of idiopathic nasal bleeding. Laryngoscope 35:899
13. Legent F, Boutet JJ, Wesolouch, Viale M, Galiba I, Beauvillain C (1986) Treatment chirurgical des epistaxis interet de la micro-chirurgie endo-nasale. Rev Laryngol Otol Rhinol (Bord) 107:31-33
14. Maceri DR, Makielski KH, Arbor A (1984) Intranasalligation of the maxillary artery for posterior epistaxis. Laryngoscope 94:734-741
15. Maris, C; Werth, JL (1981) Surgical management of epistaxis. Ear, Nose Throat J 60:463-466
16. Marks HW (1980) Complications of posterior epistaxis. Ear Nose Throat J 59:39-42
17. Mercurio GA Jr (1981) Anatomic considerations of nasal blood supply. Ear Nose Throat J 60:443-446
18. Montgomery WW (1979) Surgery of the upper respiratory system, 2nd edn. Lea and Febiger, Bostin, p 321
19. Montgomery WW, Reardon EJ (1980) Early vessel ligation of control of severe epistrucis. In: Snow JB (ed) Controversy in otolaryngology. Saunders, Philadelphia, pp 315-319
20. Myssiorek D, Lodespoto M (1993) Embolization of posterior epistaxis. Am J Rhinol 7:223-226
21. Navarro JAC, Toledo Filho JL, Zorzetto NL (1982) Anatomy of the maxillary artery into the pterygomaxillopalatine fossa. Anat Anz 152:413-433
22. Nicolaides A, Gray R, Pfleiderer A (1991) A new approach to the management of acute epistaxis. Clin Otolaryngol 16:59-61
23.0'Rahilly R (1978) Anatomia de cabec;:a e pescoc;:o. In: Gardner E (ed) Anatomia. Guanabara-Koogan, Rio de Janeiro, pp 656-658
24. Prechamandra DJ (1991) Management of posterior epistaxis with the use of fiberoptic nasolaryngoscope. J LaryngoIOtoI105:17-19
25. Procino ND (1978) Treatment of the posterior epistaxis. Ear Nose Throat J 57:305-308
26. Seiffert A (1928) Under bindung der arteria maxillaris interna. Z HNO 22:323-325
27. Sherrerd PS, Teet TJ (1981) Diagnosis and management of less common causes of epistaxis. Ear Nose Throat J 60:59-66
28. Silverblatt BL (1955) Epistaxis. Evaluation of surgical care. Laryngoscope 65:431
29. Small M, Maran AG (1984) Epistaxis and arterial ligation. J Laryngol Otol 98:281-284
30. Snyderman CH, Carrau RL (1997) Endoscopic ligation of the sphenophalatine artery for epistaxis. Operative Tech Otolaryngol Head Neck Surg 8:85-89
31. Spafford P, Durham JS (1992) Epistaxis: efficacy of arterial ligation and long-term outcome. J OtolaryngoI21:252-256
32. Stamm AC, Pinto JA, Neto AF, Menon AD (1985) Microsurgery in severe posterior epistaxis. Rhinology 23:321-532
33. Stamm AC, Ferreira GMP, Navarro JAC (1988) Microcirurgia transnasal no tratamento da epistaxe severa. Fed Med (Bras) 96:315-322
34. Stamm AC, Ferreira GMP, Navarro JAC (1995) Epistaxe severa - microcirurgia trans nasal. In: Stamm AC (ed) Microcirurgia naso-sinusal. Revinter, Rio de Janeiro, pp 289-297
35. Stemm RA (1981) Complications of nasal packing. Ear Nose Throat J 60:45-46
36. Vaartjes M, Striges RLM, Devries N (1992) Posterior nasal packing and sleep apnea. Am J RhinoI6:71-74
37. Ward PH (1980) Routine ligation of the internal maxillary artery is unwarranted. In: Snow JB (ed) Controversy in otolaryngology. Saunders, Philadelphia, pp 320-326
38. Wurman LH, Garry-Sack I, Flannery JV, Paulson 0 (1988) Selective endoscopic eletrocautery for posterior epistaxis. Laryngoscope 98: 1348-1349
39. Younkers AI, Glessman TM, Mercurio GA Jr, Werth JL, Blattner RE (1981) Etiology and management of epistaxis. Ear Nose Throat J 60:453-456





























