Embed Size (px)
Citation preview
Sex, drugs and health of men who have sex with men in
Vietnam
Nga Thi Thu Vu
M.D.
A thesis in the fulfilment of the requirements for the degree of
Doctor of Philosophy
Centre for Social Research in Health
Faculty of Arts and Social Sciences
November, 2017
Page| vi
PLEASE TYPETHE UNIVERSITY OF NEW SOUTH WALES
Thesis/Dissertation Sheet
Surname or Family name: VU
First name: NGA THI THU Other name/s:
Abbreviation for degree as given in the University calendar: Ph.D
School: Centre for Social Research in Health Faculty: Arts and Social Sciences
Title: SEX, DRUGS AND HEALTH OF MEN WHO HAVE SEX WITH MEN IN VIETNAM
Abstract 350 words maximum: (PLEASE TYPE)
This thesis assessed patterns of amphetamine-type-stimulants (ATS) use and their association with condomless anal intercourse (CAI), HIV infection and mental health issues, particularly depression, among men who have sex with men (MSM) in Vietnam. The thesis employed a socio-ecological framework with a community-based survey conducted in 2014 in Hanoi and Ho Chi Minh City, Vietnam and a systematic review and meta-analysis of the relationship between ATS use and HIV infection in MSM. A substantial proportion of Vietnamese men (30.4%) had used ATS and 20.3% had used ATS recently. Methamphetamine was the most popular substance. The majority of recent methamphetamine and ecstasy users were classified as moderate to high-risk users, according to WHO guidelines. Methamphetamine use was associated with higher sexual sensation seeking, engagement in recent sex work and the perception that methamphetamine use was popular among other MSM. A high prevalence of CAI with male partners in the last three months (75.7%) was reported. CAI was associated with methamphetamine use before or during sex, higher sexual sensation seeking, and belief in the safety of withdrawal as an HIV prevention strategy. Voluntary HIV tests conducted for 210 men in Hanoi found a moderate HIV prevalence of 6.7%. Men who used methamphetamine before or during sex, who had engaged in sex work and perceived more homosexuality-related stigma were more likely to have an HIV positive test. A sizable proportion of men (11.3%) were classified as having major depression which was associated with ever having used ATS and higher enacted (i.e. experienced) homosexuality-related stigma. The systematic review and meta-analysis demonstrated a significant pooled estimate of ATS use and HIV infection in MSM across longitudinal, case-control and cross-sectional studies, but not for ecstasy use in cross-sectional studies. Methodological shortcomings of current studies of drug use and sexual behaviour were identified. This thesis suggests a comprehensive HIV prevention package, that includes treatment for methamphetamine use, is needed for MSM in Vietnam to address drug use and the risks of HIV at the individual, community and societal levels. Recommendations for further research on drug use and sexual behaviours are suggested, including periodic assessment of ATS use.
Declaration relating to disposition of project thesis/dissertation
I hereby grant to the University of New South Wales or its agents the right to archive and to make available my thesis or dissertation in whole or in part in the University libraries in all forms of media, now or here after known, subject to the provisions of the Copyright Act 1968. I retain all property rights, such as patent rights. I also retain the right to use in future works (such as articles or books) all or part of this thesis or dissertation.
I also authorise University Microfilms to use the 350 word abstract of my thesis in Dissertation Abstracts International (this is applicable to doctoral theses only).
…………………………………………………………… Signature
……………………………………..……………… Witness Signature
……….……………………...…….… Date
The University recognises that there may be exceptional circumstances requiring restrictions on copying or conditions on use. Requests for restriction for a period of up to 2 years must be made in writing. Requests for a longer period of restriction may be considered in exceptional circumstances and require the approval of the Dean of Graduate Research.
FOR OFFICE USE ONLY Date of completion of requirements for Award:
Page| vii
ORIGINALITY STATEMENT
‘I hereby declare that this submission is my own work and to the best of my knowledge, it
contains no materials previously published or written by another person, or substantial
proportion of material which have been accepted for the award of any other degree or diploma
at UNSW or any other educational institution, except where due acknowledgement is made in
the thesis. Any contribution made to the research by others, with whom I have worked at
UNSW or elsewhere, is explicitly acknowledged in the thesis. I also declare that the intellectual
content of this thesis is the product of my own work, except to the extent that assistance from
others in the project’s designs and conception or in style, presentation and linguistic
expression is acknowledged.’
Nga Thi Thu Vu
27th June, 2017
Page| viii
Submission of a doctoral thesis as a series of publications
Publications in this thesis arise from a systematic review and meta-analysis and a
community-based cross-sectional study conducted in two major cities in Vietnam in
late 2014. In recognition of the study’s collaborators’ contributions (and as is typical
with standard journal publications), multiple co-authors are listed.
However, the author of this thesis was primarily responsible for all of these
publications, including leading the work on study design, conducting the data analyses
and preparing the manuscripts. This contribution is recognised by the candidate’s
primary author role on all of these publications. For each publication, all the co-authors
have acknowledged that the author of this thesis was responsible for at least 50% of
the contribution to the paper, and have agreed to the submission of the papers as part
of this doctoral thesis.
Given four publications included in this thesis are from the cross-sectional survey in
Vietnam, the readers are advised that there is some repetition in these publications in
the methods sections, as would be expected in a series of papers from a single study.
Page| ix
COPYRIGHT STATEMENT
‘I hereby grant the University of New South Wales or its agents the right to archive and
to make available my thesis or dissertation in whole or part in the University libraries
in all forms of media, now or here after known, subject to the provisions of the Copyright
Act 1968. I retain all proprietary rights, such as patent rights. I also retain the right to use
in future works (such as articles or books) all or part of this thesis or dissertation.
I also authorise University Microfilms to use the 350 word abstract of my thesis in
Dissertation Abstract International (this is applicable to doctoral theses only).
I have either used no substantial portions of copyright material in my thesis or I have
obtained permission to use copyright material; where permission has notbeen granted
I have applied/will apply for a partial restriction of the digital copy of my thesis or
dissertation.'
Nga Thi Thu Vu
27th June, 2017
Page| x
AUTHENTICITY STATEMENT
‘I certify that the Library deposit digital copy is a direct equivalent of the final officially
approved version of my thesis. No emendation of content has occurred and if there are
any minor variations in formatting, they are the result of the conversion to digital format.’
Nga Thi Thu Vu
27th June, 2017
Page| xi
SUPERVISOR STATEMENT
I hereby certify that the student (Nga Thi Thu Vu) is responsible for at least 50% of the
contribution to all papers included as chapters in this thesis; all co-authors of the published
papers agree to Nga Thi Thu Vu submitting those papers as part of her Doctoral Thesis.
Professor John De Wit
27th June, 2017
Page| xii
Table of contents
Thesis dissertation sheet…………………………………………………………………………i
Originality statement……………………………………………………………………………...ii
Submission of a doctoral thesis as a series of publications………………………………….iii
Copyright statement……………………………………………………………………………..iv
Authenticity statement……………………………………………………………………………v
Supervisor statement…………………………………………………………………………….vi
Thesis abstract…………………………………………………………………………………...ix
Thesis structure…………………………………………………………………………………...x
List of publications and presentations from this thesis………………………………………xiii
List of abbreviations……………………………………………………………………………..xv
List of tables……………………………………………………………………………………..xvi
List of figures…………………………………………………………………………………...xviii
Acknowledgement……………………………………………………………………………...xix
Chapter 1. Introduction and literature review…………………………………………………1
Amphetamine-type-stimulants (ATS)………………………………………………………3
Health vulnerabilities of MSM……………………………………………………………….6
Correlates of health vulnerabilities among MSM………………………………………..11
Sex, drugs use and the HIV epidemic among MSM in Vietnam……………………….21
A socio-ecological approach to studying health and well-being……………………….31
Research questions and study objectives………………………………………………..36
Chapter 2. Methodology of the cross-sectional survey in Vietnam and the systematic
review and meta-anlysis………………………………………………………………………..70
The community-based, cross-sectional survey of MSM in Hanoi and Ho Chi Minh City,
Vietnam……………………………………………………………………………………...71
The systematic review and meta-analysis of the association between ATS use and HIV
infection……………………………………………………………………………………...80
Chapter 3. Amphetamine-type-stimulant use among men who have sex with men (MSM)
in Vietnam: Results from a socio-ecological, community-based study…………………….85
Page| xiii
Chapter 4. The relationship between methamphetamine use, sexual sensation seeking and
condomless anal intercourse among men who have sex with men in Vietnam: results from
a community-based, cross-sectional study……………………………………………………95
Chapter 5. Amphtamine-type-stimulants and HIV infection among men who have sex with
men: implications on HIV research and prevention from a systematic review and meta-
analysis…………………………………………………………………………………………109
Chapter 6. The prevalence and correlates of HIV and undiagnosed infection among men
who have sex with men in Hanoi, Vietnam: findings from a cross-sectional, biobehavioural
study…………………………………………………………………………………………….124
Chapter 7. Amphetamine-type-stimulants (ATS) use and homosexuality-related enacted
stigma are associated with depression among men who have sex with men (MSM) in two
major cities in Vietnam in 2014………………………………………………………………136
Chapter 8. Discussion and Conclusion………………………………………………………147
Key findings………………………………………………………………………………..148
Lessons learned, limitations and future directions……………………………………..154
Recommendations for HIV interventions in Vietnam…………………………………..157
Conclusion…………………………………………………………………………………164
Appendix 1. Support letter…………………………………………………………………………176
Appendix 2. Participants information statement and consent forms………………………….181
Appendix 3. Ethical approvals…………………………………………………………………….192
Appendix 4. The community-based, cross-sectional survey’s questionnaire……………….. 195
Appendix 5. Quality assessment checklists for the systematic review and meta-analysis..217

Page| xiv
Thesis abstract
This thesis assessed patterns of amphetamine-type-stimulants (ATS) use and their
association with condomless anal intercourse (CAI), HIV infection and mental health issues,
particularly depression, among men who have sex with men (MSM) in Vietnam.
This study employed a socio-ecological framework with a community-based survey conducted
in 2014 in Hanoi and Ho Chi Minh City, Vietnam. As part of the thesis, a systematic review
and meta-analysis of the relationship between ATS use and HIV infection in MSM was also
conducted. The survey results showed that a substantial proportion of Vietnamese men
(30.4%) had ever used any ATS and 20.3% had used ATS recently. Methamphetamine was
the most popular substance. The majority of recent methamphetamine and ecstasy users were
classified as moderate to high-risk users, according to WHO guidelines. Methamphetamine
use was associated with higher sexual sensation seeking, engagement in recent sex work and
the perception that methamphetamine use was popular among other MSM. A high prevalence
of CAI with any male partners in the last three months (75.7%) was reported. CAI was
associated with methamphetamine use before or during sex, higher sexual sensation seeking,
and belief in the safety of withdrawal as an HIV prevention strategy. Voluntary HIV tests
conducted for 210 men in Hanoi found a moderate HIV prevalence of 6.7%. Men who used
methamphetamine before or during sex, who had engaged in sex work and perceived more
homosexuality-related stigma were more likely to have an HIV positive test. Lastly, a sizable
proportion of men (11.3%) were classified as having major depression which was associated
with ever using ATS and higher enacted (i.e. experienced) homosexuality-related stigma. The
systematic review and meta-analysis demonstrated a significant pooled estimate of ATS use
associated with HIV infection in MSM across longitudinal, case-control and cross-sectional
studies, but not for ecstasy use in cross-sectional studies. The review found several
methodological shortcomings of current studies of drug use and sexual behaviour.
This thesis suggests a comprehensive HIV prevention package, that includes treatment for
methamphetamine use, is needed for MSM in Vietnam to address drug use and the risks of
HIV at the individual, community and societal levels. The thesis also recommends the inclusion
of MSM in HIV prevention, care and treatment provision. From the systematic review and
survey findings, several recommendations for further research on drug use and sexual
behaviours are suggested, including periodic assessment of ATS use.
Page| xv
THESIS STRUCTURE
Other than the introduction (Chapter 1), the thesis consists of a methods chapter (Chapter
2), five chapters based on articles published in peer-reviewed journals (Chapters 3-7) and a
discussion and conclusion chapter (Chapter 8). The articles were written by the candidate
and have all been published. At the beginning of each chapter, the citation and copyright
permission for the article is included. Where possible, supplementary materials are also
provided. As each publisher requires a different formatting style, some discrepancies in
terminology and citations may appear across chapters. The outline of the thesis is:
Chapter 1
This chapter provides an overview of ATS, including their physiological effects and
prevalence of use in different countries and regions in the world, an overview of the health
and social vulnerabilities of MSM and a review of correlations with these vulnerabilities. The
chapter also provides an overview of the evolution of a multilevel approach to understanding
health and behavioural issues, followed by a socio-ecological framework for the study of
drug use, particularly ATS use and associated harms in MSM in Vietnam. The chapter ends
by identifying research gaps and specific research questions for the thesis.
Chapter 2
This chapter provides a description of the study design, measures and fieldwork for the
community-based cross-sectional study and the systematic review and meta-analysis on
ATS use and HIV infection in MSM. Each of the published papers also includes a description
of the method used for that analysis.
Chapter 3
This chapter represents a published, original article in Drug and Alcohol Dependence with the
following details: Vu, N. T., M. Holt, H. T. Phan, H. T. Le, L. T. La, G. M. Tran, T. T. Doan, T.
N. Nguyen and J. de Wit (2016). "Amphetamine-type stimulant use among men who have sex
with men (MSM) in Vietnam: Results from a socio-ecological, community-based study." Drug
Alcohol Depend 158: 110-117.
In this chapter, with data from the community-based cross-sectional study, I assessed the
magnitude, patterns and severity of ATS use among MSM in Hanoi and Ho Chi Minh City. I
analysed the prevalence and patterns of ATS use, including methamphetamine,
amphetamine and ecstasy use. Following a socio-ecological approach, by logistic
Page| xvi
regression, I identified the individual, community and societal correlates of
methamphetamine use (the most popular substance) in the sample. From the findings, I
suggested relevant public health recommendations for methamphetamine use prevention
and treatment.
Chapter 4
This chapter represents a published, original article in AIDS and Behavior with the following
details: Vu, N. T., M. Holt, H. T. Phan, L. T. La, G. M. Tran, T. T. Doan, T. N. Nguyen and J.
de Wit (2017). "The Relationship Between Methamphetamine Use, Sexual Sensation Seeking
and Condomless Anal Intercourse Among Men Who Have Sex With Men in Vietnam: Results
of a Community-Based, Cross-Sectional Study." AIDS Behav 21(4): 1105-1116.
In this chapter, I analysed patterns of HIV-related risky sexual behaviours of MSM in Hanoi
and Ho Chi Minh City. Correlates of CAI Prevalence Ratios (PR) are analysed by generalised
linear models with modified Poisson regression and robust error variances. Since sexual
sensation seeking has been found to modify the association between alcohol use and risky
sexual behaviours, in this analysis I also hypothesized that sexual sensation seeking may be
a modifier of the association between methamphetamine use and CAI in the sample.
Accordingly, I incorporated the interaction term of methamphetamine use and sexual
sensation seeking in the model. Based on the findings, I suggested public health
recommendations for both HIV research and prevention targetting MSM in Vietnam.
Chapter 5
This chapter represents a published, original article in the Journal of International AIDS
Society (JIAS) with the following details: Vu, N. T., L. Maher and I. Zablotska (2015).
"Amphetamine-type stimulants and HIV infection among men who have sex with men:
implications on HIV research and prevention from a systematic review and meta-analysis." J
Int AIDS Soc 18: 19273.
In this chapter, I provided the results of my systematic review and meta-analysis on the
association between ATS use and HIV infection in MSM from English language, peer-reviewed
published articles. I presented the pooled estimates of the relationship between each ATS
substance, i.e. methamphetamine, amphetamine and ecstasy, with HIV infection in MSM, by
each study design, i.e. cross-sectional, case-control and longitudinal. I also conducted meta-
regression to identify the causes of heterogeneity in the findings. I discussed the shortcomings
of current drug use studies and provided recommendations for future research.
Page| xvii
Chapter 6
This chapter represents a published, original article in Frontiers in Public Health with the
following details: Vu, N. T., M. Holt, H. T. Phan, L. T. La, G. M. Tran, T. T. Doan and J. de Wit
(2016). "The Prevalence and Correlates of HIV and Undiagnosed Infection among Men Who
Have Sex with Men in Hanoi, Vietnam: Findings from a Cross-sectional, Biobehavioral Study."
Front Public Health 4: 275.
In this chapter, I analysed the correlates of HIV infection in a sub-sample of MSM from Hanoi.
This is an embedded bio-behavioural sub-component of my cross-sectional study. I presented
HIV prevalence identified via laboratory testing and the correlates with HIV-related risky sexual
and drug use behaviours, particularly ATS use. I analysed societal, community and individual
correlates of HIV infection and suggest relevant interventions for methamphetamine use and
HIV prevention targetting MSM.
Chapter 7
This chapter represents a published, original article in Substance Use and Misuse with the
following details: Vu, N. T., M. Holt, H. T. Phan, L. T. La, G. M. Tran, T. T. Doan, T. N. Nguyen
and J. de Wit (2017). “The Prevalence and Correlates of HIV and Undiagnosed Infection
among Men Who Have Sex with Men in Hanoi, Vietnam: Findings from a Cross-sectional, Bio-
behavioural Study”. Substance Use and Misuse (In Press).
This chapter presents my work on depression and its associated factors in the sample. I
analysed the prevalence of depression classified by the Patient Health Questionnaire (PHQ-
9) and correlates of depression using logistic regression. From the findings, I suggested
relevant changes to a comprehensive HIV prevention and provide recommendations for future
research targetting MSM in Vietnam.
Chapter 8
In this chapter, I summarised the major findings of my study. I compare my findings with the
results of previous studies in other settings and in Vietnam and discuss any discrepancies and
divergent findings. I also discussed the strengths and weaknesses of my current study and
provide suggestions for future research. Based on my findings, I made recommendations for
interventions to address ATS use and HIV prevention among MSM in Vietnam.
Page| xviii
List of publications and presentations arising from this thesis
Journal paper publications
1. Vu, N. T., M. Holt, H. T. Phan, H. T. Le, L. T. La, G. M. Tran, T. T. Doan, T. N.
Nguyen and J. de Wit (2016). "Amphetamine-type stimulant use among men who
have sex with men (MSM) in Vietnam: Results from a socio-ecological, community-
based study." Drug Alcohol Depend 158: 110-117.
2. Vu, N. T., M. Holt, H. T. Phan, L. T. La, G. M. Tran, T. T. Doan, T. N. Nguyen and J.
de Wit (2017). "The Relationship Between Methamphetamine Use, Sexual Sensation
Seeking and Condomless Anal Intercourse Among Men Who Have Sex With Men in
Vietnam: Results of a Community-Based, Cross-Sectional Study." AIDS Behav 21(4):
1105-1116.
3. Vu, N. T., L. Maher and I. Zablotska (2015). "Amphetamine-type stimulants and HIV
infection among men who have sex with men: implications on HIV research and
prevention from a systematic review and meta-analysis." J Int AIDS Soc 18: 19273.
4. Vu, N. T., M. Holt, H. T. Phan, L. T. La, G. M. Tran, T. T. Doan and J. de Wit (2016).
"The Prevalence and Correlates of HIV and Undiagnosed Infection among Men Who
Have Sex with Men in Hanoi, Vietnam: Findings from a Cross-sectional,
Biobehavioral Study." Front Public Health 4: 275.
5. Vu, N. T., M. Holt, H. T. Phan, L. T. La, G. M. Tran, T. T. Doan, T. N. Nguyen and J.
de Wit (2017). “The Prevalence and Correlates of HIV and Undiagnosed Infection
among Men Who Have Sex with Men in Hanoi, Vietnam: Findings from a Cross-
sectional, Bio-behavioural Study”. Substance Use and Misuse (In Press).
Conference presentations
1. Vu, N. T., M. Holt, H. T. Phan, L. T. La, G. M. Tran, T. T. Doan, T. N. Nguyen and J.
de Wit (2016). Methamphetamine use increases the likelihood of condomless anal
intercourse (CAI) among Vietnamese men who have sex with men (MSM) who have
low sexual sensation seeking score. Paper presented at the 2016 Australasian
HIV/AIDS Conference, Adelaide, Australia
2. Vu, N. T., M. Holt, H. T. Phan, L. T. La, G. M. Tran, T. T. Doan, T. N. Nguyen and J.
de Wit (2016). Amphetamine-type-stimulant use and HIV infection: Findings from a
cross-sectional, bio-behavioural survey of men who have sex with men in Hanoi,
Vietnam. Paper presented at the 2016 Australasian HIV/AIDS Conference, Adelaide,
Australia
3. Vu, N. T., M. Holt, H. T. Phan, L. T. La, G. M. Tran, T. T. Doan, T. N. Nguyen and J.
de Wit (2016). Methamphetamine use increases the likelihood of condomless anal

Page| xix
intercourse (CAI) among Vietnamese men who have sex with men (MSM) who have
low sexual sensation seeking score. Paper presented at the 21st International AIDS
Conference. Durban, South Africa.
4. Vu NT, Maher L, Zablotska I. (2013). The association between Amphetamine-typed-
stimulants with HIV infection among men who have sex with men: A systematic
review and Meta-analysis from cross-sectional studies. Paper presented at The 19th
Social Research in HIV, HBV and other infectious diseases, Centre for Social
Research in Health, UNSW Australia.
Page| xx
LIST OF ABBREVIATIONS
ATS Amphetamine-type-stimulants
MSM Men who have sex with men
CAI Condomless anal intercourse
US United States
UNODC The United Nations Office on Drugs and Crime
LMIC Low and middle income countries
UK United Kingdom
LGBT Lesbian, gay, bisexual and transgender
STI Sexual transmitted infections
UNAIDS The Joint United Nations Programme on HIV/AIDS
IBBS Integrated Behavioural and Biological Surveillance
RCAI Receptive condomless anal intercourse
ICAI Insertive condomless anal intercourse
EDM Erectile dysfunction medications
RDS Respondent Driven Sampling
VAAC Vietnam Administration HIV/AIDS Control Office
IDU Injecting drug users
Hanoi PAC Hanoi HIV/AIDS Prevention Centre
CHP Centre for Community Health Promotion
Life Center Centre for Promotion of Quality of Life
CBO Community-based organisations
ASSIST Alcohol, smoking and substance involvement screening test
CI Confidence Interval
PRR Prevalence Rate Ratio
OR Odds Ratio
HR Hazard Risk
RR Relative Risk
Page| xxi
LIST OF TABLES
In this thesis, the table numbers are firstly identified by the chapter number and then
by their sequential number within each chapter.
Table 3.1: Demographic and behavioural characteristics of the full sample and by
study locations for men who have sex with men in Hanoi and Ho Chi
Minh City, Vietnam, 2014 ……….........................................................92
Table 3.2: Socially involvement with other MSM and perception of the popularity
of ATS substance use among MSM network’s friends of the full sample
and by study location for men who have sex with men in Hanoi and Ho
Chi Minh City, Vietnam, 2014…………………………………………….93
Table 3.3: Patterns of amphetamine-type stimulants (ATS) and other substances
among men who have sex with men sampled in Ho Chi Minh City and
Hanoi, Vietnam, 2014……………………………………………………..93
Table 3.4: Bivariate and multivariate regression analyses of covariates of recent
methamphetamine use among men who have sex with men sampled in
Ho Chi Minh City and Hanoi, Vietnam, 2014……………………………94
Table 4.1: Demographic characteristics of MSM recruited in Hanoi and HCMC,
Vietnam, 2014…………………………………………………………….103
Table 4.2: Sexual and drug use behaviours among MSM in Hanoi and HCMC,
Vietnam, 2014…………………………………………………………….104
Table 4.3: Bivariate and multivariate analyses of any CAI with male partners in the
last 3 months among MSM recruited in Hanoi and HCMC, Vietnam,
2014………………………………………………………………………..105
Table 5.1: Articles in the analysis: description of studies and their
participants………………………………………………………………..116
Table 5.2: Stratification analysis for cross-sectional studies……………………. 121
Table 6.1: Participant characteristics……………………………………………….132
Table 6.2: Sexual and drug use behaviours………………………………………..133
Table 6.3: Bivariate and multivariate analysis of associations with HIV
infection…………………………………………………………………... 134
Table 7.1: Characteristics of MSM recruited in Hanoi and Ho Chi Minh City,
Vietnam, 2014…………………………………………………………….144
Table 7.2: Sexual and drug use behaviours of MSM recruited in Hanoi and Ho Chi
Minh City, Vietnam, 2014………………………………………………..144

Page| xxii
Table 7.3: Bivariate and multivariable analysis of correlates of depression among
MSM recruited in Hanoi and Ho Chi Minh City, Vietnam, 2014……..145
Page| xxiii
LIST OF FIGURES
In this thesis, the figure numbers are firstly identified by the chapter number and
then by their sequential number within each chapter.
Figure 1.1: Hanoi prevalence among MSM by region from 2007-2011.........9
Figure 1.2: Trends in HIV prevalence among MSM in Vietnam from 2005-
2013 from Integrated Biological and Behavioural Surveillance
(IBBS)……………………………………………………………….30
Figure 1.3: Socio-ecological framework for the study of HIV risk and alcohol
environment………………………………………………………...34
Figure 1.4: The proposed Socio-Ecological Framework for the study of ATS
use and associated harms in Vietnam…………………………..36
Figure 2.1: Participant interview protocol……………………………………..77
Figure 4.1: Differences in the probability of involving in CAI in the last three
months for sexually-related methamphetamine use versus no
methamphetamine use by sexual sensation seeking………...106
Figure 5.1: Flow chart for selection of studies with number of articles…..115
Figure 5.2: Summarized effect measure of the association between ATS
use and HIV infection, by study design………………………...119
Figure 5.3: Summarized effect measure of the association between ATS
use and HIV infection, by study design and drug type. (a) cross-
sectional study; (b) case-control studies; (c) longitudinal
studies……………………………………………………………..120
Figure 8.1: Recommendation for a comprehensive HIV prevention package
for MSM in Vietnam………………………………………………165
Page| xxiv
ACKNOWLEDGEMENT
Finally, I have completed my Ph.D. study after a challenging four-year journey. I could not
have accomplished this work without the assistance and support of my supervisors,
colleagues, friends and relatives.
First of all, I want to especially extend my sincere gratitude to Professor John De Wit and
Associate Professor Martin Holt for their courageous decision to get on board with me,
knowing that I am an international student whose English is not her mother tongue. I could not
have gone through this long, difficult journey without your extraordinary support, assistance,
guidance, and patience. I remember how patient you were with my messy drafts with lots of
grammatical and typing errors, your instructions to help me develop critical thinking and writing
skills and your attention to even the smallest of details in my writing. I have learned a lot from
you and these valuable lessons will go with me for the rest of my life. I am also very thankful
for your compassion during the times when my mother went away and there was chaos in my
family back in Vietnam. Additionally, I would also like to extend my sincere thanks to Professor
Lisa Maher and Associate Professor Iryna Zablotska, my ex-supervisors at the Kirby Institute,
UNSW. Though they were only with me for a short period of my Ph.D. journey, the systematic
review and meta-analysis I did with them was the first real challenge within my doctoral
candidature and it was an extremely exciting task. I am thankful for the opportunity they gave
me to acquire a new powerful statistical analysis technique and the overall understanding of
the topics of my research at the very beginning of my Ph.D. The skills and knowledge I gained
from this particularly helped me in my research.
Secondly, I want to express my great thanks to my colleagues in Vietnam, who supported me
to conduct my research in Vietnam: Dr. Lan Thi La, Deputy Director of Hanoi HIV/AIDS
Prevention and Control Center; Dr. Gioi Minh Tran, Director of the Centre for Community
Health Promotion and Ms Trang Nguyen Nhu Nguyen, Director of the Centre for Quality of
Life Promotion. I want to especially thank Tung Thanh Doan, Thanh Le and members of all
COBs in Ho Chi Minh City for their wonderful contributions, collaboration and support during
my survey work in Hanoi and Ho Chi Minh City. I could not have conducted my fieldwork
without their agreement to collaborate with me in this study, their referral to the networks of
community-based-organisations of MSM in Hanoi and Ho Chi Minh City, and their kind offer
of various locations for meetings, interviewer training, and interviews, and most importantly,
their thoughtful contributions to this study. It is so inspiring to have come in contact with their
work and to have got to know them all on a personal basis. I also want to send my sincere
thanks to all the men who bravely came and shared their information and their life experiences.
I am grateful for the opportunity they gave me to gain an insight into the difficulties of being in
Page| xxv
a minority and how brave they are in constructing their identity in a heterosexist-dominant
society. I thank my colleagues and students at Hanoi Medical University and Ho Chi Minh
University of Pharmacy and Medicine for their great work with me during my fieldwork. Their
enthusiasm, time, hard work and wonderful interviews with the men in my study meant a lot to
me.
Thirdly, I am very much thankful to the staff and other academics at the Centre for Social
Research in Health, UNSW, particularly Carla Treolar, Christy Newman, Loren Brener, Limin
Mao and Ann Whitelaw for their great administrative and academic support, their constructive
advice, and the wonderful study conditions that they gave me. I also want to thank my fellow
Ph.D. candidates who created a friendly and supportive learning environment in our 206 lab,
at level 2 of the John Goodsell Building, UNSW Kensington campus. All of the fun moments I
spent with them helped to reduce my stress levels during the course of my research.
Last but not least, I am very grateful for the support of my ex-husband- Duy Trung Nguyen,
my little sons-Hieu and Chip and other loved ones in my extended family. Many thanks to Duy
for taking care of our sons when I had to go away. Although we are not able to spend the rest
of our lives together, I feel very relieved that we will share the endless love, caring, and
responsibilities of our children, Hieu and Chip. I know it was not easy for the children when I
was not with them and they missed me so much. Nothing can compensate for the fact they
had to grow up without their mother, especially as they were entering their teenage years.
Finally, to my mother and father, thank you so much for your encouragement and support of
me. I feel guilty that I could not take care of you and be with you, especially when you were
sick or during our traditional Tet. Mum, I love you and I hope you rest in peace now. This work
is my compliment to you and I hope you feel proud of me.
CHAPTER 1
INTRODUCTION AND LITERATURE REVIEW
1
My study focuses on the use of amphetamine-type-stimulants (ATS) and its potential
associated harms, including risky sexual behaviours, HIV infection and psychological
problems, particularly depression, among men who have sex with men (MSM) in
Vietnam. In this chapter, I provide a rationale for why I conducted this study and I assess
previous research and gaps in the existing knowledge.
In the first section of this chapter, I provide an overview of ATS including their
physiological effects and the prevalence of their use in different countries. Following this,
I explain the particular social and health vulnerabilities of MSM. I discuss homosexuality-
related stigma and discrimination, how stigma and discrimination affects MSM and the
prevalence of common health issues, including depression, risky sexual behaviours and
HIV infection. Next, I present a literature review of recent research, mostly published in
the past five years, on the correlates of drug use, particularly ATS use, risky sexual
behaviours, notably condomless anal intercourse (CAI), HIV infection and depression
among MSM.
I continue the chapter with an overview of the theoretical framework I used in my study
of ATS use and its associated harms among MSM. Specifically, I report a brief review of
previous public health research approaches and how these approaches were adapted
to develop frameworks for the study of health-related issues. I then propose an adapted
theoretical framework for my study of ATS use and its associated harms among MSM in
Vietnam.
Next, I consider the context of Vietnam and current knowledge about ATS use and
associated harms in Vietnamese MSM, including risky sexual behaviours, HIV infection
and depression. In this section, I describe how homosexuality is situated in
contemporary Vietnamese society, as well as illicit drug use in Vietnam and the
Vietnamese HIV epidemic. I then review recent research on ATS use, risky sexual
behaviours, HIV infection and depression among Vietnamese MSM. After this literature
review, I discuss the gaps and limitations of recent research in Vietnam.
I then present my overall research objective and specific research aims, as well as my
research questions, and briefly describe the study design. I conclude the chapter with an
outline of the other chapters in the thesis.
2
AMPHETAMINE-TYPE-STIMULANTS (ATS)
This section begins with background information about ATS, their classification, how they
are referred to by drug users, and a description of the biological mechanisms of the
action of ATS. The section continues with an explanation of the various physical,
psychological and sexual effects of ATS, followed by epidemiological evidence regarding
their use globally. The section concludes with information regarding the extent of ATS
use among MSM in different parts of the world.
What are ATS?
ATS are synthetic psycho-stimulants (1), that are often classified into two groups: the
amphetamine-group substances which includes ephedrine, methylphenidate, ∆-
amphetamine, L-amphetamine, amphetamine sulphate, amphetamine hydrochloride,
methamphetamine, and methcathinone, and the ecstasy-group substances which
include 3, 4-methylenedioxy-N-methylamphetamine (MDMA), N-ethyl-3, 4-methylene-
dioxyamphetamine (MDEA) and 3, 4-methylenedioxyamphetamine (MDA) (1-3). In the
amphetamine substance group, amphetamine and methamphetamine are the most
commonly used drugs (4). Methamphetamine has different street names in different parts
of the world, including “meth”, “speed”, “crystal meth”, “ice”, “batu”, “shabu”,”glass”, “tina”,
”crank”, ”go-fast”, “stove top”, and “yaba” (5). In Vietnam, methamphetamine’s street
names include (but are not limited to) “hồng phiến”, “ viên chúa” for tablets/pills and “hàng
đá” or “ice” for crystal (6). Ecstasy is the most commonly used drug in the ecstasy
substance group, with various street names, including “eva”, “adam” and “love” (3). In
Vietnam, ecstasy is called “thuốc lắc” or “ viên tình yêu” (6), or referred to by the icon
stamped on the tablets.
Between the 1940s and 1980s, methamphetamine was prescribed for various medical
conditions, particularly weight reduction (5). Currently, methamphetamine is still
indicated for the treatment of narcolepsy, and for treatment of the symptoms of attention
deficit hyperactivity disorder in children (3). Ecstasy group substances have never been
officially prescribed for medical purposes (1). Since the late twentieth century,
amphetamine and ecstasy group substances have been labelled as club or party drugs
as they are often used in dance clubs, circuit parties or raves (7). This type of recreational
use is typically classified as illegal.
In many illicit drug markets, including Vietnam, ecstasy is commonly produced as a
tablet, normally containing MDMA and other ecstasy-type substances, often stamped
with a symbol (1, 8, 9). Methamphetamine is available in the market in various forms
3
such as crystals, crushable tablets, liquids or powder, usually combined with other
substances and with varying purity (5). Both amphetamine and ecstasy substances can
be used in various ways, including oral ingestion, injection, inhalation, smoking or
“shafting” (inserting in the anus) (4, 5, 7).
How do ATS substances work and what are their effects?
Both amphetamine and ecstasy-group substances are classified as neuro-stimulants,
while ecstasy-group substances are also classified as hallucinogenic (1, 3, 5). In the
central nervous system, amphetamine substances affect the release of
neurotransmitters (i.e. dopamine), and inhibit the re-uptake of catecholamines (i.e.
adrenaline) (3), while ecstasy substances increase the release of serotonin, which is
responsible for psychological effects, and inhibit the uptake of adrenaline, which is
responsible for physical effects (1, 3). Because of their long half-life, both amphetamine
and ecstasy-type stimulants can have physiological and psychological effects which may
last up to 3-6 hours for ecstasy or 10-12 hours for methamphetamine (3, 7, 10). The
effects of ATS may be affected by the individual’s physiology and psychological state,
the dose taken, the route of administration of the drug, the user’s prior experience with
the drug, expectations of what it will do, and contextual and environmental factors, such
as where and with whom the drug is used (11, 12).
ATS tend to increase heart rate, blood pressure, body temperature, alertness,
wakefulness, endurance and energy, and decrease feelings of fatigue and sleepiness
(1, 3, 9). Users of amphetamine substances tend to report experiences of euphoria,
arousal, positive mood, behavioural disinhibition, enhancement of cognition and
increased self-esteem (11, 13). Ecstasy substance users also report experiences of
euphoria and a positive mood, as well as a sense of wellbeing, sociability, extraversion,
and closeness to other people (1, 9). Potential adverse effects of amphetamine
substances include convulsions, coma, cerebral haemorrhage and death (3), and those
of ecstasy substances include muscle pain, heighted body temperature, headache,
nausea, reduced appetite, blurred vision, dry mouth, insomnia, anxiety and psychosis (1,
9). Long-term use of methamphetamine can result in toxic effects and a variety of
psychological and/or psychiatric conditions, such as psychosis, depression, anxiety,
violent behaviour and suicide (3, 5, 11, 14). Long-term use of ecstasy substances can
result in neurotoxic effects and adverse physical, psychological and psychiatric
conditions, such as tooth grinding, muscle ache, circulatory problems, cognitive
impairment, greater impulsivity, paranoia, hallucinations, psychosis, depression and
death (1, 9).
4
A number of qualitative studies have described the motivations for methamphetamine
use and its effects on sexual behaviour from the user’s perspective. Narratives from both
HIV-positive and HIV-negative MSM in major cities in the United States (US) described
the sexual effects of methamphetamine as some of the most important reasons for MSM
to use the drugs (15-22). However, studies have also revealed numerous personal,
interpersonal and social reasons for its use. Methamphetamine can be used to enhance
sexual experience and achieve prolonged sexual encounters, heighten sexual feelings,
reduce anxiety and sexual inhibitions and increase openness about homosexuality (16,
18, 20-22). Methamphetamine may be used by MSM to socialize with other gay men or
to approach sexual partners in gay-oriented venues (16, 18, 21), and to avoid or reduce
social pressure, conflicts or rejection because of being homosexual or HIV positive (16,
18, 20-22). It may also be used to avoid psychological distress (23), and for functional
purposes, including losing weight, improving work performance, enhancing mood and
reducing fatigue (4).
In relation to ecstasy use, there are contradictory reports about its sexual effects from
both gay and bisexual men and other users in high-income countries. Qualitative
research with gay and bisexual men in New York and ecstasy users in Belfast described
some users feeling enhanced sensitivity to touch, increased affection or sensuality,
emotional closeness to others (24, 25) or just relaxation or enhanced socialisation (26).
It may also improve a sense of well-being, relationship satisfaction or increased
enjoyment of music and dancing (27) . However, other men reported sexual arousal,
increased sexual desire, and sexual disinhibition (24, 25, 28). A review of both
quantitative and qualitative studies with young recreational ecstasy users found similar
effects on sexual sensation and arousal (29).
ATS use globally and among MSM
In the recent World Drug Reports, the United Nations Office on Drugs and Crime
(UNODC) has identified ATS as the second most commonly used type of illicit drug
during the period 2011 to 2015, after cannabis (30-34). The agency estimated that
during 2011-2015, approximately 0.6% -1.3% of the global population aged 15 to 64
years used amphetamines in the previous year and 0.2% - 0.6% used ecstasy (30, 34).
Since the late 2000s, the use of ATS has been stable or has decreased slightly in North
America, Europe and some Southeast Asian countries, such as Thailand, Malaysia and
Singapore. However, ATS use has increased substantially in other countries in
Southeast Asia (30), such as Vietnam, Laos, Cambodia and Myanmar (35) and there
may be emerging markets in Africa (32). East and Southeast Asia have been identified
5
as the regions with the biggest markets for amphetamine substances, particularly
methamphetamine during the first part of the 2010s (30-34, 36).
Drug use in general and ATS use in particular have been reported at relatively high levels
among MSM in high-income countries, particularly in America, Australia and Western
Europe. It has consistently been found that ATS use is more prevalent among MSM
compared to other population groups (4, 7, 37). National and large-scale surveys in high
income countries have found relatively high rates of ATS use among MSM. In the early
2000s, national and large-scale studies in the US reported amphetamine substance use
ranging from 6% to 20% and ecstasy use from 10% to 19% among MSM (38, 39). In
some cities, such as New York City, the rate of life-time ecstasy use among MSM was
found to be as high as 84% (40). In England, a national survey of MSM in 2004 found
that the rate of ecstasy use in the last year was 18.5%, while amphetamine use was
reported as 7.2% and methamphetamine use as 2.8% (41). A large-scale survey
conducted in 2010 among gay and bisexual men in 44 cities in Europe found relatively
high life-time rates of ATS use, among which amphetamines were the most commonly
used ATS (40.0%), followed by ecstasy (20.0%) and crystal methamphetamine (10.0%)
(42). In Australia, behavioural surveys in major cities in 2014 found a high level of ATS
use among MSM, in which the prevalence of recent amphetamine (speed) use was
10.2% and 11.4% for methamphetamine (43). Recent studies in high income countries
have found inconsistent trends in ATS use. A repeated cross-sectional study that
followed 5599 substance-using MSM in the US from 2008 to 2011 reported an upward
trend in methamphetamine use in the last 30 days, from 23.7% in 2008 to 27.4% in 2011
(44). However, behavioural surveillance in Australia has observed a downward trend in
methamphetamine use from 15.6% in 2005 to 11.4% in 2014 (43, 45).
Most studies on ATS use among MSM to date have been conducted in English-speaking
high-income countries, notably the United States (US), England, other European
countries and Australia. Evidence from low and middle income countries (LMIC) is
lacking (4, 7). There has been only one published study addressed drug use among
MSM in 12 countries in Asia. This study reported an overall prevalence of any
recreational drug use of 16.7%, with ecstasy being the most commonly used drug,
reported by 8.1% (46).
HEALTH VULNERABILITIES OF MSM
MSM may experience adverse physical and mental health outcomes related to social
stigma and discrimination, as well as from specific sexual and drug-related practices. In
6
this section, I present the health vulnerabilities that MSM may face, beginning with
homosexuality-related stigma and discrimination, followed by mental health disparities
and sex and drug use behaviours which may increase the risk of HIV. The section
concludes with a consideration of the HIV burden faced by MSM.
Homosexuality-related stigma and discrimination
MSM include homosexual or gay men, bisexual men, heterosexual men who have sex
with men and any other men who have sex with men. The term only reflects the
behavioural aspect of sexuality while ignoring sexual attraction and sexual identity.
Despite continuous efforts to advocate for homosexual rights across the globe,
particularly in high-income countries, homosexuality-related stigma and discrimination
towards gay men and other MSM remain prevalent in many parts of the world (47, 48).
Even in high income countries such as the US, United Kingdom (UK) and Australia, many
MSM still experience negative stereotypes, prejudice and discrimination in various social
settings, including the home, school, workplace, health care services and the community
(49-51). Homosexuality-related stigma and discrimination toward MSM can be
expressed in various ways, including unpleasant treatment, verbal abuse and physical
violence (52, 53) and have been outlawed in some countries (47). In the literature,
homosexuality-related stigma and discrimination are often referred to as homophobia,
meaning the dislike or fear of homosexuality and beliefs that homosexuality is wrong or
abnormal (51, 54). Homosexuality-related stigma may be classified into three main types
(55): experienced or enacted stigma, perceived stigma and internalised homophobia.
Enacted stigma includes men’s experiences of stigmatising or discriminating behaviours
by others, perceived stigma refers to men’s perceptions of societal attitudes towards
homosexuality, and internalised homophobia is men’s self-blaming or stigmatising of
their homosexuality as a result of hostile societal attitudes (56).
Homosexuality-related stigma and discrimination can affect many aspects of MSM’s
lives, and adversely affect their physical and mental health. Importantly, MSM who
experience internalised stigma, typically referred to as internalised homophobia, have
been found to be more likely to have a higher risk of acquiring HIV, because they may
be more likely to engage in HIV-related risky sexual behaviours (57), including CAI (58)
and having sex under the influence of drugs (52, 58). Additionally, MSM who experience
internalised homophobia are less likely to be aware of or utilise HIV prevention programs,
including individual, group and community behavioural change interventions and HIV
testing, and are less likely to change their behaviours when participating in such HIV
prevention programs (57, 59). At the same time, experienced stigma and/or internalised
7
homophobia can adversely affect MSM’s mental health. Studies have reported that MSM
who report internalised homophobia are more likely to be socially isolated (60), have
higher rates of depression and lower self-esteem (57, 60), and are more likely to use
illicit drugs (61).
Depression
MSM are disproportionately affected by mental health problems, including depression
and anxiety (50, 62). Generally, sexual minority populations, including lesbian, gay,
bisexual and transgender (LGBT) people, report higher rates of suicide attempts,
depression, anxiety disorders and illicit drug use, compared to their heterosexual peers
(63). In the US, the prevalence of depression among MSM is up to ten times higher than
among heterosexual men (64), and, together with other health concerns such as HIV
and other sexually transmitted infections (STIs), depression and other mental health
problems have been noted as major health issues among MSM (65).
High rates of depression among MSM have been reported in a range of settings. Recent
studies of MSM in in the US have found that rates of depression ranged from 23% to
34% (66-68), and up to 42% among HIV-positive MSM (69). In Europe, the prevalence
of depression was reported to be 32% among MSM in Estonia (70) and 29% among
MSM in Belgium (71). In Australia, one third of MSM attending general medical practices
in Sydney and Adelaide were found to experience major depressive disorder (72). In
Africa, major depression was found to affect 16% of MSM in Lesotho and Kenya (73, 74)
and over half of MSM in Cape Town, South Africa (75). In Asia, recent studies have
investigated psychological disorders and sexual behaviours among MSM and male sex
workers in a number of countries, including India, Nepal, China, Taiwan, Cambodia,
Thailand and Vietnam (55, 76-82). While the prevalence of depression among MSM in
India was moderate (11%) (76), in East and Southeast Asia countries, several studies
targetting subgroups of MSM such as HIV-positive MSM or male sex workers (MSW),
reported a high proportion (43%-58%) suffering from depression (78, 79, 81, 82).
HIV infection
MSM are disproportionately affected by HIV in all countries where data are available. In
the period from 2000 to 2006, the global pooled HIV prevalence among MSM in LMIC
reportedly was 12.8%, with the prevalence of HIV among MSM in Central and South
America ranging from 7.9%-25.6%, in Africa from 0.01%-21.5%, and in Southeast Asia
from 2.8%-24.6% (83). In the period from 2007 to 2011, the pooled HIV prevalence
among MSM was reported to be as high as 25.4% in the Caribbean region, and the HIV
8
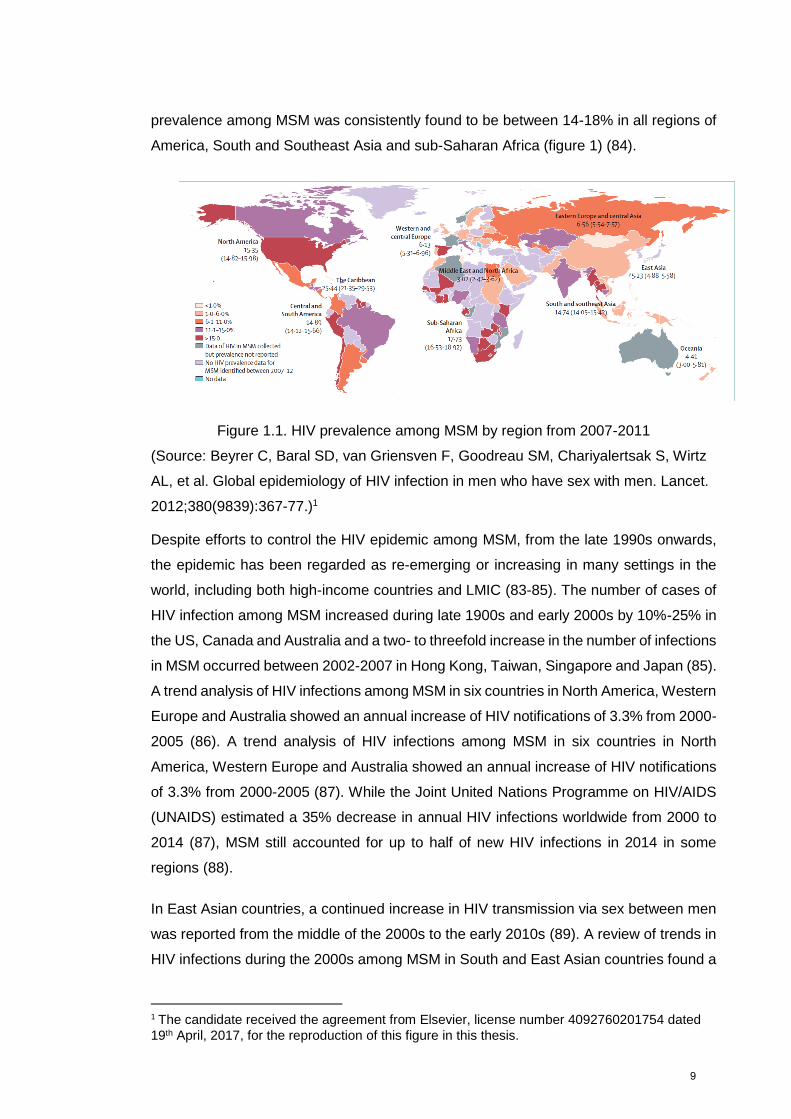
prevalence among MSM was consistently found to be between 14-18% in all regions of
America, South and Southeast Asia and sub-Saharan Africa (figure 1) (84).
Figure 1.1. HIV prevalence among MSM by region from 2007-2011
(Source: Beyrer C, Baral SD, van Griensven F, Goodreau SM, Chariyalertsak S, Wirtz
AL, et al. Global epidemiology of HIV infection in men who have sex with men. Lancet.
2012;380(9839):367-77.)1
Despite efforts to control the HIV epidemic among MSM, from the late 1990s onwards,
the epidemic has been regarded as re-emerging or increasing in many settings in the
world, including both high-income countries and LMIC (83-85). The number of cases of
HIV infection among MSM increased during late 1900s and early 2000s by 10%-25% in
the US, Canada and Australia and a two- to threefold increase in the number of infections
in MSM occurred between 2002-2007 in Hong Kong, Taiwan, Singapore and Japan (85).
A trend analysis of HIV infections among MSM in six countries in North America, Western
Europe and Australia showed an annual increase of HIV notifications of 3.3% from 2000-
2005 (86). A trend analysis of HIV infections among MSM in six countries in North
America, Western Europe and Australia showed an annual increase of HIV notifications
of 3.3% from 2000-2005 (87). While the Joint United Nations Programme on HIV/AIDS
(UNAIDS) estimated a 35% decrease in annual HIV infections worldwide from 2000 to
2014 (87), MSM still accounted for up to half of new HIV infections in 2014 in some
regions (88).
In East Asian countries, a continued increase in HIV transmission via sex between men
was reported from the middle of the 2000s to the early 2010s (89). A review of trends in
HIV infections during the 2000s among MSM in South and East Asian countries found a
1 The candidate received the agreement from Elsevier, license number 4092760201754 dated
19th April, 2017, for the reproduction of this figure in this thesis.
9
two-digit HIV prevalence in many major cities in the region: 14% in Taiwan in 2000-2001,
10%-13% in Chongqing, China, in 2006-2007, 9%-25% in several districts of India in
2006-2007, and 24%-35% in Yangon and Mandalay, Myanmar, in 2007 (90) . In
Southeast Asia, HIV was found to be highly prevalent among MSM in Cambodia (14%
in Phnom Penh in 2000), Thailand (increasing from 17% to 30% during 2003-2007 in
Bangkok; 15% in Chiang Mai in 2005), and Vietnam (9% in Hanoi in 2006) (90). From
2006 to 2011, the number of all HIV cases diagnosed in MSM increased from 2.5% to
13.7% in China, and from 23.5% to 77.2% in Taiwan (89). Since 2004, the HIV epidemic
has re-emerged among MSM in Hong Kong and a new HIV epidemic has been reported
in MSM in Mongolia (91). In Vietnam, HIV prevalence among MSM has increased
significantly, from 9% in 2006 to 20% in 2011 (92). Integrated behavioural and biological
surveillance (IBBS) conducted in Vietnam in 2009 found that HIV was most prevalent
among MSM in major cities, ranging from 14% to 20% (93).
Risky sexual behaviours
A considerable amount of research has found a high prevalence of risky sexual
behaviours, particularly CAI among MSM across the globe, both in high-income countries
and LMIC (84). A recent online survey among more than ten thousand MSM in twelve
Asian countries found that more than two fifths of MSM practiced insertive or receptive
CAI with their male partners, although the review did not distinguish between casual and
regular partners (94). A recent systematic review of studies of HIV and sexual risk
behaviours among MSM in the Mekong subregion and China conducted during the
2000s reported that the rate of CAI ranged from 31% to 72% in Cambodia, China,
Thailand and Vietnam, across different types of sexual partners and recall periods (90).
Furthermore, sizeable proportions of MSM in these countries reported having multiple
male sexual partners (31%-54%), engaging in sex work (9%-24%) and having female
sexual partners (25%-33%) (90). In China, a recent review of national and international
studies and grey literature found that only 20%, 30% and 58% of MSM practiced
consistent condom use with their regular, casual and commercial sex partners,
respectively (95). The pooled estimates from recent studies in China indicate that the
majority of HIV-positive MSM (>70%) engaged in some CAI with men and 68% had
condomless vaginal sex with women (96). A systematic review of research conducted
between 2003 and 2007 regarding homosexual behaviours among MSM in LMIC found
that the rate of condom use during the last anal sex encounter with another man was
limited and varied by geographical setting, ranging from 6%-47% in Southeast Africa,
32%-63% in East Asia, 30-82% in Southeast Asia, 37-58% in Eastern Europe and
Central Asia, and 47-61% in Latin America. Consistent condom use with another man in
10
the previous year ranged from 12-18% in Southeast Africa, 0-40% in East Asia, 54% in
the Caribbean, and 64% in Latin America (97).
The research presented above indicates high levels of high infection and low levels of
consistent condom use by MSM in LMIC, particularly East and Southeast Asia. To
improve HIV prevention, it is necessary to understand the influences on HIV infection
and sexual behaviour among MSM in these settings.
CORRELATES OF HEALTH VULNERABILITIES AMONG MSM
This section provides an overview of research published mostly in the last five years on
correlates of drug use, in particular ATS use, and associated health-related harms,
including CAI and other sexual behaviours, HIV infection and psychological distress,
notably depression, among MSM.
For each health vulnerability of interest (drug use, CAI, HIV infection and depression),
associations with these conditions are grouped into the following categories (depending
on the availability in the literature): i) socio-demographic factors, ii) personal
dispositions including mental health problems (i.e. depression) and personal traits such
as sexual sensation-seeking, iii) behavioural correlates such as drug use and sexual
behaviour, iv) environmental or contextual correlates such as access to gay venues or
HIV services, v) community/interpersonal factors (i.e. men’s involvement in a MSM
community) and lastly, vi) societal and cultural factors (i.e. homosexuality-related
stigma and discrimination).
Correlates of drug use, including ATS
Drug use has been a great concern in research with MSM because of its potential
association with risky sexual behaviours and, consequently, HIV infection. During the
past three decades of the HIV epidemic, a great deal of literature has suggested that
substance use, particularly ATS use, is a multifaceted problem which involves personal,
interpersonal, contextual, cultural and societal factors.
Socio-demographical characteristics
Previous studies reported diverse demographic profiles of MSM who used recreational
drugs, including ATS. Depending on the study’s contexts and sampling methods, the
demographic characteristics of men who used drugs varied in terms of age, education,
occupation and income. However, many studies in different settings have consistently
11
found that drug use is more likely common in younger men compared to older men (98-
105) and among HIV-positive men compared to HIV-negative men (99, 101, 105-109).
Dispositions correlates
Drug use by MSM may be shaped by personal dispositions such as comorbid health
conditions (e.g. depression) or personality characteristics such as sexual sensation
seeking or sexual compulsivity. A number of studies have found that MSM who
experienced depression or depressed mood are more likely to use drugs, including
methamphetamine (101, 105, 107, 110). Several studies have found that personal traits,
such as sexual sensation seeking, the propensity to seek novel, optimal sexual
excitement and to engage in novel sexual experiences (111), was directly associated
with both drug use and risky sexual behaviours and can mediate the association between
the two (112-116). There has also been research that has found that the sexual
compulsivity scale, which measures preoccupations with sexual acts and episodes, is
associated with an increased likelihood to use drugs in MSM (105). Drug use or sexual
behaviours could be seen as an expression of personal traits, or on the other hand,
personal traits, might affect the relationship between drug use and risky sexual
behaviours (117). However, the exploration of these factors’ effects in relation to sexual
or drug use behaviours has not received substantial attention in the literature.
Behavioural correlates
Consistently, previous studies conducted in different settings have found that MSM are
more likely than their heterosexual peers to use different drugs, such as marijuana,
inhalants, (crack) cocaine, psychedelics or hallucinogens, tranquilisers or heroin (20-22,
40, 43, 107, 118-121). Alcohol consumption and poly-drug use in the context of
methamphetamine use is very common in different populations of MSM (22, 101, 106,
107, 122, 123). Concurrent use of multiple drugs could, of course, make it difficult to
understand the effect of individual drugs, particularly the effects on risky sexual
behaviours and HIV infection. However, most of this research on the correlates of ATS
use has been conducted in high-income countries, while evidence from LMIC is lacking.
Environmental or contextual correlates
Much of the current literature has explored the influences of environmental and
contextual factors on drug use behaviours of MSM. Thus far, available evidence
highlights the widespread use of recreational drugs in gay-specific, sexual-oriented
venues and events such as gay bars, bathhouses, dance clubs, circuit or sex parties (4,
20, 22, 37, 101, 106, 124, 125). Notably, for example, in the sexual subculture of gay-
specific venues and events in New York, researchers have found that recreational drug
12
use, particularly methamphetamine use is very prevalent (18, 20, 22, 126). A study of
MSM in four cities in the US in the early 2000s also found that men who go to sex venues
were more likely to use party drugs, including methamphetamine, ecstasy and poppers
compared to men who frequent these venues less often (127).Besides physical venues,
there has been an increasing use of the internet and mobile phones by MSM to
communicate, make friends and find sexual partners (128-132). Studies have found that
drug use, including ATS use, is more prevalent among MSM who use the internet to seek
sexual partners compared to men who seek partners from other channels (102, 103,
129-132). Exploring how MSM engage with and meet other MSM in particular locations
may assist in understanding patterns of drug use and sexual behaviours by MSM.
Community/Interpersonal correlates
Studies have found that gay men who have a strong attachment to the gay community
may be more likely to take drugs to enhance sexual performance and subsequently
might engage in risky sexual behaviours (133). High involvement in the gay community
and more socialising with gay friends can also be associated with more drug use and
poly drug use (134). How interpersonal relationships among MSM and the local MSM
subculture influence drug use and sexual behaviours should therefore be taken into
account in studies of drug use and other MSM’s health behaviours.
Societal and cultural correlates
As suggested by the minority stress model (50), MSM may experience social stigma and
discrimination in relation to homosexuality, including internalised homophobia, which can
contribute to a stressful social environment, resulting in a greater risk of mental health
issues, including alcohol and substance use problems. Men who experience
discrimination against their sexual orientation alone or in combination with racism and
gender discrimination, have been found to have higher rates of substance use and
alcohol use (135-137). Furthermore, homosexual men who have internalised
homophobia have been found to be more likely to use drugs than other men (50, 138).
Nonetheless, the assessment of homosexuality-related stigma and discrimination has
not been widely included in previous studies of drug use, both in high-income countries
and in LMIC.
Correlates of condomless anal intercourse (CAI)
MSM who practice risky sexual behaviour are at risk of acquiring STI, including HIV.
These risky practices include having multiple regular and casual sexual partners,
participating in group sex, transactional sex, and having receptive condomless anal
13
intercourse (RCAI) or insertive condomless anal intercourse (ICAI). CAI, particularly
RCAI is consistently identified as a risk factor for HIV infection. Understanding local risk
factors and the correlates of CAI can assist in the formulation of HIV prevention
interventions targetting MSM in specific contexts. This section compiles the available
evidence on the correlates of risky sexual behaviours among MSM.
Socio-demographical characteristics
Associations between socio-demographic characteristics and engaging in CAI among
MSM vary, depending on the design of studies, sampling methods and recruitment
locations. Some studies have found that CAI is less frequent among men who are older,
highly educated or with higher incomes (77, 139, 140), while other studies report
opposing findings or find no associations (141, 142). Some studies have found that CAI
is more frequently reported by homosexual or gay-identified men compared to bisexual
or heterosexual MSM (143, 144). (143, 144). A number of studies have found that HIV-
positive MSM are more likely to practise CAI compared with HIV-negative or status
unknown MSM (94, 99, 140, 145, 146). An understanding of how CAI practice is
distributed by socio-demographic correlates is one of the essential steps in studies of
sexual behaviour since it provides important information about who safe sex
interventions should target.
Dispositions correlates
Few studies have assessed the association between personality traits (i.e. sexual
sensation seeking) or comorbid conditions (i.e. depression) and the likelihood of
participating in CAI by MSM. Nonetheless, findings suggest men who are more sexual
sensation seeking are more likely to engage in risky sexual behaviours, particularly CAI,
and that sensation seeking may moderate the relationship between alcohol or drug use
and CAI (113, 115, 116). Furthermore, previous studies have also found that having a
risk-taking personality (147), a higher level of sexual impulsivity (148), or having higher
trait anxiety (characterised by feelings of apprehension, tension, nervousness, or worry)
(149) were associated with a higher odds of CAI with HIV-positive or unknown status
partners. However, to the best of my knowledge, there has not been assessment of the
role of sexual sensation-seeking on the relationship between ATS use, particularly
methamphetamine use, and CAI in MSM.
Moreover, MSM who have comorbid mental health conditions, such as stress and
depression, are more likely to practice CAI (68, 149, 150). A recent study found that
depression was a significant modifier of the association between methamphetamine use
and CAI (151). While some previous findings reflect the fact that while some men engage
14
in CAI for enjoyment or enhanced sexual pleasure purposes, other practiced CAI
because they were anxious or depressed. Exploring the underlying cause of CAI,
therefore, is important to HIV prevention.
Behavioural correlates
A handful of literature has assessed the behavioural correlates of CAI, including
recreational or club drug use and alcohol consumption. Most studies, including those
from both high-income countries and LMIC, have found a statistically significant
association between CAI and alcohol consumption, including ‘binge drinking’ (141, 145,
152-155). Previous studies have also found that MSM who drink large quantities of
alcohol (‘binge drinking’) have more CAI partners and are more likely to engage in
transactional sex (4, 156).
Previous studies using different designs, i.e. cross-sectional or longitudinal studies or
studies using event-level measurement of drug use, have found that club drug use,
including methamphetamine and amphetamine use was associated with higher rates of
practicing RCAI and ICAI among both HIV negative and HIV positive MSM (4, 15, 23,
37, 68, 77, 94, 98, 122, 140, 143-149, 152, 156-171). Studies from high-income countries
indicate that methamphetamine use increases the likelihood of practicing RCAI or ICAI
with male partners (4, 15, 37, 43, 120, 122, 139, 149, 153, 165-167, 171-174). As such,
drug use, including ATS use, could facilitate the transmission of HIV and STIs.
It has been also reported that recreational or club drug use, including ATS use was
related to other sexual behaviours, such as having a higher number of sexual partners
(4, 37, 43, 98, 120, 121, 165, 166, 173, 175), and having sex with HIV positive partners
(107, 119-121, 165, 166, 172). Methamphetamine use in particular has been found to be
associated with having a higher number of sexual partners (4, 37, 43, 120, 121, 165,
166, 173), engaging in sexual marathons (4, 16, 18, 20, 37, 176) and participating in
group sex (16, 37, 43), having risky sex with casual or anonymous sexual partners with
whom they would never have had sex without the drugs (15, 16, 18, 43, 120, 166, 173)
and engaging in transactional sex or selling sex (4, 7, 37, 166). Co-administration of
methamphetamine with other illicit drugs may increase the likelihood of having sex with
many casual partners, anonymous or paid sexual partners (118), and having more RCAI
or ICAI with unknown status casual partners (119). Several studies suggest that gay or
bisexual men who use ecstasy are more likely to have more partners, have more one
night stand sex and practiced CAI (25, 177, 178). Furthermore, MSM who practiced CAI
are more likely to have high number of sexual partners, particularly having many casual
15
sexual partners (141, 142, 145, 147, 149, 174), participate in sex work (140, 169, 174,
179) and participate in group sex (145).
Overall, this research suggests a significant association between drug use and CAI and
other sexual behaviours, although evidence of causal relationships is lacking. However,
the findings can be variable, with some studies finding no evidence of an association
between drug use and CAI (4), possibly because of the difference in study designs,
sampling methodology, measurement of drug use and sexual behaviour and the potential
for underlying factors, such as contextual influences on drug use or confounding (117).
Nonetheless, understanding the association between drug use, particularly ATS use and
CAI practice, and other sexual behaviours is one of the essential components of any
study of drug use in MSM.
Environmental and situational factors
A number of studies have reported that MSM who frequent gay-specific sex venues,
such as bathhouses, saunas, gay bars and public cruising areas, are more likely to
engage in CAI (127, 140, 147, 180-182). Additionally, in the context of the popular
availability of the internet and social networking applications on smartphones, recent
studies have found that MSM who find sexual partners online are more likely to report
CAI, and have more sexual partners, particularly casual partners (73, 94, 131, 143, 183-
189). A recent meta-analysis of 11 observational studies found that MSM who initiated
sexual encounters online were more likely to participate in CAI or group sex (190). At the
environmental level, evidence has demonstrated that accessing HIV testing and other
HIV prevention services can be associated with a reduced likelihood of risky sexual
behaviours by MSM, if they receive safe sex counselling, (141, 191), while other studies
find that men who access HIV testing may report higher levels of CAI (142, 168, 192). In
either case, access to or uptake of HIV prevention and testing appears to be an influence
on the likelihood of CAI by MSM (193).
Cultural, societal correlates
Studies have analysed the relationships between societal and cultural factors and CAI.
Several studies have found that MSM who experienced homosexuality-related stigma
and discrimination (140, 194-196), internalised homophobia (197) or social isolation
(146) were more likely to report CAI. Additionally, MSM who suffered from social stress
(149) were more likely to report CAI. Moreover, MSM who perceived higher social norms
of condom use were less likely to report CAI (146), while MSM who had weaker safe-
sex norms were more likely to practice CAI (158, 198, 199). Lastly, research has shown
that MSM’s beliefs in the effectiveness of different HIV prevention strategies (such as
16
serosorting, strategic positioning and withdrawal) may affect their sexual practices. MSM
who practice strategic positioning and withdrawal or who believe that HIV treatment
reduces transmission are more likely to report CAI (140).
Correlations of HIV infection
This sub-section provides an overview of recent research regarding factors associated
with the risk of HIV infection among MSM. This includes studies with different designs,
including longitudinal, case-control and cross-sectional studies.
Socio-demographical characteristics
Studies from both high-income countries and LMIC have found socio-demographic
differences between HIV-positive and HIV-negative MSM. Some studies found that HIV-
positive MSM are more likely to be older (200-210), from lower socio-economic
backgrounds, including lower education levels (200, 202, 211-217), are unemployed
(206), or have low incomes (203). Conversely, some other studies found that HIV was
more prevalent among MSM younger than 25 years (200, 213, 218, 219) or MSM who
have higher incomes (220). Research more consistently finds that identifying as
homosexual or gay or exclusively having sex with men is associated with a higher risk of
HIV infection (203, 220-222). These findings suggest a diversity of socio-demographical
correlates of HIV infection, reflecting different epidemiological distributions of HIV
infection and variations in the ways studies were designed.
Sexual risk behaviours
Many studies have assessed the relationship between risky sexual behaviours, notably
CAI, and HIV infection. Both prospective and retrospective longitudinal studies have
consistently found that CAI, particularly RCAI, is the main risk factor for HIV
seroconversion among MSM (200, 205, 209, 214, 219, 221, 223) and it is also a strong
covariate of HIV prevalence in cross-sectional studies (203, 204, 206, 222, 224-230).
Position during anal sex may also be associated with HIV infection risk; longitudinal
studies have reported that MSM who practice receptive or versatile positions during anal
sex are more likely to get HIV infection than men who are exclusively insertive (200, 212,
231). Other behavioural risks of HIV infection in high-income and LMIC include having
a higher number of male sexual partners (205, 213, 214, 219, 231), participation in group
sex (200, 221), having sex with HIV-positive or unknown status partners (205, 219, 232)
and engaging in sex work (212). All of these risk factors have also been identified as
covariates of HIV prevalence in cross-sectional studies (203, 208, 215, 222, 224, 227,
233-237).
17
Previous studies have further found that MSM with a recent history of STIs and other
blood-borne infections, including syphilis, gonorrhoea, signs of genital ulcers and
hepatitis B or C virus are more likely to be infected with HIV (200, 205, 212-214, 221).
Findings from a number of cross-sectional studies also show a significantly higher rate
of STIs among HIV-positive MSM (203, 209, 210, 222, 228, 236, 238, 239), although
these STIs may occur after diagnosis of HIV.
Drug use behavioural correlates
Other widely reported behavioural correlates of HIV infection in MSM include drug use.
Longitudinal studies have found that MSM who use drugs generally or use drugs before
or during sex are associated with a higher likelihood of HIV infection (200, 240). Further,
evidence from longitudinal and case-control studies has demonstrated that erectile
dysfunction medications (EDM) and poppers (amyl nitrite) use increased the likelihood
of HIV seroconversion (200, 217, 219, 240). There is also some evidence that alcohol,
particularly binge drinking, increases the likelihood of getting HIV (241) and that
hazardous alcohol consumption in the last year was associated with HIV prevalence
(215). Additionally, drug use behaviour has been found to be correlated with HIV
prevalence in a number of cross-sectional studies (203, 210, 211, 226, 229, 242, 243),
although it is not clear if this drug use occurred before or after HIV infection. Injecting
drug use has also been found to be a risk factor of HIV seroconversion in a longitudinal
study (205) or a covariate of HIV prevalence in cross-sectional studies (83, 229, 236).
Regarding the association of ATS use and HIV infection, studies in the early period of
the HIV epidemic reported inconsistent findings. While almost all longitudinal and case-
control studies find that methamphetamine or amphetamine was a risk factor for HIV
seroconversion (200, 217, 219, 229, 239, 244-253), some cross-sectional studies did not
find this relationship (254, 255). In regard to ecstasy use and HIV infection, some studies
found significant associations between ecstasy use and HIV infection (196, 250-252),
while others found no relationship (217, 223, 247, 254, 256). The mechanism of how
drug use, particularly ATS use, may be associated with HIV infection is unclear.
However, because drug use and CAI are often associated, studying the influence of drug
use and particularly ATS use on HIV infection in MSM is still needed for informed HIV
interventions. Lastly, almost all studies of ATS use and HIV infection have been
conducted in high-income countries, while the evidence from LMIC is limited.
Other correlations
While the majority of studies focus on behavioural correlates, which could identify how
HIV is transmitted in a particular population, there have been few studies exploring other
18
correlates of HIV infection, which include interpersonal, environmental and cultural and
societal correlates of HIV infection.
As regards to interpersonal influences, some studies have shown that MSM who have
older sexual partners tended to have a higher risk of HIV infection (204, 223). Moreover,
disclosure of HIV status or agreement to have unprotected sex with sexual partners has
been found to be associated with a higher probability of HIV infection (223, 224). Studies
also found that HIV infection was more likely among men who had disclosed their sexual
orientation to family members or health care providers (220, 226).
In relation to environmental factors, HIV testing is regarded as one of the most important
components of a comprehensive HIV prevention package (257). Available evidence
suggests that accessibility to and uptake of HIV testing services or other HIV prevention
services increases the rate of diagnosis of HIV infection (200, 204, 211, 218, 220, 226).
Additionally, some studies have found that MSM recruited from parks and other venues
are more likely to be infected with HIV (232) possibly because MSM recruited in these
locations may be more likely to engage in sex work (258). Lastly, studies indicate that
MSM who have experienced sexual abuse or coercion may be more likely to be infected
with HIV (200, 206, 215).
Last but not least is how cultural and societal factors affect risks of HIV infection. Previous
studies have found that experiencing HIV- or homosexuality-related stigma and
discrimination or internalised homophobia is positively correlated with HIV infection (201,
215). Experience or perception of either HIV- or homosexuality-related stigma and
discrimination may prevent MSM from practising safe sex, or accessing HIV prevention
and treatment services (193, 257, 259), thus fuelling the transmission of HIV in this
population
Correlations of depression among MSM
Numerous studies have been conducted to understand the correlates of depression in
MSM. Many studies focus on exploring the correlation between socio-demographic,
behavioural, interpersonal and cultural, and societal factors with depression.
Socio-demographic characteristics
Although findings have been mixed, studies in both high-income countries and LMIC
have found that depression is more prevalent among MSM who are younger (55, 72,
260, 261), have lower levels of education (66, 67, 262, 263), are unemployed (263), have
low incomes (66, 72, 263) or are experiencing financial hardship
19
(70), are single (262, 264) or married to a woman (74, 262). Other personal
characteristics that have been found to be associated with depression among MSM
include being HIV-positive (68, 73, 76, 105, 262, 265, 266), not having any recent sex or
reporting sexual dysfunction (72, 262, 264), experiencing significant adverse events (72),
having a history of attempted suicide (264) and having low levels of self-esteem (261).
Behavioural correlates
A number of studies have been conducted to explore the relationship between
depression and HIV-related risky sexual and drug use behaviours. Findings have been
mixed in term of the significance of the association, however, numerous studies in MSM
in different settings have found an association between depression and CAI (55, 66, 68,
69, 71, 80, 265, 267-270). MSM who have depression have been found to have more
regular sexual partners than other MSM (70), to be more likely to have engaged in sex
work (269) or perceive themselves to be at high risk of HIV infection (269).
Additionally, MSM who have depression, particularly men who are also HIV-positive, are
more likely to consume alcohol or other drugs (67, 68, 73, 76, 82, 105, 271). Specifically,
in a recent comprehensive review, depression was identified as one of the psychological
harms of regular methamphetamine use (14). Syndemic conditions, where there is a
comorbidity of several psychological disorders, may have synergistic effects on risky
sexual behaviours (265, 272-274). Lastly, some studies have found a significant
association between depression and being diagnosed with STIs, particularly syphilis (73,
275).
MSM with depression and other mental health problems may be less likely to benefit
from HIV prevention interventions (276). Further, mental health problems, particularly
depression can also compromise MSM’s access to and uptake of HIV prevention and
treatment services (272, 274).
Interpersonal correlates
Several studies focused on exploring community or interpersonal-related correlations of
depression in the MSM population. One of the most interpersonal factors which have
been studied relatively widely is the level of engagement with and social support received
from the gay community and network. The level of connection to the gay community and
emotional or social support received from other MSM peers in their gay friend network
have been found to be protective factors for depression in the MSM population (72, 73,
79, 261, 264, 277). On the other hand, there has been evidence that men who suffer
interpersonal isolation or withdraw from social opportunities have a higher probability of
having depression symptomology (72). Additionally, some available evidence has
20
reported that MSM who experienced CSA or maltreatment during childhood were more
likely to experience depression in their adult years (67, 264, 265, 278). Moreover, CSA
can result in long term adverse physical health problems such as negative perceptions
of overall well-being. CSA may also result in psychological disorders, such as anxiety,
low self-esteem and feelings of helplessness, anger, fear, shame, isolation, and a
negative perception of self (279-281). Several studies also reported that depression was
associated with disclosure of being MSM to other people (277) or disclosure of being
HIV-positive (76). As already presented, interpersonal factors, particularly engagement
or attachment with the gay community and gay friendship networks, may strengthen or
promote men practicing safe or risky drug use or sexual behaviours. Attending to the
specifics of these relationships is therefore important.
Cultural, societal correlates
Numerous studies have paid attention to the cultural and societal correlates of
depression. Previous studies in both high-income countries and LMIC consistently report
that MSM who suffer from racism, HIV-or homosexuality-related stigma, are more likely
to report depression and anxiety, maybe because of subsequent associated hostile
environments (55, 67, 69, 73, 74, 264, 277, 282-286). A recent study in China found that
homosexuality-related stigma was indirectly associated with depression and anxiety
among MSM (283). Another study in Australia found that internalised homophobia and
perceived and experienced stigma were related to psychological distress and suicidal
ideation among LGBT people (286). One study in India found that gender-nonconformity
stigma and HIV-related stigma were associated with a higher degree of depression
among MSM (285). A study in the US found that experiencing racism was associated
with depression among ethnic minority MSM (282).
To summarise, stigma and discrimination, including that related to homosexuality, is
correlated with HIV infection and risky drug use and sexual behaviours. Stigma and
discrimination may also be associated with mental health problems, particularly
depression, among MSM.
SEX, DRUGS USE AND THE HIV EPIDEMIC AMONG MSM IN VIETNAM
Vietnam at a glance
Vietnam is a country located in the Southeast Asia region, bordering China, Cambodia
and Laos. The estimated population in 2013 was 92.5 million, with 47% of people working
in the agricultural sector and 21% working in the industrial sector. The reported Gross
21
Domestic Product (GDP) per capita in 2013 was US$1785(287). As of 2014, Vietnam
had 64 provincial or cities level administrative units and approximately 33% of the
population was estimated to be living in urban areas. The literacy level among people
aged 15 years or older was 94.7%, with slightly higher levels of literacy among men than
women (96% versus 93%). In 2014, the unemployment rate among working-aged people
was 3.4% with lower rates in urban areas (1.2%), particularly Hanoi (0.99%) and Ho Chi
Minh City (0.3%) (288).
Vietnam was under Chinese imperial rule for approximately 1000 years until it reclaimed
its independence in 938 AD. In 1867, France colonised Vietnam and set about ‘civilising’
and modernising what the colonial regime perceived to be Vietnam’s old and primitive
society. During this time, Vietnam underwent dramatic political, economic and social
changes (289). Vietnam retained a feudal regime until 1945, when Vietnam’s Revolution
Movement, under the leadership of the Vietnamese Communist party, liberated Vietnam
from French Colonial governance and the Nguyen dynasty. During the feudal regime
period, Vietnamese culture and society were profoundly influenced by Chinese
Confucian ideology and culture (289). After the 1945 revolution, Vietnam was at war with
France until the1954 Geneva Agreement divided the country into the North (following
socialist ideology and supported by the Soviet Union and China) and the South (ruled by
a US-backed government). In the 1960s a war broke out between the Vietnam
Democratic Republic Government in the North and the Government of the Republic of
Vietnam in the South, in which the US government became involved. This war is known
as either the Vietnam War or, in Vietnam, the American war. During the Vietnam war,
South Vietnam experienced significant economic and social changes toward capitalism
and Western freedoms (289). However, traditional Confucian beliefs and practices were
still observed in both parts of the country.
After the national reunion in 1975, when the American war ended, until the middle of the
1980s, Vietnam had a subsidised, centrally managed, state-owned economy. This
changed substantially after 1986 when a socialism oriented, open-market economy was
introduced in the reform period known as “Doi Moi” (290). This reform, together with the
lifting of economic embargoes imposed on Vietnam after the reunification of the country
in 1975 until the late 1990s, has resulted in dramatic social and economic changes, with
increased cultural exchanges and trade between Vietnam and other countries, increased
production, growth of gross domestic product, reduced poverty, and increased life
expectancy (291) . These dramatic changes in recent years have substantially affected
the position of male homosexuality in Vietnamese society.
22
Male homosexuality history in Vietnam
Over a decade ago, Blanc published a seminal analysis of the historical position of male
homosexuality in Vietnamese society (292). Blanc noted that throughout Vietnam’s
history from the ancient period under Chinese rule until today , Vietnamese culture,
family and gender roles have been profoundly influenced by Chinese Confucian
ideology, particularly in rural provinces (293). With regard to gender, Vietnam has
traditionally been a patriarchal society that assumes there are two genders (male and
female) and in which men have more power than women. Historically, homosexuality
was largely invisible because of Confucian influences, according to which
heterosexuality was normative in order to maintain families and bloodlines (292).
Therefore, during Chinese rule and the Vietnamese feudal period, there was little visibility
or discussion of homosexuality. Some “shaman” and “medium” roles in spiritual and/or
religious settings appear to have been exceptions to this limited visibility. These
“shamen” or “mediums” performed ritual worship and songs and dances to communicate
with God or ancestral spirits in temples. In these roles, men could adopt non-gender-
conforming roles that allowed for expression of homosexuality. At the same time, these
men acquired relatively high social and religious status and earnings. However, there
was little discussion or recording of sexual relationships or behaviours of these “shamen”
and “mediums” (292).
Vietnam was exposed to Western ways of living and concepts with the arrival of the
French in the mid-19th century and the Americans in South Vietnam during the mid-20th
century. The contemporary globalisation process has also contributed to significant
social and cultural changes, including changes in perceptions and practices of
homosexuality (292). During the French colonial period, and subsequently in
contemporary Vietnam, exposure to Western modernity increased the visibility and
expression of homosexuality. However, at the same time, gender inequality set out in
Confucian ideology was reinforced with the introduction of Judeo-Christian moral
standards. Since the colonial period, male homosexuality was seen as a disease or
disability, or a moral failing or deviance, imported by Western men. Homosexuality was
sometimes misunderstood by both the general public and health providers to be limited
to emotional closeness between men, without sexual relations (292). Homosexuality
remained relatively invisible before Doi Moi and was not particularly discussed or
stigmatised. Since its visibility increased, however, people who express their
homosexuality have become targets for social stigma and discrimination (294).
23

From the Doi Moi period, Vietnam has rapidly increased the extent of social, cultural and
economic exchange with the rest of the world. Homosexuality has also become more
visible in society. Gay-specific venues such as cafés, bars and discotheques have been
established, and road sides and parks where men meet are easier to recognise in urban
settings, particularly in big cities such as Ho Chi Minh City and Hanoi, These various
venues attract local MSM as well as foreign visitors (292). Websites, online forums and,
more recently, social media such as Facebook, are easy for gay men and other MSM to
access and have become important channels for men to network, exchange information
and date, as well as to advertise or obtain sex work.
In recent years, there has been a movement to promote and advocate for the rights of
LGBT people in Vietnam. LGBT people have become visible in mainstream Vietnamese
media and on the websites of government agencies. As an alternative to derogatory,
slang words to describe homosexual practices and identities, some non-governmental
organisations such as The Institute for Studies of Society, Economics and Environment
(http://www.isee.org.vn/en/Home/About) or ICS (https://www.facebook.com/icsvn) have
promoted a classification that is aligned with Western typology. According to this system,
sexual orientations in Vietnam are defined as dong tinh (gay/homosexual), song tinh
(bisexual) and di tinh (heterosexual). Currently, almost all published studies about MSM
in Vietnam use this sexual orientation classification system, as it is readily understood
overseas (266, 295-297). I have used this classification system in my research with MSM
in Vietnam as Vietnamese gay, bisexual and MSM regard these labels as acceptable
and non-stigmatising
Drug use in Vietnam
Vietnam is located in a region that is recognised for the production, smuggling and use
of illicit drugs, including opium, heroin and, increasingly in recent years, ATS (30-34,
298). As reported by UNODC, in almost all countries in the South East Asia region, the
smuggling and use of methamphetamine pills, crystal methamphetamine and ecstasy
has increased steadily in the period from 2008 to 2012 (298).
Like other countries in the region, Vietnam has viewed the use and production of illicit
drugs as important problems for decades (299). In 2012, it was reported that there were
172,000 current drug users in Vietnam, mostly using heroin or opium, followed by
synthethic drugs (i.e. ATS) and other illicit drugs (298). A recent Government report
noted that the number of reported recent illicit drug users in Vietnam had increased from
143,196 in 2010 to 204,377 in 2014 (300). The 2012 UNODC report, which drew on data
24
provided from the Vietnam Government, noted that nearly half of the drug users were
young people (16 to 30 years old) and most of the drug users (96%) were male (298).
The dominance of men in drug use in Vietnam probably reflects gender norms and
prejudice against women using alcohol, tobacco and other substances. The UNODC
(2012) also highlighted that the most popular routes of administration of illicit drugs in
Vietnam included smoking and injecting, with injecting being the most common method
for heroin use.
The use of opium has been dominant in the country, especially in the Northern
mountainous areas, from the 19th century until the middle of the 1990s. Since then, a
shift has occurred to heroin use and then from the early 2000s, to ATS use (299). In
2010, ATS, including methamphetamine pills, crystal methamphetamine and ecstasy,
were ranked the second most commonly used drugs in Vietnam, after heroin (298). The
drug use reporting and monitoring system in Vietnam has typically focused on the harder,
more potent drugs such as morphine and heroin. However, conversations with key
informants and experts suggest that many new drug users in Vietnam are perceived to
be ATS users. Therefore, the drug monitoring and reporting system may have
underreported the use of ATS and other recreational drugs. Nevertheless, the prevention
and treatment of ATS use have been recognised as key objectives of Vietnam’s Illicit
Drugs Prevention and Control Program for the period 2016 to 2020 (300).
MSM and drug use in Vietnam
There was little information about drug use among MSM in Vietnam, particularly before
2010. Studies conducted in early the 2000s in Ho Chi Minh City found a low prevalence
of lifetime drug use, of 2% to 6%, in MSM (296, 301). In the late 2000s, studies in different
parts of the country found levels of drug use, including ecstasy and methamphetamine
use, ranging from 16% to 30%, reflecting different recall periods (81, 297, 302).
Since 2006, the Vietnam Government has implemented periodic monitoring of HIV
behavioural and biological indicators called IBBS in Vietnam. Three rounds of IBBS have
been conducted. The IBBS is different from community-based and online studies in the
way it recruits participants. Participants of IBBS are recruited by Respondent Driven
Sampling (RDS). Additionally, participants who engage in sex work are targetted.
Reports from IBBBs found higher levels of lifetime drug use in MSM samples in Hanoi
and Ho Chi Minh City, ranging from 21-23% in 2006 and 25-32% in 2011 (303, 304).
Although data from IBBS also showed a relatively low proportion of men who had injected
drugs (less than 10%), the sampling approach appeared more likely to reach subgroups
25
of MSM who used illicit drugs than that of community-based studies. All of these earlier
studies, however, used nonspecific indicators of drug use (i.e. ‘any drug use’) that does
not provide information on use of ATS or specific types of drugs.
From 2010 onwards, studies began reporting on ATS use in MSM. A study of male sex
workers in three cities reported a prevalence of amphetamine or methamphetamine use
in the last 30 days of 17% and of ecstasy use of 12% (305). Another study conducted
among MSM in 12 Southern provinces who reported ever having used drugs found that
18% had ever used ecstasy and 7% had ever used methamphetamine (210). Studies
also found a high prevalence (>50%) of lifetime or current alcohol use in MSM, across
time and geographical locations (210, 296, 305, 306).
Despite using different measures and designs, the data suggests that drug use by MSM
in Vietnam has increased during the past 20 years, particularly in the Southern provinces
and larger cities. It may also reflect the fact that recent studies, particularly IBBS,
sampled subgroups of MSM who consumed more drugs. Nevertheless, data on drug use
by MSM remains scarce.
Correlates of drug use in MSM in Vietnam
There are relatively few accessible, published studies on the correlates of drug use,
particularly ATS use, by MSM in Vietnam. There have only been two published
quantitative studies in which drug use is the primary outcome found in PubMed. A study
conducted with MSM in a Southern province of Vietnam found only a few significant
behavioural covariates of injection drug use, including having partners who injected
drugs, alcohol use, and having sex with non-paying female sexual partners in the last six
months (307). Another study found that any recent drug use in MSM was significantly
associated with depression (81). A qualitative study on substance use among drug-using
MSM in Vietnam found that participating MSM used different types of drugs, including
heroine, methamphetamine, ecstasy, ketamine, and marijuana. Any drug use was
related to not using condoms during sex and overcoming social stigma towards
homosexuality and sex work in those who were involved in selling sex (308).
In the context that drug use by MSM appears to have increased in recent years,
particularly the use of ATS, evidence regarding the magnitude of drug use and its
correlations is urgently needed to provide information for effective and targetted drug use
interventions for MSM in Vietnam.
26
HIV-related risky sexual behaviours in MSM
There is a body of literature on the extent of HIV-related risky sexual behaviours,
particularly CAI, among MSM in Vietnam. At least 16 quantitative studies have reported
various measures of risky sexual behaviours (81, 295-297, 301, 302, 305-307, 309-315).
Data on HIV-related sexual behaviours is also available from IBBS reports. Some
qualitative research provides valuable supplementary insights on HIV-related sexual
behaviours among MSM in Vietnam.
In the early 2000s, community-based studies with MSM in big cities in Vietnam (i.e. Ho
Chi Minh City and Hanoi), as well as studies conducted in smaller provincial towns, found
a relatively high proportion (41-67%) of men had engaged in CAI with different sexual
partners in the last month and a high proportion (32-71%) reported CAI at their last sexual
encounter (295, 296, 301). A study reported in 2010 found that many (50%) young MSM
in Hanoi men scored high on a combined index of risky sexual practices which included
the number of sexual partners, use of condom during anal sex and consistent use of
condom during any sexual intercourse in the last 30 days (307). More recent studies
conducted online find high proportions (64-69%) of MSM reporting CAI with casual and
regular partners in the last month (311), in the last six months (41-63%) (310) (310), as
well as with any male partners in the last three months (36%) (36%) (312). Studies have
also found that rates of CAI during recent transactional sex, either with paid or paying
partners, are generally lower (21-33%) (81, 311).
IBBS findings in Hanoi and Ho Chi Minh City suggest that reports of CAI with regular and
casual partners in the last month have reduced from 63-71% in 2006 to 46-70% in 2011,
and 41%-60% in 2013, as has CAI with transactional sexual partners in the last month,
from 77-96% in 2006 to 41%-85% in 2011, and 1%-44% in 2013 (303, 304, 316).
However, findings from community-based studies, online studies and IBBS may not be
directly comparable because of different study designs and sampling methods. Because
IBBS surveys in Vietnam recruit participants by RDS and by sex work status, these
surveys may reach networks of MSM who are more likely to report high levels of CAI
(although rates have declined in the IBBS rounds). Community-based and online studies
suggest rates of CAI may have remained high in other groups of MSM in Vietnam.
Correlates of CAI practice
Correlates of CAI among MSM population in Vietnam are not well researched. Some
studies found that there were higher rates of CAI among MSM in Vietnam with higher
income level (312), more alcohol consumption before or during sex (305, 311), higher
27
perceived risk of HIV infection (311), and a history of sexual violence and childhood
sexual abuse (81). CAI was less likely among MSM who found casual sexual partners
on the internet, who had paid sexual partners in the last six months and who had multiple
casual sexual partners in the last six months (311).
When being treated as a covariate in the analysis of other health outcomes, CAI has
been found to be positively associated with enacted (i.e. experienced) homosexuality-
related stigma, being classified as having depression and having used drugs in the last
30 days (302), alcohol dependence and childhood sexual abuse (81). However, CAI was
not found to be associated with having never tested for HIV, willingness to use the
internet for seeking HIV prevention services or sex work related stigma (309, 310, 317).
In addition, several qualitative and review papers provide valuable insights into the
sexual practices of MSM in Vietnam. Qualitative data showed that MSM in Vietnam tend
to have concurrent, short-term sexual relationships and casual partners when they are
seeking new and interesting sexual experiences, or when they are not in a romantic
relationship with another man (318-322). MSM’s narratives from qualitative studies also
suggest that inconsistent condom use is pervasive among MSM because condoms are
perceived as a sign of a lack of trust between sexual partners, particularly men who are
in long-term relationships (318, 320, 321). Condoms are also perceived with a loss of
sexual pleasure and are less likely to be used with sexual partners who are perceived to
be healthy (319-321). A review of Vietnamese MSM vulnerabilities to HIV infection
reported similar findings (323).
Apparently, there is a lack of knowledge in terms of the correlations associated with CAI
by MSM in Vietnam, particularly in relation to evidence from quantitative studies.
HIV epidemic among MSM in Vietnam
HIV was first reported in Vietnam in the early 1990s (324), and since then the epidemic
has rapidly spread in different parts of the country during the last 30 years, being reported
in all provinces and cities from 1999 (325). In its early stages, the HIV epidemic was
concentrated in specific key populations, in particular people who inject drugs and female
sex workers. Injection drug use initially was the dominant route of HIV transmission,
accounting for over 88% of new cases during the late 1990s (325, 326). As reported by
the Vietnam Administration HIV/AIDS Control Office (VAAC), at the end of 2015, the
national, cumulative number of people diagnosed with HIV was 227,154, of whom 85,194
had progressed to AIDS and 86,176 had died of AIDS (327).
28
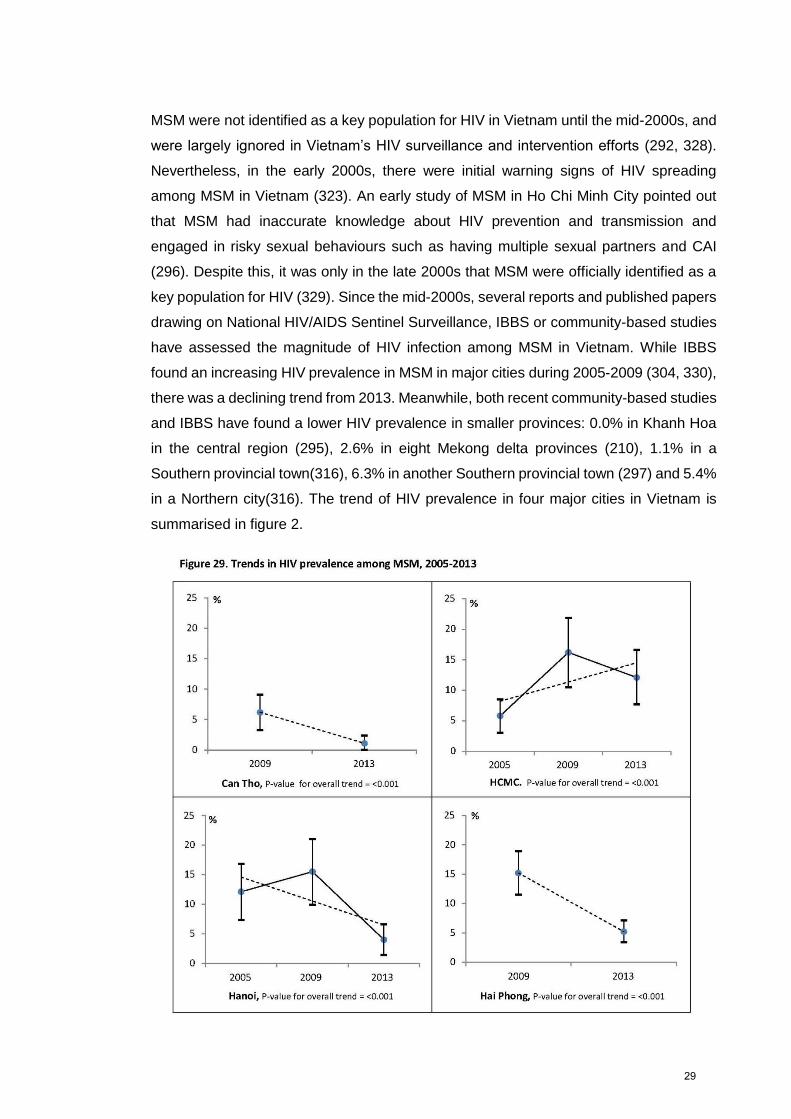
MSM were not identified as a key population for HIV in Vietnam until the mid-2000s, and
were largely ignored in Vietnam’s HIV surveillance and intervention efforts (292, 328).
Nevertheless, in the early 2000s, there were initial warning signs of HIV spreading
among MSM in Vietnam (323). An early study of MSM in Ho Chi Minh City pointed out
that MSM had inaccurate knowledge about HIV prevention and transmission and
engaged in risky sexual behaviours such as having multiple sexual partners and CAI
(296). Despite this, it was only in the late 2000s that MSM were officially identified as a
key population for HIV (329). Since the mid-2000s, several reports and published papers
drawing on National HIV/AIDS Sentinel Surveillance, IBBS or community-based studies
have assessed the magnitude of HIV infection among MSM in Vietnam. While IBBS
found an increasing HIV prevalence in MSM in major cities during 2005-2009 (304, 330),
there was a declining trend from 2013. Meanwhile, both recent community-based studies
and IBBS have found a lower HIV prevalence in smaller provinces: 0.0% in Khanh Hoa
in the central region (295), 2.6% in eight Mekong delta provinces (210), 1.1% in a
Southern provincial town(316), 6.3% in another Southern provincial town (297) and 5.4%
in a Northern city(316). The trend of HIV prevalence in four major cities in Vietnam is
summarised in figure 2.
29
Figure 1.2. Trends in HIV prevalence among MSM in Vietnam from 2005-2013 from
Integrated Biological and Behavioural Surveillances (IBSS)
(Source: National Institute of Hygiene and Epidemiology (Vietnam Ministry of Health).
HIV/STI Integrated Biological and Behavioural Surveillance (IBBS) in Vietnam. Results
from Round III and trends across three rounds (2005-2009-2013) of the survey)2
Because of different study designs, sampling methods, different subjects’ inclusion
criteria, findings from IBBSs and community-based studies are hard to compare. Other
factors such as HIV–related mortality and migration might have affected the HIV
prevalence. Therefore, it is difficult to conclude if there has truly been a decrease of HIV
prevalence among the MSM population in Vietnam, particularly in big cities (i.e. Hanoi
and Ho Chi Minh City).
Correlates of HIV infection among MSM in Vietnam
Because MSM in Vietnam were only considered as a population at risk of HIV infection
during the mid-2000s (328, 331), there have been few published studies exploring the
associated factors and/or risk factors of HIV infection among this population. Though
IBBS have collected both behavioural data and delivered HIV testing, there has only
been one analysis of the relationship between behavioural data and HIV prevalence
among MSM (332). A systematic review of available papers in PubMed found five
published papers that analysed the correlations of HIV infection in MSM since the
beginning of the epidemic in Vietnam (295, 301, 314, 332, 333). All of these studies were
conducted in Southern provinces and cities; two were conducted during early 2000s
(295, 301) and the other three were conducted during the late 2000s (297, 332) and/or
early 2010s (314).
In the first study of the correlations of HIV infection among MSM in Ho Chi Minh City
conducted in 2004 (301), Nguyen et al found being older, having lower education levels,
currently participating in selling sex, injecting drugs in the past 12 months and having
more than five male sexual partners in the past month were associated with HIV
infection. Another analysis using IBBS data for MSM in Ho Chi Minh City in 2009 (332)
reported similar findings of the association between older age, lower education levels
and a high number of sexual partners with HIV infection. Studies in the late 2000s
reported that HIV was more prevalent among men who had sexual partners who injected
drugs, who felt at risk of HIV infection, or who were injecting drug users (IDU) (297, 314).
Other factors positively associated with HIV infection among MSM in Vietnam include
2 The candidate received agreement from the National Institute of Hygiene and Epidemiology, Vietnam Ministry of Health for the reproduction of this figure in this thesis.
30
ever having used recreational drugs, particularly ATS and heroin, alcohol consumption
in relation to sex, ever having had sex with foreign sexual partners, being diagnosed with
syphilis (314), having CAI with female sexual partners and being transgender versus
cisgender (297). In agreement with other studies, consistent condom use during anal sex
was associated with a lower risk of HIV infection (314). While published research has
found no evidence of associations between HIV infection and occupation, employment,
or income levels among MSM, findings have been mixed with respect to associations
between HIV infection and sexually transmitted infections (STI), sex work and sexual
orientation (210, 297, 301, 332). In agreement with other studies, consistent condom use
during anal sex was associated with a lower risk of HIV infection (314).
As of note, all published literature on the associations with HIV among Vietnamese MSM
was conducted in the Southern provinces and cities during the 2000s. Updated evidence
is needed on the correlations of HIV infection, for example ATS use, particularly in the
Northern provinces and cities of Vietnam.
A SOCIO-ECOLOGICAL APPROACH TO STUDYING HEALTH AND WELL-BEING
Multilevel influences on health outcomes
Health conditions are often caused by multiple factors at different levels from individual
characteristics and pre-conditions to cultural and societal influences. Therefore, a holistic
understanding of the range of influences over health conditions can assist us in designing
effective interventions. It has been already argued that any study of people’s health
behaviours conducted in separation from the study of the wider environment and the
societal and cultural context is incomplete and insufficient to comprehend the complex
causes of human health and illness (334). Several epidemiologists have advised that
without considering structural factors that include societal and cultural influences, the
application of behavioural interventions to solve public health problems is unlikely to
result in successful outcomes (334, 335). Additionally, the heterogeneity of disease
patterns and socioeconomic variations in disease distribution found in previous studies
highlights the fact that there are rarely single, explanatory determinants or interventions
for health problems and as such, a multilevel approach is useful for understanding poorly
researched health issues (336). Lastly, it has been proposed that patterns of health and
disease in the population can be explained by a complex matrix of various interconnected
risks and protective factors, sometimes referred to as a “web of causation” (337).
31
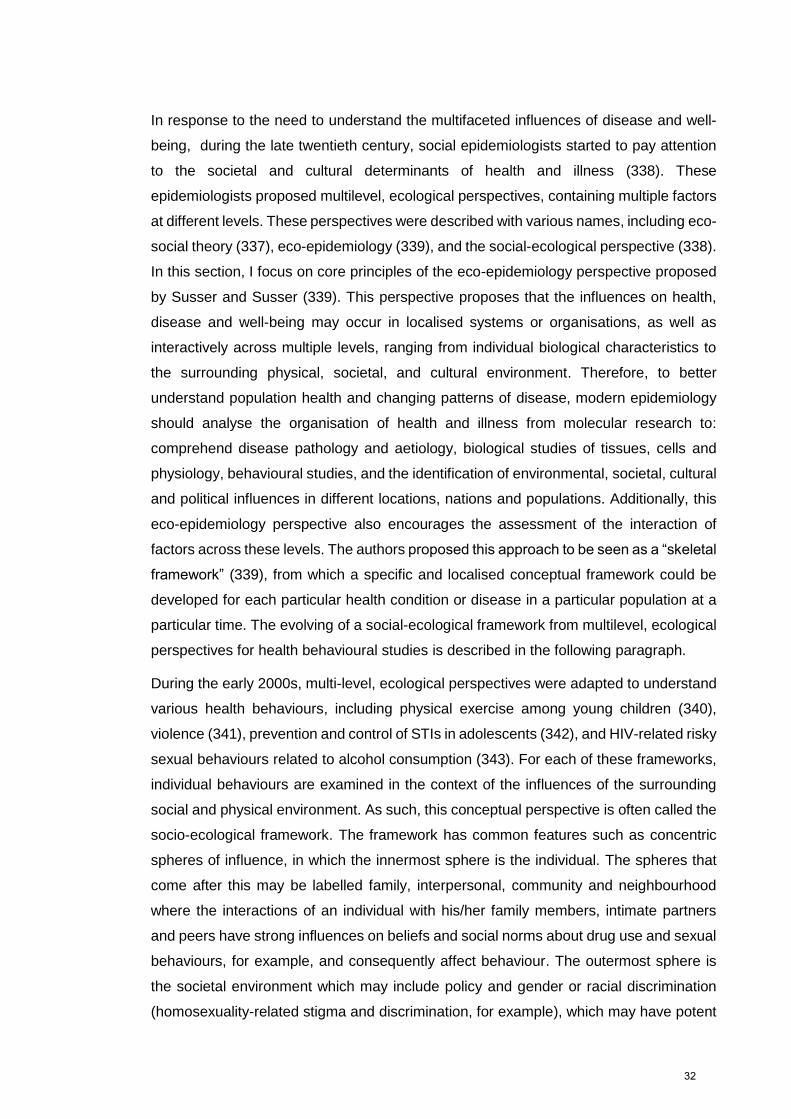
In response to the need to understand the multifaceted influences of disease and well-
being, during the late twentieth century, social epidemiologists started to pay attention
to the societal and cultural determinants of health and illness (338). These
epidemiologists proposed multilevel, ecological perspectives, containing multiple factors
at different levels. These perspectives were described with various names, including eco-
social theory (337), eco-epidemiology (339), and the social-ecological perspective (338).
In this section, I focus on core principles of the eco-epidemiology perspective proposed
by Susser and Susser (339). This perspective proposes that the influences on health,
disease and well-being may occur in localised systems or organisations, as well as
interactively across multiple levels, ranging from individual biological characteristics to
the surrounding physical, societal, and cultural environment. Therefore, to better
understand population health and changing patterns of disease, modern epidemiology
should analyse the organisation of health and illness from molecular research to:
comprehend disease pathology and aetiology, biological studies of tissues, cells and
physiology, behavioural studies, and the identification of environmental, societal, cultural
and political influences in different locations, nations and populations. Additionally, this
eco-epidemiology perspective also encourages the assessment of the interaction of
factors across these levels. The authors proposed this approach to be seen as a “skeletal
framework” (339), from which a specific and localised conceptual framework could be
developed for each particular health condition or disease in a particular population at a
particular time. The evolving of a social-ecological framework from multilevel, ecological
perspectives for health behavioural studies is described in the following paragraph.
During the early 2000s, multi-level, ecological perspectives were adapted to understand
various health behaviours, including physical exercise among young children (340),
violence (341), prevention and control of STIs in adolescents (342), and HIV-related risky
sexual behaviours related to alcohol consumption (343). For each of these frameworks,
individual behaviours are examined in the context of the influences of the surrounding
social and physical environment. As such, this conceptual perspective is often called the
socio-ecological framework. The framework has common features such as concentric
spheres of influence, in which the innermost sphere is the individual. The spheres that
come after this may be labelled family, interpersonal, community and neighbourhood
where the interactions of an individual with his/her family members, intimate partners
and peers have strong influences on beliefs and social norms about drug use and sexual
behaviours, for example, and consequently affect behaviour. The outermost sphere is
the societal environment which may include policy and gender or racial discrimination
(homosexuality-related stigma and discrimination, for example), which may have potent
32
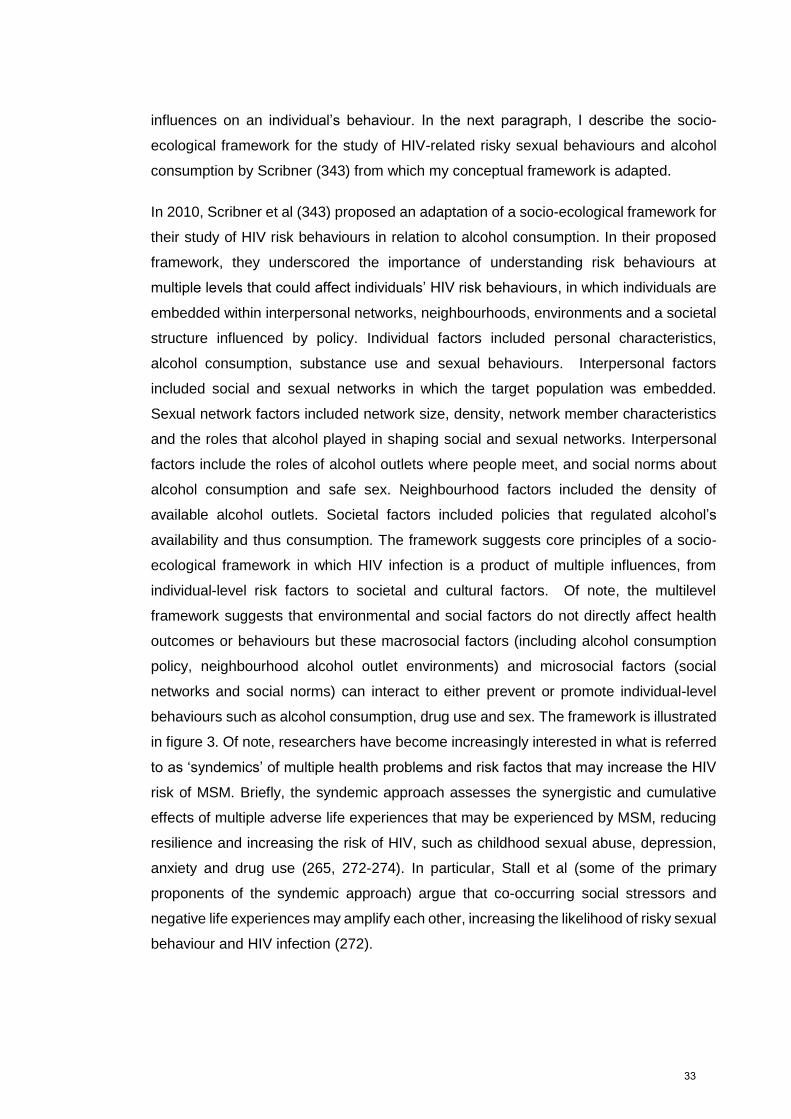
influences on an individual’s behaviour. In the next paragraph, I describe the socio-
ecological framework for the study of HIV-related risky sexual behaviours and alcohol
consumption by Scribner (343) from which my conceptual framework is adapted.
In 2010, Scribner et al (343) proposed an adaptation of a socio-ecological framework for
their study of HIV risk behaviours in relation to alcohol consumption. In their proposed
framework, they underscored the importance of understanding risk behaviours at
multiple levels that could affect individuals’ HIV risk behaviours, in which individuals are
embedded within interpersonal networks, neighbourhoods, environments and a societal
structure influenced by policy. Individual factors included personal characteristics,
alcohol consumption, substance use and sexual behaviours. Interpersonal factors
included social and sexual networks in which the target population was embedded.
Sexual network factors included network size, density, network member characteristics
and the roles that alcohol played in shaping social and sexual networks. Interpersonal
factors include the roles of alcohol outlets where people meet, and social norms about
alcohol consumption and safe sex. Neighbourhood factors included the density of
available alcohol outlets. Societal factors included policies that regulated alcohol’s
availability and thus consumption. The framework suggests core principles of a socio-
ecological framework in which HIV infection is a product of multiple influences, from
individual-level risk factors to societal and cultural factors. Of note, the multilevel
framework suggests that environmental and social factors do not directly affect health
outcomes or behaviours but these macrosocial factors (including alcohol consumption
policy, neighbourhood alcohol outlet environments) and microsocial factors (social
networks and social norms) can interact to either prevent or promote individual-level
behaviours such as alcohol consumption, drug use and sex. The framework is illustrated
in figure 3. Of note, researchers have become increasingly interested in what is referred
to as ‘syndemics’ of multiple health problems and risk factos that may increase the HIV
risk of MSM. Briefly, the syndemic approach assesses the synergistic and cumulative
effects of multiple adverse life experiences that may be experienced by MSM, reducing
resilience and increasing the risk of HIV, such as childhood sexual abuse, depression,
anxiety and drug use (265, 272-274). In particular, Stall et al (some of the primary
proponents of the syndemic approach) argue that co-occurring social stressors and
negative life experiences may amplify each other, increasing the likelihood of risky sexual
behaviour and HIV infection (272).
33
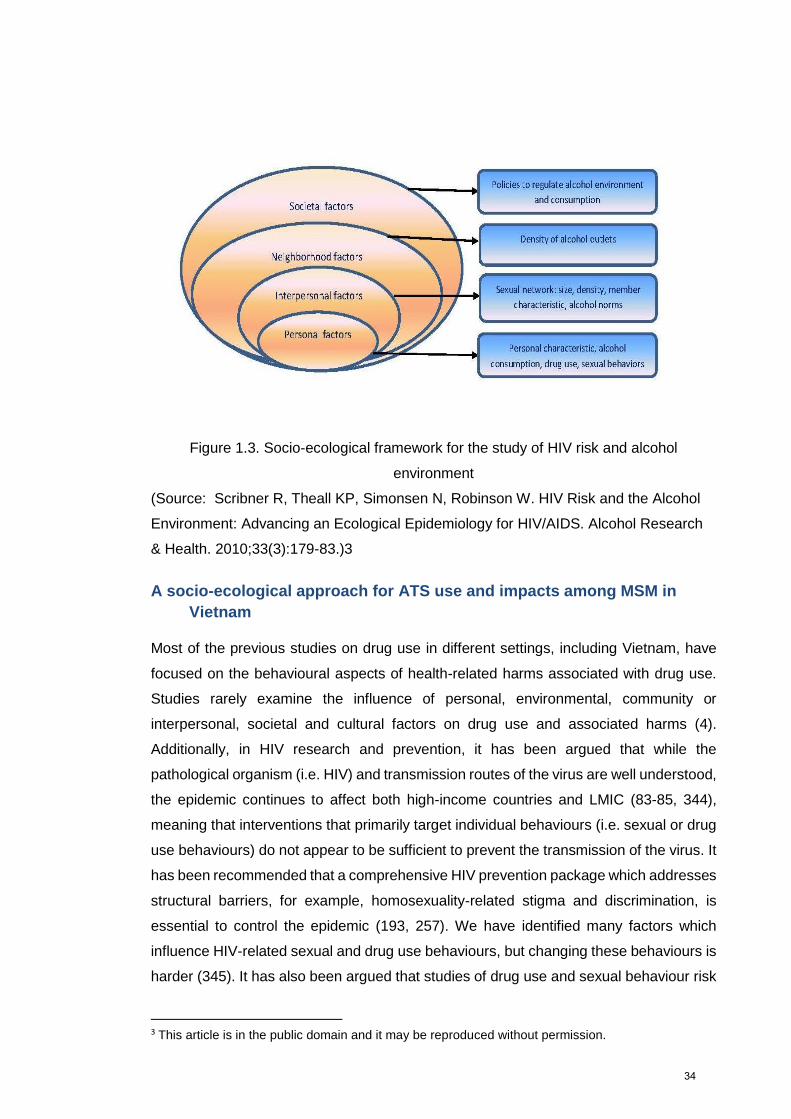
Figure 1.3. Socio-ecological framework for the study of HIV risk and alcohol
environment
(Source: Scribner R, Theall KP, Simonsen N, Robinson W. HIV Risk and the Alcohol
Environment: Advancing an Ecological Epidemiology for HIV/AIDS. Alcohol Research
& Health. 2010;33(3):179-83.)3
A socio-ecological approach for ATS use and impacts among MSM in
Vietnam
Most of the previous studies on drug use in different settings, including Vietnam, have
focused on the behavioural aspects of health-related harms associated with drug use.
Studies rarely examine the influence of personal, environmental, community or
interpersonal, societal and cultural factors on drug use and associated harms (4).
Additionally, in HIV research and prevention, it has been argued that while the
pathological organism (i.e. HIV) and transmission routes of the virus are well understood,
the epidemic continues to affect both high-income countries and LMIC (83-85, 344),
meaning that interventions that primarily target individual behaviours (i.e. sexual or drug
use behaviours) do not appear to be sufficient to prevent the transmission of the virus. It
has been recommended that a comprehensive HIV prevention package which addresses
structural barriers, for example, homosexuality-related stigma and discrimination, is
essential to control the epidemic (193, 257). We have identified many factors which
influence HIV-related sexual and drug use behaviours, but changing these behaviours is
harder (345). It has also been argued that studies of drug use and sexual behaviour risk
3 This article is in the public domain and it may be reproduced without permission.
34
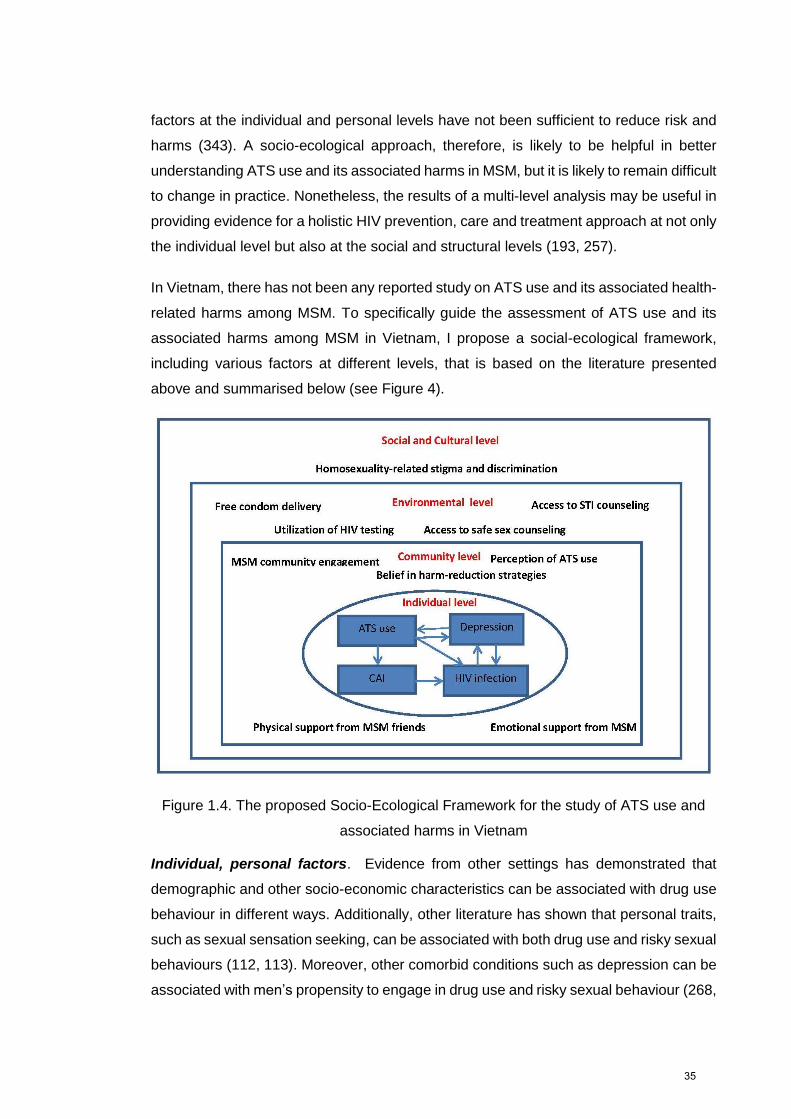
factors at the individual and personal levels have not been sufficient to reduce risk and
harms (343). A socio-ecological approach, therefore, is likely to be helpful in better
understanding ATS use and its associated harms in MSM, but it is likely to remain difficult
to change in practice. Nonetheless, the results of a multi-level analysis may be useful in
providing evidence for a holistic HIV prevention, care and treatment approach at not only
the individual level but also at the social and structural levels (193, 257).
In Vietnam, there has not been any reported study on ATS use and its associated health-
related harms among MSM. To specifically guide the assessment of ATS use and its
associated harms among MSM in Vietnam, I propose a social-ecological framework,
including various factors at different levels, that is based on the literature presented
above and summarised below (see Figure 4).
Figure 1.4. The proposed Socio-Ecological Framework for the study of ATS use and
associated harms in Vietnam
Individual, personal factors. Evidence from other settings has demonstrated that
demographic and other socio-economic characteristics can be associated with drug use
behaviour in different ways. Additionally, other literature has shown that personal traits,
such as sexual sensation seeking, can be associated with both drug use and risky sexual
behaviours (112, 113). Moreover, other comorbid conditions such as depression can be
associated with men’s propensity to engage in drug use and risky sexual behaviour (268,
35
269). In my study, individual factors include socio-demographic characteristics, sexual
sensation seeking and depression.
Community/interpersonal factors. Men’s engagement with the MSM community may
impact ATS use as well as sexual behaviours. Attachment to the gay community can
be associated with drug use and sexual behaviours among MSM in negative or positive
ways (134, 346). Interpersonal factors such as social support can also be associated
with sexual behaviour (342) and with beliefs about the effectiveness of different HIV
prevention strategies. Moreover, interpersonal interactions among men in gay social
networks might also shape their perception of how popular drug use is in the network
(134). There has been no evidence of the relationship between attachment to the gay
community, the level of social support and perceptions of ATS use and sexual
behaviours in MSM in Vietnam. This study is the first to assess these relationships.
Environmental factors. Previous evidence in both high-income and LMIC countries
has shown that utilisation of HIV prevention services, particularly HIV testing services,
can be associated with either increased or decreased probability to engage in risky
sexual behaviours (141, 174, 191) and HIV infection (200). Additionally, HIV testing is
generally regarded as an essential component in any HIV prevention package (257). In
my study, I assessed the use of HIV prevention services, including free condoms, HIV
testing, safe sex counselling and STI diagnosis and treatment.
Cultural, societal factors. Homosexuality-related stigma and discrimination can
create a hostile environment which is subsequently associated with psychological
distress including drug use and depression (50). Additionally, homosexuality-related
stigma and discrimination may also increase men’s propensity to engage in risky
sexual behaviour including CAI (140) and prevent men from accessing HIV prevention
services (257). Homosexuality-related stigma and discrimination is being regarded as a
structural barrier to HIV prevention (257). I therefore assessed homosexuality-related
stigma and discrimination, including enacted (experienced) stigma, perceived stigma
and internalised homophobia.
RESEARCH QUESTIONS AND STUDY OBJECTIVES
Research gaps in drug use, risky sexual behaviours and HIV infection in
MSM in literature
There are several gaps in the understanding of drug use behaviours, including ATS use,
and their relationship with risky sexual behaviour and HIV infection, particularly in MSM
in the current literature. Firstly, most of the current literature is from high-income
36
countries and literature about drug use, particularly ATS use among MSM in LMIC
countries, including Vietnam is limited (4, 7). Secondly, most of the current quantitative
studies on drug use, including ATS use in this population (68, 98, 146, 148, 160-162,
175), except for a few studies which measured specific types of drug use before or during
sex (149, 157, 158, 163-165), often combine all drugs together to make a composite
drug use index. As such, understanding the correlates of individual drug use is difficult
to achieve. Thirdly, most of the studies, particularly studies from LMIC countries, often
measure overall drug use with different recall periods and separately examine sexual
behaviours. More than 20 years ago, Leigh and Stall suggested stronger, more rigorous
measurements for drug use, including contextual, sex-related drug use (i.e. drug use
before or during sex) and event-level drug use (i.e. drug use in specific sexual events)
(347). Last but not least, in almost all of the current studies looking at drug use, including
ATS use, and its relations to HIV-related risky sexual behaviours, these behaviours have
not been assessed in a broader interpersonal, contextual, cultural and societal
perspective (334-337). To contribute to a much needed holistic understanding of drug
use, in particular ATS use among MSM in Vietnam, a multifaceted assessment from a
socio-ecological perspective has been undertaken.
Research gaps in drug use, risky sexual behaviours and HIV infection in
Vietnam
To date, knowledge of the correlations or risk factors of drug use, sexual behaviours and
HIV infection in MSM in Vietnam remains limited. While studies with MSM in Vietnam
have placed considerable emphasis on identifying risky sexual behaviours, there has
been little research on drug use behaviours among Vietnamese MSM, particularly the
recent emerging use of ATS. Knowledge of the popularity of drugs and correlations of
drug use, particularly ATS use, in MSM in Vietnam is limited. Additionally, studies have
often used simple indices of drug use, such as ‘any drug use’, but have not specifically
measured the use of individual drugs. Additionally, as elsewhere, studies undertaken in
Vietnam have often used composite indices of drug use, such as ‘any drug use’, but have
not specifically assessed the use of specific drugs. Furthermore, in the context of
increasing use of ATS and other stimulants in Vietnam, particularly among MSM,
knowledge of ATS use and its association with HIV-related sexual risk behaviours and
HIV infection, as well as its potential psychological harms, particularly depression, is
much needed. Currently it is unknown if ATS use among MSM in Vietnam has any
relationship with HIV-related sexual risk behaviours and HIV infection, and if ATS use is
associated with mental health problems in MSM, including depression. Previous
research seems to have mostly focused on mapping sexual risk behaviour among MSM
37
in Vietnam, in particular in Ho Chi Minh City and southern provinces of Vietnam; evidence
is lacking from the northern province cities, notably Hanoi. Furthermore, understanding
of the multilevel influences on sexual risk behaviours in MSM in Vietnam has remained
limited. Some experiential evidence is available from qualitative studies in small samples
of MSM, but quantitative, correlational data is lacking. The majority of studies on drug
use, sexual risk behaviours and HIV infection has focused on behavioural correlates and
has not addressed interpersonal, cultural, and societal factors.
Rationale for this study
The shortcomings and gaps in research into the drug use, particularly ATS use, sexual
risk behaviour, HIV infection and wellbeing among MSM in Vietnam create challenges
with respect to the development of targetted, effective HIV prevention interventions in
the context of emerging ATS use among MSM in Vietnam. Accordingly, I have conducted
this study to answer the following research questions:
▪ What is the magnitude of ATS use among MSM in Vietnam?
▪ What are the patterns and correlates of ATS use among MSM in Vietnam?
▪ Is ATS use associated with HIV-related risky sexual behaviours, particularly CAI,
among MSM in Vietnam?
▪ Is ATS use associated with HIV infection among MSM in Vietnam?
▪ Is there any relationship between ATS use and psychological distress, namely
depression, among MSM in Vietnam?
To answer my research questions, I conducted an integrated research project, including
a community-based, cross-sectional survey in major cities in Vietnam and a systematic
review and meta-analysis of the relationship between ATS use and HIV infection in MSM.
This research is the first to investigate ATS use in depth in the MSM population in
Vietnam. The findings of this study are designed to help understand associations
between ATS use and sexual behaviour, and HIV risk and associated psychological
disorders, particularly depression symptomology, among MSM in Vietnam. The findings
will assist with identifying appropriate, integrated interventions to reduce the harms
potentially associated with ATS use among MSM, especially harms that can lead to HIV
and other STIs. In such a way it will contribute to preventing the spread of HIV and other
harms among MSM – a marginalised and key population in Vietnam. Additionally, this
research suggests 1urther research priorities related to drug use, sexual behaviour, HIV
infection and mental health among MSM in Vietnam.
38
References
1. Kalant H. The pharmacology and toxicology of "ecstasy" (MDMA) and related
drugs. CMAJ : Canadian Medical Association journal = journal de l'Association
medicale canadienne. 2001;165(7):917-28.
2. Ministerial Council on Drug Strategy. National Amphetamine-Type Stimulants
Strategy, 2008-2011. Australia, 2008.
3. World Health Organization (WHO). Neuroscience of psychoactive substance
use and dependence. Geneva, Switzland 2004.
4. Colfax G, Santos GM, Chu P, Vittinghoff E, Pluddemann A, Kumar S, et al.
Amphetamine-group substances and HIV. Lancet (London, England).
2010;376(9739):458-74.
5. Vearrier D, Greenberg MI, Miller SN, Okaneku JT, Haggerty DA.
Methamphetamine: history, pathophysiology, adverse health effects, current trends,
and hazards associated with the clandestine manufacture of methamphetamine.
Disease-a-month : DM. 2012;58(2):38-89.
6. United Nations Office on Drugs and Crime (UNODC). Amphetamine Type
Stimulants in Vietnam. A Review of the Availibility, Use and Implications for Health and
Security in Vietnam 2012. Hanoi, Vietnam: 2012.
7. Colfax G, Guzman R. Club drugs and HIV infection: a review. Clinical infectious
diseases : an official publication of the Infectious Diseases Society of America.
2006;42(10):1463-9.
8. United Nations Office on Drugs and Crime (UNODC). Amphetamine type
stimulants in Vietnam. A review of the availability, use and implications for health and
security in Vietnam. Hanoi, Vietnam: 2012.
9. Parrott AC. Human psychopharmacology of Ecstasy (MDMA): a review of 15
years of empirical research. Human psychopharmacology. 2001;16(8):557-77.
10. Nordahl TE, Salo R, Leamon M. Neuropsychological effects of chronic
methamphetamine use on neurotransmitters and cognition: a review. The Journal of
neuropsychiatry and clinical neurosciences. 2003;15(3):317-25.
11. Scott JC, Woods SP, Matt GE, Meyer RA, Heaton RK, Atkinson JH, et al.
Neurocognitive effects of methamphetamine: a critical review and meta-analysis.
Neuropsychology review. 2007;17(3):275-97.
12. Zinberg NE. Drug, set and setting. The basis for controlled. 1984.
39
13. Courtney KE, Ray LA. Methamphetamine: an update on epidemiology,
pharmacology, clinical phenomenology, and treatment literature. Drug and alcohol
dependence. 2014;143:11-21.
14. Darke S, Kaye S, McKetin R, Duflou J. Major physical and psychological harms
of methamphetamine use. Drug and alcohol review. 2008;27(3):253-62.
15. Kurtz SP. Post-circuit blues: motivations and consequences of crystal meth use
among gay men in Miami. AIDS and behavior. 2005;9(1):63-72.
16. Semple SJ, Patterson TL, Grant I. Motivations associated with
methamphetamine use among HIV+ men who have sex with men. Journal of
substance abuse treatment. 2002;22(3):149-56.
17. Dew BJ. Toward a Better Understanding of Non-Addicted, Methamphetamine-
Using, Men who Have Sex with Men (MSM) in Atlanta. The open AIDS journal.
2010;4:141-7.
18. Halkitis PN, Fischgrund BN, Parsons JT. Explanations for methamphetamine
use among gay and bisexual men in New York City. Substance use & misuse.
2005;40(9-10):1331-45.
19. Jerome RC, Halkitis PN, Siconolfi DE. Club drug use, sexual behavior, and HIV
seroconversion: a qualitative study of motivations. Substance use & misuse.
2009;44(3):431-47.
20. Halkitis PN, Green KA, Mourgues P. Longitudinal investigation of
methamphetamine use among gay and bisexual men in New York City: findings from
Project BUMPS. Journal of urban health : bulletin of the New York Academy of
Medicine. 2005;82(1 Suppl 1):i18-25.
21. Halkitis PN, Mukherjee PP, Palamar JJ. Multi-level modeling to explain
methamphetamine use among gay and bisexual men. Addiction (Abingdon, England).
2007;102 Suppl 1:76-83.
22. Halkitis PN, Parsons JT, Wilton L. An Exploratory Study of Contextual and
Situational Factors Related to Methamphetamine Use among Gay and Bisexual Men in
New York City. Journal of Drug Issues. 2003;33(2):413-32.
23. Garofalo R, Mustanski B, Johnson A, Emerson E. Exploring factors that
underlie racial/ethnic disparities in HIV risk among young men who have sex with men.
Journal of Urban Health. 2010;87(2):318-23.
24. Palamar JJ, Kiang MV, Storholm ED, Halkitis PN. A Qualitative Descriptive
Study of Perceived Sexual Effects of Club Drug Use in Gay and Bisexual Men.
Psychology and sexuality. 2014;5(2):143-60.
25. McElrath K. MDMA and sexual behavior: ecstasy users' perceptions about
sexuality and sexual risk. Substance use & misuse. 2005;40(9-10):1461-77.
40
26. Bahora M, Sterk CE, Elifson KW. Understanding recreational ecstasy use in the
United States: a qualitative inquiry. The International journal on drug policy.
2009;20(1):62-9.
27. Meyer JS. 3,4-methylenedioxymethamphetamine (MDMA): current
perspectives. Substance abuse and rehabilitation. 2013;4:83-99.
28. Zemishlany Z, Aizenberg D, Weizman A. Subjective effects of MDMA
('Ecstasy') on human sexual function. European psychiatry : the journal of the
Association of European Psychiatrists. 2001;16(2):127-30.
29. Peters GJ, Kok G. A structured review of reasons for ecstasy use and related
behaviours: pointers for future research. BMC public health. 2009;9:230.
30. United Nations Office on Drugs and Crime (UNODC). World Drugs Report
2011. Vienna, Austria: 2011.
31. United Nations Office on Drugs and Crime (UNODC). World Drugs Report
2012. Vienna, Austria: 2012.
32. United Nations Office on Drugs and Crime (UNODC). World Drugs Report
2013. Vienna, Austria: 2013.
33. United Nations Office on Drugs and Crime (UNODC). World Drugs Report
2014. Vienna, Austria: 2014
34. United Nations Office on Drugs and Crime (UNODC). World Drug Report 2015.
Vienna, Austria: 2015.
35. United Nations Office on Drugs and Crime (UNODC). Ecstasy and
Amphetamines Global Survey 2003. Vienna, Austria: 2003.
36. United Nations Office on Drugs and Crime (UNODC). World Drug Report 2010.
Vienna, Austria: 2010.
37. Halkitis PN, Parsons JT, Stirratt MJ. A double epidemic: crystal
methamphetamine drug use in relation to HIV transmission among gay men. Journal of
homosexuality. 2001;41(2):17-35.
38. Koblin BA, Chesney MA, Husnik MJ, Bozeman S, Celum CL, Buchbinder S, et
al. High-risk behaviors among men who have sex with men in 6 US cities: baseline
data from the EXPLORE Study. American journal of public health. 2003;93(6):926-32.
39. Thiede H, Valleroy LA, MacKellar DA, Celentano DD, Ford WL, Hagan H, et al.
Regional patterns and correlates of substance use among young men who have sex
with men in 7 US urban areas. American journal of public health. 2003;93(11):1915-21.
40. Halkitis P, Pollock J, Pappas M, Dayton A, Moeller RW, Siconolfi D, et al.
Substance Use in the MSM Population of New York City during the Era of HIV/AIDS.
Subst Use Misuse. 2011;46(2-3):264-73.
41
41. Hickson F. Consuming passions: Findings from the United Kingdom gay men's
sex survey 2005: Sigma research; 2007.
42. Schmidt AJ, Bourne A, Weatherburn P, Reid D, Marcus U, Hickson F. Illicit drug
use among gay and bisexual men in 44 cities: Findings from the European MSM
Internet Survey (EMIS). The International journal on drug policy. 2016;38:4-12.
43. Lea T, Mao L, Hopwood M, Prestage G, Zablotska I, de Wit J, et al.
Methamphetamine use among gay and bisexual men in Australia: Trends in recent and
regular use from the Gay Community Periodic Surveys. The International journal on
drug policy. 2016;29:66-72.
44. Reback CJ, Fletcher JB, Shoptaw S, Grella CE. Methamphetamine and other
substance use trends among street-recruited men who have sex with men, from 2008
to 2011. Drug and alcohol dependence. 2013;133(1):262-5.
45. Lea T, Reynolds R, de Wit J. Alcohol and other drug use, club drug
dependence and treatment seeking among lesbian, gay and bisexual young people in
Sydney. Drug and alcohol review. 2013;32(3):303-11.
46. Wei CY, Guadamuz TE, Lim S, Huang YX, Koe S. Patterns and levels of illicit
drug use among men who have sex with men in Asia. Drug and alcohol dependence.
2012;120(1):246-9.
47. Altman D, Aggleton P, Williams M, Kong T, Reddy V, Harrad D, et al. Men who
have sex with men: stigma and discrimination. Lancet (London, England).
2012;380(9839):439-45.
48. Chard AN, Finneran C, Sullivan PS, Stephenson R. Experiences of
homophobia among gay and bisexual men: results from a cross-sectional study in
seven countries. Culture, health & sexuality. 2015;17(10):1174-89.
49. Callender KA. Understanding antigay bias from a cognitive-affective-behavioral
perspective. Journal of homosexuality. 2015;62(6):782-803.
50. Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and
bisexual populations: conceptual issues and research evidence. Psychological bulletin.
2003;129(5):674-97.
51. Herek GM. Beyond "homophobia": a social psychological perspective on
attitudes toward lesbians and gay men. Journal of homosexuality. 1984;10(1-2):1-21.
52. Diaz RM, Ayala G, Bein E. Sexual risk as an outcome of social oppression: data
from a probability sample of Latino gay men in three U.S. cities. Cultural diversity &
ethnic minority psychology. 2004;10(3):255-67.
53. Kwok DK, Wu J. Chinese attitudes towards sexual minorities in Hong Kong:
Implications for mental health. International review of psychiatry (Abingdon, England).
2015;27(5):444-54.
42
54. Zervoulis K, Lyons E, Dinos S. Stigma and self-esteem across societies:
avoiding blanket psychological responses to gay men experiencing homophobia.
BJPsych bulletin. 2015;39(4):167-73.
55. Deuba K, Ekstrom AM, Shrestha R, Ionita G, Bhatta L, Karki DK. Psychosocial
health problems associated with increased HIV risk behavior among men who have
sex with men in Nepal: a cross-sectional survey. PloS one. 2013;8(3):e58099.
56. Neilands TB, Steward WT, Choi KH. Assessment of stigma towards
homosexuality in China: a study of men who have sex with men. Archives of sexual
behavior. 2008;37(5):838-44.
57. Huebner DM, Davis MC, Nemeroff CJ, Aiken LS. The impact of internalized
homophobia on HIV preventive interventions. American journal of community
psychology. 2002;30(3):327-48.
58. Ross MW, Kajubi P, Mandel JS, McFarland W, Raymond HF. Internalized
homonegativity/homophobia is associated with HIV-risk behaviours among Ugandan
gay and bisexual men. International journal of STD & AIDS. 2013;24(5):409-13.
59. Andrinopoulos K, Hembling J, Guardado ME, de Maria Hernández F, Nieto AI,
Melendez G. Evidence of the Negative Effect of Sexual Minority Stigma on HIV Testing
Among MSM and Transgender Women in San Salvador, El Salvador. AIDS and
behavior. 2015;19(1):60-71.
60. Diaz RM, Ayala G, Bein E, Henne J, Marin BV. The impact of homophobia,
poverty, and racism on the mental health of gay and bisexual Latino men: findings from
3 US cities. American journal of public health. 2001;91(6):927-32.
61. Lee JH, Gamarel KE, Bryant KJ, Zaller ND, Operario D. Discrimination, Mental
Health, and Substance Use Disorders Among Sexual Minority Populations. LGBT
health. 2016;3(4):258-65.
62. Safren SA, Blashill AJ, O'Cleirigh CM. Promoting the sexual health of MSM in
the context of comorbid mental health problems. AIDS and behavior. 2011;15 Suppl
1:S30-4.
63. King M, Semlyen J, Tai SS, Killaspy H, Osborn D, Popelyuk D, et al. A
systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay
and bisexual people. BMC psychiatry. 2008;8:70.
64. Frost DM, LeBlanc AJ. Nonevent stress contributes to mental health disparities
based on sexual orientation: evidence from a personal projects analysis. The American
journal of orthopsychiatry. 2014;84(5):557-66.
65. Gee R. Primary care health issues among men who have sex with men. Journal
of the American Academy of Nurse Practitioners. 2006;18(4):144-53.
43
66. De Santis JP, Colin JM, Provencio Vasquez E, McCain GC. The relationship of
depressive symptoms, self-esteem, and sexual behaviors in a predominantly Hispanic
sample of men who have sex with men. American journal of men's health.
2008;2(4):314-21.
67. Klein H. Depression and HIV Risk Taking among Men Who Have Sex with
Other Men (MSM) and Who Use the Internet to Find Partners for Unprotected Sex.
Journal of gay & lesbian mental health. 2014;18(2):164-89.
68. Fendrich M, Avci O, Johnson TP, Mackesy-Amiti ME. Depression, substance
use and HIV risk in a probability sample of men who have sex with men. Addictive
behaviors. 2013;38(3):1715-8.
69. Wilson PA, Stadler G, Boone MR, Bolger N. Fluctuations in depression and
well-being are associated with sexual risk episodes among HIV-positive men. Health
psychology : official journal of the Division of Health Psychology, American
Psychological Association. 2014;33(7):681-5.
70. Parker RD, Lohmus L, Valk A, Mangine C, Ruutel K. Outcomes associated with
anxiety and depression among men who have sex with men in Estonia. Journal of
affective disorders. 2015;183:205-9.
71. Wim VB, Christiana N, Marie L. Syndemic and other risk factors for unprotected
anal intercourse among an online sample of Belgian HIV negative men who have sex
with men. AIDS and behavior. 2014;18(1):50-8.
72. Mao L, Kidd MR, Rogers G, Andrews G, Newman CE, Booth A, et al. Social
factors associated with Major Depressive Disorder in homosexually active, gay men
attending general practices in urban Australia. Australian and New Zealand journal of
public health. 2009;33(1):83-6.
73. Stahlman S, Grosso A, Ketende S, Sweitzer S, Mothopeng T, Taruberekera N,
et al. Depression and Social Stigma Among MSM in Lesotho: Implications for HIV and
Sexually Transmitted Infection Prevention. AIDS and behavior. 2015;19(8):1460-9.
74. Secor AM, Wahome E, Micheni M, Rao D, Simoni JM, Sanders EJ, et al.
Depression, substance abuse and stigma among men who have sex with men in
coastal Kenya. AIDS (London, England). 2015;29 Suppl 3:S251-9.
75. Tucker A, Liht J, de Swardt G, Jobson G, Rebe K, McIntyre J, et al.
Homophobic stigma, depression, self-efficacy and unprotected anal intercourse for
peri-urban township men who have sex with men in Cape Town, South Africa: a cross-
sectional association model. AIDS care. 2014;26(7):882-9.
76. Tomori C, McFall AM, Srikrishnan AK, Mehta SH, Solomon SS, Anand S, et al.
Diverse Rates of Depression Among Men Who Have Sex with Men (MSM) Across
44
India: Insights from a Multi-site Mixed Method Study. AIDS and behavior.
2016;20(2):304-16.
77. Yi S, Tuot S, Chhoun P, Pal K, Tith K, Brody C. Factors Associated with
Inconsistent Condom Use among Men Who Have Sex with Men in Cambodia. PloS
one. 2015;10(8):e0136114.
78. Wu YL, Yang HY, Wang J, Yao H, Zhao X, Chen J, et al. Prevalence of suicidal
ideation and associated factors among HIV-positive MSM in Anhui, China. International
journal of STD & AIDS. 2015;26(7):496-503.
79. Yan H, Wong FY, Zheng T, Ning Z, Ding Y, Nehl EJ, et al. Social support and
depressive symptoms among 'money' boys and general men who have sex with men in
Shanghai, China. Sexual health. 2014;11(3):285-7.
80. Shiu CS, Chen YC, Tseng PC, Chung AC, Wu MT, Hsu ST, et al. Curvilinear
relationship between depression and unprotected sexual behaviors among men who
have sex with men. The journal of sexual medicine. 2014;11(10):2466-73.
81. Biello KB, Colby D, Closson E, Mimiaga MJ. The syndemic condition of
psychosocial problems and HIV risk among male sex workers in Ho Chi Minh City,
Vietnam. AIDS and behavior. 2014;18(7):1264-71.
82. Goldsamt LA, Clatts MC, Giang LM, Yu G. Prevalence and Behavioral
Correlates of Depression and Anxiety Among Male Sex Workers in Vietnam.
International journal of sexual health : official journal of the World Association for
Sexual Health. 2015;27(2):145-55.
83. Baral S, Sifakis F, Cleghorn F, Beyrer C. Elevated risk for HIV infection among
men who have sex with men in low- and middle-income countries 2000-2006: a
systematic review. PLoS medicine. 2007;4(12):e339.
84. Beyrer C, Baral SD, van Griensven F, Goodreau SM, Chariyalertsak S, Wirtz
AL, et al. Global epidemiology of HIV infection in men who have sex with men. Lancet
(London, England). 2012;380(9839):367-77.
85. van Griensven F, de Lind van Wijngaarden JW, Baral S, Grulich A. The global
epidemic of HIV infection among men who have sex with men. Current opinion in HIV
and AIDS. 2009;4(4):300-7.
86. Sullivan PS, Hamouda O, Delpech V, Geduld JE, Prejean J, Semaille C, et al.
Reemergence of the HIV Epidemic Among Men Who Have Sex With Men in North
America, Western Europe, and Australia, 1996–2005. Annals of Epidemiology.
2009;19(6):423-31.
87. Joint United Nations Programs on HIV/AIDS (UNAIDS). AIDS by the numbers
2015 [cited 2016 15th September]. Available from:
45
http://www.unaids.org/sites/default/files/media_asset/AIDS_by_the_numbers_2015_en.
pdf.
88. Joint United Nations Programs on HIV/AIDS (UNAIDS). Global AIDS update
2016 [Available from: http://www.unaids.org/sites/default/files/media_asset/global-
AIDS-update-2016_en.pdf.
89. Frits van Griensven JWdLvW. A review of the epidemiology of HIV infection and
prevention responses among MSM in Asia. AIDS (London, England). 2010;24(3):S30-
S40.
90. de Lind van Wijngaarden JW, Brown T, Girault P, Sarkar S, van Griensven F.
The epidemiology of human immunodeficiency virus infection, sexually transmitted
infections, and associated risk behaviors among men who have sex with men in the
Mekong Subregion and China: implications for policy and programming. Sexually
transmitted diseases. 2009;36(5):319-24.
91. Suguimoto SP, Techasrivichien T, Musumari PM, El-saaidi C, Lukhele BW,
Ono-Kihara M, et al. Changing patterns of HIV epidemic in 30 years in East Asia.
Current HIV/AIDS reports. 2014;11(2):134-45.
92. Garcia MC, Meyer SB, Ward P. Elevated HIV prevalence and risk behaviours
among men who have sex with men (MSM) in Vietnam: a systematic review. BMJ
open. 2012;2(5).
93. Ministry of Health Vietnam. The results from the HIV/STI intergrated biological
andbehavioral surveillance (IBBS) in Vietnam-Round II 2009. 2011.
94. Lim SH, Guadamuz TE, Wei C, Chan R, Koe S. Factors associated with
unprotected receptive anal intercourse with internal ejaculation among men who have
sex with men in a large Internet sample from Asia. AIDS and behavior.
2012;16(7):1979-87.
95. Chow EP, Lau JT, Zhuang X. HIV prevalence trends, risky behaviours, and
governmental and community responses to the epidemic among men who have sex
with men in China. 2014;2014:607261.
96. He Q, Peng WJ, Zhang JQ, Wang BX, Wang J. Prevalence of unprotected anal
intercourse and unprotected vaginal intercourse among HIV-positive men who have
sex with men in China: a meta-analysis. Sexually transmitted infections.
2012;88(3):229-33.
97. Caceres CF, Konda K, Segura ER, Lyerla R. Epidemiology of male same-sex
behaviour and associated sexual health indicators in low- and middle-income countries:
2003-2007 estimates. Sexually transmitted infections. 2008;84 Suppl 1:i49-i56.
98. Xu JJ, Zhang C, Hu QH, Chu ZX, Zhang J, Li YZ, et al. Recreational drug use
and risks of HIV and sexually transmitted infections among Chinese men who have sex
46
with men: Mediation through multiple sexual partnerships. BMC infectious diseases.
2014;14:642.
99. Sanchez TH, Sineath RC, Kahle EM, Tregear SJ, Sullivan PS. The Annual
American Men's Internet Survey of Behaviors of Men Who Have Sex With Men in the
United States: Protocol and Key Indicators Report 2013. JMIR public health and
surveillance. 2015;1(1):e3.
100. Daskalopoulou M, Rodger A, Thornton A, Phillips A, Sherr L, Gilson R, et al.
Sexual behaviour, recreational drug use and hepatitis C co-infection in HIV-diagnosed
men who have sex with men in the United Kingdom: results from the ASTRA study.
Journal of the International AIDS Society. 2014;17(4 Suppl 3):19630.
101. Stall R, Paul JP, Greenwood G, Pollack LM, Bein E, Crosby GM, et al. Alcohol
use, drug use and alcohol-related problems among men who have sex with men: the
Urban Men's Health Study. Addiction (Abingdon, England). 2001;96(11):1589-601.
102. Chen X, Li X, Zheng J, Zhao J, He J, Zhang G, et al. Club Drugs and HIV/STD
Infection: An Exploratory Analysis among Men Who Have Sex with Men in Changsha,
China. PloS one. 2015;10(5):e0126320.
103. Xu JJ, Qian HZ, Chu ZX, Zhang J, Hu QH, Jiang YJ, et al. Recreational drug
use among Chinese men who have sex with men: a risky combination with unprotected
sex for acquiring HIV infection. BioMed research international. 2014;2014:725361.
104. Balan IC, Carballo-Dieguez A, Dolezal C, Marone R, Pando MA, Barreda V, et
al. High prevalence of substance use among men who have sex with men in Buenos
Aires, Argentina: implications for HIV risk behavior. AIDS and behavior.
2013;17(4):1296-304.
105. Carrico AW, Pollack LM, Stall RD, Shade SB, Neilands TB, Rice TM, et al.
Psychological processes and stimulant use among men who have sex with men. Drug
and alcohol dependence. 2012;123(1-3):79-83.
106. Greenwood GL, White EW, Page-Shafer K, Bein E, Osmond DH, Paul J, et al.
Correlates of heavy substance use among young gay and bisexual men: The San
Francisco Young Men's Health Study. Drug and alcohol dependence. 2001;61(2):105-
12.
107. Halkitis PN, Moeller RW, Siconolfi DE, Jerome RC, Rogers M, Schillinger J.
Methamphetamine and poly-substance use among gym-attending men who have sex
with men in New York City. Annals of behavioral medicine : a publication of the Society
of Behavioral Medicine. 2008;35(1):41-8.
108. Yu G, Wall MM, Chiasson MA, Hirshfield S. Complex drug use patterns and
associated HIV transmission risk behaviors in an Internet sample of U.S. men who
have sex with men. Archives of sexual behavior. 2015;44(2):421-8.
47
109. Wei C, Guadamuz TE, Lim SH, Huang Y, Koe S. Patterns and levels of illicit
drug use among men who have sex with men in Asia. Drug and alcohol dependence.
2012;120(1-3):246-9.
110. Kecojevic A, Wong CF, Corliss HL, Lankenau SE. Risk factors for high levels of
prescription drug misuse and illicit drug use among substance-using young men who
have sex with men (YMSM). Drug and alcohol dependence. 2015;150:156-63.
111. Kalichman SC, Johnson JR, Adair V, Rompa D, Multhauf K, Kelly JA. Sexual
sensation seeking: scale development and predicting AIDS-risk behavior among
homosexually active men. Journal of personality assessment. 1994;62(3):385-97.
112. Kalichman SC, Heckman T, Kelly JA. Sensation seeking as an explanation for
the association between substance use and HIV-related risky sexual behavior.
Archives of sexual behavior. 1996;25(2):141-54.
113. Kalichman SC, Simbayi L, Jooste S, Vermaak R, Cain D. Sensation seeking
and alcohol use predict HIV transmission risks: prospective study of sexually
transmitted infection clinic patients, Cape Town, South Africa. Addictive behaviors.
2008;33(12):1630-3.
114. Chng CL, Geliga-Vargas J. Ethnic identity, gay identity, sexual sensation
seeking and HIV risk taking among multiethnic men who have sex with men. AIDS
education and prevention : official publication of the International Society for AIDS
Education. 2000;12(4):326-39.
115. Heidinger B, Gorgens K, Morgenstern J. The effects of sexual sensation
seeking and alcohol use on risky sexual behavior among men who have sex with men.
AIDS and behavior. 2015;19(3):431-9.
116. Newcomb ME, Clerkin EM, Mustanski B. Sensation seeking moderates the
effects of alcohol and drug use prior to sex on sexual risk in young men who have sex
with men. AIDS and behavior. 2011;15(3):565-75.
117. Stall R, Leigh B. Understanding the relationship between drug or alcohol use
and high risk sexual activity for HIV transmission: where do we go from here? Addiction
(Abingdon, England). 1994;89(2):131-4.
118. Semple SJ, Strathdee SA, Zians J, Patterson TL. Sexual risk behavior
associated with co-administration of methamphetamine and other drugs in a sample of
HIV-positive men who have sex with men. The American journal on addictions /
American Academy of Psychiatrists in Alcoholism and Addictions. 2009;18(1):65-72.
119. Fisher DG, Reynolds GL, Ware MR, Napper LE. Methamphetamine and Viagra
use: relationship to sexual risk behaviors. Archives of sexual behavior. 2011;40(2):273-
9.
48
120. Forrest DW, Metsch LR, LaLota M, Cardenas G, Beck DW, Jeanty Y. Crystal
methamphetamine use and sexual risk behaviors among HIV-positive and HIV-
negative men who have sex with men in South Florida. Journal of urban health :
bulletin of the New York Academy of Medicine. 2010;87(3):480-5.
121. Lyons A, Pitts M, Grierson J. Methamphetamine use in a nationwide online
sample of older Australian HIV-positive and HIV-negative gay men. Drug and alcohol
review. 2013;32(6):603-10.
122. Daskalopoulou M, Rodger A, Phillips AN, Sherr L, Speakman A, Collins S, et al.
Recreational drug use, polydrug use, and sexual behaviour in HIV-diagnosed men who
have sex with men in the UK: results from the cross-sectional ASTRA study. The lancet
HIV. 2014;1(1):e22-31.
123. Paul JP, Boylan R, Gregorich S, Ayala G, Choi KH. Substance use and
experienced stigmatization among ethnic minority men who have sex with men in the
United States. Journal of ethnicity in substance abuse. 2014;13(4):430-47.
124. Bochow M. The importance of contextualizing research: an analysis of data
from the German gay press surveys. Journal of Psychology & Human Sexuality.
1998;10(3-4):37-58.
125. Lewis LA, Ross MW. A select body: The gay dance party subculture and the
HIV/AIDS pandemic: Burns & Oates; 1995.
126. Theodore PS, Achiro RP, Duran RE, Antoni MH. Body dissatisfaction and
methamphetamine use among HIV-positive gay and bisexual men: a pilot study.
Substance use & misuse. 2011;46(14):1745-9.
127. Binson D, Woods WJ, Pollack L, Paul J, Stall R, Catania JA. Differential HIV
risk in bathhouses and public cruising areas. American journal of public health.
2001;91(9):1482-6.
128. Bien CH, Best JM, Muessig KE, Wei C, Han L, Tucker JD. Gay Apps for
Seeking Sex Partners in China: Implications for MSM Sexual Health. AIDS and
behavior. 2015;19(6):941-6.
129. Beymer MR, Weiss RE, Bolan RK, Rudy ET, Bourque LB, Rodriguez JP, et al.
Sex on demand: geosocial networking phone apps and risk of sexually transmitted
infections among a cross-sectional sample of men who have sex with men in Los
Angeles County. Sexually transmitted infections. 2014;90(7):567-72.
130. Blackwell CW. Men who have sex with men and recruit bareback sex partners
on the internet: implications for STI and HIV prevention and client education. American
journal of men's health. 2008;2(4):306-13.
49
131. Ko NY, Koe S, Lee HC, Yen CF, Ko WC, Hsu ST. Online sex-seeking,
substance use, and risky behaviors in Taiwan: results from the 2010 Asia Internet MSM
Sex Survey. Archives of sexual behavior. 2012;41(5):1273-82.
132. Wei C, Lim SH, Guadamuz TE, Koe S. Virtual versus physical spaces: which
facilitates greater HIV risk taking among men who have sex with men in East and
South-East Asia? AIDS and behavior. 2014;18(8):1428-35.
133. Green AI, Halkitis PN. Crystal methamphetamine and sexual sociality in an
urban gay subculture: an elective affinity. Culture, health & sexuality. 2006;8(4):317-33.
134. Carpiano RM, Kelly BC, Easterbrook A, Parsons JT. Community and drug use
among gay men: the role of neighborhoods and networks. Journal of health and social
behavior. 2011;52(1):74-90.
135. McKirnan DJ, Peterson PL. Psychosocial and cultural factors in alcohol and
drug abuse: An analysis of a homosexual community. Addictive behaviors.
1989;14(5):555-63.
136. McCabe SE, Bostwick WB, Hughes TL, West BT, Boyd CJ. The Relationship
Between Discrimination and Substance Use Disorders Among Lesbian, Gay, and
Bisexual Adults in the United States. American journal of public health.
2010;100(10):1946-52.
137. Mizuno Y, Borkowf C, Millett G, Bingham T, Ayala G, Stueve A. Homophobia
and Racism Experienced by Latino Men Who Have Sex with Men in the United States:
Correlates of Exposure and Associations with HIV Risk Behaviors. AIDS Behav.
2012;16(3):724-35.
138. Williamson IR. Internalized homophobia and health issues affecting lesbians
and gay men. Health education research. 2000;15(1):97-107.
139. Pines HA, Gorbach PM, Weiss RE, Reback CJ, Landovitz RJ, Mutchler MG, et
al. Individual-Level, Partnership-Level, and Sexual Event-Level Predictors of Condom
Use During Receptive Anal Intercourse Among HIV-Negative Men Who Have Sex with
Men in Los Angeles. AIDS and behavior. 2015.
140. Kramer SC, Schmidt AJ, Berg RC, Furegato M, Hospers H, Folch C, et al.
Factors associated with unprotected anal sex with multiple non-steady partners in the
past 12 months: results from the European Men-Who-Have-Sex-With-Men Internet
Survey (EMIS 2010). BMC public health. 2016;16:47.
141. Zhang H, Lu H, Pan SW, Xia D, Zhao Y, Xiao Y, et al. Correlates of unprotected
anal intercourse: the influence of anal sex position among men who have sex with men
in Beijing, china. Archives of sexual behavior. 2015;44(2):375-87.
142. Cheng W, Tang W, Zhong F, Babu GR, Han Z, Qin F, et al. Consistently high
unprotected anal intercourse (UAI) and factors correlated with UAI among men who
50
have sex with men: implication of a serial cross-sectional study in Guangzhou, China.
BMC infectious diseases. 2014;14:696.
143. Chow EP, Chen X, Zhao J, Zhuang X, Jing J, Zhang L. Factors associated with
self-reported unprotected anal intercourse among men who have sex with men in
Changsha city of Hunan province, China. AIDS care. 2015;27(10):1332-42.
144. Rocha GM, Kerr LR, de Brito AM, Dourado I, Guimaraes MD. Unprotected
receptive anal intercourse among men who have sex with men in Brazil. AIDS and
behavior. 2013;17(4):1288-95.
145. Holtz TH, Pattanasin S, Chonwattana W, Tongtoyai J, Chaikummao S,
Varangrat A, et al. Longitudinal analysis of key HIV-risk behavior patterns and
predictors in men who have sex with men, Bangkok, Thailand. Archives of sexual
behavior. 2015;44(2):341-8.
146. Mimiaga MJ, Reisner SL, Cranston K, Isenberg D, Bright D, Daffin G, et al.
Sexual mixing patterns and partner characteristics of black MSM in Massachusetts at
increased risk for HIV infection and transmission. Journal of urban health : bulletin of
the New York Academy of Medicine. 2009;86(4):602-23.
147. Mor Z, Davidovich U, Bessudu-Manor N, McFarlane M, Feldshtein G, Chemtob
D. High-risk behaviour in steady and in casual relationships among men who have sex
with men in Israel. Sexually transmitted infections. 2011;87(6):532-7.
148. Woolf-King SE, Rice TM, Truong HM, Woods WJ, Jerome RC, Carrico AW.
Substance use and HIV risk behavior among men who have sex with men: the role of
sexual compulsivity. Journal of urban health : bulletin of the New York Academy of
Medicine. 2013;90(5):948-52.
149. Pantalone DW, Huh D, Nelson KM, Pearson CR, Simoni JM. Prospective
predictors of unprotected anal intercourse among HIV-seropositive men who have sex
with men initiating antiretroviral therapy. AIDS and behavior. 2014;18(1):78-87.
150. Li D, Li C, Wang Z, Lau JT. Prevalence and associated factors of unprotected
anal intercourse with regular male sex partners among HIV negative men who have
sex with men in China: a cross-sectional survey. PloS one. 2015;10(3):e0119977.
151. Fletcher JB, Reback CJ. Depression mediates and moderates effects of
methamphetamine use on sexual risk taking among treatment-seeking gay and
bisexual men. Health psychology : official journal of the Division of Health Psychology,
American Psychological Association. 2015;34(8):865-9.
152. Julio RS, Friedman RK, Cunha CB, De Boni RB, Cardoso SW, Torres T, et al.
Unprotected sexual practices among men who have sex with women and men who
have sex with men living with HIV/AIDS in Rio de Janeiro. Archives of sexual behavior.
2015;44(2):357-65.
51
153. Santos GM, Coffin PO, Das M, Matheson T, DeMicco E, Raiford JL, et al. Dose-
response associations between number and frequency of substance use and high-risk
sexual behaviors among HIV-negative substance-using men who have sex with men
(SUMSM) in San Francisco. Journal of acquired immune deficiency syndromes (1999).
2013;63(4):540-4.
154. Jones-Webb R, Smolenski D, Brady S, Wilkerson M, Rosser BR. Drinking
settings, alcohol consumption, and sexual risk behavior among gay men. Addictive
behaviors. 2013;38(3):1824-30.
155. Bruce D, Kahana S, Harper GW, Fernandez MI. Alcohol use predicts sexual
risk behavior with HIV-negative or partners of unknown status among young HIV-
positive men who have sex with men. AIDS care. 2013;25(5):559-65.
156. Hess KL, Chavez PR, Kanny D, DiNenno E, Lansky A, Paz-Bailey G. Binge
drinking and risky sexual behavior among HIV-negative and unknown HIV status men
who have sex with men, 20 US cities. Drug and alcohol dependence. 2015;147:46-52.
157. Mayer KH, O'Cleirigh C, Skeer M, Covahey C, Leidolf E, Vanderwarker R, et al.
Which HIV-infected men who have sex with men in care are engaging in risky sex and
acquiring sexually transmitted infections: findings from a Boston community health
centre. Sexually transmitted infections. 2010;86(1):66-70.
158. Bedoya CA, Mimiaga MJ, Beauchamp G, Donnell D, Mayer KH, Safren SA.
Predictors of HIV transmission risk behavior and seroconversion among Latino men
who have sex with men in Project EXPLORE. AIDS & Behavior. 2012;16(3):608-17.
159. Fan W, Lu R, Wu G, Yousuf MA, Feng L, Li X, et al. Alcohol drinking and HIV-
related risk among men who have sex with men in Chongqing, China. Alcohol
(Fayetteville, NY). 2016;50:1-7.
160. Ludford KT, Vagenas P, Lama JR, Peinado J, Gonzales P, Leiva R, et al.
Screening for drug and alcohol use disorders and their association with HIV-related
sexual risk behaviors among men who have sex with men in Peru. PloS one.
2013;8(8):e69966.
161. Darrow WW, Biersteker S, Geiss T, Chevalier K, Clark J, Marrero Y, et al. Risky
sexual behaviors associated with recreational drug use among men who have sex with
men in an international resort area: challenges and opportunities. Journal of urban
health : bulletin of the New York Academy of Medicine. 2005;82(4):601-9.
162. Hatfield LA, Horvath KJ, Jacoby SM, Simon Rosser BR. Comparison of
substance use and risky sexual behavior among a diverse sample of urban, HIV-
positive men who have sex with men. Journal of addictive diseases. 2009;28(3):208-
18.
52
163. Celentano DD, Valleroy LA, Sifakis F, MacKellar DA, Hylton J, Thiede H, et al.
Associations between substance use and sexual risk among very young men who have
sex with men. Sexually transmitted diseases. 2006;33(4):265-71.
164. Garofalo R, Mustanski BS, McKirnan DJ, Herrick A, Donenberg GR.
Methamphetamine and young men who have sex with men: understanding patterns
and correlates of use and the association with HIV-related sexual risk. Archives of
pediatrics & adolescent medicine. 2007;161(6):591-6.
165. Freeman P, Walker BC, Harris DR, Garofalo R, Willard N, Ellen JM.
Methamphetamine use and risk for HIV among young men who have sex with men in 8
US cities. Archives of pediatrics & adolescent medicine. 2011;165(8):736-40.
166. Colfax G, Shoptaw S. The methamphetamine epidemic: implications for HIV
prevention and treatment. Current HIV/AIDS reports. 2005;2(4):194-9.
167. Hoenigl M, Chaillon A, Moore DJ, Morris SR, Smith DM, Little SJ. Clear Links
between Starting Methamphetamine and Increasing Sexual Risk Behavior: a cohort
study among Men who have Sex with Men. Journal of acquired immune deficiency
syndromes (1999). 2015.
168. Barron-Limon S, Semple SJ, Strathdee SA, Lozada R, Vargas-Ojeda A,
Patterson TL. Correlates of unprotected anal sex among men who have sex with men
in Tijuana, Mexico. BMC public health. 2012;12:433.
169. Cunha CB, De Boni RB, Guimaraes MR, Yanavich C, Veloso VG, Moreira RI, et
al. Unprotected sex among men who have sex with men living with HIV in Brazil: a
cross-sectional study in Rio de Janeiro. BMC public health. 2014;14:379.
170. Cai Y, Lau JT. Multi-dimensional factors associated with unprotected anal
intercourse with regular partners among Chinese men who have sex with men in Hong
Kong: a respondent-driven sampling survey. BMC infectious diseases. 2014;14:205.
171. Melendez-Torres GJ, Hickson F, Reid D, Weatherburn P, Bonell C. Nested
Event-Level Case-Control Study of Drug Use and Sexual Outcomes in Multipartner
Encounters Reported by Men Who Have Sex with Men. AIDS and behavior.
2016;20(3):646-54.
172. Halkitis PN, Mukherjee PP, Palamar JJ. Longitudinal modeling of
methamphetamine use and sexual risk behaviors in gay and bisexual men. AIDS and
behavior. 2009;13(4):783-91.
173. Shoptaw S, Reback CJ. Associations between methamphetamine use and HIV
among men who have sex with men: a model for guiding public policy. Journal of urban
health : bulletin of the New York Academy of Medicine. 2006;83(6):1151-7.
53
174. Morineau G, Nugrahini N, Riono P, Nurhayati, Girault P, Mustikawati DE, et al.
Sexual risk taking, STI and HIV prevalence among men who have sex with men in six
Indonesian cities. AIDS and behavior. 2011;15(5):1033-44.
175. Fernandez MI, Bowen GS, Varga LM, Collazo JB, Hernandez N, Perrino T, et
al. High rates of club drug use and risky sexual practices among Hispanic men who
have sex with men in Miami, Florida. Substance use & misuse. 2005;40(9-10):1347-62.
176. Semple SJ, Patterson, T.L., Grant, I. Motivations associated with
methamphetamine use among HIV+ men who have sex with men. Journal of
substance abuse treatment. 2002;22(3):149-56.
177. Klitzman RL, Greenberg JD, Pollack LM, Dolezal C. MDMA ('ecstasy') use, and
its association with high risk behaviors, mental health, and other factors among
gay/bisexual men in New York City. Drug and alcohol dependence. 2002;66(2):115-25.
178. Klitzman RL, Pope HG, Jr., Hudson JI. MDMA ("Ecstasy") abuse and high-risk
sexual behaviors among 169 gay and bisexual men. The American journal of
psychiatry. 2000;157(7):1162-4.
179. Friedman MR, Kurtz SP, Buttram ME, Wei C, Silvestre AJ, Stall R. HIV risk
among substance-using men who have sex with men and women (MSMW): findings
from South Florida. AIDS and behavior. 2014;18(1):111-9.
180. Kerr ZY, Pollack LM, Woods WJ, Blair J, Binson D. Use of multiple sex venues
and prevalence of HIV risk behavior: identifying high-risk men who have sex with men.
Archives of sexual behavior. 2015;44(2):443-51.
181. Zhao J, Chen L, Cai WD, Tan JG, Tan W, Zheng CL, et al. HIV infection and
sexual behaviors among non-commercial men who have sex with men at different
venues. Archives of sexual behavior. 2014;43(4):801-9.
182. Verre MC, Peinado J, Segura ER, Clark J, Gonzales P, Benites C, et al.
Socialization patterns and their associations with unprotected anal intercourse, HIV,
and syphilis among high-risk men who have sex with men and transgender women in
Peru. AIDS and behavior. 2014;18(10):2030-9.
183. Bolding G, Davis M, Sherr L, Hart G, Elford J. Use of gay Internet sites and
views about online health promotion among men who have sex with men. AIDS care.
2004;16(8):993-1001.
184. Bull SS, McFarlane M, Lloyd L, Rietmeijer C. The process of seeking sex
partners online and implications for STD/HIV prevention. AIDS care. 2004;16(8):1012-
20.
185. Kakietek J, Sullivan PS, Heffelfinger JD. You've got male: internet use, rural
residence, and risky sex in men who have sex with men recruited in 12 U.S. cities.
54
AIDS education and prevention : official publication of the International Society for
AIDS Education. 2011;23(2):118-27.
186. Mustanski BS. Are sexual partners met online associated with HIV/STI risk
behaviours? Retrospective and daily diary data in conflict. AIDS care. 2007;19(6):822-
7.
187. Broaddus MR, DiFranceisco WJ, Kelly JA, St Lawrence JS, Amirkhanian YA,
Dickson-Gomez JD. Social Media Use and High-Risk Sexual Behavior Among Black
Men Who Have Sex with Men: A Three-City Study. AIDS and behavior. 2015;19 Suppl
2:90-7.
188. Abara W, Annang L, Spencer SM, Fairchild AJ, Billings D. Understanding
internet sex-seeking behaviour and sexual risk among young men who have sex with
men: evidences from a cross-sectional study. Sexually transmitted infections.
2014;90(8):596-601.
189. Holloway IW, Pulsipher CA, Gibbs J, Barman-Adhikari A, Rice E. Network
Influences on the Sexual Risk Behaviors of Gay, Bisexual and Other Men Who Have
Sex with Men Using Geosocial Networking Applications. AIDS and behavior. 2015;19
Suppl 2:112-22.
190. Lewnard JA, Berrang-Ford L. Internet-based partner selection and risk for
unprotected anal intercourse in sexual encounters among men who have sex with men:
a meta-analysis of observational studies. Sexually transmitted infections.
2014;90(4):290-6.
191. Lim SH, Bazazi AR, Sim C, Choo M, Altice FL, Kamarulzaman A. High rates of
unprotected anal intercourse with regular and casual partners and associated risk
factors in a sample of ethnic Malay men who have sex with men (MSM) in Penang,
Malaysia. Sexually transmitted infections. 2013;89(8):642-9.
192. Kelly JA, DiFranceisco WJ, St Lawrence JS, Amirkhanian YA, Anderson-Lamb
M. Situational, partner, and contextual factors associated with level of risk at most
recent intercourse among Black men who have sex with men. AIDS and behavior.
2014;18(1):26-35.
193. Mayer KH, Wheeler DP, Bekker LG, Grinsztejn B, Remien RH, Sandfort TG, et
al. Overcoming biological, behavioral, and structural vulnerabilities: new directions in
research to decrease HIV transmission in men who have sex with men. Journal of
acquired immune deficiency syndromes (1999). 2013;63 Suppl 2:S161-7.
194. Arnold MP, Struthers H, McIntyre J, Lane T. Contextual correlates of per
partner unprotected anal intercourse rates among MSM in Soweto, South Africa. AIDS
and behavior. 2013;17 Suppl 1:S4-11.
55
195. Choi KH, Hudes ES, Steward WT. Social discrimination, concurrent sexual
partnerships, and HIV risk among men who have sex with men in Shanghai, China.
AIDS and behavior. 2008;12(4 Suppl):S71-7.
196. Jeffries WLt, Marks G, Lauby J, Murrill CS, Millett GA. Homophobia is
associated with sexual behavior that increases risk of acquiring and transmitting HIV
infection among black men who have sex with men. AIDS and behavior.
2013;17(4):1442-53.
197. Ross MW, Berg RC, Schmidt AJ, Hospers HJ, Breveglieri M, Furegato M, et al.
Internalised homonegativity predicts HIV-associated risk behavior in European men
who have sex with men in a 38-country cross-sectional study: some public health
implications of homophobia. BMJ open. 2013;3(2).
198. Calabrese SK, Reisen CA, Zea MC, Poppen PJ, Bianchi FT. The pleasure
principle: the effect of perceived pleasure loss associated with condoms on
unprotected anal intercourse among immigrant Latino men who have sex with men.
AIDS patient care and STDs. 2012;26(7):430-5.
199. Kramer SC, Drewes J, Kruspe M, Marcus U. Factors associated with sexual risk
behaviors with non-steady partners and lack of recent HIV testing among German men
who have sex with men in steady relationships: results from a cross-sectional internet
survey. BMC public health. 2015;15:702.
200. Griensven Fv, Thienkrua W, McNicholl J, Wimonsate W, Chaikummao S,
Chonwattana W, et al. Evidence of an explosive epidemic of HIV infection in a cohort of
men who have sex with men in Thailand. AIDS (London, England). 2013;27(5):825-32.
201. Hladik W, Barker J, Ssenkusu JM, Opio A, Tappero JW, Hakim A, et al. HIV
infection among men who have sex with men in Kampala, Uganda--a respondent
driven sampling survey. PLoS ONE [Electronic Resource]. 2012;7(5):e38143.
202. Merrigan M, Azeez A, Afolabi B, Chabikuli ON, Onyekwena O, Eluwa G, et al.
HIV prevalence and risk behaviours among men having sex with men in Nigeria.
Sexually transmitted infections. 2011;87(1):65-70.
203. Lane T, Raymond H, Dladla S, Rasethe J, Struthers H, McFarland W, et al.
High HIV prevalence among men who have sex with men in Soweto, South Africa:
Results from the Soweto Men's Study. AIDS and behavior. 2011;15(3):626-34.
204. Joseph HA, Marks G, Belcher L, Millett GA, Stueve A, Bingham TA, et al. Older
partner selection, sexual risk behaviour and unrecognised HIV infection among black
and Latino men who have sex with men. Sexually transmitted infections.
2011;87(5):442-7.
56
205. Guy RJ, Spelman T, Stoove M, El-Hayek C, Goller J, Fairley CK, et al. Risk
factors for HIV seroconversion in men who have sex with men in Victoria, Australia:
results from a sentinel surveillance system. Sexual health. 2011;8(3):319-29.
206. Baral S, Burrell E, Scheibe A, Brown B, Beyrer C, Bekker LG. HIV risk and
associations of HIV infection among men who have sex with men in peri-urban Cape
Town, South Africa. BMC public health. 2011;11:766.
207. Pedrana AE, Hellard ME, Guy R, Wilson K, Stoove M. The difference in self-
reported and biological measured HIV prevalence: Implications for HIV prevention.
AIDS and behavior. 2012;16(6):1454-63.
208. Wang B, Li X, Stanton B, Liu Y, Jiang S. Socio-demographic and behavioral
correlates for HIV and syphilis infections among migrant men who have sex with men
in Beijing, China. AIDS care. 2013;25(2):249-57.
209. Wang QQ, Chen XS, Yin YP, Liang GJ, Zhang RL, Jiang N, et al. HIV
prevalence, incidence and risk behaviours among men who have sex with men in
Yangzhou and Guangzhou, China: a cohort study. Journal of the International AIDS
Society. 2014;17:18849.
210. Nguyen TV, Van Khuu N, Nguyen PD, Tran HP, Phan HT, Phan LT, et al.
Sociodemographic Factors, Sexual Behaviors, and Alcohol and Recreational Drug Use
Associated with HIV Among Men Who Have Sex with Men in Southern Vietnam. AIDS
and behavior. 2016;20(10):2357-71.
211. Balaji AB, Bowles KE, Le BC, Paz-Bailey G, Oster AM. High HIV incidence and
prevalence and associated factors among young MSM, 2008. AIDS (London, England).
2013;27(2):269-78.
212. Price MA, Rida W, Mwangome M, Mutua G, Middelkoop K, Roux S, et al.
Identifying at-risk populations in Kenya and South Africa: HIV incidence in cohorts of
men who report sex with men, sex workers, and youth. JAIDS Journal of Acquired
Immune Deficiency Syndromes. 2012;59(2):185-93.
213. Li D, Li S, Liu Y, Gao Y, Yu M, Yang X, et al. HIV incidence among men who
have sex with men in Beijing: A prospective cohort study. BMJ open. 2012;2(6).
214. Jansen IA, Geskus RB, Davidovich U, Jurriaans S, Coutinho RA, Prins M, et al.
Ongoing HIV-1 transmission among men who have sex with men in Amsterdam: A 25-
year prospective cohort study. AIDS (London, England). 2011;25(4):493-501.
215. Sandfort TG, Lane T, Dolezal C, Reddy V. Gender Expression and Risk of HIV
Infection Among Black South African Men Who Have Sex with Men. AIDS and
behavior. 2015.
216. Saha MK, Mahapatra T, Biswas S, Ghosh P, Mahapatra S, Deb AK, et al.
Sociobehavioral correlates of HIV risk among men who have sex with men in
57
Chhattisgarh, India: analysis of sentinel surveillance data. Japanese journal of
infectious diseases. 2015;68(1):38-44.
217. Carey JW, Mejia R, Bingham T, Ciesielski C, Gelaude D, Herbst JH, et al. Drug
use, high-risk sex behaviors, and increased risk for recent HIV infection among men
who have sex with men in Chicago and Los Angeles. AIDS and behavior.
2009;13(6):1084-96.
218. Baral S, Sifakis F, Peryskina A, Mogilnii V, Masenior NF, Sergeyev B, et al.
Risks for HIV infection among gay, bisexual, and other men who have sex with men in
Moscow and St. Petersburg, Russia. AIDS Research and Human Retroviruses.
2012;28(8):874-9.
219. Ackers ML, Greenberg, A. E., Lin, C. Y., Bartholow, B. N., Goodman, A. H.,
Longhi, M. Gurwith, M. High and persistent HIV seroincidence in men who have sex
with men across 47 U.S. cities. PLoS ONE [Electronic Resource]. 2012;7(4):e34972.
220. Millett GA, Ding H, Marks G, Jeffries WLt, Bingham T, Lauby J, et al. Mistaken
assumptions and missed opportunities: correlates of undiagnosed HIV infection among
black and Latino men who have sex with men. Journal of Acquired Immune Deficiency
Syndromes: JAIDS. 2011;58(1):64-71.
221. Sanders EJ, Okuku HS, Smith AD, Mwangome M, Wahome E, Fegan G, et al.
High HIV-1 incidence, correlates of HIV-1 acquisition, and high viral loads following
seroconversion among MSM. AIDS (London, England). 2013;27(3):437-46.
222. Rispel LC, Metcalf CA, Cloete A, Reddy V, Lombard C. HIV prevalence and risk
practices among men who have sex with men in two South African Cities. Journal of
Acquired Immune Deficiency Syndromes. 2011;57(1):69-76.
223. Oster AM, Dorell CG, Mena LA, Thomas PE, Toledo CA, Heffelfinger JD. HIV
risk among young African American men who have sex with men: a case-control study
in Mississippi. American journal of public health. 2011;101(1):137-43.
224. Pedrana AE, Hellard ME, Wilson K, Guy R, Stoove M. High rates of
undiagnosed HIV infections in a community sample of gay men in Melbourne,
Australia. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2012;59(1):94-9.
225. Berry M, Wirtz AL, Janayeva A, Ragoza V, Terlikbayeva A, Amirov B, et al. Risk
factors for HIV and unprotected anal intercourse among men who have sex with men
(MSM) in Almaty, Kazakhstan. PloS one. 2012;7(8).
226. Xu JJ, Reilly KH, Lu CM, Ma N, Zhang M, Chu ZX, et al. A cross-sectional study
of HIV and syphilis infections among male students who have sex with men (MSM) in
northeast China: implications for implementing HIV screening and intervention
programs. BMC public health. 2011;11:287.
58
227. Kanter J, Koh C, Razali K, Tai R, Izenberg J, Rajan L, et al. Risk behaviour and
HIV prevalence among men who have sex with men in a multiethnic society: A venue-
based study in Kuala Lumpur, Malaysia. International journal of STD & AIDS.
2011;22(1):30-7.
228. Hoenigl M, Chaillon A, Morris SR, Little SJ. HIV Infection Rates and Risk
Behavior among Young Men undergoing community-based Testing in San Diego.
Scientific reports. 2016;6:25927.
229. Holt M, Lea T, Asselin J, Hellard M, Prestage G, Wilson D, et al. The
prevalence and correlates of undiagnosed HIV among Australian gay and bisexual
men: results of a national, community-based, bio-behavioural survey. Journal of the
International AIDS Society. 2015;18:20526.
230. Carneiro M, Cardoso FA, Greco M, Oliveira E, Andrade J, Greco DB, et al.
Determinants of human immunodeficiency virus (HIV) prevalence in homosexual and
bisexual men screened for admission to a cohort study of HIV negatives in Belo
Horizonte, Brazil: Project Horizonte. Memorias do Instituto Oswaldo Cruz.
2003;98(3):325-9.
231. Chen YJ, Lin YT, Chen M, Huang SW, Lai SF, Wong WW, et al. Risk Factors
for HIV-1 seroconversion among Taiwanese men visiting gay saunas who have sex
with men. BMC infectious diseases. 2011;11(334).
232. Neaigus A, Jenness SM, Hagan H, Murrill CS, Torian LV, Wendel T, et al.
Estimating HIV incidence and the correlates of recent infection in venue-sampled men
who have sex with men in New York City. AIDS and behavior. 2012;16(3):516-24.
233. Rice CE, Maierhofer C, Fields KS, Ervin M, Lanza ST, Turner AN. Beyond Anal
Sex: Sexual Practices of Men Who Have Sex With Men and Associations With HIV and
Other Sexually Transmitted Infections. The journal of sexual medicine. 2016;13(3):374-
82.
234. Oster AM, Wiegand RE, Sionean C, Miles IJ, Thomas PE, Melendez-Morales L,
et al. Understanding disparities in HIV infection between Black and White MSM in the
United States. AIDS (London, England). 2011;25(8):1103-12.
235. Mor Z, Dan M. Knowledge, attitudes, sexual practices and STI/HIV prevalence
in male sex workers and other men who have sex in Tel Aviv, Israel: A cross-sectional
study. Sexually transmitted infections. 2012;88(8):574-80.
236. Dahoma M, Johnston LG, Holman A, Miller LA, Mussa M, Othman A, et al. HIV
and related risk behavior among men who have sex with men in Zanzibar, Tanzania:
results of a behavioral surveillance survey. AIDS & Behavior. 2011;15(1):186-92.
59
237. Saha MK, Mahapatra T, Biswas S, Ghosh P, Kire M. Burden and correlates of
HIV risk among men who have sex with men in Nagaland, India: analysis of sentinel
surveillance data. PloS one. 2015;10(2):e0117385.
238. Chen X, Jiang N, Wang B. HIV/STI prevalence among men who have sex with
men in 4 cities, China and associated risk factors for HIV infection. Sexually transmitted
infections. 2011;87:A50.
239. Pitpitan EV, Goodman-Meza D, Burgos JL, Abramovitz D, Chavarin CV, Torres
K, et al. Prevalence and correlates of HIV among men who have sex with men in
Tijuana, Mexico. Journal of the International AIDS Society. 2015;18:19304.
240. van Griensven F, Holtz TH, Thienkrua W, Chonwattana W, Wimonsate W,
Chaikummao S, et al. Temporal trends in HIV-1 incidence and risk behaviours in men
who have sex with men in Bangkok, Thailand, 2006-13: an observational study. The
lancet HIV. 2015;2(2):e64-70.
241. Sander PM, Cole SR, Stall RD, Jacobson LP, Eron JJ, Napravnik S, et al. Joint
effects of alcohol consumption and high-risk sexual behavior on HIV seroconversion
among men who have sex with men. AIDS (London, England). 2013;27(5):815-23.
242. Li Y, Baker JJ, Korostyshevskiy VR, Slack RS, Plankey MW. The association of
intimate partner violence, recreational drug use with HIV seroprevalence among MSM.
AIDS and behavior. 2012;16(3):491-8.
243. Yan H, Ding Y, Wong FY, Ning Z, Zheng T, Nehl EJ, et al. Epidemiological and
molecular characteristics of HIV infection among money boys and general men who
have sex with men in Shanghai, China. Infection, genetics and evolution : journal of
molecular epidemiology and evolutionary genetics in infectious diseases. 2015;31:135-
41.
244. Koblin BA, Husnik MJ, Colfax G, Huang YJ, Madison M, Mayer K, et al. Risk
factors for HIV infection among men who have sex with men. AIDS (London, England).
2006;20(5):731-9.
245. Buchbinder SP, Vittinghoff E, Heagerty PJ, Celum CL, Seage GR, III, Judson
FN, et al. Sexual Risk, Nitrite Inhalant Use, and Lack of Circumcision Associated With
HIV Seroconversion in Men Who Have Sex With Men in the United States. JAIDS
Journal of Acquired Immune Deficiency Syndromes. 2005;39(1):82-9.
246. Buchbinder SP, Douglas JM, Jr., McKirnan DJ, Judson FN, Katz MH,
MacQueen KM. Feasibility of human immunodeficiency virus vaccine trials in
homosexual men in the United States: risk behavior, seroincidence, and willingness to
participate. Journal of Infectious Diseases. 1996;174(5):954-61.
60
247. Weber AE, Craib KJP, Chan K, Martindale S, Lou Miller M, Cook DA, et al.
Determinants of HIV serconversion in an era of increasing HIV infection among young
gay and bisexual men. AIDS (London, England). 2003;17(5):774-7.
248. Plankey MW, Ostrow DG, Stall R, Cox C, Li XH, Peck JA, et al. The relationship
between methamphetamine and popper use and risk of HIV seroconversion in the
multicenter AIDS cohort study. JAIDS, Journal of Acquired Immune Deficiency
Syndromes. 2007;45(1):85-92.
249. Prestage G, Jin F, Kippax S, Zablotska I, Imrie J, Grulich A. Use of illicit drugs
and erectile dysfunction medications and subsequent HIV infection among gay men in
Sydney, Australia. The journal of sexual medicine. 2009;6(8):2311-20.
250. Macdonald N, Elam G, Hickson F, Imrie J, McGarrigle CA, Fenton KA, et al.
Factors associated with HIV seroconversion in gay men in England at the start of the
21st century. Sexually transmitted infections. 2008;84(1):8-13.
251. Thiede H, Jenkins RA, Carey JW, Hutcheson R, Thomas KK, Stall RD, et al.
Determinants of recent HIV infection among Seattle-area men who have sex with men.
American journal of public health. 2009;99 Suppl 1:S157-64.
252. Drumright LN, Gorbach PM, Little SJ, Strathdee SA. Associations between
substance use, erectile dysfunction medication and recent HIV infection among men
who have sex with men. AIDS and behavior. 2009;13(2):328-36.
253. Hoenigl M, Chaillon A, Moore DJ, Morris SR, Smith DM, Little SJ. Clear Links
Between Starting Methamphetamine and Increasing Sexual Risk Behavior: A Cohort
Study Among Men Who Have Sex With Men. Journal of acquired immune deficiency
syndromes (1999). 2016;71(5):551-7.
254. Fuller CM, Absalon J, Ompad DC, Nash D, Koblin B, Blaney S, et al. A
comparison of HIV seropositive and seronegative young adult heroin- and cocaine-
using men who have sex with men in New York City, 2000-2003. Journal of Urban
Health. 2005;82(1 Suppl 1):i51-61.
255. Ruiz J, Facer M, Sun RK. Risk factors for human immunodeficiency virus
infection and unprotected anal intercourse among young men who have sex with men.
Sexually transmitted diseases. 1998;25(2):100-7.
256. Raymond H, Bingham T, McFarland W. Locating unrecognized HIV infections
among men who have sex with men: San Francisco and Los Angeles. AIDS Education
and Prevention. 2008;20(5):408-19.
257. Beyrer C. Global prevention of HIV infection for neglected populations: men
who have sex with men. Clinical infectious diseases : an official publication of the
Infectious Diseases Society of America. 2010;50 Suppl 3:S108-13.
61
258. Guo Y, Li X, Fang X, Lin X, Song Y, Jiang S, et al. A comparison of four
sampling methods among men having sex with men in China: implications for HIV/STD
surveillance and prevention. Aids Care-Psychol Socio-Med Asp Aids-Hiv.
2011;23(11):1400-9.
259. Beyrer C, Sullivan PS, Sanchez J, Dowdy D, Altman D, Trapence G, et al. A
call to action for comprehensive HIV services for men who have sex with men. Lancet
(London, England). 2012;380(9839):424-38.
260. Salomon EA, Mimiaga MJ, Husnik MJ, Welles SL, Manseau MW, Montenegro
AB, et al. Depressive symptoms, utilization of mental health care, substance use and
sexual risk among young men who have sex with men in EXPLORE: implications for
age-specific interventions. AIDS and behavior. 2009;13(4):811-21.
261. Sivasubramanian M, Mimiaga MJ, Mayer KH, Anand VR, Johnson CV,
Prabhugate P, et al. Suicidality, clinical depression, and anxiety disorders are highly
prevalent in men who have sex with men in Mumbai, India: findings from a community-
recruited sample. Psychology, health & medicine. 2011;16(4):450-62.
262. Hirshfield S, Wolitski RJ, Chiasson MA, Remien RH, Humberstone M, Wong T.
Screening for depressive symptoms in an online sample of men who have sex with
men. AIDS care. 2008;20(8):904-10.
263. Pakula B, Marshall BD, Shoveller JA, Chesney MA, Coates TJ, Koblin B, et al.
Gradients in Depressive Symptoms by Socioeconomic Position Among Men Who Have
Sex With Men in the EXPLORE Study. Journal of homosexuality. 2016.
264. Mills TC, Paul J, Stall R, Pollack L, Canchola J, Chang YJ, et al. Distress and
depression in men who have sex with men: the Urban Men's Health Study. The
American journal of psychiatry. 2004;161(2):278-85.
265. Chakrapani V, Newman PA, Shunmugam M, Logie CH, Samuel M. Syndemics
of depression, alcohol use, and victimisation, and their association with HIV-related
sexual risk among men who have sex with men and transgender women in India.
Global public health. 2015:1-16.
266. Mimiaga MJ, Reisner SL, Closson EF, Perry N, Perkovich B, Nguyen T, et al.
Self-perceived HIV risk and the use of risk reduction strategies among men who
engage in transactional sex with other men in Ho Chi Minh City, Vietnam. AIDS care.
2013;25(8):1039-44.
267. Alvy LM, McKirnan DJ, Mansergh G, Koblin B, Colfax GN, Flores SA, et al.
Depression is associated with sexual risk among men who have sex with men, but is
mediated by cognitive escape and self-efficacy. AIDS and behavior. 2011;15(6):1171-
9.
62
268. Mimiaga MJ, Biello KB, Sivasubramanian M, Mayer KH, Anand VR, Safren SA.
Psychosocial risk factors for HIV sexual risk among Indian men who have sex with
men. AIDS care. 2013;25(9):1109-13.
269. Safren SA, Thomas BE, Mimiaga MJ, Chandrasekaran V, Menon S,
Swaminathan S, et al. Depressive symptoms and human immunodeficiency virus risk
behavior among men who have sex with men in Chennai, India. Psychology, health &
medicine. 2009;14(6):705-15.
270. Tucker A, Liht J, de Swardt G, Jobson G, Rebe K, McIntyre J, et al. An
exploration into the role of depression and self-efficacy on township men who have sex
with men's ability to engage in safer sexual practices. AIDS care. 2013;25(10):1227-35.
271. Bousman CA, Cherner M, Ake C, Letendre S, Atkinson JH, Patterson TL, et al.
Negative mood and sexual behavior among non-monogamous men who have sex with
men in the context of methamphetamine and HIV. Journal of affective disorders.
2009;119(1-3):84-91.
272. Stall R, Mills TC, Williamson J, Hart T, Greenwood G, Paul J, et al. Association
of co-occurring psychosocial health problems and increased vulnerability to HIV/AIDS
among urban men who have sex with men. Am J Public Health. 2003;93(6):939-42.
273. Mustanski B, Garofalo R, Herrick A, Donenberg G. Psychosocial health
problems increase risk for HIV among urban young men who have sex with men:
preliminary evidence of a syndemic in need of attention. Annals of Behavioral
Medicine. 2007;34(1):37-45.
274. Safren SA, Reisner SL, Herrick A, Mimiaga MJ, Stall RD. Mental health and HIV
risk in men who have sex with men. Journal of acquired immune deficiency syndromes
(1999). 2010;55 Suppl 2:S74-7.
275. Reisner SL, Mimiaga MJ, Skeer M, Bright D, Cranston K, Isenberg D, et al.
Clinically significant depressive symptoms as a risk factor for HIV infection among
black MSM in Massachusetts. AIDS and behavior. 2009;13(4):798-810.
276. O'Cleirigh C, Newcomb ME, Mayer KH, Skeer M, Traeger L, Safren SA.
Moderate levels of depression predict sexual transmission risk in HIV-infected MSM: a
longitudinal analysis of data from six sites involved in a "prevention for positives" study.
AIDS and behavior. 2013;17(5):1764-9.
277. Gibbs JJ, Rice E. The Social Context of Depression Symptomology in Sexual
Minority Male Youth: Determinants of Depression in a Sample of Grindr Users. Journal
of homosexuality. 2016;63(2):278-99.
278. Bourne A, Reid D, Hickson F, Torres-Rueda S, Weatherburn P. Illicit drug use
in sexual settings ('chemsex') and HIV/STI transmission risk behaviour among gay men
63
in South London: findings from a qualitative study. Sexually transmitted infections.
2015;91(8):564-8.
279. Schafer KR, Gupta S, Dillingham R. HIV-infected men who have sex with men
and histories of childhood sexual abuse: implications for health and prevention. The
Journal of the Association of Nurses in AIDS Care : JANAC. 2013;24(4):288-98.
280. Irish L, Kobayashi I, Delahanty DL. Long-term physical health consequences of
childhood sexual abuse: a meta-analytic review. Journal of pediatric psychology.
2010;35(5):450-61.
281. O'Cleirigh C, Safren SA, Mayer KH. The pervasive effects of childhood sexual
abuse: challenges for improving HIV prevention and treatment interventions. Journal of
acquired immune deficiency syndromes (1999). 2012;59(4):331-4.
282. Choi KH, Paul J, Ayala G, Boylan R, Gregorich SE. Experiences of
discrimination and their impact on the mental health among African American, Asian
and Pacific Islander, and Latino men who have sex with men. American journal of
public health. 2013;103(5):868-74.
283. Choi KH, Steward WT, Miege P, Hudes E, Gregorich SE. Sexual Stigma,
Coping Styles, and Psychological Distress: A Longitudinal Study of Men Who Have
Sex With Men in Beijing, China. Archives of sexual behavior. 2015.
284. Thomas B, Mimiaga MJ, Mayer KH, Perry NS, Swaminathan S, Safren SA. The
influence of stigma on HIV risk behavior among men who have sex with men in
Chennai, India. AIDS care. 2012;24(11):1401-6.
285. Logie CH, Newman PA, Chakrapani V, Shunmugam M. Adapting the minority
stress model: associations between gender non-conformity stigma, HIV-related stigma
and depression among men who have sex with men in South India. Social science &
medicine (1982). 2012;74(8):1261-8.
286. Lea T, de Wit J, Reynolds R. Minority stress in lesbian, gay, and bisexual young
adults in Australia: associations with psychological distress, suicidality, and substance
use. Archives of sexual behavior. 2014;43(8):1571-8.
287. United Nations Statistics Devision. Vietnam Country Profile 2016 [23 May,
2016]. Available from: http://data.un.org/CountryProfile.aspx?crName=Viet%20Nam.
288. General Statistics Office of Vietnam. Statistical Yearbook of Vietnam 2014.
Hanoi, Vietnam: 2014.
289. Huong PL, Fry GW. Education and Economic, Political, and Social Change in
Vietnam. Educational Research for Policy and Practice. 2004;3(3):199-222.
290. Irvin G. Vietnam: Assessing the Achievements of Doi Moi. The Journal of
Development Studies. 1995;31(5):725-50.
64
291. Dollar D. Economic reform, openness, and Vietnam's entry into ASEAN.
ASEAN Economic Bulletin. 1996;13(2):169-84.
292. Blanc M-E. Social construction of male homosexualities in Vietnam. Some keys
to understanding discrimination and implications for HIV prevention strategy.
International Social Science Journal. 2005;57(186):661-73.
293. BUI HN, MORASH M. Domestic Violence in the Vietnamese Immigrant
Community: An Exploratory Study. Violence Against Women. 1999;5(7):769-95.
294. Horton P. 'I thought I was the only one': the misrecognition of LGBT youth in
contemporary Vietnam. Culture, health & sexuality. 2014;16(8):960-73.
295. Colby D, Minh TT, Toan TT. Down on the farm: homosexual behaviour, HIV risk
and HIV prevalence in rural communities in Khanh Hoa province, Vietnam. Sexually
transmitted infections. 2008;84(6):439-43.
296. Colby DJ. HIV knowledge and risk factors among men who have sex with men
in Ho Chi Minh City, Vietnam. Journal of acquired immune deficiency syndromes
(1999). 2003;32(1):80-5.
297. Pham QD, Nguyen TV, Hoang CQ, Cao V, Khuu NV, Phan HT, et al.
Prevalence of HIV/STIs and associated factors among men who have sex with men in
An Giang, Vietnam. Sexually transmitted diseases. 2012;39(10):799-806.
298. United Nations Office on Drugs and Crime (UNODC). Patterns and Trends of
Amphetamine-Type-Stimulants and Other Drugs: Challenges for Asia and the Pacifics.
2013.
299. Nguyen VT, Scannapieco M. Drug abuse in Vietnam: a critical review of the
literature and implications for future research. Addiction (Abingdon, England).
2008;103(4):535-43.
300. Vietnam Ministry of Police. Report on the Implementation of the National Target
Program for Illicit Drugs Prevention and Control in the period 2011-2015 and the
Proposed Plan for the period 2016-2020. Hanoi, Vietnam: 2016.
301. Nguyen TA, Nguyen HT, Le GT, Detels R. Prevalence and risk factors
associated with HIV infection among men having sex with men in Ho Chi Minh City,
Vietnam. AIDS and behavior. 2008;12(3):476-82.
302. Ha H, Risser JM, Ross MW, Huynh NT, Nguyen HT. Homosexuality-related
stigma and sexual risk behaviors among men who have sex with men in Hanoi,
Vietnam. Archives of sexual behavior. 2015;44(2):349-56.
303. Vietnam Ministry of Health. Results from the HIV/STI Intergrated Biological and
Behavioural Surveillance (IBBS) in Vietnam, 2005-2006: Hanoi, Vietnam: Ministry of
Health, 2006; 2006.
65
304. Vietnam Ministry of Health. Results from the HIV/STI Biological and Behavioral
Surveillance (Ibbs) in Vietnam- Round II 2009. Hanoi, Vietnam: 2011.
305. Yu G, Clatts MC, Goldsamt LA, Giang le M. Substance use among male sex
workers in Vietnam: prevalence, onset, and interactions with sexual risk. The
International journal on drug policy. 2015;26(5):516-21.
306. Mimiaga MJ, Closson EF, Biello KB, Nguyen H, Nguyen QH, Oldenburg CE, et
al. A Group-Based Sexual Risk Reduction Intervention for Men Who Have Sex With
Men in Ho Chi Minh City, Vietnam: Feasibility, Acceptability, and Preliminary Efficacy.
Archives of sexual behavior. 2016;45(6):1493-500.
307. Pham QD, Nguyen TV, Nguyen PD, Le SH, Tran AT, Nguyen LT, et al. Men
who have sex with men in southern Vietnam report high levels of substance use and
sexual risk behaviours but underutilise HIV testing services: a cross-sectional study.
Sexually transmitted infections. 2015;91(3):178-82.
308. Vu BN, Mulvey KP, Baldwin S, Nguyen ST. HIV risk among drug-using men
who have sex with men, men selling sex, and transgender individuals in Vietnam.
Culture, health & sexuality. 2012;14(2):167-80.
309. Garcia MC, Duong QL, Mercer LE, Meyer SB, Ward PR. 'Never testing for HIV'
among men who have sex with men in Viet Nam: results from an Internet-based cross-
sectional survey. BMC public health. 2013;13:1236.
310. Justumus P, Colby D, Mai Doan Anh T, Balestre E, Becquet R, Orne-Gliemann
J. Willingness to use the Internet to seek information on HIV prevention and care
among men who have sex with men in Ho Chi Minh City, Vietnam. PloS one.
2013;8(8):e71471.
311. Garcia MC, Duong QL, Mercer LC, Meyer SB, Koppenhaver T, Ward PR.
Patterns and risk factors of inconsistent condom use among men who have sex with
men in Viet Nam: Results from an Internet-based cross-sectional survey. Global public
health. 2014;9(10):1225-38.
312. Bengtsson L, Lu X, Liljeros F, Thanh HH, Thorson A. Strong propensity for HIV
transmission among men who have sex with men in Vietnam: behavioural data and
sexual network modelling. BMJ open. 2014;4(1):e003526.
313. Garcia MC, Duong QL, Meyer SB, Ward PR. Multiple and concurrent sexual
partnerships among men who have sex with men in Viet Nam: results from a National
Internet-based Cross-sectional Survey. Health promotion international. 2016;31(1):133-
43.
314. Nguyen TV, Van Khuu N, Nguyen PD, Tran HP, Phan HT, Phan LT, et al.
Sociodemographic Factors, Sexual Behaviors, and Alcohol and Recreational Drug Use
66
Associated with HIV Among Men Who Have Sex with Men in Southern Vietnam. AIDS
and behavior. 2016.
315. Oldenburg CE, Le B, Huyen HT, Thien DD, Quan NH, Biello KB, et al.
Antiretroviral pre-exposure prophylaxis preferences among men who have sex with
men in Vietnam: results from a nationwide cross-sectional survey. Sexual health. 2016.
316. National Institute of Hygiene and Epidemioloty (Vietnam Ministry of Health).
HIV/STI Intergrated Biological and Behavioural Surveillance (IBBS) in Vietnam. Results
from Round III and trends across three round (2005-2009-2013) of survey. Hanoi,
Vietnam: 2014.
317. Oldenburg CE, Biello KB, Colby D, Closson EF, Mai T, Nguyen T, et al. Stigma
related to sex work among men who engage in transactional sex with men in Ho Chi
Minh City, Vietnam. International journal of public health. 2014;59(5):833-40.
318. Bengtsson L, Thorson A, Thanh VP, Allebeck P, Popenoe R. Sexual
relationships among men who have sex with men in Hanoi, Vietnam: a qualitative
interview study. BMC public health. 2013;13:108.
319. Ngo DA, Ross MW, Phan H, Ratliff EA, Trinh T, Sherburne L. Male homosexual
identities, relationships, and practices among young men who have sex with men in
Vietnam: implications for HIV prevention. AIDS education and prevention : official
publication of the International Society for AIDS Education. 2009;21(3):251-65.
320. Vu BN, Girault P, Do BV, Colby D, Tran LT. Male sexuality in Vietnam: the case
of male-to-male sex. Sexual health. 2008;5(1):83-8.
321. Wilson D, Cawthorne P. 'Face up to the truth': helping gay men in Vietnam
protect themselves from AIDS. International journal of STD & AIDS. 1999;10(1):63-6.
322. Berry MC, Go VF, Quan VM, Minh NL, Ha TV, Mai NV, et al. Social
environment and HIV risk among MSM in Hanoi and Thai Nguyen. AIDS care.
2013;25(1):38-42.
323. Colby D, Cao NH, Doussantousse S. Men who have sex with men and HIV in
Vietnam: a review. AIDS education and prevention : official publication of the
International Society for AIDS Education. 2004;16(1):45-54.
324. Nguyen TH, Wolffers I. HIV infection in Vietnam. Lancet (London, England).
1994;343(8894):410.
325. Quan VM, Chung A, Long HT, Dondero TJ. HIV in Vietnam: the evolving
epidemic and the prevention response, 1996 through 1999. Journal of acquired
immune deficiency syndromes (1999). 2000;25(4):360-9.
326. Nguyen TH, Nguyen TL, Trinh QH. HIV/AIDS epidemics in Vietnam: evolution
and responses. AIDS education and prevention : official publication of the International
Society for AIDS Education. 2004;16(3 Suppl A):137-54.
67
327. Viet Nam Administration of HIV/AIDS Control Office (VAAC). HIV/AIDS
Prevention and Control Report for 2015 Hanoi, Vietnam2016 [cited 23 May, 2016.
Available from:
http://vaac.gov.vn/Cms_Data/Contents/Vaac/Folders/Solieubaocao/Solieu/~contents/B
CG2DGP6NQ77KBCX/Bao-cao-2015_so-lieu_Final.pdf.
328. The Social Republicd of Vietnam. HIV/AIDS Second Country Report on
following up to the Declarat5ion of Committment on HIV/AIDS. Declaration of
Committment on HIV/AIDS adopted at the 26th United Nations General Assembly
Special Session in June 2001 (UNGASS). Reporting period: January 2003 – December
2005 Hanoi, Vietnam: 2006.
329. The Socialist Republic of Vietnam. Reporting period: January 2008 – December
2009. Declaration of Commitment on HIV and AIDS adopted at the 26th United Nations
General Assembly Special Session in June 2001 (UNGASS). Hanoi: 3/20102010.
330. Vietnam Ministry of Health. Results from the HIV/STI Intergrated Biological and
Behavioural Surveillance (IBBS) in Vietnam, 2005-2006. Hanoi, Vietnam: 2006.
331. Blanc ME. Social construction of male homosexualities in Vietnam. Some keys
to understanding discrimination and implications for HIV prevention strategy. Int Soc
Sci J. 2005;57(4):661-+.
332. Le TM, Lee PC, Stewart DE, Long TN, Quoc CN. What are the risk factors for
HIV in men who have sex with men in Ho Chi Minh City, Vietnam?- A cross-sectional
study. BMC public health. 2016;16(1):406.
333. Quang Duy P, Thuong Vu N, Cuong Quoc H, Van C, Nghia Van K, Huong Thu
Thi P, et al. Prevalence of HIV/STIs and associated factors among men who have sex
with men in An Giang, Vietnam. Sexually transmitted diseases. 2012;39(10):799-806.
334. Glass TA, McAtee MJ. Behavioral science at the crossroads in public health:
Extending horizons, envisioning the future. Social Science and Medicine.
2006;62(7):1650-71.
335. O'Donoghue G, Perchoux C, Mensah K, Lakerveld J, van der Ploeg H,
Bernaards C, et al. A systematic review of correlates of sedentary behaviour in adults
aged 18-65 years: a socio-ecological approach. BMC public health. 2016;16(1):163.
336. Kaplan GA, Everson SA, Lynch JW. The contribution of social and behavioral
research to an understanding of the distribution of disease: a multilevel approach.
2000.
337. Krieger N. Epidemiology and the web of causation: has anyone seen the
spider? Social science & medicine (1982). 1994;39(7):887-903.
68
338. McMichael AJ. Prisoners of the proximate: loosening the constraints on
epidemiology in an age of change. American journal of epidemiology.
1999;149(10):887-97.
339. Susser M, Susser E. Choosing a future for epidemiology: II. From black box to
Chinese boxes and eco-epidemiology. American journal of public health.
1996;86(5):674-7.
340. Mehtala MA, Saakslahti AK, Inkinen ME, Poskiparta ME. A socio-ecological
approach to physical activity interventions in childcare: a systematic review. The
international journal of behavioral nutrition and physical activity. 2014;11:22.
341. Etienne G. Krug LLD, James A. Mercy, Anthony B. Zwi and Rafael Lozano.
Violence -a global public health problem. In: Etienne G. Krug LLD, James A. Mercy,
Anthony B. Zwi and Rafael Lozano, editor. World report on violence and health.
Geneva, Switzerland: World Health Organization; 2002.
342. DiClemente RJ, Salazar LF, Crosby RA, Rosenthal SL. Prevention and control
of sexually transmitted infections among adolescents: the importance of a socio-
ecological perspective--a commentary. Public health. 2005;119(9):825-36.
343. Scribner R, Theall KP, Simonsen N, Robinson W. HIV Risk and the Alcohol
Environment: Advancing an Ecological Epidemiology for HIV/AIDS. Alcohol Research
& Health. 2010;33(3):179-83.
344. Beyrer C, Sullivan P, Sanchez J, Baral SD, Collins C, Wirtz AL, et al. The
increase in global HIV epidemics in MSM. AIDS (London, England). 2013;27(17):2665-
78.
345. Susser M, Susser E. Choosing a future for epidemiology: I. Eras and
paradigms. American journal of public health. 1996;86(5):668-73.
346. Southgate E. The role of folk pharmacology and lay experts in harm reduction :
Sydney gay drug using networks. International Journal of Drug Policy. 2001;12(4):321-
35.
347. Leigh BC, Stall R. Substance use and risky sexual behavior for exposure to
HIV. Issues in methodology, interpretation, and prevention. The American psychologist.
1993;48(10):1035-45.
69
CHAPTER 2
METHODOLOGY OF THE CROSS-SECTIONAL SURVEY IN VIETNAM
AND THE SYSTEMATIC REVIEW AND META-ANALYSIS
70
In this chapter, I describe the research protocol for the community-based survey in
Vietnam and the systematic review and meta-analysis that I conducted. Please note that
the study design and analytical strategy are also described in each of the published
manuscripts.
COMMUNITY-BASED, CROSS-SECTIONAL SURVEY OF MSM IN HANOI
AND HO CHI MINH CITY, VIETNAM
Study design. The cross-sectional, community-based study was conducted in
collaboration with Hanoi HIV/AIDS Prevention Centre (Hanoi PAC), the Centre for
Community Health Promotion (CHP) in Hanoi, and the Centre for Promotion of Quality
of Life (Life Centre) in Ho Chi Minh City, Vietnam, and community-based organisations
(CBO) of MSM in the two cities during September–December 2014. Supporting letters
from the local collaborating organisations can be found in Appendix 1. These
organisations have experience in working with MSM and delivering HIV prevention
though USAID and Global Fund supported projects. HIV prevention services, including
behavioural counselling, educational materials, and free condoms and lubricant are
delivered via peers from local CBOs. These CBOs provide social and emotional support,
HIV prevention education and referral to HIV treatment for MSM in their localities. Peer
outreach workers of these CBOs were engaged to reach a large number of MSM in the
two cities.
The collaborating organisations assisted with recruiting potential participants and
contributed in-kind resources, such as coordinating fieldwork activities, providing venues
for interviews and offering free HIV testing (for a subsample of participants in Hanoi).
Interview venues were arranged in different parts of the cities to facilitate easy access
by participants.
Sampling method. MSM remain a hidden, hard-to-reach population in Vietnam because
of social stigma and discrimination regarding homosexuality (1, 2). Accordingly,
developing a randomised sampling frame is impossible. A non-random, convenience
sampling method was used to recruit participants for the study. Recruitment was
continued until the expected sample size was reached. The study recruited participants
using several approaches:
▪ Staff and/or peer outreach workers of local collaborating organisations and CBOs
helped to recruit initial participants for the study via MSM groups. Initial potential
participants were referred to the research team for eligibility screening and
71
interviewing. Since each CBO targets different subgroups of MSM, it was
anticipated that initial participants in each of the two cities would come from
different socio-demographic backgrounds.
▪ Peer referral recruitment. Once interviews were completed, participants were
asked to invite other MSM they knew who might be interested in participating in
the study. They were provided with invitation letters (see Appendix 2A) which
they could give to other potential participants. Peer outreach workers of the local
collaborating organisations could also refer other MSM to the study during
fieldwork. The invitation letter contained brief information about the study,
including its purpose, ethical aspects and rights of the participants, the phone
number of the local study coordinator and the addresses of interview venues.
Interested potential participants were encouraged to contact the local study
coordinator to book a time for an interview.
This is entirely a convenience sample with men referred to the study by either: i) peer
educators of collaborating CBOs or ii) other men who already participated in the study.
We did not track the number of men referred by each of the sampling strategies,
however, the majority of men were referred to the study by CBO’s field staff.
Sample size: I used the findings regarding the prevalence of methamphetamine use,
the prevalence of ecstasy use and the prevalence of CAI with any male partner in the
last 3 months to calculate the expected sample size. The calculation of sample size was
based on the WHO formula for hypothesis testing with respect to a population proportion
with a power of 80% and two-tailed type-I error of 5% (i.e., two-tailed significance
p<0.05). Indicators used to calculate the sample size were taken from previous studies
by Bengtsson et al (3) and UNODC’s Vietnam report (4). From this calculation, it was
expected that 600 MSM would need to be recruited for the community study. With this
sample size, 95% of the CAI prevalence from the study was expected to lie in the range
of 30% to 40%; 95% of the methamphetamine use prevalence found in the study would
lie in the range of 24% to 36% and 95% of the ecstasy use prevalence was expected to
be found in the range from 34% to 46% with the power of the test at 80%.
Eligible criteria: men were eligible to participate in the study if they had Vietnamese
citizenship, were aged 18 or older, had good comprehension of Vietnamese; reported
sex with another man in the last 3 months and consented to participate. Due to the small
number of transgender women who participated in the study (less than 10), it was
decided to exclude this group and focus the primary analyses for the study on MSM,
participants who reported that they were assigned male gender at birth, who identified
72

as male at the time of the study and who identified as gay or bisexual orientation or were
sexually interested in men.
Data collection. The face to face interviews were administered by trained, experienced
interviewers from Hanoi Medical University. MSM connected to local CBOs who had
experience in conducting interviews in other studies were also invited to be interviewers
for this study. The interviews were organised at the venues arranged by the local
collaborating organisations. Each interview lasted between 35-50 minutes and interviews
were arranged from 8 am to 8pm and during weekends to accommodate men who
worked during the week.
The data collection process consisted of three steps, as illustrated in Figure 4 below:
1. Welcome: there was a host from the study team to receive study participants once
they arrived at the interview venue. The host explained the study purpose, interview
process and ethical considerations, including confidentiality, and access to
counselling and other services, if the participants needed them. Once men agreed to
participate, they were asked to sign the Participant Information and Consent form to
confirm their agreement. This form can be found in Appendix 2B. In this consent form,
men were informed that they can withdraw at any time during the interview. Men were
screened by the study host to ensure that they were eligible to participate. Men who
were not eligible were informed thereof, received compensation for their time and
were offered HIV educational materials and access to HIV-related services, if they
were requested. The study host provided eligible men with their study ID.
2. Interview: Research in different settings has shown that interview questions of a
sensitive nature, such as those related to sexual practices and drug use, may be
affected by over-reporting or under-reporting of behavior. Over-reporting may occur,
for example, when participants are incentivised (paid) to participate in research, while
under-reporting may occur if the behaviours in question are socially stigmatised.
Participants received a modest monetary compensation equivalent to US$5. The
value of this compensation was equal to that of similar studies in Vietnam. Also, as
drug use and same-sex behaviours are stigmatised in Vietnam, findings may be
affected by over-reporting as well as under-reporting biases. To minimize these
potential biases, we took several preventive measures. Firstly, all the interviewers,
including peer recruiters, participated in training on the questionnaire, and effective
techniques in asking sensitive questions about personal and confidential information,
including communicating with MSM in ways that were trustworthy, respectful and
designed to put participants at ease. Secondly, participants were given the
73
opportunity to select the interviewer they felt most comfortable talking to (e.g. a man
or a woman, a peer or a researcher). Thirdly, the questionnaire did not collect
personally identifying information, such as full name, date of birth or address. Lastly,
interviews were conducted in private (i.e. meeting rooms or offices) to ensure privacy
and confidentiality. Each interview lasted for 35-50 minutes.
3. Completion: After completing the interview, participants returned to reception and
met with the study host to receive compensation and invitation letters to circulate to
other potential participants. Each participant received compensation equal to US$5,
similar to the level used in other studies conducted with Vietnamese MSM. The
compensation was for transportation and the time taken to participate in an interview.
All participants were offered HIV prevention materials, including a list of all local HIV
service providers. Participants who expressed concern or interest in accessing any
HIV-related services were referred to appropriate service providers. Participants who
expressed mental health problems or distress were referred to appropriate mental
health support, counselling or treatment services (particularly those provided by local
partner organisations). Men could also be referred to relevant MSM groups for peer-
support and counselling.
Optional HIV testing: In Hanoi, men who wished to test for HIV were referred to an
on-site testing team provided by the Hanoi PAC. Trained staff explained the
procedure for testing, answered any questions and explained that the test result
could be linked to their questionnaire data for research purposes only, if participants
agreed. Participants could choose to test without their data being linked (consistent
with the principles of voluntary testing). Those who agreed to data linkage signed an
additional informed consent form to allow the research team to access their HIV test
results using their study ID (see Appendix 2D). Men who consented to test for HIV
and data linkage could later withdraw consent for the study team to access their HIV
test result. In this case, men were asked to sign a separate Revocation of consent
form (Appendix 2E). For consenting participants, blood samples were labelled with
the participant’s study ID. Once their blood was collected, participants were given a
letter indicating the time and location where they could obtain their test results. When
participants collected their results, they were referred to HIV care and support
services, as required, by the Hanoi PAC staff, particularly if they received an HIV
positive test result. The testing procedure follows the Vietnamese Ministry of Health
HIV testing protocol. Testing was carried out in a separate room at the collaborating
community organisation, to ensure privacy and infection control. Because of resource
constraints, optional HIV testing was delivered to the first 210 men participating in
Hanoi only.
74
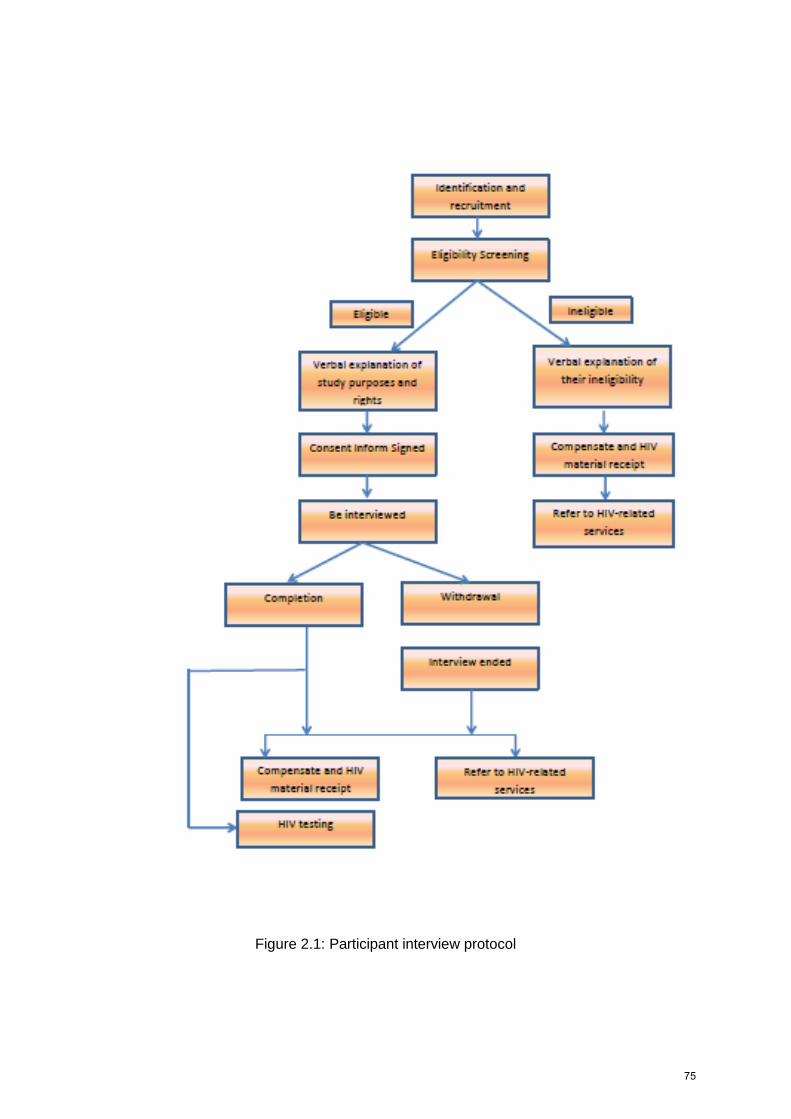
Figure 2.1: Participant interview protocol
75

Once interviews were completed, questionnaires were given to a local supervisor for its
completeness, possible missing data and the accuracy of recording checking, and safe
storage. There was a brief reflection meeting at the end of each working day for
interviewers to discuss any difficulties or challenges they faced during the interview
process and to seek suggestions and advice from peers. The local supervisor identified
errors and inconsistencies in the questionnaires and discussed the correct way to record
information in the questionnaire in such situations.
Ethical considerations. Because homosexuality-related stigma and discrimination is
still common in Vietnam, we took several steps to protect the participants’ confidentiality.
Participants were not asked for their full name or address. During the fieldwork in
Vietnam, all study documents were securely stored in a locked cabinet at Hanoi Medical
University. Data entry was conducted on password-protected laptops owned by the study
team, and the data did not contain any personally identifying information of participants.
Once data entry was completed, the data was then transferred to UNSW Australia and
stored on a secure server of UNSW, only accessible by the study team. All the study
documents, including signed consent forms, are stored securely at the Centre for Social
Research in Health, UNSW Sydney. All study team members who accessed participants’
information signed a confidentiality agreement (see Appendix 2F). The survey received
ethical approval from the Human Research Ethical Committee of the University of New
South Wales, Sydney, Australia and Hanoi University of Public Health (see Appendix 3).
Questionnaire: A structured questionnaire was used to gather the following information,
based on the study’s socio-ecological framework. The questionnaire was developed in
English and translated into Vietnamese. Two separate consultation meetings were held,
one in Hanoi and one in Ho Chi Minh City, with a total of approximately 20
representatives from local MSM organisations, to seek input into the questionnaire and
colloquial terms for sexual orientation, drug use and sexual behaviours commonly used
by MSM.The representatives also commented on the user-friendliness and social and
cultural acceptability of the questionnaire. The questionnaire was pilot-tested with ten
MSM in Hanoi and revised as required. Pilot testing was used to make sure that all terms
used in the questionnaire were easily understood. Pilot testing indicated that men had
no difficulty understanding the terms used to describe specific drugs, including drugs
with which they had little or no personal experience. In addition, the training for
recruitment staff and interviewers included discussion of local street names used by
MSM for drugs, so that they could correctly capture the experience of MSM who
participated and, if necessary, translate the chemical names for drugs into street terms
76
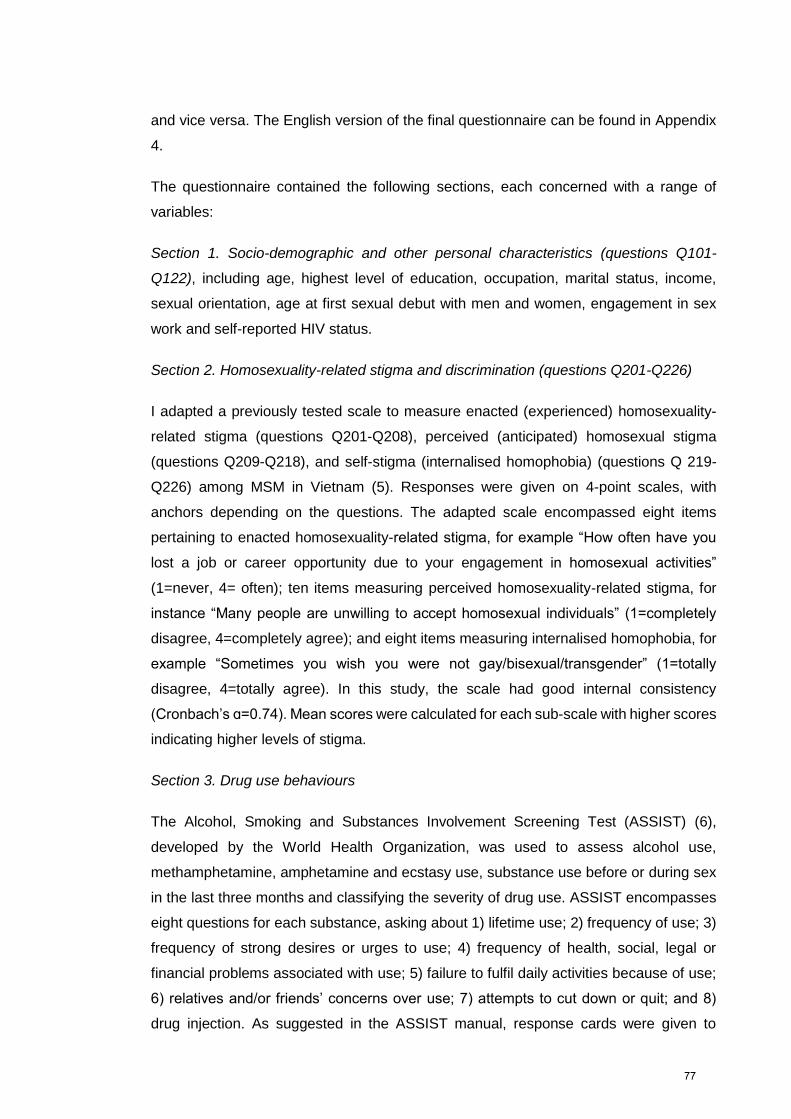
and vice versa. The English version of the final questionnaire can be found in Appendix
4.
The questionnaire contained the following sections, each concerned with a range of
variables:
Section 1. Socio-demographic and other personal characteristics (questions Q101-
Q122), including age, highest level of education, occupation, marital status, income,
sexual orientation, age at first sexual debut with men and women, engagement in sex
work and self-reported HIV status.
Section 2. Homosexuality-related stigma and discrimination (questions Q201-Q226)
I adapted a previously tested scale to measure enacted (experienced) homosexuality-
related stigma (questions Q201-Q208), perceived (anticipated) homosexual stigma
(questions Q209-Q218), and self-stigma (internalised homophobia) (questions Q 219-
Q226) among MSM in Vietnam (5). Responses were given on 4-point scales, with
anchors depending on the questions. The adapted scale encompassed eight items
pertaining to enacted homosexuality-related stigma, for example “How often have you
lost a job or career opportunity due to your engagement in homosexual activities”
(1=never, 4= often); ten items measuring perceived homosexuality-related stigma, for
instance “Many people are unwilling to accept homosexual individuals” (1=completely
disagree, 4=completely agree); and eight items measuring internalised homophobia, for
example “Sometimes you wish you were not gay/bisexual/transgender” (1=totally
disagree, 4=totally agree). In this study, the scale had good internal consistency
(Cronbach’s ɑ=0.74). Mean scores were calculated for each sub-scale with higher scores
indicating higher levels of stigma.
Section 3. Drug use behaviours
The Alcohol, Smoking and Substances Involvement Screening Test (ASSIST) (6),
developed by the World Health Organization, was used to assess alcohol use,
methamphetamine, amphetamine and ecstasy use, substance use before or during sex
in the last three months and classifying the severity of drug use. ASSIST encompasses
eight questions for each substance, asking about 1) lifetime use; 2) frequency of use; 3)
frequency of strong desires or urges to use; 4) frequency of health, social, legal or
financial problems associated with use; 5) failure to fulfil daily activities because of use;
6) relatives and/or friends’ concerns over use; 7) attempts to cut down or quit; and 8)
drug injection. As suggested in the ASSIST manual, response cards were given to
77
participants to assist them with answering these questions. For each substance, a
summary score was calculated by adding scores on questions two to seven. Severity of
ATS use was classified using ASSIST guidelines, according to which scores from 0-3
were classified as low-risk use, scores from 4-26 were classified as moderate-risk use,
and scores of 27 and higher were classified as high-risk use. The ASSIST screening test
has demonstrated validity in assessing the severity of alcohol, tobacco and psychoactive
drug use (7). Participants were also asked about their age when they first used drugs
(question Q302), routes of administration for drugs (question Q303 and Q304), people
they had used drugs with (question Q305), lifetime use of drugs (question Q301), and
lifetime sex-related use of alcohol and the followings drugs: alcohol, heroin, cannabis,
ketamine, methamphetamine, amphetamine (‘speed’), ecstasy, poppers (amyl nitrite)
and EDM (question Q306). ATS use in the last three months was asked by question
Q307. The severity of ATS use was measured by questions from Q307 to Q 313.
Section 4. Sexual behaviours (question Q401a-Q462)
Participants were asked about sexual behaviours and sexual partners over their lifetime,
in the previous three months and with respect to the three most recent instances of anal
or vaginal sex with regular and casual male and female partners. Regular sexual partners
were defined as sexual partners with whom participants had had sex more than once.
Casual partners were sexual partners with whom participants had had sex only once.
For each recall period and sexual partner type, participants were asked about the
number of sexual partners, their knowledge of their partners’ HIV status, how they met
these partners, positions during sex (i.e., insertive/receptive) and the use of condoms.
Participants were also asked about participation in group sex with more than two people
in the last twelve months, the places where these sexual encounters occurred, the types
of sexual partners involved, including HIV status, sexual positions during the encounters
and the use of condoms.
Additionally, in this section, sexual sensation-seeking was assessed using a scale
developed by Kalichman et al. (8). Ten items assessed the propensity to seek out
exciting and novel sexual experiences, for instance “I like wild, uninhibited sexual
encounters”. Participants provided their answers on 5-point scales, ranging from 1 (not
at all like me) to 4 (very much like me). Internal consistency of the items was sufficient
(Cronbach’s ɑ = 0.72). Item scores were averaged, with higher scores indicating more
sexual sensation-seeking.
Section 5. Involvement with MSM (question Q501-Q515)
78
Participants were asked about their use of MSM websites, accessing internet-based
MSM social networks, frequenting MSM-specific venues, participating in activities with
MSM in their city, and being active in MSM groups in the city where they lived. Reponses
were given on four-point scales (1=never, to 4=often). We also asked participants how
many gay/MSM friends they had. All variables assessing involvement with other gay
men/MSM were treated as binary variables (1=any involvement, 0=no involvement). The
number of gay/MSM friends was categorised into a 3-level categorical variable based on
the distribution of responses.
In this section, we also asked participants to respond to two statements assessing
participants’ perception of the popularity of methamphetamine use and ecstasy use in
the context of sex in their MSM social network. Responses were given on 4-point
scales (1=totally disagree, 4=totally agree).
Section 6. Depression assessment (question Q601-Q609)
Depression was assessed with the Patient Health Questionnaire 9 item scale (PHQ-9),
which has been used with MSM in other studies (9, 10). The scale consists of nine
items, such as “In the last two weeks, how often have you had trouble falling or staying
asleep, or sleeping too much?” Participants provided their answers on a scale ranging
from 0 (not having the problem at all) to 3 (having the problem nearly every day). The
items had good internal consistency in this study (Cronbach’s ɑ= 0.80). Participants
were categorised as having major depressive disorder if they scored 10 or more (11).
Section 7. Accessibility and uptake of HIV prevention services (question Q701-Q712)
We asked participants if they had recently tested for HIV (i.e., testing for HIV at least
once in the last 12 months) and if they had recently received safe sex counselling (i.e.,
engaging with safe sex counselling in the last 12 months) and sexual transmitted
diseases (STI) assessment and treatment. Participants were also asked where they
accessed these HIV prevention services.
Section 8. Belief in HIV prevention strategies (question Q801-Q809)
Participants were asked how effective they thought different strategies were in
preventing HIV transmission: use of condoms, antiretroviral treatment of HIV, taking the
insertive (top) position during anal sex, and withdrawal before ejaculation. Response
options ranged from 1 (totally disagree) to 4 (totally agree). Belief in the efficacy of
79
each HIV prevention method was dichotomised into disagreement (scores 1 and 2)
versus agreement (scores 3 and 4).
HIV testing
All blood samples were screened for HIV by the Murex HIV Ag/Ab combination assay
(Diasorin S.p.A, Italia). Samples that were reactive during screening were tested again
using confirmatory tests (Serodia® HIV, Fujirebio, Japan; DetermineTM HIV1/2, Alere
Medical, US). The main outcome variable was HIV status as confirmed by testing (HIV-
negative or HIV-positive). We referred to participants’ self-reported HIV status (HIV-
negative, untested/unknown or HIV-positive) to identify participants who tested HIV-
positive but were unaware of their infection before the study.
SYSTEMATIC REVIEW AND META-ANALYSIS OF THE ASSOCIATION
BETWEEN ATS USE AND HIV INFECTION
Search strategies
Electronic databases. A systematic search was undertaken of MEDLINE, EMBASE,
GLOBAL HEALTH and PsycINFO to identify relevant English, peer-reviewed journal
articles reporting quantitative studies published between 1980 and 25 April 2013.
Extended citation search. Reference lists of identified studies were screened to identify
further relevant studies.
Search terms. The search used a combination of free terms and Medline subject
headings, including:
▪ MSM OR men who have sex with men OR homosexual men OR bisexual men
OR gay men OR male homosexual OR bisexual male OR homosexuality OR
bisexuality AND
▪ Risk factors OR determinants OR associations OR correlates OR correlations
OR predictors OR high risk behaviours OR predictor variables AND
▪ HIV prevalence OR HIV incidence OR HIV sero-conversion OR HIV status OR
human immunodeficiency virus OR human immunodeficiency virus
prevalence/infection.
Inclusion criteria. Articles were eligible for inclusion in the review if the study and report
satisfied all of the following criteria:
▪ Published in a peer-reviewed English language journal;
80
▪ MSM were the target population;
▪ Cross-sectional, case-control or longitudinal study design;
▪ Quantitative assessment of ATS use and HIV infection;
▪ Crude quantitative measures of association between ATS use and HIV infection
were provided, or data to calculate this; and
▪ Participants’ HIV status was confirmed by a standardised laboratory method.
Screening process. First, electronic databases were searched using the defined key
words and/or Medical Subject Heading terms. Articles identified in this step were
downloaded to Endnote and duplicates removed. The screening process for the
remaining article was as follows:
▪ Title screening: all studies with irrelevant titles (i.e. different from the review
question) were excluded and recorded.
▪ Abstract screening: abstracts of the remaining studies were screened to
exclude irrelevant studies.
▪ The full texts of remaining studies were reviewed for availability of estimates of
the association between ATS use and prevalence and/or incidence of HIV/STI
infection.
▪ Authors of articles in which estimates of association or data to calculate it were
not provided were contacted via email to see if data could be obtained. If no
reply was received after 4 weeks, then the articles were excluded from the
review list.
▪ Authors of articles for which the full text was not accessible were also contacted
via email to ask for the full text. After 4 weeks, if no reply was received, then the
articles were excluded. Full texts provided by the author were screened as
described above.
▪ Reference lists of articles included in review were screened to identify additional
relevant articles.
Quality assessment. Quality of the included studies and reports was assessed using
quality assessment criteria adapted from Boyle for cross-sectional studies (12), and
from Wells et al. for case-control and longitudinal studies (13). The checklists can be
found in Appendix 5. Studies and reports were assigned a summative score on a scale
from 0 to 9 for cross-sectional studies, 0-10 for case-control studies and 0-11 for
longitudinal studies. All scores were categorised as high and low quality, based on a
cut off of 50%.
81

Data extraction. Extracted information included: the primary author, year of
publication, country of research, sampling method(s), sample size, type of drug(s)
examined and recall periods, basic participant characteristics (e.g., age, sexual
identification) and either a crude measure of association with 95% confidence intervals
(CI) or data to calculate this.
If articles reported on more than one drug or assessed more than one recall period,
each measure of drug use was extracted as a separate record. Measures of
association reported without 95% CIs were not extracted. Extracted data from cross-
sectional and case-control studies were used to calculate prevalence rate ratios (PRR)
(14), and odds ratios (OR), respectively. For longitudinal studies, hazard ratios (HR) or
relative risk (RR) of ATS use and new HIV seroconversion with 95% CIs were taken
directly from articles. Data extraction was carried out by two people to avoid potential
extraction bias.
82
References
1. Horton P. 'I thought I was the only one': the misrecognition of LGBT youth in
contemporary Vietnam. Culture, health & sexuality. 2014;16(8):960-73.
2. Ha H, Risser JM, Ross MW, Huynh NT, Nguyen HT. Homosexuality-related
stigma and sexual risk behaviors among men who have sex with men in Hanoi,
Vietnam. Archives of sexual behavior. 2015;44(2):349-56.
3. Bengtsson L, Lu X, Liljeros F, Thanh HH, Thorson A. Strong propensity for HIV
transmission among men who have sex with men in Vietnam: behavioural data and
sexual network modelling. BMJ Open. 2014;4(1):e003526.
4. United Nations Office on Drugs and Crime (UNODC). Amphetamine-type
stimulants in Vietnam. Review of the availibility, use and implications for health and
security. UNODC: 2012; 2012.
5. Ha H, Ross MW, Risser JM, Nguyen HT. Measurement of Stigma in Men Who
Have Sex with Men in Hanoi, Vietnam: Assessment of a Homosexuality-Related
Stigma Scale. Journal of sexually transmitted diseases. 2013;2013:174506.
6. World Health Organization. The Alcohol, Smoking and Substance Involvement
Screening Test (ASSIST). Geneva, Switzerland2010.
7. Humeniuk R, Ali R, Babor TF, Farrell M, Formigoni ML, Jittiwutikarn J, et al.
Validation of the Alcohol, Smoking And Substance Involvement Screening Test
(ASSIST). Addiction (Abingdon, England). 2008;103(6):1039-47.
8. Kalichman SC, Rompa D. Sexual sensation seeking and Sexual Compulsivity
Scales: reliability, validity, and predicting HIV risk behavior. Journal of personality
assessment. 1995;65(3):586-601.
9. Hirshfield S, Wolitski RJ, Chiasson MA, Remien RH, Humberstone M, Wong T.
Screening for depressive symptoms in an online sample of men who have sex with
men. AIDS care. 2008;20(8):904-10.
10. Mao L, Kidd MR, Rogers G, Andrews G, Newman CE, Booth A, et al. Social
factors associated with Major Depressive Disorder in homosexually active, gay men
attending general practices in urban Australia. Australian and New Zealand journal of
public health. 2009;33(1):83-6.
11. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression
severity measure. Journal of general internal medicine. 2001;16(9):606-13.
12. Boyle MH. Guidelines for evaluating prevalence studies. Evidence Based
Mental Health. 1998;1(2):37-9.
83
13. Wells G, Shea B, O’connell D, Peterson J, Welch V, Losos M, et al. The
Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in
meta-analyses. 2000.
14. Skov T, Deddens J, Petersen MR, Endahl L. Prevalence proportion ratios:
estimation and hypothesis testing. Int J Epidemiol. 1998;27(1):91-5.
84
CHAPTER 3
AMPHETAMINE-TYPE-STIMULANT USE AMONG MEN WHO HAVE
SEX WITH MEN (MSM) IN VIETNAM: RESULTS FROM A SOCIO-
ECOLOGICAL, COMMUNITY-BASED STUDY
Author Contributions
Nga Thi Thu VU1,2, Martin HOLT1, Huong Thi Thu PHAN3, Huong Thi LE2, Lan
Thi LA4, Gioi Minh TRAN5, Tung Thanh DOAN5, Trang Nhu Nguyen NGUYEN6
and John de Wit1
1: Center for Social Research in Health, University of New South Wales, Sydney,
New South Wales, Australia; 2: Institute of Preventive Medicine and Public Health,
Hanoi Medical University, Hanoi, Vietnam; 3: Vietnam Administration for
HIV/AIDS Prevention and Control, Hanoi, Vietnam; 4: Hanoi Center of HIV/AIDS
Prevention and Control, Hanoi, Vietnam; 5: Center for Community Health
Promotion, Hanoi, Vietnam; 6: Center for Promotion of Quality of Life, Ho Chi Minh
City, Vietnam.
Reference
Vu NT, Holt M, Phan HT, Le HT, La LT, Tran GM, et al. Amphetamine-type
stimulant use among men who have sex with men (MSM) in Vietnam: Results
from a socio-ecological, community-based study. Drug and alcohol dependence.
2016;158:110-7.
Declaration
I certify that this publication was a direct result of my research toward this PhD,
and that reproduction in this thesis does not breach copyright regulations.
Nga Thi Thu Vu June 2017
85
Copyright permission
The candidate is the first author of the present article, therefore, she retains the
right to include the article in a thesis or dissertation. This is an accepted
manuscript of an article published by Elsevier in journal Drug and Alcohol
Dependence on 10th November, 2015, available online:
http://doi.org/10.1016/j.drugalcdep.2015.11.016.
As this is a retained right, no written permission from Elsevier is necessary.
86

Amc
NGa
b
c
d
e
f
a
ARR1AA
KAPCMVS
1
tc2
S
j
h0
Drug and Alcohol Dependence 158 (2016) 110–117
Contents lists available at ScienceDirect
Drug and Alcohol Dependence
j ourna l ho me pa g e: www.e l sev ier .com/ locate /druga l cdep
mphetamine-type stimulant use among men who have sex withen (MSM) in Vietnam: Results from a socio-ecological,
ommunity-based study
ga Thi Thu Vua,b,∗, Martin Holta, Huong Thi Thu Phanc, Huong Thi Leb, Lan Thi Lad,ioi Minh Trane, Tung Thanh Doane, Trang Nhu Nguyen Nguyenf, John de Wita,∗∗
Centre for Social Research in Health, UNSW Australia, Sydney 2032, NSW, AustraliaInstitute of Preventive Medicine and Public Health, Hanoi Medical University, No. 1 Ton That Tung Street, HaNoi, VietnamVietnam Administration for HIV/AIDS Prevention and Control, Ministry of Health, 135/3 Nui Truc Street, Hanoi, VietnamHanoi Centre of HIV/AIDS Prevention and Control, Khu Hanh Chinh Moi, Ha Dong, Hanoi, VietnamCenter for Community Health Promotion, Suite 117-120, Block B17, Kim Lien Diplomatic Compound, Dong Da, Hanoi, VietnamCentre for Promotion of Quality of Life, 140, Street No. 7, Trung Son Area, Binh Chanh District, Ho Chi Minh City, Vietnam
r t i c l e i n f o
rticle history:eceived 10 October 2015eceived in revised form0 November 2015ccepted 10 November 2015vailable online 22 November 2015
eywords:mphetamine-type stimulantsrevalenceorrelatesen who have sex with menietnamocio-ecological perspective
a b s t r a c t
Introduction: Amphetamine-type-stimulants (ATS) use is associated with HIV-related sexual riskbehaviours and is an emergent problem among men who have sex with men (MSM) in Vietnam. Thepurpose of this study is to describe ATS use patterns and understand the correlates of recent metham-phetamine use from a socio-ecological perspective.Methods: From September through December, 2014, 622 MSM were recruited in Hanoi and Ho Chi MinhCity, Vietnam. We collected information on demographic characteristics, HIV testing behaviours, useof ATS and other recreational drugs (ever and recently), sexual sensation seeking, depressive mood,experienced and internalized stigma related to homosexuality, social involvement with other MSM, andperceptions of ATS use in MSM networks. We performed descriptive statistics to describe ATS use patternsand multivariate logistic regression to establish independent correlates of recent methamphetamine use.Results: Nearly one-third (30.4%) had ever used ATS, including 23.6% who had used methamphetamine,4.3% who had used amphetamine (‘speed’) and 20.9% who had used ecstasy. 20.1% and 11.9% had everused methamphetamine and ecstasy, respectively, during sex. Eighteen percent of methamphetamineusers were classified as engaged in high-risk use. Recent methamphetamine use (in the last 3 months)
was associated with participants perceiving more methamphetamine use in their MSM network, recentsex work, and higher sexual sensation seeking scores.Conclusions: ATS use is relatively prevalent among MSM sampled in Vietnam’s main cities. Interventionsto address methamphetamine are warranted for MSM in Vietnam. Methamphetamine treatments areneeded for high-risk users.. Introduction
Internationally, amphetamine type stimulants (ATS) are
he second most commonly used type of illicit drugs, afterannabis/marijuana (United Nations Office on Drugs and Crime,010, 2013b). In 2009, the United Nations Office on Drugs and∗ Corresponding author at: Centre for Social Research in Health, UNSW Australia,ydney 2032, NSW, Australia. Tel.: +61 2 9385 6776.∗∗ Corresponding author. Tel.: +61 2 9385 6799.
E-mail addresses: [email protected] (N.T.T. Vu),[email protected] (J. de Wit).
ttp://dx.doi.org/10.1016/j.drugalcdep.2015.11.016376-8716/© 2015 Elsevier Ireland Ltd. All rights reserved.
© 2015 Elsevier Ireland Ltd. All rights reserved.
Crime (UNODC) estimated that worldwide there were 13.7 to 52.9million people aged 15–64 (equivalent to 0.3% to 1.2% of the totalworld population in those age groups) who had ever used any kindof ATS (United Nations Office on Drugs and Crime, 2010). ATS canbe classified into two groups: the amphetamine substance groupand the ecstasy substance group (United Nations Office on Drugsand Crime, 2010). The substances in both groups can be ingested,injected, inhaled, snorted or smoked and can have immediate accel-erated physiological and psychological effects which may last up
to ten to 12 h for amphetamines or three to 6 h for ecstasy (Colfaxand Guzman, 2006; Nordahl et al., 2003). While amphetamines areclassified as psychoactive stimulants, ecstasy can have both psy-choactive and hallucinogenic effects in high doses (World Health87

ol Dep
OcoTbt(222sgHamcHi
imdlm2siat3c(2remse(
hrrpctsCmpIMbAt(tnts
2
wH(
N.T.T. Vu et al. / Drug and Alcoh
rganization, 2004). Regular ATS use has been found to be asso-iated with long-term adverse health impacts such as depressionr psychosis (United Nations Office on Drugs and Crime, 2013a).he use of ATS, particularly methamphetamine, has been found toe associated with an increased prevalence of sexual behaviourshat may increase the risk of HIV or sexually transmitted infectionsSTIs) such as condomless sex (Beyrer et al., 2004; Celentano et al.,006; Colfax et al., 2010, 2004; Colfax et al., 2001; Klitzman et al.,002; Koblin et al., 2003, 2007; Mansergh et al., 2006; Rusch et al.,004), having more sexual partners (Molitor et al., 1998), havingex with anonymous partners (Parry et al., 2008), or participating inroup sex (Prestage et al., 2011). Injection of ATS can also facilitateIV or hepatitis infection if unsafe or unsterile injecting practicesre practiced (Colfax et al., 2010; Martin et al., 2010). A recenteta-analysis of 35 studies from nine countries found a statisti-
ally significant relationship between methamphetamine use andIV infection among men who have sex with men (MSM), mainly
n high income countries (Thu Vu et al., 2015).Studies undertaken in the last ten years report different trends
n ATS use among gay, bisexual and other men who have sex withen in different places in the world. A study using 2008–2011
rug use surveillance data of substance using MSM in Los Ange-es (Reback et al., 2013) reported a significant upward trend in
ethamphetamine use in the previous 30 days (23.7% in 2008 to7.4% in 2011). In contrast, a study drawing on annual behaviouralurveillance data of MSM in Sydney, Melbourne and Queenslandn Australia observed a downward trend in ATS use between 2004nd 2011. However, the self-reported rates of ATS use were high inhis study; ecstasy was the most commonly used ATS, reported by6.2% in 2004 and 25.7% in 2011; methamphetamine was the leastommonly used ATS, reported by 15.4% in 2004 and 10.0% in 2011Lea et al., 2013). A cross-sectional study undertaken in 2011 with54 MSM attending sexual health clinics in London, UK, found lowates of ATS use in the last previous 30 days; 5.5% reported usingcstasy, 0.8% reported using amphetamine, and 1.2% reported usingethamphetamine. However, rates of ever having used ATS were
ubstantially higher, with 40.8% reported ever using ecstasy, 29.8%ver using amphetamine and 16.9% ever using methamphetamineHunter et al., 2014).
Few studies have been conducted on ATS use and associatedarms among MSM in low income or middle income countries. Aecent published study from Mexico found that 16.9% of 191 MSMecruited by respondent driven sampling had ever used metham-hetamine in the previous month (Pitpitan et al., 2015). A studyonducted in 2011 among MSM in Shenyang province, China foundhat 4% had ever used methamphetamine (Xu et al., 2014a). Anothertudy conducted in 2012–2013 among 3830 MSM from six cities inhina also reported a low prevalence of recent ATS use in the last sixonths, with 2.8% having used ecstasy, 2.5% having used metham-
hetamine, and 0.7% having used amphetamine (Xu et al., 2014b).n Thailand, the rate of ever having used methamphetamine among
SM visiting a sexual health clinic during 2008–2009 was found toe 12.6% (Chariyalertsak et al., 2011). In Vietnam, no recent study ofTS use has been reported, but a study undertaken in 2004 reported
hat 4% of MSM in Ho Chi Minh City had ever used amphetaminesNguyen et al., 2008). Therefore, we conducted this study to explorehe rate of ATS use among MSM in the two main cities of Viet-am (i.e., Hanoi and Ho Chi Minh City), and examine correlates ofhe most common form of ATS use identified in our study from aocio-ecological perspective.
. Methods
This was a cross-sectional, community-based study, conducted in collaborationith Hanoi HIV/AIDS Prevention Center (Hanoi PAC), the Center for Communityealth Promotion (CHP) in Hanoi, and the Centre for Promotion of Quality of Life
Life Center) in Ho Chi Minh City, Vietnam during September–December, 2014. A
endence 158 (2016) 110–117 111
non-random, convenience sampling method was used to recruit participants asMSM remain a relatively hidden, hard-to-reach population in Vietnam because ofhomosexuality-related stigma and discrimination (Vu et al., 2008). Potential partic-ipants were referred to the study by outreach workers of CHP and the Life Center,via local community-based organizations/groups of MSM and through peer refer-ral of MSM who had participated in the study. Men were eligible if they were 18years or older at the time of the study, reported having anal sex with at least oneman in the previous three months, had good command of listening to and read-ing the Vietnamese language and consented to participate in the study. The studyreceived approval from the Human Research Ethics Committee of the University ofNew South Wales (UNSW) Australia (reference HC14130) and from the InstitutionalReview Board of the Hanoi School of Public Health (reference 014 262/DD-YTCC).
2.1. Data collection
We adapted the socio-ecological model proposed by DiClemente et al. (2005),which proposes that people’s behaviours are influenced by their psychologicalcharacteristics as well as socio-ecological factors that reflect the surrounding envi-ronment, ranging from the proximal community/peer level to the distal societallevel. Our adapted socio-ecological model includes three levels: the individual, com-munity/peer and society levels. At the individual level, we assessed participants’demographic characteristics, HIV testing, HIV status, use of alcohol and other drugs,level of sexual sensation-seeking, and depression. Community/peer-level variablesincluded participants’ social involvement with other MSM, and their perceptionof the popularity of ATS use in their MSM social network. Societal-level variablesencompassed enacted, perceived and internalized homosexuality-related stigmaand discrimination and sex work behaviours (although a recognized economic activ-ity, sex work is illegal and stigmatized in Vietnam).
Face-to-face, structured interviews using a questionnaire were administered bystaff from Hanoi Medical University and by MSM peers, all trained by the study team.To ensure confidentiality, interviews were conducted in private rooms at locationsconvenient for participants, arranged by Hanoi PAC and CHP/Life Center. Interviewswere conducted between 8 am and 8 pm on weekdays or during weekends to accom-modate MSM who could not participate during office hours. Potential participantsreceived information about the study, were briefed on ethical considerations andconsent, screened for eligibility and provided with a unique, anonymous study ID ifthey met the inclusion criteria and signed a written consent form. Interviews lastedfor approximately 35–50 min. We took several steps to protect the participants’ con-fidentiality. Participants were not asked for their full name or address. During thefieldwork in Vietnam, all study documents were kept securely in a locked cabinet atHanoi Medical University. Data entry was conducted on password-protected laptopsowned by the study team; the dataset does not contain any personally identifyinginformation about participants. Once data entry was completed, the dataset wasthen transferred to Australia and stored on a secure server of UNSW, only accessibleby the study team. All the study’s documents, including signed consent forms, arestored securely at the Centre for Social Research in Health, UNSW Australia. After theinterviews, men received a reimbursement of 100.000 Vietnam Dong (VND) (equiv-alent to US$5) for their time and expenses, were provided with HIV preventionmaterials and referred to voluntary HIV testing. Men were also referred to supportservices, if appropriate or requested.
2.2. Measurement
The questionnaire was developed in English and translated into Vietnamese.Two separate consultation meetings were held, one in Hanoi and one in Ho ChiMinh City, with a total of approximately 20 representatives from local MSM organi-zations and researchers, to seek input into the questionnaire and colloquial termsfor drug use, sexual orientation and sexual behaviours commonly used by MSM.The representatives also commented on the user-friendliness and acceptability ofthe questionnaire. The questionnaire was pilot-tested with ten MSM in Hanoi andrevised as required.
2.2.1. Demographic and behavioural characteristics. We collected the participants’age, education, occupation, monthly income, time living in their city of residence,sexual orientation, gender of sexual partners, age at first sex with men and women,engaging in sex work (ever and in the last 3 months), and self-reported HIV status.Participants were categorized as regular sex workers if they (i) reported ever sellingsex and (ii) currently worked in a MSM-specific sauna or massage parlour wheretransactional sex occurs.
2.2.2. HIV testing. We asked participants if they had recently tested for HIV (havingat least one HIV test in the last 12 months). Participants also self-reported their HIVstatus.
2.2.3. Alcohol and drug use. For ATS and other substances, participants were asked
about having ever used them, and, if they had, age at first use, routes of administra-tion, peoples they had used with, and use in the context of sex. Substances assessedincluded: alcohol, heroin, cannabis, ketamine, methamphetamine, amphetamine(‘speed’), ecstasy, poppers (amyl nitrite) and erectile dysfunction medications(EDM); participants also had the option of reporting use of any other substance.88

1 ol De
THtitfoaamtol4as
2raiaIw
2tctattd
2pfoogmmvnpc(
2mp2qhotp4ed(i
2
Dwcf[ttLuppmsd
12 N.T.T. Vu et al. / Drug and Alcoh
he Alcohol, Smoking and Substances Involvement Screening Test (ASSIST; Worldealth Organization, 2010), developed by the World Health Organization, was used
o measure recent alcohol use, methamphetamine, amphetamine and ecstasy usen the last three months and classify the severity of drug use. ASSIST has eight ques-ions for each substance, asking about (1) lifetime use; (2) frequency of use; (3)requency of strong desires or urges to use; (4) frequency of health, social, legalr financial problems associated with use; (5) frequency of failure to fulfil dailyctivities because of use; (6) relatives and/or friends’ concerns over use; (7) failedttempts to cut down or quit; and (8) drug injection. As suggested in the ASSISTanual, response cards were given to participants to assist them with answering
hese questions. For each substance, a summary score is calculated by adding scoresn questions two to seven. Severity of ATS use was classified using ASSIST guide-ines, according to which scores from 0–3 are classified as low-risk use, scores from
to 26 are classified as moderate-risk use, and scores of 27 and higher are classifieds high-risk use. The ASSIST screening test has demonstrated validity in assessingeverity of alcohol, tobacco and psychoactive drug use (Humeniuk et al., 2008).
.2.4. Sexual sensation-seeking. The questionnaire included an adaptation of theevised sexual sensation-seeking scale (Kalichman and Rompa, 1995). Ten itemsssessed the propensity to seek out exciting and novel sexual experiences, fornstance “I like wild, uninhibited sexual encounters”. Participants provided theirnswers on 5-point scales, ranging from 1 (not at all like me) to 4 (very much like me).nternal consistency of the items was sufficient (Cronbach’s ̨ = 0.72). Item scores
ere averaged, with higher scores indicating more sexual sensation-seeking.
.2.5. Depression. This was assessed with the short form of the Patient Health Ques-ionnaire previously used with MSM (Hirshfield et al., 2008; Mao et al., 2009), whichonsisted of nine items, such as “In the last two weeks, how often have you hadrouble falling or staying asleep, or sleeping too much?” Participants provided theirnswers on a scale ranging from 0 (not having the problem at all) to 3 (havinghe problem nearly every day). In this study, the scale had good internal consis-ency (Cronbach’s ̨ = 0.80), and participants were categorized as having a depressiveisorder if they had a score of 2 on at least four items.
.2.6. Involvement with other gay men/MSM. Using six items, we assessed whetherarticipants used MSM websites, accessed internet-based MSM social networks,requented MSM-specific venues, participated in activities with MSM in their city,r were active in MSM groups in the city where they lived. Reponses were givenn four-point scales (1 = never, to 4 = often). We also asked participants how manyay/MSM friends they had. All variables assessing involvement with other gayen/MSM were treated as binary variables (1 = any involvement, 0 = no involve-ent). The number of gay/MSM friends was categorized into a 3-level categorical
ariable based on the distribution of responses. Perceptions of ATS use among MSMetwork: We asked participants to respond to two statements assessing partici-ants’ perception of the popularity of methamphetamine use and ecstasy use in theontext of sex in their MSM social network. Responses were given on 4-point scales1 = totally disagree, 4 = totally agree).
.2.7. Stigma and discrimination related to homosexuality. We adapted Ha’s scale toeasure enacted (experienced) homosexuality-related stigma, perceived (antici-
ated) homosexual stigma, and self-stigma (internalized homophobia) (Ha et al.,013). Responses were given on 4-point scales, with anchors depending on theuestions. The adapted scale encompassed eight items pertaining to enactedomosexuality-related stigma, for example “How often have you lost a job or careerpportunity due to your engaging in homosexual activities” (1 = never, 4 = often);en items measuring perceived homosexuality-related stigma, for instance “Manyeople are unwilling to accept homosexual individuals” (1 = completely disagree,
= completely agree); and eight items measuring internalized homophobia, forxample “Sometimes you wish you were not gay/bisexual/transgender” (1 = totallyisagree, 4 = totally agree). In this study, the scale had good internal consistencyCronbach’s ̨ = 0.74). Means score were calculated for each sub-scale; higher scorendicate higher levels of stigma.
.3. Data analysis
To minimize data entry errors, questionnaire data was double entered using Epi-ata 3.1. The two versions of the dataset were compared to detect inconsistencies,hich were then checked and corrected. Descriptive and analytical statistics were
alculated using Stata version 13.0 (Stata Corp, College Station, TX, USA). We reportrequencies and percentages for categorical variables and means (standard deviationSD]) or medians (inter quartile range [IQR]) for continuous variables. We comparedhe distributions of categorical variables using Chi-square tests or Fisher’s exactests, and compared means using t-tests or Mann–Whitney tests, as appropriate.ogistic regression analysis was used to identify the correlates of methamphetaminese, after it was found to be the most commonly used ATS in the sample. First, we
erformed bivariate logistic regression analyses to assess relationships between therimary outcome variable, recent methamphetamine use (i.e., use in the last threeonths), and potential covariates, including demographic characteristics, sellingex, recent HIV testing, use of alcohol and other drugs, sexual sensation seeking,epression, involvement with other gay men/MSM, perception of the popularity of
pendence 158 (2016) 110–117
methamphetamine use or ecstasy use for sexual arousal purpose in their MSM socialnetwork, and enacted, perceived and internalized homosexuality-related stigma.Variables related to methamphetamine use in the last three months at a bivariatelevel (p < 0.10) were included in a multivariate logistic regression model to iden-tify independent associations (significance level p < 0.05) (Hosmer et al., 2013). Wechecked the final model for model specification errors, goodness-of-fit and multi-collinearity.
3. Results
3.1. Sample characteristics
Approximately 5% of men referred to the study did not meetthe inclusion criteria, so were not interviewed (reported by recruit-ment staff). Two out of 643 men who were eligible and consented toparticipate did not complete the interview; therefore, the final sam-ple included 622 men. Demographic characteristics of participantsare presented in Table 1. Overall, participants had a median age of24.1 years (IQR: 18.1 to 49.7) with the majority in their twenties(63.2%). Most participants had completed university undergradu-ate education or higher (54.1%); a minority (17.4%) had completedonly secondary school education. One third of participants werelow-skilled, self-employed, freelance labourers, and nearly 15% ofparticipants worked in hospitality industry jobs such as in cafés,restaurants, bathhouses, or massage parlours; 23.5% of participantswere students. Participants’ median monthly income was five mil-lion VND (equivalent to approximately US$250), and 14.8% hada monthly income of less than three million VND (equivalent toUS$150). Over half of participants (51.6%) had migrated from otherprovinces to live in Hanoi or Ho Chi Minh City, and the median timethat participants had lived in either Hanoi or Ho Chi Minh City was18.5 years (IQR: 0.2–48.7 years).
The majority of men described themselves as “ –d `̂ong tính”(gay/homosexual) (74%), 18.7% self-reported as “song tính” (bisex-ual), and the remaining said they were “di. tính/trai th�̆ang”(heterosexual) or indicated another sexual orientation. Two-thirdsof men exclusively had sex with other men (71.7%), and the remain-der had sex with both men and women. Over a quarter of men hadever sold sex (29.1%), and nearly a quarter (23.4%) had sold sexin the last three months. A minority of participants (7.2%) reportedthat they were regular sex workers. In relation to HIV testing, 45.5%reported that they had recent tested for HIV in the last twelvemonths, and 39.2% did not know their HIV status.
In terms of social involvement with other MSM, the mediannumber of MSM friends was 30 (IQR: 2.0–900.0). The majority ofmen reported visiting MSM specific websites (81.5%), accessingMSM online social networks (74.6%), frequenting MSM-specificvenues (84.4%), participating in MSM community activities (68.8%),and participating in MSM groups (63.3%). Participants reported thatmethamphetamine use was moderately popular in their MSM net-work (mean 2.2, SD: 0.8), as was ecstasy use (mean 2.2, SD: 0.8)(Table 2).
Participants in Hanoi and in Ho Chi Minh City were similar withrespect to age, occupation, and age of first sex with either men orwomen. There were significant differences between the subsam-ples from the two cities in terms of education, income, length oftime living in the city, sexual orientation, gender of sexual partners,selling sex, having recent HIV testing, having depression signs andsexual sensation seeking score. More men in Ho Chi Minh City hadcompleted only secondary education or lower (23.2% vs. 11.3%),and fewer had an income of more than 5 million VND per month(50.2% vs. 59.7%). Additionally, fewer participants in Ho Chi Minh
City reported having sex with both men and women comparedto men in Hanoi (17.5% vs. 39.6%), and a larger proportion of HoChi Minh City participants reported ever or recently selling sex(38.2% vs. 19.5% and 31.0% vs. 14.9%, respectively). More men in89
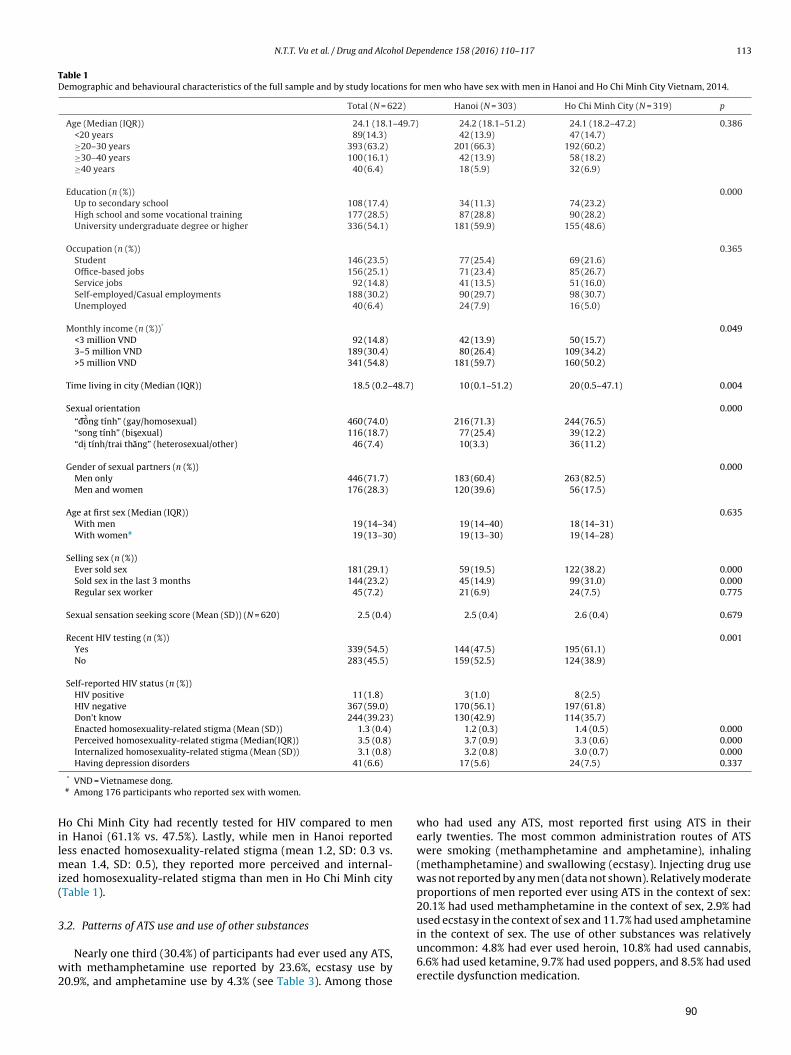
N.T.T. Vu et al. / Drug and Alcohol Dependence 158 (2016) 110–117 113
Table 1Demographic and behavioural characteristics of the full sample and by study locations for men who have sex with men in Hanoi and Ho Chi Minh City Vietnam, 2014.
Total (N = 622) Hanoi (N = 303) Ho Chi Minh City (N = 319) p
Age (Median (IQR)) 24.1 (18.1–49.7) 24.2 (18.1–51.2) 24.1 (18.2–47.2) 0.386<20 years 89(14.3) 42 (13.9) 47 (14.7)≥20–30 years 393 (63.2) 201 (66.3) 192 (60.2)≥30–40 years 100 (16.1) 42 (13.9) 58 (18.2)≥40 years 40 (6.4) 18 (5.9) 32 (6.9)
Education (n (%)) 0.000Up to secondary school 108 (17.4) 34 (11.3) 74 (23.2)High school and some vocational training 177 (28.5) 87 (28.8) 90 (28.2)University undergraduate degree or higher 336 (54.1) 181 (59.9) 155 (48.6)
Occupation (n (%)) 0.365Student 146 (23.5) 77 (25.4) 69 (21.6)Office-based jobs 156 (25.1) 71 (23.4) 85 (26.7)Service jobs 92 (14.8) 41 (13.5) 51 (16.0)Self-employed/Casual employments 188 (30.2) 90 (29.7) 98 (30.7)Unemployed 40 (6.4) 24 (7.9) 16 (5.0)
Monthly income (n (%))* 0.049<3 million VND 92 (14.8) 42 (13.9) 50 (15.7)3–5 million VND 189 (30.4) 80 (26.4) 109 (34.2)>5 million VND 341 (54.8) 181 (59.7) 160 (50.2)
Time living in city (Median (IQR)) 18.5 (0.2–48.7) 10 (0.1–51.2) 20 (0.5–47.1) 0.004
Sexual orientation 0.000“ –d `̂ong tính” (gay/homosexual) 460 (74.0) 216 (71.3) 244 (76.5)“song tính” (bisexual) 116 (18.7) 77 (25.4) 39 (12.2)“di. tính/trai th�̆ang” (heterosexual/other) 46 (7.4) 10(3.3) 36 (11.2)
Gender of sexual partners (n (%)) 0.000Men only 446 (71.7) 183 (60.4) 263 (82.5)Men and women 176 (28.3) 120 (39.6) 56 (17.5)
Age at first sex (Median (IQR)) 0.635With men 19 (14–34) 19 (14–40) 18 (14–31)With women# 19 (13–30) 19 (13–30) 19 (14–28)
Selling sex (n (%))Ever sold sex 181 (29.1) 59 (19.5) 122 (38.2) 0.000Sold sex in the last 3 months 144 (23.2) 45 (14.9) 99 (31.0) 0.000Regular sex worker 45 (7.2) 21 (6.9) 24 (7.5) 0.775
Sexual sensation seeking score (Mean (SD)) (N = 620) 2.5 (0.4) 2.5 (0.4) 2.6 (0.4) 0.679
Recent HIV testing (n (%)) 0.001Yes 339 (54.5) 144 (47.5) 195 (61.1)No 283 (45.5) 159 (52.5) 124 (38.9)
Self-reported HIV status (n (%))HIV positive 11 (1.8) 3 (1.0) 8 (2.5)HIV negative 367 (59.0) 170 (56.1) 197 (61.8)Don’t know 244 (39.23) 130 (42.9) 114 (35.7)Enacted homosexuality-related stigma (Mean (SD)) 1.3 (0.4) 1.2 (0.3) 1.4 (0.5) 0.000Perceived homosexuality-related stigma (Median(IQR)) 3.5 (0.8) 3.7 (0.9) 3.3 (0.6) 0.000Internalized homosexuality-related stigma (Mean (SD)) 3.1 (0.8) 3.2 (0.8) 3.0 (0.7) 0.000Having depression disorders 41 (6.6) 17 (5.6) 24 (7.5) 0.337
Hilmi(
3
w2
* VND = Vietnamese dong.# Among 176 participants who reported sex with women.
o Chi Minh City had recently tested for HIV compared to menn Hanoi (61.1% vs. 47.5%). Lastly, while men in Hanoi reportedess enacted homosexuality-related stigma (mean 1.2, SD: 0.3 vs.
ean 1.4, SD: 0.5), they reported more perceived and internal-zed homosexuality-related stigma than men in Ho Chi Minh cityTable 1).
.2. Patterns of ATS use and use of other substances
Nearly one third (30.4%) of participants had ever used any ATS,ith methamphetamine use reported by 23.6%, ecstasy use by
0.9%, and amphetamine use by 4.3% (see Table 3). Among those
who had used any ATS, most reported first using ATS in theirearly twenties. The most common administration routes of ATSwere smoking (methamphetamine and amphetamine), inhaling(methamphetamine) and swallowing (ecstasy). Injecting drug usewas not reported by any men (data not shown). Relatively moderateproportions of men reported ever using ATS in the context of sex:20.1% had used methamphetamine in the context of sex, 2.9% hadused ecstasy in the context of sex and 11.7% had used amphetamine
in the context of sex. The use of other substances was relativelyuncommon: 4.8% had ever used heroin, 10.8% had used cannabis,6.6% had used ketamine, 9.7% had used poppers, and 8.5% had usederectile dysfunction medication.90
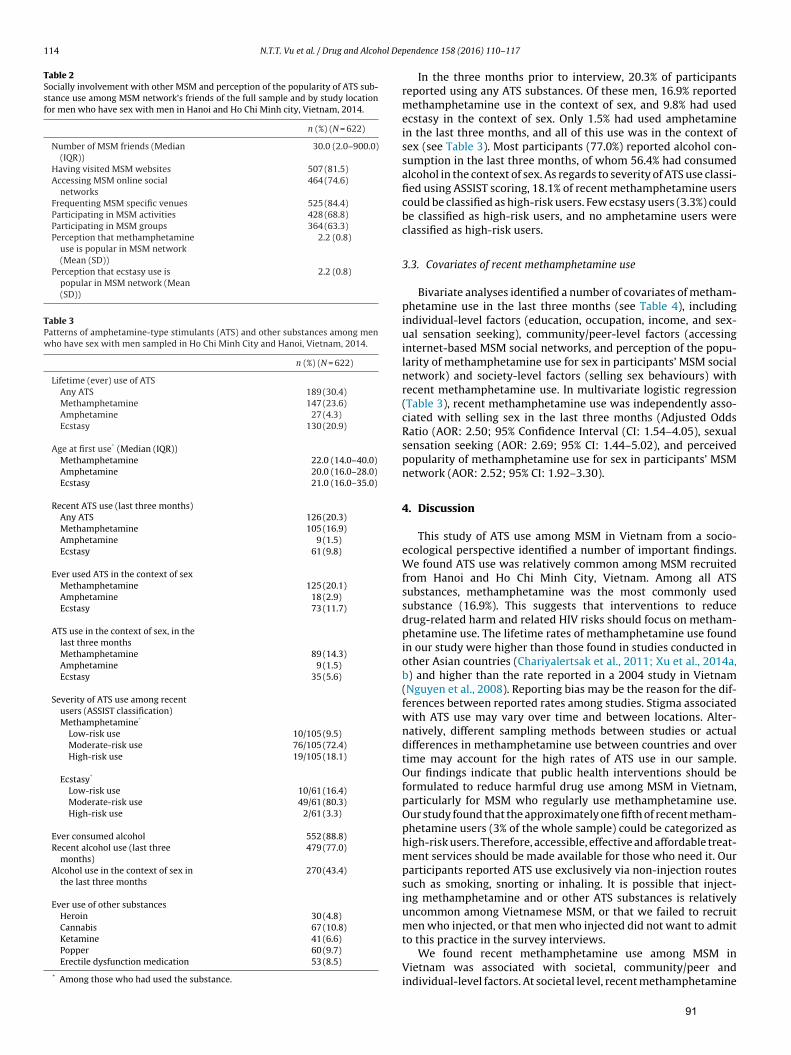
114 N.T.T. Vu et al. / Drug and Alcohol De
Table 2Socially involvement with other MSM and perception of the popularity of ATS sub-stance use among MSM network’s friends of the full sample and by study locationfor men who have sex with men in Hanoi and Ho Chi Minh city, Vietnam, 2014.
n (%) (N = 622)
Number of MSM friends (Median(IQR))
30.0 (2.0–900.0)
Having visited MSM websites 507 (81.5)Accessing MSM online social
networks464 (74.6)
Frequenting MSM specific venues 525 (84.4)Participating in MSM activities 428 (68.8)Participating in MSM groups 364 (63.3)Perception that methamphetamine
use is popular in MSM network(Mean (SD))
2.2 (0.8)
Perception that ecstasy use ispopular in MSM network (Mean(SD))
2.2 (0.8)
Table 3Patterns of amphetamine-type stimulants (ATS) and other substances among menwho have sex with men sampled in Ho Chi Minh City and Hanoi, Vietnam, 2014.
n (%) (N = 622)
Lifetime (ever) use of ATSAny ATS 189 (30.4)Methamphetamine 147 (23.6)Amphetamine 27 (4.3)Ecstasy 130 (20.9)
Age at first use* (Median (IQR))Methamphetamine 22.0 (14.0–40.0)Amphetamine 20.0 (16.0–28.0)Ecstasy 21.0 (16.0–35.0)
Recent ATS use (last three months)Any ATS 126 (20.3)Methamphetamine 105 (16.9)Amphetamine 9 (1.5)Ecstasy 61 (9.8)
Ever used ATS in the context of sexMethamphetamine 125 (20.1)Amphetamine 18 (2.9)Ecstasy 73 (11.7)
ATS use in the context of sex, in thelast three monthsMethamphetamine 89 (14.3)Amphetamine 9 (1.5)Ecstasy 35 (5.6)
Severity of ATS use among recentusers (ASSIST classification)Methamphetamine*
Low-risk use 10/105 (9.5)Moderate-risk use 76/105 (72.4)High-risk use 19/105 (18.1)
Ecstasy*
Low-risk use 10/61 (16.4)Moderate-risk use 49/61 (80.3)High-risk use 2/61 (3.3)
Ever consumed alcohol 552 (88.8)Recent alcohol use (last three
months)479 (77.0)
Alcohol use in the context of sex inthe last three months
270 (43.4)
Ever use of other substancesHeroin 30 (4.8)Cannabis 67 (10.8)Ketamine 41 (6.6)Popper 60 (9.7)Erectile dysfunction medication 53 (8.5)
* Among those who had used the substance.
pendence 158 (2016) 110–117
In the three months prior to interview, 20.3% of participantsreported using any ATS substances. Of these men, 16.9% reportedmethamphetamine use in the context of sex, and 9.8% had usedecstasy in the context of sex. Only 1.5% had used amphetaminein the last three months, and all of this use was in the context ofsex (see Table 3). Most participants (77.0%) reported alcohol con-sumption in the last three months, of whom 56.4% had consumedalcohol in the context of sex. As regards to severity of ATS use classi-fied using ASSIST scoring, 18.1% of recent methamphetamine userscould be classified as high-risk users. Few ecstasy users (3.3%) couldbe classified as high-risk users, and no amphetamine users wereclassified as high-risk users.
3.3. Covariates of recent methamphetamine use
Bivariate analyses identified a number of covariates of metham-phetamine use in the last three months (see Table 4), includingindividual-level factors (education, occupation, income, and sex-ual sensation seeking), community/peer-level factors (accessinginternet-based MSM social networks, and perception of the popu-larity of methamphetamine use for sex in participants’ MSM socialnetwork) and society-level factors (selling sex behaviours) withrecent methamphetamine use. In multivariate logistic regression(Table 3), recent methamphetamine use was independently asso-ciated with selling sex in the last three months (Adjusted OddsRatio (AOR: 2.50; 95% Confidence Interval (CI: 1.54–4.05), sexualsensation seeking (AOR: 2.69; 95% CI: 1.44–5.02), and perceivedpopularity of methamphetamine use for sex in participants’ MSMnetwork (AOR: 2.52; 95% CI: 1.92–3.30).
4. Discussion
This study of ATS use among MSM in Vietnam from a socio-ecological perspective identified a number of important findings.We found ATS use was relatively common among MSM recruitedfrom Hanoi and Ho Chi Minh City, Vietnam. Among all ATSsubstances, methamphetamine was the most commonly usedsubstance (16.9%). This suggests that interventions to reducedrug-related harm and related HIV risks should focus on metham-phetamine use. The lifetime rates of methamphetamine use foundin our study were higher than those found in studies conducted inother Asian countries (Chariyalertsak et al., 2011; Xu et al., 2014a,b) and higher than the rate reported in a 2004 study in Vietnam(Nguyen et al., 2008). Reporting bias may be the reason for the dif-ferences between reported rates among studies. Stigma associatedwith ATS use may vary over time and between locations. Alter-natively, different sampling methods between studies or actualdifferences in methamphetamine use between countries and overtime may account for the high rates of ATS use in our sample.Our findings indicate that public health interventions should beformulated to reduce harmful drug use among MSM in Vietnam,particularly for MSM who regularly use methamphetamine use.Our study found that the approximately one fifth of recent metham-phetamine users (3% of the whole sample) could be categorized ashigh-risk users. Therefore, accessible, effective and affordable treat-ment services should be made available for those who need it. Ourparticipants reported ATS use exclusively via non-injection routessuch as smoking, snorting or inhaling. It is possible that inject-ing methamphetamine and or other ATS substances is relativelyuncommon among Vietnamese MSM, or that we failed to recruitmen who injected, or that men who injected did not want to admit
to this practice in the survey interviews.We found recent methamphetamine use among MSM inVietnam was associated with societal, community/peer andindividual-level factors. At societal level, recent methamphetamine
91
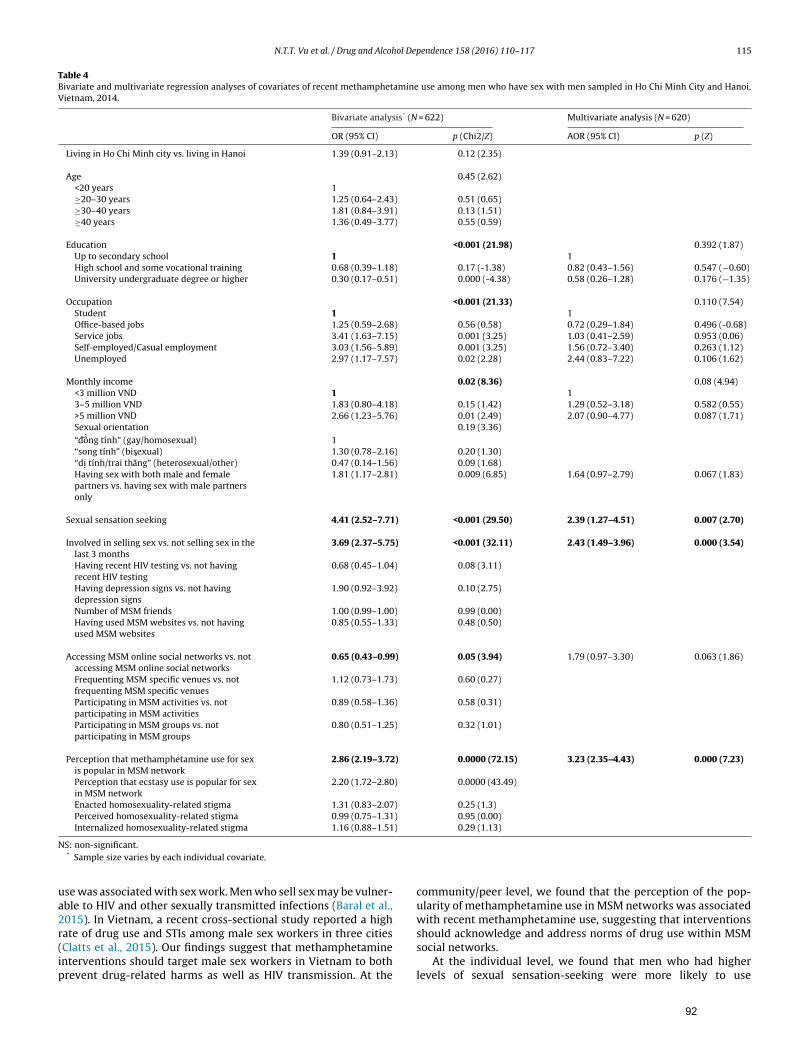
N.T.T. Vu et al. / Drug and Alcohol Dependence 158 (2016) 110–117 115
Table 4Bivariate and multivariate regression analyses of covariates of recent methamphetamine use among men who have sex with men sampled in Ho Chi Minh City and Hanoi,Vietnam, 2014.
Bivariate analysis* (N = 622) Multivariate analysis (N = 620)
OR (95% CI) p (Chi2/Z) AOR (95% CI) p (Z)
Living in Ho Chi Minh city vs. living in Hanoi 1.39 (0.91–2.13) 0.12 (2.35)
Age 0.45 (2.62)<20 years 1≥20–30 years 1.25 (0.64–2.43) 0.51 (0.65)≥30–40 years 1.81 (0.84–3.91) 0.13 (1.51)≥40 years 1.36 (0.49–3.77) 0.55 (0.59)
Education <0.001 (21.98) 0.392 (1.87)Up to secondary school 1 1High school and some vocational training 0.68 (0.39–1.18) 0.17 (-1.38) 0.82 (0.43–1.56) 0.547 (−0.60)University undergraduate degree or higher 0.30 (0.17–0.51) 0.000 (-4.38) 0.58 (0.26–1.28) 0.176 (−1.35)
Occupation <0.001 (21.33) 0.110 (7.54)Student 1 1Office-based jobs 1.25 (0.59–2.68) 0.56 (0.58) 0.72 (0.29–1.84) 0.496 (-0.68)Service jobs 3.41 (1.63–7.15) 0.001 (3.25) 1.03 (0.41–2.59) 0.953 (0.06)Self-employed/Casual employment 3.03 (1.56–5.89) 0.001 (3.25) 1.56 (0.72–3.40) 0.263 (1.12)Unemployed 2.97 (1.17–7.57) 0.02 (2.28) 2.44 (0.83–7.22) 0.106 (1.62)
Monthly income 0.02 (8.36) 0.08 (4.94)<3 million VND 1 13–5 million VND 1.83 (0.80–4.18) 0.15 (1.42) 1.29 (0.52–3.18) 0.582 (0.55)>5 million VND 2.66 (1.23–5.76) 0.01 (2.49) 2.07 (0.90–4.77) 0.087 (1.71)Sexual orientation 0.19 (3.36)“ –d `̂ong tính” (gay/homosexual) 1“song tính” (bisexual) 1.30 (0.78–2.16) 0.20 (1.30)“di. tính/trai th�̆ang” (heterosexual/other) 0.47 (0.14–1.56) 0.09 (1.68)Having sex with both male and femalepartners vs. having sex with male partnersonly
1.81 (1.17–2.81) 0.009 (6.85) 1.64 (0.97–2.79) 0.067 (1.83)
Sexual sensation seeking 4.41 (2.52–7.71) <0.001 (29.50) 2.39 (1.27–4.51) 0.007 (2.70)
Involved in selling sex vs. not selling sex in thelast 3 months
3.69 (2.37–5.75) <0.001 (32.11) 2.43 (1.49–3.96) 0.000 (3.54)
Having recent HIV testing vs. not havingrecent HIV testing
0.68 (0.45–1.04) 0.08 (3.11)
Having depression signs vs. not havingdepression signs
1.90 (0.92–3.92) 0.10 (2.75)
Number of MSM friends 1.00 (0.99–1.00) 0.99 (0.00)Having used MSM websites vs. not havingused MSM websites
0.85 (0.55–1.33) 0.48 (0.50)
Accessing MSM online social networks vs. notaccessing MSM online social networks
0.65 (0.43–0.99) 0.05 (3.94) 1.79 (0.97–3.30) 0.063 (1.86)
Frequenting MSM specific venues vs. notfrequenting MSM specific venues
1.12 (0.73–1.73) 0.60 (0.27)
Participating in MSM activities vs. notparticipating in MSM activities
0.89 (0.58–1.36) 0.58 (0.31)
Participating in MSM groups vs. notparticipating in MSM groups
0.80 (0.51–1.25) 0.32 (1.01)
Perception that methamphetamine use for sexis popular in MSM network
2.86 (2.19–3.72) 0.0000 (72.15) 3.23 (2.35–4.43) 0.000 (7.23)
Perception that ecstasy use is popular for sexin MSM network
2.20 (1.72–2.80) 0.0000 (43.49)
Enacted homosexuality-related stigma 1.31 (0.83–2.07) 0.25 (1.3)Perceived homosexuality-related stigma 0.99 (0.75–1.31) 0.95 (0.00)Internalized homosexuality-related stigma 1.16 (0.88–1.51) 0.29 (1.13)
N
ua2r(ip
S: non-significant.* Sample size varies by each individual covariate.
se was associated with sex work. Men who sell sex may be vulner-ble to HIV and other sexually transmitted infections (Baral et al.,015). In Vietnam, a recent cross-sectional study reported a high
ate of drug use and STIs among male sex workers in three citiesClatts et al., 2015). Our findings suggest that methamphetaminenterventions should target male sex workers in Vietnam to bothrevent drug-related harms as well as HIV transmission. At thecommunity/peer level, we found that the perception of the pop-ularity of methamphetamine use in MSM networks was associatedwith recent methamphetamine use, suggesting that interventions
should acknowledge and address norms of drug use within MSMsocial networks.At the individual level, we found that men who had higherlevels of sexual sensation-seeking were more likely to use
92

1 ol De
msapdtftiaeaMnIa
sotppatsuvmai
Mnutctspn
R
fsAFs
faps
C
pasmTNm
16 N.T.T. Vu et al. / Drug and Alcoh
ethamphetamine. Previous research has found that sexualensation-seeking is associated with drug use for sex (Kalichmannd Rompa, 1995). Interventions to reduce harmful metham-hetamine use among Vietnamese MSM should, therefore, beesigned to be culturally acceptable to men who engage in ‘adven-urous’ sex and drug-based sex. In Australia, previous researchound that subgroups of gay men who engaged in sexually adven-urous activities (drug-related sex, group sex, condomless analntercourse and esoteric sex practices such as sadomasochismnd fisting) were at increased risk of HIV seroconversion (Kippaxt al., 1998). To conclude, our findings suggest that interventionsddressing ATS use, specifically methamphetamine use amongSM in Vietnam, should address individual, social and commu-
ity/peer factors in order to be culturally acceptable and effective.nterventions that address personal, community and societal levelsre more likely to be successful (Hong et al., 2015).
Our study had several limitations. First, though the study teamtrived to recruit a diversified sample of MSM in the two cities,ur sample was largely a peer-referred, convenience sample, andherefore unlikely to be representative of the Vietnamese MSMopulation. As such, generalization of our findings to the broaderopulation of MSM in Hanoi and in Ho Chi Minh City should bepproached with caution. Second, because of the stigma relatedo ATS use, homosexuality and HIV, MSM who participated in ourtudy might have under-reported their drug use behaviours andnsafe sexual practices. Lastly, to avoid the weaknesses of con-enience and peer-referred sampling methods, we recommendedore rigorous, random-based sampling recruitment methods such
s respondent driven sampling or time location sampling to be usedn future studies of MSM in Vietnam.
Our study confirms a moderate prevalence of ATS use amongSM recruited from the two main metropolitan areas of Viet-
am. We found a moderate proportion of MSM who recentlysed methamphetamine reported heavy or problematic use andhat recent methamphetamine use was associated with individual,ommunity/peer-level and societal-level factors. We recommendhat interventions addressing harmful ATS/methamphetamine usehould focus on these factors to provide culturally appropriate sup-ort for the minority of Vietnamese MSM who are in immediateeed.
ole of funding resources
Nga TT Vu has received the Australian Award Scholarship (AAS)or her PhD study at UNSW Australia. The study received financialupport from the Faculty of Arts and Social Sciences (FASS), UNSWustralia under FASS Postgraduate Essential Research Programunding scheme and FASS External Research Program Fundingcheme.
The Centre for Social Research in Health is supported by fundingrom the Australian Government Department of Health. Fundinggencies were not involved in the development of the researchrotocol, data collection, data analysis, interpretation or the dis-emination of research findings.
ontributors
Nga Thi Thu Vu contributed to the development of the researchrotocol, data collection, data analysis and the manuscript draftingnd finalization. John De Wit and Martin Holt provided oversightupervision and valuable inputs for the whole process and the
anuscript drafting and finalization. Huong Thi Thu Phan, Huonghi Le, Lan Thi La, Gioi Minh Tran, Tung Thanh Doan and Tranghu Nguyen Nguyen provided inputs for the data collection andanuscript drafting and finalization.
pendence 158 (2016) 110–117
Conflict of interest statement
No conflict declared.
Acknowledgements
We acknowledge great support and inputs from staff of theInstitute of Preventive Medicine and Public Health, Hanoi Medi-cal University, Hanoi Centre of HIV/AIDS Prevention and Control,Center for Community Health Promotion, Center for Promotion ofQuality of Life and leaders and representatives of community-basedorganizations of MSM in Ho Chi Minh City during data collectionprocess in Hanoi and Ho Chi Minh City.
References
Baral, S.D., Friedman, M.R., Geibel, S., Rebe, K., Bozhinov, B., Diouf, D., Sabin, K.,Holland, C.E., Chan, R., Caceres, C.F., 2015. Male sex workers: practices,contexts, and vulnerabilities for HIV acquisition and transmission. Lancet(London, England) 385, 260–273, http://dx.doi.org/10.1016/s0140-6736(14)60801-1.
Beyrer, C., Razak, M.H., Jittiwutikarn, J., Suriyanon, V., Vongchak, T., Srirak, N.,Kawichai, S., Tovanabutra, S., Rungruengthanakit, K., Sawanpanyalert, P.,Sripaipan, T., Celentano, D.D., 2004. Methamphetamine users in northernThailand: changing demographics and risks for HIV and STD amongtreatment-seeking substance abusers. Int. J. STD AIDS 15, 697–704.
Celentano, D.D., Valleroy, L.A., Sifakis, F., MacKellar, D.A., Hylton, J., Thiede, H.,McFarland, W., Shehan, D.A., Stoyanoff, S.R., LaLota, M., Koblin, B.A., Katz, M.H.,Torian, L.V., 2006. Associations between substance use and sexual risk amongvery young men who have sex with men. Sex. Transm. Dis. 33, 265–271, http://dx.doi.org/10.1097/01.olq.0000187207.10992.4e.
Chariyalertsak, S., Kosachunhanan, N., Saokhieo, P., Songsupa, R., Wongthanee, A.,Chariyalertsak, C., Visarutratana, S., Beyrer, C., 2011. HIV incidence, risk factors,and motivation for biomedical intervention among gay, bisexual men, andtransgender persons in Northern Thailand. PLoS ONE 6, e24295, http://dx.doi.org/10.1371/journal.pone.0024295.
Clatts, M.C., Goldsamt, L.A., Giang, L.M., Yu, G., 2015. Sexual practices, partnerconcurrency and high rates of sexually transmissible infections among malesex workers in three cities in Vietnam. Sex Health 12, 39–47, http://dx.doi.org/10.1071/sh14101.
Colfax, G., Guzman, R., 2006. Club drugs and HIV infection: a review. Clin. Infect.Dis. 42, 1463–1469, http://dx.doi.org/10.1086/503259.
Colfax, G., Santos, G.M., Chu, P., Vittinghoff, E., Pluddemann, A., Kumar, S., Hart, C.,2010. Amphetamine-group substances and HIV. Lancet (London England) 376,458–474, http://dx.doi.org/10.1016/s0140-6736(10)60753-2.
Colfax, G., Vittinghoff, E., Husnik, M.J., McKirnan, D., Buchbinder, S., Koblin, B.,Celum, C., Chesney, M., Huang, Y., Mayer, K., Bozeman, S., Judson, F.N., Bryant,K.J., Coates, T.J., 2004. Substance use and sexual risk: a participant- andepisode-level analysis among a cohort of men who have sex with men. Am. J.Epidemiol. 159, 1002–1012, Retrieved from〈http://aje.oxfordjournals.org/content/159/10/1002.full.pdf〉.
Colfax, G.N., Mansergh, G., Guzman, R., Vittinghoff, E., Marks, G., Rader, M.,Buchbinder, S., 2001. Drug use and sexual risk behavior among gay andbisexual men who attend circuit parties: a venue-based comparison. J. Acquir.Immune Defic. Syndr. 28, 373–379.
DiClemente, R.J., Salazar, L.F., Crosby, R.A., Rosenthal, S.L., 2005. Prevention andcontrol of sexually transmitted infections among adolescents: the importanceof a socio-ecological perspective—a commentary. Public Health 119, 825–836,http://dx.doi.org/10.1016/j.puhe.2004.10.015.
Ha, H., Ross, M.W., Risser, J.M., Nguyen, H.T., 2013. Measurement of stigma in menwho have sex with men in Hanoi, Vietnam: assessment of ahomosexuality-related stigma scale. J. Sex. Transm. Dis., http://dx.doi.org/10.1155/2013/174506 (174506).
Hirshfield, S., Wolitski, R.J., Chiasson, M.A., Remien, R.H., Humberstone, M., Wong,T., 2008. Screening for depressive symptoms in an online sample of men whohave sex with men. AIDS Care 20, 904–910, http://dx.doi.org/10.1080/09540120701796892.
Hong, J., Voisin, D., Crosby, S., 2015. A review of STI/HIV interventions fordelinquent and detained juveniles: an application of the social–ecologicalframework. J. Child Fam. Stud. 24, 2769–2778, http://dx.doi.org/10.1007/s10826-014-0080-8.
Hosmer, D.W., Lemeshow, S., Sturdivant, R.X., 2013. Applied Logistic Regression,Retrieved from 〈http://unsw.eblib.com/patron/FullRecord.aspx?p=1138225〉.
Humeniuk, R., Ali, R., Babor, T.F., Farrell, M., Formigoni, M.L., Jittiwutikarn, J., deLacerda, R.B., Ling, W., Marsden, J., Monteiro, M., Nhiwatiwa, S., Pal, H.,
Poznyak, V., Simon, S., 2008. Validation of the Alcohol Smoking and SubstanceInvolvement Screening Test (ASSIST). Addiction 103, 1039–1047, http://dx.doi.org/10.1111/j.1360-0443.2007.02114.x.Hunter, L.J., Dargan, P.I., Benzie, A., White, J.A., Wood, D.M., 2014. Recreational druguse in men who have sex with men (MSM) attending UK sexual health services
93
ol Dep
K
K
K
K
K
L
M
M
M
M
N
X., Yan, H.J., Zhuang, M.H., Jiang, Y.J., Geng, W.Q., Vermund, S.H., Shang, H.,Qian, H.Z., 2014b. Recreational drug use and risks of HIV and sexually
N.T.T. Vu et al. / Drug and Alcoh
is significantly higher than in non-MSM. Postgrad. Med. J. 90, 133–138, http://dx.doi.org/10.1136/postgradmedj-2012-131428.
alichman, S.C., Rompa, D., 1995. Sexual sensation seeking and SexualCompulsivity Scales: reliability, validity, and predicting HIV risk behavior. J.Pers. Assess. 65, 586–601, http://dx.doi.org/10.1207/s15327752jpa6503 16.
ippax, S., Campbell, D., Van de Ven, P., Crawford, J., Prestage, G., Knox, S., Culpin,A., Kaldor, J., Kinder, P., 1998. Cultures of sexual adventurism as markers of HIVseroconversion: a case control study in a cohort of Sydney gay men. AIDS Care10, 677–688, http://dx.doi.org/10.1080/09540129848307.
litzman, R.L., Greenberg, J.D., Pollack, L.M., Dolezal, C., 2002. MDMA (‘ecstasy’) use,and its association with high risk behaviours, mental health, and other factorsamong gay/bisexual men in New York City. Drug Alcohol Depend. 66, 115–125,Retrieved from 〈http://www.drugandalcoholdependence.com/article/S0376-8716(01)00189-2/Abstract〉.
oblin, B.A., Chesney, M.A., Husnik, M.J., Bozeman, S., Celum, C.L., Buchbinder, S.,Mayer, K., McKirnan, D., Judson, F.N., Huang, Y., Coates, T.J., 2003. High-riskbehaviours among men who have sex with men in 6 US cities: baseline datafrom the EXPLORE Study. Am. J. Public Health 93, 926–932, Retrieved from〈http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1447872/pdf/0930926.pdf〉.
oblin, B.A., Murrill, C., Camacho, M., Xu, G., Liu, K.L., Raj-Singh, S., Torian, L., 2007.Amphetamine use and sexual risk among men who have sex with men: resultsfrom the National HIV Behavioural Surveillance study—New York City. Subst.Use Misuse 42, 1613–1628.
ea, T., Prestage, G., Mao, L., Zablotska, I., de Wit, J., Holt, M., 2013. Trends in druguse among gay and bisexual men in Sydney, Melbourne and Queensland,Australia. Drug Alcohol Rev. 32, 39–46, http://dx.doi.org/10.1111/j.1465-3362.2012.00494.x.
ansergh, G., Shouse, R.L., Marks, G., Guzman, R., Rader, M., Buchbinder, S., Colfax,G.N., 2006. Methamphetamine and sildenafil (Viagra) use are linked tounprotected receptive and insertive anal sex, respectively, in a sample of menwho have sex with men. Sex. Transm. Infect. 82, 131–134, http://dx.doi.org/10.1136/sti.2005.017129.
ao, L., Kidd, M.R., Rogers, G., Andrews, G., Newman, C.E., Booth, A., Saltman, D.C.,Kippax, S.C., 2009. Social factors associated with Major Depressive Disorder inhomosexually active, gay men attending general practices in urban Australia.Aust. N. Z. J. Public Health 33, 83–86, http://dx.doi.org/10.1111/j.1753-6405.2009.00344.x.
artin, M., Vanichseni, S., Suntharasamai, P., Mock, P.A., van Griensven, F.,Pitisuttithum, P., Tappero, J.W., Chiamwongpaet, S., Sangkum, U., Kitayaporn,D., Gurwith, M., Choopanya, K., 2010. Drug use and the risk of HIV infectionamongst injection drug users participating in an HIV vaccine trial in Bangkok,1999–2003. Int. J. Drug Policy 21, 296–301, http://dx.doi.org/10.1016/j.drugpo.2009.12.002.
olitor, F., Truax, S.R., Ruiz, J.D., Sun, R.K., 1998. Association of methamphetamineuse during sex with risky sexual behaviours and HIV infection amongnon-injection drug users. West. J. Med. 168, 93–97, Retrieved from〈http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1304836/pdf/westjmed00329-
0019.pdf〉.guyen, T.A., Nguyen, H.T., Le, G.T., Detels, R., 2008. Prevalence and risk factorsassociated with HIV infection among men having sex with men in Ho Chi MinhCity, Vietnam. AIDS Behav. 12, 476–482, http://dx.doi.org/10.1007/s10461-007-9267-y.
endence 158 (2016) 110–117 117
Nordahl, T.E., Salo, R., Leamon, M., 2003. Neuropsychological effects of chronicmethamphetamine use on neurotransmitters and cognition: a review. J.Neuropsychiatry Clin. Neurosci. 15, 317–325.
Parry, C., Petersen, P., Dewing, S., Carney, T., Needle, R., Kroeger, K., Treger, L., 2008.Rapid assessment of drug-related HIV risk among men who have sex with menin three South African cities. Drug Alcohol Depend. 95, 45–53, http://dx.doi.org/10.1016/j.drugalcdep.2007.12.005.
Pitpitan, E.V., Goodman-Meza, D., Burgos, J.L., Abramovitz, D., Chavarin, C.V.,Torres, K., Strathdee, S.A., Patterson, T.L., 2015. Prevalence and correlates ofHIV among men who have sex with men in Tijuana, Mexico. J. Int. AIDS Soc. 18,19304, http://dx.doi.org/10.7448/ias.18.1.19304.
Prestage, G., Down, I., Grulich, A., Zablotska, I., 2011. Sex partying among gay menin Sydney, Melbourne and Brisbane, Australia. AIDS Behav. 15, 298–304, http://dx.doi.org/10.1007/s10461-010-9824-7.
Reback, C.J., Fletcher, J.B., Shoptaw, S., Grella, C.E., 2013. Methamphetamine andother substance use trends among street-recruited men who have sex withmen, from 2008 to 2011. Drug Alcohol Depend. 133, 262–265,http://dx.doi.org/10.1016/j.drugalcdep.2013.06.007.
Rusch, M., Lampinen, T.M., Schilder, A., Hogg, R.S., 2004. Unprotected analintercourse associated with recreational drug use among young men who havesex with men depends on partner type and intercourse role. Sex. Transm. Dis.31, 492–498.
Thu Vu, N.T., Maher, L., Zablotska, I., 2015. Amphetamine-type stimulants and HIVinfection among men who have sex with men: implications on HIV researchand prevention from a systematic review and meta-analysis. J. Int. AIDS Soc.18, 19273, http://dx.doi.org/10.7448/ias.18.1.19273.
United Nations Office on Drugs and Crime, 2010. World Drug Report 2010. UnitedNations Office on Drugs and Crime, Vienna, Austria.
United Nations Office on Drugs and Crime, 2013a. Ecstasy and AmphetaminesGlobal Survey 2003. United Nations Office on Drugs and Crime, Vienna, Austria.
United Nations Office on Drugs and Crime, 2013b. World Drug Report 2013. UnitedNations Office on Drugs and Crime, Vienna, Austria.
Vu, B.N., Girault, P., Do, B.V., Colby, D., Tran, L.T., 2008. Male sexuality in Vietnam:the case of male-to-male sex. Sex. Health 5, 83–88, Retrieved from〈http://www.publish.csiro.au/index.cfm?paper=SH07064〉.
World Health Organization, 2004. Neurosciences of Psychoactive Substance Useand Dependence. World Health Organization, Geneva, Switzerland.
World Health Organization, 2010. The Alcohol, Smoking and SubstanceInvolvement Screening Test (ASSIST). World Health Organization, Geneva,Switzerland.
Xu, J.J., Qian, H.Z., Chu, Z.X., Zhang, J., Hu, Q.H., Jiang, Y.J., Geng, W.Q., Zhang, C.M.,Shang, H., 2014a. Recreational drug use among Chinese men who have sexwith men: a risky combination with unprotected sex for acquiring HIVinfection. Biomed. Res. Int., http://dx.doi.org/10.1155/2014/725361 (725361).
Xu, J.J., Zhang, C., Hu, Q.H., Chu, Z.X., Zhang, J., Li, Y.Z., Lu, L., Wang, Z., Fu, J.H., Chen,
transmitted infections among Chinese men who have sex with men:Mediation through multiple sexual partnerships. BMC Infect. Dis. 14, 642,http://dx.doi.org/10.1186/s12879-014-0642-9.
94
CHAPTER 4
THE RELATIONSHIP BETWEEN METHAMPHETAMINE USE, SEXUAL
SENSATION SEEKING AND CONDOMLESS ANAL INTERCOURSE
AMONG MEN WHO HAVE SEX WITH MEN IN VIETNAM: RESULTS
FROM A COMMUNITY-BASED, CROSS-SECTIONAL STUDY
Author Contributions
Nga Thi Thu VU1,2, Martin HOLT1, Huong Thi Thu PHAN3, Lan Thi LA4, Gioi Minh
TRAN5, Tung Thanh DOAN5, Trang Nhu Nguyen NGUYEN6 and John de Wit1
1: Center for Social Research in Health, University of New South Wales, Sydney,
New South Wales, Australia; 2: Institute of Preventive Medicine and Public Health,
Hanoi Medical University, Hanoi, Vietnam; 3: Vietnam Administration for
HIV/AIDS Prevention and Control, Hanoi, Vietnam; 4: Hanoi Center of HIV/AIDS
Prevention and Control, Hanoi, Vietnam; 5: Center for Community Health
Promotion, Hanoi, Vietnam; 6: Center for Promotion of Quality of Life, Ho Chi Minh
City, Vietnam.
Reference
Vu NT, Holt M, Phan HT, La LT, Tran GM, Doan TT, et al. The Relationship
Between Methamphetamine Use, Sexual Sensation Seeking and Condomless
Anal Intercourse Among Men Who Have Sex With Men in Vietnam: Results of a
Community-Based, Cross-Sectional Study. AIDS and Behavior.
2017;21(4):1105-16.
Declaration
I certify that this publication was a direct result of my research toward this PhD,
and that reproduction in this thesis does not breach copyright regulations.
Nga Thi Thu Vu June 2017
95
Copyright permission
As the first author of the original article, the candidate has the right to include this
article in this thesis. This is an accepted manuscript of an article published by
Springer in journal AIDS and Behavior on 28th June, 2016, available online:
https://link.springer.com/article/10.1007%2Fs10461-016-1467-x
The candidate received permission from Springer to reuse this article in her
thesis. The license number is 4093960721033, issued in 21st April, 2017.
96

ORIGINAL PAPER
The Relationship Between Methamphetamine Use, SexualSensation Seeking and Condomless Anal Intercourse Among MenWho Have Sex With Men in Vietnam: Results of a Community-Based, Cross-Sectional Study
Nga Thi Thu Vu1,2• Martin Holt1
• Huong Thi Thu Phan3• Lan Thi La4
•
Gioi Minh Tran5• Tung Thanh Doan5
• Trang Nhu Nguyen Nguyen6•
John de Wit1,7
Published online: 28 June 2016
� Springer Science+Business Media New York 2016
Abstract This study assessed the relationship between
methamphetamine use and condomless anal intercourse
(CAI) among men who have sex with men (MSM) in Hanoi
and Ho Chi Minh City, Vietnam. Of 622 MSM partici-
pants, 75.7% reported any CAI in the last three months,
23.2% reported engaging in sex work in the last three
months, 21.1% reported group sex in the last twelve
months (21.1%) and 14.3% had used methamphetamine for
sex in the last three months. CAI was associated with living
in Ho Chi Minh City vs. Hanoi, being versatile during anal
sex, a greater degree of sexual sensation-seeking, and more
strongly agreeing that withdrawal before ejaculation is
effective in preventing HIV. Effect-modification analysis
showed that recent sex-related methamphetamine use was
related to a higher probability of CAI for men with low
sexual sensationseeking scores. Methamphetamine assess-
ment and/or interventions should be incorporated into HIV
prevention and research with Vietnam’s MSM population.
Keywords Sex-related methamphetamine use � Sexualsensation seeking � Condomless anal sex � Men who have
sex with men � Vietnam
Introduction
Men who have sex with men (MSM) are disproportionately
affected by HIV worldwide, and the size of HIV epidemics
is either stable or increasing among MSM in different
countries [1, 2]. Condomless anal intercourse (CAI) is the
primary risk factor for HIV transmission among MSM.
Studies in low- and middle-income countries (LMIC) have
found that 27–78 % of MSM report CAI during their recent
or last sexual encounter [3–7]. In Vietnam, recent online
studies have found that 45 % of MSM report CAI during
their last sexual encounter [8], and 36 % report at least one
instance of CAI in the previous 3 months [9]. A community-
based cross-sectional study of MSM in Southern Vietnam
found that 34 % of participants had CAI with more than two
male partners in the month before the study and the overall
rate of CAI in the last month was 74 % [10].
In previous studies conducted mostly in high-income
countries, CAI among MSM has been found to be associ-
ated with numerous factors. CAI among MSM was less
likely among MSM who were exposed to HIV prevention
[11], but was found to be more likely for men who had
higher numbers of sexual partners [12], identified as
& Nga Thi Thu Vu
& John de Wit
1 Centre for Social Research in Health, UNSW Australia,
Sydney, NSW 2032, Australia
2 Institute of Preventive Medicine and Public Health, Hanoi
Medical University, No 1 Ton That Tung Street, Hanoi,
Vietnam
3 Vietnam Administration for HIV/AIDS Prevention and
Control, Ministry of Health, 135/3 Nui Truc Street, Hanoi,
Vietnam
4 Hanoi Centre of HIV/AIDS Prevention and Control, Khu
Hanh Chinh Moi, Ha Dong, Hanoi, Vietnam
5 Center for Community Health Promotion, Suite 117-120,
Block B17, Kim Lien Diplomatic Compound, Dong Da,
Hanoi, Vietnam
6 Centre for Promotion of Quality of Life, 140, Street No. 7,
Trung Son Area, Binh Chanh District, Ho Chi Minh City,
Vietnam
7 Utrecht University, Heidelberglaan 1, 3584 CS Utrecht,
Netherland
123
AIDS Behav (2017) 21:1105–1116
DOI 10.1007/s10461-016-1467-x
97
bisexual rather than gay [13], reported adverse psycho-
logical conditions (e.g., depression, psychological distress
and negative mood) [12, 14, 15], experienced internalized
homophobia [16], had financial difficulties [16], used club
drugs [12, 17], had sex with primary versus non-primary
partners [18], and were more sexual sensation seeking
[19, 20]. Drug use among MSM, particularly the use of
methamphetamine, and associations with CAI, is of par-
ticular interest to HIV research and prevention in many
settings.
Methamphetamine is a psychostimulant that can be
orally ingested, smoked, inhaled, snorted, injected or
shafted (inserted into the anus) [21]. Among MSM,
methamphetamine is a popular drug. In the US, the
prevalence of its use was found to be ten times greater
among MSM than in the general population [22].
Methamphetamine use can enhance stamina and sexual
pleasure [22, 23], promote sexual disinhibition and facili-
tate experimentation [24, 25], and heighten euphoria, sex-
ual pleasure and impulsiveness [23]. A recent case–control
study found that using methamphetamine decreased self-
control over sexual activities [26].
Studies in some high-income countries have found that
methamphetamine use by MSM is associated with con-
domless sex, high numbers of sexual partners and HIV
infection [22, 23, 27]. A systematic review and meta-
analysis of 35 published studies into the association
between amphetamine-type substances and HIV infection
among MSM showed that methamphetamine was signifi-
cantly associated with higher HIV prevalence or incidence
[28]. Recent studies have continued to find significant
associations between methamphetamine use and CAI
among MSM [26, 29, 30].
Findings are, however, mixed with respect to a relationship
between methamphetamine use and sexual risk behaviors
such as CAI. One US-based study found an association
between methamphetamine use and the frequency of con-
domless insertive and receptive anal intercourse among gay
and bisexual men, but could not confirm the temporal
sequence of drug use and sexual behaviours [31]. In Australia,
increasing methamphetamine use among MSM in Sydney
during 2002–2005 was not associated with an increase in
condomless sex [32]. Additionally, several published papers
included in a recent meta-analysis [28] did not find that
methamphetamine use was associated with increased risk of
HIV infection. Moreover, most previous studies assessed the
relationship between CAI and any use of methamphetamine
[28], regardless of whether drug use occurred in conjunction
with sex or not. A more stringent approach would be to
specifically examine the relationship between CAI and
methamphetamine use before or during sex.
While studies of methamphetamine use and its associ-
ation with HIV infection among MSM are relatively
common in high-income countries, to date few studies have
been conducted in LMIC, especially in East Asia and South
East Asia. A study in Thailand conducted in 2008–2009
found that 13.6 % of MSM attending a sexual health clinic
in Chiang Mai had ever used methamphetamine [33]. Two
studies of MSM in China conducted between 2011 and
2013 found that 3–4 % had ever used methamphetamine
[6, 34]. A study in Indonesia found that methamphetamine
use was associated with a higher likelihood of HIV infec-
tion in MSM [35], while a study conducted with gay,
bisexual and transgendered people in Thailand found no
relationship [33].
In Vietnam, there have been few studies of metham-
phetamine use by MSM and its association with sexual
behavior and risk of HIV. A study conducted in 2004
found that 4 % of MSM had ever used methamphetamine
[36]. Other studies on drug use by MSM in Vietnam used
composite measures of drug (any drug use vs. none)
[36–38], and cannot differentiate the specific effect of
methamphetamine use on sexual behavior or risk for HIV.
The use of methamphetamine by MSM may have
increased recently in major cities in Vietnam [39], and
there is concern that this has increased the likelihood of
CAI and risk of HIV infection. However, no previous
studies in MSM in Vietnam have reported this
association.
Recent studies among MSM in high-income countries
have found that sexual sensation-seeking may modify the
association between risky sexual behaviors and substance
use, in particular alcohol use [40, 41]. Notably, previous
research has found that among men with higher levels of
sexual sensation-seeking, men who drank alcohol were
more likely to engage in CAI compared to those who did
not drink alcohol [40]. In another study, high levels of
sexual sensation-seeking were found to strengthen the
positive association between alcohol or other drug use with
sex partners and the likelihood of CAI among young MSM
[41]. This study also found that drug use with sex partners
increased the likelihood of CAI among men who had low
sexual sensation-seeking, suggesting that in some circum-
stances drug use before or during sex is a stronger influence
on risk-taking than sexual sensation-seeking. Sexual sen-
sation-seeking might also modify the association between
methamphetamine use and CAI, but such an assessment
has not been reported.
We conducted the present study to examine the rela-
tionship between methamphetamine use and CAI and
among MSM in the two main cities of Vietnam—Hanoi
and Ho Chi Minh City (HCMC). Taking into account the
mixed findings of previous research, we assessed the
association between CAI and sex-related metham-
phetamine use, and examined the potential modification
effect of sexual sensation-seeking.
1106 AIDS Behav (2017) 21:1105–1116
123
98

Methods
This was a cross-sectional, community-based study, con-
ducted in collaboration with Hanoi HIV/AIDS Prevention
Center (Hanoi PAC), the Center for Community Health
Promotion (CHP) in Hanoi, and the Centre for Promotion
of Quality of Life (Life Center) in HCMC, Vietnam, during
September-December 2014. CHP and Life Centre have
outreach networks of MSM who are students, white-collar
workers, male sex workers, or self-employed professionals
who can reach diverse subgroups of MSM. A detailed
description of the study design can be found elsewhere
[39]. In summary, a non-random, convenience sampling
method was used to recruit participants, as MSM remain a
relatively hidden, hard-to-reach population in Vietnam,
because of homosexuality-related stigma and discrimina-
tion [42]. Potential participants were referred by outreach
workers of CHP and the Life Center, via local community-
based organizations/groups of MSM, and through partici-
pant referral. Men were eligible if they were Vietnamese
citizens, 18 years or older at the time of the study, had anal
sex with at least one man in the previous 3 months, had
good comprehension of the Vietnamese language, and
consented to participate in the study. A total of 622 MSM
were recruited. Before the study, we estimated the sample
size based on expert opinion and previous research, which
suggested that the prevalence of recent CAI would be 36 %
among MSM in Vietnam [9]. Our sample size, based on
90 % power and a 95 % significant level, was sufficient to
detect a prevalence of CAI that was 6 % higher than the
previously found prevalence of CAI.
Data Collection
Face-to-face, structured interviews using a self-report
questionnaire were administered by experienced data col-
lectors from Hanoi Medical University and by trained MSM
peers. To ensure confidentiality, interviews were conducted
in private rooms at locations convenient for participants,
arranged by Hanoi PAC and CHP in Hanoi and Life Center
in HCMC. Interviews were conducted between 8 am and
8 pm on weekdays and weekends to accommodate MSM
who could not participate during office hours. Potential
participants received information about the study, were
briefed on ethical considerations and informed consent,
screened for eligibility, and provided with a unique,
anonymous study ID if they met the inclusion criteria and
consented to participate. Interviews lasted for approximately
35–50 min. Participation in the study was entirely voluntary
and study participants were informed that they could with-
draw from the study at any time, without giving a reason and
without prejudice. After the interview, men received a
reimbursement of 100,000 Vietnam Dong (VND; equivalent
to US$5) for their time and expenses, were provided with
HIV prevention materials, and were referred to voluntary
HIV testing. Men were also referred to support services, if
appropriate or requested.
Measures
The questionnaire was developed in English and translated
into Vietnamese, confirming the quality of the translation
with MSM peers and Vietnamese colleagues. Two separate
consultation meetings were held, one in Hanoi and one in
HCMC, with a total of approximately 20 representatives
from local MSM organizations and researchers, to seek
input into the appropriateness of the questions and collo-
quial terms for drug use, sexual orientation and sexual
behaviors commonly used by MSM. The representatives
also commented on the user-friendliness and acceptability
of the questionnaire. The questionnaire was pilot-tested
with ten MSM in Hanoi and subsequently refined.
Demographic Characteristics
We collected information regarding age, education, occu-
pation, monthly income, self-reported sexual orientation,
age of first sex with men and women, and self-reported
HIV status.
HIV Testing and Safe Sex Counseling
We asked participants if they had recently tested for HIV
(i.e., having tested for HIV at least once in the last
12 months) and if they had recent safe sex counseling (i.e.,
having received safe sex counseling at least once in the last
12 months).
Sexual Behaviors
Participants were asked about ever having engaged in sex
work and having engaging in sex work in the last 3 months,
their number of regular and casual male and female part-
ners in the last 3 and 12 months, their position during anal
sex with male partners, the use of condoms during sexual
intercourse with male or female partners in the last
3 months and the use of condom during group sex in the
last 12 months. Regular sexual partners were defined as
sexual partners with whom participants had had sex more
than once, while sexual partners with whom participants
had had sex once were considered casual partners. Because
numbers of different types of sexual partners were skewed,
we undertook logarithmic or square root transformations of
these variables, as appropriate. Receptive condomless anal
AIDS Behav (2017) 21:1105–1116 1107
123
99

intercourse (RCAI) was defined as not or inconsistently
using a condom during anal sex with the participant in the
receptive (bottom) position; insertive condomless anal
intercourse (ICAI) was defined as not or inconsistently
using a condom during anal sex with the participant in the
insertive (top) position. Any recent CAI defined as
reporting either RCAI or ICAI in the past three months,
was the primary outcome of interest. CAI during group sex
in the last 12 months was defined as having had CAI (in the
insertive or receptive position) while engaging in sex with
two or more male partners at the same time.
Alcohol and Drug Use
Participants were asked questions about any use of
methamphetamine, amphetamine, ecstasy, alcohol and
other substance use (i.e., ketamine, erectile dysfunction
medications and amyl nitrite [‘poppers’]) before or during
sex in the last 3 months. Previously methamphetamine was
available in Vietnam mostly in the form of tablets. How-
ever, recently and commonly it is available in crystal form
[43]. We, therefore, asked about the use of crystal
methamphetamine. Answers to questions about substance
use were dichotomized (any use vs. none). Metham-
phetamine use before or during sex was considered as the
primary independent variable.
Depression
This was assessed with the Patient Health Questionnaire 9
scale, which has been used with MSM in other studies
[44, 45]. The scale consists of nine items, such as ‘‘In the
last 2 weeks, how often have you had trouble falling or
staying asleep, or sleeping too much?’’ Participants pro-
vided their answers on a scale ranging from 0 (not having
the problem at all) to 3 (having the problem nearly every
day). The items had good internal consistency (Cronbach’s
a = 0.80). Participants were categorized as having a
depressive disorder if they had a score equal or larger than
ten [46].
Sexual Sensation-Seeking
We adapted the revised sexual sensation-seeking scale by
Kalichman [47] for our study population and included ten
items assessing the propensity to seek exciting, novel and
stimulating sexual experiences, for instance ‘‘I like wild,
uninhibited sexual encounters’’. Participants provided their
answers on 4-point Likert-type scale ranging from 1 (not at
all like me) to 4 (very much like me). Internal consistency
of the items was adequate (Cronbach’s a = 0.72), and item
scores were averaged; a higher score indicated a higher
level of sexual sensation-seeking.
Belief in the Efficacy of HIV Risk Reduction Strategies
Participants were asked how effective they thought dif-
ferent strategies were in preventing HIV transmission:
antiretroviral treatment of HIV, taking the insertive (top)
position during anal sex, and withdrawal before ejacula-
tion. Answer options ranged from 1 (totally disagree) to 4
(totally agree). Belief in the efficacy of each HIV preven-
tion method was dichotomized into disagreement (scores 1
and 2) versus agreement (scores 3 and 4).
Data Analysis
To minimize data entry errors, questionnaire data was
double entered using EPIDATA 3.1. The two versions of
the dataset were compared to detect inconsistencies, which
were then checked and corrected. Descriptive and analyt-
ical statistics were calculated using STATA version 13.0
(Stata Corp, College Station, TX, USA). We reported fre-
quencies and percentages for categorical variables and
means and standard deviations (SD) or medians and inter
quartile ranges (IQR) for continuous variables. We com-
pared the distribution of demographic variables by
methamphetamine use. Categorical variables were com-
pared using Chi Square tests or Fisher’s exact tests, and
continuous variables were compared by t-tests or Mann–
Whitney tests, as appropriate. Previous studies on CAI
among MSM in Vietnam suggested that the prevalence of
CAI was relatively high, ranging from 36 to 74 % [8–10].
We therefore calculated Prevalence Ratios instead of
Prevalence Odds Ratios [48]. We first tested the bivariate
relationship between any CAI with male partners in the last
3 months and methamphetamine use before or during anal
sexual intercourse in the last 3 months. We subsequently
tested for associations between other potential covariates
and recent CAI with male partners, including demographic
characteristics, HIV testing and safe sex counseling, other
aspects of sexual behavior (i.e., number of sexual partners,
position during anal sex), other drug use during sex,
depression, sexual sensation-seeking, and belief in different
HIV prevention methods. Factors significantly (p\ .05)
associated with the outcome variable in bivariate analyses
were entered into a multivariate regression model. The
final model included only covariates significantly (p\ .05)
associated with CAI. Previous research has found that
sexual sensation-seeking may modify the association
between substance use and CAI [40, 41]. We therefore
tested if sexual sensation-seeking was an effect modifier of
the association between recent sex-related metham-
phetamine use and recent CAI as reflected in the signifi-
cance of the interaction term of sex-related
methamphetamine use and sexual sensation-seeking, con-
sistent with a previously suggested method [49]. For all
1108 AIDS Behav (2017) 21:1105–1116
123
100
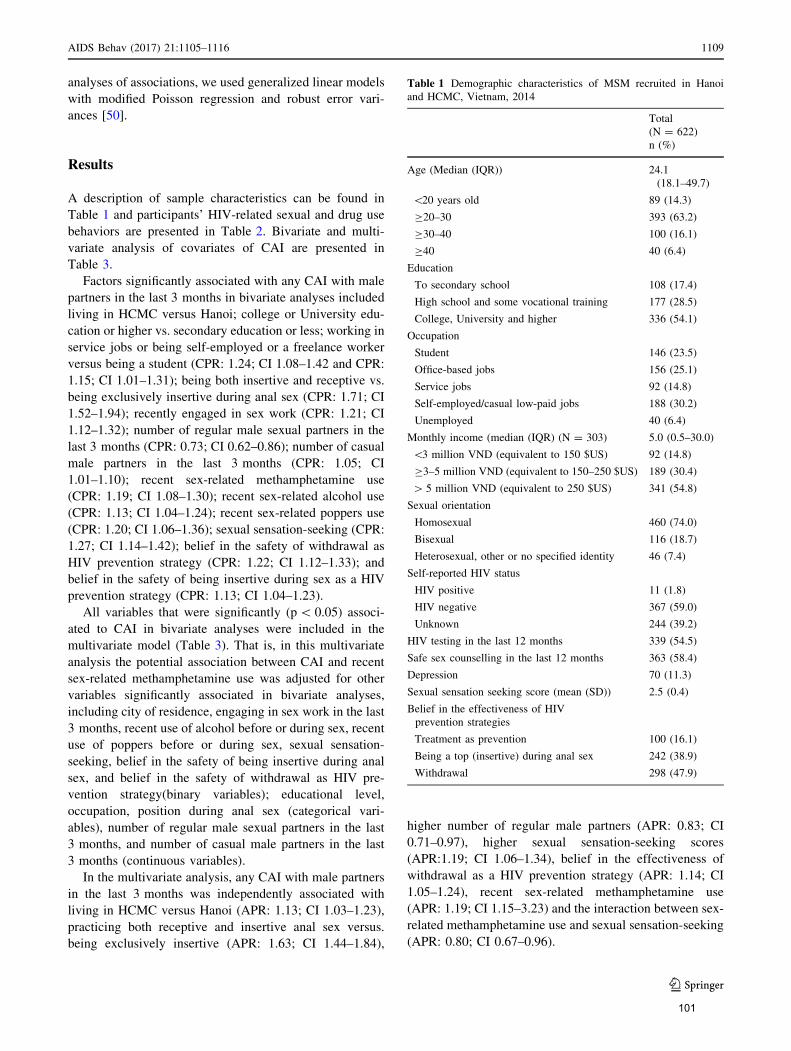
analyses of associations, we used generalized linear models
with modified Poisson regression and robust error vari-
ances [50].
Results
A description of sample characteristics can be found in
Table 1 and participants’ HIV-related sexual and drug use
behaviors are presented in Table 2. Bivariate and multi-
variate analysis of covariates of CAI are presented in
Table 3.
Factors significantly associated with any CAI with male
partners in the last 3 months in bivariate analyses included
living in HCMC versus Hanoi; college or University edu-
cation or higher vs. secondary education or less; working in
service jobs or being self-employed or a freelance worker
versus being a student (CPR: 1.24; CI 1.08–1.42 and CPR:
1.15; CI 1.01–1.31); being both insertive and receptive vs.
being exclusively insertive during anal sex (CPR: 1.71; CI
1.52–1.94); recently engaged in sex work (CPR: 1.21; CI
1.12–1.32); number of regular male sexual partners in the
last 3 months (CPR: 0.73; CI 0.62–0.86); number of casual
male partners in the last 3 months (CPR: 1.05; CI
1.01–1.10); recent sex-related methamphetamine use
(CPR: 1.19; CI 1.08–1.30); recent sex-related alcohol use
(CPR: 1.13; CI 1.04–1.24); recent sex-related poppers use
(CPR: 1.20; CI 1.06–1.36); sexual sensation-seeking (CPR:
1.27; CI 1.14–1.42); belief in the safety of withdrawal as
HIV prevention strategy (CPR: 1.22; CI 1.12–1.33); and
belief in the safety of being insertive during sex as a HIV
prevention strategy (CPR: 1.13; CI 1.04–1.23).
All variables that were significantly (p\ 0.05) associ-
ated to CAI in bivariate analyses were included in the
multivariate model (Table 3). That is, in this multivariate
analysis the potential association between CAI and recent
sex-related methamphetamine use was adjusted for other
variables significantly associated in bivariate analyses,
including city of residence, engaging in sex work in the last
3 months, recent use of alcohol before or during sex, recent
use of poppers before or during sex, sexual sensation-
seeking, belief in the safety of being insertive during anal
sex, and belief in the safety of withdrawal as HIV pre-
vention strategy(binary variables); educational level,
occupation, position during anal sex (categorical vari-
ables), number of regular male sexual partners in the last
3 months, and number of casual male partners in the last
3 months (continuous variables).
In the multivariate analysis, any CAI with male partners
in the last 3 months was independently associated with
living in HCMC versus Hanoi (APR: 1.13; CI 1.03–1.23),
practicing both receptive and insertive anal sex versus.
being exclusively insertive (APR: 1.63; CI 1.44–1.84),
higher number of regular male partners (APR: 0.83; CI
0.71–0.97), higher sexual sensation-seeking scores
(APR:1.19; CI 1.06–1.34), belief in the effectiveness of
withdrawal as a HIV prevention strategy (APR: 1.14; CI
1.05–1.24), recent sex-related methamphetamine use
(APR: 1.19; CI 1.15–3.23) and the interaction between sex-
related methamphetamine use and sexual sensation-seeking
(APR: 0.80; CI 0.67–0.96).
Table 1 Demographic characteristics of MSM recruited in Hanoi
and HCMC, Vietnam, 2014
Total
(N = 622)
n (%)
Age (Median (IQR)) 24.1
(18.1–49.7)
\20 years old 89 (14.3)
C20–30 393 (63.2)
C30–40 100 (16.1)
C40 40 (6.4)
Education
To secondary school 108 (17.4)
High school and some vocational training 177 (28.5)
College, University and higher 336 (54.1)
Occupation
Student 146 (23.5)
Office-based jobs 156 (25.1)
Service jobs 92 (14.8)
Self-employed/casual low-paid jobs 188 (30.2)
Unemployed 40 (6.4)
Monthly income (median (IQR) (N = 303) 5.0 (0.5–30.0)
\3 million VND (equivalent to 150 $US) 92 (14.8)
C3–5 million VND (equivalent to 150–250 $US) 189 (30.4)
[ 5 million VND (equivalent to 250 $US) 341 (54.8)
Sexual orientation
Homosexual 460 (74.0)
Bisexual 116 (18.7)
Heterosexual, other or no specified identity 46 (7.4)
Self-reported HIV status
HIV positive 11 (1.8)
HIV negative 367 (59.0)
Unknown 244 (39.2)
HIV testing in the last 12 months 339 (54.5)
Safe sex counselling in the last 12 months 363 (58.4)
Depression 70 (11.3)
Sexual sensation seeking score (mean (SD)) 2.5 (0.4)
Belief in the effectiveness of HIV
prevention strategies
Treatment as prevention 100 (16.1)
Being a top (insertive) during anal sex 242 (38.9)
Withdrawal 298 (47.9)
AIDS Behav (2017) 21:1105–1116 1109
123
101
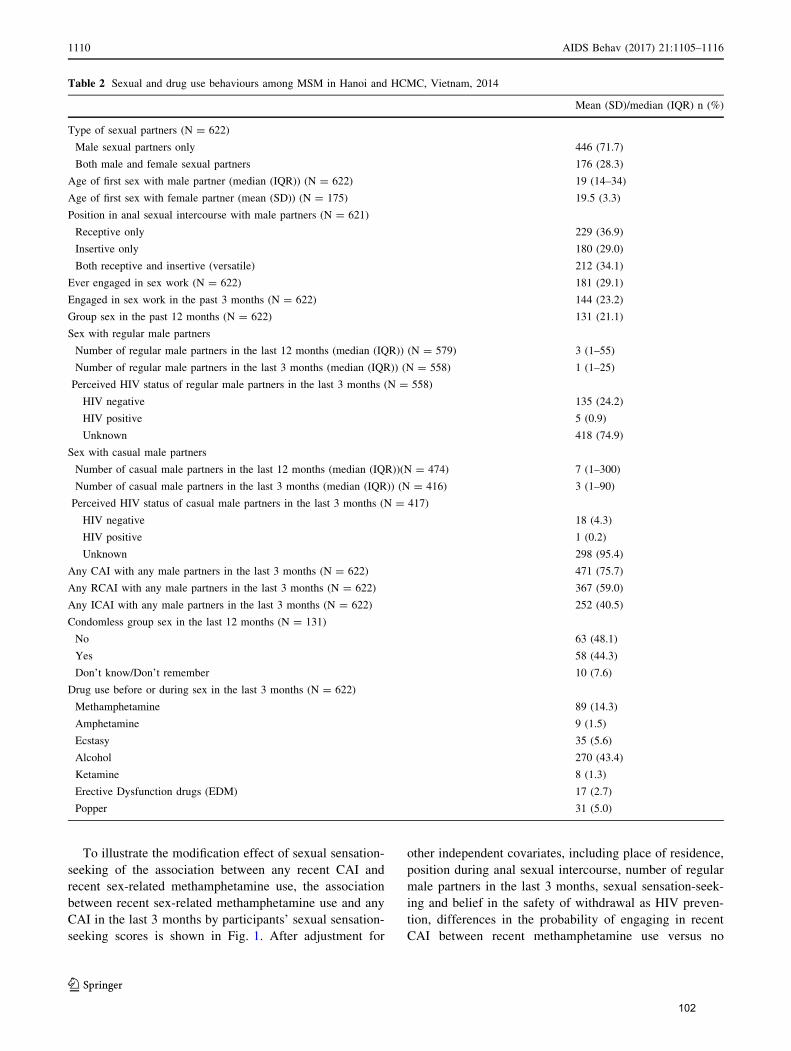
To illustrate the modification effect of sexual sensation-
seeking of the association between any recent CAI and
recent sex-related methamphetamine use, the association
between recent sex-related methamphetamine use and any
CAI in the last 3 months by participants’ sexual sensation-
seeking scores is shown in Fig. 1. After adjustment for
other independent covariates, including place of residence,
position during anal sexual intercourse, number of regular
male partners in the last 3 months, sexual sensation-seek-
ing and belief in the safety of withdrawal as HIV preven-
tion, differences in the probability of engaging in recent
CAI between recent methamphetamine use versus no
Table 2 Sexual and drug use behaviours among MSM in Hanoi and HCMC, Vietnam, 2014
Mean (SD)/median (IQR) n (%)
Type of sexual partners (N = 622)
Male sexual partners only 446 (71.7)
Both male and female sexual partners 176 (28.3)
Age of first sex with male partner (median (IQR)) (N = 622) 19 (14–34)
Age of first sex with female partner (mean (SD)) (N = 175) 19.5 (3.3)
Position in anal sexual intercourse with male partners (N = 621)
Receptive only 229 (36.9)
Insertive only 180 (29.0)
Both receptive and insertive (versatile) 212 (34.1)
Ever engaged in sex work (N = 622) 181 (29.1)
Engaged in sex work in the past 3 months (N = 622) 144 (23.2)
Group sex in the past 12 months (N = 622) 131 (21.1)
Sex with regular male partners
Number of regular male partners in the last 12 months (median (IQR)) (N = 579) 3 (1–55)
Number of regular male partners in the last 3 months (median (IQR)) (N = 558) 1 (1–25)
Perceived HIV status of regular male partners in the last 3 months (N = 558)
HIV negative 135 (24.2)
HIV positive 5 (0.9)
Unknown 418 (74.9)
Sex with casual male partners
Number of casual male partners in the last 12 months (median (IQR))(N = 474) 7 (1–300)
Number of casual male partners in the last 3 months (median (IQR)) (N = 416) 3 (1–90)
Perceived HIV status of casual male partners in the last 3 months (N = 417)
HIV negative 18 (4.3)
HIV positive 1 (0.2)
Unknown 298 (95.4)
Any CAI with any male partners in the last 3 months (N = 622) 471 (75.7)
Any RCAI with any male partners in the last 3 months (N = 622) 367 (59.0)
Any ICAI with any male partners in the last 3 months (N = 622) 252 (40.5)
Condomless group sex in the last 12 months (N = 131)
No 63 (48.1)
Yes 58 (44.3)
Don’t know/Don’t remember 10 (7.6)
Drug use before or during sex in the last 3 months (N = 622)
Methamphetamine 89 (14.3)
Amphetamine 9 (1.5)
Ecstasy 35 (5.6)
Alcohol 270 (43.4)
Ketamine 8 (1.3)
Erective Dysfunction drugs (EDM) 17 (2.7)
Popper 31 (5.0)
1110 AIDS Behav (2017) 21:1105–1116
123
102
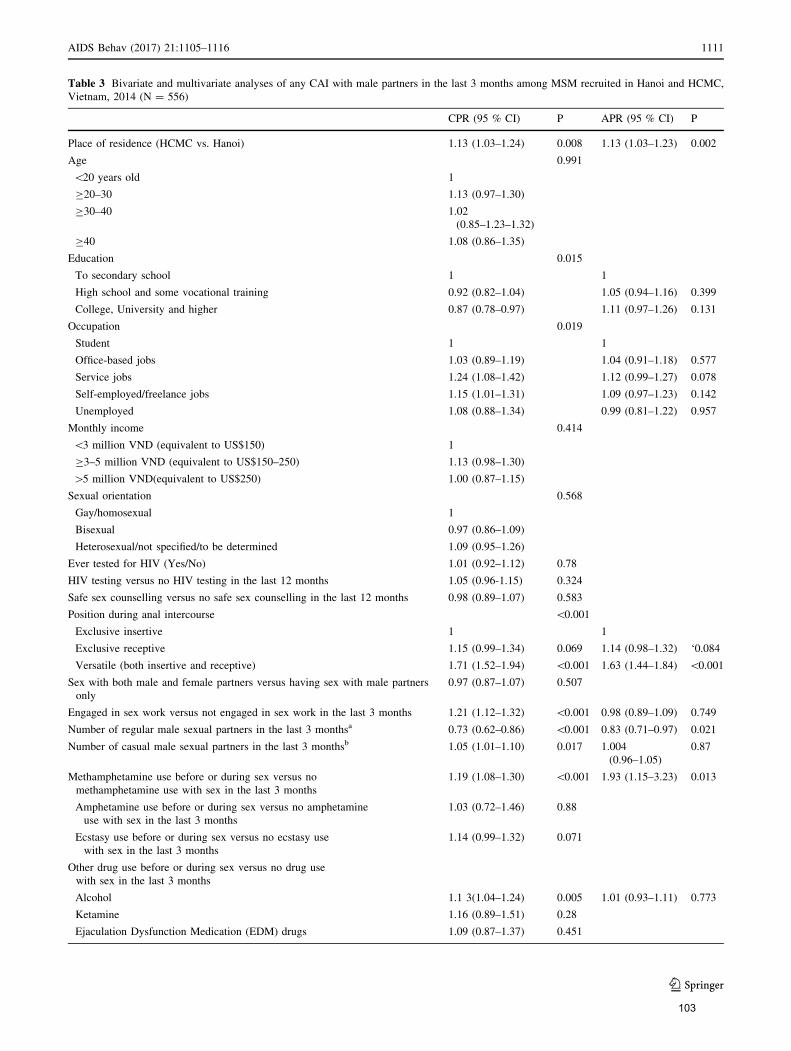
Table 3 Bivariate and multivariate analyses of any CAI with male partners in the last 3 months among MSM recruited in Hanoi and HCMC,
Vietnam, 2014 (N = 556)
CPR (95 % CI) P APR (95 % CI) P
Place of residence (HCMC vs. Hanoi) 1.13 (1.03–1.24) 0.008 1.13 (1.03–1.23) 0.002
Age 0.991
\20 years old 1
C20–30 1.13 (0.97–1.30)
C30–40 1.02
(0.85–1.23–1.32)
C40 1.08 (0.86–1.35)
Education 0.015
To secondary school 1 1
High school and some vocational training 0.92 (0.82–1.04) 1.05 (0.94–1.16) 0.399
College, University and higher 0.87 (0.78–0.97) 1.11 (0.97–1.26) 0.131
Occupation 0.019
Student 1 1
Office-based jobs 1.03 (0.89–1.19) 1.04 (0.91–1.18) 0.577
Service jobs 1.24 (1.08–1.42) 1.12 (0.99–1.27) 0.078
Self-employed/freelance jobs 1.15 (1.01–1.31) 1.09 (0.97–1.23) 0.142
Unemployed 1.08 (0.88–1.34) 0.99 (0.81–1.22) 0.957
Monthly income 0.414
\3 million VND (equivalent to US$150) 1
C3–5 million VND (equivalent to US$150–250) 1.13 (0.98–1.30)
[5 million VND(equivalent to US$250) 1.00 (0.87–1.15)
Sexual orientation 0.568
Gay/homosexual 1
Bisexual 0.97 (0.86–1.09)
Heterosexual/not specified/to be determined 1.09 (0.95–1.26)
Ever tested for HIV (Yes/No) 1.01 (0.92–1.12) 0.78
HIV testing versus no HIV testing in the last 12 months 1.05 (0.96-1.15) 0.324
Safe sex counselling versus no safe sex counselling in the last 12 months 0.98 (0.89–1.07) 0.583
Position during anal intercourse \0.001
Exclusive insertive 1 1
Exclusive receptive 1.15 (0.99–1.34) 0.069 1.14 (0.98–1.32) ‘0.084
Versatile (both insertive and receptive) 1.71 (1.52–1.94) \0.001 1.63 (1.44–1.84) \0.001
Sex with both male and female partners versus having sex with male partners
only
0.97 (0.87–1.07) 0.507
Engaged in sex work versus not engaged in sex work in the last 3 months 1.21 (1.12–1.32) \0.001 0.98 (0.89–1.09) 0.749
Number of regular male sexual partners in the last 3 monthsa 0.73 (0.62–0.86) \0.001 0.83 (0.71–0.97) 0.021
Number of casual male sexual partners in the last 3 monthsb 1.05 (1.01–1.10) 0.017 1.004
(0.96–1.05)
0.87
Methamphetamine use before or during sex versus no
methamphetamine use with sex in the last 3 months
1.19 (1.08–1.30) \0.001 1.93 (1.15–3.23) 0.013
Amphetamine use before or during sex versus no amphetamine
use with sex in the last 3 months
1.03 (0.72–1.46) 0.88
Ecstasy use before or during sex versus no ecstasy use
with sex in the last 3 months
1.14 (0.99–1.32) 0.071
Other drug use before or during sex versus no drug use
with sex in the last 3 months
Alcohol 1.1 3(1.04–1.24) 0.005 1.01 (0.93–1.11) 0.773
Ketamine 1.16 (0.89–1.51) 0.28
Ejaculation Dysfunction Medication (EDM) drugs 1.09 (0.87–1.37) 0.451
AIDS Behav (2017) 21:1105–1116 1111
123
103
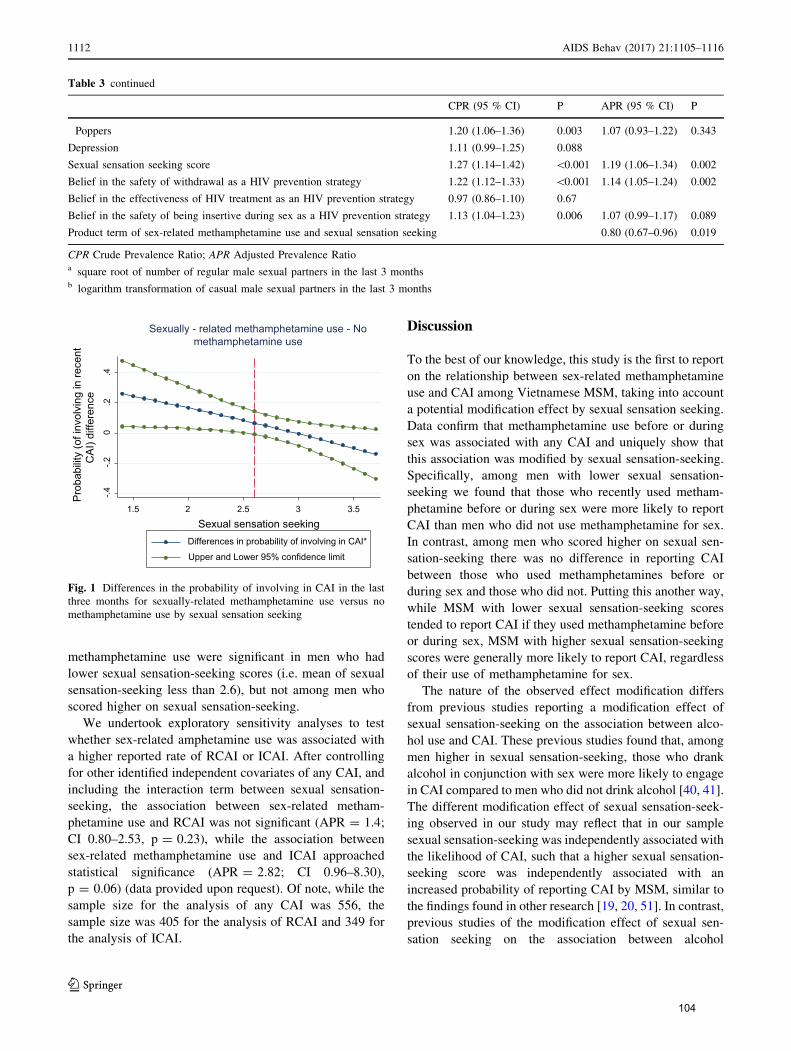
methamphetamine use were significant in men who had
lower sexual sensation-seeking scores (i.e. mean of sexual
sensation-seeking less than 2.6), but not among men who
scored higher on sexual sensation-seeking.
We undertook exploratory sensitivity analyses to test
whether sex-related amphetamine use was associated with
a higher reported rate of RCAI or ICAI. After controlling
for other identified independent covariates of any CAI, and
including the interaction term between sexual sensation-
seeking, the association between sex-related metham-
phetamine use and RCAI was not significant (APR = 1.4;
CI 0.80–2.53, p = 0.23), while the association between
sex-related methamphetamine use and ICAI approached
statistical significance (APR = 2.82; CI 0.96–8.30),
p = 0.06) (data provided upon request). Of note, while the
sample size for the analysis of any CAI was 556, the
sample size was 405 for the analysis of RCAI and 349 for
the analysis of ICAI.
Discussion
To the best of our knowledge, this study is the first to report
on the relationship between sex-related methamphetamine
use and CAI among Vietnamese MSM, taking into account
a potential modification effect by sexual sensation seeking.
Data confirm that methamphetamine use before or during
sex was associated with any CAI and uniquely show that
this association was modified by sexual sensation-seeking.
Specifically, among men with lower sexual sensation-
seeking we found that those who recently used metham-
phetamine before or during sex were more likely to report
CAI than men who did not use methamphetamine for sex.
In contrast, among men who scored higher on sexual sen-
sation-seeking there was no difference in reporting CAI
between those who used methamphetamines before or
during sex and those who did not. Putting this another way,
while MSM with lower sexual sensation-seeking scores
tended to report CAI if they used methamphetamine before
or during sex, MSM with higher sexual sensation-seeking
scores were generally more likely to report CAI, regardless
of their use of methamphetamine for sex.
The nature of the observed effect modification differs
from previous studies reporting a modification effect of
sexual sensation-seeking on the association between alco-
hol use and CAI. These previous studies found that, among
men higher in sexual sensation-seeking, those who drank
alcohol in conjunction with sex were more likely to engage
in CAI compared to men who did not drink alcohol [40, 41].
The different modification effect of sexual sensation-seek-
ing observed in our study may reflect that in our sample
sexual sensation-seeking was independently associated with
the likelihood of CAI, such that a higher sexual sensation-
seeking score was independently associated with an
increased probability of reporting CAI by MSM, similar to
the findings found in other research [19, 20, 51]. In contrast,
previous studies of the modification effect of sexual sen-
sation seeking on the association between alcohol
Table 3 continued
CPR (95 % CI) P APR (95 % CI) P
Poppers 1.20 (1.06–1.36) 0.003 1.07 (0.93–1.22) 0.343
Depression 1.11 (0.99–1.25) 0.088
Sexual sensation seeking score 1.27 (1.14–1.42) \0.001 1.19 (1.06–1.34) 0.002
Belief in the safety of withdrawal as a HIV prevention strategy 1.22 (1.12–1.33) \0.001 1.14 (1.05–1.24) 0.002
Belief in the effectiveness of HIV treatment as an HIV prevention strategy 0.97 (0.86–1.10) 0.67
Belief in the safety of being insertive during sex as a HIV prevention strategy 1.13 (1.04–1.23) 0.006 1.07 (0.99–1.17) 0.089
Product term of sex-related methamphetamine use and sexual sensation seeking 0.80 (0.67–0.96) 0.019
CPR Crude Prevalence Ratio; APR Adjusted Prevalence Ratioa square root of number of regular male sexual partners in the last 3 monthsb logarithm transformation of casual male sexual partners in the last 3 months
-.4-.2
0.2
.4
Pro
babi
lity
(of i
nvol
ving
in re
cent
CA
I) di
ffere
nce
1.5 2 2.5 3 3.5
Sexual sensation seekingDifferences in probability of involving in CAI*
Upper and Lower 95% confidence limit
Sexually - related methamphetamine use - No methamphetamine use
Fig. 1 Differences in the probability of involving in CAI in the last
three months for sexually-related methamphetamine use versus no
methamphetamine use by sexual sensation seeking
1112 AIDS Behav (2017) 21:1105–1116
123
104
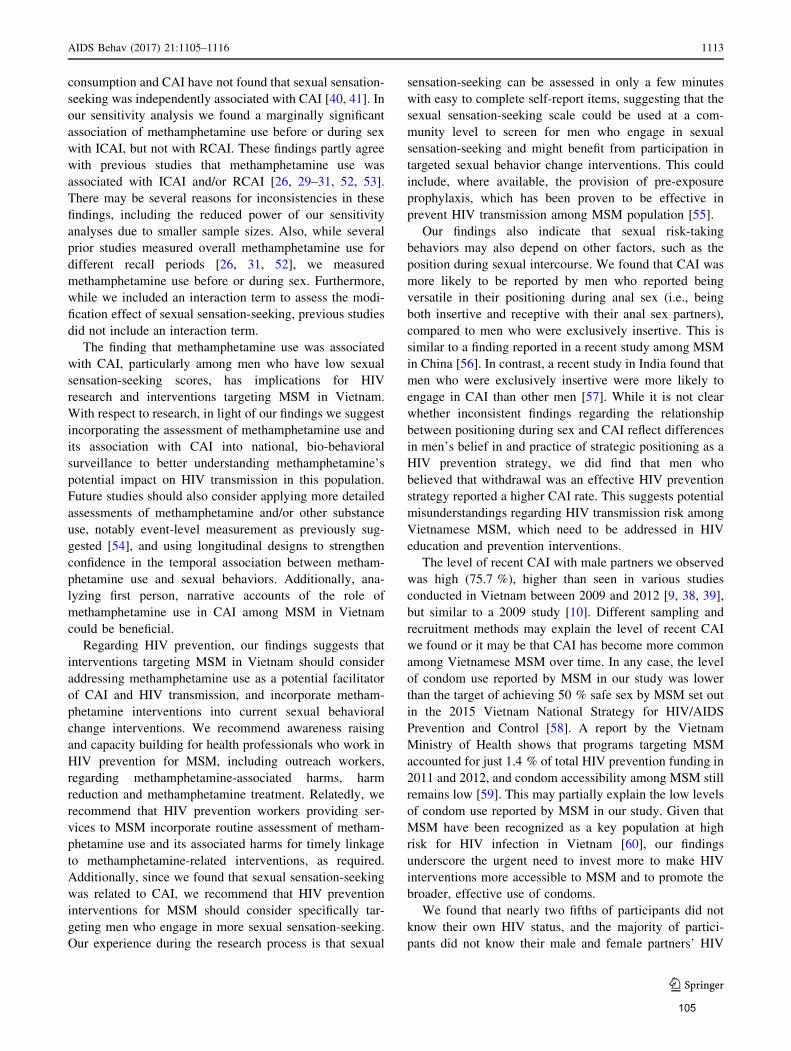
consumption and CAI have not found that sexual sensation-
seeking was independently associated with CAI [40, 41]. In
our sensitivity analysis we found a marginally significant
association of methamphetamine use before or during sex
with ICAI, but not with RCAI. These findings partly agree
with previous studies that methamphetamine use was
associated with ICAI and/or RCAI [26, 29–31, 52, 53].
There may be several reasons for inconsistencies in these
findings, including the reduced power of our sensitivity
analyses due to smaller sample sizes. Also, while several
prior studies measured overall methamphetamine use for
different recall periods [26, 31, 52], we measured
methamphetamine use before or during sex. Furthermore,
while we included an interaction term to assess the modi-
fication effect of sexual sensation-seeking, previous studies
did not include an interaction term.
The finding that methamphetamine use was associated
with CAI, particularly among men who have low sexual
sensation-seeking scores, has implications for HIV
research and interventions targeting MSM in Vietnam.
With respect to research, in light of our findings we suggest
incorporating the assessment of methamphetamine use and
its association with CAI into national, bio-behavioral
surveillance to better understanding methamphetamine’s
potential impact on HIV transmission in this population.
Future studies should also consider applying more detailed
assessments of methamphetamine and/or other substance
use, notably event-level measurement as previously sug-
gested [54], and using longitudinal designs to strengthen
confidence in the temporal association between metham-
phetamine use and sexual behaviors. Additionally, ana-
lyzing first person, narrative accounts of the role of
methamphetamine use in CAI among MSM in Vietnam
could be beneficial.
Regarding HIV prevention, our findings suggests that
interventions targeting MSM in Vietnam should consider
addressing methamphetamine use as a potential facilitator
of CAI and HIV transmission, and incorporate metham-
phetamine interventions into current sexual behavioral
change interventions. We recommend awareness raising
and capacity building for health professionals who work in
HIV prevention for MSM, including outreach workers,
regarding methamphetamine-associated harms, harm
reduction and methamphetamine treatment. Relatedly, we
recommend that HIV prevention workers providing ser-
vices to MSM incorporate routine assessment of metham-
phetamine use and its associated harms for timely linkage
to methamphetamine-related interventions, as required.
Additionally, since we found that sexual sensation-seeking
was related to CAI, we recommend that HIV prevention
interventions for MSM should consider specifically tar-
geting men who engage in more sexual sensation-seeking.
Our experience during the research process is that sexual
sensation-seeking can be assessed in only a few minutes
with easy to complete self-report items, suggesting that the
sexual sensation-seeking scale could be used at a com-
munity level to screen for men who engage in sexual
sensation-seeking and might benefit from participation in
targeted sexual behavior change interventions. This could
include, where available, the provision of pre-exposure
prophylaxis, which has been proven to be effective in
prevent HIV transmission among MSM population [55].
Our findings also indicate that sexual risk-taking
behaviors may also depend on other factors, such as the
position during sexual intercourse. We found that CAI was
more likely to be reported by men who reported being
versatile in their positioning during anal sex (i.e., being
both insertive and receptive with their anal sex partners),
compared to men who were exclusively insertive. This is
similar to a finding reported in a recent study among MSM
in China [56]. In contrast, a recent study in India found that
men who were exclusively insertive were more likely to
engage in CAI than other men [57]. While it is not clear
whether inconsistent findings regarding the relationship
between positioning during sex and CAI reflect differences
in men’s belief in and practice of strategic positioning as a
HIV prevention strategy, we did find that men who
believed that withdrawal was an effective HIV prevention
strategy reported a higher CAI rate. This suggests potential
misunderstandings regarding HIV transmission risk among
Vietnamese MSM, which need to be addressed in HIV
education and prevention interventions.
The level of recent CAI with male partners we observed
was high (75.7 %), higher than seen in various studies
conducted in Vietnam between 2009 and 2012 [9, 38, 39],
but similar to a 2009 study [10]. Different sampling and
recruitment methods may explain the level of recent CAI
we found or it may be that CAI has become more common
among Vietnamese MSM over time. In any case, the level
of condom use reported by MSM in our study was lower
than the target of achieving 50 % safe sex by MSM set out
in the 2015 Vietnam National Strategy for HIV/AIDS
Prevention and Control [58]. A report by the Vietnam
Ministry of Health shows that programs targeting MSM
accounted for just 1.4 % of total HIV prevention funding in
2011 and 2012, and condom accessibility among MSM still
remains low [59]. This may partially explain the low levels
of condom use reported by MSM in our study. Given that
MSM have been recognized as a key population at high
risk for HIV infection in Vietnam [60], our findings
underscore the urgent need to invest more to make HIV
interventions more accessible to MSM and to promote the
broader, effective use of condoms.
We found that nearly two fifths of participants did not
know their own HIV status, and the majority of partici-
pants did not know their male and female partners’ HIV
AIDS Behav (2017) 21:1105–1116 1113
123
105

status. Informal conversations with participants suggest
that it remains unusual for MSM to disclose or ask about
the HIV status of their partner(s), because HIV remains
highly stigmatized in Vietnam. HIV status disclosure can
be an important factor in the prevention of HIV trans-
mission [61]. Our findings indicate a need for culturally
appropriate interventions to promote HIV testing and HIV
status disclosure among MSM as part of a comprehensive
approach to prevent HIV transmission among MSM in
Vietnam. Only half of our participants had tested for HIV
in the previous 12 months and nearly a third had never
been tested for HIV. In order to achieve the target of
80 % MSM tested for HIV in 2020 [58], our findings
underscore the importance of promoting HIV testing
among MSM.
Several limitations should be borne in mind when
interpreting the results of our study. Although we included
contextual, sex-related assessments of methamphetamine
use, our study had a cross-sectional survey design, so we
cannot confirm the temporal relationship between
methamphetamine use and CAI. We used a convenience,
peer referral sampling method which is unlikely to have
resulted in a sample representative of the larger population
of MSM in Vietnam. Additionally, since same-sex sexual
practices and drug use are stigmatized in Vietnam, our data
may underestimate the true level of HIV-related sexual
behaviors and drug use among MSM, although our findings
are comparable with previous studies. Our results may have
been affected by recall and reporting bias and hidden
confounders.
Conclusion
Our study found a high prevalence of CAI with male
partners among MSM in Hanoi and HCMC, Vietnam.
Importantly, CAI was associated with recent sex-related
methamphetamine use and this association was found to be
modified by sexual sensation-seeking. Notably, while men
higher in sexual sensation seeking were more likely to
report CAI than men lower in sexual sensation seeking,
sex-related methamphetamine use increased the risk of
CAI among men with low sexual sensation seeking scores.
HIV prevention interventions targeting MSM in Vietnam
should therefore consider incorporating interventions for
methamphetamine use.
Acknowledgments We acknowledge the great support and input
from staff of the Institute of Preventive Medicine and Public Health,
Hanoi Medical University, Hanoi Centre of HIV/AIDS Prevention
and Control, Center for Community Health Promotion, Center for
Promotion of Quality of Life and leaders and representatives of
community-based organizations of MSM in Ho Chi Minh City during
the data collection process.
Funding Nga Thi Thu Vu received Australian Award Scholarship for
her PhD study in UNSW Australia. The study received financial
support from the Faculty of Arts and Social Sciences (FASS), UNSW
Australia under its Postgraduate Essential Research Program Funding
scheme and External Research Program Funding schemes. The Centre
for Social Research in Health is supported by funding from the
Australian Government Department of Health. Funding agencies were
not involved in the development of the research protocol, data col-
lection, data analysis, interpretation or the dissemination of research
findings.
Author’s contribution Nga Thi Thu Vu contributed to the devel-
opment of the research protocol, data collection, data analysis and the
manuscript drafting and finalization. John De Wit and Martin Holt
provided supervision of the research process and provided advice
during data analysis and the drafting of manuscript. Huong Thi Thu
Phan, Lan Thi La, Gioi Minh Tran, Tung Thanh Doan and Trang Nhu
Nguyen Nguyen provided inputs for the development of the research
protocol and manuscript drafting and finalization.
Compliance with Ethical Standards
Conflict of interest The authors declare that they have no conflict of
interest.
Research involving Human Participants and/or Animals The
study received approval from the Human Research Ethics Committee
of UNSW Australia (reference HC14130), and from the Institutional
Review Board of the Hanoi School of Public Health (reference
014_262/DD-YTCC). All procedures performed in studies involving
human participants were in accordance with the ethical standards of
the institutional and/or national research committee and with the 1964
Helsinki declaration and its later amendments or comparable ethical
standards.
Informed consent Informed consent was obtained from all individ-
ual participants included in the study.
References
1. Beyrer C, Baral SD, van Griensven F, et al. Global epidemiology
of HIV infection in men who have sex with men. Lancet.
2012;380(9839):367–77.
2. Beyrer C, Sullivan P, Sanchez J, et al. The increase in global HIV
epidemics in MSM. Aids. 2013;27(17):2665–78.
3. Chow EP, Chen X, Zhao J, Zhuang X, Jing J, Zhang L. Factors
associated with self-reported unprotected anal intercourse among
men who have sex with men in Changsha city of Hunan province,
China. AIDS Care. 2015;27(10):1332–42.
4. Deuba K, Ekstrom AM, Shrestha R, Ionita G, Bhatta L, Karki
DK. Psychosocial health problems associated with increased HIV
risk behavior among men who have sex with men in Nepal: a
cross-sectional survey. PLoS One. 2013;8(3):e58099.
5. Nyoni JE, Ross MW. Condom use and HIV-related behaviors in
urban Tanzanian men who have sex with men: a study of beliefs,
HIV knowledge sources, partner interactions and risk behaviors.
AIDS Care. 2013;25(2):223–9.
6. Xu JJ, Zhang C, Hu QH, et al. Recreational drug use and risks of
HIV and sexually transmitted infections among Chinese men who
have sex with men: mediation through multiple sexual partner-
ships. BMC Infect Dis. 2014;14:642.
7. Yi S, Tuot S, Chhoun P, Pal K, Tith K, Brody C. Factors asso-
ciated with inconsistent condom use among men who have sex
with men in cambodia. PLoS One. 2015;10(8):e0136114.
1114 AIDS Behav (2017) 21:1105–1116
123
106
8. Garcia MC, Duong QL, Mercer LC, Meyer SB, Koppenhaver T,
Ward PR. Patterns and risk factors of inconsistent condom use
among men who have sex with men in Vietnam: results from an
Internet-based cross-sectional survey. Glob Public Health.
2014;9(10):1225–38.
9. Bengtsson L, Lu X, Liljeros F, Thanh HH, Thorson A. Strong
propensity for HIV transmission among men who have sex with
men in Vietnam: behavioural data and sexual network modelling.
BMJ Open. 2014;4(1):e003526.
10. Pham QD, Nguyen TV, Nguyen PD, et al. Men who have sex
with men in southern Vietnam report high levels of substance use
and sexual risk behaviours but underutilise HIV testing services:
a cross-sectional study. Sex Transm Infect. 2015;91(3):178–82.
11. Lim SH, Bazazi AR, Sim C, Choo M, Altice FL, Kamarulzaman
A. High rates of unprotected anal intercourse with regular and
casual partners and associated risk factors in a sample of ethnic
Malay men who have sex with men (MSM) in Penang, Malaysia.
Sex Transm Infect. 2013;89(8):642–9.
12. Akin M, Fernandez MI, Bowen GS, Warren JC. HIV risk
behaviors of Latin American and Caribbean men who have sex
with men in Miami, Florida, USA. Rev Panam Salud Publica.
2008;23(5):341–8.
13. Csepe P, Amirkhanian YA, Kelly JA, McAuliffe TL, Mocsonoki
L. HIV risk behaviour among gay and bisexual men in Budapest,
Hungary. Int J STD AIDS. 2002;13(3):192–200.
14. Bousman CA, Cherner M, Ake C, et al. Negative mood and
sexual behavior among non-monogamous men who have sex with
men in the context of methamphetamine and HIV. J Affect
Disord. 2009;119(1–3):84–91.
15. Parsons JT, Halkitis PN, Wolitski RJ, Gomez CA. Correlates of
sexual risk behaviors among HIV-positive men who have sex
with men. AIDS Educ Prev. 2003;15(5):383–400.
16. Choi K-H, Hudes ES, Steward WT. Social discrimination, con-
current sexual partnerships, and HIV risk among men who have
sex with men in Shanghai, China. AIDS Behave. 2008;12(Suppl
1):S71–7.
17. Don O, Kyung-Hee C, Priscilla C, et al. Prevalence and correlates
of substance use among young Asian Pacific Islander men who
have sex with men. Prev Sci. 2006;7(1):19–29.
18. Crepaz N, Marks G, Mansergh G, Murphy S, Miller LC, Appleby
PR. Age-related risk for HIV infection in men who have sex with
men: examination of behavioral, relationship, and serostatus
variables. AIDS Educ Prev. 2000;12(5):405–15.
19. Chng CL, Geliga-Vargas J. Ethnic identity, gay identity, sexual
sensation seeking and HIV risk taking among multiethnic men
who have sex with men. AIDS Educ Prev. 2000;12(4):326–39.
20. Kalichman SC, Heckman T, Kelly JA. Sensation seeking as an
explanation for the association between substance use and HIV-
related risky sexual behavior. Arch Sex Behav.
1996;25(2):141–54.
21. Colfax G, Guzman R. Club drugs and HIV infection: a review.
Clin Infect Dis. 2006;42(10):1463–9.
22. Colfax G, Shoptaw S. The methamphetamine epidemic: impli-
cations for HIV prevention and treatment. Curr HIV/AIDS Rep.
2005;2(4):194–9.
23. Halkitis PN, Parsons JT, Stirratt MJ. A double epidemic: crystal
methamphetamine drug use in relation to HIV transmission
among gay men. J Homosex. 2001;41(2):17–35.
24. Kurtz SP. Post-circuit blues: motivations and consequences of
crystal meth use among gay men in Miami. AIDS Behav.
2005;9(1):63–72.
25. Semple SJ, Patterson TL, Grant I. Motivations associated with
methamphetamine use among HIV? men who have sex with
men. J Subst Abuse Treat. 2002;22(3):149–56.
26. Melendez-Torres GJ, Hickson F, Reid D, Weatherburn P, Bonell
C. Nested event-level case-control study of drug use and sexual
outcomes in multipartner encounters reported by men who have
sex with men. AIDS Behav. 2016;20(3):646–54.
27. Shoptaw S, Reback CJ. Methamphetamine use and infectious dis-
ease-related behaviors inmenwho have sexwithmen: implications
for interventions. Addiction. 2007;102(Suppl 1):130–5.
28. Thu Vu NT. Maher L, Zablotska I. Amphetamine-type stimulants
and HIV infection among men who have sex with men: impli-
cations on HIV research and prevention from a systematic review
and meta-analysis. J Int AIDS Soc. 2015;18(1):19273.
29. Gorbach PM, Weiss RE, Jeffries R, et al. Behaviors of recently
HIV-infected men who have sex with men in the year postdiag-
nosis: effects of drug use and partner types. J Acquir Immune
Defic Syndr. 2011;56(2):176–82.
30. Pines HA, Gorbach PM, Weiss RE, et al. Individual-Level,
partnership-level, and sexual event-level predictors of condom
use during receptive anal intercourse among HIV-negative men
who have sex with men in Los Angeles. AIDS Behav.
2016;20(6):1315–26.
31. Halkitis PN, Mukherjee PP, Palamar JJ. Longitudinal modeling of
methamphetamine use and sexual risk behaviors in gay and
bisexual men. AIDS Behav. 2009;13(4):783–91.
32. Rawstorne P, Digiusto E, Worth H, Zablotska I. Associations
between crystal methamphetamine use and potentially unsafe
sexual activity among gay men in Australia. Arch Sex Behav.
2007;36(5):646–54.
33. Chariyalertsak S, Kosachunhanan N, Saokhieo P, et al. HIV
incidence, risk factors, and motivation for biomedical interven-
tion among gay, bisexual men, and transgender persons in
Northern Thailand. PLoS One. 2011;6(9):e24295.
34. Xu JJ, Qian HZ, Chu ZX, et al. Recreational drug use among
Chinese men who have sex with men: a risky combination with
unprotected sex for acquiring HIV infection. Biomed Res Int.
2014;2014:725361.
35. Morineau G, Nugrahini N, Riono P, et al. Sexual risk taking, STI
and HIV prevalence among men who have sex with men in six
Indonesian cities. AIDS Behav. 2011;15(5):1033–44.
36. Nguyen TA, Nguyen HT, Le GT, Detels R. Prevalence and risk
factors associated with HIV infection among men having sex with
men in Ho Chi Minh City, Vietnam. AIDS Behav.
2008;12(3):476–82.
37. Ha H, Risser JM, Ross MW, Huynh NT, Nguyen HT. Homo-
sexuality-related stigma and sexual risk behaviors among men
who have sex with men in Hanoi, Vietnam. Arch Sex Behav.
2015;44(2):349–56.
38. Pham QD, Nguyen TV, Hoang CQ, et al. Prevalence of HIV/STIs
and associated factors among men who have sex with men in An
Giang, Vietnam. Sex Transm Dis. 2012;39(10):799–806.
39. Vu NT, Holt M, Phan HT, et al. Amphetamine-type stimulant use
among men who have sex with men (MSM) in Vietnam: results
from a socio-ecological, community-based study. Drug Alcohol
Depend. 2016;158:110–7.
40. Heidinger B, Gorgens K, Morgenstern J. The effects of sexual
sensation seeking and alcohol use on risky sexual behavior
among men who have sex with men. AIDS Behav.
2015;19(3):431–9.
41. Newcomb ME, Clerkin EM, Mustanski B. Sensation seeking
moderates the effects of alcohol and drug use prior to sex on
sexual risk in young men who have sex with men. AIDS Behav.
2011;15(3):565–75.
42. Berry MC, Go VF, Quan VM, et al. Social environment and HIV
risk among MSM in Hanoi and Thai Nguyen. AIDS Care.
2013;25(1):38–42.
43. United Nations Office on Drugs and Crime (UNODC). Amphe-
tamine type stimulants in Vietnam. A review of the availibility,
use and implications for health and security in Vietnam 2012.
Hanoi, Vietnam: 2012.
AIDS Behav (2017) 21:1105–1116 1115
123
107
44. Hirshfield S,Wolitski RJ, ChiassonMA, Remien RH, Humberstone
M,WongT. Screening for depressive symptoms in an online sample
of men who have sex with men. AIDS Care. 2008;20(8):904–10.
45. Mao L, Kidd MR, Rogers G, et al. Social factors associated with
Major Depressive Disorder in homosexually active, gay men
attending general practices in urban Australia. Aust N Z J Public
Health. 2009;33(1):83–6.
46. Kroenke K, Spitzer RL,Williams JB. The PHQ-9: validity of a brief
depression severity measure. J Gen InternMed. 2001;16(9):606–13.
47. Kalichman SC, Rompa D. Sexual sensation seeking and Sexual
Compulsivity Scales: reliability, validity, and predicting HIV risk
behavior. J Pers Assess. 1995;65(3):586–601.
48. Thompson ML, Myers JE, Kriebel D. Prevalence odds ratio or
prevalence ratio in the analysis of cross sectional data: what is to
be done? Occup Environ Med. 1998;55(4):272–7.
49. Hosmer DW. In: Lemeshow S, Sturdivant RX, editors. Applied
logistic regression. 3rd ed. Hoboken: Wiley; 2013.
50. Zou G. A modified poisson regression approach to prospective
studies with binary data. Am J Epidemiol. 2004;159(7):702–6.
51. Kalichman SC, Simbayi L, Jooste S, Vermaak R, Cain D. Sen-
sation seeking and alcohol use predict HIV transmission risks:
prospective study of sexually transmitted infection clinic patients,
Cape Town, South Africa. Addict Behav. 2008;33(12):1630–3.
52. Spindler HH, Scheer S, Chen SY, et al. Viagra, metham-
phetamine, and HIV risk: results from a probability sample of
MSM, San Francisco. Sex Transm Dis. 2007;34(8):586–91.
53. Mansergh G, Shouse RL, Marks G, et al. Methamphetamine and
sildenafil (Viagra) use are linked to unprotected receptive and
insertive anal sex, respectively, in a sample of men who have sex
with men. Sex Transm Infect. 2006;82(2):131–4.
54. Leigh BC, Stall R. Substance use and risky sexual behavior for
exposure to HIV. Issues in methodology, interpretation, and
prevention. Am Psychol. 1993;48(10):1035–45.
55. Spinner CD, Boesecke C, Zink A, et al. HIV pre-exposure pro-
phylaxis (PrEP): a review of current knowledge of oral systemic
HIV PrEP in humans. Infection. 2016;44(2):151–8.
56. Zhang H, Lu H, Pan SW, et al. Correlates of unprotected anal
intercourse: the influence of anal sex position among men who
have sex with men in Beijing, China. Arch Sex Behav.
2015;44(2):375–87.
57. Hemmige V, Snyder H, Liao C, et al. Sex position, marital status,
and HIV risk among Indian men who have sex with men: clues to
optimizing prevention approaches. AIDS Patient Care STDS.
2011;25(12):725–34.
58. Vietnam National Committee on AIDS Drugs and Prostitute
Control. National Strategy for HIV/AIDS Prevention and Control
to 2020 with the vision to 2030. Hanoi, Vietnam: 2012.
59. Vietnam Ministry of Health. Optimizing Vietnam’s Hiv
Response: An Investment Case. Hanoi, Vietnam: 2015.
60. Vietnam Ministry of Health. Results from the HIV/STI Biologi-
cal and Behavioral Surveillance (Ibbs) in Vietnam- Round II
2009. Hanoi, Vietnam: 2011.
61. Thoth CA, Tucker C, Leahy M, Stewart SM. Self-disclosure of
serostatus by youth who are HIV-positive: a review. J Behav
Med. 2014;37(2):276–88.
1116 AIDS Behav (2017) 21:1105–1116
123
108
CHAPTER 5
AMPHETAMINE-TYPE-STIMULANTS AND HIV INFECTION AMONG
MEN WHO HAVE SEX WITH MEN: IMPLICATIONS ON HIV
RESEARCH AND PREVENTION FROM A SYSTEMATIC REVIEW AND
META-ANALYSIS
Author Contributions Nga Thi Thu VU1,2, Lisa Maher and Iryna Zablotska
1: The Kirby Institute, The University of New South Wales Australia, Sydney, New
South Wales, Australia; 2: Center for Social Research in Health, The University
of New South Wales Australia, Sydney, New South Wales, Australia;
Reference
Vu NT, Maher L, Zablotska I. Amphetamine-type stimulants and HIV infection
among men who have sex with men: implications on HIV research and
prevention from a systematic review and meta-analysis. Journal of the
International AIDS Society. 2015;18:19273.
Declaration
I certify that this publication was a direct result of my research toward this PhD,
and that reproduction in this thesis does not breach copyright regulations.
Nga Thi Thu Vu June 2017
Copyright permission
This article was published in the Journal of the International AIDS Society
(JIAS), an open-access journal, available online:
http://www.jiasociety.org/index.php/jias/article/view/19273.
No copyright permission, therefore, is needed for reusing it in this thesis
dissertation.
109
Research article
Amphetamine-type stimulants and HIV infection among men who
have sex with men: implications on HIV research and prevention
from a systematic review and meta-analysis
Nga Thi Thu Vu§,1,2, Lisa Maher1 and Iryna Zablotska1
§Corresponding author: Nga Thi Thu Vu, The Kirby Institute, The University of NSW Australia, Sydney, NSW 2052, Australia. Tel: �61 431691214,
Fax: �61 2 9385 6455. ([email protected])
Abstract
Introduction: HIV infections and the use of amphetamine-type stimulants (ATS) among men who have sex with men (MSM) have
been increasing internationally, but the role of ATS use as a co-factor for HIV infection remains unclear. We aimed to summarize
the association between ATS use and HIV infection among MSM.
Methods: We conducted a systematic search of MEDLINE, EMBASE, GLOBAL HEALTH and PsycINFO for relevant English, peer-
reviewed articles of quantitative studies published between 1980 and 25 April 2013. Pooled estimates of the association �prevalence rate ratios (PRR, cross-sectional studies), odds ratio (OR, case-control studies) and hazard ratio (HR, longitudinal
studies), with 95% Confidence Intervals (CI) � were calculated using random-effects models stratified by study design and ATS
group (meth/amphetamines vs. ecstasy).We assessed the existence of publication bias in funnel plots and checked for sources of
heterogeneity using meta-regression and subgroup analysis.
Results: We identified 6710 article titles, screened 1716 abstracts and reviewed 267 full text articles. A total of 35 publications
were eligible for data abstraction and meta-analysis, resulting in 56 records of ATS use. Most studies (31/35) were conducted in
high-income countries. Published studies used different research designs, samples and measures of ATS use. The pooled
association between meth/amphetamine use and HIV infection was statistically significant in all three designs (PRR�1.86; 95%
CI: 1.57�2.17; OR�2.73; 95% CI: 2.16�3.46 and HR�3.43; 95% CI: 2.98�3.95, respectively, for cross-sectional, case-control andlongitudinal studies). Ecstasy use was not associated with HIV infection in cross-sectional studies (PRR�1.15; 95% CI: 0.88�1.49;OR�3.04; 95% CI: 1.29�7.18 and HR�2.48; 95% CI: 1.42�4.35, respectively, for cross-sectional, case-control and longitudinal
studies). Results in cross-sectional studies were highly heterogeneous due to issues with ATS measurement and different
sampling frames.
Conclusions: While meth/amphetamine use was significantly associated with HIV infection among MSM in high-income
countries in all study designs, evidence of the role of ecstasy in HIV infection was lacking in cross-sectional studies. Cross-
sectional study design, measurement approaches and source populations may also be important modifiers of the strength and
the direction of associations. Event-specific measure of individual drug is required to establish temporal relationship between
ATS use and HIV infection. HIV prevention programmes targeting MSM should consider including interventions designed to
address meth/amphetamine use.
Keywords: HIV; amphetamine-type stimulants; MSM; systematic review; meta-analysis; risk behaviour; meth/amphetamine;
ecstasy.
To access the supplementary material to this article please see Supplementary Files under ‘Article Tools’.
Received 12 May 2014; Revised 2 November 2014; Accepted 28 November 2014; Published 2 February 2015
Copyright: – 2015 Nga Thi Thu Vu et al; licensee International AIDS Society. This is an Open Access article distributed under the terms of the Creative Commons
Attribution 3.0 Unported (CC BY 3.0) License (http://creativecommons.org/licenses/by/3.0/), which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
IntroductionAmphetamine-type stimulants (ATS) are the second most
popular group of illegal drugs globally and are increasingly
used in different populations and in different parts of the
world [1,2]. ATS can be classified into two main subgroups:
meth/amphetamines, which include amphetamine sulphate,
amphetamine hydrochloride, methamphetamine and meth-
cathinone, and ecstasy subgroup, which comprises MDMA
(3,4-methylenedioxy-N-methylamphetamine) and its analogue
(called meth/amphetamines and ecstasy hereafter) [1,3].
Both groups are synthetic neurotropic stimulants that can
be ingested orally, injected, inhaled, smoked or ‘‘shafted’’
(inserted in the anus) and have immediate accelerated
physical and psychological effects which last up to 10�12hours (meth/amphetamines) or 3�6 hours (ecstasy) [4,5].
Ecstasy is the most common street name for MDMA [6]. As to
Nga Thi Thu Vu et al. Journal of the International AIDS Society 2015, 18:19273
http://www.jiasociety.org/index.php/jias/article/view/19273 | http://dx.doi.org/10.7448/IAS.18.1.19273
1
110

methamphetamine, its street slang names vary geographi-
cally, and some of them ‘‘crystal,’’ ‘‘speed,’’ ‘‘ice,’’ ‘‘crank,’’
‘‘batu,’’ ‘‘glass,’’ ‘‘chalk’’ and ‘‘go-fast’’ [7,8].
In relation to sex, meth/amphetamine and ecstasy have been
documented to have different effects. Meth/amphetamines
are often used to increase sexual desire, make intercourse
more pleasurable, facilitate sexual experimentation and
decrease sexual inhibition [9,10]. Meth/amphetamines may
increase sexual pleasure, help prolong sexual performance,
facilitate sexual marathons, make anal intercourse easier and
less painful, particularly during more forceful and traumatic
sexual penetration [11]. Such attributes have been valued in
more sexually adventurous gay community subcultures [12].
Meth/amphetamine use clearly affects both physiological
and psychological aspects of sexual behaviour and may
facilitate risky sexual practices, including unprotected sex,
thereby increasing the risk of HIV transmission.
While some studies suggest that ecstasy use may also
increase sexual satisfaction, prolong and enhance sexual
arousal [13�17], other studies found no effect on sexual
desire in penetrative sexual intercourse [18,19]. Ecstasy has
also been reported to increase feelings of sensuality and
emotional closeness [20,21]. Therefore, it may be used in the
context of less risky sex and its impact on HIV transmission is
less well defined.
In the past decade, ATS use has become increasingly
popular among men who have sex with men (MSM) in North
America, Asia, Western and South Western Europe [22�33].In high-income countries such as the United Kingdom and the
United States, the prevalence of recent (past 12 months)
amphetamine use among MSM was reported to be between
7.2 and 18.8% [22,23], recent meth/amphetamine use �between 2.8 and 18.0% [23�25] and recent ecstasy use �between 18.5 and 36.7% [23,34,35]. The prevalence of
lifetime use of these substances among MSM in seven US
cities was found to be much higher [26,32,33]. An online
study of drug use among MSM in 12 countries in Asia in 2010
reported an overall prevalence of recreational drug use over
a six-month period of 16.7%, with ecstasy the most com-
monly used drug (8.1%) [30]. Data from studies assessing
drug use during specific gay community events and venues in
Western countries, (e.g. circuit parties, dance clubs, bars and
bathhouses) have found the prevalence of both meth/
amphetamine and ecstasy use to be even higher [34,36].
A growing body of literature documents significant asso-
ciations between meth/amphetamine and ecstasy use and
unprotected anal intercourse (UAI), including receptive UAI �a practice which carries the highest risk of HIV infection
[11,22,28,32,37�43]. ATS use and UAI are co-occurring risk
behaviours with the potential to facilitate HIV transmission
among MSM. Since ATS can also be administered parenter-
ally, exposure to HIV can also occur via unsafe injecting
practices [44,45].
A number of studies have directly focused on the asso-
ciation between ATS use and HIV infection or included mea-
sures of ATS use in their analyses of associates/risk factors of
HIV infection among MSM [8,25,42,46�77]. However, the
results of these studies have been inconsistent as to the sig-
nificance of this association. Furthermore, the interpretation
of their findings may be complicated given the variety of
study designs, sampling frames and measures of ATS use. The
main objective of this systematic review and meta-analysis
was to evaluate and summarize the association between ATS
use and HIV infection among MSM in different study designs
and by ATS subgroup (meth/amphetamines and ecstasy).
MethodsThis paper followed the guidelines for reporting a meta-
analysis of observational studies (MOOSE) proposed by
Stroup et al. [78].
Search strategy
We conducted a systematic search in MEDLINE, EMBASE,
GLOBAL HEALTH and PsysINFO for relevant publications from
1980 until 25 April 2013. The search used a combination
of free terms and the Medline subject headings, including
(1) MSM OR homosexual men OR bisexual men OR gay men
OR male homosexual OR bisexual male OR homosexuality OR
bisexuality AND (2) risk factors OR determinants OR associa-
tions OR correlates OR correlations OR predictors OR high-risk
behaviours OR predictor variables AND (3) HIV prevalence OR
HIV incidence OR HIV seroconversion OR HIV status OR human
immunodeficiency virus OR human immunodeficiency virus
prevalence/infection. Some articles reported only a combined
drug use measure, did not specify the drug(s) used, did not
provide a quantitative effect measure with an associated 95%
confidence interval (95% CI) and did not include the original
data. In these instances, we contacted the corresponding
authors by email to obtain the effect measure or a descriptive
tabulation of ATS use and HIV infection. If no reply was
received within four weeks, the corresponding articles were
excluded from further review. The search was carried out by
Nga Thi Thu Vu and Julia Kennedy.
Inclusion and exclusion criteria
Articles were eligible for inclusion in the review if they
satisfied all of the following criteria: 1) cross-sectional, case-
control or longitudinal study design; 2) quantitative data
collection; 3) MSM as a target population; 4) the article
reported a crude quantitativemeasure of association between
ATS use and HIV infection or provided data to calculate it; 4)
HIV status of participants was confirmed by a standardized
laboratory method, and 5) the article was published in a peer-
reviewed English language journal. Studies were excluded if:
1) they applied only qualitative methods or mathematical
modelling; 2) specifically targeted only HIV positive MSM or
only ATS users; 3) quantitative data could not be extracted
and/or were not provided by the authors; 4) HIV status of
participants was self-reported; 5) the publication included
only conference proceedings; and 6) was published in a
language other than English. These inclusion and exclusion
criteria aimed to minimize any classification bias as to HIV
status and to exclude articles which did not provide a
quantitative measure of the association between ATS use
and HIV infection.
Quality assessment
The article quality was assessed using quality assessment
criteria adapted for cross-sectional studies from Boyle [79]
Nga Thi Thu Vu et al. Journal of the International AIDS Society 2015, 18:19273
http://www.jiasociety.org/index.php/jias/article/view/19273 | http://dx.doi.org/10.7448/IAS.18.1.19273
2
111

and for case-control and longitudinal studies from Wells et al.
[80] (the checklist is provided in Supplementary 1). According
to these quality criteria, a score of 1 was assigned for each of
the items included and articles were assigned a summative
score on a scale of 0 to 9 for cross-sectional studies, 0�10for case-control studies and 0�11 for longitudinal studies.
All scores were categorized into high- and low-quality groups
based on the cut off of 50%.
Data extraction
Extracted information included the primary author, year of
publication, country of research, sampling method(s), sample
size, type of drug(s) examined and recall periods, basic
participant characteristics (e.g. age, sexual identification) and
either a crude measure of association with 95% CI or data to
calculate it. If articles reported more than one drug or used
more than one recall period, each measure of drug use
at each recall period was extracted as a separate record.
Measures of association reported without 95% CIs were not
extracted. Extracted data from cross-sectional and case-
control studies were used to calculate prevalence rate ratios
(PRR) [81] and odds ratios (OR), respectively. For longitudinal
studies, we directly extracted hazard ratios (HR) or relative
risk (RR) with 95% CI as a measure of association between
ATS use and HIV seroconversion. Data extraction was carried
out by Nga Thi Thu Vu and Julia Kennedy.
Statistical analysis
Meta-analysis was performed using STATA 13.0 (StataCorp,
College Station, TX, USA) and was stratified by study design
and ATS subgroup (meth/amphetamine vs. ecstasy). We
did not combine effect measures (i.e. PRR, OR and HR) of
all selected studies because of differences in the nature and
calculation methods for each of these measures. In the group
of longitudinal studies, all articles reported HR as a measure
of association, and only Burcham et al. [74] used RR. We
treated this RR as equivalent to HR. The pooled estimates
of the association and their 95% CI were estimated using
random-effects models, as suggested by DerSimonian and
Laird. Heterogeneity was defined by Q statistic when p�0.1
as Hardy et al. [82] had previously reported this method to
have low power. Based on the I2 classification suggested by
Higgins and Thompson [83], we used the cut-offs of 25, 50
and 75% to define low, medium and high levels of hetero-
geneity, respectively [84]. Sources of heterogeneity were
checked using subgroup analysis and meta-regression [85].
The variables for meta-regression included the study quality
score (high vs. low), ATS group (meth/amphetamines vs.
ecstasy) and study location (high vs. low- and middle-income
countries (LMIC), as according to World Bank income classi-
fication, sampling location (clinic based vs. other), drug use
recall period (recent use vs. lifetime use), injecting drug use
reporting (Yes vs. No) and other specific drug use measure-
ments, that is, nitrite inhalants, heroin, cocaine and EDM use
(Yes vs. No). Injecting drug use, specifically needle and
syringe sharing and these specific drug use behaviours were
assessed because they were found to be associated with
HIV infection and/ or unprotected risky sexual behaviours
[45,69,72,86,87], therefore, may be confounders of the
association between ATS use and sexually transmitted HIV
infection. Sensitivity analysis was performed by the Compre-
hensive Meta-Analysis software V2.0 (Biostat, Englewood,
New Jersey) to explore any possible influence of abnormal or
outlier data on pooled estimates. Publication bias and the
effects of small sample sizes were evaluated in a funnel plot
[88]. Asymmetry of the funnel plot was tested as recom-
mended by Egger et al. [89].
ResultsThe flow of the review process is shown in Figure 1. We
identified 6710 unique article titles, 262 of which progressed
to full text screening, resulting in 42 articles relevant for this
review (list of excluded articles is provided upon request).
The review yielded six additional articles: two from reference
lists [69,77] and four from corresponding authors of articles
reporting only composite measures of drug use [46,47,53,59].
We contacted by email 30 authors of manuscripts which re-
ported composite drug use measures and received seven
responses: four [46,47,53,59] responded with tabulations of
ATS use and HIV infection and three clarified that ATS had not
been measured in their study or was not analyzed [90�92].Seven articles provided a descriptive tabulation of ATS and
HIV without analysis of the association with HIV infection
[25,42,49,54,64,65,72]. Because some articles reported more
than one drug used and/or more than one recall period, 58
records were extracted from 36 articles [8,25,42,46�77]. Tworecords were excluded from analysis because of a 0 cell for a
2x2 table [49,93]. Finally, 56 records from 35 studies were
retained for meta-analysis. Records from Van Griensven et al.
[46], Menza et al. [54] and Chesney et al. [69] were taken
from the baseline data of their longitudinal studies; there-
fore, these records were treated as a cross-sectional design
such that PRR was calculated for these records. The HR
reported in Chesney [69] were not comparable with that
measurement in other studies; therefore, these HR were not
included in the analysis.
Description of the selected studies and their participants
Among 35 selected articles, only five were from low- and
middle-income countries (LMIC), while 30 were from the
United States and other high-income countries, specifically
The Netherlands, Australia and the United Kingdom. The
majority of studies (30/35) used convenience, non-random
sampling, and recruited participants using such approaches as
advertising, community outreach, referrals from gay commu-
nity and networks, clients of MSM-specific clinics or HIV
testing centres. Nine studies used purely clinic-based recruit-
ment, sixteen used community-based recruitment and ten
used both. Most of the articles (26/35) reported a global
measure of drug use with different recall periods, including
1, 3, 6, or 12 months and lifetime use; five articles
[8,51,55,58,63] reported a contextual measure of ATS use in
relation to sex, and the remaining articles did not specify the
recall period. Almost all of the study had a quality score larger
than 50%, only seven studies, among which one from the
LMIC countries, had a quality score lower than 50%.
Table 1 presents the characteristics of studies selected for
meta-analysis and their participants. Regarding ATS use, the
majority of articles reported the use of methamphetamine
Nga Thi Thu Vu et al. Journal of the International AIDS Society 2015, 18:19273
http://www.jiasociety.org/index.php/jias/article/view/19273 | http://dx.doi.org/10.7448/IAS.18.1.19273
3
112
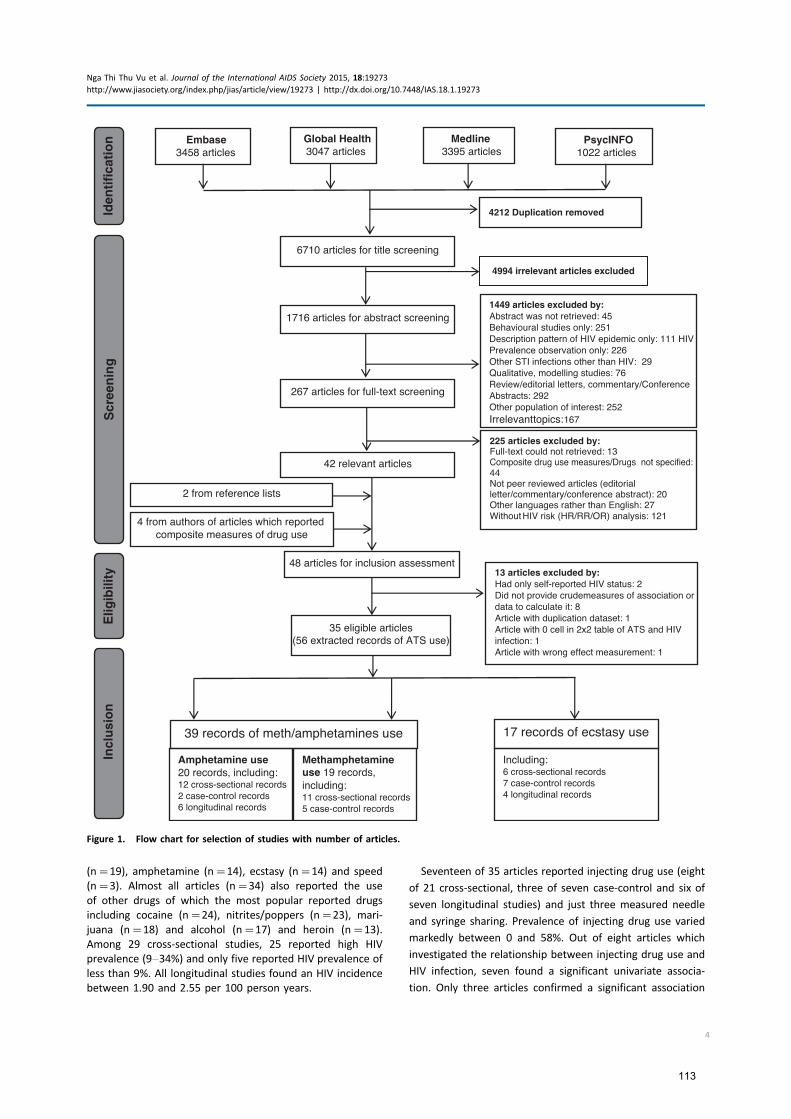
(n�19), amphetamine (n�14), ecstasy (n�14) and speed
(n�3). Almost all articles (n�34) also reported the use
of other drugs of which the most popular reported drugs
including cocaine (n�24), nitrites/poppers (n�23), mari-
juana (n�18) and alcohol (n�17) and heroin (n�13).
Among 29 cross-sectional studies, 25 reported high HIV
prevalence (9�34%) and only five reported HIV prevalence of
less than 9%. All longitudinal studies found an HIV incidence
between 1.90 and 2.55 per 100 person years.
Seventeen of 35 articles reported injecting drug use (eight
of 21 cross-sectional, three of seven case-control and six of
seven longitudinal studies) and just three measured needle
and syringe sharing. Prevalence of injecting drug use varied
markedly between 0 and 58%. Out of eight articles which
investigated the relationship between injecting drug use and
HIV infection, seven found a significant univariate associa-
tion. Only three articles confirmed a significant association
Elig
ibili
tyId
enti
fica
tio
nS
cree
nin
gIn
clu
sio
n
42 relevant articles
Embase3458 articles
Global Health3047 articles
Medline3395 articles
PsycINFO1022 articles
6710 articles for title screening
1716 articles for abstract screening
267 articles for full-text screening
48 articles for inclusion assessment
2 from reference lists
4 from authors of articles which reported composite measures of drug use
Article with wrong effect measurement: 1
35 eligible articles(56 extracted records of ATS use)
Amphetamine use 20 records, including:12 cross-sectional records2 case-control records6 longitudinal records
Including:6 cross-sectional records7 case-control records4 longitudinal records
Methamphetamine use 19 records, including:11 cross-sectional records5 case-control records
39 records of meth/amphetamines use 17 records of ecstasy use
4212 Duplication removed
1449 articles excluded by:Abstract was not retrieved: 45 Behavioural studies only: 251Description pattern of HIV epidemic only: 111 HIV Prevalence observation only: 226Other STI infections other than HIV: 29Qualitative, modelling studies: 76Review/editorial letters, commentary/Conference Abstracts: 292Other population of interest: 252Irrelevant topics: 167
225 articles excluded by:Full-text could not retrieved: 13Composite drug use measures/Drugs not specified: 44Not peer reviewed articles (editorial letter/commentary/conference abstract): 20 Other languages rather than English: 27 Without HIV risk (HR/RR/OR) analysis: 121
13 articles excluded by:Had only self-reported HIV status: 2Did not provide crudemeasures of association or data to calculate it: 8Article with duplication dataset: 1Article with 0 cell in 2x2 table of ATS and HIV infection: 1
4994 irrelevant articles excluded
Figure 1. Flow chart for selection of studies with number of articles.
Nga Thi Thu Vu et al. Journal of the International AIDS Society 2015, 18:19273
http://www.jiasociety.org/index.php/jias/article/view/19273 | http://dx.doi.org/10.7448/IAS.18.1.19273
4
113
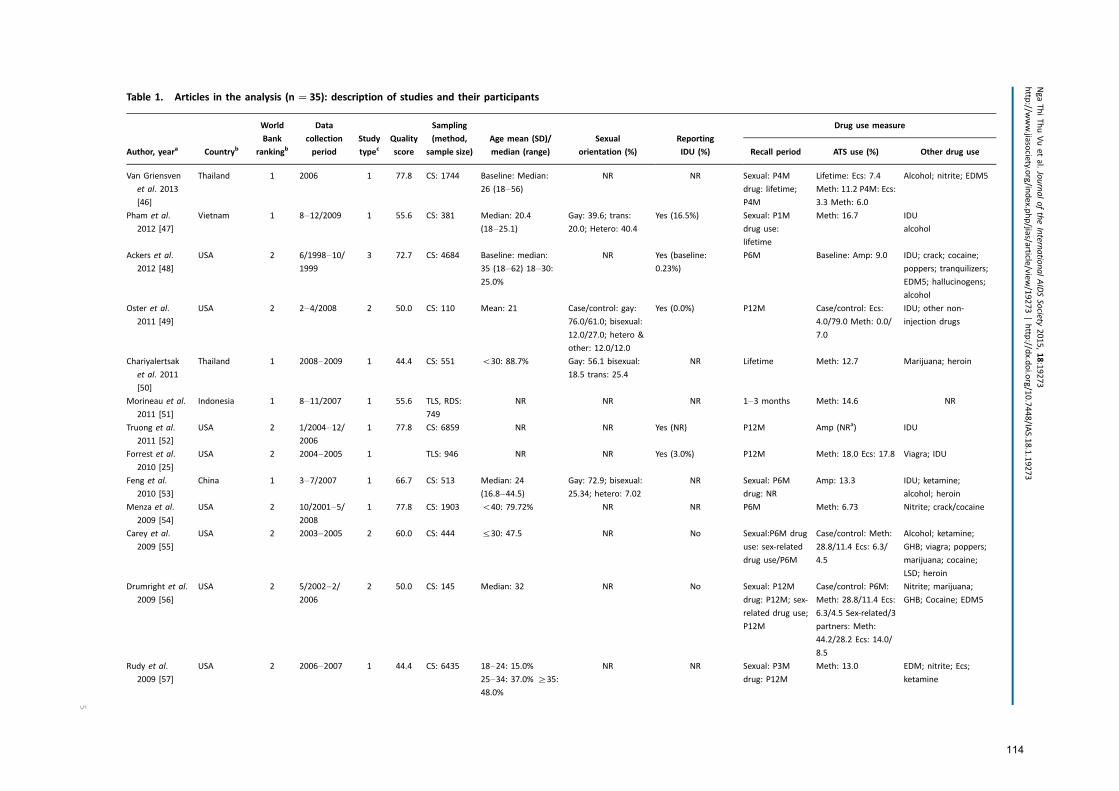
Table 1. Articles in the analysis (n �35): description of studies and their participants
Author, yeara Countryb
World
Bank
rankingb
Data
collection
period
Study
typecQuality
score
Sampling
(method,
sample size)
Age mean (SD)/
median (range)
Sexual
orientation (%)
Reporting
IDU (%)
Drug use measure
Recall period ATS use (%) Other drug use
Van Griensven
et al. 2013
[46]
Thailand 1 2006 1 77.8 CS: 1744 Baseline: Median:
26 (18�56)NR NR Sexual: P4M
drug: lifetime;
P4M
Lifetime: Ecs: 7.4
Meth: 11.2 P4M: Ecs:
3.3 Meth: 6.0
Alcohol; nitrite; EDM5
Pham et al.
2012 [47]
Vietnam 1 8�12/2009 1 55.6 CS: 381 Median: 20.4
(18�25.1)Gay: 39.6; trans:
20.0; Hetero: 40.4
Yes (16.5%) Sexual: P1M
drug use:
lifetime
Meth: 16.7 IDU
alcohol
Ackers et al.
2012 [48]
USA 2 6/1998�10/1999
3 72.7 CS: 4684 Baseline: median:
35 (18�62) 18�30:25.0%
NR Yes (baseline:
0.23%)
P6M Baseline: Amp: 9.0 IDU; crack; cocaine;
poppers; tranquilizers;
EDM5; hallucinogens;
alcohol
Oster et al.
2011 [49]
USA 2 2�4/2008 2 50.0 CS: 110 Mean: 21 Case/control: gay:
76.0/61.0; bisexual:
12.0/27.0; hetero &
other: 12.0/12.0
Yes (0.0%) P12M Case/control: Ecs:
4.0/79.0 Meth: 0.0/
7.0
IDU; other non-
injection drugs
Chariyalertsak
et al. 2011
[50]
Thailand 1 2008�2009 1 44.4 CS: 551 B30: 88.7% Gay: 56.1 bisexual:
18.5 trans: 25.4
NR Lifetime Meth: 12.7 Marijuana; heroin
Morineau et al.
2011 [51]
Indonesia 1 8�11/2007 1 55.6 TLS, RDS:
749
NR NR NR 1�3 months Meth: 14.6 NR
Truong et al.
2011 [52]
USA 2 1/2004�12/2006
1 77.8 CS: 6859 NR NR Yes (NR) P12M Amp (NRa) IDU
Forrest et al.
2010 [25]
USA 2 2004�2005 1 TLS: 946 NR NR Yes (3.0%) P12M Meth: 18.0 Ecs: 17.8 Viagra; IDU
Feng et al.
2010 [53]
China 1 3�7/2007 1 66.7 CS: 513 Median: 24
(16.8�44.5)Gay: 72.9; bisexual:
25.34; hetero: 7.02
NR Sexual: P6M
drug: NR
Amp: 13.3 IDU; ketamine;
alcohol; heroin
Menza et al.
2009 [54]
USA 2 10/2001�5/2008
1 77.8 CS: 1903 B40: 79.72% NR NR P6M Meth: 6.73 Nitrite; crack/cocaine
Carey et al.
2009 [55]
USA 2 2003�2005 2 60.0 CS: 444 530: 47.5 NR No Sexual:P6M drug
use: sex-related
drug use/P6M
Case/control: Meth:
28.8/11.4 Ecs: 6.3/
4.5
Alcohol; ketamine;
GHB; viagra; poppers;
marijuana; cocaine;
LSD; heroin
Drumright et al.
2009 [56]
USA 2 5/2002�2/2006
2 50.0 CS: 145 Median: 32 NR No Sexual: P12M
drug: P12M; sex-
related drug use;
P12M
Case/control: P6M:
Meth: 28.8/11.4 Ecs:
6.3/4.5 Sex-related/3
partners: Meth:
44.2/28.2 Ecs: 14.0/
8.5
Nitrite; marijuana;
GHB; Cocaine; EDM5
Rudy et al.
2009 [57]
USA 2 2006�2007 1 44.4 CS: 6435 18�24: 15.0%25�34: 37.0% ]35:
48.0%
NR NR Sexual: P3M
drug: P12M
Meth: 13.0 EDM; nitrite; Ecs;
ketamine
NgaThiThuVuetal.JournaloftheInternatio
nalAIDSSocie
ty2015,18:19273
http
://www.jia
socie
ty.org/in
dex.p
hp/jia
s/article
/view/19273|http
://dx.d
oi.org/10.7448/IA
S.18.1.19273
5
114
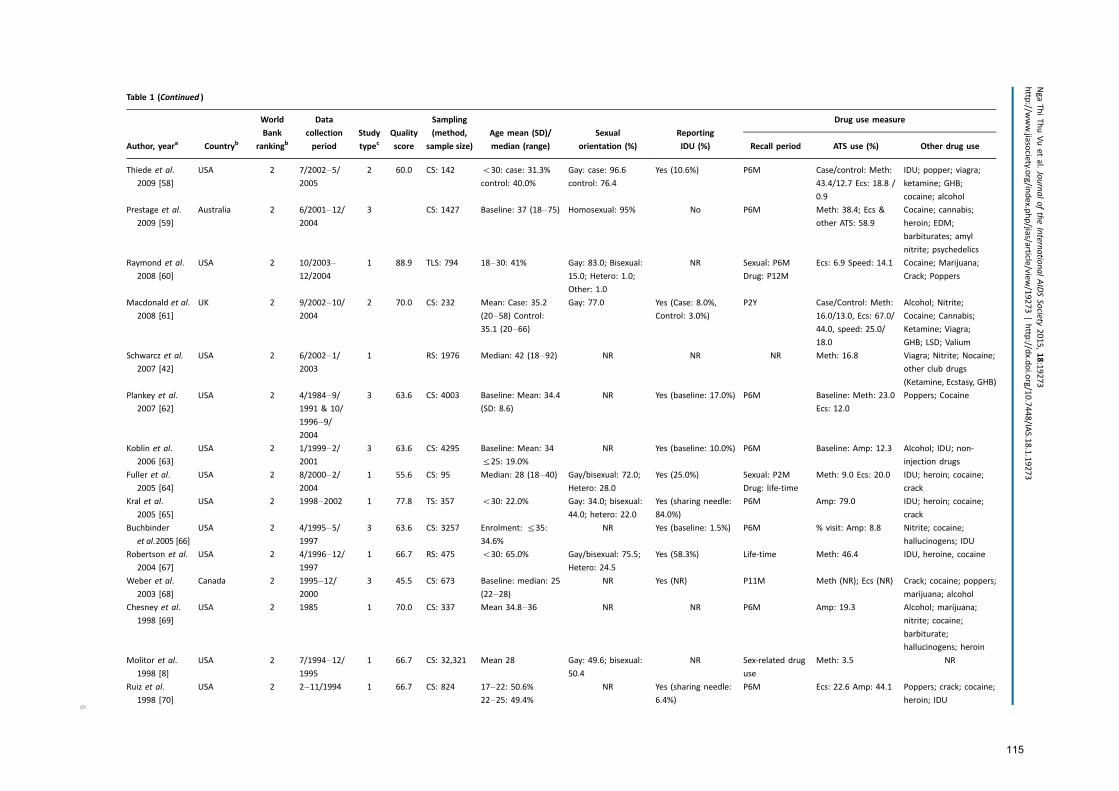
Table 1 (Continued )
Author, yeara Countryb
World
Bank
rankingb
Data
collection
period
Study
typecQuality
score
Sampling
(method,
sample size)
Age mean (SD)/
median (range)
Sexual
orientation (%)
Reporting
IDU (%)
Drug use measure
Recall period ATS use (%) Other drug use
Thiede et al.
2009 [58]
USA 2 7/2002�5/2005
2 60.0 CS: 142 B30: case: 31.3%
control: 40.0%
Gay: case: 96.6
control: 76.4
Yes (10.6%) P6M Case/control: Meth:
43.4/12.7 Ecs: 18.8 /
0.9
IDU; popper; viagra;
ketamine; GHB;
cocaine; alcohol
Prestage et al.
2009 [59]
Australia 2 6/2001�12/2004
3 CS: 1427 Baseline: 37 (18�75) Homosexual: 95% No P6M Meth: 38.4; Ecs &
other ATS: 58.9
Cocaine; cannabis;
heroin; EDM;
barbiturates; amyl
nitrite; psychedelics
Raymond et al.
2008 [60]
USA 2 10/2003�12/2004
1 88.9 TLS: 794 18�30: 41% Gay: 83.0; Bisexual:
15.0; Hetero: 1.0;
Other: 1.0
NR Sexual: P6M
Drug: P12M
Ecs: 6.9 Speed: 14.1 Cocaine; Marijuana;
Crack; Poppers
Macdonald et al.
2008 [61]
UK 2 9/2002�10/2004
2 70.0 CS: 232 Mean: Case: 35.2
(20�58) Control:35.1 (20�66)
Gay: 77.0 Yes (Case: 8.0%,
Control: 3.0%)
P2Y Case/Control: Meth:
16.0/13.0, Ecs: 67.0/
44.0, speed: 25.0/
18.0
Alcohol; Nitrite;
Cocaine; Cannabis;
Ketamine; Viagra;
GHB; LSD; Valium
Schwarcz et al.
2007 [42]
USA 2 6/2002�1/2003
1 RS: 1976 Median: 42 (18�92) NR NR NR Meth: 16.8 Viagra; Nitrite; Nocaine;
other club drugs
(Ketamine, Ecstasy, GHB)
Plankey et al.
2007 [62]
USA 2 4/1984�9/1991 & 10/
1996�9/2004
3 63.6 CS: 4003 Baseline: Mean: 34.4
(SD: 8.6)
NR Yes (baseline: 17.0%) P6M Baseline: Meth: 23.0
Ecs: 12.0
Poppers; Cocaine
Koblin et al.
2006 [63]
USA 2 1/1999�2/2001
3 63.6 CS: 4295 Baseline: Mean: 34
525: 19.0%
NR Yes (baseline: 10.0%) P6M Baseline: Amp: 12.3 Alcohol; IDU; non-
injection drugs
Fuller et al.
2005 [64]
USA 2 8/2000�2/2004
1 55.6 CS: 95 Median: 28 (18�40) Gay/bisexual: 72.0;
Hetero: 28.0
Yes (25.0%) Sexual: P2M
Drug: life-time
Meth: 9.0 Ecs: 20.0 IDU; heroin; cocaine;
crack
Kral et al.
2005 [65]
USA 2 1998�2002 1 77.8 TS: 357 B30: 22.0% Gay: 34.0; bisexual:
44.0; hetero: 22.0
Yes (sharing needle:
84.0%)
P6M Amp: 79.0 IDU; heroin; cocaine;
crack
Buchbinder
et al.2005 [66]
USA 2 4/1995�5/1997
3 63.6 CS: 3257 Enrolment: 535:
34.6%
NR Yes (baseline: 1.5%) P6M % visit: Amp: 8.8 Nitrite; cocaine;
hallucinogens; IDU
Robertson et al.
2004 [67]
USA 2 4/1996�12/1997
1 66.7 RS: 475 B30: 65.0% Gay/bisexual: 75.5;
Hetero: 24.5
Yes (58.3%) Life-time Meth: 46.4 IDU, heroine, cocaine
Weber et al.
2003 [68]
Canada 2 1995�12/2000
3 45.5 CS: 673 Baseline: median: 25
(22�28)NR Yes (NR) P11M Meth (NR); Ecs (NR) Crack; cocaine; poppers;
marijuana; alcohol
Chesney et al.
1998 [69]
USA 2 1985 1 70.0 CS: 337 Mean 34.8�36 NR NR P6M Amp: 19.3 Alcohol; marijuana;
nitrite; cocaine;
barbiturate;
hallucinogens; heroin
Molitor et al.
1998 [8]
USA 2 7/1994�12/1995
1 66.7 CS: 32,321 Mean 28 Gay: 49.6; bisexual:
50.4
NR Sex-related drug
use
Meth: 3.5 NR
Ruiz et al.
1998 [70]
USA 2 2�11/1994 1 66.7 CS: 824 17�22: 50.6%22�25: 49.4%
NR Yes (sharing needle:
6.4%)
P6M Ecs: 22.6 Amp: 44.1 Poppers; crack; cocaine;
heroin; IDU
NgaThiThuVuetal.JournaloftheInternatio
nalAIDSSocie
ty2015,18:19273
http
://www.jia
socie
ty.org/in
dex.p
hp/jia
s/article
/view/19273|http
://dx.d
oi.org/10.7448/IA
S.18.1.19273
6
115
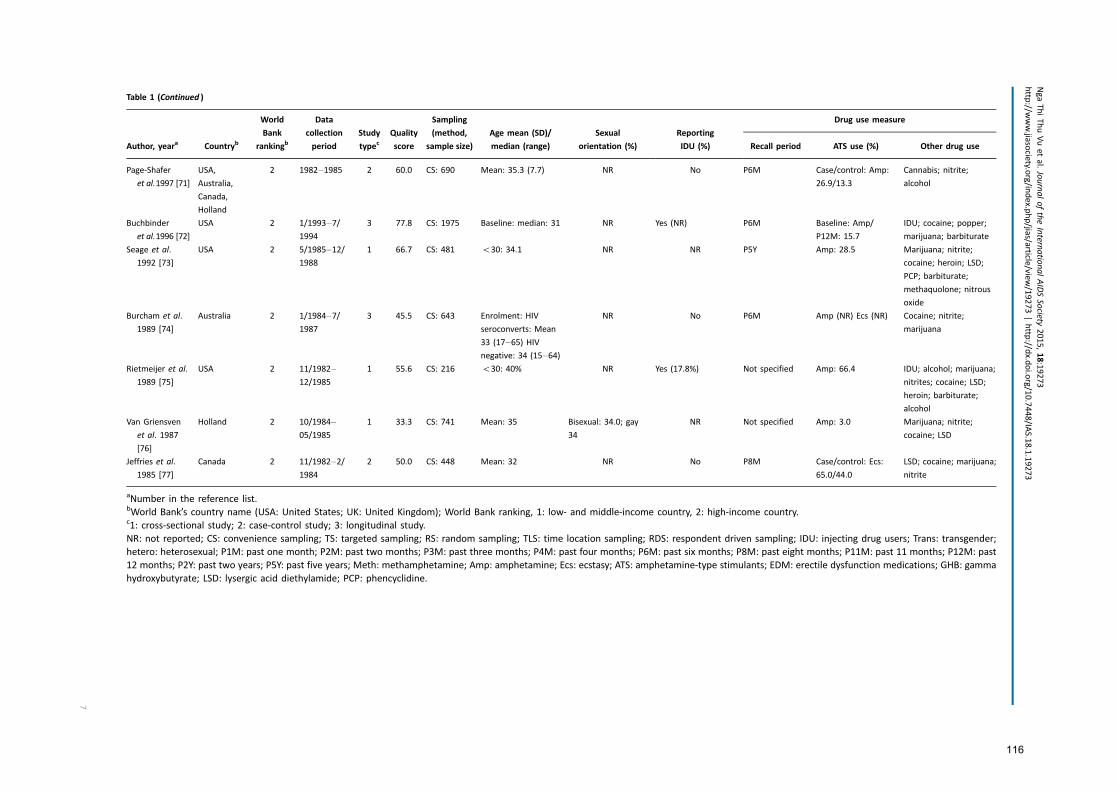
Table 1 (Continued )
Author, yeara Countryb
World
Bank
rankingb
Data
collection
period
Study
typecQuality
score
Sampling
(method,
sample size)
Age mean (SD)/
median (range)
Sexual
orientation (%)
Reporting
IDU (%)
Drug use measure
Recall period ATS use (%) Other drug use
Page-Shafer
et al.1997 [71]
USA,
Australia,
Canada,
Holland
2 1982�1985 2 60.0 CS: 690 Mean: 35.3 (7.7) NR No P6M Case/control: Amp:
26.9/13.3
Cannabis; nitrite;
alcohol
Buchbinder
et al.1996 [72]
USA 2 1/1993�7/1994
3 77.8 CS: 1975 Baseline: median: 31 NR Yes (NR) P6M Baseline: Amp/
P12M: 15.7
IDU; cocaine; popper;
marijuana; barbiturate
Seage et al.
1992 [73]
USA 2 5/1985�12/1988
1 66.7 CS: 481 B30: 34.1 NR NR P5Y Amp: 28.5 Marijuana; nitrite;
cocaine; heroin; LSD;
PCP; barbiturate;
methaquolone; nitrous
oxide
Burcham et al.
1989 [74]
Australia 2 1/1984�7/1987
3 45.5 CS: 643 Enrolment: HIV
seroconverts: Mean
33 (17�65) HIVnegative: 34 (15�64)
NR No P6M Amp (NR) Ecs (NR) Cocaine; nitrite;
marijuana
Rietmeijer et al.
1989 [75]
USA 2 11/1982�12/1985
1 55.6 CS: 216 B30: 40% NR Yes (17.8%) Not specified Amp: 66.4 IDU; alcohol; marijuana;
nitrites; cocaine; LSD;
heroin; barbiturate;
alcohol
Van Griensven
et al. 1987
[76]
Holland 2 10/1984�05/1985
1 33.3 CS: 741 Mean: 35 Bisexual: 34.0; gay
34
NR Not specified Amp: 3.0 Marijuana; nitrite;
cocaine; LSD
Jeffries et al.
1985 [77]
Canada 2 11/1982�2/1984
2 50.0 CS: 448 Mean: 32 NR No P8M Case/control: Ecs:
65.0/44.0
LSD; cocaine; marijuana;
nitrite
aNumber in the reference list.bWorld Bank’s country name (USA: United States; UK: United Kingdom); World Bank ranking, 1: low- and middle-income country, 2: high-income country.c1: cross-sectional study; 2: case-control study; 3: longitudinal study.
NR: not reported; CS: convenience sampling; TS: targeted sampling; RS: random sampling; TLS: time location sampling; RDS: respondent driven sampling; IDU: injecting drug users; Trans: transgender;
hetero: heterosexual; P1M: past one month; P2M: past two months; P3M: past three months; P4M: past four months; P6M: past six months; P8M: past eight months; P11M: past 11 months; P12M: past
12 months; P2Y: past two years; P5Y: past five years; Meth: methamphetamine; Amp: amphetamine; Ecs: ecstasy; ATS: amphetamine-type stimulants; EDM: erectile dysfunction medications; GHB: gamma
hydroxybutyrate; LSD: lysergic acid diethylamide; PCP: phencyclidine.
NgaThiThuVuetal.JournaloftheInternatio
nalAIDSSocie
ty2015,18:19273
http
://www.jia
socie
ty.org/in
dex.p
hp/jia
s/article
/view/19273|http
://dx.d
oi.org/10.7448/IA
S.18.1.19273
7
116
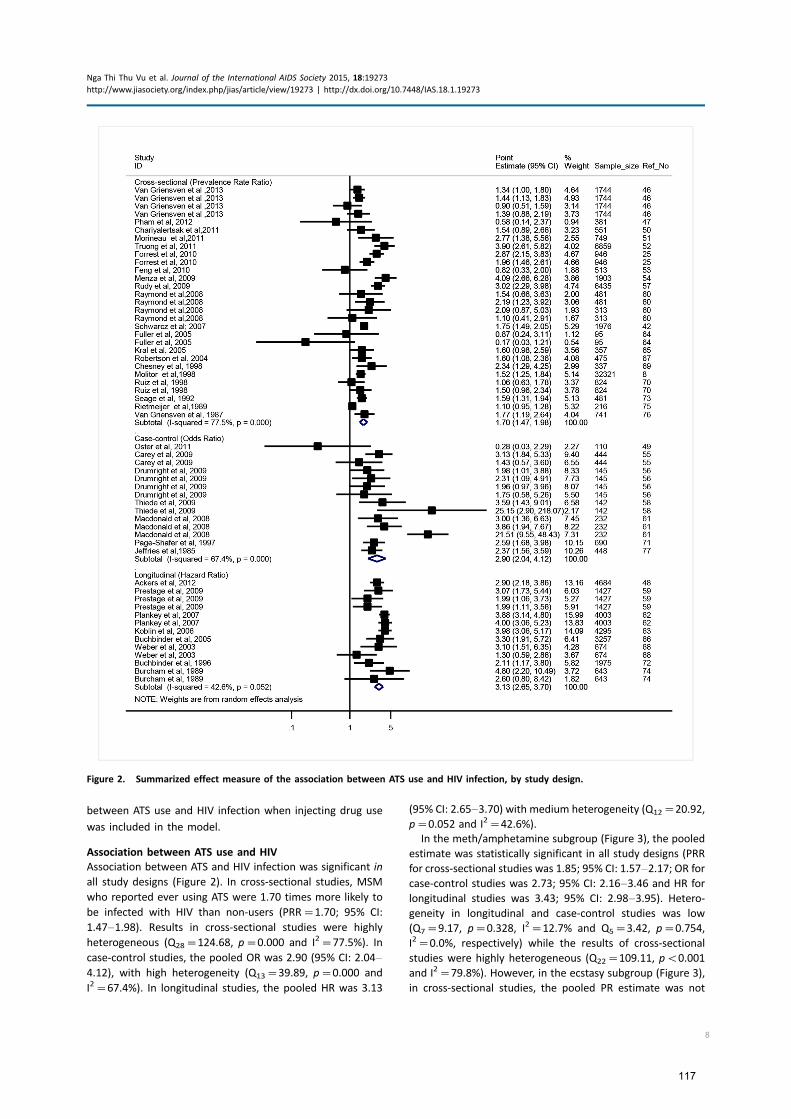
between ATS use and HIV infection when injecting drug use
was included in the model.
Association between ATS use and HIV
Association between ATS and HIV infection was significant in
all study designs (Figure 2). In cross-sectional studies, MSM
who reported ever using ATS were 1.70 times more likely to
be infected with HIV than non-users (PRR�1.70; 95% CI:
1.47�1.98). Results in cross-sectional studies were highly
heterogeneous (Q28�124.68, p�0.000 and I2�77.5%). In
case-control studies, the pooled OR was 2.90 (95% CI: 2.04�4.12), with high heterogeneity (Q13�39.89, p�0.000 and
I2�67.4%). In longitudinal studies, the pooled HR was 3.13
(95% CI: 2.65�3.70) with medium heterogeneity (Q12�20.92,
p�0.052 and I2�42.6%).
In the meth/amphetamine subgroup (Figure 3), the pooled
estimate was statistically significant in all study designs (PRR
for cross-sectional studies was 1.85; 95% CI: 1.57�2.17; OR for
case-control studies was 2.73; 95% CI: 2.16�3.46 and HR for
longitudinal studies was 3.43; 95% CI: 2.98�3.95). Hetero-geneity in longitudinal and case-control studies was low
(Q7�9.17, p�0.328, I2�12.7% and Q5�3.42, p�0.754,
I2�0.0%, respectively) while the results of cross-sectional
studies were highly heterogeneous (Q22�109.11, pB0.001
and I2�79.8%). However, in the ecstasy subgroup (Figure 3),
in cross-sectional studies, the pooled PR estimate was not
Figure 2. Summarized effect measure of the association between ATS use and HIV infection, by study design.
Nga Thi Thu Vu et al. Journal of the International AIDS Society 2015, 18:19273
http://www.jiasociety.org/index.php/jias/article/view/19273 | http://dx.doi.org/10.7448/IAS.18.1.19273
8
117
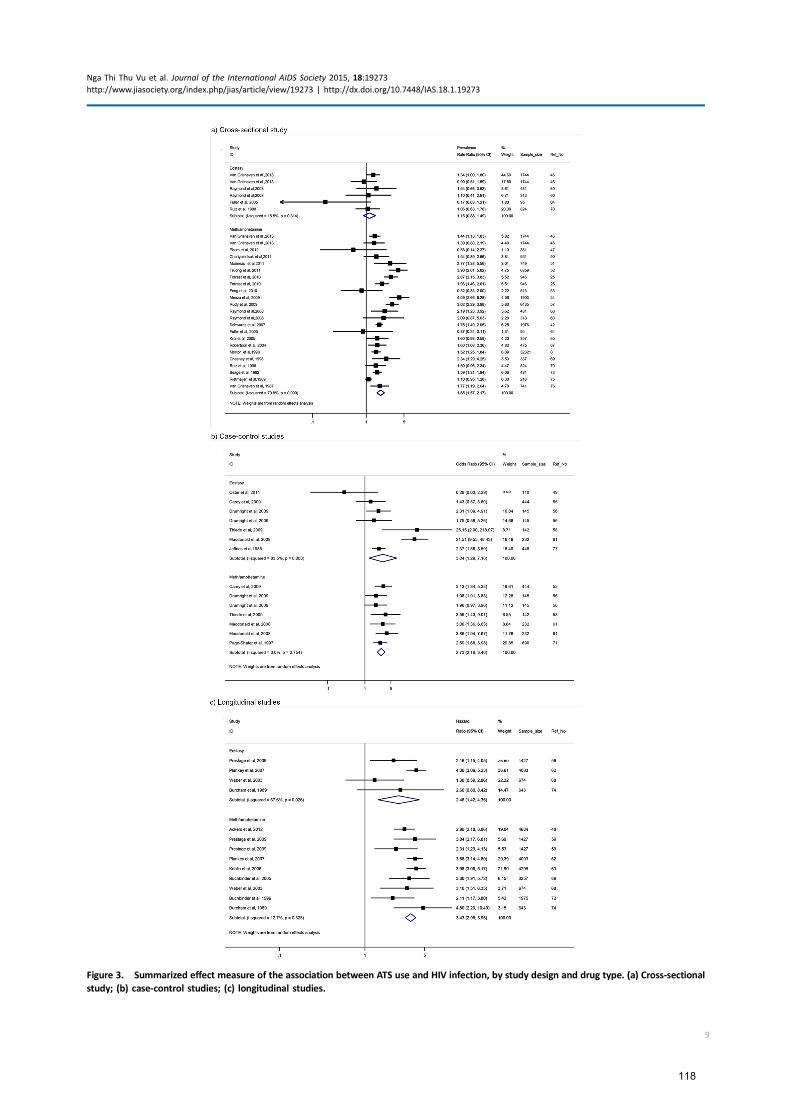
Figure 3. Summarized effect measure of the association between ATS use and HIV infection, by study design and drug type. (a) Cross-sectional
study; (b) case-control studies; (c) longitudinal studies.
Nga Thi Thu Vu et al. Journal of the International AIDS Society 2015, 18:19273
http://www.jiasociety.org/index.php/jias/article/view/19273 | http://dx.doi.org/10.7448/IAS.18.1.19273
9
118

statistically significant (PR�1.15; 95% CI: 0.88�1.49), withlow heterogeneity (Q5�5.92, p�0.314 and I2�15.5%). In
case-control studies, the pooled OR estimate was significant
(OR�3.04 (95% CI: 1.29�7.18), with high heterogeneity
(Q5�36.33, p�0.000 and I2�83.5%). Similarly, the pooled
HR estimate was statistically significant (HR�2.48; 95% CI:
1.42�4.35), with high heterogeneity (Q3�9.26, p�0.026
and I2�67.6%). Sources of heterogeneity among cross-
sectional studies were presented in Table 2. Due to the
limited number of selected case-control and longitudinal
articles and because of low power of Q statistic [82],
the test of heterogeneity in these study designs was not
conducted.
Sources of heterogeneity in cross-sectional studies
The results of subgroup analysis are presented in Table 2.
Sampling locations, ATS subgroup, recall period for drug use,
reporting EDM use and alcohol consumption were respon-
sible for a high heterogeneity of the results in cross-sectional
studies. The pooled estimates of the association between ATS
use and HIV were significantly higher in studies which re-
cruited participants in clinics rather than in other locations;
used measures of recent versus lifetime drug use; reported
EDM use (yes vs. no) or alcohol consumption (yes vs. no).
Finally, the pooled PRR is higher in studies that reported
meth/amphetamine use versus ecstasy use.
Sensitivity analysis
None of the individual study results noticeably affected the
pooled estimate for longitudinal and cross-sectional studies.
In relation to case-control studies, the pooled OR decreased
by 13.6% (from OR�2.9; 95% CI: 2.04�4.11 to OR�2.51;
95% CI: 2.02�3.12) when one high OR of a record of ecstasy
use reported by Macdonald et al. [61] was excluded from the
analysis. This record explained 50.4% of the heterogeneity of
the results.
When restricted to the ecstasy subgroup among case-
control studies, the pooled estimate of the association with
HIV infection was also noticeably affected by the same
record, which was responsible for 34.9% of the heterogeneity.
After excluding this record, the pooled OR decreased by
32.2% (from OR�3.04; 95% CI: 1.29�7.18 to OR�2.06; 95%
CI: 1.19�3.58).
Publication bias
The funnel plot of all selected studies (Supplementary 2)
indicates potential publication bias. However, the result of
the test for symmetry of the funnel plot was not statistically
significant, suggesting no small sample size effect.
DiscussionOur review andmeta-analysis of the published evidence found
a statistically significant relationship between ATS use and HIV
infection. The use of meth/amphetamines was significantly
associated with HIV infection in all study designs, while ecstasy
use was not associated with HIV in cross-sectional studies. The
pooled estimate from case-control studies had low hetero-
geneity and the significant pooled HR from longitudinal
studies was affected by studies with large samples and highly
significant results [62]. The pooled estimates of case-control
studies were affected by a record from study of Macdonald
et al. [61]; however, while the exclusion of this record in the
analysis resulted in decreasing the effect size; it did not change
the significance of the overall effect size.The pooled estimates
of cross-sectional studies were heterogeneous as a result of
sampling location approach, different drug use recall periods
and the diversity of different drug use measurement. Our
findings of the relationship between ATS and HIV infection are
consistent with results from a previous review by Drumright
et al. [45]; that review covered fewer studies. It found that
Table 2. Stratification analysis for cross-sectional studies
Study
characteristic
No. of
records
Meta-regression
(b, p-value)aPooled PR
(95% CI)b
Study location
LMIC countries 8 b�0.72, p�0.086 1.36 (1.12�1.65)
High-income
countries
21 1.85 (1.54�2.21)
Study quality
Low 3 b�1.34, p�0.289 2.10 (1.36�3.27)
High 26 1.66 (1.42�1.94)
Sampling
locations
Clinic-based
sample
6 b�1.66, p�0.005 2.53 (1.70�3.77)
Other venues 23 1.52 (1.32�1.76)
Drug use recall
period
Recent use 19 b�1.42, p�0.047 1.93 (1.57�2.37)
Lifetime use 9 1.38 (1.19�1.61)
Reported injecting
drugs
No 20 b�1.02, p�0.914 1.70 (1.46�1.97)
Yes 9 1.62 (1.09�2.42)
Type of ATS
Amphetamines 23 b�0.59, p�0.02 1.85 (1.57�2.17)
Ecstasy 6 1.15 (0.88�1.49)
Reported alcohol
use
No 21 b�0.69, p�0.039 1.90 (1.61�2.45)
Yes 8 1.30 (1.10�1.54)
Cocaine use
No 13 b�0.74, p�0.106 1.78 (1.40�2.25)
Yes 16 1.63 (1.34�1.98)
Heroin use
No 17 b�1.04, p�0.84 1.96 (1.63�2.36)
Yes 12 1.35 (1.12�1.64)
EDM use
No 21 b�0.60, p�0.003 1.67 (1.37�2.03)
Yes 8 1.77 (1.40�2.24)
aSignificant p-value indicates significant source of heterogeneity.
Results from meta-regression analysis.bResults from subgroup analysis.
LMIC: low- and middle-income countries.
Nga Thi Thu Vu et al. Journal of the International AIDS Society 2015, 18:19273
http://www.jiasociety.org/index.php/jias/article/view/19273 | http://dx.doi.org/10.7448/IAS.18.1.19273
10
119

meth/amphetamine use was associatedwith HIV infection and
reported insufficient evidence of an association between
ecstasy and HIV infection. More recently, a meta-analysis of
the relationship between ecstasy use and risky sexual behavi-
our by Hittner et al. found ecstasy use to be significantly
associated with behaviours associated with HIV infection [20],
but that review combined different sexual outcomes and
did not specifically focus on MSM. Our finding of consis-
tently significant pooled estimates of the association between
meth/amphetamine use and HIV infection in all study designs
proves the robustness of this association and echoes the
finding of Vosburgh et al. [87] that methamphetamine
was associated with event-level measurement of sexual risk
behaviour among MSM.
Differences in the relationship between meth/amphetamine
and ecstasy with HIV infection can potentially be explained
by their different sexual behavioural effects. Previous re-
search has found that meth/amphetamines facilitate sexual
disinhibition and experimentation [9], increase sexual desire
and facilitate sexual marathons [11] in which men practice
prolonged sexual encounters with different sexual par-
tners for hours and days [94]. Prestage et al. found that
meth/amphetamines have often been combined with orally
administered erectile dysfunction medications to further
enhance sexual performance [59]. Unprotected sex is com-
mon in these contexts, as are lesions due to forceful sexual
penetration and increased likelihood of condom failure, all of
which can increase the risk of sexual transmission of HIV [94].
Furthermore, high dose of methamphetamine was found to
increase anal sensation for receptive partners, thus promoting
receptive positioning in anal sex which is the practice of
highest risk in sexual transmission of HIV among MSM [44]. In
relation to ecstasy, where reported effects include improved
sexual performance and satisfaction [13,14], participants
also reported enhanced sensuality rather than sexuality [17]
and increased feelings of intimacy and emotional closeness
[20,21]. Such effects may compensate for the negative effects
associated with condom use such as decreased sensuality and
sexual satisfaction. These effects may account for the lack of
consistency of findings in relation to ecstasy observed across
different studies included in our review. However, it is
important to acknowledge that the pooled estimate of
association between ecstasy and HIV infection was signifi-
cant in case-control and longitudinal studies which provided
stronger evidence than cross-sectional studies. This find-
ing may suggest that a more robust approach to study the
relationship between ecstasy and HIV infection should be
explored in future studies.
Our review highlights the methodological limitations of
current research. First, many studies used composite mea-
sures of drug use (e.g. any drug use) which ignore the different
effects of specific drugs on sexual behaviour and ultimately on
HIV transmission. Second, most studies used global measures
of ATS use (that is measures unrelated to sexual encounters)
with various recall periods from one month to lifetime use.
Only five articles [8,51,55,58,63] reported situational or
contextual drug use in which ATS were taken before or during
sexual intercourse, but not during a specific event. As early as
1993, Leigh and Stall [95] recommended the use of event-
specific measures of ATS use in relation to sexual encounters
to enable assessment of the causal relationship between ATS
use and HIV infection. Our review, conducted in 2013, was
unable to find any studies which used the recommended
measures. Third, a number of studies, including reviews,
explored the relationship between ATS use and HIV infection
[5,45,96] but not its nature or pathway; therefore, the
question about causality of this relationship remains largely
unanswered. Future research should take into account the
methodological limitations of current studies on ATS use.
Studies should adopt study designs, sampling methods and
ATS use measures which would allow investigating and better
understanding the temporal relationship between ATS use and
HIV infection among MSM. Our analysis found that most
studies were also based on opportunistic samples recruited
from different source populations. Our finding of a higher
pooled prevalence ratio in cross-sectional studies using
samples purely recruited from clinical settings, compared to
studies which relied on community-based and/or other
recruitment approaches may be explained by the higher
prevalence of ATS use and HIV infection among clinic patients.
Our review also identified an important gap in current
research. While ATS use and HIV infections among MSM are
increasing in many settings, there is little published research
from LMIC. We excluded 27 articles published in languages
other than English. Since 25 of them were from studies
conducted in LMIC countries, it is possible that research from
these countries is underrepresented in this analysis. We were
not able to assess whether these studies investigated the
association between ATS use and HIV infection. We found
only five studies published in English language conducted
in LMIC compared to 30 in high-income countries (all five
studies were cross-sectional in design). As such, general-
ization of the relationship between ATS use and HIV infection
to LMIC may not be appropriate. Further investigation is
warranted in regions where ATS use is highly prevalent, such
as South East Asia, and may be an important co-factor in
increasing HIV transmission among MSM [97].
Our study has limitations that should be born in mind in
interpreting the results. As with all meta-analyses, we were
restricted to data from reports written in English [88]. Our
meta-analysis cannot improve the quality of the results
reported by the original studies and depends on their validity.
The study diversity with respect to designs, sampling frames,
populations, ATS use measures and other drug use measure-
ment, and the heterogeneity of their results, particularly in
cross-sectional and longitudinal studies, may have implica-
tions for our pooled estimates of the association between ATS
use and HIV infection. We assessed heterogeneity of cross-
sectional studies but unfortunately we were not able to do
the same analysis for other study designs due to the small
number of published articles from the longitudinal and case-
control studies. They leave a potential for biased results and
limit their generalizability. An inherent limitation of meta-
analysis is that we could only analyze the role of ATS use in
explaining the variance in HIV infections, and could not
account for the possibility of various confounding factors
which could also explain the association between ATS use and
HIV infections (e.g. the concurrent injecting of drugs, specific
Nga Thi Thu Vu et al. Journal of the International AIDS Society 2015, 18:19273
http://www.jiasociety.org/index.php/jias/article/view/19273 | http://dx.doi.org/10.7448/IAS.18.1.19273
11
120

sexual practices and characteristics of MSM and their net-
works which are the known risk factors for HIV infection). We
should also acknowledge that the cross-sectional or case-
control studies pooled together do not provide information
about the temporal sequence between ATS use and HIV
infection and, therefore, cannot attest to the causality of this
relationship.
ConclusionsThe findings from our meta-analysis confirmed the significant
association between meth/amphetamine use and HIV infec-
tion in all study designs, but there is lack of evidence
(particularly in cross-sectional studies) regarding the role of
ecstasy in HIV infection. Our review and meta-analysis also
revealed important methodological limitations as to the
currently used measures of drug use and their ability to
establish the causal relationship between ATS use and HIV
infection. Finally, our results have implications for policy and
practice. Because ATS are often used in the context of high-
risk unprotected sex, particularly among more adventurous
MSM [11], and a significant number of HIV infections happen
in these contexts [98], HIV prevention programmes targeting
MSM should take into account the role of ATS use, particularly
meth/amphetamines, in HIV transmission. They should also
consider including interventions designed to address meth/
amphetamine use in this population and adopt novel HIV
prevention approaches for MSM at high risk for HIV.
Authors’ affiliations1The Kirby Institute, The University of NSW Australia, Sydney, NSW, Australia;2Centre for Social Research in Health, The University of NSW Australia, Sydney,
NSW, Australia
Competing interests
No declared competing interests.
Authors’ contributions
Nga Thi Thu Vu contributed significant efforts in the development and conduct
of the review, performance of the statistical analysis and drafting of the
manuscript. Iryna Zablotska and Lisa Maher provided oversight in the design,
implementation and interpretation of findings and provided significant input
into the preparation of this manuscript. All authors have seen and approved
the final version of this paper.
Acknowledgements
We are grateful to Julia Kennedy for assistance with reviewing the abstracts,
Eric Chow for assistance with data extraction and Lei Zhang for advice on the
methods of meta-analysis.We thank the researchers who provided information
and further data on our request, including Frits van Griensven, Sarika
Pattanasin and Timothy H. Holtz (Thailand MOPH � US CDC Collaboration,
TUC); Ying Li and Michael W. Plankey (Department of Medicine, Division of
Infectious Diseases, Georgetown University); Quang Duy Pham (Pasteur
Institute, Ho Chi Minh city, Vietnam and Kirby Institute, University of New
South Wales, Australia); Garrett Prestage and Jeff Jin (Kirby Institute, University
of New South Wales); Yuji Feng (Department of Epidemiology, School of Public
Health, University of California, Los Angeles, CA, USA); Alexa Oster (Incidence
and Viral Resistance Team, Division of HIV/AIDS Prevention Centers for Disease
Control and Prevention, USA); Wolfgang Hladik (CGH/DGHA, Centers for
Disease Control and Prevention, USA) and Hillard Weinstock (Surveillance and
Special Studies Team, Epidemiology and Surveillance Branch, Division of STD
Prevention, Centers for Disease Control and Prevention, USA).
Funding
This study was carried out without funding.
References
1. United Nations Office on Drugs and Crime. World drug report 2010.
New York: United Nations; 2010.
2. United Nations Office on Drugs and Crime. World drug report 2013.
New York: United Nations; 2013.
3. Ministerial Council on Drug Strategy. National amphetamine-type stimu-
lants strategy, 2008�2011. Australia: Ministerial Council on Drug Strategy;
2008.
4. Colfax G, Guzman R. Club drugs and HIV infection: a review. Clin Infect Dis.
2006;42(10):1463�9.5. Colfax G, Santos GM, Chu P, Vittinghoff E, Pluddemann A, Kumar S, et al.
Amphetamine-group substances and HIV. Lancet. 2010;376(9739):458�74.6. Davison D, Parrott A. Ecstasy (MDMA) in recreational users: self-reported
psychological and physiological effects. Hum Psychopharmacol Clin Exp. 1997;
12(3):221�6.7. Hall JN, Broderick PM. Community networks for response to abuse out-
breaks of methamphetamine and its analogs. NIDA Res Monogr. 1991;115:
109�20.8. Molitor F, Truax SR, Ruiz JD, Sun RK. Association of methamphetamine use
during sex with risky sexual behaviors and HIV infection among non-injection
drug users. West J Med. 1998;168(2):93�7.9. Semple SJ, Patterson TL, Grant I. Motivations associated with methamphe-
tamine use among HIV� men who have sex with men. J Subst Abuse Treat.
2002;22(3):149�56.10. Kurtz SP. Post-circuit blues: motivations and consequences of crystal meth
use among gay men in Miami. AIDS Behav. 2005;9(1):63�72.11. Prestage G, Grierson J, Bradley J, Hurley M, Hudson J. The role of drugs
during group sex among gay men in Australia. Sex Health. 2009;6(4):310�7.12. Green AI, Halkitis PN. Crystal methamphetamine and sexual sociality in
an urban gay subculture: an elective affinity. Cult Health Sex. 2006;8(4):
317�33.13. Zemishlany Z, Aizenberg D, Weizman A. Subjective effects of MDMA
(‘Ecstasy’) on human sexual function. Eur Psychiatry. 2001;16(2):127�30.14. Baylen CA, Rosenberg H. A review of the acute subjective effects of
MDMA/ecstasy. Addiction. 2006;101(7):933�47.15. Solowij N, Hall W, Lee N. Recreational MDMA use in Sydney: a profile of
‘Ecstacy’ users and their experiences with the drug. Br J Addict. 1992;87(8):
1161�72.16. Cohen RS. Subjective reports on the effects of the MDMA (‘ecstasy’)
experience in humans. Prog Neuropsychopharmacol Biol Psychiatry. 1995;
19(7):1137�45.17. Parrott AC. Human psychopharmacology of ecstasy (MDMA): a review of
15 years of empirical research. Hum Psychopharmacol. 2001;16(8):557�77.18. McElrath K. MDMA and sexual behavior: ecstasy users’ perceptions about
sexuality and sexual risk. Subst Use Misuse. 2005;40(9�10):1461�77.19. Schilder AJ, Lampinen TM, Miller ML, Hogg RS. Crystal methamphetamine
and ecstasy differ in relation to unsafe sex among young gay men. Can J Public
Health. 2005;96(5):340�3.20. Hittner JB, Schachne ER. Meta-analysis of the association between ecstasy
use and risky sexual behavior. Addict Behav. 2012;37(7):790�6.21. Baggaley RF, White RG, Boily MC. HIV transmission risk through anal
intercourse: systematic review, meta-analysis and implications for HIV preven-
tion. Int J Epidemiol. 2010;39(4):1048�63.22. Koblin BA, Murrill C, Camacho M, Xu G, Liu KL, Raj-Singh S, et al.
Amphetamine use and sexual risk among men who have sex with men: results
from the National HIV Behavioral Surveillance study�New York City. Subst Use
Misuse. 2007;42(10):1613�28.23. Hichson F, Weatherburn P, Reid D, Jessup K, Hammond G. Consuming
passions: findings from the United Kingdom Gay Men’s Sex Survey 2005.
London: Sigma Research; 2007.
24. Spindler HH, Scheer S, Chen SY, Klausner JD, Katz MH, Valleroy LA, et al.
Viagra, methamphetamine, and HIV risk: results from a probability sample of
MSM, San Francisco. Sex Transm Dis. 2007;34(8):586�91.25. Forrest DW, Metsch LR, LaLota M, Cardenas G, Beck DW, Jeanty Y. Crystal
methamphetamine use and sexual risk behaviors among HIV-positive and HIV-
negative men who have sex with men in South Florida. J Urban Health.
2010;87(3):480�5.26. Thiede H, Valleroy LA, MacKellar DA, Celentano DD, Ford WL, Hagan H,
et al. Regional patterns and correlates of substance use among young
men who have sex with men in 7 US urban areas. Am J Public Health.
2003;93(11):1915�21.
Nga Thi Thu Vu et al. Journal of the International AIDS Society 2015, 18:19273
http://www.jiasociety.org/index.php/jias/article/view/19273 | http://dx.doi.org/10.7448/IAS.18.1.19273
12
121

27. Hirshfield S, Remien RH, Humberstone M, Walavalkar I, Chiasson MA.
Substance use and high-risk sex among men who have sex with men: a
national online study in the USA. AIDS Care. 2004;16(8):1036�47.28. Klitzman RL, Greenberg JD, Pollack LM, Dolezal C. MDMA (‘ecstasy’) use,
and its association with high risk behaviors, mental health, and other factors
among gay/bisexual men in New York City. Drug Alcohol Depend. 2002;
66(2):115�25.29. Stall R, Paul JP, Greenwood G, Pollack LM, Bein E, Crosby GM, et al.
Alcohol use, drug use and alcohol-related problems among men who have
sex with men: the Urban Men’s Health Study. Addiction. 2001;96(11):
1589�601.30. Wei C, Guadamuz TE, Lim SH, Huang Y, Koe S. Patterns and levels of illicit
drug use among men who have sex with men in Asia. Drug Alcohol Depend.
2012;120(1�3):246�9.31. Wei C, Guadamuz TE, Lim SH, Koe S. Sexual transmission behaviors and
serodiscordant partnerships among HIV-positive men who have sex with men
in Asia. Sex Transm Dis. 2012;39(4):312�5.32. Colfax G, Coates TJ, Husnik MJ, Huang Y, Buchbinder S, Koblin B, et al.
Longitudinal patterns of methamphetamine, popper (amyl nitrite), and cocaine
use and high-risk sexual behavior among a cohort of San Francisco men who
have sex with men. J Urban Health. 2005;82(Suppl 1):62�70.33. Rawstorne P, Digiusto E,Worth H, Zablotska I. Associations between crystal
methamphetamine use and potentially unsafe sexual activity among gay men
in Australia. Arch Sex Behav. 2007;36(5):646�54.34. Mansergh G, Colfax GN, Marks G, Rader M, Guzman R, Buchbinder S. The
Circuit Party Men’s Health Survey: findings and implications for gay and
bisexual men. Am J Public Health. 2001;91(6):953�8.35. Greenwood GL,White EW, Page-Shafer K, Bein E, Osmond DH, Paul J, et al.
Correlates of heavy substance use among young gay and bisexual men: The
San Francisco Young Men’s Health Study. Drug Alcohol Depend. 2001;61(2):
105�12.36. Colfax GN, Mansergh G, Guzman R, Vittinghoff E, Marks G, Rader M, et al.
Drug use and sexual risk behavior among gay and bisexual men who attend
circuit parties: a venue-based comparison. J Acquir Immune Defic Syndr.
2001;28(4):373�9.37. Darrow WW, Biersteker S, Geiss T, Chevalier K, Clark J, Marrero Y, et al.
Risky sexual behaviors associated with recreational drug use among men who
have sex with men in an international resort area: challenges and opportu-
nities. J Urban Health. 2005;82(4):601�9.38. Mansergh G, Shouse RL, Marks G, Guzman R, Rader M, Buchbinder S, et al.
Methamphetamine and sildenafil (Viagra) use are linked to unprotected
receptive and insertive anal sex, respectively, in a sample of men who have
sex with men. Sex Transm Infect. 2006;82(2):131�4.39. Rusch M, Lampinen TM, Schilder A, Hogg RS. Unprotected anal intercourse
associated with recreational drug use among young men who have sex with
men depends on partner type and intercourse role. Sex Transm Dis. 2004;
31(8):492�8.40. Woody GE, Donnell D, Seage GR, Metzger D, Marmor M, Koblin BA, et al.
Non-injection substance use correlates with risky sex among men having sex
with men: data from HIVNET. Drug Alcohol Depend. 1999;53(3):197�205.41. Colfax G, Vittinghoff E, Husnik MJ, McKirnan D, Buchbinder S, Koblin B,
et al. Substance use and sexual risk: a participant- and episode-level analysis
among a cohort of men who have sex with men. Am J Epidemiol. 2004;
159(10):1002�12.42. Schwarcz S, Scheer S, McFarland W, Katz M, Valleroy L, Chen S, et al.
Prevalence of HIV infection and predictors of high-transmission sexual risk
behaviors among men who have sex with men. Am J Public Health. 2007;
97(6):1067�75.43. Clatts MC, Goldsamt LA, Yi H. Drug and sexual risk in four men who have
sex with men populations: evidence for a sustained HIV epidemic in New York
City. J Urban Health. 2005;82(Suppl 1):i9�17.44. Halkitis PN, Parsons JT, Stirratt MJ. A double epidemic: crystal metham-
phetamine drug use in relation to HIV transmission among gay men.
J Homosex. 2001;41(2):17�35.45. Drumright LN, Patterson TL, Strathdee SA. Club drugs as causal risk factors
for HIV acquisition among men who have sex with men: a review. Subst Use
Misuse. 2006;41(10�12):1551�601.46. Van Griensven F, Thienkrua W, McNicholl J, Wimonsate W, Chaikummao S,
Chonwattana W, et al. Evidence of an explosive epidemic of HIV infec-
tion in a cohort of men who have sex with men in Thailand. AIDS.
2013;27(5):825�32.
47. Pham QD, Nguyen TV, Hoang CQ, Cao V, Khuu NV, Phan HT, et al.
Prevalence of HIV/STIs and associated factors among men who have sex with
men in An Giang, Vietnam. Sex Transm Dis. 2012;39(10):799�806.48. Ackers ML, Greenberg AE, Lin CY, Bartholow BN, Goodman AH, Longhi M,
et al. High and persistent HIV seroincidence in men who have sex with men
across 47 U.S. cities. PLoS One. 2012;7(4):34972.
49. Oster AM, Dorell CG, Mena LA, Thomas PE, Toledo CA, Heffelfinger JD. HIV
risk among young African American men who have sex with men: a case-
control study in Mississippi. Am J Public Health. 2011;101(1):137�43.50. Chariyalertsak S, Kosachunhanan N, Saokhieo P, Songsupa R, Wongthanee
A, Chariyalertsak C, et al. HIV incidence, risk factors, and motivation for
biomedical intervention among gay, bisexual men, and transgender persons in
Northern Thailand. PLoS One. 2011;6(9):24295.
51. Morineau G, Nugrahini N, Riono P, Nurhayati , Girault P, Mustikawati DE,
et al. Sexual risk taking, STI and HIV prevalence among men who have sex with
men in six Indonesian cities. AIDS Behav. 2011;15(5):1033�44.52. Truong HM, Kellogg TA, McFarland W, Louie B, Klausner JD, Philip SS, et al.
Sentinel surveillance of HIV-1 transmitted drug resistance, acute infection and
recent infection. PLoS One. 2011;6(10):25281.
53. Feng Y, Wu Z, Detels R, Qin G, Liu L, Wang X, et al. HIV/STD prevalence
among men who have sex with men in Chengdu, China and associated risk
factors for HIV infection. J Acquir Immune Defic Syndr. 53 Suppl. 2010;1:
S74�80.54. Menza TW, Hughes JP, Celum CL, Golden MR. Prediction of HIV acquisition
among men who have sex with men. Sex Transm Dis. 2009;36(9):547�55.55. Carey JW, Mejia R, Bingham T, Ciesielski C, Gelaude D, Herbst JH, et al.
Drug use, high-risk sex behaviors, and increased risk for recent HIV infection
among men who have sex with men in Chicago and Los Angeles. AIDS Behav.
2009;13(6):1084�96.56. Drumright LN, Gorbach PM, Little SJ, Strathdee SA. Associations between
substance use, erectile dysfunction medication and recent HIV infection among
men who have sex with men. AIDS Behav. 2009;13(2):328�36.57. Rudy ET, Shoptaw S, Lazzar M, Bolan RK, Tilekar SD, Kerndt PR.
Methamphetamine use and other club drug use differ in relation to HIV
status and risk behavior among gay and bisexual men. Sex Transm Dis.
2009;36(11):693�5.58. Thiede H, Jenkins RA, Carey JW, Hutcheson R, Thomas KK, Stall RD, et al.
Determinants of recent HIV infection among Seattle-area men who have sex
with men. Am J Public Health. 2009;99(Suppl 1):S157�64.59. Prestage G, Jin F, Kippax S, Zablotska I, Imrie J, Grulich A. Use of illicit drugs
and erectile dysfunction medications and subsequent HIV infection among gay
men in Sydney, Australia. J Sex Med. 2009;6(8):2311�20.60. Raymond HF, Bingham T, McFarland W. Locating unrecognized HIV
infections among men who have sex with men: San Francisco and Los Angeles.
AIDS Educ Prev. 2008;20(5):408�19.61. Macdonald N, Elam G, Hickson F, Imrie J, McGarrigle CA, Fenton KA, et al.
Factors associated with HIV seroconversion in gay men in England at the start
of the 21st century. Sex Transm Infect. 2008;84(1):8�13.62. Plankey MW, Ostrow DG, Stall R, Cox C, Li X, Peck JA, et al. The relationship
between methamphetamine and popper use and risk of HIV seroconversion in
the multicenter AIDS cohort study. J Acquir Immune Defic Syndr. 2007;45(1):
85�92.63. Koblin BA, Husnik MJ, Colfax G, Huang Y, Madison M, Mayer K, et al. Risk
factors for HIV infection among men who have sex with men. AIDS. 2006;
20(5):731�9.64. Fuller CM, Absalon J, Ompad DC, Nash D, Koblin B, Blaney S, et al. A
comparison of HIV seropositive and seronegative young adult heroin- and
cocaine-using men who have sex with men in New York City, 2000�2003.J Urban Health. 2005;82(Suppl 1):i51�61.65. Kral AH, Lorvick J, Ciccarone D, Wenger L, Gee L, Martinez A, et al. HIV
prevalence and risk behaviors among men who have sex with men and inject
drugs in San Francisco. J Urban Health. 2005;82(Suppl 1):i43�50.66. Buchbinder SP, Vittinghoff E, Heagerty PJ, Celum CL, Seage GR, 3rd, Judson
FN, et al. Sexual risk, nitrite inhalant use, and lack of circumcision associated
with HIV seroconversion in men who have sex with men in the United States.
J Acquir Immune Defic Syndr. 2005;39(1):82�9.67. Robertson MJ, Clark RA, Charlebois ED, Tulsky J, Long HL, Bangsberg DR,
et al. HIV seroprevalence among homeless and marginally housed adults in San
Francisco. Am J Public Health. 2004;94(7):1207�17.68. Weber AE, Craib KJ, Chan K, Martindale S, Miller ML, Cook DA, et al.
Determinants of HIV serconversion in an era of increasing HIV infection among
young gay and bisexual men. AIDS. 2003;17(5):774�7.
Nga Thi Thu Vu et al. Journal of the International AIDS Society 2015, 18:19273
http://www.jiasociety.org/index.php/jias/article/view/19273 | http://dx.doi.org/10.7448/IAS.18.1.19273
13
122

69. Chesney MA, Barrett DC, Stall R. Histories of substance use and risk
behavior: precursors to HIV seroconversion in homosexual men. Am J Public
Health. 1998;88(1):113�6.70. Ruiz J, Facer M, Sun RK. Risk factors for human immunodeficiency virus
infection and unprotected anal intercourse among young men who have sex
with men. Sex Transm Dis. 1998;25(2):100�7.71. Page-Shafer K, Veugelers PJ, Moss AR, Strathdee S, Kaldor JM, van
Griensven GJ. Sexual risk behavior and risk factors for HIV-1 seroconversion
in homosexual men participating in the Tricontinental Seroconverter Study,
1982�1994. Am J Epidemiol. 1997;146(7):531�42.72. Buchbinder SP, Douglas JM, Jr., McKirnan DJ, Judson FN, Katz MH,
MacQueen KM. Feasibility of human immunodeficiency virus vaccine trials in
homosexual men in the United States: risk behavior, seroincidence, and
willingness to participate. J Infect Dis. 1996;174(5):954�61.73. Seage GR, 3rd, Mayer KH, Horsburgh CR, Jr, Holmberg SD, Moon MW,
Lamb GA. The relation between nitrite inhalants, unprotected receptive anal
intercourse, and the risk of human immunodeficiency virus infection. Am J
Epidemiol. 1992;135(1):1�11.74. Burcham JL, Tindall B, Marmor M, Cooper DA, Berry G, Penny R. Incidence
and risk factors for human immunodeficiency virus seroconversion in a cohort
of Sydney homosexual men. Med J Aust. 1989;150(11):634�9.75. Rietmeijer CA, Penley KA, Cohn DL, Davidson AJ, Horsburgh CRJr., Judson
FN. Factors influencing the risk of infection with human immunodeficiency
virus in homosexual men, Denver 1982�1985. Sex Transm Dis. 1989;16(2):
95�102.76. Van Griensven GJ, Tielman RA, Goudsmit J, van der Noordaa J, de Wolf F,
de Vroome EM, et al. Risk factors and prevalence of HIV antibodies in
homosexual men in the Netherlands. Am J Epidemiol. 1987;125(6):1048�57.77. Jeffries E, Willoughby B, Boyko WJ, Schechter MT,Wiggs B, Fay S, et al. The
Vancouver Lymphadenopathy-AIDS Study: 2. Seroepidemiology of HTLV-III
antibody. Can Med Assoc J. 1985;132(12):1373�7.78. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al.
Meta-analysis of observational studies in epidemiology: a proposal for
reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE)
group. JAMA. 2000;283(15):2008�12.79. Boyle MH. Guidelines for evaluating prevalence studies. Evid Base Ment
Health. 1998;1(2):37�9.80. Wells G, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The
Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised
studies in meta-analyses. 2000. [cited 2015 Jan 15]. Available from: http://
www.ohri.ca/programs/clinical_epidemiology/oxford.asp
81. Skov T, Deddens J, Petersen MR, Endahl L. Prevalence proportion ratios:
estimation and hypothesis testing. Int J Epidemiol. 1998;27(1):91�5.82. Hardy RJ, Thompson SG. Detecting and describing heterogeneity in meta-
analysis. Stat Med. 1998;17(8):841�56.83. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis.
Stat Med. 2002;21(11):1539�58.
84. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in
meta-analyses. BMJ. 2003;327(7414):557�60.85. Egger M, Smith GD, Altman DG, editors. Systematic reviews in health care:
meta-analysis in context. 2nd ed. London: BMJ Publishing Group; 2001.
86. Baral S, Sifakis F, Cleghorn F, Beyrer C. Elevated risk for HIV infection
among men who have sex with men in low- and middle-income countries
2000�2006: a systematic review. PLoS Med. 2007;4(12):339.
87. Vosburgh HW, Mansergh G, Sullivan PS, Purcell DW. A review of the
literature on event-level substance use and sexual risk behavior among men
who have sex with men. AIDS Behav. 2012;16(6):1394�410.88. Rothstein HR, Sutton AJ, Borenstein M, editors. Publication bias in meta-
analysis: prevention, assessment and adjustments. Chichester: John Wiley &
Sons, Ltd; 2005.
89. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis
detected by a simple, graphical test. BMJ. 1997;315(7109):629�34.90. Hladik W, Barker J, Ssenkusu JM, Opio A, Tappero JW, Hakim A, et al. HIV
infection among men who have sex with men in Kampala, Uganda � a
respondent driven sampling survey. PLoS One. 2012;7(5):38143.
91. Oster AM, Wiegand RE, Sionean C, Miles IJ, Thomas PE, Melendez-Morales
L, et al. Understanding disparities in HIV infection between black and white
MSM in the United States. AIDS. 2011;25(8):1103�12.92. Weinstock H, Sweeney S, Satten GA, Gwinn M. HIV seroincidence and risk
factors among patients repeatedly tested for HIV attending sexually trans-
mitted disease clinics in the United States, 1991 to 1996. STD Clinic HIV
Seroincidence Study Group. J Acquir Immune Defic Syndr Hum Retrovirol.
1998;19(5):506�12.93. Li Y, Baker JJ, Korostyshevskiy VR, Slack RS, Plankey MW. The association of
intimate partner violence, recreational drug use with HIV seroprevalence
among MSM. AIDS Behav. 2012;16(3):491�8.94. Semple S, Zians J, Strathdee S, Patterson T. Sexual marathons and
methamphetamine use among HIV-positive men who have sex with men.
Arch Sex Behav. 2009;38(4):583�90.95. Leigh BC, Stall R. Substance use and risky sexual behavior for exposure
to HIV. Issues in methodology, interpretation, and prevention. Am Psychol.
1993;48(10):1035�45.96. Degenhardt L, Mathers B, Guarinieri M, Panda S, Phillips B, Strathdee SA,
et al. Meth/amphetamine use and associated HIV: implications for global policy
and public health. Int J Drug Policy. 2010;21(5):347�58.97. Fischer A, Curruthers S, Power R, Allsop S, Degenhardt L. The link between
amphetamine-type stimulant use and the transmission of HIV and other blood-
borne viruses in the Southeast Asia region. Canberra: Australian National
Council on Drugs; 2012.
98. Poynten IM, Jin F, Prestage GP, Kaldor JM, Kippax S, Grulich AE. Defining
high HIV incidence subgroups of Australian homosexual men: implications for
conducting HIV prevention trials in low HIV prevalence settings. HIV Med.
2010;11(10):635�41.
Nga Thi Thu Vu et al. Journal of the International AIDS Society 2015, 18:19273
http://www.jiasociety.org/index.php/jias/article/view/19273 | http://dx.doi.org/10.7448/IAS.18.1.19273
14
123
CHAPTER 6
THE PREVALENCE AND CORRELATES OF HIV AND UNDIAGNOSED
INFECTION AMONG MEN WHO HAVE SEX WITH MEN IN HANOI,
VIETNAM: FINDINGS FROM A CROSS-SECTIONAL, BIOBEHAVIORAL
STUDY.
Author Contributions Nga Thi Thu VU1,2, Martin HOLT1, Huong Thi Thu PHAN3, Lan Thi LA4, Gioi Minh
TRAN5, Tung Thanh DOAN5, Trang Nhu Nguyen NGUYEN6 and John de Wit1
1: Center for Social Research in Health, University of New South Wales, Sydney,
New South Wales, Australia; 2: Institute of Preventive Medicine and Public Health,
Hanoi Medical University, Hanoi, Vietnam; 3: Vietnam Administration for
HIV/AIDS Prevention and Control, Hanoi, Vietnam; 4: Hanoi Center of HIV/AIDS
Prevention and Control, Hanoi, Vietnam; 5: Center for Community Health
Promotion, Hanoi, Vietnam; 6: Center for Promotion of Quality of Life, Ho Chi Minh
City, Vietnam.
Reference
Vu NT, Holt M, Phan HT, La LT, Tran GM, Doan TT, et al. The Prevalence and
Correlates of HIV and Undiagnosed Infection among Men Who Have Sex with
Men in Hanoi, Vietnam: Findings from a Cross-sectional, Biobehavioral Study.
Frontiers in public health. 2016;4:275.
Declaration
I certify that this publication was a direct result of my research toward this PhD,
and that reproduction in this thesis does not breach copyright regulations.
Nga Thi Thu Vu June 2017
124
Copyright permission
This article was published in Frontiers in Public Health, an open-access journal,
available online:
http://journal.frontiersin.org/article/10.3389/fpubh.2016.00275/full.
No copyright permission, therefore, is needed for reusing it in this thesis
dissertation.
125
December 2016 | Volume 4 | Article 2751
Original researchpublished: 19 December 2016
doi: 10.3389/fpubh.2016.00275
Frontiers in Public Health | www.frontiersin.org
Edited by: Tak Fai Joseph Lau,
The Chinese University of Hong Kong, Hong Kong
Reviewed by: Gerjo Kok,
Maastricht University, Netherlands Zixin Wang,
The Chinese University of Hong Kong, Hong Kong
*Correspondence:Nga Thi Thu Vu
[email protected]; John de Wit
Specialty section: This article was submitted to
HIV and AIDS, a section of the journal
Frontiers in Public Health
Received: 02 August 2016Accepted: 02 December 2016Published: 19 December 2016
Citation: Vu NTT, Holt M, Phan HTT, La LT,
Tran GM, Doan TT and de Wit J (2016) The Prevalence and Correlates
of HIV and Undiagnosed Infection among Men Who Have Sex with Men
in Hanoi, Vietnam: Findings from a Cross-sectional, Biobehavioral Study.
Front. Public Health 4:275. doi: 10.3389/fpubh.2016.00275
The Prevalence and correlates of hiV and Undiagnosed infection among Men Who have sex with Men in hanoi, Vietnam: Findings from a cross-sectional, Biobehavioral studyNga Thi Thu Vu1,2*, Martin Holt1, Huong Thi Thu Phan3, Lan Thi La4, Gioi Minh Tran5, Tung Thanh Doan5 and John de Wit1,6*
1 Centre for Social Research in Health, UNSW Australia, Sydney, NSW, Australia, 2 Institute of Preventive Medicine and Public Health, Hanoi Medical University, Hanoi, Vietnam, 3 Vietnam Administration for HIV/AIDS Prevention and Control, Ministry of Health, Hanoi, Vietnam, 4 Hanoi Centre of HIV/AIDS Prevention and Control, Hanoi, Vietnam, 5 Center for Community Health Promotion, Hanoi, Vietnam, 6 Utrecht University, Utrecht, Netherlands
introduction: Men who have sex with men (MSM) are a key population for HIV infection in Vietnam, and the use of amphetamine type substances (ATS) is prevalent and possibly increasing in this population. The reported analysis examines the association between ATS use before or during sex and HIV infection among MSM in Hanoi, Vietnam.
Methods: This cross-sectional study of 210 MSM was conducted in Hanoi, Vietnam, in late 2014. Men tested for HIV and answered questions about demographic char-acteristics, sexual sensation seeking, depression, belief in HIV prevention strategies, homosexuality-related stigma and discrimination, recent accessing of HIV prevention services, sexual behaviors and ATS, and other drug use behaviors. We performed logis-tic regression to assess correlates of HIV infection.
results: HIV prevalence was 6.7% (14/210), and 85.7% (12/14) of HIV-positive men were not aware of their HIV status. Of the 210 participants, 10.5, 2.9, and 3.8% of men had used methamphetamine, amphetamine, and ecstasy before or during sex in the last 3 months. In multivariable analysis, HIV infection was associated with recent sex-related methamphetamine use [adjusted odds ratio (AOR): 5.03, 95% confidence interval (CI): 1.35–18.68], engaging in recent sex work (AOR: 3.55, 95% CI: 1.07–11.75), and homosexuality-related perceived stigma (AOR: 2.32, 95% CI: 0.98–5.47).
conclusion: Findings underscore the importance of integrating methamphetamine use interventions into HIV prevention services and scaling-up of gay-friendly, non-stigmatiz-ing HIV testing services for MSM in Hanoi. We recommend the routine assessment of ATS use and undiagnosed infection in this population.
Keywords: hiV prevalence, amphetamine type stimulants, men who have sex with men, undiagnosed hiV, hanoi—Vietnam
126

2
Vu et al. Correlates of HIV Infection among MSM in Hanoi
Frontiers in Public Health | www.frontiersin.org December 2016 | Volume 4 | Article 275
inTrODUcTiOn
The HIV epidemic was first described in Vietnam in the early 1990s (1), and in the last 30 years, the epidemic has spread to dif-ferent parts of the country. Since 1999, HIV has been reported in all provinces and cities of Vietnam (2). Although men who have sex with men (MSM) have been recognized as a key population affected by HIV in different parts of the world (3), in Vietnam, they were only identified as a priority population for HIV preven-tion in the last decade (4), despite warning signs in the early 2000s that HIV was spreading in this population (5, 6).
A study conducted only in Ho Chi Minh City in 2004 reported an HIV prevalence of 8% in a sample of MSM recruited in MSM-specific venues (7). The first, national integrated biological behavioral surveillance (IBBS) conducted in 2006 reported that the HIV prevalence among MSM in Ho Chi Minh City and Hanoi was 5 and 9%, respectively (8). In the second IBBS conducted in 2009, HIV prevalence exceeded 10% in Hanoi (19.8%) and Ho Chi Minh City (14.3%), as well as in Haiphong (16.6%), the country’s third largest city (9), suggesting HIV prevalence had increased substantially among MSM in major cities across Vietnam. A more recent study found an HIV prevalence of 14.8% among MSM in Ho Chi Minh City (10). A better understanding of the individual, social, and structural factors that affect HIV risks is, therefore, needed to prevent further transmission of HIV in the MSM population in Vietnam.
Previous studies have found that HIV infection among MSM in Vietnam is associated with younger age, lower education and injecting drug use (7, 11), a higher number of recent sexual part-ners (5, 7), and sex work and inconsistent condom use (5). MSM in Vietnam have consistently reported low levels of condom use with casual and regular male partners (8, 9).
Amphetamine type stimulants (ATS) are commonly used drugs by MSM, and their use has been found to be associated with condomless anal intercourse (CAI) and HIV infection (12). A recent meta-analysis found a significant association between methamphetamine and amphetamine use and HIV infection across 35 studies (13). However, most previous studies have been conducted in high-income countries, and evidence regarding the association between ATS use and HIV infection among MSM is lacking in low- and middle-income countries (13), particularly Vietnam. It was reported that ATS use, particularly metham-phetamine use is prevalent among MSM in Vietnam (14). The relationship between ATS use and HIV infection among MSM in Vietnam, however, remains to be assessed.
In Vietnam, homosexuality remains socially stigmatized (15), despite recent activism to protect the rights of lesbian, gay, bisexual, and transgender people. Previous international research underscores that homosexuality-related stigma and discrimina-tion are associated with a higher risk of depression (16, 17). Depression has been found to be highly prevalent among MSM, particularly HIV-positive men (18, 19), and is considered a major health issue among MSM (20). Furthermore, homosexuality-related stigma, discrimination, and depression have been found to be associated with engaging in HIV-related risky behaviors such as CAI (21–23), drug use (24, 25), having sex while on drugs (26), less awareness and underutilization of HIV prevention services
(27–29), and experiencing less benefit from participating in HIV prevention interventions (27).
Previous studies of HIV infection among MSM in Vietnam have mainly focused on individual-level covariates rather than examining social and structural barriers to HIV prevention, such as homosexuality-related stigma and discrimination. Evidence from previous studies indicates that sexual sensation seeking is associated with an increased likelihood of CAI among MSM (30–33) and that sexual sensation seeking can modify or strengthen the association between alcohol or drug use and HIV-related sexual behaviors (34, 35). However, the effect of sexual sensation seeking on HIV risk among MSM in Vietnam has not been previously investigated.
Previous research in Vietnam has found relatively high rates of CAI between MSM (8, 9), and international research has found that MSM may use various strategies to reduce HIV transmission risk during CAI, such as serosorting (having sex with partners of the same perceived HIV status), strategic positioning (HIV-negative men being insertive during CAI), withdrawal before ejaculation, or limiting CAI to HIV-positive partners who are virally suppressed (36, 37). However, belief in the efficacy of these strategies has not been previously assessed among Vietnamese MSM.
To improve HIV prevention among MSM in Vietnam, we sought to assess the prevalence of HIV and undiagnosed infec-tion among MSM in Hanoi and examined factors associated with HIV infection, including homosexuality-related stigma and discrimination, depression, sexual sensation seeking, belief in the efficacy of risk reduction strategies, and drug use, particularly ATS use.
MaTerials anD MeThODs
Participants included in this analysis were part of a larger con-venience sample of 303 MSM recruited into a cross-sectional, community-based study in Hanoi, Vietnam, from September to October 2014. The study received approval from the Human Research Ethics Committee of the University of New South Wales, Australia, and from the Institutional Review Board of the Hanoi School of Public Health. A description of the study has been previously published (14). In short, the study was conducted in collaboration with the Hanoi Center for HIV/AIDS Prevention and Control (Hanoi PAC), the Center for Community Health Promotion (CHP), and MSM community-based organizations (CBOs). MSM are a relatively hidden population in Vietnam, and developing a randomized sam-pling frame is impossible. Convenience sampling was hence used to recruit participants. First, staff and outreach workers of collaborating organizations referred potential participants to the study. Additionally, peers of collaborating CBOs referred men from their social networks. Finally, participated men were asked to invite their peers who might be interested in the study.
Men were eligible to participate if they were 18 years or older at the time of the study, reported having anal sex with at least one man in the previous 3 months, had a good command of the Vietnamese language, and provided consent. Men were screened
127

3
Vu et al. Correlates of HIV Infection among MSM in Hanoi
Frontiers in Public Health | www.frontiersin.org December 2016 | Volume 4 | Article 275
for eligibility and were interviewed after provided written consent. Upon interview completion, men were informed about optional HIV testing.
Men who chose to be tested were referred to an on-site test-ing team provided by Hanoi PAC. Separate written consent was obtained for HIV testing. Venous blood samples were collected by technicians from Hanoi PAC. Blood samples were assigned a unique, anonymous ID code enabling linkage to participants’ questionnaires (and for participants to get results). Due to resource constraints, we could only offer 210 free HIV tests to participants.
confidentiality and PrivacyBeing identified as a MSM or drug user in Vietnam may result in social stigma and discrimination (38). As such, MSM partici-pants, particularly those who use drugs, may underreport sexual and drug use behaviors. We took several steps to mitigate this potential bias. First, all interviewers were trained to be supportive and non-judgmental of MSM. Second, MSM participants were not asked to provide personal details that could reveal their identity. Third, all interviews were conducted in private rooms. Finally, all field staff signed a confidentiality agreement.
hiV Testing and statusBlood samples were tested for HIV at the Hanoi PAC labora-tory, following Vietnamese Ministry of Health guidelines. All blood samples were screened for HIV by the Murex HIV Ag/Ab combination assay (DiaSorin S.p.A., Italy). Samples that were reactive during screening were tested again using confirmatory tests (Serodia® HIV, Fujirebio, Japan; Determine™ HIV1/2, Alere Medical, USA). The main outcome variable was HIV status as confirmed by testing (HIV negative or HIV positive). We also referred to participants’ self-reported HIV status (HIV negative, untested/unknown, or HIV positive) to identify participants who tested HIV positive but were unaware of their infection. The self-report information collected through the questionnaire has previously been described (14) and contained the questions described below.
Demographic characteristicsWe asked participants about their self-reported HIV status, sexual orientation, age, place of birth, education, occupation, and monthly income.
sexual sensation seekingWe adapted a measure of sexual sensation seeking for a Vietnamese sample (39). Ten items assessed the propensity to seek out exciting and novel sexual experiences, for instance “I like wild, uninhibited sexual encounters.” Participants provided their answers on 5-point scales, ranging from 1 (not at all like me) to 4 (very much like me). Internal consistency of the items was sufficient (Cronbach’s α = 0.72). Item scores were averaged, with higher scores indicating more sexual sensation seeking.
DepressionThis was assessed with the Patient Health Questionnaire 9 scale, which has been used with MSM in other studies (40, 41). The
scale consists of nine items, such as “in the last two weeks, how often have you had trouble falling or staying asleep, or sleeping too much?” Participants provided their answers on a scale rang-ing from 0 (not having the problem at all) to 3 (having the prob-lem nearly every day). The items had good internal consistency (Cronbach’s α = 0.80). Participants were categorized as having a depressive disorder if they had a score equal or larger than 10, as previously described (42).
Belief in hiV Prevention strategiesParticipants were asked how effective they thought different strategies were in preventing HIV transmission: antiretroviral treatment of HIV, HIV-negative men taking the insertive (top) position during anal sex, and withdrawal before ejaculation. Answer options ranged from 1 (totally disagree) to 4 (totally agree). Belief in the efficacy of each HIV prevention method was dichotomized into disagreement (scores 1 and 2) versus agree-ment (scores 3 and 4).
Perceived stigma and DiscriminationWe adapted a scale to measure enacted (experienced) homosex-uality-related stigma, perceived (anticipated) homosexuality-related stigma, and self-stigma (internalized homophobia) (22). Responses were given on 4-point scales, with anchors depending on the questions. The adapted scale encompassed eight items pertaining to enacted homosexuality-related stigma, for example “how often have you lost a job or career opportunity due to your engaging in homosexual activities” (1 = never, 4 = often); 10 items measuring perceived homosexuality-related stigma, for instance “many people are unwilling to accept homosexual individuals” (1 = completely disagree, 4 = completely agree); and eight items measuring internalized homophobia, for example “sometimes you wish you were not gay/bisexual/transgender” (1 = totally disagree, 4 = totally agree). In this study, the scale had good internal consistency (Cronbach’s α = 0.74). Mean scores were calculated for each sub-scale; higher scores indicated higher levels of stigma.
recent accessing of hiV Prevention servicesWe asked participants if they had recently tested for HIV (i.e., at least once in the last 12 months) and if they had recently received safe sex counseling (i.e., at least once in the last 12 months).
sexual BehaviorsWe asked about the gender of sexual partners and age at first sex with men and women. Participants were asked about ever engaging in sex work (selling sex), recent sex work (in the last 3 months), their number of regular and casual male partners in the last 3 and 12 months, and the use of condoms during anal sexual intercourse with regular and casual male partners. Because numbers of different types of sexual partners were skewed, we undertook logarithmic or square root transformations of these variables, as appropriate. Any CAI was defined as not or incon-sistently using a condom during anal sex (assessed for regular and casual male partners in the previous 3 months).
128

4
Vu et al. Correlates of HIV Infection among MSM in Hanoi
Frontiers in Public Health | www.frontiersin.org December 2016 | Volume 4 | Article 275
aTs and Other Drug UseParticipants were asked questions about ever having used ATS, alcohol, and other substances (i.e., ketamine, erectile dysfunction medications, and amyl nitrite “poppers”), any recent use of these substances (in the last 3 months) and any use of these substances before or during sex in the last 3 months. Answers to these ques-tions were dichotomized (any use versus none).
Data analysisDescriptive and correlational statistical analyses were performed using STATA version 13.1 (StataCorp, College Station, TX, USA). We report frequencies and percentages for categorical variables and medians with interquartile ranges (IQR) for continuous variables. We tested bivariate associations between laboratory-confirmed HIV status and potential covariates using logistic regression. Factors associated with the outcome variable at p < 0.25 were subsequently entered into a multivariate regression model to identify independent covariates. We used a stepwise procedure as previously suggested (43) to develop the final multivariate model with independent covariates, which retained statistical significance (p < 0.05).
resUlTs
A total of 222 men were referred to the study as potential partici-pants, among whom nine men did not meet selection criteria, two men chose not to complete an interview, and one man refused to be tested. As such, the following analysis includes 210 men who completed an interviewer-administered questionnaire and agreed to be tested for HIV and release their HIV test result. We compared the sociodemographic characteristics of men who did and did not undertake HIV testing (analysis not shown). Men who tested for HIV and consented to release their HIV test results were significantly younger, had lower incomes, and were more likely to be students or self-employed. Men who did and didn’t undertake HIV testing were similar in terms of place of birth, education level, sexual orientation, and perceived HIV status.
sample characteristicsTable 1 presents the demographic characteristics of the 210 MSM who participated. The majority of the sample reported being homosexual (73.3%), 22.4% bisexual, and the remainder (3.8%) heterosexual or other sexual orientation. The median age of the sample was 22.7 years (IQR: 20.6–25.5); 90.0% were younger than 30 years. The majority of men had a college or university educa-tion (57.9%), 30.1% had high school or vocational training, and only 12.0% had secondary or lower education. Approximately 30.0% of the sample was students, 9.0% were unemployed, and the remainder had office-based jobs, service jobs, or were in self-employed, casual, or freelance jobs. Participants had a median monthly income of 5 million Vietnamese Dong (approximately US$228) (IQR: 3.0–8.0 million). The median sexual sensation-seeking score was 2.5 (IQR: 1.4–3.5). A minority of men (14.3%) were categorized as having depression. In relation to belief in different HIV prevention strategies, 9.5% men believed in the effectiveness of HIV treatment as prevention, 28.6% believed in
the safety of being insertive during sex, and 38.6% men believed that withdrawal was effective. The median score regarding homosexuality-related enacted stigma was 1.1 (IQR: 1.0–2.4); scores for perceived stigma and internalized homophobia were 4.0 (IQR: 1.20–5.0) and 3.4 (IQR: 1.0–4.6), respectively.
sex and Drug Use BehaviorsTable 2 presents HIV-related sex and drug use behaviors. Approximately 63% men self-reported having sex with men only; the remainder reported having sex with both men and women. The median age of first homosexual sex was 19.0 (IQR: 18.0–21.0), and the median age of first heterosexual sex was 18.0 (12.0–30.0). Of the 210 participants, 73.8% reported any recent CAI with male partners (66.2% with regular part-ners and 32.4% with casual partners). The median number of regular male sexual partners in the last 3 months was 1 (IQR: 1.0–80.0), and the median number of casual male sexual part-ners in the last 3 months was 3.0 (IQR: 1.0–100.0). Of the 210 participants, 26.2% reported having ever engaged in sex work and 21.4% reported recent sex work. One in five participants (22.9%) reported ever having used methamphetamine, 14.8% reported recent use, and 10.5% reported recent sex-related use. The corresponding rates for amphetamine use were 7.6, 2.9, and 2.9%, respectively. Rates for ecstasy they were 20.0, 8.6, and 3.8%. Men reported higher levels of alcohol use: 90.0% had ever drunk alcohol, 76.2% had recently consumed alcohol, and 39.5% reported sex-related alcohol use in the last 3 months.
hiV Testing resultsFourteen men out of 210 [6.7%, 95% confidence interval (CI): 3.7–10.9] tested HIV-antibody positive (see Table 1) and 12 of these 14 HIV-positive men (85.7%) were not aware of their HIV status. Just over half (52.4%) of all participating men had ever tested for HIV, and just under half (46.6%) did not know their HIV status, including 29.5% who had ever tested for HIV but did not know their test result and 17.1% who had never tested for HIV. Out of the 210 men who were tested, approximately 10 men returned for their results, including one man who was previously undiagnosed with HIV.
correlates of hiV infectionThe results of bivariate and multivariate analyses of associa-tions between HIV infection and other covariates are presented in the Table 3. Potential independent covariates identified in bivariate analysis included occupation, sexual sensation seek-ing, belief in the safety of being insertive during sex as a HIV prevention strategy, homosexuality-related perceived stigma, engaging in recent sex work, number of regular male sexual partners, any recent CAI with casual male sexual partners, recent methamphetamine or amphetamine use before or dur-ing sex, and having a HIV test in the last 12 months. In the final multivariate logistic regression model, HIV infection was more likely among MSM who reported recent sex work or the use of methamphetamine before or during sex. Additionally, HIV infection was marginally associated with homosexuality-related perceived stigma.
129
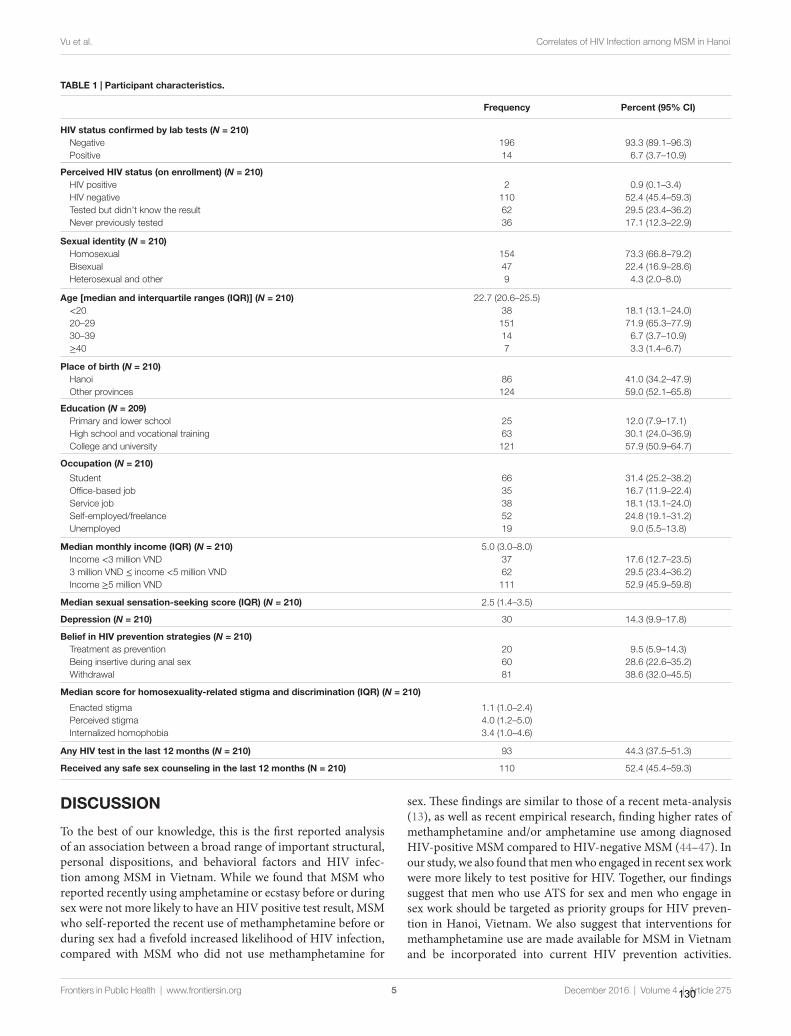
TaBle 1 | Participant characteristics.
Frequency Percent (95% ci)
hiV status confirmed by lab tests (N = 210) Negative 196 93.3 (89.1–96.3) Positive 14 6.7 (3.7–10.9)
Perceived hiV status (on enrollment) (N = 210) HIV positive 2 0.9 (0.1–3.4) HIV negative 110 52.4 (45.4–59.3) Tested but didn’t know the result 62 29.5 (23.4–36.2) Never previously tested 36 17.1 (12.3–22.9)
sexual identity (N = 210) Homosexual 154 73.3 (66.8–79.2) Bisexual 47 22.4 (16.9–28.6) Heterosexual and other 9 4.3 (2.0–8.0)
age [median and interquartile ranges (iQr)] (N = 210) 22.7 (20.6–25.5) <20 38 18.1 (13.1–24.0) 20–29 151 71.9 (65.3–77.9) 30–39 14 6.7 (3.7–10.9) ≥40 7 3.3 (1.4–6.7)
Place of birth (N = 210) Hanoi 86 41.0 (34.2–47.9) Other provinces 124 59.0 (52.1–65.8)
education (N = 209) Primary and lower school 25 12.0 (7.9–17.1) High school and vocational training 63 30.1 (24.0–36.9) College and university 121 57.9 (50.9–64.7)
Occupation (N = 210)
Student 66 31.4 (25.2–38.2) Office-based job 35 16.7 (11.9–22.4) Service job 38 18.1 (13.1–24.0) Self-employed/freelance 52 24.8 (19.1–31.2) Unemployed 19 9.0 (5.5–13.8)
Median monthly income (iQr) (N = 210) 5.0 (3.0–8.0) Income <3 million VND 37 17.6 (12.7–23.5) 3 million VND ≤ income <5 million VND 62 29.5 (23.4–36.2) Income ≥5 million VND 111 52.9 (45.9–59.8)
Median sexual sensation-seeking score (iQr) (N = 210) 2.5 (1.4–3.5)
Depression (N = 210) 30 14.3 (9.9–17.8)
Belief in hiV prevention strategies (N = 210) Treatment as prevention 20 9.5 (5.9–14.3) Being insertive during anal sex 60 28.6 (22.6–35.2) Withdrawal 81 38.6 (32.0–45.5)
Median score for homosexuality-related stigma and discrimination (iQr) (N = 210)
Enacted stigma 1.1 (1.0–2.4) Perceived stigma 4.0 (1.2–5.0) Internalized homophobia 3.4 (1.0–4.6)
any hiV test in the last 12 months (N = 210) 93 44.3 (37.5–51.3)
received any safe sex counseling in the last 12 months (n = 210) 110 52.4 (45.4–59.3)
5
Vu et al. Correlates of HIV Infection among MSM in Hanoi
Frontiers in Public Health | www.frontiersin.org December 2016 | Volume 4 | Article 275
DiscUssiOn
To the best of our knowledge, this is the first reported analysis of an association between a broad range of important structural, personal dispositions, and behavioral factors and HIV infec-tion among MSM in Vietnam. While we found that MSM who reported recently using amphetamine or ecstasy before or during sex were not more likely to have an HIV positive test result, MSM who self-reported the recent use of methamphetamine before or during sex had a fivefold increased likelihood of HIV infection, compared with MSM who did not use methamphetamine for
sex. These findings are similar to those of a recent meta-analysis (13), as well as recent empirical research, finding higher rates of methamphetamine and/or amphetamine use among diagnosed HIV-positive MSM compared to HIV-negative MSM (44–47). In our study, we also found that men who engaged in recent sex work were more likely to test positive for HIV. Together, our findings suggest that men who use ATS for sex and men who engage in sex work should be targeted as priority groups for HIV preven-tion in Hanoi, Vietnam. We also suggest that interventions for methamphetamine use are made available for MSM in Vietnam and be incorporated into current HIV prevention activities.
130
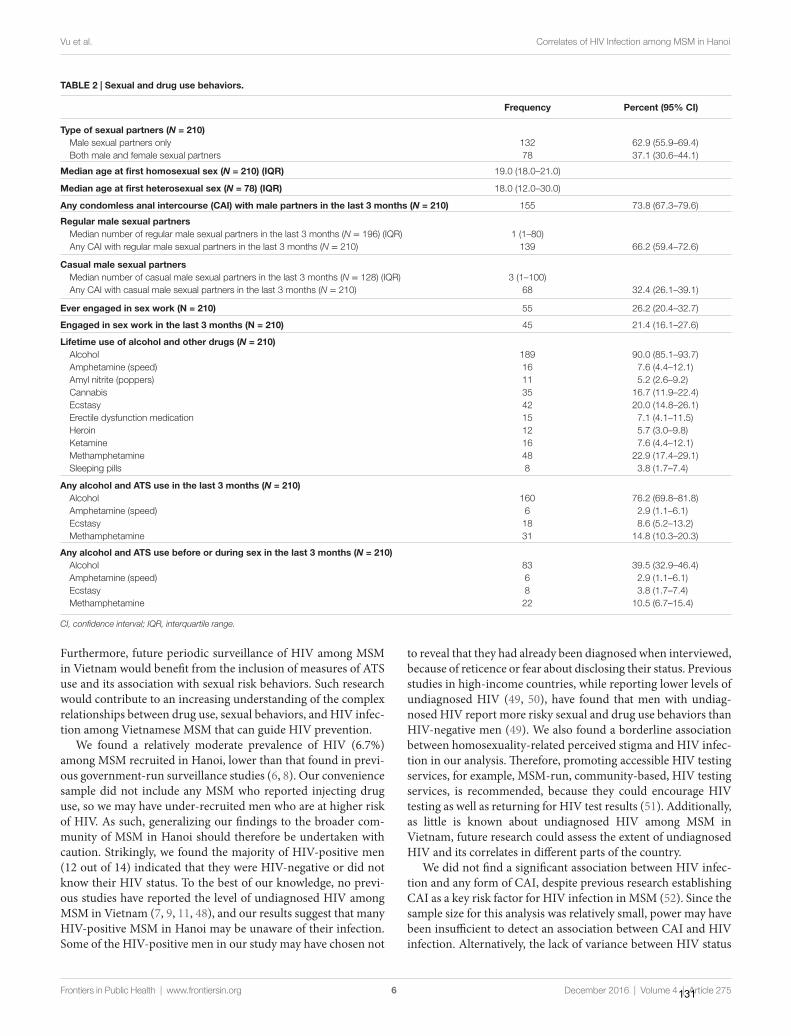
TaBle 2 | sexual and drug use behaviors.
Frequency Percent (95% ci)
Type of sexual partners (N = 210) Male sexual partners only 132 62.9 (55.9–69.4) Both male and female sexual partners 78 37.1 (30.6–44.1)
Median age at first homosexual sex (N = 210) (iQr) 19.0 (18.0–21.0)
Median age at first heterosexual sex (N = 78) (iQr) 18.0 (12.0–30.0)
any condomless anal intercourse (cai) with male partners in the last 3 months (N = 210) 155 73.8 (67.3–79.6)
regular male sexual partners Median number of regular male sexual partners in the last 3 months (N = 196) (IQR) 1 (1–80) Any CAI with regular male sexual partners in the last 3 months (N = 210) 139 66.2 (59.4–72.6)
casual male sexual partners Median number of casual male sexual partners in the last 3 months (N = 128) (IQR) 3 (1–100) Any CAI with casual male sexual partners in the last 3 months (N = 210) 68 32.4 (26.1–39.1)
ever engaged in sex work (n = 210) 55 26.2 (20.4–32.7)
engaged in sex work in the last 3 months (n = 210) 45 21.4 (16.1–27.6)
lifetime use of alcohol and other drugs (N = 210) Alcohol 189 90.0 (85.1–93.7) Amphetamine (speed) 16 7.6 (4.4–12.1) Amyl nitrite (poppers) 11 5.2 (2.6–9.2) Cannabis 35 16.7 (11.9–22.4) Ecstasy 42 20.0 (14.8–26.1) Erectile dysfunction medication 15 7.1 (4.1–11.5) Heroin 12 5.7 (3.0–9.8) Ketamine 16 7.6 (4.4–12.1) Methamphetamine 48 22.9 (17.4–29.1) Sleeping pills 8 3.8 (1.7–7.4)
any alcohol and aTs use in the last 3 months (N = 210) Alcohol 160 76.2 (69.8–81.8) Amphetamine (speed) 6 2.9 (1.1–6.1) Ecstasy 18 8.6 (5.2–13.2) Methamphetamine 31 14.8 (10.3–20.3)
any alcohol and aTs use before or during sex in the last 3 months (N = 210) Alcohol 83 39.5 (32.9–46.4) Amphetamine (speed) 6 2.9 (1.1–6.1) Ecstasy 8 3.8 (1.7–7.4) Methamphetamine 22 10.5 (6.7–15.4)
CI, confidence interval; IQR, interquartile range.
6
Vu et al. Correlates of HIV Infection among MSM in Hanoi
Frontiers in Public Health | www.frontiersin.org December 2016 | Volume 4 | Article 275
Furthermore, future periodic surveillance of HIV among MSM in Vietnam would benefit from the inclusion of measures of ATS use and its association with sexual risk behaviors. Such research would contribute to an increasing understanding of the complex relationships between drug use, sexual behaviors, and HIV infec-tion among Vietnamese MSM that can guide HIV prevention.
We found a relatively moderate prevalence of HIV (6.7%) among MSM recruited in Hanoi, lower than that found in previ-ous government-run surveillance studies (6, 8). Our convenience sample did not include any MSM who reported injecting drug use, so we may have under-recruited men who are at higher risk of HIV. As such, generalizing our findings to the broader com-munity of MSM in Hanoi should therefore be undertaken with caution. Strikingly, we found the majority of HIV-positive men (12 out of 14) indicated that they were HIV-negative or did not know their HIV status. To the best of our knowledge, no previ-ous studies have reported the level of undiagnosed HIV among MSM in Vietnam (7, 9, 11, 48), and our results suggest that many HIV-positive MSM in Hanoi may be unaware of their infection. Some of the HIV-positive men in our study may have chosen not
to reveal that they had already been diagnosed when interviewed, because of reticence or fear about disclosing their status. Previous studies in high-income countries, while reporting lower levels of undiagnosed HIV (49, 50), have found that men with undiag-nosed HIV report more risky sexual and drug use behaviors than HIV-negative men (49). We also found a borderline association between homosexuality-related perceived stigma and HIV infec-tion in our analysis. Therefore, promoting accessible HIV testing services, for example, MSM-run, community-based, HIV testing services, is recommended, because they could encourage HIV testing as well as returning for HIV test results (51). Additionally, as little is known about undiagnosed HIV among MSM in Vietnam, future research could assess the extent of undiagnosed HIV and its correlates in different parts of the country.
We did not find a significant association between HIV infec-tion and any form of CAI, despite previous research establishing CAI as a key risk factor for HIV infection in MSM (52). Since the sample size for this analysis was relatively small, power may have been insufficient to detect an association between CAI and HIV infection. Alternatively, the lack of variance between HIV status
131
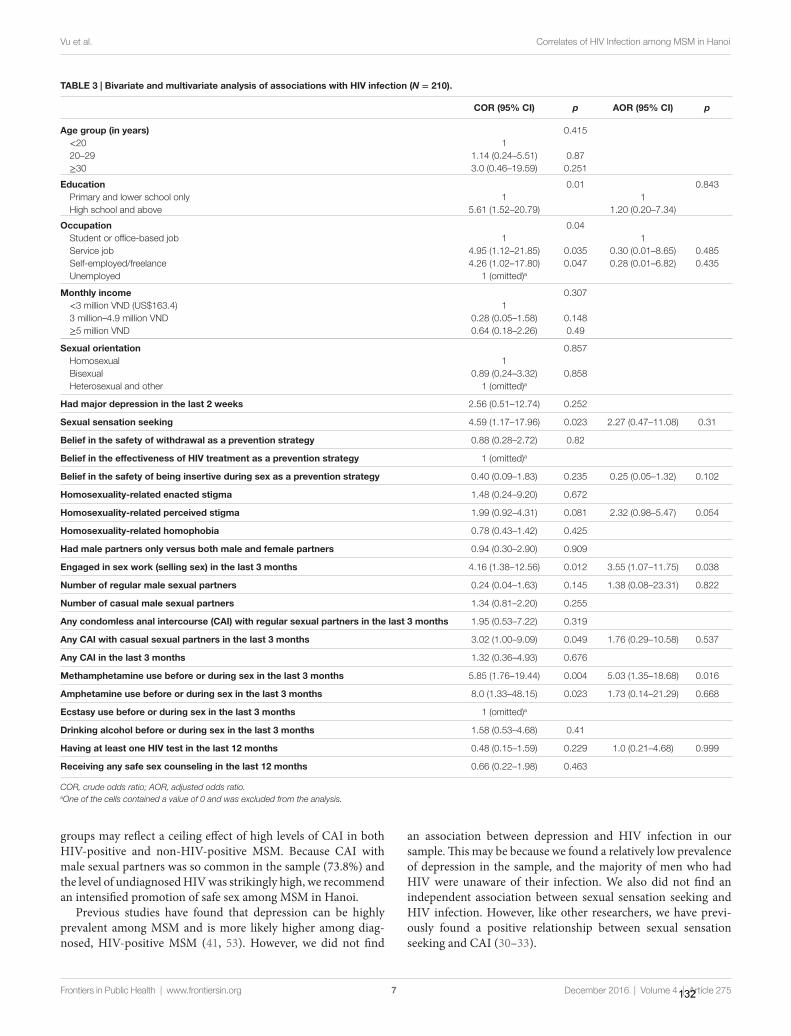
TaBle 3 | Bivariate and multivariate analysis of associations with hiV infection (N = 210).
cOr (95% ci) p aOr (95% ci) p
age group (in years) 0.415 <20 1 20–29 1.14 (0.24–5.51) 0.87 ≥30 3.0 (0.46–19.59) 0.251
education 0.01 0.843 Primary and lower school only 1 1 High school and above 5.61 (1.52–20.79) 1.20 (0.20–7.34)
Occupation 0.04 Student or office-based job 1 1 Service job 4.95 (1.12–21.85) 0.035 0.30 (0.01–8.65) 0.485 Self-employed/freelance 4.26 (1.02–17.80) 0.047 0.28 (0.01–6.82) 0.435 Unemployed 1 (omitted)a
Monthly income 0.307 <3 million VND (US$163.4) 1 3 million–4.9 million VND 0.28 (0.05–1.58) 0.148 ≥5 million VND 0.64 (0.18–2.26) 0.49
sexual orientation 0.857 Homosexual 1 Bisexual 0.89 (0.24–3.32) 0.858 Heterosexual and other 1 (omitted)a
had major depression in the last 2 weeks 2.56 (0.51–12.74) 0.252
sexual sensation seeking 4.59 (1.17–17.96) 0.023 2.27 (0.47–11.08) 0.31
Belief in the safety of withdrawal as a prevention strategy 0.88 (0.28–2.72) 0.82
Belief in the effectiveness of hiV treatment as a prevention strategy 1 (omitted)a
Belief in the safety of being insertive during sex as a prevention strategy 0.40 (0.09–1.83) 0.235 0.25 (0.05–1.32) 0.102
homosexuality-related enacted stigma 1.48 (0.24–9.20) 0.672
homosexuality-related perceived stigma 1.99 (0.92–4.31) 0.081 2.32 (0.98–5.47) 0.054
homosexuality-related homophobia 0.78 (0.43–1.42) 0.425
had male partners only versus both male and female partners 0.94 (0.30–2.90) 0.909
engaged in sex work (selling sex) in the last 3 months 4.16 (1.38–12.56) 0.012 3.55 (1.07–11.75) 0.038
number of regular male sexual partners 0.24 (0.04–1.63) 0.145 1.38 (0.08–23.31) 0.822
number of casual male sexual partners 1.34 (0.81–2.20) 0.255
any condomless anal intercourse (cai) with regular sexual partners in the last 3 months 1.95 (0.53–7.22) 0.319
any cai with casual sexual partners in the last 3 months 3.02 (1.00–9.09) 0.049 1.76 (0.29–10.58) 0.537
any cai in the last 3 months 1.32 (0.36–4.93) 0.676
Methamphetamine use before or during sex in the last 3 months 5.85 (1.76–19.44) 0.004 5.03 (1.35–18.68) 0.016
amphetamine use before or during sex in the last 3 months 8.0 (1.33–48.15) 0.023 1.73 (0.14–21.29) 0.668
ecstasy use before or during sex in the last 3 months 1 (omitted)a
Drinking alcohol before or during sex in the last 3 months 1.58 (0.53–4.68) 0.41
having at least one hiV test in the last 12 months 0.48 (0.15–1.59) 0.229 1.0 (0.21–4.68) 0.999
receiving any safe sex counseling in the last 12 months 0.66 (0.22–1.98) 0.463
COR, crude odds ratio; AOR, adjusted odds ratio.aOne of the cells contained a value of 0 and was excluded from the analysis.
7
Vu et al. Correlates of HIV Infection among MSM in Hanoi
Frontiers in Public Health | www.frontiersin.org December 2016 | Volume 4 | Article 275
groups may reflect a ceiling effect of high levels of CAI in both HIV-positive and non-HIV-positive MSM. Because CAI with male sexual partners was so common in the sample (73.8%) and the level of undiagnosed HIV was strikingly high, we recommend an intensified promotion of safe sex among MSM in Hanoi.
Previous studies have found that depression can be highly prevalent among MSM and is more likely higher among diag-nosed, HIV-positive MSM (41, 53). However, we did not find
an association between depression and HIV infection in our sample. This may be because we found a relatively low prevalence of depression in the sample, and the majority of men who had HIV were unaware of their infection. We also did not find an independent association between sexual sensation seeking and HIV infection. However, like other researchers, we have previ-ously found a positive relationship between sexual sensation seeking and CAI (30–33).
132

8
Vu et al. Correlates of HIV Infection among MSM in Hanoi
Frontiers in Public Health | www.frontiersin.org December 2016 | Volume 4 | Article 275
Our study had several limitations. Since MSM are a hid-den population in Vietnam, we used a convenience sampling approach, as a result of which our findings may not be rep-resentative of the broader MSM population in Hanoi. Our sample is more likely to be representative of young MSM in urban settings in Vietnam who are students or self-employed and have lower incomes. As MSM are a hidden population in Vietnam, previous studies have also used a variety of non-random convenience sampling methods and, as in many high income countries, no randomized samples of MSM have been recruited in Vietnam (8, 9, 38, 54–56). Also, although we tried to eliminate reporting bias during the interview process, our findings might reflect underreporting of sexual and drug use behaviors and other socially sensitive issues. Additionally, men who engaged in transactional sex were disproportionately affected by HIV (57). As one fifth of the sample engaged in sex work, assessing sex practices with their sexual partners would have been useful but no such assessment was included in our study.
cOnclUsiOn
We found a moderate prevalence of HIV infection among MSM in Hanoi, Vietnam, and most of the men who tested HIV-positive seemed to be unaware of infection. HIV infection was associated with sex-related methamphetamine use and engagement in sex work. Our analytical and descriptive findings point to several recommendations. For HIV prevention, we recommend an integration of interventions for methamphetamine use into HIV prevention, an intensified promotion of safe sex, and implemen-tation of community-based, MSM-run, or MSM-friendly HIV testing services in Hanoi, Vietnam. In research, we recommend the routine assessment of ATS use in national HIV surveillance and research to enable analysis of trends in ATS use and associa-tions with sexual behaviors. We also recommend further study of
men’s beliefs and practices with respect to various harm reduction strategies. Finally, we urge examination of the extent of undiag-nosed HIV infection in MSM in different parts of Vietnam.
aUThOr cOnTriBUTiOns
NV led the development of the research protocol and data collec-tion tools, undertook data collection and data analysis, wrote the initial draft of the manuscript, and prepared the final manuscript. JW and MH guided and supervised the development of the research protocol, data collection and analysis, and contributed to the writing of the manuscript. HP, LL, GT, and TD provided advice and guidance on the research protocol and data collection and contributed to the manuscript.
acKnOWleDgMenTs
We acknowledge the great support and input from staff of the Institute of Preventive Medicine and Public Health, Hanoi Medical University, Hanoi Centre of HIV/AIDS Prevention and Control, Center for Community Health Promotion, Center for Promotion of Quality of Life and leaders and representatives of community-based organizations of MSM in Hanoi during the data collection process.
FUnDing
NV was supported by an Australia Awards Scholarship to study at UNSW Australia. The study received financial support from the Faculty of Arts and Social Sciences, UNSW Australia. The Centre for Social Research in Health is supported by the Australian Government Department of Health. Funding agencies were not involved in the development of the research protocol, data collection, data analysis, interpretation, or the dissemination of research findings.
reFerences
1. Nguyen TH, Wolffers I. HIV infection in Vietnam. Lancet (1994) 343(8894):410. doi:10.1016/S0140-6736(94)91239-4
2. Quan VM, Chung A, Long HT, Dondero TJ. HIV in Vietnam: the evolv-ing epidemic and the prevention response, 1996 through 1999. J Acquir Immune Defic Syndr (2000) 25(4):360–9. doi:10.1097/00126334-200012010- 00011
3. Sullivan PS, Hamouda O, Delpech V, Geduld JE, Prejean J, Semaille C, et al. Reemergence of the HIV epidemic among men who have sex with men in North America, Western Europe, and Australia, 1996-2005. Ann Epidemiol (2009) 19(6):423–31. doi:10.1016/j.annepidem.2009.03.004
4. Socialist Republic of Vietnam. Vietnam AIDS Response Progress Report 2014. Following up the 2011 Political Declaration on HIV/AIDS. Hanoi, Vietnam (2014).
5. Colby D, Cao NH, Doussantousse S. Men who have sex with men and HIV in Vietnam: a review. AIDS Educ Prev (2004) 16(1):45–54. doi:10.1521/aeap.16.1.45.27722
6. Garcia MC, Meyer SB, Ward P. Elevated HIV prevalence and risk behaviours among men who have sex with men (MSM) in Vietnam: a systematic review. BMJ Open (2012) 2(5). doi:10.1136/bmjopen-2012-001511
7. Nguyen TA, Nguyen HT, Le GT, Detels R. Prevalence and risk factors asso-ciated with HIV infection among men having sex with men in Ho Chi Minh City, Vietnam. AIDS Behav (2008) 12(3):476–82. doi:10.1007/s10461-007- 9267-y
8. Vietnam Ministry of Health. Results from the HIV/STI Intergrated Biological and Behavioural Surveillance (IBBS) in Vietnam, 2005-2006. Hanoi, Vietnam: Ministry of Health (2006).
9. Vietnam Ministry of Health. Results from the HIV/STI Biological and Behavioral Surveillance (Ibbs) in Vietnam – Round II 2009. Hanoi, Vietnam: Ministry of Health (2011).
10. Le TM, Lee PC, Stewart DE, Long TN, Quoc CN. What are the risk factors for HIV in men who have sex with men in Ho Chi Minh City, Vietnam? A cross-sectional study. BMC Public Health (2016) 16(1):406. doi:10.1186/s12889-016-3088-8
11. Pham QD, Nguyen TV, Hoang CQ, Cao V, Khuu NV, Phan HT, et al. Prevalence of HIV/STIs and associated factors among men who have sex with men in An Giang, Vietnam. Sex Transm Dis (2012) 39(10):799–806. doi:10.1097/OLQ.0b013e318265b180
12. Colfax G, Santos GM, Chu P, Vittinghoff E, Pluddemann A, Kumar S, et al. Amphetamine-group substances and HIV. Lancet (2010) 376(9739):458–74. doi:10.1016/S0140-6736(10)60753-2
13. Thu Vu NT, Maher L, Zablotska I. Amphetamine-type stimulants and HIV infection among men who have sex with men: implications on HIV research and prevention from a systematic review and meta-analysis. J Int AIDS Soc (2015) 18(1):19273. doi:10.7448/IAS.18.1.19273
14. Vu NT, Holt M, Phan HT, Le HT, La LT, Tran GM, et al. Amphetamine-type stimulant use among men who have sex with men (MSM) in Vietnam: results from a socio-ecological, community-based study. Drug Alcohol Depend (2016) 158:110–7. doi:10.1016/j.drugalcdep.2015.11.016
133
9
Vu et al. Correlates of HIV Infection among MSM in Hanoi
Frontiers in Public Health | www.frontiersin.org December 2016 | Volume 4 | Article 275
15. Horton P. ‘I thought I was the only one’: the misrecognition of LGBT youth in contemporary Vietnam. Cult Health Sex (2014) 16(8):960–73. doi:10.1080/13691058.2014.924556
16. Secor AM, Wahome E, Micheni M, Rao D, Simoni JM, Sanders EJ, et al. Depression, substance abuse and stigma among men who have sex with men in coastal Kenya. AIDS (2015) 29(Suppl 3):S251–9. doi:10.1097/QAD.0000000000000846
17. Mills TC, Paul J, Stall R, Pollack L, Canchola J, Chang YJ, et al. Distress and depression in men who have sex with men: the Urban Men’s Health Study. Am J Psychiatry (2004) 161(2):278–85. doi:10.1176/appi.ajp.161.2.278
18. Klein H. Depression and HIV risk taking among men who have sex with other men (MSM) and who use the internet to find partners for unprotected sex. J Gay Lesbian Ment Health (2014) 18(2):164–89. doi:10.1080/19359705.2013. 834858
19. Fendrich M, Avci O, Johnson TP, Mackesy-Amiti ME. Depression, substance use and HIV risk in a probability sample of men who have sex with men. Addict Behav (2013) 38(3):1715–8. doi:10.1016/j.addbeh.2012.09.005
20. Gee R. Primary care health issues among men who have sex with men. J Am Acad Nurse Pract (2006) 18(4):144–53. doi:10.1111/j.1745-7599.2006. 00117.x
21. Ross MW, Berg RC, Schmidt AJ, Hospers HJ, Breveglieri M, Furegato M, et al. Internalised homonegativity predicts HIV-associated risk behavior in European men who have sex with men in a 38-country cross-sectional study: some public health implications of homophobia. BMJ Open (2013) 3(2):e001928. doi:10.1136/bmjopen-2012-001928
22. Deuba K, Ekstrom AM, Shrestha R, Ionita G, Bhatta L, Karki DK. Psychosocial health problems associated with increased HIV risk behavior among men who have sex with men in Nepal: a cross-sectional survey. PLoS One (2013) 8(3):e58099. doi:10.1371/journal.pone.0058099
23. De Santis JP, Colin JM, Provencio Vasquez E, McCain GC. The relationship of depressive symptoms, self-esteem, and sexual behaviors in a predominantly Hispanic sample of men who have sex with men. Am J Mens Health (2008) 2(4):314–21. doi:10.1177/1557988307312883
24. Lee JH, Gamarel KE, Bryant KJ, Zaller ND, Operario D. Discrimination, men-tal health, and substance use disorders among sexual minority populations. LGBT Health (2016) 3(4):258–65. doi:10.1089/lgbt.2015.0135
25. Darke S, Kaye S, McKetin R, Duflou J. Major physical and psychological harms of methamphetamine use. Drug Alcohol Rev (2008) 27(3):253–62. doi:10.1080/09595230801923702
26. Diaz RM, Ayala G, Bein E. Sexual risk as an outcome of social oppression: data from a probability sample of Latino gay men in three U.S. cities. Cultur Divers Ethnic Minor Psychol (2004) 10(3):255–67. doi:10.1037/1099-9809.10. 3.255
27. Huebner DM, Davis MC, Nemeroff CJ, Aiken LS. The impact of internalized homophobia on HIV preventive interventions. Am J Community Psychol (2002) 30(3):327–48. doi:10.1023/A:1015325303002
28. Andrinopoulos K, Hembling J, Guardado ME, de Maria Hernández F, Nieto AI, Melendez G. Evidence of the negative effect of sexual minority stigma on HIV testing among MSM and transgender women in San Salvador, El Salvador. AIDS Behav (2015) 19(1):60–71. doi:10.1007/s10461-014-0813-0
29. O’Cleirigh C, Newcomb ME, Mayer KH, Skeer M, Traeger L, Safren SA. Moderate levels of depression predict sexual transmission risk in HIV-infected MSM: a longitudinal analysis of data from six sites involved in a “pre-vention for positives” study. AIDS Behav (2013) 17(5):1764–9. doi:10.1007/s10461-013-0462-8
30. Vu NT, Holt M, Phan HT, La LT, Tran GM, Doan TT, et al. The relationship between methamphetamine use, sexual sensation seeking and condomless anal intercourse among men who have sex with men in Vietnam: results of a community-based, cross-sectional study. AIDS Behav (2016). doi:10.1007/s10461-016-1467-x
31. Chng CL, Geliga-Vargas J. Ethnic identity, gay identity, sexual sensation seeking and HIV risk taking among multiethnic men who have sex with men. AIDS Educ Prev (2000) 12(4):326–39.
32. Kalichman SC, Heckman T, Kelly JA. Sensation seeking as an explana-tion for the association between substance use and HIV-related risky sexual behavior. Arch Sex Behav (1996) 25(2):141–54. doi:10.1007/BF0 2437933
33. Kalichman SC, Simbayi L, Jooste S, Vermaak R, Cain D. Sensation seeking and alcohol use predict HIV transmission risks: prospective study of sexually
transmitted infection clinic patients, Cape Town, South Africa. Addict Behav (2008) 33(12):1630–3. doi:10.1016/j.addbeh.2008.07.020
34. Heidinger B, Gorgens K, Morgenstern J. The effects of sexual sensation seeking and alcohol use on risky sexual behavior among men who have sex with men. AIDS Behav (2015) 19(3):431–9. doi:10.1007/s10461-014-0871-3
35. Newcomb ME, Clerkin EM, Mustanski B. Sensation seeking moderates the effects of alcohol and drug use prior to sex on sexual risk in young men who have sex with men. AIDS Behav (2011) 15(3):565–75. doi:10.1007/s10461-010-9832-7
36. Parsons JT, Schrimshaw EW, Wolitski RJ, Halkitis PN, Purcell DW, Hoff CC, et al. Sexual harm reduction practices of HIV-seropositive gay and bisexual men: serosorting, strategic positioning, and withdrawal before ejac-ulation. AIDS (2005) 19(Suppl 1):S13–25. doi:10.1097/01.aids.0000167348. 15750.9a
37. Holt M, Lea T, Mao L, Zablotska I, Prestage G, de Wit J. Brief report: HIV prevention by Australian gay and bisexual men with casual partners: the emergence of undetectable viral load as one of a range of risk reduction strategies. J Acquir Immune Defic Syndr (2015) 70(5):545–8. doi:10.1097/QAI.0000000000000787
38. Ha H, Risser JM, Ross MW, Huynh NT, Nguyen HT. Homosexuality-related stigma and sexual risk behaviors among men who have sex with men in Hanoi, Vietnam. Arch Sex Behav (2015) 44(2):349–56. doi:10.1007/s10508-014-0450-8
39. Kalichman SC, Rompa D. Sexual sensation seeking and Sexual Compulsivity Scales: reliability, validity, and predicting HIV risk behavior. J Pers Assess (1995) 65(3):586–601. doi:10.1207/s15327752jpa6503_16
40. Mao L, Kidd MR, Rogers G, Andrews G, Newman CE, Booth A, et al. Social factors associated with major depressive disorder in homosexually active, gay men attending general practices in urban Australia. Aust N Z J Public Health (2009) 33(1):83–6. doi:10.1111/j.1753-6405.2009.00344.x
41. Hirshfield S, Wolitski RJ, Chiasson MA, Remien RH, Humberstone M, Wong T. Screening for depressive symptoms in an online sample of men who have sex with men. AIDS Care (2008) 20(8):904–10. doi:10.1080/ 09540120701796892
42. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depres-sion severity measure. J Gen Intern Med (2001) 16(9):606–13. doi:10.1046/ j.1525-1497.2001.016009606.x
43. Hosmer DW. Chapter 4: Model-building strategies and methods for logistic regression. In: Lemeshow S, Sturdivant RX, editors. Applied Logistic Regression. 3rd ed. Hoboken, NJ: Wiley (2013). p. 89–151.
44. Morineau G, Nugrahini N, Riono P, Nurhayati, Girault P, Mustikawati DE, et al. Sexual risk taking, STI and HIV prevalence among men who have sex with men in six Indonesian cities. AIDS Behav (2011) 15(5):1033–44. doi:10.1007/s10461-009-9590-6
45. Lyons A, Pitts M, Grierson J. Methamphetamine use in a nationwide online sample of older Australian HIV-positive and HIV-negative gay men. Drug Alcohol Rev (2013) 32(6):603–10. doi:10.1111/dar.12072
46. Truong HM, Kellogg TA, McFarland W, Louie B, Klausner JD, Philip SS, et al. Sentinel surveillance of HIV-1 transmitted drug resistance, acute infection and recent infection. PLoS One (2011) 6(10):e25281. doi:10.1371/journal.pone.0025281
47. Kral AH, Lorvick J, Ciccarone D, Wenger L, Gee L, Martinez A, et al. HIV prevalence and risk behaviors among men who have sex with men and inject drugs in San Francisco. J Urban Health (2005) 82(1 Suppl 1):i43–50. doi:10.1093/jurban/jti023
48. Nguyen TV, Van Khuu N, Nguyen PD, Tran HP, Phan HT, Phan LT, et al. Sociodemographic factors, sexual behaviors, and alcohol and recreational drug use associated with HIV among men who have sex with men in Southern Vietnam. AIDS Behav (2016) 20(10):2357–71. doi:10.1007/s10461-015-1265-x
49. Holt M, Lea T, Asselin J, Hellard M, Prestage G, Wilson D, et al. The prevalence and correlates of undiagnosed HIV among Australian gay and bisexual men: results of a national, community-based, bio-behavioural survey. J Int AIDS Soc (2015) 18:20526. doi:10.7448/IAS.18.1.20526
50. Ferrer L, Furegato M, Foschia JP, Folch C, Gonzalez V, Ramarli D, et al. Undiagnosed HIV infection in a population of MSM from six European cities: results from the Sialon project. Eur J Public Health (2015) 25(3):494–500. doi:10.1093/eurpub/cku139
51. World Health Organization (WHO). Consolidated Guidelines on HIV Testing Services. Geneva, Switzerland: World Health Organization (2015).
134

10
Vu et al. Correlates of HIV Infection among MSM in Hanoi
Frontiers in Public Health | www.frontiersin.org December 2016 | Volume 4 | Article 275
52. Beyrer C. HIV epidemiology update and transmission factors: risks and risk contexts – 16th International AIDS Conference epidemiology plenary. Clin Infect Dis (2007) 44(7):981–7. doi:10.1086/512371
53. Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull (2003) 129(5):674–97. doi:10.1037/0033-2909.129.5.674
54. National Institute of Hygiene and Epidemioloty (Vietnam Ministry of Health). HIV/STI Intergrated Biological and Behavioural Surveillance (IBBS) in Vietnam. Results from Round III and Trends Across Three Round (2005-2009-2013) of Survey. Hanoi, Vietnam: National Institute of Hygiene and Epidemiology (2014).
55. Bengtsson L, Lu X, Liljeros F, Thanh HH, Thorson A. Strong propensity for HIV transmission among men who have sex with men in Vietnam: behavioural data and sexual network modelling. BMJ Open (2014) 4(1):e003526. doi:10.1136/bmjopen-2013-003526
56. Garcia MC, Duong QL, Meyer SB, Ward PR. Multiple and concurrent sexual partnerships among men who have sex with men in Viet Nam: results from a National Internet-based Cross-sectional Survey. Health Promot Int (2016) 31(1):133–43. doi:10.1093/heapro/dau097
57. Oldenburg CE, Perez-Brumer AG, Reisner SL, Mimiaga MJ. Transactional sex and the HIV epidemic among men who have sex with men (MSM): results from a systematic review and meta-analysis. AIDS Behav (2015) 19(12):2177–83. doi:10.1007/s10461-015-1010-5
Conflict of Interest Statement: The authors declare that the research was con-ducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer ZW and handling Editor declared their shared affiliation, and the handling Editor states that the process nevertheless met the standards of a fair and objective review.
Copyright © 2016 Vu, Holt, Phan, La, Tran, Doan and de Wit. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
135
CHAPTER 7
AMPHETAMINE-TYPE-STIMULANTS (ATS) USE AND
HOMOSEXUALITY-RELATED ENACTED STIGMA ARE ASSOCIATED
WITH DEPRESSION AMONG MEN WHO HAVE SEX WITH MEN
(MSM) IN TWO MAJOR CITIES IN VIETNAM IN 2014
Author Contributions Nga Thi Thu VU1,2, Martin HOLT1, Huong Thi Thu PHAN3, Lan Thi LA4, Gioi
Minh TRAN5, Tung Thanh DOAN5, Trang Nhu Nguyen NGUYEN6 and John de
Wit1
1: Center for Social Research in Health, University of New South Wales,
Sydney, New South Wales, Australia; 2: Institute of Preventive Medicine and
Public Health, Hanoi Medical University, Hanoi, Vietnam; 3: Vietnam
Administration for HIV/AIDS Prevention and Control, Hanoi, Vietnam; 4: Hanoi
Center of HIV/AIDS Prevention and Control, Hanoi, Vietnam; 5: Center for
Community Health Promotion, Hanoi, Vietnam; 6: Center for Promotion of
Quality of Life, Ho Chi Minh City, Vietnam.
Reference
Vu NTT, Holt M, Phan HTT, La LT, Tran GM, Doan TT, et al. Amphetamine-
Type-Stimulants (ATS) Use and Homosexuality-Related Enacted Stigma Are
Associated With Depression Among Men Who Have Sex With Men (MSM) in
Two Major Cities in Vietnam in 2014. Substance use & misuse. 2017:1-9.
Declaration
I certify that this publication was a direct result of my research toward this PhD,
and that reproduction in this thesis does not breach copyright regulations.
Nga Thi Thu Vu June 2017
136

Copyright permission
As the first author of the original article, the candidate has the right to include
this article in this thesis. This is an accepted manuscript of an article published
by Taylor and Francis in journal Substance Use and Misuse on 24th April, 2017,
available online
http://www.tandfonline.com/doi/full/10.1080/10826084.2017.1284233
137

SUBSTANCE USE & MISUSEhttp://dx.doi.org/./..
ORIGINAL ARTICLE
Amphetamine-Type-Stimulants (ATS) Use and Homosexuality-Related EnactedStigma Are Associated With Depression Among Men Who Have Sex With Men(MSM) in Two Major Cities in Vietnam in
Nga Thi Thu Vua,b, Martin Holta, Huong Thi Thu Phanc, Lan Thi Lad, Gioi Minh Trane, Tung Thanh Doane,Trang Nguyen Nhu Nguyenf, and John de Wit a
aCentre for Social Research in Health, University of New South Wales, Sydney, Australia; bInstitute of Preventive Medicine and Public Health,Hanoi Medical University, Hanoi, Vietnam; cVietnam Administration for HIV/AIDS Prevention and Control, Ministry of Health, Hanoi, Vietnam;dHanoi Centre of HIV/AIDS Prevention and Control, Hanoi, Vietnam; eCenter for Community Health Promotion, Hanoi, Vietnam; fCentre forPromotion of Quality of Life, Ho Chi Minh City, Vietnam
KEYWORDSMen who have sex with men;amphetamine-type-stimulants;homosexuality-relatedstigma and discrimination;depression; Vietnam
ABSTRACTBackground: Men who have sex with men (MSM) are disproportionately affected by mental healthconcerns, including depression. Amphetamine-type-stimulants (ATS) use and homosexuality-relatedstigma and discrimination have been found associated with depression among MSM. Objectives: Toassess the prevalence of depression and its associations with ATS use and homosexuality-relatedstigma and discrimination among MSM in Vietnam. Methods: 622 MSM were conveniently recruitedin Hanoi and Ho Chi Minh city, Vietnam, from September to December 2014. We collected informationon demographic characteristics, ATS, alcohol and other drug use, sexual behaviors, homosexuality-related and discrimination stigma, and sexual sensation-seeking. Depression and suicidal thoughtswere assessed by the Patient Health Questionnaire (PHQ-9). We assessed associations of depressionwith ATS use and homosexuality-related stigma and discrimination using logistic regression. Results:Of 622 sampled MSM, 11.3% were classified as having major depression, 9.8% reported any suicidalthoughts in the last two weeks, 30.4% ever had used any ATS, 88.8% ever ad drank alcohol and 21.5%had ever used any other drugs. In multivariate analysis, depression was significantly associated withATS use (Adjusted Odds Ratio [AOR: 2.20; (95% Confidence Interval (CI): 1.32–3.67], younger age ofsexual debut with another man (AOR: 0.09; 95% CI: 0.02–0.50), and greater enacted homosexuality-related stigma (AOR: 1.97; 95% CI: 1.19–3.26). Conclusions: We found a moderate prevalence of depres-sion among sampled MSM, which was associated with ATS use and enacted homosexuality-relatedstigma. We recommend integrating assessment and interventions regarding depression and metham-phetamine use into gay-friendly, culturally adapted holistic HIV prevention for MSM in Vietnam.
Men who have sex with men (MSM) have been foundto be disproportionately affected by psychological dis-orders, including depression and anxiety (Meyer, 2003;Safren, Blashill, & O’Cleirigh, 2011). Depression andrelated forms of psychological distress have been identi-fied as priority health issues among men who have sexwith men (Gee, 2006; Sullivan et al., 2009). In the UnitedSates, as well as other parts of the world, the prevalenceof depression among MSM is found to be higher thanamong heterosexual men (Frost & LeBlanc, 2014; Meyer,2003). In the United States and in European countriessuch as Belgium and Estonia, recent studies have reporteda prevalence of depression of approximately 30% amongMSM (De Santis, Colin, Provencio Vasquez, & McCain,2008; Parker, Lohmus, Valk, Mangine, & Ruutel, 2015;Wim, Christiana, & Marie, 2014). Recent studies from
CONTACT Nga Thi Thu Vu [email protected] Center for Social Research in Health, Level John Goodsell Building, UNSW Sydney, Kensington,Sydney , Australia.
Supplemental data for this article can be accessed at http://dx.doi.org/./...
the Asia-Pacific region report varying levels of depressionamong MSM: 11% in India (Tomori et al., 2016), 46% inChina (Yan et al., 2014) and 61% in Nepal (Deuba et al.,2013). In Vietnam, recent studies have found a high levelof depression among a subgroup of MSM, male sex work-ers, ranging from 47% to 58% (Biello, Colby, Closson, &Mimiaga, 2014; Goldsamt, Clatts, Giang, & Yu, 2015; Old-enburg et al., 2014). A recently published study reporteda prevalence of depression of 68% among young MSM inHanoi (Ha, Risser, Ross, Huynh, & Nguyen, 2015).
Previous studies in different country settings havefound that MSM experiencing depression are more likelyto use stimulant drugs, including methamphetamine(Carrico et al., 2012; Stall et al., 2001), possibly as a meansto reduce anxiety and other symptoms, or to escape oravoid negative psychological states (Carrico et al., 2012).
© Taylor & Francis Group, LLC
138

2 N. T. T. VU ET AL.
Research also suggests that amphetamine-type-stimulant(ATS) use can result in psychological problems suchas depression (Darke, Kaye, McKetin, & Duflou, 2008;Folkman & Lazarus, 1988; Parrott, 2001). Use of stim-ulants, including methamphetamine or amphetamine, isalso associated with HIV infection (Thu Vu, Maher, &Zablotska, 2015). To achieve better outcomes in HIV pre-vention, it has been suggested to incorporate interven-tions for mental health problems alongside interventionsthat address the social and structural determinants ofrisky sexual behavior and HIV infection (Mayer et al.,2013; Safren, Reisner, Herrick, Mimiaga, & Stall, 2010).
In many parts of the world, despite efforts to promoteand protect the rights of sexual minority populations,social stigma and discrimination persist against MSM(Altman et al., 2012). Homosexuality-related stigma anddiscrimination can result in adverse psychological, phys-ical, and social outcomes (Mayer et al., 2013; Safrenet al., 2011). The Minority Stress Theory suggests thatsexual minorities tend to have higher levels of men-tal illness, including depression, because they experi-ence excess social and psychological stress (Meyer, 2003).Various studies have found that homosexuality-relatedsocial stigma does indeed increase the probability ofmental health problems in MSM in low, middle andhigh income countries, including anxiety, depression,and suicidal ideation (Choi, Steward, Miege, Hudes, &Gregorich, 2016; Gibbs & Rice, 2016; Mayer et al., 2013;Secor et al., 2015; Stahlman et al., 2015). MSM are alsodisproportionately affected by sexually transmitted infec-tions, including HIV (Beyrer et al., 2012; Gee, 2006).Previous studies have found direct and indirect associa-tions between homosexuality-related stigma, depressionand risky sexual behaviors among MSM, with depressionincreasing the risk of engaging in condomless anal inter-course (CAI) (Chakrapani, Newman, Shunmugam, Logie,& Samuel, 2017; Deuba et al., 2013; Mimiaga et al., 2013;Safren et al., 2011; Shiu et al., 2014; Tucker et al., 2014).
In Vietnam, a study conducted in 2011 foundthat a minority (21%) of MSM had ever experiencedhomosexuality-related stigma and discrimination (Haet al., 2015). Nevertheless, this study also found anassociation between homosexuality-related stigma anddiscrimination and risky sexual behavior, particularlyan increased number of sexual partners and engaging ininconsistent condom use (Ha et al., 2015). Recent studieshave found a relatively high level of CAI (Bengtsson, Lu,Liljeros, Thanh, & Thorson, 2014; Garcia et al., 2014;Pham et al., 2015), and a moderate level of ATS useamong MSM in Vietnam (Vu et al., 2016). Recent studiesin Vietnam have also found high a prevalence of depres-sion (68%) among MSM and male sex workers (58%)(Goldsamt et al., 2015; Ha et al., 2015). Recently, a study
on psychological disorders among male sex workers in HoChi Minh city reported that depression was significantlyassociated with sex work-related stigma, any recent druguse and experiencing sexual violence (Biello et al., 2014;Oldenburg et al., 2014). To date, however, no studies fromVietnam have assessed the correlates of depression in abroader sample of MSM. As part of a study assessing ATSuse, sexual risk behavior and HIV infection of MSM inHanoi and Ho Chi Minh City, the current analyses wereundertaken to assess the prevalence of depression and itsassociations with ATS use, homosexuality-related stigmaand discrimination and other correlates.
Methods
This was a cross-sectional, community-based study,conducted in collaboration with the Hanoi HIV/AIDSPrevention Center (Hanoi PAC), the Center for Commu-nity Health Promotion (CHP) in Hanoi, and the Cen-tre for Promotion of Quality of Life (Life Center) in HoChi Minh City (HCMC), Vietnam, during September-December 2014. CHP and Life Centre have outreach net-works that reach various subgroups of MSM. Because ofsocial stigma and discrimination towards homosexual-ity (Blanc, 2005; Ha et al., 2015), MSM are still a hid-den population in Vietnam and, as elsewhere, developinga sampling frame for a representative sample of MSM isnot possible. Therefore, a community-based, conveniencesampling method was used to recruit participants for thestudy. Study participants were recruited via several strate-gies at the same time. First, staff and peer outreach work-ers of the local collaborating organizations assisted withrecruiting participants via those organizations and groupsof MSM. Second, participants were asked to refer otherMSM to the study. Men were eligible to participate if theywere 18 years or older at the time of the study, reportedhaving anal sex with at least one man in the previous3 months, had a good command of the Vietnamese lan-guage and consented to participate. Men were screenedfor eligibility and interviewed after they had signed theParticipant Information and Consent Forms. A detaileddescription of the study design can be found elsewhere(Vu et al., 2016). The study received approval from theHuman Research Ethics Committee of UNSW Australia(reference HC14130), and from the Institutional ReviewBoard of the Hanoi School of Public Health (reference014_262/DD-YTCC).
Study locations
The study was conducted in the two biggest cities in Viet-nam: Hanoi in the Northern region and Ho Chi Minh City
139

SUBSTANCE USE & MISUSE 3
in the Southern part of Vietnam, where large communi-ties of MSM can be found. While homosexuality-relatedstigma and discrimination occur across Vietnam, Ho ChiMinh City is regarded as a more socially tolerant location,while Hanoi is considered a location where MSM canface more social stigma (Blanc, 2005).
Measures
Face-to-face, structured interviews using a self-reportquestionnaire were administered by experienced data col-lectors from Hanoi Medical University and by trainedMSM peers. The questionnaire was developed in Englishand translated into Vietnamese by the first author. Twomeetings with MSM informants were organized in Hanoiand Ho Chi Minh City to review the appropriateness ofthe language and acceptability of the questions. Men werealso asked to confirm colloquial terms used by MSM fordrug use, sexual orientation and sexual behavior in Viet-nam. The questionnaire was pilot-tested with ten MSM inHanoi and refined afterwards.
Dependent variableDepression was assessed with the Patient Health Ques-tionnaire 9 item scale (PHQ-9), which has been used withMSM in other studies (Hirshfield et al., 2008; Mao et al.,2009). The scale consists of nine items, such as “In thelast two weeks, how often have you had trouble falling orstaying asleep, or sleeping too much?” Participants pro-vided their answers on a scale ranging from 0 (not hav-ing the problem at all) to 3 (having the problem nearlyevery day). The items had good internal consistency inthis study (Cronbach’s ɑ = 0.80). Participants were cate-gorized as having major depressive disorder if they scored10 or more (Kroenke, Spitzer, & Williams, 2001).
Explanatory variablesDemographic characteristics. We collected informationregarding age, education, occupation, monthly income,self-reported sexual orientation, and self-reported HIVstatus. Men’s ages were calculated by subtracting date ofbirth from date of interview. The highest level of edu-cation men had completed was categorized as following:up to secondary school, high school, or vocational train-ing, and university or higher degree. Mens’ current occu-pation was grouped into five categories: student, office-based jobs, service jobs (working in restaurants, cafés,bars, discotheques, bathhouses or similar facilities), self-employed (or casually employed), and unemployed. Menwere asked to report their total monthly income from allsources and were classified into three groups: less than
3 million Vietnam Dong (VND) (equivalent to approxi-mately US$150 at the time of interviews), from 3 millionVND to 5 million VND and above 5 million VND.
HIV testing. Men were asked about their HIV testingbehaviors in the last 12 months. Men were categorized ashaving previously tested for HIV if they self-reported atleast one HIV test during the last 12 months.
ATS use, alcohol consumption and other drug use. Par-ticipants were asked questions about having used anymethamphetamine, amphetamine, ecstasy, alcohol orother substances (i.e., heroine, ketamine, marijuana, andamyl nitrite [‘poppers’]) during their lifetime (ever havingused ATS, alcohol or other drugs) and in the last threemonths (recently use). Men were also asked about theirrecent use of any ATS substance or alcohol before or dur-ing sex in the last three months (recently used ATS oralcohol before or during sex). Only measures of lifetime(ever) use were included in this analysis.
Sexual behaviors. Participants were asked about theirage at first sex with a man or a woman, ever havingengaged in sex work, having engaged in sex work in thelast 3 months, and the use of condoms during sexual inter-course with regular or casual male partners in the lastthree months.
Sexual sensation-seeking. We adapted the sexualsensation-seeking scale (Kalichman & Rompa, 1995)for our study population. The scale was reviewed andadapted for language appropriateness during our consul-tation meetings with MSM informants, and tested andrevised before interviews. One item from the originalscale was dropped and ten items assessing the propensityto seek exciting, novel and stimulating sexual expe-riences, for instance “I like wild, uninhibited sexualencounters”, were retained. The adapted scale can befound in the online supplemental material. Participantsprovided their answers on 4-point Likert-type scalesranging from 1 (not at all like me) to 4 (very much likeme). The items had good internal consistency in thisstudy (Cronbach’s ɑ = 0.72) and item scores were aver-aged; a higher score indicating a higher level of sexualsensation-seeking.
Stigma and discrimination related to homosexuality.We adapted an existing scale previously validated inan MSM population in Vietnam, to measure perceived(anticipated) homosexual stigma, enacted (experienced)homosexuality-related stigma and self-stigma (internal-ized homophobia) (Ha, Ross, Risser, & Nguyen, 2013).
140

4 N. T. T. VU ET AL.
The scale was reviewed and adapted for language appro-priateness during our consultation meetings with infor-mant MSM. After consultation, one item from theenacted stigma subscale and one item from the perceivedstigma subscale were dropped. The adapted scale encom-passed ten items measuring perceived homosexuality-related stigma, for instance “Many people are unwilling toaccept homosexual individuals” (1 = completely disagree,4 = completely agree); eight items pertaining to enactedhomosexuality-related stigma, for example “How oftenhave you lost a job or career opportunity due to yourengaging in homosexual activities” (1 = never, 4 =often); and eight items measuring internalized homo-phobia, for example “Sometimes you wish you were notgay/bisexual” (1 = totally disagree, 4 = totally agree).Responses were given on 4-point scales, with anchorsdepending on the questions. The full scale had goodoverall internal consistency in this study (Cronbach’sɑ = 0.74) and internal consistency for the subscales was0.66 (enacted sigma), 0.74 (perceived stigma) and 0.74(internal homophobia). Mean scores were calculated foreach sub-scale and higher scores indicated higher levelsof stigma.
Data analysis
To minimize data entry errors, questionnaire data wasdouble entered using EPIDATA 3.1. The two versionsof the dataset were compared to detect inconsistencies,which were checked and corrected. Descriptive and ana-lytical statistics were calculated using STATA version 13.0(Stata Corp, College Station, TX, USA). We report fre-quencies and percentages for categorical variables andmeans and standard deviations (SD), or medians andinterquartile ranges (IQR), for continuous variables. Wetested potential correlates of depression using logisticregression modeling, including demographic character-istics (age, education, income and occupation), life-timeuse of any ATS substances, life-time alcohol consump-tion and other drug use, recent HIV-related risky sex-ual behaviors, homosexuality-related stigma and discrim-ination and sexual sensation-seeking. Factors associatedwith depression (p < .10) were entered into a multi-variable logistic regression model. A final model includ-ing only covariates significantly associated with depres-sion (p < .05) was built using the strategy suggested byHosmer (2013). First, a base model containing all signifi-cant covariates identified in bivariable analyses was devel-oped. The least significant variable was eliminated fromthe base model and the nested model was compared withthe base model with a likelihood ratio test as suggestedby Vittinghoff and colleagues (Vittinghoff, Glidden, &Shiboski, 2012). If the test was nonsignificant (i.e. the
eliminated variable did not significantly contribute to thebase model) the nested model was retained. This elimi-nation process was continued until the final model wasreached, including only significant (p < .05) covariates.
Results
The final sample of participants included 622 men, amongwhom 303 men were recruited in Hanoi and the rest fromHo Chi Minh City; 30 men were referred to the studyteam but did not meet inclusion criteria, and two othermen were eligible and consented to participate but didnot complete their interviews. The demographic char-acteristics of the study participants have been describedelsewhere (Vu et al., 2016). This was a sample of youngMSM with a median age of 24 years (interquartile range[IQR]: 18.1–49.7; 77.5% were younger than 30 years old).Men had relatively high education levels (82.6% hadcompleted high school or higher education). The major-ity of sampled MSM were students or office-based staff(48.6%), and 54.8% had an average monthly income ofover five million Vietnam Dong or higher (approximatelyUS$ 250 or more). The majority of men (74.0%) self-identified as gay/homosexual, 18.7% identified as bisexualand the remainder reported being heterosexual or hav-ing another (unspecified) sexual orientation. The medianage of men at sexual debut with another man or womanwas 19.0 years. In the last 12 months, 54.5% had at leastone HIV test; nearly two-fifths of men did not know theirHIV status, with the majority (59.0%) self-reporting thatthey were HIV-negative. Men had a median score of per-ceived homosexuality-related stigma of 3.6 (IQR: 1.5–5),of enacted homosexuality-related stigma of 1.1 (IQR: 1–3), and of internalized homosexuality-related stigma of3.1 (SD: 0.8) (see Table 1). Men had an average sexualsensation-seeking score of 2.5 (SD: 0.4). Over one in tenmen (11.3%) were classified as having major depression atthe time of the survey (PHQ-9 score � 10).
Sexual and drug use behaviors of the sample are pre-sented in Table 2. Of the 622 men, 30.4% had ever usedany ATS use, 88.8% had ever drunk alcohol, and 21.5%had ever used any other drugs (ketamine, cannabis, hero-ine or poppers). In the last three months, 20.3% of par-ticipants had used any ATS, 77.0% had drunk alcoholand 15.8% had used any other drugs. In relation to self-reported engagement in sex work, 29.1% of men had everengaged in sex work (i.e. selling sex), and 23.2% hadengaged in sex work in the last three months. In the lastthree months, men had a median of 1 casual male sexualpartner (IQR: 1–90), and a median of 3 regular male part-ners (IQR: 1–25). The majority of participants (75.7%)self-reported any CAI in the past three months (68.3%had CAI with regular male sexual partners and 38.7% had
141
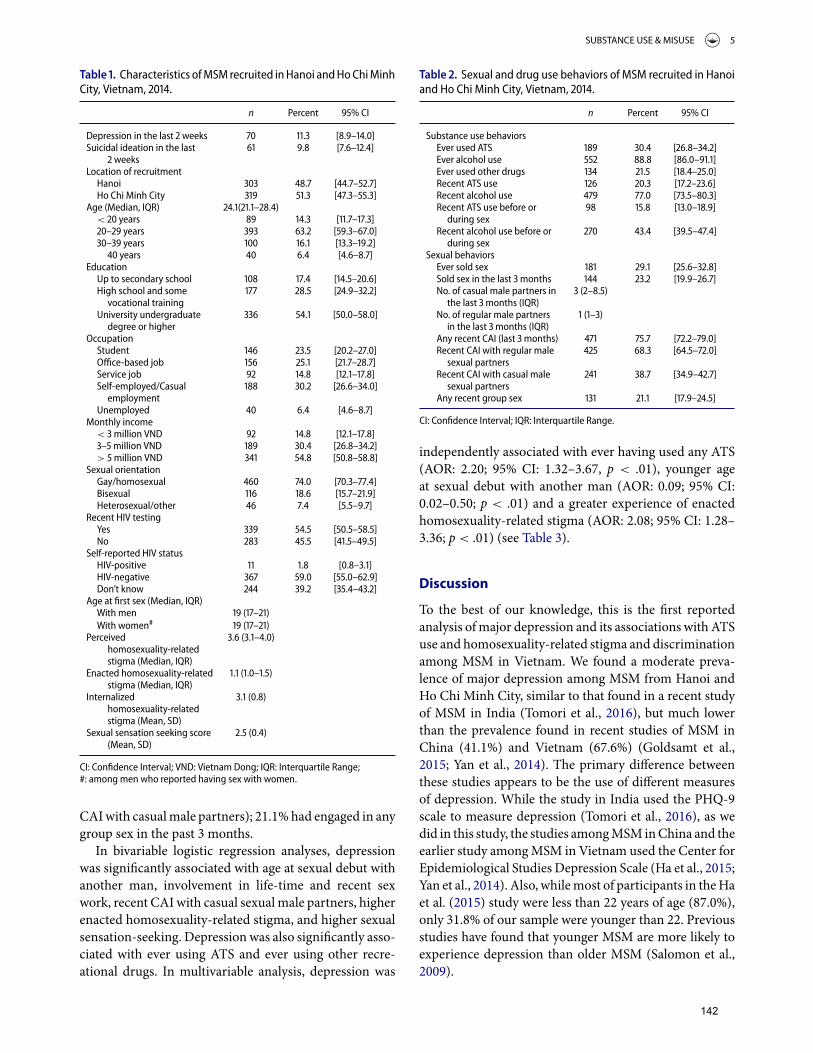
SUBSTANCE USE & MISUSE 5
Table . Characteristics of MSM recruited in Hanoi and Ho Chi MinhCity, Vietnam, .
n Percent % CI
Depression in the last weeks . [.–.]Suicidal ideation in the last
weeks . [.–.]
Location of recruitmentHanoi . [.–.]Ho Chi Minh City . [.–.]
Age (Median, IQR) .(.–.)< years . [.–.]– years . [.–.]– years . [.–.]� years . [.–.]
EducationUp to secondary school . [.–.]High school and some
vocational training . [.–.]
University undergraduatedegree or higher
. [.–.]
OccupationStudent . [.–.]Office-based job . [.–.]Service job . [.–.]Self-employed/Casual
employment . [.–.]
Unemployed . [.–.]Monthly income
< million VND . [.–.]– million VND . [.–.]> million VND . [.–.]
Sexual orientationGay/homosexual . [.–.]Bisexual . [.–.]Heterosexual/other . [.–.]
Recent HIV testingYes . [.–.]No . [.–.]
Self-reported HIV statusHIV-positive . [.–.]HIV-negative . [.–.]Don’t know . [.–.]
Age at first sex (Median, IQR)With men (–)With women# (–)
Perceivedhomosexuality-relatedstigma (Median, IQR)
. (.–.)
Enacted homosexuality-relatedstigma (Median, IQR)
. (.–.)
Internalizedhomosexuality-relatedstigma (Mean, SD)
. (.)
Sexual sensation seeking score(Mean, SD)
. (.)
CI: Confidence Interval; VND: Vietnam Dong; IQR: Interquartile Range;#: among men who reported having sex with women.
CAI with casual male partners); 21.1% had engaged in anygroup sex in the past 3 months.
In bivariable logistic regression analyses, depressionwas significantly associated with age at sexual debut withanother man, involvement in life-time and recent sexwork, recent CAI with casual sexual male partners, higherenacted homosexuality-related stigma, and higher sexualsensation-seeking. Depression was also significantly asso-ciated with ever using ATS and ever using other recre-ational drugs. In multivariable analysis, depression was
Table . Sexual and drug use behaviors of MSM recruited in Hanoiand Ho Chi Minh City, Vietnam, .
n Percent % CI
Substance use behaviorsEver used ATS . [.–.]Ever alcohol use . [.–.]Ever used other drugs . [.–.]Recent ATS use . [.–.]Recent alcohol use . [.–.]Recent ATS use before or
during sex . [.–.]
Recent alcohol use before orduring sex
. [.–.]
Sexual behaviorsEver sold sex . [.–.]Sold sex in the last months . [.–.]No. of casual male partners in
the last months (IQR) (–.)
No. of regular male partnersin the last months (IQR)
(–)
Any recent CAI (last months) . [.–.]Recent CAI with regular male
sexual partners . [.–.]
Recent CAI with casual malesexual partners
. [.–.]
Any recent group sex . [.–.]
CI: Confidence Interval; IQR: Interquartile Range.
independently associated with ever having used any ATS(AOR: 2.20; 95% CI: 1.32–3.67, p < .01), younger ageat sexual debut with another man (AOR: 0.09; 95% CI:0.02–0.50; p < .01) and a greater experience of enactedhomosexuality-related stigma (AOR: 2.08; 95% CI: 1.28–3.36; p < .01) (see Table 3).
Discussion
To the best of our knowledge, this is the first reportedanalysis of major depression and its associations with ATSuse and homosexuality-related stigma and discriminationamong MSM in Vietnam. We found a moderate preva-lence of major depression among MSM from Hanoi andHo Chi Minh City, similar to that found in a recent studyof MSM in India (Tomori et al., 2016), but much lowerthan the prevalence found in recent studies of MSM inChina (41.1%) and Vietnam (67.6%) (Goldsamt et al.,2015; Yan et al., 2014). The primary difference betweenthese studies appears to be the use of different measuresof depression. While the study in India used the PHQ-9scale to measure depression (Tomori et al., 2016), as wedid in this study, the studies among MSM in China and theearlier study among MSM in Vietnam used the Center forEpidemiological Studies Depression Scale (Ha et al., 2015;Yan et al., 2014). Also, while most of participants in the Haet al. (2015) study were less than 22 years of age (87.0%),only 31.8% of our sample were younger than 22. Previousstudies have found that younger MSM are more likely toexperience depression than older MSM (Salomon et al.,2009).
142
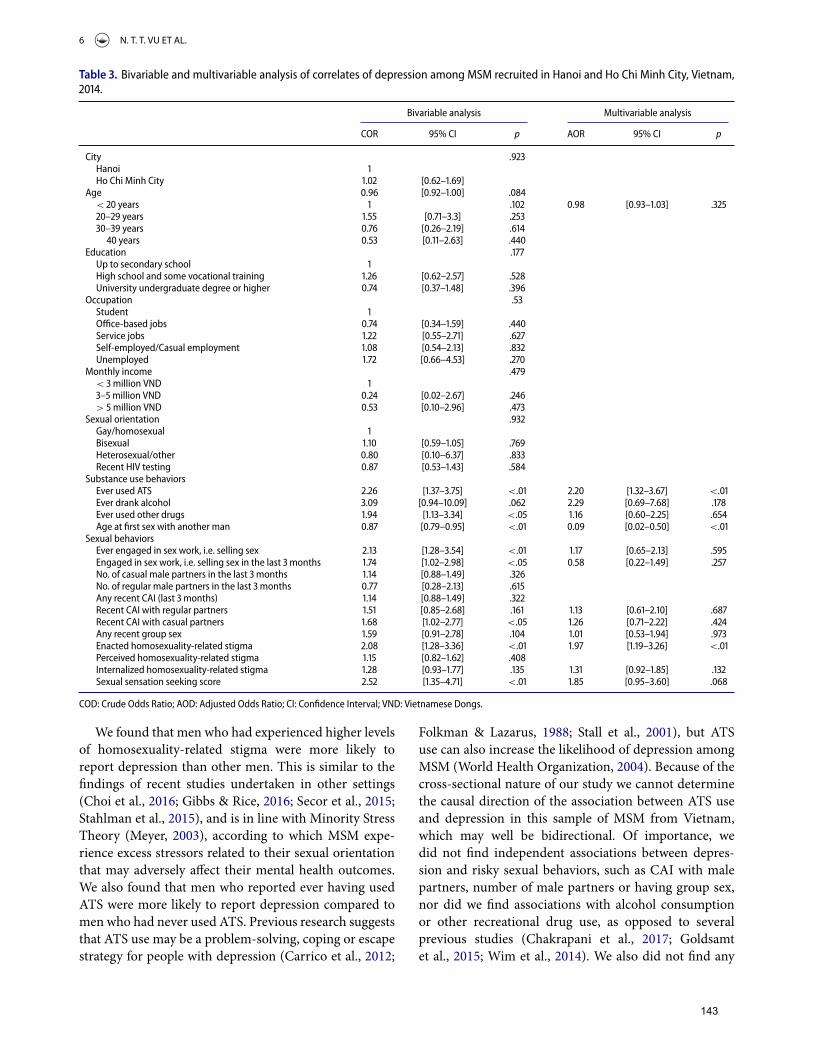
6 N. T. T. VU ET AL.
Table . Bivariable and multivariable analysis of correlates of depression among MSM recruited in Hanoi and Ho Chi Minh City, Vietnam,.
Bivariable analysis Multivariable analysis
COR % CI p AOR % CI p
City .Hanoi Ho Chi Minh City . [.–.]
Age . [.–.] .< years . . [.–.] .– years . [.–.] .– years . [.–.] .� years . [.–.] .
Education .Up to secondary school High school and some vocational training . [.–.] .University undergraduate degree or higher . [.–.] .
Occupation .Student Office-based jobs . [.–.] .Service jobs . [.–.] .Self-employed/Casual employment . [.–.] .Unemployed . [.–.] .
Monthly income .< million VND – million VND . [.–.] .> million VND . [.–.] .
Sexual orientation .Gay/homosexual Bisexual . [.–.] .Heterosexual/other . [.–.] .Recent HIV testing . [.–.] .
Substance use behaviorsEver used ATS . [.–.] <. . [.–.] <.Ever drank alcohol . [.–.] . . [.–.] .Ever used other drugs . [.–.] <. . [.–.] .Age at first sex with another man . [.–.] <. . [.–.] <.
Sexual behaviorsEver engaged in sex work, i.e. selling sex . [.–.] <. . [.–.] .Engaged in sex work, i.e. selling sex in the last months . [.–.] <. . [.–.] .No. of casual male partners in the last months . [.–.] .No. of regular male partners in the last months . [.–.] .Any recent CAI (last months) . [.–.] .Recent CAI with regular partners . [.–.] . . [.–.] .Recent CAI with casual partners . [.–.] <. . [.–.] .Any recent group sex . [.–.] . . [.–.] .Enacted homosexuality-related stigma . [.–.] <. . [.–.] <.Perceived homosexuality-related stigma . [.–.] .Internalized homosexuality-related stigma . [.–.] . . [.–.] .Sexual sensation seeking score . [.–.] <. . [.–.] .
COD: Crude Odds Ratio; AOD: Adjusted Odds Ratio; CI: Confidence Interval; VND: Vietnamese Dongs.
We found that men who had experienced higher levelsof homosexuality-related stigma were more likely toreport depression than other men. This is similar to thefindings of recent studies undertaken in other settings(Choi et al., 2016; Gibbs & Rice, 2016; Secor et al., 2015;Stahlman et al., 2015), and is in line with Minority StressTheory (Meyer, 2003), according to which MSM expe-rience excess stressors related to their sexual orientationthat may adversely affect their mental health outcomes.We also found that men who reported ever having usedATS were more likely to report depression compared tomen who had never used ATS. Previous research suggeststhat ATS use may be a problem-solving, coping or escapestrategy for people with depression (Carrico et al., 2012;
Folkman & Lazarus, 1988; Stall et al., 2001), but ATSuse can also increase the likelihood of depression amongMSM (World Health Organization, 2004). Because of thecross-sectional nature of our study we cannot determinethe causal direction of the association between ATS useand depression in this sample of MSM from Vietnam,which may well be bidirectional. Of importance, wedid not find independent associations between depres-sion and risky sexual behaviors, such as CAI with malepartners, number of male partners or having group sex,nor did we find associations with alcohol consumptionor other recreational drug use, as opposed to severalprevious studies (Chakrapani et al., 2017; Goldsamtet al., 2015; Wim et al., 2014). We also did not find any
143

SUBSTANCE USE & MISUSE 7
association between depression and men’s age or demo-graphic characteristics, including education, income andoccupation. It is possible that depression is distributedsimilarly across different demographic strata of MSM inVietnam and that differences in antecedents and con-sequences reflect the specific social contexts of variousstudies. Future research may provide additional evi-dence and contribute to understanding these differencesfindings.
Several limitations should be born in mind when inter-preting our findings. Since we recruited a conveniencesample of participants, the sample may not be representa-tive of the broader communities of MSM in Hanoi or HoChi Minh City. Also, because of the cross-sectional natureof our study, no conclusions can be drawn regarding thetemporal or causal relationship between depression, ATSuse or and other correlates. As data were self-reported, thestudy could also be subject to reporting bias.
Our findings nevertheless have several implicationsfor HIV prevention research and interventions target-ing MSM in Vietnam. To better understand the tem-poral and causal relationship between ATS use, depres-sion and other correlates among MSM in Vietnam, futureresearch could make use of longitudinal or case-controldesigns. Previous analyses of the same dataset show thatmethamphetamine use before or during sex was associ-ated with CAI among MSM in Vietnam (Vu et al., 2017),and a sizeable subgroup of MSM in Vietnam are still con-fronted with homosexuality-related stigma and discrim-ination (Ha et al., 2015). Together these findings sug-gest that a comprehensive, gay-friendly, culturally adaptedHIV prevention package for MSM in Vietnam may beindicated. This could include psychological counselingand treatment for depression, interventions for metham-phetamine use, interventions addressing homosexuality-related stigma and discrimination, and behavior changeapproaches to reduce risky sexual behaviors and promoteHIV testing, as previously suggested (Mayer et al., 2013;Safren et al., 2010).
Acknowledgments
We acknowledge great support and inputs from staff of the Insti-tute of Preventive Medicine and Public Health, Hanoi MedicalUniversity, Hanoi Centre of HIV/AIDS Prevention and Con-trol, Center for Community Health Promotion, Center for Pro-motion of Quality of Life and leaders and representatives ofcommunity-based organizations of MSM in Ho Chi Minh Cityduring data collection process in Hanoi and Ho Chi Minh City.Nga Thi Thu Vu contributed to the development of the researchprotocol, data collection, data analysis and the manuscript draft-ing and finalization. John de Wit and Martin Holt providedoversight supervision and valuable inputs for the whole pro-cess and the manuscript drafting and finalization. Huong ThiThu Phan, Lan Thi La, Gioi Minh Tran, Tung Thanh Doan, and
Trang Nguyen Nhu Nguyen provided input for the data collec-tion and manuscript drafting and finalization.
Declaration of interest
The authors report no conflict of interest.
Funding
Nga Thi Thu Vu received Australian Award Scholarship for herPhD study in UNSW Australia. The study received financialsupport from the Faculty of Arts and Social Sciences (FASS),UNSW Australia under its Postgraduate Essential Research Pro-gram Funding scheme and External Research Program Fundingschemes. The Centre for Social Research in Health is supportedby funding from the Australian Government Department ofHealth. Funding agencies were not involved in the developmentof the research protocol, data collection, data analysis, interpre-tation or the dissemination of research findings.
ORCID
John de Wit http://orcid.org/0000-0002-5895-7935
References
Altman, D., Aggleton, P., Williams, M., Kong, T., Reddy, V.,Harrad, D., … Parker, R. (2012). Men who have sex withmen: stigma and discrimination. The Lancet, 380(9839),439–445. doi:10.1016/S0140-6736(12)60920-9
Bengtsson, L., Lu, X., Liljeros, F., Thanh, H. H., & Thorson,A. (2014). Strong propensity for HIV transmission amongmen who have sex with men in Vietnam: Behavioural dataand sexual network modelling. BMJ Open, 4(1), e003526.doi:10.1136/bmjopen-2013-003526
Beyrer, C., Baral, S. D., Van Griensven, F., Goodreau, S. M.,Chariyalertsak, S., Wirtz, A. L., & Brookmeyer, R. (2012).Global epidemiology of HIV infection in men who have sexwith men. Lancet, 380(9839), 367–377. doi:10.1016/s0140-6736(12)60821-6
Biello, K. B., Colby, D., Closson, E., & Mimiaga, M. J. (2014).The syndemic condition of psychosocial problems and HIVrisk among male sex workers in Ho Chi Minh City, Vietnam.AIDS and Behavior, 18(7), 1264–1271. doi:10.1007/s10461-013-0632-8
Blanc, M. E. (2005). Social construction of male homosexuali-ties in Vietnam. Some keys to understanding discriminationand implications for HIV prevention strategy. InternationalSocial Science Journal, 57(4), 661–673.
Carrico, A. W., Pollack, L. M., Stall, R. D., Shade, S. B.,Neilands, T. B., Rice, T. M., … Moskowitz, J. T. (2012). Psy-chological processes and stimulant use among men whohave sex with men. Drug Alcohol Depend, 123(1–3), 79–83.doi:10.1016/j.drugalcdep.2011.10.020
Chakrapani, V., Newman, P. A., Shunmugam, M., Logie, C. H.,& Samuel, M. (2017). Syndemics of depression, alcohol use,and victimisation, and their association with HIV-relatedsexual risk among men who have sex with men and trans-gender women in India. Global Public Health, 12, 250–265.doi:10.1080/17441692.2015.1091024
144
8 N. T. T. VU ET AL.
Choi, K. H., Steward, W. T., Miege, P., Hudes, E., & Gregorich,S. E. (2016). Sexual stigma, coping styles, and psychologicaldistress: A longitudinal study of men who have sex with menin Beijing, China. Archives of Sexual Behavior, 45, 1483–1491. doi:10.1007/s10508-015-0640-z
Darke, S., Kaye, S., McKetin, R., & Duflou, J. (2008).Major physical and psychological harms of metham-phetamine use. Drug and Alcohol Review, 27(3), 253–262.doi:10.1080/09595230801923702
De Santis, J. P., Colin, J. M., Provencio Vasquez, E., &McCain, G. C. (2008). The relationship of depressivesymptoms, self-esteem, and sexual behaviors in a pre-dominantly Hispanic sample of men who have sex withmen. American Journal of Men’s Health, 2(4), 314–321.doi:10.1177/1557988307312883
Deuba, K., Ekstrom, A. M., Shrestha, R., Ionita, G., Bhatta, L.,& Karki, D. K. (2013). Psychosocial health problems asso-ciated with increased HIV risk behavior among men whohave sex with men in Nepal: a cross-sectional survey. PLoSOne, 8(3), e58099. doi:10.1371/journal.pone.0058099
Folkman, S., & Lazarus, R. S. (1988). The relationship betweencoping and emotion: implications for theory and research.Social Science & Medicine, 26(3), 309–317.
Frost, D. M., & LeBlanc, A. J. (2014). Nonevent stress contributesto mental health disparities based on sexual orientation: evi-dence from a personal projects analysis. American Journal ofOrthopsychiatry, 84(5), 557–566. doi:10.1037/ort0000024
Garcia, M. C., Duong, Q. L., Mercer, L. C., Meyer, S. B.,Koppenhaver, T., & Ward, P. R. (2014). Patterns and riskfactors of inconsistent condom use among men who havesex with men in Viet Nam: Results from an Internet-basedcross-sectional survey. Global Public Health, 9(10), 1225–1238. doi:10.1080/17441692.2014.948481
Gee, R. (2006). Primary care health issues among men whohave sex with men. Journal of the American Academyof Nurse Practitioners, 18(4), 144–153. doi:10.1111/j.1745-7599.2006.00117.x
Gibbs, J. J., & Rice, E. (2016). The social context of depres-sion symptomology in sexual minority male youth:Determinants of depression in a sample of Grindrusers. Journal of Homosexuality, 63(2), 278–299.doi:10.1080/00918369.2015.1083773
Goldsamt, L. A., Clatts, M. C., Giang, L. M., & Yu, G.(2015). Prevalence and behavioral correlates of depres-sion and anxiety among male sex workers in Vietnam.International Journal of Sexual Health, 27(2), 145–155.doi:10.1080/19317611.2014.947055
Ha, H., Risser, J. M., Ross, M. W., Huynh, N. T., & Nguyen,H. T. (2015). Homosexuality-related stigma and sexualrisk behaviors among men who have sex with men inHanoi, Vietnam. Archives of Sexual Behavior, 44(2), 349–356. doi:10.1007/s10508-014-0450-8
Ha, H., Ross, M. W., Risser, J. M., & Nguyen, H. T. (2013).Measurement of stigma in men who have sex with menin Hanoi, Vietnam: Assessment of a homosexuality-relatedstigma scale. Journal of Sexually Transmitted Diseases, 2013,174506. doi:10.1155/2013/174506
Hirshfield, S., Wolitski, R. J., Chiasson, M. A., Remien, R.H., Humberstone, M., & Wong, T. (2008). Screeningfor depressive symptoms in an online sample of menwho have sex with men. AIDS Care, 20(8), 904–910.doi:10.1080/09540120701796892
Hosmer, D. W. (2013). Applied logistic regression (3rd ed.).Hoboken, NJ: Wiley.
Kalichman, S. C., & Rompa, D. (1995). Sexual sensation seek-ing and Sexual Compulsivity Scales: reliability, validity, andpredicting HIV risk behavior. Journal of Personality Assess-ment, 65(3), 586–601. doi:10.1207/s15327752jpa6503_16
Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). ThePHQ-9: Validity of a brief depression severity mea-sure. Journal of General Internal Medicine, 16(9),606–613.
Mao, L., Kidd, M. R., Rogers, G., Andrews, G., Newman, C. E.,Booth, A., … Kippax, S. C. (2009). Social factors associ-ated with major depressive disorder in homosexually active,gay men attending general practices in urban Australia.Australian and New Zealand Journal of Public Health, 33(1),83–86. doi:10.1111/j.1753-6405.2009.00344.x
Mayer, K. H., Wheeler, D. P., Bekker, L. G., Grinsztejn, B.,Remien, R. H., Sandfort, T. G., & Beyrer, C. (2013). Over-coming biological, behavioral, and structural vulnerabili-ties: new directions in research to decrease HIV transmis-sion in men who have sex with men. Journal of AcquiredImmune Deficiency Syndromes, 63(Suppl 2), S161–167.doi:10.1097/QAI.0b013e318298700e
Meyer, I. H. (2003). Prejudice, social stress, and mental healthin lesbian, gay, and bisexual populations: Conceptual issuesand research evidence. Psychological Bulletin, 129(5), 674–697. doi:10.1037/0033-2909.129.5.674
Mimiaga, M. J., Biello, K. B., Sivasubramanian, M., Mayer,K. H., Anand, V. R., & Safren, S. A. (2013). Psychoso-cial risk factors for HIV sexual risk among Indian menwho have sex with men. AIDS Care, 25(9), 1109–1113.doi:10.1080/09540121.2012.749340
Oldenburg, C. E., Biello, K. B., Colby, D., Closson, E. F., Mai,T., Nguyen, T., … Mimiaga, M. J. (2014). Stigma related tosex work among men who engage in transactional sex withmen in Ho Chi Minh City, Vietnam. International Journalof Public Health, 59(5), 833–840. doi:10.1007/s00038-014-0562-x
Parker, R. D., Lohmus, L., Valk, A., Mangine, C., &Ruutel, K. (2015). Outcomes associated with anxietyand depression among men who have sex with men inEstonia. Journal of Affective Disorders, 183, 205–209.doi:10.1016/j.jad.2015.05.014
Parrott, A. C. (2001). Human psychopharmacology ofEcstasy (MDMA): a review of 15 sources of empiricalresearch. Human Psychopharmacology, 16(8), 557–577.doi:10.1002/hup.351
Pham, Q. D., Nguyen, T. V., Nguyen, P. D., Le, S. H., Tran, A. T.,Nguyen, L. T., … Zhang, L. (2015). Men who have sex withmen in southern Vietnam report high levels of substanceuse and sexual risk behaviours but underutilise HIV testingservices: a cross-sectional study. Sexually Transmitted Infec-tions, 91(3), 178–182. doi:10.1136/sextrans-2014-051574
Safren, S. A., Blashill, A. J., & O’Cleirigh, C. M. (2011). Promot-ing the sexual health of MSM in the context of comorbidmental health problems. AIDS Behav, 15(Suppl 1), S30–34.doi:10.1007/s10461-011-9898-x
Safren, S. A., Reisner, S. L., Herrick, A., Mimiaga, M. J.,& Stall, R. D. (2010). Mental health and HIV riskin men who have sex with men. Journal of AcquiredImmune Deficiency Syndromes, 55(Suppl 2), S74–77.doi:10.1097/QAI.0b013e3181fbc939
145

SUBSTANCE USE & MISUSE 9
Salomon, E. A., Mimiaga, M. J., Husnik, M. J., Welles, S. L.,Manseau, M. W., Montenegro, A. B., … Mayer, K. H.(2009). Depressive symptoms, utilization of mental healthcare, substance use and sexual risk among young men whohave sex with men in EXPLORE: implications for age-specific interventions. AIDS and Behavior, 13(4), 811–821.doi:10.1007/s10461-008-9439-4
Secor, A. M., Wahome, E., Micheni, M., Rao, D., Simoni, J.M., Sanders, E. J., & Graham, S. M. (2015). Depression,substance abuse and stigma among men who have sexwith men in coastal Kenya. AIDS, 29(Suppl 3), S251–259.doi:10.1097/qad.0000000000000846
Shiu, C. S., Chen, Y. C., Tseng, P. C., Chung, A. C., Wu, M.T., Hsu, S. T., & Ko, N. Y. (2014). Curvilinear relation-ship between depression and unprotected sexual behav-iors among men who have sex with men. Journal of SexualMedicine, 11(10), 2466–2473. doi:10.1111/jsm.12638
Stahlman, S., Grosso, A., Ketende, S., Sweitzer, S., Mothopeng,T., Taruberekera, N., … Baral, S. (2015). Depression andsocial stigma among MSM in Lesotho: Implications for HIVand sexually transmitted infection prevention. AIDS Behav,19(8), 1460–1469. doi:10.1007/s10461-015-1094-y
Stall, R., Paul, J. P., Greenwood, G., Pollack, L. M., Bein, E.,Crosby, G. M., … Catania, J. A. (2001). Alcohol use, druguse and alcohol-related problems among men who have sexwith men: The Urban Men’s Health Study. Addiction, 96(11),1589–1601. doi:10.1080/09652140120080723
Sullivan, P. S., Hamouda, O., Delpech, V., Geduld, J. E., Prejean,J., Semaille, C., … The Annecy MSM Epidemiology StudyGroup. (2009). Reemergence of the HIV epidemic amongmen who have sex with men in North America, WesternEurope, and Australia, 1996–2005. Annals of Epidemiology,19(6), 423–431. doi:10.1016/j.annepidem.2009.03.004
Thu Vu, N. T., Maher, L., & Zablotska, I. (2015). Amphetamine-type stimulants and HIV infection among men whohave sex with men: implications on HIV research andprevention from a systematic review and meta-analysis.Journal of the International AIDS Society, 18(1), 19273.doi:10.7448/ias.18.1.19273
Tomori, C., McFall, A. M., Srikrishnan, A. K., Mehta, S. H.,Solomon, S. S., Anand, S., … Celentano, D. D. (2016).
Diverse rates of depression among men who have sexwith men (MSM) across India: Insights from a multi-sitemixed method study. AIDS and Behavior, 20(2), 304–316.doi:10.1007/s10461-015-1201
Tucker, A., Liht, J., De Swardt, G., Jobson, G., Rebe, K., McIn-tyre, J., & Struthers, H. (2014). Homophobic stigma, depres-sion, self-efficacy and unprotected anal intercourse for peri-urban township men who have sex with men in Cape Town,South Africa: A cross-sectional association model. AIDSCare, 26(7), 882–889. doi:10.1080/09540121.2013.859652
Vittinghoff, E., Glidden, D. V., & Shiboski, S. C. (2012).Regression methods in biostatistics: Linear, logistic, sur-vival, and repeated measures models. Retrieved fromhttp://unsw.eblib.com/patron/FullRecord.aspx?p=973179
Vu, N. T., Holt, M., Phan, H. T., La, L. T., Tran, G. M., Doan, T.T., … De Wit, J. (2017). The relationship between metham-phetamine use, sexual sensation seeking and condomlessanal intercourse among men who have sex with men in Viet-nam: Results of a community-based, cross-sectional study.AIDS and Behavior, 21, 1105–1116. doi:10.1007/s10461-016-1467-x
Vu, N. T., Holt, M., Phan, H. T., Le, H. T., La, L. T., Tran,G. M., … De Wit, J. (2016). Amphetamine-type stim-ulant use among men who have sex with men (MSM)in Vietnam: Results from a socio-ecological, community-based study. Drug and Alcohol Dependence, 158, 110–117.doi:10.1016/j.drugalcdep.2015.11.016
Wim, V. B., Christiana, N., & Marie, L. (2014). Syndemicand other risk factors for unprotected anal intercourseamong an online sample of Belgian HIV negative menwho have sex with men. AIDS and Behav, 18(1), 50–58.doi:10.1007/s10461-013-0516-y
World Health Organization. (2004). Neuroscience of psy-choactive substance use and dependence. Retrieved fromhttp://www.who.int/substance_abuse/publications/en/Neuroscience.pdf
Yan, H., Wong, F. Y., Zheng, T., Ning, Z., Ding, Y., Nehl, E.J., … He, N. (2014). Social support and depressive symp-toms among “money” boys and general men who have sexwith men in Shanghai, China. Sex Health, 11(3), 285–287.doi:10.1071/sh14017
146

CHAPTER 8
DISCUSSION AND CONCLUSION
147
During the past several decades, the use of ATS has become more common among
MSM in different parts of the world (1-3). In high-income countries, particularly in settings
where HIV disproportionately affects MSM, the use of ATS, particularly
methamphetamine, has been found to be associated with a higher probability of
engagement in risky sexual behaviours (4-9) and HIV infection (10-19). Additionally,
there is evidence that the use of ATS, particular methamphetamine, can contribute to
mental health problems, such as depression and anxiety (20-25). Nevertheless, most of
the research on ATS, HIV and MSM is from high-income countries, and there is a lack
of knowledge about ATS use and its associated harms from LMIC (26), particularly
Southeast Asian countries such as Vietnam.
This PhD thesis is the first in-depth investigation of the magnitude and patterns of ATS
use and associated harms in MSM in Vietnam. The foundation of this thesis is a series
of five published manuscripts in English language, peer-reviewed journals. A cross-
sectional, community-based survey was conducted in Hanoi and Ho Chi Minh City,
Vietnam from September 2014 to December 2014 to investigate ATS use by MSM and
related harms, and a systematic review and a meta-analysis of the available literature on
the relationship between ATS use and HIV infection among MSM was conducted.
This chapter summarises the main findings of the PhD study, the implications of these
results for drug use interventions and HIV prevention, and recommendations for further
research. The chapter also discusses limitations in the study design and data analysis.
KEY FINDINGS
Chapter 3 presented an analysis of the magnitude, patterns and correlates of ATS use
among MSM from two major cities in Vietnam, using an adapted socio-ecological
approach. It showed that ATS use was relatively common by Vietnamese MSM, and
methamphetamine was the most popular substance, followed by ecstasy and
amphetamine. ATS were generally used by smoking, snorting and inhaling. Men reported
starting ATS use during their early 20s and a notable proportion of men had recently
consumed methamphetamine or ecstasy before or during sex. The majority of men who
used methamphetamine or ecstasy were classified as moderate to high rate users on
the WHO ASSIST scale. The patterns of ATS use among Vietnamese MSM appeared
similar to patterns of ATS use by MSM in high-income countries (26, 27). However, the
prevalence of ATS use, including methamphetamine use, was higher than that found in
neighbouring countries such as China and Thailand (28-30) and higher than that found
148
in earlier studies conducted in Vietnam (31). The high rate of ATS use, particularly
methamphetamine use, may reflect the actual level of ATS use among Vietnamese MSM
or it could relate to differences in reporting due to stigma, other reporting biases or
sampling methods. Nevertheless, these findings indicate that an intervention for ATS
use, particularly methamphetamine use, might be needed for MSM in Vietnam.
Moreover, the finding that the majority of methamphetamine use could be classified as
moderate or high-risk suggests that treatment for methamphetamine abuse or
dependence should be available and accessible to people who need it.
I found that recent methamphetamine use in the sample was associated with a range of
factors, including sexual sensation-seeking, involvement in sex work and perceiving that
methamphetamine use was common in MSM networks. The study was the first to find
that higher sexual sensation-seeking was associated with higher levels of
methamphetamine use. Previous studies have found that sexual sensation-seeking is
associated with a higher rate of practicing risky sexual behaviours (32) and may modify
the relationship between alcohol consumption, drug use and CAI (33, 34). Assessment
of sexual sensation-seeking, therefore, could help in identifying subgroups of men who
are involved in riskier drug use and sexual behaviours for specific HIV prevention
interventions, such as PrEP. I also found that methamphetamine use was more prevalent
among MSM who had engaged in sex work. Previous studies in Vietnam have found that
up to 44% of MSM have engaged in sex work (31, 35-37). In other studies in Vietnam,
ATS use and risky sexual behaviours have been found to be commonly reported by
Vietnamese male sex workers (31, 35, 36, 38).
The last correlation with methamphetamine use that I found was the perception that
methamphetamine use was popular in MSM networks. This finding is similar to findings
of previous research which shows that perceiving a high level of alcohol use among
peers is associated with higher alcohol consumption (39-41). Sociological studies of drug
use suggest that when drug use becomes normalised (perceived as common and
accepted by the community), then there is a greater chance of substance use (42). My
study did not assess whether ATS use is accepted by MSM in Vietnam. The level of
lifetime use of ATS in our sample (at 30%) was high but still lower than the level regarded
as a sign of normalisation (40%) (43), suggesting that ATS use may not yet be
normalised among MSM in Vietnam. However, from our findings it is not clear the extent
of ATS use normalisation and what the motivations are for ATS use by MSM in Vietnam.
Further research is needed to understand these factors.
149
To my knowledge, this is the first ever socio-ecological analysis of the correlations of
ATS use that has been conducted in Vietnam. The findings indicate the correlates of
ATS at multiple levels related to individuals, community norms and the social
environments of MSM. As such, our results imply that interventions addressing ATS use,
particularly methamphetamine use, among MSM in Vietnam could be more successful if
they address factors at different levels, including personal, community and social levels.
Chapter 4 presented an analysis of HIV-related sexual behaviours by MSM and
correlations with CAI. The analysis found a very high level of recent CAI (78%) by MSM
in Hanoi and Ho Chi Minh City. This level of CAI is higher than that found in other studies
conducted in Vietnam (44-47), although different study designs, sampling methods and
recall periods were used. Although the results may not be directly comparable,
collectively the studies underline that there are low levels of consistent condom use by
MSM in Vietnam. In 2012, Vietnam's National Strategy for HIV/AIDS prevention and
control set a target that 50% of MSM should consistently practice safe sex (48). However,
a recent government report indicates that the allocation for HIV prevention targetting
MSM only accounts for a small proportion (1.4%) of total national HIV funding and
condom accessibility remains poor (49). It is unlikely that the above target could be
achieved unless greater resources are allocated for HIV prevention with MSM, including
a more intense focus on safe sex counselling and easy access to condoms.
In the analysis of correlations of CAI, I found that methamphetamine use before or during
sex was significantly associated with CAI. This relationship was modified by sexual
sensation-seeking in that men with lower sexual sensation-seeking scores who used
methamphetamine for sex were significantly more likely to practise CAI than men who
did not use methamphetamine. For men with higher sexual sensation seeking scores,
there was no difference in the likelihood of CAI between men who used
methamphetamine or not. Men who had higher sexual sensation seeking scores tended
to report both risky sexual and drug use behaviours. Previous studies have found a
modification effect of sexual sensation seeking on the relationship between alcohol
consumption and CAI (32-34). Our finding that men who used methamphetamine use
before or during sex were more likely to have CAI is similar to findings of previous studies
conducted in high-income settings (9, 50-55). I also found that sexual sensation-seeking
and belief in withdrawal as an effective HIV prevention strategy were significantly
associated with higher levels of CAI. These findings again imply that assessing sexual
sensation-seeking could identify men who are involved in risky sexual behaviours, and
may have a higher risk of acquiring or transmitting HIV infection. Additionally, because
methamphetamine use is associated with higher CAI, HIV prevention for MSM in
150
Vietnam could achieve greater outcomes if interventions for methamphetamine use were
developed and integrated into existing HIV prevention services.
The findings also showed that many men had never been tested for HIV (approximately
30%), and only half of the sample had tested for HIV in the last 12 months, despite high
levels of CAI. Other studies in Vietnam have also found that a high proportion of MSM
have not been tested for HIV (ever or recently) (37, 56).
This analysis has several strengths. It was the first to analyse sex-related drug use by
MSM in Vietnam and its relationship with CAI. This type of measurement is not as strong
as event-level measurement (57, 58), but it provides contextual measures for drug use
and sexual behaviour. This research also represents the first interaction modification
analysis of sexual sensation-seeking and the relationship between methamphetamine
use and CAI, having been inspired by previous research on sexual sensation-seeking
and alcohol consumption (33, 34).
Chapter 5 presented the findings of a systematic review and meta-analysis of the
relationship between ATS use and HIV infection in MSM. The meta-analysis included 35
publications using different study designs with various types of drug use measurement
and sampling. The pooled estimates from random-effect models demonstrate that
collectively, ATS use was associated with higher levels of HIV infection. While
methamphetamine use was associated with HIV infection in all study designs, ecstasy
use was only associated with HIV infection among MSM in case-control and longitudinal
studies. The analysis demonstrated that the meta-analysis was reliable and valid and
there was no evidence of publication bias.
The systematic review and meta-analysis of the relationship between ATS use and HIV
infection is the first published report of its kind. It covered all accessible, published
studies from the beginning of the HIV epidemic to the time of analysis. It pooled estimates
for each ATS subgroup and study design, enabling an assessment of each ATS
substance as a risk factor for HIV seroconversion (from longitudinal and case-control
studies) and as a correlation with HIV infection (in cross-sectional studies). Additionally,
several efforts were made during data extraction to include not only the association
estimates of ATS use and HIV infection but also descriptive data for manual calculation
of these estimates. I also separately extracted the use of each ATS from studies which
measured more than one ATS to maximise the number of studies in the analysis.
The systematic review and meta-analysis highlighted several limitations of current
research on ATS use and HIV in MSM. Firstly, throughout the HIV epidemic, the study
151
of ATS use and HIV has predominantly been conducted in high-income countries. The
systematic review only found five studies from LMIC. Others have called for research on
ATS use and HIV infection in these settings (26, 27). Secondly, the majority of studies
measured global drug use with different recall periods, from lifetime use to monthly use,
and sexual behaviour was measured separately. Thirdly, studies used cumulative
measures of drug use, making it difficult to identify the effects of individual drugs. Lastly,
many studies recruited MSM from clinics or HIV testing sites. These men may have been
at higher HIV infection risk compared with men from community-based samples. Indeed,
the meta-regression analysis found significantly higher pooled estimates of ATS use and
HIV infection in studies with clinic-based samples.
Chapter 6 presented an analysis of HIV prevalence (confirmed by biological testing)
among MSM in Hanoi and an analysis of the correlates of HIV infection. The participants
had a moderate HIV prevalence of 6.7% but a strikingly high proportion of HIV-positive
men (85.7%) were unaware of or did not disclose their HIV status. The HIV prevalence
of 6.7% is lower than that found in previous IBBS surveys in 2006 and 2011 (59, 60) but
higher than in the more recent 2013 IBBS (47). It is not clear if HIV prevalence in MSM
in Hanoi has decreased from 2006 to 2013; however, there are several possible
explanations for the discrepant findings. Firstly, my sample used a peer-referred,
convenience sample while IBBS recruited participants by respondent- driven sampling
(RDS). Secondly, there were no MSM who injected drugs in my sample, while the IBBS
included a sizeable proportion of MSM who injected (47, 59, 60). RDS samples can vary
dramatically depending on where initial seeds are recruited from, i.e. MSM who inject or
MSW. Nevertheless, to date, because MSM are a hidden, hard-to-reach population in
Vietnam, almost all published studies have used non-random sampling methods, such
as peer referral, time-location sampling, RDS or online recruitment (31, 36, 46, 61-63).
There was a strikingly high proportion of undiagnosed HIV among HIV-positive MSM in
my study. This may have occurred for several reasons. A recent qualitative study
reported high levels of HIV-related stigma and discrimination as barriers to testing,
treatment uptake and retention among MSM in Hanoi (64). Previously diagnosed men
may have not wanted to disclose their HIV status to the study team during interviews.
Other research indicates a lack of MSM-specific HIV testing and counselling services in
Vietnam remains a barrier to HIV testing uptake (65), and therefore many of the men in
the sample may have avoided testing. HIV-positive MSM who are unaware of their
infection can unknowingly transmit the virus to others (66-68). Evidence from overseas
has shown that undiagnosed MSM may report riskier sexual and drug use behaviours
compared to HIV-negative men (68-70). This finding has important implications for HIV
152
prevention in Vietnam. Promoting greater HIV testing uptake by MSM and subsequent
referrals to treatment could prevent further transmission of the virus in this population.
The analysis of the correlates of HIV infection identified a range of social and behavioural
factors associated with HIV, which are similar to findings of previous research in other
settings, including the use of methamphetamines before or during sex (9, 50, 53, 55,
71-73), recent sex work (74-77) and perceiving a higher level of homosexuality-related
stigma (76, 78). A previous study in MSM in Ho Chi Minh City also reported a positive
relationship between involvement in sex work and HIV infection (31). Additionally, the
analysis showed that many MSM reported recent CAI (74%), particularly with regular
sexual partners (66%).
A recent qualitative study in HIV-positive MSM in Hanoi revealed that after diagnosis with
HIV, men often engaged in less sex and CAI (64). However, most of the HIV-positive
men in my analysis were undiagnosed (and therefore could not be expected to have
altered their behaviour as a result of knowing their HIV status). My analysis did not find
a significant association between CAI and HIV infection. This lack of variance between
HIV-positive men (whether diagnosed or not) and HIV-negative men may reflect a ceiling
effect of high levels of CAI in both groups. The analysis didn’t find any significant
associations between other individual, community, interpersonal or environmental
factors and HIV. The lack of other significant associations, including CAI, may have
resulted from the relatively small sample size (n=210) for this analysis.
Chapter 7 presented an analysis of the prevalence of depression and its correlations
among men recruited from both Hanoi and Ho Chi Minh City. The prevalence of
depression found in my study is lower than that found in a 2010 study conducted with
young MSM in Hanoi (68%) (63), and lower than the prevalence found among MSW in
Hanoi and Ho Chi Minh City (79-81). Previous evidence suggests that younger MSM are
more likely to report depression (82). While Ha’s study recruited mostly young MSM
(87% younger than 22 years old), only 32% in my sample were aged less than 22.
Alternatively, while my study used the classification of major depression versus not
having major depression (83), Ha's study reported men who had any form of depression
(including moderate depression). Additionally, while the study with young MSM in Hanoi
used the Centre for Epidemiologic Studies Depression Scale with 20 items, I used the
Patient Health Questionnaire with nine items to identify depression. Therefore,
differences in sampling and measurement may account for the differences in the
prevalence of depression in these studies. My finding that a sizable proportion of MSM
in Hanoi and Ho Chi Minh City had major depression and that depression was related to
153
ATS use suggests that mental health assessment and treatment should be incorporated
into HIV care and treatment services.
The analysis of correlates of depression found two factors associated with a higher
likelihood of depression: any ATS use and enacted homosexuality-related stigma.
Meanwhile, we found that men who reported earlier sex with another man were less likely
to have depression compared to men who had sex with another man at a later age. ATS
can be used to cope with isolation and loneliness, and deal with boredom, unpleasant
feelings and conflict (1, 84, 85). At the same time, use of ATS can result in mental health
problems, including depression (21). However, because of the cross-sectional nature of
my study, the analysis could not identify if depression or ATS use occurred first (or
whether another cause influenced both drug use and mental health).
I found that enacted (experienced) homosexuality-related stigma was associated with a
higher likelihood of depression. This result is similar to previous studies in settings
outside Vietnam (86-89). It accords with the minority stress theory which outlines how
sexual minority groups may experience social pressure based on their sexual identity or
orientation, leading to adverse events, including mental health problems (90). Though
there has been intensive activism for lesbian, gay, bisexual and transgender rights in
recent years (91), homosexuality-related stigma and discrimination are still common in
many parts of Vietnam, including major urban areas (63, 92). Other analyses in this study
found perceived homosexuality-related stigma is associated with recent
methamphetamine use (Chapter 2) and HIV prevalence (Chapter 5). Therefore,
addressing homosexuality-related stigma and discrimination could not only be beneficial
in reducing harmful drug use but could also improve the mental health of MSM in Vietnam
and contribute to the prevention of HIV transmission in this population.
LESSONS LEARNED, LIMITATIONS AND FUTURE DIRECTIONS
Lessons learned
My study was one of the first studies in Vietnam where academic researchers
collaborated with governmental agencies, non-governmental organisations and
community-based organisations of MSM. This collaboration had several benefits. Firstly,
while MSM remains a hidden, hard-to-reach population in Vietnam, the collaboration with
NGOs and CBOs facilitated my access to networks of MSM in Hanoi and Ho Chi Minh
City. Additionally, the collaboration allowed the full participation of key informants who
were MSM during the study. Key informants provided important suggestions about how
154
the study should be conducted, such as the screening/eligibility process and using
appropriate language to reflect sexual orientation, sexual behaviour and the street
names of drugs. Moreover, this collaboration assisted with reaching subgroups of MSM
who are usually difficult to reach, such as highly educated, professionally employed
MSM. The sample included many subgroups of MSM who may have never been included
in previous research in Vietnam. The collaboration with government agencies allowed
us to leverage resources beyond those available in a PhD project, such as accessing
offices for interviews and providing free HIV testing in Hanoi. The other lesson learned
from the study was the need for extended interview hours and flexible interview locations.
Working hours were extended to evenings and weekends to facilitate interviews with
MSM who could not participate during office hours or weekdays. Additionally, a range of
interview locations was offered to facilitate accessibility, while still ensuring the privacy
and confidentiality of participants.
Limitations
My study had several limitations that should be acknowledged. These range from study
design to data analysis.
Firstly, the sample was a convenience, peer-referred sample and therefore may not
represent the broader population of MSM in Hanoi and Ho Chi Minh City. Nevertheless,
no other studies in Vietnam have achieved random samples of MSM (31, 36, 37, 45-47,
59, 60, 62) . Secondly, the survey data relied upon self-reporting of past events. As such,
the data could have been affected by recall bias. Additionally, because drug use and
homosexuality are socially stigmatised in Vietnam (93), the data could have been
affected by information bias or social desirability bias. Participants could have under-
reported some behaviours, and therefore the study estimates could have underestimated
ATS use and CAI by MSM. The cross-sectional study design could identify correlations,
but not identify risk factors that led to ATS use, CAI, depression or HIV. Thirdly, although
sex-related measures of ATS use were employed, these measures could not identify the
temporal relationship between ATS and CAI.
My study analysed correlations with ATS use using an adapted socio-ecological
framework which involved several levels of factors from the individual to the societal level
(94). It has been suggested that interactions within and between levels of the socio-
ecological framework should be conducted (95). However, I could only perform within-
level interaction analysis in my study. In the study, environmental influences were
indirectly measured by participants reporting engagement with HIV testing, safe sex
155
counselling and STD services. The study could have better assessed the environmental
availability of HIV prevention services by directly measuring the number of services
available within each study location, or participants’ awareness of these services.
Future research directions
In the context of the increasing use of ATS by MSM in Vietnam, periodic HIV surveillance
is encouraged to integrate assessment of the magnitude and patterns of ATS use,
particularly methamphetamine use, and its associated harms to monitor change over
time. Additionally, since quantitative designs can rarely provide deep insights into the
contexts and social networks in which ATS are used, or the meanings attached to ATS
use by MSM, I recommend further qualitative or ethnographic work to explore the social,
environmental, interpersonal and personal dynamics of ATS use. This may be
particularly useful for understanding the role of peer norms in supporting or discouraging
methamphetamine use. Lastly, because of the high level of undiagnosed HIV among
HIV-positive men in my study, I recommend further studies to measure the prevalence
of undiagnosed HIV and its correlates in different parts of Vietnam.
MSM remain a hidden, hard-to-reach population in Vietnam and therefore achieving a
random, representative sample is unlikely to be possible. Evidence from other settings
has demonstrated that convenience sampling methods, including peer outreach,
informal referral through social networks, online and venue-based sampling, can yield
samples which significantly differ in socio-demographic characteristics, sexual behaviour
and HIV/STD prevalence (96). Other probability-based sampling methods have their own
limitations: time-location sampling can consume a large amount of resources and time
(97), while RDS tends to recruit men from lower socio-demographic backgrounds and
under-recruits men from higher education and income levels (98, 99). My
recommendation is that studies with MSM in Vietnam should consider several concurrent
recruitment methods, including time-location sampling, peer-referral and online
sampling, to reach men from diverse backgrounds (96). With peer-referral or snowball
sampling, a diverse group of initial seeds is needed to reach men from a range of
subgroups (97).
Regarding the correlation between drug use and risky sexual behaviours, establishing a
causal relationship is rare, outside of prospective studies (57, 58). However, a temporal
relationship between drug use and risky sexual behaviours may be identified in
longitudinal studies with event-level measurement of drug use. Recording other
contextual factors via diaries and sexual behaviour logs might also reduce the recall bias
156
for past events (57, 100). Measurement should be designed so events with drug use can
be compared to events without drug use to facilitate and obtain within-person analyses
(57). Additionally, the use of specific drugs should be measured to differentiate each
drug's relationship to sexual behaviours. Moreover, since multiple drug use is popular in
MSM (93, 101-103), polydrug use or concurrent drug use should be measured.
Alternatively, as previously suggested, studies could consider implementing an
intervention for drug use, to see if a reduction in drug use is paralleled with a reduction
in risky sexual behaviours, suggesting an association between the two sets of behaviours
(58).
Lastly, research on the correlates of HIV prevalence should not only focus on the
individual risks of HIV infection but should include the assessment of homosexuality-
related stigma and discrimination and access to HIV prevention services (104). From my
study experience, I recommend that future research on drug use and risky sexual
behaviours should take into account not only individual factors, including the underlying
causes of health behaviours such as personality traits, but also a broader range of
factors, including community, environmental, social and cultural influences. As
previously suggested, any study of people’s health behaviours conducted in separation
from the study of wider cultural, social and environmental contexts is incomplete and
insufficient to comprehend the complex causes of diseases and health behaviours (105).
A holistic understanding of the range of influences over health can assist in designing
effective interventions.
RECOMMENDATIONS FOR HIV INTERVENTIONS IN VIETNAM
In this section, I discuss the implications and recommendations from the study’s findings
as well as current international practice.
Interventions for ATS use
The finding that ATS use, particularly methamphetamine use is relatively widespread
(Chapter 3) and that sex-related methamphetamine use is related to a higher prevalence
of CAI (Chapter 4) and HIV infection (Chapter 6) suggests that interventions for ATS use,
particularly methamphetamine use, should be developed and integrated with existing
HIV prevention, care and treatment services for MSM in Vietnam. Firstly, I recommend
that health care workers who work in HIV prevention services are sensitized about ATS
use and its potential to drive HIV transmission in MSM in Vietnam. Secondly, ATS use,
particularly methamphetamine use, and its associated risky sexual behaviours should be
assessed in both HIV prevention outreach programs and counselling at HIV testing and
157
or sexually transmitted infections (STI) services to identify men who use it who may be
involved in riskier HIV-related sexual behaviours. Thirdly, I recommend the
dissemination of accurate knowledge of ATS use, indications of harm and ways to reduce
harm to encourage harm reduction strategies among MSM networks in Vietnam. A
previous study overseas has shown that gay men can develop a so-called "folk
pharmacology" to provide information and knowledge to each other about how to reduce
the harms of drug use (106). I hope that with proper knowledge of ATS, its potential
harms and harm reduction strategies, MSM in Vietnam could minimise the adverse
impacts of ATS use, particularly methamphetamine use, and develop their own
strategies for safer use.
Additionally, my finding that the majority of methamphetamine use could be classified as
moderate or high-risk use by WHO’s ASSIST scale suggests that treatment for
methamphetamine abuse or dependence should be available and accessible to MSM
who need it. Currently, there are no available effective pharmacotherapies for
methamphetamine dependence treatment (107-109). Public health managers in Vietnam
could consider psychological therapies, such as cognitive behavioural therapy or
contingency management, which have proven to be effective in addressing
methamphetamine use and dependence (110). In my survey, I found that
methamphetamine use before or during sex was more prevalent among HIV-positive
men. A previous study in the US found most methamphetamine use occurred after an
HIV positive diagnosis, possibly to deal with the emotional consequences related to
diagnosis (111). Human and animal studies have demonstrated that methamphetamine
use may lower HIV treatment adherence and exacerbate HIV disease progression, thus
altering the effectiveness of ARV treatment (112-114). Altogether, I recommend that the
assessment of methamphetamine use and associated harms should not only be routinely
conducted at the community outreach and prevention programs but should also be
integrated into existing HIV clinics, and treatment for methamphetamine use should be
available through these services. The assessment of ATS use, particularly
methamphetamine use, at HIV clinics could contribute to the prevention of risky sexual
behaviours among HIV-positive men but may also improve mental health and prevent
problems in HIV treatment.
Greater promotion of condom use and safe sex
My survey in Vietnam found a high prevalence of CAI among MSM (Chapter 4) after
more than 10 years of HIV prevention efforts with this population. I recommend a greater
promotion of condom use and behavioural change communication in community
158
outreach programs. HIV prevention programming in Vietnam should consider applying
successful interventions from overseas which have been found to be effective in reducing
HIV-related risky sexual behaviours, including group-based interventions and
community-based interventions (115), although these would need to be adapted to the
local context to be effective. Additionally, behavioural change communication strategies
for MSM in Vietnam might gain better results by using evidence-based community
models such as the popular opinion leader model (116). In this model, popular, well-
respected MSM are recruited from the local community and trained in HIV prevention,
sexual health and harm reduction. These leaders then outreach to MSM in their social
networks, correcting misunderstandings about HIV prevention and drug use, and
describing strategies for effective HIV prevention and harm reduction. This intervention
is designed to influence the community’s norms in regard to drug use, safe sex and harm
reduction. (116). However, to have the best chance of success, these overseas models
would need to be adapted for local use in Vietnam, with training, support, community
ownership and oversight (117, 118) .
Integration of mental health (particularly depression) assessment and treatment
My finding that a sizable proportion of MSM in Hanoi and Ho Chi Minh City were classified
as having major depression and that depression was related to ATS use (chapter 7)
suggests that mental health assessment and accessible treatment are needed for
Vietnamese MSM. International research has found that MSM have a higher probability
of developing mental health problems, including depression (90, 119, 120). Given ATS
use, particularly methamphetamine use, is associated with CAI and HIV infection
(Chapter 3 and 5), I recommend that assessment and treatment for depression and other
mental health problems should be incorporated into HIV care and treatment services,
along with evaluation and treatment for methamphetamine use. Internationally
recommendations suggest that a successful response to HIV should not only provide
HIV prevention and treatment, STI diagnosis and treatment and support for mental health
problems, but also needs to address the root causes of these health disparities (120).
Vietnam's public health managers should consider developing and piloting clinics where
an integrated, holistic package of clinical care for HIV, STD, depression, and
methamphetamine use is delivered to MSM, as has already been suggested elsewhere
(120).
Targetting men who engage in sex work
Male sex work may be associated with financial hardship, and younger male sex workers
(MSW) may experience power imbalances with older, male clients and offer sex in
159
exchange for food, gifts, drugs, shelter or economic support (121, 122). Previous studies
in Vietnam have found that up to 44% of MSM have engaged in sex work (31, 35-37). In
other studies, ATS use and risky sexual behaviours have been found to be common
among Vietnamese MSW (31, 35, 36, 38). A qualitative study exploring the needs of
MSW in Ho Chi Minh City highlighted the need for alcohol and drug use interventions
and alternative income generation opportunities (35). Globally, male sex workers are
generally found to be at high risk of HIV (121). From my study’s finding that men who
engaged in sex work were more likely to use methamphetamine (Chapter 3) and test
positive for HIV (Chapter 6), I recommend that this subgroup of MSM should be a priority
group for ATS use interventions and HIV prevention in Vietnam. I recommend that drug
use and HIV prevention interventions should be delivered with other complementary
supports, such as income generation opportunities.
Assessing personality traits and referral to Pre-exposure prophylaxis (PrEP)
My finding that sexual sensation-seeking was positively related to methamphetamine
use (Chapter 3), CAI (Chapter 4) and modified the relationship between
methamphetamine use and CAI underlines the importance of assessing personal traits
that may affect behavioural change strategies for safer drug use and sexual behaviour.
As noted above, I recommend the assessment of sexual sensation-seeking in outreach
activities and during counselling at HIV testing services. Screening for sexual sensation-
seeking could be considered by services to identify men who may be at high risk of HIV
infection, and to identify candidates for harm reduction interventions. Further
assessment of risky sexual and drug use behaviors as recommended by WHO, CDC
and/or national guidelines should be strictly followed, including taking sexual histories
and drug use histories in a sensitive and supportive manner that protects clients’
confidentiality. However, caution should be exercised to ensure that screening tools are
not misused to label and stigmatise MSM because of their behaviour or personal traits.
This would create an unwelcome and additional barrier to health-seeking behaviour.
MSM attending services should be provided with sufficient counselling and information
about available and affordable HIV prevention services so that they can make well-
informed decisions about the most appropriate and effective HIV prevention method(s)
that would suit them, supported by their health care provider. Men identified with higher
levels of sexual sensation-seeking and who engage in risky drug use and sexual
behaviour might be considered a priority group for alternative, evidence-based
interventions, such as PrEP. A recent study in Vietnam reported that the majority of MSM
were interested in and willing to use PrEP (123). PrEP has been proven to be effective
in preventing the transmission and infection of HIV in MSM (124).WHO recommends
160
making PrEP available to people at substantial risk of infection, and this subset of men
in Vietnam may be appropriate candidates (125).
Expand HIV testing accessibility and uptake
I found that a sizable proportion of MSM had never accessed HIV testing (Chapter 4)
and a striking proportion of men were unaware of having undiagnosed HIV (Chapter 6),
suggesting that an expansion of HIV testing and counselling services is needed. I
recommend piloting peer-controlled HIV testing services at a community level, as
suggested by WHO (126). Additionally, to empower and promote HIV testing for high-
risk people and people with undiagnosed HIV in the context of high levels of stigma and
discrimination, Vietnam’s public health managers should also consider piloting HIV self-
testing in the country, also suggested by WHO (127). Recent research in Vietnam shows
MSM's explicit needs for MSM-friendly HIV testing and counselling services and their
fears of confidentiality being breached (65). As such, to encourage men to access and
use HIV testing, government-run HIV testing services should be strengthened to be
MSM-friendly and culturally appropriate. This could be done by organising homosexuality
sensitization workshops for health care providers who work in HIV facilities to raise their
awareness about homosexuality and the importance of issues like confidentiality for
MSM. As such, I hope that HIV prevention, care, and treatment services can become
friendlier to and more supportive of MSM, increasing uptake and retention in care.
Strengthened, diversified and expanded HIV testing services for MSM may encourage
more men to seek testing. Health care managers should consider expanding HIV testing
options not only for MSM but also for other key populations at high risk of HIV in Vietnam
(e.g. female sex workers, people who inject drugs). This may assist Vietnam in reaching
the UNAIDS 90-90-90 diagnosis, treatment and viral suppression targets by 2020, to
which the Vietnamese government has already committed.
Tackling homosexuality-related stigma and discrimination
Homosexuality-related stigma and discrimination were associated with both depression
and HIV infection in the study (Chapter 5 and 6). Because of social stigma, MSM have a
higher probability of developing mental health problems, including depression (90, 119,
120). As such, it is suggested that a successful response to HIV should not only provide
HIV prevention and treatment, STI diagnosis and treatment and support for mental health
problems, but also needs to address the root causes of these health disparities, i.e.
homosexuality-related stigma and discrimination (120). As such, I want to recommend
NGOs and CBOs for MSM and other sexual minority groups continue their efforts to
protect and promote the rights of LGBT communities in Vietnamese society, as they have
161
been doing in recent years (91). Moreover, homosexuality sensitization workshops as
mentioned above should be organised for health care providers, particularly those who
work in HIV prevention, care and treatment facilities. Reports from different settings in
the world have shown that to be successful in engaging and retaining MSM in HIV
prevention, care and treatment, health care providers should be trained to provide
culturally appropriate counselling and care (120). Lastly, I believe that tackling
homosexuality-related stigma and discrimination will not only improve the overall health
and well-being of MSM but also contribute to the prevention of HIV transmission in
Vietnam.
Inclusion of MSM in HIV prevention, care and treatment interventions
HIV prevention practice in different settings demonstrates the benefits of the active
involvement of gay, bisexual and other MSM in the design and delivery of HIV prevention,
treatment and care programs (104). I recommend CBOs of MSM actively participate in
a number of different HIV prevention activities.
First of all, I recommend MSM’s active delivery of HIV prevention outreach programs to
promote condom use, encourage the accessibility and uptake of HIV testing and other
HIV prevention services (i.e. STI diagnosis and treatment). As there is a high prevalence
of ATS use, particularly methamphetamine use, in MSM, I encourage CBOs for MSM to
disseminate proper knowledge of ATS and its associated harms and potential harm
reduction strategies. I believe that MSM in Vietnam might be able to develop a “folk
pharmacology” to minimise harms associated with ATS use. Additionally, routine
assessment of ATS use, particularly methamphetamine, together with associated risky
sexual behaviours is encouraged in community outreach work to monitor changes in
patterns of ATS use and associated harms. Further, peer educators could also do rapid
assessments of sexual sensation-seeking to identify men with a higher tendency to
engage in risky drug use and sexual behaviours for advanced HIV prevention
interventions such as PrEP.
Secondly, I recommend the inclusion of CBOs of MSM in delivering HIV testing services,
PrEP interventions and other HIV care and treatment services. Particularly, with political
support and proper training, I believe CBOs of MSM could deliver trusted, MSM-friendly
peer-based HIV testing and self-testing, as recommended by WHO (126, 127). This
diversification of HIV testing, prevention and care and treatment services, together with
strengthened government-based HIV prevention services, would create more MSM-
friendly service provision and encourage men to access and use HIV prevention, care
and treatment services.
162
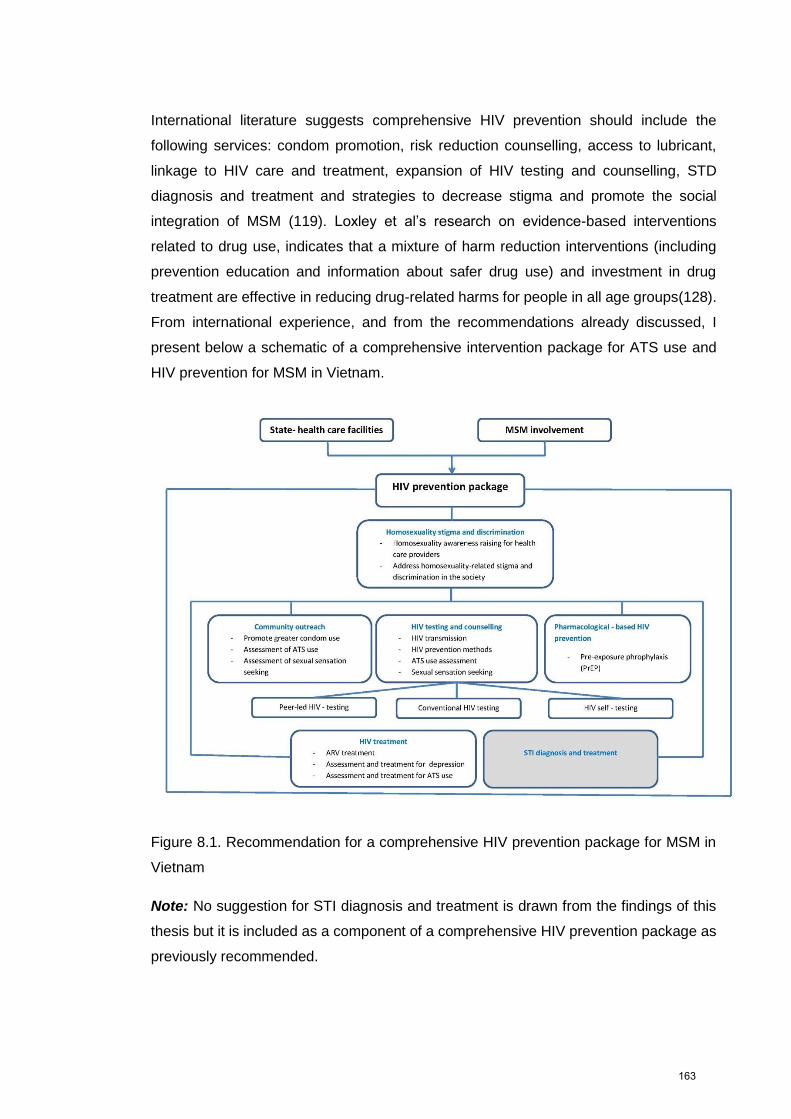
International literature suggests comprehensive HIV prevention should include the
following services: condom promotion, risk reduction counselling, access to lubricant,
linkage to HIV care and treatment, expansion of HIV testing and counselling, STD
diagnosis and treatment and strategies to decrease stigma and promote the social
integration of MSM (119). Loxley et al’s research on evidence-based interventions
related to drug use, indicates that a mixture of harm reduction interventions (including
prevention education and information about safer drug use) and investment in drug
treatment are effective in reducing drug-related harms for people in all age groups(128).
From international experience, and from the recommendations already discussed, I
present below a schematic of a comprehensive intervention package for ATS use and
HIV prevention for MSM in Vietnam.
Figure 8.1. Recommendation for a comprehensive HIV prevention package for MSM in
Vietnam
Note: No suggestion for STI diagnosis and treatment is drawn from the findings of this
thesis but it is included as a component of a comprehensive HIV prevention package as
previously recommended.
163

CONCLUSION
This thesis has contributed a range of novel research findings and suggested a number
of recommendations that would improve HIV prevention, care and harm reduction
practice and research for MSM in Vietnam. The thesis demonstrates an interplay among
sex-related methamphetamine use, risky sexual behaviour, HIV infection and depression
among MSM which requires an integrated, multilevel response. I recommend addressing
drug use at individual and community levels, promoting condom use, diversifying HIV
testing options and developing mental health services for MSM, particularly subgroups
of men with riskier drug use and sexual behaviours. My thesis recommends the inclusion
of MSM in the provision of HIV prevention, care and treatment services, particularly HIV
testing. The thesis also highlights that tackling social stigma and discrimination toward
MSM could yield beneficial outcomes not only for HIV prevention but also improving the
mental health and wellbeing of MSM in Vietnam. Lastly, I believe my thesis provides
valuable recommendations to strengthen future research on drug use, sexual behaviour
and HIV infection in MSM who use ATS, and who remain at risk of HIV.
164
References
1. Halkitis PN, Parsons JT, Stirratt MJ. A double epidemic: crystal
methamphetamine drug use in relation to HIV transmission among gay men. Journal of
homosexuality. 2001;41(2):17-35.
2. United Nations Office on Drugs and Crime (UNODC). Patterns and Trends of
Amphetamine-Type-Stimulants and Other Drugs: Challenges for Asia and the Pacifics.
2013.
3. United Nations Office on Drugs and Crime (UNODC). Amphetamine Type
Stimulants in Vietnam. A Review of the Availibility, Use and Implications for Health and
Security in Vietnam 2012. Hanoi, Vietnam: 2012.
4. Pantalone DW, Huh D, Nelson KM, Pearson CR, Simoni JM. Prospective
predictors of unprotected anal intercourse among HIV-seropositive men who have sex
with men initiating antiretroviral therapy. AIDS and behavior. 2014;18(1):78-87.
5. Daskalopoulou M, Rodger A, Phillips AN, Sherr L, Speakman A, Collins S, et al.
Recreational drug use, polydrug use, and sexual behaviour in HIV-diagnosed men who
have sex with men in the UK: results from the cross-sectional ASTRA study. The lancet
HIV. 2014;1(1):e22-31.
6. Pines HA, Gorbach PM, Weiss RE, Reback CJ, Landovitz RJ, Mutchler MG, et
al. Individual-Level, Partnership-Level, and Sexual Event-Level Predictors of Condom
Use During Receptive Anal Intercourse Among HIV-Negative Men Who Have Sex with
Men in Los Angeles. AIDS and behavior. 2015.
7. Santos GM, Coffin PO, Das M, Matheson T, DeMicco E, Raiford JL, et al. Dose-
response associations between number and frequency of substance use and high-risk
sexual behaviors among HIV-negative substance-using men who have sex with men
(SUMSM) in San Francisco. Journal of acquired immune deficiency syndromes (1999).
2013;63(4):540-4.
8. Melendez-Torres GJ, Hickson F, Reid D, Weatherburn P, Bonell C. Nested
Event-Level Case-Control Study of Drug Use and Sexual Outcomes in Multipartner
Encounters Reported by Men Who Have Sex with Men. AIDS and behavior. 2015.
9. Morineau G, Nugrahini N, Riono P, Nurhayati, Girault P, Mustikawati DE, et al.
Sexual risk taking, STI and HIV prevalence among men who have sex with men in six
Indonesian cities. AIDS and behavior. 2011;15(5):1033-44.
10. Beyrer C, Baral SD, van Griensven F, Goodreau SM, Chariyalertsak S, Wirtz AL,
et al. Global epidemiology of HIV infection in men who have sex with men. Lancet
(London, England). 2012;380(9839):367-77.
165
11. Carey JW, Mejia R, Bingham T, Ciesielski C, Gelaude D, Herbst JH, et al. Drug
use, high-risk sex behaviors, and increased risk for recent HIV infection among men who
have sex with men in Chicago and Los Angeles. AIDS and behavior. 2009;13(6):1084-
96.
12. Ackers ML, Greenberg, A. E., Lin, C. Y., Bartholow, B. N., Goodman, A. H.,
Longhi, M. Gurwith, M. High and persistent HIV seroincidence in men who have sex with
men across 47 U.S. cities. PLoS ONE [Electronic Resource]. 2012;7(4):e34972.
13. Koblin BA, Husnik MJ, Colfax G, Huang YJ, Madison M, Mayer K, et al. Risk
factors for HIV infection among men who have sex with men. Aids. 2006;20(5):731-9.
14. Buchbinder SP, Vittinghoff E, Heagerty PJ, Celum CL, Seage GR, III, Judson FN,
et al. Sexual Risk, Nitrite Inhalant Use, and Lack of Circumcision Associated With HIV
Seroconversion in Men Who Have Sex With Men in the United States. JAIDS Journal of
Acquired Immune Deficiency Syndromes. 2005;39(1):82-9.
15. Buchbinder SP, Douglas JM, Jr., McKirnan DJ, Judson FN, Katz MH, MacQueen
KM. Feasibility of human immunodeficiency virus vaccine trials in homosexual men in
the United States: risk behavior, seroincidence, and willingness to participate. Journal of
Infectious Diseases. 1996;174(5):954-61.
16. Weber AE, Craib KJP, Chan K, Martindale S, Lou Miller M, Cook DA, et al.
Determinants of HIV serconversion in an era of increasing HIV infection among young
gay and bisexual men. Aids. 2003;17(5):774-7.
17. Weber AE, Chan K, George C, Hogg RS, Remis RS, Martindale S, et al. Risk
factors associated with HIV infection among young gay and bisexual men in Canada.
JAIDS, Journal of Acquired Immune Deficiency Syndromes. 2001;28(1):81-8.
18. Macdonald N, Elam G, Hickson F, Imrie J, McGarrigle CA, Fenton KA, et al.
Factors associated with HIV seroconversion in gay men in England at the start of the
21st century. Sexually Transmitted Infections. 2008;84(1):8-13.
19. Hoenigl M, Chaillon A, Moore DJ, Morris SR, Smith DM, Little SJ. Clear Links
Between Starting Methamphetamine and Increasing Sexual Risk Behavior: A Cohort
Study Among Men Who Have Sex With Men. Journal of acquired immune deficiency
syndromes (1999). 2016;71(5):551-7.
20. Darke S, Kaye S, McKetin R, Duflou J. Major physical and psychological harms
of methamphetamine use. Drug and alcohol review. 2008;27(3):253-62.
21. World Health Organization (WHO). Neuroscience of psychoactive substance use
and dependence. Geneva, Switzland 2004.
22. Vearrier D, Greenberg MI, Miller SN, Okaneku JT, Haggerty DA.
Methamphetamine: history, pathophysiology, adverse health effects, current trends, and
166
hazards associated with the clandestine manufacture of methamphetamine. Disease-a-
month : DM. 2012;58(2):38-89.
23. Scott JC, Woods SP, Matt GE, Meyer RA, Heaton RK, Atkinson JH, et al.
Neurocognitive effects of methamphetamine: a critical review and meta-analysis.
Neuropsychology review. 2007;17(3):275-97.
24. Parrott AC. Human psychopharmacology of Ecstasy (MDMA): a review of 15
years of empirical research. Human psychopharmacology. 2001;16(8):557-77.
25. Parrott AC. Human psychobiology of MDMA or 'Ecstasy': an overview of 25 years
of empirical research. Human psychopharmacology. 2013;28(4):289-307.
26. Colfax G, Santos GM, Chu P, Vittinghoff E, Pluddemann A, Kumar S, et al.
Amphetamine-group substances and HIV. Lancet (London, England).
2010;376(9739):458-74.
27. Colfax G, Shoptaw S. The methamphetamine epidemic: implications for HIV
prevention and treatment. Current HIV/AIDS reports. 2005;2(4):194-9.
28. Chariyalertsak S, Beyrer C, Kosachunhanan N, Saokhieo P, Songsupa R,
Wongthanee A, et al. Prevalence, incidence, risk factors and willingness to participate in
HIV vaccine trials among gay and bisexual men and transgender persons seeking HI.
AIDS Research and Human Retroviruses. 2011;27 (10):A55.
29. Xu JJ, Qian HZ, Chu ZX, Zhang J, Hu QH, Jiang YJ, et al. Recreational drug use
among Chinese men who have sex with men: a risky combination with unprotected sex
for acquiring HIV infection. BioMed research international. 2014;2014:725361.
30. Xu JJ, Zhang C, Hu QH, Chu ZX, Zhang J, Li YZ, et al. Recreational drug use
and risks of HIV and sexually transmitted infections among Chinese men who have sex
with men: Mediation through multiple sexual partnerships. BMC infectious diseases.
2014;14:642.
31. Nguyen TA, Nguyen HT, Le GT, Detels R. Prevalence and risk factors associated
with HIV infection among men having sex with men in Ho Chi Minh City, Vietnam. AIDS
and behavior. 2008;12(3):476-82.
32. Kalichman SC, Simbayi L, Jooste S, Vermaak R, Cain D. Sensation seeking and
alcohol use predict HIV transmission risks: prospective study of sexually transmitted
infection clinic patients, Cape Town, South Africa. Addictive behaviors.
2008;33(12):1630-3.
33. Heidinger B, Gorgens K, Morgenstern J. The effects of sexual sensation seeking
and alcohol use on risky sexual behavior among men who have sex with men. AIDS and
behavior. 2015;19(3):431-9.
167
34. Newcomb ME, Clerkin EM, Mustanski B. Sensation seeking moderates the
effects of alcohol and drug use prior to sex on sexual risk in young men who have sex
with men. AIDS and behavior. 2011;15(3):565-75.
35. Mimiaga MJ, Reisner SL, Closson EF, Perry N, Perkovich B, Nguyen T, et al.
Self-perceived HIV risk and the use of risk reduction strategies among men who engage
in transactional sex with other men in Ho Chi Minh City, Vietnam. AIDS care.
2013;25(8):1039-44.
36. Colby DJ. HIV knowledge and risk factors among men who have sex with men in
Ho Chi Minh City, Vietnam. Journal of acquired immune deficiency syndromes (1999).
2003;32(1):80-5.
37. Pham QD, Nguyen TV, Nguyen PD, Le SH, Tran AT, Nguyen LT, et al. Men who
have sex with men in southern Vietnam report high levels of substance use and sexual
risk behaviours but underutilise HIV testing services: a cross-sectional study. Sex
Transm Infect. 2015;91(3):178-82.
38. Yu G, Clatts MC, Goldsamt LA, Giang le M. Substance use among male sex
workers in Vietnam: prevalence, onset, and interactions with sexual risk. The
International journal on drug policy. 2015;26(5):516-21.
39. Simons-Morton B, Haynie D, Liu D, Chaurasia A, Li K, Hingson R. The Effect of
Residence, School Status, Work Status, and Social Influence on the Prevalence of
Alcohol Use Among Emerging Adults. Journal of studies on alcohol and drugs.
2016;77(1):121-32.
40. Perkins HW. Misperceptions of peer drinking norms in Canada: another look at
the "reign of error" and its consequences among college students. Addictive behaviors.
2007;32(11):2645-56.
41. Rice R. College Drinking: Norms vs. Perceptions. The Scientist. 2006;20(2):54-
5.
42. Parker H, Williams L, Aldridge J. The normalization of 'sensible' recreational drug
use: Further evidence from the north west England longitudinal study. Sociol-J Brit Sociol
Assoc. 2002;36(4):941-64.
43. Sznitman SR, Kolobov T, Bogt TT, Kuntsche E, Walsh SD, Boniel-Nissim M, et
al. Exploring substance use normalization among adolescents: a multilevel study in 35
countries. Social science & medicine (1982). 2013;97:143-51.
44. Justumus P, Colby D, Mai Doan Anh T, Balestre E, Becquet R, Orne-Gliemann
J. Willingness to use the Internet to seek information on HIV prevention and care among
men who have sex with men in Ho Chi Minh City, Vietnam. PloS one. 2013;8(8):e71471.
45. Garcia MC, Duong QL, Mercer LC, Meyer SB, Koppenhaver T, Ward PR.
Patterns and risk factors of inconsistent condom use among men who have sex with men
168
in Viet Nam: Results from an Internet-based cross-sectional survey. Global public health.
2014;9(10):1225-38.
46. Bengtsson L, Lu X, Liljeros F, Thanh HH, Thorson A. Strong propensity for HIV
transmission among men who have sex with men in Vietnam: behavioural data and
sexual network modelling. BMJ open. 2014;4(1):e003526.
47. National Institute of Hygiene and Epidemioloty (Vietnam Ministry of Health).
HIV/STI Intergrated Biological and Behavioural Surveillance (IBBS) in Vietnam. Results
from Round III and trends across three round (2005-2009-2013) of survey. Hanoi,
Vietnam: 2014.
48. Vietnam National Committee on AIDS Drugs and Prostitute Control. National
Strategy for Hiv/Aids Prevention and Control to 2020 with the Vision to 2030. Hanoi,
Vietnam: 2012.
49. Vietnam Ministry of Health. Optimizing Vietnam's Hiv Response: An Investment
Case. Hanoi, Vietnam: 2015.
50. Rudy ET, Shoptaw S, Lazzar M, Bolan RK, Tilekar SD, Kerndt PR.
Methamphetamine use and other club drug use differ in relation to HIV status and risk
behavior among gay and bisexual men. Sexually transmitted diseases. 2009;36(11):693-
5.
51. Forrest DW, Metsch LR, LaLota M, Cardenas G, Beck DW, Jeanty Y. Crystal
methamphetamine use and sexual risk behaviors among HIV-positive and HIV-negative
men who have sex with men in South Florida. Journal of urban health : bulletin of the
New York Academy of Medicine. 2010;87(3):480-5.
52. Menza TW, Hughes JP, Celum CL, Golden MR. Prediction of HIV acquisition
among men who have sex with men. Sexually transmitted diseases. 2009;36(9):547-55.
53. Molitor F, Truax SR, Ruiz JD, Sun RK. Association of methamphetamine use
during sex with risky sexual behaviors and HIV infection among non-injection drug users.
Western Journal of Medicine. 1998;168(2):93-7.
54. Schwarcz S, Scheer S, McFarland W, Katz M, Valleroy L, Chen S, et al.
Prevalence of HIV infection and predictors of high-transmission sexual risk behaviors
among men who have sex with men. American journal of public health. 2007;97(6):1067-
75.
55. Robertson MJ, Clark RA, Charlebois ED, Tulsky J, Long HL, Bangsberg DR, et
al. HIV Seroprevalence Among Homeless and Marginally Housed Adults in San
Francisco. American journal of public health. 2004;94(7):1207-17.
56. Garcia MC, Duong QL, Mercer LE, Meyer SB, Ward PR. 'Never testing for HIV'
among men who have sex with men in Viet Nam: results from an Internet-based cross-
sectional survey. BMC public health. 2013;13:1236.
169
57. Leigh BC, Stall R. Substance use and risky sexual behavior for exposure to HIV.
Issues in methodology, interpretation, and prevention. The American psychologist.
1993;48(10):1035-45.
58. Stall R, Leigh B. Understanding the relationship between drug or alcohol use and
high risk sexual activity for HIV transmission: where do we go from here? Addiction
(Abingdon, England). 1994;89(2):131-4.
59. Vietnam Ministry of Health. Results from the HIV/STI Biological and Behavioral
Surveillance (Ibbs) in Vietnam- Round II 2009. Hanoi, Vietnam: 2011.
60. Vietnam Ministry of Health. Results from the HIV/STI Intergrated Biological and
Behavioural Surveillance (IBBS) in Vietnam, 2005-2006. Hanoi, Vietnam: 2006.
61. Pham QD, Nguyen TV, Hoang CQ, Cao V, Khuu NV, Phan HT, et al. Prevalence
of HIV/STIs and associated factors among men who have sex with men in An Giang,
Vietnam. Sexually transmitted diseases. 2012;39(10):799-806.
62. Nguyen TV, Van Khuu N, Nguyen PD, Tran HP, Phan HT, Phan LT, et al.
Sociodemographic Factors, Sexual Behaviors, and Alcohol and Recreational Drug Use
Associated with HIV Among Men Who Have Sex with Men in Southern Vietnam. AIDS
and behavior. 2016;20(10):2357-71.
63. Ha H, Risser JM, Ross MW, Huynh NT, Nguyen HT. Homosexuality-related
stigma and sexual risk behaviors among men who have sex with men in Hanoi, Vietnam.
Archives of sexual behavior. 2015;44(2):349-56.
64. Bui HT, Le GM, Mai AQ, Zablotska-Manos I, Maher L. Barriers to access and
uptake of antiretroviral therapy among HIV-positive men who have sex with men in
Hanoi, Vietnam: from HIV testing to treatment. Culture, health & sexuality. 2017:1-14.
65. Hoang HT, Mai TD, Nguyen NA, Thu NT, Van Hiep N, Le B, et al. Needs
Assessment on the Use of Health Services Among Men Who Have Sex with Men in Ho
Chi Minh City, Vietnam. LGBT health. 2015;2(4):341-5.
66. Punyacharoensin N, Edmunds WJ, De Angelis D, Delpech V, Hart G, Elford J, et
al. Modelling the HIV epidemic among MSM in the United Kingdom: quantifying the
contributions to HIV transmission to better inform prevention initiatives. Aids.
2015;29(3):339-49.
67. Burns DN, DeGruttola V, Pilcher CD, Kretzschmar M, Gordon CM, Flanagan EH,
et al. Toward an endgame: finding and engaging people unaware of their HIV-1 infection
in treatment and prevention. AIDS Res Hum Retroviruses. 2014;30(3):217-24.
68. Marks G, Crepaz N, Senterfitt JW, Janssen RS. Meta-analysis of high-risk sexual
behavior in persons aware and unaware they are infected with HIV in the United States:
implications for HIV prevention programs. Journal of acquired immune deficiency
syndromes (1999). 2005;39(4):446-53.
170
69. Holt M, Lea T, Asselin J, Hellard M, Prestage G, Wilson D, et al. The prevalence
and correlates of undiagnosed HIV among Australian gay and bisexual men: results of a
national, community-based, bio-behavioural survey. Journal of the International AIDS
Society. 2015;18:20526.
70. Marks G, Crepaz N, Janssen RS. Estimating sexual transmission of HIV from
persons aware and unaware that they are infected with the virus in the USA. Aids.
2006;20(10):1447-50.
71. Raymond H, Bingham T, McFarland W. Locating unrecognized HIV infections
among men who have sex with men: San Francisco and Los Angeles. AIDS Education
and Prevention. 2008;20(5):408-19.
72. Seage IGR, Mayer KH, Horsburgh Jr CR, Holmberg SD, Moon MW, Lamb GA.
The relation between nitrite inhalants, unprotected receptive anal intercourse, and the
risk of human immunodeficiency virus infection. American Journal of Epidemiology.
1992;135(1):1-11.
73. Rietmeijer CAM, Penley KA, Cohn DL, Davidson AJ, Horsburgh CR, Jr., Judson
FN. Factors influencing the risk of infection with human immunodeficiency virus in
homosexual men, Denver 1982-1985. Sexually transmitted diseases. 1989;16(2):95-
102.
74. Dahoma M, Johnston LG, Holman A, Miller LA, Mussa M, Othman A, et al. HIV
and related risk behavior among men who have sex with men in Zanzibar, Tanzania:
results of a behavioral surveillance survey. AIDS & Behavior. 2011;15(1):186-92.
75. Mor Z, Dan M. Knowledge, attitudes, sexual practices and STI/HIV prevalence in
male sex workers and other men who have sex in Tel Aviv, Israel: A cross-sectional
study. Sexually Transmitted Infections. 2012;88(8):574-80.
76. Sandfort TG, Lane T, Dolezal C, Reddy V. Gender Expression and Risk of HIV
Infection Among Black South African Men Who Have Sex with Men. AIDS and behavior.
2015.
77. Saha MK, Mahapatra T, Biswas S, Ghosh P, Kire M. Burden and correlates of
HIV risk among men who have sex with men in Nagaland, India: analysis of sentinel
surveillance data. PloS one. 2015;10(2):e0117385.
78. Hladik W, Barker J, Ssenkusu JM, Opio A, Tappero JW, Hakim A, et al. HIV
infection among men who have sex with men in Kampala, Uganda--a respondent driven
sampling survey. PLoS ONE [Electronic Resource]. 2012;7(5):e38143.
79. Biello KB, Colby D, Closson E, Mimiaga MJ. The syndemic condition of
psychosocial problems and HIV risk among male sex workers in Ho Chi Minh City,
Vietnam. AIDS and behavior. 2014;18(7):1264-71.
171
80. Goldsamt LA, Clatts MC, Giang LM, Yu G. Prevalence and Behavioral Correlates
of Depression and Anxiety Among Male Sex Workers in Vietnam. International journal of
sexual health : official journal of the World Association for Sexual Health.
2015;27(2):145-55.
81. Oldenburg CE, Biello KB, Colby D, Closson EF, Mai T, Nguyen T, et al. Stigma
related to sex work among men who engage in transactional sex with men in Ho Chi
Minh City, Vietnam. International journal of public health. 2014;59(5):833-40.
82. Salomon EA, Mimiaga MJ, Husnik MJ, Welles SL, Manseau MW, Montenegro
AB, et al. Depressive symptoms, utilization of mental health care, substance use and
sexual risk among young men who have sex with men in EXPLORE: implications for
age-specific interventions. AIDS and behavior. 2009;13(4):811-21.
83. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression
severity measure. Journal of general internal medicine. 2001;16(9):606-13.
84. Semple SJ, Patterson TL, Grant I. Motivations associated with
methamphetamine use among HIV+ men who have sex with men. Journal of substance
abuse treatment. 2002;22(3):149-56.
85. Kurtz SP. Post-circuit blues: motivations and consequences of crystal meth use
among gay men in Miami. AIDS and behavior. 2005;9(1):63-72.
86. Gibbs JJ, Rice E. The Social Context of Depression Symptomology in Sexual
Minority Male Youth: Determinants of Depression in a Sample of Grindr Users. Journal
of homosexuality. 2016;63(2):278-99.
87. Secor AM, Wahome E, Micheni M, Rao D, Simoni JM, Sanders EJ, et al.
Depression, substance abuse and stigma among men who have sex with men in coastal
Kenya. Aids. 2015;29 Suppl 3:S251-9.
88. Wilson PA, Stadler G, Boone MR, Bolger N. Fluctuations in depression and well-
being are associated with sexual risk episodes among HIV-positive men. Health
psychology : official journal of the Division of Health Psychology, American Psychological
Association. 2014;33(7):681-5.
89. Klein H. Depression and HIV Risk Taking among Men Who Have Sex with Other
Men (MSM) and Who Use the Internet to Find Partners for Unprotected Sex. Journal of
gay & lesbian mental health. 2014;18(2):164-89.
90. Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual
populations: conceptual issues and research evidence. Psychological bulletin.
2003;129(5):674-97.
91. Horton P, Rydstrom H, Tonini M. Contesting heteronormativity: the fight for
lesbian, gay, bisexual and transgender recognition in India and Vietnam. Culture, health
& sexuality. 2015;17(9):1059-73.
172
92. Berry MC, Go VF, Quan VM, Minh NL, Ha TV, Mai NV, et al. Social environment
and HIV risk among MSM in Hanoi and Thai Nguyen. AIDS care. 2013;25(1):38-42.
93. Vu BN, Mulvey KP, Baldwin S, Nguyen ST. HIV risk among drug-using men who
have sex with men, men selling sex, and transgender individuals in Vietnam. Culture,
health & sexuality. 2012;14(2):167-80.
94. Susser M, Susser E. Choosing a future for epidemiology: II. From black box to
Chinese boxes and eco-epidemiology. American journal of public health.
1996;86(5):674-7.
95. Susser M. The logic in ecological: I. The logic of analysis. American journal of
public health. 1994;84(5):825-9.
96. Guo Y, Li X, Fang X, Lin X, Song Y, Jiang S, et al. A comparison of four sampling
methods among men having sex with men in China: implications for HIV/STD
surveillance and prevention. Aids Care-Psychol Socio-Med Asp Aids-Hiv.
2011;23(11):1400-9.
97. Icard L. Reaching African-American Men on the "Down Low": Sampling Hidden
Populations: Implications for HIV Prevention. J Homosex. 2008;55(3):437-49.
98. Iguchi MY, Ober AJ, Berry SH, Fain T, Gorbach PM, Heckathorn DD, et al.
Simultaneous recruitment of drug users and men who have sex with men in the united
states and Russia using respondent-driven sampling: Sampling methods and
implications. Journal of Urban Health. 2009;86(1):S5.
99. Kendall C, Kerr L, Gondim RC, Werneck G, Macena R, Pontes M, et al. An
empirical comparison of respondent-driven sampling, time location sampling, and
snowball sampling for behavioral surveillance in men who have sex with men, Fortaleza,
Brazil. AIDS behav. 2008;12(4):S97-S104.
100. Saltzmann SP, Stoddard AM, McCusker J, Moon MW, Mayer KH. Reliability of
self-reported sexual behavior risk factors for HIV infection in homosexual men. Public
Health Reports. 1987;102(6):692-7.
101. Halkitis PN, Fischgrund BN, Parsons JT. Explanations for methamphetamine use
among gay and bisexual men in New York City. Substance use & misuse. 2005;40(9-
10):1331-45.
102. Semple SJ, Strathdee SA, Zians J, Patterson TL. Sexual risk behavior associated
with co-administration of methamphetamine and other drugs in a sample of HIV-positive
men who have sex with men. The American journal on addictions / American Academy
of Psychiatrists in Alcoholism and Addictions. 2009;18(1):65-72.
103. Fisher DG, Reynolds GL, Ware MR, Napper LE. Methamphetamine and Viagra
use: relationship to sexual risk behaviors. Archives of sexual behavior. 2011;40(2):273-
9.
173

104. Stahlman S, Beyrer C, Sullivan PS, Mayer KH, Baral SD. Engagement of Gay
Men and Other Men Who Have Sex with Men (MSM) in the Response to HIV: A Critical
Step in Achieving an AIDS-Free Generation. AIDS and behavior. 2016.
105. Glass TA, McAtee MJ. Behavioral science at the crossroads in public health:
Extending horizons, envisioning the future. Social Science and Medicine.
2006;62(7):1650-71.
106. Southgate E. The role of folk pharmacology and lay experts in harm reduction :
Sydney gay drug using networks. International Journal of Drug Policy. 2001;12(4):321-
35.
107. Brackins T, Brahm NC, Kissack JC. Treatments for methamphetamine abuse: a
literature review for the clinician. Journal of pharmacy practice. 2011;24(6):541-50.
108. Brensilver M, Heinzerling KG, Shoptaw S. Pharmacotherapy of amphetamine-
type stimulant dependence: an update. Drug and alcohol review. 2013;32(5):449-60.
109. Elkashef A, Vocci F, Hanson G, White J, Wickes W, Tiihonen J.
Pharmacotherapy of methamphetamine addiction: an update. Substance abuse.
2008;29(3):31-49.
110. Lee NK, Rawson RA. A systematic review of cognitive and behavioural therapies
for methamphetamine dependence. Drug and alcohol review. 2008;27(3):309-17.
111. Halkitis PN, Levy MD, Solomon TM. Temporal relations between
methamphetamine use and HIV seroconversion in gay, bisexual, and other men who
have sex with men. Journal of health psychology. 2016;21(1):93-9.
112. Mata MM, Napier TC, Graves SM, Mahmood F, Raeisi S, Baum LL.
Methamphetamine decreases CD4 T cell frequency and alters pro-inflammatory cytokine
production in a model of drug abuse. European journal of pharmacology. 2015;752:26-
33.
113. Carrico AW, Woolf-King SE, Neilands TB, Dilworth SE, Johnson MO. Stimulant
use and HIV disease management among men in same-sex relationships. Drug and
alcohol dependence. 2014;139:174-7.
114. Carrico AW, Shoptaw S, Cox C, Stall R, Li X, Ostrow DG, et al. Stimulant use
and progression to AIDS or mortality after the initiation of highly active antiretroviral
therapy. Journal of acquired immune deficiency syndromes (1999). 2014;67(5):508-13.
115. Lorimer K, Kidd L, Lawrence M, McPherson K, Cayless S, Cornish F. Systematic
review of reviews of behavioural HIV prevention interventions among men who have sex
with men. AIDS care. 2013;25(2):133-50.
116. Kelly JA, St Lawrence JS, Diaz YE, Stevenson LY, Hauth AC, Brasfield TL, et al.
HIV risk behavior reduction following intervention with key opinion leaders of population:
an experimental analysis. American journal of public health. 1991;81(2):168-71.
174
117. Kelly JA, Somlai AM, DiFranceisco WJ, Otto-Salaj LL, McAuliffe TL, Hackl KL, et
al. Bridging the gap between the science and service of HIV prevention: transferring
effective research-based HIV prevention interventions to community AIDS service
providers. American journal of public health. 2000;90(7):1082-8.
118. Wilson BD, Miller RL. Examining strategies for culturally grounded HIV
prevention: a review. AIDS education and prevention : official publication of the
International Society for AIDS Education. 2003;15(2):184-202.
119. Mayer KH, Wheeler DP, Bekker LG, Grinsztejn B, Remien RH, Sandfort TG, et
al. Overcoming biological, behavioral, and structural vulnerabilities: new directions in
research to decrease HIV transmission in men who have sex with men. Journal of
acquired immune deficiency syndromes (1999). 2013;63 Suppl 2:S161-7.
120. Mayer KH, Bekker LG, Stall R, Grulich AE, Colfax G, Lama JR. Comprehensive
clinical care for men who have sex with men: an integrated approach. Lancet (London,
England). 2012;380(9839):378-87.
121. Baral SD, Friedman MR, Geibel S, Rebe K, Bozhinov B, Diouf D, et al. Male sex
workers: practices, contexts, and vulnerabilities for HIV acquisition and transmission.
Lancet (London, England). 2015;385(9964):260-73.
122. Minichiello V. Male sex work and society. New York: Harrington Park Press;
2014.
123. Oldenburg CE, Le B, Huyen HT, Thien DD, Quan NH, Biello KB, et al.
Antiretroviral pre-exposure prophylaxis preferences among men who have sex with men
in Vietnam: results from a nationwide cross-sectional survey. Sexual health. 2016.
124. Spinner CD, Boesecke C, Zink A, Jessen H, Stellbrink HJ, Rockstroh JK, et al.
HIV pre-exposure prophylaxis (PrEP): a review of current knowledge of oral systemic
HIV PrEP in humans. Infection. 2016;44(2):151-8.
125. Pialoux G, Delaugerre C, Cotte L, Raffi F, Cua E, Molina JM. Pre-exposure
prophylaxis: a useful tool to prevent human immunodeficiency virus infection? Clinical
microbiology and infection : the official publication of the European Society of Clinical
Microbiology and Infectious Diseases. 2016;22(9):757-67.
126. HIV testing. WHO recommends HIV testing by lay providers [press release].
2015.
127. HIV testing services. WHO recommends HIV self-testing [press release]. 2016.
128. Loxley W, Toumbourou J, Stockwell T, Haines B, Scott K, Godfrey C, et al. The
prevention of substance use, risk and harms in Australia: a review of evidence. Autralia
2004.
175
APPENDIX 1
LETTERS OF SUPPORT
176
177
Human Research Ethics CommitteeThe University of NSWHigh StreetKensington NSW 2052
TO WHOM IT MAY CONCERN
Hanoi HIV/AIDS Prevention CenterAdd: Khu hinh chlnh m0i eu0n Hd D6ngHa Dong, Hanoi, VietnamTel: +84.433.512.746
Fax: +84.433.512.741
E-mail: [email protected]
I write in reference to ethics application for the research project entifled ,sex, Drug and Health of Men who have sex withmen in Vietnam'.
Hanoi Hlv/AIDS Prevention. Center (PAC) is the authorized lo-cal agency responsible for all Hlv+elated programs In theHanoi region. Hanoi PAC,,is the.managbment body.of .ail HtV teiiing'sitei-titV ctinics, .in.i rrrr,Lity_based HtVprevention programs and other H|V*elated services in the locality,
By this letter, I would like to confirm that Hanoi PAC is willing to carry out blood sampling procedures and Hlv and hepatitisc testing for participants of this study, who are interested inletting tested. rne pnc routinely conducts HIV testing and wehave a mobile testing service which. we are willing to provideiree oi cnirje to ttre stuly, as we are supportive of the study,saims and the data it will provide- Having revieried ihe protocol, I undirstand that Hlv/hepatitis C testing is a votuntaryservice that will be offered by PAC staff to men who have'sex *yt|',. *91 9191inrv't rrr been intervieweo torine main study.PAc will undertake this testing. following the vietnam Mli:try of Heaitn irr,roij rirrrt.rting protocot, *1'i.t .*pnrrises thattesting should be informed, voluntary and anonymous, if the'subject *.h.* t,i remain so]Rttid;i.i;;; il;larticipate inthe collection of blood samples are well kained and have exiensive .rpuii*.r in pre and post-test counselling andvenepuncture technlques. T.h: trTpl3 collection process willshictty follow'standard infbction ili;i G;tions to avoidharm to participants and PAC staff. To allow the linkage of test re'sufts witn questionnaire data collected in the research
study, I understand that participants.will sign a consentiorm ano provioe pnC lturi *itn , ,n(r. riro,, io ,, tiirt their testresults can be matched later on. No research staff will be invoived in conouc'ting Htv tests or ,iiiii#gi;rt resutts toparticipantd'once blood is collected, participants will be given a letter indicater ir,i tiru and location wndre tney can gettheir test.results'when participants collect their results, thiy will be linked to care ano support r."iru., u, ,rquired, by thePAC staff.
As part of my representative role for Hanoi PAC, I am supportive of the proposed study. The option of providing free l-uVtesting and counselling for participants of the above mentioned stuoy nas ttrJ irrr rrpport of the Hanoi pAC, subject to theindividual consent of the potential participants in the study.
Hanoi HIV/AIDS Prevention Centre
178
179

CENTER FOR COMMUNITY HEALTH PROMOTION
____________________________________________________________________
TO WHOM IT MAY CONCERN
I write in reference to ethics application for the research project entitled ‘Behaviors and Health of Men who have sex with men in Vietnam (BHMV)’.
Center for Community Health Promotion (CHP) is a Vietnamese non-governmental organization (NGO) established in 2006. Since the establishment, HIV/AIDS prevention and care and support services have been a key focus area for CHP. Via its community-based projects funded by different international donors such as PEPPAR, GLOBAL FUND, CHP’s goal is to improve the quality of life of individuals living with and affected by HIV/AIDS, to decrease HIV infection rate among most at risk population (MARP) groups and community, to improve the quality of life for people living with HIV/AIDS and orphan and vulnerable children and build capacity and promote for positive living for people living with HIV/AIDS and vulnerable populations.
By this letter, I would like to confirm that CHP commits to support BHMV study team to conduct their study in Vietnam. CHP will provide inputs and contributions to BHMV study in kinds of reviewing and commenting for the development of the research protocol and data collection tools and subsequently published manuscripts, piloting the quantitative questionnaire and coordinating the data collection in Vietnam by contributing human for interviews and recruitment of study participants.
As part of my representative role for CHP, I am charged with ensuring that the conduct of this study is acceptable to CHP supported community-based groups of MSM. This project has the full support of the CHP, subject to the individual consent of the potential participants in the study.
Yours sincerely, Tran Minh Gioi
Director Center for Community Health Promotion
180
APPENDIX 2
PARTICIPANTS INFORMATION STATEMENT AND CONSENT FORMS
181
1
Study title: SEX, DRUGS AND HEALTH OF MEN WHO HAVE SEX WITH MEN IN VIETNAM STUDY FLYER
We are researchers from The Centre for Social Research in Health (CSRH), University of New South
Wales, Australia and The Institute of Preventive Medicine and Public Health, Hanoi Medical University.
We are conducting a study about the behaviours and health of men who have sex with men (MSM) in
Vietnam. In particular, we are interested in understanding more about the use of amphetamine
(stimulant)-type drugs and how this may affect sexual behaviours. Our findings will help to facilitating
the formulation of appropriate drug education and HIV prevention programs for MSM in Vietnam.
Taking part involves being interviewed (for up to 45 minutes) about your sex life, drug use,
relationships with other MSM and general health. All men who have had sex with another man in the
past year and who are aged 18 or older are eligible to take part.
If you are interested in participating:
▪ You should contact our research assistant to make an appointment. We are interviewing
people between 8am and 8pm every day.
▪ You will be screened to see if you are eligible to participate in our study
▪ If you are eligible, you will be interviewed by an experienced, friendly interviewer for
about 30 to 45 minutes.
If you participate in our study, you will receive:
▪ $5 to compensate you for your travel costs and your time
▪ HIV prevention materials, including free condoms
▪ Access to HIV, STI and support facilities if you want them, including HIV testing
Our contact details and locations of interviews
Research assistant name: Contact number:
Location of interviews:
182
Study “Sex, Drugs and Health of Men who have sex with men in Vietnam”
1
THE UNIVERSITY OF NEW SOUTH WALES
PARTICIPANT INFORMATION STATEMENT AND CONSENT FORM
Study “Sex, Drugs and Health of Men who have sex with men in Vietnam”
FACE-TO-FACE INTERVIEW
QUANTITATIVE STUDY
About the Study
We are researchers from The Centre for Social Research in Health (CSRH), University of New South
Wales, Australia and The Institute of Preventive Medicine and Public Health, Hanoi Medical
University. We are conducting a study about the behaviours and health of men who have sex with men
(MSM) in Vietnam. This study aims to understand amphetamine type stimulant (ATS) use among men
who have sex with men (MSM) in Vietnam. In this part of the study, we are particularly interested in
behaviours that could facilitate the transmission of viruses such as HIV. We will ask you questions
about your demographic background, your drug use and sexual behaviours, your beliefs about ATS use,
your mental health, your experience of sexuality-related stigma and discrimination and your access to
HIV prevention services where you live.
Who is Being Asked to Respond?
You have been selected as a potential participant in this study because you are male, reside in Vietnam,
are gay, bisexual or other MSM and are aged 18 or older.
What Would We Like You To Do?
If you decide to participate, before you are interviewed, you will be screened for eligibility. If you
eligible and consent to take part, you will be interviewed for between thirty to forty five minutes. The
interview involves a structured questionnaire which is administered by a trained and experienced
interviewer. You can select an interviewer of your preference among the on-site interviewers.
You will receive $5 to compensate for your travelling costs and your time.
Anonymity and Consent
Participation in the study is entirely voluntary. You can withdraw from the project at any time without
giving a reason and without prejudice. If you decide not to participate in this project, there will be no
consequences of not participating in our study.
183

2
Study “Sex, Drugs and Health of Men who have sex with men in Vietnam”
A number of measures will be put in place to ensure that you remain anonymous and cannot be
identified. The questionnaire does not include questions which could reveal your personal identity. The
questionnaire with your answers will be stored in a secure database on a password protected computer
and only the investigators will have access to it.
We will only publish aggregated (combined) data from this part of the study. If you give us your
permission by signing this document, we plan to present the results at scientific meetings and
conferences and to publish the findings in academic books and journals. In any publication, information
will be provided in such a way that you cannot be identified.
Risks
The risks to participants in this study are considered minimal. All participants are offered HIV
prevention materials, including the list of all HIV service providers in the locality. Participants who
express concern or interest in accessing any HIV-related services will be referred to the relevant service
providers. If you experience distress or require support we can refer you to a local relevant support
organisation.
Feedback
Direct benefits. All participants who report or express psychological distress during an interview or
questionnaire will be referred to a relevant local support service that can offer free, confidential and
culturally appropriate support and treatment. Men who are interested in peer support can also be
referred to relevant local MSM groups. Participants who expressed concerns or difficulties in
accessing HIV-related services will be provided with list of all relevant service providers in the
locality and referral as needed.
Indirect benefits. The study findings may indirectly help participants by facilitating the formulation of
appropriate drug use and HIV prevention interventions that may improve the health and well-being of
MSM in Vietnam.
Inquiries
Complaints may be directed to the Ethics Secretariat, The University of New South Wales, SYDNEY
2052 AUSTRALIA . Any complaint you make will be investigated promptly and you will be
informed out the outcome.
If you decide to participate, you are free to withdraw your consent and to discontinue participation at
any time without prejudice.
If you have any questions, please feel free to ask the study team. If you have any additional questions
later, Dr. Vu Thi Thu Nga will be happy to answer them.
You will be given a copy of this form to keep.
184
Study “Sex, Drugs and Health of Men who have sex with men in Vietnam”
3
You are making a decision whether or not to participate. Your signature indicates that, having
read the information provided above, you have decided to participate in this study.
…………………………………………………… .……………………………………………..
Signature of Research Participant Signature of Witness
…………………………………………………… .…………………………………………….
(Please PRINT name) (Please PRINT name)
…………………………………………………… .…………………………………………….
Date Nature of Witness
185
1
REVOCATION OF CONSENT
Study “Sex, Drugs and Health of Men who have sex with men in Vietnam”
I hereby wish to WITHDRAW my consent to participate in the research titled “Sex, Drugs and Health of Men who have sex with men in Vietnam” and understand that such withdrawal WILL NOT jeopardise any services I receive or my relationship with University of New South Wales and Hanoi Medical University.
By signing into this form, I understand that the research team will keep my interview information confidentially and securely in the research office at Hanoi Medical University and my information will not be included in any forms of disseminations of the research’s findings, including abstracts to scientific conferences or meetings or publications to scientific journals or textbooks.
…………………………………………………… .……………………………………………… Signature Date
…………………………………………………… Please PRINT Name
The section for Revocation of Consent should be forwarded to:
Dr.Nga Thi Thu Vu Centre for Social Research in Health, UNSW Australia Institute of Preventive Medicine and Public Health, Hanoi Medical University Mobile: Email:
Or
Dr.Huong Thi Le Institute of Preventive Medicine and Public Health, Hanoi Medical University Mobile: Email:
186
Study “Sex, Drugs and Health of Men who have sex with men in Vietnam”
1
THE UNIVERSITY OF NEW SOUTH WALES
PARTICIPANT INFORMATION STATEMENT AND CONSENT FORM
Study “Sex, Drugs and Health of Men who have sex with men in Vietnam”
OPTIONAL, VOLUNTEERING HIV AND HCV TEST
AND ACCESS TO TEST RESULTS
About the complementary, voluntary HIV testing
This HIV testing is a voluntary, optional component to the study “Sex, Drugs and Health of men who
have sex with men in Vietnam” offered free of charge by Hanoi HIV/AIDS Prevention Center. You
should discuss with the PAC staff whether you want or need an HIV test. This testing is anonymous
and Hanoi PAC staffs do not require any personally identifying information from you. If you do not
want to get HIV test, you are not obliged to do so and your relationship with the study or the study
partners is not affected.
All the testing procedures follow Vietnam Ministry of Health (MOH) testing procedures. All
technicians who participate in the collection of blood samples are from HIV testing clinics in Hanoi,
are well trained and have extensive experience in pre and post-test counselling and venepuncture
techniques. The sample collection process will strictly follow infection control precautions to avoid
harm to you or PAC staff. If you agree to be tested, your blood sample will be tested for HIV.
You can choose to be tested for HIV and collect your results independently of the study. However, if
you agree, we can link your HIV test results with your questionnaire data. Linking your test results with
the information we gather from the questionnaire will help us to better understanding the association
between drug use, sexual behaviors and HIV infection among MSM. To link your test results and
questionnaire data, you do not need to provide personally identifying information; we will use your
anonymous study ID.
Who is Being Asked to Respond?
You are offered this testing because you have already participated in the above mentioned study.
However, this testing component is not compulsory. If you do not want to have your blood tested for
HIV, you are not required to do so, nor are you required to link your test results with your questionnaire.
Please decide on the best option for you.
What Would We Like You To Do?
If you decide to get your blood tested for HIV, an experienced, trained technician from will take a small
blood sample from you. If you agree for your sample to be linked to your questionnaire, your blood
sample will be labelled with your study ID. You will be given a letter indicating the time and location
187

Study “Sex, Drugs and Health of Men who have sex with men in Vietnam”
2
where you can get your test results and post-test counselling. You will not receive any compensation
for this testing but you do not have to pay for this testing (it is free).
Anonymity and Consent
Participation in the testing is entirely voluntary and anonymous. You can withdraw from this testing
component at any time without giving a reason and without prejudice. There is a revocation form for
you to sign if you want to withdraw from the testing. If you decide not to participate in this testing,
there will be no consequences to your participation in the overall study. You can choose to be tested for
HIV but not provide your test results to the study. In this case, there will be no consequences to you and
your relationship to the study partners will not be affected.
If you agree to allow us to use your test result, you should provide us two signatures: one is for
agreement to get your blood tested for HIV and the other is for allowing us to use your test results. If
you just want to have your blood tested, you will provide one signature for the testing only.
If you give us your permission to use your test results, we will connect it with your questionnaire data.
We plan to present the results of our study at scientific meetings and conferences and to publish the
findings in academic books and journals. In any publication, information will be provided in such a way
that you cannot be identified.
Risks
Measures are taken to minimize the risk of this testing component. Standard infection control
procedures are used to minimize the risk for you and for Hanoi PAC staff. If your HIV test result is
positive, this is likely to be a stressful experience. If you are not ready to receive a test result, we advise
that you consider testing at another time. Staffs who deliver the results at the PAC will provide you
advice and support, and you can be referred to an HIV treatment service near to you. Participants who
experience distress or require further information or support can be referred to relevant local support,
counselling or treatment services and/or community-based groups of people living with HIV/AIDS
(PLHIV) or MSM.
Feedback
Direct benefits. All participants who report or express psychological distress during an interview or
questionnaire will be referred to a relevant local support service that can offer free, confidential and
culturally appropriate support and treatment. Men who are interested in peer support can also be
referred to relevant local MSM groups. Participants who expressed concerns or difficulties in
accessing HIV-related services will be provided with list of all relevant service providers in the
locality and referral as needed.
Indirect benefits. The study findings may indirectly help participants by facilitating the formulation of
appropriate drug use and HIV prevention interventions that may improve the health and well-being of
MSM in Vietnam.
Inquiries
Complaints may be directed to the Ethics Secretariat, The University of New South Wales, SYDNEY
2052 AUSTRALIA (phone 9385 4234, fax 9385 6648, email [email protected]). Any
complaint you make will be investigated promptly and you will be informed out the outcome.
188
3
Study “Sex, Drugs and Health of Men who have sex with men in Vietnam”
If you decide to participate, you are free to withdraw your consent and to discontinue participation at
any time without prejudice.
If you have any questions, please feel free to ask the study team. If you have any additional questions
later, Dr. Vu Thi Thu Nga will be happy to answer them.
You will be given a copy of this form to keep.
Your signature below indicates that, having read the information provided above, you have
decided to participate in this HIV and HCV testing component.
…………………………………………………… .……………………………………………..
Signature of Research Participant Signature of Witness
…………………………………………………… .…………………………………………….
(Please PRINT name) (Please PRINT name)
…………………………………………………… .…………………………………………….
Date Nature of Witness
Your signature below indicates that, having read the information provided above, you have
decided to allow the study team to use your HIV testing results for our study purpose.
…………………………………………………… .……………………………………………..
Signature of Research Participant Signature of Witness
…………………………………………………… .…………………………………………….
(Please PRINT name) (Please PRINT name)
…………………………………………………… .…………………………………………….
Date Nature of Witness
189
1
REVOCATION OF CONSENT
Study “Sex, Drugs and Health of Men who have sex with men in Vietnam” HIV and HCV testing component
I hereby wish to WITHDRAW my consent to participate in the complement, voluntary testing component of the research titled “Sex, Drugs and Health of Men who have sex with men in Vietnam” and understand that such withdrawal WILL NOT jeopardise any treatment or my relationship with University of New South Wales Australia and Hanoi Medical University.
By signing into this form, I understand that the research team will keep my interview information confidentially and securely in the research office at Hanoi Medical University and my information will not be included in any forms of disseminations of the research’s findings, including abstracts to scientific conferences or meetings or publications to scientific journals or textbooks.
…………………………………………………… .……………………………………………… Signature Date
…………………………………………………… Please PRINT Name
The section for Revocation of Consent should be forwarded to:
Dr.Nga Thi Thu Vu Centre for Social Research in Health, UNSW Australia Institute of Preventive Medicine and Public Health, Hanoi Medical University Mobile: Email:
Or
Dr.Huong Thi Le Institute of Preventive Medicine and Public Health, Hanoi Medical University Mobile: Email:
190
1
THE UNIVERSITY OF NEW SOUTH WALES
CONFIDENTIALITY STATEMENT FOR PERSONS
ACCESSING RECORDS CONTAINING SENSITIVE INFORMATION
Study “Sex, Drugs and Health of Men who have sex with men in Vietnam”
By signing this letter, I commit to:
* Keep confidential any personal information I have access to in taking part in the research project “Sex,
Drugs and Health of Men who have sex with men in Vietnam”; confidential information includes
interview records and personal information divulged by participants to me while working as: i) a research
assistant; ii) interviewer; or iii) transcriber;
* Not discuss or divulge any of that information to anyone outside the research team;
* Not use the information for any other purpose other than accurately recording the data for the research
project;
* Not access any other information from the records other than that required for the research project and
approved by the Human Research Ethics Committee;
* Ensure that I keep secure the records and information extracted from those records whilst in my
possession;
* Ensure that any waste paper I generate whilst accessing the records and recording the information
required will be destroyed in a manner which is permanent and which ensures the participants’
confidentiality, e.g. by shredding.
Name:……………………………………......................Signature:…………………………………….
Date:…………………………………………………….
191
APPENDIX 3
ETHICAL APPROVALS
192
HREC Ref: # HC14130
Sex, Drugs, and Health of Men Who Have Sex With Men In Vietnam
The Human Research Ethics Committee considered the above protocol at its meeting held on 24-Jun-
2014 and is pleased to advise it is satisfied that this protocol meets the requirements as set out in the
National Statement on Ethical Conduct in Human Research*. Having taken into account the advice of
the Committee, the Deputy Vice-Chancellor (Research) has approved the project to proceed.
Would you please note:-
• approval is valid from 24-Jun-2014 to 24-Jun-2019;
• you will be required to provide annual reports on the studys progress to the HREC, as
recommended by the National Statement;
• you are required to immediately report to the Ethics Secretariat anything which might warrant
review of ethical approval of the protocol (National Statement 3.3.22, 5.5.7:
http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/e72.pdf) including:
▪ serious or unexpected outcomes experienced by research participants (using the Serious
Adverse Event proforma on the University website at
http://research.unsw.edu.au/human-ethics-forms-and-proformas ;
▪ proposed changes in the protocol; and
▪ unforeseen events or new information (eg. from other studies) that might affect
continued ethical acceptability of the project or may indicate the need for amendments
to the protocol;
• any modifications to the project must have prior written approval and be ratified by any other
relevant Human Research Ethics Committee, as appropriate;
• if there are implantable devices, the researcher must establish a system for tracking the
participants with implantable devices for the lifetime of the device (with consent) and report
any device incidents to the TGA;
• if the research project is discontinued before the expected date of completion, the researcher is
required to inform the HREC and other relevant institutions (and where possible, research
participants), giving reasons. For multi-site research, or where there has been multiple ethical
review, the researcher must advise how this will be communicated before the research begins
(National Statement 3.3.22, 5.5.7:
http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/e72.pdf);
• consent forms are to be retained within the archives of the HIVSRC - National Centre in HIV
Social Research and made available to the Committee upon request.
Sincerely,
Professor Heather Worth
Presiding Member
Human Research Ethics Committee
* http://www.nhmrc.gov.au
193
194
APPENDIX 4
THE COMMUNITY-BASED, CROSS-SECTIONAL SURVEY’S
QUESTIONNAIRE
195
1
QUESTIONNAIRE
SEX, DRUGS AND HEALTH OF MEN WHO HAVE SEX WITH MEN IN
VIETNAM 2014
001 QUESTIONNAIRE IDENTIFICATION NUMBER: |___|___|___|___|___|
002 CITY OF INTERVIEW: 1 HANOI 2 HOCHIMINH CITY
003 NAME OF INTERVIEWER:…………………………………………SIGNATURE
004 DATE OF INTERVIEW: __/ ____ / ____
005 SUPERVISOR CHECK:
Supervisor name:……………………………………………Signature
Date of checking: __/ ____ / ____
DATA MANAGEMENT
Check and Clean
by
1st Data entry by 2nd Data entry by Checked by
Name
Date
196
2
SESSION 1. DEMOGRAPHIC AND OTHER PERSONAL INFORMATION
A. DEMOGRAPHIC INFORMATION
Q101.IN WHAT MONTH AND YEAR WERE YOU BORN?
Month [__|__] Don’t remember 99
Year [__|__|__|__] Don’t remember 99
Q102. IN WHAT PROVINCE/CITY WERE YOU BORN?
Q103. HOW LONG HAVE YOU BEEN LIVING IN THIS CITY?
Month [__|__] Year [__|__] Less than 1 month □ 99. Don’t remember
Q104. WHAT IS YOUR ETHNICITY? (cirlce the only one appropriate option”)
1. Kinh 2. Tày 3. Thái 4. Mường 5. Kh-me
6. Hoa 7. Nùng 8. Mông 9. Dao 10. Other
Q105 WHAT IS YOUR HIGHEST EDUCATION LEVEL? (circle the only one appropriate option”)
1. No schooling 2. Primary 3. Secondary 4. High school
5. Vocational training 6. College 7. Undergrad 8. Postgrad
9. Other
Q106. HAVE YOU EVER MARRIED OR CO-LIVING WITH A WOMAN?? 1.Yes 0. No
Q107. CURRENTLY, WHO DO YOU LIVE WITH? (do not read out the options, circle the only one
appropriate option)
1. Alone 2. Male partner 3. Male friend(s) who
is(are) gay
4. Male friend(s) who is
(are) not gay
5. Wife/Girld friend 6. Family
(mum/dad/siblings)
7. Homeless 8. Other (specify)
Q108. WHAT IS YOUR MAIN OCCUPATION WHICH YOU SPEND MOST OF YOUR TIME FOR? (do not
read out the options, circle the only one appropriate option)
1. Student 2. Gov. employee 3. Private company
employee
4. Foreign-investment
company employee
5. Self-employ 6. Army officer 7. Fine Art-related
occupations
8. Entertainment
venues’ employee
9. Freelance 10. Farmer 11. Unemployment 12. Other (specify)
Q109. WHAT IS YOUR AVERAGE MONTHLY INCOME FROM ALL SOURCES? (including monthly
allowance from parent if you are a student)? VNĐ
B. HEALTH AND SEXUAL LIFE
Q110. DO YOU THINK IF YOU ARE A GAY/HOMOSEXUAL MAN, BISEXUAL MAN,
HETEROSEXUAL MAN OR TRANSGENDER? (read out all options, circle the only one appropriate option)
1. Gay 2. Bisexual 3. Heterosexual 4. Transgender 5. Other
(specify)
Q111.WHO HAVE YOU BEEN HAVING SEX WITH? (read out all options, circle the only one appropriate
option) 1. Only with men 2. With both men
and women
3. Only with
women
4. Other (specify)
If answer: 1- ask Q112 2-ask Q112 and Q113 3- ask Q113
Q112 AT WHAT AGE DID YOU HAVE 1ST SEX WITH A MAN?..................age 99. Don’t
remember
Q113. AT WHAT AGE DID YOU HAVE 1ST SEX WITH A WOMAN?................age 99. Don’t remember
197
3
Q114. HAVE YOU EVER HAD SEX FOR MONEY? 0. No, I haven’t 1. Yes, I have
(If answer NO, move to Q118)
Q115. HAVE YOU HAD SEX FOR MONEY IN THE LAST 3 MONTHS? 0. No, I haven’t 1. Yes, I have
Q116. FOR HOW LONG HAVE YOU BEEN INVOLVED IN HAVING SEX FOR MONEY
(CUMULATIVELY)?....................year
Q117. WHAT IS THE AVERAGE AMOUNT OF MONEY YOU RECEIVE FROM A TRANSEXUAL SEX?
.........................VNĐ
Q118. WHAT IS YOUR HIV STATUS? (If HIV negative or don’t know, move to Q122) (circle the only one
appropriate option) 1. HIV positive 2. HIV negative
3. Never had HIV test before 99. Don’t know/Don’t remember/Don’t answer
Q119. WHEN DO YOU KNOW YOU ARE HIV POSITIVE?
Q120. ARE YOU ON HIV TREATMENT? 0. No, I don’t 1. Yes, I do
Q121. WHAT IS YOUR RECENT CD4 TEST RESULT?.............. cell/mm 99. Don’t know/Don’t remember
Q122. HAVE YOU PARTICIPATED IN ANY STUDY RELATED TO DRUG USE, SEXUAL BEHAVIOURS
AND/OR HIV INFECTION DURING THE LAST TWO YEARS?
0. No, I haven’t 1. Yes, I do
SESSION 2. HOMOSEXUALITY-RELATED STIGMA AND DISCRIMINATION
2A. EXPERIENCED HOMOSEXUALITY-RELATED STIGMA (Use prompt card # 1)
Question
Nev
er
Occ
atio
nal
ly
Som
etim
e
Usu
ally
Q201. Have you ever lost your job or job opportunity because you are found to
be homosexual or being engaging in homosexual activities? 1 2 3 4
Q202. Have you ever been rejected/isolated/disregarded by your family because
of your homosexuality/engaging in homosexual activities 1 2 3 4
Q203. Have you ever lost your friend(s) because they know about your
homosexuality or your engaging in homosexual activities? 1 2 3 4
Q204. Have you ever been hit/beaten because you are a homosexual or your
engaging in homosexual activities? 1 2 3 4
Q205. Have you ever changed your school or being kicked out of your school
because you are homosexual or your engaging in homosexual activities? 1 2 3 4
Q206. Have you ever changed your accommodation because you are a
homosexual or your engaging in homosexual activities? 1 2 3 4
Q207. Have you ever been refused health care services because of your
homosexual or your engaging in homosexual activities? 1 2 3 4
Q208. Have you ever felt ambarrassed or afraid of seeking health care services
because of your homosexuality or your engaging in homosexual activities? 1 2 3 4
2B. PERCEIVED HOMOSEXUALITY-RELATED STIGMA (Use prompt card # 2)
198
4
Question
Sto
rng
ly
dis
agre
e
Dis
agre
e
Ag
ree
Str
ong
ly a
gre
e
Q209. Many people unwilling to accept homosexual men/men engage in
homosexual activities 1 2 3 4
Q210. Homosexual men would lose their heterosexual girlfriend/wife if they
knew their homosexual status/activities 1 2 3 4
Q211. Many employers would underestimate homosexual men due to his
homosexuality/homosexual activities regardless of his appropriate qualifications
for the job
1 2 3 4
Q212. Many people curse or tease homosexual men 1 2 3 4
Q213. Many people have negative attitude toward homosexual men/men with
homosexual activities 1 2 3 4
Q214. Many people don’t see homosexual men/men with homosexual activities
as a normal man 1 2 3 4
Q215. Many families are disappointed having a homosexual son/ a son with
homosexual activities 1 2 3 4
Q216. Many people believe homosexual men/men with homosexual activities
are not normal people 1 2 3 4
Q217. Nhiều cán bộ y tế thường tỏ thái độ không thoải mái hoặc không tích cực
với người MSM (nam QHTD đồng giới) Many health care providers show
unpleasant or negative attitude toward homosexual men/men with homosexual
activities
1 2 3 4
Q218. Many people believe that homosexual activities are transmitted 1 2 3 4
2C. INTERNALIZED HOMOPHOBIA (Use prompt card # 2)
Items
Str
ongly
dis
agre
e
Dis
agre
e
Agre
e
Dis
agre
e Q219. Sometimes you wish you are not gay/a man with homosexual activities 1 2 3 4
Q220. Sometimes you think you would be happier if you were not gay/a man
with homosexual activities 1 2 3 4
Q221. Sometime to hide your homosexuality/homosexual activities you have to
conceal your interest/being attracted to other men in pubic places 1 2 3 4
Q222. Sometimes you wish you could be sexually attracted to a woman 1 2 3 4
Q223. Sometimes you think your homosexual preference is your weakness 1 2 3 4
Q224. Sometimes you feel ashame of your homosexual orientation 1 2 3 4
Q225. You ar afraid that your family and/or friends know about your sexual
preference 1 2 3 4
Q226. You try to look masculine in order to avoid other stigma/rejection 1 2 3 4
199
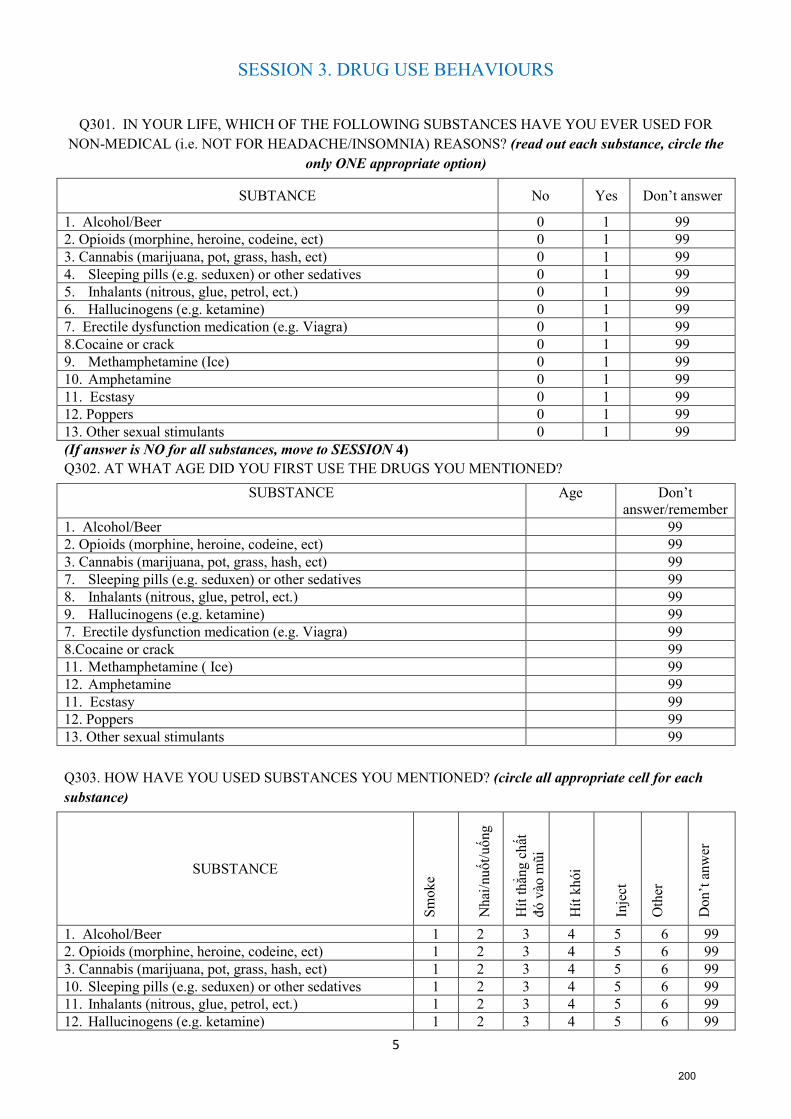
5
SESSION 3. DRUG USE BEHAVIOURS
Q301. IN YOUR LIFE, WHICH OF THE FOLLOWING SUBSTANCES HAVE YOU EVER USED FOR
NON-MEDICAL (i.e. NOT FOR HEADACHE/INSOMNIA) REASONS? (read out each substance, circle the
only ONE appropriate option)
SUBTANCE No Yes Don’t answer
1. Alcohol/Beer 0 1 99
2. Opioids (morphine, heroine, codeine, ect) 0 1 99
3. Cannabis (marijuana, pot, grass, hash, ect) 0 1 99
4. Sleeping pills (e.g. seduxen) or other sedatives 0 1 99
5. Inhalants (nitrous, glue, petrol, ect.) 0 1 99
6. Hallucinogens (e.g. ketamine) 0 1 99
7. Erectile dysfunction medication (e.g. Viagra) 0 1 99
8.Cocaine or crack 0 1 99
9. Methamphetamine (Ice) 0 1 99
10. Amphetamine 0 1 99
11. Ecstasy 0 1 99
12. Poppers 0 1 99
13. Other sexual stimulants 0 1 99
(If answer is NO for all substances, move to SESSION 4)
Q302. AT WHAT AGE DID YOU FIRST USE THE DRUGS YOU MENTIONED?
SUBSTANCE Age Don’t
answer/remember
1. Alcohol/Beer 99
2. Opioids (morphine, heroine, codeine, ect) 99
3. Cannabis (marijuana, pot, grass, hash, ect) 99
7. Sleeping pills (e.g. seduxen) or other sedatives 99
8. Inhalants (nitrous, glue, petrol, ect.) 99
9. Hallucinogens (e.g. ketamine) 99
7. Erectile dysfunction medication (e.g. Viagra) 99
8.Cocaine or crack 99
11. Methamphetamine ( Ice) 99
12. Amphetamine 99
11. Ecstasy 99
12. Poppers 99
13. Other sexual stimulants 99
Q303. HOW HAVE YOU USED SUBSTANCES YOU MENTIONED? (circle all appropriate cell for each
substance)
SUBSTANCE
Sm
ok
e
Nh
ai/n
uốt/
uố
ng
Hít
th
ẳng
ch
ất
đó
vào
mũi
Hít
kh
ói
Inje
ct
Oth
er
Do
n’t
an
wer
1. Alcohol/Beer 1 2 3 4 5 6 99
2. Opioids (morphine, heroine, codeine, ect) 1 2 3 4 5 6 99
3. Cannabis (marijuana, pot, grass, hash, ect) 1 2 3 4 5 6 99
10. Sleeping pills (e.g. seduxen) or other sedatives 1 2 3 4 5 6 99
11. Inhalants (nitrous, glue, petrol, ect.) 1 2 3 4 5 6 99
12. Hallucinogens (e.g. ketamine) 1 2 3 4 5 6 99
200
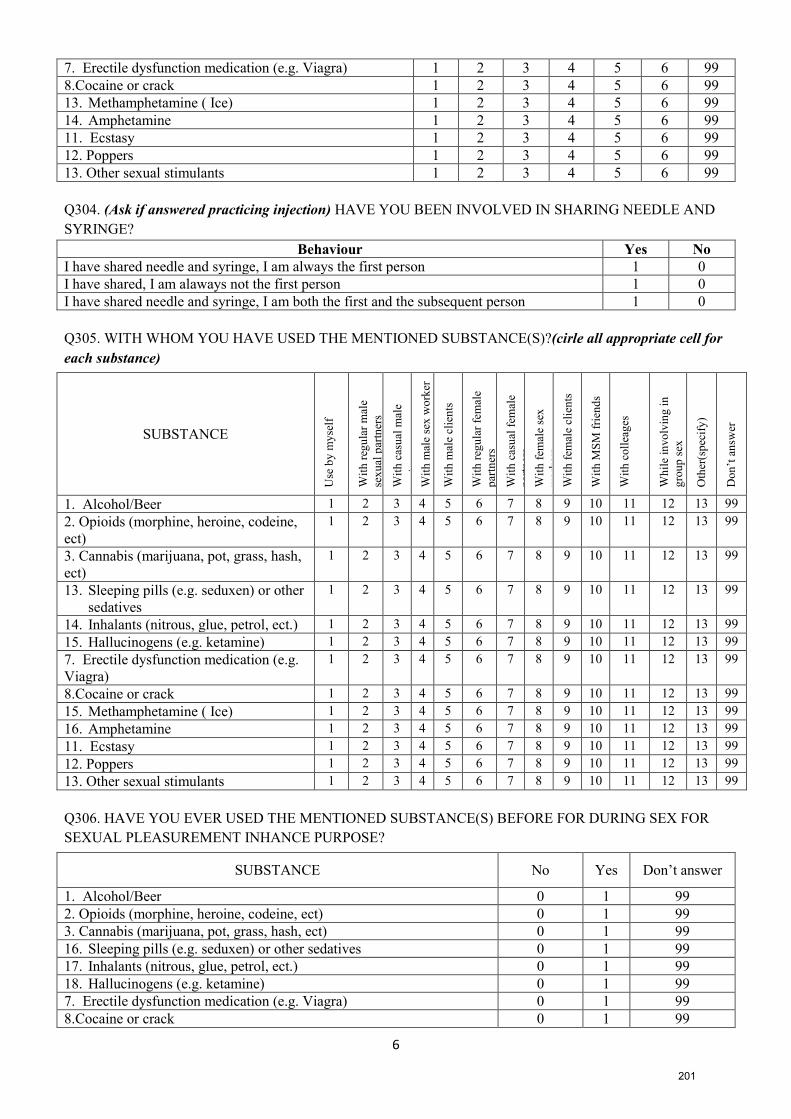
6
7. Erectile dysfunction medication (e.g. Viagra) 1 2 3 4 5 6 99
8.Cocaine or crack 1 2 3 4 5 6 99
13. Methamphetamine ( Ice) 1 2 3 4 5 6 99
14. Amphetamine 1 2 3 4 5 6 99
11. Ecstasy 1 2 3 4 5 6 99
12. Poppers 1 2 3 4 5 6 99
13. Other sexual stimulants 1 2 3 4 5 6 99
Q304. (Ask if answered practicing injection) HAVE YOU BEEN INVOLVED IN SHARING NEEDLE AND
SYRINGE?
Behaviour Yes No
I have shared needle and syringe, I am always the first person 1 0
I have shared, I am alaways not the first person 1 0
I have shared needle and syringe, I am both the first and the subsequent person 1 0
Q305. WITH WHOM YOU HAVE USED THE MENTIONED SUBSTANCE(S)?(cirle all appropriate cell for
each substance)
SUBSTANCE
Use
by
my
self
Wit
h r
egu
lar
mal
e
sex
ual
par
tner
s
Wit
h c
asu
al m
ale
par
tner
s
Wit
h m
ale
sex
wo
rker
Wit
h m
ale
clie
nts
Wit
h r
egu
lar
fem
ale
par
tner
s
Wit
h c
asu
al f
emal
e
par
tner
s
Wit
h f
emal
e se
x
wo
rker
s
Wit
h f
emal
e cl
ien
ts
Wit
h M
SM
fri
end
s
Wit
h c
oll
eag
es
Wh
ile
invo
lvin
g i
n
gro
up
sex
Oth
er(s
pec
ify
)
Do
n’t
an
swer
1. Alcohol/Beer 1 2 3 4 5 6 7 8 9 10 11 12 13 99
2. Opioids (morphine, heroine, codeine,
ect)
1 2 3 4 5 6 7 8 9 10 11 12 13 99
3. Cannabis (marijuana, pot, grass, hash,
ect)
1 2 3 4 5 6 7 8 9 10 11 12 13 99
13. Sleeping pills (e.g. seduxen) or other
sedatives
1 2 3 4 5 6 7 8 9 10 11 12 13 99
14. Inhalants (nitrous, glue, petrol, ect.) 1 2 3 4 5 6 7 8 9 10 11 12 13 99
15. Hallucinogens (e.g. ketamine) 1 2 3 4 5 6 7 8 9 10 11 12 13 99
7. Erectile dysfunction medication (e.g.
Viagra)
1 2 3 4 5 6 7 8 9 10 11 12 13 99
8.Cocaine or crack 1 2 3 4 5 6 7 8 9 10 11 12 13 99
15. Methamphetamine ( Ice) 1 2 3 4 5 6 7 8 9 10 11 12 13 99
16. Amphetamine 1 2 3 4 5 6 7 8 9 10 11 12 13 99
11. Ecstasy 1 2 3 4 5 6 7 8 9 10 11 12 13 99
12. Poppers 1 2 3 4 5 6 7 8 9 10 11 12 13 99
13. Other sexual stimulants 1 2 3 4 5 6 7 8 9 10 11 12 13 99
Q306. HAVE YOU EVER USED THE MENTIONED SUBSTANCE(S) BEFORE FOR DURING SEX FOR
SEXUAL PLEASUREMENT INHANCE PURPOSE?
SUBSTANCE No Yes Don’t answer
1. Alcohol/Beer 0 1 99
2. Opioids (morphine, heroine, codeine, ect) 0 1 99
3. Cannabis (marijuana, pot, grass, hash, ect) 0 1 99
16. Sleeping pills (e.g. seduxen) or other sedatives 0 1 99
17. Inhalants (nitrous, glue, petrol, ect.) 0 1 99
18. Hallucinogens (e.g. ketamine) 0 1 99
7. Erectile dysfunction medication (e.g. Viagra) 0 1 99
8.Cocaine or crack 0 1 99
201
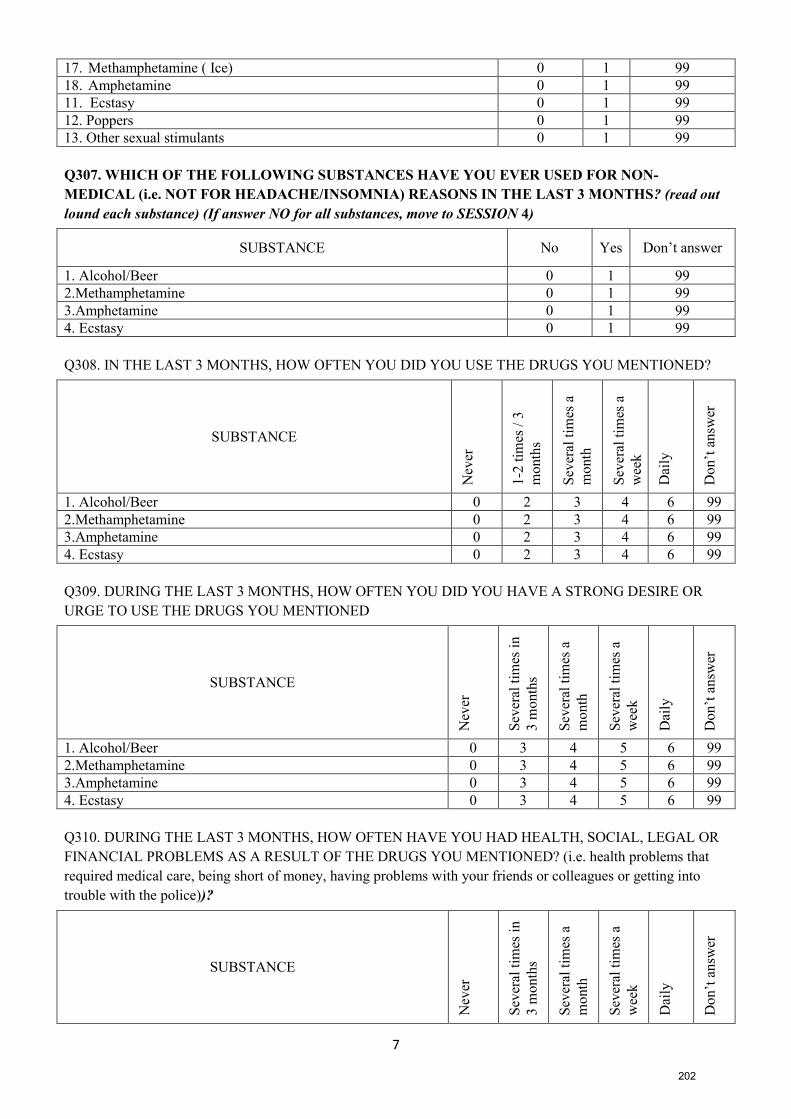
7
17. Methamphetamine ( Ice) 0 1 99
18. Amphetamine 0 1 99
11. Ecstasy 0 1 99
12. Poppers 0 1 99
13. Other sexual stimulants 0 1 99
Q307. WHICH OF THE FOLLOWING SUBSTANCES HAVE YOU EVER USED FOR NON-
MEDICAL (i.e. NOT FOR HEADACHE/INSOMNIA) REASONS IN THE LAST 3 MONTHS? (read out
lound each substance) (If answer NO for all substances, move to SESSION 4)
SUBSTANCE No Yes Don’t answer
1. Alcohol/Beer 0 1 99
2.Methamphetamine 0 1 99
3.Amphetamine 0 1 99
4. Ecstasy 0 1 99
Q308. IN THE LAST 3 MONTHS, HOW OFTEN YOU DID YOU USE THE DRUGS YOU MENTIONED?
SUBSTANCE
Nev
er
1-2
tim
es /
3
month
s
Sev
eral
tim
es a
month
Sev
eral
tim
es a
wee
k
Dai
ly
Don’t
answ
er
1. Alcohol/Beer 0 2 3 4 6 99
2.Methamphetamine 0 2 3 4 6 99
3.Amphetamine 0 2 3 4 6 99
4. Ecstasy 0 2 3 4 6 99
Q309. DURING THE LAST 3 MONTHS, HOW OFTEN YOU DID YOU HAVE A STRONG DESIRE OR
URGE TO USE THE DRUGS YOU MENTIONED
SUBSTANCE
Nev
er
Sev
eral
tim
es i
n
3 m
onth
s
Sev
eral
tim
es a
month
Sev
eral
tim
es a
wee
k
Dai
ly
Don’t
answ
er
1. Alcohol/Beer 0 3 4 5 6 99
2.Methamphetamine 0 3 4 5 6 99
3.Amphetamine 0 3 4 5 6 99
4. Ecstasy 0 3 4 5 6 99
Q310. DURING THE LAST 3 MONTHS, HOW OFTEN HAVE YOU HAD HEALTH, SOCIAL, LEGAL OR
FINANCIAL PROBLEMS AS A RESULT OF THE DRUGS YOU MENTIONED? (i.e. health problems that
required medical care, being short of money, having problems with your friends or colleagues or getting into
trouble with the police))?
SUBSTANCE
Nev
er
Sev
eral
tim
es i
n
3 m
onth
s
Sev
eral
tim
es a
month
Sev
eral
tim
es a
wee
k
Dai
ly
Don’t
answ
er
202
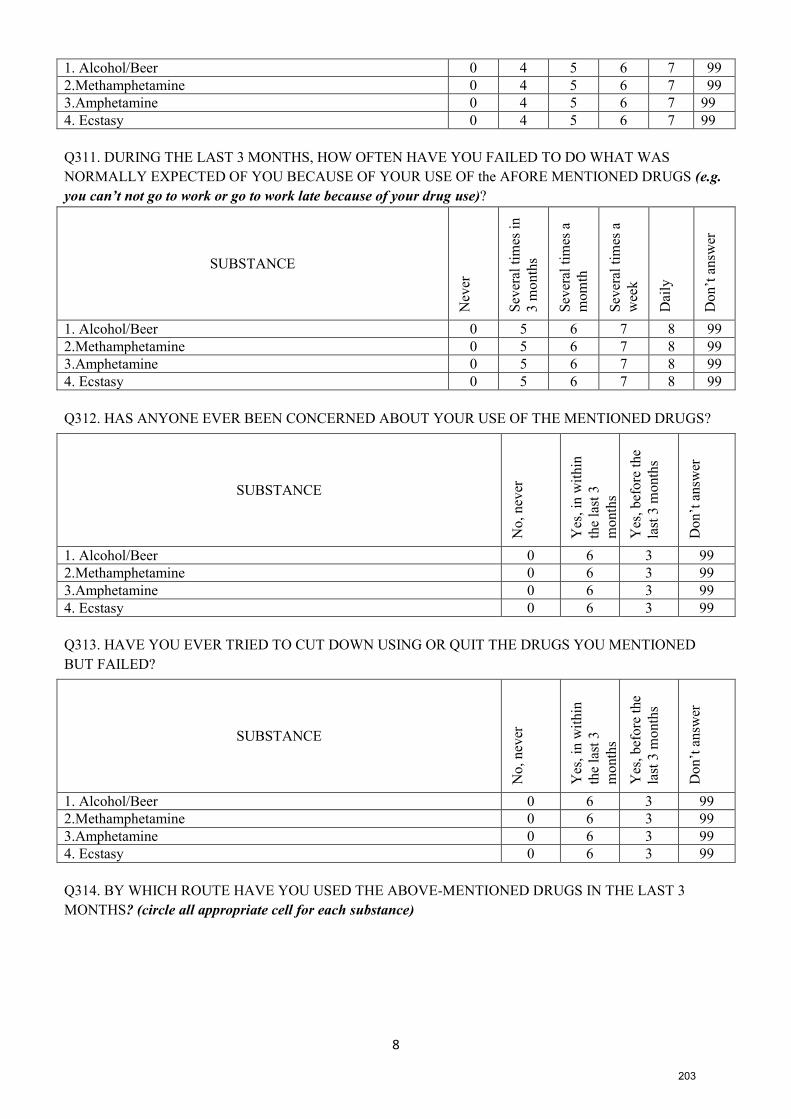
8
1. Alcohol/Beer 0 4 5 6 7 99
2.Methamphetamine 0 4 5 6 7 99
3.Amphetamine 0 4 5 6 7 99
4. Ecstasy 0 4 5 6 7 99
Q311. DURING THE LAST 3 MONTHS, HOW OFTEN HAVE YOU FAILED TO DO WHAT WAS
NORMALLY EXPECTED OF YOU BECAUSE OF YOUR USE OF the AFORE MENTIONED DRUGS (e.g.
you can’t not go to work or go to work late because of your drug use)?
SUBSTANCE
Nev
er
Sev
eral
tim
es i
n
3 m
onth
s
Sev
eral
tim
es a
mom
th
Sev
eral
tim
es a
wee
k
Dai
ly
Do
n’t
an
swer
1. Alcohol/Beer 0 5 6 7 8 99
2.Methamphetamine 0 5 6 7 8 99
3.Amphetamine 0 5 6 7 8 99
4. Ecstasy 0 5 6 7 8 99
Q312. HAS ANYONE EVER BEEN CONCERNED ABOUT YOUR USE OF THE MENTIONED DRUGS?
SUBSTANCE
No,
nev
er
Yes
, in
wit
hin
the
last
3
month
s
Yes
, bef
ore
the
last
3 m
onth
s
Don’t
answ
er
1. Alcohol/Beer 0 6 3 99
2.Methamphetamine 0 6 3 99
3.Amphetamine 0 6 3 99
4. Ecstasy 0 6 3 99
Q313. HAVE YOU EVER TRIED TO CUT DOWN USING OR QUIT THE DRUGS YOU MENTIONED
BUT FAILED?
SUBSTANCE
No,
nev
er
Yes
, in
wit
hin
the
last
3
month
s
Yes
, bef
ore
the
last
3 m
onth
s
Don’t
answ
er
1. Alcohol/Beer 0 6 3 99
2.Methamphetamine 0 6 3 99
3.Amphetamine 0 6 3 99
4. Ecstasy 0 6 3 99
Q314. BY WHICH ROUTE HAVE YOU USED THE ABOVE-MENTIONED DRUGS IN THE LAST 3
MONTHS? (circle all appropriate cell for each substance)
203
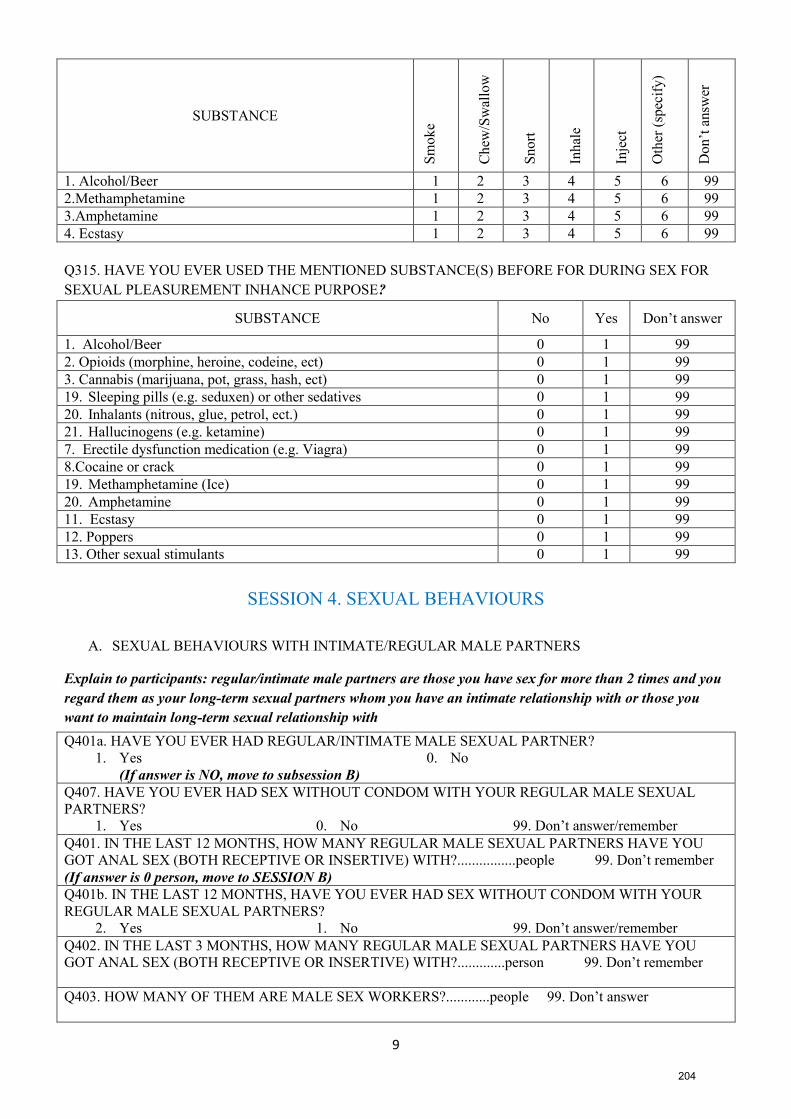
9
SUBSTANCE
Sm
ok
e
Ch
ew/S
wal
low
Sn
ort
Inh
ale
Inje
ct
Oth
er (
spec
ify)
Do
n’t
an
swer
1. Alcohol/Beer 1 2 3 4 5 6 99
2.Methamphetamine 1 2 3 4 5 6 99
3.Amphetamine 1 2 3 4 5 6 99
4. Ecstasy 1 2 3 4 5 6 99
Q315. HAVE YOU EVER USED THE MENTIONED SUBSTANCE(S) BEFORE FOR DURING SEX FOR
SEXUAL PLEASUREMENT INHANCE PURPOSE?
SUBSTANCE No Yes Don’t answer
1. Alcohol/Beer 0 1 99
2. Opioids (morphine, heroine, codeine, ect) 0 1 99
3. Cannabis (marijuana, pot, grass, hash, ect) 0 1 99
19. Sleeping pills (e.g. seduxen) or other sedatives 0 1 99
20. Inhalants (nitrous, glue, petrol, ect.) 0 1 99
21. Hallucinogens (e.g. ketamine) 0 1 99
7. Erectile dysfunction medication (e.g. Viagra) 0 1 99
8.Cocaine or crack 0 1 99
19. Methamphetamine (Ice) 0 1 99
20. Amphetamine 0 1 99
11. Ecstasy 0 1 99
12. Poppers 0 1 99
13. Other sexual stimulants 0 1 99
SESSION 4. SEXUAL BEHAVIOURS
A. SEXUAL BEHAVIOURS WITH INTIMATE/REGULAR MALE PARTNERS
Explain to participants: regular/intimate male partners are those you have sex for more than 2 times and you
regard them as your long-term sexual partners whom you have an intimate relationship with or those you
want to maintain long-term sexual relationship with
Q401a. HAVE YOU EVER HAD REGULAR/INTIMATE MALE SEXUAL PARTNER?
1. Yes 0. No
(If answer is NO, move to subsession B)
Q407. HAVE YOU EVER HAD SEX WITHOUT CONDOM WITH YOUR REGULAR MALE SEXUAL
PARTNERS?
1. Yes 0. No 99. Don’t answer/remember
Q401. IN THE LAST 12 MONTHS, HOW MANY REGULAR MALE SEXUAL PARTNERS HAVE YOU
GOT ANAL SEX (BOTH RECEPTIVE OR INSERTIVE) WITH?................people 99. Don’t remember
(If answer is 0 person, move to SESSION B)
Q401b. IN THE LAST 12 MONTHS, HAVE YOU EVER HAD SEX WITHOUT CONDOM WITH YOUR
REGULAR MALE SEXUAL PARTNERS?
2. Yes 1. No 99. Don’t answer/remember
Q402. IN THE LAST 3 MONTHS, HOW MANY REGULAR MALE SEXUAL PARTNERS HAVE YOU
GOT ANAL SEX (BOTH RECEPTIVE OR INSERTIVE) WITH?.............person 99. Don’t remember
Q403. HOW MANY OF THEM ARE MALE SEX WORKERS?............people 99. Don’t answer
204
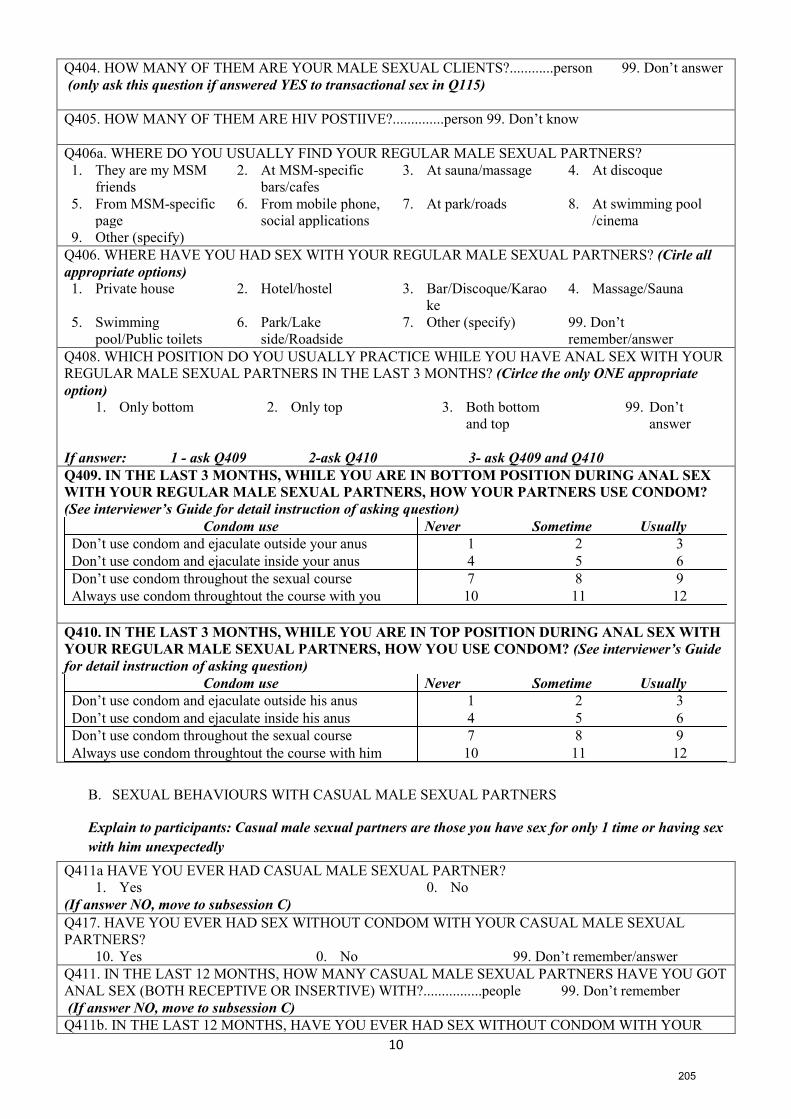
10
Q404. HOW MANY OF THEM ARE YOUR MALE SEXUAL CLIENTS?............person 99. Don’t answer
(only ask this question if answered YES to transactional sex in Q115)
Q405. HOW MANY OF THEM ARE HIV POSTIIVE?..............person 99. Don’t know
Q406a. WHERE DO YOU USUALLY FIND YOUR REGULAR MALE SEXUAL PARTNERS?
1. They are my MSM
friends
2. At MSM-specific
bars/cafes
3. At sauna/massage 4. At discoque
5. From MSM-specific
page
6. From mobile phone,
social applications
7. At park/roads 8. At swimming pool
/cinema
9. Other (specify)
Q406. WHERE HAVE YOU HAD SEX WITH YOUR REGULAR MALE SEXUAL PARTNERS? (Cirle all
appropriate options)
1. Private house 2. Hotel/hostel 3. Bar/Discoque/Karao
ke
4. Massage/Sauna
5. Swimming
pool/Public toilets
6. Park/Lake
side/Roadside
7. Other (specify) 99. Don’t
remember/answer
Q408. WHICH POSITION DO YOU USUALLY PRACTICE WHILE YOU HAVE ANAL SEX WITH YOUR
REGULAR MALE SEXUAL PARTNERS IN THE LAST 3 MONTHS? (Cirlce the only ONE appropriate
option)
1. Only bottom 2. Only top 3. Both bottom
and top
99. Don’t
answer
If answer: 1 - ask Q409 2-ask Q410 3- ask Q409 and Q410
Q409. IN THE LAST 3 MONTHS, WHILE YOU ARE IN BOTTOM POSITION DURING ANAL SEX
WITH YOUR REGULAR MALE SEXUAL PARTNERS, HOW YOUR PARTNERS USE CONDOM?
(See interviewer’s Guide for detail instruction of asking question)
Condom use Never Sometime Usually
Don’t use condom and ejaculate outside your anus 1 2 3
Don’t use condom and ejaculate inside your anus 4 5 6
Don’t use condom throughout the sexual course 7 8 9
Always use condom throughtout the course with you 10 11 12
Q410. IN THE LAST 3 MONTHS, WHILE YOU ARE IN TOP POSITION DURING ANAL SEX WITH
YOUR REGULAR MALE SEXUAL PARTNERS, HOW YOU USE CONDOM? (See interviewer’s Guide
for detail instruction of asking question)
Condom use Never Sometime Usually
Don’t use condom and ejaculate outside his anus 1 2 3
Don’t use condom and ejaculate inside his anus 4 5 6
Don’t use condom throughout the sexual course 7 8 9
Always use condom throughtout the course with him 10 11 12
B. SEXUAL BEHAVIOURS WITH CASUAL MALE SEXUAL PARTNERS
Explain to participants: Casual male sexual partners are those you have sex for only 1 time or having sex
with him unexpectedly
Q411a HAVE YOU EVER HAD CASUAL MALE SEXUAL PARTNER?
1. Yes 0. No
(If answer NO, move to subsession C)
Q417. HAVE YOU EVER HAD SEX WITHOUT CONDOM WITH YOUR CASUAL MALE SEXUAL
PARTNERS?
10. Yes 0. No 99. Don’t remember/answer
Q411. IN THE LAST 12 MONTHS, HOW MANY CASUAL MALE SEXUAL PARTNERS HAVE YOU GOT
ANAL SEX (BOTH RECEPTIVE OR INSERTIVE) WITH?................people 99. Don’t remember
(If answer NO, move to subsession C)
Q411b. IN THE LAST 12 MONTHS, HAVE YOU EVER HAD SEX WITHOUT CONDOM WITH YOUR
205
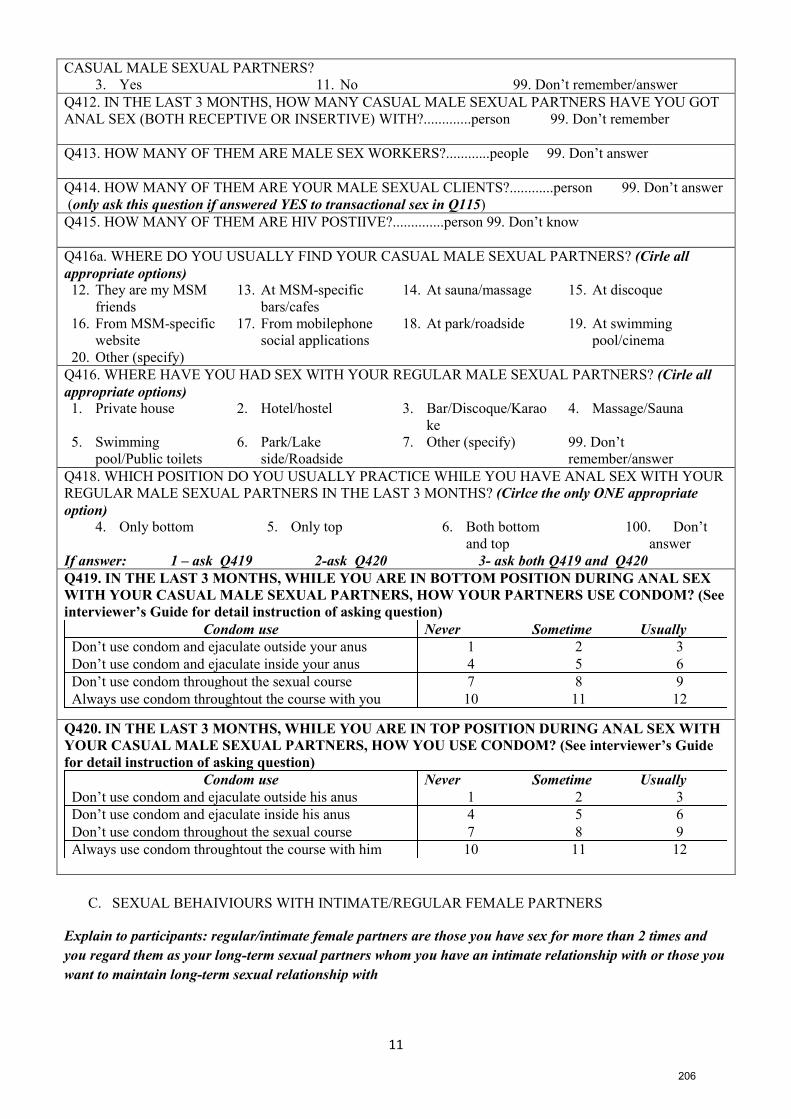
11
CASUAL MALE SEXUAL PARTNERS?
3. Yes 11. No 99. Don’t remember/answer
Q412. IN THE LAST 3 MONTHS, HOW MANY CASUAL MALE SEXUAL PARTNERS HAVE YOU GOT
ANAL SEX (BOTH RECEPTIVE OR INSERTIVE) WITH?.............person 99. Don’t remember
Q413. HOW MANY OF THEM ARE MALE SEX WORKERS?............people 99. Don’t answer
Q414. HOW MANY OF THEM ARE YOUR MALE SEXUAL CLIENTS?............person 99. Don’t answer
(only ask this question if answered YES to transactional sex in Q115)
Q415. HOW MANY OF THEM ARE HIV POSTIIVE?..............person 99. Don’t know
Q416a. WHERE DO YOU USUALLY FIND YOUR CASUAL MALE SEXUAL PARTNERS? (Cirle all
appropriate options)
12. They are my MSM
friends
13. At MSM-specific
bars/cafes
14. At sauna/massage 15. At discoque
16. From MSM-specific
website
17. From mobilephone
social applications
18. At park/roadside 19. At swimming
pool/cinema
20. Other (specify)
Q416. WHERE HAVE YOU HAD SEX WITH YOUR REGULAR MALE SEXUAL PARTNERS? (Cirle all
appropriate options)
1. Private house 2. Hotel/hostel 3. Bar/Discoque/Karao
ke
4. Massage/Sauna
5. Swimming
pool/Public toilets
6. Park/Lake
side/Roadside
7. Other (specify) 99. Don’t
remember/answer
Q418. WHICH POSITION DO YOU USUALLY PRACTICE WHILE YOU HAVE ANAL SEX WITH YOUR
REGULAR MALE SEXUAL PARTNERS IN THE LAST 3 MONTHS? (Cirlce the only ONE appropriate
option)
4. Only bottom 5. Only top 6. Both bottom
and top
100. Don’t
answer
If answer: 1 – ask Q419 2-ask Q420 3- ask both Q419 and Q420
Q419. IN THE LAST 3 MONTHS, WHILE YOU ARE IN BOTTOM POSITION DURING ANAL SEX
WITH YOUR CASUAL MALE SEXUAL PARTNERS, HOW YOUR PARTNERS USE CONDOM? (See
interviewer’s Guide for detail instruction of asking question)
Condom use Never Sometime Usually
Don’t use condom and ejaculate outside your anus 1 2 3
Don’t use condom and ejaculate inside your anus 4 5 6
Don’t use condom throughout the sexual course 7 8 9
Always use condom throughtout the course with you 10 11 12
Q420. IN THE LAST 3 MONTHS, WHILE YOU ARE IN TOP POSITION DURING ANAL SEX WITH
YOUR CASUAL MALE SEXUAL PARTNERS, HOW YOU USE CONDOM? (See interviewer’s Guide
for detail instruction of asking question)
Condom use Never Sometime Usually
Don’t use condom and ejaculate outside his anus 1 2 3
Don’t use condom and ejaculate inside his anus 4 5 6
Don’t use condom throughout the sexual course 7 8 9
Always use condom throughtout the course with him 10 11 12
C. SEXUAL BEHAIVIOURS WITH INTIMATE/REGULAR FEMALE PARTNERS
Explain to participants: regular/intimate female partners are those you have sex for more than 2 times and
you regard them as your long-term sexual partners whom you have an intimate relationship with or those you
want to maintain long-term sexual relationship with
206
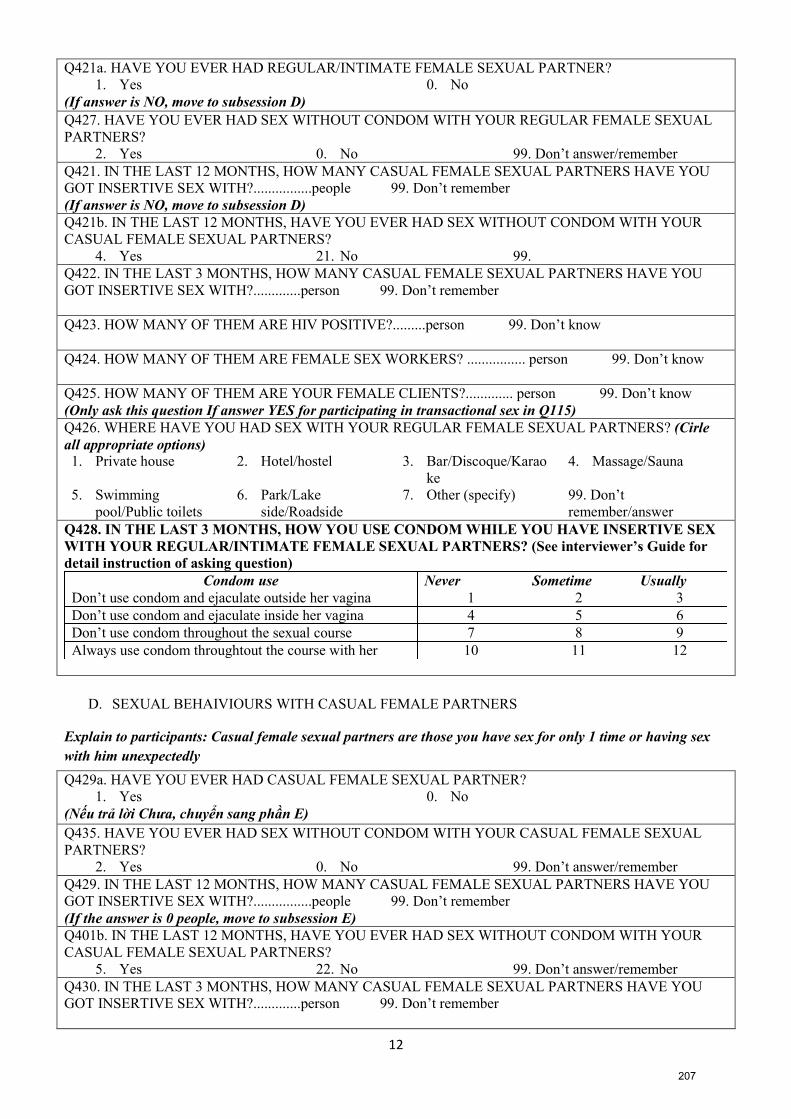
12
Q421a. HAVE YOU EVER HAD REGULAR/INTIMATE FEMALE SEXUAL PARTNER?
1. Yes 0. No
(If answer is NO, move to subsession D)
Q427. HAVE YOU EVER HAD SEX WITHOUT CONDOM WITH YOUR REGULAR FEMALE SEXUAL
PARTNERS?
2. Yes 0. No 99. Don’t answer/remember
Q421. IN THE LAST 12 MONTHS, HOW MANY CASUAL FEMALE SEXUAL PARTNERS HAVE YOU
GOT INSERTIVE SEX WITH?................people 99. Don’t remember
(If answer is NO, move to subsession D)
Q421b. IN THE LAST 12 MONTHS, HAVE YOU EVER HAD SEX WITHOUT CONDOM WITH YOUR
CASUAL FEMALE SEXUAL PARTNERS?
4. Yes 21. No 99.
Q422. IN THE LAST 3 MONTHS, HOW MANY CASUAL FEMALE SEXUAL PARTNERS HAVE YOU
GOT INSERTIVE SEX WITH?.............person 99. Don’t remember
Q423. HOW MANY OF THEM ARE HIV POSITIVE?.........person 99. Don’t know
Q424. HOW MANY OF THEM ARE FEMALE SEX WORKERS? ................ person 99. Don’t know
Q425. HOW MANY OF THEM ARE YOUR FEMALE CLIENTS?............. person 99. Don’t know
(Only ask this question If answer YES for participating in transactional sex in Q115)
Q426. WHERE HAVE YOU HAD SEX WITH YOUR REGULAR FEMALE SEXUAL PARTNERS? (Cirle
all appropriate options)
1. Private house 2. Hotel/hostel 3. Bar/Discoque/Karao
ke
4. Massage/Sauna
5. Swimming
pool/Public toilets
6. Park/Lake
side/Roadside
7. Other (specify) 99. Don’t
remember/answer
Q428. IN THE LAST 3 MONTHS, HOW YOU USE CONDOM WHILE YOU HAVE INSERTIVE SEX
WITH YOUR REGULAR/INTIMATE FEMALE SEXUAL PARTNERS? (See interviewer’s Guide for
detail instruction of asking question)
Condom use Never Sometime Usually
Don’t use condom and ejaculate outside her vagina 1 2 3
Don’t use condom and ejaculate inside her vagina 4 5 6
Don’t use condom throughout the sexual course 7 8 9
Always use condom throughtout the course with her 10 11 12
D. SEXUAL BEHAIVIOURS WITH CASUAL FEMALE PARTNERS
Explain to participants: Casual female sexual partners are those you have sex for only 1 time or having sex
with him unexpectedly
Q429a. HAVE YOU EVER HAD CASUAL FEMALE SEXUAL PARTNER?
1. Yes 0. No
(Nếu trả lời Chưa, chuyển sang phần E)
Q435. HAVE YOU EVER HAD SEX WITHOUT CONDOM WITH YOUR CASUAL FEMALE SEXUAL
PARTNERS?
2. Yes 0. No 99. Don’t answer/remember
Q429. IN THE LAST 12 MONTHS, HOW MANY CASUAL FEMALE SEXUAL PARTNERS HAVE YOU
GOT INSERTIVE SEX WITH?................people 99. Don’t remember
(If the answer is 0 people, move to subsession E)
Q401b. IN THE LAST 12 MONTHS, HAVE YOU EVER HAD SEX WITHOUT CONDOM WITH YOUR
CASUAL FEMALE SEXUAL PARTNERS?
5. Yes 22. No 99. Don’t answer/remember
Q430. IN THE LAST 3 MONTHS, HOW MANY CASUAL FEMALE SEXUAL PARTNERS HAVE YOU
GOT INSERTIVE SEX WITH?.............person 99. Don’t remember
207
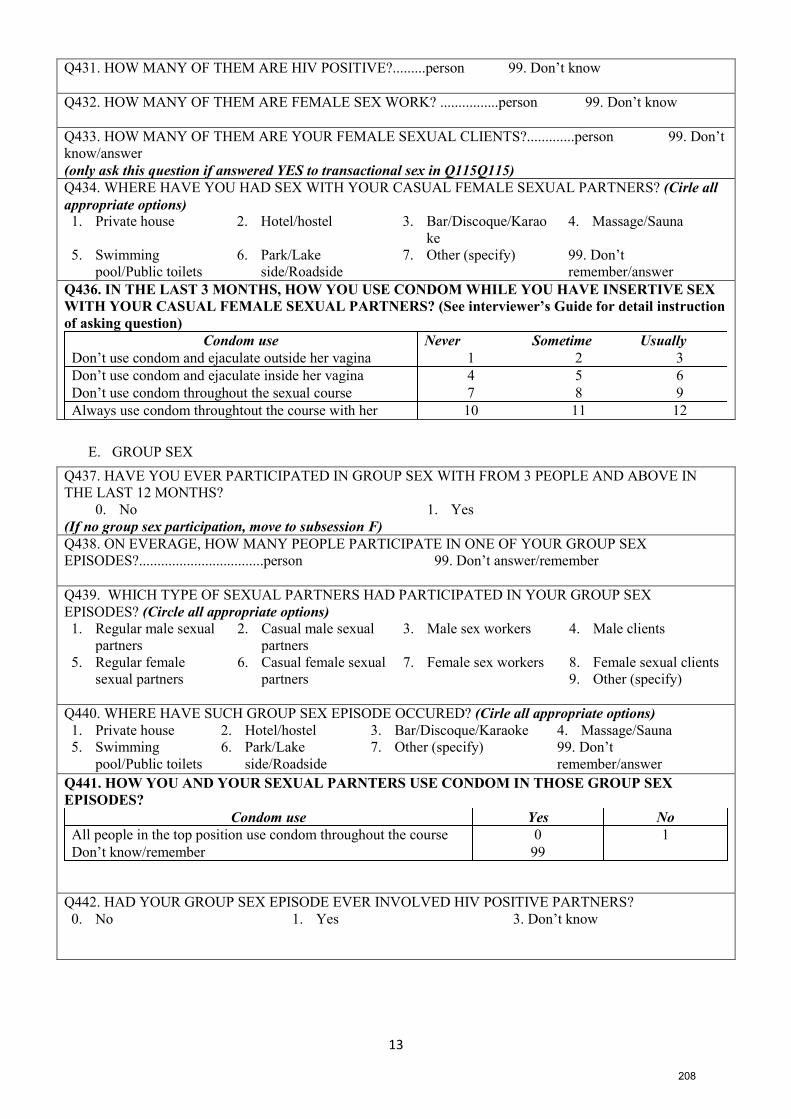
13
Q431. HOW MANY OF THEM ARE HIV POSITIVE?.........person 99. Don’t know
Q432. HOW MANY OF THEM ARE FEMALE SEX WORK? ................person 99. Don’t know
Q433. HOW MANY OF THEM ARE YOUR FEMALE SEXUAL CLIENTS?.............person 99. Don’t
know/answer
(only ask this question if answered YES to transactional sex in Q115Q115)
Q434. WHERE HAVE YOU HAD SEX WITH YOUR CASUAL FEMALE SEXUAL PARTNERS? (Cirle all
appropriate options)
1. Private house 2. Hotel/hostel 3. Bar/Discoque/Karao
ke
4. Massage/Sauna
5. Swimming
pool/Public toilets
6. Park/Lake
side/Roadside
7. Other (specify) 99. Don’t
remember/answer
Q436. IN THE LAST 3 MONTHS, HOW YOU USE CONDOM WHILE YOU HAVE INSERTIVE SEX
WITH YOUR CASUAL FEMALE SEXUAL PARTNERS? (See interviewer’s Guide for detail instruction
of asking question)
Condom use Never Sometime Usually
Don’t use condom and ejaculate outside her vagina 1 2 3
Don’t use condom and ejaculate inside her vagina 4 5 6
Don’t use condom throughout the sexual course 7 8 9
Always use condom throughtout the course with her 10 11 12
E. GROUP SEX
Q437. HAVE YOU EVER PARTICIPATED IN GROUP SEX WITH FROM 3 PEOPLE AND ABOVE IN
THE LAST 12 MONTHS?
0. No 1. Yes
(If no group sex participation, move to subsession F)
Q438. ON EVERAGE, HOW MANY PEOPLE PARTICIPATE IN ONE OF YOUR GROUP SEX
EPISODES?..................................person 99. Don’t answer/remember
Q439. WHICH TYPE OF SEXUAL PARTNERS HAD PARTICIPATED IN YOUR GROUP SEX
EPISODES? (Circle all appropriate options)
1. Regular male sexual
partners
2. Casual male sexual
partners
3. Male sex workers 4. Male clients
5. Regular female
sexual partners
6. Casual female sexual
partners
7. Female sex workers 8. Female sexual clients
9. Other (specify)
Q440. WHERE HAVE SUCH GROUP SEX EPISODE OCCURED? (Cirle all appropriate options)
1. Private house 2. Hotel/hostel 3. Bar/Discoque/Karaoke 4. Massage/Sauna
5. Swimming
pool/Public toilets
6. Park/Lake
side/Roadside
7. Other (specify) 99. Don’t
remember/answer
Q441. HOW YOU AND YOUR SEXUAL PARNTERS USE CONDOM IN THOSE GROUP SEX
EPISODES?
Condom use Yes No
All people in the top position use condom throughout the course 0 1
Don’t know/remember 99
Q442. HAD YOUR GROUP SEX EPISODE EVER INVOLVED HIV POSITIVE PARTNERS?
0. No 1. Yes 3. Don’t know
208
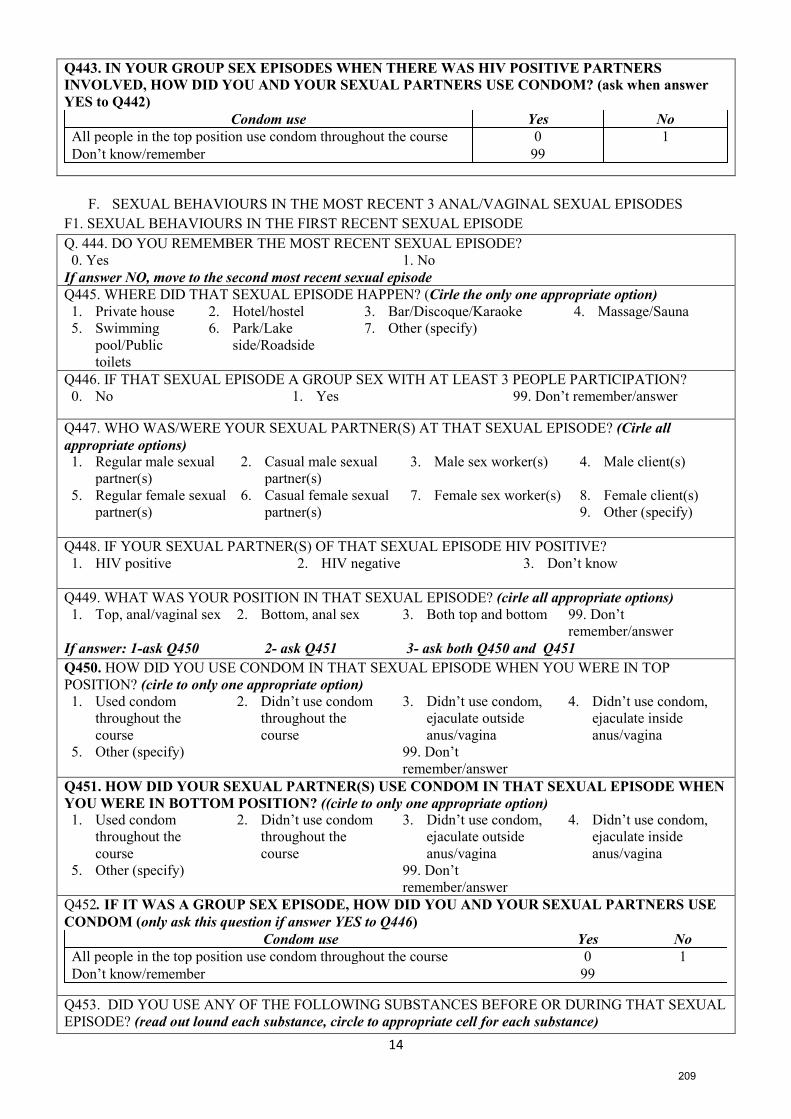
14
Q443. IN YOUR GROUP SEX EPISODES WHEN THERE WAS HIV POSITIVE PARTNERS
INVOLVED, HOW DID YOU AND YOUR SEXUAL PARTNERS USE CONDOM? (ask when answer
YES to Q442)
Condom use Yes No
All people in the top position use condom throughout the course 0 1
Don’t know/remember 99
F. SEXUAL BEHAVIOURS IN THE MOST RECENT 3 ANAL/VAGINAL SEXUAL EPISODES
F1. SEXUAL BEHAVIOURS IN THE FIRST RECENT SEXUAL EPISODE
Q. 444. DO YOU REMEMBER THE MOST RECENT SEXUAL EPISODE?
0. Yes 1. No
If answer NO, move to the second most recent sexual episode
Q445. WHERE DID THAT SEXUAL EPISODE HAPPEN? (Cirle the only one appropriate option)
1. Private house 2. Hotel/hostel 3. Bar/Discoque/Karaoke 4. Massage/Sauna
5. Swimming
pool/Public
toilets
6. Park/Lake
side/Roadside
7. Other (specify)
Q446. IF THAT SEXUAL EPISODE A GROUP SEX WITH AT LEAST 3 PEOPLE PARTICIPATION?
0. No 1. Yes 99. Don’t remember/answer
Q447. WHO WAS/WERE YOUR SEXUAL PARTNER(S) AT THAT SEXUAL EPISODE? (Cirle all
appropriate options)
1. Regular male sexual
partner(s)
2. Casual male sexual
partner(s)
3. Male sex worker(s) 4. Male client(s)
5. Regular female sexual
partner(s)
6. Casual female sexual
partner(s)
7. Female sex worker(s) 8. Female client(s)
9. Other (specify)
Q448. IF YOUR SEXUAL PARTNER(S) OF THAT SEXUAL EPISODE HIV POSITIVE?
1. HIV positive 2. HIV negative 3. Don’t know
Q449. WHAT WAS YOUR POSITION IN THAT SEXUAL EPISODE? (cirle all appropriate options)
1. Top, anal/vaginal sex 2. Bottom, anal sex 3. Both top and bottom 99. Don’t
remember/answer
If answer: 1-ask Q450 2- ask Q451 3- ask both Q450 and Q451
Q450. HOW DID YOU USE CONDOM IN THAT SEXUAL EPISODE WHEN YOU WERE IN TOP
POSITION? (cirle to only one appropriate option)
1. Used condom
throughout the
course
2. Didn’t use condom
throughout the
course
3. Didn’t use condom,
ejaculate outside
anus/vagina
4. Didn’t use condom,
ejaculate inside
anus/vagina
5. Other (specify) 99. Don’t
remember/answer
Q451. HOW DID YOUR SEXUAL PARTNER(S) USE CONDOM IN THAT SEXUAL EPISODE WHEN
YOU WERE IN BOTTOM POSITION? ((cirle to only one appropriate option) 1. Used condom
throughout the
course
2. Didn’t use condom
throughout the
course
3. Didn’t use condom,
ejaculate outside
anus/vagina
4. Didn’t use condom,
ejaculate inside
anus/vagina
5. Other (specify) 99. Don’t
remember/answer
Q452. IF IT WAS A GROUP SEX EPISODE, HOW DID YOU AND YOUR SEXUAL PARTNERS USE
CONDOM (only ask this question if answer YES to Q446)
Condom use Yes No
All people in the top position use condom throughout the course 0 1
Don’t know/remember 99
Q453. DID YOU USE ANY OF THE FOLLOWING SUBSTANCES BEFORE OR DURING THAT SEXUAL
EPISODE? (read out lound each substance, circle to appropriate cell for each substance)
209
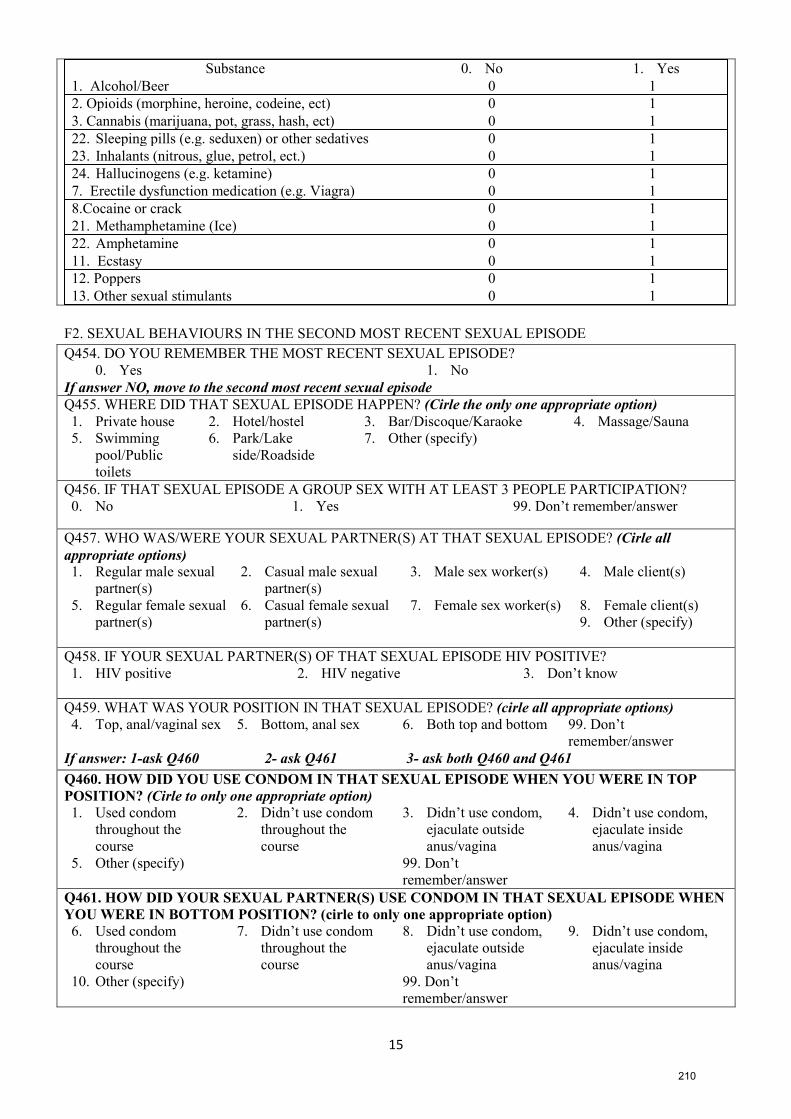
15
Substance 0. No 1. Yes
1. Alcohol/Beer 0 1
2. Opioids (morphine, heroine, codeine, ect) 0 1
3. Cannabis (marijuana, pot, grass, hash, ect) 0 1
22. Sleeping pills (e.g. seduxen) or other sedatives 0 1
23. Inhalants (nitrous, glue, petrol, ect.) 0 1
24. Hallucinogens (e.g. ketamine) 0 1
7. Erectile dysfunction medication (e.g. Viagra) 0 1
8.Cocaine or crack 0 1
21. Methamphetamine (Ice) 0 1
22. Amphetamine 0 1
11. Ecstasy 0 1
12. Poppers 0 1
13. Other sexual stimulants 0 1
F2. SEXUAL BEHAVIOURS IN THE SECOND MOST RECENT SEXUAL EPISODE
Q454. DO YOU REMEMBER THE MOST RECENT SEXUAL EPISODE?
0. Yes 1. No
If answer NO, move to the second most recent sexual episode
Q455. WHERE DID THAT SEXUAL EPISODE HAPPEN? (Cirle the only one appropriate option)
1. Private house 2. Hotel/hostel 3. Bar/Discoque/Karaoke 4. Massage/Sauna
5. Swimming
pool/Public
toilets
6. Park/Lake
side/Roadside
7. Other (specify)
Q456. IF THAT SEXUAL EPISODE A GROUP SEX WITH AT LEAST 3 PEOPLE PARTICIPATION?
0. No 1. Yes 99. Don’t remember/answer
Q457. WHO WAS/WERE YOUR SEXUAL PARTNER(S) AT THAT SEXUAL EPISODE? (Cirle all
appropriate options)
1. Regular male sexual
partner(s)
2. Casual male sexual
partner(s)
3. Male sex worker(s) 4. Male client(s)
5. Regular female sexual
partner(s)
6. Casual female sexual
partner(s)
7. Female sex worker(s) 8. Female client(s)
9. Other (specify)
Q458. IF YOUR SEXUAL PARTNER(S) OF THAT SEXUAL EPISODE HIV POSITIVE?
1. HIV positive 2. HIV negative 3. Don’t know
Q459. WHAT WAS YOUR POSITION IN THAT SEXUAL EPISODE? (cirle all appropriate options)
4. Top, anal/vaginal sex 5. Bottom, anal sex 6. Both top and bottom 99. Don’t
remember/answer
If answer: 1-ask Q460 2- ask Q461 3- ask both Q460 and Q461
Q460. HOW DID YOU USE CONDOM IN THAT SEXUAL EPISODE WHEN YOU WERE IN TOP
POSITION? (Cirle to only one appropriate option) 1. Used condom
throughout the
course
2. Didn’t use condom
throughout the
course
3. Didn’t use condom,
ejaculate outside
anus/vagina
4. Didn’t use condom,
ejaculate inside
anus/vagina
5. Other (specify) 99. Don’t
remember/answer
Q461. HOW DID YOUR SEXUAL PARTNER(S) USE CONDOM IN THAT SEXUAL EPISODE WHEN
YOU WERE IN BOTTOM POSITION? (cirle to only one appropriate option) 6. Used condom
throughout the
course
7. Didn’t use condom
throughout the
course
8. Didn’t use condom,
ejaculate outside
anus/vagina
9. Didn’t use condom,
ejaculate inside
anus/vagina
10. Other (specify) 99. Don’t
remember/answer
210
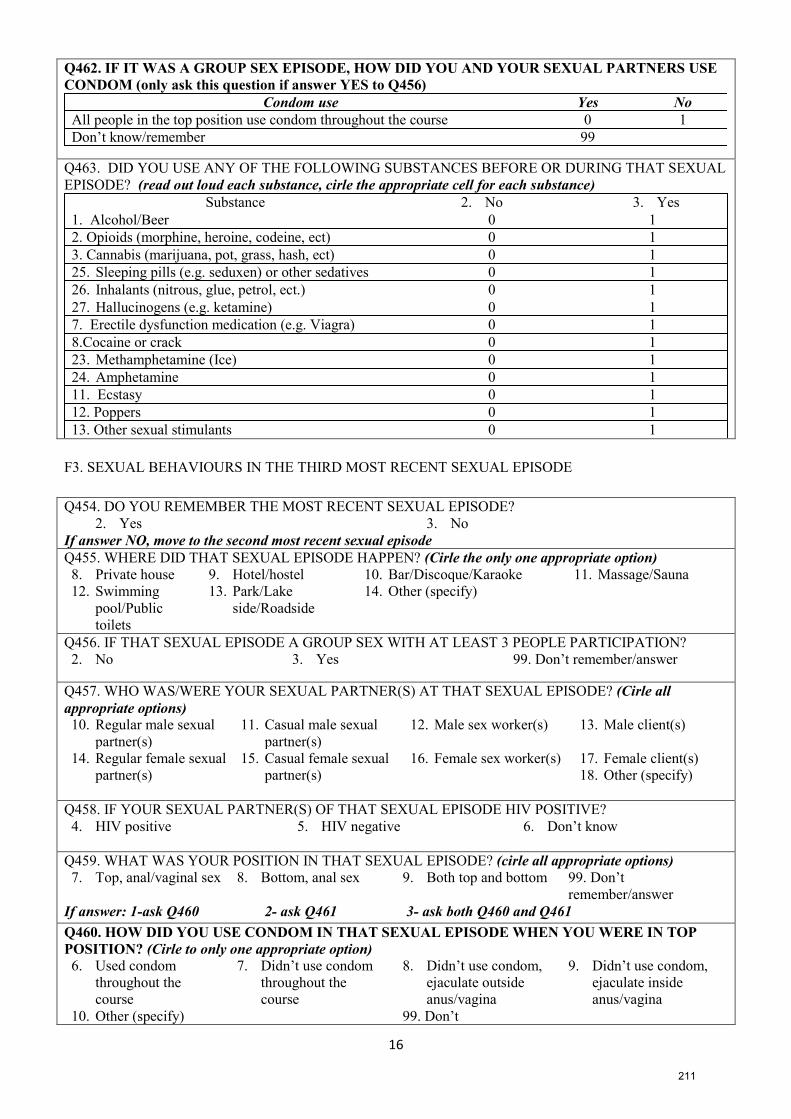
16
Q462. IF IT WAS A GROUP SEX EPISODE, HOW DID YOU AND YOUR SEXUAL PARTNERS USE
CONDOM (only ask this question if answer YES to Q456)
Condom use Yes No
All people in the top position use condom throughout the course 0 1
Don’t know/remember 99
Q463. DID YOU USE ANY OF THE FOLLOWING SUBSTANCES BEFORE OR DURING THAT SEXUAL
EPISODE? (read out loud each substance, cirle the appropriate cell for each substance)
Substance 2. No 3. Yes
1. Alcohol/Beer 0 1
2. Opioids (morphine, heroine, codeine, ect) 0 1
3. Cannabis (marijuana, pot, grass, hash, ect) 0 1
25. Sleeping pills (e.g. seduxen) or other sedatives 0 1
26. Inhalants (nitrous, glue, petrol, ect.) 0 1
27. Hallucinogens (e.g. ketamine) 0 1
7. Erectile dysfunction medication (e.g. Viagra) 0 1
8.Cocaine or crack 0 1
23. Methamphetamine (Ice) 0 1
24. Amphetamine 0 1
11. Ecstasy 0 1
12. Poppers 0 1
13. Other sexual stimulants 0 1
F3. SEXUAL BEHAVIOURS IN THE THIRD MOST RECENT SEXUAL EPISODE
Q454. DO YOU REMEMBER THE MOST RECENT SEXUAL EPISODE?
2. Yes 3. No
If answer NO, move to the second most recent sexual episode
Q455. WHERE DID THAT SEXUAL EPISODE HAPPEN? (Cirle the only one appropriate option)
8. Private house 9. Hotel/hostel 10. Bar/Discoque/Karaoke 11. Massage/Sauna
12. Swimming
pool/Public
toilets
13. Park/Lake
side/Roadside
14. Other (specify)
Q456. IF THAT SEXUAL EPISODE A GROUP SEX WITH AT LEAST 3 PEOPLE PARTICIPATION?
2. No 3. Yes 99. Don’t remember/answer
Q457. WHO WAS/WERE YOUR SEXUAL PARTNER(S) AT THAT SEXUAL EPISODE? (Cirle all
appropriate options)
10. Regular male sexual
partner(s)
11. Casual male sexual
partner(s)
12. Male sex worker(s) 13. Male client(s)
14. Regular female sexual
partner(s)
15. Casual female sexual
partner(s)
16. Female sex worker(s) 17. Female client(s)
18. Other (specify)
Q458. IF YOUR SEXUAL PARTNER(S) OF THAT SEXUAL EPISODE HIV POSITIVE?
4. HIV positive 5. HIV negative 6. Don’t know
Q459. WHAT WAS YOUR POSITION IN THAT SEXUAL EPISODE? (cirle all appropriate options)
7. Top, anal/vaginal sex 8. Bottom, anal sex 9. Both top and bottom 99. Don’t
remember/answer
If answer: 1-ask Q460 2- ask Q461 3- ask both Q460 and Q461
Q460. HOW DID YOU USE CONDOM IN THAT SEXUAL EPISODE WHEN YOU WERE IN TOP
POSITION? (Cirle to only one appropriate option) 6. Used condom
throughout the
course
7. Didn’t use condom
throughout the
course
8. Didn’t use condom,
ejaculate outside
anus/vagina
9. Didn’t use condom,
ejaculate inside
anus/vagina
10. Other (specify) 99. Don’t
211
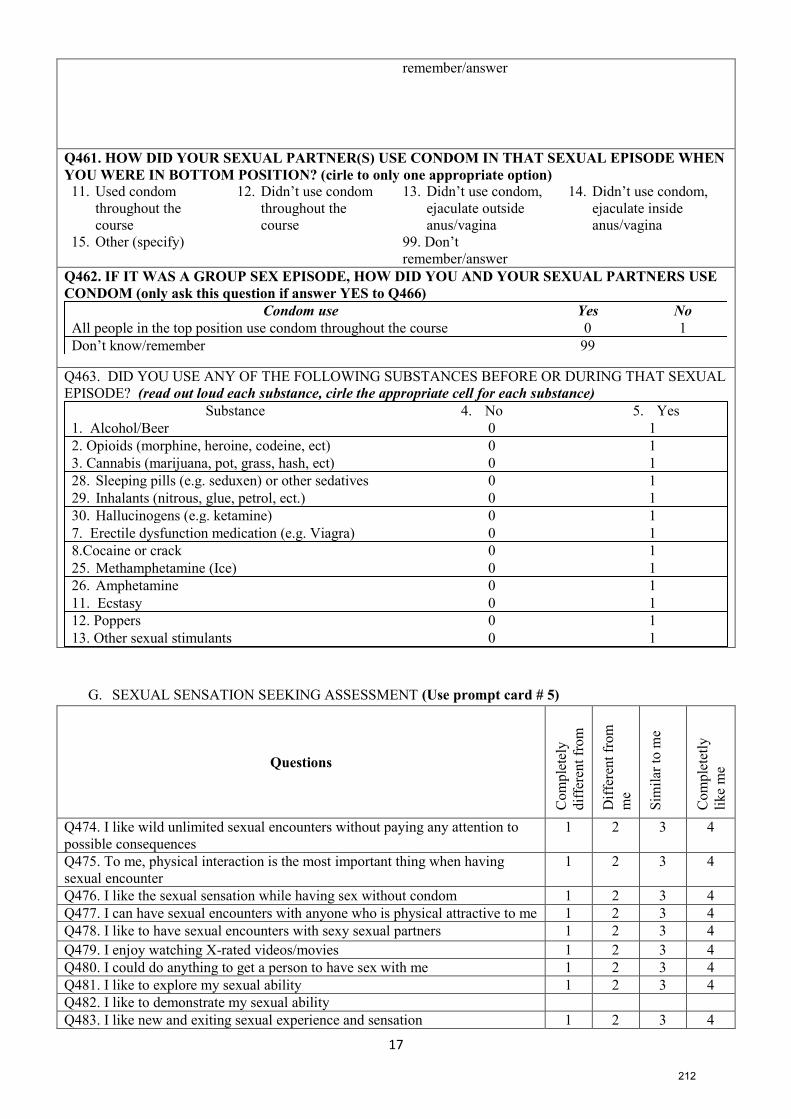
17
remember/answer
Q461. HOW DID YOUR SEXUAL PARTNER(S) USE CONDOM IN THAT SEXUAL EPISODE WHEN
YOU WERE IN BOTTOM POSITION? (cirle to only one appropriate option) 11. Used condom
throughout the
course
12. Didn’t use condom
throughout the
course
13. Didn’t use condom,
ejaculate outside
anus/vagina
14. Didn’t use condom,
ejaculate inside
anus/vagina
15. Other (specify) 99. Don’t
remember/answer
Q462. IF IT WAS A GROUP SEX EPISODE, HOW DID YOU AND YOUR SEXUAL PARTNERS USE
CONDOM (only ask this question if answer YES to Q466)
Condom use Yes No
All people in the top position use condom throughout the course 0 1
Don’t know/remember 99
Q463. DID YOU USE ANY OF THE FOLLOWING SUBSTANCES BEFORE OR DURING THAT SEXUAL
EPISODE? (read out loud each substance, cirle the appropriate cell for each substance)
Substance 4. No 5. Yes
1. Alcohol/Beer 0 1
2. Opioids (morphine, heroine, codeine, ect) 0 1
3. Cannabis (marijuana, pot, grass, hash, ect) 0 1
28. Sleeping pills (e.g. seduxen) or other sedatives 0 1
29. Inhalants (nitrous, glue, petrol, ect.) 0 1
30. Hallucinogens (e.g. ketamine) 0 1
7. Erectile dysfunction medication (e.g. Viagra) 0 1
8.Cocaine or crack 0 1
25. Methamphetamine (Ice) 0 1
26. Amphetamine 0 1
11. Ecstasy 0 1
12. Poppers 0 1
13. Other sexual stimulants 0 1
G. SEXUAL SENSATION SEEKING ASSESSMENT (Use prompt card # 5)
Questions
Co
mple
tely
dif
fere
nt
from
me
Dif
fere
nt
from
me
Sim
ilar
to m
e
Co
mple
tetl
y
like
me
Q474. I like wild unlimited sexual encounters without paying any attention to
possible consequences
1 2 3 4
Q475. To me, physical interaction is the most important thing when having
sexual encounter
1 2 3 4
Q476. I like the sexual sensation while having sex without condom 1 2 3 4
Q477. I can have sexual encounters with anyone who is physical attractive to me 1 2 3 4
Q478. I like to have sexual encounters with sexy sexual partners 1 2 3 4
Q479. I enjoy watching X-rated videos/movies 1 2 3 4
Q480. I could do anything to get a person to have sex with me 1 2 3 4
Q481. I like to explore my sexual ability 1 2 3 4
Q482. I like to demonstrate my sexual ability
Q483. I like new and exiting sexual experience and sensation 1 2 3 4
212
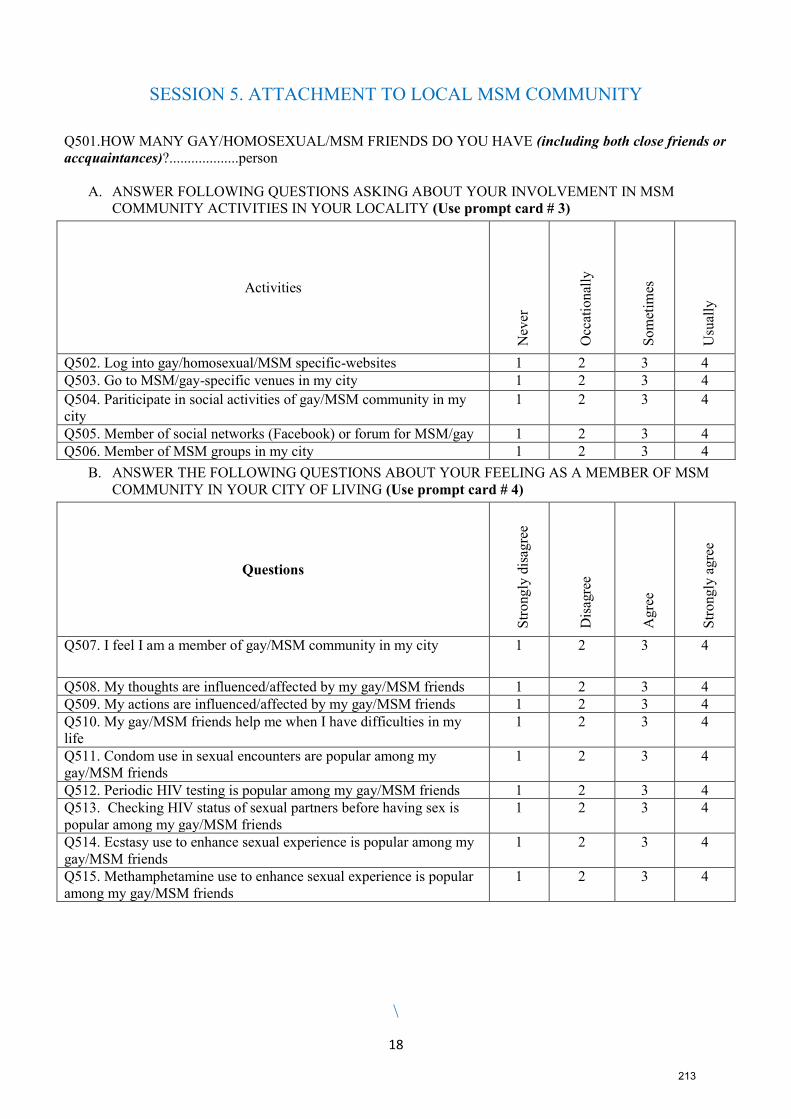
18
SESSION 5. ATTACHMENT TO LOCAL MSM COMMUNITY
Q501.HOW MANY GAY/HOMOSEXUAL/MSM FRIENDS DO YOU HAVE (including both close friends or
accquaintances)?...................person
A. ANSWER FOLLOWING QUESTIONS ASKING ABOUT YOUR INVOLVEMENT IN MSM
COMMUNITY ACTIVITIES IN YOUR LOCALITY (Use prompt card # 3)
Activities
Nev
er
Occ
atio
nal
ly
So
met
imes
Usu
ally
Q502. Log into gay/homosexual/MSM specific-websites 1 2 3 4
Q503. Go to MSM/gay-specific venues in my city 1 2 3 4
Q504. Pariticipate in social activities of gay/MSM community in my
city
1 2 3 4
Q505. Member of social networks (Facebook) or forum for MSM/gay 1 2 3 4
Q506. Member of MSM groups in my city 1 2 3 4
B. ANSWER THE FOLLOWING QUESTIONS ABOUT YOUR FEELING AS A MEMBER OF MSM
COMMUNITY IN YOUR CITY OF LIVING (Use prompt card # 4)
Questions
Str
ongly
dis
agre
e
Dis
agre
e
Agre
e
Str
ongly
agre
e
Q507. I feel I am a member of gay/MSM community in my city 1 2 3 4
Q508. My thoughts are influenced/affected by my gay/MSM friends 1 2 3 4
Q509. My actions are influenced/affected by my gay/MSM friends 1 2 3 4
Q510. My gay/MSM friends help me when I have difficulties in my
life
1 2 3 4
Q511. Condom use in sexual encounters are popular among my
gay/MSM friends
1 2 3 4
Q512. Periodic HIV testing is popular among my gay/MSM friends 1 2 3 4
Q513. Checking HIV status of sexual partners before having sex is
popular among my gay/MSM friends
1 2 3 4
Q514. Ecstasy use to enhance sexual experience is popular among my
gay/MSM friends
1 2 3 4
Q515. Methamphetamine use to enhance sexual experience is popular
among my gay/MSM friends
1 2 3 4
\
213
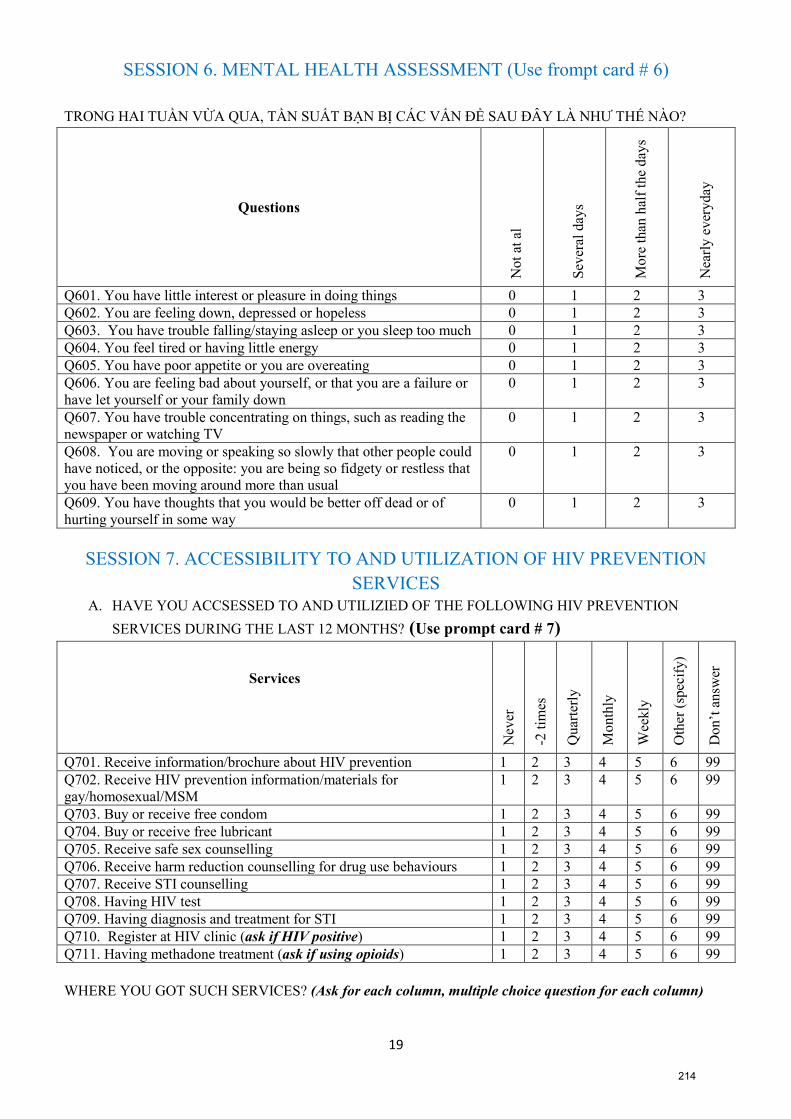
19
SESSION 6. MENTAL HEALTH ASSESSMENT (Use frompt card # 6)
TRONG HAI TUẦN VỪA QUA, TẦN SUẤT BẠN BỊ CÁC VẤN ĐỀ SAU ĐÂY LÀ NHƯ THẾ NÀO?
Questions
No
t at
al
Sev
eral
day
s
Mo
re t
han
hal
f th
e d
ays
Nea
rly
ev
ery
day
Q601. You have little interest or pleasure in doing things 0 1 2 3
Q602. You are feeling down, depressed or hopeless 0 1 2 3
Q603. You have trouble falling/staying asleep or you sleep too much 0 1 2 3
Q604. You feel tired or having little energy 0 1 2 3
Q605. You have poor appetite or you are overeating 0 1 2 3
Q606. You are feeling bad about yourself, or that you are a failure or
have let yourself or your family down
0 1 2 3
Q607. You have trouble concentrating on things, such as reading the
newspaper or watching TV
0 1 2 3
Q608. You are moving or speaking so slowly that other people could
have noticed, or the opposite: you are being so fidgety or restless that
you have been moving around more than usual
0 1 2 3
Q609. You have thoughts that you would be better off dead or of
hurting yourself in some way
0 1 2 3
SESSION 7. ACCESSIBILITY TO AND UTILIZATION OF HIV PREVENTION
SERVICES A. HAVE YOU ACCSESSED TO AND UTILIZIED OF THE FOLLOWING HIV PREVENTION
SERVICES DURING THE LAST 12 MONTHS? (Use prompt card # 7)
Services
Nev
er
-2 t
imes
Quar
terl
y
Month
ly
Wee
kly
Oth
er (
spec
ify)
Don’t
answ
er
Q701. Receive information/brochure about HIV prevention 1 2 3 4 5 6 99
Q702. Receive HIV prevention information/materials for
gay/homosexual/MSM
1 2 3 4 5 6 99
Q703. Buy or receive free condom 1 2 3 4 5 6 99
Q704. Buy or receive free lubricant 1 2 3 4 5 6 99
Q705. Receive safe sex counselling 1 2 3 4 5 6 99
Q706. Receive harm reduction counselling for drug use behaviours 1 2 3 4 5 6 99
Q707. Receive STI counselling 1 2 3 4 5 6 99
Q708. Having HIV test 1 2 3 4 5 6 99
Q709. Having diagnosis and treatment for STI 1 2 3 4 5 6 99
Q710. Register at HIV clinic (ask if HIV positive) 1 2 3 4 5 6 99
Q711. Having methadone treatment (ask if using opioids) 1 2 3 4 5 6 99
WHERE YOU GOT SUCH SERVICES? (Ask for each column, multiple choice question for each column)
214
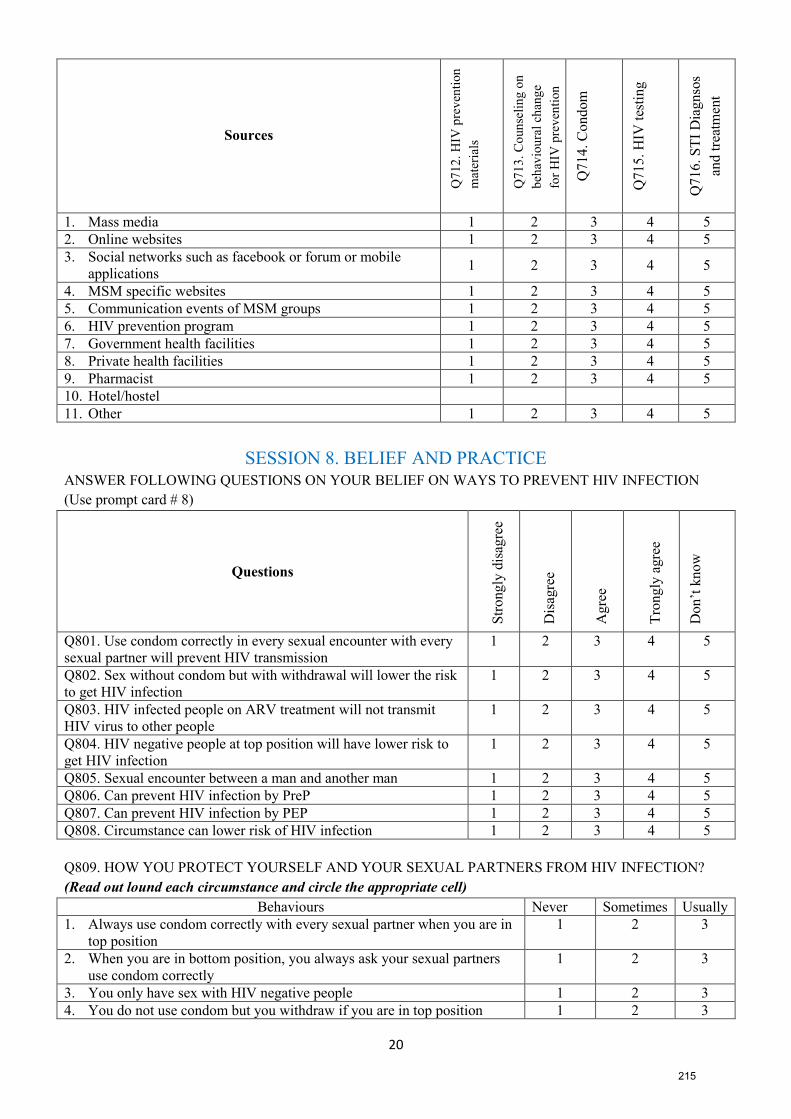
20
Sources
Q7
12
. H
IV p
rev
enti
on
mat
eria
ls
Q7
13
. C
oun
seli
ng
on
beh
avio
ura
l ch
ang
e
for
HIV
pre
ven
tion
Q7
14
. C
on
dom
Q7
15
. H
IV t
esti
ng
Q7
16
. S
TI
Dia
gn
sos
and
tre
atm
ent
1. Mass media 1 2 3 4 5
2. Online websites 1 2 3 4 5
3. Social networks such as facebook or forum or mobile
applications1 2 3 4 5
4. MSM specific websites 1 2 3 4 5
5. Communication events of MSM groups 1 2 3 4 5
6. HIV prevention program 1 2 3 4 5
7. Government health facilities 1 2 3 4 5
8. Private health facilities 1 2 3 4 5
9. Pharmacist 1 2 3 4 5
10. Hotel/hostel
11. Other 1 2 3 4 5
SESSION 8. BELIEF AND PRACTICE ANSWER FOLLOWING QUESTIONS ON YOUR BELIEF ON WAYS TO PREVENT HIV INFECTION
(Use prompt card # 8)
Questions
Str
ongly
dis
agre
e
Dis
agre
e
Agre
e
Tro
ngly
agre
e
Don’t
know
Q801. Use condom correctly in every sexual encounter with every
sexual partner will prevent HIV transmission
1 2 3 4 5
Q802. Sex without condom but with withdrawal will lower the risk
to get HIV infection
1 2 3 4 5
Q803. HIV infected people on ARV treatment will not transmit
HIV virus to other people
1 2 3 4 5
Q804. HIV negative people at top position will have lower risk to
get HIV infection
1 2 3 4 5
Q805. Sexual encounter between a man and another man 1 2 3 4 5
Q806. Can prevent HIV infection by PreP 1 2 3 4 5
Q807. Can prevent HIV infection by PEP 1 2 3 4 5
Q808. Circumstance can lower risk of HIV infection 1 2 3 4 5
Q809. HOW YOU PROTECT YOURSELF AND YOUR SEXUAL PARTNERS FROM HIV INFECTION?
(Read out lound each circumstance and circle the appropriate cell)
Behaviours Never Sometimes Usually
1. Always use condom correctly with every sexual partner when you are in
top position
1 2 3
2. When you are in bottom position, you always ask your sexual partners
use condom correctly
1 2 3
3. You only have sex with HIV negative people 1 2 3
4. You do not use condom but you withdraw if you are in top position 1 2 3
215
21
5. You ask your sexual partners to withdraw if you are in bot position and
your sexual partners do not use condom
1 2 3
6. You can have sex with a HIV positive but on ARV treatment 1 2 3
7. You only have sex in top position 1 2 3
8. You take PEP for HIV prevention 1 2 3
9. You take Prep for HIV prevention 1 2 3
10. You only wear dondom when you ejaculate 1 2 3
11. You only have sex with looking healthy, handsome, clean sexual
partner(s)
1 2 3
12. You check your sexual partners penis 1 2 3
13. Other (specify) 1 2 3
216
APPENDIX 5
QUALITY ASSESSMENT CHECKLIST FOR THE SYSTEMATIC REVIEW
AND META-ANALYSIS
217
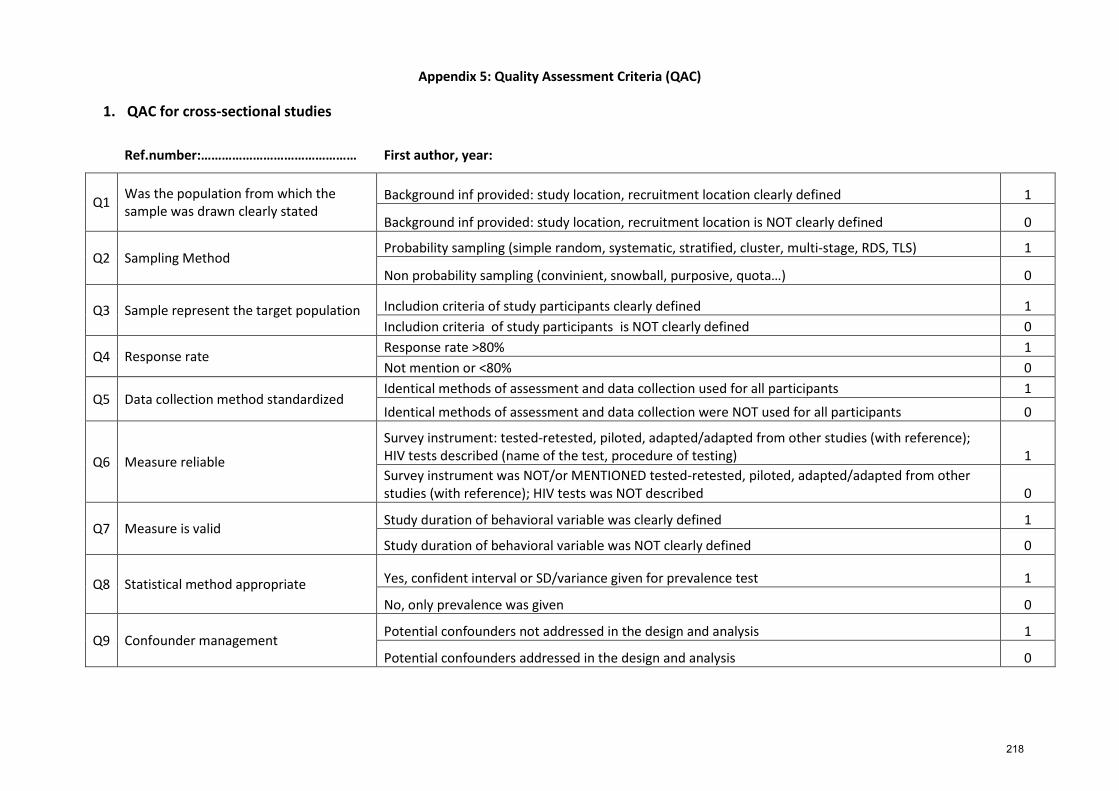
Appendix 5: Quality Assessment Criteria (QAC)
1. QAC for cross-sectional studies
Ref.number:……………………………………… First author, year:
Q1 Was the population from which the sample was drawn clearly stated
Background inf provided: study location, recruitment location clearly defined 1
Background inf provided: study location, recruitment location is NOT clearly defined 0
Q2 Sampling Method Probability sampling (simple random, systematic, stratified, cluster, multi-stage, RDS, TLS) 1
Non probability sampling (convinient, snowball, purposive, quota…) 0
Q3 Sample represent the target population Includion criteria of study participants clearly defined 1
Includion criteria of study participants is NOT clearly defined 0
Q4 Response rate Response rate >80% 1
Not mention or <80% 0
Q5 Data collection method standardized Identical methods of assessment and data collection used for all participants 1
Identical methods of assessment and data collection were NOT used for all participants 0
Q6 Measure reliable
Survey instrument: tested-retested, piloted, adapted/adapted from other studies (with reference); HIV tests described (name of the test, procedure of testing) 1
Survey instrument was NOT/or MENTIONED tested-retested, piloted, adapted/adapted from other studies (with reference); HIV tests was NOT described 0
Q7 Measure is valid Study duration of behavioral variable was clearly defined 1
Study duration of behavioral variable was NOT clearly defined 0
Q8 Statistical method appropriate Yes, confident interval or SD/variance given for prevalence test 1
No, only prevalence was given 0
Q9 Confounder management Potential confounders not addressed in the design and analysis 1
Potential confounders addressed in the design and analysis 0
218
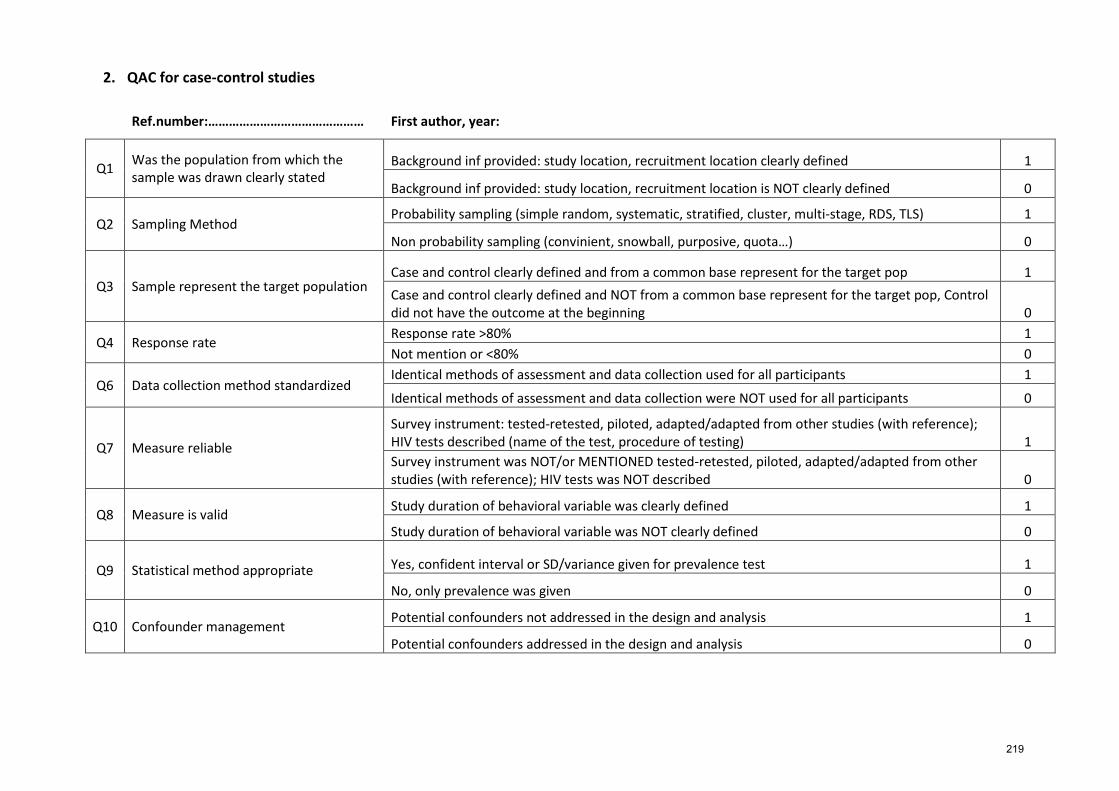
2. QAC for case-control studies
Ref.number:……………………………………… First author, year:
Q1 Was the population from which the sample was drawn clearly stated
Background inf provided: study location, recruitment location clearly defined 1
Background inf provided: study location, recruitment location is NOT clearly defined 0
Q2 Sampling Method Probability sampling (simple random, systematic, stratified, cluster, multi-stage, RDS, TLS) 1
Non probability sampling (convinient, snowball, purposive, quota…) 0
Q3 Sample represent the target population Case and control clearly defined and from a common base represent for the target pop 1
Case and control clearly defined and NOT from a common base represent for the target pop, Control did not have the outcome at the beginning 0
Q4 Response rate Response rate >80% 1
Not mention or <80% 0
Q6 Data collection method standardized Identical methods of assessment and data collection used for all participants 1
Identical methods of assessment and data collection were NOT used for all participants 0
Q7 Measure reliable
Survey instrument: tested-retested, piloted, adapted/adapted from other studies (with reference); HIV tests described (name of the test, procedure of testing) 1
Survey instrument was NOT/or MENTIONED tested-retested, piloted, adapted/adapted from other studies (with reference); HIV tests was NOT described 0
Q8 Measure is valid Study duration of behavioral variable was clearly defined 1
Study duration of behavioral variable was NOT clearly defined 0
Q9 Statistical method appropriate Yes, confident interval or SD/variance given for prevalence test 1
No, only prevalence was given 0
Q10 Confounder management Potential confounders not addressed in the design and analysis 1
Potential confounders addressed in the design and analysis 0
219
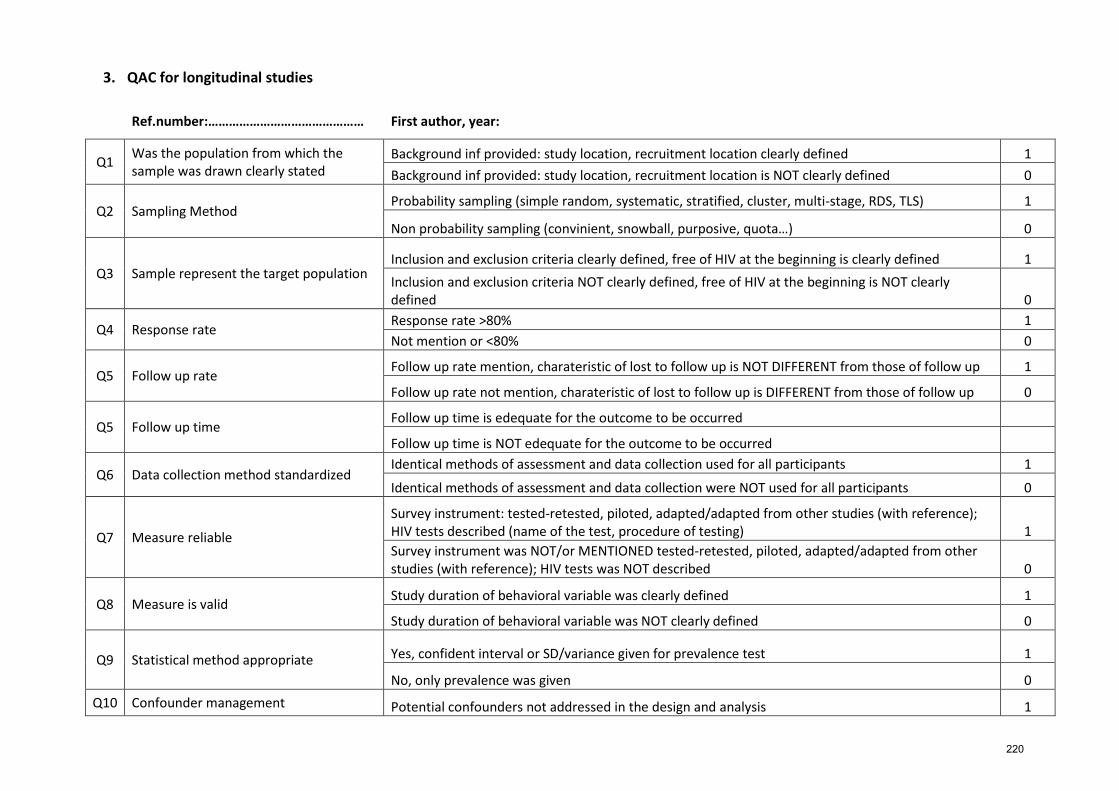
3. QAC for longitudinal studies
Ref.number:……………………………………… First author, year:
Q1 Was the population from which the sample was drawn clearly stated
Background inf provided: study location, recruitment location clearly defined 1
Background inf provided: study location, recruitment location is NOT clearly defined 0
Q2 Sampling Method Probability sampling (simple random, systematic, stratified, cluster, multi-stage, RDS, TLS) 1
Non probability sampling (convinient, snowball, purposive, quota…) 0
Q3 Sample represent the target population Inclusion and exclusion criteria clearly defined, free of HIV at the beginning is clearly defined 1
Inclusion and exclusion criteria NOT clearly defined, free of HIV at the beginning is NOT clearly defined 0
Q4 Response rate Response rate >80% 1
Not mention or <80% 0
Q5 Follow up rate Follow up rate mention, charateristic of lost to follow up is NOT DIFFERENT from those of follow up 1
Follow up rate not mention, charateristic of lost to follow up is DIFFERENT from those of follow up 0
Q5 Follow up time Follow up time is edequate for the outcome to be occurred
Follow up time is NOT edequate for the outcome to be occurred
Q6 Data collection method standardized Identical methods of assessment and data collection used for all participants 1
Identical methods of assessment and data collection were NOT used for all participants 0
Q7 Measure reliable
Survey instrument: tested-retested, piloted, adapted/adapted from other studies (with reference); HIV tests described (name of the test, procedure of testing) 1
Survey instrument was NOT/or MENTIONED tested-retested, piloted, adapted/adapted from other studies (with reference); HIV tests was NOT described 0
Q8 Measure is valid Study duration of behavioral variable was clearly defined 1
Study duration of behavioral variable was NOT clearly defined 0
Q9 Statistical method appropriate Yes, confident interval or SD/variance given for prevalence test 1
No, only prevalence was given 0
Q10 Confounder management Potential confounders not addressed in the design and analysis 1
220
Potential confounders addressed in the design and analysis 0
221



![HERITAGE ROAD & PARADISE OF CENTRAL VIETNAM Vietnam Tourism VITOURS JSC., VIETNAM DISCOVER [2014-2015 EDITION] Vietnam Tourism VITOURS Top Ten Travel Agents in Vietnam Page 2 INTINERARY](https://img.pdfslide.net/doc/110x75/631aea28d43f4e176304a8e9/heritage-road-paradise-of-central-vietnam-vietnam-tourism-vitours-jsc-vietnam.jpg)

























