Embed Size (px)
Citation preview

1550-7289/14/$http://dx.doi.org
*CorrespondMancha CentroAlcázar de San
E-mail: cms
Surgery for Obesity and Related Diseases ] (2014) 00–00
Review article
Single-incision laparoscopic bariatric surgery: a systematic reviewCarlos Moreno-Sanz, M.D., Ph.D., F.A.C.S.a,*, Antonio Morandeira-Rivas, M.D., Ph.D.a,
Cristina Sedano-Vizcaino, M.D.a, Jose María Tenías-Burillo, M.D., Ph.D.b,Carmén Román-Ortíz, M.D., Ph.D.b, Juan Bautista Muñoz de la Espada, M.D., Ph.D.a
aDepartment of Surgery, La Mancha Centro General Hospital, San Juan, SpainbResearch Support Unit, La Mancha Centro General Hospital, San Juan, Spain
Received August 17, 2013; accepted November 27, 2013
Abstract Background: Single-incision laparoscopic surgery has sparked a great deal of interest in the sur-
– see/10.10
ence:GeneJuanurgery
gical community in recent years, including bariatric surgery. However, we still do not definitivelyknow if this type of surgical approach provides benefits over conventional techniques withoutincreasing morbidity and mortality.Objective: To evaluate the safety and efficacy of single-incision laparoscopic bariatric surgery(SILBS) compared with conventional laparoscopic bariatric surgery (CLBS).Materials and Methods: We searched the most important databases. Randomized clinical trialsand observational studies comparing SILBS with CLBS were included. This systematic review wasperformed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations.Results: Fourteen studies complied with the inclusion criteria for our analysis, which included2357 patients (1179 SILBS group versus 1178 CLBS group). The duration of surgery was longer inthe SILBS group and no major intraoperative complications were observed in these series. A smallimprovement in postoperative pain was indicated in the SILBS group. The overall morbidity ratewas 5% in the SILBS group and 4.8% in the CLBS. There was 1 perioperative death in 1 study,which occurred in an adjustable gastric banding (AGB) group, at .1% of all cases of AGB and.005% of all SILBS cases. When cosmesis was evaluated, patients in the SILBS group were moresatisfied with the scar outcome.Conclusion: SILBS is a feasible technique to use in selected patients. However, there is insufficientevidence to recommend its widespread use compared with a conventional approach. More studiesare needed to analyze the safety of this technique and its possible benefits. (Surg Obes Relat Dis2014;]:00–00.) r 2014 American Society for Metabolic and Bariatric Surgery. All rights reserved.
Keywords: Single-incision adjustable gastric banding; Single-incision sleeve gastrectomy; Single-incision; Roux-en-Y
gastric bypass; Single-incision bariatric surgery; Systematic; reviewThe expansion of new minimally invasive surgical (MIS)techniques and technologies in recent years has been basedon achieving one of the primary “ideal” goals of modernsurgery: surgery without visible scars. Surgery involving
front matter r 2014 American Society for Metabolic and16/j.soard.2013.11.013
Carlos Moreno-Sanz, Department of Surgery, Laral Hospital, Avd. de la Constitución nº 3, 13600(Ciudad Real), [email protected]
zero or minimal trauma to the abdominal wall would, atleast in theory, imply all the advantages of MIS. In thiscontext, natural orifice transluminal endoscopic surgerycould be considered as a paradigm of this type of develop-ment, although despite proven feasibility, its widespreadimplementation has been limited by a lack of development[1]. However, the innovation resulting from research intonatural orifice transluminal endoscopic surgery techniqueshas allowed for the development of current surgical
Bariatric Surgery. All rights reserved.

Fig. 1. Study flow chart.
C. Moreno-Sanz et al. / Surgery for Obesity and Related Diseases ] (2014) 00–002
techniques geared toward the concept of reducing accesssurgery. A series of bridge technologies have facilitated thisdevelopment under high standards of safety and efficacy,with single-incision laparoscopic surgery (SILS) being themost attractive of the techniques currently available. SILShas been used for various abdominal procedures includingcholecystectomy [2], appendectomy [3], and colectomy[4,5] and recently this technique has also been applied tobariatric surgery [6].In an attempt to improve the results of bariatric surgery, a
number of single-incision laparoscopic bariatric surgery(SILBS) procedures have been developed, including adjust-able gastric banding (AGB), sleeve gastrectomy (SG), andRoux-en-Y gastric bypass (RYGB) [7].The objective of this review was to evaluate the
feasibility and safety of SILBS and compare its potentialadvantages with conventional laparoscopic bariatric surgery(CLBS).
Materials and Methods
This systematic review was conducted in accordance withPreferred Reporting Items for Systematic Reviews andMeta-Analyses recommendations [8].
Search parameters
We took into account all studies published between 1985and February 2013, with no limitations based on thelanguage of publication. The standard major medical data-bases were accessed: Embase, PubMed, and CochraneCentral Register of Controlled Trials. In our searches,we used the MeSH “bariatric surgery,” the word roots“endoscop*,” “laparoscop*,” and “laparoendoscop*,” andthe keywords “single incision,” “single site,” “single port,”“single access,” “single trocar,” “one trocar,” “one port,”“one wound,” “transumbilical,” “embryonic,” and“embryologic.”
Study selection and data collection
Randomized controlled trials (RCTs) and observationalstudies comparing SILBS with CLBS were included. Wealso reviewed the reference lists of these articles to findadditional information. Duplicated publications and reviewarticles were excluded. The results from each study weretransferred into our data set by 2 independent reviewers(A. M-R., C. S-V.), and a third reviewer (C.M-S.) collabo-rated for a final decision in the case of any discrepancies.We assessed the methodologic quality of all included
studies according to the Cochrane methodology for RCTsand the Newcastle-Otawa Quality Assessment Scale forobservational studies [9,10].The primary objective of our analysis was to evaluate
feasibility and safety of SILBS and to compare its potentialbenefits over CLBS.
Results
We identified a total of 262 studies for review based ontitle and abstract. After excluding duplicated articles andthose that did not comply with the inclusion criteria, weobtained a total of 20 studies that were reviewed in depth.Finally, 4 studies did not contain a control group and 2 werereview articles, all of which were excluded. The flow chartof this selection process is summarized in Fig. 1. Fourteenstudies with a total of 2357 patients, 1179 in the SILBSgroup and 1178 in the CLBS group, were included forqualitative synthesis [11–24]. These included 13 cohortstudies [11–19,21–24] and 1 RCT [20] (Table 1).
Quality of studies
The general characteristics of the studies are summarizedin Table 1. There was only 1 RCT, published by Lakdawalaet al. [20], a preliminary study comparing 50 single-incisionand 50 conventional SGs. This study had no adequate
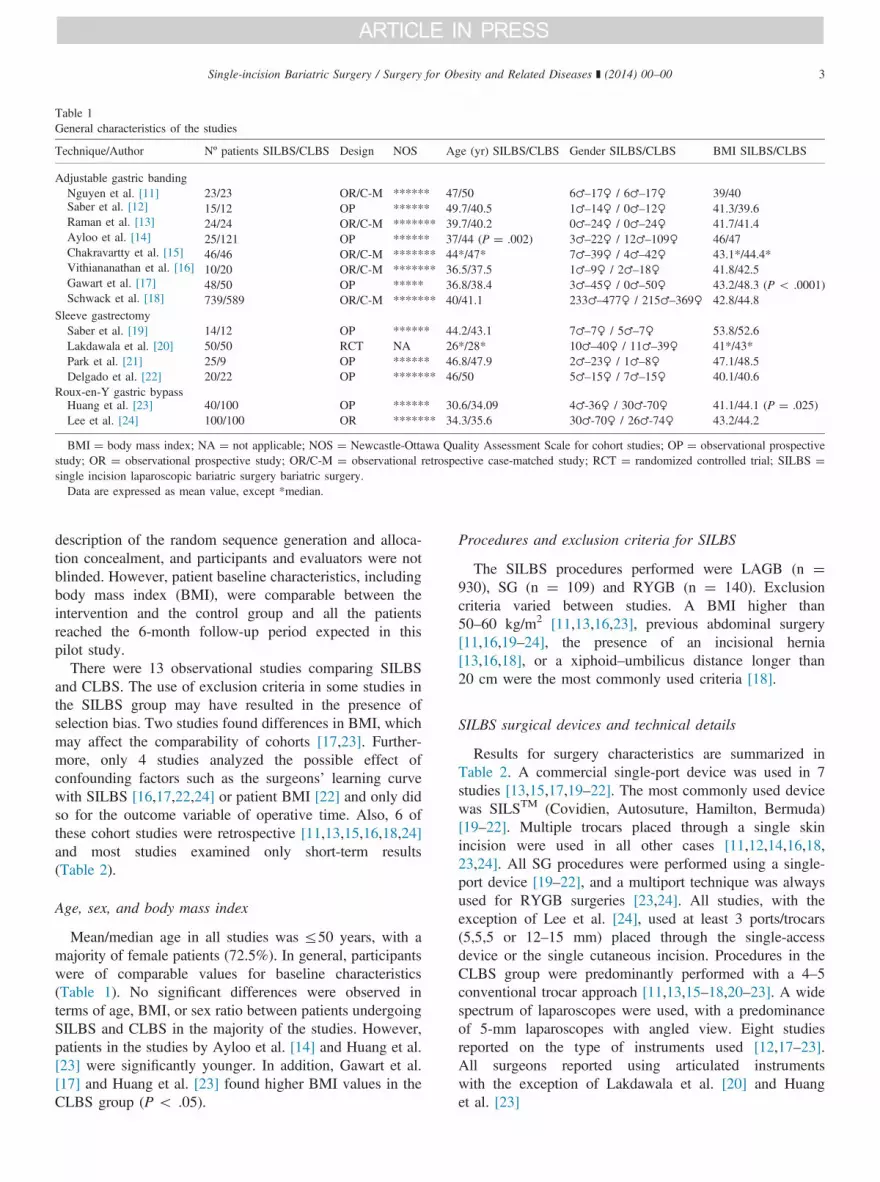
Table 1General characteristics of the studies
Technique/Author Nº patients SILBS/CLBS Design NOS Age (yr) SILBS/CLBS Gender SILBS/CLBS BMI SILBS/CLBS
Adjustable gastric bandingNguyen et al. [11] 23/23 OR/C-M ****** 47/50 6♂–17♀ / 6♂–17♀ 39/40Saber et al. [12] 15/12 OP ****** 49.7/40.5 1♂–14♀ / 0♂–12♀ 41.3/39.6Raman et al. [13] 24/24 OR/C-M ******* 39.7/40.2 0♂–24♀ / 0♂–24♀ 41.7/41.4Ayloo et al. [14] 25/121 OP ****** 37/44 (P ¼ .002) 3♂–22♀ / 12♂–109♀ 46/47Chakravartty et al. [15] 46/46 OR/C-M ******* 44*/47* 7♂–39♀ / 4♂–42♀ 43.1*/44.4*Vithiananathan et al. [16] 10/20 OR/C-M ******* 36.5/37.5 1♂–9♀ / 2♂–18♀ 41.8/42.5Gawart et al. [17] 48/50 OP ***** 36.8/38.4 3♂–45♀ / 0♂–50♀ 43.2/48.3 (P o .0001)Schwack et al. [18] 739/589 OR/C-M ******* 40/41.1 233♂–477♀ / 215♂–369♀ 42.8/44.8
Sleeve gastrectomySaber et al. [19] 14/12 OP ****** 44.2/43.1 7♂–7♀ / 5♂–7♀ 53.8/52.6Lakdawala et al. [20] 50/50 RCT NA 26*/28* 10♂–40♀ / 11♂–39♀ 41*/43*Park et al. [21] 25/9 OP ****** 46.8/47.9 2♂–23♀ / 1♂–8♀ 47.1/48.5Delgado et al. [22] 20/22 OP ******* 46/50 5♂–15♀ / 7♂–15♀ 40.1/40.6
Roux-en-Y gastric bypassHuang et al. [23] 40/100 OP ****** 30.6/34.09 4♂-36♀ / 30♂-70♀ 41.1/44.1 (P ¼ .025)Lee et al. [24] 100/100 OR ******* 34.3/35.6 30♂-70♀ / 26♂-74♀ 43.2/44.2
BMI ¼ body mass index; NA ¼ not applicable; NOS ¼ Newcastle-Ottawa Quality Assessment Scale for cohort studies; OP ¼ observational prospectivestudy; OR ¼ observational prospective study; OR/C-M ¼ observational retrospective case-matched study; RCT ¼ randomized controlled trial; SILBS ¼single incision laparoscopic bariatric surgery bariatric surgery.Data are expressed as mean value, except *median.
Single-incision Bariatric Surgery / Surgery for Obesity and Related Diseases ] (2014) 00–00 3
description of the random sequence generation and alloca-tion concealment, and participants and evaluators were notblinded. However, patient baseline characteristics, includingbody mass index (BMI), were comparable between theintervention and the control group and all the patientsreached the 6-month follow-up period expected in thispilot study.There were 13 observational studies comparing SILBS
and CLBS. The use of exclusion criteria in some studies inthe SILBS group may have resulted in the presence ofselection bias. Two studies found differences in BMI, whichmay affect the comparability of cohorts [17,23]. Further-more, only 4 studies analyzed the possible effect ofconfounding factors such as the surgeons’ learning curvewith SILBS [16,17,22,24] or patient BMI [22] and only didso for the outcome variable of operative time. Also, 6 ofthese cohort studies were retrospective [11,13,15,16,18,24]and most studies examined only short-term results(Table 2).
Age, sex, and body mass index
Mean/median age in all studies was r50 years, with amajority of female patients (72.5%). In general, participantswere of comparable values for baseline characteristics(Table 1). No significant differences were observed interms of age, BMI, or sex ratio between patients undergoingSILBS and CLBS in the majority of the studies. However,patients in the studies by Ayloo et al. [14] and Huang et al.[23] were significantly younger. In addition, Gawart et al.[17] and Huang et al. [23] found higher BMI values in theCLBS group (P o .05).
Procedures and exclusion criteria for SILBS
The SILBS procedures performed were LAGB (n ¼930), SG (n ¼ 109) and RYGB (n ¼ 140). Exclusioncriteria varied between studies. A BMI higher than50–60 kg/m2 [11,13,16,23], previous abdominal surgery[11,16,19–24], the presence of an incisional hernia[13,16,18], or a xiphoid–umbilicus distance longer than20 cm were the most commonly used criteria [18].
SILBS surgical devices and technical details
Results for surgery characteristics are summarized inTable 2. A commercial single-port device was used in 7studies [13,15,17,19–22]. The most commonly used devicewas SILSTM (Covidien, Autosuture, Hamilton, Bermuda)[19–22]. Multiple trocars placed through a single skinincision were used in all other cases [11,12,14,16,18,23,24]. All SG procedures were performed using a single-port device [19–22], and a multiport technique was alwaysused for RYGB surgeries [23,24]. All studies, with theexception of Lee et al. [24], used at least 3 ports/trocars(5,5,5 or 12–15 mm) placed through the single-accessdevice or the single cutaneous incision. Procedures in theCLBS group were predominantly performed with a 4–5conventional trocar approach [11,13,15–18,20–23]. A widespectrum of laparoscopes were used, with a predominanceof 5-mm laparoscopes with angled view. Eight studiesreported on the type of instruments used [12,17–23].All surgeons reported using articulated instrumentswith the exception of Lakdawala et al. [20] and Huanget al. [23]

Table 2Operative technical details
Author Single-incision system Incision Incisionlengh (cm)
Laparoscope Instruments
Device SI ports Extra incisions Tip Diameter(mm)
Angledvision
Adjustable gastric bandingNguyen et al. [11] Multiport 4 (5,5,5,15) or 3
(5,5,15)No or 1 (5)
umbilicalBetween xiphoidand umbilicus
3.5-4.5 Flexible 5 — NA
Saber et al. [12] Multiport 3 (5,5,12) 1 (5) subxiphoid Umbilical NA Flexible 5 — ArticulatedRaman et al. [13] SILSTM 3 (5,5,5) No Umbilical 2.5 NA NA NA NAAyloo et al. [14] Multiport 3 (5,5,15) Optional (5)
subxiphoidSupraumbilical 5–6 NA NA NA NA
Chakravartty et al.[15]
Multichanelport
4 No Between xiphoidand umbilicus
NA NA NA NA NA
Vithiananthanet al. [16]
Multiport 3 (5,5,15) 1 (3) subxiphoid Left subcostal 5–6 Rigid NA 45º NA
Gawart et al. [17] Multichanelport
NA 1 (2) subxiphoid NA NA Flexible 5 — Articulated
Schwack et al.[18]
Multiport 3 (5,5,12) Optional (3)subxiphoid
Umbilical 3–4 Rigid NA 30 º Articulated
Sleeve gastrectomySaber et al. [19] SILSTM 3 (5,5,15) No Umbilical 2.5 NA NA NA ArticulatedLakdawala et al.[20]
SILSTM 3 (5,5,12) No Umbilical 2.5 Rigid 5 30º Straight
Park et al. [21] SILSTM 3 (5,5,12) No Umbilical 2.5 Flexible 5 — ArticulatedDelgado et al. [22] SILSTM/
LESSTM3 (5,5,12) 1 (2) subxiphoid Umbilical 2.5 Rigid 5 30º Articulated
Roux-en-Y gastric bypassHuang et al. [23] Multiport 3 (5, 12,15) No Umbilical 6 Rigid 10 30º StraightLee et al. [24] Multiport 2 (10,12) 1 (5) Umbilical NA Rigid 10 30º NA
NA ¼ data not available; SI ¼ single incision.Data in parenthesis represent diameter in mm.
C. Moreno-Sanz et al. / Surgery for Obesity and Related Diseases ] (2014) 00–004
When reported, the skin incision for the insertion ofsingle-port devices initially measured 2.5 cm [13,19–22]. Incontrast, a 3–6 cm cutaneous incision was necessary for themultiport technique [11,14,16,18,23]. With the exception ofHuang et al. [23] (3.5 cm), none of the studies mentionedthe final scar length. The incision was mainly transumbilical[12,13,18–24] or placed between the xiphoid and theumbilicus [11,14,15]. Only Vithiananthan et al. [16] usedan incision outside of the midline (left subcostal). In 6studies no additional trocars were used [13,15,19–21,23]. Asubxiphoid trocar (2–5 mm) was routinely placed in 5 studies[12,16,17,22,24] and only when required in 2 [14,18].Nguyen et al. [11] used an optional 5-mm umbilical trocar.All studies used liver retraction. A retraction device
placed through the additional trocar was used in 4 studies[11,22] and was inserted through the single-access point in4 [14,21]. A percutaneus liver retractor (Nathanson) wasused in 5 studies [13–15,16,18,19]. Gawart et al. [17] used aMiniLap device (Mini-Lap Technologies, Stryker, CA,USA). Finally, transparietal sutures were used in somestudies [18,19,20,23,24].Regarding the specific bariatric techniques used, AGBs
were performed using a standard pars flaccida technique.
SGs were created at a distance of 4–6 cm from the pylorusover a 32–36F bougie. Oversewing or reinforcement of thestaple line was not routinely used [19–22]. Finally, a 15–25cm3 pouch was created for the RYGB. Huang et al. [23]used a 150–200 cm alimentary limb, whereas Lee et al. [24]preferred a 100-cm limb length. In both studies, a 100-cmbiliary limb was created.
Surgical characteristics
Operative parameters are summarized in Table 3. Con-version to CLBS was reported in 4 studies in the LAGBgroup, with a global conversion rate of 2.4%, ranging from0% to 13% [11,15–17]. The conversion rate among all 109cases of SG was 1.83% and ranged from 0% to 5% [19–21].There were no conversions among the RYGB patients[23,24]. The use of an additional trocar to finish theprocedure was reported in 3 studies of AGB (0%–10%)[15–17], 1 of SG (20%) [22], and 1 of RYGB (20%) [24].The mean/median estimated blood loss ranged from 8.4
mL to 78 mL (n ¼ 5 studies), slightly higher in the SILBSgroup, but this difference was only statistically significant inthe study by Lee et al. [24]. Interestingly, Saber et al. [19]

Table 3Perioperative parameters
Author Operative time(SILBS / CLBS)
Estimated bloodloss (mL)
Additionalports
Conversion toCLBS
Morbidity (%)(SILBS / CLBS)
Reoperation (%)(SILBS / CLBS)
Mortality (%)(SILBS / CLBS)
Adjustable gastric bandingNguyen et al.[11] 65 / 66 22 / 2.4 NA 3 (13%) 0 / 0 0 / 0 0 / 0
Saber et al.[12]
118 / 78.8(P ¼ .005) NA NA NA 0 / 0 0 / 0 0 / 0
Raman et al.[13]
62.6 / 51,5(P ¼ .03) NA NA NA 0 / 0 0 / 0 0 / 0
Ayloo et al.[14] 78 / 76 8.4 / 9 NA NA 12 / 14 4 / 0 0 / 0
Chakravarttyet al. [15] 70* / 61.5* NA 4 (9%)
0 (0%) 2.2 / 0 0 / 0 0 / 0
Vithiananthanet al. [16]
106.6 / 100.9 NA 1 (10%) 0 (0%) 10 / 5 0 / 0 0 / 0
Gawart et al.[17]
76.8 / 64.4(P ¼ .001)
NA 0 (0%) 0 (0%) 0 / 0 0 / 0 0 / 0
Schwack et al.[18]
44.3 / 51.1(P o .001)
NA NA NA 6.4 / 5.9 0.9 / 1.5 0.14 / 0
Sleeve gastrectomySaber et al.[19]
128 / 110(P ¼ .055)
78 / 93 NA 0 (0%) 0 / 0 0 / 0 0 / 0
Lakdawalaet al. [20]
50* / 45* 20* / 28* NA 0 (0%) 0 / 0 0 / 0 0 / 0
Park et al. [21] 118.4 / 101.1 NA NA 1 4 / 0 0 / 0 0 / 0Delgado et al.[22]
79.2 / 54.1(P ¼ .002)
NA 4 (20%) 1 (5%) 10 / 4.5 10 / 4.5 0 / 0
Roux-en-Y gastric bypassHuang et al.[23]
101.1 / 81.1(P o .001)
NA NA NA 5 / 1 0 / 0 0 / 0
Lee et al. [24] 143.7 / 110.1(P ¼ .000)
55.6 / 40.3 (P ¼.008)
20 (20%) 0 (0%) 3 / 2 3 / 0 0 / 0
CLBS ¼ conventional laparoscopic bariatric surgery; NA ¼ data not available; SILBS ¼ single-incision laparoscopic bariatric surgery.Data are expressed as mean value, except * median.
Single-incision Bariatric Surgery / Surgery for Obesity and Related Diseases ] (2014) 00–00 5
and Lakdawala et al. [20] observed a higher estimated bloodloss in the conventional laparoscopic SG group.The duration of the surgical procedure was longer in the
SILBS group in 12 [12,17,19,24] of the 14 studiesanalyzed, but only 11 involved significant differences[12,13,17,22–24]. In 2 studies of AGB [11,18] the operativetime favored the SILBS technique, resulting in significantdifferences in the study by Schwack et al. [18].No major intraoperative complications were observed in
these studies.
Pain and hospital stay
Postoperative pain was assessed using a visual analoguescale in 5 studies [12,14,19–21] (Table 4). In the AGBstudies, Saber et al. [12] observed statistically significantdifferences that favored the SILBS group. In studies onSG, Saber et al. [19] and Lakdawala et al.[20] also observedthe same results. However, Park et al. [21] only foundbetter pain results in the SILBS group at 1 hour afterthe operation, a tendency that was inverted in thefollowing hours.
Consumption of analgesics and duration of analgesictreatment were assessed in 8 studies (Table 4). In all studies[12,13,15,19,20,24] except 2 [21,23] the results favoredSILBS, but only 4 of these found significant differences[13,15,20,24].The mean/median length of hospital stay (LOS) varied
from .5 to 4.5 days (n = 11 studies). There was a smallvariability in the LOS among different types of SILBS, withthe exception of the study by Huang et al. [23] in which themean LOS was notably short (1.12 days). Only Ayloo et al.[14] reported a significantly longer LOS in the CLBS group(Table 3).
Morbidity and reoperations
The overall morbidity rate was 5% in the SILBS groupand 4.8% in the CLBS group. Table 5 summarizes thenumber and type of complications in each group. Apredominance of minor complications was found amongthe SILBS cases and minor complications or port compli-cations in the CLBS group.

Table 4Postoperative pain, analgesic use, and follow-up
Author Pain (VAS) SILBS / CLBS Analgesic use SILBS / CLBS %EWL SILBS / CLBS Follow-up (mo)SILBS / CLBS
Adjustable gastric bandingNguyen et al. [11] NA NA NA NASaber et al. [12] Postop. 4.8 � 1.6/5 � 1.4
Opiate use (%) 87/100 29 � 13 / 26 � 8 5.6 � 4.4 / 7.8 � 4.9Overall 2.5 � .5/3.5 � 1.2(P ¼ 0.012)
Raman et al. [13]
NA
Opiate use (mg) 33 � 19.2 / 49 � 23.78(P ¼ .01) 8.92 � 6.97‡/
9.35 � 7.87‡4.2 � 2.8 / 4.8 � 3
Analgesic duration (d) 2 � 3 / 5.7 � 7.7(P ¼ .03)
Ayloo et al. [14] At discharge 2.5 / 2.4 NA NA NAChakravartty et al. [15] NA Opiate use (mg) 10 (0–20)* / 17
(0–90)* (P o .01)34 (�15–116)* /31(5–93)*
12.5 (1–29)* / 14(5–25)*
Vithiananthan et al.[16]
NA NA 38 � 3.8 / 29.6 � 15.4 12 / 12
Gawart et al. [17] NA NA 11.2 / 12.5 3 / 3Schwack et al. [18] NA NA 54.4 � 16.3 / 46.4 � 16.1 24 / 24
Sleeve gastrectomySaber et al. [19] 4 / 6.5 (P ¼ .003) Opiate use (%) 71.4 / 91.6 25.7 / 22.6 2.8 / 1.6Lakdawala et al. [20] 4 hr postop. (P 4 .05) Analgesics 24 hr after surgery (%) 52 (39–68)* / 50.8 6 / 6
8 hr postop. (P o .05, favorsSILBS)
6 / 24 (P o .0001) (27–70)*
Park et al. [21] 1 hr postop. 3.6 / 5.8(P ¼ .039)
Opiate dose (mg) 5.6 � 3 /6.4 � 2.6
37.2 / 39.9 6 / 6
12 hr postop. 1.2 / .9 Analgesic duration (d) 1.8 � .7 / 1.7 � .224 hr postop. .6 / .3
Delgado et al. [22] NA NA 60.1 / 61.9 6 / 6Roux-en-Y gastric bypassHuang et al. [23] NA Opiate administration 2.4 � 1.9 / 1.9 � 1.6 75.4 � 8.45 / 78.20 � 10.3 12 / 12Lee et al. [24] NA Opiate dose (mg) 62.5 (29.1–142.8)† /
78.4 (16.8–99.9) )† (P ¼ .021)NA NA
CLBS ¼ conventional laparoscopic bariatric surgery; EWL ¼ excess weight loss; NA ¼ data not available; SILBS ¼ single-incision laparoscopic bariatricsurgery; VAS ¼ visual analog scale.Data are expressed as mean value, except * median. Data are expressed as mean � standard deviation, except*median (range)†mean (range)‡mean EWL
C. Moreno-Sanz et al. / Surgery for Obesity and Related Diseases ] (2014) 00–006
Two studies of gastric banding registered reoperations inthe SILBS group (4% and .9%) [14,18]. Ayloo et al. [14]reported 1 case of a stoma obstruction, and Schwack et al.[18] reported 1 stoma obstruction, 1 omental hemorrhage, 1small bowel injury, 2 wound complications, and 2 cases ofexploratory laparoscopy/laparotomy without significantfindings. It is remarkable that in this study [18] thereoperation rates were higher in the CLBS group, althoughthis difference was not statistically significant (Table 3).Delgado et al. [22] performed 2 reoperations (10%) forhemoperitoneum after single-access SG. Finally, in thestudy by Lee et al. [24] 3 cases of single-access RYGB(3%) required reoperation for incomplete pouch division orleakage.
Mortality
Only in 1 study [18] in the AGB group was perioperativemortality observed (1/739; .14%), at .1% of all cases of
gastric banding and .005% of all SILBS cases. Pulmonaryembolism was identified as the cause of death in thispatient.
Follow-up, percentage excess weight loss, and co-morbidities
Mean/median follow-up periods ranged from 3 to 24months and percentage excess weight loss (%EWL) washighly variable (n ¼ 11 studies) [12,13,15–23]. The %EWLwas higher in the SILBS group in 6 studies [12,15,16–20]and higher in the CLBS group in 5 [13,17,21–23]. The highheterogeneity found in these results hinders our ability todetect any tendencies.Finally, only Raman et al. [13] considered the time to
return to work (9.54 days in SILBS versus 10.69 days inCLBS), but this difference was not statistically significant.Resolution of co-morbidities at different follow-up peri-
ods were compared in 5 studies [12,16,19,22]. The majority

Table 5Postoperative complications
Complications SILBS CLBS
Adjustable gastric bandingSmall bowel injury 1 1Stoma obstruction requiring reoperation 2 4Exploratory laparoscopy or laparotomy 2 1Gastric ulcer 0 1Port complications 1 13Bleeding omentum 1 1Wound infection 4 6Wound seroma 1 0Minor complications not specified 40 26Total 52 (5.6%) 53 (5.9%)Sleeve gastrectomyPulmonary embolus 1 0Hemoperitoneum 2 1Total 3 (2.7%) 1 (1.1%)Roux-en-Y gastric bypassIncomplete division of the gastric pouch 1 0Leakage 2 1Wound seroma 2 0Complications not specified 0 2Total 5 (3.6%) 3 (1.5%)
CLBS ¼ conventional laparoscopic bariatric surgery; SILBS ¼ single-incision laparoscopic bariatric surgery.
Single-incision Bariatric Surgery / Surgery for Obesity and Related Diseases ] (2014) 00–00 7
of obesity-related co-morbidities improved or wereresolved, with no differences between groups.
Cosmetics
Cosmetic results were evaluated by Huang et al. [23] andLee et al. [24] in the 2 studies in the RYGB group. In bothstudies, patients with SILBS were more satisfied with thescar outcome (P o .05).
Cost
Ayloo et al. [14] included a cost analysis that favored theCLBS group but without statistically significant differences.
Discussion
In this systematic review of the medical literature, wehave identified and analyzed 13 observational comparativestudies and 1 RCT with a total of 2357 patients operated on,comparing the results between SILBS and CLBS. The SILStechnique was first described 420 years ago when Pelosiperformed supracervical hysterectomies through a singleumbilical incision [25]. In the late 1990s the scope of SILSexpanded to general surgery. Esposito [26] reported the useof a single-incision technique for appendectomy andNavarra et al. [27] reported the first cholecystectomy in1997. Later, SILS broadened to more complex surgeries andprogressively gained substantial interest among the surgicalcommunity [28,29]. Morbid obesity was initially consideredas a detractor to SILS in several procedures. However, with
the expansion of this approach, SILS was first included inbariatric surgeries in the year 2008 and early case reportswere published. Nguyen et al. [30] described the first casesof AGB, and Saber et al. [31] published the first experienceswith single-incision SG. Finally, in 2009, Saber et al. [32]and Huang et al. [33] reported the first single-access RYGB.Patient selection is of paramount importance when
performing SILS [34]. Based on our review, super-obesity,previous abdominal surgery, the presence of an incisionalhernia, or a xiphoid–umbilicus distance longer than 20 cmcould be exclusion criteria for this approach, or at leastserve as a warning for technical difficulty, although it isdifficult to suggest any recommendation in the case ofSILBS. However, some authors do not exclude the latter forSILBS but state that in these cases the incision should beoutside the umbilicus [11,14–16].Regarding surgical devices, instruments, and equipment,
SILBS can be performed with commercial single-portdevices or with multiple trocars placed through a single-skin incision, but it is difficult to detect any trends of useand it is not possible to make any recommendations in thisregard. However, the use of a single-port device would behelpful when a surgical specimen must be extracted. In ourreview, all the SG procedures were performed using asingle-port device [19–22].Although SILS can be performed with conventional 10-
mm front-view laparoscopes and straight instruments,crowding over the working area decreases the freedom ofmotion for the surgeon and assistant. Furthermore, limitedtriangulation increases the difficulty of tissue exposure anddissection [1]. The use of 5-mm laparoscopes with angled-view and articulated instruments improves exposure andmanipulation [1,7], a tendency that can be seen in most ofthe studies selected for this review [11,12,17–20]. Addi-tional ports, retractors, and transparietal sutures were usedroutinely or when needed in all studies [11,13–24]. In obesepatients, one of the biggest surgical difficulties is due toenlarged livers, and retraction continues to present aconstant challenge. A wide variety of liver retraction solutionshave been proposed, mainly represented by percutaneousdevices [13–15,16–19], retractors inserted through the umbil-ical [14,21] or an additional trocar [11,22], and transparietalsutures [18,19,20,23,24]. The use of the abovementionedresources will provide an improvement in visibility andexposure of the surgical field and assist in adequate tissuemanagement. Finally, regarding the specific bariatric techni-ques used, all the procedures were performed using standardtechniques without significant differences with respect to theconventional laparoscopic approach.Rates of conversion to CLBS were extremely low in
AGB (2.4%) and SG (1.8%) groups, with no conversionsamong RYGB patients. The use of additional trocars couldexplain these rates. Another possible reason for this is thatthese procedures were performed on selected patients andby experienced laparoscopic bariatric surgeons.

C. Moreno-Sanz et al. / Surgery for Obesity and Related Diseases ] (2014) 00–008
Finally, SILBS may be used as a hybrid approachbecause of the technical difficulties inherent to single-access points in obese patients and the amount of assistanceneeded to perform this surgery.Operative times were longer in almost all SILBS groups
of patients [12–17,19–24], with statistical differences inmost of them [12,13,17,22–24]. No major intraoperativecomplications were observed in these studies, and perhaps alimited experience with the SILBS techniques wouldexplain these differences. In this sense the study with thegreatest number of patients indicated a significant reductionin SILBS operative times [18] and an improvement ofoperative times could be expected as experience is gained.All SILBS groups presented relatively low rates of
overall morbidity (0%–12%). The global incidence ofcomplications in the overall SILBS group was 4.8%,somewhat lower than the 13% observed in a previousmulticenter registry of SILS [7]. We did not observesignificant differences between groups in terms of theglobal incidence of complications [11–24]. Finally, therewere no differences in morbidity when complications weresummarized by type of surgery, and most of them wereminor complications.Morbidity associated with the abdominal wall has also
garnered a great deal of interest during the development ofSILS. Theoretically, the use of a single incision should becorrelated with a lower number of complications. In contrast,many authors defend that a larger incision size, a more severeparietal contusion, and a longer duration of the surgicalprocedure can be associated with an increase in woundinfection and incisional hernia rates [35], as indicated in arecent study of single-incision cholecystectomy [36]. In ourreview, we observed no differences in the incidence ofwound complications. Moreover, no incisional hernias wereregistered in this systematic review, although the follow-upperiod in the majority of these studies was short.Regarding reoperations, Delgado et al. [22] performed 2
reoperations (10%) after single-access SG and 1 after usinga conventional approach (4.5%) as a result of hemoperito-neum. These rates are higher than those reported in theliterature for this complication (2%) [37]. Finally, Lee et al.[24] reported 1 case of incomplete pouch division and 2cases of leakage (2%), a complication with an incidencethat ranges from 0% to 5.6% in large series [38]. Althoughthese studies evaluated initial experiences, reoperationsare always of clinical significance and this fact must beconsidered as a word of caution when evaluating aninnovation.In general, the mortality rate of bariatric surgery is low,
and in the case of adjustable gastric banding it is remarkablylow. The in-hospital mortality rate for this procedure is only.02%, and the risk adjusted mortality index is .4%,compared with .08% and .7%, respectively, for laparoscopicRYGB [39]. In our review, although the mortality in the
SILBS AGB group was higher (.14%), the cause of deathwas not associated with the surgical technique.One of the theoretical advantages to reducing the number
of incisions is the decrease in postoperative pain andanalgesic consumption. The results from this systematicreview favor SILBS, although it is remarkable that data arevery heterogeneous regarding the time after surgery whenthe postoperative pain was evaluated and the methods usedto analyze analgesic consumption.Length of stay varied among the types of surgery, with an
average stay of 24 hours in the majority of AGB cases,o72 hours in the SG group, and close to 5 days in theRYGB group, with no significant differences amonggroups. Only Ayloo et al. [14] reported a significantlylonger LOS in the CLBS group, but they failed to explainthe criteria used for discharging patients.Efficacy is a very important issue when evaluating new
procedures. The percentage of weight loss among groupsindicated small differences, with studies favoring SILBS[12,15,16,18–20] and CLBS [13,17,21–23]. In any case,%EWL was always comparable between groups and thehigh heterogeneity found could be explained by the differ-ences in the follow-up among studies. Finally, resolution ofco-morbidities was comparable among groups when it wastaken into account. In our opinion, bariatric techniquesperformed through SILBS should not be different whether asingle-port or a conventional procedure is performed, andfor this reason results must be comparable.The cosmetic result can be an important outcome to
consider in the bariatric population, where there is apredominance of young women [14], as in our review. Infact, Yeung et al. [40] recently published the results of asurvey and visual analog scale scores, which found thatpatients preferred an umbilical single-incision for hyster-ectomy. In the 2 studies in which the cosmetic result wasevaluated, this aspect was better rated among patients whounderwent SILBS [23,24], although these studies evaluatedcosmetic result shortly after surgery (1 and 3 months).Besides, in our opinion, bariatric patients have more severeaesthetic problems than the small trocar incisions and it isnot uncommon that some of them have to undergo furtheroperations for skin resections. In this context, cosmeticreasons for using a SILBS are not really convincing in thisgroup of patients.Cost is always an important issue when a new technology
is evaluated. The initial increases in operative costs relatedto MIS are mitigated by a reduction in morbidity and LOS.Because SILBS requires access devices and special instru-ments and equipment, demonstration of any economicbenefit over CLBS can be difficult. In our review, onlyAyloo et al. [14] included a cost analysis, and the overalldirect operative costs were similar between the 2 groupswith a difference of only $150, which was not statisticallysignificant. However, if lower morbidity rates, reoperations,

Single-incision Bariatric Surgery / Surgery for Obesity and Related Diseases ] (2014) 00–00 9
and LOS are associated with SILBS, it will probably makeit this the more cost-effective technique.Our review does involve certain limitations. The fact that
the majority of the studies included initial experiences anddata from selected patients might be inconvenient whenextrapolating these results. There was also only onerandomized controlled trial. Meta-analysis was not consid-ered appropriate due to heterogeneity in the bariatricsurgical techniques and the limited number of comparativestudies, which were mostly observational. Other limitationsinclude the heterogeneity among the different studies interms of the types of surgical techniques and differentaccess devices, instruments, and equipment used in theSILBS group. Finally, most studies have a follow-up of o1year, a short period to study the incidence of incisionalhernia and to evaluate the %EWL.Given our results, we consider SILBS to be a feasible
option in selected patients when performed in a controlledenvironment of expert bariatric surgeons familiar with theuse of reduced access surgery tools. However, there isinsufficient evidence to recommend its widespread usecompared with CLBS. As in other studies evaluating SILS[33], the available evidence suggests that the primarybenefit of this approach could be the cosmetic result, withno clear differences in terms of postoperative pain and LOS.The incidence of complications was small and similarbetween SILBS and CLBS, although SILBS is associatedwith prolonged surgical times.Finally, RCTs are needed after the initial period of
implementation and learning curve to analyze the safetyof these SILBS techniques, the long-term results in weightloss, and the resolution of co-morbidities and their possiblebenefits.
Disclosures
This study was supported by a 2012 grant from Funda-cion Mutua Madrileña, Madrid, Spain.
References
[1] Moreno Sanz C, Noguera Aguilar JF, Herrero Bogajo ML, et al.Single incision laparoscopic surgery. Cir Esp 2010;88:12–7.
[2] Trastulli S, Cirocchi R, Desiderio J, et al. Systematic review andmeta-analysis of randomized clinical trials comparing single-incisionversus conventional laparoscopic cholecystectomy. Br J Surg 2013Jan;100:191–208.
[3] Gill RS, Shi X, Al-Adra DP, Birch DW, Karmali S. Single-incisionappendectomy is comparable to conventional laparoscopic appendec-tomy: a systematic review and pooled analysis. Surg Laparosc EndoscPercutan Tech 2012 Aug;22:319–27.
[4] Makino T, Milsom JW, Lee SW. Feasibility and safety of single-incision laparoscopic colectomy: a systematic review. Ann Surg2012;255:667–76.
[5] Fung AK, Aly EH. Systematic review of single-incision laparoscopiccolonic surgery. Br J Surg 2012;99:1353–64.
[6] Saber AA, Elgamal MH, Itawi EA, Rao AJ. Single incisionlaparoscopic sleeve gastrectomy (SILS): a novel technique. ObesSurg 2008;18:1338–42.
[7] Moreno-Sanz C, Morandeira-Rivas A, Morales-Conde S, et al. Singleincision laparoscopic surgery: analysis of the national register. CirEsp 2012;90:298–309.
[8] Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items forsystematic reviews and meta-analyses: the PRISMA statement. Int JSurg 2010;8:336–41.
[9] Higgins JPT, Green S, editors. Cochrane handbook for systematicreviews of interventions version 5.1.0. Oxford, UK: The CochraneColloboration; 2011.
[10] Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale(NOS) for assessing the quality of nonrandomised studies in meta-analyses [cited 2013 April 1]. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
[11] Nguyen NT, Slone J, Reavis K. Comparison study of conventionallaparoscopic gastric banding versus laparoendoscopic single sitegastric banding. Surg Obes Relat Dis 2010;6:503–7.
[12] Saber AA, El-Ghazaly TH, Elain A, Dewoolkar AV. Single-incisionlaparoscopic placement of an adjustable gastric band versus conven-tional multiport laparoscopic gastric banding: a comparative study.Am Surg 2010;76:1328–32.
[13] Raman SR, Franco D, Holover S, Garber S. Does transumbilicalsingle incision laparoscopic adjustable gastric banding result indecreased pain medicine use? A case-matched study. Surg ObesRelat Dis 2011;7:129–33.
[14] Ayloo SM, Buchs NC, Addeo P, Bianco FM, Giulianotti PC.Traditional versus single-site placement of adjustable gastric band-ing: a comparative study and cost analysis. Obes Surg 2011;21:815–9.
[15] Chakravartty S, Murgatroyd B, Ashton D, Patel A. Single andmultiple incision laparoscopic adjustable gastric banding: a matchedcomparison. Obes Surg 2012;22:1695–700.
[16] Vithiananthan S, Gero D, Zhang JY, Machan JT. A case-controlledmatched-pair cohort study of single-incision and conventional laparo-scopic gastric band patients in a single US center with 1-year follow-up. Surg Endosc 2012;26:3467–75.
[17] Gawart M, Dupitron S, Lutfi R. Laparoendoscopic single-site gastricbands versus standard multiport gastric bands: a comparison oftechnical learning curve measured by surgical time. Am J Surg2012;203:327–9.
[18] Schwack BF, Novack R, Youn H, Fielding CR, Kurian MS, FieldingGA. Single-incision laparoscopic adjustable gastric banding is effec-tive and safe: 756 cases in an academic medical center. Obes Surg2013 Mar;23:332–7.
[19] Saber AA, El-Ghazaly TH, Dewoolkar AV, Slayton SA. Single-incision laparoscopic sleeve gastrectomy versus conventional multi-port laparoscopic sleeve gastrectomy: technical considerations andstrategic modifications. Surg Obes Relat Dis 2010;6:658–64.
[20] Lakdawala MA, Muda NH, Goel S, Bhasker A. Single-incision sleevegastrectomy versus conventional laparoscopic sleeve gastrectomy—arandomised pilot study. Obes Surg 2011;21:1664–70.
[21] Park K, Afthinos JN, Lee D, Koshy N, McGinty JJ, Teixeira JA.Single port sleeve gastrectomy: strategic use of technology to re-establish fundamental tenets of multiport laparoscopy. Surg ObesRelat Dis 2012;8:450–7.
[22] Delgado S, Ibarzabal A, Adelsdorfer C, et al. Transumbilical single-port sleeve gastrectomy: initial experience and comparative study.Surg Endosc 2012;26:1247–53.
[23] Huang CK, Lo CH, Houng JY, Chen YS, Lee PH. Surgical results ofsingle-incision transumbilical laparoscopic Roux-en-Y gastric bypass.Surg Obes Relat Dis 2012;8:201–7.
[24] Lee WJ, Chen JC, Yao WC, Taou JJ, Lee YC, Ser KH. Transumbil-ical 2-site laparoscopic Roux-en-Y gastric bypass: initial results of

C. Moreno-Sanz et al. / Surgery for Obesity and Related Diseases ] (2014) 00–0010
100 cases and comparison with traditional laparoscopic technique.Surg Obes Relat Dis 2012;8:208–13.
[25] Pelosi MA, Pelosi MA 3rd. Laparoscopic supracervical hysterectomyusing a single-umbilical puncture (mini-laparoscopy). J Reprod Med1992;37:777–84.
[26] Esposito C. One-trocar appendectomy in pediatric surgery. SurgEndosc 1998;12:177–8.
[27] Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I.One-wound laparoscopic cholecystectomy. Br J Surg 1997;84:695.
[28] Sabar AA, El-Ghazaly AA, Dewoolkar AV. Single-incision laparo-scopic bariatric surgery: a comprehensive review. Surg Obes RelatDis 2010;6:575–82.
[29] Ahmed I, Paraskeva P. A clinical review of single-incision laparo-scopic surgery. Surgeon 2011;9:341–51.
[30] Nguyen NT, Hinojosa MW, Smith BR, Reavis KM. Single laparo-scopic incision transabdominal (SLIT) surgery-adjustable gastricbanding: a novel minimally invasive surgical approach. Obes Surg2008;18:1628–31.
[31] Saber AA, Elgamal MH, Itawi EA, Rao AJ. Single incisionlaparoscopic sleeve gastrectomy (SILS): a novel technique. ObesSurg 2008 Oct;18:1338–42.
[32] Saber AA, El-Ghazaly TH, Minnick DB. Single port access tran-sumbilical laparoscopic Roux-en-Y gastric bypass using the SILSPort: first reported case. Surg In nov 2009;16:343–7.
[33] Huang CK, Houng JY, Chiang CJ, Chen YS, Lee PH. Single incisiontransumbilical laparoscopic Roux-en-Y gastric bypass: a first casereport. Obes Surg 2009;19:1711–5.
[34] Arezzo A, Scozzari G, Famiglietti F, Passera R, Morino M. Is single-incision laparoscopic cholecystectomy safe? Results of a systematicreview and meta-analysis. Surg Endosc 2013;27:2293–304.
[35] Alptekin H, Yilmaz H, Acar F, et al. Incisional hernia rate mayincrease after single-port cholecystectomy. J Laparoendosc Adv SurgTech A 2012;22:731–7.
[36] Marks JM, Phillips MS, Tacchino R, et al. Single-incision laparo-scopic cholecystectomy is associated with improved cosmesis scoringat the cost of significantly higher hernia rates: 1-year results of aprospective randomized, multicenter, single-blinded trial of traditionalmultiport laparoscopic cholecystectomy vs single-incision laparo-scopic cholecystectomy. J Am Coll Surg 2013;216:1037–47.
[37] Brethauer SA. Sleeve gastrectomy. Surg Clin North Am 2011;91:1265–79.
[38] Al Harakeh AB. Complications of laparoscopic Roux-en-Y gastricbypass. Surg Clin North Am 2011;91:1225–37.
[39] Snow JM, Severson PA. Complications of adjustable gastric banding.Surg Clin North Am 2011;91:1249–64.
[40] Yeung PP Jr, Bolden CR, Westreich D, Sobolewski C. Patientpreferences of cosmesis for abdominal incisions in gynecologicsurgery. J Minim Invasive Gynecol 2013;20:79–84.














![[Laparoscopic adrenalectomy]](https://img.pdfslide.net/doc/110x75/635b67f44028fc5adf01ad9d/laparoscopic-adrenalectomy.jpg)

![[Results of bariatric surgery. Experience over 18 years]](https://img.pdfslide.net/doc/110x75/633733dd1c5ab7fce205968a/results-of-bariatric-surgery-experience-over-18-years.jpg)












