Embed Size (px)
Citation preview
Social support and socialnetwork as intermediary socialdeterminants of dental caries inadolescents
Fontanini H, Marshman Z, Vettore M. Social support and social network asintermediary social determinants of dental caries in adolescents. CommunityDent Oral Epidemiol 2014. © 2014 John Wiley & Sons A/S. Published by JohnWiley & Sons Ltd.
Abstract – Objective: The aim of this study was to investigate the associationbetween intermediary social determinants, namely social support and socialnetwork with dental caries in adolescents. Methods: An adapted version of theWHO social determinants of health conceptual framework was used toorganize structural and intermediary social determinants of dental caries intosix blocks including perceived social support and number of social networks. Across-sectional study was conducted with a representative sample of 542students between 12 and 14 years of age in public schools located in the city ofDourados, Brazil in 2012. The outcome variables were caries experience(DMFT ≥ 1) and current dental caries (component D of DMFT ≥ 1) recorded bya calibrated dentist. Individual interviews were performed to collect data onperceived social support and numbers of social networks from family andfriends and covariates. Multivariate Poisson regressions using hierarchicalmodels were conducted. Results: The prevalence of adolescents with cariesexperience and current dental caries was 55.2% and 32.1%, respectively.Adolescents with low numbers of social networks and low levels of socialsupport from family (PR 1.47; 95% CI = 1.01–2.14) were more likely to haveDMFT ≥ 1. Current dental caries was associated with low numbers of socialnetworks and low levels of social support from family (PR 2.26; 95% CI = 1.15–4.44). Conclusion: Social support and social network were influentialpsychosocial factors to dental caries in adolescents. This finding requiresconfirmation in other countries but potentially has implications forprogrammes to promote oral health.
Humberto Fontanini1, Zoe Marshman2
and Mario Vettore2
1Family Health Strategy, Municipal Health
Secretariat of Dourados Dourados, Brazil,2Unit of Dental Public Health, School of
Clinical Dentistry, University of Sheffield
Sheffield, UK
Key words: dental caries; social support,social network, social determinants ofhealth, psychosocial factors
Mario V. Vettore, Unit of Dental PublicHealth, School of Clinical Dentistry,University of Sheffield, Claremont Crescent,Sheffield, S10 2TA, UKTel.: +44-0114-2265325Fax: +44-0114-2717843e-mail: [email protected]
Submitted 7 March 2014;accepted 15 October 2014
Dental caries remains a public health problem in
most countries not only because of its high prev-
alence but also because of its impact on overall
well-being and quality of life (1–3). Until
recently, most research has focused on the indi-
vidual behavioural risk factors of dental caries.
However, this does not take into account the
underlying social, economic and environmental
aspects related to the distribution of the disease
(1, 4, 5).
Societal processes and socioeconomic character-
istics are considered the underlying determinants
of oral health because they can influence proximal
risk factors of oral diseases, such as shaping oral
health-related behaviours and modifying lifestyle
(4–6). The importance of structural and intermedi-
ary social determinants of dental caries in children
and adolescents has been well established (4, 7–10).The World Health Organization Commission
on the Social Determinants of Health (CSDH)
doi: 10.1111/cdoe.12139 1
Community Dent Oral EpidemiolAll rights reserved
� 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd

developed a conceptual framework demonstrating
how structural determinants of health inequities
(e.g. socioeconomic position, income and occupa-
tion) shape intermediary determinants, including
material and psychosocial circumstances, behavio-
ural and biological factors and health services,
which in turn shape health outcomes (11). While
some research has investigated the aetiology of
dental caries by examining behavioural and biolog-
ical factors (4, 6–8), there has been a paucity of
research exploring the links between psychosocial
circumstances such as social network and social
support and inequalities in dental caries and how
these specific intermediary determinants relate to
other intermediary and structural determinants of
dental caries in adolescents.
Social networks can be defined as the web of
identified social relationships that surround an
individual and the characteristics of those linkages.
It is the set of people with whom one maintains
social contact or some form of social bond that may
offer help or support in a variety of situations (12).
Social networks are considered the structure
through which social support is provided. Social
support refers to the perceived available resources
from people who individuals trust and on whom
they can rely (13). Social support is also related to
individual’s perceptions of the degree to which
social relations offer different forms of resources
(functions) such as material aid or emotional sup-
port (12, 14). Social networks and social support
have been associated with psychological and
physical well-being, self-esteem, performance at
school and use of dental services during adoles-
cence (15, 16).
The possible influence of social support and
social networks on oral health has mainly been
investigated in adults and older people (17–23).Few studies have evaluated the association
between social networks and social support and
oral health in adolescents (24, 25). Poor self-rated
oral health was predicted by socioeconomic char-
acteristics and untreated dental caries but not by
emotional and network support in a large sample
of Brazilian school adolescents (24). In another
study involving 1451 adolescents attending sec-
ondary schools in East London, multivariate analy-
sis showed that social support was negatively
related to caries (25). No study has assessed the
possible role of social support and social networks
as intermediary determinants of health on dental
caries in adolescents within the social determinants
of health conceptual framework.
The aim of this study was to investigate the asso-
ciation of social support and social network with
adolescents’ dental caries using an adapted version
of the WHO social determinants of health concep-
tual framework.
Methods
Study design and populationA cross-sectional study was carried out in the city
of Dourados, Brazil in 2012. Data were collected
through individual interviews and dental clinical
examinations of adolescents as well as from infor-
mation provided by questionnaires completed by
their parents. The study was approved by the
Committee of Ethics and Research of the National
School of Public Health – Oswaldo Cruz Founda-
tion (Protocol no. 0297.0.031.000-11). All partici-
pants and their parents provided informed consent
to participate in the study.
The inclusion criteria to take part in the study
were adolescents between 12 and 14 years of age
(born between 1998 and 2000) at the time of study
enrolled in public schools located in the urban area
in the city of Dourados, Brazil. All eligible students
were invited to take part in the study.
Dourados is a middle-size city with a population
of 196 035 inhabitants located in the Central-West
geographical region of Brazil, along the border with
Paraguay. It is a predominantly urban developed
city with Human Development Index of 0.788 and
with moderate level of income inequality as the
GINI Index was 0.460. Adolescents between 12 and
14 years old represent 8.82% of the population and
97.2% of them were regularly enrolled in schools
according to the 2010 Brazilian National Census.
The city has had fluoridated public water since 1992.
Theoretical frameworkA theoretical framework was adapted from WHO
Conceptual Framework for Action on the Social
Determinants of Health (11) (Fig. 1). The indepen-
dent variables were classified into the two hierarchi-
cal levels. The structural level of social determinants
of health was composed of variables related to
family socioeconomic position and demographic
characteristics of the adolescents. Intermediary
determinants were material circumstances, oral
health-related behaviours and psychosocial factors
and dental healthcare system. The explanatory vari-
ables social support and social network were consid-
ered psychosocial factors at the intermediary level.
2
Fontanini et al.

Sampling and power calculationsThe sample size was estimated as 495 adolescents
based on the prevalence of 69% of caries, consider-
ing DMFT > 1 (26) to detect a 8% of the differences
between groups, design effect of 1.5, with a signifi-
cance level of 5% and power of 95% (27). A study
with 15% of nonacceptance rate required 569
participants.
The sample was recruited in two stages to
ensure representativeness with respect to all urban
public schools of the city; these were considered
the primary units of selection (PUS). There are 66
public-funded schools for adolescents between 12
and 14 years of age. Of them, 21 were initially
excluded as they were located in nonurban areas
of the city. On average, there are 1.5 classes per
school and approximately 20 students per class
for this age group. In the first stage, a random
sample of 18 from the 45 schools located in the
urban area of the city was drawn without replace-
ment, considering the proportional probability to
the population size of the corresponding school.
The list of schools containing the pre-established
age group selected for this study was obtained
from the schools’ directors after formal agreement.
These 18 schools, secondary units of selection,
were randomly selected to ensure disaggregation
of schools considered for recruitment and repre-
sentativeness of PUS. In the second stage, a sys-
tematic sample of 30 school classes, tertiary units
of selection, was selected from those containing
students between 12 and 14 years of age. In this
stage, all individuals recruited across each school
class were approached for interview.
Dental caries assessment and groups ofcomparisonDental caries was assessed using the DMFT index
(28). Two binary outcomes related to dental caries
were considered in this study: at least one tooth
with current carious lesion or previous caries
experience (DMFT ≥ 1) and at least one tooth with
current carious lesion (component D of
DMFT ≥ 1).
Perceived social supportPerceived social support is a theoretical construct
based on the cognitive appraisal of one’s connec-
tions to others. The central aspect of perceived
social support is that not all social connectedness
between individuals results in social support. In
addition, the level of confidence and availability of
support when it is required by the individual are
core elements of perceived social support (29). The
validated version of Social Support Appraisals
(SSA) questionnaire for Brazilian adolescents was
used to assess social support. SSA questionnaire
focuses on the different sources of support and
consists of 30 items comprising 4 dimensions of
social support: ‘friends’, ‘teachers’, ‘family’ and
‘others’ (30, 31). In this study, the dimensions ‘fam-
ily’ and ‘friends’ of social support were used
because they are related to the social networks
investigated.
The participants were then categorized into three
equal groups according to tertiles of the social sup-
port score. Friends social support: low (from 0 to
32), moderate (from 33 to 35) and high (36 and
over); family social support: low (from 0 to 41),
moderate (from 42 to 44) and high (45 and over).
Social networkSocial network is the ‘web’ of social connectivity
and their characteristics surrounding the individ-
ual, including contacts with friends and relatives
(32). The Brazilian version of the social network
Medical Outcomes Study (MOS) questionnaire
was used to evaluate social networks (33). The ori-
ginal version was tested with adolescents because
it was developed for adults. No changes were
needed. The questionnaire to assess social net-
works consisted of two questions on the person’s
Fig. 1. Theoretical model for the study ofstructural and intermediary social deter-minants of dental caries in adolescents(Adapted fromWHO 2010).
3
Social support, social network and caries

relationships with family and friends. The adoles-
cents were asked to state how many family mem-
bers and friends they feel comfortable with and
who they can talk to about almost everything. The
participants were categorized into three equal
groups according to tertiles of the number of
friends and family social networks as follows: low
(from 0 to 1), moderate (2) and high (3 or more).
CovariatesDemographic data included adolescents’ sex and
ethnicity. Ethnicity was based on self-perception of
skin colour (White; Yellow; Indigenous; Brown;
Black). Family socioeconomic and material circum-
stances were obtained from parental-completed
structured questionnaires. All questionnaires were
returned, and 75% of the participants were moth-
ers. The variables included years of schooling of
the parent (0–4 years; 5–8 years; 9 or more years),
family income [less than 1 Brazilian Minimal Wage
(BMW); 1 to 4 BMW; more than 4 BMW] – one
BMW corresponded to US$ 245.00 in 2012 (stan-
dard value) – and house ownership (own; rented;
borrowed).
The oral health-related behaviours assessed were
frequency of toothbrushing (do not brush teeth; 1
time per day; 2 times per day; 3 times per day) and
number of days eating sweets during the last week
(none; 1 to 3 days; 4 to 6 days; all days). The sweets
listed in the questionnaire included sweet biscuits,
crackers, candies and chocolate bars. Information
about dental health care included time since last
dental visit (<1 year; 1 to 2 years; > 2 years) and
offer of dental treatment within the school (yes; no).
Calibration and assessment of reliabilityOne examiner was calibrated in the use of DMFT
index. Kappa coefficients for DMFT and its compo-
nents were DMFT = 0.709, D = 0.728, M = 1.00
and F = 0.927.
The internal consistency and reliability of the
social support scale and its dimensions were evalu-
ated by the Cronbach’s a coefficient and intraclass
correlation coefficient (ICC). The Cronbach’s a for
social support subscales ‘friends’ and ‘family’ was,
respectively, 0.859 and 0.714. ICC for the social
support subscales ‘friends’ ‘and ‘family’ was,
respectively, 0.992 (95% CI 0.980–0.997) and 0.994
(95% CI 0.985–0.998).
Statistical analysisThe frequencies of independent variables were pre-
sented for the whole sample and according to the
two dental caries outcomes: DMFT ≥ 1 and compo-
nent D of DMFT ≥ 1. The comparison of social sup-
port and social network between family income
groups was assessed using chi-square test.
Unadjusted associations between independent
variables related to structural and intermediary
determinants and dental caries were estimated
through prevalence ratio and 95% confidence inter-
vals (CI). The interaction between family and
friends social support and social network on dental
caries was tested. Evidence of interaction was
found for both outcomes when regression models
with and without the interaction terms were com-
pared using likelihood ratio tests (DMFT ≥ 1,
P = 0.0446 and component D of DMFT ≥ 1,
P = 0.0204).
Multivariate Poisson regression using hierarchi-
cal models was used to test the association of
Table 1. Demographic and socioeconomic characteris-tics, psychosocial factors (social network and social sup-port) of the participants
Variables N (%)
Demographic and socioeconomic characteristicsAge12 years 185 (31.5)13 years 196 (39.8)14 years 161 (28.7)SexMale 274 (55.1)Female 268 (44.9)EthnicityWhite 169 (24.0)Yellow 4 (2.2)Indigenous 15 (4.5)Brown 328 (64.4)Black 26 (4.9)Family income<1 BMW 91 (13.1)1 to <4 BMW 412 (81.5)4 to 6 BMW 39 (5.4)
Psychosocial factorsNumber of social network of familyLow (0 to 1) 134 (18.2)Moderate (2) 165 (32.4)High (3 or more) 243 (49.3)Number of social network of friendsLow (0 to 1) 164 (29.8)Moderate (2) 114 (18.3)High (3 or more) 264 (51.9)Social support from familyLow (1st tertile) 200 (35.9)Moderate (2nd tertile) 220 (47.2)High (3rd tertile) 122 (16.9)Social support from friendsLow (1st tertile) 200 (50.1)Moderate (2nd tertile) 190 (27.3)High (3rd tertile) 152 (22.6)
4
Fontanini et al.

Table 2. Unadjusted association of structural and intermediary social determinants with DMFT and dental caries
Decayedteeth = 0 N (%)
Decayedteeth ≥ 1 N (%) PR 95% CI
DMFT = 0N (%)
DMFT ≥ 1N (%) PR 95% CI
Structural determinantsFamily socioeconomic conditionsYears of schooling of the respondent≥9 170 (46.2) 82 (47.2) 1 114 (46.9) 138 (46.2) 15 to 8 164 (44.6) 62 (35.6) 0.84 (0.64–1.11) 109 (44.9) 117 (39.1) 0.95 (0.80–1.12)0 to 4 34 (9.2) 30 (17.2) 1.44 (1.05–1.98)* 20 (8.2) 44 (14.7) 1.26 (1.03–1.53)*
Family income4 to 6 BMW 31 (8.4) 8 (4.6) 1 19 (7.8) 20 (6.7) 11 to <4 BMW 281 (76.4) 131 (75.3) 1.55 (0.82–2.92) 190 (78.2) 222 (74.2) 1.05 (0.76–1.45)<1 BMW 56 (15.2) 35 (20.1) 1.88 (0.96–3.67) 34 (14.0) 57 (19.1) 1.22 (0.87–1.72)
Demographic characteristicsSexMale 191 (51.9) 83 (47.7) 1 125 (51.4) 149 (49.8) 1Female 177 (48.1) 91 (52.3) 1.12 (0.88–1.43) 118 (48.6) 150 (50.2) 1.03 (0.88–1.20)EthnicityWhite 121 (32.9) 48 (27.6) 1 83 (34.2) 86 (28.8) 1Yellow 3 (0.8) 1 (0.6) 0.88 (0.16–4.89) 3 (1.2) 1 (0.3) 0.49 (0.09–2.70)Indigenous 10 (2.7) 5 (2.9) 1.17 (0.55–2.50) 5 (2.1) 10 (3.3) 1.31 (0.89–1.93)
Brown 220 (59.8) 108 (62.0) 1.16 (0.87–1.54) 143 (58.8) 185 (61.9) 1.11 (0.93–1.32)Black 14 (3.8) 12 (6.9) 1.63 (1.01–2.62)* 9 (3.7) 17 (5.7) 1.29 (0.94–1.76)
Intermediary determinantsMaterial circumstancesType of houseOwn 289 (78.5) 130 (74.8) 1 198 (81.5) 221 (73.9) 1Rented 58 (15.8) 30 (17.2) 1.10 (0.80–1.52) 35 (14.4) 53 (17.7) 1.14 (0.94–1.38)Borrowed 21 (5.7) 14 (8.0) 1.29 (0.84–1.98) 10 (4.1) 25 (8.4) 1.35 (1.08–1.70)*
Psychosocial factorsSocial support and social networkNumber of social networks of familyHigh (3 or more) 183 (49.7) 60 (34.5) 1 125 (51.4) 118 (39.5) 1Moderate (2) 109 (29.6) 56 (32.2) 1.38 (1.01–1.87)* 74 (30.5) 91 (30.4) 1.14 (0.94–1.37)Low (0 to 1) 76 (20.7) 58 (33.3) 1.75 (1.31–2.35)* 44 (18.1) 90 (30.1) 1.38 (1.16–1.65)*
Number of social networks of friendsHigh (3 or more) 193 (52.5) 71 (40.8) 1 124 (51.1) 140 (46.8) 1Moderate (2) 74 (20.1) 40 (23.0) 1.31 (0.95–1.80) 56 (23.0) 58 (19.4) 0.96 (0.78–1.19)Low (0 to 1) 101 (27.4) 63 (36.2) 1.43 (1.08–1.89)* 63 (25.9) 101 (33.8) 1.16 (0.98–1.37)Social support from familyHigh (3rd tertile) 88 (23.9) 34 (19.5) 1 57 (23.5) 65 (21.7) 1Moderate (2nd tertile) 156 (42.4) 64 (36.8) 1.04 (0.73–1.49) 114 (46.9) 106 (35.5) 0.90 (0.73–1.12)Low (1st tertile) 124 (33.7) 76 (43.7) 1.36 (0.97–1.91) 72 (29.6) 128 (42.8) 1.20 (0.99–1.46)Social support from friendsHigh (3rd tertile) 101 (27.4) 51 (29.2) 1 72 (29.6) 80 (26.8) 1Moderate (2nd tertile) 143 (38.9) 47 (27.0) 0.74 (0.53–1.03) 98 (40.4) 92 (30.8) 0.92 (0.75–1.14)Low (1st tertile) 124 (33.7) 76 (43.8) 1.13 (0.85–1.51) 73 (30.0) 127 (42.4) 1.21 (1.01–1.45)*
Health-related behavioursToothbrushing frequency≥3 times/day 206 (56.0) 91 (52.3) 1 142 (58.4) 155 (51.8) 12 times per day 136 (37.0) 68 (39.1) 1.09 (0.84–1.41) 83 (34.2) 121 (40.5) 1.14 (0.97–1.33)Once a day 23 (6.2) 13 (7.5) 1.18 (0.74–1.88) 15 (6.2) 21 (7.0) 1.12 (0.83–1.50)Do not brush teeth 3 (0.8) 2 (1.1) 1.31 (0.44–3.87) 3 (1.2) 2 (0.7) 0.77 (0.26–2.26)Number of days eating sweets during the last weekNone day 43 (11.7) 12 (6.9) 1 32 (13.2) 23 (7.7) 11 to 3 days 135 (36.6) 61 (35.0) 1.43 (0.83–2.45) 89 (36.6) 107 (35.8) 1.31 (0.93–1.83)4 to 6 days 93 (25.3) 48 (27.6) 1.56 (0.90–2.71) 60 (24.7) 81 (27.1) 1.37 (0.98–1.94)All days 97 (26.4) 53 (30.5) 1.62 (0.94–2.79) 62 (25.5) 88 (29.4) 1.40 (1.01–1.97)*
Healthcare systemLast dental visit< 1 year 252 (73.9) 100 (59.2) 1 172 (77.1) 180 (62.7) 11 to 2 years 80 (23.5) 58 (34.3) 1.08 (0.70–1.68) 43 (19.3) 95 (33.1) 0.90 (0.66–1.23)
5
Social support, social network and caries
structural and intermediary determinants with the
outcomes (34). Prevalence ratio (PR) with 95% CI
and P values were estimated. Stepwise forward
selection of variables in six blocks was conducted
according to the theoretical framework (Fig. 1)
(11). The first block included family socioeconomic
position variables (family income and years of
schooling of the parents) and the second block con-
sisted of demographic characteristics of the adoles-
cent (gender and ethnicity). The third and fourth
blocks included material circumstances (house
ownership) and oral health-related behaviours (fre-
quency of toothbrushing and frequency of inade-
quate diet). Psychosocial factors (social support
and social network) composed the fifth block, and
dental health system (time since last dental visit
and dental treatment offered within the school)
was the sixth block. Independent variables of each
block were adjusted for each other and those that
remained significant at 20% (P < 0.20) were
retained in the analysis for adjustment (34). This
approach reduces the discrepancy between the
data and the model to reach an economic model
with few parameters (35).
Sample weights were used to adjust for sam-
pling complexity. Weighted data were obtained by
using a complex sample plan and were submitted
to the complex samples analysis in SPSS version
22.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
Of the 18 schools randomly selected, one was
replaced because the head of the school did not
agree to participate. Initially, 569 students from 30
school classes were invited to participate in the
study. The nonresponse rate was 4.8% (N = 27)
resulting in a sample of 542 adolescents between
12 and 14 years of age.
The prevalence of adolescents with at least one
tooth with caries experience (DMFT ≥ 1) and at
least one decayed tooth with current carious lesion
(component D of DMFT ≥ 1) was 55.2% and 32.1%,
respectively. The mean DMFT and decayed teeth
of the sample were 2.20 (SD = 1.92) and 1.17
(SD = 0.68). Adolescents’ social support and social
network did not differ between family income
groups (P > 0.05).
Demographic and socioeconomic characteristics
and information on social support and social net-
work of the participants are presented in Table 1.
The frequency of individuals in the age groups and
sex categories was similar and in terms of ethnicity
Table 2 Continued
Decayedteeth = 0 N (%)
Decayedteeth ≥ 1 N (%) PR 95% CI
DMFT = 0N (%)
DMFT ≥ 1N (%) PR 95% CI
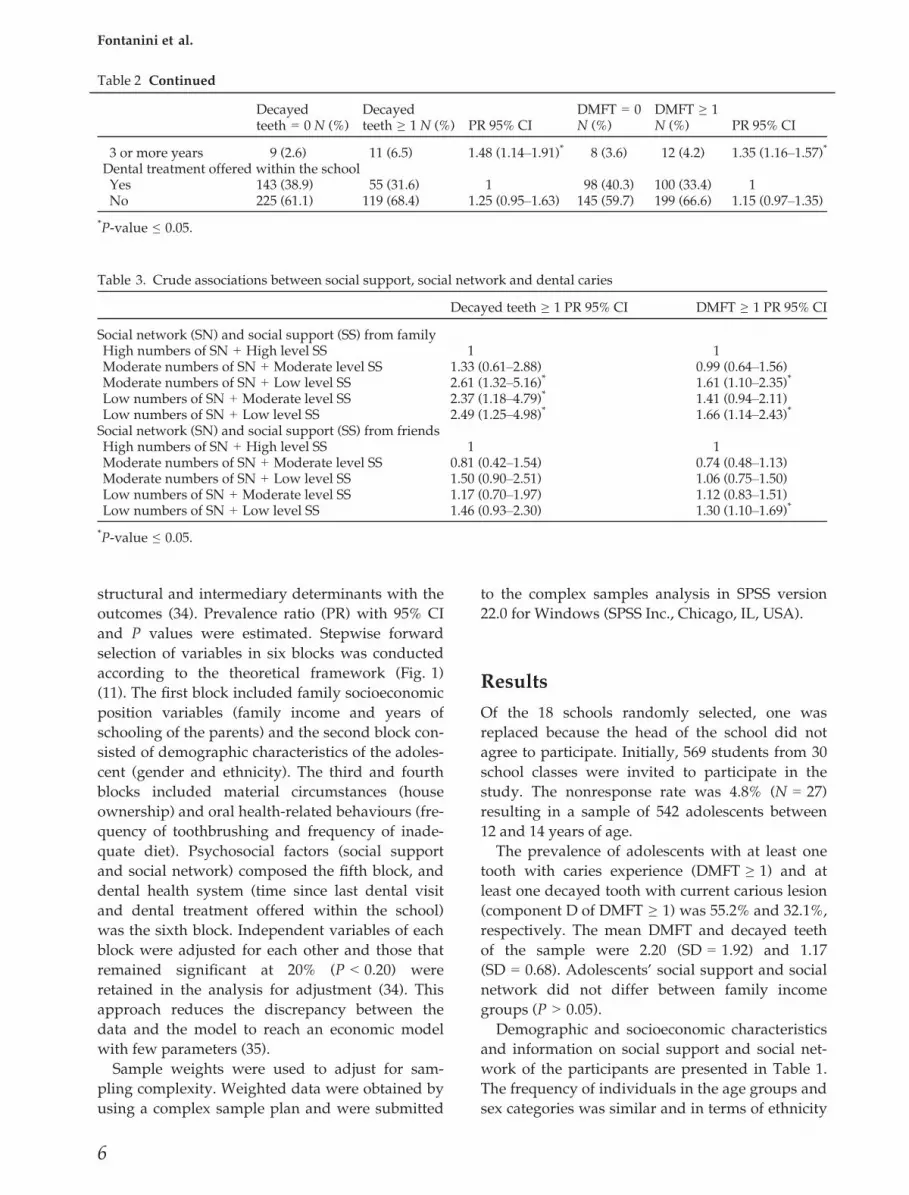
3 or more years 9 (2.6) 11 (6.5) 1.48 (1.14–1.91)* 8 (3.6) 12 (4.2) 1.35 (1.16–1.57)*
Dental treatment offered within the schoolYes 143 (38.9) 55 (31.6) 1 98 (40.3) 100 (33.4) 1No 225 (61.1) 119 (68.4) 1.25 (0.95–1.63) 145 (59.7) 199 (66.6) 1.15 (0.97–1.35)
*P-value ≤ 0.05.
Table 3. Crude associations between social support, social network and dental caries
Decayed teeth ≥ 1 PR 95% CI DMFT ≥ 1 PR 95% CI
Social network (SN) and social support (SS) from familyHigh numbers of SN + High level SS 1 1Moderate numbers of SN + Moderate level SS 1.33 (0.61–2.88) 0.99 (0.64–1.56)Moderate numbers of SN + Low level SS 2.61 (1.32–5.16)* 1.61 (1.10–2.35)*
Low numbers of SN + Moderate level SS 2.37 (1.18–4.79)* 1.41 (0.94–2.11)Low numbers of SN + Low level SS 2.49 (1.25–4.98)* 1.66 (1.14–2.43)*
Social network (SN) and social support (SS) from friendsHigh numbers of SN + High level SS 1 1Moderate numbers of SN + Moderate level SS 0.81 (0.42–1.54) 0.74 (0.48–1.13)Moderate numbers of SN + Low level SS 1.50 (0.90–2.51) 1.06 (0.75–1.50)Low numbers of SN + Moderate level SS 1.17 (0.70–1.97) 1.12 (0.83–1.51)Low numbers of SN + Low level SS 1.46 (0.93–2.30) 1.30 (1.10–1.69)*
*P-value ≤ 0.05.
6
Fontanini et al.

Table 4. Multivariate Poisson regression between social support, social network and DMFT ≥ 1 adjusted for covariates(prevalence ratio and 95% confidence intervals)
Model 1PR 95% CI
Model 2PR 95% CI
Model 3PR 95% CI
Model 4PR 95% CI
Model 5PR 95% CI
Model 6PR 95% CI
Structural determinants
Family socioeconomic conditions
Years of schooling of the respondent
≥ 9 1 1 1 1 1
5 to 8 0.92 (0.78–1.10) 0.92 (0.77–1.09) 0.90 (0.76–1.07) 0.89 (0.75–1.06)* 0.95 (0.80–1.13)
0 to 4 1.19 (0.96–1.48)* 1.19 (0.97–1.47)* 1.16 (0.94–1.44)* 1.13 (0.91–1.40) 1.12 (0.90–1.40)
Family income
4 to 6 BMW 1
1 to <4 BMW 1.06 (0.76–1.47)
<1 BMW 1.19 (0.83–1.72)
Demographic characteristics
Sex
Male 1
Female 1.01 (0.87–1.18)
Ethnicity
White 1 1 1 1
Yellow 0.50 (0.09–2.84) 0.51 (0.09–2.95) 0.62 (0.11–3.46) 0.63 (0.13–3.20)
Indigenous 1.28 (0.86–1.90) 1.25 (0.85–1.85) 1.30 (0.86–1.96) 1.16 (0.81–1.68)
Brown 1.11 (0.93–1.33) 1.11 (0.93–1.33) 1.11 (0.93–1.33) 1.08 (0.90–1.29)
Black 1.26 (0.92–1.73)* 1.24 (0.90–1.72)* 1.25 (0.91–1.71)* 1.16 (0.84–1.61)
Intermediary determinants
Material circumstances
Type of house
Own 1 1 1 1
Rented 1.13 (0.93–1.37)* 1.13 (0.93–1.35) 1.16 (0.96–1.39)* 1.13 (0.93–1.36)
Borrowed 1.32 (1.05–1.66)** 1.35 (1.07–1.70)** 1.38 (1.09–1.75)** 1.45 (1.15–1.84)**
Health-related behaviours
Toothbrushing frequency
≥3 times/day 1
2 times per day 0.84 (0.28–2.54)
Once a day 1.07 (0.80–1.42)
Do not brush teeth 1.11 (0.94–1.29)
Number of days eating sweets during the last week
None day 1 1 1
1 to 3 days 1.34 (0.96–1.88)* 1.36 (0.97–1.89)* 1.35 (0.99–1.84)*
4 to 6 days 1.36 (0.97–1.92)* 1.42 (1.02–1.99)** 1.43 (1.04–1.96)**
All days 1.39 (1.00–1.95)* 1.37 (0.99–1.91)* 1.38 (1.01–1.90)*
Psychosocial factors
Social network (SN) and social support (SS) from family
High numbers of SN + High level SS 1 1
Moderate numbers of SN + Moderate level SS 0.95 (0.61–1.48) 0.91 (0.59–1.41)
Moderate numbers of SN + Low level SS 1.45 (1.01–2.15)** 1.44 (0.99–2.08)*
Low numbers of SN + Moderate level SS 1.34 (0.88–2.02)* 1.32 (0.89–1.97)*
Low numbers of SN + Low level SS 1.49 (1.02–2.20)** 1.47 (1.01–2.14)**
Social network (SN) and social support (SS) from friends
High numbers of SN + High level SS 1 1
Moderate numbers of SN + Moderate level SS 0.71 (0.47–1.08) 0.67 (0.45–1.01)
Moderate numbers of SN + Low level SS 1.00 (0.70–1.42) 0.97 (0.68–1.38)
Low numbers of SN + Moderate level SS 1.05 (0.78–1.43) 1.02 (0.76–1.39)
Low numbers of SN + Low level SS 1.22 (0.93–1.60)* 1.13 (0.86–1.49)
Healthcare system
Last dental visit
<1 year 1
1 to 2 years 0.88 (0.65–1.20)
3 or more years 1.32 (1.13–1.54)**
Dental treatment offered within the school
Yes 1
No 1.10 (0.94–1.30)
*P-value < 0.20.**P-value ≤ 0.05.
7
Social support, social network and caries

64.4% were Brown. Only 5.4% of the sample had
family income ≥4 Brazilian minimal wages. Nearly
half of the sample reported three or more social
networks from family and friends. Around 36%
and 50% of the individuals were classified as with
low levels of social support from family and
friends, respectively (Table 1).
Table 2 presents the unadjusted associations of
structural and intermediary social determinants,
including social support and social network, with
dental caries. Low years of schooling of the parents,
lower numbers of social networks from family and
longer time since last dental visit were more com-
mon for both dental caries outcomes. Black ethnicity
and lower numbers of social networks from friends
were associated with current dental caries. Individ-
uals with caries experience had worse material cir-
cumstances, lower levels of social support from
friends and a more cariogenic diet. Sex, levels of
social support from family, frequency of tooth-
brushing and offer of dental treatment within the
school were similar across groups (Table 2).
Table 3 includes the crude analysis on the associ-
ation between interaction terms of social support
and social network from family and friends with
dental caries. In that analysis, adolescents with
high levels of social support and higher numbers
of social networks were the reference category.
Moderate and low levels of social support and
social networks from family were associated with
current dental caries while adolescents with lower
levels of social support and low numbers of social
networks from family and friends were more likely
to have previous caries experience.
Poisson hierarchical models investigated the asso-
ciation of social support and social network from
family and friends with DMFT (Table 4). In models
1 and 2, family socioeconomic conditions and
demographic variables were not associated with
DMFT. Type of housing (borrowed house) in Model
3 and cariogenic diet in Model 4 predicted DMFT
and remained associated with DMFT afterwards.
The prevalence of DMFT ≥ 1 was significantly
higher for adolescents with moderate social net-
work and low social support from family and low
social network and low social support from family
(Model 5). In the final model (Model 6), low num-
bers of social networks and low levels social sup-
port from family were associated with DMFT ≥ 1
(PR 1.47; 95% CI = 1.01–2.14). Time since last dental
visit was also associated with DMFT.
Table 5 summarizes the same analyses for cur-
rent dental caries (component D of DMFT ≥ 1).
Family socioeconomic conditions, demographic
variables, material circumstances and health-
related behaviours were not associated with cur-
rent dental caries (Models 1, 2, 3 and 4). Moderate
and low social network and social support from
family increased the prevalence of current decayed
tooth in Models 5 and 6. Individuals with low
numbers of social networks and moderate levels of
social support from family (PR 2.24; 95%
CI = 1.13–4.41), those with moderate numbers of
social networks and low levels of social support
(PR 2.42; 95% CI = 1.25–4.68) and those with low
numbers of social networks and low levels of social
support (PR 2.26; 95% CI = 1.15–4.44) from family
were more likely to have dental caries. Time since
last dental visit was also associated with current
dental caries in the final model.
Discussion
In the present study, adolescents with low num-
bers of social networks and low levels of social
support from family had more current dental car-
ies as well as more caries experience. Therefore,
social support and social networks from family
were psychosocial factors related to dental caries in
adolescents. The stratified analysis illustrated the
modifying effect of social support. The prevalence
of current dental caries was higher among adoles-
cents with lower levels of social networks of family
with lower levels of social support compared with
those with higher levels of social support. The
combined effect of low levels of social support and
low numbers of social networks of family appears
to be relevant for the occurrence of dental caries. In
addition to that, inadequate use of oral health care
was also associated with caries.
There are potential direct and indirect mecha-
nisms that explain the influence of lower levels of
social support and social network on oral health
outcomes. Direct pathways suggest that oral dis-
eases can be affected by social support and social
network through psychological mechanisms. They
operate through cognitive and emotional processes
including the development and strengthening of
trust, well-being, self-efficacy, social integration,
self-steem and mutual cooperation (36, 37).
Behavioural pathways have been implicated in the
indirect effects of unsupportive social connections
and oral health. Oral health-related behaviours in
adolescents (e.g. smoking and eating a more cario-
genic diet) are strongly related to social influence
8
Fontanini et al.
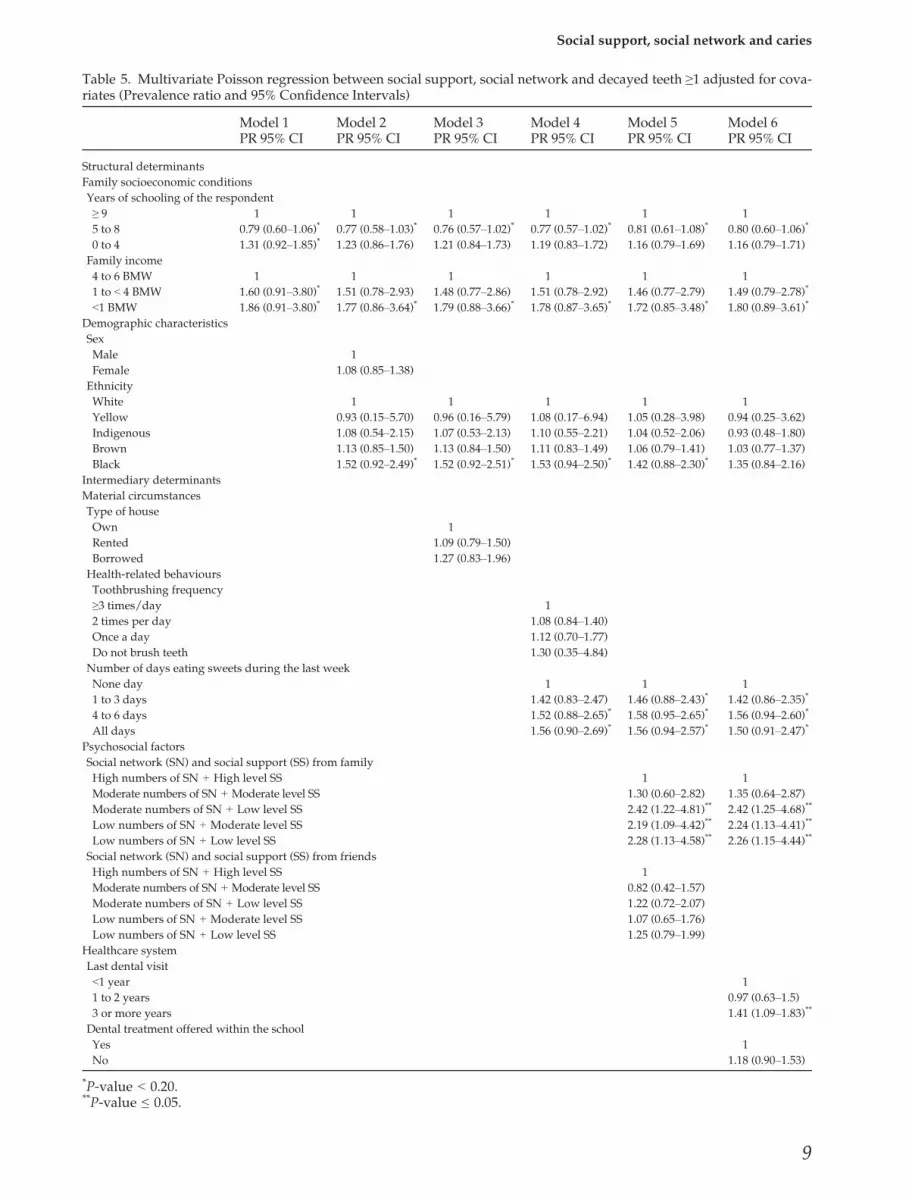
Table 5. Multivariate Poisson regression between social support, social network and decayed teeth ≥1 adjusted for cova-riates (Prevalence ratio and 95% Confidence Intervals)
Model 1PR 95% CI
Model 2PR 95% CI
Model 3PR 95% CI
Model 4PR 95% CI
Model 5PR 95% CI
Model 6PR 95% CI
Structural determinants
Family socioeconomic conditions
Years of schooling of the respondent
≥ 9 1 1 1 1 1 1
5 to 8 0.79 (0.60–1.06)* 0.77 (0.58–1.03)* 0.76 (0.57–1.02)* 0.77 (0.57–1.02)* 0.81 (0.61–1.08)* 0.80 (0.60–1.06)*
0 to 4 1.31 (0.92–1.85)* 1.23 (0.86–1.76) 1.21 (0.84–1.73) 1.19 (0.83–1.72) 1.16 (0.79–1.69) 1.16 (0.79–1.71)
Family income
4 to 6 BMW 1 1 1 1 1 1
1 to < 4 BMW 1.60 (0.91–3.80)* 1.51 (0.78–2.93) 1.48 (0.77–2.86) 1.51 (0.78–2.92) 1.46 (0.77–2.79) 1.49 (0.79–2.78)*
<1 BMW 1.86 (0.91–3.80)* 1.77 (0.86–3.64)* 1.79 (0.88–3.66)* 1.78 (0.87–3.65)* 1.72 (0.85–3.48)* 1.80 (0.89–3.61)*
Demographic characteristics
Sex
Male 1
Female 1.08 (0.85–1.38)
Ethnicity
White 1 1 1 1 1
Yellow 0.93 (0.15–5.70) 0.96 (0.16–5.79) 1.08 (0.17–6.94) 1.05 (0.28–3.98) 0.94 (0.25–3.62)
Indigenous 1.08 (0.54–2.15) 1.07 (0.53–2.13) 1.10 (0.55–2.21) 1.04 (0.52–2.06) 0.93 (0.48–1.80)
Brown 1.13 (0.85–1.50) 1.13 (0.84–1.50) 1.11 (0.83–1.49) 1.06 (0.79–1.41) 1.03 (0.77–1.37)
Black 1.52 (0.92–2.49)* 1.52 (0.92–2.51)* 1.53 (0.94–2.50)* 1.42 (0.88–2.30)* 1.35 (0.84–2.16)
Intermediary determinants
Material circumstances
Type of house
Own 1
Rented 1.09 (0.79–1.50)
Borrowed 1.27 (0.83–1.96)
Health-related behaviours
Toothbrushing frequency
≥3 times/day 1
2 times per day 1.08 (0.84–1.40)
Once a day 1.12 (0.70–1.77)
Do not brush teeth 1.30 (0.35–4.84)
Number of days eating sweets during the last week
None day 1 1 1
1 to 3 days 1.42 (0.83–2.47) 1.46 (0.88–2.43)* 1.42 (0.86–2.35)*
4 to 6 days 1.52 (0.88–2.65)* 1.58 (0.95–2.65)* 1.56 (0.94–2.60)*
All days 1.56 (0.90–2.69)* 1.56 (0.94–2.57)* 1.50 (0.91–2.47)*
Psychosocial factors
Social network (SN) and social support (SS) from family
High numbers of SN + High level SS 1 1
Moderate numbers of SN + Moderate level SS 1.30 (0.60–2.82) 1.35 (0.64–2.87)
Moderate numbers of SN + Low level SS 2.42 (1.22–4.81)** 2.42 (1.25–4.68)**
Low numbers of SN + Moderate level SS 2.19 (1.09–4.42)** 2.24 (1.13–4.41)**
Low numbers of SN + Low level SS 2.28 (1.13–4.58)** 2.26 (1.15–4.44)**
Social network (SN) and social support (SS) from friends
High numbers of SN + High level SS 1
Moderate numbers of SN + Moderate level SS 0.82 (0.42–1.57)
Moderate numbers of SN + Low level SS 1.22 (0.72–2.07)
Low numbers of SN + Moderate level SS 1.07 (0.65–1.76)
Low numbers of SN + Low level SS 1.25 (0.79–1.99)
Healthcare system
Last dental visit
<1 year 1
1 to 2 years 0.97 (0.63–1.5)
3 or more years 1.41 (1.09–1.83)**
Dental treatment offered within the school
Yes 1
No 1.18 (0.90–1.53)
*P-value < 0.20.**P-value ≤ 0.05.
9
Social support, social network and caries

from friends and relatives and access to material
goods and resources (38, 39).
The association of poor social support and low
numbers of social networks with oral conditions
has been consistently highlighted (17–25). How-
ever, little attention has been placed on the possible
influence of social relationships on dental caries as
most of the previous studies focused on subjective
oral health outcomes (17, 21, 23, 24). Furthermore,
adults and elderly people have been the most
investigated population groups in this topic and
few studies have involved adolescents. Early stud-
ies assessed the association between social support
and oral health in adolescents and reported differ-
ent findings (24, 25). Emotional and network sup-
port were not associated with poor self-rated oral
health in Brazilian adolescents (24). Similar to our
findings, social support was related to caries expe-
rience (25). Nevertheless, social support from a
special person was more important for the absence
of dental caries compared to family and friends.
However, the terminology ‘special person’ is non-
specific and can represent a variety of forms of
social connectedness.
Positive aspects of this study include the use of
the WHO social determinants of health concep-
tual framework (11) and the hierarchical model-
ling regressions. Thus, the nature and hierarchy
of the predictors for dental caries were consid-
ered in the data analysis. Social support was
assessed using a valid instrument for the studied
population. The limitations of this study include
the cross-sectional design, which restricts causal
inferences. Recruiting adolescents from public
schools might affect the generalizability of our
findings resulting in a homogeneous sample from
low socioeconomic background. In addition, the
WHO social determinants of health conceptual
framework (11) were not fully addressed in the
present study because contextual socioeconomic
and political determinants were not assessed.
This study was also subject to information bias
because frequency of tooth brushing; diet and
dental attendance are information that requires
memory and some notion of quantity, which
might be influenced by the age of the group
investigated. The questionnaire used to assess
social networks was originally developed and
tested in adults and adapted for adolescents in
this study (33). Although the validity of the social
networks measures might be questionable, the
positive association between social support and
social network and dental caries suggests that at
least there is low probability of nondifferential
bias.
Based on our findings, potential recommenda-
tions for programmes to improve the oral health of
adolescents can be suggested. Psychosocial inter-
ventions focusing on enhancing social networks
from family and strengthening the social support
from relatives may bring benefits to oral health.
Nonetheless, such interventions should be devel-
oped based on appropriate psychological theories
and tested to confirm their benefits to oral health.
However, as levels of social support and numbers
of social networks are influenced by aspects of cul-
ture, further research in other countries should be
conducted to confirm our findings.
This is the first study to evaluate the combined
effect of social support and social networks on den-
tal caries and to report the modifying effect of
social support. This finding is expected and theo-
retically plausible because social support and
social network are interconnected. Furthermore,
the different types of social support are embedded
within an individual’s social networks, and social
networks is the way the social support can be
expressed and perceived (13, 40). Our findings sug-
gest that adolescents’ oral health is independently
influenced by the number of social networks from
family as well as by the levels of perceived social
support originated from family networks.
References1. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day
S, Ndiaye C. The global burden of oral diseases andrisks to oral health. Bull World Health Organ2005;83:661–9.
2. Nurelhuda NM, Ahmed MF, Trovik TA, �AstrømAN. Evaluation of oral health-related quality of lifeamong Sudanese schoolchildren using Child-OIDPinventory. Health Qual Life Outcomes 2010;23:152.
3. Krisdapong S, Prasertsom P, Rattanarangsima K,Sheiham A. Sociodemographic differences in oralhealth-related quality of life related to dental cariesin thai school children. Community Dent Health2013;30:112–8.
4. Locker D. Deprivation and oral health: a review.Community Dent Oral Epidemiol 2000;28:161–9.
5. Watt RG. Emerging theories into the social determi-nants of health: implications for oral healthpromotion. Community Dent Oral Epidemiol2002;30:241–7.
6. Baelum V. Dentistry and population approaches forpreventing dental diseases. J Dent 2011;39(Suppl. 2):S9–19.
7. Gratrix D, Holloway P. Factors of deprivation associ-ated with dental caries in young children. Commu-nity Dent Health 1994;11:66–70.
10
Fontanini et al.

8. Amstutz R, Rozier G. Community risk indicatorsfor dental caries in young children: an ecologicstudy. Community Dent Oral Epidemiol 1995;23:129–37.
9. Peres MA, de Oliveira Latorre Mdo R, Sheiham A,Peres KG, Barros FC, Hernandez PG et al. Social andbiological early life influences on severity of dentalcaries in children aged 6 years. Community DentOral Epidemiol 2005;33:53–63.
10. Antunes JL, Peres MA, de Campos Mello TR, Wald-man EA. Multilevel assessment of determinants ofdental caries experience in Brazil. Community DentOral Epidemiol 2006;34:146–52.
11. WHO. A conceptual framework for action on thesocial determinants of health. World Health Organi-zation: Geneva; 2010.
12. Bowling A Measuring social networks and socialsupport. In: Bowling A, editor. Measuring health: areview of quality of life measurements scales, 2ndedn. Buckingham: Open University, 1997; 91–109.
13. Berkman LF, Kawachi I. Social epidemiology. NewYork: Oxford University Press, 2000.
14. Due P, Holstein B, Lund R, Modvig J, Avlund K.Social relations: network, support and relationalstrain. Soc Sci Med 1999;48:661–73.
15. Harter S, Waters P, Whitesell NR. Relational self-worth: differences in perceived worth as a personacross interpersonal contexts among Adolescents.Child Dev 1998;69:756–66.
16. Wentzel KR. Social relationships and motivation inmiddle school: the role of parents, teachers, andpeers. J Educ Psychol 1998;90:202–9.
17. Petersen PE, N€ortov B. General and dental health inrelation to life-style and social network activityamong 67-year-old Danes. Scand J Prim Health Care1989;7:225–30.
18. Hanson BS, Liedberg B, Owall B. Social network,social support and dental status in elderly Swedishmen. Community Dent Oral Epidemiol 1994;22:331–7.
19. Aida J, Hanibuchi T, Nakade M, Hirai H, Osaka K,Kondo K. The different effects of vertical social capi-tal and horizontal social capital on dental status: amultilevel analysis. Soc Sci Med 2009;69:512–8.
20. Aida J, Kuriyama S, Ohmori-Matsuda K, HozawaA, Osaka K, Tsuji I. The association betweenneighborhood social capital and self-reported den-tate status in elderly Japanese – The OhsakiCohort 2006 Study. Community Dent Oral Epi-demiol 2011;39:239–49.
21. Furuta M, Ekuni D, Takao S, Suzuki E, Morita M,Kawachi I. Social capital and self-rated oral healthamong young people. Community Dent Oral Epi-demiol 2012;40:97–104.
22. Sabbah W, Tsakos G, Chandola T, Newton T, Kaw-achi I, Sheiham A et al. The relationship betweensocial network, social support and periodontal dis-ease among older Americans. J Clin Periodontol2011;38:547–52.
23. Lamarca GA, Leal Mdo C, Leao AT, Sheiham A,Vettore MV. Oral health related quality of life inpregnant and post partum women in two social net-work domains; predominantly home-based and
work-based networks. Health Qual Life Outcomes2012;10:5.
24. Pattussi MP, Olinto MT, Hardy R, Sheiham A. Clini-cal, social and psychosocial factors associated withself-rated oral health in Brazilian adolescents. Com-munity Dent Oral Epidemiol 2007;35:377–86.
25. Bernab�e E, Stansfeld SA, Marcenes W. Roles of dif-ferent sources of social support on caries experienceand caries increment in adolescents of East London.Caries Res 2011;45:400–7.
26. Brasil. Minist�erio da Sa�ude/SAS. Projeto SB-Brasil2003: condic�~oes de sa�ude bucal da populac�~ao brasile-ira 2002-2003. Bras�ılia, DF: Minist�erio da Sa�ude; 2004.
27. Fleiss JL. Statistical Methods for rates and propor-tions. New York: John Wiley & Sons, 1981; 2.
28. World Health Organization. Oral health surveys – basicmethods. Geneva: World Health Organization, 1997.
29. Streeter CL, Franklin C. Defining and MeasuringSocial Support: guidelines for Social Work Practitio-ners. Res Soc Work Pract 1992;2:81–98.
30. Vaux A, Philips J, Holly L, Thompson B, Williams D,Stewart D. The social support appraisals (SSA) scale:studies of reliability and validity. Am J CommunityPsychol 1986;14:195–220.
31. Squassoni CE, Matsukura TS. Suporte Social:Adaptac�~ao Transcultural do Social SupportAppraisals e Desenvolvimento Socioemocional deCrianc�as e Adolescentes. Dissertac�~ao apresentada aoprograma de p�os-graduac�~ao em Educac�~ao Especialda Universidade Federal de S~ao Carlos – UFSCar,2009; P�ag. 211.
32. Berkman L, Syme S. Social networks, host resistanceand mortality: a nine year follow-up study of Ala-meda County residents. Am J Epidemiol1979;109:186–204.
33. Chor D, Griep R, Lopes C, Faerstein E. Medidas derede e apoio social no Estudo Pr�o-Sa�ude: pr�e-testes eestudo piloto. Cad Saude Publica 2001;17:887–96.
34. Victora CG, Huttly SR, Fuchs SC, Olinto MTA. Therole of conceptual frameworks in epidemiologicalanalysis: a hierarchical approach. Int J Epidemiol1997;26:224–7.
35. Kleinbaum DG. Epidemiologic research: principlesand quantitative methods. California: LifetimeLearning Publications, 1982.
36. Umberson D. Family status and health behaviors:social control as a dimension of social integration.J Health Soc Behav 1987;28:306.
37. Phongsavan P, Chey T, Bauman A, Brooks R, SiloveD. Social capital, socio-economic status and psycho-logical distress among Australian adults. Soc SciMed 2006;63:2546–61.
38. Sisson KL. Theoretical explanations for socialinequalities in oral health. Community Dent Oral Ep-idemiol 2007;35:81–8.
39. Berkman LS, Glass T. Social integration, social net-works, social support, and health. In: Marmot M,Wilkinson RG, editors. Social determinants of health.London, UK: Oxford University Press, 2006; 137–73.
40. McDowell I. Measuring health: a guide to ratingscales and questionnaires. New York: OxfordUniversity Press, 2006.
11
Social support, social network and caries





























