Embed Size (px)
Citation preview
State of CaliforniaOffice of Administrative Law
In re:California Health Benefit Exchange
Regu9atory Action:
Title 10, California Code of Regulations
Adopt sections: 6432Amend sections:Repeal sections:
NOTICE OF APPROVAL OF EMERGENCYREGULATORY ACTION
Government Code Sections 11346.1 and11349.6
OAL Matter Number: 2015-0603-02
OAL Matter Type: Emergency Readopt (EE)
This action re-adopts and amends the 2016 Standard Benefit Design, whichstandardizes the way health insurers design their health plans.
OAL approves this emergency regulatory action pursuant to sections 11346.1 and11349.6 of the Government Code.
This emergency regulatory action is effective on 6/15/2015 and will expire on 2/22/2017.The Certificate of Compliance for this action is due no later than 2/21/2017.
Date: June 15, 2015Mark StormSenior Attorney
For: DEBRA M. CORNEZDirector
Original: Peter LeeCopy: Andrea Rosen
STA'.'= OF CALIFORNIA—OFFICE OF ADMI RATI For use by Secretary of State onlyNOTICE PUBLICATI instructions on
reverse)
OAL FILE NOTICE FILE NUMBER REGULATORY ACTION NUMBER EMERGENCY NUMBERNUMBERS Z-
~ s-a 6 o3-oaEFor use by Office of Administrative Law (OAL) only
ENDORS~D -FILEDin the office of t#~e Secretary of State
of the State of Cal'rfomia~ ~
~~~~,~ ~~~~ ~, !JUN _15 201a
~~ ~~~~NOTICE REGULATIONS
AGENCY WITHRULEMAKINGAUTXORITY AGENCY FILE NUMBER (If any)California Health Benefit Exchange
A. PUBLICATION OF NOTItE (Complete for publication in Notice Register)1. SUBJECT OF NOTICE TITLES) ' FIRST SECTION AFFECTED 2. REQUESTED PUBLICATION DATE
3. NOTICE TYPE 4. AGENCY CONTACT PERSON TELEPHONE NUMBER FAX NUMBER (Optional)Notice re Proposed❑ Re ulator Action ❑ether
OAL USE ACTION ON PROPOSEDNOTICE NOTICE REGISTER NUMBER PUBLICATION DATE
ONLY ~ Approved as ❑ Approved as ~ Disapproved/Submitted Modified Withdr8wn
B. SUBMISSION OF REGULATIONS (Complete when submitting regulations)1a. SUBJECT OF REGULATIONS) 1b. ALL PREVIOUS RELATED OAL REGULATORY ACTION NUMBERS)2016 Standard Benefit Design 2015-0209-03E; 2015-0312-07 EE2. SPECIFY CALIFORNIA CODE OF REGULATIONSTITLE(5) AND SECTIONS) (Including title 26, if toxics related) -
SECTION(S)AFFECTED ADOPT
(List all section numbers) 6432
individually. Attach AMEND
additional sheet if needed.)TITLES)
10
3. TYPE OF FILING
Regular Rulemaking (Gov. ~ Certificate of Compliance: The agency officer named Emer enc Reado t (Gov.Code §11346) Q 9 y P ~ Changes Without Regulatorybelow certifies that this agency complied with the Code, §71346.1(h)) Effect (Cal. Code Regs., title❑ Resubmittal of disapproved or provisions of Gov. Code 4§11346.2-113473 either
1, §100)withdrawn nonemergency before the emergency regulation was adopted orfiling (Gov. Code §§113493, within the time period required by statute. ~ File &Print ~ Print Only11349.4)
Emergency (Gov. Code, ~ Resubmittal of disapproved or withdrawn ~ Other (Specify)§11346.1(b)) emergency filing (Gov. Code, 411346.1)
4. ALL BEGINNING AND ENDING DATES OF AVAILABILITY OF MODIFIED REGULATIONS AND/OR MATERIAL ADDED TO THE RULEMAKING FILE (Cal. Lode Regs. title 1, §44 and Gov. Code §11347.1)
5. EFFECTIVE DATE OF CHANGES (Gov. Code, 4§ 11343.4, 11346.1(d); Cal. Code Regs., title 1, §700 )Effective January 1, April 1, July 1, or X Effective on filing with §700 Changes Without EffectiveOctober 1 (Gov. Code §11343.4(a)) ~ Secretary of State ~ Regulatory Effect ~ other (Specify)
6. CHECK IF THESE REGULATIONS REQUIRE NOTICE TO, OR REVIEW, CONSULTATION, APPROVAL OR CONCURRENCE BY, ANOTHER AGENCY OR ENTITYDepartment of Finance (Form STD. 399) (SAM §6660) ~ Fair Political Practices Commission ~ State Fire Marshal
OF /~£NCY HEAD
JUN 1 5 2015NAME AND TITLE OF SIGNATORY V
Peter V. Lee, Executive Director ~e~ Qf (jCg ~ Ad1Y11111StfatlVe LaW
8• I certify that the attached copy of the regulations) is a true and correct copy For use by Office of Administrative Law (OAL) onlyof the regulations) identified on this form, that the information specified on this form ENppRSED APPROVEis true and ,and that I am the head of the agency taking this action,or a gn of the head~,f the agency, and am a~orized to make this certification.
STATE OF CALIFORNIA
NOTICE PUBLICATION/REGULATIONS SUBMISSION
STD. 400 (REV. 01-2013) (REVERSE)
INSTRUCTIONS FOR PUBLICATION OF NOTICE
AND SUBMISSION OF REGULATIONS
Use the form STD. 400 for submitting notices for publication and regulations for Office of Administrative Law (OAL) review.
ALL FILINGSEnter the name of the agency with the rulemaking authority and
agency's file number, if any.
NOTICESComplete Part A when submitting a notice to OAL for publica-
tion in the California Regulatory Notice Register. Submit two
(2) copies of the STD. 400 with four (4) copies of the notice
and, if a notice of proposed regulatory action, one copy each of
the complete text of the regulations and the statement of
reasons. Upon receipt of the notice, OAL will place a number in
the box mazked "Notice File Number." If the notice is approved,
OAL will return the STD. 400 with a copy of the notice and
will check "Approved as Submitted" or "Approved as
Modified." If the notice is disapproved or withdrawn, that will
also be indicated in the space marked "Action on Proposed
Notice." Please submit a new form STD. 400 when
resubmitting the notice.
REGULATIONSWhen submitting regulations to OAL for review, fill out-STD.
400, Part B. Use the form that was previously submitted with
the notice of proposed regulatory action which contains the
"Notice File Number" assigned, or, if a new STD. 400 is used,
please include the previously assigned number in the box
marked "Notice File Number." In filling out Part B, be sure to
complete the certification including the date signed, the title and
typed name of the signatory. The following must be submitted
when filing regulations: seven (7) copies of the regulations
with a copy of the STD. 400 attached to the front of each (one
copy must bear an original signature on the certification) and
the complete rulemaking file with index and sworn statement.
(See Gov. Code § 11347.3 for rulemaking file contents.)
RESUBMITTAL OF DISAPPROVED OR WITHDRAWN
REGULATIONSWhen resubmitting previously disapproved or withdrawn regu-
lations to OAL for review, use a new STD. 400 and fill out Part
B, including the signed certification. Enter the OAL file
numbers) of all previously disapproved or withdrawn filings in
the box marked "All Previous Related OAL Regulatory Action
Number(s)" (box lb. of Part B). Submit seven (7) copies of the
regulation to OAL with a copy of the STD. 400 attached to the
front of each (one copy must bear an original signature on the
certification). Be sure to include an index, sworn statement,
and (if returned to the agency) the complete rulemaking file.
(See Gov. Code §§ 11349.4 and 113473 for more specific
requirements.)
EMERGENCY REGULATIONS
Fill out only Part B, including the signed certification, and
submit seven (7) copies of the regulations with a copy of the
STD. 400 attached to the front of each (one copy must bear an
original signature on the certification). (See Gov. Code.
§ 11346.1 for other requirements.)
NOTICE FOLLOWING EMERGENCY ACTION
When submitting a notice of proposed regulatory action after an
emergency filing, use a new STD. 400 and complete Part A
and insert the OAL file numbers) for the original emergency
filings) in the box marked "All Previous Related OAL
Regulatory Action Number(s)" (box lb. of Part B). OAL will
return the STD. 400 with the notice upon approval or
disapproval. If the notice is disapproved, please fill out a new
form when resubmitting for publication.
CERTIFICATE OF COMPLIANCE
When filing the certificate of compliance for emergency regula-
tions, fill out Part B, including the signed certification, on the
form that was previously submitted with the notice. If a new
STD. 400 is used, fill in Part B including the signed
certification, and enter the previously assigned notice file
number in the boz mazked "Notice File Number" at the top of
the form. T'he materials indicated in these instructions for
"REGULATIONS" must also be submitted.
EMERGENCY REGULATIONS - READOPTION
When submitting previously approved emergency regulations
for readoprion, use a new STD. 400 and fill out Part B,
including the signed certification, and insert the OAL file
numbers) related to the original emergency filing in the box
marked "All Previous Related OAL Regulatory Action Number
(s)" (box lb. of Part B)..
CHANGES WITHOUT REGULATORY EFFECT
When submitting changes without regulatory effect pursuant to
California Code of Regulations, Title 1, section 100, complete
Part B, including marking the appropriate box in both B3. and
B.S.
ABBREVIATIONS .Cal. Code Regs. -California Code of Regulations
Gov. Code -Government Code
SAM -State Administrative Manual
For questions regarding this form or the procedure for filing notices or submitting regulations to OAL for review, please contact the
Office of Administrative Law Reference Attorney at (916) 323-6815.
Title 10, California Code of Regulations
Re-adopt Section 6432:
SECTION 6432: 2016 STANDARD BENEFIT PLAN DESIGNS
(a) For plan year and calendar year 2016, The California Health Benefit Exchangeadopts the Standard Benefit Plan Designs identified as the 2016 Standard BenefitPlan Designs dated '~^, ~~^, ''n ~n~ ~ Mav 21, 2015 which are incorporated byreference.
Authority: Government Code Section 100504
Reference: Government Code Sections 100503 and 100504(c); Health and Safety CodeSection 1366.6(e) and Insurance Code Section 10112.3(e)
2016 Standard Benefit Plan Designs
.► •. ~
Mav 21, 2015
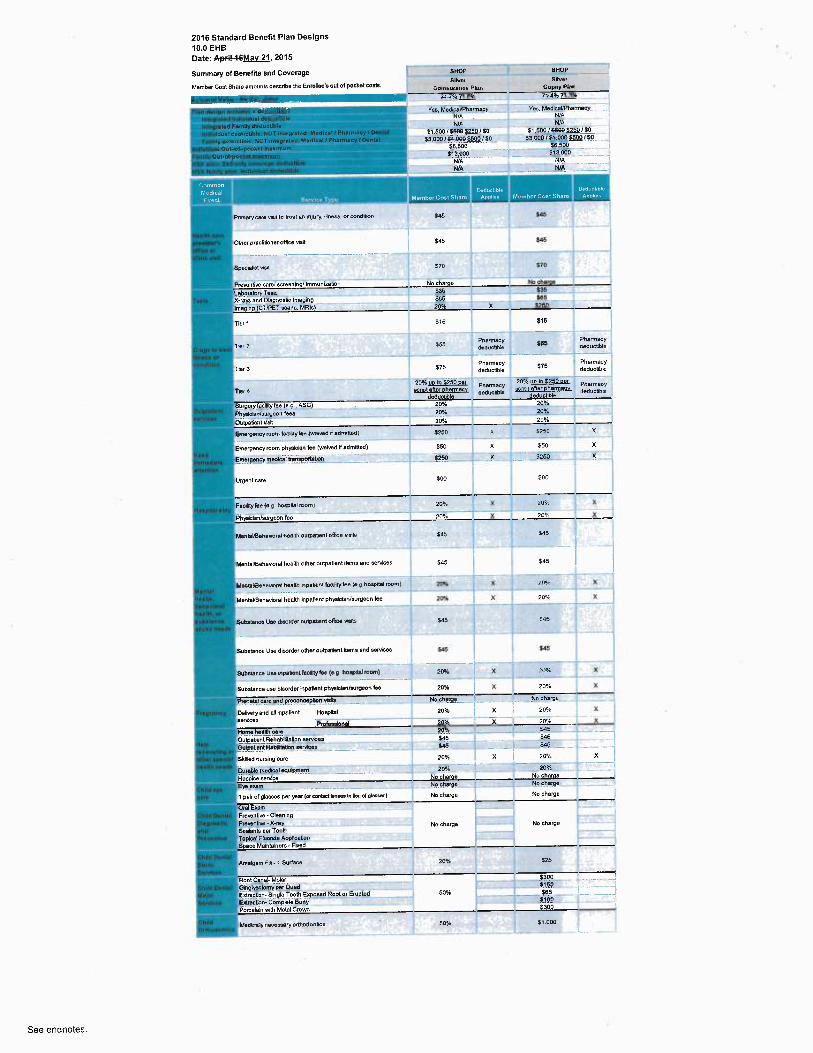
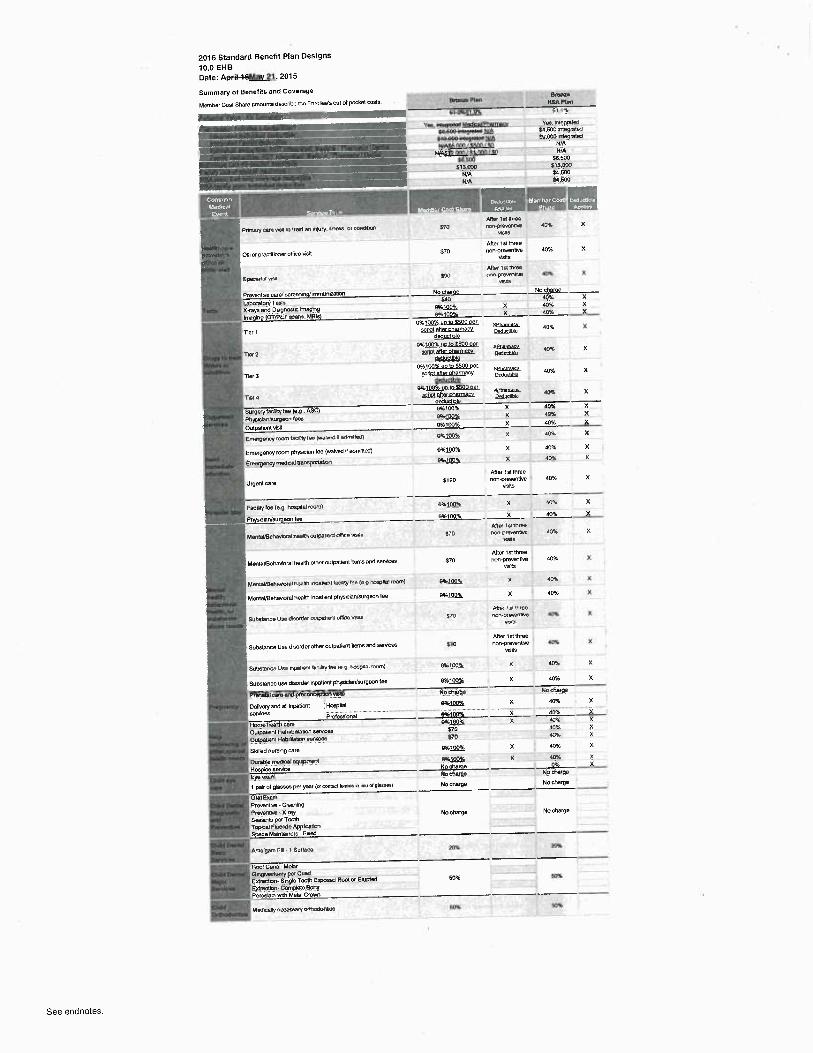
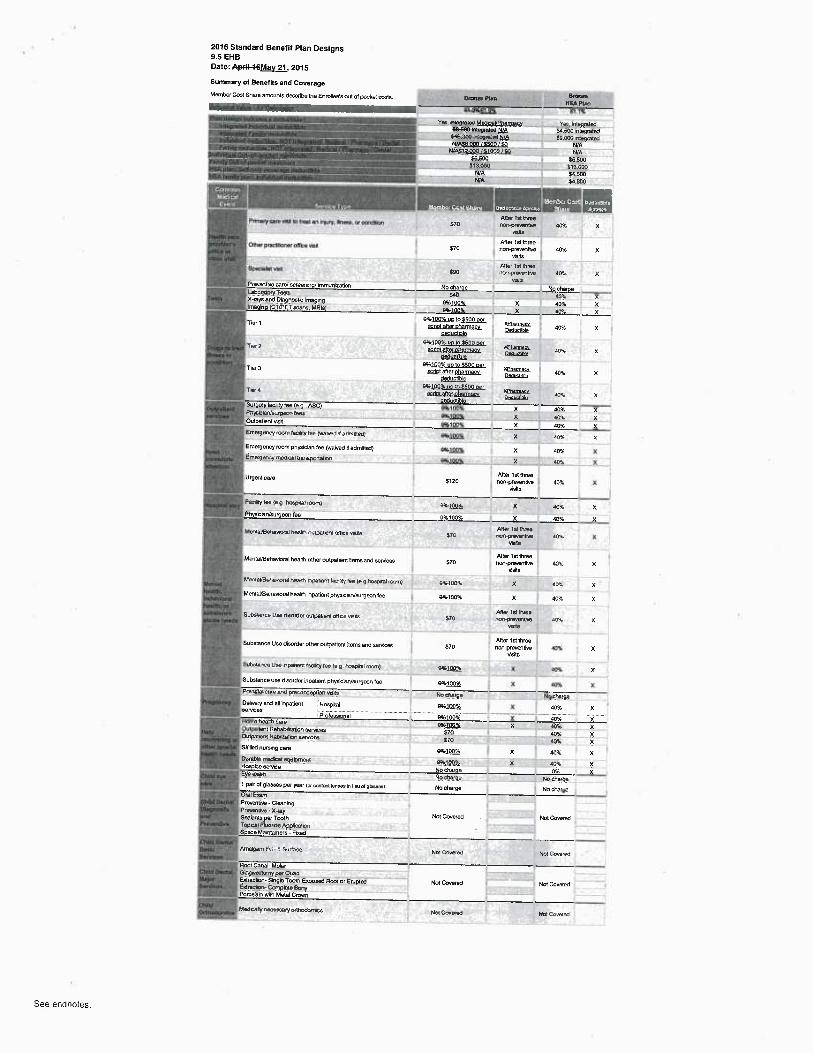
2016 Standard Benefit Plan Designs10.0 EHB
Date: AryFiNbMav 21, 2015
Summery of BenetRs and Coverage
Member Cost Share ertwunis tlasCriCe the EnmIIBe's wl of pocket Co51s.
~—
Prrreryoere vb1 b treat an Yqury. v~ese. or mntlibn
Other pra~.td'aner office Ysu
Speoal~l Mstl
1
Emwgary room taaury tee (wavee I admmxa)
Emergency room physiclar~ fee (warved'rf admMed)Emmgency medcainuwpona~wn
Ufgent care
FecEry fa (e.9. ~D~~ rooml
PMentknM~imwnnim
MemaVBahnwral nealp~ ouyetnnt attre vK~~
MenlaVBehavioralhaats other outpatient dams acid earvices b~ 420
MMteWMavnral prsW hC~enl lecXAY fae le.g ~oeptlel roam) 10% 5250 Der EaY Wto 6 Caye
Mentat~Hehaviorel ~eaM inpatient physbun/wrgeon tee 10% $40
buoemrke uae amorAe. anpetiem mrce vbtn S20 820
Substance Uaa d'~.sorder other wyalient flans end services
SuOstance Wse npatient WCJM1y lee (e g hmP~nt loom)
Substance use tlisortler iipalieM phys~kWsurgeon lee
Prana~m cai0 aM preconcaptbn vleAa
DeMery end all k~peGent !Hoapialaervicaz ................. ....._._.............
' ProfembnelHoma tieAMh damOutpatent RenebYnatron eeMcesOu~petrN Hebdlaton ~ervicm
Skilled nursng care
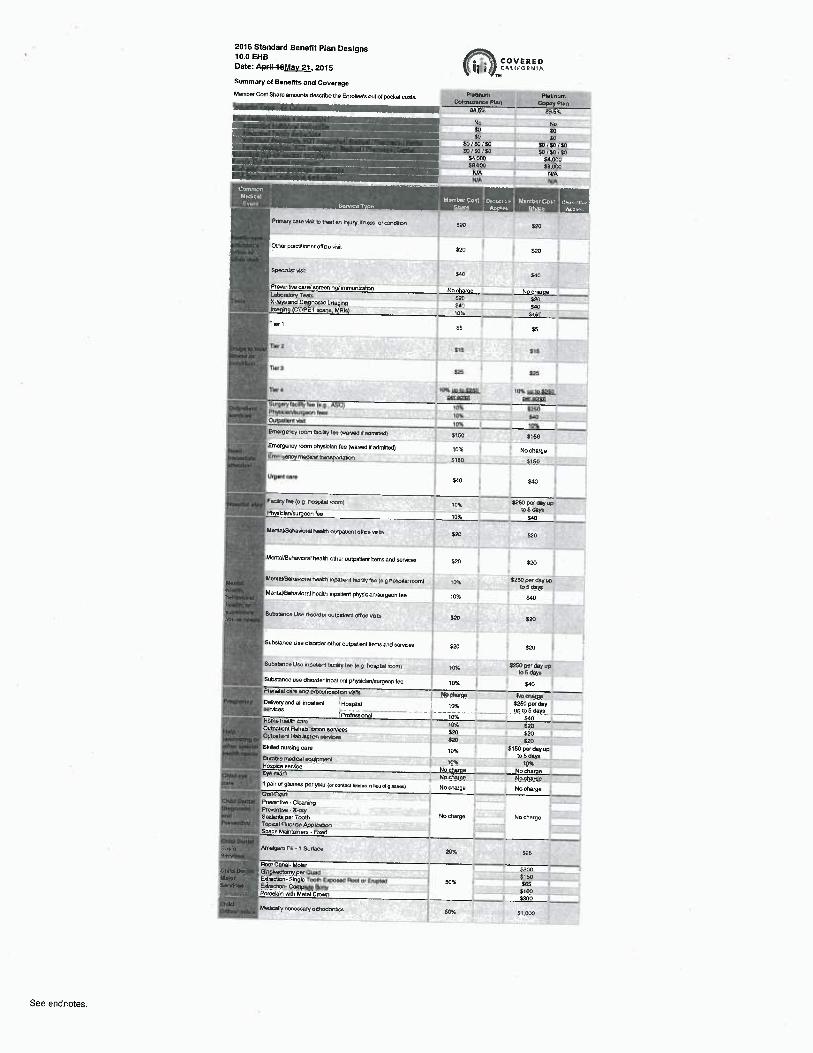
COVERED~~~+~ CAIiFGtR Nilt
Gl~tlnan WatlnumCdnsunna Plm Copry Vlm
B8 5'x 89.5%
No NoEo SOm ~
SO/E~/SO — .—_~ SO/SD/EOSO/SO/SO ~ f0/5{1l f054.000 .. _. J_.__.___._S<.00058.000 _~8~00Wn + WnWA .._.._......__.__..NIA
'~. Mwnbar Cost aa~rc~mro Namber Costsnso npm« stura nppnw
52~ E2o
F~ID
540 E<0
No cherae No charoe52b S~Sno Sao10% S4W
$5 $5
E15 516
$25 $25
7oaL w.~o szso tout ~oma25oQBL5Itl1
10% E25010% §~010% 10%
5150 5150
10% Na charge
St60 5150
54~ $4~
ion szs° °e` °ay ~°to 5 08ye
10% ¢IO
510 S20
52o S2o
tiox s2s~axmrwb6dey~
70% SW
No dm%fl.? ~P10% 5260 per day
....._......_._..... ._up Jo 5 dapn..10% ~40104: S20SZO S20420 E20~~ E150 per day up
to 6 tlaye109: ipK
No charge No tharaeNo chazpe No ehprpeNo charge No Che~get
Child OMtX ~Prerenfre-CleanngUMgna~~k . Piea~trve ~ %-ray
No charge No Margead Sealants per 7oM~P~rantlw Top~cel FluorW APplwtpn
_. Spsta Mab~lHners - FaetlCNkl Oontil 'oasis .mm~gem Fa-19urtece lox Say~+.vieyg~
Fool Cenel-Molar $,a00ChNd GYM/+ lomypm ~ue0 5150M~{or. EMracwn-~5hgle TaoN E~osetl Rorn or Eruptetl 50% 3659 E~aceom GanpMe Bmy FtsOFaroelart~ with Metal Grown E300--.x
CN1d Me0icalN nereesa~Y oMw4wNcaOAhakxr~+e~ Sow St.0a0
1 pair of glasses per year 1«coma knm n Geu a 9iasam)
See endnotes.
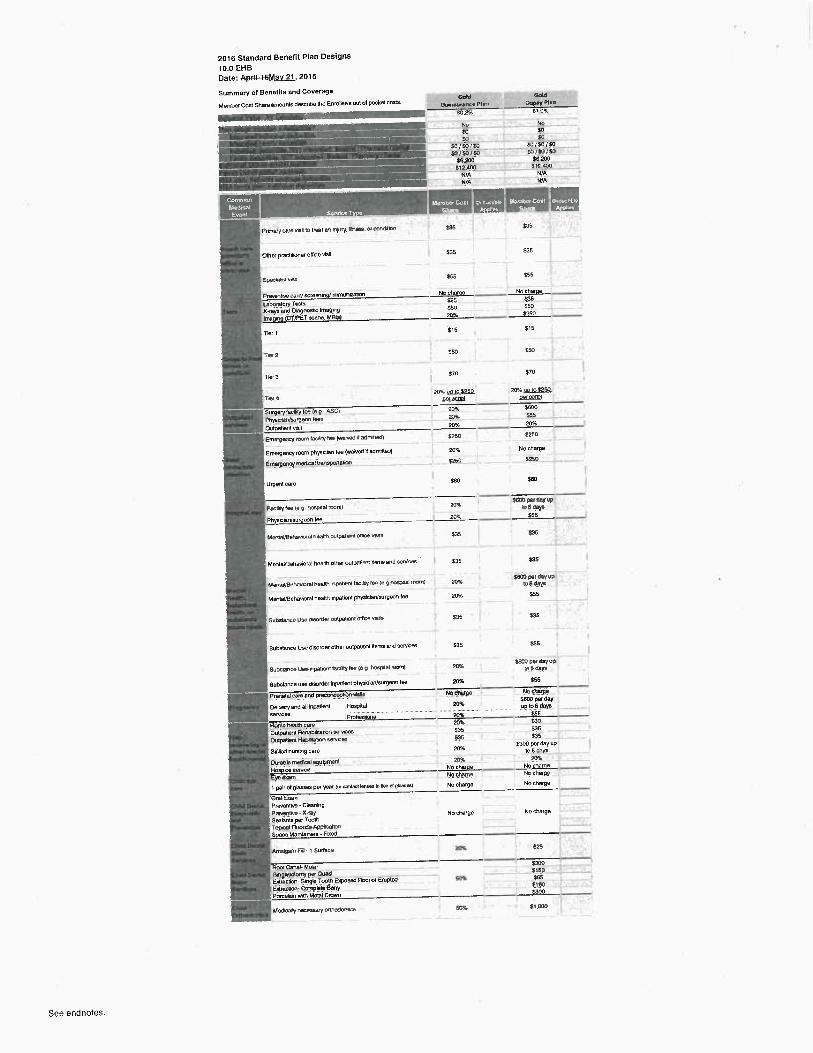
2076 Standard Benefit Plan Designs
10.0 EHB
Date: A~iI~6Mav 21, 2015
Summary of BenefNs and Coverage
Member Coral Share amoume tlescrlbe fie Enrollee's out of pocket costa. ~ ~~
Goinvane~P6n f:op~y Plv~
_. _. ,T~ B02% Bt 09c
No No
EO So
__ SO EO
SO/SO/Eo SO/S~/54
w~mr~ soiigisu
S6,2oo E6200
St4A00 i12.~o0
N!A N/A
dUA NIA
~-
yc. ~~~
Prt~uryfare vme b n ai an n~~ry. d+eay. a cone~m E35 b5
Other practAioner office Volt $35 535
Spectv6sl vae 566 E55
Pra+emte car~acreen~ngi enmun¢atan No eheroe No charoe
leboretoryTasb S35 §35
%-raya end Deyrwstc imagng SSo Aso
hrogng (CT/PET e~ene. MRI~ 2pA E250
Tief 1 S15 515
Tsar 2 E50 E~0
T1M 3 570 570
Tea 2M. uo m525o 20%w10 S25L
➢ffi.6~ PHL~3GI
Surgery(acPry tee (e q.. nSC) 40% Shoo
P~yaCOrVeurgeOn l¢9e pq~ E55
Outpatient eitit 20% 20%
Emerperwy noun IaC~Gly fee (warvatl 1 atlmmetl~ E26U E250
Emergency room physlclen fee (warveC M etlmMled) ZO% No charge
EmerBerwy medralirenaponetan ;250 f25o
Urgent care Sfi0 $60
-
Facity Iea la e rasoaa~ mom) M+s
E600 ~ ~vwb 5 Eaye
Phye'c'arJsu~geon fee 20% E55
MaVnyBeMKxelM1w~n wipeteM OMae vkte bJ5 E3b
Men~aVBehavioral healUi other outpa~lent Mems arM services X35 S35
4ernelrt3enawre~neeM npamnc faculY tar (n9 nmpea~r~.vn1 Zp9',
S6~OOatEryYpIo6Aey~
MemaVBahavbral healU~ npa~lem physklaMeurgeon lee 20% 555
SuOsiance Use Oreo~der wlpetwH aMcn Nsae y35 S35
Substance Use disorder other ouq~slian Hems end services
SuEsmnca Uee npannrrt iaciery iee (e q. losyaai roan!
Substance used'~sorder npatienl phyeiciuUwrgean Ice
Prenatal care aM ptetoneepticn NW
De@,ery arM all inpetlent Hoepilal
Ou1pm4M FeheOtlrtabon aervces
Oulpetien~ Hadmalun aervcm
Sk1AeO nunhg care
1 pairof glazaes par year (or c«um~ b~ h neu w g~m~
Orel EmmPre/enlNe - ClBerlhp
PreapM • X-taySealanm per ToothTopwl Fluwda AppNitbn
Soece Mantaners - FueO
M1YIppn F➢ ~ 1 S~rtece
NeObeBy neceaeery ortnodont~
Roof or En~ptetl
S35 E35
~ E600per tleyWro 8 tleya
20% ¢56
No j~ No Uwrp_e
20% S~ ~ ~Y........................._...
...up to 5 daYs.. ....._......._.
20% ....................
E55
2091 q0
y35 S35
E3b .Zia...̀
~ 5300 P~ ~Y ~Pto 5 days
10`K 207L
No charoe No cAarae
N.4nn ~aa
No charge No dmrpe
No charge No charge
209: E25
5300j160
50'K S85f1805300
sax si.aoo
See endnotes.
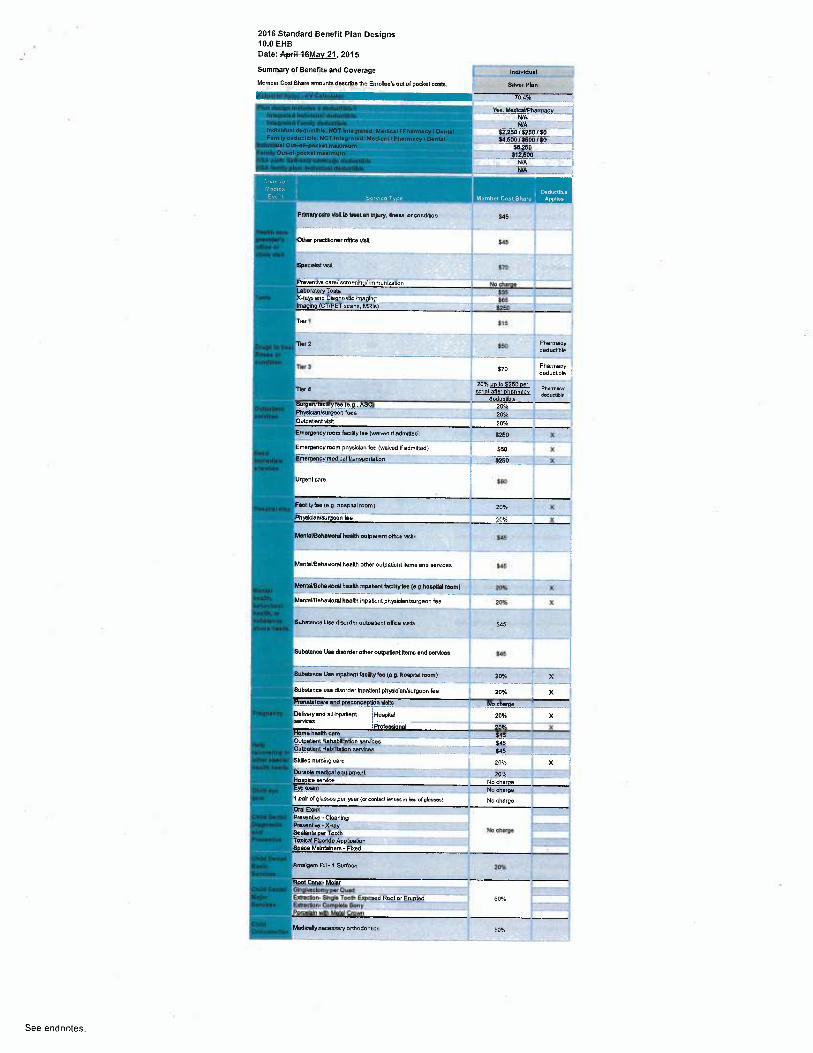
2016 Standard Benefit Plan Designs10.0 EHBDate: Apr+l-3&Mav 21.2015
Summary of Benefits and Coverage ~narvmuaiMamber Post Share amounts describe the Enrollee's oW of Dockel coats. SUv.r Plan
'AcWariel Valua • AV Calculator X0.4
Phn drlpn Mcludr ~ C~dudlAl~i [ Yea. MedkaYPharmaey.InYOnNdlndirWud dWuel6M WA
._..—_
In1~p~Yd Fancy MduN3M N!AMdWkual tNduelMM. NOT h~Ypal $2.250 / 3250! $0. __ .
sa.soo ~ uoo i so-- - — . _se,zso
-----aiz;s`oo — —_ _
.— WA—_. _____._'_
Nn~ry can NNlb Usot an lnJury. ilnean. orwndRbn S45
Iher D~~~~er oflke Nett $qg
»awscwsn --- - -- - - a~
s~ronMro ur./wroanlny Mmunmtion ~..-'- --- No eh~rae ~--~~— ;iboMonTwb 535nYs and D40nostk Im~Oha -'
—_ _ _ __..- ~ -
Tbr 1 $75
TNr2 - ~ 55G P~ermacydetlucLbk
Tbr 3 ~ $~~ Pharmacyaea~~uma
20% uo to 5250 oe~ P~~y7bl< ecrl0l eflef DhertneCV ~uceble
deductlbleurperytac0ity fee (e.g., ASC) 20%
Phyaicbnhurgean fees 20%ouaa~~~ ~ zo r.Emergency room feality fee (waiwa dadmilted) 5250 X
Emergency room physician fee (wei~,ed Hedmitled) $50 X
Emergency medkal transportation y250 X
Ufgenl wre $80
Factlttytee (e g nospiwi room> 20°ro X ~
Ph IcieNsurgeon fee 20% X
Menl9WeheNorel hanitn oulpalrent oflwe Nsits ; 54'. j `
"' _ "_~" __ _ ~'_ ___ 1
MenteVBehavioralhaalth other outpatient Rems and aeMcea ~ sq6
Mente4BlhBNotelhMMe~pa6Mf1fiG4gke (e.g hoapil8l room) 20%
Manlel/BeheNorel healtl~ k~patienl Dhyslclan/surgeon fee _—~ 20Yo X
Sueslenca use tlisordai oubatnni office was yq5
Subelance Uae dleorder otlia oulpNMnl items and eerNces , T g45
8ubat~~~ce Uae npaGem feclAtyfee (a.p. hospRel room) 70 i~ X'__ _ . _ _ .__.. _ .._'—_'—iSubetence use disorder InDaUenl Dhyswianlaurgaon (ee 20 % X
' Renetel care erM preconcepWn wXa Na charge i
Delivery end all inpetbnl ',Hospital 20% X a
Profemional ZO% XHome haeMh care yM.__ _ _..Ou~atlent Rehebllitetlon eerNces -- ..- - - --~ - - ~—Ou etlent Hebi9leWnearvices
~ .____J~ ..
Skilled nunlnq taro 10Ne ~ X ~
Durabb medfcalaqugment .yps5. _.H ke eervke No chugs
cram .. Nc ch!!➢e1 Deir of glassa9 per ye9r (a wnlect bnnec In Irou ci pinasa) No charge
Off ExamPrewntiva - CleenmgPrevenUw - Xtey
No chargeSealants per ToothTopkal FWoride ApplicationSDate Maintainers - FU(ed
Amegem Fni- t Surface 20°r~
Root Cana4 Molaromvt~~wmvv~,owa __
-.
6Ereclion-Single Toots F~ossd Root or Erupted 50Enaction- Compble Bony ._._.Porcelain with Melel Crown
Med~elly necessary annodonUcs 50 r~
See endnotes.
2016 Standard Benefit Plan Designs
10.0 EHB
Date: ApriF~6M6 av 21, 2015
Summary o1 Benefits and Coverage - sHov eHOP
Member Coat Shere amounts deactlbe the Enrollee's oul of pocket cosU. S~h'°r 9INs.
Cmnsunnw PVn Gopay PWn
ita95 18 71.4% 1 3°,
Yes, MadwaVPharmee~ Yes. Medica~/PhertnecyWA N/A
WA N!A
_ 51,500/i69G~,¢Q./50 $1,60o /8608 ~Q/$0
S9,000 I~S;000_/SO E3,000 /iiA9B~~lSO
SE 500 56,500 ,~"_
119000 ~ ~ 513,000 _
µA ~~1
Prvnerycere ywt m vmt en ~n~ury. wneae. or cantlnan S45 E45
Other precOUonor office visll $45 S45
8pecrelut Han E)0 h0
Pre~enuw care/careening/Immunization No charge No chnce
Laboratory Testu S35 _. __~_
X-rays antl Dlagnostic Ime9~~G S85 505 _
Tbr'I E15 516
Pnartnecy _-' _'_ PharmacyTiv2 Su deaucUbb ~ dedutllbb
Pharmacy ~ ~ -". _J..-_' PharmacyTbr3 $75 daductl6b $75 deductible
20% VD b $250 oe~ P~~~Y 20°k UD to $250 oBt pM1B~~y
71er4 ecnot after oharmacr deaucubb ~^o~efler ohartnacv daductlEM
deducWle deductible
urpery ecniy ea (e.e., c zoi zoi
Phyablen/Nryfon fees 20% iov
Ou~atienl Nall 20% 20%
Emergency room lxiNy/ae (waiwtlrf Amrtbd) 5450 k E250 X
Emerg cy room physlclen fee (wai d NedmHletl) $50 X $50 X
~Em rp cy medical trenaportatbn ~ ~ ~ $250 X $250 X
Urgent care ~ iB0 SBO
FeCYltyhe (e9 hoapll8~room) $~ x 10°i. K i
Phyaklen/au eon fee 20% X 20 % X
MenbUBsheonrN heats oumaLent oftws vane 645 bt5
MenteVBehavioralhealth other outpatianl Ilems end eaMus ~ Sq5 ~ $45 '
MM~LVBe~evp~el heats mDet~eni faaltty tea (e p Ii44lpW 100111) _— IIpj _— —X.."" "~— 70Wi X ~
MentalrBeheNoral heeMh Inpatient physician/surgeon he 20% X 20 % X
SubNp~u Ua AMONarouWauem ott~ce teats ~y 8a5
Substance Uee disorder other outpatient Items and aervkes J s0.5 ~ $45
SuDNanw Use hpa6enl bolAlyfer (a p noapnei room) ~-~ pOM _~ 20°/. ̀ X
Subatanu use disorder hp~tlenl physklan/aurgaon ise p 20% % 20% X
Prenelel care antl D!~?~~n Mite No charge. •._ Fb~ ..._ _ __ _ _
DeNery end ell inpatlent ;Hoapilel 20% X ZOS4 _1 X
Profesaionel 20'h X ZO X
Home hearth care _._. _ .__ ___.-' .. ZOX__~._ _. __ _ _-.~._.___
OutpeOenl RehabAttebon eerNces S45 _ ~ S06 _ _ _
Ou~i~Benl HabWtemn aeMcea _ ~ _ _ ._ _ ~ -_ _ _. .. ~--_..
SkMed nureing care 2055 K 20% X~
CirtWkmadkal e9 P ant _. _'__ _. _ _2QK - 2~'_.. __. __'__i
l pelr o(plaeeea Der year (oremi.eebmes Mibu a(pVsms) No ehupe No charge
Oral ExamPreventive - CbaningPreventive - %+aY No oharps No charge -SealanLs Der Tooth ~~ ~ —
TopkelFWondeApppcatlonSpace Melntainers -Fixed
Amalgam F~0 - 1 SuAace 20%. E25
Root Cane4 Molar $300 __ ___~
QN,piveclamy Der hued $~ 50 _ '—_
EzUactlon-Singk Taolh E~osad Root or Erupted 50% $85_. ..
ErtraelbM Compbte Bony 5180
Porcekin wits Metal Crown $300
MedmeAy neaeeseryoMadontice 60•h 57.000
See endnotes
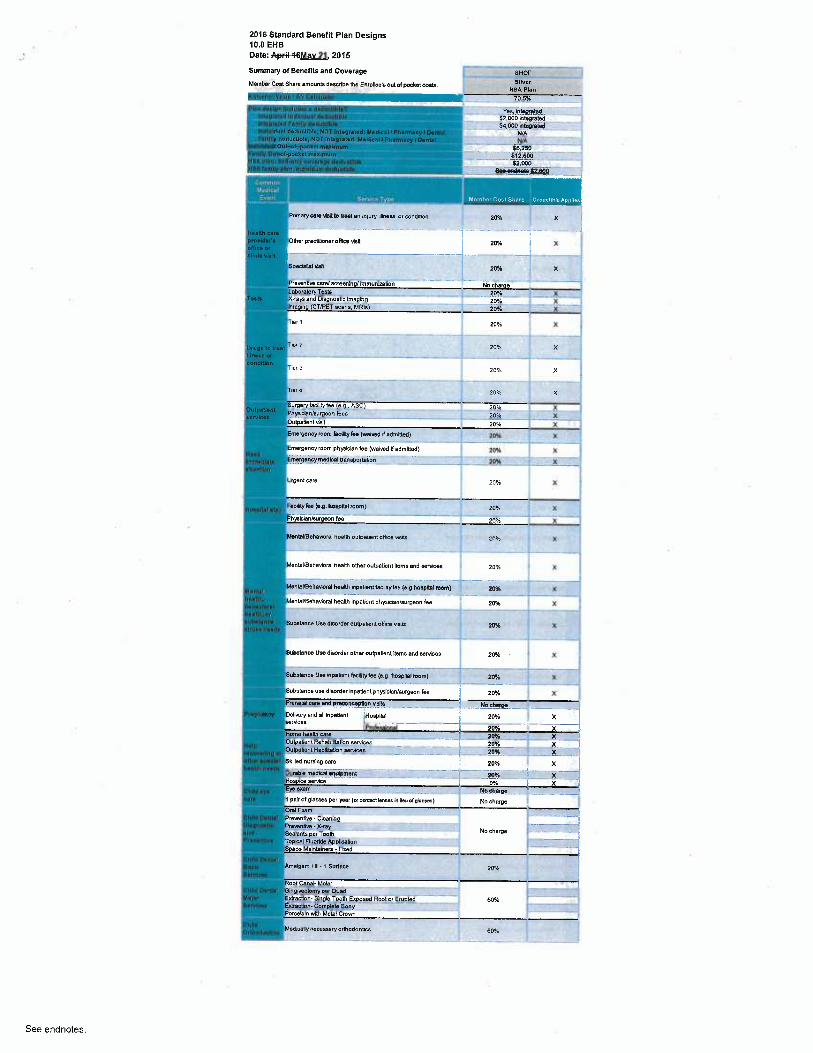
2016 Standard Benefit Plan Designs10.0 EHBDate: AryFrl-46Mav 21.2015
Summary of eeneflts and Coverage SHOP
Member Cost Share amounts describe the Fnroiina's out of pocket coats. 81~a~ X9A PknActuarial Value -AV Cnlculawr ..s̀ue. 70.5%
{'Inn das lgn Includun o deductil~bl _ Yee, integratedIntop~afocl lntlividual doductlhla SY,000 Integratedin1oB~~~o4 Fnmlly tleductlbN $4,000IntegratedIndNtdunl doAuctible, NDT InNO~~Nd: M~tliccl I P~amuryl W nlal WAfamily doductlbb, NOT Inl~pr+tad: Medical/PAumary l0~ = WA
1-pocket rtwlmum y8,2S0i'amlly Ouhof~pockel m~xlmum 612,600HSA Inn: SoNronl ---'--.--_~..~....- ..p ycovmm{p deductible §$,000IISA family glen: Individual doduc~ible ~ V_szeoo____ _
- -.~_s. ~Pnmary care ~.rett to veal en injury, Jlneas or condroon p0°h X
Ha~Nh urnprorN~Is Other practitioner oNwe Nsi[ 20% i XoHic~ orcn~m van ------- -- -
soec~,i~st vise zox x
Praventiee carol aersenln lhnmuntratlon WWuLaboreto Teete_ ___ _. 20%_ _ _._ %
1~sb Xrays anU Diepnaatlo Imaging _~ 20Yo -:.__'_. _X _....__~
Ima9in9 (CT/PET 0G6ne, MRIs "'-- '- ' '-'-. _.20% X
Trer ~ 20% _. X
upa l0 4•M T~~ ? 20% Xn~~t a _ _'_"_. _____'
Tbr 3 ppg; J(
Tbr a ppSS x
utP~ _ urperyfactity ..e s.q.. ASC) _ _ ___- -.. ?~..._.__ _- X-PhyeblerJwrpsonfan 20% X Jrvlo~c __ __.._'____ _ ..__.._. _____~._~;,o~b.ue~iwsa zoss xEmergency mom iao9ltyfee (xrolved H~dmlged) ppy. X ~~
Emergency room Dhyslclan fee (waked tl edmttted) ppg5 { X
Imm~dl~t• Emergency mad~cel bansporfatlon _ ___~~ > ~(rllenflon
UrBenl care 20% X '.
/IwPiut~uy faaliryfee (o.g ~oepnal room) ppq: X
MantaVBenevarel neanh ouWa~entoMce u~ens ZO% ; X
a Men4UBehavbnl health other outpatient uems end saMces ~~ p~ 1 xf
Montal ~~°h°Nonl health npatiantfacnnylae ~e.g.hosplld room) 2M,~ _~
ho.lth, MenlaVBehavbral heahh Inpatient physkian/swgaon lee pp?5 7(boh~vlor~l ~ ~ha~Hh,oa uhatanea Subefence Usn disortler outpalrenl oHre Nsils jQ~g X,n~~F~ ~..a.
SuWt~rrce UaedWrder otlier oulpelbnt l0ema and aeMcas I ypy ~ X
9ubelance Uae MpatlencficAttylae (eg hoapnel room) ~ _ ppy. _ --_X -~
Substance uae disorder lnpatlenl DhyslclaNsurgeon fee pp!5 X
Preneletum and prsoorw~e¢6on vlNls __No ah_atge__'_~' ____. _-.Pnpn~ncy Delivery end all MDaUent ~Hoepllel 20% ~ X
eeMcas —_. _... _-___-'-__"-_Pmkatlonal 20% X
Home heetlh care ppg5 X
Haig Outpetlanl Rehebliiletbn aeMcas 20% ..._....7(___'. .. _
rocovetlnp or Outpellent Habilnatbn eervices 20% __. X
other ~p~clal Skilled nuraing care 20% Xhealth n~~d~
Durabb medical equlpmmt 20°!o XHospice service . .... 0% X
Child eye Eye exam No chargeears ipelr of glasaea per ye9r(a eanbet bnaea in lle~Mpiesaes) No charge
Olel ExamCniM Dental Pmwn6~e-CleaningUiapno~lk PrownUw-X~raY
No charge ~ -'~'•ntl Sealants per ToothPnvanura ToDkal Fluoride Appllcetlon
Space Mainteinen • Fbcetl
C hlld Don41Q~~It Amalgam FBI. 1 SuAace 20%Sorvlc~~
Root Canal- MokrChIIA Denial GlnQiwCWmyper Cued . _. ..MnJw Ebrection-Single Toots E~oaetl Rool or 6u~ted_ _ _ 50%Seniors 6erection-ComDbte Bony - ~ `- --~-~-' -~~ 1
Porcelain vAth Metal Crovm -.~..-.. __. _ '~
Ghlld MedweM neeessBry aMotlonLcs ypSSo~u~odo~ua
See endnotes.
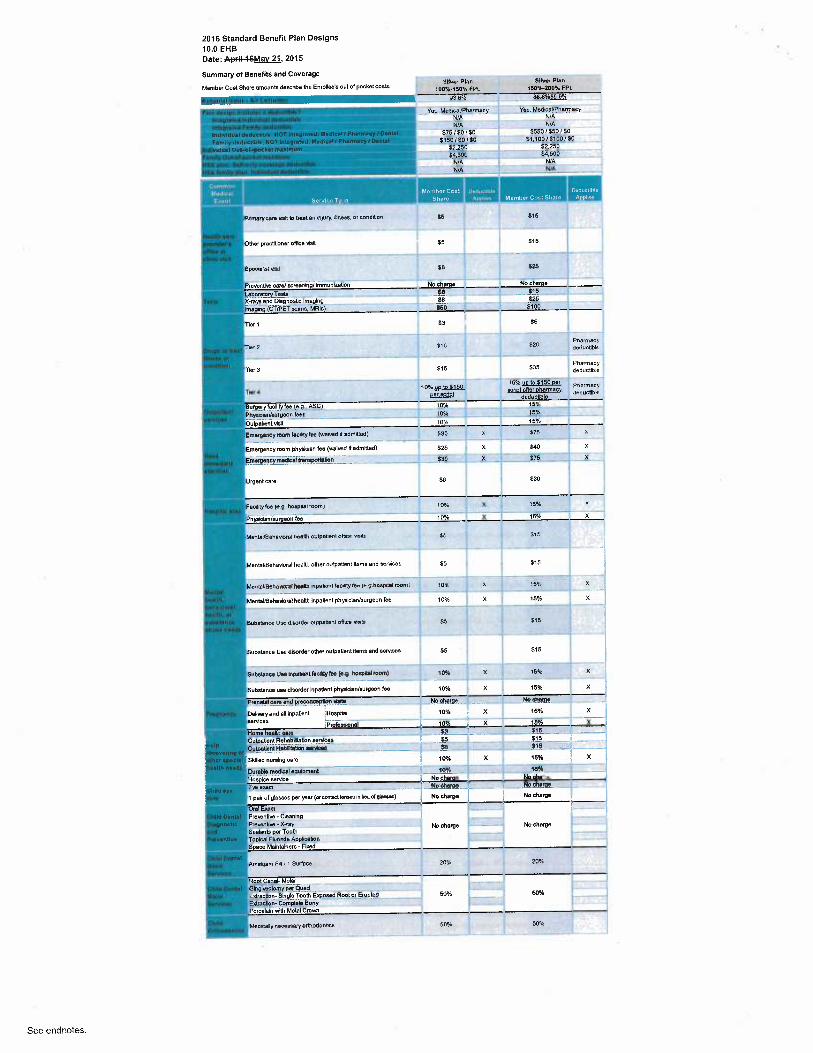
2076 Standard Benefit Plan Designs
10.0 EHBDate: A6Mav 27.2015
Summary of BenefRs and Coverage
Member Casl Shere amounk dexribe the Enrolbe's oul of pocket coats. 91w" ~~°~
8~iwr Plan
100°/x'150%FPl 160%~2009b FPL
83.8% 88-8%~e B°~
Vm AAetlleaVPhNnacy Yec, Medical/PhartnetyWA _ N/A
WA N/A$75 /E0 /SO 5550/$50/SO
$160150 /SO S'I,t00/$100/50
52.250 52,250
¢1,500 54.500
'-"'IJ/A N/A
--~- WA WA
Member Cost pad~~ctihle Dwluctinle
Share Ann~~es Memher Cost Share_ anr~~>s
Pnmary care Nsn ro treat an mryry. ~li~eaa. or conOroon ~5 S~ 6
OtherprectMlonar oHka Wit $5 E15
SPsw4~ wa ~ i8 _
_ _ __tt6 _ - _ _~_ __
P~ewntNe can/ecresnin /Ynmuntratlan —N-o a~he~°~ No dome
k.ab~T~sta _ _~^ __ . - - _.. _ t1d _.__~_ _.
X-reys end Diaenoatb ImNInO_ ...SB _ _. ( _ y25_. _ _
ImaOinp (CT/PET scene, MRIs) f60 5100
Tler 1 Z3 SSi
Tr2 t70 E20 ~a~~y—.. "_ _~--~ - _-_ deductb4
Tiara E15 535 Pharmacydeductible
15%uc io~sl5o ner
Tb.a ~ ce~xMnt - wnot afrer harmacv de0uctlbbdaductlble
Surgery acllity ee (e.p., ASC) 10°k 15%,.. __Phyafcian/surgeon tees 10°k 1551_.. _o~beu~~~ ~n ~ o i ~ s
Emerpenay room 6coryM(xanee asammetl) Eso z a7s x
EmarpencY~m phydcien fea (vrelvad Hadmltted) y25 X 540 X
Emerpenoymedkeltnneporfatlon $30 X E75 %
Urgent care $6 $30
Fac~IM1y tee (ep hoag181 loom) SOW. X 15H~ K
Phynklen/wrpeon tee 70% X 75% X
MsnlWBehawral hseXh outpaWnl ofliw aetls &. Si5
MenhVBeheNorel health otl~er outpatient ttems and services g5 515
MenuYBeMvw~e~ neah/~ inoxire~t hcartytoe (e v hoapnel moml 10~ x 'S9~ X
MentaVBehavioral health lnpatlent physkNn/surgeon fee 10% X 75°/< X
Subelence Uce duoedm outnmm~l ofice N~ S5 E15
Substance Use disorder other aulpelienl llama and eeMcea $5 $15
_—_'_ "_~
Substance Use fnpaSenlhaMytr (~.p hogNal room) to% X i54~ X `
Subetence use dlsorJer lnpatiant phyekkn/surgeon lee 70% X 15%
Prenatal care and preconq~tbn +lake No charge No charge
DaNvery anO eA inpatlant HosD~l 70% X 15% X
~~e IProfesslonal 10% X 15% %
Home health taro _S3 _E75___ i-
N'~P ~ Outpatient RehabNiletbn sarrices $5 S15 _
Outpatient HebAibLon serncea __ 5.', _~16 _
Skilled nureing care 10% X 16% X
Durabb medkal equipment _'____'______ 1a% 16%..
Ho ka eefYfte No charge No cherpe
E~ exam ,._ . __ _ _~ ____ "_ __ _. .., No charge No charge
1 pa4 of glasses per year (a cai0w~bna«In hualpWas) No charge No charge
Orol EwmPreventive-Cbanlnp .. __
~`~~'X'~Y No charge No charge lSealants per Tooth t'" '" " -
ToDkal FluoMe APGAcetion ~
S acs Mainfalnars-FLred _~
Amalgam FYI. t Surlece 20%~ 2U°.~
Root CeneF MoWrOingiveclomy Oer Quad `
6ctrection-Single Taolh E~osed Rool or EruO~. 50% 50% S
F~ctrectwn- Compbb BonyPorcelain with Metal Crown
Meawairy neceasaN oMotlonnce 60% 50%
See endnotes.
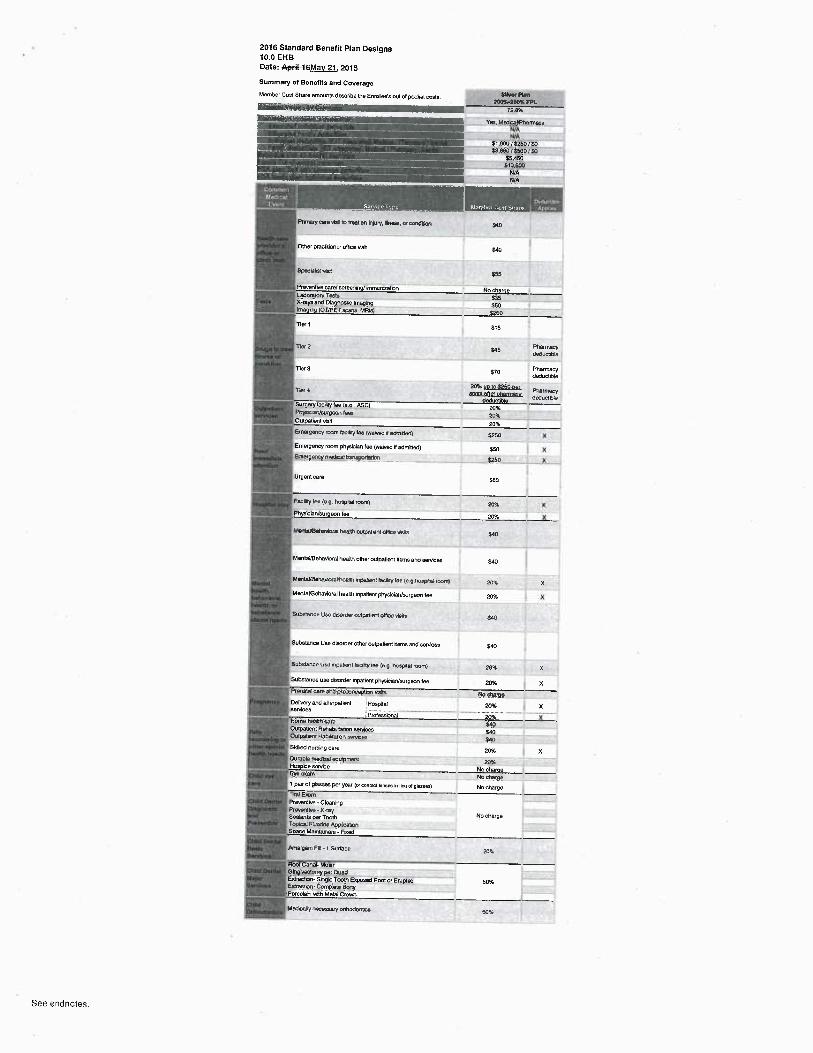
2016 Standard Benefit Plan Designs10.0 EHBDate: A~r~H6Mav 27.2015
Summary of Benefits and CoverageMertbar Cost Sara emairtls tleacrbe tl» EnmAae's an of pmke~ wets. ~~` ~nt00T.-p609: FPL
l2 8'k
Vm~ Meticat~Pne~macyN/A
- tdlAE1.900 / 5250 / 5053.80015bU0/SO
55.450510,90DN/AN/A
Prmary me vbI b VaBI en Yyu~•. Iheae. a Gmtltbn j40
ONer pracYfwnar once visit $CO
bpechlet vka 355
PreeMive carN acraening/ Ynmun¢ation No chargeLabora~ory Tds S35X-2ytl entl DO~nosuC Ime¢X1g $50Imnghg (C7}P~'f Beane. Mqb) 5250
Tier 1 $16
Tier2 ¢75 ~~~~~am~,c~ae
Tler3 S70 Pharmacydedudble
zoo ~o ioseso-nee ~~,71ara ~rtn after ol~ermacv tleduGNe
P~yscarJsurgeon feae 20%Outpetbnl vstl 20%
Emer9a~tY room lao~My lee M'arvaClaEmfleN 5250 %
Emergency room physblan fee (waNed'R adminetl) $5p XEmOrgaity medcat UanSppnalpn §260 %
UIQeM care $BO
Feclly len (a.9 ~Prtal+oom) 20% %PhysceNsurgeon fea 20% %
MentaYBeMw~ai MaM wq~nt'nnt once vNs ¢7p
MentaVBeheviorel headh other outpafrent hems and eer~es $cp
MenlBbBeheuwgl he9M npat6nt feclNy lee (e g MBp1181 room) 20'4 X
MentayBehaVioral heeM inpa~ienl physiciarJwrgeonfae 20% X
SuOetence Use tlmrder wlpetieM dhv vbb Sao
Substance Uae tlisoNer other outpetientXans arM services $ea
bLbstancn Use npat~t tauM1ry Me (e g hosPeal mom) 20% %
Substance use tlisortler hpe~iant physicien/argeon tee 20% XPrenetaltare YM ptecoi~cePtion vlvEs No thargeDelNery end all Mpeflent Ho6pLel 20% XmMcea _..... ........__._ .. .. ....._.. .........P ofassional ~20% %HomaM1a tlF Dare $WON~at4n1 RBhabJ~a~on aemc~ $6pOuipelc~n McDtlletun nemctr gqp.. _ _.Skilletl nuraMig care 20% XDuraOr maor.~ equpmery zacHoapbe service No chargeEye e+iam No, dvrpg1 pair at gla65e5 per year («worst braes h lieu d glraea) No ehargeoyPreenfhe -Cleaning
P~~~~ ~ X~~ No chargeSeaW~ffi per Tooth
F0-1 &uAece 20A
Egwseo Root or ErupleO 50%
IAadcaAY tgewsary onFroEontles 60Y.
See endnotes.
2016 Standard Benefit Plan Designs
10.0 EHB
Date: A~~iHSMav 2t, 2075
Summary of Benefits and Coverage
Member Coal Share anrounls tlexrWe lie Enmlleo's out of pocket Coals. Bm~Plan ~~~~
HfiA P{wl
~ 911&
.• vw, ~Megrele9Y vee. rnegrate0
f~ 54.500 ritegmtetl
Cs3.BBB~Megroled.~ E8.000 tHeg~eted
N//1~y~{q / E500 / Eo NIA
NN SY2000 l~~)OOOISO NfA
Es.Soo ..... _ 56.500
(13.000 :18:000
WA '. . _ - 54.500
WA E4~500
~-.. ~AR9~ la N2a
Prmary taa waE b Deal an ryury. Mew. or mEuon $70 nonyt YllM1a <0# X
~E6a
Afler isl Mree
Other prectkbner oR eHsil $70 rwn-pre.9ntA9 40% X
veils
Alter iq Nree
S4eeel~v~m E90 mn9~e~Me a0Y %
~+ane
Pre~enlve cerN ecreenn4/mmun¢alon No charne No c~erae
Labo~aloryTmts S~ 'a?~ K
X-gays erM~D'mg~wstic unegnq ev6100w, x ao9c X
I.meB4B ~T~PET acBM, MAi6) Bb700% X 40 A', %
B%100% uo is 5500 oer
r r i scr:>~ en~r onar~,~~ ' aox x
mua
ew~oo~, uo ro ssoo oar ~,~ ~,
Tier 2 pg~g„Q~g~y, ~Q~ <0% X
QR~LC1~9B%100% uo ro S50o oar ~na~~
T r 3 script ever ohermaw 40% X
O~u~b~6%],QO% w b E500 per
nee a scao~ ever onerma~ ao~ X
oeauab~
Surgery tacJlly tee (e.~. ASC1 0v.100% x 40% X
P~~mbYnreur9eon teen 6~bJ,J~pyy X a0% %
oucpe~ern viaii ew,1m44 x aox x
Emagpwy ~aam Iacnity tw (werw~G r aamnetl~ e~ry~ x aaa x
Emergency room phyablan fee (waNed H edmmed) B%100% X 40 % K
Emerpaicy med~lberaponatm lws,~jQ,~ x aov. X
Alter tat three
Urgent care 5120 rwn-preaeniive 40% X
visM1s
Fecdlylem (e g hoaG~el roortl) B%1 W R K Mi %
P~ysclBri/surgeon tea B%100% X 40% %
M& 1tl91fB6
MBntaUHNavn,al heats wlpe~W o~M1Cn vsOa STO nonCra.9~4w W4. X
VbAa
Alter 1M Mree
MentaVBehavbral heaXh aher outpatient items antl eervices $7o rwnyresnTrva 40% X
visA9
Men~eVBeMNof8l tiealP~ Mellen: UeYM1y tea (e p 1~IRaI mOm) B%1Q4_ % 60Y6 %
MeriiayBehevioral heats npelieM physkiaNwrgeon fee BA6100% X 40% X
Ma t9 tnrge
$Ub918nce Use EsoNer aulpatia~i oflbe vela SIO nOn-ptB~+nAv CPK X
vp~s
After tat three
Substance U%disorder oMer oulpatleni Gems arts services E70 non-preWnitie 40% X
visRs
9une~ance us.. nceia,~ iec~M ree 1. 9 ~Wai ~onml ex~ x aox X
Su Wbnce use disoMer hpatient phyaiciaNsurgeon tee B9ci W% % 4096 X
Prerotelcere antl praonception Helm No chgrpe No char{p
Deltre~y entl all t~pat t HoepW 9%]QQ96. % d0% X
aervkes ~.... _....._._.. ...... ... ... .............. ._....... ...._. .... ... .......
-Proteubnal B%t00% X 40% X
Hang Mash cin 9K,~Q,~ % b9L X
Outpet~ent RehebBnatpn aemcas y70 40% X
Out~gllaN Hebiflazon aervices 470 d09~ %
Skilletl nursing care 0%jff~ % 40% X
Durobb meQieel eyuprfent BY. % W°6 %
H~a be eervbe No charoe 0% X
-Eye eum No,[email protected] No charqu
1 pek of glaxea per year (n comae rues ti Gw a gam) No cher9a No charge
Oiel£vemPrereMhe - Cleennq
P~~° ~ x"~ No charge No charge
Sealants per Tooth
1 Surface 1~ti ?o%
Eq»setl Root ar E~uptetl 50% 50%
McCrally rieCe6m'Y ar1lMConUq 60'Y. SO%
See endnotes.
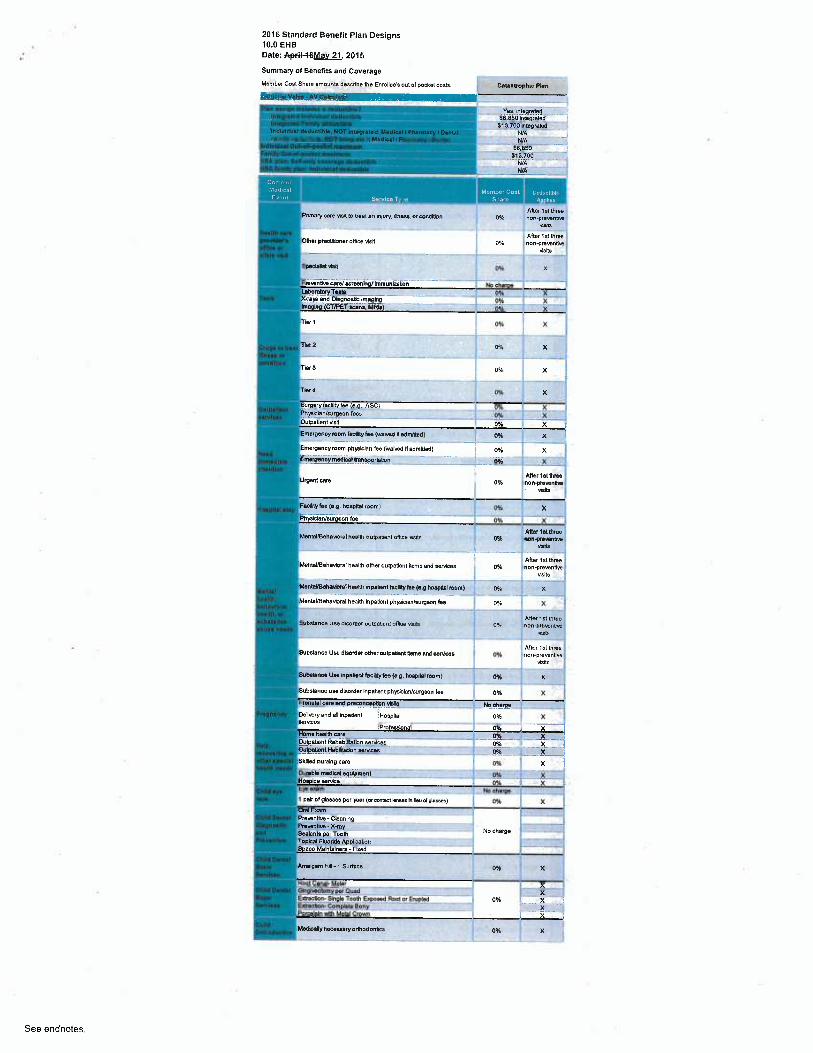
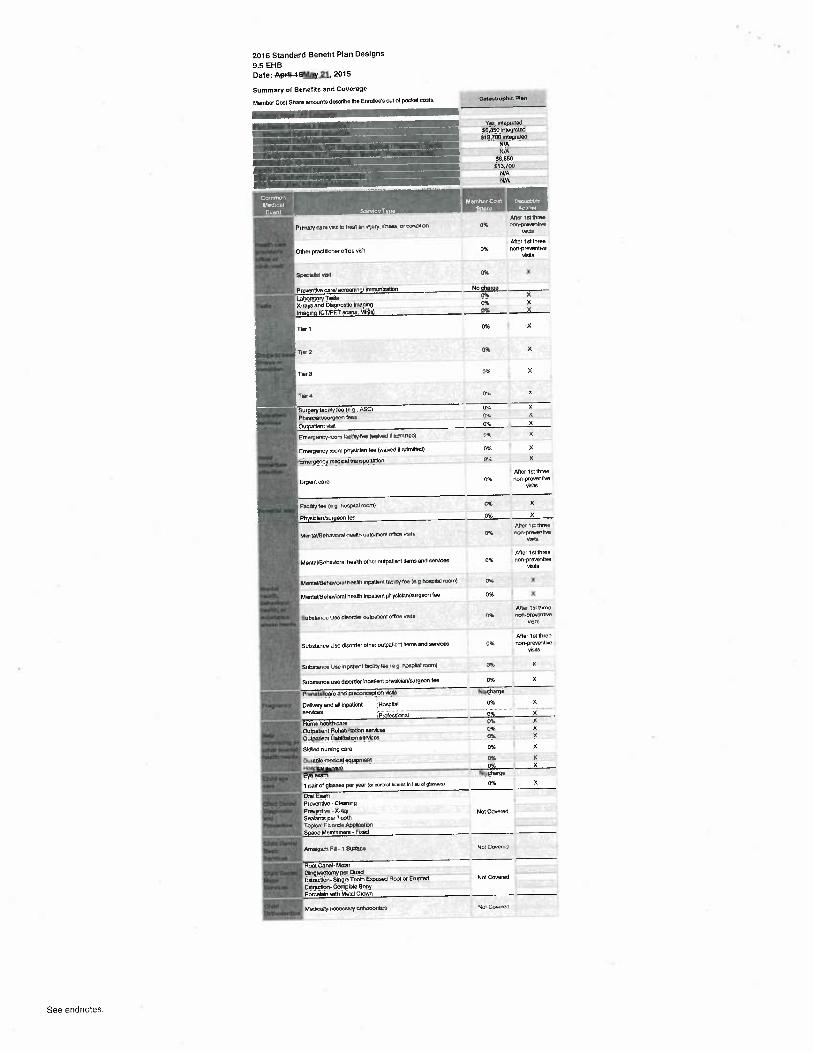
2016 Standard Benefit Plan Designs10.0 EHBDate: AryFiF46Mav 21.2015
Summary of Benefits antl Coverage
Member Cost Shere amounts describe tha Enrollee's out of Docket costa, Cabatrophb Flan
Ves, .ntugrated$6,850 Integrated$13,7001ntepreted
N/qN/A
$6,&50$13,700
-- N/AWA
Aller t ai threery cera Ksit to treat an m~ury Jlnoss, or wntlttpn OX non-prewnb~e
Hw~t
After lst NraeprecWonar olflce Nstt M/o non-praventive
Nsils
3ASI vivt
____
0% ~ ... k
X~nyc and D4pnoatle ImpNp 0 % X _im h crm~r sans; ~s o ~ z
TNr7- --'- -' 0% X _~
Tix 2 OW. X
Tkr3 0% X i
TNr4 0% %
Surparyfadliry fee (e.g.,ASC) 0% X jPhyabien/surgeon kes 0% XO~ipaue~i wsa - - of x-- R
Emergency room lecilRy fee lwerved dedmmed) ~ 0°h X
:Emergency room Dhysician fee (walveE NedmXled) ~ 0/ X
Emergency medical transpo~tetion ~ Ok %
~~~ ~ After isl threeUrgent cars 0% non-preventive
Nsils
F~c9M~ (e.g. ho~plW room) D i x
Ph~ kMaurpeon tae __. . ___. _
0 % X
Afte~7el tiveaMenteUBehexo.el heann outcxuent office vans 0% non-p~B~.enLw
Nsits
ARer 1 st threeMen~aVBeheWoral health other oulpatiantileme and eeMeea 0% non-preventive
visHs
MenteYBehavbral heats inpabsnf hG~lyfie(e.phwplW room) o% x
ManlaUBehavloral hearth InpalNnl ph)miclan/surgeon fee o % X
After 151 NroeSubspnce Use tlisortler oulpalieM ofllce waits 0°ir non-pre~enbva
v..ub.
After 1st threeSub~t~nce Use dkoNer otheroulp~tlenl kema and wrvkea o% non-vrevenuve
Nsits
SuEelenee Uee InpatleM tpollafae (s.p. hoeppal mom) 0 i X
Substance use dleorder Inpatient physicleNsurpeon tae 0% X
Pnnehl care and pnconceptlon NWs No charge_ _ _ __...
DeH~wryand all inpatbnl jHospNel 096 XsaMces i.-__-' ___ __... __..__.....
Profseabn I 0% XHome health care Mfe X __Outpetlent Rehabibtetion serNces ~ py. XOu~atient HabAnalbn earvfLYs ."'_---- .__ 0~._. _ _. X.'__1~ySkilled nurinp wro 0% X i
Durebb medNsl et~ul~m_ent _~ p% XHo Ice servke . _ __ _— _ X
ye eram i_ .. ~
1 palr of glasses per year (a correct bn~s m lieu d v~~) 0% XOral Evam ___'",_".jProventive-Cbening _~P~evenN.e.X-raY No charge -~- ---SeelanffiDerTooNTopical Fluoride ApplkationS ace Mainfsinere •Flied
Amepam Fq-t Sudecc pq~ X
Root CaneF Molar Xorpi~m~,Yw,a~w xF~actlon _Slnyb Tooth_E~oeedRoot or Erupted 0% X_ ____IE~actlon-Comybls_Bony 7(.. ._.. _.Porcelek~ with AAelai Crown X
~Medkalynacesaery oModonUca 0°i x
See endnotes.
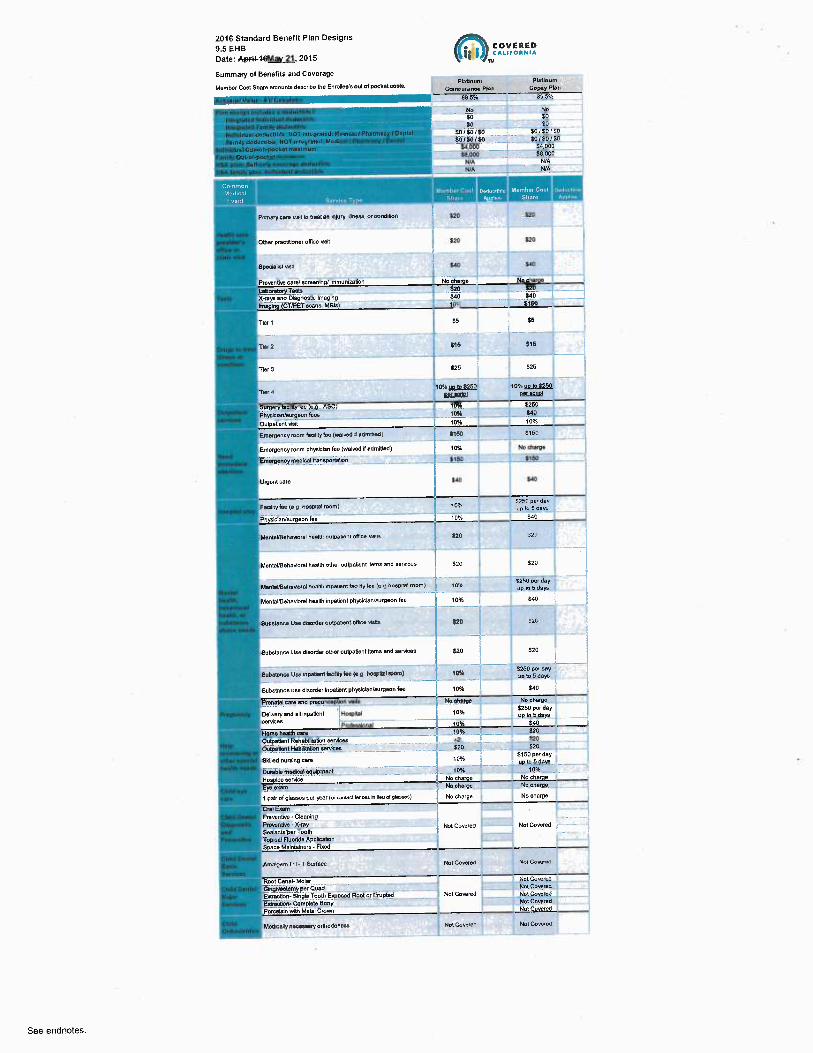
~ COVBtIED'~ ' CAlliOlNIA
~u
Pladnum PhtlnumCarouranu PNn CopyPlan
885% BB.S%
Nc NoEO $0
EO EOSO/EO/SO $0/SO/SO
~_ soraorso.--- - _ .soi_so/ao. _..._._ _ a°_°°° __ _ sd.000 ,
ie,000 sauuu
Plvnery care Halt to head en mlury J~ness. o~ co~Eltlon $20 $20 ~ _--
Othef practilloner oflka Nsit $20 $20
bbeCiahaf Wp E40 Y10
Prewntlra card acreenNg/ Ynmunimtlon No oha No theme
Luton Tab ._i20 _ _ _ 520_ _
X-reya and Dia9noatic Imepin9_ SIO _ E40. _ _ _..
Im - In ~ CTIPET wane, MRIa 1 E760 i
Tbr 1 SS SS
TW 7 i'16 E7S
Tbr3 S~6 525}
TW 6 Y10% uo b E2b0 10°ia yo to 8250•
per BCrio~ aD (6~f101
~reery cnny e a.9..nsc> ,o% alsoPh~aicAn/eur9~n ieee 10% S<o
Oulpatbnt NeR 1Mh 10%
Fmerpancy room fu~tyiee {rsned a.a1nmea) 516o a~so
Emergency room phyekkn tea (weiwd H edmiLLed) 10% No charye
EmeiOen?Y medkal tren rintbn _.. ._ ._-_ -- _ _ _ ."____
. ... __' Wo _ ___— _'_.§~~__~,_.__.t _~~._
Urgent care t/0 ~ S40
Fkmlyfee p.p ~oaWbl room) 7Mi I ~~~yup b 6 d~~
Ph Ian/aurBeon ke 10% E40
MsnbVBe~aworei ~ealM ouWeve~i oPoce vans fp0 i20 ~
Menlel~BeheNorel health other outpetlanl ttema and eervices {20 i20
Menbl~Hehe.~wal heeuh mpabem lectlHyM (e.p.hWpttal room) --1p9~ '--"' ~~~_. —~ uRbSd'~y~.
1MenmlrBehevbrel heeNh Inoatient physicieNwrpson fee 10% E40
Subalanw Uee agoNer outpe4ant Wlwe Neaa fR0 EYO
3ubelance Use disorder oMer oulpatientltems and services S20 E20
Subeience Use npe0enl fealyM (s p hoeplW room) tp% '5430 per Gy
.... _ —_ '__ _ _ ._ . _ ..~.._.. uV W 5 deW .....
'Substance use disorder lnpetbnt ph~ablan/surgeon fee 10% Z $40 ~
Pronetal care and preconcevtion He~tr. No die W che(ge_
Deliveryand ell inpatlenl Hospital 10% E250 pardeyup WSdeys ~__ _ '
Professional 10 E40
Fiume heaidi care 10% _'_ _ _ "~0 ~_'
Ou~petient R h b0lation services _ _ ~0_ ~ _ _ _ 520 i
Oulpallent HabJitation aervicas _ __,.#0 ~__ ~. __.,~20
Skilled nursi gcare ~~v,~ i S~`.~Dar day
____~_'_' _ up b 5 deya..
Durable medical e4uipmanl __ _ _ 10%. _ _. 70%. ._._ _ ..
Hos Ice serNce No charge No theme
ye e~ram _ _ _ _ No charge Nocharge
1 pair o18~~s per year (« rnrnact bnnea in Yeu d dam) No charge No charge
ExamPreventive - Cbaning
Pro~enlNa-X-raY Not Covered _.... Not Cowrad --SeaWntsgerTooN '~
TODkaI Fluoride App4ca~onSoece Melnleinars - FWd
gr~a~em cn ~ i sur~au r»~ co~rae Nm cow~dn
Root Cena4 Molar Not Coe~ared
ONplveCtomy px Oued Nol Covered
Extraction- SInOb Tooth E~oaed Rool ar Erupbd Nol Covered Not Covered
E~drecllan-Complete Bony Nal Coesred
Porcelain with Metal Crown Not Covered
MedroaAy nacayseryoMo0on4es Not CowrPe Noi Govu~eE
See endnotes.
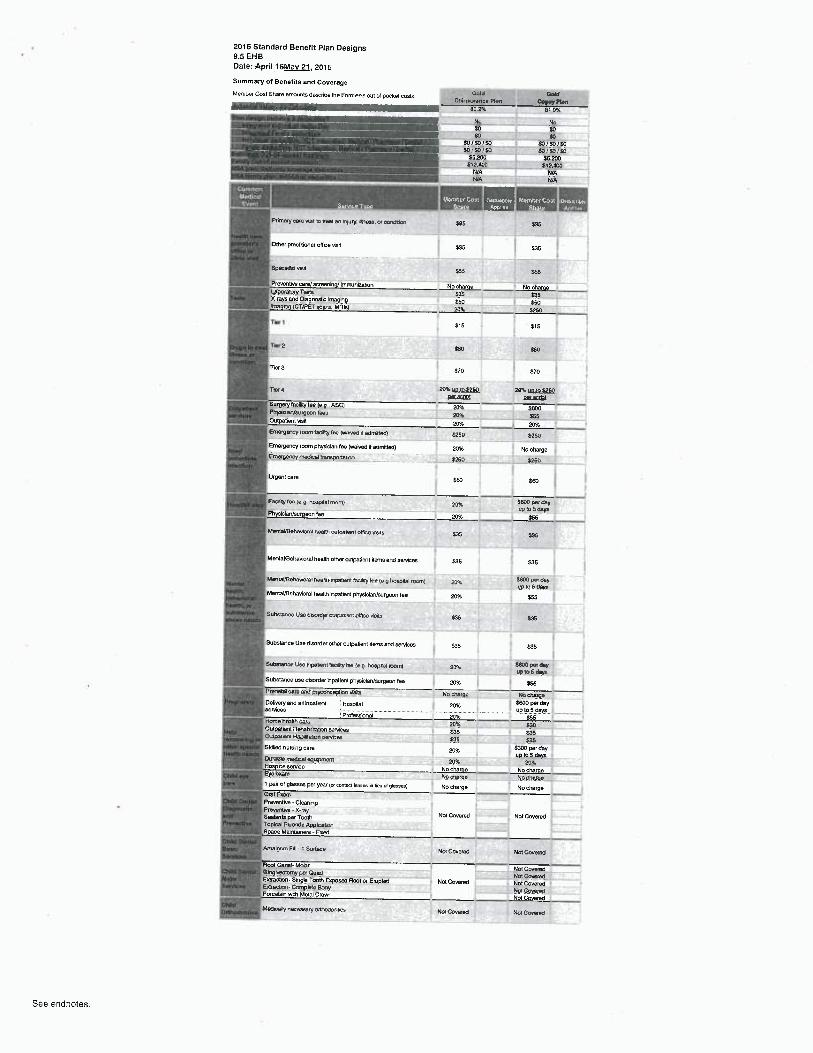
2016 Standard Benefit Plan Designs
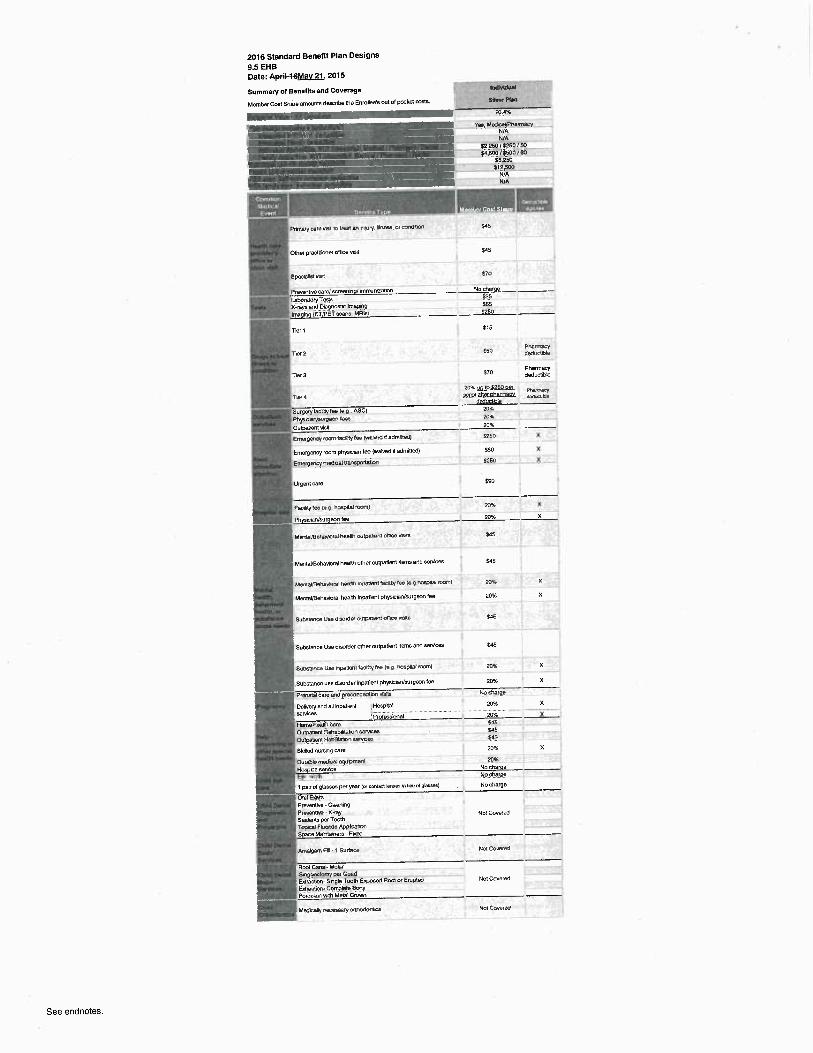
9.5 EHBDate: A{~iFi6Mav 21, 2015
Summary of Benefits and Coverage
Membor Cod Share emountn dencribo the Enrollee's out of pocket costs.
2016 Standard Benefit Plan Designs9.5 EHBDate: Apr~FibMav 21.2015
Summary of Bene(Rs and Coverage
Member Cost Share amounts desaba Ne Enrollee's out of pocket cons. ~ ~Coin~v~v PNn Copvy PlanBO 2% 01 ~s
~~ No No~~ ~~ ~ ~
~ ~EO/SOlSa EO/SD/EDSoiioiso Eo~sorsoss.zoo Sszoas+e..no a~x,eooWA N/AWA WA
~S.!dlly
Prmery~wve~btreat nn ryury. iB'~~s.wcaWaan b5 S35
Otllet precCA'onef olficeWsil §35 $35
SpeEhl6I NeM1 $55 %6
Pre~ernFae eara~ecreenny hnmuntraton No charge No chargeLeDnWoryl"uece S36 E36Xrdys end Di~9nosle Mnege~g S50 S50knagng (CT/PET ecero, MFI~ 20% 5250
ller 1 §15 $15
Tler2 y$p §50
T 3 E70 $70
11er~ zOx wroaxso tot uo wszso~.~',IOI 40C.vGlGI
Surgaryfacd4y lee (eq .ASC) ?p94 $BOo~c6Murpeon Iwa 40% 555Outpatient ~nsN ZO% 20%Emergercy room tanAty lee ~warwC ~ atlmne0) a2bo E25o
Emergerxy room physkAan fee (waived tt atlmittetl) 209E No rherge ~ ~Emprpency madc91van5Portetm X260 5450
Urgent care S6o S~
FeCtlgy Iae (e g ho9pnal roOr~) 20% E~ ~ ~up to 5 daysPnyscmNwrgeon iee 2o5c yss
Mer+~eVHM~avbmllipalEi outpatwN dM1te vs~s 535 E35
MentaVBehavioralheaM other anpetient gansand aervicaa g35 S35
MnWUBenavoral health Webar~i tecilty Ieo le B ~cai roan) 204e 5~ Var EaYup io 6 E@yR
MentaVBehavioralhealC~npaT~ant physiciaNaurgeon fee 20%, 555
Subctanca Use EisorC~r o~nW+~ent ottco veee 535 E35
Substance Use disoNer other oulpaGent flans and services $35 535
9ubatenoe Use npetan MCMy feo leg noapt~ roarn) 20'4 ~ W~ ~Yup b 6 daar~
Substar~ce use dsoNer npatienl phyaclaNwrgeon fee 20% $55PrenelalwrenrW geoerwro~tlpn v~elb No clurpe No cherypDefrery end all inpatient iFbepYel 20% ~~~dBYservices ......... _up toy days .. .................
': Profeasbnal .... 20%.... _.. E5.5FianaheaMh care '~py~ pbOutpateM Rehablaatnn services 535 E35Outpaten Nabme~on eeNcee ASS i3bSklllad nursng ears 20% 5300 Parday
~v ~o s mye~uratib meGcat qupment 20% Z9%Hospce service No charoe No charue,.yaepm
No c„Asrpe NQ dlal.!N1 pair M glasses per y~r (n cmtm fences e~ ilea d glwea) No charge No chargeOrel'Erum
Preventhe-CleenngPrevailrw - K-my
Not Covaied Not CovetedSaalenta per ToothTopical F~orda AppkauonSpace MaManers - Faetl
Amalgam FU - t Sw~ca NW Covaretl Not Cwe~BO
Root Cenel-Mohr NotCWereOohgaeo~ar~y par alga Na cgyeredEvracwn- Sngla Tootle E~osetl Root or E~uptetl Not Cweretl NM CoveretlEzraenon~ Compkro Bony MolCwemEPorcelal'~ wah Metal Crovm Not Co~etl
McCceOy irecaeaery oMoOoritlp Na CwereO Not Goveretl
See endnotes.
2016 Standard Benefit Plan Designs
9.5 EHB
Date: 11~riH6Mav 21, 2015
Summary of Benefks and Coverage Mv1e~W
Member Coet Share ar~wunts daccribe tl~e Enrollee's out of pocket msGs. Si7w PW~
7p.nat
~~~ ~ ~ vea~ MedcaVPnelmacY
WAN/A
E2,250 /5250 / $0S<.5W /6511U / S4
E8250512.500
IJ/AN/A
Pmia~y care vW n vmt en rqury, 11ria9s, or cmtlRm
Other practp'aner once Hstt
SpeoeMt vma
Tkr7
Tier 3
rw ~
Surgery iacriry iee le q ns~)PhyeClONBuNeon lase
ougie~~em Oren
Ertrerga~cy marvlacsryfea (wan.3e rt aammed~
Emergency roan physklan tee (wawaa X admMed)
Emma envy medcal aarieponaibn
Urgent care
FaomY~es h9 final rooml
Sab
E45
570
S~1250
E15
Eso °^81"'x'ems
570 P~~ytleductDla
20'%uoroE25ooer ~r~t.rmi abler oha aem~e~~—
zo%]Osszo%
5260 %
y50 X
5250 %
590
zaa x
zow x
MeiVayBntmwral haxM wlpe~eN o11ee Wts §OS
MenlayHehavbrelheatth other o~npatient items antl servkas $45
McMaVBBMW~rel heats ~Wa~lent fe[iUy}ee leylW~ael roon+l 20% %
McMaVBehevioral health inpatient physlcfaNwrgeon fee ~ pp96 X
SuCs~enca Uce tlreordx a✓~euen~ottce race ya5
Substance Use disoNer other outpa[ t Rems aM services
9R»~nn U90 M~~en~ hclYlY lee (a q I+o%Wei iaanl
Substance use tlLvoNer npatient physbmrJwrgeon fee
arenetelceieeM,Preco.!maPebn Nsne
DeMeryantl all Inpallait ; Hospkelserrices ........ ..._._.__.......__.........
'Prafess'ronalHome l~llh careONpat~ent Re~e6nnauan semces
Outpel~eM HaDYpalun Nrvca~
Sklllatl nursng pre
1 pelt of gleeeee per year lu canlact lewaa in Ilev a 9lazsazl
Oia~ EmnPreveMNe -CleaningPre~41IM ~ X-raysea~u vex roomTopmJIF1~MEe AppACetnnSpace Maelteners - Faetl
M~Igam FW ~ 1 6urteca
Root or E~uptea
McEkepy nece68eryo~noEorrtim
Sas
2096 %
20% X
N„oet~rpa _
20% X
20% XSdbE<559b
ZO% X
2096No chargeNo cf~vpe
No charge
Not Coveretl
Not Coveiee
Not Covaretl
Not Cwe~ea
See endnotes.

2016 Standard Benefit Plan Designs9.5 EHBDate: ApFi1~6Mav 21.2015
Summary of Benefits antl Coverage sifoa sHoaMember Coat Sharo emounla dascMe the EnroAee's out of Docket cosh.
BINe. SilverCoinsurance Plan Copey Plan
71:74' 71~B%4. 11.496 71'3 %
~ ' Vea. Madicel~Phermecy V s. MedkaWharmacy _.le WA N/A
Ndividual tlaductlEk,NOT lnleprnfod: Modicrll PhermacylD~n41 51.500 /i6YB,~~$Q/SO _ 37,50DIi6B0_~~i /_EOFamily detluclibl~, NOT Int~pr~led: Medimll PhartneryfD~n _ E3_000/ZhYG6__~/60 _ __S~9 _OODlti~Y09_/S0 . _
wl OuW1-pocket mulmum j8.6(10 SB,Spp'_4~bJlD11~ '_'___.__ N8.000.. ~_.. .__._.~___—.__. ES8000 .:
._ __'_.I
b WA WA___._ _ _ w~.._ ._ ... _ __._ WA
' ~~~~ ' .
Pmmerycaro Nat to Vaet an nryry. Nneu, o. condlaon yqg yqs
Otl~ar practitioner oflka Nsit $qs { sq$
'A+~~ E70 X70
Prewntlw wro/ ecreenln hnmuntr~tbn No eheme . - No eharosLabonb Testa 836 5,96Xyeye and DleOnoatic Imapinp y66 Sp6
C7fPET wna~MRh -------. .pp!5 j( ~ ~0
Tier 1 $15 E18
Pharmacy NnarmacyTlfZ ~5 Eadutt@le ~ aetlucbbk
Tler3 ._ ~.. Pharmacy "— Pharmacy$75 deductl6te $76 deductlble
20%uob E250 oar ZO%uob5250 oei o~ermac~7llertnacyTIV~N4 6Ll~~l BhBf ~hBIR18CV 6C(iD~eNBf Dheft118E~
deductible tleductlDk
detluctlCle aeduchbk
ryery Iliry a (e.p.. AS) 20~ ~ 20Ph1~ioW✓wroeon bee '-. ._ _. ._.
_.... ..—____.._. 20X ~ 201.Ou~Datlant Nett 20X ~—__—~— 20%Emsrpsnoy room hc4giee (vroNetl ll ~dmlttad) E250 X 6460 X
Emarpencyroom phyeiclen fee (waived If edmlded) E60 X ~ E50 X
EmeNencY medical tran Ntlon. —'-_—"'.'— ""__.. ~. _ ._.. ___' "."__ _ _'._....___ ..~"_
Urgent care $BO ~ 590
FacYnylee lop nosv~~~ room) 2044 X ZO% t X J
Phyakknlnurgaon fee 20% X 204. X
MentevBaheNmel nea~m omnanem oflice vises i ~ :qg
_f~.. ------- ~ ----- --- - i-- _J~MenleUBeheNoral health other oulpetlanl tteme end eeMces y~,5 f y~,5
—_ _. _. _. _ _ _ __ _ ____j_'_____._— '_.~._MenteVBehavwrel heelih mpabentlae6rtyfee (e.ghoepNlmmmj Zp,S ~ X PO% X ~i
MentaVBehallorel hea1N Inpatient Ohyslclen/surgeon fee 2055 ~ X 20% X '~
Substance Ube disoNer oubeAent office u,aiu ~$ jq$ '~
Substance Use dlmrder other outpatlent Items and aerNces ~ gq5 E45
SuDabnu Use Fpatiant IecAM~e (e.p. hapdal room) 20% % 20% X
Subatenoe use disorder bpetlent Dhyslclan/wipeon be ~ 20% X 2DX X
Prenatal aaro and pnconwptlon via~n.. _ .. _ _ __ _ No therBP _ _._'_No th~Jrp _ - ..—Defvaryendelllnpalbnl ~;Hoaplld 20% X 20% XeeMces -_. ._. ___ __—~_.. _. .._.
iProfeaeb a 20 ~ X 20% XHome health care _ _ ~ _ , q5 __Wtpatlant Rahablldati arNces {45 y15Oumatbnt HabAtta4on Mcee ~.~,5 y~,5
SkAbd nurNnp care 20 % X 10 % XWrebk medkel equipment 20% 20%Fk ke eendce No charoa No charcaEto exam No cher0e No cherpe. _.~ pair of pleases per year (a eonmct lens in lieu Nplassee) No charge No cherpeOral E~mmProventi~e - Cbening
~°NBn~-%may Not Covered Nol Coverod ~ ~----Sealante per Tooth ...._Topical Fluoride ApplicationS~ ce Ma~nlelnars-FMed
Amelpam Fm-~SuAace Not CovereC Not Cowrod
Root Canal-Molar ! Not CoveredGngi~eclomy per Ouetl ~~~ ~ Np~rpy~EbrecGon-Singb Tooth E~oaed Rool or Erupted Nol Covered j ~.W~~w~6dra tlon-ComPble Bony Z _.. ~S.~?wrW _ ~ "'_.Porceleln with Mefel Crovm i Not Cowrod
Medically neceesery orthoConUCc Not Covered NOI Co~arod
See endnotes.
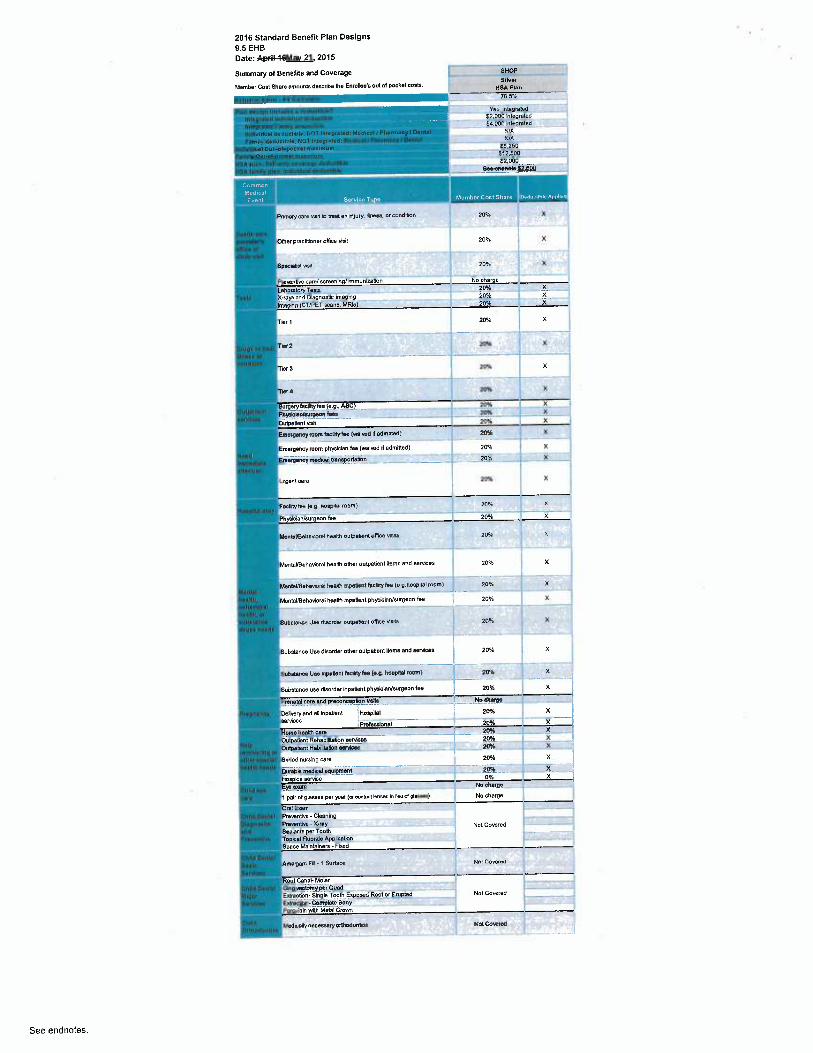
2016 Standard Benefit Plan Designs
9.5 EHB
Date: AryFiF9&Mav 21.2015
Summary of Benet)ts and Coverage SHOP
Member Cost Shere amounts describe Iha Enrolba s out of Dookel weta. g~NB~H8A Plan
705%
Yee~inlegreted -'-"---.._.. §2.000 Nlegraletl
'. Qj,-000 InteOreledWP
.._.__. WA58,250612,300§2,000
6~ndnsl ._ . _
~~~
PIMIiry CBn vlsn b vans an ml~~v. ~~~~ nr contlttroff ~ Qpx X
_. _ ...._
ONer practitioner oMce Nsit 20% X
SDeorbtxW 20% X
Prasnntiw care/acroenln Fnmunlutbn No ch~rpe
X-rayn end Dlegnoatic Imaging __ 20% __ _ X
Ima n CTIPET wns, MRk 20R X
Tbr1 IOX~
Z 2M6 Xi
Tier 3 20% ~ X
Trorc 20W X
SurgeryfacllHy lee (e.B~. P.SC) 20°h
Ph~nicienlwrBeon fees 20% X
o~a~re~i~n soi x
Emet9 groom hcllGy tee (welvea If tlmNed) 20 h X
Eme ge cy room phyek~en fee (welwd Nadmltted) 20 % X
Emergency medical tra portetan ~~ 2oh X
ureentcaro 2o°h
F~dMYfeeN p.IwWgel loom) 20% x ~.
Ph ...__n/awpeon he 20% X i
AlsnrVBahaw~W heal0~ oum.Usnt oflka aeM _..— 70% x
Mental9ehesiorel heeNh other outpeGenl ttems end services 2056 X
t2 __—~' _'
MsnlaYBehevbnl heelQ~+np~oent kcWtyM (e p.~oeprcal room) Zp% x
MenlWBeheNonlhNlXi lnpalNnl Phyakkn/aurgean fee _~ 20% X
Sues~enco Uae duoMe~ oubetbn~ office Hsro ~ Y09L x
Subatence Use dleorder olheroulpetient Nems and neMces 20Yo % i
Manor Um Y~WMntfioWYfes fag hoWaal room) _ - --yM1~--_. X
Substance use dleorder Mpatbnt physiclen/aurgaon fee 20% X 1_~~
Pra~atal ears u~d Preooncevtbn wNs ~ lb oAWs.. _._.,
DeOwryand aA Inpatient Hospital ~ 20% X
neMcas . _........__—____"_- ___—"._. _ _Prolesslonal Z X
-- -ouaeu~~~ aanaeurc~uo~ ~~as _ _
zon x ____,Outpallenl Habillletlon §snits§ -' ...'~-" --- -- ~ 2Mb X
SkAbd nursing taro '20% X '~
Dunbb medbel equpment 20% X
Ho ke aerAce - - .. - 0% X
Ep sum ___'.._~_~... No Wv:He ~
l pak of glessea per yoer(o wnbctlenm In Reudpuroe) No charge ~
Oral mPnwnOve-Cbeninp _
Sealenb TooUi Not Covered ;.--.. _.--1
Pei ___ . _
Toplaal Fluoride APPGutlanS ace Malnteinere-Fbcad
Amalgam FM • 1 Surlata Nol Co~9rod
Root Cane4 Molar _
Olnpivecmmy per OuedF~Grection-Slnpb Tooth E~osed Raol ar Erupted Not Covered
FHiaction• 6ompkte_BonyPoroeleln with Metal Crovm
reea~canv ~ecoanery ormoaonu~a ruoi co~an
See endnotes
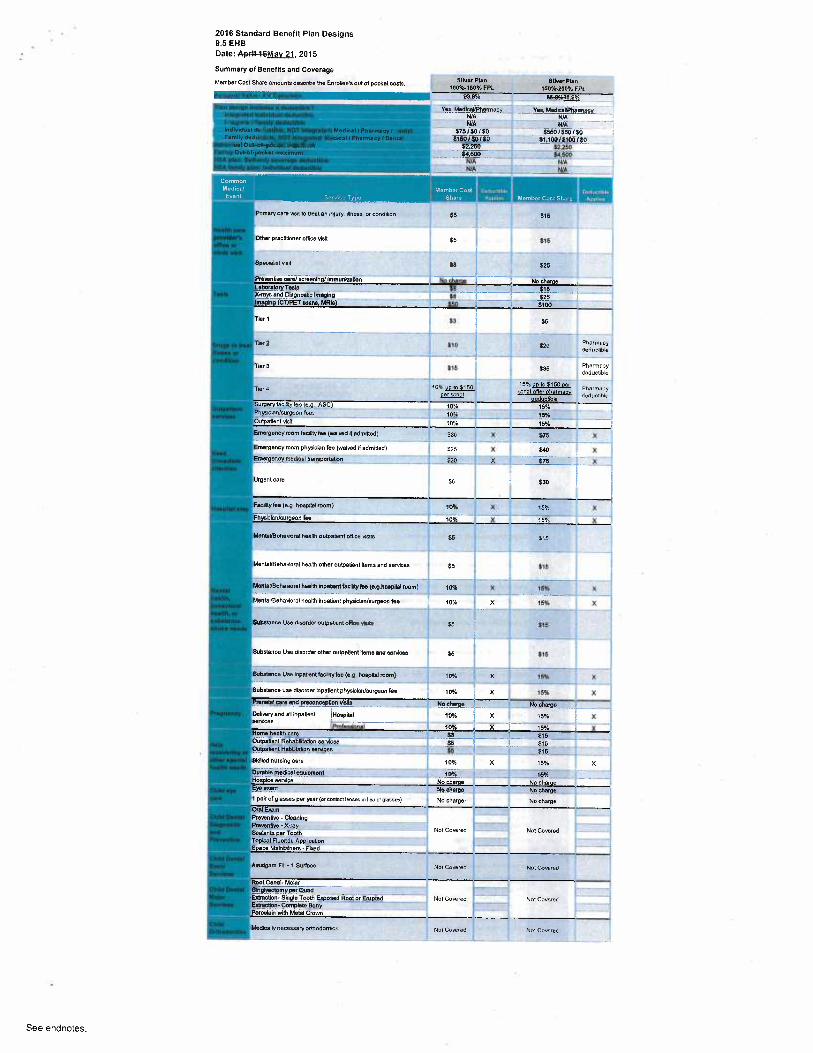
2016 Standard Benefit Plan Designs9.5 EHBDate: A~iF466Mav 21, 2015
Summary of Benefits and Coverage
Mambar Cost Share emounta descMe Ne Enrollee's out of Dockel eoeb. SHvar Pk~ SINer Plan
1009o-150Ye FPl 760%•20096 FPL83.8% 8&8%8,8%
_ Yas̀ Metllcei/Phermecy Vas, MedlcaWhemiacy_ WA WA
NIA WA575%SU/50 Z_ 5550/S50/5ot~aoito~to s,,~oo~s~ooiac
--- sz,zso--- --- --- _ _ ss;2su,_,__ .$4.600 _"_.' '.' _"_ ~4~500
WA WA_. wA _ _ _ _ __ _ WA
Pnmary care Hsn fo veal en m~ury. 4nesa or contlmon S5 S76
Otlier practitioner office visll --~ S5 `-- 315
SpecuGet we y9 ~ y~
Prs~entlw taro/xroenin %Ynmuniratbn - No ch No oharueUboobryTeele_.._.___ .. '______. ~_ ,_'___516.___ __X+ays and Dlepnoatk knepinp fB S25Ime In CT/PET u:am MRIa -~ --'-~ ~"- ~p - —'~-' --~ -~-~pp
YTbf 7 $3 y$
_ _ _. __ _...___ ___--. _. -~_ --_u _
~2 t10 ~ S20 Pharmacytleductlbb
Tler3 S1b ~ Y S35 PharmacyOaductlbla
i 5 % yo to Et50 oarTM~d 10% m 15 - u~ot after ohertn P~e~macy
oar unot deduetible eC dedueODb
Surgery fecllityfee (e.g., ASC) 70% 15%_.. _.... _..Phyeiclen/surgeon fees 10% 15% jOutpe4enl Nsit - 70% 15% _~FEmegency mom fecillty tee (waived Aadmmed~ j3p ~{~ % E75 X
Emergency room physlclan fee (waived rfadmitted) $25 1 X 540 XiEmsrpsncy medical trenaporlafwn _ $30 ~_ X 575_ X
Uryent oaro f9 ~ - $30
F~eRy1s~(~.p. hoeplui room) ~pq~ x is°/< x
PhY+kunhuNwn tse ~ ----10%~ x 15 % X
MenpllBeheworai heats oulpauanl oNice ante ~5 ~ g~„
_' ... ~
MenlaVBehalloral heeNh other outpatient lama and eeruices $5 ~ $15 - -~'~'
__'..._ _'__ __ _ _ Y..'.___MmYVBeheNonl healB~InD~~thcAtyhs (e.phoepnel room) 10% X t5% X
MsntaVBeh~Norol heats t~patbnl physician/aurpeon fee 10% j X 15% X_ __ _ ' '_'_'_ ' _ _ _- _ _ __ _. --t— _' --
Subaience use tl~sorder outpenen~otfice wN E,5 i g15 i
"~_—'.~
SSubWnu Use dborder other outpatlent Meme and aervkes s5 ~ 515 r
BuEstanu Use InDatlentfiUlRyba (e.8 hoepllnl room) 1046 K 75% X
Subatenu use disorder lnpatlont physicleNaurgaon ke 70°h ! X 75% X
RanaW aro and_~eaonoeptlon Nelle No chupe _ ~ No throe
DaM~eryand Nhpatlenl ~~Hop~Mel 109L X j 15% X
~~~ IProtesslonN ~0% ~-~- i5% XHoms hw are 53 - _¢16 _Ou1p~Uen1 RehahWtetbn wMese -- - $5 —_ ~- }Oub~tlml H~blBlaibn seM¢es _ y5 _' __ S15 __._ ..-.--_._SkAkd ureing car 10/ X 15% XDurable medkel equipment t 0 % 15%.Hoeplce eeMce No charge No themeEye erem No charge _ No charge1 pelt of glasses per year (ar wntacl lenses In lieu of pbsaes) No charge No cher8eOrai ExamPrownuve - cbaningPr°~°~6~e ~x-raY
Not Covered Not Covered ~ --Sealenbpar TootsTopkal Fluoride AODllcelionSpecs Melnlalnera -Fixed
Amegem Fdl-t Surfeu not Co~erec Not Co~.eretl
Root Canh Molar6hyAeotomyper quad _E~~ctbn• Single Toots El~osed Root or Eiupbd - Nat Covered Not CoveredEtttraotbn• ComPbte Bon.Y.. _._'__'Po~eelain with Metal Crown
McCpalry necessary oMotlontcx Not Corere0 Nol Coveretl
See endnotes.
2016 Standard Benefit Plan Designs
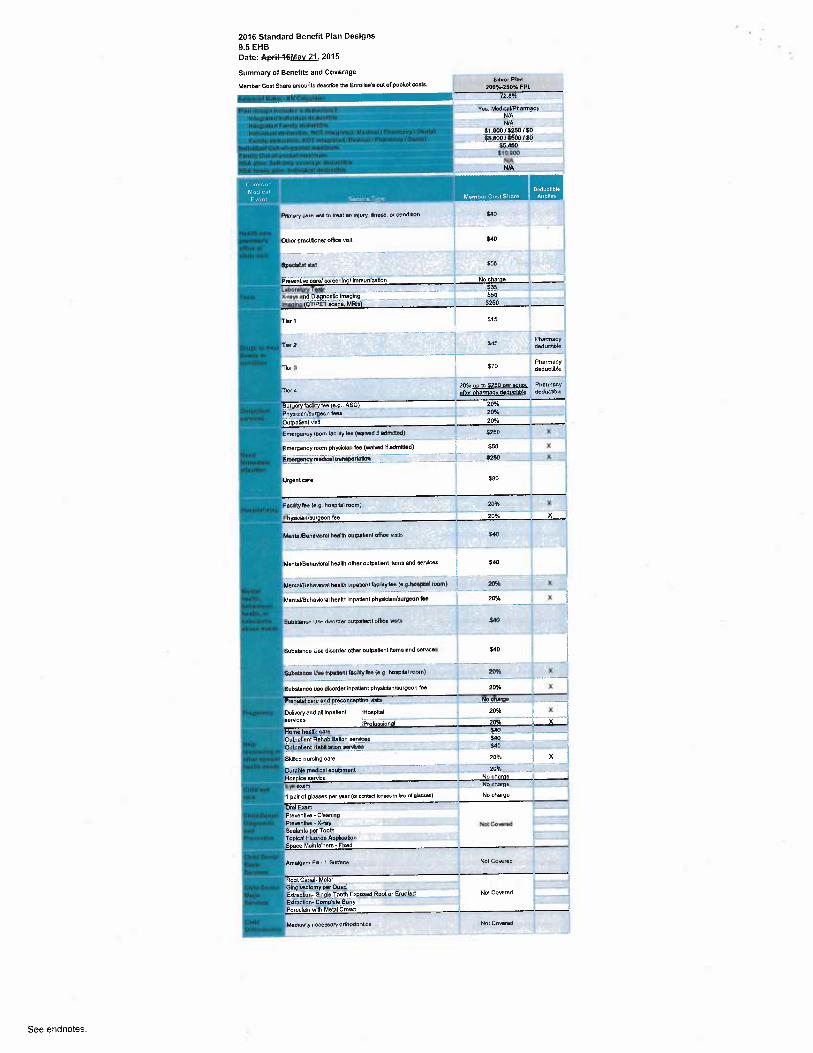
9.5 EHB
Date: April-9&Mav 21, 2015
Summary of Benefits antl Coverage
Member Coet Share amounts describe the Enrollee's out o! pocket costs. 6Mer Plan
I00%-250% FPL
72 B%
Yes. Medwal/Pharmacy _N/AWA
Ind:vinunl doducibb. NOS lnlaprsl. d: Midi<a11 PA.~maryfDan~nl S1,B0015250/$0 ,
f9~B00/d600/EO._._._.—~-55.450
__`. .. __._
._ t1Q00D—.—. _._._,.
WA
Mary ~~ wn m alai a~ ~i~ry ~o~,, o. co~eroo~ Eao
~erDrecWoner office visit yd0 ~ '
~ 4
16Y61 vYY S65
wntlw uro/ acreeninp/ Immunlratbn No charoe
~oCfb~eHe. _._ _ _ _____ _ - ~'-_. ..
Tbr1 S75
Tv 2
—_—. . _—'.'_' _-- ~ Pharmacy
Oeducbbb
Tier3 ~~" .` _. $70 Phartnecydeductlbla
T~ 4 20% uo b 5250 oer stmt PhaimetyeAeroharmecvdeducGbk eeducubk
Surgery fecllitytee (e.g., ASC) 20%
Phyaiclen/eurpeon lees 20N~
Outpatient Natt 20%
E ryancy room laW~ry lee lwa~wC nadmrcleC) jp5p %
E erBancy room phys clan (ee (waived N edmided) ~ y60 X
~Emergencymedleel tre aportdtlo -__` f260 X
urye~i Dare ~ aeo j
fsW0.ytee (e.p. hoapinl room) 20% X
~Phyeklen/aurpeon he - .._ YOSL ~- X
MentBUBehnvroral neel~h outpa0e~t oflke was j40
Manlal/BeheNoral health other outpatient items and services t aA0}3
MenuVBenaHo~ni nea1N np~§enifklyfea ~e p.hoplW mom) p~ X
MentsUBehavbralhsats Inpatlent ph~alcknhurgeon fee 2091 X
Subalence Use OieoMe~ outuebant office vaN `40
dSubatnnce Use disorder other oulpatlenl items and saMcae ~ §40
Subamnw Uss hpUNnt txMyfee (s.0 noapnei room) 20li X
Subelnnce use dieortler lnpatbnt Dhyskienfaurgaon fee 20%s X
Pronatal are ana preCo~pBon_ Wile _. No ohafQs. __.
DaliNeryanE aA inpatlent ~Hoapilel 20% X
services _ .. "' _'_"_—_ —~--'_' —_
Profeaelonal 20
Nome heeHh taro ,.__ ____ _~___
Outpatient Rehebllitelion eervkes y40 _
OutpaUenl Heblilaoon eervicea ._ S40 _ __r,
Skilled nureing care ~ 20% X
bureble metlicel equipment _ _ _ 20°h
Has ke caMce No charge
Eye eram Pkcherge
1 pair of gleasas per year (a canlact bnsea In 11eu d 9~~) No charge
n ErsmPrewnave • Cleanlnp _
Prewnma ~ X-ray Nol CawredSealenfa per TootsTopical fWoride ADP~celion
S ace Malntalners-Fbced
Amapem Fb -1 Surteoe Not Corored
Root CanaF MoWrOMgrvecbmy Oa quad~Edracuon-Single TooN E~oeetl Root or Eruvtad Nol Cowrad __._._ _..6A~eclion- Compbb Bony
Not Co~eratl
See endnotes.
2016 Standard Benefit Plan Designs
9.5 EHB
Date: A~iN&Mav 21.2015
Summary of Benef%s and Coverage
Member Cost Share artwurns tleurlbe Ne EnroDee's out of pocket costs. Biaw Ulan `"'—IIRAPI.n
642K~1„9~9p 61 S9G
Yom. ~fl'~~ ~Q.kW' .UAdFT Vag. hMpteled~~ 54.50U inegratetl
E9.000 eveQteleENM56.Oo0 /.5500 / SO N/AP(~AS]2~ 1510001 SO WA
56.500._ 56.500313,obo 573.000N/A 54,500WA j4,590
~■~~~~~AI19r Iat ll+eaBPmurymre vhf b treat an hryry. 0mae. of cona~bn E70 ro+praenuo» ao% K
~aMc
After tef MreeOther precf9'ioner olfiCe vis@ $7o non-preventi~9 40% XaicAs
Auer 1 A R+RBfipecOBat Jsd .490 nmy~eenfrve a09'. %vans
Preventive carN screennp/ wnmun2aton No charoe No cheroelaCo'aloryTee{e $db 1091 Xx r~y~ ~a oagno~s u~gng eas~gq, x aaz xkrrephg (CF~PET acana, MRle) 6%toob X 90% X
BA6100% VD t0 E500 oarr~r ~ scam an~r d,err~~ '~ aox x
4~LCIDle
au~iooa. ~o m ssoo ~rTrer 2 xrirn attar darrt~acv ~~a <ws %
0%10 %uo to 550D oarTler3 Griot alter oturtnecv ~ AO'% X
dadudbleGY.IOOA uo b 5500 perTer 4 ~,gy, a0% %
deduel'bla
-Surgery tactiry tee (e.g.. ASC) ea,i00% x aovc xPhy¢cmNeu~geon fees pp,~~ X ~0% XOutpatient visR BW,100% X 40% %Emerge y roan taatm~ tac twamM ~ atlmmedl avetoo~ X X046 x
Emergeney mom physician fce (wahrea M etlmmed) BW100% X 40% XEmet9enc•me0ralVarePor121ron B~y~1 ~~ % W~% X
After 1 tt~reeUfgeni Care 8120 non~feuBnlive 40% %
Wspe
Facmry tea le q. no~Aa~roam) 9u;,t 009n X 405 XP~yseaNsurgeon fee BY6100% X CO% X
Af1x tm rtveaMervaVBenavwa~ nnaim oup~aen~ off.-e vcls $i0 nan~prwentr v X01 X~bY
After 1sttreeMentaUHehavioral ~eaM other anpatient tlans and aernces y70 non~preientne 40% XNeXa
MentaVBaharnrel heaR~npeteni lxCn~y lee (pg noepeai,00ml pge100'A. X 905. X
MerrtiVBehevglelheaM hpefiBni phySCiaN9urgeon lee Bq:100% X 40% X
Aha~ /Bf I!1roeSuOstanw Uw o~soNer anpet~erq oMce vaea 57o rw~-p~erenlie a.5v. xarts
ARer tst threeSUWtance Use disoNer other wq~atienl Xems arM services X70 nonprevenMe 40% XJsils
suosmnca usa npauam mcWry lee lap noaPeai raoml eacyQQ~ x ao°,. x
Substance usa dhortlar inpatient physlcieNwrgeontee p%tm% X 40~ X~Prenet~cary aM PreconcepNan NWe No cFurge
_......
No ha~,ga
..
Defrvery antl ell npatiern .Hoeplal 0%]gq,y, X 40% Xservieaz :.... .__... .. _.._.... . __._._ .............. .. _ _...... ........iProfa99ional 896100% % 40% XHone hearth care B9y 100% % ~pW~ XOulpetfeni Rehabtl0atpn s¢rvxm $]0 40% XOuyiazeM Hadnaibn eemcm E7o ui% K.... __ _
Sklbtl nursing care 9%~ X 40% XDureE4 matlNat equhmen~ 6Y„]gy,~ X W9c %Hospice service No charoe 0% X
-Eya ~ No rh2rPe N.q rhsrpo1 pas of glasses per yeas ~« cmmu ~ensas n nee a gmam~ No charge No MargeDrat Eimm
Preventive ~ Cleaning
P~~~~ ~ X~Y Not CAvared Nod CoveredSeal nis oar Toot
FW ~ 7 9uAaae Nm Carereo Not Coee,M
El~o9e0 Root or ENpletl Na Coveretl Not Covere0
McOeeRy namsary orUntlonHca Nod Covered Not Ccw~wt
See endnotes.
2016 Standard Benefit Plan Designs
9.5 EHB
Date: A~iFi6Mav 21, 2015
Summary of Benelils end Coverage
Member Cost Shve amounts tlaacribe the Enrollee's out of pocket costs. CaLsbopF4c Pha
YeO, MB,prat0dSs,eso n~egre~eaSt3,700 Mepimed
WA
W~ss,esotaa5ooWAN!A
~~~Arts tp Uiree
Prkiery~an vmbveat s~tgury. 6+ea~. or eanaton 09L nan9~ea~tneOman
After 1st three
Other practLLbnar once vbX pg5 riwi-prevenlHevales
SpalY.ort 0# %
PreeeniNa care/ecreenhy Ynmun¢atbn No eharge
126oralory Tm~9 Ox x
X-~ayseM. Diaerwstb lmegng 0% X
Ima9ng (CT1PET scene, MRW OA, X
r~r i ox, x
Tier 2 0~ x
Tier 3 0% X
Ter a oY, X
Sur9erytacYlry fee (eq, ASCU o% X
anyecrrvs„~eonrw. e~ x
oucpa~~ent vmn - o% x
EmaveKvmom lx9N re. tweNee l.annea) ar. x
Emergency room phyelclen fee (warvetl ii edmXled) 0% X
EmergencX medcd ear poneaon ox x
After 1 t three
Urgent care 0% iwn-preenlrvev~97ts
Fecflrytae (a 9 ~~a~ ~~0 0% X
PnysbleNsurgeon fee 0% ~%
Mer 1 W ttlrea
MaRAUBWgvnRliveall~oulD~b~t olM1ce ~6ls 0'A non-P~eenlneweae
After 1s1 three
MenleVHehavbrelheaM When ou~palieni M1emse~sendC~ 0% non-prarenHvevisits
MentaVBennw~x~naelm rpe~Ym; recurty tee-(epfwsprtN ~ooni) 09. x
MenisUBahevioral heats npatent physken/surgeon tee 0% X
Ma Iel mree
suw~„n, yea enorae~o~ncei~ionc<.~~s o+. rontxea,,.w~~
After tat Mree
Substartce Uee tlKo~dar other outpeller~ilwns arts aervtcaty 0% rgnyrevBnWaYisile
3ubemnce Uea npel~ent mdXy tee l0 9 ~Ot~ ~) 0! X
Substance uee tlaorder hpef tphyslcieNargeon fee 0% %
Prgra~el care aM p~eoonceplgn'Veb NoU+erge
Defrve~y anC en k~petient ~HoapNal o% X
OW(~a9entflehaOYllef services 0% %
Wf(mlent HeENYetCn eerulcea OA. x
Sk111Bd numhg care 0% X
DuRbIB m9Aoel eQY~~ Oi %
H 0% %ce aervce
EyB exmn No charpa
1 pair Of glasses per year (w conteci Ames n I'wu m gmsses) oM, X
Oral ExamPfeva~~hre - Cleanng
Preen itiw - X~rey Not CoveretlSealants per ToothTopcal FWorE~ AypkYtion
Specs Mamtanars - Foced
Amelgt+m FY ~ t SuthG NW Covaad
Raot Cane4 Mpler
~^9..:.. yon!Y per Ouoe'
Etlractlon-Shgle Toolli F~osed Root a E~upteG Not Covered
M~~~M^ Y NotCovered
See endnotes.
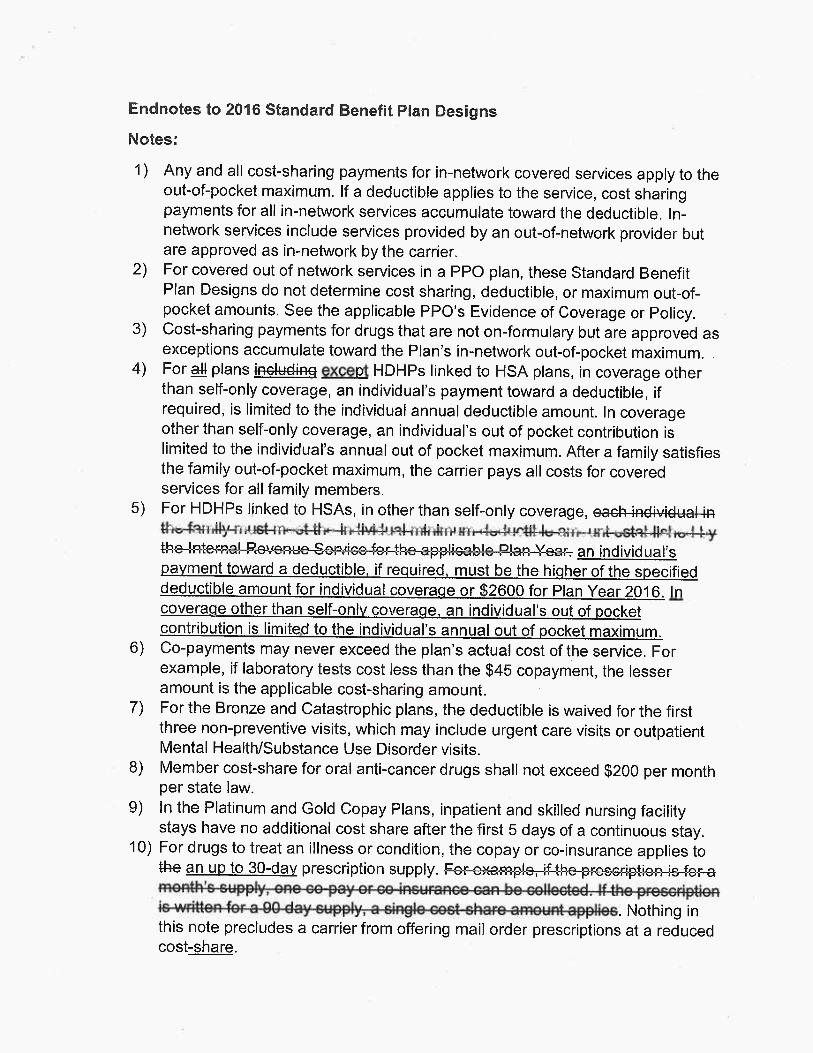
Endnotes to 2016 Standard Benefit Plan Designs
Notes:
1) Any and all cost-sharing payments for in-network covered services apply to theout-of-pocket maximum. If a deductible applies to the service, cost sharingpayments for all in-network services accumulate toward the deductible. In-network services include services provided by an out-of-network provider butare approved as in-network by the carrier.
2) For covered out of network services in a PPO plan, these Standard BenefitPlan Designs do not determine cost sharing, deductible, or maximum out-of-pocketamounts. See the applicable PPO's Evidence of Coverage or Policy.
3) Cost-sharing payments for drugs that are not on-formulary but are approved asexceptions accumulate toward the Plan's in-network out-of-pocket maximum.
4) For ail plans ~ except HDHPs linked to HSA plans, in coverage otherthan self-only coverage, an individual's payment toward a deductible, ifrequired, is limited to the individual annual deductible amount. In coverageother than self-only coverage, an individual's out of pocket contribution islimited to the individual's annual out of pocket maximum. After a family satisfiesthe family out-of-pocket maximum, the carrier pays all costs for coveredservices for all family members.
5) For HDHPs linked to HSAs, in other than self-only coverage,
. an individual'spayment toward a deductible, if required, must be the higher of the specifieddeductible amount for individual coverage or $2600 for Plan Year 2016. Incoverage other than self-only coverage, an individual's out of pocketcontribution is limited to the individual's annual out of pocket maximum.
6) Co-payments may never exceed the plan's actual cost of the service. Forexample, if laboratory tests cost less than the $45 copayment, the lesseramount is the applicable cost-sharing amount.
7) For the Bronze and Catastrophic plans, the deductible is waived for the firstthree non-preventive visits, which may include urgent care visits or outpatientMental Health/Substance Use Disorder visits.
8) .Member cost-share for oral anti-cancer drugs shall not exceed $200 per monthper state law.
9) In the Platinum and Gold Copay Plans, inpatient and skilled nursing facilitystays have no additional cost share after the first 5 days of a continuous stay.
10) For drugs to treat an illness or condition, the copay or co-insurance applies to#-fie an uq to 30-dav prescription supply. ,
.Nothing inthis note precludes a carrier from offering mail order prescriptions at a reducedcost-share.
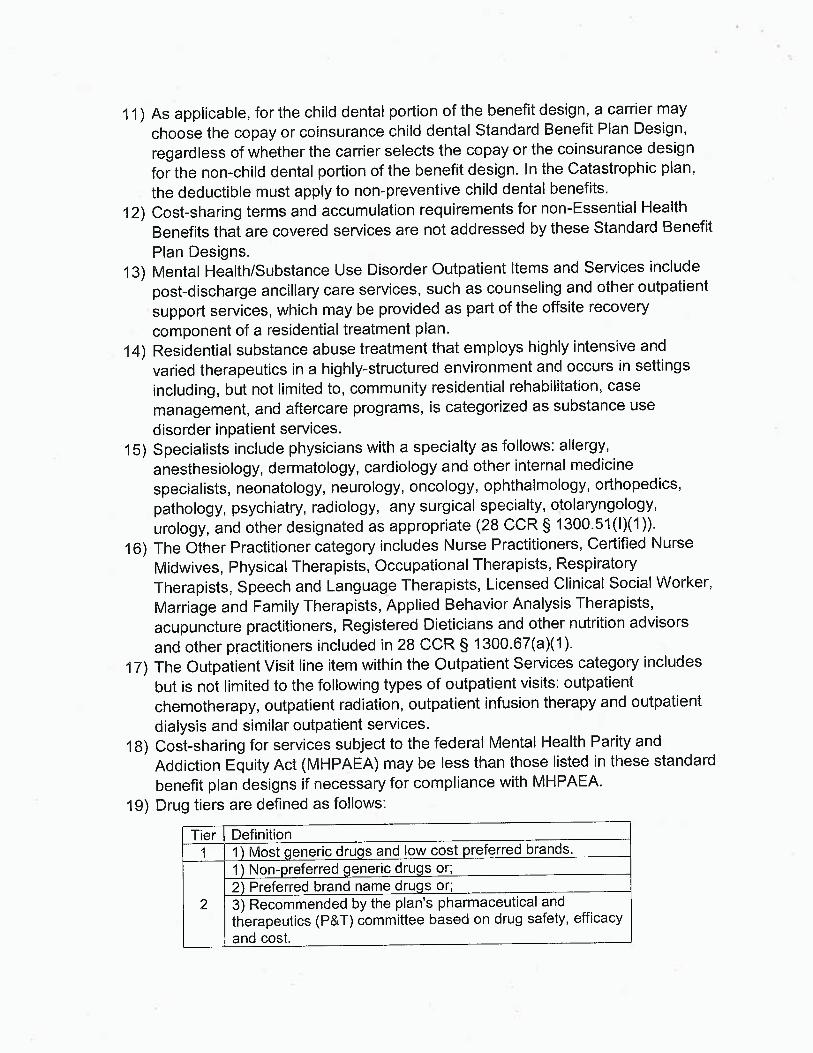
11) As applicable, for the child dental portion of the benefit design, a carrier may
choose the copay or coinsurance child dental Standard Benefit Plan Design,
regardless of whether the carrier selects the copay or the coinsurance design
for the non-child dental portion of the benefit design. In the Catastrophic plan,
the deductible must apply to non-preventive child dental benefits.
12) Cost-sharing terms and accumulation requirements for non-Essential Health
Benefits that are covered services are not addressed by these Standard Benefit
Plan Designs.
13) Mental Health/Substance Use Disorder Outpatient Items and Services include
post-discharge ancillary care services, such as counseling and other outpatient
support services, which may be provided as part of the offsite recovery
component of a residential treatment plan.
14) Residential substance abuse treatment that employs highly intensive and
varied therapeutics in ahighly-structured environment and occurs in settings
including, but not limited to, community residential rehabilitation, case
management, and aftercare programs, is categorized as substance use
disorder inpatient services.
15) Specialists include physicians with a specialty as follows: allergy,
anesthesiology, dermatology, cardiology and other internal medicine
specialists, neonatology, neurology, oncology, ophthalmology, orthopedics,
pathology, psychiatry, radiology, any surgical specialty, otolaryngology,
urology, and other designated as appropriate (28 CCR § 1300.51(1)(1)).
16) The Other Practitioner category includes Nurse Practitioners, Certified Nurse
Midwives, Physical Therapists, Occupational Therapists, Respiratory
Therapists, Speech and Language Therapists, Licensed Clinical Social Worker,
Marriage and Family Therapists, Applied Behavior Analysis Therapists,
acupuncture practitioners, Registered Dieticians and other nutrition advisors
and other practitioners included in 28 CCR § 1300.67(a)(1).
17) The Outpatient Visit line item within the Outpatient Services category includes
but is not limited to the following types of outpatient visits: outpatient
chemotherapy, outpatient radiation, outpatient infusion therapy and outpatient
dialysis and similar outpatient services.
18) Cost-sharing for services subject to the federal Mental Health Parity and
Addiction Equity Act (MHPAEA) may be less than those listed in these standard
benefit plan designs if necessary for compliance with MHPAEA.
19) Drug tiers are defined as follows:
Tier Definition1 1 Most eneric dru sand low cost referred brands.
1 Non- referred eneric dru s or;2 Preferred brand name dru s or;
2 3) Recommended by the plan's pharmaceutical andtherapeutics (P&T) committee based on drug safety, efficacyand cost.
1 Non- referred brand name dru s or;2) Recommended by P&T committee based on drug safety,
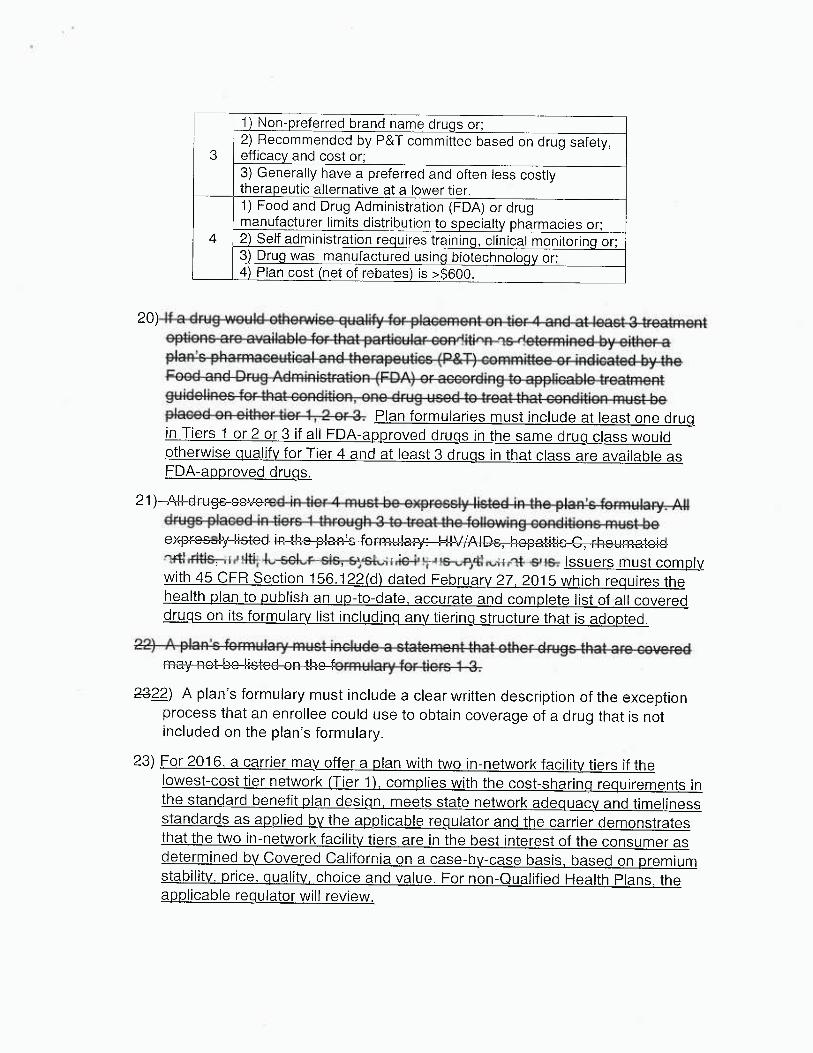
3 efficac and cost or;3) Generally have a preferred and often less costlythera eutic alternative at a lower tier.1) Food and Drug Administration (FDA) or drugmanufacturer limits distribution to s ecialt harmacies or;
4 2 Self administration re uires trainin ,clinical monitorin or;3 Dru was manufactured usin biotechnolo or;4 Plan cost net of rebates is >$600.
20)~n+ir~nc nrn ~~mil~hln fir+hit nor+in~il~r nnnrJi+inn ~c rlotarminocl h~i~ith~r n
0
Cr~nrl nni-! flr~in Arlminictr~+ir~ri r~nn~ nr ~nr~nrrlinn to ~nnlinohlo tro~tmnntrn iilJ~linnc fir +ham+ nnr~rJiti~ri nn~ rJri in i icon +n +rn~+ +hnt nnr~rlitinn mi ict ho
,~^~~~~T+;or' ̀' ̂ Y ~. Plan formularies must include at least one drugin Tiers 1 or 2 or 3 if all FDA-approved drugs in the same drug class wouldotherwise aualifv for Tier 4 and at least 3 druas in that class are available asFDA-approved drugs.
21) 'rin inc nlnnniJ in +i~rc i thr~~ ~nh 4 to +r~o+ ?ho fnlln~niinn nnnrli+i~nc m~ pct ho
~ qv ~iTCT+~Vr~l in Oho r~lnn'c fnrmiil~ni• I-II\//Alflc hor,oti+ic (` rho~im~tnirl. ~J, .~~., o e
. issuers must comKwith 45 CFR Section 156.122(d~ dated February 27, 2015 which requires thehealth plan to publish an up-to-date, accurate and complete list of all covereddrugs on its formulary list including any tiering structure that is adopted.
X322) A plan's formulary must include a clear written description of the exceptionprocess that an enrollee could use to obtain coverage of a drug that is notincluded on the plan's formulary.
23) For 2016, a carrier may offer a plan with two in-network facility tiers if thelowest-cost tier network (Tier 1), complies with the cost-sharing requirements inthe standard benefit plan design, meets state network adequacy and timelinessstandards as applied bathe applicable regulator and the carrier demonstratesthat the two in-network facility tiers are in the best interest of the consumer asdetermined by Covered California on a case-by-case basis, based on premiumstability, price, quality, choice and value. For non-Qualified Health Plans, theapplicable regulator will review.
• ~ GO~/~RE~'; ' CALIFtlRN1A
Yid
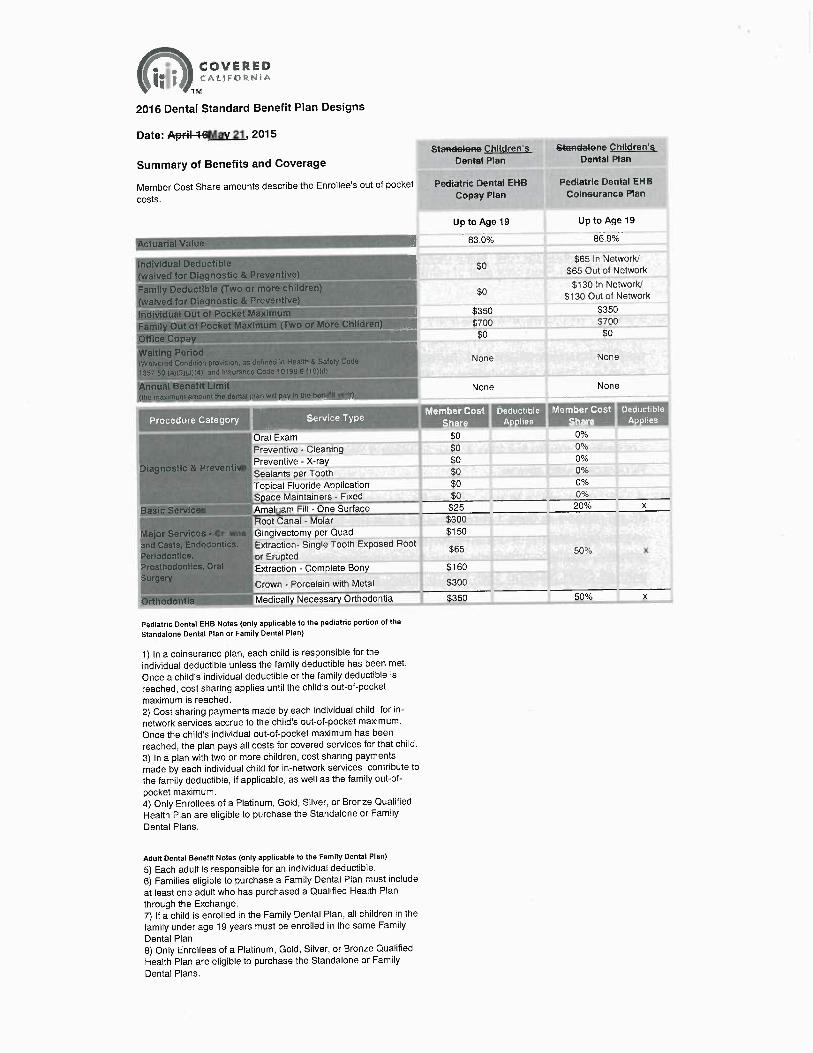
2016 Dental Standard Benefit Plan Designs
Date: ~lpr+~1-6Mav 21, 2015
Summary of Benefits and CoverageStawdaier+e Children's SFa~daler~e Ch7)dren's
Dental Plan Denial Plan
Member Cost Share amounts describe the Enrollee's out of pocket Pediatric Dental EHB Pediatric Dental EHB
costs. Copay Plan Coinsurance Plan
Actuarial Value
Individual Deductible $~
(waived for Diagnostic & Preventivo)
Family Deductible (fwo or more children) - $p
(waived for Diagnostic $c Preventive)
Individual Out of Packet Maximum ''~,~ $350
Family Out of Pocket Maximum {Two or More Children} ~ $700
Otilce Copay .,~ $0
Waiting PeriodIWoivarod Contlitlon provision, as d~Gned in Heath 6 Safety Cado - ~~ ~ NOf18
X357 50 (a)(3J~J)(4) and ~nsuranco Code t0i98 6 (i0)(0}
Annual Benefit Limit None¢he maximum amount tho donial plan will pay in the bo~jt)
•, . E71I~ I
" " Oral Exam $0
Preventive -Cleaning $0
diagnostic & Preventi Preventive - X-ray $0
k ~ Sealants per Tooth $0
Topical Fluoride Application $0
Space Maintainers -Fixed $0
Basic Services Amal am Fill -One Surface $25
Root Canal -Molar $300
Major Servicos -Crown Gingivectomy per Quad $150
and Casts, Endodontics. • Extraction- Single Tooth Exposed Root
periodon[ica, t of Erupted $65
Prosthodontics, Oral Extraction -Complete Bony $160Surgery
Crown -Porcelain with Metal $300
Orthodontia Medically Necessary Orthodontia $350
Up to Age 19 Up to Age 19
83.0% 86.8%
Pediatric Dental EHB Notes (only applicable to the pediatric portion of the
Standalone Dental Plan or Family Dental Plan)
1) In a coinsurance plan, each child is responsible for the
individual deductible unless the family deductible has been met.
Once a child's individual deductible or the family deductible is
reached, cost sharing applies until the child's out-of-pocket
maximum is reached.2) Cost sharing payments made by each individual child for in-
network services accrue to the child's out-of-pocket maximum.
Once the child's individual out-of-pocket maximum has been
reached, the plan pays all costs for covered services for that child.
3) in a plan with two or more children, cost sharing payments
made by each individual child for in-network services contribute to
the family deductible, if applicable, as well as the family out-of-
pocket maximum.4) Only Enrollees of a Platinum, Gold, Silver, or Bronze Qualified
Health Ptan are eligible to purchase the Standalone or Family
Dental Plans.
Adult Dental Benefit Notes (only applicable to the Family Dental Plan)
5) Each adult is responsible for an individual deductible.
6) Families eligible to purchase a Family Dental Plan must include
at least one adult who has purchased a Qualified Health Plan
through the Exchange.
7) If a child is enrolled in the Family Dental Plan, all children in the
family under age 19 years must be enrolled in the same Family
Dental Plan.8) Only Enrollees of a Platinum, Gold, Silver, or Bronze qualified
Health Plan are eligible to purchase the Standalone or Family
Dental Plans.
$65 In Network/
$65 Out of Network
$130 In Network/
$130 Out of Network
$350$goo$0
None
None
0%0%0%0%0°i20% x
50°o x
50% x
• •r~ CO~i'~~~D~;f' CALIFORNIA
TM
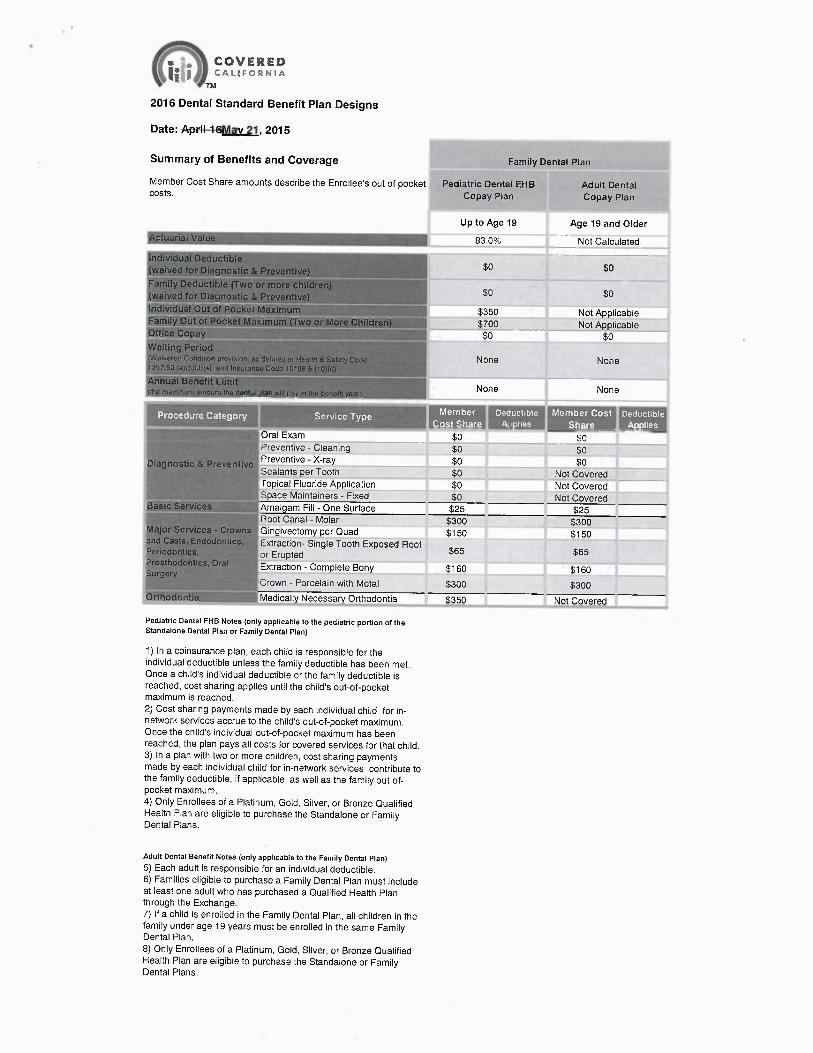
2016 Dental Standard Benefit Plan Designs
Date: A~i1-a-6Mav 21, 2015
Summary of Benefits and Coverage Family Dental Pian
Member Cost Share amounts describe the Enrollee's out of pocket Pediatric Dental EHB Adult Dentaicosts. Copay Plan Copay Plan
Up to Age 19 Age 19 and Older
Actuarial Value ?' 83.0% Not Calculated
Individual Deductible g0 $0(waived for Diagnostic & Prevontive)
Fatuity Deductible (T'wo or morn children} -(waived for Diagnostic &Preventive} $0 $0
lndividua! Out of Pocket Maximum ~ $350 Not ApplicableFamily Out of Pocket Maximum (Two or More Children} `~ $700 Not ApplicableOffice Copay ~ $0 $0Waiting Period(Waivorc~tl Condi~io~ provision, as delined in Health 8 Sn(ory• Coda NOf1@ NOf18 -7357.50 (a)(3)W)(4) and Insurance; CoUe t6~88.6 (7 D)(d)
Annual Benefit Limit None Nonephe maximum amount tha tlantal plan will pay m Use ~enufrt yo2r)
Oral Exam $0 $0Preventive -Cleaning $0 $0
Diagnostic &Preventive Preventive - X-ray $0 $0Sealants per Tooth $0 Not CoveredTopical Fluoride Application $0 Not CoveredSpace Maintainers -Fixed $0 Not Covered
Basic Services Amalgam Fill -One Surface $25 $25Root Canal -Molar $300 $300
Major Services -Crowns Gingiveciomy per Quad $150 $150and Casts, Endodontics, Extraction- Single Tooth Exposed RootPeriodontics, or Erupted $65 $65Proschodontics, Oral Extraction -Complete Bony $160 $160Surgery
Crown -Porcelain with Metal $300 $300Orthodontia Medically Necessary Orthodontia $350 Not Covered
Pediatric Dental EHB Notes (only applicable to the pediatric portion of theStandalone Dental Plan or Family Dental Plan)
1) In a coinsurance plan, each child is responsible for theindividual deductible unless the family deductible has been met.Once a child's individual deductible or the family deductible isreached, cost sharing applies until the child's out-of-pocketmaximum is reached.2) Cost sharing payments made by each individual child for in-network services accrue to the child's out-of-pocket maximum.Once the child's individual out-of-pocket maximum has beenreached, the plan pays all costs for covered services for that child.3) In a plan with two or more children, cost sharing paymentsmade by each individual child for in-network services contribute tothe family deductible, if applicable, as well as the family out-of-pocketmaximum.4) Only Enrollees of a Platinum, Gold, Silver, or Bronze QualifiedHealth Plan are eligible to purchase the Standalone or FamilyDental Plans.
Adult Dental Benefit Notes (only applicable to the Family Dental Plan)5) Each adult is responsible for an individual deductible.6) Families eligible to purchase a Family Dental Plan must includeat Ieast one adult who has purchased a Qualified Health Planthrough the Exchange.7) If a child is enrolled in the Family Dental Plan, all children in thefamily under age 19 years must be enrolled in the same FamilyDental Plan.8) Only Enrollees of a Platinum, Gold, Silver, or Bronze QualifiedHealth Plan are eligible to purchase the Standalone or FamilyDental Plans.
. ~~ COV~R~~.f1~t'~ ca~rFoaNia
Tu
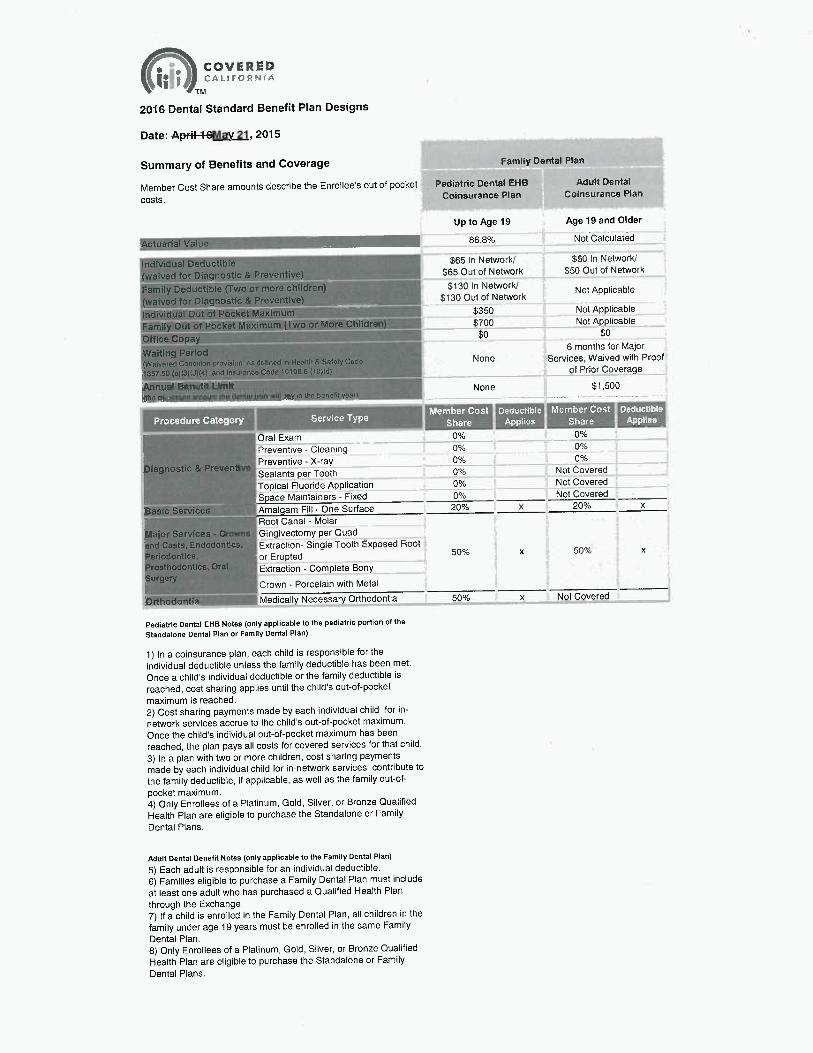
2016 Dental Standard Benefit Pian Designs
Date: ~6Mav 21, 2015
Summary of Benefits and Coverage Family Derrtal Play
Member Cost Share amounts describe the Enrollee's out of pocket Pediatric Dental EHB Adult Dental
costs. Coinsurance PFan Coinsurance Plan
Actuarial Value
Individual Deductible
(waived for Diagnostic &Preventive)
Family Deductible (Two or more cfifidren
(waived for Diagnostic &Preventive)
individual Out of Pocket Maximum
Family Out of Pocket Maximum (Two or
Office Copay
Waging Per(od
Up to Age 19 Age 19 and Older
86.8% Not Calculated
$65 In Network/ $50 In Network/
$65 Out of Network $50 Out of Network
$130 In Network/ Not Applicable$130 Out of Network
$350 Not Applicable
$700 Not Applicable
$0 $0
6 months for Major
{Wnivereu CandNon provisinn, ;+s dc+finod in Hoalth R Sntoty Coue None Services, Waived with Proof
1357.50 (a)(3)(J)(a) and Insuranw Cole t0~98b (10y(d~ ~ of Prior Coverage
Mnual Benefit Limit None $1,500(tie mrsximum amoum iho aunial plan wail pay m she DB~,O,ar~
.,. ~ ,~~
Oral Exam 0% 0%
Preventive - Cleaning 0% 0°/,
Diagnostic &Preventive Preventive - X-ray 0~% 0%
Sealants per Tooth 0 /o Not Covered
Topical Fluoride Application 0°/a Not Covered
Space Maintainers -Fixed 0% Not Covered
Basic Services Amalgam Fill -One Surface 20% x 20% x
Root Canal -Molar
Major Services -Crowns Gingivectomy per quad
and Casts, Endodontics, Extraction- Single Tooth Exposed Root
Periodontics, or Erupted 50% x 50°~6 x
Prosthodontics, Or Extraction -Complete BonySurgery ,
,' Crown -Porcelain with Metal
Orthodontia i+i~ Medically Necessary Orthodontia 50 % x Not Covered
Pediatric Dental EHB Notes (only applicable to the pediatric portion of the
Standalone Dental Plan or Family Dental Plan)
1) In a coinsurance plan, each child is responsible for the
individual deductible unless the family deductible has been met.
Once a child's individual deductible or the family deductible is
reached, cost sharing applies until the child's out-of-pocket
maximum is reached.
2) Cost sharing payments made by each individual child for in-
network services accrue to the child's out-of-pocket maximum.
Once the child's individual out-of-pocket maximum has been
reached, the plan pays all costs for covered services for that child.
3) In a plan with two or more children, cost sharing payments
made by each individual child for in-network services contribute to
the family deductible, if applicable, as wail as the family out-of-
pocket maximum.4) Only Enrollees of a Platinum, Gold, Silver, or Bronze Qualified
Health Plan are eligible to purchase the Standalone or Family
Dental Plans.
Adult Dental Benefit Notes (only applicable to the Family Dental Plan)
5) Each adult is responsible for an individual deductible.
6) Families eligible to purchase a Family Dental Plan must include
at least one adult who has purchased a Qualified Health Plan
through the Exchange.
7) If a child is enrolled in the Family Dental Plan, all children in the
family under age 19 years must be enrolled in the same Family
Dental Plan.
8) Only Enrollees of a Platinum, Gold, Silver, or Bronze Qualified
Health Plan are eligible to purchase the Standalone or Family
Dental Plans.





























