Embed Size (px)
Citation preview

Abstract Gamma irradiation from Cobalt 60
sources has been used to terminally sterilize bone
allografts for many years. Gamma radiation
adversely affects the mechanical and biological
properties of bone allografts by degrading the
collagen in bone matrix. Specifically, gamma rays
split polypeptide chains. In wet specimens irra-
diation causes release of free radicals via radiol-
ysis of water molecules that induces cross-linking
reactions in collagen molecules. These effects are
dose dependent and give rise to a dose-dependent
decrease in mechanical properties of allograft
bone when gamma dose is increased above
25 kGy for cortical bone or 60 kGy for cancellous
bone. But at doses between 0 and 25 kGy (stan-
dard dose), a clear relationship between gamma
dose and mechanical properties has yet to be
established. In addition, the effects of gamma
radiation on graft remodelling have not been
intensively investigated. There is evidence that
the activity of osteoclasts is reduced when they
are cultured onto irradiated bone slices, that
peroxidation of marrow fat increases apoptosis of
osteoblasts; and that bacterial products remain
after irradiation and induce inflammatory bone
resorption following macrophage activation.
These effects need considerably more investiga-
tion to establish their relevance to clinical out-
comes. International consensus on an optimum
dose of radiation has not been achieved due to a
wide range of confounding variables and indi-
vidual decisions by tissue banks. This has resulted
in the application of doses ranging from 15 to
35 kGy. Here, we provide a critical review on the
effects of gamma irradiation on the mechanical
and biological properties of allograft bone.
Keywords Allograft bone Æ Bone allograft
healing/remodelling Æ Allograft osteoinduction ÆDose-dependent effect Æ Gamma radiation ÆMechanical properties Æ Terminal sterilization
Introduction
Bone banks supply a wide range of tissue,
including massive bone allografts cortical bone
allografts, and milled bone. These products play
an important role in filling bone defects during
surgery aimed at improving the mobility of pa-
H. Nguyen Æ M. R. Forwood (&)Department of Anatomy and DevelopmentalBiology, The University of Queensland, School ofBiomedical Sciences, Brisbane, Qld 4072, Australiae-mail: [email protected]
D. A. F. MorganThe University of Queensland, Brisbane PrivateHospital, Brisbane, Australia 4000
H. Nguyen Æ D. A. F. MorganQueensland Bone Bank, Brisbane, Australia
Cell Tissue Banking (2007) 8:93–105
DOI 10.1007/s10561-006-9020-1
123
REVIEW PAPER
Sterilization of allograft bone: effects of gamma irradiationon allograft biology and biomechanics
Huynh Nguyen Æ David A. F. Morgan ÆMark R. Forwood
Received: 18 December 2005 / Accepted: 10 May 2006 / Published online: 25 October 2006� Springer Science+Business Media B.V. 2006
tients, and reducing the disability associated with
bone and joint diseases. However, the use of bone
allografts carries a risk of transferring bacteria,
viruses or prions from donor to recipient. To
eliminate potential infection, donor screening is
important along with aseptic surgical technique
during tissue retrieval, processing and storage
(AATB 2002; Andre and Liz 2000; Angermann
and Jepsen 1991; Boyce et al. 1999; Eastlund and
Strong 2003; IAEA 2002). Following tissue pro-
cessing, many banks consider it essential for
allografts to be terminally sterilized using gamma
irradiation from Cobalt 60 sources (Kennedy
et al. 2005). This issue has become controversial
in the bone bank community as the industry
debates whether it is necessary to use radiation to
sterilize bone. If so, the question is whether
25 kGy (standard dose) is justified as a gold
standard, or whether a lower dose for sterilization
can still minimize the risk of infection but reduce
the adverse effects of radiation? The aim of this
paper is to critically analyse the effects of gamma
radiation on mechanical and biological properties
of banked bones.
Effects of gamma radiation on mechanical
properties of bone allografts
When massive bone allografts are implanted, they
replace the functions of the removed bone. They
are often used to provide a scaffold to support
weak parts of the skeleton, to act as a bridge to
cover bone defects, and to provide a frame for
modeling new bone (Triantafyllou et al. 1975). It
usually takes several months, or even years, for
grafts to incorporate and be remodelled into new
bone. Therefore, mechanical properties of the
bone allografts must be as close as possible to the
original bone to reproduce its mechanical support
and structural integrity.
Multiple factors contribute to the biomechan-
ical performance of bone allografts (Davy 1999).
These may be the properties of the graft itself, the
interfaces between grafts and the host bone, and
the nature of the applied loads to the graft-host
bone complex. Unfortunately, in the process of
sterilization, the mechanical properties of bone
allografts can be impaired by gamma radiation
(Anderson et al. 1992; Cornu et al. 2000; Currey
et al. 1997; Gibbons et al. 1991; Hamer et al.
1996; Rasmussen et al. 1994; Vastel et al. 2004);
and these effects are dose-dependent (Fideler
et al. 1995; Hamer et al. 1996; Salehpour et al.
1995). The mechanism of mechanical impairment
has been explained, but the degree of change
varies among reports.
Mechanism of tissue damage by gamma
radiation
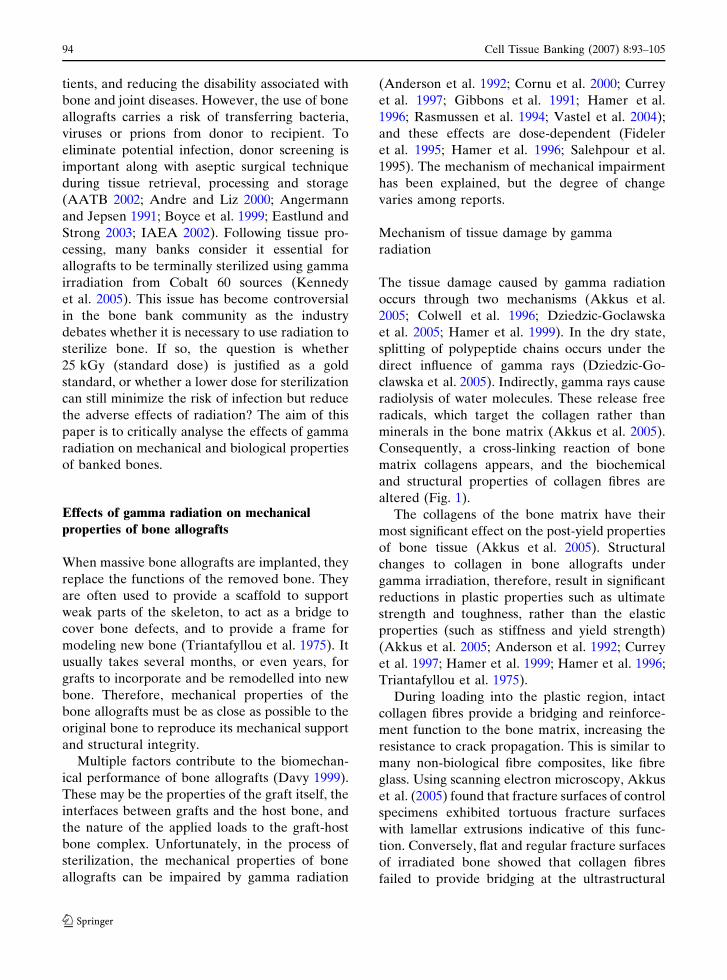
The tissue damage caused by gamma radiation
occurs through two mechanisms (Akkus et al.
2005; Colwell et al. 1996; Dziedzic-Goclawska
et al. 2005; Hamer et al. 1999). In the dry state,
splitting of polypeptide chains occurs under the
direct influence of gamma rays (Dziedzic-Go-
clawska et al. 2005). Indirectly, gamma rays cause
radiolysis of water molecules. These release free
radicals, which target the collagen rather than
minerals in the bone matrix (Akkus et al. 2005).
Consequently, a cross-linking reaction of bone
matrix collagens appears, and the biochemical
and structural properties of collagen fibres are
altered (Fig. 1).
The collagens of the bone matrix have their
most significant effect on the post-yield properties
of bone tissue (Akkus et al. 2005). Structural
changes to collagen in bone allografts under
gamma irradiation, therefore, result in significant
reductions in plastic properties such as ultimate
strength and toughness, rather than the elastic
properties (such as stiffness and yield strength)
(Akkus et al. 2005; Anderson et al. 1992; Currey
et al. 1997; Hamer et al. 1999; Hamer et al. 1996;
Triantafyllou et al. 1975).
During loading into the plastic region, intact
collagen fibres provide a bridging and reinforce-
ment function to the bone matrix, increasing the
resistance to crack propagation. This is similar to
many non-biological fibre composites, like fibre
glass. Using scanning electron microscopy, Akkus
et al. (2005) found that fracture surfaces of control
specimens exhibited tortuous fracture surfaces
with lamellar extrusions indicative of this func-
tion. Conversely, flat and regular fracture surfaces
of irradiated bone showed that collagen fibres
failed to provide bridging at the ultrastructural
94 Cell Tissue Banking (2007) 8:93–105
123
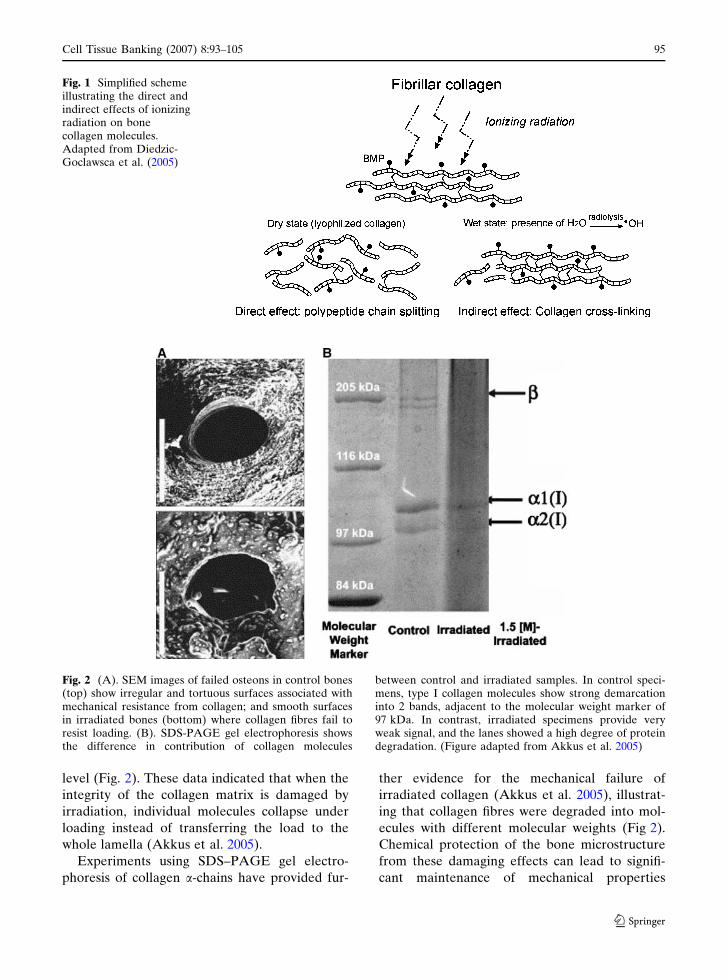
level (Fig. 2). These data indicated that when the
integrity of the collagen matrix is damaged by
irradiation, individual molecules collapse under
loading instead of transferring the load to the
whole lamella (Akkus et al. 2005).
Experiments using SDS–PAGE gel electro-
phoresis of collagen a-chains have provided fur-
ther evidence for the mechanical failure of
irradiated collagen (Akkus et al. 2005), illustrat-
ing that collagen fibres were degraded into mol-
ecules with different molecular weights (Fig 2).
Chemical protection of the bone microstructure
from these damaging effects can lead to signifi-
cant maintenance of mechanical properties
Fig. 1 Simplified schemeillustrating the direct andindirect effects of ionizingradiation on bonecollagen molecules.Adapted from Diedzic-Goclawsca et al. (2005)
Fig. 2 (A). SEM images of failed osteons in control bones(top) show irregular and tortuous surfaces associated withmechanical resistance from collagen; and smooth surfacesin irradiated bones (bottom) where collagen fibres fail toresist loading. (B). SDS-PAGE gel electrophoresis showsthe difference in contribution of collagen molecules
between control and irradiated samples. In control speci-mens, type I collagen molecules show strong demarcationinto 2 bands, adjacent to the molecular weight marker of97 kDa. In contrast, irradiated specimens provide veryweak signal, and the lanes showed a high degree of proteindegradation. (Figure adapted from Akkus et al. 2005)
Cell Tissue Banking (2007) 8:93–105 95
123
(Grieb et al. 2005), but the safety of such radio-
protectants for use in humans needs greater
scrutiny in comparison to simply reducing the
radiation dose.
Mechanical changes in irradiated allograft
bone—a controversial issue
The effects of gamma radiation on biomechanical
properties of bone allografts are well documented,
and irradiation is suspected as the most damaging
factor for mechanical properties of bone allografts
during processing and sterilization (Triantafyllou
et al., 1975). For example, frozen bovine cortical
bone specimens (sized 8 · 0.5 · 0.5 cm), irradi-
ated at a dose of 30 ± 3 kGy, display reductions in
strength of 25–50% compared to control bone;
and similar reductions in maximum torque and
stress of rabbit tibiae of 23 and 25%, respectively,
have been observed (Godette et al. 1996),
Currey et al. (1997) reported that the standard
dose of 25 kGy significantly reduces bone
strength. They observed minimal differences in
the elastic Young’s modulus, but progressive
decreases in the plastic behaviour between bones
irradiated at 29.5 kGy and control specimens.
The bending strength of bone irradiated at the
standard dose, for example, was around 20–30%
lower than control groups. More importantly,
irradiation severely diminished work-to-fracture
by more than 70%. The results support the fact
that irradiation has little influence on the stiffness
of bone, but that brittleness is significantly
increased (Currey et al. 1997). This pattern of
failure is consistently observed (Akkus et al.
2005; Cornu et al. 2003; Hamer et al. 1999). For
example, Hamer et al. (1996) reported decreases
in the energy absorption capacity and bone
strength at doses between 28–30 kGy, while the
elastic properties were only mildly affected. The
maximum load declined by 36% and the work to
fracture by 68%, while the yield strength was only
reduced by 17%. Similarly, post-yield properties
such as work to fracture and post-yield energy of
the grafts were reduced by 70 and 87%, respec-
tively, following irradiation at 36.4 kGy, while
elastic energy was decreased by only 26% com-
pared to control (Akkus et al. 2005). Irradiation
also affects the fatigue behaviour of allografts
with evidence that it causes dramatic reductions
of 87% in fatigue life (cycles/1,000) at 36.4 kGy
(Akkus and Belaney 2005), and reduces the
resistance of bone to crack propagation (Mitchell
et al. 2004).
In clinical practice, of course, what is important
is the performance of the allograft during its
working life in patients. In a 3 year follow-up of
127 massive allografts sterilized by gamma irra-
diation (25 kGy), the rates of mechanical com-
plications such as fracture and non-union were
only 6 and 5.5%, respectively (Hernigou et al.
1993). These did not differ from other reports
using non-irradiated grafts. They concluded,
therefore, that irradiating allograft bone 25 kGy
was the most convenient and acceptable method
for sterilization. In contrast, Lietman et al. (2000)
found that the fracture rate in a patient group
implanted with irradiated grafts was more than
double that of a control group (38% vs. 18%).
Although they may have some observational rel-
evance, such case control studies are less rigorous
than clinically controlled trials, and more difficult
to interpret. This is because they are confounded
by factors such as recipient age, types of graft,
stage of original diseases, adjuvant therapy, fixa-
tion techniques, co-morbidity and weight bearing,
rather than gamma radiation alone (Hornicek
et al. 2001).
The use of massive osteochondral allografts
such as the proximal femur, distal femur and
proximal tibia is increasing in clinical practice.
These allografts contain both cortical and can-
cellous bone and are indicated for reconstruction
of large joints such as the hip and knee. In these
cases, cancellous bone is predominately loaded in
compression (Anderson et al. 1992). Therefore,
the effects of irradiation on mechanical properties
of cancellous bone also need to be considered.
Cancellous bone is more resistant to gamma
irradiation than cortical bone. Using cancellous
bone cubes from the tibial plateau, Anderson
et al. (1992) found no significant differences
between a control group and groups irradiated at
10, 31 and 51 kGy in failure stress. The failure
stress of these groups remained 78.9, 88.5 and 102
% of control value, respectively. However, it was
significantly reduced when radiation dose
increased to 60 kGy, only 23.9%. Similarly, iliac
96 Cell Tissue Banking (2007) 8:93–105
123
crest wedges irradiated up to 20–25 kGy showed
minimal change in elastic modulus, compressive
strength and strain to failure, compared to non-
irradiated bone (Zhang et al. 1994).
With lower doses, such as 15–20 kGy, there is
very little affect of radiation on the properties of
bone allografts (Jinno et al. 2000; Pelker et al.
1989). When irradiated at 15 kGy, bone allografts
implanted into rat femora showed no deleterious
change in the bone strength after 4 months post-
transplantation (Jinno et al. 2000). Furthermore,
the strength of processed allogeneic grafts was
significantly higher than fresh allogeneic grafts.
Similarly, the force for screw pullout between
control and irradiated grafts (15.7–18.7 kGy) is
not significantly different (Simonian et al. 1994).
Unfortunately, the range of studies using doses
less than 25 kGy, is relatively small and further
work is required to verify the effects of lower
doses, while still achieving adequate sterilization.
The dose-response range, therefore, requires
further scrutiny.
Dose-dependent effect of irradiation
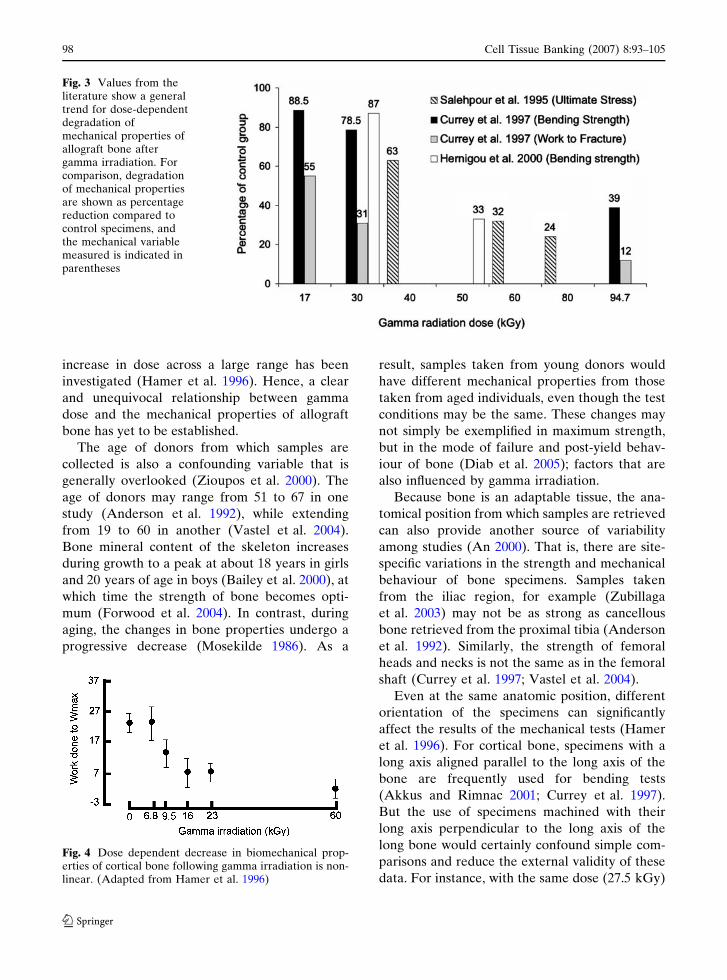
There is a general consensus that the strength of
allograft bone decreases in a dose-dependent
manner (Anderson et al. 1992; Currey et al. 1997;
Fideler et al. 1995; Gibbons et al. 1991; Hamer
et al. 1996; Salehpour et al. 1995) (Fig. 3).
For example, the bending strength of bone
allografts decreased by 10%, 20% and more than
50% as the gamma dose increased from 17 kGy
(low dose), to 29.5 kGy (standard) and 94.7 kGy
(high), respectively (Currey et al. 1997). More-
over, work-to-fracture decreased by 30–40%,
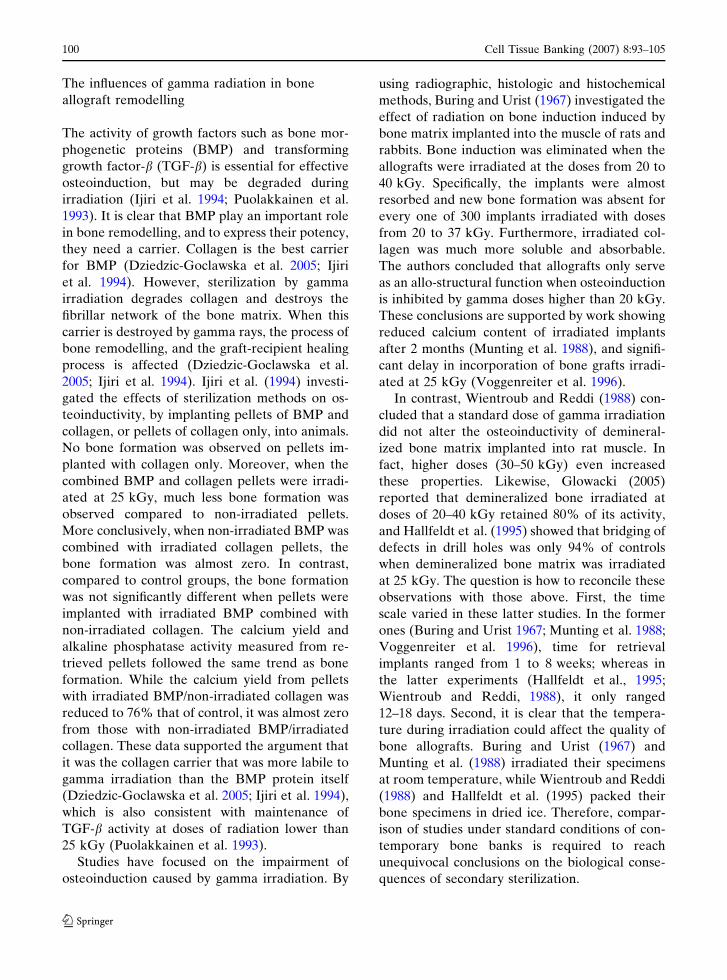
50–60%, and 90%. With a lower dose series, 0,
6.8, 9.5, 16, 23 and 60 kGy, a small dose-response
reduction was observed in work done to ultimate
stress up to 23 kGy, but a bigger decrease was
observed at 60 kGy (Fig. 4). (Hamer et al., 1996).
Similar trends have been observed from bone-
tendon-bone allografts in which the maximum
stress decreased by 37% for those irradiated at
40 kGy, 68% at 60 kGy and 76% at 80 kGy
(Salehpour et al. 1995); whereas lower doses of 20
and 30 kGy reduced the ultimate strength by
11–27% compared with controls (Gibbons et al.
1991; Hernigou et al. 2000). Increasing the
gamma dose with numerous small increments
shows that this relationship is non-linear with a
dose of 27 kGy causing a reduction in strength of
20%, but a dose of 37 kGy causing a reduction of
65% (Loty et al. 1990).
This dose-response reduction in allograft
strength is not only observed ex vivo, but affects
the success of the implanted bone. After being
implanted in rabbits for 6 weeks, the non-union
rate of irradiated graft-host bone was positively
related to the irradiation dose of the allografts
with rates increasing from 0 to 12.5 and 33% as
the gamma dose increased from 0 to 25 and
75 kGy (Godette et al. 1996).
Confounding variables for interpretation of
biomechanical studies
The evidence is consistent that gamma irradiation
causes a dose-response reduction in the mechanical
properties of allograft bone. Nonetheless, while
most authors agree that high doses of gamma
radiation (e.g. 40–60 kGy or more) cause deleteri-
ous effects, the influence of lower doses remains
debatable. Furthermore, interpretation of data is
confounded by the range of gamma doses applied,
and by other factors such as the age and sex of
donors, anatomical position of specimens, size of
specimens and especially direction of specimen and
type of mechanical tests (Zioupos et al. 2000).
Interpretation of different studies is very
difficult when the range of gamma doses, and the
definition of ‘‘standard dose’’, is very wide. The use
of ‘‘standard dose’’ has varied from 25–35 kGy,
with some authors adopting 25–30 kGy (Cornu
et al. 2000; Currey et al. 1997; Hamer et al. 1996;
Smith et al. 1996), but others reporting even
higher ‘‘standard’’ doses (Akkus and Rimnac 2001;
Dziedzic-Goclawska et al. 1991). The higher doses
adopted are those expected to eliminate viral
infection, with doses ranging from 40 to 50, 60 and
even 94 kGy (Campbell and Li 1999; Currey et al.
1997; Hernigou et al. 2000). This is because the
D10 value of HIV virus was very different among
studies. It may range from 4 to 8.3 kGy depending
on the irradiation environment (Dziedzic-
Goclawska et al. 1991). Moreover, there are
limited studies in which a small, but continuous,
Cell Tissue Banking (2007) 8:93–105 97
123
increase in dose across a large range has been
investigated (Hamer et al. 1996). Hence, a clear
and unequivocal relationship between gamma
dose and the mechanical properties of allograft
bone has yet to be established.
The age of donors from which samples are
collected is also a confounding variable that is
generally overlooked (Zioupos et al. 2000). The
age of donors may range from 51 to 67 in one
study (Anderson et al. 1992), while extending
from 19 to 60 in another (Vastel et al. 2004).
Bone mineral content of the skeleton increases
during growth to a peak at about 18 years in girls
and 20 years of age in boys (Bailey et al. 2000), at
which time the strength of bone becomes opti-
mum (Forwood et al. 2004). In contrast, during
aging, the changes in bone properties undergo a
progressive decrease (Mosekilde 1986). As a
result, samples taken from young donors would
have different mechanical properties from those
taken from aged individuals, even though the test
conditions may be the same. These changes may
not simply be exemplified in maximum strength,
but in the mode of failure and post-yield behav-
iour of bone (Diab et al. 2005); factors that are
also influenced by gamma irradiation.
Because bone is an adaptable tissue, the ana-
tomical position from which samples are retrieved
can also provide another source of variability
among studies (An 2000). That is, there are site-
specific variations in the strength and mechanical
behaviour of bone specimens. Samples taken
from the iliac region, for example (Zubillaga
et al. 2003) may not be as strong as cancellous
bone retrieved from the proximal tibia (Anderson
et al. 1992). Similarly, the strength of femoral
heads and necks is not the same as in the femoral
shaft (Currey et al. 1997; Vastel et al. 2004).
Even at the same anatomic position, different
orientation of the specimens can significantly
affect the results of the mechanical tests (Hamer
et al. 1996). For cortical bone, specimens with a
long axis aligned parallel to the long axis of the
bone are frequently used for bending tests
(Akkus and Rimnac 2001; Currey et al. 1997).
But the use of specimens machined with their
long axis perpendicular to the long axis of the
long bone would certainly confound simple com-
parisons and reduce the external validity of these
data. For instance, with the same dose (27.5 kGy)
Fig. 3 Values from theliterature show a generaltrend for dose-dependentdegradation ofmechanical properties ofallograft bone aftergamma irradiation. Forcomparison, degradationof mechanical propertiesare shown as percentagereduction compared tocontrol specimens, andthe mechanical variablemeasured is indicated inparentheses
Fig. 4 Dose dependent decrease in biomechanical prop-erties of cortical bone following gamma irradiation is non-linear. (Adapted from Hamer et al. 1996)
98 Cell Tissue Banking (2007) 8:93–105
123

and from the same donors, the work-to-fracture
of transverse specimens was as low as 38% com-
pared to controls, but was up to 51% in specimens
with the axis aligned longitudinally with the bone
axis (Akkus and Rimnac 2001). Therefore, the
results from Currey’s study (Currey et al. 1997),
using longitudinal beams is more difficult to
compare with Hamer et al. (1996), who used
transverse sections.
In conclusion, gamma irradiation causes a
dose-dependent decrease in mechanical proper-
ties of allograft bone when the doses are signifi-
cantly and highly increased. However, at doses
between 0 and 25 kGy (our standard dose), a
clear relationship between gamma dose and
mechanical properties has not been established,
partly due to a range of confounding variables.
Therefore, there is still considerable justification
for further studies on the influence of gamma
irradiation on the mechanical properties of allo-
graft bone in which variability due to age, sex,
anatomical position, and range of gamma doses
has been controlled.
The correlation between bone allograft biology
and gamma radiation sterilization
Mechanism of bone allograft healing/
remodelling
To replace the functions of removed bone, the
mineralized allograft must facilitate biological
activity at the graft site. This activity includes the
provision of an osteoconductive surface for
remodelling, incorporation with the host skeleton,
facilitation of bone resorption and formation
phases of remodelling and biological acceptability
with the host. The biology of bone graft healing
has been well investigated (Aspenberg et al. 1996;
Enneking and Campanacci 2001; Enneking and
Mindell 1991; Heiple et al. 1987; Heyligers and
Klein-Nulend 2005; Kalfas 2001; Khan et al. 2005;
Kingsmill et al. 1999; Lee et al. 2000), but the role
of gamma irradiation on these biological functions
has not been clearly established in the literature.
Two processes occur during repair of massive
bone allografts: surface repair and internal repair.
Both of them start with bone resorption, in which
the activation of osteoclasts plays a central role.
During this process, un-resorbed surfaces of the
allograft serve as an anchor for the attachment of
the host soft tissues. Within the first 6 months, a thin
seam of appositional lamellar bone forms from the
host, and continues to cover about half of the outer
cortical surface by the end of the first year (Enne-
king and Campanacci 2001; Enneking and Mindell
1991). The other half of the surface is resorbed and
covered by new lamellar bone by remodelling dur-
ing the second year. Overall, resorption only re-
moves several millimetres of superficial cortical
bone. Therefore, the graft is not completely re-
placed by the new bone, and its remaining tissue is
surrounded by new lamellae (Enneking and Cam-
panacci 2001; Enneking and Mindell 1991). At that
time, the walls of Haversian canals start to be
remodeled and then filled with new bone formation.
This pattern replaces the allograft bone by viable
host bone (Schachar et al. 2002).
The repair of bone allografts described above
involves both osteoinduction and osteoconduction
(Kalfas 2001; Khan et al. 2005). Osteoinduction
refers to the adhesion of host mesenchymal stem
cells onto graft surfaces to differentiate and start
the remodeling process. Osteoconductivity is the
ability of the graft to provide a scaffold for bone
healing by recruitment of the mesenchymal stem
cells of the host, to stabilize on their bone surfaces
and stimulate cell differentiation and subsequent
remodelling (Kalfas 2001; Khan et al. 2005). Mej-
dahl et al. (1998) hypothesized that signals from
the allograft bone matrix are mediated by the
interaction of adhesion molecules with osteoblast-
like cells forming contacts with the graft surface.
These cells release factors that signal the osteo-
clastic cell-line and initiate bone resorption. When
bone mineral is resorbed, matrix-derived growth
factors from the graft, such as bone morphogenetic
protein –2, –4 and –7, are released to activate and
amplify the osteoinduction process (Kalfas 2001;
Khan et al. 2005).
Obviously, allografts in optimum condition
contribute to the success of transplantation sur-
geries. Although a great focus is placed on new
bone formation, the ability of the graft to be re-
sorbed by osteoclasts plays a crucial role in the
incorporation of bone allografts, because this is the
primary step in remodeling (Kluger et al. 2003).
Cell Tissue Banking (2007) 8:93–105 99
123
The influences of gamma radiation in bone
allograft remodelling
The activity of growth factors such as bone mor-
phogenetic proteins (BMP) and transforming
growth factor-b (TGF-b) is essential for effective
osteoinduction, but may be degraded during
irradiation (Ijiri et al. 1994; Puolakkainen et al.
1993). It is clear that BMP play an important role
in bone remodelling, and to express their potency,
they need a carrier. Collagen is the best carrier
for BMP (Dziedzic-Goclawska et al. 2005; Ijiri
et al. 1994). However, sterilization by gamma
irradiation degrades collagen and destroys the
fibrillar network of the bone matrix. When this
carrier is destroyed by gamma rays, the process of
bone remodelling, and the graft-recipient healing
process is affected (Dziedzic-Goclawska et al.
2005; Ijiri et al. 1994). Ijiri et al. (1994) investi-
gated the effects of sterilization methods on os-
teoinductivity, by implanting pellets of BMP and
collagen, or pellets of collagen only, into animals.
No bone formation was observed on pellets im-
planted with collagen only. Moreover, when the
combined BMP and collagen pellets were irradi-
ated at 25 kGy, much less bone formation was
observed compared to non-irradiated pellets.
More conclusively, when non-irradiated BMP was
combined with irradiated collagen pellets, the
bone formation was almost zero. In contrast,
compared to control groups, the bone formation
was not significantly different when pellets were
implanted with irradiated BMP combined with
non-irradiated collagen. The calcium yield and
alkaline phosphatase activity measured from re-
trieved pellets followed the same trend as bone
formation. While the calcium yield from pellets
with irradiated BMP/non-irradiated collagen was
reduced to 76% that of control, it was almost zero
from those with non-irradiated BMP/irradiated
collagen. These data supported the argument that
it was the collagen carrier that was more labile to
gamma irradiation than the BMP protein itself
(Dziedzic-Goclawska et al. 2005; Ijiri et al. 1994),
which is also consistent with maintenance of
TGF-b activity at doses of radiation lower than
25 kGy (Puolakkainen et al. 1993).
Studies have focused on the impairment of
osteoinduction caused by gamma irradiation. By
using radiographic, histologic and histochemical
methods, Buring and Urist (1967) investigated the
effect of radiation on bone induction induced by
bone matrix implanted into the muscle of rats and
rabbits. Bone induction was eliminated when the
allografts were irradiated at the doses from 20 to
40 kGy. Specifically, the implants were almost
resorbed and new bone formation was absent for
every one of 300 implants irradiated with doses
from 20 to 37 kGy. Furthermore, irradiated col-
lagen was much more soluble and absorbable.
The authors concluded that allografts only serve
as an allo-structural function when osteoinduction
is inhibited by gamma doses higher than 20 kGy.
These conclusions are supported by work showing
reduced calcium content of irradiated implants
after 2 months (Munting et al. 1988), and signifi-
cant delay in incorporation of bone grafts irradi-
ated at 25 kGy (Voggenreiter et al. 1996).
In contrast, Wientroub and Reddi (1988) con-
cluded that a standard dose of gamma irradiation
did not alter the osteoinductivity of demineral-
ized bone matrix implanted into rat muscle. In
fact, higher doses (30–50 kGy) even increased
these properties. Likewise, Glowacki (2005)
reported that demineralized bone irradiated at
doses of 20–40 kGy retained 80% of its activity,
and Hallfeldt et al. (1995) showed that bridging of
defects in drill holes was only 94% of controls
when demineralized bone matrix was irradiated
at 25 kGy. The question is how to reconcile these
observations with those above. First, the time
scale varied in these latter studies. In the former
ones (Buring and Urist 1967; Munting et al. 1988;
Voggenreiter et al. 1996), time for retrieval
implants ranged from 1 to 8 weeks; whereas in
the latter experiments (Hallfeldt et al., 1995;
Wientroub and Reddi, 1988), it only ranged
12–18 days. Second, it is clear that the tempera-
ture during irradiation could affect the quality of
bone allografts. Buring and Urist (1967) and
Munting et al. (1988) irradiated their specimens
at room temperature, while Wientroub and Reddi
(1988) and Hallfeldt et al. (1995) packed their
bone specimens in dried ice. Therefore, compar-
ison of studies under standard conditions of con-
temporary bone banks is required to reach
unequivocal conclusions on the biological conse-
quences of secondary sterilization.
100 Cell Tissue Banking (2007) 8:93–105
123
Dziedzic-Goclawska et al. (1991) compared the
effect of irradiation on osteoinduction of bone
allografts preserved by lyophilization or deep-
freezing. Samples were irradiated at 35 or 50 kGy
at room temperature for lyophilization, and on dry
ice for frozen groups and then implanted into
parietal bones of adult rabbits. After 12 weeks,
deep-frozen bone was much more resorbed, and
then replaced, by new bone than lyophilized bone.
Fifty percent of frozen implants were resorbed
and replaced with new bone, compared to 20%
resorption and 10% new bone formation in
lyophilized implants. After 26 weeks, 70% of
frozen allografts were remodeled and compared
to less than 40% for the lyophilized bone
(Dziedzic-Goclawska et al. 1991).
In frozen massive bone allografts, the lipid
content of the marrow cavity is not removed. This
may change their properties after exposure to
gamma irradiation, causing them to become toxic
to the osteoblasts (Moreau et al. 2000). When
osteoblast-like cells are cultured with irradiated
bone slices, considerable cell death is induced
around the bone slices, when compared to non-
irradiated bone (Moreau et al. 2000). Biochemi-
cal analysis revealed that the peroxidized lipids:
total lipids ratio was 2–3 times higher in the
gamma irradiation group. This analysis provided
evidence that bone marrow lipids were peroxi-
dized by gamma radiation, a process that releases
free radicals that can induce necrosis and osteo-
blast death. Peroxidation, therefore, may be
another mechanism by which remodelling of
allograft bone is impaired by gamma irradiation.
Moreover, peroxidation of lipids may also induce
giant cell reactions to release cytokines and
prostaglandins, leading to an inflammatory med-
iated bone resorption (Moreau et al. 2000).
Although experimental studies provide evidence
for a degradation of biological properties of allo-
grafts, this does not appear to be translated into
worse clinical outcomes. Clinically, there is evi-
dence that rates of non-union or fracture in bone
grafted with irradiated bone (25 kGy) do not differ
from those reported for non-irradiated grafts
(Hernigou et al. 1993; Lietman et al. 2000). The
apparent maintenance of osteoinductive properties
at 25 kGy is observed in mineralized bone allo-
grafts (Hernigou et al. 1993), as well as deminer-
alized bone matrix (Urist and Hernandez 1974;
Wientroub and Reddi 1988). Although these data
suggest that the osteoinduction and osteoconduc-
tion of bone allografts are not altered by irradia-
tion, it is difficult to compare with experimental
studies without strong evidence from randomized
controlled trials. Until these are performed, or
irradiated allografts are compared in well-designed
studies in large animals, the clinical performance of
irradiated allografts remains equivocal.
Where allograft bone has been grafted into ani-
mal models, a dose-dependent effect is generally
observed (Godette et al. 1996; Jinno et al. 2000;
Urist and Hernandez 1974; Voggenreiter et al.
1996). For example, allograft bone sterilized at
15 kGy did not compromise allograft incorporation
at 4 or 6 months following surgery (Jinno et al.
2000); yet, bone grafts irradiated at 25 kGy and
implanted into rabbit femora or rat tibiae showed
dramatically reduced rates of incorporation when
compared to fresh frozen specimens (Godette et al.
1996; Voggenreiter et al. 1996). These data are
more highly controlled than human clinical obser-
vations and provide evidence for dose-related
impairment of allograft performance, but would be
strengthened by experiments in a large animal
model, and randomised controlled trials in humans.
Changes in osteoconduction of irradiated
allografts
Resorption is the first stage of bone remodeling
during the incorporation of bone allografts.
Osteoclasts, therefore, play an initial and essen-
tial role (Kluger et al. 2003). Moreover, the cells
coordinate with osteoblasts to stimulate bridging
and facilitate union (Akkus and Rimnac 2001;
Chapman and Villar 1992; Enneking and Cam-
panacci 2001). Therefore, the effectiveness of
graft-host incorporation depends on effective
bone resorption by osteoclasts recruited from the
host. The better the quality of bone allografts, the
more host cells will be attracted and remodelling
facilitated (Kluger et al. 2003).
However, studies utilizing osteoclasts to
determine the quality of irradiated bone are few.
Using the resorption assay on bone slices Kluger
et al. (2003) investigated the effects of irradiation
on osteoclast activity. Transverse femoral cortical
Cell Tissue Banking (2007) 8:93–105 101
123
bone slices, 8–10 mm, were irradiated at 25 kGy,
and then incubated with osteoclasts isolated from
rabbit bone for 50 h. Full processing of bone
allografts, including de-fatting, freeze-drying and
gamma irradiation reduced osteoclast activity by
57% compared with fresh frozen bone. They also
recognized that processing damaged bone matrix
proteins such as integrins, which lead to the
impairment of osteoclast attachment and resorp-
tion (Kluger et al. 2003).
In short, sterilization by gamma irradiation af-
fects bone allograft remodelling by impairing the
organic components of allografts such as proteins
and lipids. However, the levels of damage differ
among the studies. These differences are caused by
variations in studies such as temperature conditions,
allograft materials and gamma dose. In addition,
aspects of bone formation have been more inten-
sively studied than those of bone resorption, al-
though bone resorption and osteoclast activation
play a fundamental role in bone remodelling.
The role of macrophages in bone allograft
implantation
When implanted into the new host, allograft tissue
stimulates cellular immune reactions (Muldashev
et al. 2005). These reactions appear as important
factors initiating osteoclast activation and trans-
plant resorption. During allograft remodelling, re-
lease of TNFa and activation of macrophages play a
key role in the resorption and formation process of
biomaterial implantation (Muldashev et al. 2005).
In infectious bone disease, products released
from bacteria may cause chronic inflammation
and subsequence bone loss (Jiang et al. 2002).
There is sound evidence for the hypothesis that
this bone resorption is bacteria-mediated (Hong
et al. 2004; Jiang et al. 2002; Meghji et al. 1998;
Moreau et al. 2000; Nair et al. 1995; Nair et al.
1996; Schuster et al. 2000). Nair and colleagues
have listed three mechanisms of bacterially
induced bone destruction (Nair et al. 1995, 1996):
1. The bone matrix is directly resorbed by
release of acids and proteases from bacteria.
2. The osteoclastic cell line is stimulated by
bacterial products; and
3. Bacterial products inhibit bone formation.
Of these, the two latter ones play a more
important role in bone loss, given that bacteria
can release many capsule factors during lysis.
Lipopolysaccharide (LPS) secreted from gram-
negative bacteria can promote bone resorption by
triggering macrophages to release osteolytic
mediators (Hong et al. 2004; Jiang et al. 2002).
LPS also directly stimulates the formation of
osteoclast-like cells without the involvement of
osteoblasts, and these cells form resorption pits in
vitro on bone slices (Jiang et al. 2002). Moreover,
this inflammatory bone resorption is bacterial
dose-dependent.
Surface-associated proteins (SAPs) from some
gram-positive bacteria such as Staphylococcus
epidermidis and aureus can also promote bone
resorption by directly activating osteoclasts
(Arora et al. 1998; Meghji et al. 1998; Meghji
et al. 1997a, 1997b; Nair et al. 1995). These bac-
terial infections, in orthopaedic clinics, are asso-
ciated with rapid bone loss. These gram-positive
anaerobic cocci rarely cause infectious diseases in
healthy humans, but it has emerged as an
important pathogen in foreign body implantation
(James and Gower 2002; Liu et al. 2002; Som-
merville et al. 2000).
Several experiments have used bone resorption
assays and calcium release to investigate the
osteoclast activation potential of SAPs extracted
from S. epidermidis and S. areaus (Arora et al.
1998; Meghji et al. 1998; Meghji et al. 1997a).
These bacterial products caused a dose-depen-
dent stimulation of calcium release and pit
resorption. Furthermore, there is evidence that
LPS and SAPs prevent osteoblasts from synthe-
sizing bone matrix (Schuster et al. 2000). The
mechanism of this inhibition is still not clear, but
proteins from certain bacteria can inhibit cell-
cycle progression by blocking cells in the G2
phase of the cell cycle. These experiments also
demonstrated that the bacterial products were
easily released by elution in saline solutions, and
were also heat and trypsin sensitive (Meghji et al.
1998; Meghji et al. 1997a).
Therefore, when irradiation is used for sterili-
zation of bone allografts, the destruction of bac-
teria may also release these products. Given that
the gamma dose is high enough to kill all bacteria
present in the bone allograft, their products may
102 Cell Tissue Banking (2007) 8:93–105
123

still remain. If the grafts are heavily contami-
nated, it could contain a large amount of bacterial
particles following irradiation. Consequently, we
hypothesize that the particles could activate a
cellular immune reaction and cause excess bone
resorption. To date there are no published studies
testing this hypothesis.
In conclusion, bone allografts provide replace-
ment and reinforcement for defective skeletal
structures caused by bone disease, and act as a
stimulus for new bone remodelling. For optimal
activation of these processes, biological and bio-
mechanical properties of bone allografts must be
preserved. However, the risk of disease transmis-
sion leads to the use of terminal/secondary sterili-
zation using gamma irradiation. This sterilization
method negatively alters the properties of bone al-
lografts. While the biomechanical properties of
bone allografts irradiated by gamma rays have been
widely studied, the biological properties such as the
ability for bone resorption and formation have not
been equally considered. Due to developments in
the bone bank industry, manufacturing procedures
have markedly improved bone quality. Therefore,
the trend towards application of lower gamma do-
ses for terminal sterilization is becoming a greater
concern in tissue banking. However, to substantiate
the lower dose, there is a need for global investi-
gation of bone allograft qualities such as sterility,
mechanical properties and biological functions
after gamma irradiation. Such studies should be
undertaken using a wide range of doses and under
tightly controlled conditions of bone banking in
which non-irradiation factors can be minimized.
References
AATB (ed) (2002) Standards for tissue banking, AmericanAssociation of Tissue Banking, MD
Akkus O, Belaney RM (2005) Sterilization by gammaradiation impairs the tensile fatigue life of cortical boneby two orders of magnitude. J Orthop Res 23:1054–1058
Akkus O, Belaney RM, Das P (2005) Free radical scav-enging alleviates the biomechanical impairment ofgamma radiation sterilized bone tissue. J Orthop Res23:838–845
Akkus O, Rimnac CM (2001) Fracture resistance ofgamma radiation sterilized cortical bone allografts. JOrthop Res 19:927–934
An HY (2000) Mechanical properties of bone. In: An HY,Draughn AR (eds) Mechanical testing of bone and bone-implant interface. CRC Press, Boca Raton, pp 41–63
Anderson MJ, Keyak JH, Skinner HB (1992) Compressivemechanical-properties of human cancellous bone aftergamma-irradiation. J Bone Joint Surg-Am 74A:747–752
Andre LP, Liz AG-ER (2000) Proposed donor screeningquestionnaire. Cell Tissue Bank 1:149–153
Angermann P, Jepsen OB (1991) Procurement, bankingand decontamination of bone and collagenous tissueallografts: guidelines for infection control. J HospInfect 17:159–169
Arora M, Shah N, Meghji S, et al (1998) Effect of Staph-ylococcus aureus extracellular proteinaceous fractionin an isolated osteoclastic resorption assay. J BoneMiner Metab 16:158–161
Aspenberg P, Tagil M, Kristensson C, Lidin S (1996) Bonegraft proteins influence osteoconduction—a titaniumchamber study in rats. Acta Orthop Scand 76:377–382
Bailey DA, Martin AD, McKay HA, Whiting S, MirwaldR (2000) Calcium accretion in girls and boys duringpuberty: a longitudinal analysis. J Bone Miner Res15:2245–50
Boyce T, Edwards J, Scarborough N (1999) Allograftbone—the influence of processing on safety and per-formance. Orthop Clin North Am 30:571–581
Buring K, Urist RM (1967) Effects of ionizing radiation onthe bone induction principle in the matrix of boneimplants. Clin Orthop 55:225–234
Campbell DG, Li P. (1999) Sterilization of HIV withirradiation: relevance to infected bone allografts. AustNZ J Surg 69:517–521
Chapman PG, Villar RN (1992) The bacteriology of boneallografts. J Bone Joint Surg Br 74:398–399
Colwell A, Hamer A, Blumsohn A, Eastell R (1996) Todetermine the effects of ultraviolet light, natural lightand ionizing radiation on pyridinium cross-links inbone and urine using high-performance liquid chro-matography. Eur J Clin Invest 26:1107–1114
Cornu O, Banse X, Docquier PL, Luyckx S, Delloye C(2000) Effect of freeze-drying and gamma irradiationon the mechanical properties of human cancellousbone. J Orthop Res 18:426–431
Cornu O, Bavadekar A, Godts B, et al (2003) Impactionbone grafting with freeze-dried irradiated bone. Part IIChanges in stiffness and compactness of morselizedgrafts—experiments in cadavers. Acta Orthop Scand74:553–558
Currey JD, Foreman J, Laketic I, et al (1997) Effects ofionizing radiation on the mechanical properties ofhuman bone. J Orthop Res 15:111–117
Davy DT (1999) Biomechanical issues in bone transplan-tation. Orthop Clin N Am 30:553–563
Diab T, Condon KW, Burr DB, Vashishth D (2005) Age-related change in the damage morphology of humancortical bone and its role in bone fragility bone
Dziedzic-Goclawska A, Kaminski A, Uhrynowska-Tys-zkiewicz I, Stachowicz W (2005) Irradiation as asafety procedure in tissue banking. Cell Tissue Bank6:201–219
Cell Tissue Banking (2007) 8:93–105 103
123
Dziedzic-Goclawska A, Ostrowski K, Stachowicz W,Michalik J, Grzesik W (1991) Effect of radiationsterilization on the osteoinductive properties and therate of remodeling of bone implants preserved bylyophilization and deep-freezing. Clin Orthop 30–37
Eastlund DT, Strong DM (2003) Infectious disease trans-mission through tissue transplantation. In: PhillipsGO (ed) Advances in tissue banking. World ScientificPublishing, Singapore, pp 51–131
Enneking WE, Campanacci DA (2001) Retrieved humanallografts—a clinicopathological study. J Bone JointSurg Am 83A:971–986
Enneking WF, Mindell ER (1991) Observations on mas-sive retrieved human allografts. J Bone Joint Surg Am73A:1123–1142
Fideler BM, Vangsness CT Jr, Lu B, Orlando C, Moore T(1995) Gamma irradiation: effects on biomechanicalproperties of human bone-patellar tendon-bone allo-grafts. Am J Sports Med 23:643–646
Forwood MR, Bailey DA, Beck TJ, et al (2004) Sexualdimorphism of the femoral neck during the adolescentgrowth spurt: a structural analysis. Bone 35:973–981
Gibbons MJ, Butler DL, Grood ES, et al (1991) Effects ofgamma-irradiation on the initial mechanical andmaterial properties of goat bone-patellar tendon-boneallografts. J Orthop Res 9:209–218
Godette GA, Kopta JA, Egle DM (1996) Biomechanicaleffects of gamma irradiation on fresh frozen allograftsin vivo. Orthopedics 19:649–653
Grieb TA, Forng R-Y, Stafford RE, et al (2005) Effectiveuse of optimized, high-dose (50 kGy) gamma irradi-ation for pathogen inactivation of human bone allo-grafts. Biomaterials 26:2033–2042
Hallfeldt KKJ, Stutzle H, Puhlmann M, Kessler S, Schwei-berer L (1995) Sterilization of partially demineralizedbone-matrix—the effects of different sterilizationtechniques on osteogenetic properties. J Surg Res59:614–620
Hamer AJ, Stockley I, Elson RA (1999) Changes in allo-graft bone irradiated at different temperatures. JBone Joint Surg Br 81:342–344
Hamer AJ, Strachan JR, Black MM, et al. (1996) Biome-chanical properties of cortical allograft bone using anew method of bone strength measurement—a com-parison of fresh, fresh-frozen and irradiated bone. JBone Joint Surg Br 78B:363–368
Heiple KG, Goldberg VM, Powell AE, Bos GD, Zika JM(1987) Biology of cancellous bone-grafts. Orthop ClinN Am 18:179–185
Hernigou P, Delepine G, Goutallier D, Julieron A (1993)Massive allografts sterilised by irradiation. Clinicalresults J Bone Joint Surg Br 75:904–913
Hernigou P, Gras G, Marinello G, Dormont D (2000)Inactivation of HIV by application of heat and radi-ation: implication in bone banking with irradiatedallograft bone. Acta Orthop Scand 71:508–512
Heyligers IC, Klein-Nulend J (2005) Detection of livingcells in non-processed but deep-frozen bone allo-grafts. Cell Tissue Bank 6:25–31
Hong CY, Lin SK, Kok SH, et al (2004) The role oflipopolysaccharide in infectious bone resorption ofperiapical lesion. J Oral Pathol Med 33:162–169
Hornicek FJ, Gebhardt MC, Tomford WW, et al (2001)Factors affecting nonunion of the allograft-host junc-tion. Clin Orthop 87–98
IAEA (2002) International standards on tissue bank-ing—first meeting of the IAEA technical advisorycommittee. In: Committee ITA (ed) The IAEA pro-gramme in radiation and tissue banking. IAEA,Boston, USA, pp 44
Ijiri S, Yamamuro T, Nakamura T, Kotani S, Notoya K(1994) Effect of sterilization on bone morphogeneticprotein. J Orthop Res 12:628–636
James LA, Gower A. (2002) The clinical significance offemoral head culture results in donors after hiparthroplasty—a preliminary report. J Arthroplasty17:355–358
Jiang YL, Mehta CK, Hsu TY, Alsulaimani FFH (2002)Bacteria induce osteoclastogenesis via an osteoblast-independent pathway. Infect Immun 70:3143–3148
Jinno T, Miric A, Kirk S, Davy D, Stevenson S (2000) Theeffects of processing and low dose irradiation oncortical bone grafts. J Clin Orthopa Relat Res375:275–285
Kalfas I (2001) Principles of bone healing Neurosurg.Focus 10:1–4
Kennedy JF, Phillips GO, Williams PA (2005) Sterilisationof tissues using ionising radiation. CRC Press LLC,Boca Raton, Florida
Khan SN, Cammisa FP, Sandha HS, et al (2005) Thebiology of bone grafting. J Am Acad Orthop Surg13:77–86
Kingsmill VJ, Boyde A, Jones SJ (1999) The resorption ofvital and devitalized bone in vitro: significance forbone grafts. Calcif Tissue Int 64:252–256
Kluger R, Bouhon W, Freudenberger H, et al (2003) Re-moval of the surface layers of human cortical boneallografts restores in vitro osteoclast function reducedby processing and frozen storage. Bone 32:291–296
Lee FYI, Hazan EJ, Gebhardt MC, Mankin HJ (2000)Experimental model for allograft incorporation andallograft fracture repair. J Orthop Res 18:303–306
Lietman AS, Tomford WW, Gebhardt CM, SpringfieldSD, Mankin JM (2000) Complications os irradiatedallografts in orthopaedic tumor surgery. J ClinOrthopaedic Relat Res 375:214–217
Liu JW, Chao LH, Su LH, Wang JW, Wang CJ (2002)Experience with a bone bank operation and allograftbone infection in recipients at a medical centre insouthern Taiwan. J Hosp Infect 50:293–297
Loty B, Courpied JP, Tomeno B, et al. (1990) Bone allo-grafts sterilised by irradiation. Biological properties,procurement and results of 150 massive allografts. IntOrthop 14:237–242
Meghji S, Crean SJ, Hill PA, et al. (1998) Surface-associ-ated protein from Staphylococcus aureus stimulatesosteoclastogenesis: possible role in S-aureus-inducedbone pathology. Br J Rheumatol 37:1095–1101
104 Cell Tissue Banking (2007) 8:93–105
123
Meghji S, Crean SJ, Nair S, et al. (1997a) Staphylococcusepidermidis produces a cell-associated proteinaceousfraction which causes bone resorption by a prosta-noid-independent mechanism: Relevance to thetreatment of infected orthopaedic implants. Br JRheumatol 36:957–963
Meghji S, Henderson B, Nair SP, Tufano MA (1997b)Bacterial porins stimulate bone resorption. InfectImmun 65:1313–1316
Mitchell EJ, Stawarz AM, Kayacan R, Rimnac CM (2004)The effect of gamma radiation sterilization on thefatigue crack propagation resistance of human corticalbone. Bone Joint Sur 86-A:2648–2657
Moreau MF, Gallois Y, Basle MF, Chappard D (2000)Gamma irradiation of human bone allografts altersmedullary lipids and releases toxic compounds forosteoblast-like cells. Biomaterials 21:369–376
Mosekilde L (1986) Normal vertebral body size andcompressive strength: relations to age and to vertebraland iliac trabecular bone compressive strength. Bone7:207–212
Muldashev ER, Muslimov SA, Musina LA, NigmatulinRT, Lebedeva AI (2005) The role of macrophage inthe tissue regeneration stimulated by the biomaterials.Cell Tissue Bank 6:99–107
Munting E, Wilmart JF, Wijne A, Hennebert P, Delloye C(1988) Effect of sterilization on osteoinduc-tion—comparison of 5 methods in demineralized ratbone. Acta Orthop Scand 59:34–38
Nair S, Song Y, Meghji S, et al (1995) Surface-associatedproteins from Staphylococcus-aureus demonstratepotent bone-resorbing activity. J Bone Miner Res10:726–734
Nair SP, Meghji S, Wilson M, et al. (1996) Bacterially in-duced bone destruction: mechanisms and misconcep-tions. Infect Immun 64:2371–2380
Pelker RR, McKay J, Troiano N, Panjabi MM, Friedla-ender GE (1989) Allograft incorporation—a biome-chanical evaluation in a rat model. J Orthop Res7:585–589
Puolakkainen PA, Ranchalis JE, Strong DM, TwardzikDR (1993) The effect of sterilization on transforminggrowth-factor-beta isolated from demineralizedhuman bone transfusion (Paris). 33:679–685
Rasmussen TJ, Feder SM, Butler DL, Noyes FR (1994)The effects of 4 mrad of gamma-irradiation on theinitial mechanical-properties of bone patellar tendonbone-grafts arthroscopy, 10:188–197
Salehpour A, Butler DL, Proch E, et al. (1995) Dose-dependent response of gamma irradiation onmechanical properties and related biochemical com-position of coat bone-patellar tendon-bone allografts.J Orthop Res 13:898–906
Schachar N, Fennel C, Otsuka T, Ladd A (2002) Bonegrafts and bone subtitutes. In: R., F. H., H., K. and A.,M. L. (eds) Orthopaedics. St. Louis, Mosby, pp186–194
Schuster JM, Avellino AM, Mann FA, et al (2000) Use ofstructural allografts in spinal osteomyelitis: a reviewof 47 cases. J Neurosurg 93:8–14
Simonian PT, Conrad EU, Chapman JR, Harrington RM,Chansky HA (1994) Effect of sterilization and storagetreatments on screw pullout strength in human allo-graft bone. Clin Orthop 290–296
Smith CW, Young IS, Kearney JN (1996) Mechanicalproperties of tendons: changes with sterilizationand preservation. J Biomech Eng-Trans Asme118:56–61
Sommerville SMM, Johnson N, Bryce SL, Journeaux SF,Morgan DAF (2000) Contamination of banked fem-oral head allograft: incidence, bacteriology and donorfollow up. Aust N Z J Surg 70:480–484
Triantafyllou E, Sotiropoulos E, Triantafyllou JN (1975)The mechanical properties of the lymphylized andIrradiated bone grafts. Acta Orthopeadica Belgica41:35–44
Urist, MR, Hernandez, A. (1974) Excitation transfer inbone. Deleterious effects of cobalt 60 radiation-ster-ilization of bank bone. Arch Surg 109:586–593
Vastel L, Meunier A, Siney H, Sedel L, Courpied JP(2004) Effect of different sterilization processingmethods on the mechanical properties of humancancellous bone allografts. Biomaterials 25:2105–2110
Voggenreiter G, Ascherl R, Blumel G, SchmitNeuerburgKP (1996) Extracorporeal irradiation and incorpora-tion of bone grafts- autogeneic cortical grafts studiedin rats. Acta Orthop Scand 67:583–588
Wientroub S, Reddi HA (1988) Influence of irradiation onthe osteoindictive potential of demineralized bonematrix calcif. Tissue Int 42:255–260
Zhang YX, Homsi D, Gates K, et al. (1994) A compre-hensive study of physical parameters, biomechanicalproperties, and statistical correlations of iliac crestbone wedges used in spinal-fusion surgery 4. Effect ofgamma-irradiation on mechanical and material prop-erties Spine 19:304–308
Zioupos P, Smith WC, An HY (2000) Factors effectingmechanical properties of bone. In: An HY, DraughnAR (eds) Mechanical testing of bone and bone-im-plant interface. pp 65–85
Zubillaga G, Von Hagen S, Simon BI, Deasy MJ (2003).Changes in alveolar bone height and width followingpost-extraction ridge augmentation using a fixed bio-absorbable membrane and demineralized freeze-driedbone osteoinductive graft. J Periodontol 74:965–975
Cell Tissue Banking (2007) 8:93–105 105
123





























