Embed Size (px)
Citation preview

Stress, glucocorticoids and liquorice in human pregnancy:Programmers of the offspring brain
K. RAIKKONEN1, J. R. SECKL2, A.-K. PESONEN1, A. SIMONS3,
& B. R. H. VAN DEN BERGH3
1Institute of Behavioural Sciences, University of Helsinki, Helsinki, Finland, 2Centre for Cardiovascular Science, The Queen’s
Medical Research Institute, University of Edinburgh, Edinburgh, UK, and 3Developmental Psychology, Tilburg University,
Tilburg, The Netherlands
(Received 18 January 2011; revised 4 April 2011; accepted 4 May 2011)
AbstractA suboptimal prenatal environment may induce permanent changes in cells, organs and physiology that alter social, emotionaland cognitive functioning, and increase the risk of cardiometabolic and mental disorders in subsequent life (“developmentalprogramming”). Although animal studies have provided a wealth of data on programming and its mechanisms, including onthe role of stress and its glucocorticoid mediators, empirical evidence of these mechanisms in humans is still scanty. We reviewthe existing human evidence on the effects of prenatal maternal stress, anxiety and depression, glucocorticoids and intake ofliquorice (which inhibits the placental barrier to maternal glucocorticoids) on offspring developmental outcomes including,for instance, alterations in psychophysiological and neurocognitive functioning and mental health. This work lays thefoundations for biomarker discovery and affords opportunities for prevention and interventions to ameliorate adverseoutcomes in humans.
Keywords: Child, glucocorticoids, human, liquorice, mood, offspring
Introduction
Mounting epidemiological evidence suggests that
smaller body size at birth and/or a shorter length of
gestation increase the risk of poorer physical health
later in life (Barker et al. 1989; Eriksson et al. 2006,
2007). The brain is particularly affected, manifesting
as altered cognitive and affective functioning and as
an increased risk of mental health disorders. These
associations may not be linear, as children born at the
upper end of the birth weight distribution may also be
at a higher risk for poorer health later in life (Gunnell
et al. 2003). These findings can be best understood
within the framework of prenatal “programming” or
developmental origins of health and disease (DOHaD;
Barker 1998). According to the DOHaD paradigm,
adverse environmental experiences during critical
periods of early development can permanently alter
or programme the structure and function of cells,
organs and physiological systems. Recent research has
shown that the influences of programming may not be
limited to the prenatal period, but may extend across
the entire human growth period from preconception
to adulthood (Barker et al. 2005). The effects of
programming are not limited to development in
childhood, but are influential across the life span
(Barker et al. 1989; Eriksson et al. 2006, 2007;
Raikkonen et al. 2007, 2008a, 2009a).
Recently, much interest has been focused on
whether developmental programming—as reflected
in alterations in body size at birth and length of
gestation—plays a role in determining individual
differences in cognitive, social and emotional func-
tioning, including characteristic traits of temperament
and personality, in neuroendocrine and autonomic
Correspondence: K. Raikkonen, Institute of Behavioural Sciences, University of Helsinki, PO Box 9, 00014 University of Helsinki, Finland.Tel: 358 9 19129501. Fax: 358 9 19129521. E-mail: [email protected]
Stress, November 2011; 14(6): 590–603q Informa Healthcare USA, Inc.ISSN 1025-3890 print/ISSN 1607-8888 onlineDOI: 10.3109/10253890.2011.602147
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.

nervous system (ANS) functioning and in mental
health. A series of studies have shown that smaller
body size at birth and/or shorter length of gestation
associate, for instance, with alterations in hypothala-
mic–pituitary–adrenocortical (HPA) axis and ANS
functioning during daily living and under psychosocial
stress (Reynolds et al. 2001; IJzerman et al. 2003;
Wust et al. 2005; Jones et al. 2006, 2007; Phillips and
Jones 2006; Feldt et al. 2007; Kajantie et al. 2007) and
with increased risks of depression (Raikkonen et al.
2007, 2008b), suicide (Barker et al. 1995), schizo-
phrenia (Wahlbeck et al. 2001), personality disorders
(Lahti et al. 2010b), schizotypal personality traits
(Lahti et al. 2009), hostility (Raikkonen et al. 2008a),
behavioural symptoms of attention deficit/hyperactiv-
ity disorder (Lahti et al. 2006; Strang-Karlsson et al.
2008b; Heinonen et al. 2010), poorer cognitive
functioning (Gale et al. 2004; Heinonen et al. 2008;
Broekman et al. 2009; Raikkonen et al. 2009a)
internalizing and externalizing behaviour problems
(Schlotz et al. 2008), poorer sleep (Strang-Karlsson
et al. 2008a; Pesonen et al. 2009) and negative and
positive affectivity characteristics of temperament and
personality (Pesonen et al. 2006, 2008a, Schlotz et al.
2008, Schmidt et al. 2008; Lahti et al. 2010a). These
associations may not be linear as children born with
higher birth weights may display higher levels of
anxiety (Lahti et al. 2010a) and distress (Cheung
2002), and be at an increased risk for psychosis later in
life (Gunnell et al. 2003). The extent to which the
associations with higher birth weight reflect maternal
obesity, poorer health and pregnancy disorders, such
as maternal diabetes/glucose intolerance, is not clear.
In addition to the original empirical studies, several
papers exist that have reviewed the evidence linking
smaller body size at birth and/or shorter length of
gestation with psychological and psychophysiological
functioning and mental health later in life (Shenkin
et al. 2004; Gluckman et al. 2005, 2008, 2009; Seckl
and Meaney 2006; Seckl and Holmes 2007; Hanson
and Gluckman 2008; Kajantie 2008; Seckl 2008;
Raikkonen and Pesonen 2009; Kajantie and Raikko-
nen 2010).
Despite the increasing evidence pointing to the
importance of early life programming in inducing
alterations in psychological and psychophysiological
functioning and mental health, the mechanisms
through which these prenatal influences operate
remain largely unknown. Two major hypotheses have
been advanced to explain the link between events
in utero and the later risk of neuropsychiatric and
cardiometabolic disorders: maternal malnutrition and
foetal overexposure to glucocorticoid stress hormones
(Barker 1991; Edwards et al. 1993). These notions
have been extensively explored in preclinical studies.
In a range of experimental species, maternal malnu-
trition (global undernutrition or selective protein
deficiency) reduces birth weight and reliably leads to
higher blood pressure, glucose levels, altered beha-
viour and HPA axis function in adult offspring
(Warner and Ozanne 2010). Similarly, maternal stress
or administration of glucocorticoids, such as dexa-
methasone or betamethasone that freely crosses the
placenta, also reduces birth weight and produces a
similar or identical phenotype in the adult offspring
(Seckl and Holmes 2007). Similar effects occur in
non-human primates exposed to glucocorticoids in
the last half of gestation (de Vries et al. 2007). The two
hypotheses may be linked. Thus, circulating levels of
physiological glucocorticoids (cortisol and corticos-
terone) are much higher in the maternal than in the
foetal blood. This gradient is ensured by a placental
enzyme, 11b-hydroxysteroid dehydrogenase type 2
(11b-HSD2), that catalyzes the rapid inactivation of
glucocorticoids to their inert 11-keto forms (corti-
sone, 11-dehydrocorticosterone), thus forming a
physiological “barrier” to maternal glucocorticoids.
Liquorice contains compounds, such as glycyrrhizic
acid and glycyrrhetinic acid, that potently inhibit 11b-
HSDs. Maternal administration of these agents or the
derived drug carbenoxolone (Lindsay et al. 1996a,b)
or genetic knock out of the enzyme (Holmes et al.
2006) reduces birth weight and generates similar
programmed CNS and peripheral outcomes in the
adult offspring. Moreover, maternal protein malnu-
trition selectively lowers placental 11b-HSD2 (Lang-
ley-Evans et al. 1996), affording a possible link
between the proposed mechanisms. Maternal stress in
rodents also downregulates placental 11b-HSD2
(Mairesse et al. 2007), perhaps delimited by genotype
(Lucassen et al. 2009), suggesting a double hit of
elevated maternal glucocorticoids and reduced pla-
cental barrier function.
Despite this increasingly coherent body of evidence
in model organisms, understanding the key mechan-
isms of programming in humans has been much less
explored. Figure 1 outlines the mechanisms that are
potentially involved. A series of human studies have
demonstrated that prenatal environmental adversities,
such as exposure to malnutrition (Roseboom et al.
2001), maternal pre-pregnancy overweight (Rodri-
guez 2010), pregnancy disorders, such as hyperten-
sion (Tuovinen et al. 2010, 2011), tobacco (Cornelius
and Day 2009; Espy et al. 2011; Heinonen et al.
2011), cannabis (El Marroun et al. 2009) and alcohol
exposure (Hellemans et al. 2010), have the potential
to induce alterations in the offspring growth, birth
anthropometry, development and adult functions. In
this paper, we concentrate on reviewing the existing
human evidence of programming induced by prenatal
maternal stress, depression and anxiety, maternal
glucocorticoid therapy and intake of liquorice during
pregnancy.
Stress, glucocorticoids and liquorice in human pregnancy 591
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.

Exposure to prenatal maternal stress, depression and
anxiety: Overview of results of studies, examining offspring
behaviour with questionnaires, standardized observations,
neurocognitive tasks, EEG, MRI and fMRI
Prenatal maternal stress, depression and anxiety may
exert effects on offspring development through
multiple pathways. These pathways, which include
alterations, for instance, in maternal lifestyle, physio-
logical stress-regulatory mechanisms and placental
function, are outlined in Figure 1 and described in
more detail in previous reviews (O’Regan et al. 2001;
Seckl 2001, 2008; Seckl and Meaney 2004b; Van den
Bergh et al. 2005b; Seckl and Holmes 2007).
In humans, prospective follow-up studies have
provided accumulating evidence for an association
between prenatal exposure to high levels of maternal
stress, anxiety and depression and altered neurodeve-
lopment in the offspring at stages ranging from birth
up to 20 years of age. Importantly, these associations
persisted after controlling for postnatal maternal
Fetal genomeand epigenome
Maternalnutrition
Maternalstress
Pregnancydisorders
Placentalfunction
Fetal programming leading to life-long changes in:
Organ structureand function- Muscle tissue- Fat tissue- Pancreas- Liver- Brain
Hormonalfunction/axes - HPAA- Thyroid
Autonomicnervoussystem
Neurotransmittersystems
Glucose metabolismBody compositionLipid metabolismInsulin sensitivity
Stress responsiveness
Other factors(e.g., hormonal,growth factors)
Nutrient andoxygen
availability
Sympathoadrenalfunction
Glucocorticoidexposure
HPAA andAutonomic
nervous systemfunction
Physical health, e.g.,CHD
StrokeType 2 diabetes
Mental health Other stress-related bodily
disorders
Other healthoutcomes
- Social, emotional, cognitive functioning- Temperemant- Personality- Behavior
Figure 1. Mechanisms involved in the offspring programming. (Modified from Raikkonen et al. 2008b).
K. Raikkonen et al.592
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.

mood and/or other potentially important pre- and
postnatal confounders, such as alcohol consumption
and smoking, during pregnancy, birth weight and
socio-economic status, and in some studies also use of
medication, such as antidepressants, have been taken
into account. Results of the studies reviewed here are
described in Table I. The studies are organized by the
age of the offspring at the final follow-up assessment.
In newborn babies, maternal prenatal stress was
associated with neurodevelopmental alterations
manifesting as less optimal scores on the Brazelton
Neonatal Assessment Scale (Brouwers et al. 2001;
Rieger et al. 2004; Hernandez-Reif et al. 2006) and on
quantitative neurological examination (Lou et al.
1994). The newborn babies also displayed higher
cardiac vagal tone, lower Apgar score (Ponirakis et al.
1998), less optimal behavioural states (Van den Bergh
1990, 1992) and higher cortisol levels 1 week
postpartum (Diego et al. 2004). In the study of
Harvison et al. (2009), neonates of mothers scoring
lower on perinatal anxiety displayed more negative
frontal slow wave amplitudes in response to their
mother’s voice compared to a female stranger’s voice,
while neonates of mothers scoring higher on perinatal
anxiety showed the opposite pattern. The latter results
indicate that maternal anxiety may induce neurophy-
siologically based differences in attentional allocation,
processes known to be crucial to an infant’s ability to
maintain homoeostasis.
Infants of mothers scoring higher on prenatal stress
were rated by an observer as having poorer inter-
actions with their mother (Field et al. 1985), being
more irritable (DiPietro et al. 2008) and reactive
(Davis et al. 2004, 2007), having problems with
regulation of attention (Huizink et al. 2002, 2003) and
having poorer language abilities and a lower IQ
(Laplante et al. 2004, 2008). Their mothers rated
them as having more sleeping, feeding and activity
problems (Van den Bergh 1990, 1992), and being
more irritable, difficult and showing more negative
affectivity characteristics of temperament (Vaughn
et al. 1987; Van den Bergh 1990, 1992; Huizink et al.
2002, 2003; Austin et al. 2005; Pesonen et al. 2005;
McGrath et al. 2008; Henrichs et al. 2009) and crying
more excessively (van der Wal et al. 2007). Scores on
the Bayley Scales of Infant Development were worse at
8 and 24 months (Brouwers et al. 2001; Huizink et al.
2002, 2003; Laplante et al. 2004), but not in another
study of 7-month-old infants (Van den Bergh 1990,
1992). Methodological differences, such as differ-
ences in sample size and variables that were used as
covariates, may explain the conflicting findings
between the studies using the Bayley Scales. Dawson
and colleagues found that during mother–infant
interaction, children of depressed mothers showed
higher than normal heart rates and higher levels of
cortisol, and reduced activity in brain regions that
mediate positive approach behaviour. The authors
indicate that there is suggestive evidence from their
follow-up study that the postnatal experience with the
mother may have had more effect on infant frontal
EEG than on prenatal factors (Dawson and Ashman
2000; Dawson et al. 2001).
Pre-school children and children were rated by their
mothers (Martin et al. 1999; O’Connor et al. 2002,
2003; Niederhofer and Reiter 2004; Van den Bergh
and Marcoen 2004), teachers (Niederhofer and Reiter
2004; Rodriguez and Bohlin 2005), an external
observer (Van den Bergh and Marcoen 2004) or
themselves (Van den Bergh and Marcoen 2004) as
showing poorer attention, hyperactivity, behavioural
and emotional problems, and they were rated by their
teacher as having lower school grades and problem
behaviour (Niederhofer and Reiter 2004). O’Connor
et al. (2002) found that the effects of antenatal anxiety
were stronger than the effects of antenatal depression.
Finally, the results of Obel et al. (2003)indicated that
stressful life events in the mother during pregnancy
increased the risk for ADHD problems in pre-
adolescence between ages, 9–11 years.
Adolescents showed problems with cognitive control
when performing computerized cognitive tasks
measuring prefrontal cortex functioning and scored
lower on intelligence subtests at the age of 14–15 and
17 years (Mennes et al. 2006; Van den Bergh et al.
2005a, 2006). Girls displayed higher levels of
depressive symptoms (Van den Bergh et al. 2008).
Mennes et al. (2009) showed that 17-year-old
children of mothers who were more anxious between
12 and 22 weeks of gestation displayed changes in
event-related potentials (ERP) measured with EEG,
when performing a gambling task, requiring endogen-
ous control. Functional magnetic resonance (fMRI)
measures revealed that in the 20-year-old offspring,
differences related to the level of antenatal maternal
anxiety were found in the activation patterns of several
important prefrontal regions (Mennes 2008). Buss
et al. (2009) showed in a MRI study that high
pregnancy-specific anxiety in mid gestation, but not
later, is associated with decreased grey matter density
in specific brain areas, in 8-year-old children.
Some evidence also suggests that the major life
events inducing severe prenatal stress, such as death of
a close relative during pregnancy, may be associated
with stillbirth (Wisborg et al. 2008), low birth weight
and smallness for gestational age status (Khashan et al.
2008b), cerebral palsy (Li et al. 2009b) and
schizophrenia (Khashan et al. 2008a) in the offspring.
One study has linked such events also with the risk of
autism in the offspring (Kinney et al. 2008), but
another study failed to replicate this association (Li
et al. 2009a).
In humans, birth anthropometry associates with
subsequent HPA axis function. Higher plasma and
urinary glucocorticoid levels are found in children and
adults who were of lower birth weight (Clark et al.
Stress, glucocorticoids and liquorice in human pregnancy 593
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.

Table
I.S
tud
ies
test
ing
ass
oci
ati
on
sbet
wee
npre
nata
lm
ate
rnal
stre
ss,
an
xie
tyan
dd
epre
ssio
nw
ith
off
spri
ng
dev
elopm
ent.
Age
of
child
Mea
sure
or
type
of
pre
nata
lex
posu
re
Pre
nata
lti
min
g
wee
ks
ges
tati
on
Ou
tcom
em
easu
re(s
)R
efer
ence
(s)
2–
3d
ays
An
xie
ty(s
tate
&tr
ait
);S
tres
s(P
SS
)20;
30
NB
AS
:habit
uati
on
,so
cial
inte
ract
ion
,m
oto
r
syst
em,
state
org
an
izati
on
,st
ate
regu
lati
on
,
au
ton
om
icsy
stem
Her
nan
dez
-Rei
fet
al.
(2008)
3–
5d
ays
Tota
ld
istr
ess
,20;
30
–34
Reg
ula
tion
pro
ble
ms
(NB
AS
)R
ieger
etal.
(2004)
1w
eek
Per
inata
ld
epre
ssio
n26
Cort
isol
leve
lD
iego
etal.
(2004)
Neo
nate
An
xie
ty(g
ener
al)
40*
Au
dit
ory
evoked
resp
on
ses
(AE
R)
Harv
ison
etal.
(2009)
12
day
sD
epre
ssio
nN
ot
rep
ort
edA
tten
tiven
ess
(NB
AS
)H
ern
an
dez
-Rei
fet
al.
(2006)
4–
14
day
sL
ife
even
tsst
ress
Mid
ges
tati
on
Bir
thw
eight,
hea
dci
rcu
mfe
ren
ce,
Pre
chtl
’s
neu
rolo
gic
al
obse
rvati
on
Lou
etal.
(1994)
Bir
th,
1d
ay,
3–
4w
eeks
An
xie
ty(s
tate
an
dtr
ait
)#
16;
32
–34
Med
ical
reco
rds
(e.g
.A
pgar
scale
),ca
rdia
c
vagal
ton
e(E
KG
Porg
es’
met
hod
)
Pon
irakis
etal.
(1998)
6w
eeks
Foet
al
react
ivit
yto
mate
rnal
stim
ula
tion
(vie
win
gof
vid
eo)
32
Infa
nt
neg
ati
vere
act
ivit
yd
uri
ng
a
stan
dard
ized
lab
pro
ced
ure
DiP
ietr
oet
al.
(2008)
3m
on
ths
Dep
ress
ion
15
–28;
29
–40
Infa
nt
cort
isol
leve
lp
rean
dp
ost
infa
nt
stre
ss
test
Ober
lan
der
etal.
(2008)
4m
on
ths
An
xie
ty(s
tate
)an
dd
epre
ssio
n32
Beh
avio
ura
lre
act
ivit
y(H
IBR
P)
Dav
iset
al.
(2004)
2,
6m
on
ths
Dep
ress
ion
Th
ird
trim
este
rT
emp
eram
ent
rati
ngs
McG
rath
etal.
(2008)
3–
5m
on
ths
Str
ess
an
dd
epre
ssio
n28
–40
Face
-to-f
ace
pla
yin
tera
ctio
ns
(CC
TI)
Fie
ldet
al.
(1985)
3–
6m
on
ths
Dep
ress
ive
sym
pto
ms,
an
xie
ty
(pre
gn
an
cy-s
pec
ific)
,pare
nti
ng
stre
ss;
job
stra
in
7–
40
Exce
ssiv
ecr
yin
gva
nd
erW
al
etal.
(2007)
4–
6m
on
ths
An
xie
ty(t
rait
);d
epre
ssio
n,
life
even
tsst
ress
Thir
dtr
imes
ter
(32)
Dif
ficu
ltte
mper
am
ent
(SIT
Q)
Au
stin
etal.
(2005)
6m
on
ths
Dep
ress
ion
an
dan
xie
ty26
Infa
nt
cort
isol
leve
lpre
an
dpost
infa
nt
stre
ss
test
Bre
nn
an
etal.
(2008)
6m
on
ths
Str
ess
exper
ien
ce1st
wee
kpost
part
um
Tem
per
am
ent
(IB
Q);
neg
ati
ve
an
dover
all
tem
per
am
enta
lre
act
ivit
y
Pes
on
enet
al.
(2005)
6m
on
ths
An
xie
ty(p
regn
an
cy-s
pec
ific;
gen
eral)
12;
20
Tem
per
am
ent
(IB
Q-R
);in
fan
td
iffi
cult
ies
Hen
rich
set
al.
(2009)
1w
eek,
12
wee
ks,
7m
on
ths
An
xie
ty(s
tate
an
dtr
ait
)12
–22;
23
–31;
32
–40
Pre
chtl
’sn
euro
logic
al
obse
rvati
on
,b
eha-
vio
ura
lst
ate
ob
serv
ati
on
,fe
edin
gsc
ore
,
moth
er–
infa
ntin
tera
ctio
n(I
TQ
,IC
Q,B
SID
)
Van
den
Ber
gh
,(1
990;1
992)
7m
on
ths
An
xie
ty36
–39*
Cort
isol
leve
lof
the
child
,p
rean
dp
ost
still
face
pro
ced
ure
Gra
nt
etal.
(2009)
4–
8m
on
ths
An
xie
ty(t
rait
)21;
26
–34,
35
Tem
per
am
ent
(IT
Q-r
evis
ed)
Vau
gh
net
al.
(1987)
8m
on
ths
Daily
hass
les
15
–17,
27
–28,
37
–38
Men
tal
dev
elopm
ent
(BS
ID-M
DI)
Hu
izin
ket
al.
(2002,
2003)
9m
on
ths
9/1
1N
ot
rep
ort
edT
emp
eram
ent
(IB
Q)
Bra
nd
etal.
(2006)
9m
on
ths
9/1
128
–40
Cort
isol
leve
lof
the
child
Yeh
ud
aet
al.
(2005)
1.5
yea
rsL
ife
even
tsst
ress
(i.e
.re
lati
on
ship
pro
ble
ms)
14
mon
ths
post
part
um
*C
ogn
itiv
ed
evel
opm
ent
(BS
ID-M
DI)
,fe
ar
react
ivit
y(L
ab
-TA
B)
Ber
gm
an
etal.
(2007)
2yea
rsA
nxie
ty(g
ener
al:
PO
MS
an
dS
TA
I),st
ress
(DS
I,
PS
S);
dep
ress
ion
(PO
MS
,C
ES
-D);
pre
gn
an
cy-s
pec
ific
stre
ss(P
ES
)
24,
28,
32
BS
ID:
MD
I,P
DI;
IBR
Dip
ietr
oet
al.
(2006)
3w
eeks;
1yea
r;2
yea
rsA
nxie
ty(s
tate
an
dtr
ait
)32
Ori
enta
tion
(NB
AS
),C
ogn
itiv
ed
evel
opm
ent
(BS
ID-M
DI)
,T
ask
ori
enta
tion
an
dm
oto
r
co-o
rdin
ati
on
(IB
R)
Bro
uw
ers
etal.
(2001)
K. Raikkonen et al.594
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.

TA
BL
EI
–continued
Age
of
child
Mea
sure
or
typ
eof
pre
nata
lex
posu
re
Pre
nata
lti
min
g
wee
ks
ges
tati
on
Ou
tcom
em
easu
re(s
)R
efer
ence
(s)
2yea
rsP
erce
ived
stre
sspre
gn
an
cy-r
elate
dan
xie
ty15
–38
Beh
avio
ura
lpro
ble
ms
(CB
CL
)te
mper
am
ent
(IC
Q),
att
enti
on
regu
lati
on
(BS
ID)
Gu
ttel
ing
etal.
(2005b)
13
–15
an
d42
mon
ths
Dep
ress
ion
Mon
thly
,fr
om
con
cepti
on
on
ward
s
Fro
nta
lan
dp
ari
etal
EE
Gasy
mm
etry
score
sD
awso
nan
dA
shm
an
(2000);
Daw
son
etal.
(2001)
14
–54
mon
ths
An
xie
ty,
dep
ress
ion
Each
trim
este
rB
ehav
iou
ral
an
dem
oti
on
al
pro
ble
ms
(CB
CL
);sa
liva
cort
isol
aft
erst
ress
ors
de
Bru
ijn
etal.
(2009a,b
)
6m
on
ths,
5yea
rsP
sych
olo
gic
al
dis
tres
s1
–16;
17
–28;
29
–40
Tem
per
am
ent
(IT
Q,
PT
Q)
Mart
inet
al.
(1999)
2yea
rsIc
est
orm
4–
24
Cogn
itiv
ed
evel
opm
ent
(BS
ID-M
DI)
,
lan
gu
age
pro
du
ctio
n(M
CD
I)
Lap
lan
teet
al.
(2004)
5.5
yea
rs–
IQ(W
ISC
)L
ap
lan
teet
al.
(2008)
6m
on
ths,
6yea
rsP
regn
an
cyri
sks
16
–20
Tem
per
am
ent
(IT
Q),
sch
ool
gra
des
an
d
mark
s
Nie
der
hofe
ran
dR
eite
r(2
004)
4–
6ye
ars
Daily
hass
les,
an
xie
ty,
per
ceiv
ed
stre
ss,
life
even
ts
16
Cort
isol
level
of
the
child
at
firs
tsc
hool
day
;
aft
erin
ocu
lati
on
mem
ory
(TO
MA
L)
Gu
ttel
ing
etal.
(2004,
2005a,
2006)
4an
d7
years
An
xie
ty18,
32
Em
oti
on
al
an
db
ehav
iou
ral
pro
ble
ms
(SD
Q)
O’C
on
nor
etal.
(2002,
2003)
7–
8ye
ars
Per
ceiv
edst
ress
10,
12,
20,
28,
32,
36
AD
HD
(DS
M-I
V)
Rod
rigu
ezan
dB
ohlin
(2005)
6–
9ye
ars
An
xie
ty(p
regn
an
cysp
ecifi
c)19,2
5,3
1G
rey
matt
erd
ensi
ty(M
RI
stu
dy)
Bu
sset
al.
(2009)
10
yea
rsS
elf
rate
dan
xie
ty18,
32
Cort
isol
level
of
the
child
O’C
on
nor
etal.
(2005)
10
yea
rs!
Dea
thof
acl
ose
rela
tive
0–
12
Sch
izophre
nia
(IC
D8/I
CD
10)
Khash
an
etal.
(2008)
14
yea
rsC
her
nob
yl
14
!D
epre
ssio
n/M
DD
(C-S
SA
GA
-A:
DS
M-I
II-
R)
AD
HD
Hu
izin
ket
al.
(2007)
8–
9ye
ars
,14
–15,
17
yea
rs
An
xie
ty(s
tate
an
dtr
ait
)12
–22
AD
HD
(CB
CL
,T
RF
),co
mp
ute
rize
d
enco
din
gta
skan
dst
op
task
,vo
cabu
lary
an
d
blo
ckd
esig
n(W
ISC
-R),
sust
ain
edatt
enti
on
(CP
T),
dep
ress
ion
(CD
I),
cued
att
enti
on
,
N-b
ack
,G
o/N
oG
o,
du
al
task
(ER
P),
resp
on
se-s
hif
tin
g.
Van
den
Ber
gh
an
dM
arc
oen
(2004);
Van
den
Ber
gh
etal.
(2005,
2006,
2008),
Men
nes
etal.
(2006,
2009)
25
yea
rsS
ever
elife
even
tsO
nave
rage
25
years
post
part
um
*
Cort
isol
an
dA
CT
Hle
vel
sE
ntr
inger
etal.
(2009)
–H
urr
ican
e24
–40
Au
tism
(DS
M-I
I-R
/DS
M-I
V)
Kin
ney
etal.
(2008)
Note
:A
DH
D,
att
enti
on
defi
cit
hyper
act
ivit
yd
isord
er;
AE
R,
Au
dit
ory
Evo
ked
Res
pon
ses;
BS
ID,
Bay
ley
Sca
les
of
Infa
nt
Dev
elopm
ent;
CB
CL
,C
hild
Beh
avio
ur
Chec
klist
;C
CT
I,C
olo
rad
oC
hild
Tem
per
am
ent
Inven
tory
;C
DI,
child
dep
ress
ion
inve
nto
ry;C
PT
,co
nti
nu
ou
sper
form
an
ceta
sk;C
-SS
AG
A-A
-,ch
ild
sem
i-st
ruct
ure
dass
essm
ent
of
gen
eti
csan
dalc
oholism
;D
SI,
Daily
Str
ess
Inven
tory
;
DS
M-R
,D
iagn
ost
ican
dS
tati
stic
al
Man
ual-
revis
ed;
EC
G,
elec
troca
rdio
gra
m;
ER
P,
even
t-re
late
dpote
nti
al;
HIB
RP,
Harv
ard
Infa
nt
Beh
avio
ura
lR
eact
ivit
yP
roto
col;
IBQ
,In
fan
tB
ehav
iou
r
Qu
esti
on
nair
e;IB
R,
Infa
nt
Beh
avio
ur
Rec
ord
;IC
D,
Inte
rnati
on
al
Cla
ssifi
cati
on
of
Dis
ease
s;IC
Q,
Infa
nt
Chara
cter
isti
csQ
ues
tion
nair
e;IT
Q,
Infa
nt
Tem
per
am
ent
Qu
esti
on
nair
e;IQ
,In
tellig
ence
Qu
oti
ent;
MC
DI,
MacA
rth
ur
Com
mu
nic
ati
veD
evel
opm
ent
Inven
tory
;M
DD
,M
ajo
rD
epre
ssiv
eD
isord
er;
MD
I,M
enta
lD
evel
opm
ent
Ind
ex;
Lab
-TA
B,
lab
ora
tory
tem
per
am
ent
ass
essm
ent
Batt
ery;
NB
AS
,B
raze
lton
neo
nata
lbeh
avio
ura
lass
essm
ent
scale
;P
ES
,P
regn
an
cyE
xper
ien
ceS
cale
;P
OM
S,P
rofi
leof
Mood
sS
cale
;P
SS
,P
erce
ived
Str
ess
Sca
le;P
DI,
Psy
chom
oto
rD
evel
opm
ent
Ind
ex;P
TQ
,
Pre
school
Tem
per
am
ent
Qu
esti
on
nair
e;S
DQ
,S
tren
gth
san
dD
iffi
cult
ies
Qu
esti
on
nair
e;S
ITQ
:S
hort
Infa
nt
Tem
per
am
ent
Qu
esti
on
nair
e;T
OM
AL
,T
est
of
Mem
ory
an
dL
earn
ing;
TR
F,
Tea
cher
’s
Rep
ort
Form
;W
ISC
,W
ech
sler
Inte
llig
ence
Sca
lefo
rC
hild
ren
;W
PP
SI,
Wec
hsl
erP
resc
hool
an
dP
rim
ary
Sca
leof
Inte
llig
ence
;*
Ret
rosp
ecti
ve.
Stress, glucocorticoids and liquorice in human pregnancy 595
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.

1996; Phillips et al. 1998). Cortisol responses to
ACTH stimulation are exaggerated in those of low
birth weight (Levitt et al. 2000; Reynolds et al. 2001,
2007). This occurs in myriad populations (Phillips
et al. 2000; Kajantie and Raikkonen 2010) and
precedes overt adult disease (Levitt et al. 2000). It is
well known that psychological stress causes activation
of the HPA axis with a consequent elevation in the
levels of cortisol. Elevated levels of cortisol are also
among the most consistently demonstrated biological
abnormalities found in depression (Knorr et al. 2010),
and in some contexts in anxiety (Roelofs et al. 2009).
As maternal and foetal levels of cortisol are correlated
(Gitau et al. 1998; O’Keane et al. 2011), the
experience of stress and higher levels of depression
and anxiety during pregnancy may directly result in
higher foetal exposure to maternal cortisol. In a recent
study, Sarkar et al. (2008) demonstrated that the
correlation between amniotic fluid cortisol (reflecting
foetal exposure) and maternal plasma cortisol
becomes stronger the higher with levels of maternal
prenatal anxiety, while maternal prenatal anxiety
correlated with higher plasma cortisol levels of the
mother, it was not directly related to amniotic fluid
cortisol (Glover et al. 2009).
As a consequence of this biology, a number of
studies have explored the effects of maternal
psychopathology on offspring HPA axis function,
mainly observing the effects by comparing the
offspring of high vs. low anxiety, stressed or depressed
pregnant women (Glover et al. 2010). Prenatal
maternal anxiety and depression are in general
associated with raised cortisol in the offspring, but
infants of mothers exposed to the trauma of 9/11 who
themselves developed symptoms of posttraumatic
stress disorder (PTSD) had lower cortisol levels,
though this is a common finding in PTSD (Yehuda
et al. 2005). One study has provided evidence that an
altered cortisol diurnal profile in the offspring
associated with prenatal maternal anxiety was also
associated with an altered behavioural phenotype, i.e.
with depressed mood (Van den Bergh et al. 2008).
Differences have been reported throughout the
lifespan from infancy, ages 1 week to 9 months
(Diego et al. 2004; Yehuda et al. 2005; Brennan et al.
2008; Oberlander et al. 2008; Grant et al. 2009),
4–15 years of age (Gutteling et al. 2004, 2005;
O’Connor et al. 2005; Huizink et al. 2008; Van den
Bergh et al. 2008) and in adults (Entringer et al.
2009). These data suggest that, as in animal models,
the HPA axis is a prime target for prenatal influences
and programming.
The studies on prenatal maternal stress, anxiety and
depression, even when controlling for postnatal
maternal stress, anxiety and depression, cannot
overrule a possibility that a shared genetic basis may
underlie the associations with offspring neurodevelop-
mental outcomes. Most evidence pointing to a
hereditary component comes from the studies of
depression (Belmaker and Agam 2008). It is, however,
unlikely that individual differences in offspring
neurodevelopmental outcomes could be attributed
to a single genetic, epigenetic or pre- or postnatal
environmental factor. Multiple mechanisms do exist
(see Figure 1), and these may act in concert. Further
studies on the exact underlying mechanisms through
which maternal stress, depression and anxiety induce
programming of the offspring are clearly warranted.
Maternal glucocorticoid therapy
In humans, therapeutic treatment with synthetic
glucocorticoids is common in women at risk of
preterm delivery, serving to accelerate foetal lung
maturation and thus reduce neonatal morbidity and
mortality (Seckl and Meaney 2004a). The long-term
effects of this treatment are not fully determined,
although there are suggestions that foetal growth and
subsequent development may be impaired (for a
review see Bolt et al. 2001). Glucocorticoid treatment
during pregnancy typically reduces birth weight (for a
review see Sloboda et al. 2005), but long-term follow
up studies are few. Antenatal glucocorticoid admin-
istration has been linked with higher blood pressure in
adolescence (Doyle et al. 2000) and higher insulin
levels in adulthood (Dalziel et al. 2005). Studies
aimed at establishing the long-term neurological and
developmental effects of antenatal glucocorticoid
therapy are complicated by the frequency of neuro-
logical sequelae common in such children anyway.
However, in a group of 6-year-old children, antenatal
glucocorticoid exposure is associated with subtle
effects on neurological function, including reduced
visual closure and visual memory (MacArthur et al.
1982). Multiple doses of antenatal glucocorticoids
given to women at risk of preterm delivery reduced
birth weight and head circumference in the offspring
(French et al. 1999). There are also effects on
behaviour: three or more courses of glucocorticoids
associate with an increased risk of externalizing
behaviour problems, distractibility and inattention
(Yeh et al. 2004), and children exposed to a longer
(.24 h to delivery) relative to a shorter duration
(,24 h to delivery) of a single, repeat dose of
betamethasone were rated by their mothers as more
impulsive at the age of 3 years (Pesonen et al. 2009a).
Children exposed to dexamethasone in early preg-
nancy because of risk of congenital adrenal hyperpla-
sia and born at term showed increased emotionality,
unsociability, avoidance and behavioural problems
(Trautman et al. 1995). Postnatally, dexamethasone
in premature babies lowers later IQ and other higher
brain functions (Yeh et al. 2004). Overall, whilst far
from complete, evidence indicates that exposure of the
foetus (or premature neonate) to excess glucocorti-
coids that readily cross the placental and foetal tissue
K. Raikkonen et al.596
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.

barriers to physiological cortisol (because they are
poor substrates for 11b-HSD2) may induce altera-
tions in the developing CNS.
Maternal intake of liquorice
If glucocorticoid exposure underpins some develop-
mental effects on the foetus, what does 11b-HSD2
do? Rare children homozygous for deleterious
mutations of the HSD11B2 gene encoding 11b-
HSD2 are of substantially lower birth weight than
their siblings, many of whom will be heterozygous for
the mutations (Dave-Sharma et al. 1998). In humans,
as in rodents (Benediktsson et al. 1993), placental
11b-HSD2 activity correlates with birth weight in
some (Stewart et al. 1995), but not all studies
(Rogerson et al. 1997). However, such correlations
are weak and mechanisms can only be inferred.
A handful of recent studies have focused on prenatal
maternal intake of liquorice confectionery as a natural
experimental platform to address mechanisms of
programming. These have been conducted in Finland
where consumption of large quantities of liquorice
confectionery is common among young women:
nearly half of the pregnant women consume at least
some liquorice (Raikkonen et al. 2009b; Strandberg
et al. 2001). Glycyrrhizin (3b-D-diglucuronyl-18b-
glycyrrhetinic or -glycyrrhizic acid) is a natural
constituent of liquorice. Its hemisuccinate synthetic
analogue, carbenoxolone, was a clinical drug formerly
used to treat peptic ulcers. Its water solubility makes it
attractive for use in preclinical and human studies
(Welberg et al. 2000). These agents are potent (low
nanomolar Ki) inhibitors of 11b-HSD2. Though they
also potently inhibit 11b-HSD type 1, this is little
expressed in the foetus at least in rodents (Speirs et al.
2004). In normal circumstances, this placental
enzyme metabolizes up to 80–90% of maternal active
cortisol to inactive cortisone, a function inhibited by
carbenoxolone, at least in intact placenta ex vivo
(Benediktsson et al. 1997).
In 1998, a project was initiated to test whether
varying levels of maternal consumption of glycyrrhizin
in liquorice during pregnancy was associated
with body size at birth and length of gestation. In
over 1000 pregnant women, prenatal exposure to high
(.500 mg/wk) compared to zero-low (0–249 mg/wk)
or moderate (250–499 mg/wk) glycyrrhizin in
liquorice was associated with a slightly shorter
duration of gestation (Strandberg et al. 2001).
Glycyrrhizin intake during pregnancy was not
significantly associated with birth anthropometry.
The findings on shorter length of gestation were
replicated in another Finnish cohort: high intake of
glycyrrhizin during pregnancy was associated with
over a twofold increased risk in the rate of preterm
delivery (Strandberg et al. 2002).
In a follow-up study, the long-term effects of
maternal intake of liquorice during gestation on
8-year-old offspring psychological development,
mental health and psychophysiological functioning
were determined. In comparison to the group whose
mothers had zero-low glycyrrhizin exposure, those
with high exposure scored significantly lower on verbal
and visuo-spatial abilities and in narrative memory. In
addition, children in the high-exposure group had
significant 2.4–3.0-fold increased risk of externalizing
symptoms, attention, rule breaking, aggression pro-
blems and DSM IV-based symptoms of obsessive
defiant disorder (Raikkonen et al. 2009b). The effects
on cognitive performance appeared dose-related.
None of the associations were affected by birth weight
or duration of gestation and other pre- and perinatal,
maternal and child characteristics implicated as risks
for pregnancy and/or cognitive and psychiatric
outcomes.
The HPA axis of these children was also affected.
Children of mothers consuming high levels of
glycyrrhizin had a higher salivary cortisol peak and
area under the curve upon awakening and higher
overall salivary cortisol throughout a Trier Social
Stress Test for Children (TSST-C; Raikkonen et al.
2010c). The associations with salivary cortisol peak
and salivary cortisol baseline during the TSST-C were
dose-related. As far as could be ascertained, the results
were not due to confounding factors such as maternal
health during pregnancy, including blood pressure
levels, obesity and pregnancy disorders, birth anthro-
pometry and length of gestation, maternal social class
at birth and in a follow-up at the child’s age of 8 years,
maternal smoking and alcohol consumption during
pregnancy, and child characteristics, such as sex,
growth in height, head circumference and difficulties
in cognitive functioning that might interfere with
cognitive performance, associate with psychiatric
symptomatology, and alter performance in the
TSST-C. We have previously reported, in this
same sample of 8-year-old children, that shorter
sleep duration and lower sleep efficiency (percent time
spent asleep whilst in bed) are associated with
alterations in the diurnal salivary cortisol pattern and
in salivary cortisol responses during the TSST-C
(Raikkonen et al. 2010b). Poorer sleep may thus
introduce another factor that may confound the
associations between liquorice consumption and
HPA axis activity. Maternal intake of liquorice during
pregnancy is, however, not associated with the
children’s sleep patterns (Raikkonen, unpublished
data). Thus, when we further controlled the associ-
ations of maternal liquorice intake during pregnancy
and their children’s HPA axis function for the
children’s sleep duration and sleep efficiency, the
associations remained identical.
These findings suggest that high maternal liquorice
consumption during pregnancy may exert deleterious
Stress, glucocorticoids and liquorice in human pregnancy 597
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.

effects upon cognitive and psychiatric outcomes and
HPAA functioning in children paralleling the effects
seen in preclinical models. Whilst it remains to be
ascertained whether the dose of liquorice consumed
affects placental 11b-HSD2 function appreciably
in vivo (mice lacking one copy of the gene encoding
11b-HSD2 have intermediate reductions in birth
weight), it is plausible to suggest that this may occur
and that placental glucocorticoid “leakiness” may
have an impact on foetal brain development during
periods critical for affective and cognitive develop-
ment with persisting impacts. If humans resemble
rodents, then maternal stress-related disorders may
further lower placental glucocorticoid barrier
function.
Conclusion
This review shows, first, that accumulating evidence
exists suggesting that maternal negative emotions
during pregnancy are linked with the long-term
behaviour and physiology of her child, even after
controlling for relevant covariates. The range of
maternal “stressors” that predict the child outcomes
is quite wide. Moreover, a wide range of different
outcomes have been found to be affected by these
maternal stressors (Glover et al. 2010). This should
come as no surprise. In terms of mechanisms, we are
far from understanding how and when the early
hormonal environment may affect the refinement of
neural circuits in specific brain layers and areas which
will later determine the way in which sensory-
cognitive, motor, arousal and emotional structure–
function relationships are affected (Van den Bergh
et al. 2005a; Fox et al. 2010).
Second, this review shows that there are links
between prenatal maternal intake of glucocorticoids
and of liquorice confectionery and long-term beha-
viour and physiology of her child, even after
controlling for relevant covariates. These findings
may not generalize merely to intake of liquorice
confectionery.
Because of its sweetening (50–200 times sweeter
than refined sugar) and flavouring capacity, glycyr-
rhizin is also used as a natural sweetener and is also
found in other foodstuffs, including some candies and
chewing gum, herbal teas, alcoholic and non-alcoholic
drinks, tobacco and some traditional (e.g. cough
medicine) as well as some herbal medicine (to treat
stomach ulcers, sore throat and viral infections).
Hence, not surprisingly, according to some estimates
the daily consumption levels of glycyrrhizin range
from 1.6 to 215.2 mg (Isbrucker and Burdock 2006).
This estimate was derived from the USA where
consumption of liquorice confectionery is not popular.
Glycyrrhizin is generally recognized as safe for use
in foods, though the European Community’s
Scientific Committee on Food and the FAO/WHO
Expert Committee (http://ec.europa.eu/food/fs/sc/scf/
out186_en.pdf) have considered that a consumption
of 100 mg/day may be a reasonable upper limit for the
majority of the population, and the FDA recommends
that if glycyrrhizin-containing foods are not consumed
in excess or by sensitive individuals, these foods do not
pose a health hazard (http://www.accessdata.fda.gov/
scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr ¼ 184.
1408). The findings reviewed here suggest that
consumption of large quantities of glycyrrhizin in
foodstuffs may alter offspring’s brain development and
subsequent function, and therefore, it may be prudent
to inform pregnant women of the potential hazards of
eating large quantities of liquorice.
Future studies should try to increase knowledge
about mechanisms underlying the effect of prenatal
influences on social-emotional, cognitive and beha-
vioural problems, particularly about whether prenatal
stress and gene-environment interactions affecting the
HPA-axis play a role in early developmental processes.
It has become increasingly clear that epigenetic
changes, including DNA methylation and histone
modifications, are causally involved in a range of
developmental processes by affecting transcriptional
activity. For the future, it is important that these
epigenetic processes, that take place also in the
placenta, are integrated in the studies of prenatal
stress. They provide “a physical basis for the influence
of the perinatal environmental signals over the life of
the individual” (Meaney 2010). Moreover, the
eventual moderating influence of other environmental
factors, such as the postnatal caregiving environment,
should also be studied. There is evidence that severe
early life stress may carry consequences on a wide
range of developmental outcomes, including physical
and mental health, psychophysiological functioning
and cognitive abilities and attained social class in
adulthood (Pesonen et al. 2007, 2008b, 2010, 2011;
Alastalo et al. 2009; Raikkonen et al. 2011). Whether
the postnatal environmental influences buffer or add
to the prenatal influences is little studied. Results of
these research efforts would open the way for the
development of targeted pre- and perinatal prevention
and intervention strategies that could reduce the risk
that prenatal environmental adversities carry for early
functioning and later mental health of children, and
have significant consequences for the long-term health
and well-being of the children.
Declaration of interest: This work was sponsored by
the grants from the European Science Foundation,
Stress and Mental Health programme (EuroS-
TRESS), the Finnish Academy, the Medical Research
Council (UK), The Netherlands Organisation for
Scientific Research (NWO). The authors report no
conflicts of interest. The authors alone are responsible
for the content and writing of the paper.
K. Raikkonen et al.598
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.

References
Alastalo H, Raikkonen K, Pesonen A-K, Osmond C, Barker DJ,
Kajantie E, Heinonen K, Forsen TJ, Eriksson JG. 2009.
Cardiovascular health of Finnish war evacuees 60 years later.
Ann Med 41:66–72.
Austin MP, Hadzi-Pavlovic D, Leader L, Saint K, Parker G. 2005.
Maternal trait anxiety, depression and life event stress in
pregnancy: Relationships with infant temperament. Early Hum
Dev 81:183–190.
Barker DJ. 1991. The intrauterine environment and adult
cardiovascular disease. Ciba Found Symp 156:3–10, discussion
10–6.
Barker DJ. 1998. In utero programming of chronic disease. Clin Sci
(Lond) 95:115–128.
Barker DJ, Winter PD, Osmond C, Margetts B, Simmonds SJ.
1989. Weight in infancy and death from ischaemic heart disease.
Lancet 2:577–580.
Barker DJ, Osmond C, Rodin I, Fall CH, Winter PD. 1995. Low
weight gain in infancy and suicide in adult life. Br Med J 311:
1203.
Barker DJ, Osmond C, Forsen TJ, Kajantie E, Eriksson JG. 2005.
Trajectories of growth among children who have coronary events
as adults. N Engl J Med 353:1802–1809.
Belmaker RH, Agam G. 2008. Major depressive disorder. N Engl J
Med 358:55–68.
Benediktsson R, Lindsay RS, Noble J, Seckl JR, Edwards CR. 1993.
Glucocorticoid exposure in utero: New model for adult
hypertension. Lancet 341:339–341.
Benediktsson R, Calder AA, Edwards CR, Seckl JR. 1997. Placental
11 beta-hydroxysteroid dehydrogenase: A key regulator of fetal
glucocorticoid exposure. Clin Endocrinol (Oxf) 46:161–166.
Bergman K, Sarkar P, O’Connor TG, Modi N, Glover V. 2007.
Maternal stress during pregnancy predicts cognitive ability and
fearfulness in infancy. J Am Acad Child Adolesc Psychiatry 46:
1454–1463.
Bolt RJ, van Weissenbruch MM, Lafeber HN, Delemarre-van de
Waal HA. 2001. Glucocorticoids and lung development in the
fetus and preterm infant. Pediatr Pulmonol 32:76–91.
Brand SR, Engel SM, Canfield RL, Yehuda R. 2006. The effect of
maternal PTSD following in utero trauma exposure on behavior
and temperament in the 9-month-old infant. Ann N Y Acad Sci
1071:454–458.
Brennan PA, Pargas R, Walker EF, Green P, Newport DJ, Stowe Z.
2008. Maternal depression and infant cortisol: Influences of
timing, comorbidity and treatment. J Child Psychol Psychiatry
49:1099–1107.
Broekman BF, Chan YH, Chong YS, Quek SC, Fung D, Low YL,
Ooi YP, Gluckman PD, Meaney MJ, Wong TY, Saw SM. 2009.
The influence of birth size on intelligence in healthy children.
Pediatrics 123:e1011–e1016.
Brouwers EPM, van Baar AL, Pop VJM. 2001. Maternal anxiety
during pregnancy and subsequent infant development. Inf Behav
Dev 24:95–106.
Buss C, Davis EP, Muftuler LT, Head K, Sandman CA. 2009. High
pregnancy anxiety during mid-gestation is associated with
decreased gray matter density in 6–9-year-old children.
Psychoneuroendocrinology 35:141–153.
Cheung YB. 2002. Early origins and adult correlates of psychoso-
matic distress. Soc Sci Med 55:937–948.
Clark PM, Hindmarsh PC, Shiell AW, Law CM, Honour JW, Barker
DJP. 1996. Size at birth and adrenocortical function in
childhood. Clin Endocrinol 45:721–726.
Cornelius MD, Day NL. 2009. Developmental consequences of
prenatal tobacco exposure. Curr Opin Neurol 22:121–125.
Dalziel SR, Walker NK, Parag V, Mantell C, Rea HH, Rodgers A,
Harding JE. 2005. Cardiovascular risk factors after antenatal
exposure to betamethasone: 30-year follow-up of a randomised
controlled trial. Lancet 365:1856–1862.
Dave-Sharma S, Wilson RC, Harbison MD, Newfield R, Azar MR,
Krozowski ZS, Funder JW, Shackleton CH, Bradlow HL, Wei
JQ, Hertecant J, Moran A, Neiberger RE, Balfe JW, Fattah A,
Daneman D, Akkurt HI, De Santis C, New MI. 1998.
Examination of genotype and phenotype relationships in 14
patients with apparent mineralocorticoid excess. J Clin
Endocrinol Metab 83:2244–2254.
Davis EP, Snidman N, Wadhwa PD, Glynn LM, Schetter CD,
Sandman CA. 2004. Prenatal maternal anxiety and depression
predict negative behavioral reactivity in infancy. Infancy 6:
319–331.
Davis EP, Glynn LM, Schetter CD, Hobel C, Chicz-Demet A,
Sandman CA. 2007. Prenatal exposure to maternal depression
and cortisol influences infant temperament. J Am Acad Child
Adolesc Psychiatry 46:737–746.
Dawson G, Ashman SB. 2000. On the origins of a vulnerability to
depression: The influence of the early social environment on the
development of psychobiological systems related to risk for
affective disorder. Mahwah, NJ: Erlbaum.
Dawson G, Ashman SB, Hessl D, Spieker S, Frey K, Panagiotides
H, Embry L. 2001. Autonomic and brain electrical activity in
securely- and insecurely-attached infants of depressed mothers.
Inf Behav Dev 24:135–149.
de Bruijn ATCE, van Bakel HJA, van Baar AL. 2009a. Sex
differences in the relation between prenatal maternal emotional
complaints and child outcome. Early Hum Dev 85:319–324.
de Bruijn ATCE, van Bakel HJA, Wijnen H, Pop VJM, van Baar AL.
2009b. Prenatal maternal emotional complaints are associated
with cortisol responses in toddler and preschool aged girls. Dev
Psychobiol 51:553–563.
de Vries A, Holmes MC, Heijnis A, Seier JV, Heerden J, Louw J,
Wolfe-Coote S, Meaney MJ, Levitt NS, Seckl JR. 2007. Prenatal
dexamethasone exposure induces changes in nonhuman primate
offspring cardiometabolic and hypothalamic–pituitary–adrenal
axis function. J Clin Invest 117:1058–1067.
Diego MA, Field T, Hernandez-Reif M, Cullen C, Schanberg S,
Kuhn C. 2004. Prepartum, postpartum, and chronic depression
effects on newborns. Psychiatry 67:63–80.
DiPietro JA, Ghera MM, Costigan KA. 2008. Prenatal origins of
temperamental reactivity in early infancy. Early Hum Dev 84:
569–575.
Doyle LW, Ford GW, Davis NM, Callanan C. 2000. Antenatal
corticosteroid therapy and blood pressure at 14 years of age in
preterm children. Clin Sci 98:137–142.
Edwards CR, Benediktsson R, Lindsay RS, Seckl JR. 1993.
Dysfunction of placental glucocorticoid barrier: Link between
fetal environment and adult hypertension? Lancet 341:355–357.
El Marroun H, Tiemeier H, Steegers EA, Jaddoe VW, Hofman A,
Verhulst FC, van den Brink W, Huizink AC. 2009. Intrauterine
cannabis exposure affects fetal growth trajectories: The
generation R study. J Am Acad Child Adolesc Psychiatry
48(12):1173–1181.
Entringer S, Kumsta R, Hellhammer DH, Wadhwa PD, Wust S.
2009. Prenatal exposure to maternal psychosocial stress and
HPA axis regulation in young adults. Horm Behav 55:292–298.
Eriksson JG, Osmond C, Kajantie E, Forsen TJ, Barker DJ. 2006.
Patterns of growth among children who later develop type 2
diabetes or its risk factors. Diabetologia 49:2853–2858.
Eriksson JG, Forsen TJ, Kajantie E, Osmond C, Barker DJ. 2007.
Childhood growth and hypertension in later life. Hypertension
49:1415–1421.
Espy KA, Fang H, Johnson C, Stopp C, Wiebe SA, Respass J. 2011.
Prenatal tobacco exposure: Developmental outcomes in the
neonatal period. Dev Psychol 47:153–156.
Feldt K, Raikkonen K, Eriksson JG, Andersson S, Osmond C,
Barker DJ, Phillips DI, Kajantie E. 2007. Cardiovascular
reactivity to psychological stressors in late adulthood is predicted
by gestational age at birth. J Hum Hypertens 21:401–410.
Stress, glucocorticoids and liquorice in human pregnancy 599
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.

Field T, Sandberg D, Garcia R, Vega-Lahr N, Goldstein S, Guy L.
1985. Pregnancy problems, postpartum depression, and early
mother–infant interactions. Dev Psychol 21:1152–1156.
Fox SE, Levitt P, Nelson CA, 3rd. 2010. How the timing and quality
of early experiences influence the development of brain
architecture. Child Dev 81:28–40.
French NP, Hagan R, Evans SF, Godfrey M, Newnham JP. 1999.
Repeated antenatal corticosteroids: Size at birth and subsequent
development. Am J Obstet Gynecol 180:114–121.
Gale CR, O’Callaghan FJ, Godfrey KM, Law CM, Martyn CN.
2004. Critical periods of brain growth and cognitive function in
children. Brain 127:321–329.
Gitau R, Cameron A, Fisk NM, Glover V. 1998. Fetal exposure to
maternal cortisol. Lancet 352:707–708.
Glover V, Bergman K, Sarkar P, O’Connor TG. 2009. Association
between maternal and amniotic fluid cortisol is moderated by
maternal anxiety. Psychoneuroendocrinology 34:430–435.
Glover V, O’Connor TG, O’Donnell K. 2010. Prenatal stress and
the programming of the HPA axis. Neurosci Biobehav Rev 35:
17–22.
Gluckman PD, Hanson MA, Pinal C. 2005. The developmental
origins of adult disease. Matern Child Nutr 1:130–141.
Gluckman PD, Hanson MA, Cooper C, Thornburg KL. 2008.
Effect of in utero and early-life conditions on adult health and
disease. N Engl J Med 359:61–73.
Gluckman PD, Hanson MA, Bateson P, Beedle AS, Law CM,
Bhutta ZA, Bhutta ZA, Anokhin KV, Bougneres P, Chandak
GR, Dasgupta P, Smith GD, Ellison PT, Forrester TE, Gilbert
SF, Jablonka E, Kaplan H, Prentice AM, Simpson SJ, Uauy R,
West-Eberhard MJ. 2009. Towards a new developmental
synthesis: Adaptive developmental plasticity and human disease.
Lancet 373:1654–1657.
Grant KA, McMahon C, Austin MP, Reilly N, Leader L, Ali S.
2009. Maternal prenatal anxiety, postnatal caregiving and
infants’ cortisol responses to the still-face procedure. Dev
Psychobiol 51:625–637.
Gunnell D, Rasmussen F, Fouskakis D, Tynelius P, Harrison G.
2003. Patterns of fetal and childhood growth and the
development of psychosis in young males: A cohort study. Am
J Epidemiol 158:291–300.
Gutteling BM, de Weerth C, Buitelaar JK. 2004. Maternal prenatal
stress and 4–6 year old children’s salivary cortisol concentrations
pre- and post-vaccination. Stress 7:257–260.
Gutteling BM, de Weerth C, Buitelaar JK. 2005. Prenatal stress and
children’s cortisol reaction to the first day of school.
Psychoneuroendocrinology 30:541–549.
Gutteling BM, de Weerth C, Willemsen-Swinkels SH, Huizink AC,
Mulder EJ, Visser GH, Buitelaar JK. 2005b. The effects of
prenatal stress on temperament and problem behavior of
27-month-old toddlers. Eur Child Adolesc Psychiatry 14:41–51.
Gutteling BM, de Weerth C, Zandbelt N, Mulder EJ, Visser GH,
Buitelaar JK. 2006. Does maternal prenatal stress adversely
affect the child’s learning and memory at age six? J Abnorm
Child Psychol 34:789–798.
Hanson MA, Gluckman PD. 2008. Developmental origins of health
and disease: New insights. Basic Clin Pharmacol Toxicol 102:
90–93.
Harvison KW, Molfese DL, Woodruff-Borden J, Weigel RA. 2009.
Neonatal auditory evoked responses are related to perinatal
maternal anxiety. Brain Cogn 71:369–374.
Heinonen K, Raikkonen K, Pesonen AK, Kajantie E, Andersson S,
Eriksson JG, Niemela A, Vartia T, Peltola J, Lano A. 2008.
Prenatal and postnatal growth and cognitive abilities at 56
months of age: A longitudinal study of infants born at term.
Pediatrics 121:e1325–e1333.
Heinonen K, Raikkonen K, Pesonen AK, Andersson S, Kajantie E,
Eriksson JG, Wolke D, Lano A. 2010. Behavioural symptoms of
attention deficit/hyperactivity disorder in preterm and term
children born small and appropriate for gestational age: A
longitudinal study. BMC Pediatr 15:10–91.
Heinonen K, Raikkonen K, Pesonen AK, Andersson S, Kajantie E,
Eriksson JG, Wolke D, Lano A. 2011. Longitudinal study of
smoking cessation before pregnancy and children’s cognitive
abilities at 56 months of age. Early Hum Dev 87(5):353–359.
Hellemans KG, Sliwowska JH, Verma P, Weinberg J. 2010. Prenatal
alcohol exposure: Fetal programming and later life vulnerability
to stress, depression and anxiety disorders. Neurosci Biobehav
Rev 34:791–807.
Henrichs J, Schenk JJ, Schimdt HG, Velders FP, Hofman A, Jaddoe
VWV, Verhulst FC, Tiemeier H. 2009. Maternal pre- and
postnatal anxiety and infant temperament. The generation R
study. Inf Child Dev 18:556–572.
Hernandez-Martinez C, Arija V, Balaguer A, Cavalle P, Canals J.
2008. Do the emotional states of pregnant women affect
neonatal behaviour? Early Hum Dev 84:745–750.
Hernandez-Reif M, Field T, Diego M, Ruddock M. 2006. Greater
arousal and less attentiveness to face/voice stimuli by neonates of
depressed mothers on the Brazelton Neonatal Behavioral
Assessment Scale. Inf Child Dev 29:594–598.
Holmes MC, Abrahamsen CT, French KL, Paterson JM, Mullins
JJ, Seckl JR. 2006. The mother or the fetus? 11beta-
hydroxysteroid dehydrogenase type 2 null mice provide evidence
for direct fetal programming of behavior by endogenous
glucocorticoids. J Neurosci 26:3840–3844.
Huizink AC, de Medina PG, Mulder EJ, Visser GH, Buitelaar JK.
2002. Psychological measures of prenatal stress as predictors of
infant temperament. J Am Acad Child Adolesc Psychiatry 41:
1078–1085.
Huizink AC, Robles de Medina P, Mulder EJ, Visser GH, Buitelaar
JK. 2003. Stress during pregnancy is associated with develop-
mental outcome in infancy. J Child Psychol Psychiatry 44:
810–818.
Huizink AC, Bartels M, Rose RJ, Pulkkinen L, Eriksson CJ, Kaprio
J. 2008. Chernobyl exposure as stressor during pregnancy and
hormone levels in adolescent offspring. J Epidemiol Community
Health 62:e5.
IJzerman R, Stehouwer CD, de Geus EJ, van Weissenbruch MM,
Delemarre-van de Waal HA, Boomsma DI. 2003. Low birth
weight is associated with increased sympathetic activity:
Dependence on genetic factors. Circulation 108:566–571.
Isbrucker RA, Burdock GA. 2006. Risk and safety assessment on the
consumption of Licorice root (Glycyrrhiza sp.), its extract and
powder as a food ingredient, with emphasis on the pharmacology
and toxicology of glycyrrhizin. Regul Toxicol Pharmacol 46:
167–192.
Jones A, Godfrey KM, Wood P, Osmond C, Goulden P, Phillips DI.
2006. Fetal growth and the adrenocortical response to
psychological stress. J Clin Endocrinol Metab 91:1868–1871.
Jones A, Beda A, Ward AM, Osmond C, Phillips DI, Moore VM,
Simpson DM. 2007. Size at birth and autonomic function
during psychological stress. Hypertension 49:548–555.
Kajantie E. 2008. Early-life events. Effects on aging. Hormones
(Athens) 7:101–113.
Kajantie E, Raikkonen K. 2010. Early life predictors of the
physiological stress response later in life. Neurosci Biobehav Rev
35:23–32.
Kajantie E, Feldt K, Raikkonen K, Phillips DI, Osmond C,
Heinonen K, Pesonen AK, Andersson S, Barker DJ, Eriksson
JG. 2007. Body size at birth predicts hypothalamic–pituitary–
adrenal axis response to psychosocial stress at age 60 to 70 years.
J Clin Endocrinol Metab 92:4094–4100.
Khashan AS, Abel KM, McNamee R, Pedersen MG, Webb RT,
Baker PN, Kenny LC, Mortensen PB. 2008a. Higher risk of
offspring schizophrenia following antenatal maternal exposure to
severe adverse life events. Arch Gen Psychiatry 65:146–152.
Khashan AS, McNamee R, Abel KM, Pedersen MG, Webb RT,
Kenny LC, Mortensen PB, Baker PN. 2008b. Reduced infant
K. Raikkonen et al.600
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.

birthweight consequent upon maternal exposure to severe life
events. Psychosom Med 70:688–694.
Kinney DK, Miller AM, Crowley DJ, Huang E, Gerber E. 2008.
Autism prevalence following prenatal exposure to hurricanes and
tropical storms in Louisiana. J Autism Dev Disord 38:481–488.
Knorr U, Vinberg M, Kessing LV, Wetterslev J. 2010. Salivary
cortisol in depressed patients versus control persons: A
systematic review and meta-analysis. Psychoneuroendocrinology
35:1275–1286.
Lahti J, Raikkonen K, Kajantie E, Heinonen K, Pesonen AK,
Jarvenpaa AL, Strandberg T. 2006. Small body size at birth and
behavioural symptoms of ADHD in children aged five to six
years. J Child Psychol Psychiatry 47:1167–1174.
Lahti J, Raikkonen K, Sovio U, Miettunen J, Hartikainen AL, Pouta
A, Taanila A, Joukamaa M, Jarvelin MR, Veijola J. 2009. Early-
life origins of schizotypal traits in adulthood. Br J Psychiatry 195:
132–137.
Lahti J, Raikkonen K, Pesonen AK, Heinonen K, Kajantie E,
Forsen T, Osmond C, Barker DJ, Eriksson JG. 2010a. Prenatal
growth, postnatal growth, and trait anxiety in late adulthood—
the Helsinki Birth Cohort Study. Acta Psychiatr Scand 121:
227–235.
Lahti M, Raikkonen K, Wahlbeck K, Heinonen K, Forsen T,
Kajantie E, Pesonen AK, Osmond C, Barker DJ, Eriksson JG.
2010b. Prenatal origins of hospitalization for personality
disorders: The Helsinki birth cohort study. Psychiatry Res 179:
226–230.
Langley-Evans SC, Phillips GJ, Benediktsson R, Gardner DS,
Edwards CR, Jackson AA, Seckl JR. 1996. Protein intake in
pregnancy, placental glucocorticoid metabolism and the
programming of hypertension in the rat. Placenta 17:169–172.
Laplante DP, Barr RG, Brunet A, Galbaud du Fort G, Meaney ML,
Saucier JF, Zelazo PR, King S. 2004. Stress during pregnancy
affects general intellectual and language functioning in human
toddlers. Pediatr Res 56:400–410.
Laplante DP, Brunet A, Schmitz N, Ciampi A, King S. 2008.
Project Ice Storm: Prenatal maternal stress affects cognitive and
linguistic functioning in 5 1/2-year-old children. J Am Acad
Child Adolesc Psychiatry 47:1063–1072.
Levitt NS, Lambert EV, Woods D, Hales CN, Andrew R, Seckl JR.
2000. Impaired glucose tolerance and elevated blood pressure in
low birth weight, nonobese, young south african adults: Early
programming of cortisol axis. J Clin Endocrinol Metab 85:
4611–4618.
Li J, Vestergaard M, Obel C, Christensen J, Precht DH, Lu M,
Olsen J. 2009a. A nationwide study on the risk of autism after
prenatal stress exposure to maternal bereavement. Pediatrics
123:1102–1107.
Li J, Vestergaard M, Obel C, Precht DH, Christensen J, Lu M,
Olsen J. 2009b. Prenatal stress and cerebral palsy: A nationwide
cohort study in Denmark. Psychosom Med 71:615–618.
Lindsay RS, Lindsay RM, Edwards CR, Seckl JR. 1996a. Inhibition
of 11-beta-hydroxysteroid dehydrogenase in pregnant rats and
the programming of blood pressure in the offspring. Hyperten-
sion 27:1200–1204.
Lindsay RS, Lindsay RM, Waddell BJ, Seckl JR. 1996b. Prenatal
glucocorticoid exposure leads to offspring hyperglycaemia in the
rat: Studies with the 11 beta-hydroxysteroid dehydrogenase
inhibitor carbenoxolone. Diabetologia 39:1299–1305.
Lou HC, Hansen D, Nordentoft M, Pryds O, Jensen F, Nim J,
Hemmingsen R. 1994. Prenatal stressors of human life affect
fetal brain development. Dev Med Child Neurol 36:826–832.
Lucassen PJ, Bosch OJ, Jousma E, Kromer SA, Andrew R, Seckl JR,
Neumann ID. 2009. Prenatal stress reduces postnatal neurogen-
esis in rats selectively bred for high, but not low, anxiety: Possible
key role of placental 11beta-hydroxysteroid dehydrogenase type
2. Eur J Neurosci 29:97–103.
MacArthur BA, Howie RN, Dezoete JA, Elkins J. 1982. School
progress and cognitive development of 6-year-old children
whose mothers were treated antenatally with betamethasone.
Pediatrics 70:99–105.
Mairesse J, Lesage J, Breton C, Breant B, Hahn T, Darnaudery M,
Dickson SL, Seckl J, Blondeau B, Vieau D, Maccari S, Viltart O.
2007. Maternal stress alters endocrine function of the feto-
placental unit in rats. Am J Physiol Endocrinol Metab 292:
E1526–E1533.
Martin RP, Noyes J, Wisenbaker J, Huttunen M. 1999. Prediction of
early childhood negative emotionality and inhibition from
maternal distress during pregnancy. Merrill-Palmer Q 45:
370–391.
McGrath JM, Records K, Rice M. 2008. Maternal depression and
infant temperament characteristics. Infant Behav Dev 31:71–80.
Meaney MJ. 2010. Epigenetics and the biological definition of
gene £ environment interactions. Child Dev 81:41–79.
Mennes M. 2008. Longitudinal study on the effects of maternal
anxiety during pregnancy: Neuropsychological and neurophy-
siological examination of cognitive control in the adolescent
offspring. Leuven: Katholieke Universiteit Leuven.
Mennes M, Stiers P, Lagae L, Van den Bergh BR. 2006. Long-term
cognitive sequelae of antenatal maternal anxiety: Involvement of
the orbitofrontal cortex. Neurosci Biobehav Rev 30:1078–1086.
Mennes M, Van den Bergh BR, Lagae L, Stiers P. 2009.
Developmental brain alterations in 17 year old boys are related
to antenatal maternal anxiety. Clin Neurophysiol 120:
1116–1122.
Niederhofer H, Reiter A. 2004. Prenatal maternal stress, prenatal
fetal movements and perinatal temperament factors influence
behavior and school marks at the age of 6 years. Fetal Diagn
Ther 19:160–162.
Obel C. 2003. Epidemiological studies of stress during pregnancy
and fetal brain development. Denmark: University of Aarhus.
Oberlander TF, Weinberg J, Papsdorf M, Grunau R, Misri S, Devlin
AM. 2008. Prenatal exposure to maternal depression, neonatal
methylation of human glucocorticoid receptor gene (NR3C1)
and infant cortisol stress responses. Epigenetics 3:97–106.
O’Connor TG, Heron J, Golding J, Beveridge M, Glover V. 2002.
Maternal antenatal anxiety and children’s behavioural/emotional
problems at 4 years. Report from the Avon Longitudinal Study
of Parents and Children. Br J Psychiatry 180:502–508.
O’Connor TG, Heron J, Golding J, Glover V. 2003. Maternal
antenatal anxiety and behavioural/emotional problems in
children: A test of a programming hypothesis. J Child Psychol
Psychiatry 44:1025–1036.
O’Connor TG, Ben-Shlomo Y, Heron J, Golding J, Adams D,
Glover V. 2005. Prenatal anxiety predicts individual differences
in cortisol in pre-adolescent children. Biol Psychiatry 58:
211–217.
O’Keane V, Lightman S, Marsh M, Pawlby S, Papadopoulos AS,
Taylor A, Moore R, Patrick K. 2011. Increased pituitary–
adrenal activation and shortened gestation in a sample of
depressed pregnant women: A pilot study. J Affect Disord 130:
300–305.
O’Regan D, Welberg LL, Holmes MC, Seckl JR. 2001.
Glucocorticoid programming of pituitary–adrenal function:
Mechanisms and physiological consequences. Semin Neonatol
6:319–329.
Pesonen AK, Raikkonen K, Strandberg TE, Jarvenpaa AL. 2005.
Continuity of maternal stress from the pre- to the postnatal
period: Associations with infant’s positive, negative and overall
temperamental reactivity. Inf Behav Devel 28:36–47.
Pesonen AK, Raikkonen K, Kajantie E, Heinonen K, Strandberg
TE, Jarvenpaa AL. 2006. Fetal programming of temperamental
negative affectivity among children born healthy at term. Dev
Psychobiol 48:633–643.
Pesonen AK, Raikkonen K, Heinonen K, Kajantie E, Forsen T,
Eriksson JG. 2007. Depressive symptoms in adults separated
from their parents as children: A natural experiment during
World War II. Am J Epidemiol 166:1126–1133.
Stress, glucocorticoids and liquorice in human pregnancy 601
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.
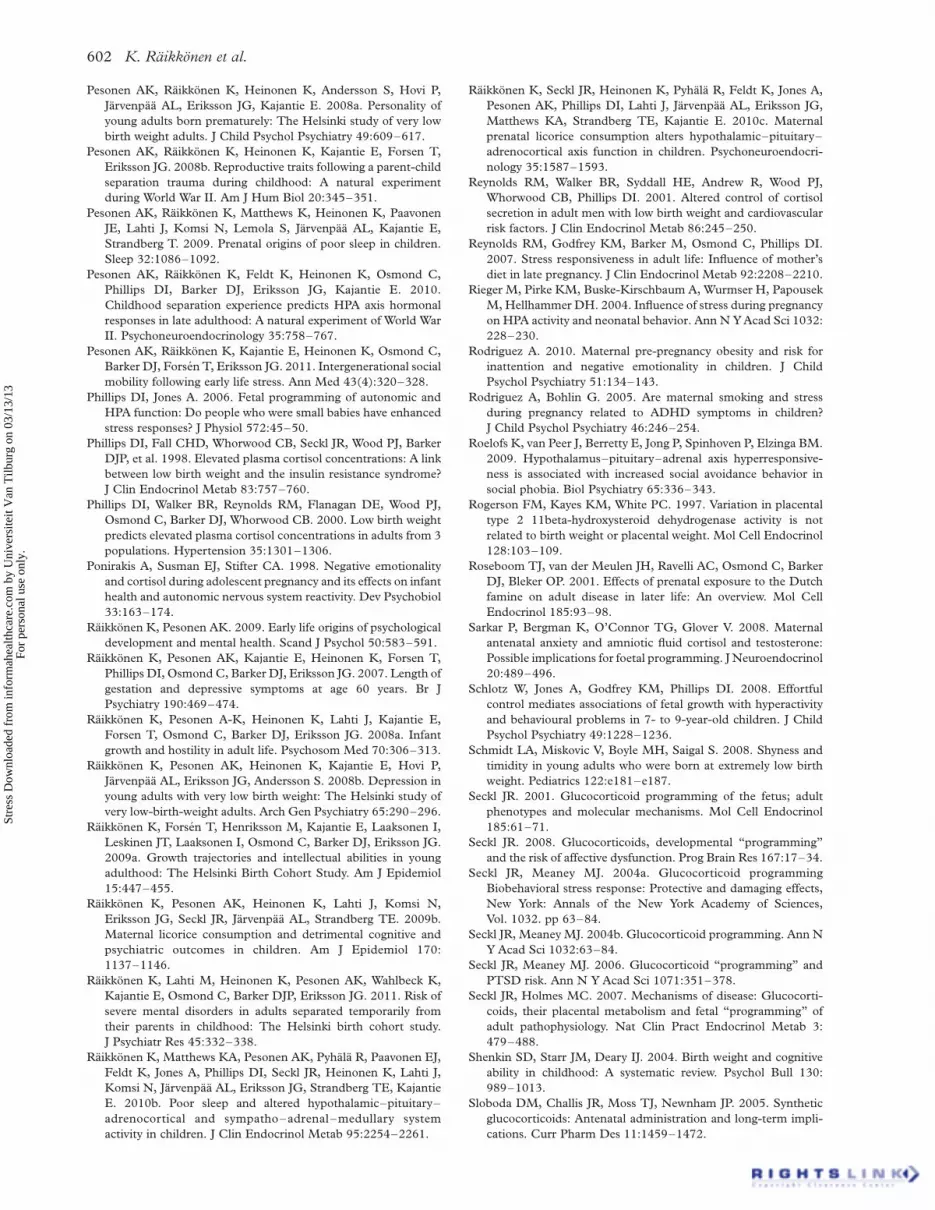
Pesonen AK, Raikkonen K, Heinonen K, Andersson S, Hovi P,
Jarvenpaa AL, Eriksson JG, Kajantie E. 2008a. Personality of
young adults born prematurely: The Helsinki study of very low
birth weight adults. J Child Psychol Psychiatry 49:609–617.
Pesonen AK, Raikkonen K, Heinonen K, Kajantie E, Forsen T,
Eriksson JG. 2008b. Reproductive traits following a parent-child
separation trauma during childhood: A natural experiment
during World War II. Am J Hum Biol 20:345–351.
Pesonen AK, Raikkonen K, Matthews K, Heinonen K, Paavonen
JE, Lahti J, Komsi N, Lemola S, Jarvenpaa AL, Kajantie E,
Strandberg T. 2009. Prenatal origins of poor sleep in children.
Sleep 32:1086–1092.
Pesonen AK, Raikkonen K, Feldt K, Heinonen K, Osmond C,
Phillips DI, Barker DJ, Eriksson JG, Kajantie E. 2010.
Childhood separation experience predicts HPA axis hormonal
responses in late adulthood: A natural experiment of World War
II. Psychoneuroendocrinology 35:758–767.
Pesonen AK, Raikkonen K, Kajantie E, Heinonen K, Osmond C,
Barker DJ, Forsen T, Eriksson JG. 2011. Intergenerational social
mobility following early life stress. Ann Med 43(4):320–328.
Phillips DI, Jones A. 2006. Fetal programming of autonomic and
HPA function: Do people who were small babies have enhanced
stress responses? J Physiol 572:45–50.
Phillips DI, Fall CHD, Whorwood CB, Seckl JR, Wood PJ, Barker
DJP, et al. 1998. Elevated plasma cortisol concentrations: A link
between low birth weight and the insulin resistance syndrome?
J Clin Endocrinol Metab 83:757–760.
Phillips DI, Walker BR, Reynolds RM, Flanagan DE, Wood PJ,
Osmond C, Barker DJ, Whorwood CB. 2000. Low birth weight
predicts elevated plasma cortisol concentrations in adults from 3
populations. Hypertension 35:1301–1306.
Ponirakis A, Susman EJ, Stifter CA. 1998. Negative emotionality
and cortisol during adolescent pregnancy and its effects on infant
health and autonomic nervous system reactivity. Dev Psychobiol
33:163–174.
Raikkonen K, Pesonen AK. 2009. Early life origins of psychological
development and mental health. Scand J Psychol 50:583–591.
Raikkonen K, Pesonen AK, Kajantie E, Heinonen K, Forsen T,
Phillips DI, Osmond C, Barker DJ, Eriksson JG. 2007. Length of
gestation and depressive symptoms at age 60 years. Br J
Psychiatry 190:469–474.
Raikkonen K, Pesonen A-K, Heinonen K, Lahti J, Kajantie E,
Forsen T, Osmond C, Barker DJ, Eriksson JG. 2008a. Infant
growth and hostility in adult life. Psychosom Med 70:306–313.
Raikkonen K, Pesonen AK, Heinonen K, Kajantie E, Hovi P,
Jarvenpaa AL, Eriksson JG, Andersson S. 2008b. Depression in
young adults with very low birth weight: The Helsinki study of
very low-birth-weight adults. Arch Gen Psychiatry 65:290–296.
Raikkonen K, Forsen T, Henriksson M, Kajantie E, Laaksonen I,
Leskinen JT, Laaksonen I, Osmond C, Barker DJ, Eriksson JG.
2009a. Growth trajectories and intellectual abilities in young
adulthood: The Helsinki Birth Cohort Study. Am J Epidemiol
15:447–455.
Raikkonen K, Pesonen AK, Heinonen K, Lahti J, Komsi N,
Eriksson JG, Seckl JR, Jarvenpaa AL, Strandberg TE. 2009b.
Maternal licorice consumption and detrimental cognitive and
psychiatric outcomes in children. Am J Epidemiol 170:
1137–1146.
Raikkonen K, Lahti M, Heinonen K, Pesonen AK, Wahlbeck K,
Kajantie E, Osmond C, Barker DJP, Eriksson JG. 2011. Risk of
severe mental disorders in adults separated temporarily from
their parents in childhood: The Helsinki birth cohort study.
J Psychiatr Res 45:332–338.
Raikkonen K, Matthews KA, Pesonen AK, Pyhala R, Paavonen EJ,
Feldt K, Jones A, Phillips DI, Seckl JR, Heinonen K, Lahti J,
Komsi N, Jarvenpaa AL, Eriksson JG, Strandberg TE, Kajantie
E. 2010b. Poor sleep and altered hypothalamic–pituitary–
adrenocortical and sympatho–adrenal–medullary system
activity in children. J Clin Endocrinol Metab 95:2254–2261.
Raikkonen K, Seckl JR, Heinonen K, Pyhala R, Feldt K, Jones A,
Pesonen AK, Phillips DI, Lahti J, Jarvenpaa AL, Eriksson JG,
Matthews KA, Strandberg TE, Kajantie E. 2010c. Maternal
prenatal licorice consumption alters hypothalamic–pituitary–
adrenocortical axis function in children. Psychoneuroendocri-
nology 35:1587–1593.
Reynolds RM, Walker BR, Syddall HE, Andrew R, Wood PJ,
Whorwood CB, Phillips DI. 2001. Altered control of cortisol
secretion in adult men with low birth weight and cardiovascular
risk factors. J Clin Endocrinol Metab 86:245–250.
Reynolds RM, Godfrey KM, Barker M, Osmond C, Phillips DI.
2007. Stress responsiveness in adult life: Influence of mother’s
diet in late pregnancy. J Clin Endocrinol Metab 92:2208–2210.
Rieger M, Pirke KM, Buske-Kirschbaum A, Wurmser H, Papousek
M, Hellhammer DH. 2004. Influence of stress during pregnancy
on HPA activity and neonatal behavior. Ann N Y Acad Sci 1032:
228–230.
Rodriguez A. 2010. Maternal pre-pregnancy obesity and risk for
inattention and negative emotionality in children. J Child
Psychol Psychiatry 51:134–143.
Rodriguez A, Bohlin G. 2005. Are maternal smoking and stress
during pregnancy related to ADHD symptoms in children?
J Child Psychol Psychiatry 46:246–254.
Roelofs K, van Peer J, Berretty E, Jong P, Spinhoven P, Elzinga BM.
2009. Hypothalamus–pituitary–adrenal axis hyperresponsive-
ness is associated with increased social avoidance behavior in
social phobia. Biol Psychiatry 65:336–343.
Rogerson FM, Kayes KM, White PC. 1997. Variation in placental
type 2 11beta-hydroxysteroid dehydrogenase activity is not
related to birth weight or placental weight. Mol Cell Endocrinol
128:103–109.
Roseboom TJ, van der Meulen JH, Ravelli AC, Osmond C, Barker
DJ, Bleker OP. 2001. Effects of prenatal exposure to the Dutch
famine on adult disease in later life: An overview. Mol Cell
Endocrinol 185:93–98.
Sarkar P, Bergman K, O’Connor TG, Glover V. 2008. Maternal
antenatal anxiety and amniotic fluid cortisol and testosterone:
Possible implications for foetal programming. J Neuroendocrinol
20:489–496.
Schlotz W, Jones A, Godfrey KM, Phillips DI. 2008. Effortful
control mediates associations of fetal growth with hyperactivity
and behavioural problems in 7- to 9-year-old children. J Child
Psychol Psychiatry 49:1228–1236.
Schmidt LA, Miskovic V, Boyle MH, Saigal S. 2008. Shyness and
timidity in young adults who were born at extremely low birth
weight. Pediatrics 122:e181–e187.
Seckl JR. 2001. Glucocorticoid programming of the fetus; adult
phenotypes and molecular mechanisms. Mol Cell Endocrinol
185:61–71.
Seckl JR. 2008. Glucocorticoids, developmental “programming”
and the risk of affective dysfunction. Prog Brain Res 167:17–34.
Seckl JR, Meaney MJ. 2004a. Glucocorticoid programming
Biobehavioral stress response: Protective and damaging effects,
New York: Annals of the New York Academy of Sciences,
Vol. 1032. pp 63–84.
Seckl JR, Meaney MJ. 2004b. Glucocorticoid programming. Ann N
Y Acad Sci 1032:63–84.
Seckl JR, Meaney MJ. 2006. Glucocorticoid “programming” and
PTSD risk. Ann N Y Acad Sci 1071:351–378.
Seckl JR, Holmes MC. 2007. Mechanisms of disease: Glucocorti-
coids, their placental metabolism and fetal “programming” of
adult pathophysiology. Nat Clin Pract Endocrinol Metab 3:
479–488.
Shenkin SD, Starr JM, Deary IJ. 2004. Birth weight and cognitive
ability in childhood: A systematic review. Psychol Bull 130:
989–1013.
Sloboda DM, Challis JR, Moss TJ, Newnham JP. 2005. Synthetic
glucocorticoids: Antenatal administration and long-term impli-
cations. Curr Pharm Des 11:1459–1472.
K. Raikkonen et al.602
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.

Speirs HJ, Seckl JR, Brown RW. 2004. Ontogeny of glucocorticoid
receptor and 11beta-hydroxysteroid dehydrogenase type-1 gene
expression identifies potential critical periods of glucocorticoid
susceptibility during development. J Endocrinol 181:105–116.
Stewart PM, Whorwood CB, Mason JI. 1995. Type 2 11 beta-
hydroxysteroid dehydrogenase in foetal and adult life. J Steroid
Biochem Mol Biol 55:465–471.
Strandberg TE, Jarvenpaa AL, Vanhanen H, McKeigue PM. 2001.
Birth outcome in relation to licorice consumption during
pregnancy. Am J Epidemiol 153:1085–1088.
Strandberg TE, Andersson S, Jarvenpaa AL, McKeigue PM. 2002.
Preterm birth and licorice consumption during pregnancy. Am J
Epidemiol 156:803–805.
Strang-Karlsson S, Raikkonen K, Kajantie E, Andersson S, Hovi P,
Heinonen K, Pesonen AK, Jarvenpaa AL, Eriksson JG,
Paavonen EJ. 2008a. Sleep quality in young adults with very
low birth weight—the Helsinki study of very low birth weight
adults. J Pediatr Psychol 33:387–395.
Strang-Karlsson S, Raikkonen K, Pesonen AK, Kajantie E,
Paavonen EJ, Lahti J, Hovi P, Heinonen K, Jarvenpaa AL,
Eriksson JG, Andersson S. 2008b. Very low birth weight and
behavioral symptoms of attention deficit hyperactivity disorder
in young adulthood: The Helsinki study of very-low-birth-weight
adults. Am J Psychiatry 165:1345–1353.
Trautman PD, Meyer-Bahlburg HFL, Postelnek J, New MI. 1995.
Effects of early prenatal dexamethasone on the cognitive and
behavioral development of young children: Results of a pilot
study. Psychoneuroendocrinology 20:439–449.
Tuovinen S, Raikkonen K, Kajantie E, Pesonen AK, Heinonen K,
Osmond C, Barker DJ, Eriksson JG. 2010. Depressive
symptoms in adulthood and intrauterine exposure to pre-
eclampsia: The Helsinki Birth Cohort Study. Br J Obstet
Gynaecol 117:1236–1242.
Tuovinen SH, Raikkonen K, Kajantie E, Lehtinen J, Henriksson M,
Pesonen AK, Heinonen K, Osmond C, Barker D, Eriksson JG.
2011. Hypertensive disorders in pregnancy and intellectual
abilities in the offspring in young adulthood: The Helsinki birth
cohort study. Ann Med. Apr 15. [Epub ahead of print].
Van den Bergh BR. 1990. The influence of maternal emotions
during pregnancy on fetal and neonatal behavior, Win, 1990.
J Prenatal Perinatal Psychol Health 5:119–130.
Van den Bergh BR. 1992. Maternal emotions during pregnancy and
fetal and neonatal behavior. Oxford University Press: Oxford,
UK.
Van den Bergh BR, Marcoen A. 2004. High antenatal maternal
anxiety is related to ADHD symptoms, externalizing problems,
and anxiety in 8- and 9-year-olds. Child Dev 75:1085–1097.
Van den Bergh BR, Mennes M, Oosterlaan J, Stevens V, Stiers P,
Marcoen A, Lagae L. 2005a. High antenatal maternal anxiety is
related to impulsivity during performance on cognitive tasks in
14- and 15-year-olds. Neurosci Biobehav Rev 29:259–269.
Van den Bergh BR, Mulder EJ, Mennes M, Glover V. 2005b.
Antenatal maternal anxiety and stress and the neurobehavioural
development of the fetus and child: Links and possible
mechanisms. A review. Neurosci Biobehav Rev 29:237–258.
Van den Bergh BR, Mennes M, Stevens V, van der Meere J, Borger
N, Stiers P, Marcoen A, Lagae L. 2006. ADHD deficit as
measured in adolescent boys with a continuous performance task
is related to antenatal maternal anxiety. Pediatr Res 59:78–82.
van der Wal MF, van Eijsden M, Bonsel GJ. 2007. Stress and
emotional problems during pregnancy and excessive infant
crying. J Dev Behav Pediatr 28:431–437.
Van den Bergh BR, Van Calster B, Smits T, Van Huffel S, Lagae L.
2008. Antenatal maternal anxiety is related to HPA-axis
dysregulation and self-reported depressive symptoms in
adolescence: A prospective study on the fetal origins of depressed
mood. Neuropsychopharmacology 33:536–545.
Vaughn B, Bradley C, Joffe L, Seifer R, Barglow P. 1987. Maternal
characteristics measured prenatally are predictive of ratings of
temperamental “difficulty” on the Carey Infant Temperament
Questionnaire. Dev Psychol 23:152–161.
Wahlbeck K, Forsen T, Osmond C, Barker DJ, Eriksson JG. 2001.
Association of schizophrenia with low maternal body mass index,
small size at birth, and thinness during childhood. Arch Gen
Psychiatry 58:48–52.
Warner MJ, Ozanne SE. 2010. Mechanisms involved in the
developmental programming of adulthood disease. Biochem J :
427.
Welberg LA, Seckl JR, Holmes MC. 2000. Inhibition of 11beta-
hydroxysteroid dehydrogenase, the foeto-placental barrier to
maternal glucocorticoids, permanently programs amygdala GR
mRNA expression and anxiety-like behaviour in the offspring.
Eur J Neurosci 12:1047–1054.
Wisborg K, Barklin A, Hedegaard M, Henriksen TB. 2008.
Psychological stress during pregnancy and stillbirth: Prospective
study. BJOG: Int J Obstet Gynaecol 115:882–885.
Wust S, Entringer S, Federenko IS, Schlotz W, Hellhammer DH.
2005. Birth weight is associated with salivary cortisol responses
to psychosocial stress in adult life. Psychoneuroendocrinology
30:591–598.
Yeh TF, Lin YJ, Lin HC, Huang CC, Hsieh WS, Lin CH, Tsai CH.
2004. Outcomes at school age after postnatal dexamethasone
therapy for lung disease of prematurity. N Engl J Med 350:
1304–1313.
Yehuda R, Engel SM, Brand SR, Seckl J, Marcus SM, Berkowitz
GS. 2005. Transgenerational effects of posttraumatic stress
disorder in babies of mothers exposed to the World Trade Center
attacks during pregnancy. J Clin Endocrinol Metab 90:
4115–4118.
Stress, glucocorticoids and liquorice in human pregnancy 603
Stre
ss D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsite
it V
an T
ilbur
g on
03/
13/1
3Fo
r pe
rson
al u
se o
nly.





























