Embed Size (px)
Citation preview

A multicentre randomiSed controlled TRial of IntraVEnous immunoglobulin (IVIG) versus standard therapy for the
treatment of transverse myelitis in adults and children
Ming Lim
Children’s Neurosciences, Evelina Children’s Hospital,
Kings Health Partner’s AHSC
Background
UK TM Conference 2011
Wyboston Lakes
Transverse Myelitis
• Immune-mediated myelitis affecting both children and adults
• Estimated annual incidence 3-7/millionYoung et al., 2009 Mult Scler 15:1295-302
Absoud et al., 2013 Mult Scler 19(1): 76-86
• Diagnosis - TM Consortium Working Group criteria 2002Neurology 2002 59:499-505
• Relapse in 17% with a diagnosis of MS or NMODeiva et al., 2015 Neurology 84(4):341-9
• Outcome is poor– 50% good recovery in children
– Poorer in adults
Reviewed in Absoud et al., 2013
Neuromyelitis optica
Recurrent episodes of optic neuritis and myelitis
B cell mediated, AQP-4 Ab in majority of patientsJacob et al., 2013 J Neurol Neurosurg Psychiatry. 84(8):922-30
Wingerchuk Criteria – initial presentation may be as transverse myelitisNeurology. 2006; 66(10):1485-9.
Management of TM/NMO
• Current best practice is treatment with corticosteroids
– Based on Class IV evidence of case series and extrapolations from clinical trials of adult MS – treatment shortens relapse duration and speeds recovery
• Plasma Exchange is also used
– Effective as second line in 1 RCT of adults with CNS demyelination
– Single centre retrospective cohort found benefit in TM in combination with steroids
– BUT invasive, expensive, not universally available
Weinshenker et al.,1999.Ann Neurol; 46:878-86.Greenberg et al., 2007 Neurology ;68:1614-7.Scott et al., 2011 Neurology ;77:2128-34.
Why IVIG?
• IVIG increasingly used in the clinical setting in a variety of neurological disorders including TM
• RCTs in other conditions have demonstrated benefit
• Case series in TM have observed benefit
• Opportunity for RCT to help establish an evidence base for treatment
– Standardised diagnostic tools and outcome measures
– Prospective follow-up
Banwell et al., 2007 Lancet Neurol 6:887-902Hughes et al., 2009 Clin Exp Immunol 158 Suppl 1, 34-42. Elsone et al., 2014. Mult Scler. 20(4):501-4.
Overview of thoughts
• Does addition of IVIG to standard therapy (steroids), improve outcome at 6 months?
• If so, what are the cost implications?
• What are the long-term health outcomes and are there any prognostic indicators?
• Biobanking samples for future basic science research
King CTU Dr Jennifer Hellier
Prof Andrew Pickles, Prof Paul McCrone
Joanna KellyDr Caroline Murphy.
Ming Lim, Michael Absoud and Anu Jacob
PAEDIATRICS
Dr Mike Pike
ADULT Prof Neil Robertson
Prof Gavin GiovannoniDr Jackie Palace
Dr Peter BrexDr Olga Cicarelli
MS SocietyGuthy Jackson foundation
TM Society
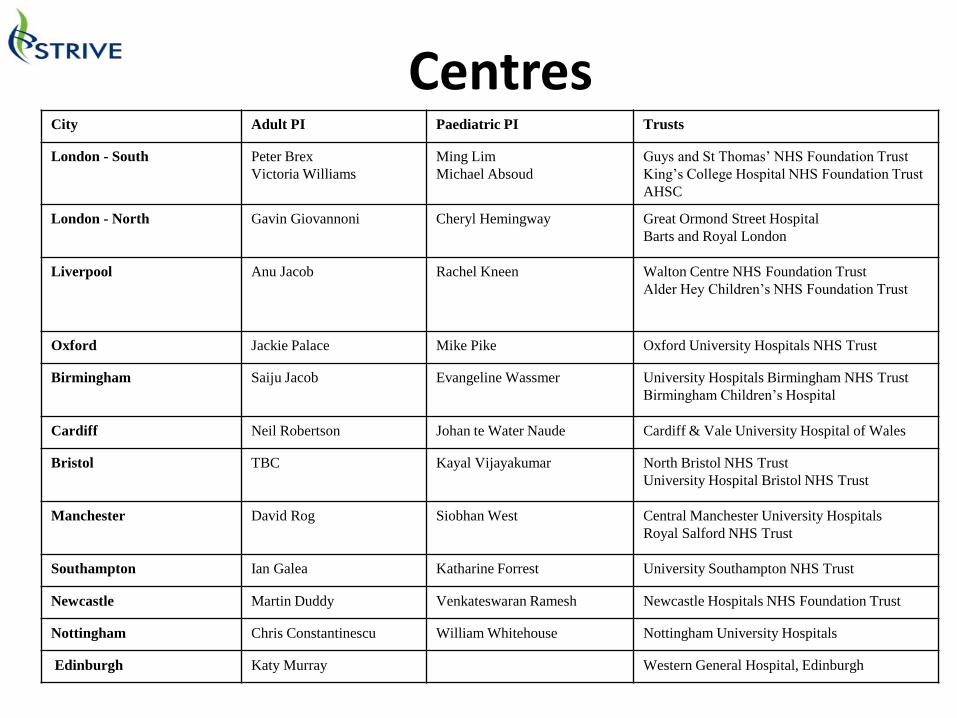
City Adult PI Paediatric PI Trusts
London - South Peter Brex
Victoria Williams
Ming Lim
Michael Absoud
Guys and St Thomas’ NHS Foundation Trust
King’s College Hospital NHS Foundation Trust
AHSC
London - North Gavin Giovannoni Cheryl Hemingway Great Ormond Street Hospital
Barts and Royal London
Liverpool Anu Jacob Rachel Kneen Walton Centre NHS Foundation Trust
Alder Hey Children’s NHS Foundation Trust
Oxford Jackie Palace Mike Pike Oxford University Hospitals NHS Trust
Birmingham Saiju Jacob Evangeline Wassmer University Hospitals Birmingham NHS Trust
Birmingham Children’s Hospital
Cardiff Neil Robertson Johan te Water Naude Cardiff & Vale University Hospital of Wales
Bristol TBC Kayal Vijayakumar North Bristol NHS Trust
University Hospital Bristol NHS Trust
Manchester David Rog Siobhan West Central Manchester University Hospitals
Royal Salford NHS Trust
Southampton Ian Galea Katharine Forrest University Southampton NHS Trust
Newcastle Martin Duddy Venkateswaran Ramesh Newcastle Hospitals NHS Foundation Trust
Nottingham Chris Constantinescu William Whitehouse Nottingham University Hospitals
Edinburgh Katy Murray Western General Hospital, Edinburgh
Centres
Purpose of study
To conduct a multi-centre, single blind, parallel group randomised-controlled trial to generate
evidence to inform clinical and health economics decisions of IVIG use in adults and
children with TM
Primary Objective
• Is additional and early treatment with IVIG of extra benefit in TM and 1st episode NMO when compared to the current standard therapy of intravenous steroids?
– ≥2 point change in ASIA Impairment scale (classified A-E) at 6 months post randomisation
ASIA Impairment Scale
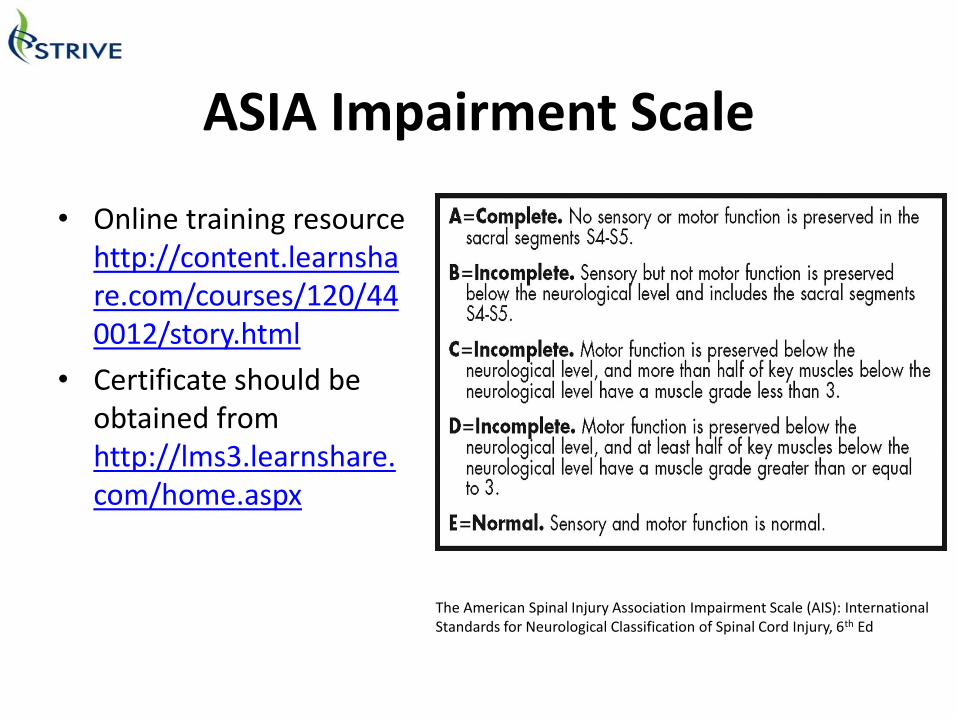
• Online training resource http://content.learnshare.com/courses/120/440012/story.html
• Certificate should be obtained from http://lms3.learnshare.com/home.aspx
The American Spinal Injury Association Impairment Scale (AIS): International Standards for Neurological Classification of Spinal Cord Injury, 6th Ed

Secondary Objectives
• Obtain clinical and para-clinical data, including identification of early predictors of poor outcome
• Change in ASIA motor and sensory scales, Kurtzke EDSS, EQ-5D, SCI QoL, CSRI at 6 months
• Biobank samples for future research
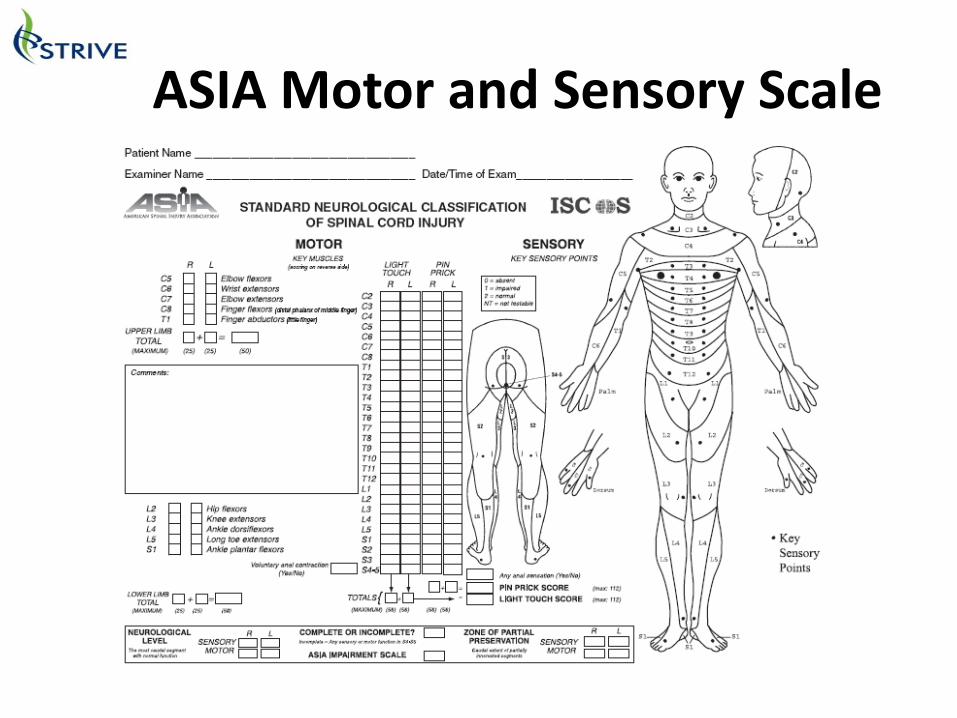
ASIA Motor and Sensory Scale
EDSS, EQ-5D, SCI QoL, CSRI
http://www.neurostatus.net/scoring/index.php
Tertiary measures at 6 months
• International SCI bladder/bowel data set
• Peds QL
• International SCI pain data set
Patient recruitment
• Recruitment is through individual site neurologists, though patients can also be
recruited through rapid GP referral and district general hospitals.
• Recruitment target for the trial is 170 patients
No site specific target is set, TM and NMO are ‘rare diseases’ (+- 350
cases per year in the UK)
Total duration of the trial is expected to be 3.5 years, with recruitment
in the initial 2.5 years
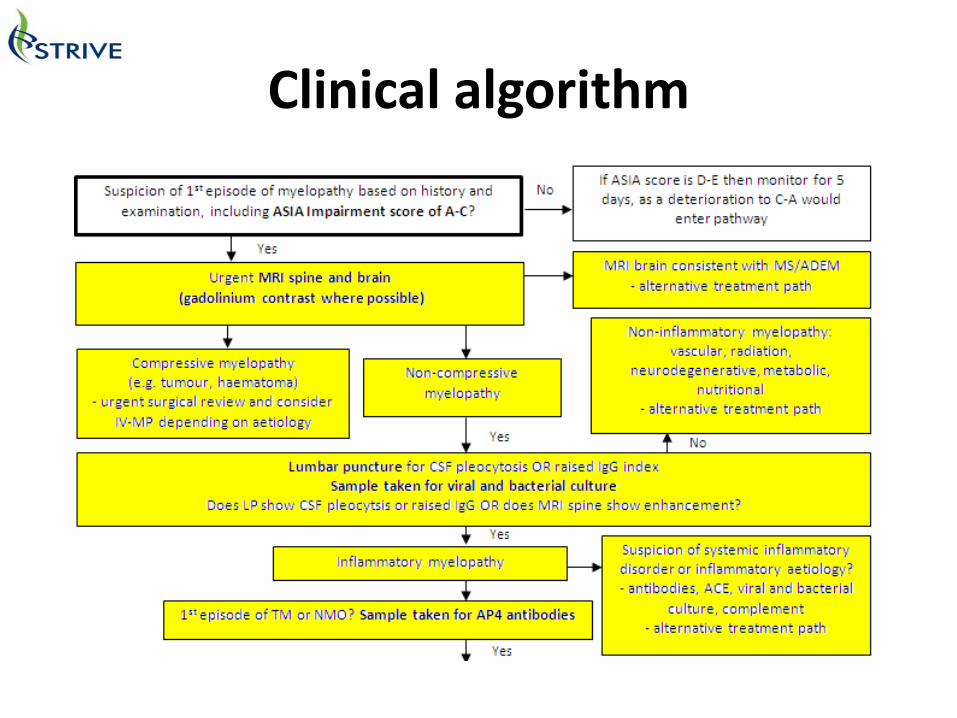
Clinical algorithm
Inclusion Criteria 1/3
Patients will be eligible for inclusion on the trial if on presentation they:
Are aged 1 year or over
Have been diagnosed with:
EITHER acute first onset transverse myelitis
The TM CONSORTIUM WORKING GROUP 2002 criteria for probable TM will
be used. Hence, patients will be diagnosed to have TM if they meet all the
following criteria:
Sensory, motor, or autonomic dysfunction attributable to spinal cord
disease
Bilateral signs and/or symptoms (not necessarily symmetric)
Sensory level (except in young children <5 years where this is difficult
to evaluate)
Lack of MRI brain criteria consistent with MS (McDonald 2010 space
criteria)
Progression to nadir between 4 h and 21 days)
OR Have been diagnosed with first presentation of neuromyelitis optica.
(Patients with definite modified NMO will meet the following criteria (Wingerchuck
et al, 2006).
Absolute criteria, both:
Optic neuritis
Acute myelitis
Plus two out of three supportive criteria:
Brain MRI not meeting criteria for MS at disease onset
Spinal cord MRI with contiguous T2-weighted signal abnormality extending
over three or more vertebral segments, indicating a relatively large lesion in
the spinal cord
Aquaporin 4 seropositive status
Inclusion Criteria 2/3
Diagnosed with TM or NMO
Have an ASIA Impairment score of A, B or C
Have commenced steroid treatment but will be
randomised no later than day 5 of steroids, and if
definitely known, randomisation will not exceed 21 days
from the onset of symptoms
Give assent(<16 years)/consent to participate in the trial
Inclusion Criteria 3/3
Patients will be excluded if they show evidence of:
o Contraindication to IVIg as stated in the product SmPC, or receiving
IVIg for other reasons
o Previously known systemic autoimmune disease (eg systemic lupus
erythematosus) or any evidence of systemic inflammation during
current presentation.
o Direct infectious aetiology (eg varicella zoster)
o Previous episode of CNS inflammatory demyelination
o Acute disseminated encephalomyelitis (ADEM)
o Other causes of myelopathy not thought to be due to myelitis (eg
nutritional, ischaemic, tumour etc.)
o Other disease which would interfere with assessment of outcome
measures
o Known pregnancy
o Circumstances which would prevent follow-up for 12 months
Exclusion Criteria
Dosing• Control arm
– IV methylprednisolone in line with local clinical practice (variations will be recorded)
• 30mg/kg/day or 500mg/m2/day (max dose of 1g/day) for 5 days
• Intervention arm
– Above treatment plus IVIG
• Adults + children >41.2kg: IVIG - total dose 2g/kg, divided into 5 daily doses
• Children <41.2kg: IVIG – total dose 2g/kg, divided into 2 daily doses
Rescue therapy• Treatment failure if no improvement after 14 days from
presentation or 5 days after completion of treatment arm
• Patients in either arm not responding to treatment should have rescue therapy, such as PLEX.
• Standardised PLEX treatment
– 5 cycles with >75% plasma volume exchanged
– 24-48 hours between each cycle
– Additional course of IV-MP may be given between decision to start PLEX and therapy initiation
Steroid Weaning Regimen
• Steroid weaning dosing will be recommended Child (<16): Steroids continued at a dose of 1-2 mg/kg
(capped at 60mg) for 4 weeks followed by a 4 week taper
Adults: Steroids continued at a dose of 60 mg for 4 weeks followed by a 4 week taper
• All variation of steroid weaning regimens should be documented in the eCRF
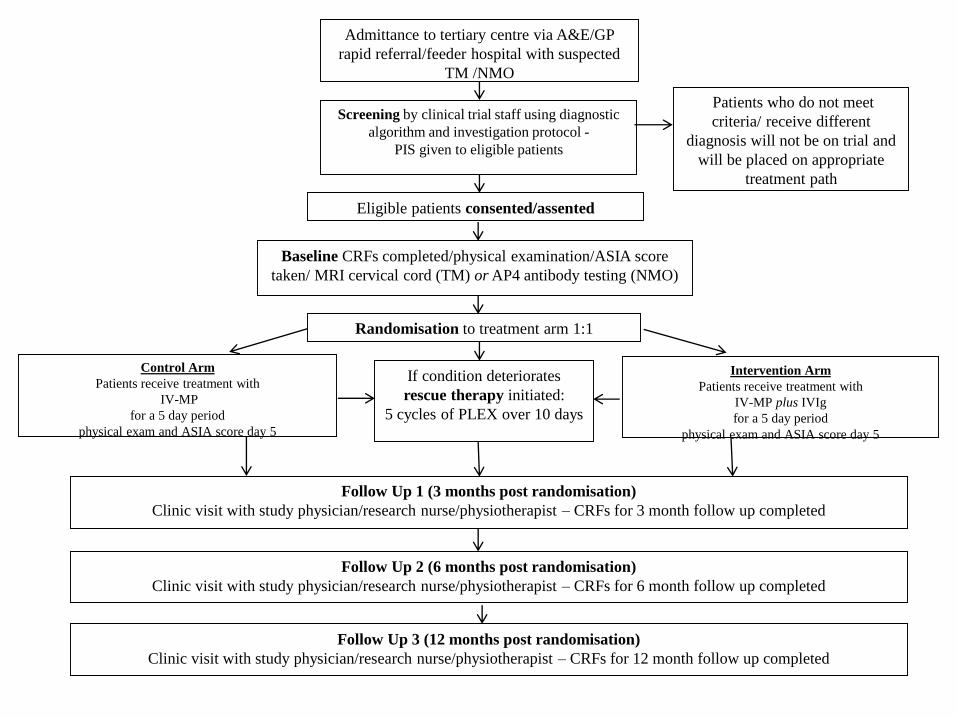
Admittance to tertiary centre via A&E/GP
rapid referral/feeder hospital with suspected
TM /NMO
Intervention Arm
Patients receive treatment with
IV-MP plus IVIg
for a 5 day period
physical exam and ASIA score day 5
Screening by clinical trial staff using diagnostic
algorithm and investigation protocol -
PIS given to eligible patients
Control Arm
Patients receive treatment with
IV-MP
for a 5 day period
physical exam and ASIA score day 5
Baseline CRFs completed/physical examination/ASIA score
taken/ MRI cervical cord (TM) or AP4 antibody testing (NMO)
Patients who do not meet
criteria/ receive different
diagnosis will not be on trial and
will be placed on appropriate
treatment path
Eligible patients consented/assented
Randomisation to treatment arm 1:1
If condition deteriorates
rescue therapy initiated:
5 cycles of PLEX over 10 days
Follow Up 1 (3 months post randomisation)
Clinic visit with study physician/research nurse/physiotherapist – CRFs for 3 month follow up completed
Follow Up 3 (12 months post randomisation)
Clinic visit with study physician/research nurse/physiotherapist – CRFs for 12 month follow up completed
Follow Up 2 (6 months post randomisation)
Clinic visit with study physician/research nurse/physiotherapist – CRFs for 6 month follow up completed
Page 27
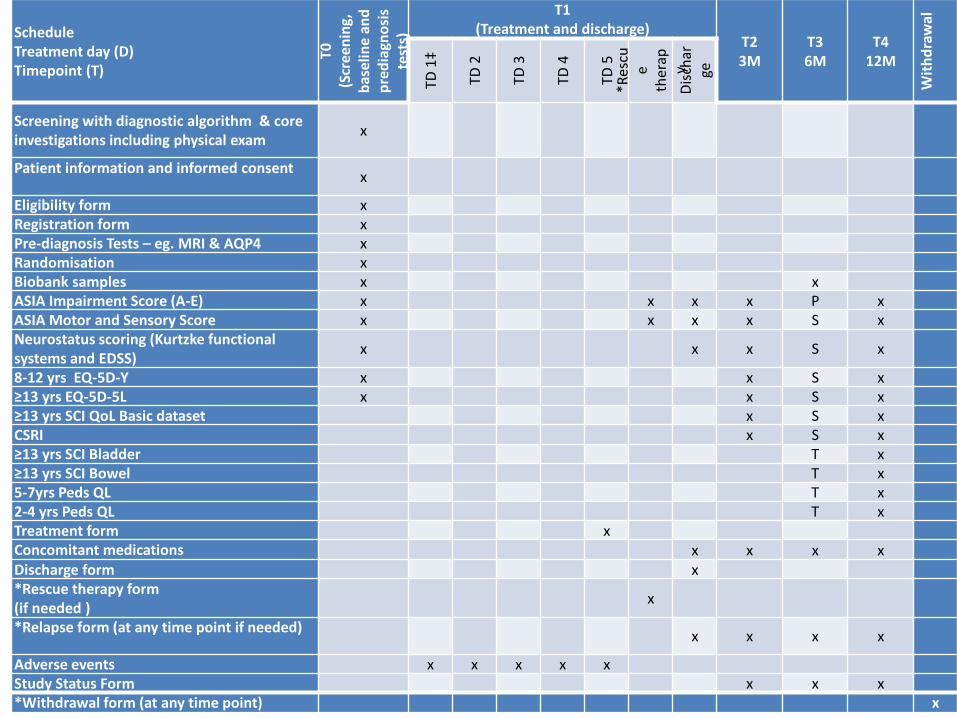
ScheduleTreatment day (D)Timepoint (T)
T0(S
cree
nin
g,
bas
elin
e an
d
pre
dia
gno
sis
test
s)
T1 (Treatment and discharge)
T23M
T36M
T412M
Wit
hd
raw
al
TD 1
‡
TD 2
TD 3
TD 4
TD 5
*Res
cue
ther
apy
Dis
char
ge
Screening with diagnostic algorithm & core investigations including physical exam
x
Patient information and informed consentx
Eligibility form xRegistration form xPre-diagnosis Tests – eg. MRI & AQP4 xRandomisation xBiobank samples x xASIA Impairment Score (A-E) x x x x P xASIA Motor and Sensory Score x x x x S xNeurostatus scoring (Kurtzke functional systems and EDSS)
x x x S x
8-12 yrs EQ-5D-Y x x S x≥13 yrs EQ-5D-5L x x S x≥13 yrs SCI QoL Basic dataset x S xCSRI x S x≥13 yrs SCI Bladder T x≥13 yrs SCI Bowel T x5-7yrs Peds QL T x2-4 yrs Peds QL T xTreatment form xConcomitant medications x x x xDischarge form x*Rescue therapy form(if needed )
x
*Relapse form (at any time point if needed)x x x x
Adverse events x x x x xStudy Status Form x x x*Withdrawal form (at any time point) x
Trial Timeline
Multi-centre, single blind, parallel group randomised-controlled trial
• Funding: NIHR and Biotest
• Recruitment starts March 2015 – run for 3.5 years
• GSTT open
• All London sites next
• 2 trust/month
• August 2015 all sites open

Collaborators: Dr Michael Absoud, Dr Peter Brex, Dr Olga Cirrarelli, Prof Gavin Giovannoni, Dr Jennifer Hellier, Dr Anu Jacob, Dr Ming
Lim, Prof Paul McCrone, Dr Caroline Murphy, Dr Jackie Palace, Prof Andrew Pickles, Dr Mike Pike, Prof Neil Robertson.
TSC: Professor Richard Hughes, DrClaire Lundy, Barbara Babcock, Lew
Gray, Dr Martin Kappler, Dr Mark Sanders
DMEC: Professor John Zajicek, DrSarah Cotterill, Dr Alasdair Parker
https://www.nets.nihr.ac.uk/projects/hta/11129148
EudraCT (REF: 2014-002335-34); and ISRCTN (REF: 12127581).
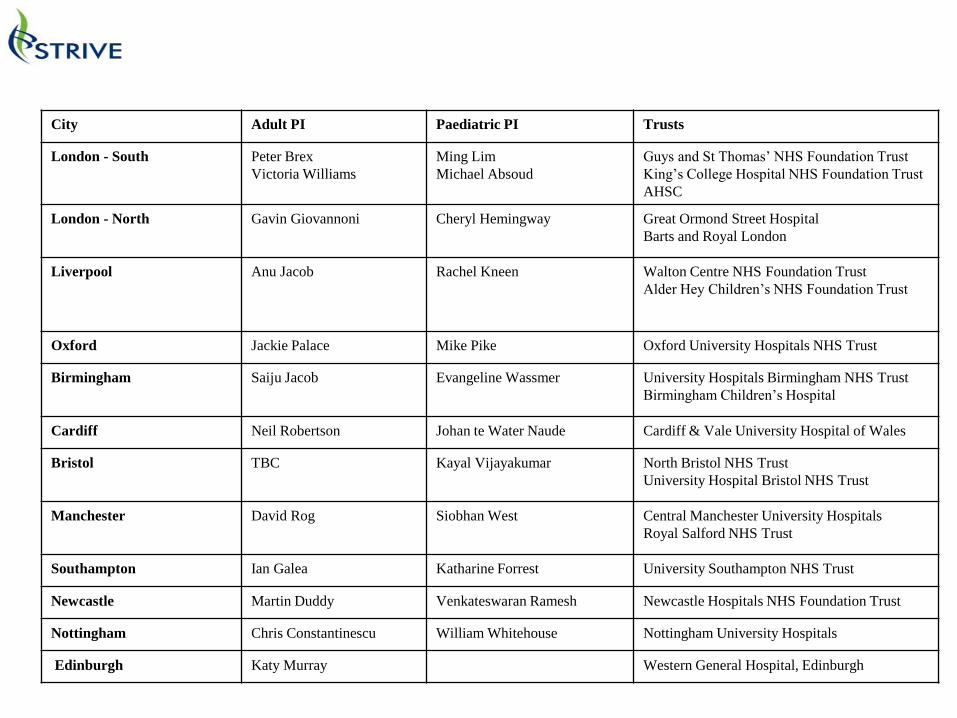
City Adult PI Paediatric PI Trusts
London - South Peter Brex
Victoria Williams
Ming Lim
Michael Absoud
Guys and St Thomas’ NHS Foundation Trust
King’s College Hospital NHS Foundation Trust
AHSC
London - North Gavin Giovannoni Cheryl Hemingway Great Ormond Street Hospital
Barts and Royal London
Liverpool Anu Jacob Rachel Kneen Walton Centre NHS Foundation Trust
Alder Hey Children’s NHS Foundation Trust
Oxford Jackie Palace Mike Pike Oxford University Hospitals NHS Trust
Birmingham Saiju Jacob Evangeline Wassmer University Hospitals Birmingham NHS Trust
Birmingham Children’s Hospital
Cardiff Neil Robertson Johan te Water Naude Cardiff & Vale University Hospital of Wales
Bristol TBC Kayal Vijayakumar North Bristol NHS Trust
University Hospital Bristol NHS Trust
Manchester David Rog Siobhan West Central Manchester University Hospitals
Royal Salford NHS Trust
Southampton Ian Galea Katharine Forrest University Southampton NHS Trust
Newcastle Martin Duddy Venkateswaran Ramesh Newcastle Hospitals NHS Foundation Trust
Nottingham Chris Constantinescu William Whitehouse Nottingham University Hospitals
Edinburgh Katy Murray Western General Hospital, Edinburgh
• Key Contacts:• CI - Dr Ming Lim• Evelina Children’s Hospital, LondonTel 02071884002, Fax
02071884269• [email protected]
• Paediatric Lead – Dr Michael Absoud, Evelina Children’s Hospital, London
• Tel 02071883995, Fax 02071884665• [email protected]
• Adult Lead – Dr Anu Jacob, The Walton Centre, Liverpool• Tel 01515295420, Fax 01515295513• [email protected]
• STRIVE Trial Manager – Rosemary Howe, King’s CTU• [email protected]





























