Embed Size (px)
Citation preview

Suicide Attempts in Women With Eating Disorders
Emily M. Pisetsky and Laura M. ThorntonUniversity of North Carolina at Chapel Hill
Paul Lichtenstein and Nancy L. PedersenKarolinska Institutet
Cynthia M. BulikUniversity of North Carolina at Chapel Hill
We evaluated whether the prevalence of lifetime suicide attempts/completions was higher in women witha lifetime history of an eating disorder than in women with no eating disorder and assessed whether eatingdisorder features, comorbid psychopathology, and personality characteristics were associated withsuicide attempts in women with anorexia nervosa, restricting subtype (ANR), anorexia nervosa, binge-purge subtype (ANBP), lifetime history of both anorexia nervosa and bulimia nervosa (ANBN), bulimianervosa (BN), binge eating disorder (BED), and purging disorder (PD). Participants were part of theSwedish Twin study of Adults: Genes and Environment (N � 13,035) cohort. Lifetime suicide attemptswere identified using diagnoses from the Swedish National Patient and Cause of Death Registers. Generallinear models were applied to evaluate whether eating disorder category (ANR, ANBP, ANBN, BN,BED, PD, or no eating disorder [no ED]) was associated with suicide attempts and to identify factorsassociated with suicide attempts. Relative to women with no ED, lifetime suicide attempts were significantlymore common in women with all types of eating disorder. None of the eating disorder features or personalityvariables was significantly associated with suicide attempts. In the ANBP and ANBN groups, the prevalenceof comorbid psychiatric conditions was higher in individuals with than without a lifetime suicide attempt. Theodds of suicide were highest in presentations that included purging behavior (ANBN, ANBN, BN, and PD),but were elevated in all eating disorders. To improve outcomes and decrease mortality, it is critical to bevigilant for suicide and identify indices for those who are at greatest risk.
Keywords: suicide, eating disorders, anorexia, bulimia, binge eating disorder
Eating disorders (EDs) are serious mental illnesses that occur in1–5% of women (Hudson, Hiripi, Pope, & Kessler, 2007) and canhave poor long-term outcomes (Berkman et al., 2006; Hudson etal., 2007). A comprehensive meta-analysis of mortality in EDsincluding 36 studies reported standardized mortality ratios (SMRs)of 5.86 (95% CI [4.17, 8.26]) for anorexia nervosa (AN) and 1.93(95% CI [1.44, 2.59]) for bulimia nervosa (BN; Arcelus, Mitchell,Wales, & Nielsen, 2011), suggesting that individuals with eitherdisorder are at increased risk of death compared with their age- andgender-matched peers.
Suicide is a common cause of this elevated mortality in EDs. Ameta-analysis by Preti, Rocchi, Sisti, Camboni, and Miotto (2011)analyzed data from 40 studies comprising 16,342 patients with ANfollowed over a mean of 11.1 years and yielded an SMR � 31.0.
A companion analysis of 16 studies on BN comprising 1,768patients, with a mean follow-up of 7.5 years, yielded an SMR �7.5 (Preti et al., 2011). Only three studies examining suicide inindividuals with binge eating disorder (BED) were available forinclusion in this meta-analysis. With only 246 patients, no com-pleted suicides were identified and an SMR could not be calcu-lated. Purging disorder (PD), characterized by purging in the absenceof binge eating behavior, is described in depth by Keel and Striegel-Moore (2009) and is included as a named condition in the Diagnosticand Statistical Manual of Mental Disorders (5th ed.; DSM–5) in theOther Specified Feeding and Eating Disorders section (AmericanPsychiatric Association, 2013). To our knowledge, there are no pub-lished data on completed suicides in individuals with PD.
Suicide attempts in individuals with AN are also common, withestimates of lifetime attempts ranging from 3.0% to 29.7% (Buliket al., 2008; Forcano et al., 2011; Franko & Keel, 2006). Further-more, these attempts are often serious and are associated with theintention to die. In a sample of 432 non–treatment-seeking partic-ipants with AN, of those who had attempted suicide, 78.3% wantedto die from their attempt(s), and 56.5% thought that they would die asa result of the attempt(s). Over half of these attempts required medicalattention (Bulik et al., 2008). In another study of a treatment-seekingsample, 79% of those who had attempted suicide endorsed “moderateor severe intent” to die (Bulik, Sullivan, & Joyce, 1999).
Suicide attempts are also common in BN, with between 15%and 40% of individuals indicating a lifetime history of at least onesuicide attempt (Bulik et al., 1999; Corcos et al., 2002; Favaro &
Emily M. Pisetsky and Laura M. Thornton, Department of Psychiatry,University of North Carolina at Chapel Hill; Paul Lichtenstein and NancyL. Pedersen, Department of Medical Epidemiology and Biostatistics, Karo-linska Institutet, Stockholm, Sweden; Cynthia M. Bulik, Department ofPsychiatry, University of North Carolina at Chapel Hill.
This study was supported by Grants CA-085739 (P.I.: P. F. Sullivan) andAI-056014 (P.I.: P. F. Sullivan) from the National Institutes of Health. TheSwedish Twin Registry is supported by grants from the Swedish Depart-ment of Higher Education and the Swedish Research Council.
Correspondence concerning this article should be addressed to CynthiaBulik, CB #7160, University of North Carolina at Chapel Hill, Chapel Hill,NC 27599. E-mail: [email protected]
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
Journal of Abnormal Psychology © 2013 American Psychological Association2013, Vol. 122, No. 4, 1042–1056 0021-843X/13/$12.00 DOI: 10.1037/a0034902
1042

Santonastaso, 1997; Forcano et al., 2009; Franko & Keel, 2006;Milos, Spindler, Hepp, & Schnyder, 2004). Of individuals with BNwho attempted suicide, 34.1% had a “serious” or “extreme” firstattempt; the proportion of “serious” or “extreme” attempts in-creased with the number of attempts. More than 60% of individ-uals with BN were hospitalized as a result of their first suicideattempt, and 100% of those who endorsed an “extreme” suicideattempt were hospitalized (Corcos et al., 2002).
Whether the risk of suicide attempts across ED subtypes differsremains a matter of some disagreement, with some studies report-ing no difference in the prevalence of attempts (Bulik et al., 1999;Herzog et al., 1999; Milos et al., 2004), some reporting higherprevalence of suicide attempts in individuals with BN than in thosewith AN (Favaro & Santonastaso, 1996, 1997), and others report-ing higher prevalence of suicide attempts in individuals with ANthan in those with BN (Franko et al., 2004). The differences arelikely attributable to differences in subtyping diagnostics, althoughone fairly consistent finding is higher risk among the binge-purgesubtype of AN than individuals with the restricting subtype (Buliket al., 2008; Favaro, Tenconi, & Santonastaso, 2006; Franko &Keel, 2006). However, most of the research has focused on dif-ferences in prevalence of suicide attempts across AN subtypes andBN. Research on the prevalence of suicide attempts in individualswith BED or PD is extremely limited. One recent study of patientswith BED presenting for outpatient treatment found that 12.5%had a lifetime history of a suicide attempt, providing initial indi-cation of elevated risk of suicide attempts in this populationcompared with individuals with no ED (Carano et al., 2012). PDhas not been included in any of the large studies of suicideattempts in women with EDs. Additional studies are needed tofurther clarify the prevalence of suicide attempts in individualswith BED and individuals with PD and compare suicide risk in theother ED groups. Large population-based studies have the poten-tial to clarify differences in suicide risk across the ED diagnosticcategories, particularly in these understudied disorders, and informrisk assessment in treatment settings.
Reports have been inconsistent when addressing whether spe-cific patient profiles or characteristics are associated with suicideattempts in individuals with EDs. Factors identified as associatedwith suicide attempts in isolated studies of AN include older age,longer duration of illness, lower body mass index (BMI), depres-sion, greater number of past treatments, antidepressant use, ele-vated phobic anxiety, and drug and alcohol abuse (Favaro &Santonastaso, 1997; Forcano et al., 2009). For BN, associatedfactors include greater general psychopathology; greater numberof past treatments; antidepressant use; lower education; lowerminimum BMI; family history of alcohol abuse; increased impul-sive behaviors including self-injury; lower self-directedness, co-operativeness, and reward dependence; and higher harm avoidance(Favaro & Santonastaso, 1997; Forcano et al., 2009). Currentevidence suggests that suicidality is associated with anxious per-sonality traits such as harm avoidance and neuroticism in variouspsychiatric and community samples of individuals with EDs (Bu-lik et al., 1999; Engström, Brandstrom, Sigvardsson, Cloninger, &Nylander, 2004; McGirr, Paris, Lesage, Renaud, & Turecki, 2007;Ruchkin, Schwab-Stone, Koposov, Vermeiren, & King, 2003; vanHeeringen et al., 2003). Moreover, impulsivity, high novelty seek-ing, and low self-directedness have also been reported (Forcano etal., 2009; McGirr et al., 2007; Zouk, Tousignant, Seguin, Lesage,
& Turecki, 2006). The coexistence of anxious and impulsive traitsmay converge to increase suicidal risk.
Several comorbid psychiatric disorders have been associated withsuicide attempts in individuals who have an ED, including a lifetimehistory of major depression (Anderson, Carter, McIntosh, Joyce, &Bulik, 2002; Bulik et al., 2008; Corcos et al., 2002; Favaro &Santonastaso, 1997), with more than 80% of individuals with AN whoattempted suicide reporting that their worst or only attempt occurredduring an active episode of major depressive disorder (Bulik et al.,2008). In addition, anxiety disorders (e.g., posttraumatic stress disor-der, panic disorder, and a broad diagnosis of “any anxiety disorder”;Bulik et al., 2008; Milos et al., 2004), substance abuse, and alcoholabuse (Anderson et al., 2002; Corcos et al., 2002; Franko et al., 2004)have been associated with suicide attempts in AN and BN.
The present study clarifies and extends this body of research byemploying data from the population-based Swedish Twin Registry inconjunction with the Swedish National Patient Register and the Na-tional Cause of Death Register. Conducting research with nationalregisters is a valuable methodological approach, especially in Nordiccountries (Allebeck, 2009) where data are reliable and participants areless likely to be lost to follow-up. Moreover, all deaths and hospital-izations in Sweden are captured in national registers (Ludvigsson etal., 2011; National Board of Health and Welfare, 2010). Using Swed-ish national registers, we evaluated whether suicide attempts/comple-tions were more prevalent in individuals with AN subtypes, BN,lifetime history of both AN and BN (ANBN), BED, and PD than inindividuals without EDs and explored whether there were specificpsychopathological, temperament, and personality features that wereassociated with suicide attempts in individuals with EDs.
Method
Participants
Participants were female twins born between 1959 and 1985 andassessed as part of the Swedish Twin study of Adults: Genes andEnvironment (STAGE; N � 13,035; Furberg et al., 2008; Lichten-stein et al., 2006). STAGE data were collected in 2005 using Web-based questionnaires and phone interviews (response rate for fullSTAGE data set � 59.6%). Questionnaires assessed demographicinformation; medical history; presence of psychiatric disorders includ-ing detailed information on EDs and alcohol and illicit substance use;and personality variables including neuroticism, extraversion, perfec-tionism, and self-directedness. Participants were between 20 and 47years of age at the time of assessment.
Determination of zygosity was based on responses to standardtwin similarity questions, which were validated with a panel of 47single-nucleotide polymorphisms in a random sample of 198 twinpairs. Ninety-five percent (n � 188) were correctly classified. Thiszygosity algorithm has also previously been validated with similarresults (Lichtenstein et al., 2002). Of the twins included in thepresent study, 42.4% were from monozygotic twin pairs, 30.2%were from same-sex dizygotic twin pairs, 25.2% were fromopposite-sex twin pairs, and 2.3% were of unknown zygosity.
Identification of Attempted and Completed Suicide
All Swedish citizens since 1947 and, therefore, all participantsin STAGE, have an assigned unique personal identification num-
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1043SUICIDE ATTEMPTS IN WOMEN WITH EATING DISORDERS

ber (national registration number; Ludvigsson, Otterblad-Olausson, Pettersson, & Ekbom, 2009). Via this number, theSTAGE database can be linked to any Swedish national register.To identify all recorded suicide attempts and completions, STAGEwas linked with following registers:
National Patient Register. The National Board of Health andWelfare maintains the National Patient Register (National Boardof Health and Welfare, 2010), which covers all public inpatienthospitalizations in Sweden. Each record contains admission anddischarge dates, primary discharge diagnosis, and up to eightsecondary diagnoses using the International Classification of Dis-eases (ICD)-8, ICD-9, or ICD-10 depending on the year of hospi-talization (World Health Organization, 1967, 1978, 1992). Theattending physician documented the diagnoses. This register cap-tures all inpatient psychiatric care in Sweden since 1973. Theregister also routinely captures suicide attempts using ICD codes(codes E950–E959 in ICD-8 and ICD-9 and X60–X84 in ICD-10). This register was searched for any discharge diagnoses indi-cating suicide attempts.
Cause of Death Register. All deaths in Sweden from 1958 to2009 are contained in the Cause of Death Register (National Boardof Health and Welfare, 2010). The diagnoses and causes of deathare coded according to ICD codes. The register routinely codessuicide as a cause of death. This database was searched to identifyall cases of death by suicide (ICD-10 X60–X84 for years 2005–2009).
Suicide attempts/completions. Information on suicide at-tempts was extracted from the National Patient Register for theyears 1969–2009. Therefore, all suicide attempts not resulting indeath prior to participation in STAGE and suicide attempts afterparticipation in STAGE were captured. To participate in STAGE,individuals needed to be alive in 2005 and suicide information wasavailable up to 2009. As such, information on completed suicideswas available only for the interval between 2005 and 2009. Giventhe restricted interval to capture completed suicides, the number ofcompleted suicides was hypothesized a priori to be too small to beadequately powered to conduct independent analyses acrossgroups. Therefore, we created a composite variable that includedsuicide attempts and completions. In addition, the number ofindividuals with an initial suicide attempt subsequent to theirparticipation in STAGE was hypothesized a priori to be too smallto compose a sufficiently large group to be examined indepen-dently (i.e., suicide attempt prior to STAGE participation vs. afterSTAGE participation). For this reason, we identified the presenceor absence of lifetime suicide attempts as the primary outcomevariable.
ED Diagnosis
Narrow. Two sets of diagnostic criteria were used to defineEDs. The first reflected narrow definitions from the Diagnosticand Statistical Manual of Mental Disorders (4th ed.; DSM–IV;American Psychiatric Association, 2000). Specifically, AN wascoded if a participant (a) indicated that she had a period of timewhen she weighed much less than other people thought she shouldweigh and reported a BMI � 17.55, (b) indicated being very orextremely afraid of gaining weight or becoming fat, and (c) indi-cated feeling very or extremely fat when at low weight. Amenor-rhea was not required for the diagnosis as it is an unreliable
diagnostic criterion for AN (American Psychiatric Association,1994; Bulik, Sullivan, & Kendler, 2000) and was ultimately elim-inated in the DSM–5 (American Psychiatric Association, 2013).Information about binge eating (eating an unusually large amountof food in a short period of time with at least slight loss of control)and purging (defined as vomiting, diuretic use, or laxative useduring the time when binge eating was occurring or at leastweekly) was also collected and used to further classify women asAN, restricting subtype (ANR; absence of both lifetime bingeeating and purging) or AN, binge-purge subtype, (ANBP; presenceof lifetime binge eating and or purging).
Narrow BN was defined as meeting DSM–IV Criteria A (bingeeating), B (inappropriate compensatory behaviors), C (binge eatingepisodes occur at least eight times a month for at least 3 months),and D (body weight or shape are important or the most importantfactors in self-evaluation).
Narrow BED was defined as meeting DSM–IV Criteria A (bingeeating), B (endorsing at least three of the following symptoms:eating faster than usual, eating until uncomfortably full, eatinglarge amounts of food when not hungry, eating alone due toembarrassment, and feeling disgusted/depressed/guilty after over-eating), C (distress or upset over binge episodes), D (at least eightbinge episodes a month for at least 3 months), and E (did notengage in inappropriate compensatory behaviors during the timewhen they were binge eating). A diagnosis of BED was not madeif the participant had a history of either AN or BN.
If a participant indicated that she engaged in vomiting, laxativeuse, or diuretic use at least weekly, indicated that body weight orshape are important or the most important factors in self-evaluation, had no history of binge eating, and did not have alifetime history of AN, she was scored positive for narrow PD.
In addition to the specific questions described above, partici-pants were also asked the general prompt “Do you have or haveyou ever had any of the following problems?” and one of the listedproblems was “anorexia/bulimia/eating disorders” as part of amedical checklist (n � 11,117). Participants responded “yes” or“no” to this question. This question was used in the present studyonly to identify agreement between the response on the medicalchecklist and ED diagnosis as established by the diagnostic algo-rithms (� � 0.40). Most individuals who responded yes to thechecklist item were also given an ED diagnosis (n � 261). Of the10,391women who were not classified as meeting a narrow diag-nosis for an ED, 642 (6.10%) self-identified as having an ED.There were 50 individuals who said no to the checklist item, butwere classified as having an ED diagnosis by the algorithms.
Broad. For the broad diagnoses, the criteria were modified foreach disorder. Specifically, AN was coded if a participant (a)indicated that she had a period of time when she weighed muchless than other people thought she should weigh and had a BMI �18.55; (b) indicated being slightly, somewhat, very, or extremelyafraid of gaining weight or becoming fat; and (c) indicated feelingslightly, somewhat, very, or extremely fat when at low weight. Forbroad BN, Criterion C was modified: A reduced frequency ofbinge eating of four or more times per month was required. Inaddition, Criterion D was defined as body weight or shape at leastmoderately influences self-evaluation. This definition has beenused previously (Root et al., 2010) and has been shown to improvethe detection of binge eating behavior without significantly in-creasing the prevalence of the disorder (Trace et al., 2012). Broad
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1044 PISETSKY ET AL.

BED was defined as meeting DSM–IV criteria with a reducedfrequency of at least four binge eating episodes in a 1-monthperiod (broadened Criterion D). For broad PD, vomiting, laxativeuse, or diuretic use had to occur at least weekly and body weightor shape at least moderately influenced self-evaluation.
Agreement between those identified as having a broadly definedED diagnosis from the above-described criteria and those whoself-identified as having an ED on the medical checklist wascalculated (� � 0.60). Many individuals identified by the algo-rithms as having an ED diagnosis also answered yes to the EDquestion on the medical checklist (n � 524). However, 202 womenmet criteria for an ED using the algorithms but responded no to thechecklist item. Of those who were not classified as meeting a broaddiagnosis for an ED, 407 self-identified as having an ED.
The ED categories used in the analyses were nonoverlapping.For both the narrow and broad definitions, each person was clas-sified as either having a lifetime diagnosis of ANR, lifetimediagnosis of ANBP (the respondent was scored as positive forbinge eating, defined below, and/or indicated engaging in at leastone purging behavior weekly or daily), lifetime diagnosis of BN,lifetime diagnosis of BED, lifetime diagnosis of PD, or no lifetimediagnosis of an ED (no ED). Any participant who had a lifetimehistory of both AN and BN (narrow definition, n � 23; broaddefinition, n � 103) was classified as ANBN. Participants whomet broad criteria for an ED but not narrow criteria (n � 388) wereexcluded from the analyses for the narrow diagnoses, as thoseindividuals could not be considered cases or controls. Therefore,the final sample size for the analyses of the broad definitions ofillness was 13,035.
ED Features
Binge eating. The main binge eating question was “Have youever had binges when you ate what most people would regard asan unusually large amount of food in a short period of time?” withresponse options yes, no, and don’t know/refuse. Positive re-sponses were followed by “When you were having eating binges,did you feel your eating was out of control?” Response optionswere not at all, slightly, moderately, very much, extremely, anddon’t know/don’t wish to answer. Binge eating was scored aspresent if the individual responded yes to the first question andindicated feeling slightly, moderately, very much, or extremely outof control.
ED behaviors. Two questions evaluated weight control meth-ods. Individuals who endorsed binge eating were asked whetherthey engaged in compensatory behaviors (vomiting, laxative use,diuretic use, diet pills) during the time of binge eating. Those whoresponded that they engaged in compensatory behaviors during thetime of binge eating were scored as positive for the respectivemethod. Individuals who did not endorse binge eating were askedwhether they ever engaged in vomiting, laxative use, diuretic use,or diet pill use at any point in their lifetime to control shape orweight. Response options were never, once or twice, weekly, ordaily. Those who engaged in any of the behaviors weekly or dailywere scored as positive for the respective weight control method.
Each participant was asked whether she ever fasted to controlher shape or weight or had not eaten for 24 hr or more (present/absent). Excessive exercise reflected exercising more than 2 hr per
day to control shape and weight. Those who endorsed daily werescored positive for excessive exercise.
Amenorrhea. Women were asked to recall age at menarche.Those who got their first period at age 16 or later, those who hadnot yet experienced menarche prior to AN onset, and those whoreported missing three or more periods were classified as havingamenorrhea.
BMI. Each participant reported lowest weight in kilograms(kg) since age 18 and current height in meters (m). For womenwho did not have a history of AN, lowest adult BMI (kg/m2) wascalculated. For women with a history of AN, lowest BMI wascalculated from lowest weight during AN and height at the time oflow weight. Current BMI was calculated using current height (m)and participant-reported current weight (kg). Highest BMI wascalculated using current height (m) and participant-reported high-est weight (not including pregnancy; kg). BMI difference wascalculated by subtracting the lowest BMI value from the highestBMI value.
Age of onset. Age of onset of ANR was defined as age atlowest illness-related weight. Age of onset of BN and of BED wasdefined as age at first binge. Age of onset of ANBP and ANBNwas defined as age at first binge or age at lowest illness-relatedweight, which ever was younger. No age of onset information wasprovided for inappropriate compensatory behaviors, so these dataare unavailable for participants with PD.
Psychiatric Comorbidity
Other psychiatric disorders were assessed using detailed self-report questionnaires based on the Structured Clinical Interviewfor DSM–IV (First, Spitzer, Gibbon, & Williams, 2002). Depres-sion was coded as present if Criterion A (five symptoms ofdepression, including depressed mood and/or anhedonia, associ-ated with a change of functioning) and Criterion C (significantimpairment caused by the symptoms) were met. Participantsneeded to endorse the symptoms of depression for 2 or more weeksin a row and experience these symptoms all day long or most of theday to be coded as meeting criteria for depression. Participantswere also asked whether they “have or have ever had . . . depres-sion” with a response option of yes or no. Agreement betweenthose identified as having lifetime depression from the above-described algorithm and those self-identified as having lifetimedepression from the yes–no question was calculated (� � 0.56).
Generalized anxiety disorder (GAD) was considered present ifDiagnostic and Statistical Manual of Mental Disorders (4th ed.,text rev.; American Psychiatric Association, 2000) Criteria A(excessive anxiety and worry) and C (at least three symptomsresulting from anxiety and worry) were met. Lifetime prevalenceof specific phobias, obsessive–compulsive disorder (OCD), andpanic disorder was assessed with the question “Have you ever hadany of the following problems?” Each disorder was then listed andresponse options were “yes” and “no.” A composite “any anxietydisorder” variable was also assessed: If the participant had ahistory of GAD, phobias, OCD, or panic disorder, she was scoredpositive for any anxiety disorder.
Alcohol abuse/dependence was assigned based on DSM–IV cri-teria (American Psychiatric Association, 1994); participants wereasked about the presence (and frequency where appropriate) ofeach abuse and dependence criterion. If a participant responded
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1045SUICIDE ATTEMPTS IN WOMEN WITH EATING DISORDERS

positively to one abuse criterion or three or more dependencecriteria, she was given a positive diagnosis for alcohol abuse/dependence. Substance use was defined as using marijuana/hash,opioids, stimulants, hallucinogens, sedatives, and/or hormones 10times or more in 1 month.
Temperament and Personality
Concern over mistakes (� � .82), personal standards (� � .81),and doubts about actions (� � .90) were each evaluated using fouritems from the subscales of the Frost Multidimensional Perfection-ism Scale (Frost, Marten, Lahart, & Rosenblate, 1990). Extraver-sion was evaluated using nine items (� � .78) and neuroticism wasevaluated using 18 items (� � .90) of the Eysenck PersonalityInventory (Schapiro et al., 2001). Self-directedness was measuredusing five items (� � .84) from the Temperament and CharacterInventory (Cloninger, 1994).
Statistical Analyses
All data management and analyses were conducted using SAS9.2. The STAGE database was first linked with the SwedishNational Patient Register and the Swedish National Cause ofDeath Register. For each individual, the total number of lifetimesuicide attempts resulting in hospitalization was based on thenumber of unique dates of hospital discharge entries into theSwedish National Patient Register with a suicide attempt code.Individuals who died as a result of a suicide attempt were identi-fied from a cause of death code for suicide in the Swedish NationalCause of Death Register. Identified completed suicides were addedto the number of suicide attempts generated from the SwedishHospital Discharge Register if the date of the death was differentfrom the last Swedish National Patient Register entry.
Each individual’s age at first attempt was calculated from thedate of discharge or death. ICD codes were used to categorize themethod used for each attempt. Methods were classified as “vio-lent” (e.g., stabbing, hanging, jumping from a high place) and“nonviolent” (see Table 1 for classification by ICD code). Anyparticipant who had more than one suicide attempt with at leastone attempt classified as violent was coded as having had a violentattempt. The prevalence of at least one lifetime suicide attempt andof a violent suicide attempt among those who had ever attemptedsuicide was computed for ANR, ANBP, ANBN, BN, BED, PD,and no ED groups by narrow and broad ED definitions. Means andstandard deviations for number of attempts and age at first attemptwere calculated for all groups.
Logistic regression analyses (using PROC GENMOD in SAS)with generalized estimating equations (GEEs) were applied toassess differences in the prevalence of suicide attempts/completionacross the ANR, ANBP, ANBN, BN, BED, PD, and no ED groups.GEE was used to account for the nesting of the data within twinpairs in this and all subsequent full-model analyses. GEE assumesa relationship within clusters (twin pairs), and this relationship ismodeled and treated as a nuisance variable. For our analyses, theexchangeable correlation matrix was used to model the relation-ship for the analyses of the ANR, ANBP, ANBN, and PD groupsand for the personality features for the BN and BED groups. Theidentity matrix was used for the analyses of the ED features andcomorbidity in the BN groups because the models for these groups
would not converge. Models for the ED features and comorbidityfor the BED group could not be applied. Age at assessment wasentered as a covariate in all models. Type 3 score statistics wereused to determine the significance of the independent variable inthe models. Post hoc contrasts, which use adjusted means, wererequested to assess pairwise group differences for the omnibustests that were significant. The score statistics are presented as �2
for all analyses. We used the guidelines presented by Chen, Cohen,and Chen (2010): Odds ratios of 1.68, 3.47, and 6.71 are consid-ered equivalent to Cohen’s d � 0.2 (small), 0.5 (medium), and 0.8(large), respectively. Therefore, odds ratios greater than 1.68 in-dicate a small effect size and are presented even if the model didnot reach significance.
Among those who ever attempted suicide, differences in theprevalence of violent suicide attempts and in age at first suicideattempt across ED category were assessed using general linearmodels with GEE corrections. To determine whether ED categorywas associated with the total number of lifetime suicide attempts,we conducted a Poisson regression with GEE corrections.
Associations between suicide attempts and lifetime lowest BMI,age of onset of ED, specific ED features (including history ofvomiting, laxative use, diet pill use, diuretic use, excessive exer-cise, fasting, other inappropriate compensatory behaviors, andamenorrhea), psychiatric comorbidity, and personality traits wereevaluated for each ED group separately using general linear mod-els with GEE corrections. All p values of omnibus tests werecorrected for multiple testing using the methods of false discovery(pfdr) (Benjamini & Hochberg, 1995).
In addition, sign tests were conducted to evaluate whether therewas a systematic difference in reporting of comorbid conditionsbetween individuals with a history of suicide attempts and thosewho had never attempted suicide. Specifically, we evaluatedwhether those with suicide attempts reported higher prevalencesacross a majority of comorbid conditions than those without sui-cide attempts. These analyses were stratified by ED group, wereone-tailed, and were not corrected for multiple testing.
Results
Demographics
Narrow diagnostic groups. Demographic information is pre-sented across the narrow ED categories in the top panel of Table2. There were no differences in age at assessment across the EDgroups. BMI at time of assessment differed across EDs (�2 �48.79, p � .0001). Post hoc analyses revealed that the BED grouphad a significantly higher mean BMI at assessment than all of theother ED categories. In addition, the mean BMIs at assessment forthe ANR and ANBP groups were significantly lower than those forthe BN, PD, and no ED groups. Education level differed acrossgroups (�2 � 15.38, p � .02); post hoc analyses revealed thateducation levels differed between the BN and no ED groups. Civilstatus differed across groups (�2 � 13.83, p � .04). The preva-lence of being married or cohabiting with a partner was lower inthe BN and BED groups than the no ED group.
Broad diagnostic groups. The bottom panel of Table 2 pres-ents the demographic information across the broadly defined EDcategories. There were no differences in age at assessment acrossthe ED groups. BMI at time of assessment differed across ED
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1046 PISETSKY ET AL.

groups (�2 � 99.57, p � .0001). Post hoc analyses revealed thatthe BED group had a significantly higher mean BMI than all of theother ED categories and the mean BMI for the ANBN group waslower than those for the BN, PD, and no ED groups. Educationlevel differed across groups (�2 � 19.89, p � .01), with post hocanalyses revealing differences between the BN group and both thePD and no ED groups. Civil status differed across groups (�2 �19.32, p � .04). The prevalence of being married or cohabitingwith a partner was lower in the BN group than the PD and no EDgroups.
Prevalence of Suicide Attempts
Narrow diagnostic groups. Suicide attempts were identifiedin 260 of the 12,647 (2.06%) individuals included in the analysisapplying the narrow ED diagnoses, representing 11.99% of indi-
viduals with EDs and 1.74% of the referent group. Three individ-uals died subsequent to their participation in STAGE as a result ofa suicide attempt: One had a lifetime diagnosis of narrowly definedBN and two had no lifetime ED diagnosis.
Table 3 presents the lifetime prevalence of suicide attemptsacross the ANR, ANBP, ANBN, BN, BED, PD, and no ED groupsfor narrow and broad definitions of illness. The prevalence ofsuicide attempts was significantly different across narrow EDgroups (�2 � 31.39, pfdr � .004). Suicide attempts were signifi-cantly more common in all ED groups than in the referent group(see Table 4). There were no other significant pairwise differencesacross the narrow ED groups.
Characteristics of the suicide attempts among those with narrowdiagnostic classifications who attempted suicide are presented inTable 5. No significant differences emerged across the narrow ED
Table 1International Classification of Diseases (ICD) Codes Used to Identify Suicide Attempts and Completions and the ViolenceCategorization for Each Code
Code DefinitionViolence
categorization
ICD-8 and ICD-9E950 Suicide and self-inflicted poisoning by solid or liquid substances NonviolentE951 Suicide and self-inflicted poisoning by gases in domestic use NonviolentE952 Suicide and self-inflicted poisoning by other gases and vapors NonviolentE953 Suicide and self-inflicted injury by hanging, strangulation, and suffocation ViolentE954 Suicide and self-inflicted injury by submersion (drowning) ViolentE955 Suicide and self-inflicted injury by firearms, air guns, and explosives ViolentE956 Suicide and self-inflicted injury by cutting and piercing instrument ViolentE957 Suicide and self-inflicted injuries by jumping from high place ViolentE958 Suicide and self-inflicted injury by other and unspecified means NonviolentE959 Late effects of self-inflicted injury Nonviolent
ICD-10X60 Intentional self-poisoning by and exposure to nonopioid analgesics, antipyretics, and antirheumatics NonviolentX61 Intentional self-poisoning by and exposure to antiepileptic, sedative-hypnotic, anti-Parkinsonism,
and psychotropic drugs, not elsewhere classifiedNonviolent
X62 Intentional self-poisoning by and exposure to narcotics and psychodysleptics [hallucinogens], notelsewhere classified
Nonviolent
X63 Intentional self-poisoning by and exposure to other drugs acting on the autonomic nervous system NonviolentX64 Intentional self-poisoning by and exposure to other and unspecified drugs, medicaments and
biological substancesNonviolent
X65 Intentional self-poisoning by and exposure to alcohol NonviolentX66 Intentional self-poisoning by and exposure to organic solvents and halogenated hydrocarbons and
their vaporsNonviolent
X67 Intentional self-poisoning by and exposure to other gases and vapors NonviolentX68 Intentional self-poisoning by and exposure to pesticides NonviolentX69 Intentional self-poisoning by and exposure to other and unspecified chemicals and noxious
substancesNonviolent
X70 Intentional self-harm by hanging, strangulation, and suffocation ViolentX71 Intentional self-harm by drowning and submersion ViolentX72 Intentional self-harm by handgun discharge ViolentX73 Intentional self-harm by rifle, shotgun, and larger firearm discharge ViolentX74 Intentional self-harm by other and unspecified firearm discharge ViolentX75 Intentional self-harm by explosive material ViolentX76 Intentional self-harm by smoke, fire, and flames ViolentX77 Intentional self-harm by steam, hot vapors, and hot objects ViolentX78 Intentional self-harm by sharp object ViolentX79 Intentional self-harm by blunt object NonviolentX80 Intentional self-harm by jumping from a high place ViolentX81 Intentional self-harm by jumping or lying before moving object ViolentX82 Intentional self-harm by crashing of motor vehicle ViolentX83 Intentional self-harm by other specified means NonviolentX84 Intentional self-harm by unspecified means Nonviolent
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1047SUICIDE ATTEMPTS IN WOMEN WITH EATING DISORDERS

groups and the referent group in terms of the percentage ofindividuals who experienced violent suicide attempts (see Table5). The age at first attempt for individuals with at least one suicideattempt ranged from 13 to 50 years and did not differ across
narrow ED and referent groups (see Table 5). The total number ofsuicide attempts ranged from one to 34 (see Table 5). Although thenumber of suicide attempts did not differ across groups, there wasa small effect observed for the ANBN group (OR � 1.92, 95% CI[0.87, 2.98]) having a higher mean number of attempts than thereferent group.
Broad diagnostic groups. Suicide attempts were identified in270 of 13,035 (2.07%) individuals included in the analyses whenapplying broad diagnoses, representing 9.13% of individuals withEDs and 1.56% of the referent group. The prevalence of suicideattempts was also significantly different across the broad EDgroups (�2 � 51.88, pfdr � .004). Post hoc pairwise comparisons(see Table 4) revealed that suicide attempts were significantlymore common in all broad ED groups than in the referent group.In addition, suicide attempts were significantly more prevalent inthe ANBN, BN, and PD groups than in the ANR group.
No significant differences emerged across the broad ED groupsand the referent group in terms of the percentage of individualswho experienced violent suicide attempts (see Table 5). The age atfirst attempt for all individuals with at least one suicide attemptranged from 13 to 50 years and did not differ across broad ED andreferent groups (see Table 5). The total number of suicide attemptsranged from 1 to 43 and also did not differ across all groups (seeTable 5).
ED Features Associated With Suicide Attempts
Narrow diagnostic groups. The top panel of Table 6 presentsdescriptive statistics for ED features by ED diagnosis for individ-uals with narrow EDs with and without suicide attempts. None ofthe ED features was significantly associated with suicide attempts
Table 2Age and Body Mass Index (BMI) at Time of Swedish Twin study of Adults: Genes and Environment Assessment and Education andRelationship Status by Eating Disorder
Variable ANR ANBP ANBN BN BED PD No ED
Narrow eating disorder defiitionn 65 75 23 124 22 83 12,255Mean (SD) age at assessment (years) 32.20 (7.78) 30.68 (7.32) 30.09 (6.09) 32.59 (7.14) 33.09 (7.32) 31.78 (7.36) 33.59 (7.65)Mean (SD) BMI at assessment 21.37 (4.05) 21.07 (2.89) 22.94 (4.99) 22.76 (3.76) 28.72 (7.18) 23.07 (3.83) 23.17 (3.90)Education, n (%)
Some secondary or secondary graduate 26 (40.63) 26 (34.67) 7 (30.43) 36 (29.27) 6 (27.27) 36 (43.90) 5,113 (42.16)University graduate 30 (46.88) 38 (50.67) 12 (52.17) 66 (53.66) 12 (54.55) 29 (35.37) 5,603 (46.20)Other (military, vocational, or folk) 8 (12.50) 11 (14.67) 4 (17.39) 21 (17.07) 4 (18.18) 17 (20.73) 1,412 (11.64)
Civil status, n (%)Married or cohabiting 39 (61.90) 41 (55.41) 12 (52.17) 68 (54.84) 10 (45.45) 54 (66.67) 8,283 (68.40)Living alone 24 (38.10) 33 (44.59) 11 (47.83) 56 (45.16) 12 (54.55) 27 (33.33) 3,826 (31.60)
Broad eating disorder defiitionn 242 127 103 251 64 89 12,159Mean (SD) age at assessment (years) 31.93 (7.52) 30.96 (7.35) 32.10 (7.40) 31.77 (7.19) 30.95 (7.59) 31.92 (7.42) 33.67 (7.65)Mean (SD) BMI at assessment 21.28 (3.82) 21.57 (3.47) 21.74 (3.75) 23.46 (4.62) 26.20 (6.02) 23.49 (3.79) 23.18 (3.87)Education, n (%)
Some secondary or secondary graduate 88 (37.29) 50 (39.37) 30 (29.41) 81 (32.40) 20 (31.25) 41 (46.59) 5,087 (42.33)University graduate 123 (52.12) 61 (48.03) 54 (52.94) 137 (54.80) 34 (53.13) 31 (35.23) 5,506 (45.81)Other (military, vocational, or folk) 25 (10.59) 16 (12.60) 18 (17.65) 32 (12.80) 10 (15.63) 16 (18.18) 1,425 (11.86)
Civil status, n (%)Married or cohabiting 144 (60.76) 71 (56.80) 67 (65.05) 135 (53.78) 34 (53.13) 59 (67.05) 8,251 (68.77)Living alone 93 (39.24) 54 (43.20) 36 (34.95) 116 (46.22) 30 (46.88) 29 (32.95) 3,747 (31.23)
Note. ANR � restricting subtype anorexia nervosa; ANBP � binge-purge subtype anorexia nervosa; ANBN � lifetime diagnosis of both anorexia nervosaand bulimia nervosa; BN � bulimia nervosa; BED � binge eating disorder; PD � purging disorder; No ED � no eating disorder.
Table 3Lifetime Prevalence of at Least One Suicide Attempt by EatingDisorder Group for Narrow and Broad EatingDisorder Definitions
Group
No lifetimesuicide attempt
n (%)
Lifetime suicideattemptn (%)
NarrowANR (n � 65) 60 (92.31) 5 (7.69)ANBP (n � 75) 65 (86.67) 10 (13.33)ANBN (n � 23) 19 (82.61) 4 (17.39)BN (n � 124) 108 (87.10) 16 (12.90)BED (n � 22) 19 (86.36) 3 (13.64)PD (n � 83) 74 (89.16) 9 (10.84)No ED (n � 12,255) 12,042 (98.26) 213 (1.74)
BroadANR (n � 242) 232 (95.87) 10 (4.13)ANBP (n � 127) 116 (91.34) 11 (8.66)ANBN (n � 103) 90 (87.38) 13 (12.62)BN (n � 251) 222 (88.45) 29 (11.55)BED (n � 64) 59 (92.19) 5 (7.81)PD (n � 89) 77 (86.52) 12 (13.48)No ED (n � 12,159) 11,969 (98.44) 190 (1.56)
Note. ANR � restricting subtype anorexia nervosa; ANBP � binge-purge subtype anorexia nervosa; ANBN � lifetime diagnosis of bothanorexia nervosa and bulimia nervosa; BN � bulimia nervosa; BED �binge eating disorder; PD � purging disorder; No ED � no eating disorder.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1048 PISETSKY ET AL.

in any of the ED groups. Although all of the models investigatingthe association between ED features and suicide attempts in eachof the ED groups failed to reach statistical significance, several ofthe models produced medium and large effect sizes. The Cohen’sd for BMI difference was 0.52 and for age of ED onset was 1.24in the ANR group, with women with suicide attempts having agreater BMI difference and an older age of onset. For the ANBNgroup, women with suicide attempts had lower lowest BMI values(Cohen’s d � 0.60), higher highest BMI values (Cohen’s d �0.63), greater BMI differences (Cohen’s d � 0.63), and an olderage of ED onset (Cohen’s d � 0.87). A greater BMI difference wasalso observed for women with suicide attempts in the BN group(Cohen’s d � 0.57). In the BED group, women with suicide
attempts had higher lowest BMI values (Cohen’s d � 1.04) andhigher highest BMI values (Cohen’s d � 0.75) than women whohad no suicide attempts. In the PD group, those with suicideattempts had higher highest BMI values (Cohen’s d � 0.74) and agreater BMI difference (Cohen’s d � 0.84). The remaining modelsdid not produce a remarkable effect size or did not converge.Models that did not converge are indicated in Table 6.
Broad diagnostic groups. The bottom panel of Table 6 pres-ents descriptive statistics for ED features by group for individualswith broad EDs with and without suicide attempts. None of the EDfeatures was significantly associated with suicide attempts in anyof the ED groups. Regarding effect sizes, results were similar tothose for the narrow ED definitions: Cohen’s d � 0.80 for age of
Table 4Results of Post Hoc Pairwise Comparison Evaluating Differences in Suicide Prevalence Between Eating Disorder Groups for Narrowand Broad Eating Disorder Definitions
Comparison eatingdisorder group Referent group
Narrow Broad
OR [95% CI] �2 (p) OR [95% CI] �2 (p)
ANR No ED 4.77 [1.94, 11.72] 11.56 (.001) 2.70 [1.40, 5.20] 8.79 (.003)ANBP No ED 7.92 [3.86, 16.20] 32.07 (.001) 5.79 [3.04, 10.95] 28.81 (.001)ANBN No ED 10.74 [3.70, 31.25] 19.03 (.001) 8.46 [4.53, 15.81] 44.80 (.001)BN No ED 8.12 [4.50, 14.65] 48.34 (.001) 7.83 [5.07, 12.09] 86.41 (.001)BED No ED 7.84 [2.08, 29.59] 9.25 (.003) 5.09 [1.99, 13.06] 11.47 (.001)PD No ED 6.59 [3.18, 13.65] 25.72 (.001) 9.16 [4.81, 17.45] 45.46 (.001)ANBP ANR 1.66 [0.54, 5.10] 0.79 (.376) 2.14 [0.88, 5.19] 2.84 (.093)ANBN ANR 2.26 [0.57, 8.97] 1.33 (.249) 3.14 [1.31, 7.54] 6.53 (.011)BN ANR 1.70 [0.59, 4.90] 0.98 (.324) 2.90 [1.37, 6.17] 7.71 (.006)BED ANR 1.65 [0.33, 8.08] 0.38 (.542) 1.89 [0.60, 5.93] 1.19 (.277)PD ANR 1.38 [0.44, 4.31] 0.31 (.577) 3.40 [1.40, 8.28] 7.25 (.008)ANBN ANBP 1.36 [0.38, 4.83] 0.22 (.637) 1.47 [0.62, 3.48] 0.75 (.387)BN ANBP 1.03 [0.42, 2.53] 0.00 (.956) 1.36 [0.65, 2.85] 0.65 (.420)BED ANBP 0.99 [0.22, 4.40] 0.00 (.991) 0.88 [0.29, 2.71] 0.05 (.827)PD ANBP 0.83 [0.31, 2.26] 0.13 (.719) 1.59 [0.66, 3.83] 1.06 (.304)BN ANBN 0.76 [0.23, 2.52] 0.21 (.649) 0.93 [0.45, 1.90] 0.04 (.833)BED ANBN 0.73 [0.13, 3.98] 0.13 (.716) 0.60 [0.20, 1.84] 0.79 (.374)PD ANBN 0.61 [0.17, 2.20] 0.57 (.453) 1.08 [0.45, 2.59] 0.03 (.858)BED BN 0.97 [0.23, 4.03] 0.00 (.963) 0.65 [0.24, 1.79] 0.69 (.406)PD BN 0.81 [0.32, 2.03] 0.20 (.656) 1.17 [0.55, 2.47] 0.17 (.682)PD BED 0.84 [0.21, 3.44] 0.06 (.809) 1.80 [0.62, 5.25] 1.15 (.283)
Note. ANR � restricting subtype anorexia nervosa; ANBP � binge-purge subtype anorexia nervosa; ANBN � lifetime diagnosis of both anorexia nervosaand bulimia nervosa; BN � bulimia nervosa; BED � binge eating disorder; PD � purging disorder; No ED � no eating disorder.
Table 5Suicide Characteristics in Women Who Attempted Suicide by Eating Disorder and Results for Models Assessing Differences in TheseFeatures Across Eating Disorder for Both Narrow and Broad Eating Disorder Definitions
Variable Definition ANR ANBP ANBN BN BED PD No EDResults�2 (pfdr)
n Narrow 5 10 4 16 3 9 213Broad 10 11 13 29 5 12 190
Violent attempt, n (%) Narrow 2 (40.00) 3 (30.00) 3 (75.00) 3 (18.75) 0 (0.00) 1 (11.11) 30 (14.08) 12.33 (.147)a
Broad 3 (30.00) 2 (18.18) 4 (30.77) 4 (13.79) 1 (20.00) 3 (25.00) 27 (14.21) 3.34 (.766)Mean (SD) age at first
attempt (years)Narrow 30.40 (4.93) 22.90 (6.26) 25.25 (9.63) 24.20 (6.39) 28.00 (10.82) 31.11 (10.41) 25.73 (8.48) 6.56 (.492)Broad 28.90 (4.48) 20.55 (5.82) 25.77 (8.27) 24.11 (6.75) 23.80 (9.73) 29.08 (9.89) 26.07 (8.64) 5.95 (.492)
Mean (SD) totalnumber of attempts
Narrow 2.60 (3.05) 5.80 (6.64) 15.50 (18.95) 4.56 (5.50) 1.00 (0.00) 2.33 (1.41) 2.25 (3.78) 8.85 (.366)Broad 2.20 (2.20) 4.00 (6.20) 6.85 (11.63) 3.34 (4.53) 1.60 (0.89) 2.50 (1.93) 2.31 (3.95) 6.33 (.492)
Note. ANR � restricting subtype anorexia nervosa; ANBP � binge-purge subtype anorexia nervosa; ANBN � lifetime diagnosis of both anorexia nervosaand bulimia nervosa; BN � bulimia nervosa; BED � binge eating disorder; PD � purging disorder; No ED � no eating disorder; pfdr � p-value aftercorrecting for multiple comparisons using the method of false discovery.a Model applied without correcting for nonindependence of the sample.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1049SUICIDE ATTEMPTS IN WOMEN WITH EATING DISORDERS

ED onset for the ANR group; Cohen’s d � 0.68 for lowest BMIand Cohen’s d � 0.64 for BMI difference for the ANBN group;Cohen’s d � 0.52 for BMI difference for the BN group; Cohen’sd � 0.71 for lowest BMI and Cohen’s d � 0.68 for highest BMIfor the BED group; and, for the PD group, Cohen’s d � 0.62 forlowest BMI (those with suicide attempts had lower lowest BMIvalues), Cohen’s d � 0.58 for highest BMI, and Cohen’s d � 0.78for BMI difference. The remaining models produced effect sizesless than 0.50 or did not converge. Models that did not convergeare indicated in Table 6.
Psychiatric Comorbidity and Personality FeaturesAssociated With Suicide Attempts
Narrow diagnostic groups. The top panel of Table 7 presentscomorbid psychiatric disorders and personality variables acrossnarrow ED groups by the presence or absence of suicide attempts.None of the comorbid psychiatric disorders was significantly as-sociated with suicide attempts. None of the models yielded me-dium or large effect sizes. Models that did not converge areindicated in Table 7.
Although there were no significant differences in the individualcomorbid conditions, the sign test indicated that, in the ANBP and
ANBN groups, the prevalence of all seven conditions was signif-icantly higher in the group with suicide attempts compared withthe group without suicide attempts (ps � .008).
None of the personality measures was significantly associatedwith suicide attempts in any of the ED groups. However, several ofthese measures had medium or large effect sizes. Specifically,concern over mistakes was greater in those with suicide attemptsthan those without attempts in the ANBP (Cohen’s d � 0.73) andBN (Cohen’s d � 0.85) groups, as were doubts about actions in theANBP group (Cohen’s d � 0.61) and neuroticism in the BEDgroup (Cohen’s d � 0.69). Personal standards was lower in thosewith suicide attempts than in those without attempts in the ANBN(Cohen’s d � 0.66) and PD (Cohen’s d � 0.70) groups. Extraver-sion was also lower in those with suicide attempts in the ANBP(Cohen’s d � 0.58), ANBN (Cohen’s d � 0.93), and BED (Co-hen’s d � 1.25) groups. Those with suicide attempts in the ANR,BED, and PD groups also had lower self-directedness (Cohen’sd � 0.88, 1.26, and 0.56, respectively).
Broad diagnostic groups. The bottom panel of Table 7 pres-ents comorbid psychiatric disorders and personality variablesacross broad ED groups by the presence or absence of suicideattempts. None of the comorbid psychiatric disorders was signif-
Table 6Lifetime Prevalence of Eating Disorder Features and Characteristics of Women With a Lifetime History of a Suicide Attempt byEating Disorder
Variable ANR ANBP ANBN
Narrow eating disorder definitionn 65 75 23Suicide attempt, n (%) No: 60 (92.31) Yes: 5 (7.69) No: 65 (86.67) Yes: 10 (13.33) No: 19 (82.61) Yes: 4 (17.39)Eating disorder features, n (%)
Vomiting NA NA 50 (76.92) 9 (90.00) 17 (89.47)a 4 (100.00)a
Laxative use NA NA 15 (23.08) 3 (30.00) 6 (31.58) 3 (75.00)Diuretic use NA NA 5 (7.69) 2 (20.00) 7 (36.84) 1 (25.00)Diet pill use 2 (3.33)a 0 (0.00)a 6 (9.23) 4 (40.00) 5 (26.32) 1 (25.00)Fasting 20 (33.33) 3 (60.00) 40 (61.54) 6 (66.67) 10 (52.63)a 4 (100.00)a
Excessive exercise 17 (28.33) 4 (80.00) 46 (70.77) 4 (40.00) 13 (68.42)a 4 (100.00)a
Amenorrhea 31 (65.96) 4 (80.00) 37 (67.27) 5 (55.56) 15 (83.33) 2 (66.67)Mean (SD) lowest BMI 15.09 (1.91) 14.50 (2.42) 15.20 (1.74) 14.90 (1.45) 15.69 (1.26) 14.36 (2.86)Mean (SD) highest BMI 22.93 (3.58) 26.16 (10.98) 23.69 (3.64) 24.88 (6.34) 26.32 (6.95) 31.44 (9.20)Mean (SD) BMI difference (highest – lowest) 7.80 (3.98) 11.66 (9.60) 8.49 (4.11) 9.86 (6.75) 10.48 (6.96) 16.50 (11.54)Mean (SD) age of eating disorder onset (years) 17.63 (4.06) 25.80 (8.35) 17.71 (4.23) 19.30 (2.98) 17.26 (3.23) 20.75 (4.65)
Broad eating disorder definition
n 242 127 103Suicide attempt, n (%) No: 232 (95.87) Yes: 10 (4.13) No: 116 (91.34) Yes: 11 (8.66) No: 90 (87.38) Yes: 13 (12.62)Eating disorder features, n (%)
Vomiting NA NA 84 (72.41) 10 (90.91) 68 (75.56) 12 (92.31)Laxative use NA NA 20 (17.24) 3 (27.27) 24 (26.67) 7 (53.85)Diuretic use NA NA 11 (9.48) 2 (18.18) 15 (16.67) 3 (23.08)Diet pill use 8 (3.45)a 0 (0.00)a 11 (9.48) 4 (36.36) 10 (11.11) 4 (30.77)Fasting 44 (18.97) 4 (40.00) 59 (50.86) 8 (72.73) 48 (53.33) 6 (50.00)Excessive exercise 42 (18.10) 5 (50.00) 62 (53.45) 3 (27.27) 56 (62.22) 8 (61.54)Amenorrhea 88 (46.32) 5 (55.56) 46 (52.27) 4 (40.00) 53 (60.92) 5 (45.45)
Mean (SD) lowest BMI 16.45 (1.89) 15.55 (2.37) 16.36 (1.53) 16.01 (1.73) 16.36 (1.82) 15.01 (2.16)Mean (SD) highest BMI 23.12 (3.93) 24.35 (8.11) 24.39 (4.36) 25.43 (5.97) 24.23 (4.14) 26.84 (7.50)Mean (SD) BMI difference (highest – lowest) 6.64 (4.12) 8.56 (7.75) 8.05 (4.44) 9.20 (6.69) 7.84 (4.55) 11.90 (7.79)Mean (SD) age of eating disorder onset (years) 18.94 (5.25) 24.10 (7.43) 18.69 (4.16) 20.18 (4.75) 17.48 (3.44) 18.69 (5.36)
Note. ANR � restricting subtype anorexia nervosa; ANBP � binge-purge subtype anorexia nervosa; ANBN � lifetime diagnosis of both anorexia nervosaand bulimia nervosa; BN � bulimia nervosa; BED � binge eating disorder; PD � purging disorder; BMI � body mass index.a The model evaluating the association with the variable and suicide attempt for the specific group did not converge.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1050 PISETSKY ET AL.
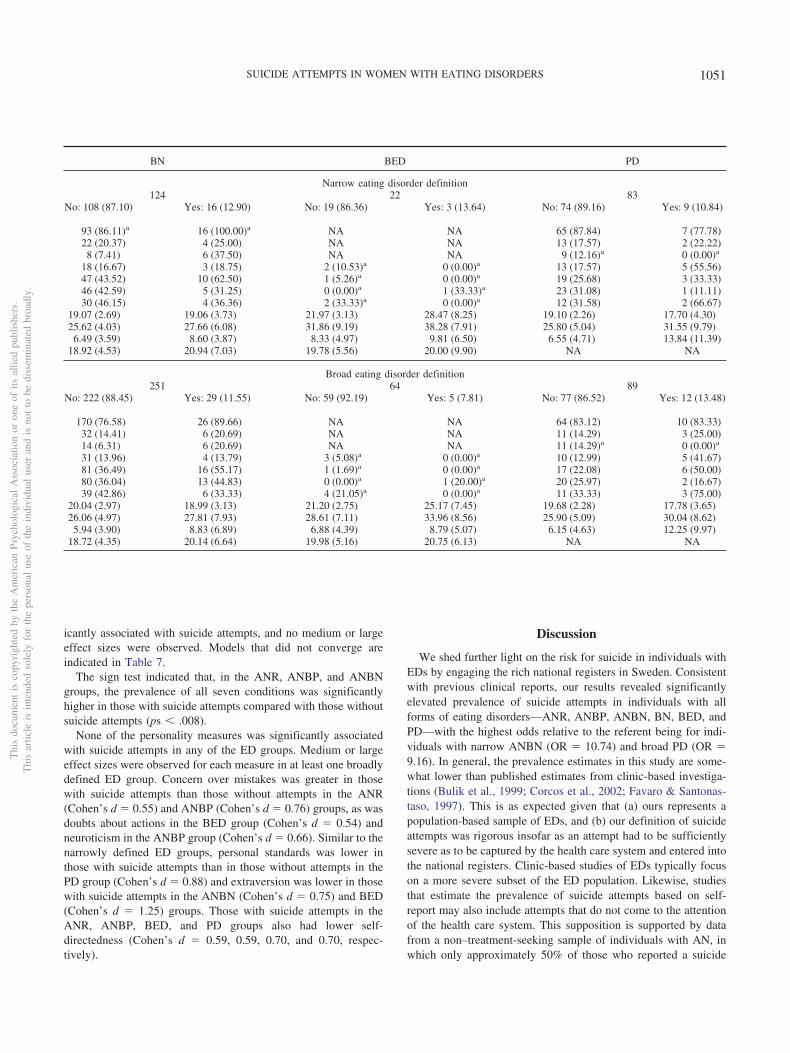
icantly associated with suicide attempts, and no medium or largeeffect sizes were observed. Models that did not converge areindicated in Table 7.
The sign test indicated that, in the ANR, ANBP, and ANBNgroups, the prevalence of all seven conditions was significantlyhigher in those with suicide attempts compared with those withoutsuicide attempts (ps � .008).
None of the personality measures was significantly associatedwith suicide attempts in any of the ED groups. Medium or largeeffect sizes were observed for each measure in at least one broadlydefined ED group. Concern over mistakes was greater in thosewith suicide attempts than those without attempts in the ANR(Cohen’s d � 0.55) and ANBP (Cohen’s d � 0.76) groups, as wasdoubts about actions in the BED group (Cohen’s d � 0.54) andneuroticism in the ANBP group (Cohen’s d � 0.66). Similar to thenarrowly defined ED groups, personal standards was lower inthose with suicide attempts than in those without attempts in thePD group (Cohen’s d � 0.88) and extraversion was lower in thosewith suicide attempts in the ANBN (Cohen’s d � 0.75) and BED(Cohen’s d � 1.25) groups. Those with suicide attempts in theANR, ANBP, BED, and PD groups also had lower self-directedness (Cohen’s d � 0.59, 0.59, 0.70, and 0.70, respec-tively).
Discussion
We shed further light on the risk for suicide in individuals withEDs by engaging the rich national registers in Sweden. Consistentwith previous clinical reports, our results revealed significantlyelevated prevalence of suicide attempts in individuals with allforms of eating disorders—ANR, ANBP, ANBN, BN, BED, andPD—with the highest odds relative to the referent being for indi-viduals with narrow ANBN (OR � 10.74) and broad PD (OR �9.16). In general, the prevalence estimates in this study are some-what lower than published estimates from clinic-based investiga-tions (Bulik et al., 1999; Corcos et al., 2002; Favaro & Santonas-taso, 1997). This is as expected given that (a) ours represents apopulation-based sample of EDs, and (b) our definition of suicideattempts was rigorous insofar as an attempt had to be sufficientlysevere as to be captured by the health care system and entered intothe national registers. Clinic-based studies of EDs typically focuson a more severe subset of the ED population. Likewise, studiesthat estimate the prevalence of suicide attempts based on self-report may also include attempts that do not come to the attentionof the health care system. This supposition is supported by datafrom a non–treatment-seeking sample of individuals with AN, inwhich only approximately 50% of those who reported a suicide
BN BED PD
Narrow eating disorder definition124 22 83
No: 108 (87.10) Yes: 16 (12.90) No: 19 (86.36) Yes: 3 (13.64) No: 74 (89.16) Yes: 9 (10.84)
93 (86.11)a 16 (100.00)a NA NA 65 (87.84) 7 (77.78)22 (20.37) 4 (25.00) NA NA 13 (17.57) 2 (22.22)8 (7.41) 6 (37.50) NA NA 9 (12.16)a 0 (0.00)a
18 (16.67) 3 (18.75) 2 (10.53)a 0 (0.00)a 13 (17.57) 5 (55.56)47 (43.52) 10 (62.50) 1 (5.26)a 0 (0.00)a 19 (25.68) 3 (33.33)46 (42.59) 5 (31.25) 0 (0.00)a 1 (33.33)a 23 (31.08) 1 (11.11)30 (46.15) 4 (36.36) 2 (33.33)a 0 (0.00)a 12 (31.58) 2 (66.67)
19.07 (2.69) 19.06 (3.73) 21.97 (3.13) 28.47 (8.25) 19.10 (2.26) 17.70 (4.30)25.62 (4.03) 27.66 (6.08) 31.86 (9.19) 38.28 (7.91) 25.80 (5.04) 31.55 (9.79)6.49 (3.59) 8.60 (3.87) 8.33 (4.97) 9.81 (6.50) 6.55 (4.71) 13.84 (11.39)
18.92 (4.53) 20.94 (7.03) 19.78 (5.56) 20.00 (9.90) NA NA
Broad eating disorder definition251 64 89
No: 222 (88.45) Yes: 29 (11.55) No: 59 (92.19) Yes: 5 (7.81) No: 77 (86.52) Yes: 12 (13.48)
170 (76.58) 26 (89.66) NA NA 64 (83.12) 10 (83.33)32 (14.41) 6 (20.69) NA NA 11 (14.29) 3 (25.00)14 (6.31) 6 (20.69) NA NA 11 (14.29)a 0 (0.00)a
31 (13.96) 4 (13.79) 3 (5.08)a 0 (0.00)a 10 (12.99) 5 (41.67)81 (36.49) 16 (55.17) 1 (1.69)a 0 (0.00)a 17 (22.08) 6 (50.00)80 (36.04) 13 (44.83) 0 (0.00)a 1 (20.00)a 20 (25.97) 2 (16.67)39 (42.86) 6 (33.33) 4 (21.05)a 0 (0.00)a 11 (33.33) 3 (75.00)
20.04 (2.97) 18.99 (3.13) 21.20 (2.75) 25.17 (7.45) 19.68 (2.28) 17.78 (3.65)26.06 (4.97) 27.81 (7.93) 28.61 (7.11) 33.96 (8.56) 25.90 (5.09) 30.04 (8.62)5.94 (3.90) 8.83 (6.89) 6.88 (4.39) 8.79 (5.07) 6.15 (4.63) 12.25 (9.97)
18.72 (4.35) 20.14 (6.64) 19.98 (5.16) 20.75 (6.13) NA NA
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1051SUICIDE ATTEMPTS IN WOMEN WITH EATING DISORDERS

attempt had ever sought medical treatment for the attempt (Buliket al., 2008). However, the percentage of individuals seekingtreatment for a suicide attempt was only slightly higher in atreatment-seeking sample of individuals with EDs (60%; Corcos etal., 2002).
Our results underscore the value of the recommendation ofFranko and Keel (2006), who emphasized the importance of sub-typing AN into ANR and ANBP when assessing the prevalence ofsuicide attempts. Risk is elevated in both AN subtypes, narrowlyand broadly defined, compared with the no ED group. Althoughthere was no significant difference in prevalence of suicide at-tempts between the ANR and ANBP groups, either narrowly orbroadly defined, the broad ANR group had a significantly lowerprevalence of suicide attempts than the broad ANBN, BN, and PDgroups.
It has long been known that diagnostic crossover is a commonoccurrence in individuals with AN, with around 50% of those with
initial ANR migrating to a bulimic presentation at some pointduring the course of their illness (Bulik, Sullivan, Fear, & Pick-ering, 1997; Eddy et al., 2008; Fichter & Quadflieg, 2007; Tozzi etal., 2005). Suicide risk may fluctuate as the clinical presentationmigrates between restricting and binge-purge forms. It is notewor-thy that the highest prevalence of suicide attempts (17.39%) andthe highest mean number of lifetime suicide attempts (15.50)in the present sample were in the narrow ANBN group, indi-cating that individuals who experience diagnostic crossovermay be at particularly elevated risk. More granular investiga-tions of longitudinal risk are required to confirm whether sui-cide risk fluctuates with symptom evolution or is more stronglyrelated to trait factors.
We further extend our understanding of suicide and EDs bydemonstrating significantly elevated risk for suicide in individualswith BED. Although the number of cases of BED was smaller thanwould have been expected on the basis of U.S. population data
Table 7Lifetime Prevalence of Comorbid Psychiatric Disorders and Temperament Characteristics by Eating Disorder and by Lifetime SuicideAttempt/Completion Status
Variable ANR ANBP ANBN
Narrow eating disorder definitionn 65 75 23Suicide attempt/completion, n (%) No: 60 (92.31) Yes: 5 (7.69) No: 65 (86.67) Yes: 10 (13.33) No: 19 (82.61) Yes: 4 (17.39)Psychiatric comorbidity, n (%)
Major depression 27 (50.94) 3 (60.00) 39 (63.93)a 10 (100.00)a 12 (70.59)a 4 (100.00)a
Generalized anxiety disorder 2 (5.41) 1 (50.00) 10 (25.00) 3 (42.86) 4 (33.33) 2 (66.67)Specific phobia 5 (12.82) 1 (50.00) 8 (18.18) 3 (60.00) 3 (23.08) 2 (66.67)Obsessive–compulsive disorder 7 (13.46)a 0 (0.00)a 12 (23.08) 2 (25.00) 3 (20.00) 1 (33.33)Panic disorder 18 (34.62)a 0 (0.00)a 17 (32.69) 7 (77.78) 6 (40.00) 2 (66.67)Any anxiety disorder 21 (56.76)a 2 (100.00)a 29 (70.73)a 7 (100.00)a 10 (76.92) 3 (75.00)Alcohol abuse/dependence 7 (11.67) 2 (40.00) 10 (15.38) 4 (40.00) 5 (27.78) 2 (50.00)Substance use 6 (10.00) 2 (40.00) 4 (6.15) 6 (60.00) 3 (15.79) 2 (50.00)
Mean (SD) personality featuresConcern over mistakes (MPS) 12.05 (4.02) 11.50 (2.89) 11.51 (4.47) 14.67 (4.18) 15.20 (2.86) 15.33 (1.15)Doubts about actions (MPS) 8.77 (3.15) 10.00 (1.82) 9.34 (3.76) 11.78 (4.24) 12.60 (4.14) 11.33 (2.08)Personal standards (MPS) 14.38 (2.90) 14.25 (3.50) 13.57 (3.24) 13.78 (2.68) 17.40 (1.72) 15.75 (3.10)Extraversion (EPI) 5.43 (2.10) 5.50 (1.73) 5.07 (2.19) 3.88 (1.89) 5.29 (1.90) 3.00 (2.94)Neuroticism (EPI) 6.92 (4.23) 7.25 (5.50) 8.88 (5.15) 10.57 (5.88) 10.62 (4.96) 12.00 (6.08)Self-directedness (TCI) 19.25 (2.88) 16.00 (4.36) 17.65 (3.28) 16.00 (4.15) 15.40 (2.75) 15.75 (3.10)
Broad eating disorder definition
n 242 127 103Suicide attempt/completion, n (%) No: 232 (95.87) Yes: 10 (4.13) No: 116 (91.34) Yes: 11 (8.66) No: 90 (87.38) Yes: 13 (12.62)Psychiatric comorbidity, n (%)
Major depression 94 (44.98) 7 (70.00) 59 (55.14)a 11 (100.00)a 43 (53.75) 12 (92.31)Generalized anxiety disorder 24 (14.63) 3 (60.00) 14 (18.92) 4 (50.00) 13 (22.41) 5 (55.56)Specific phobia 21 (12.73) 1 (20.00) 18 (21.95) 1 (25.00) 13 (20.97) 4 (57.14)Obsessive–compulsive disorder 19 (9.18) 1 (14.29) 17 (17.89) 2 (22.22) 13 (17.81) 3 (30.00)Panic disorder 57 (27.67) 4 (57.14) 28 (29.79) 8 (88.89) 30 (40.54) 7 (63.64)Any anxiety disorder 83 (53.55)a 6 (100.00)a 47 (62.67)a 8 (100.00)a 40 (64.52) 9 (90.00)Alcohol abuse/dependence 24 (10.53) 2 (20.00) 13 (11.40) 4 (36.36) 18 (20.22) 6 (46.15)Substance use 21 (9.05) 2 (20.00) 9 (7.76) 6 (54.55) 8 (8.89) 7 (53.85)
Mean (SD) personality featuresConcern over mistakes (MPS) 11.42 (3.98) 13.50 (3.51) 11.14 (4.28) 14.14 (3.63) 12.96 (4.26) 13.18 (4.38)Doubts about actions (MPS) 8.95 (3.66) 10.38 (2.72) 8.99 (3.59) 10.29 (3.59) 10.66 (4.11) 12.09 (3.33)Personal standards (MPS) 13.46 (3.59) 13.86 (3.24) 13.39 (3.41) 13.00 (1.73) 14.36 (3.21) 13.83 (3.38)Extraversion (EPI) 5.07 (2.28) 5.29 (1.60) 4.92 (2.29) 4.29 (2.56) 5.01 (2.26) 3.45 (1.86)Neuroticism (EPI) 7.60 (4.53) 9.71 (5.82) 8.30 (4.72) 11.43 (4.76) 9.28 (5.06) 10.22 (6.12)Self-directedness (TCI) 18.48 (3.14) 16.67 (3.01) 17.92 (3.28) 15.57 (4.54) 16.49 (3.02) 15.25 (2.83)
Note. ANR � restricting subtype anorexia nervosa; ANBP � binge-purge subtype anorexia nervosa; ANBN � lifetime diagnosis of both anorexia nervosaand bulimia nervosa; BN � bulimia nervosa; BED � binge eating disorder; PD � purging disorder; MPS � Frost Multidimensional Perfectionism Scale;EPI � Eysenck Personality Inventory; TCI � Temperament and Character Inventory.a The model evaluating the association with the variable and suicide attempt/completion for the specific group did not converge.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1052 PISETSKY ET AL.

(Hudson et al., 2007), suicide risk was significantly elevated inindividuals with both narrow and broad BED diagnoses. As ad-justments are made worldwide secondary to BED being a bonafide diagnostic category in DSM–5, clinicians should remain vig-ilant for suicide risk in individuals with this disorder.
An additional extension of the knowledge base is the observa-tion that individuals with broadly defined PD had elevated risk forsuicide attempts relative to individuals with no ED (OR � 9.16)and ANR (OR � 3.40). These initial results are consistent withobservations that, within those with AN and those with BN,individuals who purge are at greater risk for suicide attempts thanthose who do not purge (Favaro & Santonastaso, 1997) and high-light the need for additional research to better understand thishigh-risk yet understudied population.
Unlike previous investigations, we did not identify specificfeatures of EDs that were associated with suicide attempts. The
small cell sizes for some of the suicide groups most likelyprecluded the detection of significant effects. However, theoverall pattern of results indicates that the highest odds ratiosfor suicide were observed in presentations that included purging(ANBP, ANBN, ANBP, and PD). This observation is consistentwith findings that individuals who engage in purging behaviorare at particularly elevated risk for suicide attempts.
Also consistent with previous reports, our results confirmthat greater comorbid psychiatric burden (i.e., increased prev-alence across seven comorbid conditions) is associated withelevated risk for suicide in individuals with ANBP and ANBN(Franko & Keel, 2006). By nature of having an ED presentationwith both AN and BN features, these individuals already expe-rience elevated comorbidity burden. Individuals who presentwith a clinical picture of both low weight plus binge eatingand/or purging are at increased risk for adverse medical out-
BN BED PD
Narrow eating disorder definition124 22 83
No: 108 (87.10) Yes: 16 (12.90) No: 19 (86.36) Yes: 3 (13.64) No: 74 (89.16) Yes: 9 (10.84)
66 (65.35) 14 (93.33) 12 (66.67)a 3 (100.00)a 37 (56.06)a 9 (100.00)a
19 (29.69) 8 (66.67) 4 (33.33)a 2 (100.00)a 15 (28.30) 1 (20.00)14 (22.58)a 0 (0.00)a 2 (18.18)a 0 (0.00)a 10 (20.41)a 0 (0.00)a
21 (25.30) 4 (36.36) 1 (6.67)a 0 (0.00)a 4 (6.56)a 0 (0.00)a
40 (47.62)a 11 (100.00)a 6 (40.00)a 2 (100.00)a 16 (26.67) 5 (62.50)55 (78.57)a 15 (100.00)a 8 (57.14)a 2 (100.00)a 29 (64.44) 5 (71.43)29 (27.88) 5 (31.25) 5 (26.32)a 0 (0.00)a 10 (13.70) 2 (25.00)12 (11.11) 8 (50.00) 3 (15.79) 2 (66.67) 11 (14.86) 4 (44.44)
12.39 (4.39) 15.54 (2.84) 12.44 (5.20) 12.50 (0.71) 11.15 (4.16) 9.50 (4.28)10.76 (4.14) 12.67 (4.96) 9.25 (3.64) 10.00 (2.83) 8.12 (3.75) 9.17 (4.49)13.19 (3.24) 14.17 (3.97) 12.25 (4.60) 10.50 (3.54) 12.96 (3.24) 10.00 (5.06)4.53 (2.20) 4.09 (2.26) 4.75 (2.77) 2.00 (1.41) 5.25 (1.99) 5.80 (1.30)
10.61 (4.70) 12.83 (4.22) 9.00 (4.43) 12.00 (4.24) 7.76 (4.05) 9.57 (3.31)16.31 (2.83) 14.92 (3.20) 16.56 (4.03) 12.50 (2.12) 17.63 (3.65) 15.33 (4.46)
Broad eating disorder definition251 64 89
No: 222 (88.45) Yes: 29 (11.55) No: 59 (92.19) Yes: 5 (7.81) No: 77 (86.52) Yes: 12 (13.48)
117 (57.92) 23 (85.19) 30 (53.57)a 5 (100.00)a 40 (57.97) 9 (81.82)29 (20.71) 8 (47.06) 8 (18.60)a 2 (100.00)a 13 (24.07) 1 (20.00)27 (19.71) 2 (15.38) 5 (12.82) 1 (50.00) 10 (18.87)a 0 (0.00)a
27 (15.17) 4 (19.05) 6 (12.24)a 0 (0.00)a 3 (4.48)a 0 (0.00)a
60 (33.52) 14 (66.67) 15 (30.61)a 3 (100.00)a 20 (29.85) 6 (60.00)91 (65.00) 19 (95.00) 22 (53.66)a 3 (100.00)a 30 (60.00) 6 (75.00)48 (22.43) 5 (17.24) 9 (15.52) 1 (25.00) 12 (15.79) 2 (18.18)16 (7.21) 9 (31.03) 4 (6.78) 3 (60.00) 9 (11.69) 5 (41.67)
11.41 (4.16) 13.14 (4.05) 11.90 (4.42) 11.50 (5.45) 10.75 (4.48) 9.62 (3.26)9.39 (4.21) 10.65 (4.62) 9.29 (3.83) 11.75 (5.19) 8.23 (3.78) 8.25 (4.17)
12.52 (3.40) 13.22 (3.70) 12.26 (3.62) 11.50 (4.36) 12.95 (3.08) 9.62 (4.34)4.83 (2.26) 3.90 (2.43) 4.70 (2.55) 3.75 (2.22) 5.26 (2.09) 5.43 (1.51)9.48 (4.85) 10.61 (4.15) 9.07 (4.59) 10.00 (5.29) 7.65 (4.34) 9.25 (3.20)
16.83 (3.30) 16.17 (2.71) 16.27 (3.34) 14.25 (2.36) 17.85 (3.67) 15.25 (3.81)
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1053SUICIDE ATTEMPTS IN WOMEN WITH EATING DISORDERS

comes (Takakura et al., 2006) and psychiatric comorbidity(Peat, Mitchell, Hoek, & Wonderlich, 2009). Our results revealthat this pattern holds in population-based samples as wellclinical samples. In aggregate, these results underscore thecritical importance of flagging these individuals in the clinicalsetting as high risk for an array of adverse outcomes, includingsuicide attempts.
Unlike previous studies of women who sought treatment forEDs, we did not find clear differences in personality measuresbetween those who did and did not attempt suicide. This may be anartifact of the fact that the personality measures in STAGE werenot necessarily completed contemporaneously with the suicideattempts, whereas measurements in treatment-seeking samplescapture extremes of personality evident during the acute phase ofillness (Perkins et al., 2005). Moreover, some of the personalitymeasures assessed in the STAGE cohort are not ones commonlyassociated with suicide risk (e.g., perfectionism).
Our sample is uniquely informative by referencing apopulation-based register to identify ED cases. This approacheliminates the biases inherent in relying on samples of individ-uals seeking treatment for an ED, which skews observationstoward the extreme. By coupling this population-based samplewith hospital and cause of death registers, we were able tocapture those suicide attempts that were sufficiently severe towarrant medical attention. This methodology yields a clearpicture of risk of suicide attempts individuals with EDs in thegeneral population. As there is no evidence of elevated risk ofsuicide in twins (Statham et al., 1998), our results from theSTAGE sample are likely to generalize to the nontwin popula-tion.
Strengths
One strength of this study is the sample, which was large andpopulation-based. Such a sample decreases the biases inherent inusing treatment-seeking populations that are likely to have a moresevere ED and be more psychologically distressed. EDs, particu-larly BN, often go undetected in the community (Hoek, 1991;Hudson et al., 2007). Therefore, a woman is likely to seek treat-ment if (a) her disorder is sufficiently severe to be noticed byothers who encourage treatment, (b) she is highly distressed by herdisorder, (c) she has a comorbid disorder for which she is seekingtreatment, or (d) she is hospitalized for a suicide attempt and thenreferred for treatment of her ED. Therefore, the previous relianceon samples of individuals seeking treatment for an ED may haveinflated the estimates of the prevalence of suicide attempts.
By estimating the prevalence of suicide attempts from hospitaldischarge registers and cause of death registers, we opted for aconservative estimate not subject to self-report bias. Furthermore, theuse of the cause of death register, albeit for a restricted interval,allowed for the identification of completed suicides. A longer obser-vation period would allow for direct comparisons of those individualswho completed assessments at a point in time after a suicide attemptwith individuals who attempted suicide after completing assessments.
Limitations
Although this study makes a significant contribution to theliterature, several limitations should be noted. First, the study is of
Swedish twins. Although twin registers are often used to conductresearch about the general population, twins may differ from thegeneral population in significant ways. The population of Swedenis also fairly homogeneous in terms of racial and ethnic demo-graphics. Therefore, results must be interpreted within the contextof limited generalizability.
By estimating the prevalence of suicide attempts via the hospitalregister, we were unable to identify those suicide attempts that didnot warrant medical attention. This yields a conservative estimate;thus, the findings of this study may apply primarily to individualswith more severe suicide attempts.
STAGE was chosen for this study because of the large sample sizeand detailed information about ED behaviors. However, we werenonetheless faced with fairly small cell sizes—especially in ANR andBED—which left us underpowered for some comparisons. In addi-tion, as only the lifetime presence of ED behaviors and diagnoseswere assessed, we did not have information on illness duration orstatus of illness (currently ill or recovered) at the time of assessment.
The STAGE assessment covers a wide range of physical andpsychological variables. Unfortunately, given the large number ofvariables being assessed, not all of the constructs were assessed indepth. For example, Criterion B of GAD, difficulty controlling worry,was not assessed and therefore not required for participants to receivea diagnosis of GAD. Specific phobia, OCD, and panic disorderwere assessed with a single yes–no self-report item, limiting thevalidity of these diagnoses. Age of onset and status of illness(currently ill or recovered) at the time of assessment were notassessed for any of the comorbid diagnoses, which precluded theinvestigation of temporal precedence of eating disorders, comorbiddisorders, and suicide attempts. Furthermore, personality disorderswere not assessed.
Conclusion
Suicide attempts in women with EDs in the general populationare concerningly common. Suicide risk is elevated in all EDsstudied here—ANR, ANBP, ANBN, BN, PD, and BED. To im-prove outcomes and decrease mortality, it is critical to identifyindividuals who, within this patient population, experience psy-chological suffering so intense that they feel compelled to taketheir own lives.
References
Allebeck, P. (2009). The use of population-based registers in psychiatricresearch. Acta Psychiatrica Scandinavica, 120, 386–391. doi:10.1111/j.1600-0447.2009.01474.x
American Psychiatric Association. (1994). Diagnostic and statisticalmanual of mental disorders (4th ed.). Washington, DC: Author.
American Psychiatric Association. (2000). Diagnostic and statisticalmanual of mental disorders (4th ed., text rev.). Washington, DC:Author.
American Psychiatric Association. (2013). Diagnostic and statistical man-ual of mental disorders (5th ed.). Washington, DC: Author.
Anderson, C. B., Carter, F. A., McIntosh, V. V., Joyce, P. R., & Bulik,C. M. (2002). Self-harm and suicide attempts in individuals with bulimianervosa. Eating Disorders: Journal of Treatment and Prevention, 10,227–243. doi:10.1002/erv.472
Arcelus, J., Mitchell, A. J., Wales, J., & Nielsen, S. (2011). Mortality ratesin patients with anorexia nervosa and other eating disorders: A meta-
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1054 PISETSKY ET AL.

analysis of 36 studies. Archives of General Psychiatry, 68, 724–731.doi:10.1001/archgenpsychiatry.2011.74
Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discoveryrate: A practical and powerful approach to multiple testing. Journal ofthe Royal Statistical Society: Series B, 57, 289–300.
Berkman, N. D., Bulik, C. M., Brownley, K. A., Lohr, K. N., Sedway,J. A., Rooks, A., & Gartlehner, G. (2006). Management of eatingdisorders (Evidence Report: Technology Assessment No. 135). Rock-ville, MD: U.S. Department of Health and Human Services.
Bulik, C. M., Sullivan, P. F., Fear, J., & Pickering, A. (1997). Predictors ofthe development of bulimia nervosa in women with anorexia nervosa.Journal of Nervous and Mental Disease, 185, 704–707. doi:10.1097/00005053-199711000-00009
Bulik, C. M., Sullivan, P. F., & Joyce, P. R. (1999). Temperament,character and suicide attempts in anorexia nervosa, bulimia nervosa andmajor depression. Acta Psychiatrica Scandinavica, 100, 27–32. doi:10.1111/j.1600-0447.1999.tb10910.x
Bulik, C. M., Sullivan, P. F., & Kendler, K. S. (2000). An empirical studyof the classification of eating disorders. The American Journal of Psy-chiatry, 157, 886–895. doi:10.1176/appi.ajp.157.6.886
Bulik, C. M., Thornton, L., Pinheiro, A. P., Plotnicov, K., Klump, K. L.,Brandt, H., . . . Kaye, W. H. (2008). Suicide attempts in anorexianervosa. Psychosomatic Medicine, 70, 378 –383. doi:10.1097/PSY.0b013e3181646765
Carano, A., De Berardis, D., Campanella, D., Serroni, N., Ferri, F., Di Iorio,G., . . . Di Giannantonio, M. (2012). Alexithymia and suicide ideation in asample of patients with binge eating disorder. Journal of Psychiatric Prac-tice, 18, 5–11. doi:10.1097/01.pra.0000410982.08229.99
Chen, H., Cohen, P., & Chen, S. (2010). How big is a big odds ratio?Interpreting the magnitudes of odds ratios in epidemiological studies.Communications in Statistics—Simulation and Computation, 39, 860–864. doi:10.1080/03610911003650383
Cloninger, C. R. (1994). Temperament and personality. Current Opinion inNeurobiology, 4, 266–273. doi:10.1016/0959-4388(94)90083-3
Corcos, M., Taieb, O., Benoit-Lamy, S., Paterniti, S., Jeammet, P., &Flament, M. F. (2002). Suicide attempts in women with bulimia nervosa:Frequency and characteristics. Acta Psychiatrica Scandinavica, 106,381–386. doi:10.1034/j.1600-0447.2002.02318.x
Eddy, K. T., Dorer, D. J., Franko, D. L., Tahilani, K., Thompson-Brenner,H., & Herzog, D. B. (2008). Diagnostic crossover in anorexia nervosaand bulimia nervosa: Implications for DSM–V. The American Journal ofPsychiatry, 165, 245–250. doi:10.1176/appi.ajp.2007.07060951
Engström, C., Brandstrom, S., Sigvardsson, S., Cloninger, C. R., & Ny-lander, P. O. (2004). Bipolar disorder: III. Harm avoidance a risk factorfor suicide attempts. Bipolar Disorders, 6, 130–138. doi:10.1111/j.1399-5618.2004.00101.x
Favaro, A., & Santonastaso, P. (1996). Purging behaviors, suicide attempts,and psychiatric symptoms in 398 eating disordered subjects. Interna-tional Journal of Eating Disorders, 20, 99 –103. doi:10.1002/(SICI)1098-108X(199607)20:1�99::AID-EAT11�3.0.CO;2-E
Favaro, A., & Santonastaso, P. (1997). Suicidality in eating disorders:Clinical and psychological correlates. Acta Psychiatrica Scandinavica,95, 508–514. doi:10.1111/j.1600-0447.1997.tb10139.x
Favaro, A., Tenconi, E., & Santonastaso, P. (2006). Perinatal factors andthe risk of developing anorexia nervosa and bulimia nervosa. Archives ofGeneral Psychiatry, 63, 82–88. doi:10.1001/archpsyc.63.1.82
Fichter, M. M., & Quadflieg, N. (2007). Long-term stability of eatingdisorder diagnoses. International Journal of Eating Disorders,40(Suppl. 3), S61–S66. doi:10.1002/eat.20443
First, M. B., Spitzer, R., Gibbon, M., & Williams, J. B. (2002). StructuredClinical Interview for DSM–IV–TR Axis I Disorders, Research Version,Patient Edition (SCID-I/P). New York, NY: Biometrics Research, NewYork State Psychiatric Institute.
Forcano, L., Alvarez, E., Santamaria, J. J., Jimenez-Murcia, S., Granero,R., Penelo, E., . . . Fernandez-Aranda, F. (2011). Suicide attempts inanorexia nervosa subtypes. Comprehensive Psychiatry, 52, 352–358.doi:10.1016/j.comppsych.2010.09.003
Forcano, L., Fernandez-Aranda, F., Alvarez-Moya, E., Bulik, C., Granero,R., Gratacos, M., . . . Estivill, X. (2009). Suicide attempts in bulimianervosa: Personality and psychopathological correlates. European Psy-chiatry, 24, 91–97. doi:10.1016/j.eurpsy.2008.10.002
Franko, D., & Keel, P. (2006). Suicidality in eating disorders: Occurrence,correlates, and clinical implications. Clinical Psychology Review, 26,769–782. doi:10.1016/j.cpr.2006.04.001
Franko, D., Keel, P., Dorer, D., Blais, M., Delinsky, S., Eddy, K., . . .Herzog, D. (2004). What predicts suicide attempts in women with eatingdisorders? Psychological Medicine, 34, 843– 853. doi:10.1017/S0033291703001545
Frost, R., Marten, P., Lahart, C., & Rosenblate, R. (1990). The dimensionsof perfectionism. Cognitive Therapy and Research, 14, 449–468. doi:10.1007/BF01172967
Furberg, H., Lichtenstein, P., Pedersen, N. L., Thornton, L., Bulik, C. M.,Lerman, C., & Sullivan, P. F. (2008). The STAGE cohort: A prospectivestudy of tobacco use among Swedish twins. Nicotine & Tobacco Re-search, 10, 1727–1735. doi:10.1080/14622200802443551
Herzog, D. B., Dorer, D. J., Keel, P. K., Selwyn, S. E., Ekeblad, E. R.,Flores, A. T., . . . Keller, M. B. (1999). Recovery and relapse in anorexiaand bulimia nervosa: A 7.5-year follow-up study. Journal of the Amer-ican Academy of Child & Adolescent Psychiatry, 38, 829–837. doi:10.1097/00004583-199907000-00012
Hoek, H. W. (1991). The incidence and prevalence of anorexia nervosa andbulimia nervosa in primary care. Psychological Medicine, 21, 455–460.doi:10.1017/S0033291700020560
Hudson, J. I., Hiripi, E., Pope, H. G., Jr., & Kessler, R. C. (2007). Theprevalence and correlates of eating disorders in the National Comorbid-ity Survey Replication. Biological Psychiatry, 61, 348 –358. doi:10.1016/j.biopsych.2006.03.040
Keel, P. K., & Striegel-Moore, R. H. (2009). The validity and clinicalutility of purging disorder. International Journal of Eating Disorders,42, 706–719. doi:10.1002/eat.20718
Lichtenstein, P., De Faire, U., Floderus, B., Svartengren, M., Svedberg, P.,& Pedersen, N. (2002). The Swedish Twin Registry: A unique resourcefor clinical, epidemiological and genetic studies. Journal of InternalMedicine, 252, 184–205. doi:10.1046/j.1365-2796.2002.01032.x
Lichtenstein, P., Sullivan, P. F., Cnattingius, S., Gatz, M., Johansson, S.,Carlstrom, E., . . . Pedersen, N. L. (2006). The Swedish Twin Registryin the third millennium: An update. Twin Research and Human Genet-ics, 9, 875–882. doi:10.1375/twin.9.6.875
Ludvigsson, J. F., Andersson, E., Ekbom, A., Feychting, M., Kim, J. L.,Reuterwall, C., . . . Olausson, P. O. (2011). External review and vali-dation of the Swedish National Inpatient Register. BMC Public Health,11, 450. doi:10.1186/1471-2458-11-450
Ludvigsson, J. F., Otterblad-Olausson, P., Pettersson, B. U., & Ekbom, A.(2009). The Swedish personal identity number: Possibilities and pitfallsin healthcare and medical research. European Journal of Epidemiology,24, 659–667. doi:10.1007/s10654-009-9350-y
McGirr, A., Paris, J., Lesage, A., Renaud, J., & Turecki, G. (2007). Riskfactors for suicide completion in borderline personality disorder: Acase–control study of Cluster B comorbidity and impulsive aggression.Journal of Clinical Psychiatry, 68, 721–729. doi:10.4088/JCP.v68n0509
Milos, G., Spindler, A., Hepp, U., & Schnyder, U. (2004). Suicide attemptsand suicidal ideation: Links with psychiatric comorbidity in eatingdisorder subjects. General Hospital Psychiatry, 26, 129 –135. doi:10.1016/j.genhosppsych.2003.10.005
National Board of Health and Welfare. (2010). Causes of death 2008.Stockholm, Sweden: Author. Retrieved from http://www.socialstyrelsen.se/register/halsodataregister/patientregistret/inenglish
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1055SUICIDE ATTEMPTS IN WOMEN WITH EATING DISORDERS

Peat, C., Mitchell, J. E., Hoek, H. W., & Wonderlich, S. A. (2009). Validityand utility of subtyping anorexia nervosa. International Journal ofEating Disorders, 42, 590–594. doi:10.1002/eat.20717
Perkins, P. S., Klump, K. L., Iacono, W. G., McGue, M. (2005). Person-ality traits in women with anorexia nervosa: evidence for a treatment-seeking bias? International Journal of Eating Disorders, 37, 32–7.
Preti, A., Rocchi, M. B., Sisti, D., Camboni, M. V., & Miotto, P. (2011).A comprehensive meta-analysis of the risk of suicide in eating disorders.Acta Psychiatrica Scandinavica, 124, 6–17. doi:10.1111/j.1600-0447.2010.01641.x
Root, T. L., Pisetsky, E. M., Thornton, L., Lichtenstein, P., Pedersen, N. L.,& Bulik, C. M. (2010). Patterns of co-morbidity of eating disorders andsubstance use in Swedish females. Psychological Medicine, 40, 105–115. doi:10.1017/S0033291709005662
Ruchkin, V. V., Schwab-Stone, M., Koposov, R. A., Vermeiren, R., &King, R. A. (2003). Suicidal ideations and attempts in juvenile delin-quents. Journal of Child Psychology and Psychiatry, 44, 1058–1066.doi:10.1111/1469-7610.00190
Schapiro, I. R., Ross-Petersen, L., Saelan, H., Garde, K., Olsen, J. H., &Johansen, C. (2001). Extroversion and neuroticism and the associatedrisk of cancer: A Danish cohort study. American Journal of Epidemiol-ogy, 153, 757–763. doi:10.1093/aje/153.8.757
Statham, D. J., Heath, A. C., Madden, P. A., Bucholz, K. K., Bierut, L.,Dinwiddie, S. H., . . . Martin, N. G. (1998). Suicidal behaviour: Anepidemiological and genetic study. Psychological Medicine, 28, 839–855. doi:10.1017/S0033291798006916
Takakura, S., Nozaki, T., Nomura, Y., Koreeda, C., Urabe, H., Kawai, K.,. . . Kubo, C. (2006). Factors related to renal dysfunction in patients withanorexia nervosa. Eating and Weight Disorders, 11, 73–77.
Tozzi, F., Thornton, L., Klump, K., Bulik, C., Fichter, M., Halmi, K., . . .Kaye, W. (2005). Symptom fluctuation in eating disorders: Correlates ofdiagnostic crossover. The American Journal of Psychiatry, 162, 732–740. doi:10.1176/appi.ajp.162.4.732
Trace, S. E., Thornton, L. M., Root, T. L., Mazzeo, S. E., Lichtenstein, P.,Pedersen, N. L., & Bulik, C. M. (2012). Effects of reducing the fre-quency and duration criteria for binge eating on lifetime prevalence ofbulimia nervosa and binge eating disorder: Implications for DSM–5.International Journal of Eating Disorders, 45, 531–536. doi:10.1002/eat.20955
van Heeringen, C., Audenaert, K., Van Laere, K., Dumont, F., Slegers, G.,Mertens, J., & Dierckx, R. A. (2003). Prefrontal 5-HT2a receptor bind-ing index, hopelessness and personality characteristics in attemptedsuicide. Journal of Affective Disorders, 74, 149–158. doi:10.1016/S0165-0327(01)00482-7
World Health Organization. (1967). International classification of diseases(8th rev. ed.). Geneva, Switzerland: Author.
World Health Organization. (1978). International classification of diseases(9th rev. ed.). Geneva, Switzerland: Author.
World Health Organization. (1992). International classification of diseases(10th rev. ed.). Geneva, Switzerland: Author.
Zouk, H., Tousignant, M., Seguin, M., Lesage, A., & Turecki, G. (2006).Characterization of impulsivity in suicide completers: Clinical, behav-ioral and psychosocial dimensions. Journal of Affective Disorders, 92,195–204. doi:10.1016/j.jad.2006.01.016
Received January 7, 2013Revision received October 1, 2013
Accepted October 1, 2013 �
New Editors Appointed, 2015–2020
The Publications and Communications Board of the American Psychological Association an-nounces the appointment of 6 new editors for 6-year terms beginning in 2015. As of January 1,2014, manuscripts should be directed as follows:
● Behavioral Neuroscience (http://www.apa.org/pubs/journals/bne/), Rebecca Burwell, PhD,Brown University
● Journal of Applied Psychology (http://www.apa.org/pubs/journals/apl/), Gilad Chen, PhD,University of Maryland
● Journal of Educational Psychology (http://www.apa.org/pubs/journals/edu/), Steve Graham,EdD, Arizona State University
● JPSP: Interpersonal Relations and Group Processes (http://www.apa.org/pubs/journals/psp/),Kerry Kawakami, PhD, York University, Toronto, Ontario, Canada
● Psychological Bulletin (http://www.apa.org/pubs/journals/bul/), Dolores Albarracín, PhD,University of Pennsylvania
● Psychology of Addictive Behaviors (http://www.apa.org/pubs/journals/adb/), Nancy M. Petry,PhD, University of Connecticut School of Medicine
Electronic manuscript submission: As of January 1, 2014, manuscripts should be submittedelectronically to the new editors via the journal’s Manuscript Submission Portal (see the websitelisted above with each journal title).
Current editors Mark Blumberg, PhD, Steve Kozlowski, PhD, Arthur Graesser, PhD, JeffrySimpson, PhD, Stephen Hinshaw, PhD, and Stephen Maisto, PhD, will receive and consider newmanuscripts through December 31, 2013.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
1056 PISETSKY ET AL.





























