Embed Size (px)
Citation preview
ORIGINAL CONTRIBUTION
Sumatriptan-Naproxen for Acute Treatmentof MigraineA Randomized TrialJan Lewis Brandes, MDDavid Kudrow, MDStuart R. Stark, MDC. Phillip O’Carroll, MDJames U. Adelman, MDFrancis J. O’Donnell, DOW. James Alexander, MD, MPHSusan E. Spruill, MSPamela S. Barrett, PharmDShelly E. Lener, PharmD
MIGRAINE IS A PREVALENT,often debilitating dis-ease manifested by at-tacks of bilateral or uni-
lateral headache and associatedsymptoms, such as nausea, vomiting,and sensitivity to light and sound.1-3 Thepast 15 years have witnessed advancesin migraine therapy with the introduc-tion in the United States of several ef-fective agents, including 7 triptans.However, therapeutic shortfalls re-main. Some patients do not achieveheadache relief by 2 hours after ingest-ing oral migraine medications, and re-currence of headache within 24 hoursof initial dosing is common.4 Many pa-tients treated with migraine-specifictherapy are less than fully satisfied withtreatment.5,6
The challenges in optimizing effi-cacy of migraine pharmacotherapy arepartly attributed to the complex patho-physiology of migraine. None of the cur-rently available monotherapeutic agentsprovides broad coverage of the mul-tiple pathogenic processes in migraine,which is thought to involve multipleneural pathways that appear to be se-
Author Affiliations: Nashville Neuroscience Group,Nashville, Tenn (Dr Brandes); California Medical Clinicfor Headache, Santa Monica (Dr Kudrow); The Inno-vative Clinical Research Center, Alexandria, Va (DrStark); Headache Institute, Newport Beach, Calif (DrO’Carroll); Headache Wellness Center, Greensboro,NC (Dr Adelman); OrthoNeuro, Columbus, Ohio
(Dr O’Donnell); Pozen Inc, Chapel Hill, NC (Dr Alex-ander and Ms Spruill); and GlaxoSmithKline, Re-search Triangle Park, NC (Drs Barrett and Lener).Corresponding Author: Jan Lewis Brandes, MD, Nash-ville Neuroscience Group, 300 20th Ave N, #603, Nash-ville, TN 37203 ([email protected]).
Context Multiple pathogenic mechanisms may be involved in generating the mi-graine symptom complex, and multimechanism-targeted therapy may confer advan-tages over monotherapy.
Objective To evaluate the efficacy and safety of a fixed-dose tablet containing su-matriptan succinate and naproxen sodium relative to efficacy and safety of each mono-therapy and placebo for the acute treatment of migraine.
Design, Setting, and Participants Two replicate, randomized, double-blind, single-attack, parallel-group studies conducted among 1461 (study 1) and 1495 (study 2)patients at 118 US clinical centers who were diagnosed as having migraine and re-ceived study treatment for a moderate or severe migraine attack.
Interventions Patients were randomized in a 1:1:1:1 ratio to receive a single tabletcontaining sumatriptan, 85 mg, and naproxen sodium, 500 mg; sumatriptan, 85 mg(monotherapy); naproxen sodium, 500 mg (monotherapy); or placebo, to be used af-ter onset of a migraine with moderate to severe pain.
Main Outcome Measures Primary outcome measures included the percentages ofpatients with headache relief 2 hours after dosing, absence of photophobia, absence ofphonophobia, andabsenceofnausea for thecomparisonbetweensumatriptan–naproxensodium and placebo, and the percentages of patients with sustained pain-free responsefor the comparison between sumatriptan–naproxen sodium and each monotherapy.
Results Sumatriptan–naproxen sodium was more effective than placebo for headacherelief at 2 hours after dosing (study 1, 65% vs 28%; P�.001 and study 2, 57% vs 29%;P�.001), absence of photophobia at 2 hours (58% vs 26%; P�.001 and 50% vs 32%;P�.001),andabsenceofphonophobiaat2hours (61%vs38%;P�.001and56%vs34%;P�.001).Theabsenceofnausea2hoursafterdosingwashigherwithsumatriptan–naproxensodium than placebo in study 1 (71% vs 65%; P=.007), but in study 2 rates of absence ofnausea did not differ between sumatriptan–naproxen sodium and placebo (65% vs 64%;P=.71). For 2- to 24-hour sustained pain-free response, sumatriptan–naproxen sodiumwassuperioratP�.01(25%and23%instudies1and2, respectively) tosumatriptanmono-therapy(16%and14%instudies1and2),naproxensodiummonotherapy(10%and10%in studies 1 and 2), and placebo (8% and 7% in studies 1 and 2). The incidence of adverseeventswas similarbetweensumatriptan–naproxensodiumandsumatriptanmonotherapy.
Conclusion Sumatriptan, 85 mg, plus naproxen sodium, 500 mg, as a single tablet foracute treatment of migraine resulted in more favorable clinical benefits compared witheither monotherapy, with an acceptable and well-tolerated adverse effect profile.
Trial Registration clinicaltrials.gov Identifiers: NCT00434083 (study 1); NCT00433732(study 2)JAMA. 2007;297:1443-1454 www.jama.com
©2007 American Medical Association. All rights reserved. (Reprinted) JAMA, April 4, 2007—Vol 297, No. 13 1443
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

quentially activated and sensitized as amigraine attack develops.3,7 Early in thecourse of a migraine attack, trigeminalnerve endings, possibly stimulated bycortical spreading depression, release va-soactive and inflammatory substances,including calcitonin gene-related pep-tide and kinins. Calcitonin gene-related peptide causes meningeal vaso-dilation, and kinins induce inflammatoryprostaglandins.8 The resulting menin-geal and vascular inflammation and va-sodilation cause peripheral sensitiza-tion and stimulate trigeminal nociceptorsto activate ascending pain pathways.9
The initial activation of central path-ways during the early stages of a mi-graine attack depends on incoming painsignals from the periphery; without pe-ripheral input, central activation ceases.With prolonged nociceptive stimula-tion, glia surrounding the trigeminalnucleus caudalis become activated andrelease neuromodulators, includingprostaglandins. The prostaglandins mayamplify the pain signal and, with othersubstances, cause trigeminal nucleuscaudalis neurons to fire in a sustained,continuous manner that is characteris-tic of the central sensitization hypoth-esized to underlie a full-blown mi-graine attack.10,11 Unlike initial activationof central pathways during the earlystages of a migraine attack, central sen-sitization appears to be independent ofperipheral neural input.12-16
Because multiple pathogenic mecha-nisms are putatively involved in gen-eration of the migraine symptom com-plex, multimechanism-targeted therapymay confer advantages over indi-vidual monotherapy. Drugs within 2classes of migraine pharmacotherapy—triptans and nonsteroidal anti-inflammatory drugs (NSAIDs)—target distinct aspects of the vascularand inflammatory processes hypoth-esized to underlie migraine. Triptans re-duce calcitonin gene-related peptide–mediated vasodilation, inhibit releaseof inflammatory mediators from tri-geminal nerves, and decrease transmis-sion of pain impulses to the trigemi-nal nucleus caudalis.9,11 Data fromanimal models and studies in mi-
graine patients suggest that triptans in-hibit synaptic transmission between theperipheral and central neurons andthereby interrupt activation of centralpathways during the early stages of amigraine attack—before central sensi-tization, which is independent of pe-ripheral input, has developed.14,15
NSAIDs inhibit the synthesis of pros-taglandins and may mitigate menin-geal inflammation while preventing orreversing central sensitization arisingfrom activation of glial cells in the brainstem.17 In a recent study, the NSAIDnaproxen suppressed sensitization ofcentral trigeminovascular neurons inthe spinal trigeminal nucleus in an ani-mal model of intracranial pain.18
Together, a triptan and an NSAID hy-pothetically alter both peripheral acti-vation of central pathways during theearly stages of a migraine attack and thelater developing central sensitization thatis independent of peripheral input. Re-sults of several clinical studies supportthis possibility,19-22 particularly with theconcomitant use of sumatriptan succi-nate and naproxen sodium. Data sug-gest that the combination of sumatrip-tan succinate and naproxen sodium maybe useful both in enhancing acute re-lief and conferring a prolonged thera-peutic response.19,20 The latter finding isconsistent both with the aforemen-tioned mechanistic considerations andwith the long half-life (12-17 hours) ofnaproxen.23
A tablet specifically formulated withsumatriptan succinate, equivalent to su-matriptan, 85 mg, and naproxen so-dium, 500 mg (hereafter sumatriptan–naproxen sodium), has been developedfor the acute treatment of migraine. Thetechnology used in the formulation ofsumatriptan is a fast-disintegrating,rapid-release formulation designed to fa-cilitate tablet disintegration and drug dis-persion and mitigate the effects of gas-tric stasis that can accompany migraine.Development of a combination therapywas motivated by the rationale that con-comitant use of a triptan and an NSAIDmight confer additive efficacy relative tothat with use of either triptans orNSAIDs alone.19,20 This article de-
scribes the results of 2 replicate random-ized, double-blind clinical trials con-ducted to evaluate the efficacy and safetyof sumatriptan–naproxen sodium com-pared with placebo and with mono-therapy with sumatriptan succinate ornaproxen sodium in the acute treat-ment of migraine.
METHODSPatients
Men and nonpregnant, nonlactatingwomen were eligible for the studies ifthey were between 18 and 65 years ofage, had at least a 6-month history ofmigraine with or without aura as de-fined by the International Headache So-ciety criteria,24,25 had an average of 2 to6 moderate or severe migraine epi-sodes monthly during the 3 monthspreceding the screening visit, and coulddistinguish migraine episodes fromother types of headache. Women hadto be physiologically incapable of be-coming pregnant or, if they could be-come pregnant, had to agree to prac-tice adequate contraception during thestudy. Site personnel asked each par-ticipant to self-identify their race andethnicity and, if needed, the choicesand/or further clarification would beprovided to assist in the process. If theparticipant did not self-identify with anycategory, “other” or “unknown” was en-tered. For the purposes of this article,the categories were collapsed to white,black, and other.
Patients were excluded if they hadmore than 6 migraine attacks monthlyduring either of the 2 months beforescreening; chronic daily headache (�15days per month of nonmigraine head-aches during each of the 3 months be-fore screening); uncontrolled hyper-tension (diastolic blood pressure �95mm Hg or systolic blood pressure �160mm Hg); confirmed or suspected car-diovascular or cerebrovascular dis-ease; a history of cardiac arrhythmiasrequiring medication or clinically sig-nificant electrocardiogram abnormali-ties that, in the investigator’s opinion,contraindicated study participation; orbasilar or hemiplegic migraine. Otherexclusion criteria included current use
SUMATRIPTAN–NAPROXEN SODIUM FOR MIGRAINE TREATMENT
1444 JAMA, April 4, 2007—Vol 297, No. 13 (Reprinted) ©2007 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

or use within 3 months before screen-ing of migraine prophylactic medica-tion containing ergotamine, an ergot de-rivative, or methysergide; use of amonoamine oxidase inhibitor within 2weeks or preparations containing StJohn’s wort within 4 weeks beforescreening; and regular use of any anti-coagulant or NSAID (except aspirin,�325 mg/d, for cardiovascularprophylaxis).
Patients were eligible for the stud-ies regardless of whether they were trip-tan-naive. All patients provided writ-ten informed consent prior to studyparticipation.
Procedures
The protocols for these multicenterstudies were approved by ethics com-mittees or institutional review boardsfor each of the 118 US study sites. Studysites included primary care practices,neurology clinics, and headache clin-ics. Patient recruitment methods in-cluded advertisements, regular officevisits, and chart reviews. The studies,which were identically designed andconducted, consisted of a screening visitfollowed by outpatient treatment of asingle migraine attack and a follow-upvisit occurring 1 to 5 days after treat-ment. At the screening visit, patientsmeeting eligibility criteria were ran-domized 1:1:1:1 to receive one of thefollowing: a single tablet containing su-matriptan–naproxen sodium; a singletablet containing sumatriptan, 85 mg;a single tablet of naproxen sodium, 500mg; or placebo; and were dispensedblinded study medication. Patients wereinstructed to treat a migraine attackwith study medication when pain in-tensity was moderate or severe. Pa-tients were to treat a migraine within6 weeks of the screening visit. If a pa-tient failed to treat a migraine withinthese 6 weeks, he/she was allowed toreturn for rescreening and given an-other 6 weeks to treat. Patients were al-lowed to rescreen only once. Dosingregimens of migraine prophylaxis couldnot be changed (added, withdrawn, ordose changed) during the 2 weeks priorto treatment, including the use of cal-
cium channel blockers, tricyclic anti-depressants, �-blockers, or serotoner-gic medications for any other indication.No NSAIDs (except aspirin, �325mg/d, for cardiovascular prophy-laxis); analgesics containing mor-phine, codeine, or opioid derivatives;ergotamine-containing compounds; orserotonin agonists could be takenwithin 24 hours before treatment withstudy medication. No analgesics oracute migraine treatment (including an-tiemetics) could be taken within 6 hoursbefore treatment with study medica-tion. Patients were permitted to takerescue medication beginning 2 hoursafter dosing, as prescribed or recom-mended by their physicians, withthe exception of ergot-containingmedications, serotonin agonists, orNSAID-containing products. A sec-ond dose of study medication was notpermitted.
Patients recorded on diary cards de-tails about the migraine they treatedwith study medication and any use ofstudy medication or concomitant medi-cation. Pain severity was rated imme-diately before dosing; 0.5, 1, and 1.5hours after dosing; and hourly from 2to 24 hours after dosing on a 4-pointscale (0=none; 1=mild; 2=moderate;3=severe). Presence and absence ofnausea, photophobia, and phonopho-bia were also recorded at these points.At 24 hours after dosing, patients in-dicated whether they had vomited anytime during the 24-hour postdose pe-riod. Patients were required to stayawake to record pain and symptom as-sessments for the first 2 postdose hours.Sleeping was permitted between post-dose hours 2 and 4 as long as patientsawakened to record assessments at the3- and 4-hour points. After 4 hours af-ter dosing, patients were required tocomplete diary-card assessments onlywhen awake. If a patient missed any re-cording time, the last recorded obser-vation was carried forward to fill in themissed recording.
Outcome Measures
The primary objectives of the studieswere (1) to determine the efficacy of su-
matriptan–naproxen sodium vs pla-cebo as assessed by headache relief andthe incidences of photophobia, phono-phobia, and nausea 2 hours after dos-ing as primary outcome measures and(2) to evaluate the efficacy of suma-triptan–naproxen sodium comparedwith each monotherapy, using sus-tained pain-free response as the out-come measure.
There were 6 primary outcome mea-sures. The primary outcome measureswere chosen because they represent thespectrum of the key symptoms respon-sible for disability in migraine and mea-sure both the early (2-hour) and sus-tained (24-hour) relief of thesesymptoms. The first 4 of these out-come measures, which compared su-matriptan–naproxen sodium with pla-cebo, were the percentages of patientswho had headache relief 2 hours afterdosing (ie, the reduction of pain frommoderate/severe intensity to mild/nopain without use of rescue medicationat each of the prespecified time points),absence of photophobia, absence ofphonophobia, and absence of nausea.The other 2 outcome measures, whichcompared sumatriptan–naproxen so-dium with its individual components,were the percentages of patients withsustained pain-free response (ie, mod-erate or severe pain at treatment re-duced to no pain from 2 hours through24 hours after dosing with no use of res-cue medication).
A secondary efficacy outcome mea-sure 2 hours after dosing was the per-centage of patients with pain-free re-sponse (moderate or severe pain attreatment reduced to no pain). Second-ary efficacy outcome measures also in-cluded the percentages of patients withsustained headache relief (ie, moder-ate or severe pain at treatment re-duced to mild or no pain from 2 hoursthrough 24 hours after dosing, with nouse of rescue medication); sustainedfreedom from nausea, photophobia, andphonophobia from 2 through 24 hoursafter dosing; use of rescue medicationthrough 24 hours after dosing; andheadache recurrence (ie, return of mod-erate or severe pain within 24 hours of
SUMATRIPTAN–NAPROXEN SODIUM FOR MIGRAINE TREATMENT
©2007 American Medical Association. All rights reserved. (Reprinted) JAMA, April 4, 2007—Vol 297, No. 13 1445
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013
dosing among patients with headacherelief 2 hours after dosing). The inci-dence of any vomiting through 24 hoursafter dosing was also evaluated.
Clinical safety was assessed by cal-culating the incidence of specific ad-verse events, defined as any untowardmedical occurrences, regardless of theirsuspected cause, that were reported bya patient or noted by a clinician dur-ing the study.
Statistical AnalysesEfficacy data were analyzed for the in-tention-to-treat population, defined asrandomized participants who tookstudy medication, recorded baselinepain as moderate or severe, and had atleast 1 postbaseline efficacy evalua-tion. Participants who were random-ized but who did not have an oppor-tunity to treat a migraine during thestudy period were omitted from any
analysis of safety or efficacy, includ-ing the intention-to-treat analysis.
Baseline migraine characteristics andeach of the efficacy outcome measures(except recurrence, which was summa-rized with descriptive statistics only)were analyzed using the Cochran-Mantel-Haenszel test with 2 outcome cat-egories and with pooled investigator sitesas strata. Analyses of the outcome mea-sures at 2 hours after dosing were ad-
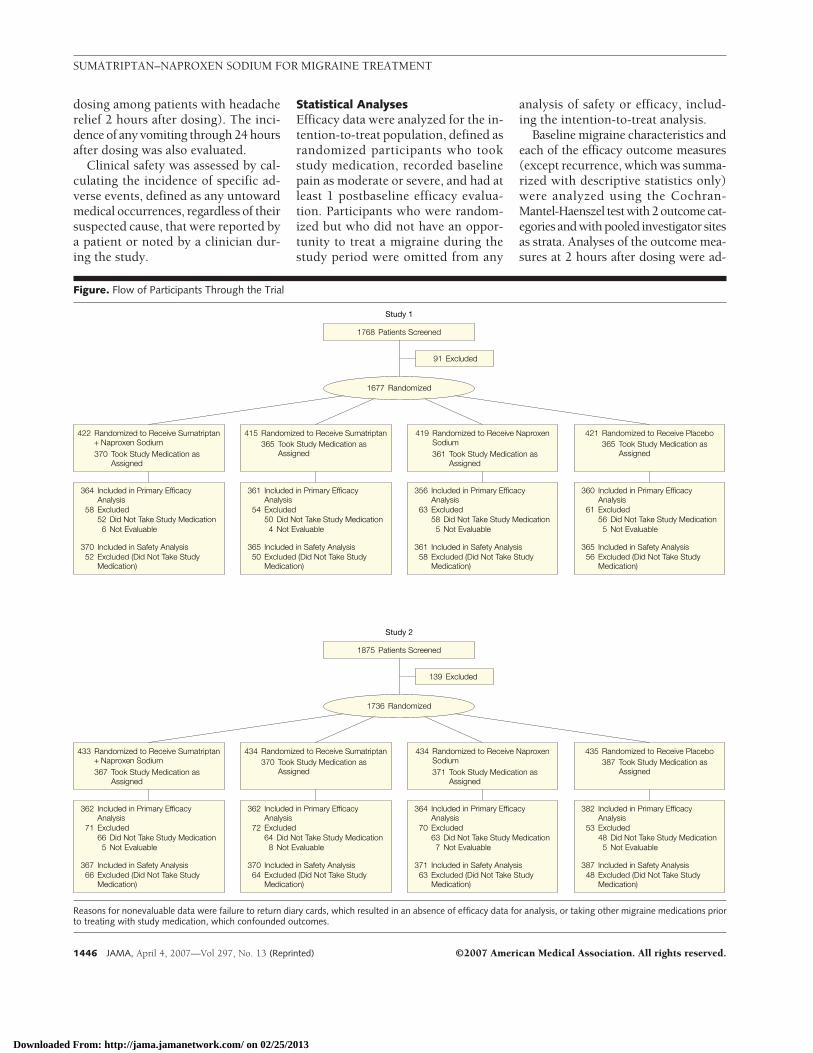
Figure. Flow of Participants Through the Trial
1677 Randomized
1768 Patients Screened
Study 1
370 Included in Safety Analysis52 Excluded (Did Not Take Study
Medication)
364 Included in Primary EfficacyAnalysis
58 Excluded52 Did Not Take Study Medication6 Not Evaluable
365 Included in Safety Analysis50 Excluded (Did Not Take Study
Medication)
361 Included in Primary EfficacyAnalysis
54 Excluded50 Did Not Take Study Medication4 Not Evaluable
361 Included in Safety Analysis58 Excluded (Did Not Take Study
Medication)
356 Included in Primary EfficacyAnalysis
63 Excluded58 Did Not Take Study Medication5 Not Evaluable
365 Included in Safety Analysis56 Excluded (Did Not Take Study
Medication)
360 Included in Primary EfficacyAnalysis
61 Excluded56 Did Not Take Study Medication5 Not Evaluable
367 Included in Safety Analysis66 Excluded (Did Not Take Study
Medication)
362 Included in Primary EfficacyAnalysis
71 Excluded66 Did Not Take Study Medication5 Not Evaluable
370 Included in Safety Analysis64 Excluded (Did Not Take Study
Medication)
362 Included in Primary EfficacyAnalysis
72 Excluded64 Did Not Take Study Medication8 Not Evaluable
371 Included in Safety Analysis63 Excluded (Did Not Take Study
Medication)
364 Included in Primary EfficacyAnalysis
70 Excluded63 Did Not Take Study Medication7 Not Evaluable
387 Included in Safety Analysis48 Excluded (Did Not Take Study
Medication)
382 Included in Primary EfficacyAnalysis
53 Excluded48 Did Not Take Study Medication5 Not Evaluable
422 Randomized to Receive Sumatriptan+ Naproxen Sodium370 Took Study Medication as
Assigned
419 Randomized to Receive NaproxenSodium361 Took Study Medication as
Assigned
415 Randomized to Receive Sumatriptan365 Took Study Medication as
Assigned
421 Randomized to Receive Placebo365 Took Study Medication as
Assigned
433 Randomized to Receive Sumatriptan+ Naproxen Sodium367 Took Study Medication as
Assigned
434 Randomized to Receive NaproxenSodium371 Took Study Medication as
Assigned
434 Randomized to Receive Sumatriptan370 Took Study Medication as
Assigned
435 Randomized to Receive Placebo387 Took Study Medication as
Assigned
91 Excluded
139 Excluded
1736 Randomized
1875 Patients Screened
Study 2
Reasons for nonevaluable data were failure to return diary cards, which resulted in an absence of efficacy data for analysis, or taking other migraine medications priorto treating with study medication, which confounded outcomes.
SUMATRIPTAN–NAPROXEN SODIUM FOR MIGRAINE TREATMENT
1446 JAMA, April 4, 2007—Vol 297, No. 13 (Reprinted) ©2007 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013
justed for anybaseline imbalancesamongtreatment groups for the symptoms of in-terest. For key secondary efficacy out-come measures, a hierarchical step-down procedure was used to control formultiplicity.26-30 Outcome measures weretested in the order specified below, withthe requirement that once the P value fora test on an outcome measure exceeded.05, outcome measures further down inthe order were not considered to be sta-tistically significant. The secondary com-parisons were tested in the following or-der: pain-free response at 2 hours forsumatriptan–naproxen sodium vs pla-cebo, sustained pain relief for sumatrip-tan–naproxen sodium vs placebo, sus-tained pain relief for sumatriptan–naproxen sodium vs sumatriptan,sustained freedom from symptoms forsumatriptan–naproxen sodium vs su-matriptan, use of rescue medication forsumatriptan–naproxen sodium vs su-matriptan, time to rescue for sumatrip-tan–naproxen sodium vs sumatriptan,pain relief at 4 hours for sumatriptan–naproxen sodium vs sumatriptan, free-dom from symptoms at 4 hours for su-matriptan–naproxen sodium vssumatriptan, pain relief at 2 hours for su-matriptan–naproxen sodium vs suma-triptan, and freedom from symptoms at2 hours for sumatriptan–naproxen so-dium vs sumatriptan. For the fourth sec-ondary outcome measure of sustainedfreedom from symptoms, the outcomemeasures were adjusted for rescue medi-cation and 3 separate analyses were per-formed. For patients who used rescuemedication, the worst possible score(symptoms present) was substituted forthe actual scores at the time of rescue andfor all subsequent time points. For thehierarchical step-down procedure, sta-tistically significant improvement withsumatriptan–naproxen sodium treat-ment in the associated symptoms (pho-tophobia, phonophobia, and nausea)considered together was interpreted asmeeting the significance criterion.
The sumatriptan–naproxen sodiumgroup was compared with placebo instatistical analyses of all outcome mea-sures except headache recurrence. Thesumatriptan–naproxen sodium group
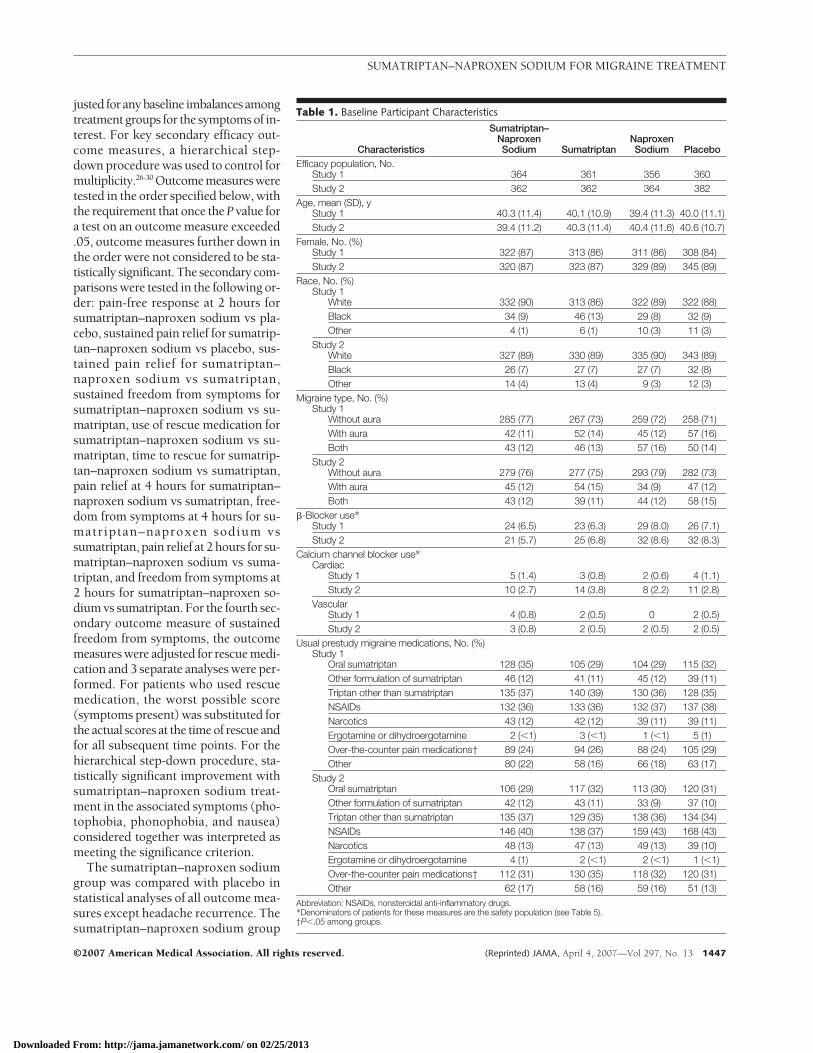
Table 1. Baseline Participant Characteristics
Characteristics
Sumatriptan–NaproxenSodium Sumatriptan
NaproxenSodium Placebo
Efficacy population, No.Study 1 364 361 356 360Study 2 362 362 364 382
Age, mean (SD), yStudy 1 40.3 (11.4) 40.1 (10.9) 39.4 (11.3) 40.0 (11.1)Study 2 39.4 (11.2) 40.3 (11.4) 40.4 (11.6) 40.6 (10.7)
Female, No. (%)Study 1 322 (87) 313 (86) 311 (86) 308 (84)Study 2 320 (87) 323 (87) 329 (89) 345 (89)
Race, No. (%)Study 1
White 332 (90) 313 (86) 322 (89) 322 (88)Black 34 (9) 46 (13) 29 (8) 32 (9)Other 4 (1) 6 (1) 10 (3) 11 (3)
Study 2White 327 (89) 330 (89) 335 (90) 343 (89)Black 26 (7) 27 (7) 27 (7) 32 (8)Other 14 (4) 13 (4) 9 (3) 12 (3)
Migraine type, No. (%)Study 1
Without aura 285 (77) 267 (73) 259 (72) 258 (71)With aura 42 (11) 52 (14) 45 (12) 57 (16)Both 43 (12) 46 (13) 57 (16) 50 (14)
Study 2Without aura 279 (76) 277 (75) 293 (79) 282 (73)With aura 45 (12) 54 (15) 34 (9) 47 (12)Both 43 (12) 39 (11) 44 (12) 58 (15)
�-Blocker use*Study 1 24 (6.5) 23 (6.3) 29 (8.0) 26 (7.1)Study 2 21 (5.7) 25 (6.8) 32 (8.6) 32 (8.3)
Calcium channel blocker use*Cardiac
Study 1 5 (1.4) 3 (0.8) 2 (0.6) 4 (1.1)Study 2 10 (2.7) 14 (3.8) 8 (2.2) 11 (2.8)
VascularStudy 1 4 (0.8) 2 (0.5) 0 2 (0.5)Study 2 3 (0.8) 2 (0.5) 2 (0.5) 2 (0.5)
Usual prestudy migraine medications, No. (%)Study 1
Oral sumatriptan 128 (35) 105 (29) 104 (29) 115 (32)Other formulation of sumatriptan 46 (12) 41 (11) 45 (12) 39 (11)Triptan other than sumatriptan 135 (37) 140 (39) 130 (36) 128 (35)NSAIDs 132 (36) 133 (36) 132 (37) 137 (38)Narcotics 43 (12) 42 (12) 39 (11) 39 (11)Ergotamine or dihydroergotamine 2 (�1) 3 (�1) 1 (�1) 5 (1)Over-the-counter pain medications† 89 (24) 94 (26) 88 (24) 105 (29)Other 80 (22) 58 (16) 66 (18) 63 (17)
Study 2Oral sumatriptan 106 (29) 117 (32) 113 (30) 120 (31)Other formulation of sumatriptan 42 (12) 43 (11) 33 (9) 37 (10)Triptan other than sumatriptan 135 (37) 129 (35) 138 (36) 134 (34)NSAIDs 146 (40) 138 (37) 159 (43) 168 (43)Narcotics 48 (13) 47 (13) 49 (13) 39 (10)Ergotamine or dihydroergotamine 4 (1) 2 (�1) 2 (�1) 1 (�1)Over-the-counter pain medications† 112 (31) 130 (35) 118 (32) 120 (31)Other 62 (17) 58 (16) 59 (16) 51 (13)
Abbreviation: NSAIDs, nonsteroidal anti-inflammatory drugs.*Denominators of patients for these measures are the safety population (see Table 5).†P�.05 among groups.
SUMATRIPTAN–NAPROXEN SODIUM FOR MIGRAINE TREATMENT
©2007 American Medical Association. All rights reserved. (Reprinted) JAMA, April 4, 2007—Vol 297, No. 13 1447
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013
was compared prospectively with thegroup given sumatriptan mono-therapy in statistical analyses of all ef-ficacy outcome measures except pain-free response 2 hours after dosing, anyvomiting through 24 hours after dos-ing, and headache recurrence. The su-matriptan–naproxen sodium group wascompared prospectively with the groupgiven naproxen sodium monotherapyfor the primary efficacy outcome mea-sures 2 hours after dosing.
Adverse event data were summa-rized for the safety population, de-fined as all patients who took studymedication and had available data. TheFisher exact test was used to compareincidences of adverse events in the su-matriptan–naproxen sodium groupwith those in the sumatriptan mono-therapy group, the naproxen mono-therapy group, and the placebo group.Only the incidences of overall adverseevents and overall events considered to
be treatment related were analyzed fortreatment group differences. All analy-ses of efficacy and safety were con-ducted using SAS software, version 9.1(SAS Institute Inc, Cary, NC).
RESULTSPatients
The FIGURE summarizes the disposi-tion of patients in each study. The num-bers of patients screened for the studywere 1768 in study 1 and 1875 in study2. Of those screened, the numbers ofpatients randomized to receive treat-ment were 1677 in study 1 and 1736in study 2. Safety analyses included the1461 patients in study 1 and 1495 pa-tients in study 2 who took study medi-cation and had evaluable safety data. Ef-ficacy analyses included 1441 patientsin study 1 and 1470 patients in study2 who took study medication, re-corded baseline pain as moderate or se-vere, and had at least 1 postbaseline ef-
ficacy evaluation. Among randomizedpatients, the primary reason that 216patients in study 1 and 241 in study 2were not included in the safety and ef-ficacy populations was because they didnot have the opportunity to treat aqualifying migraine episode before thestudies were concluded.
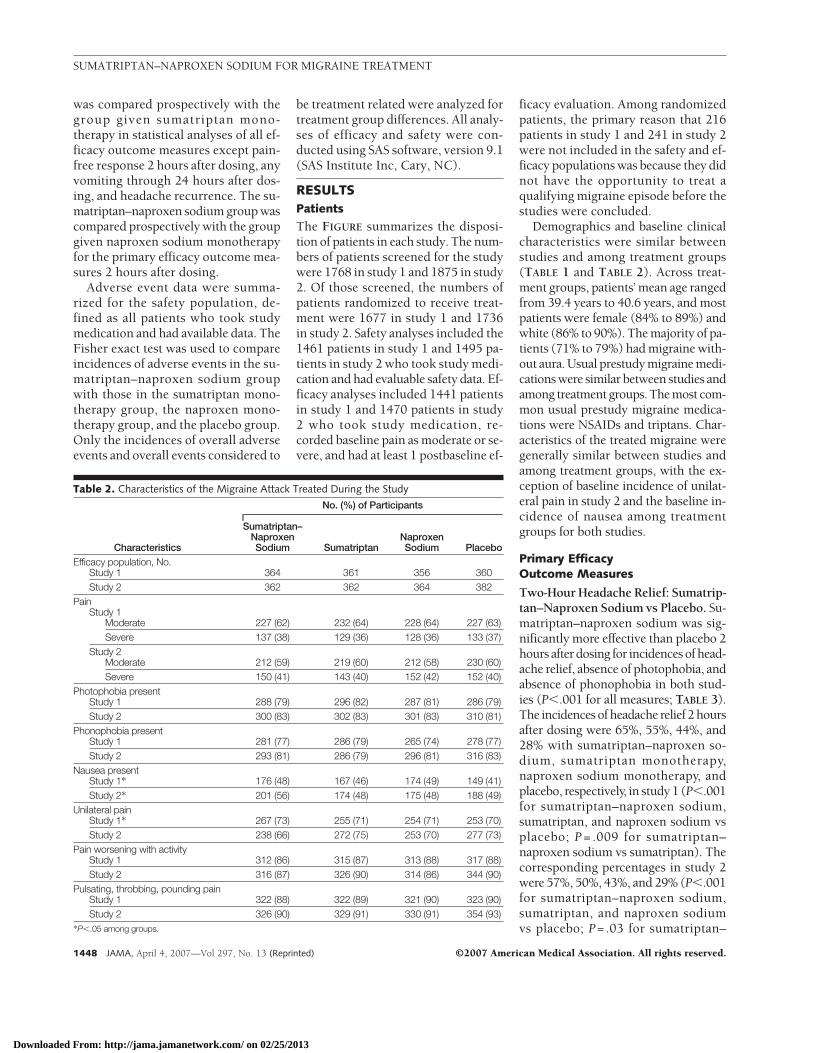
Demographics and baseline clinicalcharacteristics were similar betweenstudies and among treatment groups(TABLE 1 and TABLE 2). Across treat-ment groups, patients’ mean age rangedfrom 39.4 years to 40.6 years, and mostpatients were female (84% to 89%) andwhite (86% to 90%). The majority of pa-tients (71% to 79%) had migraine with-out aura. Usual prestudy migraine medi-cations were similar between studies andamong treatment groups. The most com-mon usual prestudy migraine medica-tions were NSAIDs and triptans. Char-acteristics of the treated migraine weregenerally similar between studies andamong treatment groups, with the ex-ception of baseline incidence of unilat-eral pain in study 2 and the baseline in-cidence of nausea among treatmentgroups for both studies.
Primary EfficacyOutcome Measures
Two-Hour Headache Relief: Sumatrip-tan–Naproxen Sodium vs Placebo. Su-matriptan–naproxen sodium was sig-nificantly more effective than placebo 2hours after dosing for incidences of head-ache relief, absence of photophobia, andabsence of phonophobia in both stud-ies (P�.001 for all measures; TABLE 3).The incidences of headache relief 2 hoursafter dosing were 65%, 55%, 44%, and28% with sumatriptan–naproxen so-dium, sumatriptan monotherapy,naproxen sodium monotherapy, andplacebo, respectively, in study 1 (P�.001for sumatriptan–naproxen sodium,sumatriptan, and naproxen sodium vsplacebo; P = .009 for sumatriptan–naproxen sodium vs sumatriptan). Thecorresponding percentages in study 2were 57%, 50%, 43%, and 29% (P�.001for sumatriptan–naproxen sodium,sumatriptan, and naproxen sodiumvs placebo; P= .03 for sumatriptan–
Table 2. Characteristics of the Migraine Attack Treated During the Study
Characteristics
No. (%) of Participants
Sumatriptan–NaproxenSodium Sumatriptan
NaproxenSodium Placebo
Efficacy population, No.Study 1 364 361 356 360Study 2 362 362 364 382
PainStudy 1
Moderate 227 (62) 232 (64) 228 (64) 227 (63)Severe 137 (38) 129 (36) 128 (36) 133 (37)
Study 2Moderate 212 (59) 219 (60) 212 (58) 230 (60)Severe 150 (41) 143 (40) 152 (42) 152 (40)
Photophobia presentStudy 1 288 (79) 296 (82) 287 (81) 286 (79)Study 2 300 (83) 302 (83) 301 (83) 310 (81)
Phonophobia presentStudy 1 281 (77) 286 (79) 265 (74) 278 (77)Study 2 293 (81) 286 (79) 296 (81) 316 (83)
Nausea presentStudy 1* 176 (48) 167 (46) 174 (49) 149 (41)Study 2* 201 (56) 174 (48) 175 (48) 188 (49)
Unilateral painStudy 1* 267 (73) 255 (71) 254 (71) 253 (70)Study 2 238 (66) 272 (75) 253 (70) 277 (73)
Pain worsening with activityStudy 1 312 (86) 315 (87) 313 (88) 317 (88)Study 2 316 (87) 326 (90) 314 (86) 344 (90)
Pulsating, throbbing, pounding painStudy 1 322 (88) 322 (89) 321 (90) 323 (90)Study 2 326 (90) 329 (91) 330 (91) 354 (93)
*P�.05 among groups.
SUMATRIPTAN–NAPROXEN SODIUM FOR MIGRAINE TREATMENT
1448 JAMA, April 4, 2007—Vol 297, No. 13 (Reprinted) ©2007 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013
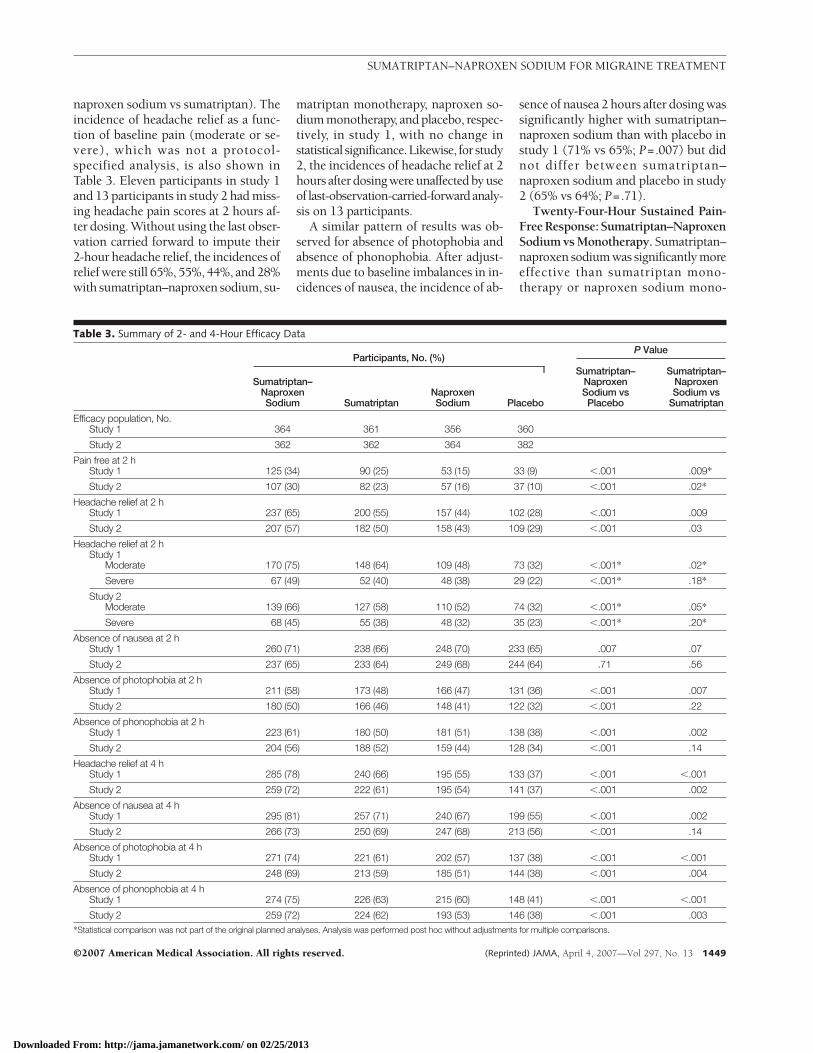
naproxen sodium vs sumatriptan). Theincidence of headache relief as a func-tion of baseline pain (moderate or se-vere), which was not a protocol-specified analysis, is also shown inTable 3. Eleven participants in study 1and 13 participants in study 2 had miss-ing headache pain scores at 2 hours af-ter dosing. Without using the last obser-vation carried forward to impute their2-hour headache relief, the incidences ofrelief were still 65%, 55%, 44%, and 28%with sumatriptan–naproxen sodium, su-
matriptan monotherapy, naproxen so-dium monotherapy, and placebo, respec-tively, in study 1, with no change instatistical significance.Likewise, for study2, the incidences of headache relief at 2hours after dosing were unaffected by useof last-observation-carried-forwardanaly-sis on 13 participants.
A similar pattern of results was ob-served for absence of photophobia andabsence of phonophobia. After adjust-ments due to baseline imbalances in in-cidences of nausea, the incidence of ab-
sence of nausea 2 hours after dosing wassignificantly higher with sumatriptan–naproxen sodium than with placebo instudy 1 (71% vs 65%; P=.007) but didnot differ between sumatriptan–naproxen sodium and placebo in study2 (65% vs 64%; P=.71).
Twenty-Four-Hour Sustained Pain-FreeResponse:Sumatriptan–NaproxenSodium vs Monotherapy. Sumatriptan–naproxen sodium was significantly moreeffective than sumatriptan mono-therapy or naproxen sodium mono-
Table 3. Summary of 2- and 4-Hour Efficacy Data
Participants, No. (%)P Value
Sumatriptan–NaproxenSodium Sumatriptan
NaproxenSodium Placebo
Sumatriptan–NaproxenSodium vsPlacebo
Sumatriptan–NaproxenSodium vs
Sumatriptan
Efficacy population, No.Study 1 364 361 356 360
Study 2 362 362 364 382
Pain free at 2 hStudy 1 125 (34) 90 (25) 53 (15) 33 (9) �.001 .009*
Study 2 107 (30) 82 (23) 57 (16) 37 (10) �.001 .02*
Headache relief at 2 hStudy 1 237 (65) 200 (55) 157 (44) 102 (28) �.001 .009
Study 2 207 (57) 182 (50) 158 (43) 109 (29) �.001 .03
Headache relief at 2 hStudy 1
Moderate 170 (75) 148 (64) 109 (48) 73 (32) �.001* .02*
Severe 67 (49) 52 (40) 48 (38) 29 (22) �.001* .18*
Study 2Moderate 139 (66) 127 (58) 110 (52) 74 (32) �.001* .05*
Severe 68 (45) 55 (38) 48 (32) 35 (23) �.001* .20*
Absence of nausea at 2 hStudy 1 260 (71) 238 (66) 248 (70) 233 (65) .007 .07
Study 2 237 (65) 233 (64) 249 (68) 244 (64) .71 .56
Absence of photophobia at 2 hStudy 1 211 (58) 173 (48) 166 (47) 131 (36) �.001 .007
Study 2 180 (50) 166 (46) 148 (41) 122 (32) �.001 .22
Absence of phonophobia at 2 hStudy 1 223 (61) 180 (50) 181 (51) 138 (38) �.001 .002
Study 2 204 (56) 188 (52) 159 (44) 128 (34) �.001 .14
Headache relief at 4 hStudy 1 285 (78) 240 (66) 195 (55) 133 (37) �.001 �.001
Study 2 259 (72) 222 (61) 195 (54) 141 (37) �.001 .002
Absence of nausea at 4 hStudy 1 295 (81) 257 (71) 240 (67) 199 (55) �.001 .002
Study 2 266 (73) 250 (69) 247 (68) 213 (56) �.001 .14
Absence of photophobia at 4 hStudy 1 271 (74) 221 (61) 202 (57) 137 (38) �.001 �.001
Study 2 248 (69) 213 (59) 185 (51) 144 (38) �.001 .004
Absence of phonophobia at 4 hStudy 1 274 (75) 226 (63) 215 (60) 148 (41) �.001 �.001
Study 2 259 (72) 224 (62) 193 (53) 146 (38) �.001 .003*Statistical comparison was not part of the original planned analyses. Analysis was performed post hoc without adjustments for multiple comparisons.
SUMATRIPTAN–NAPROXEN SODIUM FOR MIGRAINE TREATMENT
©2007 American Medical Association. All rights reserved. (Reprinted) JAMA, April 4, 2007—Vol 297, No. 13 1449
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013
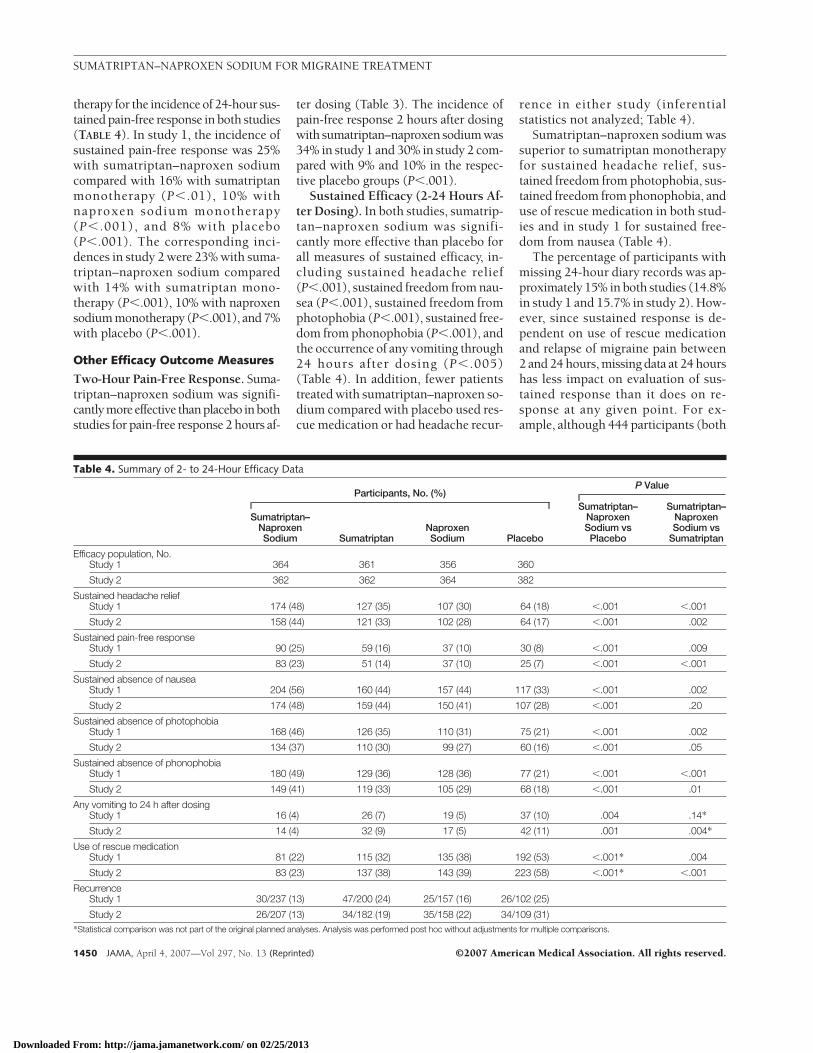
therapy for the incidence of 24-hour sus-tained pain-free response in both studies(TABLE 4). In study 1, the incidence ofsustained pain-free response was 25%with sumatriptan–naproxen sodiumcompared with 16% with sumatriptanmonotherapy (P�.01), 10% withnaproxen sodium monotherapy(P� .001), and 8% with placebo(P�.001). The corresponding inci-dences in study 2 were 23% with suma-triptan–naproxen sodium comparedwith 14% with sumatriptan mono-therapy (P�.001), 10% with naproxensodium monotherapy (P�.001), and 7%with placebo (P�.001).
Other Efficacy Outcome Measures
Two-Hour Pain-Free Response. Suma-triptan–naproxen sodium was signifi-cantlymoreeffective thanplacebo inbothstudies for pain-free response 2 hours af-
ter dosing (Table 3). The incidence ofpain-free response 2 hours after dosingwith sumatriptan–naproxen sodium was34% in study 1 and 30% in study 2 com-pared with 9% and 10% in the respec-tive placebo groups (P�.001).
Sustained Efficacy (2-24 Hours Af-ter Dosing). In both studies, sumatrip-tan–naproxen sodium was signifi-cantly more effective than placebo forall measures of sustained efficacy, in-cluding sustained headache relief(P�.001), sustained freedom from nau-sea (P�.001), sustained freedom fromphotophobia (P�.001), sustained free-dom from phonophobia (P�.001), andthe occurrence of any vomiting through24 hours after dosing (P� .005)(Table 4). In addition, fewer patientstreated with sumatriptan–naproxen so-dium compared with placebo used res-cue medication or had headache recur-
rence in either study (inferentialstatistics not analyzed; Table 4).
Sumatriptan–naproxen sodium wassuperior to sumatriptan monotherapyfor sustained headache relief, sus-tained freedom from photophobia, sus-tained freedom from phonophobia, anduse of rescue medication in both stud-ies and in study 1 for sustained free-dom from nausea (Table 4).
The percentage of participants withmissing 24-hour diary records was ap-proximately 15% in both studies (14.8%in study 1 and 15.7% in study 2). How-ever, since sustained response is de-pendent on use of rescue medicationand relapse of migraine pain between2 and 24 hours, missing data at 24 hourshas less impact on evaluation of sus-tained response than it does on re-sponse at any given point. For ex-ample, although 444 participants (both
Table 4. Summary of 2- to 24-Hour Efficacy Data
Participants, No. (%)P Value
Sumatriptan–NaproxenSodium Sumatriptan
NaproxenSodium Placebo
Sumatriptan–NaproxenSodium vsPlacebo
Sumatriptan–NaproxenSodium vs
Sumatriptan
Efficacy population, No.Study 1 364 361 356 360
Study 2 362 362 364 382
Sustained headache reliefStudy 1 174 (48) 127 (35) 107 (30) 64 (18) �.001 �.001
Study 2 158 (44) 121 (33) 102 (28) 64 (17) �.001 .002
Sustained pain-free responseStudy 1 90 (25) 59 (16) 37 (10) 30 (8) �.001 .009
Study 2 83 (23) 51 (14) 37 (10) 25 (7) �.001 �.001
Sustained absence of nauseaStudy 1 204 (56) 160 (44) 157 (44) 117 (33) �.001 .002
Study 2 174 (48) 159 (44) 150 (41) 107 (28) �.001 .20
Sustained absence of photophobiaStudy 1 168 (46) 126 (35) 110 (31) 75 (21) �.001 .002
Study 2 134 (37) 110 (30) 99 (27) 60 (16) �.001 .05
Sustained absence of phonophobiaStudy 1 180 (49) 129 (36) 128 (36) 77 (21) �.001 �.001
Study 2 149 (41) 119 (33) 105 (29) 68 (18) �.001 .01
Any vomiting to 24 h after dosingStudy 1 16 (4) 26 (7) 19 (5) 37 (10) .004 .14*
Study 2 14 (4) 32 (9) 17 (5) 42 (11) .001 .004*
Use of rescue medicationStudy 1 81 (22) 115 (32) 135 (38) 192 (53) �.001* .004
Study 2 83 (23) 137 (38) 143 (39) 223 (58) �.001* �.001
RecurrenceStudy 1 30/237 (13) 47/200 (24) 25/157 (16) 26/102 (25)
Study 2 26/207 (13) 34/182 (19) 35/158 (22) 34/109 (31)*Statistical comparison was not part of the original planned analyses. Analysis was performed post hoc without adjustments for multiple comparisons.
SUMATRIPTAN–NAPROXEN SODIUM FOR MIGRAINE TREATMENT
1450 JAMA, April 4, 2007—Vol 297, No. 13 (Reprinted) ©2007 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013
studies) had missing data at the 24-hour point, only 14 (7 in study 1 and7 in study 2) could not be evaluated for24-hour sustained response without useof last-observation-carried-forwardanalysis. Excluding these participantsfrom the sustained analyses did not al-ter the overall incidences or statisticalinterpretation of the treatment differ-ences.
Clinical Safety
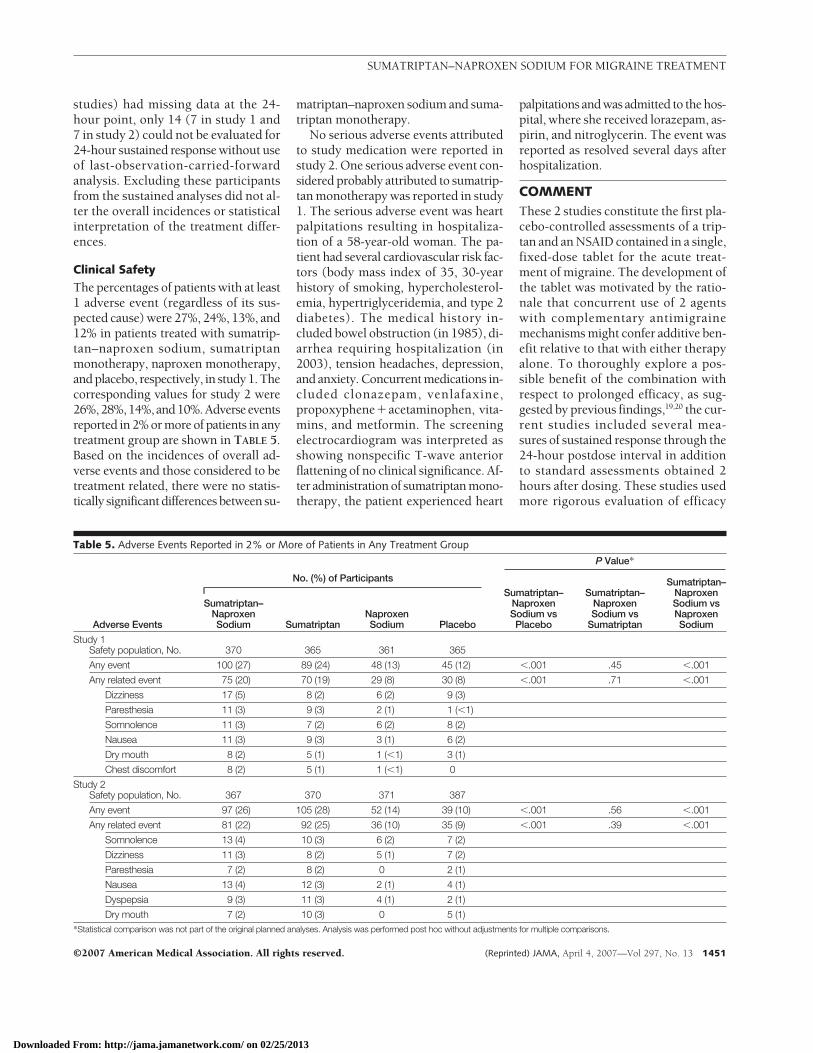
The percentages of patients with at least1 adverse event (regardless of its sus-pected cause) were 27%, 24%, 13%, and12% in patients treated with sumatrip-tan–naproxen sodium, sumatriptanmonotherapy, naproxen monotherapy,and placebo, respectively, in study 1. Thecorresponding values for study 2 were26%,28%,14%,and10%.Adverseeventsreported in 2% or more of patients in anytreatment group are shown in TABLE 5.Based on the incidences of overall ad-verse events and those considered to betreatment related, there were no statis-tically significant differences between su-
matriptan–naproxen sodium and suma-triptan monotherapy.
No serious adverse events attributedto study medication were reported instudy 2. One serious adverse event con-sidered probably attributed to sumatrip-tan monotherapy was reported in study1. The serious adverse event was heartpalpitations resulting in hospitaliza-tion of a 58-year-old woman. The pa-tient had several cardiovascular risk fac-tors (body mass index of 35, 30-yearhistory of smoking, hypercholesterol-emia, hypertriglyceridemia, and type 2diabetes). The medical history in-cluded bowel obstruction (in 1985), di-arrhea requiring hospitalization (in2003), tension headaches, depression,and anxiety. Concurrent medications in-cluded clonazepam, venlafaxine,propoxyphene�acetaminophen, vita-mins, and metformin. The screeningelectrocardiogram was interpreted asshowing nonspecific T-wave anteriorflattening of no clinical significance. Af-ter administration of sumatriptan mono-therapy, the patient experienced heart
palpitations and was admitted to the hos-pital, where she received lorazepam, as-pirin, and nitroglycerin. The event wasreported as resolved several days afterhospitalization.
COMMENTThese 2 studies constitute the first pla-cebo-controlled assessments of a trip-tan and an NSAID contained in a single,fixed-dose tablet for the acute treat-ment of migraine. The development ofthe tablet was motivated by the ratio-nale that concurrent use of 2 agentswith complementary antimigrainemechanisms might confer additive ben-efit relative to that with either therapyalone. To thoroughly explore a pos-sible benefit of the combination withrespect to prolonged efficacy, as sug-gested by previous findings,19,20 the cur-rent studies included several mea-sures of sustained response through the24-hour postdose interval in additionto standard assessments obtained 2hours after dosing. These studies usedmore rigorous evaluation of efficacy
Table 5. Adverse Events Reported in 2% or More of Patients in Any Treatment Group
Adverse Events
No. (%) of Participants
P Value*
Sumatriptan–NaproxenSodium Sumatriptan
NaproxenSodium Placebo
Sumatriptan–NaproxenSodium vsPlacebo
Sumatriptan–NaproxenSodium vs
Sumatriptan
Sumatriptan–NaproxenSodium vsNaproxenSodium
Study 1Safety population, No. 370 365 361 365
Any event 100 (27) 89 (24) 48 (13) 45 (12) �.001 .45 �.001
Any related event 75 (20) 70 (19) 29 (8) 30 (8) �.001 .71 �.001
Dizziness 17 (5) 8 (2) 6 (2) 9 (3)
Paresthesia 11 (3) 9 (3) 2 (1) 1 (�1)
Somnolence 11 (3) 7 (2) 6 (2) 8 (2)
Nausea 11 (3) 9 (3) 3 (1) 6 (2)
Dry mouth 8 (2) 5 (1) 1 (�1) 3 (1)
Chest discomfort 8 (2) 5 (1) 1 (�1) 0
Study 2Safety population, No. 367 370 371 387
Any event 97 (26) 105 (28) 52 (14) 39 (10) �.001 .56 �.001
Any related event 81 (22) 92 (25) 36 (10) 35 (9) �.001 .39 �.001
Somnolence 13 (4) 10 (3) 6 (2) 7 (2)
Dizziness 11 (3) 8 (2) 5 (1) 7 (2)
Paresthesia 7 (2) 8 (2) 0 2 (1)
Nausea 13 (4) 12 (3) 2 (1) 4 (1)
Dyspepsia 9 (3) 11 (3) 4 (1) 2 (1)
Dry mouth 7 (2) 10 (3) 0 5 (1)*Statistical comparison was not part of the original planned analyses. Analysis was performed post hoc without adjustments for multiple comparisons.
SUMATRIPTAN–NAPROXEN SODIUM FOR MIGRAINE TREATMENT
©2007 American Medical Association. All rights reserved. (Reprinted) JAMA, April 4, 2007—Vol 297, No. 13 1451
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

than any approved acute migraine treat-ment to date, with the incorporation of6 primary outcomes, all of which shouldbe statistically significant, as opposedto the usual single primary outcome ofheadache relief 2 hours after dosing.Previous studies used a combination of2 separate tablets rather than a singlefixed-dose tablet. Clinically, the lack ofa single fixed-dose tablet may lead tovariability in dosing and potentiallyhigher levels of sumatriptan; ie, suma-triptan tablets and naproxen sodiumtablets are each available in 3 doses, po-tentially resulting in numerous com-binations, and if not administered con-currently, may lead to the suboptimal“step care approach” to treatment. Thislack of standardization poses prob-lems with extrapolation of the previ-ously reported pharmacokinetic ben-efits of sumatriptan–naproxen sodium31
and the current safety profile.The combination tablet uses a su-
matriptan dosage strength of 85 mg anda naproxen sodium dosage strength of500 mg. The dosages of the 2 compo-nents of the combination are within therespective ranges of the lowest andhighest single daily doses recom-mended for use by adults in the UnitedStates. Whether a different combina-tion of doses of sumatriptan andnaproxen sodium might be more effi-cacious has not been studied. Suma-triptan and naproxen sodium doses forthe combination tablet were chosen onthe basis of known risks and benefitsof the separate drugs. Benefits and riskswere based on results of numerousother clinical trials in which, by con-vention, risks were not subjected to sta-tistical analysis but the incidence wasreported above the usual cutoff of morethan 1% or 2%.
The superior efficacy of sumatriptan–naproxen sodium compared with su-matriptan monotherapy might be ex-plained by its targeting of multiplepathogenic mechanisms in migraine. Itis hypothesized that migraine attacksarise from neurally induced cranial va-sodilation that produces painful inflam-mation of the surrounding nerves.3 Pe-ripheral and central pain pathways
appear to be sequentially recruited andsensitized as a migraine attack devel-ops.12-16 Peripheral pain pathways origi-nating from neurons with cell bodies inthe trigeminal ganglion are recruited andsensitized first, then the peripheral nerveactivity contributes to sensitization ofcentral pain pathways originating fromneurons with cell bodies in the dorsalhorn of the spinal cord. The initial pe-ripheral sensitization is thought to bringabout the mild, often throbbing pain as-sociated with the onset of a migraineattack, while central sensitization isthought to underlie a full-blown mi-graine attack. Whereas initiation of cen-tral sensitization depends on input fromperipheral pathways, central sensitiza-tion can be maintained independentlyof peripheral input.13 Data from animalmodels and studies in persons with mi-graine suggest that triptans can alter ini-tial peripheral sensitization but cannotappreciably affect central sensitiza-tion.14,15,32 NSAIDs, conversely, affectcentral sensitization.18,32 A triptan-NSAID combination, sumatriptan–naproxen sodium putatively affects bothperipheral and central sensitization to al-ter a broader range of pathogenic pro-cesses involved in migraine than eithermedication administered as mono-therapy.
The pharmacokinetic profile ofnaproxen when given as sumatriptan–naproxen sodium might also contrib-ute to the superior efficacy of suma-triptan–naproxen sodium relative tosumatriptan monotherapy, particu-larly for measures of sustained re-sponse. When administered as suma-triptan, 85 mg, � naproxen sodium,500 mg, sumatriptan is absorbed rela-tively quickly to confer rapid therapeu-tic response.31 With administration ofsumatriptan–naproxen sodium rela-tive to administration of naproxen so-dium alone, the time to maximum con-centration of naproxen is delayed(median, 6 hours vs 1 hour) and themaximum plasma concentration is re-duced by approximately 26%.31 Differ-ences in naproxen pharmacokineticprofiles observed between the suma-triptan–naproxen sodium and the
naproxen sodium groups may possi-bly arise from the presence of suma-triptan succinate in the combinationproduct. Sumatriptan has been reportedto cause a delay in gastric empty-ing.33,34 The delay in naproxen maxi-mum concentration and its long half-life of 12 to 17 hours23 may contributeto sustained efficacy.
The distinct pharmacokinetic pro-file of this single fixed-dose tablet of su-matriptan–naproxen sodium likely con-tributes to the acute and sustainedefficacy demonstrated in these stud-ies. Although the combination tabletsubstantially improved sustained pain-free response relative to the monothera-pies, approximately one quarter of pa-tients given active treatment hadsustained pain-free response regard-less of treatment group. Whether modi-fying treatment variables could im-prove the rate of sustained pain-freeresponse is being investigated in otherstudies. For example, the impact ofearly intervention (ie, treating a mi-graine attack while pain is still mild in-stead of waiting for pain to becomemoderate or severe) on sustained pain-free response and other outcome mea-sures is being evaluated with sumatrip-tan–naproxen sodium.
The incidences of adverse eventsoverall and of specific adverse eventswere low across treatment groups, al-though all active treatments were as-sociated with more frequent adverseevents than placebo. While the inci-dence of adverse events was low acrosstreatment groups, sumatriptan–naproxen sodium was associated withapproximately twice the incidence ofany adverse event as placebo. No spe-cific adverse event or group of adverseevents accounted for this difference.The nature of adverse events follow-ing treatment with sumatriptan–naproxen sodium did not differ mean-ingfully from events associated withsumatriptan monotherapy or naproxensodium monotherapy in previously re-ported controlled trials,35-38 nor fromthose reported in a long-term, open-label safety study of sumatriptan-naproxen sodium.39
SUMATRIPTAN–NAPROXEN SODIUM FOR MIGRAINE TREATMENT
1452 JAMA, April 4, 2007—Vol 297, No. 13 (Reprinted) ©2007 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013

The results of these studies shouldbe interpreted in the context of theirlimitations. Patients’ most common pre-study migraine medications wereNSAIDs and triptans, which are amongthe most common medications takenby persons with migraine generally. Thedegree to which the efficacy data fromthese studies can be extrapolated toNSAID- and triptan-naive patients andto patients with migraine refractory toNSAIDs and/or triptans is unknown. Asecond limitation is the inclusion of pri-marily white patients in the study. Thedegree to which the results generalizeto other race/ethnicity groups is notknown. However, there is no evidenceto suggest that response to the combi-nation or its components would be ex-pected to differ by race or ethnicity. Fi-nally, we did not compare sumatriptan–naproxen sodium with sumatriptan andnaproxen sodium taken together asseparate tablets. However, for patientsin whom adherence to taking 2 pills isan issue, the combination pill has ob-vious advantages.
In conclusion, sumatriptan, 85 mg,plus naproxen sodium, 500 mg, admin-istered as a single, fixed-dose tablet foracute treatment of migraine, resulted insuperior clinical benefits over mono-therapy with either sumatriptan ornaproxen sodium and was well toler-ated, as evidenced by the adverse eventprofile. Targeting multiple mecha-nisms of migraine with a specifically for-mulated single tablet of sumatriptan–naproxen sodium resulted in morefavorable 2-hour pain relief and 24-hour sustained pain-free responses vs su-matriptan or naproxen sodium alone.Author Contributions: Dr Brandes, as principal inves-tigator, had full access to all of the data in the studyand takes responsibility for the integrity of the dataand the accuracy of the data analysis.Study concept and design: Brandes, Adelman, Spruill,Barrett, Lener.Acquisition of data: Brandes, Kudrow, Stark, O’Carroll,Adelman, O’Donnell, Spruill.Analysis and interpretation of data: Brandes, Kudrow,Stark, O’Carroll, Adelman, O’Donnell, Alexander,Spruill, Barrett, Lener.Drafting of the manuscript: Brandes, Kudrow, Stark,O’Donnell, Spruill.Critical revision of the manuscript for important in-tellectual content: Brandes, Kudrow, Stark, O’Carroll,Adelman, O’Donnell, Alexander, Spruill, Barrett, Lener.Statistical analysis: Spruill.Obtained funding: Barrett, Lener.
Administrative, technical, or material support: Brandes,Kudrow.Study supervision: Brandes, Adelman, Alexander,Barrett, Lener.Financial Disclosures: Dr Brandes reports having re-ceived clinical research or educational support fromMerck, GlaxoSmithKline, UCB Pharma, Allergan,Johnson & Johnson, AstraZeneca, Pfizer, Bristol-Myers Squibb, Winston Laboratories, Sanofi-Aventis, Elan Pharmaceuticals, Novartis, Endo, POZEN,Vernalis, Ortho-McNeil, Advanced Bionics, ForestLaboratories, MedPointe Pharmaceuticals, and Ara-digm Corp. Dr Kudrow reports having received re-search grants f rom Ortho-McNei l , P f i zer ,GlaxoSmithKline, Merck, and Eisai and has served onthe speaker’s bureau for Pfizer and GlaxoSmithKline.Dr Stark reports having received clinical research oreducational support from GlaxoSmithKline, Proeth-ics, Allergan, Ortho-McNeil, Pfizer, and Merck. DrO’Carroll reports having received clinical research oreducational support from Allergan, GlaxoSmithKline,Merck, Pfizer, Eli Lilly, Sanofi-Aventis, Cephalon, For-est Pharmaceutical, AstraZeneca, Ortho-McNeil,POZEN, and Ligand Pharmaceuticals. Dr Adelman re-ports having received clinical research support fromGlaxoSmithKline and POZEN and having servedon advisory boards or speaker’s bureaus forGlaxoSmithKline, AstraZeneca, Pfizer, Merck, andOrtho-McNeil. Dr O’Donnell reports having re-ceived research support from Merck, GlaxoSmithKline,and Allergan; having served as a consultant forMerck, GlaxoSmithKline, and Ortho-McNeil; and hav-ing received speaker’s honoraria from Merck,GlaxoSmithKline, Pfizer, and Ortho-McNeil. Dr Alex-ander is a previous employee and shareholder ofPOZEN. Ms Spruill is a previous employee of and cur-rently serves as a consultant to POZEN. Ms Barrett isa previous employee of GlaxoSmithKline, serves as aconsultant to GlaxoSmithKline, and is a stockholderin Pfizer. Ms Lener is an employee of GlaxoSmithKline.MT400-301 Study Group: Alabama: Birmingham:Gregory M. Flippo, MD; Radiant Research, Birming-ham, Gordon T. Connor, MD; Montgomery: Drug Re-search and Analysis Corp, Norman A. Garrison, Jr, MD;Arizona: Tucson: Northwest NeuroSpecialists PLLC,Jeanette Wendt; Arkansas: Hot Springs: PalmettoClinical Research, Richard G. Pellegrino, MD; LittleRock: Clinical Study Centers LLC, Gordon L. Gibson,MD;California: San Diego: Medical Center for Clini-cal Research, William D. Koltun, MD; Santa Monica:California Medical Clinic for Headache, David Kud-row, MD; Oceanside: The Neurology Center, Benja-min M. Frishberg, MD; Walnut Creek: NeurologicalResearch Institute of the East Bay, Michael Stein, MD;Florida:Hialeah: Medical Research Unlimited, StevenD. Wheeler, MD; Melbourne: Comprehensive Neu-roscience Inc, Murray A. Kimmel, DO; Miami: MiamiResearch Associates Inc, Bruce Kohrman, MD; PalmBeach Gardens: Palm Beach Neurological Center,Michael M. Tuchman, MD; Plantation: NeurologyClinical Research Inc, Richard P. Singer, MD; Port Or-ange: Coastal Medical Research, Alex White, MD; WestPalm Beach: Premiere Research Institute, Paul K. Win-ner, DO; Georgia: Augusta: Walton Headache Cen-ter, Marc Husid; Decatur: Neurology and HeadacheSpecialists of Atlanta, Sarah E. DeRossett; Illinois:Chi-cago: Diamond Headache Clinic, Merle Lea Dia-mond, MD; Indiana: Evansville: MediSphere Medi-cal Research Center LLC, Steven K. Elliott, MD;Research Solutions, Jennifer S. Wahle, MD; India-napolis: Midwest Institute for Clinical Research, PhillipD. Toth, MD; Louisiana: Lake Charles: The Clinic, AlanSconzert, MD, PhD; Metairie: New Orleans MedicalInstitute, Robert B. De Trinis, MD; Massachusetts:Milford: Milford Emergency Associates Inc, AnthonyPuopolo, MD; North Dartmouth: Northeast MedicalResearch Associates Inc, S. David Miller, MD; Worces-ter: New England Regional Headache Center, Her-
bert G. Markley, MD;Michigan: Ann Arbor: Michi-gan Head-Pain and Neurological Institute, Todd Rozen,MD; Kalamazoo: Westside Family Medical Center, GaryRuoff, MD; Missouri: St. Louis: Mercy Health Re-search, Timothy R. Smith, MD; Radiant Research Inc,Mohammed Z. Abudalu, MD; Nevada: Las Vegas:Lovelace Scientific Resources, James Snyder, MD;NewMexico: Albuquerque: Lovelace Scientific Re-sources, Lydia Lawson, MD;NewYork: Endwell: Re-gional Clinical Research Inc, Victor A. Elinoff, MD; NewYork City: Analgesic Development Ltd, Abraham Sun-shine, MD; New York Headache Center, AlexanderMauskop, MD; North Carolina: Charlotte: Char-lotte Clinical Research Inc, Greg V. Collins, MD; Greens-boro: Headache Wellness Center, James U. Adel-man, MD; Raleigh: Multi-Specialty Research Associatesof North Carolina, John Rubino, MD; Ohio: Cincin-nati: Community Research, Bruce C. Corser, MD; Ra-diant Research Inc, Michael J. Noss, MD; Okla-homa: Tulsa: Neurological Associates of Tulsa Inc,Harvey J. Blumenthal, MD, James Dean, MD; Or-egon: Portland: Radiant Research Inc, Keith D. Klatt,MD; The Neurology Clinic, Hubert A. Leonard, MD,PhD; Pennsylvania: Lancaster: Oyster Point FamilyHealth Center Research Across America, Michael War-ren, MD; Philadelphia: Jefferson Headache Center,Stephen D. Silberstein, MD; Rhode Island: War-wick: Omega Medical Research, David L. Fried, MD;South Carolina: Mt Pleasant: Coastal Carolina Re-search Center, Cynthia Strout, MD; Summerville: Pal-metto Clinical Research, Michael Otruba, DO; Ten-nessee:Nashville: Nashville Neuroscience Group PC,Jan Lewis Brandes, MD; Texas:Austin: Benchmark Re-search Austin, Teresa L. Coats, MD; Fort Worth: Bench-mark Research, William Seger, MD; San Angelo: WestTexas Medical Associates, Darrell T. Herrington, DO;San Antonio: Integra Clinical Research LLC, SusanneK. Gazda, MD; Radiant Research, San Antonio, Wil-liam P. Jennings, MD; Richardson: KRK Medical Re-search, Roy S. Kiser, MD; Virginia: Roanoke: BlueRidge Research Center, Gordon Burch, MD;Wiscon-sin: Milwaukee: Advanced Healthcare SC, Daniel J.Thompson, MD.MT400-302 Study Group:Alabama: Huntsville: Am-Doc Inc, Medical Affiliated Research Center Inc, HarryLee McDaris, M.D; Mobile: USA Neurology, John F.Rothrock, MD; Arizona: Phoenix: Lovelace ScientificResources Inc, Philip B. James, MD, Richard V. Al-bery, MD; Valley Neurological Headache Clinic, CarolFoster, MD; Scottsdale: Radiant Research-Scottsdale, Timm McCarty, MD; Tucson: Radiant Re-search-Tucson, Frank Dunlap, MD, Robert Hirsch, MD;Arkansas: Little Rock: Little Rock Family Practice Clinic,Kevin Roberts, MD; California: Carlsbad: SanjeevSharma, MD; Irvine: Radiant Research-Irvine, SidRosenblatt, MD; Newport Beach: Christopher PhilipO’Carroll, MD; Northridge: Northridge NeurologicalCenter; Ronald B. Ziman, MD; Redondo Beach: GeorgeJ. Rederich, MD, PhD;Colorado: Denver: Radiant Re-search Inc, Leslie Moldauer, MD;Connecticut: Stam-ford: The New England Center for Headache, Alan M.Rapoport, MD; Stratford: Clinical Research Consult-ants Inc, Selwyn A. Cohen, MD; Florida: Clearwa-ter: Tampa Bay Medical Research Inc, Steven C. Bow-man, MD; Coral Gables: Clinical Research of SouthFlorida, Jeffrey B. Rosen, MD; Ft Myers: Internal Medi-cine Associates-Department of Research, Stephen R.Zellner, MD; Gainesville: Florida Medical Research In-stitute PA, C. Richard King, MD; St Petersburg: Com-prehensive NeuroScience Inc, Margarita Nunez, MD;Meridian Research, Mildred (Mimi) Farmer, MD;Geor-gia: Atlanta: Child Neurology Associates LLC, FrankBerenson, MD; Illinois: Peoria: NTouch Research,Daniel Brune, MD; Maryland: Towson: Interna-tional Research Center, Alberto Yataco, MD;Minne-sota: Plymouth: Clinical Research Institute, Gary Ber-man, MD; Missouri: Kansas City: The Center forPharmaceutical Research, John Ervin, MD; Spring-
SUMATRIPTAN–NAPROXEN SODIUM FOR MIGRAINE TREATMENT
©2007 American Medical Association. All rights reserved. (Reprinted) JAMA, April 4, 2007—Vol 297, No. 13 1453
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013
field: Headache Care Center, Roger Cady, MD;NewHampshire: Lebanon: Neurology Studies Group, Dart-mouth-Hitchcock Medical Center, Thomas N. Ward,MD; New Jersey: Morristown: Neuroscience Centerof Northern New Jersey, Stuart W. Fox, MD; Prince-ton: Global Medical Institute, Jeffrey Apter, MD; Ridge-wood: Neurology Group of Bergen County, PA, Ken-neth A. Levin, MD;NewYork: Albany: Upstate ClinicalResearch, James P. Wymer, MD; Manlius: Central NewYork Clinical Research, Douglas P. Zmolek, MD;NorthCarolina: Raleigh: North Carolina Clinical Research,Craig F. LaForce, MD; Winston-Salem: PiedmontMedical Research Associates, Thomas Littlejohn, MD;Ohio: Cleveland: Health Research Associates, Rob-ert S. Kunkel, MD; Columbus: Columbus Neurologi-cal Group Inc, Kenneth A. Mankowski, MD; RadiantResearch Inc, Douglas Schumacher, MD; Mogadore:Radiant Research Inc, Dennis C. McCluskey, MD; To-ledo: Headache Center of Ohio, Gary Gerard, MD;West Chester: ClinExcel Research, Lisa K. Mannix, MD;Westerville: Ortho Neuro Inc, Francis O’Donnell, DO;Pennsylvania: Philadelphia: Radiant Research-Einstein Center One, Barry Packman, MD; SouthCaro-lina: Anderson: Radiant Research Inc, Harry I. Geis-berg, MD; Greer: Radiant Research-Greer, WilliamTravis Ellison, MD; Statesville: Statesville Research In-stitute, Neil M. Kassman, MD; Tennessee: Mem-phis: Wesley Headache Clinic, Stephen H. Landy, MD;Nashville: Clinical Research Associates Inc, StephenC. Sharp, MD; Texas: Dallas: Harold Urschel, MD;Houston: The Houston Headache Clinic, Ninan T.Mathew, MD; Lubbock: Bhupesh Dihenia, MD; SanAntonio: Texas Association of Pediatric Neurology PA,Jerry Tomasovic, MD;Utah: Salt Lake City: Jean BrownResearch-JBA Research Inc, Gilbert Podolsky, MD;Ver-mont: Burlington: Department of Neurology, Col-lege of Medicine, University of Vermont, Robert Sha-piro, MD;Virginia: Alexandria: The Innovative ClinicalResearch Center, Stuart R. Stark, MD;Washington:Spokane: Rockwood Research Department, TimothyW. Powell, MD, Steven Pugh, MD; Tacoma: Neurol-ogy and Neurosurgery Associates of Tacoma, JohnHuddlestone, MD; Wenatchee: Clinical Research-Wenatchee Valley Medical Center, James R. Cook, MD.Funding/Support: The 2 clinical trials (MT-400:301 andMT-400:302) described in this article were funded byGlaxoSmithKline in partnership with POZEN, the INDsponsor of the investigational drug MT-400 (suma-triptan–naproxen sodium).Role of the Sponsors: GlaxoSmithKline and Pozen Incprovided financial and material support, monitoring,data collection and management, and data analysisto the authors and study investigators.Independent Statistical Analysis: Eugene Laska, PhD(director, Statistical Sciences Laboratory, Nathan S. KlineInstitute forPsychiatricResearch, andprofessor,Depart-ment of Psychiatry, New York University School ofMedicine, Orangeburg), had full access to all of theefficacy data and was provided the SAS programs andstatistical outputproducedbyPOZEN/GlaxoSmithKline.Dr Laska reviewed the appropriateness of the ana-lytic approach to the analysis of the primary efficacymeasures and select secondary outcomes, suggestedadditional analyses, and verified the primary resultsreported in the article. POZEN/GlaxoSmithKline Phar-maceutical Research and Development paid Dr Laskafor the time he spent on the review. Research assis-tance was provided to Dr Laska by Joseph Wander-ling, a research scientist at the Nathan S. Kline Insti-tute for Psychiatric Research.Acknowledgment: We acknowledge Meredith A. Cu-cuel, BA, of Nashville Neuroscience Group, Nash-ville, Tenn, for editorial assistance, Michael H. Ames,PhD, of GlaxoSmithKline, Research Triangle Park, NC,for statistical input, Jane Saiers, PhD, of The Write-
Medicine Inc, Chapel Hill, NC, for assistance withpreparation of the manuscript, and Susan A. McDonald,MA, of GlaxoSmithKline, Research Triangle Park, NC,for critical review of the manuscript. Ms Cucuel’s workon the manuscript was funded by Nashville Neuro-science Group and Dr Saiers’ work on the manuscriptwas funded by GlaxoSmithKline.
REFERENCES
1. Lipton RB, Stewart WF, Diamond S, et al. Preva-lence and burden of migraine in the United States: datafrom the American Migraine Study II. Headache. 2001;41:646-657.2. Lipton RB, Bigal ME. The epidemiology of migraine.Am J Med. 2005;118(suppl 1):3S-10S.3. Goadsby PJ, Lipton RB, Ferrari MD. Migraine—current understanding and treatment. N Engl J Med.2002;346:257-270.4. Ferrari MD, Roon KI, Lipton RB, et al. Oral trip-tans in acute migraine treatment: a meta-analysis of53 trials. Lancet. 2001;358:1668-1675.5. Gendolla A. Part I: what do patients really need andwant from migraine treatment? Curr Med Res Opin.2005;21(suppl 3):S3-S7.6. Lipton RB, Hamelsky SW, Dayno JM. What do pa-tients with migraine want from acute migrainetreatment? Headache. 2002;42(suppl 1):3-9.7. Hargreaves RJ, Shepheard SL. Pathophysiology ofmigraine-new insights. Can J Neurol Sci. 1999;26:S12-S19.8. Goadsby PJ. Current concepts of the pathophysi-ology of migraine. Neurol Clin. 1997;15:27-42.9. Moskowitz MA, Cutrer FM. Sumatriptan: a receptor-targeted treatment for migraine. Annu Rev Med. 1993;44:145-154.10. Watkins LR, Milligan ED, Maiser SF. Glial proin-flammatory cytokines mediate exaggerated pain states:implications for clinical pain. Adv Exp Med Biol. 2003;521:1-21.11. Burstein R. Deconstructing migraine headache intoperipheral and central sensitization. Pain. 2001;89:107-110.12. Burstein R, Yarnitsky D, Goor-Aryeh I, et al. Anassociation between migraine and cutaneous allodynia.Ann Neurol. 2000;47:614-624.13. Burstein R, Cutrer MF, Yarnitsky D. The devel-opment of cutaneous allodynia during a migraineattack: clinical evidence for the sequential recruit-ment of spinal and supraspinal nociceptive neuronsin migraine. Brain. 2000;123:1703-1709.14. Burstein R, Jakubowski M. Analgesic triptan ac-tion in an animal model of intracranial pain: a raceagainst the development of central sensitization. AnnNeurol. 2004;55:27-36.15. Burstein R, Collins B, Jakubowski M. Defeatingmigraine pain with triptans: a race against the devel-opment of cutaneous allodynia. Ann Neurol. 2004;55:19-26.16. Yarnitsky D, Goor-Aryeh I, Bajwa ZH, et al. 2003Wolff Award: possible parasympathetic contribu-tions to peripheral and central sensitization duringmigraine. Headache. 2003;43:704-714.17. Burstein R, Jakubowski M. Implications of multi-mechanism therapy: when to treat? Neurology. 2005;64(suppl 2):S16-S20.18. Burstein R, Jakubowski M, Levy D. Naproxen sup-presses sensitization in of central trigeminovascular neu-rons—implication for migraine therapy [abstract].Neurology. 2006;66(suppl 2):A69.19. Krymchantowski AV. Naproxen sodium de-creases migraine recurrence when administered withsumatriptan. Arq Neuropsiquiatr. 2000;58:428-430.
20. Smith TR, Sunshine A, Stark SR, et al. Sumatrip-tan and naproxen sodium for the acute treatment ofmigraine. Headache. 2005;45:983-991.21. Krymchantowski AV, Bigal ME. Rizatriptan ver-sus rizatriptan plus rofecoxib versus rizatriptan plus tolf-enamic acid in the acute treatment of migraine. BMCNeurol. 2004;4:10.22. Krymchantowski AV, Barbosa JS. Rizatriptan com-bined with rofecoxib vs rizatriptan for the acute treat-ment of migraine: an open-label pilot study.Cephalalgia. 2002;22:309-312.23. Naprosyn Complete Prescribing Information. Nut-ley, NJ: Roche Laboratories Inc; January 2006.24. Headache Classification Committee of the Inter-national Headache Society. Classification of head-ache disorders, cranial neuralgias and facial pain.Cephalalgia. 1988;8(suppl 7):1-96.25. Headache Classification Subcommittee of the In-ternational Headache Society. The international clas-sification of headache disorders: 2nd edition.Cephalalgia. 2004;24(suppl 1):9-160.26. Holm S. A simple sequentially rejective Bonfer-roni test procedure. Scand J Stat. 1979;6:65-70.27. Shaffer JP. Modified sequentially rejective mul-tiple test procedures. J Am Stat Assoc. 1986;81:826-831.28. Holland BS, Copenhaver MD. An improved se-quentially rejective Bonferroni test procedure.Biometrics. 1987;43:417-424.29. Hochberg Y, Tamhane AC. Multiple Compari-son Procedures. New York, NY: John Wiley & SonsInc; 1987.30. Hochberg Y. A sharper Bonferroni procedure formultiple significance testing Biometrika. 1988;75:800-803.31. Kori S, Littlefield D, Taylor D, et al. Pharmacoki-netics of a single-tablet formulation of sumatriptan RTTechnology™ and naproxen sodium [abstract].Cephalalgia. 2005;25:933.32. Jakubowski M, Levy D, Goor-Aryeh I, et al. Ter-minating migraine with allodynia and ongoingcentral sensitization using parenteral administrationof COX1/COX2 inhibitors. Headache. 2005;45:850-861.33. Cipolla G, Sacco S, Crema F, et al. Gastric motoreffects of triptans: open questions and futureperspectives. Pharmacol Res. 2001;43:205-210.34. Houghton LA, Fowler P, Keene ON, et al. Effectof sumatriptan, a new selective 5HT1-like agonist, onliquid gastric emptying in man. Aliment PharmacolTher. 1992;6:685-691.35. Treves TA, Streiffler M, Korczyn AD. Naproxensodium versus ergotamine tartrate in the treatmentof acute migraine attacks. Headache. 1992;32:280-282.36. Pradalier A, Rancurel G, Dordain G, et al. Acutemigraine attack therapy: comparison of naproxen so-dium and an ergotamine tartrate compound.Cephalalgia. 1985;5:107-113.37. Carpay J, Schoenen J, Ahmad F, et al. Efficacy andtolerabil ity of sumatriptan tablets in a fast-disintegrating, rapid-release formulation for the acutetreatment of migraine: results of a multicenter, ran-domized, placebo-controlled study. Clin Ther. 2004;26:214-223.38. Sheftell FD, Dahlof CG, Brandes JL, et al. Two rep-licate randomized, double-blind, placebo-controlledtrials of the time to onset of headache relief in the acutetreatment of migraine with a fast-disintegrating/rapid-release formulation of sumatriptan tablets. Clin Ther.2005;27:407-417.39. Winner P, Cady RK, Ruoff GE, et al. Twelve-month tolerability and safety of sumatriptan andnaproxen sodium for the treatment of acute migraine.Mayo Clin Proc. 2007;82:61-68.
SUMATRIPTAN–NAPROXEN SODIUM FOR MIGRAINE TREATMENT
1454 JAMA, April 4, 2007—Vol 297, No. 13 (Reprinted) ©2007 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 02/25/2013





























