Embed Size (px)
Citation preview

Neurosurg. Rev. 17 (1994) 145-150
Surgical t reatment of s y m p t o m a t i c s u b e p e n d y m o m a of the nervous system. R e p o r t of f ive cases
Faruk ildan, Erdal .Cetinalp, Hiiseyin Ba~dato~lu, Nurdan Tunall, Gulfiliz G6nlii.sen, and Askm Karadayl
Cukurova University, Faculty of Medicine, Department of Neurosurgery, Balcah, Adana, Ttirkey
Abstract
Subependymomas are uncommon and relatively benign tumors with a distinctive histological appearance. They are generally asymptomatic and most of them are found incidentally at postmortem examination. These tumors are usually located in the fourth and lateral ventricle, and sometimes in the spinal cord. The authors present a series of 5 pure subependymomas of the central nervous system all of which were symptomatic and all of which were treated by microsurgical removal. The clinico- pathological findings and the results of microsurgical treatment in this series are presented.
Keywords: Brain tumor, ependymoma, subependym- o m a .
1 Introduction
Subependymoma was first described as a distinc- tive pathological entity by SCHEINKER [13] in 1945. Before his original description, early case reports of gliomas with features of subeper/dym- oma were scattered in the literature [2]. Since that original description, approximately 110 cases of subependymoma of the central nervous system (CNS) have been reported. Subependymomas are neuroectodermal tumors. The majority of them are small and asymptomatic and are encountered incidentally at postmortem examination [12]. They are localised mainly in the fourth and lateral ventricles [5, 16]. Their histological appearances do not include malignant features [1, 12, 14].
We have presented our experience of five micro- surgically treated subependymomas which form
part of a series 96 ependymomas in the period 1976-1992. Clinical presentation, radiological appearance, microsurgical treatment and histopa- thological characteristics are discussed in an ef- fort to identify further prognostic indicators.
2 Clinical material
2.1 Clinical features
Between 1981 and 1992, five patients underwent operation for the lateral ventricle and fourth ven- tricle tumor which were later diagnosed histologi- cally as subependymoma. The series included three men and two women, ranging in age from 32 to 48 (mean 39 years). The duration of symp- toms prior to presentation ranged from 5 months to 4 years (mean 2,5 years). The most common presenting symptom was headache and this find- ing usually preceded other complaints by many months. Other main symptoms were ataxi, nausea and vomiting. These symptoms, particularly nau- sea and vomiting occured early in the course and tended to be episodic. The clinical symptoms and neurological signs are summerized in tables I and II.
2.2 Radiological findings
Plain skull x-rays were obtained in all patients, but were not contributory to the diagnosis in the series.
�9 1994 by Walter de Gruyter & Co. Berlin - New York
146 lldan et al, Surgical treatment of symptomatic subependyoma of the nervous system
Table I. Symptoms in 5 patients with subependymoma
Case no Age/sex Site Symptoms
1 39 M Fourth ventricle 2 48 F Rt and Lf lateral ventricle 3 45 M Fourth ventricle 4 32 M Fourth ventricle 5 34 F Rt ventricle and in part Lf
lateral ventricle
Table II. Neurological signs and surgical outcome in 5 cases of CNS subependymoma
Case no Neurological signs Therapy Follow-up
Headache, diplopia, nausea, vomiting Headache, mental disturbance Headache, ataxi, nystagmus, nausea Headache, ataxi, nytagmus incontinance Mental disturbance, headache, nausea vomiting
1 Papilledema, ataxi deficj~left 6 Total exc. Good, 6 years 2 Papilledema, personality change Total exc. Good, 1 year 3 Papilledema, dysmetria, dysdiadochokinesia Total exc. Died, postop. 4 Papilledema, dysmetria, dysdiadochokinesia Subtotal exc. Moderate, 6 months 5 Papilledema, personality change Total exc. Good, 8 months
exc. = excision good = no neurological deficit moderate = minimal neurological deficit but general health good postop. = postoperatively
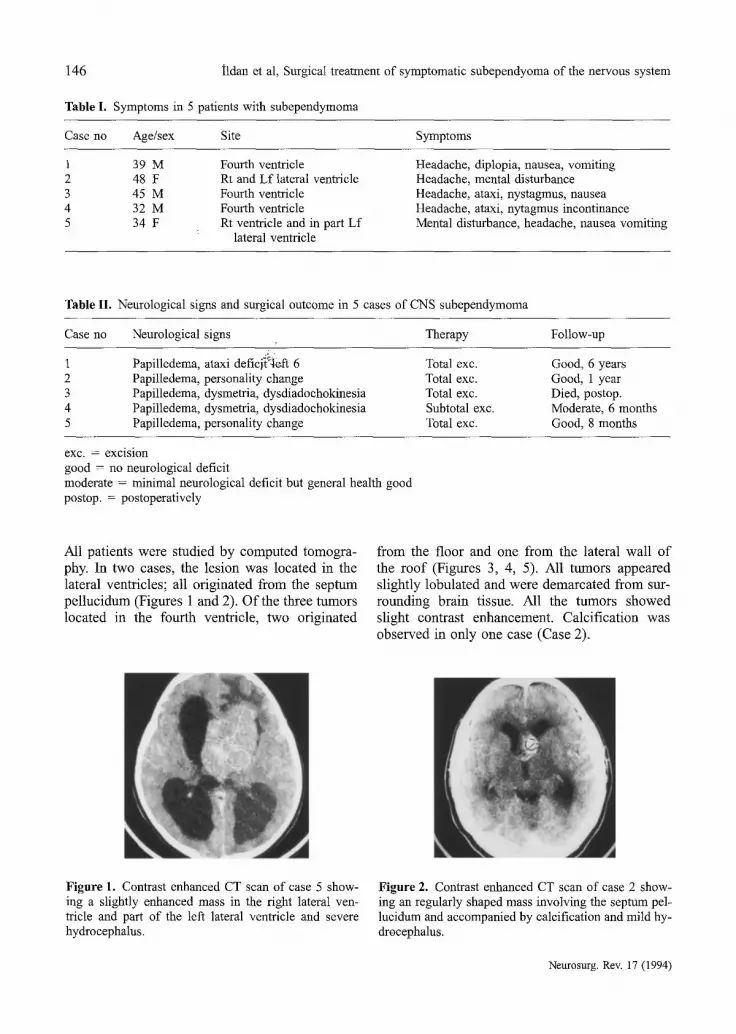
All patients were studied by computed tomogra- phy. In two cases, the lesion was located in the lateral ventricles; all originated from the septum pellucidum (Figures 1 and 2). Of the three rumors located in the fourth ventricle, two originated
from the floor and one from the lateral wall of the roof (Figures 3, 4, 5). All tumors appeared slightly lobulated and were demarcated from sur- rounding brain tissue. All the tumors showed slight contrast enhancement. Calcification was observed in only one case (Case 2).
Figure 1. Contrast enhanced CT scan of case 5 show- ing a slightly enhanced mass in the right lateral ven- tricle and part of the left lateral ventricle and severe hydrocephalus.
Figure 2. Contrast enhanced CT scan of case 2 show- ing an regularly shaped mass involving the septum pel- lucidum and accompanied by calcification and mild hy- drocephalus.
Neurosurg. Rev. 17 (1994)

Hdan et al, Surgical treatment of symptomatic subependyoma of the nervous system 147
Figure 3. Contrast enhanced CT scan of case 3 show- ing a slightly high density tumor within the fourth ven- tricle along with the presence of edema and mild hydro- cephalus.
Figure 4. Contrast enhanced CT scan of case 1 show- ing a well-demarcated, lobulated, fourth ventricular mass with peritumoral edema.
2.3 Operative findings
The surgical approaches included suboccipital median craniectomy in three cases, and anterior interhemispheric transcallosal route in two. In the patient (Case 4) with the tumor in the fourth ven- tricle, removal was subtotal, because there was a little portion of the tumor which was invaded the neighboring brain tissue. In all the other cases, excision was total in the fourth ventricle location. Resection was complete in two cases with subep- endymoma located in the lateral ventricles. The tumor generally presented as a greyish or white- yellowish solid mass. The bulk of the tumor was well demarcated from the surrounding tissue ex- cept in case 4. The tumor tissue nearly always included hemorrhagic and microcystic parts.
Figure 5. Contrast enhanced CT scan of case 4 show- ing a lobulated fourth ventricular mass.
2.4 Results
The postoperative course was complicated in the patient with the complete tumor excision in the fourth ventricle. The patient could not respond to verbal commands after recovery from anestesia. On the second day after the operation, this patient became less responsive and died from a respirat- ory problem. This was the only postoperative death in this series (Case 3). The other patients with complete and incomplete excision of the tumor in the fourth ventricle had no postoperative complications or evidence of recurrence of the tumor during the follow-up period. These patients were in good general health although the one with incomplet excision had objective evidence of minimal deficits related to the brain stem. The postoperative course was uneventful in the patients whose tumors were located in the lateral ventricles and removed totally, There has been no evidence of tumor recurrence in these patients in the follow-up periods (Table II).
2.5 Pathological findings
The basic histological features of subependym- omas were similar in all cases located in the fourth and lateral ventricles. They were charac- terized by scattered clusters of fairly uniform cells with oval nuclei surrounded by a matrix of dense fibrillary material (Figures 6a+b). The nu- clei were of regular round to oval shape. Lobular architecture and hypocellularity were prominent in any case. Microcysts were present in the ma- jority of the specimens and were prominent in
Neurosurg. Re~ 17 (1994)

148 ildan et al, Surgical treatment of symptomatic subependyoma of the nervous system
Figure 6. Typical histological pattern of subependym- dant fibrillary matrix at higher magnification oma at low magnification (A : 100 • Note the abun- (B : 250 • (haematoxylin & Eosin Stain).
three instance. Astrocytic differentiation was noted in two cases. The vast majority of tumors were hypovascular. Necrosis in association with hemorrhage was noted in one instance. Degener- ative changes were frequently present, and in- cluded vascular sclerosis in two cases, vascular thrombosis in two, hemorrhage in one, hemosid- erin deposition in two, microcalcification in two (abundant in one), particularly in large examples. Mitotic figures were not identified in any of the samples.
3 Discussion
The subependymoma is a tumor rarely found in neurosurgical practice. It is commonly considered a slowly growing tumor generally located in the wall of the lateral or fourth ventricles and found incidentally at necropsy [12].
Occasionally they reach a size big enough to block the cerebro-spinal fluid (CSF) pathways and become symptomatic [14]. Therefore, the most important clinical sign is intracranial hyper- tension which is caused by hydrocephalus due to blocking of the CSF pathways. Other neurologi- cal findings, including irritation and/or deficit de- pend on the location of the tumor. Subependym- omas have a distinctive histological appearance, but histogenesis of this uncommon tumor has been a matter of some controversy. The histologi- cal picture of the tumor is being considered to be composed of subependymal glia [1, 10] of astro- cytes of the subependymal plate [4, 13], of epen-
dymal cells [12] or of a mixture of astrocytic and ependymal cells [3, 14]. The histogenesis is due, in part, to the various proportions of astrocytes and ependymal cells in those transitional tumors with mixed areas of ependymoma and subepen- dymoma. The combined type of the tumor should be distinguished from pure subependymoma from the clinical point of view, because it is biologi- cally rather malignant and tends to occur in the first decade of life [14]. Current opinion is that subependymomas are of mixed composition and originate from the pluripotential cells of the sub- ependymal layer [1, 3]. Ependymal cells are usu- ally the predominant component in this lesion.
It has been reported that ependymomas occured in the infratentorial location in more than 70% of cases and arised most frequently from the floor or roof of the fourth ventricle [14]. The tumor originated from the floor in two of our cases and from the roof in one case in our series.
Most subependymomas are clinically silent and are only incidentally found at autopsy. ScrIEIT- HAUER [14] reported that the most important fac- tors that determine whether a subependymoma is symptomatic or not are the size and location of the lesion. In his series, all symptomatic lesions were larger than 4 cm in diameter.
The characteristic appearance of subependymoma on CT scan shows a "well-demarcated, slightly lobulated intra or periventricular tumor with or without distrofic calcifications and cystic por- tions. Although calcification is a common finding
Neurosurg. Rev. 17 (1994)

ildan et al, Surgical treatment of symptomatic subependyoma of the nervous system 149
in this tumor [8], it was visible on the CT scan in only one case (Case 2) and was not visible on skull x-rays in our series. The lobulated asym- metrical appearance, uniform radiodensity, slight contrast enhancement, calcifications and cystic formation are reliable diagnostic criteria. In fact, however no preoperative diagnosis of subependy- morea was made according to CT scan appear- ance in our series. We think that difficulties in diagnosis may have originated from the rarity of subependymoma.
LOBATO et al. [8] and STEVENS et al. [15J reported that CT findings in symptomatic subependymoma are close to those of ependymoma. Therefore, preoperative diagnosis according to those of the CT findings is uncertain.
We have no experience with magnetic resonance imaging (MR/) in this disease. MRI character- istics of subependymomas have been reported re- cently [7, 11]. Long T1 and T2 times or isointens- ity of the tumor were thought to be of diagnostic importance but not as prominent findings as seen in other benign astrocytomas [11]. Astrocytomas ofl:en show more intense signal intensity on T2- weighted MRI image [6]. Although MRI was su- perior to CT scan, especially the sagittal scan, for the planning of the operation, further studies are required.
W]henever possible, complete removal of the sub- ependymomas is recommended due to their avas-
cularity and their good demarcation. Total re- moval of this lesion usually results in complete recovery [4, 9]. Complete resection of ependy- momas in the lateral ventricle arising from the septum pellucidum is often achieved. However, complete resection is not advisable in fourth ven- tricle lesions. This tumor arises from the floor of the fourth ventricle so that total removal is haz- ardous due to the delicate structures involved. In our series, alteration of vital signs occured during dissection in two cases in which the subependym- oma were attached to the floor of the ventricle (cases 3 and 4). In the fatal case in our series, the tumor was located in the fourth ventricle and involved the delicate structures.
Radiation therapy for subependymomas has not been routinely applied. Some authors advocated radiation therapy in the mixed of ependymomas subependymomas, but considered it obsolete for pure subependymomas [4]. None of our patients received radiotherapy even in the case of subtotal removal in the fourth ventricle.
These tumors are generally totally removable par- ticularly in the lateral ventricle location. Total ex- cision with modem neurosurgical techniques may provide cure in this location. Therefore the sur- geon should not hesitate to make total excision. Radical operation in the fourth ventricle location carries the risk of morbidity and mortality. In these cases, debulking or subtotal resection is ad- visible to restore CSF flow.
References
[1] AZZARELLI B, HL REKATE, V ROESSMANN: Sub- ependymoma: case report with ultrastructural study. Acta Neuropathol (Berl) 40 (1977) 279- 282
[2] Cox LB: The cytology of the glioma group with special references to the inclusion of cells derived from the invaded tissue. Am J Pathol 9 (1933) 839-898
[3] Fu YS, ATL CHEN, S KAY, HF YOUNG: IS subep- endymoma (subependymal glomeate astrocytoma) an astrocytoma or ependymoma? A comparative ultrastructural and tissue culture study. Cancer 34 (1974) 1992-2008
[4] GODWIN JT: Subependymal glomerate astro- cytoma. Report of two cases. J Neurosurg 16 (1959) 385-389
[5] JOOMA R, MJ TORRENS, J BRADSHAW, B BROWNELL: Subependymomas of the fourth ven- tricle. Surgical treatment in 12 cases. J Neurosurg 62 (1985) 508-512
[6] Just M, M THELEN: Tissue characterization with T1, T2 and proton density values: results in 160 patients with brain tumor. Radiology 169 (1988) 779-785
[7] KALFAS IH, J HAHN: Symptomatic subependym- oma in a 14 year old girl diagnosed by NMR scan. Child Nerv Syst 2 (1986) 44-46
[8] LOBATO RD, M SARABIA, S CASTRO, J ESPARZA, F CORDOBES, JM PORTILLO, JJ PdVAS: Symptomatic subependymoma. Report of four new cases studied with computed tomography and review of the lit- erature. Neurosurgery 19 (1986) 594-598
Neurosurg. Rev. 17 (1994)

150 ildan et al, Surgical treatment of symptomatic subependyoma of the nervous system
[9] LOBATO RD, A CABELLO, JJ CARMENA, M DE LA FUBNTE, MJ MUNOZ: Subependymoma of the lat- eral ventricle. Surg Neurol 15 (1980) 144-147
[10] Moss TH: Observations on the nature of subepen- dymomas an electron microscoping study. Neuro- pathol Appl Neurobiol 10 (1984) 63-75
[11] PETERMANN SB, RE STEINER, GM BYDDER, DJ THOMAS~ JS TOBIAS, IR YOUNG: Nuclear magnetic resonance imaging (NMR), (MRI) of brain stem tumours. Neuroradiology 27 (1985) 202-207
[12] RUSSELL DS, LJ RUBINSTEIN: Pathology of Tu- mours of the Nervous System, ed 4. London Ed- ward Arnold 1977
[13] SCrmINKER IM: Subependymoma: a newly recog- nized tumor of subependymal derivation. J Neuro- surg 2 (1945) 232-240
[14] SCHE~THAU~R BW: Symptomatic subependym- oma. Report of 21 cases with review of the litera- ture. J Neurosurg 49 (1978) 689-696
[15] STEVENS JM, BE KENDALL, S LOVE: Radiological features of subependymoma with emphasis on computed tomography. Neuroradiology 26 (1984) 223 -228
[16] VAQUERO J, J HERRERO, JM CABEZUDO: Sympto- matic subependymomas of the lateral ventricles. Acta Neurochir (Wien) 53 (1980) 99-105
Submitted October 6, 1992. Accepted March 23, 1993.
Faruk [ldan, M.D. Cukurova University School of Medicine Department of Neurosurgery Balcah, Adana Turkey
Neurosurg. Rev. 17 (1994)





























