Embed Size (px)
Citation preview

TACTICAL MEDICINE—COMPETENCY-BASED GUIDELINES
Richard Bruce Schwartz, MD, John G. McManus, Jr., MD, MCR, John Croushorn, MD,Gina Piazza, DO, Phillip L. Coule, MD, Mark Gibbons, Glenn Bollard, MD, David Ledrick, MD,
Paul Vecchio, E. Brooke Lerner, PhD
ABSTRACT
Background. Tactical emergency medical support (TEMS)is a rapidly growing area within the field of prehospitalmedicine. As TEMS has grown, multiple training programshave emerged. A review of the existing programs demon-strated a lack of competency-based education. Objective.To develop educational competencies for TEMS as a firststep toward enhancing accountability. Methods. As an ini-tial attempt to establish accepted outcome-based competen-cies, the National Tactical Officers Association (NTOA) con-vened a working group of subject matter experts. Results.This working group drafted a competency-based educationalmatrix consisting of 18 educational domains. Each domainincluded competencies for four educational target audiences(operator, medic, team commander, and medical director).The matrix was presented to the American College of Emer-gency Physicians (ACEP) Tactical Emergency Medicine Sec-tion members. A modified Delphi technique was utilized forthe NTOA and ACEP groups, which allowed for additionalexpert input and consensus development. Conclusion. Theresultant matrix can serve as the basic educational standardaround which TEMS training organizations can design pro-grams of study for the four target audiences. Key words:tactical medicine; tactical combat casualty care; hemorrhagecontrol
PREHOSPITAL EMERGENCY CARE 2011;Early Online:1–15
INTRODUCTION
Over the course of the last 40 years, law enforcementunits have identified the need for specialized teams
Received February 26, 2010, from the Department of EmergencyMedicine (PLC) and the Center of Operational Medicine (PV), Medi-cal College of Georgia (RBS, GP), Augusta, Georgia; the Departmentof Emergency Medicine (JGMcM, JC), Brooke Army Medical Center,Fort Sam Houston, Texas; the National Tactical Officers Association(MG), Baltimore, Maryland; the Department of Emergency Medicine(DL), Saint Vincent’s Mercy Medical Center, Toledo, Ohio; the De-partment of Emergency Medicine (EBL), Medical College of Wiscon-sin, Milwaukee, Wisconsin; and TEMS Section (GB), American Col-lege of Emergency Physicians, Irving, Texas. Revision received June17, 2010; accepted for publication June 22, 2010.
The authors report no conflicts of interest. The authors alone are re-sponsible for the content and writing of the paper.
Address correspondence and reprint requests to: Richard BruceSchwartz, MD, Medical College of Georgia, 1120 15th Street, Au-gusta, GA 30912. e-mail: [email protected]
doi: 10.3109/10903127.2010.514092
to deal with unique problems.1 These teams have de-veloped a variety of subject matter experts in nego-tiations, weapons, explosives, and medicine. Thosewho provide medical support during tactical opera-tions represent a unique segment of prehospital careproviders, working in hazardous and austere environ-ments. This type of prehospital medicine, known astactical medicine, is an evolving discipline.
Tactical medicine is broad based and includes careprovided not only by traditional medical providers(emergency medical technicians [EMTs], physicians,physician assistants, and nurses), but also by the op-erators themselves. Additionally, it impacts the tacti-cal and medical command structure in which the unitoperates. The goal of effective tactical medicine sup-port is to enable law enforcement to operate more ef-ficiently, more effectively, and with reduced risk. Tra-ditional emergency medical services (EMS), nursing,and medicine require practitioners to undergo stan-dardized testing and licensure procedures. In addi-tion, various standardized educational curricula havebeen developed for aspects of medical care such as theuse of Advanced Cardiac Life Support (ACLS) for themanagement of cardiac arrest. No such standardizedcurricula exist for tactical emergency medical support(TEMS). There is a need for defined and consistent skillcompetencies that are expected for TEMS providers.The lack of a tool of this nature has limited standard-ization through our nation’s law enforcement organi-zations. Consistency with regard to core competencieswould provide standards from which training and pro-tocols could be developed.
The provision of trauma care in the tactical envi-ronment has been guided by the U.S. Defense HealthBoard Committee for Tactical Combat Casualty Care(TCCC). This committee comprises military and civil-ian subject matter experts in tactical medicine. Thecommittee meets regularly to update and incorporatebattlefield experience and research into best practicesfor traumatic casualty care in the tactical environment.The American College of Surgeons (ACS) and the Na-tional Association of Emergency Medical Technicians(NAEMT) have endorsed the military’s guidelines forTCCC. This set of best practices for military care on thebattlefield is published in the manual PHTLS: Prehos-pital Trauma Life Support, sixth edition.2 The guide-lines specify the trauma care to be delivered in a hostileenvironment to mitigate the risks inherent in combatand are utilized as a base for most tactical medicine
1
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.

2 PREHOSPITAL EMERGENCY CARE JANUARY/MARCH 2011 VOLUME EARLY ONLINE / NUMBER 1
training programs. These TCCC best practices couldbe developed into competency-based TEMS educa-tion programs; however, they are limited and do notaddress other areas that are considered to be es-sential for the delivery of a comprehensive TEMSprogram.1,3–10 Therefore, a more broadly defined com-petency base is needed for TEMS training curricula.
Currently many well-experienced providers andeducators share the desire to see best practicesbrought into this aspect of prehospital emergencycare. Several tactical medicine training courses ex-ist. However, the educational model has been basedon a process-oriented educational model ratherthan a competency-based, outcome-oriented educa-tional model. Competency-based training is describedas a way to produce reliable and reproducibleroles and responsibilities.11,12 Process-oriented train-ing is focused on the delivery of material, whereascompetency-based training focuses on the attain-ment of specific educational objectives. For instance,process-oriented training would assign credit for at-tending a one-hour lecture on hemorrhage control. Al-ternatively, a competency-based program would focuson the student’s ability to demonstrate the identifica-tion of hemorrhage, the proper application of a tourni-quet, and the application of combat gauze to a woundwith life-threatening hemorrhage. It is essentially thedifference between receiving a card or certificate forcourse attendance after attaining a certain level of per-formance on a written test and receiving a card or cer-tificate for course completion after the demonstrationof skills in a simulated environment. When no demon-stration of skills or knowledge is required, the attendeemay or may not have gained the ability to performthe skills that were taught. As an example, in train-ing physicians, the Accreditation Council for Gradu-ate Medical Education (ACGME) recently adopted sixcore competencies to ensure that residents in trainingconformed to uniform guidelines. This transition tocompetency-based education has changed the focus ofeducation from course or process completion to task orcompetency completion.
Competency can be broadly defined as the habitualand judicious use of communication, knowledge, tech-nical skills, clinical reasoning, emotions, values, andreflection in daily practice for the benefit of the indi-vidual and community being served.13 Competencyis context dependent. A physician’s rank in medicalschool, a pilot’s rank in flight school, or an officer’sstanding at a military academy will not predict how heor she will perform with a given patient, during an in-flight emergency, or in a unique tactical situation. At-taining acceptable grades on a normative test or com-pletion of a course of study alone does not necessar-ily prove that the practitioner has the needed skills.Rather, a demonstration of mastery of a set of crite-ria forms the basis for qualification and the mark of a
competent provider. Competency-based training mayallow for greater standardization of training with a fo-cus on outcomes.11–13
The National Tactical Officers Association (NTOA)and its academic partners assert that tactical medicineprograms should be developed utilizing competency-based, outcome-oriented education programs. Further,if accountability is to be enhanced, objectives, stan-dards, and criteria must be clearly stated and openfor inspection by colleagues, administration, experts,and students.14 The goal of this project was to de-velop educational competencies for TEMS as a firststep toward enhancing accountability. The same ap-proach was taken by the ACGME in 1999 through itsOutcomes Project.15
METHODS
To meet this need, the NTOA assembled an 11-memberworking group of subject matter experts to review ex-isting course curricula, to identify gaps, and to assem-ble a competency-based educational framework forTEMS curricula. This working group was made up offour physicians, one physician assistant, and six out-of-hospital providers (Appendix 1). All members ofthe working group had previously collaborated in thedevelopment of national level TEMS curricula (NTOATEMS curricula and the Tactical Operator Care [TOC]curriculum that was developed for the Federal Bu-reau of Investigation [FBI]). The working group wasselected by the leadership of the NTOA based on theirnational reputation and to ensure that there was rep-resentation from all stakeholder groups (physicians,EMS, law enforcement, military, fire rescue). The TEMSexperience of the group included military as well aslocal, state, and federal civilian law enforcement. Themembers of the working group are listed in Appendix1 along with the individual expertise of each member.
Prior to initiating their work, the members of theworking group reviewed the Core Competencies forHealth Professionals in a Disaster developed by theAmerican Medical Association (AMA) under a grantfrom the Assistant Secretary for Preparedness andResponse (ASPR) as an example of how to developcompetencies for selected population groups.16 Theworking group then drafted a TEMS competencymatrix utilizing a similar methodology as the priorAMA work. They incorporated the practices from theTCCC guidelines into the matrix along with additionalcompetencies relevant to the civilian law enforcementenvironment. The draft TEMS competency matrixwas then reviewed by the American College ofEmergency Physicians (ACEP) Tactical EmergencyMedicine Section using a modified Delphi procedure.The Delphi procedure is a method for obtaininggroup consensus by making revisions to a list ordocument based on group feedback until all agree
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.

Schwartz et al. TACTICAL MEDICINE COMPETENCY-BASED GUIDELINES 3
that the final list or document is complete or a setnumber of feedback cycles are completed. The Delphiprocedure is based on the assumption that the con-sensus from a structured group is more accurate thanthat from an unstructured group. A “mini” Delphiprocedure (also called talk estimate talk) has beendeveloped for use during face-to-face meetings. Thisproject used a modified Delphi procedure by utilizingboth the traditional Delphi procedure (ACEP TEMSleadership and general membership) and the miniDelphi procedure (NTOA working group).
The specific steps for this project are provided in de-tail. An initial draft of the competencies was developedby a single author (RBS), who then acted as the facilita-tor for the modified Delphi review. The competencieswere provided in written form to the NTOA workinggroup and they had a face-to-face meeting where sev-eral rounds of review were facilitated until consensuson the competencies was achieved.
The revised competency document was then pro-vided to the leadership of the ACEP TEMS Section.The leaders of the TEMS Section reviewed the docu-ment and provided suggested revisions. The facilitator(RBS) reviewed the recommendations and integratedthem into the competency document. The revised doc-ument was provided to the leaders of the TEMS Sec-tion for a review and approval that that version shouldbe sent to the general membership of the ACEP TEMSSection for review. Once the revised document was ap-proved by the section leaders, it was provided via e-mail to the general membership the ACEP TEMS Sec-tion, which consists of 275 physicians. All feedbackwas reviewed by the facilitator (RBS) and integratedinto the document. The revised document was sent tothe general membership of the section for review andconcurrence that consensus was established. The doc-ument was then circulated among the NTOA workinggroup for a final review, and there was agreement thatthe document was complete.
RESULTS
The initial draft document included 11 competency do-mains along with 30 separate core crosscutting com-petencies. The core crosscutting competencies were in-tended to apply to all levels of TEMS providers. Theinitial draft document also included 184 specific com-petencies for TEMS providers. These were competen-cies that would apply to a given target audience. Thespecific target audiences were operator/agent/officer,medical provider, team commander, and medical di-rector.
The expert NTOA working group utilized the miniDelphi procedure to modify the initial draft document.They increased the number of competency domains to14. They also increased the core crosscutting compe-tencies to 43, and the specific competencies to 285.
TABLE 1. The 18 Identified Competency Domains
1. Tactical Combat Casualty Care Methodology2. Remote Assessment and Rescue/Extraction3. Hemostasis4. Airway5. Breathing6. Circulation7. Vascular Access8. Medication Administration9. Casualty Immobilization
10. Medical Planning11. Human Performance Factors/Health Surveillance12. Environmental Factors13. Explosions and Blast Injuries14. Injury Patterns and Evidence Preservation15. Hazardous Materials Management16. Remote/Surrogate Treatment17. Less Lethal Injuries18. Special Populations
The leadership of the ACEP TEMS Section used theDelphi procedure and increased the number of com-petency domains to 17, along with the number of corecrosscutting competencies to 46 and the number ofspecific competencies to 314.
Finally, on review by the ACEP TEMS Section gen-eral membership, using the Delphi procedure, one ad-ditional domain was added, along with two core cross-cutting competencies and 44 specific competencies.
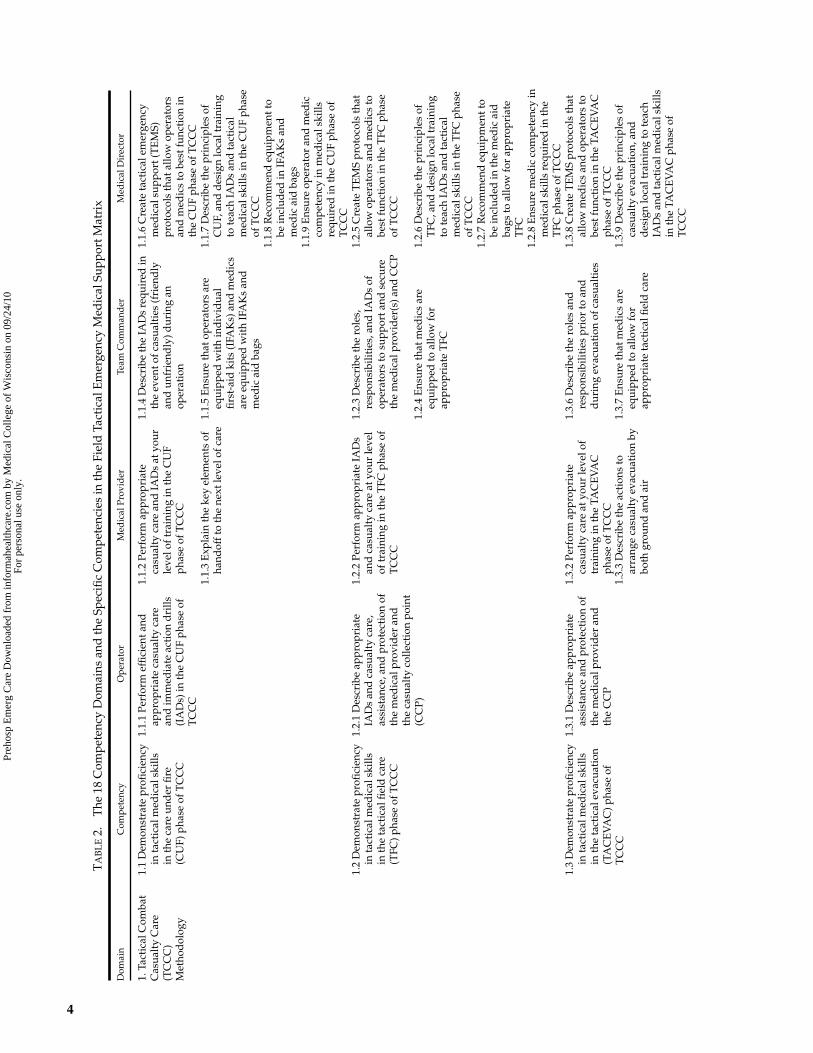
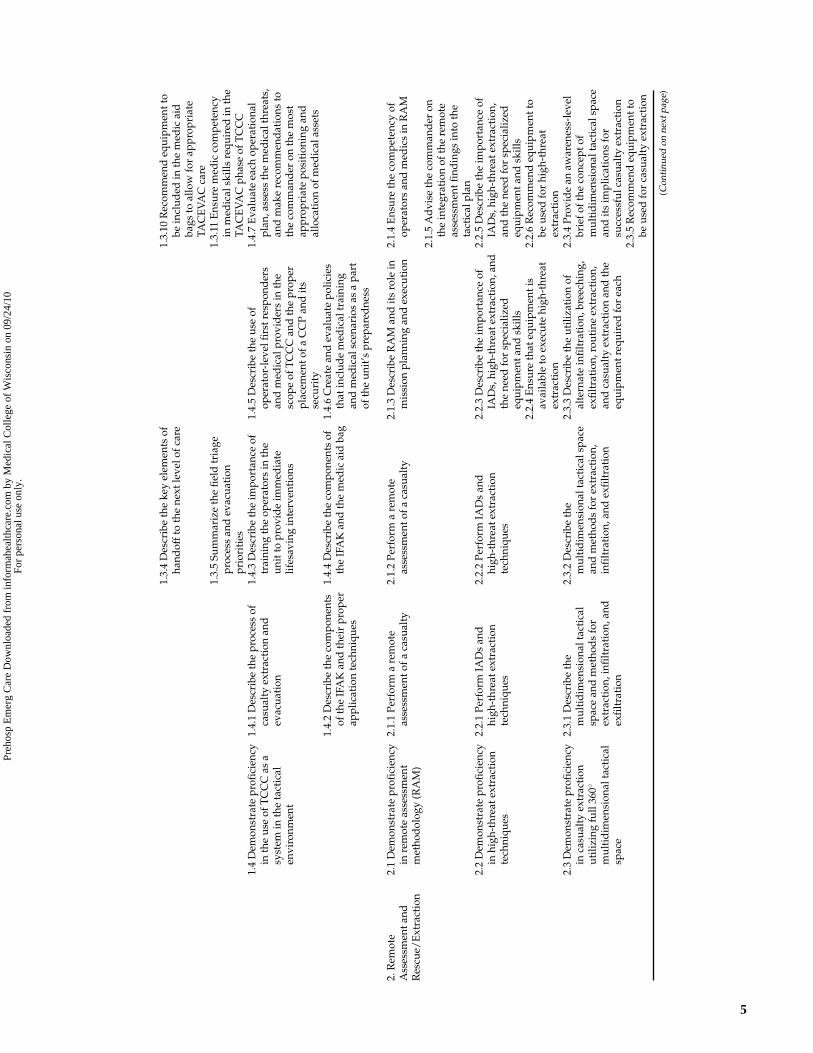
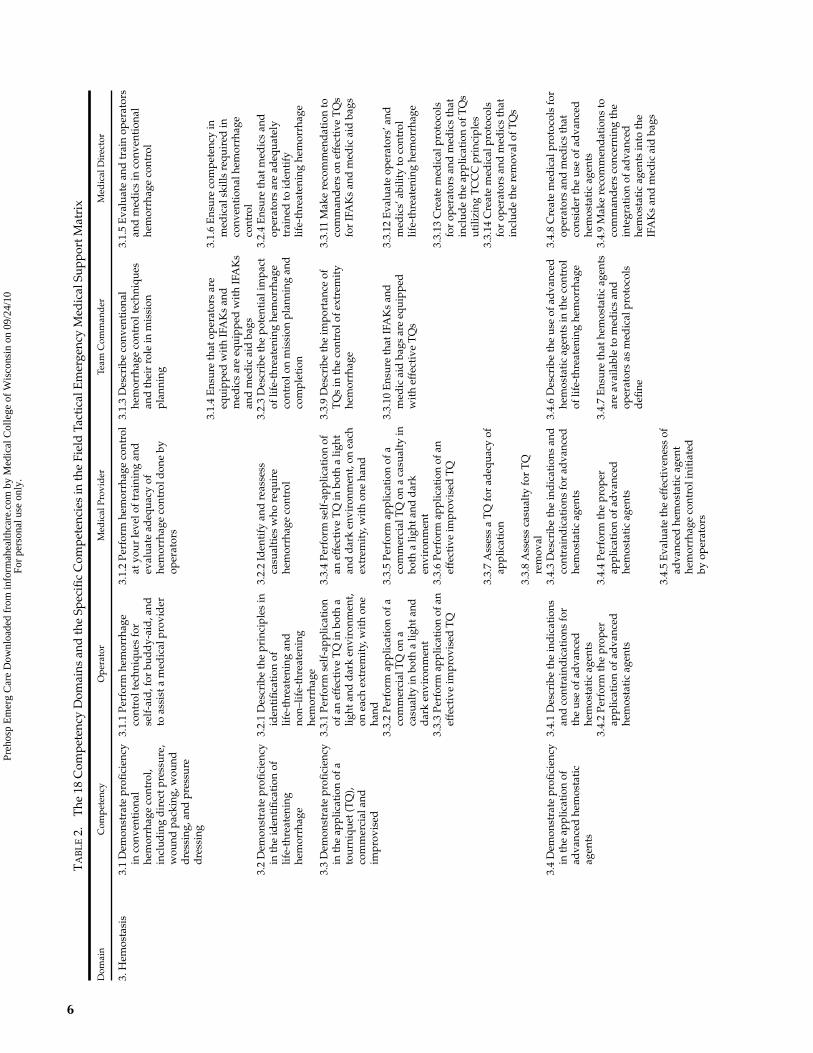
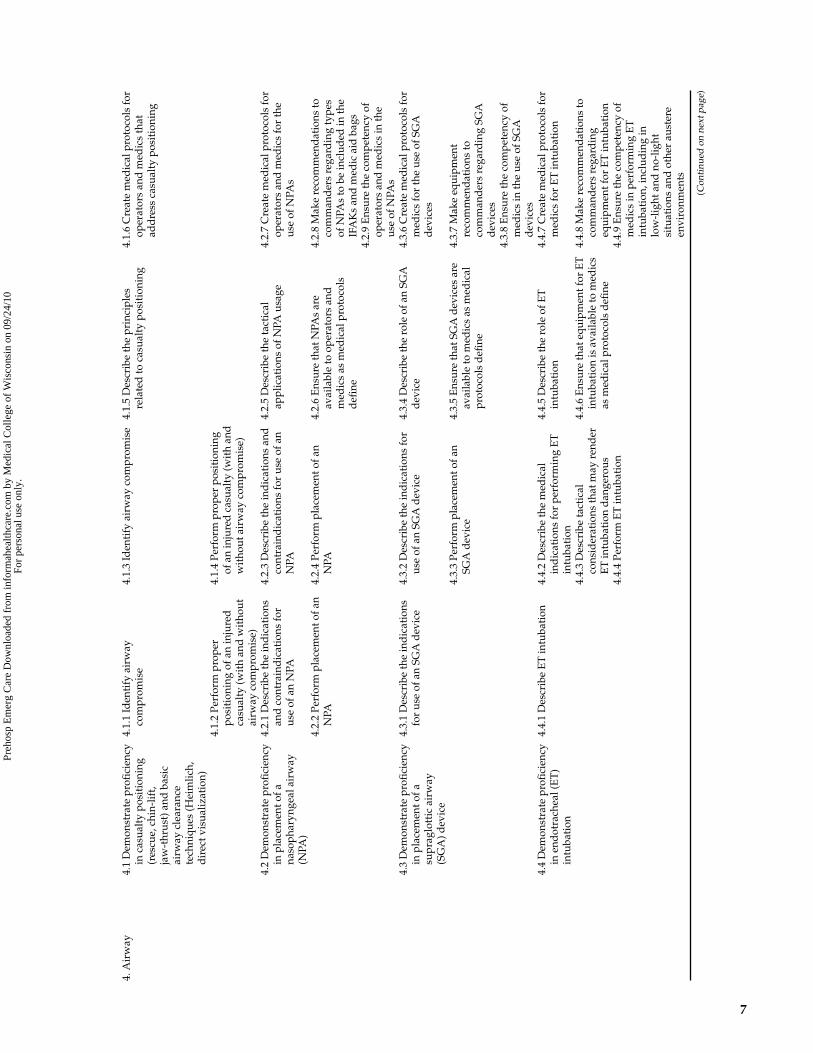
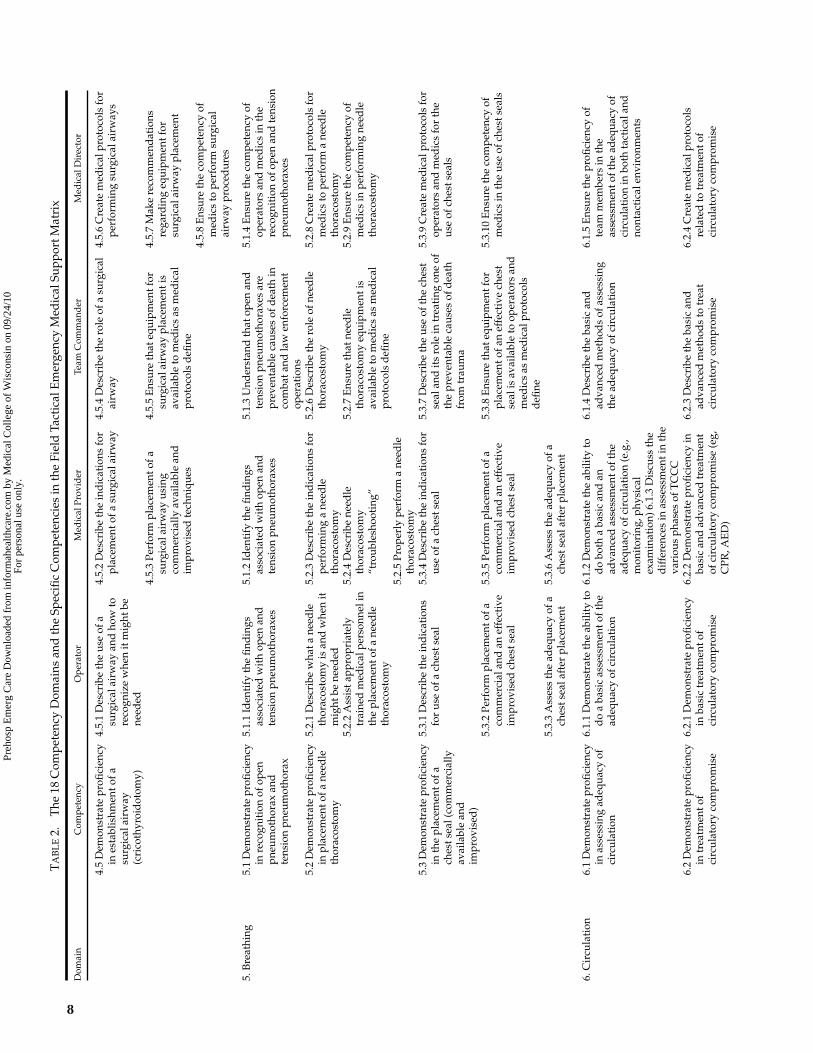
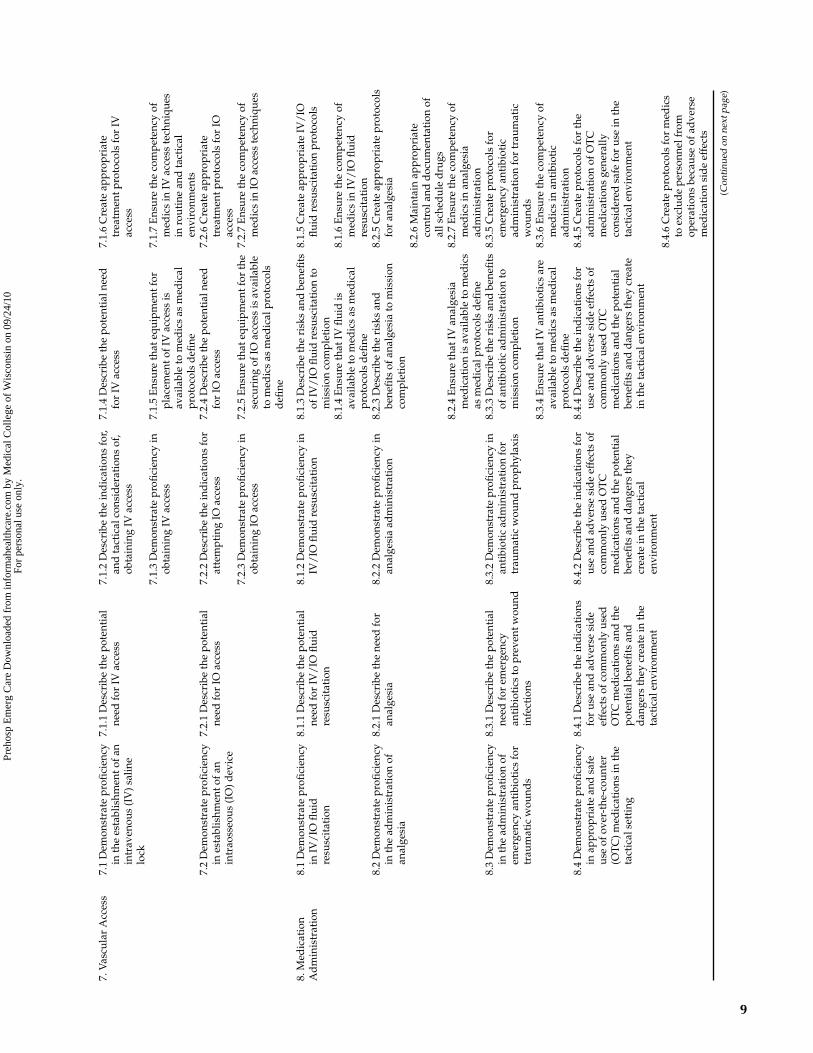
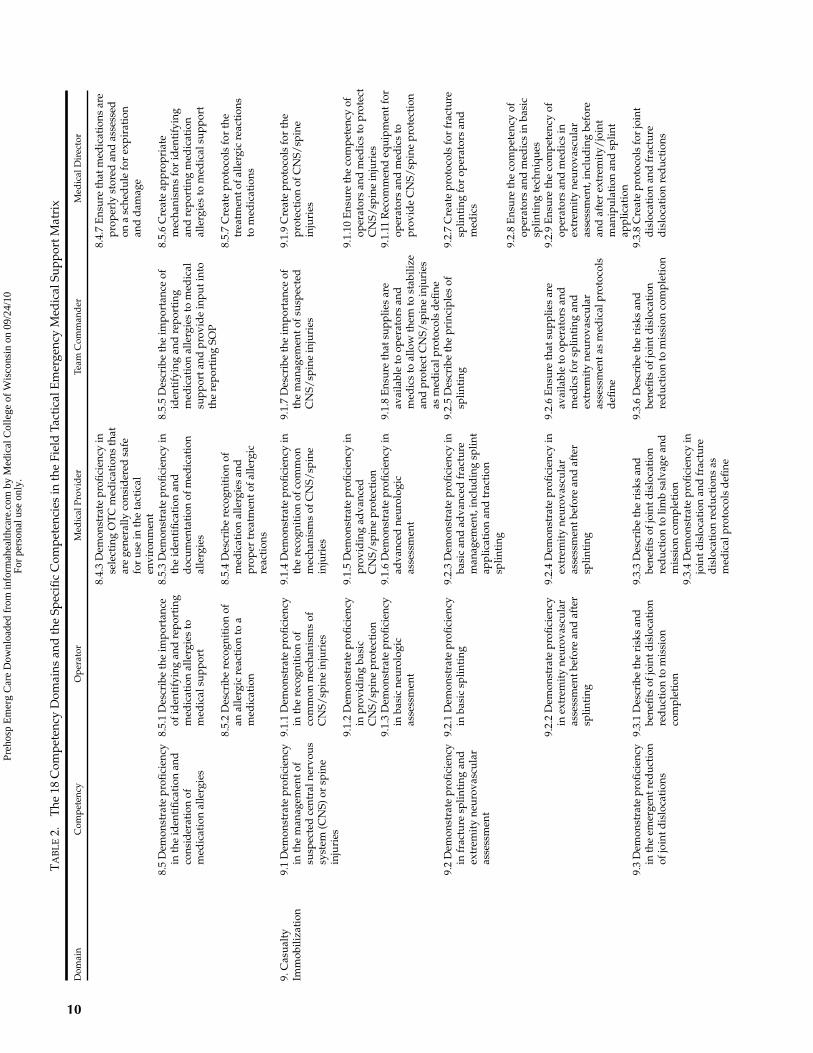
The final TEMS competency matrix includes 18competency domains (see Table 1), 48 core cross-cutting competencies, and 358 specific competencies.As shown in Table 2, the specific competencies aredefined for each level of TEMS provider: opera-tor/agent/officer, medical provider, team commander,and medical director.
The competencies were defined to represent basictasks and information for which the different providertypes are responsible. In some instances, the tasks per-tain to medical procedures and skills. For the comman-der and medical director, unique tasks address specificcommand functions. For example, one role defined forthe commander is ensuring that key equipment andtraining are available. Recurring medical director tasksinclude ensuring competency in the performance ofmedical skills by operators and medical providers, cre-ating medical protocols, and advising the team com-mander.
DISCUSSION
This competency-based matrix represents the initialversion of a dynamic document meant to change andgrow with the evolution of medical technology, as wellas with the collective experience of those who practicemedicine in this unique environment. The matrix rep-resents a framework on which training curricula andmedical protocols can be based.
There is an inherent inability to routinely em-ploy traditional assets (i.e., ambulances, EMTs, and
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.
TA
BL
E2.
The
18C
ompe
tenc
yD
omai
nsan
dth
eSp
ecifi
cC
ompe
tenc
ies
inth
eFi
eld
Tact
ical
Em
erge
ncy
Med
ical
Supp
ortM
atri
x
Dom
ain
Com
pete
ncy
Ope
rato
rM
edic
alPr
ovid
erTe
amC
omm
and
erM
edic
alD
irec
tor
1.Ta
ctic
alC
omba
tC
asua
lty
Car
e(T
CC
C)
Met
hod
olog
y
1.1
Dem
onst
rate
profi
cien
cyin
tact
ical
med
ical
skill
sin
the
care
und
erfi
re(C
UF)
phas
eof
TC
CC
1.1.
1Pe
rfor
mef
ficie
ntan
dap
prop
riat
eca
sual
tyca
rean
dim
med
iate
acti
ond
rills
(IA
Ds)
inth
eC
UF
phas
eof
TC
CC
1.1.
2Pe
rfor
map
prop
riat
eca
sual
tyca
rean
dIA
Ds
atyo
urle
velo
ftra
inin
gin
the
CU
Fph
ase
ofT
CC
C
1.1.
4D
escr
ibe
the
IAD
sre
quir
edin
the
even
tofc
asua
ltie
s(f
rien
dly
and
unfr
iend
ly)d
urin
gan
oper
atio
n
1.1.
6C
reat
eta
ctic
alem
erge
ncy
med
ical
supp
ort(
TE
MS)
prot
ocol
sth
atal
low
oper
ator
san
dm
edic
sto
best
func
tion
inth
eC
UF
phas
eof
TC
CC
1.1.
3E
xpla
inth
eke
yel
emen
tsof
hand
offt
oth
ene
xtle
velo
fcar
e1.
1.5
Ens
ure
that
oper
ator
sar
eeq
uipp
edw
ith
ind
ivid
ual
first
-aid
kits
(IFA
Ks)
and
med
ics
are
equi
pped
wit
hIF
AK
san
dm
edic
aid
bags
1.1.
7D
escr
ibe
the
prin
cipl
esof
CU
F,an
dd
esig
nlo
calt
rain
ing
tote
ach
IAD
san
dta
ctic
alm
edic
alsk
ills
inth
eC
UF
phas
eof
TC
CC
1.1.
8R
ecom
men
deq
uipm
entt
obe
incl
uded
inIF
AK
san
dm
edic
aid
bags
1.1.
9E
nsur
eop
erat
oran
dm
edic
com
pete
ncy
inm
edic
alsk
ills
requ
ired
inth
eC
UF
phas
eof
TC
CC
1.2
Dem
onst
rate
profi
cien
cyin
tact
ical
med
ical
skill
sin
the
tact
ical
fiel
dca
re(T
FC)p
hase
ofT
CC
C
1.2.
1D
escr
ibe
appr
opri
ate
IAD
san
dca
sual
tyca
re,
assi
stan
ce,a
ndpr
otec
tion
ofth
em
edic
alpr
ovid
eran
dth
eca
sual
tyco
llect
ion
poin
t(C
CP)
1.2.
2Pe
rfor
map
prop
riat
eIA
Ds
and
casu
alty
care
atyo
urle
vel
oftr
aini
ngin
the
TFC
phas
eof
TC
CC
1.2.
3D
escr
ibe
the
role
s,re
spon
sibi
litie
s,an
dIA
Ds
ofop
erat
ors
tosu
ppor
tand
secu
reth
em
edic
alpr
ovid
er(s
)and
CC
P
1.2.
5C
reat
eT
EM
Spr
otoc
ols
that
allo
wop
erat
ors
and
med
ics
tobe
stfu
ncti
onin
the
TFC
phas
eof
TC
CC
1.2.
4E
nsur
eth
atm
edic
sar
eeq
uipp
edto
allo
wfo
rap
prop
riat
eT
FC
1.2.
6D
escr
ibe
the
prin
cipl
esof
TFC
,and
des
ign
loca
ltra
inin
gto
teac
hIA
Ds
and
tact
ical
med
ical
skill
sin
the
TFC
phas
eof
TC
CC
1.2.
7R
ecom
men
deq
uipm
entt
obe
incl
uded
inth
em
edic
aid
bags
toal
low
for
appr
opri
ate
TFC
1.2.
8E
nsur
em
edic
com
pete
ncy
inm
edic
alsk
ills
requ
ired
inth
eT
FCph
ase
ofT
CC
C1.
3D
emon
stra
tepr
ofici
ency
inta
ctic
alm
edic
alsk
ills
inth
eta
ctic
alev
acua
tion
(TA
CE
VA
C)p
hase
ofT
CC
C
1.3.
1D
escr
ibe
appr
opri
ate
assi
stan
cean
dpr
otec
tion
ofth
em
edic
alpr
ovid
eran
dth
eC
CP
1.3.
2Pe
rfor
map
prop
riat
eca
sual
tyca
reat
your
leve
lof
trai
ning
inth
eTA
CE
VA
Cph
ase
ofT
CC
C
1.3.
6D
escr
ibe
the
role
san
dre
spon
sibi
litie
spr
ior
toan
dd
urin
gev
acua
tion
ofca
sual
ties
1.3.
8C
reat
eT
EM
Spr
otoc
ols
that
allo
wm
edic
san
dop
erat
ors
tobe
stfu
ncti
onin
the
TAC
EV
AC
phas
eof
TC
CC
1.3.
3D
escr
ibe
the
acti
ons
toar
rang
eca
sual
tyev
acua
tion
bybo
thgr
ound
and
air
1.3.
7E
nsur
eth
atm
edic
sar
eeq
uipp
edto
allo
wfo
rap
prop
riat
eta
ctic
alfi
eld
care
1.3.
9D
escr
ibe
the
prin
cipl
esof
casu
alty
evac
uati
on,a
ndd
esig
nlo
calt
rain
ing
tote
ach
IAD
san
dta
ctic
alm
edic
alsk
ills
inth
eTA
CE
VA
Cph
ase
ofT
CC
C
4
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.
1.3.
4D
escr
ibe
the
key
elem
ents
ofha
ndof
fto
the
next
leve
lofc
are
1.3.
10R
ecom
men
deq
uipm
entt
obe
incl
uded
inth
em
edic
aid
bags
toal
low
for
appr
opri
ate
TAC
EV
AC
care
1.3.
5Su
mm
ariz
eth
efi
eld
tria
gepr
oces
san
dev
acua
tion
prio
riti
es
1.3.
11E
nsur
em
edic
com
pete
ncy
inm
edic
alsk
ills
requ
ired
inth
eTA
CE
VA
Cph
ase
ofT
CC
C1.
4D
emon
stra
tepr
ofici
ency
inth
eus
eof
TC
CC
asa
syst
emin
the
tact
ical
envi
ronm
ent
1.4.
1D
escr
ibe
the
proc
ess
ofca
sual
tyex
trac
tion
and
evac
uati
on
1.4.
3D
escr
ibe
the
impo
rtan
ceof
trai
ning
the
oper
ator
sin
the
unit
topr
ovid
eim
med
iate
lifes
avin
gin
terv
enti
ons
1.4.
5D
escr
ibe
the
use
ofop
erat
or-l
evel
first
resp
ond
ers
and
med
ical
prov
ider
sin
the
scop
eof
TC
CC
and
the
prop
erpl
acem
ento
faC
CP
and
its
secu
rity
1.4.
7E
valu
ate
each
oper
atio
nal
plan
,ass
ess
the
med
ical
thre
ats,
and
mak
ere
com
men
dat
ions
toth
eco
mm
and
eron
the
mos
tap
prop
riat
epo
siti
onin
gan
dal
loca
tion
ofm
edic
alas
sets
1.4.
2D
escr
ibe
the
com
pone
nts
ofth
eIF
AK
and
thei
rpr
oper
appl
icat
ion
tech
niqu
es
1.4.
4D
escr
ibe
the
com
pone
nts
ofth
eIF
AK
and
the
med
icai
dba
g1.
4.6
Cre
ate
and
eval
uate
polic
ies
that
incl
ude
med
ical
trai
ning
and
med
ical
scen
ario
sas
apa
rtof
the
unit
’spr
epar
edne
ss
2.R
emot
eA
sses
smen
tand
Res
cue/
Ext
ract
ion
2.1
Dem
onst
rate
profi
cien
cyin
rem
ote
asse
ssm
ent
met
hod
olog
y(R
AM
)
2.1.
1Pe
rfor
ma
rem
ote
asse
ssm
ento
faca
sual
ty2.
1.2
Perf
orm
are
mot
eas
sess
men
tofa
casu
alty
2.1.
3D
escr
ibe
RA
Man
dit
sro
lein
mis
sion
plan
ning
and
exec
utio
n2.
1.4
Ens
ure
the
com
pete
ncy
ofop
erat
ors
and
med
ics
inR
AM
2.1.
5A
dvi
seth
eco
mm
and
eron
the
inte
grat
ion
ofth
ere
mot
eas
sess
men
tfind
ings
into
the
tact
ical
plan
2.2
Dem
onst
rate
profi
cien
cyin
high
-thr
eate
xtra
ctio
nte
chni
ques
2.2.
1Pe
rfor
mIA
Ds
and
high
-thr
eate
xtra
ctio
nte
chni
ques
2.2.
2Pe
rfor
mIA
Ds
and
high
-thr
eate
xtra
ctio
nte
chni
ques
2.2.
3D
escr
ibe
the
impo
rtan
ceof
IAD
s,hi
gh-t
hrea
text
ract
ion,
and
the
need
for
spec
ializ
edeq
uipm
enta
ndsk
ills
2.2.
5D
escr
ibe
the
impo
rtan
ceof
IAD
s,hi
gh-t
hrea
text
ract
ion,
and
the
need
for
spec
ializ
edeq
uipm
enta
ndsk
ills
2.2.
4E
nsur
eth
ateq
uipm
enti
sav
aila
ble
toex
ecut
ehi
gh-t
hrea
tex
trac
tion
2.2.
6R
ecom
men
deq
uipm
entt
obe
used
for
high
-thr
eat
extr
acti
on2.
3D
emon
stra
tepr
ofici
ency
inca
sual
tyex
trac
tion
utili
zing
full
360◦
mul
tid
imen
sion
alta
ctic
alsp
ace
2.3.
1D
escr
ibe
the
mul
tid
imen
sion
alta
ctic
alsp
ace
and
met
hod
sfo
rex
trac
tion
,infi
ltra
tion
,and
exfi
ltra
tion
2.3.
2D
escr
ibe
the
mul
tid
imen
sion
alta
ctic
alsp
ace
and
met
hod
sfo
rex
trac
tion
,in
filt
rati
on,a
ndex
filt
rati
on
2.3.
3D
escr
ibe
the
utili
zati
onof
alte
rnat
ein
filt
rati
on,b
reec
hing
,ex
filt
rati
on,r
outi
neex
trac
tion
,an
dca
sual
tyex
trac
tion
and
the
equi
pmen
treq
uire
dfo
rea
ch
2.3.
4Pr
ovid
ean
awar
enes
s-le
vel
brie
foft
heco
ncep
tof
mul
tid
imen
sion
alta
ctic
alsp
ace
and
its
impl
icat
ions
for
succ
essf
ulca
sual
tyex
trac
tion
2.3.
5R
ecom
men
deq
uipm
entt
obe
used
for
casu
alty
extr
acti
on
(Con
tinu
edon
next
page
)
5
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.
TA
BL
E2.
The
18C
ompe
tenc
yD
omai
nsan
dth
eSp
ecifi
cC
ompe
tenc
ies
inth
eFi
eld
Tact
ical
Em
erge
ncy
Med
ical
Supp
ortM
atri
x
Dom
ain
Com
pete
ncy
Ope
rato
rM
edic
alPr
ovid
erTe
amC
omm
and
erM
edic
alD
irec
tor
3.H
emos
tasi
s3.
1D
emon
stra
tepr
ofici
ency
inco
nven
tion
alhe
mor
rhag
eco
ntro
l,in
clud
ing
dir
ectp
ress
ure,
wou
ndpa
ckin
g,w
ound
dre
ssin
g,an
dpr
essu
red
ress
ing
3.1.
1Pe
rfor
mhe
mor
rhag
eco
ntro
ltec
hniq
ues
for
self
-aid
,for
bud
dy-
aid
,and
toas
sist
am
edic
alpr
ovid
er
3.1.
2Pe
rfor
mhe
mor
rhag
eco
ntro
lat
your
leve
loft
rain
ing
and
eval
uate
adeq
uacy
ofhe
mor
rhag
eco
ntro
ldon
eby
oper
ator
s
3.1.
3D
escr
ibe
conv
enti
onal
hem
orrh
age
cont
rolt
echn
ique
san
dth
eir
role
inm
issi
onpl
anni
ng
3.1.
5E
valu
ate
and
trai
nop
erat
ors
and
med
ics
inco
nven
tion
alhe
mor
rhag
eco
ntro
l
3.1.
4E
nsur
eth
atop
erat
ors
are
equi
pped
wit
hIF
AK
san
dm
edic
sar
eeq
uipp
edw
ith
IFA
Ks
and
med
icai
dba
gs
3.1.
6E
nsur
eco
mpe
tenc
yin
med
ical
skill
sre
quir
edin
conv
enti
onal
hem
orrh
age
cont
rol
3.2
Dem
onst
rate
profi
cien
cyin
the
iden
tifi
cati
onof
life-
thre
aten
ing
hem
orrh
age
3.2.
1D
escr
ibe
the
prin
cipl
esin
iden
tifi
cati
onof
life-
thre
aten
ing
and
non–
life-
thre
aten
ing
hem
orrh
age
3.2.
2Id
enti
fyan
dre
asse
ssca
sual
ties
who
requ
ire
hem
orrh
age
cont
rol
3.2.
3D
escr
ibe
the
pote
ntia
lim
pact
oflif
e-th
reat
enin
ghe
mor
rhag
eco
ntro
lon
mis
sion
plan
ning
and
com
plet
ion
3.2.
4E
nsur
eth
atm
edic
san
dop
erat
ors
are
adeq
uate
lytr
aine
dto
iden
tify
life-
thre
aten
ing
hem
orrh
age
3.3
Dem
onst
rate
profi
cien
cyin
the
appl
icat
ion
ofa
tour
niqu
et(T
Q),
com
mer
cial
and
impr
ovis
ed
3.3.
1Pe
rfor
mse
lf-a
pplic
atio
nof
anef
fect
ive
TQ
inbo
tha
light
and
dar
ken
viro
nmen
t,on
each
extr
emit
y,w
ith
one
hand
3.3.
4Pe
rfor
mse
lf-a
pplic
atio
nof
anef
fect
ive
TQ
inbo
tha
light
and
dar
ken
viro
nmen
t,on
each
extr
emit
y,w
ith
one
hand
3.3.
9D
escr
ibe
the
impo
rtan
ceof
TQ
sin
the
cont
rolo
fext
rem
ity
hem
orrh
age
3.3.
11M
ake
reco
mm
end
atio
nto
com
man
der
son
effe
ctiv
eT
Qs
for
IFA
Ks
and
med
icai
dba
gs
3.3.
2Pe
rfor
map
plic
atio
nof
aco
mm
erci
alT
Qon
aca
sual
tyin
both
alig
htan
dd
ark
envi
ronm
ent
3.3.
5Pe
rfor
map
plic
atio
nof
aco
mm
erci
alT
Qon
aca
sual
tyin
both
alig
htan
dd
ark
envi
ronm
ent
3.3.
10E
nsur
eth
atIF
AK
san
dm
edic
aid
bags
are
equi
pped
wit
hef
fect
ive
TQ
s
3.3.
12E
valu
ate
oper
ator
s’an
dm
edic
s’ab
ility
toco
ntro
llif
e-th
reat
enin
ghe
mor
rhag
e
3.3.
3Pe
rfor
map
plic
atio
nof
anef
fect
ive
impr
ovis
edT
Q3.
3.6
Perf
orm
appl
icat
ion
ofan
effe
ctiv
eim
prov
ised
TQ
3.3.
13C
reat
em
edic
alpr
otoc
ols
for
oper
ator
san
dm
edic
sth
atin
clud
eth
eap
plic
atio
nof
TQ
sut
ilizi
ngT
CC
Cpr
inci
ples
3.3.
7A
sses
sa
TQ
for
adeq
uacy
ofap
plic
atio
n3.
3.14
Cre
ate
med
ical
prot
ocol
sfo
rop
erat
ors
and
med
ics
that
incl
ude
the
rem
oval
ofT
Qs
3.3.
8A
sses
sca
sual
tyfo
rT
Qre
mov
al3.
4D
emon
stra
tepr
ofici
ency
inth
eap
plic
atio
nof
adva
nced
hem
osta
tic
agen
ts
3.4.
1D
escr
ibe
the
ind
icat
ions
and
cont
rain
dic
atio
nsfo
rth
eus
eof
adva
nced
hem
osta
tic
agen
ts
3.4.
3D
escr
ibe
the
ind
icat
ions
and
cont
rain
dic
atio
nsfo
rad
vanc
edhe
mos
tati
cag
ents
3.4.
6D
escr
ibe
the
use
ofad
vanc
edhe
mos
tati
cag
ents
inth
eco
ntro
lof
life-
thre
aten
ing
hem
orrh
age
3.4.
8C
reat
em
edic
alpr
otoc
ols
for
oper
ator
san
dm
edic
sth
atco
nsid
erth
eus
eof
adva
nced
hem
osta
tic
agen
ts3.
4.2
Perf
orm
the
prop
erap
plic
atio
nof
adva
nced
hem
osta
tic
agen
ts
3.4.
4Pe
rfor
mth
epr
oper
appl
icat
ion
ofad
vanc
edhe
mos
tati
cag
ents
3.4.
7E
nsur
eth
athe
mos
tati
cag
ents
are
avai
labl
eto
med
ics
and
oper
ator
sas
med
ical
prot
ocol
sd
efine
3.4.
9M
ake
reco
mm
end
atio
nsto
com
man
der
sco
ncer
ning
the
inte
grat
ion
ofad
vanc
edhe
mos
tati
cag
ents
into
the
IFA
Ks
and
med
icai
dba
gs3.
4.5
Eva
luat
eth
eef
fect
iven
ess
ofad
vanc
edhe
mos
tati
cag
ent
hem
orrh
age
cont
roli
niti
ated
byop
erat
ors
6
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.
4.A
irw
ay4.
1D
emon
stra
tepr
ofici
ency
inca
sual
typo
siti
onin
g(r
escu
e,ch
in-l
ift,
jaw
-thr
ust)
and
basi
cai
rway
clea
ranc
ete
chni
ques
(Hei
mlic
h,d
irec
tvis
ualiz
atio
n)
4.1.
1Id
enti
fyai
rway
com
prom
ise
4.1.
3Id
enti
fyai
rway
com
prom
ise
4.1.
5D
escr
ibe
the
prin
cipl
esre
late
dto
casu
alty
posi
tion
ing
4.1.
6C
reat
em
edic
alpr
otoc
ols
for
oper
ator
san
dm
edic
sth
atad
dre
ssca
sual
typo
siti
onin
g
4.1.
2Pe
rfor
mpr
oper
posi
tion
ing
ofan
inju
red
casu
alty
(wit
han
dw
itho
utai
rway
com
prom
ise)
4.1.
4Pe
rfor
mpr
oper
posi
tion
ing
ofan
inju
red
casu
alty
(wit
han
dw
itho
utai
rway
com
prom
ise)
4.2
Dem
onst
rate
profi
cien
cyin
plac
emen
tofa
naso
phar
ynge
alai
rway
(NPA
)
4.2.
1D
escr
ibe
the
ind
icat
ions
and
cont
rain
dic
atio
nsfo
rus
eof
anN
PA
4.2.
3D
escr
ibe
the
ind
icat
ions
and
cont
rain
dic
atio
nsfo
rus
eof
anN
PA
4.2.
5D
escr
ibe
the
tact
ical
appl
icat
ions
ofN
PAus
age
4.2.
7C
reat
em
edic
alpr
otoc
ols
for
oper
ator
san
dm
edic
sfo
rth
eus
eof
NPA
s
4.2.
2Pe
rfor
mpl
acem
ento
fan
NPA
4.2.
4Pe
rfor
mpl
acem
ento
fan
NPA
4.2.
6E
nsur
eth
atN
PAs
are
avai
labl
eto
oper
ator
san
dm
edic
sas
med
ical
prot
ocol
sd
efine
4.2.
8M
ake
reco
mm
end
atio
nsto
com
man
der
sre
gard
ing
type
sof
NPA
sto
bein
clud
edin
the
IFA
Ks
and
med
icai
dba
gs4.
2.9
Ens
ure
the
com
pete
ncy
ofop
erat
ors
and
med
ics
inth
eus
eof
NPA
s4.
3D
emon
stra
tepr
ofici
ency
inpl
acem
ento
fasu
prag
lott
icai
rway
(SG
A)d
evic
e
4.3.
1D
escr
ibe
the
ind
icat
ions
for
use
ofan
SGA
dev
ice
4.3.
2D
escr
ibe
the
ind
icat
ions
for
use
ofan
SGA
dev
ice
4.3.
4D
escr
ibe
the
role
ofan
SGA
dev
ice
4.3.
6C
reat
em
edic
alpr
otoc
ols
for
med
ics
for
the
use
ofSG
Ad
evic
es
4.3.
3Pe
rfor
mpl
acem
ento
fan
SGA
dev
ice
4.3.
5E
nsur
eth
atSG
Ad
evic
esar
eav
aila
ble
tom
edic
sas
med
ical
prot
ocol
sd
efine
4.3.
7M
ake
equi
pmen
tre
com
men
dat
ions
toco
mm
and
ers
rega
rdin
gSG
Ad
evic
es4.
3.8
Ens
ure
the
com
pete
ncy
ofm
edic
sin
the
use
ofSG
Ad
evic
es4.
4D
emon
stra
tepr
ofici
ency
inen
dot
rach
eal(
ET
)in
tuba
tion
4.4.
1D
escr
ibe
ET
intu
bati
on4.
4.2
Des
crib
eth
em
edic
alin
dic
atio
nsfo
rpe
rfor
min
gE
Tin
tuba
tion
4.4.
5D
escr
ibe
the
role
ofE
Tin
tuba
tion
4.4.
7C
reat
em
edic
alpr
otoc
ols
for
med
ics
for
ET
intu
bati
on
4.4.
3D
escr
ibe
tact
ical
cons
ider
atio
nsth
atm
ayre
nder
ET
intu
bati
ond
ange
rous
4.4.
6E
nsur
eth
ateq
uipm
entf
orE
Tin
tuba
tion
isav
aila
ble
tom
edic
sas
med
ical
prot
ocol
sd
efine
4.4.
8M
ake
reco
mm
end
atio
nsto
com
man
der
sre
gard
ing
equi
pmen
tfor
ET
intu
bati
on4.
4.4
Perf
orm
ET
intu
bati
on4.
4.9
Ens
ure
the
com
pete
ncy
ofm
edic
sin
perf
orm
ing
ET
intu
bati
on,i
nclu
din
gin
low
-lig
htan
dno
-lig
htsi
tuat
ions
and
othe
rau
ster
een
viro
nmen
ts
(Con
tinu
edon
next
page
)
7
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.
TA
BL
E2.
The
18C
ompe
tenc
yD
omai
nsan
dth
eSp
ecifi
cC
ompe
tenc
ies
inth
eFi
eld
Tact
ical
Em
erge
ncy
Med
ical
Supp
ortM
atri
x
Dom
ain
Com
pete
ncy
Ope
rato
rM
edic
alPr
ovid
erTe
amC
omm
and
erM
edic
alD
irec
tor
4.5
Dem
onst
rate
profi
cien
cyin
esta
blis
hmen
tofa
surg
ical
airw
ay(c
rico
thyr
oid
otom
y)
4.5.
1D
escr
ibe
the
use
ofa
surg
ical
airw
ayan
dho
wto
reco
gniz
ew
hen
itm
ight
bene
eded
4.5.
2D
escr
ibe
the
ind
icat
ions
for
plac
emen
tofa
surg
ical
airw
ay4.
5.4
Des
crib
eth
ero
leof
asu
rgic
alai
rway
4.5.
6C
reat
em
edic
alpr
otoc
ols
for
perf
orm
ing
surg
ical
airw
ays
4.5.
3Pe
rfor
mpl
acem
ento
fasu
rgic
alai
rway
usin
gco
mm
erci
ally
avai
labl
ean
dim
prov
ised
tech
niqu
es
4.5.
5E
nsur
eth
ateq
uipm
entf
orsu
rgic
alai
rway
plac
emen
tis
avai
labl
eto
med
ics
asm
edic
alpr
otoc
ols
defi
ne
4.5.
7M
ake
reco
mm
end
atio
nsre
gard
ing
equi
pmen
tfor
surg
ical
airw
aypl
acem
ent
4.5.
8E
nsur
eth
eco
mpe
tenc
yof
med
ics
tope
rfor
msu
rgic
alai
rway
proc
edur
es
5.B
reat
hing
5.1
Dem
onst
rate
profi
cien
cyin
reco
gnit
ion
ofop
enpn
eum
otho
rax
and
tens
ion
pneu
mot
hora
x
5.1.
1Id
enti
fyth
efin
din
gsas
soci
ated
wit
hop
enan
dte
nsio
npn
eum
otho
raxe
s
5.1.
2Id
enti
fyth
efin
din
gsas
soci
ated
wit
hop
enan
dte
nsio
npn
eum
otho
raxe
s
5.1.
3U
nder
stan
dth
atop
enan
dte
nsio
npn
eum
otho
raxe
sar
epr
even
tabl
eca
uses
ofd
eath
inco
mba
tand
law
enfo
rcem
ent
oper
atio
ns
5.1.
4E
nsur
eth
eco
mpe
tenc
yof
oper
ator
san
dm
edic
sin
the
reco
gnit
ion
ofop
enan
dte
nsio
npn
eum
otho
raxe
s
5.2
Dem
onst
rate
profi
cien
cyin
plac
emen
tofa
need
leth
orac
osto
my
5.2.
1D
escr
ibe
wha
tane
edle
thor
acos
tom
yis
and
whe
nit
mig
htbe
need
ed
5.2.
3D
escr
ibe
the
ind
icat
ions
for
perf
orm
ing
ane
edle
thor
acos
tom
y
5.2.
6D
escr
ibe
the
role
ofne
edle
thor
acos
tom
y5.
2.8
Cre
ate
med
ical
prot
ocol
sfo
rm
edic
sto
perf
orm
ane
edle
thor
acos
tom
y5.
2.2
Ass
ista
ppro
pria
tely
trai
ned
med
ical
pers
onne
lin
the
plac
emen
tofa
need
leth
orac
osto
my
5.2.
4D
escr
ibe
need
leth
orac
osto
my
“tro
uble
shoo
ting
”
5.2.
7E
nsur
eth
atne
edle
thor
acos
tom
yeq
uipm
enti
sav
aila
ble
tom
edic
sas
med
ical
prot
ocol
sd
efine
5.2.
9E
nsur
eth
eco
mpe
tenc
yof
med
ics
inpe
rfor
min
gne
edle
thor
acos
tom
y
5.2.
5Pr
oper
lype
rfor
ma
need
leth
orac
osto
my
5.3
Dem
onst
rate
profi
cien
cyin
the
plac
emen
tofa
ches
tsea
l(co
mm
erci
ally
avai
labl
ean
dim
prov
ised
)
5.3.
1D
escr
ibe
the
ind
icat
ions
for
use
ofa
ches
tsea
l5.
3.4
Des
crib
eth
ein
dic
atio
nsfo
rus
eof
ach
ests
eal
5.3.
7D
escr
ibe
the
use
ofth
ech
est
seal
and
its
role
intr
eati
ngon
eof
the
prev
enta
ble
caus
esof
dea
thfr
omtr
aum
a
5.3.
9C
reat
em
edic
alpr
otoc
ols
for
oper
ator
san
dm
edic
sfo
rth
eus
eof
ches
tsea
ls
5.3.
2Pe
rfor
mpl
acem
ento
faco
mm
erci
alan
dan
effe
ctiv
eim
prov
ised
ches
tsea
l
5.3.
5Pe
rfor
mpl
acem
ento
faco
mm
erci
alan
dan
effe
ctiv
eim
prov
ised
ches
tsea
l
5.3.
8E
nsur
eth
ateq
uipm
entf
orpl
acem
ento
fan
effe
ctiv
ech
est
seal
isav
aila
ble
toop
erat
ors
and
med
ics
asm
edic
alpr
otoc
ols
defi
ne
5.3.
10E
nsur
eth
eco
mpe
tenc
yof
med
ics
inth
eus
eof
ches
tsea
ls
5.3.
3A
sses
sth
ead
equa
cyof
ach
ests
eala
fter
plac
emen
t5.
3.6
Ass
ess
the
adeq
uacy
ofa
ches
tsea
laft
erpl
acem
ent
6.C
ircu
lati
on6.
1D
emon
stra
tepr
ofici
ency
inas
sess
ing
adeq
uacy
ofci
rcul
atio
n
6.1.
1D
emon
stra
teth
eab
ility
tod
oa
basi
cas
sess
men
toft
head
equa
cyof
circ
ulat
ion
6.1.
2D
emon
stra
teth
eab
ility
tod
obo
tha
basi
can
dan
adva
nced
asse
ssm
ento
fthe
adeq
uacy
ofci
rcul
atio
n(e
.g.,
mon
itor
ing,
phys
ical
exam
inat
ion)
6.1.
3D
iscu
ssth
ed
iffe
renc
esin
asse
ssm
enti
nth
eva
riou
sph
ases
ofT
CC
C
6.1.
4D
escr
ibe
the
basi
can
dad
vanc
edm
etho
ds
ofas
sess
ing
the
adeq
uacy
ofci
rcul
atio
n
6.1.
5E
nsur
eth
epr
ofici
ency
ofte
amm
embe
rsin
the
asse
ssm
ento
fthe
adeq
uacy
ofci
rcul
atio
nin
both
tact
ical
and
nont
acti
cale
nvir
onm
ents
6.2
Dem
onst
rate
profi
cien
cyin
trea
tmen
tof
circ
ulat
ory
com
prom
ise
6.2.
1D
emon
stra
tepr
ofici
ency
inba
sic
trea
tmen
tof
circ
ulat
ory
com
prom
ise
6.2.
2D
emon
stra
tepr
ofici
ency
inba
sic
and
adva
nced
trea
tmen
tof
circ
ulat
ory
com
prom
ise
(eg,
CPR
,AE
D)
6.2.
3D
escr
ibe
the
basi
can
dad
vanc
edm
etho
ds
totr
eat
circ
ulat
ory
com
prom
ise
6.2.
4C
reat
em
edic
alpr
otoc
ols
rela
ted
totr
eatm
ento
fci
rcul
ator
yco
mpr
omis
e
8
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.
7.V
ascu
lar
Acc
ess
7.1
Dem
onst
rate
profi
cien
cyin
the
esta
blis
hmen
tofa
nin
trav
enou
s(I
V)s
alin
elo
ck
7.1.
1D
escr
ibe
the
pote
ntia
lne
edfo
rIV
acce
ss7.
1.2
Des
crib
eth
ein
dic
atio
nsfo
r,an
dta
ctic
alco
nsid
erat
ions
of,
obta
inin
gIV
acce
ss
7.1.
4D
escr
ibe
the
pote
ntia
lnee
dfo
rIV
acce
ss7.
1.6
Cre
ate
appr
opri
ate
trea
tmen
tpro
toco
lsfo
rIV
acce
ss
7.1.
3D
emon
stra
tepr
ofici
ency
inob
tain
ing
IVac
cess
7.1.
5E
nsur
eth
ateq
uipm
entf
orpl
acem
ento
fIV
acce
ssis
avai
labl
eto
med
ics
asm
edic
alpr
otoc
ols
defi
ne
7.1.
7E
nsur
eth
eco
mpe
tenc
yof
med
ics
inIV
acce
sste
chni
ques
inro
utin
ean
dta
ctic
alen
viro
nmen
ts7.
2D
emon
stra
tepr
ofici
ency
ines
tabl
ishm
ento
fan
intr
aoss
eous
(IO
)dev
ice
7.2.
1D
escr
ibe
the
pote
ntia
lne
edfo
rIO
acce
ss7.
2.2
Des
crib
eth
ein
dic
atio
nsfo
rat
tem
ptin
gIO
acce
ss7.
2.4
Des
crib
eth
epo
tent
ialn
eed
for
IOac
cess
7.2.
6C
reat
eap
prop
riat
etr
eatm
entp
roto
cols
for
IOac
cess
7.2.
3D
emon
stra
tepr
ofici
ency
inob
tain
ing
IOac
cess
7.2.
5E
nsur
eth
ateq
uipm
entf
orth
ese
curi
ngof
IOac
cess
isav
aila
ble
tom
edic
sas
med
ical
prot
ocol
sd
efine
7.2.
7E
nsur
eth
eco
mpe
tenc
yof
med
ics
inIO
acce
sste
chni
ques
8.M
edic
atio
nA
dm
inis
trat
ion
8.1
Dem
onst
rate
profi
cien
cyin
IV/
IOfl
uid
resu
scit
atio
n
8.1.
1D
escr
ibe
the
pote
ntia
lne
edfo
rIV
/IO
flui
dre
susc
itat
ion
8.1.
2D
emon
stra
tepr
ofici
ency
inIV
/IO
flui
dre
susc
itat
ion
8.1.
3D
escr
ibe
the
risk
san
dbe
nefit
sof
IV/
IOfl
uid
resu
scit
atio
nto
mis
sion
com
plet
ion
8.1.
5C
reat
eap
prop
riat
eIV
/IO
flui
dre
susc
itat
ion
prot
ocol
s
8.1.
4E
nsur
eth
atIV
flui
dis
avai
labl
eto
med
ics
asm
edic
alpr
otoc
ols
defi
ne
8.1.
6E
nsur
eth
eco
mpe
tenc
yof
med
ics
inIV
/IO
flui
dre
susc
itat
ion
8.2
Dem
onst
rate
profi
cien
cyin
the
adm
inis
trat
ion
ofan
alge
sia
8.2.
1D
escr
ibe
the
need
for
anal
gesi
a8.
2.2
Dem
onst
rate
profi
cien
cyin
anal
gesi
aad
min
istr
atio
n8.
2.3
Des
crib
eth
eri
sks
and
bene
fits
ofan
alge
sia
tom
issi
onco
mpl
etio
n
8.2.
5C
reat
eap
prop
riat
epr
otoc
ols
for
anal
gesi
a
8.2.
6M
aint
ain
appr
opri
ate
cont
rola
ndd
ocum
enta
tion
ofal
lsch
edul
ed
rugs
8.2.
4E
nsur
eth
atIV
anal
gesi
am
edic
atio
nis
avai
labl
eto
med
ics
asm
edic
alpr
otoc
ols
defi
ne
8.2.
7E
nsur
eth
eco
mpe
tenc
yof
med
ics
inan
alge
sia
adm
inis
trat
ion
8.3
Dem
onst
rate
profi
cien
cyin
the
adm
inis
trat
ion
ofem
erge
ncy
anti
biot
ics
for
trau
mat
icw
ound
s
8.3.
1D
escr
ibe
the
pote
ntia
lne
edfo
rem
erge
ncy
anti
biot
ics
topr
even
twou
ndin
fect
ions
8.3.
2D
emon
stra
tepr
ofici
ency
inan
tibi
otic
adm
inis
trat
ion
for
trau
mat
icw
ound
prop
hyla
xis
8.3.
3D
escr
ibe
the
risk
san
dbe
nefit
sof
anti
biot
icad
min
istr
atio
nto
mis
sion
com
plet
ion
8.3.
5C
reat
epr
otoc
ols
for
emer
genc
yan
tibi
otic
adm
inis
trat
ion
for
trau
mat
icw
ound
s8.
3.4
Ens
ure
that
IVan
tibi
otic
sar
eav
aila
ble
tom
edic
sas
med
ical
prot
ocol
sd
efine
8.3.
6E
nsur
eth
eco
mpe
tenc
yof
med
ics
inan
tibi
otic
adm
inis
trat
ion
8.4
Dem
onst
rate
profi
cien
cyin
appr
opri
ate
and
safe
use
ofov
er-t
he-c
ount
er(O
TC
)med
icat
ions
inth
eta
ctic
alse
ttin
g
8.4.
1D
escr
ibe
the
ind
icat
ions
for
use
and
adve
rse
sid
eef
fect
sof
com
mon
lyus
edO
TC
med
icat
ions
and
the
pote
ntia
lben
efits
and
dan
gers
they
crea
tein
the
tact
ical
envi
ronm
ent
8.4.
2D
escr
ibe
the
ind
icat
ions
for
use
and
adve
rse
sid
eef
fect
sof
com
mon
lyus
edO
TC
med
icat
ions
and
the
pote
ntia
lbe
nefit
san
dd
ange
rsth
eycr
eate
inth
eta
ctic
alen
viro
nmen
t
8.4.
4D
escr
ibe
the
ind
icat
ions
for
use
and
adve
rse
sid
eef
fect
sof
com
mon
lyus
edO
TC
med
icat
ions
and
the
pote
ntia
lbe
nefit
san
dd
ange
rsth
eycr
eate
inth
eta
ctic
alen
viro
nmen
t
8.4.
5C
reat
epr
otoc
ols
for
the
adm
inis
trat
ion
ofO
TC
med
icat
ions
gene
rally
cons
ider
edsa
fefo
rus
ein
the
tact
ical
envi
ronm
ent
8.4.
6C
reat
epr
otoc
ols
for
med
ics
toex
clud
epe
rson
nelf
rom
oper
atio
nsbe
caus
eof
adve
rse
med
icat
ion
sid
eef
fect
s
(Con
tinu
edon
next
page
)
9
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.
TA
BL
E2.
The
18C
ompe
tenc
yD
omai
nsan
dth
eSp
ecifi
cC
ompe
tenc
ies
inth
eFi
eld
Tact
ical
Em
erge
ncy
Med
ical
Supp
ortM
atri
x
Dom
ain
Com
pete
ncy
Ope
rato
rM
edic
alPr
ovid
erTe
amC
omm
and
erM
edic
alD
irec
tor
8.4.
3D
emon
stra
tepr
ofici
ency
inse
lect
ing
OT
Cm
edic
atio
nsth
atar
ege
nera
llyco
nsid
ered
safe
for
use
inth
eta
ctic
alen
viro
nmen
t
8.4.
7E
nsur
eth
atm
edic
atio
nsar
epr
oper
lyst
ored
and
asse
ssed
ona
sche
dul
efo
rex
pira
tion
and
dam
age
8.5
Dem
onst
rate
profi
cien
cyin
the
iden
tifi
cati
onan
dco
nsid
erat
ion
ofm
edic
atio
nal
lerg
ies
8.5.
1D
escr
ibe
the
impo
rtan
ceof
iden
tify
ing
and
repo
rtin
gm
edic
atio
nal
lerg
ies
tom
edic
alsu
ppor
t
8.5.
3D
emon
stra
tepr
ofici
ency
inth
eid
enti
fica
tion
and
doc
umen
tati
onof
med
icat
ion
alle
rgie
s
8.5.
5D
escr
ibe
the
impo
rtan
ceof
iden
tify
ing
and
repo
rtin
gm
edic
atio
nal
lerg
ies
tom
edic
alsu
ppor
tand
prov
ide
inpu
tint
oth
ere
port
ing
SOP
8.5.
6C
reat
eap
prop
riat
em
echa
nism
sfo
rid
enti
fyin
gan
dre
port
ing
med
icat
ion
alle
rgie
sto
med
ical
supp
ort
8.5.
2D
escr
ibe
reco
gnit
ion
ofan
alle
rgic
reac
tion
toa
med
icat
ion
8.5.
4D
escr
ibe
reco
gnit
ion
ofm
edic
atio
nal
lerg
ies
and
prop
ertr
eatm
ento
falle
rgic
reac
tion
s
8.5.
7C
reat
epr
otoc
ols
for
the
trea
tmen
tofa
llerg
icre
acti
ons
tom
edic
atio
ns
9.C
asua
lty
Imm
obili
zati
on9.
1D
emon
stra
tepr
ofici
ency
inth
em
anag
emen
tof
susp
ecte
dce
ntra
lner
vous
syst
em(C
NS)
orsp
ine
inju
ries
9.1.
1D
emon
stra
tepr
ofici
ency
inth
ere
cogn
itio
nof
com
mon
mec
hani
sms
ofC
NS/
spin
ein
juri
es
9.1.
4D
emon
stra
tepr
ofici
ency
inth
ere
cogn
itio
nof
com
mon
mec
hani
sms
ofC
NS/
spin
ein
juri
es
9.1.
7D
escr
ibe
the
impo
rtan
ceof
the
man
agem
ento
fsus
pect
edC
NS/
spin
ein
juri
es
9.1.
9C
reat
epr
otoc
ols
for
the
prot
ecti
onof
CN
S/sp
ine
inju
ries
9.1.
2D
emon
stra
tepr
ofici
ency
inpr
ovid
ing
basi
cC
NS/
spin
epr
otec
tion
9.1.
5D
emon
stra
tepr
ofici
ency
inpr
ovid
ing
adva
nced
CN
S/sp
ine
prot
ecti
on
9.1.
10E
nsur
eth
eco
mpe
tenc
yof
oper
ator
san
dm
edic
sto
prot
ect
CN
S/sp
ine
inju
ries
9.1.
3D
emon
stra
tepr
ofici
ency
inba
sic
neur
olog
icas
sess
men
t
9.1.
6D
emon
stra
tepr
ofici
ency
inad
vanc
edne
urol
ogic
asse
ssm
ent
9.1.
8E
nsur
eth
atsu
pplie
sar
eav
aila
ble
toop
erat
ors
and
med
ics
toal
low
them
tost
abili
zean
dpr
otec
tCN
S/sp
ine
inju
ries
asm
edic
alpr
otoc
ols
defi
ne
9.1.
11R
ecom
men
deq
uipm
entf
orop
erat
ors
and
med
ics
topr
ovid
eC
NS/
spin
epr
otec
tion
9.2
Dem
onst
rate
profi
cien
cyin
frac
ture
splin
ting
and
extr
emit
yne
urov
ascu
lar
asse
ssm
ent
9.2.
1D
emon
stra
tepr
ofici
ency
inba
sic
splin
ting
9.2.
3D
emon
stra
tepr
ofici
ency
inba
sic
and
adva
nced
frac
ture
man
agem
ent,
incl
udin
gsp
lint
appl
icat
ion
and
trac
tion
splin
ting
9.2.
5D
escr
ibe
the
prin
cipl
esof
splin
ting
9.2.
7C
reat
epr
otoc
ols
for
frac
ture
splin
ting
for
oper
ator
san
dm
edic
s
9.2.
8E
nsur
eth
eco
mpe
tenc
yof
oper
ator
san
dm
edic
sin
basi
csp
linti
ngte
chni
ques
9.2.
2D
emon
stra
tepr
ofici
ency
inex
trem
ity
neur
ovas
cula
ras
sess
men
tbef
ore
and
afte
rsp
linti
ng
9.2.
4D
emon
stra
tepr
ofici
ency
inex
trem
ity
neur
ovas
cula
ras
sess
men
tbef
ore
and
afte
rsp
linti
ng
9.2.
6E
nsur
eth
atsu
pplie
sar
eav
aila
ble
toop
erat
ors
and
med
ics
for
splin
ting
and
extr
emit
yne
urov
ascu
lar
asse
ssm
enta
sm
edic
alpr
otoc
ols
defi
ne
9.2.
9E
nsur
eth
eco
mpe
tenc
yof
oper
ator
san
dm
edic
sin
extr
emit
yne
urov
ascu
lar
asse
ssm
ent,
incl
udin
gbe
fore
and
afte
rex
trem
ity/
join
tm
anip
ulat
ion
and
splin
tap
plic
atio
n9.
3D
emon
stra
tepr
ofici
ency
inth
eem
erge
ntre
duc
tion
ofjo
intd
islo
cati
ons
9.3.
1D
escr
ibe
the
risk
san
dbe
nefi
tsof
join
tdis
loca
tion
red
ucti
onto
mis
sion
com
plet
ion
9.3.
3D
escr
ibe
the
risk
san
dbe
nefi
tsof
join
tdis
loca
tion
red
ucti
onto
limb
salv
age
and
mis
sion
com
plet
ion
9.3.
6D
escr
ibe
the
risk
san
dbe
nefi
tsof
join
tdis
loca
tion
red
ucti
onto
mis
sion
com
plet
ion
9.3.
8C
reat
epr
otoc
ols
for
join
td
islo
cati
onan
dfr
actu
red
islo
cati
onre
duc
tion
s
9.3.
4D
emon
stra
tepr
ofici
ency
injo
intd
islo
cati
onan
dfr
actu
red
islo
cati
onre
duc
tion
sas
med
ical
prot
ocol
sd
efine
10
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.
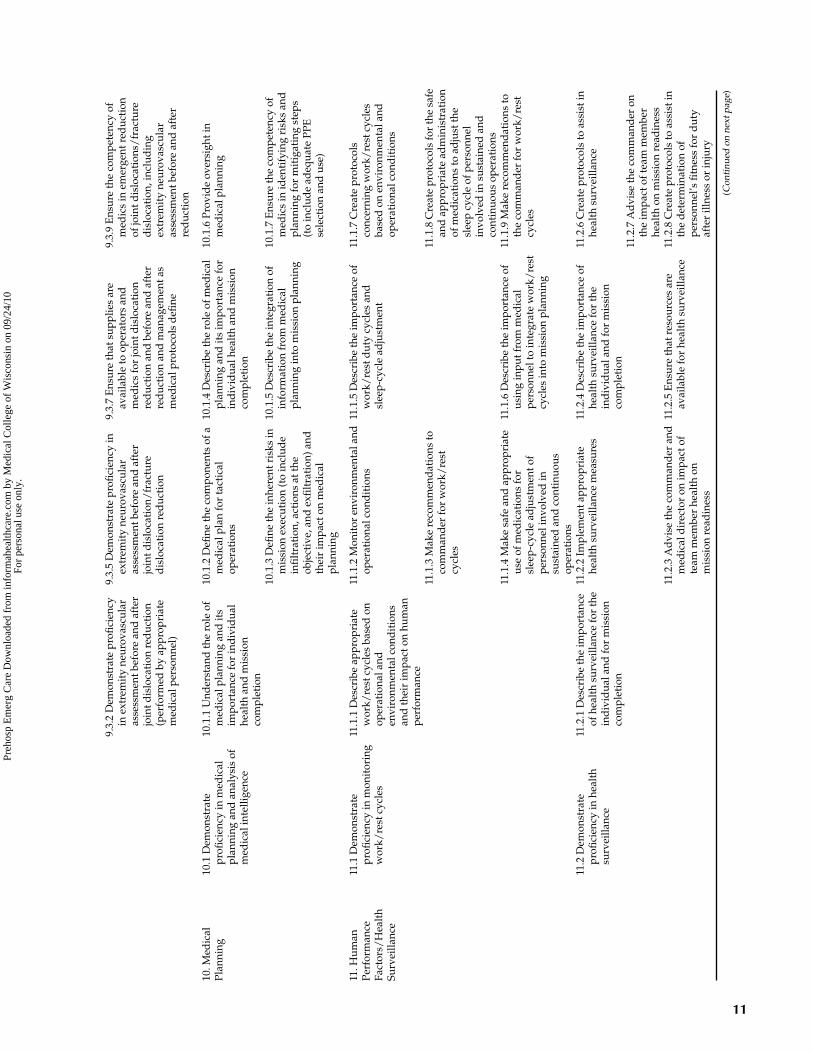
9.3.
2D
emon
stra
tepr
ofici
ency
inex
trem
ity
neur
ovas
cula
ras
sess
men
tbef
ore
and
afte
rjo
intd
islo
cati
onre
duc
tion
(per
form
edby
appr
opri
ate
med
ical
pers
onne
l)
9.3.
5D
emon
stra
tepr
ofici
ency
inex
trem
ity
neur
ovas
cula
ras
sess
men
tbef
ore
and
afte
rjo
intd
islo
cati
on/
frac
ture
dis
loca
tion
red
ucti
on
9.3.
7E
nsur
eth
atsu
pplie
sar
eav
aila
ble
toop
erat
ors
and
med
ics
for
join
tdis
loca
tion
red
ucti
onan
dbe
fore
and
afte
rre
duc
tion
and
man
agem
enta
sm
edic
alpr
otoc
ols
defi
ne
9.3.
9E
nsur
eth
eco
mpe
tenc
yof
med
ics
inem
erge
ntre
duc
tion
ofjo
intd
islo
cati
ons/
frac
ture
dis
loca
tion
,inc
lud
ing
extr
emit
yne
urov
ascu
lar
asse
ssm
entb
efor
ean
daf
ter
red
ucti
on
10.M
edic
alPl
anni
ng10
.1D
emon
stra
tepr
ofici
ency
inm
edic
alpl
anni
ngan
dan
alys
isof
med
ical
inte
llige
nce
10.1
.1U
nder
stan
dth
ero
leof
med
ical
plan
ning
and
its
impo
rtan
cefo
rin
div
idua
lhe
alth
and
mis
sion
com
plet
ion
10.1
.2D
efine
the
com
pone
nts
ofa
med
ical
plan
for
tact
ical
oper
atio
ns
10.1
.4D
escr
ibe
the
role
ofm
edic
alpl
anni
ngan
dit
sim
port
ance
for
ind
ivid
ualh
ealt
han
dm
issi
onco
mpl
etio
n
10.1
.6Pr
ovid
eov
ersi
ghti
nm
edic
alpl
anni
ng
10.1
.3D
efine
the
inhe
rent
risk
sin
mis
sion
exec
utio
n(t
oin
clud
ein
filt
rati
on,a
ctio
nsat
the
obje
ctiv
e,an
dex
filt
rati
on)a
ndth
eir
impa
cton
med
ical
plan
ning
10.1
.5D
escr
ibe
the
inte
grat
ion
ofin
form
atio
nfr
omm
edic
alpl
anni
ngin
tom
issi
onpl
anni
ng
10.1
.7E
nsur
eth
eco
mpe
tenc
yof
med
ics
inid
enti
fyin
gri
sks
and
plan
ning
for
mit
igat
ing
step
s(t
oin
clud
ead
equa
tePP
Ese
lect
ion
and
use)
11.H
uman
Perf
orm
ance
Fact
ors/
Hea
lth
Surv
eilla
nce
11.1
Dem
onst
rate
profi
cien
cyin
mon
itor
ing
wor
k/re
stcy
cles
11.1
.1D
escr
ibe
appr
opri
ate
wor
k/re
stcy
cles
base
don
oper
atio
nala
nden
viro
nmen
talc
ond
itio
nsan
dth
eir
impa
cton
hum
anpe
rfor
man
ce
11.1
.2M
onit
oren
viro
nmen
tala
ndop
erat
iona
lcon
dit
ions
11.1
.5D
escr
ibe
the
impo
rtan
ceof
wor
k/re
std
uty
cycl
esan
dsl
eep-
cycl
ead
just
men
t
11.1
.7C
reat
epr
otoc
ols
conc
erni
ngw
ork/
rest
cycl
esba
sed
onen
viro
nmen
tala
ndop
erat
iona
lcon
dit
ions
11.1
.3M
ake
reco
mm
end
atio
nsto
com
man
der
for
wor
k/re
stcy
cles
11.1
.8C
reat
epr
otoc
ols
for
the
safe
and
appr
opri
ate
adm
inis
trat
ion
ofm
edic
atio
nsto
adju
stth
esl
eep
cycl
eof
pers
onne
lin
volv
edin
sust
aine
dan
dco
ntin
uous
oper
atio
ns11
.1.4
Mak
esa
fean
dap
prop
riat
eus
eof
med
icat
ions
for
slee
p-cy
cle
adju
stm
ento
fpe
rson
neli
nvol
ved
insu
stai
ned
and
cont
inuo
usop
erat
ions
11.1
.6D
escr
ibe
the
impo
rtan
ceof
usin
gin
putf
rom
med
ical
pers
onne
lto
inte
grat
ew
ork/
rest
cycl
esin
tom
issi
onpl
anni
ng
11.1
.9M
ake
reco
mm
end
atio
nsto
the
com
man
der
for
wor
k/re
stcy
cles
11.2
Dem
onst
rate
profi
cien
cyin
heal
thsu
rvei
llanc
e
11.2
.1D
escr
ibe
the
impo
rtan
ceof
heal
thsu
rvei
llanc
efo
rth
ein
div
idua
land
for
mis
sion
com
plet
ion
11.2
.2Im
plem
enta
ppro
pria
tehe
alth
surv
eilla
nce
mea
sure
s11
.2.4
Des
crib
eth
eim
port
ance
ofhe
alth
surv
eilla
nce
for
the
ind
ivid
uala
ndfo
rm
issi
onco
mpl
etio
n
11.2
.6C
reat
epr
otoc
ols
toas
sist
inhe
alth
surv
eilla
nce
11.2
.7A
dvi
seth
eco
mm
and
eron
the
impa
ctof
team
mem
ber
heal
thon
mis
sion
read
ines
s11
.2.3
Ad
vise
the
com
man
der
and
med
ical
dir
ecto
ron
impa
ctof
team
mem
ber
heal
thon
mis
sion
read
ines
s
11.2
.5E
nsur
eth
atre
sour
ces
are
avai
labl
efo
rhe
alth
surv
eilla
nce
11.2
.8C
reat
epr
otoc
ols
toas
sist
inth
ed
eter
min
atio
nof
pers
onne
l’sfi
tnes
sfo
rd
uty
afte
rill
ness
orin
jury
(Con
tinu
edon
next
page
)
11
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.
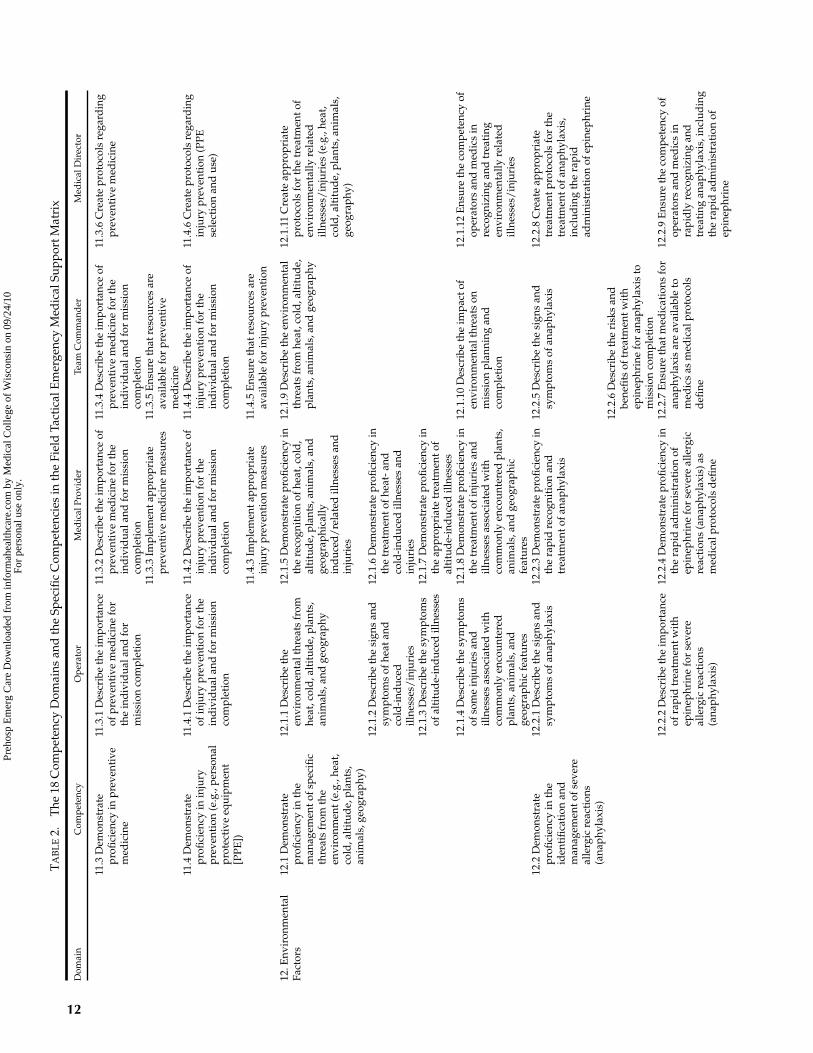
TA
BL
E2.
The
18C
ompe
tenc
yD
omai
nsan
dth
eSp
ecifi
cC
ompe
tenc
ies
inth
eFi
eld
Tact
ical
Em
erge
ncy
Med
ical
Supp
ortM
atri
x
Dom
ain
Com
pete
ncy
Ope
rato
rM
edic
alPr
ovid
erTe
amC
omm
and
erM
edic
alD
irec
tor
11.3
Dem
onst
rate
profi
cien
cyin
prev
enti
vem
edic
ine
11.3
.1D
escr
ibe
the
impo
rtan
ceof
prev
enti
vem
edic
ine
for
the
ind
ivid
uala
ndfo
rm
issi
onco
mpl
etio
n
11.3
.2D
escr
ibe
the
impo
rtan
ceof
prev
enti
vem
edic
ine
for
the
ind
ivid
uala
ndfo
rm
issi
onco
mpl
etio
n
11.3
.4D
escr
ibe
the
impo
rtan
ceof
prev
enti
vem
edic
ine
for
the
ind
ivid
uala
ndfo
rm
issi
onco
mpl
etio
n
11.3
.6C
reat
epr
otoc
ols
rega
rdin
gpr
even
tive
med
icin
e
11.3
.3Im
plem
enta
ppro
pria
tepr
even
tive
med
icin
em
easu
res
11.3
.5E
nsur
eth
atre
sour
ces
are
avai
labl
efo
rpr
even
tive
med
icin
e11
.4D
emon
stra
tepr
ofici
ency
inin
jury
prev
enti
on(e
.g.,
pers
onal
prot
ecti
veeq
uipm
ent
[PPE
])
11.4
.1D
escr
ibe
the
impo
rtan
ceof
inju
rypr
even
tion
for
the
ind
ivid
uala
ndfo
rm
issi
onco
mpl
etio
n
11.4
.2D
escr
ibe
the
impo
rtan
ceof
inju
rypr
even
tion
for
the
ind
ivid
uala
ndfo
rm
issi
onco
mpl
etio
n
11.4
.4D
escr
ibe
the
impo
rtan
ceof
inju
rypr
even
tion
for
the
ind
ivid
uala
ndfo
rm
issi
onco
mpl
etio
n
11.4
.6C
reat
epr
otoc
ols
rega
rdin
gin
jury
prev
enti
on(P
PEse
lect
ion
and
use)
11.4
.3Im
plem
enta
ppro
pria
tein
jury
prev
enti
onm
easu
res
11.4
.5E
nsur
eth
atre
sour
ces
are
avai
labl
efo
rin
jury
prev
enti
on
12.E
nvir
onm
enta
lFa
ctor
s12
.1D
emon
stra
tepr
ofici
ency
inth
em
anag
emen
tofs
peci
ficth
reat
sfr
omth
een
viro
nmen
t(e.
g.,h
eat,
cold
,alt
itud
e,pl
ants
,an
imal
s,ge
ogra
phy)
12.1
.1D
escr
ibe
the
envi
ronm
enta
lthr
eats
from
heat
,col
d,a
ltit
ude,
plan
ts,
anim
als,
and
geog
raph
y
12.1
.5D
emon
stra
tepr
ofici
ency
inth
ere
cogn
itio
nof
heat
,col
d,
alti
tud
e,pl
ants
,ani
mal
s,an
dge
ogra
phic
ally
ind
uced
/re
late
dill
ness
esan
din
juri
es
12.1
.9D
escr
ibe
the
envi
ronm
enta
lth
reat
sfr
omhe
at,c
old
,alt
itud
e,pl
ants
,ani
mal
s,an
dge
ogra
phy
12.1
.11
Cre
ate
appr
opri
ate
prot
ocol
sfo
rth
etr
eatm
ento
fen
viro
nmen
tally
rela
ted
illne
sses
/in
juri
es(e
.g.,
heat
,co
ld,a
ltit
ude,
plan
ts,a
nim
als,
geog
raph
y)
12.1
.2D
escr
ibe
the
sign
san
dsy
mpt
oms
ofhe
atan
dco
ld-i
nduc
edill
ness
es/
inju
ries
12.1
.6D
emon
stra
tepr
ofici
ency
inth
etr
eatm
ento
fhea
t-an
dco
ld-i
nduc
edill
ness
esan
din
juri
es12
.1.3
Des
crib
eth
esy
mpt
oms
ofal
titu
de-
ind
uced
illne
sses
12.1
.7D
emon
stra
tepr
ofici
ency
inth
eap
prop
riat
etr
eatm
ento
fal
titu
de-
ind
uced
illne
sses
12.1
.4D
escr
ibe
the
sym
ptom
sof
som
ein
juri
esan
dill
ness
esas
soci
ated
wit
hco
mm
only
enco
unte
red
plan
ts,a
nim
als,
and
geog
raph
icfe
atur
es
12.1
.8D
emon
stra
tepr
ofici
ency
inth
etr
eatm
ento
finj
urie
san
dill
ness
esas
soci
ated
wit
hco
mm
only
enco
unte
red
plan
ts,
anim
als,
and
geog
raph
icfe
atur
es
12.1
.10
Des
crib
eth
eim
pact
ofen
viro
nmen
talt
hrea
tson
mis
sion
plan
ning
and
com
plet
ion
12.1
.12
Ens
ure
the
com
pete
ncy
ofop
erat
ors
and
med
ics
inre
cogn
izin
gan
dtr
eati
ngen
viro
nmen
tally
rela
ted
illne
sses
/in
juri
es
12.2
Dem
onst
rate
profi
cien
cyin
the
iden
tifi
cati
onan
dm
anag
emen
tofs
ever
eal
lerg
icre
acti
ons
(ana
phyl
axis
)
12.2
.1D
escr
ibe
the
sign
san
dsy
mpt
oms
ofan
aphy
laxi
s12
.2.3
Dem
onst
rate
profi
cien
cyin
the
rapi
dre
cogn
itio
nan
dtr
eatm
ento
fana
phyl
axis
12.2
.5D
escr
ibe
the
sign
san
dsy
mpt
oms
ofan
aphy
laxi
s12
.2.8
Cre
ate
appr
opri
ate
trea
tmen
tpro
toco
lsfo
rth
etr
eatm
ento
fana
phyl
axis
,in
clud
ing
the
rapi
dad
min
istr
atio
nof
epin
ephr
ine
12.2
.6D
escr
ibe
the
risk
san
dbe
nefi
tsof
trea
tmen
twit
hep
inep
hrin
efo
ran
aphy
laxi
sto
mis
sion
com
plet
ion
12.2
.2D
escr
ibe
the
impo
rtan
ceof
rapi
dtr
eatm
entw
ith
epin
ephr
ine
for
seve
real
lerg
icre
acti
ons
(ana
phyl
axis
)
12.2
.4D
emon
stra
tepr
ofici
ency
inth
era
pid
adm
inis
trat
ion
ofep
inep
hrin
efo
rse
vere
alle
rgic
reac
tion
s(a
naph
ylax
is)a
sm
edic
alpr
otoc
ols
defi
ne
12.2
.7E
nsur
eth
atm
edic
atio
nsfo
ran
aphy
laxi
sar
eav
aila
ble
tom
edic
sas
med
ical
prot
ocol
sd
efine
12.2
.9E
nsur
eth
eco
mpe
tenc
yof
oper
ator
san
dm
edic
sin
rapi
dly
reco
gniz
ing
and
trea
ting
anap
hyla
xis,
incl
udin
gth
era
pid
adm
inis
trat
ion
ofep
inep
hrin
e
12
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.
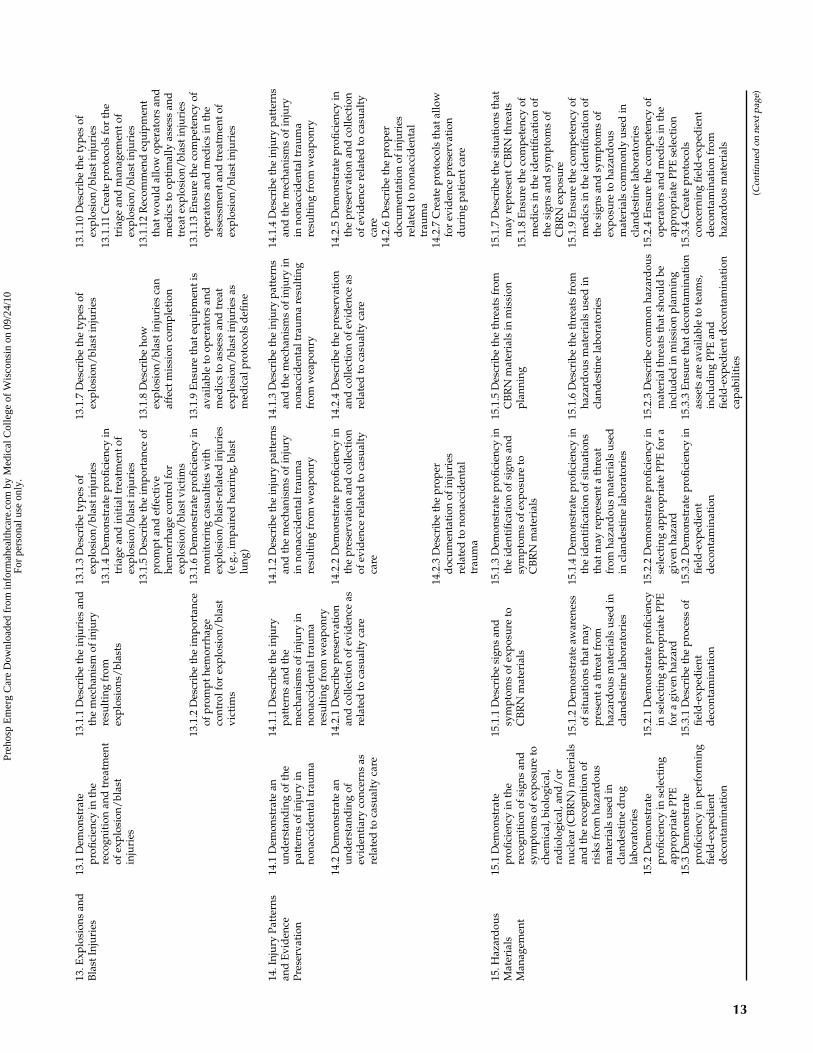
13.E
xplo
sion
san
dB
last
Inju
ries
13.1
Dem
onst
rate
profi
cien
cyin
the
reco
gnit
ion
and
trea
tmen
tof
expl
osio
n/bl
ast
inju
ries
13.1
.1D
escr
ibe
the
inju
ries
and
the
mec
hani
smof
inju
ryre
sult
ing
from
expl
osio
ns/
blas
ts
13.1
.3D
escr
ibe
type
sof
expl
osio
n/bl
asti
njur
ies
13.1
.7D
escr
ibe
the
type
sof
expl
osio
n/bl
asti
njur
ies
13.1
.10
Des
crib
eth
ety
pes
ofex
plos
ion/
blas
tinj
urie
s13
.1.4
Dem
onst
rate
profi
cien
cyin
tria
gean
din
itia
ltre
atm
ento
fex
plos
ion/
blas
tinj
urie
s
13.1
.11
Cre
ate
prot
ocol
sfo
rth
etr
iage
and
man
agem
ento
fex
plos
ion/
blas
tinj
urie
s13
.1.5
Des
crib
eth
eim
port
ance
ofpr
ompt
and
effe
ctiv
ehe
mor
rhag
eco
ntro
lfor
expl
osio
n/bl
astv
icti
ms
13.1
.8D
escr
ibe
how
expl
osio
n/bl
asti
njur
ies
can
affe
ctm
issi
onco
mpl
etio
n
13.1
.12
Rec
omm
end
equi
pmen
tth
atw
ould
allo
wop
erat
ors
and
med
ics
toop
tim
ally
asse
ssan
dtr
eate
xplo
sion
/bl
asti
njur
ies
13.1
.2D
escr
ibe
the
impo
rtan
ceof
prom
pthe
mor
rhag
eco
ntro
lfor
expl
osio
n/bl
ast
vict
ims
13.1
.6D
emon
stra
tepr
ofici
ency
inm
onit
orin
gca
sual
ties
wit
hex
plos
ion/
blas
t-re
late
din
juri
es(e
.g.,
impa
ired
hear
ing,
blas
tlu
ng)
13.1
.9E
nsur
eth
ateq
uipm
enti
sav
aila
ble
toop
erat
ors
and
med
ics
toas
sess
and
trea
tex
plos
ion/
blas
tinj
urie
sas
med
ical
prot
ocol
sd
efine
13.1
.13
Ens
ure
the
com
pete
ncy
ofop
erat
ors
and
med
ics
inth
eas
sess
men
tand
trea
tmen
tof
expl
osio
n/bl
asti
njur
ies
14.I
njur
yPa
tter
nsan
dE
vid
ence
Pres
erva
tion
14.1
Dem
onst
rate
anun
der
stan
din
gof
the
patt
erns
ofin
jury
inno
nacc
iden
talt
raum
a
14.1
.1D
escr
ibe
the
inju
rypa
tter
nsan
dth
em
echa
nism
sof
inju
ryin
nona
ccid
enta
ltra
uma
resu
ltin
gfr
omw
eapo
nry
14.1
.2D
escr
ibe
the
inju
rypa
tter
nsan
dth
em
echa
nism
sof
inju
ryin
nona
ccid
enta
ltra
uma
resu
ltin
gfr
omw
eapo
nry
14.1
.3D
escr
ibe
the
inju
rypa
tter
nsan
dth
em
echa
nism
sof
inju
ryin
nona
ccid
enta
ltra
uma
resu
ltin
gfr
omw
eapo
nry
14.1
.4D
escr
ibe
the
inju
rypa
tter
nsan
dth
em
echa
nism
sof
inju
ryin
nona
ccid
enta
ltra
uma
resu
ltin
gfr
omw
eapo
nry
14.2
Dem
onst
rate
anun
der
stan
din
gof
evid
enti
ary
conc
erns
asre
late
dto
casu
alty
care
14.2
.1D
escr
ibe
pres
erva
tion
and
colle
ctio
nof
evid
ence
asre
late
dto
casu
alty
care
14.2
.2D
emon
stra
tepr
ofici
ency
inth
epr
eser
vati
onan
dco
llect
ion
ofev
iden
cere
late
dto
casu
alty
care
14.2
.4D
escr
ibe
the
pres
erva
tion
and
colle
ctio
nof
evid
ence
asre
late
dto
casu
alty
care
14.2
.5D
emon
stra
tepr
ofici
ency
inth
epr
eser
vati
onan
dco
llect
ion
ofev
iden
cere
late
dto
casu
alty
care
14.2
.6D
escr
ibe
the
prop
erd
ocum
enta
tion
ofin
juri
esre
late
dto
nona
ccid
enta
ltr
aum
a14
.2.3
Des
crib
eth
epr
oper
doc
umen
tati
onof
inju
ries
rela
ted
tono
nacc
iden
tal
trau
ma
14.2
.7C
reat
epr
otoc
ols
that
allo
wfo
rev
iden
cepr
eser
vati
ond
urin
gpa
tien
tcar
e
15.H
azar
dou
sM
ater
ials
Man
agem
ent
15.1
Dem
onst
rate
profi
cien
cyin
the
reco
gnit
ion
ofsi
gns
and
sym
ptom
sof
expo
sure
toch
emic
al,b
iolo
gica
l,ra
dio
logi
cal,
and
/or
nucl
ear
(CB
RN
)mat
eria
lsan
dth
ere
cogn
itio
nof
risk
sfr
omha
zard
ous
mat
eria
lsus
edin
clan
des
tine
dru
gla
bora
tori
es
15.1
.1D
escr
ibe
sign
san
dsy
mpt
oms
ofex
posu
reto
CB
RN
mat
eria
ls
15.1
.3D
emon
stra
tepr
ofici
ency
inth
eid
enti
fica
tion
ofsi
gns
and
sym
ptom
sof
expo
sure
toC
BR
Nm
ater
ials
15.1
.5D
escr
ibe
the
thre
ats
from
CB
RN
mat
eria
lsin
mis
sion
plan
ning
15.1
.7D
escr
ibe
the
situ
atio
nsth
atm
ayre
pres
entC
BR
Nth
reat
s15
.1.8
Ens
ure
the
com
pete
ncy
ofm
edic
sin
the
iden
tifi
cati
onof
the
sign
san
dsy
mpt
oms
ofC
BR
Nex
posu
re15
.1.2
Dem
onst
rate
awar
enes
sof
situ
atio
nsth
atm
aypr
esen
tath
reat
from
haza
rdou
sm
ater
ials
used
incl
and
esti
nela
bora
tori
es
15.1
.4D
emon
stra
tepr
ofici
ency
inth
eid
enti
fica
tion
ofsi
tuat
ions
that
may
repr
esen
tath
reat
from
haza
rdou
sm
ater
ials
used
incl
and
esti
nela
bora
tori
es
15.1
.6D
escr
ibe
the
thre
ats
from
haza
rdou
sm
ater
ials
used
incl
and
esti
nela
bora
tori
es
15.1
.9E
nsur
eth
eco
mpe
tenc
yof
med
ics
inth
eid
enti
fica
tion
ofth
esi
gns
and
sym
ptom
sof
expo
sure
toha
zard
ous
mat
eria
lsco
mm
only
used
incl
and
esti
nela
bora
tori
es15
.2D
emon
stra
tepr
ofici
ency
inse
lect
ing
appr
opri
ate
PPE
15.2
.1D
emon
stra
tepr
ofici
ency
inse
lect
ing
appr
opri
ate
PPE
for
agi
ven
haza
rd
15.2
.2D
emon
stra
tepr
ofici
ency
inse
lect
ing
appr
opri
ate
PPE
for
agi
ven
haza
rd
15.2
.3D
escr
ibe
com
mon
haza
rdou
sm
ater
ialt
hrea
tsth
atsh
ould
bein
clud
edin
mis
sion
plan
ning
15.2
.4E
nsur
eth
eco
mpe
tenc
yof
oper
ator
san
dm
edic
sin
the
appr
opri
ate
PPE
sele
ctio
n15
.3D
emon
stra
tepr
ofici
ency
inpe
rfor
min
gfie
ld-e
xped
ient
dec
onta
min
atio
n
15.3
.1D
escr
ibe
the
proc
ess
offie
ld-e
xped
ient
dec
onta
min
atio
n
15.3
.2D
emon
stra
tepr
ofici
ency
infie
ld-e
xped
ient
dec
onta
min
atio
n
15.3
.3E
nsur
eth
atd
econ
tam
inat
ion
asse
tsar
eav
aila
ble
tote
ams,
incl
udin
gPP
Ean
dfi
eld
-exp
edie
ntd
econ
tam
inat
ion
capa
bilit
ies
15.3
.4C
reat
epr
otoc
ols
conc
erni
ngfie
ld-e
xped
ient
dec
onta
min
atio
nfr
omha
zard
ous
mat
eria
ls
(Con
tinu
edon
next
page
)
13
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.
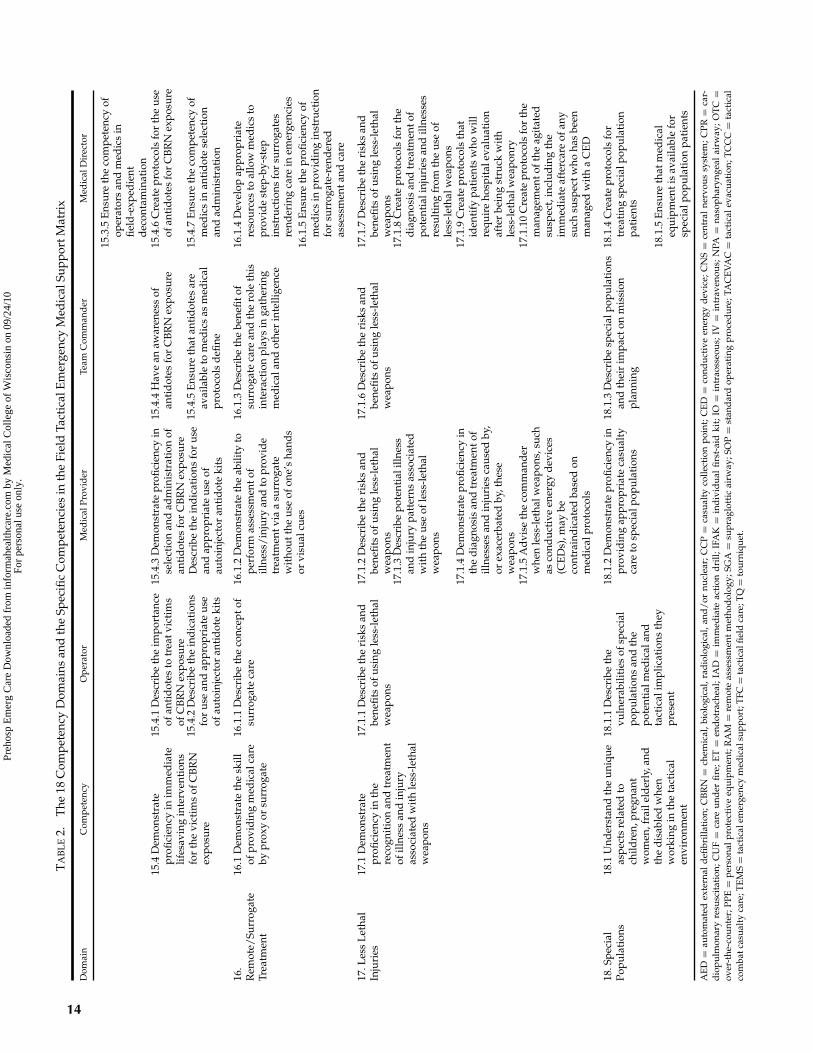
TA
BL
E2.
The
18C
ompe
tenc
yD
omai
nsan
dth
eSp
ecifi
cC
ompe
tenc
ies
inth
eFi
eld
Tact
ical
Em
erge
ncy
Med
ical
Supp
ortM
atri
x
Dom
ain
Com
pete
ncy
Ope
rato
rM
edic
alPr
ovid
erTe
amC
omm
and
erM
edic
alD
irec
tor
15.3
.5E
nsur
eth
eco
mpe
tenc
yof
oper
ator
san
dm
edic
sin
field
-exp
edie
ntd
econ
tam
inat
ion
15.4
Dem
onst
rate
profi
cien
cyin
imm
edia
telif
esav
ing
inte
rven
tion
sfo
rth
evi
ctim
sof
CB
RN
expo
sure
15.4
.1D
escr
ibe
the
impo
rtan
ceof
anti
dot
esto
trea
tvic
tim
sof
CB
RN
expo
sure
15.4
.3D
emon
stra
tepr
ofici
ency
inse
lect
ion
and
adm
inis
trat
ion
ofan
tid
otes
for
CB
RN
expo
sure
Des
crib
eth
ein
dic
atio
nsfo
rus
ean
dap
prop
riat
eus
eof
auto
inje
ctor
anti
dot
eki
ts
15.4
.4H
ave
anaw
aren
ess
ofan
tid
otes
for
CB
RN
expo
sure
15.4
.6C
reat
epr
otoc
ols
for
the
use
ofan
tid
otes
for
CB
RN
expo
sure
15.4
.2D
escr
ibe
the
ind
icat
ions
for
use
and
appr
opri
ate
use
ofau
toin
ject
oran
tid
ote
kits
15.4
.5E
nsur
eth
atan
tid
otes
are
avai
labl
eto
med
ics
asm
edic
alpr
otoc
ols
defi
ne
15.4
.7E
nsur
eth
eco
mpe
tenc
yof
med
ics
inan
tid
ote
sele
ctio
nan
dad
min
istr
atio
n
16.
Rem
ote/
Surr
ogat
eTr
eatm
ent
16.1
Dem
onst
rate
the
skill
ofpr
ovid
ing
med
ical
care
bypr
oxy
orsu
rrog
ate
16.1
.1D
escr
ibe
the
conc
epto
fsu
rrog
ate
care
16.1
.2D
emon
stra
teth
eab
ility
tope
rfor
mas
sess
men
tof
illne
ss/
inju
ryan
dto
prov
ide
trea
tmen
tvia
asu
rrog
ate
wit
hout
the
use
ofon
e’s
hand
sor
visu
alcu
es
16.1
.3D
escr
ibe
the
bene
fitof
surr
ogat
eca
rean
dth
ero
leth
isin
tera
ctio
npl
ays
inga
ther
ing
med
ical
and
othe
rin
telli
genc
e
16.1
.4D
evel
opap
prop
riat
ere
sour
ces
toal
low
med
ics
topr
ovid
est
ep-b
y-st
epin
stru
ctio
nsfo
rsu
rrog
ates
rend
erin
gca
rein
emer
genc
ies
16.1
.5E
nsur
eth
epr
ofici
ency
ofm
edic
sin
prov
idin
gin
stru
ctio
nfo
rsu
rrog
ate-
rend
ered
asse
ssm
enta
ndca
re
17.L
ess
Let
hal
Inju
ries
17.1
Dem
onst
rate
profi
cien
cyin
the
reco
gnit
ion
and
trea
tmen
tof
illne
ssan
din
jury
asso
ciat
edw
ith
less
-let
hal
wea
pons
17.1
.1D
escr
ibe
the
risk
san
dbe
nefit
sof
usin
gle
ss-l
etha
lw
eapo
ns
17.1
.2D
escr
ibe
the
risk
san
dbe
nefit
sof
usin
gle
ss-l
etha
lw
eapo
ns
17.1
.6D
escr
ibe
the
risk
san
dbe
nefit
sof
usin
gle
ss-l
etha
lw
eapo
ns
17.1
.7D
escr
ibe
the
risk
san
dbe
nefit
sof
usin
gle
ss-l
etha
lw
eapo
ns17
.1.3
Des
crib
epo
tent
iali
llnes
san
din
jury
patt
erns
asso
ciat
edw
ith
the
use
ofle
ss-l
etha
lw
eapo
ns
17.1
.8C
reat
epr
otoc
ols
for
the
dia
gnos
isan
dtr
eatm
ento
fpo
tent
iali
njur
ies
and
illne
sses
resu
ltin
gfr
omth
eus
eof
less
-let
halw
eapo
ns17
.1.4
Dem
onst
rate
profi
cien
cyin
the
dia
gnos
isan
dtr
eatm
ento
fill
ness
esan
din
juri
esca
used
by,
orex
acer
bate
dby
,the
sew
eapo
ns
17.1
.9C
reat
epr
otoc
ols
that
iden
tify
pati
ents
who
will
requ
ire
hosp
ital
eval
uati
onaf
ter
bein
gst
ruck
wit
hle
ss-l
etha
lwea
ponr
y17
.1.5
Ad
vise
the
com
man
der
whe
nle
ss-l
etha
lwea
pons
,suc
has
cond
ucti
veen
ergy
dev
ices
(CE
Ds)
,may
beco
ntra
ind
icat
edba
sed
onm
edic
alpr
otoc
ols
17.1
.10
Cre
ate
prot
ocol
sfo
rth
em
anag
emen
toft
heag
itat
edsu
spec
t,in
clud
ing
the
imm
edia
teaf
terc
are
ofan
ysu
chsu
spec
twho
has
been
man
aged
wit
ha
CE
D
18.S
peci
alPo
pula
tion
s18
.1U
nder
stan
dth
eun
ique
aspe
cts
rela
ted
toch
ildre
n,pr
egna
ntw
omen
,fra
ilel
der
ly,a
ndth
ed
isab
led
whe
nw
orki
ngin
the
tact
ical
envi
ronm
ent
18.1
.1D
escr
ibe
the
vuln
erab
iliti
esof
spec
ial
popu
lati
ons
and
the
pote
ntia
lmed
ical
and
tact
ical
impl
icat
ions
they
pres
ent
18.1
.2D
emon
stra
tepr
ofici
ency
inpr
ovid
ing
appr
opri
ate
casu
alty
care
tosp
ecia
lpop
ulat
ions
18.1
.3D
escr
ibe
spec
ialp
opul
atio
nsan
dth
eir
impa
cton
mis
sion
plan
ning
18.1
.4C
reat
epr
otoc
ols
for
trea
ting
spec
ialp
opul
atio
npa
tien
ts
18.1
.5E
nsur
eth
atm
edic
aleq
uipm
enti
sav
aila
ble
for
spec
ialp
opul
atio
npa
tien
ts
AE
D=
auto
mat
edex
tern
ald
efibr
illat
ion;
CB
RN
=ch
emic
al,b
iolo
gica
l,ra
dio
logi
cal,
and
/or
nucl
ear;
CC
P=
casu
alty
colle
ctio
npo
int;
CE
D=
cond
ucti
veen
ergy
dev
ice;
CN
S=
cent
ral
nerv
ous
syst
em;C
PR=
car-
dio
pulm
onar
yre
susc
itat
ion;
CU
F=
care
und
erfi
re;E
T=
end
otra
chea
l;IA
D=
imm
edia
teac
tion
dri
ll;IF
AK
=in
div
idua
lfir
st-a
idki
t;IO
=in
trao
sseo
us;I
V=
intr
aven
ous;
NPA
=na
soph
aryn
geal
airw
ay;O
TC
=ov
er-t
he-c
ount
er;P
PE=
pers
onal
prot
ecti
veeq
uipm
ent;
RA
M=
rem
ote
asse
ssm
ent
met
hod
olog
y;SG
A=
supr
aglo
ttic
airw
ay;S
OP
=st
and
ard
oper
atin
gpr
oced
ure;
TAC
EV
AC
=ta
ctic
alev
acua
tion
;TC
CC
=ta
ctic
alco
mba
tcas
ualt
yca
re;T
EM
S=
tact
ical
emer
genc
ym
edic
alsu
ppor
t;T
FC=
tact
ical
field
care
;TQ
=to
urni
quet
.
14
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.
Schwartz et al. TACTICAL MEDICINE COMPETENCY-BASED GUIDELINES 15
paramedics) in law enforcement operations due to thehazardous environment and risk involved in activelaw enforcement operations. Because of these risks, itcould be argued that without tactical medicine, thestandard of care practiced in the prehospital environ-ment is not consistently applied in the tactical environ-ment. There is a pressing need to provide a mechanismby which the standard of prehospital care can be deliv-ered in this environment.
The provision of tactical medicine allows all mem-bers of our society access to the best available prac-tices of prehospital care by specially trained individ-uals, prepared and equipped for the unique hazardsof the tactical environment. Defining the roles and re-sponsibilities of these providers and creating educa-tional programs of study based on a set of competency-based standards will aid in ensuring the provisionquality care. While these competencies will allow forcompetency-based training programs, the applicationof the training is obviously also subject to appropriatestate law and local protocols.
CONCLUSION
The TEMS competency matrix presented here canprovide a structure around which competency-basedTEMS courses for four target audiences (operator,medic, team commander, and medical director) can bedeveloped.
References
1. Carmona RH. The history and evolution of tactical emergencymedical support and its impact on public safety. Top EmergMed. 2003;25:277–81.
2. Prehospital Trauma Life Support Committee of the NationalAssociation of Emergency Medical Technicians, in cooperationwith the Committee on Trauma of the American College ofSurgeons. PHTLS: Prehospital Trauma Life Support, 6th ed. St.Louis, MO: Mosby Elsevier, 2007.
3. Croushorn JM, Carmona R. Tactical medical support. TopEmerg Med, 2003;25:273–351.
4. Schwartz RB, McManus JG, Swienton RE. Tactical EmergencyMedicine. 1st ed. Philadelphia, PA: Lippincott Williams &Wilkins, 2008.
5. Vayer JS, Schwartz RB. Developing a tactical emergency medi-cal support program. Top Emerg Med. 2003;25:282–93.
6. Tang NF, Fabbri W. Medical direction and integration with ex-isting EMS infrastructure. Top Emerg Med. 2003;25:326–32.
7. Rathbun DJ. The clinical practice of tactical medicine and careunder fire: medical decision making and the role of the tac-tical emergency medical support provider. Top Emerg Med.2003;25:306–15.
8. Heck JJ. The role of preventive medicine in TEMS. Top EmergMed. 2003;25:299–305.
9. Dressler FL. Operational planning for the law enforcementmedic. Top Emerg Med. 2003;25:333–6.
10. Rinnert KJ, Hall WL 2nd. Tactical emergency medical support.Emerg Med Clin North Am. 2002;20:929–52.
11. Sullivan R. The Competency-Based Approach to Training. JH-PIEGO Policy Paper for USAID. September 1995.
12. Dubois DR, W. Competency-based or a traditional approach totraining? A new look at ISD models and an answer to the ques-tion, What’s the best approach? April 2004.
13. Epstein RM, Hundert EM. Defining and assessing professionalcompetence. JAMA. 2002;287:226–35.
14. Dilendik JR. Assumptions underlying criterion referenced as-sessment are educationally sound. Education. 2001;99(1):89–96.
15. Bradley FM. Competency-based resident education. Otolaryn-gol Clin North Am. 2007;40:1215–25.
16. Subbarao I, Lyznicki JM, Hsu EB, et al. A consensus-basededucational framework and competency set for the disciplineof disaster medicine and public health preparedness. DisasterMed Public Health Prep. 2008;2(1):57–68.
APPENDIX 1National Tactical Officers AssociationWorking Group Participants
Brent Bronson, EMT-P (18 years’ experience—EMS ed-ucation, fire rescue education, TEMS education)
Phillip Coule, MD, FACEP (23 years’experience—EMS, EMS education, federal lawenforcement, diving medicine)
John Croushorn, MD, FACEP (10 years’experience—military medicine, federal law en-forcement, aviation medicine, TEMS education)
Mark Gibbons, EMT-P (25 years’ experience—TEMSeducation, aviation medicine, EMS education, local,state, and federal law enforcement)
Sean McKay, EMT-P (14 years’ experience—fire res-cue education, TEMS education, EMS education, locallaw enforcement)
Gina Piazza, DO, FACEP (8 years’ experience—EMSeducation, TEMS education, local and federal law en-forcement)
David Rathbun, EMT-P (40 years’ experience—locallaw enforcement, TEMS education)
Richard Schwartz, MD, FACEP (20 years’experience—military medicine, local and federallaw enforcement, aviation medicine, wildernessmedicine education, diving medicine education,TEMS education)
Robert Soto, EMT-P (17 years’ experience—EMS ed-ucation, fire/rescue education, TEMS education)
Charles Studley, PA-C, 18D/18Z (29 years’experience—military medicine, federal law enforce-ment, TEMS education, diving medicine education)
Paul Vecchio, 18D/18B/18F/18Z (27 years’experience—military medicine, federal law en-forcement, TEMS education)
Preh
osp
Em
erg
Car
e D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
edic
al C
olle
ge o
f W
isco
nsin
on
09/2
4/10
For
pers
onal
use
onl
y.





























