Embed Size (px)
Citation preview
What Is EPT?Expedited partner therapy (EPT) is an innovative treatment option for people diagnosed with the sexually trans-mitted diseases chlamydia or gonorrhea. EPT has been proved to increase treatment rates and decrease the num-ber of people who are reinfected. With EPT:
Patients deliver either medications or prescriptions to their sexual partners.
The doctor does not examine the partner.
In 2005, the Centers for Disease Control and Prevention (CDC) recommended using EPT as an option for treating patients diagnosed with chlamydia or gonorrhea.
How Is EPT Different Than Traditional Treatment Practices? There are several different traditional ways to get a patient’s sexual partners treated, including:
Direct contact by the doctor with a patient’s sexual partner(s);
A patient encouraging his/her partner(s) to visit a doctor; or
A patient providing the name(s) of his/her partner(s) to public health officials to contact.
But the high number of cases, combined with decreased financial and personnel resources in public health pro-grams, caused researchers to investigate other options to assure partners received treatment to prevent reinfection of the orginal patient and to prevent the further spread of the disease.
Chlamydia and Gonorrhea Are the Two Most Commonly Reported Notifiable Diseases Almost 1 million cases of chlamydia were reported in 2005, an increase of 5.1 percent from the previous year.1
Almost 340,000 cases of gonorrhea were reported in 2005.1
Both Diseases Can Be CostlyIt costs an estimated $763 million (2006 dollars) to treat chlamydia and gonorrhea every year.4
If untreated, nearly 40 percent of chlamydia cases can develop into a more serious infection called pelvic inflam-matory disease (PID), resulting in additional treatment costs of $1,167 per patient (1998 dollars).2 Gonorrhea also is a common cause of PID.3
Both chlamydia and gonorrhea increase a person’s chances they will contract HIV if exposed.3,5
n
n
n
n
n
n
n
n
n
n
R
R
R
Talking Points:Expedited Partner Therapy for Sexually Transmitted Diseases
R
What Disparities Are Associated with Chlamydia and Gonorrhea?In 2005:
About 68 percent of the gonorrhea cases reported to CDC were among African–Americans. That was 18 times higher than among whites.1
The gonorrhea rate for Hispanics was two times higher than whites.1
Almost 42 percent of all chlamydia cases occurred among African–Americans.1
The rate of chlamydia among African–American females was more than seven times higher than among white females. The rate of chlamydia among African–American males was more than 11 times higher than among white males.1
How Well Does EPT Work?In one study involving patients diagnosed with gonorrhea or chlamydia in King County, Wash., patients who received EPT were:
Significantly more likely to report that all of their sexual partners were treated than those who were told to refer their partners for treatment;
Less likely to report having sex with an untreated partner; and
Less likely to be diagnosed with another infection at a follow–up visit.6
What Can State Legislators Do?EPT can be a challenging topic for policymakers, since each state has different laws and regulations regarding medical practice. In some states, regulations by medical boards prohibit doctors prescribing medicine to patients they haven’t seen. In others, laws may stand in the way. A tool on the CDC’s Web site (available at http://www.cdc.
gov/std/ept/legal/default.htm) can help legislators begin to understand the legal landscape in their state. In addition, state legislators can:
Learn more. Talk to your state’s STD director to discuss what statutory or regulatory barriers stand in the way of implementing EPT.
Become an advocate. Educate other policymakers and the public about how many people are infected with chla-mydia and gonorrhea and the consequences that can result from persistent infections.
Take action. If statutes stand in the way of implementing EPT, consider legislation that will remove the road-blocks. If regulations are the problem, begin a discussion with the state medical board about the issue.
n
n
n
n
n
n
n
n
n
n
R
R
R
If you would like more information, references, or to explore this topic in greater depth, please:
send your inquiry to http://www.healthystates.csg.org/ (keyword: inquiry) or
call the CSG Health Policy Group at (859) 244–8000.
This Healthy States publication is funded by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, under Cooperative Agreement U38/CCU424348. Points of view in this document are those of the author and do not necessarily represent the official position or policies of the U.S. government.
n
n

Sources:
1 Centers for Disease Control and Prevention. "Sexually Transmitted Disease Surveillance, 2005". Atlanta, GA: U.S. Department of Health and Human Services, November 2006.2 Rein, D.; Kassler, W.; Irwin, K., et al. “Direct medical cost of pelvic inflammatory disease and its sequelae: decreasing, but still substantial.” Obstetrics and Gynecology 2000: 95(3):397–402.3 Centers for Disease Control and Prevention. “Gonorrhea – CDC Fact Sheet.” Accessed from http://www.cdc.gov/std/Gonorrhea/STDFact–gonorrhea.htm March 1, 2007. 4 Chesson, H.W.; Blandford, J.M.; Gift, T.L.; Tao, G.; Irwin, K.L. “The estimated direct medical costs of STDs among American youth, 2000.” Abstract P075. 2004 National STD Prevention Conference. Philadelphia, PA. March 8–11, 2004.5 Centers for Disease Control and Prevention. “Chlamydia – CDC Fact Sheet.” Accessed from http://www.cdc.gov/std/chlamydia/STDFact–Chlamydia.htm#complications March 1, 2007.6 Golden, Matthew R., et al. “Effects of Expedited Treatment of Sex Partners on Recurrent of Persistent Gonorrhea or Chlamydia Infection.” The New Eng-land Journal of Medicine, 2005; 352:7, 676–85.7 Kissinger, Patricia, et al. “Patient–Delivered Partner Treatment for Male Urethritis: A Randomized, Controlled Trial.” Clinical Infectious Diseases, 2005; 41:623–9.
Why Is Routine HIV Testing Recommended?ß Anestimated1.2millionpeoplearelivingwithHIV/AIDSintheUnitedStatestoday.Ofthese,25per-
centdonotknowtheyareinfectedandcanspreaditunknowinglytoothers.
ß Peoplewhoareinfectedbutnotawareoftheirconditioncannotaccessandbenefitfromtreatmentandmaynottakestepstoprotecttheirsexualordrug-usingpartners.
ß HIVinfectionisaseriousconditionthatcanbediagnosedpriortothedevelopmentofsymptomsthroughreliable,inexpensiveandnoninvasivescreeningtests.
ß Infectedpeoplecanlivelonglivesiftreatmentisstartedearly.
ß Onestudyestimatedthatinhigh-riskpopulations,aone-timescreeningcansavelivesandcostsbypre-ventingadditionaltransmissionsofthevirus.Forevery100,000peopleinthisgroupwhoarescreened,anestimated300fewerpeoplewillbecomeinfectedwithHIV.
ß ScreeninghasbeenshowntobeeffectiveindetectingHIVinfectionamongmothersandinpreventingtransmissionbetweenmotherandchildbeforeorduringbirthorthroughbreast-feedingafterbirth.
How Costly Are HIV/AIDS Infections?ß CurrentaveragelifetimecostofcareforapatientwithHIVinfectionis$200,000.
ß Thetotal lifetimecostforAmericansnewlydiagnosedwithHIV/AIDSduring2002wasapproxi-mately$36.4billion,whichincludesalmost$7billionindirectmedicalcostsandalmost$30billioninproductivitylosses.
ß Thefederalgovernmentisestimatedtohavespent$21billiononHIV/AIDSduringthe2006fiscalyear,whichincludestreatment,research,housingassistance,preventionandinternationalefforts.
What Does the Centers for Disease Control and Prevention Recommend?ItisimportantpeoplelearnoftheirHIVinfectionearlysinceresearchhasshownthatoncepeopleareawareofinfection,theytendtotakestepstoreducespreadingittoothers.InSeptember2006,CDCreviseditsrecommendationsforHIVtestinginhealthcaresettingsinanefforttoreducethestigmasurroundingHIVtestingandmakeitamoreroutinepartofmedicalcare.Therecommendationsare:
ß Allpatientsages13to64inhealthcaresettingsshouldbetestedforHIV.
ß Patientsshouldbeabletooptoutoftesting,whichmeanstheyshouldbeinformedthatHIVtestingwillbeconductedunlesstheydecline.
ß Testingproceduresshouldbesimplifiedbyeliminatingpre-testcounselingandaseparate,writtencon-sent.Consentcanbeincludedinthegeneralconsentformedicalcare.PreventioncounselingisstronglyencouragedforpeopleathighriskforHIVinsettingsinwhichriskbehaviorsareassessedroutinely(i.e.STDclinics),butshouldnotberequiredasapartoftesting.
R
R
Talking Points:Making HIV Testing Routine
R
celebrating
ß Screenallpregnantwomenaspartofnormalfirsttrimesterbloodtests.Also,womenwhoareathighriskofHIVorwhoreceivehealthcareinareaswithhighHIV/AIDSincidenceshouldberetestedinthethirdtrimester.TherapidHIVtestshouldbeusedduringlaborforallwomenwhosestatusisunknown.
SomestatesmayneedtopassnewlegislationtochangecurrentlawsoninformedconsentorcounselingthatpreventtheimplementationofCDC’snewrecommendations.
What Can State Legislators Do?ß TalkwiththeAIDSdirectorinyourstatehealthdepartmenttoseeifanylegalbarriersstandintheway
ofimplementingthenewHIVtestingrecommendationsfromCDC.
ß ConsiderlegislationtoovercomeexistingobstaclestoimplementingCDC’snewtestingrecommendations.
ß ConsiderincludingHIVtestinginMedicaid,privateandstateemployeehealthbenefitcoverageifyourstatehasn’talreadydonesotomakeitaffordable.
ß Facilitateorhelppromotecoalitionsofsocialservicegroups,communityorganizationsandfaith-basedorganizationsthatcanhelppromoteawarenessoftheimportanceofHIVtesting.
ß MakeHIV/AIDSawarenessahighpriorityinyourstatebytalkingtootherlegislatorsandincludingitinnewsletters,yourWebsiteandspeeches.
ß Considerworkingwithyourstatehealthdepartmenttomakesuretestingsitesareavailableinethnically,raciallyandeconomicallydiverseareas.
ß BeawarethattheremaybeobjectionstochangingstatelawsorregulationsregardingHIV/AIDStesting.Someoftheissuesraisedmayinclude:
† Informedconsent:Ifseparate,writtenconsentiseliminated,peoplemaybetestedwithouttheirknowl-edge,especiallyinurgent-caresettings.Therealsoareconcernsthatthosewhochoosetooptoutoftestingmayfacenegativerepercussionsfromhealthcareproviders.
† Eliminatingpretestcounseling:Ifmandatorypretestcounselingiseliminated,doctorsmaymissacriti-calopportunitytotalktopatientsabouthowtoreducetheirriskofacquiringHIV.
Bepreparedtodiscusstheseandotherconcernsinanopensettingandtoencouragestakeholderstohelpseeksolutions.
R
To find state-by-state statistics on HIV in your state, go to The Kaiser Family Foundation: http://www.statehealthfacts.org/cgi-bin/healthfacts.cgi?action=compare&welcome=1&category=HIV%2fAIDS
If you would like to receive more information, references, or to explore this topic in greater depth, please:Send your inquiry to http://www.healthystates.csg.org/ (keyword: questions/comments), orCall the CSG Health Policy Group at (859) 244-8000.
This Healthy States publication is funded by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, under Cooperative Agree-ment U38/CCU424348. Points of view in this document are those of the author and do not necessarily represent the official position or policies of the U.S. government.
n
n
Why Should State Legislators Be Concerned?ß The number of people with curable sexually transmitted diseases is increasing across the country.
ß Chlamydia, gonorrhea and syphilis are easily treated and cured with antibiotics, but untreated STDs can lead to serious health problems. Inaddition,studiessuggestthepresenceofSTDsmakesanindividualmorelikelytoacquireHIV.
ß STDs disproportionately affect racial and ethnic minority populations.African-Americanshavethehighestratesofchlamydia,gonorrheaandsyphilis,followedbyHispanicsandAmericanIndians/AlaskanNatives.
How Large Are the Disparities in Sexually Transmitted Diseases?ß Chlamydia infections are the most common bacterial STD and affect African-Americans more
frequently than whites. Infectionratesincreasedbyabout6percentfrom2005to2006toslightlymorethan1milliondocumentedcases.Comparedtowhites,chlamydiaratesare:
† MorethaneighttimeshigherforAfrican-Americans;
† MorethanfivetimeshigherforAmericanIndians/AlaskanNatives;and
† SlightlymorethanthreetimeshigherforHispanics.
ß Gonorrhea infections have greater health disparities than any other reportable disease. ThedocumentednumberofAmericanswithgonorrhearoseabout6percentfrom2005to2006tonearly360,000.Comparedtowhites:
† African-Americansare18timesmorelikelytohaveareporteddiagnosisofgonorrhea,makingitthelargesthealthdisparitytobeaddressedbytheU.S.DepartmentofHealthandHumanServices’HealthyPeople2010objectives.
† AmericanIndians/AlaskanNativesareaboutfour timesmorelikely tohaveareporteddiagnosisofgonorrhea;and
† Hispanicsaretwiceaslikelytohaveareporteddiagnosis.
ß After years of decline, syphilis is now affecting more Americans and is increasing in all racial and ethnic groups.Reportedsyphiliscasesincreasedacrossalltypesofthediseaseby11percentbetween2005and2006toalmost37,000reportedinfections.Comparedtowhites:
† African-Americansarenearlysixtimesmorelikelytohaveareporteddiagnosisofsyphilis;and
† Hispanics andAmerican Indian/AlaskanNativesareeachnearly twiceas likely tohavea reporteddiagnosisofsyphilis.
What Causes Racial and Ethnic Disparities in STDs?ß Factors that contribute to STD disparities include socioeconomic status, individual risk behavior,
social environment, and access and availability of health care.
ß Individual risk behavior does not fully explain why STD disparities exist.Evenwhenindividualriskbehaviorissimilar,African-AmericansarestillmorelikelytocontractSTDsthanwhitesbecausetheratesofthediseasearealreadymuchhigherinAfrican-Americancommunities.
R
R
Talking Points:Confronting Disparities in
Sexually Transmitted Diseases
celebrating
R
What Can State Legislators Do?PolicysolutionsareaimedatencouragingSTDscreeningforpeopleaswellastreatmentiftheyhaveaninfection.Statelegislatorscanleadamulti-prongedapproachthatencouragesstakeholdersto:
ß Cooperate with others who have an interest in STD disparities.
† WorkwithstatehealthdepartmentofficialsandcommunityleaderstoidentifytheareasinyourstatethataremostimpactedbySTDdisparities;and
† EngagestakeholderswhohaveaninterestinreducingSTDdisparities
ß Educate the public and providers on STD screening and treatment.
† Assurethateducationalmessagesareculturallyappropriateforthespecificcommunitieswheredisparitiesexist;
† EncouragepeopletobescreenedforSTDsandtogettreatmentiftheyareinfected.Inparticular,encouragesexuallyactivewomenunderage26togettestedforchlamydiaeachyear;and
† Educatehealthcareprovidersontheneedforexpandedtestingandtreatment,suchascouplingchla-mydiatestswithPaptests,andexpandedscreeningforgonorrheaandsyphilistoimprovehealthcareaccessandqualityinminoritycommunities.
ß Support state efforts to identify and treat those affected.
† SupportpublichealthfundingforSTDscreeningandtreatment,includingsyphilisandgonorrhea,forlow-incomeanduninsuredpopulations;
† Supportlegislationrequiringinsurancecompaniestocoverannualchlamydiascreenings;and
† Removelegalandadministrativebarrierstoimplementingexpeditedpartnertherapy(makingtreat-mentmoreavailableforsexpartners).
R
For more information see these Healthy States publications available at http://www.healthystates.csg.org/Publications/.† HIV/STDs Tool Kit† Chlamydia Screening and Treatment Policy Brief† Expedited Partner Therapy Talking Points
If you would like more information or references:
Send your inquiry to http://www.healthystates.csg.org/ (keyword: questions/comments) orCall the CSG Health Policy Group at (859) 244–8000.
This Healthy States publication is funded by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, under Cooperative Agree-ment U38/CCU424348. Points of view in this document are those of the author and do not necessarily represent the official position or policies of the U.S. government.
n
n
healthy states br iefCSG’s par tnership to promote publ ic health
Kids in middle school and high school hav-ing sex—it’s not something parents, teach-ers or community leaders want to think about. But public health experts warn that ignoring risky youth sexual behaviors is likely to be counterproductive. They are urging parents, teachers and community leaders to work with state and local policymakers to develop sex education programs that can gain community acceptance and be effective in protecting kids from the harm of risky sex behavior.
Consequences and CostsAnyone not convinced that youth sexual
behavior is worth worrying about should consider the following facts:
n Approximately 50 percent of high school age students in the United States have engaged in sexual intercourse;1
n One in four sexually active teens con-tracts a sexually transmitted disease (STD) each year ;2
n Although the teen pregnancy rate is dropping, about 880,000 teen girls get pregnant every year ;3
n About 78 percent of these pregnancies, in girls 15 to 19 years old, are unin-tended, with about 45 percent ending in abortion;4
n There are approximately 19 million new STD infections in the United States ev-ery year, and almost half of them are among those aged from 15 to 24;5
n An estimated 38,490 young people in the United States were diagnosed with AIDS in 2003.6
“If those numbers aren’t reason enough (to worry about risky youth sexual behav-iors), the cost of HIV infection, other STDs and unintended pregnancies among teenag-ers is another good reason,” says Dr. Jennifer Galbraith, a behavioral scientist at the Cen-
ters for Disease Control and Prevention’s (CDC) HIV/AIDS prevention division.
Prevention Efforts Do WorkAlthough education to curb risky sexual
behavior among teens is controversial, there is clear evidence that efforts to prevent HIV and other STDs and to reduce teen pregnan-cies are not only effective, but can translate to cost-savings for states. For example, accord-ing to Galbraith, for every dollar invested in Safer Choices, a school-based HIV, STD and pregnancy prevention program, $2.65 is saved in terms of medical and social costs.7 Consid-ering that in some states up to 90 percent of teenage births are paid for by Medicaid, implementing prevention strategies will have fiscal as well as social benefits.
What States are DoingStates know they can’t afford to ignore
the risks associated with sexual behavior
Protecting America’s Youth: Schools and Communities Tackle Youth Sexual Risk Behaviors
Vol. 1, No. 7 May 2006
The Council of State Governments (CSG) is the premier multibranch organization forecasting policy trends for the community of states, commonwealths and territories on a national and regional basis.
among young people, and they have been actively engaged in prevention efforts. Near-ly all states require that public schools teach some form of sex or HIV/STD education, yet just what that education entails varies dramatically from state to state.
Sex education is mandated in 21 states and STD/HIV prevention education is man-dated in 37 states. The majority of states that offer sex or HIV/STD education require that abstinence be stressed as part of the required content, even if it is not mandated by state law. Only a few require that contra-ception be covered. Additionally, the major-ity of states—regardless of whether sex and STD/HIV education is mandatory—have an opt-out option clause, which allows parents to remove students from instruction they find objectionable.8 For example, Delaware mandates sex and STD/HIV education cover both abstinence and contraception and does not allow for an opt-out option.
healthy states issue brief: youth sexual risk behaviorsThis issue brief is based on an Oct. 17, 2005, Healthy States Web conference titled “Protecting America’s Youth: Schools and Communities Tackle Youth Sexual Risk Behaviors.” Access an archive of this Web conference and others in this Healthy States series at www.healthystates.csg.org, key-word: web conferences.

North Carolina and Tennessee, on the other hand, mandate sex and STD/HIV education, stress abstinence, do not cover contracep-tion and allow for an opt-out option (For a more detailed look at a state STD/HIV pre-vention education program, see the article on Michigan’s curriculum, page 4.).
Challenges Faced by LegislatorsDespite the real political and policy chal-
lenges they face, public health champions say state legislators play a key role in develop-ing and implementing effective sex educa-tion curricula—the kind of curricula that will actually protect kids from risky sexual behavior.
According to public health experts like Galbraith, the main challenge for legisla-tors is crafting school district guidelines that stress the importance of teaching medically accurate and science-based programs, while allowing for strong parental involvement and local input.
Washington state Rep. Shay Schual-Berke agrees with that assessment. “We legislators have an important role in promoting effective prevention strategies for teen sexual risk be-havior,” says Schual-Berke, a parent and retired physician who has championed developing an evidence-based sex education curriculum in her state. “These roles include understanding
National Youth Risk Behavior Survey, 1991–2003
2 May 2006 Healthy States Brief: Youth Sexual Risk Behaviors
the needs of your state, understanding which strategies are medically and scientifically ac-curate and developing a broad coalition of stakeholders and crafting legislation that is flexible and meets the needs of all constitu-encies.” (See page 3 for more information about Washington state’s efforts.)
Keys to Effective Prevention EffortsAccording to Schual-Berke and other
public health experts, there are three key components to developing an effective, ac-cepted sex education curriculum:
n Use evidence-based, medically ac-curate strategies. This means that the programs have undergone an evaluation process to determine their effectiveness and medical accuracy. Researchers, in-cluding some at CDC, have conducted various studies of school health educa-tion curricula and programs aimed at reducing youth’s risk behavior. By un-derstanding which strategies are known to be effective, legislators can encour-age the adoption of these programs thereby maintaining the positive trend of reduced risky sex behavior.
n Avoid “one size fits all” approach. Sen-sitivities of the community need to be taken into account when proposing sex education programs. By understanding what the community wants and needs in its individual program, different constitu-encies can come together to find a solu-tion that will best fit the needs of their young people. To help identify need, the CDC has surveillance data that tracks cases of HIV and other STDs that can be used as a starting point to determine the incidence of HIV/STDs and teen pregnancy rates in communities.
n Bring everybody to the table. Legisla-tors also have a critical role in bringing everybody to the table when designing sex education curricula. While most of the controversy surrounding sex educa-tion focuses on the use of abstinence-only versus abstinence-plus methods, policymakers can find creative solutions that address both constituencies.
Promising TrendsSchual-Berke says there’s a reason why
some state legislators take the lead in cre-ating effective sex education curricula—be-cause it makes a positive difference.
And there is evidence to back her up. Ac-cording to the National Youth Risk Behavior Survey, 1991-2003, developed by the CDC to help monitor youth risk behaviors, there has been a significant decrease in youth who report they have engaged in sexual inter-course. This is down from 54 percent in 1991 to 47 percent in 2003.
There is also promising news regarding youth engaging in sexual activities with mul-tiple partners. In 1991, 19 percent of youth reported having sex with multiple partners. In 2003, 14 percent made the same claim. The use of condoms among youth has in-creased from 46 percent in 1991 to 63 percent in 2003. However, the percentage of sexually active youth who report using drugs and/or alcohol before a sexual en-counter rose from 22 percent to 25 percent over the 12-year period.
“If it is done right—if we can implement a medically and scientifically accurate curricu-lum that gains buy-in from parents—we can do a better job of protecting our kids,” says Schual-Berke. “And we owe it to our kids to do our best.”
Definitions
STDs or sexually transmitted diseases are caused by more than 25 infectious organ-isms that are transmitted primarily through sexual activity. Among the most common STDs are genital human papillomavirus (HPV), chlamydia, gonorrhea and syphilis.
HIV or human immunodeficiency virus is the virus that causes AIDS. HIV infection is commonly spread by unprotected sexual contact with an infected person.
AIDS or acquired immunodeficiency syn-drome is the most severe and life-threat-ening manifestation of the HIV infection.
100
80
60
40
20
01991 1993 1995 1997 1999 2001 2003
Multiple Partners
AIc/Drug before SexCondom Use
Ever Had Sex63
4725
14
5446
2219
Perc
enta
ge o
f Hig
h Sc
hool
Stu
dent
s Trends in Sex Risks
Healthy States Brief: Youth Sexual Risk Behaviors May 2006 3
How to Build a Broad Coalition to Prevent Risky Teen BehaviorAdvice from a Veteran Legislator
Washington state Rep. Shay Schual-Berke is a parent and a retired physician. She is also a veteran legislator, having served since 1994 in Washington’s House of Representatives. She is keenly aware of both the need to protect children from risky sexual behavior and the need to build broad coalitions to sup-port effective sex education policies.
Responding to concerns of parents and students about the quality and accuracy of the HIV/STD and sex education being taught in school, Schual-Berke spearheaded a broad coalition to develop new state guidelines for sexual health and disease prevention education. Based on that experience—which in-volved a retreat from requiring schools to adopt a specific sex education curriculum to allowing them to develop their own guidelines—Schual-Berke offers this advice to legislators who want to take action to reduce the impacts of youth sexual risk behaviors in their states:n Assess where your state is. It is important to understand the unique needs of your state. “We are all very, very different and you need to know whether your own state requires this education, whether there is remodel curricula available or not,” says Schual-Berke.n Develop a nonpartisan/bipartisan coalition of stakehold-ers. With sensitive issues such as sex education where different viewpoints can lead to political stalemates, it is important to encourage discussion. “It always helps in a legislative arena to develop a very broad coalition of stakeholders who cross party
lines and who are able to keep at the fore the well-being of students,” she says. In Washington, this coalition consisted of the state departments of health and education and many local organizations.n Legislation should be flexible and evidence-based. Schual-Berke ex-plains, “As we worked through this, it became clear that legislation does have to meet the needs of all constituencies. So for example, in our voluntary guidelines, we do emphasize the necessity and the utility of ab-stinence, but we recognize that we have to go beyond that. We think it’s very important that it be evidence-based and I think as legislators work through that, the need for the evidence base becomes very obvious.”n Be happy with incremental change. When dealing with difficult issues like sex education, do not expect huge changes overnight. As Schual-Berke says, “this is a great example of in-cremental progress, where in our case, we’re moving forward with voluntary guidelines and then we’ll get more information and take further steps as needed. So this is a situation where incremental progress is a very worthwhile progress.”
What WorksTen Components of Effective Sex Education Programs
1. Reinforce a clear message to teens about abstinence as the only sure way to avoid unintended pregnancy and STDs and about how to use condoms and other forms of contraception for those who are sexually active.
2. Focus on getting teens to reduce one or more sexual behaviors that lead to unintended pregnancy or HIV/STD infection.
3. Base programs on approaches that have been demonstrated to be effective in influenc-ing other health-risk behaviors.
4. Provide basic information about the risks of adolescent sexual behavior and about methods of avoiding intercourse or using protection against pregnancy and STDs.
5. Include activities that address how teens can handle social pressures to engage in sexual behavior.
6. Provide modeling and practice of communication, negotiation and refusal skills for teens.
7. Employ a variety of teaching methods designed to involve the teens and have them personalize the information.
8 Incorporate behavioral goals, teaching methods and materials that are appropriate to the age, sexual experience and culture of the students.
9. Ensure programs last a sufficient length of time to have a measurable impact on behavior.
10. Select educators who believe in the program they are implementing and provide them with quality professional development so they are competent to deliver the material.
Source: Adapted from Guidelines for Sexual Health Information and Disease Prevention, The Washing-ton State Department of Health & The Office of Superintendent of Public Instruction, 2005. Down-load the guidelines at www.k12.wa.us/CurriculumInstruct/healthfitness/default.aspx.
Notes1Grunbaum JA, Kann L, Kinchen S, Ross J, Hawkins J,
Lowry R, et al. Youth Risk Behavior Surveillance—United States, 2003. Morbidity and Mortality Weekly Report 2004; 53 (SS-2): 1-95
2Alan Guttmacher Institute. (1994). Sex and America’s Teenagers. New York
3Henshaw SK (2003). U.S. teenage pregnancy statistics with comparative statistics for women aged 20-24. New York: The Alan Guttmacher Institute. http://www.guttmach-er.org/pubs/teen_stats.html (accessed April 18, 2006).
4Ibid,http://www.guttmacher.org/pubs/teen_stats.html (accessed April 18, 2006).
5Weinstock H, Berman S, Cates W. Sexually trans-mitted diseases among American youth: Incidence and prevalence estimates, 2000. Perspectives on Sexual and Reproductive Health 2004;36(1):6-10.
6CDC. HIV/AIDS Surveillance Report. 2003. Vol. 15 Atlanta: US Department of Health and Human Services; 2004: 1-40
7Wang, LY, Davis, M, Robin, L, Collins, J, Coyle, K and Baumler, Elizabeth. Economic Evaluation of Safer Choices: A school-based human immunodeficiency virus, other sexually transmitted diseases, and pregnancy prevention program. Archives of Pediatric & Adolescent Medicine: October 2000. 154:1017-1024,
8Alan Guttmacher Institute. State Policies in Brief: Sex and STD/HIV Education. www.guttmacher.org/statecenter/spibs/spib_SE.pdf (accessed April 18, 2006).

healthy states briefThe Council of State GovernmentsP.O. Box 11910Lexington, KY 40578-1910
www.healthystates.csg.org
Nonprofit Organization
U.S. Postage
PAID
Lexington, KY 40578
Permit No. 355
resourcesCenters for Disease Control and Prevention HIV/AIDS and STD Web sitewww.cdc.gov/std/hiv/default.htm
American Social Health Associationwww.ashastd.org
Education Training Research Associates (ETR) Resource Center for Adolescent Pregnancy Preventionwww.etr.org/recapp/
Kaiser Family Foundationwww.kff.org/hivaids/index.cfm
The Council of Chief State School Officerswww.ccsso.org
The National Association of State Boards of Educationwww.nasbe.org/healthy_schools
The National Campaign to Prevent Teen Pregnancywww.teenpregnancy.org
Youth Risk Behavior Survey Surveillance Systemwww.cdc.gov/HealthyYouth/yrbs/index.htm
HIV/AIDS Prevention Education in MichiganHealth and education departments work to create model curriculum
In June 2004, Michigan’s HIV/AIDS and sex education laws were changed significantly, and school districts looked to state for assis-tance. One helpful resource was a model curriculum developed jointly by the state’s health and education departments.
The curriculum consists of skill-based content, and local school districts can adopt it as written, adapt it to meet their needs, or dis-regard it and create their own material. At the elementary level, one to two lessons are provided for each grade. At the middle school level, eight lessons are provided, and high school students will receive more than 20 lessons.
“The curriculum is based on the latest science about what’s ef-fective in terms of programs and includes a lot of chances for the students to practice the skills that are necessary in terms of HIV prevention,” said Laurie Bechhofer, an HIV/STD consultant with Michigan’s education department.
Under the law, local advisory boards review all materials and cur-ricula. The law requires that half of each local board be comprised of parents with students currently enrolled in a district’s schools. Accord-ing to Bechhofer, this membership requirement ensures all viewpoints are represented from the broader parental community. Other mem-bers include students, educators, clergy and health professionals.
Under the law, schools may also offer—but not require—sexuality education classes which provide such content as family planning, hu-man sexuality and family life education. Parents also have the option to receive notification of any sex education courses and are allowed to review course content in advance. Parents may choose to exempt
their kids from any part of the instruction. For more information about Michigan’s model curriculum, go to
www.emc.cmich.edu/mm/default.htm.
healthy states brief
Volume 1, Number 7
Healthy States Briefs highlight trends and promising practices in state public health policy.
The Healthy States Initiative is a partnership among The Council of State Governments, the National Black Caucus of State Legislators and the National Hispanic Caucus of State Legisla-tors. The initiative is supported by the Centers for Disease Control and Prevention.
This Healthy States Brief was written by Pam Goins, senior education policy analyst, and Lizeth Fowler, health policy analyst at The Council of State Governments. Pam can be reached at [email protected].
www.healthystates.csg.org
Funding for CSG’s Healthy States Initiative is provided by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, under Cooperative Agreement U38/CCU424348. The contents of this Healthy States Brief are the responsibil-ity of CSG’s Healthy States Initiative and do not necessarily represent the official views of the CDC or CSG.
Chlamydia Screening
and Treatment
Legislator Policy Brief
TheHealthyStatesInitiativehelpsstateleadersaccesstheinformationtheyneedtomakeinformeddecisions
onpublichealthissues.Theinitiativebringstogetherstatelegislators,CentersforDiseaseControlandPreven-
tion (CDC)officials, statehealthdepartmentofficialsandpublichealthexperts to share informationand to
identifyinnovativesolutions.
TheCouncilofStateGovernments’partnersintheinitiativearetheNationalBlackCaucusofStateLegislators
(NBCSL)andtheNationalHispanicCaucusofStateLegislators(NHCSL).Theseorganizationsenhanceinfor-
mation–sharingwithstatelegislatorsandpolicymakersoncriticalpublichealthissues.
FundingforthispublicationisprovidedbytheU.S.DepartmentofHealthandHumanServices,Centers
forDiseaseControlandPrevention,underCooperativeAgreementU38/CCU424348.Pointsofviewinthis
documentarethoseoftheauthoranddonotnecessarilyrepresenttheofficialpositionorpoliciesoftheU.S.
government.
Why public health? Statelegislatorsplayavitalroleindeterminingthestructureandresourcesavailabletostateandlocalagen-
ciesdedicatedtoprotectingthepublic’shealth.Publichealthagencieseducatethepublicandofferinterventions
acrossawidespectrumofpublichealthissuesincluding:
Ensuringthatchildrenandat–riskadultsareimmunizedagainstdeadlydiseases;
Assistingvictimsofchronicconditionssuchascancer,heartdiseaseandasthma;
Preventingdiseaseanddisabilityresultingfrominteractionsbetweenpeopleandtheenvironment;
ResearchinghowHIV/AIDSinfectionsandothersexuallytransmitteddiseasescanbeprevented;
Promotingthehealthandwell–beingofpeoplewithdisabilities;and
Workingwithschoolstopreventriskybehavioramongchildren,adolescentsandyoungadults.
Information resources for state policymakers Newinformationresourcesproducedunderthisinitiativeinclude:
HealthyStatesWebsite.ThisuniqueWebsiteoffersinformationandresourcesonmanypublichealthissues.Visithttp://www.healthystates.csg.org togetinformation,signupforpublicationsandviewotherinformationontheinitiative.
HealthPolicyHighlightsandHealthyStatese–weekly.Eachweek,thisfreeweeklyelectronicnewsletterbringsthelatestpublichealthnews,resources,reportsandupcomingeventsstraighttoyourinbox.
HealthyStatesQuarterly.CSGpublishesa freequarterlynewslettercoveringpublichealth legislativeandpolicytrends,innovativebestpracticesfromtheexecutiveandlegislativebranches,currentresearch
andinformationonHealthyStatesactivities.
ForumsandWebConferences.Webconferencesareofferedtoallowpublichealthexperts,legislatorsand
legislativestafftointeractonprioritypublichealthissues.Forumsincludeeducationalsessionsonpublichealthissues,newlegislatortrainingandroundtablediscussionswithpeersandpublichealthexperts.
HealthyStatesPublications.Newresourceswillassiststatelegislatorsinterestedinpublichealthtopics,includingobesityandchronicdiseaseprevention,HIV/AIDSandsexuallytransmitteddiseasepreven-tion,vaccines,healthdisparitiesandschoolhealth.
For more information IfyouareinterestedinthelearningopportunitiesavailablethroughtheHealthyStatesInitiative,visithttp://
www.healthystates.csg.org, http://www.nbcsl.org or http://www.nhcsl.org.
n
n
n
n
n
n
n
n
n
n
n
The
Hea
lthy
Stat
es In
itiat
ive
A pa
rtne
rshi
p to
pro
mot
e pu
blic
hea
lth
Chlamydia Screening and Treatment Overview
With nearly a million new cases reported in 2005, chlamydia is the most frequently reported sexually transmitteddisease(STD)intheUnitedStates.1,2Chlamydiaiscausedbyabacterialinfectionandiseasilytreatedwithantibiotics.Theeffectsofuntreatedchlamydiacanincludeirreversibledamagetowomen’sreproductiveorgans,pregnancycompli-cations,infertility,andchronicpain.3,4Overall,anestimated2.8millionnewcasesofchlamydiaoccureachyear,5atanestimatedcostof$598million.6
Thisbriefinformsstatepolicymakersaboutchlamydiaanditseffectsonpublichealth,alongwithcost-effectivepreventionstrategiesthatstatesareimplementing.
What Legislators Need to Know About Chlamydia TheCentersforDiseaseControlandPrevention(CDC)reportsthatnearlyonein20sexuallyactivewomenbetweentheagesof14and19—agroupparticularlyvulnerabletothedevastatingcomplicationsofthisinfection—isinfectedwithchlamydia.7Additionally,chlamydiainfectionsaremorecommonlyfoundamongyoungadults,urbanresidents,African-Americansandsocioeconomicallydisadvantagedpopulations.3,8
Annualchlamydiascreeningisrecommendedforallsexuallyactivewomenage25oryounger,andforwomenolderthan25withspecificriskfactorssuchasanewsexpartnerormultiplesexpartners.ThisrecommendationisendorsedbytheCDC,allleadinghealthandmedicalassociationsandtheU.S.PreventiveServicesTaskForce.Chlamydiascreeningisoneofthemostcost-effectiveyetunderusedpreventionservicesavailable.9
Screeningandearlydetectionareprovenhigh-valueservicesthatarecriticaltocontainingchlamydiaanditslong-termeffects.10Butchlamydiaisoftena“silent”infection,offeringnowarningsignsorsymptoms;therefore,individualstendnottoseektreatment.Publicoutreachandeducationaboutthisinfectionandtheimportanceofscreeningarecorestrategiesinreducingtheburdenofchlamydia—particularlysincethisinfectioncanbeeasilyandeffectivelytreatedandcostlysideeffectscanbeavoided.
Onceanindividualistreated,hisorhersexpartnersmustalsobetreated.Thismaybeachievedbyhealthcareprovid-erscontactingidentifiedpartnersandprovidingpublichealthservices.Butthelargenumberofcasesofchlamydia,andtherefore,partnersinfectedwiththedisease,typicallymakesthisimpossibleorimpracticalforprovidersandpublichealthdepartments.Analternatepracticeisexpeditedpartnertherapy,orEPT,inwhichhealthcareprovidersgiveprescriptionsormedicationtothepatienttheyaretreatingforhim/hertodelivertohis/hersexualpartner.Inadditiontodispensingmedicationandprovidingcounselingandinstructionoftheproperuseofthemedicine,providersencouragepatientstourgetheirpartnerstoseekevaluationandcare.11
What Can State Legislators Do to Help Prevent Chlamydia?
Sponsororsupportlegislationrequiringinsurerstocoverannualchlamydiascreening.
Serveonorsupportlegislativetaskforcesandfocusgroupsthathelptoinformandmotivatecolleagues,raiseawareness
andsupportpublicadvocacyforscreeningandtreatmentservices.
Promotefundingforchlamydiascreeningandtreatmentforlow-incomeanduninsuredpopulations.
Supportor sponsorchlamydiapreventionalliancesamongstateand localdepartmentsofhealthandhealthcare
professionals.
n
n
n
n
Legislator Policy Brief Chlamydia Screening and Treatment 1
Actions for State Legislators
Demonstrate Leadership
CreateorserveonastatewidetaskforceonSTDeducationandcontroltoincreaseawarenessforpreventionofSTDs
includingchlamydia.
Request,supportorparticipateincommunityfocusgroupstoexploreobstaclesandinnovativesolutionstoencour-
age screeningand treatment for chlamydia, and to identifyopportunities forpublicandprofessionaloutreachand
education.Considerwaystoreachouttothosepeoplethediseasemorecommonlyaffects,includingyoungadultsand
African-Americans.
TheConnecticutHealthPolicyProjectconductedafocusgrouptoexploresolutionsforreducingtheincidenceof
chlamydia in the state. Focus group participants represented policy experts, adolescents, educators, health care
professionalsandlegislators.Findingsfromthefocusgroupinclude:proposinglegislationtosupportchlamydia
testing,coordinatingwithstateandlocalhealthdepartmentsonpublicandprovideroutreachandeducation,and
fundinglocalorganizationstoexpandaccesstotestingandtreatmentforchlamydia.12,13
Formpartnershipswithcommunityandfaith-basedorganizations,andwomen’shealthandreproductivehealthadvo-
catestoraiseawarenessabouttheimportanceofchlamydiascreening,particularlyinminorityandat-riskpopulations.
Support Comprehensive Screening and Education Programs
Sponsororsupportlegislationto:
Requirepublicandprivatehealthinsurerstocoverthecostofannualchlamydiascreeningamongadolescents
andyoungadults;
CoverscreeningforchlamydiaandotherSTDsforallpatientsofpublicorstate-supportedmedicalservices;10
Supporttrainingforprimaryhealthcareproviderstotestpatientsforchlamydiaaccordingtonationalguidelines,
andsupportpaymentincentivesthatencourageproviderstoofferchlamydiascreeningtotheirpatients;
Fundpublicinformationcampaignsontheeffectsofchlamydiainfectionandthebenefitsofannualscreeningfor
youngwomen;and
Encourageage-appropriatecomprehensiveSTDpreventioneducationinschools.
Promotefundingtoprovidechlamydiascreeningservicesforuninsured,at-riskpopulationsinnontraditionalsettings
suchasworksites,prisonsandhalfwayhouses.14
Workwithlocaladvocacyorganizationstoreducedisparitiesintheincidenceofchlamydia:
Createandsupportculturallyappropriatepubliceducationcampaignsthatencouragewomentogetscreenedfor
chlamydia;
Encouragelocalcommunityhealthcenterstoofferchlamydiascreeningservicestolowincomeuninsuredpatients;and
Supportprovidingscreeningforthosewithoutaccesstomedicalservices.
n
n
®
n
n
®
®
®
®
®
n
n
®
®
®
2 Chlamydia Screening and Treatment Legislator Policy Brief
Contribute to State and Local Efforts to Identify and Treat Those Affected
Supportlegislationorregulatorychangetoallowexpeditedpartnertherapy(EPT),whichallowshealthcareproviders
togivemedicationoraprescriptiontoapatienttodelivertohisorhersexualpartner.
WorkwithyourstateSTDdirector,pharmacyboard,medicalboardandotherappropriatepublichealthentitiesto
determineifbarrierstoimplementingEPTexistinyourstate—regulatory,statutory,policyorpractice;and
Developplanstoreducethesebarriers.ToreviewthelegalissuesrelatedtoadoptionofEPTinyourstate,see:
http://www.cdc.gov/std/ept/legal/default.htm.
Support funding for health departments to encourage pediatricians, family practitioners and other primary care
providerstoscreenforchlamydiaandtreatchlamydiapatientscomprehensively.
Supportlegislationforpublicandprivateinsurerstocover:
Counselingandretestingofchlamydiapatients;and
Medicationstotreatboththepatientandhis/herpartner(s)throughEPTtopreventreinfection.
Supportfundingforstateandlocalhealthdepartmentstoestablishstrategicallylocatedtreatmentsiteswithconvenient
(evenings,weekends)hoursofoperation.Forexample,establishsatelliteSTD/chlamydiaclinicstobringservicesto
morecitizensinmorelocationsattimesthatdonotconflictwithworkhours.
Supportcollaborativeeffortswiththemedicalandpharmacyboardsandstatemedicalsocietytoestablishstanding
ordersthatpermitnonphysicianhealthcareproviders(physicianassistants,nursepractitioners) toadministerchla-
mydiascreeningandtreatmentservices(includingEPT)inmedicallyunderservedareas,suchasindustrialworkplaces
orgeographicallyremotelocations.
Participateincoalitionsofprivatehealthproviders,women’sandreproductivehealthorganizations,andstateandlocal
publichealthpersonneltoassurethatallcomponentsofhighqualitychlamydiascreeningandtreatmentservicesare
availableinthecommunity,specifically:
Preventionandmonitoringcomponentssuchasscreenings,partnernotificationandcasereporting;
Medicationandcounselingservicesforthoseaffectedbychlamydiaandtheirpartners;and
Ongoingeducationandtrainingofprivatehealthprovidersandpublichealthpersonnel.15
n
®
®
n
n
®
®
n
n
n
®
®
®
Legislator Policy Brief Chlamydia Screening and Treatment 3
State Policy Examples
Chlamydia Prevention and Control in California AmultifacetedpublichealthinterventionprogramtocontrolchlamydiawaslaunchedinCaliforniain2000.TheCaliforniaSTDControlBranchandotherpublichealthleadersgarneredpoliticalsupportandconvenedkeystakeholdersthroughtheCaliforniaChlamydiaActionCoalition(CCAC),apublic-privatepartnershipledbytheCaliforniaDepartmentofHealthSer-vices,theCaliforniaHealthCareFoundationandtheUniversityofCalifornia,SanFrancisco.TheCCACrecruitedstakeholdersfrombothpublicandprivatesectorsandinitiatedactivitiesonseveralfronts,includingscreening,partnerservices,awarenesscampaignsandtracking.
Inacoordinatedeffort,SB648,sponsoredbySen.DeborahOrtiz,wasenactedonJan.1,2001,amendingstatelawtoallowphysicians toprescribeandphysicianassistants,nursepractitioners, andcertifiednursemidwives todispenseantibiotictherapyforthesexpartnersofindividualsinfectedwithchlamydia—evenifunabletoperformadirectexamofthepatient’spartner.
ResearchconductedsinceSB648wassignedintolawfoundthatpatient-deliveredtherapy(oneformofEPT)wasas-sociatedwithreducedratesofinfection.16Achlamydia“toolbox”supportedbyon-sitetrainingwasdevelopedtoraiseproviderawarenessandimprovescreeningandtreatmentofthoseaffectedandtheirpartners.Additionally,achlamydiainformationclearinghousewasestablishedtoprovidedatatomanagedcareorganizationsandpublichealthagenciesfordiseasereportingpurposes.
http://www.ucsf.edu/castd/chlamydia_coalition.html
Increasing Screening in Tennessee In2001,theTennesseeDepartmentofHealthmetwithmanagedcareorganizationsthatprovideservicesforthestate’sMedicaidpopulation.Workingtogetherwiththequalityassurancearmoftheorganizations,thestatewasabletohavechlamydiascreeningofsexuallyactivefemalesages15to24includedasaquality-of-caremeasurement.
Tofurtherexpandthepopulationbeingtested,thestatestartedscreeningallfemalesreceivingapregnancytestinthestate’sfamilyplanningclinics.Furthermore,in2006,thestateDepartmentofHealthfundedagranttoKnoxCountytoscreeneveryonebookedinthejuveniledetentioncenter.Allofthescreeningtestsuseaurine-basedtesttoscreenforbothchlamydiaandgonorrhea.
Tennesseealsoisoneofthefewstatesinthecountrytohaveclearedlegalorregulatorybarrierstoexpeditedpartnertherapy.In2002,themedicalpracticerulesoftheBoardofMedicalExaminerswereamendedtoallowphysicianstodis-penseantibioticsforthepartnersofthoseinfectedwithchlamydiaeveniftheywerenotexamined.Healthcareproviderscanwriteaprescriptionbothforthepatientandhisorherpartnerwithin60daysfromonsetofsymptomsorpositivetestresults.
http://health.state.tn.us/health/std/field.htm
4 Chlamydia Screening and Treatment Legislator Policy Brief
New Mexico Health Department and Medical Society Collaboration Aboutsixyearsago,theNewMexicoHealthDepartmentandtheNewMexicoStateMedicalSocietyjointlyformedtheClinicalPreventionInitiative(CPI).Thegoalofthegroupwastohelpthestate’sdoctors,nursesandotherhealthcarepro-vidersimplementclinicallyproveninterventions—basedontheU.S.PreventiveServicesTaskForcerecommendation—intheirpractices.Asteeringcommitteehelpedguidetheworkandincludedrepresentativesfrommanagedcareorganizationsandotherhealthorganizations,suchastheAmericanCancerSociety.
CPIfocuseditseffortsonincreasingroutinechlamydiascreeningforallsexuallyactivewomen25yearsoryounger;men or women with more than one sexual partner or a recently diagnosed STD regardless of age; and all pregnantwomen.CPIdevelopedinformationalhandoutsforpatientsaboutthesymptomsandrisksofchlamydia.ThegroupalsohelpeddevelopaDearColleagueletterandtrainingforhealthcareproviderstoinformthemofthereasoningbehindthenewtestingguidelines,recommendedtreatmentsforinfectionsandthecostsandreimbursementratesfordifferenttestingmethods.
“Basicallyinthepublicsector,we’vebeenscreeningforchlamydiaformanyyears,”saidDr.BruceTrigg,medicaldirectoroftheSTDProgram,Regions1and3,NewMexicoDepartmentofHealth.“It’srelativelyrecentthatscreeninghasbecomeprevalentintheprivatesector.It’sabout50to60percentofwomenwhoshouldbescreenedarebeingscreened.ComparedtoPapsmears,there’salongwaytogo.”
http://www.swcp.com/nmms/subpages/NMMS_CPI.htm
Reaching African-American Teens in Texas TheTexasDepartmentofStateHealthServices(DSHS)launchedamediacampaigndesignedtoincreaseawarenessofSTDsandtheneedfortestingamongsexuallyactiveAfrican-Americanfemalesages15–19.TheDSHSBureauofHIVandSTDPrevention’ssuccessfulcampaignreceivedtheNationalPublicHealthInformationCoalition’sBronzeAwardforexcellenceinPublicHealthCommunication.
TheSTDAwarenessMediaCampaign,developedbythebureauwithapublicrelationsagency,usedtargetedtelevision,radioandbillboardstobringSTDawarenessandpreventionmessagestoAfrican-AmericanadolescentgirlsinthecitiesofTylerandLongview.Thecampaign’stoolsincludedaninteractiveCD-ROMtoolkittitled“CDCynergy,”forhealthcareproviderstouseindesigningpublichealthcommunications.
Surveysofadolescentsafterthepilotcampaignindicatedthatawarenessofchlamydiaasasexuallytransmitteddiseasemorethandoubled.Ofthosewhosawthecampaignads,69percentsaidtheadsmadethemthinkmoreaboutSTDsthantheyhadbefore,28percentsaidtheytalkedtosomeoneaboutSTDsbecauseoftheads,and19percentsaidtheygottestedforanSTDotherthanHIVbecauseoftheads.17TheadscontinuetobeusedbypublichealthdepartmentsthroughoutTexasforpublicinformationcampaigns.
http://www.dshs.state.tx.us/hivstd/info/stdmedia.shtm
http://www.cdc.gov/std/healthcomm/cdcynergy.htm
Legislator Policy Brief Chlamydia Screening and Treatment 5

Sen.NanGroganOrrock’s20years intheGeorgialegislaturehaveincludedsuccessfulinitiativesonfamilymedicalleaveandequityforcontraceptives.Orrockalsosponsoredthe1998ChlamydiaScreeningAct(HB1565).Theactrequireshealthinsurerstocoveranannualchlamydiascreeningtestforwomenunderage30,whichresultsinphysiciansroutinelytestingwomenatriskfortheinfectiononatimelybasis.Orrockcreditstheact’ssuccesstolegislators’commitmenttoprotectingthehealthofyoungwomenandobtainingstrongevidencethatchlamydiascreeningwouldsavemoneyandimprovehealthinlocaljurisdictionsacrossthestate.
OrrockworkedcloselywiththeGeorgiaDivisionofPublicHealthdirector,whowantedtoreducechlamydiaanditsseverecomplicationsthroughwideuseofscreeningprogramsandaconvenientone-timeantibiotictreatment.Publichealthstatisticsfrom265sitesacrossthestateindicatedthatthosewhoweredisproportionatelyaffectedbychlamydiaincludedwomenunder20,African-Americansandresidentsofsomeareasofthestate.
WiththehelpofOrrock—whowasatthattimearepresentative—andotherlegislativechampions,statelegislatorswereeducatedabouttheincreasingcasesofchlamydiaacrossthestateandthesuccessofchlamydiascreeningandtreatmentprogramsinotherstates.AlegislativestudycommitteeandmeetingswiththeWomen’sCaucus,HealthCommittee,Ap-propriationsCommitteeandthefullHousehelpedbuildsupport for the legislation.PublichealthofficialsalsoworkedwiththestateMedicaidagencytoreimbursephysiciansforadministeringtheconvenientsingledoseantibiotictopatientsimmediatelyupondiagnosis.
Her Advice to State Legislators:
Do your homework.Havethefactsonthepotentialcost-savingsandhealthbenefitsforyoungwomenandhavethe
statisticsforthoseaffectedinlocaljurisdictionsacrossthestate.Usepublichealthexpertstorespondtoquestionson
testing,medicalconditionsandtreatment.Showpotentialcost-savingsifectopicpregnanciesinMedicaidpatientswere
prevented.Havingthefactsallowslegislatorstofocusonpolicydecisionsforthesesensitiveissues,whichcanbedif-
ficulttoaddress.
Build a broad base of support.Buildlegislatorsupportforchlamydiascreeningacrossgenderandpartylines.Awomen’s
caucusisagreatresourceinbuildingthesealliances,asaregroupscommittedtoreducinghealthdisparities.
Know the costs.Bepreparedforobjectionsmandating insurancebenefits;showthesignificantcost-savingspossible
throughincreasedchlamydiascreeningandtreatment.
Appeal to the common sense of the legislators.“Anounceofprevention”forthecostlyeffectsofchlamydia,suchas
pelvicinflammatorydisease,isworthwhile.Thediseaseis“silent”for75percentofinfectedwomen,sothoseaffected
oftendon’tknowtoseektreatment.Also,theavailabilityofaone-timemedicationcureassuresthatthoseaffectedwill
receivetreatmentimmediately.
See: Georgia Department of Human Resources, Division of Public Health, “An Overview, Gonorrhea and Chlamydia, Georgia,” avail-able at: http://health.state.ga.us/pdfs/epi/hivstd/gonorrhea_chlamydia.pdf.
n
n
n
n
Advice from a State LegislatorRequiring Health Insurance Coverage for Chlamydia Screening
Nan Grogan OrrockGeorgia Senate
6 Chlamydia Screening and Treatment Legislator Policy Brief

Establishingpositiveworkingrelationshipsbetweenstateagencies,medicalsoci-etiesandhealthcareprovidersiscriticalwhenconfrontingdifficultissues,saidDr.BruceTrigg,medicaldirectoroftheSTDProgramintheNewMexicoDepartmentofHealth.Forexample,implementingEPTinastatecanbechallenging:manystatesfaceuncertaintyoverwhetherthepracticeislegal,whetherregulatoryorstatutorychangesarenecessarytopermititandevenwhichagencyhasauthority.
TheprocesshasbeenmadeeasierinNewMexicothroughtheClinicalPreventionInitiative(CPI),ajointeffortoftheNewMexicoHealthDepartmentandtheNewMexicoStateMedicalSocietytoencourageuseofpreventionservices.WhenCPIofficialsbeganworkingonexpandingguidelinesforchlamydiatesting,theydiscoveredEPTwasbannedbytheMedicalPracticeAct.OfficialsbelievediftheycouldconvincetheNewMexicoMedicalBoardtosupportchangingtheregulations,theymightbeabletoremovethebarrierstoimplementingEPT.
Cooperation,agoodworkingrelationshipandawillingnesstotalkhelpedmovetheprocessforward.“Whenwefirstapproachedthem(theNewMexicoMedicalBoard),theywereextremelynegative,”Triggsaid.“…Theysawthisasanerosionofmedicalcontroloverprescriptionmedications.”
TheCPIgroupsoughtendorsementoftheproposedchangefromitstwosponsors,theNewMexicoMedicalSocietyandtheDepartmentofHealth.Thepublichealthdepartmentsupportedthiseffort,butthemedicalsocietywashesitantatfirst.Afterfurtherdiscussionbetweenthehealthdepartmentandthemedicalsociety,theproposalwasendorsedunanimously.
TheNewMexicoMedicalBoardreactedpositivelywhenpublichealthandthemedicalsocietycollaboratedtoproposetheregulatorychange.AccordingtoTrigg,theywereabletosay,“Thisistheconsensusofthemedicalandpublichealthcommunityandhere’sallthestudiesandCDCrecommendations(infavorofEPT).”
Asaresult,sinceearly2007newEPTregulationsallowdoctorsandphysicianassistantstoprescribemedicineforthepartnersofpatientswhohavebeendiagnosedwithasexuallytransmitteddisease,withoutexaminingthepartner(s).
His Advice to State Legislators: Trigghadtwosuggestionsforlegislatorswantingtoincreasethenumberofconstituentsbeingscreenedforchlamydia:
First, talk to their state’s STD program director.“Ithinkitissomethingstatelegislatorsneedtospeaktotheirstatehealth
peopleabout”toidentifythebarrierstoincreasingscreeningintheirstate,Triggsaid.
Increase funding.Triggsaiditisessentialtoincreasingthenumberofpeoplewhoarescreened.“…Ourlimitationright
nowisfundingtobeabletogointocorrectionalfacilitiesortheschools,”hesaid.“That’swherethechlamydiais,in
youngpeople.Insomeways,toprovidefundingforthescreeningofyoungpeopleisimperativeforlegislators.That’s
keepingusfromaddressingtheepidemic.”
n
n
Dr. Bruce TriggMedical Director of the STD Program
Regions 1 and 3, New Mexico Department of Health
Advice from a Public Health OfficialImplementing Expedited Partner Therapy to Reduce Chlamydia Infection
Legislator Policy Brief Chlamydia Screening and Treatment 7
Key Facts and Terms
Health Impact of Chlamydia Infection
Chlamydiaisthemostfrequentlyreportedbacterialsexuallytransmitteddisease(STD)intheUnitedStates.Chlamydia
infectionoftenhasnosymptoms,soCDCrecommendsannualscreeningforchlamydiaforsexuallyactivewomen25
andyounger.Chlamydiainfectioniseasilydiagnosedbyalaboratorytestusingeitherurineoraspecimenobtained
duringaPaptestandiseasilytreatedwithasingledoseofantibiotics.Completetreatmentalsoincludescounseling
patientsonpreventingtransmissionandreinfection,encouragingpatientstoinformtheirpartnersandtestingfor
reoccurrenceoftheinfection.4
Expertsestimatethatthenearly1millioncasesofchlamydiareportedtoCDCin2005representonlyaboutone-third
theactualnumberofinfections.1Only25percentofwomenandabout50percentofmeninfectedwithchlamydia
experiencesymptomsofinfection,whichtypicallywouldbegenitaldischarge,burningordiscomfort.
Anestimated2.8millionnewcasesofchlamydiaoccureachyear,5atanestimatedcostof$598million.6Under-reporting
ofchlamydiaissignificantsincemanypeopleareunawareoftheirinfectionsanddonotseektesting.
Nearly40percentofuntreatedchlamydiacasesdevelopintomoreseriousinfection,resultinginadditionaltreatment
costsof$1,167perpatient.18Untreatedchlamydiacanleadtoirreversibledamagetowomen’sreproductiveorgans,
recurringinfection,pregnancycomplications,infertilityandchronicpain.
Health Disparities
Chlamydiainfectionsaremorecommonlyfoundamongyoungadults,urbanresidents,African-Americansandsocioeco-
nomicallydisadvantagedpopulations.3,8Culturalbarriersmustbeaddressedwheneducatingonchlamydiaprevention.
African-American,HispanicandAmericanIndianwomenallhavehigherratesofchlamydiathanwhitewomen.African-
AmericanwomenhavemorethanseventimesandAmericanIndianwomenhavenearlyfivetimesthechlamydiarate
ofwhitewomen.19
Keybarrierstochlamydiascreeningandtreatmentinminoritycommunitiesincludelackofaccesstocare,insurance
coverage,andfundsforpaymentforservicesandinadequateinformationandeducation.20
Sexual Partner Services
Topreventreinfectionbytheirsexualpartner(s),chlamydiapatientsareaskedtonotifytheirpartner(s)thattreatment
isnecessary,althoughthisapproachhasbeenonlymodestlysuccessful.11Anotheralternative,askingthepatientforthe
nameofhisorhersexpartnerforfollow-upbythestatehealthdepartment,alsoencountersdifficultiesduetostafftime
constraintsandthepatient’sdiscomfortinrevealinghisorherpartner’sname.
Expeditedpartnertherapy(EPT)allowshealthcareproviderstogivemedicationorprescriptionstothepatienttheyare
treatingtodelivertohisorhersexpartnertoreducereinfection.Inadditiontodispensingthemedication,providers
offercounselingandinstructiononproperuseofthemedicine,andrecommendthatpatientsencouragetheirpartner(s)
tobetestedforchlamydia.
n
n
n
n
n
n
n
n
n
8 Chlamydia Screening and Treatment Legislator Policy Brief
What Scientific Research Says
Chlamydia Screening Is a Proven But Underused Strategy
Identifyingandtreatingchlamydiaearlyisaneffectiveandcost-savingapproachbecauseitstopsthespreadofinfection
andreducesriskofseriouscomplications.9,10
Althoughannualchlamydiascreeningisrecommendedforallsexuallyactivewomenage25oryounger,lessthanhalf
ofyoungwomenreceivescreeningtests.In2005,sexuallyactivewomenwerescreenedattheserates:
Ages16–20yearsold:49percentwithMedicaid,and34percentwithcommercialinsurance;and
Ages21–25yearsold:52percentwithMedicaid,and35percentwithcommercialinsurance.21
Ongoingeducationandtrainingofhealthcareprovidersisneededtoimprovethechlamydiascreeningrates.
Behavior Change Is Crucial
Effectivechlamydiaprevention requireschanging thebehaviors thatplacepeopleat risk,andencouraging those
behaviorsthatreducerisk,suchaspracticingabstinence,usingcondoms,limitingthenumberofsexpartnersand
modifyingsexualbehaviors.22
Preventioneffortsdemandsustainedoutreachandeducation—bothofwhichhavebeenproventoreducetheriskof
individualsbecominginitiallyinfected,infectingothersorexperiencingmoreseveremedicalcomplications.23
Expedited Partner Therapy (EPT) Demonstrates Promise
EPTcanalleviatesomeofthehealthandfiscalburdensofchlamydiabyreachingmoreinfectedindividuals.CDC
sponsoredstudiesfoundthatEPTismedicallyeffective,cost-effectiveandcost-saving.11,24
EPT isnotwithoutbarriers to implementation.Healthcareprovidersareoftenhesitantornot legallypermitted to
dispensemedicationforanindividualtheyhavenotexamined,evaluatedandcounseled.Thepotentialrisksforthe
partner includeallergicreactions,medicationtakenimproperlyandundiagnosedSTDsorothermedicalconditions
thatmightcontradicttheuseofaspecificantibiotic.11,24
Astudyoflawsin50states,PuertoRicoandtheDistrictofColumbiasuggeststhatEPTisprohibitedin13states.In
theremainderofthestates,thepracticeisclearlypermittedorispotentiallyallowable,subjecttointerpretationor
clarificationofambiguitiesinstatelaw.25(Foranassessmentofeachstate’sstatus,see:http://www.cdc.gov/std/ept/le-
gal/default.htm)
n
n
®
®
n
n
n
n
n
n
Want to Know More?We’ll help you find experts to talk to about this topic
If you would like to explore this topic in greater depth, contact us at the Healthy States Initiative and we’ll help you connect with:
an expert on this issue from the CDC.
fellow state legislators who have worked on this issue.
other public health champions or officials who are respected authorities on this issue.
Send your inquiry to http://www.healthystates.csg.org/ (keyword: inquiry) or call the health policy group at (859) 244–8000 and let us help you find the advice and resources you need.
n
n
n
References
1CentersforDiseaseControlandPrevention(CDC).“SexuallyTransmittedSurveillance2005Supplement,ChlamydiaPrevalenceMonitoringProject.”Atlanta,GA:U.S.DepartmentofHealthandHumanServices.December2006.Accessedfromhttp://www.cdc.gov/std/Chlamydia2005/CTSurvSupp2005Short.pdfApril14,2007.2AlexanderLJ,CatesJR,HerndonN,etal.“SexuallyTransmittedDiseaseinAmerica:HowManyCasesandatWhatCost?”AmericanSocialHealthAs-sociation,ResearchTrianglePark,NC.December1998.3CaliforniaSTDInitiatives,ChlamydiaCoalition.“ChlamydiaFacts.”Accessedfromhttp://www.ucsf.edu/castd/std_statistics.html and http://www.ucsf.edu/castd/chlamydia_coalition.htmlSeptember7,2006.4CDC.“ChlamydiaFactSheet.”Atlanta,GA:U.S.DepartmentofHealthandHumanServices.Accessedfromhttp://www.cdc.gov/std/Chlamydia/STDFact-Chlamydia.htmSeptember7,2006.5WeinstockH,BermanS,CatesWJr.“SexuallyTransmittedDiseasesamongAmericanYouth:IncidenceandPrevalenceEstimates,2000.”Perspectives on Sexual and Reproductive Health2004:36(1):6–10.6Costestimateadaptedfrom:ChessonHW,BlandfordJM,GiftTL,TaoG,andIrwinKL.“TheEstimatedDirectMedicalCostofSexuallyTransmittedDiseasesamongAmericanYouth,2000.”Perspectives on Sexual and Reproductive Health2004,36(1):11–19andWeinstockH,BermanS,CatesWJr.“SexuallyTransmittedDiseasesamongAmericanYouth:IncidenceandPrevalenceEstimates,2000.”Perspectives on Sexual and Reproductive Health2004;36:6–10.7CDC.“NewDataShowHeavyImpactofChlamydiaonU.S.MenandWomen,ParticularlyYoungPeople.”July12,2005.Accessedfromhttp://www.cdc.gov/od/oc/media/pressrel/r050712.htmJune15,2007.8eMedicineHealth.“Chlamydia.”Accessedfromhttp://www.emedicinehealth.com/chlamydia/article_em.htmDecember13,2006.9MaciosekMV,CoffieldAB,EdwardsNM,etal.“PrioritiesamongEffectiveClinicalPreventiveServicesResultsofaSystematicReviewandAnalysis.”American Journal of Preventive Medicine2006:31(1):52–61,Accessedfromhttp://www.prevent.org/images/stories/clinicalprevention/article%201669p.pdfDecem-ber18,2006.10 Partnership for Prevention. “Priorities forAmerica’s Health: Capitalizing on Life-Saving, Cost-Effective Preventive Services, Public Policy Maker’sGuide.”Washington,DC:PartnershipforPrevention,2006.Accessedfromhttp://www.prevent.org/images/stories/clinicalprevention/policymakers%20guide.pdfSeptember7,2006.11CDC.“ExpeditedPartnerTherapy in theManagementofSexuallyTransmittedDiseases:ReviewandGuidance.”Atlanta,GA:U.S.DepartmentofHealthandHumanServices,2006.Accessedfromhttp://www.cdc.gov/std/treatment/EPTFinalReport2006.pdfSeptember7,2006.12ConnecticutHealthPolicyProject.“InformationforPolicymakers:ChlamydiaFocusGroupReport,March10,2001.”Accessedfromhttp://www.cthealth-policy.org/policy/chlamydia.htmSeptember7,2006.13PersonalcommunicationfromConnecticutSen.ToniN.Harp,Sept.8,2006.14CoalitionforChlamydiaControlinCalifornia.“ChallengesandOpportunities:ActionAgendaforChlamydiaPreventionandControlinCalifornia:AFiveYearPlan.”January1999.Accessedfromhttp://www.ucsf.edu/castd/CAR_full.htmlSeptember7,2006.15AmericanSocialHealthAssociation.“STDPreventionPartnershipPositionStatement:CriticalComponentsofSTDPreventionandControl.”Accessedfromhttp://www.ashastd.org/involve/involve_adv_critcom1.cfmJune13,2007.16SchillingerJ,KissingerP,BermanS,etal.“ARandomizedTrialofPatient-DeliveredTherapytoPreventRecurrentChlamydialInfectionamongAdoles-centandYoungWomen.”NationalSTDPreventionConference.Milwaukee,2000.17CommunicationfromGregBeets,PublicInformationCoordinator,HIV/STDComprehensiveServicesBranch,TexasDepartmentofStateHealthSer-vices,March8,2007.18ReinD,KasslerW,IrwinK,etal.“DirectMedicalCostofPelvicInflammatoryDiseaseanditsSequelae:Decreasing,butStillSubstantial.”Obstetrics and Gynecology2000;95(3):397–402.19CDC.“TrendsinReportableSexuallyTransmittedDiseasesintheUnitedStates,2005.”Accessedfromhttp://www.cdc.gov/std/stats/05pdf/trends-2005.pdf December13,2006.20McRaeD.“OvercomingtheEpidemic:RacialDisparitiesinHIVandSTDs.”Washington,DC:NationalBlackCaucusofStateLegislators.Accessedfromhttp://www.healthystates.csg.orgSeptember7,2006.21 National Committee for Quality Assurance. “The State of Health Care Quality: 2006.” Washington, DC. Accessed from http://web.ncqa.org/Default.aspx?tabid=447April14,2007.22CDC.“SexuallyTransmittedDiseasesTreatmentGuidelines,2006.”Morbidity and Mortality Weekly Report2006;55(No.RR-11)Availableat:http://www.cdc.gov/std/treatment/2006/rr5511.pdf.23CDC.“ProgramOperations.GuidelinesforSTDPrevention:CommunityandIndividualBehaviorChangeInterventions.”Atlanta,GA:U.S.Dept.ofHealthandHumanServices.Accessedfromhttp://www.cdc.gov/std/program/community.pdfSeptember7,2006.24KlausnerJD,ChawJK.“Patient-deliveredTreatmentforChlamydia:PuttingResearchintoPractice.”Sexually Transmitted Diseases2003;30(6):509–11.25CDC.“LegalStatusofExpeditedPartnerTherapy(EPT).”Accessedfromhttp://www.cdc.gov/std/ept/legal/default.htmJune13,2007.
10 Chlamydia Screening and Treatment Legislator Policy Brief

Resources
Centers for Disease Control and Prevention
Infertility and STDs http://www.cdc.gov/std/infertility/default.htm
Chlamydia Fact Sheethttp://www.cdc.gov/std/Chlamydia/STDFact-Chlamydia.htm
Legal Status of Expedited Partner Therapy (EPT)http://www.cdc.gov/std/ept/legal/default.htm
CDC National Prevention Information Networkhttp://www.cdcnpin.org
Other Sources
American Social Health Association: Chlamydial Infectionshttp://www.ashastd.org/learn/learn_chlamydia_facts.cfm
Action Agenda for Chlamydia Prevention and Control in California: A Five Year Planhttp://www.ucsf.edu/castd/CAR_full.html
Chlamydia facts from the California Chlamydia Coalition http://www.ucsf.edu/castd/chlamydia_coalition.html
National Coalition of STD Directors: State Program Siteshttp://www.ncsddc.org/programsites.htm
Connecticut Health Policy Project, Information for Policymakers on Chlamydia Focus Group http://www.cthealthpolicy.org/policy/chlamydia.htm
Council of State Governments’ Healthy States Web site http://www.healthystates.csg.org
CSG’s Tool Kit on HIV and STD Prevention http://www.healthystates.csg.org/Publications
Partnership for Prevention: Chlamydia Screeninghttp://www.prevent.org/content/view/69/96/http://www.prevent.org
Legislator Policy Brief Chlamydia Screening and Treatment 11
Preventing Diseases:Policies that work based on the research evidence
1) Promote healthy eating. Policiesthatgivekidshealthierfoodchoicesatschoolcanhelpcurbrisingratesofyouthobesity.EnsuringthateveryneighborhoodhasaccesstohealthyfoodswillimprovethenutritionofmanyAmericans.
2) Get people moving. Policiesthatencouragemorephysicalactivityamongkidsandadultshavebeenproventoreduceratesofobesityandtohelppreventotherchronicdiseases.
3) Discourage smoking. Policies that support comprehensive tobacco controlprograms—thosewhich combine school–based, community–basedandmediainterventions—areextremelyeffectiveatcurbingsmokingandreducingtheincidenceofcancerandheartdisease.
4) Encourage prevention coverage. Policiesthatencouragehealthinsurerstocoverthecostsofrecommendedpreventivescreenings,testsandvaccinationsareproventoincreasetheratesofpeopletakingpreventiveaction.
5) Promote health screenings. Policiesthatpromote—throughworksitewellnessprogramsandmediacampaigns—theimportanceofhealthscreen-ingsinprimarycaresettingsareproventohelpreduceratesofchronicdisease.
6) Protect kids’ smiles. Policiesthatpromotetheuseofdentalsealantsforkidsinschoolsandcommunitywaterfluoridationareproventodramaticallyreduceoraldiseases.
7) Require childhood immunizations. Requiringimmunizationsforschoolandchildcaresettingsreducesillnessandpreventsfurthertransmissionofthosediseasesamongchildren.Scientific,economicandsocialconcernsshouldbeaddressedwhenpoliciestomandateim-munizationsareconsidered.
8) Encourage immunizations for adults. Policiesthatsupportandencourageimmunizationsofadults,includingcollegestudentsandhealthcareworkers,re-duceillness,hospitalizationsanddeaths.
9) Make chlamydia screenings routine. Screeningandtreatingchlamydia,themostcommonsexuallytransmittedbacterialinfection,willhelpprotectsexu-allyactiveyoungwomenagainst infertilityandothercomplicationsofpelvic inflammatorydisease(PID)thatarecausedbychlamydia.
10) Promote routine HIV testing. MakingHIVtestingpartofroutinemedicalcareforthoseaged13to64canfosterearlierdetectionofHIVinfectionamongthequarterofamillionAmericanswhodonotknowtheyareinfected.
Learnmoreabouttheseandotherprovenpreventionstrategiesathttp://www.ahrq.gov/clinic/uspstfix.htm,http://www.thecommu-nityguide.org/policymakers.htmlandhttp://www.prevent.org/images/stories/health_policy.pdf.
12 Chlamydia Screening and Treatment Legislator Policy Brief

The Centers for Disease Control and Prevention (CDC) is part of the United States Department ofHealthandHumanServices,whichisthemainfederalagencyforprotectingthehealthandsafetyofallAmericans.Sinceitwasfoundedin1946tohelpcontrolmalaria,CDChasremainedattheforefrontofpublichealtheffortstopreventandcontrolinfectiousandchronicdiseases,injuries,workplacehazards,disabilitiesandenvironmentalhealththreats.
Helpingstategovernmentsenhancetheirownpublichealthefforts isakeypartofCDC’smission.Everyyear,CDCprovidesmillionsingrantstostateandlocalhealthdepartments.Somefundsareintheformofcategoricalgrantsdirectedatspecificstatutorily–determinedhealthconcernsoractivities.Otherfundsaredistributedasgeneralpurposeblockgrants,whichtheCDChasmoreflexibilityindecidinghowtodirectanddistribute.
TheCDCdoesnotregulatepublichealthinthestates.Rather,itprovidesstateswithscientificadviceinfieldsrangingfromdiseasepreventiontoemergencymanagement.Italsomonitorsstateandlocalhealthexperiencesinsolvingpublichealthproblems,studieswhatworks,providesscientificassistancewithinvestigationsandreportsthebestpracticesbacktopublicagenciesandhealthcarepractitioners.
Forstatelegislatorswhoareinterestedinimprovingtheirstate’spublichealth,theCDCoffersawealthofresources,including:
Recommendationsforprovenpreventionstrategies;
Examplesofeffectivestateprograms;
AccesstotoppublichealthexpertsattheCDC;
Meetingsspecificallyaimedatstatelegislativeaudiences;
Factsheetsonpoliciesthatpreventdiseases;and
State–specificstatisticsontheincidenceandcostsofdisease.
ThispublicationfromtheHealthyStatesInitiativeisalsoanexampleofCDC’seffortstohelpstates.TheHealthyStatesInitiativeisfundedbyacooperativeagreementwiththeCDC.
TheCDChasdevelopedpartnershipswithnumerouspublicandprivateentities—amongthemmedicalprofessionals,schools,nonprofitorganizations,businessgroupsandinternationalhealthorganizations—butitscooperativeworkwithstateandlocalhealthdepartmentsandthelegislativeandexecutivebranchesofstategovernmentremainscentraltoitsmission.
n
n
n
n
n
n
What the CD
C Does for States
The Council of State Governments' (CSG) Healthy States Initiativeisdesignedtohelpstateleadersmakeinformeddecisionsonpublichealthissues.Theenterprisebringstogetherstatelegislators,officialsfrom the Centers for Disease Control and Prevention, state healthdepartmentofficials,andpublichealthexpertstoshareinformation,analyzetrends,identifyinnovativeresponses,andprovideexpertad-viceonpublichealth issues.CSG'spartners in the initiativeare theNationalBlackCaucusofStateLegislatorsandtheNationalHispanicCaucusofStateLegislators.
Fundingfor thispublication isprovidedbytheU.S.DepartmentofHealthandHumanServices,CentersforDiseaseControlandPrevention,underCooperativeAgreementU38/CCU424348.PointsofviewinthisdocumentarethoseoftheauthoranddonotnecessarilyrepresenttheofficialpositionorpoliciesoftheU.S.government.
Published August 2007
Preventing HIV/AIDS & Sexually Transmitted Diseases Tool Kit:ßPolicy OverviewßPopulations At RiskßPrevention ProgramsßHow Legislators Can ActßTalking PointsßResourcesßHealthy States Initiative Fact Sheet
�
Sexuallytransmitteddiseases(STDs)refertothemorethan25infectiousorganismstransmit-tedprimarilythroughsexualactivity.Despitetheburdens,costs,complicationsandpreventablenatureofSTDs,theyremainasignificantpublichealthproblemthatislargelyunrecognizedbythepublic,policymakersandhealthcareprofessionalsintheUnitedStates.ManySTDsareeasilytreated,butifleftuntreatedtheycancauseharmful,oftenirreversibleandcostlyclinicalcomplicationssuchasinfertility,canceranddeath. TheCentersforDiseaseControlandPrevention(CDC)estimatesthateachyear40,000newHIVinfectionsarediagnosed,andhundredsofthousandsmorepeoplearediagnosedwithotherSTDs. If leftuntreated,HIV/AIDSandsyphiliscan lead todeath.Untreatedgonorrheaandchlamydiainwomencanleadtopelvicinflammatorydisease(PID),whichcanleadtoectopicpregnancy,chronicpelvicpainandinfertility. Thereareeconomicaswellashealthconsequences.Thefederalgovernmentbudgetedmorethan$21billioninHIV/AIDScareforfiscalyear2006.1CDCestimatestheannualdirectmedi-calcostsofallSTDs(includingHIV)are$13billion(2003dollars).2,3
What Are HIV/AIDS and STDs, Their Causes and Whom Do They Affect?
HIV/AIDS
HIV(humanimmunodeficiencyvirus)andAIDS(acquiredimmunodeficiencysyndrome)aretermsusedtodescribethevirusthatcausesinfection(HIV)andthesyndromeorsetofsymp-tomsthatcandevelopasaresultofinfection(AIDS). AIDSisthemostseveremanifestationofHIVinfection.CDChasdocumentedmanyoppor-tunisticinfectionsandcancersthatdetermineifanHIV-infectedpersonmeetsthedefinitionforadiagnosisofAIDS.Apatient’swhitebloodcellcount,whichsignalsthestrengthofaperson’simmunesystem,alsoisusedtodiagnoseAIDS. Since1996,theintroductionofpowerfulanti-retroviralmedicationshasdramaticallyslowedthe progress of HIV infection intoAIDS. Prior to 1996, 50 percent of those infected withHIVwereexpected todevelopAIDS.Arecentstudyofhighlyactiveanti-retroviral therapy(HAART)suggeststhatthesedrugsnowreducetheriskofdyingordevelopingAIDSby86percentcomparedtothosereceivingnotreatment.4
STDs
In addition toHIV, there aremore than25other infections transmittedprimarily throughsexualactivity.CDCestimatesthatthereare19millionnewinfectionseveryyearintheUnitedStates,almosthalfofthemamongyoungpeopleages15to24.Thethreemajornationallyre-portableSTDsarechlamydia,gonorrheaandsyphilis.ThesethreearebacterialSTDsthatcanbetreatedandcured. Chlamydiaandgonorrheausuallyhavefewornosymptomsand,ifleftuntreatedinwomen,canleadtopelvicinflammatorydisease(PID),whichcanleadtochronicpelvicpain,ectopicpregnancyandinfertility. Syphilisiseasilycuredinitsearlystages,butifleftuntreatedcanleadtoseriouslong-termcomplicationsincludingnerve,cardiovascularandorgandamageandevendeath.Congenital
Policy Overview:
Preventing HIV/AIDS & Sexually Transmitted Diseases
HIV/AIDS STD K
Preventing HIV/AIDS and STDs
�
syphilis(mother-to-childtransmission)cancausestillbirthordeathsoonafterbirthandphysicaldefor-mityandneurologicalcomplicationsinchildrenwhosurvive.Inaddition,infectionwithchlamydia,gonorrheaorsyphilisincreasestheriskofbecominginfectedwithHIVatleasttwo-tofivefold. Genitalhumanpapillomavirus(HPV)is themostcommonSTDintheUnitedStates;at least50percentofsexuallyactivepeoplewillhaveHPVsometimeintheirlives.ThereisnocureforgenitalHPV,butahealthyimmunesystemcanusuallyfightthevirusoffonitsown.TherearetreatmentsforthehealthproblemsthatgenitalHPVcancause,suchasgenitalwarts,cervicalcellchangesandcervi-calcancer. InJune2006,theFoodandDrugAdministrationlicensedthefirstHPVvaccine.ItprotectsagainstfourtypesofHPV,includingtwothatcausemostcervicalcancers(70percent)andtwothatcausemostgenitalwarts(90percent).AlsoinJune2006,theCDC’sAdvisoryCommitteeonImmunizationPrac-tices(ACIP)recommendedthevaccineberoutinelygiventogirls11–12yearsofage.Thevaccinealsoisrecommendedforwomen13to26yearsofagewhohavenotbeenvaccinatedandmaybeusedingirlsasyoungas9.Thevaccineisdeliveredthroughaseriesofthreeinjectionsoverasix-monthperiod.5
Causes
ThespreadofHIVandotherSTDsismostcommonlyattributedtounprotectedsexwithaninfectedpartner.However,HIValsocanbecontractedthroughriskybehaviorssuchassharingdrugneedlesorsyringes.OtherwaysHIVisspreadincludecontactwithinfectedblood(i.e.bloodtransfusions),andmother-to-childtransmissionduringpregnancy,birthorbreastfeeding.6
Who’s Affected
It is estimated that 1 millionAmericans today are infected with HIV, one-quarter of whom areunawareoftheirinfection.Thereare40,000newHIVcasesandmorethan45,000newAIDScasesreported in theUnitedStates annually,7with communities of color beingmost adversely affected.ForSTDs, includingHIV/AIDS,African-Americansare thehardesthitwithnewinfections.OthergroupsdisproportionatelyaffectedincludeHispanics,youngwomen,andmenwhohavesexwithmen(MSM). AccordingtodatareleasedbytheCDC,althoughtheestimatednumberofnewHIV/AIDScasesdecreasedintheAfrican-Americancommunitybetween2001and2004,African-Americansstillac-countedfor50percentofallnewcasesin2004.Duringthatsametimeperiod,thenumberofHIV/AIDScasesincreasedamongMSM,accountingfor47percentofallnewinfections.8Otherstartlingstatisticsinclude:
�
In2002,HIV/AIDSwasthethirdandfourthleadingcauseofdeathamongAfrican-Ameri-canmenandwomen(25–54years)respectively.ItwastheleadingcauseofdeathforAfri-can-Americanwomen25–34yearsoldduringthistime.9African-AmericanshavethehighestratesofHIV/AIDSinfectionsofallracialcategoriesintheUnitedStates.In2004,therewereanestimated97casesper100,000people.Thiscomparestojust11casesper100,000forwhites.10Attheendof2004,HispanicshadthesecondgreatestnumberofpeopleestimatedtobeinfectedwithHIV/AIDS,with39casesper100,000.11
Inrecentyears,datafromacrosstheUnitedStatessuggestthatanincreasingnumberofMSMareacquiringSTDs,andthatyoungpeopleareathigherriskforacquiringSTDsforacombina-tionofbehavioral,biologicalandculturalreasons.Thefollowingdatafrom2004underscorethesepoints:
In2004,youngAfrican-Americanfemalesaged15–24hadthehighest rates of chlamydia infections, followed byAmericanIndian/Alaska Native females aged 15–24 and Hispanic fe-malesaged15–24.Gonorrhearateswerehighestamongwomen15–24,followedbywomen20–24.Aswithchlamydia,ratesofreportedgon-orrhea were highest among African-American women aged15–19.CDC estimates that in 2004, MSM comprised 64 percent ofnewprimaryandsecondary(P&S)syphiliscases,upfromanestimated5percentin1999.12
Youngpeople (13 to24yearsold) are atparticularlyhigh riskofcontractingHIV.In2004,anestimated5,000youngpeoplere-ceivedanewdiagnosisofHIV/AIDS,representing13percentofthenewpositivediagnosesinthatyear.13 In2001,theCDCreportedthatAfrican-Americanyouthwerethelargestgroupofyoungpeo-pleaffectedbyHIV;accountingfor56percentofallHIVinfectionseverreportedamongtheyouthagegroup.Transmissioninthisagegroupisprimarilyduetoheterosexualcontact,whereyoungminor-itywomenareatanincreasedriskduetobiologicalvulnerability,lackofrecognitionofapartner’sriskfactorsandhavingsexwitholdermen.ForyoungMSM,risksareassociatedwiththosewhodonotdisclose theirsexualorientationand if infected,may transmitthevirustobothwomenandmen.14 The higher rate of STDs among adolescents reflects multiplebarrierstoqualitySTDpreventionservices,includinglackofin-suranceorabilitytopay, lackof transportation,discomfortwithfacilities and services designed for adults, and concerns aboutconfidentiality.15
The Costs of Infections PreventingandcontrollingthespreadofHIV/AIDSandSTDsisbothapublichealthandaneconomicconcern.ThelifetimedirectmedicalcostsofHIV/AIDSandSTDsareestimatedat$13billionannually.Thistotalcostdoesnotincludelostwagesandproductiv-ity,out-of-pocketexpensesorthecostsassociatedwithtransmissionofdiseasestoinfants.16 Federal and state governments are responsible for some of thecosts of treating poor and elderly HIV/AIDS patients, and theyalso must deal with the loss of income and productivity that canresultwhenHIV/AIDSpatientsareunabletocontinueworking.Tolower these costs, prevention is essential. However, themajorityoffederalfundinggoestotreatment.IntheFY2006federalbud-get,$21billionisallottedforHIV/AIDS.Ofthat,60percentisforcare—whichincludes$6.3billionforMedicaidand$3.2billionfor
n
n
n
n
n
n Reduce barriers to screening for HIV that
prevent people from getting tested, such as written consent requirements before test-ing and limitations on spousal/partner noti-fication.
Reduce barriers to STD prevention activi-ties and support basic STD prevention in high-risk populations.
Support HIV screening tests as part of rou-tine medical care through policy support or legislation.
Require insurance coverage for HIV and STD screening programs through Medic-aid and state employee health benefits and consider requiring private insurers to offer coverage.
Require changing to confidential name-based reporting of HIV cases if your state is not already doing so.
Support expedited partner therapy treat-ment for selected STDs through adjust-ments to practices, regulations or legislation, depending on the barriers in your state.
Support state education department tools for HIV/AIDS and STD prevention educa-tion through collaboration with school dis-tricts, parent organizations and community groups so youth are educated about pre-venting sexually transmitted diseases.
n
n
n
n
n
n
n
What State Legislators Can Do: Advancing Prevention Efforts Through Legislation and Regulation
�
Medicare.Just4percentisearmarkedforprevention,whichislessthantheamountdesignatedforresearch,globalAIDSprogramsandhousingassistance.17 Also,whilenewdrugshaveincreasedthelifespanofindividualswithAIDS,medicationsareexpensiveandmorepatientsareseekinghelptopayforthem.TheAIDSDrugAssistanceProgram(ADAP)providesfinancialhelpwithmedicationsforpeoplewhohavenoorlimitedprescriptiondrugcoverage.Themainsourceoffundingisthefederalgovernment,althoughstategovernmentsanddrugcompaniesalsoprovidemoney. Eachyear,ADAPprovideshelpto136,000people—orapproximately30percentofthetotalnumberofpeoplewithHIV/AIDSwhoarereceivingmedicalcare.Between1996and2004,thenumberofpeopleusingADAPincreasedby217percentinthe41statesreportingdatadur-ingthatperiod.Theamountofmoneyspentonmedicationsroseduringthesametime,increas-ing591percent.TheaveragecostperHIV/AIDSprescriptioninJune2004was$257.18
How Do States Monitor Infection Rates? CDC,throughtheNationalCenterforHIV/AIDS,STDandTBPrevention(NCHSTP)istheprimaryfederalagencythatprovidessupporttostatesforHIV/AIDSandSTDsurveillanceandpreventionprograms.CDC’sSTDsurveillanceconsistsofnationalnotifiablediseasereporting,sentinelsurveillance,specialsurveysandprevalencemonitoring:
Nationalnotifiablediseasereporting:Thissystemcollectscasereportsofchlamydia,gon-orrhea,syphilisandchancroidinfectionsreportedfromalljurisdictions.SentinelSurveillance:Sentinelsurveillancesystemscollectdatafromalimitednumberofparticipating facilities thatperformspecific,andsometimesnonroutine,STD testingamongaparticularpopulation.OnesuchsystemistheGonococcalIsolateSurveillanceProject(GISP),whichmonitorstheantimicrobialdrugresistanceofstrainsofgonorrhea.Specialsurveys:Specialsurveysusepopulation-basedsamplesandprovidetheonlymeansbywhichanaccuratenationalestimateofdiseaseprevalencecanbeobtained.TheNationalHealthandNutritionExaminationSurvey(NHANES)examinesabout5,000peopleeachyearfromacrossthecountrytofocusonavarietyofhealthandnutritionalmeasurementstomeetemergingneeds.Prevalencemonitoring:Prevalencemonitoringprovidesdataonprevalencetrendsindis-easeamongdefinedpopulationsovertime.Prevalencemonitoringfocusesonpopulations,suchasMSMoradolescents,or takesplace inparticular settings, suchas correctionalfacilitiesandfamilyplanningclinicsSTDSurveillanceNetwork:ThisisanetworkoflocalenhancedSTDsurveillancesystemstoimprovethecapacityofnational,stateandlocalSTDprogramstodetect,monitorandrespondtotrends.
ThesesurveillancesystemsarecriticalforunderstandinganddescribingtheburdenofSTDson thehealthofAmericans,particularlyyoungAmericans; formonitoringnationaldiseasetrendsandhealthdisparities;andforevaluatingtheimpactofimportantnationalprograms,such as the Infertility Prevention Program and the Syphilis Elimination Effort. The dataare alsoused tohelp target resources for specificpopulations andhealth jurisdictions andfor specificdiseasecontrol activities, suchaspartnernotificationand screening. NationalrecommendationsforthetreatmentofgonorrheacontinuetorelyoninformationfromGISP,andsurveillancedatahavetriggeredCDCinvestigations,oftenresultinginincreasedtargetedpublichealtheffortsinlocalareas. CDCusesothersurveillancesystemstomonitorbehaviorsrelatedtoHIV/AIDStransmis-sionandservicesprovidedtoHIV-infectedpatients.Thosesystemsinclude:
MorbidityMonitoringProject(MMP):Thisisanewsurveillancesystemdesignedtocol-lectinformationfromHIV/AIDSpatientswhoreceivedcarefromrandomlyselectedHIVcareproviders.MMPcollectsinformationaboutaccesstoanduseofHIVcare,treatment,preventionservicesandprevalenceofbehaviorsthatcanresultinHIVtransmissionandaffectdiseaseoutcomes(likeadherencetotherapy).NationalHIVBehavioralSurveillanceSystem(NHBS):SurveysareconductedincitieswithhighlevelsofHIV/AIDSamonghigh-riskpopulations(suchasinjectiondrugusers)todeterminetheirriskbehavior,testingbehavioranduseofpreventionservices.
CDCalsocontinuestoadaptsurveillancesystemstomatchchangesintheepidemics.Inthe
n
n
n
n
n
n
n
�
earlyyearsoftheHIV/AIDSepidemicinthe1980s,theCDCrequestedstatesandlocalhealthdepartmentstoreportAIDScasestotheCDC.19Since1996,duetotheincreasedlifespanofthoseinfectedwithHIV,reportingAIDScasesprovedtobeinsufficienttotrackthescopeoftheepidemic. InJuly2005,CDCformallyrecommendedthatallstatesandterritoriesadoptaconfidentialname-basedsurveillancesystemtoreportHIVinfections.Name-basedHIVreportingprovidesamoreaccurateandreliablereportingoftheepidemic.AsofJune2006,44statesandtheU.S.territorieswereusingconfidentialname-basedreportingofHIVinfection.Theremainingstatehealthdepartmentsuseotherreportingmethods.20,21 The2000RyanWhiteComprehensiveAIDSResourcesEmergencyAct (RWCA)—whichhelpsmeetthecareneedsofthoselivingwithHIV/AIDS—requiresthatfundingbedeterminedbythenumberofHIVcases(notAIDScases)reportedtotheCDCbynolaterthan2007.22CDConlyacceptsname-basedHIVreporting.Thus,statesstandtolosefundingunderRWCAiftheyhavenotadoptedaname-basedHIVsurveillancesystem.
What Are the Federal and State Prevention Programs for HIV/AIDS and STDs?
Federal Programs
ThefederalgovernmentplaysakeyroleinthepreventionandtreatmentofHIV/AIDSandSTDs. Federal health agencies recommend policies, set screening and treatment guidelinesbasedonscientificevidence,providefundsforresearch,financehealthservicesandprovidetechnicalassistance.TheU.S.DepartmentofHealthandHumanServices(DHHS)hastheleadroleinpublichealthprogramstoaddressHIV/AIDSandSTDs,includingresearchonpreven-tionandtreatmentofHIVandfinancingtreatmentservices. ForHIV/AIDS,thevastmajorityofmoneyisspentonmedicaltreatment,whichcomesmain-lyfromtheHealthResourcesandServicesAdministrationthroughtheRWCA.Since1990,theRWCAhasprovidedfortheneedsofindividualsandfamilieslivingwithHIVorAIDS,anddirectedfederalfundingtoareasdisproportionatelyaffectedbytheepidemic.23Itsmainfocusistoprovideprimarycare,treatmentandsupportservices. TheCentersforMedicareandMedicaidServices(CMS)alsospendsasignificantamountofmoneyonHIV/AIDScare.MedicaidisthelargestsourceoffederalfundingforHIV/AIDStreatmentinthecountry.CMSestimatesthatinFY2005,Medicaidspent$5.7billiononHIV/AIDStreatment.ForFY2006,thatnumberisexpectedtoincreaseto$6.3billion.24 CDC, through the National Center for HIV/AIDS, STD andTB Prevention, provides themajorityoffundingtostatesforHIV/AIDSandSTDpreventionandsurveillance-morethan$600millioninFY2005. CDCprovidesfundingandtechnicalassistanceto65stateandlocalhealthdepartmentstoconductHIV/AIDScasesurveillancetotracktheepidemicandidentifythosegroupsmostatriskofcontractingthevirusandtodevelopprogramsandinterventionstocontrolthespreadofthedisease.Fundingalsoisprovidedtocommunity-andfaith-basedorganizations,whichtailorprevention,counselingandtestingprogramstomatchlocalneeds. CDCalsohasanactive role inSTDpreventionefforts. Itprovides leadership throughre-search,surveillance,policydevelopmentandfinancialandpersonnelassistancetostates,ter-ritoriesandlocalhealthdepartments.TwomajorSTDprogramareasarepreventinginfertilityinwomenandeliminatingsyphilis. TheInfertilityPreventionProgram—whichfundschlamydiascreeningandtreatmentservic-esforlow-income,sexuallyactivewomenattendingfamilyplanning,STDandotherwomen’shealthcareclinics—hasproventhatroutinescreeningofwomencanreducetheprevalenceofchlamydiaandPID. TheNationalPlantoEliminateSyphilis,launchedin1999andupdatedin2006,improvesac-cesstohigh-quality,community-basedpreventiveandcareservices;provideseducationaboutthepreventionofsyphilisandotherSTDstoaffectedcommunities;andstrengthensoutbreakresponseandpreparedness. STDsurveillanceandpreventionare twoof thewaysstatehealthdepartmentsfulfill theirresponsibilitiesofpreventingdiseaseandinjury,promotinghealthybehaviorsandensuringac-cesstohealthcareservices.State-by-stateprofilesofHIVandSTDpreventionactivitiescanbeaccessedat:www.cdc.gov/nchstp/od/stateprofiles/usmap.htm.
�
State Programs
Statehealthdepartmentsalsoreceivefundingthroughstatebudgets,userfeesandfines,andspecialfundssuchastobaccosettlementfunding.Eachstatereceivessomefundingfromavarietyofgrantsandorganizations,thoughthisalsovariesfromstatetostateandyeartoyear. Preventionprogramscreatedbystatesvarybasedontheirlocalpolitical,socialanddemographiccontext;howevertheyshouldbebasedonsoundscientificprinciples.SpecificrecommendationsforstateHIV/AIDSprogramsinclude:
HIVpreventionprogramsmustbescience-basedandusemessages,techniquesandinterventionsthathavebeenscientificallydemonstratedtoeffectivelyreduceHIVtransmission.Fundingmustbeflexibleandsufficienttoallowcreative,uniqueandinnovativeHIVpreventionprograms,usingavarietyofmethodstoreachhigh-riskgroups.Preventionprogramsshouldbeculturallycompetentandaddresstheuniqueneedsofthetargetedpopulation.PartnercounselingandreferralservicestopreventfurtherinfectionshouldbeanintegralpartofcomprehensiveHIVpreventionprograms.25
What Can State Legislators Do to Promote HIV/AIDS and STD Prevention Efforts? Statelegislatorsacrossthecountryhavebeenintroducing,debatingandpassinglegislationaimedatpreventingHIV/AIDSandSTDs.ManystateshaverecentlypassedlegislationestablishingHPVandcervicalcancertaskforces.ManyareconsideringrequiringMedicaidandstateemployeehealthben-efitcoverageforHIV/AIDSandSTDscreenings.Somearetargetingeffortsatparticularpopulationstoeliminatehealthdisparities. Individualstatelegislatorslookingforwaystofurtheradvancepreventioneffortsintheirownstatescanchoosefromanumberofroles—fromsupportinglegislativeandregulatorychangestoservingasacommunityleaderontheissue.Onthelegislativeandregulatoryfront,forexample,statelawmak-erscanadvancepreventioneffortsbyreviewingstatelawsandregulationsforbarriersthatpreventpeoplefromgettingtestedforHIV.LegislationalsocanaddressexpandingMedicaid,privateandstateemployeehealthbenefitcoveragetoincludechlamydiascreeningandHIVscreeningorsupportcon-fidentialname-basedreportingofHIVtoensuretheaccuratetrackingofHIV-infectedpopulations. Inadditiontolegislativeandregulatoryefforts,statelegislatorscanplayacommunityleadershiprole inkeepingHIV/AIDSandSTDpreventionat the forefrontofpublicawareness.State legisla-torscancallforcommitteehearingsonpreventioneffortsandholdtownhallmeetings.ByspeakingpubliclyabouttheimportanceofHIV/AIDSandSTDprevention,theycanhelpadvanceawarenessofandsupportforpreventionefforts.Lawmakersmayalsoprovideleadershiptohelpneighborhoodsandcommunitiesmobilizeresourcesinacoalitiontosupportlocalpreventionefforts.
n
n
n
n
�
Endnotes 1 KaiserFamilyFoundation. “ThePresident’sFY2006BudgetProposal:OverviewandBriefingcharts.” Accessed from www.kff.org/uninsured/upload/The-President-s-FY-2006-Budget-Proposal-Overview-and-Briefing-Charts.pdfApril11,2006.2Chesson,HarrellW.;Blandford,JohnM.;Gift,ThomasL.;Tao,Guoyu;andIrwin,KathleenL.“TheEstimatedDirectMedicalCostsofSexuallyTransmittedDiseasesAmongAmericanYouth,2000.”Perspectives on Sexual and Reproductive Health,2004,36(1)11–19.3 Weinstock,H.;Berman,S.;CatesJr.,W.“SexuallytransmitteddiseasesamongAmericanyouth:incidenceandprevalenceestimates,2000.”Perspectives on Sexual and Reproductive Health,2004,36:6–10.4 Smith,Michael. “HAARTCutsRiskofHIVProgression toAIDSorDeathby86%.”Medpage Today,July28,2005.Accessedfromwww.medpagetoday.com/InfectiousDisease/HIVAIDS/tb1/1448 April11,2006.5CentersforDiseaseControlandPrevention.“HPVVaccineQuestionsandAnswers.”Accessedfromwww. cdc.gov/std/hpv/STDFact-HPV-vaccine.htm#vaccineJune5,20066NationalInstituteofAllergyandInfectionsDisease,NationalInstitutesofHealth.“HIVInfectionandAIDS:AnOverview.”Accessedfromwww.niaid.nih.gov/factsheets/hivinf.htmApril11,2006.7 Centers forDiseaseControl andPrevention.HIV/AIDSSurveillanceReport, 2004.Vol.16.At-lanta:U.S.DepartmentofHealthandHumanServices,CentersforDiseaseControlandPrevention;2005:[6].Alsoavailableat:www.cdc.gov/hiv/stats/hasrlink.htm.8CentersforDiseaseControlandPrevention.“HIV/AIDSamongAfricanAmericans.”Accessedfromwww.cdc.gov/hiv/topics/aa/resources/factsheets/pdf/aa.pdfFebruary7,2006.9Ibid.10 CentersforDiseaseControlandPrevention.HIV/AIDSSurveillanceReport,2004.Vol.16.At-lanta:U.S.DepartmentofHealthandHumanServices,CentersforDiseaseControlandPrevention;2005:[6].Alsoavailableat:www.cdc.gov/hiv/stats/hasrlink.htm.11Ibid.12CentersforDiseaseControlandPrevention.SexuallyTransmittedDiseaseSurveillance,2004.At-lanta,GA:U.S.DepartmentofHealthandHumanServices,September2005.Alsoavailableat:www.cdc.gov/std/stats/13 CentersforDiseaseControlandPrevention.HIV/AIDSSurveillanceReport,2004.Vol.16.At-lanta:U.S.DepartmentofHealthandHumanServices,CentersforDiseaseControlandPrevention;2005:[6].Alsoavailableat:www.cdc.gov/hiv/stats/hasrlink.htm.14DivisionofHIV/AIDSPrevention,TheCentersforDiseaseControlandPrevention.“HIV/AIDSAmongYouth.Accessedfromwww.cdc.gov/hiv/pubs/facts/youth.htmFebruary7,2006.15CentersforDiseaseControlandPrevention.SexuallyTransmittedDiseaseSurveillance,2004.At-lanta,GA:U.S.DepartmentofHealthandHumanServices,September2005.Alsoavailableat:www.cdc.gov/std/stats/16KaiserFamilyFoundation,“SexuallyTransmittedDiseasesinAmerica:HowManyCasesandatWhatCost?”Accessedfromwww.kff.org/womenshealth/1445-std_rep3.cfmFebruary7,2006.17 KaiserFamilyFoundation. “ThePresident’sFY2006BudgetProposal:OverviewandBriefingCharts.” Accessed from www.kff.org/uninsured/upload/The-President-s-FY-2006-Budget-Proposal-Overview-and-Briefing-Charts.pdfApril11,2006.18 KaiserFamilyFoundation.“NationalADAPMonitoringProjectannualreport,April2005.”Ac-cessedfromwww.kff.org/hivaids/7288.cfmApril11,2006.19LouChibarroJr.,Lou.“HIVNamesReportingGaininginPopularity.”Washington Blade(Decem-ber 2, 2005).Accessed from www.washingtonblade.com/print.cfm?content_id=7063 December 27,2005.20CentersforDiseaseControlandPreventionHIV/STD/TBPreventionNewsUpdate.“AIDS:NotAnonymous?”Accessedfromwww.cdcnpin.org/scripts/locates/LocateNews.aspJanuary5,2006.21TheKaiserFamilyFoundation.“HIVName/Code-BasedReportingPolicies,2005.”Accessedfromwww.statehealthfacts.kff.org/cgi-bin/healthfacts.cgi?action=compare&category=HIV%2fAIDS&subcategory=HIV+Testing&topic=Name%2fCode%2dBased+ReportingFebruary1,2006.22NationalAllianceofStateandTerritorialHealthDirectors,“CAREActReauthorizationWatch,”September 6, 2005. Accessed from www.nastad.org/documents/public/reauth_watch/Volume3ver-sion2.docDecember27,2005.
�
23U.S.DepartmentofHealthandHumanServices,HealthResourcesandServicesAdministration.“RyanWhiteCAREAct:PurposeoftheCAREAct.”Accessedfromhttp://hab.hrsa.gov/history.htm February7,2006.24TheKaiserFamilyFoundation,“FederalFundingforHIV/AIDS:TheFY2005BudgetRequest.”Accessed from www.kff.org/hivaids/upload/Federal-Funding-for-HIV-AIDS-The-FY-2005-Budget-Request.pdfDecember15,2005.25AssociationofStateandTerritorialHealthOfficials,“HIV/AIDSPolicyoftheAssociationofStateandTerritorialHealthOfficials.”Accessedfromwww.astho.org/policy_statements/HIVAIDS%20Policy.pdfJanuary26,2006.
�
HIV/AIDSandsexuallytransmitteddiseases(STDs)continuetoposeamajorproblemintheUnitedStates.Morethan20yearsafterthefirstdiagnosedcaseofAIDS,theCentersforDiseaseControlandPrevention(CDC)estimatesthat40,000peopleareinfectedwithHIVev-eryyear,andhundredsofthousandsmorearediagnosedwithanSTD.Withtoday’spreventioneffortsandtreatmentoptions,manyoftheseinfectionscanbeaverted. Inthissection,youwillfindthebasicsaboutHIV/AIDSandthemostcommonSTDs,thepopulationsmostaffected,theimpactofthesediseasesonminoritycommunitiesandthecostsoftheseinfections.
What is HIV/AIDS? HIV(humanimmunodeficiencyvirus)isthevirusthatcausesAIDS(acquiredimmunode-ficiency syndrome). HIV is commonly spread by sexual contact or by sharing needles andsyringes,primarilyfordruginjection,withsomeonewhoisinfected.HIVislesscommonlytransmittedthroughtransfusionsofinfectedbloodorbloodclottingfactors.Also,babiesborntoHIV-infectedwomencanbecomeinfectedbeforeorduringbirth,orthroughbreast-feedingfollowingbirth.1
AIDSstandsforAcquiredImmunodeficiencySyndrome.Acquiredmeansthatthediseaseisnothereditary,butdevelopsafterbirthfromcontactwithadisease-causingagent,inthiscase,HIV.Immunodeficiencymeansthatthediseaseischaracterizedbyaweakeningoftheimmunesystem,andsyndromereferstoagroupofsymptomsthatcollectivelyindicateorcharacterizeadisease. InthecaseofAIDS,thiscanincludethedevelopmentofcertaininfectionsandcancers,aswellasadecreaseinthenumberofdisease-fightingcellsinaperson’simmunesystem.CDClistsnumerousopportunisticinfectionsandcancersthatcanhelpdetermineifanHIV-infectedpersonhasAIDS.ThoselivingwithAIDSoftenhaveinfectionsofthelungs,brain,eyesandotherorgans,andfrequentlysufferdebilitatingweightloss,diarrheaandatypeofcancercalledKaposi’ssarcoma.2
What are STDs? Inaddition toHIV, therearemore than25other infections transmittedprimarily throughsexualactivity.CDCestimatesthatthereare19millionnewinfectionseveryyearintheUnitedStates,almosthalfofthemamongyoungpeopleages15to24.Thethreemajornationallyre-portableSTDsarechlamydia,gonorrheaandsyphilis. Chlamydia is causedbybacteriaandcandamageawoman’s reproductiveorgans. Ithasbeen called a “silent” disease, because about three-quarters of infected women and half ofinfectedmenhavenosymptoms.Althoughanysexuallyactivewomanisatriskofcontractingchlamydia,teenagegirlsandyoungwomenareparticularlysusceptiblebecausethecervixhasnotfullymatured.3 If leftuntreated, the infectioncanspreadintotheuterusorfallopiantubesandcausepel-vicinflammatorydisease(PID).Thedamagecanleadtochronicpelvicpain,infertilityandapotentiallyfatalectopicpregnancy.Inpregnantwomen,thereissomeevidencethatuntreatedinfectionscanleadtoprematuredelivery.WomeninfectedwithchlamydiaarealsouptofivetimesmorelikelytobecomeinfectedwithHIVifexposed.4
Populations at Risk
Preventing HIV/AIDS & Sexually Transmitted Diseases
HIV/AIDS STD K
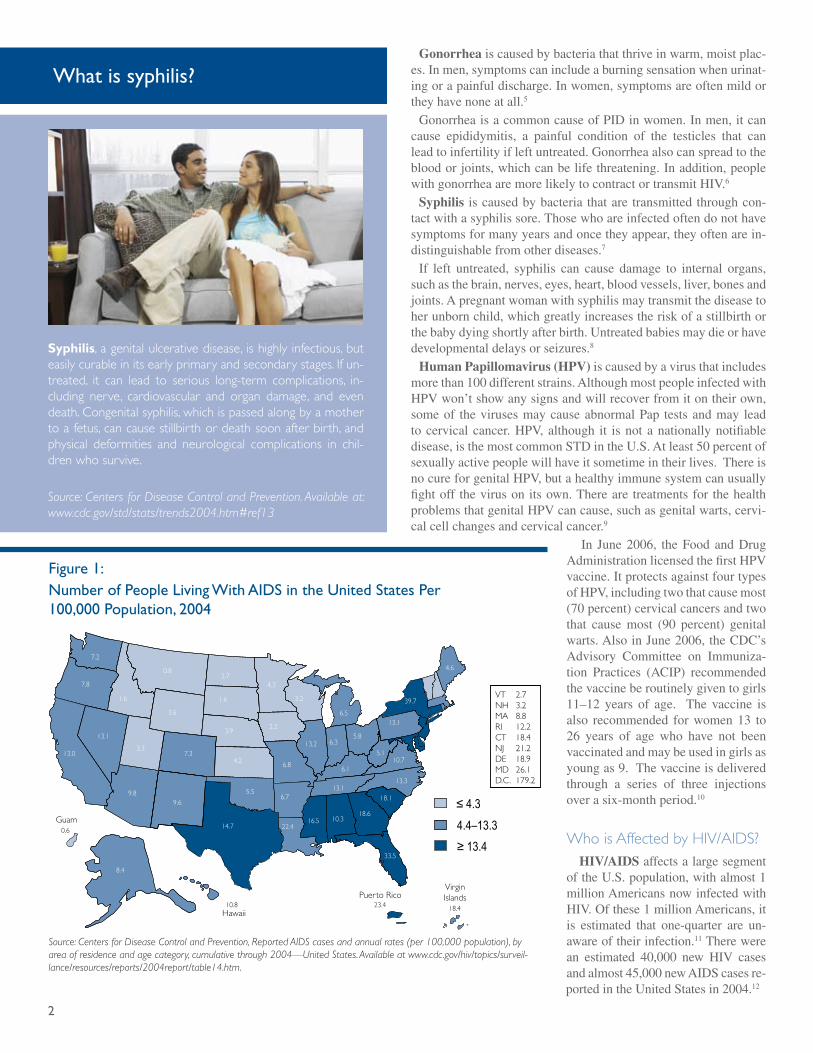
�
Gonorrheaiscausedbybacteriathatthriveinwarm,moistplac-es.Inmen,symptomscanincludeaburningsensationwhenurinat-ingorapainfuldischarge.Inwomen,symptomsareoftenmildortheyhavenoneatall.5 GonorrheaisacommoncauseofPIDinwomen.Inmen,itcancause epididymitis, a painful condition of the testicles that canleadtoinfertilityifleftuntreated.Gonorrheaalsocanspreadtothebloodorjoints,whichcanbelifethreatening.Inaddition,peoplewithgonorrheaaremorelikelytocontractortransmitHIV.6 Syphilis iscausedbybacteriathataretransmittedthroughcon-tactwithasyphilissore.Thosewhoareinfectedoftendonothavesymptomsformanyyearsandoncetheyappear,theyoftenarein-distinguishablefromotherdiseases.7 If left untreated, syphilis can cause damage to internal organs,suchasthebrain,nerves,eyes,heart,bloodvessels,liver,bonesandjoints.Apregnantwomanwithsyphilismaytransmitthediseasetoherunbornchild,whichgreatlyincreasestheriskofastillbirthorthebabydyingshortlyafterbirth.Untreatedbabiesmaydieorhavedevelopmentaldelaysorseizures.8 Human Papillomavirus (HPV)iscausedbyavirusthatincludesmorethan100differentstrains.AlthoughmostpeopleinfectedwithHPVwon’tshowanysignsandwillrecoverfromitontheirown,someof thevirusesmaycauseabnormalPap testsandmay leadtocervicalcancer.HPV,although it isnotanationallynotifiabledisease,isthemostcommonSTDintheU.S.Atleast50percentofsexuallyactivepeoplewillhaveitsometimeintheirlives.ThereisnocureforgenitalHPV,butahealthyimmunesystemcanusuallyfightoff thevirusonitsown.Therearetreatmentsfor thehealthproblemsthatgenitalHPVcancause,suchasgenitalwarts,cervi-calcellchangesandcervicalcancer.9
In June2006, theFoodandDrugAdministrationlicensedthefirstHPVvaccine.ItprotectsagainstfourtypesofHPV,includingtwothatcausemost(70percent)cervicalcancersandtwothat cause most (90 percent) genitalwarts.AlsoinJune2006,theCDC’sAdvisory Committee on Immuniza-tion Practices (ACIP) recommendedthevaccineberoutinelygiventogirls11–12 years of age. The vaccine isalso recommended forwomen13 to26 years of age who have not beenvaccinatedandmaybeusedingirlsasyoungas9.Thevaccineisdeliveredthrough a series of three injectionsoverasix-monthperiod.10
Who is Affected by HIV/AIDS? HIV/AIDSaffectsalargesegmentoftheU.S.population,withalmost1millionAmericansnowinfectedwithHIV.Ofthese1millionAmericans,itis estimated that one-quarter are un-awareoftheirinfection.11Therewerean estimated 40,000 new HIV casesandalmost45,000newAIDScasesre-portedintheUnitedStatesin2004.12
Figure �: Number of People Living With AIDS in the United States Per �00,000 Population, �004
≤ 4.3
4.4–13.3
≥ 13.4
7.2
13.1
13.0
7.8
1.6
0.8
3.6
3.3
9.8
8.4
9.6
7.3
3.9
1.6
2.74.3
2.2
6.8
6.7
22.416.5 10.3
18.6
33.5
18.113.1
6.1
13.2 6.35.8
6.5
3.2
13.1
39.7
4.6
5.110.7
13.3
4.2
5.5
14.7
10.8 23.4
0.6
18.4
VT 2.7NH 3.2MA 8.8RI 12.2CT 18.4NJ 21.2DE 18.9MD 26.1D.C. 179.2
Guam
Hawaii
Virgin IslandsPuerto Rico
Source: Centers for Disease Control and Prevention, Reported AIDS cases and annual rates (per 100,000 population), by area of residence and age category, cumulative through 2004—United States. Available at www.cdc.gov/hiv/topics/surveil-lance/resources/reports/2004report/table14.htm.
Syphilis, a genital ulcerative disease, is highly infectious, but easily curable in its early primary and secondary stages. If un-treated, it can lead to serious long-term complications, in-cluding nerve, cardiovascular and organ damage, and even death. Congenital syphilis, which is passed along by a mother to a fetus, can cause stillbirth or death soon after birth, and physical deformities and neurological complications in chil-dren who survive.
Source: Centers for Disease Control and Prevention. Available at: www.cdc.gov/std/stats/trends2004.htm#ref13
What is syphilis?
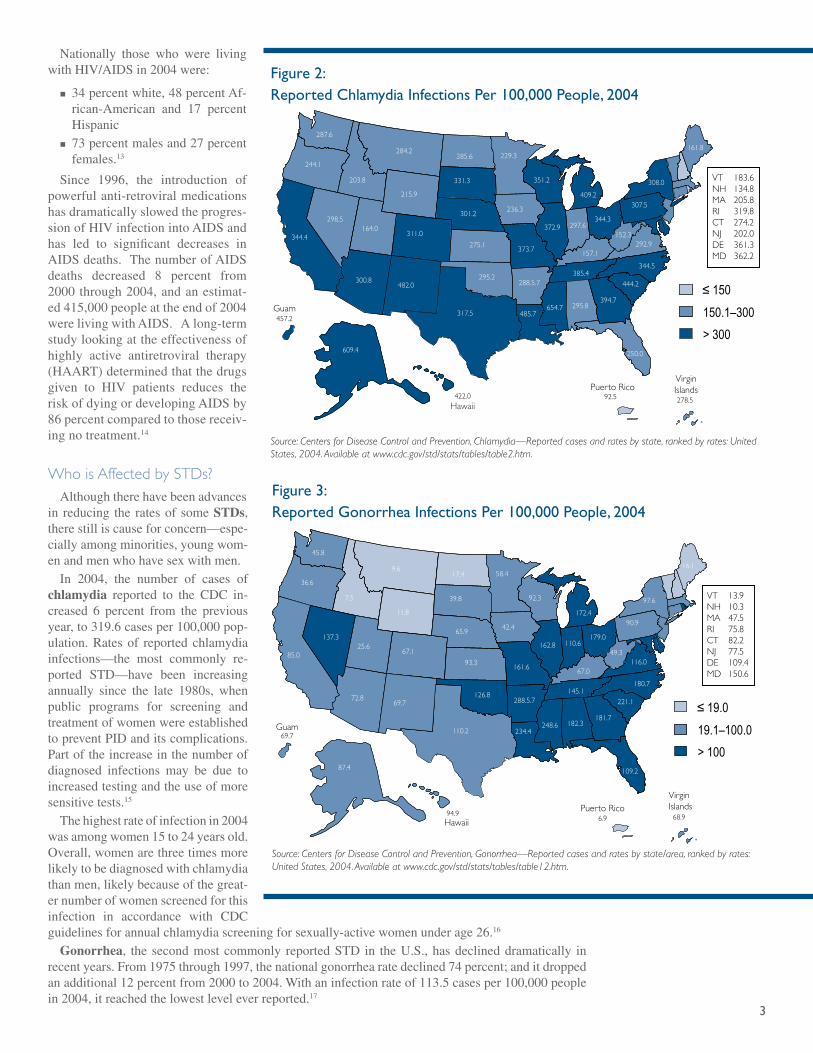
�
Nationally those who were livingwithHIV/AIDSin2004were:
34percentwhite,48percentAf-rican-American and 17 percentHispanic73percentmalesand27percentfemales.13
Since 1996, the introduction ofpowerfulanti-retroviralmedicationshasdramaticallyslowedtheprogres-sionofHIVinfectionintoAIDSandhas led to significant decreases inAIDSdeaths.ThenumberofAIDSdeaths decreased 8 percent from2000through2004,andanestimat-ed415,000peopleattheendof2004werelivingwithAIDS.Along-termstudylookingattheeffectivenessofhighly active antiretroviral therapy(HAART)determinedthatthedrugsgiven to HIV patients reduces theriskofdyingordevelopingAIDSby86percentcomparedtothosereceiv-ingnotreatment.14
Who is Affected by STDs? Althoughtherehavebeenadvancesin reducing the ratesof someSTDs,therestilliscauseforconcern—espe-ciallyamongminorities,youngwom-enandmenwhohavesexwithmen. In 2004, the number of cases ofchlamydia reported to the CDC in-creased 6 percent from the previousyear,to319.6casesper100,000pop-ulation.Ratesof reportedchlamydiainfections—the most commonly re-ported STD—have been increasingannually since the late 1980s, whenpublic programs for screening andtreatmentofwomenwereestablishedtopreventPIDanditscomplications.Partoftheincreaseinthenumberofdiagnosed infections may be due toincreasedtestingandtheuseofmoresensitivetests.15 Thehighestrateofinfectionin2004wasamongwomen15to24yearsold.Overall,womenarethreetimesmorelikelytobediagnosedwithchlamydiathanmen,likelybecauseofthegreat-ernumberofwomenscreenedforthisinfection in accordance with CDCguidelinesforannualchlamydiascreeningforsexually-activewomenunderage26.16 Gonorrhea, thesecondmostcommonly reportedSTD in theU.S.,hasdeclineddramatically inrecentyears.From1975through1997,thenationalgonorrhearatedeclined74percent;anditdroppedanadditional12percentfrom2000to2004.Withaninfectionrateof113.5casesper100,000peoplein2004,itreachedthelowestleveleverreported.17
n
n
Figure �: Reported Chlamydia Infections Per �00,000 People, �004
≤ 150
150.1–300
> 300
287.6
298.5
344.4
244.1
203.8
284.2
215.9
164.0
300.8
609.4
422.0
482.0
311.0
301.2
331.3
285.6 229.3
236.3
373.7
288.5.7
485.7654.7 295.8
394.7
250.0
444.2385.4
157.1
372.9 297.6344.3
409.2
351.2
307.5
308.0
161.8
152.3292.9
344.5
275.1
295.2
317.5457.2
92.5 278.5
VT 183.6NH 134.8MA 205.8RI 319.8CT 274.2NJ 202.0DE 361.3MD 362.2
Guam
Hawaii
Virgin IslandsPuerto Rico
Source: Centers for Disease Control and Prevention, Chlamydia—Reported cases and rates by state, ranked by rates: United States, 2004. Available at www.cdc.gov/std/stats/tables/table2.htm.
Figure �: Reported Gonorrhea Infections Per �00,000 People, �004
≤ 19.0
19.1–100.0
> 100
45.8
137.3
85.0
36.6
7.5
9.6
11.8
25.6
72.8
87.4
94.9
69.7
69.7
67.1
65.9
39.8
17.4 58.4
42.4
161.6
288.5.7
234.4248.6 182.3
181.7
68.96.9
109.2
221.1145.1
67.0
162.8 110.6179.0
172.4
92.3
90.9
97.6
16.1
49.3116.0
180.7
93.3
126.8
110.2
VT 13.9NH 10.3MA 47.5RI 75.8CT 82.2NJ 77.5DE 109.4MD 150.6
Guam
Hawaii
Virgin IslandsPuerto Rico
Source: Centers for Disease Control and Prevention, Gonorrhea—Reported cases and rates by state/area, ranked by rates: United States, 2004. Available at www.cdc.gov/std/stats/tables/table12.htm.
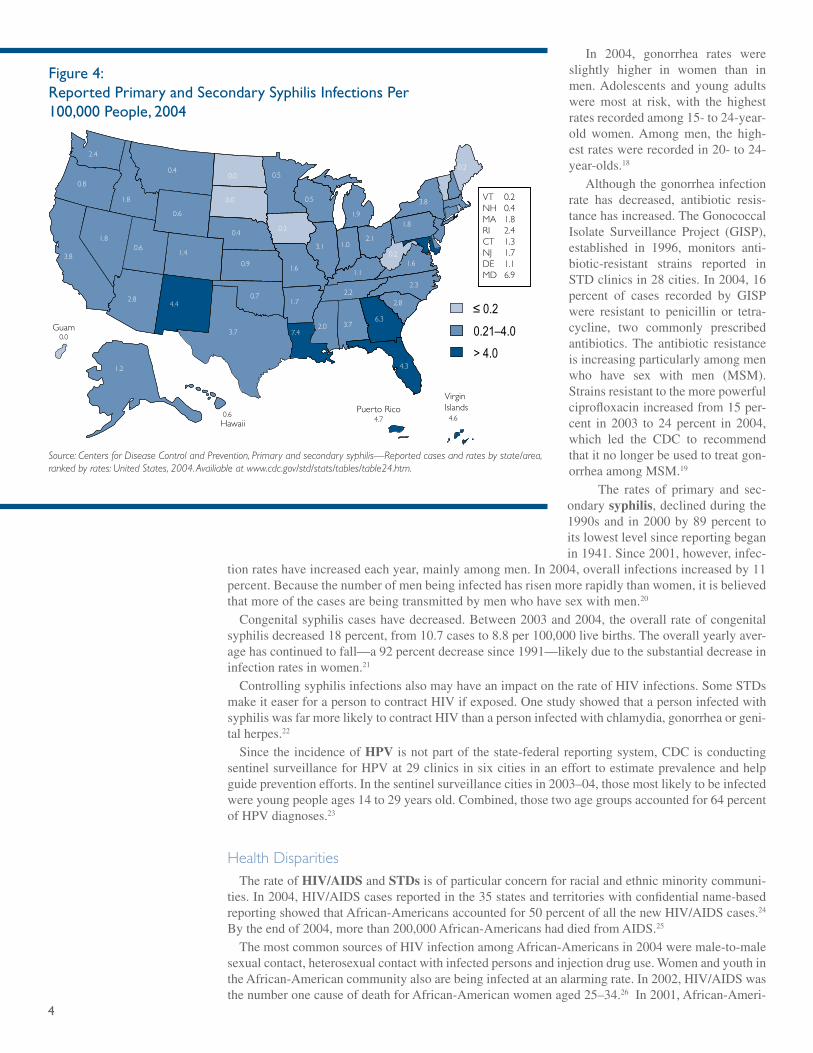
4
In 2004, gonorrhea rates wereslightly higher in women than inmen.Adolescents and young adultswere most at risk, with the highestratesrecordedamong15-to24-year-old women.Among men, the high-estrateswererecordedin20-to24-year-olds.18Althoughthegonorrheainfectionrate has decreased, antibiotic resis-tancehasincreased.TheGonococcalIsolate Surveillance Project (GISP),established in 1996, monitors anti-biotic-resistant strains reported inSTDclinicsin28cities.In2004,16percent of cases recorded by GISPwere resistant to penicillin or tetra-cycline, two commonly prescribedantibiotics.The antibiotic resistanceisincreasingparticularlyamongmenwho have sex with men (MSM).Strainsresistanttothemorepowerfulciprofloxacinincreasedfrom15per-cent in 2003 to 24 percent in 2004,which led the CDC to recommendthatitnolongerbeusedtotreatgon-orrheaamongMSM.19 The rates of primary and sec-ondarysyphilis,declinedduringthe1990sand in2000by89percent toitslowestlevelsincereportingbeganin1941.Since2001,however,infec-
tionrateshaveincreasedeachyear,mainlyamongmen.In2004,overallinfectionsincreasedby11percent.Becausethenumberofmenbeinginfectedhasrisenmorerapidlythanwomen,itisbelievedthatmoreofthecasesarebeingtransmittedbymenwhohavesexwithmen.20 Congenitalsyphiliscaseshavedecreased.Between2003and2004,theoverallrateofcongenitalsyphilisdecreased18percent,from10.7casesto8.8per100,000livebirths.Theoverallyearlyaver-agehascontinuedtofall—a92percentdecreasesince1991—likelyduetothesubstantialdecreaseininfectionratesinwomen.21 ControllingsyphilisinfectionsalsomayhaveanimpactontherateofHIVinfections.SomeSTDsmakeiteaserforapersontocontractHIVifexposed.OnestudyshowedthatapersoninfectedwithsyphiliswasfarmorelikelytocontractHIVthanapersoninfectedwithchlamydia,gonorrheaorgeni-talherpes.22 SincetheincidenceofHPV isnotpartofthestate-federalreportingsystem,CDCisconductingsentinelsurveillanceforHPVat29clinicsinsixcitiesinanefforttoestimateprevalenceandhelpguidepreventionefforts.Inthesentinelsurveillancecitiesin2003–04,thosemostlikelytobeinfectedwereyoungpeopleages14to29yearsold.Combined,thosetwoagegroupsaccountedfor64percentofHPVdiagnoses.23
Health Disparities TherateofHIV/AIDSandSTDsisofparticularconcernforracialandethnicminoritycommuni-ties.In2004,HIV/AIDScasesreportedinthe35statesandterritorieswithconfidentialname-basedreportingshowedthatAfrican-Americansaccountedfor50percentofallthenewHIV/AIDScases.24Bytheendof2004,morethan200,000African-AmericanshaddiedfromAIDS.25 ThemostcommonsourcesofHIVinfectionamongAfrican-Americansin2004weremale-to-malesexualcontact,heterosexualcontactwithinfectedpersonsandinjectiondruguse.WomenandyouthintheAfrican-Americancommunityalsoarebeinginfectedatanalarmingrate.In2002,HIV/AIDSwasthenumberonecauseofdeathforAfrican-Americanwomenaged25–34.26In2001,African-Ameri-
Figure 4: Reported Primary and Secondary Syphilis Infections Per �00,000 People, �004
≤ 0.2
0.21–4.0
> 4.0
2.4
1.8
3.8
0.8
1.8
0.4
0.6
0.6
2.8
1.2
0.6
0.0
4.4
1.4
0.4
0.0
0.0 0.5
0.2
1.6
1.7
7.42.0 3.7
6.3
4.64.7
4.3
2.82.2
1.1
3.1 1.02.1
1.9
0.5
1.8
3.8
0.2
0.21.6
2.3
0.9
0.7
3.7
VT 0.2NH 0.4MA 1.8RI 2.4CT 1.3NJ 1.7DE 1.1MD 6.9
Guam
Hawaii
Virgin IslandsPuerto Rico
Source: Centers for Disease Control and Prevention, Primary and secondary syphilis—Reported cases and rates by state/area, ranked by rates: United States, 2004. Availiable at www.cdc.gov/std/stats/tables/table24.htm.
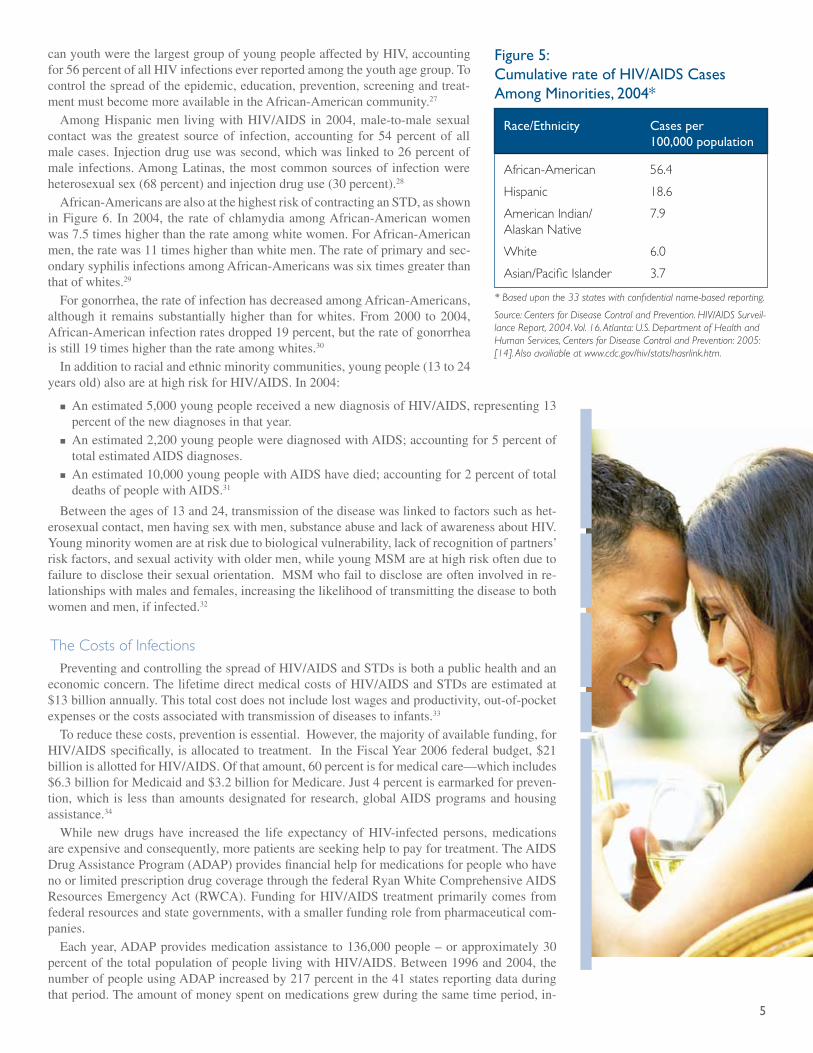
�
canyouthwerethelargestgroupofyoungpeopleaffectedbyHIV,accountingfor56percentofallHIVinfectionseverreportedamongtheyouthagegroup.Tocontrolthespreadoftheepidemic,education,prevention,screeningandtreat-mentmustbecomemoreavailableintheAfrican-Americancommunity.27 AmongHispanicmen livingwithHIV/AIDSin2004,male-to-malesexualcontactwas thegreatest sourceof infection, accounting for54percentof allmalecases.Injectiondrugusewassecond,whichwaslinkedto26percentofmale infections.AmongLatinas, themostcommonsourcesof infectionwereheterosexualsex(68percent)andinjectiondruguse(30percent).28 African-AmericansarealsoatthehighestriskofcontractinganSTD,asshowninFigure6. In2004, the rateofchlamydiaamongAfrican-Americanwomenwas7.5timeshigherthantherateamongwhitewomen.ForAfrican-Americanmen,theratewas11timeshigherthanwhitemen.Therateofprimaryandsec-ondarysyphilisinfectionsamongAfrican-Americanswassixtimesgreaterthanthatofwhites.29 Forgonorrhea,therateofinfectionhasdecreasedamongAfrican-Americans,although it remains substantiallyhigher than forwhites.From2000 to2004,African-Americaninfectionratesdropped19percent,buttherateofgonorrheaisstill19timeshigherthantherateamongwhites.30 Inadditiontoracialandethnicminoritycommunities,youngpeople(13to24yearsold)alsoareathighriskforHIV/AIDS.In2004:
Anestimated5,000youngpeoplereceivedanewdiagnosisofHIV/AIDS,representing13percentofthenewdiagnosesinthatyear.Anestimated2,200youngpeoplewerediagnosedwithAIDS;accountingfor5percentoftotalestimatedAIDSdiagnoses.Anestimated10,000youngpeoplewithAIDShavedied;accountingfor2percentoftotaldeathsofpeoplewithAIDS.31
Betweentheagesof13and24,transmissionofthediseasewaslinkedtofactorssuchashet-erosexualcontact,menhavingsexwithmen,substanceabuseandlackofawarenessaboutHIV.Youngminoritywomenareatriskduetobiologicalvulnerability,lackofrecognitionofpartners’riskfactors,andsexualactivitywitholdermen,whileyoungMSMareathighriskoftenduetofailuretodisclosetheirsexualorientation.MSMwhofailtodiscloseareofteninvolvedinre-lationshipswithmalesandfemales,increasingthelikelihoodoftransmittingthediseasetobothwomenandmen,ifinfected.32
The Costs of Infections PreventingandcontrollingthespreadofHIV/AIDSandSTDsisbothapublichealthandaneconomicconcern.ThelifetimedirectmedicalcostsofHIV/AIDSandSTDsareestimatedat$13billionannually.Thistotalcostdoesnotincludelostwagesandproductivity,out-of-pocketexpensesorthecostsassociatedwithtransmissionofdiseasestoinfants.33 Toreducethesecosts,preventionisessential.However,themajorityofavailablefunding,forHIV/AIDSspecifically,isallocatedtotreatment.IntheFiscalYear2006federalbudget,$21billionisallottedforHIV/AIDS.Ofthatamount,60percentisformedicalcare—whichincludes$6.3billionforMedicaidand$3.2billionforMedicare.Just4percentisearmarkedforpreven-tion,which is less thanamountsdesignatedfor research,globalAIDSprogramsandhousingassistance.34 While new drugs have increased the life expectancy of HIV-infected persons, medicationsareexpensiveandconsequently,morepatientsareseekinghelptopayfortreatment.TheAIDSDrugAssistanceProgram(ADAP)providesfinancialhelpformedicationsforpeoplewhohavenoorlimitedprescriptiondrugcoveragethroughthefederalRyanWhiteComprehensiveAIDSResourcesEmergencyAct(RWCA).FundingforHIV/AIDStreatmentprimarilycomesfromfederalresourcesandstategovernments,withasmallerfundingrolefrompharmaceuticalcom-panies. Eachyear,ADAPprovidesmedicationassistanceto136,000people–orapproximately30percentofthetotalpopulationofpeoplelivingwithHIV/AIDS.Between1996and2004,thenumberofpeopleusingADAPincreasedby217percentinthe41statesreportingdataduringthatperiod.Theamountofmoneyspentonmedicationsgrewduringthesametimeperiod,in-
n
n
n
Race/Ethnicity Cases per �00,000 population
African-American 56.4
Hispanic 18.6
American Indian/ 7.9Alaskan Native
White 6.0
Asian/Pacific Islander 3.7
* Based upon the 33 states with confidential name-based reporting.
Source: Centers for Disease Control and Prevention. HIV/AIDS Surveil-lance Report, 2004. Vol. 16. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention: 2005: [14]. Also availiable at www.cdc.gov/hiv/stats/hasrlink.htm.
Figure �: Cumulative rate of HIV/AIDS Cases Among Minorities, �004*

�
creasing591percent.TheaveragecostperprescriptionforHIV/AIDStreatmentinJune2004was$257permonth.35
Conclusion Despiteadvancesinpreventionandtreatment,HIV/AIDSandotherSTDsremainanimportanthealthconcern,particularlythedisproportionateimpactoftheepidemicsonracialandethnicmi-noritypopulations.IncreasedfocusonHIVandSTDpreventioneffortsisnecessarytocontrolthespreadofthediseasesandre-ducetheeconomicandhealthcosts.ThecostsofdrugsusedtotreatHIV/AIDShaveincreasedandthenumberofpeopleseekingfederalassistancetooffsetcostshasfollowed.ThedirectmedicalcostsofHIV/AIDSandotherSTDsareestimatedat$13billionannually(2003dollars).36,37Toencouragethedevelopmentofeffectivepreventionmessagesand better targeted efforts, legislators should be aware of localpopulationsmostaffected.Chlamydiaismostoftendiagnosedinyoungwomen,andgonorrhearatesareslightlyhigherinwomenthanmen.Syphilis rates,however,havebeen increasingamongmenand themajorityof those livingwithHIV/AIDSaremen.PreventionmessagesmustaddressthespecificconcernsofAfri-can-Americans,Hispanics,youngwomenandMSM. Legislators should also be aware of how HIV/AIDS data arecollectedintheirstate.Statesthathavenotyetadoptedconfiden-tialname-basedsurveillancesystemsforreportingHIVinfectionscouldpotentiallyfacemajorreductionsinfundingfortreatmentthroughRWCAresources. HIV/AIDSandotherSTDsarepreventable.Legislatorswhoareawareof theepidemicsand informedof their local impactcanbechampionsforprevention,testingandeducationaleffortsfocusedonthesediseases.
Race/Ethnicity Chlamydia Gonorrhea P&S Syphilis
African-American 1,209.4 629.6 9.0
American Indian/ 705.8 117.7 3.2Alaskan Native
Hispanic 436.1 71.3 3.2
White 143.6 33.3 1.6
Asian/Pacific Islander 133.7 21.4 1.2
Source: Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveil-lance, 2004. Atlanta, GA: U.S. Department of Health and Human Services, September 2005.
Figure �: Reported Infection Rate of STDs Among Minorities Per �00,000 Population, �004
�
Endnotes1NationalInstituteofAllergyandInfectiousDisease,NationalInstitutesofHealth.“HowHIVCausesAIDS.”Accessedfromwww.niaid.nih.gov/factsheets/howhiv.htmApril11,2006.2Ibid.3 Centers forDiseaseControlandPrevention.“Chlamydia.”Accessedfrom www.cdc.gov/std/chla-mydia/default.htmDecember20,2005.4Ibid.5CentersforDiseaseControlandPrevention.“Gonorrhea.”Accessedfromwww.cdc.gov/std/Gonor-rhea/default.htmDecember20.2005.6Ibid.7CentersforDiseaseControlandPrevention.“Syphilis.”Accessedfromwww.cdc.gov/std/syphilis/de-fault.htmDecember20,2005.8Ibid.9CentersforDiseaseControlandPrevention.“HumanPapillomavirus(HPV)Infection.”Accessedfromwww.cdc.gov/std/hpv/default.htmDecember20,2005.10CentersforDiseaseControlandPrevention.“HPVVaccineQuestionsandAnswers.”Accessedfromwww.cdc.gov/std/hpv/STDFact-HPV-vaccine.htm#vaccineJune5,2006.11NationalInstituteofAllergyandInfectiousDisease,NationalInstitutesofHealth“HIVInfectionandAIDS:AnOverview.”Accessedfromwww.niaid.nih.gov/factsheets/hivinf.htmApril11.2006.12CentersforDiseaseControlandPrevention.HIV/AIDS Surveillance Report, 2004.Vol.16.Atlanta:U.S.DepartmentofHealthandHumanServices,CentersforDiseaseControlandPrevention;2005.Alsoavailableat:www.cdc.gov/hiv/stats.hasrlink.htm13Ibid.14 Smith,Michael. “HAARTCutsRiskofHIVProgression toAIDSorDeathby86%”Medpage Today,July28,2005.Accessedfromwww.medpagetoday.com/InfectiousDisease/HIVAIDS/tb1/1448April11,2006.15CentersforDiseaseControlandPrevention,Sexually Transmitted Disease Surveillance, 2004.At-lanta,GA:U.S.DepartmentofHealthandHumanServices,September2005.Thisreportalsoisavail-ablebyInternetviatheCDChomepageat:www.cdc.gov/std/stats/16Ibid.17Ibid.18Ibid.19Ibid.20Ibid.21Ibid.22Chesson,HarrellW.;Pinkerton,StevenD.“SexuallyTransmittedDiseasesandtheIncreasedRiskforHIVTransmission:ImplicationsforCost-EffectivenessAnalysesofSexuallyTransmittedDiseasePreventionInterventions.”Journal of Acquired Immune Deficiency Syndrome(May1,2000).23Ibid.24CentersforDiseaseControlandPrevention.HIV/AIDS Surveillance Report, 2004.Vol.16.Atlanta:U.S.DepartmentofHealthandHumanServices,CentersforDiseaseControlandPrevention;2005.Availableat:www.cdc.gov/hiv/stats/hasrlink.htm.25Ibid.26CentersforDiseaeControlandPrevention.“AfricanAmericans:Overview.”Accessedfromwww.cdc.gov/hiv/topics/aa/index.htmMay4,2006.27Ibid.28CentersforDiseaseControlandPrevention.HIV/AIDS Surveillance Report, 2004.Vol.16.Atlanta:U.S.DepartmentofHealthandHumanServices,CentersforDiseaseControlandPrevention;2005.Availableat:www.cdc.gov/hiv/stats/hasrlink.htm.29CentersforDiseaseControlandPrevention,Sexually Transmitted Disease Surveillance, 2004.At-lanta,GA:U.S.DepartmentofHealthandHumanServices,September2005.Thisreportalsoisavail-ablebyInternetviatheCDChomepageat:www.cdc.gov/std/stats/30Ibid.31Ibid.32CentersforDiseaseControlandPrevention,DivisionofHIV/AIDSPrevention.“HIV/AIDSamongYouth.”Accessedfromwww.cdc.gov/hiv/pubs/facts/youth.htmApril11,2006.33KaiserFamilyFoundation,“SexuallyTransmittedDiseasesinAmerica:HowManyCasesandatWhatCost?”Accessedfromwww.kff.org/womenshealth/1445-std_rep3.cfmFebruary7,2006.34 Kaiser Family Foundation, “The President’s FY 2006 Budget Proposal: Overview and Briefing
�
Charts.”Availableat:www.kff.org/uninsured/upload/The-President-s-FY-2006-Budget-Propos-al-Overview-and-Briefing-Charts.pdf35KaiserFamilyFoundation.“NationalADAPMonitoringProjectAnnualReport,April2005.”Availableat:www.kff.org/hivaids/7288.cfm36Chesson,HarrellW.;Blandford,JohnM.;Gift,ThomasL.;Tao,Guoyu;andIrwin,KathleenL.“TheEstimatedDirectMedicalCostsofSexuallyTransmittedDiseasesAmongAmericanYouth,2000.”Perspectives on Sexual and Reproductive Health,2004,36(1)11–19.37Weinstock,H.;Berman,S.;CatesJr.,W.“SexuallytransmitteddiseasesamongAmericanyouth: incidenceandprevalence estimates, 2000.”Perspectives on Sexual and Reproductive Health,2004,36:6–10.
�
TopreventthespreadofHIV/AIDSandothersexuallytransmitteddiseases(STDs),stateandfederalgovernmentsworkinpartnershipwithcommunity-basedprovidersandorganizations.Because these infectionsare sexually transmitted,privacy issues, fearsofembarrassmentorexposureandmoralityconcernshavecreatedobstaclestoinstitutingprovenpreventionefforts,suchasmakingtestingapartofroutinemedicalcare. Preventionprograms inAfrican-AmericanandHispaniccommunities faceparticularchal-lenges, includinga lackofproven interventions thatareculturally sensitiveandspecificallydesignedtoreachthesepopulations.ForHispanics, thediversityoftheLatinopopulationintheUnitedStatesfurthercomplicatesoutreacheffortsbecauseregionalandculturaldifferences,socioeconomicstatusandbehavioralriskallimpactHIV/AIDSstatus.1Distrustofgovernmenthealthdepartments,fearofdeportation,languagebarriersandlackofrepresentationinplanningprocessesfurthercomplicateeffectiveSTDandHIV/AIDSprevention.Culturallycompetentpreventionprogramsshouldtakeallthesefactorsintoaccount. Governmentpolicyseekstopreventfurtherspreadofthediseasesby:
Encouraging individuals tobe tested so theyknow if theyhave a sexually transmitteddisease;Counselingandeducating thosewhoare infected regarding their role inpreventing thespreadofthedisease;Generatingsupportforpreventionandtreatmenteffortsamonghealthcareprovidersandothercommunity-basedpartnerssuchasschoolsandfaith-basedorganizations;Understandingthepopulationsmostaffectedbythediseases,includinghowthediseasesaretransmittedandhowwelltreatmentsareworking;andUsingdatatohelpdevelopmoretargetedpreventionandtreatmentefforts.
Thefollowingsectionswilldescribehowthefederalgovernmentworkswithstateandlocalgovernmentsandcommunityagenciestoimplementprogramsthatreinforcethesepreventionstrategies.
What Role Does the Federal Government Play in Prevention and Treatment of HIV/AIDS and STDs? ThefederalgovernmentplaysakeyroleinthepreventionandtreatmentofHIV/AIDSandSTDs. Federal health agencies recommend policies, set screening and treatment guidelinesbasedonscientificevidence,providefundsforresearch,financehealthservicesandprovidetechnicalassistance.TheDepartmentofHealthandHumanServiceshastheleadroleinover-seeingpublichealthprogramsthataddressHIV/AIDSandSTDs,includingresearchonpreven-tionandtreatmentofHIVandfinancingtreatmentservices. CDCprovidesfundingtostateandlocalhealthdepartmentsforSTDcontrolandpreventionthroughitsComprehensiveSTDPreventionSystemscooperativeagreements,whichincludesfundingfortheInfertilityPreventionProgramandSyphilisEliminationEffort.ThesefederalfundsareusedinlocalcommunitiesforSTDclinicalandpreventionservices.CDCalsopro-videsdirectpersonnelandtechnicalassistancetostatehealthdepartments.Inadditiontopro-vidinghumanandfinancialresourcestostates,theCDCmonitorsdiseasetrendsthroughsur-
n
n
n
n
n
Prevention Programs:State, Federal & Community-Based
Preventing HIV/AIDS & Sexually Transmitted Diseases
HIV/AIDS STD K

�
veillanceefforts,conductsresearchandevaluatesprogramstodevelopimprovedtoolsforcontrollingSTDs. ForHIV/AIDS,mostfederalfundingisspentonmedicaltreatment,whichcomesmainlyfromtheHealthResourcesandServicesAdminis-trationthroughtheRyanWhiteComprehensiveAIDSResourcesEmer-gencyAct(RWCA).Since1990,theRWCAhasprovidedfortheneedsofindividualsandfamilieslivingwithHIV/AIDSanddirectedfederalfundingtoareasdisproportionatelyaffectedbytheepidemic.2Itsmainfocusistoprovideprimarycare,treatmentandsupportservices.Morethan 2,700 providers who receive RWCA funding reach more than500,000peopleeachyear—whichisabouthalfofallofthoseestimatedtobelivingwithHIV/AIDSintheUnitedStates.3 TheCentersforMedicareandMedicaidServices(CMS)alsospendsasignificantamountofmoneyonHIV/AIDScare.Medicaidisthelarg-estsourceof federal fundingforHIV/AIDStreatment in thecountry.CMSestimatesthatinFiscalYear(FY)2005,Medicaidspent$5.7bil-liononHIV/AIDStreatment.ForFY2006,thatnumberisexpectedtoincreaseto$6.3billion.4 CDCprovidesmostofthefundsspentonHIVpreventionbystateand local health departments and community-based organizations.CDCprovidesHIVpreventionfundingto65stateandlocaljurisdic-tions.Eachstatecontributessomelocalfundingtobothpreventionandtreatment,althoughtheamountvariesfromyeartoyearandfromstatetostate.
Federal Surveillance Systems
CDC,throughtheNationalCenterforHIV/AIDS,STDandTBPre-vention(NCHSTP)istheprimaryfederalagencythatprovidessupporttostatesforHIV/AIDSandSTDsurveillanceandpreventionprograms.CDC’sSTDsurveillanceconsistsofnationalnotifiablediseasereport-ing,sentinelsurveillance,specialsurveys,andprevalencemonitoring:
Nationalnotifiablediseasereporting:Thissystemcollectscasere-ports of chlamydia, gonorrhea, syphilis and chancroid infectionsreportedfromalljurisdictions.Sentinel surveillance:Sentinel surveillancesystemscollectdatafromalimitednumberofparticipatingfacilitiesthatperformspe-cific,andsometimesnonroutine,STDtestingamongaparticularpopulation.Onesuchsystemis theGonococcal IsolateSurveil-lanceProject(GISP),whichmonitorstheantimicrobialdrugre-sistanceofstrainsofgonorrhea.Specialsurveys:Specialsurveysusepopulation-basedsamplesandprovidetheonlymeansbywhichanaccuratenationalestimateofdiseaseprevalencecanbeobtained.TheNationalHealthandNutri-tionExaminationSurvey(NHANES)examinesabout5,000peopleeachyearfromacrossthecountrytofocusonavarietyofhealthandnutritionalmeasurementstomeetemergingneeds.Prevalence monitoring: Prevalence monitoring provides data onprevalencetrendsindiseaseprevalenceamongdefinedpopulationsover time.Prevalencemonitoringfocusesonavarietyofpopula-tions,suchasmenwhohavesexwithmen(MSM)oradolescents,ortakesplaceinparticularsettings,suchascorrectionalfacilitiesandfamilyplanningclinics.STDSurveillanceNetwork:This is a networkof local enhancedSTDsurveillancesystemstoimprovethecapacityofnational,stateandlocalSTDprogramstodetect,monitorandrespondtotrends.
Thesesurveillancesystemsarecriticalforunderstandinganddescrib-ingtheburdenofSTDsonthehealthofAmericans,particularly,youngAmericans; formonitoringnationaldisease trendsandhealthdispari-
n
n
n
n
n
Effective clinical management of patients with treatable sexually transmitted diseases (STDs) re-quires treatment of the patients’ current sex part-ners to prevent reinfection and stop further trans-mission. The standard approach to partner treatment has included clinical evaluation in a health care setting, with partner notification accomplished by the pa-tient, the provider or an agent of the provider, or a combination of these methods. Provider-assisted referral is considered the op-timal strategy for partner treatment, but is not available to most patients with gonorrhea or chla-mydial infection because of resource limitations. The usual alternative is to advise patients to refer their partners for treatment. In recent years, research supported by CDC evaluated expedited partner therapy (EPT), an approach where partners are treated without an intervening clinical assessment. EPT typically is accomplished by patients delivering either medica-tions or prescriptions to their partners. Based on evidence from randomized control studies and surveys of practice, CDC has concluded that EPT is a useful option to facilitate partner man-agement, particularly for treatment of male partners of women with chlamydial infection or gonorrhea. EPT is permissible in only five states, though it may be possible in as many as 33 additional states with some regulatory or administrative action. Since 2005, the CDC has strongly encouraged lo-cal and state health departments and policymakers interested in STD prevention to work together to resolve the outstanding legal issues and find ways to implement this proven prevention strategy. EPT is a promising practice for treating infected sexual partners of those diagnosed with chlamydia, but implementation likely requires policy or legislative action in most states. Some states, such as California, have passed legislation to permit EPT; other states, such as Tennessee, have implemented regulations to permit the practice.
Source: Centers for Disease Control and Prevention. “Expedited Partner Therapy in the Management of Sexually Transmitted Disease.” Available at: www.cdc.gov/std/treatment/EPTFinalReport2006.pdf
Expedited Partner Therapy (EPT): An Innovative Approach
�
ties;andforevaluatingtheimpactofimportantnationalprograms,suchastheInfertilityPreventionProgramandtheSyphilisEliminationEffort.Thedataarealsousedtohelptargetresourcesforspe-cificpopulationsandhealth jurisdictionsandforspecificdiseasecontrolactivities, suchaspartnernotificationandscreening.NationalrecommendationsforthetreatmentofgonorrheacontinuetorelyoninformationfromGISP,andsurveillancedatahavetriggeredCDCinvestigations,oftenresultinginincreasedtargetedpublichealtheffortsinlocalareas. CDCusesadditionalsurveillancesystemstomonitorbehaviorsrelatedtoHIV/AIDSinfectionsandtheservicesprovidedtothosepatients.Thosesystemsinclude:
MorbidityMonitoringProject(MMP):InformationiscollectedfromHIV/AIDSpatientsreceiv-ingcarefromrandomlyselectedprovidersaboutaccesstoanduseofHIVtreatmentandpreven-tionservices,aswellas theirbehaviors thatcanresult inHIVtransmissionandaffectdiseaseoutcomes(likeadherencetotherapy).NationalHIVBehavioralSurveillanceSystem(NHBS):SurveysareconductedincitieswithhighlevelsofHIV/AIDSamonghigh-riskpopulations(suchasinjectiondrugusers)todeterminetheirriskbehavior,testingbehavioranduseofpreventionservices.5
Federal HIV/AIDS Prevention Initiatives
CDCprovidesgrantstoall50statehealthdepartmentsforpreventionandreportingofHIV/AIDScases and targeted funding for special surveillanceactivities forprioritypopulationsorbehavioralinterventionsin29states. CDCfundingsupportsstateeffortstostrengthenorganizationalinfrastructure,improveandevaluateinterventionsthatpreventHIV,especiallyinhigh-riskpopulations,andworkwithcommunityrepre-sentativesfromhigh-riskethnicandracialminoritygroupstoimprovecommunityaccessanduseofHIVpreventionandrisk-reductionactivities. AdvancingHIVPrevention(AHP):InApril2003,CDC,inpartnershipwithotherU.S.DepartmentofHealthandHumanServices(HHS)agenciesandothergovernmentalagencies,launchedtheirnewinitiative,“AdvancingHIVPrevention:NewStrategiesforaChangingEpidemic.”TheinitiativewasbegunbecausetheannualnewHIVinfectionratehadremainedrelativelystableforaboutadecade
n
n

�
andaboutaquarteroftheestimated1millionHIV-infectedpeoplehadnotbeentested.Also,makingpeopleawarethattheywerecarryingthevirusbecameaprioritybecauseCDCresearchdemonstratedthatonceapersonlearnsoftheirinfectiontheytendtotakestepstoreducetransmissiontopartners. AHPfocusesonfourprovenstrategies:
MakingvoluntaryHIVtestingaroutinepartofmedicalcare;ImplementingnewmodelsfordiagnosingHIVinfectionsoutsidemedicalsettings;PreventingnewinfectionsbyworkingwithHIV-infectedpersonsandtheirpartners;andFurtherdecreasingperinatalHIVtransmission.6
AHPalsofocusesonencouragingfacilitiestoconductrapidHIVtesting,whichprovidesresultsin20minutesandcanbedoneinanon-clinicalsetting.Non-rapidHIVtestscantakeseveraldaysandresearchhasshownthatabout30percentofthepeoplewhotestpositiveinCDC-fundedsitesdonotreturntogettheirresults.7Between2003and2005,theCDCpurchasedanddistributedmorethan500,000rapidHIVtestingkitsforstateandlocaluseandconductedtrainingsessionsonhowtoprop-erlyusethem.8
TheAHPinitiativepromotesincludingHIVtestingaspartofroutinemedicalcareinclinicalset-tingssuchashospitalsandemergencyrooms.ThepurposeofthisstrategyistoincreasetheproportionofpeoplewhoknowtheirHIVstatusandtoeliminatebarrierstovoluntarytestingsuchaspre-testcounselingrequirements. However,manyphysiciansareconcernedaboutroutinelytestingtheirpatientsforHIV,preferringtotestonlythosewhohaveatraditionalriskfactor.9Researchersareevaluatingthecostbenefitofwidespreadpopulationscreeningprograms.Onestudyestimatedthatinhigh-riskpopulationswheremorethan40percenthavealifetimeriskofbecominginfectedwithHIV,eachHIV-positivepersonidentifiedcost$32,000,butfurthertransmissionto300otherswasaverted.10 MinorityAIDS Initiative (MAI): Since 1999, HHS agencies, including the CDC, have receivedresourcesfromtheMinorityAIDSInitiative(MAI)toenhancepreventionofHIVinfectionsinracialandethnicminoritycommunities,particularlyinAfrican-AmericanandHispanic/Latinopopulations.
n
n
n
n
�
MAIresourcesareappropriatedannuallybyCongress.Theinitiativesupportscommunity-basedHIVpreventionprogramsandtargetededucationefforts.Usingthesefunds,CDCconductsad-ditionalsurveillancetodefinethemagnitudeoftheprobleminracialandethniccommunities,andtoresearch,developandrefineculturallyrelevantinterventionsandprograms.11
Federal STD Prevention Initiatives
CDC’sComprehensiveSTDPreventionSystems(CSPS)providessupportto65projectareasin50states,sixcities,seventerritories,theDistrictofColumbiaandPuertoRicotodesign,im-plementandevaluatehighquality,comprehensivestateandlocalSTDpreventionandtreatmentprogramsthatintegrateHIVservices.ExamplesofcollaborativeactivitiesincludeencouragingmedicalproviderstoprovideHIV,hepatitisandSTDscreeninginhigh-prevalencesettings;sup-portingthedevelopmentandexpansionofHIVcounseling,testing,referralandpartnerservices;andintegratingHIV,hepatitisandSTDpreventionmessagesintoeducationalmaterials. FourimportantCDCSTDpreventionprogramsare: InfertilityPreventionProgram.Chlamydiaandgonorrheaarethemostimportantpreventablecausesofinfertilityandpotentiallyfataltubalpregnancy.Ifnotadequatelytreated,upto40per-centofwomeninfectedwitheitherdiseasewilldeveloppelvicinflammatorydisease(PID),thecriticallinktoinfertility.Becausemostinfectedwomenandatleasthalfofinfectedmenhavenosymptoms,manyinfectionsgoundetectedandarenotreportedorcounted. CDC, incollaborationwith theOfficeofPopulationAffairs,supportsanationalInfertilityPrevention Program that funds chlamydia screening and treatment services for low-income,sexually-activewomenattendingfamilyplanning,STDandotherwomen’shealthcareclinics.TheprogramwasauthorizedbyCongressin1993andhasdemonstratedthatroutinescreeningofwomencanreducechlamydiaprevalenceandPIDincidenceinwomen. Syphilis Elimination Effort (SEE). When CDC launched the National Plan to EliminateSyphilisin1999,theepidemicofinfectioussyphiliswasatanhistoriclowandwascontainedinlimitedgeographicalareas,makingtheeliminationgoalof1,000orfewercasesfeasible.Atthetimeofthelaunch,syphiliswasmainlyfoundindisadvantagedandunderservedAfrican-Americancommunitieswherepovertyandaccesstohealthcarewerekeyfactorsallowingittopersist.In1998,theprimaryandsecondarysyphilis(P&Ssyphilis)rateforAfrican-Americanswas34timesgreaterthantherateforwhites. AsasupplementtotheCSPSgrants,39SEEprojectsin31states,sevencitiesandPuertoRicowerefundedin2005inareaswithhighsyphilismorbidity.TheSEEprogramimprovesaccesstohigh-quality,community-basedpreventiveandcareservices,provideseducationaboutpreventionofsyphilisandotherSTDs toaffectedcommunitiesandstrengthensoutbreak re-sponsepreparedness.Theprogramalsobuildsandstrengthenspartnershipswithpublichealthorganizations,theprivatemedicalcommunityandotherpublicandprivatepartnersinSTDandHIVprevention. SEEallowstheCDCandstatestotargetresourcesandprogramsinareaswiththehighestratesofdisease.Suchtargetinghasresultedinsignificantdeclinesinsyphilisamongkeypopu-lationsatrisk.Forexample,between1999and2004,P&SsyphilisratesamongAfrican-Ameri-cansdecreased37percent;theblack-whitedisparityinsyphilisratesfellfrom28.6:1to5.6:1;syphilisratesamongwomendecreased60percent;andcongenitalsyphilis(transmissionfrommothertochild)ratesdeclined39percent.12Overall,therehasbeena92percentdecreaseincasesofcongenitalsyphilissince1991.13 Thenationalplanwasupdatedin2006toaddresstheincreasingratesofsyphilisamongmenwhohavesexwithmen.More than60percentofnew infectionsnowarediagnosedamongMSM.Theeffortwillincludeenhancingsurveillance,includingaskingforthegenderofsexualpartners,advocatingroutinesyphilisscreeningamongMSMbyHIVcareproviders,developingInternet-basedinterventionsandincreasingfundingtocommunity-basedorganizationsinhigh-prevalenceareastomoreeffectivelytargetat-riskpopulations.14 STD/HIVpreventiontraining.TheNationalNetworkofSTD/HIVPreventionTrainingCen-tersisagroupof18CDC-fundedregionalcenters.Tenprovideclinicalandlabtraining,fourprovidebehavioralinterventionstrainingandfourprovidepartnerservicestraining.Theywerecreatedinpartnershipwithhealthdepartmentsanduniversitiesthatprovidestate-of-the-artedu-cationforhealthprofessionalsintheareasofsexualandreproductivehealth. Supportingscreeningsaspartofroutinemedicalcare.Itisanationalhealthprioritytodiag-noseandtreatindividualsassoonafterinfectionaspossible.ButbecausesomeoftheSTDs

�
havefewornosymptoms,theCDCrecommendsregularscreeningsbecomeapartofroutinepatientcare.CDCandotherprofessionalhealthcareorganizationsrecommendannualchla-mydia screening of sexually active women 25 years old or younger in order to avert PID,whichcanleadtoinfertility,ectopicpregnancyandchronicpain.Becausesyphiliscanhavedevastatingeffectsonunbornchildren,CDCandotherprofessionalhealthcareorganizationsrecommendprenatalscreeningofallpregnantwomenforsyphilis.AndaswithHIV/AIDS,counselingalsoisrecommendedtopreventnewinfectionsortransmissionofthediseasetopartners.
How Do State and Local Health Departments Work to Prevent HIV/AIDS and STDs?
State health departments
Statehealthdepartmentsareresponsibleforprotectingthehealthoftheirstate’spopulation.Theirprimaryrolesincludepreventingdiseasesandinjuries,protectingagainstenvironmentalhazards,respondingtodisasters,promotinghealthybehaviorsandensuringaccesstohealthcareservices.Theactivitiesofhealthdepartmentsintegratetheseprioritieswiththerequire-mentsoffederalandothergrantfunding.State-by-stateprofilesofHIVandSTDpreventionactivitiescanbeaccessedatwww.cdc.gov/nchstp/od/stateprofiles/usmap.htm. InFY2005,CDCprovidedmorethan$600millioningrantstostatesforHIV/AIDSandSTDsurveillanceandprevention.Statehealthdepartmentsalsoreceivefundingthroughstatebudgets,userfees,finesandspecialfunds,suchastobaccosettlementfunding. EachstatehealthdepartmentdeterminesitsownapproachtomeetingtherequirementsoftheCDCfundingtomonitorthenumberofpatientsdiagnosedwithHIV,AIDSandSTDsaswellastoimplementinitiativestomeettheirownpriorities.Somestatehealthdepartmentsalsofundtheactivitiesofthelocalhealthdepartments. StatesreportcasesofHIV/AIDSandSTDstotheCDC.Nationalsurveillancedataareusedtohelppolicymakersdecidewhatactionstotaketoaddresstheareasoftheirstateorsegmentsoftheirpopulationmostat-riskofcontractingHIVoranSTD. AnexampleofHIVsurveillancedataprovidingtheimpetusforpolicyactionoccurredinAlabama,wherethedatashowedthatwhileonly26percentofthestate’spopulationisAfrican-American,morethan70percentofnewlyreportedHIVinfectionsoccurredinAfrican-Ameri-cans.This information led to a multi-year initiative, including declaration by the governorof anAfrican-AmericanHIV/AIDSAwarenessDay,whichwaspaid for throughadditionalfederal funding.The initiativesought toencourageAfrican-Americans tobe testedforHIVandsuppliedfundingtofaith-basedandminorityorganizationstobuildcommunitycoalitionstoconfronttheproblem.15 Completeandaccuratestatedataareessential todevelopingeffectiveactionson thefed-eral, state and local level to combat HIV and STDs. For example, case reports inWesternstatesidentifiedmethamphetamineuseasacontributortounsafesexualpracticesandincreasedtransmissionofSTDs,particularlyamongMSM.AdditionalreportingandanalysisalertedthepublichealthagenciestotheproblemastheuseofmethamphetaminespreadtotheEasternstates.EastCoaststatesnowareusingtheexperiencesofWesternstatesasaframeworkforformulatingtheirownprogramstoaddresstheissue.16
Local health departments
Organization and fundingof local healthdepartments varies.Some serve cities, countiesortownships.Insomestates,theyareindependentfromthestatehealthdepartmentsbutarerequiredtoconformtostateregulations.Inotherstates,fundingmaybecompletelyorpartiallystate provided. State regulations grant authority to the local health departments to quaran-tine, investigate disease outbreaks and regulate facilities, and to require supportive actionsfrommedicalcareproviderssuchasreportingindividualsinfectedwithHIV/AIDSandcertainSTDs.17 Usingtheguidanceofbroadfederalinitiatives,stateandlocalprogramstargettheiractivitiesaccordingtothoselocalpopulationsmostaffectedbytheepidemics.Someexamplesare:
Baseduponsurveillancedata,theWyomingRuralAIDSPreventionProject(WRAPP)isfindingnewwaystotargetpreventioneffortsforMSMinthelargelyruralstate.Because
n

�
thereislittlegay-identifiedcultureinWyoming,WRAPPislookingfornewwaystousetheIn-ternettogetitspreventionmessageacrosstoMSM.18InSanFrancisco,patientsnowcanordersyphilistestsandgettheresultsonline,eliminatingtheneedforwaitingatclinicsandencouragingmorepeopletobetested.Inaddition,thehealthde-partmentalsohostsaWebsitethatallowspatientstosende-cardstopartnerstoletthemknowthattheymayhavebeenexposedtoanSTDandtheyneedtobetested.Follow-upresearchhasshownthattheWebsitehelpedhealthofficialsdetect20casesofsyphilisthatprobablyotherwisewouldnothavebeendiagnosed.SanFrancisco’sinitialinvestmenttosetuptheWebsitewas$20,000andmonthlymaintenancecosts$40.19TheWilliamF.RyanCommunityHealthCenterinNewYorkCityconductstargetedstreetandcommunityoutreachforAfrican-AmericansandLatinostoreducetheirriskofbecominginfectedwithHIV.One-on-oneandgroupsessionsoffereducationalmaterialsandcounseling.Clientsur-veysareusedtoassistinplanningfutureactivities.20During2004,theIllinoisDepartmentofPublicHealthSTDProgram,incollaborationwiththeChicagoDepartmentofPublicHealth,helpedfundroutinechlamydiaandgonorrheascreeningattheCookCountyJail.Allfemaledetaineeswereofferedchlamydiaandgonorrheatestingatthetimeofbooking.Atotalof12,447womenweretestedforchlamydia,resultingintheidentifica-tionandtreatmentof1,297infectedwomen.Atotalof12,479femalesweretestedforgonorrhea,whichresultedin1,046womenbeingidentifiedandtreated.Becauseofthesuccessofthepro-gram,routinetestingbeganin2005formalesatincreasedriskofinfection.21
What Other Local Programs and Resources Work On HIV/AIDS and STD Prevention?
Health care providers
Privateandpublichealthcare,mentalhealthandsubstanceabuseproviders,emergencyroomsandhospitalsofferinformationaboutHIV/AIDSandSTDs,andprovidescreeningtestsandreferralsto
n
n
n

�
treatmentandcounselingservices.Freeorreduced-costeducationalandtesting/counselingprogramsareofferedtocommunities,particularlyminorityandunderservedpopulations,toaddresstheseepi-demics.LocalcommunitymedicalclinicsfundedbystateorfederalinitiativesprovideopportunitiesforcommunitymemberstoreceivetestingandcounselingservicesforHIVandotherSTDs.
School and youth-based programs
Localschoolboardsandschoolsmakedecisionsonhowtoincorporatehealthandsexeducation,includingpreventionofHIV/AIDSandotherSTDs, intoschoolcurricula.Schoolboardsarefacedwithbalancinglocalpreferencesforeducationonsexualriskbehaviorsandthedesiretoprotectthehealthoftheirstudents,withparents’rightstocontrolinformationpresentedtotheirchildren.Manyapproacheshavebeenimplementedacrossthestatestodealwiththeselocalissues. CDC’sDivisionofAdolescentandSchoolHealthprovidesfundingtostatedepartmentsofeduca-tiontoimplementHIV/AIDSpreventioneducationprograms.TheseprogramsprimarilyemphasizeabstinencefromsexualintercoursetoprotectteensfromHIV,otherSTDsandunintendedpregnan-cy.Sincea2005studyreportedthat47percentofhighschoolstudentshavehadsexualintercourseandonly63percentofthemusedacondomduringtheirmostrecentintercourse,thereisacontinu-ingcauseforconcernabouteducationandpreventionforteens.22Insomestates,thestatedepart-mentsofeducationhavecurricularelatedtoHIVandSTDprevention,whichisusedbyschoolsatthediscretionoftheschoolboardandwithparentalinvolvementintheapprovalofschool-basedprograms. InMichigan,a2004statelawgivesabroadoutlineofwhatschoolsshouldteachinacomprehen-sivesexeducationcourse,butitalsoallowsforagreatdealoflocalcontrolsoitcanbemodifiedtofitcommunitystandards.Undertheregulations,sexeducationcannotbetaughtunlessacommunitysexeducationadvisoryboardisestablished.Atleasthalfoftheboard’smembersmustbeparentswhohavechildrenthatattendaschoolinthedistrict.Theadvisoryboarddecideswhatistaughtwithinthe
�
confinesofthelaw,whichregulatesthatallinformationshouldbeage-appropriateandmedicallyac-curate.Parentsareallowedtoexcludetheirchildrenfromtheclasses. Whileabstinenceistheonly100percenteffectivewaytopreventHIV,otherSTDsandunintendedpregnancy,theMichiganStateBoardofEducationrequiresstudentstobeeducatedaboutotherwaystoreducetheriskofinfection.Thestatealsohasdevelopedmodelcurriculaforusebylocalschoolboardsforelementary,middleschoolandhighschoolstudents.23,24FormoreinformationaboutMich-igan’slaw,seethearchiveofaWebconferencehostedbyTheCouncilofStateGovernmentstitled,“ProtectingAmerica’sYouth:SchoolsandCommunitiesTackleYouthSexualRiskBehaviors,”avail-ableatwww.healthystates.csg.org/Events+and+Conferences/Web+Conferences/Teen+Sexual+Risk+Behavior+Web+Conference.htm. Aschooldistrict’simpactcangobeyondeducation.Todealwithagrowingnumberofteensdi-agnosedwithchlamydiaandgonorrhea,theSchoolDistrictofPhiladelphiapartneredwiththelocalhealthdepartmenttoofferoptionalurinescreeningsforstudents.In1995,thePhiladelphiaDepartmentofHealthrecorded7,946casesofchlamydiaforallagesthroughoutthecity.Thisnumberdoubledto14,605by2002,andthecaseratefor15-to19-year-oldgirlswas8,251.8per100,000.Theseinfectionratesindicatedagrowingchlamydiaepidemicdisproportionaltootherlargecities.TheCommissionerofHealthsuggestedestablishingafirstannualschoolsystem-wideSTDscreeningprograminhighschoolsinhighmorbidityareas.ThechiefexecutiveofficerofthePhiladelphiaSchoolDistrictdirect-edallhighschoolstoparticipatetoavoidstigmatizinganygroupofschools.In2003,CDCprovidedfundingforthescreeningprogram. Duringthefirstyear,thehealthdepartmentpresentededucationalsessionstostudentsin53ofthecity’s 54 public high schools.Voluntary urine-based screening was offered immediately followingeachpresentationand treatmentwasprovided ineachschoolapproximately7-to-10daysafter thescreening.Duringthe2004–05schoolyear,thethirdyearoftheprogram,16,378studentsweretested;ofthose,680or4.2percentwerepositiveforchlamydia,gonorrheaorboth,adecreaseof21percentfromthe5.3percentwhotestedpositivein2002–03.25
Faith- and Community-Based Initiatives
Faith-basedeffortshavebeenasuccessfulapproach toreachingminoritycommunities—particu-larlyAfrican-Americancommunities.Localchurchesbringalevelofcomfortwhentheyaddresstherisingepidemicthatisdisproportionatelyaffectingminorities. Community-basedorganizations, like faith-basedorganizations, canprovidehighly tailoredpro-gramstomeetthespecificneedsofthecommunity.Someexamplesinclude:
InstituteforPublicHealthFaithCollaboration/InterfaithHealthProgram(IHP)buildsanddevel-opsbroadnetworksforlearningwithinandacrosshealthandfaithsystemslocally,nationallyandglobally. Interdisciplinary academic working groups link government, religious organizations,academicinstitutions,foundationsandcommunitypartnerstoconfrontissuessuchasteenpreg-nancy,HIV,elderissuesandcancer.26
TheBalminGileadisanonprofit,nongovernmentalorganizationthatbringstogethermorethan17 major church denominations, caucuses, coalitions and independent churches to respond totheAIDScrisisintheAfrican-Americancommunity.IthasestablishedandcontinuestodevelopeducationalandtrainingprogramstomeettheneedsofAfrican-AmericanchurchesthatstrivetobecomecentersforAIDSministry,educationandcompassion.27TheNationalLatinaHealthNetworkbeganin1989asagroupofLatinaprofessionalsinpublichealthwhowantedawaytoinvolveLatinaleaders inHIVprevention.Therearecurrentlysixregional offices and more than 1,500 members, including health professionals, educators andthemedia.SeveraloftheprogramstopromoteHIV/AIDSawarenessinvolvepeereducatorsandstorytelling—atraditioninHispaniccommunities—tospreadawareness.Ayouthadvisorygroupmadeupofyoungwomenages16–24helpensureallmaterialsareageappropriate.28TheHealingLodgeisafaith-basedecumenicalorganizationlocatedinRobesonCounty,N.C.,thatreceivesSEEsupportforsyphilisscreening.Ithasbeeninstrumentalinprovidingrisk-reduc-tioncounselinganddrugrehabilitationservicesforwomenengagedinhigh-risksexualactivities.Asaresult,therateofinfectioussyphilisin2004inthecountywas12.7per100,000people,downfrom47per100,000in2000.29
n
n
n
n
�0
Conclusion LegislatorscanjoinwithothergroupstoaddresslocalHIVandSTDpreventioneffortstargetingpopulationsmostatriskintheirstatesorcommunities.WhiletherearemanyprovenHIVandSTDpreventionstrategies,therearealsochallengestoimplementingthem,includingstigma,privacycon-cernsandstatelawsrestrictingsomeeffortssuchaspartnernotification.LegislatorsshouldbeawareofSTDtrendsamongpopulationsintheircommunitiesandtheobstaclestopeoplegettingpreventionandtreatmentservices. Whilethefederalandstategovernmentsplayamajorroleinpreventionandtreatmentefforts,therearemanyothergroupswhocanplayarole.Localhealthdepartments,physicians,schoolsandfaith-basedorganizationscanbeinvitedtothetabletohelpplanandimplementpreventionprograms.Leg-islatorscanserveasfacilitatorsofthesecoordinatedefforts.
��
Endnotes1NationalAllianceofStateandTerritorialHealthDirectors.“AddressingHIV/AIDS…La-tinoPerspectives&PolicyRecommendations.”Accessedfromwww.nastad.org/pro_hiv_pre-vention.asp?menu=proJanuary30,2006.2U.S.DepartmentofHealthandHumanServices,HealthResourcesandServicesAdminis-tration.“RyanWhiteCareAct.”Accessedfromhttp://hab.hrsa.gov/history.htmJanuary30,2006.3U.S.DepartmentofHealthandHumanServicesHealthResourcesandServicesAdminis-tration,HIV/AIDSBureau.“TheAIDSEpidemicandtheRyanWhiteCAREAct.”Accessedfromhttp://hab.hrsa.gov/publications/progress05/December28,2005.4TheKaiserFamilyFoundation.“HIV/AIDSPolicyFactSheet.”Accessedfromwww.kff.org/hivaids/treatment.htmDecember15,2005.5CentersforDiseaseControlandPrevention.“TheChangingEpidemic:HowisCDCRe-sponding?”Accessedfromwww.cdc.gov/hiv/resources/reports/hiv3rddecade/print/chapter3.htmApril7,2006.6 Centers for Disease Control and Prevention. “Questions andAnswers:Advancing HIVPrevention.”Accessedfromwww.cdc.gov/hiv/topics/prev_prog/AHP/resources;qa/question.htmApril7,2006.7 Centers forDiseaseControlandPrevention.Accessedfromwww.cdc.gov/hiv/ partners/question.htmNovember11,2005.8 Centers for Disease Control and Prevention.Accessed from www.cdc.gov/hiv/partners/AHP/Progress_2005.htmNovember11,2005.9Elliott,VictoriaStagg.“Morebackingforbroad,routineHIVtesting..”American Medical News(March28,2005):25–28.10Paltiel,A.David;Weinstein,MiltonC.;Kimmel,AprilD.;Seage,GeorgeR.III;Losina,Elena;Zhang,Hong;Freedberg,KennethA.;Walensky,RochelleP.“ExpandedScreeningforHIVintheUnitedStates–AnAnalysisofCost-Effectiveness.”The New England Journal of Medicine(February10,2005).11CentersforDiseaseControlandPrevention.“MinorityAIDSInitiative.”Accessedfromwww.cdc.gov/programs/hiv08.htmApril7,2006.12CentersforDiseaseControlandPrevention.“FACTSHEET-CDC’sUpdatePlantoElimi-nateSyphilisintheUnitedStates.”Accessedfromwww.cdc.gov/stdconference/2006/media/SEE-fact-sheet.htmJuly10,2006.13CentersforDiseaseControlandPrevention.SexuallyTransmittedDiseaseSurveillance,2004.Atlanta,GA:U.S.DepartmentofHealthandHumanServices,September2005.ThisreportisalsoavailablebyInternetviatheCDChomepageat:www.cdc.gov/std/stats/.14CentersforDiseaseControlandPrevention.“FACTSHEET-CDC’sUpdatedPlantoElim-inateSyphilisintheUnitedStates.”Accessedfromwww.cdc.gov/stdconference/2006/media/SEE-fact-sheet.htmJune6,2006.15AssociationofStateandTerritorialHealthOfficials.“TheUseofHIV/AIDSSurveillanceDataforPrevention,Care,Policy,ResearchandEvaluation:AFocusonFlorida,Washington,Alabama,andWyoming.”Accessedfromwww.astho.orgJanuary25,2006.16AssociationofStateandTerritorialHealthOfficials.“BreakingtheGlass:PublicHealthStrategiestoConfronttheEvolvingEpidemicsofHIVandSTDTransmissionandMetham-phetamineUseAmongMenWhoHaveSexwithMen.”Accessedfromwww.astho.org/pubs/MSM_MethSept05.pdfFebruary2,2006.17Hooker,T.andSpeissegger,S.PublicHealth,ALegislator’sGuide.NationalConferenceofStateLegislatures,Denver,CO,2002.18Ibid.19Elliott,VictoriaStagg.“OnlineservicesofferSTDtests,accesstoresults.”American Med-ical News(April18,2005):38.20CentersforDiseaseControlandPrevention,DivisionofHIV/AIDS,STDandTBPreven-tion.NewYorkStateProfile.Accessedfromwww.cdc.gov/nchstp/od/stateprofiles/usmap.htmJune6,2006.21 CentersforDiseaseControlandPrevention,DivisionofHIV/AIDS,STDandTBPre-vention.Illinoisstateprofile.Accessedfromwww.cdc.gov/nchstp/od/stateprofiles/usmap.htmJune6,2006.22CentersforDiseaseControlandPrevention.“YouthRiskBehaviorSurveillance—YouthOnline:ComprehensiveResults,2005.”Accessedfromhttp://apps.nccd.cdc.gov/yrbss/Cat-egoryQuestions.asp?Cat=4&desc=Sexual%20BehaviorsJuly13,2006.
��
23EducationalMaterialsCenter.“2004ComparisonofPreviousandCurrentLaws.”Accessedfromwww.emc.cmich.edu/HIV/pdf/comparison.pdfJanuary26,2006.24EducationalMaterialsCenter.“PolicytoPromoteHealthandPreventDiseaseandPregnancy,StateofMichiganStateBoardofEducation.”Accessedfrom:www.emc.cmich.edu/HIV/pdf/D.pdfJanuary26,2006.25 Fisman, David N.; Spain, C.Victor;Asbel, Lenore; Goldberg, Martin; Salmon, Melinda; andNewbern,E.Claire;“HighSchool-BasedScreeningforChlamydiainPhiladelphia:IdentificationofCost-SavingsUsingaDynamicTransmissionModel.”Presentationatthe2005annualmeetingoftheSocietyforMedicalDecisionMaking.Accessedfromhttp://smdm.confex.com/smdm/2005ca/techpro-gram/P1953.htmJanuary26,2006.26IHPNet.“TheInterfaithHealthProgram:Whoweare,whatwebelieve,andwhyweexist.”Ac-cessedfromwww.ihpnet.org/4about.htmJanuary30,2006.27TheBalminGileadInc.Accessedfromwww.balmingilead.org/about/about.aspFebruary1,2006.28NationalLatinaHealthNetwork.Accessedfromwww.nlhn.net/index.phpFebruary6,2006.29TheHealingLodge.Accessedfromwww.thehealinglodge.org/July10,2006.
�
HIV/AIDS and STD Prevention Efforts:How Legislators Can Act
Preventing HIV/AIDS & Sexually Transmitted Diseases
HIV/AIDS STD K
ü
ü
ü
State legislatorscanadvanceefforts topreventandcontrolHIV/AIDSandother sexuallytransmitteddiseases(STDs)inanumberofways—fromsupportinglegislativechangestobe-cominganadvocatefortheconstituentsaffectedbyorinvolvedinpreventionefforts.HereareeightwayslegislatorscanmakeadifferenceinHIV/AIDSandSTDprevention.
The Prevention Checklist for State Health Policymakers
Become Informed About State Policies Affecting HIV and STD Prevention EverystatepublichealthdepartmenthasastateAIDSdirectorandastatedirectorforSTDPreventionwhoisknowledgeableaboutthelaws,regulationsandpracticesthatinfluencehowHIV/AIDSandSTDcasesarereportedandhowpreventionactivitiesarecarriedoutintheirstate.CentersforDiseaseControl(CDC)summariesofstate-by-statepreventionactivitiesandcontactscanbeobtainedat:www.cdc.gov/nchstp/od/stateprofiles/usmap.htm. Onenotableactivitybeingimplementedineverystate is the“AdvancingHIVPrevention:NewStrategiesforaChangingEpidemic”Initiative.InApril2003,CDC,inpartnershipwithotherfederalagencies,launchedthisinitiativeconsistingoffourkeysstrategies:
MakevoluntaryHIVtestingaroutinepartofmedicalcare.ImplementnewmodelsfordiagnosingHIVinfectionsoutsidemedicalsettings.PreventnewinfectionsbyworkingwithpersonsdiagnosedwithHIVandtheirpartners.FurtherdecreaseperinatalHIVtransmission.
Throughyourstatehealthdepartment,youcandeterminehowthiscomprehensiveinitiativeisbeingimplementedinyourstate.
Reduce Barriers to Screening for HIV Through Legislative or Regulatory Change BarriersthatpreventpeoplefromgettingtestedforHIV,suchaswrittenconsentrequirementsbeforetestingandlimitationsonpartnernotification,maybemodifiedthroughregulatoryorlegislativechange.Forexample:
FloridaSB186 (enacted2005) allowed rapid testing, testingwithoutwritten consent ofpregnantwomenandthereportingofHIV-exposedinfantsafterbirth.
Make HIV Testing A Routine Part of Medical Care StatehealthpolicymakerscansupporteffortstomakeHIVtestingapartofroutinemedicalcareby:
Workingcloselywithandeducatinghealthcareprovidersabouttheimportanceofincor-poratingHIVtestingintocurrentservices,particularlyproviderstreatingpatientsathighriskofHIVinfection;1
Conductingeducationalandanti-stigmaprogramstoencouragethepublictobetestedforHIVinfectionandknowtheirHIVstatus;2and
n
n
n
n
n
n
n
�
ü
ü
ü
WorkingwithstatecorrectionalfacilitiestotestforandtreatHIVinfectionsamonginmates.
Legislatorsalsocanhelpmakescreeningtestsapartofroutinemedicalcarethroughsupportforpoliciesorlegislationthattargetsspecialorhigh-riskpopulations.Forexample:
NewJerseyHB164(proposed2005)supportedinsurancecoverageforcounselingservicesforpregnantwomenwhotestpositiveforHIV,allowingforfollow-upcareaftertesting.CaliforniaAB1142(enactedin2005)establishedastatewideinitiativetoaddressthedispropor-tionateimpactofHIV/AIDSonthehealthofAfrican-Americansthroughcoordinatedpreventionandserviceprovidernetworksinthestate,andtoincreasethecapacityoftheseserviceproviders.Toencouragescreeningofhigh-riskpopulations,MinnesotaHB1373(introduced2005)soughttocreateandfundanAIDSpreventioninitiativeforAfrican-bornMinnesotans,andOhioHB44(introduced2005)proposedcreatingaminorityHIV/AIDS task force todevelopapreventionprogramtargetingat-riskgroups.
Require Insurance Coverage for HIV and STD Screening Programs ConsiderexpandingMedicaidandstateemployeehealthbenefitcoveragetoincludescreeningsandconsiderrequiringprivateinsurerstoprovidecoveragetosupportCDC’srecommendationsfor:
HIVtestingforallat-riskpopulationsinthestate;Prenatal screening of all pregnant women for syphilis, which can have devastating effects onunbornchildren;andAnnualchlamydiascreeningforallsexuallyactivewomenage25andyoungertoavertpelvicinflammatorydisease,whichcanleadtoinfertility,ectopicpregnancyandchronicpain.Currently,onlythreestatesrequirecoverage—Georgia,MarylandandTennessee.3
Require Use of Confidential Name-based HIV Reporting If Your State Does Not Have This System AfterapositiveHIVdiagnosis ismade,stateandnationalsurveillancesystemsrelyonaccuratereportingofpositivecases.Toenableaccuratetrackingofaffectedpopulations,CDCrecommendsaconfidentialname-basedsurveillancesystemtoreportHIVinfections.AsofJune2006,44statesandtheU.S. territorieswereusingconfidentialname-based reportingofHIV infection.The remainingstatehealthdepartmentsuseothermethodsofreporting.4,5 The RyanWhite ComprehensiveAIDS Resources EmergencyAct (RWCA)—federal legislationwhichhelpsmeettheneedsofthoselivingwithHIV/AIDS—requiresthatbynolaterthan2007,fund-ingwillbedeterminedbythenumberofHIVcases(notAIDScases)reportedtotheCDC.Asare-sult,severalstatesarenowconsideringchangingfromcode-basedtoname-basedHIVcasereporting.Name-basedHIVreportingprovidesamoreaccurateandreliablepictureoftheepidemic.BecauseCDConlyacceptsname-basedHIVreporting,statesstandtolosefundingunderRWCAiftheyfailtoadoptthesesystems. FloridaaddedtoitsHIVcasereportingrequirementsthrough2005legislationthatrequiresreport-inglabresultsthatindicatehowfarthediseasehasprogressedtowardAIDS.ItalsoallowsthestatetoreportHIVexposureinnewborns.ThisenablespolicymakerstohavemorespecificinformationonwhoisaffectedbyHIVintheirstatesandtoplanappropriateaction.
Remove Legislative and Regulatory Barriers To Expedited Partner Therapy for Treatment of Partners of Patients Diagnosed With Some STDs EffectiveclinicalmanagementofpatientswithtreatableSTDsrequirestreatmentof thepatients’currentsexpartners toprevent reinfectionandstopfurther transmission.Thestandardapproach topartnertreatmenthasincludedclinicalevaluationinahealthcaresetting,witheitherthepatientorhealthcareprovideralertingpartnersof theirpotentialexposure.Theusualalternative is toadvisepatientstorefertheirpartnersfortreatment. In recent years, research supported by the CDC has evaluated expedited partner therapy (EPT),anapproachwherepartnersaretreatedwithoutaninterveningclinicalassessment.EPTtypicallyisaccomplishedbypatientsdeliveringeithermedicationsorprescriptionstotheirpartners.EPTisper-missibleinonlyfivestates,thoughitmaybepossibleinasmanyas33additionalstateswithsomeregulatoryoradministrativeaction.
n
n
n
n
n
n
n
�
When working with community organizations, it is important to include all the relevant organi-zations, keep the discussion progressing toward a specific outcome and have a timetable to com-plete the work and determine next steps. Key participants in a prevention coalition include:
Local health department staff and state health department program experts who will know the number of affected individuals in the com-munity and the populations at high risk for contracting and transmitting the diseases.Representatives from community-based HIV and STD prevention programs, which provide educational and testing/counseling services, or those that are directed to particular segments of the community, such as parents of African-American youth. Private health care providers, such as family physicians and obstetrician-gynecologists, psy-chotherapists and counselors, dentists and so-cial workers who identify and report cases of HIV or STD infection.Representatives of local drug treatment cen-ters, who have experience reaching out to drug users.Instructors or administrators of school and youth-based programs who are sensitive to local concerns about sexual risk behaviors among youth.Faith-based leaders, who are effective in reaching minority communities in prevention efforts and can bring a level of comfort to those unaccustomed to addressing the rising epidemic that disproportionately affects mi-nority communities.
n
n
n
n
n
n
Key People to Include in a Coalition to Support Prevention
ü
ü
Since 2005, the CDC has strongly encouraged local and state healthdepartmentsandpolicymakersinterestedinSTDpreventiontoworkto-gethertoresolvetheoutstandinglegalissuesandfindwaystoimplementthis proven prevention strategy. Some states, such as California, havepassed legislation topermitEPT;other states, such asTennessee, haveimplementedregulationstopermitthepractice.
Assure That Youth Are Educated About HIV/AIDS and STD Prevention Schooldistrictscanauthorizeschools toprovideage-appropriateandmedicallyaccurateHIVandSTDpreventioneducationaspartofcompre-hensivehealtheducation.Districtsalsocanbeencouragedtocollaboratewithparentgroupsandcommunityorganizationsondeterminingthescopeandcontentofcurricula.Stateeducationdepartmentsprovideleadershipfor theseeffortsbysupporting interagencypartnershipsandcurriculumdevelopment,andrequiringaccountabilityforlearningoutcomes. Atthelocallevel,legislatorscanprovideleadershipforthesecollabora-tions,whichmayincludeparentorganizations,healthdepartments,hos-pitals,medicalproviders,communityandfaith-basedorganizations,busi-nessesandeducationalorganizations.Somestatelegislatureshavetakenspecificactiontosupporttheseefforts:
In2004,Michiganstrengthenedtheroleofparentsinoverseeingsex-ualityeducationin theirchildren’sschools throughparentadvisoryboards.TheMichiganDepartmentofEducationdevelopedaparents’surveyforschooldistrictstousetoassessopinions.Italsoprovidesmodelcurriculafordifferentgradelevelsandrequiresthedistrictstosetgoalsandobjectivesforstudentknowledgeandskills.6In2004,WashingtondirectedtheDepartmentsofEducationandHealthtodevelopvoluntaryguidelines for school districts on sexual healthinformationanddiseaseprevention.Completedin2005,theguidelinesweredevelopedtoassurethatmedicallyaccurateinformationwasin-cludedinthecurriculum.
Work Locally To Keep HIV/AIDS and STD Prevention On Your State’s Public Health Agenda Inadditiontolegislativeandregulatoryefforts,statelegislatorsalsocantakeimportantleadershiprolesinkeepingHIV/AIDSandSTDpreventionissuesontheirstate’spublichealthagenda.Forexample,legislatorscan:
Usetheirpowertoconvene.Aselectedpublicofficials,statelegisla-tors arepositioned to call ongovernment, business andcommunityleaderstoworktogethertobringattentiontoanissueandtosearchforcommonsolutions.Statelegislatorscancallforcommitteehear-ingsonpreventioneffortsandholdtownhallmeetingsontheissue.By speakingpubliclyabout the importanceofHIV/AIDSandSTDprevention,theycanhelpadvanceawarenessofandsupportforpre-ventionefforts.Help neighborhoods and communities mobilize resources. In anylocal community, state legislators canhelp tobuilda coalitionofcommunity support for prevention efforts by bringing togetherneighborhoodleaders,healthcareproviders,educators,faith-basedorganizationsandpublicofficials.7
WorkingwithindividualswhohavebeeninfectedwithHIVorotherSTDsisimportantwhenplanningcommunity-basedprogramstomeettheirneedsandwhenenlisting theircooperation inpreventionefforts.Programsneedtobeculturallyappropriateforthosegroupsdispropor-tionatelyaffected.
n
n
n
n

�
Summary LegislatorscanhaveapositiveimpactinthepreventionandcontrolofHIV/AIDSandotherSTDs.TheycaneducateothersaboutthecurrentissuessurroundingHIVandSTDs,helpformtaskforcesorcommitteestoidentifysolutionsanddraftlegislationtoaddresstheissues.Al-though theproblemspresentedby thesediseases are serious, approaches such as expeditedpartner therapy, routinescreeningandbasicSTDpreventionprogramscanhelp.Legislatorsmustsimplymakeanefforttohelpraiseawareness,focusscarceresourcesandleadlocalandstatecommunitypartnerships.
Endnotes1 AssociationofStateandTerritorialHealthOfficialsIssueReport.“MakingHIVTestingaRoutinePartofMedicalCare:TheStateHealthAgencyRole.”February2005.Availableatwww.astho.org.2Ibid.3KaiserFamilyFoundation.“StateMandatedBenefits:AnnualChlamydiaScreening,2001.”Accessed from www.statehealthfacts.org/cgi-bin/healthfacts.cgi?action=compare&category=Women%27s+Health&subcategory=Mandated+Benefits+in+Private+Insurance&topic=Chlamydia+ScreeningJune6,2006.4CentersforDiseaseControlandPreventionHIV/STD/TBPreventionNewsUpdate.“AIDS:NotAnonymous?”Accessed from www.cdcnpin.org/scripts/locates/LocateNews.asp January5,2006.5 The Kaiser Family Foundation. “HIV Name/Code-Based Reporting Policies, 2005.”Ac-cessedfromwww.statehealthfacts.kff.org/cgi-bin/healthfacts.cgi?action=compare&category=HIV%2fAIDS&subcategory=HIV+Testing&topic=Name%2fCode%2dBased+Reporting Feb-ruary1,2006.6CouncilofChiefStateSchoolOfficers,“WhatEducationLeadersShouldKnowaboutForm-ing Partnerships to Prevent Sexual Risk Behaviors in SchoolAgedYouth,” 2005.Accessedfromwww.ccsso.org/content/pdfs/HIVFactsheetPartnerships.pdfFebruary5,2006.7Carlson,ChristineandWolf,Greg.“ThePowertoConvene,”State News,November/Decem-ber2005.
�
HundredsofthousandsofAmericansarediagnosedeachyearwithanSTD.Chlamydia infections reported to the Centers for Disease Control and Prevention (CDC) rose to more than 929,000 cases in 2004. This was an almost 6 percent increase from 2003. The number of primary and secondary syphilis infections has increased yearly since 2000, with almost 8,000 cases reported in 2004, an increase of 11 percent from 2003. Early treat-ment of these cases can save lives.The number of reported cases of gonorrhea dropped in 2004 to its lowest level ever—about 330,000 cases.
Althoughsustainedtreatmenteffortsoverthepast20yearshavereduced thenumberofAIDScasesanddeaths,HIVandAIDSarestillmajor problemsintheUnitedStates.
CDC estimates that currently 1 to 1.2 million people in the U.S. are infected with HIV, the virus that causes AIDS. Although the number of people dying from AIDS has decreased due to new drug thera-pies, the number of people being infected yearly with HIV—an estimated 40,000—has remained stable for more than a decade despite ongoing prevention efforts.
CommunitiesofcolorarethehardesthitbyHIV/AIDSandotherSTDs.African-Americans accounted for 50 percent of all new HIV/AIDS diagnoses in 2004, with African-American women and youth increasingly at risk of infection. In 2002, HIV/AIDS was the number one cause of death for African-American women age 25–34 years. In 2001, African-American youth were the largest group of young people affected by HIV, accounting for 56 percent of all HIV infections ever reported among the youth age group.In 2004, compared to whites, African-Americans were: six times more likely to have pri-mary or secondary syphilis; eight times more likely to have chlamydia; 16 times more likely to have congenital syphilis; and 19 times more likely to have gonorrhea.In 2004, compared to whites, Hispanics were: twice as likely to have primary or second-ary syphilis; twice as likely to have contracted gonorrhea; three times more likely to have chlamydia; and nine times more likely to have congenital syphilis.
HIV/AIDSandotherSTDshavetakenaheavytollonthosewhoareinfected andstategovernments,whicharebearingpartofthecostsfortreatment.
More than 500,000 people have died from AIDS through 2004.If left untreated in pregnant women, syphilis results in the death of the fetus in up to 40 per-cent of cases.The direct medical costs of HIV/AIDS and STDs are estimated at $13 billion annually. This total does not include lost wages and productivity, out-of-pocket expenses or the costs associ-ated with transmission of diseases to infants.
n
n
n
n
n
n
n
n
n
n
n
n
n
Talking Points:HIV/AIDSandSTDPrevention
Preventing HIV/AIDS & Sexually Transmitted Diseases
HIV/AIDS STD K
þ
þ
þ
þ

2
What State Legislators Can Do: Advance Prevention Efforts Through Legislation and Regulation
Reduce barriers to screening for HIV, such as written consent requirements before testing and limitations on partner notification stipulated by state laws and regulations.
Support STD prevention activities, such as annual chlamydia screening for sexually active women under age 26.
Support HIV testing as part of routine medical care through policy or legislation.
Provide insurance coverage for HIV and STD screening through Medicaid and state em-ployee health benefits, and consider requiring private insurers to offer coverage.
Explore changing to confidential name-based reporting of HIV cases if your state is not already doing so. Although this is recommended by the CDC, only 44 states were using this system as of June 2006. States could potentially receive reduced funding in Ryan White CARE resources in 2007 if they are not using an integrated name-based HIV/AIDS report-ing system.
Support expedited partner therapy for STD treatment as recommended by CDC through adjustments to practices, regulations or laws, depending on the specific barriers present in your state.
Support state education department tools for HIV/AIDS and STD prevention education through collaboration with school districts, parent organizations and community groups.
Take On Community Leadership Roles to Support Prevention
Use the power to convene. State legislators are positioned to call on government, business and community leaders to work together to bring attention to an issue and search for com-mon solutions. State legislators can call for committee hearings on prevention efforts and hold town hall meetings. By speaking publicly about the importance of HIV/AIDS and STD prevention, they can help advance awareness of and support for prevention efforts.
Help neighborhoods and communities by mobilizing resources. In any local community, state legislators can help to build a coalition of community support for prevention efforts by bringing together neighborhood leaders, health care providers, educators, faith-based orga-nizations and public officials.
n
n
n
n
n
n
n
n
n
�
Centers for Disease Control and Prevention ResourcesNational Center for HIV, STD and TB Prevention (NCHSTP), Centers for Disease Control and Preventionwww.cdc.gov/nchstp/od/nchstp.html
The mission of the Division of HIV/AIDS Prevention at the Centers for Disease Controland Prevention is to prevent HIV infection and reduce the incidence of HIV-related illnessanddeath,incollaborationwithcommunity,stateandnationalpartners.TheDivisionofSTDPreventionprovidesnationalleadershipthroughresearch,policydevelopmentandsupportofeffectiveservicestopreventsexuallytransmitteddiseasesandtheircomplications.
State profiles:Toviewaprofileofyourstate,whichincludesthenumberofSTDandAIDScases,howyourstaterankswhencomparedtotherestofthecountry,programsfundedbytheCDCandwhotocontactformoreinformation,visit:www.cdc.gov/nchstp/od/statepro-files/usmap.htm.
National Network of STD/HIV Prevention Training Centers http://depts.washington.edu/nnptc/
TheNationalNetworkofSTD/HIVPreventionTrainingCenters(PTCs)isaCDC-fundedgroupofregionalcenterscreatedinpartnershipwithhealthdepartmentsanduniversities.ThePTCsarededicatedtoincreasingtheknowledgeandskillsofhealthprofessionalsintheareasofsexualandreproductivehealth.
National Prevention Information Network (NPIN)www.cdcnpin.org/scripts/index.asp
TheNationalPreventionInformationNetwork(NPIN)isaserviceoftheCDCandservesasthenation’slargestcollectionofinformationandresourcesonHIV,STDandTBprevention.
Other Health and Human Services Resources
Health Resources and Services Administration (HRSA)www.hrsa.gov
TheHIV/AIDSBureau(HAB)oftheHealthResourcesandServicesAdministration(HRSA)wasformedinAugust1997toconsolidateallprogramsfundedundertheRyanWhiteCompre-hensiveAIDSResourcesEmergencyAct.ThisprogramfundstreatmentservicesforHIV/AIDSpatientsinthestates.Informationonstateagenciesbenefitingfromfunding,examplesoffund-ingopportunitiesandmoreisavailableat:www.hab.hrsa.gov/tools/progressreport/ and www.hrsa.gov/grants/preview.
n
Resource List
Preventing HIV/AIDS & Sexually Transmitted Diseases
HIV/AIDS STD K
�
The Leadership Campaign on AIDSwww.osophs.dhhs.gov/aids/tlcapage1.html
In 1999, theOfficeofHIV/AIDSPolicy in theU.S.Department ofHealth andHumanServiceslaunchedTheLeadershipCampaignonAIDS(TLCA),whichworkswithbothprivatesectorpartnersandfederalagenciestosupportthefightagainstHIV/AIDSincommunitiesofcolor.
National Institutes of Health-National Institutes of Allergy and Infectious Diseases (NIAID)www.niaid.nih.gov
NIAIDsupportscomprehensiveclinicalresearchtoevaluatetreatmentandpreventionstrategiesforHIV/AIDSanditsassociatedcomplicationsandco-infectionssuchasSTDs.
Office on Minority Health Resource Center (OMHRC)www.omhrc.gov
ThemissionoftheOfficeofMinorityHealthistoimproveandprotectthehealthofracialandethnicminoritypopulationsthroughthedevelopmentofhealthpoliciesandprogramsthateliminatehealthdisparities.ItadvisesthesecretaryoftheU.S.DepartmentofHealthandHumanServicesandtheOfficeofPublicHealthandScienceonactivitiesaffectingAmericanIndiansandAlaskaNatives,AsianAmeri-cans,Blacks/African-Americans,Hispanics/Latinos,NativeHawaiiansandotherPacificIslanders.
Substance Abuse & Mental Health Services Administration (SAMHSA)www.samhsa.gov
SAMHSA’smissionistobuildresilienceandfacilitaterecoveryforpeoplewithoratriskforsub-stanceabuseandmentalillness.SAMHSAaddressesincreasedaccesstohealthcarethroughSAMH-SA’sRapidHIVTestingInitiative(RHTI);theMentalHealthHIVServiceCollaborative(MHHSC)Program;andtargetedcapacityexpansioninitiativesforSubstanceAbusePrevention(SAP)andHIVpreventioninminoritycommunities.
�
National Professional Organizations
American Social Health Association (ASHA)www.ashastd.org
Since1914, theAmericanSocialHealthAssociationhasdedicated itself to improving thehealthofindividuals,familiesandcommunities,withafocusonpreventingsexuallytransmitteddiseasesandinfectionsandtheirharmfulconsequences.
Association of State and Territorial Health Officials (ASTHO)www.astho.org
TheAssociationofStateandTerritorialHealthOfficials(ASTHO)isthenationalnonprofitorganizationrepresentingstateandterritorialpublichealthagenciesoftheUnitedStates,U.S.territoriesand theDistrictofColumbia.ASTHOisdedicated to formulatingand influencingsoundpublichealthpolicyandassuringexcellenceinstate-basedpublichealthpractice.
National Coalition of STD Directorswww.ncsddc.org
TheNationalCoalitionofSTDDirectors,basedinWashington,D.C.,representsthe65di-rectorsofpublichealthsexuallytransmitteddiseasepreventionprogramsinstates,largecities/countiesandterritoriesoftheUnitedStates.Thegroup’sgoalistomakeSTDprogramsstrongerbyadvocatingeffectivepolicies,strategiesandsufficientresourcesandbyincreasingawarenessoftheirmedicalandsocialimpact.
National Alliance of State and Territorial AIDS Directors (NASTAD)www.nastad.org
NASTADisanonprofitnationalassociationofstatehealthdepartmentHIV/AIDSprogramdirectorsbasedinWashington,D.C.,thatprovidesHIV/AIDShealthcare,prevention,educationandsupportservicesprograms.Itisfundedbystateandfederalgovernments.
National Association of County and City Health Officials (NACCHO)www.naccho.org
NACCHOisthenationalorganizationbasedinWashington,D.C.,thatrepresentslocalpublichealthagencies. Itworks tosupportefforts thatprotectand improve thehealthofallpeopleandallcommunities.ItoffersaModelPracticeDatabase,whichisasearchablecollectionofpracticesacrosspublichealthareas,allowsprofessionalstolearnwhatworksandtoensurethatresourcesareusedwiselyoneffectiveprograms.
Other Organizations
The Ark of Refuge: HIV/AIDS Ministrywww.arkofrefuge.org
TheArkofRefuge, based inCalifornia, is a program targetinghigh-riskgroupsdesignedforpromotingAIDSeducationintheAfrican-Americancommunity.AnendeavoroftheCityofRefugeCommunityChurch,UnitedChurchofChrist,itwasdevelopedasanAIDSserviceorganizationthatrecognizestheroleofspiritualityintheAfrican-AmericancommunityandthenecessityofsustaininghopeforeveryoneaffectedbytheHIVepidemic.ItsgoalistoreducetheincidenceofHIVinfectionamongAfrican-AmericansbyempoweringchurchleaderstomeettheHIV/AIDSpreventionneedsoftheirmembers.
�
The Balm In Gileadwww.balmingilead.org/home.asp
TheBalmInGilead isanonprofit,nongovernmentalorganizationbased inNewYork thatbringstogethermorethan17majorchurchdenominations,caucuses,coalitionsandindependentchurchestorespondtotheAIDScrisisintheblackcommunity.Ithasestablishedandcontinuestodevelopeduca-tionalandtrainingprogramstomeettheneedsofblackchurchesthatstrivetobecomecompassionatecentersforAIDSministryandeducation.
Black AIDS Institutewww.blackaids.org
TheBlackAIDSInstitute,basedinCalifornia,isthefirstblackHIV/AIDSpolicycenterdedicatedtoreducingHIV/AIDShealthdisparitiesbymobilizingblackinstitutionsandindividualsineffortstoconfronttheepidemicintheircommunities.
Institute for Youth Developmentwww.youthdevelopment.org
TheInstituteforYouthDevelopment(IYD)isanonpartisan,nonprofitorganizationbasedinWash-ington,D.C.,dedicatedtoensuringthebestpossiblefutureforAmerica’schildrenbypromotingposi-tivechoicesandbehaviors.IYDwasawardedagrantfromthefederalU.S.DepartmentofHealthandHumanServicesundertheCompassionCapitalFundtoassistfaith-basedandcommunityorganiza-tionsincompetingforfederalgrants.
Kaiser Family Foundationwww.kff.org
TheHenryJ.KaiserFamilyFoundation,basedinWashington,D.C.,isanonprofit,privatelyoperatedfoundationfocusingonthemajorhealthcareissuesfacingthenation.Thefoundationsponsorspublica-tionsandprogramsonissuessuchasHIVPolicyProgram,theRace/EthnicityandHealthCareProgramandtheNationalAIDSDrugAssistanceProgramMonitoring.
National Minorities AIDS Council (NMAC)www.nmac.org
TheNationalMinorityAIDSCouncilisanationalorganizationbasedinWashington,D.C.,thatisdedicatedtodevelopingleadershipwithinthecommunitiesofcolortoaddressthechallengesofHIV/AIDS.
CSG’s Healthy States Initiative
Trends analysis, innovative responses and expert advice on critical public health issues for states.
www.healthystates.csg.org859.244.8000
CSG’s Healthy States InitiativeThe Council of State Governments’ (CSG) Healthy States Initiative is designed to help state leaders make informed decisions on public issues. The enterprise brings together state legislators, officials from the Centers for Disease Control and Prevention, state health department officials, and public health experts to share information, analyze trends, identify innovative responses, and provide expert advice on public health issues. CSG’s partners in the initiative are the National Black Caucus of State Legislators and the National Hispanic Caucus of State Legislators.
Funding for this publication is provided by the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, under
cooperative agreement U38/CCU424348.