Embed Size (px)
Citation preview

e413Intravitreal Ranibizumab in venous occlusion treatment
Testing the effectiveness of intravitreal Ranibizumab during
12 months of follow-up in venous occlusion treatmentE. Pacella¹, F. Pacella¹, G. La Torre², D. Impallara¹, K. Malarska¹, C. Brillante¹, P Turchetti³, M. De Giusti²
¹Department of Sense Organs, Faculty of Medicine and Dentistry, Sapienza University of Rome, ²Department of Public Health and
Infectious Diseases, Faculty of Pharmacy and Medicine, Sapienza University of Rome; ³National Institute for Health, Migration and
Poverty (INMP/NIHMP), Rome, Italy
Original article Clin Ter 2012; 163 (6):e413-422
Correspondence: Dr.ssa Elena Pacella. Department of Sense Organs, Faculty of Medicine and Dentistry, Sapienza University of Rome, Viale del
Policlinico, 00161 Rome, Italy. Tel.: +39.06.4997.5303; +39.336.783409; Fax: +39.06.49975304. E-mail: [email protected]
Copyright © Società Editrice Universo (SEU)
Introduction
Retinal vein occlusion (RVO) causes anatomical al-
terations of either an ischemic (ischemic or hemorrhagic
form) or non-ischemic nature (non-ischemic form or venous
stasis) in retinal tissue. We can divide RVO into two types:
branch retinal vein occlusion (BRVO) and central retinal
vein occlusion (CRVO).
Abstract
Aims. To determine the effectiveness and safety of treatment of
intravitreal Ranibizumab for Central Retinal Vein Occlusion.
Patients and Methods. This non-randomized observational clinical
study was comprised of a round of therapy with three IVI. Twenty eyes
affected by CRVO were recruited. The average age was 65.06 ± 15
years and criterion for inclusion: age >18 years, best Corrected Visual
Acuity (BCVA) from 5 to 40 letters and macular edema with thickness
greater than 275 µm. The criteria used for reinjection were: CMT> 150
µm, ETDRS <10 letters and LogMAR <0.2. The statistical analysis
for continuous variables (ETDRS, logMar and CMT) was conducted
calculating median and range (min-max), since these variables, due
to sample size, were not normally distributed.Time trends of these
variables were plotted with boxplot and differences.
Events between T0 and T12 were assessed using the analysis of
variance (ANOVA) for repeated measurements and the F test (Pillai’s
trace). The statistical significance was set at p ≤0.05.
Results. All of the patients showed improvement. In fact, the
ETDRS went from a median of 20.00 to 28.50, LogMAR went from
a median of 0.75 to 0.55 and the values for CMT went from a median
of 556.00 µm to 390.00 µm. The drug reaches maximum effectiveness
after two months of therapy, with T2 remaining constant from the third
injection at T3 until the end of 12 months at T12.
Conclusions. The results produced by our study indicate that Ra-
nibizumab is a valid treatment for CRVO. Clin Ter 2012; 163(6):e413-
422
Key words: Macular edema, Ranibizumab, Retinal vein and
vascular occlusion
International prevalence of RVO, standardized for age
and sex, is equivalent to 0.52% (0.442% for BRVO and
0.08% for CRVO) (1).
The risk of RVO reoccurring in the same eye is 0.9%
within two years and 7.7% in the contralateral eye (2).
Ninety percent of patients are over 50 years of age and this
could be explained by the strong relationship vein occlusion
has with pathologies typically discovered in people over
50: cardiovascular diseases (70% of cases), atherosclerosis
(50% of cases), diabetes mellitus (30% of cases) (3), arterial
hypertension (60%-65% of cases) (4) and glaucoma (20%
of cases).
These listed conditions, along with other risk factors
such as smoking and hyperlipidemia (5), are at the begin-
ning of a series of events that make up the pathogenesis of
vein occlusion. In fact, the first cause is the decrease in the
size of vein lumen followed by turbulence in blood flow
and vein thrombosis. The result is an increase in central
pressure, hemorrhage, ischemia and production of vascular
endothelial growth factor (VEGF) which, in turn, stimulates
capillary neoangiogenesis with the formation of macular
edema due to endothelial damage and rupturing of blood-
retinal membranes (6).
Macular edema results in the accumulation of fluid in the
outer plexiform and inner nuclear layers of the perifoveal
area and is responsible for the increase in macular thickness
and the reduction of visual acuity (7).
In scientific literature, different therapeutic approaches
have been reported especially for handling complications
secondary to macular edema: laser (8), systemic (9-10)
or surgical treatments (11-15); topical steroids (16, 17);
intravitreal injections with steroids (18-20); or intravitreal
injections with anti-VEGF (2).
Our study takes into consideration the intravitreal admi-
nistration of Ranibizumab as an anti-VEGF molecule (21).
Ranibizumab is a humanized antibody fragment directed
towards vascular endothelial growth factor A (VEGF-A)
(22) with high binding affinity for the isoforms VEGF110,
VEGF121 and VEGF165. Its pharmacodynamic action in-
volves blocking the binding of these factors to VEGFR-1 and

e414 E. Pacella, et al.
VEGFR-2 receptors, therefore preventing the proliferation
of endothelial cells, neovascularization, and the increase of
vessel permeability.
The objective of this study is to evaluate the effectiveness
and safety of macular edema treatment secondary to CRVO
during 12 months of follow-up.
Patients and Methods
We conducted a non-randomized clinical study upon
receiving approval from the ethics committee at the Reti-
na Center at the Umberto I General Hospital, “Sapienza”
University of Rome, Italy). In particular, 20 patients were
recruited (for a total of 20 eyes) including: 9 males and 11
females with an average age of 65.06 ± 15 years who had
been suffering from central retinal vein occlusion for 4
weeks to 3 months.
Inclusion criteria
– Willingness to provide signed Informed Consent Form
– Age ≥18 years
– For sexually active women of childbearing potential, use
of an appropriate form of contraception (or abstinence)
for the duration of the study
– Ability and willingness to return for all scheduled visits
and assessments.
Ocular inclusion criteria and injection criteria (Study Eye)
– Foveal center-involved macular edema secondary to
CRVO
– BCVA using ETDRS charts of 20/40 to 20/320 (Snellen
equivalent)
– Mean central subfield thickness ≥ 250 µm on two optical
coherence tomography (OCT) measurements (at scree-
ning [confirmed by the central reading center] and Day
0 [confirmed by the evaluating physician])
– Media clarity, pupillary dilation, and participant coope-
ration sufficient to obtain adequate fundus photographs
with visual acuity from five letters (corresponding to
1/10, LogMar 1.0 or higher) to 40 letters (corresponding
to 5/10, LogMar 0.3 or less) and macular edema with
thickness over 275 µm. Before the first injection (T0),
initial best-corrected visual acuity (BCVA) had a median
of 20 letters (LogMar 0.75) and central macular thickness
(CMT) had a median of 556 µm. An eye exam at T0
showed superficial hemorrhages in the four quadrants,
macular edema, cotton-like snowballs, venous turgidity
and coiling and signs of A-V crossing. Five patients
showed moderate edema of the optic disc.
Intravitreal injection with Ranibizumab was carried out
without distinction between ischemic and non-ischemic
forms of CRVO since the FAG was performed two months
after onset for patients suffering less than four weeks. Me-
anwhile, retinal alterations made it impossible to distinguish
between the type of occlusion in patients who had been
suffering for more than four weeks.
Exclusion criteria
– History of cerebral vascular accident or myocardial
infarction within 3 months prior to Day 0; any anti-
vascular endothelial growth factor (VEGF) or treatment
in the fellow eye within 3 months prior to Day 0; any
systemic anti-VEGF or pro-VEGF treatment within 6
months prior to Day 0; allergy to fluorescein; allergy
to Ranibizumab injection or related molecule
– Relevant systemic disease that may be associated with
increased systemic VEGF levels (namely, all active ma-
lignancies); history of successfully treated malignancies
is not an exclusion criterion.
– Uncontrolled blood pressure
– Pregnancy or lactation
– Any condition that, in the opinion of the investigator,
would preclude participation in the study (e.g., chronic
alcoholism or drug abuse, personality disorder or use
of major tranquilizers, indicated difficulty in long-term
follow-up, and likelihood of survival of less than 1
year)
– Participation in an investigational trial within 30 days
prior to Day 0 that involved treatment with any drug
(excluding vitamins and minerals) or device that has not
received regulatory approval at time of study entry
Ocular exclusion criteria
– Prior episode of retinal vein occlusion (RVO)
– Brisk afferent pupillary defect
– History of radial optic neurotomy or sheathotomy; age-
related macular degeneration (AMD; dry or wet form);
any anti-VEGF treatment in the study eye within 3 mon-
ths prior to Day 0; laser photocoagulation for macular
edema within 4 months prior to Day 0; panretinal scatter
photocoagulation or sector laser photocoagulation within
3 months prior to randomization or anticipated within
the next 4 months following randomization; intraocular
corticosteroid use within 3 months prior to Day 0; pars
plana vitrectomy; intraocular surgery (including cataract
extraction, scleral buckle, etc.) within 2 months prior to
Day 0 or anticipated within the next 7 months following
Day 0; yttrium-aluminum-garnet capsulotomy performed
within 2 months prior to Day 0; herpetic ocular infection,
ocular toxoplasmosis, rhegmatogenous retinal detach-
ment, idiopathic central serous chorioretinopathy
– Previous filtration surgery in the study eye
– Evidence upon examination of vitreoretinal interface
disease (e.g., vitreomacular traction, epiretinal mem-
brane), either on clinical examination or OCT, thought
to be contributing to macular edema
– An eye that, in the investigator’s opinion, would not
benefit from resolution of macular edema, such as eyes
with foveal atrophy, dense pigmentary changes, or dense
subfoveal hard exudates
– Presence of an ocular condition that, in the opinion of the
investigator, might affect macular edema or alter visual
acuity during the study (e.g., uveitis or other ocular in-
flammatory disease, neovascular glaucoma, Irvine-Gass
syndrome, or prior macula-off rhegmatogenous retinal
detachment)
– Visually significant hemorrhage obscuring the fovea and
felt to be a major contributor to reduced visual acuity
– Presence of a substantial cataract that, in the opinion of
the investigator, is likely to be decreasing visual acuity
by 3 lines or more (i.e., a 20/40 cataract)
e415Intravitreal Ranibizumab in venous occlusion treatment
– Aphakia
– Relevant ocular disease that may be associated with
increased intraocular VEGF levels (namely, uveitis,
neovascular glaucoma, neovascular AMD, diabetic
retinopathy, diabetic maculopathy, or ocular ischemic
syndrome)
– Improvement of >10 letters on best corrected visual
acuity (BCVA) between screening and Day 0.
Medical history
The following was carried out on all patients: a thorough
look at general pre-operative medical history, cardiology
exam, ECG and hematochemical testing. The presence of
possible changes in homocysteine and the Leiden factor
was also particularly evaluated. In no cases were these
factors shown to be pathological. General medical history
highlighted the presence of risk factors such as smoking
(seven patients admitted to being habitual smokers) and
associated pathologies such as diabetes mellitus (in three
patients), essential arterial hypertension (in ten patients),
hypertriglyceridemia (in six patients) and hypercholestero-
lemia (in nine patients) (Table 1).
Treatment
Treatment was administered in the operating room
under sterile conditions injecting 0.5 mg of Ranibizumab
through the pars plana in the inferior-temporal sector, after
preparing the conjunctiva with povidone-iodine 50% solu-
tion, topical anesthesia with Ropivacaine and positioning
of the eyelid.
Re-injection criteria
– A round of therapy included three intravitreal injections
(one injection every four weeks) for all subjects.
– The criteria used for reinjection were: CMT >150 µm,
ETDRS <10 letters and LogMAR <0.2.
Evaluation
During the follow-up all patients underwent slit lamp
biomicroscopy and binocular indirect ophthalmoscopy.
IOP was evaluated using the Goldmann applanation
tonometer.
The BCVA score based on the ETDRS visual acuity
charts (number of correct letters) and assessed at a starting
distance of 4 meters.
Macular thickness and morphology were monitored at
T0- T1- T2- T3- T6- T9- T12 with OCT (OCT Spectralis
HRA-OCT from Heidelberg Engineering with a 512 x 49
volume scan) followed by color fundus photos.
Macular thickness and morphology were monitored
every four weeks (from T0 to T12) in patients with persistent
or recurring macular edema.
Generality
patients
included
General conditions associated INITIAL BCVA
Age Sex Smoking Hypercolesterolemia HypetrigliceridemiaDiabetes
mellitusHyertension
Etdrs
(letters)LogMAR
CMT
( µm)
54 M • • • • • 25 0,6 869
67 M • • • • 20 1 1042
54 M • • • 35 0,5 390
72 M • • • 25 0,7 510
65 M • • 54 0,2 329
59 M • • 19 1 1040
80 F • • • 7 1 900
56 F • • 21 1 1038
69 M • • • 24 0,6 860
57 M • • 26 0,7 506
70 F • • • 53 0,2 327
66 F • • • 18 1 1036
79 M • • • 8 1 902
63 M • • • 35 0,5 391
55 M • • • 25 0,7 503
73 M • • 24 0,6 862
64 F • • • • 20 1 1030
53 M • • • • 53 0,2 325
51 F • • • 18 1 1034
61 F • • • 20 1 1045
Age
average
63.4
±8.623
M/F
13/7
Total
patients
10
Total
patients
11
Total
patients
10
Total
patients
20
Total
patients
9
Average
etdrs
26.50
±
13.387
Average
logmar
0.7 ±
0.295
Average
CMT
746.95
±293.601
Table 1. General conditions.
e416 E. Pacella, et al.
The study group underwent 12 scheduled follow-ups (at
T0 upon admittance, three follow-ups after one week’s time
from each intravitreal injection at T1, T2 and T3, and nine
follow-ups during the following months after every four weeks
at T4, T5, T6, T7, T8, T9, T10, T11 and T12 respectively).
At T0, the following specific tests were carried out: visual
acuity examination, slit lamp biomicroscopy, tonometry,
direct and indirect ophthalmoscopy of the ocular fundus
and OCT.
Patients underwent ophthalmoscopy and tonometry
testing the day after injections.
During all follow-ups (from T1 to T12), the following
were evaluated: BCVA, biomicroscopy of the anterior and
posterior segments, and tonometry testing.
Safety
We can divide ocular implications related to intravitreal
administration of Lucentis into three categories: preopera-
tive, intraoperative and postoperative. Preoperative compli-
cations (tied to anesthesia by injection) are: perforation of
the ocular bulb, optic nerve lesions, eye muscle lesions and
palpebral, periocular or retrobulbar hemorrhages.
During treatment conjuctival lacerations, lesions of the
crystalline lens and vitreous and choroidal hemorrhage
may occur.
The postoperative complications are as follows: retinal
or choroidal detachment, endophthalmitis, alterations of the
macula, retinal and/or vitreous hemorrhages, vitreoretinal
proliferation, cataract, scleral rupture and scleromalacia,
hypertonia, the permanent or temporary reduction in eye
pressure, reduction of visual acuity, visual field defects,
strabismus, diplopia, myodesopsia, palpebral ptosis, optic
nerve atrophy and glaucoma.
Statistical analysis
The statistical analysis for continuous variables (ET-
DRS®, LogMar and CMT) was conducted calculating me-
dian and range (min-max), since these variables were not
normally distributed due to sample size.
Time trends of these variables were plotted with box plot
and differences between T0 and T12 were assessed using
the analysis of variance (ANOVA) for repeated measure-
ments using the F test (Pillai’s trace) (Table 2). Moreover,
the impact of the following factors was evaluated: gender,
diabetes mellitus, hypertriglyceridemia, hypercholestero-
lemia and arterial hypertension. The statistical significance
was set at p ≤0.05.
Results
Effectiveness
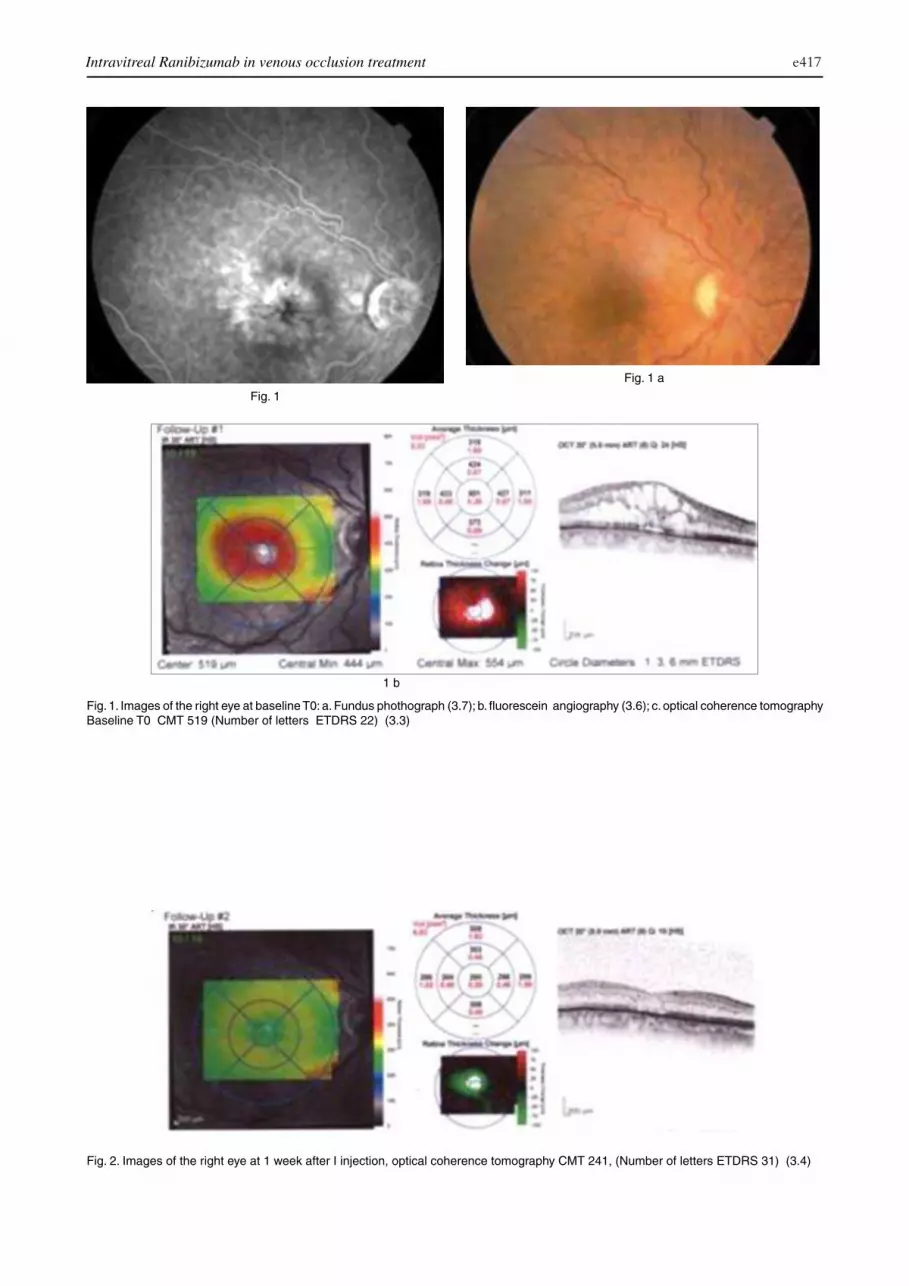
After one week from the first intravitreal injection (IVI)
at T1, visual acuity had a median of 29.50 (LogMar average
of 0.55) and CMT average of 44.60 µm (Fig. 1a and 1b and
Fig. 2).
After the second IVI (after five weeks of follow-up at
T2), we were able to observe a significant improvement in
function along with a consistent reduction of macular thick-
ness (ETDRS with a median of 35.00, LogMar value of 0.40
and CMT with a median of 301.50 µm) (Fig .3).
Following the third IVI (after nine weeks of follow-up
at T3), we found values for ETDRS with a median of 37.50,
LogMar at 0.40 and CMT with a median of 284.00 µm (Fig.
4a and 4b).
Patients, after being re-evaluated after 24 weeks from
the first IVI (after six months of follow-up at T6), were
observed to have values of ETDRS with a median of 35.00,
LogMar at 0.40 and CMT with a median of 313.50 µm (Fig.
5a and 5b).
During the follow-up after 36 weeks from the first IVI
(nine months of follow-up at T9), we found: ETDRS with a
median of 35.00, LogMar at 0.40 and CMT with a median
of 395.00 µm (Fig. 6a and 6b).
At T12 (12 months of follow-up), re-evaluation of all
parameters showed an overall worsening of both anatomic
and functional conditions (ETDRS with a median of 28.50,
LogMar at 0.55 and CMT with a median of 390.00 µm).
The response to treatment was independent of age, sex
and concomitant pathologies. The final reading of data has
allowed us to compare the variations in visual acuity and
CMT from T0 to T6. ETDRS went from a median of 20.00
to 28.50, LogMar went from a median of 0.75 to 0.55 and
CMT went from a median of 556.00 µm to 390.00 µm.
Safety
We did not encounter any preoperative, intraoperative or
postoperative complications in any of the patients.
ANOVA for repeated measurements
The ANOVA for repeated measurements revealed that
differences between T0 and T12 were statistically significant
for all the three variables considered (Table 2) (p <0.001;
Table 2. F-test (Pillai’s trace) and p-values for factor variables influencing trends of ETRDS, LogMAR and CMT.
Variables ETRDS logMAR CMT
Hypercholesterolemia 1.212 (p = 0.286) 0.764 (p = 0.685) 0.444 (p = 0.818)
Hypertriglyceridemia 0.941 (p = 0.510) 0.994 (p = 0.460) 1.151 (p = 0.493)
Diabetes mellitus 0.785 (p = 0.665) 0.585 (p = 0.849) 0.300 p = (0.903)
Hypertension 1.106 (p = 0.364) 0.774 (p = 0.676) 0.567 (p = 0.746)
Gender 0.575 (p = 0.858) 0.381 (p = 0.967) 2.145 (p = 0.284)
e417Intravitreal Ranibizumab in venous occlusion treatment
1 b
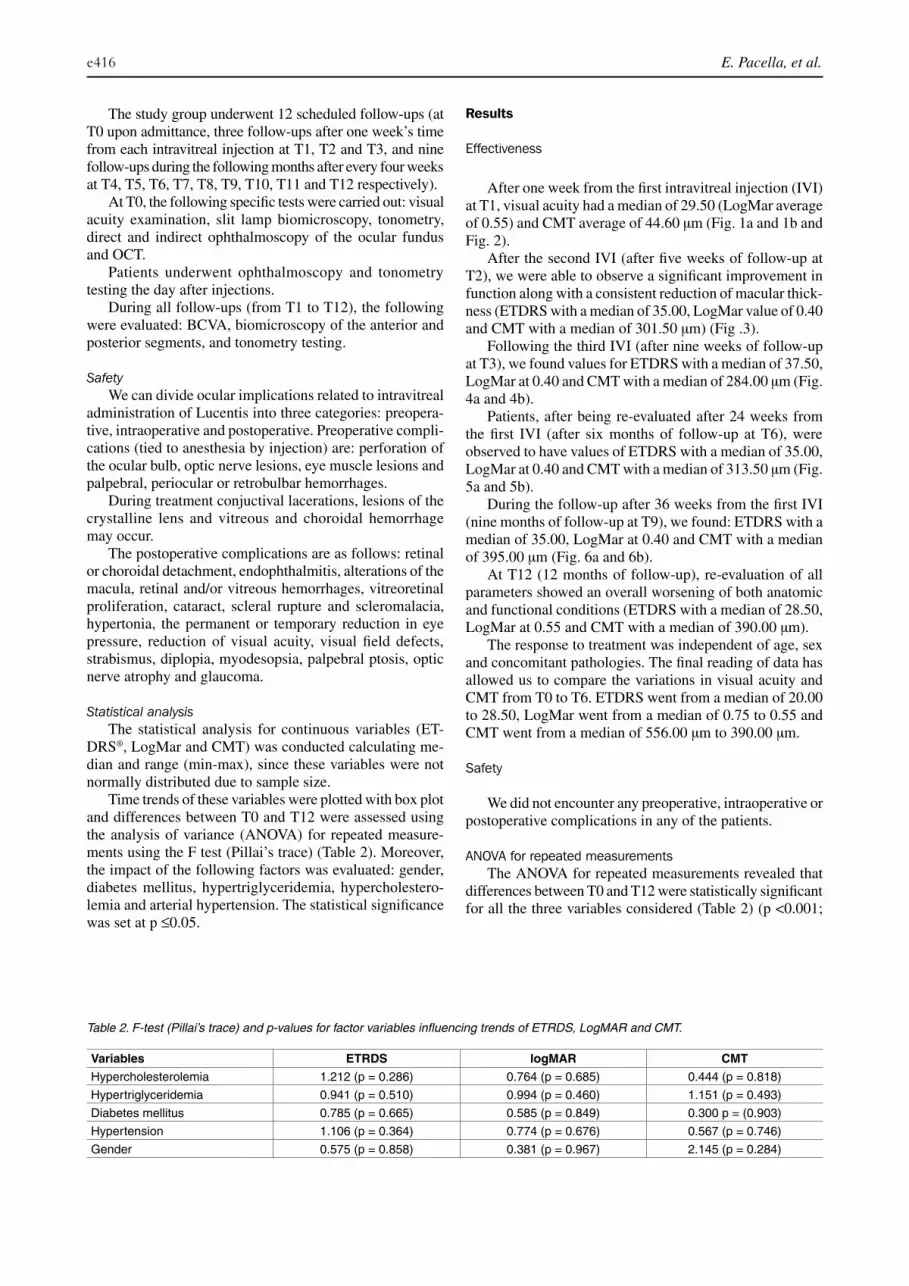
Fig. 1. Images of the right eye at baseline T0: a. Fundus phothograph (3.7); b. fluorescein angiography (3.6); c. optical coherence tomography
Baseline T0 CMT 519 (Number of letters ETDRS 22) (3.3)
Fig. 1
Fig. 1 a
Fig. 2. Images of the right eye at 1 week after I injection, optical coherence tomography CMT 241, (Number of letters ETDRS 31) (3.4)

e418 E. Pacella, et al.
Fig. 3. Images of the right eye at II injection after 5 weeks CMT 226 ( Number of letters ETDRS 35) (3.5).
Fig. 4a
Fig. 4b
Fig. 4. Images of the right eye at II injection after III injection 9
weeks: a. Fundus phothograph (3.7); b. fluorescein angiography
(3.6); c. optical coherence tomography CMT 228 (Number of letters
ETDRS 36) (3.8).

e419Intravitreal Ranibizumab in venous occlusion treatment
Fig. 5 Fig. 5a
Fig. 5. Images of the right eye at IV injection after IV injection 24 weeks: a. Fundus phothograph (3.10); b. fluorescein angiography (3.9);
c. optical coherence tomography CMT 365 (Number of letters ETDRS 28) CMT (3.11).
Fig. 6 Fig. 6a

e420 E. Pacella, et al.
p <0.001 and p =0.017 for ETRDS, LogMar and CMT,
respectively).
None of the considered factors (gender, diabetes mellitus,
hypertriglyceridemia, hypercholesterolemia, arterial hyper-
tension) have an impact on the time trends of the variables
considered (Table 1).
Discussion
The pathogenesis of macular edema secondary to CRVO
is determined by altered vascular permeability and neoangio-
genesis deriving from post-thrombotic hypoxic damage. The
leading cause of the accumulation of intra- and subretinal
fluid is due to the liberation of VEGF and other proinflam-
matory cytokines such as IL-6 and IL-8.
The goal of treatments geared towards stopping and re-
ducing the formation of edema is to increase patients’ visual
acuity and prevent the development of any complications
related to neoangiogenesis.
Available data in scientific literature shows that patients
suffering from CRVO have a higher intravitreal concentra-
tion of VEGF with regards to that of healthy subjects or
subjects suffering from other types of retinal pathologies
(2). These factors have lead to the use of anti-VEGF drugs,
such as Ranibizumab, for treating the pathology under
examination.
The CRUISE study reported that 260 patients treated
with 0.3 mg or 0.5 mg of intravitreal Ranibizumab (or
sham injection) showed an improvement in visual acuity
after six months along with a significant and continuous
reduction of macular edema measured in terms of central
retinal thickness (23).
The study “Ranibizumab for macular edema following
central retinal vein occlusion: six-month primary end point
results of a phase III study” carried out on 392 patients
treated with 0.3 mg or 0.5 mg doses of Ranibizumab (24)
also reported improvements of visual acuity along with a
reduction in macular thickness (23).
The results derived from our study altogether highlight
a clear improvement of BCVA after administration of Ra-
nibizumab accompanied by a reduction of CMT that went
from a median of 556 µm at T0 to a median of 313.5 µm
at T6 (after six months from the beginning of treatment).
Nonetheless, it was necessary to repeat IVI in four patients
(20%) due to a recurrence of edema, and persistent edema
in two other patients (10%).
Specifically, three patients with recurring macular edema
received four injections, one patient with recurring macular
edema received five injections and two patients with per-
sistent macular edema received seven injections (with an
average number of 5.16 injections).
The study “Ranibizumab for macular edema due to
retinal vein occlusions: implication of VEGF as a critical
stimulator” looked at 20 eyes with CRVO observed during
a short follow-up of only three months with the goal of eva-
luating the effectiveness of three consecutive injections of
Ranibizumab with two different doses (0.3 mg or 0.5 mg).
After three months of observation, significant improvements
were seen for visual acuity (a gain >14 letters for the group
that received doses of 0.5 mg and >17 letters for the group
that received doses of 0.3mg) including a reduction of CMT
by 90% (25).
The prospective randomized study “Pieramici-Rabena”
was conducted on ten eyes with CRVO with nine months of
follow-up. The use of Ranibizumab lead to an improvement
of BCVA of 12±20 letters after three months, 3±21 letters
after six months, and 1±24 letters plus a reduction of CMT
(from 272±244 to 119±153 micron) after nine months of
therapy, with respect to pre-treatment values. Nonetheless,
the authors confirm that the effectiveness of treatment is
invalidated by the great variability in data (high standard
deviation) and the excessive number of injections necessary
to maintain the same results that had been obtained with
only one round of therapy (three injections of Ranibizu-
mab) (2).
After looking at results derived from our study, we ob-
served a rapid response to the drug after the first week of
treatment (T1), followed by moderate improvement of visual
acuity and a substantial reduction in macular thickness after
both the first and second injections at T1 and T2. However,
after the third administration (T3), data showed average
Fig. 6. Images of the right eye 36 weeks: a. Fundus phothograph (3.13); b. fluorescein angiography (3.12); c. optical coherence tomography
CMT 244 (Number of letters ETDRS 38) (3.14)

e421Intravitreal Ranibizumab in venous occlusion treatment
values of ETDRS, LogMar and CMT that were analogous to
previous values observed at T2. When re-evaluating patients
between T4 and T12, the data highlights a slight decline in
the values of the three parameters that were examined when
compared to those from T3 (one week after the third IVI).
Out of the group’s 20 patients, reinjection due to a decline
in conditions was not necessary for 14 patients (70%) during
the 12 months of follow-up.
The remaining six subjects (30%) underwent reinjection
because of a decline in visual acuity and persistent or recur-
ring edema. In fact, regardless of the additional administra-
tions of Ranibizumab, the group’s CMT values at T12 were
the same or had increased with respect to T0 most likely
due to the effectiveness of treatment being correlated to the
great variability of implied factors (correlated pathologies
and risk factors). This study has demonstrated the correlation
between a negative outcome and certain chronic pathologies
such as: essential hypertension (found in 100% of patients)
and diabetes mellitus (found in 33.3% of patients).
In accordance with data found in scientific literature,
Ranibizumab guarantees rapid improvement of patients’
clinical conditions after just the first week of treatment
(T1) and maximum efficacy is reached after two months of
treatment (T2) (2, 26, 27).
After the third intravitreal injection (T3), and with re-
gards to the initial effectiveness of treatment, we observed
a slight decline in results that had been achieved during the
second month as gathered from the average reduction in
visual acuity and the average increase of CMT.
Nonetheless, the final values (obtained at T12) were,
on average, better than initial values recorded (T0), which
demonstrates that, in any case, patients had benefitted from
treatment with Ranibizumab.
The turnaround of progression may most likely be ex-
plained by anti-VEGF drug limitations, such as the limited
vitreal half-life of Ranibizumab (less than nine days), the
lack of a predefined protocol for therapy regarding admi-
nistration procedures, doses and the number of injections
necessary, the possibility of a rebound effect (consistent in
an increase of macular edema secondary to upregulation of
VEGF receptors in the retina caused by the drug’s inhibitory
mechanism) (28), the possible negative effect on the survival
of retinal neurons (VEGF agents are neuroprotective) and
the variability of factors that cause CRVO.
Other than this, we must take into consideration that
VEGF agents do not represent the only factor in the etio-
pathogenesis of the retinal vein occlusion. Other cytokines
(IL-1a, IL-6 and IL-8) and growth factors may have a role
in the formation of pathological neoangiogenesis and an
inflammatory response (29).
In conclusion, the results obtained from this study have
led us to confirm that intravitreal treatment with Ranibizu-
mab represents a valid therapeutic option for retinal vein
occlusion due to the fact that it has shown to immediately
improve all morphofunctional parameters as well as clini-
cal and subjective conditions (Fig. 3 and 4). This has also
resulted in a high level of patient compliance.
In order to most likely achieve higher effectiveness, it
would be ideal to include other therapeutic strategies along
with intravitreal treatment with anti-VEGF agents, such as
laser treatment, as has been reported recently in an interna-
tional case series prospective (with 12 months of follow-
up). Twenty eyes with CRVO were studied. On average,
8.5 injections of Ranibizumab followed by panretinal laser
treatment (PRN) showed to greatly improve visual acuity
(from 45.8 to 64.3 letters) and macular thickness was redu-
ced (from 574 to 186 micron with respect to initial values)
(2), or with intravitreal injection with steroids.
To this end, we believe it is necessary to increase the
number of subjects and the duration of the follow-up.
References
1. Rogers S, McIntosh RL, Cheung N, et al. The prevalence of
retinal vein occlusion: pooled data from population studies
from the United States, Europe, Asia, and Australia. Ophthal-
mology 2010; 117:313-9
2. Klein R, Klein BEK, Moss SE, et al. The epidemiology of
retinal vein occlusion: the Beaver Dam Eye Study. Trans Am
Ophthalmol Soc 2000; 98:133-43
3. Cheung N, Klein R, Wang JJ, et al. Traditional and novel
cardiovascular risk factors for retinal vein occlusion: the
multiethnic study of atherosclerosis. Invest Ophthalmol Vis
Sci 2008; 49:4297-302
4. O’Mahoney PR, Wong DT, Ray JG. Retinal vein occlusion
and traditional risk factors for atherosclerosis. Arch Ophthal-
mol 2008; 126:692-9
5. Janssen MC, den Heijer M, Cruysberg JR, et al. Retinal vei-
nocclusion: a form of venous thrombosis or a complication
of atherosclerosis? A meta-analysis of thrombophilic factors.
Thromb Haemost 2005; 93:1021-6
6. Alexander LJ. The implications and management of retinal
vaso-occlusive disease. J Optom 1986; 2:20-34
7. Coscas G, (ed), Macular Edema. Dev Ophthalmol. Basel,
Karger, 2010; 47: 10-26
8. Aref AA, Scott IU. Managment of macula edema secondary
to retinal vein occlusion: an evidence-based update Adv Ther
2011; 28(1):28-39
9. Farahvash MS, Farahvash MM, Moradimogadam M, et al.
Longterm effect of dalteparin in the prevention of neovascu-
larization of iris in recent-onset central retinal vein occlusion.
Arch Iran Med 2008; 11:539-43
10. Parodi MB, Lanzetta P, Guarnaccia G, et al. Surgical treat-
ments of central retinal vein occlusion. Semin Ophthalmol
2003; 18:142-6
11. Sharma A, D’Amico DJ. Medical and surgical management
of central retinal vein occlusion. Int Ophthalmol Clin 2004;
44:1-16
12. Quiroz-Mercado H, Sánchez-Buenfil E, Guerrero-Naranjo JL,
et al. Successful erbium:YAG laser-induced chorioretinal
venous anastomosis for the management of ischemic central
retinal vein occlusion. A report of two cases. Graefes Arch
Clin Exp Ophthalmol 2001; 239:872-5
13. Opremcak EM, Bruce RA, Lomeo MD, et al. Radial optic
neurotomy for central retinal vein occlusion: a retrospective
pilot study of 11 consecutive cases. Retina 2001; 21:408-
15
14. Lahey JM, Fong DS, Kearney J. Intravitreal tissue plasmi-
nogen activator for acute central retinal vein occlusion.
Ophthalmic Surg Lasers 1999; 30:427-34
15. Weiss JN, Bynoe LA. Injection of tissue plasminogen acti-
vator into a branch retinal vein in eyes with central retinal
vein occlusion. Ophthalmology 2001; 108:2249-57

e422 E. Pacella, et al.
16. Leopold IH. Nonsteroidal and Steroidal Anti-Inflammatory
Agents. Surgical Pharmacology of the Eye. M. Sears and A.
Tarkkanen (Eds), New York: Raven Press, 1985
17. Iwao K, Inatani M, Kawaji T, et al. Frequency and risk factors
for intraocular pressure elevation after posterior sub-Tenon
capsule triamcinolone acetonide injection. J Glaucoma 2007;
16:251-6
18. Saleh M, Gaucher D, Letsch J, Bourcier T, Speeq-Schatz C.
Efficacy of early injection of intravitreal triancinolone ace-
tonide (IVTA) versus delayed injection for macular edema
resulting from retinalvein occlusion.J Fr Ophtalmom 201;
34(6):355-61
19. Coscas G, Coscas F, Zucchiatti I, et al. SD-OCT pattern of
retinal venous occlusion with cystoid macular edema treated
with Ozurdex®. Eur J Ophthalmol 2011; 21(5):631-6
20. Rossi-Cuomo-Riccardi. Farmacologia, principi di base e
applicazioni terapeutiche”. Min Med; Torino 2005; 726
21. Goodman-Gilman. Le Basi Farmacologiche della Terapia,
XI Ed. Mc Graw-Hill, Milan 2006; 1379
22. Gschwind-Fischer-Ullrichin. The discovery of recertor tyro-
sine kinases: targets for cancer therapy, National Rev Cancer
2004; 361-70
23. Keane PA, Sadda SR. Retinal vein occlusion and macular
edema - critical evaluation of the clinical value of ranibizu-
mab. NIHR Biomedical Research Centre for Ophthalmology,
Moorfields Eye Hospital NHS Foundation Trust and UCL
Institute of Ophthalmology, London, UK; Clin Ophthalmol
2011; 5:771-81
24. Brown DM, Campochiaro PA, Singh RP, et al. Ranibizumab
for macular edema following central retinal vein occlusion:
six-month primary end point results of a phase III study.
Ophthalmology 2010; 117(6):1124-33
25. Campochiaro PA, Hafiz G, Shah SM, et al. Ranibizumab for
macular edema due to retinal vein occlusions: implication of
VEGF as a critical stimulator. Mol Ther 2008; 16:791-9
26. Risard SM, Pieramici DJ, Rabena MD, et al. Intravitreal rani-
bizumab for macular edema secondary to central retinal vein
occlusion. From the California Retina Research Foundation,
Santa Barbara, California. Retina 2011;31(6):1060-7
27. Pieramici DJ, Rabena M, Castellarin AA, et al. Ranibizumab
for the treatment of macular edema associated with perfu-
sed central retinal vein occlusions. Ophthalmology 2008;
115:e47-54
28. Matsumoto Y, Freund KB, Peiretti E, et al. Rebound macular
edema following bevacizumab (Avastin) therapy for retinal
venous occlusive disease. Retina 2007; 27:426-31
29. Funk M, Kriechbaum K, Prager F, et al. Intraocular con-
centrations of growth factors and cytokines in retinal vein
occlusion and the effect of therapy with bevacizumab. Invest
Ophthalmol Vis Sci 2009; 50:1025-32




























