Embed Size (px)
Citation preview

October • 2013 167
CCC
the Behavior TherapistI S S N 0 2 7 8 - 8 4 0 3
VOLUME 36, NO. 7 • OCTOBER 2013
ContentsPresident’s MessageStefan G. Hofmann The Future of ABCT • 167
At ABCTDebra Hope and Denise Davis ABCT Operational Assessment Yields Important Insights • 169
Research-Practice LinksChristina M. Gilliam, Melissa M. Norberg, Christina E. Ryan, David F. Tolin Understanding Afghanistan and Iraq Veterans’ TreatmentPreferences and Perceptions of Stigma • 172
Clinical ForumArthur Freeman, Angela Breitmeyer, and Melissa Flint The Challenges in Diagnosing Narcissistic PersonalityDisorder: Difficult to Define, but “We Know It When WeSee It” • 179
Past Presidents SeriesAlayna Schreier and David J. Hansen Perspectives From Past Presidents: Foundations ofBehaviorism and Studying Behavior Change • 184
Classified • 185
ASSOCIATION FOR BEHAVIORALAND COGNITIVE THERAPIES
[continued on p. 169]
President’s Message
The Future of ABCTStefan G. Hofmann, Boston University
CBT is a growing and matur-ing field. As one of the pre-mier organizations represent-ing this dominant approachto mental health, ABCTneeds to be responsive andproactive to the many currentand future challenges. As the
leader in the field, we have the obligation toreevaluate on a regular basis our own leadershipstructure, our goals, and our mission in order toassure that we remain an active player in theever-changing field of mental health care.
To deal with these challenges, we decided toseek the assessment of an objective and knowl-edgeable third-party consulting firm. After acareful screening process, we decided to workwith McKinley Advisors, a well-respected con-sulting firm that also served the AmericanPsychological Association and other professionalorganizations. We chose this firm because of thecompany’s extensive knowledge and expertise atthe intersection of business and nonprofit orga-nizations.
McKinley interviewed some of our members,including many past presidents, and some of thecentral office staff. We were very satisfied withtheir service and pleased with the product. Theadvisors provided us with concrete recommen-dations on how to further improve our alreadyexcellent organization in order to position our-selves in the best possible situation for the fu-ture. The following article by Deb Hope andDenise Davis summarizes some of the importantinsights that we gained from this experience.
As you can imagine, this was a time-consum-ing enterprise and I want to thank everybodywho participated, especially the central officestaff. We all agree that it was well worth the timeand money. In fact, many of us believe that it
Call for 2014 Award Nominations • 186
Call for 2014 Continuing Education Sessions • 188
Call for 2014 Officer Nominations • 189
Welcome, New Members • 192

168
the Behavior TherapistPublished by the Association for
Behavioral and Cognitive Therapies305 Seventh Avenue - 16th Floor
New York, NY 10001-6008(212) 647-1890 /Fax: (212) 647-1865
www.abct.org
EDITOR · · · · · · · · · · Kathleen GunthertEditorial Assistant . . . . . . . . Melissa ThemBehavior Assessment . . . . . . Matthew TullBook Reviews · · · · · · · · · · · C. Alix TimkoClinical Forum · · · · · · · · · · · · · Kim GratzClinical Dialogues . . . . . . . Brian P. MarxClinical Training Update . . .Steven E. BruceInstitutional Settings. . . . . . Dennis CombsLighter Side · · · · · · · · · · · · Elizabeth MooreMedical and Health Care Settings . . . . . . . . . . . . . . Laura E. DreerNews and Notes. . . . . . . . Nicholas Forand
James W. SturgesSusan Wenze
Shannon Wiltsey-StirmanePublic Health Issues. . . . . . . . . Giao TranResearch-Practice Links· · · · · · · · · · · · · · · · David J. HansenResearch-Training Links · · · · · · · · · · · · · · · · · · · · Dan StrunkScience Forum· · · · · · · · · · · Jeffrey M. LohrSpecial Interest Groups · · · · · · · · · · · · · · Aleta AngelosanteStudent Forum · · · · · · · · · · David DiLilloTechnology Update. . . . . . . Zach Rosenthal
ABCT President . . . . . . Stefan G. HofmannExecutive Director · · · · · · Mary Jane EimerDirector of Education &Meeting Services . . . . . . Mary Ellen BrownDirector of Communications David TeislerManaging Editor . . . . . Stephanie Schwartz
Copyright © 2013 by the Association for Behavioraland Cognitive Therapies. All rights reserved. Nopart of this publication may be reproduced or trans-mitted in any form, or by any means, electronic ormechanical, including photocopy, recording, or anyinformation storage and retrieval system, withoutpermission in writing from the copyright owner.
Subscription information: the Behavior Therapist ispublished in 8 issues per year. It is provided free toABCT members. Nonmember subscriptions areavailable at $40.00 per year (+$32.00 airmailpostage outside North America).
Change of address: 6 to 8 weeks are required foraddress changes. Send both old and new addresses tothe ABCT office.
ABCT is committed to a policy of equal opportu-nity in all of its activities, including employment.ABCT does not discriminate on the basis of race,color, creed, religion, national or ethnic origin, sex,sexual orientation, gender identity or expression,age, disability, or veteran status.
All items published in the Behavior Therapist,including advertisements, are for the information ofour readers, and publication does not imply endorse-ment by the Association.
The Association for Behavioral andCognitive Therapies publishes the BehaviorTherapist as a service to its membership.Eight issues are published annually. Thepurpose is to provide a vehicle for the rapiddissemination of news, recent advances,and innovative applications in behaviortherapy.
Feature articles that are approximately16 double-spaced manuscript pages maybe submitted.
Brief articles, approximately 6 to 12double-spaced manuscript pages, arepreferred.
Feature articles and brief articlesshould be accompanied by a 75- to100-word abstract.
Letters to the Editor may be used torespond to articles published in theBehavior Therapist or to voice a profes-sional opinion. Letters should be lim-ited to approximately 3 double-spacedmanuscript pages.
Submissions must be accompanied bya Copyright Transfer Form (a form isprinted on p. 35 of the February 2011issue of tBT, or download a form from ourwebsite): submissions will not be reviewedwithout a copyright transfer form. Prior topublication authors will be asked to sub-mit a final electronic version of their man-uscript. Authors submitting materials totBT do so with the understanding that thecopyright of the published materials shallbe assigned exclusively to ABCT.Electronic submissions are preferred andshould be directed to the editor at [email protected]. Please in-clude the phrase tBT submission and theauthor’s last name (e.g., tBT Submission -
Smith et al.) in the subject line of your e-mail. Include the corresponding author'se-mail address on the cover page of themanuscript attachment. Please also in-clude, as an attachment, the completedcopyright transfer document.
INSTRUCTIONS Ñçê AUTHORS
“Every student deserves to be treated
as a potential genius.” —Anton Ehrenzweig
ABCT’s Mentorship Directory connects exceptional students with
the best mentors that psychology has to offer. Promote your lab,
and allow your next student to find you by name, interest, loca-
tion, or program. Signing up is easy and takes just 3 minutes!
Join the ABCT Mentorship Directory
http://www.abct.org/Mentorship
entorship
directory
Mgraduate

should be one of many such self-study exer-cises in years to come to help us navigatethe ever-changing landscape of CBT.
. . .
Correspondence to Stefan G. Hofmann,Ph.D., Department of Psychology, BostonUniversity, 648 Beacon Street, 6th Fl.,Boston, MA 02215; [email protected]
In November 2012, the ABCT Board ofDirectors commissioned an in-depthstudy of our organization’s perfor-
mance. The primary objective of this “oper-ational assessment,” as it came to be known,was to evaluate ABCT’s strengths and op-portunities, as well as its weaknesses andthreats relative to other comparable organi-zations and in context with our mission, vi-sion, and values. As ABCT has continued togrow and evolve, the Board thought that itwas an appropriate time to take a step backand assess the key functions of the associa-tion. The study, the first of its kind thatABCT has conducted, was designed to pro-vide input and analysis across several keyoperational areas, including finance, humanresources, governance, membership, andtechnology.
The project was guided by the Ad HocOperations Review Committee (theCommittee), which was co-chaired by theauthors and included several other currentmembers of the Board of Directors, and in-formed by the work of McKinley Advisors(McKinley)1, an independent associationconsulting firm headquartered inWashington, DC. McKinley consultants in-terviewed current and past ABCT leaders,senior staff, and others to gain insight onimportant questions related to ABCT’s op-
erations. The firm also analyzed ABCT’sperformance in context with key associationindustry ratios and Form 990 financial datacompiled from several comparable scientificand professional associations. Final recom-mendations from the report were presentedto the ABCT Finance Committee in NewYork during its May 2013 meeting.
Through this project, ABCT has gainedimportant insight into many long-standingquestions about the relative health and per-
formance of our organization. Following theconclusion of the project, the Board came toconsensus that an organizational review ofthis kind is a sound practice for an organiza-tion of ABCT’s scope, and that we shouldconduct updates on a periodic basis with afrequency to be determined.
McKinley’s findings and recommenda-tions from the project were organized intothree main categories:
• Governance, strategy, and leadership• Internal processes, staffing, and
performance• Delivering member value
Key findings from the project include thefollowing:
ABCT is fiscally sound, with several ofits key financial ratios meeting or exceedingassociation-industry benchmarks for perfor-mance, a noteworthy finding given theseverity of the recent recession and rela-
47th Annual ConventionNovember 21–24, 2013 | Nashville
www.abct.orgRegister now!
At ABCT
ABCT Operational Assessment YieldsImportant InsightsDebra Hope, University of Nebraska–Lincoln
Denise Davis, Vanderbilt University
Key Revenue Ratios
ABCTForm 990
Form 990Research PeerGroup Average
(N = 6)
Operating Ratio Report*Assns with Revenues of $1-2 M
All Assns (N = 616)
IMOs**(N = 275)
Total revenue
Membership duesrevenue as % oftotal revenue
Non-dues revenue as a % of total revenue
Conference/meeting revenueas a % of totalrevenue
$1,854,379
30.3%
69.7%
42.6% 26.2% 24.4% 22.1%
73% 61.5% 65.4%
27% 38.5% 34.6%
$2,317,295 $1,448,039 $1,459,134
*ASAE, Operating Ratio Report, 12th Edition, 2012; **IMOs = individual membership organizations that are the most appropriate comparable organizations for ABCT.
1The full committee was comprised of DebHope and Denise Davis (co-chairs), Bob Klepac,Stefan Hofmann, and Dean McKay.
October • 2013 169

170 the Behavior Therapist
tively slow rebound of the global economy.Because the association’s main revenuesources are diversified—membership dues,conference, and publications—we have asolid financial foundation for ABCT to con-tinue to invest in mission-related programsand services. In fact, the consultants sug-gested that ABCT may be able to consider a“strategic investment fund,” which could beused to develop new programs, services, orresources that enhance member value.
The organizational structure, staffingmodel, and relative costs of operation arewell within association-industry norms.Specifically, the location of the ABCT officein New York does not have a material im-pact on the cost to operate the organization.In fact, due to the association’s ownerhip ofits physical space, occupancy costs and re-lated expenses are lower than many otherscenarios. While some amount of cost re-duction could be possible from moving theheadquarters to another location, theCommittee concluded that the disruptionto the organization would greatly outweighthe benefit of any potential cost savings.
Many of the challenges faced by ABCTare common in the association community,particularly the difficulty of sustainingmembership growth, developing meaning-ful sources of nondues revenue, and expand-ing public awareness of our field. McKinleyencouraged ABCT to consider strategicpartnerships with other organizations whosupport our science-based approach and of-fered specific guidance on how to best pro-ceed with our dissemination efforts.
In addtion to these contextual findings,the consultants provided a series of more
specific recommendations, including thefollowing:
• Improve and enhance continuity in lead-ership and nurture the board/staff part-nership. Strategies include developing anew “board development workshop” toengage leadership in a discussion of therole they will play in promoting strate-gic, generative, and fiduciary gover-nance practices to advance theorganization. The training and onboard-ing program should include an externalperspective from outside the associationon a regular basis to coincide with theterms of office for elected leaders.
• Develop and implement a clear strategyto fuel membership growth, as an ex-panded membership base is central tothe association’s future goals and objec-tives.
• Encourage innovation and expand tech-nological capabilities on staff through aneffort to align competencies, roles, andresponsibilities for future intiatives.
• Develop a succession plan to ensure asmooth transfer of institutional knowl-edge from tenured leaders to futureABCT staff and volunteers.
• Add rigor to the tools and methods usedfor performance assessment to increaseaccountability and objectivity. By creat-ing a thoughtful set of review criteriaand performance metrics, the associa-tion can better understand the progressit is making toward strategic and opera-tional goals and objectives.
Finally, one of the most important out-comes of the assessment was a decision to
pursue a more rigorous and impactfulstrategic planning process, which will be in-formed by the comprehensive ABCT mem-ber survey that was fielded in August. Weare thrilled to report that nearly 1,000ABCT members participated in the survey,and while detailed results are not availableat press time, we will share key findings ofthe survey, as well as the outcomes of theBoard’s fall strategic planning retreat, in afuture issue of tBT. A central topic of dis-cussion at the retreat will be how the associ-ation can continue to enhance its value toour members and the field.
We think we can safely speak for the en-tire Committee and Board when we say thatwe found the project to be extremely illumi-nating, valuable, and an important step inunderstanding where ABCT is today, andhow we can most effectively lead our field inthe future. The research and analysis con-ducted for the project was thorough, yield-ing a large repository of actionable data thatABCT can continue to utilize to help guideour next phase of development.
Should you have any questions about theproject, its outcomes, or implications,please do not hesitate to get in touch.
. . .
Correspondence to Debra Hope, Ph.D.,University of Nebraska–Lincoln, Departmentof Psychology, 238 Burnett Hall, Lincoln, NE68588 ([email protected]); or DeniseDavis, Ph.D., Vanderbilt University,Department of Psychology, PMB 407817,2301 Vanderbilt Place, Nashville, TN 37240([email protected]).
Articulate ABCT’s vision, purpose, and identity to encourage membership
Mentor individuals through the process ofpresenting at the annual convention ortransitioning into leadership positions
Act as the eyes and earsof the association locally
m e s s e n g e r
g u i d e
s i g n i f y
Learn howyou can
become anAmbassador
for ABCT.
ContactLisa Yarde,
Membership Services
Manager,[email protected]
�
�
Become an ABCT
Ambassador

October • 2013 171
Hogrefe Publishing · 30 Amberwood Parkway · Ashland, OH 44805 Tel: (800) 228 3749 · Fax: (419) 281 6883 E-Mail: [email protected]
Order online at www.hogrefe.com or call toll-free (800) 228-3749 (US only)
See sample pages at www.hogrefe.com
Visit our booth #306 to find out more!
See our new releases at the ABCT’s 47th Annual Convention 2013!

172 the Behavior Therapist
The extremely stressful demands ofwar can lead to maladaptive symp-toms in even the best-prepared mili-
tary personnel. Prevalence rates for mentalhealth disorders range as high as 20% to42% among returning Operation EnduringFreedom (OEF) and Operation IraqiFreedom (OIF) soldiers and veterans, withposttraumatic stress disorder (PTSD) citedas one of the most common problemsamong this population (Milliken,Auchterlonie, & Hoge, 2007; Seal et al.,2010). Despite the efforts of the VeteransAdministration to increase access to mentalhealth treatment for OEF/OIF veterans,many OEF/OIF veterans with mentalhealth conditions do not seek or participatein an adequate amount of treatment (Seal etal.). In fact, OEF/OIF veterans who havethe greatest number and the most severesymptoms may be the least willing to seekhelp (Hoge et al., 2004).
Mixed findings regarding veterans’ andsoldiers’ barriers to help seeking havecaused confusion. In some studies, bothstigma and negative perceptions of mentalhealth care (e.g., beliefs that treatment is in-effective or mental health professionals areuntrustworthy) were identified as barriersto help seeking (Hoge et al., 2004; Sayer etal., 2009; Stecker, Fortney, Hamilton, &Ajzen, 2007), whereas one study found aninverse relationship between negative per-ceptions of mental health care and helpseeking (Kim, Britt, Klocko, Riviere, &Adler, 2011). Yet another study indicatesthat neither negative beliefs about mentalhealth care nor perceived stigma predicthelp-seeking behavior (Rosen et al., 2011).Paradoxically, other studies have shownthat greater perceived stigma is associatedwith greater interest in seeking mentalhealth treatment (Brown et al., 2011) and
longer psychotherapy attendance (Rosen etal.). One possible reason for these mixedfindings may be that previous studies onthese barriers to mental health treatmentassessed mental health treatments broadly;veterans or returning soldiers were ques-tioned about their views on psychotherapyand/or pharmacologic intervention in gen-eral, without a specific definition or expla-nation of either of these types of treatments.In order to understand and increase accep-tance of mental health treatments, it maybe more informative to examine veterans’views and preferences for specific mentalhealth treatments.
Civilians queried about their preferencefor PTSD treatment consistently choosepsychotherapy over pharmacotherapy(Cochran, Pruitt, Fukuda, Zoellner, &Feeny, 2008; Feeny, Zoellner, & Kahana,2009; Feeny, Zoellner, Mavissakalian, &Roy-Byrne, 2009; Roy-Byrne, Berliner,Russo, Zatzick, & Pitman, 2003; Zoellner,Feeny, & Bittinger, 2009; Zoellner, Feeny,Cochran, & Pruitt, 2003) and when queriedabout types of psychotherapy, they consis-tently choose prolonged exposure (PE) overpsychodynamic therapy (Becker, Darius, &Schaumberg, 2007; Tarrier, Liversidge, &Gregg, 2006) and technology-based treat-ments, such as virtual reality exposure ther-apy (VRET; Tarrier, et al., 2006). Further,civilians often report greater credibility fortheir preferred treatments than their non-preferred treatments (Zoellner et al., 2009).It is yet unclear whether veterans share sim-ilar preferences for the treatment of PTSD.There is some suggestion that veterans mayexperience greater stigma about seekingmental health treatment due to the militaryculture’s emphasis on emotional strength(Nash, Silva, & Litz, 2009; Vogt, 2011) aswell as the added concern about how seek-
ing treatment will affect their careers(Owens, Herrera, & Whitesell, 2009;Vogt).
These civilian findings led us to examineOEF/OIF veterans’ treatment preferencesand factors (stigma and credibility) thatmay influence their preferences. We exam-ined veterans’ perceptions of PE, VRET,peer support groups (PSG), and pharma-cotherapy with sertraline (SER). We choseto examine OEF/OIF veterans’ preferencesfor PE and SER as several studies have sup-ported their effectiveness (Boudewyns,Hyer, Woods, Harrison, & McCranie, 1990;Brady et al., 2000; Cooper & Clum, 1989;Davidson, Rothbaum, van der Kolk, Sikes,& Farfel, 2001; Keane, Fairbank, Caddell,& Zimering, 1989; Pitman et al., 1996;Tolin & Foa, 1999). We chose VRET be-cause of the growing support for its efficacy(Gerardi, Rothbaum, Ressler, Heekin, &Rizzo, 2008; McLay, McBrien, Wiederhold,& Wiederhold, 2010; McLay et al., 2011;Reger & Gahm, 2008; Rizzo et al., 2009;Rizzo et al., 2008a; Wood et al., 2007;Wood et al., 2008) and because research hasidentified that a third of active-duty soldierswho are unwilling to seek face-to-face psy-chotherapy may be willing to seek technol-ogy-based mental health care (Wilson,2008). We chose to examine PSG as evi-dence suggests that social support mayserve as a protective factor against the de-velopment of PTSD (Brewin, Andrews, &Valentine, 2000; Coker et al., 2002;Pietrzak et al., 2010; Pietrzak, Johnson,Goldstein, Malley, & Southwick, 2009),while poor social support following a trau-matic event may increase the risk of PTSD(Armenian et al., 2000; Gregurek et al.,2001; Ozer, Best, Lipsey, & Weiss, 2003).Further, peer-based interventions mayallow veterans to talk to someone whomthey feel can understand their problems(Stecker, et al., 2007).
Method
Participants
Twenty-eight OEF/OIF veterans en-rolled in the study. We recruited partici-pants via newspaper, Internet, radioadvertisements, and flyers posted in thegreater Hartford, CT, area. All OEF/OIFveterans were eligible for the study, regard-less of mental health symptoms, treatmenthistory, or combat exposure. Initially wetried to recruit OEF/OIF veterans withPTSD, but as we were unable to reach thisgroup, we chose to enroll any OEF/OIF vet-eran. While not ideal, there is a precedent ofconducting analog studies on treatment
Research-Practice Links
Understanding Afghanistan and IraqVeterans’ Treatment Preferences andPerceptions of StigmaChristina M. Gilliam, The Institute of Living
Melissa M. Norberg, Macquarie University
Christina E. Ryan, The Institute of Living
David F. Tolin, The Institute of Living and Yale University School of Medicine

October • 2013 173
newharbingerpub l i ca t i ons, i n c .1-800-748-6273 / newharbinger.com
Effective Resources for Well-Being
Read an excerpt at
newharbinger.com/thinking-traps
Workbook for Teens
“…I highly recommend this book for those
receiving the diagnosis, as well as for those with
family members or friends with BPD.”
—TIMOTHY J. TRULL, PhD, curators' professor of
psychological sciences at the University of Missouri
ISBN: 978-1608827060 US $15.95
ISBN: 978-1608826087 US $16.95
ISBN: 978-1608826568 US $16.95
ISBN: 978-1608827527 US $16.95
“An excellent resource for students, educators and families. …I will defi nitely use this as a tool to help our students succeed in the area of executive functioning!”—LISA KOENECKE, WisconsinSchool Counselor Association President
“…Micki Fine shines a clear light on our
habits of seeking approval, and off ers
meditations that free us to live from
our own natural compassion and
intelligence.” —TARA BRACH, PhD, author
of Radical Acceptance and True Refuge
"…Stosny’s guide to healing the heartache of betrayal is the most helpful I have seen in twenty-fi ve years of clinical practice."—RONALD J. COUGHLIN, EdD, licensed psychologist with twenty-fi ve years in full-time private practice
From the Newly Diagnosed Series
174 the Behavior Therapist
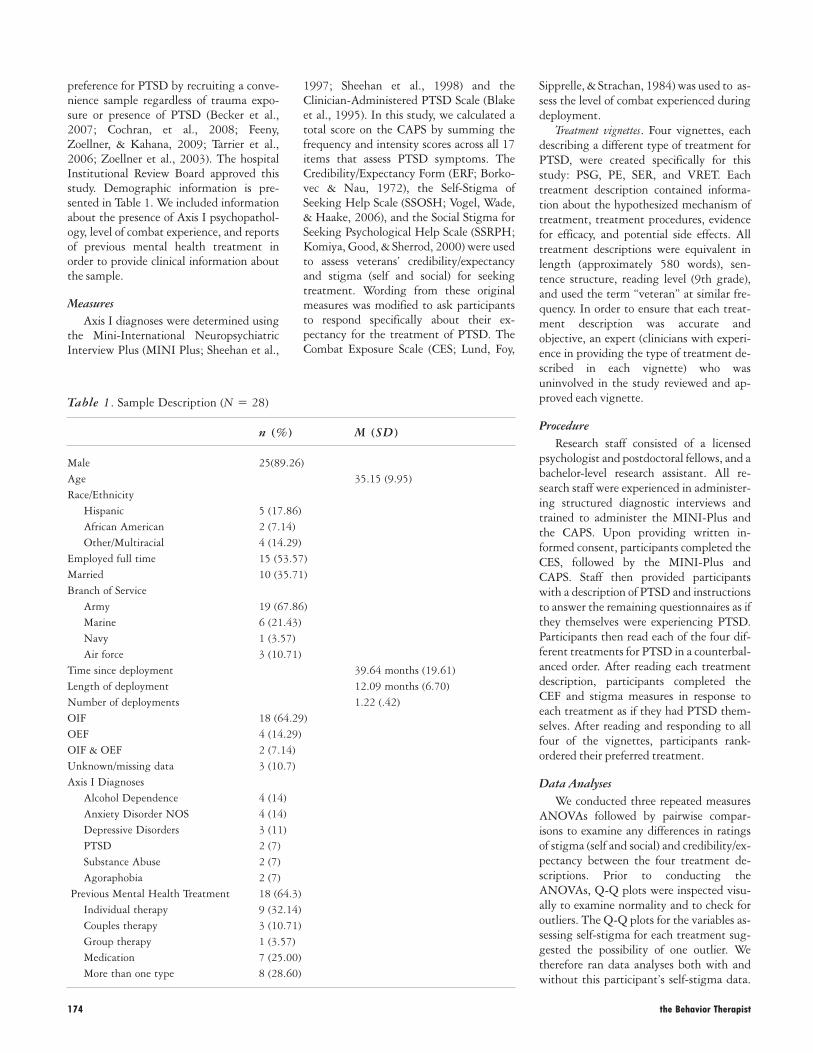
preference for PTSD by recruiting a conve-nience sample regardless of trauma expo-sure or presence of PTSD (Becker et al.,2007; Cochran, et al., 2008; Feeny,Zoellner, & Kahana, 2009; Tarrier et al.,2006; Zoellner et al., 2003). The hospitalInstitutional Review Board approved thisstudy. Demographic information is pre-sented in Table 1. We included informationabout the presence of Axis I psychopathol-ogy, level of combat experience, and reportsof previous mental health treatment inorder to provide clinical information aboutthe sample.
Measures
Axis I diagnoses were determined usingthe Mini-International NeuropsychiatricInterview Plus (MINI Plus; Sheehan et al.,
1997; Sheehan et al., 1998) and theClinician-Administered PTSD Scale (Blakeet al., 1995). In this study, we calculated atotal score on the CAPS by summing thefrequency and intensity scores across all 17items that assess PTSD symptoms. TheCredibility/Expectancy Form (ERF; Borko-vec & Nau, 1972), the Self-Stigma ofSeeking Help Scale (SSOSH; Vogel, Wade,& Haake, 2006), and the Social Stigma forSeeking Psychological Help Scale (SSRPH;Komiya, Good, & Sherrod, 2000) were usedto assess veterans’ credibility/expectancyand stigma (self and social) for seekingtreatment. Wording from these originalmeasures was modified to ask participantsto respond specifically about their ex-pectancy for the treatment of PTSD. TheCombat Exposure Scale (CES; Lund, Foy,
Sipprelle, & Strachan, 1984) was used to as-sess the level of combat experienced duringdeployment.
Treatment vignettes. Four vignettes, eachdescribing a different type of treatment forPTSD, were created specifically for thisstudy: PSG, PE, SER, and VRET. Eachtreatment description contained informa-tion about the hypothesized mechanism oftreatment, treatment procedures, evidencefor efficacy, and potential side effects. Alltreatment descriptions were equivalent inlength (approximately 580 words), sen-tence structure, reading level (9th grade),and used the term “veteran” at similar fre-quency. In order to ensure that each treat-ment description was accurate andobjective, an expert (clinicians with experi-ence in providing the type of treatment de-scribed in each vignette) who wasuninvolved in the study reviewed and ap-proved each vignette.
Procedure
Research staff consisted of a licensedpsychologist and postdoctoral fellows, and abachelor-level research assistant. All re-search staff were experienced in administer-ing structured diagnostic interviews andtrained to administer the MINI-Plus andthe CAPS. Upon providing written in-formed consent, participants completed theCES, followed by the MINI-Plus andCAPS. Staff then provided participantswith a description of PTSD and instructionsto answer the remaining questionnaires as ifthey themselves were experiencing PTSD.Participants then read each of the four dif-ferent treatments for PTSD in a counterbal-anced order. After reading each treatmentdescription, participants completed theCEF and stigma measures in response toeach treatment as if they had PTSD them-selves. After reading and responding to allfour of the vignettes, participants rank-ordered their preferred treatment.
Data Analyses
We conducted three repeated measuresANOVAs followed by pairwise compar-isons to examine any differences in ratingsof stigma (self and social) and credibility/ex-pectancy between the four treatment de-scriptions. Prior to conducting theANOVAs, Q-Q plots were inspected visu-ally to examine normality and to check foroutliers. The Q-Q plots for the variables as-sessing self-stigma for each treatment sug-gested the possibility of one outlier. Wetherefore ran data analyses both with andwithout this participant’s self-stigma data.
Male 25(89.26)Age 35.15 (9.95)Race/Ethnicity
Hispanic 5 (17.86)African American 2 (7.14)Other/Multiracial 4 (14.29)
Employed full time 15 (53.57)Married 10 (35.71)Branch of Service
Army 19 (67.86)Marine 6 (21.43)Navy 1 (3.57)Air force 3 (10.71)
Time since deployment 39.64 months (19.61)Length of deployment 12.09 months (6.70)Number of deployments 1.22 (.42)OIF 18 (64.29)OEF 4 (14.29)OIF & OEF 2 (7.14)Unknown/missing data 3 (10.7)Axis I Diagnoses
Alcohol Dependence 4 (14)Anxiety Disorder NOS 4 (14)Depressive Disorders 3 (11)PTSD 2 (7)Substance Abuse 2 (7)Agoraphobia 2 (7)
Previous Mental Health Treatment 18 (64.3)Individual therapy 9 (32.14)Couples therapy 3 (10.71)Group therapy 1 (3.57)Medication 7 (25.00)More than one type 8 (28.60)
Table 1. Sample Description (N = 28)
n (%) M (SD)

October • 2013 175
Celebrat ing I ts 40th Anniversary
Steven T. Fishman, Ph.D., ABPP | Barry S. Lubetkin, Ph.D., ABPP
Directors and FoundersSince 1971, our professional staff has treated over 20,000 patients with compassionate, empirically-based CBT.
Our specialty programs include: OCD, Social Anxiety Disorder, Panic Disorder, Depression, Phobias, Personality
Disorders, and ADHD-Linked Disorders, and Child/Adolescent/Parenting Problems.
Our externs, interns, post-doctoral fellows and staff are from many of the area’s most prestigious universities
specializing in CBT, including: Columbia, Fordham, Hofstra, Rutgers, Stony Brook, St. John’s, and Yeshiva
Universities.
Conveniently located in the heart of Manhattan just one block from Grand Central Station. Fees are affordable,
and a range of fees are offered.
We are pleased to announce the Oct. 2013 opening of our new Post-traumatic Stress & Relationship TherapyCenter, focusing on the full range of trauma-related difficulties and directed by Heidi Kar, Ph.D.
New York City
INSTITUTE for BEHAVIOR THERAPY
For referrals and/or information, please call: (212) 692-9288
110 East 40th St., Suite 206, New York, NY 10016
e-mail: [email protected] | web: www.ifbt.com
Last, we used the Friedman rank test to as-sess participants’ preferences for treatment,and the Wilcoxon test to compare two-paired groups following a significantFriedman’s statistic.
Results
Descriptive Information
Ten (36%) met criteria for an Axis I dis-order. Types of diagnoses are presented inTable 1. Those diagnosed with anxiety dis-order NOS reported clinically significantsymptoms consistent with PTSD, but didnot meet full criteria for PTSD at the timeof the study. Type of previous mental healthtreatment is listed in Table 1. No partici-pant reported participating in PE or VRET.One participant endorsed participating ingroup therapy, but did not specify whetherthis group was specifically for veterans. Themean score for the CES was 18.11 (SD =8.67), suggesting that this sample experi-enced moderate levels of combat duringtheir deployment(s).
Stigma and Expectancy/Credibility
We conducted three repeated measuresanalysis of variance (ANOVAs) to examine
any differences in ratings of credibility/ex-pectancy and stigma (self and social) be-tween the four treatment descriptions. Wefound significant differences across the fourtreatments in ratings of credibility/ex-pectancy, Wilks’s Λ= .60, F(3, 25) = 5.46,p < .01, ηp2 = .40, and social stigma,Wilks’s Λ = .49, F(3, 25) = 8.77, p <.001, ηp2 = .51, but not self-stigma, re-gardless of whether the one outlier’s datawere included or not (Outlier included:Wilks’s Λ = .86, F[3, 24] = .30, p = .82,ηp2 = .04; Outlier excluded: Wilks’s Λ =.86, F[3, 25] = .30, p = .28, ηp2 = .14).
Bonferroni corrected pairwise compar-isons revealed that veterans rated SER sig-nificantly lower in credibility/expectancycompared to PE (p < .05, d = .67) andVRET (p = .03, d = .62). Veterans alsorated SER higher in social stigma comparedto PE (p = .01, d = .38), VRET (p < .01, d= .61), and PSG (p =.02, d = .43).
Due to the small sample size we lackedstatistical power to examine differences inratings of stigma and credibility betweenveterans with or without an Axis I disorder,or between veterans with and without a re-ported history of mental health treatment.Means and standard deviations of stigma
and credibility for the entire sample, as wellas those of veterans with and without anAxis I disorder, and with and without a re-ported history of mental health treatmentare presented in Table 2 for descriptive pur-poses.
Treatment Preference
We conducted a Friedman test to evalu-ate differences in rankings among VRET(median rank = 2.10), PE (median rank =2.27), PSG (median rank = 2.48) and SER(median rank= 3.15). The test was signifi-cant, χ2(3, N = 26) = 10.09, p > 0.02)The Kendall coefficient of concordance was.13. We conducted follow-up pairwise com-parisons using a Wilcoxon test and control-ling for the Type I errors across thesecomparisons at the .05 level using the LSDprocedure. The ranks for VRET (p = .006)and PE (p = .02) were significantly greaterthan the rank for SER. Analyses revealed noother significant differences in preferredranking of treatments.
DiscussionThis is one of the first studies to system-
atically compare OEF/OIF veterans’ per-ceptions of different treatment modalities

for PTSD. Results of this study suggest thatveterans may prefer and believe PE andVRET to be more credible than SER. In ad-dition, they may find SER to be more so-cially stigmatizing than the other threetreatments (PE, VRET, or PSG). This find-ing is consistent with results found in civil-ian studies of treatment preference in whichparticipants generally showed a bias againstthe use of SER (Cochran et al., 2008; Feeny,Zoellner, & Kahana, 2009; Feeny, Zoellner,Mavissakalian, et al., 2009; Roy-Byrne etal., 2003; Zoellner et al., 2009; Zoellner etal., 2003) In fact, in at least one study, re-ceiving detailed information about SER, in-cluding treatment mechanism, strength-ened participants’ bias against the use ofSER for PTSD treatment (Feeny, Zoellner,& Kahana, 2009). Thus, despite its evi-dence of efficacy, it may be beneficial to offerother treatment options besides pharma-cotherapy (such as sertraline) to OEF/OIFveterans. Simply providing psychoeduca-tion about the medication may not increaseits credibility or veterans’ preference for it.
No significant differences emerged intreatment preference or ratings of socialstigma or credibility/expectancy betweenthe three psychosocial treatments (PE,VRET, or PSG). Although small sample sizemay account for these null findings, it also ispossible that veterans do not distinguishdifferences between psychosocial treat-ments. Research on the acceptability andpreference for technology-based interven-
tions appear to be mixed. While there arereports that consumers find computer-assisted therapy acceptable (Gavin,Cuijpers, Craske, McEvoy, & Titov, 2010;MacGregor, Hayward, Peck, & Wilkes,2009), there is some evidence that attritionmay be higher in those participating incomputer-assisted treatments compared totreatment as usual (de Graaf, Huibers,Riper, Gerhards, & Arntz, 2009; Waller &Gilbody, 2009). Undergraduate studentsrated technology-based treatments, includ-ing VRET, as the least preferred treatmentsamong 14 possible treatments for PTSD(Tarrier et al., 2006) and one-fifth of pa-tients refused computer-aided treatment foranxiety and depression when it was offeredto them (Marks et al., 2003). Thus, the pur-ported advantage of VRET as being morecredible and acceptable than traditionalface-to-face psychotherapy (Rizzo et al.,2008b) may not hold true.
In this study, perceptions of self-stigmafor seeking treatment did not differ be-tween the four types of treatments, suggest-ing that social stigma may play a more vitalrole in veterans’ treatment seeking.However, in a recent study of veterans (N =490) that included OEF/OIF veterans (n =248), veterans identified both types ofstigma (self and social) as barriers to care forPTSD (Ouimette et al., 2011). In this study,Ouimette et al. used a study-specific mea-sure to assess the two types of stigma.Examination of the items shows that
Ouimette et al.’s self-stigma items assessmore the emotional discomfort associatedwith treatment than one’s self-esteem beingdevalued from seeking treatment. Thus,study differences may be the result of howself-stigma was measured in the two stud-ies.
The results of this study should be inter-preted with caution due to significant limi-tations of the study. First, null findings mayhave been due to lack of power associatedwith the small sample size. Veterans in thissample were also self-selected, and most didnot meet criteria for PTSD or any Axis I dis-order. Therefore, their perceptions of treat-ments for PTSD may differ from thoseveterans with PTSD or other mental healthconditions. Although we asked veterans torespond as if they themselves were experi-encing symptoms, asking people to imaginehaving a mental health problem, such asPTSD, is not the same as getting the opin-ion of those who do have mental healthproblems. Further, more than half (61%) ofthe sample reported a history of mentalhealth treatment; thus, the results of thisstudy may not generalize to those naïve tomental health treatment, which may be alarge portion of OEF/OIF veterans. Futureresearch is needed to examine the impact ofthe presence of mental health disorders andprevious mental health treatment historyon treatment preference and perceptions oftreatment credibility and stigma. Finally,the participants’ familiarity with the four
Self-StigmaPeer Support GroupProlonged ExposureSertralineVirtual Reality
Social StigmaPeer Support GroupProlonged ExposureSertralineVirtual Reality
Credibility/ExpectancyPeer Support GroupProlonged ExposureSertralineVirtual Reality
25.29 (5.91)26.29 (3.43)27.04 (2.63)27.02 (3.77)
5.86 (3.27)5.93 (3.68)7.21 (3.05)5.39 (2.95)
25.46 (9.13)27.54 (7.65)22.36 (7.85)27.42 (8.43)
26.80 (5.75)26.40 (2.32)26.80 (2.35)26.87 (2.69)
6.30 (2.87)6.50 (3.41)7.30 (2.67)5.20 (1.81)
23.00 (9.65)23.40 (7.86)21.00 (8.31)26.00 (9.75)
24.44 (5.99)26.22 (3.98)27.17 (2.83)27.10 (4.34)
5.61 (3.53)5.61 (3.88)7.17 (3.31)5.50 (3.47)
26.83 (8.81)29.83 (6.68)23.11 (7.71)28.21 (7.78)
25.06 (6.61)25.89 (4.00)26.78 (3.14)26.32 (4.25)
5.61 (3.65)5.72 (4.08)7.11 (3.41)5.22 (3.41)
26.06 (8.12)27.89 (7.21)22.56 (8.33)27.04 (8.99)
25.70 (4.69)27.00 (2.05)27.50 (1.35)28.27 (2.43)
6.30 (2.58)6.30 (2.98)7.40 (2.41)5.70 (2.00)
24.40 (11.13)26.90 (8.76)22.00 (6.09)28.10 (7.72)
Table 2. Means and Standard Deviations for Stigma Measures (N = 28)
Measure M (SD)EntireSample(N = 28)
M (SD)With Axis 1a
(n = 10)
M (SD)WithoutAxis 1b
(n = 18)
M (SD)WithPrevious txc
(n = 18)
M (SD)WithoutPrevious txd
(n = 10)
Note. aParticipants who met criteria for an Axis I disorder. bParticipants who did not meet criteria for any Axis I disorder. cParticipants whoreported previous mental health treatment. dParticipants who did not report any previous mental health treatment.
176 the Behavior Therapist

October • 2013 177
types of treatment also may have influencedparticipants’ responses. Although theVeterans Administration has made efforts toincrease availability of evidence-based psy-chological treatments for PTSD (e.g., pro-longed exposure and cognitive processingtherapy) in recent years (Department ofVeterans Affairs, Veterans HealthAdministration, 2010; Karlin et al., 2010),the participants in this study may not havebeen as aware of the availability of PE at theVeterans Administration health care facili-ties compared to pharmacotherapy, groupcounseling, or general (i.e., unspecified) in-dividual counseling. Further most VAhealth care facilities likely do not have thenecessary equipment for providing VRET.Thus, the perceived novelty of PE andVRET compared to pharmacotherapy andgroup counseling may have influenced par-ticipants’ responses.
Overall, the results of this study suggestthat OEF/OIF veterans, like civilians, mayhave a preference for psychosocial treat-ment over pharmacotherapy, even after re-ceiving information about SER’seffectiveness. This study, along with civilianresearch, shows that simply educating po-tential clients about the availability and ef-fectiveness of treatments may not increaseits uptake. Instead, it may be more benefi-cial to offer multiple treatment options sothat veterans may select a treatment that isconsistent with their personal beliefs. In ad-dition to interventions to reduce perceivedself-stigma regarding mental health treat-ment, efforts to reduce treatment-stigma inloved ones and colleagues may facilitatetreatment-seeking in OEF/OIF veteransgiven some evidence that encouragement toparticipate in treatment from others ap-pears to increase treatment-seeking behav-iors, despite the presence of other barriers tocare (e.g., having negative beliefs abouttreatment; Sayer et al., 2009). Future re-search should examine how local policiesimpact treatment seeking and treatmenttype and how educating the friends andfamilies of veterans affects perceived stigmaand help seeking among veterans. Futurestudies on treatment preference and stigmafor PTSD among OEF/OIF veterans needto be replicated with a sample of those diag-nosed with PTSD, as we were unable to re-cruit such a sample.
ReferencesArmenian, H. K., Morikawa, M., Melkonian, A.
K., Hovanesian, A. P., Haroutunian, N.,Saigh, P. A., . . . Akiskal, H. (2000). Loss as adeterminant of PTSD in a cohort of adultsurvivors of the 1988 earthquake in
Armenia: implications for policy. ActaPsychiatrica Scandinavica, 102(1), 58-64.
Becker, C. B., Darius, E., & Schaumberg, K.(2007). An analog study of patient prefer-ences for exposure versus alternative treat-ments for posttraumatic stress disorder.Behaviour Research and Therapy, 45(12), 2861-2873. doi: S0005-7967(07)00111-8 [pii]10.1016/j.brat.2007.05.006
Blake, D. D., Weathers, F. W., Nagy, L. M.,Kaloupek, D. G., Gusman, F. D., Charney,D. S., & Keane, T. M. (1995). The develop-ment of a Clinician-Administered PTSDScale. Journal of Traumatic Stress, 8(1), 75-90.
Borkovec, T. D., & Nau, S. D. (1972).Credibility of analogue therapy rationales.Journal of Behavior Therapy and ExperimentalPsychiatry, 3, 257-260.
Boudewyns, P. A., Hyer, L., Woods, M. G.,Harrison, W. R., & McCranie, E. (1990).PTSD among Vietnam Veterans: An earlylook at treatment outcome using direct ther-apeutic exposure. Journal of Traumatic Stress,3(3), 359-368.
Brady, K., Pearlstein, T., Asnis, G. M., Baker, D.,Rothbaum, B., Sikes, C. R., & Farfel, G. M.(2000). Efficacy and safety of sertraline treat-ment of posttraumatic stress disorder: A ran-domized controlled trial. Journal of theAmerican Medical Association, 283(14), 1837-1844.
Brewin, C. R., Andrews, B., & Valentine, J. D.(2000). Meta-analysis of risk factors for post-traumatic stress disorder in trauma-exposedadults. Journal of Consulting and ClinicalPsychology, 68(5), 748-766.
Brown, M. C., Creel, A. H., Engel, C. C.,Herrell, R. K., & Hoge, C. W. (2011).Factors associated with interest in receivinghelp for mental health problems in combatveterans returning from deployment to Iraq.Journal of Nervous and Mental Disease,199(10), 797-801. doi: 10.1097/NMD.0b013e31822fc9bf00005053-201110000-00012 [pii]
Cochran, B. N., Pruitt, L., Fukuda, S., Zoellner, L.A., & Feeny, N. C. (2008). Reasons underlyingtreatment preference: an exploratory study.Journal of Interpersonal Violence, 23(2), 276-291. doi: 23/2/276 [pii]10.1177/0886260507309836
Coker, A. L., Davis, K. E., Arias, I., Desai, S.,Sanderson, M., Brandt, H. M., & Smith, P.H. (2002). Physical and mental health ef-fects of intimate partner violence for men andwomen. American Journal of PreventativeMedicine, 23(4), 260-268. doi: S0749379702005147 [pii]
Cooper, N. A., & Clum, G. A. (1989). Imaginalflooding as a supplementary treatment forPTSD in combat veterans: A controlledstudy. Behavior Therapy, 20(3), 381-391.
Davidson, J. R. T., Rothbaum, B. O., van derKolk, B. A., Sikes, C. R., & Farfel, G. M.(2001). Multicenter, double-blind compari-son of Sertraline and placebo in the treat-ment of posttraumatic stress disorder.Archives of General Psychiatry, 58(5), 485-492.
de Graaf, L. E., Huibers, M. J., Riper, H.,Gerhards, S. A., & Arntz, A. (2009). Use andacceptability of unsupported online comput-erized cognitive behavioral therapy for de-pression and associations with clinicaloutcome. Journal of Affective Disorders, 116(3),227-231. doi: S0165-0327(08)00487-4 [pii]10.1016/j.jad.2008.12.009
Department of Veterans Affairs, Veterans HealthAdministration. (2010). Programs for veteranswith post-traumatic stress disorder (PTSD).(VHA Handbook No. 1160.03).
Feeny, N. C., Zoellner, L. A., & Kahana, S. Y.(2009). Providing a treatment rationale forPTSD: does what we say matter? BehaviourResearch and Therapy, 47(9), 752-760. doi:S0005-7967(09)00141-7 [pii]10.1016/j.brat.2009.06.007
Feeny, N. C., Zoellner, L. A., Mavissakalian, M.R., & Roy-Byrne, P. P. (2009). What wouldyou choose? Sertraline or prolonged exposurein community and PTSD treatment seekingwomen. Depression and Anxiety, 26(8), 724-731. doi: 10.1002/da.20588
Gavin, A., Cuijpers, P., Craske, M. G., McEvoy,P., & Titov, N. (2010). Computer therapy forthe anxiety and depressive disorders is effec-tive, acceptable, and practical health care: Ameta-analysis. PloS one, 5(10), e13196.
Gerardi, M., Rothbaum, B. O., Ressler, K.,Heekin, M., & Rizzo, A. (2008). Virtual real-ity exposure therapy using a virtual Iraq: casereport. Journal of Traumatic Stress, 21(2), 209-213.
Gregurek, R., Pavic, L., Vuger-Kovacic, H.,Potrebica, S., Bitar, Z., Kovacic, D., . . .Klain, E. (2001). Increase of frequency ofpost-traumatic stress disorder in disabledwar veterans during prolonged stay in a reha-bilitation hospital. Croatian Medical Journal,42(2), 161-164.
Hoge, C. W., Castro, C. A., Messer, S. C.,McGurk, D., Cotting, D. I., & Koffman, R.L. (2004). Combat duty in Iraq andAfghanistan, mental health problems, andbarriers to care. New England Journal ofMedicine, 351(1), 13-22.
Karlin, B. E., Ruzek, J. I., Chard, K. M.,Eftekhari, A., Monson, C. M., Hembree, E.A., & Foa, E. B. (2010). Dissemination of ev-idence-based psychological treatments forposttraumatic stress disorder in the VeteransHealth Administration. Journal of TraumaticStress, 23, 663–673.
Keane, T. M., Fairbank, J. A., Caddell, J. M., &Zimering, R. T. (1989). Implosive (flooding)therapy reduces symptoms of PTSD inVietnam combat veterans. Behavior Therapy,20, 254-260.
Kim, P. Y., Britt, T. W., Klocko, R. P., Riviere, L.A., & Adler, A. W. (2011). Stigma, negativeattitudes about treatment, and utilization ofmental health care among soldiers. MilitaryPsychology, 23, 65-81.
Komiya, N., Good, G. E., & Sherrod, N. B.(2000). Emotional openness as a predictor ofcollege students' attitudes toward seeking

178 the Behavior Therapist
psychological help. Journal of CounselingPsychology, 47, 138-143.
Lund, M., Foy, D., Sipprelle, C., & Strachan, A.(1984). The Combat Exposure Scale: A sys-tematic assessment of trauma in the VietnamWar. Journal of Clinical Psychology, 40, 1323-1328.
MacGregor, A. D., Hayward, L., Peck, D. F., &Wilkes, P. (2009). Empirically groundedclinical interventions clients' and referrers'perceptions of computer-guided CBT(FearFighter). Behavioural and CognitivePsychotherapy, 37(1), 1-9. doi: S135246580800492X[pii]10.1017/S135246580800492X
Marks, I. M., Mataix-Cols, D., Kenwright, M.,Cameron, R., Hirsch, S., & Gega, L. (2003).Pragmatic evaluation of computer-aided self-help for anxiety and depression. BritishJournal of Psychiatry, 183, 57-65.
McLay, R. N., McBrien, C., Wiederhold, M. D., &Wiederhold, B. K. (2010). Exposure therapywith and without virtual reality to treatPTSD while in the combat theater: a parallelcase series. Cyberpsychology, Behavior, and SocialNetworking, 13(1), 37-42. doi: 10.1089/cyber.2009.0346 [pii]
McLay, R. N., Wood, D. P., Webb-Murphy, J. A.,Spira, J. L., Wiederhold, M. D., Pyne, J. M.,& Wiederhold, B. K. (2011). A randomized,controlled trial of virtual reality-graded ex-posure therapy for post-traumatic stress dis-order in active duty service members withcombat-related post-traumatic stress disor-der. Cyberpsychology, Behavior, and SocialNetworking, 14(4), 223-229. doi:10.1089/cyber.2011.0003
Milliken, C. S., Auchterlonie, J. L., & Hoge, C.W. (2007). Longitudinal assessment of mentalhealth problems among active and reservecomponent soldiers returning from the Iraqwar. Journal of the American MedicalAssociation, 298(18), 2141-2148.
Nash, W. P., Silva, C., & Litz, B. T. (2009). Thehistoric origins of military and veteran mentalhealth stigma and the stress injury model as ameans to reduce it. Psychiatric Analysis, 39,789-794.
Ouimette, P., Vogt, D., Wade, M., Tirone, V.,Greenbaum, M. A., Kimerling, R., . . .Rosen, C. S. (2011). Perceived barriers to careamong veterans health administration pa-tients with posttraumatic stress disorder.Psychological Services, 8(3), 212-223.
Owens, G. P., Herrera, C. J., & Whitesell, A. A.(2009). A preliminary investigation of men-tal health needs and barriers to mental healthcare for female veterans of Iraq andAfghanistan. Traumatology, 15, 31-37.
Ozer, E. J., Best, S. R., Lipsey, T. L., & Weiss, D.S. (2003). Predictors of posttraumatic stressdisorder and symptoms in adults: A meta-analysis. Psychological Bulletin, 129(1), 52-73.
Pietrzak, R. H., Johnson, D. C., Goldstein, M.B., Malley, J. C., Rivers, A. J., Morgan, C. A.,& Southwick, S. M. (2010). Psychosocialbuffers of traumatic stress, depressive symp-toms, and psychosocial difficulties in veter-
ans of Operations Enduring Freedom andIraqi Freedom: the role of resilience, unitsupport, and postdeployment social support.Journal of Affective Disorders, 120(1-3), 188-192. doi: S0165-0327(09)00164-5 [pii]10.1016/j.jad.2009.04.015
Pietrzak, R. H., Johnson, D. C., Goldstein, M.B., Malley, J. C., & Southwick, S. M. (2009).Psychological resilience and postdeploymentsocial support project against traumaticstress and depressive symptoms in soldiersreturning from Operations EnduringFreedom and Iraqi Freedom. Journal of SpecialOperations Medicine, 9(3), 67-73.
Pitman, R. K., Orr, S. P., Altman, B., Longpre,R. E., Poire, R. E., Macklin, M. L., . . .Steketee, G. S. (1996). Emotional processingand outcome of imaginal flooding therapy inVietnam veterans with chronic posttrau-matic stress disorder. Comprehensive Psychiatry,37(6), 409-418.
Reger, G. M., & Gahm, G. A. (2008). Virtual re-ality exposure therapy for active duty sol-diers. Journal of Clinical Psychology, 64(8),940-946.
Rizzo, A. A., Difede, J., Rothbaum, B. O.,Johnston, S., McLay, R. N., Reger, G., . . .Pair, J. (2009). VR PTSD exposure therapyresults with active duty OIF/OEF combat-ants. Studies in Health Technology andInformatics, 142, 277-282.
Rizzo, A. A., Graap, K., Perlman, K., McLay, R.N., Rothbaum, B. O., Reger, G., . . . Pair, J.(2008a). Virtual Iraq: Initial results from aVR exposure therapy application for combat-related PTSD. Studies in Health Technology andInformatics, 132, 420-425.
Rizzo, A. A., Graap, K., Perlman, K., McLay, R.N., Rothbaum, B. O., Reger, G., . . . Pair, J.(2008b). Virtual Iraq: initial results from aVR exposure therapy application for combat-related PTSD. Studies in Health Technology &Informatics, 132, 420-425.
Rosen, C. S., Greenbaum, M. A., Fitt, J. E.,Laffaye, C., Norris, V. A., & Kimerling, R.(2011). Stigma, help-seeking attitudes, anduse of psychotherapy in veterans with diag-noses of posttraumatic stress disorder. Journalof Nervous and Mental Disease, 199(11), 879-885. doi: 10.1097/NMD.0b013e3182349ea500005053-201111000-00011 [pii]
Roy-Byrne, P., Berliner, L., Russo, J., Zatzick, D.,& Pitman, R. K. (2003). Treatment prefer-ences and determinants in victims of sexualand physical assault. Journal of Nervous andMental Disease, 191(3), 161-165. doi:10.1097/01.NMD.0000055343.62310.73
Sayer, N. A., Friedemann-Sanchez, G., Spoont,M., Murdoch, M., Parker, L. E., Chiros, C., &Rosenheck, R. (2009). A qualitative study ofdeterminants of PTSD treatment initiationin veterans. Psychiatry: Interpersonal andBiological Processes, 72(3), 238-255. doi:10.1521/psyc.2009.72.3.23810.1521/psyc.2009.72.3.238 [pii]
Seal, K. H., Maguen, S., Cohen, B., Gima, K. S.,Metzler, T. J., Ren, L., . . . Marmar, C. R.(2010). VA mental health services utilization
in Iraq and Afghanistan veterans in the firstyear of receiving new mental health diag-noses. Journal of Traumatic Stress, 23(1), 5-16.doi: 10.1002/jts.20493
Sheehan, D. V., Lecrubier, Y., Harnett-Sheehan,K., Janavs, J., Weiller, E., Bonora, L. I., et al.(1997). Reliability and validity of the MINIInternational Neuropsychiatric Interview(M.I.N.I.): According to the SCID-P.European Psychiatry, 12, 232-241.
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H.,Amorim, P., Janavs, J., Weiller, E., et al.(1998). The Mini-International Neuropsychiatric Interview (M.I.N.I.): The devel-opment and validation of a structured diag-nostic psychiatric interview for DSM-IV andICD-10. Journal of Clinical Psychiatry, 59Suppl 20, 22-33..
Stecker, T., Fortney, J. C., Hamilton, F., & Ajzen,I. (2007). An assessment of beliefs aboutmental health care among veterans whoserved in Iraq. Psychiatric Services, 58(10),1358-1361. doi: 58/10/1358[pii]10.1176/appi.ps.58.10.1358
Tarrier, N., Liversidge, T., & Gregg, L. (2006).The acceptability and preference for the psy-chological treatment of PTSD. BehaviourResearch and Therapy, 44(11), 1643-1656.doi: S0005-7967(05)00267-6 [pii]10.1016/j.brat.2005.11.012
Tolin, D. F., & Foa, E. B. (1999). Treatment of apolice officer with PTSD using prolonged ex-posure. Behavior Therapy, 30, 527-538.
Vogel, D. L., Wade, N. G., & Haake, S. (2006).Measuring the self-stigma associated withseeking psychological help. Journal ofCounseling Psychology, 53, 325-337.
Vogt, D. (2011). Mental health-related beliefs asa barrier to service use for military personneland veterans: a review. Psychiatric Services,62(2), 135-142. doi: 62/2/135 [pii]10.1176/appi.ps.62.2.135
Waller, R., & Gilbody, S. (2009). Barriers to theuptake of computerized cognitive behav-ioural therapy: a systematic review of thequantitative and qualitative evidence.Psychological Medicine, 39(5), 705-712. doi:S0033291708004224 [pii]10.1017/S0033291708004224
Wilson, J. A. B., Onorati, K., Mishkind, M.,Reger, M. A., Gahm, G. A. (2008). Soldierattitudes about technology-based ap-proaches to mental health care.CyberPsychology & Behavior, 11(6), 767-769.
Wood, D. P., Murphy, J., Center, K., McLay, R.,Reeves, D., Pyne, J., . . . Wiederhold, B. K.(2007). Combat-related post-traumaticstress disorder: a case report using virtual re-ality exposure therapy with physiologicalmonitoring. Cyberpsychology & Behavior, 10(2),309-315.
Wood, D. P., Murphy, J. A., Center, K. B., Russ,C., McLay, R. N., Reeves, D., . . .Wiederhold, B. K. (2008). Combat relatedpost traumatic stress disorder: a multiplecase report using virtual reality graded expo-sure therapy with physiological monitoring.

October • 2013 179
Studies in Health Technology and Informatics,132, 556-561.
Zoellner, L. A., Feeny, N. C., & Bittinger, J. N.(2009). What you believe is what you want:Modeling PTSD-related treatment prefer-ences for sertraline or prolonged exposure.Journal of Behavior Therapy and ExperimentalPsychiatry, 40(3), 455-467. doi: S0005-7916(09)00028-7 [pii]10.1016/j.jbtep.2009.06.001
Zoellner, L. A., Feeny, N. C., Cochran, B., &Pruitt, L. (2003). Treatment choice forPTSD. Behaviour Research and Therapy, 41(8),879-886. doi: S0005796702001006 [pii]
. . .
Christina E. Ryan is now at Zucker HillsideHospital Psychiatry Research Department.
This study was funded by a HartfordHospital grant. We thank the veterans fortheir participation. We would like to thank
Sara Whiting for her assistance on this study.We also thank Scott Hannan, ElizabethMoore, John Goethe, and Gwendolyn Bassettfor reviewing the treatment descriptions andMichael Moravecek for his consultations for participant recruitment.
Correspondence to Christina M. Gilliam,Ph.D., Anxiety Disorders Center, TheInstitute of Living/ Hartford Hospital, 200Retreat Avenue, Hartford, CT 06106;[email protected]
I shall not today attempt further to define thekinds of material I understand to be em-braced within that shorthand description;and perhaps I could never succeed in intelligi-bly doing so. But I know it when I see it…and the motion picture involved in this case isnot that.
—Justice Potter Stewart, concurringopinion in Jacobellis v. Ohio 378 U.S.184 (1964), regarding possible ob-scenity in The Lovers
The quote by Justice Potter Stewart(1964), “I know it when I see it,”while originally in reference to the
use of explicit images, could also be used todescribe the common experience of clini-cians when diagnosing individuals with nar-cissistic personality disorder (NPD). Manyof us who have treated individuals withNPD, or any Axis II pathology, can resonatewith the idea of “having that feeling,” “hav-ing a ‘gut’ reaction,” or simply “knowing itwhen we see it.”
The controversy, difficulty, and reluc-tance of assigning Axis II diagnoses have
been well documented (Miller & Campbell,2010; Pincus, 2011; Ronningstam, 2011).In the Diagnostic and Statistical Manual ofMental Disorders (2000, p. 717; DSM-IV-TR), narcissistic personality disorder is de-fined by the following criteria (boldfacetype indicates what we believe to be the op-erative or troubling word or phrase in eachcriterion):
A pervasive pattern of grandiosity (infantasy or behavior), need for admiration,and lack of empathy, beginning by earlyadulthood and present in a variety of con-texts, as indicated by five (or more) of thefollowing:
(1) has a grandiose sense of self-impor-tance (e.g., exaggerates achievementsand talents, expects to be recognized assuperior without commensurateachievements)
(2) is preoccupied with fantasies ofunlimited success, power, brilliance,beauty, or ideal love
(3) believes that he or she is “special”and unique and can only be understood
by, or should associate with, other specialor high-status people (or institutions)
(4) requires excessive admiration (5) has a sense of entitlement, i.e., un-
reasonable expectations of especially fa-vorable treatment or automaticcompliance with his or her expectations
(6) is interpersonally exploitative, i.e.,takes advantage of others to achieve hisor her own ends
(7) lacks empathy: is unwilling to rec-ognize or identify with the feelings andneeds of others
(8) is often envious of others or believesthat others are envious of him or her
(9) shows arrogant, haughty behav-iors or attitudes
In reviewing the DSM-IV-TR criteria, weknow what it says, but what exactly does itmean? While aspects of defining NPD areoften controversial, per DSM-IV-TR, thehallmark feature of the disorder is grandios-ity.
Merriam-Webster defines grandiosity(www.merriam-webster.com) as (a) charac-terized by affectation of grandeur or splen-dor or by absurd exaggeration or (b)impressive because of uncommon largeness,scope, effect, or grandeur. According to theDSM-IV-TR, this grandiosity manifests it-self in three primary ways: (a) an inflatedsense of self-importance, (b) limitless fan-tasies, and (c) extreme behaviors. The firsttwo aspects of self-importance and fantasyoccur more internally, yet tend to be mani-fested externally in the individual’s behav-ior. For instance, suppose a young woman,new to her job in the corporate world, be-
Clinical Forum
The Challenges in Diagnosing NarcissisticPersonality Disorder: Difficult to Define, but “We Know It When We See It”
Arthur Freeman, Angela Breitmeyer, and Melissa Flint, Midwestern University
Meet ABCT’s Featured Therapists
What is the last book you read?“The Political Brain by Drew Weston, aclinical psychologist. This is very muchworth reading by any cognitive behav-ior therapist interested in how emotionsare engaged to influence (and can beused to alter) cognitions and behavior,in this case the thoughts and actions ofvoters.”
―Gerald Stein, Ph.D., ABCT Featured Therapist
www.abct.org/Public/?m=mPublic&fa=ClinicianMonth
Don’t miss these in-depth interviews at

180 the Behavior Therapist
lieves she is the most valuable asset to hercompany (inflated sense of self-importance).She firmly believes that within months, sheis going to begin her “climb of the corporateladder” and will eventually be named CEO,recognized by Fortune 500, and interna-tionally known (limitless fantasies).Consequently, she sees herself parking inthe CEO’s reserved parking space and de-mands that she be assigned a personal assis-tant for her entry-level position. However,her work has been criticized by her supervi-sor as being superficial and incomplete.Rather than taking the feedback and cor-recting her work, she makes an appoint-ment with her supervisor’s supervisor aboutbiased and inappropriate feedback becauseshe views her work as excellent. Thus, herexternal behaviors of parking in the CEO’sreserved space and demanding a personalassistant are an outward manifestation ofher internal high regard for herself.
Although grandiosity is clearly definedthrough Merriam-Webster, other wordswithin the definition are somewhat vague.Below are proposed descriptors of each ofthese terms:
Pervasive: This implies that the behaviorin part is manifested throughout the indi-vidual’s life experience (e.g., work, inter-personal relationships, family life).
Need: The pattern of seeking specialtreatment is not simply a desire, wish, oraspiration, but something that involves acraving.
Lack: The term “lack” seems to denote anabsence of empathy rather than a limitedfund of empathy; it is rarely an all-or-nothing issue.
Exaggerate: Exaggeration can involve asmall embellishment, inflation, or over-statement or a powerful and unrealisticamplification.
Without commensurate achievement:The issue of what is commensurate is de-batable. Who judges whether an achieve-ment warrants special notice?
Preoccupied: A question to ask wouldbe, is the preoccupation pervasive or tran-sient?
Unlimited: This is an unrealistic criterioninasmuch as most narcissists do havesome idea of limits and boundaries. If theindividual’s view is, indeed, unlimited andthat is required for the diagnosis, it wouldleave far fewer individuals being diag-nosed with this disorder.
Special and unique: One can make thecase that we are all special and unique,
and that specialness defines the issue ofdiversity.
Excessive: A question to ask would be, Isthe excess also pervasive or more attachedto specific issues, persons, opportunities,and settings?
Unreasonable expectations: What maybe deemed as unreasonable by one personmay not be seen by others as unreason-able.
Takes advantage of others: What is notspecified is how, when, why, and wherethe manipulation or misuse occurs. Whatis the cost to the individual that is beingmistreated?
Lacks empathy: Here, again, the issue isnot a total lack of empathy but a misuseof the empathic process or limited empa-thy.
Arrogant, haughty behaviors or atti-tudes: For the observer of specific behav-iors, any lack of humility may be viewedas arrogant and inappropriate.
In addition to the terms containedwithin the diagnostic criteria, the clinicalliterature on NPD is largely abstract, theo-retical, and general (Ashmun, 2004). Thus,what we propose is viewing NPD through alens on three fronts. First, we need to estab-lish that there are several subcategories ofNPD which will be identified and expli-cated. For the purposes of this article, we areproposing ten distinct narcissistic subtypes,as originally proposed by Freeman and Fox(2012): positive self-esteem; healthy;group; helpful; real; compensated; oblivi-ous; ruthless; hypervigilant; and helpless.Thus, our approach would be categorical—however, we view the different subtypes on acontinuum of severity and “normal.” Whiletwo proposed subtypes (i.e., positive self-es-teem and healthy narcissism) would not beconsidered pathological per se, these classi-fications serve as “anchor points” to concep-tualize the full spectrum of narcissism, froma “normal” baseline through severe pathol-ogy. Second, there is a need to identify theunique manifestation as a primarily inter-nalizing disorder, primarily externalizingdisorder, or combined type (Krueger,McGue, & Iacono, 2001). Thus, our ap-proach would be dimensional. Finally, eachsubtype would receive a severity ratingfrom 1 to 4 based upon the level of func-tional impairment. Thus, our approachwould be hierarchical. All of these factorscombined—i.e., the categories, dimensions,and hierarchy—would yield a more specific
diagnosis and lead the clinician to be able todo specific treatment planning.
In order to fully capture the broad ex-panse of possible human experience with re-gard to the narcissistic spectrum (rangingfrom “normal” behaviors to those consid-ered to be more pathological), we suggestdividing behaviors into 10 subclassificationsnoted above. Depending on the situation-specific cultural implications, some of thesebehaviors and subclassifications might beviewed as normal cultural experiences ofsome diverse groups; however, for others,these behaviors might be seen as clearly dif-ferent from the cultural expectations of thepredominant culture in their area. Takingthat into account, these classifications focuson the phenomenological experience of thatperson and those around him/her. This willallow us to view narcissism through thesedifferent lenses. It also warrants that weconceptualize and treatment plan based onthe levels of severity, which require specifictherapeutic approaches (Freeman & Fox,2012), which be discussed in the next tBTarticle on this topic. The subtypes can bedefined as follows:
Subtype 1: “Positive Self-Esteem”When looking at the full continuum of
any issue, we must include what some maysuggest is “normal” or “expected.” For ex-ample, if one were to hear Michael Phelpsdeclare that he was the most decoratedOlympian of all time, not only would he bereciting fact, he would be expected to showa great deal of pride in the accomplishmentat hand. When there is evidence that the as-sertion is correct, we call this positive or“healthy” self-esteem, rather than labelingit negative in any way. Therefore, it anchorsthe least deviant or “normal” end of thespectrum. Typical automatic thoughts forthis subtype are: “I am proud of my accom-plishments,” “I have achieved great things,”“I am pleased with what I have done,” and“Hard work and practice pay off.”
Case Example
Jason is a 30-year-old male who wasasked to give a college commencementspeech at his alma mater, StanfordUniversity. Jason takes great pride in his ac-complishment of earning his Ph.D. atStanford at age 24. He is not waving a flag orbragging that he went to a better schoolthan others—he is stating, matter of fact,what he has earned. The key word is that hehas earned his degree through effort, dedi-cation, and hard work.

October • 2013 181
Subtype 2: “Healthy” NarcissismCertainly there are people who have gifts
and/or outstanding attributes. While theyare “special” in this sense, they do not ap-pear to have a need or desire to flaunt this toothers. They may give to charities that areclose to them, but they do not go on prime-time television to do so. As mentioned inFreeman and Fox (2012), an example ofsuch a person is Bill Gates. Despite his for-tune, he remains fairly quiet and humble inthe public eye (to date). Typical automaticthoughts for this subtype are: “My accom-plishments set me apart from others,” “Ihave achieved at a higher level than mostmy age,” and “I recognize that I work hardand do great work.” Typical automaticthoughts for this subtype are: “I am proudof myself,” “It is not necessary to shout outmy accomplishments but I would be proudto discuss them,” or “There is no need forfalse humility.”
Case Example
Margaret is a 47-year-old retired AirForce officer. She received a military honorin which she was awarded a medal and alapel pin. Every day, she wears her lapel pin“proudly, but not loudly.” Everyone whocomes in contact with her will see her pin,but she will not go out of her way to make apoint of announcing her honor.
Subtype 3: “Group” NarcissismThe “specialness” of these individuals
was bestowed upon them because of theirmembership in an organization or group.With the definition of a group being quiteopen, this could refer to a gang, family sys-tem, school, social club, work organization,or even religious group. If the group were tono longer exist, the elevated status wouldalso disperse. For example, if one was in-vited into a specific club based on living in acertain gated community, “outsiders”would be unwelcome because they mightbe considered to be of “lesser” status. If amember was to move from that commu-nity, their membership would also be void.Typical automatic thoughts of this subtypeare: “Others wish they could be me,” “I ama member of a powerful group,” and“People should feel special to associate withme.”
Case Example
Timothy is a 16-year-old teenager whorecently joined a powerful local gang. As agang member, he saw himself as more spe-cial than nongang members and deservingof prestige and status. He also recognizedthe benefits and “safety” of this gang out-
weighed the disadvantages and were worththe risk. One day, he forgot to wear the sig-nature red and black colors of his gang anddid not receive the typical recognition hehad come to expect. After that day, he wassure to remember to wear the gang’s colors,as that offered him a sense of protection andprestige.
Subtype 4: “Helpful” NarcissismPersons with characteristics of helpful
narcissism are often unaware that theirguiding and correcting of others is per-ceived to be negative. This person feels freeto correct family, peers, colleagues and evenstrangers without invitation. Their “offer”of help, even when overtly rejected, is con-tinued despite pleas from those involved forthe “help” to stop. In other words, their per-ception is that they are “on a mission” tohelp others, whether called upon or not.Thus, their personal identity is based onhow helpful they are to others, which canonly be defined internally. One example ofsuch behavior may occur within the boundsof an adult child’s marriage. The “helpful”parent might comment on the child rearingor housekeeping skills of the adult child.Despite requests to cease such behavior, theparent continues, interjecting their ideas,perhaps going as far as moving items in thehome and/or changing household rules withregard to the children. Typical automaticthoughts of this subtype are: “If people lis-tened to me, they would get things doneright,” “Others would be lost without me,”“I play an important role in ensuring thatthings run smoothly,” or, “If I really wantedyour opinion I would tell you what thatopinion should be.”
Case Example
Helen, a 69-year-old female, lives acrosstown from her son and his wife and threechildren. She comes to their home almostdaily, lets herself in with her key, mightcome at very early hours, helps herself totheir home, insisting that she is the expertin all things, especially child rearing andhomemaking. This, of course, causes a greatdeal of turmoil within the family. One ex-ample of her “helpfulness” included a tutor-ial on the only way to appropriately vacuuma living room in the most aesthetic way.
Subtype 5: “Real” NarcissismThe superiority asserted by those who
have characteristics of “real” narcissism re-quires that they be constantly justified byothers and validated to maintain their per-ceived elite status. They are quite openabout the unique attributes that they (and
often only they) can bring to the situationfor which others around them should bethankful. Typical automatic thoughts forthis subtype are: “I am superior to others,”“My accomplishments well exceed those ofeveryone else,” and “People should be hon-ored to be in my presence.”
Case Example
Jennifer is a 31-year-old woman whopresents to therapy at the request of her em-ployer as a contingency of her professionaldevelopment plan. She is quite angry aboutthis plan and declares several times that she“doesn’t need to be here.” She identifies thatshe has been falsely accused of being “ver-bally aggressive” and “overbearing” to-wards lateral peers and managers alike. Shefeels that they lack appreciation for all shebrings to the table and wonders what willhappen when the “whole place falls apartwhen she leaves over this [explicative]” be-cause “without [her], nothing will getdone!”
Subtype 6: “Compensated” NarcissismThis person creates a superhero façade to
cover up for perceived failures. As describeddecades ago by Horney (1937), this individ-ual feels the need to inflate him- or herself toappear competent while demeaning and de-grading others. Typical automatic thoughtsfor this subtype are: “Other people are so in-competent,” “I am truly powerful,” and“Others should recognize my superiority.”
Case Example
Tom is a 40-year-old male who, in de-scribing his family-of-origin experience,identified himself as the “runt of the litter,”the “dummy,” the “loser,” and the “failure ofthe family.” Tom is a community collegedropout; his siblings have completed med-ical, law, and doctorate degrees. In Tom’sdescription of others at work, he declaredhimself to be “superman” and consistentlydegraded others, labeling them “incompe-tent” and “stupid.” It appears that Tomraises himself above others, not throughperformance but by standing upon theirbacks.
Subtype 7: “Oblivious” NarcissismQuite literally, these individuals are
oblivious to their impact on others. Theyare often so offensive that they are excludedfrom events or groups, only to complainthat they have no idea why they have beenexcluded. They may not intentionally setout to offend, but they do—repeatedly.With no awareness that “the foot has beeninserted into the mouth” yet again, they

182 the Behavior Therapist
move forward through life with a path ofdevastation in their wake. Typical auto-matic thoughts for this subtype are: “Peoplecannot handle the truth,” “I wish peoplewould just realize their incompetence,” and“I cannot understand why someone wouldnot want to be with me.”
Case Example
Sarah is pleased and proud of what shedescribes as her caustic wit and her ability to“cut to the chase” and call a “spade a spade.”She is often at a loss to explain why she hasfew friends, fewer dates, and, at age 37, hasnever had a relationship that lasted morethan 3 months. When asked to explain thisstate of affairs, she states, “People just don’tlike to hear it like it really is.”
Subtype 8: “Hypervigilant” NarcissismIndividuals who struggle with the hy-
pervigilant subtype may often be seen asparanoid. They are constantly on guard forwhomever might be the next assailant ontheir integrity. They tend to be “on guard24/7” and easily provoked to counterattackwhen presented with the most nonthreat-ening of discourse. Typical automaticthoughts for this subtype are: “Why arepeople always out to get me?” “I wish otherswould not be so hostile towards me,” and“What is it with people these days?”
Case Example
Patty, a 19-year-old woman, was expect-ing a phone call from her friend at 7:00 P.M.At 7:20, Patty’s friend called her, explainingthat she was stuck in traffic. Patty statedthat she “didn’t want to hear any more ex-cuses” and exclaimed, “How dare you for-get about our phone call!”
Subtype 9: “Ruthless” NarcissismThis type of narcissism describes the per-
son who actually gains satisfaction or enjoy-ment from being party to the humiliation ofothers. They may bully, insult, tease, pointout flaws in others, and gain satisfaction inembarrassing others publically. At times,they may even find this humorous and at-tempt to have others join in on the “fun”against an identified victim. They appear tolack empathy. Typical automatic thoughtsfor this subtype are: “It does not matterwhat other people think of me,” “I do notcare about the feelings of others,” and“People better get out of my way.”
Case Example
Eddie is a 42-year-old man who was at-tending his weekly poker night. One of hisfriends brought along his brother-in-law,who came from a small farming town.
Within minutes of his arrival, Eddie offeredup a toast, followed by a joke that wasderogatory toward farmers, insinuatingthat they were “stupid” and “backwards.”Despite others’ obvious discomfort, Eddiecontinued to make offensive remarks, stat-ing, “Wait ’til you hear this one, guys . . .”Several of the men left the poker table,clearly offended, while Eddie continued toverbally badger the guest.
Subtype 10: “Helpless” NarcissismIn clinical practice, these clients are
often (mis)diagnosed as having refractoryanxiety or refractory depression. The “win”in therapy for this client involves not allow-ing him- or herself to be helped. The uncon-scious mantra, “neither therapist normodality, nor hospital nor medication, canhelp,” defines what may be a rather longand complicated history. If they are refusedcare, or feel as if they are about to be re-jected, they may beg you to help them be-cause you might be “the one” who canfinally break through. Typical automaticthoughts for this subtype are: “I cannot behelped,” “My problems are far too great,”and “I wish I could find someone who trulyunderstands how bad things really are forme.”
Case Example
Carol, a 52-year-old woman, sought thehelp of a renowned psychologist as a last re-sort after countless therapy experienceswith the most highly regarded doctors. As acollege graduate and daughter of an accom-plished surgeon, she had the best opportu-nities afforded to her. Despite this, she isunemployed, lives at home, and her motheris her only friend. She has no dating historyand her life consists of walking the dog andwatching television with her mother. Hermother caters to her every whim and re-quires no remuneration in return. “You’remy only hope, doctor! Do you think youcan help me?”
In addition to the 10 proposed subtypes, wesuggest a further classification system, typi-cally used when diagnosing children (i.e.,internalizing versus externalizing disor-ders). This distinction originated from re-search on the manifestation of psycho-pathology in children suggestive of a two-factor structure (Achenbach & Edelbrock,1984). Within the context of NPD, thereare internalizing components related tonegative cognitions and externalizing com-ponents related to a lack of behavioral con-straint. Common to both internalizing andexternalizing disorders is emotional distress,
which is directed inward when individualshave appropriate levels of impulse control,and directed outward when such distress isaccompanied by a lack of impulse control(Krueger & Tackett, 2003).
Perhaps the most logical emphasisshould be on the individual’s tangible, iden-tifiable, external behaviors. For example, ifwe assign each of the 9 criteria for NPD aseither internal, external, or both, it wouldappear then that the majority of the criteriaare external: (4) requires excessive admira-tion; (6) is interpersonally exploitative; (7)lacks empathy; and (9) shows arrogant,haughty behaviors or attitudes. Three of thecriteria would be internal: (2) is preoccupiedwith fantasies of unlimited success, power,brilliance, beauty, or ideal love; (3) believesthat he or she is “special” and unique andcan only be understood by, or should associ-ate with, other special or high-status peo-ple; and (8) is often envious of others orbelieves that others are envious of him orher. Two of the criteria would be both inter-nal and external: (1) has a grandiose sense ofself-importance, exaggerating achieve-ments and expecting to be recognized as su-perior; and (5) has a sense of entitlement,i.e., unreasonable expectations or automaticcompliance.
Depending on the combination and per-mutation of criteria within clients, we candescribe various subcategories of NPD. Forinstance, if a client possessed all five of theexternal criteria, then that would be onetype of narcissism. Likewise, if a client pos-sessed all of the internal criteria, then thatwould be a second type of narcissism.Finally, if a client possessed a combinationof internal and external criteria, then thatwould be a third type of narcissism (i.e.,combined). Furthermore, narcissistic pat-terns may be a result of a diathesis-stressmodel. Individuals may have a genetic pre-disposition towards narcissistic behavior. Itis, however, in our view, the experiences inone’s family of origin and subsequent envi-ronmental reinforcement that will then dic-tate how the possible predisposition isactualized. Finally, in discussing narcissismas an externalizing behavioral pattern, par-ticularly one that is learned, there is the pos-sibility that such a pattern can beunlearned, which offers some hope in thetreatment of individuals with NPD. Forclarity, it might be helpful to consider a verycondensed version of the DSM-IV-TR crite-ria in Table 1:
In addition to an emphasis on the externalbehaviors of narcissism, another proposed

approach to the multidimensional issue ofnarcissism is to explicitly describe the sub-categories of the disorder and the relativeseverity that each category holds. The per-
son demonstrating symptoms on the mildside of the continuum within any one sub-type may be only mildly problematic tothose around him/her. However, as wemove towards the more severe side of thespectrum, the pattern of behavior becomesmore and more detrimental, not only forthe individual (although they may beg todiffer), but for the persons in both theirwork and social/ familial spheres.
Finally, a proposed severity index wouldoffer finer graduations and more opera-tional definitions of narcissistic behaviors.Essentially, this index would involve a 4-point scale, ranging from mild to severe(similar to how other disorders, such asmajor depressive disorder, are coded in theDSM-IV-TR). Below is the proposed sever-ity index:
1. Noticeable: Behavior is noticeable, butdoes not interfere with functioning. Suchindividuals would be perceived as “annoy-ing.” An example would be bragging aboutone’s accomplishments.
2. Occasional: Behavior occasionallycauses problems for the individual. In thisinstance, narcissism may intersect withother Axis II (Cluster B) pathology. For in-stance, one’s partner may perceive the indi-vidual as selfish and contemplate endingthe relationship with the individual.
3. Frequent: Behavior frequently causesproblems for the individual. For example,this individual’s sense of entitlement mayresult in problems with the law and inter-personal relationships, e.g., disciplinary ac-tions at work.
4. Severe: Behavior is severe and debili-tating, significantly impairing one’s func-tioning. This individual would not be able
to successfully maintain relationships, em-ployment, or fulfill important obligations.
Although this multifaceted systemmight present challenges at first, in the endit will yield a more specific criteria set, amore comprehensive diagnostic system,and better treatment planning. To illustratethis point, we conclude with one final caseexample.
Ferdinand, a 43-year-old married man,seeks therapy in an attempt to have thetherapist “help his family learn to mind[him] better.” He reports a history of unful-filling interpersonal relationships beginningin late adolescence (at home and in theworkplace) and several extramarital affairs.He spends every spare moment in the gym,working out (excessively?) to maintain his“Mr. Universe” physique. Furthermore, hereports that his wife is getting “a littleflabby” and that she should “hit the gym”to work on her “trouble areas.” He reportsthat his children (Ben, aged 14, and Olivia,aged 17) want “nothing to do with him.”His wife works at a full-time job, with apart-time job evenings and weekends,which Ferdinand feels limits her “availabil-ity” to cook, clean, and do her “wifely du-ties.” Over the past weekend, he reportsthat he confronted her about her lack of “at-tention” to his needs, stating, “You shouldconsider yourself lucky to have a husbandlike me! There is nobody as special as mewho would put up with someone as drab asyou!” When she failed to respond with dot-ing admiration, he made sure to inform herthat “ALL the girls in the gym tell me howbuff I am. THEY appreciate me!”
Ferdinand holds a midmanagement po-sition at a local bank and is angry over being“passed by” for several promotions. He hasrecently been reprimanded by his supervi-sor for delegating tasks to his peers, actingas if he is their supervisor when he is not.Despite these reprimands, he continues todelegate to his peers, stating that it is in the“company’s best interests.” He reportsbeing “baffled” that he is continually not in-vited to special events, parties, and outsideactivities with his coworkers because he issure he would be the “life of the party.”
In considering this case example, we willapply our system of classification illustrat-ing the use of subtype, subcategory, andseverity. According to the DSM-IV-TR cri-teria, Ferdinand clearly demonstrates thehallmark criteria of a pervasive pattern ofgrandiosity, need for admiration, and lack ofempathy (beginning by early adulthoodand present in a variety of contexts), in ad-dition to: (1) a grandiose sense of self-im-
portance, (2) a preoccupation with fantasiesof unlimited beauty, or ideal love, (4) requir-ing excessive admiration, (5) a grandiosesense of entitlement, (7) lacking empathy,and (9) showing arrogant, haughty behav-iors or attitudes. Based on the specificsymptom presentation, he meets the estab-lished criteria for the DSM-IV-TR diagnosisof NPD.
To further classify using our comprehen-sive diagnostic system, Ferdinand demon-strates a complete lack of awareness abouthis impact on others, i.e., the Oblivious sub-type. He is offensive to others and conse-quently is not included in parties, activities,and plans; however, he displays no aware-ness as to why he is excluded. For example,we have information that his children havelittle interaction with him, presumably be-cause of this type of behavior, and that hiscoworkers would rather not see him outsideof the office. Ferdinand may not intend tobe intentionally hurtful towards others, butthat is often how he comes across. For ex-ample, telling his wife to go to the gym islikely cruel in his present communicationstyle.
In addition to applying the subtype clas-sification, we also propose to use a subcate-gory classification of internal, external, andcombined. In Table 2, you will note that hehas the following combined criteria of self-importance and entitlement; the followinginternal criterion of fantasies; and the fol-lowing external criteria of admiration, lackof empathy, and arrogance. Thus, it is evi-dent that Ferdinand’s narcissism manifestsitself more externally than internally.
The last step would be applying theseverity index. When applying the severitycriteria, it is clear that Ferdinand has fre-quent problems as a result of his narcissism.Persons who fall into the frequent severitycategory display behavior that often causesproblems for the individual. For example,this individual’s sense of entitlement mayresult in problems with the law and inter-personal relationships (e.g., disciplinary ac-
1 self-importance C2 fantasies I3 special/ unique I4 admiration E5 entitlement C6 exploitative E7 lacks empathy E8 envious I9 arrogance E
Table 1
Note. C = combined; I = internalizing; E = externalizing.
1 self-importance C √2 fantasies I √3 special/ unique I4 admiration E √5 entitlement C √6 exploitative E7 lacks empathy E √8 envious I9 arrogance E √
Table 2
Note. C = combined; I = internalizing; E = externalizing.
October • 2013 183

184 the Behavior Therapist
tions at work). Thus, with Ferdinand’s over-all clinical presentation, he would be diag-nosed with NPD, oblivious subtype,primarily externalizing, frequent severity.
As shown in the example above, our sys-tem provides a much richer diagnostic pic-ture of an individual presenting with thisdisorder. Using subtypes, it allows a clini-cian to further categorize the unique mani-festation of NPD for an individual. Usingdimensions, it allows a clinician to deter-mine whether the symptoms are primarilyinternalizing, externalizing, or both. Usinga severity index, it allows a clinician to assessthe level of functional impairment. Thus,our approach could be considered categori-cal, dimensional, and hierarchical.Although not currently substantiated em-pirically, a potential future direction wouldbe to implement clinical trials in whichtherapists utilized this diagnostic system incomparison to more traditional means of di-agnostic assessment.
The DSM-IV-TR criteria provide aframework for additional classification, cat-egorization, and severity criteria. Such acomprehensive system allows the clinicianto direct care that would be specific to aclient’s unique symptom manifestation andconstellation. We are able to more ade-quately and accurately address the uniquesymptoms of clients with NPD. Now, we
not only “. . . know it when we see it” but wecan now say…“We know it when we see it, sowe can help to modify it!”
References
Achenbach, T.M., & Edelbrock, C.S. (1984).Psychopathology of childhood. AnnualReview of Psychology, 35, 227 – 256. doi:10.1146/annurev.ps.35.020184.001303
American Psychiatric Association. (2000).Diagnostic and statistical manual of mental disor-ders (4th ed., text rev.). Washington, DC:Author.
Ashmun, J. (2004). What is a personality disorder?Narcisstic Personality Disorder. Retrieved from:http://www.halcyon.com/jmashmun/npd/dsm-iv.html
Freeman, A., & Fox, S. (2012). Cognitive behav-ioral perspectives on the theory and treat-ment of narcissistic character. In J.Ogrodniczuk (Ed.), Understanding and treat-ing pathological narcissism. Washington, DC:American Psychological Association.
Krueger, R.F., McGue, M., & Iacono, W.G.(2001). The higher-order structure of com-mon DSM mental disorders: Internalization,externalization, and their connections to per-sonality. Personality and Individual Differences,30, 1245–1259. doi:10.1016/S0191-8869(00)00106-9
Krueger, R.F., & Tackett, J.L. (2003). Personalityand psychopathology: working toward thebigger picture. Journal of Personality Disorders,
17(2), 109–128. doi: 10.1521/pedi.17.2.109.23986
Miller, J.D., & Campbell, W.K. (2010). The casefor using research on trait narcissism as abuilding block for understanding narcissticpersonality disorder. Personality Disorders:Theory, Research, and Treatment, 1(3), 180–191. doi: 10.1037/a0018229
Pincus, A.L. (2011). Some comments on nomol-ogy, diagnostic process, and narcisstic per-sonality disorder in the DSM-5 proposal forpersonality and personality disorders.Personality Disorders: Theory, Research, andTreatment, 2(1), 41-53. doi: 10.1037/a0021191
Ronningstam, E. (2011). Narcisstic personalitydisorder in DSM V: In support of retaining asignificant diagnosis. Journal of PersonalityDisorders, 25(2), 248–259. doi: 10.1521/pedi.2011.25.2.248
. . .
Correspondence to Arthur Freeman,Ed.D., Midwestern University, Departmentof Behavioral Medicine, 555 31st St.,Downers Grove, IL 60515;[email protected]
This brief article is the first in a four-part series that provides recommen-dations on relevant literature and
resources from expert researchers and clini-cians: past presidents of the Association forBehavioral and Cognitive Therapies(ABCT). Past presidents were surveyed fortheir perspectives on research articles, theo-retical articles, books, websites, and self-help books they would recommend tomembers of ABCT and to readers of theBehavior Therapist. This provided an oppor-tunity to connect readers to the expertise ofsome of the leaders in our field. After an ex-amination of the responses, it seemed most
informative to organize their recommenda-tions based on content rather than medium.The following suggestions are foundationaltexts and resources in the field and scienceof behaviorism and the study of behaviorchange, beginning with broad historicaltexts and followed by more specific applica-tions.
Science and Human Behavior (Skinner,1953) is a classic text that provides a closeexamination of human behavior anddemonstrates ways such behavior can bechanged and controlled through experi-mental science. Dr. Thomas Ollendick,president of ABCT from 1994–1995,
stated that this book laid “the foundationfor behavior therapy and cognitive behaviortherapy.” This text, cited over 9,200 times,provided an overview of behaviorism, in-cluding reflexes, operant behavior, discrimi-nation, and punishment. It then arguedthat this science, which had until this pointbeen used primarily with animals, can beemployed to influence and control humanbehavior, and introduced the role of self-control, groups of people, and broaderagencies in the maintenance of this control.Dr. Ollendick also recommended anotherfoundational text in Bandura’s (1977) SocialLearning Theory. This book, cited over22,000 times, explored the behavioral as-pects of social learning theory while empha-sizing cognitions and the role of theindividual.
Dr. Philip Kendall, president from1989–1990, recommended a text focusedon understanding aggressive behaviorthrough behavioral principles. Frustrationand Aggression (Dollard, Doob, Miller,Mowrer, & Sears, 1939) explored the as-sumption that “aggression is always a con-sequence of frustration” (p. 1). Chaptersfocus on the role of aggression in socializa-
Past Presidents Series
Perspectives From Past Presidents:Foundations of Behaviorism and StudyingBehavior ChangeAlayna Schreier and David J. Hansen, University of Nebraska-Lincoln

October • 2013 185
tion, adolescence, criminality, and democ-racy, along with more dated references tofascism, Marxism, and communism. Dr.Kendall recommended this early text as a“great theoretical document, infused withresearch-based information.”
A text that extends the theoretical prin-ciples of behaviorism to applications of be-havior change was recommended by Dr.David Barlow, president from 1978–1979.Bandura’s (1969) Principles of BehaviorModification provided a specific emphasis onthe vicarious, symbolic, and self-regulatoryprocesses involved in social learning andtheir role in increasing and decreasing be-haviors. This text focused on the basic prin-ciples of behavior modification, butextended the field through an examinationof conditions under which these principlescould be utilized for self-enhancement.
Some of the most commonly used be-havior modification programs have beenbased on applied behavior analysis (ABA).Dr. Michel Hersen, president from1979–1980, recommended an article byBaer, Wolf, and Risley (1968) that exam-ined various dimensions of ABA. This man-uscript cited over 2,300 times, describedthe primary components of ABA and in-cluded an additional focus on appropriateprocedural descriptions of effective tech-niques, the practical importance of theseskills, and the generalizability of skillslearned through ABA.
Dr. Ollendick recommended anothertext (co-authored by another ABCT pastpresident, Gerald Davison) that demon-strated the use of behavioral principles inclinical practice. Goldfried and Davison’s(1976) Clinical Behavior Therapy approachedbehavior therapy as an emphasis withinclinical work that was closely tied to basicpsychological research and social psycho-logical theory. Specific therapeutic tech-niques included behavioral assessment,
relaxation training, behavior rehearsal, cog-nitive relabeling, and problem solving.Goldfried and Davison emphasized the im-portance of cognitive processes to behaviorchange, clearly outlining the cognitive be-havioral therapy the field is familiar withtoday.
Applications of behavior change in clini-cal practice have also led to examinations oftherapeutic outcomes. Dr. Anne MarieAlbano, president of ABCT from2007–2008, recommended an article (au-thored by past president Alan Kazdin) thatprovided a conceptualization of behaviorchange, focusing on response covariationinstead of symptom substitution. Kazdin(1982) argued that behavioral responses arerelated, and treatment of one behavior mayresult in changes in other behaviors. The ar-ticle proposed a new conceptual frameworkwith which to explore behavior change inthe context of psychotherapy. Dr. Albanorecommended this text to aid in under-standing how “theories are developed andideas are vetted via the empirical literature.”
Dr. Debra Hope, president from2010–2011, and Dr. Barlow recommendedanother text that focused on the examina-tion of behavior change and behaviorism.Sidman’s (1960) Tactics of Scientific Research:Evaluating Experimental Data in Psychologyhas been instrumental in the evaluation ofbehavior analysis and behavior therapy. Dr.Barlow explained that this text focused onwithin-subject research design, identifyingthe “philosophy and theory of how to focuson the individual in psychological research.”The research methodology outlined inSidman’s text provided the basis for manyof the studies that have supported behavior-ism and behavior therapy and will continueto influence the study of behavior change.
These books and articles on the founda-tions of behaviorism and behavior changehave set the stage for the empirical and clin-
ical work that is currently being donewithin ABCT. Past presidents have pro-vided their expert recommendations ofthese seminal texts for the continued educa-tion of professionals, educators, students,and readers of the Behavior Therapist. Futurearticles in this series will include additionalrecommendations from Drs. J. Gayle Beck,Steven Hollon, Rosemery Nelson-Gray, andJacqueline Persons, and will address themessuch as assessment and evidence-basedpractice and data analysis and research de-sign.
References
Baer, D. M, Wolf, M. M., & Risley, T. R. (1968).Some current dimensions of applied behavioranalysis. Journal of Applied Behavior Analysis,1, 91-97.
Bandura, A. (1969). Principles of behavior modifica-tion. New York, NY: Holt, Rinehart, &Winston.
Bandura, A. (1977). Social learning theory.Englewood Cliffs, NJ: Prentice-Hall.
Dollard, J., Doob, L. W., Miller, N. E., Mowrer,O. H., & Sears, R. R. (1939). Frustration andaggression. New Haven, CT: Yale UniversityPress.
Goldfried, M. R., & Davison, G. C. (1976).Clinical behavior therapy. New York, NY:Wiley.
Kazdin, A. (1982). Symptom substitution, gen-eralization, and response covariation:Implications for psychotherapy outcome.Psychological Bulletin, 91, 349-365.
Sidman, M. (1960). Tactics of scientific research:Evaluating experimental data in psychology. NewYork, NY: Basic Books.
Skinner, B. F. (1953). Science and human behavior.New York, NY: Macmillan.
. . .
Correspondence to Alayna Schreier,Department of Psychology, University ofNebraska-Lincoln, Lincoln, NE 68588-0308;[email protected]
Classified
FELLOWSHIPS IN ADVANCED COGNI-TIVE THERAPY WITH AARON T. BECK,M.D. The Aaron T. Beck PsychopathologyResearch Center in the Perelman School ofMedicine at the University of Pennsylvania isseeking applicants for two types of PostdoctoralFellowship positions: (1) Ruth L. KirschsteinNational Research Service PostdoctoralFellowship Award from the National Institute ofMental Health and (2) Aaron T. Beck EndowedFellowship (see www.aaronbeckcenter.org).Fellows will have the opportunity to participatein cutting-edge CT projects that include re-search or training in collaboration with Dr.Aaron T. Beck and core faculty, Drs. Greg
Brown, Torrey Creed, and Paul Grant. Successfulcandidates may focus on (1) schizophrenia, (2)implementation and dissemination of CT, or (3)suicide prevention. Populations may includechildren, adults and older adults. Applicantsshould have earned a Ph.D., Psy.D., or equiva-lent in psychology or related field and had previ-ous training in CT, severe mental illness, ordissemination/implementation. We especiallyencourage bilingual candidates to apply.
Please email curriculum vita, cover letter,and two letters of recommendation to Aaron T.Beck, M.D.: [email protected] University of Pennsylvania is an EqualOpportunity/Affirmative Action Employer.Applications will be accepted until November30, 2013.
Classified ads are only $4.00 per line.For a free price estimate, attach thetext of your ad in the form of a Worddocument and email StephanieSchwartz at sschwartz@abct. For infor-mation on display ads, deadlines, andrates, contact S. Schwartz at the emailabove or visit our website atwww.abct.org and click on ADVERTISE.
ADVERTISING in tBT

186 the Behavior Therapist
Call for AwardNominat ions
The ABCT Awards and Recognition Committee, chaired by Shireen L. Rizvi, Ph.D., of Rutgers University, is pleased to announce the 2014 awards program, to be presented at the 48th Annual Convention in
Philadelphia. Nominations are requested in all categories listed below. Please see the specific nominationinstructions in each category. Please note that award nominations may not be submitted by current
members of the ABCT Board of Directors.
20th Annual Awards & Recognition
Career/Lifetime Achievement Eligible candidates for this award should be members ofABCT in good standing who have made significant contri-butions over a number of years to cognitive and/or behav-ior therapy. Applications should include a letter of nomina-tion, three letters of support, and a curriculum vitae of thenominee. Past recipients of this award include David H.Barlow, G. Alan Marlatt, Antonette M. Zeiss, Alan E.Kazdin, and Thomas H. Ollendick. Please complete thenomination form found online at www.abct.org. Then e-mail the completed form and associated materials as one pdfdocument to [email protected]. Include “Career/Lifetime Achievement” in the subject line. Also, mail a hardcopy of your submission to ABCT, Career/LifetimeAchievement, 305 Seventh Ave., New York, NY 10001.■ Nomination deadline: March 3, 2014
Mid-Career Innovator This year we are introducing a new award category.Eligible candidates for the Mid-Career Innovator Award aremembers of ABCT in good standing who are at the associ-ate professor level or equivalent mid-career level, and whohave made significant innovative contributions to clinicalpractice or research on cognitive and/or behavioral modal-ities. The 2014 Mid-Career Innovator Award will be givenin honor of Alan Marlatt. Please complete the nominationform found online at www.abct.org. Then e-mail the com-pleted form and associated materials as one pdf documentto [email protected]. Include “Mid-Career Innova-tor” in the subject line. Also, mail a hard copy of your sub-mission to ABCT, Career/Lifetime Achievement, 305Seventh Ave., New York, NY 10001.■ Nomination deadline: March 3, 2014
Outstanding MentorThis year we are seeking eligible candidates for theOutstanding Mentor award who are members of ABCT ingood standing who have encouraged the clinical and/oracademic and professional excellence of psychology gradu-ate students, interns, postdocs, and/or residents.Outstanding mentors are considered those who have pro-vided exceptional guidance to students through leadership,advisement, and activities aimed at providing opportunitiesfor professional development, networking, and futuregrowth. Appropriate nominators are current or past stu-dents of the mentor. Previous recipients of this award areRichard Heimberg, G. Terence Wilson, Richard J. McNally,and Mitchell J. Prinstein. Please complete the nominationform found online at www.abct.org. Then e-mail the com-pleted form and associated materials as one pdf documentto [email protected]. Include “Outstanding Mentor”in your subject heading. Also, mail a hard copy of your sub-mission to ABCT, Outstanding Training Program, 305Seventh Ave., New York, NY 10001.■ Nomination deadline: March 3, 2014
Distinguished Friend to Behavior Therapy Eligible candidates for this award should NOT be membersof ABCT, but are individuals who have promoted the mis-sion of cognitive and/or behavioral work outside of ourorganization. Applications should include a letter of nomi-nation, three letters of support, and a curriculum vitae ofthe nominee. Past recipients of this award include TheHonorable Erik K. Shinseki, Michael Gelder, and Mark S.Bauer. Please complete the nomination form found online atwww.abct.org. Then e-mail the completed form and associ-ated materials as one pdf document to awards.abct@gmail.

October • 2013 187
com. Include “Distinguished Friend to BT” in the subjectline. Also, mail a hard copy of your submission to ABCT,Distinguished Friend to BT, 305 Seventh Ave., New York,NY 10001.■ Nomination deadline: March 3, 2014
Student Dissertation Awards• Virginia A. Roswell Student Dissertation Award ($1,000) • Leonard Krasner Student Dissertation Award ($1,000) • John R. Z. Abela Student Dissertation Award ($500) Each award will be given to one student based on his/herdoctoral dissertation proposal. Accompanying this honorwill be a monetary award (see above) to be used in supportof research (e.g., to pay participants, to purchase testingequipment) and/or to facilitate travel to the ABCT conven-tion. Eligibility requirements for these awards are as fol-lows: (a) candidates must be student members of ABCT; (b)topic area of dissertation research must be of direct rele-vance to cognitive-behavioral therapy, broadly defined; (c)the dissertation must have been successfully proposed; and(d) the dissertation must not have been defended prior toNovember 2013. Proposals with preliminary results includ-ed are preferred. To be considered for the Abela Award,research should be relevant to the development, mainte-nance, and/or treatment of depression in children and/ oradolescents. Self-nominations are accepted or a student'sdissertation mentor may complete the nomination.Nominations must be accompanied by a letter of recom-mendation from the dissertation advisor. Please completethe nomination form found online at www.abct.org. Then e-mail the completed form and associated materials as one pdfdocument to [email protected]. Include candidate’slast name and “Student Dissertation Award” in the subjectline. Also, mail a hard copy of your submission to ABCT,Student Dissertation Award, 305 Seventh Ave., New York,NY 10001.■ Nomination deadline: March 3, 2014
Student Travel Award This award is designed to recognize excellence among ourstudent presenters and to aid in allaying some of the sig-nificant travel costs associated with presenting at the con-vention. Accompanying this honor will be a monetaryaward ($500) to be used to facilitate travel to the ABCTconvention. Eligibility requirements for this award specifythat nominees must be (a) speaking at the 2014 conventionas a symposium presenter (i.e., first author on a symposiumtalk), panel participant, or moderator; (b) student membersof ABCT in good standing; (c) currently enrolled as a stu-dent, including individuals on predoctoral internships inthe 2014-2015 year but excluding postbaccalaureates.Information about the nomination form and application willbe available following announcement of conference accep-tances. ■ Nomination deadline: August 1, 2014
. . .
Nominations for the following award are solicited from membersof the ABCT governance:
Outstanding Service to ABCTPlease complete the nomination form found online atwww.abct.org. Then e-mail the completed form and associ-ated materials as one pdf document to [email protected]. Include “Outstanding Service” in the subject line.Also, mail a hard copy of your submission to ABCT,Outstanding Service to ABCT, 305 Seventh Ave., NewYork, NY 10001.■ Nomination deadline: March 3, 2014
President’s New Researcher AwardABCT’s 2013–2014 President, Dean McKay, Ph.D., invitessubmissions for the 36th Annual President’s NewResearcher Award. The winner will receive a certificate anda cash prize of $500. The award will be based upon an earlyprogram of research that reflects factors such as: consis-tency with the mission of ABCT; independent work pub-lished in high-impact journals; and promise of developingtheoretical or practical applications that represent clearadvances to the field. While nominations consistent withthe conference theme are particularly encouraged, submis-sions will be accepted on any topic relevant to cognitivebehavior therapy, including but not limited to topics such asthe development and testing of models, innovative prac-tices, technical solutions, novel venues for service delivery,and new applications of well-established psychologicalprinciples. Submissions must include the nominee’s currentcurriculum vita and one exemplary paper. Eligible papersmust (a) be authored by an individual with five years or lessposttraining experience (e.g., post-Ph.D. or post-residency);and (b) have been published in the last two years or cur-rently be in press. Submissions will be judged by a reviewcommittee consisting of Dean McKay, Ph.D., Stefan G.Hofmann, Ph.D., and Jonathan D. Abramowitz, Ph.D.(ABCT’s President, Immediate Past-President, andPresident-Elect). Submissions must be received by Monday,August 4, 2014, and must include four copies of both thepaper and the author’s vita and supporting letters if the lat-ter are included. Send submissions to ABCT President’sNew Researcher Award, 305 Seventh Ave., 16th floor, NewYork, NY 10001. ■ Submission deadline: August 4, 2014
NOMINATE ONLINE: www.abct.org
188 the Behavior Therapist
Workshops and Mini WorkshopsWorkshops cover concerns of the practitioner/educator/
researcher. Workshops are 3 hours long, are generally limited
to 60 attendees, and are scheduled for Friday and Saturday.
Please limit to no more than FOUR presenters.
Mini Workshops address direct clinical care or training at a broad
introductory level. They are 90 minutes long and are scheduled
throughout the convention.
Please limit to no more than FOUR presenters.
When submitting for Workshops or Mini Workshop, please indicatewhether you would like to be considered for the other format as well.
Barbara Kamholz, Workshop Committee [email protected]
InstitutesInstitutes, designed for clinical practitioners, are 5 hours or
7 hours long, are generally limited to 40 attendees, and are
scheduled for Thursday.
Please limit to no more than FOUR presenters.
Lauren Weinstock, Institute Committee [email protected]
Master Clinician SeminarsMaster Clinician Seminars are opportunities to hear the
most skilled clinicians explain their methods and show
taped demonstrations of client sessions. They are 2 hours
long, are limited to 40 attendees, and are scheduled Friday
through Sunday.
Sarah Kertz, Master Clinician Seminar Committee [email protected]
Continuing Education Sessions
call48th Annual Convention | November 20–23, 2014 | Philadelphia
for
Please send a 250-word
abstract and a CV
for each presenter.
For submission
requirements and
information on the CE
session selection
process, please see the
Frequently Asked
Questions section of
the ABCT Convention
page at www.abct.org.
for Submission : February 1, 2014D E A D L I N E

October • 2013 189
I nominate the following individuals:
P R E S I D E N T- E L E C T ( 2 0 1 4 – 2 0 1 5 )
R E P R E S E N TAT I V E -AT- L A R G E ( 2 0 1 4 – 2 0 1 7 )
N A M E ( p r i n t e d )
S I G N AT U R E ( r e q u i r e d )
2014 Call for NominationsNOMINATE the Next Candidates for ABCT Office
Every nomination counts! Encourage colleagues to runfor office or consider running yourself. Nominate as manyfull members as you like for each office. The results will betallied and the names of those individuals who receive themost nominations will appear on the election ballot nextApril. Only those nomination forms bearing a signatureand postmark on or before February 1, 2014, will becounted.
Nomination acknowledges an individual's leadershipabilities and dedication to behavior therapy and/or cogni-tive therapy, empirically supported science, and to ABCT.When completing the nomination form, please take intoconsideration that these individuals will be entrusted torepresent the interests of ABCT members in important pol-icy decisions in the coming years. Contact the Leadershipand Elections Chair for more information about servingABCT or to get more information on the positions.
Please complete, sign, and send this nomination formto Christopher Martell, Ph.D., Leadership & ElectionsChair, ABCT, 305 Seventh Ave., New York, NY 10001.
�
We are approaching the nomina-tions period for ABCT’s electedleadership positions. Profession
al organizations are as strong as their mem-bers’ participation. ABCT belongs to all ofus and the selection of leaders represents thesingle most important task that membersaccomplish. Please take ownership of yourassociation and participate in the leadershipselection process. Make this the year youguide your professional home and make acontribution by running for office or take anactive role in selecting our leaders. If youask members who have previously served ina leadership role in ABCT why they partici-pated, they all share similar reasons for par-ticipating in the leadership: they wanted tomake a difference, and they did. Will you orsomeone you know run for office? In addi-tion to the inherent satisfaction achievedfrom contributing to ABCT, you have theopportunity to develop new friendshipswhile reconnecting with old ones.
This coming year we need nominationsfor two elected positions: President-Elect
and Representative-at-Large. Those mem-bers who receive the most nominations willappear on the ballot. In April, members ingood standing vote for the candidates oftheir choice to serve for 3 years. ThePresident-Elect serves in that function from2014-2015, then as President from 2015-2016, and then as Past President from2016-2017.
Each representative serves as a liaison toone of the branches of the association. Therepresentative position up for 2014 electionwill serve as the liaison to the MembershipIssues Coordinator. The Coordinator workswith a wide variety of committees devotedto membership and membership services.These include the Membership Committee;Committee on Student Members; Leader-ship and Elections; List Serve; the ClinicalDirectory and Referral Issues, which just re-vamped our on-line referral network, Find aCBT Therapist; Social Networking MediaCommittee, responsible for our Facebookpage; and our ever-growing Special InterestGroups Committee. This representative
serves a crucial role working with theCoordinator to ensure these committeeshave clear job descriptions that are in keep-ing with the ABCT mission statement andkeep the Board updated on their activitiesthroughout the year. All full members ingood standing are eligible to be nominated,and there is no limit to the number of mem-bers you can nominate for any of the posi-tions.
Electioneering starts at the AnnualConvention. So if you are interested in run-ning for office, or if you have a candidate inmind, start the campaign now with thenominations and go to the AnnualConvention and start making your case tothe electorate.
How to Nominate: Three Ways
�Mail the form to the ABCT office (address below)
� Fill out the nomination form by handand fax it to the office at 212-647-1865
� Fill out the nomination form by handand then scan the form as a PDF file andemail the PDF as an attachment to ourcommittee: [email protected].
The nomination form with your orig-inal signature is required, regardless ofhow you get it to us.
Good governance requires participationof the membership. ABCT needs you par-ticipation to insure good governance and tocontinue to thrive as an organization.
At ABCT
Nominations for ABCT Officers: Get in on Choosing the LeadersChristopher Martell, Chair, Leadership and Elections Committee

190 the Behavior Therapist
Learning doesn't need to stop at the Convention! ABCT is proudto provide online Continuing Education (CE) webinars for psy-chologists and other mental health professionals. Our webinarscan be attended live or viewed online at your convenience. Thewebinar series offers opportunities to learn about evidence-based treatments and latest research while earning CE creditsfrom the comfort and convenience of your own home/office.
Resick | CPT for PTSDCognitive Processing Therapy for PTSD: Does Child Sexual or Physical Abuse Make a Difference?
Herbert | ACTAcceptance and Commitment Therapy: A Radically Different yet Remarkably Familiar Approach to Behavior Change
Albano | CBT for Adolescent AnxietyAdolescents, Anxiety and Development: A Family-Focused CBT Approach
Harvey | CBT for Insomnia (CBT-I)Cognitive Behavioral Therapy for Insomnia and Transdiagnostic Sleep Problems in Clinical Practice
Tirch | Compassion-Focused TherapyAn Introduction to Compassion Focused Therapy
Brown | CBT for Child TraumaCBT for Traumatized Youth: Components of Evidence-Based Practice
Friday, September 20, 201311:00 a.m. EST
Jeffrey E. Barnett, Psy.D., ABPPEthical, Legal, and ClinicalConsiderations in BehavioralTelehealth
Friday, December 13, 201311:00 a.m. EST
Alec Miller, Psy.D.DBT With Adolescents: Research and Clinical Developments
Thursday, February 6, 201311:00 a.m. EST
Jonathan Abramowitz, Ph.D.Exposure Therapy for OCD Symptom Dimensions
ABCT ONLINE CE
WEBINARS
w w w . a b c t . o r g
UpcomingWebinars
Register today at www.abct.org | Earn CE all year long!
Watch Instantly
ABCT’s webinars empower and support
you to learn and train enduringly, from
the comfort of home or office.

October • 2013 191
The most recent issues of ABCT’s journals are online at ScienceDirect.Your ABCT membership gives you free online access to both journals.BEHAVIOR THERAPY Volume 44, #3, Sept. 2013
Taylor et al.. Epidemiology of Insomnia in College Students:Relationship With Mental Health, Quality of Life, andSubstance Use Diff iculties
Capron et al. Distress Tolerance and Anxiety SensitivityCognitive Concerns: Testing the Incremental Contributions of Affect Dysregulation Constructs on Suicidal Ideation andSuicide Attempt
Ammerman et al. A Clinical Trial of In-Home CBT forDepressed Mothers in Home Visitation
Desrosiers, Klemanski, & Nolen-Hoeksema. MappingMindfulness Facets Onto Dimensions of Anxiety andDepression
Martinelli, Cavanagh, & Dudley. The Impact of Rumination on State Paranoid Ideation in a Nonclinical Sample
Abramowitz et al. Treating OCD in Intimate Relationships: A Pilot Study of Couple-Based Cognitive-Behavior Therapy
Levy et al. Characteristics of Individuals Seeking Treatment for Obsessive-Compulsive Disorder
Boswell et al. Anxiety Sensitivity and Interoceptive Exposure: A Transdiagnostic Construct and Change Strategy
Oser et al. Differential Associations Between Perceived andObjective Measurement of Distress Tolerance in Relation toAntiretroviral Treatment Adherence and Response AmongHIV-Positive Individuals
Ortiz & Del Vecchio. Cultural Diversity: Do We Need a NewWake-Up Call for Parent Training?
Bardeen, Fergus, & Orcutt. Experiential Avoidance as aModerator of the Relationship Between Anxiety Sensitivity and Perceived Stress
Levinson, Langer, & Rodebaugh. Reactivity to ExclusionProspectively Predicts Social Anxiety Symptoms in YoungAdults
Hawkins & Cougle. Effects of Interpretation Training onHostile Attribution Bias and Reactivity to Interpersonal Insult
Choi et al. Depression in Homebound Older Adults: Problem-Solving Therapy and Personal and Social Resourcefulness
Krieger et al. Self-Compassion in Depression: AssociationsWith Depressive Symptoms, Rumination, and Avoidance inDepressed Outpatients
Feldner et al. Initial Evaluation of an Integrated Treatment for Comorbid PTSD and Smoking Using a Nonconcurrent,Multiple-Baseline Design
Zaki et al. Emotion Differentiation as a Protective FactorAgainst Nonsuicidal Self-Injury in Borderline PersonalityDisorder
COGNITIVE AND BEHAVIORAL PRACTICEVolume 20, #3, August 2013
COGNITIVE-BEHAVIORAL CASE CONFERENCERobichaud. A Clinical Case of Generalized Anxiety Disorder
CONTAINS VIDEO | Robichaud. Cognitive Behavior TherapyTargeting Intolerance of Uncertainty: Application to a ClinicalCase of Generalized Anxiety Disorder
CONTAINS VIDEO | Hayes-Skelton et al. An Acceptance-BasedBehavioral Therapy for Individuals With Generalized AnxietyDisorder
CONTAINS VIDEO | Fresco et al. Emotion Regulation Therapyfor Generalized Anxiety Disorder
Hjemdal et al. Metacognitive Therapy for Generalized AnxietyDisorder: Nature, Evidence and an Individual Case Illustration
FEATURED ARTICLE WITH ACCOMPANYING COMMENTARIESTARGET ARTICLE | Koons et al. Negotiating for ImprovedReimbursement for Dialectical Behavior Therapy: A SuccessfulProject
COMMENTARY | Rizvi. When Insurance Companies andClinicians Pay Attention to Data, Everybody Wins: ACommentary on Koons, O’Rourke, Carter, and Erhardt
COMMENTARY | Wisniewski & Altman. Commentary on Koons et al.’s “Negotiating for Improved Reimbursement forDialectical Behavior Therapy: A Successful Project”
COMMENTARY | Jacobo et al. “Stay in the Game”: CollectingData on Symptom Improvement in Naturalistic Settings inOrder to Increase Reimbursement Rates
REGULAR ARTICLESBagner et al. Home-Based Preventive Parenting Interventionfor at-Risk Infants and Their Families: An Open Trial
Spuij et al. Cognitive-Behavioral Therapy for Prolonged Griefin Children: Feasibility and Multiple Baseline Study
Calzada, Basil, & Fernandez. What Latina Mothers Think ofEvidence-Based Parenting Practices: A Qualitative Study ofTreatment Acceptability
McIlvain, Walter, & Chard. Using Cognitive ProcessingTherapy–Cognitive in a Residential Treatment Setting With an OEF/OIF Veteran With PTSD and a History of SevereTraumatic Brain Injury: A Case Study
BOOK REVIEWHofmann, S. G. (2012). An Introduction to Modern CBT:Psychological Solutions to Mental Health ProblemsReviewed by Kristalyn Salters-Pedneault

192 the Behavior Therapist
Welcome, New Members
Full MembersAnne C. AveryAnna Bardone-Cone Jeffrey BarnettKaren Caplovitz BarrettSheaLynne Baus Erica Bennett Shaindy BondiKeri Raelyn BrownMartina De GiorgisEdrick H. DorianLisa Elwood Gregory Fabiano Jonathan FaderLara Fielding Randi FredricksRex Paul Gatto Elizabeth GoodsiteDiana Corwin GordonKathryn Grant David Scott GreenawayCynthia Gross Nate Gruner Kurt HahlwegShannon Michelle HarveyJonathan HershfieldHunter Hoffman Ricky M. HornblassLisa Huber Patricia A. HunterJeremy D. Jewell Kim Allen Jones A.B. Kaplan Joseph LaBrie Carol Larach Winnie LeungKenneth Lichstein Michelle Lilly Carmen LynasPriscilla Valerie Marotta Suzanne MeunierDesiree W Murray Julie Orris Tonya Palermo Rachel Blumstein PosnerMaryanne Reilly-Spong Kevin RooneyChelsea RothschildMegan Marie RussellNatalia SalinasJohn Edward ScaliseRyan SharmaTimothy Sisemore
Erica Smith-LynchKristen E. Smith-Simon Katherine Simpson SpencerEmily SternSuzanne StoneDavid Street David James UdelfStephanie Vaughn Amanda Vaught James Vermilyea Mairin McCarthy WeinerJan WillerAbraham W. Wolf
New Professional 1Lindsay CummingsDebra Marie DominczakKathleen HerzigAmanda Louise HollyMarie-Josee LessardBrooke Arin RaskinSeema SaigalMeredith SchreierAndrea S. StarsiakE. Samuel WinerPearl McGee-Vincent Mindy Slovinsky
PostbaccalaureateZakieh Bigio Krystal CashenNicholas DemasMary Caitlin FertittaElizabeth Cope FeurerJessie Fitts Hannah FrankKaren T. Garelik Michael GiordanoChelsea GoldenGizem Iskenderoglu Alex Eve KellerKerry KinneyJeannette Lewis Leah LucidArwen Michelle MarkerKatherine McMahonKatherine OdomElizabeth Danielle ReeseEffua Erica SosooMarlene Vernette Strege Kristin Louise ToffeyMatthew P. TraficanKelsey WoodsXin Yu
StudentGuillermo Perez AlgortaRawya Al-Jabari Kaylie AllenJennifer AltmanAnjali P. Arora Sara Beth Austin J. Ben Barnes Gregory BaronKellie Lynn BartonErik Benau Eleanor BennerMarc Patrick BennettRandi BennettJennifer Bernier-ColemanKatie Lee Binns Denis G. Birgenheir Jennifer M BirnkrantStacey L. Blase Jenna Nicole BlewisJoseph William Boffa Alice BorodianskyJaclyn Bowes Emily BrackmanJames Derek BroussardAnnaBelle BryanJennifer Bryan Christine BurbankRoslyn DeVon Burton-
Robertson Cherelle CarringtonAriana Andrea CastroRobert CaveraJaime ChangCourtney ChappuisPhilippe Charles Alyssa ChimiklisErica ChinMichelle Andrea ClementiAmelia D. CoffmanLior CohenCrystal Cole Caitlin ConditColleen Lurel CookGraham Elliot Cooper Christopher CranstonMark Andrew CrossenJeremy Cummings Holly Curran Pooja DaveJessica DavisMolly Faye DavisStephanie Davis
Mariah Lillian DeSerisy Jessica Dietch David Disabato Seth Gordon DisnerAriadne DonnellShannon Diane DonofryTyler DorityErika DotySusan Jamie DoyleKelley L. Drayer Luci DumasEeva Edds Sarah Ehlke Johannes ChristopherEichstaedt Jamal Hussein EssayliLaura Failla Jennifer Lyn FeibelmanMargaret Feuille Christine Ann Fiore Lindsey FreeKaitlin P. GalloPamela M. GarciaKerrianne M. Gardner-Dixit Sheila GarlandJami Michelle GauthierKaren Sue Glenn Alison Goers Lauren GreenbergKaren GuanEvan GuidryAustin HahnChristine HansenAnna HawleyJenna J. HeroldCatherine HilcheyRyan Michael HillMarchion Hinton Jessica HoffmannJudy Hong Hannah M. Hueneke Barbara HuntNadia HuqDavid William Hutsell Nicholas Taylor James Jeremy Jinkerson Adriana Brya JosephNicole KatzJordan Keller Lori Jean Kellner-Schoelles Jessica Kenny Alexander Malik Khaddouma Smith E. Kidkarndee

October • 2013 193
Welcome, New Members
Vincent Shumpert Kinsey Megan Kirouac Douglas Ray KnutsonKirstin KramerZed Kramer David KronemyerYoonhee C. KyungKatherine LawrenceChristine LeeJennifer Lehmann Meaghan LehmannCrissa Draper LevinBrittany LewnoNicole Llewellyn Ishmael Israel Lopez Matthew Thomas LucianoKellina LupasKelsey MacKenzie Ann MacklinJennifer MadowitzNicole Eva Mahrer Raegan MazurkaPatricia McDaniel Hannah McKillopKathryn McLeanLidia Meshesha Johanna Marie MeyerCaroline Leslee MikelsonAdam Bryant MillerAmanda MintzerDaniel Mirtenbaum Frances MitchellSean Mitchell Tessa Katherine Mooney Kayla Moorer Meghan MoreanJared C. MoserLana Mousessian Ashley Neuhauser Audrey NguyenMelissa Ann Noelle Jennifer PazMaria PentchevaAmy PetersJoanna PiedmonJennifer PinkRandi Pochtar Barbara Prempeh Kristi Ensor Pruiksma Victoria Elena Quinones Michelle Christine QuistChelsea Gilts Ratcliff
C. Beth ReadyBrittany RemmertMargaret Reuland Rachel A. ReyesLindsey RodriguezMelanie RodriguezAna Teresa RondonStephanie RossLiza M. RubensteinKatrina A. RufinoGina Marie SacchettiCindy F. SchmidtBrent W. Schneider Anna V. SheedyZahid H. Sheikh Stacie Danielle ShiversJoanne Beverley ShurlandLaura Smart Katherine Sosna Simona Daniela StefanigaCesalie T. StepneyJessica SternLaurie StickneyMegan SySamantha Synett Sarah M. Taber-ThomasIsabel Tada Kathleen TallonKelli Taylor Rachel Terry Stephen Justin ThomasJulie Diane Thompson Marsha TriceAndrea TrubanovaJessica UlmerHelen Valenstein Margo VillarosaScott Wagoner Jennifer WallerMonica Danielle Walling Allison D. WalshCatherine Pittaway WalshJennifer WardLuisa Weiner Chelsey R. Wilks Jacquelyne WongShondrea WoodsMina YadegarChelsie Marie YoungMiryam YusufovaStacey ZarembaZhuoying Zhu
in-press article
archive
A Case Study Illustrating Therapist-Assisted Internet Cognitive BehaviorTherapy for Depression“Also readily apparent in theclient-therapist email exchangesis that the therapist was not ableto use the typical visual cues toconvey her reactions, such as eyecontact, body language, or facialexpressions. In some instances,however, keyboard techniqueswere used to enhance communi-cation to make the emails lookand feel more like an in-personencounter (e.g., quotes, italics,bold text).”
Pugh et al. Cognitive and Behavioral Practicein press, accepteddoi:10.1016/j.cbpra.2013.08.002
online47th Annual ConventionRegister now! If you register byOctober 15, you will receive yourprogram book in the mail.
“… part of the universe isenclosed within the organism’sown skin.”
B. F. Skinner, 1953Science and Human Behavior
https://www.abct.org/conv13
n w

PRSRT STD
U.S. POSTAGE
PAID
Hanover, PA
Permit No. 4
the Behavior TherapistAssociation for Behavioral and Cognitive Therapies305 Seventh Avenue, 16th floorNew York, NY 10001-6008212-647-1890 | www.abct.org
ADDRESS SERV ICE REQUESTED
Convention Planner
http://www.abct.org/conv2013/
itinerary
by topic, presenter,
session type, day/time
November 21–24 | Nashville
Search
Browse
by day and view the entire
program in time/day
order





























