Embed Size (px)
Citation preview
The Canadian ConsensusConference on Menopause
and Osteoporosis
2002 UpdateOriginally printed in JOGC
September 2001, Volume 23, Number 9
October 2001, Volume 23, Number 10
November 2001, Volume 23, Number 11
December 2001, Volume 23, Number 12
Revised October 2002, Volume 24, Number 10
following Advisory Committee Review
* The Canadian Consensus Conference on Menopause and Osteoporosis has been reviewed and approved bythe Executive and Council Committees of the Society of Obstetricians and Gynaecologists of Canada
The following companies have provided unrestricted educational grants to the SOGC for the development of this consensus: Berlex Canada Inc., Merck Frosst Canada Inc., Novartis Pharmaceutical Canada Inc.,Novo Nordisk Canada Inc., Pfizer Canada Inc., Schering Canada Inc., and Wyeth-Ayerst Canada Inc.
THE SOCIETY OFOBSTETRICIANS AND
GYNAECOLOGISTS OF CANADA
LA SOCIÉTÉDES OBSTÉTRICIÉNSET GYNÉCOLOGUES
DU CANADA
THE CANADIAN CONSENSUS CONFERENCE
ON MENOPAUSE AND OSTEOPOROSIS - 2002 UPDATE
Consensus Conference Participants ..................................................................................................4
Executive Summary ................................................................................................................................5
Perimenopause ....................................................................................................................................12
Menopause: Healthy Living ................................................................................................................18
Menopause and Sexual Function......................................................................................................25
Hormone Replacement Therapy and Cardiovascular Disease ................................................29
Osteoporosis ........................................................................................................................................35
Urogenital Health ................................................................................................................................46
Medical and Special Conditions........................................................................................................51
Hormones and the Brain ..................................................................................................................56
Pharmacotherapy ................................................................................................................................59
Hormone Replacement Therapy and Cancer ..............................................................................69
Complementary Approaches ............................................................................................................74
Evaluation, Decision Making and Follow-up ..................................................................................84
JOGC OCTOBER 20024
These guidelines reflect emerging clinical and scientific advances as of the date issued and are subject to change.The information should not be construed asdictating an exclusive course of treatment or procedure to be followed. Local institutions can dictate amendments to these opinions.They should be well doc-umented if modified at the local level. None of the contents may be reproduced in any form without prior written permission of SOGC.
No. 108, October 2002
CONSENSUS EDITORTimothy Rowe, MB, BS, FRCSC,Vancouver, BC
CONFERENCE EDITORSSerge Bélisle, MD, MSc, FRCSC, Montreal, QCChristine Derzko, MD, FRCSC, Toronto, ONMargo R. Fluker, MD, FRCSC,Vancouver, BCGillian R. Graves, MD, FRCSC, Halifax, NS
CONFERENCE CHAIRRobert H. Lea, MD, FRCSC, Halifax, NS
CONFERENCE COORDINATORElke Henneberg, Montreal, QC
FACULTYJennifer M. Blake, MD, FRCSC, Toronto, ONJacques P. Brown, MD, FRCPC, Ste-Foy, QCElizabeth Contestabile, RN, BScN, Ottawa, ONEma Ferreira, MSc, PharmD, Montreal, QCMichel Fortier, MD, FRCSC, Ste-Foy, QCShawna L. Johnston, MD, FRCSC, Kingston, ONDavid L. Kendler, MD, FRCPC,Vancouver, BCAliya Khan, MD, FRCPC, FACP, Oakville, ONSuzanne Montemuro, MD, CCFP,Vancouver, BCJune Rogers, Toronto, ONBarbara B. Sherwin, PhD, Montreal, QCThirza Smith, MD, FRCSC, Saskatoon, SKMichèle A. Turek, MD, FRCPC, Ottawa, ONChui Kin Yuen, MD, FRCSC, FACOG, Winnipeg, MB
CONTRIBUTING AUTHORSThomas E.R. Brown, PharmD, Toronto, ONGisèle Bourgeois-Law, MD, FRCSC, Winnipeg, MB
THE CANADIAN CONSENSUS ON
MENOPAUSE AND OSTEOPOROSIS - 2002 UPDATE
The original Consensus document was prepared and reviewed by the Committee on Menopause and Osteoporosis,approved by Executive and Council of the Society of Obstetricians and Gynaecologists of Canada,and endorsed by the Osteoporosis Society of Canada.
This 2002 Update reflects revised recommendations after the findings of the WHI study were reviewed.

JOGC OCTOBER 20025
AbstractObjectives: To define the standard of care for menopausal
women in Canada. To assist women and their caretakers inmaking informed choices to improve their quality of life bypromoting health and preventing disease.
Options: The areas of perimenopause and menopause wereexplored under the headings of healthy living; sexual health;hormone replacement therapy in relation to cardiovasculardisease, cancer, and the brain; osteoporosis; urogenital health;medical and special conditions; pharmacotherapy; comple-mentary approaches; and evaluation, decision-making, andfollow-up.
Outcomes: Improved health and quality of life for perimenopausal,menopausal, and postmenopausal women in Canada.
Values: References were collected through Medline searches andcomparison made to existing current guidelines and consen-sus documents for consistency.
Evidence: The level of evidence has been determined using thecriteria described by the Canadian Task Force on the PeriodicHealth Examination.
Benefits, Harms, and Costs: Utilization of the information andrecommendations by Canadian health professionals willenhance the health and quality of life for perimenopausal,menopausal, and postmenopausal women in Canada.
Recommendations: Recommendations were grouped accord-ing to section themes. A detailed list of recommendations isavailable in the Executive Summary.
Validation: Recommendations were reviewed and revised bythe Canadian Consensus Conference on the Menopause andthe SOGC Council, and endorsed by the OsteoporosisSociety of Canada.
Sponsor: The Society of Obstetricians and Gynaecologists ofCanada.
INTRODUCTION
The Society of Obstetricians and Gynaecologists of Canada(SOGC) is committed to delivering the highest standards ofhealth care to Canadian women. The management of healthduring menopause and the postmenopausal years continuesto be a major focus of women and health care providers. Thefield of menopause and osteoporosis is rapidly evolving andthere is increased public demand for accurate information.The Mission Statement of the 2001 Canadian MenopauseConsensus Committee remains unchanged from its inceptionin 1994:
• To define the standard of care for menopausal women inCanada.
• To assist women and their caregivers in making informedchoices to improve their quality of life by promoting healthand preventing disease.1
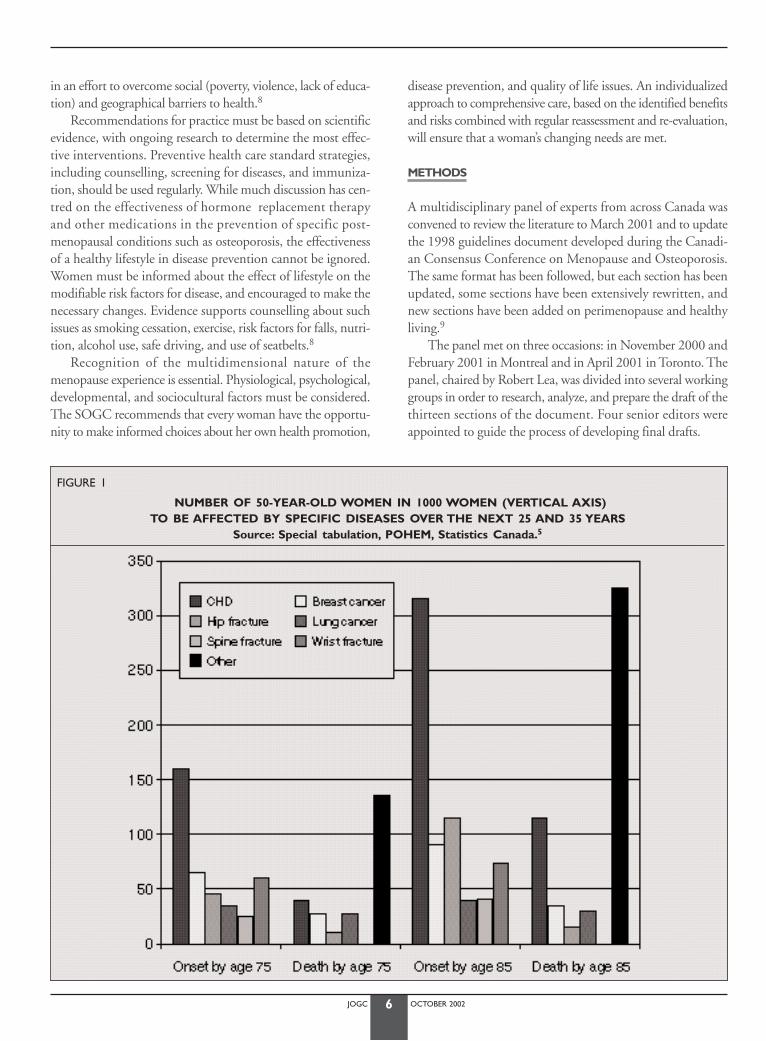
Canadian statistics show an increase in life expectancy formenopausal women. In 1922, a 50-year-old woman lived, onaverage, until age 75.2 Today, a woman the same age can expectto live until her mid-80s.3 In the year 2000, it was estimatedthat more than 4.75 million women (17% of the population)were aged 50 or older in Canada;4 by 2006, this number is pro-jected to be 5.6 million.5 The increasing number of women over70 are particularly vulnerable to conditions listed in Figure 1.
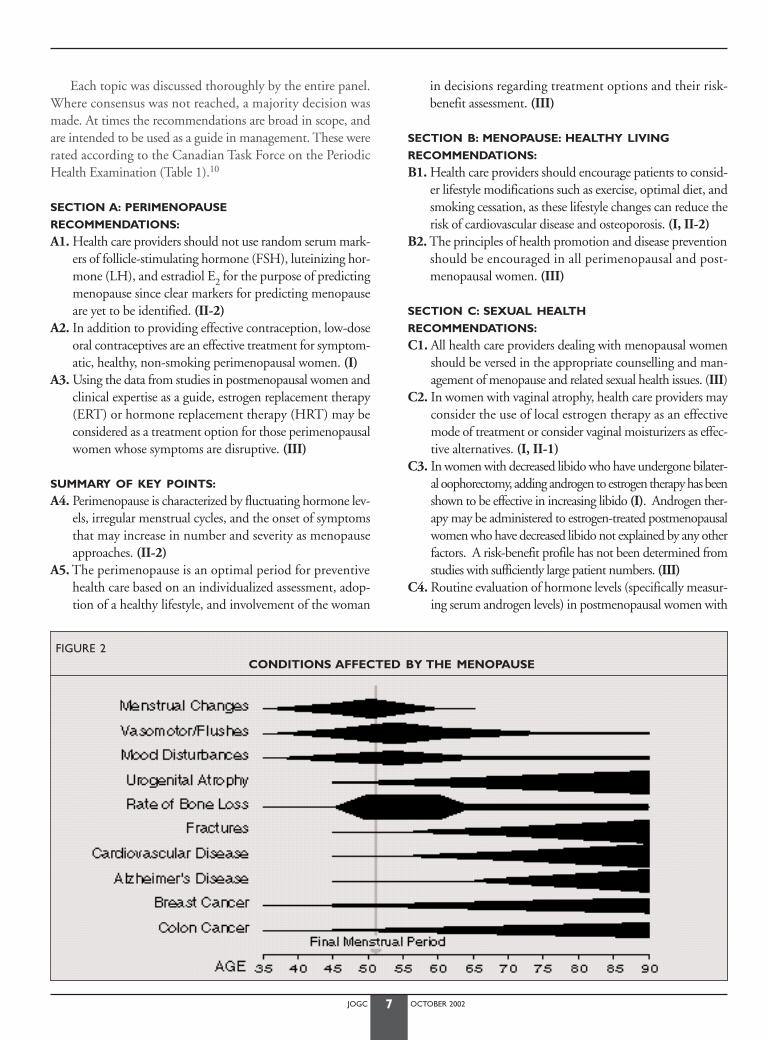
The average age at menopause of 51 years has remainedremarkably constant throughout the centuries, apparently unaffected by improving nutrition and reduction of disease.However, certain chemotherapeutic agents, radiation, smoking,and hysterectomy can contribute to an earlier onset ofmenopause.6 Many younger women have had their ovaries sur-gically removed, and a smaller number, who have prematureovarian failure, undergo menopause before the age of 40.6 Theincreasing number of women dealing with conditions affectedby menopause, early or otherwise (Figure 2), has resulted in are-examination of the traditional approaches to mature women’shealth care. The experience and the reporting of symptoms varywidely among individuals and cultures. While usually not a seri-ous threat to health, symptoms may negatively affect quality oflife. Notably, the majority of women experience menopause asa normal event without significant difficulty.
The traditional approach of diagnosing and treating dis-ease is no longer sufficient; health promotion and disease pre-vention strategies must be incorporated into every practice.
Health promotion and disease prevention provide the foun-dation for the comprehensive management of women’s health,and are critical strategies for the responsible allocation of limit-ed health care resources. It is also important to recognize thatmedical care determines only a small portion of the health of asociety. Both individual and population-or society-based initia-tives must be developed for effective health promotion. Con-sideration must be given to the determinants of health, includingthe social and physical environment as well as individual genet-ic and physiologic characteristics in combination with lifestyleand behaviour. By focusing on disease prevention and early inter-vention, health care providers can help women to avoid muchdisability.7 Health care providers can also advocate for women
EXECUTIVE SUMMARYThirza Smith, MD, FRCSC,1 Elizabeth Contestabile, RN, BScN2
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
1 Saskatoon, SK2 Ottawa, ON
JOGC OCTOBER 20026
in an effort to overcome social (poverty, violence, lack of educa-tion) and geographical barriers to health.8
Recommendations for practice must be based on scientificevidence, with ongoing research to determine the most effec-tive interventions. Preventive health care standard strategies,including counselling, screening for diseases, and immuniza-tion, should be used regularly. While much discussion has cen-tred on the effectiveness of hormone replacement therapyand other medications in the prevention of specific post-menopausal conditions such as osteoporosis, the effectivenessof a healthy lifestyle in disease prevention cannot be ignored.Women must be informed about the effect of lifestyle on themodifiable risk factors for disease, and encouraged to make thenecessary changes. Evidence supports counselling about suchissues as smoking cessation, exercise, risk factors for falls, nutri-tion, alcohol use, safe driving, and use of seatbelts.8
Recognition of the multidimensional nature of themenopause experience is essential. Physiological, psychological,developmental, and sociocultural factors must be considered.The SOGC recommends that every woman have the opportu-nity to make informed choices about her own health promotion,
disease prevention, and quality of life issues. An individualizedapproach to comprehensive care, based on the identified benefitsand risks combined with regular reassessment and re-evaluation,will ensure that a woman’s changing needs are met.
METHODS
A multidisciplinary panel of experts from across Canada wasconvened to review the literature to March 2001 and to updatethe 1998 guidelines document developed during the Canadi-an Consensus Conference on Menopause and Osteoporosis.The same format has been followed, but each section has beenupdated, some sections have been extensively rewritten, andnew sections have been added on perimenopause and healthyliving.9
The panel met on three occasions: in November 2000 andFebruary 2001 in Montreal and in April 2001 in Toronto. Thepanel, chaired by Robert Lea, was divided into several workinggroups in order to research, analyze, and prepare the draft of thethirteen sections of the document. Four senior editors wereappointed to guide the process of developing final drafts.
FIGURE 1
NUMBER OF 50-YEAR-OLD WOMEN IN 1000 WOMEN (VERTICAL AXIS) TO BE AFFECTED BY SPECIFIC DISEASES OVER THE NEXT 25 AND 35 YEARS
Source: Special tabulation, POHEM, Statistics Canada.5
JOGC OCTOBER 20027
Each topic was discussed thoroughly by the entire panel.Where consensus was not reached, a majority decision wasmade. At times the recommendations are broad in scope, andare intended to be used as a guide in management. These wererated according to the Canadian Task Force on the PeriodicHealth Examination (Table 1).10
SECTION A: PERIMENOPAUSE
RECOMMENDATIONS:
A1. Health care providers should not use random serum mark-ers of follicle-stimulating hormone (FSH), luteinizing hor-mone (LH), and estradiol E2 for the purpose of predictingmenopause since clear markers for predicting menopauseare yet to be identified. (II-2)
A2. In addition to providing effective contraception, low-doseoral contraceptives are an effective treatment for symptom-atic, healthy, non-smoking perimenopausal women. (I)
A3. Using the data from studies in postmenopausal women andclinical expertise as a guide, estrogen replacement therapy(ERT) or hormone replacement therapy (HRT) may beconsidered as a treatment option for those perimenopausalwomen whose symptoms are disruptive. (III)
SUMMARY OF KEY POINTS:
A4. Perimenopause is characterized by fluctuating hormone lev-els, irregular menstrual cycles, and the onset of symptomsthat may increase in number and severity as menopauseapproaches. (II-2)
A5. The perimenopause is an optimal period for preventivehealth care based on an individualized assessment, adop-tion of a healthy lifestyle, and involvement of the woman
in decisions regarding treatment options and their risk-benefit assessment. (III)
SECTION B: MENOPAUSE: HEALTHY LIVING
RECOMMENDATIONS:
B1. Health care providers should encourage patients to consid-er lifestyle modifications such as exercise, optimal diet, andsmoking cessation, as these lifestyle changes can reduce therisk of cardiovascular disease and osteoporosis. (I, II-2)
B2. The principles of health promotion and disease preventionshould be encouraged in all perimenopausal and post-menopausal women. (III)
SECTION C: SEXUAL HEALTH
RECOMMENDATIONS:
C1. All health care providers dealing with menopausal womenshould be versed in the appropriate counselling and man-agement of menopause and related sexual health issues. (III)
C2. In women with vaginal atrophy, health care providers mayconsider the use of local estrogen therapy as an effectivemode of treatment or consider vaginal moisturizers as effec-tive alternatives. (I, II-1)
C3. In women with decreased libido who have undergone bilater-al oophorectomy, adding androgen to estrogen therapy has beenshown to be effective in increasing libido (I). Androgen ther-apy may be administered to estrogen-treated postmenopausalwomen who have decreased libido not explained by any otherfactors. A risk-benefit profile has not been determined fromstudies with sufficiently large patient numbers. (III)
C4. Routine evaluation of hormone levels (specifically measur-ing serum androgen levels) in postmenopausal women with
FIGURE 2CONDITIONS AFFECTED BY THE MENOPAUSE
JOGC OCTOBER 20028
psychosexual problems is not recommended. (III)C5. Sildenafil citrate does not appear to improve sexual response
in estrogenized women (III). However, it may do so inwomen with decreased libido associated with use of selec-tive serotonin re-uptake inhibitors (SSRIs) (III).
SECTION D: HRT AND CARDIOVASCULAR DISEASE
RECOMMENDATIONS:
D1. Hormone replacement therapy (oral continuous-combinedconjugated equine estrogens [CEE] and medroxyproges-terone acetate [MPA]) (I) or other regimens (III) shouldnot be initiated or continued for the sole purpose of pre-venting future cardiovascular events (primary and sec-ondary prevention). (I)
D2. All women should be counselled about the beneficialeffects of lifestyle modifications on reducing the risk offuture cardiovascular events. Appropriate modificationsinclude consumption of a heart-healthy diet, cessationof smoking, moderate daily exercise, and maintenance ofhealthy body weight. (II)
D3. To prevent future cardiovascular events, women should beprescribed therapies for which there is abundant scientificevidence, such as antihypertensive and lipid-lowering med-ications, β-adrenergic blockers, antiplatelet agents, andangiotensin-converting enzyme (ACE) inhibitors, with dueattention to the potential risks or adverse effects of any ofthese therapies. (I)
SECTION E: OSTEOPOROSIS
RECOMMENDATIONS:
E1. Evaluation of fracture risk in postmenopausal womenshould include the assessment of risk factors, with bonemineral density measurement for those at increased risk.
a) Central (hip and spine) measurements by dual energy X-ray absorptiometry (DEXA) are the mostaccurate and precise measurements of bone densityavailable, making them useful for both risk assessmentand follow-up. (I)
b) Peripheral bone mass measurements (e.g., ulrasoundor DEXA measurements in the radius, phalanx, orheel) is useful for fracture risk assessment, but cannotbe used for follow-up. (I)
E2. Physicians should be aware that a prevalent vertebral ornon-vertebral fragility fracture markedly increases the riskof future fracture. (I)
E3. Markers of bone resorption, while useful in documentinggroup responses in large clinical trials, have no clear placein the evaluation of follow-up of individual patients. (II)
E4. Women should be encouraged to have adequate intake ofcalcium and vitamin D, good nutrition and exercise, avoid-ance of negative lifestyle habits (smoking, alcohol). A nor-mal exposure to estrogen during reproductive life andexercise contribute to optimal achievement and main-tenance of genetically determined peak bone mass. Theserecommendations are applicable to all women (II); for earlypostmenopausal women, adequate calcium and vitamin Dintake alone is not sufficient to maintain bone mass. (I)
E5. Although combination of antiresorptive therapies may be
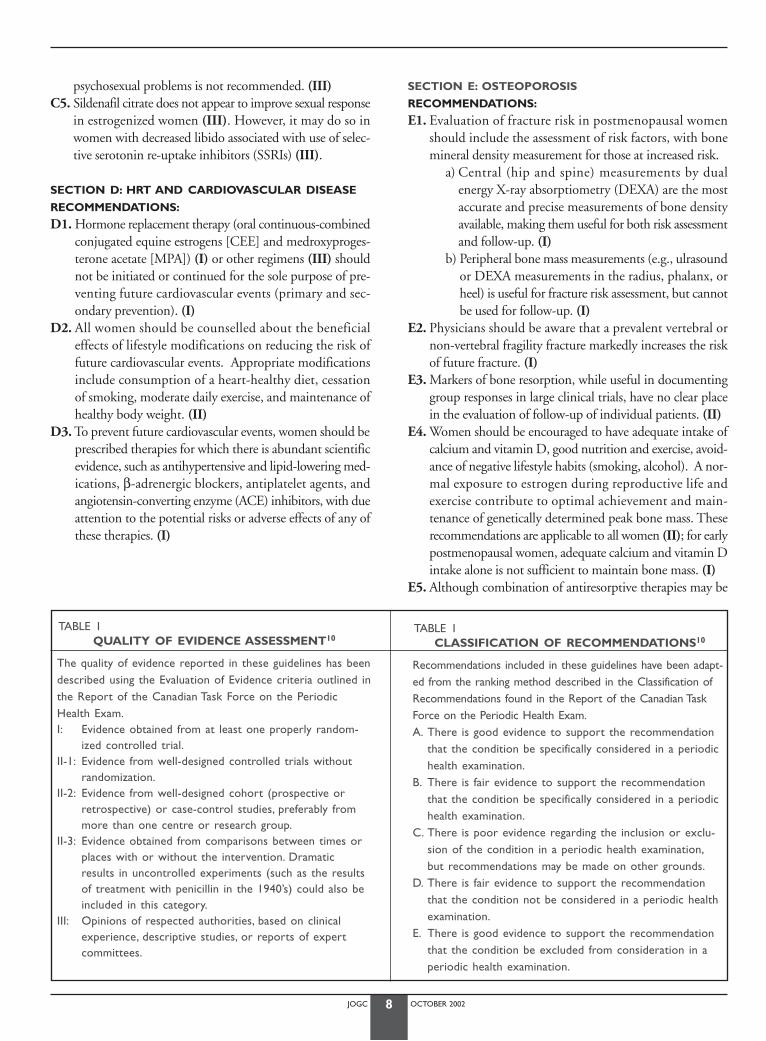
TABLE 1QUALITY OF EVIDENCE ASSESSMENT10
The quality of evidence reported in these guidelines has beendescribed using the Evaluation of Evidence criteria outlined inthe Report of the Canadian Task Force on the PeriodicHealth Exam.I: Evidence obtained from at least one properly random-
ized controlled trial.II-1: Evidence from well-designed controlled trials without
randomization.II-2: Evidence from well-designed cohort (prospective or
retrospective) or case-control studies, preferably frommore than one centre or research group.
II-3: Evidence obtained from comparisons between times orplaces with or without the intervention. Dramaticresults in uncontrolled experiments (such as the resultsof treatment with penicillin in the 1940’s) could also beincluded in this category.
III: Opinions of respected authorities, based on clinicalexperience, descriptive studies, or reports of expertcommittees.
TABLE 1CLASSIFICATION OF RECOMMENDATIONS10
Recommendations included in these guidelines have been adapt-ed from the ranking method described in the Classification ofRecommendations found in the Report of the Canadian TaskForce on the Periodic Health Exam.A. There is good evidence to support the recommendation
that the condition be specifically considered in a periodichealth examination.
B. There is fair evidence to support the recommendationthat the condition be specifically considered in a periodichealth examination.
C. There is poor evidence regarding the inclusion or exclu-sion of the condition in a periodic health examination,but recommendations may be made on other grounds.
D. There is fair evidence to support the recommendationthat the condition not be considered in a periodic healthexamination.
E. There is good evidence to support the recommendationthat the condition be excluded from consideration in aperiodic health examination.
JOGC OCTOBER 20029
synergistic in increasing bone mineral density, their effecton fracture has not been proven. Combination therapyshould be reserved for patients not responding to single-agent antiresorptive therapy. (I)
SUMMARY OF KEY POINTS:
E6. The goal of osteoporosis management is the prevention offracture. This may or may not be associated with signifi-cant increases in bone mineral density. (I)
E7. Postmenopausal bone loss can be effectively prevented by antiresorptive therapy such as estrogen replacement, selective estrogen receptor modulator, or bisphosphonatetherapy. (I)
E8. Treatment with alendronate or risedronate has beendemonstrated to decrease both vertebral and non-vertebralfractures including hip fractures (I); treatment with ralox-ifene, or calcitonin, has been demonstated to reduce ver-tebral fractures (I); treatment with estrogen or etidronateappears to reduce vertebral fracture (II). Physicians shouldconsider a range of treatment options for osteoporosis.
E9. According to the WHI study, continuous combined HRTwas effective in reducing the risk of hip fractures (5 fewercases per 10,000 women per year). Vertebral and other frac-tures were also reduced.
SECTION F: UROGENITAL HEALTH
RECOMMENDATIONS:
F1. Urodynamic studies should be performed prior to inconti-nence surgery or when there is mixed incontinence. (II-3)
SUMMARY OF KEY POINTS:
F2. Urogenital aging may result in urinary urge and stressincontinence, recurrent urinary tract infection, and pelvicorgan prolapse.
F3. There is no objective benefit from estrogen replacementtherapy for postmenopausal urinary stress incontinence. (I)
F4. There is neither objective nor subjective benefit from estro-gen replacement therapy for postmenopausal urge inconti-nence. (I)
F5. Estrogen therapy decreases the incidence of recurrent uri-nary tract infections in postmenopausal women. (I)
SECTION G: MEDICAL AND SPECIAL CONDITIONS
No specific recommendations.
SECTION H: HORMONES AND THE BRAIN
SUMMARY OF KEY POINTS:
H1. Estrogen positively influences brain structures and func-tions that are known to be critical for memory. (I)
H2. In healthy postmenopausal women, estrogen protectsagainst the deterioration in short- and long-term memorythat occurs with normal aging. (I)
H3. Estrogen replacement is associated with a reduction in therisk of developing Alzheimer’s disease in postmenopausalwomen (II-2), but does not affect the progression of dete-rioration in women with diagnosed Alzheimer’s disease. (I)
H4. Estrogen effectively enhances mood in women with dys-phoria or mood lability (I), but there is no evidence that estro-gen alone is an effective treatment for clinical depression. Theaddition of progestin may attenuate the beneficial effect ofestrogen on mood and on cognition in some women. (I)
H5. At present, there is no evidence that raloxifene influencescognitive functioning or mood. (I)
SECTION I: PHARMACOTHERAPY
RECOMMENDATIONS:
I1. The route of estrogen delivery should be primarily deter-mined by patient preference, with the objective of using thelowest effective dose. (III)
I2. Physicians should consider alternate routes of administra-tion such as vaginal and transdermal administration. (III)
I3. Physicians should be aware that women who wish to usecontinuous combined HRT long term (five or more years)should be re-evaluated annually. (III)
SECTION J:
HORMONE REPLACEMENT THERAPY AND CANCER
RECOMMENDATIONS:
J1. No estrogen-progestin regimen is completely protectiveagainst endometrial carcinoma, and all unscheduled uterinebleeding should be investigated. (II-2)
J2. Estrogen-progestin therapy should not be withheld fromwomen with treated stage 1 and 2, grade 1 or 2 adeno-carcinoma of the endometrium who have moderate tosevere menopausal symptoms. (II-3)
J3. According to the WHI study, physicians should inform theirpatients that the use of estrogen-progestin treatment increas-es the risk of breast cancer after 5 years of use but not in astatistically significant way. The risk returns to baseline after5 years of stopping therapy. (I)
J4. There should be increased breast surveillance for womenwho are at high risk of developing breast cancer when usingestrogen-progestin therapy. (III)
J5. In very special circumstances, women at increased risk ofdeveloping breast cancer or who have been treated for breastcancer may be prescribed low dose estrogen-progestin ther-apy for severe symptoms unrelieved by effective alternativetherapies, after risks and benefits have been extensively dis-cussed. The duration of therapy should be regularlyreviewed; there is no preventative role for estrogen therapyin this population. (III)
J6. Physicians should be aware that the reported effects of estrogen-progestin therapy on ovarian cancer have been inconsistent. A possible increased risk may occur in women
JOGC OCTOBER 200210
on long-term estrogen-only therapy (10 or more years). (I)
SUMMARY OF KEY POINTS:
J7. Unopposed estrogen therapy substantially increases the riskof developing atypical endometrial hyperplasia (I) andendometrial carcinoma (II-2). The appropriate dose andduration of progestin therapy will reduce these estrogen-associated risks.
J8. Continuous combined HRT was associated with a reductionin the risk of colorectal cancer, which failed to reach statisti-cal significance (6 fewer cases per 10,000 women per year). (I)
SECTION K:
MENOPAUSE: COMPLEMENTARY APPROACHES
RECOMMENDATIONS:
K1. Physicians and their patients should be more aware of com-plementary therapies in order to effectively consider treat-ment options. (III)
K2. Patients should be informed that lifestyle changes, includ-ing dietary modifications, exercise (I), reduction of stress,and cessation of smoking can benefit the emotional andphysical health of women in midlife. (II-1)
SECTION L:
EVALUATION, DECISION-MAKING, AND FOLLOW-UP
RECOMMENDATIONS:
L1. The assessments recommended by the Canadian Task Forceon the Periodic Health Examination should be included inthe evaluation and follow-up of perimenopausal and post-menopausal women. (III)
L2. Routine abdominal or transvaginal ultrasonography of thepelvis should not be used in healthy asymptomatic post-menopausal women. (II-1)
L3. Postmenopausal women with abnormal bleeding patternsshould undergo a review of their estrogen-progestin thera-py administration (where appropriate), a pelvic examina-tion, and an endometrial biopsy (II-1). Transvaginalultrasonography is an alternative when endometrial sam-pling is not possible or the results are inconclusive. If thesituation remains unclear, tissue sampling with or withouthysteroscopy is recommended. (II)
L4. The majority of women wish to participate in the decision-making process, and health care providers should encour-age them to do so. (III)
L5. Decisions should be based on an individual assessment ofsymptoms, risk factor analysis, and discussion of the risksand benefits of each option. The decision should be re-evaluated as new information becomes available. (III)
L6. Health care providers should actively advocate for public-
funded educational programs to increase knowledge aboutmenopause and osteoporosis for both women and theirhealth care providers. (III)
GLOSSARY
To provide consistency and to clarify any confusion surround-ing the terminology associated with the menopause, the fol-lowing set of definitions published in the World HealthOrganization Technical Report11 are included.*
Natural menopause:The permanent cessation of menstruation resulting from theloss of ovarian follicular activity. Natural menopause is recog-nized to have occurred after 12 consecutive months of amen-orrhoea for which there is no other obvious pathological orphysiological cause. Menopause occurs with the final menstru-al period (FMP), which is known with certainty only in retro-spect one year or more after the event. An adequate independentbiological marker for the event does not exist.
Perimenopause:Includes the period immediately prior to menopause (whenthe endocrinological, biological, and clinical features ofapproaching menopause commence) and the first year aftermenopause. The term “climacteric” should be abandoned toavoid confusion.
Menopausal transition:Reserved for that time before the FMP when variability in themenstrual cycle is usually increased.
Premenopause:The whole of the reproductive period prior to menopause.
Induced menopause:Cessation of menstruation that follows either surgical removalof both ovaries (with or without hysterectomy) or iatrogenicablation of ovarian function (by chemotherapy or radiation).
Simple hysterectomy:Hysterectomy with conservation of at least one ovary. Womenwho undergo a simple hysterectomy will have continuing ovar-ian function for a variable period after surgery.
Postmenopause:The period of time dating from the FMP, regardless of whetherthe menopause was induced or spontaneous.
* These are also used by the Council of Affiliated Menopause Societies(CAMS), the International Menopause Society (IMS), and the North Ameri-can Menopause Society (NAMS, www.menopause.org).

JOGC OCTOBER 200211
Premature menopause:Menopause that occurs at an age more than two standard devi-ations below the mean age of menopause in the reference pop-ulation. In practice, without reliable estimates of the distributionof age at natural menopause in developing countries, the age of40 years is used frequently as an arbitrary cut-off point, belowwhich menopause is said to be premature.
J Obstet Gynaecol Can 2001;23(9)829-35.
REFERENCES
1. Society of Obstetricians and Gynaecologists of Canada. CanadianMenopause Consensus Conference. J Soc Obstet Gynaecol Can1994;16:4-40.
2. Nagnur D. Longevity and Historical Life Tables 1921B1981 (abridged),Canada and the Provinces. Ottawa: Statistics Canada, 1986. Cat. No. 89-2056.
3. Life Tables, Canada and Provinces, 1990B1992. Ottawa: Statistics Cana-da, 1992. Cat. No. 84-537.
4. CANSIM, Matrix 6367 Ottawa: Statistics Canada. www.statscan.ca 5. CANSIM, Matrix 6900 Ottawa: Statistics Canada. www.statscan.ca6. McKinlay SM, Brambilla DJ, Posner JG.The normal menopause
transition. Maturitas 1992;14:103-15.7. Taylor DL,Woods NF. Changing women’s health, changing nursing prac-
tice. JOGNN 1996;25:791-802.8. Patterson C, Feightner J. Promoting the health of senior citizens. Can
Med Assoc J 1997;157:1107-13.9. Genuis SJ, Genuis SK, Chang WC.The Well-being of women in the post-
menopausal Years. J Soc Obstet Gynaecol Can 2000;22(2):141-50.10. Woolf SH, Battista RN,Angerson GM, Logan AG, Eel W. Canadian Task
Force on the Periodic Health Exam. Ottawa:Canada CommunicationGroup, 1994;xxxvii.
11. WHO Scientific Group on Research on the Menopause in the 1990s.WHO Technical Report Series. Geneva, Switzerland, 1996:866.

JOGC OCTOBER 200212
INTRODUCTION
Our aging population has focused attention on postmenopausalhealth issues. However, far less is known about the peri-menopause. This transition period between reproductive andpost-reproductive life is characterized by fluctuations in hormonelevels, irregularities in the menstrual cycle, and several other signsand symptoms. It can be a perplexing time for women and clin-icians because of insufficient data from clinical trials for the devel-opment of evidence-based treatment guidelines.
The Society of Obstetricians and Gynaecologists of Cana-da (SOGC) concurs with the World Health Organization(WHO) and the North American Menopause Society(NAMS) in defining perimenopause as the two to eight yearspreceding menopause and the first year after the final men-strual period.1 It typically begins in the fifth decade when theendocrinological, biological, and clinical features of approach-ing menopause are first noticed.2
CLINICAL AND PHYSIOLOGIC CHANGES ASSOCIATED WITH PERIMENOPAUSE
The following clinical, endocrinological, and biological changesassociated with perimenopause have been identified:2-4
• menstrual cycle pattern variations • accelerated rate of follicular depletion• erratic variations in circulating estrogen levels (it is only in the
year or so before final menses that levels fall substantially)• lower circulating progesterone levels with short or insufficient
luteal phases, often preceding anovulation• gradually increasing serum follicle-stimulating hormone (FSH)
levels, while luteinizing hormone (LH) levels remain normal• decreased serum levels of inhibin A and B (responsible for
suppression of FSH), possibly as a result of follicular agingand diminishing follicular competence.
VARIATIONS IN THE MENSTRUAL CYCLE
Longitudinal studies4-7 have shown that the perimenopausaltransition average age of onset is 45.1 years (39-51 years) and
the average duration is five years (2-8 years) (mean, 95% CI).The majority of women experience four to eight years ofchanges in the menstrual cycle before menopause, with only 10 percent reporting abrupt cessation of menstruation.
Three distinct stages of the menopausal transition are iden-tified in the Seattle Midlife Women’s Health Study:8
1. Early menopausal transition: menstrual cycles continue tobe regular, but changes in the amount and length of flow orin cycle length are noted;
2. Middle menopausal transition: onset of menstrual cycleirregularity without skipping of periods;
3. Late menopausal transition: skipping of menstrual bleedsoccurs, with periods often two or more months apart.
Although there was an age progression across these stages, agewas not a consistent predictor of the type of menstrual cyclechange. Several patterns of cycle change were also noted, includ-ing forward progression from stage to stage, no change in stage,and switching back and forth between stages.8
ABNORMAL UTERINE BLEEDING
Clinicians must differentiate between irregular bleeding andabnormal uterine bleeding, a more serious concern that war-rants further investigation. This topic is discussed in Section L,*
as well as in SOGC guidelines for Evaluation and Managementof Abnormal Uterine Bleeding.9,10
FERTILITY AND PREGNANCY
Women may be uncertain about their reproductive status becauseof the unpredictable nature of hormone production and the irreg-ularity of their menstrual cycles during the perimenopause. Fer-tility in perimenopausal women is decreased, with fewer oocytesavailable for recruitment and ovulation. A significant number ofthese oocytes are chromosomally abnormal. The result is anincrease in infertility and reduced success rates with infertility treat-ment for women age 40 years and over.11
Pregnancy in the perimenopause is associated with increasedobstetrical and genetic risks, including spontaneous abortion,fetal anomalies, and perinatal and maternal mortality.11
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
Elizabeth Contestabile RN, BScN1; Christine Derzko, MD, FRCSC2
1 Ottawa ON2 Toronto ON
PERIMENOPAUSE
* Evaluation, Decision-Making, and Follow-up, J Obstet Gynaecol Can 2001;23(12).

JOGC OCTOBER 200213
CONTRACEPTION
During perimenopause, periods of ovarian failure are inter-spersed with periods of ovarian function. Isolated hormonemeasurements are not reliable for assessing reproductive status.A laboratory marker to predict the onset of menopause has yetto be identified.12 Contraception should be recommended untilmenopause is confirmed clinically, usually when amenorrheahas been present for one year.
SYMPTOMS OF PERIMENOPAUSE
Women report increasing symptoms during the peri- and post-menopausal period (Table 1).13-15 The most prevalent symp-toms attributed to fluctuating hormone production includevasomotor symptoms, breast tenderness, vaginal dryness, andsleep disturbances.3,7,13
Much of the current knowledge about the symptoms asso-ciated with perimenopause and menopause is limited becausestudy populations have consisted mainly of Caucasian womenover the age of 45. These issues are being addressed in the Studyof Women and Health in the Nation (SWAN),15 which isexamining the natural history of menopause in a multiracialand multiethnic population of women 40 to 55 years of age.
VASOMOTOR SYMPTOMS
Hot flushes and night sweats are common names for the vaso-motor instability reported by as many as 85 percent of peri-menopausal women. Defined as recurrent, transient episodesof flushing, sweating, and a sensation of heat, flushes are oftenaccompanied by palpitations and feelings of anxiety, and maybe followed by chills. While only a minor annoyance for many,flushes cause major disruptions in sleep and daily activities in
about 15 percent of perimenopausal women.16 These symp-toms often begin before the cessation of menses, increase in fre-quency and intensity as menopause approaches, and persist forsome time afterwards.7,13-15
It has generally been assumed that vasomotor symptomsare a result of the effect of low estrogen levels at the ther-moregulatory centre in the hypothalamus. This theory is sup-ported by the demonstrated efficacy of estrogen in relievingvasomotor symptoms.17 However, most postmenopausalwomen have consistently low levels of estradiol and do notexperience hot flushes after the initial transition. Similarly, pre-pubertal girls do not have hot flushes. An alternate hypothesisis that it is the withdrawal of estrogen, or a decreasing abilityof estrogen to bind to estrogen receptors, that precipitates hotflushes.3,17 This would explain the frequent occurrence of hotflushes in the perimenopause when fluctuations from relative-ly high to low or normal levels of estrogen occur.
Numerous other factors contribute to hot flushes, including:epilepsy, infection, carcinoid syndromes, thyroid disease, insuli-noma, pheochromocytoma, pancreatic tumours, hematologicmalignancies, autoimmune disorders, and mast-cell disorders.18
Appropriate investigation is required when vasomotor symptomsdo not respond to hormone replacement therapy (HRT).4Whenthe clinical situation is not clear, documentation of an elevatedserum follicle stimulating hormone (FSH) level may be helpfulfor confirming menopausal change.
SLEEP DISTURBANCES
Sleep disturbances are common in the perimenopausal period,and are often related to vasomotor symptoms.7,13,19 The patternof difficulty in sleeping differs from other symptoms ofmenopause, suggesting that it may not be a direct effect of hor-monal changes but rather a result of many factors.13 Insomnia canresult in excessive daytime fatigue, irritability, and impaired learn-ing and cognition. Since there are many possible causes of insom-nia other than those specifically associated with perimenopause,further investigation is warranted, especially for insomnia thatoccurs nightly and is long-lasting.19
BREAST TENDERNESS
Mastalgia is often cyclic in nature, occurring in the luteal phaseof the menstrual cycle, and is common in the premenopausaland early perimenopausal period. A decrease in prevelance isnoted in the late perimenopause and postmenopause as ovula-tion ceases and cyclical hormone production stops.13
UROGENITAL SYMPTOMS
Vaginal dryness is occasionally reported by perimenopausalwomen and may increase over time, becoming more of a con-cern postmenopausally.13 Often the first change noted isdecreased lubrication with sexual arousal.20
Other symptoms related to urogenital aging, such as urinary
TABLE 1
COMMONLY REPORTED SYMPTOMS OF THE PERIMENOPAUSE13,14
Associated with hormonal status:• Vasomotor symptoms: hot flushes, night sweats• Vaginal dryness, dyspareunia• Mastalgia
Potentially associated with hormonal status:• Fatigue, lack of energy, insomnia, sleep disturbances• Backache, joint and muscle pain• Mood swings, depression, irritability, anxiety, memory loss,
changes in libido• Urinary incontinence• Headaches
Not associated with hormonal status:• Major depression• Weight gain

JOGC OCTOBER 200214
incontinence, may be common but are not frequently reportedunless specifically addressed during evaluation. The prevalenceof stress incontinence is highest in perimenopause, while theprevalence of urge incontinence increases after menopause.21**
SEXUAL FUNCTION
Perimenopausal women may express concerns about changesin sexual function, including a decreased interest in and capac-ity for sexual activity. The level of sexual function a woman hasat the time of menopause correlates with her current health andactivity level, her sexual adjustment in the premenopausal years,and her personal and cultural expectations of sexual functionafter menopause. Ongoing population studies such as SWAN15
will help to determine the associations between menopausal sta-tus, aging, sociocultural factors, and sexual function.22†
PSYCHOLOGICAL EFFECTS
Depression and anxiety are more frequently reported during peri-menopause. Greater psychological stress is experienced during themenopause transition than in the postmenopausal years. Transientdepressed mood during the perimenopause is associated with
depressed mood before menopause, a longer transition tomenopause, and more severe menopausal symptoms.23,24 Currentevidence does not support an association between estrogen levelsduring the menopausal transition and the onset of clinical depres-sion.13,24 Women who have major depression at the time ofmenopause are likely to have had prior depressive episodes, post-partum affective syndromes or premenstrual dysphoric disorder.25
Women who seek care for symptoms during the peri-menopausal period may be more vulnerable to symptom distress.Studies report that these women were less healthy, had more psy-chosomatic complaints and vasomotor reactions,23,26 and weremore likely to have a history of premenstrual symptoms.25
Women who report the development or exacerbation ofpremenstrual syndrome (PMS) or premenstrual dysphoric dis-order (PDD) may be confusing the symptoms with onset ofperimenopause. Monitoring of symptoms will help to deter-mine if they are confined to the luteal phase of the cycle andmeet the criteria for PMS/PDD.25
Some of the somatic and psychological symptoms associatedwith the perimenopause may be difficult to differentiate from themanifestations of a depressive disorder. Clinical evaluation, includ-ing a detailed history, confirmation of perimenopausal or post-menopausal status, and the use of standardized mood-rating scales,will help to clarify the diagnosis.27
Mild depressive symptoms may respond to treatment withestrogen alone, but more severe depression or a failure torespond to estrogen treatment alone are clear indications forstandard psychopharmacologic therapy.27*
EVALUATION OF THE PERIMENOPAUSAL WOMAN
Evaluation of the perimenopausal woman should focus onthree areas: assessment of menopause status and the severity ofsymptoms, assessment of current health status, and assessmentof risk factors for disease. Random serum measurements ofFSH, lutenizing hormone (LH), and estradiol to determinemenopause status are of no use in menstruating women. Theymay be helpful to determine menopause status in women whohave undergone hysterectomy, when premature ovarian failureis suspected, or for other clinical concerns. They may also beused to predict ovarian reserve in older women desiring preg-nancy. The most meaningful results are obtained in the earlyfollicular phase. Amenorrhea in women under 50 years shouldnot be presumed to be a result of menopause. The possibilityof pregnancy and other causes should be considered. A men-strual calendar is a useful tool for monitoring bleeding patterns,for identifying abnormal uterine bleeding, and for determin-ing the need for further investigation. The elements of a com-prehensive evaluation are explained in Section L.***
TABLE 2
NON-HORMONAL OPTIONS FOR SYMPTOM CONTROL
Vasomotor symptoms:*
Antidepressants ClonidineBellergal™Regular aerobic exercisePeriodic deep breathing exercisesDietary phytoestrogensBlack cohosh
Vaginal dryness:†
Vaginal moisturizer (Replens™)Vaginal lubricantsContinued regular sexual activity
Sleep Disturbances:Prescription pharmacotherapy (hypnotics)19
Valerian*
Behavioural treatments‡
Mild to Moderate Depression:Prescription antidepressants27
Psychotherapy27
St. John’s Wort*
* Menopause: complementary approaches,J Obstet Gynaecol Can 2001;23(11)
† Menopause and sexual function,J Obstet Gynaecol Can 2001;23(9):849-52
‡ Menopause: healthy living,J Obstet Gynaecol Can 2001;23(9):842-8
* Pharmacotherapy, J Obstet Gynaecol Can 2001;23(11).*** Evaluation, Decision-Making and Follow-up, J Obstet Gynaecol Can 2001;23(12).
** Urogenital health, J Obstet Gynaecol Can 2001;23(10).† Menopause and sexual function, J Obstet Gynaecol Can 2001;23(9)849-52.

JOGC OCTOBER 200215
THERAPEUTIC OPTIONS FOR THE PERIMENOPAUSAL YEARS
The perimenopausal years provide an excellent opportunity todevelop an individualized plan for disease prevention andhealth promotion. Objectives include the maintenance of opti-mal physical, mental, and social activity, the early detection ofchronic diseases, and a smooth transition to the post-menopausal years.4 A comprehensive assessment, reassur-ance, and counselling may be all that healthy perimenopausalwomen require.
HEALTHY LIFESTYLE
A healthy lifestyle is a prerequisite for any program to promotehealth and prevent disease. The fundamentals include the avoid-ance of smoking, maintenance of a healthy weight, regular phys-ical activity, a healthy diet, and limited alcohol intake. This topicis discussed in more detail in Section B.*
NON-HORMONAL THERAPIES
FOR SYMPTOM CONTROL
Non-hormonal options with evidence of effectiveness in con-trolling symptoms are listed in Table 2.
HORMONAL THERAPIES FOR SYMPTOM CONTROL
ORAL CONTRACEPTIVE THERAPY
Low-dose oral contraceptives (OCs) containing 20 to 35 µg ofethinyl estradiol offer many benefits for the perimenopausalwoman (Table 3). An OC containing 20 µg of ethinyl estra-diol has been shown to provide effective contraception, reducemenstrual cycle irregularity, decrease bleeding, and relievemenopausal symptoms.28 Important additional benefits of such
treatment include a decrease in the risk for ovarian andendometrial cancer, reduced dysmenorrhea, reduced menor-rhagia, a lower risk of functional ovarian cysts, and possiblyincreased bone density.4,9,29,30 Women taking an OC mayexperience a return of symptoms during the hormone-freeinterval, although supplementation during that time with alow dose of estrogen may be helpful. Alternatively, the OC maybe taken continuously.
Risks associated with the use of OCs include an increasedrisk for venous thromboembolism (VTE) and acute myocar-dial infarction.31 The risk for ischemic stroke appears to be lowfor users of low-dose OCs who do not have additional risk fac-tors.32 The risk for cardiovascular disease increases further withage, smoking, a positive family history of premature heart dis-ease or VTE, and other cardiac risk factors.31,32 After the ageof 35, OC use should be considered only for healthy non-smoking women.
Oral contraceptive use is associated with a slightly increasedrisk of developing breast cancer, which returns to baseline 10years after cessation. Breast cancers diagnosed in OC users tendto be less clinically advanced than those found in non-users.33
It should be noted that the risks associated with OC usehave been identified from older studies and meta-analyses thatusually involved younger women and higher doses of estrogen.Further studies are needed to determine the risks of low-doseOC use by perimenopausal women.
TABLE 3EFFECTS OF ESTROGEN IN CONTROLLING
MENOPAUSAL SYMPTOMS
Vasomotor symptoms:• dose-related decrease in incidence and severity 37-40
• efficacy may be altered by the estrogen preparation,route of administration, or concomitant progestin4
Sleep disturbances:• estrogen therapy improves restlessness, ability
to fall asleep and nocturnal awakenings41
Sexual function:• estrogen therapy increases blood flow to the genital area• relief of dyspareunia and vaginal dryness with either
systemic or local administration42
Psychological effects:• estrogen therapy improves mood in depressed peri-
menopausal women, independent of its effect on flushes43
* Menopause: healthy living, J Obstet Gynaecol Can 2001;23(9)842-8.
FIGURE 1
ALGORITHM FOR DISCONTINUING ORALCONTRACEPTIVES
IN PERIMENOPAUSAL/MENOPAUSAL WOMEN30
Age 51-52
Serum FSH on day 7 of pill-free week
FSH > 30 IU/L FSH < 30 IU/L
Discontinue OC Serum E2, FSH:LH+/- switch to ratio on day 7 of
HRT pill-free week OR Continue OC x 12 months
E2 < 73 pmol/lFSH:LH ratio > 1
From: Case AM, Reid RL. Diagnosis of menopause in peri-menopausal women taking oral contraceptives. J Soc ObstetGynaecol Can 1998;20:1159-62.

JOGC OCTOBER 200216
Serum FSH measurements on day 7 of the pill-free inter-val may not have sufficient sensitivity to diagnose menopause.Figure 1 provides guidelines for discontinuing the OC and ini-tiating HRT.
PROGESTIN THERAPY
Cyclic progestin therapy (5-10 mg of medroxyprogesteroneacetate daily, 10-14 days of each month) has been used to reg-ulate anovulatory bleeding and reverse endometrial hyperpla-sia.4,9 Synthetic progestins such as medroxyprogesterone acetate(20 mg daily by mouth)34 and megestrol acetate (20 mg twicedaily)35 can offer an effective alternative for the treatment ofvasomotor symptoms in postmenopausal women.
A progesterone-releasing intrauterine system (Mirena™)has been approved in Canada for contraception. It reduces theamount and duration of menstrual flow and may be an effec-tive option for the control of menorrhagia.36
The progestogen-only contraceptive pill (POP) provides effec-tive contraception for perimenopausal women without increasingrisk for cardiovascular disease. Compared to the combined estro-gen-progestin OC, the POP is associated with a higher rate of spot-ting and breakthrough bleeding, may be less effective for relief ofvasomotor symptoms, and may worsen depressed mood.29 Prog-estin therapy is further discussed in Section H.*
HORMONE REPLACEMENT THERAPY
The use of HRT or estrogen replacement therapy (ERT) pro-vides the most effective relief of vasomotor and othermenopausal symptoms (Table 3). However, HRT and ERThave not been well studied in the perimenopausal interval. Inaddition, HRT and ERT cannot be assumed to provide con-traception for the perimenopausal woman, and may not pro-vide cycle control in women still having spontaneous menses.
RECOMMENDATIONS:
A1. Health care providers should not use random serummarkers of follicle-stimulating hormone (FSH),luteinizing hormone (LH), and estradiol E2 for the pur-pose of predicting menopause since clear markers forpredicting menopause are yet to be identified. (II-2)
A2. In addition to providing effective contraception, low-dose oral contraceptives are an effective treatment forsymptom-atic, healthy, non-smoking perimenopausalwomen. (I)
A3. Using the data from studies in postmenopausal womenand clinical expertise as a guide, estrogen replacementtherapy (ERT) or hormone replacement therapy (HRT)may be considered as a treatment option for those perimenopausal women whose symptoms are disrup-tive. (III)
SUMMARY OF KEY POINTS:
A4. Perimenopause is characterized by fluctuating hormonelevels, irregular menstrual cycles, and the onset of symp-toms that may increase in number and severity asmenopause approaches. (II-2)
A5. The perimenopause is an optimal period for preventivehealth care based on an individualized assessment,adoption of a healthy lifestyle, and involvement of thewoman in decisions regarding treatment options andtheir risk-benefit assessment. (III)
CONCLUSION
Emerging evidence about perimenopause provides informationabout the associated clinical, endocrinological, and biologicalchanges, as well as effective treatment options for troublesomesymptoms. The clinical encounter between a woman and herhealth care provider presents an excellent opportunity for dis-cussion about perimenopausal issues, individualized assessment,counselling, and shared decision-making. Continued research isneeded to support further understanding and the developmentof evidence-based management guidelines for the perimenopause.
J Obstet Gynaecol Can 2001;23(9)836-41
REFERENCES
1. WHO Scientific Group on Research on the Menopause in the 1990s.WHO Technical Report Series. Geneva, Switzerland:WHO, 1996;p.866.
2. Clinical challenge of the perimenopause: consensus opinion of TheNorth American Menopause Society. Menopause 2000;7:5-13.
3. Prior JC. Perimenopause: the complex endocrinology of themenopausal transition. Endoc Rev 1998;19:398-428.
4. Speroff L. Management of the perimenopausal transition. ContempObstet Gynecol 2000;10:14-37.
5. Treolar AE, Boynton RE, Behn BG,Variation of the human menstrualcycle through reproductive life. Int J Fertil 1967;12:77-126.
6. Treolar AE. Menstrual cyclicity and the pre-menopause. Maturitas1981;3:249-64.
7. McKinlay SM, Brambilla DJ, Posner JG.The normal menopausetransition. Maturitas 1992;14:103-15.
8. Mitchell ES,Woods NF, Mariella A.Three stages of the menopausal tran-sition from the Seattle Midlife Women’s Health Study: toward a moreprecise definition. Menopause 2000;7:334-49.
9. Derzko CM. Perimenopausal dysfunctional uterine bleeding: physiologyand management. J Soc Obstet Gynaecol Can 1997;19:589-600.
10. Brand A. Diagnosis of endometrial cancer in women with abnormalvaginal bleeding. Practice guideline no. 86. J Soc Obstet Gynaecol Can2000;22(2):102-4.
11. Hosseinzadeh M, Jolly EE. Fertility in the mature woman. J Soc ObstetGynaecol Can 1997;19:611-18.
12. Burger HG, Dudley EC, Hopper JL, Groome N, Guthrie JR, Green A,et al. Prospectively measured levels of serum follicle-stimulatinghormone, estradiol, and the dimeric inhibins during the menopausaltransition in a population-based cohort of women. J Clin EndocrinolMetab 1999;84:4025-30.
13. Dennerstein L, Dudley EC, Hopper JL, Guthrie JR, Burger HG.Aprospective population-based study of menopausal symptoms. Obstet
* Hormones and the brain, J Obstet Gynaecol Can 2001;23(11).
JOGC OCTOBER 200217
Gynecol 2000;96:351-8.14. Avis NE, Kaufert PA, Lock M, McKinlay S,Vass K.The evolution of
menopausal symptoms. Baillieres Clin Endocrinol Metab 1993;7:17-32.15. Gold EB, Sternfeld B, Kelsey JL, Brown C, Mouton C, Reame N, et al.
Relation of demographic and lifestyle factors to symptoms in a multi-racial/ethnic population of women 40-55 years of age.Am J Epidemiol2000;152:463-73.
16. Kronenberg F. Hot Flashes. In:Lobo RA (ed).Treatment of thePostmenopausal Woman: Basic and Clinical Aspects. 2nd edition.Philadelphia: Lippincott,Williams & Wilkins, 1999;pp.157-77.
17. Andrews MC. Hormonal Changes in the Perimenopause and ClinicalConsequences. In:Eskin BA (ed).The Menopause: Comprehensive Man-agement. 4th edition. New York: Parthenon, 2000;pp.79-86.
18. Scully RE, Mark EJ, McNeely WF, McNeely BU (eds). Case records of theMassachusetts General Hospital: weekly clinicopathological exercises,case 7-1992. N Engl J Med 1992;326:472-81.
19. Shaver JL. Sleep problems II: assessment and treatment. MenopauseManagement 2000;9:14-8.
20. Bachmann G. Urogenital ageing: an old problem newly recognised.Maturitas 1995;22(suppl):1-5.
21. Drutz H, Bachmann G, Bouchard C, Morris B.Towards a better recogni-tion of urogenital aging. J Soc Obstet Gynaecol Can 1996;18:1017-31.
22. Obermeyer CM. Menopause across cultures: a review of the evidence.Menopause 2000;7:184-92.
23. Stewart DE, Boydell K, Derzko C, Marshall V. Psychologic distress dur-ing the menopausal years in women attending a menopause clinic. Int JPsychiatry Med 1992;22:213-20.
24. Avis NE, Brambilla D, McKinlay SM,Vass K. A longitudinal analysis of theassociation between menopause and depression: results from the Mass-achusetts Women’s Health Study.Ann Epidemiol 1994;4:214-21.
25. Pearlstein TB. Hormones and depression: what are the facts about pre-menstrual syndrome, menopause, and hormone replacement therapy?Am J Obstet Gynecol 1995;173:646-53.
26. Kuh DL,Wadsworth M, Hardy R.Women’s health in midlife: theinfluence of the menopause, social factors and health in earlier life. Br JObstet Gynaecol 1997;104:923-33.
27. Meguid AS,Wise TN. Depressive disorders and the menopause.Menopause Management 2001;10:10-20.
28. Casper RF, Dodin S, Reid RL, and Study Investigators.The effect of 20 µgethinyl estradiol/ 1 mg norethindrone acetate (MinestrinJ), a low doseoral contraceptive, on vaginal bleeding patterns, hot flashes, and qualityof life in symptomatic perimenopausal women. Menopause 1997;4:139-47.
29. Shaaban MM.The perimenopause and contraception. Maturitas1996;23:181-92.
30. Case AM,Reid RL.Diagnosis of menopause in perimenopausal womentaking oral contraceptives. J Soc Obstet Gynaecol Can 1998;20:1159-62.
31. Collins JA, Gunby J. Oral contraceptive use and the cardiovascularhealth of Canadian women. J Soc Obstet Gynaecol Can 1997;19:125-37.
32. Goldstein LB,Adams R, Becker K, Furberg CD, Gorelick PB,Hademenos G, et al. Primary prevention of ischemic stroke: a statementfor healthcare professionals from the Stroke Council of the AmericanHeart Association. Stroke 2001;32:280-99.
33. Collaborative Group on Hormonal Factors in Breast Cancer. Breastcancer and hormonal contraceptives: collaborative reanalysis of individ-ual data on 53,297 women with breast cancer and 100,239 womenwithout breast cancer from 54 epidemiological studies. Lancet1996;347:1713-27.
34. Schiff I,Tulchinsky D, Cramer D, Ryan K. Oral medroxyprogesterone in the treatment of postmenopausal symptoms. J Am Med Assoc1980;244:1443-5.
35. Loprinzi CL, Michalak JC, Quella SK, O’Fallon JR, Hatfield AK, et al.Megesterol acetate for the prevention of hot flashes. N Engl J Med1994;331:247-52.
36. Sturridge F, Guillebaud J.A risk-benefit assessment of the levonor-gestrel-releasing intrauterine system. Drug Safety 1996;15:430-440.
37. Greendale GA, Reboussin BA, Hogan P, Barnabei VM, Shumaker S,Johnson S. et al. Symptom relief and side effects of postmenopausal hormones: results from the Postmenopausal Estrogen/progestin Interventions Trial. Obstet Gynecol 1998;92:982-8.
38. Notelevitz M, Cassel D, Hille D, Furst KW, Dain MP,VandePol C, et al.Efficacy of continuous sequential transdermal estradiol and norethin-drone acetate in relieving vasomotor symptoms associated withmenopause.Am J Obstet Gynecol 2000;182 (1 Pt 1):7-12.
39. Utian WH, Burry KA,Archer DF, Gallagher JC, Boyeit RL, Guy MP, et al.Efficacy and safety of low, standard, and high doses of estradioltransdermal system (Esclim) compared with placebo on vasomotorsymptoms in highly symptomatic menopausal patients.The Esclim StudyGroup.Am J Obstet Gynecol 1995;181:71-9.
40. Speroff L,Whitcomb RW, Kempfert NJ, Boyd RA, Paulissen JB, Rowan JP.Efficacy and local tolerance of a low-dose, 7-day matrix estradiol trans-dermal system in the treatment of menopausal vasomotor symptoms.Obstet Gynecol 1996;88:587-92.
41. Polo-Kantola P, Erkkola R, Helenins H, Irjala K, Polo O.When doesestrogen replacement therapy improve sleep quality? Am J ObstetGynecol 1998;178:1002-9.
42. Notelevitz M. Estrogen therapy in the management of problems associ-ated with urogenital aging: a simple diagnostic test and the effect of theroute of administration. Maturitas 1995;22(suppl):31-3.
43. Schmidt PJ, Nieman L, Danaceau MA,Tobin MB, Roca CA, Murphy JH,et al. Estrogen replacement in perimenopause-related depression: apreliminary report.Am J Obstet Gynecol 2000;183:414-20.

T K
JOGC OCTOBER 200218
INTRODUCTION
The transition through perimenopause and menopause pro-vides an ideal opportunity to focus women’s attention onlifestyle choices that can improve their overall health. This isoften a time of high motivation, during which health careproviders can encourage lifestyle modifications involving nutri-tion, exercise, weight management, stress reduction, smokingcessation, and the limitation of alcohol and caffeine intake. TheNurses’ Health Study showed an 83 percent reduction in coro-nary events in women who adhered to a healthy lifestyle involv-ing diet, exercise, and abstinence from smoking. The numbersof women in this category were small (3%), but they under-score the enormous potential for intervention in this area.1
DIET
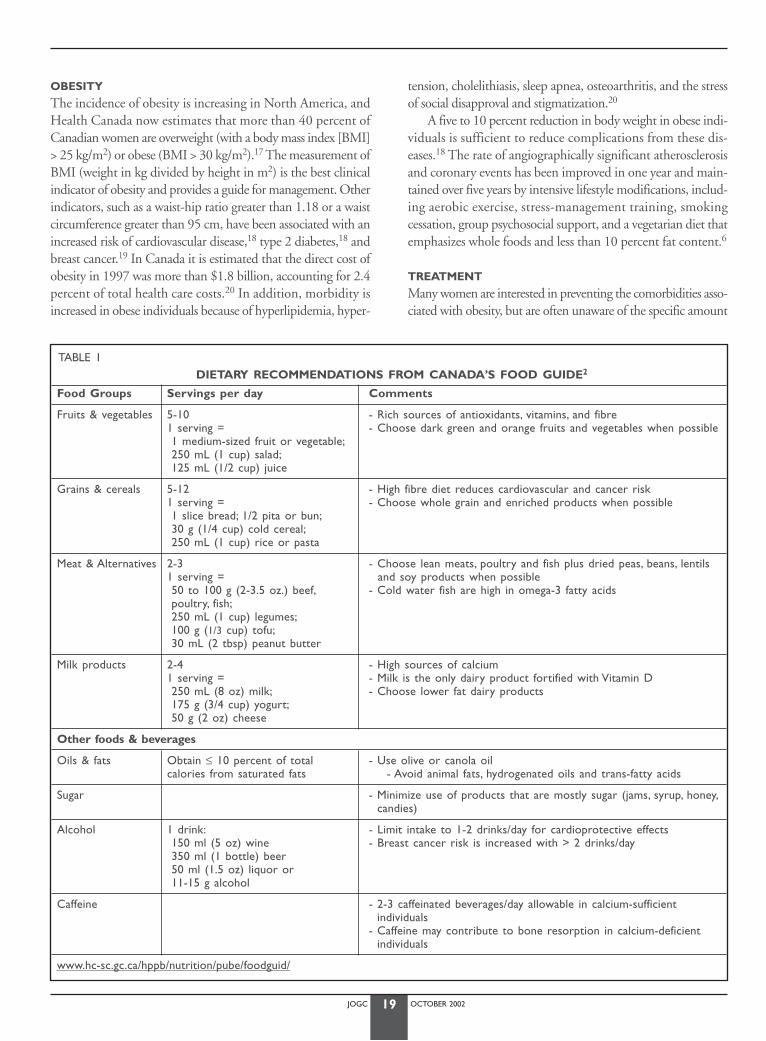
Canada’s Food Guide2 recommends a diet rich in plant-basedfoods, low in saturated and trans-fatty acids, high in dietaryfibre, and accompanied by six to eight glasses of water perday (Table 1). This diet provides adequate nutrients and vita-mins for most menopausal women, unless specific diseases ormalabsorption problems are present. It may, however, be diffi-cult to obtain optimal amounts of select nutrients such as cal-cium, vitamin D, and folate from diet alone (Table 2).
Women with medical conditions such as hypertension,dyslipidemia, and diabetes mellitus should consult a dietitianfor specific dietary advice.3-5 Additional information about var-ious nutritional issues can be obtained from resources listed atthe end of this section and from the Canadian recommenda-tions for the management and treatment of dyslipidemia.4
EXERCISE
The simplest and most effective way to maintain good health isthrough regular exercise. Among the many benefits of exerciseare improvements in serum lipids and weight, and protectionfrom cardiovascular disease, diabetes, and breast cancer.6,7
Women who exercise regularly report lower levels of stress, lighterperiods, and fewer menopausal symptoms.8 Regular exercise canalso decrease bone loss, improve balance and strength, and pro-vide protection from falls and fractures.9-11
Exercise must be tailored to a woman’s age, ability, and indi-vidual preference. A sedentary woman should be advised to startslowly and progress gradually. A minimum of 20 to 30 minutesof weight-bearing exercise on most days is recommended by theOsteoporosis Society of Canada to promote bone health. Theaddition of muscle-strengthening exercise involving the upper andlower limbs, abdomen, and back muscles for 30 to 60 minutesthree times per week can help to improve bone mass and decreaseback pain.11 Flexibility training (stretch classes, tai chi, yoga)improves balance and helps to prevent muscular injuries and falls.12
Thirty minutes of moderate aerobic exercise (which may be bro-ken into 10 minute sessions three times daily) on most days is rec-ommended by the Canadian Medical Association and the Heartand Stroke Foundation for its cardioprotective effects. The HealthCanada Activity Guide13 is a useful resource.
WEIGHT GAIN
Perimenopausal weight gain is common but not inevitable. Theaverage amount of weight gained during the perimenopauseranges from 2.25 to 4.19 kg.14 This weight gain is not relatedto hormone replacement therapy or menopause itself, but to anage-associated reduction in the metabolic rate resulting fromthe shift in ratio of fat-to-lean body composition.15
Most menopausal women are more accepting of their bodyimage and size, and do not pursue drastic weight-loss diets.However, many are surprised and dismayed when they expe-rience midlife weight gain, and will seek advice from theirhealth-care practitioner on how to minimize adverse healthconsequences. A recent 54 month randomized controlled trialindicated that perimenopausal weight gain and elevations inlow-density lipoprotein (LDL) cholesterol could be minimizedby ingestion of a low-fat diet with moderate calorie restriction,combined with a modest increase in exercise.16
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
Suzanne Montemuro, MD, CCFP,1 Margo Fluker, MD, FRCSC,2 June Rogers,3 Christine Derzko, MD, FRCSC4
1 Vancouver BC2 Vancouver BC3 Toronto ON4 Toronto ON
MENOPAUSE: HEALTHY LIVING
JOGC OCTOBER 200219
OBESITY
The incidence of obesity is increasing in North America, andHealth Canada now estimates that more than 40 percent ofCanadian women are overweight (with a body mass index [BMI]> 25 kg/m2) or obese (BMI > 30 kg/m2).17 The measurement ofBMI (weight in kg divided by height in m2) is the best clinicalindicator of obesity and provides a guide for management. Otherindicators, such as a waist-hip ratio greater than 1.18 or a waistcircumference greater than 95 cm, have been associated with anincreased risk of cardiovascular disease,18 type 2 diabetes,18 andbreast cancer.19 In Canada it is estimated that the direct cost ofobesity in 1997 was more than $1.8 billion, accounting for 2.4percent of total health care costs.20 In addition, morbidity isincreased in obese individuals because of hyperlipidemia, hyper-
tension, cholelithiasis, sleep apnea, osteoarthritis, and the stressof social disapproval and stigmatization.20
A five to 10 percent reduction in body weight in obese indi-viduals is sufficient to reduce complications from these dis-eases.18 The rate of angiographically significant atherosclerosisand coronary events has been improved in one year and main-tained over five years by intensive lifestyle modifications, includ-ing aerobic exercise, stress-management training, smokingcessation, group psychosocial support, and a vegetarian diet thatemphasizes whole foods and less than 10 percent fat content.6
TREATMENT
Many women are interested in preventing the comorbidities asso-ciated with obesity, but are often unaware of the specific amount
TABLE 1DIETARY RECOMMENDATIONS FROM CANADA’S FOOD GUIDE2
Food Groups Servings per day Comments
Fruits & vegetables 5-10 - Rich sources of antioxidants, vitamins, and fibre1 serving = - Choose dark green and orange fruits and vegetables when possible1 medium-sized fruit or vegetable;250 mL (1 cup) salad;125 mL (1/2 cup) juice
Grains & cereals 5-12 - High fibre diet reduces cardiovascular and cancer risk1 serving = - Choose whole grain and enriched products when possible1 slice bread; 1/2 pita or bun;30 g (1/4 cup) cold cereal;250 mL (1 cup) rice or pasta
Meat & Alternatives 2-3 - Choose lean meats, poultry and fish plus dried peas, beans, lentils 1 serving = and soy products when possible 50 to 100 g (2-3.5 oz.) beef, - Cold water fish are high in omega-3 fatty acidspoultry, fish;250 mL (1 cup) legumes;100 g (1/3 cup) tofu;30 mL (2 tbsp) peanut butter
Milk products 2-4 - High sources of calcium1 serving = - Milk is the only dairy product fortified with Vitamin D250 mL (8 oz) milk; - Choose lower fat dairy products175 g (3/4 cup) yogurt;50 g (2 oz) cheese
Other foods & beverages
Oils & fats Obtain ≤ 10 percent of total - Use olive or canola oilcalories from saturated fats - Avoid animal fats, hydrogenated oils and trans-fatty acids
Sugar - Minimize use of products that are mostly sugar (jams, syrup, honey,candies)
Alcohol 1 drink: - Limit intake to 1-2 drinks/day for cardioprotective effects150 ml (5 oz) wine - Breast cancer risk is increased with > 2 drinks/day350 ml (1 bottle) beer50 ml (1.5 oz) liquor or 11-15 g alcohol
Caffeine - 2-3 caffeinated beverages/day allowable in calcium-sufficient individuals
- Caffeine may contribute to bone resorption in calcium-deficientindividuals
www.hc-sc.gc.ca/hppb/nutrition/pube/foodguid/

JOGC OCTOBER 200220
of weight loss required to improve their health. They may also haveinadequate or inaccurate information about weight-loss programs.Health care professionals play an important role in assessing individual readiness for weight management measures, in educat-ing women about sensible approaches, and in providing long-termfollow-up and encouragement.
The initial goal is to reduce body weight by approximate-ly 10 percent from baseline over six to 12 months. The mostsuccessful treatment to date includes a controlled diet with adeficit of 500 to 1000 Kcal per day, reducing dietary fat intaketo less than 30 percent of total energy intake, regular physicalactivity, and behaviour modification.21
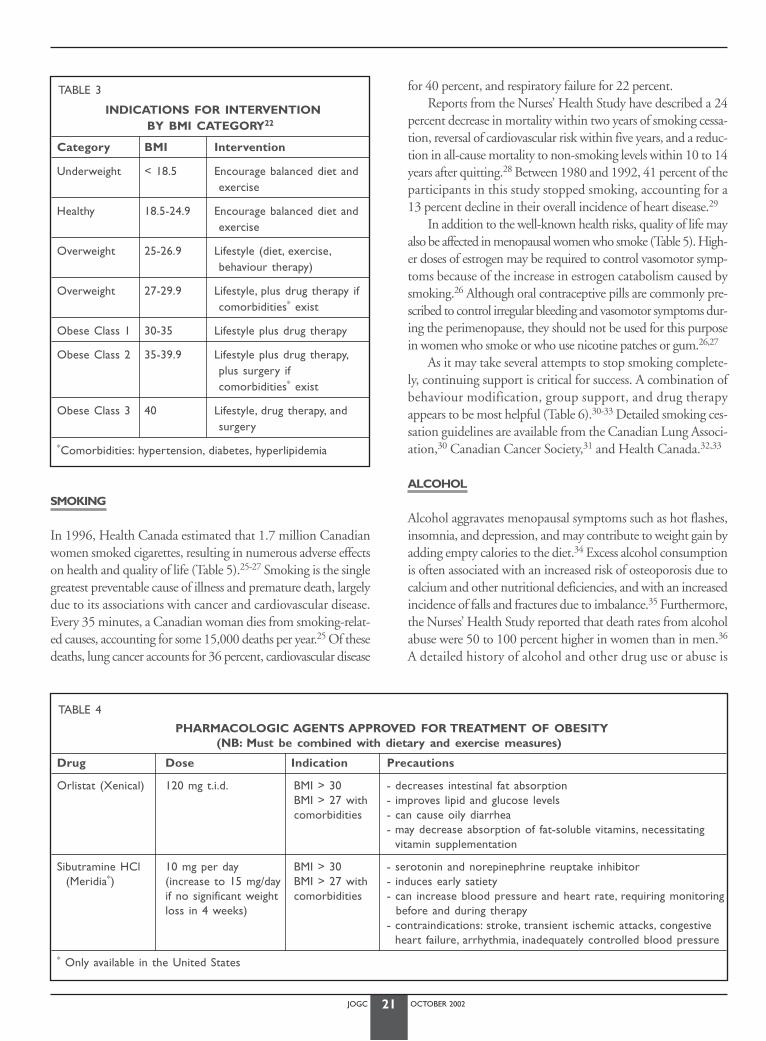
Individual and group support (Dietitians, Weight Watchers,Overeaters Anonymous, Take Off Pounds Sensibly [TOPS]),medication, and surgery all play a role in facilitating weight loss.The level of intervention required depends on the BMI catego-ry and the presence of comorbidities (Table 3).22 Drug therapy(orlistat or sibutramine) should only be used when diet and exer-cise have failed in individuals with a BMI greater than 30 or BMIgreater than 27 with comorbidities (Table 4).23
The National Institute of Health has a detailed website out-lining the Clinical Guidelines on the Identification, Evaluation andTreatment of Overweight and Obesity in Adults. It also contains BMItables and the evidence tables used to construct the guidelines.
STRESS
Women face many challenging stressors during midlife and themenopausal transition. Stress significantly affects quality of life,may result in a variety of somatic symptoms, and may aggravatevarious underlying medical conditions. Stress has been causallyrelated to cardiovascular disease, particularly in women. Notonly has stress been reported to trigger ischemia and acutemyocardial infarction (MI), but marital stress triples the risk ofsudden death after an MI in women.24 Stress reduction strate-gies that may benefit all individuals include regular exercise, yoga,tai chi, massage, meditation, paced respiration, biofeedback,relaxation techniques, and behaviour-modification techniques.Some of these techniques have also been helpful in relieving vaso-motor symptoms (Section K*).
TABLE 2
DIETARY REFERENCE INTAKES (DRI) OF SELECTED NUTRIENTS2
Vitamins and Minerals DRI Comments
Vitamin D Function: Required for optimal calcium absorption- premenopausal 200 IU Sources: Daily intake of 3-4 oz fish or one litre fortified milk, or exposure to 15-20 - age 50-65 400 IU minutes sunshine without suncreen- age 65+ 800 IU Caution: Deficiency common in northern climates (including all of Canada), elderly and
housebound. Supplements often required to achieve adequate intake in these circumstances.
Calcium (elemental) Function: Required to maintain calcium homeostasis, cellular function and bone premenopausal 1000 mg mineralizationpostmenopausal Food sources: Most plentiful in milk products- on antiresorptive therapy 1000 mg Comment: Prerequisite for effective anti-resorptive therapy- not on anti-resorptive 1500 mg
therapy
Iron Function: Required for red blood cell (RBC) formation- premenopausal 18 mg Food sources: Most plentiful in red meat. Also found in fruits, vegetables and grains.- postmenopausal 8 mg
Vitamin B6 (serotonin) 1.5 mg Function: Needed for production of RBCs and seritonin and for metabolism of proteinand fatFood sources: Whole grains, green vegetables, beans, nuts, meatsCaution: Doses > 100 mg may be neurotoxic
Vitamin B12 2.4 µg Function: Needed for RBC formation and neurological function(cyanocobalamin) Food sources: Milk products and protein-rich foods
Caution: Absorption decreases with age and gastric hypoacidity
Folate (Folic Acid) 400 µg Function: B vitamin that affects cell division and RBC formation and lowers homocysteine levelsFood sources: Fruits, vegetables, and grains
www.hc-sc.gc.ca/hppb/nutrition/pube/foodguid/
* Menopause: complementary approaches,J Obstet Gynaecol Can 2001;23(12).
JOGC OCTOBER 200221
SMOKING
In 1996, Health Canada estimated that 1.7 million Canadianwomen smoked cigarettes, resulting in numerous adverse effectson health and quality of life (Table 5).25-27 Smoking is the singlegreatest preventable cause of illness and premature death, largelydue to its associations with cancer and cardiovascular disease.Every 35 minutes, a Canadian woman dies from smoking-relat-ed causes, accounting for some 15,000 deaths per year.25 Of thesedeaths, lung cancer accounts for 36 percent, cardiovascular disease
for 40 percent, and respiratory failure for 22 percent.Reports from the Nurses’ Health Study have described a 24
percent decrease in mortality within two years of smoking cessa-tion, reversal of cardiovascular risk within five years, and a reduc-tion in all-cause mortality to non-smoking levels within 10 to 14years after quitting.28 Between 1980 and 1992, 41 percent of theparticipants in this study stopped smoking, accounting for a13 percent decline in their overall incidence of heart disease.29
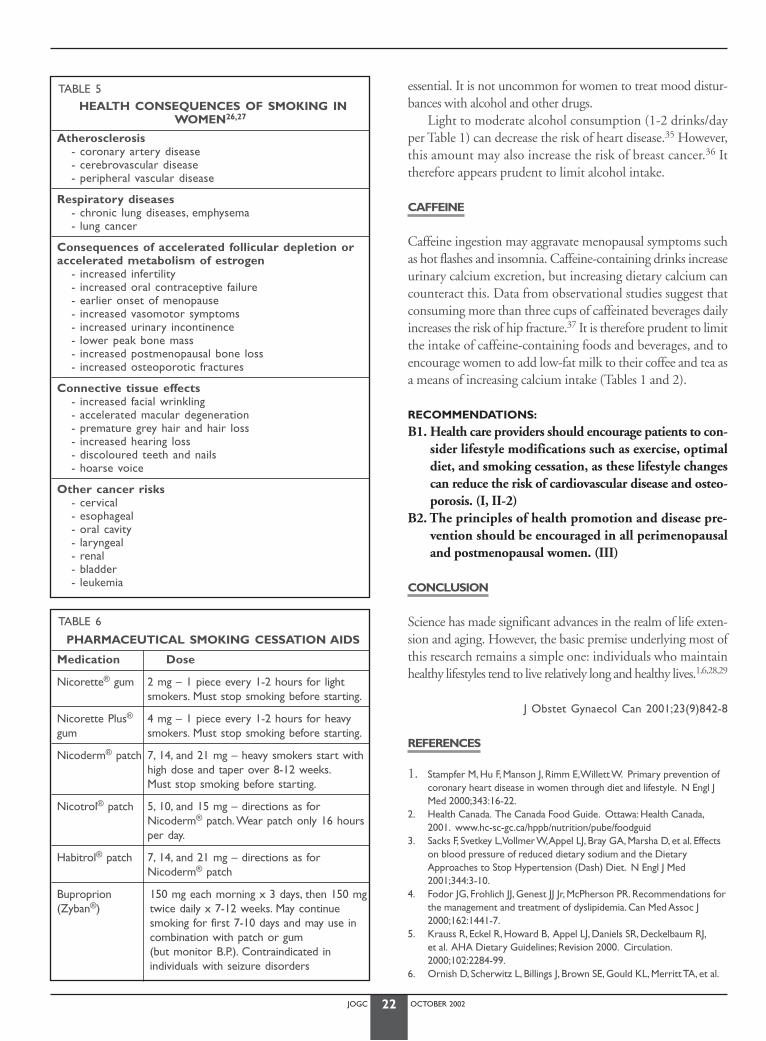
In addition to the well-known health risks, quality of life mayalso be affected in menopausal women who smoke (Table 5). High-er doses of estrogen may be required to control vasomotor symp-toms because of the increase in estrogen catabolism caused bysmoking.26 Although oral contraceptive pills are commonly pre-scribed to control irregular bleeding and vasomotor symptoms dur-ing the perimenopause, they should not be used for this purposein women who smoke or who use nicotine patches or gum.26,27
As it may take several attempts to stop smoking complete-ly, continuing support is critical for success. A combination ofbehaviour modification, group support, and drug therapyappears to be most helpful (Table 6).30-33 Detailed smoking ces-sation guidelines are available from the Canadian Lung Associ-ation,30 Canadian Cancer Society,31 and Health Canada.32,33
ALCOHOL
Alcohol aggravates menopausal symptoms such as hot flashes,insomnia, and depression, and may contribute to weight gain byadding empty calories to the diet.34 Excess alcohol consumptionis often associated with an increased risk of osteoporosis due tocalcium and other nutritional deficiencies, and with an increasedincidence of falls and fractures due to imbalance.35 Furthermore,the Nurses’ Health Study reported that death rates from alcoholabuse were 50 to 100 percent higher in women than in men.36
A detailed history of alcohol and other drug use or abuse is
TABLE 3
INDICATIONS FOR INTERVENTION BY BMI CATEGORY22
Category BMI Intervention
Underweight < 18.5 Encourage balanced diet andexercise
Healthy 18.5-24.9 Encourage balanced diet andexercise
Overweight 25-26.9 Lifestyle (diet, exercise,behaviour therapy)
Overweight 27-29.9 Lifestyle, plus drug therapy ifcomorbidities* exist
Obese Class 1 30-35 Lifestyle plus drug therapy
Obese Class 2 35-39.9 Lifestyle plus drug therapy,plus surgery if comorbidities* exist
Obese Class 3 40 Lifestyle, drug therapy, andsurgery
*Comorbidities: hypertension, diabetes, hyperlipidemia
TABLE 4
PHARMACOLOGIC AGENTS APPROVED FOR TREATMENT OF OBESITY(NB: Must be combined with dietary and exercise measures)
Drug Dose Indication Precautions
Orlistat (Xenical) 120 mg t.i.d. BMI > 30 - decreases intestinal fat absorption BMI > 27 with - improves lipid and glucose levelscomorbidities - can cause oily diarrhea
- may decrease absorption of fat-soluble vitamins, necessitating vitamin supplementation
Sibutramine HCl 10 mg per day BMI > 30 - serotonin and norepinephrine reuptake inhibitor(Meridia*) (increase to 15 mg/day BMI > 27 with - induces early satiety
if no significant weight comorbidities - can increase blood pressure and heart rate, requiring monitoring loss in 4 weeks) before and during therapy
- contraindications: stroke, transient ischemic attacks, congestiveheart failure, arrhythmia, inadequately controlled blood pressure
* Only available in the United States
JOGC OCTOBER 200222
essential. It is not uncommon for women to treat mood distur-bances with alcohol and other drugs.
Light to moderate alcohol consumption (1-2 drinks/dayper Table 1) can decrease the risk of heart disease.35 However,this amount may also increase the risk of breast cancer.36 Ittherefore appears prudent to limit alcohol intake.
CAFFEINE
Caffeine ingestion may aggravate menopausal symptoms suchas hot flashes and insomnia. Caffeine-containing drinks increaseurinary calcium excretion, but increasing dietary calcium cancounteract this. Data from observational studies suggest thatconsuming more than three cups of caffeinated beverages dailyincreases the risk of hip fracture.37 It is therefore prudent to limitthe intake of caffeine-containing foods and beverages, and toencourage women to add low-fat milk to their coffee and tea asa means of increasing calcium intake (Tables 1 and 2).
RECOMMENDATIONS:
B1. Health care providers should encourage patients to con-sider lifestyle modifications such as exercise, optimaldiet, and smoking cessation, as these lifestyle changescan reduce the risk of cardiovascular disease and osteo-porosis. (I, II-2)
B2. The principles of health promotion and disease pre-vention should be encouraged in all perimenopausaland postmenopausal women. (III)
CONCLUSION
Science has made significant advances in the realm of life exten-sion and aging. However, the basic premise underlying most ofthis research remains a simple one: individuals who maintainhealthy lifestyles tend to live relatively long and healthy lives.1,6,28,29
J Obstet Gynaecol Can 2001;23(9)842-8
REFERENCES
1. Stampfer M, Hu F, Manson J, Rimm E,Willett W. Primary prevention ofcoronary heart disease in women through diet and lifestyle. N Engl JMed 2000;343:16-22.
2. Health Canada. The Canada Food Guide. Ottawa: Health Canada,2001. www.hc-sc-gc.ca/hppb/nutrition/pube/foodguid
3. Sacks F, Svetkey L,Vollmer W,Appel LJ, Bray GA, Marsha D, et al. Effectson blood pressure of reduced dietary sodium and the DietaryApproaches to Stop Hypertension (Dash) Diet. N Engl J Med2001;344:3-10.
4. Fodor JG, Frohlich JJ, Genest JJ Jr, McPherson PR. Recommendations forthe management and treatment of dyslipidemia. Can Med Assoc J2000;162:1441-7.
5. Krauss R, Eckel R, Howard B, Appel LJ, Daniels SR, Deckelbaum RJ,et al. AHA Dietary Guidelines; Revision 2000. Circulation.2000;102:2284-99.
6. Ornish D, Scherwitz L, Billings J, Brown SE, Gould KL, Merritt TA, et al.
TABLE 5HEALTH CONSEQUENCES OF SMOKING IN
WOMEN26,27
Atherosclerosis- coronary artery disease- cerebrovascular disease- peripheral vascular disease
Respiratory diseases- chronic lung diseases, emphysema- lung cancer
Consequences of accelerated follicular depletion or accelerated metabolism of estrogen
- increased infertility- increased oral contraceptive failure- earlier onset of menopause- increased vasomotor symptoms- increased urinary incontinence- lower peak bone mass- increased postmenopausal bone loss- increased osteoporotic fractures
Connective tissue effects- increased facial wrinkling- accelerated macular degeneration- premature grey hair and hair loss- increased hearing loss- discoloured teeth and nails- hoarse voice
Other cancer risks- cervical- esophageal- oral cavity- laryngeal- renal- bladder- leukemia
TABLE 6
PHARMACEUTICAL SMOKING CESSATION AIDS
Medication Dose
Nicorette® gum 2 mg – 1 piece every 1-2 hours for lightsmokers. Must stop smoking before starting.
Nicorette Plus® 4 mg – 1 piece every 1-2 hours for heavygum smokers. Must stop smoking before starting.
Nicoderm® patch 7, 14, and 21 mg – heavy smokers start withhigh dose and taper over 8-12 weeks.Must stop smoking before starting.
Nicotrol® patch 5, 10, and 15 mg – directions as forNicoderm® patch.Wear patch only 16 hoursper day.
Habitrol® patch 7, 14, and 21 mg – directions as forNicoderm® patch
Buproprion 150 mg each morning x 3 days, then 150 mg(Zyban®) twice daily x 7-12 weeks. May continue
smoking for first 7-10 days and may use incombination with patch or gum (but monitor B.P.). Contraindicated in individuals with seizure disorders
JOGC OCTOBER 200223
Intensive lifestyle changes for reversal of coronary heart disease. J AmMed Assoc 1998;280:2001-7.
7. Lee I-M, Rexrode KM, Cook NR, Manson JE, Buring JE. Physical activityand coronary heart disease in women: is “no pain, no gain” passe? J AmMed Assoc 2001;285:1447-54.
8. Hammer M, Berg G, Lindgren R. Does physical exercise influence thefrequency of postmenopausal hot flushes? Acta Obstet Gynecol Scand1990;167:436-9.
9. Layne JE, Nelson ME. The effects of progressive resistance training onbone density: a review. Med Sci Sports Exerc 1999;31:25-30.
10. Province MA, Hadley EC, Hornbrook MC, Lipsitz LA, Miller JP, MulrowCD, et al. The effects of exercise on falls in elderly patients. J Am MedAssoc 1995;273:1341-7.
TABLE 7
SELECTED RESOURCES
Topic Organization Website
Breast Cancer Risk National Cancer Institute Breast Cancer Risk Assessment Tool http//brca.nci.nih.gov/brc/
Heart and Stroke Heart and Stroke Foundation of Canada (includes heart, stroke and dietary information plus individual risk www.hsf.ca (1-888-HSF-INFO)assessment and smoking cessation guidelines)
Menopause Society of Obstetricians and Gynecologists of Canada www.sogc.org(includes Consumer Education brochures, Clinical Practice Guidelines,and Consensus Conference Reports)
North American Menopause Society (includes Consensus Opinions,surveys, and Consumer Education materials) www.menopause.org
Nutrition Canada’s Food Guide www.hc-sc.gc.ca/hppb/nutrition/pube/foodguid/
www.hc-sc.gc.ca/hppb/la-nutrition/
Dietitians of Canada www.dieticians.ca/eatwell
Osteoporosis Osteoporosis Society of Canada (includes osteoporosis diagnosis, www.osteoporosis.caprevention & treatment plus Calcium Calculator)
National Osteoporosis Foundation (includes NOF guidelines plus www.nof.org/professional and patient information on osteoporosis)
Smoking Cessation Canadian Lung Association (includes Smoking Cessation Support Group www.sk.lung.ca/smoking/ oron the Web, information on provincial stop smoking programs) www.lung.ca
Canadian Cancer Society (includes smoking cessation support programs www.cancer.ca/tobacco& links to other smoking cessation web sites) (1-888-939-3333)
Health Canada (website includes smoking cessation programs and www.infotobacco.com/index2.htmlinformation about smoking in Canada)
Smoking Cessation Guidelines: from the University of Toronto www.hc-sc.gc.ca/hppb/cessation/Department of Family & Community Medicine Contact: Shirley Crum
1-905-812-4104
Weight Management National Institute of Health Clinical Guidelines on the Identification, www.nhlb.nih.gov/guidelines/Evaluation and Treatment of Overweight and Obesity in Adults obesity/ob_home.htm(includes BMI calculator, evidence tables, tip sheets)
Exercise Health Canada Physical Activity Guide www.hc-sc.gc.ca/hppb/paguide
JOGC OCTOBER 200224
11. Wolff I, van Croonenborg JJ, Kemper HCG, Kostense PJ,Twisk JWR.Theeffect of exercise training programs on bone mass: a meta-analysis ofpublished controlled trials in pre-and postmenopausal women. Osteo-porosis Int 1999;9:1-12.
12. Marcus R. Exercise: moving in the right direction. J Bone Min Res1998;13:1793-6.
13. Health Canada. The Health Canada Physical Activity Guide. Ottawa:Health Canada, 2001. www.hc-sc.gc.ca/hppb/paguide
14. Wing RR, Matthews KA, Kuller LH, Meilahn EN, Plantinga, PL. Weightgain at the time of menopause. Arch Int Med 1991;151: 97-102.
15. Norman RJ, Flight IH, Rees MC. Estrogen and progestin hormonereplacement therapy for peri-menopausal and post-menopausalwomen: weight and body fat distribution. Cochrane Database Syst Rev2000;(2):CD001018.
16. Kuller LH, Simkin-Silverman LR,Wing RR, Meilahn EN, Ives DG.Women’s Healthy Lifestyle Project: a randomized clinical trial: results at54 months. Circulation 2001;103:32-7.
17. National Population Health Survey, 1994-1995. Ottawa: Statistics Cana-da, 1995. Catalogue no. 82-F0001XCB.
18. Rexrode KM, Carey V, Hennekens CH,Walters EE, Colditz GA, StampfMJ, et al. Abdominal adiposity and coronary heart disease in women. JAm Med Assoc 1998;280:1843-8.
19. Wu AH, Pike MC, Stram DO. Meta-analysis: dietary fat intake, serumestrogen levels, and the risk of breast cancer. J Natl Cancer Inst1999;l91:529-34.
20. Birmingham CL, Muller JL, Palepu A, Spinelli J,Anis A. The cost of obesi-ty in Canada. Can Med Assoc J 1999;160:483-8.
21. Lau DC. Call for action: preventing and managing the expansive andexpensive obesity epidemic. Can Med Assoc J 1999;160:503-5.
22. Arnonne L. Weight gain during the perimenopause: the case for earlyintervention. Menopause Management 1999;8:6-11.
23. Davidson MH, Hauptman J, DiGirolamo M, Foreyt JP, Halsted CH,Heber D, et al. Weight control and risk factor reduction in obese sub-jects treated for 2 years with orlistat: a randomized controlled trial. JAm Med Assoc 1999;281:235-42.
24. Orth-Gomer K,Wamala S, Horsten M, Schenck-Gustafsson K, Schnei-derman N, Mittleman M. Marital stress worsens prognosis in womenwith coronary heart disease. J Am Med Assoc 2000;284:3008-14
25. Makomaski Illing E, Kaiserman M. Mortality attributable to tobacco usein Canada and its regions, 1994-1996. Health Canada 20(3);1999.
26. Nusbaum M, Gordon M, Nusbaum D, Mcarthy M,Vasilakis D. Smokealarm: a review of the clinical impact of smoking on women. Prim CareUpdate Ob Gyn 2000;7:207-14.
27. Tajada D, Liesa F,Arenas L, et al. The effect of tobacco consumption onacoustic voice analysis. Acta Otorinolaringol Esp 1999;50:448-52.
28. Kawachi I, Colditz GA, Stampfer MJ,Willet WC, Manson JE, Rosner B,et al. Smoking cessation and time course of decreased risks ofcoronary heart disease in middle-aged women. Arch Intern Med1994;154:169-75.
29. Hu FB, Stampfer MJ, Manson JE, Grodstein F, Colditz GA, Speizer, FE,et al. Trends in the incidence of coronary heart disease and changes in diet and lifestyle in women. N Engl J Med 2000;343:530-7.
30. Canadian Lung Association. Smoking Cessation Program on the WorldWide Web. 2001. www.sk.lung.ca/smoking
31. Canadian Cancer Society. Tobacco and cancer. 2001.www.cancer.ca/tobacco
32. Health Canada. Infotobacco. 2001. www.infotobacco.com/index2.html33. Health Canada. Smoking cessation: living smoke free. 2001. www.hc-
sc.gc.ca/hppb/cessation34. Spickard A.Advances in the epidemiology, diagnosis and intervention of
alcohol and drugs. Yearbook of Medicine. St. Louis: Mosby Yearbook,1991;p.391.
35. Fuchs CS, Stampfer MJ, Colditz GA, Giovannucci EL, Manson JE,Kawachi I, et al. Alcohol consumption and mortality among women.N Engl J Med 1995;332:1245-50.
36. Smith-Warner SA, Spiegelman D,Yaun S, von den Brandt PA, Folson AR,Goldbohn RA, et al. Alcohol and breast cancer in women: a pooledanalysis of cohort studies. J Am Med Assoc 1998;279:535-40.
37. Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM, Ensrud KE,et al. Risk factors for hip fracture in white women. Study ofOsteoporotic Fractures Research Group. N Engl J Med 1995;332:767-73.

T K
INTRODUCTION
Sexual concerns are often an issue for women in the peri-menopausal years and beyond. Health care providers have to beaware of these issues and provide a nonjudgemental approachto sexual health based on mutual trust and respect. It is impor-tant to remember that personal, relationship,1 and societal2 fac-tors play an important role in menopausal sexuality. The healthcare provider’s time limitations and experience and the natureof the problem may warrant referral for counselling.
EFFECTS ON SEXUALITY
HORMONAL CHANGES
Lack of estrogen leads to urogenital atrophy and resultant dys-pareunia, as well as to decreased blood flow and reduced sensa-tion.3 Estrogen replacement increases blood flow to the genitalarea and relieves vaginal dryness and dyspareunia.3 Through itspositive effects on mood and wellbeing, estrogen replacementmay also affect sexuality.4
Lack of progesterone has no adverse effect on sexual func-tion. Progestin replacement, whether cyclic or continuous, canhave a negative influence on mood and wellbeing as well as causea decrease in sexual activity when associated with frequent break-through bleeding. Lack of testosterone, particularly in womenwith surgical menopause, has been associated with decreasedlibido.5 Levels of testosterone were reduced by more than 40 per-cent in women undergoing bilateral oophorectomy.6
HYSTERECTOMY
The majority of women experience no adverse effects on sexualfunction from a hysterectomy. In the two year MarylandWomen’s Health Study, sexual function was not impaired andmost women reported that their sexual activity and overall libidoimproved after hysterectomy.7 In many cases, freedom fromheavy or irregular bleeding or from pelvic pain and dyspareunialeads to enjoyable sexual activity for the first time in many years.In a minority of women, hysterectomy can adversely affect coitalfunction, either because of shortened vaginal length or becauseof a painful vaginal vault scar.7 For most women, orgasm is unaf-fected; however, orgasmic function may be altered if loss of
uterine contractions leads to decreased pleasurable sensations orif loss of cervical tapping eliminates the woman’s particular trig-ger for orgasm.8 Possible changes in sexual function associatedwith gynaecological surgery should be discussed with patientsprior to the procedure.
OOPHORECTOMY
As with hysterectomy, many women experience no adverse effectson their sexual function after oophorectomy. However, bilateraloophorectomy is associated with a reduction in serum estrogenand testosterone levels that, in some women, may lead to decreasedlibido or a decreased sense of wellbeing.9 Physicians should askabout changes in sexual function in follow-up visits after surgery.9
HORMONAL TREATMENTS
Estrogen therapy increases mucosal thickness and vaginal ruga-tion,3 and restores vaginal fluid volume, moisture, and pH lev-els. It can be administered either systemically or locally inestrogen vaginal cream, a sustained-release vaginal ring or vagi-nal tablets (not yet available in Canada). Some women experi-ence troublesome atrophic urogenital symptoms despitestandard systemic estrogen therapy. These symptoms respondwell to the addition of vaginal estrogen therapy.3
TOPICAL ESTROGEN THERAPY
Vaginally administered estrogen can be absorbed systemically,but circulating levels are only 25 percent of those seen withequivalent doses orally ingested. Daily doses of 0.3 mg conju-gated estrogens or less do not produce changes in serum estro-gen levels (equivalent to 0.5 g or 1/8 applicator of Premarin®
cream).11 This dose-related absorption has not been consistent-ly proven to provide relief of vasomotor symptoms bone pro-tection, but may be sufficient to cause endometrial hyperplasia.11
The vaginal ring incurs lower serum estrogen levels than vaginalestrogen cream, but the therapeutic efficacy for urogenital atro-phy is equivalent.12 Although no data have yet been published,the fact that serum estradiol levels are undetectable 48 hours afterinsertion of the vaginal ring suggests its possible use in womenfor whom systemic estrogen therapy is contraindicated.
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
Gillian Graves, MD, FRCSC,1 Robert Lea, MD, FRCSC,2 Gisele Bourgeois-Law, MD, FRCSC3
MENOPAUSE AND SEXUAL FUNCTION
JOGC OCTOBER 200225
1 Halifax NS2 Halifax NS3 Winnipeg MB

ANDROGEN THERAPY
A trial of androgen therapy should be considered in women withdecreased libido following bilateral oophorectomy if adequateestrogen therapy has been given and the problem persists.13-15 Atrial of androgen therapy may also be appropriate following nat-ural cessation of ovarian function for women on hormone replace-ment therapy (HRT) with no other explanation for their loss oflibido or for women with other symptoms of androgen deficien-cy (Table 1).16 Clinical factors rather than serum hormone levelsinfluence the discussion of androgen supplementation. There isno role for testosterone therapy in premenopausal women.
SIDE-EFFECTS OF ANDROGEN THERAPY IN WOMEN
Symptoms of androgen excess such as hirsutism, voice changes,and clitoromegaly can occur in women treated with testosterone,and these symptoms may be irreversible. The incidence is less thanfive percent in women on low-dose therapy. Since androgens mayhave adverse effects on blood lipid levels, androgen therapy shouldnot be given without concomitant estrogen therapy. Testosteroneis partly metabolized to estrogen, and it is therefore prudent to usea progestin to protect the endometrium from hyperplasia.18
Hepatotoxicity is a theoretical concern with oral adminis-tration of methyltestosterone, but it has not been observed withthe replacement doses of testosterone used in women. A recentreview of the side-effects of testosterone therapy concluded thatthe adverse effects associated with the supraphysiologic dosesused in men did not occur with the much lower doses used incombination with estrogen for HRT in women.18
ANDROGEN PREPARATIONS
There are no data on the optimal preparation, dosage, length oftreatment or long-term safety of testosterone replacement. Cur-rently used preparations and suggested dosages are listed in Table 2.
Preliminary results from the use of testosterone unde-canoate (Andriol®) in women have been reported.19 To date,no hepatotoxicity has been reported with use of low-dosetestosterone undecanoate. Supraphysiologic testosterone con-centrations following testosterone undecanoate administrationwith 40 mg on alternate days have been reported, but indi-vidual variations are considerable.19 Expanded pharmacoki-netic and clinical studies are required.
To reduce the risk of virilizing side-effects, clinicians mayadminister reduced dosages of intramuscular testosterone enan-thate (Climacteron® or Delatestryl®). Use of the 1.0 ml doserecommended in the past should be discouraged, since it is asso-ciated with hirsutism and virilization.20 In order to ensure ade-quate estrogen for symptom relief, these testosterone enanthatepreparations can be administered in combination with 0.5 mlof estradiol valerate (Delestrogen®) in the same syringe. Anec-dotal reports have suggested that patients may be reluctant todiscontinue androgen therapy due to its positive effect on ener-gy and well-being.
Tibolone (Livial®) is a synthetic steroid with estrogenic,progestogenic, and androgenic properties.21 It is not current-ly available in Canada. Tibolone was found to have a greaterpositive effect on libido than an estrogen-norethisterone com-bination after one year of treatment.21 A comparison oftibolone and conjugated estrogen therapy over six monthsshowed no difference between the treatments in recovery oflibido.21 There was no evidence of virilizing side-effects.21
In oophorectomized women with low libido, transdermaltestosterone (300 µg daily) added to estrogen replacement ther-apy (ERT) led to increased desire, increased frequency of sex-ual activity, and increased orgasmic functioning.22 Transdermaladministration of testosterone appears to result in more sta-ble serum levels than oral testosterone undecanoate23 or sub-cutaneous implants of testosterone.23
Further studies are necessary to determine the optimaldose, formulation, and duration of all androgen-containingtreatment plans.
JOGC OCTOBER 200226
TABLE 1
SYMPTOMS OF ANDROGEN DEFICIENCY SYNDROME (ADS)17
• loss of sexual desire• loss of sensation in clitoris and nipples• difficulty reaching orgasm• thinning and loss of pubic hair• loss of vitality• diminished sense of well-being• reduction in muscle tone
TABLE 2
ANDROGEN PREPARATIONS AVAILABLE IN CANADA*
Preparation Dose
Oral
Methyl testosterone 1/4 or 1/8 of a 10 mg tablet (Metandren®)
Testosterone undecanoate 40 mg daily or on alternate (Andriol®) days
Intramuscular
Testosterone enanthate 0.5 ml intramuscularly(in combination with estrogen every 4-6 weeksas Climacteron® injection, or without as Delatestryl®)
* Pharmacotherapy, J Obstet Gynaecol Can 2001;23(12)

JOGC OCTOBER 200227
MONITORING WOMEN
RECEIVING ANDROGEN THERAPY
Symptoms should be re-evaluated after an initial two to threemonth trial of therapy. If the degree of symptom relief warrantscontinued androgen therapy, it is prudent to re-evaluate thelipid profile after three to six months of therapy. If the lipid pro-file is normal, then the guidelines from the Canadian Consen-sus on Cholesterol* should be followed. If the lipid profile isabnormal, then androgen therapy should be discontinued andadditional investigation and possible treatment of the lipidabnormality is warranted. The results of liver function testsshould remain normal.
SILDENAFIL CITRATE (VIAGRA™)
There was no increase in sexual response in a large randomizedcontrolled trial of sildenafil citrate in estrogenized women withsexual dysfunction that included female sexual arousal disor-der.24 However, sildenafil citrate therapy may benefit a subsetof women experiencing delayed orgasm during therapy withselective serotonin re-uptake inhibitors (SSRIs).25
NON-HORMONAL TREATMENTS
Regular sexual activity maintains genital blood flow and helps toprevent vaginal dryness and atrophy. A lubricant can be used dur-ing sexual activity to decrease dyspareunia. A polycarbophil-basedvaginal moisturizer has been shown to provide beneficial effectssimilar to those of vaginal estrogen cream on vaginal moisture,fluid volume, elasticity, and pH after 12 weeks of treatment.10
NON-HORMONAL SEXUAL ISSUES IN THE PERI- AND POSTMENOPAUSAL PERIOD
Numerous lifestyle and non-hormonal issues can influence sex-ual health. Contraception should be assumed necessary to pre-vent pregnancy until the diagnosis of menopause has beenestablished. It should be remembered that women with pre-mature menopause can occasionally retain ovarian function andspontaneous ovulation. A woman with a new sexual partnershould be counselled about safe sex practices. Coital inconti-nence may be helped by emptying the bladder just prior tointercourse, or by using an antimuscarinic (such as oxybutynin4 mg) one hour prior to intercourse.26
Depression may be associated with a loss of sexual interest.While antidepressants may improve libido as a function of improv-ing the depression, many antidepressants have sexual side-effects.These include loss of libido and, in the case of selective serotoninreuptake inhibitors (SSRIs), orgasmic dysfunction. Sexual side-effects are less prevalent with certain antidepressants (nefazodone,moclobemide), but other factors may be more important in deter-
mining the appropriate choice of antidepressant. The orgasmicdysfunction but not the decreased libido induced by SSRIs can beameliorated by using cyproheptadine two to four mg prior to sex-ual activity.27 Physicians should be aware of the sexual side-effectsof prescribed and over-the-counter medications.28
The lack of a sexually functioning partner is the most com-mon sexual problem in older women. Some couples areunaware of the normal changes in sexual function associatedwith aging, including the need in older men for direct penilestimulation to achieve an erection. As in any couple’s life as wellas during menopause, relationship difficulties can also havenegative effects on a woman’s sexual wellbeing.
ASSESSMENT OF SEXUAL
CONCERNS IN MENOPAUSAL WOMEN
The depth of inquiry into factors listed in Table 3 should reflectthe woman’s level of concern. For example, if anorgasmia is nota problem for a particular woman, nothing needs to be doneapart from ensuring that it is not a symptom of an underlyingmedical condition. Conversely, every woman, regardless of ageor health, deserves the opportunity to have her sexual concernsappropriately evaluated and treated.
REFERRAL TO A SEX THERAPIST
In most cases, a patient’s sexual concerns can be discussed bya concerned and informed family physician or gynaecologist,1
especially if a long-standing relationship exists. A referral to aspecialist in sex therapy is appropriate if there continues to beno improvement in sexual issues despite adequate hormonereplacement, if there are difficult relationship issues, or if thereare chronic issues such as unresolved sexual abuse or sexualproblems spanning most of the woman’s life or relationship.
If possible, both partners should be referred. Sexual diffi-culties, by their very nature, involve more than one person,
TABLE 3
COMPONENTS OF THE SEXUAL ASSESSMENT IN PERI- AND POSTMENOPAUSAL WOMEN
• Libido (desire) • Depression• Arousal (lubrication) • Medical conditions and • Orgasm medications• Hormonal status • Body image• Lifestyle weight gain
fatigue agingdistractions (work, • Partner’s sexual functionchildren, caring for • Motivation – does she wantelderly parents) to be sexual:
• Relationship issues why or why not? including abuse • Fear of pregnancy
* Hormone replacement therapy and cardiovascular disease,J Obstet Gynaecol Can 2001;23(10).

regardless of with whom the problem originated. Referral as acouple also avoids the perception by the woman or her part-ner that there is something “wrong” with her and that sheneeds to be “fixed.”
RECOMMENDATIONS:
C1. All health care providers dealing with menopausalwomen should be versed in the appropriate counsellingand management of menopause and related sexualhealth issues. (III)
C2. In women with vaginal atrophy, health care providersmay consider the use of local estrogen therapy as aneffective mode of treatment or consider vaginal mois-turizers as effective alternatives. (I, II-1)
C3. In women with decreased libido who have undergonebilateral oophorectomy, adding androgen to estrogentherapy has been shown to be effective in increasinglibido (I). Androgen therapy may be administered toestrogen-treated postmenopausal women who havedecreased libido not explained by any other factors. Arisk-benefit profile has not been determined from stud-ies with sufficiently large patient numbers. (III)
C4. Routine evaluation of hormone levels (specifically mea-suring serum androgen levels) in postmenopausalwomen with psychosexual problems is not recom-mended. (III)
C5. Sildenafil citrate does not appear to improve sexualresponse in estrogenized women (III). However, it maydo so in women with decreased libido associated withuse of selective serotonin re-uptake inhibitors (SSRIs)(III).
J Obstet Gynaecol Can 2001;23(9)849-52
REFERENCES
1. Basson R. Perimenopausal sexuality. J Soc Obstet Gynaecol Can1997;19(4)(suppl);1-7.
2. Winn R, Newton N. Sexuality in aging: a study of 106 cultures.Arch SexBehav 1982;11:283-98.
3. Notelovitz M. Estrogen therapy in the management of problems associ-ated with urogenital aging: a simple diagnostic test and the effect of theroute of hormone administration. Maturitas 1995;22 (suppl):31-3.
4. Zweifel JE, O’Brien WH. A meta-analysis of the effect of hormonereplacement therapy on depressed mood. Psychoneuroendocrinology1997;22:189-212.
5. Cawood EHH, Bancroft J. Steroid hormones, the menopause, sexualityand well being of women. Psychol Med 1996;26:925-36.
6. Laughlin GA, Barrett-Connor E, Kritz-Silverstein D, von Muhlen D.Hysterectomy, oophorectomy, and endogenous sex hormone levels in older women: the Rancho Bernardo study. J Clin Endocrinol Metab2000;85:645-51.
7. Rhodes JC, Kjerulff KH, Langenberg PW, Guzinski GM. Hysterectomyand sexual functioning. J Am Med Assoc 1999; 282:1934-41.
8. Lamont JA. Hysterectomy: the removal of a sex organ? ContemporaryOb/Gyn 1997;1:8-9.
9. Avis N, Stellato R, Crawford S, Johannes C, Longcope C. Is there anassociation between menopause status and sexual functioning?Menopause 2000;7(5):297-309.
10. Nachtigall LE. Comparative study: Replens 7 versus local estrogen inmenopausal women. Fertil Steril 1994;61(1):178-80.
11. Mandel FP, Geola FL, Meldrum DR, et al. Biological effects of variousdoses of vaginally administered conjugated equine estrogen inpostmenopausal women. J Clin Endocrinol Metab 1983;57:133-8.
12. Nachtigall LE. Clinical trial of the estradiol vaginal ring in the US. Matu-ritas 1995;22(suppl):43-7.
13. Sherwin BB, Gelfand MM, Bender W.Androgen enhances sexual motiva-tion in females: a prospective, cross-over study of sex steroid adminis-tration on surgical menopause. Psychosom Med 1985;47:339-51.
14. Casson PR, Carson SA.Androgen replacement therapy in women:myths and realities. Int J Fertil 1996;41:412-22.
15. Myers LS. Methodological review and meta-analysis of sexuality andmenopause research. Neurosci Biobehavioral Rev 1995;19:331-41.
16. Sarrel PM, Dobay B,Witta B. Estrogen and estrogen-androgen replace-ment in post-menopausal women dissatisfied with estrogen only. JReprod Med 1998;43:847-56.
17. Rako S.The Hormone of Desire:The Truth About Sexuality, Menopauseand Testosterone. New York: Harmony, 1996.
18. Gelfand MM,Wiita B.Androgen and estrogen-androgen hormonereplacement therapy: a review of the safety literature 1941-1996.Clin Ther 1997;19:383-404.
19. Floter A, Caristrom K, von Schoultz B, Nathorst-Boos J.Administrationof testosterone undecanoate in postmenopausal women: effects onandrogens, estradiol and gonadotrophins. Menopause 2000;7:251-6.
20. Urman B, Pride SM,Yuen BH. Elevated serum testosterone, hirsutismand virilism associated with combined androgen-estrogen hormonereplacement therapy. Obstet Gynecol 1991;77:595-8.
21. Moore RA. Livial:A review of clinical studies Br J Obs Gyn1999;106(S19):1-21.
22. Shifren JL, Braunstein GD, Simon JA, et al.Transdermal testosteronetreatment in women with impaired sexual function after oophorecto-my. N Engl J Med 2000;343:682-8.
23. Buckler HM, Robertson WR,Wu FC.Which androgen replacementtherapy for women? J Clin Endocrinol Metab 1998;83(11):3920-4.
24. Basson R, McInnes R, Smith MD, Hodgson G, Spain T, Koppiker N.Efficacy and safety of sildenafil in estrogenized women with sexual dysfunction associated with female sexual arousal disorder. ObstetGynecol 2000 April; 95 Suppl (4):S54.
25. Shen WW, Urosevich Z, Clayton DO. Br Med J Reprod Med 1999;44:535-42.
26. Cardozo L. Sex and the bladder. Br Med J 1988;296:587-8.27. Maxmen JS,Ward N. Psychotropic Drugs: Fast Facts. 2nd edition.
New York:WW Norton, 1995:p.118.28. Crenshaw T, Goldberg J. Sexual Pharmacology. NewYork:WW Norton,
1996:587-8.
JOGC OCTOBER 200228
INTRODUCTION
Cardiovascular disease (CVD) is a leading cause of morbidity andmortality in postmenopausal women (Figure 1). Half of all post-menopausal women will develop coronary artery disease (CAD)and one-third will die from this disease. A majority of womenhave at least one risk factor for CAD.1 The risk for CVD riseswith age and increases significantly after menopause. Prematuremenopause provides additional risk. These observations haveprompted suggestions that estrogen-progestin treatment (EPT)might reduce CVD risk in postmenopausal women. Evidencefrom two randomized controlled trials (RCTs) indicates, how-ever, that EPT is not effective for either primary or secondaryprevention of CAD events in women with few or nomenopausal symptoms.2,3
Estrogen has both rapid and longer-term actions on thecardiovascular system.4 These rapid actions are non-genomicand cause vasodilatation. The longer-term actions are genom-ic, mediated by estrogen receptors, and affect vascular injuryresponses and atherosclerosis. Some estrogen effects may bebeneficial (effects on lipoproteins, fibrinolysis, antioxidant,endothelial function) whereas some are considered to be detri-mental (pro-inflammatory, prothrombotic).
This document reviews clinical and biological evidenceabout the known or potential balance of the cardiovascularbenefits and risks, including the case when estrogen is takenwith or without progestin shortly after the menopause for thetreatment of menopausal symptoms. This type of use was notthe target of either the HERS or the WHI study.2,3
EFFECTS OF ESTROGEN AND PROGESTINS
LIPOPROTEIN METABOLISM
Elevated total serum cholesterol and low-density lipoprotein cho-lesterol (LDL) levels are important coronary risk factors inwomen. Low levels of high-density lipoprotein cholesterol (HDL)are a strong independent risk factor.5 The effect of high serumtriglycerides is not as clear, since this is also associated with otherrisk factors such as diabetes and obesity.6 Alterations in other lipidfractions, such as an increase in levels of lipoprotein(a) [Lp(a)],are also associated with the risk of CAD in women. Levels of
Lp(a) are lowered with estrogen, regardless of the route of admin-istration. In part, the beneficial effects of HRT on CVD risk canbe attributed to effects of these plasma lipoproteins (Table 1).
The specific lipid effect depends on the type of hormonesadministered and the route of administration. For example, theaddition of medroxyprogesterone acetate (MPA) attenuates thebeneficial effects of estrogen on HDL, whereas the addition ofmicronized progesterone does not.7 Oral estrogen therapy hasa greater beneficial effect upon HDL and LDL than does trans-dermal therapy, whereas transdermal estrogen has a morefavourable effect on serum triglyceride levels (Table 1 ).8-10
These effects may not be clinically relevant, except in thosewomen with hypertriglyceridemia or low HDL levels.8
ENDOTHELIAL EFFECTS OF ESTROGEN
Endothelial function is impaired in postmenopausal women.11
Estrogen administration results in up-regulation of estrogenreceptors on the vessel wall.4 Short-term estrogen administra-tion enhances endothelial-dependent flow-mediated vasodi-latation in healthy women, mediated mostly by nitric oxide(NO).12 The exposure of arterial endothelium to estrogensappears to induce an estrogen receptor-mediated antioxidanteffect, which enhances the biological activity of NO. The effectof the addition of a progestin to estrogen replacement therapy(ERT) on vascular reactivity is uncertain. In addition, few stud-ies have examined the effects of long-term estrogen in womenwith established atherosclerosis using standard tests of vasodi-latation.4
ANTITHROMBOTIC AND
PRO-INFLAMMATORY EFFECTS
C-reactive protein (CRP), an acute phase reactant protein anda marker of inflammation, is associated with future coronaryevents in postmenopausal women.13 HRT increases circulatinglevels of CRP.14 Markers of thrombosis are also adversely affect-ed by currently used regimens of HRT (Table 2). However,serum homocysteine levels (a marker for cardiovascular risk) arelower in users of HRT.15 The effects of lower doses of oral estro-gen and transdermal estrogen on inflammatory and pro-coagulant markers are currently being investigated.
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
Michele A.Turek, MD, FRCPC,1 Christine Derzko, MD, FRCSC2
1 Ottawa, ON2 Toronto, ON
HORMONE REPLACEMENT THERAPY
AND CARDIOVASCULAR DISEASE
JOGC OCTOBER 200229
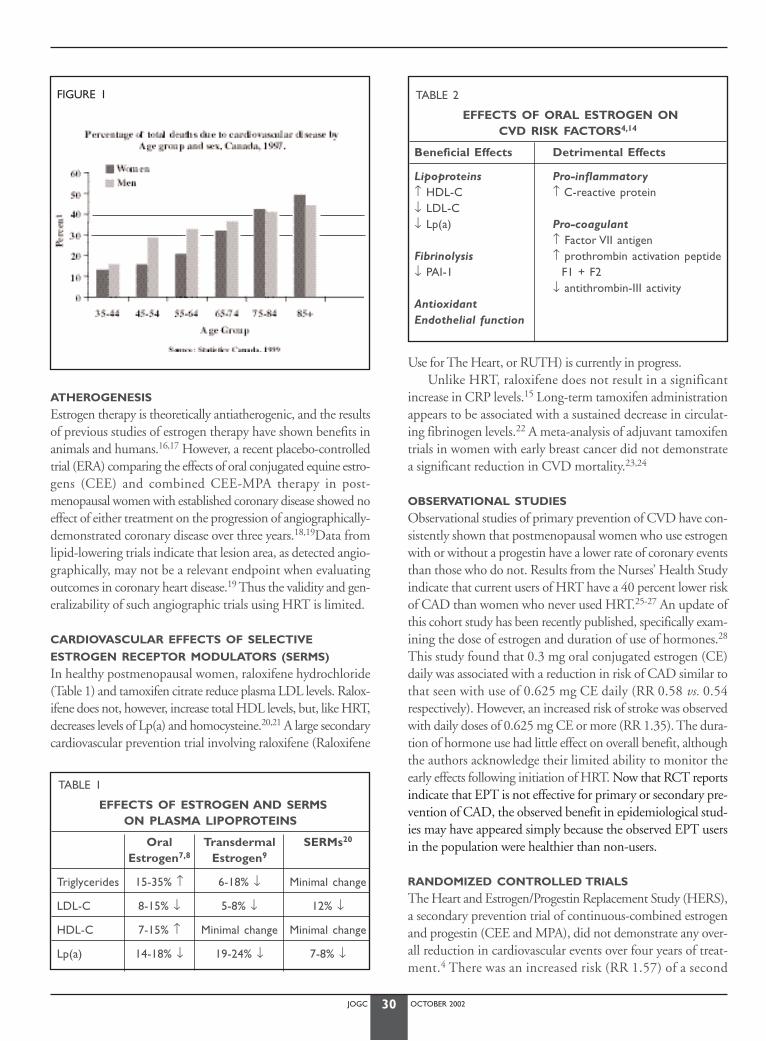
JOGC OCTOBER 200230
ATHEROGENESIS
Estrogen therapy is theoretically antiatherogenic, and the resultsof previous studies of estrogen therapy have shown benefits inanimals and humans.16,17 However, a recent placebo-controlledtrial (ERA) comparing the effects of oral conjugated equine estro-gens (CEE) and combined CEE-MPA therapy in post-menopausal women with established coronary disease showed noeffect of either treatment on the progression of angiographically-demonstrated coronary disease over three years.18,19Data fromlipid-lowering trials indicate that lesion area, as detected angio-graphically, may not be a relevant endpoint when evaluatingoutcomes in coronary heart disease.19 Thus the validity and gen-eralizability of such angiographic trials using HRT is limited.
CARDIOVASCULAR EFFECTS OF SELECTIVE
ESTROGEN RECEPTOR MODULATORS (SERMS)
In healthy postmenopausal women, raloxifene hydrochloride(Table 1) and tamoxifen citrate reduce plasma LDL levels. Ralox-ifene does not, however, increase total HDL levels, but, like HRT,decreases levels of Lp(a) and homocysteine.20,21 A large secondarycardiovascular prevention trial involving raloxifene (Raloxifene
Use for The Heart, or RUTH) is currently in progress.Unlike HRT, raloxifene does not result in a significant
increase in CRP levels.15 Long-term tamoxifen administrationappears to be associated with a sustained decrease in circulat-ing fibrinogen levels.22 A meta-analysis of adjuvant tamoxifentrials in women with early breast cancer did not demonstratea significant reduction in CVD mortality.23,24
OBSERVATIONAL STUDIES
Observational studies of primary prevention of CVD have con-sistently shown that postmenopausal women who use estrogenwith or without a progestin have a lower rate of coronary eventsthan those who do not. Results from the Nurses’ Health Studyindicate that current users of HRT have a 40 percent lower riskof CAD than women who never used HRT.25-27 An update ofthis cohort study has been recently published, specifically exam-ining the dose of estrogen and duration of use of hormones.28
This study found that 0.3 mg oral conjugated estrogen (CE)daily was associated with a reduction in risk of CAD similar tothat seen with use of 0.625 mg CE daily (RR 0.58 vs. 0.54respectively). However, an increased risk of stroke was observedwith daily doses of 0.625 mg CE or more (RR 1.35). The dura-tion of hormone use had little effect on overall benefit, althoughthe authors acknowledge their limited ability to monitor theearly effects following initiation of HRT. Now that RCT reportsindicate that EPT is not effective for primary or secondary pre-vention of CAD, the observed benefit in epidemiological stud-ies may have appeared simply because the observed EPT usersin the population were healthier than non-users.
RANDOMIZED CONTROLLED TRIALS
The Heart and Estrogen/Progestin Replacement Study (HERS),a secondary prevention trial of continuous-combined estrogenand progestin (CEE and MPA), did not demonstrate any over-all reduction in cardiovascular events over four years of treat-ment.4 There was an increased risk (RR 1.57) of a second
TABLE 1
EFFECTS OF ESTROGEN AND SERMS ON PLASMA LIPOPROTEINS
Oral Transdermal SERMs20
Estrogen7,8 Estrogen9
Triglycerides 15-35% ↑ 6-18% ↓ Minimal change
LDL-C 8-15% ↓ 5-8% ↓ 12% ↓
HDL-C 7-15% ↑ Minimal change Minimal change
Lp(a) 14-18% ↓ 19-24% ↓ 7-8% ↓
TABLE 2
EFFECTS OF ORAL ESTROGEN ON CVD RISK FACTORS4,14
Beneficial Effects Detrimental Effects
Lipoproteins Pro-inflammatory↑ HDL-C ↑ C-reactive protein↓ LDL-C↓ Lp(a) Pro-coagulant
↑ Factor VII antigenFibrinolysis ↑ prothrombin activation peptide↓ PAI-1 F1 + F2
↓ antithrombin-III activityAntioxidantEndothelial function
FIGURE 1

JOGC OCTOBER 200231
cardiovascular event in the first year of treatment, followed by anon-significant reduction in risk in the last two years (RR 0.67).The downward trend in risk was statistically significant (p < 0.009). The increased risk in the first year encompassed car-diac death, nonfatal myocardial infarction, and a three timesgreater risk of venous thromboembolism. In a subgroup analy-sis, the highest risk of cardiac events occurred in those womenwith low Lp(a) levels, and the greatest benefit was seen in thosewith the highest Lp(a) levels.29 Recently, although not a ran-domized trial, the Nurses’ Health Study has provided prospec-tive cohort data regarding secondary prevention that is consistentwith HERS.30 In a subject of women with previous coronary dis-ease, there was an increase in cardiovascular events (RR 1.25 [CI,0.78-2.00]) among short-term hormone users (defined as cur-rent use less than one year). However, there was a significantdecrease in risk (RR 0.38 [CI, 0.22-0.66]) with longer-term use(defined as current hormone use more than 2 years).
Because estrogen has demonstrated beneficial effects onmany cardiovascular risk factors, and because observationalstudies show an association between estrogen therapy and car-dioprotection, the reasons for an apparent lack of benefit inrandomized trials of HRT are unknown. Proposed theoriesinclude a reduced expression of estrogen receptors in athero-sclerotic arteries, or the development of a milieu that enhancesestrogen’s pro-inflammatory and pro-coagulant effects.Additionally, the secondary prevention trials enrolled elderlywomen who were postmenopausal for many years beforebeginning HRT. It is possible that the duration of HERS maynot have been long enough to demonstrate the cardioprotec-tion that has been shown with long-term HRT in observationalcohort studies. Extended follow-up of HERS participants hasshown no evidence of cardiovascular benefit associated withEPT treatment during 6.8 years of observations.31,32
The Women’s Health Initiative (WHI)33is a nine-year pri-mary prevention study, with approximately 27,000 post-menopausal women randomized to treatment with placebo,CEE alone (for those without a uterus), or CEE and MPA (inthose with an intact uterus). This randomized, double-blind-ed, controlled trial recruited predominantly healthy post-menopausal women aged 50 to 79 years. There was a 1.29-foldincrease in CAD events (95% CI 1.02, 1.63), with 37 eventsin the EPT group and 30 in the placebo group per 10,000women per annum.34 The small number of excess eventsoccurred despite a significant 13% reduction in low-densitylipoprotein cholesterol and 7% increase in high-density lipopro-tein cholesterol with EPT compared to placebo. Thus, EPT isnot indicated for the primary prevention of coronary heart dis-ease. The WHI estrogen only study continues because the ben-efits and risks have not yet been established.2
Another primary prevention trial, the WISDOM study(Women’s International Study of Long Duration of Estrogenafter Menopause) is also in progress.
CLINICAL INDICATIONS AND CONTRAINDICATIONSFOR HORMONE REPLACEMENT THERAPY
PRIMARY PREVENTION OF ISCHEMIC
(CORONARY) HEART DISEASE
Primary prevention strategies are designed to prevent coronarydisease, including myocardial infarction, angina, or angiographicevidence of coronary disease, in those healthy women who havenot yet manifested the disease. The WHI study results indicatethat EPT is not effective for the primary prevention of coronaryartery disease (CAD). Further large long-term trials are neededto evaluate whether EPT taken soon after the menopause forsymptom relief has any effect on CAD. The first line of thera-py should include lifestyle modifications, the use of acetycsali-cylic acid (ASA) in high-risk women, and antihypertensive andlipid-lowering agents,35 all of which have been shown in RCTsto decrease cardiovascular risk and improve outcome.
SECONDARY PREVENTION OF ISCHEMIC
(CORONARY) HEART DISEASE
Secondary prevention strategies are designed to lower the riskof subsequent events in those women who already have mani-fest coronary artery disease (a history of myocardial infarction,angina with documented disease, or having undergone coro-nary artery bypass surgery or percutaneous coronary angio-plasty). As data from the available randomized trials fail toprovide evidence that starting HRT provides effective secondaryprevention of CVD, it should not be initiated as a means ofdecreasing the risk of further cardiovascular events.
At present, proven therapies such as ASA, β-adrenergicblockers, ACE inhibitors, and lipid-lowering agents are rec-ommended.36
HISTORY OF DEEP VEIN THROMBOSIS
Postmenopausal women with a history of deep vein thrombo-sis (DVT) should be cautioned about the risk of venous throm-boembolic events (VTEs), including pulmonary embolism,associated with use of HRT.37-39 In addition to a personal his-tory of DVT or pulmonary embolism, other risk factors shouldbe considered prior to initiation of HRT (Table 3). Suggestedinvestigations for a patient with a history of idiopathic VTE arelisted in Table 4.
In the WHI study, venous thromboembolism risk in thefirst year of use was 3.6-fold higher for EPT users comparedwith placebo users.2 Although the relative hazard declined withtime, the overall risk during more than 5 years of use remainedsignificantly elevated (RH 2.11, 95% CI 1.26, 3.55).
The HERS results indicated that, in postmenopausalwomen with known CAD, use of HRT is associated with athree times greater risk for venous thrombosis (four events per1000 women-years).40 In HERS, most of these events occurredin women at risk for VTE because of cancer, lower extremity
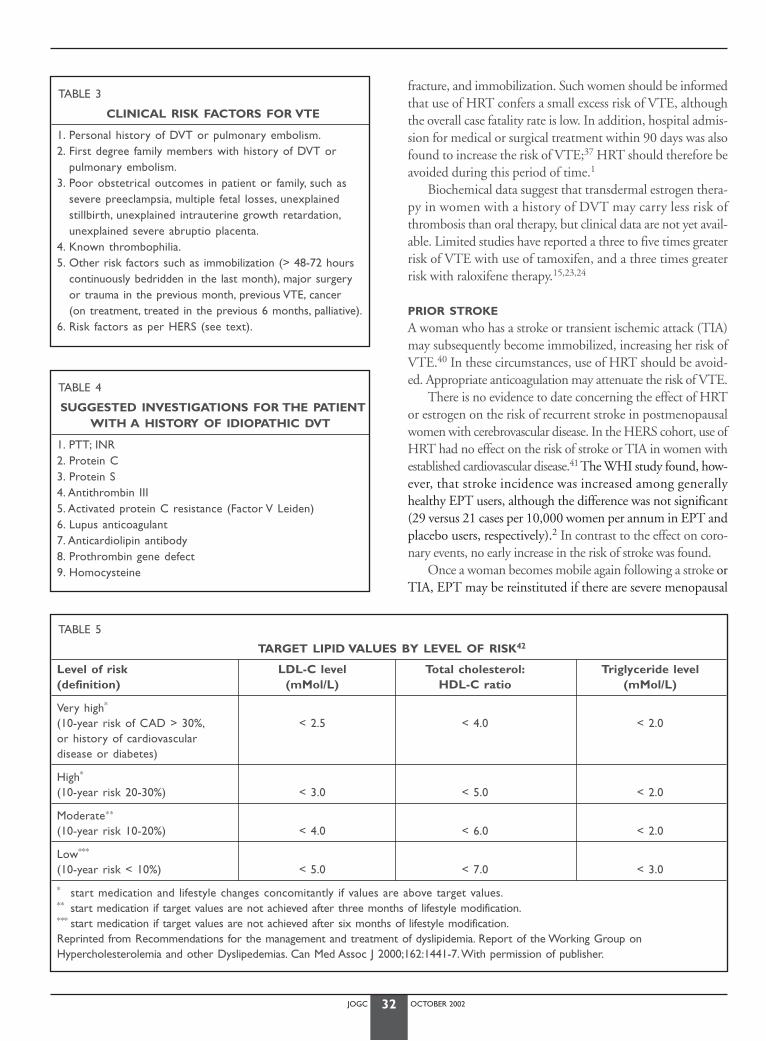
JOGC OCTOBER 200232
fracture, and immobilization. Such women should be informedthat use of HRT confers a small excess risk of VTE, althoughthe overall case fatality rate is low. In addition, hospital admis-sion for medical or surgical treatment within 90 days was alsofound to increase the risk of VTE;37 HRT should therefore beavoided during this period of time.1
Biochemical data suggest that transdermal estrogen thera-py in women with a history of DVT may carry less risk ofthrombosis than oral therapy, but clinical data are not yet avail-able. Limited studies have reported a three to five times greaterrisk of VTE with use of tamoxifen, and a three times greaterrisk with raloxifene therapy.15,23,24
PRIOR STROKE
A woman who has a stroke or transient ischemic attack (TIA)may subsequently become immobilized, increasing her risk ofVTE.40 In these circumstances, use of HRT should be avoid-ed. Appropriate anticoagulation may attenuate the risk of VTE.
There is no evidence to date concerning the effect of HRTor estrogen on the risk of recurrent stroke in postmenopausalwomen with cerebrovascular disease. In the HERS cohort, use ofHRT had no effect on the risk of stroke or TIA in women withestablished cardiovascular disease.41 The WHI study found, how-ever, that stroke incidence was increased among generallyhealthy EPT users, although the difference was not significant(29 versus 21 cases per 10,000 women per annum in EPT andplacebo users, respectively).2 In contrast to the effect on coro-nary events, no early increase in the risk of stroke was found.
Once a woman becomes mobile again following a stroke orTIA, EPT may be reinstituted if there are severe menopausal
TABLE 3
CLINICAL RISK FACTORS FOR VTE
1. Personal history of DVT or pulmonary embolism.2. First degree family members with history of DVT or
pulmonary embolism.3. Poor obstetrical outcomes in patient or family, such as
severe preeclampsia, multiple fetal losses, unexplained stillbirth, unexplained intrauterine growth retardation,unexplained severe abruptio placenta.
4. Known thrombophilia.5. Other risk factors such as immobilization (> 48-72 hours
continuously bedridden in the last month), major surgery or trauma in the previous month, previous VTE, cancer (on treatment, treated in the previous 6 months, palliative).
6. Risk factors as per HERS (see text).
TABLE 4
SUGGESTED INVESTIGATIONS FOR THE PATIENTWITH A HISTORY OF IDIOPATHIC DVT
1. PTT; INR2. Protein C3. Protein S4. Antithrombin III5. Activated protein C resistance (Factor V Leiden)6. Lupus anticoagulant7. Anticardiolipin antibody8. Prothrombin gene defect9. Homocysteine
TABLE 5
TARGET LIPID VALUES BY LEVEL OF RISK42
Level of risk LDL-C level Total cholesterol: Triglyceride level(definition) (mMol/L) HDL-C ratio (mMol/L)
Very high*
(10-year risk of CAD > 30%, < 2.5 < 4.0 < 2.0or history of cardiovascular disease or diabetes)
High*
(10-year risk 20-30%) < 3.0 < 5.0 < 2.0
Moderate∗∗
(10-year risk 10-20%) < 4.0 < 6.0 < 2.0
Low***
(10-year risk < 10%) < 5.0 < 7.0 < 3.0
* start medication and lifestyle changes concomitantly if values are above target values.** start medication if target values are not achieved after three months of lifestyle modification.*** start medication if target values are not achieved after six months of lifestyle modification.Reprinted from Recommendations for the management and treatment of dyslipidemia. Report of the Working Group onHypercholesterolemia and other Dyslipedemias. Can Med Assoc J 2000;162:1441-7.With permission of publisher.

JOGC OCTOBER 200233
symptoms. Randomized trials specifically targeted to stroke pre-vention currently in progress will provide more information.
HRT AND DYSLIPIDEMIA
The choice of HRT prescribed for menopausal symptoms maybe influenced by the lipid profile. A lipid screen should berepeated three to six months after beginning HRT, particularlyif the initial serum triglyceride level was 2.5 mmol/L or greater.Asymptomatic (low-risk) women should undergo a full lipidscreen (serum total cholesterol, HDL, LDL, triglycerides) everyfive years after the age of 50 or at menopause, whichever comesfirst. Routine screening should occur when women develop clin-ical evidence of CAD, peripheral vascular disease, carotid ather-osclerosis, stroke, diabetes mellitus, stigmata of dyslipidemia, ormore than one risk factor for CAD. Target lipid levels are deter-mined according to a patient’s level of risk. Most women withclinical CAD or diabetes (classified as “very high risk”) willrequire lipid-lowering drugs. The reader is referred to the recent-ly published lipid guidelines (Table 5).42
HYPERTENSION
Large controlled trials such as the PEPI trial have found no sig-nificant change in blood pressure with oral administration ofHRT.7 A study comparing transdermal and oral HRT foundno change in blood pressure in treated women over two years,whereas the placebo group showed an increase.43 In the Nurse’sHealth Study, hypertensive women who used HRT had adecreased risk of coronary artery disease.26 Therefore, the pres-ence of hypertension is not a contraindication to HRT use, andit may in fact have a favourable effect on blood pressure due tobeneficial changes in thromboxane and prostacyclin activity.
RECOMMENDATIONS:
D1. Hormone replacement therapy (oral continuous-combined conjugated equine estrogens [CEE] andmedroxy-progesterone acetate [MPA]) (I) or other reg-imens (III) should not be initiated or continued for thesole purpose of preventing future cardiovascular events(primary and secondary prevention). (I)
D2. All women should be counselled about the beneficialeffects of lifestyle modifications on reducing the riskof future cardiovascular events. Appropriate modifi-cations include consumption of a heart-healthy diet,cessation of smoking, moderate daily exercise, andmaintenance of healthy body weight. (II)
D3. To prevent future cardiovascular events, women shouldbe prescribed therapies for which there is abundant sci-entific evidence, such as antihypertensive and lipid-low-ering medications, b-adrenergic blockers, antiplateletagents, and angiotensin-converting enzyme (ACE)inhibitors, with due attention to the potential risks oradverse effects of any of these therapies. (I)
CONCLUSION
In contrast to results obtained from earlier long-term observa-tional studies, the available RCT data provides clear evidence thatestrogen, with or without progestin, does not reduce cardiovas-cular events either in healthy women or in those with establishedcoronary disease; nor does it slow the progression of atheroscle-rosis as detected by angiography. The reason for the differencebetween observational and RCT findings appears to be the lowervalidity of the observational study design methodology.
Based on the available data, HRT in any form is not rec-ommended to reduce cardiovascular events or to prevent coro-nary heart disease. Other proven methods for risk reductionshould be strongly encouraged, including the adoption of aheart-healthy lifestyle (including daily moderate to vigorousphysical activity, not smoking, maintaining a normal bodymass index, and good dietary habits) and modification ofcardiovascular risk factors.35 Evidence-based treatment, in theform of lipid-lowering therapy, ASA therapy, use of b-adren-ergic blockers, and angiotensin-converting enzyme (ACE)inhibitors, should also be considered since there is reliable evi-dence that such treatments are effective.36
J Obstet Gynaecol Can 2001;23(10):966-72.
REFERENCES
1. Heart and Stroke Foundation of Canada.The Changing Face of Heart Dis-ease and Stroke in Canada 2000.Prepared in collaboration with Laborato-ry Centre for Disease Control,Health Canada;Statistics Canada;CanadianInstitute for Health Information;Canadian Cardiovascular Society;Canadi-an Stroke Society;Heart and Stroke Foundation of Canada.
2 Writing Group for the Women’s Health Initiative Investigators. JAMA2002;28:321-33
3. Hulley S, Grady D, Bush T, Furberg K, Herrington D, Riggs B,Vittinghoff E for the Heart and Estrogen/Progestin Replacement Study(HERS) Research Group. Randomized trial of estrogen plus progestinfor secondary prevention of coronary heart disease in postmenopausalwomen. J Am Med Assoc 1998;280:605-13.
4. Mendelsohn ME, Karas RH.The protective effects of estrogen on thecardiovascular system. N Engl J Med 1999;340:1801-11.
5. Castelli WP, Garrison RJ,Wilson PWF,Abbott RD, Kalousdian S, KannelWB. Incidence of coronary heart disease and lipoprotein cholesterollevels: the Framingham study. J Am Med Assoc 1986;256:2835-8.
6. Criqui MH, Heiss G, Cohn R, Cowan LD, Suchindran CM, Bangdiwala S,et al. Plasma triglyceride level and mortality from coronary heartdisease. N Engl J Med 1993;328:1220-5.
7. The Postmenopausal Estrogen/Progestin Interventions (PEPI) trial.Effects of estrogen or estrogen/progestin regimens on heart disease riskfactors in postmenopausal women. J Am Med Assoc 1995;273:199-208.
8. Walsh BW, Schiff I, Rosner B, Greenberg L, Ravnikar V, Sacks FM. Effectsof postmenopausal estrogen replacement on the concentrations andmetabolism of plasma lipoproteins. N Engl J Med 1991;325:1196-1204.
9. Sacks F, McPherson R,Walsh BW. Effects of estrogen replacement ther-apy on plasma concentrations of lipoprotein(a) and cholesterol estertransfer protein.Arch Intern Med 1994;154:1107-10.
10. Crook D, Cust MP, Ganger KF,Worthington M, Hillard TC, StevensonJC, et al. Comparison of transdermal and oral estrogen-progestinreplacement therapy: effects on serum lipids and lipoproteins.Am JObstet Gynecol 1992;166:950-955.
JOGC OCTOBER 200234
11. Taddei S,Virdis A, Ghiadoni L, Mattei P, Sudano I, Bernini G, et al.Menopause is associated with endothelial dysfunction in women.Hypertension 1996;28:576-82.
12. Gerhard M,Walsh BW,Tawakol A, Haley EA, Creager SJ, Seely EW, et al.Estradiol therapy combined with progesterone and endothelium-dependent vasodilatation in postmenopausal women. Circulation1998;98:1158-63.
13. Ridker PM, Buring JE, Shih J, Matias M, Hennekens CH.A prospectivestudy of C-reactive protein and the risk of future cardiovascular eventsamong apparently healthy women. Circulation 1998;98:731-3.
14. Cushman M, Legault C, Barrett-Connor E, Stefanick ML, Kessler C, JuddHL, et al. Effect of postmenopausal hormones on inflammation-sensi-tive proteins.The Postmenopausal Estrogen/Progestin Interventions(PEPI) Study. Circulation 1999;100:717-22.
15. Walsh BW, Paul S,Wild RA, Dean RA,Tracy RP, Cox DA, et al.Theeffects of HRT and raloxifene on C-reactive protein and homocysteinein healthy postmenopausal women: a randomized controlled trial. J ClinEndocrinol Metab 2000;85:214-8.
16. Westendorp IC,Veld BA, Bots ML, et al. Hormone replacement therapyand intima-media thickness of common carotid artery: the Rotterdamstudy. Stroke 1999;12:2562-7.
17. Dubuisson JT,Wagenknecht LE, D’Agostina RB, et al.Association ofhormone replacement therapy and carotid wall thickness in womenwith and without diabetes. Diabetes Care 1998;11:1790-6.
18. Herrington DM, Resboussin DM, Brosnihan KB, Sharp PC, ShumakerSA, Snyder TE, et al. Effects of estrogen replacement on the progressionof coronary artery atherosclerosis. N Engl J Med 2000;343:522-9.
19. Nabel EG. Coronary heart disease in women: an ounce of prevention.N Engl J Med 2000;343:572-4.
20. Walsh BW, Kuller LH,Wild RA, Paul S, Farmer M, Lawrence JB, et al.Effects of raloxifene on serum lipids and coagulation factors in healthypostmenopausal women. J Am Med Assoc 1998;279:1445-50.
21. Conrad JC, Bjarnason NH, Cohen FJ, Shah A, Lindsay R, Mitlak BH, et al.Long-term effects of raloxiphene on bone mineral density, boneturnover, and serum lipid levels in early postmenopausal women.ArchIntern Med 2000;160:3444-50.
22. Love RR,Wiebe DA, Feyzi JM, Newcomb PA, Chappell RJ. Effects oftamoxifen on cardiovascular risk factors in postmenopausal womenafter 5 years of treatment. J Natl Cancer Inst 1994;86:1534-9.
23. Early Breast Cancer Trialists’ Collaborative Group.Tamoxifen for earlybreast cancer: an overview of the randomised trials. Lancet1998;351:1451-67.
24. Reis SE, Constantino JP,Wickerham DL,Tan-Chiu E,Wang J, Kavana M.Cardiovascular effects of tamoxifen in women with and without heartdisease: breast cancer prevention trial. National Surgical AdjuvantBreast and Bowel Project Cancer Prevention Trial Investigators. J NatlCancer Inst 2001;93:16-21
25. Stampfer MJ,Willett WC, Colditz GA, Rosner B, Speizer FE, HennekensGH.A prospective study of postmenopausal estrogen therapy andcoronary heart disease. N Engl J Med 1985;313:1044-9.
26. Stampfer MJ, Colditz GA,Willett WC, Manson JE, Rosner B, Speizer FE,et al. Postmenopausal estrogen therapy and cardiovascular disease: tenyear follow-up from the Nurses’ Health Study. N Engl J Med1991;325:756-62.
27. Grodstein F, Stampfer MJ, Manson JE, Colditz GA,Willett WC, RosnerB, et al. Postmenopausal estrogen and progestin use and the risk of car-diovascular disease. N Engl J Med 1996;335:453-61.
28. Grodstein F, Manson JE, Colditz GA,Willett WC, Speizer FE, StampferMJ.A prospective, observational study of postmenopausal hormonetherapy and primary prevention of cardiovascular disease.Ann InterMed 2000;133:933-41.
29. Shlipak MG, Simon JA,Vittinghoff E, Lin F, Barrett-Connor E, Knopp RH,et al. Estrogen and progestin, lipoprotein(a), and the risk of recurrentcoronary heart disease events after menopause. J Am Med Assoc2000;283:1845-52.
30. Grodstein F, Manson JE, Stamfer MJ. Post menopausal hormone use andsecondary prevention of coronary events in the Nurses’ Health Study:a prospective, observational study.Ann Intrn Med 2001;135:1-8.
31. Hulley S, Furburg C, Barrett-Connor E, Cauley J, Grady D, Haskill W et al. Non-Cardiovascular Disease Outcomes During 6.8 Years of Hormone Replacement Therapy: Heart and Estrogen/ProgestinReplacement Study Follow-up (HERS II). JAMA 2002;288:58-66.
32. Grady D, Herrington D, Bittner V, Blumenthal R, Davidson M, Hlatky Met al. Cardiovascular Disease Outcomes During 6.8 Years of Hormone Replacement Therapy: Heart and Estrogen/ProgestinReplacement Study Follow-up (HERS II). JAMA 2002;288:49-57.
33. The Women’s Health Initiative Study Group. Design of the Women’sHealth Initiative clinical trial and observational study. Control Clin Trials1998;19:61-109.
34. Lenfant C. Statement from Claude Lenfant, MD, Director, NationalHeart, Lung, and Blood Institute, on preliminary trends in the Women’sHealth Initiative. National Heart, Lung, and Blood Institute Communica-tions Office. 3 April, 2000.
35. Stampfer MJ, Hu FB, Manson JE, Rimm EB,Willett WC. Primary preven-tion of coronary heart disease in women through diet and lifestyle. NEngl J Med 2000;343:16-22.
36. Mosca L, Grundy SM, Judelson D, King K, Limacher M, Oparil S, et al.Guide to preventive cardiology for women. Circulation 1999;99:2480-4.
37. Daly E,Vessey MP, Hawkins MM, Carson JL, Gough P, Marsh S. Risk ofvenous thrombo-embolism in users of hormone replacement therapy.Lancet 1996;348:977-80.
38. Jick H, Derby LE, Myers MW,Vasilakis C, Newton KM. Risk of hospitaladmission for idiopathic venous thrombo-embolism among users ofpostmenopausal estrogens. Lancet 1996;348:981-3.
39. Grodstein F, Stampfer MJ, Goldhaber SZ, Manson JE, Colditz GA, Speiz-er FE, et al. Prospective study of exogenous hormones and risk of pul-monary embolism in women. Lancet 1996;348:983-7.
40. Grady D,Wenger NK, Herrington D, Khan S, Furberg C, HunninghakeD, et al for the Heart and Estrogen/progestin Replacement StudyResearch Group. Postmenopausal hormone therapy increases risk forvenous thromboembolic disease.Ann Intern Med 2000;132:689-96.
41. Simon JA, Hsia J, Cauley JA, Richards C, Harris F, Fong J, et al., for theHERS Research Group. Postmenopausal hormone therapy and risk ofstroke. Circulation 2001;103:638-42.
42. Fodor JG, Frohlich JJ, Genest Jr JJG, McPherson PR, for the WorkingGroup on Hypercholesterolemia and Other Dyslipidemias. Recommen-dations for the management and treatment of dyslipidemia. Can MedAssoc J 2000;162:1441-7.
43. Khaw KT.Women, hormones and blood pressure. Can J Cardiol1996;12:9D-12D.

JOGC OCTOBER 200235
INTRODUCTION
Osteoporosis is a skeletal disease characterized by low bonemass and microarchitectural deterioration of bone tissue, witha consequent increase in bone fragility and susceptibility tofracture.1 Loss of bone mineral density is silent until fractureoccurs. Postmenopausal status and advanced age account forabout 80 percent of cases of osteoporosis.2 Secondary osteo-porosis refers to bone loss that is due to identifiable causes suchas diseases, drugs or immobility.
EPIDEMIOLOGY, FRACTURE RISK
Over 70 percent of all fractures in people aged 45 or over aredue to osteoporosis.3 It has been estimated that two millionCanadian women have osteoporosis.3 With the aging of theCanadian population, this number will increase rapidly.Women are particularly at risk for osteoporotic fracture, havingan incidence of fracture three times that of men.4 The average50-year-old woman has a lifetime osteoporosis fracture risk of17.5 percent for the hip, 15.6 percent for the vertebra, 16 per-cent for the distal forearm, and almost 40 percent for any site.4
Occult vertebral fractures are common in elderly post-menopausal women and indicate a three to five times greaterrisk of future vertebral fracture, as well as an increased risk ofhip fracture.5 An incident vertebral fracture in a patient withosteoporosis confers a 20 percent risk of subsequent vertebralfracture in the following year.6
SOCIAL AND MEDICAL OUTCOMES OF FRACTURE
The medical and social consequences of fractures make osteo-porosis an important public health problem. About 20 percentof women and 40 percent of men die within one year after hipfracture.7 It has been estimated that 50 percent of women whosustain a hip fracture become functionally dependent in theirdaily activities, and 19 percent require long-term nursing homecare because of the fracture.7 Vertebral fractures appear to beassociated with similar five-year mortality.8-10 Only one-thirdof all vertebral fractures are clinically diagnosed.11
In addition to health care costs, vertebral fractures causeback pain, loss of height, depression, and low self-esteem.12
Wrist and other fractures have considerable morbidity that isnot usually captured in osteoporosis cost estimates.
The total costs of osteoporosis are difficult to assess and arebased on many assumptions. It is estimated that the total acutecare costs attributable to osteoporosis in Canada (hospitalization,outpatient care, and drug therapy) approached 1.3 billion dollarsin 1993.3 With the aging of the population, the frequency of osteo-porotic fractures will increase in both men and women. In addi-tion, it is likely that the population explosion in developingcountries will change the demography of osteoporosis; for exam-ple, the incidence of hip fracture (and presumably other osteo-porotic fractures) is expected to increase four-fold worldwideduring the next 50 years, and the attendant costs will threaten theviability of the health care systems of many countries.13
PREVENTION OF OSTEOPOROSIS
Because of the high prevalence of osteoporosis, we must adopta cost-economic approach to preventing osteoporosis. Popula-tion strategies for primary prevention of osteoporosis, includ-ing interventions in childhood and young adult life to maximizepeak bone mass and prevent premenopausal decline in bonemass, are essential.
BUILDING AND MAINTAINING SKELETAL HEALTH
THROUGHOUT LIFE
Bone size, strength, and mineralization increase during devel-opment, with a peak in the third decade of life.14 Those withthe highest peak bone mass have a protective advantage fromthe reductions in bone density that occur with increasing age,illness, and decreased sex-steroid activity. Genetic factors are thepredominant predictors of peak bone mass,14 with physiologi-cal, environmental, and modifiable lifestyle factors also havinga significant role.14
Adequate and appropriate nutrition is important for all indi-viduals, but diet alone is not sufficient to prevent bone loss inwomen who experience early menopause.15,16 Supplementationof calcium and vitamin D may be necessary, especially in those
Chui Kin Yuen, MD, FRCSC,1 David Kendler, MD, FRCPC,2 Aliya Khan, MD, FRCSC,3
Jacques Brown, MD, FRCPC,4 Michel Fortier, MD, FRCSC4
OSTEOPOROSIS
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
1 Winnipeg, MB2 Vancouver, BC3 Oakville, ON4 Quebec, QC
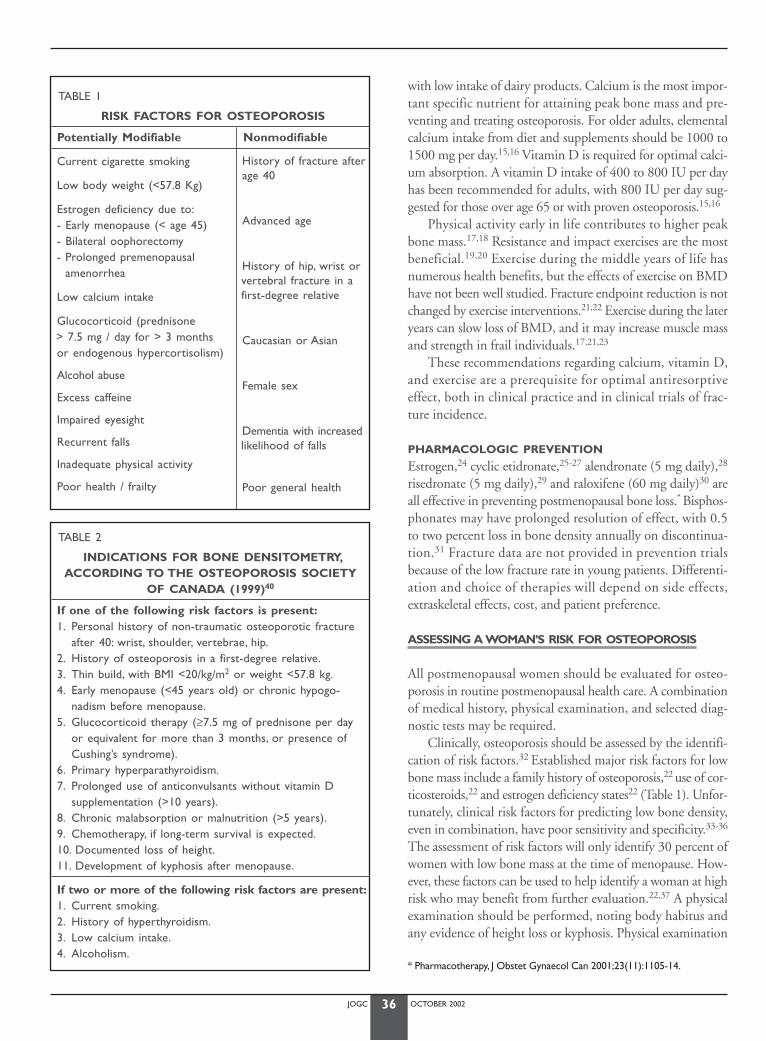
JOGC OCTOBER 200236
with low intake of dairy products. Calcium is the most impor-tant specific nutrient for attaining peak bone mass and pre-venting and treating osteoporosis. For older adults, elementalcalcium intake from diet and supplements should be 1000 to1500 mg per day.15,16 Vitamin D is required for optimal calci-um absorption. A vitamin D intake of 400 to 800 IU per dayhas been recommended for adults, with 800 IU per day sug-gested for those over age 65 or with proven osteoporosis.15,16
Physical activity early in life contributes to higher peakbone mass.17,18 Resistance and impact exercises are the mostbeneficial.19,20 Exercise during the middle years of life hasnumerous health benefits, but the effects of exercise on BMDhave not been well studied. Fracture endpoint reduction is notchanged by exercise interventions.21,22 Exercise during the lateryears can slow loss of BMD, and it may increase muscle massand strength in frail individuals.17,21,23
These recommendations regarding calcium, vitamin D,and exercise are a prerequisite for optimal antiresorptiveeffect, both in clinical practice and in clinical trials of frac-ture incidence.
PHARMACOLOGIC PREVENTION
Estrogen,24 cyclic etidronate,25-27 alendronate (5 mg daily),28
risedronate (5 mg daily),29 and raloxifene (60 mg daily)30 areall effective in preventing postmenopausal bone loss.* Bisphos-phonates may have prolonged resolution of effect, with 0.5to two percent loss in bone density annually on discontinua-tion.31 Fracture data are not provided in prevention trialsbecause of the low fracture rate in young patients. Differenti-ation and choice of therapies will depend on side effects,extraskeletal effects, cost, and patient preference.
ASSESSING A WOMAN’S RISK FOR OSTEOPOROSIS
All postmenopausal women should be evaluated for osteo-porosis in routine postmenopausal health care. A combinationof medical history, physical examination, and selected diag-nostic tests may be required.
Clinically, osteoporosis should be assessed by the identifi-cation of risk factors.32 Established major risk factors for lowbone mass include a family history of osteoporosis,22 use of cor-ticosteroids,22 and estrogen deficiency states22 (Table 1). Unfor-tunately, clinical risk factors for predicting low bone density,even in combination, have poor sensitivity and specificity.33-36
The assessment of risk factors will only identify 30 percent ofwomen with low bone mass at the time of menopause. How-ever, these factors can be used to help identify a woman at highrisk who may benefit from further evaluation.22,37 A physicalexamination should be performed, noting body habitus andany evidence of height loss or kyphosis. Physical examination
TABLE 1
RISK FACTORS FOR OSTEOPOROSIS
Potentially Modifiable Nonmodifiable
Current cigarette smoking
Low body weight (<57.8 Kg)
Estrogen deficiency due to:- Early menopause (< age 45)- Bilateral oophorectomy- Prolonged premenopausal
amenorrhea
Low calcium intake
Glucocorticoid (prednisone > 7.5 mg / day for > 3 monthsor endogenous hypercortisolism)
Alcohol abuse
Excess caffeine
Impaired eyesight
Recurrent falls
Inadequate physical activity
Poor health / frailty
TABLE 2
INDICATIONS FOR BONE DENSITOMETRY,ACCORDING TO THE OSTEOPOROSIS SOCIETY
OF CANADA (1999)40
If one of the following risk factors is present:1. Personal history of non-traumatic osteoporotic fracture
after 40: wrist, shoulder, vertebrae, hip.2. History of osteoporosis in a first-degree relative.3. Thin build, with BMI <20/kg/m2 or weight <57.8 kg.4. Early menopause (<45 years old) or chronic hypogo-
nadism before menopause.5. Glucocorticoid therapy (≥7.5 mg of prednisone per day
or equivalent for more than 3 months, or presence ofCushing’s syndrome).
6. Primary hyperparathyroidism.7. Prolonged use of anticonvulsants without vitamin D
supplementation (>10 years).8. Chronic malabsorption or malnutrition (>5 years).9. Chemotherapy, if long-term survival is expected.10. Documented loss of height.11. Development of kyphosis after menopause.
If two or more of the following risk factors are present:1. Current smoking.2. History of hyperthyroidism.3. Low calcium intake.4. Alcoholism.
* Pharmacotherapy, J Obstet Gynaecol Can 2001;23(11):1105-14.
History of fracture after age 40
Advanced age
History of hip, wrist orvertebral fracture in afirst-degree relative
Caucasian or Asian
Female sex
Dementia with increasedlikelihood of falls
Poor general health

JOGC OCTOBER 200237
will also help exclude secondary causes of osteoporosis. Factorsassociated with an increased risk of falls, such as an impairedsensorium, muscle weakness, and instability, should be noted.
INDICATIONS FOR DUAL
ENERGY X-RAY ABSORPTIOMETRY
BMD is only one of several determinants of fracture risk,accounting for the overlap in the distribution of BMD for indi-viduals who have and have not sustained fractures. Neverthe-less, it is the single most predictive test for the identification ofa population at risk, and it has been used as the entry criteri-on for clinical trials of pharmacologic agents. A fragility frac-ture is, by itself, sufficient for the diagnosis of osteoporosis,regardless of BMD.
BMD testing is indicated only in patients in whom theinformation might lead to a change in management. Cost-economic BMD testing, such as dual energy X-ray absorp-tiometry (DEXA) of the hip and spine, is appropriate forwomen over the age of 65, or for women over the age of 55with one or more additional risk factors for osteoporotic frac-ture besides menopause.38,39
The Osteoporosis Society of Canada (OSC) has recentlyupdated its indications for BMD testing, summarized in Table 2.40
ROLE OF PERIPHERAL BONE DENSITY TESTING
Peripheral BMD can be measured by DEXA, ultrasound orsingle X-ray absorptiometry at several skeletal sites (radius, pha-lanx, calcaneus, tibia, metatarsal). These technologies are almostas accurate as DEXA of the hip and spine in predicting futurefracture risk,41,42 but they cannot be used at the present timefor follow-up. Peripheral testing may play an important rolefor women in underserviced areas and in raising awarenessabout osteoporosis. However, these services may be providedby unregulated practitioners, which raises concerns about quality control.
INTERPRETING THE RESULTS OF BMD TESTING
A study group of the World Health Organization (WHO) hasproposed guidelines for the interpretation of BMD by DEXA
at the hip and spine in postmenopausal Caucasian women(Table 3).43,44 These guidelines are based on fracture prevalencein this population. Their relevance to other populations, toother BMD technologies (such as ultrasound), or to sites otherthan hip and spine is not determined.45 A T-score is used tocompare the patient’s BMD to a normal young woman’s BMD.
In 30 percent of cases, an imperfect correlation existsbetween BMD measurements at different sites.46 When thereare discrepancies between sites, the lowest value should be usedfor diagnosis. Ordinarily, BMD in the lumbar spine can bemeasured with more precision, and early postmenopausalchanges are more readily detected there than at other sites.16
In elderly women, degenerative changes in the lumbar spinemay artefactually elevate spinal BMD.47 Therefore, the totalhip BMD measurement may be the best test for assessingBMD in women over age 65. Even with a precision error aslow as one percent, serial BMD measurements require a min-imum follow-up interval of one to two years to detect a boneloss of two to three percent (the average loss per year for a nor-mal woman at menopause). A longer interval (5 years) isrequired for repeat BMD testing when normal values areobtained.
BLOOD AND URINE TESTS
In patients with diagnosed osteoporosis, blood tests to rule outsecondary osteoporosis are essential, and are documented inTable 4.15
Although blood and urine tests may be useful in large clin-ical trials to determine the level of bone turnover, they have verylimited clinical utility at present. Individual patients show a largevariability in tests from one day to the next.48 Markers of boneformation (such as bone specific alkaline phosphatase) and boneresorption (urinary N-telopeptide or deoxypyridinoline, uri-nary or serum C-telopeptide) may show elevated levels in post-menopausal women.49 The levels of markers in postmenopausalwomen on antiresorptive therapy may be reduced.50 Elevatedmarker levels cannot be used to identify patients for therapy,and in an individual patient they are not useful for monitoringthe response to therapy.
TABLE 3
WORLD HEALTH ORGANIZATION (WHO) GUIDELINES FOR THE INTERPRETATION OF BMD READINGS43,44
BMD T- Score* standard deviations Change in fracture risk WHO categorization
> -1 — Normal
-1 to -2.5 4-fold increase Osteopenia
< -2.5 8-fold increase Osteoporosis
With one or more fragility fractures 20-fold increase Severe osteoporosiswith or without low BMD
*Results (T-score) are compared with the mean for young adult normal female controls.Derived from a WHO Study Group report. WHO Tech Rep Ser 1994;843:1-129.
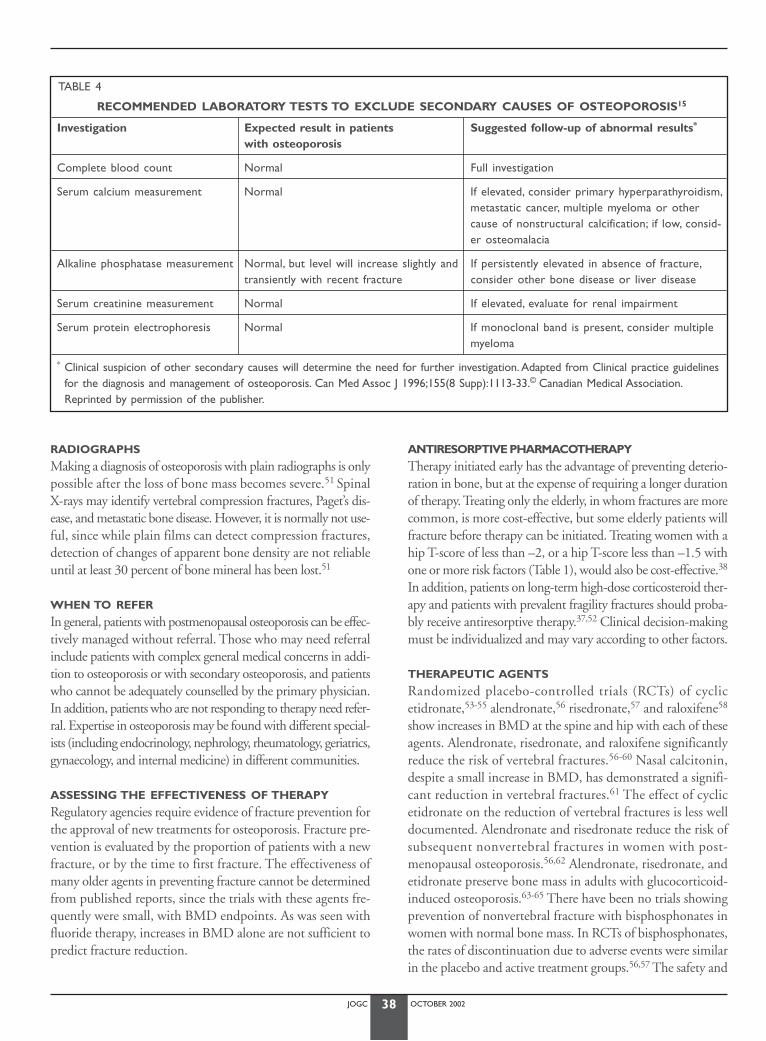
JOGC OCTOBER 200238
RADIOGRAPHS
Making a diagnosis of osteoporosis with plain radiographs is onlypossible after the loss of bone mass becomes severe.51 Spinal X-rays may identify vertebral compression fractures, Paget’s dis-ease, and metastatic bone disease. However, it is normally not use-ful, since while plain films can detect compression fractures,detection of changes of apparent bone density are not reliableuntil at least 30 percent of bone mineral has been lost.51
WHEN TO REFER
In general, patients with postmenopausal osteoporosis can be effec-tively managed without referral. Those who may need referralinclude patients with complex general medical concerns in addi-tion to osteoporosis or with secondary osteoporosis, and patientswho cannot be adequately counselled by the primary physician.In addition, patients who are not responding to therapy need refer-ral. Expertise in osteoporosis may be found with different special-ists (including endocrinology, nephrology, rheumatology, geriatrics,gynaecology, and internal medicine) in different communities.
ASSESSING THE EFFECTIVENESS OF THERAPY
Regulatory agencies require evidence of fracture prevention forthe approval of new treatments for osteoporosis. Fracture pre-vention is evaluated by the proportion of patients with a newfracture, or by the time to first fracture. The effectiveness ofmany older agents in preventing fracture cannot be determinedfrom published reports, since the trials with these agents fre-quently were small, with BMD endpoints. As was seen withfluoride therapy, increases in BMD alone are not sufficient topredict fracture reduction.
ANTIRESORPTIVE PHARMACOTHERAPY Therapy initiated early has the advantage of preventing deterio-ration in bone, but at the expense of requiring a longer durationof therapy. Treating only the elderly, in whom fractures are morecommon, is more cost-effective, but some elderly patients willfracture before therapy can be initiated. Treating women with ahip T-score of less than –2, or a hip T-score less than –1.5 withone or more risk factors (Table 1), would also be cost-effective.38
In addition, patients on long-term high-dose corticosteroid ther-apy and patients with prevalent fragility fractures should proba-bly receive antiresorptive therapy.37,52 Clinical decision-makingmust be individualized and may vary according to other factors.
THERAPEUTIC AGENTS
Randomized placebo-controlled trials (RCTs) of cyclicetidronate,53-55 alendronate,56 risedronate,57 and raloxifene58
show increases in BMD at the spine and hip with each of theseagents. Alendronate, risedronate, and raloxifene significantlyreduce the risk of vertebral fractures.56-60 Nasal calcitonin,despite a small increase in BMD, has demonstrated a signifi-cant reduction in vertebral fractures.61 The effect of cyclicetidronate on the reduction of vertebral fractures is less welldocumented. Alendronate and risedronate reduce the risk ofsubsequent nonvertebral fractures in women with post-menopausal osteoporosis.56,62 Alendronate, risedronate, andetidronate preserve bone mass in adults with glucocorticoid-induced osteoporosis.63-65 There have been no trials showingprevention of nonvertebral fracture with bisphosphonates inwomen with normal bone mass. In RCTs of bisphosphonates,the rates of discontinuation due to adverse events were similarin the placebo and active treatment groups.56,57 The safety and
TABLE 4
RECOMMENDED LABORATORY TESTS TO EXCLUDE SECONDARY CAUSES OF OSTEOPOROSIS15
Investigation Expected result in patients Suggested follow-up of abnormal results*
with osteoporosis
Complete blood count Normal Full investigation
Serum calcium measurement Normal If elevated, consider primary hyperparathyroidism,metastatic cancer, multiple myeloma or othercause of nonstructural calcification; if low, consid-er osteomalacia
Alkaline phosphatase measurement Normal, but level will increase slightly and If persistently elevated in absence of fracture,transiently with recent fracture consider other bone disease or liver disease
Serum creatinine measurement Normal If elevated, evaluate for renal impairment
Serum protein electrophoresis Normal If monoclonal band is present, consider multiplemyeloma
* Clinical suspicion of other secondary causes will determine the need for further investigation. Adapted from Clinical practice guidelinesfor the diagnosis and management of osteoporosis. Can Med Assoc J 1996;155(8 Supp):1113-33.© Canadian Medical Association.Reprinted by permission of the publisher.

JOGC OCTOBER 200239
efficacy of this therapy in children and young adults has notbeen evaluated. Patients in clinical trials may not always be rep-resentative of a community population.
HORMONE REPLACEMENT THERAPY
Hormone replacement therapy (HRT) is the traditionalapproach for osteoporosis prevention, as demonstrated by manystudies with BMD as the primary measure.66-68 Both oral andtransdermal estrogen therapy decrease bone loss.66-68 Estrogentherapy that is begun after age 60 and continued also offers bone-conserving benefit.69,70 Lower doses of estrogen taken in com-bination with calcium may be equally protective.71 BMD risesin women who begin estrogen therapy within five years aftermenopause;66-68 stabilization of BMD is expected in olderwomen who begin therapy 10 years or more after menopause.70
Observational studies show a reduction in the rate of hip frac-ture in women who choose to take long-term HRT and remainon therapy.69,70 The Women’s Health Initiative randomized con-trolled trial is the first trial with definitive data supporting the abil-ity of postmenopausal hormones to prevent fractures at the hip,vertebrae, and other sites.72 The additional benefits and risks ofHRT are important to an individual woman in making a choiceof therapy. HRT is inexpensive, and dosing is convenient.
BISPHOSPHONATES
There are two major classes of bisphosphonates approved forthe prevention and treatment of osteoporosis in Canada: non-nitrogen-containing bisphosphonates such as cyclic etidronate,and nitrogen-containing bisphosphonates such as alendronateand risedronate. These classes differ in their molecular mecha-nism of action, and clinical trials demonstrate differences in frac-ture and bone density protection when compared to placebo.There have been no head-to-head trials of these agents.
NON-NITROGEN-CONTAINING BISPHOSPHONATES:
CYCLIC ETIDRONATE
Trials with cyclic etidronate (etidronate 400 mg daily for twoweeks every three months) were powered for BMD endpointsonly.53,54,73 Discernible increases in BMD are seen in the spineand, to a lesser extent, the hip. Non-responders are frequent.Reduction in vertebral fracture risk can be seen only in high-risk subgroups of the etidronate clinical trials. Data on non-vertebral fracture prevention have only been reported fromobservational studies.74 It is also approved for the prevention ofcorticosteroid-induced osteoporosis.65
Cyclic etidronate is inexpensive and well-tolerated, with raregastrointestinal upset and bone pain reported as side effects.54,73
It is administered either two hours before eating or two hoursafter eating. Low-dose cyclic therapy is required because contin-uous therapy impairs mineralization.75
Etidronate acts by forming toxic metabolites of adenosinetriphosphate (ATP) and consequently inhibiting osteoclasticbone resorption.76 This mode of action differs from that ofnitrogen-containing bisphosphonates, which act on the meva-lonic acid pathway.77
NITROGEN-CONTAINING BISPHOSPHONATES:
ALENDRONATE
Alendronate, in doses of 10 mg daily78 or 70 mg once week-ly,79 leads to detectable increases in bone mineral density atboth spine and hip. A reduction in vertebral fracture risk is seenwith use of alendronate 10 mg daily, both in patients with priorvertebral fractures56 and patients with no prior vertebral frac-tures.59 Significant reductions in rates of non-vertebral and hipfractures are seen as soon as 12 to 18 months after commen-cing therapy. Alendronate is approved for the prevention andtreatment of corticosteroid-induced osteoporosis. Side effectsof therapy are frequently associated with misdosing. Rarely,gastrointestinal upset and bone pain occurs, but there is noimpairment of mineralization.80 Studies confirm long-termefficacy and safety, with continuing increases in bone densityto the end of seven years. Alendronate must be taken withwater, 30 minutes before breakfast, with the patient subse-quently remaining upright for 30 minutes.
The 70 mg once-weekly dosing regimen of alendronate hasbeen shown to provide patients with a more convenient, thera-peutically equivalent alternative to daily dosing.79 It may enhancecompliance and long-term persistence with therapy. Dosing with70 mg once weekly is equivalent to 10 mg daily in safety andBMD efficacy, but no fracture data is available.79
NITROGEN-CONTAINING BISPHOSPHONATES:
RISEDRONATE
Administration of risedronate 5 mg daily leads to significantBMD increases at the spine and hip.60 A reduction in vertebralfracture rate is seen in patients who have prevalent vertebral frac-tures.60 Morphometric vertebral fracture reduction at one yearof therapy has been demonstrated.57,60 Significant reductions innon-vertebral and hip fractures have been reported in a recentstudy;62 this is the only study recording hip fracture as a prima-ry endpoint. Risedronate rarely causes gastrointestinal upset andbone pain. No impairment of mineralization is seen.60 It mustalso be taken after fasting, with water only, either 30 minutesbefore breakfast, or at least two hours before or after food, andthe patient must subsequently remain upright for 30 minutes.
SELECTIVE ESTROGEN RECEPTOR MODULATORS
Selective estrogen receptor modulators (SERMs) have been animportant advance in osteoporosis therapy. The goal of theseagents is to maximize the beneficial effect of estrogen on boneand to minimize or antagonize the effects of estrogen on thebreast and endometrium. Modest BMD increases are seen at the
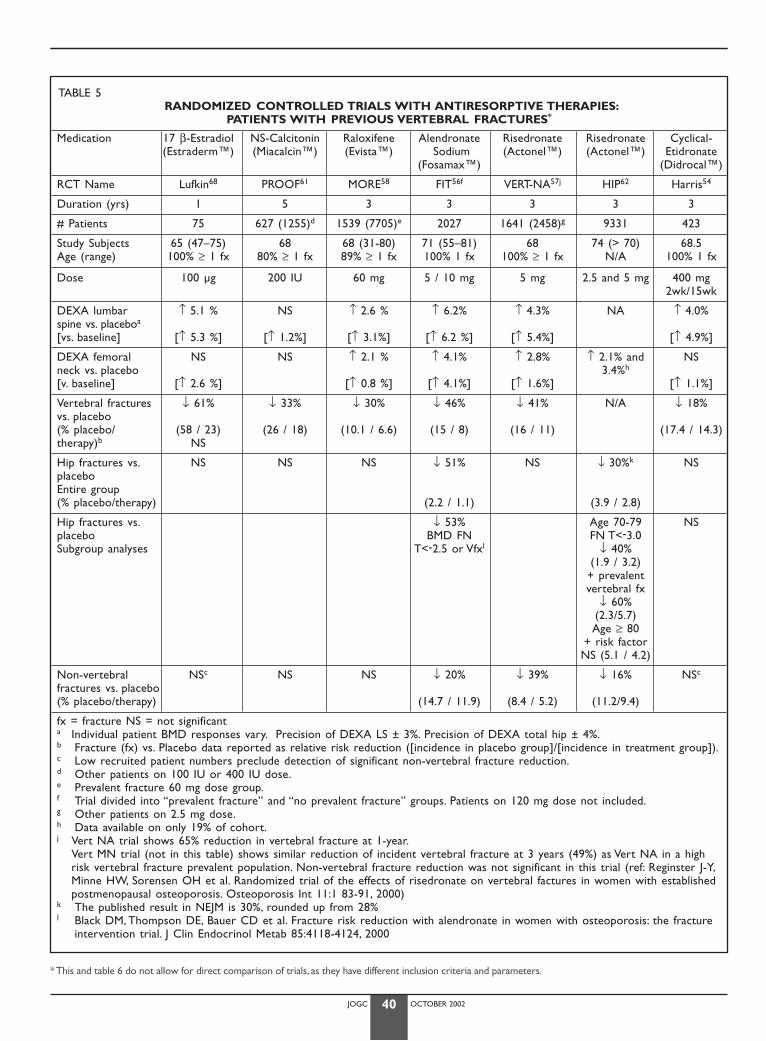
JOGC OCTOBER 200240
* This and table 6 do not allow for direct comparison of trials, as they have different inclusion criteria and parameters.
TABLE 5RANDOMIZED CONTROLLED TRIALS WITH ANTIRESORPTIVE THERAPIES:
PATIENTS WITH PREVIOUS VERTEBRAL FRACTURES*
Medication 17 β-Estradiol NS-Calcitonin Raloxifene Alendronate Risedronate Risedronate Cyclical-(Estraderm™) (Miacalcin™) (Evista™) Sodium (Actonel™) (Actonel™) Etidronate
(Fosamax™) (Didrocal™)
RCT Name Lufkin68 PROOF61 MORE58 FIT56f VERT-NA57j HIP62 Harris54
Duration (yrs) 1 5 3 3 3 3 3
# Patients 75 627 (1255)d 1539 (7705)e 2027 1641 (2458)g 9331 423
Study Subjects 65 (47–75) 68 68 (31-80) 71 (55–81) 68 74 (> 70) 68.5Age (range) 100% ≥ 1 fx 80% ≥ 1 fx 89% ≥ 1 fx 100% 1 fx 100% ≥ 1 fx N/A 100% 1 fx
Dose 100 µg 200 IU 60 mg 5 / 10 mg 5 mg 2.5 and 5 mg 400 mg 2wk/15wk
DEXA lumbar ↑ 5.1 % NS ↑ 2.6 % ↑ 6.2% ↑ 4.3% NA ↑ 4.0%spine vs. placeboa
[vs. baseline] [↑ 5.3 %] [↑ 1.2%] [↑ 3.1%] [↑ 6.2 %] [↑ 5.4%] [↑ 4.9%]
DEXA femoral NS NS ↑ 2.1 % ↑ 4.1% ↑ 2.8% ↑ 2.1% and NSneck vs. placebo 3.4%h
[v. baseline] [↑ 2.6 %] [↑ 0.8 %] [↑ 4.1%] [↑ 1.6%] [↑ 1.1%]
Vertebral fractures ↓ 61% ↓ 33% ↓ 30% ↓ 46% ↓ 41% N/A ↓ 18%vs. placebo(% placebo/ (58 / 23) (26 / 18) (10.1 / 6.6) (15 / 8) (16 / 11) (17.4 / 14.3)therapy)b NS
Hip fractures vs. NS NS NS ↓ 51% NS ↓ 30%k NSplaceboEntire group(% placebo/therapy) (2.2 / 1.1) (3.9 / 2.8)
Hip fractures vs. ↓ 53% Age 70-79 NSplacebo BMD FN FN T<-3.0Subgroup analyses T<-2.5 or Vfxl ↓ 40%
(1.9 / 3.2)+ prevalentvertebral fx
↓ 60%(2.3/5.7)Age ≥ 80
+ risk factorNS (5.1 / 4.2)
Non-vertebral NSc NS NS ↓ 20% ↓ 39% ↓ 16% NSc
fractures vs. placebo (% placebo/therapy) (14.7 / 11.9) (8.4 / 5.2) (11.2/9.4)
fx = fracture NS = not significanta Individual patient BMD responses vary. Precision of DEXA LS ± 3%. Precision of DEXA total hip ± 4%.b Fracture (fx) vs. Placebo data reported as relative risk reduction ([incidence in placebo group]/[incidence in treatment group]).c Low recruited patient numbers preclude detection of significant non-vertebral fracture reduction.d Other patients on 100 IU or 400 IU dose.e Prevalent fracture 60 mg dose group.f Trial divided into “prevalent fracture” and “no prevalent fracture” groups. Patients on 120 mg dose not included.g Other patients on 2.5 mg dose.h Data available on only 19% of cohort.j Vert NA trial shows 65% reduction in vertebral fracture at 1-year.
Vert MN trial (not in this table) shows similar reduction of incident vertebral fracture at 3 years (49%) as Vert NA in a highrisk vertebral fracture prevalent population. Non-vertebral fracture reduction was not significant in this trial (ref: Reginster J-Y,Minne HW, Sorensen OH et al. Randomized trial of the effects of risedronate on vertebral factures in women with establishedpostmenopausal osteoporosis. Osteoporosis Int 11:1 83-91, 2000)
k The published result in NEJM is 30%, rounded up from 28%l Black DM, Thompson DE, Bauer CD et al. Fracture risk reduction with alendronate in women with osteoporosis: the fracture
intervention trial. J Clin Endocrinol Metab 85:4118-4124, 2000
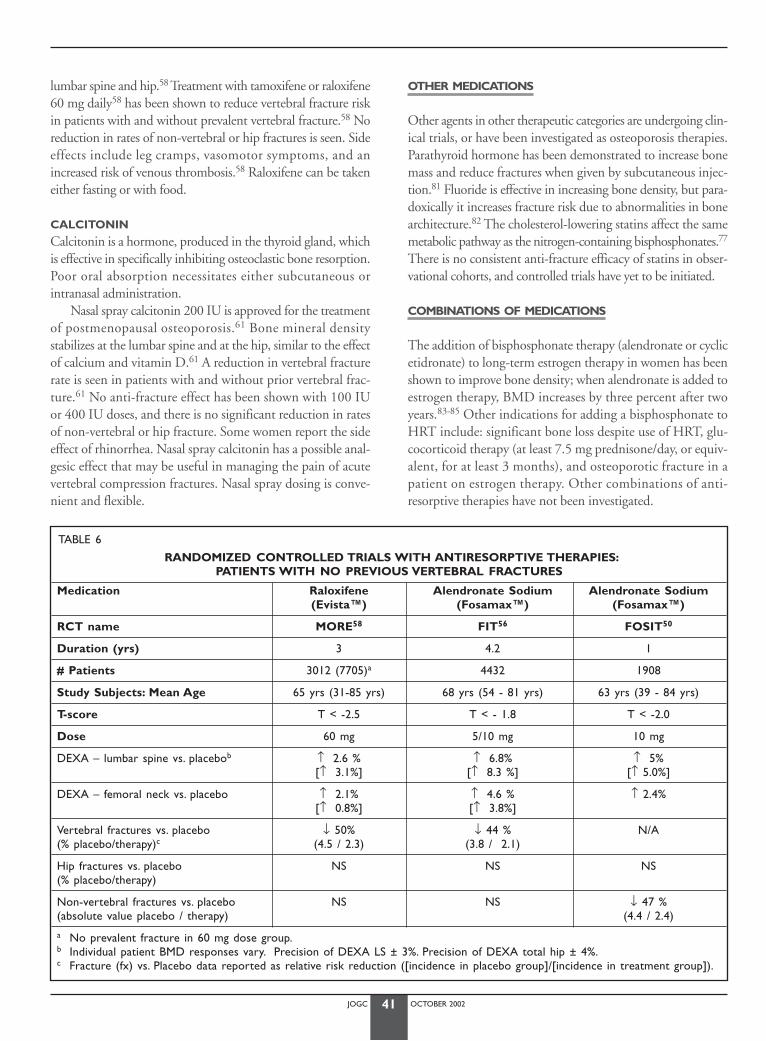
JOGC OCTOBER 200241
lumbar spine and hip.58 Treatment with tamoxifene or raloxifene60 mg daily58 has been shown to reduce vertebral fracture riskin patients with and without prevalent vertebral fracture.58 Noreduction in rates of non-vertebral or hip fractures is seen. Sideeffects include leg cramps, vasomotor symptoms, and anincreased risk of venous thrombosis.58 Raloxifene can be takeneither fasting or with food.
CALCITONIN
Calcitonin is a hormone, produced in the thyroid gland, whichis effective in specifically inhibiting osteoclastic bone resorption.Poor oral absorption necessitates either subcutaneous orintranasal administration.
Nasal spray calcitonin 200 IU is approved for the treatmentof postmenopausal osteoporosis.61 Bone mineral density stabilizes at the lumbar spine and at the hip, similar to the effectof calcium and vitamin D.61 A reduction in vertebral fracturerate is seen in patients with and without prior vertebral frac-ture.61 No anti-fracture effect has been shown with 100 IUor 400 IU doses, and there is no significant reduction in ratesof non-vertebral or hip fracture. Some women report the sideeffect of rhinorrhea. Nasal spray calcitonin has a possible anal-gesic effect that may be useful in managing the pain of acutevertebral compression fractures. Nasal spray dosing is conve-nient and flexible.
OTHER MEDICATIONS
Other agents in other therapeutic categories are undergoing clin-ical trials, or have been investigated as osteoporosis therapies.Parathyroid hormone has been demonstrated to increase bonemass and reduce fractures when given by subcutaneous injec-tion.81 Fluoride is effective in increasing bone density, but para-doxically it increases fracture risk due to abnormalities in bonearchitecture.82 The cholesterol-lowering statins affect the samemetabolic pathway as the nitrogen-containing bisphosphonates.77
There is no consistent anti-fracture efficacy of statins in obser-vational cohorts, and controlled trials have yet to be initiated.
COMBINATIONS OF MEDICATIONS
The addition of bisphosphonate therapy (alendronate or cyclicetidronate) to long-term estrogen therapy in women has beenshown to improve bone density; when alendronate is added toestrogen therapy, BMD increases by three percent after twoyears.83-85 Other indications for adding a bisphosphonate toHRT include: significant bone loss despite use of HRT, glu-cocorticoid therapy (at least 7.5 mg prednisone/day, or equiv-alent, for at least 3 months), and osteoporotic fracture in apatient on estrogen therapy. Other combinations of anti-resorptive therapies have not been investigated.
TABLE 6
RANDOMIZED CONTROLLED TRIALS WITH ANTIRESORPTIVE THERAPIES:PATIENTS WITH NO PREVIOUS VERTEBRAL FRACTURES
Medication Raloxifene Alendronate Sodium Alendronate Sodium (Evista™) (Fosamax™) (Fosamax™)
RCT name MORE58 FIT56 FOSIT50
Duration (yrs) 3 4.2 1
# Patients 3012 (7705)a 4432 1908
Study Subjects: Mean Age 65 yrs (31-85 yrs) 68 yrs (54 - 81 yrs) 63 yrs (39 - 84 yrs)
T-score T < -2.5 T < - 1.8 T < -2.0
Dose 60 mg 5/10 mg 10 mg
DEXA – lumbar spine vs. placebob ↑ 2.6 % ↑ 6.8% ↑ 5%[↑ 3.1%] [↑ 8.3 %] [↑ 5.0%]
DEXA – femoral neck vs. placebo ↑ 2.1% ↑ 4.6 % ↑ 2.4%[↑ 0.8%] [↑ 3.8%]
Vertebral fractures vs. placebo ↓ 50% ↓ 44 % N/A(% placebo/therapy)c (4.5 / 2.3) (3.8 / 2.1)
Hip fractures vs. placebo NS NS NS(% placebo/therapy)
Non-vertebral fractures vs. placebo NS NS ↓ 47 % (absolute value placebo / therapy) (4.4 / 2.4)
a No prevalent fracture in 60 mg dose group.b Individual patient BMD responses vary. Precision of DEXA LS ± 3%. Precision of DEXA total hip ± 4%.c Fracture (fx) vs. Placebo data reported as relative risk reduction ([incidence in placebo group]/[incidence in treatment group]).

JOGC OCTOBER 200242
AGE FOR BEGINNING ANTIRESORPTIVE THERAPY
Although the management of osteoporosis should focus on pre-vention of the first fracture, the treatment of large numbers ofyoung menopausal women is not cost-effective due to the lowshort-term incidence of fractures in this population. All womenwould benefit from adequate calcium, vitamin D, and lifestyleadvice.* It is reasonable to discuss the risks and benefits of estro-gen therapy with young postmenopausal women, and reservethe assessment of osteoporosis by BMD measurement for thewoman 55 years of age or older with a risk factor, or the woman65 years of age or older with no specific risk factor (Table 2).
MONITORING TREATMENT FOR ESTABLISHEDPOSTMENOPAUSAL OSTEOPOROSIS
Periodic evaluation of bone density by DEXA at intervals of 1.5to two years represents the best way to monitor the clinicalresponse to medical intervention.47 Once the clinical condi-tion is stabilized, there is no need to repeat DEXA assessmentsthroughout life. When monitoring skeletal status with serialDEXA, it is important to understand the magnitude of biolog-ical change expected at the site measured, as well as the instru-ment precision at that site. The spine will change most rapidlyafter menopause, and with nitrogen-containing bisphosphonatetherapy, the magnitude of change could be three to five percentafter the first year of treatment (precision ± 3%).56 However, hipchanges are slower (2% at one year) and machine precision is less(4%),47 mandating a longer interval between tests. Total hipmeasurements are more precise than other hip regions for fol-lowing patients serially. The purpose of monitoring patients onmedications that are not expected to produce detectable positiveeffects on BMD (calcitonin, raloxifene) is to identify any patientswho may be losing bone mass on therapy.
USING BMD CHANGES TO MODIFY THERAPY
Increases in BMD on antiresorptive therapy may be more markedwith one agent than another. Fracture prevention may or may notbe associated with detectable increases in bone density, and a reduc-tion in fracture risk may result from beneficial effects on bonearchitecture. Patients who lose bone density on therapy (by morethan the precision of the instrument at that site) should have theirdosing instructions reinforced, and secondary causes of osteo-porosis should be excluded. The possibility of changes to therapy,or the addition of therapy, should be considered. Patients with sta-ble or increasing bone density on therapy should continue untilthe clinical risk of fracture has diminished.
LENGTH OF THERAPY FOR OSTEOPOROSIS
We do not have long-term experience with most approvedtherapies for osteoporosis. Consequently, questions concern-
ing fracture risk in patients who discontinue therapy remainunanswered. We can advise patients that anti-fracture efficacypersists three to seven years (the length of follow-up in the clin-ical trials),86 and that bone density changes may plateau orincrease slowly after the first two to three years of therapy.86
The decisions about duration of therapy must, however, remainclinical judgements based upon individual patient factors.
RECOMMENDATIONS:
E1. Evaluation of fracture risk in postmenopausal womenshould include the assessment of risk factors, with bonemineral density measurement for those at increased risk.
a) Central (hip and spine) measurements by dual energy X-ray absorptiometry (DEXA) are themost accurate and precise measurements of bonedensity available, making them useful for bothrisk assessment and follow-up. (I)
b) Peripheral bone mass measurements (e.g., ultra-sound or DEXA measurements in the radius, pha-lanx, or heel) is useful for fracture risk assessment,but cannot be used for follow-up. (I)
E2. Physicians should be aware that a prevalent vertebral ornon-vertebral fragility fracture markedly increases therisk of future fracture. (I)
E3. Markers of bone resorption, while useful in documentinggroup responses in large clinical trials, have no clear placein the evaluation of follow-up of individual patients. (II)
E4. Women should be encouraged to have adequate intakeof calcium and vitamin D, good nutrition and exercise,avoidance of negative lifestyle habits (smoking, alco-hol). A normal exposure to estrogen during reproduc-tive life and exercise contribute to optimal achievementand maintenance of genetically determined peak bonemass. These recommendations are applicable to allwomen (II); for early postmenopausal women, adequatecalcium and vitamin D intake alone is not sufficient tomaintain bone mass. (I)
E5. Although combination of antiresorptive therapies maybe synergistic in increasing bone mineral density, theireffect on fracture has not been proven. Combinationtherapy should be reserved for patients not respondingto single-agent antiresorptive therapy. (I)
SUMMARY OF KEY POINTS:
E6. The goal of osteoporosis management is the preventionof fracture. This may or may not be associated with sig-nificant increases in bone mineral density. (I)
E7. Postmenopausal bone loss can be effectively prevented by antiresorptive therapy such as estrogen replacement, selective estrogen receptor modulator, or bisphosphonatetherapy. (I)
* Menopause:healthy living, J Obstet Gynaecol Can 2001;23(9):842-8.

JOGC OCTOBER 200243
E8. Treatment with alendronate or risedronate has beendemonstrated to decrease both vertebral and non-ver-tebral fractures including hip fractures (I); treatmentwith raloxifene, or calcitonin, has been demonstated toreduce vertebral fractures (I); treatment with estrogenor etidronate appears to reduce vertebral fracture (II).Physicians should consider a range of treatmentoptions for osteoporosis.
E9. According to the WHI study, continuous combinedHRT was effective in reducing the risk of hip fractures(5 fewer cases per 10,000 women per year). Vertebraland other fractures were also reduced.
CONCLUSION
For premenopausal women with normal estrogen levels, notreatment except calcium and vitamin D should be offered.Bone mineral density testing should be delayed until aftermenopause. Patients on glucocorticoid therapy represent a dif-ferent clinical situation,* and they must be investigated andappropriately treated for osteoporosis.31-36, 40-53
The best therapy is the one that takes into account the totalbenefits for a patient. In considering a patient’s need for phar-macotherapy and choosing between the therapeutic options,an individualized approach is necessary. If the patient requiresmore than skeletal effects, such as relief from hot flushes, estro-gen preparations may be the best option. If the patient is pri-marily at short-term risk for hip or non-vertebral fracture, abisphosphonate is probably the best option. If the patient hasspecific intolerance to a medication, or other conditions suchas a history of venous thrombosis or esophageal stricture, theclinician might favour one medication over another. Patientswill also consider factors of cost, access through formularies,and dosing convenience.
J Obstet Gynaecol Can 2001;23(10):978-8.
REFERENCES
1. Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosis.Am J Med 1993;94:646-50.
2. Barrett-Connor E.The economic and human cost of osteoporotic fracture. Am J Med 1995;98(24):24-35.
3. Goeree ROB, Pettitt D B, Cuddy L, Ferraz M,Adachi J.An assessment of the burden of illness due to osteoporosis in Canada. J Soc ObstetGynaecol Can 1996:15-24.
4. Melton LJ III, Chrischilles EA, Cooper C, Lane AW, Riggs BL.Perspective. How many women have osteoporosis? J Bone Miner Res 1992;7:1005-10.
5. Black DM,Arden NK, Palermo L, Pearson J, Cummings SR. Prevalentvertebral deformities predict hip fractures and new vertebral deformi-ties but not wrist fractures. Study of Osteoporotic Fractures ResearchGroup. J Bone Miner Res 1999;14:821-8.
6. Lindsay R, Silverman SL, Cooper C, Hanley DA, Barton I, Broy SB, et al.Risk of new vertebral fracture in the year following a fracture. J AmMed Assoc 2001;285:320-3.
7. Chrischilles EA, Butler CD, Davis CS,Wallace RB. A model of lifetimeosteoporosis impact. Arch Intern Med 1991;151:2026-32.
8. Cauley JA,Thompson DE, Ensrud KC, Scott JC, Black DM. Risk of mor-tality following clinical fractures. Osteoporos Int 2000;11:556-61.
9. Cooper C,Atkinson EJ, Jacobsen SJ, O'Fallon WM, Melton LJ.Population-based study of survival after osteoporotic fractures.Am J Epidemiol 1993;137:1001-5.
10. Center JR, Nguyen TV, Schneider D, Sambrook PN, Eisman JA. Mortalityafter all major types of osteoporotic fracture in men and women: anobservational study. Lancet 1999;353:878-82.
11. Cooper C,Atkinson EJ, O'Fallon WM, Melton LJ III. Incidence of clinical-ly diagnosed vertebral fractures: a population-based study in Rochester,Minnesota, 1985-1989. J Bone Miner Res 1992;7:221-7.
12. Gold DT.The clinical impact of vertebral fractures: quality of life inwomen with osteoporosis. Bone 1996;18:185S-189S.
13. Riggs BL, Melton LJ.The worldwide problem of osteoporosis: insightsafforded by epidemiology. Bone 1995;17:505S-511S.
14. Becker RR, Davies KM, Hinders SM, Heaney RP. Bone gain in youngadult women. J Am Med Assoc 1992;268:2403-8.
15. Scientific Advisory Board, Osteoporosis Society of Canada. Clinicalpractice guidelines for the diagnosis and management of osteoporosis.Can Med Assoc J 1996;155:1113-33.
16. Murray TM. Prevention and management of osteoporosis: consensusstatements from the Scientific Advisory Board of the OsteoporosisSociety of Canada. 4. Calcium nutrition and osteoporosis. Can MedAssoc J 1996;155:935-9.
17. Smith EL.The role of exercise in the prevention and treatment ofosteoporosis [review].Tap Geriatr Rehab 1995;10:55-63.
18. Jaglal SB, Kreiger N, Darlington G. Past and recent physical activity andrisk of hip fracture. Am J Epidemiol 1993;138:107-18.
19. Kerr DA, Prince RL, Morton A, Dick I. Does high resistance weighttraining have a greater effect on bone mass than low resistance weighttraining? [abstract, 128]. J Bone Miner Res 1994;9(suppl 1):S152.
20. Dalsky GP, Stocke KS, Ehsani AA, Slatopolsky E, Lee WC, Birge SJ Jr.Weight-bearing exercise training and lumbar bone mineral content inpostmenopausal women. Ann Intern Med 1998;108:824-8.
21. Harrison JE, Chow R, Dornan J, Goodwin S, Strauss A. Evaluation of aprogram for rehabilitation of osteoporotic patients (PRO): 4-year fol-low-up.The Bone and Mineral Group of the University of Toronto.Osteoporos Int 1993;3:13-7.
22. Cummings SR,Nevitt MC,Browner WS, Stone K, Fox KM,Ensrud KE, etal. Risk factors for hip fracture in white women. Study of OsteoporoticFractures Research Group.N Engl J Med 1995;332:767-73.
23. Chow R, Harrison JE, Notarius C. Effect of two randomised exerciseprogrammes on bone mass of healthy postmenopausal women. Br MedJ 1987;295:1441-4.
24. Cauley JA, Seeley DG,Browner WS, Ensrud K,Kuller LH, Lipschutz RC,et al. Estrogen replacement therapy and mortality among older women.The study of osteoporotic fractures. Arch Intern Med 1997;157:2181-7.
25. Meunier PJ, Confavreux E,Tupinon I, Hardouin C, Delmas PD, Balena R.Prevention of early postmenopausal bone loss with cyclical etidronatetherapy (a double-blind, placebo-controlled study and 1-year follow-up).J Clin Endocrinol Metab 1997;82:2784-91.
26. Herd RJ, Balena R, Blake GM, Ryan PJ, Fogelman I.The prevention ofearly postmenopausal bone loss by cyclical etidronate therapy: a 2-year,double-blind, placebo-controlled study. Am J Med 1997;103:92-9.
27. Pouilles JM,Tremollieres F, Roux C, Sebert JL,Alexandre C, Goldberg D,et al. Effects of cyclical editronate therapy on bone loss in earlypostmenopausal women who are not undergoing hormonalreplacement therapy. Osteoporos Int 1997;7:213-8.
28. Hosking D, Chilvers CE, Christiansen C, Ravn P,Wasnich R, Ross P, et al.Prevention of bone loss with alendronate in postmenopausal womenunder 60 years of age. Early Postmenopausal Intervention CohortStudy Group. N Engl J Med 1998;338:485-92.
* Pharmacotherapy. J Obstet Gynaecol Can. 2001;11:1105-14.
JOGC OCTOBER 200244
29. Mortensen L, Charles P, Bekker PJ, Digennaro J, Johnston CC.Risedronate increases bone mass in an early postmenopausal population: two years of treatment plus one year of follow-up. J ClinEndocrinol Metab 1998;83:396-402.
30. Delmas PD, Bjarnason NH, Mitlak BH, Ravoux AC, Shah AS, Huster WJ,et al. Effects of raloxifene on bone mineral density, serum cholesterolconcentrations, and uterine endometrium in postmenopausal women.N Engl J Med 1997;337:1641-7.
31. Ravn P,Weiss SR, Rodriguez-Portales JA, McClung MR,Wasnich RD,Gilchrist NL, et al.Alendronate in early postmenopausal women: effectson bone mass during long-term treatment and after withdrawal.Alen-dronate Osteoporosis Prevention Study Group. J Clin EndocrinolMetab 2000;85:1492-7.
32. Kreiger N,Bentvelsen K,Tenenhouse A.The Epidemiology ofOsteoporotic Fracture. J Soc Obstet Gynaecol Can 1997;19:1059-74.
33. Lydick E,Zimmerman SI,Yawn B, Love B,Kleerekoper M,Ross P, et al.Development and validation of a discriminative quality of lifequestionnaire for osteoporosis (the OPTQoL). J Bone Miner Res1997;12:456-63.
34. Cadarette SM, Jaglal SB, Murray TM.Validation of the simple calculatedosteoporosis risk estimation (SCORE) for patient selection for bonedensitometry. Osteoporos Int 1999;10:85-90.
35. Cadarette SM, Jaglal SB, Kreiger N, McIsaac WJ, Darlington GA,Tu JV.Development and validation of the Osteoporosis Risk AssessmentInstrument to facilitate selection of women for bone densitometry.Can Med Assoc J 2000;162:1289-94.
36. Cadarette SM, et al. Evaluation of decisions for referrring women forbone densitometry by dual-energy ray absorpitometry. J Am Med Assoc2001;286:57-63.
37. Torgerson DJ, Campbell MK,Thomas RE, Reid DM. Prediction of peri-menopausal fractures by bone mineral density and other risk factors.J Bone Miner Res 1996;11:293-7.
38. Osteoporosis: review of the evidence for prevention, diagnosis andtreatment and cost-effectiveness analysis. Introduction. Osteoporos Int1998;8:S7-80.
39. Osteoporosis: review of the evidence for prevention, diagnosis andtreatment and cost-effectiveness analysis. Executive summary. Osteo-poros Int 1998;8:S3-6.
40. Josse R, Hanley D, Lentle B. Diagnostic technologies:A position state-ment from the Osteoporosis Society of Canada. Osteoporosis Update1999;3.
41. Bauer DC, Gluer CC, Cauley JA,Vogt TM, Ensrud KE, Genant HK, et al.Broadband ultrasound attenuation predicts fractures strongly and inde-pendently of densitometry in older women. A prospective study. Studyof Osteoporotic Fractures Research Group. Arch Intern Med1997;157:629-34.
42. Hans D, Dargent-Molina P, Schott AM, Sebert JL, Cormier C, Kotzki PO,et al. Ultrasonographic heel measurements to predict hip fracture inelderly women: the EPIDOS prospective study. Lancet 1996;348:511-4.
43. World Health Organization (WHO) guidelines for the interpretation ofBMD readings.WHO Study Group Report.WHO Tech Rep Ser1994;843:1-129.
44. Kanis JA, Melton LJ, Christiansen C, Johnston CC, Khaltaev N.The diag-nosis of osteoporosis. J Bone Miner Res 1994;9:1137-41.
45. Kanis JA,Gluer CC. An update on the diagnosis and assessment ofosteoporosis with densitometry.Committee of Scientific Advisors, Inter-national Osteoporosis Foundation.Osteoporos Int 2000;11:192-202.
46. Greenspan SL, Bouxsein ML, Melton ME, Kolodny AH, Clair JH, DeluccaPT, et al. Precision and discriminatory ability of calcaneal bone assess-ment technologies. J Bone Miner Res 1997;12:1303-13.
47. Sturtridge W, Lentle B, Hanley DA. The use of bone density measure-ment in the diagnosis and management of osteoporosis. Can MedAssoc J 1996; 155(7):924-9.
48. Uebelhart D,Schlemmer A, Johansen JS,Gineyts E,Christiansen C,Delmas PD.Effect of menopause and hormone replacement therapy on theurinary excretion of pyridiium cross-links.Clin Endocrinol Metab199;72:367-73.
49. Prestwood KM, Pilbeam CC, Burleson JA,Woodiel FN, Delmas PD,Deftos LJ, et al.The short-term effects of conjugated estrogen on boneturnover in older women. JCEM 1994;79(2):366-71.
50. Pols HA, Felsenberg D, Hanley DA, Stepan J, Munoz-Torres M,Wilkin TJ,et al. Multinational, placebo-controlled, randomized trial of the effectsof alendronate on bone density and fracture risk in postmenopausalwomen with low bone mass: results of the FOSIT study. Foxamax International Trial Study Group. Osteoporos Int 1999;9:461-8.
51. Johnson CC, et al.Clinical, biochemical, radiographic epidemiologic andeconomic features of osteoporosis.Orthop Clin N Am 1981;12:559-69.
52. Adachi JD, Olszynski WP, Hanley DA, Hodsman AB, Kendler DL,Siminoski KG, et al.“Management of Corticosteroid-InducedOsteoporosis.” Seminars in Arthritis and Rheumatism,Vol 29, No. 4,228-51. (2000).
53. Watts NB, Harris ST, Genant HK,Wasnich RD, Miller PD, Jackson RD,et al. Intermittent cyclical etidronate treatment of postmenopausalosteoporosis. N Engl J Med 1990;323:73-9.
54. Harris ST,Watts NB, Jackson RD, Genant HK,Wasnich RD, Ross P, et al.Four-year study of intermittent cyclic etidronate treatment ofpostmenopausal osteoporosis: three years of blinded therapy followedby one year of open therapy. Am J Med 1993;95:557-67.
55. Miller PD,Watts NB, Licata AA, Harris ST, Genant HK,Wasnich RD,et al. Cyclical etidronate in the treatment of postmenopausalosteoporosis: efficacy and safety after seven years of treatment.Am J Med 1997;103:468-76.
56. Black DM, Cummings SR, Karpf DB,Cauley JA,Thompson DE, NevittMC, et al. Randomised trial of effect of alendronate on risk of fracturein women with existing vertebral fractures. Fracture Intervention TrialResearch Group. Lancet 1996;348:1535-41.
57. Harris ST,Watts NB, Genant HK, McKeever CD, Hangartner T, Keller M,et al. Effects of risedronate treatment on vertebral and nonvertebralfractures in women with postmenopausal osteoporosis: a randomizedcontrolled trial.Vertebral Efficacy With Risedronate Therapy (VERT)Study Group. J Am Med Assoc 1999;282:1344-52.
58. Ettinger B, Black DM, Mitlak BH, Knickerbocker RK, Nickelsen T,Genant HK, et al. Reduction of vertebral fracture risk in postmeno-pausal women with osteoporosis treated with raloxifene: results from a3-year randomized clinical trial. Multiple Outcomes of Raloxifene Evalu-ation (MORE) Investigators. J Am Med Assoc 1999;282:637-45.
59. Cummings SR,Black DM,Thompson DE,Applegate WB,Barrett-Connor E,Musliner TA,et al. Effect of alendronate on risk of fracture inwomen with low bone density but without vertebral fractures: resultsfrom the Fracture Intervention Trial. J Am Med Assoc 1998;280:2077-82.
60. Reginster J, Minne HW, Sorensen OH, Hooper M, Roux C, Brandi ML,et al. Randomized trial of the effects of risedronate on vertebral frac-tures in women with established postmenopausal osteoporosis.Verte-bral Efficacy with Risedronate Therapy (VERT) Study Group.Osteoporos Int 2000;11:83-91.
61. Chesnut CH 3rd, Silverman S,Andriano K, Genant G, Gimona A,Harris S, et al.A randomized trial of nasal spray salmon calcitonin inpost-menopausal women with established osteoporosis: the preventrecurrence of osteoporotic fractures study. PROOF Study Group.Am J Med 2000;109:267-76.
62. McClung MR, Geusens P, Miller PD, Zippel H, Bensen WG, Roux C, etal. Effect of risedronate on the risk of hip fracture in elderly women.Hip Intervention Program Study Group. N Engl J Med 2001;344:333-40.
63. Wallach S, Cohen S, Reid DM, Hughes RA, Hosking DJ, Laan RF, et al.Effects of risedronate treatment on bone density and vertebral fracturein patients on corticosteroid therapy. Calcif Tissue Int 2000;67:277-85.
64. Saag KG, Emkey R, Schnitzer TJ, Brown JP, Hawkins F, Goemaere S, et al.Alendronate for the prevention and treatment of glucocorticoid-induced osteoporosis. Glucocorticoid-Induced Osteoporosis Interven-tion Study Group. N Engl J Med 1998;339:292-9.
65. Adachi JD, Bensen WG, Brown J, Hanley D, Hodsman A, Josse R, et al.Intermittent etidronate therapy to prevent corticosteroid-inducedosteoporosis. N Engl J Med 1997;337:382-7.
JOGC OCTOBER 200245
66. Ettinger B, Genant HK, Cann CE. Long-term estrogen replacementtherapy prevents bone loss and fractures. Ann Intern Med1985;102:319-24.
67. Nachtigall LE, Nachtigall RH, Nachtigall RD, Beckman EM. Estrogenreplacement therapy I: a 10-year prospective study in the relationshipto osteoporosis. Obstet Gynecol 1979;53:277-81.
68. Lufkin EG,Wahner HW, O'Fallon WM, Hodgson SF, Kotowica MA,Lane AW, et al.Treatment of postmenopausal osteoporosis with trans-dermal estrogen. Ann Intern Med 1992;117:1-9.
69. Grodstein F, Stampfer MJ, Colditz GA,Willett WC, Manson JE, Joffe M,et al. Postmenopausal hormone therapy and mortality. N Engl J Med1997;336:1769-75.
70. Schneider DL, Barrett-Connor EL, Morton DJ.Timing of postmeno-pausal estrogen for optimal bone mineral density.The Rancho BernardoStudy. J Am Med Assoc 1997;277:543-7.
71. Genant HK, Lucas J,Weiss S,Akin M, Emkey R, McNaney-Flint H, et al.Low-dose esterified estrogen therapy: effects on bone, plasma estradiolconcentrations, endometrium, and lipid levels. Estratab/OsteoporosisStudy Group. Arch Intern Med 1997;157:2609-15.
72. Writing Group for the Women’s Health Initiative Investigators. JAMA,2002;288:321-33.
73. Storm T,Thamsborg G, Steiniche T, Genant HK, Sorensen OH. Effect ofintermittent cyclical etidronate therapy on bone mass and fracture ratein women with postmenopausal osteoporosis. N Engl J Med1990;322:1265-71.
74. van Staa TP, Abenhaim L, Cooper C. Use of cyclical etidronate and pre-vention of non-vertebral fractures. Br J Rheumatol 1998;37:87-94.
75. Boyce BF, Smith L, Fogelman I, Johnston E, Ralston S, Boyle H. Focalosteomalacia due to low dose diphosphonate therapy in Paget'sdisease. Lancet 1984;1:821-4.
76. Frith J, Monkkonen J, Blackburn GM, Russell RG, Rogers MJ. Clodronateand liposome-encapsulated clodronate are metabolized to a toxic ATPanalog adenosine 5'- (beta, gamma-dichloromethylene) triphosphate, bymammali cells in vitro. J Bone Miner Res 1997;12:1358-67.
77. Luckman SP, Hughes DE, Coxon FP, Graham R, Russell G, Rogers MJ.Nitrogen-containing bisphosphonates inhibit the mevalonic acid path-way and prevent post-translational prenylation of GTP binding proteinsincluding Ras. J Bone Miner Res 1998;13:581-9.
78. Liberman UA,Weiss SR, Broll J, Minne HW, Quan H, Bell NH, et al.Effect of oral alendronate on bone mineral density and the incidence offractures in postmenopausal osteoporosis.The Alendronate Phase IIIOsteoporosis Treatment Study Group. N Engl J Med 1995;333:1437-43.
79. Schnitzer T, Bone HG, Crepaldi G,Adami S, McClung M, Kiel D, et al.Therapeutic equivalence of alendronate 70 mg once-weekly and alen-dronate 10 mg daily in the treatment of osteoporosis. AlendronateOnce-Weekly Study Group. Aging (Milano) 2000;12:1-12.
80. Rodan GA, Fleisch HA. Bisphosphonates: mechanism of action. J ClinInvest 1996;97:2692-6.
81. Cosman F, Nieves J,Woelfert L, Forrnica C, Gordon S, Shen V, et al.Parathyroid hormone added to established hormone therapy: effects on vertebral fracture and maintenance of bone mass after parathyroidhormone withdrawal. J Bone Miner Res 2001;16(5):925-31.
82. Riggs BL, Hodgson SF, O'Fallon WM, Chao EY,Wahner HW, Muhs JM, etal. Effect of fluoride treatment on the fracture rate in postmenopausalwomen with osteoporosis. N Engl J Med 1990;322:802-9.
83. Bone HG, Greenspan SL, McKeever C, Bell N, Davidson M, Downs RW,et al. Alendronate and estrogen effects in postmenopausal women withlow bone mineral density. Alendronate/Estrogen Study Group. J ClinEndocrinol Metab 2000;85:720-6.
84. Lindsay R, Cosman F, Lobo RA,Walsh BW, Harris ST, Reagan JE, et al.Addition of alendronate to ongoing hormone replacement therapy inthe treatment of osteoporosis: a randomized, controlled clinical trial.J Clin Endocrinol Metab 1999;84:3076-81.
85. Wimalawansa SJ. Combined therapy with estrogen and etidronate hasan additive effect on bone mineral density in the hip and vertebrae:four-year randomized study. Am J Med 1995;99:36-42.
86. Tonino RP, Meunier PJ, Emkey R, Rodriguez-Portales JA, Menkes CJ,Wasnich RD, et al. Skeletal benefits of alendronate: 7-year treatment of postmenopausal osteoporotic women. Phase III Osteoporosis Treatment Study Group. J Clin Endocrinol Metab 2000;85:3109-15.

JOGC OCTOBER 200246
INTRODUCTION
Urinary complaints, including stress incontinence, urge inconti-nence, and recurrent urinary tract infection, are common amongwomen in their postmenopausal years. They result at least partlyfrom urogenital aging, a progressive and variable condition thatoccurs as a result of both estrogen deprivation and tissue aging itself.1
The female introitus, vagina, bladder, and urethra are allderived from the primitive urogenital sinus. Estrogen recep-tors have been found in all of these structures2 and possibly inthe pelvic floor musculature1 and anorectum3 as well. Theshared embryology of these organs accounts for their similarhormonal responsiveness.
In the markedly estrogen-reduced state of menopause, uro-genital epithelial and subepithelial tissues become thinned andflattened. Urethral mucosal thickness and blood vessel engorge-ment decline, resulting in a reduction in mean urethral clo-sure pressure.4 Urethral collagen content and elasticity alsodecrease,5 further compromising function and favouring thedevelopment of urethral sphincter incompetence. In the blad-der, mucosal thinning with estrogen loss lowers the sensorythreshold for detrusor contraction, resulting in irritative symp-toms including urinary frequency, nocturia, and urge inconti-nence.6 Alterations in the natural vaginal and urethral flora anda rise in vaginal pH are thought to contribute to an increasedincidence of lower urinary tract infection.7 Finally, estrogendeprivation may contribute to a loss of pelvic floor tone8 andcollagen content,9 weakening musculofascial support for thepelvic organs and vaginal walls. Pelvic organ prolapse can thusbe considered a consequence of urogenital aging, though this isa multifactorial problem not solely related to hypoestrogenism.
Studies on human tissues have not consistently docu-mented the presence of progesterone receptors in either thebladder or the urethra.2 If progesterone receptors are indeedpresent in the human urinary tract, their number is low. Prog-estins, in either high or low levels, would thus not be expect-ed to exert any effects on urethral or bladder function.
Urinary incontinence of all forms has been reported in 10 to30 percent of postmenopausal women.10,11 The prevalence of urgeincontinence seems to increase with the number of years aftermenopause. In contrast, the prevalence of stress incontinence ishighest in the perimenopausal years, with no marked increasethereafter (Figures 1 and 2).12 Ten to 15 percent of post-menopausal women suffer from recurrent urinary tract infections.7
UROGENITAL AGING
SYMPTOMS
Studies of the prevalence of urogenital symptoms in post-menopausal women are limited. Affected individuals may notreport symptoms, or their complaints may be deferred orignored. The true extent of the problem of urogenital aging istherefore difficult to assess.
Symptoms related to urogenital aging may precede physi-cal findings (Table 1). The first symptom reported is oftenreduced lubrication on sexual arousal.13 Superficial dyspareu-nia is common, and postcoital bleeding may occur.13 Additionalsymptoms include pruritus, dysuria, and vaginal discharge relat-ed to inflammation or infection.13 Urinary symptoms includeincontinence, urgency, frequency, nocturia, and dysuria.1,13
Incontinence may be related to physical effort (stress) or tourgency, but is often mixed. Coital incontinence may occur,which may further contribute to sexual dysfunction.13 Symp-toms of pelvic organ prolapse include pelvic heaviness andintroital bulging.14 Voiding difficulty from urethral kinking15
or fecal incontinence16 can be associated with prolapse.
PHYSICAL FINDINGS
Due to a loss of rugae, the postmenopausal hypoestrogenic vagi-na is foreshortened, smooth, and narrowed. The vulvovaginalepithelium is comparatively pale, thin, and friable. Decreasedtissue elasticity may cause introital narrowing and limited vagi-nal mobility. Pelvic floor relaxation with prolapse of the vaginalwalls or uterus is often present. Estrogen deficiency results in arelative degree of narrowing and retraction of the urethral mea-tus toward the introitus.13 Urethral prolapse can occur. Like thevagina, the urethral and bladder mucosa appear pale and thin atthe time of cystoscopy, especially in the area of the trigone.
INVESTIGATING URINARY INCONTINENCE
Urinary incontinence affects each woman’s quality of life dif-ferently. Decisions regarding investigation and treatmentshould be patient-motivated. After a complete history andphysical examination, initial evaluation of the incontinentfemale should include a screening urine culture and a mea-surement of residual urine volume. Urine cytology and cys-toscopy should be reserved for those patients with irritativesymptoms, recurrent infection or hematuria. Urodynamic testsshould be performed when urinary symptoms are mixed (both
Shawna Johnston, MD, FRCSC1
1 Kingston ON
UROGENITAL HEALTH
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
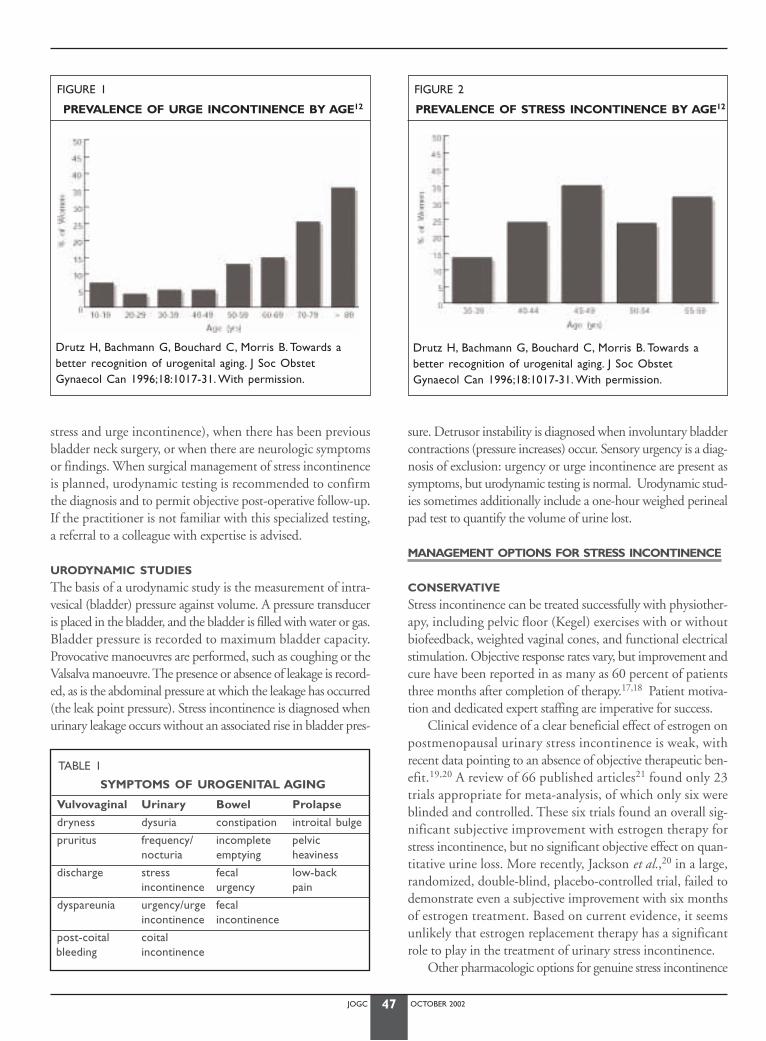
JOGC OCTOBER 200247
stress and urge incontinence), when there has been previousbladder neck surgery, or when there are neurologic symptomsor findings. When surgical management of stress incontinenceis planned, urodynamic testing is recommended to confirmthe diagnosis and to permit objective post-operative follow-up.If the practitioner is not familiar with this specialized testing,a referral to a colleague with expertise is advised.
URODYNAMIC STUDIES
The basis of a urodynamic study is the measurement of intra-vesical (bladder) pressure against volume. A pressure transduceris placed in the bladder, and the bladder is filled with water or gas.Bladder pressure is recorded to maximum bladder capacity.Provocative manoeuvres are performed, such as coughing or theValsalva manoeuvre. The presence or absence of leakage is record-ed, as is the abdominal pressure at which the leakage has occurred(the leak point pressure). Stress incontinence is diagnosed whenurinary leakage occurs without an associated rise in bladder pres-
sure. Detrusor instability is diagnosed when involuntary bladdercontractions (pressure increases) occur. Sensory urgency is a diag-nosis of exclusion: urgency or urge incontinence are present assymptoms, but urodynamic testing is normal. Urodynamic stud-ies sometimes additionally include a one-hour weighed perinealpad test to quantify the volume of urine lost.
MANAGEMENT OPTIONS FOR STRESS INCONTINENCE
CONSERVATIVE
Stress incontinence can be treated successfully with physiother-apy, including pelvic floor (Kegel) exercises with or withoutbiofeedback, weighted vaginal cones, and functional electricalstimulation. Objective response rates vary, but improvement andcure have been reported in as many as 60 percent of patientsthree months after completion of therapy.17,18 Patient motiva-tion and dedicated expert staffing are imperative for success.
Clinical evidence of a clear beneficial effect of estrogen onpostmenopausal urinary stress incontinence is weak, withrecent data pointing to an absence of objective therapeutic ben-efit.19,20 A review of 66 published articles21 found only 23trials appropriate for meta-analysis, of which only six wereblinded and controlled. These six trials found an overall sig-nificant subjective improvement with estrogen therapy forstress incontinence, but no significant objective effect on quan-titative urine loss. More recently, Jackson et al.,20 in a large,randomized, double-blind, placebo-controlled trial, failed todemonstrate even a subjective improvement with six monthsof estrogen treatment. Based on current evidence, it seemsunlikely that estrogen replacement therapy has a significantrole to play in the treatment of urinary stress incontinence.
Other pharmacologic options for genuine stress incontinence
FIGURE 1
PREVALENCE OF URGE INCONTINENCE BY AGE12
FIGURE 2
PREVALENCE OF STRESS INCONTINENCE BY AGE12
TABLE 1
SYMPTOMS OF UROGENITAL AGING
Vulvovaginal Urinary Bowel Prolapse
dryness dysuria constipation introital bulge
pruritus frequency/ incomplete pelvicnocturia emptying heaviness
discharge stress fecal low-backincontinence urgency pain
dyspareunia urgency/urge fecalincontinence incontinence
post-coital coitalbleeding incontinence
Drutz H, Bachmann G, Bouchard C, Morris B. Towards a better recognition of urogenital aging. J Soc Obstet Gynaecol Can 1996;18:1017-31. With permission.
Drutz H, Bachmann G, Bouchard C, Morris B. Towards a better recognition of urogenital aging. J Soc Obstet Gynaecol Can 1996;18:1017-31. With permission.
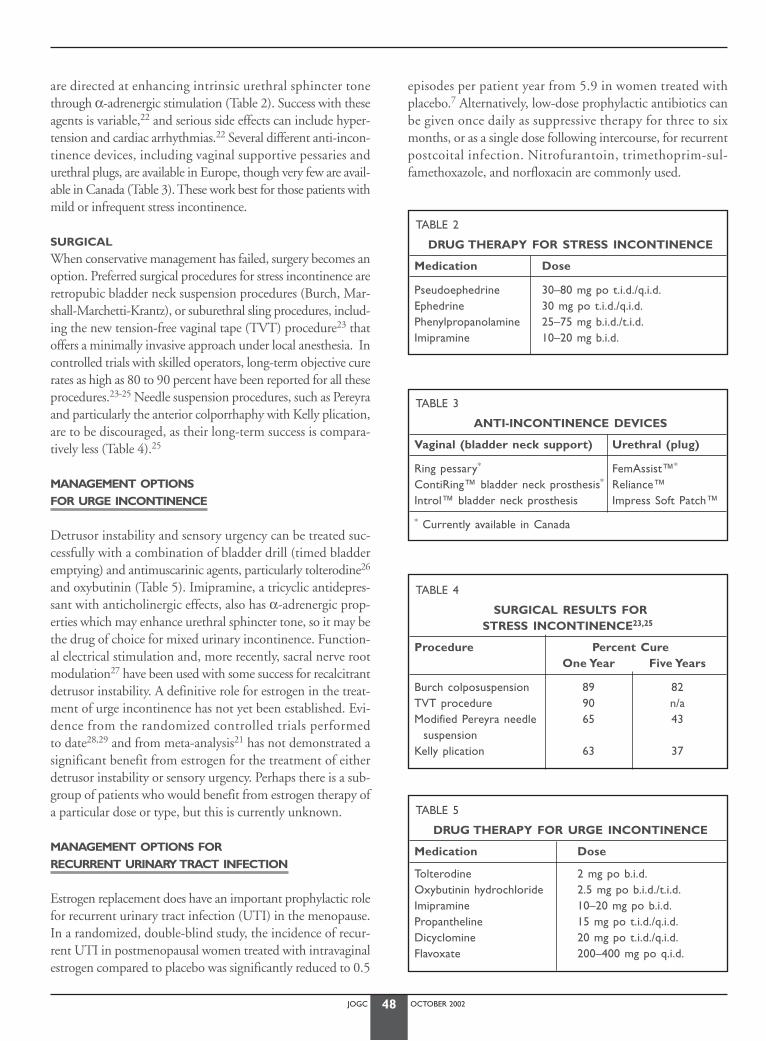
JOGC OCTOBER 200248
are directed at enhancing intrinsic urethral sphincter tonethrough α-adrenergic stimulation (Table 2). Success with theseagents is variable,22 and serious side effects can include hyper-tension and cardiac arrhythmias.22 Several different anti-incon-tinence devices, including vaginal supportive pessaries andurethral plugs, are available in Europe, though very few are avail-able in Canada (Table 3). These work best for those patients withmild or infrequent stress incontinence.
SURGICAL
When conservative management has failed, surgery becomes anoption. Preferred surgical procedures for stress incontinence areretropubic bladder neck suspension procedures (Burch, Mar-shall-Marchetti-Krantz), or suburethral sling procedures, includ-ing the new tension-free vaginal tape (TVT) procedure23 thatoffers a minimally invasive approach under local anesthesia. Incontrolled trials with skilled operators, long-term objective curerates as high as 80 to 90 percent have been reported for all theseprocedures.23-25 Needle suspension procedures, such as Pereyraand particularly the anterior colporrhaphy with Kelly plication,are to be discouraged, as their long-term success is compara-tively less (Table 4).25
MANAGEMENT OPTIONS FOR URGE INCONTINENCE
Detrusor instability and sensory urgency can be treated suc-cessfully with a combination of bladder drill (timed bladderemptying) and antimuscarinic agents, particularly tolterodine26
and oxybutinin (Table 5). Imipramine, a tricyclic antidepres-sant with anticholinergic effects, also has α-adrenergic prop-erties which may enhance urethral sphincter tone, so it may bethe drug of choice for mixed urinary incontinence. Function-al electrical stimulation and, more recently, sacral nerve rootmodulation27 have been used with some success for recalcitrantdetrusor instability. A definitive role for estrogen in the treat-ment of urge incontinence has not yet been established. Evi-dence from the randomized controlled trials performed to date28,29 and from meta-analysis21 has not demonstrated asignificant benefit from estrogen for the treatment of either detrusor instability or sensory urgency. Perhaps there is a sub-group of patients who would benefit from estrogen therapy ofa particular dose or type, but this is currently unknown.
MANAGEMENT OPTIONS FOR RECURRENT URINARY TRACT INFECTION
Estrogen replacement does have an important prophylactic rolefor recurrent urinary tract infection (UTI) in the menopause.In a randomized, double-blind study, the incidence of recur-rent UTI in postmenopausal women treated with intravaginalestrogen compared to placebo was significantly reduced to 0.5
episodes per patient year from 5.9 in women treated withplacebo.7 Alternatively, low-dose prophylactic antibiotics canbe given once daily as suppressive therapy for three to sixmonths, or as a single dose following intercourse, for recurrentpostcoital infection. Nitrofurantoin, trimethoprim-sul-famethoxazole, and norfloxacin are commonly used.
TABLE 2
DRUG THERAPY FOR STRESS INCONTINENCE
Medication Dose
Pseudoephedrine 30–80 mg po t.i.d./q.i.d.Ephedrine 30 mg po t.i.d./q.i.d.Phenylpropanolamine 25–75 mg b.i.d./t.i.d.Imipramine 10–20 mg b.i.d.
TABLE 3
ANTI-INCONTINENCE DEVICES
Vaginal (bladder neck support) Urethral (plug)
Ring pessary* FemAssist™*
ContiRing™ bladder neck prosthesis* Reliance™Introl™ bladder neck prosthesis Impress Soft Patch™
* Currently available in Canada
TABLE 4
SURGICAL RESULTS FOR STRESS INCONTINENCE23,25
Procedure Percent CureOne Year Five Years
Burch colposuspension 89 82TVT procedure 90 n/aModified Pereyra needle 65 43
suspensionKelly plication 63 37
TABLE 5
DRUG THERAPY FOR URGE INCONTINENCE
Medication Dose
Tolterodine 2 mg po b.i.d.Oxybutinin hydrochloride 2.5 mg po b.i.d./t.i.d.Imipramine 10–20 mg po b.i.d.Propantheline 15 mg po t.i.d./q.i.d.Dicyclomine 20 mg po t.i.d./q.i.d.Flavoxate 200–400 mg po q.i.d.

JOGC OCTOBER 200249
ESTROGEN IN THE TREATMENT OF PROLAPSE
Pelvic organ prolapse is managed with a pessary or with surgery.When a pessary is used in the menopausal patient, maintenancetherapy with estrogen (local or systemic) may be helpful in pre-venting vaginal ulceration and infection. The value of estrogenitself in maintaining or improving pelvic support remainsunclear, although the presence of estrogen receptors in theendopelvic fascia and pelvic floor musculature suggests a poten-tial beneficial effect. Skin thickness and dermal collagen contentdecline after menopause.30 These changes are reversed in part byestrogen replacement. A similar situation may exist for the col-lagen of the pelvic floor and vaginal fascia;31 if so, estrogen ther-apy may help to maintain existing collagen or reverse thesecollagen changes. Preliminary evidence points to a decrease indescent of the bladder base, demonstrated by videourodynam-ics, after estrogen administration in postmenopausal women.8
Additional unresolved questions include whether or notestrogen administered before vaginal surgery can improve tissue planes and promote mucosal healing. Mikklesen etal.32 reported that rates of recurrent prolapse after surgery weresimilar in women receiving intravaginal estradiol or placebopreoperatively.
ESTROGEN IN THE TREATMENT OF FECAL INCONTINENCE
Fecal incontinence is reported in 15 to 26 percent of womenwith urinary incontinence,33 likely because both conditions arisefrom pelvic floor neuromuscular dysfunction. As with urinaryincontinence, fecal incontinence may be partly due to alteredhormonal factors that include lower estrogen levels aftermenopause. Estrogen receptors are present in high number inthe anorectum,3 suggesting that these tissues are also a targetsite for estrogen action. To date, limited observational data showsubjective improvement in flatal incontinence and fecal stain-ing after estrogen treatment, with objective improvement inanal resting and squeeze pressures.16 Further study is neededbefore a therapeutic role for estrogen in postmenopausal fecalincontinence can be established.
RECOMMENDATIONS:
F1. Urodynamic studies should be performed prior toincontinence surgery or when there is mixed inconti-nence. (II-3)
SUMMARY OF KEY POINTS:
F2. Urogenital aging may result in urinary urge and stressincontinence, recurrent urinary tract infection, andpelvic organ prolapse.
F3. There is no objective benefit from estrogen replacementtherapy for postmenopausal urinary stress incontinence. (I)
F4. There is neither objective nor subjective benefit fromestrogen replacement therapy for postmenopausal urgeincontinence. (I)
F5. Estrogen therapy decreases the incidence of recurrenturinary tract infections in postmenopausal women. (I)
CONCLUSION
Urinary incontinence of all types is common amongmenopausal women. At least in part, it is the consequence ofurogenital aging. Many effective treatment options are avail-able, including both conservative (non-surgical) and surgicalapproaches. Based on the current available literature, however,there is no proven benefit from estrogen replacement therapyfor the treatment of urinary incontinence. Estrogen replacementhas a proven role as a prophylactic agent for recurrent urinarytract infection in postmenopausal women. Its role in the pre-vention or treatment of pelvic organ prolapse and fecal incon-tinence is largely unstudied and thus unknown.
J Obstet Gynaecol Can 2001;23(10):973-7.
REFERENCES
1. Griebling TL, Nygaard IE. The role of estrogen replacement therapy inthe management of urinary incontinence and urinary tract infection inpostmenopausal women. Endocrinol Metab Clin North Amer1997;26:347-60.
2. Iosif CS, Batra SC, Ek A, Astedt Bl. Estrogen receptors in the humanfemale urinary tract. Am J Obstet Gynecol 1981;141:817-820.
3. Oettling G, Franz HB. Mapping of androgen, estrogen andprogesterone receptors in the anal continence organ. Eur J ObstetGynecol Reprod Biol 1998;77:211-6.
4. Hilton P, Stanton SL.The use of intravaginal estrogen cream in genuinestress incontinence. Br J Obstet Gynaecol 1983;90:940-4.
5. Versi E, Cardozo L, Brincat M, Cooper D, Montgomery J, Stuno JW.Correlation of urethral physiology and skin collagen in post-menopausal women. Br J Obstet Gynaecol 1988; 95:147-52.
6. Fantl JA,Wyman JF,Anderson RL, Matt DW, Bump RC. Postmenopausalurinary incontinence: a comparison between non-estrogen-supplemented and estrogen-supplemented females. Obstet Gynecol1988;71:823-8.
7. Raz R, Stamm W. A controlled trial of intravaginal estriol inpostmenopausal women with recurrent urinary tract infections.N Engl J Med 1993:329:753-6.
8. Cardozo LD. Role of estrogens in the treatment of female urinaryincontinence. J Am Geriatr Soc 1990;38:326-8.
9. Falconer C, Ekman G, Malmstrom A, Ulmsten U. Decreased collagensynthesis in stress incontinent women. Obstet Gynecol 1994;84:583-6.
10. Mallet VT, Bump RC.The epidemiology of female pelvic floor dysfunction. Curr Opin Obstet Gynecol 1994;6:308-12.
11. Milsom I, Ekelund P,Molander U, Arvidsson L, Areskoug B. Theinfluence of age, parity, oral contraception, hysterectomy and menopause on the prevalence of urinary incontinence in women.J Urol 1993;149:1459-62.
12. Drutz H,Bachmann G,Bouchard C,Morris B.Towards a better recognition of urogenital aging. J Soc Obstet Gynaecol Can1996;18:1017:31.
JOGC OCTOBER 200250
13. Bachmann G. Urogenital aging: an old problem newly recognised.Maturitas 1995;22(suppl):1-5.
14. Harrison BP, Cespedes RD. Pelvic organ prolapse. Emerg Med ClinNorth Am 2001;19(3):781-97.
15. Versi E, Lyell DJ, Griffiths DJ. Videourodynamic diagnosis of occult genuine stress incontinence in patients with anterior vaginal wall relaxation. J Soc Gynecol Investig 1998;5(6):327-30.
16. Donnelly V, O’Connell PR, O’Herlihy C. The influence of oestrogenreplacement on faecal incontinence in postmenopausal women.Br J Obstet Gynaecol 1997;104:311-5.
17. Bo K, Hagen RH, Kvarstein B, Jorgensen J, Larsen S. Pelvic floor muscleexercise for the treatment of female stress urinary incontinence: III.Effects of two different degrees of pelvic floor muscle exercises.Neurol Urodyn 1990:489-502.
18. Sand PK, Richardson DA, Staskin DR, Swift SE, Appell RA,WhitmoreKE, et al. Pelvic floor electrical stimulation in the treatment of genuine stress incontinence: a multicenter, placebo-controlled trial.Am J Obstet Gynecol 1995;173:72-9.
19. Fantl JA, Bump RC, Robinson D, McClish DK,Wyman J. Efficacy ofestrogen supplementation in the treatment of urinary incontinence.Obstet Gynecol 1996;88:745-9.
20. Jackson S, Shepherd A, Brookes S,Abrams P. The effect of oestrogensupplementation on post-menopausal urinary stress incontinence: adouble-blind placebo-controlled trial. Br J Obstet Gynaecol1999;106:711-8.
21. Fantl JA, Cardozo L, McClish DK. Estrogen therapy in the managementof urinary incontinence in postmenopausal women: a meta-analysis.First report of the Hormones and Urogenital Therapy Committee.Obstet Gynecol 1994;83:12-18.
22. Sullivan J, Abrams P. Pharmacological management of incontinence.Eur Urol 1999;36:89-95.
23. Ulmsten U, Johnson P, Rezapour M. A three-year follow up of tensionfree vaginal tape for surgical treatment of female stress urinary incontinence. Br J Obstet Gynaecol 1999;106:345-50.
24. Weber AM,Walters MD. Burch procedure compared with sling forstress urinary incontinence: a decision analysis. Obstet Gynecol2000;96:867-73.
25. Bergman A, Elia G.Three surgical procedures for genuine stress incontinence: five-year follow-up of a prospective randomized study.Am J Obstet Gynecol 1995;173:66-71.
26. Appell RA. Clinical efficacy and safety of tolterodine in the treatmentof overactive bladder: a pooled analysis. Urology 1997;50(6A Suppl):90-6; discussion 97-9.
27. Appell RA. Electrical stimulation for the treatment of urinary incontinence. Urology 1998;51(2A suppl):24-6.
28. Cardozo LD, Rekers H,Tapp A, Barnick C, Shepherd A, Schussler B,et al. Oestriol in the treatment of postmenopausal urgency:a multicentre study. Maturitas 1993;18:47-53.
29. Cardozo LD, Kelleher CJ. Sex hormones, the menopause and urinaryproblems. Gynecol Endocrinol 1995;9:75-84.
30. Brincat M, Moniz CJ, Studd JWW, Darby A, Magos A, Emburey G, et al.Long-term effects of the menopause and sex hormones on skin thickness. Br J Obstet Gynaecol 1985;92:256-59.
31. Hughes PN, Jackson SR.The scientific basis of prolapse. The Obstetri-cian and Gynaecologist 2000;2:10-15.
32. Mikklesen AL, Felding C, Clausen HV. Clinical effects of preoperativeoestradiol treatment before vaginal repair operation. A double-blind,randomised trial. Gynaecol Obstet Invest 1995;40:125-8.
33. Khullar V, Damiano R,Tooz-Hobson P, Cardozo L. Prevalence of faecalincontinence among women with urinary incontinence. Br J ObstetGynaecol 1998;105:1211-3.

JOGC OCTOBER 2002
DIABETES MELLITUS
Hormone replacement therapy (HRT) should be discussed withpostmenopausal women who have diabetes mellitus, particu-larly as diabetes is itself a risk factor for cardiovascular disease.1
A recent study recently demonstrated an improvement inglycemic control and serum lipoproteins in postmenopausalType II diabetics after eight weeks of conjugated estrogen (CEE)therapy.2 Estrogens alter glucose and insulin metabolism in dif-ferent ways, depending on the compound used and the routeof delivery.3 Estradiol-17β reduces insulin resistance throughimprovements in insulin sensitivity and elimination. Hyper-triglyceridemia may occur in some diabetic women and, as thiscan be aggravated with oral estrogen therapy, the transdermalroute of estrogen delivery is preferable in these cases.
At present, no data suggest that hormone replacement ther-apy alters the risk of developing diabetes mellitus.
MIGRAINE
Various internal and external factors may trigger migraineheadache. Genetic predisposition may set a lower threshold forthese triggers.4 In women, fluctuating or falling levels of estro-gen appear to be a trigger:5 some women have a history of men-strual migraine, and migraine incidence may increase in themenopausal years.6 Although the influence of HRT on migrainevaries with the individual woman, most evidence suggests aworsening of headaches with use of HRT.7 The constant dailyhormone doses of a continuous-combined regimen may thusbe better tolerated than those of a cyclical regimen. Transder-mal estrogen may similarly afford more steady-state dosing andthus less provocation of migraine headache.
Women with a history of atypical migraines provoked byoral contraceptives will be concerned about the risk of eitherprovoking headaches with HRT or causing a permanent neu-rological abnormality. There are few relevant studies for guid-ance. If neurological symptoms or signs develop or worsen withuse of HRT, it is advisable to withdraw treatment and seek neu-rological consultation for assessment of any abnormality. If it isdetermined that this is atypical migraine, reintroduction of
HRT at a lower dose may be attempted if warranted by thepotential benefits.7 Informed consent for treatment is essential.
SYSTEMIC LUPUS ERYTHEMATOSUS
Data from the Nurses’ Health Study show that postmenopausalHRT is associated with a two-fold increase in the risk of deve-loping systemic lupus erythematosus (SLE).8 The role of estro-gen in exacerbating pre-existing SLE is unclear to date, althoughthe large randomized placebo-controlled SELENA trial study-ing the safety of HRT in SLE is currently under way.9 HRTmay also exacerbate the prothrombotic tendency that exists inpatients with antiphospholipid antibody syndrome.9 At pre-sent, most authors recommend that HRT be used with cautionin patients with active disease.
ARTHRITIS
RHEUMATOID ARTHRITIS
Hormone replacement therapy has not been shown to preventthe development of rheumatoid arthritis in postmenopausalwomen.10,11 Similarly, data from double-blind, randomized, con-trolled trials have shown no convincing effect of HRT on the clin-ical course or disease markers of rheumatoid arthritis.12,13 Womenwith rheumatoid arthritis have diminished bone mass for sever-al reasons, including use of corticosteroids and immobility, andhave an increased risk of fracture.13 Postmenopausal osteoporo-sis further exacerbates these conditions. Treatment options forosteoporosis should be strongly considered in these patients.
OSTEOARTHRITIS
It is still unclear if estrogen withdrawal is implicated in the devel-opment or clinical course of osteoarthritis in women, althoughmost prospective studies suggest HRT may help prevent devel-opment of osteoarthritis in the hip and knee,14 and may have abeneficial modulating effect on clinical and radiological diseaseprogression.15 However, while present epidemiologic evidenceis strongly suggestive of a preventive and therapeutic role forHRT, data from randomized controlled trials is still lacking.
51
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
Shawna L. Johnston, MD, FRCSC,1 Gillian R. Graves, MD, FRCSC,2 David L. Kendler, MD, FRCPC,3
Margo R. Fluker, MD, FRCSC3
1 Kingston ON2 Halifax NS3 Vancouver BC
MEDICAL AND SPECIAL CONDITIONS

PREMATURE OVARIAN FAILURE
Premature ovarian failure (POF) affects one percent of womenunder the age of 40.16 In the absence of a clear cause, such aschromosome abnormalities, chemotherapy, radiation to theovaries or surgical ovarian trauma, a high incidence of bio-chemical, clinical or familial auto-immune disorders leads tothe presumptive diagnosis of autoimmune POF.16,17 Evaluationfor other autoimmune diseases, including thyroid, parathyroidand adrenal disorders, systemic lupus erythematosus, and dia-betes mellitus, is recommended as clinically warranted.18
Between five and 25 percent of women with idiopathicor presumed autoimmune POF will undergo at least one spon-taneous remission.16,17 In the absence of a spontaneous remis-sion, oocyte donation offers the best potential for allowingconception. Due to the risk of premature osteoporosis, long-term HRT should be offered to all women with POF. In theseyounger women, higher doses of estrogen may be needed forrelief of symptoms than are usually required in older post-menopausal women. As women with POF will generally beexposed to lower monthly estrogen levels but much longerduration of HRT than their non-POF peers, the long-termeffects of this therapy on such disorders as breast cancer remainunclear. It seems prudent to reevaluate the individual HRTrisk-benefit balance when a woman with POF enters the usualmenopausal age range.
THYROID DISEASE
Autoimmune hypothyroidism is approximately ten times morecommon in women than in men, with an exponential rise inits occurrence after menopause.19 It is unclear whether thisincrease has any relationship to the withdrawal of circulatingestrogen at menopause, or whether the incidence is lower inwomen who use estrogen replacement therapy. Since hypothy-roidism in women is frequently underdiagnosed, screeningstrategies for those at highest risk have been proposed. Recentcross-sectional data suggest that symptoms are more frequentand cholesterol levels are higher in women with subclinicalhypothyroidism.20 Longitudinal data suggest that there maybe significant risk of cardiovascular morbidity if hypothy-roidism is not treated.21
Since hypothyroidism is treated with thyroxine supple-ments, it is also reasonable to consider the effects of thyroxinesupplementation on bone density and fractures. In addition tocross-sectional reports of lower bone density in women on thy-roxine,22 recent data suggest that risk of fracture is alsoincreased.23 In a large cohort of women over 65 years of age,hip fracture risk was also increased in women with previouslydiagnosed Graves’ disease (RR 1.8).24
Women on thyroxine supplements should be monitored bytitration of serum TSH levels.25 Free thyroxine levels can give aless precise indication of the adequacy of thyroxine supplements.25
Serum total thyroxine levels should not be relied upon in womenusing oral estrogen, since the elevation of serum levels of thyroidbinding globulin will lead to misleading elevations of total thy-roxine levels, but normal free thyroxine and normal TSH levels.25
Thyroid nodularity becomes more prevalent in post-menopausal women than in men of similar age.19 The associa-tion between thyroid nodularity and estrogen withdrawal isnot understood. Most of the nodules are benign, and, if pal-pable, should at most be investigated with fine needle aspira-tion biopsy.
ENDOMETRIOSIS
Combined estrogen and progestin replacement therapy in stan-dard doses does not appear to cause regrowth of endometrio-sis in menopausal women, or in young women receivingestrogen-progestin “addback” therapy following medicaloophorectomy with GnRH analogues.26 A small subgroup ofwomen may experience recurrence of pain and other symp-toms during unopposed estrogen therapy, particularly if resid-ual disease remains following definitive surgery. In the absenceof evidence from randomized studies, this appears to be one ofthe few clinical indications for progestin therapy following hys-terectomy, either as part of a continuous-combined regimenor as progestin-only therapy. There are no convincing data tosupport the prophylactic use of progestin-only therapy or thewithholding of estrogen for six months following definitivesurgery in order to allow regression of residual disease.
There are anecdotal reports of endometrial cancer deve-loping in residual endometriosis in women receiving unop-posed estrogen therapy following abdominal hysterectomy andbilateral salpingo-oophorectomy for endometriosis.27,28 Theavailable data does not indicate whether women with residualendometriosis following such surgery should be treated withcombined estrogen-progestin therapy.
FIBROIDS
Although uterine fibroids do not constitute a contraindicationto HRT, HRT should be used with caution in women knownto have fibroids. Both estrogen and progestins can influencefibroid growth; however, the doses in conventional HRT reg-imens are usually not sufficient to cause enlargement offibroids. However, rapid growth or abnormal bleeding from asubmucous fibroid requires investigation* and possibly surgi-cal intervention.
JOGC OCTOBER 200252
* Evaluation, decision-making, and follow-up. J Obstet Gynaecol Can2001;23(12).

JOGC OCTOBER 200253
LIVER DISEASE AND GALLBLADDER DISEASE
The use of oral estrogen may carry a 1.5- to two-fold increase inthe risk of gallbladder disease.29 The risk of cholecystectomyappears to increase with dose and duration of use, and to persistfor five or more years after stopping treatment.29 The transdermalroute of estrogen administration had been thought to exert noeffect on gallbladder disease, but a recent study documented sim-ilar changes in bile lipids and cholesterol following use of oral ortransdermal estradiol, suggesting that both routes of administra-tion may increase gallstone formation.30
HRT in standard doses is not associated with significantliver injury, nor is it contraindicated in patients with chronicliver disease who have normal liver function tests.31 In womenwith pre-existing liver disease, it may be advantageous to deli-ver estrogen by a non-oral route in order to avoid alterationsin liver metabolism.
PREOPERATIVE STATE
The SOGC’s Policy and Practice Guidelines Committee hasdrafted guidelines for prevention and treatment of thrombo-embolic disease in gynaecological surgery.32 These guidelinessuggest that, in the absence of data from randomized studies,HRT should be considered as constituting a risk for postoper-ative venous thromboembolism. Women who undergo surgerywith postoperative immobilization without discontinuingHRT should be given specific anticoagulant prophylaxis, evenif the excess risk is likely to be small. In some circumstances,surgical candidates will have additional risk factors for venousthromboembolism, such as age or malignancy, and will clear-ly need to receive prophylaxis.
WOUND HEALING
Venous ulcers, pressure sores, and burns occur frequently inelderly institutionalized women. Animal and limited humanstudies suggest that wound healing may accelerate with estro-gen replacement therapy, improving the inflammatory and pro-liferative phase of wound repair, as well as tissue angiogenesis.33
Growth factors play an integral role in modulating woundrepair. Preliminary human study shows that levels of trans-forming growth factor-β1 (TGF-β1) increase after HRTadministration.34 Further investigation in this field is needed.
MASTALGIA
Pre-existing mastalgia is not a contraindication to the use ofHRT, although it is prudent in this situation to use the lowesteffective doses of estrogen and progestin. Mastalgia developingafter initiation of HRT may improve with a reduction in the
dose of estrogen or progestin, or both, or with use of cyclic reg-imens involving estrogen-free days each month.
WEIGHT GAIN
As women age, resting metabolic rate gradually declines andbody weight tends to increase.35 A number of studies haveshown that weight gain is greatest in the perimenopause.*
Although HRT is often blamed for this weight gain, combinedHRT has in fact been shown to prevent an increase in centralbody fat mass and fat redistribution after menopause.36 In thePostmenopausal Estrogen/Progestin Interventions (PEPI) trial,37
the mean weight gain was higher in the placebo group than inany of the HRT groups. Appropriate counselling is important,as it is estimated that as many as 20 percent of women discon-tinue HRT because of perceived weight gain.36
THE SKIN
Soon after menopause, skin collagen content and skin thick-ness decline38 and abrupt increases in skin laxity and wrinklingoccur.39 Skin elasticity is decreased.40 Estrogen replacement lim-its the extent of skin collagen loss and helps to maintain skinthickness.39 Significant increases in skin collagen and thicknesswere demonstrated in women using oral estrogen comparedwith use of placebo.41 Facial fine wrinkling has been reportedto improve with estrogen therapy.42,43 Less skin extensibility wasdocumented in postmenopausal women treated with estrogenthan in untreated women, although no change in skin visco-elastic properties was found between groups.39
Whether elastic fibres can be preserved or repaired with theuse of HRT remains controversial.40 Preliminary evidence sug-gests that estrogen has a beneficial effect on at least some of themechanical properties of the skin, so that it may slow theprogress of intrinsic cutaneous aging.34 Present evidence doesnot yet support instituting estrogen replacement for its poten-tial benefits on skin alone. Such possible cosmetic benefits mayenhance adherence to prescribed therapy.
THE EYES
Animal studies have shown that estrogen provides protectionagainst cataract formation.44 In humans, preliminary reportshave suggested a similar protective effect in postmenopausalwomen using estrogen.45,46 Current epidemiological evidencesuggests a possible preventative role for estrogen in the deve-lopment of early age-related macular degeneration.47 Thesymptom of dry eyes (keratoconjunctivitis sicca) may also beimproved with the use of estrogen.48 Intraocular pressuredecreased in a cohort of 25 postmenopausal women after 12weeks of HRT.49
* Perimenopause. J Obstet Gynaecol Can 2001;23(9):836-41.
JOGC OCTOBER 200254
ORAL HEALTH
Oral alveolar bone loss is correlated with poor oral hygiene,50
and also with osteoporosis.50 The beneficial effects on skeletalbone mass attributed to estrogen are also seen on oral (maxil-lary and mandibular) bone and teeth. Tooth loss and the needfor dentures are much reduced in postmenopausal estrogenusers compared to non-users: a benefit which correlates posi-tively with the duration of estrogen use.51,52 There may alsobe a reduction in gingival inflammation and bleeding in womenusing estrogen replacement therapy.53
OLDER POSTMENOPAUSAL WOMEN (60 AND OLDER)
HRT may be of particular benefit for the prevention of suchage-associated conditions as osteoporosis, cognitive decline, andAlzheimer’s disease. Continuous-combined therapy is the pre-ferred regimen for the older woman with a uterus, as the returnof cyclic menses is usually poorly tolerated and thus leads topoor compliance. Breakthrough bleeding on this regimen isuncommon in older hypoestrogenic women. In order to min-imize mastalgia and other estrogenic side effects, it is advisableto start therapy with the lowest possible estrogen dose, givendaily or on alternate days, followed by slow increases to the min-imal effective dose.
There are at present no data to support reducing estab-lished doses of hormone replacement therapy simply becauseof a woman’s advancing age. As with all patients, the decisionsregarding long-term use of hormone replacement therapy mustbe individualized and based on good counselling provided bywell-informed health care practitioners.
OTHER SPECIAL CONSIDERATIONS
Stroke, hypertension, pulmonary embolism, and the hyper-coagulable state are examined in Section D.*
RECOMMENDATIONS
No specific recommendations.
J Obstet Gynaecol Can 2001;23(11):1096-1101.
REFERENCES
1. Dunaif A, Utian WH, Brandenburg SL, Gerhard M, Lobo RA, SolomonCG, et al. Effects of menopause and estrogen replacement therapy orhormone replacement therapy in women with diabetes mellitus: con-sensus opinion of the North American Menopause Society. Menopause2000;7:87-95.
2. Friday KE, Dong C, Fontenot RU. Conjugated equine estrogenimproves glycemic control and blood lipoproteins in postmenopausalwomen with Type II diabetes. J Clin Endocrinol Metab 2001;86:48-52.
3. Miller-Bass K,Adashi EY. Current status and future prospects of trans-dermal estrogen replacement therapy. Fertil Steril 1990;53:961-74.
4. Fettes I. Migraine in the Menopause. Neurol 1999;53(Suppl 1):S29-S33.5. Silberstein S, Merriam G. Sex hormones and headache 1999 (menstrual
migraine). Neurol 1999;53(Suppl 1):S3-S13.6. Neri I, Graneela F, Nappi R. Characteristics of headache at menopause:
a clinico-epidemiologic study. Maturitas 1993;17:31-7.7. Bousser M-G. Migraine, female hormones, and stroke. Cephalalgia
1999;19:75-9.8. Sanchez-Guerrero J, Liang MH, Karlson EW, Hunter DJ, Colditz GA.
Postmenopausal estrogen therapy and the risk for developing systemiclupus erythematosus.Ann Intern Med 1995;122:430-3.
9. Buton JP. Hormone replacement therapy in postmenopausal womenwith systemic lupus erythematosus. J Am Med Womens Assoc1998;53(1):13-7.
10. Van Vollenhoven RF, McGuire JL. Estrogen, progesterone, andtestosterone: can they be used to treat autoimmune disease? CleveClin J Med 1994;61:276-84.
11. Hernandez-Avila M, Liang MH,Willet WC, Stampfer MJ, Colditz GA,Rosner B, et al. Exogenous sex hormones and the risk of rheumatoidarthritis.Arthritis Rheum 1990;33:947-53.
12. Bijlsma JW,Van den Brink HR. Estrogens and rheumatoid arthritis.Am JReprod Med 1992;28:231-4.
13. MacDonald AG, Murphy EA, Capell HA, Bankowska UZ, Ralston SH.Effects of hormone replacement therapy in rheumatoid arthritis: a dou-ble blind placebo-controlled study. Ann Rheum Dis 1994;53:54-7.
14. Nevitt MC, Felson DT. Sex hormones and the risk of osteoarthritis inwomen: epidemiological evidence. Ann Rheum Dis 1996;55:673-6.
15. Zhang Y, McAlindon TE, Hannan MT, Chaisson CE, Klein R,Wilson PW,et al. Estrogen replacement therapy and worsening of radiographicknee osteoarthritis: the Framingham study. Arthritis Rheum1998;41:1867-73.
16. Coulam C. Immunology of ovarian failure. Am J Reprod Immunol1991;25:169-74.
17. Rebar RW, Connelly HV. Clinical features of young women with hyper-gonadotropic amenorrhea. Fertil Steril 1990;53:804-8.
18. Speroff L, Glass RH, Kase NG. Clinical Gynecologic Endocrinology andInfertility. Baltimore:Williams and Wilkins; 1994, p.412-4.
19. Vanderpump MP,Tunbridge WM, French JM,Appleton D, Bates D, ClarkF, et al.The incidence of thyroid disorders in the community: a twenty-year follow-up of the Whickham Survey. Clin Endocrinol 1995;43:55-68.
20. Canaris GJ, Manowitz NR, Mayor G, Ridgway EC.The Colorado thyroiddisease prevalence study. Arch Intern Med 2000;160:526-34.
21. Hak AE, Pols HAP,Visser TJ, Drexhage HA, Hofman A,Witteman JCM.Subclinical hypothyroidism is an independent risk factor for atheroscle-rosis and myocardial infarction in elderly women:The Rotterdam Study.Ann Intern Med 2000;132:270-8.
22. Uzzan B, Campos J, Cucherat M, Nony P, Boissel JP, Perret GY. Effectson bone mass of long term treatment with thyroid hormones: a meta-analysis. J Clin Endocrinol Metab 1996;81(12):4278-89.
23. Bauer DC, Ettinger B, Nevitt MC, Stone KL, for the Study ofOsteoporotic Fractures Research Group. Risk for fracture in womenwith low serum levels of thyroid-stimulating hormone.Ann Int Med2001;134:561-8.
24. Cummings SR, Nevitt MC, Browner WS, Stone K, Fox KM, Ensrud KE,et al. Risk factors for hip fracture in white women. Study of Osteo-porotic Fractures Research Group. N Engl J Med 1995;332:767-73.
25. Cooper DS. Clinical practice: subclinical hypothyroidism. N Engl J Med2001;345(4):260-6.
26. Schlaff WD, Moghissi K, Lemay A,Yuzpe AA, Petty SR, Ferdousi T. Multi-center trial comparing 3.6 mg Zoladex therapy with or withouthormone replacement therapy for the treatment of endometriosis.
* Hormone replacement therapy and cardiovascular disease. J ObstetGynaecol Can 2001;23(10):966-72.
JOGC OCTOBER 200255
Abstract 0-21. Fertil Steril 1995;64:S11-S12.27. Reimnitz C, Brand E, Nieberg RK, Hacker NF. Malignancy arising in
endometriosis associated with unopposed estrogen replacement.Obstet Gynecol 1988;71(3 pt 2):444-7.
28. Heaps JM, Nieberg RK, Berek JS. Malignant neoplasm arising inendometriosis. Obstet Gynecol 1990;75:1023-8.
29. Grodstein F, Colditz GA, Stampfer MJ. Postmenopausal hormone useand cholecystectomy in a large prospective study. Obstet Gynecol1994;83:5-11.
30. Uhler ML, Marks JW, Judd HL. Estrogen replacement therapy and gall-bladder disease in postmenopausal women. Menopause 2000;7:162-6.
31. Hartmann BW, Huber JC. The mythology of hormone replacementtherapy. Br J Obstet Gynaecol 1997;104:163-8.
32. Dubuc-Lissoir J, Ehlen T, Heywood M, Plante M. Prevention and treat-ment of thrombo-embolic disease in gynaecologic surgery. J SocObstet Gynaecol Can 1999;81:1-8.
33. Calvin M. Oestrogens and wound healing. Maturitas 2000;34:195-210.34. Brincat MP. Hormone replacement therapy and the skin. Maturitas
2000;35:107-17.35. Poehlman ET, Goran MI, Gardner AW,Ades PA,Arciero PJ, Katzmann-
Rooks SM, et al. Determinants of decline in resting metabolic rate inageing females. Am J Physiol 1993;264:E450-5.
36. van Seumeren I. Weight gain and hormone replacement therapy: arewomen’s fears justified? Maturitas 2000;34(Suppl 1):S3-S8.
37. Espeland MA, Stefanick ML, Kritz-Silverstein D, Fineberg SE,WaclawiwMA, James MK, et al. Effect of postmenopausal hormone therapy onbody weight and waist and hip girths. Postmenopausal Estrogen/Prog-estin Interventions Study Investigators. J Clin Endocrinol Metab1997;82:1549-56.
38. Brincat M, Moniz CF, Studd JWW, Darby AJ, Magos AL, Cooper DJ.Sex hormones and skin collagen in post-menopausal women. BMJ1983;287:1337-8.
39. Pierard GE, Letawe C, Dowlati A, Pierard-Franchimont C. Effect of hor-mone replacement therapy for menopause on the mechanical proper-ties of skin. J Am Geriatr Soc1995;43:662-5.
40. Punnonen R,Vaajalahti P,Tiesala K. Local oestradiol treatment improvesthe structure of elastic fibres in the skin of postmenopausal women.Ann Chir Gynaecol 1987;76(Suppl 202):39-41.
41. Maheux R, Naud F, Rioux M. A randomized, double-blind, placebo-con-trolled study on the effect of conjugated estrogens on skin thickness.Am J Obstet Gynecol 1994;170:642-9.
42. Creidi P, Faivre B,Agache P, Richard E, Haudiquet V, Sauvanet JP. Effect ofa conjugated oestrogen (Premarin) cream on aging facial skin: acomparative study with a placebo cream. Maturitas 1994;19:211-23.
43. Henry F, Pierard-Franchimont C, Cauwenbergh G, Pierard GE. Age-related changes in facial skin contours and rheology. J Am Geritr Soc1997;45:220-2.
44. Hales AM, Chamberlain CG, Murphy CR, McAvoy JW. Estrogen protectsagainst cataract induced by transforming growth factor (TGFbeta). JExp Med 1997;185:273-80.
45. Cumming RG, Mitchell P. Hormone replacement therapy, reproductivefactors, and cataract.The Blue Mountains Eye Study. Am J Epidemiol1997;145:242-9.
46. Benitez del Castillo JM, del Rio T, Garcia-Sanchez J. Effects of estrogenuse on transmittance in postmenopausal women. Ophthalmology1997;104:970-3.
47. Smith W, Mitchell P,Wang JJ. Gender, oestrogen, hormone replacementand age-related macular degeneration: results from the Blue MountainsEye Study. Aust NZ J Ophthalmol 1997;25 Suppl 1(9):S13-15.
48. Wenderlein M, Mattes S.The “dry eye” phenomenon and ovarian func-tion. Study of 700 pre- and post-menopausal women. Zentralbl Gynakol1996;118:643-9.
49. Sator MO, Joura EA, Frigo P, Kurz C, Metka M, Hommer A, Huber JC.Hormone replacement therapy and intraocular pressure. Maturitas1997;28:55-8.
50. von Wowern N. General and oral aspects of osteoporosis: a review.Clin Oral Investig 2001;5(2):71-82.
51. Paganini-Hill A.The benefits of estrogen replacement therapy on oralhealth.The Leisure World cohort. Arch Intern Med 1995;155:2325-9.
52. Grodstein F, Colditz GA, Stampfer MJ. Post-menopausal hormone useand tooth loss: a prospective study. J Am Dent Assoc 1996;127:370-7.
53. Speroff L. Unpublicized effects of postmenopausal hormone therapy.Ob/Gyn Clinic Alert 1996 (May):6-8.

JOGC OCTOBER 2002
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
56
INTRODUCTION
Although cognitive performance is thought to decline withincreasing age, the available evidence suggests that age-relateddeficits develop only in specific skills. Whereas no changes inperformance are seen in tasks involving very short-term mem-ory or in distant, remote memory in aging individuals, there aredecreases in the ability of older people to acquire, encode, andretrieve new material.1 Thus, the ability to learn new associa-tions or to remember new facts becomes compromised withincreasing age, regardless of gender or hormonal status.
ESTROGEN AND BRAIN FUNCTION
Several different effects of estrogen on brain structure and func-tion could explain its ability to maintain aspects of memory. Forexample, estrogen potentiates neurite outgrowth, dendritic spineformation, and synapse formation.2 Regions of the brainresponsible for learning and memory, including the basal fore-brain (the origin of ascending cholinergic pathways) and thehippocampus (a critical brain structure), contain nuclear recep-tors for estrogen.3 Estrogen also increases cerebral blood flow,4
modulates cerebral glucose utilization,5 and possesses antioxi-dant properties.6 In adult female rats, ovariectomy causes a sig-nificant decrease in the number of dendritic spines in the CA1area of the hippocampus, and the density of spines is restoredby the administration of estrogen.2 Thus, estrogen increases thenumber of synapses in this area of the brain, thereby enhanc-ing neuronal communication and, presumably, enhancingmemory functions.
ESTROGEN REPLACEMENT AS
PROTECTION AGAINST COGNITIVE
DECLINE IN HEALTHY WOMEN
Most7-10 but not all11 large epidemiological studies of elderly post-menopausal women (age approximately 65 years or older) foundthat women who had been taking estrogen replacement therapy(ERT) had higher scores on tests of cognitive functioning thandid women of similar age who had not used ERT. Physician andpatient biases may have influenced these results because of a lackof randomization. However, the majority of the randomized,prospective, double-blind, placebo-controlled trials (RCTs)12-15
have confirmed observational study findings7-10 that post-menopausal women who received treatment with estrogen per-formed significantly better on tests of cognitive function,especially on tests of short- and long-term verbal memory. Thishas clinical importance because verbal memory, which appearsto be preferentially maintained by ERT,13-15 is the cognitive func-tion that shows the greatest decline with normal aging.16 The con-sistency of the RCT findings on estrogen use and cognitivefunction strongly suggests that ERT protects short- and long-termmemory in healthy, aging postmenopausal women.
ESTROGEN REPLACEMENT AS PROTECTION
AGAINST ALZHEIMER’S DISEASE
Alzheimer’s disease (AD), the most common cause of demen-tia, affects 1.5 to three times as many women as men, even afteradjusting for increased longevity in women.17 Because the find-ings from basic neuroscience research and from RCTs in healthypostmenopausal women provide strong evidence that estrogenhelps to preserve memory in aging women, much attention hasrecently been focused on investigating whether ERT may lowerthe risk of AD. Sizable cohort studies have consistently foundthat current estrogen use is significantly lower among womenwith AD than among healthy women of comparable age andeducation,18 suggesting that women taking ERT have a sub-stantially reduced risk of AD.
In a recent community-based cohort, postmenopausalestrogen-users had a 50 percent reduction in the incidence ofAD compared to non-users (OR 0.5, 95% CI = 0.2-0.9).19
These case-control and cohort studies suggest that ERT mayreduce a woman’s risk of later developing Alzheimer’s diseaseby between 40 and 60 percent.
ESTROGEN REPLACEMENT AS AN EFFECTIVE
TREATMENT FOR ALZHEIMER’S DISEASE
Several open-label clinical trials have reported selective cogni-tive improvements in women with dementia who receivedERT.20-22 The findings from these early treatment studies mustbe interpreted cautiously, however, since the studies were uncon-trolled, short-term, and relatively small. Recently, two RCTsinvestigated the possible benefit of ERT for women with mildto moderate Alzheimer’s disease.23-24 Women with AD whowere treated with estrogen for 16 weeks showed no change in
Barbara B. Sherwin, PhD1
1 Montreal QC
HORMONES AND THE BRAIN

tests of cognitive function compared to those who were givenplacebo.23 Similarly, estrogen had no effect on slowing diseaseprogression or improving cognitive outcomes in women withmild to moderate AD when treatment lasted for one year.24
Although preliminary evidence suggests that estrogenpotentiates the effect of the cholinesterase inhibitor tacrine,used to treat women with mild to moderate AD,25 thesefindings need to be replicated in controlled studies.
ESTROGEN AND MOOD FLUCTUATIONS
Estrogen up-regulates the serotonergic system whose dysfunc-tion is implicated in mood disorders.26 In prospective, con-trolled studies of postmenopausal women, ERT wasconsistently effective in relieving dysphoric mood,27-29 but notmood disorders that met criteria for a diagnosis of clinicaldepression.30 In a recent RCT of perimenopausal women diag-nosed with either major or minor depression, a full or partialtherapeutic response was seen in 80 percent of women whoreceived estradiol and 22 percent of those given a placebo.31
However, the finding that feelings of sadness improved whileother symptoms such as disturbed sleep, feelings of unreality,emotional detachment, and somatic preoccupation were unaf-fected suggests that estrogen alone is not effective in alleviat-ing the totality of symptoms that constitute a depressivesyndrome. Therefore, the mood lability, dysphoria, and irri-tability that some women report specifically during themenopausal transition may be stabilized or alleviated by initi-ation of ERT.
PROGESTINS,TESTOSTERONE, SELECTIVE ESTROGEN RECEPTOR MODULATORS (SERMS) AND COGNITION OR MOOD
Several observational studies and one randomized study showthat the addition of a progestin to an estrogen replacement reg-imen attenuates the beneficial effect of estrogen on mood.32
This negative effect of progestin on mood might be mitigat-ed by a higher estrogen-progestin dose ratio. In a recent study,the beneficial association between unopposed estrogen use andthe rate of change in cognitive functioning in older women wasopposed by the addition of a progestin,33 suggesting that com-bined therapy might negate the beneficial effect of estrogen oncognition. Although one study found a positive effect of a com-bined estrogen-androgen drug on aspects of cognition,13 it isnot known whether this was a direct effect of the androgen, orwhether it occurred due to the aromatization of testosteroneto estrogen. The only randomized study of raloxifene, a selec-tive estrogen receptor modulator, showed that treatment ofpostmenopausal women for one year was not associated withany change in their scores on tests of cognitive functioning orof mood.34
SUMMARY OF KEY POINTS:
H1. Estrogen positively influences brain structures andfunctions that are known to be critical for memory. (I)
H2. In healthy postmenopausal women, estrogen protectsagainst the deterioration in short- and long-term memory that occurs with normal aging. (I)
H3. Estrogen replacement is associated with a reduction inthe risk of developing Alzheimer’s disease in post-menopausal women (II-2), but does not affect the pro-gression of deterioration in women with diagnosedAlzheimer’s disease. (I)
H4. Estrogen effectively enhances mood in women withdysphoria or mood lability (I), but there is no evidencethat estrogen alone is an effective treatment for clinicaldepression. The addition of progestin may attenuatethe beneficial effect of estrogen on mood and on cog-nition in some women. (I)
H5. At present, there is no evidence that raloxifene influ-ences cognitive functioning or mood. (I)
CONCLUSION
Estrogen replacement prevents deterioration of aspects of cog-nition in older women that occurs with normal aging. There isalso compelling evidence that ERT prevents or delays the onsetof Alzheimer’s disease in women who are at risk for genetic orenvironmental reasons. However, once a woman has a diagno-sis of Alzheimer’s disease, there is no evidence that ERT in thedoses conventionally used for postmenopausal women will beeffective in influencing the course of the disease. More defini-tive information on estrogen and cognition in postmenopausalwomen will be available in 2005 when the results of the multi-centre, randomized trials of the Women’s Health InitiativeMemory Study (WHIMS) and the Women’s Health InitiativeStudy on Cognitive Aging (WHISCA) become available.
J Obstet Gynaecol Can 2001;23(11):1102-4.
REFERENCES
1. Craik FIM. Age Differences in Human Memory. In: Birren JE, SchaieKW (eds). Handbook of the Psychology of Aging. New York: Van Nostrand Reinhold, 1977;pp.384-420.
2. Wooley CS, McEwen BS. Roles of estradiol and progesterone in regula-tion of hippocampal dendritic spine density during the estrous cycle inthe rat. J Comp Neurol 1993;336:293-306.
3. Loy R, Gerlach JL, McEwen BS. Autoradiographic localization of estradi-ol binding neurons in the rat hippocampal formation and entorhinalcortex. Dev Brain Res 1988;39:245-51.
4. Belfort MA, Saade GR, Snabes M, Dunn R, Moise KJ Jr., Cruz A, et al.Hormonal status affects the reactivity of the cerebral vasculature.Am J Obstet Gynecol 1995;172:1273-8.
5. Bishop J, Simpkins JW. Role of estrogens in peripheral and cerebral glucose utilization. Rev Neurosci 1992;3:121-37.
6. Mooradian AD. Antioxidant properties of steroids. J Steroid BiochemMol Biol 1993;45:509-11.
JOGC OCTOBER 200257
JOGC OCTOBER 200258
7. Jacobs DM,Tang MX, Stern Y, Sano M, Marder K, Bell KL, et al. Cognitivefunction in nondemented older women who took estrogen aftermenopause. Neurology 1998;50:368-73.
8. Yaffee K, Sawaya G, Leiberberg L, Grady D. Estrogen therapy inpostmenopausal women: effects on cognitive function and dementia.J Am Med Assoc 1998;279:685-95.
9. Robinson D, Friedman L, Marcus R,Tinklenberg J,Yesavage J. Estrogenreplacement therapy and memory in older women. J Am Geriatr Soc1994;42:919-22.
10. Resnick SM, Metter J, Zonderman AB. Estrogen replacement therapyand longitudinal decline in visual memory: a possible protective effect?Neurology 1997;49:1491-7.
11. Barrett-Connor E, Kritz-Silverstein D. Estrogen replacement therapyand cognitive function in older women. J Am Med Assoc1993;269;2637-41.
12. Fedor-Freyberg P. The influence of oestrogens in the well being andmental performance in postmenopausal women. Acta Obstet GynecolScand 1977;64:3-69.
13. Sherwin BB. Estrogen and/or androgen replacement therapy and cognitive functioning in surgically menopausal women. Psychoneuro-endocrinology 1988;13:345-57.
14. Sherwin BB, Phillips SM. Estrogen and cognitive functioning in surgicallymenopausal women. Ann NY Acad Sci 1990;592:474-5.
15. Phillips SM, Sherwin BB. Effects of estrogen on memory function insurgically menopausal women. Psychoneuroendocrinology1992;17:485-95.
16. Small SA.Age-related memory decline: current concepts and futuredirections.Arch Neurol 2001;58:360-4.
17. Jorm AF, Korten AE, Henderson AS.The prevalence of dementia:a quantitative intergration of the literature. Acta Psychiatr Scand1987;76:465-79
18. Henderson VW. Estrogen, cognition and a woman’s risk of Alzheimer’sdisease. Am J Med 1997;103:115-85.
19. Tang MX, Jacobs D, Stern Y,Marder K, Schofield P,Gurland B, et al. Effectof oestrogen during menopause on risk and age on onset of Alzheimer’sdisease. Lancet 1996;348:429-32.
20. Filit H,Weinreb H, Cholst I, Luine V, McEwen B,Amador R, et al.Observations in a preliminary open trial of estradiol therapy for senile dementia — Alzheimer’s type. Psychoneuroendocrinology1986;11:337-45.
21. Honjo H, Ogino Y, Naitoh K, Urabe M, Kitawaki J,Yasuda J, et al. In vivoeffects by estrone sulfate on the central nervous system–senile demen-tia (Alzheimer’s type). J Steroid Biochem 1989;34:521-5.
22. Ohkura T, Isse K, Hamamoto M,Yaoi Y, Hagino N. Low dose estrogenreplacement therapy for Alzheimer disease in women. Menopause1994;1:125-30.
23. Henderson VW, Paganini-Hill A, Miller BL, Elbe RJ, Reyes PF, Shoupe D,et al. Estrogen for Alzheimer’s disease in women. Neurology2000;54:295-301.
24. Mulnard RA, Cotman CW, Kawas C, van Dyck CH, Sano M, Doody R,et al. Estrogen replacement therapy for treatment of mild to moderateAlzheimer’s disease. J Am Med Assoc 2000;283:1007-15.
25. Schneider LS, Farlow MR, Henderson VW, Pogoda JM. Effects of estrogen replacement therapy on response to tacrine in patients with Alzheimer’s disease. Neurology 1996;46:1580-4.
26. Price WA, Giannini AJ. Antidepressant effects of estrogen. J Clin Psychiatr 1985;46:506-10.
27. Sherwin BB. Affective changes with estrogen and androgenreplacement therapy in surgically menopausal women.J Affect Disord 1988;14:177-87.
28. Ditkoff LC, Crary WG, Cristo M, Lobo RA. Estrogen improves psychological function in asymptomatic postmenopausal women.Obstet Gynaecol 1991;178:991-5
29. Sherwin BB, Suranyi-Cadotte BE. Up-regulatory effect of estrogen onplatelet 3H-imipramine binding sites in surgically menopausal women.Biol Psychiatr 1990;28:339-48.
30. Schneider MA, Brotherton PL, Hailes J. The effect of exogenous oestrogens on depression in menopausal women. Med J Aust1977;2:162-3.
31. Schmidt PJ, Nieman L, Danaceau MA,Tobin MB, Roca CA, Murphy JH,et al. Estrogen replacement in perimenopausal-related depression:a preliminary report.Am J Obstet Gynecol 2000;183:414-20.
32. Sherwin BB. Progestogens used in menopause: side effects, mood andquality of life. J Reprod Med 1999;44:227-32.
33. Rice MM, Graves AB, McCurry SM, Gibbons LE, et al. Postmenopausalestrogen and estrogen-progestin use and 2-year rate of cognitivechange in a cohort of Japanese American women.Arch Int Med2000;160:1641-9.
34. Nickelsen T, Lufkin EG, Riggo BL, Cox DA, Crook TH. Raloxifene hydro-chloride, a selective estrogen receptor modulator: safety assessment ofeffects on cognitive function and mood in postmenopausal women. Psy-choneuroendocrinology 1986;11:337-45.

JOGC OCTOBER 200259
INTRODUCTION
The first pharmaceutical agent to treat menopausal complaintswas developed in the late 1920s. Since then, several discover-ies have led to the development of compounds for improvingthe health and quality of life in postmenopausal women. Nostandard therapeutic regimen exists, but a variety of compounds,routes of administration, and dosages can be used to assist theindividual woman desiring treatment.
Every woman should be informed of the potential benefitsand adverse reactions associated with any treatment option sheconsiders. It is the responsibility of the health care profession-al to provide the most current information.
ESTROGENS
The terminology of natural versus synthetic is often used to dis-tinguish between different estrogens; however, this can be con-fusing or misleading. While some use the term “natural” to referto the source of the preparation (plant or animal), others usethe term to refer to the chemical structure (identical to humanestrogens). However, the only truly “natural” estrogens are thoseproduced and secreted within a woman’s body: estrone (E1) andestradiol (E2). The critical determinant of an estrogen prepara-tion’s usefulness is not its origin, but its biological effectiveness.The most potent naturally occurring estrogen is 17β-estradi-ol, followed by estrone and estriol.1
Approximate biological equivalents of the estrogens current-ly available for hormone replacement therapy (HRT) are listed inTable 1.2,3 These standard doses have approximately one-quarterto one-sixth the potency of the standard estrogen doses in low-dose oral contraceptive pills. Estrogen preparations used in Cana-da for HRT are listed in Table 2.
ABSORPTION
Estrone and estradiol are not readily absorbed by the gastrointesti-nal tract. Rapid conversion of E2 to E1 occurs in the intestinalmucosa.1 Further metabolism and conjugation occur in the liver,with glucuronidation of up to 30 percent of the initial oral doseoccurring in the “first pass” through the liver, followed by rapid
urinary and biliary excretion.1 To enhance oral bioavailability andprevent degradation, estrogens can be conjugated and delivered assodium sulphates, or stabilized by adding piperazine or an estergroup.1 Estrogens may also be micronized, creating very small par-ticles that result in an increase in surface area and rapid absorption.1
Orally ingested estrogens produce more biologically activesubstances in the liver than transdermal estrogens due to the“first pass” effect.1 Oral administration is associated with rapidincreases in levels of high-density lipoprotein (HDL)-choles-terol and triglycerides, whereas transdermal estrogen therapyhas less effect on the lipoprotein profile and may have afavourable effect on triglycerides.* Transdermal administrationdoes not produce high levels of the drug in the portal circula-tion, which may explain why the oral and transdermal routesare associated with different effects on lipoprotein profile.1 Intheory, transdermal estrogen therapy should have less effect oncoagulation factors and gallbladder disease,4 but this has notyet been demonstrated clinically.
SMOKING
Smoking increases the clearance of estrogen in the liver. Muchlower serum concentrations of estrone and estradiol have beenfound in smokers than in non-smokers after oral administra-tion of estrogen, with a consequent reduction in the effect ofestrogen on lipid levels and bone mineral content.5 No differ-ence in serum estrogen concentrations between smokers andnon-smokers has been observed after transdermal therapy.5
Conjugated EstrogensConjugated estrogens are a blend of estrogens that can bechemically produced or derived from plant or animal sources.Under current Canadian regulations, conjugated estrogentablets must contain specific proportions of sodium estrone sul-phate, sodium equilin sulphate, and 17α-dihydroequilin sul-phate. Conjugated equine estrogens (CEE) contain suchadditional bioactive estrogens as delta 8-9-dehydroestrone sul-phate. Other conjugated estrogens may not be pharmacologic-ally identical to conjugated equine estrogens, and their use couldresult in a change in therapeutic effectiveness.3
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
Ema Ferreira, MSc, PharmD,1 Thomas E. R. Brown, PharmD2
1 Montreal QC2 Toronto ON
PHARMACOTHERAPY
* Hormone replacement therapy and cardiovascular disease, J Obstet Gynaecol Can2001;23(10):966-72.
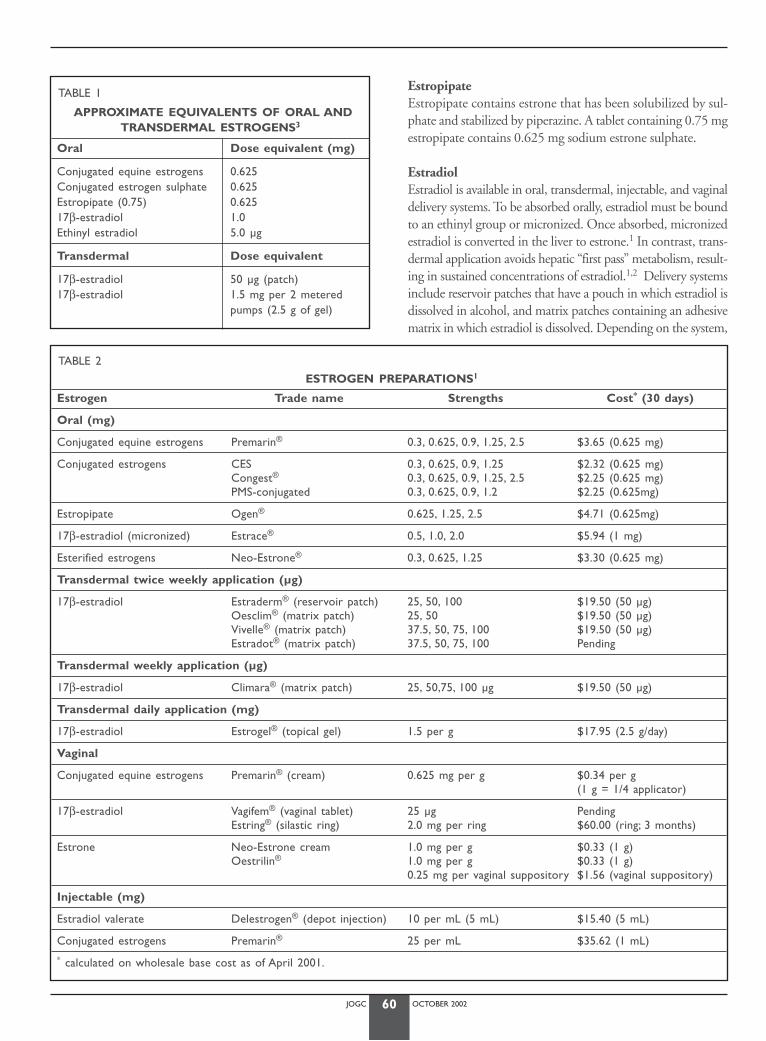
JOGC OCTOBER 200260
EstropipateEstropipate contains estrone that has been solubilized by sul-phate and stabilized by piperazine. A tablet containing 0.75 mgestropipate contains 0.625 mg sodium estrone sulphate.
EstradiolEstradiol is available in oral, transdermal, injectable, and vaginaldelivery systems. To be absorbed orally, estradiol must be boundto an ethinyl group or micronized. Once absorbed, micronizedestradiol is converted in the liver to estrone.1 In contrast, trans-dermal application avoids hepatic “first pass” metabolism, result-ing in sustained concentrations of estradiol.1,2 Delivery systemsinclude reservoir patches that have a pouch in which estradiol isdissolved in alcohol, and matrix patches containing an adhesivematrix in which estradiol is dissolved. Depending on the system,
TABLE 1
APPROXIMATE EQUIVALENTS OF ORAL ANDTRANSDERMAL ESTROGENS3
Oral Dose equivalent (mg)
Conjugated equine estrogens 0.625Conjugated estrogen sulphate 0.625Estropipate (0.75) 0.62517β-estradiol 1.0Ethinyl estradiol 5.0 µg
Transdermal Dose equivalent
17β-estradiol 50 µg (patch) 17β-estradiol 1.5 mg per 2 metered
pumps (2.5 g of gel)
TABLE 2
ESTROGEN PREPARATIONS1
Estrogen Trade name Strengths Cost* (30 days)
Oral (mg)
Conjugated equine estrogens Premarin® 0.3, 0.625, 0.9, 1.25, 2.5 $3.65 (0.625 mg)
Conjugated estrogens CES 0.3, 0.625, 0.9, 1.25 $2.32 (0.625 mg)Congest® 0.3, 0.625, 0.9, 1.25, 2.5 $2.25 (0.625 mg)PMS-conjugated 0.3, 0.625, 0.9, 1.2 $2.25 (0.625mg)
Estropipate Ogen® 0.625, 1.25, 2.5 $4.71 (0.625mg)
17β-estradiol (micronized) Estrace® 0.5, 1.0, 2.0 $5.94 (1 mg)
Esterified estrogens Neo-Estrone® 0.3, 0.625, 1.25 $3.30 (0.625 mg)
Transdermal twice weekly application (µg)
17β-estradiol Estraderm® (reservoir patch) 25, 50, 100 $19.50 (50 µg)Oesclim® (matrix patch) 25, 50 $19.50 (50 µg)Vivelle® (matrix patch) 37.5, 50, 75, 100 $19.50 (50 µg)Estradot® (matrix patch) 37.5, 50, 75, 100 Pending
Transdermal weekly application (µg)
17β-estradiol Climara® (matrix patch) 25, 50,75, 100 µg $19.50 (50 µg)
Transdermal daily application (mg)
17β-estradiol Estrogel® (topical gel) 1.5 per g $17.95 (2.5 g/day)
Vaginal
Conjugated equine estrogens Premarin® (cream) 0.625 mg per g $0.34 per g(1 g = 1/4 applicator)
17β-estradiol Vagifem® (vaginal tablet) 25 µg PendingEstring® (silastic ring) 2.0 mg per ring $60.00 (ring; 3 months)
Estrone Neo-Estrone cream 1.0 mg per g $0.33 (1 g)Oestrilin® 1.0 mg per g $0.33 (1 g)
0.25 mg per vaginal suppository $1.56 (vaginal suppository)
Injectable (mg)
Estradiol valerate Delestrogen® (depot injection) 10 per mL (5 mL) $15.40 (5 mL)
Conjugated estrogens Premarin® 25 per mL $35.62 (1 mL)
* calculated on wholesale base cost as of April 2001.
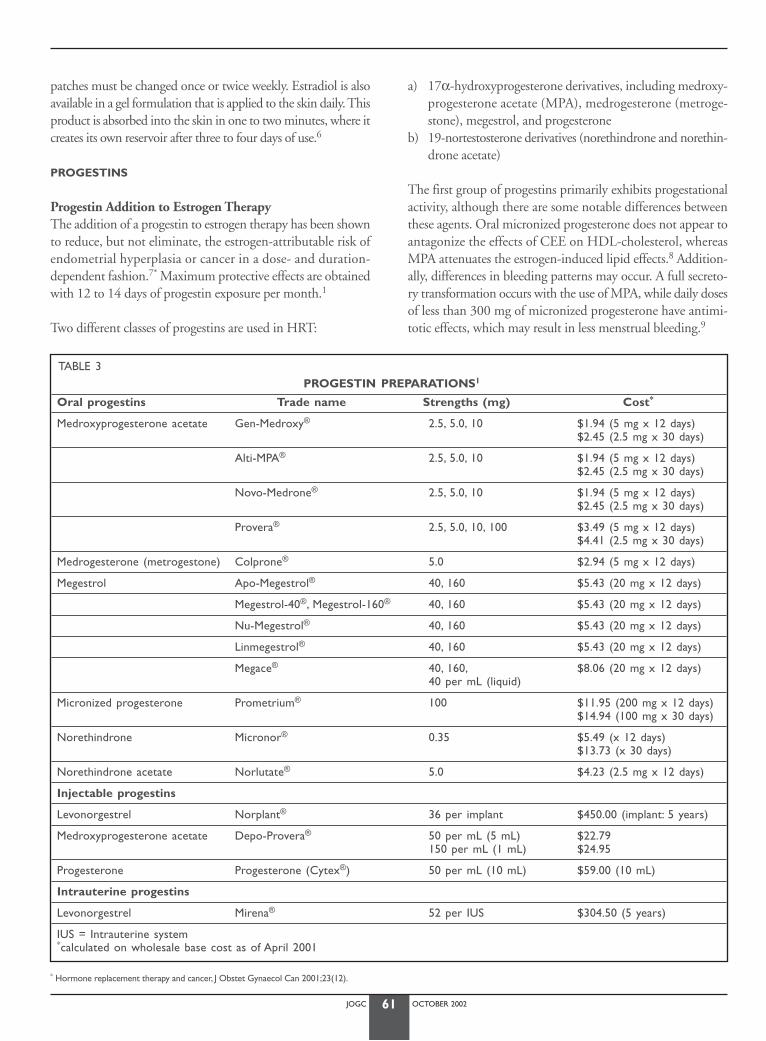
JOGC OCTOBER 200261
patches must be changed once or twice weekly. Estradiol is alsoavailable in a gel formulation that is applied to the skin daily. Thisproduct is absorbed into the skin in one to two minutes, where itcreates its own reservoir after three to four days of use.6
PROGESTINS
Progestin Addition to Estrogen TherapyThe addition of a progestin to estrogen therapy has been shownto reduce, but not eliminate, the estrogen-attributable risk ofendometrial hyperplasia or cancer in a dose- and duration-dependent fashion.7* Maximum protective effects are obtainedwith 12 to 14 days of progestin exposure per month.1
Two different classes of progestins are used in HRT:
a) 17α-hydroxyprogesterone derivatives, including medroxy-progesterone acetate (MPA), medrogesterone (metroge-stone), megestrol, and progesterone
b) 19-nortestosterone derivatives (norethindrone and norethin-drone acetate)
The first group of progestins primarily exhibits progestationalactivity, although there are some notable differences betweenthese agents. Oral micronized progesterone does not appear toantagonize the effects of CEE on HDL-cholesterol, whereasMPA attenuates the estrogen-induced lipid effects.8 Addition-ally, differences in bleeding patterns may occur. A full secreto-ry transformation occurs with the use of MPA, while daily dosesof less than 300 mg of micronized progesterone have antimi-totic effects, which may result in less menstrual bleeding.9
TABLE 3PROGESTIN PREPARATIONS1
Oral progestins Trade name Strengths (mg) Cost*
Medroxyprogesterone acetate Gen-Medroxy® 2.5, 5.0, 10 $1.94 (5 mg x 12 days)$2.45 (2.5 mg x 30 days)
Alti-MPA® 2.5, 5.0, 10 $1.94 (5 mg x 12 days)$2.45 (2.5 mg x 30 days)
Novo-Medrone® 2.5, 5.0, 10 $1.94 (5 mg x 12 days)$2.45 (2.5 mg x 30 days)
Provera® 2.5, 5.0, 10, 100 $3.49 (5 mg x 12 days)$4.41 (2.5 mg x 30 days)
Medrogesterone (metrogestone) Colprone® 5.0 $2.94 (5 mg x 12 days)
Megestrol Apo-Megestrol® 40, 160 $5.43 (20 mg x 12 days)
Megestrol-40®, Megestrol-160® 40, 160 $5.43 (20 mg x 12 days)
Nu-Megestrol® 40, 160 $5.43 (20 mg x 12 days)
Linmegestrol® 40, 160 $5.43 (20 mg x 12 days)
Megace® 40, 160, $8.06 (20 mg x 12 days)40 per mL (liquid)
Micronized progesterone Prometrium® 100 $11.95 (200 mg x 12 days)$14.94 (100 mg x 30 days)
Norethindrone Micronor® 0.35 $5.49 (x 12 days)$13.73 (x 30 days)
Norethindrone acetate Norlutate® 5.0 $4.23 (2.5 mg x 12 days)
Injectable progestins
Levonorgestrel Norplant® 36 per implant $450.00 (implant: 5 years)
Medroxyprogesterone acetate Depo-Provera® 50 per mL (5 mL) $22.79150 per mL (1 mL) $24.95
Progesterone Progesterone (Cytex®) 50 per mL (10 mL) $59.00 (10 mL)
Intrauterine progestins
Levonorgestrel Mirena® 52 per IUS $304.50 (5 years)
IUS = Intrauterine system*calculated on wholesale base cost as of April 2001
* Hormone replacement therapy and cancer, J Obstet Gynaecol Can 2001;23(12).
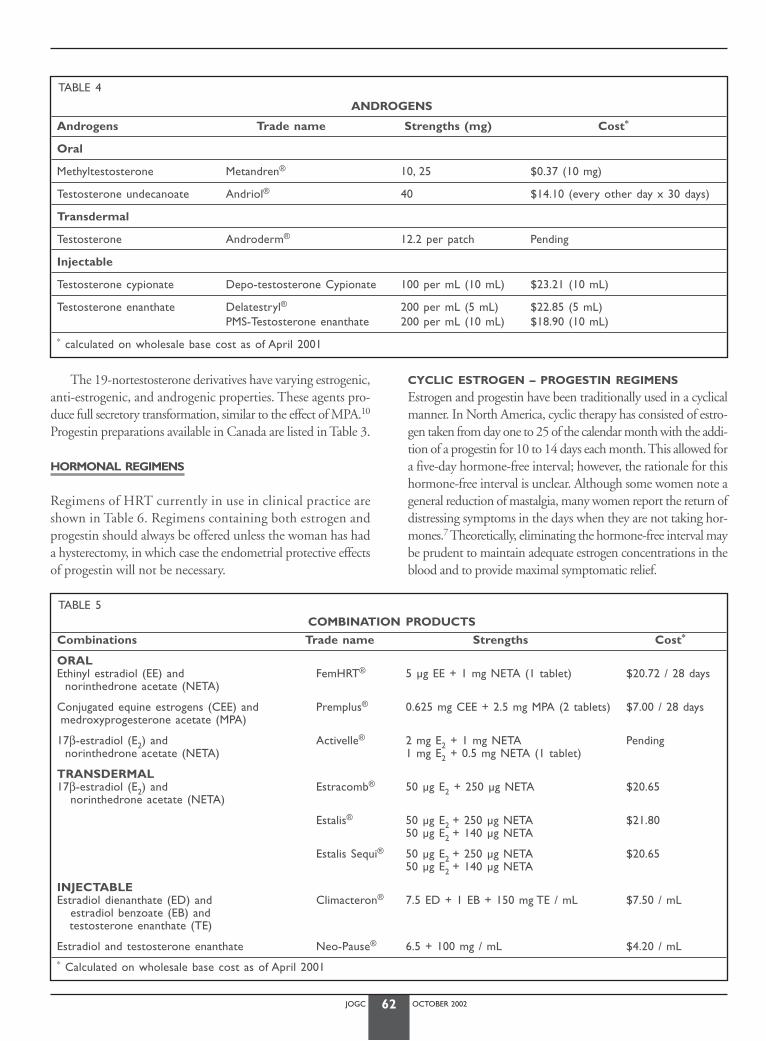
JOGC OCTOBER 200262
The 19-nortestosterone derivatives have varying estrogenic,anti-estrogenic, and androgenic properties. These agents pro-duce full secretory transformation, similar to the effect of MPA.10
Progestin preparations available in Canada are listed in Table 3.
HORMONAL REGIMENS
Regimens of HRT currently in use in clinical practice areshown in Table 6. Regimens containing both estrogen andprogestin should always be offered unless the woman has hada hysterectomy, in which case the endometrial protective effectsof progestin will not be necessary.
CYCLIC ESTROGEN – PROGESTIN REGIMENS
Estrogen and progestin have been traditionally used in a cyclicalmanner. In North America, cyclic therapy has consisted of estro-gen taken from day one to 25 of the calendar month with the addi-tion of a progestin for 10 to 14 days each month. This allowed fora five-day hormone-free interval; however, the rationale for thishormone-free interval is unclear. Although some women note ageneral reduction of mastalgia, many women report the return ofdistressing symptoms in the days when they are not taking hor-mones.7 Theoretically, eliminating the hormone-free interval maybe prudent to maintain adequate estrogen concentrations in theblood and to provide maximal symptomatic relief.
TABLE 4
ANDROGENS
Androgens Trade name Strengths (mg) Cost*
Oral
Methyltestosterone Metandren® 10, 25 $0.37 (10 mg)
Testosterone undecanoate Andriol® 40 $14.10 (every other day x 30 days)
Transdermal
Testosterone Androderm® 12.2 per patch Pending
Injectable
Testosterone cypionate Depo-testosterone Cypionate 100 per mL (10 mL) $23.21 (10 mL)
Testosterone enanthate Delatestryl® 200 per mL (5 mL) $22.85 (5 mL)PMS-Testosterone enanthate 200 per mL (10 mL) $18.90 (10 mL)
* calculated on wholesale base cost as of April 2001
TABLE 5COMBINATION PRODUCTS
Combinations Trade name Strengths Cost*
ORALEthinyl estradiol (EE) and FemHRT® 5 µg EE + 1 mg NETA (1 tablet) $20.72 / 28 days
norinthedrone acetate (NETA)
Conjugated equine estrogens (CEE) and Premplus® 0.625 mg CEE + 2.5 mg MPA (2 tablets) $7.00 / 28 daysmedroxyprogesterone acetate (MPA)
17β-estradiol (E2) and Activelle® 2 mg E2 + 1 mg NETA Pendingnorinthedrone acetate (NETA) 1 mg E2 + 0.5 mg NETA (1 tablet)
TRANSDERMAL17β-estradiol (E2) and Estracomb® 50 µg E2 + 250 µg NETA $20.65
norinthedrone acetate (NETA)
Estalis® 50 µg E2 + 250 µg NETA $21.8050 µg E2 + 140 µg NETA
Estalis Sequi® 50 µg E2 + 250 µg NETA $20.6550 µg E2 + 140 µg NETA
INJECTABLEEstradiol dienanthate (ED) and Climacteron® 7.5 ED + 1 EB + 150 mg TE / mL $7.50 / mL
estradiol benzoate (EB) and testosterone enanthate (TE)
Estradiol and testosterone enanthate Neo-Pause® 6.5 + 100 mg / mL $4.20 / mL* Calculated on wholesale base cost as of April 2001
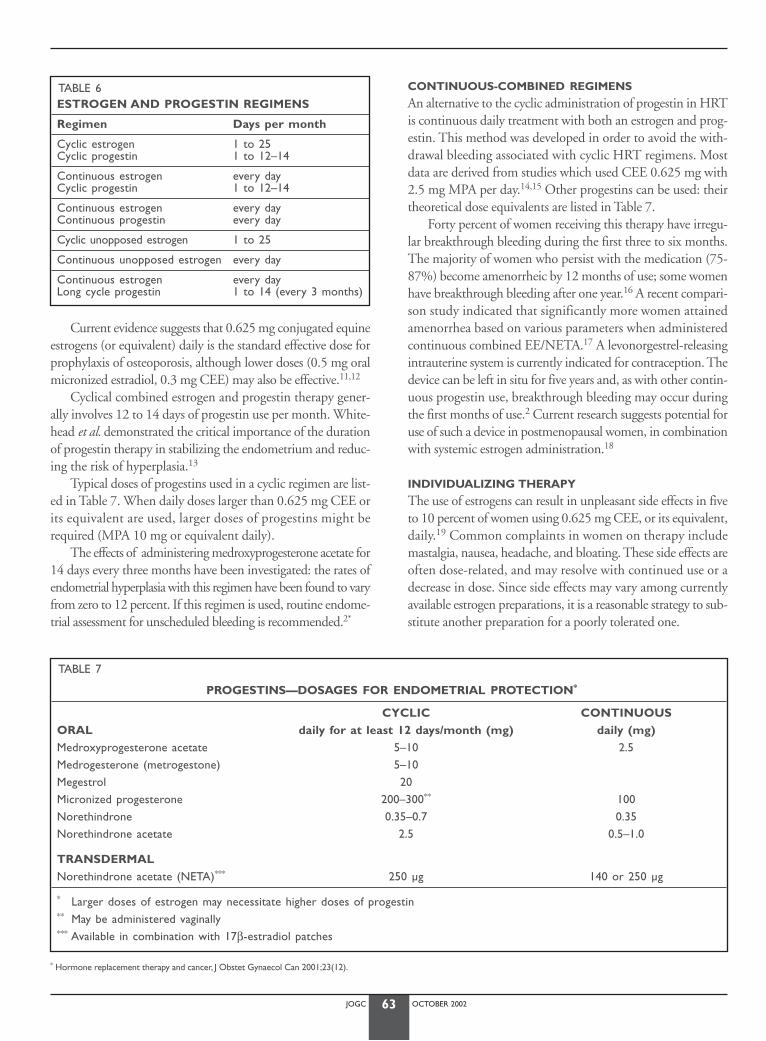
JOGC OCTOBER 200263
Current evidence suggests that 0.625 mg conjugated equineestrogens (or equivalent) daily is the standard effective dose forprophylaxis of osteoporosis, although lower doses (0.5 mg oralmicronized estradiol, 0.3 mg CEE) may also be effective.11,12
Cyclical combined estrogen and progestin therapy gener-ally involves 12 to 14 days of progestin use per month. White-head et al. demonstrated the critical importance of the durationof progestin therapy in stabilizing the endometrium and reduc-ing the risk of hyperplasia.13
Typical doses of progestins used in a cyclic regimen are list-ed in Table 7. When daily doses larger than 0.625 mg CEE orits equivalent are used, larger doses of progestins might berequired (MPA 10 mg or equivalent daily).
The effects of administering medroxyprogesterone acetate for14 days every three months have been investigated: the rates ofendometrial hyperplasia with this regimen have been found to varyfrom zero to 12 percent. If this regimen is used, routine endome-trial assessment for unscheduled bleeding is recommended.2*
CONTINUOUS-COMBINED REGIMENS
An alternative to the cyclic administration of progestin in HRTis continuous daily treatment with both an estrogen and prog-estin. This method was developed in order to avoid the with-drawal bleeding associated with cyclic HRT regimens. Mostdata are derived from studies which used CEE 0.625 mg with2.5 mg MPA per day.14,15 Other progestins can be used: theirtheoretical dose equivalents are listed in Table 7.
Forty percent of women receiving this therapy have irregu-lar breakthrough bleeding during the first three to six months.The majority of women who persist with the medication (75-87%) become amenorrheic by 12 months of use; some womenhave breakthrough bleeding after one year.16 A recent compari-son study indicated that significantly more women attainedamenorrhea based on various parameters when administeredcontinuous combined EE/NETA.17 A levonorgestrel-releasingintrauterine system is currently indicated for contraception. Thedevice can be left in situ for five years and, as with other contin-uous progestin use, breakthrough bleeding may occur duringthe first months of use.2 Current research suggests potential foruse of such a device in postmenopausal women, in combinationwith systemic estrogen administration.18
INDIVIDUALIZING THERAPY
The use of estrogens can result in unpleasant side effects in fiveto 10 percent of women using 0.625 mg CEE, or its equivalent,daily.19 Common complaints in women on therapy includemastalgia, nausea, headache, and bloating. These side effects areoften dose-related, and may resolve with continued use or adecrease in dose. Since side effects may vary among currentlyavailable estrogen preparations, it is a reasonable strategy to sub-stitute another preparation for a poorly tolerated one.
TABLE 7
PROGESTINS—DOSAGES FOR ENDOMETRIAL PROTECTION*
CYCLIC CONTINUOUS ORAL daily for at least 12 days/month (mg) daily (mg)Medroxyprogesterone acetate 5–10 2.5Medrogesterone (metrogestone) 5–10Megestrol 20Micronized progesterone 200–300** 100Norethindrone 0.35–0.7 0.35Norethindrone acetate 2.5 0.5–1.0
TRANSDERMALNorethindrone acetate (NETA)*** 250 µg 140 or 250 µg
* Larger doses of estrogen may necessitate higher doses of progestin** May be administered vaginally*** Available in combination with 17β-estradiol patches
TABLE 6ESTROGEN AND PROGESTIN REGIMENS
Regimen Days per month
Cyclic estrogen 1 to 25Cyclic progestin 1 to 12–14
Continuous estrogen every dayCyclic progestin 1 to 12–14
Continuous estrogen every dayContinuous progestin every day
Cyclic unopposed estrogen 1 to 25
Continuous unopposed estrogen every day
Continuous estrogen every day Long cycle progestin 1 to 14 (every 3 months)
* Hormone replacement therapy and cancer, J Obstet Gynaecol Can 2001;23(12).

JOGC OCTOBER 200264
Estrogen doses may be titrated to achieve control of symp-toms. Residual vasomotor symptoms or vaginal dryness may indi-cate a need to increase the dose, or to change the preparation orroute of administration. Breast tenderness or leukorrhea mayrequire a reduction in medication dose. Side effects of progestinsinclude alterations in mood, mastalgia, and bloating. Switchingfrom one progestin formulation to another may reduce thesesymptoms.2 Adverse reactions to progestins are more frequentwhen progestins are given with estrogen therapy.20
Cyclic progestin-associated side effects may be reduced or elim-inated by switching to a continuous-combined regimen. Likeestrogens, each progestin preparation has a different side-effectprofile. For example, micronized progesterone can cause seda-tion,21 and should therefore be administered at bedtime. Themicronized progesterone formulation Prometrium® containspeanut oil and is contraindicated in women allergic to peanuts.
The potential benefits of androgen treatment have beenobserved with the administration of relatively large doses ofandrogens. Androgen therapy is associated with virilizing effects(acne, alopecia, and hirsutism) and an adverse effect on thecholesterol-lipoprotein profile; potential benefits from this ther-apy must be weighed against the unwanted effects.2
ESTROGEN-ONLY THERAPY
Estrogen without the endometrial protective effect of a progestinis recommended only in women who do not have a uterus. Therole of unopposed estrogen in the development of endometrialneoplasia has been well documented.8* Infrequently, a woman witha uterus may elect to take unopposed estrogen, usually because ofprevious bleeding problems or adverse progestin-related side effects.However, these women need close follow-up and evaluation.†
Endometrial assessment, preferably by biopsy, should be per-formed annually, and may also be prudent as a baseline in womenwith other risk factors for endometrial cancer.
PROGESTIN-ONLY THERAPY
Progestins can be used to control vasomotor symptoms inwomen with contraindications to estrogen. Schiff et al.22
demonstrated the efficacy of MPA 20 mg daily in controllingvasomotor symptoms, while Loprinzi et al.23 used megestrol20 mg twice daily to relieve hot flushes. The obese patient isable to produce endogenous estrogen by peripheral conversionof androstendione to estrone in adipose tissue.24 In addition,obese women have low serum concentrations of sex hormone-binding globulin (SHGB), resulting in a further increase in cir-culating free estrogen.24 These women have high concen-trations of unopposed free estrogen, and are at risk of devel-oping endometrial neoplasia.*
ESTROGEN-ANDROGEN HORMONE
REPLACEMENT THERAPY
A woman’s total estrogen production after menopause decreasesby 80 percent and androgen production decreases by as muchas 50 percent.2 Following bilateral oopherectomy, serum estro-gen and androgen concentrations drop precipitously. Thepotential indications for estrogen-androgen therapy are out-lined in Section C*, while the androgen preparations used forHRT are listed in Table 4.
CONTRAINDICATIONS TO ESTROGEN USE
The number of contraindications continues to decrease, as bothknowledge and use of estrogen replacement therapy (ERT)increase. Special considerations regarding the use of ERT arediscussed in Section G.†
The following conditions are usually considered absolute con-traindications to ERT: 1. unexplained vaginal bleeding prior to investigation2. acute liver disease3. active thromboembolic disease4. known or suspected carcinoma of the breast§
The risk posed by estrogen use in a patient with a past his-tory of thrombosis is variable.‡ The risk of recurrence of breastcancer following estrogen therapy is also unknown.§ Cautionis recommended in patients with a history of cardiovasculardisease and hypertriglyceridemia.11 For all patients, the sever-ity of menopausal symptoms must be considered in light of theknown risks and potential benefits of therapy.
CONTRAINDICATIONS TO PROGESTIN USE
The contraindications to use of progestins are:1. known or suspected carcinoma of the breast2. undiagnosed vaginal bleeding3. pregnancy
There is insufficient evidence to support a contraindica-tion to the use of progestins in patients with a past history ofthromboembolic disorders.
CONTRAINDICATIONS TO ANDROGEN USE
The use of androgen is contraindicated in women with exten-sive cardiac, hepatic or renal disease.25
SELECTIVE ESTROGEN
RECEPTOR MODULATORS (SERMS)
Estrogen binds intracellularly to an estrogen receptor, and the
* Hormone replacement therapy and cancer, J Obstet Gynaecol Can 2001;23(12).† Evaluation, decision-making, and follow-up, J Obstet Gynaecol Can 2001;23(12).
* Menopause and sexual function, J Obstet Gynaecol Can 2001;23(9):849-52.† Medical and special conditions, J Obstet Gynaecol Can 2001;23(11):1096-1101.‡ Hormone replacement therapy and cardiovascular disease, J Obstet Gynaecol Can
2001;23(10), 966-72.§ Hormone replacement therapy and cancer, J Obstet Gynaecol Can 2001;23(12).

JOGC OCTOBER 200265
estrogen-receptor complex in turn binds to DNA, thus activating target genes. Different estrogen receptor subtypes indifferent tissues have allowed the development of selectiveestrogen receptor modulators (SERMs), which can act as estro-gen agonists in some tissues and as estrogen antagonists in othertissues. Ideally, SERMs would have favourable effects on boneand liver while being antagonistic in the uterus and breast.
TamoxifenTamoxifen, first synthesized in 1966, has been found to havesome estrogen agonist effect in the endometrium and estrogenantagonist effect in the breast.26 This agent is useful as adju-vant therapy in patients with estrogen receptor-positive breastcancer,27 and as a primary prevention in patients who are atvery high risk for breast cancer.28 Endometrial stimulation andan increased long-term risk of endometrial carcinoma remainsignificant concerns regarding its use.
RaloxifeneRaloxifene reduces the risk of new vertebral fractures by 30 to50 percent.29-31 No significant reduction in non-vertebral orhip fracture was seen in a very large trial.30 Although LDL-cho-lesterol levels are reduced and triglyceride levels not increasedwith raloxifene therapy, HDL-cholesterol levels are notincreased, in contrast to the effect of oral estrogen therapy.29
As yet there are no data to prove any reduction in cardiovas-cular disease with use of raloxifene. The side effects of SERMsinclude exacerbation of vasomotor symptoms and vaginal dry-ness, leg cramps, and an increase in the risk of venous throm-boembolism similar to that seen with estrogen therapy.29
CONTRAINDICATIONS TO SERMS
Contraindications to tamoxifen and raloxifene are listed inTable 8.
NON-HORMONAL MEDICATIONS
BISPHOSPHONATES
Bisphosphonates are physiologic inhibitors of crystallization. Theirbasic structure is phosphorus-carbon-phosphorus, which cannotbe degraded in humans. Consequently, the molecules are excretedunchanged in the urine and have a half-life in the organism pro-portional to the affinity they have for bone.29,32 The agents with avery high affinity for bone, such as etidronate and alendronate, mayhave half-lives in the skeleton of up to 15 years.25
Three bisphosphonates are approved for the preventionand treatment of osteoporosis: etidronate, alendronate, andrisedronate. There is a need to distinguish between nitrogen-containing bisphosphonates (alendronate, risedronate) andnon-nitrogen bisphosphonates (etidronate), as the molecularmechanism of action and the clinical effects of the two classesare significantly different.
Non-nitrogen bisphosphonates inhibit osteoclasts by form-ing toxic metabolites of adenosine triphosphate (ATP). By rea-son of their affinity for bone, they are selective in inhibitingosteoclast action. Etidronate is a bisphosphonate that caninhibit mineralization when given continously; it must there-fore only be given cyclically.25
Nitrogen-containing bisphosphonates inhibit protein preny-lation, a step along the mevalonic acid pathway.25
Alendronate and risedronate have very low bioavailability, and
TABLE 8COMMON SIDE EFFECTS AND CONTRAINDICATIONS OF DRUGS USED IN OSTEOPOROSIS25,29
Drug Common side effects Contraindications
Alendronate • Abdominal pain • Abnormalities of the esophagus• Nausea • Inability to sit/stand upright for 30 minutes• Diarrhea • Hypersensitivity to the drug
• Women of childbearing potential• Renal insufficiency (< 30 mL/min)
Etidronate • Diarrhea • Clinically overt osteomalacia• Nausea • Hypersensitivy to the drug• Constipation • Women of childbearing potential
• Renal insufficiency (< 30 mL/min)
Nasal calcitonin • Rhinitis • Hypersensitivity to the drug• Nasal dryness • Women of childbearing potential• Epistaxis
Raloxifene • Vasodilatation (flushing) • History of venous thromboembolic events• Leg cramps • Hypersensitivity to the drug
• Women of childbearing potential
Risedronate • Abdominal pain • Abnormalities of the esophagus• Nausea • Inability to sit/stand upright for 30 minute• Diarrhea • Hypersensitivity to the drug
• Women of childbearing potential• Renal insufficiency (< 30 mL/min)
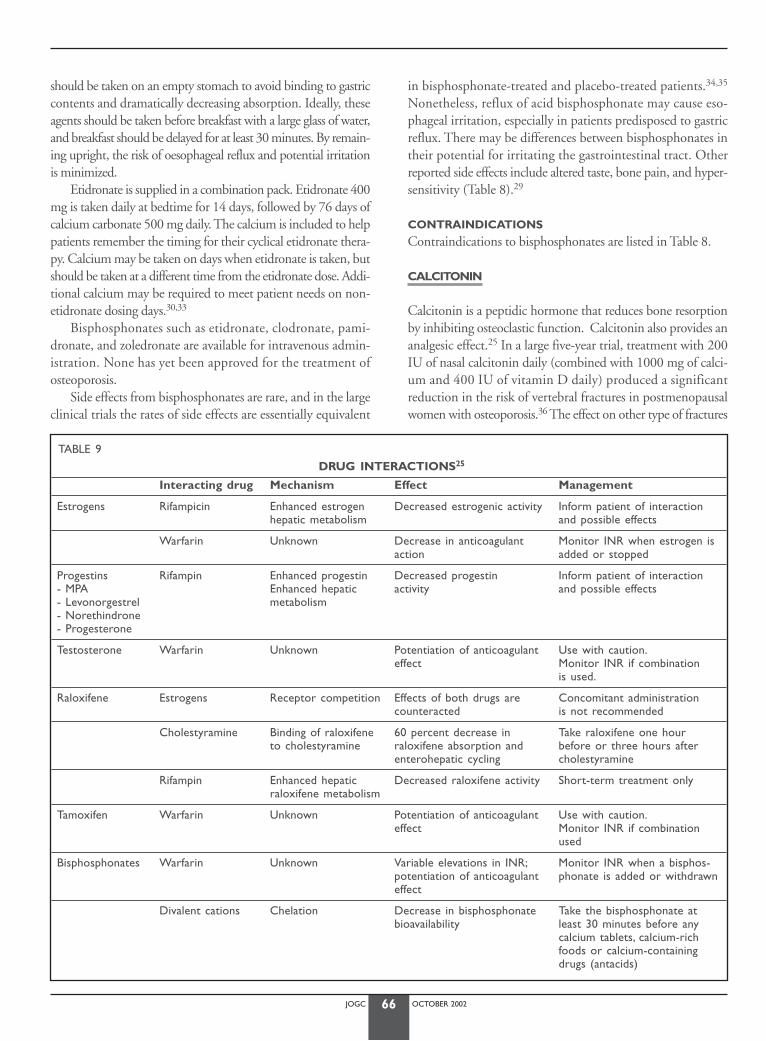
JOGC OCTOBER 200266
should be taken on an empty stomach to avoid binding to gastriccontents and dramatically decreasing absorption. Ideally, theseagents should be taken before breakfast with a large glass of water,and breakfast should be delayed for at least 30 minutes. By remain-ing upright, the risk of oesophageal reflux and potential irritationis minimized.
Etidronate is supplied in a combination pack. Etidronate 400mg is taken daily at bedtime for 14 days, followed by 76 days ofcalcium carbonate 500 mg daily. The calcium is included to helppatients remember the timing for their cyclical etidronate thera-py. Calcium may be taken on days when etidronate is taken, butshould be taken at a different time from the etidronate dose. Addi-tional calcium may be required to meet patient needs on non-etidronate dosing days.30,33
Bisphosphonates such as etidronate, clodronate, pami-dronate, and zoledronate are available for intravenous admin-istration. None has yet been approved for the treatment ofosteoporosis.
Side effects from bisphosphonates are rare, and in the largeclinical trials the rates of side effects are essentially equivalent
in bisphosphonate-treated and placebo-treated patients.34,35
Nonetheless, reflux of acid bisphosphonate may cause eso-phageal irritation, especially in patients predisposed to gastricreflux. There may be differences between bisphosphonates intheir potential for irritating the gastrointestinal tract. Otherreported side effects include altered taste, bone pain, and hyper-sensitivity (Table 8).29
CONTRAINDICATIONS
Contraindications to bisphosphonates are listed in Table 8.
CALCITONIN
Calcitonin is a peptidic hormone that reduces bone resorptionby inhibiting osteoclastic function. Calcitonin also provides ananalgesic effect.25 In a large five-year trial, treatment with 200IU of nasal calcitonin daily (combined with 1000 mg of calci-um and 400 IU of vitamin D daily) produced a significantreduction in the risk of vertebral fractures in postmenopausalwomen with osteoporosis.36 The effect on other type of fractures
TABLE 9DRUG INTERACTIONS25
Interacting drug Mechanism Effect Management
Estrogens Rifampicin Enhanced estrogen Decreased estrogenic activity Inform patient of interactionhepatic metabolism and possible effects
Warfarin Unknown Decrease in anticoagulant Monitor INR when estrogen is action added or stopped
Progestins Rifampin Enhanced progestin Decreased progestin Inform patient of interaction- MPA Enhanced hepatic activity and possible effects- Levonorgestrel metabolism- Norethindrone- Progesterone
Testosterone Warfarin Unknown Potentiation of anticoagulant Use with caution.effect Monitor INR if combination
is used.
Raloxifene Estrogens Receptor competition Effects of both drugs are Concomitant administration counteracted is not recommended
Cholestyramine Binding of raloxifene 60 percent decrease in Take raloxifene one hour to cholestyramine raloxifene absorption and before or three hours after
enterohepatic cycling cholestyramine
Rifampin Enhanced hepatic Decreased raloxifene activity Short-term treatment onlyraloxifene metabolism
Tamoxifen Warfarin Unknown Potentiation of anticoagulant Use with caution.effect Monitor INR if combination
used
Bisphosphonates Warfarin Unknown Variable elevations in INR; Monitor INR when a bisphos-potentiation of anticoagulant phonate is added or withdrawneffect
Divalent cations Chelation Decrease in bisphosphonate Take the bisphosphonate atbioavailability least 30 minutes before any
calcium tablets, calcium-richfoods or calcium-containing drugs (antacids)
JOGC OCTOBER 200267
is uncertain.36 The most frequent side effects reported with useof nasal calcitonin are nasal dryness, epistaxis, and rhinitis.29
NEW THERAPIES
Tibolone is a steroid with estrogenic, progestational, and andro-genic activity. It has been used in Europe for treatment ofmenopausal symptoms and sexual functioning. It is not cur-rently available in Canada.
In addition to new compounds, different formulations ofestrogens and progestins are in development. These includetransdermal delivery systems, gels, subdermal pellets for im-plantation, and vaginal tablets. Newer SERMs, which mayhave differing effects on target tissues depending on their selec-tivity and potency, are also in development.
DRUG INTERACTIONS
HRT might interact with several drugs. Table 9 lists the mostimportant interactions. Since other interactions might occur,it is advisable to consult a pharmacist or a drug interaction ref-erence when adding a new therapy to a patient receiving HRTor osteoporosis medications.
RECOMMENDATIONS:
I1. The route of estrogen delivery should be primarily deter-mined by patient preference, with the objective of usingthe lowest effective dose. (III)
I2. Physicians should consider alternate routes of administra-tion such as vaginal and transdermal administration. (III)
I3. Physicians should be aware that women who wish to usecontinuous combined HRT long term (five or moreyears) should be re-evaluated annually. (III)
CONCLUSIONSeveral products are available to treat menopause-related prob-lems. Every woman should be informed of the potential bene-fits and adverse reactions with any treatment option considered.Health professionals play a key role in providing the most cur-rent information for each patient.
J Obstet Gynaecol Can 2001;23(11):1105-14.
REFERENCES
1. Williams CL, Stancel GM. Estrogens and Progestins. In: Hardman JG,Limbird LE (eds). The Pharmacological Basis of Therapeutics. 9th edi-tion. Toronto: McGraw-Hill, 1996;pp.1411-40.
2. Speroff L, Glass RH, Kase NG. Clinical Gynecologic Endocrinology andInfertility. 6th edition. Philadelphia: Lippincott Williams & Wilkins, 1999.
3. Ansbacher R. Bioequivalence of conjugated estrogen products. ClinPharmacokinet 1993;24:271-4.
4. Judd HL.Transdermal estradiol: a potentially improved method of hor-mone replacement. J Reprod Med 1994;39:343-52.
5. Jensen J, Christiansen C. Effects of smoking on serum lipoproteins andbone mineral content during postmenopausal hormone replacementtherapy.Am J Obstet Gynecol 1988;159: 820-5.
6. Jarvinen A, Nykanen S, Paasiniemi L.Absorption and bioavailability ofoestradiol from a gel, a patch and a tablet. Maturitas 1999;32:103-13.
7. Beresford SA,Weiss NS,Voigt LF, McKnight B. Risk of endometrial can-cer in relation to use of estrogen combined with cyclic progestin thera-py in women. Lancet 1997;349:458-61.
8. The Postmenopausal Estrogen/Progestin Interventions (PEPI) TrialInvestigators. Effects of estrogen or estrogen/progestin regimens onheart disease risk factors in postmenopausal women: the postmeno-pausal estrogen/progestin interventions (PEPI) trial. J Am Med Assoc1995;273:199-208.
9. Moyer DL, de Lignieres B, Driguez P, Pez JP. Prevention of endometrialhyperplasia by progesterone during long-term estradiol replacement:influence of bleeding pattern and secretory changes. Fertil Steril1993;59:992-7.
10. Padwick ML, Pryse-Davies J,Whitehead Ml.A simple method for deter-mining the optimal dosage of progestin in postmenopausal womenreceiving estrogens. N Eng J Med 1986;315:930-4.
11. Stevenson JC, Cust MP, Gangar KF, Hillard TC, Lees B,Whitehead MI.Effects of transdermal versus oral hormone replacement therapy onbone density in spine and proximal femur in postmenopausal women.Lancet 1990;336:265-9.
12. Genant HK, Lucas J,Weiss S et al. Low-dose esterified estrogen therapy:effects on bone, plasma estradiol concentrations, endometrium, andlipid levels. Estratab/Osteoporosis Study Group.Arch Intern Med.1997;157:2609-15.
13. Whitehead MI,Townsend PT, Pryse-Davies J, Ryder T, Lane G, SiddleNC, et al. Effects of various types and dosages of progesterones on thepostmenopausal endometrium. J Reprod Med 1982;27;539-48.
14. Weinstein L. Efficacy of a continuous estrogen progestin regimen in themenopausal patient. Obstet Gynecol 1987;69:1534-9.
15. Weinstein L, Bewtra G, Gallagher JC. Evaluation of a continuous com-bined low dose regimen of estrogen/progestin for treatment of themenopausal patient.Am J Obstet Gynecol 1990;162:1534-9.
16. Archer DF, Pickar JH, Bottiglioni F. Bleeding patterns in postmenopausalwomen taking continuous combined or sequential regimens of conju-gated estrogens with medroxyprogesterone acetate. Obstet Gynecol1994;83:686-92.
17. Simon J.A., Symonds J.P. Unscheduled bleeding during initiation of con-tinuous combined hormone replacement therapy: a direct comparisonof two combinations of norethindrone acetate and ethinyl estradiol tomedroxyprogesterone acetate and conjugated equine estrogens.Menopause 2001;8(5):321-7.
18. Sturridge F, Guillebaud J.A risk-benefit assessment of the levonor-gestrel-releasing intrauterine system. Drug Saf 1996; 15: 430-40.
19. Grady D, Rubin SM, Petitti DB, Fox CS, Black D, Ettinger B, et al.Hormone replacement to prevent disease and prolong life inpostmenopausal women.Ann Intern Med 1992;117:1016-37.
20. Prior JC,Alojado N, McKay DW,Vigna YM. No adverse effects ofmedroxyprogesterone treatment without estrogen in postmenopausalwomen: double-blind, placebo-controlled, crossover trial. ObstetGynecol 1994;83:24-8.
21. Frishman GN, Klock SC, Luciano AA, Nulsen JC. Efficacy of oral micro-nized progesterone in the treatment of luteal phase defects. J ReprodMed 1995;40:521-4.
22. Schiff I,Tulchinsky D, Cramer D, Ryan K. Oral medroxyprogesterone inthe treatment of postmenopausal symptoms. J Am Med Assoc 1980;244:1443-5.
23. Loprinzi CL, Michalak JC, Quella SK, O’Fallon JR, Hatfield AK, MelimarkRA et al. Megestrol acetate for the prevention of hot flashes. N Engl JMed 1994;331:247-52.
24. Macdonald PC, Siiteri PK.The relationship between extraglandular pro-duction of estrone and the occurrence of endometrial neoplasia.Gynecol Oncol 1974;2(2-3):259-63.
25. Hutchison TA, Shahan DR & Anderson ML, eds. DRUGDEX® System.Micromedex Inc., Englewood, Colorado (CD-ROM).

JOGC OCTOBER 200268
26. Dutertre M, Smith CL. Molecular mechanisms of selective estrogen receptor modulator (SERM) action. J Pharmacol Exp Ther 2000;295:431-7.
27. Early Breast Cancer Trialists Group. Systemic treatment of early breastcancer by hormonal, systemic or immune therapy: 133 randomized trials involving 31,000 recurrences and 24,000 deaths among 75,000women. Lancet 1992:339:71-85.
28. Vogel VG. Reducing the risk of breast cancer with tamoxifen in womenat increased risk. J Clin Oncol 2001;19:87S-92S.
29. No authors listed. Médicaments pour la prévention et le traitement del’ostéoporose postménopausique. Lettre Médicale 2000;24:69-72.
30. Gambacciani M, Ciaponi M. Postmenopausal osteoporosismanagement. Curr Opin Obstet Gynecol 2000;12:189-97.
31. Ettinger B, Black DM, Mitlak BH, et al. Reduction of vertebral fracturerisk in postmenopausal with osteoporosis treated with raloxifene:results from a 3-year randomised clinical trial. J Am Med Assoc1999;282:637-45.
32. Williams CL, Stancel GM. Estrogens and Progestins. In: Hardman JG,Limbird LE (eds). The Pharmacological Basis of Therapeutics. 9th edi-tion. Toronto: McGraw-Hill, 1996:pp.1537-42.
33. Estell R. Treatment of postmenopausal osteoporosis. N Engl J Med1993;338:736-46.
34. Hosking D, Chilvers CE, Christiansen C et al. Prevention of bone losswith alendronate in postmenopausal women under 60 years of age.Early Postmenopausal Intervention Cohort Study Group. N Engl J Med1998;338:485-92.
35. McClung MR, Geusens P, Miller PD, et al. Effect of risedronate on therisk of hip fracture women. Hip Intervention Program Study Group. NEngl J Med 2001;344:333-40.
36. Chesnut CH III, Silverman S,Andriano K, et al. A randomized trial ofnasal spray salmon calcitonin in postmenopausal women withestablished osteoporosis: the prevent recurrence of osteoporotic fractures study. PROOF Study Group. Am J Med 2000;109:267-76.
JOGC OCTOBER 2002
INTRODUCTION
The fact that several risk factors for breast and endometrial can-cer are associated with increased endogenous estrogen expo-sure1-4 suggests that exogenous estrogen might also increase theincidence of these cancers.4 Repeated gonadotropic stimulationmay also be a risk factor for ovarian cancer,5 whereas estrogensare generally accepted as promoters of endometrial and breastepithelial cell proliferation, but their actions within the ovariesare less well known.
The association between progesterone, progestins, and can-cer remains controversial. In the endometrium, progesteronemostly functions as an anti-estrogen by decreasing the num-ber of nuclear estrogen receptors6 and introducing 17β-hydroxysteroid dehydrogenase.7 Most in vitro studies of can-cer cell lines and cultured normal cells show progesterone tohave an inhibitory effect on proliferation in the breast, but invivo experiments with normal breast tissue show a high mitot-ic index during the luteal phase.8 Similarly, synergistic effectsof progestins in combination with estrogen have been found.9
ENDOMETRIAL CANCER
UNOPPOSED ESTROGEN
Several lines of evidence indicate that unopposed estrogenreplacement therapy (ERT) increases the risk of endometrialcancer.1,2 Epidemiological studies have shown a five to 10-fold increased risk of endometrial cancer in women takingERT;9 this risk is related to estrogen dose and duration of ther-apy.10 Furthermore, this increased risk of developing endome-trial carcinoma persists for at least five years after unopposedERT has ceased.10 In the PEPI trial, unopposed ERT has alsobeen shown to cause atypical endometrial hyperplasia in up to30 percent of study subjects.11
Whereas the risk of developing endometrial cancer is sig-nificantly elevated after at least five years of therapy,10 the riskof developing invasive cancer or of dying from endometrialcancer while taking ERT remains uncertain. Although moststudies report no excess deaths due to endometrial canceramong ERT users,10 one meta-analysis has shown an increasedrisk for late-stage, high grade invasive tumours.12
COMBINED PROGESTIN AND
ESTROGEN REPLACEMENT
Adding progestins or progesterone to an ERT regimen marked-ly reduces the risk of developing both endometrial hyperpla-sia11 and cancer,10 although no hormone replacement therapy(HRT) regimen has proven completely protective. Various reg-imens using different dosages of progestins for a minimum of12 to 14 days per month13 have been proposed. While the doseof progestin should be individualized, as a general rule higherprogestin doses should accompany higher-dose estrogenadministration. In keeping with the observation that the dura-tion of progestin therapy is more important than the actualdose,14 continuous therapy with low-dose progestin may offerendometrial protection equivalent or superior to that of cyclic-al therapy.
Limited experience suggests that 14 days of progestin ther-apy every three months may not be completely protective againstatypical endometrial hyperplasia.15 Limited data also suggest thatdaily micronized progesterone for 25 to 30 days may be protec-tive against hyperplasia.16 Long-term follow-up data on endome-trial cancer are not yet available with these regimens.
HRT FOR WOMEN PREVIOUSLY
TREATED FOR ENDOMETRIAL CANCER
HRT has traditionally been withheld from women after treat-ment for endometrial cancer, based on the belief that HRTmight increase the risk of recurrence. This belief has never beensubstantiated, and two recent retrospective studies have ques-tioned it.17,18 Based on these limited studies, a committee opin-ion of the American College of Obstetricians and Gyne-cologists concluded that HRT may be used by women whohave been treated for endometrial cancer and who fall into alow-risk group, defined as women with stage I disease, grade 1or 2 histiology, and less than 50 percent depth of myometrialinvasion.19 Estrogen administration is commonly begun post-operatively when the patient is ambulatory. It remains unde-termined whether progestin should be added to the regimenin these patients. The use of androgens in these patients is con-troversial, because androgens may undergo aromatization toestrogen.20
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
Serge Bélisle, MSc, MD, FRCSC,1 Christine Derzko, MD, FRCSC2
1 Montreal QC2 Toronto ON
HORMONE REPLACEMENT THERAPY AND CANCER
69
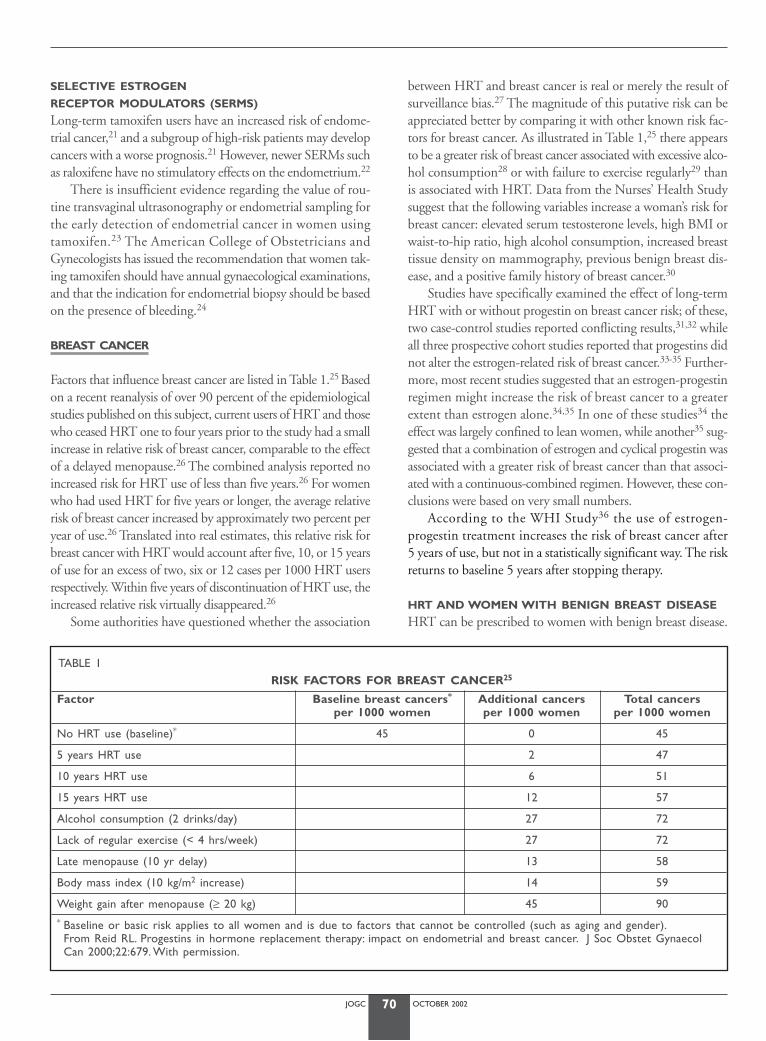
SELECTIVE ESTROGEN
RECEPTOR MODULATORS (SERMS)
Long-term tamoxifen users have an increased risk of endome-trial cancer,21 and a subgroup of high-risk patients may developcancers with a worse prognosis.21 However, newer SERMs suchas raloxifene have no stimulatory effects on the endometrium.22
There is insufficient evidence regarding the value of rou-tine transvaginal ultrasonography or endometrial sampling forthe early detection of endometrial cancer in women usingtamoxifen.23 The American College of Obstetricians andGynecologists has issued the recommendation that women tak-ing tamoxifen should have annual gynaecological examinations,and that the indication for endometrial biopsy should be basedon the presence of bleeding.24
BREAST CANCER
Factors that influence breast cancer are listed in Table 1.25 Basedon a recent reanalysis of over 90 percent of the epidemiologicalstudies published on this subject, current users of HRT and thosewho ceased HRT one to four years prior to the study had a smallincrease in relative risk of breast cancer, comparable to the effectof a delayed menopause.26 The combined analysis reported noincreased risk for HRT use of less than five years.26 For womenwho had used HRT for five years or longer, the average relativerisk of breast cancer increased by approximately two percent peryear of use.26 Translated into real estimates, this relative risk forbreast cancer with HRT would account after five, 10, or 15 yearsof use for an excess of two, six or 12 cases per 1000 HRT usersrespectively. Within five years of discontinuation of HRT use, theincreased relative risk virtually disappeared.26
Some authorities have questioned whether the association
between HRT and breast cancer is real or merely the result ofsurveillance bias.27 The magnitude of this putative risk can beappreciated better by comparing it with other known risk fac-tors for breast cancer. As illustrated in Table 1,25 there appearsto be a greater risk of breast cancer associated with excessive alco-hol consumption28 or with failure to exercise regularly29 thanis associated with HRT. Data from the Nurses’ Health Studysuggest that the following variables increase a woman’s risk forbreast cancer: elevated serum testosterone levels, high BMI orwaist-to-hip ratio, high alcohol consumption, increased breasttissue density on mammography, previous benign breast dis-ease, and a positive family history of breast cancer.30
Studies have specifically examined the effect of long-termHRT with or without progestin on breast cancer risk; of these,two case-control studies reported conflicting results,31,32 whileall three prospective cohort studies reported that progestins didnot alter the estrogen-related risk of breast cancer.33-35 Further-more, most recent studies suggested that an estrogen-progestinregimen might increase the risk of breast cancer to a greaterextent than estrogen alone.34,35 In one of these studies34 theeffect was largely confined to lean women, while another35 sug-gested that a combination of estrogen and cyclical progestin wasassociated with a greater risk of breast cancer than that associ-ated with a continuous-combined regimen. However, these con-clusions were based on very small numbers.
According to the WHI Study36 the use of estrogen-progestin treatment increases the risk of breast cancer after 5 years of use, but not in a statistically significant way. The riskreturns to baseline 5 years after stopping therapy.
HRT AND WOMEN WITH BENIGN BREAST DISEASE
HRT can be prescribed to women with benign breast disease.
JOGC OCTOBER 200270
TABLE 1RISK FACTORS FOR BREAST CANCER25
Factor Baseline breast cancers* Additional cancers Total cancersper 1000 women per 1000 women per 1000 women
No HRT use (baseline)* 45 0 45
5 years HRT use 2 47
10 years HRT use 6 51
15 years HRT use 12 57
Alcohol consumption (2 drinks/day) 27 72
Lack of regular exercise (< 4 hrs/week) 27 72
Late menopause (10 yr delay) 13 58
Body mass index (10 kg/m2 increase) 14 59
Weight gain after menopause (≥ 20 kg) 45 90 * Baseline or basic risk applies to all women and is due to factors that cannot be controlled (such as aging and gender).From Reid RL. Progestins in hormone replacement therapy: impact on endometrial and breast cancer. J Soc Obstet Gynaecol Can 2000;22:679. With permission.

JOGC OCTOBER 200271
Women with a personal history of premalignant disease of thebreast are at increased risk for breast cancer.37 The relative riskof developing breast cancer is 1.8 in women with a history ofproliferative breast disease without atypical hyperplasia, and 3.6in those with atypical hyperplasia,38 compared to women withnon-proliferative benign histology. These risks are not affectedby the use of HRT.39
RISK OF BREAST CANCER IN WOMEN
CONSIDERING HRT WITH A HISTORY
OF ORAL CONTRACEPTIVE USE
Previous use of oral contraceptives (OCs) does not furtherincrease the HRT-related risk for breast cancer. Neither long-term past use nor use prior to menopause confers any appre-ciable increase in the risk of HRT-related breast carcinoma.40
HRT AND WOMEN WITH RISK
FACTORS FOR BREAST CANCER
HRT can be prescribed for women with a history of breast can-cer after proper counselling. Women with a history of breastcancer in a first-degree relative carry a two to four timesincreased risk of developing breast cancer.41 This risk increaseseven further if two first-degree relatives are affected or if the can-cer occurs premenopausally.41 The available data suggest thatthe addition of HRT does not further increase this risk.41
HRT can also be prescribed to women with a genetic pre-disposition to breast or ovarian cancer, after bilateral prophy-lactic oophorectomy (BPO) and after proper counselling.Three to five percent of these women carry a specific geneticmutation (BRCA1 or 2) that confers a 60 to 80 percent life-time risk of developing breast cancer.42 Some of the womenmay elect to undergo BPO, which raises concerns about use ofHRT after surgical menopause. The effects of HRT on womencarrying BRCA1 or 2 genes have not been well studied.Rebbeck et al.43 reported that ever-use or never-use of HRTwas not a significant independent predictor of breast canceroutcome, in a model that included BPO. Exclusion of womenwho had HRT exposure after BPO43 did not significantly affectthe risk reduction conferred by BPO. The use of newer syn-thetic antiestrogens such as raloxifene is an option that mayalso be considered for prevention of osteoporosis.
HRT AND WOMEN WITH BREAST CANCER
It remains unclear whether HRT can be prescribed to women pre-viously treated for breast cancer. All women should receive expertindividualized counselling which takes into account prognosticfactors for breast cancer (stage of disease, estrogen receptor statusof the tumour, and time since diagnosis of breast cancer), imme-diate quality of life issues related to estrogen deficiency, risk factors
for future osteoporotic fractures, and other options for control ofsymptoms and disease prevention. At present, the risks and ben-efits of HRT in breast cancer survivors are poorly defined.44,45
Recruitment bias is a major factor in interpreting outcome reports,and most study subjects to date had favourable prognostic factors.A mean of 7.4 percent (range 0–9%) of women with localizedbreast cancer showed recurrence of disease equivalent to the pre-dicted rate of recurrence.46 The National Cancer Institute of theUnited States has initiated a randomized prospective trial of HRTfollowing treatment of breast cancer in women with stage I and IIdisease to clarify some of these issues.
There is no reliable information about the influence ofHRT on cancer progression in a woman found to have breastcancer while taking HRT. In general, the current practice is tostop HRT until proper staging and therapy are completed.
Breast cancer survivors frequently report such symptoms ashot flashes, vaginal dryness, and decreased libido, especially if thecancer occurred premenopausally and was followed by chemother-apy. For such patients, non-hormonal medications have beenproven more effective than placebo in reducing hot flashes.47* Sim-ilarly, high doses of progestins are effective in alleviating vasomo-tor symptoms, although their safety has not been established inwomen previously treated for breast cancer.† Certain forms of top-ical estrogen therapy, such as sustained-release estradiol vaginalrings or low-dose vaginal cream (equivalent to 0.5 g or one-eighthapplicator of CEE cream daily) will control hypo-estrogenic vagi-nal symptoms with minimal systemic absorption. The vaginalmucosa will readily absorb higher dosages of estrogenic vaginalcream.‡ Other approaches may also be considered, including theuse of lubricants or gels.
In women with reduced libido, androgen therapy may beconsidered, although the same concerns exist as for HRT becauseandrogens may be aromatized into estrogens.20 There is present-ly no evidence to support or refute the usefulness of addingandrogens to an HRT regimen in breast cancer survivors.
OTHER CANCERS
HRT AND COLO-RECTAL CANCER
Most case-control and cohort studies in current HRT users haveshown a decrease in the incidence of colo-rectal cancers.48,49
Moreover, two recent meta-analyses summarizing the results ofthese studies show that the risk is reduced by one-third in cur-rent and recent (within one year of assessment) users ofHRT.48,49 According to the WHI Study36 continuous-com-bined treatment with HRT was associated with a reduction inthe risk of colorectal cancer, which failed to reach statistical sig-nificance (6 fewer cases/10,000 women/year). The benefit didnot appear until after three years of use.
* Complementary approaches, J Obstet Gynaecol Can 2001;23(12):1204-13.† Pharmacotherapy, J Obstet Gynaecol Can 2001;23(11):1105-14.‡ Urogenital health, J Obstet Gynaecol Can 2001;23(10):973-7.
JOGC OCTOBER 200272
HRT AND OTHER CANCERS
OF THE REPRODUCTIVE TRACT
There is too little information to comment on any relationshipbetween HRT use and cancers of the cervix, vagina or vulva.50 Arecent epidemiological study reported that long-term use of unop-posed estrogens was associated with an increased risk of ovarian can-cer, but data were not available on the hormone regimens used.51
OTHER CANCERS PRECLUDING THE USE OF HRT
Melanoma, especially the cutaneous form, is considered to bepotentially hormone-sensitive, but it is not possible to commenton any relationship between melanoma and HRT because ofinsufficient data, and the confounding factor of quantity ofexposure to ultraviolet light.50
Although OCs are associated with an increased risk ofhepatocellular cancer, no data supports an association. Thy-roid carcinoma is quite prevalent in postmenopausal women,but available data again shows no association between ever-useof HRT and this malignancy.52
RECOMMENDATIONS:
J1. No estrogen-progestin regimen is completely protectiveagainst endometrial carcinoma, and all unscheduled uter-ine bleeding should be investigated. (II-2)
J2. Estrogen-progestin therapy should not be withheld fromwomen with treated stage 1 and 2, grade 1 or 2 adeno-carcinoma of the endometrium who have moderate tosevere menopausal symptoms. (II-3)
J3. According to the WHI study, physicians should informtheir patients that the use of estrogen-progestin treat-ment increases the risk of breast cancer after 5 years ofuse but not in a statistically significant way. The riskreturns to baseline after 5 years of stopping therapy.(I)
J4. There should be increased breast surveillance for womenwho are at high risk of developing breast cancer whenusing estrogen-progestin therapy. (III)
J5. In very special circumstances, women at increased riskof developing breast cancer or who have been treated forbreast cancer may be prescribed low dose estrogen-prog-estin therapy for severe symptoms unrelieved by effec-tive alternative therapies, after risks and benefits havebeen extensively discussed. The duration of therapyshould be regularly reviewed; there is no preventativerole for estrogen therapy in this population. (III)
J6. Physicians should be aware that the reported effects of estrogen-progestin therapy on ovarian cancer have been inconsistent. A possible increased risk may occur in womenon long-term estrogen-only therapy (10 or more years). (I)
SUMMARY OF KEY POINTS:
J7. Unopposed estrogen therapy substantially increases therisk of developing atypical endometrial hyperplasia (I)
and endometrial carcinoma (II-2). The appropriate doseand duration of progestin therapy will reduce theseestrogen-associated risks.
J8. Continuous combined HRT was associated with areduction in the risk of colorectal cancer, which failedto reach statistical significance (6 fewer cases per 10,000women per year). (I)
J Obstet Gynaecol Can 2001;23(12):1198-1203.
REFERENCES
1. Beral V, Banks E, Reeves G,Appleby P. Use of HRT and the subsequentrisk of cancer. J Epidemiol Biost 1999;4(3):191-215.
2. Burger CW, Koomen I, Peters NJAB,Van Leeuwen FE, Kenemans P.Postmenopausal hormone replacement therapy and cancer of thefemale genital tract and the breast. Eur Menopause J 1997;4:23-36.
3. Brinton LA, Schairer C. ERT and breast cancer risk. Epidemiol Rev1995;15:66-79.
4. King RJB.A discussion of the roles of estrogen and progestin in humanmammary carcinogensis. J Steroid Biochem Mol Biol 1991;39:811-8.
5. Rao BR, Slotman BJ. Endocrine factors in common epithelial ovariancancer. Endocr Rev 1991;12:14-26.
6. Hsueh AJW, Peck EJ, Clark JH. Control of uterine estrogen receptorlevels by progesterone. Endocrinology 1976;98:438-44.
7. Tseng L, Gurpide E. Induction of human estradiol dehydrogenase byprogestins. Endocrinology 1975;97:825-33.
8. Speroff L. Role of progesterone in normal breast physiology. J ReprodMed 1999;44(2 Suppl):172-9.
9. Campagnoli C, Biglia N, Cantamessa C, Lesca L, Sismondi P. HRT andbreast cancer risk: a clue for interpreting the available data. Maturitas1999;33:185-90.
10. Grady D, Gebretsadik T, Kerlikowske K, Ernster V, Petitti D. Hormonereplacement therapy and endometrial cancer risk: a meta-analysis.Obstet Gynecol 1995;85:304-13.
11. Writing Group for the PEPI trial. Effects of estrogen or estrogen/prog-estin regimens on heart disease risk factors in postmenopausal women.J Am Med Assoc 1995;273:199-208.
12. Ettinger B, Golditch IM, Friedman G. Gynecologic consequences oflong-term unopposed estrogen replacement therapy. Maturitas1998;10:271-82.
13. Gibbons WE,Thorneycroft IH. Protecting the endometrium. Opposingthe hyperplasia/malignancy potential of ERT. J Reprod Med 1999;44(2Suppl):203-8.
14. Weiderpass E,Adami HO, Baron JA, Magnusson C, Bergström R, Lind-gren A, et al. Risk of endometrial cancer following estrogenreplacement with and without progestins. J Natl Cancer Inst1999;91(13):1331-7.
15. Guerin A, Heldass K, Moeller B.Adverse endometrial effects of longcycle estrogen and progestogen replacement therapy. N Engl J Med1996;334:668-9.
16. Fitzpatrick LA, Good A. Micronized progesterone: clinical indicationsand comparison with current treatments. Fertil Steril 1999;72:389-97.
17. Creasman WT, Henderson D, Hinshaw W, Clarke-Pearson D. Estrogenreplacement therapy in the patient treated for endometrial cancer.Obstet Gynecol 1986;67:326-30.
18. Lee RB, Burke TW, Park RC. Estrogen replacement therapy followingtreatment for stage I endometrial carcinoma. Gynecol Oncol1990;36(2):189-91.
19. ACOG Committee Opinion (no. 126). Estrogen Replacement Therapyand Endometrial Cancer.Washington DC:American College of Obste-tricians and Gynecologists, 1993.
20. Siiteri PK, MacDonald PC. In: Greep RO,Astwood E, editors. Handbookof physiology and endocrinology.Vol 2, pt. 1. 1973.Washington:Ameri-
JOGC OCTOBER 200273
can Physiological Society. p. 615-29.21. Bergman L. Risk and prognosis of endometrial cancer after tamoxifen
for breast cancer. Lancet 2000;356:881-7.22. Delmas PD, Bjarnason NH, Mitlak BH, Ravoux AC, Shah AS, Huster WJ,
et al. Effects of raloxifene on bone mineral density, serum cholesterolconcentrations and uterine endometrium in postmenopausal women.N Engl J Med 1997;337:1641-7.
23. Smedira HJ. Practical issues in counseling healthy women about theirbreast cancer risk and use of tamoxifen citrate. Arch Intern Med2000;160:3034-42.
24. ACOG Committee Opinion.Tamoxifen and Endometrial Cancer.Wash-ington DC:American College of Obstetricians and Gynecologists, 1996.
25. Reid RL. Progestins in hormone replacement therapy: impact onendometrial and breast cancer. J Soc Obstet Gynaecol Can2000;22:679.
26. Collaborative Group on Hormonal Factors in Breast Cancer. Breast can-cer and hormone replacement therapy: collaborative reanalysis of datafrom 51 epidemiological studies of 52,705 women with breast cancerand 108,401 women without breast cancer. Lancet 1997;350:1047-59.
27. MacLennan AH, Smith M. Hormone replacement therapy and breastcancer: what are the facts? Med J Aust 1995 6;163(9):483-5.
28. Fuchs CS, Stampfer MJ, Colditz GA, et al.Alcohol consumption andmortality among women. N Engl J Med 1995;332(19):1245-50.
29. Thune I, Brenn T, Lund E, Gaard M. Physical activity and the risk ofbreast cancer. N Engl J Med 1997;336(18):1269-75.
30. Colditz GA. Hormones and breast cancer: evidence and implicationsfor consideration of risks and benefits of HRT. J Women Health1999;8(3):349-57.
31. Schairer C, Byrne C, Keyl PM, Brinton LA, Sturgeon SR, Hoover RN.Menopausal estrogen and estrogen-progestin replacement therapy andthe risk of breast cancer (United States). Cancer Causes Control1994;5(6):491-500.
32. Stanford J,Weiss N,Voigt L, Daling L, Habel L, Rossing M. Combinedestrogen and progestin hormone replacement therapy in relation torisk of breast cancer in middle-aged women. J Am Med Assoc1995;274:137-42.
33. Grodstein F, Stampfer MJ, Colditz GA,Walter C,Willett MD.Postmenopausal hormone therapy and mortality. N Engl J Med1997;336:1769-75.
34. Schairer G, Lubin J,Troisi R, et al. Menopausal estrogen and estrogen-progestin replacement therapy and breast cancer risk. J Am Med Assoc2000;283:485-91.
35. Ross RK, Paganini-Hill A,Wan PC, Pike MC. Effect of hormonal replace-ment therapy on breast cancer risk: estrogen versus estrogen plusprogestin. J Natl Cancer Inst 2000;92:328-32.
36. Writing Group for the Women’s Health Initiative Investigators. JAMA,2002;288:321-33.
37. Colditz GA, Rosner B. HRT use increases cumulative risk of breast can-cer at age 70.Am J Epidemiol 2000;92:328-32.
38. Byrne C, Connolly JL, Colditz GA, Schnitt SJ. Biopsy confirmed benignbreast disease, postmenopausal use of exogenous female hormones,and breast carcinoma risk. Cancer 2000;89:2046-52.
39. Dupont WD, Page DL, Parl FF, Plummer WD Jr., Schuyler PA, Kasami M,et al. Estrogen replacement therapy in women with a history of prolif-erative breast disease. Cancer 1999;85:1279-83.
40. Clemons M, Gauss P. Estrogen and the risk of breast cancer. N Engl JMed 2001;344(4):276-85.
41. Hoskins KF, Stopfer JE, Calzone KA, et al.Assessment and counselingfor women with a family history of breast cancer.A guide for clinicians. JAm Med Assoc 1995;273(7):577-85.
42. Whittemore AS, Gong G, Itnyre J. Prevalence and contribution ofBRCA1 mutations in breast cancer and ovarian cancer: results fromthree U.S. population-based case-control studies of ovarian cancer.Am JHum Genet 1997;60(3):496-504.
43. Rebbeck TR, Levin AM, Eisen A, et al. Breast cancer risk after bilateralprophylactic oophorectomy in BRCA-1 mutation carriers. J Natl Can-cer Inst 1999;91(17):1475-9.
44. Vassilopoulou-Sellin R,Theriault R, Klein MJ. Estrogen replacement ther-apy in women with prior diagnosis and treatment for breast cancer.Gynecol Oncol 1997;65:89-93.
45. Disaia PJ, Grosen EA, Kurosaki T, Gildea M, Cohen B, Culver HA. Hor-mone replacement therapy in breast cancer survivors: a cohort study.Am J Obstet Gynecol 1996;174:1494-8.
46. Vassilopoulou-Sellin R,Asmar L, Hortobagyi GN, Klein MJ, McNeese M,Singletary SE, et al. Estrogen replacement therapy after localized breastcancer. J Clin Oncol 1999;17:1482-7.
47. Loprinzi CL, Kugler JW, Sloan JA, Mailliard JA, LaVasseur BI, Barton DL,et al.Venlafaxine in management of hot flashes in survivors of breastcancer: a randomized controlled trial. Lancet 2000;356(9247):2059-63.
48. Nanda K, Bastian LA, Hasselblad V, Simel DL. Hormone replacementtherapy and the risk of colorectal cancer: a meta-analysis. ObstetGynecol 1999;93(5 Pt 2):880-8.
49. Grodstein F, Newcomb PA, Stampfer MJ. Postmenopausal hormonetherapy and the risk of colo-rectal cancer: a review and meta-analysis.Am J Med 1999;106:574-82.
50. Beral V, Banks E, Reeves G,Appleby P. Use of HRT and the subsequentrisk of cancer. J Epidemiol 1999;4(3):191-215.
51. Rodriguez C, Patel AV, Calle EE, Jacob EJ,Thun MJ. Estrogen replacementtherapy and ovarian cancer mortality in a large prospective study of USwomen. J Am Med Assoc 2001;285(11):1460-5.
52. Persson T,Yuen J, Bergkvist L, Schaimer C. Cancer incidence and mortal-ity in women receiving HRT: long-term follow-up. Intl J Cancer1996;67:327-33.

JOGC OCTOBER 2002
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
74
INTRODUCTION
There is a strong consumer-driven need for health care providersto be knowledgeable about complementary treatments formenopausal symptoms. While conventional hormone replace-ment therapy (HRT) is effective for the treatment ofmenopausal symptoms and prevention of such diseases as osteo-porosis, adherence rates for HRT are low. Data from the Mass-achusetts Women’s Health Survey of 2500 postmenopausalwomen indicated that 20 percent of women stopped takingHRT within nine months, predominantly due to fear of can-cer and dissatisfaction with uterine bleeding.1 Another 10 per-cent used HRT intermittently, while 20 to 30 percent neverfilled their prescriptions. Women frequently combined HRTwith herbal remedies, yet 60 to 70 percent of them failed toinform their physicians of this use.1,2
An estimated 46 percent of the American population con-sulted an alternative care provider in 1997, amounting to over600 million visits, and exceeding the number of visits to allAmerican primary care physicians.2 In a 1997 survey conduct-ed by the North American Menopause Society in Canada andthe United States, 80 percent of respondents reported the useof interventions other than prescription medication (Table 1).3
In the largest survey to date, more than 46,000 subscribersof Consumer Reports magazine assessed standard and alternativetherapies for common medical problems.4 Alternative therapiesincluded use of megavitamins, herbal and nutritional supple-ments, deep-tissue massage, chiropractic manipulation, acu-pressure, meditation, and relaxation therapy. Almost 35 percent(more than 16,000 readers) had used alternative therapies; ninepercent used them alone while 25 percent used them in com-bination with conventional therapies. They used alternativetherapies predominantly for the relief of troublesome symptomsthat had not responded to conventional therapy. In contrastto previous surveys,2 more than 60 percent of those who usedalternative therapies informed their doctors about it, and weremore likely to report good results when they tried alternative(especially herbal) treatments on the advice of their health pro-fessional or alternative practitioner than when they simply treat-ed themselves. Reassuringly, for nearly all of the 43 medical
conditions reported, respondents obtained the best results fromprescription drugs (50% much improved) and from surgerywhen it was recommended (75% much improved).
As mainstream medical journals begin to publish researchabout alternative therapies, health care providers face both thechallenge and the opportunity to incorporate evidence-basedalternative therapies into their practices. Despite the clear ben-efits of therapies involving dietary and lifestyle modifications,adherence rates are regrettably low.
DIET AND LIFESTYLE INFLUENCE ON MIDLIFE HEALTH
Many of the leading causes of death are influenced by modifi-able factors such as cigarette smoking, diet, exercise, and obesi-ty. Cigarette smoking is a strong independent risk factor forcardiovascular disease, stroke, peripheral vascular disease, osteo-porosis, and certain forms of cancer.5-8 The cardioprotective andanticancer effects of a diet low in saturated and trans-unsatu-rated fats and high in fibre cannot be overemphasized.5-8
Weight-bearing exercise enhances wellbeing, promotes balanceand agility, and has positive effects on cardiovascular functionand in the skeleton.5-8*
DIETARY PHYTOESTROGENS
Phytoestrogens are non-steroidal plant compounds withestrogen-like biological activity and a chemical structure simi-lar to that of estrogen.9 They have mixed estrogen agonist andantagonist effects in different target tissues related to their weakcompetitive binding to the estrogen receptor.9
Phytoestrogens may also activate “orphan” receptors thatare distinct from the recognized estrogen receptors (ER-α andER-β), and may have non-receptor-mediated effects on enzymeactivity, growth factor action, angiogenesis, and cell growth.9
The three principal varieties of phytoestrogens are isoflavones(genistein, daidzein), coumestans, and lignans. Phytoestrogensmay possess anticancer properties, likely related to the antiox-idant properties of genistein and to genistein-mediated inhi-bition of the enzyme tyrosine kinase, which is involved withcell growth and regulation.9-11
Phytoestrogens are present in the highest concentrations
Margo R. Fluker, MD, FRCSC, Suzanne Montemuro, MD, CCFP
COMPLEMENTARY APPROACHES
Vancouver BC
* Menopause, healthy living, J Obstet Gynaecol Can 2001;23(9):942-8;Hormone replacement therapy and cardiovascular disease,J Obstet Gynaecol Can 2001;23(10):966-72.Osteoporosis, J Obstet Gynaecol Can 2001;23(10):978-88.

JOGC OCTOBER 200275
in soybean and linseed (flaxseed) products. In addition to thecommonly known soy foods (tofu, tempeh, miso, soy milk),newer products more palatable to Western taste have beenintroduced. Fruits, vegetables, cereals, and seeds contain com-paratively trivial amounts of phytoestrogens, although anappreciable cumulative intake may be obtained from a com-bination of several sources (Table 2).
Although there are few specific recommendations aboutdose and formulation, the epidemiological evidence regardingphytoestrogens is derived from a typical Asian diet, which con-tains 20 to 150 mg isoflavones, or 20 to 50 g soy protein, perday (Table 2).9-11 The recent United States Food and DrugAdministration guidelines suggest a health benefit from thedaily intake of approximately 50 mg isoflavones, or 25 g soyprotein.12 The benefits attributable to phytoestrogens may bederived, at least in part, from their incorporation into a low-fat, high-fibre Asian diet. It is unknown whether increasingthe phytoestrogen content in a relatively high fat, processedWestern diet will have the same benefit, or whether there is anybenefit from over-the-counter phytoestrogen or isoflavone sup-plements. The production of these supplements is currentlynot regulated or standardized.
The phytoestrogen or isoflavone content of foods varies sig-nificantly, due to varying conditions of cultivation and industrialprocessing. There may be marked individual and sex-related dif-ferences in the absorption of various phytoestrogens, and it is notclear whether interactions with other foods, or competition withexogenous or endogenous estrogens for the same receptors, willalter the potential effects of phytoestrogens.9
The role of isoflavones in menopausal health has beenextensively reviewed in a recent Consensus Opinion statementfrom the North American Menopause Society.12
LIPIDS AND CARDIOVASCULAR DISEASE
Primate and in vitro studies have shown that soy protein orisoflavone extracts reduce atherosclerotic plaque progression, whilehuman trials have shown an increase in arterial compliance with
isoflavone treatment, similar to that seen in other studies of long-term estrogen use.12
A meta-analysis of 38 controlled clinical trials13 reported avariable but significant decrease in total cholesterol, low-den-sity lipoprotein (LDL) cholesterol and triglyceride levels fol-lowing a high dietary intake of soy protein. The proposedmechanisms are thought to involve up-regulation of LDL-cholesterol receptors, increased clearance of cholesterol, andinhibition of cholesterol synthesis.
The best evidence for the positive health effects of phy-toestrogens is derived from the lipid effects. However, it seemspossible that the beneficial effects are derived only from wholefoods and soy proteins, because purified isoflavone extractsappear to have inconsistent or absent lipid effects.12
BONE DENSITY
A review of randomized clinical trials involving a potent syntheticphytoestrogen derivative (ipriflavone) reported a positive effecton bone density, although the doses used were much higher thanthose achievable through dietary phytoestrogen intake.14 Morerecently, a large randomized trial reported no improvement inbone density and no change in vertebral fracture risk after 36months of treatment with 600 mg ipriflavone daily versus place-bo.15 Studies involving dietary soy proteins and isoflavone extractshave varied in their results and methodological strength.12 Frac-ture data are not available and further study is needed.
BREAST CANCER
Phytoestrogens appear to have antiangiogenic, antiestrogenic, andantiproliferative properties in animal models and human breastcancer cell-lines.10,12,16 Epidemiological evidence suggests an asso-ciation between dietary phytoestrogens and a reduced breast can-cer risk or improved breast cancer survival, although prepubertalexposure may be required. Case-control studies demonstrate asoy protein-related reduction in breast cancer risk, particularly inAsian and premenopausal women, although not necessarily inpostmenopausal women. The use of phytoestrogen supplements
TABLE 1
REPORTED PAST OR CURRENT USE OF SUPPLEMENTS OR ALTERNATIVES TO PRESCRIPTION HRT—RESULTS OF THE 1997 NORTH AMERICAN MENOPAUSE SOCIETY (NAMS) SURVEY (N = 605)3
Healthy Eating 85%Healthy Weight 77%Regular Exercise 75%Vitamins 70%Calcium Supplements 58%Smoking Cessation 28%Herbal Therapies 27%Relaxation/Yoga 25%
Menopause: Complementary approaches. Canadian Consensus Conference on Menopause and Osteoporosis. J Soc Obstet GynaecolCan 1998;20(13):55-63. Table 1. With permission.
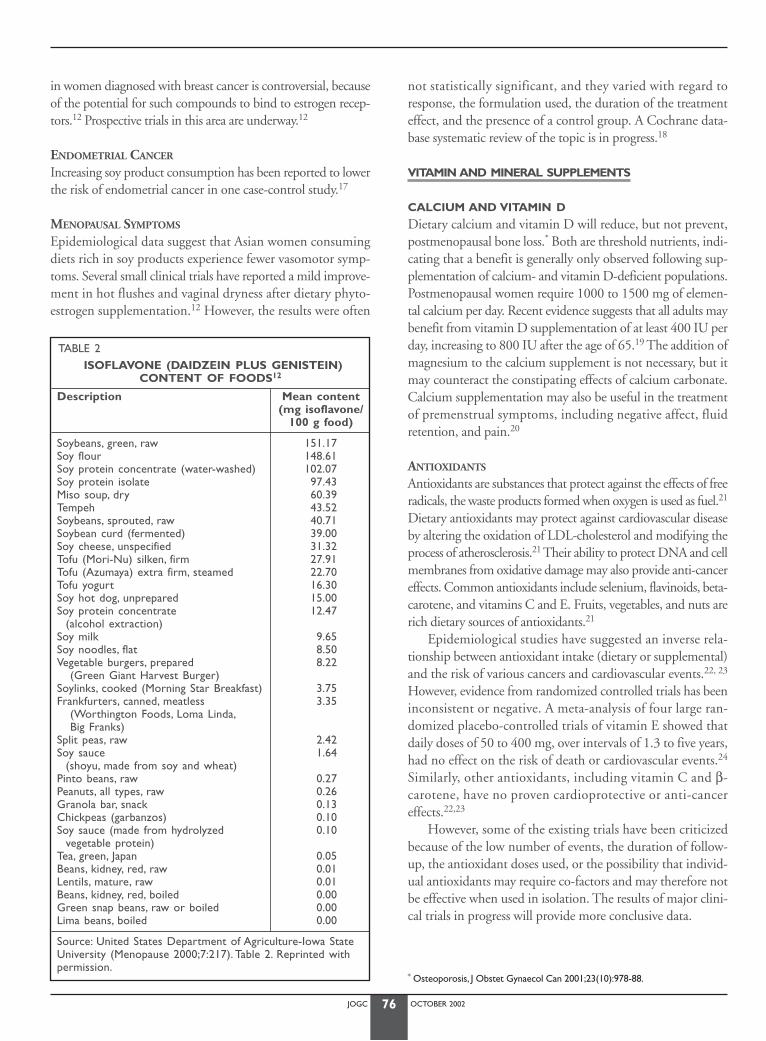
JOGC OCTOBER 200276
in women diagnosed with breast cancer is controversial, becauseof the potential for such compounds to bind to estrogen recep-tors.12 Prospective trials in this area are underway.12
ENDOMETRIAL CANCER
Increasing soy product consumption has been reported to lowerthe risk of endometrial cancer in one case-control study.17
MENOPAUSAL SYMPTOMS
Epidemiological data suggest that Asian women consumingdiets rich in soy products experience fewer vasomotor symp-toms. Several small clinical trials have reported a mild improve-ment in hot flushes and vaginal dryness after dietary phyto-estrogen supplementation.12 However, the results were often
not statistically significant, and they varied with regard toresponse, the formulation used, the duration of the treatmenteffect, and the presence of a control group. A Cochrane data-base systematic review of the topic is in progress.18
VITAMIN AND MINERAL SUPPLEMENTS
CALCIUM AND VITAMIN D
Dietary calcium and vitamin D will reduce, but not prevent,postmenopausal bone loss.* Both are threshold nutrients, indi-cating that a benefit is generally only observed following sup-plementation of calcium- and vitamin D-deficient populations.Postmenopausal women require 1000 to 1500 mg of elemen-tal calcium per day. Recent evidence suggests that all adults maybenefit from vitamin D supplementation of at least 400 IU perday, increasing to 800 IU after the age of 65.19 The addition ofmagnesium to the calcium supplement is not necessary, but itmay counteract the constipating effects of calcium carbonate.Calcium supplementation may also be useful in the treatmentof premenstrual symptoms, including negative affect, fluidretention, and pain.20
ANTIOXIDANTS
Antioxidants are substances that protect against the effects of freeradicals, the waste products formed when oxygen is used as fuel.21
Dietary antioxidants may protect against cardiovascular diseaseby altering the oxidation of LDL-cholesterol and modifying theprocess of atherosclerosis.21 Their ability to protect DNA and cellmembranes from oxidative damage may also provide anti-cancereffects. Common antioxidants include selenium, flavinoids, beta-carotene, and vitamins C and E. Fruits, vegetables, and nuts arerich dietary sources of antioxidants.21
Epidemiological studies have suggested an inverse rela-tionship between antioxidant intake (dietary or supplemental)and the risk of various cancers and cardiovascular events.22, 23
However, evidence from randomized controlled trials has beeninconsistent or negative. A meta-analysis of four large ran-domized placebo-controlled trials of vitamin E showed thatdaily doses of 50 to 400 mg, over intervals of 1.3 to five years,had no effect on the risk of death or cardiovascular events.24
Similarly, other antioxidants, including vitamin C and β-carotene, have no proven cardioprotective or anti-cancereffects.22,23
However, some of the existing trials have been criticizedbecause of the low number of events, the duration of follow-up, the antioxidant doses used, or the possibility that individ-ual antioxidants may require co-factors and may therefore notbe effective when used in isolation. The results of major clini-cal trials in progress will provide more conclusive data.
TABLE 2ISOFLAVONE (DAIDZEIN PLUS GENISTEIN)
CONTENT OF FOODS12
Description Mean content (mg isoflavone/
100 g food)
Soybeans, green, raw 151.17Soy flour 148.61Soy protein concentrate (water-washed) 102.07Soy protein isolate 97.43Miso soup, dry 60.39Tempeh 43.52Soybeans, sprouted, raw 40.71Soybean curd (fermented) 39.00Soy cheese, unspecified 31.32Tofu (Mori-Nu) silken, firm 27.91Tofu (Azumaya) extra firm, steamed 22.70Tofu yogurt 16.30Soy hot dog, unprepared 15.00Soy protein concentrate 12.47
(alcohol extraction)Soy milk 9.65Soy noodles, flat 8.50Vegetable burgers, prepared 8.22
(Green Giant Harvest Burger)Soylinks, cooked (Morning Star Breakfast) 3.75Frankfurters, canned, meatless 3.35
(Worthington Foods, Loma Linda,Big Franks)
Split peas, raw 2.42Soy sauce 1.64
(shoyu, made from soy and wheat)Pinto beans, raw 0.27Peanuts, all types, raw 0.26Granola bar, snack 0.13Chickpeas (garbanzos) 0.10Soy sauce (made from hydrolyzed 0.10
vegetable protein)Tea, green, Japan 0.05Beans, kidney, red, raw 0.01Lentils, mature, raw 0.01Beans, kidney, red, boiled 0.00Green snap beans, raw or boiled 0.00Lima beans, boiled 0.00
Source: United States Department of Agriculture-Iowa StateUniversity (Menopause 2000;7:217). Table 2. Reprinted withpermission.
* Osteoporosis, J Obstet Gynaecol Can 2001;23(10):978-88.

JOGC OCTOBER 200277
VITAMIN B6
Any effectiveness of vitamin B6 for the treatment of peri-menopausal symptoms similar to those of premenstrual syndrome(PMS) remains controversial. Conclusions from a systematicreview of nine trials involving 940 patients were limited by thelow quality of most of the trials, but did suggest that doses of vi-tamin B6 up to 100 mg per day may have a beneficial effect onPMS and premenstrual depression.25 A Cochrane database sys-tematic review of the topic is in progress.26 Care should be takento calculate the total vitamin B6 dose obtained from varioussources, as doses over 100 mg per day may be neurotoxic.
HERBAL REMEDIES
QUALITY CONTROL
The use of herbal remedies to treat menopausal symptoms, oras an adjunct to HRT, is growing rapidly in Canada and theUnited States.2-4 Many prescription drugs originate from plantsources, including digitalis (foxglove), acetylsalicylic acid (ASA)(white willow), vincristine (periwinkle), and estrogen-progestinpreparations (soybeans and Mexican wild yams). Because notherapeutic claims are made for most natural health productsand herbal remedies, they are classified as food or dietary sup-plements, not as drugs. As such, they may be consumed asdesired because of the presumed absence of pharmacologicproperties. Consumers often consider them to be inherentlysafe, even though they may contain biologically active com-pounds with the potential for side effects and drug interactions.
On 26 March 1999, Health Canada’s Office of NaturalHealth Products was created to oversee areas such as regula-tion, labelling, standards development, product licensing, post-approval monitoring, and research involving natural healthproducts.* However, there is still no routine surveillance byHealth Canada for product quality.27 Several hundred herbalproducts have undergone scrutiny by the Therapeutic Prod-ucts Program of Health Canada, and have been issued DrugIdentification Numbers (DIN) or General Public numbers(GP), which indicate that there has been a review of a prod-uct’s formulation, labelling, and instructions, but which do notconfirm bioactivity or clinical efficacy. Because the DIN or GPdoes not refer to the herbal product in general but to a partic-ular manufacturer’s preparation, consumers are advised to pur-chase only those brands with appropriate DIN or GP labelling.
SOURCES OF ACCURATE INFORMATION
Table 3 lists general references for researching herbal remedies.The Canadian Medical Association and Canadian PharmacistsAssociation recently published an authoritative, practical, evi-dence-based guide to herbal products.27 It contains an exten-sive appendix of general references, as well as a detailed literaturereview on each of 57 individual herbal products. The book alsoprovides information about reporting adverse drug reactions(ADRs) to drug products or herbal medicines via regional ADRcentres, Health Canada’s Web site,† or the form in the ClinicalInformation section of the Compendium of Pharmaceuticals andSpecialties (CPS).
TABLE 3SELECTED GENERAL REFERENCES FOR RESEARCHING HERBAL MEDICINES
Organization Reference
American Herbal Pharmacopoeia American Herbal Pharmacopoeia and therapeutic compendium.Quality control, analytical and therapeutic monographs.
Canadian Pharmacists Association and Herbs: Everyday reference for health professionals.Canadian Medical Association Chandler, F (ed). Ottawa; 2000.
www.cma.ca or www.cdnpharm.ca
European Scientific Cooperative on ESCOP monographs on the medicinal uses of plant drugs.Phytotherapy (ESCOP) Fascicules 1-5. Exeter, UK; ESCOP; 1996-7.
European Phytojournal (official newsletter of ESCOP)www.exeter.ac.uk/phytonet
World Health Organization WHO monographs on selected medicinal plants. Vol 1.Geneva: The World Health Organization; 1999.
American Botanical Council, Austin TX HerbalGramwww.herbalgram.org
Herbal Hall www.herb.com
National Center for Complementary and www.nccam.nih.gov/Alternative Medicine, Bethesda MD
Office of Dietary Supplements, www.odp.od.nih.gov/ods/National Institutes of Health, Bethesda MD
* www.hc-sc.gc.ca/hpb/onhp†www.hc-sc.gc.ca/hpb-dgps/therapeut/zfiles/english/forms/advers_e.pdf
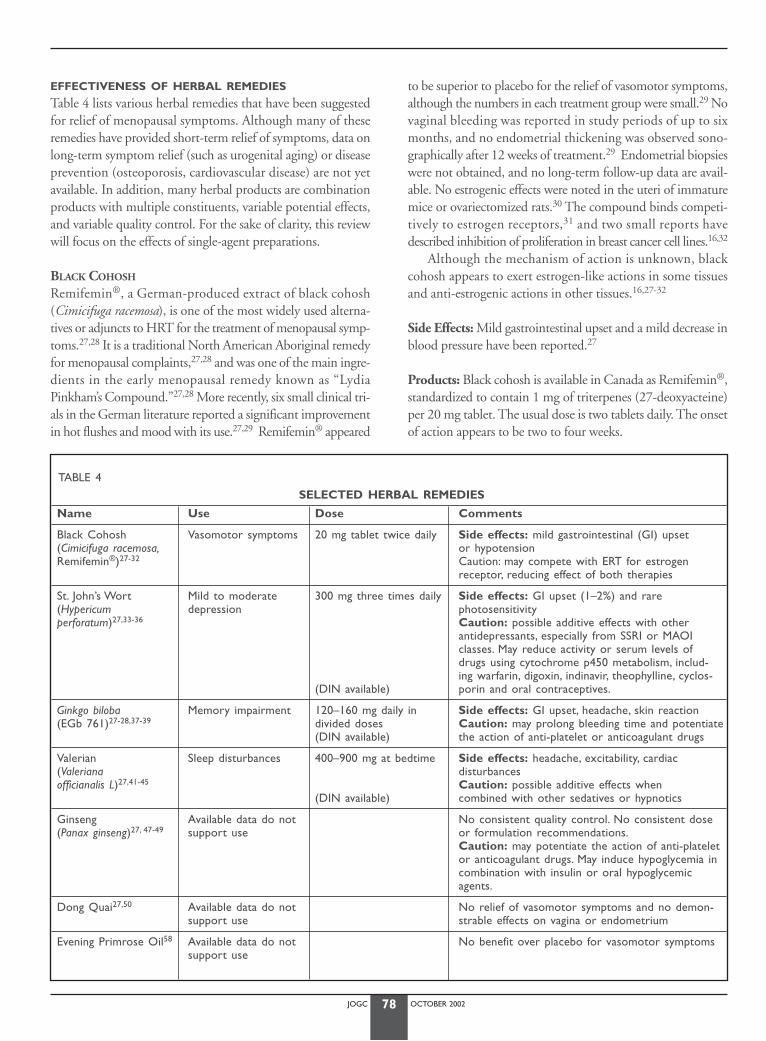
JOGC OCTOBER 200278
EFFECTIVENESS OF HERBAL REMEDIES
Table 4 lists various herbal remedies that have been suggestedfor relief of menopausal symptoms. Although many of theseremedies have provided short-term relief of symptoms, data onlong-term symptom relief (such as urogenital aging) or diseaseprevention (osteoporosis, cardiovascular disease) are not yetavailable. In addition, many herbal products are combinationproducts with multiple constituents, variable potential effects,and variable quality control. For the sake of clarity, this reviewwill focus on the effects of single-agent preparations.
BLACK COHOSH
Remifemin®, a German-produced extract of black cohosh(Cimicifuga racemosa), is one of the most widely used alterna-tives or adjuncts to HRT for the treatment of menopausal symp-toms.27,28 It is a traditional North American Aboriginal remedyfor menopausal complaints,27,28 and was one of the main ingre-dients in the early menopausal remedy known as “LydiaPinkham’s Compound.”27,28 More recently, six small clinical tri-als in the German literature reported a significant improvementin hot flushes and mood with its use.27,29 Remifemin® appeared
to be superior to placebo for the relief of vasomotor symptoms,although the numbers in each treatment group were small.29 Novaginal bleeding was reported in study periods of up to sixmonths, and no endometrial thickening was observed sono-graphically after 12 weeks of treatment.29 Endometrial biopsieswere not obtained, and no long-term follow-up data are avail-able. No estrogenic effects were noted in the uteri of immaturemice or ovariectomized rats.30 The compound binds competi-tively to estrogen receptors,31 and two small reports havedescribed inhibition of proliferation in breast cancer cell lines.16,32
Although the mechanism of action is unknown, blackcohosh appears to exert estrogen-like actions in some tissuesand anti-estrogenic actions in other tissues.16,27-32
Side Effects: Mild gastrointestinal upset and a mild decrease inblood pressure have been reported.27
Products: Black cohosh is available in Canada as Remifemin®,standardized to contain 1 mg of triterpenes (27-deoxyacteine)per 20 mg tablet. The usual dose is two tablets daily. The onsetof action appears to be two to four weeks.
TABLE 4SELECTED HERBAL REMEDIES
Name Use Dose Comments
Black Cohosh Vasomotor symptoms 20 mg tablet twice daily Side effects: mild gastrointestinal (GI) upset (Cimicifuga racemosa, or hypotensionRemifemin®)27-32 Caution: may compete with ERT for estrogen
receptor, reducing effect of both therapies
St. John’s Wort Mild to moderate 300 mg three times daily Side effects: GI upset (1–2%) and rare (Hypericum depression photosensitivityperforatum)27,33-36 Caution: possible additive effects with other
antidepressants, especially from SSRI or MAOI classes. May reduce activity or serum levels ofdrugs using cytochrome p450 metabolism, includ-ing warfarin, digoxin, indinavir, theophylline, cyclos-
(DIN available) porin and oral contraceptives.
Ginkgo biloba Memory impairment 120–160 mg daily in Side effects: GI upset, headache, skin reaction(EGb 761)27-28,37-39 divided doses Caution: may prolong bleeding time and potentiate
(DIN available) the action of anti-platelet or anticoagulant drugs
Valerian Sleep disturbances 400–900 mg at bedtime Side effects: headache, excitability, cardiac (Valeriana disturbancesofficianalis L)27,41-45 Caution: possible additive effects when
(DIN available) combined with other sedatives or hypnotics
Ginseng Available data do not No consistent quality control. No consistent dose(Panax ginseng)27, 47-49 support use or formulation recommendations.
Caution: may potentiate the action of anti-plateletor anticoagulant drugs. May induce hypoglycemia incombination with insulin or oral hypoglycemicagents.
Dong Quai27,50 Available data do not No relief of vasomotor symptoms and no demon-support use strable effects on vagina or endometrium
Evening Primrose Oil58 Available data do not No benefit over placebo for vasomotor symptomssupport use

Impression: Remifemin® may be a useful alternative for theshort-term relief of menopausal symptoms. Further study is jus-tified, particularly to determine its effect on human endometri-um, bone, lipid profiles, and breast tissue.
ST. JOHN’S WORT
Extracts of St. John’s wort (Hypericum perforatum) have beenused for the treatment of mild to moderate depression since thetime of Hippocrates. A Cochrane database review of 29 trialsinvolving 2291 patients, two subsequent randomized controlledtrials, and post-marketing surveillance data involving 3250patients all indicate that St. John’s wort is superior to placebo,and as effective as standard antidepressants, in the short-termtreatment (2-8 weeks) of mild to moderate depression.33-36 Alarge multicentre trial of St. John’s wort sponsored by the Unit-ed States National Institute of Mental Health is in progress.
The exact mechanism of action is unclear, but the compoundmay include interaction with gamma-aminobutyric acid, sigmaand serotonin receptors.33-36
Side Effects: St. John’s wort should not be used concurrentlywith full doses of other prescription antidepressants because ofthe potential for serotonin syndrome, hypomania, or other seri-ous interactions, particularly with drugs of the monoamine oxi-dase inhibitor (MAOI) and selective serotonin reuptake inhibitor(SSRI) classes. Decreased activity or decreased serum levels ofwarfarin, dixogin, theophylline, indinavir, cyclosporin, and phen-procoumon, as well as breakthrough bleeding on oral contra-ceptives, have been reported.27,36 These actions are likely due toinduction of hepatic cytochrome p450 activity and appear sim-ilar in magnitude to that of grapefruit juice. The most commonside effects are gastrointestinal symptoms, dizziness, and rest-lessness occurring in one to two percent of patients, similar toplacebo. Rarely, photosensitivity has been reported in fair-skinned individuals taking more than 1800 mg daily.27,36 Thedrug does not cause sedation, impair concentration or drivingability, affect libido or potentiate the effects of alcohol.27, 35
Products: St. John’s wort is available in Canada as an aqueous-phenolic extract in capsules of 300 mg standardized to containfive percent hyperforin, 0.3 percent hypericin, or both. Theusual dose is 900 mg per day in three divided doses, althoughthis may be increased to 1800 mg if required and decreased to300 to 600 mg daily for maintenance therapy. The onset ofaction is two to four weeks.27
Impression: St. John’s wort may be a useful herbal alternativefor the short-term treatment of mild to moderate depression.Additional studies are needed to characterize the precise mech-anism of action and the long-term effects of the compound.
GINKGO BILOBA
An extract of Ginkgo biloba (EGb 761) appears to be effectivein the treatment of dementia, mood disorders associated withpoor memory, and intermittent claudication.37 Three recentrandomized controlled trials38-40 demonstrated modest but sig-nificant improvement in cognitive performance and social func-tioning among patients with memory impairment, Alzheimer’sdisease, and multi-infarct dementia. However, the treatmenteffect was small and may not be clinically meaningful.
The mechanism of action of Ginkgo biloba includes antag-onism of platelet-activating factor in addition to antioxidantand vasoregulatory properties, which appear to increase toler-ance to cerebral hypoxia.40
Side Effects: Gastrointestinal upset, headache, and allergic skinreactions have been reported.27 Caution should be used inpatients taking ASA, non-steroidal anti-inflammatory drugs(NSAIDs), and anticoagulants, as Gingko biloba may prolongthe bleeding time.27,28
Products: Ginkgo biloba is available in Canada as an extractstandardized to contain 40 mg of Ginkgo (24% ginkgohetero-sides) per capsule. The recommended dose is 120 to 160 mgper day in divided doses.
Impression: More research is needed to determine the fullmechanism of action and therapeutic potential of Ginkgo bilo-ba. To date, evidence suggests that it may be a useful alternativefor some postmenopausal women experiencing difficulties withmemory.
VALERIAN
Valerian (Valeriana officianalis L) has been used for over 1000 yearsas a tranquilizer and sedative.41-45 Five small placebo-controlledtrials reported a variable decrease in sleep latency scores, improve-ment in sleep quality, and increase in slow-wave sleep.41-45
Side Effects: The drug is generally well tolerated, althoughheadaches, excitability, and cardiac disturbances have beenreported, possibly due to other unidentified active ingredientsor inappropriate doses.28 Valerian does not appear to producea morning hangover.27 It should not be mixed with other seda-tives because of the possibility of additive effects.
Products: Valerian is available as a standardized extract of 0.8percent valerenic acid. The studied doses are 400 to 900 mgorally at bedtime.
Impression: Valerian appears to exert a mild dose-dependenthypnotic effect, and may be useful for short-term therapy ofmenopausal sleep disturbances.
JOGC OCTOBER 200279

JOGC OCTOBER 200280
GINSENG
Ginseng is perhaps the most widely recognized plant used in tra-ditional Chinese medicine. It plays a major role in the herbal healthcare market, although there are few well-controlled human trials.28
A large placebo-controlled trial of 384 symptomatic post-menopausal women reported no overall effect of a standard-ized ginseng extract (Ginsana®) on vasomotor symptoms,serum estradiol or follicle-stimulating hormone levels, endome-trial thickness or vaginal maturation index. Furthermore, therewas no overall difference in three standardized quality of lifequestionnaires, although there was significant improvement inindividual subscales involving depression, general heath, andpositive well-being.46 A recent systematic review of random-ized controlled trials involving preparations of ginseng alonefound variable, but not compelling, evidence to support theuse of ginseng to enhance physical performance, psychomotorperformance, and cognitive function.47
Side Effects: Although ginseng is thought to be safe, adverseeffects including nervousness, insomnia, dizziness, and hyper-tension have been reported.27,28 Ginseng preparations may pro-long the bleeding time via antiplatelet activities and inhibitionof thromboxane formation.27 Ginseng should therefore not beused peri-operatively or in patients taking anticoagulants, ASA,NSAIDs or other compounds such as Gingko biloba that mayaffect bleeding parameters. American ginseng may inducehypoglycemic reactions when used in combination with insulinor oral hypoglycemic agents.48 Siberian ginseng may falsely ele-vate serum digoxin levels, presumably by interfering with thedigoxin assay.27
Products: Ginseng is available in a wide and confusing array ofproducts. At least six species and varieties of the genus Panaxhave been used in traditional medicine (American, Korean,Sanchi, Shuzishen, Chikusetsu, Himalayan, and dwarf ginseng).Siberian ginseng is derived from a different plant (Eleuthero-coccus senticosus). Some products have been found to contain noginsenosides at all. There are no consistent recommendationsregarding dose.
Impression: Ginseng is commonly used for a variety of com-plaints, but the available evidence does not support its use formenopausal symptoms. Additional trials are required to con-firm ginseng’s potential effect on general health and well-being.Poor quality control is a major problem for the consumer.
DONG QUAI
Dong quai (Angelica sinensis) is a coumarin-containing rootcommonly used in Chinese herbal remedies to treat a varietyof gynaecologic complaints, including menopausal symptoms,premenstrual syndrome, menstrual irregularities, dysmenor-
rhea, and infertility. The only randomized, blinded, controlledtrial to date demonstrated no difference between dong quaiand placebo in the relief of vasomotor symptoms in 73menopausal women, and no demonstrable estrogenic effectsof dong quai on the endometrium or vagina.49 The availabledata do not support the use of dong quai in the treatment ofmenopausal symptoms. It remains possible that dong quai hasa beneficial effect when it is incorporated into traditional herbalmixtures, rather than when it is used in isolation.27,49
ALTERNATIVES TO ESTROGEN THERAPY FOR THE CONTROL OF HOT FLUSHES
There is widespread interest in alternatives to estrogen replace-ment therapy for the relief of vasomotor symptoms in womenin whom estrogen therapy is not appropriate or acceptable.*
CLONIDINE
Clonidine inhibits sympathetic outflow by acting as a presynapticCNSα-2-agonist. It can decrease hot flushes.5 The initial dose is0.05 mg twice daily, but many women require at least 0.1 mgtwice daily. It may also be administered as a weekly transder-mal patch (containing 2.5 mg clonidine). Frequent side effects,including dry mouth, palpitations, drowsiness, dizziness, andhypotension, limit the usefulness of this medication.
PROGESTINS
Progestins may offer an effective alternative for the treatment ofvasomotor symptoms. Medroxyprogesterone acetate (150 mgIM every 3 months or 10–20 mg daily orally) and megestrolacetate (20–40 mg daily) may be used.5
ANTIDEPRESSANTS
One randomized controlled trial has reported a significant reduc-tion in vasomotor symptoms with venlafaxine hydrochloride(Effexor®) compared to placebo.50 Dose-response studies rangingfrom 37.5 to 150 mg daily showed that 75 mg daily was the mosteffective dose. Uncontrolled pilot studies have also reported animprovement in vasomotor symptoms over baseline with use ofparoxetine hydrochloride (Paxil®),51 fluoxetine (Prozac®),52 andsertraline (Zoloft®).53 Side effects include dry mouth, decreasedappetite, nausea, and constipation, particularly in the initial weeksof therapy.50 There is a dose-related risk of increased blood pres-sure with use of venlafaxine, affecting approximately three percentof patients using daily doses of less than 100 mg.
BLACK COHOSH
Six small clinical trials in the German literature have reporteda significant improvement in hot flushes and mood with use ofthis agent (Table 4).27,28 These reports require confirmation inlarger randomized controlled trials.
* Perimenopause, J Obstet Gynaecol Can 2001;23(9): 836-41,Table 2.

JOGC OCTOBER 200281
LIFESTYLE
Both regular aerobic exercise54,55 and periodic deep breathingexercises may result in a 40 to 50 percent reduction in hot flush-es. Weight-bearing exercise also enhances well-being, promotesbalance and agility, and has protective effects in the cardiovas-cular system and skeleton. Regrettably, few candidates persistwith regular exercise programs.
BELLERGAL
Anecdotal reports suggest that Bellergal® (a combination of phe-nobarbital, ergotamine, and belladonna) may be helpful for theshort-term relief of vasomotor symptoms, but it can cause seda-tion, and has potential for habituation.5
PHYTOESTROGENS
Several small clinical trials have demonstrated a mild improvementin hot flushes and vaginal dryness in response to dietary phyto-estrogen supplementation.12 However, the results often failed toreach statistical significance and varied with regard to response,formulation used, and duration of the treatment effect. ACochrane database systematic review of the topic is in progress.18
VITAMIN E
Although vitamin E supplements have been used empiricallyto relieve hot flushes, a randomized placebo-controlled trialshowed no statistical improvement in flushes among breast can-cer survivors using 800 IU daily for four weeks.56 Anecdotalevidence suggests that vaginal vitamin E oil may relieve vaginaldryness, itching, and irritation.
EVENING PRIMROSE OIL
A randomized controlled trial indicated that evening primroseoil was as effective as placebo for the treatment of menopausalvasomotor symptoms.57 Although it is commonly sold for avariety of “female complaints,” the available data do not sup-port the use of evening primrose oil for control of menopausalsymptoms.
ESTRIOL
Estriol is a metabolite of estradiol that has been proposed to relievevasomotor symptoms, when given in sufficient doses.59 Howev-er, a large Swedish case-control study58 found that use of oral estri-ol at doses of 1 to 2 mg daily was associated with an increasedrelative risk of endometrial neoplasia, suggesting that a progestinshould be added to estriol therapy for endometrial protection. Incontrast, there appears to be little risk of endometrial prolifera-tion following low-dose vaginal administration of estriol.58
There is no evidence to show that estriol provides any pro-tection against postmenopausal breast cancer, osteoporosis, car-diovascular disease, and colon cancer.59 Tri-est (80% estriol, 10%estrone, 10% estradiol) and Bi-est (70% estriol, 30% estradiol)
are available as tablets or creams from compounding pharmaciesin Canada. Much of their biological activity may be derived fromthe more potent estrone and estradiol components. Estrogenbioavailability after topical application of the cream is uncertain,and no clinical trials regarding the efficacy of these compoundshave been completed. These preparations are expensive, and theyappear to offer no advantage over standard HRT.
PROGESTERONE CREAMS
Numerous different progesterone creams are available over-the-counter in the United States and many are available throughcompounding pharmacies in Canada or surreptitiously throughhealth food stores. For most products, there is little consistencyor quality control. The products can be categorized as follows:
1) Those that contain no progesterone, but variable amountsof progesterone precursors that are generally obtained fromthe inedible Mexican wild yam (Dioscorea barbasco). Thereis no enzymatic process in the human body to convert theseprecursors into progesterone.
2) Those that contain progesterone that has been synthesizedin a laboratory, often from Mexican wild yam or soy pre-cursors. While these products contain variable amounts ofchemically defined progesterone, absorption through the skinis variable and usually poor.60-62
In a 12-week randomized trial, no progestational effect onthe endometrium was noted in 21 estrogen-primed womenusing standardized daily doses of 16 to 64 mg of micronizedprogesterone cream.63 In a one-year randomized controlled trial,a daily dose of 20 mg progesterone cream produced no protec-tive effect on bone density, yet produced a small but significantimprovement in vasomotor symptoms compared to placebo.64
Although these products claim to treat menopausal symp-toms, premenstrual syndrome, and osteoporosis, the amount ofprogesterone absorbed from the various preparations is highlyvariable, and should be considered inadequate to provideendometrial or bone protection.63,64 While prescription prepa-rations of progesterone and progestins are absorbed through theskin (norethindrone-containing patches) or vaginal mucosa(micronized progesterone tablets administered vaginally, proges-terone vaginal suppositories or progesterone vaginal gel), thereis insufficient evidence to conclude that transdermal absorptionof the non-prescription progesterone creams is similarly effective.*
RECOMMENDATIONS:
K1. Physicians and their patients should be more aware ofcomplementary therapies in order to effectively con-sider treatment options. (III)
* Pharmacotherapy, J Obstet Gynaecol Can 2001;23(11):1105-14.

JOGC OCTOBER 200282
K2. Patients should be informed that lifestyle changes,including dietary modifications, exercise (I), reductionof stress, and cessation of smoking can benefit the emo-tional and physical health of women in midlife. (II-1)
CONCLUSION
Various complementary therapies can benefit the health andwell-being of midlife women. Moderate or high-quality evi-dence exists to support the benefits of lifestyle changes andselected botanical preparations. Conversely, evidence has alsoaccumulated to refute the putative benefits of other alternativetherapies. Awareness of this information permits more effectivecounselling of midlife women and facilitates informed decision-making. Health care providers now face both the challenge andthe opportunity to incorporate evidence-based alternative ther-apies into their practices and their lifestyles.
J Obstet Gynaecol Can 2001;23(12):1204-13.
REFERENCES
1. Ravnikar VA. Compliance with hormone therapy.Am J Obstet Gynecol1987;156:1332-42.
2. Eisenberg D,Davis R, Ettner S,Appel S,Wilkey S,Van Rompay M,et al.Trends in alternative medicine use in the United States, 1990-1997:results of a follow-up national survey. J Am Med Assoc 1998;280:1569-75.
3. Kaufert P, Boggs PP, Ettinger B,Woods NF, Utian WH.Women inmenopause: Beliefs, attitudes and behaviours. NAMS 1997 MenopauseSurvey. Menopause 1998;4:197-202.
4. The mainstreaming of alternative medicine. Consumer Reports 2000May;17-25.
5. Kessel B.Alternatives to estrogen for menopausal women. Proc SocExper Biol Med 1998;217:38-43.
6. Hooper L, Summerbell C, Higgins J,Thompson R, Clements G, CappsN, et al. Reduced or modified dietary fat for preventing cardiovasculardisease. Cochrane Database Syst Rev 2000;(4):CD002137.
7. Hu FB, Stampfer MJ, Manson JE, Rimm E, Colditz G, Rosner B, et al.Dietary fat intake and the risk of coronary heart disease in women. NEngl J Med 1997;337:1491-9.
8. Hu F, Stampfer M, Manson J, Grodstein F, Colditz G, Speizer F, et al.Trends in the incidence of coronary heart disease and changes in dietand lifestyle in women. N Engl J Med 2000;343:530-7.
9. Tham DM, Gardner CD, Haskell WL. Potential health benefits of dietaryphytoestrogens: a review of the clinical, epidemiological and mechanisticevidence. J Clin Endocrinol Metab 1998;83:2223-35.
10. Knight DC, Eden JA.A review of the clinical effects of phytoestrogens.Obstet Gynecol 1996;87:897-904.
11. Murkies AL,Wilcox G, Davis SR. Phytoestrogens. J Clin EndocrinolMetab 1998;83:297-303.
12. The role of isoflavones in menopausal health: Consensus opinion of theNorth American Menopause Society. Menopause 2000;7:215-29.
13. Anderson JW, Johnstone B, Cook-Newell ME. Meta-analysis of theeffects of soy protein intake on serum lipids. N Engl J Med1995;333:276-82.
14. Scheiber MD, Rebar RW. Isoflavones and postmenopausal bone health: aviable alternative to estrogen therapy? Menopause 1999;6:233-41.
15. Alexandersen P,Toussaint A, Christiansen C, Devogelaer J, Roux C,Fechtenbaum J, et al. Ipriflavone in the treatment of postmenopausalosteoporosis. J Am Med Assoc 2001;285:1482-8.
16. Dixon-Shanies D, Shaikh N. Growth inhibition of human breast cancercells by herbs and phytoestrogens. Oncol Rep 1999;6:1383-7.
17. Goodman M,Wilkens LR, Hankin JH, Lyu LC,Wu AH, Kolonel LN.Asso-ciation of soy and fiber consumption with the risk of endometrial can-cer.Am J Epidemiol 1997;146:294-306.
18. Lethaby A, Kronenberg F, Roberts H, Eden J. Phytoestrogens formenopausal symptoms. In:The Cochrane Library, Issue 4, 2000. Oxford:Update Software.
19. Thomas M, Lloyd-Jones D,Thadhani R, Shaw A,Deraska D,Kitch B, et al.Hypovitaminosis D in medical inpatients.N Engl J Med 1998;338:777-83.
20. Alvir J,Thys-Jacobs S. Premenstrual and menstrual symptom clustersand response to calcium treatment. Psychopharmacology Bulletin1991;1991:145-8.
21. Hooper L, Capps N, Clements G, et al.Anti-oxidant foods orsupplements for preventing cardiovascular disease. In:The CochraneLibrary, Issue 4, 2000. Oxford: Update Software.
22. Paiva S, Russell R. Beta-carotene and other carotenoid as antioxidants. JAm Coll Nutr 1999;18:426-33.
23. Rimm E, Stampfer M.Antioxidant for vascular disease. Med Clin N Am2000;84:239-49.
24. The Heart Outcomes Prevention Evaluation Study Investigators.Vita-min E supplementation and cardiovascular events in high-risk patients.N Engl J Med 2000;342:154-60.
25. Wyatt K, Dimmock P, Jones P, O’Brien P. Efficacy of vitamin B6 in thetreatment of premenstrual syndrome: a systematic review. Br Med J1999;318:1375-81.
26. Iasco S, Castro A,Atallah A.Vitamin B6 for premenstrual syndrome. In:The Cochrane Library, Issue 4, 2000. Oxford: Update Software.
27. Chandler F, ed. Herbs: Everyday reference for health professionals.Ottawa: Canadian Pharmacists Association and the Canadian MedicalAssociation, 2000.
28. Israel D,Youngkin E. Herbal therapies for perimenopausal andmenopausal complaints. Pharmacotherapy 1997;17:970-84.
29. Liske E.Therapeutic efficacy and safety of Cimicifuga racemosa forgynecologic disorders.Adv Therapy 1998;15:43-51.
30. Einer-Jensen N, Zhao J,Andersen K, Kristoffersen K. Cimicifuga andMelbrosia lack oestrogenic effects in mice and rats. Maturitas1996;25:149-53.
31. Jarry H, Harnischfeger G, Duker E. Studies on the endocrine effects ofthe contents of Cimifuga racemosa. 2. In vitro binding of componentsto estrogen receptors. Planta Med 1983;4:316-9.
32. Nesselhut T, Schellhase C, Dietrich R, Kuhn W. Studies on mammarycarcinoma cells regarding the proliferative potential of herbal medica-tions with estrogen-like effects.Arch Gynecol Obstet 1993;254:817-8.
33. Linde K, Mulrow C. St John’s wort for depression. Cochrane DatabaseSyst Rev 2000;(2):CD000448.
34. Woelk H, for the Remotiv/Imipramine Study Group. Comparison of StJohn’s wort and imipramine for treating depression: randomised con-trolled trial. Br Med J 2000;321:536-9.
35. Philipp M, Kohnen R, Hiller K. Hypericum extract versus imipramine orplacebo in patients with moderate depression: randomised multicentrestudy of treatment for eight weeks. Br Med J 1999;319:1534-8.
36. Woelk H, Burkard G, Grunwald J. Benefits and risks of Hypericumextract LI 60; drug monitoring study with 3250 patients. J Geriatr Psy-chiatry Neurol 1994;7(Suppl 1):S34-8.
37. Kleijnen J, Knipschild P. Ginkgo biloba. Lancet 1992;340:1136-9.38. Le Bars P, Katz M, Berman N, Itil T, Freedman A, Schatzberg A.A place-
bo-controlled, double-blind, randomized trial of an extract of Ginkgobiloba for dementia. North American AGb Study Group. J Am MedAssoc 1997;278:1327-32.
39. Kanowski S, Herrmann W, Stephan K,Wierich W, Horr R. Proof of effi-cacy of the ginkgo biloba special extract Egb 761 in outpatients suffer-ing from mild to moderate primary degenerative dementia of theAlzheimer type or multi-infarct dementia. Pharmacopsychiatry1996;29:47-56.
40. Rai G, Shovlin C,Wesnes K.A double-blind placebo controlled study ofGinkgo biloba extract (‘tanakan’) in elderly out-patients with mild tomoderate memory impairment. Curr Med Res Opin 1991;12:350-5.
JOGC OCTOBER 200283
41. Leathwood P, Chauffard F, Heck E, Munoz-Box R.Aqueous extract ofValerian root (Valeriana officinalis L) improves sleep quality in man. Phar-macol Biochem Behav 1982;17:65-71.
42. Balderer G, Borbely A. Effect of Valerian on human sleep. Psychophar-macology (Berl) 1985;87:406-9.
43. Schulz H,Stolz C,Mulle R.The effect of Valerian extract on sleep poly-graphy in poor sleepers: a pilot study.Pharmacopsychiatry 1994;27:127-51.
44. Lindahl O, Lindwall L. Double blind study of a valerian preparation.Pharmacol Biochem Behav 1989;32:1065-6.
45. Donath F, Quispe S, Diefenbach K, Maurer A, Fietze I, Roots I. Criticalevaluation of the effect of Valerian extract on sleep structure and sleepquality. Pharmacopsychiatry 2000;33:47-53.
46. Wiklund I, Mattsson L-A, Lindgren R, Limoni C, for the Swedish Alterna-tive Medicine Study Group. Effects of a standardized Ginseng extract onquality of life and physiological parameters in symptomaticpostmenopausal women: a double-blind, placebo-controlled trial. Int JClin Pharm Res 1999;19:89-99.
47. Vogler B, Pittler M, Ernst E.The efficacy of ginseng.A systematic reviewof randomised clinical trials. Eur J Clin Pharmacol 1999;55:567-75.
48. Vuksa V, Sievenpiper J, Koo V.American ginseng (Panax quinquefolius L)reduces postprandial glycemia in nondiabetic subjects and subjects withtype 2 diabetes mellitus.Arch Intern Med 2000;160:1009-13.
49. Hirata J, Swiersz L, Zell B, Small R, Ettinger B. Does Dong Quai haveestrogenic effects in postmenopausal women? A double-blind placebo-controlled trial. Fertil Steril 1997;68:981-6.
50. Loprinzi C, Kugler J, Sloan J, Mailliard J, LaVasseur B, Barton D, et al.Venlafaxine in management of hot flashes in survivors of breast cancer:a randomised controlled trial. Lancet 2000;356:2059-63.
51. Stearns V, Isaacs C, Rowland J, Crawford J, Ellis M, Kramer R, et al.Apilot trial assessing the efficacy of paroxetine hydrochloride (Paxil) incontrolling hot flashes in breast cancer survivors.Ann Oncol2000;11:17-22.
52. Loprinzi C, Quella S, Sloan J. Preliminary data from a randomized evalu-ation of fluoxetine (Prozac) for treating hot flashes in breast cancer sur-vivors. Breast Cancer Res Treat 1999;57:34.
53. Trott E, Largoza M, Hansen K.An open trial of sertraline formenopausal hot flushes: potential involvement of serotonin in vasomo-tor instability. Del Med J 1997;69:481-2.
54. Hammar M, Berg G, Lindgren R. Does physical exercise influence thefrequency of postmenopausal hot flushes? Acta Obstet Gynecol Scand1990;69:409-12.
55. Freedman RR,Woodward S. Behavioral treatment of menopausal hotflushes: evaluation by ambulatory monitoring.Am J Obstet Gynecol1992;167:436-9.
56. Barton DL, Loprinzi CL, Quella SK, Sloan JA,Veeder MH, Egner JR, et al.Prospective evaluation of vitamin E for hot flashes in breast cancer sur-vivors. J Clin Oncol 1998;16:495-500.
57. Chenoy R, Hussain S,Tayob Y, O’Brien P, Moss M, Morse P. Effect of oralgamolenic acid from evening primrose oil on menopausal flushing. BrMed J 1994;308:501-3.
58. Weiderpass E, Baron J,Adami H-O, Magnusson C, Lindgren A,Bergstrom R, et al. Low-potency oestrogen and risk of endometrialcancer: a case-control study. Lancet 1999;353:1824-28.
59. Head K. Estriol: Safety and Efficacy.Alt Med Rev 1998;3:101-12.60. Cooper A, Spencer C,Whitehead M, Ross D, Barnard G, Collins W. Sys-
temic absorption of progesterone from Progest cream in postmenopa-sual women. Lancet 1998;351:1255-6.
61. Burry K, Patton P, Hermsmeyer K. Percutaneous absorption of proges-terone in postmenopausal women treated with transdermal estrogen.Am J Obstet Gynecol 1999;180:1504-11.
62. Carey B, Carey A, Patel S, Carter G, Studd J.A study to evaluate serumand urinary hormone levels following short and long term administra-tion of two regimens of progesterone cream in postmenopausalwomen. Br J Obstet Gynaecol 2000;107:1447-8.
63. Wren B, McFarland K, Edwards L. Micronised transdermalprogesterone and endometrial response. Lancet 1999;354:1447-8.
64. Leonetti H, Longo S,Anasti J.Transdermal progesterone cream for vaso-motor symptoms and postmenopausal bone loss. Obstet Gynecol1999;94:225-8.

JOGC OCTOBER 200284
CANADIAN CONSENSUS ON MENOPAUSE AND OSTEOPOROSIS
INTRODUCTION
Evaluation of peri- and postmenopausal women should be donein the context of overall health promotion. General recom-mendations for health care evaluation can be found in theCanadian Guide to Clinical Preventive Health Care,1 which hasbeen developed and endorsed by the Canadian Task Force onthe Periodic Health Examination.
The broader issues of healthy choices in menopause aredescribed in Section B.* For women with medical concerns,the reader is directed to those sections dealing with specificmedical conditions. The first two parts of this section deal withthe specific considerations to incorporate into the assessmentof menopausal women.The assessment will guide decisionsabout the range of menopausal concerns and options. A care-ful assessment and decision-making process can improve thelikelihood that a woman will make a lasting choice, or a choicethat will be reassessed appropriately.
EVALUATION
In addition to a standard clinical assessment, the history shouldinclude quality of life issues and an assessment of risk factors.The goal of risk assessment is to identify a patient’s risk for dis-ease, to determine appropriate screening and risk reductionstrategies, and to promote adherence to the recommendations.2,3
Comprehensive assessment of the peri- or postmenopausalwoman includes an evaluation both of risk factors for generaldisease4 (Table 1) and of specific risk factors for the most preva-lent diseases of the postmenopausal years, including cardio-vascular disease, osteoporosis, and cancer.† This information isobtained during the history and physical examination and fromscreening test results. Several specific screening examinationsand tests are useful for women over the age of 50. It is appro-priate to offer these or to encourage women to discuss thesewith their primary care provider.
The accuracy of the risk assessment depends on the relia-bility of the information provided by the patient, the ability of
the clinician to identify the major risk factors for disease, andre-evaluation of risk factors at regular intervals. Use of a spe-cially designed documentation form can ensure that the riskassessment is comprehensive and that the information is easyto retrieve, update, and convey to the patient.2 Compilationof a risk assessment profile identifies the areas of increased riskand provides a focus for risk-reduction strategies.
BREAST EVALUATION
BREAST CANCER RISK ASSESSMENT
The purpose of risk assessment is to identify women at high riskof developing breast cancer. Unfortunately, 76 percent of breastcancers occur in women with no identifiable risk factors.5
Women with a strong genetic predisposition for breast cancer andthose identified as being at high risk can benefit from referral todedicated clinics for closer monitoring or consideration ofchemoprophylaxis.5
The Gail model6 is a risk-assessment tool that allows awoman to predict her five-year and lifetime probability ofdeveloping breast cancer compared to women of the same agewith low risk factors. This mathematical model considers sixfactors (Table 2), but does not incorporate BRCA status orexposure to hormone supplements.7
Risk assessment tools may be helpful for women who are veryconcerned about breast cancer, provided that they understand thelimitations of the model. Computer-based software, hand calcula-tors, and user-friendly Internet sites are available for calculating risk.*
BREAST EXAMINATION
Breast examination by a clinician should be performed annu-ally. In some studies it has been found to be as effective as mam-mography in detecting abnormalities.8,9 It additionally providesan opportunity to reinforce the importance of breast self-exam-ination and to review the technique.
MAMMOGRAPHY
Recommendations about the appropriate frequency of mam-mographic examinations depend on a woman’s age and breast
Jennifer M. Blake, MD, FRCSC,1 Elizabeth Contestabile, RN, BScN,2 Michel Fortier, MD, FRCSC3
EVALUATION, DECISION-MAKING AND FOLLOW-UP
1 Toronto ON2 Ottawa ON3 Ste-Foy QC
* Menopause: Healthy Living, J Obstet Gynaecol Can 2001;23(9):842-8.† Hormone replacement therapy and cardiovascular disease, J Obstet
Gynaecol Can 2001;23(10):966-72; Osteoporosis, J Obstet Gynaecol Can2001;23(10):978-8 and Hormone replacement therapy and cancer, JObstet Gynaecol Can 2001;23(12):1198-203.
* http://brca.nci.nih.gov/brc/
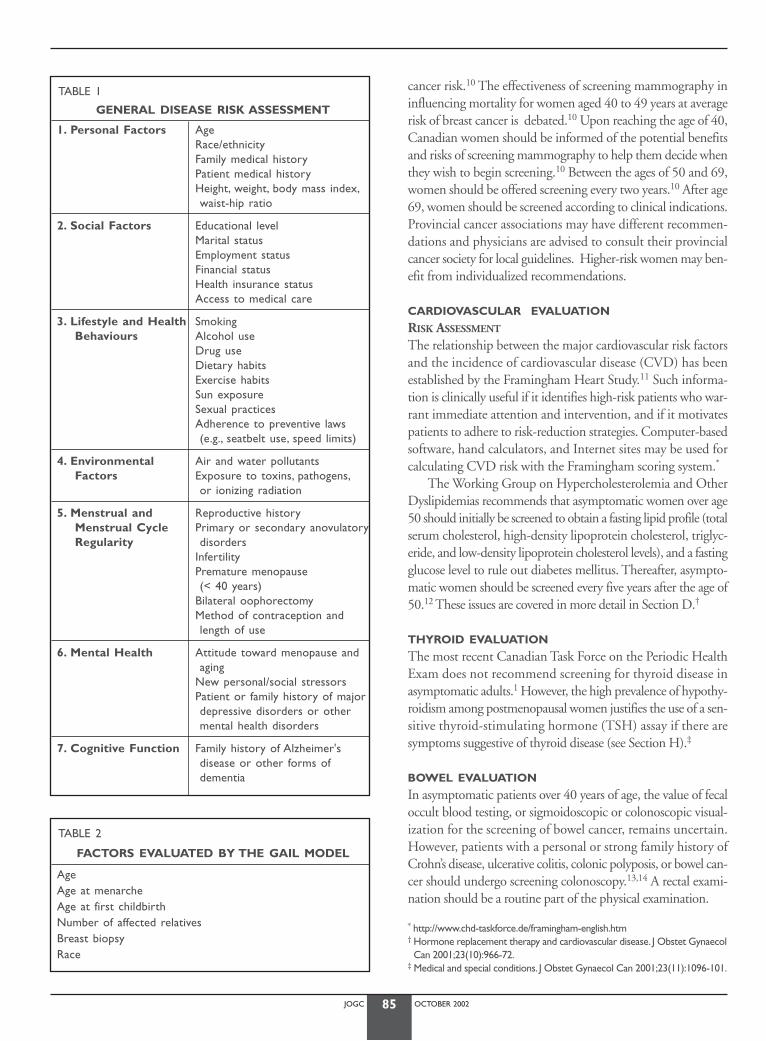
JOGC OCTOBER 200285
cancer risk.10 The effectiveness of screening mammography ininfluencing mortality for women aged 40 to 49 years at averagerisk of breast cancer is debated.10 Upon reaching the age of 40,Canadian women should be informed of the potential benefitsand risks of screening mammography to help them decide whenthey wish to begin screening.10 Between the ages of 50 and 69,women should be offered screening every two years.10 After age69, women should be screened according to clinical indications.Provincial cancer associations may have different recommen-dations and physicians are advised to consult their provincialcancer society for local guidelines. Higher-risk women may ben-efit from individualized recommendations.
CARDIOVASCULAR EVALUATION
RISK ASSESSMENT
The relationship between the major cardiovascular risk factorsand the incidence of cardiovascular disease (CVD) has beenestablished by the Framingham Heart Study.11 Such informa-tion is clinically useful if it identifies high-risk patients who war-rant immediate attention and intervention, and if it motivatespatients to adhere to risk-reduction strategies. Computer-basedsoftware, hand calculators, and Internet sites may be used forcalculating CVD risk with the Framingham scoring system.*
The Working Group on Hypercholesterolemia and OtherDyslipidemias recommends that asymptomatic women over age50 should initially be screened to obtain a fasting lipid profile (totalserum cholesterol, high-density lipoprotein cholesterol, triglyc-eride, and low-density lipoprotein cholesterol levels), and a fastingglucose level to rule out diabetes mellitus. Thereafter, asympto-matic women should be screened every five years after the age of50.12 These issues are covered in more detail in Section D.†
THYROID EVALUATION
The most recent Canadian Task Force on the Periodic HealthExam does not recommend screening for thyroid disease inasymptomatic adults.1 However, the high prevalence of hypothy-roidism among postmenopausal women justifies the use of a sen-sitive thyroid-stimulating hormone (TSH) assay if there aresymptoms suggestive of thyroid disease (see Section H).‡
BOWEL EVALUATION
In asymptomatic patients over 40 years of age, the value of fecaloccult blood testing, or sigmoidoscopic or colonoscopic visual-ization for the screening of bowel cancer, remains uncertain.However, patients with a personal or strong family history ofCrohn’s disease, ulcerative colitis, colonic polyposis, or bowel can-cer should undergo screening colonoscopy.13,14 A rectal exami-nation should be a routine part of the physical examination.
TABLE 1
GENERAL DISEASE RISK ASSESSMENT
1. Personal Factors AgeRace/ethnicityFamily medical historyPatient medical historyHeight, weight, body mass index,waist-hip ratio
2. Social Factors Educational levelMarital statusEmployment statusFinancial statusHealth insurance statusAccess to medical care
3. Lifestyle and Health SmokingBehaviours Alcohol use
Drug useDietary habitsExercise habitsSun exposureSexual practicesAdherence to preventive laws(e.g., seatbelt use, speed limits)
4. Environmental Air and water pollutantsFactors Exposure to toxins, pathogens,
or ionizing radiation
5. Menstrual and Reproductive historyMenstrual Cycle Primary or secondary anovulatoryRegularity disorders
InfertilityPremature menopause (< 40 years)
Bilateral oophorectomyMethod of contraception andlength of use
6. Mental Health Attitude toward menopause andaging
New personal/social stressorsPatient or family history of majordepressive disorders or othermental health disorders
7. Cognitive Function Family history of Alzheimer's disease or other forms of dementia
TABLE 2
FACTORS EVALUATED BY THE GAIL MODEL
AgeAge at menarcheAge at first childbirthNumber of affected relativesBreast biopsyRace
* http://www.chd-taskforce.de/framingham-english.htm† Hormone replacement therapy and cardiovascular disease. J Obstet GynaecolCan 2001;23(10):966-72.
‡ Medical and special conditions. J Obstet Gynaecol Can 2001;23(11):1096-101.

JOGC OCTOBER 200286
BONE DENSITOMETRYThis subject is discussed in Section E.* Non-modifiable risk fac-tors for osteoporosis should be identified (such as a history offracture, family history of osteoporosis, prior use of corticos-teroids), and modifiable behaviours discussed (diet, exercise,smoking). After menopause, the rate of bone loss varies amongindividuals, and bone densitometry can be useful in quantify-ing bone mass. Bone densitometry should be performed accord-ing to the guidelines published by the SOGC and theOsteoporosis Society of Canada.*
GENERAL GYNAECOLOGICAL ASSESSMENT
In the gynaecological assessment, the examiner must includeevaluations for vulvar disease and the manifestations of uro-genital aging. Screening for sexually transmitted diseases, includ-ing human immunodeficiency virus (HIV) infection, shouldbe offered in appropriate situations.
CERVICAL ASSESSMENT
Cervical cancer screening (Pap smear) should be performedaccording to Health Canada guidelines from the Cervical Can-cer Prevention Network,15 which are endorsed by theSOGC.†All women 18 years or older who have had sexual inter-course should be initially screened with two Pap smears, oneyear apart; if these smears are satisfactory, then rescreening everythree years is advised until the age of 69, if they have had no sig-nificant abnormality in the past,15 but these recommendationsare predicated on the presence of a system for recall and quali-ty assurance, and currently most provinces in Canada do nothave such a system. Thus annual screening is prudent.† Forwomen 69 years of age or older who have never been screened,two Pap smears at six-month intervals are recommended, and,if normal, they do not need to have any further smears.16 Smearscontaining atrophic cells may be misinterpreted by the cytolo-gist, and a course of vaginal estrogen before repeating thesmear may improve accuracy.15
EVALUATION OF THE ENDOMETRIUM
DURING THE MENOPAUSAL TRANSITION
Perimenopausal women with abnormal vaginal bleeding shouldbe appropriately investigated (Figure 1). Women who have riskfactors for endometrial cancer may benefit from a baseline orscreening endometrial biopsy. These risk factors include obesi-ty, diabetes, hypertension, high alcohol intake, anovulation, pro-longed oligomenorrhea or amenorrhea in an estrogenized state(for example, polycystic ovarian disease).
IN POSTMENOPAUSAL WOMEN NOT TAKING HRTAny bleeding that occurs after 12 months of amenorrhea war-rants investigation.
IN POSTMENOPAUSAL WOMEN TAKING HRTThe investigation and management of abnormal bleeding inwomen using hormone replacement therapy (HRT) must beindividualized. Vaginal bleeding may occur because of the effectsof the exogenous hormones or because of coincidental disease.
Cyclical Estrogen-ProgestinAny irregular or unscheduled bleeding should be evaluated, onceproper compliance and dosage have been confirmed. Typically,the bleeding is considered reassuring if it occurs during the finaldays of a 12- to 14-day progestin regimen, or in the week fol-lowing progestin withdrawal. Absence of withdrawal bleeding isusually not worrisome unless cervical stenosis is suspected.
Continuous-Combined Estrogen and ProgestinIrregular bleeding is common in the first six months of treat-ment, especially in recently menopausal women. Bleeding thatpersists after six months of therapy generally requires evaluationto rule out neoplasia or anatomical lesions such as polyps orfibroids. Women who continue to have irregular bleeding afterone year of therapy may benefit from an increase in progestindose or a change in regimen.
Unopposed EstrogenWomen with a uterus should only be given unopposed estro-gen therapy after discussing the associated risk of endometrialneoplasia and the need for yearly endometrial assessment. ThePostmenopausal Estrogen/Progestin Interventions (PEPI) studyshowed that 10 percent of women taking unopposed estrogentherapy will develop complex or atypical endometrial hyper-plasia within one year of beginning treatment.17
TAMOXIFEN
The place of transvaginal ultrasonography or endometrial sam-pling in the early detection of endometrial cancer in womentaking tamoxifen is undetermined.18 The American Collegeof Obstetricians and Gynecologists has recommended thatwomen taking tamoxifen have annual gynaecologic examina-tions, and that further evaluation be based on symptoms.19
METHODS OF ENDOMETRIAL EVALUATION
ENDOMETRIAL BIOPSY
Histological evaluation of the endometrium has been the goldstandard to rule out endometrial neoplasia.20 An endometrialbiopsy can usually be performed as an office procedure,although a paracervical nerve block may occasionally berequired. Plastic semi-rigid cervical dilators may be used in theoffice. Only in rare circumstances is a general anesthetic neces-sary for sampling of the endometrium.
* Osteoporosis. J Obstet Gynaecol Can 2001;23(10):978-8.† http://www.hc-sc.gc.ca/hppb/ahi/cervicalcancer/index.html
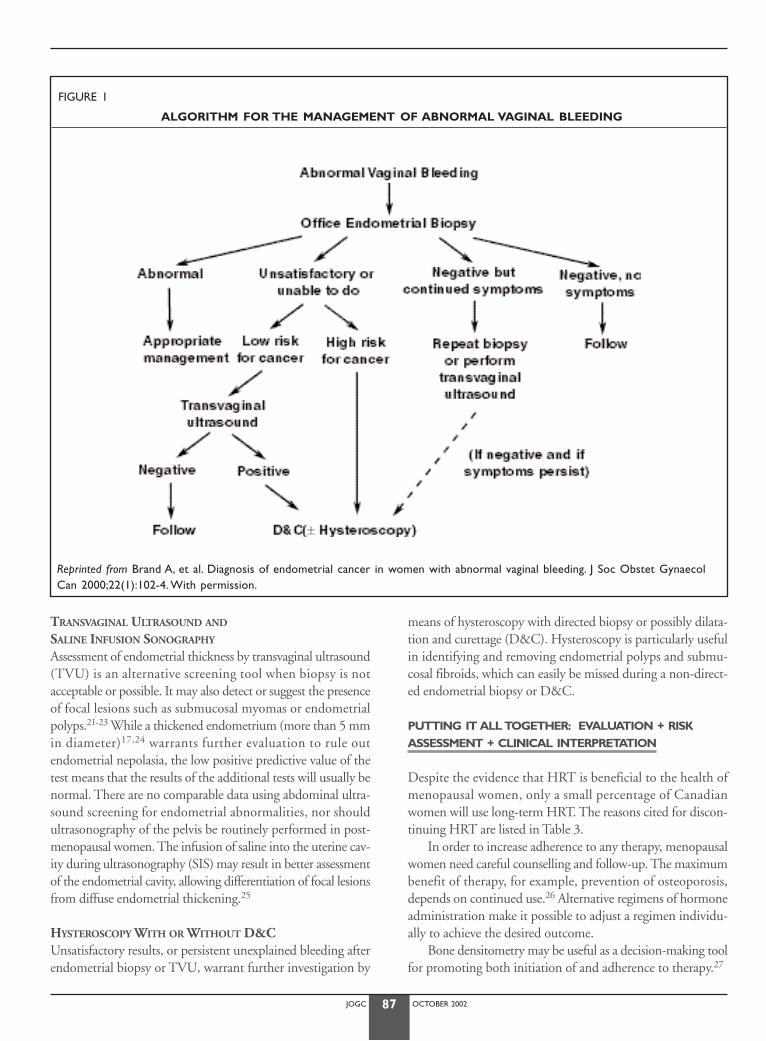
JOGC OCTOBER 200287
TRANSVAGINAL ULTRASOUND AND
SALINE INFUSION SONOGRAPHY
Assessment of endometrial thickness by transvaginal ultrasound(TVU) is an alternative screening tool when biopsy is notacceptable or possible. It may also detect or suggest the presenceof focal lesions such as submucosal myomas or endometrialpolyps.21-23 While a thickened endometrium (more than 5 mmin diameter)17,24 warrants further evaluation to rule outendometrial nepolasia, the low positive predictive value of thetest means that the results of the additional tests will usually benormal. There are no comparable data using abdominal ultra-sound screening for endometrial abnormalities, nor shouldultrasonography of the pelvis be routinely performed in post-menopausal women. The infusion of saline into the uterine cav-ity during ultrasonography (SIS) may result in better assessmentof the endometrial cavity, allowing differentiation of focal lesionsfrom diffuse endometrial thickening.25
HYSTEROSCOPY WITH OR WITHOUT D&CUnsatisfactory results, or persistent unexplained bleeding afterendometrial biopsy or TVU, warrant further investigation by
means of hysteroscopy with directed biopsy or possibly dilata-tion and curettage (D&C). Hysteroscopy is particularly usefulin identifying and removing endometrial polyps and submu-cosal fibroids, which can easily be missed during a non-direct-ed endometrial biopsy or D&C.
PUTTING IT ALL TOGETHER: EVALUATION + RISKASSESSMENT + CLINICAL INTERPRETATION
Despite the evidence that HRT is beneficial to the health ofmenopausal women, only a small percentage of Canadianwomen will use long-term HRT. The reasons cited for discon-tinuing HRT are listed in Table 3.
In order to increase adherence to any therapy, menopausalwomen need careful counselling and follow-up. The maximumbenefit of therapy, for example, prevention of osteoporosis,depends on continued use.26 Alternative regimens of hormoneadministration make it possible to adjust a regimen individu-ally to achieve the desired outcome.
Bone densitometry may be useful as a decision-making toolfor promoting both initiation of and adherence to therapy.27
FIGURE 1
ALGORITHM FOR THE MANAGEMENT OF ABNORMAL VAGINAL BLEEDING
Reprinted from Brand A, et al. Diagnosis of endometrial cancer in women with abnormal vaginal bleeding. J Soc Obstet GynaecolCan 2000;22(1):102-4. With permission.

JOGC OCTOBER 200288
Knowledge of risk is one of the factors that can help inadherence to a decision. The challenge of patient evaluation isto combine various individual risks in a clinically useful waythat assists with decision-making. A decision model has beendeveloped to compare the effects of alendronate therapy, ralox-ifene therapy, and HRT on risks of hip fracture, coronary heartdisease, breast cancer, and life expectancy, according to an indi-vidual woman’s risk factors.28
DECISION-MAKING RESOURCES
Few clinicians have the time necessary to fully educate eachwoman in their practice about the wide range of options avail-able in menopause, yet education about menopause is a prerequisite for informed decision-making. Several useful bookletsand other resource materials are available to assist the clinician.Patients can study these on their own time, and return to theirclinician to formulate a plan (Table 4).
SHARED DECISION-MAKING
A woman’s decision-making regarding HRT is primarily herown, but appears to be influenced by factors beyond risk andbenefit assessment. Physicians’ prescribing habits vary by geo-graphic region, and female physicians are more likely to pre-scribe HRT than are male physicians.32 Risk factors presented
by the patient may be less influential than the prevailing viewof the physician about the benefit of HRT in general. Clini-cal tips to help establish an appropriate system of managementare listed in Table 5.
PREVENTION DECISIONS AND
TREATMENT DECISIONS
Decisions to use HRT for the relief of symptoms are generallystraightforward, entailing short-term use of medication. Pre-ventive benefits are only measured after long-term exposure,and are measured by their impact on a population, rather thanon an individual.
Preventive decision-making involves four considerations:
1. Perceived susceptibility to the preventable condition2. Perceived severity of the preventable condition3. Perceived likelihood of benefiting from the intervention4. Risk of harm from the intervention.
Perception drives decision-making. Perceptions are formedby a complex interaction of factual knowledge, personal expe-rience, vivid anecdotes, social supports, and socially held beliefs.The Internet is a new source of opinion that also colours per-ception. Each woman will apply her own weighting, based onpersonal context and various social factors, in arriving at a deci-sion.33,34 A process to explore each dimension, enabling misconceptions to be corrected, is most likely to lead to a senseof confidence in the decision.
HIDDEN AGENDAS
Women may hesitate to disclose benefits they hope to achievefrom HRT that may not be on the physician’s list, such as con-cern with skin aging. A decision to accept risks based on suchgoals needs to be considered in the context of the relevant lit-erature and the end-points used.
TABLE 3
REASONS FOR DISCONTINUING HRT
Fear of cancer (especially breast)BleedingLack of information about benefits/risksUnnatural to take hormonesPMS-like symptomsWeight gainComplicated regimens
TABLE 4
DECISION-MAKING RESOURCES
Decision Tree on ERT/HRT Recommendation for Health CareProfessionals published by the North American MenopauseSociety29
Decision aid Making Choices: Hormones after Menopause,developed at the Ottawa Health Decision Centre in 199630,31
SOGC brochures:Menopause: Let’s Talk About It
Osteoporosis: Let’s Talk About ItDrug Therapy for Menopause and Osteoporosis:Let’s Talk About It
Heart Disease: Let’s Talk About ItHormones and Breast Cancer: Let’s Talk About ItYour Guide to Menopause
TABLE 5
CLINICAL TIPS FOR PRACTICE
• Negotiate the decision-making process and confirm thatthe process may require several office visits
• Suggest decision aids, reading materials, and Internetresources
• Suggest interaction with other health care professionalswho have special knowledge (e.g., nurses, physiotherapists,dieticians, and pharmacists)
• Engage the patient in the choice, to facilitate adherence tothe decision
• Plan certain criteria for each individual to follow (e.g., fre-quency of hot flushes, bone density)
• Provide the framework for monitoring (e.g., follow-up vis-its, a schedule for mammography)
JOGC OCTOBER 200289
FOLLOW - UP
Involving the woman in the decision-making process, antici-pating start-up problems, and arranging suitable follow-up allfacilitate adherence to treatment. The regular follow-up sched-ule should include, as a minimum, one follow-up visit threeto six months after initiating therapy, followed by annual visits.
RECOMMENDATIONS:
L1. The assessments recommended by the Canadian TaskForce on the Periodic Health Examination should beincluded in the evaluation and follow-up of peri-menopausal and postmenopausal women. (III)
L2. Routine abdominal or transvaginal ultrasonography ofthe pelvis should not be used in healthy asymptomaticpostmenopausal women. (II-1)
L3. Postmenopausal women with abnormal bleeding patternsshould undergo a review of their estrogen-progestin ther-apy administration (where appropriate), a pelvic exami-nation, and an endometrial biopsy (II-1). Transvaginalultrasonography is an alternative when endometrial sam-pling is not possible or the results are inconclusive. If thesituation remains unclear, tissue sampling with or with-out hysteroscopy is recommended. (II)
L4. The majority of women wish to participate in the deci-sion-making process, and health care providers shouldencourage them to do so. (III)
L5. Decisions should be based on an individual assessmentof symptoms, risk factor analysis, and discussion of therisks and benefits of each option. The decision shouldbe re-evaluated as new information becomes available.(III)
L6. Health care providers should actively advocate for pub-lic-funded educational programs to increase knowledgeabout menopause and osteoporosis for both womenand their health care providers. (III)
J Obstet Gynaecol Can 2001;23(12):1214-20.
REFERENCES
1. Canadian Task Force on the Periodic Health Examination. Canadianguide to clinical preventive health care. Ottawa: Health Canada;1994.
2. Mahon SM. Cancer risk assessment: conceptual considerations for clini-cal practice. Oncol Nurs Forum 1998;25:1535-47.
3. Fuster V, Gotto AM. Risk reduction. Circulation 2000;102 (20 Suppl4):IV94-IV102.
4. Byyny RL, Speroff L. Successful aging: health maintenance and preventivecare. A Clinical Guide for the Care of Older Women, 2nd ed. Philadel-phia: Lippincott Williams & Wilkins; 1996:21-30.
5. Armstrong K, Eisen A,Weber B.Assessing the risk of breast cancer. NEngl J Med 2000;342:564-71.
6. Gail MH, Benichou J.Validation studies on a model for breast cancerrisk. J Natl Cancer Inst 1994;86:573-5.
7. Rockhill B, Spiegelman D, Byrne C, Hunter DJ, Colditz GA.Validation ofthe Gail et al. Model of Breast Cancer Risk Prediction and Implicationsfor Chemoprevention. J Natl Cancer Inst 2001;93:358-66.
8. Harvey BJ, Miller AB, Baines CJ, Corey PN. Effect of breast self-examina-tion techniques on the risk of death from breast cancer. Can MedAssoc J 1997;157:1205-12.
9. Miller AB,To T, Baines CJ,Wall C. Canadian National Breast ScreeningStudy-2: 13-year results of a randomized trial in women aged 50-59years. J Natl Cancer Inst 2000;92:1490-9.
10. Ringash J. Preventive health care, 2001 update: screening mammographyamong women aged 40-49 years at average risk of breast cancer. CanMed Assoc J 2001;164:469-76.
11. Grundy SM, Pasternak R, Greenland P, Smith S, Fuster V. Assessment ofcardiovascular risk by use of multiple-risk-factor assessment equations:a statement for healthcare professionals from the American HeartAssociation and the American College of Cardiology. Circulation1999;100:1481-92.
12. Fodor JG, Frohlich JJ, Genest JR JJG, McPherson PR, for the WorkingGroup on Hypercholesterolemia and Other Dyslipidemias. Recommen-dations for the management and treatment of dyslipidemia. Can MedAssoc J 2000;162:1441-7.
13. Solomon MJ, McLeod RS. Periodic health examination, 1994 update: 2.Screening strategies for colorectal cancer. Canadian Task Force on thePeriodic Health Examination. Can Med Assoc J 1994;150:1961-70.
14. Benson AB 3rd,Chuti MA, Cohen AM et al. NCCN Practice Guidelinesfor Colorectal Cancer. Oncology (Huntingt) 2000;14:203-12(11A).
15. Programmatic Guidelines for Screening for Cancer of the Cervix inCanada. Ottawa: Health Canada; 1998.
16. Parboosingh J. Screening for cervical cancer. Canadian programmaticguidelines. Can Fam Physician 1999;45:383-93.
17. Effects of hormone replacement therapy on endometrial histology inpostmenopausal women.The Postmenopausal Estrogen/Progestin Inter-ventions (PEPI) Trial.The Writing Group for the PEPI Trial. J Am MedAssoc 1996;275:370-5.
18. Smedira HJ. Practical issues in counseling healthy women about theirbreast cancer risk and use of tamoxifen citrate.Arch Intern Med2000;160:3034-42.
19. ACOG committee opinion.Tamoxifen and the prevention of breastcancer in high-risk women. Number 224, October 1999. Committee onGynecologic Practice.American College of Obstetricians and Gynecol-ogists. Int J Gynaecol Obstet 2000;68:73-5.
20. Langer RD, Pierce JJ, O’Hanlan KA, Johnston SR, Espeland MA,Trabal JF,et al.Transvaginal ultrasonography compared with endometrial biopsyfor the detection of endometrial disease. Postmenopausal Estrogen/Progestin Interventions Trial. N Engl J Med 1997;337(25):1792-8.
21. Omodei U, Ferrazzia E, Ruggeri C, et al. Endometrial thickness and his-tological abnormalities in women on hormonal replacement therapy: atransvaginal ultrasound/hysteroscopic study. Ultrasound ObstetGynecol 2000;15:317-20.
22. Guner H,Tiras MB, Karabacak O, Sarikaya H, Erdem M,Yildirim M.Endometrial assessment by vaginal ultrasonography might reduceendometrial sampling in patients with postmenopausal bleeding: aprospective study.Aust N Z J Obstet Gynaecol 1996;36:175-8.
23. Langer RD, Pierce JJ, O’Hanlan KA, et al.Transvaginal ultrasonographycompared with endometrial biopsy for the detection of endometrialdisease. Postmenopausal Estrogen/Progestin Interventions Trial. N Engl JMed 1997;337:1792-8.
24. Neele SJ, Marchien van Baal W, van der Mooren MJ, Kessel H, Netelen-bos JC, Kenemans P. Ultrasound assessment of the endometrium inhealthy, asymptomatic early post-menopausal women: saline infusionsonohysterography versus transvaginal ultrasound. Ultrasound ObstetGynecol 2000;16:254-9.
25. Goldstein SR, Zeltser I, Horan CK, Snyder JR, Schwartz LB. Ultrasonog-raphy-based triage for perimenopausal patients with abnormal uterinebleeding.Am J Obstet Gynecol 1997;177:102-8.
26. Delmas PD,Bjarnason NH,Mitlak BH,et al. Effects of raloxifene on bonemineral density, serum cholesterol concentrations, and uterineendometrium in postmenopausal women.N Engl J Med 1997;337:1641-7.
JOGC OCTOBER 200290
27. Fitt NS, Mitchell SL, Cranney A, Gulenchyn K, Huang M,Tugwell P. Influ-ence of bone densitometry results on the treatment of osteoporosis.Can Med Assoc J 2001;164:777-805.
28. Col NF, Pauker SG, Goldberg RJ, et al. Individualizing therapy to preventlong-term consequences of estrogen deficiency in postmenopausalwomen.Arch Intern Med 1999;159:1458-66.
29. A decision tree for the use of estrogen replacement therapy orhormone replacement therapy in postmenopausal women: consensusopinion of The North American Menopause Society. Menopause2000;7:76-86.
30. O’Connor AM,Tugwell P,Wells GA, et al.A decision aid for women con-sidering hormone therapy after menopause: decision supportframework and evaluation. Patient Educ Couns 1998;33:267-79.
31. O’Connor AM,Tugwell P,Wells GA, et al. Randomized trial of aportable, self-administered decision aid for postmenopausal womenconsidering long-term preventive hormone therapy. Med Decis Making1998;18:295-303.
32. Seto TB,Taira DA, Davis RB, Safran C, Phillips RS. Effect of physician gen-der on the prescription of estrogen replacement therapy. J Gen InternMed 1996;11(4):197-203.
33. Sarrel PM. Improving adherence to hormone replacement therapy witheffective patient-physician communication.Am J Obstet Gynecol1999;180:S337-40.
34. Fisher WA,Sand M,Lewis W,Boroditsky R.Canadian menopause study - I:Understanding women’s intentions to utilise hormone replacement thera-py.Maturitas 2000;37:1-14.

In addition to previous corrections appearing in the chapters on Pharmacotherapy and Complementary Approaches, revised recommendations and relevant statements throughout the text have been incorporated in answer to the
WHI study on continuous-combined HRT. Changes have been made to the chapters on Hormone Replacement Therapyand Cardiovascular Disease, Osteoporosis, and Hormone Replacement Therapy and Cancer.

Originally printed in JOGC September 2001,Volume 23, Number 9October 2001,Volume 23, Number 10
November 2001,Volume 23, Number 11December 2001,Volume 23, Number 12
Revised October 2002,Volume 24, Number 10following Advisory Committee Review
Rogers Media777 Bay Street, 5th Floor
Toronto, Ontario M5W 1A7Tel: (416) 596-5038 Fax: (416) 596-5023
Copyright© 2002
All rights reserved. None of the contents may be reproducedin any form without prior written permission of the publisher.
The opinions expressed in this publication are those of the authors and do not necessarily reflect the opinions or recommendations of the publisher or the sponsor. 7441-7021





























![[Third National Ovarian Consensus]](https://img.pdfslide.net/doc/110x75/6355648cf4b7d3d11c0c9f9a/third-national-ovarian-consensus.jpg)