Embed Size (px)
Citation preview

THE CONTRIBUTION OF THE RIGHT PARIETAL LOBE TO OBJECT RECOGNITION
Elizabeth K. Warrington and Angela M. Taylor
(National Hospital, Queen Square, London)
INTRODUCTION
A disorder of visual recognition of pictorial material is well established in patients with right posterior cerebral lesions. Perception of photographs of faces (De Renzi and Spinnler, 1966; Warrington and James, 1967a; Benton and Van Allen, 1968), sketchy drawings of scenes (Milner, 1958; Ettlinger, 1960), fragmented drawings of objects and letters (Warrington 'and James, 1967b; Faglioni, Scotti and Spinnler, 1969), and overlapping drawings of object·s (De Renzi, Scotti and Spinnler, 1969) have ·all been shown to be impaired. Though the basis of this disorder is still obscure, certain explanations can be eliminated. Many investigations have established that the deficit is not a trivial consequence of intellectual impairment or of visual field defects (e.g., De Renzi and Spinnler, 1967). More pertinent are the studies which have shown that neither subtle visuo-sensory changes in any part of the visual field (Ettlinger, 1956), nor a failure of discrimination of a particular feature or oharacteristic of a v1sual stimulus (Warrington and Rabin, 1970; Taylor and Warrington, 1973) can account for these visual recognition deficits. There is also some evidence that this disorder of visual recognition is not merely a minor form of a more florid and clinically obvious right-parietal syndrome, i.e. of visuo~spatial agnosia (Warrington and James, 1967b; Newcombe, 1969; Warrington and Rabin, 1970).
The attainment of a meaningful percept, obviously a complex process, is increasingly being analysed in terms of hierarchical processes. However, it is still uncertain what is the appropriate breakdown of stages in this hierarchy. The problem of gestalt formation (figure from ground) is to some extent bypassed hy modern theories of perception. The possibility that the structuring of forms precedes the cla·ssification of forms (this concept will be clarified in the next paragtaph) receives tentative support from two sources. Rubel and Wiesel's analysis (1968) of their data obtained from single unit recordings proposes that hyper-complex cells aohieve ·a percept

The contribution of the right parietal lobe to object recognition 153
with the qualities of a 'figure' (but carry no information regarding which figure). Furthermore, Neisser (1966) has argued from the evidence of selective attention studies that 'figure' perception in the classical gestalt sense must precede 'recognition.' This position he cogently summarises as "the whole is prior to its parts."
The orientation, luminance and distance of objects are continually changing. The recognition of visual stimuli demands the capacity to make the same response to an infinite number of different visual patterns. An often quoted example is that all A's CA A A) are recognised as A's. Tbis, the classical problem of object recognition, has a somewhat confused nomenclature. However, 'perceptual classification' can be regarded as the most satisfactory since it describes the phenomenon briefly without any implications as to mechanisms.
This further study of patients with localised cerebral lesions considers two hypotheses, that the visual recognition deficit associated with right posterior cerebral lesions is (1) a deficit of gestalt formation or (2) a deficit of 'perceptual classification.'
MATERIAL AND METHOD
Subjects
Thirty-nine patients with right-hemisphere lesions (mean age 50.8 years) and 35 patients with left-hemisphere lesions (mean age 43.5 years) were tested. These patients were subsequently classified by a radiologist according to site of lesions as follows: 1) Anterior: patients with frontal, fronto-parietal or frontotemporal lesions; 2) Temporal: patients with lesions restricted to the temporal lobe; 3) Posterior: patients with occipital, parietal, temporo-parietal or occipitoparietal lesions.
Further information concerning this group of patients, criteria for selection and method of classification are given by Taylor and Warrington (1972). Seven out of the 74 patients did not complete the tests reported in the previous paper; nevertheless the individual patient groups in the two studies· are essentially the same. Not all patients completed all tests. Twenty patients with extra-cerebral neurological lesions were tested as controls (mean age 44.2 years).
Figure-ground discrimination
Test procedure
A test of figure-ground discrimination was devised by superimposing a fragmented letter (either 0 or X) upon a fragmented background (see Figure 1). The test stimuli were graded in difficulty by varying the ratio of black to white in the figure in relation to the ratio of black/white in the background. When the ratio of black/white in the figure and in the background was close the presence of the figure was difficult to detect by all subjects. Two versions of the test were prepared;

154 E. K. Warrington and A. M. Taylor
Fig. 1 - Figure-ground discrimination stimulus.
in one the figure was an X, in the other an O. Each version comprised 20 test cards, 12 with a figure, 8 without. The subjects' task was to detect the presence of a known letter stimulus, an X or an 0 respectively. That is, for each test stimulus he was asked whether the figure was present or absent. The number of errors was recorded.
Results
The mean error score for each patient group is given in Figure 2 (the Mann Whitney U test was used for this and all subsequent group comparisons). Although the right-hemisphere group was significantly worse than the control group, there were no significant differences between the right and left hemisphere groups, nor between any of the lesion subgroups (see Table I). It is noteworthy that the right posterior group is not impaired compared with other lesion groups.
Enlarged drawings of small objects
Test procedure
Pictorial material often represents objects as smaller than life-size, but the reverse is only rarely the case. A task comprising enlarged drawings of small objects was devised in an attempt to manipulate size changes of objects without altering any other perceptual dimensions. Pictorial representations of 20 small

TA
BL
E
I
Com
pari
son
of P
atie
nt G
roup
s on
Per
cept
ual
Task
s (V
alue
s of
Z u
sing
Man
n-W
hitn
ey U
Tes
t)
Con
trol
(N
= 20
) vs
. R
ight
he
mis
pher
e (N
= 39
) C
ontr
ol (
N =
20)
vs.
Lef
t he
mis
pher
e (N
= 35
) L
eft
hem
isph
ere
(N =
35)
vs.
Rig
ht
hem
isph
ere
(N =
39)
Ant
erio
r:
Lef
t (1
1) v
s.
Rig
ht (
1l)
T
empo
ral:
L
eft
(13)
vs.
Rig
ht (
9)
Pos
teri
or:
Lef
t (1
1)
vs.
Rig
ht
(19)
* p
< .0
5 **
p
< .0
1 **
* p <
.001
Figu
re-g
roun
d :",
225*
0.36
1.78
0.16
1.77
0.69
Enl
arge
d dr
awin
gs
Mea
sure
M
easu
re
1 2
2.65
**
2.46
*
3.07
**
2.48
*
0.08
0.
56
0.19
0.
19
0.06
0.
58
0.06
0.
98
GoU
in
figur
es
4.29
***
2.75
**
2.24
*
1.74
0.25
2.38
*
Unc
onve
ntio
nal
view
ph
otog
raph
s
Mea
sure
M
easu
re
1 2
4.07
***
4.23
***
1.93
1.
25
2.79
**
2.97
**
0.40
00
40
0.80
0.
53
2.78
**
3.16
**
~ '" B
;:;: ~ ~
~ c'
;:;: o -- S.
'" ... ~. "" .... "<
:7 '" ... ~.
~
C
<:r- '" 0- o ~ '" ~ ~ " ~ ~: c' ;:;:
......
VI
VI

156 E. K. Warrington and A. M. Taylor
10
Fig. 2 - Figure-ground discrimination mean errors scores.
objects were prepared. These were photographed and printed in 2 sizes, (a) approximating to life-size, and (b) approximately 4 X life-size (see Figure 3). Subjects were first tested on the set of enlarged drawings and then on the set of
Fig. 3 - Example of enlarged drawing.
drawings realistic in size. Subjects were required to identify each drawing, either by name or, in the case of dysphasic patients, by description, and the number of " recognition" errors was recorded.
Results
Recognition of the small drawings was not impaired in any patient group. The mean recognition error score for the set of enlarged drawings for each patient
The contribution of the right parietal lobe to obiect recognition 157
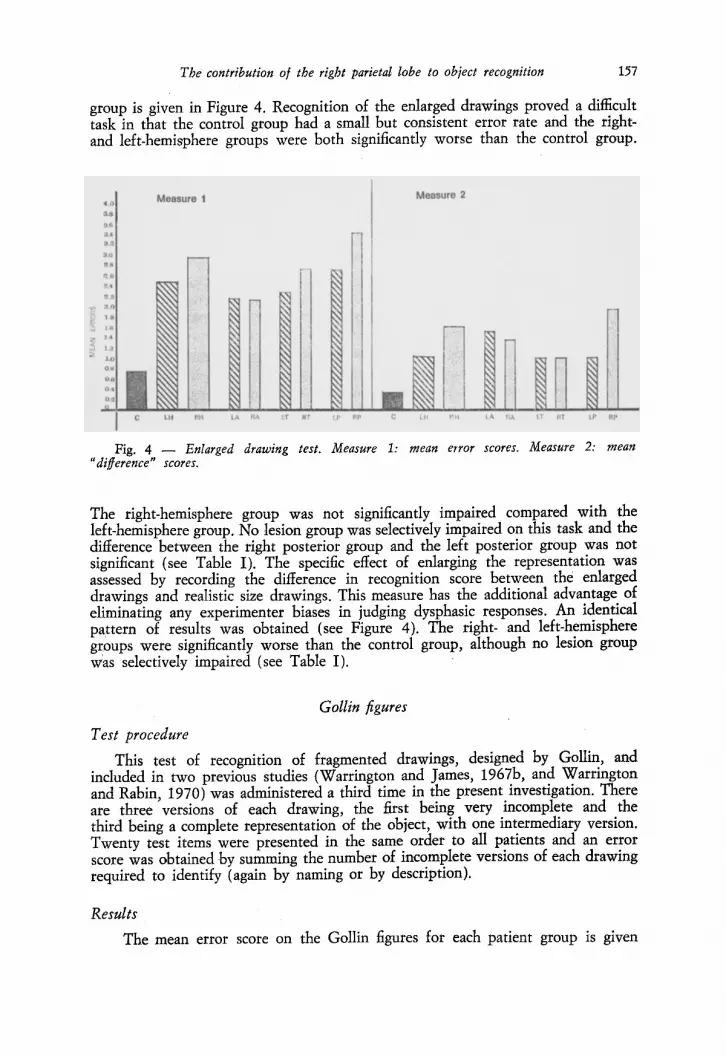
group is given in Figure 4. Recognition of the enlarged drawings proved a difficult task in that the control group had a small but consistent error rate and the rightand left-hemisphere groups were both significantly worse than the control group.
Measure 2
LA RA I:T R"r LA RA LT RT l P RP
Fig. 4 Enlarged drawing test. Measure 1: mean error scores. Measure 2: mean "difference" scores.
The right-hemisphere group was not significantly impaired compared with the left-hemisphere group. No lesion group was selectively impaired on this task and the difference between the right posterior group and the left posterior group was not significant (see Table I). The specific effect of enlarging the representation was assessed by recording the difference in recognition score between the enlarged drawings and realistic size drawings. This measure has the additional advantage of eliminating any experimenter biases in judging dysphasic responses. An identical pattern of results was obtained (see Figure 4). The right- and left-hemisphere groups were significantly worse than the control group, although no lesion group Was selectively impaired (see Table I) .
GoUin figures
Test procedure
This test of recogmtlon of fragmented drawings, designed by Gollin, and included in two previous studies (Warrington and James, 1967b, and Warrington and Rabin, 1970) was administered a third time in the present investigation. There are three versions of each drawing, the first being very incomplete and the third being a complete representation of the object, with one intermediary version. Twenty test items were presented in the same order to all patients and an error score was obtained by summing the number of incomplete versions of each drawing required to identify (again by naming or by description).
Results
The mean error score on the GoUin figures for each patient group is given

158 E. K. Warrington and A. M. Taylor
in Figure 5. Both the left- and the right-hemisphere group were significantly worse than the control group; however the right-hemisphere group was significantly worse than both the left posterior group and the right anterior group (see Table I).
2'
Fig. 5 - Gollin figures mean error scores.
The possibility that the right posterior deficit is an artefact of age differences was considered. A regression equation relating age to test score was obtained from the control data and hence an expected score for each experimental subject could be calculated. These age corrected scores (obtained, minus expected) were compared using Student's "t." Although the right-hemisphere group was not significantly worse than the left-hemisphere group (t = 1.7; P < .10), the right posterior group was significantly worse than the left posterior group (t = 2.45; P < .05).
Object recognition: conventional vs. unconventional view
Test procedure
A series of objects were photographed from two angles, from a conventional view and from an unconventional view (see Figure 6). The two views for each object were photographed by the same person under identical conditions, so that the quality and lighting of the unconventional and conventional view were identical. It is worth noting that the unconventional orientation of the object did not necessarily represent an unfamiliar view; for example, a bucket is probably as often seen from the top as the side (see Figure 6). It is possible that the conventional view would correspond to a subject's choice of ..orientation if required to draw the object from memory. Twenty objects were photographed, the conventional and unconventional orientation being arbitrarily decided.
Subjects were first shown each of the 20 photographs of unconventional view objects, followed by the conventional view objects. Subjects were requested to identify each object (either by naming or description), and errors of recognition were recorded. In addition to a recognition error score on each set of photographs, a measure of the differential effects of angle of view was used: a "difference score,"

The contribution of the right parietal lobe to ·ob;ect recognition 159
Fig. 6 - Example of conventional and unconventional view ob;ect.
the number correct on the conventional view set minus the number correct on the unconventional view set, was recorded. As with the enlarged drawings task this measure minimises any bias due to misjudging aphasic responses.
Results
The recogmtIon error rate for the conventional view objects was very low in all patient groups and no significant differences were found between any patient group. The mean recognition error score on unconventional view sets of object photographs for each patient group is given in Figure 7. The left-hemisphere
0.0
4.8
4.6
4.4
4.2
4.0
3.8
36
Measure 1
LA AA LT AT
Measure 2
lP RP LA RA LT AT LP RP
Fig. 7 - Unconventional view ob;ect. Measure 1: mean error .scores. Measure 2: mean "difference" scores.

160 E. K. Warrington and A. M. Taylor
group was not significantly worse than the control group but the right-hemisphere group was significantly impaired compared with the left-hemisphere group on the unconventional view objects. Furthermore, the right posterior lesion group obtained the highest error score and was impaired relative to the left posterior group (see Table I). The "d" scores representing the difference between performance on the conventional and unconventional views are given in Figure 7. The same pattern of results is obtained as with the recognition error score. The righthemisphere group is obtaining significantly higher "d" scores than the lefthemisphere group. Again the right posterior group is significantly worse than any other lesion group (see Table I).
Again some attempt has been made to assess the possibility that these significant results are an artefact due to age differences. Using the same statistical method as for the Gollin figures task data, the right-hemisphere group is significantly worse than the left-hemisphere group on the recognition error score (t = 2.08; P < .05). Similarly the right posterior group is significantly worse than the left posterior group (t = 2.06; P < .05).
A very clear-cut deficit has been obtained in the right posterior lesion group on this test of object recognition in which the view of the · object represented is the only critical parameter. An attempt was made to define the site of lesion with more precision than can be achieved by subdividing the 38 patients with righthemisphere lesions into 3 groups. Thirteen patients made 5 or more errors of recognition on the unconventional view objects. A radiologist drew a brain map indicating the likely extent of lesion on the lateral and medial surface for each of these patients. These 13 maps were superimposed on a brain map marked in cm squares. Thus the 13 lesions were "added" on a single brain map. The cumulative brain map of these 13 patients is given in Figure 8. The striped area represents squares in which lesions were present in 9 or more subjects. The dotted area represents the less stringent criterion of lesions in 8 subjects. In the remaining areas lesions were present in 7 or fewer subjects.
Fig. 8 - Locus of lesion giving recognition deficit on unconventional view ob;ects (see text).

The contribution of the right parietal lobe to object recognition 161
DISCUSSION
The most striking finding of this study was the differential effect of perception of conventional and unconventional views in the right posterior hemisphere group. Before discussing the significance of this finding the other main effects will be commented on briefly.
Warrington and James (1967h) reported a deficit in the right parietal group on the Gollin pictures test that Warrington and Rabin (1970) failed to replicate on testing a further series of patients. The present result, namely a sIgnificant deficit by the right posterior group on the Gollin figures test, suggests that more weight be given to the former result; that is, the perception of fragmented pictorial material may be impaired in patients with posterior right hemisphere lesions. Furthermore it seems likely that the lesion category" posterior" in this patient population is comparable with the previous inclusive "parietal " category .
In many visual recognition tasks which elicit a right posterior deficit it could be said that the signal/noise ratio is degraded (e.g., overlapping figures, fragmented letters, etc.). ToO test whether this is a critical variable it seemed appropriate to include a task which had virtually no identification or recognition component, while the signal/noise ratio was manipulated to alter the difficulty of figure/ground discrimination. The figure/ground discrimination task meets these requirements. No deficit associated with localisation of lesion was obtained on the figure/ground task (although performance was impaired in the tight-hemisphere group compared with the control group). Since there was no ceiling effect, the absence of a significant deficit in the right posterior group cannot therefore be attributed to the figure/ground test being an insensitive measure. This negative finding provides evidence that the organisation of sensory input into coherent "forms" or "gestalts" is not the critical factor. That is, the right posterior lesion group can achieve an adequate form perception from the sense data.'
If this analysis be accepted, that a failure at the level of structuring of forms (gestalt formation) cannot account for the right posterior group recognition deficit, then by elimination the perceptual classification hypothesis can be considered. Two tasks were devised in which two quite different perceptual transformations were employed, the size of the representation of an object, and the angle of view of an object. These two tasks shared one property, that the load on the "sensory" information processing was constant in the two conditions of each task. ~_ecognition of enlarged drawings of small
, This negative finding does not deny the possibility of the existence of a disorder of object recognition at this level of abstraction. Indeed Efron (1968) described a patient with intact brightness, colour and hue discrimination who was unable to match simple shapes or isolate an object from its background. This case may well represent a failure at the level of form or gestalt formation.
162 E. K. Warrington and A. M. Taylor
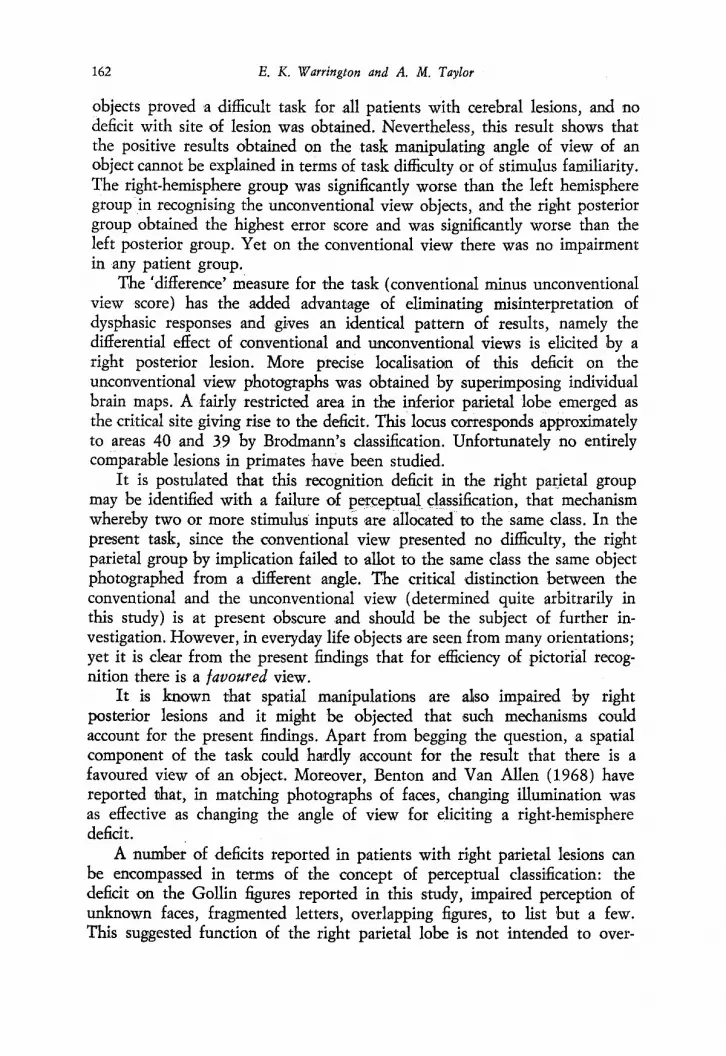
objects proved a difficult task for all patients with cerebral lesions, and no deficit with site of lesion was obtained. Nevertheless, this result shows that the positive results obtained on the task manipulating angle of view of an object cannot be explained in terms of task difficulty or of stimulus familiarity. The right-hemisphere group was significantly worse than the left hemisphere group in recognising the unconventional view objects, and the right posterior group obtained the highest error score and was significantly worse than the left posterior group. Yet on the conventional view there was no impairment in any patient group.
The 'difference' measure for the task (conventional minus unconventional view score) has the added advantage of eliminating misinterpretation of dysphasic responses and g1ves an identical pattern of results, namely the differential effect of conventional and unconventional views is elicited by a right posterior lesion. More precise localisation of this deficit on the unconventional view photographs was obtained by superimposing individual brain maps. A fairly restricted area in the inferior parietal lobe emerged as the critical site giving rise to the deficit. This locus corresponds approximately to areas 40 and 39 by Brodmann's classification. Unfortunately no entirely comparable lesions in primates have been studied.
It is postulated that this recognition deficit in the right par.ietal group may be identified with a failure of pen:eptual classification, that mechanism whereby two or more stimulus inputs 'are allocated to the same class. In the present task, since the conventional view presented no difficulty, the right parietal group by implication failed to allot to the same class the same object photographed from a different angle. The critical distinction between the conventional and the unconventional view (determined quite arbitrarily in this study) is at present obscure and should be the subject of further investigation. However, in everyday life objects are seen from many orientations; yet it is clear from the present findings that for efficiency of pictorial recognition there is a favoured view.
It is known that spatial manipulations are also impaired by right posterior lesions and it might be objected that such mechanisms could account for the present findings. Apart from begging the question, a spatial component of the task could hardly account for the result that there is a favoured view of an object. Moreover, Benton and Van Allen (1968) have reported that, in matching photographs of faces, changing illumination was as effective as changing the angle of view for eliciting a right-hemisphere deficit.
A number of deficits reported in patients with right parietal lesions can be encompassed in terms of the concept of perceptual classification: the deficit on the Gollin figures reported in this study, impaired perception of unknown faces, fragmented letters, overlapping figures, to list but a few. This suggested function of the right parietal lobe is not intended to over-

The contribution of the right parietal lobe to ob;ect recognition 163
ride other probably independent functions of the right posterior cortex such as integration of sensory data and spatial processing information. If the present formulation is ,accepted, namely that the recognition deficit in the right parietal group be identified with a failure of perceptual classification, then certain inferences, follow. First, the present findings provide neuropsychological evidence that gestalt or figure percepti9.p precedes perceptual classification. Secondly, the critical site for this deficit is the right parietal lobe, in a group whose language functions are intact. Thus it follows that perceptual classification, which has been isolated asa separate 'stage in the recognition process, must function independently of verbal hypotheses. Though the structural locus of perceptual classification may have been identified, the mechanism by which it is aohieved remains unclear. The • favoured view' finding can be accommodated by notions such as feature analysis and template matching.
SUMMARY
Visual recogmtlon of pictorial material was investigated in a group of 74 patients with localised cerebral lesions. Four tasks of visual perception, figure/ ground, fragmented drawings, enlarged drawings, and photographs of objects from an unconventional view, were administered. An unimpaired performance of the right posterior group on the figure/ground task contrasted with a marked deficit on the unconventional view objects task. It was demonstrated that there is a favoured view for efficiency of object recognition. The findings provide evidence that gestalt formation is intact whereas perceptual classification is impaired in patients with right posterior lesions. The implications of this interpretation of the data for theories of object recognition are discussed. ,
Acknowledgements. We wish to thank the Physicians and Surgeons of the . National Hospital for permission to study and report our findings on patients under their care. We are grateful to Mrs. H. E. Nelson, Dr. R.T.C. Pratt and Dr. T. Shallice for their advice in the preparation of this manuscript. Mrs. A. M. Taylor was supported by a grant from the Medical Research Council. We are particularly grateful to Dr. H. Swanson for providing us with individual brain maps.
REFERENCES
BENTON, A. 1., and VAN ALLEN, M. W. (1968) Impairment in facial recognition in patients with cerebral disease, "Cortex," 4, 344-358.
DE RENZI, E., ScOTTI, G., and SPINNLER, H. (1969) Perceptual and associative disorders of visual recognition: relationship to the site of the cerebral lesion, "Neurology," 19, 634-642.
-, and SPINNLER, H. (1966) Facial recognition in brain-damaged patients, "Neurology," 16, 145-152.
-, - (1967) Impaired performance on color tasks in patients with hemispheric damage, "Cortex," 3, 194-216.
EFRON, R. (1968) What is perception?, in Boston Studies in the Philosophy of Science, IV, ed. by R. S. Cohen and M. W. Wartofsky, Reide, Dordrecht (Holland).

164 E. K. Warrington and A. M. Taylor
ETTLINGER, G. (1956) Sensory deficits in visual agnosia, "J. Neurol., Neurosurg. Psychiat.," 19, 297-307.
- (1960) The description and interpretation of pictures in cases of brain lesions, "J. Ment. Sci.," 106, 1337-1346.
FAGLIONI, P., SCOTTI, G., and SPINNLER, H. (1969) Impaired recognition of written letters following unilateral hemisphere damage, "Cortex," 5, 327-342.
HUBEL, D. H., and WIESEL, T. N. (1968) Receptive fields and functional architecture of monkey striate cortex, "J. Physiol.," 195, 215-243.
MILNER, B. (1958) Psychological defects produced by temporal lobe excision, Proceedings of the Association for Research in Nervous and Mental Disease, 36, 244-257.
NEISSER, U. (1966) Cognitive Psychology, Appleton, New York. NEWCOMBE, F., and RUSSELL, W. R. (1969) Dissociated visual perceptual and spatial deficits
in focal lesions of the right hemisphere, "J. Neurol., Neurosurg. Psychiat.," 32, 73-81. TAYLOR, A. M., and WARRINGTON, E. K. (1973) Visual discrimination in patients with
localised cerebral lesions, "Cortex," 9, 82-93. WARRINGTON, E. K., and JAMES, M. (1967a) An experimental investigation of facial recognition
in patients with unilateral cerebral lesions, "Cortex," 3, 317-326. -, - (1967b) Disorders of visual perception in patients with localised cerebral lesions,
"Neuropsychologia," 5, 253-266. -, and RABIN, P. (1970) Perceptual matching in patients with cerebral lesions, "Neuro
psychologia," 8, 475-487.
Elizabeth K. Warrington and Angela M. Taylor, Psychology Department, The National Hospital, Queen Square, we IN 3BG, London, England.





























