Embed Size (px)
Citation preview
The University of Dodoma
University of Dodoma Institutional Repository http://repository.udom.ac.tz
Social Sciences Master Dissertations
2015
The impact of health sector reforms on
health service delivery in Tanzania: the
case of Dodoma regional referral hospital
Mathew, Asela
The University of Dodoma
Mathew, A. (2015). The impact of health sector reforms on health service delivery in Tanzania:
The case of Dodoma regional referral hospital. Dodoma: The University of Dodoma.
http://hdl.handle.net/20.500.12661/873
Downloaded from UDOM Institutional Repository at The University of Dodoma, an open access institutional repository.

THE IMPACT OF HEALTH SECTOR REFORMS ON HEALTH
SERVICE DELIVERY IN TANZANIA: THE CASE OF DODOMA
REGIONAL REFERRAL HOSPITAL
By
Asela Mathew
A Dissertation Submitted in Partial Fulfillment of the Requirements for the Master
Degree of Public Administration of the University of Dodoma
The University of Dodoma
October, 2015
i
CERTIFICATION
The undersigned certifies that he has read and hereby recommends for acceptance by
the University of Dodoma, a dissertation entitled “The Impact of Health Sector
Reforms on Health Service Delivery in Tanzania: The Case of Dodoma Regional
Referral Hospital”, in fulfillment of the requirements for the Master Degree of Public
Administration of the University of Dodoma.
………………………………………….
Dr. Ajali M. Nguyahambi
(SUPERVISOR)
Date……………………………………
ii
DECLARATION
AND
COPYRIGHT
I, Asela Mathew, declare that this dissertation is my own original work and that it has
not been presented and will not be presented to any other University for a similar or
any other degree award.
Signature………………………………………………….
No part of this dissertation may be produced, stored in any retrieval system, or
transmitted in any form or by any means without prior permission of the author or the
University of Dodoma.
iii
ACKNOWLEDGEMENT
First and foremost, I thank the Almighty God for granting me strength, health and
courage to meet the demand and rigour of graduate studies and thus, enriching my
knowledge. I extend my heartfelt thanks and appreciation to the School of Social
Science management for giving me permission to undertake studies and providing me
technical and material support for my studies.
Special thanks go to my major supervisor Dr. Ajali M. Nguyahambi for his assistance
in guidance, encouragement and commitment throughout the process of preparing this
dissertation. I appreciate his work.
I would also like to express my sincere gratitude to my parents Mr. and Mrs. Mathew
Mwaiswelo and the whole family in assisting me with unquestionable values and
morals: thank you for your love, guidance and for always believing in me throughout
my education life. I also thank them for reminding me to pray and to thank God every
day for everything. May God bless you abundantly.
In particular, I also thank much to my classmate brother Masanja Paul, Mrs. Rehema
Mginah and the whole staff of Dodoma Regional Referral Hospital who helped me a
lot in accessing data at Dodoma Regional Referral Hospital where it was my study
area. Thank you a lot and God bless you.
I extend a lot of thanks to my classmates Julius Bukobero, Lechipya Lawi, Nzunda
John and Henry Peter who gave me a lot of material support during the whole period of
preparing my dissertation. Also I express my thanks to all respondents who
participated in this study for their time spent. May God bless you.

iv
Lastly I would like to give special thanks to my beloved friends Mariam Gladson
Mwaikuju and Catherine Kiondo who assisted me and gave a lot of support during the
whole time of preparing my dissertation in Dodoma. Thank you my friends for your
hospitality and be blessed.
v
DEDICATION
This dissertation is dedicated to my beloved parents Mr. and Mrs. Mathew Mwaiswelo
and to my young Magdalena, Onesmo and Rachel. I am very grateful for their
guidance, financial support, prayers, encouragement and love during my whole life of
studying.
vi
ABSTRACT
The purpose of this study was to assess the impact of health sector reforms on health
service delivery in Tanzania. The main objective was to assess the impact of health
sector reforms on improving quality and accessibility of health services. Specific
objectives were to assess the status of health services accessibility, examine the
contribution of various actors in promoting quality and accessibility of health services
delivery and to analyze the challenges towards provision and accessibility of quality
health services. The study was carried out at Dodoma Regional Hospital as it is among
government health facilities that provide health services to the general public in the
area. This gave room for assessing the impact of health sector reforms on improving
quality and accessibility of health services.
The study employed a cross-sectional research design, and data were collected through
survey questionnaire, interview and observation methods. Data analysis employed both
qualitative and quantitative methods through computer (SPSS) program.
Research findings indicate that there is a number of challenges that need to be
addressed towards provision of improved health services in government health
facilities after health sector reforms. The study concluded that health sector reforms
have achieves its goals in improving health service delivery to some extent although
there are some weaknesses in some areas. Therefore, the study recommends that
corrective measures to be taken by government and other actors in order to ensure that
the goal of health sector reforms is achieved to the desired level, and quality, access,
equity and efficiency in the delivery of health services is guaranteed.
vii
TABLE OF CONTENTS
CERTIFICATION .............................................................................................................. i
DECLARATION AND COPYRIGHT ............................................................................ ii
ACKNOWLEDGEMENT ............................................................................................... iii
DEDICATION .................................................................................................................. v
ABSTRACT ..................................................................................................................... vi
TABLE OF CONTENTS ............................................................................................... vii
LIST OF TABLES ............................................................................................................ x
LIST OF FIGURES .......................................................................................................... xi
LIST OF ACRONYMS .................................................................................................. xii
CHAPTER ONE: INTRODUCTION AND BACKGROUND OF THE STUDY ..... 1
1.0 Introduction ................................................................................................................. 1
1.1 Background to the Problem ......................................................................................... 1
1.2 Statement of the Problem ............................................................................................ 6
1.3 Objectives of the Study ............................................................................................... 7
1.3.1 General Objective ..................................................................................................... 7
1.3.2 Specific Objectives ................................................................................................... 8
1.4 Research Questions ..................................................................................................... 8
1.5 Scope of the Study ....................................................................................................... 8
1.6 Significance of the Study............................................................................................. 8
1.7 Limitations of the Study .............................................................................................. 9
CHAPTER TWO: LITERATURE REVIEW ............................................................ 10
2.0 Introduction ............................................................................................................... 10
2.1 The Concept of Health Sector Reforms..................................................................... 10
2.2 Theoretical Review .................................................................................................... 10
2.3 Empirical Review ...................................................................................................... 19
2.3.1 Overview on Health Sector Reforms ...................................................................... 20
2.3.2 National Health Policy Framework in Tanzania .................................................... 22
2.4 Conceptual Framework ............................................................................................. 24
2.5 Research Gap ............................................................................................................. 25
viii
CHAPTER THREE: RESEARCH METHODOLOGY ............................................ 27
3.0 Introduction ............................................................................................................... 27
3.1 Research Approaches ................................................................................................ 27
3.3 Location of the Study ................................................................................................ 28
3.6 Population of the Study ............................................................................................. 30
3.7 Sample Size ............................................................................................................... 30
3.8 Methods for Data Collection ..................................................................................... 32
3.8.1 Interview ................................................................................................................. 32
3.8.2 Survey Questionnaire ............................................................................................. 32
3.8.3 Observation............................................................................................................. 33
3.9 Data Presentation ....................................................................................................... 34
3.10 Data Analysis........................................................................................................... 34
3.11 Validity and Reliability of Data .............................................................................. 34
3.12 Ethical Considerations ............................................................................................. 35
CHAPTER FOUR: DISCUSSION AND INTERPRETATION OF FINDINGS .... 36
4.0 Introduction ............................................................................................................... 36
4.1 Profile of Respondents .............................................................................................. 36
4.1.1 Sex Distribution of the Respondents ...................................................................... 36
4.1.2 Age Distribution of the Respondents ..................................................................... 37
4.1.3 Level of Education Distribution of the Respondents ............................................. 38
4.2 Status of Health Services Provision .......................................................................... 39
4.2.1 Perception on the Status of Health Services Provision .......................................... 40
4.2.2 Quality of the Health Services ................................................................................ 41
4.2.3 Level of Satisfaction ............................................................................................... 41
4.2.4 Comparison of Services between Government and Private Hospitals ................... 42
4.2.5 Level of Improvement ............................................................................................ 43
4.2.6 Extent of Accessibility in Health Services ............................................................. 45
4.2.7 User Fee in Health Services ................................................................................... 46
4.2.8 Importance of Government Hospitals .................................................................... 47
4.2.9 Appreciation of Government Health Services ........................................................ 48
4.2.9.1 Affordable Medical Price .................................................................................... 48
4.2.9.2 Geographical Coverage ....................................................................................... 49
4.2.10 Suggestions to the Government ............................................................................ 49
ix
4.2.10.1 Provision of Enough Funds ............................................................................... 49
4.2.10.2 Environmental Management and Increase Hospital Buildings ......................... 50
4.3 Contribution of Various Actors ................................................................................. 50
4.3.1 Resource Allocation Contribution .......................................................................... 51
4.3.2 Public - Private Partnerships Contribution ............................................................. 51
4.4 Challenges towards Health Services Provision and Accessibility ............................ 52
4.4.1 Resource Based Challenges .................................................................................... 52
4.4.2 Motivation Based Challenges ................................................................................. 53
4.4.3 Recruitment Based Challenges ............................................................................... 53
4.5 Ways to end Challenges ............................................................................................ 53
4.5.1 Resource Based Prospect ........................................................................................ 54
4.5.2 Motivation Based Prospect ..................................................................................... 54
4.5.3 Recruitment Based Prospect ................................................................................... 55
CHAPTER FIVE: CONCLUSION AND RECOMMENDATIONS ........................ 56
5.0 Introduction ............................................................................................................... 56
5.1 Summary of the Study ............................................................................................... 56
5.2 Summary of the Findings .......................................................................................... 57
5.3 Conclusion ................................................................................................................. 58
5.4 Recommendations ..................................................................................................... 59
5.4.1 Policy - Based Recommendations .......................................................................... 59
5.4.2 Recommendations for Further Studies ................................................................... 60
REFERENCES ................................................................................................................ 61
APPENDICES ................................................................................................................. 65

x
LIST OF TABLES
Table 1: Distribution of Respondents ........................................................................... 31
Table 2: Perception on the Status of Health Services ................................................... 40
Table 3: Quality of Health Services ............................................................................. 41
Table 4: Level of Satisfaction....................................................................................... 42
Table 5: Comparison of Services between Government and Private Hospitals ........... 43
Table 6: Importance of Government Hospitals ............................................................ 47

xi
LIST OF FIGURES
Figure 1: Conceptual Framework ................................................................................. 25
Figure 2: Sex Distribution of the Respondents............................................................. 37
Figure 3: Age Distribution of the Respondents ............................................................ 38
Figure 4: Level of Education Distribution of the Respondents .................................... 39
Figure 5: Level of Improvement ................................................................................... 44
Figure 6: Extent of Accessibility in Health Services.................................................... 45
Figure 7: User Fee in Health Services .......................................................................... 46
xii
LIST OF ACRONYMS
CHF Community Health Fund
CHMTs Council Health Management Teams
CHSB Country Health Service Board
D by D Decentralization by Devolution
DPs Development Partners
FP Family Planning
HIV/AIDS Human Immune Virus/ Acquired Immune Deficiency Syndrome
HPSS Health Promotion and System Strengthening
HSRs Health Sector Reforms
LGAs Local Government Authorities
MCH Maternal-Child Health
MoH Ministry of Health
MoHSW Ministry of Health and Social Welfare
NGOs Non-Governmental Organisations
NHIF National Health Insurance Fund
NHSSP National Health Sector Strategic Plan
NPM New Public Management
PSRP Public Sector Reform Program
PPPs Public - Private Partnerships
SAPs Structural Adjustment Programs
SPSS Statistical Package for Social Scientist
UNDP United Nations Development Program
URT United Republic of Tanzania
WHO World Health Organization
1
CHAPTER ONE
INTRODUCTION AND BACKGROUND OF THE STUDY
1.0 Introduction
The study was about the Impact of Health Sector Reforms on health service delivery in
Tanzania. The focus was to examine how Public Sector Reform Program (PSRP)
specifically Health Sector Reforms contribute in improving the quality and
accessibility of health services to the public. This part introduces the title and aims of
the study, followed by background information of the study, statement of the problem,
objectives of the study, significance of the study, scope of the study and limitations of
the study.
1.1 Background to the Problem
Many countries worldwide are devising reforms intended to bring about fundamental
and sustained change in their health sector policies, institutions and implementation
processes (World Bank, 1994). Most African countries have embarked on
comprehensive public sector reform programs, and in many cases have received
assistance from international institutions. However, despite the tremendous efforts and
resources that has been allocated to this endeavor, progress remains scant and less
impressive (Willis, 2005).
Experience from South Africa, a number of issues has stimulated reform (Mogedal, et
al, 1995). For example, people are increasingly becoming aware (because of the spread
of democratization) that quality health services need to be provided more efficiently
and equitably to larger constituencies of people. Health services are being threatened
by economic recession which is leading to cutbacks in recurrent budgets and a decline
in capital development.
2
Health care planners in South Africa who are interested in reform have to deal with
various constraints. These constraints limit the impact of health services on health
status, especially at the primary level. These include the following: Hospital care still
consumes most expenditures, salaries absorb the bulk of recurrent costs, and urban
areas get more resources than rural areas. Poor systems for budgeting, for disbursing,
for purchasing, and for monitoring expenditures that have failed to achieve an
equitable distribution of health care resources. Lack of access to health care for
populations that are disadvantaged because of such factors as location, age, sex,
poverty, unavailability of services, unemployment, and bad planning or management of
services. Services that do not respond adequately to local needs. For example, the poor
quality of many services leads to underutilization, unmotivated and poorly trained
staff, long waiting periods, inconvenient clinic hours, inadequate drug supplies, lack of
confidentiality, financial exploitation by the private sector, and lack of safeguards
against dangerous treatments. (Cassels, 1995; Zwi and Mills 1995). As all these
constraints are caused in part by a scarcity of resources, health care planners have
become preoccupied with reforms that secure more adequate financing for health care
and ensure greater value for money. Yet, while some documentation of developing
countries experience of different health financing reforms is emerging, the real impact
of these reforms remains relatively unknown (Gilson and Mills, 1995; Janovsky and
Cassels, 1996; Kutzin, 1995; Shaw and Griffin, 1995; World Bank 1994).
The combination of mechanisms used for reform and the approach adopted to address
the health sector‟s deficiencies varies in each country according to several internal
factors. Seminar participants identified such factors as, among others, the overall vision
of health service development, the existing sources of finance, the current management
of finance, the range and type of service providers, and the prevailing economic
3
conditions and other factors outside the health sector such as rural development,
literacy, the political system and local-level organization (Kutzin, 1995).
The impulse for such reforms came as a result of combination of a number of factors.
These include market determination, public dissatisfaction with service delivery,
growing demand for citizen participation in decision making and disillusion with the
standard of public sector resource management (Njunwa, 2005). Other concerns like
cost effectiveness, efficiency, accountability, focus on results, contestability of advice
and services, better performance management and decentralization of service delivery
also contribute significantly to create pressure for change and reform. Most of the
public sector reform programs that have taken place in developing countries during the
last two decades were introduced as part of the Structural Adjustment Programs (SAPs)
of the World Bank in the 1980s. However, most of the more recent reforms under the
influence of the New Public Management (NPM) have been driven by a combination
of economic, social, political and technological factors which have triggered the quest
for efficiency and for ways to cut the cost of delivering public services. Additional
factors, particularly for Africa, include lending conditionality and the increasing
emphasis on good governance (ECA, 2003).
In Kenya, Health Sector Reforms were tailored to meet Kenya‟s health sector policy
goal of providing accessible, affordable and efficient health care services to all
Kenyans. Before their implementation, it was feared that health reforms would
marginalise the poor and vulnerable in accessing health care. However, the government
of Kenya took care of this concern by introducing the system of waivers and
exemptions. Under exemptions, certain categories of patients were automatically
exempted from user fees. These included those seeking family planning, children under
4
five years, sexually transmitted disease patients and those suffering from HIV/AIDS.
Exempting children under five years was in realization of the fact that such children
have a low immunity development which predisposes them to sickness. Indeed,
statistics on malaria morbidity attests to this fact, as children under five years are the
most affected both in terms of morbidity and mortality (Walt, 1994).
Kenya‟s health policy was designed to achieve the following objectives, increase
coverage and accessibility of preventive and promotive curative health services
especially in rural areas, consolidate urban and rural curative and preventive /
promotive health services like rural-urban referral system, increase emphasis on
Maternal-Child Health (MCH) and Family Planning (FP) in order to reduce morbidity,
mortality and fertility through related public health education programmes, strengthen
the Ministry of Health‟s Health management capabilities with emphasis being placed at
the district level in order to take care of management problems such as facility
management, drug supply and transport and equipment maintenance, increase inter-
sectoral coordination between the Ministry of Health and other ministries such as
agriculture, water, education, social ser-vices, information and NGOs; increase
alternative mechanisms for financing health care programmes, improve and expand the
National Health Insurance (Owino, 1997).
Kenya‟s health care delivery system, which was charged with meeting health policy
objectives, was organised around the Ministry of Health (MoH). The Ministry of
Health headed by the Minister is charged with the responsibility of setting policies,
coordinating the activities of Non-Governmental Organisations (NGOs), and
managing, monitoring and evaluating policy implementation (Dmytracsenko, 2003).
Kenya‟s Ministry of Health is the largest provider of health care (curative, preventive
5
and promotive) and undertakes environmental protection and pollution surveillance
(Odada and Odhiambo 1989). In general, the Ministry of Health is involved in six
health related programmes, namely promotional and preventive health care, family
planning and population control, environmental protection and programme supervision,
special programmes such as disease control projects and research. The Government of
Kenya has also encouraged the plural system of health service delivery. Other
providers of health care services include local authorities which, by law, are required to
undertake public health activities, supported by public finance. They provide curative
in-patient and out-patient care. In addition, there is a for-profit private hospitals and
nursing homes that concentrate on curative services (Odada and Ayako 1989).
In 1990, the first health care policy was prepared in Tanzania. Among other things, it
offered the road map and guidelines on how health services should be delivered
equitably to meet the needs of urban populations. This is considered to be the health
reformation period in order to overcome health problems in health sector. The reason
behind the health sector reform was to overcome different problems at district level.
The vision behind was to enhance transparency and accountability of resources
allocated to health sector and improve health access by the poor (URT, 2003). In 2007,
primary health care development plan was initiated. It was intended to speed up the
construction of sufficient health care facilities such as hospitals, health centers and
dispensaries, to strengthen preventive services and to ensure availability of adequate
health professionals (Kiwanga et al, 2011 and URT, 2003). The Ministry of Health and
Social Welfare has developed a framework to reform health sector in order to improve
quality of health services at all levels in the country. The focus is on district health
services where most of the essential health services are provided close to the
communities. The thrust is to improve significantly the quality of essential health

6
services and make Council Health Management Team (CHMT), Hospitals, Health
Centers and Dispensaries health providers more accountable to the community
(MoHSW, 2009).
1.2 Statement of the Problem
Health Sector Reforms is a significant and intentional effort to improve the
performance of the health care system (Roberts et al, 2004). Health Sector Reforms has
been expected to facilitate the transformation of the health system into a system which
is effective, efficient, equitable and responsive to the needs of the society. To make this
possible, the government through the office responsible for regional administration and
local governments decided to require the participation of all key stakeholders in the
design and translation of the reforms into action (Semali, 2003 and URT, 2003).
Despite the implementation of the Health Sector Reforms and Decentralization policy
since 1990s, Tanzania experiences many problems in health facilities which included
shortage of human resources, inadequate health facilities and equipments and high
prevalence of various killer diseases such as malaria. The problems are more acute
among health facilities in terms of health services delivery especially at grass root
levels (URT 2003:2-5, Masatu, 2007:2, Fjeldstad and Semboja, 2000:22). Also, the
health services are generally characterized by shortages of essential drugs, equipment,
poor management, lack of supervision and staff motivation (MoHSW, 2009). There is
also limited coordination of different stakeholders (Development Partners) support to
the health sector despite different health reforms purposely undertaken to improve
health service delivery to all Tanzanians (Hutchinson 2002, Antwi, 2008 and MoHSW,
2009).
7
Tanzania faces serious challenges in improving the health and well-being of its people
due to poor health services offered by public service utilities. The Ministry of Health
and its partners in government, the donor community and civil society have responded
with concerted action in many cases achieving significant gains. Health systems are
inherently relational and so many of the most critical challenges for health systems are
relationship problems. Poor staff attitudes towards patients can cause dissatisfaction
with services which even good technical care may not offset. Such attitudes may, in
turn, result from de-motivating management practices and behaviors. International
concern with the weak responsiveness of health systems towards its users, particularly
in low income countries, reflects these sorts of problems (World Health Organisation,
2001). Many researchers put more emphasis on the accessibility of facilities and drugs
as well as affordability on the part of the most vulnerable groups while others have
compared health services with other services like education and come up with
realization that the satisfaction rating on health service is low. However, the challenges
facing health services delivery is a lack of capacity and personal to exercise the
responsibility for service delivery. Health workers who are the ones providing services
seem to be underrated as crucial part in service provision (Braathen, et al, 2005).
So, the aim of this study was to assess the Impact of Health Sector Reforms on
improving quality and accessibility of health services in Tanzania, and the study was
specifically carried out at Dodoma Regional Referral Hospital.
1.3 Objectives of the Study
1.3.1 General Objective
To assess the impact of health sector reforms on improving quality and accessibility of
health services in Tanzania.
8
1.3.2 Specific Objectives
i. To assess the status of health services provision and accessibility at Dodoma
Regional Referral Hospital.
ii. To examine the contribution of various actors in promoting quality and
accessibility of health services delivery at Dodoma Regional Referral Hospital.
iii. To analyze the challenges towards provision and accessibility of quality health
services at Dodoma Regional Referral Hospital.
1.4 Research Questions
i. What is the perception on the status of health services provision and accessibility at
Dodoma Regional Referral Hospital?
ii. What is the contribution of various actors in promoting quality and accessibility of
health services delivery at Dodoma Regional Referral Hospital?
iii. What are the challenges towards provision and accessibility of quality health
services at Dodoma Regional Referral Hospital?
1.5 Scope of the Study
The study was conducted at Dodoma Regional Referral Hospital focusing on the
assessment of the Impact of Health Sector Reforms on health service delivery in
Tanzania by inquiring if there is some improvements in quality and accessibility of
health services after health sector reforms so as to meet public needs.
1.6 Significance of the Study
On the accomplishment of this study, the findings have generated a number of benefits,
not only to the researcher, but also to other stakeholders like the government, health
facilities and the general public. It will cultivate interest to individuals and
organizations on further research on the topic and inform policy makers understanding
9
on what should be considered at policy level regarding better provision of the services.
The research findings also have added knowledge to other researchers in the field.
1.7 Limitations of the Study
During the field work, the researcher faced some challenges which could have
hindered the success of this research. One of the challenges was financial constraint
where the researcher needed enough money for meals, transport fare, accommodations
and stationeries to accomplish the research work. So, the researcher was required to
use money carefully to accomplish the study. Another challenge was language barrier
to some of the respondents who were the ordinary citizens where by the researcher
prepared questionnaires in English language but some of the respondents did not
understood. To make it clear, the researcher was supposed to prepare other
questionnaires in Swahili language so as to be understood by each respondent. Also
time constraint was another barrier during data collection through interview method
where respondents at field area were very busy and others were not available at all.
This made the researcher to take long time waiting for them until when they were
available. Some respondents were also not willing to fill in the questionnaires. This
constraint was solved by the researcher through educating them about the importance
of filling in the questionnaires on the topic concerned.
10
CHAPTER TWO
LITERATURE REVIEW
2.0 Introduction
This part gives the theoretical framework and background laid down by different
researchers on public social service delivery basing on health service delivery after the
Health Sector Reforms in Tanzania and theory concerning service delivery. It also
provides empirical review on the topic concerned.
2.1 The Concept of Health Sector Reforms
Mogale (2011) defines Health Sector Reforms as the sustained purposeful change to
improve the efficiency, equity, and effectiveness on health sector. The health sector has
been one of the pioneers of decentralized service delivery through Health Sector
Reforms (HSRs) starting from the early 1990s aiming at improving the quality of
health services provided to communities (URT, 2003 and Maluka et al, 2010).
Therefore, health sector reforms has been defined as a sustained process of
fundamental change in national policy and institutional arrangements led by
government and designed to improve the functioning and performance of the health
sector and ultimately the health status of the population. Health sector reforms is a
process that seeks major changes in national policies, programs and practices through
changes in health sector priorities; laws; regulations; organizational and management
structure; and financing arrangements. The central goals were most often to improve
access, equity, quality, efficiency and sustainability.
2.2 Theoretical Review
This study has been pegged on the New Public Management Theory (NPM) which is
the core theory used to understand public services delivery. Theory suggests that
11
policies may enhance the efficiency of public service delivery such as healthcare
provision for a comprehensive overview of NPM and efficiency (Andrews, 2013).
Improved responsiveness has been one of the main objectives of NPM through
providing services that correspond to individuals‟ wishes and through improving
customer friendliness. It informs our understanding and analysis of the delivery of
public services.
Osborne and Gaebler (1991) identified ten principles that represent an operational
definition of New Public Management. The first is that a government has a
responsibility to "steer" the delivery of public services in the addressing of public
issues. As such, it reflects the notion that government does not necessarily have to be
doing something in order to be responsible for the delivery of that public services.
The second principle is that government ought to be "community-owned" and that the
role of the government is to empower citizens and communities to exercise self-
governance. This notion stands in contrast to the notion that citizens are merely
recipients of public services and do not have to be actively engaged in the process of
deciding what those services would look like. Indeed, the citizens simply need to know
they were receiving the same service as that delivered to other citizens or recipients
such that no preferential treatment is being shown. The third principle involves the role
of competition. Competition is seen as inherently good such that, through competition,
the best ideas and most efficient delivery of services can emerge. Competition can
drive the newly empowered citizens and recipients to create new and better ways of
providing public goods to themselves and their fellow citizens. Sometimes competition
means that various public and private firms compete to procure the rights to deliver a
public service. It also means that departments within a government have to compete for
12
limited public resources, that communities have to compete with each other to offer
fresh and original ideas, and employees have to compete with each other in the
delivery of the services for which they are responsible.
The fourth principle is based on the notion that governments should be driven by their
missions. Far too often, the results of governmental operations were the enforcement of
rules that may or may not have been relevant to the particular cases. It should be the
purposes for which agencies are created that drive the activities of that agency, not the
rules that have been constructed around that agency. Furthermore, it is companion
principle that public agencies should be judged on the results that they generate.
Organizational processes like the budget cycle should be directed in assessing the cost
and benefits of the outputs of the units and not on the allocation of inputs (staff, space,
resources) between those units. The sixth principle relates to viewing citizens and
consumers of public goods as customers. The notion of customer is predicated on the
value of choice. Customers ought to have a right to choose between competing and
differentiated approaches that could be taken to deliver any particular public good. The
seventh principle is based on the notion that agencies (bureaucracies) “earn” their
allocation of resources by demonstrating the value in terms of the public good that will
be generated by the “investment” that elected officials would make in a particular
agency. This perspective has the units in an agency competing with each other by
“selling” to the elected officials, a greater public good than that offered by the other
agencies.
The eighth principle relates to the desirability of orienting public agencies toward
preventing rather than curing public problems. Although this particular principle has
been seen as a critique of bureaucracy is general, it is not the intention to argue that
anticipatory organizations are inherently related to NPM. It may include here for
13
completeness. The ninth principle is about maximizing the participation of the broadest
possible number of people and institutions in the decision-making process. In this
sense, it is antihierarchy and anti-bureaucratic. It is also anti-uniformity in that the way
a particular public service is delivered is a function of the local community of
participants who decide how that service will be delivered. The tenth principle relates
to leveraging market forces and utilizing market based strategies in the delivery of
public goods. It presumes that there is no one way to deliver a public good and a wide
variety of delivery mechanisms are possible.
These ten principles were translated into an implementation plan (Osborne and
Plastrik, 2000) by looking at the following five key elements for a successful
organization in New Public Management. First is the need to create clarity of aim
(core) that allows the organization to focus on the key items that will achieve its ends.
The core element in this action plan is the focusing of the activities of a public
organization on those that will best help to achieve the desired outcomes of that
organization. The phrase "clarity of aim" is used to connote the efforts that
organization must go through to communicate to affect stakeholders, employees, and
the public its vision, mission, strategic goals, outcomes and relevance. The openness of
communication and the transparency of the organization in serving its public purpose
are essential to serve this end. The tools to accomplish this task include strategic
management, performance budget systems and policy analysis/program evaluation as
feedback mechanisms.
In the New Public Management, the desired outcome is for elected officials to be
"steering" the organization, not "rowing." It also challenges the notion of a traditional
hierarchical organizational chart where the pyramid places the managers at the top and
14
the workers at the bottom. It turns that pyramid upside down, and recognizes the
workers (the ones who actually deliver the public good) the most important members
of the organization and should, therefore, be at the top. The role of management is to
support the new top of the organization.
The second key element is the need to connect consequences to the actions of
organizations, individuals and collectives so that those actions have meaning and
impact on the public. The connecting of consequences to our actions seems overly
obvious. But, on reflection, it is not necessarily the way governments and
bureaucracies have operated. Individuals, bureaucracies, collectives and communities
that take actions should do so anticipating that there will be results (consequences)
associated with their actions. It is desirable that all actions taken have positive
consequences, and it could certainly want to pursue public policies that could generate
a whole lot of positive consequences.
If the actions of any of the above actors had no consequences, it could ask activities
undertaken in the first place. If there are negative consequences, it could ask those that
generated those consequences to be held accountable for those consequences. Public
activities can be assessed for the consequences they create and the actors either
individually or collectively, should be acknowledged when they create and produce
positive consequences and penalized if they create negative consequences.
The third element focuses on acknowledgement that being a customer implies several
elements namely: (i) choice, to decide whether to engage with whom and if, at all; (ii)
equality of condition in the sense that the customer is neither superior nor subordinate
to the individual, collective, community or bureaucracy; (iii) knowledge, interest,
power may be asymmetrical, but the fundamental right of the citizen-customer to
15
participate is a choice of that customer; (iv) focus on the customer in order to recognize
that the purpose of public service is the delivery of a public good to human beings.
The fourth key element is the need to shift control from the top or center in order to
empower individuals, organizations and communities to address public problems.
Shifting control way the top and center has the effect of empowering organizations,
employees and communities to engage in deciding of the things that governments do
and the outcomes that they achieve. The act of empowering requires participation of all
parties and open and free communications to allow for the various parties to do that
which they are called upon to do. Empowering organizations allows the parts of that
organization that are best able to implement desired organizational outcomes to do so.
Empowering employees allows front-line governmental workers to use organizational
resources to achieve results. Empowering communities creates power sharing between
the government and affected communities and shifts control from bureaucracies to
those communities.
The fifth element is the need for change in the organizational culture of public agencies
by “changing the habits, touching the hearts and winning the minds” of public
employees. The culture strategy is about creating a bonded relationship between the
bureaucracy‟s employees and the agency. The desire is to create a feeling within the
organization that its employee‟s higher order psychological needs for self-actualization
can be met as the employee engages in the activities of the agency as an active
participant in the designing and implementing of the good consequences that should be
the outputs of any public agency. This requires the organization to “touch the hearts”
and “win the minds” of its employees.
16
According to Hood (2003) New Public Management has been a dominant force
shaping market based reform agenda. The protagonists recommended that the public
sector be opened up to greater private sector influence. This was to be achieved
through the implementation of panoply of practices which reflected these arguments,
ranging from the promotion of various forms of relationships with private firms such as
contracting-out or partnerships to the development of complex performance
management systems and customer service orientation. However, the benefits of NPM
related tools in healthcare delivery have been already questioned from an international
perspective.
Boston, et al, (1996) point out that, while the development of the theoretical framework
can be said to be still ongoing, it has been posted that NPM is a revival of the old
managerialist ethos, reminiscent of Taylor‟s scientific management, which has been
greatly influenced by such doctrines as homo economics and new institutional
economics. He identified nine characteristics of New Public Management.
Firstly, NPM involves large-scale privatization, corporatization and commercialization
by which government disengaged from the trading aspects of its commitments that
could best be left to the private sector, or run autonomously by agencies like private
sector businesses. Secondly, NPM entails processes of managerialism and
marketisation heralding business sector management style, where in top public
managers can exercise a great amount of discretionary power, exhibiting and using
such tools as mission statements, development plans, labour contracts and performance
agreements.
Thirdly is a shift from maintenance management to change management. Public sector
managers are no longer carrying out small-scale, localized, incremental reforms aimed
17
at maintaining standards, but they are becoming transformational change managers.
Fourthly is parsimony cutting costs and applying only the least necessary amount of
resources with the aim of achieving the maximum utility possible. This is the most
basic characteristic of all reform programmes, and it is nowadays ideology-neutral.
Fifth is a shift from input controls to output and outcome controls. Resources are
allocated on the basis of a fair assessment of the satisfactory outcome; the result must
justify the expense, irrespective of the process. Sixth is the creation of quasi-markets
and greater competition attempts to make the provision and quality of services
customer driven, and more contracting and outsourcing to stimulate contestability in
service delivery.
Seventh is devolution/decentralization involving the delegation or spreading of
management authority, organizational unbundling and the institution of new forms of
governance structures, e.g. boards of governors or chief executives. Eighth is
disaggregation involving detaching policy formulation from policy execution. A
strategic core dedicates itself to policy making while a peripheral group of managers
implements the policies. Ninth is tighter performance specification which is manifested
in widespread employment of contracts between principals and agents that specify in
detail their respective obligations, the use of performance indicators and league tables.
The implication of the theory to the study is that, public services are structurally
inefficient; markets are in all circumstances superior to public provision, if markets are
not readily available then quasi-markets or a regime of targets should be used to secure
effectiveness and value for money. A part from that, the theory builds awareness to the
people on different social problems like in the health sectors where individuals face a
lot of the challenges in health services delivery even after the health sector reforms.
Where there is poor and lack of accessibility of the health services among public health
18
centers that are currently affecting their localities, the public should be given room to
decide which challenge is to be solved first according to how the majority prioritize.
Appropriate solution can be realized when people who know their localities well are
involved in setting priorities right.
Also the theory has been a useful tool for the bureaucrats and politician to allocate the
health service and to use the revenue collected from the natural resources because by
improving health service delivery into quality and accessibility finance is needed to
support the health sectors in order to improve service delivery. It enable the
government to maintain existing health services without abandoning its policy of
achieving equity in health. We are all aware that the society has different problems or
challenges in terms of the health services after reforms. The various actors and
stakeholders may collect the choices of the public and channel to the municipal council
for action. So, government should make sure that it delivers quality services to its
individuals in order to meet public needs like in the health. Consumers of the health
services who are the patients must be satisfied with the health services given in the
hospitals.
The theory was criticized by Pollitt (2003) by elaborating on the alternative logics
posed by NPM by arguing that there is a contradictory message being presented to
public managers. When the concern over accountability and the primacy of politics,
which restricts the manager, intersects with the NPM call for letting the managers
manage through the liberation motive, the message becomes mixed. The demands for
increased performance evaluation and stakeholder participation complicate the
message even more as now the public entrepreneur is to be both creative and
responsive, transparent and measured or audited while not making any decisions that
will affect particular groups without involving those groups in the process.
19
Also Cohen and Eimicke (1995) note that since reinvention places a direct emphasis on
entrepreneurship, public administration scholars are critical of the movement for its
avoidance of constitutional law and representational democracy. Critics often argue
that real entrepreneurs cannot be created in government, that market incentives cannot
be substituted for law, and that reinventers undermine public management capacity by
eliminating management layers in the effort to empower lower levels of public
employees.
Williams (2000) contends that NPM makes contradictory prescriptions in the call for a
more business-like government while lacking a complete and historically accurate
understanding of public administration. If NPM was merely inconsistent and
inaccurate, could simply ignore it. However, NPM dispenses advice that is counter to
effective and democratic government and espouse information so misleading that it is
deceptive. Thus, he argues it cannot ignore.
2.3 Empirical Review
This part presents a review of different studies in relation to the health sector reforms
as presented by various scholars. The review based on the general overview on health
sector reforms explains how it improves the efficiency, equity and effectiveness of the
health services. It also explains the national health policy towards development of
health service delivery.
20
2.3.1 Overview on Health Sector Reforms
Khan, et al, (2003:92), Masatu (2007:163) and Lethbridge (2004:2) contend that Health
Sector Reform is the sustained purposeful change to improve the efficiency, equity and
effectiveness of the health sector. Understanding the process of reform is important for
learning how changes have taken place and also to identify critical factors for
successful policy implementation.
Varraich (2011:2) note that, in an attempt to improve health sector performance, many
countries across the developing world such as Chile, Colombia, Ethiopia, Ghana,
Kenya, Philippines, Tanzania, Thailand, Uganda, and Zambia have pursued a variety of
health sector reforms, including decentralization. Health reforms in developing
countries take place along with political reforms. This stressed the need for developing
different stakeholders‟ management skills and tools in developing countries. The active
participation of different stakeholders includes emphasis on self-reliance and
community participation. This was expected to empower households and communities
with knowledge and skills to reduce the burden of diseases (Semali, 2003:5, and
Odaro, 2012:2). Governments of the developing countries then needed to provide
conducive environments in overcoming the obstacles to improved health. The
supportive environment included strong political commitment, appropriate
organizational framework and managerial process, equitable distribution of health
resources and community involvement (Hutchinson, et al, 2011:1-7).
However, despite these appealing policy contents, performance is thwarted by several
problems. These include weakness of political commitment, inadequate financing,
technical inefficiency, hierarchical and centralized structures of the Ministry of Health
programs and policies (Varraich 2011:1-2). UNDP (2010:74) reported that, in
21
developed countries like Britain, Germany and United States of America, life
expectancy has benefited people who are older, wealthier and more educated partly
because of more effective healthcare interventions and better health services. The
reasons behind these achievements were strong economy and good practices of
decentralization policy. Chitama, et al (2011:2) add that good policy can bring positive
outcomes to a specific country in health sector. There is a consensus that, good policy
alone, even when made correctly, will not by itself produce the desired sufficient
outcome. The successful priority setting during policy implementation level will help
in achieving the desired outcomes in health sector.
Mogale (2011:9-10) note that health sector reforms are aimed at implementing
fundamental changes in the health sector that are purposeful and sustainable. The
changes consequent to health sector reforms involved re-defining priorities, refining
policies and reforming the institutions through which those policies were implemented.
Semali (2003:9-10) analyzed that, the overall goals of the health sector reforms were to
improve health status and consumer satisfaction by increasing the effectiveness and
quality of services and obtaining greater equity by improving the access of
disadvantaged groups to quality care. They are also aimed obtaining greater value for
money (cost-effectiveness) from health spending, considering improvements in both
the distribution of resources to priority activities. It is therefore evident that developing
countries still have some way to go to realize the full benefits of decentralization.
There is a need for regular assessment on the part of the government with the view to
make hard choices and adjustments when this becomes necessary (UNDP 2010:74 and
Varraich 2011:1). Reforms intend to improve service delivery by making sure the
service providers are accountable to the citizens. Change should not just be introduced
it is for the sake of it, because it is a fashion and has applied elsewhere. Any reform
22
that is introduced must be relevant to the public service (Kiragu et al, 2005). This
argument shows how important for the service providers to be committed to changes.
Otherwise these reforms will be ending theoretically without practical application.
Some of the researchers focus on services delivery in terms of their availability,
affordability and acceptability by the clients. WHO (2008) puts emphasis on physical
access or reach ability of services that meet a minimum standard, the ability of the
clients to pay for service and acceptability of the services by the clients. Staffs who are
the major providers of the services are not given priority. Hence, they are underrated as
a crucial part in service provision. The Ministry of Health and Social Welfare has
developed a framework to reform health sector in order to improve quality of health
services at all levels in the country. The focus is on District health services, where most
of the essential health services are provided close to the communities. The trust is to
improve the quality of essential health services, and make Council Health Management
Team (CHMT), Hospitals, Health Centers and Dispensaries, health providers more
accountable to the community (MoHSW, 2009).
2.3.2 National Health Policy Framework in Tanzania
The health policies are vital guides towards health sector development of any country.
The policy recognizes the challenges of consolidating the principles of the previous
health policy in community involvement, improved health services provision, access
and equity while addressing the different dimensions of reforms that take place in the
public sector (URT, 2013:1). The Tanzania National Health Policy was formulated in
1990 and provided the guidelines on how the health services will be provided. The new
developments such as proposal for health sector reform of 1994, Tanzania development
vision 2025 and poverty reduction strategy 2000, have been integrated in the new
23
health policy documents of 2003. The health policy was linked with local government
and public service reforms. Hence, the decentralization policy in health sector was
formulated to facilitate the health services provision in rural areas (Yamauchi, 2011:33,
and URT, 2003:1-5).
On the National Health Policy, the government jointly with the development partners
formulated the program of work (1999-2002) and the second health sector strategic
plan (2003-2008). The plan assured an essential health package and it revealed the role
of central government for setting policy. The plan also analyzed the roles of districts as
implementers of health policy (Yamauchi, 2011:33). Maluka, et al, (2010:755) note
that at the district level, the policy recognized the challenges of consolidating the
principles of the previous health policy in community involvement, improved health
services provision, access and equity while addressing the different dimensions of
reforms that were taking place in the public sector at that time. The health plan
identified the key constraints including lack of progress in some of the district councils,
which resulted from the differing calendars for phased implementation of government
reforms.
The studies which were conducted in Tanzania revealed that, as part of the health
sector reforms, the Council Health Management Teams (CHMTS) have been given the
task of planning and budgeting for activities needed to manage, control, coordinate and
support all health services in the district on a year-to-year basis (Maluka et al, 2010-
755). Maluka et al (2010:763 and URT 2003:1) also note that, there is shortage of
number of skilled health staff at the municipal level. Further, it is noted that, there is a
challenge in capturing the available health resources during the planning process. This
situation is contributed by lack of skilled health workers. These constraints limit the
24
provision of health services at the municipal level. The Council Health Management
Teams have to survey the priorities needed from hospitals, health centers, dispensaries
and the community before the planning period begins. However, at the municipal level
there were discrepancies between the policy guidelines and the practice of resource
allocation in the municipal. The lack of human resources is a challenge in health sector
and it was recommended to train and upgrade the health workers, to provide incentives
and hardship allowances to health workers who work in rural areas, and to recruit more
manpower. Also regarding the quality of health services at rural areas, it was
recommended to monitor and evaluate the roles of CHSB and facility health
committees‟ role on health services supervision (Semali, Savigny and Tanner, 2005:1-
5).
2.4 Conceptual Framework
A conceptual framework acts as a map that guides a researcher organized in a manner
that makes them easy to communicate to others (Kothari, 2004). It refers to pictorial
narration of the relationship between the independent variables versus dependent
variables. The researcher explains the relationship between the variables as follows: the
independent variable is health sector and the intervening variable is the management
practice in health sector. When the intervening variable is positive the outcome is good
leadership, responsiveness and finance and when it is negative the outcome is
corruption, poor leadership, favoritism and lack of motivation. The dependent variable
is health service delivery. The health service delivery depends much on the health
facility which delivers health services. Also the health service delivery can be
intervened positively as well as negatively through management practice in the health
sector. If there is positive outcome in management practice it leads to improved health
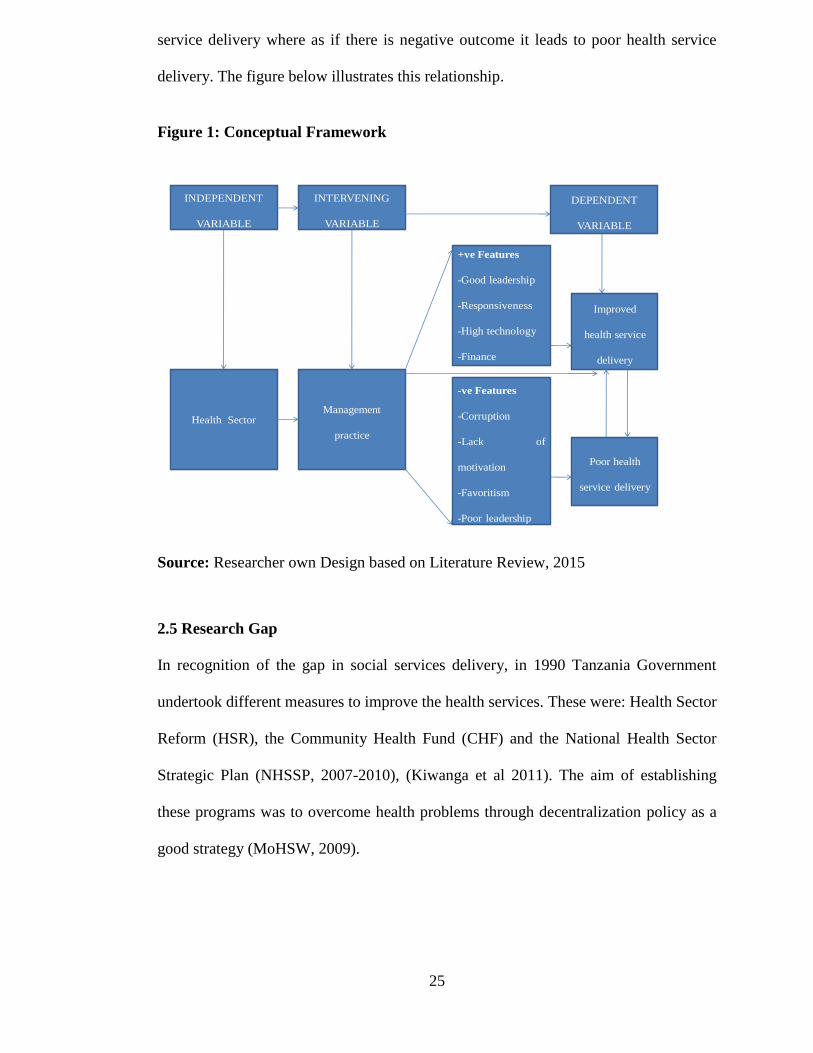
25
service delivery where as if there is negative outcome it leads to poor health service
delivery. The figure below illustrates this relationship.
Figure 1: Conceptual Framework
INDEPENDENT
VARIABLE
INTERVENING
VARIABLE
DEPENDENT
VARIABLE
Health SectorManagement
practice
+ve Features
-Good leadership
-Responsiveness
-High technology
-Finance
-ve Features
-Corruption
-Lack of
motivation
-Favoritism
-Poor leadership
Improved
health service
delivery
Poor health
service delivery
Source: Researcher own Design based on Literature Review, 2015
2.5 Research Gap
In recognition of the gap in social services delivery, in 1990 Tanzania Government
undertook different measures to improve the health services. These were: Health Sector
Reform (HSR), the Community Health Fund (CHF) and the National Health Sector
Strategic Plan (NHSSP, 2007-2010), (Kiwanga et al 2011). The aim of establishing
these programs was to overcome health problems through decentralization policy as a
good strategy (MoHSW, 2009).
26
The health services in Tanzania were recognized as the basic social services and
remain as one of the governments priorities. Saltman, et al, (2007), Smoke (2003),
Semali (2003), URT (2003) and many others argue in favour of decentralization citing
the democratizing potential of increased scope for participation and accountability of
health service delivery. There is the intrinsic value of decentralization as a desirable
goal in improving health services.
Despite all expectations of Health Sector Reforms, still there are ongoing problems
towards provision of health services among peoples in Tanzania. The arguments for the
contribution of Health Sector Reforms on health services from many studies rest
principally on a series of assumptions and theoretical justifications particularly to
developing countries (URT, 2011 and Manor, 2011). However, there are limited
studies on appropriately designed health system for health services delivery in
Tanzania. This study therefore, focused on assessing the position of health services in
government health facilities after Health Sector Reforms in order to if there is any
improvements Dodoma Regional Referral hospital as the case study.
27
CHAPTER THREE
RESEARCH METHODOLOGY
3.0 Introduction
Research methodology is a way to undertake investigation that aims at solving a
research problem. The chapter provides a frame work upon which the study is
grounded. It may be understood as a science of studying how research can be done
scientifically. In it we study the various steps that are adopted by the researcher in
studying her/his research problem along with the logic behind them (Kothari, 2004).
This chapter describes how the study was designed and conducted. It also presents the
methodological strategies which were adopted to make the study successful.
3.1 Research Approaches
The study involved both qualitative and quantitative approach. Quantitative approach
involves statistical analysis relying on numerical evidence to draw conclusion or to test
hypotheses. Qualitative approach is generally not concerned with numbers rather it
involves gathering a great deal of information about a small number of people rather
than a limited amount of information about a large number of people (Veal, 1997).
Based on meanings expressed through words where data were analyzed using content
analysis.
Quantitative data were collected through survey questionnaire by using Statistical
Package for Social Scientist (SPSS) for the results. In this study questionnaires were
distributed to the ordinary citizens who are the beneficiaries of the health services.
Respondents were able to state their perceptions on the status of health services
provision and accessibility at Dodoma Regional Referral Hospital. Results indicate that
the status of health services provision and accessibility is moderate because there are
28
still some challenges which hinder the provision and accessibility of quality health
services in government health facilities.
Qualitative data were collected through interview method whereby the management
staffs were interviewed concerning the contribution of various actors in promoting
quality and accessibility of health services delivery at Dodoma Regional Referral
Hospital. Results indicate that various actors like HPSS and AGHAKAN contributes
much in promoting quality and accessibility of health services delivery. Also nurses
and doctors were able to analyze the challenges towards provision and accessibility of
quality health services where the results indicate that still there are some challenges
which hinder the provision and accessibility of quality health services.
3.2 Research Design
A research design is the conceptual structure within which research is conducted. It
constitutes the blueprint for the collection, measurement and analysis of data (Kothari,
2003). This study employed cross-sectional research design. The rationale for using
this design is to enable the researcher to collect data based on the point of view of time
and study different groups of respondents in a single period of time.
3.3 Location of the Study
The study conducted at Dodoma Regional Referral Hospital. A criterion for selection
was based on the fact that it is among government health facilities in Tanzania which
deliver health services to the society. This gave a room to get data that helped to assess
the impact of health sector reforms on improving quality and accessibility of health
services to the community.
29
3.4 Types of Data
Types of data required were both Primary and Secondary Data. Primary data were
those which are collected afresh and for the first time, and thus happen to be original
in character (Kothari, 2004). Data were collected direct from the government health
facility in various departments at the field area by looking for the respondents who are
the management staff and the health officers at Dodoma Regional Referral Hospital
and the ordinary citizens who are the beneficiaries of the health services in Dodoma
Municipality. In collecting primary data, the interview method was employed in this
study.
The rationale for the use of this type of data collection based on the need for first hand
information from the respondents so as to meet the objective of the study. Secondary
data means data that are already available. They refer to the data which have already
been collected and analyzed by someone else (Kothari, 2004). When the researcher
utilizes secondary data, then he /she have to look into various sources from where
he/she can obtain them. These data were found from sources like journals, newspapers
and other published sources. The rationale for using secondary data was to find and
make additional information to the data collected from respondents so as to bring clear
understanding about the topic concerned.
3.5 Sampling Methods
This study employed both probability and non-probability sampling in identifying
respondents who participated in the study. Probability sampling was based on random
selection. In probability sampling, each unit in the population has an equal chance of
being in the sample (Kothari, 2004). The rationale for using probability sampling was
to make sure that each respondent get an equal chance of being selected from the
30
whole group. Probability sampling was used where each respondent in the study area
like nurses, doctors and the ordinary citizens who are the beneficiaries of health service
get a chance of being selected.
Non-probability sampling is a decision in which a researcher chooses only those
elements which he/she believes will be able to deliver the required data. The major
criterion for including a person in a sample is possession of expertise or experience
about the problem under investigation (Adam and Kamuzora, 2008). Through
interview method of data collection, this sampling was applied by choosing some
members in the study area like management staff to provide data through primary data
collection method. Non – probability sampling allowed the researcher to have a
purposive target on a group of people believed to be reliable for the study (Kombo and
Tromp, 2006).
3.6 Population of the Study
Population of the study has to fulfill the requirements of efficiency, representatives,
reliable and flexibility (Kothari, 2004). The target populations were the ordinary
citizens who are the beneficiaries of the health services in Dodoma Municipality,
management staff, nurses and doctors of Dodoma Regional Referral Hospital.
3.7 Sample Size
Sample size refers to the number of items to be selected from the universe to constitute
a sample. The size of sample should neither be excessively large, nor too small
(Kothari, 2004). It should be optimum in the sense of being able to fulfill the
requirements of efficiency, representativeness, reliability and flexibility. The sample
size is the total number of the management staff, nurses and doctors of Dodoma
Regional Referral Hospital and the ordinary citizens of Dodoma Municipality.
31
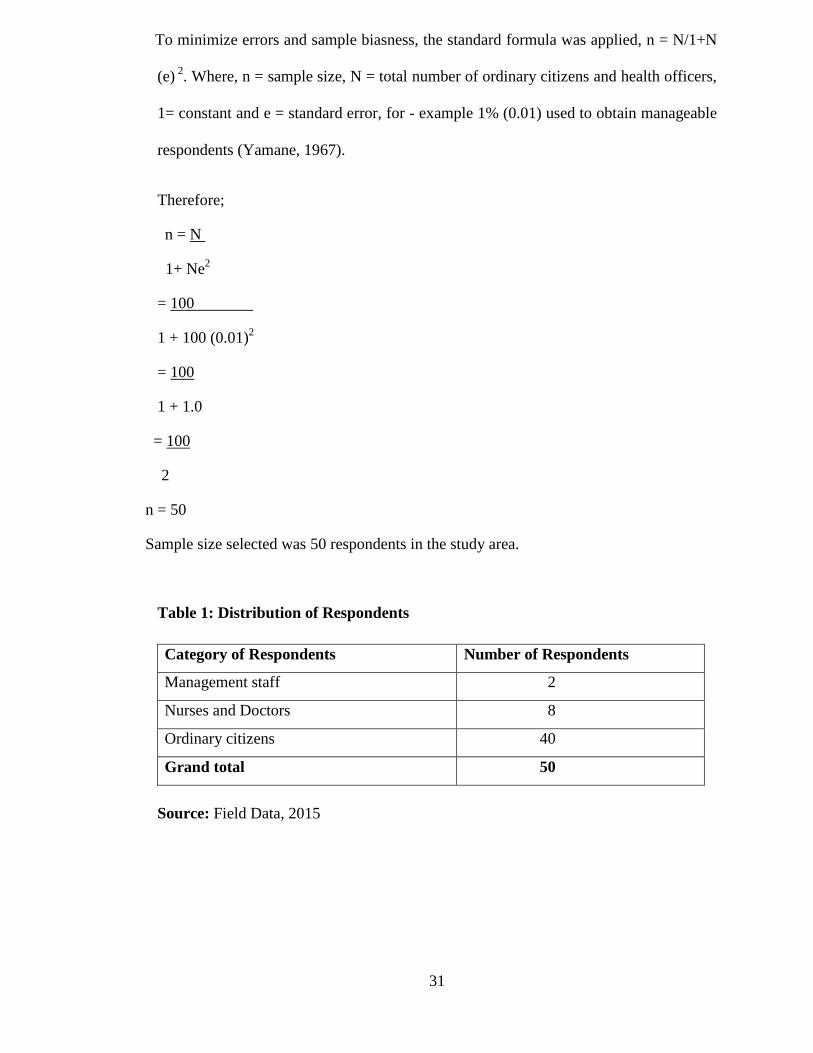
To minimize errors and sample biasness, the standard formula was applied, n = N/1+N
(e) 2
. Where, n = sample size, N = total number of ordinary citizens and health officers,
1= constant and e = standard error, for - example 1% (0.01) used to obtain manageable
respondents (Yamane, 1967).
Therefore;
n = N
1+ Ne2
= 100
1 + 100 (0.01)2
= 100
1 + 1.0
= 100
2
n = 50
Sample size selected was 50 respondents in the study area.
Table 1: Distribution of Respondents
Category of Respondents Number of Respondents
Management staff 2
Nurses and Doctors 8
Ordinary citizens 40
Grand total 50
Source: Field Data, 2015
32
3.8 Methods for Data Collection
Data collection refers to gathering specific information aimed at proving or refuting
some facts (Kombo and Tromp, 2006). Data which were collected were those which
meet the objectives of the study. Basing on this research, the researcher used the
following methods of collecting data.
3.8.1 Interview
Young (1983) as quoted in Rwegoshora (2006) defines an interview as a systematic
method by which one person enters more or less imaginatively into the inner life of
another who is generally a comparative stranger to him. He further argues that the
interview is a technique of field work which is used to watch the behavior of an
individual or individual to record statements to observe the concrete results of social or
group interaction. The tool which was used in this method of data collection was
interview guide. An interview guide was used to interview the management staff,
nurses and doctors. The rationale for using interview method was to capture the
attitudes, behaviors and perceptions of the respondents. Face to face interview was
suitable in the study because it gave a chance to probe more deeply.
3.8.2 Survey Questionnaire
According to Rwegoshora (2006), questionnaire tool for data collection is a tool which
uses a set of questions for collecting data in carrying out the social science research. In
this tool, data is collected with the help of a set of questions. In the questionnaire tool
the investigator does not collect the matter all by him/her, but rather he/she sends the
questions to the respondents and collects information on the basis of the answer sent by
them.
33
Survey is a preferable method for many studies suited for gathering descriptive
information to which the study is focused (Kothari, 2004). Survey method was
employed in questionnaire tool for data collection to investigate the opinions and
behavior of the respondents by asking them probing questions.
Both open-ended and closed-ended questions were employed in this study where in
open-ended questions, respondents were allowed to write and give details as per their
choice without any limitations while in closed-ended questions, the respondents were
limited to answer questions and provide information as per choices indicated. Both
Swahili and English Languages were used in questionnaire tool for data collection.
Questionnaires were distributed to the ordinary citizens and who are the beneficiaries of
the health services. The rationale for using questionnaire in this study was to collect
data from relatively large sample size and avoid bias. Questionnaires were also used due
to time consideration.
3.8.3 Observation
According to Veal (1997), observation is an appropriate technique to use when
knowledge of the presence of the researcher is likely to lead to unacceptable
modification of subjects‟ behaviors, and when mass patterns of behaviors not apparent
to individual subject is of interest. Seeing and listening are key to observation and
provide the opportunity to document activities, behaviors and physical aspects without
having to depend upon peoples‟ willingness and ability to respond to questions.
The rationale for using observation as a tool in data collection was to gather
information through watching and noticing the phenomenon within a study area as they
occur in nature with regard to the causes and impacts. Through observation checklist,
the researcher was able to observe what was going on in the study area in physical
34
situation like health service delivery to the patients in hospital, and how they got
services.
3.9 Data Presentation
Data were collected, organized, interpreted and analyzed by means of summarizing and
manipulating and presented through illustrations, figures and tables, where necessary
and applicable so as to provide document. Therefore, discussion of results, conclusion
and recommendations were based on the findings which were interpreted through these
forms.
3.10 Data Analysis
According to Kombo and Tromp (2006) data analysis refers to examining what has
been collected in a survey or experiment and making deductions and inferences. It
involves uncovering underlying structures, extracting important variables, detecting
any anomalies and testing any underlying assumptions. It involves scrutinizing the
acquired information and making inferences.
Thereafter, with the help of computer Statistical Package for Social Scientist (SPSS),
data were entered into the computer for analysis. In this analysis data were cross
tabulated to produce percentages of respondents on performance and effectiveness
variables by respondent‟s category. Frequency and percentages were used to determine
the respondent‟s profiles.
3.11 Validity and Reliability of Data
Validity is defined as the trust worthiness of the research and its findings. It is the
extent to which a measurement measures what it is supposed to measure (Henning, et
al, 2004). To ensure validity, the researcher tested the tools by first carrying out a pilot
35
study in a selected study area. The pilot study made the research tool relevant and
ready for use in the actual field. The results obtained by valid tools corresponded to
reality. Construct and content validity were established. Construct validity was
established through the assistance of the supervisor who administered this research in
all stages including research tools for data collection.
Reliability is defined as the extent to which results are consistent over time and an
accurate representation of the total population under study (Joppe, 2000). In this study,
reliability was maintained by checking the procedures and documentation so that they
are precise. To ensure trustworthiness, more than one method was used to gather data.
Reliability was ensured through the use of multiple methods and tools during data
collection, including interview method through interview guide, survey method
through questionnaire and observation method through observation checklist.
3.12 Ethical Considerations
Ethical issues in research are to protect human rights and privacy from being infringed
by scientific experimentation as well as to safeguard the credibility of the research
(Keya, et al, 1989). Ethics describe legitimate and illegitimate, or moral values in
research procedures. Ethical considerations employed in this study were informed
consent, confidentiality and privacy. The decision to participate or not was on free will
of the respondents. To maintain confidentiality, the identity of the respondents was
concealed through coding and labeling instead of naming. And for privacy the
respondents were given the decision on where and when an interview should be
conducted.
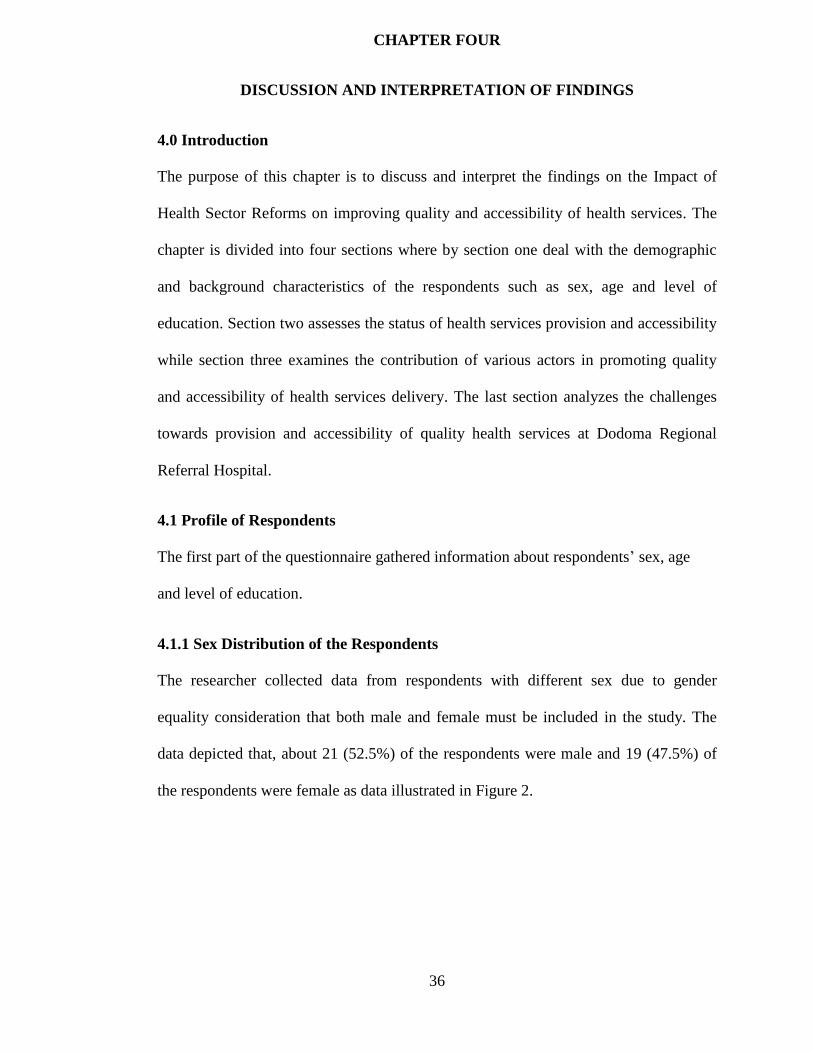
36
CHAPTER FOUR
DISCUSSION AND INTERPRETATION OF FINDINGS
4.0 Introduction
The purpose of this chapter is to discuss and interpret the findings on the Impact of
Health Sector Reforms on improving quality and accessibility of health services. The
chapter is divided into four sections where by section one deal with the demographic
and background characteristics of the respondents such as sex, age and level of
education. Section two assesses the status of health services provision and accessibility
while section three examines the contribution of various actors in promoting quality
and accessibility of health services delivery. The last section analyzes the challenges
towards provision and accessibility of quality health services at Dodoma Regional
Referral Hospital.
4.1 Profile of Respondents
The first part of the questionnaire gathered information about respondents‟ sex, age
and level of education.
4.1.1 Sex Distribution of the Respondents
The researcher collected data from respondents with different sex due to gender
equality consideration that both male and female must be included in the study. The
data depicted that, about 21 (52.5%) of the respondents were male and 19 (47.5%) of
the respondents were female as data illustrated in Figure 2.
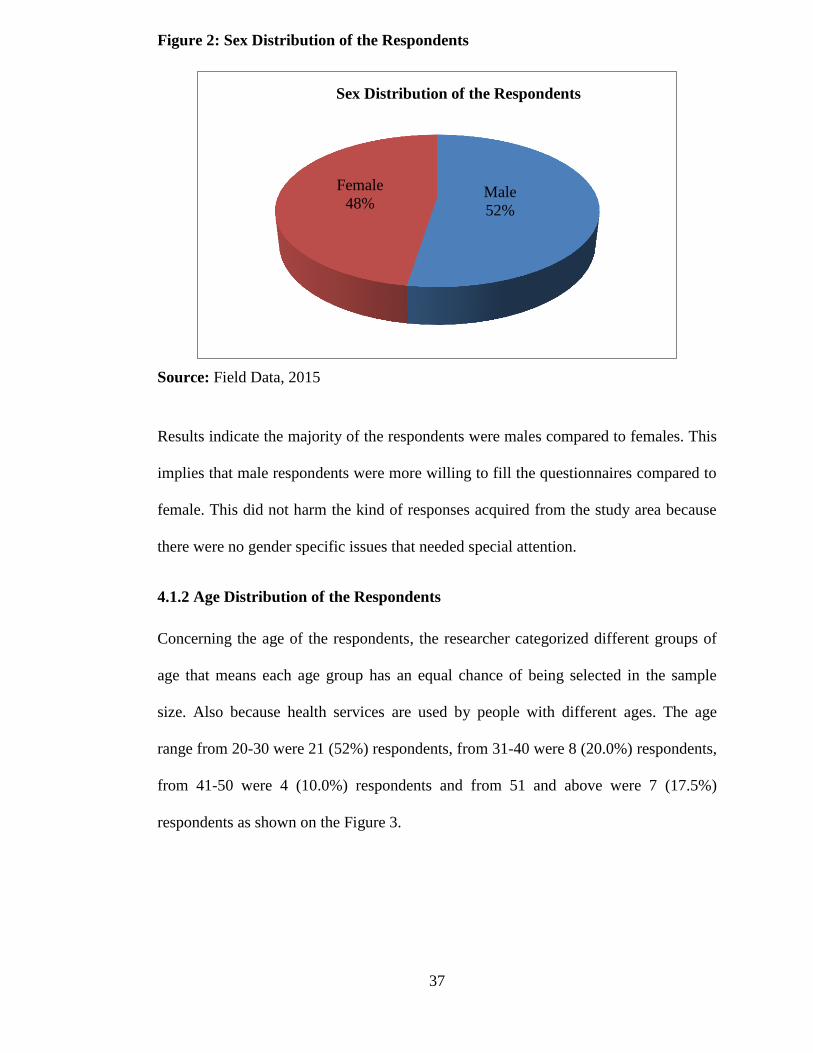
37
Figure 2: Sex Distribution of the Respondents
Source: Field Data, 2015
Results indicate the majority of the respondents were males compared to females. This
implies that male respondents were more willing to fill the questionnaires compared to
female. This did not harm the kind of responses acquired from the study area because
there were no gender specific issues that needed special attention.
4.1.2 Age Distribution of the Respondents
Concerning the age of the respondents, the researcher categorized different groups of
age that means each age group has an equal chance of being selected in the sample
size. Also because health services are used by people with different ages. The age
range from 20-30 were 21 (52%) respondents, from 31-40 were 8 (20.0%) respondents,
from 41-50 were 4 (10.0%) respondents and from 51 and above were 7 (17.5%)
respondents as shown on the Figure 3.
Male
52%
Female
48%
Sex Distribution of the Respondents
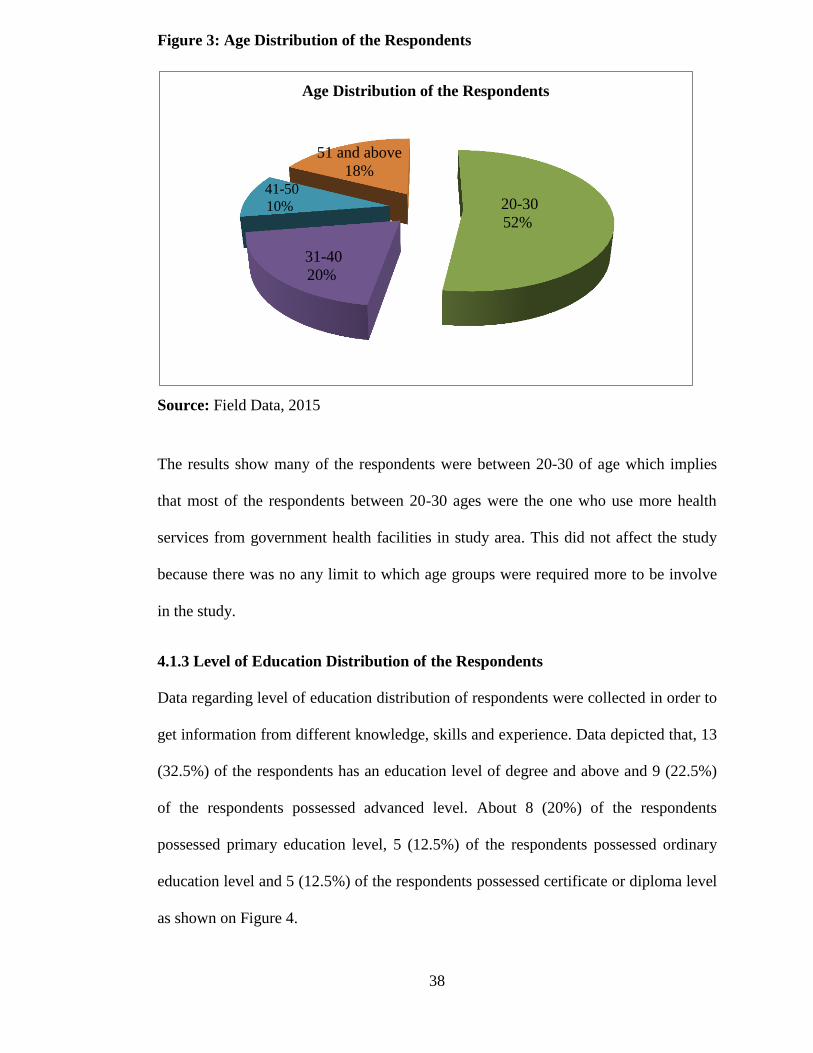
38
Figure 3: Age Distribution of the Respondents
Source: Field Data, 2015
The results show many of the respondents were between 20-30 of age which implies
that most of the respondents between 20-30 ages were the one who use more health
services from government health facilities in study area. This did not affect the study
because there was no any limit to which age groups were required more to be involve
in the study.
4.1.3 Level of Education Distribution of the Respondents
Data regarding level of education distribution of respondents were collected in order to
get information from different knowledge, skills and experience. Data depicted that, 13
(32.5%) of the respondents has an education level of degree and above and 9 (22.5%)
of the respondents possessed advanced level. About 8 (20%) of the respondents
possessed primary education level, 5 (12.5%) of the respondents possessed ordinary
education level and 5 (12.5%) of the respondents possessed certificate or diploma level
as shown on Figure 4.
20-30
52%
31-40
20%
41-50
10%
51 and above
18%
Age Distribution of the Respondents
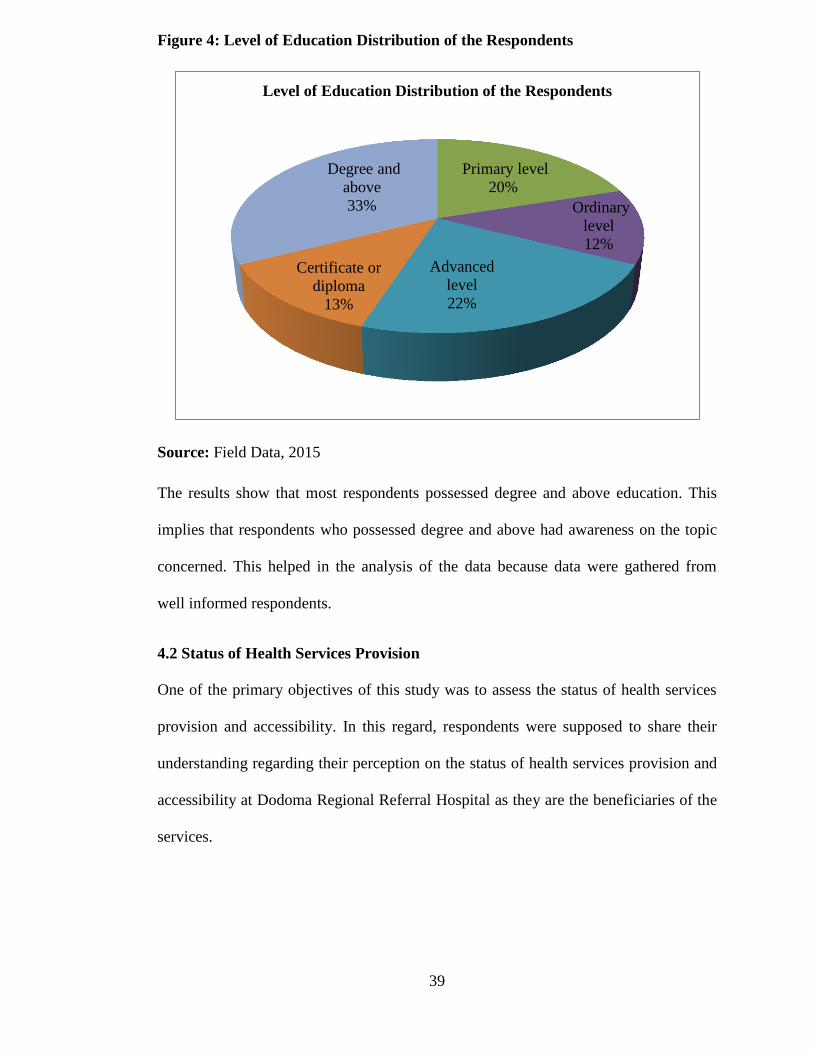
39
Figure 4: Level of Education Distribution of the Respondents
Source: Field Data, 2015
The results show that most respondents possessed degree and above education. This
implies that respondents who possessed degree and above had awareness on the topic
concerned. This helped in the analysis of the data because data were gathered from
well informed respondents.
4.2 Status of Health Services Provision
One of the primary objectives of this study was to assess the status of health services
provision and accessibility. In this regard, respondents were supposed to share their
understanding regarding their perception on the status of health services provision and
accessibility at Dodoma Regional Referral Hospital as they are the beneficiaries of the
services.
Primary level
20%
Ordinary
level
12%
Advanced
level
22%
Certificate or
diploma
13%
Degree and
above
33%
Level of Education Distribution of the Respondents
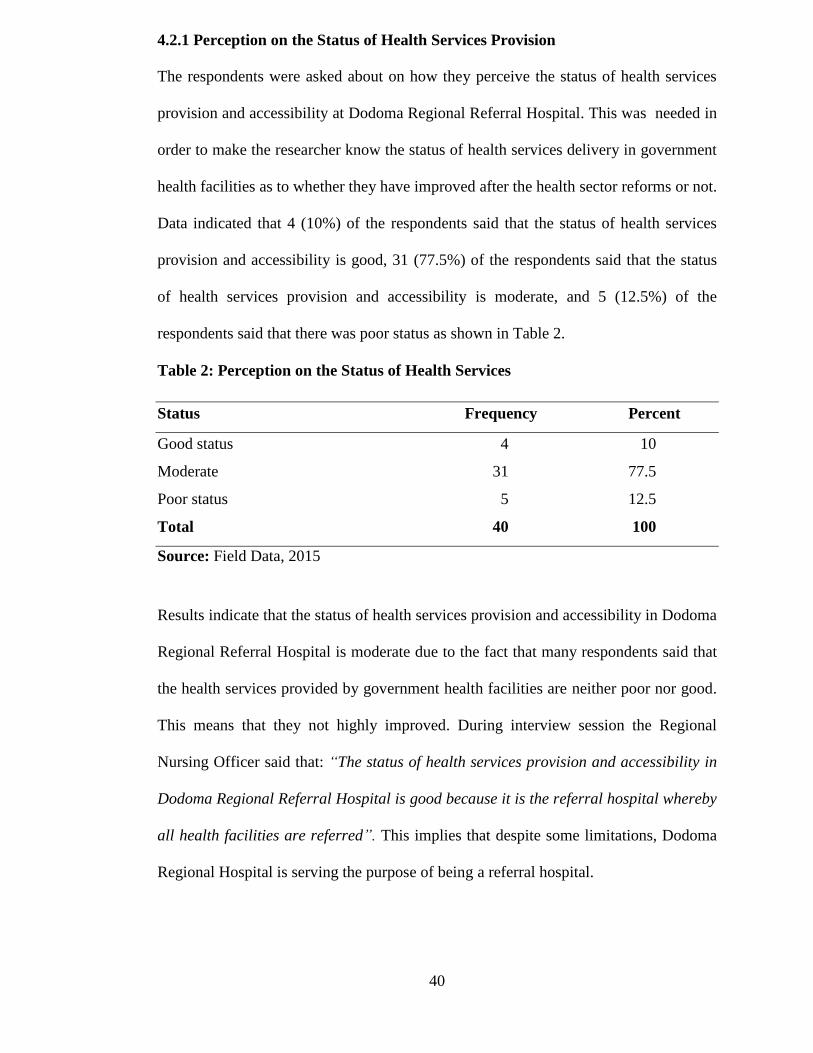
40
4.2.1 Perception on the Status of Health Services Provision
The respondents were asked about on how they perceive the status of health services
provision and accessibility at Dodoma Regional Referral Hospital. This was needed in
order to make the researcher know the status of health services delivery in government
health facilities as to whether they have improved after the health sector reforms or not.
Data indicated that 4 (10%) of the respondents said that the status of health services
provision and accessibility is good, 31 (77.5%) of the respondents said that the status
of health services provision and accessibility is moderate, and 5 (12.5%) of the
respondents said that there was poor status as shown in Table 2.
Table 2: Perception on the Status of Health Services
Status Frequency Percent
Good status 4 10
Moderate 31 77.5
Poor status 5 12.5
Total 40 100
Source: Field Data, 2015
Results indicate that the status of health services provision and accessibility in Dodoma
Regional Referral Hospital is moderate due to the fact that many respondents said that
the health services provided by government health facilities are neither poor nor good.
This means that they not highly improved. During interview session the Regional
Nursing Officer said that: “The status of health services provision and accessibility in
Dodoma Regional Referral Hospital is good because it is the referral hospital whereby
all health facilities are referred”. This implies that despite some limitations, Dodoma
Regional Hospital is serving the purpose of being a referral hospital.
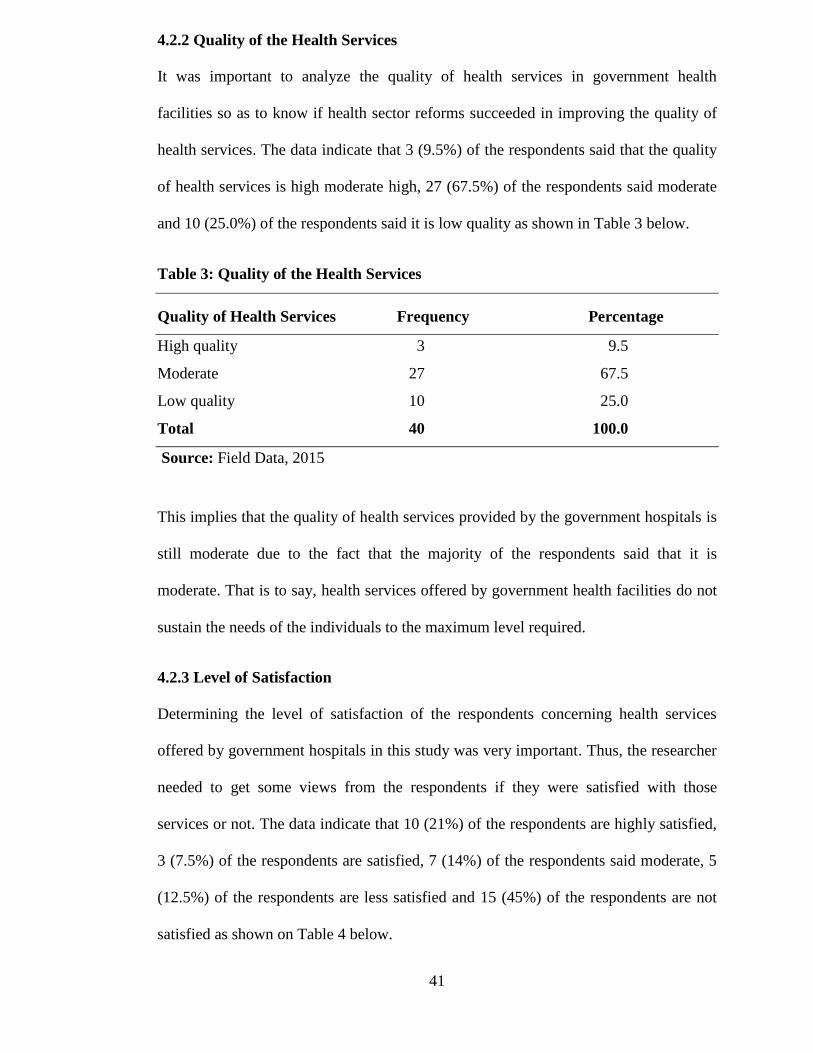
41
4.2.2 Quality of the Health Services
It was important to analyze the quality of health services in government health
facilities so as to know if health sector reforms succeeded in improving the quality of
health services. The data indicate that 3 (9.5%) of the respondents said that the quality
of health services is high moderate high, 27 (67.5%) of the respondents said moderate
and 10 (25.0%) of the respondents said it is low quality as shown in Table 3 below.
Table 3: Quality of the Health Services
Quality of Health Services Frequency Percentage
High quality 3 9.5
Moderate 27 67.5
Low quality 10 25.0
Total 40 100.0
Source: Field Data, 2015
This implies that the quality of health services provided by the government hospitals is
still moderate due to the fact that the majority of the respondents said that it is
moderate. That is to say, health services offered by government health facilities do not
sustain the needs of the individuals to the maximum level required.
4.2.3 Level of Satisfaction
Determining the level of satisfaction of the respondents concerning health services
offered by government hospitals in this study was very important. Thus, the researcher
needed to get some views from the respondents if they were satisfied with those
services or not. The data indicate that 10 (21%) of the respondents are highly satisfied,
3 (7.5%) of the respondents are satisfied, 7 (14%) of the respondents said moderate, 5
(12.5%) of the respondents are less satisfied and 15 (45%) of the respondents are not
satisfied as shown on Table 4 below.
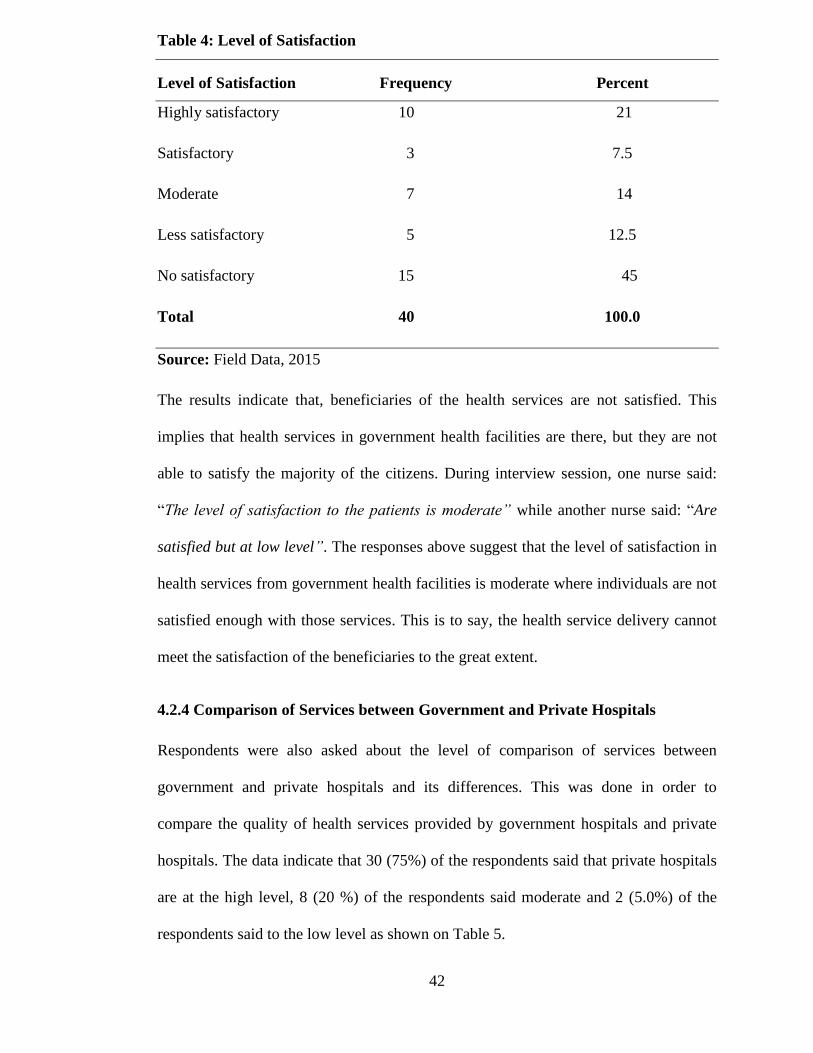
42
Table 4: Level of Satisfaction
Level of Satisfaction Frequency Percent
Highly satisfactory 10 21
Satisfactory 3 7.5
Moderate 7 14
Less satisfactory 5 12.5
No satisfactory 15 45
Total 40 100.0
Source: Field Data, 2015
The results indicate that, beneficiaries of the health services are not satisfied. This
implies that health services in government health facilities are there, but they are not
able to satisfy the majority of the citizens. During interview session, one nurse said:
“The level of satisfaction to the patients is moderate” while another nurse said: “Are
satisfied but at low level”. The responses above suggest that the level of satisfaction in
health services from government health facilities is moderate where individuals are not
satisfied enough with those services. This is to say, the health service delivery cannot
meet the satisfaction of the beneficiaries to the great extent.
4.2.4 Comparison of Services between Government and Private Hospitals
Respondents were also asked about the level of comparison of services between
government and private hospitals and its differences. This was done in order to
compare the quality of health services provided by government hospitals and private
hospitals. The data indicate that 30 (75%) of the respondents said that private hospitals
are at the high level, 8 (20 %) of the respondents said moderate and 2 (5.0%) of the
respondents said to the low level as shown on Table 5.
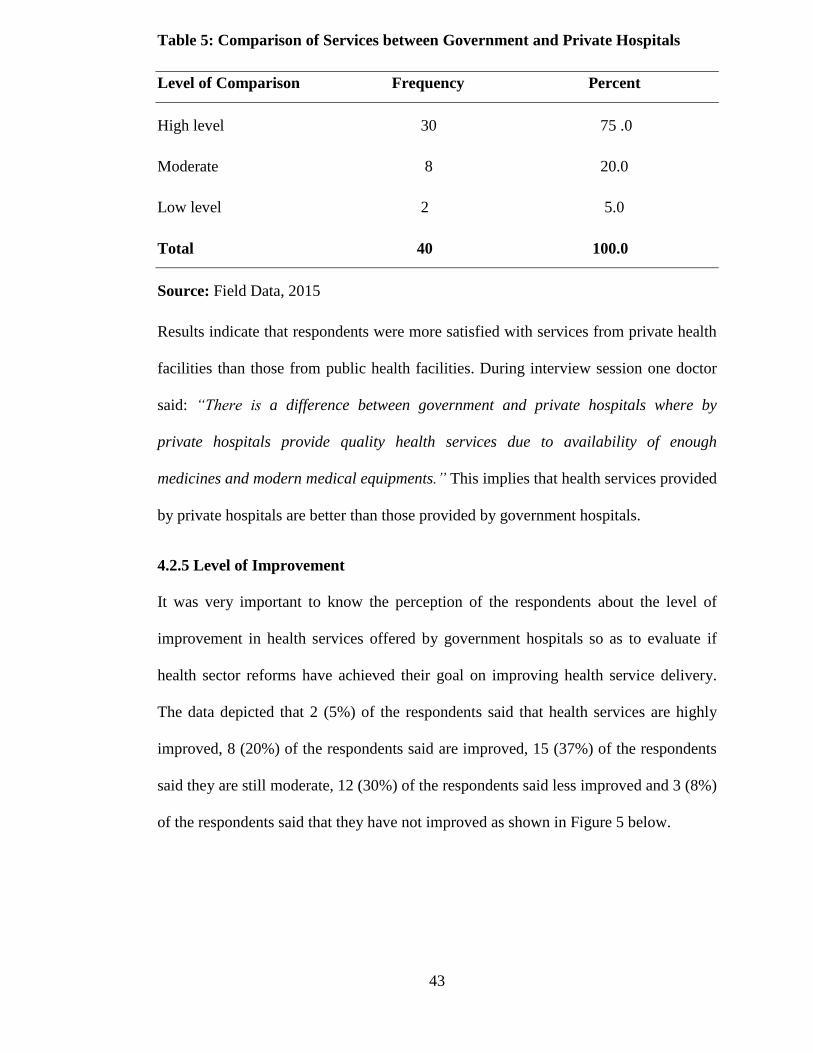
43
Table 5: Comparison of Services between Government and Private Hospitals
Level of Comparison Frequency Percent
High level 30 75 .0
Moderate 8 20.0
Low level 2 5.0
Total 40 100.0
Source: Field Data, 2015
Results indicate that respondents were more satisfied with services from private health
facilities than those from public health facilities. During interview session one doctor
said: “There is a difference between government and private hospitals where by
private hospitals provide quality health services due to availability of enough
medicines and modern medical equipments.” This implies that health services provided
by private hospitals are better than those provided by government hospitals.
4.2.5 Level of Improvement
It was very important to know the perception of the respondents about the level of
improvement in health services offered by government hospitals so as to evaluate if
health sector reforms have achieved their goal on improving health service delivery.
The data depicted that 2 (5%) of the respondents said that health services are highly
improved, 8 (20%) of the respondents said are improved, 15 (37%) of the respondents
said they are still moderate, 12 (30%) of the respondents said less improved and 3 (8%)
of the respondents said that they have not improved as shown in Figure 5 below.
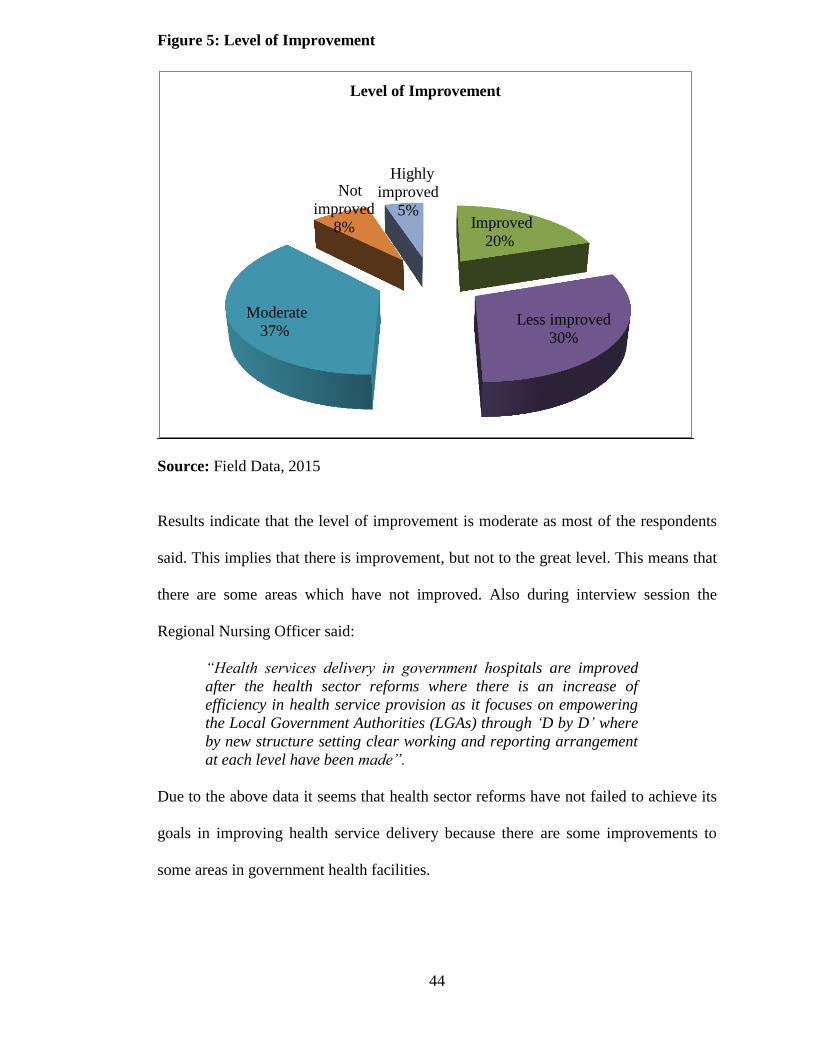
44
Figure 5: Level of Improvement
Source: Field Data, 2015
Results indicate that the level of improvement is moderate as most of the respondents
said. This implies that there is improvement, but not to the great level. This means that
there are some areas which have not improved. Also during interview session the
Regional Nursing Officer said:
“Health services delivery in government hospitals are improved
after the health sector reforms where there is an increase of
efficiency in health service provision as it focuses on empowering
the Local Government Authorities (LGAs) through „D by D‟ where
by new structure setting clear working and reporting arrangement
at each level have been made”.
Due to the above data it seems that health sector reforms have not failed to achieve its
goals in improving health service delivery because there are some improvements to
some areas in government health facilities.
Improved
20%
Less improved
30%
Moderate
37%
Not
improved
8%
Highly
improved
5%
Level of Improvement
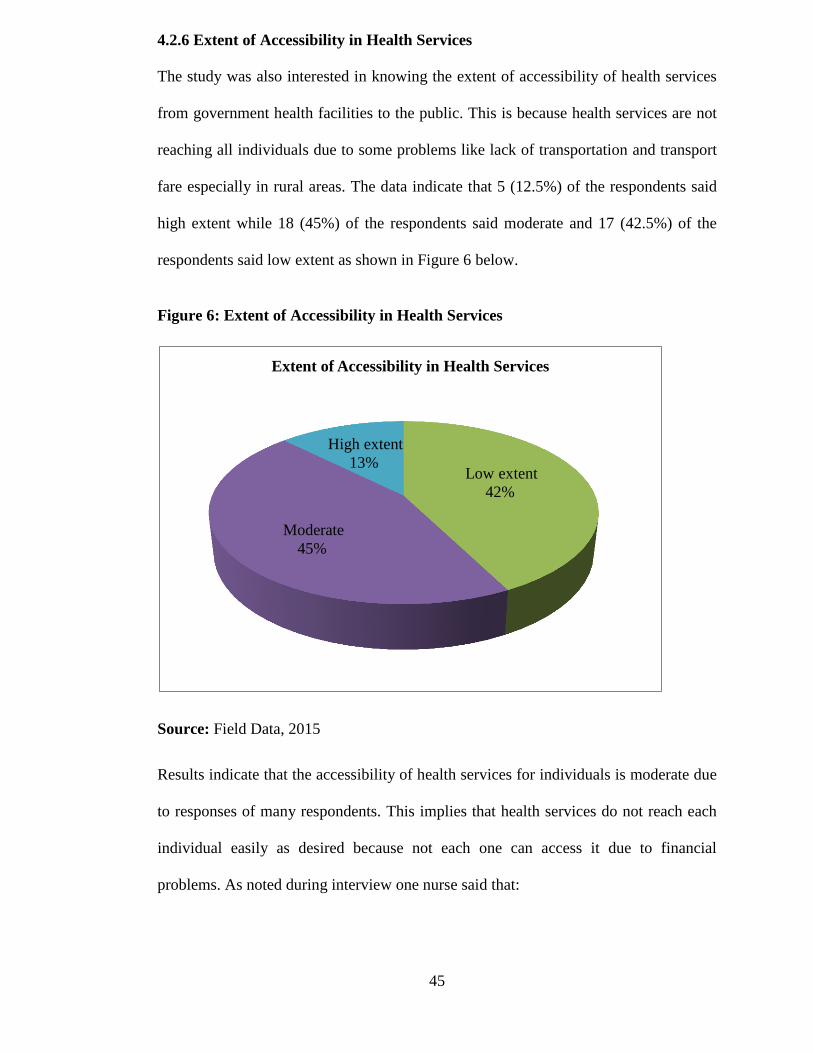
45
4.2.6 Extent of Accessibility in Health Services
The study was also interested in knowing the extent of accessibility of health services
from government health facilities to the public. This is because health services are not
reaching all individuals due to some problems like lack of transportation and transport
fare especially in rural areas. The data indicate that 5 (12.5%) of the respondents said
high extent while 18 (45%) of the respondents said moderate and 17 (42.5%) of the
respondents said low extent as shown in Figure 6 below.
Figure 6: Extent of Accessibility in Health Services
Source: Field Data, 2015
Results indicate that the accessibility of health services for individuals is moderate due
to responses of many respondents. This implies that health services do not reach each
individual easily as desired because not each one can access it due to financial
problems. As noted during interview one nurse said that:
Low extent
42%
Moderate
45%
High extent
13%
Extent of Accessibility in Health Services
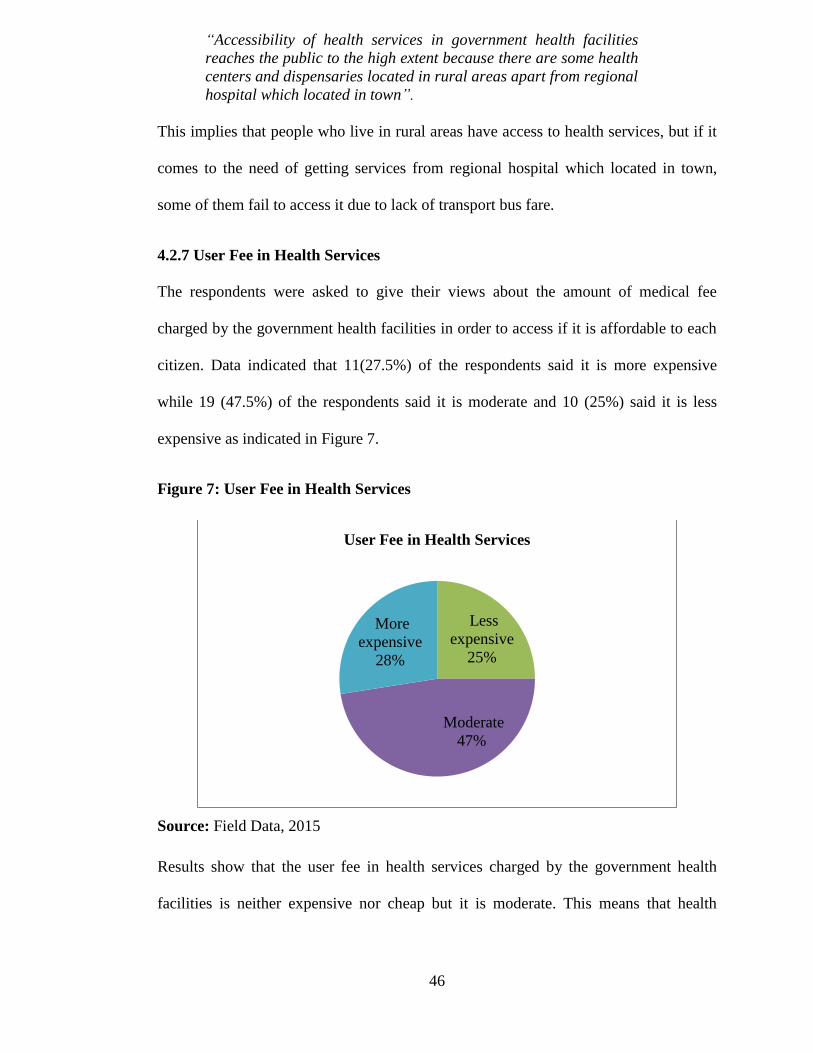
46
“Accessibility of health services in government health facilities
reaches the public to the high extent because there are some health
centers and dispensaries located in rural areas apart from regional
hospital which located in town”.
This implies that people who live in rural areas have access to health services, but if it
comes to the need of getting services from regional hospital which located in town,
some of them fail to access it due to lack of transport bus fare.
4.2.7 User Fee in Health Services
The respondents were asked to give their views about the amount of medical fee
charged by the government health facilities in order to access if it is affordable to each
citizen. Data indicated that 11(27.5%) of the respondents said it is more expensive
while 19 (47.5%) of the respondents said it is moderate and 10 (25%) said it is less
expensive as indicated in Figure 7.
Figure 7: User Fee in Health Services
Source: Field Data, 2015
Results show that the user fee in health services charged by the government health
facilities is neither expensive nor cheap but it is moderate. This means that health
Less
expensive
25%
Moderate
47%
More
expensive
28%
User Fee in Health Services
47
facilities are affordable by most beneficiaries in the area. As it was noted during
interview session, the Regional Nursing Officer said:
“User fee in government hospitals is less expensive due to cost
sharing so that most of the patients can afford. However other
patients fail to afford it although there is exemption policy for
those who fail to afford the medical fees compared to the private
hospitals. Also there is exemption to the elders from 60 years old
and above”.
The above data revealed that the government plays its role in supporting health service
delivery through the provision of NHIF and CHF to the citizens so that each one can be
able to acquire health services in government health facilities and also through
exemption policy to elders and those who fail to afford medical fees.
4.2.8 Importance of Government Hospitals
The researcher also was interested in knowing from the respondents the importance of
government hospitals in delivering health services to the society. The interest was to
know whether government hospitals have an important role to the public. The data
indicate that 24 (60%) of the respondents said that government hospitals are very
important, 10 (25%) of the respondents said moderate and 6 (15.0%) of the
respondents said less important as shown in Table 6 below.
Table 6: Importance of Government Hospitals
Level of Importance Frequency Percent
Very important 24 60.0
Moderate 10 25.0
Less important 6 15
Total 40 100.0
Source: Field Data, 2015
48
The implication of this is that, government hospitals are very important to the society
because it seems that a lot of people use them to get health services as per responses
from the respondents. During interview session one Doctor said:
“Government hospitals are very important because they cover
majority of the places in the country where there is no private
hospitals like in rural areas. Government hospitals also cover
poor people who fail to afford medical treatment through
exemption policy and Community Health Fund (CHF)”.
This implies that government health facilities have been very helpful to poor people
and to majority of the people who fail to afford medical fee charged in private health
facilities.
4.2.9 Appreciation of Government Health Services
The study on this subpart needed to understand and know the extent to which
government health services are appreciated by individuals based on the fact that health
services are improved. Apart from some weaknesses in government health facilities,
the study came with the views of respondents who appreciate those services by giving
the following factors:
4.2.9.1 Affordable Medical Price
Respondents appreciate health services provided by government health facilities due to
low cost of treatment. One respondent said: “I appreciate health services provided by
government health facilities because medical treatment is less expensive which I can
afford to pay”. Another respondent said: “I appreciate health services provided by
government health facilities because there is the government share through NHIF”.
This implies that government health facilities are helpful to individuals who have low
economic status to sustain their living standard. This is due to its affordable medical
49
treatment because not all people have enough money to pay for medical treatment in
private health facilities.
4.2.9.2 Geographical Coverage
Government health facilities cover both rural and urban areas in a country; thus,
respondents appreciate them. As the data show, one of the respondents said: “I
appreciate health services provided by government health facilities because those
services are spread and available in rural areas like health centers and dispensaries”.
Another respondent said: “I appreciate government health facilities because it reaches
many people even in rural areas where each individual can access it, and due to this
reason the death rate is decreasing to a large extent in rural areas”. This implies that
the government plays its big role and effort to make sure that health facilities are
located all over the country both in rural and urban areas .This makes the government
health facilities to be accessible to all individuals in the society.
4.2.10 Suggestions to the Government
Lastly the respondents provided their opinions on what should be done by the
government in order to improve the quality and accessibility of health services in
government health facilities.
4.2.10.1 Provision of Enough Funds
Provision of enough funds is among the ways forward which respondents suggested to
the government so as to improve quality and accessibility of health services in
government health facilities. Respondents suggested that: “The government should
increase budget to the health facilities so as to purchase adequate drugs and medical
supplies”. During interview session one nurse said: “The government should increase
budget for MOHSW and budget allocation to health facilities”. Another nurse said,

50
“The government should provide funds on time to run hospital activities”. This implies
that despite the fact that the government provides funds to health facilities; the funds
are not enough and are not provided on time. Therefore the government should provide
enough funds on time.
4.2.10.2 Environmental Management and Increase Hospital Buildings
At that point, respondents suggested that the government should manage
environmental cleanness around health facilities so as to prevent the outbreak of other
diseases and increase hospital buildings like wards to accommodate a big number of
patients. One of the respondents said that: “The government should improve hygiene
and sanitation around hospitals environment in order to avoid the spread of other
diseases”. Another respondent said: “The government should build enough wards
where patients will be admitted”. This implies that government health facilities lack
enough wards to accommodate the patients but also there is poor environmental
management around government health facilities which may lead to the outbreak of
other diseases.
4.3 Contribution of Various Actors
This was the second objective of the study done through interview method where the
researcher wanted to know from the respondents who were the management staff about
the contribution of various actors in promoting quality and accessibility of health
services delivery at Dodoma Regional Referral Hospital. It is well known that the role
of the government is to provide social services to the society like health services. Also
there are some various actors who contribute in promoting quality and accessibility of
health services delivery as follows:
51
4.3.1 Resource Allocation Contribution
In resource allocation contribution this study revealed that there are some actors who
contribute in promoting health service delivery as it was noted during interview
session, the Regional Health Secretary said that: “The various actors like HPSS
contribute in provision of drugs, medical equipments and provision of advanced CHF”
while the Regional Nursing Officer said that: “Various actors like AGHAKAN
contributes in medical supply and improve maternal child birth service”. This means
apart from government role in promoting quality and accessibility of health services
delivery through provision of medical equipments and drugs in government health
facilities also there are contributions from some actors like HPSS and AGHAKAN
who support government in promoting quality and accessibility of health service
delivery.
4.3.2 Public - Private Partnerships Contribution
Public - Private Partnerships is collaboration between the public and private sector
organizations where there is the use of private finance to facilitate the provision of
services to the public. Data revealed that public - Private Partnerships contribute in
promoting quality and accessibility of health service delivery. During interview
session, the Regional Nursing Officer said: “Public - Private Partnerships help in
reducing workload in government hospitals where private hospitals are used as
Referral Centers”. The Regional Health Secretary said: “Public - Private Partnerships
contributes in implementation of health care programs under the MoHSW and NGOs
which covers reproductive and child health, HIV AIDS and Malaria”. This means that
there is a direct relationship between government and other stakeholders in promoting
and improving quality and accessibility of health services delivery in government
health facilities.
52
4.4 Challenges towards Health Services Provision and Accessibility
The third objective of the study was to investigate the challenges towards provision
and accessibility of quality health services at Dodoma Regional Referral Hospital. This
was done through interview method where the researcher wanted to know from the
nurses and doctors about the challenges towards provision and accessibility of quality
health services and their suggestions on what to do in ending those challenges in order
to improve health services delivery. The challenges are:
4.4.1 Resource Based Challenges
Health facilities are faced with a lot of challenges which hinder the provision and
accessibility of quality health services mostly in government health facilities. The
study found that there is a challenge of inadequate fund to run health facilities activities
like purchasing modern laboratory equipments and medicines. This is due to the fact
that government health facilities lack enough laboratory equipments and modern ones.
There is also lack of enough medicines in hospitals pharmacy. During interview
session, one nurse responded to this question and said: “Lack of fund to support health
care delivery is a challenge towards provision and accessibility of quality health
services”. It seems that the government does not provide enough funds to the health
facilities so that health service delivery can be accessible and in quality. On the other
hand one doctor said: “Few laboratory equipments which are not modern and
inadequate of medical supply like dental medicine are the challenges towards
provision and accessibility of health services at my work place”. This implies that
there is a shortage of laboratory equipments in health facility and the ones which are
there are not modern. Also, there is a shortage of medicines like dental medicines
where patients are responsible for purchasing medicines on their own money.
53
4.4.2 Motivation Based Challenges
Motivation at work place is very crucial so as to increase the work performance of the
employees. If there is lack of motivation to the employees, their work performance
remains low. This was another challenge towards provision and accessibility of quality
health services. During interview session the researcher wanted to know, from the
respondents, if they were motivated so as to increase their work performance in
providing health services to the patients. One doctor responded to the question and
said:
“I am not motivated. I am doing my duty because I am employed, and I am paid”
Another doctor said: “I am not motivated because I am not promoted for a longtime”.
Data revealed that, there is lack of motivation to the health workers which makes them
to perform their duty at low performance and leads to poor health service delivery.
4.4.3 Recruitment Based Challenges
This was another challenge towards provision and accessibility of quality health
services. The study revealed that mode of recruitment is one of the challenges where
the government seems to recruit few health workers. In health facilities there is a
shortage health workers compared to a big number of the patients who need services,
but also lack of professional health workers. As it was noted during interview, one
nurse said: “Lack of subordinates to support doctors and nurses and inadequate of
professional doctors are the challenges towards provision and accessibility of quality
health services”. Data revealed that health workers are there, but they are not enough
compared to a big number of the patients, and also the professional ones are few.
4.5 Ways to end Challenges
Due to these challenges towards provision and accessibility of quality health services
in Dodoma Regional Referral Hospital, the respondents gave some prospects for the
54
improvement of health services delivery in government health facilities through
resource based prospects, motivation based prospects and recruitment based prospects.
4.5.1 Resource Based Prospect
Respondents proposed the ways to end resource based challenges by suggesting that
enough budgets from the government to the health facilities and availability of
laboratory equipments which are modern will improve the provision and accessibility
of quality health services. During interview session one Nurse said: “The government
should increase budget for MOHSW to support health facilities in purchasing enough
medicines and enough laboratory equipments which are modern”. This means if the
government provides enough budget to run health facilities, the health services delivery
can be improved because there will be enough medical supply and enough laboratory
equipments which are modern.
4.5.2 Motivation Based Prospect
Health workers in any health facility need motivation apart from their basic payments
so as to increase work performance and improve health service delivery. Respondents
suggested that management staffs who are the employers should motivate their
employees. It was noted during interview when one doctor said: “In order to improve
work performance in health service delivery, management should motivate me by
promotion, giving risk allowances, on-call allowances and on job training”. The data
revealed that motivation is a means to improve work performance of the health
workers. Through motivation to the health workers, the provision and accessibility of
quality health services will be improved.
55
4.5.3 Recruitment Based Prospect
In recruiting health workers, the government should make sure that it recruit more and
professional staff according to demand so as to reduce the workload in the health
facility due to lack of the health workers. During interview session one nurse said:
“MOHSW should employ enough health workers and enough professional doctors in
order to reduce the congestion due to a big number of patients”. This indicates that
recruitment of enough and professional health workers can improve the provision of
quality health services.
56
CHAPTER FIVE
CONCLUSION AND RECOMMENDATIONS
5.0 Introduction
This chapter presents the summary of the study, summary of the findings, conclusion
based on the research findings and gives the recommendations and suggestions for
further study.
5.1 Summary of the Study
The present study was designed to assess the impact of health sector reforms on health
service delivery in Tanzania, the case of Dodoma Regional Referral Hospital. It is
important to assess if health sector reforms achieve its goal on improving quality and
accessibility of health services so as to meet public needs.
The study was guided by three specific objectives which were set to address the main
objective of the study stated above. The first objective was to assess the status of health
services provision and accessibility which was guided by the question that asked: What
is the perception on the status of health services provision and accessibility in Dodoma
Regional Referral Hospital? The second objective was to examine the contribution of
various actors in promoting quality and accessibility of health services delivery which
was guided by the question that asked: What is the contribution of various actors in
promoting quality and accessibility of health services delivery? The third objective was
to analyze challenges towards provision and accessibility of quality health services
which was guided by the question that asked: What are the challenges towards
provision and accessibility of quality health services? The study was conducted at
Dodoma Regional Referral Hospital by including respondents like management staff,
nurses, doctors and the ordinary citizens of Dodoma Municipality. The study employed
a cross sectional design where data was collected in a single period of time. The study
57
used interviews, survey questionnaires and observation checklist as the methods for
data collection from the sampled respondents.
5.2 Summary of the Findings
The study came up with a number of major findings as per research specific objectives
as far as the research questions are concerned. The study revealed that the status of
health services provision and accessibility at Dodoma Regional Referral Hospital
seems to be neither poor status nor good. This is due to the perception of majority of
the respondents who said the status of health services is moderate. This was associated
with the reason that, due to the responses of many respondents it seems that there are
still some challenges which hinder the provision and accessibility of quality health
services in government health facilities.
Also the study discovered that there are various actors who contribute in promoting
quality and accessibility of health services at Dodoma Regional Referral Hospital apart
from government role on promoting health services. HPSS and AGHAKAN contribute
in provision of medical supplies and drugs, provision of medical equipments and
provision of advanced CHF to the community. This implies that there is a connection
between government and private health facilities in promoting health service delivery.
The findings also indicated that there are some challenges towards provision and
accessibility of quality health services at Dodoma Regional Referral Hospital. The
challenges are resource based challenge, motivation based challenge and recruitment
challenge. The study observed some potential ways to overcome these challenges so as
to improve health service delivery. This include: the government should increase
budget to health facilities for availability of resources, health workers should be
motivated so as to improve their work performance and MOHSW should recruit
58
enough and professional health workers so as to improve quality health service
delivery.
5.3 Conclusion
The study conclude that, despite the implementation of health sector reforms which
was the sustained purposeful change to improve the efficiency, equity and the
effectiveness on health sector, there are ongoing problems towards provision of health
services among people in Tanzania. This is because the study through findings
revealed that there are some weaknesses in health facilities in health service delivery
specifically in government health facilities. Therefore, it can be argued that health
sector reforms remain theoretical and not in practical form due to a lot of shortages in
health facilities.
The study also shows the relationship between the variables used in the conceptual
framework and the study results. The independent variable is health sector which
provide health facilities like hospitals. Health sector intervened with the management
practice which show the outcomes of the health services delivery if positive or
negative. When the management practice intervened positively with health sector the
study results show that by motivating the health workers through promotion, training,
giving risk allowances, on-call allowances, giving enough budget to support health
facilities in purchasing enough medicines, enough modern equipments and recruitment
enough and professional health workers the provision and accessibility of quality
health services will be improved at Dodoma Regional Referral Hospital.
When the management practice intervened negatively with the health sector the study
results show there is lack of subordinates to support nurses and doctors, inadequate of
professional health workers, lack of motivation to the health workers, lack of fund to
59
support health care delivery, few laboratory equipments which are not modern,
inadequate of medical supply like dental medicine. This will lead to poor health
services delivery at Dodoma Regional Referral Hospital.
5.4 Recommendations
The study recommends that the government as the services provider should take
corrective measures to eliminate all the weaknesses which encounter health facilities
for the improvement of health service delivery. Based on the research findings the
study provides two types of recommendations as follows:
5.4.1 Policy - Based Recommendations
The overall objective of the health policy in Tanzania is to improve the health and
well-being of all Tanzanian with a focus on those most at risk and encourage the health
system to be more responsive to the needs of the people (MoH, 1990). In order to
improve health service delivery, the government should consider the followings:
i. Ensure that health services are available and accessible to all people wherever
they are in the country, whether in urban or rural areas.
ii. Reduce infant and maternal morbidity and mortality and increase life
expectancy through the provision of adequate and equitable maternal and child
health services, promotion of adequate nutrition, control of communicable
diseases and treatment of common conditions.
iii. Sensitize the community on common preventable health problems and improve
capabilities of all levels of society to access, analyze problems and to design
appropriate action through genuine community involvement.
60
iv. Create awareness through family health promotion that the responsibility for
one‟s health rests squarely with the able-bodied individuals as an integral part
of the family.
5.4.2 Recommendations for Further Studies
The study was based on the impact of health sector reforms on health services delivery
by looking at whether the health sector reforms have achieve their goal in improving
quality and accessibility of health services to the public. The study discovered other
area for further study as follows:
i. The influence of political leaders in improving quality and accessibility of
health services delivery specifically in government hospitals. This is because
the study revealed that there is relationship between leadership accountability
and public service delivery through revenue collected from the natural
resources to support service delivery.
ii. Capacity of the Local Government Authorities in improving quality and
accessibility of health services at district level due to the reason that the health
policy was linked with local government and public service reforms in favor of
decentralization policy in health sector.
iii. The impact of public sector reforms on education services delivery as it is
among one of the public services. With every other sector, the education sector
was also reformed where by education should be delivered more efficiently and
effectively.
61
REFERENCES
Adam, J. and Kamuzora, F. (2008), Research Methods for Business and Social Studies,
Mzumbe Book Project, Morogoro.
Andrews, R. (2013), NPM and the Search for Efficiency. The Ashgate Research
Companion to New Public Management. 2ed.
Ashgante Publishing
Company.
Antwi, K. (2011), “Challenges in Building the Capacity of Human Resources
Development in Decentralized Local Governments: Evidence from
Ghana”, Social Science Journal, Vol. 31, No 7, 504-5017.
Boston, J. Martin, J. Pallot, J. & Walsh, P. (1996) Public Management: The New
Zealand Model. Auckland: Oxford University Press.
Buchanan, J.M, (1987), The Constitution of Economic Policy, Stockholm: Nobel
Foundation.
Cassels, A. (1995), “Health Sector Reform: Key Issues in Less Developed Countries.”
Journal of International Development 7(3):329.
Chitama, D. Baltussen I, R. Ketting, E. Kamazina, S. Nswilla, A and Mujinja, P.
(2011), “From Papers to Practices: District Level Priority Setting
Processes and Criteria for Family Planning, Maternal, Newborn and
Child Health (FMNCH) interventions in Tanzania”, Journal for Public
Health, Vol.11, No. 2, 1-13.
Cohen, Steven and William Eimicke, (1995). Ethics and the Public Administrator. The
Annals of the American Academy of Political and Social Science.
537(1): 96-108.
Dmytracsenko (2003), „Health Sector Reform: How it Affects Reproductive Health‟,
Population Research Bureau, Policy Brief.
Fjeldstad, O. and Semboja, J. (2000), “Dilemmas of Fiscal Decentralization: A Study
of Local Government Taxation in Tanzania”, Forum for Development
Studies, Vol. 27, No. 1, 7-41.
Gilson, L. and Mills, (1995), “Health Sector Reforms in Sub-Saharan Africa: Lessons
of the Last 10 Years.” In P. Berman, ed., Health Sector Reform in
Developing Countries: Making Health Development Sustainable.
Harvard Series on Population and International Health. Boston: Harvard
University Press.
62
Grindle, M.S, and Thomas J.W, (1991), Public Choices and Policy Change: The
Political Economy of Reform in Developing Countries, Baltimore and
London: The Johns Hopkins Press.
Hutchison, P. (2002), Decentralization in Tanzania: The View of District Health
Management Teams, University of Dar es Salaam, Dar es Salaam.
Hutchison, P. Mai, D. and Agha, S. (2011), “Measuring Client Satisfaction and the
Quality of Family Planning Services: A Comparative Analysis of Public
and Private Health Facilities in Tanzania, Kenya and Ghana”, Health
Services Research Journal, Vol.11, 3-7.
Kombo , D.K. & Tromp, D.L.A (2006), Proposal and Thesis Writing: An Introduction
Nairobi: Paulines Publications Africa.
Kothari, R. C. (2004), Research Methodology: Methods and techniques, India, New
Delhi.
Kutzin, J. (1995), Experience with Organizational and Financing Reform of the Health
Sector. Strengthening Health Services Paper No. 8. Geneva: World
Health Organization, Division of Strengthening of Health Services,
National Health Systems and Policies Unit.
Lane, J . E. (1993), The Public Sector: Concepts, Models and Approaches, London:
Sage. Lessons from Selected African Countries.” Journal of
International Development 7(3):349.
Lethbridge, J. (2004), “Public Sector Reform and Demand for Human Resources for
Health”, Journal of Public Health, Vol2, No. 2, 125-153.
Manor, J. (2011), “Perspective on Decentralization”, Swedish Journal for International
Centre of Local Democracy Sweden, Vol. 1, No, 2, 120- 185.
Masatu, C. & Leonard, L. (2007), “Variations in the Quality of Care Accessible to
Rural Communities in Tanzania, Health Affairs”.
Mogale, P. (2011), An Analysis of the Human Resource Management Function During
Decentralization of Hospital Management: Case of North West
province, Unpublished Thesis, The University of South Africa,
Johannesburg.
Mogedal, S. Steen, S. H. and G. Mpelumbe, (1995), “Health Sector Reform and
Organizational Issues at the Local Level:
MoHSW, (2009), Health Sector Strategic Plan 2009-2015, Ministry of of Health and
Social Welfare Office, Dar es Salaam.
63
MoHSW, (2009), Template for Developing Annual Health Plans for Health Centers
and Dispensaries, Unpublished report, Dar es Salaam.
Njunwa, P. (2005), Public Sector Reforms in Tanzania, Mzumbe University.
Odada, J. E. O. and Ayako A. B. (1989), Report of the Proceedings of the Workshop
on „The Impact of Structural Adjustment Policies on the Well-being of
the Vulnerable Groups in Kenya‟.
Odada, J. E. O. and Odhiambo, L. O. (1989), Report of the Proceedings of the
Workshop on „Cost-sharing in Kenya‟.
Odaro, D.E. (2012), “Causes of Poor Service Delivery in Africa and their Impact on
Development”. The journal of Sustainable Development Vol 7, No. 1,
27-28 .
Osborne, D. and Gaebler, T. (1993), Reinventing Government: How the
Entrepreneurial Spirit is Transforming the Public Sector. New York:
Penguin Books.
Osborne, D. and Plastrik, P. (2000), The Reinventor‟s Fieldbook: Tools for
Transforming Your Government. San Francisco, CA: Jossey Bass.
Owino, P. S. W. (1997), „Public Health Sector Efficiency in Kenya. Estimation and
Policy Implications‟, IPAR Discussion Papers.
Pollitt, (2003), The Essential Public Manager. Philadelphia: Open University Press.
Roberts M, Hsiao W, Berman P, Reich M (2004), Getting Health Reform Rright: A
Guide to Improving Performance and Equity. Oxford University Press,
New York, USA.
Rwegoshora, M. N. (2006), A Guide to Social Science Research, Dar es Salaam.
Saltman, B. Bankauskaite, V. and Vranboek, K. (2007), Decentralization in Health
Care, Mc Graw, Washington.
Semali, A. (2003), “Understanding Stakeholder‟s Roles in Health Sector Reform
Process in Tanzania: The Case of Decentralizing the Immunization
Program” Unpublished Thesis, The University of Basel. Switzerland.
Semali, A. Savigny, D. and Tanner, M (2005), Health Sector Reform and
Decentralization in Tanzania: The Case of the Expanded Programme on
Immunization at District Level”, Journal of Health and Population in
Developing Countries School of Public Health, Vol. 30, No. 2, 1-22.
64
Shaw, R. P, and Griffin C.C (1995), Financing Health Care in Sub-Saharan Africa
through User Fees and Insurance. Washington, D.C. World Bank.
Smoke, P. (2003), “Decentralization in Africa: Goals, Dimension, Myths and
Challenges” Journal of Development Studies, Vol. 4. No. 23, 7-16.
UNDP, (2010), Human Development Report, UNDP, New York.
URT, (2003), Tanzania National Health Policy, Ministry of Health and Social Welfare,
Dar es Salaam.
URT, (2011), “Report on the Fifty Years of Independence of Tanzania Mainland 1961-
2011”, The President‟s Office, Dar es Salaam.
Varraich, A. (2010), Decentralization; The Road to Better Quality of Government?,
University of Gothenburg, German.
Veal, A . J. (1997), Research Methods for Leisure and Tourism. London: Financial
Times, Prentice Hall.
Walt, G. (1994), Health Policy: An Introduction to Process and Power, Johannesburg,
Witwatersrand University Press.
Williams, D. (2000), Reinventing the Proverbs of Government. Public Administration
Review. p 522-535.
World Bank. (1994), Better Health in Africa: Experience and Lessons Learned.
Washington, D.C.
World Health Organization (2000), World Health Report. Geneva.
Yamauchi, T. (2011), Background Paper for the Chronic Poverty Report 2008-2009:
Assessment on Chronic Poverty in Tanzania: Focusing on the Health
and HIV/AIDS Sector, Chronic Poverty Research Centre, Dar es
Salaam.
Zwi, A. B. and Mills, A. (1995), “Health Policy in Less Developed Countries: Past
Trends and Future Directions.” Journal of International Development
7(3):299.
65
APPENDICES
APPENDIX A: QUESTIONNAIRE FOR THE ORDINARY CITIZENS
Dear participant,
I am ASELA MATHEW, a student of Master of Arts in Public Administration from
the University of Dodoma. I am doing research on “THE IMPACT OF HEALTH
SECTOR REFORMS IN HEALTH SERVICE DELIVERY IN TANZANIA. THE
CASE OF DODOMA REGIONAL REFERRAL HOSPITAL”.
The purpose of the study is to obtain information on performance of the Health Sector
Reforms in Health Service Delivery. The focus of the study is on the government
Health Sectors Reforms Program on how it contributes to improve the quality and
accessibility of health services to the public.
I request you to kindly participate in this study and provide your valuable opinions and
suggestions. The information to be provided by you will be used for academic purpose
only and will be kept confidential.
As participant, you are kindly requested to answer the following questions according to
the instructions provided. Your response and cooperation will be highly appreciated.
66
INSTRUCTIONS TO PARTICIPANT
You are requested to answer the following questions. For many questions, choices are
given. You may kindly put a tick (√) on your choice and choose the correct answer to
be filled in the brackets in case of these questions with multiple choices. For a few
other questions, you can fill the gap in the space provided.
A. PERSONAL INFORMATION
1. 1. Name (Optional)………………………………………………………..
1.2. Sex
1) Male ( )
2) Female ( )
1.3. Age
1) 20-30 ( )
2) 31-40 ( )
3) 41-50 ( )
4) 51 and above ( )
1.4. Level of education
1) Primary level ( )
2) Ordinary secondary level ( )
3) Advanced level ( )
4) Certificate or diploma level ( )
5) Degree and above ( )
67
B. DATA ABOUT THE PERCEPTION ON THE STATUS OF HEALTH
SERVICES PROVISION AND ACCESSIBILITY.
1. What is your perception on the status of health services provision and
accessibility at Dodoma Regional Referral Hospital?
a) Good status
b) Moderate ( )
c) Poor status
2. What about the quality of health services provided by the government
hospitals?
a) High quality
b) Moderate ( )
c) Low quality
3. What is your level of satisfaction concerning health services provided by the
government hospitals?
a) Highly satisfactory
b) Satisfactory
c) Moderate ( )
d) Less satisfactory
e) Not satisfactory
4. A t what level do you compare services from government and private hospitals?
a) High level
b) Moderate ( )
c) Low level
5. Since you have started to use health services from government hospitals, how
do you rate the level of improvement in health services delivery?
68
a) Highly improved
b) Improved
c) Moderate ( )
d) Less improved
e) Not improved
6. To what extent does the accessibility of health services from the government
hospitals reach the public?
a) High extent
b) Moderate ( )
c) Low extent
7. How do you rate the user fee in health services charged by the government
hospitals?
a) More expensive
b) Moderate ( )
c) Less expensive
8. What is the level of importance of the government hospitals in delivering health
services to the society?
a) Very important
b) Moderate ( )
c) Less important
9. How do you appreciate the health services provided by the government hospital
apart from weaknesses?
……………………………………………………………………………………
……………………………………………………………………………………
69
10. What do you think should be done by the government so as to improve quality
and accessibility of health services in government health facilities?
……………………………………………………………………………………
……………………………………………………………………………………
……………………………………………………………………………………
……………………………………………………………………………………
Thank you for your cooperation,
Asela Mathew
70
APPENDIX B SWAHILI VERSION: DODOSO KWA WANANCHI /
WATUMIAJI WA HUDUMA ZA AFYA.
Ndugu muhusika,
Naitwa ASELA MATHEW, ni mwanafunzi wa Shahada ya Uzamili katika kitivo cha
Uongozi na Utawala kutoka chuo kikuu cha Dodoma. Nafanya utafiti kuhusu
“MATOKEO KUTOKANA NA MABADILIKO YA SEKTA YA AFYA
KATIKA UTOAJI WA HUDUMA ZA AFYA TANZANIA. HOSPITALI YA
MKOA WA DODOMA IKIWA SEHEMU YA KUFANYIA UTAFITI”.
Dodoso hili litakuwa la msaada sana kwangu wakati huu ninapomaliza masomo yangu
ya Shahada ya uzamili ya Uongozi na Utawala. Lengo kuu ni kupata taarifa kuhusu
matokeo ya mabadiliko ya sekta ya afya katika kuimarisha upatikanaji wa huduma bora
za kiafya Tanzania. Taarifa zote zitakazokusanywa na dodoso hili zitakuwa ni siri na
zitatumika kwa ajili ya masomo tu na si vinginevyo.
71
MAELEKEZO KWA MUHUSIKA.
Unaombwa kujibu maswali yafuatayo. Maswali mengi ni ya kuchagua. Weka alama ya
vema ( √ ) katika jibu sahihi kwenye maswali ya kuchagua na chagua jibu sahihi
kujaza kwenye mabano. Kwa maswali machache jaza nafasi zilizoachwa wazi.
SEHEMU A. TAARIFA BINAFSI
1. 1. Jina (sio lazima)………………………………………………………..
1.2. Jinsia
1. Mwanaume ( )
2. Mwanamke ( )
1.3. Umri
1. 20-30 ( )
2. 31-40 ( )
3. 41-5 ( )
4. 51 na kuendelea ( )
1.4. Kiwango cha elimu
1. Elimu ya Msingi ( )
2. Elimu ya Sekondari ( )
3. Astashahada au Stashahada ( )
4. Shahada na kuendelea ( )
72
SEHEMU B: TAARIFA KUTOKA KWA WANANCHI KUHUSU
MUONEKANO / HALI YA HUDUMA ZA AFYA ZITOLEWAZO KATIKA
HOSPITALI ZA SERIKALI.
1. Unaonaje hadhi ya huduma za kiafya zitolewazo katika hospitali ya mkoa wa
Dodoma pamoja na upatikanaji wake kwa ujumla?
a) Hadhi nzuri
b) Wastani ( )
c) Hadhi mbaya
2. Unaonaje ubora wa huduma za afya zitolewazo katika hospitali za serikali?
a) Ni bora sana
b) Wastani ( )
c) Ni bora kidogo
3. Ni kwa kiasi gani unaridhishwa na huduma za kiafya zinazotolewa katika
hospitali za serikali?
a) Naridhika sana
b) Naridhika
c) Naridhika kwa wastani ( )
d) Naridhika kidogo
e) Siridhiki
4. Mbali na mapungufu yaliyopo katika hospitali za serikali ni kwa kiwango gani
unaweza kuelezea ubora wake ukilinganisha na hospitali binafsi?
a) Kiwango kikubwa
b) Wastani ( )
c) Kiwango kidogo
5. Tangu umeanza kutumia huduma za afya katika hospitali za serikali, unaonaje
maendeleo yake katika utoaji huduma hizo?
73
a) Maendeleo yapo makubwa
b) Maendeleo yapo
c) Wastani ( )
d) Maendeleo yapo kidogo
e) Hakuna maendeleo
6. Ni kwa kiwango gani upatikanaji wa huduma za afya katika hospitali za
serikali huwafikia watu?
a) Kiwango kikubwa
b) Wastani ( )
c) Kiwango kidogo
7. Unazionaje gharama za malipo ya huduma ya afya katika hospitali za serikali?
a) Gharama kubwa
b) Wastani ( )
c) Gharama ndogo
8. Je, hospitali za serikali zina umuhimu kiasi gani katika utoaji wa huduma za
kiafya kwa jamii?
a) Umuhimu mkubwa
b) Wastani ( )
c) Umuhimu mdogo
9. Ni kwa vipi unazikubali huduma za afya zinazotolewa na hospitali za serikali?
……………………………………………………………………………………
……………………………………………………………………………………
……………………………………………………………………………………
……………………………………………………………………………………

74
10. Unafikiri nini kifanyike kwa serikali ili kuimarisha ubora na upatikanaji
kirahisi wa huduma za afya katika hospitali za serikali?
……………………………………………………………………………………
……………………………………………………………………………………
……………………………………………………………………………………
……………………………………………………………………………………
Asante kwa ushirikiano wako,
Asela Mathew
75
APPENDIX C: INTERVIEW GUIDE FOR THE MANAGEMENT STAFF
A. PERSONAL INFORMATION.
1. 1. Name (Optional)………………………………………………………..
1.2. Occupation………………………………………………………………
B: DATA ABOUT THE CONTRIBUTION OF VARIOUS ACTORS IN
PROMOTING QUALITY AND ACCESSIBILITY OF HEALTH SERVICES
DELIVERY.
1. What is the contribution of various actors in promoting quality and accessibility of
health services delivery at Dodoma Regional Referral Hospital?
2. To what extent do the various actors contribute in promoting quality and
accessibility of health services delivery? If to the low extent explain how and if to
the high extent explain how.
3. What is the status of health services provision and accessibility at Dodoma
Regional Referral Hospital?
4. What is the contribution of private health facilities in promoting quality and
accessibility health services delivery?
5. What is your perception on the user fee in health services charged by the
government hospitals compared to private hospitals? How do you help patients
who fail to afford the medical fee?
6. What is the status of health services in the government health sectors after Health
Sector Reforms? Has it improved or not? If it has improved, which improvements?
7. What are the challenges which face the provision of quality health services delivery
at Dodoma Regional Referral Hospital?
76
APPENDIX D: INTERVIEW GUIDE FOR THE NURSES AND DOCTORS
A. PERSONAL INFORMATION
1. 1. Name (Optional)………………………………………………………..
1.2. Occupation………………………………………………………………
B: DATA ABOUT THE CHALLENGES TOWARDS PROVISION AND
ACCESSIBILITY OF QUALITY HEALTH SERVICES.
1. What are the challenges towards provision and accessibility of quality health
services at Dodoma Regional Referral Hospital?
2. What are the ways that you think may help in ending these challenges in order
to improve health services delivery?
3. What is the status of health services provision and accessibility at Dodoma
Regional Referral Hospital?
4. How do you rate the level of satisfaction to the health service beneficiaries in
government hospitals?
5. How the accessibility of health services from the government hospitals reach
the public?
6. What is your perception of the user fee in health services charged by the
government hospitals compared to private hospitals? How do you help patients
who fail to afford the medical fee?
7. What is the status of health services in the government health sectors after
Health Sector Reforms? Has it improved or not? If it has improved, which
improvements?
8. What is the importance of the government hospitals in delivering health
services to the society?
77
APPENDIX E: RESEARCH PERMISSION LETTER




























