Embed Size (px)
Citation preview

The Individualized Neuromuscular Quality of Life Questionnaire (INQoL); Cultural
translation and psychometric validation for the Dutch population
Femke M Seesing, MSC1§
, Lisanne EWM van Vught, BS1, Michael R Rose, MD ,PhD
2, Gea Drost, MD, PHD
1,3†, Baziel GM van
Engelen, MD, PhD, professor1 and Gert-Jan van der Wilt, PhD, professor
4
1 Department of Neurology, Radboud University Medical Centre, Reinier Postlaan 4, Nijmegen, The
Netherlands
2 Department of Neurology, Kings College Hospital, Denmark Hill, London SE5 9RU, United Kingdom
3 Department of Neurology/ Department of Neurosurgery, University Medical Centre Groningen,
University of Groningen, Hanzeplein 1, Groningen, The Netherlands
4 Department for Health Evidence, Radboud University Medical Centre, Geert Grooteplein noord 21,
Nijmegen, The Netherlands
†Study executed while working at Radboud University Medical Centre, currently working at
University Medical Centre Groningen.
§Corresponding author
Running title: Dutch INQoL validation
Correspondence: F.M. Seesing, Department of Neurology, Radboud University Medical Centre, 935
Neurology, PO BOX 9101, 6500 HB Nijmegen, The Netherlands. Tel.: +31243615213; E-mail:
Word count: 1727 excl abstract and tables
Keywords: Muscle disease, Quality of Life , INQoL, validation, outcome, patient-reported
This article has been accepted for publication and undergone full peer review but has not beenthrough the copyediting, typesetting, pagination and proofreading process which may lead todifferences between this version and the Version of Record. Please cite this article as an‘Accepted Article’, doi: 10.1002/mus.24337

Abstract
Introduction
This paper describes the translation and psychometric evaluation of the Dutch Individualized
Neuromuscular Quality of Life (INQoL) questionnaire.
Methods
Backward and forward translation of the questionnaire was executed, and psychometric properties
were assessed on the basis of reliability and validity.
Results
206 patients were included in the study. Reliability analyses resulted in Cronbach alpha values above
0.70 for all sub-domains. Known group validity showed a significant correlation between INQoL
scores and severity as well as age for the majority of sub-domains. Item-total correlation for overall
QoL was satisfactory. Concurrent validity with SF-36 and EQ-5D was good (range, Spearman
correlation coefficients: -0.43 to -0.76).
Conclusion
This study resulted in a questionnaire which is appropiate for use in the Dutch-speaking population
to measure quality of life of patients with a wide variety of muscle disorders. This confirms and
extends data obtained in the United Kingdom, US, Italy, and Serbia.
Page 2 of 18
John Wiley & Sons, Inc.
Muscle & Nerve
Introduction
Measuring quality of life (QoL) in patients with a muscle disorder is important to identify specific
areas at which to direct interventions that might help retain QoL despite illness progression 1,2
.
Muscle disorders show a wide variety of symptoms, often with a large impact on multiple aspects of
daily living, for which no curative treatments are currently available 3-5
. In contrast to generic QoL
measurement instruments, disease-specific questionnaires allow detection of differences or changes
in specific muscle disorder symptoms such as locking or weakness of the muscles or body image. This
minimizes the questionnaire burden on patients and clinicians caused by irrelevant or potentially
intrusive items and therefore facilitates their use in research and daily clinical practice6. The
Individualized Neuromuscular Quality of Life (INQoL) questionnaire is a muscle disease-specific QoL
questionnaire for patients with muscle disorders that was developed by Rose et al in 2007 7. The
psychometric properties of the INQoL have been tested and shown to be valid, reliable, and, to some
extent, responsive 7-9
. The INQoL was translated and validated for populations in the UK, USA, Italy,
and Serbia 10,7-9
. In this paper, we describe the translation and psychometric evaluation of the Dutch
INQoL questionnaire for patients with a muscle disorder. Psychometric properties were assessed on
the basis of reliability and validity (known-group validity, item-total correlation, and concurrent
validation).
Methods
INQoL questionnaire
The INQoL is constructed of 4 main domains that are divided into 12 sub-domains. Each sub-domain
is composed of questions that vary from 3 to 14 items, with responses given on a 7-point Likert scale.
Raw data are converted to a score from 0-100 for every sub-domain, a higher score indicating a
greater impact on QoL. The 4 main domains of the INQoL include symptoms (sub-domains:
weakness, locking, pain, and fatigue); life domains (sub-domains: activities, independence, social
relationships, emotions, and body image); treatment effects (sub-domains: perceived treatment
Page 3 of 18
John Wiley & Sons, Inc.
Muscle & Nerve
effects and expected treatment effects); and overall QoL, an aggregation of parts of the 5 sub-
domains (activities, independence, social relationships, emotions, and body image). The 4 main
domains are considered to properly reflect the QoL of patients with a muscle disorder7.
Cultural translation
Backward and forward translation of the questionnaire was executed independently by 2
neurologists (CH, NV). Differences were resolved by consensus. Remaining questions were submitted
to the original author (MR) to assure conceptual equivalence with the original questionnaire.
Psychometric evaluation
Psychometric properties of the Dutch INQoL questionnaire were evaluated using data collected from
a randomized controlled trial (RCT) on shared medical appointments for patients with a muscle
disorder. The RCT and the subsequent use of the data for this study were reviewed and approved by
the local medical ethics committee (reference CMO nr. 2008/224) and registered with the Dutch Trial
Register (nr NTR1412)11,12
.
Reliability was assessed by measuring the relationship (Cronbach alpha) of the items within each of
the 12 sub-domains. The internal consistency among items addressing the same underlying domains
should be higher than an alpha value 0.70 13
. Spearman correlation coefficients and interclass
correlations (single measures) were computed to assess the relation between the questions of each
domain14
.
Validity was assessed through known-group validity, item-total correlation, and concurrent validity.
Known-group validity aimed to compare the INQoL scores with demographic or disease-related
factors which are known from previous research to have a significant correlation with the INQoL.
Earlier studies showed that age and severity of disease are correlated negatively with INQoL scores
2,8. Age was divided in 3 groups: 18-35, 36-65, and 66-80 years. Severity of disease was assessed
through the Modified Rankin Scale (MRS), ranging from 0 (no symptoms) to 5 (severe disability;
Page 4 of 18
John Wiley & Sons, Inc.
Muscle & Nerve

bedridden, incontinent, and requiring constant nursing care and attention) 15
. Means and standard
deviations of the INQoL scores for the sub-groups were analyzed. P-values < 0.05 were considered
statistically significant for known-group validity. Item-total correlation was determined by the
correlation between the individual items (activities, independence, social relationships, emotions,
and body image) and overall QoL. The corresponding item was omitted in the total score. Correlation
coefficients should be between 0.20 and 0.90 in order to indicate sufficient item-total correlation 13
.
Concurrent validity was measured by the association of the 12 INQoL sub-domains with the
corresponding Short Form-36 (SF-36) and EuroQol 5D (EQ5D) questions and were expressed in terms
of Spearman correlation coefficients 16,17
Subjects and data collection
Patients were recruited from the Department of Neurology of the Radboud University Medical
Centre (Radboudumc) and identified as patients with a muscle disorder through the Dutch
neuromuscular database (CRAMP) 18
. Patients had to be aged 18 years and above and literate in the
Dutch language. In view of the RCT intervention on shared medical appointments, patients with
hearing problems and those who attended the outpatient clinic less than 6 months ago were
excluded 11
. Of the eligible patients, 70% agreed to participate in the RCT. Data were collected
through a self-administered questionnaire-booklet which contained, besides the Dutch INQoL
questionnaire, the following questionnaires: EQ5D, SF-36, General self-efficacy, social support
subscale from the Dutch Social Support List-Discrepancies, QUality Of care Through the patient’s Eyes
(QUOTE) and satisfaction with the marital relationship. The questionnaires were filled out at home.
Non-responders at 2 weeks were contacted by phone to remind them to complete the questionnaire.
SPSS version 18 was used for statistical analysis.
Results
Cultural translation
Page 5 of 18
John Wiley & Sons, Inc.
Muscle & Nerve

A noteworthy adjustment resolved by discussion with the original author (MR) concerned the English
word for “locking”, which implies myotonia. In Dutch, this is not a common lay term, therefore this
was translated as: “Do you notice that your muscles have difficulties relaxing after sustained
contraction?“. A final version of the Dutch INQoL questionnaire has been deposited with the MAPI
Research Institute Website, and inquiries regarding its use can be obtained from www.mapi-
trust.org.
Patient characteristics
In total, 206 patients with 1 of the following muscle disorders were included in the study: myotonic
dystrophy type 1 (MD), McArdle disease, facioscapulohumeral muscular dystrophy (FSHD), chronic
progressive external ophthalmoplegia (CPEO), oculopharyngeal muscular dystrophy (OPMD),
inclusion body myositis (IBM), non-dystrophic myotonias, and myositis. See table 1 for patient
characteristics. MD type 1 was the largest patient group (N=75), and chronic progressive external
ophthalmoplegia (CPEO) was the smallest (N=5). Slightly more than half of the patients were men
(54%), and the mean age was 51 years, range 18-79. Most patients reported having a slight disability,
and although unable to carry out previous activities, they were still able to look after themselves
without assistance (score 2 on MRS) (N=63).
Reliability
Table 2 shows that all internal consistency values had a Cronbach alpha above 0.70, ranging from
0.721 (relationships) to 0.903 (fatigue). The correlation coefficients ranged from 0.797 (body image)
to 0.331 (relationships). All inter-class correlation coefficients were above 0.400, ranging from 0.478
(expected treatment effects) to 0.792 (body image), except for the sub-domain relationships (0.224).
Validity
Known group validation
Page 6 of 18
John Wiley & Sons, Inc.
Muscle & Nerve

Figure 1 summarizes the relation between severity of disease (MRS) and INQoL sub-domains. The
MRS showed a significantly higher INQoL score for more severely disabled patients for 8 of the 10
sub-domains (P<0.03). Age correlated significantly with INQoL score for 4 of the 10 sub-domains
(P<0.03) (data not shown).
Item-total correlation
In table 3, the correlation between the calculated domain, overall QoL and the individual items
contributing to this score, is presented. Although some items correlated only poorly, overall QoL
correlated quite well with each of its component items. Correlation coefficients were 0.400 or higher
for all sub-domains with overall QoL, ranging from 0.448 (activity) to 0.533 (independence).
Concurrent validation
The data in table 4 show the correlation between the INQoL and the SF-36 questionnaire. The
Spearman correlation coefficient ranged from -0.453 (emotions vs. emotional well being) to -0.769
(Activities vs. Physical functioning). The concurrent validation analysis for the EQ5D VAS score and
the EQ5D index score compared to the INQoL overall QoL score resulted in Spearman correlation
coefficients of -0.472 and -0.4 respectively (data not shown)
Discussion
Main findings
These results show that the translation of the INQoL questionnaire resulted in a Dutch – language
questionnaire with adequate psychometric properties for patients with muscle disease. Reliability,
known group validity, item-total correlation, and concurrent validation were good. The questionnaire
is appropiate for use in the Dutch-speaking population to measure QoL of patients with diverse
muscle disorders. This confirms and extends data obtained in the United Kingdom, US, Italy, and
Serbia 10,7-9
.
Page 7 of 18
John Wiley & Sons, Inc.
Muscle & Nerve

Strengths and limitations
A major strength of our study was the broad range of the study population, including 8 different
diagnoses. In line with the prevalence of the various muscle diseases in the population patients with
MD and FSHD made up the largest number of subjects in this validation study. However we were not
able to detect substantial differences in psychometric properties for these subgroups. This confirms
data from Peric et al who studied the INQoL specifically for patients with MD9 Although some muscle
diseases such as limb-girdle muscular dystrophy (LGMD) were not represented, we doubt that this
weakens the validation of INQoL for muscle disease generally. LGMDs for example were present in
the US and Italian validations of INQoL, and like us, those studies did not find significant differences
between most specific muscle diseases.19,8
. Our sample reflects the Dutch national population of
patients with a muscle disorder even though this is is a single center design, as the Radboudumc is a
Dutch national referral center which sees patients with muscle disease from the whole of the
country. Our study design did not allow for the assessment of a test-retest reliability of the INQoL.
Implications and future research
The assessment of QoL of patients with a muscle disorder can help identify domains that are affected
most by the disease in individual patients. Such findings may help to guide clinical management
decisions and may be used to evaluate the impact of treatments. The INQoL questionnaire is an easy
to administer self-rating scale with an acceptable burden on patients and satisfactory psychometric
properties. It can be used both in daily clinical practice and in research. The availability of
quantitative data on minimal clinical significant differences of the INQoL questionnaire would be
imperative to make optimal use of this instrument. Responsiveness and test-retest analyses should
be performed in future research to further strengthen the validation of the Dutch-language INQoL
questionnaire.
Page 8 of 18
John Wiley & Sons, Inc.
Muscle & Nerve

Acknowledgements
The authors would like to thank Nicol Voermans, MD (NV) and Charlotte Haaxma, MD (CH) for their
contribution to the translation of the Dutch INQoL questionnaire.
Page 9 of 18
John Wiley & Sons, Inc.
Muscle & Nerve
Abbreviations
CPEO: chronic progressive external ophthalmoplegia
CRAMP: Dutch Computer Registry of All Myopathies and Polyneuropathies
EQ5D: EuroQol 5D
FSHD: Facioscapulohumeral muscular dystrophy
HRQoL: Health Related Quality of Life
IBM: Inclusion body myositis
INQoL: Individualized Neuromuscular Quality of Life
MD: Myotonic dystrophy type 1
MRS: Modified Rankin Scale
NTR: Dutch Trial Registration
OPMD: Oculopharyngeal muscular dystrophy
Radboudumc: Radboud University Medical Centre
SF-36: Short Form 36
QoL: Quality of Life
QUOTE: QUality Of care Through the patient’s Eyes
Page 10 of 18
John Wiley & Sons, Inc.
Muscle & Nerve

References
1. Rose MR, Sadjadi R, Weinman J, Akhtar T, Pandya S, Kissel JT, Jackson CE, Muscle Study G.
Role of disease severity, illness perceptions, and mood on quality of life in muscle disease. Muscle
Nerve 2012;46(3):351-359.
2. Graham CD, Rose MR, Grunfeld EA, Kyle SD, Weinman J. A systematic review of quality of life
in adults with muscle disease. Journal of neurology 2011;258(9):1581-1592.
3. Attarian S, Salort-Campana E, Nguyen K, Behin A, Andoni Urtizberea J. Recommendations for
the management of facioscapulohumeral muscular dystrophy in 2011. Revue neurologique
2012;168(12):910-918.
4. Kaminsky P, Pruna L. [A genetic systemic disease: Clinical description of type 1 myotonic
dystrophy in adults.]. La Revue de medecine interne / fondee par la Societe nationale francaise de
medecine interne 2012.
5. Smits BW, Heijdra YF, Cuppen FW, van Engelen BG. Nature and frequency of respiratory
involvement in chronic progressive external ophthalmoplegia. Journal of neurology
2011;258(11):2020-2025.
6. Burns TM, Graham CD, Rose MR, Simmons Z. Quality of life and measures of quality of life in
patients with neuromuscular disorders. Muscle Nerve 2012;46(1):9-25.
7. Vincent KA, Carr AJ, Walburn J, Scott DL, Rose MR. Construction and validation of a quality of
life questionnaire for neuromuscular disease (INQoL). Neurology 2007;68(13):1051-1057.
8. Sansone VA, Panzeri M, Montanari M, Apolone G, Gandossini S, Rose MR, Politano L,
Solimene C, Siciliano G, Volpi L, Angelini C, Palmieri A, Toscano A, Musumeci O, Mongini T, Vercelli L,
Massa R, Panico MB, Grandi M, Meola G. Italian validation of INQoL, a quality of life questionnaire for
adults with muscle diseases. European journal of neurology : the official journal of the European
Federation of Neurological Societies 2010;17(9):1178-1187.
9. Peric S, Sansone V, Lavrnica D, Meola G, Bastaa I, Miljkovica M, Rakocevic-Stojanovica V.
Serbian Validation of the Individualized Neuromuscular Quality of Life Questionnaire (INQoL) in
Adults With Myotonic Dystrophy Type 1. Journal of Neurology Research 2011;1(4):153-160.
10. Sadjadi R, Vincent KA, Carr AJ, Walburn J, Brooks VL, Pandya S, Kissel JT, Jackson CE, Rose MR,
Muscle Study G. Validation of the individualised neuromuscular quality of life for the USA with
comparison of the impact of muscle disease on those living in USA versus UK. Health Qual Life
Outcomes 2011;9:114.
11. Seesing FM, Drost G, van der Wilt GJ, van Engelen BG. Effects of shared medical
appointments on quality of life and cost-effectiveness for patients with a chronic neuromuscular
disease. Study protocol of a randomized controlled trial. BMC neurology 2011;11:106.
12. Seesing FM, Drost G, Groenewoud J, van der Wilt GJ, van Engelen BG. Shared medical
appointments improve QOL in neuromuscular patients: A randomized controlled trial. Neurology
2014.
13. Streiner DL, Norman GR. Health Measurement Scales : A practical guide to their development
and use: OUP Oxford; 2008.
14. Schouten LM, Grol RP, Hulscher ME. Factors influencing success in quality-improvement
collaboratives: development and psychometric testing of an instrument. Implementation science : IS
2010;5:84.
15. Quinn TJ, Dawson J, Walters MR, Lees KR. Reliability of the Modified Rankin Scale. Stroke
2007;38(11):e144.
16. EuroQoL EG. a new facility for the measurement of health-related quality of life. Health Policy
1990;16:199-208. Health Policy 1990;16:199-208.
17. Ware JE, Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I.
Conceptual framework and item selection. Med Care 1992;30(6):473-483.
18. van Engelen BG, van Veenendaal H, van Doorn PA, Faber CG, van der Hoeven JH, Janssen NG,
Notermans NC, van Schaik IN, Visser LH, Verschuuren JJ. The Dutch neuromuscular database CRAMP
Page 11 of 18
John Wiley & Sons, Inc.
Muscle & Nerve

(Computer Registry of All Myopathies and Polyneuropathies): development and preliminary data.
Neuromuscul Disord 2007;17(1):33-37.
19. Seyedsadjadi R, Rose M, Weinman J, Pandya S, Jackson C, Kissel J, Group MS. The relative
contributions of disease severity, mood and illness perceptions on the quality of life of those with
muscle disease. Neurology 2008;70(11):A219-A219.
Page 12 of 18
John Wiley & Sons, Inc.
Muscle & Nerve

Attachments: tables, figures
Table 1 Patient characteristics
Variable Men (N) (%) 111 (54) Age (years), Mean (SD) 51 (14.6) Diagnosis (N):
- Myotonic Dystrophy type 1 75 - McArdle disease 8 - Facioscapulohumeral Muscular Dystrophy 46 - Chronic progressive external ophthalmoplegia 5 - Oculopharyngeal Muscular Dystrophy 22 - Inclusion body myositis 9 - Non-dystrophic myotonias: chloride and sodium channelopathies 21 - Myositis: Dermatomyositis and Polymyositis 19 - Missing 1
Rankin Scale (N): - No symptoms (0) 9 - No significant disability (1) 27 - Slight disability (2) 63 - Moderate disability (3) 31 - Moderate-severe disability (4) 56 - Severe disability (5) 2 - Missing 18
Page 13 of 18
John Wiley & Sons, Inc.
Muscle & Nerve
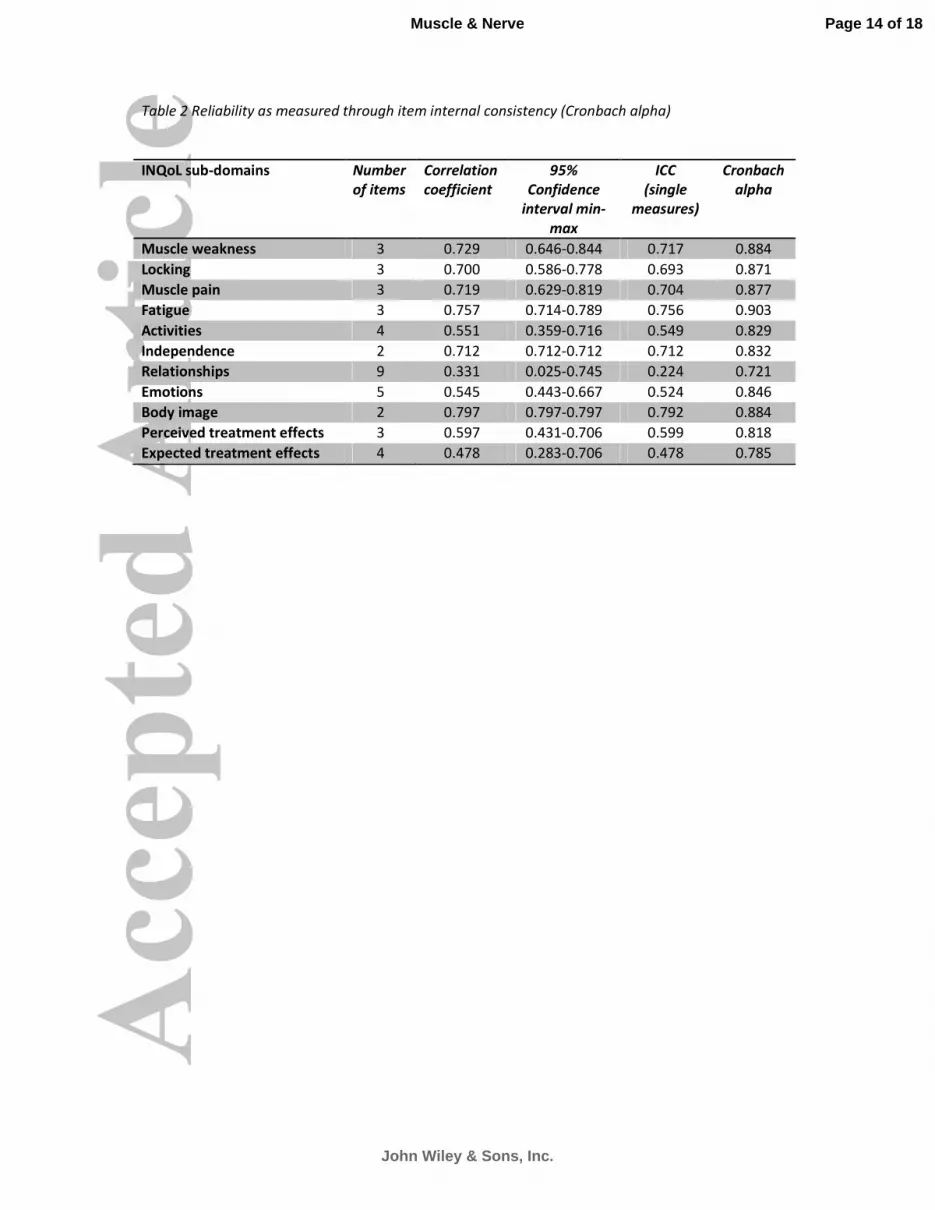
Table 2 Reliability as measured through item internal consistency (Cronbach alpha)
INQoL sub-domains Number
of items
Correlation
coefficient
95%
Confidence
interval min-
max
ICC
(single
measures)
Cronbach
alpha
Muscle weakness 3 0.729 0.646-0.844 0.717 0.884
Locking 3 0.700 0.586-0.778 0.693 0.871
Muscle pain 3 0.719 0.629-0.819 0.704 0.877
Fatigue 3 0.757 0.714-0.789 0.756 0.903
Activities 4 0.551 0.359-0.716 0.549 0.829
Independence 2 0.712 0.712-0.712 0.712 0.832
Relationships 9 0.331 0.025-0.745 0.224 0.721
Emotions 5 0.545 0.443-0.667 0.524 0.846
Body image 2 0.797 0.797-0.797 0.792 0.884
Perceived treatment effects 3 0.597 0.431-0.706 0.599 0.818
Expected treatment effects 4 0.478 0.283-0.706 0.478 0.785
Page 14 of 18
John Wiley & Sons, Inc.
Muscle & Nerve

Table 3 Item-total correlation overall QoL. Correlation coefficients
Overall
QoL
Activity Independenc
e
Relationships Emotions Body image
Overall QoL - 0.448 0.533 0.468 0.469 0.495
Activity 0.448 - 0.742 0.412 0.279 0.521
Independence 0.533 0.742 - 0.413 0.240 0.570
Relationships 0.468 0.412 0.413 - 0.336 0.313
Emotions 0.469 0.279 0.240 0.336 - 0.279
Body image 0.495 0.521 0.570 0.313 0.279 -
Page 15 of 18
John Wiley & Sons, Inc.
Muscle & Nerve

Table 4 Concurrent validity; correlation between selected INQoL domains and SF-36 items.
Spearman correlation coefficient.
INQoL SF-36 Spearman
correlation
Pain Pain -0.686
Fatigue Energy/fatigue/emotions -0.686
Independence Social functioning -0.510
Overall QoL General Health -0.453
Activities Physical functioning -0.769
Emotions Emotional well being -0.453
Relationships Social functioning -0.504
Page 16 of 18
John Wiley & Sons, Inc.
Muscle & Nerve

Figure 1. Known group validity; INQoL subdomains vs severity of disease as measured by the
Modified Rankin Scale (MRS). Mean values.
MRS 0: No symptoms (n=9); MRS 1: No significant disability (n=27); MRS 2: Slight disability (n=63);
MRS 3: Moderate disability (n=31); MRS 4: Moderate severe disability (n=56); MRS 5: Severe
disability (n=2)
Page 17 of 18
John Wiley & Sons, Inc.
Muscle & Nerve

MRS 0: No symptoms (n=9); MRS 1: No significant disability (n=27); MRS 2: Slight disability (n=63); MRS 3: Moderate disability (n=31); MRS 4: Moderate severe disability (n=56); MRS 5: Severe disability (n=2)
157x243mm (300 x 300 DPI)
Page 18 of 18
John Wiley & Sons, Inc.
Muscle & Nerve





























