Embed Size (px)
Citation preview

INT’L. J. AGING AND HUMAN DEVELOPMENT, Vol. 65(2) 149-161, 2007
THE INFLUENCE OF SPECIFIC PHYSICAL HEALTH
CONDITIONS ON RETIREMENT DECISIONS
KENNETH S. SHULTZ
California State University, San Bernardino
MO WANG
Portland State University
ABSTRACT
Physical health has consistently been shown to strongly influence the retire-
ment decision-making process. Unfortunately, “physical health” is typically
operationalized in global terms. As a result, we know little about the specific
aspects of physical health that influence the decision to retire. Therefore, in
the present study, data from three waves of the Americans’ Changing Lives
(ACL) data set was examined to determine which specific health conditions
are associated with retirement, continued work in the same job, or continued
work but in a different job. The major health conditions most strongly related
to retirement were lung disease and cancer, while only lung disease was pre-
dictive of job change at older ages. In contrast, arthritis and diabetes were
the minor health conditions most strongly related to both changing jobs and
retiring over an eight-year period. The results are discussed in terms of the
importance of better understanding why specific health factors are associated
with retirement and job changes during one’s late career.
INTRODUCTION
Researchers have consistently shown that health and wealth factors are among the
strongest influences on retirement decisions (Barnes-Farrell, 2003). That is, those
individuals with sufficient income and poor health are more likely to retire than
149
� 2007, Baywood Publishing Co., Inc.
doi: 10.2190/AG.65.2.c
http://baywood.com

individuals with insufficient (or unstable) incomes and those in good health
(Hedge, Borman, & Lammlein, 2006). Health factors have typically been the
domain of study for sociologists, demographers, and epidemiologists, while
wealth factors have been the focus of economists (Adams & Beehr, 2003).
However, psychological factors, such as job attachment, satisfaction with career
attainment, and anxieties about separation from the workplace, have also been
shown to influence retirement decisions (Adams & Beehr, 1998, 2003; Cude &
Jablin, 1992; Hansson, DeKoekkoek, Neece, & Patterson, 1997; Taylor & Shore,
1995), but their influence appears to be much weaker and less robust than health
and wealth factors (Barnes-Farrell, 2003). However, since health is typically
operationalized via a global self-rating of current health, little is known about the
specific aspects of health which influence the retirement decision (Feldman,
1994). Therefore, in this study the concept of physical health is expanded by
providing a more detailed examination of physical health, thereby allowing
us to examine the influence of specific health conditions on the retirement
decision-making and job change processes at older ages (e.g., bridge employment;
Shultz, 2003).
Health Factors
Researchers have continued to show a strong link between a mature worker’s
health and planned retirement age (Farr & Ringseis, 2002; Taylor & Shore,
1995), actual retirement behaviors (Hardy & Quadagno, 1995; Herzog, House, &
Morgan, 1991; Muller & Boaz, 1988), and post-retirement satisfaction and adjust-
ment (Shultz, Morton, & Weckerle, 1998). In most cases though, health is
typically operationalized via global self-report measures asking about a person’s
current or past overall health status. While these global self-report health measures
tend to be highly correlated to actual observed physical health limitations
(Wegman & McGee, 2004), they tend to be very broad, providing no detailed
information on specific health problems or limitations.
Feldman (1994) has noted that, “rather than looking at health status in general,
more careful attention needs to be paid to the specific illnesses and impairments
that impel older workers to leave the workforce” (p. 307). For example, is it
chronic or acute health problems that tend to be more predictive of retirement
intentions and decisions? Clearly more detailed aspects of health need to be
delineated as we move forward to try to better understand the influence of health
on retirement decisions and outcomes.
More specifically, Feldman (1994) has suggested looking within three
categories of health related concerns. First, Feldman hypothesizes that major
health conditions (e.g., cancer) would likely cause retirement age individuals to
completely exit the labor force. Similarly, Feldman predicted that functional
impairments or minor health conditions (e.g., hearing loss) would force older
individuals to exit the workforce in the form of early retirement. Finally, Feldman
150 / SHULTZ AND WANG

predicted that psychosomatic illnesses (e.g., headaches) would be unlikely to force
people to retire, but instead would foster movement to a job or occupation with
fewer demands and so reduce the likely incidence of such illnesses.
Similar to Feldman (1994), Colsher, Dorfman, and Wallace (1988) predicted
that “major health conditions” (e.g., stroke, myocardial infarction, cancer) would
lead individuals to retire. However, they predicted that “minor complaints”
(e.g., foot problems, arthritis, bladder problems) would not affect employment
status in the elderly (65+). Studying a large cohort of rural elderly in Iowa,
Colsher et al. found that in fact it was the major health conditions that distinguish
those elderly who had retired for health reasons, versus those who retired for
some “other” non-health reason or were still employed. While minor health
ailments were prominent in those who retired for health reasons, they were also
prominent in those who retired for other reasons, as well as those who remained
employed. Thus, using a more detailed breakdown of health (i.e., examining
more than just overall health status), we begin to get a better idea of why and how
health influences the retirement decision.
A recent summary of aging workforce issues by Hedge et al. (2006) also
discusses the influence of general health conditions on employment and retire-
ment decisions in late career. However, those authors were unable to point to
any research that examines specific physical health conditions and employment
related decisions at older ages. In addition, a recent exhaustive review of the
occupational health and safety literature specific to older workers by The National
Academies of Science (Wegman & McGee, 2004) does provide detailed infor-
mation on specific health conditions and how they differ for older versus younger
workers. Unfortunately, there is no discussion of how the specific health con-
ditions may influence job change and retirement decisions at older ages. Finally,
another recent comprehensive review of the occupational health and aging
literature by Jex, Wang, and Zarubin (2007) found a paucity of research examining
specific health conditions and employment/retirement related decisions of
older workers. Thus, the lack of available research on this topic further supports
the need of the present research.
Present Study
It is clear from recent comprehensive reviews of prior empirical research (e.g.,
Barnes-Farrell, 2003; Hedge et al., 2006; Jex et al., 2007; Wegman & McGee,
2004) that health factors have a strong influence on the work and retirement
decisions of older workers. However, it is not clear which specific aspects of
health are most prominent in predicting and understanding retirement decisions.
Colsher et al. (1988) provide some evidence for the greater importance of major
health conditions, however their study was cross-sectional, retrospective, and
restricted to the rural elderly (age 65+) in Iowa. Therefore, in the present study,
we expanded on the work of Colsher et al., and the propositions of Feldman
HEALTH AND RETIREMENT DECISIONS / 151

(1994), by examining a variety of health conditions. In addition, we used a large,
longitudinal (three waves of data), national, multistage area probability sample
examining health conditions separately for those who had continued in the same
job, those who had changed jobs, and those who had retired, between 1986
and 1994. Based on Colsher et al.’s findings, and the propositions provided by
Feldman, we propose several hypotheses below. However, given the paucity of
previous empirical research examining the influence of specific physical health
conditions on employment and retirement related decisions at older ages, our
hypotheses should be viewed as preliminary.
Hypothesis 1: Those participants who retired should report higher incidence
of major physical impairments (heart attacks, cancer, stroke, lung disease)
prior to retirement than those who changed jobs.
Hypothesis 2: Those participants who kept their same job should report the
lowest incidence rates of major physical impairments (heart attacks, cancer,
stroke, lung disease).
Hypothesis 3: Those participants who changed jobs should report higher
incidence of minor health conditions (arthritis, hypertension, foot prob-
lems, diabetes, incontinence, and broken bones) before changing jobs
than those who kept their same job.
Hypothesis 4: Those participants who kept their same job should report the
lowest incidence rates of minor health conditions (arthritis, hypertension,
foot problems, diabetes, incontinence, and broken bones).
METHOD
Data Source
The Americans’ Changing Lives (ACL) data set (House, 2003) was used for
the present analyses. The ACL is a multi-wave, national longitudinal panel survey
of sociological, psychological, mental, and physical health factors (see House
et al., 1992, for more details on sampling methods and procedures). Wave I data
(collected in 1986) was a multistage stratified area probability sample of 3,617
participants, with over sampling of Blacks and those 60 years of age and over
(House, 2003). As of Wave I (1986), 29.3% (N = 987) of participants were
between the ages of 47 and 64. Of this group, 569 were working when surveyed
at Wave I (1986). By Wave III (1994), 168 were still in the same job, 66 had
changed jobs, and 177 had retired. The remaining 158 participants listed their
1994 “employment” status as disabled, unemployed, keeping house, or were
“missing,” and thus were excluded from the analyses described below.
The sample was limited to ages 47 to 64 in that many company pension plans
allow individuals to retire as early as age 55, thus those age 47 in 1986 would be
152 / SHULTZ AND WANG

age 55 by 1994. In addition, much of the recent historical demographic data show
a noticeable decline in labor force participation after age 55 (Costa, 1998).
Meanwhile, by age 65 individuals were still eligible for full social security benefits
in 1994. Therefore, it was decided to limit the sample to this age group.
In addition, given that the ACL over-sampled Blacks and those over age 60
at twice the rate found in the United States, it is necessary to weight the data
when conducting multivariate analyses (cf. Schnittker, 2001). As the sample
in this study was selected based on age, we decided to only weight the current
multinomial logistic regression analyses on ethnicity using the WEIGHT function
offered by the SPSS software. It should be noted that we also conducted the
multinomial logistic regression analyses without weighting the data, which
yielded very similar results, however, only the weighted results are reported here.
Measures
A variety of physical health measures were used (see Appendix for specific
items and response scales for each measure). The physical health measures
included a list of 10 physical conditions experienced in the last 12 months at
Wave I. These were divided into “major health conditions” (heart attack, cancer,
stroke, and lung disease) and “minor health conditions” (arthritis, hypertension,
foot problems, diabetes, incontinence, and broken bones), along the lines
suggested by Colsher et al. (1988) and Feldman (1994). Unfortunately, no infor-
mation on what Feldman (1994) refers to as psychosomatic illnesses (e.g.,
headaches) were collected. While no strong rationale or theory was provided by
House (2003) as to why these specific physical conditions were included, they
are in line with previous theorizing of Feldman (1994), as well as Wegman and
McGee (2004).
RESULTS
Table 1 displays the percentage of participants, who between 1986 and 1994
kept their same job (N = 168), changed jobs (N = 66), or retired (N = 177), who
possibly suffered from 10 different chronic physical health conditions in the
previous 12 months at the time of the first survey in 1986. Looking at Table 1, we
see that 7.4% of participants suffered from cancer prior to retirement, compared
to 3.0% and 1.2% for those who changed jobs and those who kept their job,
respectively. In addition, 15.9% of participants suffered from lung disease prior to
retirement, compared to 7.6% and 1.2% for those who changed jobs and those
who kept their job, respectively. These results support hypotheses 1 and 2. The
other “major health conditions” show a somewhat similar pattern, with retirees
having the highest incidence rates among the three employment status groups.
However, due to the relatively low incidence rates in general for major health
HEALTH AND RETIREMENT DECISIONS / 153
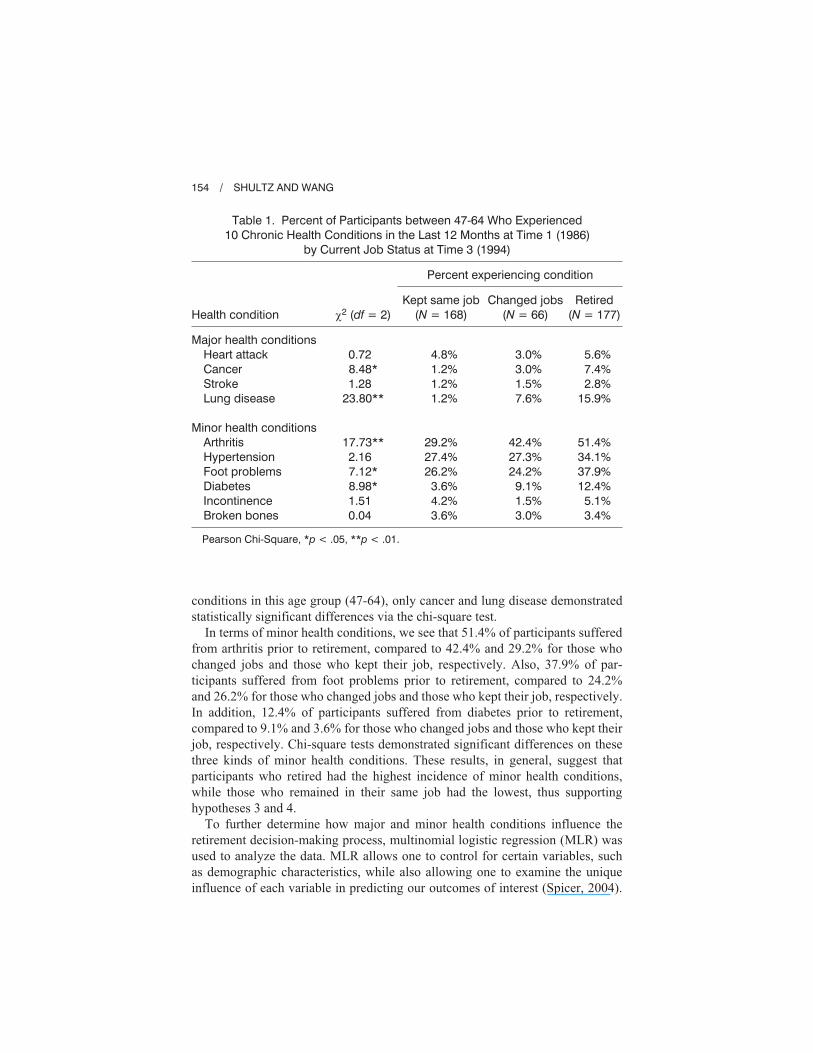
conditions in this age group (47-64), only cancer and lung disease demonstrated
statistically significant differences via the chi-square test.
In terms of minor health conditions, we see that 51.4% of participants suffered
from arthritis prior to retirement, compared to 42.4% and 29.2% for those who
changed jobs and those who kept their job, respectively. Also, 37.9% of par-
ticipants suffered from foot problems prior to retirement, compared to 24.2%
and 26.2% for those who changed jobs and those who kept their job, respectively.
In addition, 12.4% of participants suffered from diabetes prior to retirement,
compared to 9.1% and 3.6% for those who changed jobs and those who kept their
job, respectively. Chi-square tests demonstrated significant differences on these
three kinds of minor health conditions. These results, in general, suggest that
participants who retired had the highest incidence of minor health conditions,
while those who remained in their same job had the lowest, thus supporting
hypotheses 3 and 4.
To further determine how major and minor health conditions influence the
retirement decision-making process, multinomial logistic regression (MLR) was
used to analyze the data. MLR allows one to control for certain variables, such
as demographic characteristics, while also allowing one to examine the unique
influence of each variable in predicting our outcomes of interest (Spicer, 2004).
154 / SHULTZ AND WANG
Table 1. Percent of Participants between 47-64 Who Experienced
10 Chronic Health Conditions in the Last 12 Months at Time 1 (1986)
by Current Job Status at Time 3 (1994)
Percent experiencing condition
Health condition �2 (df = 2)
Kept same job
(N = 168)
Changed jobs
(N = 66)
Retired
(N = 177)
Major health conditions
Heart attack
Cancer
Stroke
Lung disease
Minor health conditions
Arthritis
Hypertension
Foot problems
Diabetes
Incontinence
Broken bones
0.72
8.48*
1.28
23.80**
17.73**
2.16
7.12*
8.98*
1.51
0.04
4.8%
1.2%
1.2%
1.2%
29.2%
27.4%
26.2%
3.6%
4.2%
3.6%
3.0%
3.0%
1.5%
7.6%
42.4%
27.3%
24.2%
9.1%
1.5%
3.0%
5.6%
7.4%
2.8%
15.9%
51.4%
34.1%
37.9%
12.4%
5.1%
3.4%
Pearson Chi-Square, *p < .05, **p < .01.

MLR also has the advantage of providing odds ratios so that the likelihood of an
event occurring (e.g., retiring) can be determined based on the unique predictive
influence of a given variable (Menard, 2001). Weighted data were used in these
analyses, as African Americans were over-sampled in the ACL. To obtain the
multinomial logistic regression coefficients, participants who kept their jobs
were designated as the reference group for each model. Age, gender, ethnicity,
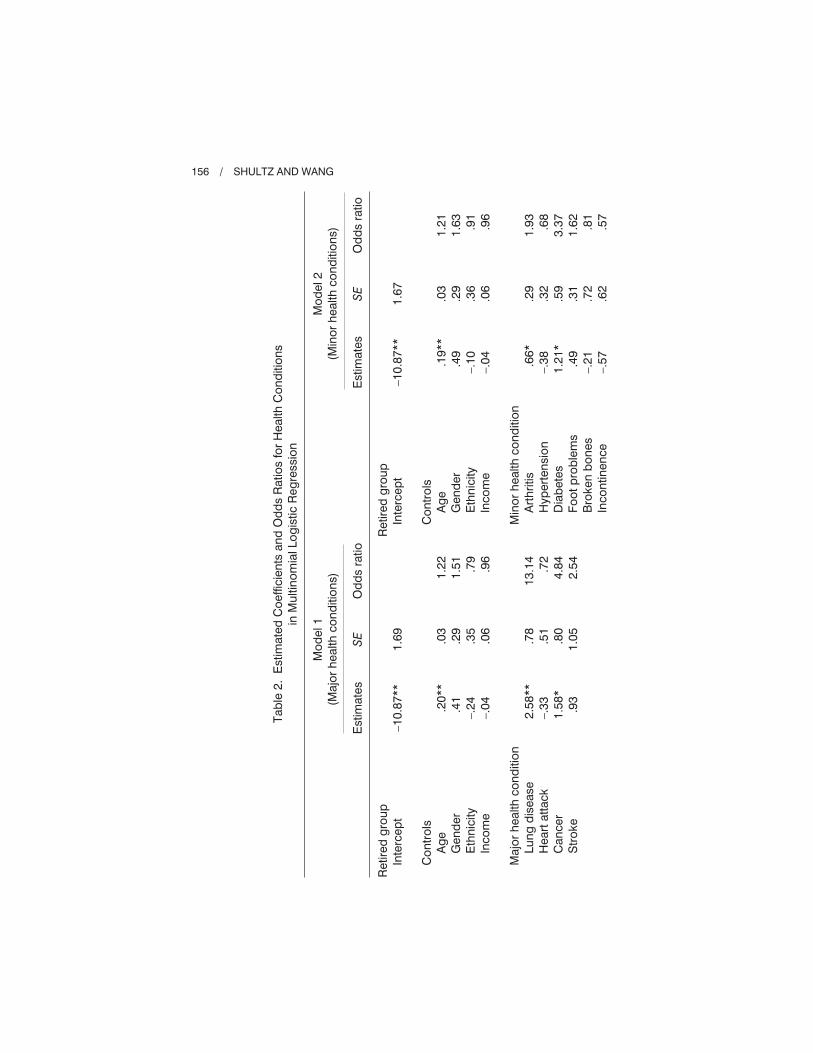
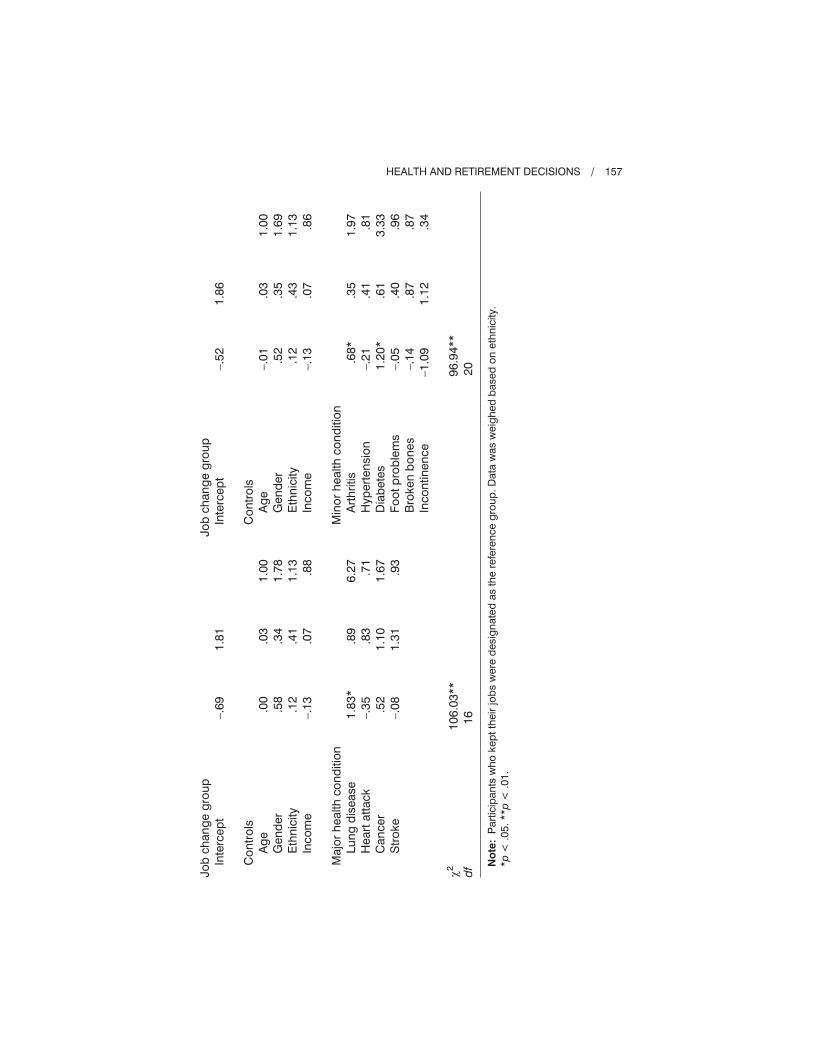
and income were treated as control variables in each model. Table 2 presents
the MLR analysis results.
In terms of the major health conditions, it was found that the incidence of lung
disease and cancer significantly predicted participants’ retirement decision.
Specifically, participants who suffered from lung disease were 13.14 times more
likely to retire than to keep their jobs. It was also found that participants who
suffered from cancer were 4.84 times more likely to retire than to keep their jobs.
In addition, participants who suffered from lung disease were 6.27 times more
likely to change their jobs than to keep their jobs. Another MLR analysis, which is
not presented in the table, revealed a marginal effect (B = 0.74, SE = 0.44, p < .10)
that participants who suffered from lung disease were 2.10 times more likely to
retire than to change their jobs (see Table 2).
For minor health conditions, it was found that the incidence of arthritis and
diabetes significantly predicted participants’ retirement decision. Specifically,
participants who suffered from arthritis were 1.93 times more likely to retire than
to keep their jobs. It was also found that participants who suffered from diabetes
were 3.37 times more likely to retire than to keep their jobs. In addition, par-
ticipants who suffered from arthritis were 1.97 times more likely to change their
jobs than to keep their jobs. Participants who suffered from diabetes were also
3.33 times more likely to change their jobs than to keep their jobs. Additional
MLR analyses, which are not presented in the table, did not find evidence that
minor health conditions differentiate participants in terms of the probability of
choosing retirement and the probability of changing jobs (see Table 2).
DISCUSSION
Beehr and Adams (2003) recently noted that, “There is much that we already
know and much yet to be learned about retirement decisions and retired life”
(p. 293). In the same edited text, Barnes-Farrell (2003) discusses a variety of
attitudinal and other variables (e.g., worker attitudes, job conditions, organi-
zational climate, social pressures) that may influence the retirement decision-
making process. So, while we have chosen to focus on specific health concerns
in this study, it should be made clear that there are a variety of factors, both
individual and contextual, that potentially influences the retirement decision.
Thus, the retirement process is indeed a complex process with many factors
potentially playing a role.
HEALTH AND RETIREMENT DECISIONS / 155
Tab
le2
.E
stim
ate
dC
oeffic
ien
tsan
dO
dd
sR
atio
sfo
rH
ealth
Co
nd
itio
ns
inM
ultin
om
ialLo
gis
tic
Reg
ressio
n
Mo
del1
(Majo
rh
ealth
co
nd
itio
ns)
Mo
del2
(Min
or
health
co
nd
itio
ns)
Estim
ate
sS
EO
dd
sra
tio
Estim
ate
sS
EO
dd
sra
tio
Retire
dg
rou
p
Inte
rcep
t
Co
ntr
ols
Ag
e
Gen
der
Eth
nic
ity
Inco
me
Majo
rh
ealth
co
nd
itio
n
Lu
ng
dis
ease
Heart
att
ack
Can
cer
Str
oke
–1
0.8
7**
.20
**
.41
–.2
4
–.0
4
2.5
8**
–.3
3
1.5
8*
.93
1.6
9
.03
.29
.35
.06
.78
.51
.80
1.0
5
1.2
2
1.5
1
.79
.96
13
.14
.72
4.8
4
2.5
4
Retire
dg
rou
p
Inte
rcep
t
Co
ntr
ols
Ag
e
Gen
der
Eth
nic
ity
Inco
me
Min
or
health
co
nd
itio
n
Art
hri
tis
Hyp
ert
en
sio
n
Dia
bete
s
Fo
ot
pro
ble
ms
Bro
ken
bo
nes
Inco
ntin
en
ce
–1
0.8
7**
.19
**
.49
–.1
0
–.0
4
.66
*
–.3
8
1.2
1*
.49
–.2
1
–.5
7
1.6
7
.03
.29
.36
.06
.29
.32
.59
.31
.72
.62
1.2
1
1.6
3
.91
.96
1.9
3
.68
3.3
7
1.6
2
.81
.57
156 / SHULTZ AND WANG
Jo
bch
an
ge
gro
up
Inte
rcep
t
Co
ntr
ols
Ag
e
Gen
der
Eth
nic
ity
Inco
me
Majo
rh
ealth
co
nd
itio
n
Lu
ng
dis
ease
Heart
att
ack
Can
cer
Str
oke
�2
df
–.6
9
.00
.58
.12
–.1
3
1.8
3*
–.3
5
.52
–.0
8
10
6.0
3**
16
1.8
1
.03
.34
.41
.07
.89
.83
1.1
0
1.3
1
1.0
0
1.7
8
1.1
3
.88
6.2
7
.71
1.6
7
.93
Jo
bch
an
ge
gro
up
Inte
rcep
t
Co
ntr
ols
Ag
e
Gen
der
Eth
nic
ity
Inco
me
Min
or
health
co
nd
itio
n
Art
hri
tis
Hyp
ert
en
sio
n
Dia
bete
s
Fo
ot
pro
ble
ms
Bro
ken
bo
nes
Inco
ntin
en
ce
–.5
2
–.0
1
.52
.12
–.1
3
.68
*
–.2
1
1.2
0*
–.0
5
–.1
4
–1
.09
96
.94
**
20
1.8
6
.03
.35
.43
.07
.35
.41
.61
.40
.87
1.1
2
1.0
0
1.6
9
1.1
3
.86
1.9
7
.81
3.3
3
.96
.87
.34
No
te:
Part
icip
an
tsw
ho
kep
tth
eir
job
sw
ere
desig
nate
das
the
refe
ren
ce
gro
up
.D
ata
was
weig
hed
based
on
eth
nic
ity.
*p
<.0
5.**p
<.0
1.
HEALTH AND RETIREMENT DECISIONS / 157

However, as Barnes-Farrell (2003) points out, “. . . it is clear that both health
and wealth play important roles in the decision to retire and the timing of
retirement, largely because they place important constraints on a worker’s ability
to carry out a preferred path of action . . . [in doing so they] mitigate the influence
of other individual and contextual variables that would otherwise lead workers
to remain on the job or retire from the workplace” (p. 159). Thus, we must better
understand how health status influences the retirement process before moving
on to examine other (secondary) factors.
Therefore, in the present study we extended previous research in several
important ways to better understand the health precursors to retirement and job
changes in late career in more detail. First, we evaluated specific health conditions
that older individuals (ages 47-64) suffer from, reporting these separately as
“major health conditions” and “minor health conditions.” In addition, these health
conditions were reported separately for those who subsequently retired, those
who remained employed in the same job, and those who changed jobs over an
eight-year period (1986 to 1994). The results of the present study strongly
support both Colsher et al.’s (1988) empirical findings and Feldman’s (1994)
propositions. That is, the major health conditions of lung disease and cancer are
more likely to lead to retirement, whereas minor health conditions of diabetes
and arthritis are more likely to lead to either retirement or job changes, at least for
those in the 47-64 age range. Future research should include what Feldman calls
psychosomatic illnesses to determine if they too are likely to results in job changes
versus retirement or continuing to work in the same job at older ages.
Interestingly, another important extension of the present research, the use of
longitudinal data, may have contributed to the fact that only half (5 of 10) of the
health conditions showed statistically significant differences (see Table 1). This
lack of statistical significance may be due in part to the low number of participants
(i.e., low power) in the “changed jobs” (N = 66) category. Future studies should
use longer time intervals and/or larger initial samples to examine these issues.
In addition, the low prevalence rate for major health conditions such as stroke
also likely contributed to the lack of power to detect significant differences.
In addition, the difficulty in defining and measuring retirement should be noted.
Feldman (1994), for example, pointed out that retirement can be defined in
self-report, labor force participation, pension receipt, and several other forms. In
the present study we used self-report of current employment status at Wave III
(1994). Thus, the same individuals currently working part-time who have “retired”
from career jobs may well report different employment statuses (Shultz, 2003). In
a similar vein, we used self-report measures of illness as well. Thus, future
researchers should try to confirm self-reported health conditions with actual
medical records. Given the increased use of electronic medical records, this may
be practical in just a few years.
Better understanding of the specific physical health related factors that
influence employment decisions at older ages would help both researchers and
158 / SHULTZ AND WANG

organizations to better predict and understand the retirement process. In particular,
specific health conditions, which put individuals at risk for premature retirement,
can be identified, as well as identifying which conditions play the greatest role in
the decision to retire (Colsher et al., 1988). However, recent preventive strategies
may already be reducing major illnesses such as heart disease (via reduced fat
diets, increased exercise, and cholesterol lowering drugs) and lung disease (via
reduced tobacco use), thus reducing the risks of the need to change jobs late in
ones career or retire early altogether. Still, retirement and employment counselors
who are aware of the health conditions associated with the need to change jobs or
retire early at later ages can provide targeted counseling to individuals deemed
to be “at risk” for such conditions.
In addition, future research should incorporate organizational factors that
might impact the relationship between health and retirement decisions. For
example, given an older employee might be experiencing a chronic major health
condition or minor health condition, what would be the impact of the loss of
health insurance upon her retirement decision? In terms of job changes, what
options exist within her organization for reduced work schedules or for light duty
assignments? What job redesign processes could be implemented to assist older
workers to remain employed versus having to retire or change jobs (Jex et al.,
2007)? What types of social supports exist in the employee’s work and home
environments that might help her to deal with her physical condition(s)? Other
psychosocial variables (e.g., job satisfaction or organizational commitment), no
doubt, interact with current health conditions to impact one’s retirement and late
career job decisions as well, and so should be examined in future research
(Barnes-Farrell, 2003).
In conclusion, although this study served as an important first step in better under-
standing how specific physical health conditions influence later life employment
decisions, it was just a first step. Additional, primary research with larger samples
and psychometrically stronger, well-established scales is clearly warranted. In
doing so, we will gain a better understanding of the specific health precursors to job
changes and early retirements at older ages, as well as eventually determine how
these specific health factors interact with other known predictors of retirement
(e.g., wealth, job commitment) in the complex retirement decision making process.
ACKNOWLEDGMENTS
This research was begun while the first author was on sabbatical and serving
as a post-doctoral fellow at the Ethel Percy Andrus Gerontology Center at
the University of Southern California. He thanks the University of Southern
California for providing financial support through a National Institute on Aging
training grant (No. T32-AG00037). The authors also thank Deborah Olson,
Elizabeth Klonoff, and two anonymous reviewers for their comments on earlier
versions of this article.
HEALTH AND RETIREMENT DECISIONS / 159
APPENDIX
Physical Health Measures
Chronic conditions experienced in the last 12 months (scored: 0 = not experi-
enced, 1 = experienced).
• arthritis/rheumatism
• lung disease
• hypertension
• heart attacks or heart trouble
• diabetes
• cancer/malignant tumor
• foot problems
• stroke
• fracture or broken bones
• incontinence
REFERENCES
Adams, G. A., & Beehr, T. A. (1998). Turnover and retirement: A comparison of their
similarities and differences. Personnel Psychology, 51, 643-665.
Adams, G. A., & Beehr, T. A. (Eds.). (2003). Retirement: Reasons, processes, and results.
New York: Springer Publishing.
Barnes-Farrell, J. L. (2003). Beyond health and wealth: Attitudinal and other influences
on retirement decision-making. In G. A. Adams & T. A. Beehr (Eds.), Retirement:
Reasons, processes, and results (pp. 159-187). New York: Springer Publishing.
Beehr, T. A., & Adams, G. A. (2003). Concluding observations and future endeavors.
In G. A. Adams & T. A. Beehr (Eds.), Retirement: Reasons, processes, and results
(pp. 293-298). New York: Springer Publishing.
Colsher, P. L., Dorfman, L. T., & Wallace, R. B. (1988). Specific health conditions and
work-retirement status among the elderly. The Journal of Applied Gerontology, 7,
485-503.
Costa, D. L. (1998). The evolution of retirement: An American economic history,
1880-1990. Chicago, IL: University of Chicago Press.
Cude, R., & Jablin, F. M. (1992). The paradoxical impact of organizational commitment.
Journal of Managerial Issues, 4, 31-45.
Farr, J. L., & Ringseis, E. L. (2002). The older worker in organizational context: Beyond
the individual. In C. L. Cooper & I. T. Robertson (Eds.), International review of
industrial and organizational psychology (Vol. 17, pp. 31-76). Chichester, England:
John Wiley.
Feldman, D. C. (1994). The decision to retire early: A review and conceptualization.
Academy of Management Review, 19, 285-311.
Hansson, R. O., DeKoekkoek, P. D., Neece, W., & Patterson, D. W. (1997). Successful
aging at work: Annual review, 1992-1996: The older worker and transitions to retire-
ment. Journal of Vocational Behavior, 51, 202-233.
Hardy, M. A., & Quadagno, J. (1995). Satisfaction with early retirement: Making choices
in the auto industry. Journals of Gerontology: Social Sciences, 50B, S217-226.
160 / SHULTZ AND WANG

Hedge, J. W., Borman, W. C., & Lammlein, S. E. (2006). The aging workforce: Realities,
myths, and implications for organizations. Washington, DC: American Psychological
Association.
Herzog, A. R., House, J. S., & Morgan, J. N. (1991). Relation of work and retirement to
health and well-being in older age. Psychology and Aging, 6, 202-211.
House, J. S. (2003). AMERICANS’ CHANGING LIVES: WAVES I, II, AND III, 1986,
1989, AND 1994 [computer file]. ICPSR version. Ann Arbor, MI: University of
Michigan, Institute for Social Research, Survey Research Center [producer], 2002. Ann
Arbor, MI: Inter-University Consortium for Political and Social Research [distributor].
House, J. S., Kessler, R. C., Herzog, A. R., Mero, R. P., Kinney, A. M, & Breslow, M. J.
(1992). Social stratification, age, and health. In K. W. Schaie, D. Blazer, & J. S. House
(Eds.), Aging, health behaviors, and health outcomes. Hillsdale, NJ: Lawrence Erlbaum
Associates, Publishers.
Jex, S. M., Wang, M., & Zarubin, A. (2007). Aging and occupational health. In K. S. Shultz
& G. A. Adams (Eds.), Aging and work in the 21st century (pp. 199-223). Mahwah, NJ:
Lawrence Erlbaum, Publishers.
Menard, S. W. (2001). Applied logistic regression analysis (2nd ed.). Sage University
Paper series on Quantitative Applications in the Social Sciences, 07-106. Thousand
Oaks, CA: Sage Publications, Inc.
Muller, C. F., & Boaz, R. F. (1988). Health as a reason or rationalization for being retired?
Research on Aging, 10, 37-55.
Schnittker, J. (2001). When is faith enough? The effects of religious involvement on
depression. Journal for the Scientific Study of Religion, 40, 393-411.
Shultz, K. S. (2003). Bridge employment: Work after retirement. In G. A. Adams &
T. A. Beehr (Eds.), Retirement: Reasons, processes, and results (pp. 214-241). New
York: Springer Publishing.
Shultz, K. S., Morton, K. R., & Weckerle, J. R. (1998). The influence of push and pull
factors on voluntary and involuntary early retirees’ retirement decision and adjustment.
Journal of Vocational Behavior, 53, 45-57.
Spicer, J. (2004). Making sense of multivariate data analysis: An intuitive approach.
Thousand Oaks, CA: Sage Publications, Inc.
Taylor, M. A., & Shore, L. M. (1995). Predictors of planned retirement age: An application
of Beehr’s model. Psychology and Aging, 10, 76-83.
Wegman, D. J., & McGee, J. P. (Eds.). (2004). Health and safety needs of older workers.
Committee on the Health and Safety Needs of Older Workers, Division of Behavioral
and Social Sciences and Education, National Research Council and the Institute of
Medicine. Washington, DC: National Academies Press.
Direct reprint requests to:
Kenneth S. Shultz
Department of Psychology
5500 University Parkway
California State University, San Bernardino
San Bernardino, CA 92407
e-mail: [email protected]
HEALTH AND RETIREMENT DECISIONS / 161





























