Embed Size (px)
Citation preview

The Millennium Development Goals and Human Rights: RealizingShared Commitments
Shyama KuruvillaFlavia BustreoPaul HuntAmarjit Singh
Human Rights Quarterly, Volume 34, Number 1, February 2012, pp.141-177 (Article)
Published by The Johns Hopkins University PressDOI: 10.1353/hrq.2012.0010
For additional information about this article
Access Provided by your local institution at 02/20/13 2:05AM GMT
http://muse.jhu.edu/journals/hrq/summary/v034/34.1.kuruvilla.html

HUMAN RIGHTS QUARTERLY
Human Rights Quarterly 34 (2012) 141–177 © 2012 by The Johns Hopkins University Press
The Millennium Development Goals and Human Rights: Realizing Shared Commitments
Shyama Kuruvilla,1 Flavia Bustreo,2 Paul Hunt,3 Amarjit Singh,4 Eric Friedman,5 Thiago Luchesi,6
1Shyama Kuruvilla is Senior Technical Officer at The Partnership for Maternal, Newborn and Child Health. She coordinated the development of the background paper on human rights for the UN Secretary-General’s Global Strategy for Women’s and Children’s Health in 2010. Her work focuses on global health policy and partnerships, and the interchange between scientific evidence and socio-political values. She previously worked at the Center for Global Health and Development, Boston University, and the London School of Hygiene and Tropical Medicine.
2Flavia Bustreo is Assistant Director-General at the World Health Organization (WHO) for Family, Women’s and Children’s Health. Previously she served as Director of The Partnership for Maternal, Newborn and Child Health. Dr. Bustreo was instrumental to the development of the UN Secretary-General’s Global Strategy for Women’s and Children’s Health in 2010. Her work has focused on policy development and implementation concerning maternal and child health, both at the domestic and global level.
3Paul Hunt is a professor of law at the University of Essex. In 2011 he served as a working group member for the Commission on Information and Accountability for Women’s and Children’s Health. Between 2002 and 2008, he was the UN Special Rapporteur on the right to the highest attainable standard of health. He is also a Member of the Human Rights Centre at the University of Essex and served as Director from 2001 to 2003. Between 1999 and 2002 he served as an independent expert on the UN Committee on Economic, Social and Cultural Rights.
4Amarjit Singh is an advocate and solicitor qualified in England and in Singapore. Currently, he is a Ph.D. candidate in the Department of Law at the London School of Economics and Political Science. His research covers: international law and regulation; compliance strategy and risks; human rights risks in international infrastructure projects; international investment law and political risk; and law of international organizations.
5 Eric Friedman is a Law Fellow at the O’Neill Institute for National and Global Health Law at Georgetown University. Previously, Friedman was Senior Global Health Policy Advisor at Physicians for Human Rights, where he focused on health systems and the global shortage of health workers, and sought to increase the extent to which U.S. global health policy incorporates the human right to health. He also served on the Board of the Global Health Workforce Alliance.
6Thiago Luchesi is a Ph.D. Candidate in International Law at the Graduate Institute, Geneva, specializing in the right to health under the Convention on the Rights of the Child. He is a Health and Human Rights Researcher at the Geneva Office of World Vision International and an active member of the Brazilian Early Childhood Forum. He has previously worked

Vol. 34142 HUMAN RIGHTS QUARTERLY
Stefan Germann,7 Kim Terje Loraas,8 Alicia Ely Yamin,9 Ximena Andion,10 Julio Frenk,11 and other members of the Working Group on the MDGs and Human Rights for the UN Secretary-General’s Global Strategy for Women’s and Children’s Health*
1. Partnership for Maternal, Newborn & Child Health (PMNCH), 2. World Health Organiza-tion (WHO), 3. University of Essex, 4. London School of Economics and Political Science, 5. Georgetown University, 6. World Vision International, 7. World Vision International, 8. Save the Children, Norway, 9. Harvard School of Public Health, 10. EQUIS: Justice for Women, 11. Harvard School of Public Health
* Other working group members in alphabetical order:
◼ Janne Andresen (Peace, Gender and Democracy Department, NORAD)◼ Berit Austveg (Norwegian Board of Health Supervision, Center for Human Rights) ◼ Reina Buijs (Ministry of Foreign Affairs, The Hague, The Netherlands)◼ Mara Bustelo (Office of the High Commissioner for Human Rights (OHCHR)) ◼ Jashodhara Dasgupta (Negotiating Rights, SAHAYOG, India)
in Brazil as a Human Rights and Policy Advisor at the Zero to Six Institute, a Brazilian NGO focusing on the rights of the child in early childhood.
7Stefan Germann is the Global Director for External Partnerships, Research & Learning of World Vision International’s Health, HIV and Nutrition team. For the past 18 years, he has been working in the field of HIV/AIDS, health, and community care of children. In 2002, he founded REPSSI, one of the leading agencies focusing on psychosocial issues for children affected by poverty, war, and AIDS.
8Kim Terje Loraas is the Advocacy Advisor at Save the Children Norway. She trained as a Social Anthropologist and has worked for over fifteen years on policy and advocacy focusing on the rights of indigenous populations and, more recently, on children’s rights.
9 Alicia Ely Yamin is the director of the Program on the Health Rights of Women and Children at the François-Xavier Bagnoud Center, Harvard School of Public Health. She is Chair of the Board of the Center for Economic and Social Rights and serves on the advisory boards of the International Initiative on Maternal Mortality and Human Rights, the Center for Policy Analysis on Trade and Health, as well as of several human rights and public health organi-zations in Latin America and internationally.
10 Ximena Andion has eleven years of experience working in the human rights field. She is currently the President and co-founder of EQUIS: Justice for Women and the Director of Strategic Development at the Information Group on Reproductive Choice. She was the International Advocacy Director at the Center for Reproductive Rights and before that she worked for the UN Office High Commissioner for Human Rights in Mexico and Guatemala.
11Julio Frenk is the Dean of the Faculty and T & G Angelopoulos Professor of Public Health and International Development at the Harvard School of Public Health and the Board Chair of The Partnership for Maternal, Newborn and Child Health. Dr. Frenk served as the Minister of Health of Mexico from 2000 to 2006. He was the founding director-general of the National Institute of Public Health in Mexico.
Acknowledgements
Special thanks to Helga Fogstad and Unni Silkoset from NORAD for convening the Work-ing Group on the MDGs and Human Rights for the UN Secretary-General’s Global Strategy for Women’s and Children’s Health, and to Carole Presern and Andres de Francisco from PMNCH for their advice on this paper.

2012 The Millennium Development Goals 143
◼ Helga Fogstad (Norwegian Agency for Development Coordination, NORAD)◼ Lynn Freedman (Mailman School of Public Health, Columbia University)◼ Helena Hofbauer (Center on Budget and Policy Priorities)◼ Claudia Garcia Moreno (World Health Organization (WHO))◼ Gill Greer (International Planned Parenthood Federation)◼ Arun Gupta (Indian International Baby Food Action Network Asia)◼ Meetali Kakad (CARE International)◼ Malcolm Langford (Norwegian Centre for Human Rights, Socio-Economic Rights
Program)◼ Jeffrey O’Malley (United Nations Development Programme)◼ Ignacio Saiz (Center for Economic and Social Rights, Spain and USA) ◼ Dan Seymour (UNICEF, Gender and Rights Unit) ◼ Unni Silkoset (NORAD)◼ Katerini Storeng (Section for International Health, University of Oslo)◼ Marta Seoane (PMNCH)◼ Tomas Solfaro (Nord Sud XXI)◼ Ann Starrs (Family Care International)◼ Marcus Stahlhofer (WHO)◼ Kim Terje Loraas (Save the Children, Norway office)◼ Kadidiatou Toure (PMNCH)◼ Claudia Trautvetter (GTZ, Germany)
AbSTRACT
Every preventable death poses a challenge to health, development, and hu-man rights initiatives. Although the Millennium Development Goals (MDGs) prioritize reducing maternal and child mortality, progress is unequal and the sustainability of related efforts beyond 2015 is a concern. Strategies that link the MDGs and human rights would facilitate more comprehensive, equitable, and sustainable progress in health and development. Strategies include: ensuring entitlements that link human rights provisions with laws and resources; building capacities for different contexts and challenges; promoting integration and innovation to catalyze progress; combating inequality and discrimination; committing to accountability for resources and results; and emphasizing sustainability.
I. INTRoDUCTIoN
Every year, over 350,000 women die from pregnancy and childbirth-related causes, and over seven million children under the age of five die, most from preventable causes.1 These preventable deaths pose a challenge to
1. World HealtH organization [WHo], Un CHildren’s FUnd [UniCeF], Un PoPUlation FUnd & tHe World Bank, trends in Maternal Mortality: 1990 to 2008 (2010), available at http://whqlibdoc.who.int/publications/2010/9789241500265_eng.pdf; UniCeF, WHo, tHe World Bank, & Un dePartMent oF eConoMiC and soCial aFFairs [Un desa], levels and trends

Vol. 34144 HUMAN RIGHTS QUARTERLY
health, development, and human rights efforts; they also reflect systematic violations of human rights. In the Millennium Declaration of 2000, world leaders committed to an unprecedented and ambitious global initiative with eight Millennium Development Goals (MDGs) to be achieved by 2015. The MDGs include the reduction of maternal and child mortality, as well as goals related to alleviating poverty and promoting sustainable develop-ment. World leaders vowed to: “spare no effort to promote . . . respect for all internationally recognized human rights.”2
The human rights framework is comprised of internationally recognized human rights, and the institutions and procedures to facilitate and monitor their implementation. There are also legally binding human rights obligations upon governments, which inform international cooperation. The Universal Declaration of Human Rights (UDHR) was adopted by the United Nations General Assembly (UNGA) in 1948.3 Building on this, and specifying different aspects of universal human rights, are nine core international treaties (Table 1). These have independent committees of experts to monitor implementa-tion and, in some cases, to address complaints.
in CHild Mortality (2011), available at http://www.unicef.org/media/files/Child_Mortal-ity_Report_2011_Final.pdf ; WHo, CoUntdoWn to 2015: taking stoCk oF Maternal, neW-Born and CHild sUrvival, 7 (2010) [hereinafter CoUntdoWn to 2015], available at http://whqlibdoc.who.int/publications/2010/9789241599573_eng.pdf.
2. United Nations Millennium Declaration, G.A. Draft Res. 55/L.2, U.N. GAOR, 55th Sess., at 6, ¶ 24, U.N. Doc. A/55/L.2 (2000).
3. Universal Declaration of Human Rights, adopted 10 Dec. 1948, G.A. Res. 217A (III), U.N. GAOR, 3d Sess., U.N. Doc. A/RES/3/217A (1948).
4. Office of the High Commission of Human Rights [OHCHR], International Law (1996–2007), available at http://www2.ohchr.org/english/law/index.htm#core.
Table 1: Core International Human Rights Treaties4
Human rights treaty or convention Acronym Date Treaty ratified body
International Convention on the ICERD 21 Dec CERD Elimination of All Forms of Racial 1965 Discrimination
International Covenant on Civil and ICCPR 16 Dec CCPR Political Rights 1966
International Covenant on Economic, ICESCR 16 Dec CESCR Social and Cultural Rights 1966
Convention on the Elimination of All Forms CEDAW 18 Dec CEDAW of Discrimination against Women 1979
Convention against Torture and Other Cruel, CAT 10 Dec CAT Inhuman or Degrading Treatment or Punishment 1984

2012 The Millennium Development Goals 145
Additionally, the International Labor Organization’s (ILO) Maternity Protection Convention is concerned with maternity leave and ensuring that pregnant women are not given tasks that could endanger their health and pregnancy.5
The international human rights treaties listed above detail other specific rights, such as: participation in public affairs; self-determination and non-discrimination; the highest attainable standard of health; just and favor-able working conditions; food; and education. The UN General Assembly continues to play a role in extending human rights protection and recently declared access to clean water to be a human right.6
There are also regional human rights bodies. These include: the African Commission on Human and Peoples’ Rights, the African Court of Human Rights, the Inter-American Commission on Human Rights, the Inter-American Court of Human Rights, the European Court of Human Rights, and the Eu-ropean Committee of Social Rights.
There are numerous other instruments relating to human rights, although not all have the same legal effect. As the United Nations Office of the High Commissioner for Human Rights (OHCHR) explains: “The legal status of these instruments varies: declarations, principles, guidelines, standard rules and recommendations have no binding legal effect, but such instruments
Table 1: continued
Human rights treaty or convention Acronym Date Treaty ratified body
Convention on the Rights of the Child CRC 20 Nov CRC 1989
International Convention on the Protection ICRMW 18 Dec CMW of the Rights of All Migrant Workers and 1990 Members of Their Families
International Convention for the Protection CPED 20 Dec CED of All Persons from Enforced Disappearance 2006
Convention on the Rights of Persons CRPD 13 Dec CRPD with Disabilities 2006
5. Maternity Protection Convention, (ILO No. C003), §§ 1–2, adopted 28 Nov. 1919 (entered into force 13 June 1921), available at http://www.ilo.org/ilolex/cgi–lex/convde.pl?C003.
6. United Nations, General Assembly Adopts Resolution Recognizing Access to Clean Water, Sanitation, adopted 28 July 2010, G.A. Res. 10967, U.N. GAOR, U.N. Doc. GA/10967 (2010), available at http://www.un.org/News/Press/docs/2010/ga10967.doc.htm.

Vol. 34146 HUMAN RIGHTS QUARTERLY
have an undeniable moral force and provide practical guidance to States in their conduct.”7
A number of core concepts or principles inform the nature of interna-tionally agreed human rights, such as the concept that human rights are interdependent and indivisible. This recognizes the fact that human rights overlap in their scope, that they are mutually reinforcing, and that none is more intrinsically valuable than another.8 Progressive realization is another important concept through which, “the international code of human rights recognizes that many human rights will be realized progressively and are subject to the availability of resources.”9 However, even if resources are limited, there is nevertheless an immediate, ongoing obligation to use all appropriate means and maximum available resources, in a non-retrogressive manner, to assure the realization of rights. This involves applying the ap-propriate priorities when it comes to resource allocation, domestically and internationally, because “maximum resources” is defined not only by refer-ence to the state’s resources, but also by reference to resources available through international assistance.10 Internationally, this requires commitments from other countries to assist—or at the very least not to undermine—the efforts of a particular state to provide for human rights. The critical challenge is to implement international human rights obligations within countries, and it is here that efforts towards achieving the MDGs can play an important role.
II. HUMAN RIGHTS AND THE MILLENNIUM DEVELopMENT GoALS
The MDGs set out specific goals within the more comprehensive human rights framework (Table 2).11
7. OHCHR, supra note 4, at 2. 8. Vienna Declaration and Programme of Action, adopted 25 June 1993, U.N. GAOR, World
Conf. on Hum. Rts., 48th Sess., 22d plen. mtg., ¶¶ 5–8, U.N. Doc. A/CONF.157/23 (1993), reprinted in 32 I.L.M. 1661 (1993).
9. oHCHr, HUMan rigHts and Poverty redUCtion: a ConCePtUal FraMeWork 22 (2004), avail-able at: http://www2.ohchr.org/english/issues/poverty/docs/povertyE.pdf.
10. Flavia Bustreo & Curtis F. J. Doebbler, Making Health an Imperative of Foreign Policy: The Value of a Human Rights Approach, 12 HealtH & HUM. rts. 47, 52–53 (2010).
11. Millennium Declaration, supra note 2; International Covenant on Economic, Social and Cultural Rights, adopted 16 Dec. 1966, G. A. Res. 2200 (XXI), U.N. GAOR, 21st Sess, art. 2, 6, 9, 11–14, U.N. Doc. A/6316 (1966), 993 U.N.T.S. 3 (entered into force 3 Jan. 1976) [hereinafter ICESCR]; Convention on the Elimination of All Forms of Discrimi-nation Against Women, adopted 18 Dec. 1979, G.A. Res. 34/180, U.N. GAOR, 34th Sess., art. 10–12, 14, U.N. Doc. A/34/46 (1980), 1249 U.N.T.S. 13 (entered into force 3 Sept. 1981); International Convention on the Elimination of All Forms of Racial Dis-crimination, adopted 21 Dec. 1965, G.A. Res. 2106 (XX), U.N. GAOR, 20th Sess., art. 5, 660 U.N.T.S. 195 (entered into force 4 Jan. 1969), reprinted in 5 I.L.M. 352 (1966); Convention on the Rights of Persons with Disabilities, adopted 13 Dec. 2006, G.A. Res. 61/106, U.N. GAOR, 61st Sess., art. 6–7, 24, U.N. Doc. A/RES/61/106 (entered into
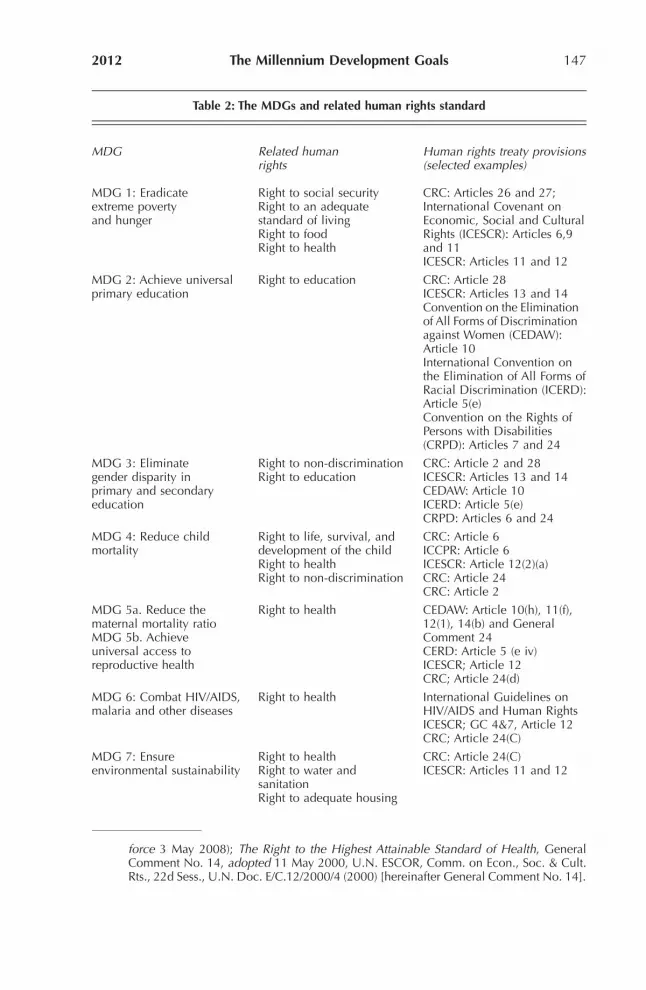
2012 The Millennium Development Goals 147
force 3 May 2008); The Right to the Highest Attainable Standard of Health, General Comment No. 14, adopted 11 May 2000, U.N. ESCOR, Comm. on Econ., Soc. & Cult. Rts., 22d Sess., U.N. Doc. E/C.12/2000/4 (2000) [hereinafter General Comment No. 14].
Table 2: The MDGs and related human rights standard
MDG Related human Human rights treaty provisions rights (selected examples)
MDG 1: Eradicate Right to social security CRC: Articles 26 and 27; extreme poverty Right to an adequate International Covenant on and hunger standard of living Economic, Social and Cultural Right to food Rights (ICESCR): Articles 6,9 Right to health and 11 ICESCR: Articles 11 and 12
MDG 2: Achieve universal Right to education CRC: Article 28 primary education ICESCR: Articles 13 and 14 Convention on the Elimination of All Forms of Discrimination against Women (CEDAW): Article 10 International Convention on the Elimination of All Forms of Racial Discrimination (ICERD): Article 5(e) Convention on the Rights of Persons with Disabilities (CRPD): Articles 7 and 24
MDG 3: Eliminate Right to non-discrimination CRC: Article 2 and 28 gender disparity in Right to education ICESCR: Articles 13 and 14 primary and secondary CEDAW: Article 10 education ICERD: Article 5(e) CRPD: Articles 6 and 24
MDG 4: Reduce child Right to life, survival, and CRC: Article 6 mortality development of the child ICCPR: Article 6 Right to health ICESCR: Article 12(2)(a) Right to non-discrimination CRC: Article 24 CRC: Article 2
MDG 5a. Reduce the Right to health CEDAW: Article 10(h), 11(f), maternal mortality ratio 12(1), 14(b) and General MDG 5b. Achieve Comment 24 universal access to CERD: Article 5 (e iv) reproductive health ICESCR; Article 12 CRC; Article 24(d)
MDG 6: Combat HIV/AIDS, Right to health International Guidelines on malaria and other diseases HIV/AIDS and Human Rights ICESCR; GC 4&7, Article 12 CRC; Article 24(C)
MDG 7: Ensure Right to health CRC: Article 24(C) environmental sustainability Right to water and ICESCR: Articles 11 and 12 sanitation Right to adequate housing

Vol. 34148 HUMAN RIGHTS QUARTERLY
Though human rights and the MDGs are clearly linked and constitute shared global commitments, in practice there is surprisingly little that con-nects them. In 2004, Philip Alston described the MDGs and human rights as “ships passing in the night,”12 and explained why the MDGs developed more momentum in capturing global attention and resources than other human rights and development efforts:
First, the Goals are limited and selective and thus prioritize certain objectives over the many others endorsed every year by the international community. Second, they are deliberately designed to be measured and thus to provide a basis for accountability. Third, they are time-bound, thereby bringing greater precision to goals that might otherwise be said only to be subject to “progressive realization.” Fourth, an extensive institutional apparatus has been set up to promote them.13
From a human rights perspective, the selectivity is problematic, as the real-ization of rights requires broad measures to change the structures, policies, and social relationships that underlie poverty. The time-bound nature of the MDGs also raises questions about what will happen after 2015 to sustain efforts. Further, equity concerns were largely invisible in the formulation of the MDGS, despite the evidence that barriers to achieving the MDGs relate to inequalities in resources to realize human rights.14 United Nations Development Programme (UNDP) Administrator Helen Clark highlights the conclusions of a 2010 International Assessment of fifty countries showing that:
Women, rural inhabitants, ethnic minorities, people with disabilities and other excluded groups often lag well behind national averages of progress on MDG targets. . . . The denial of human rights and the persistence of exclusion, dis-
Table 2: continued
MDG Related human Human rights treaty provisions rights (selected examples)
MDG 8: Global partnership Achieve international UN Charter: Article 1(3) for development cooperation to realize ICESCR: Article 2 human rights CRC : Article 4
12. Philip Alston, Ships Passing in the Night: The Current State of the Human Rights and Development Debate Seen Through the Lens of the Millennium Development Goals, 27 HUM. rts. Q. 755, 755 (2005).
13. Id. at 756. 14. Un develoPMent PrograMMe [UndP] , WHat Will it take to aCHieve tHe MillenniUM develoP-
Ment goals? an international assessMent 3–4, 16–17, 38 (2010), available at http://content.undp.org/go/cms-service/stream/asset/?asset_id=2620072.

2012 The Millennium Development Goals 149
crimination and a lack of accountability are . . . barriers to the pursuit of human development and the MDGs.15
Women’s and children’s health are a bellwether for all MDGs, and the area where there has been the least progress and where there is the most urgent need.16 In 2010, with five years left to achieve the MDGs, United Nations Secretary-General Ban Ki-moon, supported by the Partnership for Maternal, Newborn and Child Health (PMNCH), led a global consultation to develop the Global Strategy for Women’s and Children’s Health (the Global Strategy). The Global Strategy states that the MDGs represent “human needs and basic rights that every individual around the world should be able to enjoy.”17
Both the human rights and MDG communities increasingly recognize that global efforts to achieve their respective aims overlap and complement each other in many areas. There are also extensive analyses on the potential links between the MDGs and human rights, critiques on the lack of progress to realize this potential, and recommendations to strengthen linkages.18
The Global Strategy offers a significant opportunity to bring together and harness the complementarities between the MDGs and human rights commitments. To help translate this aspiration into application, this paper reviews legal and policy analyses about how the links between human rights and the MDGs can, and have, worked in practice to the mutual benefit of both systems. Recommendations on how to leverage the com-plementarities between the human rights framework and the MDGs are discussed with reference to six strategic actions: (1) assuring entitlements that operationalize human rights provisions with resources; (2) building capacities for different contexts and challenges; (3) promoting integration and innovation to catalyze progress; (4) combating inequality and discrimi-nation; (5) committing to accountability for resources and results; and (6) emphasizing sustainability.
15. OHCHR, Human Rights: Key to Keeping the MDG Promise of 2015 (2 July 2010), avail-able at http://www.ohchr.org/EN/NewsEvents/Pages/MDGNYEvent02072010.aspx.
16. Un, tHe MillenniUM develoPMent goals rePort 2010 (2010) [hereinafter MDG rePort], available at http://www.un.org/millenniumgoals/pdf/MDG%20Report%202010%20En%20r15%20-low%20res%2020100615%20-.pdf.
17. Un seCretary-general Ban ki-Moon, gloBal strategy For WoMen’s and CHildren’s HealtH (2010), available at http://www.everywomaneverychild.org/images/content/files/global_strategy/full/20100914_gswch_en.pdf.
18. Alston, supra note 12, at 755; The John D. and Catherine T. MacArthur Foundation & Paul Hunt, The Millennium Development Goals and the Right to the Highest Attainable Standard of Health 8 (2007) available at http://www.macfound.org/atf/cf/%7BB0386CE3-8B29-4162-8098-E466FB856794%7D/Hunt_Population.pdf; Paul J. Nelson, Human Rights, the Millennium Development Goals, and the Future of Development Coopera-tion, 35 World dev. 2041 (2007).

Vol. 34150 HUMAN RIGHTS QUARTERLY
A. ASSURE ENTITLEMENTS THAT opERATIoNALIzE HUMAN RIGHTS pRoVISIoNS wITH RESoURCES
Individuals have human rights—the right to health, for example—but unless the required resources are in place to access health services, one cannot enjoy these rights. Henry Shue explains this distinction:
A proclamation of a right is not the fulfillment of a right, any more than an airplane schedule is a flight. A proclamation [an example of which would be the domestic legal enactment of an international human right] may or may not be an initial step toward the fulfillment of the rights listed. It is frequently the substitute of the promise in place of the fulfillment.19
When a right is fulfilled it means the rights-holder “is enjoying the substance of the right” or, in short, enjoying or realizing the right itself.20 An example of steps for realizing human rights, translated in terms of resources and ac-tions, is set out in the Convention on Economic, Social and Cultural Rights as follows:
Each State Party to the present Covenant undertakes to take steps, individually and through international assistance and co-operation, especially economic and technical, to the maximum of its available resources, with a view to achieving progressively the full realization of the rights recognized in the pres-ent Covenant by all appropriate means, including particularly the adoption of legislative measures.21
While the MDGs are not rights in themselves, there is an overlap between a government’s MDG commitments and its human rights obligations under international law, as set out in Table 1. Entitlements forge an essential link between efforts to realize the MDGs and human rights. Amartya Sen defines the entitlements of any individual as resulting from a specification of the rights-structure and the resources and opportunities that enable an individual to access these rights.22 When governments pass legislation and allocate resources so that people can access adequate and appropriate MDG-related services, they are in effect enhancing people’s entitlements, so that people can better enjoy their rights. Of course, in any one country at any point in time, MDG gains may be incomplete or uneven, masking discrimination. However, where those gains have been made, the enjoyment of important aspects of human rights in that country has increased.23 The idea of entitle-
19. Henry sHUe, BasiC rigHts: sUBsistenCe, aFFlUenCe, and U.s. Foreign PoliCy 15 (2d ed.1996). 20. Id. at 16. 21. ICESCR supra note 11, art. 2. 22. Amartya Sen, The Right Not To Be Hungry, in volUMe 2: PHilosoPHy oF sCienCe 347–48
(Guttorm Fløistad ed., 1982); aMartya sen, Poverty and FaMines: an essay on entitleMent and dePrivation 2 (1981).
23. Nadine Sika, The Millennium Development Goals: Prospects for Gender Equality in the Arab World, 12 J. int’l WoMen’s stUd. 12 (2011).

2012 The Millennium Development Goals 151
ments therefore connects MDGs and human rights through the operational lens of the laws and resources required to enjoy the rights.
Resources that facilitate the enjoyment of rights are not only provided by governments. Many other actors, including civil society organizations and the private sector, may provide resources that enable the enjoyment of rights, and may be expected to do so. Shue explains:
A right is ordinarily a justified demand that some other people make some arrangements so that one will still be able to enjoy the substance of the right even if—actually, especially if—it is not within one’s own power to arrange on one’s own to enjoy the substance of the right. Suppose people have a right to physical security. Some of them may nevertheless choose to hire their own private guards. . . . But they would be justified, and everyone else is justified, in demanding that somebody somewhere make some effective arrangements to establish and maintain security. Whether the arrangements should be govern-mental or non-governmental; local, national, or international; participatory or non-participatory, are all difficult questions.24
As Shue summarizes, a “right is the rational basis . . . for a justified demand.”25 The importance of making the connection between MDGs and human rights lies in giving rights-holders the basis for demanding that efforts at achieving the MDGs reach them. This can be regarded as the “demand side” of human rights.26 If the connection between MDGs and human rights is made clear to people, they can demand MDG interventions as claimants of rights and not as passive recipients of government policy or foreign aid.
If a government has ratified international human rights treaties but has not given them effect in national laws and policies, accountability and enforcement are diminished. Nevertheless, human rights treaties still bind governments under international law. Therefore, internationally recognized human rights justify citizens’ claims on their government, including for the provision of services such as health care, education, and water.
Two broad consequences flow from this. First, there could be increased demand for services, which would then need to be adapted to the require-ments of target populations. Feedback from populations in this regard would also help calibrate MDG interventions to the needs of local populations, and more relevant interventions could increase buy-in and sustainability. Secondly, in their role as rights-holders, people may seek increased ac-countability from those providing MDG interventions—be they state or local governments, UN agencies, foreign or local NGOs, or the private sector. These two consequences reinforce one another, since responsiveness
24. sHUe, supra note 19, at 16. 25. Id. at 14. 26. Id. at 13.

Vol. 34152 HUMAN RIGHTS QUARTERLY
is intrinsic to the concept of accountability, and is something to which an engaged population can contribute. However, because of socio-economic and other inequalities, individuals may have equal rights, but very different resources and opportunities to claim and enjoy their rights.
The “supply side” of entitlements refers to the provision of goods and services to the right-holders by government and non-government agencies.27 These goods and services constitute the effective arrangements (with an emphasis on “effective”) made by governments and non-state actors so that people may enjoy their rights, especially if they lack the power to access these arrangements on their own. In other words, the supply side of rights is especially concerned with those rights-holders with less access to resources. Efforts made to achieve the MDGs mainly relate to the supply side of human rights and are thereby concerned with improving people’s endowments, so they can enjoy the human rights that directly relate to particular MDGs.
The 2003 health reforms in Mexico introduced a public insurance scheme known as Seguro Popular. This provides an example of how entitlements were conceptualized and made operational by linking rights to legislation and resources (Box 1).
27. See Sen, supra note 22. 28. Julio Frenk & Octavio Gomez-Dantes, Ideas and Ideals: Ethical Basis of Health Reform
in Mexico, 373 lanCet 1406 (2009).
box 1. From rights to entitlements: the example of Seguro popular in Mexico28
The right to health care has been recognized in the Mexican Constitution since 1983, but in practice not all Mexican citizens enjoyed this right. Specifically, 50 million people lacked guaranteed access to health services. Mexican citizens’ lack of access to health care represented an endowment or resource deficit that had to be addressed.
The 2003 health reforms in Mexico introduced a public insurance scheme known as Seguro Popular. Frenk and Gomez-Dantes explain how these reforms explicitly positioned health care as a social right, and not as a commodity or a privilege. To ensure that people had the required resources to enjoy their right to health care, the reform arrangements consisted of legal incentives and support, as well as two specific packages of services. The legal incentives took the form of the legal requirement that the number of families affiliated to the Seguro Popular scheme would determine state budgets. This meant that state governments had an incentive to sign up all families within the state to the scheme, ensuring universal coverage.
Arrangements were made in such a way that, once families had been signed up to the scheme, the state then had to deliver the services outlined in the two service

2012 The Millennium Development Goals 153
Recognizing the human rights dimension to MDGs can help direct MDG interventions to those with the greatest need. The human rights framework facilitates this by emphasizing that health coverage within a country needs to be non-discriminatory in law and practice, and prompts the redistribution of resources to ensure all communities are equitably served. For example, if an MDG intervention targeted only urban communities, adding the hu-man rights framework would also take account of rural communities. Since resources are limited, this may necessitate a scaling back of the range of services being delivered to the urban community in order for similar services to be delivered to the rural community. As a result, a basic set of services would be delivered throughout the country.
box 1: continued
packages. Part of each package involved making people aware that under the law those signed up to the scheme would “have access to all interventions included in both packages and to the respective drugs.” Once people were made aware of this they were empowered to access and demand these services, according to those involved in designing and implementing the Seguro Popular reform.
Interventions to boost endowments are necessarily limited by the availability of resources. Given the government’s limited resources, the two service packages in Seguro Popular were designed to be as cost-effective as possible. They were costed on the basis of “the largest amount of benefits for the available resources,” meaning that they were more often than not targeted at the poor—the group with the fewest endowments.
Given the ethical framework and values underpinning Seguro Popular, the cost-effectiveness of the interventions was buttressed by “social acceptability criteria.” These accounted for the preferences of the health profession, and of society as a whole, through a consultative process. The government also made the necessary investment to improve infrastructure, equipment, and personnel.
Finally, the endowment arrangements required every health-care facility to be accredited according to standardized protocols. This was important to ensure that coverage throughout the country was standardized not only in terms of quality but also in terms of the resources required to provide the services stipulated. Each of these arrangements was designed to boost the endowments of the individuals who joined the Seguro Popular scheme.
This health reform from Mexico illustrates how a focus on improving the enjoy-ment of rights leads to the instituting of required endowments and resources, such as the Seguro Popular law and packages. This has to be concomitant with the empowerment of people so that they can demand and enjoy their rights.

Vol. 34154 HUMAN RIGHTS QUARTERLY
As in Mexico, this outcome might be achieved by the adoption of standardized protocols and packages, demonstrating further—as mentioned above and shown in the example from Mexico—that the human rights dimension of the intervention can prompt demands and accountability for interventions. This approach also helps ensure that interventions such as the MDGs enhance endowments to enable the enjoyment of rights, and that related arrangements are more effective, because they are tailored to local demands and needs, rather than designed as one-size-fits-all interventions.
The concept of entitlements can help reconcile the potential tension between those arguing for the specific, targeted focus of the MDGs, and those arguing for health and development efforts to be situated within a human rights framework. The need to dedicate specific resources to assure citizens’ enjoyment of their rights can be linked with the principle of progres-sive realization of human rights. From this view, the MDGs form part of the continuum of endowments and achievements, which together can constitute progressive steps towards the comprehensive realization of human rights.
b. build Capacities for Different Contexts and Challenges
Another complementarity between achieving the MDGs and ensuring human rights is the fact that capacities and context matter. In health and develop-ment work, there is strong empirical evidence to support this fundamental principle. As the report of the Commission on the Social Determinants of Health of the World Health Organization (WHO) emphasizes:
Within countries there are dramatic differences in health that are closely linked with degrees of social disadvantage. Differences of this magnitude, within and between countries, simply should never happen. These inequities in health, avoidable health inequalities, arise because of the circumstances in which people grow, live, work, and age, and the systems put in place to deal with illness. The conditions in which people live and die are, in turn, shaped by political, social, and economic forces.29
Context and capacities are intrinsic, fundamental concerns in the human rights framework. They focus attention on nationally-owned efforts to improve the enjoyment of human rights, on strengthening economic, social, and po-litical systems, and on international responsibilities to support these efforts.30
29. WHo & CoMMission on soCial deterMinants oF HealtH, Closing tHe gaP in a generation: HealtH eQUity tHroUgH aCtion on tHe soCial deterMinants oF HealtH: Final rePort oF tHe CoMMission on soCial deterMinants oF HealtH (2008).
30. Amarjit Singh,“Rights-Based Approaches” to Health Policies and Programmes: Why are they Important to Use? 31 J. PUB. HealtH Pol’y 146 (2010).

2012 The Millennium Development Goals 155
The human rights framework recognizes and directly addresses the fact that countries have different capacities and contextual challenges to realize human rights and to achieve health and development goals. For instance, the Limburg Principles concerning the implementation of economic, social, and cultural rights afford States a “margin of discretion” in selecting the means to implement their human rights obligation, and take into account the fact that some constraints may be beyond a single State’s capacity to address.31 The international code of human rights also recognizes that:
Many human rights will be realized progressively and are subject to the avail-ability of resources. Accordingly, the precise obligations arising from some hu-man rights vary over time in relation to the same State (progressive realization) and from one State to another (because of differing resource availability) . . . However, despite the flexibility accorded by the acknowledgement of progres-sive realization and resource availability, States have a core obligation to ensure at least the minimum essential levels of various rights, including the rights to adequate food and housing, health protection and education.32
The principles of the “margin of discretion” and of the “progressive realiza-tion” of rights focus attention on nationally-owned efforts to improve the enjoyment of human rights of citizens and on international responsibility to support these efforts. The human rights framework underscores the need for local contexts and capacities to be taken into account, and provides a frame-work for inter-sectoral and international coordination and accountability.
One of the criticisms of the MDGs is that the emphasis on specific goals and technical strategies fails to take into consideration the broader social context and determinants of health and development.33 The concurrent lack of emphasis on strengthening the systems and services required to reach the MDGs compounds this critical gap. The Global Strategy seeks to address the problem by emphasizing the primacy of national health plans—aligned with the principles of aid effectiveness set out in the Paris Declaration and the Accra Agenda for Action.34 “Health systems strengthening” is increas-ingly a global catch phrase, and is also a key feature of the Global Strategy. However, until now it has not been an explicit feature of the MDGs.
The importance of strengthening systems and services is powerfully dem-onstrated in the “natural experiment” of Western development. Reviewing
31. Limburg Principles on the Implementation of the International Covenant on Economic, Social and Cultural Rights, adopted 8 Jan. 1987, U.N. ESCOR, Comm’n on Hum. Rts., 43d Sess., Agenda Item 8, ¶71, U.N. Doc. E/CN.4/1987/17/Annex (1987), reprinted in The Limburg Principles on the Implementation of the International Covenant on Economic, Social and Cultural Rights, 9 HUM. rts. Q. 122 (1987).
32. OHCHR, HUMan rigHts and Poverty redUCtion: a ConCePtUal FraMeWork (2004), available at http://www2.ohchr.org/english/issues/poverty/docs/povertyE.pdf.
33. Alston, supra note 12, at 762. 34. The Paris Declaration on Aid Effectiveness and the Accra Agenda for Action 2005/2008,
available at http://www.oecd.org/dataoecd/11/41/34428351.pdf.

Vol. 34156 HUMAN RIGHTS QUARTERLY
the decline of maternal mortality in Europe and North America in the nine-teenth and twentieth centuries, Alicia Yamin and Deborah Maine show that:
[M]aternal mortality was impervious to the changes in standards of living in-cluding, improvements in nutrition . . . [and] the importance of education for women in other arenas of public health . . .This decline came about with the availability of effective means to treat obstetric complications, including antibi-otics for infection, banked blood, and safer surgical techniques for hemorrhage and obstructed labor.35
To achieve the maternal and child mortality reductions set out in MDGs 4 and 5, a strategic and evidence-informed approach to strengthening health systems is required. To reduce maternal and newborn mortality, strong emergency obstetric and neonatal services are essential.36 Reducing child mortality requires a more comprehensive primary health care approach, including prevention, nutrition, immunization, and effective treatment for diseases such as pneumonia and diarrhea.37 This comprehensive approach to primary health care is set out in the Alma-Ata Declaration.38
A commitment to considering context is also critical in health systems strengthening. Lynn Freedman calls attention to this fact:
The health system is not simply a mechanical structure to deliver technical interventions the way a post office delivers a letter. Rather, health systems are core social institutions. They function at the interface between people and the structures of power that shape their broader society. Neglect, abuse and exclusion by the health system is part of the very experience of being poor. Conversely, health claims, legitimate claims of entitlement to the services and other condi-tions necessary to promote health, are assets of citizens in a democratic society.39
The human rights framework provides a comprehensive means for helping to integrate the economic, social, and cultural dimensions of health and development work.
An additional, important aspect of the human rights framework is that it focuses attention on the agency and capacities of individuals as rights-holders. Here, too, there is supporting empirical evidence. Sen and Jean Drèze have shown in several analyses how starvation and famine are not only the result of changes in food supply, but also of the inability of individuals and groups
35. Alicia Ely Yamin & Deborah Maine, Maternal Mortality as a Human Rights Issue: Measur-ing Compliance with International Treaty Obligations, 21 HUM. rts. Q. 563, 572 (1999).
36. Id. at 591. 37. Zulfiqar A. Bhutta et al., Countdown to 2015 Decade Report (2000–10): Taking Stock
of Maternal, Newborn, and Child Survival, 375 lanCet 2032, 2041 (2010). 38. Declaration of Alma-Ata: International Conference on Primary Health Care, adopted
12 Dec. 1978, WHO (1978) available at www.who.int/publications/almaata_declara-tion_en.pdf.
39. Lynn P. Freedman, Achieving the MDGs: Health Systems as Core Social Institutions, 48 dev. 19, 21 (2005).

2012 The Millennium Development Goals 157
to procure jobs and other development entitlements.40 In Nepal, a random-ized control trial showed that a combined approach of strengthening health services and facilitating women’s participation—through group meetings to identify perinatal problems and to find ways to address them in an “action-learning cycle”—resulted in significant improvements in birth outcomes.41
The “agency” of individuals is largely underemphasized in MDG strat-egies. A human rights perspective can help facilitate the participation of individuals in decisions and interventions that affect their lives, avoid purely prescriptive solutions, and directly contribute to health, development, and realization of human rights. Failures to access health, development, and human rights entitlements can occur because of shortcomings in both indi-vidual and institutional capabilities.
Claiming human rights through litigation is one way to bring pressure to bear—primarily on states—to improve the delivery of services or to desist from actively violating human rights. In a landmark case in India, petitions were filed in the Delhi High Court in response to the deaths of two women from pregnancy-related causes. The High Court judgment stated:
These two petitions highlight the deficiencies in the implementation of a cluster of schemes, funded by the Government of India, which are meant to reduce infant and maternal mortality. The issues common to both petitions concern the systemic failure resulting in denial of benefits to two mothers below the poverty line (BPL) during their pregnancy and immediately thereafter. These petitions are essentially about the protection and enforcement of the basic, fundamental and human right to life under Article 21 of the Constitution. These petitions focus on two inalienable survival rights that form part of the right to life: the right to health (which would include the right to access and receive a minimum standard of treatment and care in public health facilities) and in particular the reproductive rights of the mother. The other right which calls for immediate protection and enforcement in the context of the poor is the right to food.42
The Delhi High Court instructed the central and state governments to com-pensate the claimants, take immediate corrective action on a range of spe-cific interventions to prevent maternal and infant mortality, and to regularly monitor and improve the related implementation schemes.43 Further, the High Court raised concerns on whether “a private . . . corporate hospital [was] sufficiently sensitive and informed in the manner that BPL patients should
40. sen, Poverty and FaMines, supra note 22 at 7–8, 51; see generally Jean drèze & aMartya sen, HUnger and PUBliC aCtion (1989).
41. Zulfiqar A. Bhutta et al., Interventions to Address Maternal, Newborn, and Child Survival: What Difference Can Primary Health Care Strategies Make?, 372 lanCet 972, 974 (2008).
42. Cases of Laxmi Mandal v. Deen Dayal Harinagar Hospital and Ors. & Jaitun v. Ma-ternity Home MCD, Jangpura and Ors., (2010) (Delhi H.C.) WP(C) 8853/2008, WP(C) 10700/2009 (India).
43. Id. at 43–51.

Vol. 34158 HUMAN RIGHTS QUARTERLY
be interacted with” and that “a poor person who is sent to a private hospital cannot be assured of quality and timely health services.”44
Cases such as this highlight the possibility of not only states, but also of the private sector and other non-state actors—who have made commitments to, or are responsible for, providing resources and interventions—being held to account for their actions or inactions towards preventing maternal and child mortality.
The outcomes of legal suits may not always be favorable to the rights-holder, and even when favorable may be subject to challenge when attempts are made to enforce decisions. Enforcement issues can at least be partially addressed by instituting initiatives to train legal personnel, such as judges and lawyers, as well as community leaders and local government officials, in people’s legal rights regarding health care (and the underlying determi-nants of health).
Beyond the court system, other mechanisms exist to enforce the right to health and hold the government accountable to its obligations. These include quasi-judicial mechanisms (such as national human rights commissions), administrative means (such as human rights assessments), political means (such as parliamentary reviews of, and hearings on, the budget), and social means (such as NGO involvement in budget monitoring and health-center monitoring).45
Where such mechanisms exist, but are underutilized, the relevant train-ing and implementation will take time as will adapting or developing new mechanisms. This raises questions about the efficiency of using the human rights framework to enhance existing or forthcoming MDG efforts, since such efforts must achieve results by 2015. However, the time involved in facilitating human rights claims should be viewed from the perspective that building on the complementarity between human rights and MDG efforts is a way to sustain such efforts beyond 2015. Seen this way, we must empha-size efforts to introduce such training and accountability mechanisms—not only so they can enhance existing MDG efforts but also, and perhaps more importantly, to put a “human rights infrastructure” in place by 2015. It will then be available to sustain subsequent efforts by states to fulfill their human rights obligations. To this end, existing training and accountability mechanisms ought to be identified and developed. Where they are absent, they ought to be instituted.
Generally, the issue of claiming rights should be viewed in terms of establishing a principled dialogue between rights-holders, states, and other
44. Id. at 15, 19. 45. Helen Potts, Accountability and the Right to the Highest Attainable Standard of Health
19 (University of Essex Human Rights Centre) (2008), available at http://www.essex.ac.uk/human_rights_centre/research/rth/docs/HRC_Accountability_Mar08.pdf.

2012 The Millennium Development Goals 159
partners to develop more relevant and improved interventions.46 In fact, in many cases, such interventions already exist. The main issue is likely to be their reach, scope, and adaptation to local contexts and capacities. In this regard, the human rights perspective adds value to MDG efforts.
C. promote Integration and Innovation to Catalyze progress
The Global Strategy estimates that to strengthen health systems in forty-nine low-income countries and implement essential PMNCH interventions, the funding gap is $88 billion.47 Since the September 2010 launch of the UN Secretary-General’s Global Strategy for Women’s and Children’s Health, states and non-state actors including donors, multilateral agencies, civil society organizations, and private sector companies have committed over $40 billion towards this goal, and have made significant policy and service delivery commitments.48
It is important not only to get more money for health, but also to ensure that the monies are used effectively. To do this, integration and innovation are required.49 The Global Strategy explicitly forges links across the MDGs—between poverty, inequity, education, sustaining environments, and health.50
Egypt is one of the few countries on track to achieve both MDGs four and five by 2015. It has achieved this by integrating services within and across sectors: child health and family planning programs; improving facilities and access for safe motherhood programs; combining oral rehydration programs with the expansion of water and sanitation systems; and training health-care workers in parallel with community outreach programs.51 An international assessment by UNDP in 2010 of what it will take to achieve the MDGs emphasized that:
There are important synergies among the MDGs—acceleration in one goal often speeds up progress in others. In households where women are illiterate, child mortality is higher, implying the links between education, the empowerment of women and the health of children. Given these synergistic and multiplier
46. Christine Chinkin, The United Nations Decade for the Elimination of Poverty: What Role for International Law?, 54 CUrr. l. ProB. 553–89 (2001).
47. gloBal strategy, supra note 17. 48. PartnersHiP For Maternal, neWBorn & CHild HealtH [PMnCH), tHe PMnCH 2011 rePort:
analysing CoMMitMents to advanCe tHe gloBal strategy For WoMen’s and CHildren’s HealtH (2011), available at http://www.who.int/pmnch/topics/part_publications/PMNCH_Re-port_2011_-_29_09_2011_full.pdf.
49. gloBal strategy, supra note 17. 50. Id. 51. Oona Campbell et al., National Maternal Mortality Ratio in Egypt Halved Between
1992–93 and 2000, 83 BUll. World HealtH org. 462 (2005); save tHe CHildren, state oF tHe World’s MotHers 2007: saving tHe lives oF CHildren Under 5 (2007), available at http://www.savethechildren.net/alliance/media/newsdesk/2007-05-08.html.

Vol. 34160 HUMAN RIGHTS QUARTERLY
effects, all the goals need to be given equal attention and achieved simultane-ously. This requires multisectoral approaches and coordination among various implementing agencies.52
The human rights framework would help “guide the design and implementa-tion” of integrated policies and programs.53 The human rights principles of interdependence and indivisibility focus attention on the linkages between health, development, and human rights goals, and help promote integration of required services. The UN Committee on Economic, Social and Cultural Rights, drafted in collaboration with WHO and others, adopted General Comment 14 on the Right to Health,54 affirming that:
The right to health not only includes access to medical care, but also the under-lying determinants of health, such as safe water, adequate sanitation, a healthy environment, health-related information (including on sexual and reproductive health), and freedom from discrimination.55
Gender equality is fundamental to improving women’s and children’s health. Within the health sector, equality of access to health care needs to be assured, including affordability of services through measures such as abolishing user fees and incorporating innovative financing mechanisms, as well as improving physical access through transportation and infrastructure measures.56 Promoting gender equality also requires addressing the social, economic and political barriers to women’s participation and status in society.
The integration of health and human rights can be a powerful force. In global policy, the integration of health, development, and human rights frameworks have brought together and mobilized a range of actors. For ex-ample, Sofia Gruskin et al. note: “It was not until the late 20th century that maternal mortality started to be recognized as a public-health concern.”57 This recognition was substantiated by landmark international agreements that brought together the women’s reproductive health and human rights move-ments: the 1994 International Conference on Population and Development in Cairo58 and the 1995 Fourth World Conference on Women in Beijing.59
In MDG work, there is a tendency to adopt vertical, sector-specific ap-proaches. MDG efforts to alleviate poverty, promote education, and reduce
52. UndP, supra note 14, at iv. 53. Lynn P. Freedman, Using Human Rights in Maternal Mortality Programs: From Analysis
to Strategy, 75 gyn. & oBstetriCs 51 (2001). 54. General Comment No. 14, supra note 11, ¶ 1. 55. MacArthur Found. & Hunt, supra note 18, at 2. 56. General Comment No. 14, supra note 11, ¶¶ 8–9, 12. 57. Sofia Gruskin, et al., Using Human Rights to Improve Maternal and Neonatal Health:
History, Connection and a Proposed Practical Approach, 86 BUll. World HealtH org. 589, 592 (2008).
58. Draft Programme of Action of the International Conference on Population and Develop-ment, U.N. GAOR, Provisional Agenda Item 9, U.N. Doc. A/CONF.171/L.1 (1994).
59. Fourth World Conference on Women: Action for Equality, Development, and Peace, Beijing Declaration and Platform for Action, U.N. GAOR, U.N. Doc. A/CONF.177/20 (1995).

2012 The Millennium Development Goals 161
maternal and child mortality are often implemented independently of each other. To promote integration of rights-related efforts, UN agencies and other development agencies adopted the “Common Understanding on the Human Rights Based Approach to Development Cooperation.”60 This was built on UN reform efforts and a call from the then UN Secretary-General for all UN agencies to place human rights in the mainstream of their respective mandates.61 Perhaps linking the operational concepts of the continuum of care with the Common Understanding will provide an overarching innova-tive and integrating operational concept for MDGs and human rights efforts.
The concept of the “Continuum of Care” across maternal, newborn, and child health—and across health care at the home, community, and health facilities (Figure 1)—has been a successful integrative concept within the health sector.62 It has been influential in bringing together groups—previously working separately on maternal, newborn, and child health issues—in the Part-nership for Maternal, Newborn and Child Health. PMNCH now has over 300 partner organizations, with states and non-state actors including multilateral institutions, health-care professional associations, donors and foundations, academic, research and training institutions, and civil society organizations.63
60. UNESCO Bangkok, The Human Rights Based Approach to Development Cooperation: Towards a Common Understanding Among the UN Agencies (2003), available at http://www.unescobkk.org/fileadmin/user_upload/appeal/human_rights/UN_Common_under-standing_RBA.pdf.
61. MDG rePort, supra note 16. 62. Kate J. Kerber et al., Continuum of Care for Maternal, Newborn, and Child Health: From
Slogan to Service Delivery, 370 lanCet 1358, 1362 (2007). 63. See generally The Partnership for Maternal, Newborn and Child Health (2011), available
at http://www.who.int/pmnch/about/constituencies/en/index.html. 64. PMnCH, University oF aBerdeen, sHaring knoWledge For aCtion on Maternal, neWBorn and
CHild HealtH 47 (2010).
Figure 1. The continuum of care for reproductive, maternal, newborn, and child health64

Vol. 34162 HUMAN RIGHTS QUARTERLY
Jeremy Shiffman, in analyzing how issues become part of global agendas, underscores the importance of unifying values and ideas, around which ac-tors can mobilize. He notes that this is particularly important for maternal and child health issues, which hitherto had failed to achieve the attention they warrant on the global policy stage.65
There are a variety of options for cooperation and coordination between MDGs and human rights efforts within a country or a region, and across the UN and regional human rights bodies. Using the analogy of the continuum of care, options could be arrayed along a similar continuum, anchored at one end by actions in countries and regions, and at the other end in global collective action, perhaps integrated within the United Nations General Assembly.
The human rights framework can help further enhance the Global Strat-egy’s focus on research and innovation with a complementary emphasis on ethics and facilitating access to global public goods. Chris Beyrer and Nancy E. Kass highlight the overlap between human rights and health-research ethics:
Although the human rights movement and the sphere of research ethics have overlapping principles and goals, there has been little attempt to incorporate external political and human rights contexts into research ethics codes or ethics reviews. Every element of a research ethics review—the balance of risks and benefits, the assurance of rights for individual participants, and the fair selec-tion of research populations—can be affected by the political and human rights background in which a study is done.66
Getting “more health for the money” need not devolve into utilitarian cal-culations within the health sector. The Global Strategy’s focus on integration and innovation encourages collaborations across sectors, including economic development, nutrition, education, water and sanitation, and information technology (for example innovation and adaptation of “mobile phones and other communication tools”).67 A human rights framework would take ac-count of all such activities and provide a valid legal basis for coordinating the disparate but relevant activities of various government sectors.
Using the human rights framework to promote research and innovation would also mean ensuring equitable access to these products as global public goods. This would require inter-sectoral cooperation and commitments on is-sues such as promoting standards for interoperability of different technologies, open source applications, and equitable pricing. These might be achieved
65. Jeremy Shiffman, Issue Attention in Global Health: The Case of Newborn Survival, 375 lanCet 2045, 2048 (2010); Jeremy Shiffman & Stephanie Smith, Generation of Political Priority for Global Health Initiatives: A Framework and Case Study of Maternal Mortality, 370 lanCet 1370, 1372 (2007).
66. Chris Beyrer & Nancy E. Kass, Human Rights, Politics, and Reviews of Research Ethics, 360 lanCet 9328, 246 (2002).
67. gloBal strategy, supra note 17, at 5.

2012 The Millennium Development Goals 163
through promoting business models that create “shared value.”68 The so-called “Bottom of the Pyramid” strategy involves the profitable engagement of the private sector, even with customers who have minimal financial resources.69
D. Combat Inequality and Discrimination
Progress towards achieving MDGs 4 and 5—to reduce maternal and child mortality and to promote universal access to reproductive health—cannot be achieved unless the human rights standards of equality and non-discrim-ination are met. Around the world, women who die in childbirth, newborns who die from infections, and children who die from preventable diseases such as pneumonia and diarrhea, are usually from the most marginalized and vulnerable communities. The Countdown to 2015 data show that there are significant inequities in coverage of essential interventions for maternal, newborn, and child health across the highest and lowest socioeconomic quintiles in countries.70
In studying the health of indigenous communities, Carolyn Stephens et al. raise concerns about the MDGs’ targets:
We are concerned that major international policies such as the Millennium Development Goals might further marginalise indigenous communities through their top-down and utilitarian approach to health policy-making—encouraging targets to maximise health benefits for the majority, while at the same time potentially demoting the minority.71
In the most vulnerable communities across the world, access to essential health services is typically constrained by financial, geographic, and cultural barriers. Identifying equality and empowerment of women as one of the defining factors in making progress towards the MDGs, the UNDP interna-tional assessment highlights the fact that:
Gender equality and women’s empowerment have large multiplier effects on other MDGs. This is perhaps one of the most important linkages across the MDGs. The country-level evidence indicates that women and girls do not have equal access to goods, services and productive assets. In some communities, girls are given less food than boys, contributing to nutritional imbalances between men and women. In Nepal, for instance, reports show that food distribution is influenced by social and cultural practices. In many countries, transactional
68. Michael E. Porter & Mark R. Kramer, Creating Shared Value, Harvard BUsiness revieW, Jan. 2011.
69. See generally, C.K. PraHalad, tHe FortUne at tHe BottoM oF tHe PyraMid: eradiCating Poverty tHroUgH ProFits (2005).
70. CoUntdoWn to 2015, supra note 1, at 7, 13, 36–37. 71. Carolyn Stephens, John Porter, Clive Nettleton, & Ruth Willis, Disappearing, Displaced,
and Undervalued: A Call to Action for Indigenous Health Worldwide, 367 lanCet 2019, 2019 (2006).

Vol. 34164 HUMAN RIGHTS QUARTERLY
sex, social norms that disempower women and domestic violence are among the causes of HIV infection. Birth rates are likely to be lower in households where women are empowered, which, in turn, is associated with better health and education for children.72
Adopting equality and non-discrimination as programming standards will assist in designing health interventions that successfully reach and meet the needs of marginalized populations. This approach will contribute to achieving the MDGs by improving health outcomes among populations where such outcomes are often the worst, and will help realize the right to health and, through that, other related human rights.
Ensuring quality health care also benefits from a rights perspective. Health workers must be trained and required to respect the rights of patients to, for example, non-discrimination, confidentiality, informed consent, privacy, and access to information.73 Poor treatment—particularly of disadvantaged and vulnerable people (such those with disabilities, indigenous communi-ties, and those who are HIV-positive)—deters people from seeking health services and obstructs high-quality care. The comprehensive human rights framework can help identify gaps and focus efforts towards the progressive realization of health and development goals and human rights.
In order to identify inequalities in the provision of health care and to ensure non-discrimination, it is critical that efforts to strengthen health-information systems include improvements in the ability of countries to disaggregate data. This includes data for women and children, marginalized populations such as indigenous peoples, and people with disabilities. This will enable countries to monitor the health of these populations and the ability of health services to reach them, and to show how effectively health interventions are meeting their needs.
The challenge for governments, as described in the case of Mexico (see Box 1), is to develop an appropriate national strategy, so that interventions reach all segments of a country’s population equally. An example from South Africa illustrates this point. In 2000, a claim was brought by a group living in an informal settlement after they were evicted from land they were illegally occupying. They claimed a violation of their right to adequate hous-ing, which was enshrined in the South African Constitution.74 The South African Constitutional Court, while accepting that the government could not immediately provide housing or shelter for all people in the country without accommodation, nevertheless noted that the constitution required “the state to devise and implement within its available resources a com-prehensive and coordinated programme progressively to realise the right of
72. UndP, supra note 14, at 1. 73. PMnCH, supra note 64. 74. South Africa v. Grootboom & Others 2000 (11) BCLR (CC) 55 (S. Afr.).

2012 The Millennium Development Goals 165
access to adequate housing.”75 It went on to state that this “comprehensive and coordinated programme” must include reasonable measures to provide “for people who have no access to land, no roof over their heads, and who are living in intolerable conditions or crisis situations.”76 The Court found that the relevant state housing program had failed to make such provision and had therefore violated the constitution.77 In effect, the court directed the relevant housing authority to go back to the drawing board and produce a housing program or strategy that took into account all segments of the population, including those who were marginalized, such as the homeless.
Unless MDG interventions are also undertaken as part of such compre-hensive strategies, there is a risk they will exclude some groups. The human rights dimension would help mitigate such a risk, owing to its emphasis on meaningful participation by affected groups, including marginalized popula-tions, and its focus on equality and non-discrimination. Taking account of the human rights dimensions can therefore help MDG interventions avoid the problem identified by concerned commentators such as Stephens et al.
E. Commit to Accountability for Resources and Results
To ensure that the commitments made by state and non-state actors to the Global Strategy are met and results achieved, the UN Secretary-General established the Commission on Information and Accountability for Women’s and Children’s Health. The Commission explicitly links accountability to: “the fundamental human right of every woman and child to the highest attainable standard of health and on the critical importance of achieving equity in health.”78 Accountability here comprises monitoring, review, and action. Monitoring of core progress indicators helps track what is happen-ing where, to whom, and with what resources. Review, by an independent Expert Review Group, then asks whether or not commitments were kept and the required results achieved. Based on the independent review, remedial action to address shortcomings and facilitate progress would need to be undertaken by all relevant actors. The Commission also recommends that by 2012, all countries establish or strengthen vital registration systems and national accountability mechanisms.79
There are powerful complementarities between accountability processes for the MDGs and for human rights. MDG-related accountability augments
75. Chinkin, supra note 46; South Africa v. Grootboom & Others 2001 (1) SA 46 (CC) 88 (S. Afr.).
76. South Africa. v. Grootboom & Others 2000 (11) BCLR at 99. 77. Id. at 97. 78. WHO, CoMMission on inForMation and aCCoUntaBility For WoMen’s and CHildren’s HealtH,
keePing ProMises, MeasUring resUlts 3 (2011) [hereinafter keePing ProMises]. 79. Id. at 5.

Vol. 34166 HUMAN RIGHTS QUARTERLY
the accountability of states within the human rights framework by taking into account both state and non-state actors. The analytic and methodological developments—including benchmarks, targets, and indicators—that have evolved in monitoring the MDGs can significantly strengthen the human rights monitoring process with respect to aspects of rights.80 The human rights framework has long-established criteria and processes for monitoring, review, and remedial action that provide a foundation on which to build accountability of state and non-state actors. Human rights criteria that guide the monitoring of policies and programs are set out by the Committee on Economic, Social and Cultural Rights.81 These criteria include: availability; acceptability (in local contexts and for individuals); accessibility (physical and financial); adaptability; and quality.82 The criteria operate in three dimensions:
1. They inform the content of laws, policies and other measures adopted in relation to entitlements.
2. They represent requirements for compliance in relation to how the laws, policies and measures are brought into operation or practically instituted.
3. They encompass the objectives and goals of those laws, policies and measures, and so provide the criteria for assessing if they have been suc-cessfully met.
The precise application of these criteria will depend on the best interests of rights-holders, and on the prevailing conditions and context, as health and development goals and human rights are progressively realized.83
Monitoring is limited by the type of data available. Data on maternal, newborn, and child mortality are difficult to obtain in many countries. Some countries lack even basic systems for registering births and deaths, which severely limits the effective functioning of monitoring processes.84 The Global Strategy includes a commitment to build capacity to establish and strengthen vital registration and health information systems.85 This would boost national
80. MacArthur Found. & Hunt, supra note 18, at 4, 14–15. 81. ICESCR, supra note 11. 82. General Comment No. 14, supra note 11, ¶ 12; The Right to Adequate Food, General
Comment No. 12, U.N. ESCOR, Comm. on Econ., Soc. & Cult. Rts., 20th Sess., U.N. Doc. E/C.12/1999/5 (1999); The Right to Education, General Comment No. 13, U.N. ESCOR, Comm. on Econ., Soc. & Cult. Rts., 21st Sess., U.N. Doc. E/C.12/1999/10 (1999); Preliminary report of the Special Rapporteur on the Right to Education, Ms. Katarina Tomasevski, Submitted in Accordance with Commission on Human Rights Resolution 1998/33, U.N. ESCOR, Comm’n on Hum. Rts., 55th Sess., Provisional Agenda Item 10, U.N. Doc. E/CN4/1999/49 (1999).
83. General Comment No. 14, supra note 11. 84. Report of the Special Rapporteur on the Right of Everyone to the Enjoyment of the High-
est Attainable Standard of Health, Paul Hunt, Mission to India, U.N. GAOR, 14th Sess., Agenda Item 3, U.N. Doc. A/HRC/14/20/Add2 (2010); Katarina Tomaševski, Indicators, in eConoMiC, soCial, and CUltUral rigHts: a textBook (Asbjørn Eide, Catarina Krause, & Allan Rosas eds., 2001).
85 gloBal strategy, supra note 17.

2012 The Millennium Development Goals 167
capacity for monitoring health and development policies and practices, which is otherwise a constraint for governments in understanding the effect of efforts to improve the enjoyment of the right to health.86
Different groups of experts continue to develop more sophisticated and reliable monitoring methods. The Countdown to 2015 for Maternal, Newborn, and Child Survival regularly monitors coverage of priority interventions to achieve MDGs 4 and 5 in sixty-eight Countdown priority countries. These account for more than 95 percent of maternal and child deaths worldwide.87 In addition to indicators for MDGs 4 and 5, the Countdown analyzes equity, financing, and health policy issues that influence these health outcomes.88 Recent publications in academic journals also propose new approaches to measure progress towards reducing maternal mortality and determining the main causes of child mortality.89
If monitoring for the MDGs and human rights were integrated, states would have multiple, reinforcing incentives to improve monitoring and re-porting with regard to health and development indicators. States are legally required to submit data for international scrutiny by human rights bodies, and the MDGs have caused reporting on health and development progress to receive heightened attention and resources.90 There are efficiencies to be gained in adopting common monitoring frameworks, and there is great potential to strengthen monitoring and accountability methods and systems by combining forces and resources. Currently, the extent to which monitor-ing for the MDGs and human rights is integrated varies greatly.91 Reviewing country MDG reports for their human rights content, Alston observed:
At one end of the spectrum is the report on Bosnia and Herzegovina which, in the course of 141 pages, makes 108 references to human rights. Indeed the entire analysis of the MDG situation is located squarely within a human rights framework. . . .The report of the Philippines, a country in which a great deal has been done to promote human rights based approaches to development, contains only two references to human rights within a fifty-eight page report. . . . Many other reports lie at the end of the spectrum where human rights are completely absent from the picture. . . . An especially striking example is a lengthy report of some fifty-six pages on Afghanistan, prepared with extensive
86. Committee on Economic, Social and Cultural Rights, Report on the Third Session, General Comment No. 1, U.N. ESCOR, Comm. On Econ., Soc, & Cult. Rts., 3d Sess., U.N. Doc. E/1989/22 (1989).
87. Bhutta et al., supra note 37, at 2032. 88. Id. 89. Margaret C. Hogan et al., Maternal Mortality for 181 Countries, 1980–2008: A Systematic
Analysis of Progress Towards Millennium Development Goal 5, 365 lanCet 1609, 1610 (2010); Robert E. Black et al., Global, Regional, and National Causes of Child Mortality in 2008: A Systematic Analysis, 375 lanCet 1969, 1970 (2010).
90. See, e.g., PMNCH, supra note 48. 91. Alston, supra note 12, at 767; MacArthur Found. & Hunt, supra note 18, at 4, 14–15.

Vol. 34168 HUMAN RIGHTS QUARTERLY
assistance from UNDP, . . . despite the clear relevance of human rights to so many of the challenges faced.92
This variability is to be expected, since governments are currently not required to make reference to human rights in their MDG reports. Unless there are requirements for integration of human rights and MDG monitoring, the integration of MDGs and human rights efforts will be uneven. That is a problem, because these separate systems will fail to capitalize on the range of potential complementarities that this paper highlights.
Mechanisms to review the monitoring data are well-established in the human rights framework. While the indivisibility and interdependence of human rights is a fundamental principle, there are different bodies involved in reviewing the implementation of human rights. For example, there are several human rights treaty bodies, including Committees on Economic Social and Cultural Rights, the Elimination of Discrimination Against Women, and the Rights of the Child. There are also charter-based bodies such as the Hu-man Rights Council, which oversees about thirty thematic mandates under its special-procedures mechanism.
As an example of how the human rights review process works, to meet the terms of the Convention on the Rights of the Child (CRC), countries submit reports every five years to the Committee on the Rights of the Child, detailing their progress towards obligations.93 Governments submit a national report on progress towards education enrollment, women’s and children’s health, and other key health and development indicators. Civil society orga-nizations also submit a report, and UNICEF and other UN agencies submit inputs.94 The CRC’s eighteen-member committee of legal and technical experts meets three times a year in Geneva to assess these reports.95 Based on their analysis, the committee presents concluding observations, with recommendations to guide further implementation and evaluation towards the realization of rights.96 There are similar monitoring provisions for other human rights treaties.
Ultimately, accountability must be owed primarily to the people of countries where health and development goals are to be achieved. In rela-tion to human rights, remedy or redress is on two levels. At the inter-state level, states have to report their compliance with their treaty obligations and have to account to other states for widespread human rights violations, if any. States are also accountable to individual citizens as rights-holders
92. Alston, supra note 12, at 794–96. 93. OHCHR, Committee on the Rights of the Child, Monitoring Children’s Rights (2010)
available at http://www2.ohchr.org/english/bodies/crc/. 94. Convention on the Rights of the Child, adopted 20 Nov. 1989, G.A. Res. 44/25, U.N.
GAOR, 44th Sess., art. 19, U.N. Doc. A/RES/61/106 (2006). 95. Id. arts. 44–45. 96. Id.

2012 The Millennium Development Goals 169
both within countries and as part of the international community, through the human rights treaty bodies, such as the Committee on the Rights of the Child discussed above.
Mechanisms for state accountability include: legal suits (both domesti-cally and through regional court systems); state reporting to the international treaty bodies; parliamentary oversight and investigations; national human rights institutions; and external monitoring by media and NGO investigations. States’ responsibilities in relation to human rights issues include and extend beyond the MDGs. In this sense, MDG accountability is subsumed within the human rights accountability of states, and the UN General Assembly can provide overarching global oversight.
MDG-related accountability has features and innovations that augment state accountability. One critical innovation that the Global Strategy pro-motes is a framework designed to hold all stakeholders, not just states, to account for the commitments made in relation to the health MDGs.97 This innovation is important because it moves away from the focus on the state as the main actor from whom accountability for human rights is expected. Although the state has the primary responsibility in relation to human rights, the realization of human rights is not solely dependent on the activities of states. The activities and interventions of non-state actors also have an impact on the enjoyment of human rights.98 If the human rights framework is explicitly linked to the MDGs, it is important that this framework of ac-countability is maintained, so that non-state partners (for which there are only weak mechanisms of accountability in human rights) also can be held accountable to the,rights-holders or to citizens in states where MDG inter-ventions are being undertaken. Such accountability is important in order for such non-state actors to take account of the human rights impacts of their interventions.
To promote mutual accountability of state and non-state actors, a range of accountability measures can be used. In addition to national, regional, and international legal mechanisms and courts, community-based accountability mechanisms—such as village health committees, health facility management boards, and maternal and child death audits—can be effective. Countries should support all communities in developing and implementing strategies to hold local health services accountable. Box 2 highlights some innovative accountability mechanisms that have been developed by countries to help achieve the MDGs.
97. Press Release, United Nations, Global Strategy Launched by U.N. Millennium Develop-ment Goals Summit Draws More Than $40 Billion to Save the Lives of 16 Million Women and Children (22 Sept. 2010), http://www.un.org/News/Press/docs/2010/dev2827.doc.htm.
98. andreW ClaPHaM, HUMan rigHts oBligations oF non–state aCtors 348 (2006).

Vol. 34170 HUMAN RIGHTS QUARTERLY
There is a dynamic and powerful relationship between health and law in promoting accountability as highlighted in the following analysis of the role of law in combating the HIV/AIDS pandemic:
Laws may: (1) help to ensure that public health authorities are empowered to provide effective prevention and treatment programmes; (2) effectuate the hu-man rights to life, health, work, education and property ownership of persons living with, or at risk of, HIV/AIDS; and (3) protect persons living with HIV/AIDS from social risks, stigma and other harms by respecting privacy and prohibit-ing unwarranted discrimination. However, laws can also create legal barriers in many countries that impede effective HIV/AIDS interventions by penalizing those with HIV/AIDS through criminal sanctions or other policies. As a result, it
99. UndP, supra note 14; UNICEF, Children and the Millennium Development Goals (2007), available at http://www.unicef.org/publications/files/Children_and_the_MDGs.pdf.
box 2: promoting Accountability for MDG Acceleration99
Evidence from various countries shows significant progress towards creating systems of accountability.
Eighty-four developing countries adopted Right to Information or Freedom of Information Acts, with the recognition that informed citizenry is central to im-proving governance.
In India, in addition to the Right to Information Act, social audit mechanisms have been introduced to hold policy makers and institutions accountable for service delivery.
In the Philippines the “Promoting Procurement, Transparency and Efficiency to Achieve the MDGs” initiative helps ensure that MDG-related programs and projects are implemented in a transparent and efficient manner at national and local levels.
In Tunisia, municipal councils for children have been in place since 1987, and since 2002, there has been a children’s parliament, which works with members of the country’s parliament on a range of issues.
Gambia adopted a community scorecard scheme whereby citizens are empowered to demand and monitor service delivery.
Albania adopted MDG 9 to “establish and strengthen a good governance process.” The target is to reform overall state systems of public administration, legislation and policies in accordance with EU Standards by 2015. The country has made significant progress, albeit slowly, towards this target.

2012 The Millennium Development Goals 171
is recommended globally that laws should facilitate the prevention and treatment of HIV/AIDS consistent with scientific and public health practices and with a human rights framework. Effective use of existing laws that promote the public’s health, and reforms of laws which impede it, contribute to improved individual and communal health outcomes concerning HIV/AIDS.100
Overall, accountability for what governments, donors, and others are invest-ing in MDGs continues to be very weak. This emphasizes the importance of linking the MDGs and human rights through the concept of entitle-ments, which requires countries to adopt internationally recognized rights in national policies. In addition, for meaningful progress to be achieved, specific resources allocated to meet these rights need to be specified, and their impact needs to be monitored and accounted for by all stakeholders.
One obvious drawback of all the accountability mechanisms instituted specifically for the MDGs is that they may not be sustained beyond 2015. Sustainability in this and other domains of health and development work is a further advantage of linking the MDGs to human rights systems, and will have a more effective, long-term impact on health and development efforts.
F. Emphasize Sustainability
A fundamental advantage offered by the human rights framework is that it can help sustain MDG efforts beyond 2015. MDG interventions strengthen resources and capacities that contribute towards realizing human rights. In ensuring entitlements it is possible to promote the integration of the MDGs with the human rights framework.
The challenges and constraints targeted by the MDGs are systemic and recurring. The international regulatory framework concerning human rights was designed to address such issues, and is intended to assure continuity and constancy beyond the timeframe of individual governments or specific health and development programs. So, the human rights framework provides a ready-made means to carry on the work catalyzed by the MDGs.
International frameworks, such as the human rights framework, are designed to improve cooperation and coordination among states. However, the effectiveness of such cooperation and coordination frameworks can be undermined by the creation of parallel frameworks, and the fragmentation that this engenders.
This problem of fragmentation and accountability gaps is recognized in the Global Strategy, which calls for the increased harmonization of ef-
100. L. Gable, L. Gostin & J.G. Hodge, Jr., A Global Assessment of the Role of Law in the HIV/AIDS Pandemic, 123 PUB. HealtH 260, 260 (2009).

Vol. 34172 HUMAN RIGHTS QUARTERLY
forts towards achieving the MDGs.101 Ongoing, coordinated engagement between states, communities, and other health and development partners on longer-term goals is required to sustain the results of MDG efforts after 2015 (see Figure 2).
101. gloBal strategy, supra note 17. 102. Id.
Figure 2. Sustaining MDG Progress towards Realizing Universal Human Rights102
Just as the international regulatory framework concerning human rights can help harmonize and systematize MDG efforts, the focus on achieving the MDGs can catalyze the realization and enjoyment of human rights. Much of what governments already do contributes to achieving both the MDGs and to the realization of human rights. In relation to both issues, governments can be assisted with improved resources and capacity, and the MDGs have focused attention and action towards this end. This improved capacity—which, it appears, is being delivered in relation to MDG efforts—would also help in developing capacities for the longer-term realization of human rights. The MDGs also appear to have been a more effective mobi-lizing force for resources than have human rights treaties. Thus, when both systems converge, the effect can potentially be catalytic and far-reaching.
In advocating a role for human rights in relation to the MDGs, it is nec-essary to sound a cautionary note. The struggle to define and claim rights is a political struggle—a fact that human rights advocates often gloss over. As Freedman notes:

2012 The Millennium Development Goals 173
The ultimate role of human rights is to identify the workings of power that keep unacceptable levels of maternal mortality as they are and to use the human rights vision of dignity and social justice to work for the re-arrangements of power necessary for change.103
Freedman’s assessment refers to the structural and resource changes needed in society to bring about the legal recognition and practical enjoyment of human rights. The reconfiguration of power and resources in society is often marked by conflict and even violence. Those who currently have the power and resources will not want to lose related control.104 This dynamic of conflicting values and interests is one reason why the struggle for rights takes time—often spanning years, if not generations.105 However, while hu-man rights take time to be realized, this does not mean that the effort is not worthwhile. Instead, it means that we have to proceed responsibly and with resolve towards the longer-term vision of a world where every individual’s rights are respected, protected, and fulfilled.
This article puts forward reasons for, and advantages to be gained from, integrating the human rights framework with efforts to achieve the MDGs. With regard to time, the global community has focused on inter-generational benefits in relation to climate change and sustainable environments, and this sensibility also needs to be applied to other human rights, including the right to health.
G. Recommendations
The complementarities between human rights and MDGs identified in this paper will need to be effectively leveraged to achieve shared commitments. The following recommendations indicate how this may be achieved in rela-tion to the strategic actions discussed in this article.
1. Assure Entitlements that Operationalize Human Rights Provisions with Resources
a. States should specify their MDG and human rights commitments in their national legal and policy frameworks. They should develop plans and allocate available resources to achieve MDGs and human rights commit-ments to the extent possible. States should link their policies for achieving
103. Freedman, supra note 53. 104 Katharina Pistor, The Evolution of Legal Institutions and Economic Regime Change,
in governanCe, eQUity, and gloBal Markets: tHe annUal Bank ConFerenCe on develoPMent eConoMiCs 87 (Joseph E. Stiglitz & Pierre–Alain Muet eds., 2001).
105. US Supreme Court Justice Stephen Breyer, A Presentation on International Law, The Blum Center for Developing Economies, University of California, Berkeley (Apr. 10 2009).

Vol. 34174 HUMAN RIGHTS QUARTERLY
specific health MDGs with laws that ensure an essential level of universal health care. Progressively, quality health care should be made available, accessible, and acceptable so that all citizens can enjoy their right to the highest attainable standard of health.
b. States should enable community members to participate meaningfully in health-related planning. States and non-state actors should monitor and evaluate local health services and adapt them to meet local needs, and ensure that health policies are fully funded and effectively implemented. Approaches should include legal reform, educating health system users and health workers on patient and human rights, and establishing effective complaints procedures.
c. With the help of the international community, states should remove barriers preventing access to health-care services as soon as possible. For example, user fees should be replaced by equitable health financing mechanisms that do not disproportionately burden the poor. They should also address other obstacles to access. For example, they should minimize the time people have to spend traveling to health facilities by opening additional facilities in areas of need and improving transportation. They should use a compre-hensive approach to tackle the inequitable distribution of health workers, and should address discrimination that prevents universal access to health care, including language barriers, gender-based violence, and stigma.
2. Build Capacities for Different Contexts and Challenges
a. States should spend as much as they can afford immediately towards pro-gressively realizing the full spectrum of human rights, as well as the MDGs. This might require assessments of the current context and adjustments to priorities in national plans and budgets.
b. All development actors should collaborate to identify key implementation gaps and solutions that could bridge these gaps in different contexts. Sup-porting national plans and harmonizing development efforts in alignment with the Paris Declaration on Aid Effectiveness and the Accra Agenda for Action are fundamental to this process.
c. States and non-state actors should ensure that individuals are aware of their rights and the MDGs, and are active agents in decisions that affect their lives. Governments, NGOs, and the media should cooperate to educate people about their rights and entitlements. All actors should improve participation, particularly women’s and children’s, in local, national, and international planning efforts and program reviews, and provide mechanisms to address concerns about rights violations and failures in entitlement systems.
3. Promote Integration and Innovation to Catalyze Progress
a. States should integrate human rights principles to guide the elaboration, implementation, and evaluation of MDG-related policies and programs.

2012 The Millennium Development Goals 175
These principles include equality and non-discrimination; the interdepen-dence and indivisibility of all human rights; participation, accountability, and self-determination; and the commitment to take steps to the maximum extent of available resources.
b. A shared operational framework will facilitate the integration of diverse, intersectoral MDG and human rights efforts. Different actors can use such a framework to mobilize and coordinate their work, and to cooperate across sectors. For MDGs 4 and 5, this operational framework should be linked to the concept of the Continuum of Care.
c. States and non-state actors should support innovation in policy, financing, service, and accountability mechanisms. For example, innovative uses of technology (such as SMS messaging) could enable communities to monitor and report on the availability and quality of local health services.
4. Combat Inequality and Discrimination
a. MDG interventions and national health strategies must take account of the needs of marginalized populations to ensure non-discrimination and equal-ity, including gender equality. These populations should be fully included in helping to develop targets and strategies. Accelerating achievement of the MDGs cannot be achieved without an emphasis on non-discrimination in, among other things, access to essential services for the most vulnerable and at-risk groups, particularly with respect to reducing maternal and child mortality.
b. States and non-state actors should monitor inequalities in achieving the MDGs. All development data should be routinely and consistently disag-gregated according to wealth quintile (highlighting the poorest 20 percent), rural/urban location, ethnicity, gender, disability, legal citizenship, status as a refugee or internally displaced person, living situation, and age (children/youth/adult), alongside national averages.106
c. States and non-state actors should comprehensively review laws and poli-cies to identify any that discriminate against women, children, and mar-ginalized populations or fail to adequately protect their rights, including a full spectrum of reproductive and sexual rights. Legislative reform should be supported to replace these with laws and policies that protect rights, which should be robustly enforced. States should effectively enforce laws that protect women’s and children’s rights. All development actors should support women’s and children’s rights, and organizations that directly or indirectly promote health and human rights. Governments should ensure an environment that is conducive to the work of such organizations.
106. For instance, disaggregation according to the living situation of the child should at the very least include those in and outside parental care, and should preferably include disaggregation by as many of the following categories as possible: in parental care; in parental care but identified as vulnerable to abuse or neglect; in extended family care; in institutions; in prison; on the streets; and living with husbands, or employers, or in child-only households.

Vol. 34176 HUMAN RIGHTS QUARTERLY
5. Commit to Accountability for Resources and Results
a. Immediately, states and non-state actors should implement the recommen-dations of the Commission on Information and Accountability for Women’s and Children’s Health.107 Accountability comprises three elements: monitor-ing, review by an independent Expert Review Group, and remedial action. All actors should help strengthen vital registration and health information systems to register births and deaths and to identify causes of preventable deaths in women and children; track coverage of essential interventions for reproductive, maternal, newborn and child health; support the independent review process to determine whether related policy, financial and service commitments are being met; and then take the required remedial actions. Health workers and communities should participate in these processes, which should include regular audits of maternal, newborn, and child deaths to identify shortcomings and inform progress.
b. States and donors should include budgetary transparency as an indicator of their progress towards realizing the MDGs. This is necessary as an early indicator of whether commitments are being translated into entitlements that further progress towards global commitments to the MDGs and human rights. The Commission recommends that tracking resources at a minimum include data on: (i) total health expenditure by financing source, per capita; and (ii) total reproductive, maternal, newborn, and child health expenditure by financing source, per capita.108
c. States and non-state actors should try to integrate accountability mechanisms for the MDGs and human rights. The latter can be strengthened using the more specific indicators and methods developed for MDG monitoring. The human rights institutions can provide institutional review and remedy mechanisms for states that are sustainable beyond 2015. There are a variety of options for cooperation and coordination between MDG and human rights accountability efforts. Adopting the concept of the continuum of care, these efforts could be arrayed along a continuum, anchored at one end by integration of country and regional activities, and at the other end by overarching international collective action, for example, within the United Nations General Assembly.
6. Emphasize Sustainability
a. The international community should build on lessons learned from the MDG global effort to accelerate and sustain health and development efforts towards the progressive realization of human rights. The MDG community should think beyond 2015. The human rights framework can help ensure
107. See keePing ProMises, supra note 78, at 4–5. 108. Id.

2012 The Millennium Development Goals 177
that progress made on the MDGs is maintained, and address recurring constraints and challenges.
b. To sustain the benefits of the MDG efforts beyond 2015, states and non-state actors should coordinate on three key elements, namely: prioritizing national and global commitments and actions, ensuring ongoing monitoring and tracking of efforts and results, and providing feedback to inform future action. These elements are already part of the human rights framework and MDG efforts should be linked with and sustained through them.
c. The international community should develop long-term perspectives and commitments for maternal, newborn, and child health, aligned with the global approach adopted to address environmental change and sustainable development. A world that sustains women’s and children’s health requires political reforms, concerted joint action, innovation, new ways of thinking, and empowered, enlightened citizens. To this end, the MDG community should appreciate that attempting these changes is a difficult and unpredict-able process, and may only produce results in the long term. Future genera-tions may be the main beneficiaries of these efforts. This is a promise that our generation can try and keep for the next. In fact, the potential health and productivity of the next generation depends on our commitment today.
III. CoNCLUSIoN
Despite substantial differences, there are also important complementarities between the MDGs and the human rights framework. A significant oppor-tunity to bring them together and harness the synergies is presented by the UN Secretary-General’s Global Strategy for Women’s and Children’s Health. It would be an unforgivable waste to ignore the human rights dimensions of the MDG implementation effort, and vice versa, whereas linking the two will help realize shared global commitments.
Ultimately, the MDGs and human rights initiatives should enable every individual and community to realize their right to the highest attainable standard of health. We all have a role to play in seizing this unprecedented opportunity to achieve global health and development goals and to realize our universal human rights.





























