Embed Size (px)
Citation preview

The nitric oxide pathwayin the cardiovascular system
S. Llorens, J. Jordán and E. Nava
Facultad de Medicina de la Universidad de Castilla La Mancha y Centro Regionalde Investigaciones Biológicas, Campus de Albacete, 02071 Albacete, Spain
(Received on October 9, 2002)
S. LLORENS, J. JORDÁN and E. NAVA. The nitric oxide pathway in the car-diovascular system (minireview). J. Physiol. Biochem., 58 (3), 179-188, 2002.
The present review analyzes the role nitric oxide (NO) plays in the homeostasisof the cardiovascular system. By regulating vascular smooth muscle cell and myocytecontractility, myocardial oxygen consumption and renal tubular transport, this sim-ple molecule plays a central role in the control of vascular tone, cardiac contractilityand short and long term regulation of arterial pressure. Fifteen years ago, all we knewabout NO is that it had very similar properties as those of endothelium-derivedrelaxing factor and that its action was probably mediated by cGMP. An enormousamount of knowledge has since been amassed on the biochemical pathways that NOfollows from the moment it is synthesized from L-arginine until the physiological orpathological actions take place in the effector cells. This review intends to organizethis knowledge in a fashion that is easy to understand. We will dissect the NO path-way in different steps, focusing on the physiological and pathophysiological actionsof the isoenzymes which synthesize NO, the molecules involved in this synthesissuch as caveolins, protein kinases and cofactors, the situations in which endogenousinhibitors of NO synthase are formed from L-arginine instead of NO, the way inwhich NO exerts its physiological actions through cGMP-dependent protein kinas-es and finally, the pathological routes NO may follow when the oxidative status ofthe cell is high.
Key words: Nitric oxide, L-arginine, Nitric oxide synthase (NOS), Superoxide anion, Peroxynitrite.
J. Physiol. Biochem., 58 (3), 179-188, 2002
Nitric oxide is probably one of themost studied molecules of the last 15
years. NO is a ubiquitous mediator of cellcommunication with central roles in everysystem of the organism. The history ofdiscovery of the NO pathway has beenclosely related to the cardiovascular sys-tem. The reason for this is that the first
Correspondence to E. Nava (Tel.: 967 599200 Ext.2745 / 667 845475; Fax: 967 599327; e-mail: [email protected]).

biological role ascribed to NO was as themolecule that accounted for Furchgott’sendothelium-derived relaxing factor(EDRF) (20). Therefore, most of theresearch performed since 1987, when thisdiscovery was published (44), was focusedon vascular research. While only 385papers were published between 1988 and1989 on the topic “NO in the cardiovas-cular system”, in the last two years (2000and 2001), nearly 5000 papers werereleased. This review intends to providean overview of all the relevant discoverieson the NO pathway that relate to the car-diovascular system. Because the kidneyplays a determinant role in the regulationof arterial pressure we will include in thepresent review some comments on theroles of NO in this organ as well.
NO is a relatively highly reactive freeradical that arises from the enzymatic oxi-dation of a terminal guanidine-nitrogen ofthe semi-essential amino acid L-arginine.Once synthesized, NO undergoes threemain routes: a) activation of guanylatecyclase, which is responsible for the phys-iological effects of NO; b) reaction withoxyhemoglobin to form the stable oxida-tive metabolite, nitrate; or c) transforma-tion to peroxynitrite (OONO–) by thereaction with superoxide (O2
–) and subse-quent protein nitration, which is responsi-ble for most of the pathophysiologicaleffects of NO. Three isoenzymes of NOsynthase (NOS) synthesize NO. In thecardiovascular system, the most relevantisoenzyme for physiological purposes isendothelial NOS (eNOS or NOS III),which is constitutively present in the vas-cular endothelium (31), endocardium andmyocardium (30). Neuronal NOS (nNOSor NOS I) is another isoform, andalthough it is mainly present in the ner-vous system where it is responsible for thephysiological release of NO as a neuro-
transmitter (63), increasing roles in car-diovascular function have been ascribed tothis isoform as we will describe later.nNOS is present in various tissues ofinterest to the cardiovascular system suchas perivascular nerves (2), cardiac conduc-tion tissue (30), myocardial sarcoplasmicreticulum (65) and renal tubules (3). Final-ly, there is an isoform which is normallyexpressed only in the presence of noxiousstimuli, such as toxins. For this reason itwas named inducible NOS (iNOS orNOS II). In the cardiovascular system, itcan be induced in smooth muscle cells(19), endothelial cells (48), endocardialcells (53) and myocardium (50). It can alsobe constitutively present in various typesof renal cells (1). Because this isoform isinduced in the presence of toxins, it playsa major role in septic shock (41).
Figures 1 and 2 depict the physiologicaland pathophysiological routes of the NOpathway as focused on the cardiovascularsystem. In order to make this complexpathway easier to understand, in the pre-sent review we will divide the wholeprocess in seven stages. Namely: 1) Con-version of L-arginine into NO via eNOSand nNOS; 2) Conversion of L-arginineinto NO via iNOS; 3) Conversion of L-arginine into the endogenous inhibitor ofNOS, asymmetric dimethylarginine(ADMA) and transformation of the latterinto L-citrulline by dimethylargininedimethylaminohydrolase (DDAH); 4)Generation of O2
– by NOS under specialcircumstances; 5) Activation of solubleguanylate cyclase (sGC) and generation ofcyclic GMP; 6) Reaction of NO with O2
–
to form OONO– and subsequent tyrosinenitration to form nitrotyrosine; and 7)Release of NO from OONO– under spe-cial circumstances.
S. LLORENS, J. JORDÁN AND E. NAVA180
J. Physiol. Biochem., 58 (3), 2002
Conversion of L-arginine to NOvia eNOS and nNOS
eNOS and nNOS are calcium-depen-dent constitutive enzymes that catalyze afive-electron oxidation of L-arginine toNO and L-citrulline using NADPH asthe electron source. These enzymesrequire the presence of calmodulin to pro-vide the calcium and four cofactors:tetrahydrobiopterin (BH4), flavin adeninedinucleotide (FAD), flavin mononu-cleotide (FMN) and heme. While nNOS iscytosolic, eNOS is a membrane-boundenzyme which is now known to be specif-ically located in caveolae (38), the choles-terol-rich membrane microdomainswhich function as a strategic place formessenger processing and signal-trans-duction pathways (38). In particular, cave-olae possess large amounts of G proteins,IP3 receptors, tyrosine kinase, as well asbeing enriched in eNOS and calmodulin
and specific proteins called caveolinswhich interact with eNOS and attenuateits activity. eNOS remains inactive whileit is bound to caveolin, but when intracel-lular calcium concentration increases, thecomplex calcium-calmodulin liberateseNOS from caveolin and the enzyme istranslocated to the cytosol, free to synthe-size NO. Knock-out mice lacking caveo-lae have a high eNOS activity andincreased endothelium-dependent relax-ation (15). Although, for years calciumconcentration was considered the mostimportant stimulus for eNOS activity, anumber of alternative pathways are beingdiscovered. It is noteworthy that amongthe three isoenzymes of NOS, theentothelial is the one subjected to themost numerous regulatory mechanisms.Activation mechanisms include: a) tyro-sine phosphorylation of certain proteins;b) serine phosphorylation of eNOS byserine/threonine protein kinase Akt (pro-
NITRIC OXIDE PATHWAY IN THE CARDIOVASCULAR SYSTEM 181
J. Physiol. Biochem., 58 (3), 2002
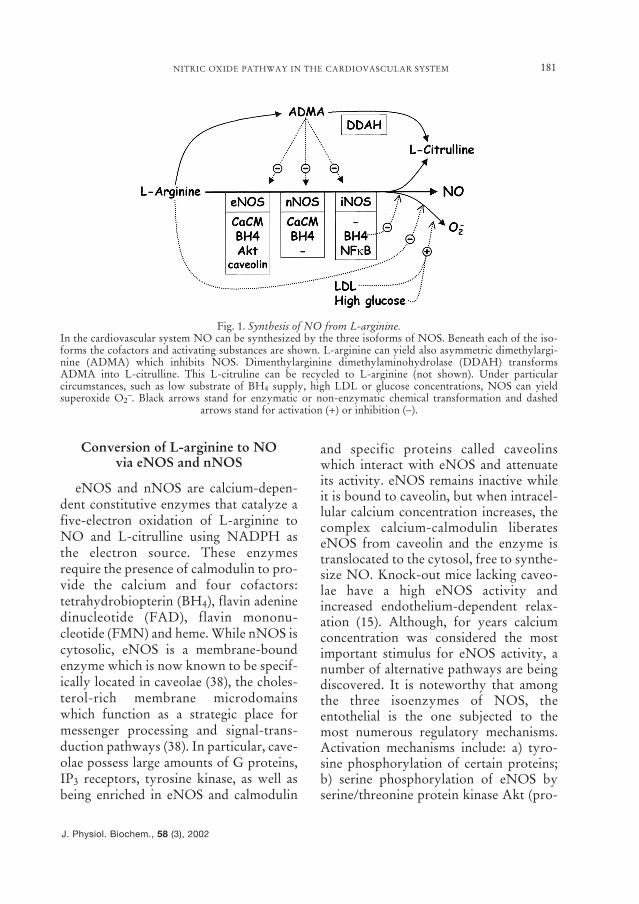
Fig. 1. Synthesis of NO from L-arginine.In the cardiovascular system NO can be synthesized by the three isoforms of NOS. Beneath each of the iso-forms the cofactors and activating substances are shown. L-arginine can yield also asymmetric dimethylargi-nine (ADMA) which inhibits NOS. Dimenthylarginine dimethylaminohydrolase (DDAH) transformsADMA into L-citrulline. This L-citruline can be recycled to L-arginine (not shown). Under particularcircumstances, such as low substrate of BH4 supply, high LDL or glucose concentrations, NOS can yieldsuperoxide O2
–. Black arrows stand for enzymatic or non-enzymatic chemical transformation and dashedarrows stand for activation (+) or inhibition (–).

er, our knowledge on the transductionpathways of the mechanical signal to theintracellular space is still rather poor. It islikely that shear forces on the endothelialcell surface are transmitted to the caveolaethrough the cytoskeleton (14) and thatcomplex G protein activation processesare involved (24).
Stimulation of eNOS and nNOS activ-ity in myocardial and renal tubular cells.–All the intracellular and extracellularmechanisms described so far have beenexplored mostly in endothelial cells, how-ever, myocardial and renal tubular cellsexpress the constitutive forms of NOS,eNOS and nNOS and possess specificmechanisms of activation. For instance,renal tubular cells upregulate eNOS andnNOS through shear stress mechanismscaused by increases in tubular flow (13).Myocardial cells are also able to synthe-size and release NO which is deeplyinvolved in the regulation of cardiac func-tion (31), but for years researchers wereunable to reach a consensus as to whetherNO increases or decreases cardiac con-tractility (24, 62). It appears clear thatmechanical forces generated by the beat-ing heart cause NO release mostly fromcoronary endothelial cells (45). Now weknow that myocardial cells have anextremely complex machinery to produceNO that involves eNOS and nNOS activ-ities. Myocardial eNOS, localizes to cave-olae and causes negative inotropy andpositive lusitropy, that is, enhances con-tractility and hastens relaxation (37). Onthe other hand, nNOS is localized in thesarcoplasmic reticulum (64) and causespositive inotropy (4). Besides theseeffects, NO also causes negativechronotropism (37) and reduces cardiacO2 consumption (35) by inhibiting mito-chondrial respiration (14)
S. LLORENS, J. JORDÁN AND E. NAVA182
J. Physiol. Biochem., 58 (3), 2002
tein kinase B), protein kinase A, AMPkinase and other kinases; c) threoninedephosphorylation of eNOS; d) intracel-lular alkalinization and e) heat shock pro-tein. Inhibitory pathways include: a)eNOS phosphorylation by PKC and b)NOS integrating protein (NOSIP). For anextensive review on eNOS regulatorymechanisms see ref. 22. In addition, a largenumber of mechanisms upregulate ordowregulate eNOS expression. For exam-ple, estrogen upregulates eNOS (22) andthe recently described endothelial dys-function inducing protein (EDIP)dowregulates eNOS expression (35).
Stimulation of eNOS activity inendothelial cells.– Endothelial cells coverthe luminal side of vascular smooth mus-cle and the cardiac cavities. These cellsexpress only eNOS in a constitutive man-ner and the released NO causes vascularsmooth muscle relaxation and, whenreleased from endocardial or coronaryendothelial cells, possibly myocardialfunction modulation. The extracellularstimuli which turn on the pathways thatultimately activate eNOS in these cells arepharmacological and mechanical. Pharma-cological stimuli include all the wellknown endothelium-dependent vasoac-tive substances like acetylcholine orbradykinin. These agents bind membranereceptors linked to G proteins that canactivate the processes to increase intracel-lular calcium, which would bind calmod-ulin, or activate the alternative eNOSphosphorylation pathways (50). Mechani-cal stimuli also activate eNOS through theaforementioned protein kinases but in analmost calcium-independent fashion (22)derived NO release. The major mechani-cal force to which endothelial cells areexposed is the shear stress of blood flow-ing along the endothelial surface, howev-
Conversion of L-arginineinto NO via iNOS
iNOS is a calcium-independent indu-cible enzyme and is not normally presentin the cells. This enzyme requires de novosynthesis or induction, which is mainlytriggered by endotoxins and cytokines ina very complex manner that involves acti-vation of nuclear factor-kB (NFkB),among other factors (52). This means thatiNOS is implicated in septic shock andother processes that activate the immunesystem (18). The requirements and cofac-tors for its activation are the same as forthe other isoenzymes with the exceptionthat iNOS, although it has a binding sitefor calmodulin, can work at calcium con-centrations well below the physiologicalones (27). Septic shock is probably thedisease in which the medical communityhas had the highest hopes for NO-basedtherapies. This disease is characterized byrefractory hypotension, generalized organmalfunction and tissue damage (18). Theinitial triggering factor of all theseprocesses is the activation of macro-phages, neutrophils and monocytes by anendotoxin that is ussually a lipopolysac-charidic component of gram negative bac-teria walls (LPS). Activated cells producecytokines like tumour necrosis factor(TNFα) or interferon (IFγ) and many oth-ers, and until the discovery of NO, it wasbelieved that the interactions of thesemediators produce the pathophysiologicalalterations of septic shock (9). The discov-ery of the induction of iNOS in septicshock (49) led to the hypothesis that anuncontrolled release of NO was theunderlying cause of this disease. This ideawas based on the following observations:a) NO is a potent vasodilator; b) whenimmunologically induced, iNOS reachesan enzymatic activity very well in excessof that of the other isoenzymes (50); and
c) the major symptom of septic shock ishypotension. Therefore, an enormouseffort has been invested in the fightagainst a presumably unwanted excess inNO produced by iNOS (18, 41), particu-larly in the quest to find a specificinhibitor of iNOS (27).
Conversion of L-arginine into ADMA
Pharmacologically designed NOSinhibitors are mainly based in methylatedderivatives of L-arginine. For example,the first and most used inhibitor ofNOS is N-monomethyl-L-arginine(L-NMMA) (27). Many years before thediscovery of the NO pathway, the exis-tence of endogenous methylated forms ofL-arginine were reported (29). In 1992, itwas reported that patients with renal fail-ure accumulate an endogenously synthe-sized methylated L-arginine, ADMA (58)and it is now known that vascular tissuepossesses an enzyme, DDAH, which con-verts ADMA into L-citrulline (36) possi-bly playing a protective role againstunwanted NOS inhibition. ExcessiveADMA formation has been reported invarious cardiovascular diseases, such asatherosclerosis (28) and hypertension(55), in which endothelial function is com-promised.
Generation of O2– by NOS
under special circumstances
Interestingly, the three isoforms ofNOS can produce O2
– in a process calleduncoupling (47, 61, 64). In this situation,electrons are not transferred to L-arginineto form NO, but to oxygen to form O2
–.This anion reacts avidly with NO, dra-matically reducint its half-life and derivat-ing NO to the dangerous ONOO- path-way. Furthermore, ONOO– oxidizesBH4 to an inactive BH2 form, thus pro-
NITRIC OXIDE PATHWAY IN THE CARDIOVASCULAR SYSTEM 183
J. Physiol. Biochem., 58 (3), 2002
moting a cycle of destruction iniciated byNOS-dependent ONOO- formation (39).Fortunately this happens only in specialcircumstances like L-arginine or BH4depletion and under the presence ofnative/oxidized LDL (59) or high glucoseconcentrations (67). These situations areof particular interest in atherosclerosis ordiabetes mellitus (26). Indeed, administra-tion of L-arginine (16) or BH4 (54) in ath-erosclerosis restores endothelium-depen-dent responses.
Activation of soluble guanylate cyclase(sGC) and generation of cyclic GMP
Cells expressing eNOS and nNOSrelease NO in the range of 50-500 nM (6,46). This NO acts in a paracrine orautocrine fashion as O2
– quickly destroysit (6). In contrast, immunologically-induced iNOS releases NO in a muchhigher rate as plasma nitrate measure-ments suggest (42). Nearly all the physio-
logical effects of NO are mediated bycGMP. NO has no membrane receptor,but binds the heme group of sGC produc-ing a conformational change, whichincreases its activity (27). sGC convertsGTP into cGMP and this would activateprotein kinase G (PKG), a cGMP-depen-dent protein phosphorylator. The resultsof PKG-mediated protein phosphoryla-tion are: a) inhibition of L-type calciumchannels in the plasma membrane (8); b)activation of Ca++-ATPase (60) and Ca++-Na+ exchanger also in the plasma mem-brane (21); c) activation of Ca++-ATPaseat the level of the sarcoplasmic reticulum(13); and d) inhibition of protein lipase C(PLC) (32). Altogether, the result is areduction of intracellular calcium, which,in the particular case of vascular smoothmuscle cells leads to relaxation. Obvious-ly, all these PKG-calcium dynamics varybetween different cell types and are par-ticularly complex in the myocyte (37).
S. LLORENS, J. JORDÁN AND E. NAVA184
J. Physiol. Biochem., 58 (3), 2002
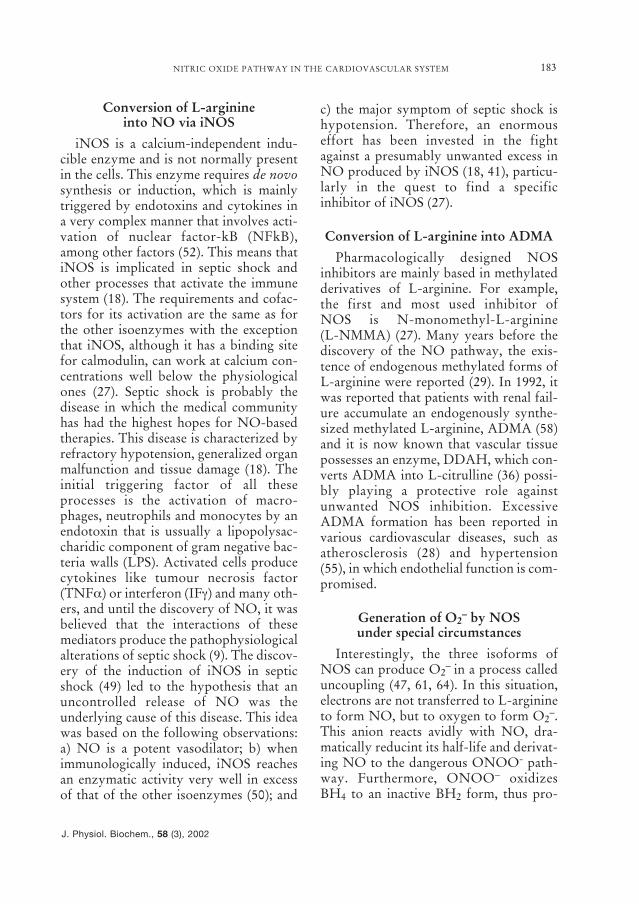
Fig. 2. NO pathways in the cardiovascular system and renal tubular epithelium.In normal conditions NO follows the cGMP route by activating soluble guanylate cyclase (sGC). cGMP caus-es the typical physiological effects of NO in the vessels, the heart and the kidney. In certain pathophysiologi-cal situations in wich the production of O2
– is enhanced, NO follows the peroxynitrite (OONO–) route andthis reactive species elicits tissue damage detectable as tyrosine nitration in various tissues. There are multiplesources of O2
–. For an extensive review on the mechanisms of O2– generation, see fev. 66 NO2-Tyr = nitroty-
rosine. Black arrows stand for enzymatic or non-enzymatic chemical transformation, dashed arrows stand foractivation (+) or inhibition (–), and thick white arrows stand for elicited effect.

Reaction of NO with O2– to form
OONO– and subsequent tyrosinenitration to form nitrotyrosine
NO can combine directly with localelectron-accepting species like oxygen,transition metal ions, or superoxide radi-cals to generate potent reactive species(e.g. N2O3, NO+ and ONOO–) thatwould S-nitrosylate sulphur-containingmolecules. Overproduction of NO cancause cellular damage by forming morecytotoxic reactive nitrogen species, suchas the one with O2
– to form peroxynitrite(NO + O2
–→ ONOO–) (6). Peroxynitriteis rapidly protonated to peroxynitrousacid (ONOO– + H+ → ONOOH). Thisacid generates a range of cytotoxic speciesthat exhibit hydroxylating, oxidizing, andnitrating activity. In particular, ONOOHrapidly oxidizes and nitrates proteins; forexample cysteine and methionine residuesare oxidized, whereas tyrosine and tryp-tophan can be nitrated (6). Measurementof 3-nitrotyrosine residues is a widelyused biomarker for ONOOH formation,although nitration can also involve otherreactive nitrogen species (25).
NO· in its singlet or high-energy statecan also react with thiol groups withinproteins (33). Formation of such S-nitro-sylated proteins is an important, post-translational modification of proteinstructure that can modulate protein func-tion. This ubiquitous regulatory mecha-nism is comparable to phosphorylationand has been shown to affect manyprocesses ranging from signal transduc-tion to DNA repair (10). Examples of thisinclude the activation or inhibition of sev-eral enzymes that are involved in numer-ous cellular processes including apoptosis(17). S-nitrosylation by NO has become avery important post-translational modifi-cation of numerous intracellular proteinsincluding Ras (56), c-Jun N-terminal
kinase/ stress-activated protein kinase(45), ornithine decarboxylase (5) andtransglutaminase (7). S-nitrosylation ofthese and other proteins may modulatetheir activity and apoptotic potential.These reactions play an important role insituations where there is a generation ofsignificantly more O2
– as seems to happenin endothelial cells in atherosclerosis,hypertension, septic shock and diabetesmellitus. In support of this is the fact thatin all these diseases, nitrotyrosine accu-mulation has been found at the level ofendothelial cells or other tissues affectedby the pathological process (57).
Release of NO from OONO–
under special circumstances
Although OONO– indeed causes tissuedamage, there are detoxification mecha-nisms designed to counteract its potentialto injure tissues. As stated above,ONOO– can react with thiol groups. Inthis line, it has been demonstrated thatOONO– can also react with compoundscontaining an alcohol functional group,such as glucose, to form an NO donorwith the same characteristics of a nitrova-sodilator (40). These protective mecha-nisms are of particular relevance inischemia-reperfusion of the heart (43).
In summary, in the cardiovascular sys-tem the conversion of L-arginine to NOis catalyzed by the three existing isoformsof NOS: a) eNOS, located in the mem-brane caveolae of endothelial cells andmyocytes, is stimulated by shear stress inthe vessels and by beating forces in theheart. Calcium-calmodulin, caveolins andvarious protein kinases are involved inthis stimulation, which causes vasodila-tion, negative inotropism and diminishesmyocardial oxygen consumption; b)nNOS, is a cytosolic enzyme and is locat-ed in perivascular nerves, myocyte sar-
NITRIC OXIDE PATHWAY IN THE CARDIOVASCULAR SYSTEM 185
J. Physiol. Biochem., 58 (3), 2002

coplasmic reticulum and renal tubularepithelium. Its stimulation causes vasodi-lation, positive inotropism and diuresis; c)iNOS, which is not normally present, canbe induced in endothelial cells, smoothmuscle cells and myocytes and is involvedin processes that activate the immune sys-tem.
Once released, NO undergoes a physi-ological route by which it exerts its nor-mal cGMP-mediated biological effects.However, NO can also follow a patholog-ical route by reacting with O2
– and gener-ating OONO– which causes protein nitra-tion and tissue damage. Reduced thiolsplay a protective role against the deletere-ous effects of OONO– by generating NOdonors.
Acknowledgements
This work was supported by the “Fondo deInvestigaciones Sanitarias” (00/0280), the “Conse-jería de Sanidad de Castilla-La Mancha” (02038-00)and CICYT (SAF2002-04721). S.L. was granted bythe “Consejería de Sanidad de Castilla-La Mancha”.
S. LLORENS, J. JORDÁN y E. NAVA.La vía del óxido nítrico en el sistema cardiovas-cular (minirrevisión). J. Physiol. Biochem., 58(3), 179-188, 2002.
Esta revisión aborda el importante papelque juega el óxido nítrico (NO) en la homeos-tasis del sistema cardiovascular. Esta simplemolécula regula la contractilidad de las célulasdel músculo liso vascular y de los miocitos, elconsumo de oxígeno del miocardio y el trans-porte tubular renal. Así pues, juega un papelclave en el control del tono vascular, en la con-tractilidad cardiaca y en la regulación a corto ylargo plazo de la presión arterial. Hace quinceaños lo único que se sabía del NO era queposeía propiedades muy similares a las del fac-tor relajante derivado del endotelio y que suacción, probablemente, estaba mediada por elGMP cíclico. A lo largo de los últimos años, seha ido recopilando mucha información relativaa las vías metabólicas que sigue el NO, desde
que es sintetizado a partir de la L-arginina,hasta que tienen lugar sus acciones fisiológicaso patológicas en las células efectoras del siste-ma cardiovascular. Esta revisión pretendeorganizar esta información de una manerafácilmente comprensible. La vía del NO sedivide en diferentes pasos, centrándose en lasacciones fisiológicas y patofisiológicas de lasisoenzimas que sintetizan NO, en las molécu-las involucradas en esta síntesis, tales como lascaveolinas, las proteín cinasas y los cofactoresde la NO sintasa (NOS). También se analizanlas situaciones en las que, a partir de la L-argi-nina, se forman inhibidores endógenos de laNOS, los mecanismos por los que el NO ejer-ce sus acciones fisiológicas a través de proteíncinasas dependientes de GMPc y, finalmente,se estudian las rutas patológicas que puedeseguir el NO cuando el estado oxidativo de lacélula es elevado.
Palabras clave: Óxido nítrico, L-arginina, Óxidonítrico sintasa (NOS), Anión superóxido, Peroxini-
trito.
References
1. Ahn, K. Y., Mohaupt, M. G., Madsen, K. M. andKone, B. C. (1994): Am. J. Physiol., 267, F 748-757.
2. Ayajiki, K., Okamura, T., Noda, K. and Toda,N. (2002): Jpn. J. Pharmacol., 89, 197-200.
3. Bachmann, S., Bosse, H. M. and Mundel, P.(1995): Am. J. Physiol., 268, F 885-898.
4. Barouch, L. A., Harrison, R. W., Skaf, M. W.,Rosas, G. O., Cappola, T. P., Kobeissi, Z. A.,Hobai, I. A., Lemmon, C. A., Burnett, A. L.,O’Rourke, B., Rodriguez, E. R., Huang, P. L.,Lima, J. A., Berkowitz, D. E. and Hare, J. M.(2002): Nature, 416, 337-339.
5. Bauer, P. M., Buga, G. M., Fukuto, J. M., Pegg,A. E. and Ignarro, L. J. (2001): J. Biol. Chem.,276, 34458-34464.
6. Beckman, J. S. and Koppenol, W. H. (1996): Am.J. Physiol., 271, C 1424-1437.
7. Bernassola, F., Rossi, A. and Melino, G. (1999):Ann. N. Y. Acad. Sci., 887, 83-91.
8. Blatter, L. A. and Wier, W. G. (1994): Cell Cal-cium, 15, 122-131.
9. Bone, R. C. (1991): Ann. Int. Med., 115, 457-469.
S. LLORENS, J. JORDÁN AND E. NAVA186
J. Physiol. Biochem., 58 (3), 2002
NITRIC OXIDE PATHWAY IN THE CARDIOVASCULAR SYSTEM 187
J. Physiol. Biochem., 58 (3), 2002
10. Broillet, M. C. (1999): Cell Mol. Life Sci., 55,1036-1042.
11. Cai, Z., Xin, J., Pollock, D. M. and Pollock, J. S.(2000): Am. J. Physiol., 279, F 270-274.
12. Clementi, E., Brown, G. C., Foxwell, N. andMoncada, S. (1999): Proc. Natl. Acad. Sci. USA,96, 1559-1562.
13. Cohen, R. A., Weisbrod, R. M., Gericke, M.,Yaghoubi, M., Bierl, C. and Bolotina, V. M.(1999): Circ. Res., 84, 210-219.
14. Davies, P. F. (1995): Physiol. Rev., 75, 519-560.15. Drab, M., Verkade, P., Elger, M., Kasper, M.,
Lohn, M., Lauterbach, B., Menne, J., Lindschau,C., Mende, F., Luft, F. C., Schedl, A., Haller, H.and Kurzchalia, T. V. (2001): Science, 293, 2449-2452.
16. Drexler, H., Zeiher, A. M., Meinzer, K. and Just,H. (1991): Lancet, 338, 1546-1550.
17. Estévez, A. and Jordán, J. (2002): Ann. N.Y.Acad. Sci., 962, 207-211.
18. Feihl, F., Waeber, B. and Liaudet, L. (2001):Crit. Care Med., 29, 2230-2231.
19. Fleming, I., Gary, G. A., Schott, C. and Stoclet,J. C. (1991): Eur. J. Pharmacol., 200, 375-376.
20. Furchgott, R. F. and Zawadzki, J. V. (1980):Nature, 28, 373-376.
21. Furukawa, K., Ohshima, N., Tawada-Iwata, Y.and Shigekawa, M. (1991): J. Biol. Chem., 266,12337-12341.
22. Govers, R. and Rabelink T. J. (2001): Am. J.Physiol., 280, H 193-206.
23. Grocott-Mason, R., Fort, S., Lewis, M. J. andShah, A. M. (1994): Am. J. Physiol., 266, H 1699-1705.
24. Gudi, S. R., Clark, C. B. and Frangos, J. A.(1996): Circ. Res., 79, 834-839.
25. Halliwell, B., Zhao, K. and Whiteman, M.(1999): Free Radic. Res., 31, 651-669.
26. Heitzer, T., Krohn, K., Albers, S. and Meinertz,T. (2000): Diabetologia, 43, 1435–1438.
27. Hobbs, A. J., Higgs, A. and Moncada, S. (1999):Annu. Rev. Pharmacol. Toxicol., 39, 191-220.
28. Ito, A., Tsao, P. S., Adimoolam, S., Kimoto, M.,Ogawa, T. and Cooke, J. P. (1999): Circulation,99, 3092-3095.
29. Kakimoto, Y. and Akazawa, S. (1970): J. Biol.Chem., 245, 5751-5758.
30. Kelly, R. A., Balligand, J. L., Smith, T. W.(1996): Circ. Res., 79, 363-380.
31. Lamas, S., Marsden, P. A., Li, G. K., Tempst, P.and Michel T. (1992): Proc. Natl. Acad. Sci. USA,89, 6348-6352.
32. Lang, D. and Lewis, M. J. (1991): Br. J. Pharma-col., 102, 277-281.
33. Lipton, S. A. and Stamler, J. S. (1994): Neu-ropharmacology, 33, 1229-1233.
34. Loke, K. E., McConnel, P. I., Tuzman, J. M.,Shesely, E. G., Smith, C. J., Stackpole, C. J.,Thompson, C. I., Kaley, G., Wolin, M. S. andHintze, T. H. (1999): Circ. Res., 84, 840-845.
35. López-Farré, A. and Casado, S. (2001): Hyper-tension, 38, 1400-1405.
36. MacAllister, R. J., Parry, H., Kimoto, M.,Ogawa, T., Russell, R. J., Hodson, H., Whitley,G. S. and Vallance, P. (1996): Br. J. Pharmacol.,119, 1533-1540.
37. Massion, P. B., Moniotte, S. and Balligand, J. L.(2001): Curr. Opin. Crit. Care, 7, 323-336.
38. Michel, T. and Feron, O. (1997): J. Clin. Invest.,9, 2146-2152.
39. Milstien, S. and Katusic, Z. (1999): Biochem.Biophys. Res. Commun., 263, 681-684.
40. Moro, M. A., Darley-Usmar, V. M., Lizasoain,I., Su, Y., Knowles, R. G., Radomski, M. W. andMoncada, S. (1995): Br. J. Pharmacol., 116, 1999-2004.
41. Nava, E., Palmer, R. M. J. and Moncada, S.(1991): Lancet, 338, 1555-1557.
42. Nava, E. and Salazar, F. J. (1997): Eur. J. Clin.Invest., 27, 673-679.
43. Nossuli, T. O., Hayward, R., Scalia, R. andLefer, A. M. (1997): Circulation, 96, 2317-24.
44. Palmer, R. M. J., Ferrige, A. G. and Moncada, S.(1987): Nature, 327, 524-526.
45. Park, H. S., Huh, S. H., Kim, M. S., Lee, S. H.and Choi, E. J. (2000): Proc. Natl. Acad. Sci.USA, 97, 14382-14387.
46. Pinsky, D. J., Patton, S., Mesaros, S.,Brovkovych, V., Kubaszewski, E., Grunfeld, S.and Malinski, T. (1997): Circ. Res., 81:372-379.
47. Pou, S., Pou, W. S., Bredt, D. S., Snyder, S. H.and Rosen, G. M. (1992): J. Biol. Chem., 267,24173-24176.
48. Radomski, M. W., Palmer, R. M. J. and Monca-da, S. (1990): Proc. Natl. Acad. Sci. USA, 87,10043-10047.
49. Rees, D. D., Cellek, S., Palmer, R. M. J. andMoncada, S. (1990): Biochem. Biophys. Res.Commun., 173, 541-547.
50. Schulz, R., Nava, E. and Moncada, S. (1992): Br.J. Pharmacol., 105, 575-580.
51. Shaul, P. W. (2002): Annu. Rev. Physiol., 64,749-774.
52. Sheenan, M., Wong, H. R., Hake, P. W., Malho-tra, V., O´Connor, M. and Zingarelli, B. (2002):Mol. Pharmacol., 61, 953-963.
53. Smith, J. A., Radomski, M. W., Schulz, R., Mon-cada, S. and Lewis, M. J. (1993): Br. J. Pharma-col., 108, 1107-1110.
54. Stroes, E., Kastelein, J., Cosentino, F., Erkelens,W., Wever, R., Koomans, H., Lüscher, T. andRabelink, T. (1997): J. Clin. Invest., 99, 41-46.
55. Surdacki, A., Nowicki, M., Sandmann, J., Tsikas,D., Boeger, R. H., Bode-Boeger, S. M., Kruszel-nicka-Kwiatkowska, O., Kokot, F., Dubiel, J. S.and Froelich, J. C. (1999): J. Cardiovasc. Phar-macol., 33, 652-658.
56. Teng, K. K., Esposito, D. K., Schwartz, G. D.,Lander, H. M. and Hempstead, B. L. (1999):J. Biol. Chem., 274, 37315-37320.
57. Turko, I. V., Marcondes, S. and Murad, F.(2001): Am. J. Physiol., 281, 2289-2294.
58. Vallance, P., Leone, A., Calver, A., Collier, J.and Moncada, S. (1992): Lancet, 329, 572-575.
59. Vergnani, L., Hatrik, S., Ricci, F., Passaro, A.,Manzoli, N., Zuliani, G., Brovkovych, V.,Fellin, R. and Malinski, T. (2000): Circulation,101, 1261-1266.
60. Vrolix, M., Raeymaekers, L., Wuytack, F., Hof-mann, F. and Casteels, R. (1988): Biochem. J.,255, 855-863.
61. Wever, R. M., van-Dam, T., van-Rijn, H. J., de-Groot, F. and Rabelink, T. J. (1997): Biochem.Biophys. Res. Commun., 237, 340-344.
62. Weyrich, A. S., Ma, X., Buerke, M., Murohara,T., Armstead, V. E., Lefer, A. M., Nicholas, J.M., Thomas, A. P., Lefer, D. J. and Vinten-Johansen, J. (1994): Circ. Res., 75, 692-700.
63. Wiklund, N. P., Cellek, S., Leone, A. M.,Iversen, H. H., Gustafsson, L. E., Brundin, L.,Furst, V. W., Flock, A. and Moncada, S. (1997):J. Neurosci. Res., 47, 224-232.
64. Xia, Y. and Zweier, J. L. (1997): Proc. Natl. Acad.Sci. USA, 94, 6954-6958.
65. Xu, K. Y., Huso, D. L., Dawson, T. M., Bredt,D. S. and Becker, L. C. (1999): Proc. Natl. Acad.Sci. USA, 96, 657-662.
66. Zalba, G., Beaumont, J., San José, G., Fortuño,A., Fortuño, M. A. and Diez, J. (2000): J. Phy-siol. Biochem., 56, 57-64.
67. Zou, M. H., Shi, C., Cohen, R. A. (2002): Diabe-tes, 51:198-203.
S. LLORENS, J. JORDÁN AND E. NAVA188
J. Physiol. Biochem., 58 (3), 2002





























