Embed Size (px)
Citation preview

Fax +41 61 306 12 34E-Mail [email protected]
Original Paper
Psychopathology 2011;44:106–115 DOI: 10.1159/000319788
The Prevalence of Delusion-LikeBeliefs Relative to Sociocultural Beliefsin the General Population Rachel!Pechey Peter!Halligan
School of Psychology, Cardiff University, Cardiff , UK
chometric properties demonstrated by the CBQ indicate that this measure is a useful tool to investigate the wider continuum of beliefs held in the general population.
Copyright © 2010 S. Karger AG, Basel
Introduction
Delusions remain one of the most powerful constructs in psychiatry, given their contribution to the diagnosis of patients considered to have lost touch with reality [1] . For Jaspers [2] delusions were ‘psychologically irreducible’, and constituted the ‘basic characteristic of madness’. While established psychiatric definitions claim that delu-sions are beliefs (i) held despite what almost everyone else believes and (ii) qualitatively distinct from those beliefs ordinarily held by members of a person’s culture, most clinicians are not in a position to know the prevalence of such beliefs within society. Thus this criterion that a de-lusion is ‘not [a belief] ordinarily accepted by other mem-bers of the person’s culture or subculture’ is typically not based on evidence of how widely accepted such beliefs are.
One pragmatic way of establishing the prevalence of culturally held beliefs is to employ large-scale market re-search polls. Previously such studies confirmed that sig-
Key Words Delusion-like belief ! Paranormal belief ! Religious belief ! Continuum
Abstract Background: Delusions are defined as false beliefs different from those that almost everyone else believes. The aim was to develop a new measure (the Cardiff Beliefs Questionnaire, CBQ) to establish the range and prevalence of delusion-like beliefs (DLB) and compare these to other types of beliefs in the general population. Sampling and Methods: A total of 1,000 participants completed the CBQ, which uniquely as-sesses a broader range of currently held beliefs [delusion-like (bizarre and non-bizarre), paranormal and religious and general political/social beliefs) using this large stratified sample. Results: Strong belief in 1 or more DLB was reported by 39% of the participants (91% reporting ‘weak’, ‘moderate’ or ‘strong’ belief in at least 1 DLB). Moreover, 25% endorsed at least 1 bizarre DLB (76% one or more at any strength). En-dorsements of DLB were strongly correlated with paranor-mal and religious beliefs but not general political/social be-liefs. Conclusions: Both bizarre and non-bizarre DLB are fre-quently found in the general population, lending support to the psychosis continuum account and need to revise key clinical criteria used to diagnose delusions. The good psy-
Received: September 28, 2009 Accepted after revision: July 29, 2010 Published online: December 24, 2010
Peter W. Halligan School of Psychology, Cardiff University Park Place Cardiff CF10 3YG (UK) Tel. +44 29 208 76911, Fax +44 29 208 74858, E-Mail HalliganPW ! @ ! cf.ac.uk
© 2010 S. Karger AG, Basel0254–4962/11/0442–0106$38.00/0
Accessible online at:www.karger.com/psp

DLB Psychopathology 2011;44:106–115 107
nificant numbers of Britons and North Americans hold surprisingly high levels of conviction about abnormal, unscientific or paranormal beliefs (e.g. over 50% of adults in the USA report believing in ghosts [3] ) ( table!1 ). In con-trast, the prevalence rates for clinical psychosis varie but were considerably less, with a major systematic review reporting median values per 1,000 persons for point and lifetime prevalence of schizophrenia of 4.6 (1.9–10.0) and 4.0 (1.6–12.1), respectively [4] . Most individuals who present at psychiatric clinics with delusions have experi-enced significant disruption to their lives and/or those of family and friends. By comparison, ‘the core symptoms of psychosis, delusions and hallucinations are much more prevalent in the general populations than their clinical counterparts’, with studies estimating a lifetime preva-lence of around 15% [ 5 , p. 53] and an average annual prev-alence rate of 5% [6] for delusions. Several researchers consider that such beliefs lie on a continuum where symp-toms do not demonstrate any significant morbidity or disability [5–10] . Indeed, the consistent finding that many non-clinical participants endorse questions relat-ing to both delusions and hallucinations implies that ‘ex-periencing symptoms of psychosis such as delusions and hallucinations is not inevitably associated with the pres-ence of disorder’ [ 6 , p. 179]. Clearly other factors such as intrusiveness, psychopathological comorbidities, illness behaviour, societal tolerance, coping and distress play a significant role in the clinical presentation of delusional beliefs.
An important issue when establishing the prevalence of psychosis-like symptoms in the general population concerns the types of measures used. A critical issue here concerns the validity of self-reported data obtained from non-clinical subjects, particularly where questions ex-
plicitly pertain to mental illness, given the understand-able unwillingness of subjects to provide honest respons-es where these could present participants in a socially un-acceptable manner [11, 12] . Stigma associated with mental illness is well recognised as an important factor influenc-ing access to mental healthcare by the general population [13] . Indeed, a study of military personnel revealed that many had not honestly answered health screening ques-tions for reasons of lack of trust in medical confidential-ity, stigmatisation and fears that the process would jeop-ardise career prospects [14] . In particular older subjects, and especially women, are more likely to respond in a so-cially desirable manner [15, 16] .
To help reduce the effects of clinical language, sever - al studies developed less clinically explicit measures of ‘delusional ideation’ [17–19] . Using this approach, stud - ies found that around 10% of non-clinical participants scored above the mean for deluded patients on the Peters et al. Delusion Inventory (PDI) [19] , a popular non-clini-cal measure, much of the content of which is taken from the Present State Examination [20] . Median scores for healthy participants on the PDI [18, 19] showed that the majority of these non-clinical samples endorsed at least one psychosis-based item.
To date, most non-clinical measures focus almost ex-clusively on the delusions commonly found in schizophre-nia, namely non-bizarre delusions (e.g. persecutory be-liefs) and some bizarre delusions concerning thought and action control. This approach (while informative) does not address the range of bizarre delusions, which – according to the DSM-IV – are ‘clearly implausible and not under-standable and do not derive from ordinary life experienc-es’ [ 20 , p. 275]. Many well-documented monothematic bi-zarre delusions (e.g. Capgras, Cotard’s, reduplicative par-
Table 1. Prevalence of selected religious and paranormal beliefs in recent British surveys
Date conducted: J an 1998 Feb 1998 Aug 2003 Oct 2004 Apr 2005 Jan 2006 Jan 2008
Co nducted by: ICM MORI MORI YouGov Populus MORI MRUK
Conducted for: Daily Mail The Sun BBC: Heavenand Earth Show
ITV:This Morning
The Sun The Sun: BritishVoters Survey
Cardiff University
Number 1,000 721 1,001 2,116 1,009 1,001 1,000Belief in, %
God 64 64 60 – 70 60 73A soul – 67 68 – 71 – 64Astrology – 38 31 – – 28 45Reincarnation 25 24 23 29 – 23 40Communication with the dead – – – 33 – – 55

Pechey/Halligan
Psychopathology 2011;44:106–115 108
amnesia, mirrored-self misidentification) ( table! 2 ) have been the subject of considerable recent research [21–24] , despite being less common than other delusions.
One aim of the present study was to describe the Car-diff Beliefs Questionnaire (CBQ), which was developed to capture a wider range of beliefs (including delusion-like beliefs, DLB) and minimise the social stigma at-tached to endorsing psychosis-like beliefs by embedding such questions in a broader range of moral, paranormal and religious beliefs. The inclusion of questions covering more common, less stigmatising beliefs served to reduce the psychiatric associations and encourage participants to engage honestly with the questions. In addition, the range of bizarre DLBs covered distinguishes the CBQ from previous measures of delusions or delusional ide-ation.
By avoiding clinical language and locating DLB with-in a broader context, it was predicted that participants might be more willing to endorse items honestly and openly, leading to higher than previously reported en-dorsements of clinical-like beliefs. By investigating a wide range of delusion-like items (including several bizarre be-liefs), the aim was to estimate and compare the prevalence of both bizarre and non-bizarre DLB in a large non-clin-ical population, with the prediction that bizarre beliefs would be reported to a lesser extent than non-bizarre be-liefs. Such data would provide clinicians with a bench-mark to compare with those holding clinically relevant
beliefs (delusions), given that a key diagnostic criterion for delusion requires that such beliefs should not be com-monly endorsed by other members of a person’s culture. Within the three different sets of beliefs an association between delusion-like and paranormal and religious be-liefs was predicted, but not with general political/social beliefs. Finally, assuming a psychosis phenotype contin-uum, it was expected that relevant demographic charac-teristics (e.g. age, gender, socioeconomic group, educa-tion and ethnicity [25] ) found in clinical groups would also be found in the non-clinical sample. The following section briefly introduces the CBQ, before describing the results of the large survey.
Method
Cardiff Beliefs Questionnaire The CBQ includes 46 questions addressing a wide range of be-
liefs. These consist of 17 DLB (10 considered bizarre by DSM cri-teria), 10 paranormal and religious beliefs, and 19 political, social and science-related beliefs (Appendix). The term ‘delusion-like belief ’ is used here, given that ‘delusional ideation’ lacks a stan-dard definition (and in any case has been used interchangeably with ‘delusion’ [26] ). Moreover, unlike other non-clinical mea-sures (PDI [18, 27] ), which use a variety of terms (e.g. ‘feel’, ‘think’ or ‘worry’) interchangeably in their questions, all relevant CBQ questions used the term ‘belief ’ to avoid ambiguity (e.g. using ‘feel’ may highlight affective features).
Table 2. Percentage of participants (n = 1,000) reporting DLB weakly, moderately or strongly in the final study
Delusion type DLB1 P ercentage reporting belief
weak moderate strong total
Cotard You are dead and/or do not exist 3.2 1.3 0.9 5.4Capgras Relatives or close friends are sometimes replaced by identical-looking impostors 3.4 2.0 0.4 5.8Somatoparaphrenia Part of your body does not belong to you 3.0 2.0 1.1 6.1Erotomania Some well-known celebrity is secretly in love with you 4.9 1.0 1.0 6.9Parasitosis You are infested by parasites 5.7 3.9 2.8 12.4Nihilism The world is about to end 7.6 3.6 1.7 12.9Mirrored-self misidentification The reflection in the mirror is sometimes not you 7.1 8.7 2.6 18.4Frégoli People you know disguise themselves as others to manipulate or influence you 10.6 9.9 4.4 24.9Reduplicative paramnesia (person) Some people are duplicated, i.e. are in 2 places at the same time 12.4 9.7 4.1 26.2Subjective doubles There is another person who looks and acts like you 13.0 14.3 5.4 32.7Controlled thoughts Your thoughts are not fully under your control 12.3 15.1 6.2 33.6Persecution Certain people are out to harm or discredit you 14.8 12.5 6.5 33.8Reference People say or do things that contain special messages for you 14.4 17.1 7.0 38.5Reduplicative paramnesia (place) Certain places are duplicated, i.e. are in 2 different locations at the same time 14.3 17.6 6.8 38.7Grandeur You are an exceptionally gifted person that others do not recognise 17.0 19.7 3.8 40.5Controlled actions You are not in control of some of your actions 15.4 18.1 10.8 44.3Body dysmorphia Your body or part of your body is misshapen or ugly 14.0 21.6 10.8 46.4
DLB = Delusion-like belief. 1 Bizarre DLB are set in italics.

DLB Psychopathology 2011;44:106–115 109
Item Selection The final version of the CBQ was developed following feed-
back from 3 iterative pilot versions, involving a total sample of 559 participants. DLB were based on the major thematic delusions found in mainstream psychotic and neuropsychiatric conditions. Items addressing DLB were adapted from the DSM-IV-TR [20] , existing clinical measures [19, 28–30] and examples from the cog-nitive neuropsychological research literature [31–33] . To ensure coverage of a broad range, items were chosen to be representative of each delusional theme. These included 5 questions relating to subtypes of delusional disorder [20] ; 1 item each for persecutory, erotomanic and grandiose ideas, and 2 different aspects of the somatic subtype (body dysmorphia and parasitosis). Two other items assessed the non-bizarre ideas of reference and nihilistic beliefs.
In addition, 10 questions specifically addressed bizarre themes. While the boundaries between what are considered bi-zarre and non-bizarre beliefs are not always clear (there is dis-agreement between experienced clinicians regarding the diagno-sis [34] ), non-bizarre delusions can be distinguished from bizarre by invoking the ‘implausibility’ criterion adopted from the DSM-IV. Thus a belief, however strange or unlikely, could be considered non-bizarre if it were physically possible. However, delusions in which the events were considered impossible or highly implausi-ble to occur in reality were deemed bizarre.
Bizarre delusions have been comparatively underresearched, perhaps due to the assumption that their implausibility makes them unlikely to be found in the general population. However, given the emphasis on the content of beliefs in the criteria for schizophrenia (with different requirements depending on the bi-zarre/non-bizarre distinction), it was important to determine the degree to which bizarre ideas were present. Bizarre items were considered to cover beliefs of external control, thought insertion, the Capgras syndrome, Cotard’s syndrome, the Frégoli syn-drome, reduplicative paramnesia (of both person and place), mir-rored-self misidentification, subjective doubles and somatopara-phrenia.
The questions addressing paranormal and religious beliefs were constructed from reviews of published market research polls [3, 35, 36] and paranormal belief measures [37–39] . Following Lin-deman and Aarnio [ 40 , pp. 586–587], we defined this cluster as ‘beliefs in physical, biological or psychological phenomena that feature fundamental or core ontological properties of another on-tological category’ (e.g. ‘do you believe that some people commu-nicate with the dead?’). Finally, the last group of beliefs included scientific, political and social items (e.g. ‘do you believe that hu-mans cause significant global warming?’). Importantly, the large number of non-clinical belief questions provided a balanced con-text aimed to encourage participants to respond truthfully and allowed exploration of the links between DLB and other belief types.
Unlike previous questionnaires, the CBQ questions always in-volved current beliefs to avoid relying on the memory of partici-pants, with respondents being offered 5 response options: ‘do not believe’ (–1); ‘don’t know’ (0); ‘weakly believe’ (1); ‘moderately be-lieve’ (2), and ‘strongly believe’ (3). The participants were explic-itly asked not to include beliefs related to the influence of drugs/alcohol.
Reliability and Validity of CBQ Test-Retest Reliability. Seventy-six participants (age: 18–48
years; mean: 21.4 years; SD: 4.91 years) completed version 2 of the CBQ on 2 occasions, on average 1 month apart. A highly signifi-cant correlation was found between participants’ responses for the 2 sessions (Pearson’s r = 0.865; p ! 0.001).
Internal Consistency. Two exploratory principal component analyses were conducted to assess the dimensionality of (1) para-normal and religious beliefs and (2) DLB. The majority of items in both categories loaded strongly onto a single component (for each group), although 3 delusion-like and 2 paranormal and reli-gious items with low factor loadings (below 0.4) were removed from the analysis to ensure a reliable scale for comparisons. Using the large sample from the general public described below (n = 1,000), both the CBQ delusion-like (n = 14) and paranormal and religious (n = 8) items demonstrated good internal consistency (Cronbach’s ! of 0.79 and 0.80, respectively). Corrected split-half reliability analysis indicated relatively good correlations of 0.82 for delusion-like and 0.81 for paranormal and religious items. Po-litical/social items, given the wide range of beliefs covered in this category, were understandably less stable, but 13 of the 19 items (6 were removed due to low item-whole correlations) nevertheless formed an adequate scale, with a Cronbach ! of 0.65 and cor-rected split-half reliability of 0.69.
Construct Validity. 169 participants completed version 3 of the CBQ and the Oxford-Liverpool Inventory of Feelings and Experiences (O-LIFE [41] ), an established measure of psychosis-proneness, previously used when evaluating the construct valid-ity of the PDI. This is divided into 4 subscales (unusual experi-ences, cognitive disorganisation, introvertive anhedonia and impulsive nonconformity), and provides a strong evaluation of construct validity. Correlations were expected between anoma-lous beliefs (in particular, DLB) and the most similar OLIFE scale (unusual experiences) but not, or at least to a lesser extent, with the other O-LIFE scales. The CBQ scores (for DLB, para-normal and religious beliefs, and political/social beliefs) were calculated by summing participants’ positive responses (i.e. rat-ings of 1–3) for the belief items that formed part of the scales described in the previous subsection Internal Consistency. These scores were correlated against all 4 O-LIFE scales, but only those significant at p ! 0.001 were considered. Congruent validity was established as the O-LIFE unusual experiences scale correlated with delusion-like and paranormal and religious be-liefs ( " = 0.35 and 0.36, respectively), but not with political/social beliefs. The less relevant O-LIFE scales did not correlate with the CBQ scores ( " varying between –0.08 and 0.19), demonstrating discriminant validity. Thus, the paranormal and religious be-liefs and DLB on the CBQ are associated with positive symptom-atology scores, in particular those relating to aberrant beliefs and experiences.
Study Design and Participants A stratified random sampling technique was used to obtain a
large sample from across Britain, with quotas set on age, gender and employment status. Computer-assisted telephone interview-ing was carried out by an experienced market research company (MRUK), using numbers generated by random digit dialling. Telephone interviews were chosen as being more conducive to frank responses than face-to-face interviews [42] . A total of 1,000 adults (aged 18 years or over) took part in the survey ( table!2 ). Of
Pechey/Halligan
Psychopathology 2011;44:106–115 110
these participants, 19.4% were aged 18–29 years, 29.2% aged 30–44 years, 24.5% aged 45–59 years and 26.9% aged 60 years or over; 52.1% were female. Socioeconomic groups (using British classifi-cations according to occupation/prior occupation) were AB (e.g. managers, administrators and professionals; 34.6%), C1 (e.g. cler-ical workers, call centre agents, nursery nurses; 21.2%), C2 (tech-nical and craft workers; 9.3%), DE (semi/unskilled manual work-ers; 20.3%) and not classified (14.6%). The study was approved by the Cardiff University School of Psychology ethics committee, and all participants gave verbal consent.
Results
Prevalence of Beliefs Delusion-Like Beliefs (DLB) The key finding was that 1 or more of the 17 DLB were
strongly endorsed (rated 3) by 38% of the participants. Moreover, 91% endorsed (rated 1–3) at least 1 DLB. It was also relatively common to endorse more than 1 DLB, 77% of the participants endorsing more than 1 at any strength. Two or more DLB were strongly endorsed by 17% of the participants. Comparing non-bizarre and bizarre DLB, the results showed both were given similar levels of en-dorsement, 1 or more being strongly endorsed by 25 and 26%, respectively. Similarly, the results for any level of conviction showed at least 1 non-bizarre DLB item was endorsed by 79% and at least 1 bizarre DLB item by 78%. Table!2 shows that beliefs in one’s body being misshapen or ugly and in not being in control of one’s actions were the most common. Even bizarre delusional themes thought of as clinically rare (and previously not much re-ported), such as those associated with Capgras syndrome
or Cotard’s syndrome, were endorsed by a surprising number of this sample.
Despite the high levels of endorsement of DLB in gen-eral, the number of reported bizarre beliefs was relatively lower than non-bizarre beliefs, as predicted.
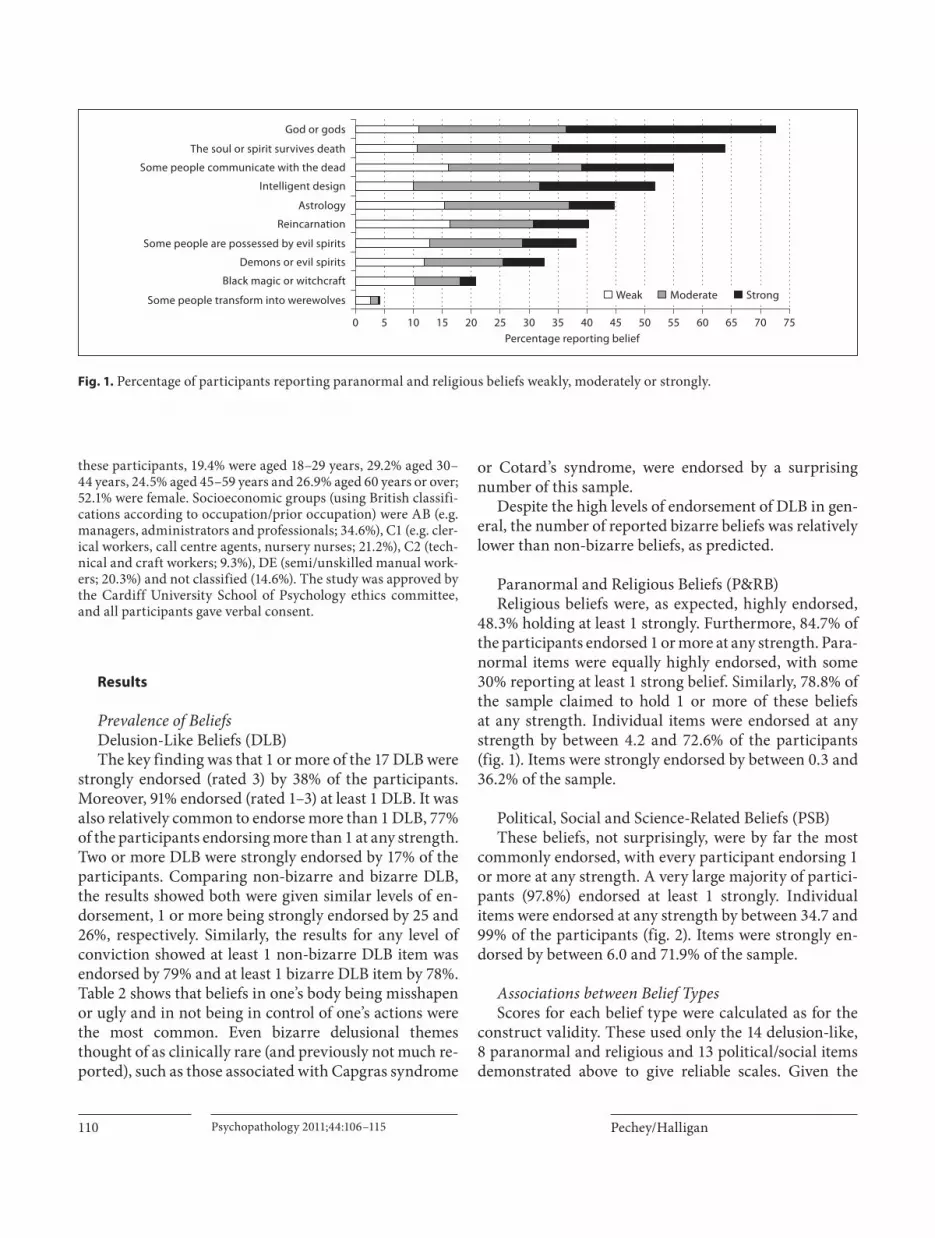
Paranormal and Religious Beliefs (P&RB) Religious beliefs were, as expected, highly endorsed,
48.3% holding at least 1 strongly. Furthermore, 84.7% of the participants endorsed 1 or more at any strength. Para-normal items were equally highly endorsed, with some 30% reporting at least 1 strong belief. Similarly, 78.8% of the sample claimed to hold 1 or more of these beliefsat any strength. Individual items were endorsed at any strength by between 4.2 and 72.6% of the participants ( fig.!1 ). Items were strongly endorsed by between 0.3 and 36.2% of the sample.
Political, Social and Science-Related Beliefs (PSB) These beliefs, not surprisingly, were by far the most
commonly endorsed, with every participant endorsing 1 or more at any strength. A very large majority of partici-pants (97.8%) endorsed at least 1 strongly. Individual items were endorsed at any strength by between 34.7 and 99% of the participants ( fig. 2 ). Items were strongly en-dorsed by between 6.0 and 71.9% of the sample.
Associations between Belief Types Scores for each belief type were calculated as for the
construct validity. These used only the 14 delusion-like, 8 paranormal and religious and 13 political/social items demonstrated above to give reliable scales. Given the
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75
Some people transform into werewolves
Black magic or witchcraft
Demons or evil spirits
Some people are possessed by evil spirits
Reincarnation
Astrology
Intelligent design
Some people communicate with the dead
The soul or spirit survives death
God or gods
Percentage reporting belief
Weak Moderate Strong
Fig. 1. Percentage of participants reporting paranormal and religious beliefs weakly, moderately or strongly.

DLB Psychopathology 2011;44:106–115 111
large size, the sample was split randomly into 4 groups of 250, and Spearman’s correlations were carried out for each of these. Significant correlations were found be-tween delusion-like and paranormal and religious beliefs for all 4 groups ( table!3 ), but no significant correlations between delusion-like and political/social beliefs or be-tween paranormal and religious and political/social be-liefs.
Demographic Variables Non-parametric tests (Kruskal-Wallis/Mann-Whit-
ney) were used (given their relative robustness and the ordinal nature of the response variable) to assess the ef-fects of relevant demographic variables [age group; gen-der; socioeconomic group; education (secondary/univer-sity/higher); ethnicity (white/other); religion (Christian/other/none); household (live with others/live alone)] on the DLB score.
Age [ # 2 (3) = 39.88] and socioeconomic group [ # 2 (3) = 32.08] were both significant factors (p ! 0.0001) related to the DLB score, whereas associations with the other variables were non-significant. Follow-up Mann-Whit-ney tests were carried out to compare between the levels of each significant demographic variable ( table!4 ). For the
purpose of calculating odds ratios for significant com-parisons, the participants were divided into above and below average DLB scores.
Eighteen- to 29-year-olds showed significantly higher DLB scores than those in each of the other age groups. No other age group comparisons were significant. Individu-als in socioeconomic group DE (semi/unskilled manual workers) had significantly higher DLB scores than those in group AB (e.g. managers, administrators and profes-sionals).
Earth has been visited by aliens from other solar systemsEarth is the centre of the universe
Animals have beliefsExtraterrestrial life
Same-sex relationships are rightIt is right to use animals for medically related research
Death penalty for serious crimesYoung children (under 6) are capable of holding beliefs
Euthanasia is rightAbortion is right
Organised religion is one of the main sources of human strifeTheory of evolution
Humans share a common ancestor with apesDemocracy is the best system of government
You have fundamental human rights that cannot be taken from youHumans cause signi"cant global warming
You have free choice or free willPositive thoughts and attitudes improve your physical wellbeing
People should help those less fortunate than themselves
Percentage reporting belief0 40 50 60 70 80 90 10010 20 30
Weak Moderate Strong
Fig. 2. Percentage of participants reporting political/social beliefs weakly, moderately or strongly.
Table 3. Spearman’s correlations between scores for each belief type
P&RB PSB
DLB 0.32–0.46 0.12–0.19P&RB 1 –0.01–0.16
P&RB = Paranormal and religious beliefs; PSB = political/so-cial beliefs.

Pechey/Halligan
Psychopathology 2011;44:106–115 112
Discussion
Delusion-Like Beliefs In this study, a substantial proportion of participants
(38%) strongly endorsed DLB (and 91% at any strength), indicating that these types of beliefs are not uncommon. This level of endorsement for currently held beliefs is higher than previous lifetime prevalence studies of delu-sion-type beliefs showed (around 15% [5] ). This was due in part to efforts to minimise the psychiatric or mental health connotations (although the degree to which these efforts were effective was not assessed) and to embed such beliefs in more generic sociocultural beliefs. The preva-lence levels for currently held beliefs were not, however, dissimilar to levels of lifetime delusional ideation found using the PDI [18] , where around 95% of the sample en-dorsed at least one item to some degree. This comparison is especially pertinent, given the similar focus of these instruments, and also the presence of a comparable num-ber of delusion-related items on both. The current study found high levels of belief when including a much wider range of beliefs, including a more varied selection of DLB due to the inclusion of more bizarre themes.
Indeed, 26% of the participants strongly endorsed bi-zarre DLB (78% at any strength), suggesting that the pres-ence of such a belief is not in itself sufficient to qualify it as a clinical delusion. Only a few of these bizarre beliefs have been investigated in any form in general population studies before. In contrast to the DSM assumption that these are so significantly different as to warrant a special set of criteria for the diagnosis of schizophrenia, it seems that these forms of belief are relatively common in non-clinical populations. This provides further support and extension of the continuum hypothesis to bizarre DLB in non-clinical samples.
Demographics Some of the demographic factors associated with high
DLB scores are worth comment. Individuals who were aged 18–29 years or belonged to the lowest socioeconom-ic group tended to report higher DLB scores. Both factors identified here have been associated with delusional be-liefs [25, 43–45] . In addition, younger age has previously been found to correlate with delusional ideation and is considered to reflect a neurodevelopmental disposition that favours the expression of psychosis proneness [17, 46] . Gender did not appear to be a significant factor in this study, despite being associated with subclinical psy-chosis in a meta-analysis by van Os et al. [6] . This may be due to the wider range of delusion-like items included – for example, the item addressing body dysmorphia is more common among females. Phillips et al. [47] report that 72% of their sample of delusional body dysmorphic disorder patients were female.
Other Belief Types This is the first study to provide an explicit compari-
son with other common beliefs, including paranormal and religious beliefs, in a large sample. Not surprisingly, these types of belief were the most commonly endorsed, with the majority being endorsed (at any strength) by over 80% of the sample. In a similar finding to that by Gallup and Newport [35] , where paranormal beliefs were endorsed by 75%, in our study 79% reported one or more beliefs of the paranormal type at any strength (not in-cluding beliefs in God or gods, intelligent design or the existence of a soul or spirit, which were judged to be mainly religious in content). These levels do not differ by any substantial degree from the results found in previous surveys ( table!3 ). Some of the variation is probably due to the differences in question phrasing. For example, in the present study, participants were offered three ‘believe’
Table 4. Demographic variables significantly associated with DLB score
Subgroup Mann-Whitney test Odds ratio 95% CI
Age group 30–44 years U (194, 292) = 21,701.0* 2.131 1.473–3.084(RG: 18–29 years) 45–59 years U (194, 245) = 18,131.0* 2.066 1.409–3.030
60+ years U (194, 269) = 17,122.5* 2.787 1.903–4.082
Socioeconomic group AB U (346, 203) = 25,179.0* 2.521 1.765–3.600(RG: DE) C1 U (212, 203) = 18,091.5 1.603 1.087–2.362
C2 U (93, 203) = 8,269.5 1.135 0.694–1.855
R G = Reference group. * p < 0.0001.

DLB Psychopathology 2011;44:106–115 113
options (strongly/moderately/weakly) rather than the yes/no choice presented in other studies. The general consistency in belief prevalence between polls suggests that the findings of the current study are reliable.
Relationships between Belief Types The relationship between paranormal and religious
beliefs and DLB suggests that the clinical descriptive boundary is far from clear, particularly given the strong and reliable association between delusional and paranor-mal beliefs [48–51] . However, a limitation of the CBQ paranormal and religious belief group is that the major-ity of these beliefs refer to some kind of spirit, and these results could be improved by taking into account a wider range of items of the paranormal type. Nonetheless, this result ties in with evidence suggesting that members of new religious movements report higher levels of delu-sional ideation than other non-clinical populations, but not the levels of distress or preoccupation found in clini-cal patients [52] . Moreover, the lack of association be-tween political/social beliefs and both paranormal belief and DLB types reinforces the distinctive nature of this relationship.
However, our study does not address why this relation-ship occurs. One potential explanation is that holding a belief may impact upon an individual’s wider belief sys-tem so that the endorsement of similar (e.g. irrational/unscientific) beliefs becomes more likely. This is in line with the web-of-belief hypothesis advocated by Quine and Ullian [53] , which suggests that a belief coheres with other beliefs held by an individual. In addition, other cog-nitive factors such as the reasoning biases associated with delusions [54, 55] may also play a role in the development of other abnormal beliefs. Similarly, anomalous experi-ences have been suggested to lead to the development of delusional beliefs [1] , and these experiences could have more wide-ranging effects on a variety of anomalous be-liefs.
To summarise, the main findings of the study confirm that it is not unusual to find large numbers of the general population endorsing DLB; 38% reported holding one or more DLB strongly (with approximately 90% at any strength). Moreover, the nature of these DLB was often bizarre (26% endorsing one or more of these items strong-ly). Thus, as previously indicated [6, 10, 18, 33, 56] , en-dorsing or holding certain beliefs per se may be necessary but not sufficient to qualify as a clinically relevant disor-der. Clinical diagnosis of any form of delusion largely de-pends on the functional consequences (e.g. distress, pre-occupation) that impact on an individual’s quality of life.
Indeed, one limitation of the CBQ is that, unlike the PDI, it does not measure these dimensions of the beliefs. How-ever, as a result, the CBQ retains its conciseness and avoids any implications, for example, that these beliefs might or should cause distress in those responding. The results also question assumptions regarding the presence of only a low level and extent of DLB in the general popu-lation and can be taken as further support for the con-tinuum hypothesis, alongside previous reports showing that DLB are not uncommon in non-clinical populations [25, 57–61] . The high levels of DLB within the normal population, and the association between DLB and para-normal and/or religious beliefs, raise important ques-tions regarding the assumption that delusions per se are distinguishable from other beliefs depending on the pro-portion of people assumed to hold them, as proposed in the DSM definition [20] .
Appendix: CBQ Questions
(Question order in parentheses)
Delusion-Like Beliefs Do you believe that your body or part of your body is mis-
shapen or ugly? (4) * Do you believe that you are an exceptionally gifted person that
others do not recognise? (6) * Do you believe that certain people are out to harm or discred-
it you? (8) Do you believe that certain places are duplicated, i.e. are in two
different locations at the same time? (10) Do you believe that people say or do things that contain special
messages for you? (12) Do you believe that the reflection in the mirror is sometimes
not you? (16) Do you believe that you are infested by parasites? (19) Do you believe that you are not in control of some of your ac-
tions? (21) Do you believe that some well-known celebrity is secretly in
love with you? (25) Do you believe that some people are duplicated, i.e. are in two
places at the same time? (28) Do you believe that the world is about to end? (30) * Do you believe that people you know disguise themselves as
others to manipulate or influence you? (32) Do you believe that your thoughts are not fully under your
control? (34) Do you believe that there is another person who looks and acts
like you? (36) Do you believe that part of your body doesn’t belong to you?
(38) Do you believe that relatives or close friends are sometimes
replaced by identical-looking impostors? (41) Do you believe that you are dead and/or do not exist? (43)

Pechey/Halligan
Psychopathology 2011;44:106–115 114
Paranormal and Religious Do you believe in astrology (i.e. that the position of the stars
and planets affects or determines your life)? (3) * Do you believe in a god or gods? (9) Do you believe that the soul or spirit survives death? (13) Do you believe in black magic or witchcraft? (15) To what extent do you believe in demons or evil spirits? (18) Do you believe in intelligent design (i.e. that the complexity of
the world suggests that it was purposefully designed by an intel-ligent creator)? (20)
Do you believe that some people communicate with the dead? (23)
Do you believe in reincarnation (i.e. that when you die your soul is reborn in another body)? (33)
Do you believe that some people transform into werewolves? (39) *
Do you believe that some people are possessed by evil spirits? (45)
Political, Social and Science-Related Do you believe that people should help those less fortunate
than themselves? (1) * Do you believe that humans cause significant global warming?
(2) Do you believe that euthanasia is right or wrong? (5) † Do you believe that democracy is the best system of govern-
ment? (7) Do you believe in extraterrestrial life? (11) Do you believe that you have fundamental rights that cannot
be taken from you? (14) Do you believe that abortion is right or wrong? (17) † To what extent do you believe that organised religion is one of
the main sources of human strife? (22) To what extent do you believe that humans share a common
ancestor with apes? (24)
Do you believe in the death penalty for serious crimes? (26) * To what extent do you believe that earth has been visited by
aliens from other solar systems? (27) Do you believe in the theory of evolution? (29) To what extent do you believe that same-sex relationships are
right or wrong? (31) † Do you believe it is right to use animals for medically related
research? (35) * , † To what extent do you believe that the earth is the centre of the
universe? (37) * To what extent do you believe that young children (under 6)
are capable of holding beliefs? (40) * Do you believe that you have free choice, or free will? (42) To what extent do you believe that animals have beliefs? (44) * Do you believe that positive thoughts and attitudes improve
your physical wellbeing? (46)
* !These questions were removed when calculating scores for comparisons due to low factor loadings and/or item-whole cor-relations.
† !To keep the scales consistent, ‘or wrong’ was omitted from these questions during the telephone interviews conducted in the study reported here.
Acknowledgements
Particular thanks to Professor Hadyn Ellis, who helped de-velop the Cardiff Beliefs Questionnaire, but sadly died beforeits completion. This work was supported by an Economic and So-cial Research Council studentship (PTA-031-2005-00352 to R.P.). MRUK carried out the telephone interviews.
References
1 Maher B: Anomalous experience and delu-sional thinking: the logic of explanations; in Oltmanns TF, Maher BA (eds): Delusional Beliefs. Chichester, Wiley, 1988, pp 15–33.
2 Jaspers K: General Psychopathology, ed 7, transl. Manchester, Manchester University Press, 1963.
3 Taylor H: The religious and other beliefs of Americans 2003. 2003. www.harrisinterac-tive.com/harris_poll/index.asp?PID=359 (accessed December 19, 2005).
4 Saha S, Chant D, Welham J, McGrath J: A systematic review of the prevalence of schizophrenia. PLoS Med 2005; 2: 413–433.
5 Rutten BPF, van Os J, Dominguez M, Krab-bendam L: Epidemiology and social factors: findings from the Netherlands Mental Health Survey and Incidence Study (NEM-ESIS); in Freeman D, Bentall R, Garety P (eds): Persecutory Delusions. Assessment, Theory, and Treatment. Oxford, Oxford University Press, 2008, pp 53–71.
6 van Os J, Linscott RJ, Myin-Germeys I, De-lespaul P, Krabbendam L: A systematicreview and meta-analysis of the psychosis continuum: evidence for a psychosis prone-ness-persistence-impairment model of psy-chotic disorder. Psychol Med 2009; 39: 179–195.
7 Strauss JS: Hallucinations and delusions as points on continua function: rating scale ev-idence. Arch Gen Psychiatry 1969; 21: 581–586.
8 Claridge G: Single indicator of risk for schizophrenia: probable fact or likely myth? Schizophr Bull 1994; 20: 151–168.
9 Crow TJ, Done DJ, Sacker A: Childhood pre-cursors of psychosis as clues to its evolution-ary origins. Eur Arch Psychiatry Clin Neu-rosci 1995; 245: 61–69.
10 Johns LC, van Os J: The continuity of psy-chotic experiences in the general population. Clin Psychol Rev 2001; 21: 1125–1141.
11 Byrne P: Stigma of mental illness and ways of diminishing it. Adv Psychiatr Treat 2000; 6: 65–72.
12 Corrigan PW: Mental health stigma as social attribution: implications for research meth-ods and attitude change. Clin Psychol Sci Pract 2000; 7: 48–67.
13 White A, Shiralkar P, Hassan T, Galbraith N, Callaghan R: Barriers to mental healthcare for psychiatrists. Psychiatr Bull 2006; 30: 382–384.
14 French C, Rona RJ, Jones M, Wessely S: Screening for physical and psychological ill-ness in the British Armed Forces. 2. Barriers to screening: learning from the opinions of service personnel. J Med Screen 2004; 11: 153–161.
15 Ray JJ, Lovejoy FH: Age-related social desir-ability responding among Australian wom-en. J Soc Psychol 2003; 143: 669–671.

DLB Psychopathology 2011;44:106–115 115
16 Thomsen DK, Mehlsen MY, Vidik A, Som-merlund B, Zachariae R: Age and gender dif-ferences in negative affect: is there a role for emotion regulation? Pers Individ Dif 2005; 38: 1935–1946.
17 Verdoux H, Maurice-Tison S, Gay B, van Os J, Salamon R, Bourgeois ML: A survey of de-lusional ideation in primary-care patients. Psychol Med 1998; 28: 127–134.
18 Peters ER, Joseph SA, Day S, Garety P: Mea-suring delusional ideation: the 21-item Pe-ters et al Delusions Inventory (PDI). Schizophr Bull 2004; 30: 1005–1022.
19 Peters ER, Joseph SA, Garety PA: The mea-surement of delusional ideation in the nor-mal population: introducing the PDI (Peters et al Delusions Inventory). Schizophr Bull 1999; 25: 553–576.
20 American Psychiatric Association: Diagnos-tic and Statistical Manual of Mental Disor-ders, ed 4, rev. Washington, American Psy-chiatric Association, 2000.
21 Coltheart M: The 33rd Sir Frederick Bartlett Lecture: cognitive neuropsychiatry and de-lusional belief. Q J Exp Psychol 2007; 60: 1041–1062.
22 Davies M, Coltheart M, Langdon R, Breen N: Monothematic delusions: towards a two-fac-tor account. Philos Psychiatr Psychol 2001; 8: 133–158.
23 Ellis HD, Lewis MB: Capgras delusion: a window on face recognition. Trends Cogn Sci 2001; 5: 149–156.
24 Stone T, Young AW: Delusions and brain in-jury: the philosophy and psychology of be-lief. Mind Lang 1997; 12: 327–364.
25 van Os J, Hanssen M, Bijl RV, Ravelli A: Strauss 1969, revisited: a psychosis continu-um in the general population? Schizophr Res 2000; 45: 11–20.
26 Wang C-K, Lee JY-Y: Monosymptomatic hy-pochondriacal psychosis complicated by self-inflicted skin ulceration, skull defect and brain abscess. Br J Dermatol 1997; 137: 299–302.
27 Stefanis NC, Hanssen M, Smirnis NK, Avramopoulos DA, Evdokimidis IK, Stefa-nis CN, Verdoux H, van Os J: Evidence that three dimensions of psychosis have a distri-bution in the general population. Psychol Med 2002; 32: 347–358.
28 Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, Hergueta T, Baker R, Dunbar GC: The Mini-Internation-al Neuropsychiatric Interview. J Clin Psychi-atry 1988; 59(suppl 20):22–33.
29 Bebbington PE, Nayani T: The Psychosis Screening Questionnaire. Int J Methods Psy-chiatr Res 1995; 5: 11–19.
30 Robins LN, Helzer JE, Croughan J, Ratcliff KA: National Institute of Mental Health Di-agnostic Interview Schedule. Arch Gen Psy-chiatry 1981; 38: 381–389.
31 Ellis HD, Young AW: Accounting for delu-sional misidentifications. Br J Psychiatry 1990; 157: 239–248.
32 Davies M, Coltheart M: Introduction: pa-thologies of belief. Mind Lang 2000; 15: 1–46.
33 Bell V, Halligan PW, Ellis HD: Explaining delusions: a cognitive perspective. Trends Cogn Sci 2006; 10: 219–226.
34 Flaum M, Arndt S, Andreasen NC: The reli-ability of ‘bizarre’ delusions. Comp Psychia-try 1991; 32: 59–65.
35 Gallup GH, Newport F: Belief in paranormal phenomena among adult Americans. Skept Inq 1991; 15: 137–146.
36 Rice TW: Believe it or not: religious and oth-er paranormal beliefs in the United States. J Sci Study Relig 2003; 421: 95–106.
37 Eckblad M, Chapman LJ: Magical ideation as an indicator of schizotypy. J Consult Clin Psychol 1983; 1: 215–225.
38 Tobacyk JJ, Milford G: Belief in paranormal phenomena: assessment instrument devel-opment and implications for personality functioning. J Pers Soc Psychol 1983; 44: 1029–1037.
39 Thalbourne MA, Delin PS: A new instru-ment for measuring the sheep-goat variable: its psychometric properties and factor struc-ture. J Am Soc Psych Res 1993; 59: 172–186.
40 Lindeman M, Aarnio K: Paranormal beliefs: their dimensionality and correlates. Eur J Pers 2006; 20: 585–602.
41 Mason O, Claridge G, Jackson M: New scales for the assessment of schizotypy. Pers Indi-vid Dif 1995; 1: 7–13.
42 Frey JH, Oishi SM: How to Conduct Inter-views by Telephone and in Person. London, Sage, 1995.
43 Tien AY: Distributions of hallucinations in the population. Soc Psychiatry Psychiatr Ep-idemiol 1991; 26: 287–292.
44 Johns LC, Cannon M, Singleton N, Murray RM, Farrell M, Brugha T, Bebbington P, Jen-kins R, Meltzer H: The prevalence and cor-relates of self-reported psychotic symptoms in the British population. Br J Psychiatry 2004; 185: 298–305.
45 Scott J, Welham J, Martin G, Bor W, Najman J, O’Callaghan M, Williams G, Aird R, Mc-Grath J: Demographic correlates of psychot-ic-like experiences in young Australian adults. Acta Psychiatr Scand 2008; 118: 230–237.
46 Lincoln TM, Keller E: Delusions and halluci-nations in students compared to the general population. Psychol Psychother 2008; 81: 231–235.
47 Phillips KA, Menard W, Pagano ME, Fay C, Stout RL: Delusional versus nondelusional body dysmorphic disorder: clinical features and course of illness. J Psychiatr Res 2006; 40: 95–104.
48 Thalbourne MA: Belief in the paranormal and its relationship to schizophrenia-rele-vant measures: a confirmatory study. Br J Clin Psychol 1994; 33: 78–80.
49 Irwin HJ, Green MJ: Schizotypal processes and belief in the paranormal: a multidimen-sional study. Eur J Parapsychol 1998; 14: 1–15.
50 Houran J, Irwin HJ, Lange R: Clinical rele-vance of the two-factor Rasch version of the Revised Paranormal Belief Scale. Pers Indi-vid Dif 2001; 31: 371–382.
51 McCreery C, Claridge G: Healthy schizo-typy: the case of out-of-the-body experienc-es. Pers Individ Dif 2002; 32: 141–154.
52 Peters E, Day S, McKenna J, Orbach G: Delu-sional ideation in religious and psychotic populations. Br J Clin Psychol 1999; 38: 83–96.
53 Quine WV, Ullian JS: The Web of Belief, ed 2. Toronto, Random House, 1970.
54 Garety PA, Hemsley DR: Delusions. Investi-gations into the Psychology of Delusional Reasoning. Oxford, Oxford University Press, 1994.
55 Linney YM, Peters ER, Ayton P: Reasoning biases in delusion-prone individuals. Br J Clin Psychol 1998; 37: 285–303.
56 Lincoln TM: Relevant dimensions of delu-sions: continuing the continuum versus cat-egory debate. Schizophr Res 2007; 93: 211–220.
57 Eaton WW, Romanoski A, Anthony JC, Nestadt G: Screening for psychosis in the general population with a self-report inter-view. J Nerv Ment Dis 1991; 179: 689–693.
58 Kendler KS, Gallagher TJ, Abelson JM, Kess-ler RC: Lifetime prevalence, demographic risk factors, and diagnostic validity of non-affective psychosis as assessed in a US com-munity sample. Arch Gen Psychiatry 1996; 53: 1022–1031.
59 Poulton R, Caspi A, Moffitt TE, Cannon M, Murray R, Harrington H: Children’s self-reported psychotic symptoms and adult schizophreniform disorder. Arch Gen Psy-chiatry 2000; 57: 1053–1058.
60 Olfson M, Lewis-Fernández R, Weissman MM, Feder A, Gameroff MJ, Pilowsky D, Fuentes M: Psychotic symptoms in an urban general medicine practice. Am J Psychiatry 2002; 159: 1412–1419.
61 Scott J, Chant D, Andrews G, McGrath J: Psy-chotic-like experiences in the general com-munity: the correlates of CIDI psychosis screen items in an Australian sample. Psy-chol Med 2006; 36: 231–238.

![El romance Mainés en su contexto sociocultural [Mainés: A Folk Ballad inside Its Sociocultural Context]](https://img.pdfslide.net/doc/110x75/631f57d163ac2c35640ac400/el-romance-maines-en-su-contexto-sociocultural-maines-a-folk-ballad-inside-its.jpg)



























